Embed Size (px)
Citation preview

Pergamon Leukemia Research Vol. 21, No. 6, pp. 575-580, 1991.
b 1997 Elsevicr Science Ltd. All rights reserved Printed in Great Britain
0145%2126/97 $17.00 + 0.00
PII: SO145-2126(97)00094-X
CASE REPORT
A MICROGRANULAR VARIANT OF ACUTE PROMYELOCYTIC LEUKEMIA WITH ATYPICAL MORPHO-CYTOCHEMICAL
FEATURES AND AN EARLY MYELOID IMMUNOPHENOTYPE
Roberto Stasi, Antonio Bruno, Adrian0 Venditti, Giovanni Del Poeta, German0 Aronica, Maria Christina Cox, Laura Maffei, Gianfranco Catalano, Daniela Zangrilli and Sergio Amadori
Chair of Hematology, University of Rome ‘Tor Vergata’, S. Eugenio Hospital, Rome, Italy
(Accepted 14 August 1996)
Abstract-This report describes a unique case of acute promyelocytic leukemia (APL) showing elusive morphologic features, an atypical pattern of cytochemical reactions, and a previously unreported immunophenotype consistent with a very early myeloid form: CD13 (+I, CD33 (+I, CD9 (+), CD2 (+), HLA-DR (-1, CD34 (+I, CD117 (+I, and TdT (+). The diagnosis of AML M3 variant was made only after genotypic analyses revealed the PML/RARc( rearrangement associated with the typical (15;17) (q22;q21) translocation. This example of ‘asynchronous differentiation’ emphasizes the need for a multiparameter approach to the diagnosis of acute leukemia. $3 1997 Elsevier Science Ltd.
Key word.s:Acute promyelocytic leukemia, morphology, cytochemistry, immunophenotype, asynchronous differ&iation.
Introduction
Acute promyelocytic leukemia (APL, FAB subtype M3) comprises approximately 10% of the acute myeloid leukemias (AMLs) in adults. Peculiar clinical and biological characteristics configure APL as a distinct entity. These include younger patient age at presenta- tion, constant occurrence of disseminated intravascular coagulation (DIC), distinctive morphology and cyto- chemistry, specific immunophenotype, specific chromo- somal abnormality, and unique response to treatment with all-trans retinoic acid (ATRA) [l]. Although the cytological features of APL provide the most rapid means for diagnosis, confusion with other types of AML can arise in cases of microgranular variant M3 (M3v) [2-71. In view of the therapeutic options and prognosis
Abbreviations: APL, acute promyelocytic leukemia; AML, acute myeloid leukemia; DZC, disseminated intravascular coagulation; ATRA, all-tram retinoic acid; M3v, M3 variant; MPO, myeloperoxidase; SBB, Sudan Black B; NASD-CAE, naphthol AS-D chloroacetate esterase; ANAE, alpha-naphthyl- acetate esterase; AZVBE, alpha-naphthyl-butyrate esterase; AcP, acid phosphatase; FISH, fluorescence in situ hybridization; RT- PCR, reverse transcriptase-polymerase chain reaction.
Correspondence to: Roberto Stasi, M.D., Via de1 Passer0 Solitario 19, 00169 Rome, Italy (Tel.: +39 360 248529; Fax: +39 6 260370, E-mail: mc2558Qmclink.it).
in APL, the detection of these cases has great relevance in clinical practice.
We describe herein a case of M3v that posed particular diagnostic problems because of atypical morphology and pattern of cytochemical reactions, and because of a previously unreported APL phenotype identified by the expression of TdT, CD34, and CD 117 (c-kit receptor) antigens.
Case Report
A 2Pyear-old man was admitted on April 1995 with a 2-week history of easy bruising, bleeding gums, and fatigue. Leukocytosis (WBC 20.9 x 103/p1), thrombo- cytopenia (Plt 27 x 109/1) and anemia (Hb 7.7 g/dl) were found upon analysis. Observation of a peripheral blood smear revealed that 97% of leukocytes were undifferentiated blasts and 3% lymphocytes. Blasts were pleomorphic elements with a heterogeneous size, a high N/C ratio, ill-defined nucleoli, agranular and basophilic cytoplasm. Nuclei were folded or reniform in 52% of cells, with 7% being clearly bilobed [Fig. l(a)]. Blood coagulation tests were suggestive of decompensated DIC: prolonged prothrombin time (INR = 1.85; n.v. = 0.9-1.15) and activated partial thomboplastin time (42.6 set; n.v. = 27-35 set), low fibrinogen levels
575

R. Stasi et al.
Fig. 1. (a) Peripheral blood smear morphology (May-Grunwald-Giemsa x 1000). Cells are type I blasts with agranular cytoplasm and a few distinct nucleoli; some present a reniform or folded nucleus.(b) NASD-CAE reaction in a bone marrow smear (x 1000). The majority of blasts are negative or faintly positive. A. single blast shows intense staining revealing numerous Auer rods (‘faggot
cell’).
(144 mg/dl; n.v. 200-400 mg/dl), and increased D- dimers (1000 rig/ml; n.v. < 200 rig/ml). Needle bone marrow aspiration was successfully performed, and samples were collected for morphology, cytochernistry, immunophenotyping, cytogenetics, and molecular biol- ogy studies. Morphologic evaluation of bone marrow preparations revealed a total replacement of normal hemopoietic cells by a population of blasts that shared the same characteristics as those found in the peripheral blood, only with a higher percentage of cells with a bilobed nucleus. Besides, about 10% of blasts showed a slightly more abundant cytoplasm with very fine
azurophilic granules. Cytochemical studies demon- strated a strong myeloperoxidase (MPO) and Sudan Black B (SBB) activity in all cells; naphthol AS-D chloroacetate esterase (NASD-CAE) was strong in lo%, weak to moderate in 35%, and completely negative in the rest of blasts; alpha-naphthyl-acetate esterase (ANAE) stained weakly in 10% of blasts, a reaction not inhibited by the addition of sodium fluoride (NaP); 10% of leukemic cells were also moderately-to-strongly positive for alpha-naphthyl-butyrate esterase (ANBE), and 15% showed a weak diffuse granular pattern with the acid phosphatase (AcP) reaction. It is noteworthy

Unique APL variant
800.
. 600. ‘.
I __.. ..: .: ‘. :. ..
:. (.. _. ‘. .:_; .._ ‘... ._ :
t ;
‘. .,_’ . . :_
400
I .M
+ 2 200.
9 T 3 .
2 RI *
7, . . I . . I . . . . I . . . . 1. . . . , 0 200 400 600 nw 1000
FSC-H\FSC-Herght - (a)
40 30 50
M1
0 4 0, -----TO IO4 IO0 IO’ IO2 103 IO4
(cl Cd)
Fig. 2. (a) Light-scatter analysis of leukemic cells.(b-d) Reactivity with monoclonal antibodies (dark histograms) against (b) CD34, (c) CD1 17 and (d) TdT. Blank histograms represent controls with isotype monoclonal antibodies. Histogram subtraction analysis was
performed with the Kolmogorov-Smimov procedure.
that both MPO/SBB and NASD-CAE enabled the detection of atypical promyelocytes containing multiple Auer rods that were not visible by conventional panoptic staining [Fig. l(b)].
Flow cytometric studies showed light-scatter char- acteristics identified by an accumulation of cells with low/intermediate forward- and low/intermediate side- scatter [Fig. 2(a)]. Immunophenotyping with a wide panel of monoclonal antibodies (see below) revealed expression of CD13 (97%), CD33 (98%) CD9 (95%), CD2 (70%), CD34 [95%, Fig. 2(b)], CD1 17 [96%, Fig. 2(c)], and TdT [46%, Fig. 2(d)]. Analysis of TdT by indirect immunofluorescence revealed a dim nuclear positivity in 40% of cells.
A diagnosis of M3v was eventually made after polymerase chain reaction (PCR) analysis of PMW RARa transcripts demonstrated the presence of a bcr-3 type PML/RARa rearrangement. This allowed patients to be assigned the appropriate treatment protocol (GIMEMA/AIEOP LAP 0493-AIDA), which included induction with oral ATRA (45 mg/m*/day from day 1 to
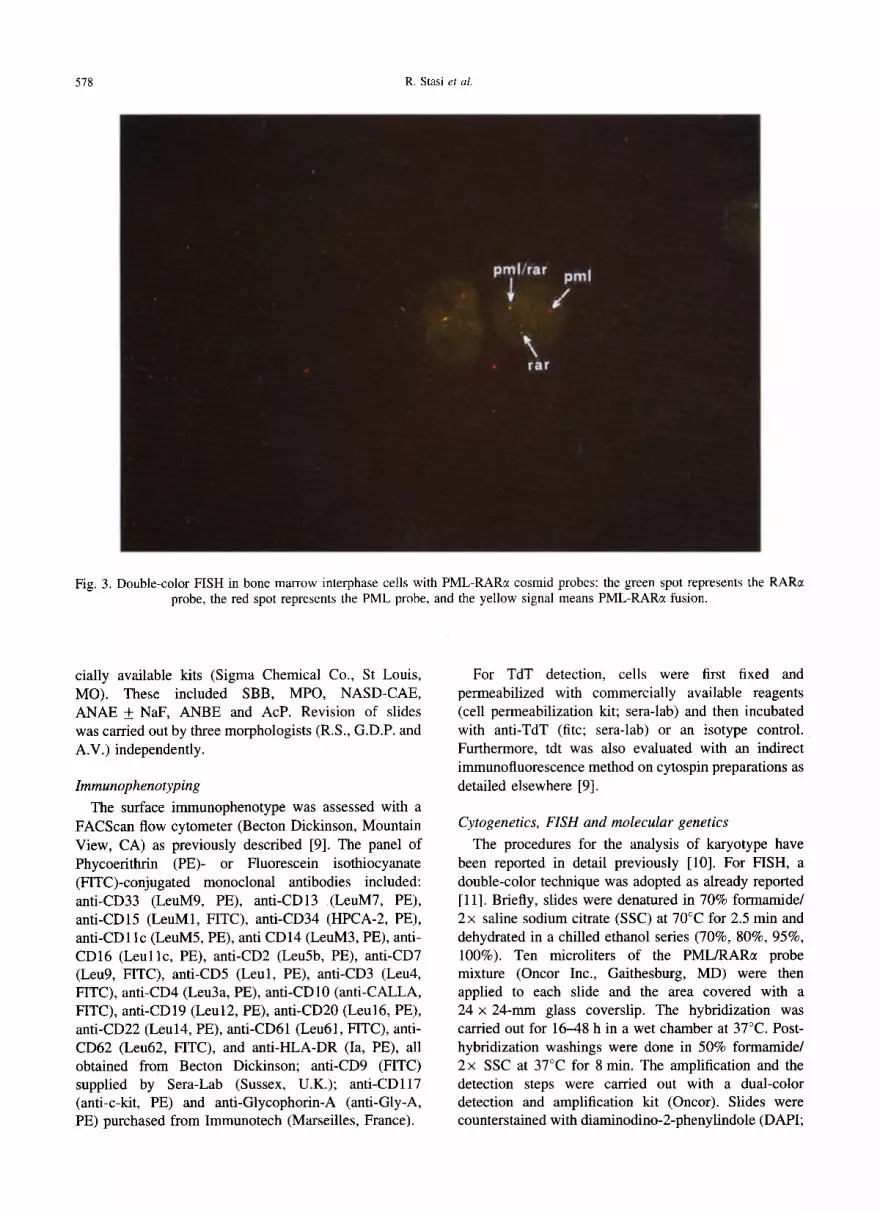
day 60) and the anthracycline Idarubicin (12 mg/m* intravenously on days 2, 4, 6, 8). The results of FISH analysis indicated a fusion signal with a PML-RARc( probe in 85% of cells (Fig. 3). Conventional cytogenetic analysis indicated a typical t(15;17) (q21;q22) in 10 out of the 20 metaphases examined, the other 10 displaying a normal karyotype. The patient tolerated therapy well and recovered quickly from the hypoplastic phase. Sixty days after the start of treatment, peripheral blood parameters were normal, bone marrow aspirate showed complete remission, and PCR did not reveal the PMW RARol rearrangement.
Materials and Methods
Morphology and cytochemistry
Bone marrow and peripheral blood smears were routinely stained and evaluated according to the revised FAB criteria [8]. Cytochemical reactions were per- formed following standard procedures with commer-
578 R. Stasi et al.
Fig. 3. Double-color FISH in bone marrow interphase cells with PML-RARE cosmid probes: the green spot represents the probe, the red spot represents the PML probe, and the yellow signal means PML-RARcx fusion.
RARa
cially available kits (Sigma Chemical Co., St Louis, MO). These included SBB, MPO, NASD-CAE, ANAE f NaF, ANBE and AcP. Revision of slides was carried out by three morphologists (RX, G.D.P. and A.V.) independently.
Immunophenotyping
The surface immunophenotype was assessed with a FACScan flow cytometer (Becton Dickinson, Mountain View, CA) as previously described [9]. The panel of Phycoerithrin (PE)- or Fluorescein isothiocyanate (FITC)-conjugated monoclonal antibodies included: anti-CD33 (LeuM9, PE), anti-CD13 (LeuM7, PE), anti-CD15 (LeuMl, FITC), anti-CD34 (HPCA-2, PE), anti-CD1 lc (LeuM5, PE), anti CD14 (LeuM3, PE), anti- CD16 (Leullc, PE), anti-CD2 (LeuSb, PE), anti-CD7 (Leu9, FITC), anti-CD5 (Leul, PE), anti-CD3 (Leu4, FITC), anti-CD4 (Leu3a, PE), anti-CD10 (anti-CALLA, FITC), anti-CD19 (Leu12, PE), anti-CD20 (Leu16, PE), anti-CD22 (Leu14, PE), anti-CD61 (Leu61, FITC), anti- CD62 (Leu62, FITC), and anti-HLA-DR (Ia, PE), all obtained from Becton Dickinson; anti-CD9 (FITC) supplied by Sera-Lab (Sussex, U.K.); anti-CD117 (anti-c-kit, PE) and anti-Glycophorin-A (anti-Gly-A, PE) purchased from Immunotech (Marseilles, France).
For TdT detection, cells were first fixed and permeabilized with commercially available reagents (cell permeabilization kit; sera-lab) and then incubated with anti-TdT (fitc; sera-lab) or an isotype control. Furthermore, tdt was also evaluated with an indirect immunofluorescence method on cytospin preparations as detailed elsewhere [9].
Cytogenetics, FISH and molecular genetics
The procedures for the analysis of karyotype have been reported in detail previously [lo]. For FISH, a double-color technique was adopted as already reported [ 111. Briefly, slides were denatured in 70% formamide/ 2x saline sodium citrate (SSC) at 70°C for 2.5 min and dehydrated in a chilled ethanol series (70%, 80%, 95%, 100%). Ten microliters of the PML/RARc( probe mixture (Oncor Inc., Gaithesburg, MD) were then applied to each slide and the area covered with a 24 x 24-mm glass coverslip. The hybridization was carried out for 16-48 h in a wet chamber at 37°C. Post- hybridization washings were done in 50% formamidel 2x SSC at 37°C for 8 min. The amplification and the detection steps were carried out with a dual-color detection and amplification kit (Oncor). Slides were counterstained with diaminodino-2-phenylindole (DAPI;

unique APL variant 579
Sigma) at 0.01 rig/ml and analyzed with a Zeiss Axioskop supplied with a dual-band pass filter.
For PML/RARa rearrangement, studies single- stranded cDNA was generated from approximately 0.5 pg of total RNA using an RT-PCR kit (Perkin Elmer Cetus, Norwalk, CT), and amplified by a two-step nested PCR in a 1.5~mM MgC12, 50-n-M KCl, lo-mM Tris-Cl-buffered solution (pH 8.3) with 200 mM dNTPs and 2.5 U Taq polymerase, using 15-30 pmol of each primer [ 121:
M4 S’AGC TGC TGG AGG CTG TGG ACG CGC GGT ACC 3
R5 5’ CCA CTA GTG GTA GCC TGA GGA CT 3’.
Five to 10 ul of the first step product (94°C 1’; 60°C 1’; 72°C l’, for 40 cycles total) were amplified with the nested primer: R8 5’ CAG AAC TGC TGC TCT GGG TCT CAA T 3’ and M4 for 30 cycles (94°C 1’; 60°C 1’; 72°C 1’) in a 1.5~mM MgC12, 5-mM KCl, IO-mM Tris- Cl buffered solution (pH 8.3) with 200~mM of dNTPs and 2.5 U Taq polymerase.
Discussion
This report emphasizes the importance of a multi- parameter approach to the diagnosis of AML. Although the appearance of the bone marrow might suggest a diagnosis of M3v to an experienced hemopathologist, this would have been highly questionable without the support of additional methods because other forms of AML can mimic the morphology of M3v [2-71. The distinction from acute myelomonocytic leukemia repre- sents the most common diagnostic problem [13]. Most of the leukemic cells of M3v have a basophilic cytoplasm with no or sparse fine granules, features that, in conjunction with the peculiar nuclear shape, are reminiscent of immature monocytes [ 131. Cytochemistry can be of greatest help in these cases, since both in the hypergranular and in the microgranular variant blasts typically display a strongly positive reaction for IWO/ SBB and, most distinctively, for NASD-CAE. In fact, a strong staining of monocytes for NASD-CAE is rarely, or never, observed [ 141. However, a degree of cytochemical heterogeneity of APL cells may be observed [7, 15-171. In our case, the reactivity for NASD-CAE was strongly positive in a small proportion of blasts, and highly reduced or completely negative in the majority. A similar pattern of cytochemical reactions has been reported in only a few other cases that possessed otherwise typical microgranular features consistent with the diagnosis of M3v [17]. Several authors [ 14-181 have also noted that leukemic cells from many patients with APL stained strongly with sodium fluoride-sensitive non-specific esterases, showing a pattern of reactivity similar to that of cases with M4
or M5 acute leukemias. Besides, a distinct entity associated with basophilic differentiation has been described [6, 151. Leukemic promyelocytes of baso- Phil-like M3 may show a metachromatic staining when stained with Toluidine Blue. Differential diagnosis of this form with MZbaso subtype and with cases of MIX or AML with basophilia (M2, M4 with t(6;9) transloca- tion) may be obtained by the use of cytochemistry, cytogenetic investigations and electron microscopy.
Recently, immunologic marker analysis has been considered to provide contirmatory diagnostic evidence in APL by virtue of a characteristic leukemic cell phenotype. The pan-myeloid markers CD33 and/or CD13 are constantly positive [19], as well as CD9 [20,21] and CD68 [21], whereas CD2 appears to be closely associated with M3v [21,22] and possibly with specific PML/RAR CI rearrangements [23]. Markers positive in early myeloid precursors that become negative by the promyelocytic stage, including HLA- DR, CD34, and TdT, are usually negative in APL [ 191. CD1 17, the product of the c-kit protooncogene and the receptor of the stem cell factor, appears to be expressed synchronously with CD34 in AML [24]. While expres- sion of HLA-DR and CD34 has been occasionally described [25-281, there is only one other case of TdT- positive [ 171 and no case at all of CD1 17positive APL in the literature. This, however, may be partly related to the fact that monoclonal antibodies against the CD1 17 antigen have been commercialized only in recent years, and data about their reactivity with AMLs are still inconspicuous. Nevertheless, in reviewing our recent database of 106 AMLs, including 9 APLs, tested with monoclonal antibodies against all these antigens, we found no other case that matched the above phenotype, and all leukemias with the concomitant expression of TdT, CD34 and CD117 belonged to either MO, Ml or M5a FAB subtypes.
In this case, the diagnosis of M3v finally rested on the results of cytogenetics and/or PCR analysis. The (15;17) (q21;q22) translocation is seen in almost every patient with APL but in no other form of malignancy and serves to fuse the PML gene on chromosome 15 to the retinoic acid receptor alpha (RARa) gene on chromosome 17 [l]. Detection of either the karyotypic abnormality or of the molecular rearrangement provides the final and unequi- vocal support to the diagnosis of APL. While cytoge- netics can provide information about additional karyotypic abnormalities, PCR appears to be a more rapid and sensitive assay [29]. This is most useful in the clinical setting not only for diagnostic purposes at presentation, since APL requires urgent specific therapy, but also over the course of treatment protocols, to assess minimal residual disease that might need a therapy to be adapted.
In summary, we have reported a unique case of M3v

580 R. Stasi et al.
that showed certain biological features of a very early myeloid precursor and may therefore represent an example of ‘asynchronous differentiation’ in leukemia. There is now ample evidence that APL is a hetero- geneous disease with respect to morphologic, cytochem- ical, immunophenotypic, and genotypic features. This heterogeneity should be considered in view of the important therapeutic implications related to the diag- nosis of AFL. Molecular analysis appears to be the most valuable tool for identifying previously unrecognized variants, PML/RARcr rearrangement representing the unifying characteristic for all cytological subtypes of AFL.
References
1. Warrell, R. P. Jr, de The, H., Wang, Z. Y. and Degos, L., Acute promyelocytic leukemia. N. Engl. J. Med., 1993, 329, 177.
2. Krause, J. R., Stoic, V., Kaplan, S. S. and Penchansky, L., Microgranular promyelocytic leukemia: a multiparameter examination. Am. J. Hematol., 1989, 30, 158.
3. Bain, B. J. (1990) Leukemia Diagnosis. A Guide to the FAB CZassiJicaticm. J. B. Lippincott, Philadelphia.
4. McKenna, R. W., Parkin, J., Bloomfield, C. D., Sundberg, R. D. and Brunning, R. D., Acute promyelocytic leukemia: a study of 39 cases with identification of a hyperbasophilic microgranular variant. Br. J. HaematoZ., 1982, 50, 201.
5. Scott, A. A., Head, D. R. and Kopecky, K. J. et al., HLA- DR-, CD33+, CD56+, CDl6- myeloid/natural killer cell acute leukemia: a previously unrecognized form of acute leukemia potentially misdiagnosed as French-American- British acute myeloid leukemia-M3. Blood, 1994, 84, 244.
6. Tallman, M. S., Hakimian, D. and Snower, D. et al., Basophilic differentiation in acute promyelocytic leukemia. Leukemia, 1993, 7, 521.
7. Castoldi, G. L., Liso, V., Specchia, G. and Tomasi, P., Acute promyelocytic leukemia: morphological aspects. Leukemia, 1994, 8, 1441.
8. Bennett, J. M., Catovsky, D. and Daniel, M. T. et al, Proposed revised criteria for the classification of acute myeloid leukemia. A. Znt. Med., 1985, 103, 620.
9. Vend&i, A., Del Poeta, G. and Stasi, R. et al., Minimally differentiated acute myeloid leukemia @ML-MO): Cyto- chemical, immunophenotypic and cytogenetic analysis of 19 cases. Br. J. Haematol., 1994, 88, 784.
10. Stasi, R., Del Poeta, G. and Masi, M. et al, Incidence of chromosome abnormalities and clinical significance of karyotype in de novo acute myeloid leukemia. Cancer Genet. Cytogenet., 1993, 67, 28.
11. Cox-Froncillo, M. C., Cantonetti, M., Masi, M., et al., Cytogenetic analysis is non-informative for assessing the remission rate in chronic myeloid leukemia (CML) patients on interferon-o: (FN-a) therapy. Cancer Genet. Cytogenet., 1995, 84, 15.
12. Biondi, A., Luciano, A. and Bassan, R. et al., CD2 expression in acute promyelocytic leukemia is associated with microgranular morphology (FAB M3v) but not with any PML gene breakpoint. Leukemia, 1995,9, 1461.
13. Bennett, J. M., Catovsky, D. and Daniel, M. T. et al, A
variant form of hypergranular promyelocytic leukemia (M3). Br. J. Haematol., 1980, 44, 169.
14. Hayhoe, F. G. J. & Quaglino, D. (1988) Hematological Cytochemistry, 2nd edition. Churchill Livingstone, Edin- burgh.
15. Tomonaga, M., Yoshida, Y. and Tagawa, M. et al., Cytochemistry of acute promyelocytic leukemia (M3): leukemic promyelocytes exhibit heterogeneous patterns in cellular differentiation. Blood, 1985, 66, 350.
16. Das Gupta, A., Sapre, R. S., Shah, A. S., Advani, S. H. and Nair, C. N., Cytochemical and immunophenotypic hetero- geneity in acute promyelocytic leukemia. Acta Haematol., 1989, 81, 5.
17. Scott, C. S., Patel, D. and Drexler, H. G. et al., Immunophenotypic and enzymatic studies do not support the concept of mixed monocytic granulocytic differentia- tion in acute promyelocytic leukemia (M3): a study of 44 cases. Br. J. Haematol., 1989, 71, 505.
18. Matsuo, T., Jain, N. C. and Bennett, J. M., Nonspecific esterase of acute promyelocytic leukemia (m3). Am. J. Hematol., 1988, 29, 148.
19. Paietta, E., Andersen, J. and Gallagher, R. et al., The immunophenotype of acute promyelocytic leukemia (APL): an ECOG study. Leukemia, 1994, 8, 1108.
20. Ferrero, D., Carlesso, N. and Gallo, E. et aZ., CD9 antigen in acute non lymphoid leukemia cells: preferential expression by promyelocytic (M3) subtype. Leuk. Res., 1991, 15, 457.
21. Erber, W. N., Asbahr, H., Rule, S. A. and Scott, C. S., Unique immunophenotype of acute promyelocytic leukae- mia as defined by CD9 and CD68 antibodies. Br. J. Haematol., 1994, 88, 101.
22. Rovelli, A., Biondi, A. and Cantu-Rajnoldi, A. et al., Microgranular variant of acute promyelocytic leukemia in children. J. clin. Oncol., 1992, 10, 1413.
23. Claxton, D. F., Reading, C. L. and Nagarajan, L. et al., Correlation of CD2 expression with PML gene breakpoints in patients with acute promyelocytic leukemia. Blood, 1992, 80, 582.
24. Muroi, K., Nakamura, M., Amemiya, Y., Suda, T. and Miura, Y., Expression of c-kit receptor (CD117) and CD34 in leukemic cells. Leuk. Lymphoma, 1995, 16, 297.
25. Lo Coca, F., Avvisati, G. and Diverio, D. et aZ., Rearrangements of the RAR-a gene in acute promyelocytic leukemia: correlations with morphology and immuno- phenotype. Br. J. Haematol., 1991, 78, 494.
26. Del Poem, G., Stasi, R. and Vend@ A. et al., Prognostic value of cell marker analysis in de nova acute myeloid leukemia. Leukemia, 1994, 8, 388.
27. McKiMey, C. D., Golden, W. L., Gemma, N. W., Swerdlow, S. H. and Williams, M. E., RARc( and PML gene rearrangements in acute promyelocytic leukemia with complex translocations and atypical features. Genes, Chromosomes & Cancer, 1994, 9, 49.
28. Paietta, E., Andersen, J. and Racevskis, J. et al., Significantly lower P-glycoprotein expression in acute promyelocytic leukemia than in other types of acute myeloid leukemia: immunological, molecular and func- tional analyses. Leukemia, 1994, 8, 968.
29. Diverio, D., Riccioni, R., Mandelli, F. and Lo Coca, F., The PML/RARu fusion gene in acute promyelcqtic leukemia. Haematologica, 1995, 80, 155.





























