Embed Size (px)
Citation preview

A Caregiving Model of Copingwith a Partner’s Depression*
Elizabeth L. Jeglic Carolyn M. Pepper** Karen A. Ryabchenko
James W. Griffith Allison B. Miller Matthew D. Johnson
Abstract: To test a caregiving model of depression in spouses, 31 married couples completed interviewand questionnaire assessments of depressive symptoms and caregiving activities. Spouses living with a part-ner with depressive symptoms had more symptoms of depression themselves. However, this associationwas found to be fully mediated by spouses� perceived level of caregiving stress and burden. Results sug-gest that feelings of stress associated with caring for a depressed spouse may lead to depressive symptomsin the caregiving spouse and should be addressed in treatment.
Key Words: caregiving burden, depression, spouse.
Spouses of depressed individuals are at risk forincreased depressive symptoms themselves(Benazon & Coyne, 2000; Coyne et al., 1987;Dudek et al., 2001). In treating depressedpatients, particularly in the context of maritaltherapy, therapists need to be aware of howdepressive symptoms in one spouse may pro-duce increased symptoms in the other spouse.Several models have been proposed to explainthis ‘‘contagion’’ effect of depression. In thepresent study, caregiver stress and burden wastested as a possible mediator of the relationshipbetween depression levels in spouses.
Coyne (1976) posited that depression has det-rimental effects on interpersonal relationships. Ina meta-analysis of the empirical literature exam-ining the interpersonal nature of depression,Joiner and Katz (1999) found substantial supportfor the contention that depressive symptoms and
negative mood are contagious. For example,studies of college roommates found elevateddepression in roommates of depressed students(Joiner, 1994), providing support for Coyne’sinterpersonal theory of depression that suggeststhat living with a depressed person could precipi-tate distress and psychiatric disturbance.
Although studies of college roommates haveilluminated the potential effects of living witha depressed person, there are notable differencesin the quality, duration, and commitment ofmarital relations in comparison with transientroommate relationships. If merely being in thepresence of a depressed person is associated withdepressive symptoms, then spouses whose livesare intertwined with their depressed partner’salso should show more depressive symptoms,perhaps to an even greater degree than in otherrelationships. Findings support this speculation,
*This project was funded in part by National Institute of Mental Health Grant 1R03MH059696-01.
**Address correspondence to Dr. Carolyn M. Pepper, Department of Psychology, University of Wyoming, Laramie, WY 82071 (cpepper@
uwyo.edu).
Family Relations, 54 (January 2005), 37–45. Blackwell Publishing. Printed in the USA.Copyright 2005 by the National Council on Family Relations.

such that studies of married couples also havefound that living with a depressed individual isassociated with higher levels of distress anddepression, lending support to the contagiousmodel of depression (Benazon, 2000). Specifi-cally, couples in which one partner was depressedreported more dysphoric and uncomfortablefeelings and negative well-being compared withnondepressed couples (Hautzinger, Linden, &Hoffman, 1982). Depressed spouses also appearto be less able to respond to a spouse’s posi-tive behavior with their own positive behavior(Johnson & Jacob, 2000). Further, Coyne et al.(1987) reported that 36%–40% of the spousesof individuals in a depressive episode had enoughdepressive symptoms themselves to meet stan-dardized criteria to warrant a referral, comparedwith 17% of spouses of previously depressedindividuals not in a depressive episode.
Caregiving and Depression
The relationship between caregiving burden anddepression is well documented within the medi-cal domain. A recent meta-analysis of 84 studiesexamining differences between caregivers andnoncaregivers on a variety of physical and psy-chological health variables found the greatestdifference between the groups on depression(Pinquart, Schiller, & Soerensen, 2003). Muchof this literature examined caring for a familymember with Alzheimer’s disease or dementia.Compared with healthcare professionals andother family members, spouses are the most vul-nerable group of caregivers because they have themost invested in the relationship (Pruchno &Resch, 1989), and Dura, Stukenberg, and Kie-colt-Glasner (1990) found that 30% of spousalcaregivers experienced a depressive disorder dur-ing the years that they provided care.
Although depression is qualitatively differentfrom Alzheimer’s disease and dementia, caregiversof depressed individuals may encounter many ofthe same stressors. For example, when in the midstof a depressive episode, the depressed individualmay require help performing the simple tasks ofdaily living, such as preparing food, paying bills,
child rearing, and housekeeping. In many cases, itis the spouse of the depressed person who assistswith these duties (Hinrichsen, 1991).
In addition, spouses of depressed peoplesometimes see their depressed partner as a bur-den (Barling, MacEwen, & Kelloway, 1994;Coyne et al., 1987). Spouses reported that theirdepressed partner’s lack of energy, feelings ofworthlessness, lack of interest, and constantworrying were a source of burden to them(Coyne et al.). Further, the level of distress evi-denced by the spouses was almost entirelyaccounted for by the degree of burden that theyreported experiencing.
Perception of burden may be more directlyrelated to health outcomes than the actualamount of care provided by the caregiver(Macera, Eaker, Jannarone, Davis, & Stoskpf,1993). Several studies have looked at the rela-tionship between subjective and objective bur-den and depression in the caregivers ofindividuals with traumatic brain injuries andAlzheimer’s disease (Marsh, Kersel, Havill, &Sleigh, 1998a, 1998b, 2002). These studiesfound that the caregiver’s level of perceived bur-den was the strongest predictor of depression,whereas the actual objective burden of caring forthe individual had little relationship to thedegree of distress that he or she felt. Importantto our study, this relationship has yet to betested in the caregivers of depressed individuals.
The Caregiving Model of Depression
Given that both depression and caregiving stressand burden are related to depressive symptomsin the nonafflicted spouse, we proposed a caregiv-ing model of spousal depression. We hypothe-sized that subjective levels of caregiver stress andburden mediate the relationship between thelevel of patient’s (individuals that were screenedin the primary care offices and met criteria forparticipation in the study) depressive symptomsand the spouse’s depressive symptoms, such thathigher levels of perceived caregiver stress andburden are associated with higher levels ofdepressive symptoms in the spouse.
Family Relations � Volume 54, Number 1 � January 200538

Method
Participants and Procedure
Participants were drawn from a larger study ofdepression in primary medical care settings.Patients were recruited from the waiting roomsof three primary care clinics in Binghamton,New York, where they completed a packet ofscreening measures. Individuals were selected toparticipate if they were currently married for atleast 1 year. Individuals were screened for all AxisI diagnoses using the Structured Clinical Inter-view for the DSM-IV (SCID; Spitzer, Gibbon,Gibbon, & Williams, 1997), and they wereexcluded from participation if they met criteriafor Bipolar I Disorder, Bipolar II Disorder, ora psychotic disorder. Patients also were excludedif they had been separated or divorced during the6 months prior to the date of the interview.
During the study period, 147 individuals com-pleted the screening measures. Of these 147 peo-ple, 87 (59%) reported that they were currentlymarried for at least 1 year. Those 87 individualswere contacted via telephone by a research assis-tant and asked to participate in a clinical inter-view. Fifty-five individuals (63%) agreed toparticipate and completed the interview. These55 individuals were asked whether their spouseor partner could be contacted to participate ina further study. Forty-two (76%) of the individu-als who were interviewed gave permission to con-tact their spouse. There was no difference on theHamilton Depression Rating Scale (HRSD;Hamilton, 1960; Williams, 1988) for those whogave permission and those who did not. Afterreceiving written consent, the spouse was con-tacted by telephone and asked to participate inthe study. Once a spouse agreed to participate inthe study, the person who had been interviewedwas entered into this study. For the purposes ofclarification, the spouse who was recruited fromthe primary care office is referred to as thepatient, and his or her partner is referred to asthe spouse. Thirty-one (74%) of the spouses whowere contacted agreed to participate. The spouses
were asked to complete a battery of question-naires and a semistructured clinical interview toassess current depressive symptoms and otherAxis I disorders. All participants were paid $20for their participation. Descriptive statistics ofdemographic variables are presented in Table 1for both patients and spouses.
Measures
Depressive symptoms. The mood disordersmodule of the SCID, nonpatient version wasadministered to both the patients and theirspouses to assess current and lifetime depressionand depressive symptoms in order to describe theparticipants and to screen out bipolar patients.Questions on the SCID are designed to corre-spond to diagnostic criteria in the DSM-IV.Graduate students administered all of the inter-views. The interviews were audiotaped with theinformed consent of the participant and werereviewed and rated for interrater reliability. For10 participants, current major depression and thepresence of a past major depressive episode wereassessed with perfect agreement (kappa ¼ 1.0).
The 17-item structured interview version ofthe HRSD (Hamilton, 1960; Williams, 1988)was administered to both patients and spousesto assess the severity of current depressive symp-toms during the week prior to the interview.Participants were asked questions about thenature of their depressed mood, and the inter-viewer then rated their responses. Questionson the HRSD include ‘‘What’s your moodbeen like this past week?’’ and ‘‘How have youbeen sleeping this past week?’’ Potts, Daniels,Burnam, and Wells (1990) found support forboth the interrater and internal consistency ofthe instrument. In this study, intraclass correla-tions for depressive symptom severity was .95.
Caregiving stress and burden. The level ofperceived burden among the caregiving spouseswas evaluated using the Caregiver Burden Scale(CBS; Macera et al., 1993), a 14-item self-report measure completed by the caregivingspouse. This questionnaire assesses 14 generalareas in which the patient may require assistance,
Caregiving Model of Depression � Jeglic et al. 39

such as housekeeping, cooking, child care, anddecision making. For each area, spouses wereasked to evaluate the amount of assistance thatthey were required to provide to the patient dur-ing the past month as a result of the patient’smood (objective burden), and whether the assis-tance they provided resulted in feelings of stressand burden (subjective burden). Spouses ratedeach of the items on a scale from 0 (not at all) to2 (daily). Items were summed to produce objec-tive and subjective burden scores. In this study,the alpha coefficient for internal consistency forboth the objective and subjective scales was .96.
Results
Description of Sample
The average scores, standard deviations, inter-correlations, and alphas on the measures ofdepression and the level of caregiving stress andburden for the spouse only are presented inTable 2. Patients experienced significantly moresymptoms of depression than spouses as mea-
sured by the SCID, t(60) ¼ 2.58, p , .05, andthe HRSD, t(60) ¼ 2.00, p ¼ .05. Eight of thepatients met full diagnostic criteria for a majordepressive episode, whereas only 1 of thespouses met criteria for current major depres-sion. There were no differences on number ofpast episodes of major depression betweenpatients and spouses. Additionally, no genderdifferences were found in depression levels ofeither the spouses or patients; thus, no furthergender comparisons were examined.
Testing the Proposed Model
The results of testing the proposed model appearin Figure 1. This model suggests that caregivingburden mediates the relationship between pa-tients� depression and spouses� depression, suchthat increased levels of caregiver stress and bur-den are associated with increased feelings ofdepression in the spouse. This model was testedusing Baron and Kenny’s (1986) guidelines forevaluating mediation. They require that each ofthe following criteria be satisfied for media-tion to occur: (a) the predictor variable (HRSD
Table 1. Demographic and Clinical Characteristics
Patient Spouse(n ¼ 31) (n ¼ 31)
Characteristics n % n %
Gender (% female) 17 55% 14 45%Ethnicity (% white) 29 94% 30 97%Previously married 16 52% 10 32%Education levelHigh school degree 13 42% 13 42%College degree 12 39% 17 55%
Employed 23 74% 22 71%Prior psychiatric treatment 11 35% 10 2%AgeM 44.7 46.2SD 11.6 12.1
GAF scoreM 70.2 77.2SD 12.1 10.6
Note. GAF ¼ Global Assessment of Functioning.
Family Relations � Volume 54, Number 1 � January 200540
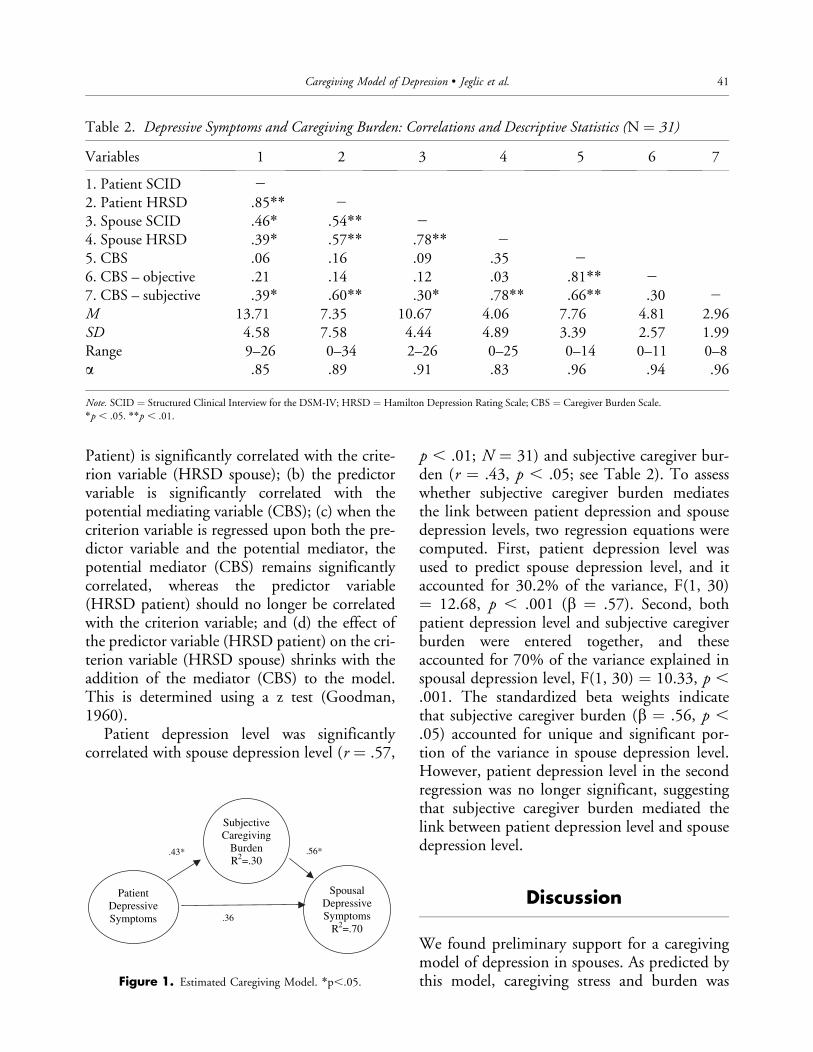
Patient) is significantly correlated with the crite-rion variable (HRSD spouse); (b) the predictorvariable is significantly correlated with thepotential mediating variable (CBS); (c) when thecriterion variable is regressed upon both the pre-dictor variable and the potential mediator, thepotential mediator (CBS) remains significantlycorrelated, whereas the predictor variable(HRSD patient) should no longer be correlatedwith the criterion variable; and (d) the effect ofthe predictor variable (HRSD patient) on the cri-terion variable (HRSD spouse) shrinks with theaddition of the mediator (CBS) to the model.This is determined using a z test (Goodman,1960).
Patient depression level was significantlycorrelated with spouse depression level (r ¼ .57,
p , .01; N ¼ 31) and subjective caregiver bur-den (r ¼ .43, p , .05; see Table 2). To assesswhether subjective caregiver burden mediatesthe link between patient depression and spousedepression levels, two regression equations werecomputed. First, patient depression level wasused to predict spouse depression level, and itaccounted for 30.2% of the variance, F(1, 30)¼ 12.68, p , .001 (b ¼ .57). Second, bothpatient depression level and subjective caregiverburden were entered together, and theseaccounted for 70% of the variance explained inspousal depression level, F(1, 30) ¼ 10.33, p ,.001. The standardized beta weights indicatethat subjective caregiver burden (b ¼ .56, p ,.05) accounted for unique and significant por-tion of the variance in spouse depression level.However, patient depression level in the secondregression was no longer significant, suggestingthat subjective caregiver burden mediated thelink between patient depression level and spousedepression level.
Discussion
We found preliminary support for a caregivingmodel of depression in spouses. As predicted bythis model, caregiving stress and burden was
Table 2. Depressive Symptoms and Caregiving Burden: Correlations and Descriptive Statistics (N ¼ 31)
Variables 1 2 3 4 5 6 7
1. Patient SCID 2
2. Patient HRSD .85** 2
3. Spouse SCID .46* .54** 2
4. Spouse HRSD .39* .57** .78** 2
5. CBS .06 .16 .09 .35 2
6. CBS – objective .21 .14 .12 .03 .81** 2
7. CBS – subjective .39* .60** .30* .78** .66** .30 2
M 13.71 7.35 10.67 4.06 7.76 4.81 2.96SD 4.58 7.58 4.44 4.89 3.39 2.57 1.99Range 9–26 0–34 2–26 0–25 0–14 0–11 0–8a .85 .89 .91 .83 .96 .94 .96
Note. SCID ¼ Structured Clinical Interview for the DSM-IV; HRSD ¼ Hamilton Depression Rating Scale; CBS ¼ Caregiver Burden Scale.
*p , .05. **p , .01.
Patient DepressiveSymptoms
SpousalDepressiveSymptoms
R2=.70
SubjectiveCaregiving
BurdenR2=.30
.36
.43* .56*
Figure 1. Estimated Caregiving Model. *p,.05.
Caregiving Model of Depression � Jeglic et al. 41

found to mediate the relationship betweendepressive symptoms in the patient and depres-sive symptoms in the spouse. That is, individu-als who reported more subjective stress andburden associated with caring for theirdepressed spouse also reported more depressivesymptoms themselves. This model is congruentwith Coyne and colleagues� (1987) findings thatsuggested that it is the spouse’s perception ofthe depressed individual as a burden that medi-ates the relationship between patient depressionand spouse depression.
Consistent with the contagion model ofdepression (Joiner, 1994), we also found thatdepressive symptoms in the patient are relatedto depressive symptoms in the spouse. However,this relationship was explained better whenspousal caregiving stress and burden wasincluded as a mediator. This is consistent withthe medical literature suggesting that caregivingburden mediates the relationship betweenpatient and spouse outcome on factors such asphysical health, depressive symptoms, andimmune system functioning in caregivers ofAlzheimer’s patients (Pinquart et al., 2003).
Although we examined both objective andsubjective caregiver burden, the model was notsignificant when both were included. However,when subjective burden was included alone,caregiving mediated the relationship betweenpatient and spousal depressive symptoms.Unlike Hinrichsen (1991), who found thatobjective burden of caring for a depressedelderly family member accounted for most ofthe variance in adjustment, our findings supportCoyne et al. (1987), who found that subjectiveburden, rather than actual burden, predicteddepression.
It may be that negative patient behavior isassociated with the increased levels of depressivesymptoms in the presence of the spouse. Thisincreased level of depressive symptoms mightlead to more negative appraisals of their spouse,and an increased perception of inequity in thehousehold. Further, partners of depressedspouses evaluate them more negatively (e.g.,Hautzinger et al., 1982). Such negative evalua-
tions from spouses, at least in cases in whichthat evaluation is consistent with one’s own self-view, are associated with greater depressivesymptoms (Katz & Beach, 1997). This suggeststhat the higher levels of caregiver burden experi-enced by those with spouses experiencing higherlevels of depressive symptoms may be an artifactof the depression rather than a result ofincreased level of caregiving duties. Our findingregarding objective burden supports this hunch.
In reviewing the literature on marital com-munication patterns in the context of a depres-sed spouse, Mead (2002) concluded that suchinteractions follow complex patterns that dif-fer depending on the gender of the spouse.Negative comments by depressed husbands aremore likely to be met with negative commentsby their wives (Hops et al., 1987; Johnson &Jacob, 1997), whereas husbands� reactions tonegative comments from depressed wives are lessnegative than those of spouses of depressed hus-bands (Biglan et al., 1985) and do not differfrom controls (Jacob & Johnson). In our study,we found no differences by gender in our pre-liminary analyses, so gender was not included intesting the model. Although the effects of sub-jective burden were not associated with gender,it is possible that communication about burdenmay differ depending on the gender of thedepressed spouse.
Although not directly measured here, otherstudies have found that burden is associatedwith excessive reassurance-seeking in depressedspouses (Joiner, 2000). In addition to seekingreassurance, some depressed individuals valueinformation that confirms their negative self-view (Katz, 2001), leading them to dismiss thereassurance. Over time, a pattern of seekingreassurance and seeking contradictory negativeinformation develops, creating interpersonalconfusion and frustration (Katz & Beach,1997). In turn, the resulting stress is associatedwith an increase in depressive symptoms in thepreviously nondepressed spouse. Our findingssuggest that physical tasks associated with care-giving, such as housekeeping and cooking, alsomay contribute to a sense of burden.
Family Relations � Volume 54, Number 1 � January 200542

Our study has several limitations that war-rant caution in interpreting the findings. First,because of the cross-sectional design, we couldnot ascertain whether depressive symptoms pre-ceded or followed increased levels of caregivingstress and burden. Determining whether caregiv-ing stress and burden was a function of the levelof patient depressive symptoms requires a longi-tudinal design. In addition, the individualscreened in the primary care office was consid-ered the patient, and his or her partner was con-sidered the spouse. However, it is plausible thatthe partner designated as the spouse was actuallythe individual who was experiencing greater de-pressive symptoms, and the individual who wasdesignated the patient was the caregiving spouse.Four of the spouses reported more depressivesymptoms than the patients, however overallpatients reported significantly more depressivesymptoms than spouses. To alleviate this prob-lem in future studies, a detailed history of theonset and offset of past depressive symptomsshould be obtained. This would aid the investi-gator in the determination of which spouseexperienced the depressive symptoms first. Basedon our findings, we may conclude only that a his-tory of depression in the patient was related tosymptoms of depression in the spouse. As a pre-liminary test of the caregiving model, the medi-ating effect of caregiving stress and burden wasexamined in a subclinical sample composed ofpatients and their spouses who were experiencingvarying levels of depressive symptoms, with fewparticipants meeting criteria for major depres-sion. Thus, the sample is more representative ofthe general population than either psychiatric orcollege roommate samples used in previous stud-ies. Finally, we found evidence for the mediatingrole of caregiving stress and burden in these31 couples. Although significant results wereobtained, replication with larger samples is nec-essary to assure the robustness of the findings.
Implications
Our findings have practical implications forclinicians who work with depressed individuals
and their spouses, because the stress associatedwith caring for a depressed partner could influ-ence the caregiver’s own emotional adjustment.Several therapies have been developed to treatco-occurring depression and marital distress. Ina recent review of these treatments, Mead(2002) concluded that Behavioral Marital Ther-apy for Depression (BMT-D) has the mostresearch supporting its efficacy, and is shown toreduce both depression and marital distress(e.g., Beach & O’Leary, 1992). This therapybegins with educating the couple about thenature of both marital distress and depression.Other goals of this therapy include increasingthe exchange of positive behaviors, increasingacceptance, and reducing blame, coercion, andaversive stimuli. Problem-solving and commu-nication skills are taught, and negative thoughtsabout the self, the partner, the world, and thefuture are challenged (Beach, Sandeen, &O’Leary, 1990). Mead also concluded that thereis some empirical support for cognitive maritaltherapy and interpersonal therapy. Cognitivemarital therapy was an efficacious treatmentfor depression in two studies, although maritalsatisfaction was not assessed as an outcome(Teichman, Bar-El, Shor, & Elizur, 1998;Teichman, Bar-El, Shor, & Sirota, 1995). Aversion of interpersonal therapy for depressiondeveloped for couples, conjoint marital ther-apy (IPT-CM (Interpersonal Psychotherapy-Conjoint Marital Treatment); Foley, Rounsaville,Weissman, Sholomaskas, & Chevron, 1989),also shows promise in reducing both depressionand marital distress. Regardless of specific treat-ment used, our findings suggest that perceptionsof burden play a greater role in the spouse’s levelof distress experienced than the actual level ofburden experienced. Whether approached froma behavioral, cognitive, or interpersonal perspec-tive, interventions should be tailored specificallyto modifying the spouses� perceptions of burdenregarding their partners� depressive symptoms.
Further, spouses should be encouraged totake advantage of available self-help books andcommunity resources to help them cope withcaregiver stress and burden. Several organiza-
Caregiving Model of Depression � Jeglic et al. 43

tions, such as the National Alliance for theMentally Ill (NAMI), the National Depressiveand Manic Depressive Association (NDMDA),and the Depression and Related Affective Disor-ders Association, have local chapters that pro-vide support groups for families of depressedindividuals. In support groups, spouses canshare their experiences with individuals who aregoing through similar experiences, and poten-tially alleviate the negative effects of caregivingon mental health (Mittelman, Ferris, Shulman,& Steinberg, 1995). Additionally, reports showthat the major impact of support groups forcaregiving spouses is on the caregiver’s percep-tion of the caregiving situation (Labrecque,Peak, & Toseland, 1992).
Self-administered treatments like bibliotherapyalso may prove to benefit the caregiving spouse.These treatments are effective in lowering symp-toms of depression and stress (Mains & Scogin,2003). Because numerous books deal with adepressed partner, therapists� awareness and useof these resources may help the caregiving spouseunderstand his or her partner and cope moreeffectively with the stressors experienced.
Our findings are an important advance in theliterature with respect to the relationshipbetween depression and the burden experiencedby the caregiving spouse. Both the interpersonaltheory of depression (Coyne, 1976) and thecontagion model (Joiner & Katz, 1999) addressthe phenomenon of promulgation of depressivesymptoms among individuals who live in closecontact with one another. We build upon theliterature examining caregiving stress and bur-den in medical populations and extend thesefindings to propose a mechanism that mediatesthe relationship between depression in thepatient and depression in the spouse.
Future research should further examine theprocesses by which perceptions of burden leadto increased symptoms in a spouse. One possi-bility is that increased burden is associated withnegative beliefs about depression. That is,spouses who believe that their depressed spouseis lazy or that the patient has volitional controlover his or her depressive behavior may more
likely feel resentment toward him or her as com-pared with spouses who view depression as anillness. Psychological interventions that empha-size educating the spouse on the nature ofdepression could be examined to see whetherthey reduce perceived burden, thereby reducingspouse symptoms. Using a randomized controlgroup design, lower levels of depression in thecaregiving spouses in the treatment group withan education component would further supportour caregiving model.
Our study highlights the important role ofperceived caregiving stress and burden as a medi-ator of depressive symptoms of one spouse, andthe development of depressive symptoms in theother spouse. As such, the role of caregiver bur-den should be addressed explicitly in couples�therapy with depressed patients, with specificattention focused on the perception of burdenand how these perceptions negatively affect thecaregiving spouse.
References
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variabledistinction in social psychological research: Conceptual, strategic, andstatistical considerations. Journal of Personality and Social Psychology,51, 1173–1182.
Barling, J., MacEwen, K. E., & Kelloway, E. K. (1994). Predictors and out-comes of elder-care-based interrole conflict. Psychology & Aging, 9,391–397.
Beach, S. R. H., & O’Leary, K. D. (1992). Treating depression in the con-text of marital discord: Outcome and predictors of response for maritaltherapy versus cognitive therapy. Behavior Therapy, 23, 507–528.
Beach, S. R. H., Sandeen, E. E., & O’Leary, K. D. (1990). Depression inmarriage: A model for etiology and treatment. New York: Guilford Press.
Benazon, N. R. (2000). Predicting negative spousal attitudes towarddepressed persons: A test of Coyne’s Interpersonal Model. Journal ofAbnormal Psychology, 109 (3), 550–554.
Benazon, N. R., & Coyne, J. C. (2000). Living with a depressed spouse.Journal of Family Psychology, 14, 70–79.
Biglan, A., Hops, H., Sherman, L., Friedman, L. S., Arthur, J., & Osteen,V. (1985). Problem-solving interactions of depressed women and theirhusbands. Behavior Therapy, 16, 431–451.
Coyne, J. C. (1976). Depression and the response of others. Journal ofAbnormal Psychology, 85, 186–193.
Coyne, J. C., Kessler, R. C., Tal, M., Turnbull, J., Wortman, C., &Greden, J. (1987). Living with a depressed person. Journal of Consultingand Clinical Psychology, 55, 347–352.
Dudek, D., Zieba, A., Jawor, M., Szymaczek, M., Opila, J., & Dattilio,F. M. (2001). The impact of depressive illness on spouses of depressedpatients. Journal of Cognitive Psychotherapy, 15, 49–57.
Dura, J. R., Stukenberg, K. W., & Kiecolt-Glasner, J. K. (1990). Chronicstress and depressive disorders in older adults. Journal of Abnormal Psy-chology, 99, 284–290.
Family Relations � Volume 54, Number 1 � January 200544

Foley, S. H., Rounsaville, B. J., Weissman, M. M., Sholomskas, D., &Chevron, E. (1989). Individual versus conjoint interpersonal psycho-therapy for depressed patients with marital disputes. International Jour-nal of Family Psychiatry, 10, 29–42.
Goodman, L. A. (1960). On the exact variance of products. Journal of theAmerican Statistical Association, 55 , 708–713.
Hamilton, M. (1960). A rating scale for depression. Journal of Neurology,Neurosurgery, and Psychiatry, 23, 56–62.
Hautzinger, M., Linden, M., & Hoffman, N. (1982). Distressed coupleswith and without a depressed partner: An analysis of their verbal inter-action. Journal of Behavior Therapy and Experimental Psychiatry, 13,307–314.
Hinrichsen, G. A. (1991). Adjustment of caregivers to depressed olderadults. Psychology and Ageing, 6, 631–639.
Hops, H., Biglan, A., Sherman, L., Arthur, J., Friedman, L., & Osteen, V.(1987). Home observations of family interactions of depressed women.Journal of Consulting and Clinical Psychology, 55, 341–346.
Johnson, S. L., & Jacob, T. (1997). Marital interactions of depressedmen and women. Journal of Consulting & Clinical Psychology, 65,15–23.
Johnson, S. L., & Jacob, T. (2000). Sequential interactions in the maritalcommunication of depressed men and women. Journal of Consultingand Clinical Psychology, 68, 4–12.
Joiner, T. E. (1994). Contagious depression: Existence, specificity todepressed symptoms, and the role of reassurance seeking. Journal ofPersonality and Social Psychology, 67, 287–296.
Joiner, T. E. (2000). Depression’s vicious scree: Self-propagating and ero-sive processes in depression chronicity. Clinical Psychology: Science andPractice, 7, 203–218.
Joiner, T. E., & Katz, J. (1999). Contagion of depressive symptoms andmood: Meta-analytic review and explanations from cognitive, behav-ioral, and interpersonal viewpoints. Clinical Psychology: Science andPractice, 6, 149–164.
Katz, J. (2001). Self-verification theory: Expanding current conceptualiza-tion of the link between marital distress and depression. In S. R. H.Beach (Ed.), Marital and family processes in depression: A scientific foun-dation for clinical practice (pp. 111–127). Washington, DC: AmericanPsychological Association.
Katz, J., & Beach, S. R. H. (1997). Self-verification and depressive symp-toms in marriage and courtship: A multiple pathway model. Journal ofMarriage and the Family, 59, 903–914.
Labrecque, M. S., Peak, T., & Toseland, R. W. (1992). Long-term effec-tiveness of a group program for caregivers of frail elderly veterans.American Journal of Orthopsychiatry, 62, 575–588.
Macera, C. E., Eaker, E. D., Jannarone, R. J., Davis, D. R., & Stoskopf,C. H. (1993). A measure of perceived burden among caregivers. Evalu-ation and the Health Professions, 16, 204–211.
Mains, J. A., & Scogin, F. R. (2003). The effectiveness of self-administeredtreatments: A practice-friendly review of the research. Journal of ClinicalPsychology, 59, 237–246.
Marsh, N. V., Kersel, D. A., Havill, J. H., & Sleigh, J. W. (1998a). Care-giver burden at 7 months following severe traumatic brain injury. BrainInjury, 12, 225–238.
Marsh, N. V., Kersel, D. A., Havill, J. H., & Sleigh, J. W. (1998b). Care-giver burden at 1 year following severe traumatic brain injury. BrainInjury, 12, 1045–1059.
Marsh, N. V., Kersel, D. A., Havill, J. H., & Sleigh, J. W. (2002). Care-giver burden during the year following severe traumatic brain injury.Journal of Clinical and Experimental Neuropsychology, 24, 434–447.
Mead, D. E. (2002). Marital distress, co-occurring depression, and maritaltherapy: A review. Journal of Marital and Family Therapy, 28, 299–314.
Mittelman, M. S., Ferris, S. H., Shulman, E., & Steinberg, G. (1995). Acomprehensive support program: Effect on depression in spouse-care-givers of AD patients. Gerontologist, 35, 792–802.
Pinquart, M., Schiller, F., & Soerensen, S. (2003). Differences betweencaregivers and noncaregivers in psychological health and physical health:A meta-analysis. Psychology & Aging, 18, 250–267.
Potts, M. K., Daniels, M., Burnam, A. M., & Wells, K. B (1990). A struc-tured interview version of the Hamilton Depression Rating Scale: Evi-dence of reliability and versatility of administration. Journal ofPsychiatric Research, 24, 335–350.
Pruchno, R. A., & Resch, N. L. (1989). Mental health of caregivingspouses: Coping as mediator, moderator, or main effect? Psychology andAging, 4, 454–463.
Spitzer, M. B., Gibbon, R. L., Gibbon, M., & Williams, J. B. W. (1997).Structured clinical interview for DSM-IV axis I disorders—non-patientedition. New York: Biometrics Research Department, New York StatePsychiatric Institute.
Teichman, Y., Bar-El, Z., Shor, H., & Elizur, A. (1998). Changes in cogni-tions, emotions, and behaviors in depressed patients and their spousesfollowing marital cognitive therapy, traditional cognitive therapy, phar-macotherapy, and no intervention. Journal of Psychotherapy Integration,8, 27–35.
Teichman, Y., Bar-El, Z., Shor, H., & Sirota, P. (1995). A comparison oftwo modalities of cognitive therapy (individual and marital) in treatingdepression. Psychiatry: Interpersonal and Biological Processes, 58, 136–148.
Williams, J. B. (1988). A structured interview guide for the HamiltonDepression Rating Scale. Archives of General Psychiatry, 45, 742–747.
Caregiving Model of Depression � Jeglic et al. 45






























