Embed Size (px)
Citation preview

A Multi-Component Intervention to Prevent Child Maltreatment:
Long-term Effects on Parenting and Child Functioning
by
Elizabeth M. Demeusy
Submitted in Partial Fulfillment of the
Requirements for the Degree
Doctor of Philosophy
Supervised by Professor Sheree L. Toth
Department of Psychology
Arts, Sciences, and Engineering
School of Arts and Sciences
University of Rochester
Rochester, New York
2020
ii
Dedication
This dissertation is dedicated to all of the children, families, and teachers who
participated in the Building Health Children (BHC) program and this follow-up study,
and to Mt. Hope Family Center staff who worked tirelessly to make the BHC program
and this study possible.

iii
Table of Contents
Biographical Sketch ...................................................................................................... v
Acknowledgements ........................................................................................................ x
Abstract ....................................................................................................................... xii
Contributors and Funding Sources ........................................................................... xiv
List of Tables ............................................................................................................... xv
List of Figures ............................................................................................................. xvi
Chapter 1: Introduction ................................................................................................ 1 Background ................................................................................................................. 1 Prevention of Child Maltreatment ................................................................................ 3
Impact of Home Visiting on Child Maltreatment & Parenting ...................................... 7 Prevention of Externalizing Behavior Problems ......................................................... 14
Mechanisms of Change ............................................................................................. 18 Rationale for Follow-up ............................................................................................. 22
Chapter 2: Hypotheses ................................................................................................ 25
Chapter 3: Methods..................................................................................................... 27 Participants ................................................................................................................ 27 Recruitment ............................................................................................................... 28
Procedures ................................................................................................................. 30 Building Healthy Children (BHC) Program ............................................................... 33
Measures ................................................................................................................... 42
Chapter 4: Results ....................................................................................................... 51 Data Preparation ........................................................................................................ 51 Preliminary Analyses................................................................................................. 52
Correlations ............................................................................................................... 55 Intervention Effects ................................................................................................... 60 Mediation Analyses ................................................................................................... 67
iv
Chapter 5: Discussion.................................................................................................. 69 Study Aim 1: Impacts on Parenting ........................................................................... 70
Study Aim 2: Impacts on Child Outcomes ................................................................. 75 Study Aim 3: Mechanisms of Change ........................................................................ 78
Qualitative Impressions ............................................................................................. 80 Strengths & Limitations ............................................................................................. 81
Future Research ......................................................................................................... 84 Conclusion ................................................................................................................ 86
References .................................................................................................................... 88
Appendix A ................................................................................................................ 103
v
Biographical Sketch
Elizabeth Demeusy was born in Sayville, New York, USA. She attended
Pennsylvania State University, graduating with honors in 2012 with a Bachelor of Arts
degree in Psychology and a minor in Spanish. Following graduation, Elizabeth worked
for one year at New York University as a Junior Research Scientist with Drs. Clancy
Blair and Cybele Raver examining the role of Early Head Start in supporting parenting
and buffering the effects of toxic stress. She spent the following year gaining clinical
experience both domestically and internationally. During this time, Elizabeth lived in
Santiago, Chile where she worked with girls who had been abused and neglected. After
returning to the United States, she worked as a therapist assistant for Hope for Youth in
New York where she served youth and families as part of a juvenile diversion program.
In 2014, Elizabeth began her doctoral studies in Clinical Psychology at the University of
Rochester under the mentorship of Dr. Sheree Toth. She earned her Master of Arts degree
in Psychology in 2017. Her thesis was titled: “Child Maltreatment and the Development
of Early Externalizing Behavior: The role of Executive Functioning.”
During her time at the University of Rochester, Elizabeth completed clinical
externships at the University Counseling Center, Mt. Hope Family Center, Industry
Residential Center, and the University of Rochester Medical Center. These clinical
experiences provided Elizabeth with strong training in evidence-based assessment and
intervention for youth and families, many of whom were from underserved populations
and had experienced trauma. Elizabeth also served as a Teaching Assistant for Research
Methods and Social and Emotional Development courses at the University.
vi
In conjunction with her clinical training, Elizabeth served in various capacities on
a variety of research projects conducted at Mt. Hope Family Center. Her program of
research is centered around the developmental psychopathology framework, with a
specific eye towards prevention. In particular, she is interested in the dissemination and
implementation of evidenced-based interventions to prevent trauma and subsequent
psychopathology in vulnerable populations. In the latter part of her graduate school
career, Elizabeth also pursued training opportunities in the translation of research to
policy. She has worked with the American Psychological Association and the National
Prevention Science Coalition to better understand how research informs policies that
impact vulnerable children and families.
The following publications and presentations were a result of work conducted
prior to and during her doctoral study:
Publications
Demeusy, E., Handley, E., Manly, J.T., Sturm, R. & Toth, S. (in press). Building Healthy
Children: A preventive intervention for high-risk young families. Development
and Psychopathology.
Toth, S., Handley, E., Manly, J.T., Sturm, R., Adams, T., Demeusy, E., Cicchetti, D. (in
press). The moderating role of child maltreatment in treatment efficacy for
adolescent depression. Journal of Abnormal Child Psychology.
vii
Demeusy, E., Handley, E., & Toth, S. (2020). Trauma and stress-related disorders in
childhood. In The Encyclopedia of Child and Adolescent Development (Vol. 4).
Hoboken, New Jersey: Wiley-Blackwell.
Petrenko, C., Demeusy, E., & Alto, M. (2019). Six-month follow-up of the Families on
Track intervention pilot trial for children with fetal alcohol spectrum disorders
and their families. Alcoholism: Clinical and Experimental Research, 43(10),
2242–2254.
Demeusy, E., Handley, E. Rogosch, F., Cicchetti, D., & Toth, S. (2018). Early neglect
and the development of aggression in toddlerhood: The role of working memory.
Child Maltreatment, 23(4), 344-354.
Presentations
Demeusy, E., Manly, J., Sturm, R., Handley, E., Toth, S. (2020) The long-term effects of
a multi-component home visiting program on parenting, child regulation and
behavior problems. Paper presentation accepted to the Society for Prevention
Research 28th Annual Meeting, Washington, D.C.
Walsh, L., Demeusy, E., Griglak, S., & Sheldon, J. C. (2020). Demographic and service
utilization of children impacted by familial substance use. Poster accepted for
presentation at the 128th annual meeting of the American Psychological
Association, Washington, D.C.
Demeusy, E., Manly, J., Sturm, R., Toth, S. (2019, September). A multi-component home
visitation program to prevent child maltreatment: Effects on parenting and child
viii
functioning. Poster accepted to the Society for Implementation Research
Collaboration’s 5th Biennial Conference, Seattle, WA.
Demeusy, E. (2019, March). Cross-lagged panel models for longitudinal data. Invited
oral presentation at the HSDg Quantitative Colloquia, Department of Clinical and
Social Sciences in Psychology, University of Rochester, NY.
Demeusy, E., Alto, M., Handley, E., Manly, J., Sturm, R., Toth, S. (2019, March).
Maternal sensitivity, self-efficacy and parenting stress in high-risk, young
mothers: Effects on child functioning. Poster presented at the Society for Research
in Child Development 2019 Biennial Meeting, Baltimore, MD.
Demeusy, E., Rogosch, F., Cicchetti, D., Toth, S. (2018, November). The effect of
maternal history of childhood maltreatment on future parenting and child
behavior. Poster presented at the International Society for Traumatic Stress
Studies 34th Annual Meeting, Washington, DC.
Demeusy, E., Handley, E., Rogosch, F., Cicchetti, D., Toth, S. (2018, June). Early
neglect and the development of aggression in toddlerhood: The role of working
memory. Poster presented at the Administration for Child and Families National
Research Conference on Early Childhood, Arlington, VA.
Petrenko, C., Demeusy, E., Alto, M. (2018, June). Findings from the 6-month post-
intervention follow-up assessment of the Families on Track intervention for
children with fasd and their families. Symposium presentation at the 41st Annual
Research Society on Alcoholism Scientific Meeting, San Diego, CA.
ix
Demeusy, E., Handley, E., Rogosch, F., Cicchetti, D., Toth, S. (2017, November).
Maternal depression and the development of externalizing behavior in early
childhood: The role of parenting stress. Poster presented at the Association of
Behavioral and Cognitive Therapies 51st Annual Convention, San Diego, CA.
Demeusy, E., Handley, E., Rogosch, F., Cicchetti, D., Toth, S. (2017, April). Child
maltreatment and the development of early externalizing behavior: The role of
executive functioning. Poster presented at the Society for Research in Child
Development 2017 Biennial Meeting, Austin, TX.
Demeusy, E., Bailey, A., Rogosch, F., Handley, E., Cicchetti, D., Toth, S. (2016, March).
The relationship between maltreatment and adolescent marijuana dependence:
The mediating role of family environment and monitoring. Poster presented at the
Society for Research on Adolescence 2016 Biennial Meeting, Baltimore, MD.
x
Acknowledgements
First, I would like to thank and acknowledge my advisor, Dr. Sheree Toth, who
played an integral part in making this study possible. Thank you for your ever-present
guidance and encouragement throughout graduate school, for the opportunity to learn
from your expertise, and for helping me make this dream a reality. A special thanks to
Dr. Jody Todd Manly and Dr. Robin Sturm for providing clinical support to this project,
and invaluable information about the BHC program and the population we strive to serve.
I would also like to thank Dr. Fred Rogosch for providing guidance and expertise on
research design and implementation, and all things IRB-related. Thank you to Dr. Linda
Alpert-Gillis for serving on my committee and providing much appreciated expertise. I
owe much gratitude to Dr. Elizabeth Handley for her unwavering statistical support and
patience throughout this project and my graduate school career. A huge thank you to
Carol Ann Dubovsky for wading through the data with me, and for being a much-
appreciated sounding board and cheerleader throughout this journey. I want to
acknowledge my three undergraduate research assistants, Hannah Wadsworth, Hailey
Palleschi, and Tahreem Kamal, whose dedication made this project possible. Finally, I
want to express a great deal of gratitude to all Mt. Hope Family Center staff. You have
played a crucial role in this project and my graduate school experience. It has been an
honor to learn from you and to work alongside you.
On a personal note, I want to express immense appreciation to my family and
friends who have been with me through my graduate school journey. I especially want to
thank my parents, who taught me I can do anything I set my mind and heart to, even a
xi
six-year-long doctoral degree. I want to thank my partner, Deven, for supporting me,
encouraging me, and loving me, even from a distance. A big thank you to my cohort –
Michelle, Jess, and Irina – for being there from the beginning, and being an incredible
support network. And to my friends, for keeping me sane and reminding me of my life
and identity outside of graduate school.
xii
Abstract
The Building Healthy Children (BHC) home visiting program was designed to
provide concrete support and evidence-based intervention to young mothers and their
infants who were at heightened risk for child maltreatment and poor developmental
outcomes. BHC flexibly delivers three evidence-based treatment models based on
individual need in conjunction with continuous outreach support. These models
addressed parenting (Parents as Teachers), attachment (Child-Parent Psychotherapy), and
maternal depression (Interpersonal Psychotherapy for Depressed Adolescents). The
current study utilized a longitudinal follow-up design to examine the long-term effects of
BHC on parenting and child behavior in elementary school. In the current study, child
maltreatment and parenting practices were assessed using the Conflict Tactics Scales:
Parent–Child Version and Parenting Practices Interview. Child externalizing behavior
and self-regulation were assessed using both parent and teacher report on the Child
Behavior Checklist/Teacher Report Form (CBCL/TRF 6-18), the Behavior Rating
Inventory of Executive Function (BRIEF-2), and the Emotion Regulation Checklist.
Maternal social support and parent-child relationship quality were also examined as
potential mechanisms of change. Data for these mediators was collected during the
original study using the Parenting Stress Index, Attachment Q-sort, Maternal Behavior Q-
sort, and Social Support Behaviors Scale.
Follow-up data was collected from 87 mothers/caregivers and 69 teachers. Main
effects of the intervention on outcome variables of interest were analyzed using
independent sample T-tests. Compared to the comparison condition, findings indicated
xiii
that BHC intervention mothers exhibited less harsh and inconsistent parenting, and
marginally less psychological aggression towards their children at follow-up.
Interestingly, there were no significant intervention effects on positive parenting. BHC
intervention children also exhibited less externalizing behavior and self-regulatory
problems at follow-up, across parent and teacher report. Finally, there were no significant
effects of the intervention on maternal social support or parent-child relationship quality,
indicating that these were not the mechanisms responsible for change in this intervention.
When delivered during infancy and early childhood, this program is effective in
preventing negative parenting practices and the onset of child behavior problems in later
childhood. Findings highlight the importance of an adaptive model of home visitation
that addresses multiple determinants of parenting and child psychopathology.
xiv
Contributors and Funding Sources
This dissertation was supervised by the following committee members: Professor
Sheree Toth (advisor), Professor Fred Rogosch, and Professor Jody Todd Manly of Mt.
Hope Family Center, Department of Psychology; Professor Linda Alpert-Gillis of the
Department of Psychiatry, Pediatrics, and Clinical Nursing; and Professor Kathryn
Douthit of the Department of Counseling and Human Development serving as Chair of
this committee. Professors Toth and Manly, in addition to Professor Robin Sturm of Mt.
Hope Family Center, provided the data and contact information from the original BHC
study for this project. Professor Elizabeth Handley provided statistical consultation for
this work. Research assistants Hannah Wadsworth, Hailey Palleschi, and Tahreem Kamal
helped to collect and input the data for this study.
The original BHC study, from which these families were recruited and data was
used, was funded by Monroe County Department of Human Services, the United Way of
Greater Rochester, and the Administration of Children and Families (90CA1772/01).
This follow-up study was additionally funded by the Society for Research in Child
Development Student and Early Career Council Dissertation Research Award, and the
American Psychological Association Division 29 Charles J. Gelso, PhD, Psychotherapy
Research Grant.
xv
List of Tables
Table 1 Baseline Characteristics 53
Table 2 Prevalence of Adverse Life Events since Post-intervention 54
Table 3 Correlations – Parent Report 58
Table 4 Correlations – Teacher Report 59
Table 5 Intervention Effects on Main Outcomes – Parent Report 64
Table 6 Intervention Effects on Main Outcomes – Teacher Report 65
xvi
List of Figures
Figure 1 BHC Pyramid 34
1
Chapter 1: Introduction
Background
Child maltreatment is both a pervasive and significant public health concern.
National data indicate that 1 in 4 children experience some form of child maltreatment in
their lifetime, commonly experiencing more than one type and/or more than one incident
(Barnett, Manly, & Cicchetti, 1993; CDC, 2014; Finkelhor, Turner, Shattuck, & Hamby,
2013; Vachon, Krueger, Rogosch, & Cicchetti, 2015). Approximately three-quarters of
the cases reported to child protective services are classified as neglect, and the youngest
children (birth to 1 year), are often the most vulnerable (National Research Council,
2014; U.S.D.H.H.S., 2020). The impact of child maltreatment is widespread and
enduring, often resulting in a cascading effect on multiple developmental domains.
Trauma experienced at the hands of a caregiver is likely to fundamentally impact a
child’s social, emotional, cognitive, and neurobiological development (Cicchetti & Toth,
2016; Cowell, Cicchetti, Rogosch, & Toth, 2015). The effects permeate various arenas of
functioning, including mental and physical health, as well as education, employment and
interpersonal relationships (National Research Council, 2014).
The cost of child maltreatment can be understood both monetarily and in terms of
the suffering experienced by the victims and those that interact with them (e.g. family,
peers, future romantic partner), the latter of which is impossible to fully quantify.
Although human suffering should be enough to justify prevention efforts, quantifying the
monetary cost is often necessary in advocating for funding to support prevention and
2
treatment. Monetarily, the lifetime economic burden of first-time child maltreatment in
the United States in 2014 was estimated to be $5.9 trillion in lifetime spending, and $2.7
trillion in lost gross domestic profit (Perryman Group, 2014). These estimates include
spending in the areas of health care, social welfare, criminal justice, and education, as
well as the reduction in earnings due to child maltreatment. A significant portion of this
cost is due to out of home placement in foster care. A past study examining Medicaid
records found that youth in foster care consume approximately half of the dollars spent
on mental health, while only comprising 4% of the population (Halfon, Berkowitz, &
Klee, 1992). Taken together, it is clear that the cost of child maltreatment makes it critical
for researchers, practitioners, and policymakers alike to focus efforts on the prevention of
these debilitating incidents before they occur.
While recognizing that no single approach can address the multitude of risk
factors associated with child maltreatment in high-risk families, the “Building Healthy
Children” program (BHC; Paradis, Sandler, Manly, & Valentine, 2013) was designed as
a multi-component preventive intervention aimed at preventing child maltreatment and
supporting healthy development in infants of young mothers. This program was
developed as a collaborative community initiative, integrating the expertise, resources,
and services of various providers. BHC uses a combination of three evidence-based
models, which are provided to families in their homes. These three models address
parenting (Parents as Teachers), trauma and attachment (Child-Parent Psychotherapy),
and maternal depression (Interpersonal Psychotherapy for Depressed Adolescents), and
each has received substantial evidentiary support (Cicchetti, Rogosch, & Toth, 2006;
3
Lieberman, Van Horn, & Ippen, 2005; Mufson, Weissman, Moreau, & Garfinkel, 1999;
Toth et al., 2013; Wagner & Clayton, 1999; Weissman, Markowitz, & Klerman, 2000). In
order to ensure efficiency and flexibility in service delivery, and to avoid overwhelming
young mothers with excessive services, the intervention models implemented were
determined based on each individual family’s interest and needs. In addition, to mitigate
contextual risk factors and to address social determinants of health, all intervention
families also received outreach services which included assistance with food, housing,
transportation, education and employment. The structure and individual components of
BHC will be discussed in the methods section of this dissertation. The objective of this
dissertation is to follow up families that have completed the BHC program in order
to ascertain whether this approach to preventive intervention has sustained effects
on the prevention of child maltreatment and harsh parenting, and the promotion of
positive parenting practices and adaptive socioemotional development through
middle childhood.
Prevention of Child Maltreatment
Child maltreatment is an umbrella term that encompasses both abuse (physical,
sexual, and emotional) and neglect (physical, emotional). Additionally, these subtypes
include acts of commission and omission. They can also be defined by Standards of
Harm, which involve demonstrable harm to the child, and Endangerment, in which a
child is put in danger but not yet harmed (Cicchetti & Toth, 2015; Sedlak et al., 2010).
Over the past decades, important advances have been made to how we define and
operationalize child maltreatment (Barnett et al., 1993; Manly, 2005). Clear and agreed
4
upon definitions of these constructs are necessary in our understanding of the prevalence,
impact, and resources needed to address this public health concern (Cicchetti &
Valentino, 2006).
The precursors and sequela of child maltreatment can be best understood through
a developmental psychopathology lens. Developmental psychopathology is an
interdisciplinary scientific framework for conceptualizing and examining the links
between normal and abnormal development (Cicchetti, 1984; Cicchetti & Toth, 2005).
For decades, our understanding of child maltreatment and its causes and consequences,
have been shaped by the theoretical underpinnings of this perspective (e.g. Cicchetti &
Toth, 1995, 2016). The concept of equifinality, derived from general systems theory, is a
guiding principle of the developmental psychopathology framework (Von Bertalanffy,
1968). Equifinality can be defined as different paths leading to the same outcome
(Cicchetti & Toth, 2017). In the context of child maltreatment, this can be understood as
a multitude of risk factors leading to the maltreatment of a child. Extant literature has
identified a number of risk factors, ranging from sociodemographic variables
(race/ethnicity, income, parent age, parent education, unplanned pregnancy), to parent-
child relationship quality (attachment, maternal sensitivity, family cohesion and conflict),
to parenting practices (parent views child as a problem, parenting stress, use of corporal
punishment), to a parent’s own mental health and caregiving history (psychopathology,
social support, history of trauma) (Dixon, Browne, & Hamilton-Giachritsis, 2005;
Hussey, Chang, & Kotch, 2006; Sidebotham, Heron, & Team, 2006; Stith et al., 2009). It
is important to note that while many studies have found disproportionate representation
5
of racial and ethnic minorities in the child welfare system, this prevalence is largely due
to sociodemographic risk (e.g. poverty) (Hussey et al., 2006).
BHC was developed to address a number of these risk factors through its selection
criteria and the models of evidence-based intervention delivered. Specifically,
participants were mothers who had their first child prior to 21 years of age, and who were
eligible to receive Temporary Assistance for Needy Families (TANF), addressing both
age and income risk factors. Although not a selection criterion, the majority of the
mothers who participated in the program identified as part of racial/ethnic minorities
groups, and a large percentage had a history of maltreatment as a child. The intervention
models incorporated into BHC address additional risk factors including parent-child
attachment, maternal sensitivity, maternal trauma history, maternal depression and social
support, exposure to violence, and knowledge of appropriate developmental expectations.
Child maltreatment has been regarded as a severe, fundamental failure of the
caregiving system to provide the essential experiences necessary to scaffold optimal
psychological development (Cicchetti & Lynch, 1995; Cicchetti & Toth, 2005).
Maltreatment during infancy and early childhood can undermine the mastery of early
developmental tasks and decrease the probability that children will access subsequent
opportunities to help them build the skills necessary for adaptive development; therefore,
propelling them on a maladaptive trajectory (Cicchetti & Toth, 1995; Jaffee &
Maikovich-Fong, 2011). Therefore, the impact of maltreatment is cascading in nature, in
that early disturbances in development affect later functioning, which can ultimately
contribute to the emergence of psychopathology.
6
Often times in early childhood, children may experience certain risk factors or
exhibit elevated levels of symptomatology without reaching the clinical level for
diagnosis. Therefore, interventions designed to counteract these risk factors or ameliorate
prodromal signs or symptoms of a problem or disorder are termed preventive
interventions (Greenberg, Domitrovich, & Bumbarger, 1999). Preventive interventions
are delivered before the onset of a problem (e.g. child maltreatment) or disorder and can
target multiple populations that vary in their level of risk. Over the past few decades,
there has been increasing interest and investment in these programs in terms of research,
practice, and policy (P. Collins et al., 2011; Weisz, Sandler, Durlak, & Anton, 2005).
Extant research has identified guidelines for effective prevention programs. These
include various treatment characteristics (theoretically-based, comprehensive, includes
varied methods of teaching, fosters positive relationships), procedural characteristics
(appropriate dosage and timing, implemented by well-trained staff, sociocultural
relevance), and design characteristics (demonstrated effectiveness, measures meaningful
outcomes) (Borkowski, Smith, & Akai, 2007). These guidelines were taken into careful
consideration in the development of the BHC program. BHC is an example of a
“selective preventive intervention,” which targets families whose risk of child
maltreatment is higher than average. This risk may be on the basis of biological,
psychological, or social factors that are known to be associated with the outcome of
interest (O’Connell, Boat, & Warner, 2009).
Child maltreatment prevention efforts have grown exponentially over the past
several decades, due to the increasing awareness of the prevalence and severity of the
7
problem, and new policies implemented which allocate resources for such services (Child
Welfare Information Gateway, 2011). A broad range of preventive interventions has been
developed in attempt to prevent the harmful acts of child abuse and neglect. These
interventions vary in type (e.g. evidence-based model used), context (e.g. home
visitation, hospital, community-based center), and target (e.g. parent, parent-child dyad,
group of parents) (MacMillan et al., 2009). Extant literature has reviewed the
effectiveness of many of these interventions. One meta-analysis examined 56 programs
designed to prevent child maltreatment (or the reoccurrence of maltreatment) and
promote family wellness (MacLeod & Nelson, 2000). Results indicated that most
interventions were successful, with an overall mean effect size of d=.41. Multi-
component and home visiting interventions displayed the largest effects sizes among
those using a proactive (prior to maltreatment) approach. Of particular relevance to the
current study, authors found that effect sizes of proactive interventions were larger at
follow-up than immediately following the completion of the intervention. This
underscores the importance of conducting follow-up studies with families who have
participated in these preventive interventions. These results support the notion that
proactive prevention efforts can break a maladaptive pattern that may result in child
maltreatment by targeting various known risk factors (Rutter, 1987).
Impact of Home Visiting on Child Maltreatment & Parenting
Home visiting is one of the most widespread, proactive approaches to preventing
child maltreatment, particularly prenatally and during infancy. The Mother, Infant, and
Early Childhood Home Visiting Program (MIECHV), established through the Patient
8
Protection and Affordable Care Act, provides home-visiting services to at-risk pregnant
women and their children from birth to five years old (Avellar & Supplee, 2013). This
federal investment has increased funding for and accessibility to these services,
specifically those that are evidence-based. Several reviews have been conducted to
examine the effectiveness of home visiting in the prevention of child maltreatment,
identifying several promising programs (Avellar & Supplee, 2013; Mikton & Butchart,
2009). Indicators of prevention can be measured by both official records (e.g. Child
Protective Services (CPS); hospital records), as well as, parent-report measures. There is
some skepticism in relying solely on substantiated CPS reports, as families receiving
these services are under more surveillance, which may increase the likelihood that a CPS
report is made (Avellar & Supplee, 2013).
Ample research has documented Nurse Family Partnership (NFP), a widely
implemented home visiting intervention that assists high-risk mothers during pregnancy
and post-delivery, as effective at preventing maltreatment and improving child outcomes
(e.g. Eckenrode et al., 2000; Olds, 2006; Olds et al., 1997). Interestingly, avoidance of
CPS was most notable during the follow-up period, between the children’s fourth and
fifteenth birthday. During this time, mothers in the NFP group were identified as
perpetrators of child maltreatment significantly less than mothers in the comparison
group (Olds et al., 1997). These results highlight the importance of conducting long-term
follow-up studies to better understand the impact of home visiting interventions over
time. BHC differs from NFP by incorporating a focus on child social-emotional
development, maternal mental health, and parent-child attachment in order to prevent
9
child maltreatment. Another effective home visiting intervention of particular relevance
to the current study is Parents as Teachers (PAT; Parents as Teachers National Center,
1999). PAT is a parent-education program, which emphasizes positive parenting behavior
as the vehicle through which adaptive functioning and healthy child development are
achieved. A main goal of the program is to prevent and reduce child abuse, and there is
some promising evidence to suggest that this program can effectively achieve that goal
(Pfannenstiel, Lambson, & Yarnell, 1996; Pfannenstiel et al., 1991; Wagner & Clayton,
1999; Wagner, Spiker, & Linn, 2002). However, additional research is needed in order to
replicate this finding.
Additional home visiting programs that have demonstrated favorable impacts on
the prevention of child abuse and neglect include Child FIRST, Early Head Start-Home
Visiting, Early Start, Health Access Nurturing Development Services (HANDS), Healthy
Families America, and SafeCare Augmented (Avellar & Supplee, 2013; Sama-Miller,
Akers, Mraz-Esposito, Coughlin, & Zukiewicz, 2017). Many of these programs are
multidimensional in order to address a range of risk factors. For example, an important
dimension of the Child FIRST model is its focus on strengthening the parent-child
relationship and attachment. Similar to BHC, this dimension was derived from Child-
Parent Psychotherapy (CPP); however, the full CPP model was not implemented (Lowell,
Carter, Godoy, Paulicin, & Briggs-Gowan, 2011). Extensive research has been conducted
on what makes home visiting programs more, or less, effective. In one review, Howard
and Brooks-Gunn (2009) found that home-visiting programs are especially effective in
child maltreatment prevention for first-time adolescent mothers, suggesting that these
10
mothers may be more receptive to intervention having never engaged in poor parenting or
child maltreatment previously. In addition, duration and frequency of visits have been
shown to impact program effectiveness, with longer programs (greater than six months),
and those that provide more frequent visits resulting in more positive outcomes
(MacLeod & Nelson, 2000; Nievar, Van Egeren, & Pollard, 2010). Finally, many home
visiting evaluations have found greater benefits for families at higher risk (e.g. low-
income, unmarried) (Olds, 2008; Wagner et al., 2002). This suggests that targeting home
visitation services to families at-risk for child maltreatment may increase the likelihood
that the family benefits and that program funding is utilized to its fullest extent.
Home visiting programs have also demonstrated favorable effects on parenting
more broadly. A review of nine widely implemented home visiting programs found that
many of these programs significantly decreased parental harshness, and/or increased
parental responsivity and sensitivity (K. S. Howard & Brooks-Gunn, 2009). In contrast to
child abuse, harsh parenting falls on the milder end of the spectrum. Harsh parenting is an
umbrella term for a range of negative parenting behavior, but often includes physically
harsh behaviors (e.g. spanking, slapping, or pinching), as well as, verbally and
psychologically harsh behaviors (e.g. verbal threats) (H. K. Kim, Pears, Fisher, Connelly,
& Landsverk, 2010; Straus, Hamby, Finkelhor, Moore, & Runyan, 1998; Webster-
Stratton, 1998). Research has found that parents who regularly exhibit a pattern of
negative affect (e.g. anger, hostility) as part of harsh parenting behavior are at increased
risk for child maltreatment (Deater-Deckard, 2008; Deater-Deckard, Wang, Chen, &
Bell, 2012; Patterson, 1997). While harsh parenting may not be as extreme as child
11
physical or emotional abuse, it too can have detrimental effects on child development.
Extant literature has linked harsh parenting to the development of externalizing behavior
problems (e.g. conduct problems, aggression, disruptive behavior) and difficulties with
emotion regulation in childhood, adolescence and beyond (Bailey, Hill, Oesterle, &
Hawkins, 2009; Chang, Schwartz, Dodge, & McBride-Chang, 2003; Gershoff, 2002;
Pinquart, 2017).
Research has found that various interventions are effective at modifying negative
parenting practices, including harsh parenting (Brotman, Gouley, Chesir-Teran, Dennis,
Klein, & Shrout, 2005; Dawson-McClure et al., 2015; Wong, Gonzales, Montaño,
Dumka, & Millsap, 2014). Mediational studies have found that this change in parenting
behavior then leads to a decrease in child externalizing behavior (Beauchaine, Webster-
Stratton, & Reid, 2005). One study examining the effect of a home visiting program
implemented with adolescent mothers, found that home visitation significantly decreased
negative parenting attitudes and child-rearing practices (Barnet, Liu, DeVoe, Alperovitz-
Bichell, & Duggan, 2007). Similar to BHC, this program focused on improving teens’
understanding of child development, improving parenting attitudes and skills, while also
attending to maternal mental health concerns. Another home visiting program (Healthy
Families New York) found a significant preventive effect on observed harsh parenting
behavior. However, this effect was only seen for those in the High Prevention
Opportunity subsample which included first-time mothers under the age of 19 that began
the program during pregnancy (M. Rodriguez, Dumont, Mitchell-Herzfeld, Walden, &
12
Greene, 2010). BHC eligibility criteria targets a similar population of young, and often
new mothers.
Home visiting has also demonstrated a beneficial impact on positive parenting.
For example, results from NFP found that home-visited mothers were more competent at
caring for their child, as evidenced by their increased responsivity (Olds, 2006). This
result was found amongst mothers who had low psychological resources (e.g. poor
mental health, low sense of control over life circumstances) (Olds, Kitzman, et al., 2007).
Despite these promising results, there is a dearth of research examining the impact of
home visiting on positive parenting practices, such as providing praise and incentives and
setting clear expectations. More research is needed to better understand the impact of
home visiting on these aspects of parenting.
Although home visiting programs have proliferated over the past decade,
additional research is needed in order to help us better understand what works for whom,
and why (Roth & Fonagy, 2013). Ultimately, the term home visitation only describes the
mechanism of service delivery; therefore, the design and content of each program can
vary significantly. Many home visiting programs include principles from evidence-based
models, while not implementing the full model. This is concerning because the efficacy
of individual models incorporated is based on the model’s implementation to fidelity.
Therefore, more research is needed on home visiting programs that implement previously
established, evidence-based treatment models (Sweet & Appelbaum, 2004). In addition,
more comprehensive preventive interventions for child maltreatment are needed,
13
specifically those that address maternal mental health and the attachment relationship
(Duggan, Berlin, Cassidy, Burrell, & Tandon, 2009; Robinson & Emde, 2004).
A recent trend in precision medicine has also been adopted in the field of home
visiting. One question being asked is whether home visiting can improve outcomes more
efficiently? To do so, researchers are being called to refine evidence-based models by
tailoring them to client’s specific needs and responses to treatment (August & Gewirtz,
2019; Supplee & Duggan, 2019). Supplee and Duggan (2019) suggest four pillars
necessary to implementing “precision home visiting” research effectively. These include
1) authentic research-practice partnerships, 2) a focus on active ingredients, 3) coherent
well-specified models, and 4) innovative research designs that accelerate building
evidence. BHC was designed to addresses the first three of these pillars. First, the
program was born out of an interagency collaborative between medical, university and
community stakeholders. In addition, it offers a menu of well-specified evidence-based
models. Finally, the original research study collected a range of measures in order to
examine potential mediators and determine the active ingredients responsible for key
outcomes, some of which will be analyzed in the current study.
Additional research is also needed to examine the effect of home visiting on child
outcomes, particularly in cases where the parent is the only, or the primary, participant in
the intervention. Extant research has found mixed results for the effect of home visiting
on child outcomes (Peacock, Konrad, Watson, Nickel, & Muhajarine, 2013). Favorable
results have been found for a variety of programs in the areas of cognitive development,
social emotional development, and behavior problems; however, these results are not
14
always consistent across program sites or measures (Avellar & Supplee, 2013). Questions
remain regarding the ability of this prevention strategy to impact child functioning and
create sustainable effects.
Prevention of Externalizing Behavior Problems
Many preventive interventions designed to prevent child maltreatment also aim to
promote adaptive functioning in children. The definition and operationalization of
adaptive functioning varies by program and outcomes measured. The second aim of this
dissertation is to examine the effect of BHC on child functioning, specifically
externalizing behavior and self-regulation. Numerous studies have found that
externalizing behavior problems develop as early as preschool and can have continued
detrimental effects on development if they persist (Broidy et al., 2003; Campbell, Shaw,
& Gilliom, 2000; Moffitt, 1993). Externalizing behavior problems in early childhood are
linked to a number of adverse outcomes during early and middle childhood, such as
academic underachievement and peer difficulties (Campbell et al., 2000; Hinshaw, 1992).
If these behavior problems persist and become chronic, children are at risk to continue
along a maladaptive trajectory (Hill, Degnan, Calkins, & Keane, 2006) which may
include violence, delinquency, and substance abuse in adolescence, followed by
criminality and mental health problems in adulthood (Babinski, Hartsough, & Lambert,
1999; Broidy et al., 2003; Miller-Johnson, Coie, Maumary-Gremaud, Lochman, & Terry,
1999; Odgers et al., 2008).
These adverse outcomes are taxing on the individual and their loved ones, and
often require costly public assistance programs or mental health services. Childhood
15
conduct problems that develop into criminality in adolescence and adulthood have high
monetary costs for society. However, encouraging results from cost-benefit analyses have
revealed that investments in early intervention programs can have preventive effects,
therefore saving society money in the long term (Aos, Phipps, Barnoski, & Lieb, 2001;
Cohen & Piquero, 2009). Because behavioral difficulties have already emerged by
preschool, interventions targeting infants and toddlers, such as home-visiting programs,
can be particularly effective. Although change is possible at every point in development,
the longer a child continues along a maladaptive trajectory, the more difficult change
becomes (Sroufe, 2013).
The development of externalizing behavior in early childhood is widely believed
to be multifactorial and transactional (Olson, Sameroff, Kerr, Lopez, & Wellman, 2005;
Sameroff, 1995). No one risk factor, biological nor environmental, is responsible for the
development of such behavior. Extant literature has outlined a range of risk factors that
can lead to the development of externalizing behavior problems, including a number of
intrapersonal, interpersonal, and contextual factors. Of particular relevance to this study,
maternal unresponsiveness, inconsistent and ineffective parental control strategies,
insecure attachment, and maternal depression are linked with externalizing behavior in
childhood (Campbell et al., 2000; Goodman et al., 2011). Various sociocultural risk
factors, such as teenage pregnancy, unplanned pregnancy and low socioeconomic status,
are also associated with these behaviors in childhood (Deater–Deckard, Dodge, Bates, &
Pettit, 1998). By utilizing a multi-component approach, BHC addresses each of these risk
factors.
16
Child self-regulation is also closely linked to externalizing behavior problems.
For the purpose of this study, the construct of self-regulation will integrate both executive
functioning and emotion regulation (Zhou, Chen, & Main, 2012). The development of
self-regulation is a critical developmental issue in infancy and early childhood, and a
central capacity that lies at the core of normal and abnormal development (Sroufe, 2013).
The capacity for self-regulation is one of the strongest predictors of outcome in
longitudinal studies examining psychopathology in children (Masten, 2004). Extant
literature has found that deficits in executive functioning and emotion regulation are
concurrently and longitudinally related to the development of externalizing behavior,
including aggression and conduct problems (Frick & Morris, 2004; Gilliom, Shaw, Beck,
Schonberg, & Lukon, 2002; Séguin & Zelazo, 2005). Longitudinal research also suggests
that improving positive parenting and the parent-child relationship, as well as addressing
maternal psychological functioning, enhances child self-regulation, which can then
decrease child externalizing behavior (Gilliom et al., 2002; S. Kim & Brody, 2005).
Therefore, the proposed study will examine the effect of BHC on childhood self-
regulation as well.
Interventions for externalizing behavior problems have generally been
concentrated after the first two years of life and have targeted children already displaying
conduct problems (Lyons-Ruth & Melnick, 2004). Often, interventions are not delivered
until a disorder has developed and significantly impacts functioning. Research has found
that delaying intervention until after aggressive and delinquent behaviors have developed
and have already resulted in secondary risk factors (e.g. academic failure, deviant peers,
17
etc.), often limits the impact of the intervention (Offord & Bennett, 1994; Webster-
Stratton & Reid, 2017). Clinical investigators of conduct disorders have called for an
increased focus on parent–infant services designed to prevent the early onset of
aggression and disruptive behavior (Tremblay, LeMarquand, & Vitaro, 1999). Webster-
Stratton & colleagues are a strong proponent of this approach, delivering a preventive
intervention (The Incredible Years) that emphasizes nonviolent, positive parenting skills
to prevent or reduce conduct problems in young children (Webster-Stratton & Hammond,
1998). However, much of the research conducted on the Incredible Years series has been
done with children already exhibiting behavioral difficulties.
An alternative approach to the prevention of externalizing behavior problems is
home visitation. Reviews of existing literature have found mixed results regarding the
effect of home visiting on this outcome (Carney, Stratford, Moore, Rojas, & Daneri,
2015; Peacock et al., 2013). A recent study examining the effect of the home visiting
program Child FIRST found a significant reduction in clinical levels of externalizing
behavior in toddlerhood. Similar to BHC, this intervention incorporates both parent
education and a focus on the parent-child relationship (Lowell et al., 2011). Relatively
fewer studies have investigated the impact of infant home-visiting services on
externalizing behavior problems (e.g. aggression) at school entry or beyond (Lyons-Ruth
& Melnick, 2004). One study found that children who engaged in a parent–infant home
visiting program during the first 18 months of life exhibited less hostile-aggressive
behavior in their kindergarten classrooms, compared to children in the control group.
This pattern was particularly evident for families that participated in home visiting
18
services weekly for at least one year (Lyons-Ruth & Melnick, 2004). The long-term
effects of home visitation on externalizing behavior have been demonstrated through
NFP. A 15-year follow-up found significant reductions in the number of arrests,
convictions, and probation violations for adolescents in the high-risk group who received
home visiting services, compared to those that did not (Olds et al., 1997). Overall, more
research is needed on the sustainability of favorable child outcomes gained from home
visitation (Carney et al., 2015).
Additionally, there is a dearth of research on the effect of home visiting on child
self-regulation. Some studies have evaluated the effect of home visiting interventions on
socioemotional competency more broadly. One meta-analysis found that children who
received home-visiting services fared better than control children in the area of
socioemotional functioning (Sweet & Appelbaum, 2004). Although this term
encompasses a range of abilities, self-regulation is one component of socioemotional
functioning. In addition, NFP has found some promising results for the long-term impact
of home visiting on child executive functioning at age nine (Olds et al., 1997). The same
program found significant effects on children’s dysregulated aggression and behavioral
regulation, in the intended direction (Olds et al., 1997; Olds et al., 2004). Additional
research is needed to more comprehensively understand the impact of home visiting on
the critical capacity of self-regulation.
Mechanisms of Change
Researchers in the field of home visiting have called for an increased
understanding of the underlying processes that produce change in home visiting programs
19
(Olds, Sadler, & Kitzman, 2007). It is imperative to examine mechanisms of change in
order to better understand why an intervention program works (Roth & Fonagy, 2013;
Shonkoff & Fisher, 2013). Therefore, the tertiary aim of this study is to examine
parent-child relationship quality and maternal social support as potential
mechanisms of change in the BHC intervention program. Specifically, a sequential
effect will be examined wherein BHC increases maternal social support, which then
fosters parent-child relationship quality, which then together act as a mechanism through
which BHC impacts parenting and child functioning.
For the purpose of this study, parent-child relationship quality will encompass
facets of maternal sensitivity and the attachment relationship. A meta-analysis of
preventive interventions designed to enhance maternal sensitivity and foster secure
attachment found that many of these preventive interventions were quite effective at
impacting these constructs (Bakermans-Kranenburg, Van Ijzendoorn, & Juffer, 2003). Of
particular relevance to this study, both IPT and CPP (components of BHC) have
demonstrated efficacy in improving parent-child relationship quality (Beeber et al., 2013;
Cicchetti et al., 2006; Mulcahy, Reay, Wilkinson, & Owen, 2010). Extant literature
suggests home visiting programs in particular can impact sensitivity and attachment, and
effectively impart positive benefits to families by way of influencing maternal practices
(K. S. Howard & Brooks-Gunn, 2009; M. Rodriguez et al., 2010). A review of nine well-
known home visiting programs found that these programs were often associated with
higher rates of maternal responsivity and sensitivity in parent-child interactions (K. S.
Howard & Brooks-Gunn, 2009).
20
Fostering a positive parent-child relationship has significant effects on child
maltreatment and functioning (Cicchetti et al., 2006; Lieberman et al., 2005). A recent
consensus purported by a number of experts in the field highlights the importance of
promoting positive parenting in order to reduce child maltreatment (Luthar & Eisenberg,
2017). Attachment insecurity is closely linked to child maltreatment; therefore, fostering
a secure attachment relationship and increasing maternal sensitivity, can reduce or
prevent the occurrence of child maltreatment (Morton & Browne, 1998; Thomas &
Zimmer-Gembeck, 2011). As reviewed by Miner and Clarke-Stewart (2008), higher rates
of maternal sensitivity and responsiveness have also been related to lower rates of child
externalizing behavior across a number of studies (e.g. Deater-Deckard, Ivy, & Petrill,
2006; Shaw, Gilliom, Ingoldsby, & Nagin, 2003; Stams, Juffer, & van IJzendoorn, 2002).
In particular, enhancing parental sensitivity appears to have a particularly positive effect
on child functioning in ethnic minority families. Researchers suggest that interventions
attempting to improve child well-being in these populations should focus on fostering
sensitivity (Mesman, van IJzendoorn, & Bakermans-Kranenburg, 2012). In addition,
ample data has supported the link between attachment and emotion regulation in children,
suggesting that a secure attachment relationship lends itself to the development of
adaptive regulatory abilities (Sroufe, 2005). There is some evidence to suggest that
changes in child functioning produced by home visitation are mediated by changes in
parenting attitudes and behaviors (Howard & Brooks-Gunn, 2009). In particular,
programs that emphasized responsive and sensitive caregiving demonstrated positive
effects on a range of child outcomes (Filene, Kaminski, Valle, & Cachat, 2013).
21
However, more research is needed to examine parent-child relationship quality as a
mechanism through which home visitation impacts child functioning.
One factor that has been shown to impact parent-child relationship quality is
maternal social support. Researchers have emphasized the importance of fostering the
well-being of caregivers via regular support in order to promote resilient adaptations
among high-risk children (Luthar & Eisenberg, 2017). Maternal social support can be
provided by any individual within the mother’s social network, be it a family member,
partner/spouse, friend, or co-worker. As reviewed by Thompson, Flood, and Goodvin
(2006), the nature of a parent’s social networks can have positive and negative impacts
on family functioning, specifically the parent-child relationship. Parental social support
has been found to positively impact attachment security, as well as other aspects of
children’s psychological well-being. Extant research supports the association between
maternal social support and mother-child interactive behavior (Crnic, Greenberg,
Ragozin, Robinson, & Basham, 1983; Goldstein, Diener, & Mangelsdorf, 1996; Shin,
Park, & Kim, 2006). In addition, families living in poverty are more likely to report that
their social networks are less supportive and, at times, more stressful than families with
more economic advantage (Ceballo & McLoyd, 2002). The positive relationship between
social support and parent-child relationship quality is evident in these populations (e.g.
impoverished; racially diverse); therefore, suggesting that this is a prime target for
intervention in a disadvantaged sample (Burchinal, Follmer, & Bryant, 1996). Although
many home visiting programs seek to create change by providing parents with social
support, few evaluations have measured this outcome and provided evidence for the
22
impact of home visitation on maternal social support (Gomby, Culross, & Behrman,
1999). Promising results suggest that social support is impacted by home visiting services
(Kendrick et al., 2000); however, more research is needed.
Rationale for Follow-up
The literature reviewed above provides the rationale for the current dissertation,
which proposes to follow-up families who previously participated in the BHC program in
order to assess the program’s ability to have sustained effects on the prevention of child
maltreatment, reduction of harsh parenting, and promotion of adaptive parent and child
functioning. Researchers have echoed the importance of continued evaluation of
preventive interventions that have been tested in efficacy trials as they are disseminated
into increasingly naturalistic conditions in the community through effectiveness trials
(Cicchetti & Toth, 2016; Flay et al., 2005; Olds, Sadler, et al., 2007). BHC is an
effectiveness trial as it incorporates multiple evidence-based interventions models that
have been proven efficacious into one home visiting model, which is then delivered
within existing community infrastructure. At this time, there have been two evaluations
on the immediate effects of BHC.
Paradis et al. (2013) examined preliminary results from the first few years that
BHC was delivered in the community. At baseline, they found that over a third of
mothers had documented histories of abuse and/or neglect in their own childhood, a
quarter of the sample had elevated depressive symptoms, and nearly two thirds were
exposed to domestic violence, indicating that the mothers engaged in this program had a
multitude of risk factors. In addition, families in the BHC group demonstrated higher
23
rates of compliance with well-child visits, compared to those in the control group. When
assessing child maltreatment, results indicated that 98% of families in the BHC group and
95% of families in the control group avoided indicated CPS reports. While this difference
is not statistically significant, these results are promising given the closer surveillance
that comes with participating in home visitation services. Long-term follow-up is needed
to determine whether this pattern is sustained, or whether a difference is evident between
groups over time, similar to the results that were found with the Nurse Family Partnership
(Olds et al., 1997).
A more recent investigation of the effects of BHC on maternal and child
functioning found promising effects of the intervention on child maltreatment, parenting
attitudes, maternal depression and child behavior (Handley, Demeusy, Manly, Sturm &
Toth, 2020, November). At the conclusion of the intervention, families in the intervention
condition exhibited significantly lower rates of maltreatment (4.8%) compared to families
in the comparison group (13.6%), as evidenced by official CPS records. In addition,
mothers in the intervention group exhibited significantly fewer depressive symptoms by
mid-intervention compared to those in the control group. This reduction in maternal
depressive symptoms significantly mediated the effect of BHC on child internalizing and
externalizing symptoms, as well as, parenting stress and self-efficacy at post-intervention.
These results highlight the importance of attending to maternal mental health needs, and
the subsequent effect that addressing these needs has on maternal and child functioning.
Although these results provide compelling evidence for the effect of BHC on maternal
and child functioning, additional research is to examine the long-term effects of this

24
preventive intervention on maltreatment, parenting and child functioning.
25
Chapter 2: Hypotheses Specific Aim #1: To ascertain whether the BHC intervention has sustainable effects on
the prevention of child maltreatment and the reduction of negative parenting practices.
Hypothesis 1a: Mothers enrolled in BHC treatment group will report lower rates
of child maltreatment at follow-up, compared to mothers in the comparison group.
Hypothesis 1b: Mothers enrolled in BHC treatment group will endorse higher
rates of positive parenting practices and lower rates of harsh and inconsistent
parenting practices at follow-up, compared to mothers in the comparison group.
Specific Aim #2: To examine the sustained effect of BHC on child functioning,
specifically externalizing behavior problems and self-regulation.
Hypothesis 2a: Mothers and teachers will report lower rates of child externalizing
behavior at follow-up for children in the BHC treatment group, compared to those
in the comparison group.
Hypothesis 2b: Mothers and teachers will report higher rates of self-regulation at
follow-up for children in the BHC treatment group, compared to those in the
comparison group.
Specific Aim #3: To examine maternal social support and parent-child relationship
quality as potential mechanisms in the BHC intervention program.
Hypothesis 3a: Mid-intervention maternal social support and post-intervention
parent-child relationship quality will act as sequential mediators in the relation
between intervention group and the parenting outcomes measured at follow-up
(positive parenting, harsh and inconsistent parenting, and child maltreatment).
26
Specifically, mothers enrolled in the BHC treatment group will report higher
levels of social support, which will predict better parent-child relationship quality,
which will then lead to more positive parenting, less harsh and inconsistent
parenting, and lower rates of child maltreatment, compared to those in the
comparison group.
Hypothesis 3b: Mid-intervention maternal social support and post-intervention
parent-child relationship quality will act as sequential mediators in the relation
between intervention group and the child functioning outcomes measured at
follow-up (externalizing behavior and self-regulation). Specifically, mothers
enrolled in the BHC treatment group will report higher levels of social support,
which will predict better parent-child relationship quality, which will then lead to
lower rates of child externalizing behavior, and higher rates of child self-
regulation, compared to those in the comparison group.
27
Chapter 3: Methods
Participants
Participants for this study were drawn from a larger randomized control trial
examining the effectiveness of the BHC program to prevent child maltreatment and
support healthy child development. Mothers and their newborns were initially recruited
from local pediatric practices by a project-funded pediatric social worker who screened
for project eligibility. These families were not treatment seeking, but instead were
identified based on eligibility criteria and then referred to the BHC program. Families
were deemed eligible if they were a resident of Monroe County, eligible to receive
Temporary Assistance for Needy Families (TANF), if the mother was under the age of 21
at the birth of her first child, and if she had a maximum of two children under the age of
three at the time of recruitment. Families were excluded if they had any indicated Child
Protective Service reports or a child that was or had been placed in foster care at the time
of initial recruitment. In addition, any children or mothers who were not able to complete
the research protocol due to extreme medical or psychiatric conditions or serious
cognitive impairments were excluded. These conditions and impairments included a
diagnosis of a thought disorder, severe depression or suicidality requiring hospitalization,
severely limited intellectual functioning (IQ less than 70), and/or maternal incarceration.
Once deemed eligible, families were then randomized to receive BHC intervention
services or the Enhanced Community Standard. These intervention conditions are
described in detail below. Involvement in the original study ranged from birth until the
child’s third birthday. Although ideally the family would be enrolled immediately
28
following the child’s birth, they could be enrolled up until the child’s first birthday (Mean
age of enrollment=4 months).
For the current dissertation, a subset of the families who participated in the BHC
program were selected for follow-up. Specifically, families who were still enrolled in the
study at the conclusion of the intervention phase (referred to as “post-intervention” or
T36 throughout this manuscript), and whose target child was 6-10 years old at the follow-
up visit were contacted. School-age was chosen for a number of reasons. First, teachers
can provide an alternative perspective of child functioning. In addition, normative
externalizing behavior typically decreases by school entry; therefore, examining children
after this developmental period allows for the differentiation between normative and
clinically-elevated externalizing behavior (Hill et al., 2006).
Recruitment
The recruited sample included 237 caregivers and children. The project
coordinator and all research assistants remained blind to intervention status throughout
this study. Families were recruited over the phone using a variety of sources for contact
information. These included the original BHC project database, other Mt. Hope Family
Center research project databases, and the University of Rochester Medical Center’s
electronic medical record system. Due to the time lapse between the conclusion of the
intervention and recruitment for this study, a number of families were unable to be
reached or uninterested in the study. Three of these families were living out of state and
therefore were not contacted. Once contact was made and families agreed to participate,
multiple methods were used to ensure completion of the visit. These included reminder
29
calls, the provision of transportation, childcare, rescheduling visits, and completing the
visit at the family’s home if necessary. If the study team lost phone contact with the
family, then home visits were made and/or letters were sent to the home in order to re-
engage families.
Overall, our research team contacted 132/237 eligible families (56%). Of the 132,
2% refused to participate, 5% scheduled a call back but contact was never made, and
94% were scheduled to attend the follow-up visit. Overall, 87 families (70% of those
scheduled) completed the follow-up visit. Eighty-five of the caregivers were the child’s
biological mother who also participated in the original study. For the other two families,
alternative primary caregivers (father, grandmother) participated. Fifty-nine percent of
the sample had been randomized to the intervention condition, while 41% had been
randomized to the Enhanced Community Standard (ECS) condition. At the time of
follow-up, maternal age ranged from 22-32 years old (M=27), and child age ranged from
6-10 years old (M=7.5). Child gender was split nearly even (42 girls, 45 boys). The
demographics of the original sample of mothers are similar to those of the Rochester City
School District in the city of Rochester, New York, where the project was conducted as
well as to the local social services population. As a result, the racial composition of the
caregivers was 64% African-American, 22% Caucasian, and 14% Biracial or Multiracial.
Additionally, 20% of the caregivers identified as Hispanic/Latino. The racial composition
of the children in the sample was similar, although a much larger percentage were
Biracial or Multiracial: 56% African-American, 14% Caucasian, 30% Biracial or
Multiracial. Additionally, 31% of children identified as Hispanic/Latino. Attrition
30
analyses were conducted on the recruitment sample to compare families who completed
the follow-up visit versus those that did not. These groups did not differ based on
maternal age, race, ethnicity, marital status, education, baseline depression, or
intervention status. Nor did they differ based on child gender, age, race, or ethnicity.
In addition, data was collected from the child’s primary teacher. The child’s
caregiver identified the child’s teacher during the follow-up visit and signed a release
form for the teacher to be contacted and provide data on the child. Teachers were then
emailed and asked to participate. We successfully collected teacher data from 69/87
families. Five caregivers requested that we did not contact the child’s teacher. One
caregiver was the child’s teacher (home-schooled) therefore teacher data was not
collected for that child. Demographic information was not collected from teachers due to
the method of data collection (online), and to minimize personal information collected
due to the waiver of documentation of consent that was utilized. This waiver was
requested in order to minimize barriers to teacher completion.
Procedures
Once caregivers were contacted over the phone and deemed eligible, they were
scheduled for a one-time visit at Mt. Hope Family Center. This visit lasted one to two
hours. At the start of the visit, the caregiver was read the informed consent and signed the
form after having any questions answered. A copy of the consent form was provided to
the caregiver for their records. Caregivers met individually with the research staff in a
private interview room. Transportation was provided to and from the center by study
staff, if needed, to facilitate participation. Childcare was also available for the family if
31
needed. If neither transportation nor childcare could facilitate center-based participation,
then visits were conducted in a private area of the family’s home. During the follow-up
visit a number of questionnaires were completed with the caregiver to assess life
stressors, previous service utilization, and child symptomatology and self-regulation. If
the caregiver was the child’s mother, they also completed the parenting questionnaires.
Alternative caregivers did not complete the parenting questionnaires because they did not
participate in the intervention stage of the original study; and therefore, we would not
expect their parenting practices to be impacted by the mother’s participation.
Given the sensitive nature of the parenting questionnaires, mothers recorded their
responses on a paper copy of the measure. The mothers’ responses to these questionnaires
were reviewed prior to the end of the visit and predetermined critical responses regarding
child maltreatment were flagged and followed up on prior to the mother completing her
visit. The project’s licensed clinical supervisor was consulted regarding critical responses
when necessary. For all other measures, research assistants read the questionnaire aloud
and marked the caregiver’s response. Caregivers had a copy of the questionnaires to
follow along and view the anchors. Data from paper measures were stored in locked file
cabinets at Mt. Hope Family Center, while electronic data was stored either in the online
REDCAP system or in the measure’s secure online scoring system (CBCL, BRIEF-2).
REDCap is a secure, HIPAA-compliant, web-based application used for data collection.
For details regarding measures, see the measures section below and/or Appendix A. After
all visit measures were completed, caregivers were asked to sign a release form for study
32
staff to contact the child’s teacher. At the completion of the visit, the caregiver received
monetary compensation ($50) for completing the study.
Following completion of the caregiver’s participation in this study, with her
consent (via the signed release form), the child’s teacher was contacted via email to
complete questionnaires regarding the child’s functioning in school. Prior to completing
the requested questionnaires, the teacher was required to review the caregiver’s signed
release form and the study’s information sheet, both sent via a secure link through the
REDCap system. A waiver of documentation of consent was approved by RSRB for the
teachers’ participation in this study. Teacher participation consisted of completing three
questionnaires, taking approximately 30 minutes in total. The questionnaires were the
same as the parent questionnaires regarding child functioning. However, they were the
teacher version and asked about the child’s behaviors, executive functioning, and
emotion regulation in the school setting. For details regarding these measures, see the
measures section below and/or Appendix A. If teachers did not complete the
questionnaires or respond to the request via REDCap within 2 weeks, subsequent follow-
up emails were sent. During the follow-up emails, we offered to mail the teachers a hard
copy of the information sheet, signed release, and questionnaires if they preferred. The
questionnaires were then returned to Mt. Hope Family Center in a pre-paid business reply
envelope provided. Teachers were compensated with a $20 Target gift card for their
participation in the study.
Finally, this study also utilized longitudinal data that was previously collected as
part of the original research study. Data was collected at baseline (birth to 12 months of
33
age), mid-intervention (approximately 24 months of age), and immediately following
completion of the BHC intervention (approximately 36 months of age) by research
assistants at Mt. Hope Family Center. This included demographic information and
maternal report of depression symptoms at baseline. In addition, data on maternal social
support collected at mid-intervention, and data on parent-child relationship quality
assessed at post-intervention were also utilized. These measures included a combination
of maternal-report and observational data. Data on child externalizing behavior was also
collected at post-intervention and was utilized in this study. For details regarding
measures by timepoints, see the measures section and/or Appendix A.
Building Healthy Children (BHC) Program
Intervention group. The BHC intervention is a multi-component, home
visitation program that combines three evidence-based interventions (Parents as Teachers
(PAT; Parents as Teachers National Center, 1999), Interpersonal Psychotherapy for
Depressed Adolescents (IPT-A; Mufson, Dorta, Moreau, & Weissman, 2004), and Child-
Parent Psychotherapy (CPP; Lieberman & Van Horn, 2005)) with outreach support.
Service delivery for the various components of the intervention is best conceptualized as
a pyramid (see Figure 1). At the bottom level, all families receive broad-based support
via persistent outreach to address concrete needs. As the pyramid builds up, the
interventions become more intensive and specialized, and are only delivered to families
based on individual interest and need.
Figure 1
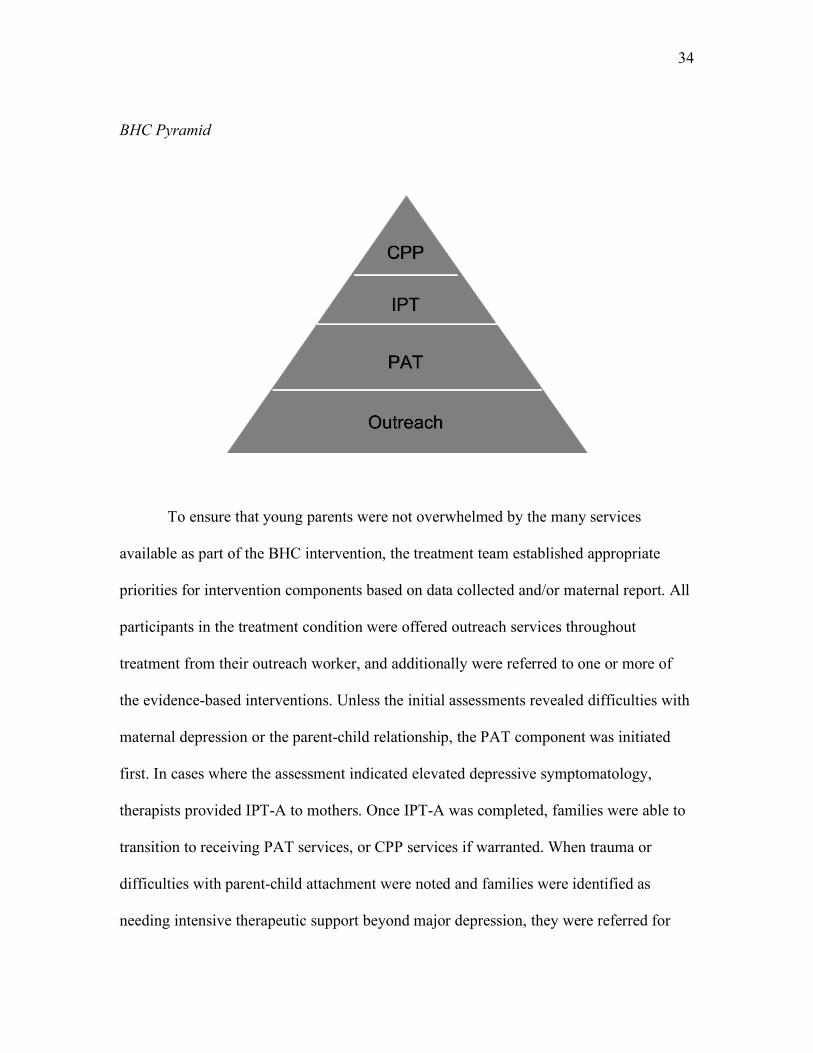
34
BHC Pyramid
To ensure that young parents were not overwhelmed by the many services
available as part of the BHC intervention, the treatment team established appropriate
priorities for intervention components based on data collected and/or maternal report. All
participants in the treatment condition were offered outreach services throughout
treatment from their outreach worker, and additionally were referred to one or more of
the evidence-based interventions. Unless the initial assessments revealed difficulties with
maternal depression or the parent-child relationship, the PAT component was initiated
first. In cases where the assessment indicated elevated depressive symptomatology,
therapists provided IPT-A to mothers. Once IPT-A was completed, families were able to
transition to receiving PAT services, or CPP services if warranted. When trauma or
difficulties with parent-child attachment were noted and families were identified as
needing intensive therapeutic support beyond major depression, they were referred for
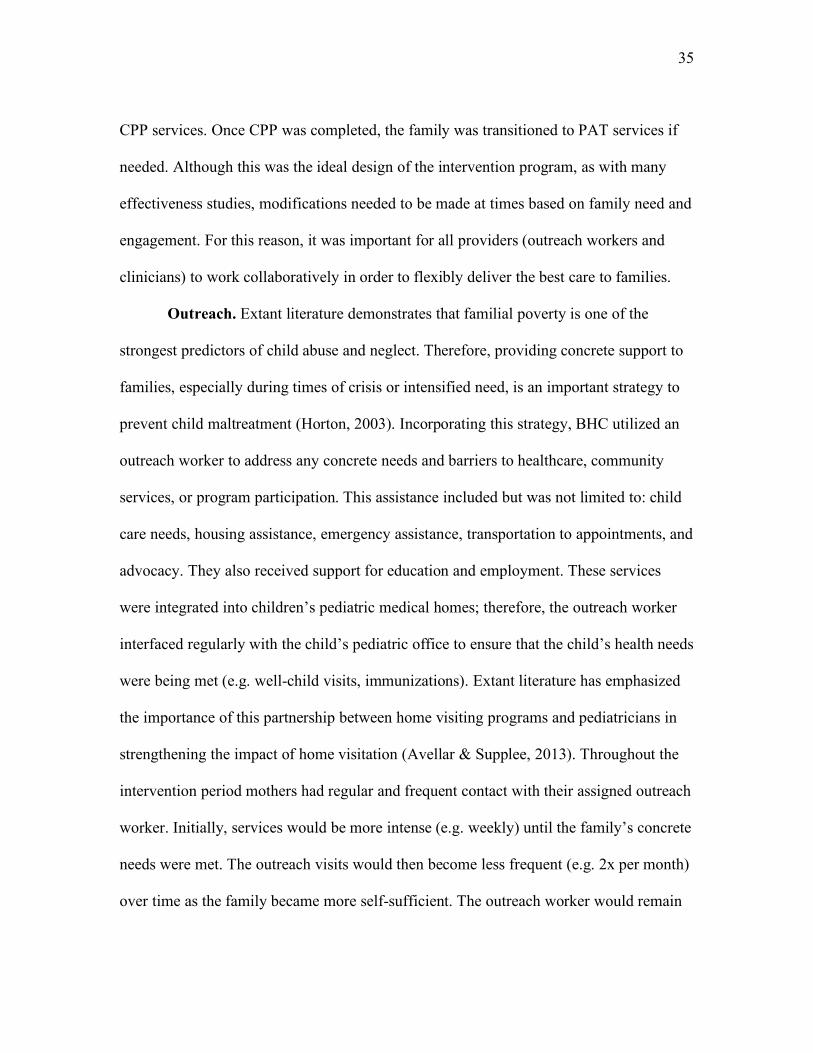
35
CPP services. Once CPP was completed, the family was transitioned to PAT services if
needed. Although this was the ideal design of the intervention program, as with many
effectiveness studies, modifications needed to be made at times based on family need and
engagement. For this reason, it was important for all providers (outreach workers and
clinicians) to work collaboratively in order to flexibly deliver the best care to families.
Outreach. Extant literature demonstrates that familial poverty is one of the
strongest predictors of child abuse and neglect. Therefore, providing concrete support to
families, especially during times of crisis or intensified need, is an important strategy to
prevent child maltreatment (Horton, 2003). Incorporating this strategy, BHC utilized an
outreach worker to address any concrete needs and barriers to healthcare, community
services, or program participation. This assistance included but was not limited to: child
care needs, housing assistance, emergency assistance, transportation to appointments, and
advocacy. They also received support for education and employment. These services
were integrated into children’s pediatric medical homes; therefore, the outreach worker
interfaced regularly with the child’s pediatric office to ensure that the child’s health needs
were being met (e.g. well-child visits, immunizations). Extant literature has emphasized
the importance of this partnership between home visiting programs and pediatricians in
strengthening the impact of home visitation (Avellar & Supplee, 2013). Throughout the
intervention period mothers had regular and frequent contact with their assigned outreach
worker. Initially, services would be more intense (e.g. weekly) until the family’s concrete
needs were met. The outreach visits would then become less frequent (e.g. 2x per month)
over time as the family became more self-sufficient. The outreach worker would remain
36
with the family throughout the entirely of their participation in the program in order to
develop a consistent and supportive relationship with the family. Researchers have
emphasized the importance of consistency in the relationship between the home visitor
and the family in rendering positive results (Gomby, 2007).
Each mother was also assigned a PAT home visitor for the duration of the
program. In addition, a mental health clinician cross-trained in IPT-A and CPP was
assigned to the family if a referral for one or more of these intervention components was
made. This allowed for families to flexibly receive services from a consistent provider as
needed. At the initiation of treatment, the outreach worker and the mental health clinician
conducted a needs assessment with the family to develop an initial service plan.
BHC evidence-based intervention components:
Parents as Teachers (PAT). All mothers randomly assigned to the BHC
treatment group were offered weekly in-home PAT services, delivered by their PAT
home visitor. PAT is a parent-education program, which emphasizes positive parenting
behavior as the precipitant of developmental gains for children. The major goals of the
PAT curriculum are to increase parents’ knowledge of normative child development,
increase school readiness, and increase parents’ sense of competence and self-efficacy in
parenting (Wagner & Clayton, 1999). A specialized curriculum for young mothers, which
extends the normal PAT curriculum with additional emphasis on interacting with peers
through group meetings, was utilized for this program (Parents as Teachers National
Center, 1999). These meetings were offered monthly to reinforce individual learning
experiences and were open to all mothers enrolled in the BHC intervention arm
37
regardless of whether they were actively enrolled in PAT at the time. Empirical support
for PAT has been demonstrated across a number of studies. Overall, positive effects on
parent knowledge, parenting attitudes (e.g. sense of competence), parenting behaviors
(e.g. appropriate play materials), and parents’ perceived social support have been
demonstrated, albeit inconsistently, across evaluations (Owen & Mulvihill, 1994;
Pfannenstiel & Seltzer, 1989; Wagner et al., 2002). In terms of child functioning, there is
evidentiary support for the effect of PAT on children’s cognitive, language, and socio-
emotional development, as well as, their school readiness and achievement (Drotar,
Robinson, Jeavons, & Lester Kirchner, 2009; Pfannenstiel & Seltzer, 1989; Wagner et al.,
2002). Finally, there is some promising evidence to suggest that engagement in PAT
services helps to reduce the likelihood of child abuse and neglect (Pfannenstiel et al.,
1996; Pfannenstiel et al., 1991; Wagner & Clayton, 1999). However, additional research
is needed in order to replicate this finding.
Interpersonal Psychotherapy for Depressed Adolescents (IPT-A). In cases
where elevated depressive symptomatology or an interest in individual therapy was
indicated, mental health clinicians referred mothers to IPT-A. This version of the
treatment is an empirically supported adaptation of the IPT model for adolescents with
depression, in order to address issues that commonly occur at this developmental stage
(e.g. separation from parents, exploration of authority in relation to parents, initial
experience with grief, peer pressure, etc.) IPT-A was chosen over IPT for this study due
to the high portion of adolescent mothers in the original sample. IPT-A is a time-limited,
individual therapy model which was delivered in accordance with the manual (IPT-A;
38
Mufson et al., 2004). Similar to IPT, IPT-A is split into three phases of treatment: Initial,
Intermediate, and Termination. Following assessment in the Initial phase, treatment was
centered around one to two problem areas identified by the clinician and mother during
the Initial phase. These focus areas can include: 1) grief, 2) role transitions (including
single-parent household), 3) role disputes, or 4) interpersonal deficits. The Termination
phase focused on prevention of recurrent depressive episodes. Empirical support for IPT-
A for adolescent depression has been demonstrated by a number of RCTs (Mufson et al.,
1999; Young, Mufson, & Davies, 2006). Results indicate that IPT-A is as effective as
CBT in reducing depressive symptoms (Horowitz, Garber, Ciesla, Young, & Mufson,
2007), and more effective than supportive treatment for depressed adolescents with co-
morbid anxiety disorders (Young et al., 2006). In addition, mothers receiving IPT have
shown significant improvement mother-child relationship quality, perceived stress, self-
efficacy, and social support (Beeber et al., 2013; Mulcahy et al., 2010; Toth et al., 2013).
Notably, IPT-A and IPT have demonstrated efficacy across racially/ethnically diverse
samples from various socioeconomic backgrounds, and in women with histories of
trauma and PTSD (Duberstein et al., 2018; Markowitz et al., 2015; Rossello & Bernal,
1999; Toth et al., 2013).
Child Parent Psychotherapy (CPP). In cases where project staff observed, or
mothers reported, traumatic experiences (including domestic violence) and/or difficulties
in the parent-child relationship, CPP services were offered. These services included
weekly home or center-based psychotherapy sessions, usually with both the mother and
child in accordance with the treatment manual (Lieberman & Van Horn, 2005;
39
Lieberman, Ippen, Van Horn, 2015). CPP is typically one year in length and focuses on
strengthening the parent-child relationship in order to restore the child’s sense of safety
and support secure attachment, which in turn fosters the child’s socioemotional
development. In addition, this model focuses on exploring the mother’s own caregiving
history to consider how it impacts her current parental functioning. Empirical research on
CPP has demonstrated that this treatment is effective at improving attachment security,
increasing mothers’ positive expectations of their child, improving child’s maternal and
self-representations, and decreasing maternal and child mental health symptoms,
including child behavior problems and PTSD symptoms (Lieberman, Ippen, & Van Horn,
2006; Lieberman et al., 2005; Toth, Maughan, Manly, Spagnola, & Cicchetti, 2002; Toth,
Rogosch, Manly, & Cicchetti, 2006). This research has largely been conducted with
impoverished and racially/ethnically diverse samples.
Fidelity. Extant intervention research has emphasized the importance of high-
quality training, and clear, coherent, guidance to support the learning of core intervention
components. The field of implementation science has regularly cited model fidelity as a
critical mediator in achieving the positive outcomes observed in research trials (Paulsell,
Del Grosso, & Supplee, 2014). For this reason, careful measures were taken to ensure
that all models were implemented to fidelity. The PAT component of the BHC
intervention was delivered by Masters-level social workers extensively trained and
certified in the curriculum. In addition, phone consultation regarding programmatic
concerns was provided by the PAT headquarters as needed. The Masters-level BHC
mental health clinicians that implemented the IPT-A and CPP components of the
40
intervention were trained by certified, doctoral-level clinicians. Certified clinicians
provided weekly individual and/or group supervision specific to each model. In addition,
supervisors and the principal investigator of the project oversaw model fidelity by
reviewing video or audiotape of sessions. Fidelity checklists were utilized to aid in this
review when provided by the treatment model.
Intervention Participation. As expected, given the long period of intervention
and diversity in family needs, there was a wide range in intervention participation. Home
visiting programs vary greatly in terms of expected participation. Some programs have
specific performance standards (e.g. weekly visit), while others are more flexible based
on the home visitors’ perception of family need. In addition, some programs may
exchange face-to-face contact for telephone contact over time as families become more
independent and self-reliant or reach specific treatment goals (Korfmacher et al., 2008).
For many programs, such as Healthy Families America, visit frequency is reduced over
time as families meet specific goals (Daro & Harding, 1999). This approach is similar to
that of the BHC intervention.
In order to provide a more detailed picture of dosage, we examined the total
number of in-person and phone sessions families received across intervention
components, across the period of intervention. It should be noted that phone sessions
were mostly used for the outreach components of the model. On average, the intervention
families in this sample attended 92 in-person sessions and 72 phone sessions across the
intervention period. We examined the in-person session count more closely and found
that 10% of families attended 32 or less visits, 25% of families attended 60 or less visits,
41
50% of families attended 87 or less visits, 75% of families attended 120 or less visits,
90% of families attended 146 or less visits.
In order to better understand which components of the intervention families were
engaging in, we examined program status for each component individually. Families
were deemed to have “completed,” “partially engaged,” or “never engaged” in each
component for which they were referred. For IPT-A or CPP, “completed” meant that
families participated in at least 10 sessions, while PAT was “completed” if they engaged
in at least the 8 foundational visits. Any engagement less than these cutoffs was deemed
“partially engaged.” “Never engaged” was reserved for families who were referred for
the intervention component but did not engage. It should be noted that the majority of
families in this sample completed more than the minimum requirement for these
interventions (84% for PAT, 56% for IPT-A, and 67% for CPP). In the current sample,
84% of families completed the outreach component, while 16% partially engaged. For
outreach, partially engaged indicated that the family did not complete the program and
may have ended services early for various reasons (e.g. move away, lack of follow
through, improved functioning). In addition, all but one family (who completed IPT-A
and CPP) were referred to receive PAT. Of those referred, 80% completed PAT, and 20%
partially engaged. Approximately half of intervention mothers were referred to receive
IPT-A (n=24). Of those referred, 67% completed this component, while 8% partially
engaged and 25% never engaged. Finally, approximately one third of intervention
families (n=17) were referred to receive CPP, and of those mothers 76% completed this
component, and 24% partially engaged. While families received a combination of
42
services based on family need, all families were referred to Outreach and at least one
intervention component (PAT, IPT-A, and/or CPP), with the large majority of families
completing both outreach and PAT.
Enhanced Community Standard (ECS). Participants randomized to the ECS
condition received screening and resource information at each assessment point, as
deemed necessary. This could range from information on food pantries, housing, or
educational opportunities, to community mental health referrals. In addition, if the
participant reported any suicidal thoughts, project staff would assist in safety planning.
Measures
Collected at baseline
Demographic Interview (Cicchetti & Carlson, 1989). Developed by Cicchetti and
Carlson (1989), this measure has been used extensively in research with underprivileged,
high-risk families. Information obtained from this measure included: date of birth,
gender, race/ethnicity, family composition, parent’s education and current occupation,
income, and use of public assistance.
Beck Depression Inventory-II (BDI-II; Beck, Steer, & Brown, 1996). The BDI-II
is a 21-item, maternal self-report measure of depressive symptoms and severity. This
measure has been used extensively across a wide range of populations and research
contexts, exhibiting good psychometric properties (Beck et al., 1996). Higher scores
indicate an increased number and/or frequency of depressive symptoms. The mean total
BDI-II score at baseline for the current sample was 8.91 (SD=8.18). Eight percent of
mothers in this sample scored above 19, indicative of clinical significance.
43
Collected at mid-intervention (T24)
Social Support Behaviors Scales (SS-B;Vaux, Riedel, & Stewart, 1987). The SS-B
is a 45-item self-report questionnaire that measures five distinct modes of support:
emotional, socializing, practical assistance, financial assistance, and advice/guidance.
Separate scales assess these modes in family and friends. This measure was collected at
mid-intervention. Past research indicates that internal consistencies for the scales have
exceeded µ=0.80 (Vaux et al., 1987). Concurrent validity has been demonstrated through
high correlations with social support network associations, support appraisals, and the
Inventory of Socially Support Behavior (Vaux & Harrison, 1985; Vaux et al., 1987).
Collected at post-intervention (T36)
Parenting Stress Index- Short Form (PSI-SF; Abidin, 1990). The PSI/SF is a self-
report measure of parenting stress for parents of children 12 years and younger. It
includes 36 items that are derived from the PSI long-form measure (Abidin, 1990). This
measure was completed post-intervention, when the child was approximately 36 months
old. Respondents rated their agreement with items on a 5-point scale from strongly
disagree to strongly agree. The measure yields a Total Stress score from three scales:
Parental Distress, Parent-Child Dysfunctional Interaction (P-CDI), and Difficult Child.
For the purpose of this study, the P-CDI scale was examined. This scale measures the
extent to which the parent perceives the child to meet their expectations and that their
interactions with the child positively reinforce their role as a parent. Strong construct,
discriminant, and predictive validity have been demonstrated for this measure (Abidin,
1990).
44
Attachment Q-Sort (Version 3.0) (AQS; Waters, 1995). The AQS consists of 90
items that describe behaviors typically observed during a parent-child interaction. The
research assistant observed the parent and child interact for approximately 1.5-2 hours in
their home over the course of the post-intervention assessment visit. Immediately
following this visit, the research assistant completed the AQS by sorting the 90 items into
a forced distribution of nine piles that ranged from “extremely uncharacteristic (1)” to
“extremely characteristic (9)” of the dyad. The distribution of items for each dyad was
then correlated with an ideal criterion distribution for attachment security previously
established by expert raters (Waters, 1995). This correlation rendered an individual score
of attachment security ranging from -1 to 1, with higher values indicating more secure
base behavior. Examples of items with high values on the security criterion include:
“Child clearly shows a pattern of using the mother as a base from which to explore” and
“If held in the mother’s arms, child stops crying and quickly recovers from being upset.”
Items with low values on the security criterion include: “When something upsets the
child, he stays where he is and cries” and “Child easily becomes angry at mother.” The
AQS has been shown to relate to attachment classifications derived from the Strange
Situation (Vaughn & Waters, 1990), as well as to parenting quality (Teti, Nakagawa, Das,
& Wirth, 1991).
Maternal Behavior Q-sort (MBQ; Pederson, Moran, & Bento, 1999). The MBQ
consists of 90 items that assess mother’s sensitive behavior towards their child. The
research assistant observed the parent and child interact for approximately 1.5-2 hours in
their home over the course of the post-intervention assessment visit. Immediately
45
following this visit, the research assistant completed the MBQ by sorting the 90 items
into a forced distribution of nine piles that ranged from “extremely uncharacteristic (1)”
to “extremely characteristic (9)” of the dyad. The distribution of items for each mother is
correlated with a previously established, ideal criterion distribution of maternal
sensitivity. This correlation rendered an individual score of maternal sensitivity ranging
from -1 to 1, with higher values indicating more sensitive behavior.
Child Behavior Checklist 1½-5 (CBCL; Achenbach & Rescorla, 2000). The
CBCL was used to assess externalizing symptomatology, by capturing maternal report of
children’s behavior problems post-intervention. The CBCL is a widely used and validated
instrument to assess symptomatology by mothers. It contains 100 total items rated for
frequency on a 3-point scale (0= not true to 2 = very true or often true). In addition, it
assesses two broadband dimensions of psychopathology: internalizing and externalizing
behavior problems. For the purpose of this study, the externalizing behavior broadband
scale was examined.
Collected at follow-up
Demographic Interview- Enhanced. In order to better understand the current
demographic and life circumstances of this sample, the Demographic Interview (Cicchetti
& Carlson, 1989) was amended and re-administered at follow-up. This version of the
questionnaire collected the same information as the original version; however, it
additionally asked whether certain life stressors had occurred between post-intervention
and the follow-up visit. These questions were adapted from the Adverse Childhood
Experiences (ACE) questionnaire (Felitti, 1998), and assessed the following domains:
46
parental separation/divorce, substance use, incarceration, loss, homelessness, domestic
violence, and community violence. The loss question asked if someone close to the
mother and/or child had passed away. The incarceration and substance use questions
asked whether the mother or anyone close to her and/or the child had struggled with these
concerns. All other questions asked directly about the mother’s and child’s experiences.
These questions were used to better understand the various life stressors families may
have experienced during the follow-up period.
Services Questionnaire. This questionnaire was developed to assess family
service utilization between post-intervention and follow-up. Mothers/caregivers reported
on mental health services (mother and child), DHS services (CPS involvement, foster
care, kinship care), and medical services (medication, hospitalization, etc.). Of
particularly interest to this study were the two questions that asked about CPS
involvement and foster care/kinship care placement.
Conflict Tactics Scales: Parent–Child Version (CTSPC; Straus, Hamby, &
Warren, 2003). The CTSPC consists of 35 items that identify abuse and neglect in
families. The items focus on the target parent and/or other caregiver behavior towards the
child. Mothers rated the frequency to which an item occurred within the past year or prior
to the past year on an 8-point Likert scale ranging (0=None to 6=More than 20 times; 7=
Not in the past year but it happened since the end of BHC intervention). For the purpose
of this study, mothers’ frequency of each behavior in the past year was analyzed. This
measure yields six subscales including, Nonviolent Discipline, Psychological Aggression,
Physical Assault, Weekly Discipline, Neglect, and Sexual Abuse. There are a variety of
47
ways to score and analyze this measure. Straus, Hamby, and Warren’s (2003)
recommendations for scoring were followed by summing the midpoints for the response
categories chosen by the mother. For example, for response option 3 (3 to 5 times) the
midpoint would be 4. Higher scores indicate increased frequency of behavior. Internal
consistency was acceptable in the current sample for the Nonviolent Discipline (a = .77)
and Psychological Aggression (a = .71) subscales. However, the Physical Assault
subscale demonstrated unacceptable internal consistency (a = .47); therefore, rendering it
invalid. This was most likely due to the very low endorsement of many of these items. In
addition, there was very low endorsement of items on the Neglect and Sexual Abuse
subscales; therefore, they were analyzed at the item level. The weekly discipline subscale
was not analyzed in this study.
Parenting Practices Interview (PPI; Webster-Stratton, 1998). The PPI is a 73-
item parent-report measure assessing positive and negative parenting strategies. This
measure was previously adapted from the Oregon Social Learning Center’s discipline
questionnaire for use with parents of young children This measure yields seven summary
scales which assess Appropriate Discipline, Harsh and Inconsistent Discipline, Positive
Verbal Discipline, Monitoring, Physical Punishment, Praise and Incentives, and Clear
expectations. For the purpose of this study, items pertaining to the monitoring subscale
were removed due to low internal reliability in past studies and lack of applicability to the
current sample. The remaining subscales were used to create two summary scores, one
for Positive Parenting (Appropriate Discipline, Positive Verbal Discipline, Clear
Expectations, Praise and Incentives) and one for Harsh and Inconsistent Parenting (Harsh
48
and Inconsistent Discipline, Physical Punishment). Higher scores indicate increased
frequency of the parenting behavior. These two summary scales demonstrated acceptable
internal consistency (a =.79 and .80 respectively).
Behavior Rating Inventory of Executive Functioning, Second edition (BRIEF-2;
Gioia, Isquith, Guy, & Kenworthy, 2016). The BRIEF-2 is an 86-item other-report
questionnaire that was completed by caregivers and teachers to assess children’s
executive functioning in the home and school environments. This measure is appropriate
for children ages 5 to 18 years old. Respondents rated the child on a 3-point scale (Never,
Sometimes, Often) based on the child’s behaviors over the previous 2 months. This
measure yields nine non-overlapping clinical scales that form a General Executive
Composite score, and three index scores: Behavior Regulation (Inhibition, Self-Monitor),
Emotion Regulation (Shift, Emotional Control), and Cognitive Regulation (Initiate,
Working Memory, Plan/Organize, Organization of Materials, and Task-Monitor). All
three indices demonstrated excellent internal consistency in this sample for both
caregiver and teacher report (a =.92-.97). This measure produces T-scores for each of the
indices which are normed based on age and gender. Higher scores indicate greater
difficulty with regulation in that domain. For this reason, index scores are labeled as
“dysregulation” in order to differentiate from the emotion regulation subscale of the
ERC.
Emotion Regulation Checklist (ERC; Shields & Cicchetti, 1995). The ERC is a
24-item other-report measure, which targets processes central to emotionality and
regulation, including affective lability, intensity, valence, flexibility, and situational
49
appropriateness of emotional expression (Shields & Cicchetti, 1998). Caregivers and
teachers rated children on a 4-point Likert scale ranging from 1 (Never) to 4 (Almost
Always), as to how characteristic each item is of the child. Factor analyses using ERC
data in a large sample of maltreated and impoverished children (6-12 years old) have
yielded a two-factor solution. The first factor, Lability/Negativity, assesses for mood
swings, angry reactivity, emotional intensity, and dysregulated positive emotions. The
second factor, Emotion Regulation, assess for processes central to adaptive regulation,
including equanimity, emotion understanding, and empathy (Shields & Cicchetti, 1997).
The Lability/Negativity subscale demonstrated good internal consistency amongst
caregiver (a=.87) and teacher (a=.93) data in this sample. The Emotion Regulation
subscale demonstrated questionable internal consistency amongst caregiver data (a= .67)
but good internal consistency for teacher data (a =.85).
Child Behavior Checklist/ 6-18 (CBCL; Achenbach & Rescorla, 2001). The
CBCL is a widely used and validated measure of child psychopathology. Caregivers
reported the frequency of each behavior over the previous 2 months on a 3-point scale
(0= not true to 2 = very true or often true). This measure contains 113 items and assesses
two broadband dimensions of psychopathology: internalizing and externalizing behavior
problems. For the purpose of this study, the externalizing behavior dimension was
examined. This subscale demonstrated excellent internal consistency in this sample
(a=.93).
Teacher Report Form/6-18 (TRF; Achenbach & Rescorla, 2001). Similar to the
CBCL, the TRF is a widely used and validated measure of child psychopathology. This
50
measure is completed by the child’s teacher and has been adapted to reflect problematic
behaviors in school. Teachers rated the child’s behavior over previous 2 months on a 3-
point frequency scale (0= not true to 2 = very true or often true). Mirroring the CBCL,
this measure contains 113 items that assess internalizing and externalizing
symptomatology. For the purpose of this study, the externalizing behavior dimension was
examined. This subscale demonstrated excellent internal consistency in this sample
(a=.95).
51
Chapter 4: Results
Data Preparation
Prior to hypothesis testing, a number of preliminary steps were taken using SPSS
Statistical Software, Version 25.0 to prepare the data for analyses. The skewness and
kurtosis of all endogenous variables was examined to assess if assumptions of normality
were met. No variables showed evidence of non-normality. In addition, all scales were
assessed to determine internal consistency. These values were reported in the measures
section. Scales that did not meet the recommended standard (α > .70) were further
examined at the item level to determine if individual items are responsible for poor
reliability. The majority of scales were well above the recommended value, although a
limited number of scales had alphas in the .63-.70 range. One scale was eliminated
(Physical Assault on the CTSPC) due to very poor internal consistency (α= .48).
Next, missing data was assessed. Fortunately, there was minimal missing data in
this study. Missing data on outcome variables measured at follow-up ranged from 0-
3.4%. Missing data on exogenous and endogenous variables at earlier timepoints
(baseline, T24, T36) ranged from 0-9.2%. Missing data was assessed by conducting
Little’s Missing Completely At Random (MCAR) test. The Chi-square test was non-
significant, indicating that the data was Missing Completely At Random, c2 (77) =
94.858, p > .05.
Finally, for hypothesis testing, significance was determined at the level of p <.05.
Marginally significant results (p <.10) are also reported given the small sample size. For
analyses examining the direct effect of the intervention on parenting outcomes (positive
52
parenting, harsh and inconsistent parenting, and child maltreatment) and child outcomes
(externalizing behavior and self-regulation), latent outcome variables were not created as
proposed due to the limited sample size. Instead, manifest outcome variables were
utilized. For analyses examining parent child-relationship quality as a mediator in the
relationship between intervention and parent and child outcomes, the proposed latent
mediator was still tested. Measurement modeling of the proposed mediator was tested
with the following as potential indicators: Attachment security, maternal sensitivity, and
dysfunctional parent-child interaction. Results from these analyses are reported below.
Preliminary Analyses
To assess for comparability on baseline characteristics between intervention and
ECS families, comparisons were made on a number of maternal (age, race, ethnicity,
education, and marital status) and child (age, gender, race, ethnicity) demographic
variables using chi-square and t-test analyses. As reported in Table 1, groups did not
differ based on maternal or child factors at follow-up. In addition, groups were compared
on presence of adverse life events between conclusion of the intervention and the follow-
up visit. This was theorized to have a potential impact on the sustainability of
intervention effects. Results indicate that groups did not differ based on the presence or
absence of these events (Table 2). It is notable that the sample did experience high rates
of adverse life events overall during this period (3-7 years post-intervention). Based on
maternal report, 67% of families experienced the death of someone close to them, 35%
experienced incarceration of themselves or someone close to them, 16% struggled with
substance use themselves or in someone close to them, 15% experienced homelessness,
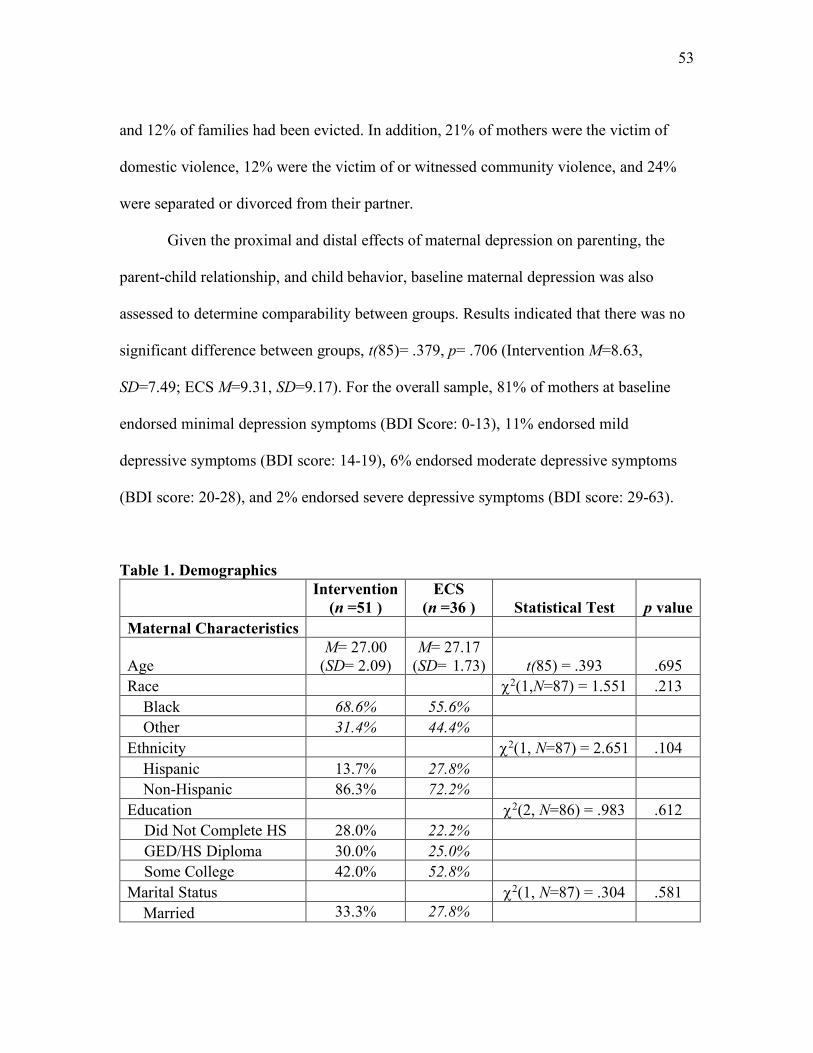
53
and 12% of families had been evicted. In addition, 21% of mothers were the victim of
domestic violence, 12% were the victim of or witnessed community violence, and 24%
were separated or divorced from their partner.
Given the proximal and distal effects of maternal depression on parenting, the
parent-child relationship, and child behavior, baseline maternal depression was also
assessed to determine comparability between groups. Results indicated that there was no
significant difference between groups, t(85)= .379, p= .706 (Intervention M=8.63,
SD=7.49; ECS M=9.31, SD=9.17). For the overall sample, 81% of mothers at baseline
endorsed minimal depression symptoms (BDI Score: 0-13), 11% endorsed mild
depressive symptoms (BDI score: 14-19), 6% endorsed moderate depressive symptoms
(BDI score: 20-28), and 2% endorsed severe depressive symptoms (BDI score: 29-63).
Table 1. Demographics
Intervention
(n =51 ) ECS
(n =36 ) Statistical Test p value Maternal Characteristics
Age M= 27.00
(SD= 2.09) M= 27.17
(SD= 1.73) t(85) = .393 .695 Race c2(1,N=87) = 1.551 .213
Black 68.6% 55.6% Other 31.4% 44.4%
Ethnicity c2(1, N=87) = 2.651 .104 Hispanic 13.7% 27.8% Non-Hispanic 86.3% 72.2%
Education c2(2, N=86) = .983 .612 Did Not Complete HS 28.0% 22.2% GED/HS Diploma 30.0% 25.0% Some College 42.0% 52.8%
Marital Status c2(1, N=87) = .304 .581 Married 33.3% 27.8%
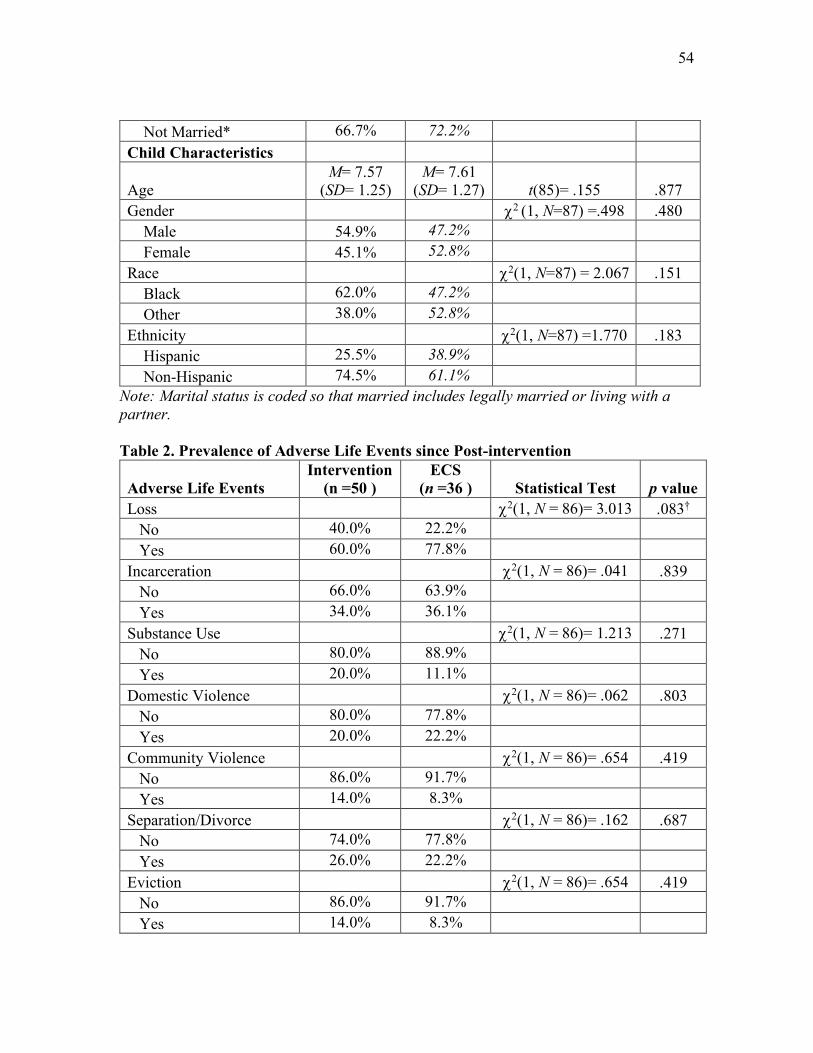
54
Not Married* 66.7% 72.2% Child Characteristics
Age M= 7.57
(SD= 1.25) M= 7.61
(SD= 1.27) t(85)= .155 .877 Gender c2 (1, N=87) =.498 .480 Male 54.9% 47.2% Female 45.1% 52.8% Race c2(1, N=87) = 2.067 .151 Black 62.0% 47.2% Other 38.0% 52.8% Ethnicity c2(1, N=87) =1.770 .183 Hispanic 25.5% 38.9% Non-Hispanic 74.5% 61.1%
Note: Marital status is coded so that married includes legally married or living with a partner. Table 2. Prevalence of Adverse Life Events since Post-intervention
Adverse Life Events Intervention
(n =50 ) ECS
(n =36 ) Statistical Test p value Loss c2(1, N = 86)= 3.013 .083† No 40.0% 22.2% Yes 60.0% 77.8% Incarceration c2(1, N = 86)= .041 .839 No 66.0% 63.9% Yes 34.0% 36.1% Substance Use c2(1, N = 86)= 1.213 .271 No 80.0% 88.9% Yes 20.0% 11.1% Domestic Violence c2(1, N = 86)= .062 .803 No 80.0% 77.8% Yes 20.0% 22.2% Community Violence c2(1, N = 86)= .654 .419 No 86.0% 91.7% Yes 14.0% 8.3% Separation/Divorce c2(1, N = 86)= .162 .687 No 74.0% 77.8% Yes 26.0% 22.2% Eviction c2(1, N = 86)= .654 .419 No 86.0% 91.7% Yes 14.0% 8.3%
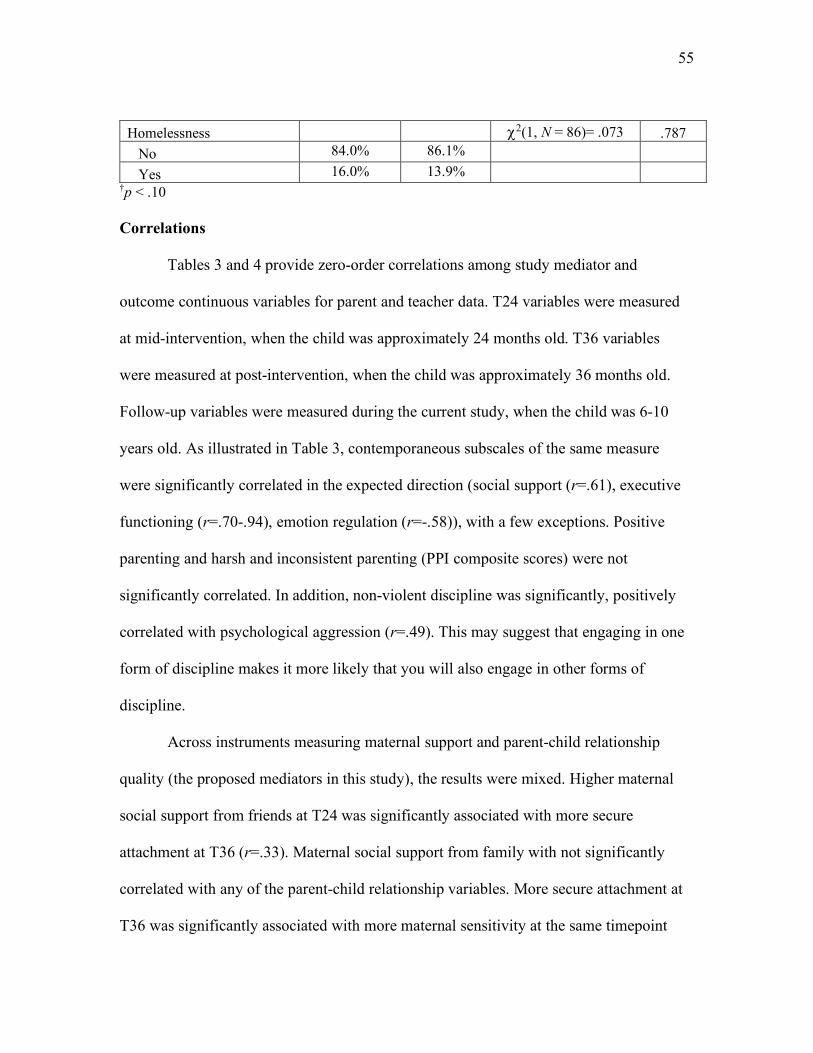
55
Homelessness c2(1, N = 86)= .073 .787 No 84.0% 86.1% Yes 16.0% 13.9%
†p < .10 Correlations
Tables 3 and 4 provide zero-order correlations among study mediator and
outcome continuous variables for parent and teacher data. T24 variables were measured
at mid-intervention, when the child was approximately 24 months old. T36 variables
were measured at post-intervention, when the child was approximately 36 months old.
Follow-up variables were measured during the current study, when the child was 6-10
years old. As illustrated in Table 3, contemporaneous subscales of the same measure
were significantly correlated in the expected direction (social support (r=.61), executive
functioning (r=.70-.94), emotion regulation (r=-.58)), with a few exceptions. Positive
parenting and harsh and inconsistent parenting (PPI composite scores) were not
significantly correlated. In addition, non-violent discipline was significantly, positively
correlated with psychological aggression (r=.49). This may suggest that engaging in one
form of discipline makes it more likely that you will also engage in other forms of
discipline.
Across instruments measuring maternal support and parent-child relationship
quality (the proposed mediators in this study), the results were mixed. Higher maternal
social support from friends at T24 was significantly associated with more secure
attachment at T36 (r=.33). Maternal social support from family with not significantly
correlated with any of the parent-child relationship variables. More secure attachment at
T36 was significantly associated with more maternal sensitivity at the same timepoint
56
(r=.53). However, neither attachment nor maternal sensitivity were significantly
correlated with parent-child dysfunctional interaction at the same timepoint.
When examining child outcomes at follow-up, results indicate that more
attachment security at post-intervention was significantly related to less child
externalizing behavior (r=-.23) and behavior dysregulation at follow-up (r=-.25). In
addition, more maternal sensitivity at post-intervention was significantly related to less
behavior dysregulation (r=-.24) and more emotion regulation at follow-up (r=.24). More
dysfunctional parent-child interaction was significantly related to more externalizing
behavior (r=.32) and self-regulation problems at follow-up (r=.27-.32). Maternal social
support was not significantly correlated with any of the child outcome variables. In
addition, higher rates of child externalizing behavior were significantly associated with
more self-regulation difficulties across measures (r=.72-.86). Emotion regulation
difficulties, as measured by the BRIEF-2, were also significantly, negatively correlated
with emotion regulation capabilities, as measured by the ERC (r=-.53).
In terms of parenting outcomes at follow-up, surprisingly, none of the proposed
mediator variables were significantly correlated with these outcome variables. In
addition, positive parenting was not significantly correlated with any of the other
parenting outcomes or the child outcomes. On the other hand, more harsh and
inconsistent parenting was significantly associated with more psychological aggression
(r=.44). More harsh and inconsistent parenting was also significantly related to more
externalizing behavior (r=.49) and self-regulation difficulties at follow-up (r=.32-.40).
More non-violent discipline was also significantly related to more externalizing behavior
57
(r= .35) and self-regulation difficulties (r=.35-.54). Finally, more psychological
aggression was significantly related to more externalizing behavior (r=.29) and self-
regulation difficulties (r=.22-.43).
As illustrated in Table 4, bivariate correlations were conducted between proposed
mediator variables and teacher outcome variables. Similar to the parent data,
contemporaneous subscales of the same measure were significantly correlated in the
expected direction (executive functioning (r=.60-.90), and emotion regulation (r=-.63)).
In addition, teacher-reported child externalizing behavior was significantly correlated
with teacher-reported self-regulation difficulties across measures (r=.52-.86). However,
unlike the parent data, the teacher outcome variables were not significantly correlated
with any of the parent mediator variables measured at mid-intervention (social support)
and post-intervention (attachment, maternal sensitivity, or dysfunctional parent-child
interaction). Interestingly, parent and teacher report for the same measure of child
behavior were all significantly and positively correlated (EXT r=.51, p<.001; GEC r=.43,
p<.001; BRI r=.57, p<.001; ERI r=.52, p<.001; CRI r=.31, p<.01; ERC Neg/Lab r=.41,
p<.001; ERC Emo Reg r=.44, p<.001).
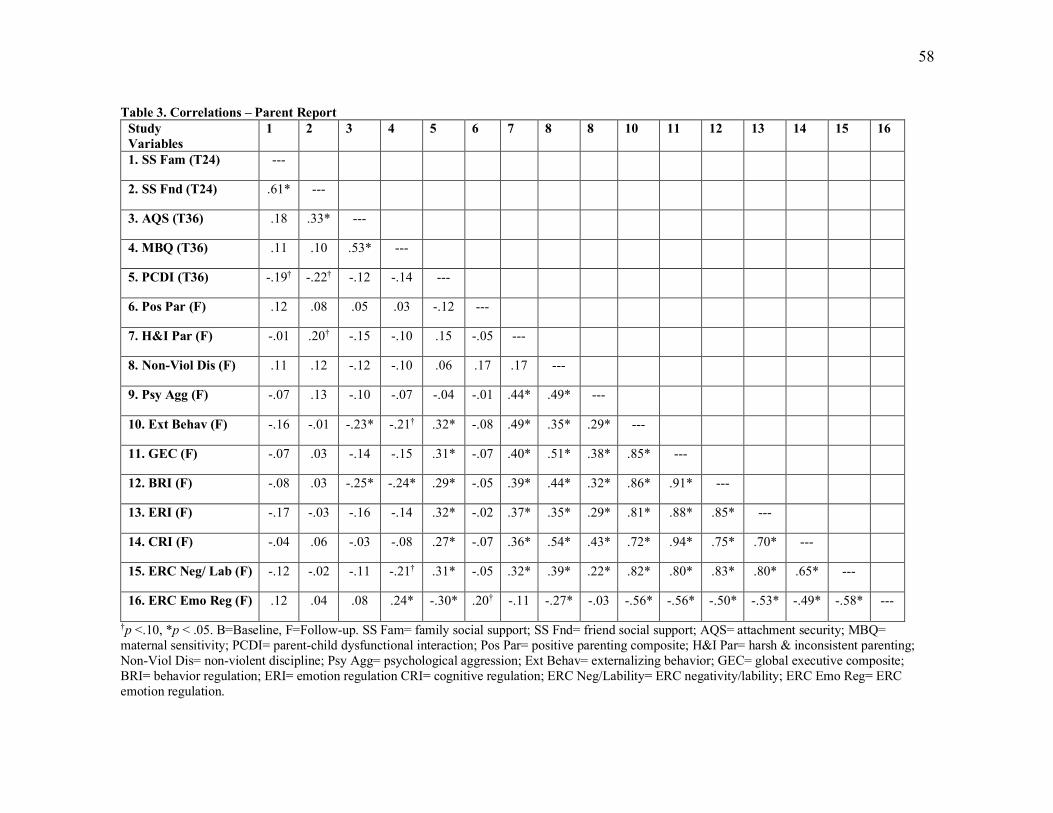
58
Table 3. Correlations – Parent Report Study Variables
1 2 3 4 5 6 7 8 8 10 11 12 13 14 15 16
1. SS Fam (T24) ---
2. SS Fnd (T24) .61* ---
3. AQS (T36) .18 .33* ---
4. MBQ (T36) .11 .10 .53* ---
5. PCDI (T36) -.19† -.22† -.12 -.14 ---
6. Pos Par (F) .12 .08 .05 .03 -.12 ---
7. H&I Par (F) -.01 .20† -.15 -.10 .15 -.05 ---
8. Non-Viol Dis (F) .11 .12 -.12 -.10 .06 .17 .17 ---
9. Psy Agg (F) -.07 .13 -.10 -.07 -.04 -.01 .44* .49* ---
10. Ext Behav (F) -.16 -.01 -.23* -.21† .32* -.08 .49* .35* .29* ---
11. GEC (F) -.07 .03 -.14 -.15 .31* -.07 .40* .51* .38* .85* ---
12. BRI (F) -.08 .03 -.25* -.24* .29* -.05 .39* .44* .32* .86* .91* ---
13. ERI (F) -.17 -.03 -.16 -.14 .32* -.02 .37* .35* .29* .81* .88* .85* ---
14. CRI (F) -.04 .06 -.03 -.08 .27* -.07 .36* .54* .43* .72* .94* .75* .70* ---
15. ERC Neg/ Lab (F) -.12 -.02 -.11 -.21† .31* -.05 .32* .39* .22* .82* .80* .83* .80* .65* ---
16. ERC Emo Reg (F) .12 .04 .08 .24* -.30* .20† -.11 -.27* -.03 -.56* -.56* -.50* -.53* -.49* -.58* ---
†p <.10, *p < .05. B=Baseline, F=Follow-up. SS Fam= family social support; SS Fnd= friend social support; AQS= attachment security; MBQ= maternal sensitivity; PCDI= parent-child dysfunctional interaction; Pos Par= positive parenting composite; H&I Par= harsh & inconsistent parenting; Non-Viol Dis= non-violent discipline; Psy Agg= psychological aggression; Ext Behav= externalizing behavior; GEC= global executive composite; BRI= behavior regulation; ERI= emotion regulation CRI= cognitive regulation; ERC Neg/Lability= ERC negativity/lability; ERC Emo Reg= ERC emotion regulation.
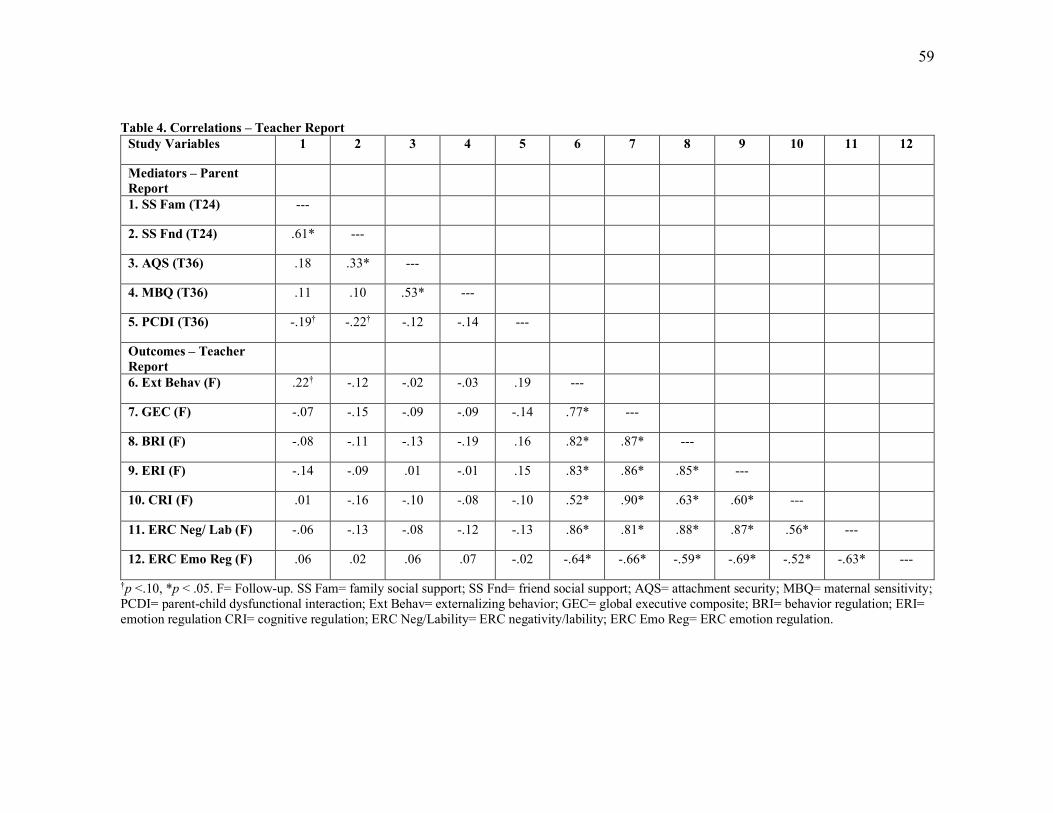
59
Table 4. Correlations – Teacher Report
Study Variables 1 2 3 4 5 6 7 8 9 10 11 12
Mediators – Parent Report
1. SS Fam (T24) ---
2. SS Fnd (T24) .61* ---
3. AQS (T36) .18 .33* ---
4. MBQ (T36) .11 .10 .53* ---
5. PCDI (T36) -.19† -.22† -.12 -.14 ---
Outcomes – Teacher Report
6. Ext Behav (F) .22† -.12 -.02 -.03 .19 ---
7. GEC (F) -.07 -.15 -.09 -.09 -.14 .77* ---
8. BRI (F) -.08 -.11 -.13 -.19 .16 .82* .87* ---
9. ERI (F) -.14 -.09 .01 -.01 .15 .83* .86* .85* ---
10. CRI (F) .01 -.16 -.10 -.08 -.10 .52* .90* .63* .60* ---
11. ERC Neg/ Lab (F) -.06 -.13 -.08 -.12 -.13 .86* .81* .88* .87* .56* ---
12. ERC Emo Reg (F) .06 .02 .06 .07 -.02 -.64* -.66* -.59* -.69* -.52* -.63* ---
†p <.10, *p < .05. F= Follow-up. SS Fam= family social support; SS Fnd= friend social support; AQS= attachment security; MBQ= maternal sensitivity; PCDI= parent-child dysfunctional interaction; Ext Behav= externalizing behavior; GEC= global executive composite; BRI= behavior regulation; ERI= emotion regulation CRI= cognitive regulation; ERC Neg/Lability= ERC negativity/lability; ERC Emo Reg= ERC emotion regulation.
60
Intervention Effects
To examine the main effects of the intervention on outcome variables of interest,
independent sample t-tests were conducted in SPSS. Prior to interpreting the t-statistic,
Leven’s Test for Equality of Variances was assessed. If this test was non-significant, the t
and p value for “equal variances assumed” was interpreted. If this test was significant, the
t and p value for “equal variances not assumed” was interpreted. Tables 5 and 6 illustrate
the group differences between the intervention and ECS groups on key mediator and
outcome variables. Prior to conducting these analyses, covariates were assessed for all
non-normed outcome variables (CBCL/TRF, and BRIEF-2 are normed for child gender
and age) to determine if they should be controlled for in the analyses. Child gender and
age were not significantly predictive of any of these outcome variables. However, child
gender was marginally predictive (p=.07) of parental psychological aggression; therefore,
this will be included as a statistical control in the regression model.
Parenting outcomes
Results from the independent sample t-tests indicate that BHC significantly
predicted parenting at follow-up. Specifically, mothers in the intervention group reported
using significantly less harsh and inconsistent parenting at follow-up (M=3.73) compared
to mothers in the ECS group (M=4.36), t(83)= 2.948, p=.004. In addition, there was a
marginally significant effect of intervention status on psychological aggression,
indicating that mothers in the intervention group reported using less psychological
aggression towards their children at follow-up (M=12.98) compared to mothers in the
ECS group (M=21.03), t(59.83)=1.93, p=.058. Child gender was then added as a
61
covariate in a regression model. The overall model was significant, F(2,82)= 4.077,
p=.021. Intervention status remained a marginally significant predictor of psychological
aggression, above and beyond the effects of child gender, b= -.202, p= .059. There were
no significant effects of the intervention on positive parenting or non-violent discipline.
In addition, parents were asked to report on Child Protective Services involvement and
foster care/kinship care placement since the conclusion of the intervention. 28% of
parents reported that they had “any involvement with Child Protective Services,”
although this does not mean that their case was substantiated. In addition, 6% of mothers
reported that their child had been placed in foster care or kinship care. There were no
statistically significant group differences on these two outcomes.
There were two additional maltreatment outcomes on the CTSPC (neglect and
child sexual abuse) that were not included due to minimal endorsement. There was one
item on the neglect subscale that was endorsed by 13% of the sample which assessed
emotional unavailability (“you were so caught up with your own problems that you were
not able to show or tell your child that you loved him or her”). There were no significant
groups differences on this item, t(83)=.372, p >.10. In addition, child sexual abuse was
quantified by only two items; therefore, these were analyzed individually. Seven percent
of mothers endorsed that their child had been the victim of inappropriate sexual touching
since the conclusion of the intervention. Chi-square analysis indicated that there was not
a significant group difference, c2(1, N=85) = .208, p > .05. Only 1 mother endorsed that
their child had been “forced to have sex by an adult or older child” since the conclusion
of the intervention, therefore, analyses were not conducted for this item.
62
Child outcomes
In order to assess the impact of BHC on child outcomes (externalizing behavior
and self-regulation), both parent and teacher report were assessed. Although a latent
variable was originally proposed which included parent and teacher indicators for each
outcome, sample size precluded this option. Creating a latent or composite variable with
parent and teacher report would have shrunk the sample size from 87 to 69 (number of
teacher reports). In addition, analyzing parent and teacher data separately can assess if
children are functioning differently in the home and school setting, as well as minimize
reporter bias by having two independent reporters.
As demonstrated in Table 5, results from parent report indicate that children in the
intervention group exhibited significantly less externalizing behavior problems at follow-
up (M=51.06) compared to children in the ECS group (M=57.14), t(58.68)= 2.219,
p=.030. In order to examine the effect of the intervention on externalizing behavior at
follow-up while controlling for externalizing behavior at post-intervention, T36
externalizing behavior was entered into a regression model, followed by follow-up
externalizing behavior. Results indicated that the effect of the intervention on
externalizing behavior at follow up was significant over and above the stability of
externalizing behavior from T36 to follow up, b= -.276, p= .009. In terms of clinical
significance, ECS children’s externalizing behavior fell in the Clinically Significant
range (T-score ³ 64) at a significantly higher rate (36%) than BHC children (12%), c2
(1)=8.90, p=.003.
63
In terms of self-regulation, parents reported that children in the intervention group
exhibited marginally significantly less difficulties with self-regulation at follow-up, as
measured by the Global Executive Composite of the BRIEF-2, t(61.14)= 1.847, p=.070
(INT M=50.51; ECS M=55.42). Specifically, parents in the intervention group reported
that their children exhibited significantly less difficulties with emotion regulation
(M=50.02) compared to children in the ECS condition (M=56.72), t(56.28)= 2.456,
p=.017. Results indicated that ECS children’s emotion dysregulation fell in the
Potentially Clinically Elevated/Clinically Elevated range (T score ³ 65) at a significantly
higher rate (28%) than BHC children (8%), c2 (1)=6.211, p=.013. This result was
marginally significant for global executive functioning, ECS=28%, BHC=12%, c2
(1)=3.605, p=.058. There were no significant group differences on measures of behavior
and cognitive dysregulation. There were also no significant differences between groups
on the two subscales of the ERC, including negativity/lability and emotion regulation
ability.
As exhibited in Table 6, results from teacher report echo many of the parent
report findings. Teachers reported that children in the intervention group exhibited
significantly less externalizing behavior at follow-up (M=59.10), compared to children in
the ECS group (M=64.37), t(67)=2.015, p=.048. ECS children’s externalizing behavior
fell in the Clinically Significant range at a marginally, significantly higher rate (39%)
than BHC children (24%), c2 (1)=3.793, p=.051. In addition, teachers reported that
children in the intervention group exhibited marginally significantly less difficulties with
self-regulation, across measures of global executive functioning (t(67)= 1.867, p=.066;
64
Intervention M=59.81; ECS M=65.67), behavior dysregulation (t(67)= 1.792, p= .078;
Intervention M=58.71; ECS M=64.37), and emotion dysregulation (t(67)= 1.845, p= .070;
Intervention M=59.24; ECS M=66.30). ECS children’s global executive functioning fell
in the Potentially Clinically Elevated/Clinically Elevated range at a significantly higher
rate (42%) than BHC children (26%), c2 (1)=4.126, p=.042. ECS children’s emotion
dysregulation also fell in the Potentially Clinically Elevated/Clinically Elevated range at
a significantly higher rate (44%) than BHC children (28%), c2 (1)=4.495, p=.034. There
was no significant difference in clinical significance rates for behavior dysregulation. In
addition, there were no significant group differences on the cognitive dysregulation
subscale. There were also no significant group differences on the two subscales of the
ERC, including negativity/lability and emotion regulation ability.
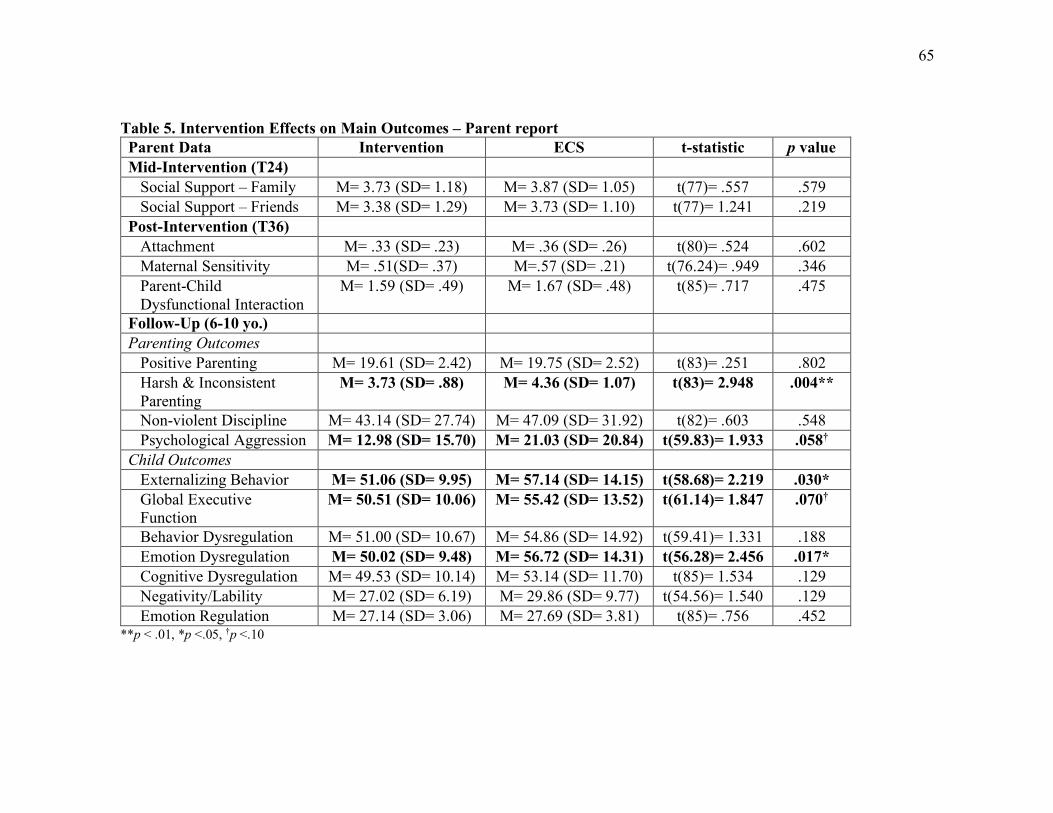
65
Table 5. Intervention Effects on Main Outcomes – Parent report Parent Data Intervention ECS t-statistic p value Mid-Intervention (T24) Social Support – Family M= 3.73 (SD= 1.18) M= 3.87 (SD= 1.05) t(77)= .557 .579 Social Support – Friends M= 3.38 (SD= 1.29) M= 3.73 (SD= 1.10) t(77)= 1.241 .219 Post-Intervention (T36) Attachment M= .33 (SD= .23) M= .36 (SD= .26) t(80)= .524 .602 Maternal Sensitivity M= .51(SD= .37) M=.57 (SD= .21) t(76.24)= .949 .346 Parent-Child Dysfunctional Interaction
M= 1.59 (SD= .49)
M= 1.67 (SD= .48)
t(85)= .717 .475
Follow-Up (6-10 yo.) Parenting Outcomes Positive Parenting M= 19.61 (SD= 2.42) M= 19.75 (SD= 2.52) t(83)= .251 .802 Harsh & Inconsistent Parenting
M= 3.73 (SD= .88) M= 4.36 (SD= 1.07) t(83)= 2.948 .004**
Non-violent Discipline M= 43.14 (SD= 27.74) M= 47.09 (SD= 31.92) t(82)= .603 .548 Psychological Aggression M= 12.98 (SD= 15.70) M= 21.03 (SD= 20.84) t(59.83)= 1.933 .058† Child Outcomes Externalizing Behavior M= 51.06 (SD= 9.95) M= 57.14 (SD= 14.15) t(58.68)= 2.219 .030* Global Executive Function
M= 50.51 (SD= 10.06) M= 55.42 (SD= 13.52) t(61.14)= 1.847 .070†
Behavior Dysregulation M= 51.00 (SD= 10.67) M= 54.86 (SD= 14.92) t(59.41)= 1.331 .188 Emotion Dysregulation M= 50.02 (SD= 9.48) M= 56.72 (SD= 14.31) t(56.28)= 2.456 .017* Cognitive Dysregulation M= 49.53 (SD= 10.14) M= 53.14 (SD= 11.70) t(85)= 1.534 .129 Negativity/Lability M= 27.02 (SD= 6.19) M= 29.86 (SD= 9.77) t(54.56)= 1.540 .129 Emotion Regulation M= 27.14 (SD= 3.06) M= 27.69 (SD= 3.81) t(85)= .756 .452
**p < .01, *p <.05, †p <.10
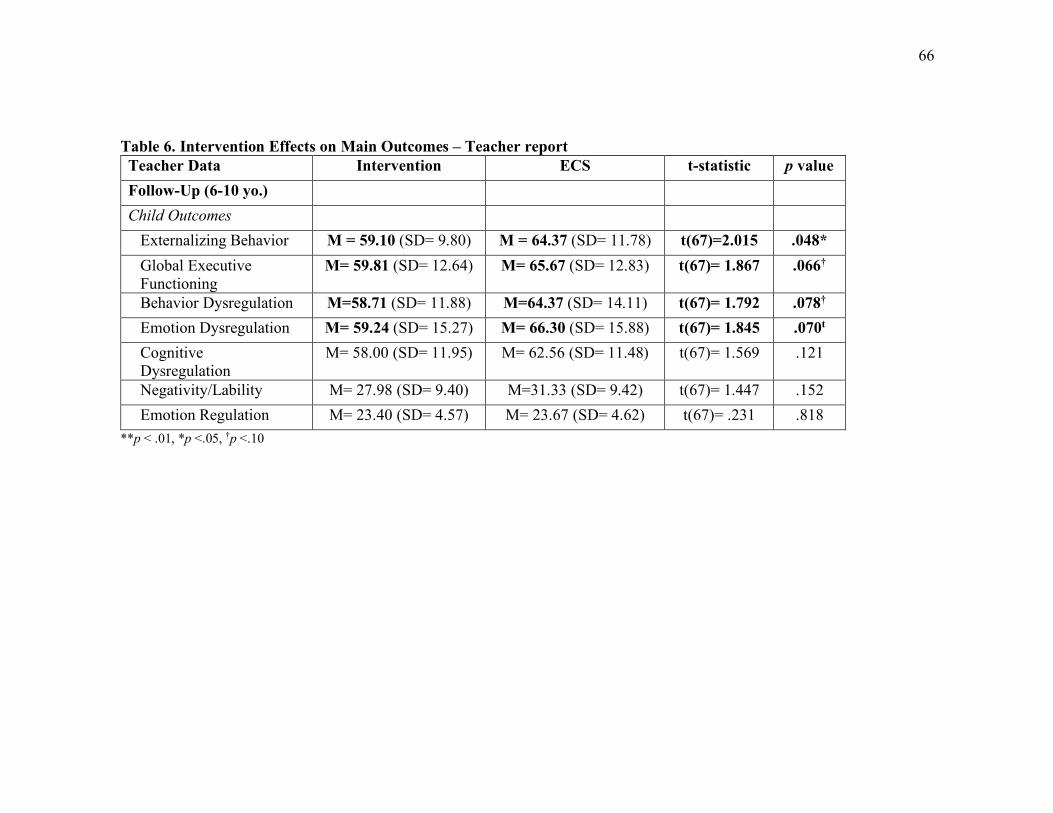
66
Table 6. Intervention Effects on Main Outcomes – Teacher report Teacher Data Intervention ECS t-statistic p value Follow-Up (6-10 yo.) Child Outcomes Externalizing Behavior M = 59.10 (SD= 9.80) M = 64.37 (SD= 11.78) t(67)=2.015 .048* Global Executive Functioning
M= 59.81 (SD= 12.64) M= 65.67 (SD= 12.83) t(67)= 1.867 .066†
Behavior Dysregulation M=58.71 (SD= 11.88) M=64.37 (SD= 14.11) t(67)= 1.792 .078†
Emotion Dysregulation M= 59.24 (SD= 15.27) M= 66.30 (SD= 15.88) t(67)= 1.845 .070t
Cognitive Dysregulation
M= 58.00 (SD= 11.95) M= 62.56 (SD= 11.48) t(67)= 1.569 .121
Negativity/Lability M= 27.98 (SD= 9.40) M=31.33 (SD= 9.42) t(67)= 1.447 .152 Emotion Regulation M= 23.40 (SD= 4.57) M= 23.67 (SD= 4.62) t(67)= .231 .818
**p < .01, *p <.05, †p <.10
67
Mediation Analyses
Measurement Modeling
In order to examine specific aim 3 and assess potential mediators in the relation
between intervention status and parent and child outcomes, a measurement model was
tested for the proposed latent variable of parent-child relationship quality using
Confirmatory Factor Analysis (CFA) in Mplus. The proposed latent variable included the
following post-intervention (T36) manifest variables: Attachment Security (AQS),
Maternal Sensitivity (MBQ), and Parent-Child Dysfunctional Interaction (PCDI; reverse
coded). Standardized factor loadings and their related p-values were then examined.
Although the AQS and MBQ loaded significantly onto the latent construct (b=.680,
p=.037, b=.781, p=.029 respectively), PCDI did not (b=.174, p=.191). Fit statistics could
not be calculated for this model because the model was fully saturated. Since a minimum
of three factors are required when analyzing only one latent variable, removing the
insignificant PCDI factor was not possible. Therefore, I analyzed the proposed mediators
as independent manifest variables instead.
Mediation analyses
The first step in mediation analysis after establishing a direct effect, is to test the
a-path (independent variable to mediator)(Baron, Kenny, & psychology, 1986; Judd &
Kenny, 1981). An empirically supported method for testing mediation is the product of
coefficients method which has been recommended for smaller sample sizes. The theory
behind this method is that mediation is dependent on the extent to which the independent
variable changes the mediator, and the mediator affects the outcome. In regards to
68
intervention research, this analysis tests the hypothesis that the intervention substantially
changes the mediator variable, which in turn changes the outcome (MacKinnon,
Fairchild, & Fritz, 2007). To test this theory, t-tests were first conducted to examine the
effect of intervention status on the proposed mediators. As reported in Table 5, results
indicated that there were no group differences between the intervention condition and
ECS condition on measures of T24 Social Support from family, t(77)=.557, p >.10, or
friends, t(77)= 1.241, p >.10. In addition, there were no group differences between the
intervention condition and the ECS condition on measures of T36 Attachment Security
(t(80)=.524, p >.10), T36 Maternal Sensitivity (t(80)=.949, p >.10, and T36
Dysfunctional Parent-Child Interaction (PCDI; t(85)= .717, p >.10). Given that none of
these a-paths were approaching significance, the additional steps to conducting
mediational analyses were not conducted.
69
Chapter 5: Discussion
Recognizing that no single approach can meet the multi-dimensional needs of
impoverished, high-risk families, the Building Healthy Children (BHC) program was
designed to provide concrete support and evidence-based intervention to young mothers
and their infants who are at heightened risk for child maltreatment and poor
developmental outcomes. BHC supports these families by flexibly delivering three
evidence-based treatment models in conjunction with outreach support. This dissertation
utilized a longitudinal mixed-method, multi-informant design to evaluate the long-term
effectiveness of this program on parenting practices and child functioning in elementary
school (ages 6-10 years). Mothers in the intervention group were hypothesized to endorse
lower rates of negative parenting practices (child maltreatment, harsh and inconsistent
parenting), and higher rates of positive parenting practices at follow-up. Children in the
intervention group were hypothesized to exhibit less externalizing behavior problems and
more adaptive self-regulation at follow-up, as rated by both their caregivers and teachers.
Finally, social support and parent-child relationship quality were hypothesized to serve as
sequential mediators in the relation between intervention group and the parent and child
outcomes of interest.
Before delving into the results of this study, it is important to understand the
context in which these children have developed and the myriad of challenges that these
families have faced. In the time between the conclusion of the intervention and the
follow-up study (3-7 years depending on family), a large portion of families experienced
significant life stressors, including loss, incarceration, substance use, homelessness and
70
violence. Extant literature has linked these adverse events with a number of negative
outcomes in childhood and adulthood, including but not limited to: internalizing and
externalizing behavior problems, problematic substance use, and chronic health issues
(Dube, Anda, Felitti, Edwards, & Croft, 2002; Evans, Davies, & DiLillo, 2008; Felitti,
1998). Despite these stressors, many children and caregivers across intervention
conditions have shown resilience. This highlights one of the main pillars of the
developmental psychopathology perspective – multifinality – or the recognition that
different outcomes can result from similar experiences. While the results presented above
clearly highlight the positive and preventive effects that the BHC intervention had on
families, it is important to note that “the pathway to either psychopathology or resilience
is influenced by a complex matrix” of multi-level influences (Curtis & Cicchetti, 2003,
pp. 778-779). In addition, regardless of whether families were in the intervention
condition or the ECS condition, all families enrolled in BHC got something. While the
intervention condition received more comprehensive, evidence-based intervention
services, the ECS condition also received screening and referrals for various resources.
Thus, the resilience evidenced may have been enhanced by the provision of even a
minimal amount of service. Without this support, some families may have exhibited more
difficulties.
Study Aim 1: Impacts on Parenting
The first aim of this study was to examine the sustained effects of BHC on a)
child maltreatment, and b) parenting practices, including harsh and inconsistent parenting
and positive parenting. While I was unable to gather an objective measure of child
71
maltreatment (e.g. DHS report), the current study examined a spectrum of negative
parenting behavior. This included mother’s report of CPS involvement and out of home
placement, harsh and inconsistent discipline, physical punishment, and the use of
psychological aggression and physical assault towards their child. Results indicated that
28% of caregivers in our follow-up sample reported CPS involvement related to the
target child since the conclusion of the intervention. Six percent of families reported that
their child was placed in foster care or with a relative during the follow-up period. There
were no significant differences between groups on these items. It is important to note that
CPS involvement does not mean that the case was ever substantiated or that the mother
was the perpetrator, therefore, this question is not a precise measure of the impact of
BHC on child maltreatment. In addition, this rate is similar, if not lower than previously
reported CPS referral rates found in the literature for similar populations (minority
race/ethnicity, low SES) (Putnam-Hornstein, Needell, King, & Johnson-Motoyama,
2013).
Child maltreatment was also assessed via the physical assault subscale on the
CTSPC. The items on this subscale ranged from “minor” assaults (e.g. slapped your
child on the hand, arm, or leg.) to “severe” (e.g. hit your child with a fist or kicked your
child hard) to “extreme” (e.g. burned or scalded your child on purpose). There was very
poor validity on this subscale, and therefore it could not be analyzed. This is most likely
due to low endorsement of a majority of these items. Only one mother endorsed any of
the items on the severe scale, and none endorsed the items on the extreme subscale. Some
mothers did endorse a few of the items on the minor assault subscale; however, many of
72
these items would be classified as corporal punishment under the law (e.g. spanking on
the bottom, slapping on the hand, arm, or leg). The low endorsement of these items may
be due to social desirability concerns (Straus et al., 2003) or to concerns related to
knowledge of mandatory reporting laws. While widely used due to lack of available
alternatives, self-report measures child maltreatment can be problematic because they are
susceptible to response bias due to fear of negative consequences (Degarmo, Reid, &
Knutson, 2006; C. Rodriguez, Cook, & Jedrziewski, 2012).
While harsh parenting (including corporal punishment) does not necessarily
equate to child maltreatment, previous literature has found that it is related to child abuse
potential (C. Rodriguez, 2010). Not surprisingly, abusive parents typically administer
excessively harsh discipline (Veltkamp & Miller, 1994). In addition, harsh parenting is
similarly associated with many of the same adverse outcomes as child maltreatment,
including externalizing behavior problems. In fact, harsh parenting is one of the strongest
correlates for childhood aggression and disruptive behavior (Erath, El-Sheikh, & Mark
Cummings, 2009; Gershoff, 2002). Results from this study found that mothers in the
intervention group reported using significantly less harsh and inconsistent parenting
(including harsh and inconsistent discipline and physical punishment) at follow-up
compared to mothers in the ECS group.
In addition, there was a marginally significant effect of the intervention on
psychological aggression, in favor of the intervention group. In this study, psychological
aggression was defined as “verbal and symbolic acts by the parent intended to cause
psychological pain or fear on the part of the child (e.g. threatening to hit your child, or
73
send them away) (Straus & Field, 2003). This construct would most likely be subsumed
under the more comprehensive construct of psychological maltreatment (also referred to
as mental, emotional, and psychological abuse and neglect) (Binggeli, Hart, & Brassard,
2001; Taskforce, 2019). Psychological aggression has been significantly associated with
greater child abuse potential (C. Rodriguez, 2010). It has also been linked to a number of
detrimental outcomes in childhood and beyond (Liu & Wang, 2015; Straus & Field,
2003). In fact, one study found that when considering physical aggression, corporal
punishment and psychological aggression simultaneously, psychological aggression
emerged as the strongest predictor of negative psychological outcomes (Miller-Perrin,
Perrin, & Kocur, 2009). Findings from a large, nationally representative study revealed a
robust association between psychological maltreatment and a wide range of clinician-
rated diagnostic symptoms and risk indicators in adolescence (e.g. depression, anxiety,
self-injurious behavior, behavior problems, academic problems). This study found that
psychological maltreatment was as, if not more, potent of a predictor for childhood
maladjustment as sexual abuse, physical abuse, and the combination of the two, across a
range of outcomes (Spinazzola et al., 2014). Psychological maltreatment has also been
associated with mood disorders, trauma symptomatology and self-deprecation in
adulthood (Higgins & McCabe, 2000). Despite the prevalence and clear detriment of
psychological maltreatment, it is often not a target of intervention (Hart & Brassard,
1987; Spinazzola et al., 2014). The results of this study, while only marginally
significant, suggest the effectiveness of a comprehensive home visiting program in
preventing the use of this detrimental parenting practice.
74
In addition to examining the effect of BHC on negative parenting practices, a
significant impact of the intervention on positive parenting was hypothesized. However,
this hypothesis was not supported by the data. This finding is consistent with other
studies of parenting interventions (e.g. Incredible Years) that have used this measure
(PPI) to detect intervention effects on parenting practices. While many of these studies
have found a significant impact on negative parenting practices (e.g. harsh and
inconsistent discipline), they have similarly had difficulty detecting group differences
amongst positive parenting subscales of this measure (e.g. Brotman, Gouley, Chesir-
Teran, Dennis, Klein, Shrout, et al., 2005; Leijten et al., 2017). One reason for this may
be social desirability. When it is easy to detect the “right” or socially desirable answer,
participants may respond in this way even if it is not an accurate representation of their
behavior. Explicit assessment of controversial constructs (e.g. parenting) can lead
respondents to intentionally misrepresent their true attitudes or even unconsciously
present a socially desirable image wanting to believe this positive self-perception (Fazio
& Olson, 2003). Alternatively, the intervention may not have specifically targeted the
positive parenting strategies being measured in this study. For example, positive
parenting items include parenting behaviors such as discussing the problem with your
child, getting your child to correct the problem, giving/removing privileges or rewards,
and brief timeout. While it is certainly possible that BHC would impact these distal
parenting behaviors, these behaviors were not a direct target of the intervention,
particularly given child age during participation (0-3 years old).
75
Other potential reasons for these null results might be the potential contributing
effects of maternal stress and/or depression. Since we did not measure maternal stress or
depression during the follow-up study, it is impossible to control for the effect that these
might have on the mothers’ positive parenting practices. However, we know from the life
stressor questions, and from literature regarding this population in general, that the
majority of these families were experiencing significant life stress. Both maternal stress
and depression have been shown to impact parenting practices (Lovejoy, Graczyk,
O'Hare, & Neuman, 2000; Morrison Gutman, McLoyd, & Tokoyawa, 2005). In addition,
maternal social support at follow-up may have impacted parenting practices as well.
Unfortunately, this was not examined at follow-up; therefore, the potential for
moderation could not be tested. Future studies could measure these potentially
moderating variables to gain a more robust understanding of the impact of BHC on
parenting.
Taken together, these results partially support the first hypothesis of this study.
Overall, mothers in the intervention group exhibited less harsh and inconsistent
parenting, and marginally less psychological aggression than those in the comparison
group. These findings suggest that an adaptive multi-component home visiting program
that addresses concrete needs as well as parenting and maternal psychopathology, is
effective in preventing the use of negative parenting strategies.
Study Aim 2: Impacts on Child Outcomes
The second aim of this dissertation was to examine the sustained effects of BHC
on child behavior, including a) externalizing behavior problems, and b) self-regulation.
76
To answer this question, I used a multi-method and multi-informant (parents and
teachers) approach in order to limit the effect of bias and better understand child
functioning across settings. As predicted, the intervention significantly impacted
externalizing behavior problems at follow-up. Children who had received the BHC
intervention in infancy and early childhood exhibited significantly less externalizing
behavior problems in elementary school. These results were significant across parent and
teacher report. Interestingly, teachers endorsed a higher rate of problems in this area for
the ECS group compared to parents. Specifically, based on teacher report, children in the
ECS group exhibited clinically significant elevations (>64) in externalizing symptoms,
while those in the intervention group fell within the normative range.
Regarding self-regulation, finding across parent and teacher report indicate
marginally significant to significant intervention effects across different domains of self-
regulation, in favor of the intervention group. According to parents, intervention children
exhibited significantly less difficulty with emotion regulation, compared to the ECS
group. However, this effect was only evident in one measure (BRIEF-2) and not the other
(ERC). This may be due to the fact that while these two measures are significantly
correlated (parent r= .80, teacher r=.87) and do overlap, they are ultimately tapping
different capabilities. The BRIEF-2 was developed to assess children’s executive
functions in an everyday setting (Gioia, Isquith, Retzlaff, & Espy, 2002). Gioia and
colleagues (2002) define executive functions as a “collection of related but distinct
abilities that direct and control goal-oriented cognitive, behavioral, and emotional
functioning” (pp. 249-250). The Emotion Regulation Index of the BRIEF-2 is composed
77
of two subcomponents that measure internalized emotional control and the ability to
flexibility shift between tasks. While the ERC measures difficulties with emotion
regulation as well, the Lability/Negativity subscale assesses a wide range of
dysregulation in affect, including mood swings, angry reactivity, emotional intensity, and
dysregulated positive emotions. Therefore, it is clear that while on the surface (and
statistically) these two constructs look highly similar, they differ conceptually.
Examining the intervention effects on self-regulation, we again see that teachers’
report of these difficulties approach the clinically significant range. According to
teachers, difficulties with self-regulation reached the “potentially clinically elevated”
range for global executive functioning and emotion regulation for children in the ECS
condition. In addition, difficulties with behavior regulation fell in the mild elevation
range for this group. However, parent report on all three of these indices fell in the
normative range. While the pattern of results was the same across parents and teachers,
and parent and teacher data was significantly correlated, it may be that children’s
externalizing behavior and difficulties with self-regulation are more disruptive and
therefore more noticeable in the school setting. Additionally, parents may be biased in
reporting their own child’s behavior.
In addition, it should be noted that for some of the subscales of the CBCL/TRF
and the BRIEF-2, the standard deviations of the T-scores were slightly larger than
expected (greater than 10). The large standard deviations indicate that the scores on some
of these subscales varied greatly among study families, according to both parent and
78
teacher data. In addition, large standard deviations can make it more difficult to detect a
significant effect, particularly in smaller samples.
Overall, these findings support hypothesis two of this study. Children who were
enrolled in the BHC intervention during infancy and early childhood exhibited
significantly less externalizing behavior and difficulty with self-regulation during
elementary school. This preventive effect is further underlined by the significant life
stressors that many of these children have experienced. Despite the fact that these
stressors are often associated with externalizing behavior problems and difficulties with
self-regulation, those that received the BHC intervention were still functioning in the
normative range compared to same-age and same-gender peers.
Study Aim 3: Mechanisms of Change
The third aim of this study was to examine social support and parent-child
relationship quality as potential mechanisms of change in the relation between
intervention group and parent and child outcomes. Specifically, it was predicted that
mothers enrolled in the intervention group would report higher levels of social support,
which would then predict better parent-child relationship quality, which would then lead
to better parent and child outcomes. Contrary to expectation, there was no evidence of
sequential mediation. Each of the manifest variables was then examined individually
(family/friend social support, attachment, maternal sensitivity, and parent-child
dysfunctional interaction) and results indicated no significant effects of the intervention
on these mediators. This was surprising given the evidence outlined above linking these
constructs to one or more of the intervention components.
79
One explanation for the null findings may be that not all mothers received the
same components of the intervention, or the same dosage outlined in the efficacy trials
for these interventions. As discussed above, BHC was designed as a menu of evidence-
based options for families based on their individual needs. Given that only half of
mothers in the intervention group received IPT-A, and only a third received CPP, the
positive effects that were expected to be derived from these intervention components may
have only occurred for a subgroup of mothers who engaged in these components.
Unfortunately, given the sample size, we could not analyze these subgroups
independently. This may especially be the case for indicators of parent-child relationship
quality as the majority of evidence supporting this as a mediator is related to IPT-A and
CPP (Beeber et al., 2013; Cicchetti et al., 2006; Mulcahy et al., 2010; Toth et al., 2013).
In addition, the measures utilized for the parent-child relationship quality
mediator might also explain the insignificant intervention results. While the Attachment
Q-sort can be used with a broad age range (12-48 months old), research has shown the
this measure is more valid (based on its concurrent validity with the gold standard
Strange Situation Procedure) for younger children (less than 18 months) than older
children. It has also demonstrated better validity when the sort is based on an observation
that is longer that 3 hours (Van Ijzendoorn, Vereijken, Bakermans-Kranenburg & Riksen-
Walraven, 2004). In the current study, the sort was based on an observation of 1.5-2
hours.
An alternative explanation centers around the shift from efficacy trials to
effectiveness studies. Sometimes the results that we see under optimal and controlled
80
conditions (efficacy) are not the same as those that we see in the real-world setting
(effectiveness)(Flay et al., 2005; Nathan, Stuart, & Dolan, 2000). While fidelity was
carefully monitored for the implementation of this program, changes to how the EBP was
administered (e.g. number of sessions) as part of this effectiveness study may explain
some of the null effects for the proposed mediators. These results might suggest that
certain program components need to be strengthened or measurements of these mediating
variables need to be improved (MacKinnon et al., 2007). In addition, many efficacy trials
examine the intervention condition compared to a control group (e.g. waitlist, treatment
as usual). However, this study used an enhanced community standard comparison group
which included screening and provision of resources. Doing so can make it more difficult
to detect group differences, especially given the study’s sample size.
Qualitative Impressions
While we did not directly measure mother’s satisfaction or perspective on the
impact of BHC, there were many mothers who spoke highly of the program during the
follow-up visit multiple years later. A number of mothers asked to say hello to their
outreach worker/clinician and wanted to thank them for the impact the program had on
their lives. Multiple mothers reported that the program helped provide them with the
knowledge, resources, and support that they needed at that time. One mother
affectionately referred to her home visitor(s) as “like family,” while another mother said
that BHC “taught me so many things. I was 17 when I had my son, I didn’t know what I
was doing.” These anecdotes underscore the impact that this program had on the
individual lives of these mothers and children.
81
In addition, the follow-up visit conducted when children were school-age also
served as more than just a point for data collection. At the conclusion of the visit,
multiple caregivers were provided with resources ranging from community mental health
agencies to more concrete resources such as clothing, toys, or a list for affordable housing
options. While we do not know if caregivers used the resources provided, the majority of
mothers expressed appreciation for them. In addition, the follow-up visit provided a touch
point to emotionally support parents. At the conclusion of the visit, I often validated
parents’ experiences and the difficulty of parenting, praising them for their efforts and
their attempts to engage in more positive parenting strategies than negative ones.
Strengths & Limitations
This study is characterized by several notable strengths, as well as a number of
limitations. In terms of strengths, this study utilized a multi-informant, multi-method
longitudinal design. Because of its longitudinal design, I was able to capture the temporal
precedence necessary to examine intervention effects and potential mechanisms of
change. Having both parent and teachers report of child behavior also strengthened the
results of this study, as it controls for potential bias and generalizes results across settings
(home and school). In addition, this study provides a long-term follow up of a prevention
program which is actually quite rare in the literature. Researchers have emphasized the
importance of longer term follow-up in order to examine sustainability of program effects
and the prevention of psychological disorders (Gillham, Shatté, & Reivich, 2001). While
examining child behavior at post-intervention (approximately 3 years old) is informative,
we know from the literature that externalizing behavior often doesn’t stabilize until
82
approximately five years of age (Hill et al., 2006). Therefore, examining this construct
after this developmental plateau allows us to better assess the impact of BHC on long-
term functioning. Additionally, this study utilized a racially and ethnically diverse
(African American; Hispanic/Latino) sample. This is especially important since these
groups have typically been underrepresented in academic research, including intervention
research. This makes these results generalizable to other similar, often-underrepresented
populations. Given that there is often stigma surrounding mental health and service
utilization within these populations, BHC’s flexible delivery approach helps to reduce
this stigma. By recruiting families from their established medical home and by delivering
services in their homes, tailored to their individual interests and needs, BHC’s model of
service delivery actively works to reduce the stigma associated with traditional outpatient
service delivery, and partner with parents and children to support healthy development.
Another strength of this study is the flexible design of the intervention and its
real-world application. Researchers have stressed the importance of continued evaluation
of preventive interventions along the continuum from efficacy trials to effectiveness
studies, in order to better understand the utility of our interventions in the real world
(Cicchetti & Toth, 2016; Flay et al., 2005; Olds, Sadler, et al., 2007). BHC was
specifically developed with this in mind, balancing fidelity to evidence-based models
(PAT, IPT-A, CPP) with adaptation to the demands of widespread community
implementation and individual family need. This approach is aligned with the burgeoning
field of precision medicine. As Supplee and Duggan (2019) highlight, precision public
health uses this approach on a larger scale to match communities’ specific needs with the
83
most efficient and cost-effective investment. Doing so means offering those with less risk
factors less intensive (and less costly) interventions, and those at higher risk more
intensive (and more costly) interventions. Recently, the field of prevention science has
supported the precision approach, calling for interventions that are more tailored to
specific client needs (August & Gewirtz, 2019). As part of this call, the field of home
visiting has begun actively conducting research on precision home visiting (e.g. Home
Visiting Applied Research Collaborative).
Although this study has several notable strengths, it is important to acknowledge
its limitations as well. First, the relatively small sample size may have affected the
statistical power to detect certain significant effects, especially for the proposed
mediators. For example, according to the Fritz and MacKinnon (2007)’s power
simulation for mediation, a sample size of 148 or more would be required for sufficient
power (.80) to detect a small-medium effect from intervention to parent-child relationship
quality (e.g. maternal sensitivity (Geeraert, Van den Noortgate, Grietens, & Onghena,
2004; Mulcahy et al., 2010) and a small-medium effect from parent-child relationship
quality to externalizing behavior (Alink et al., 2009; Fearon, Bakermans-Kranenburg,
Van IJzendoorn, Lapsley, & Roisman, 2010) using the proposed bias-corrected bootstrap
method. However, these are only estimated effect sizes considering that the intervention
(BHC specifically) to mediator path has not been measured in past literature.
Another limitation to consider is sample bias. Given the length of time between
the intervention period and the follow-up visit (3-7 years) and the transience of this
population, we decided to only recruit families that were still enrolled at the conclusion
84
of the intervention (T36). While this improved recruitment feasibility, it does bias the
sample. Families that were still enrolled at T36 are likely to differ from those that
dropped out after baseline or mid-intervention. It is likely that those still enrolled at T36
had higher program satisfaction or perceived effectiveness than those who dropped out,
therefore making them more likely to come back for a follow-up visit. These are
important factors to consider when thinking about the generalizability of these results.
A final limitation of this study is the probability of alpha inflation (also known as
familywise error or cumulative Type-I error). When multiple tests are conducted on the
same dataset (t-tests in this case), the probability of Type-I error increases. In order to
help decrease the likelihood of this, comparisons were planned in advance, and included
only a subset of all possible comparisons (Howell, 2009). For example, instead of
running a t-test on all of the individual subscales of each measure, composite scores
(PPI), dimension scores (CBCL/TRF), and index scores (BRIEF-2) were used when
possible.
Future Research
While the results of this dissertation highlight the effectiveness of a multi-
component home visiting program on parent and child outcomes, future research could
make important contributions to the fields of home visiting and prevention science. Given
the sample size utilized in this study, replication with a larger sample is recommended.
This would allow for more sophisticated mediation analyses in order to identify active
ingredients responsible for impacts on key outcomes. In addition, further research could
utilize innovative research designs in order to more precisely determine effective
85
treatment pathways tailored to individual needs. One such method is the Sequential
Multiple Assignment Randomized Trial (SMART) method, which examines the
effectiveness of different sequences or combinations of intervention components (L. M.
Collins, Murphy, & Strecher, 2007; M. C. Howard & Jacobs, 2016).
In addition, future research examining BHC or similar interventions could look at
alternative ways to measure parenting constructs, especially harsh parenting. While self-
report is the most widely available and feasible option, responses may be biased due to
social desirability and fear of repercussions. Substituting or supplementing self-report
measures with behavioral observation would be advantageous and allow us to draw
stronger conclusions regarding the impact of this intervention. In addition, alternative
mediators could be examined that more closely align with the common factors received
by all mothers in the intervention. For example, since nearly all mothers engaged in the
outreach and PAT components, a measure of concrete support and/or parenting
attitudes/behaviors (a focus of PAT) could be examined as a mechanism of change.
Finally, this study provides further evidence that efficacious interventions can be
adapted and implemented in real world settings effectively and with long-term success.
More effectiveness research is needed to determine how alternative interventions can be
adapted and delivered in more naturalistic settings. For example, an intervention designed
to improve child behavior outcomes could also incorporate an outreach component.
Alternatively, researchers could adjust the length of an intervention to make it more
amendable to combination and/or more feasible for widespread implementation. One
example of this research is a current evaluation of CPP being conducted by the
86
TRANSFORM (Translational Research that Adapts New Science FOR Maltreatment
Prevention) center at the University of Rochester. This evaluation compares the typical
year-long model, with a more concise 6-month model. Given the current session limits in
many community-based settings, this research is vital to the widespread dissemination of
this evidence-based model.
Conclusion
In conclusion, this dissertation demonstrates the effectiveness of a multi-
component preventive intervention which offers outreach support and a menu of
evidence-based models tailored to individual family need. When delivered during infancy
and toddlerhood, this program is effective in preventing negative parenting practices and
the onset of child behavior problems in later childhood. Given the long-term detrimental
effect of harsh parenting and externalizing behavior, this evidence highlights the
importance of early intervention to prevent the onset of these behaviors in high-risk
families. Due to the stigma towards mental health and the social and economic burden
many of these families face, it is likely that many of these behaviors would not have been
identified until school-age or later. Rather than waiting for problems to develop, BHC
takes a preventive approach by reaching a non-treatment seeking population within their
medical home and providing a flexible approach to service delivery. This study moves us
away from a “one size fits all” approach to intervention and towards a better
understanding of “what works for whom and why” (Roth & Fonagy, 2013), in order to
increase efficiency and cost-effectiveness for families, providers, and community
stakeholders. These findings support the current trend in precision home visiting and

87
implementation science, and encourage future researchers to not only consider the
efficacy of their interventions, but their effectiveness in real world settings as well.

88
References Abidin, R. R. (1990). Parenting stress index-short form: Pediatric Psychology Press
Charlottesville, VA. Achenbach, T. M., & Rescorla, L. A. (2000). Manual for the ASEBA preschool forms &
profiles: An integrated system of multi-informant assessment; Child behavior checklist for ages 1 1/2-5; Language development survey; Caregiver-teacher report form: University of Vermont.
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA school-age forms & profiles: an integrated system of multi-informant assessment Burlington, VT: University of Vermont. Research Center for Children, Youth, & Families.
Alink, L. R., Mesman, J., Van Zeijl, J., Stolk, M. N., Juffer, F., Bakermans-Kranenburg, M. J., . . . Koot, H. M. (2009). Maternal sensitivity moderates the relation between negative discipline and aggression in early childhood. Social Development, 18(1), 99-120.
Aos, S., Phipps, P., Barnoski, R., & Lieb, R. (2001). The Comparative Costs and Benefits of Programs To Reduce Crime. Version 4.0.
August, G. J., & Gewirtz, A. (2019). Moving toward a precision-based, personalized framework for prevention science: Introduction to the special issue. Prevention Science, 20(1), 1-9.
Avellar, S. A., & Supplee, L. H. (2013). Effectiveness of home visiting in improving child health and reducing child maltreatment. Pediatrics, 132(Supplement 2), S90-S99.
Babinski, L. M., Hartsough, C. S., & Lambert, N. M. (1999). Childhood Conduct Problems, Hyperactivity-Impulsivity, and Inattention as Predictors of Adult Criminal Activity. Journal of Child Psychology and Psychiatry, 40(3), 347-355.
Bailey, J. A., Hill, K. G., Oesterle, S., & Hawkins, J. D. (2009). Parenting practices and problem behavior across three generations: monitoring, harsh discipline, and drug use in the intergenerational transmission of externalizing behavior. Developmental Psychology, 45(5), 1214.
Bakermans-Kranenburg, M. J., Van Ijzendoorn, M. H., & Juffer, F. (2003). Less is more: meta-analyses of sensitivity and attachment interventions in early childhood. Psychological Bulletin, 129(2), 195.
Barnet, B., Liu, J., DeVoe, M., Alperovitz-Bichell, K., & Duggan, A. K. (2007). Home visiting for adolescent mothers: Effects on parenting, maternal life course, and primary care linkage. The Annals of Family Medicine, 5(3), 224-232.
Barnett, D., Manly, J. T., & Cicchetti, D. (1993). Defining child maltreatment: The interface between policy and research. Child Abuse, Child Development, and Social Policy, 8, 7-73.
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173.
Beauchaine, T. P., Webster-Stratton, C., & Reid, M. J. (2005). Mediators, moderators, and predictors of 1-year outcomes among children treated for early-onset conduct

89
problems: a latent growth curve analysis. Journal of Consulting and Clinical Psychology, 73(3), 371.
Beck, A. T., Steer, R. A., & Brown, G. K. J. S. A. (1996). Beck depression inventory-II. 78(2), 490-498.
Beeber, L. S., Schwartz, T. A., Holditch-Davis, D., Canuso, R., Lewis, V., & Hall, H. W. (2013). Parenting enhancement, interpersonal psychotherapy to reduce depression in low-income mothers of infants and toddlers: A randomized trial. Nursing Research, 62(2), 82.
Binggeli, N. J., Hart, S. N., & Brassard, M. R. (2001). Psychological maltreatment of children: Sage.
Borkowski, J. G., Smith, L. E., & Akai, C. E. (2007). Designing effective prevention programs: How good science makes good art. Infants & Young Children, 20(3), 229-241.
Broidy, L. M., Nagin, D. S., Tremblay, R. E., Bates, J. E., Brame, B., Dodge, K. A., . . . Laird, R. (2003). Developmental trajectories of childhood disruptive behaviors and adolescent delinquency: a six-site, cross-national study. Developmental Psychology, 39(2), 222.
Brotman, L. M., Gouley, K. K., Chesir-Teran, D., Dennis, T., Klein, R. G., & Shrout, P. (2005). Prevention for preschoolers at high risk for conduct problems: Immediate outcomes on parenting practices and child social competence. Journal of Clinical Child & Adolescent Psychology, 34(4), 724-734.
Brotman, L. M., Gouley, K. K., Chesir-Teran, D., Dennis, T., Klein, R. G., Shrout, P. (2005). Prevention for preschoolers at high risk for conduct problems: Immediate outcomes on parenting practices and child social competence. Journal of Clinical Child and Adolescent Psychology, 34(4), 724-734.
Burchinal, M. R., Follmer, A., & Bryant, D. M. (1996). The relations of maternal social support and family structure with maternal responsiveness and child outcomes among African American families. Developmental Psychology, 32(6), 1073.
Campbell, S. B., Shaw, D. S., & Gilliom, M. (2000). Early externalizing behavior problems: Toddlers and preschoolers at risk for later maladjustment. Development and Psychopathology, 12(03), 467-488.
Carney, R., Stratford, B., Moore, K., Rojas, A., & Daneri, M. (2015). What works for reducing problem behaviors in early childhood: Lessons from experimental evaluations. Retrieved from: http://www.childtrends.org/wp-content/uploads/2015/08/2015-32WhatWorksProblemBehaviors.pdf
Ceballo, R., & McLoyd, V. C. (2002). Social support and parenting in poor, dangerous neighborhoods. Child Development, 73(4), 1310-1321.
Centers for Disease Control and Prevention. (2014). Child maltreatment: Facts at a glance. Atlanta, GA: Centers for Disease Control and Prevention.
Chang, L., Schwartz, D., Dodge, K. A., & McBride-Chang, C. (2003). Harsh parenting in relation to child emotion regulation and aggression. Journal of Family Psychology, 17(4), 598.
90
Child Welfare Information Gateway. (2011). Child maltreatment prevention: Past, present, and future. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau.
Cicchetti, D. (1984). The emergence of developmental psychopathology. Child Development, 1-7.
Cicchetti, D., & Carlson, V. (1989). Child maltreatment: Theory and research on the causes and consequences of child abuse and neglect: Cambridge University Press.
Cicchetti, D., & Lynch, M. (1995). Failures in the expectable environment and their impact on individual development: The case of child maltreatment. In D. Cicchetti & D. Cohen (Eds.), Developmental Psychopathology: Vol. 2. Risk, disorder and adaptation (Vol. 2, pp. 32-71). New York Wiley.
Cicchetti, D., Rogosch, F. A., & Toth, S. L. (2006). Fostering secure attachment in infants in maltreating families through preventive interventions. Development and Psychopathology, 18(03), 623-649.
Cicchetti, D., & Toth, S. L. (1995). A developmental psychopathology perspective on child abuse and neglect. Journal of the American Academy of Child & Adolescent Psychiatry, 34(5), 541-565.
Cicchetti, D., & Toth, S. L. (2005). Child maltreatment. Annual Review of Clinical Psychology, 1, 409-438.
Cicchetti, D., & Toth, S. L. (2015). Child maltreatment. In R. M. Lerner (Ed.), Handbook of child psychology and developmental science (7 ed., Vol. 3): John Wiley & Sons, Inc.
Cicchetti, D., & Toth, S. L. (2016). Child maltreatment and developmental psychopathology: A multilevel perspective. Developmental Psychopathology, Maladaptation and Psychopathology, 3, 457.
Cicchetti, D., & Toth, S. L. (2017). Using the science of developmental psychopathology to inform child and adolescent psychotherapy. In J. R. Weisz & A. E. Kazdin (Eds.), Evidence-based psychotherapies for children and adolescents (3 ed., pp. 484-500). New York, NY: Guilford Press.
Cicchetti, D., & Valentino, K. (2006). An ecological-transactional perspective on child maltreatment: Failure of the average expectable environment and its influence on child development. Developmental Psychopathology, Second Edition, 129-201.
Cohen, M. A., & Piquero, A. R. (2009). New evidence on the monetary value of saving a high risk youth. Journal of Quantitative Criminology, 25(1), 25-49.
Collins, L. M., Murphy, S. A., & Strecher, V. (2007). The multiphase optimization strategy (MOST) and the sequential multiple assignment randomized trial (SMART): new methods for more potent eHealth interventions. American journal of Preventive Medicine, 32(5), S112-S118.
Collins, P., Patel, V., Joestl, S., March, D., Insel, T., Daar, A., . . . Fairburn, C. (2011). Grand challenges in global mental health. Nature, 475(7354), 27-30.
Cowell, R. A., Cicchetti, D., Rogosch, F. A., & Toth, S. L. (2015). Childhood maltreatment and its effect on neurocognitive functioning: Timing and chronicity matter. Development and Psychopathology, 27(2), 521-533.

91
Crnic, K. A., Greenberg, M. T., Ragozin, A. S., Robinson, N. M., & Basham, R. B. (1983). Effects of stress and social support on mothers and premature and full-term infants. Child Development, 209-217.
Curtis, W. J., & Cicchetti, D. (2003). Moving research on resilience into the 21st century: Theoretical and methodological considerations in examining the biological contributors to resilience. Development and Psychopathology, 15(3), 773-810.
Daro, D. A., & Harding, K. A. J. T. F. o. C. (1999). Healthy Families America: Using research to enhance practice. The Future of Children, 9(1), 152-176.
Dawson-McClure, S., Calzada, E., Huang, K.-Y., Kamboukos, D., Rhule, D., Kolawole, B., . . . Brotman, L. M. (2015). A population-level approach to promoting healthy child development and school success in low-income, urban neighborhoods: impact on parenting and child conduct problems. Prevention Science, 16(2), 279-290.
Deater-Deckard, K. (2008). Parenting stress: Yale University Press. Deater-Deckard, K., Ivy, L., & Petrill, S. A. (2006). Maternal warmth moderates the link
between physical punishment and child externalizing problems: A parent-offspring behavior genetic analysis. Parenting: Science and Practice, 6(1), 59-78.
Deater-Deckard, K., Wang, Z., Chen, N., & Bell, M. A. (2012). Maternal executive function, harsh parenting, and child conduct problems. Journal of Child Psychology and Psychiatry, 53(10), 1084-1091.
Deater–Deckard, K., Dodge, K. A., Bates, J. E., & Pettit, G. S. (1998). Multiple risk factors in the development of externalizing behavior problems: Group and individual differences. Development and Psychopathology, 10(03), 469-493.
Degarmo, D. S., Reid, J. B., & Knutson, J. F. (2006). Direct laboratory observations and analog measures: In research definitions of child maltreatment. In Child abuse and neglect: Definitions, classifications, and a framework for research. (pp. 293-328). Baltimore, MD, US: Paul H Brookes Publishing Co.
Dixon, L., Browne, K., & Hamilton-Giachritsis, C. (2005). Risk factors of parents abused as children: a mediational analysis of the intergenerational continuity of child maltreatment (Part I). Journal of child Psychology and Psychiatry, 46(1), 47-57.
Drotar, D., Robinson, J., Jeavons, L., & Lester Kirchner, H. (2009). A randomized, controlled evaluation of early intervention: The Born to Learn curriculum. Child: Care, Health and Development, 35(5), 643-649.
Dube, S. R., Anda, R. F., Felitti, V. J., Edwards, V. J., & Croft, J. B. J. A. b. (2002). Adverse childhood experiences and personal alcohol abuse as an adult. Addictive Behaviors, 27(5), 713-725.
Duberstein, P. R., Ward, E. A., Chaudron, L. H., He, H., Toth, S. L., Wang, W., ... & Talbot, N. L. (2018). Effectiveness of interpersonal psychotherapy-trauma for depressed women with childhood abuse histories. Journal of consulting and clinical psychology, 86(10), 868.
Duggan, A. K., Berlin, L. J., Cassidy, J., Burrell, L., & Tandon, S. D. (2009). Examining maternal depression and attachment insecurity as moderators of the impacts of home visiting for at-risk mothers and infants. Journal of Consulting and Clinical Psychology, 77(4), 788.
92
Eckenrode, J., Ganzel, B., Henderson Jr, C. R., Smith, E., Olds, D. L., Powers, J., . . . Sidora, K. (2000). Preventing child abuse and neglect with a program of nurse home visitation: The limiting effects of domestic violence. Jama, 284(11), 1385-1391.
Erath, S. A., El-Sheikh, M., & Mark Cummings, E. (2009). Harsh parenting and child externalizing behavior: Skin conductance level reactivity as a moderator. Child development, 80(2), 578-592.
Evans, S. E., Davies, C., & DiLillo, D. (2008). Exposure to domestic violence: A meta-analysis of child and adolescent outcomes. Aggression and Violent Behavior, 13(2), 131-140.
Fazio, R. H., & Olson, M. A. (2003). Implicit measures in social cognition research: Their meaning and use. Annual Review of Psychology, 54(1), 297-327.
Fearon, R., Bakermans-Kranenburg, M. J., Van IJzendoorn, M. H., Lapsley, A. M., & Roisman, G. I. (2010). The significance of insecure attachment and disorganization in the development of children’s externalizing behavior: a meta-analytic study. Child Development, 81(2), 435-456.
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Marks, J. S. . (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. American Journal of Preventive Medicine, 14(4), 245-258.
Filene, J. H., Kaminski, J. W., Valle, L. A., & Cachat, P. (2013). Components associated with home visiting program outcomes: A meta-analysis. Pediatrics, 132(Supplement 2), S100-S109.
Finkelhor, D., Turner, H. A., Shattuck, A., & Hamby, S. L. (2013). Violence, crime, and abuse exposure in a national sample of children and youth: an update. JAMA Pediatrics, 167(7), 614-621.
Flay, B. R., Biglan, A., Boruch, R. F., Castro, F. G., Gottfredson, D., Kellam, S., . . . Ji, P. (2005). Standards of evidence: Criteria for efficacy, effectiveness and dissemination. Prevention Science, 6(3), 151-175.
Frick, P. J., & Morris, A. S. (2004). Temperament and developmental pathways to conduct problems. Journal of Clinical Child and Adolescent Psychology, 33(1), 54-68.
Fritz, M. S., & MacKinnon, D. P. (2007). Required sample size to detect the mediated effect. Psychological Science, 18(3), 233-239.
Geeraert, L., Van den Noortgate, W., Grietens, H., & Onghena, P. (2004). The effects of early prevention programs for families with young children at risk for physical child abuse and neglect: A meta-analysis. Child Maltreatment, 9(3), 277-291.
Gershoff, E. T. (2002). Corporal punishment by parents and associated child behaviors and experiences: a meta-analytic and theoretical review. Psychological Bulletin, 128(4), 539.
Gillham, J. E., Shatté, A. J., & Reivich, K. (2001). Needed for prevention research: Long-term follow up and the Evaluation of mediators, moderators, and lay providers. Prevention & Treatment, 4(1), Article 9c.
93
Gilliom, M., Shaw, D. S., Beck, J. E., Schonberg, M. A., & Lukon, J. L. (2002). Anger regulation in disadvantaged preschool boys: strategies, antecedents, and the development of self-control. Developmental Psychology, 38(2), 222.
Gioia, G. A., Isquith, P. K., Guy, S. C., & Kenworthy, L. (2016). Behavior rating inventory of executive function, (BRIEF-2): Lutz, FL: Psychological Assessment Resource.
Gioia, G. A., Isquith, P. K., Retzlaff, P. D., & Espy, K. A. (2002). Confirmatory factor analysis of the Behavior Rating Inventory of Executive Function (BRIEF) in a clinical sample. Child Neuropsychology, 8(4), 249-257.
Goldstein, L. H., Diener, M. L., & Mangelsdorf, S. C. (1996). Maternal characteristics and social support across the transition to motherhood: Associations with maternal behavior. Journal of Family Psychology, 10(1), 60.
Gomby, D. S. (2007). The promise and limitations of home visiting: implementing effective programs. Child Abuse & Neglect.
Gomby, D. S., Culross, P. L., & Behrman, R. E. (1999). Home visiting: Recent program evaluations: Analysis and recommendations. The Future of Children, 4-26.
Goodman, S. H., Rouse, M. H., Connell, A. M., Broth, M. R., Hall, C. M., & Heyward, D. (2011). Maternal depression and child psychopathology: A meta-analytic review. Clinical Child and Family Psychology Review, 14(1), 1-27.
Greenberg, M. T., Domitrovich, C. E., & Bumbarger, B. (1999). Preventing mental disorders in school-age children: A review of the effectiveness of prevention programs. Prevention Research Center for the Promotion of Human Development, College of Health and Human Development, Pennsylvania State University.
Halfon, N., Berkowitz, G., & Klee, L. (1992). Mental health service utilization by children in foster care in California. Pediatrics, 89(6), 1238-1244.
Handley, E.D., Demeusy, E.M., Manly, J.T., Sturm, R., & Toth, S.T. (2020, November). An examination of the effectiveness of home visiting program “Building Healthy Children” at preventing child maltreatment and fostering positive child outcomes. Paper accepted for presentation at the 2020 SRCD Special Topic Workshop: The State of Research on Prevention of Child Maltreatment: Current Knowledge and Future Directions to Inform Policy and Practice, St. Louis, MO.
Hart, S. N., & Brassard, M. R. (1987). A major threat to children's mental health: Psychological maltreatment. American Psychologist, 42(2), 160.
Higgins, D. J., & McCabe, M. P. (2000). Relationships between different types of maltreatment during childhood and adjustment in adulthood. Child Maltreatment, 5(3), 261-272.
Hill, A., Degnan, K. A., Calkins, S. D., & Keane, S. P. (2006). Profiles of externalizing behavior problems for boys and girls across preschool: the roles of emotion regulation and inattention. Developmental Psychology, 42(5), 913.
Hinshaw, S. P. (1992). Externalizing behavior problems and academic underachievement in childhood and adolescence: causal relationships and underlying mechanisms. Psychological Bulletin, 111(1), 127.

94
Horowitz, J. L., Garber, J., Ciesla, J. A., Young, J. F., & Mufson, L. (2007). Prevention of depressive symptoms in adolescents: a randomized trial of cognitive-behavioral and interpersonal prevention programs. Journal of Consulting and Clinical Psychology, 75(5), 693.
Horton, C. (2003). Protective factors literature review: Early care and education programs and the prevention of child abuse and neglect: Center for the Study of Social Policy.
Howard, K. S., & Brooks-Gunn, J. (2009). The role of home-visiting programs in preventing child abuse and neglect. The future of Children, 19(2), 119-146.
Howard, M. C., & Jacobs, R. R. (2016). The multiphase optimization strategy (MOST) and the sequential multiple assignment randomized trial (SMART): two novel evaluation methods for developing optimal training programs. Journal of Organizational Behavior, 37(8), 1246-1270.
Howell, D. C. (2009). Statistical methods for psychology (seventh ed.). Belmont, CA: Cengage Learning.
Hussey, J. M., Chang, J. J., & Kotch, J. B. (2006). Child maltreatment in the United States: prevalence, risk factors, and adolescent health consequences. Pediatrics, 118(3), 933-942.
Jaffee, S. R., & Maikovich-Fong, A. K. (2011). Effects of chronic maltreatment and maltreatment timing on children’s behavior and cognitive abilities. Journal of Child Psychology and Psychiatry, 52(2), 184-194.
Judd, C. M., & Kenny, D. A. J. E. r. (1981). Process analysis: Estimating mediation in treatment evaluations. Evaluation Review, 5(5), 602-619.
Kendrick, D., Elkan, R., Hewitt, M., Dewey, M., Blair, M., Robinson, J., . . . Brummell, K. (2000). Does home visiting improve parenting and the quality of the home environment? A systematic review and meta analysis. Archives of Disease in Childhood, 82(6), 443-451.
Kim, H. K., Pears, K. C., Fisher, P. A., Connelly, C. D., & Landsverk, J. A. (2010). Trajectories of maternal harsh parenting in the first 3 years of life. Child Abuse & Neglect, 34(12), 897-906.
Kim, S., & Brody, G. H. (2005). Longitudinal pathways to psychological adjustment among Black youth living in single-parent households. Journal of Family Psychology, 19(2), 305.
Korfmacher, J., Green, B., Staerkel, F., Peterson, C., Cook, G., Roggman, L., . . . Schiffman, R. (2008). Parent involvement in early childhood home visiting. Paper presented at the Child & Youth Care Forum.
Leijten, P., Raaijmakers, M. A., Orobio de Castro, B., van den Ban, E., & Matthys, W. (2017). Effectiveness of the incredible years parenting program for families with socioeconomically disadvantaged and ethnic minority backgrounds. Journal of Clinical Child & Adolescent Psychology, 46(1), 59-73..
Lieberman, A. F., Ippen, C. G., & Van Horn, P. (2006). Child-parent psychotherapy: 6-month follow-up of a randomized controlled trial. Journal of the American Academy of Child & Adolescent Psychiatry, 45(8), 913-918.
95
Lieberman, A.F., Ippen, C. G., & Van Horn, P. (2015). Don’t hit my mommy: A manual for Child-Parent Psychotherapy with young children exposed to violence and other trauma, Second Edition. Washington, DC: Zero to Three.
Lieberman, A. F., & Van Horn, P. (2005). Don't hit my mommy!: A manual for child-parent psychotherapy with young witnesses of family violence. Washington, DC: Zero to Three.
Lieberman, A. F., Van Horn, P., & Ippen, C. G. (2005). Toward evidence-based treatment: Child-parent psychotherapy with preschoolers exposed to marital violence. Journal of the American Academy of Child & Adolescent Psychiatry, 44(12), 1241-1248.
Liu, L., & Wang, M. (2015). Parenting stress and children’s problem behavior in China: The mediating role of parental psychological aggression. Journal of Family Psychology, 29(1), 20.
Lovejoy, M. C., Graczyk, P. A., O'Hare, E., & Neuman, G. (2000). Maternal depression and parenting behavior: A meta-analytic review. Clinical Psychology Review, 20(5), 561-592.
Lowell, D. I., Carter, A. S., Godoy, L., Paulicin, B., & Briggs-Gowan, M. J. (2011). A randomized controlled trial of Child FIRST: A comprehensive home-based intervention translating research into early childhood practice. Child Development, 82(1), 193-208.
Luthar, S. S., & Eisenberg, N. (2017). Resilient Adaptation Among At-Risk Children: Harnessing Science Toward Maximizing Salutary Environments. Child Development, 88(2), 337-349.
Lyons-Ruth, K., & Melnick, S. (2004). Dose–response effect of mother–infant clinical home visiting on aggressive behavior problems in kindergarten. Journal of the American Academy of Child & Adolescent Psychiatry, 43(6), 699-707.
MacKinnon, D. P., Fairchild, A. J., & Fritz, M. S. (2007). Mediation analysis. Annual Review of Psychology, 58, 593-614.
MacLeod, J., & Nelson, G. (2000). Programs for the promotion of family wellness and the prevention of child maltreatment: A meta-analytic review. Child Abuse & Neglect, 24(9), 1127-1149.
MacMillan, H. L., Wathen, C. N., Barlow, J., Fergusson, D. M., Leventhal, J. M., & Taussig, H. N. (2009). Interventions to prevent child maltreatment and associated impairment. The Lancet, 373(9659), 250-266.
Manly, J. T. (2005). Advances in research definitions of child maltreatment. Child Abuse & Neglect, 29(5), 425-439.
Markowitz, J. C., Petkova, E., Neria, Y., Van Meter, P. E., Zhao, Y., Hembree, E., . . . Marshall, R. D. (2015). Is exposure necessary? A randomized clinical trial of interpersonal psychotherapy for PTSD. American Journal of Psychiatry, 172(5), 430-440.
Masten, A. S. (2004). Regulatory processes, risk, and resilience in adolescent development. Annals of the New York Academy of Sciences, 1021(1), 310-319.
Mesman, J., van IJzendoorn, M. H., & Bakermans-Kranenburg, M. J. (2012). Unequal in opportunity, equal in process: Parental sensitivity promotes positive child

96
development in ethnic minority families. Child Development Perspectives, 6(3), 239-250.
Mikton, C., & Butchart, A. (2009). Child maltreatment prevention: a systematic review of reviews. Bulletin of the World Health Organization, 87(5), 353-361.
Miller-Johnson, S., Coie, J. D., Maumary-Gremaud, A., Lochman, J., & Terry, R. (1999). Relationship between childhood peer rejection and aggression and adolescent delinquency severity and type among African American youth. Journal of Emotional and Behavioral Disorders, 7(3), 137-146.
Miller-Perrin, C. L., Perrin, R. D., & Kocur, J. L. (2009). Parental physical and psychological aggression: Psychological symptoms in young adults. Child Abuse & Neglect, 33(1), 1-11.
Miner, J. L., & Clarke-Stewart, K. A. (2008). Trajectories of externalizing behavior from age 2 to age 9: relations with gender, temperament, ethnicity, parenting, and rater. Developmental Psychology, 44(3), 771.
Moffitt, T. E. (1993). Adolescence-limited and life-course-persistent antisocial behavior: a developmental taxonomy. Psychological Review, 100(4), 674.
Morrison Gutman, L., McLoyd, V. C., & Tokoyawa, T. (2005). Financial strain, neighborhood stress, parenting behaviors, and adolescent adjustment in urban African American families. Journal of Research on Adolescence, 15(4), 425-449.
Morton, N., & Browne, K. D. (1998). Theory and observation of attachment and its relation to child maltreatment: A review. Child Abuse & Neglect, 22(11), 1093-1104.
Mufson, L., Dorta, K. P., Moreau, D., & Weissman, M. M. (2004). Interpersonal psychotherapy for depressed adolescents (second ed.). New York: Guilford Press.
Mufson, L., Weissman, M. M., Moreau, D., & Garfinkel, R. (1999). Efficacy of interpersonal psychotherapy for depressed adolescents. Archives of General Psychiatry, 56(6), 573-579.
Mulcahy, R., Reay, R. E., Wilkinson, R. B., & Owen, C. (2010). A randomised control trial for the effectiveness of group interpersonal psychotherapy for postnatal depression. Archives of Women's Mental Health, 13(2), 125-139.
Nathan, P. E., Stuart, S. P., & Dolan, S. L. (2000). Research on psychotherapy efficacy and effectiveness: Between Scylla and Charybdis? Psychological Bulletin, 126(6), 964.
National Research Council (2014). New directions in child abuse and neglect research: National Academies Press.
Nievar, M. A., Van Egeren, L. A., & Pollard, S. (2010). A meta-analysis of home visiting programs: Moderators of improvements in maternal behavior. Infant Mental Health Journal, 31(5), 499-520.
O’Connell, M. E., Boat, T., & Warner, K. E. (2009). Committee on the Prevention of Mental Disorders and Substance Abuse Among Children, Youth, and Young Adults: Research Advances and Promising Interventions.
Odgers, C. L., Moffitt, T. E., Broadbent, J. M., Dickson, N., Hancox, R. J., Harrington, H., . . . Caspi, A. (2008). Female and male antisocial trajectories: From childhood origins to adult outcomes. Development and Psychopathology, 20(02), 673-716.

97
Offord, D. R., & Bennett, K. J. (1994). Conduct disorder: Long-term outcomes and intervention effectiveness. Journal of the American Academy of Child & Adolescent Psychiatry, 33(8), 1069-1078.
Olds, D. L. (2006). The nurse–family partnership: An evidence-based preventive intervention. Infant Mental Health Journal, 27(1), 5-25.
Olds, D. L. (2008). Preventing child maltreatment and crime with prenatal and infancy support of parents: The nurse-family partnership. Journal of Scandinavian Studies in Criminology and Crime Prevention, 9(S1), 2-24.
Olds, D. L., Eckenrode, J., Henderson, C. R., Kitzman, H., Powers, J., Cole, R., . . . Luckey, D. (1997). Long-term effects of home visitation on maternal life course and child abuse and neglect: Fifteen-year follow-up of a randomized trial. Jama, 278(8), 637-643.
Olds, D. L., Kitzman, H., Cole, R., Robinson, J., Sidora, K., Luckey, D. W., . . . Holmberg, J. (2004). Effects of nurse home-visiting on maternal life course and child development: age 6 follow-up results of a randomized trial. Pediatrics, 114(6), 1550-1559.
Olds, D. L., Kitzman, H., Hanks, C., Cole, R., Anson, E., Sidora-Arcoleo, K., . . . Tutt, R. A. (2007). Effects of nurse home visiting on maternal and child functioning: age-9 follow-up of a randomized trial. Pediatrics, 120(4), e832-e845.
Olds, D. L., Sadler, L., & Kitzman, H. (2007). Programs for parents of infants and toddlers: recent evidence from randomized trials. Journal of Child Psychology and Psychiatry, 48(3-4), 355-391.
Olson, S. L., Sameroff, A. J., Kerr, D. C., Lopez, N. L., & Wellman, H. M. (2005). Developmental foundations of externalizing problems in young children: The role of effortful control. Development and Psychopathology, 17(01), 25-45.
Owen, M. T., & Mulvihill, B. A. (1994). Benefits of a parent education and support program in the first three years. Family Relations, 206-212.
Paradis, H. A., Sandler, M., Manly, J. T., & Valentine, L. (2013). Building healthy children: Evidence-based home visitation integrated with pediatric medical homes. Pediatrics, 132(Supplement 2), S174-S179.
Parents as Teachers National Center (1999). Born to Learn curriculum (prenatal to 3 years). St. Louis, MO: Author.
Patterson, G. R. (1997). Performance models for parenting: A social interactional perspective. In Parenting and children's internalization of values: A handbook of contemporary theory. (pp. 193-226). Hoboken, NJ, US: John Wiley & Sons Inc.
Paulsell, D., Del Grosso, P., & Supplee, L. (2014). Supporting replication and scale-up of evidence-based home visiting programs: Assessing the implementation knowledge base. American journal of public health, 104(9), 1624-1632.
Peacock, S., Konrad, S., Watson, E., Nickel, D., & Muhajarine, N. (2013). Effectiveness of home visiting programs on child outcomes: a systematic review. BMC Public Health, 13(1), 17.
Pederson, D. R., Moran, G., & Bento, S. (1999). Maternal behaviour Q-sort manual version 3.1. Department of Psychology, University of Western Ontario.

98
Perryman Group (2014). Suffer the Little Children: An Assessment of the Economic Cost of Child Maltreatment. The Perryman Group. Retrieved from: https://www.perrymangroup.com/media/uploads/reports/perryman-suffer-the-little-children-11-2014.pdf.
Pfannenstiel, J., Lambson, T., & Yarnell, V. (1996). The Parents as Teachers program: Longitudinal followup to the Second Wave Study. In: Overland Park, KS: Resarch & Training Associates.
Pfannenstiel, J., Lambson, T., Yarnell, V., Research, Inc., T. A., & America, U. S. o. (1991). Second wave study of the Parents as Teachers program: Executive summary. St. Louis, MO: Parents as Teachers National Center.
Pfannenstiel, J., & Seltzer, D. (1989). New parents as teachers: Evaluation of an early parent education program. Early Childhood Research Quarterly, 4(1), 1-18.
Pinquart, M. (2017). Associations of parenting dimensions and styles with externalizing problems of children and adolescents: An updated meta-analysis. Developmental Psychology, 53(5), 873.
Putnam-Hornstein, E., Needell, B., King, B., & Johnson-Motoyama, M. (2013). Racial and ethnic disparities: A population-based examination of risk factors for involvement with child protective services. Child Abuse & Neglect, 37(1), 33-46.
Robinson, J. L., & Emde, R. N. (2004). Mental health moderators of Early Head Start on parenting and child development: Maternal depression and relationship attitudes. Parenting: Science and Practice, 4(1), 73-97.
Rodriguez, C. (2010). Parent–child aggression: Association with child abuse potential and parenting styles. Violence and Victims, 25(6), 728-741.
Rodriguez, C., Cook, A., & Jedrziewski, C. (2012). Reading between the lines: Implicit assessment of the association of parental attributions and empathy with abuse risk. Child Abuse & Neglect, 36(7-8), 564-571.
Rodriguez, M., Dumont, K., Mitchell-Herzfeld, S. D., Walden, N., & Greene, R. (2010). Effects of Healthy Families New York on the promotion of maternal parenting competencies and the prevention of harsh parenting. Child Abuse & Neglect, 34(10), 711-723.
Rossello, J., & Bernal, G. (1999). The efficacy of cognitive-behavioral and interpersonal treatments for depression in Puerto Rican adolescents. Journal of Consulting and Clinical Psychology, 67(5), 734.
Roth, A., & Fonagy, P. (2013). What works for whom?: a critical review of psychotherapy research: Guilford Publications.
Rutter, M. (1987). Psychosocial resilience and protective mechanisms. American Journal of Orthopsychiatry, 57(3), 316.
Sama-Miller, E., Akers, L., Mraz-Esposito, A., Coughlin, R., & Zukiewicz, M. (2017). Home visiting evidence of effectiveness review: Executive summary. Retrieved from
Sameroff, A. J. (1995). General systems theories and developmental psychopathology. Sedlak, A. J., Mettenburg, J., Basena, M., Peta, I., McPherson, K., & Greene, A. (2010).
Fourth national incidence study of child abuse and neglect (NIS-4). Washington, DC: US Department of Health and Human Services. Retrieved on July, 9, 2010.

99
Séguin, J. R., & Zelazo, P. D. (2005). Executive Function in Early Physical Aggression. In R. E. Tremblay, W. W. Hartup, & J. Archer (Eds.), Developmental Origins of Aggression (p. 307–329). The Guilford Press.
Shaw, D. S., Gilliom, M., Ingoldsby, E. M., & Nagin, D. S. (2003). Trajectories leading to school-age conduct problems. Developmental Psychology, 39(2), 189.
Shields, A., & Cicchetti, D. (1995). The development of an emotion regulation assessment battery: Reliability and validity among at-risk grade-school children. Paper presented at the Poster presented at the Society for Research in Child Development. Indianapolis, IN.
Shields, A., & Cicchetti, D. (1997). Emotion regulation among school-age children: The development and validation of a new criterion Q-sort scale. Developmental Psychology, 33(6), 906.
Shields, A., & Cicchetti, D. (1998). Reactive aggression among maltreated children: The contributions of attention and emotion dysregulation. Journal of Clinical Child Psychology, 27(4), 381-395.
Shin, H., Park, Y. J., & Kim, M. J. (2006). Predictors of maternal sensitivity during the early postpartum period. Journal of Advanced Nursing, 55(4), 425-434.
Shonkoff, J. P., & Fisher, P. A. (2013). Rethinking evidence-based practice and two-generation programs to create the future of early childhood policy. Development and Psychopathology, 25(4pt2), 1635-1653.
Sidebotham, P., Heron, J., & Team, A. S. (2006). Child maltreatment in the “children of the nineties”: A cohort study of risk factors. Child Abuse & Neglect, 30(5), 497-522.
Spinazzola, J., Hodgdon, H., Liang, L.-J., Ford, J. D., Layne, C. M., Pynoos, R., . . . Kisiel, C. (2014). Unseen wounds: The contribution of psychological maltreatment to child and adolescent mental health and risk outcomes. Psychological Trauma: Theory, Research, Practice, and Policy 6(S1), S18.
Sroufe, L. A. (2005). Attachment and development: A prospective, longitudinal study from birth to adulthood. Attachment & Human Development, 7(4), 349-367.
Sroufe, L. A. (2013). The promise of developmental psychopathology: Past and present. Development and Psychopathology, 25(4pt2), 1215-1224.
Stams, G.-J. J., Juffer, F., & van IJzendoorn, M. H. (2002). Maternal sensitivity, infant attachment, and temperament in early childhood predict adjustment in middle childhood: The case of adopted children and their biologically unrelated parents. Developmental Psychology, 38(5), 806.
Stith, S. M., Liu, T., Davies, L. C., Boykin, E. L., Alder, M. C., Harris, J. M., . . . Dees, J. (2009). Risk factors in child maltreatment: A meta-analytic review of the literature. Aggression and Violent Behavior, 14(1), 13-29.
Straus, M. A., & Field, C. J. (2003). Psychological aggression by American parents: National data on prevalence, chronicity, and severity. Journal of Marriage and Family, 65(4), 795-808.
Straus, M. A., Hamby, S. L., Finkelhor, D., Moore, D. W., & Runyan, D. (1998). Identification of child maltreatment with the Parent-Child Conflict Tactics Scales:

100
Development and psychometric data for a national sample of American parents. Child Abuse & Neglect, 22(4), 249-270.
Straus, M. A., Hamby, S. L., & Warren, W. L. (2003). The conflict tactics scales handbook: Revised Conflict Tactics Scales (CTS2): CTS: Parent-Child Version (CTSPC): Western Psychological Services.
Supplee, L. H., & Duggan, A. (2019). Innovative research methods to advance precision in home visiting for more efficient and effective programs. Child Development Perspectives, 13(3), 173-179.
Sweet, M. A., & Appelbaum, M. I. (2004). Is home visiting an effective strategy? A meta-analytic review of home visiting programs for families with young children. Child Development, 75(5), 1435-1456.
Taskforce, A. (2019). The Investigation and Determination of Suspected Psychological Maltreatment in Children and Adolescents. Retrieved from https://www.apsac.org/guidelines.
Teti, D. M., Nakagawa, M., Das, R., & Wirth, O. (1991). Security of attachment between preschoolers and their mothers: Relations among social interaction, parenting stress, and mother's sorts of the Attachment Q-Set. Developmental Psychology, 27(3), 440.
Thomas, R., & Zimmer-Gembeck, M. J. (2011). Accumulating evidence for parent–child interaction therapy in the prevention of child maltreatment. Child Development, 82(1), 177-192.
Thompson, R. A., Flood, M. F., & Goodvin, R. (2006). Social support and developmental psychopathology. Developmental Psychopathology, 3, 1-37.
Toth, S. L., Maughan, A., Manly, J. T., Spagnola, M., & Cicchetti, D. (2002). The relative efficacy of two interventions in altering maltreated preschool children's representational models: Implications for attachment theory. Development and Psychopathology, 14(4), 877-908.
Toth, S. L., Rogosch, F. A., Manly, J. T., & Cicchetti, D. (2006). The efficacy of toddler-parent psychotherapy to reorganize attachment in the young offspring of mothers with major depressive disorder: a randomized preventive trial. Journal of Consulting and Clinical Psychology, 74(6), 1006.
Toth, S. L., Rogosch, F. A., Oshri, A., Gravener-Davis, J., Sturm, R., & Morgan-López, A. A. (2013). The efficacy of interpersonal psychotherapy for depression among economically disadvantaged mothers. Development and Psychopathology, 25(4pt1), 1065-1078.
Tremblay, R. E., LeMarquand, D., & Vitaro, F. (1999). The prevention of oppositional defiant disorder and conduct disorder. In Handbook of Disruptive Behavior Disorders (pp. 525-555): Springer.
U.S. Department of Health & Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2020). Child Maltreatment 2018. Available from https://www.acf.hhs.gov/cb/research-data-technology /statistics-research/child-maltreatment.

101
Vachon, D. D., Krueger, R. F., Rogosch, F. A., & Cicchetti, D. (2015). Different forms of child maltreatment have comparable consequences among children from low-income families. JAMA psychiatry, 72(11), 1135.
Van Ijzendoorn, M. H., Vereijken, C. M., Bakermans-Kranenburg, M. J., & Marianne Riksen-Walraven, J. (2004). Assessing attachment security with the attachment Q sort: Meta-analytic evidence for the validity of the observer AQS. Child Development, 75(4), 1188-1213.
Vaughn, B. E., & Waters, E. (1990). Attachment behavior at home and in the laboratory: Q-sort observations and strange situation classifications of one-year-olds. Child Development, 61(6), 1965-1973.
Vaux, A., & Harrison, D. (1985). Support network characteristics associated with support satisfaction and perceived support. American Journal of Community Psychology, 13(3), 245-265.
Vaux, A., Riedel, S., & Stewart, D. (1987). Modes of social support: The social support behaviors (SS-B) scale. American Journal of Community Psychology, 15(2), 209-232.
Veltkamp, L. J., & Miller, T. W. (1994). Clinical handbook of child abuse and neglect: International Universities Press, Inc.
Von Bertalanffy, L. (1968). General system theory. New York, 41973(1968), 40. Wagner, M., & Clayton, S. (1999). The Parents as Teachers program: Results from two
demonstrations. The Future of Children, 91-115. Wagner, M., Spiker, D., & Linn, M. I. (2002). The effectiveness of the Parents as
Teachers program with low-income parents and children. Topics in Early Childhood Special Education, 22(2), 67-81.
Waters, E. (1995). Appendix A: The attachment Q-set (version 3.0). Monographs of the Society for Research in Child Development, 234-246.
Webster-Stratton, C. (1998). Preventing conduct problems in Head Start children: strengthening parenting competencies. Journal of Consulting and Clinical Psychology, 66(5), 715.
Webster-Stratton, C., & Hammond, M. (1998). Conduct problems and level of social competence in Head Start children: Prevalence, pervasiveness, and associated risk factors. Clinical Child and Family Psychology Review, 1(2), 101-124.
Webster-Stratton, C., & Reid, M. J. (2017). A multifaceted treatment approach for young children with conduct problems. Evidence-Based Psychotherapies for Children and Adolescents. 3rd ed. New York: Guildford, 122-141.
Weissman, M. M., Markowitz, J. C., & Klerman, G. L. (2000). Comprehensive guide to interpersonal psychotherapy. Basic Books.
Weisz, J. R., Sandler, I. N., Durlak, J. A., & Anton, B. S. (2005). Promoting and protecting youth mental health through evidence-based prevention and treatment. American Psychologist, 60(6), 628.
Wong, J. J., Gonzales, N. A., Montaño, Z., Dumka, L., & Millsap, R. E. (2014). Parenting intervention effects on parental depressive symptoms: Examining the role of parenting and child behavior. Journal of Family Psychology, 28(3), 267-277.

102
Young, J. F., Mufson, L., & Davies, M. (2006). Efficacy of Interpersonal Psychotherapy-Adolescent Skills Training: an indicated preventive intervention for depression. Journal of Child Psychology and Psychiatry, 47(12), 1254-1262.
Zhou, Q., Chen, S. H., & Main, A. (2012). Commonalities and Differences in the Research on Children’s Effortful Control and Executive Function: A Call for an Integrated Model of Self-Regulation. Child Development Perspectives, 6(2), 112-121.
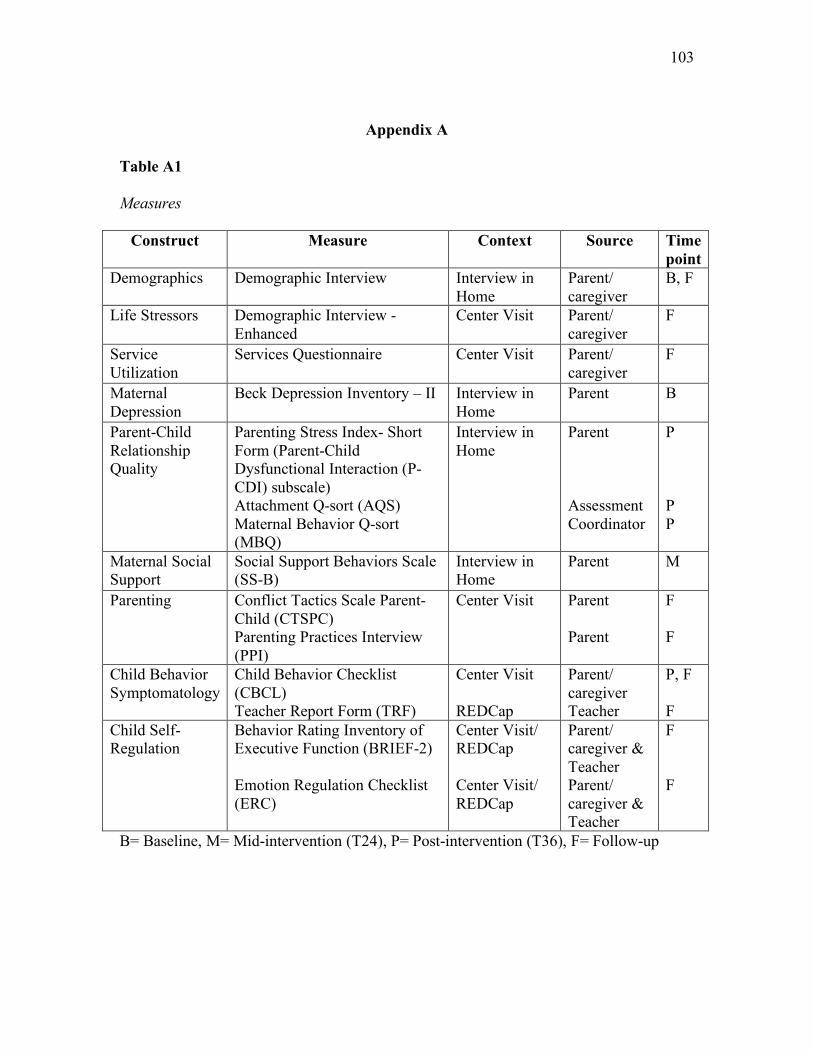
103
Appendix A
Table A1 Measures
Construct Measure Context Source Time point
Demographics Demographic Interview Interview in Home
Parent/ caregiver
B, F
Life Stressors Demographic Interview - Enhanced
Center Visit Parent/ caregiver
F
Service Utilization
Services Questionnaire Center Visit Parent/ caregiver
F
Maternal Depression
Beck Depression Inventory – II Interview in Home
Parent B
Parent-Child Relationship Quality
Parenting Stress Index- Short Form (Parent-Child Dysfunctional Interaction (P-CDI) subscale) Attachment Q-sort (AQS) Maternal Behavior Q-sort (MBQ)
Interview in Home
Parent Assessment Coordinator
P P P
Maternal Social Support
Social Support Behaviors Scale (SS-B)
Interview in Home
Parent M
Parenting Conflict Tactics Scale Parent-Child (CTSPC) Parenting Practices Interview (PPI)
Center Visit Parent Parent
F F
Child Behavior Symptomatology
Child Behavior Checklist (CBCL) Teacher Report Form (TRF)
Center Visit REDCap
Parent/ caregiver Teacher
P, F F
Child Self-Regulation
Behavior Rating Inventory of Executive Function (BRIEF-2) Emotion Regulation Checklist (ERC)
Center Visit/ REDCap Center Visit/ REDCap
Parent/ caregiver & Teacher Parent/ caregiver & Teacher
F F
B= Baseline, M= Mid-intervention (T24), P= Post-intervention (T36), F= Follow-up





























