Embed Size (px)
Citation preview

s9tb
C
NS
Peer-Review Reports
A New Bilayer Chitosan Scaffolding as a Dural Substitute: Experimental EvaluationJosé Humberto Sandoval-Sánchez1, Rodrigo Ramos-Zúñiga2, Sonia Luquín de Anda2, Fernando López-Dellamary2,
Rocío Gonzalez-Castañeda2, Juan De la Cruz Ramírez-Jaimes3, Guadalupe Jorge-Espinoza2
ChcamCoHgai
lmwrdgao(
1isarsacmb
M
IEu3(ts
ctdpflt
�n
bw
INTRODUCTION
At the end of a neurosurgical procedure, aninadequate dural closure exposes patientsto cerebrospinal fluid (CSF) fistula, infec-tions, neural tissue herniation, hypertensivepneumocephalus, pseudomeningocele, andadhesions (3, 4, 21, 31, 37). For these rea-sons, a watertight dural closure with autol-ogous dura mater is recommended; how-ever, in some situations it is necessary touse dural substitutes. These situations in-clude replacement of dura mater loss, en-largement of the intradural compartment,and difficult closures owing to tearing orshrinkage of the dural edges during longoperations (4, 17, 38, 42). Numerous duralubstitutes have been implemented (1, 4-6,, 25, 30, 32, 33, 45); however, these substi-utes lack suitable characteristics and have
Key words� Biomaterials� Chitosan� Dura mater� Duraplasty� Graft� Tissue engineering
Abbreviations and AcronymsBChS: Bilayer chitosan scaffolding
M: Collagen matrixCSF: Cerebrospinal fluid
From the 1Department of Neurosurgery,Hospital de Especialidades, Centro Médico
acional de Occidente, Instituto Mexicano del Seguroocial, Guadalajara, Jalisco, México; 2Laboratory of
Neuroscience, Department of Neuroscience, CentroUniversitario de Ciencias de la Salud, Universidad deGuadalajara, Guadalajara, Jalisco, México; and3Department of Neuropathology, Gomez-Farías Hospital,ISSSTE, Guadalajara, Jalisco, México
To whom correspondence should be addressed:Rodrigo Ramos-Zúñiga, M.D., Ph.D.[E-mail: [email protected]]
Citation: World Neurosurg. (2012).DOI: 10.1016/j.wneu.2011.07.007
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter © 2012 Elsevier Inc.All rights reserved.
een associated with complications such as a
WORLD NEUROSURGERY xx [x]: xxx, MON
SF fistula, aseptic meningitis, infections,ydrocephalus, pseudomeningocele, corti-al inflammation, adhesions, and bleeding,mong others (8, 10, 12, 13, 24). Collagenatrix (CM) (Duragen; Integra LifeSciencesorporation, Plainfield, New Jersey, USA) isne of the most common dura substitutes.owever, CM has poor resistance to elon-
ation, it cannot be sutured, and it is notlways available in undeveloped countries;n addition, it is very expensive (25, 30, 40).
Chitosan, a substance obtained by deacety-ation of chitin, stimulates macrophages, che-
oattracts neutrophils, and helps accelerateound healing (20, 27, 34, 43). Chitosan de-
ivatives limit scar formation and retractionuring healing (2). They are versatile, biode-radable, and nontoxic; offer a wide range ofpplications; and can be formulated in vari-us forms, including powders, gels, and films18). They have been used in skin regeneration
� OBJECTIVE: To evaluate whetherprovide a watertight dural closure anexperimental in vivo model.
� METHODS: In the in vitro phase,haracteristics were evaluated: pore s
ensile strength, strain, and toughnurectomized New Zealand rabbits wlasty groups with autologous dura, couid leakage pressure was measured
o regeneration was evaluated throug
RESULTS: BChS was standardizedonporous layer and a porous layer. T
was 400 �m, strain was 57.8%, and tencharacteristics of BChS allowed duralleak. There were no differences in fludura, and CM groups. Histologic anadequate dural regeneration.
� CONCLUSIONS: BChS is an idealecause it can be sutured, and it inducithout evidence of fibrosis.
nd for orthopedic tissue engineering (2, 7, a
TH 2012
4, 15). Nevertheless, pure chitosan bilayer orts derivatives have not been evaluated as duralubstitutes (11). Because of the lack of a suit-ble dural substitute, we designed, elabo-ated, and characterized a bilayer chitosancaffolding (BChS). Then we evaluated thebility of BChS to provide a watertight durallosure over the course of different experi-ental times and permit colonization by fi-
roblasts in an experimental model in vivo.
ETHODS
n Vitro Phaselaboration of Bilayer Chitosan Scaffolding. Wesed chitosan with a molecular weight of58 kDa and deacetylation degree of 80.8%Vanson Laboratory, Redmond, Washing-on, USA). First, we elaborated acetic acidolution by dissolving chitosan (3 gr) in
er chitosan scaffolding (BChS) canrmit regeneration by fibroblasts in an
was elaborated and the followingthickness, water absorption capacity,
In the second in vivo phase, 27randomly assigned into three dura-n matrix (CM), or BChS. In all groups,
0, 21, or 180 days. Histology responsematoxylin and eosin stain.
obtain bilayer scaffoldings with aore size was 10 �m, total thickness
strength was 5.5 gr/mm2. The physicalure without cerebrospinal fluid (CSF)akage pressures between the BChS,
is showed fibroblast migration with
native for a watertight dural closurerganized regeneration with fibroblasts
bilayd pe
BChSize,ess.ere
llageat 1
h he
tohe psileclosid lealys
alteres o
cetic acid (2 ml) and distilled water (100
www.WORLDNEUROSURGERY.org 1

WabcbteaaCmempwr(tls
E
T
Wabo(
altin
ClmidWaeet
SW
PEER-REVIEW REPORTS
JOSÉ HUMBERTO SANDOVAL-SÁNCHEZ ET AL. CHITOSAN AS A DURAL SUBSTITUTE
mL). This solution was filtered to removethe insoluble content. To obtain the nonpo-rous layer, we poured 3 gr of the solutioninto a flat round mold 4.3 cm in diameter;later we evaporated the solvent in a vacuumoven at room temperature for 24 hours. Toelaborate the porous layer, we poured aceticacid solution (2 gr) into the mold contain-ing the dry nonporous chitosan layer at itsbottom. We immediately froze the mold at�196°C and then lyophilized it in a freeze-dryer for 5 hours (FTS Systems Inc, NewYork, New York, USA) to give a poroussponge layer over the nonporous layer. Wewashed the BChS with distilled water to ob-tain an alkaline pH.
Characterization of Bilayer Chitosan Scaffold-ing. We coated the BChS and CM (Duragen)with an ultrathin layer of gold salts in a coat-ing apparatus. We measured pore diameter,porous layer, nonporous layer, and totalthickness with a scanning electron micro-scope (Jeol JSM-5400LV; JEOL Ltd, Tokyo,Japan).
Later, we immersed samples of BChS andCM in a phosphate-buffered saline solutionfor 24 hours to evaluate water retention. Weplaced samples in filter paper, and weweighed and registered them as Wwet.Twenty-four hours later, we dried, weighed,and recorded as Wdry. Water retention wascalculated according to the following for-mula:
Water retention ( % ) � ��Wwet �
Wdry� ⁄ Wdry� � 100%
e also measured tensile strength (forcepplied to a biomaterial needed to producereakup of the biomaterial); strain (modifi-ation in the length of the biomaterial untilreakup as a result of a tensile force); and
oughness (capacity of a material to absorbnergy before breaking; this includes therea under the curve and reflects fragilitynd hardness on their ends) in BChS andM samples. We placed samples of 5 � 5m in a device that held the samples by the
dges. One edge was in contact with a dyna-ometer (maximum capacity of 1 kg). We
erformed traction on this edge slowly,hile the other edge was fixed to a table. We
egistered area, initial length, final lengthlength at rupture), and strength applied athe time of rupture. Subsequently, we calcu-ated elongation percentage and tensiletrength with the following formulas:
longation % � fL ⁄ iL � 100
2 www.SCIENCEDIRECT.com
ensile strength � S/A
here elongation % is elongation percent-ge, fL is final length, iL is initial lengthefore traction, S is strength (gr) at the timef rupture, and A is area of biomaterialmm2). Finally, a stress-strain curve was
made.
In Vivo PhaseThis study was approved by the local Com-mittee for Animal Experimentation, Centrode Investigación Biomédica de Occidente,and by the bioethical committee from Cen-tro Universitario de Ciencias de la Saludof University of Guadalajara, Mexico. Thestudy was performed in accordance withNOM ZOO099, Mexican law for care andmanagement of experimental animals.
Surgical Procedure. We used adult New Zea-land rabbits weighing 3 kg. For all invasiveprocedures, we injected xylazine 10% (3mg/kg body weight, Sedazine; LaboratoriesFort Dodge, Mexico City, Mexico), intra-muscularly as premedication, followed by 1mg of atropine. We used a mixture of 3.5mL of 10% ketamine and 0.45 mL of 10%xylazine dissolved in 40 mL of 0.9% sodiumchloride, administered intravenously at in-fusion rate of 10 –15 mL/hr, for general an-esthesia. We intubated the rabbits to allowbreathing. Next, we fixed the head andshaved the scalp. We made a scalp incisionin the midline of the cranium and, using anelectric drill, performed a craniectomy mea-suring 1.5 � 1 cm in the right parietal re-gion. We opened the dura with a small knifeunder microscopic observation and re-moved a 4 � 4 mm section of the dura.
At this point, rabbits were randomly as-signed into nine groups of three rabbitseach: groups 1a, 1b, and 1c (duraplasty withautologous dura mater and measurement offluid leakage pressure at 10, 21, or 180 dayslater); groups 2a, 2b, and 2c (duraplastywith CM [Duragen] and measurement offluid leakage pressure at 10, 21, or 180 dayslater); and groups 3a, 3b, and 3c (duraplastywith BChS and measurement of fluid leak-age pressure at 10, 21, or 180 days later).Wepositioned a 5 � 5 mm graft of autologousdura mater, CM, or BChS and fixed the graftwith four 10-0 polyamide sutures (Ethilon;Ethicon, Inc, Somerville, New Jersey, USA).We used round needles with noncutting mi-
crotips to prevent a lack of tightness of theWORLD NEUROSURGE
duraplasty caused by the suture holes (CMwas not sutured because the material didnot permit suturing). Finally, we fixed thebone flap with nylon 4-0 suture (AtramatIntern; Internacional Farmaceutica, MexicoCity, Mexico) and closed the scalp with 3-0nylon sutures (Atramat).
Postoperative Care and Postoperative Complica-tions. Rabbits were housed in individualcages exposed to daylight with free accessto food and water. We monitored the rab-bits for the presence of fever, CSF fistula,and infection from the immediate postop-erative period until performance of fluidleakage pressure test.
Fluid Leakage Pressure Test. At 10, 21, or 180days after surgery, we anesthetized the ani-mals, removed the bone flap, and infused asolution of 0.9% sodium chloride into thesubarachnoidal space under microscopicguidance and measured the fluid leakagepressure (in cm H2O) at the interface of thegraft and surrounding dura mater. A 22-Fcatheter was inserted and connected to asystem for measuring central venous pres-sure. The system contained a connection tothe subarachnoid space, another to the col-umn of a water measurement (cm H2O),
nd one more for the injection of saline so-ution. The measurement was registered athe time of leakage of liquid through thenterface of the implant, and the value wasoted in cm H2O.
olonization by Fibroblasts. After the fluideakage pressure test, we obtained speci-
ens of repaired areas for histologic exam-nation. We fixed specimens in paraformal-ehyde and blocked them in paraffin wax.e stained specimens with hematoxylin
nd eosin and performed light microscopicxamination. Then the specimens werevaluated by a pathologist who was blindedo assigned groups.
tatistical Analysise used �2 and Fisher exact test for cate-
gorical variables. To determine statisticalsignificance among groups, we used theKruskal-Wallis and Mann-Whitney U test.All analyses were performed using R for Li-nux software (R Development Core Team,Auckland, New Zealand); P values � 0.05
were considered significant.RY, DOI:10.1016/j.wneu.2011.07.007
fp
m
Fw
t68(awf
IPsC
FmgH
cg1wr
(
Cciccpacwouca
D
Ttawtidh
rvdCtbfirttan(pt
rous
PEER-REVIEW REPORTS
JOSÉ HUMBERTO SANDOVAL-SÁNCHEZ ET AL. CHITOSAN AS A DURAL SUBSTITUTE
RESULTS
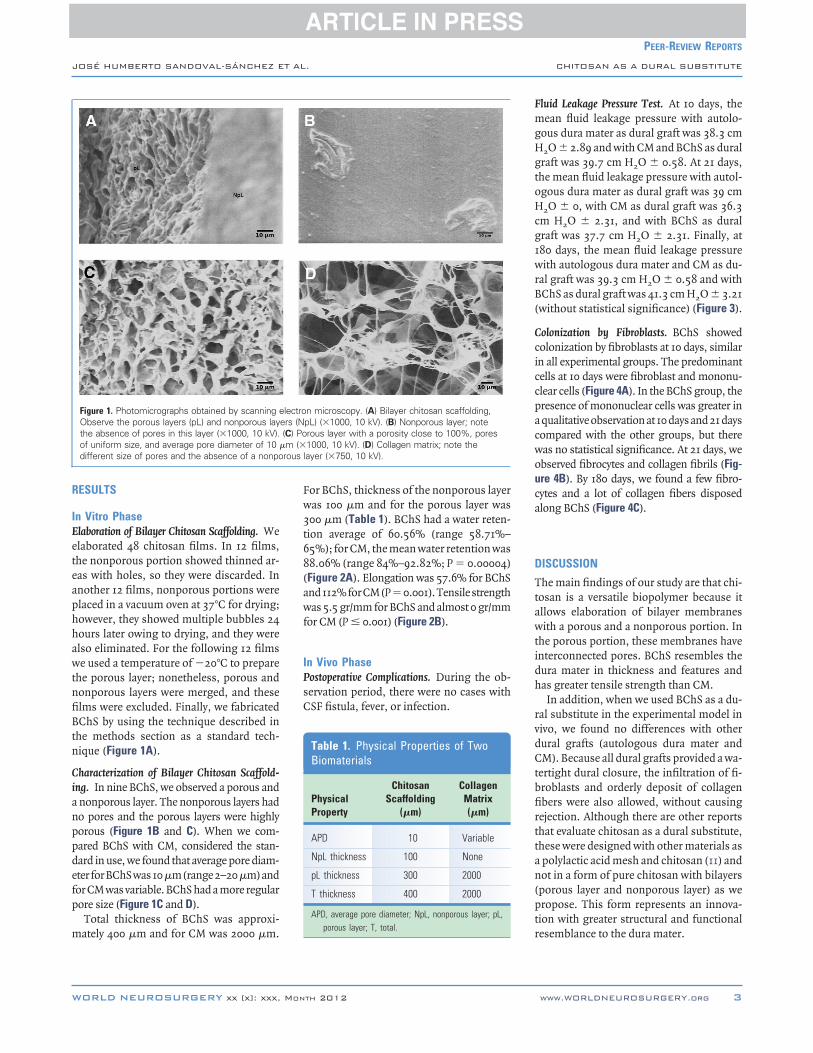
In Vitro PhaseElaboration of Bilayer Chitosan Scaffolding. Weelaborated 48 chitosan films. In 12 films,the nonporous portion showed thinned ar-eas with holes, so they were discarded. Inanother 12 films, nonporous portions wereplaced in a vacuum oven at 37°C for drying;however, they showed multiple bubbles 24hours later owing to drying, and they werealso eliminated. For the following 12 filmswe used a temperature of �20°C to preparethe porous layer; nonetheless, porous andnonporous layers were merged, and thesefilms were excluded. Finally, we fabricatedBChS by using the technique described inthe methods section as a standard tech-nique (Figure 1A).
Characterization of Bilayer Chitosan Scaffold-ing. In nine BChS, we observed a porous anda nonporous layer. The nonporous layers hadno pores and the porous layers were highlyporous (Figure 1B and C). When we com-pared BChS with CM, considered the stan-dard in use, we found that average pore diam-eter for BChS was 10�m (range 2–20�m) andor CM was variable. BChS had a more regularore size (Figure 1C and D).
Total thickness of BChS was approxi-
Figure 1. Photomicrographs obtained by scanning eObserve the porous layers (pL) and nonporous laythe absence of pores in this layer (�1000, 10 kV).of uniform size, and average pore diameter of 10different size of pores and the absence of a nonpo
ately 400 �m and for CM was 2000 �m.
WORLD NEUROSURGERY xx [x]: xxx, MON
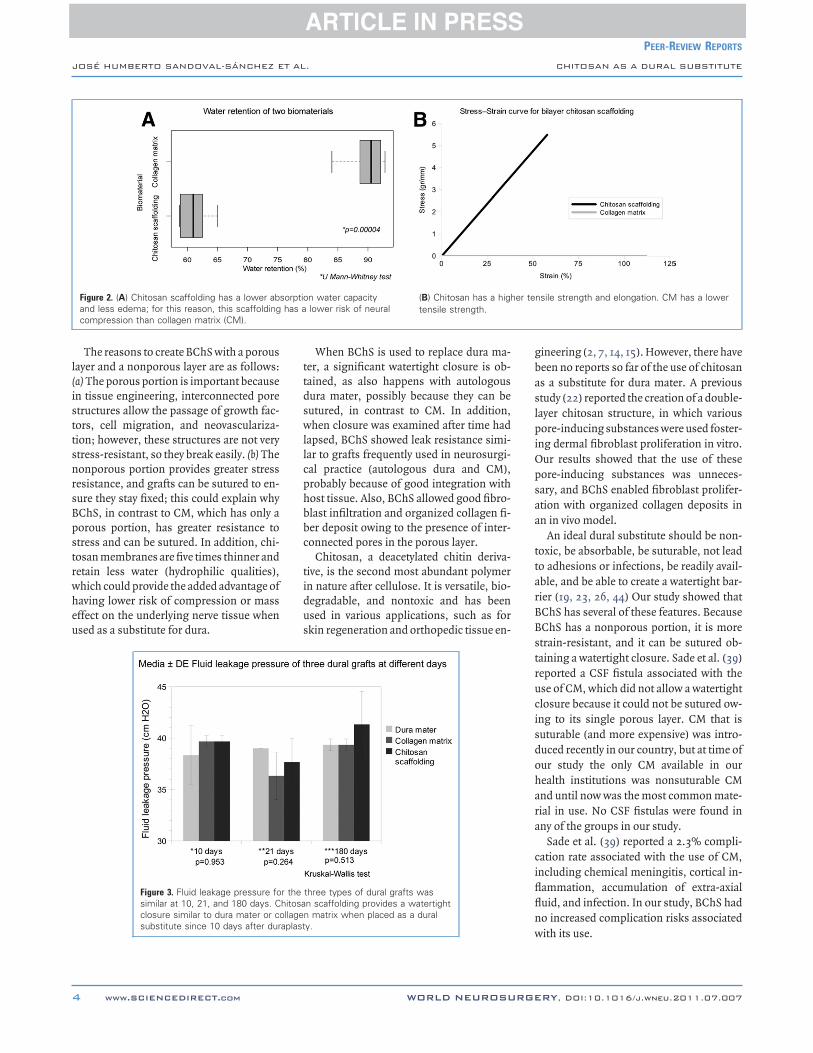
or BChS, thickness of the nonporous layeras 100 �m and for the porous layer was
300 �m (Table 1). BChS had a water reten-ion average of 60.56% (range 58.71%–5%); for CM, the mean water retention was8.06% (range 84%–92.82%; P � 0.00004)Figure 2A). Elongation was 57.6% for BChSnd 112% for CM (P�0.001). Tensile strengthas 5.5 gr/mm for BChS and almost 0 gr/mm
or CM (P � 0.001) (Figure 2B).
n Vivo Phaseostoperative Complications. During the ob-ervation period, there were no cases withSF fistula, fever, or infection.
n microscopy. (A) Bilayer chitosan scaffolding,pL) (�1000, 10 kV). (B) Nonporous layer; noterous layer with a porosity close to 100%, pores1000, 10 kV). (D) Collagen matrix; note the
layer (�750, 10 kV).
Table 1. Physical Properties of TwoBiomaterials
PhysicalProperty
ChitosanScaffolding
(�m)
CollagenMatrix(�m)
APD 10 Variable
NpL thickness 100 None
pL thickness 300 2000
T thickness 400 2000
APD, average pore diameter; NpL, nonporous layer; pL,
rporous layer; T, total.
TH 2012
luid Leakage Pressure Test. At 10 days, theean fluid leakage pressure with autolo-
ous dura mater as dural graft was 38.3 cm
2O � 2.89 and with CM and BChS as duralgraft was 39.7 cm H2O � 0.58. At 21 days,the mean fluid leakage pressure with autol-ogous dura mater as dural graft was 39 cmH2O � 0, with CM as dural graft was 36.3
m H2O � 2.31, and with BChS as duralraft was 37.7 cm H2O � 2.31. Finally, at80 days, the mean fluid leakage pressureith autologous dura mater and CM as du-
al graft was 39.3 cm H2O � 0.58 and withBChS as dural graft was 41.3 cm H2O � 3.21without statistical significance) (Figure 3).
olonization by Fibroblasts. BChS showedolonization by fibroblasts at 10 days, similarn all experimental groups. The predominantells at 10 days were fibroblast and mononu-lear cells (Figure 4A). In the BChS group, theresence of mononuclear cells was greater inqualitative observation at 10 days and 21 daysompared with the other groups, but thereas no statistical significance. At 21 days, webserved fibrocytes and collagen fibrils (Fig-re 4B). By 180 days, we found a few fibro-ytes and a lot of collagen fibers disposedlong BChS (Figure 4C).
ISCUSSION
he main findings of our study are that chi-osan is a versatile biopolymer because itllows elaboration of bilayer membranesith a porous and a nonporous portion. In
he porous portion, these membranes haventerconnected pores. BChS resembles theura mater in thickness and features andas greater tensile strength than CM.
In addition, when we used BChS as a du-al substitute in the experimental model inivo, we found no differences with otherural grafts (autologous dura mater andM). Because all dural grafts provided a wa-
ertight dural closure, the infiltration of fi-roblasts and orderly deposit of collagenbers were also allowed, without causing
ejection. Although there are other reportshat evaluate chitosan as a dural substitute,hese were designed with other materials aspolylactic acid mesh and chitosan (11) andot in a form of pure chitosan with bilayers
porous layer and nonporous layer) as weropose. This form represents an innova-
ion with greater structural and functional
lectroers (N(C) Po
�m (�
esemblance to the dura mater.
www.WORLDNEUROSURGERY.org 3
ttdswllcphbbc
tidus
gbaslpiOpsaa
ttarBBst
PEER-REVIEW REPORTS
JOSÉ HUMBERTO SANDOVAL-SÁNCHEZ ET AL. CHITOSAN AS A DURAL SUBSTITUTE
The reasons to create BChS with a porouslayer and a nonporous layer are as follows:(a) The porous portion is important becausein tissue engineering, interconnected porestructures allow the passage of growth fac-tors, cell migration, and neovasculariza-tion; however, these structures are not verystress-resistant, so they break easily. (b) Thenonporous portion provides greater stressresistance, and grafts can be sutured to en-sure they stay fixed; this could explain whyBChS, in contrast to CM, which has only aporous portion, has greater resistance tostress and can be sutured. In addition, chi-tosan membranes are five times thinner andretain less water (hydrophilic qualities),which could provide the added advantage ofhaving lower risk of compression or masseffect on the underlying nerve tissue whenused as a substitute for dura.
Figure 2. (A) Chitosan scaffolding has a lower aband less edema; for this reason, this scaffoldingcompression than collagen matrix (CM).
Figure 3. Fluid leakage pressure fosimilar at 10, 21, and 180 days. Cclosure similar to dura mater or c
substitute since 10 days after duraplast4 www.SCIENCEDIRECT.com
When BChS is used to replace dura ma-er, a significant watertight closure is ob-ained, as also happens with autologousura mater, possibly because they can beutured, in contrast to CM. In addition,hen closure was examined after time had
apsed, BChS showed leak resistance simi-ar to grafts frequently used in neurosurgi-al practice (autologous dura and CM),robably because of good integration withost tissue. Also, BChS allowed good fibro-last infiltration and organized collagen fi-er deposit owing to the presence of inter-onnected pores in the porous layer.
Chitosan, a deacetylated chitin deriva-ive, is the second most abundant polymern nature after cellulose. It is versatile, bio-egradable, and nontoxic and has beensed in various applications, such as forkin regeneration and orthopedic tissue en-
n water capacitylower risk of neural
(B) Chitosan has a hightensile strength.
three types of dural grafts wasn scaffolding provides a watertightn matrix when placed as a dural
y.WORLD NEUROSURGE
ineering (2, 7, 14, 15). However, there haveeen no reports so far of the use of chitosans a substitute for dura mater. A previoustudy (22) reported the creation of a double-ayer chitosan structure, in which variousore-inducing substances were used foster-
ng dermal fibroblast proliferation in vitro.ur results showed that the use of theseore-inducing substances was unneces-ary, and BChS enabled fibroblast prolifer-tion with organized collagen deposits inn in vivo model.
An ideal dural substitute should be non-oxic, be absorbable, be suturable, not leado adhesions or infections, be readily avail-ble, and be able to create a watertight bar-ier (19, 23, 26, 44) Our study showed thatChS has several of these features. BecauseChS has a nonporous portion, it is moretrain-resistant, and it can be sutured ob-aining a watertight closure. Sade et al. (39)
reported a CSF fistula associated with theuse of CM, which did not allow a watertightclosure because it could not be sutured ow-ing to its single porous layer. CM that issuturable (and more expensive) was intro-duced recently in our country, but at time ofour study the only CM available in ourhealth institutions was nonsuturable CMand until now was the most common mate-rial in use. No CSF fistulas were found inany of the groups in our study.
Sade et al. (39) reported a 2.3% compli-cation rate associated with the use of CM,including chemical meningitis, cortical in-flammation, accumulation of extra-axialfluid, and infection. In our study, BChS hadno increased complication risks associated
nsile strength and elongation. CM has a lower
sorptiohas aer te
r thehitosaollage
with its use.
RY, DOI:10.1016/j.wneu.2011.07.007

ib
ifimo5
scaf ) can
PEER-REVIEW REPORTS
JOSÉ HUMBERTO SANDOVAL-SÁNCHEZ ET AL. CHITOSAN AS A DURAL SUBSTITUTE
Several studies have reported that CMworks like a scaffold for fibroblast infil-trates and neovascularization (16, 28). Dur-ing the time course of our study, we foundthat BChS adapted to the defect and at-tached to the host tissue borders. From the10th day on, fibroblast and other cells infil-trated the area showing organized collagenfiber deposits and neovascularization. Sub-sequently, fibroblasts turned into maturecells. Finally, the number of cells decreased,and collagen fibers increased, with no evi-dence of fibrosis or abnormal healing orepidural or subdural adhesions.
Another desirable feature is thickness sim-ilar to human dura, reported close to 300 �m(35, 36). The double-layer chitosan mem-brane had a total thickness of 400 �m (ie, fivetimes thinner than CM, which is a dura sub-stitute often used in clinical practice accord-ing to several studies) (28, 29, 41).
When hydrated, BChS absorbed less waterthan CM. Under wet conditions, it does notexpand much, reducing the likelihood ofcompressing tissue. Even though CM is mar-keted as totally absorbable, even at 42 monthsthere are remnants of this matrix, as reportedin 1995 by Narotam et al. (28). BChS showedgradual absorption up to 6 months, withoutdisturbing the regenerative process of duraltissue. Apart from production challenges,BChS is brittle and hard, but if it is hydratedbefore placement as a dural substitute it be-comes softer and malleable.
It is unknown whether BChS are totallyabsorbed, as we still found chitosan rem-nants after 6 months. Future studies shouldextend the follow-up period to confirm ifBChS is totally absorbed and assess the un-
Figure 4. Photomicrographs of chitosan scaffoldinhematoxylin and eosin after placement as a duraZealand rabbits (�400). (A) Chitosan scaffoldingas a dural substitute; colonization by fibroblastscells (arrowheads) can be observed. (B) Chitosan
derlying nerve tissue to rule out neurotoxic-
WORLD NEUROSURGERY xx [x]: xxx, MON
ty from the membrane. Also, its hardnessefore hydration must be improved.
An additional advantage is the cost includ-ng inexpensive production. An approximatenancial cost per unit, excluding the invest-ent for its production, is around 300 USD to
btain 10 segments of a film of chitosan of� 5 cm square. We hope there will be more
publications in the future about the economi-cal impact and use, particularly in communi-ties without resources for access to the mate-rials available on the market. Considering afuture stage of marketing, the impact of thecost will not be as expensive as other substi-tutes of dura mater.
CONCLUSIONS
BChS holds promise as an ideal dural sub-stitute because it can be sutured and pro-vides a watertight dural closure; also, it actsas scaffolding that promotes the regenera-tion of the dura. This regeneration is char-acterized initially by scaffolding infiltratedwith fibroblasts. Later deposits of orga-nized collagen fibers are observed withoutevidence of infection or abnormal healing.BchS is inexpensive, it is thin, and it doesnot compress neural tissue. Although chi-tosan tends to be brittle and tough, is apromising alternative for use as a dural sub-stitute.
REFERENCES
1. Abuzayed B, Kafadar AM, Oguzoglu SA, Canbaz B,Kaynar MY: Duraplasty using autologous fascia lata
ined withstitute in Newys after placements) and mononuclear
folding 21 days after
placement as a dural scolonizing the scaffoldscaffolding can be obsplacement as a dural scollagen fibers (arrows
reenforced by on-site pedicled muscle flap: techni-cal note. J Craniofac Surg 20:435-438, 2009.
TH 2012
2. Azad AK, Sermsintham N, Chandrkrachang S, Ste-vens WF: Chitosan membrane as a wound-healingdressing: characterization and clinical application. JBiomed Mater Res B Appl Biomater 69:216-222,2004.
3. Becker SS, Jackler RK, Pitts LH: Cerebrospinal fluidleak after acoustic neuroma surgery: a comparisonof the translabyrinthine, middle fossa, and retrosig-moid approaches. Otol Neurotol 24:107-112, 2003.
4. Biroli F, Fusco M, Bani GG, Signorelli A, Esposito F,de Divitiis O, Cappabianca P, Cavallo LM: Novelequine collagen-only dural substitute. Neurosur-gery 62:273-274, 2008.
5. Caroli E, Rocchi G, Salvati M, Delfini R: Duraplasty:our current experience. Surg Neurol 61:55-59, 2004.
6. Chappell ET, Pare L, Salehpour M, Mathews M,Middlehof C: GORE PRECLUDE MVP dura substi-tute applied as a nonwatertight “underlay” graft forcraniotomies: product and technique evaluation.Surg Neurol 71:126-128, 2009.
7. Di Martino A, Sittinger M, Risbud MV: Chitosan: aversatile biopolymer for orthopaedic tissue-engi-neering. Biomaterials 26:5983-5990, 2005.
8. Ekseth K, Boström S. Late complications of Silasticduraplasty: low-virulence infections. Case report. JNeurosurg 90:559-562, 1999.
9. Filippi R, Schwarz M, Voth D, Reisch R, Grunert P,Perneczky A: Bovine pericardium for duraplasty:clinical results in 32 patients. Neurosurg Rev 24:103-107, 2001.
10. Gudmundsson G, Søgaard I: Complications to theuse of vicryl-collagen dural substitute. Acta Neuro-chir (Wien) 132:145-147, 1995.
11. Guo W, Guo Q, Zhang S, Li J: Manufacturing ofartificial dura mater with chitosan polylactic acid.Chin J Clin Rehabil 9:24-25, 2005.
12. Hoffman CE, Souweidane MM: Cerebrospinal fluid-related complications with autologous duraplasty
ute. Numerous fibrocytes (arrowheads)d collagen fibers (arrows) arranged along the. (C) Chitosan scaffolding 180 days afterute. A few fibrocytes (arrowheads) andbe observed.
g stal sub10 da(arrow
ubstiting anervedubstit
and arachnoid sparing in type I Chiari malforma-tion. Neurosurgery 62:156-160, 2008.
www.WORLDNEUROSURGERY.org 5
2
2
2
2
2
3
3
3
3
3
3
3
PEER-REVIEW REPORTS
JOSÉ HUMBERTO SANDOVAL-SÁNCHEZ ET AL. CHITOSAN AS A DURAL SUBSTITUTE
13. Hoover DA, Mahmood A: Ossification of autologouspericranium used in duraplasty: Case report. J Neu-rosurg 95:350-352, 2001.
14. Jin R, Moreira Teixeira LS, Dijkstra PJ, Karperien M,van Blitterswijk CA, Zhong ZY, Feijen J: Injectablechitosan-based hydrogels for cartilage tissue engi-neering. Biomaterials 30:2544-2551, 2009.
15. Kawai T, Yamada T, Yasukawa A, Koyama Y, MunetaT, Takakuda K: Biological fixation of fibrous mate-rials to bone using chitin/chitosan as a bone forma-tion accelerator. J Biomed Mater Res B Appl Biom-ater 88:264-270, 2009.
16. Khorasani L, Kapur RP, Lee C, Avellino AM: Histo-logical analysis of DuraGen in a human subject: casereport. Clin Neuropathol 27:361-364, 2008.
17. Kikuta K, Hojo M, Gomi M, Hashimoto N, NozakiK: Expansive duraplasty for the treatment of spinalextradural arachnoid cysts: case report. J NeurosurgSpine 4:251-255, 2006.
18. Kiyozumi T, Kanatani Y, Ishihara M, Saitoh D, Shi-mizu J, Yura H, Suzuki S, Okada Y, Kikuchi M: Me-dium (DMEM/F12)-containing chitosan hydrogel asadhesive and dressing in autologous skin grafts andaccelerator in the healing process. J Biomed MaterRes B Appl Biomater 79:129-136, 2006.
19. Knopp U, Christmann F, Reusche E, Sepehrnia A: Anew collagen biomatrix of equine origin versus acadaveric dura graft for the repair of dural de-fects—a comparative animal experimental study.Acta Neurochir (Wien) 147:877-887, 2005.
20. Kojima K, Okamoto Y, Kojima K, Miyatake K, FujiseH, Shigemasa Y, Minami S: Effects of chitin andchitosan on collagen synthesis in wound healing. JVet Med Sci 66:1595-1598, 2004.
21. Kuhn J, Hofmann B, Knitelius H, Coenen H, Bewer-meyer H: Bilateral subdural haematoma and lumbarpseudomeningocele due to a chronic leakage of li-quor cerebrospinalis after a lumbar discectomy withthe application of ADCON-L gel. J Neurol Neuro-surg Psychiatry 76:1031-1033, 2005.
22. Ma J, Wang H, He B, Chen J: A preliminary in vitrostudy on the fabrication and tissue engineering ap-plications of a novel chitosan bilayer material as ascaffold of human neofetal dermal fibroblasts. Bio-materials 22:331-336, 2001.
23. Maher CO, Anderson RE, McClelland RL, Link MJ:Evaluation of a novel propylene oxide-treated colla-gen material as a dural substitute. J Neurosurg 99:1070-1076, 2003.
24. Malliti M, Page P, Gury C, Chomette E, Nataf F,
Roux FX: Comparison of deep wound infectionrates using a synthetic dural substitute (neuro-6 www.SCIENCEDIRECT.com
patch) or pericranium graft for dural closure: aclinical review of 1 year. Neurosurgery 54:599-603,2004.
5. McCall TD, Fults DW, Schmidt RH: Use of resorb-able collagen dural substitutes in the presence ofcranial and spinal infections—report of 3 cases.Surg Neurol 70:92-96, 2008.
6. Mello LR, Feltrin LT, Fontes Neto PT, Ferraz FA:Duraplasty with biosynthetic cellulose: an experi-mental study. J Neurosurg 86:143-150, 1997.
7. Mori T, Murakami M, Okumura M, Kadosawa T,Uede T, Fujinaga T: Mechanism of macrophage ac-tivation by chitin derivatives. J Vet Med Sci 67:51-56,2005.
8. Narotam PK, van Dellen JR, Bhoola KD: A clinico-pathological study of collagen sponge as a duralgraft in neurosurgery. J Neurosurg 82:406-412,1995.
9. Narotam PK, van Dellen JR, Bhoola K, Raidoo D:Experimental evaluation of collagen sponge as a du-ral graft. Br J Neurosurg 7:635-641, 1993.
0. Narotam PK, Qiao F, Nathoo N: Collagen matrixduraplasty for posterior fossa surgery: evaluation ofsurgical technique in 52 adult patients. J Neurosurg111:380-386, 2009.
1. Nutik SL, Korol HW: Cerebrospinal fluid leak afteracoustic neuroma surgery. Surg Neurol 43:553-556,1995.
2. Parízek J, Husek Z, Mericka P, Téra J, Nemecek S,Spacek J, Nemecková J, Suba P: Ovine pericardium:a new material for duraplasty. J Neurosurg 84:508-513, 1996.
3. Parízek J, Mericka P, Husek Z, Suba P, Spacek J,Nemecek S, Nemecková J, Sercl M, Eliás P: Detailedevaluation of 2959 allogeneic and xenogeneic denseconnective tissue grafts (fascia lata, pericardium,and dura mater) used in the course of 20 years forduraplasty in neurosurgery. Acta Neurochir (Wien)139:827-838, 1997.
4. Park CJ, Gabrielson NP, Pack DW, Jamison RD,Wagoner Johnson AJ: The effect of chitosan on themigration of neutrophil-like HL60 cells, mediatedby IL-8. Biomaterials 30:436-444, 2009.
5. Reina MA, De Leon Casasola O, López A, De AndrésJA, Mora M, Fernández A: The origin of the spinalsubdural space: ultrastructure findings. AnesthAnalg 94:991-995, 2002.
6. Reina MA, López-García A, Dittmann M, de AndrésJA: [Structural analysis of the thickness of human
dura mater with scanning electron microscopy].Rev Esp Anestesiol Reanim 43:135-137, 1996.WORLD NEUROSURGE
37. Reynolds MR, Blackburn SL, Smyth MD: Ossifiedpseudomeningocele following Chiari decompres-sion surgery in a patient with Kleeblattschädel de-formity. J Neurosurg Pediatr 2:203-206, 2008.
38. Ruf B, Heckmann M, Schroth I, Hügens-Penzel M,Reiss I, Borkhardt A, Gortner L, Jödicke A: Earlydecompressive craniectomy and duraplasty for re-fractory intracranial hypertension in children: re-sults of a pilot study. Crit Care 7:R133-R138, 2003.
39. Sade B, Oya S, Lee JH: Non-watertight dural recon-struction in meningioma surgery: results in 439consecutive patients and a review of the literature. JNeurosurg 114:714-718, 2011.
40. Stendel R, Danne M, Fiss I, Klein I, Schilling A,Hammersen S, Pietilae T, Jänisch W, HopfenmüllerW: Efficacy and safety of a collagen matrix for cra-nial and spinal dural reconstruction using differentfixation techniques. J Neurosurg 109:215-221, 2008.
41. Tatsui CE, Martinez G, Li X, Pattany P, Levi AD:Evaluation of DuraGen in preventing peridural fi-brosis in rabbits. J Neurosurg Spine 4:51-59, 2006.
42. Tazbir J, Marthaler MT, Moredich C, Keresztes P:Decompressive hemicraniectomy with duraplasty: atreatment for large-volume ischemic stroke. J Neu-rosci Nurs 37:194-199, 2005.
43. Ueno H, Nakamura F, Murakami M, Okumura M,Kadosawa T, Fujinag T: Evaluation effects of chi-tosan for the extracellular matrix production by fi-broblasts and the growth factors production bymacrophages. Biomaterials 22:2125-2130, 2001.
44. Yamada K, Miyamoto S, Nagata I, Kikuchi H, IkadaY, Iwata H, Yamamoto K: Development of a duralsubstitute from synthetic bioabsorbable polymers. JNeurosurg 86:1012-1017, 1997.
45. Yano S, Tsuiki H, Kudo M, Kai Y, Morioka M,Takeshima H, Yumoto E, Kuratsu J: Sellar repairwith resorbable polyglactin acid sheet and fibringlue in endoscopic endonasal transsphenoidal sur-gery. Surg Neurol 67:59-64, 2007.
Conflict of interest statement: The authors declare that thearticle content was composed in the absence of anycommercial or financial relationships that could beconstrued as a potential conflict of interest.
received 03 March 2011; accepted 07 July 2011
Citation: World Neurosurg. (2012).DOI: 10.1016/j.wneu.2011.07.007
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter © 2012 Elsevier Inc.All rights reserved.
RY, DOI:10.1016/j.wneu.2011.07.007





























