Embed Size (px)
Citation preview

A multicenter randomized trial of computer-driven protocolized weaning from
mechanical ventilation
François Lellouche,1 Jordi Mancebo,2 Philippe Jolliet,3 Jean Roeseler,4 Fréderique Schortgen,5
Michel Dojat,6 Belen Cabello,2 Lila Bouadma,5 Pablo Rodriguez,1 Salvatore Maggiore,7 Marc
Reynaert,4 Stefan Mersmann,8 Laurent Brochard1
1 Réanimation Médicale, AP-HP, Hôpital Henri Mondor, Unité INSERM U 651, Université
Paris XII, Créteil, France
2 Servei Medicina Intensiva, Hospital Sant Pau, Barcelona, Spain
3 Soins Intensifs de Médecine, Hôpital Cantonal Universitaire, Genève, Suisse
4 Soins Intensifs - Unité médico-chirurgicale. Cliniques Universitaires Saint-Luc, Bruxelles,
Belgique
5 Réanimation Médicale et Infectieuse, AP-HP, Hôpital Bichat, Paris, France
6 INSERM / UJF U594, Neuro-imagerie Fonctionelle et Métabolique, LRC CEA 30V, CHU
de Grenoble, France
7 Istituto di Anestesiologia e Rianimazione - Università Cattolica Policlinico A.Gemelli,
Rome, Italie
8 Dräger Medical AG & Co.KG, Research & Development Critical Care, Lübeck, Germany
Correspondence : Prof. Laurent Brochard, Service de Réanimation Médicale, Hôpital Henri
Mondor, 51 av. du Maréchal de Lattre de Tassigny, 94010 Créteil, France
Phone: 33 1 49 81 23 84; Fax: 33 1 42 07 99 43
E-mail: [email protected]
Descriptor: 6. Mechanical ventilation: controlled trials
AJRCCM Articles in Press. Published on July 13, 2006 as doi:10.1164/rccm.200511-1780OC
Copyright (C) 2006 by the American Thoracic Society.

Running title: Automated ventilation
Word count (body of text only): 3302
Abstract word count: 249
This article has an online data supplement, which is accessible from this issue's table of
content online at www.atsjournals.org.

3
ABSTRACT
Rationale and objectives: Duration of weaning from mechanical ventilation may be reduced by the
use of a systematic approach. We assessed whether a closed-loop knowledge-based algorithm
introduced in a ventilator to act as a computer-driven weaning protocol can improve patient
outcomes as compared to usual care.
Methods and measurements: We conducted a multicenter randomized controlled study with
concealed allocation to compare usual care for weaning to computer-driven weaning. The
computerized protocol included an automatic gradual reduction in pressure support, automatic
performance of spontaneous breathing trials (SBT), and generation of an incentive message when a
SBT was successfully passed. One hundred forty-four patients were enrolled before weaning
initiation. They were randomly allocated to computer-driven weaning or to physician-controlled
weaning according to local guidelines. Weaning duration until successful extubation and total
duration of ventilation were the primary endpoints.
Main results: Weaning duration was reduced in the computer-driven group from a median of 5 to 3
days (P=0.01) and total duration of mechanical ventilation from 12 to 7.5 days (P=0.003).
Reintubation rate did not differ (23 vs 16 %, P=0.40). Computer-driven weaning also decreased
median intensive-care-unit stay duration from 15.5 to 12 days (P=0.02) and caused no adverse
events. The amount of sedation did not differ between groups. In the usual care group compliance
to recommended modes and to SBT was estimated respectively at 96% and 51%.
Conclusions: The specific computer-driven system used in this study can reduce mechanical
ventilation duration and intensive-care-unit length of stay, as compared to physician-controlled
weaning process.

4
Keywords: mechanical ventilation, weaning protocols, computers, knowledge-based system,
extubation

5
INTRODUCTION
The weaning process accounts for approximately forty percent of the total duration of
mechanical ventilation.(1, 2) Undue prolongation of mechanical ventilation can lead to an
increased risk of infectious complications, mainly nosocomial pneumonia,(3, 4) but premature
extubation followed by reintubation is associated with increased morbidity and mortality.(5) Thus,
a major goal is to recognize readiness for extubation as soon and as reliably as possible. Clinical
judgment is far from perfect and often tends to prolong mechanical ventilation.(6-8) Thus, studies
have shown that the duration of mechanical ventilation, and most notably of the weaning period,
can be shortened by using a systematic approach for reducing the level of assistance and testing the
possibility to resume spontaneous breathing.(6, 9)
A closed-loop knowledge-based system has been developed and tested over the last few
years as a method for driving pressure-support ventilation.(10) This system interprets clinical data
in real-time and provides continuous adjustment of the level of assistance delivered to intubated or
tracheotomized patients. The system has been described elsewhere (10-14). In brief, it is embedded
in a standard ventilator and adapts the level of pressure support to continuously recorded data on
patient’s ventilatory needs, with the goal of keeping the patient within a “comfort” zone. Comfort
is defined primarily as a respiratory rate that can vary freely in the 15-30 breaths-per-minute range
(up to 34 in patients with neurological disease), a tidal volume above a minimum threshold, and an
end-tidal CO2 level below a maximum threshold. The level of pressure support is periodically
adapted by the system (10, 13) in steps of 2 to 4 cm of water. The system automatically tries to
reduce the pressure level down to a minimal value. At this value, a trial of “spontaneous breathing”
with the minimal low pressure support is performed. When successful, a message on the screen
recommends separation from the ventilator.

6
It therefore adapts and reduces the level of assistance at a pace tailored to the individual
patient’s needs and evaluates the patient’s ability to be separated from the ventilator. Such a
system has previously been shown to reduce the duration of ventilation spent with excessive levels
of respiratory work,(13) and to improve extubation readiness prediction.(11) Such a system can be
used safely over prolonged periods of mechanical ventilation (15).
Applying guidelines to real-life clinical practice has been found difficult.(16, 17) The
closed-loop system constitutes an automated, continuous, protocol-driven ventilation and weaning
process that may help to improve compliance with guidelines, including a prompt to physiscians
when readiness testing is successful. Although it may not outperform a strictly followed and
aggressive weaning protocol, it may be better than usual care. We tested this hypothesis in a
multicenter randomized controlled trial versus usual weaning processes. This work has been
presented in abstract form (18).

7
METHODS (628 words)
A detailed methods section is available in the on-line supplement.
Patients
This study was conducted in five teaching-hospital medical-surgical intensive care units in
Barcelona (Spain), Brussels (Belgium), Créteil (France), Geneva (Switzerland), and Paris (France).
Each center obtained approval of the study from the ethics committee. Signed informed consent
was obtained from each patient or next of kin.
Patients under mechanical ventilation for at least 24 hours and ventilated using an assisted
mode were screened for eligibility at an early stage, before usual criteria for weaning readiness
were present (Figure 1). Enrolment criteria required absence of the following: do-not-
resuscitate order, expected poor short-term prognosis, tracheostomy, and cardiac arrest with a poor
neurological prognosis. Inclusion criteria were pulse oximetry > 90 percent with a fraction of
inspired oxygen ≤ 50 percent, positive end-expiratory pressure level ≤ 8 cm of water, no need for
epinephrine or norepinephrine at a rate >1 mg per hour, body temperature between 36 °C and 39
°C, and a stable neurological status with little or no sedation.
Study protocol
As soon as patients met the inclusion criteria, a pre-inclusion test with pressure support at ≥
15 cm of water was performed to assess the patient’s ability to tolerate this mode. The test was
positive at 30 minutes if the patient remained clinically stable, with no hemodynamic or respiratory
distress.
Patients were then allocated at random to ventilation with an Evita 4 ventilator (Dräger,
Lübeck, Germany) equipped with the system or to the usual care (control) group. In the usual care
arm, weaning was conducted according to usual local practice (guidelines were available in four

8
units). In all centers, weaning was conducted based on written guidelines, as follows (i) Once daily
or more, screening for criteria to decide for a SBT (T-piece or PSV±PEEP) had to be performed,
(ii) SBT might be performed as soon as criteria were present (iii) after succeeding a SBT,
standardized extubation criteria were used. These principles and the local guidelines are detailed in
the online supplement. We did not assess compliance to guidelines not to influence practice. In this
group, ventilatory settings were chosen by the physician in charge of the patient.
Randomization was concealed and generated by an electronic-mail system. The
randomization was stratified by center and on the presence of an underlying disease (chronic
obstructive pulmonary disease, central neurological disease, or none).
Identical criteria were used in both groups to switch back to assist-control ventilation in
case of worsening. The patient was then retested, and returned to the same arm when the test was
positive.
End-points
The primary end-points were the time to successful extubation, defined as the time from
inclusion until successful extubation (followed by 72 hours without ventilator support) and the
total duration of mechanical ventilation.
Secondary end-points were the duration of ventilatory support until first extubation, length
of intensive care unit and hospital stay, number of complications in the intensive care unit, number
of nosocomial pneumonia, and mortality rates in the intensive care unit and hospital.
Statistical analysis
The sample size of 75 in each group was chosen to give power of 0.80 to detect a reduction
in weaning time of 2 days (from 7 to 5 days, 30%), assuming a standard deviation of 5 days and a

9
two-sided test at the 0.05 level. The analysis was performed in the two groups as treated. Results
are given as medians (25th-75th interquartile ranges). Proportions were compared using the chi-
square test or the Fisher exact test when required. The Mann-Whitney U test was used to analyze
mechanical ventilation durations or length of stay. The cumulative probability of remaining on
mechanical ventilation was analysed by the Kaplan-Meier method and a log-rank test was used to
assess differences. P values smaller than 0.05 were considered significant. All the P values were
two-sided.

10
RESULTS
Patients
Patients were enrolled from September 1st, 2002, to July 12th, 2003. Mean duration of
participation per center was 171 days; 40 patients were enrolled in Brussels, 39 in Barcelona, 34 in
Créteil, 18 in Geneva, and 16 in Paris. Figure 1 indicates the number of patients receiving invasive
mechanical ventilation in the study centers, and the 147 patients included. Two patients were
extubated before being randomized to the computer-driven weaning group, due to a delay in the
electronic randomization procedure, and one control group patient was excluded because the
family withdrew their consent. This left 144 patients for the data analysis, 74 in the intervention
group and 70 in the control group.
Patient characteristics at baseline are shown in Table 1. Patients were similar for most
characteristics, including the number of patients with chronic obstructive pulmonary disease or
central neurological disorders. Duration of mechanical ventilation before inclusion was similar in
the two groups. The values used for the pressure-support test, including the positive end-expiratory
pressure and fraction of inspired oxygen, were also similar.
Outcome
The main results are shown in Table 2. The weaning time was greatly reduced with the
computer-driven weaning as compared to usual weaning, whether or not the time on post-
extubation noninvasive ventilation was counted. The total duration of mechanical ventilation and
the duration of the intensive-care-unit stay were also significantly reduced with the computer-
driven weaning, when considering the total population as well as patients alive at ICU discharge
(Table E1). No difference was found for hospital length of stay.

11
Mortality in the intensive care unit was similar in the computer-driven weaning group and
the usual group (21.6 vs. 22.9 percent, P=1.0), as was hospital mortality (37.8 vs. 28.6 percent,
P=0.29). Mortality while connected to the ventilator during the weaning phase was also similar in
the computer-driven weaning and control groups (6 and 5 patients, respectively, P=0.70).
The probability of remaining on mechanical ventilation is shown in Figure 2, and was
significantly reduced with the computer-driven weaning (log-rank test P=0.015). Data concerning
survivors only are shown in Table E1 in the on-line supplement.
Complications
Complications are reported in Table 3. The need for noninvasive ventilation was almost
halved in the group. The total number of ventilation-related complications (reintubation, self-
extubation, need for noninvasive ventilation, mechanical ventilation longer than 21 days, and
tracheotomy) was reduced by 30 percent with the computer-driven weaning compared to the usual
group. In the computer-driven weaning and control groups, ventilator-associated pneumonia
occurred in 13 and 11 patients, and pneumothorax in 0 and 2 patients respectively.
Mechanical ventilation
Patients were ventilated with pressure support for 392 days in the usual weaning group and
293 days in the computer-driven weaning group. The modes of ventilation recommended in the
guidelines (PS for the weaning phase and ACV in case of worsening) were used 92 and 96% of the
time after inclusion in the computer driven weaning group and in the usual weaning group
respectively. Alternatively, SIMV was used in 8% and 4% of the time (Table E2). A T-piece trial
was performed 124 times in the usual weaning group and 12 times (in 8 patients) in the computer-
driven weaning group. In the usual care group, we estimated compliance to recommendations for

12
using spontaneous breathing trials: T-piece trials were performed 51% of the days of ventilation
with PSV or SIMV at FiO2 below 50% in the usual weaning group. In the computer-driven
weaning group, the mean time from display of the message recommending separation from the
ventilator to extubation was 0.6 ± 2.65 days (median 1, 25th - 75th 0-2), minimum of 0 days, and
maximum of 15 days. Only 42% of the patients were extubated the day of the message.
Technical problems recorded with the computer-driven weaning were as follows. In five
patients, a total of eleven episodes of transient system interruption occurred over a total of 293
days of ventilation using this system. During the interruptions, ventilatory assistance was delivered
in standard pressure-support mode. In 10 patients, the system was voluntarily stopped because
worsening of the clinical condition required assist-control ventilation. In five patients, a manual
increase in pressure support was deemed necessary by the physician, and a manual decrease in
three patients. Two instances of CO2 sensor dysfunction requiring removal of the computer-driven
weaning system occurred in one center.
The amount of sedatives used did not differ between the groups during the intubation-to-
inclusion period and the inclusion-to-extubation period (see Table 4 and Table E3 in the on-line
supplement). Use of steroids and neuromuscular blocking agents before and after inclusion was
also similar in the two groups.

13
DISCUSSION
In this study, a computer-driven weaning protocol performed better than usual care based
on written weaning guidelines. Weaning time was nearly halved with the computer-driven weaning
as compared to usual weaning. The system used in this study was developed several years ago and
has been repeatedly evaluated since then .(10-14) It ensures that the desired ventilation protocol is
applied. In the usual weaning group, weaning was performed according to local guidelines,
representing the usual care in these university centers involved in respiratory and weaning
research. The reduction in weaning duration was associated with decreases in both the total
duration of mechanical ventilation, and the intensive care unit length of stay.
Weaning protocols or guidelines recommending a systematic approach have been shown to
reduce the duration of weaning and mechanical ventilation (6, 9) and are often recommended.(19)
In a randomized controlled study, Ely et al. showed that routine daily screening and identification
of the patients able to breathe spontaneously reduced weaning duration from a median of 3 days to
1 day and the total duration of mechanical ventilation from 6 days to 3.5 days.(6) Kollef et al. also
showed a reduction in the duration of mechanical ventilation in patients weaned using protocols,
from a median of 1.8 to 1.4 days.(9) The implementation of protocols, however, is time-
consuming,(16) requires staff training, is not always followed faithfully,(17) and varies in efficacy
according to all these factors.(20-22) Protocols may even not be necessary in well-staffed centres
(20) . In the present study, written weaning guidelines were compared to a closed-loop knowledge-
based ventilation. The duration of weaning was significantly decreased, from a median of 5 days to
3 days in the computer-driven weaning group, and the total duration of mechanical ventilation
decreased from 12 to 7.5 days. The duration of weaning was slightly longer in the present study
than in the previously mentioned studies. This is in part because the type of patients was
different,(9) and also because patients were included at an early stage, as soon as they were able to

14
tolerate moderate to high pressure support levels and before they met criteria for readiness testing
and weaning.
In our study, several reasons may explain the reduction of mechanical ventilation duration
in the computer-driven weaning group. Automation of the weaning protocol may explain an
essential part of the results. The system is designed to perform several tasks comparable to a
weaning protocol 24 hours a day and 7 days a week: to automatically and gradually reduce the
ventilatory assistance, to automatically perform the equivalent of a spontaneous breathing trial and
to display an incentive message when the patient is deemed ready to breathe spontaneously.
Although the reduction in pressure support applied by the system is gradual, complete weaning can
be obtained in less than 24 hours, thus allowing rapid detection of readiness for extubation. This
computer-driven weaning protocol has advantages compared to a human-driven protocol. The
computer-driven weaning protocol does not depend on the willingness or availability of the staff,
and full compliance with the weaning protocol is therefore ensured. A permanent evaluation and
adjustment of ventilatory support can not be continuously performed by care-givers, and the
system has the ability to determine more easily and rapidly than usual care the time for a possible
separation from the ventilator. It is likely that the message delivered by the system also constitutes
a strong incentive for the clinician to consider a possible extubation. This visual prompt constitutes
an important aspect of the “computer-driven protocol”.
Other specific features of the computerized protocol used in the study, which may differ
from human directed protocols, should be underlined. The computerized protocol used in the
study, takes into account the history of breathing pattern and the previous modifications of the
assistance level to decide for the setting. One important feature is that the decision process of the
system is designed to accept transient instabilities, such as a short increase in respiratory
frequency, without changing the ventilation classification. The system is also able to perform the

15
final test at any time and to repeat it whenever possible, increasing the opportunity to find a
successful test. This temporal reasoning may differ from an automated or even a human-driven
approach where one single measurement or test is performed.
It is possible, however, that the rigor with which weaning assessment was performed in the
control group was suboptimal (e.g. with less assessment on week-ends or in case of major
variations in overall workload in the units), as often observed in the real life. Such a suboptimal
approach could also participate in the difference between the two groups, but our design did not
allow addressing this question.
The need for reintubation within 72 hours after extubation tended to be lower with the
computer-driven weaning (16.2 vs. 22.9 percent), but not significantly. This failure rate is in the
higher end of the reported range. In recent studies, reintubation rates were 11 percent,(23) 15.7
percent,(24) 23.5 percent,(25) and 14.5 percent.(26) A relatively high extubation rate was expected
because patients on mechanical ventilation for less than 24 hours were not included in the study.
The need for noninvasive ventilation after extubation was reduced to 18.9 percent in the computer-
driven weaning group as compared to 37.1 percent in the usual group. The rate of respiratory
failure after extubation with a potential need for noninvasive ventilation was 23 percent in the
study by Keenan et al.(27) and 22.5 percent in the study by Esteban et al.(28) The difference with
our study may be ascribable to differences in patient selection, with higher severity scores in our
population, and to the experience of the centers with this technique.
The trend for a reduction in reintubation and in the need for non-invasive ventilation in the
computer-driven weaning group may be explained by physiological benefits of the system
previously demonstrated, since adjusting the level of assistance to the breathing pattern may avoid
periods of excessive work of breathing. In a previous study,(13) patients were ventilated
successively with the computer-driven weaning and with standard pressure support. The time spent

16
in the comfort zone of ventilation was 93±8 percent with automatic pressure support and 66±24
percent with standard pressure support (p<0.05). The time spent with a high airway occlusion
pressure (suggesting excessive work of breathing) was significantly lower with automatic pressure
support. The level of pressure support was modified 56±40 times over a 24-hour period in the
computer-driven weaning group versus 1±2 times in the standard pressure support group. Repeated
periods of excessive workload during mechanical ventilation may slow recovery from
diaphragmatic fatigue and/or aggravate diaphragm weakness, a frequent finding in difficult-to-
wean patients.(29)
This study has limitations. The results can not be generalized to all patients since only a
small proportion of eligible patients were randomized (14%). The rationale, however, extends at
least to patients with a short weaning duration and further studies will be needed including this
group. In a few patients, the closed-loop was interrupted, either for technical reasons or because
the clinicians disagreed with the settings. More work is needed to determine which patients may be
poor candidates for ventilation with the system. Another limitation is that blinding of the
investigators was not feasible, which may have favored the computer-driven weaning group. The
selection of controls is an important issue in randomized trials of mechanical ventilation and has
recently been a focus of debate.(30) It has been suggested that usual care should be applied in the
control group when feasible,(31) as in the study by Ely et al.(6) The control group in our study was
managed based on written weaning guidelines used routinely in each center. These guidelines had
been in use for several years in all study centers and included daily screening and spontaneous
breathing tests. Compliance with guidelines, however, was not evaluated in the usual weaning
group, as our goal was to keep usual weaning practices unchanged. Compliance with weaning
protocols is frequently relatively low.(17, 22, 32) In the study by Ely et al., after the training
period, compliance was 81 percent in medical intensive care units and 63 percent in surgical units,

17
and poor compliance was often related to the T-piece trial.(17) With the computer-driven weaning,
T-piece trials are not required to test the patient’s readiness for extubation, as the spontaneous
breathing trials are automatically carried out with low levels of pressure support. In the present
study, 12 T-piece trials were nevertheless performed in the computer-driven weaning arm, as
compared to 124 in the usual weaning group. In the usual weaning group, we estimated from the
number of performed T-piece trials that compliance with recommendations for testing spontaneous
breathing with trials was about 51%. This calculation, however, only takes into account
spontaneous breathing trials performed with T-piece, and not those performed in pressure support,
which were not recorded. The level of compliance may then have been underestimated by this
estimation. In the future, comparison with protocolized weaning rather than usual care may be
required.
In conclusion, we have shown in the present study that weaning duration from mechanical
ventilation could be reduced using a system which automatically drives the level of pressure
support, automatically performs spontaneous breathing trials and displays an incentive message
when the trial is successfully passed. Milic-Emili asked whether weaning was an art or a
science.(33) Science is gaining ground as knowledge accumulates from physiological studies and
randomized trials. We think that incorporation of this knowledge into a computer-driven weaning
system is a step forward in a scientific approach to weaning.

18
Acknowledgment, conflict of interest and source of funding
Stefan Mersmann is employed by Dräger Medical. Laurent Brochard, as head of the clinical
research group, has received funding through research contracts with Dräger for the conduct of
clinical trials concerning the system. Dräger Medical has provided the centers with the equipment
necessary for the study (including the ventilators (EVITA 4) equipped with the Evita Weaning
System), and has provided a grant necessary to cover insurance costs, Ethics Committee’s
administrative fees, organization of meetings for the investigators and for monitoring purposes.

19
REFERENCES
1. Esteban A., Alia I., Ibanez J., Benito S., and Tobin M. J. Modes of mechanical ventilation
and weaning. A national survey of Spanish hospitals. The Spanish Lung Failure Collaborative
Group. Chest 1994; 106:1188-93.
2. Esteban A., Anzueto A., Frutos F., Alia I., Brochard L., Stewart T. E., Benito S., Epstein S.
K., Apezteguia C., Nightingale P., Arroliga A. C., and Tobin M. J. Characteristics and outcomes in
adult patients receiving mechanical ventilation: a 28-day international study. Jama 2002; 287:345-
55.
3. Torres A., Aznar R., Gatell J. M., Jimenez P., Gonzalez J., Ferrer A., Celis R., and
Rodriguez-Roisin R. Incidence, risk, and prognosis factors of nosocomial pneumonia in
mechanically ventilated patients. Am Rev Respir Dis 1990; 142:523-8.
4. Fagon J. Y., Chastre J., Domart Y., Trouillet J. L., Pierre J., Darne C., and Gibert C.
Nosocomial pneumonia in patients receiving continuous mechanical ventilation. Prospective
analysis of 52 episodes with use of a protected specimen brush and quantitative culture techniques.
Am Rev Respir Dis 1989; 139:877-84.
5. Epstein S. K., and Ciubotaru R. L. Independent effects of etiology of failure and time to
reintubation on outcome for patients failing extubation. Am J Respir Crit Care Med 1998;
158:489-93.
6. Ely E. W., Baker A. M., Dunagan D. P., Burke H. L., Smith A. C., Kelly P. T., Johnson M.
M., Browder R. W., Bowton D. L., and Haponik E. F. Effect on the duration of mechanical
ventilation of identifying patients capable of breathing spontaneously. N Engl J Med 1996;
335:1864-9.

20
7. Coplin W. M., Pierson D. J., Cooley K. D., Newell D. W., and Rubenfeld G. D.
Implications of extubation delay in brain-injured patients meeting standard weaning criteria. Am J
Respir Crit Care Med 2000; 161:1530-6.
8. Stroetz R. W., and Hubmayr R. D. Tidal volume maintenance during weaning with pressure
support. Am J Respir Crit Care Med 1995; 152:1034-40.
9. Kollef M. H., Shapiro S. D., Silver P., St John R. E., Prentice D., Sauer S., Ahrens T. S.,
Shannon W., and Baker-Clinkscale D. A randomized, controlled trial of protocol-directed versus
physician-directed weaning from mechanical ventilation. Crit Care Med 1997; 25:567-74.
10. Dojat M., Brochard L., Lemaire F., and Harf A. A knowledge-based system for assisted
ventilation of patients in intensive care units. Int J Clin Monit Comput 1992; 9:239-50.
11. Dojat M., Harf A., Touchard D., Laforest M., Lemaire F., and Brochard L. Evaluation of a
knowledge-based system providing ventilatory management and decision for extubation. Am J
Respir Crit Care Med 1996; 153:997-1004.
12. Dojat M., Pachet F., Guessoum Z., Touchard D., Harf A., and Brochard L. NeoGanesh: a
working system for the automated control of assisted ventilation in ICUs. Artif Intell Med 1997;
11:97-117.
13. Dojat M., Harf A., Touchard D., Lemaire F., and Brochard L. Clinical evaluation of a
computer-controlled pressure support mode. Am J Respir Crit Care Med 2000; 161:1161-6.
14. Dojat M., and Brochard L. Knowledge-based systems for automatic ventilatory
management. Respir Care Clin N Am 2001; 7:379-96, viii.
15. Bouadma L., Lellouche F., Cabello B., Taille S., Mancebo J., Dojat M., and Brochard L.
Computer-driven management of prolonged mechanical ventilation and weaning: a pilot study.
Intensive Care Med 2005; 31:1446-50.

21
16. Vitacca M., Clini E., Porta R., and Ambrosino N. Preliminary results on nursing workload
in a dedicated weaning center. Intensive Care Med 2000; 26:796-9.
17. Ely E. W., Bennett P. A., Bowton D. L., Murphy S. M., Florance A. M., and Haponik E. F.
Large scale implementation of a respiratory therapist-driven protocol for ventilator weaning. Am J
Respir Crit Care Med 1999; 159:439-46.
18. Lellouche F., Mancebo J., Roesler J., Jolliet P., Schortgen F., Cabello M., Bouadma L.,
Rodriguez P., Maggiore S., Qader S., Taille S., and Brochard L. Computer-driven ventilation
reduces duration of weaning: a multicenter randomized controlled study. Intensive Care Medecine
2004; 30:S1-S234.
19. MacIntyre N. R., Cook D. J., Ely E. W., Jr., Epstein S. K., Fink J. B., Heffner J. E., Hess
D., Hubmayer R. D., and Scheinhorn D. J. Evidence-based guidelines for weaning and
discontinuing ventilatory support: a collective task force facilitated by the American College of
Chest Physicians; the American Association for Respiratory Care; and the American College of
Critical Care Medicine. Chest 2001; 120:375S-95S.
20. Krishnan J. A., Moore D., Robeson C., Rand C. S., and Fessler H. E. A Prospective,
Controlled Trial of a Protocol-based Strategy to Discontinue Mechanical Ventilation. Am J Respir
Crit Care Med 2004; 169:673-678.
21. Namen A. M., Ely E. W., Tatter S. B., Case L. D., Lucia M. A., Smith A., Landry S.,
Wilson J. A., Glazier S. S., Branch C. L., Kelly D. L., Bowton D. L., and Haponik E. F. Predictors
of successful extubation in neurosurgical patients. Am J Respir Crit Care Med 2001; 163:658-64.
22. Randolph A. G., Wypij D., Venkataraman S. T., Hanson J. H., Gedeit R. G., Meert K. L.,
Luckett P. M., Forbes P., Lilley M., Thompson J., Cheifetz I. M., Hibberd P., Wetzel R., Cox P.
N., and Arnold J. H. Effect of mechanical ventilator weaning protocols on respiratory outcomes in
infants and children: a randomized controlled trial. Jama 2002; 288:2561-8.

22
23. Brochard L., Rauss A., Benito S., Conti G., Mancebo J., Rekik N., Gasparetto A., and
Lemaire F. Comparison of three methods of gradual withdrawal from ventilatory support during
weaning from mechanical ventilation. Am J Respir Crit Care Med 1994; 150:896-903.
24. Esteban A., Frutos F., Tobin M. J., Alia I., Solsona J. F., Valverdu I., Fernandez R., de la
Cal M. A., Benito S., Tomas R., and et al. A comparison of four methods of weaning patients from
mechanical ventilation. Spanish Lung Failure Collaborative Group. N Engl J Med 1995; 332:345-
50.
25. Torres A., Gatell J. M., Aznar E., el-Ebiary M., Puig de la Bellacasa J., Gonzalez J., Ferrer
M., and Rodriguez-Roisin R. Re-intubation increases the risk of nosocomial pneumonia in patients
needing mechanical ventilation. Am J Respir Crit Care Med 1995; 152:137-41.
26. Epstein S. K., Ciubotaru R. L., and Wong J. B. Effect of failed extubation on the outcome
of mechanical ventilation. Chest 1997; 112:186-92.
27. Keenan S. P., Powers C., McCormack D. G., and Block G. Noninvasive Positive-Pressure
Ventilation for Postextubation Respiratory Distress. JAMA 2002; 287:3238-3244.
28. Esteban A., Frutos-Vivar F., Ferguson N. D., Arabi Y., Apezteguia C., Gonzalez M.,
Epstein S. K., Hill N. S., Nava S., Soares M. A., D'Empaire G., Alia I., and Anzueto A.
Noninvasive positive-pressure ventilation for respiratory failure after extubation. N Engl J Med
2004; 350:2452-60.
29. Laghi F., Cattapan S. E., Jubran A., Parthasarathy S., Warshawsky P., Choi Y. S., and
Tobin M. J. Is weaning failure caused by low-frequency fatigue of the diaphragm? Am J Respir
Crit Care Med 2003; 167:120-7.
30. Silverman H. J., and Miller F. G. Control group selection in critical care randomized
controlled trials evaluating interventional strategies: An ethical assessment. Crit Care Med 2004;
32:852-7.

23
31. Tobin M. Of Principles of Protocols and Weaning. Am J Respir Crit Care Med 2004;
169:661-662.
32. Iregui M., Ward S., Clinikscale D., Clayton D., and Kollef M. H. Use of a handheld
computer by respiratory care practitioners to improve the efficiency of weaning patients from
mechanical ventilation. Crit Care Med 2002; 30:2038-43.
33. Milic-Emili J. Is weaning an art or a science? Am Rev Respir Dis 1986; 134:1107-1108.
34. Higgins T. L., Yared J. P., Estafanous F. G., Coyle J. P., Ko H. K., and Goodale D. B.
Propofol versus midazolam for intensive care unit sedation after coronary artery bypass grafting.
Crit Care Med 1994; 22:1415-23.
35. Jacobi J., Fraser G. L., Coursin D. B., Riker R. R., Fontaine D., Wittbrodt E. T., Chalfin D.
B., Masica M. F., Bjerke H. S., Coplin W. M., Crippen D. W., Fuchs B. D., Kelleher R. M., Marik
P. E., Nasraway S. A., Jr., Murray M. J., Peruzzi W. T., and Lumb P. D. Clinical practice
guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med
2002; 30:119-41.

24
FIGURE LEGENDS
Figure 1: Flow chart of the study. This chart shows the results of daily screening for study
inclusion in the five participating centers during the study period. Mean duration of center
participation was 171 days (range, 79 to 284 days).
PS denotes pressure support and CDW computer-driven weaning.
Figure 2: Kaplan-Meier analysis of weaning time until successful extubation or death after
inclusion for all included patients, in each study group.
CDW denotes computer-driven weaning.

25
Tables
CDW denotes computer-driven weaning, SAPS II simplified acute physiologic score II, LODS
logistic organ dysfunction score, COPD chronic obstructive pulmonary disease, PS pressure
support, and PEEP positive end expiratory pressure. Values are expressed as medians (interquartile
range), or numbers (percentage). †The duration of invasive mechanical ventilation before inclusion is the time on endotracheal
mechanical ventilation prior to study inclusion.
PValue
Age - yr 0.76Sex Male/Female (no.) 0.99
SAPS II at amission 0.89LODS at admission 0.65LODS at inclusion 0.65
Mc Cabe no. (%) 1 2 0.97 3
Admission type no. (%) Medical Elective surgery Emergent surgery
Comorbidities no. (%) COPD 0.68 Restrictive respiratory insufficiency 0.71 Asthma 0.99 Ischemic heart disease 0.21 Hypertensive heart disease 0.76 Valvular heart disease 0.56 Peripheral neurological disorder 0.20 Central neurological disorder 0.56 Psychiatric disorder 0.40 Immunosuppression 0.79 At least one comorbidities 0.48
Pressure support test at inclusion Level of PS (cmH 2 O) 0.14 Level of PEEP (cmH 2 O) 0.52 Level of FiO 2 (%) 0.95
Duration of invasive mechanical ventilation before inclusion (Days) † 0.08
35 (30-40) 35 (30-40)
3.50 (2-6) 4 (3-7)
18 (15-20) 16 (15-20) 5 (5-6) 5 (5-6)
51 (69) 43 (63)
9 (12) 5 (7)8 (11) 9 (13)
1 (1) 4 (6)8 (11) 5 (7)
5 (7) 6 (9)5 (7) 7 (10)
2 (3) 1 (1)12 (16) 6 (9)
16 (22) 13 (19) 3 (4) 4 (6)
0.9311 (15) 10 (14) 12 (16) 13 (19)
5 (7) 5 (7)
51 (68) 47 (67)
38 (51) 37 (53) 31 (42) 28 (40)
7 (5-9) 7 (5 -10) 5 (3-7) 5 (3-7)
47/27 45/25
49 (39 - 57) 47.50 (38 - 50)
60 (51-74) 62 ( 52 - 72)
TABLE 1.
VARIABLE group (N = 74)
Usual weaning group
(N = 70)
CDW
BASELINE CHARACTERISTICS OF THE STUDY PATIENTS

26
CDW denotes computer-driven weaning. †The time to first extubation is the time from study
inclusion (first positive pressure-support test) to first extubation. *The time to successful
extubation is the time from study inclusion (first positive pressure-support test) to last successful
extubation. Total duration of mechanical ventilation is the time from intubation to first or last
successful extubation. Data are expressed as medians (25th-75th interquartile range).
OUTCOME median no. of days (interquartile range)
PValue
Time to first extubation † 0.02Duration of mechanical ventilation until first extubation † 0.03
Time to successful extubation * 0.01Total duration of mechanical ventilation * 0.003
Intensive care length of stay 0.02Hospital length of stay 0.22
TABLE 2. COMPARISON OF THE OUTCOMES IN THE TWO GROUPS
group (N = 74)
Usual weaning group
(N = 70)
2.00 (1.75-6.25) 4.00 (2.00-8.25)
6.50 (3.00-12.25) 9.00 (5.75-16.00)
3.00 (2.00-8.00) 5.00 (2.00-12.00)
30.00 (17.00-54.75) 35.00 (21.00-60.25)
7.50 (4.00-16.00) 12.00 (7.00-26.00)
12.00 (6.00-22.00) 15.50 (9.00-33.00)
CDW

27
CDW denotes computer-driven weaning. Figures denote number of patients (percentage).
COMPLICATION PValue
Reintubation within 72 h 0.40Any reintubation 0.20Need for non invasive ventilation 0.02Self-extubation 0.99Tracheostomy 0.83Mechanical ventilation duration > 14 d 0.11Mechanical ventilation duration > 21 d 0.11
TABLE 3. COMPLICATIONS OF MECHANICAL VENTILATION
CDWgroup (N = 74)
Usual weaning group (N = 70)
no. of patients (%)12 (16) 16 (23) 17 (23) 23 (33) 14 (19) 26 (37) 8 (11) 7 (10)
5 (7) 11 (16)
12 (16) 13 (19) 12 (16) 20 (29)

28
Table 4.
Usual weaning group
(N = 70)
Pvalue
Sedative agentsCumulative daily dosage (midazolam-equivalent, mg)Before inclusion 46 (28-81) 0.74After inclusion 0.7 (0-16) 0.14
OpioidsCumulative daily dosage (fentanyl-equivalent, µg)Before inclusion 170 (0-1312) 0.51After inclusion 0 (0-100) 0.08
Neuromuscular blockers% of days with NMBs before inclusion 0 (0-0) 0.10% of days with NMBs after inclusion 0 (0-0) 0.25
Corticosteroids% of days with corticosteroids before inclusion 0 (0-62) 0.49% of days with corticosteroids after inclusion 0 (0-34) 0.36
0 (0-33)0 (0-0)
0 (0-0)0 (0-0)
TABLE 4. USE OF OPIOIDS, SEDATIVES, NEUROMUSCULAR BLOCKERS, AND CORTICOSTEROIDS*
49 (25-81)0 (0-8)
CDW group
(N = 74)
100 (0-795)0 (0-50)
Opioids, sedatives, neuromuscular blocking agents (NMB), and corticosteroids used in each
group. This table shows the cumulative daily dosages of sedatives per patient (in mg midazolam
equivalent) (34) and opioids (in µg fentanyl equivalent) (35) and the percentage of days under
neuromuscular blockers and corticosteroids. These data are given for the periods of ventilation
before and after study inclusion. Data are expressed as medians (25th-75th interquartile range).*
CDW denotes computer-driven weaning, NMB neuromuscular blockers

29
Figure 1:
Patients on mechanical ventilation(n=1014)
CDW group(n=74)
Usual weaning group
(n=70)
Included patients (n=147)
Mechanical ventilation duration < 24H (n=304)
Presence of non inclusion criteria (n=283)
Death during mechanical ventilation before evaluation
(n=48)
no CDW ventilator available (n=6)
Weaning before evaluation (n=169)
Miscellanous (self extubation , other protocol, absence of consent)
(n=56)
• 2 patients excluded because extubation occurred before electronic assignment
• 1 patient excluded after retraction of consent
Randomization
Analysis (n=144)
Non Included patients (n=866)
Inclusion criteria present, PS test positive

30
Figure 2:
140120100806040200
Days of mechanical ventilation until outcome
1,0
0,8
0,6
0,4
0,2
0,0
Prob
abili
ty o
f rem
aini
ng o
n m
echa
nica
l ven
tilat
ion
Log-rank test p=0.015
Usual Weaning
CDW
Usual WeaningCDW
70
74
23
13
9
4
2
1
Days of mechanical ventilation
Prob
ablil
ty o
f rem
aini
ng o
n m
echa
nica
l ven
tilat
ion
0,0
0,2
0,6
0,4
0,8
1,0
0 20 40 60 80 100 120 1401
1
1
p=0.015

31
ON-LINE DATA SUPPLEMENT
A multicenter randomized trial of computer-driven protocolized weaning from mechanical
ventilation
François Lellouche, Jordi Mancebo, Philippe Jolliet, Jean Roeseler, Frédérique Schortgen, Michel
Dojat, Belen Cabello, Lila Bouadma, Pablo Rodriguez, Salvatore Maggiore, Marc Reynaert, Stefan
Mersmann, Laurent Brochard
Contents:
Complete Methods
Supplementary results
Information on the computer-driven ventilation
References
Figure legend
Tables
Figure
Appendix: Weaning guidelines (control group)

32
Complete Methods
Protocol
Patients
This study was conducted in five university medico-surgical intensive care units: Créteil (France),
Barcelona (Spain), Geneva (Switzerland), Brussels (Belgium), and Paris (France). Two ventilators
equipped with the computer-driven weaning system (Evita Weaning system, Dräger Evita 4,
Lübeck, Germany) were available at each center. These ventilators were well known to the nurses
and healthcare workers. Each center could include 40 patients at the most, to homogenize the
distribution of inclusions. Each center obtained approval of the study from the ethics committee.
Signed informed consent was obtained from each patient or next of kin.
Patients on mechanical ventilation for at least 24 hours and ventilated with an assisted mode
(assist-control, intermittent mandatory ventilation with pressure support, or pressure-support
ventilation) were considered for enrolment in the study. Enrolment criteria required age younger
than 18 or older than 85 years, and absence of the following: do-not-resuscitate order, expected
poor short-term prognosis, tracheostomy, and cardiac arrest with a poor neurological prognosis,
and pregnancy. Patients could be enrolled at an early stage, before usual criteria for weaning
readiness were present, when they reached the following criteria: plateau pressure below 30 cm of
water with a tidal volume of 8 ml per kilogram of body weight on assist-control ventilation,
positive end-expiratory pressure level lower than or equal to 8 cm of water, a ratio of partial
pressure of arterial oxygen over the fraction of inspired oxygen of 150 or higher or arterial oxygen
saturation higher than 90 percent with a fraction of inspired oxygen lower than or equal to 50
percent, epinephrine or norepinephrine requirement no greater than 1 mg per hour, body

33
temperature above 36 °C and below 39 °C, and stable neurological status with a Glasgow Coma
Scale above 4 with little or no sedation.
Study protocol
Data on all ventilated patients in the study centers were recorded daily. As shown in figure E1, as
soon as the inclusion criteria were met and after informed consent was obtained, a pre-inclusion
test with a level of pressure support of 15 cm of water or higher, but an inspiratory pressure no
greater than 30 cm of water (pressure-support level plus positive end-expiratory pressure) was
performed to evaluate patient tolerance of this ventilation mode; the test was repeated daily until
positive. The test could be stopped before 30 minutes if the patient showed evidence of
hemodynamic or respiratory distress (heart rate increase by more than 30 beats per minute as
compared to baseline, systolic arterial pressure lower than 80 mm Hg or higher than 160 mm Hg,
or respiratory rate higher than 40 breaths per minute). The test was considered positive when, after
30 minutes, the patient remained clinically stable with a respiratory rate lower than 35 breaths per
minute and an expiratory tidal volume of at least 6 ml per kilogram of body weight within the
authorized pressure-support range, and with an arterial oxygen saturation no lower than 90 percent
when the fraction of inspired oxygen was no greater than 50 percent.
When the pressure-support test was positive, the patient was assigned at random either to the
computer-driven weaning group or to the control group. Patients assigned to the computer-driven
weaning were connected to an Evita 4 equipped with the system. In the usual care arm, ventilation
and weaning was conducted according to the usual practice introduced several years ago in each
unit. Written guidelines were available in four of the five units, and educational sessions were
performed on a regular basis.

34
In the control group, the patients were returned to the ventilation mode used before randomization.
Every effort was made to minimize potential study-induced changes in usual ventilation and
weaning procedures in the control arm. We choose not to assess the protocol compliance in order
not to influence practice.
A random allocation sequence was generated by a computer by blocks of six. Randomization was
concealed and generated by an electronic-mail system. Randomization was also stratified by
center, and also on presence of a central neurological disorder, a chronic obstructive pulmonary
disease, or absence of both factors. When both factors were present, the neurological disorder was
given priority. This stratification was designed to ensure even distribution of patients with these
three factors between the two treatment groups. The randomization process was centralized.
For subsequent changes in ventilation mode, the same criteria were used in the two groups. Thus,
controlled or assist-control ventilation could be used when a procedure requiring sedation was
performed (surgery or invasive diagnostic or therapeutic procedure) or when the clinical status
deteriorated, with a respiratory rate higher than 40 breaths per minutes, clinical discomfort, and
hypoxemia (need for a fraction of inspired oxygen higher than 60 percent and need for positive
end-expiratory pressure higher than 8 cm of water to obtain an arterial oxygen saturation higher
than 90 percent). In both groups, patients who were switched to controlled ventilation were
evaluated daily with pressure-support tests. When the pressure support test became positive again,
the patient was again ventilated with mode assigned by the randomization process throughout the
rest of the time on ventilation.

35
In the control arm, the following weaning principles were used in the participating centers (see
specific guidelines used by each center)
- At least daily screening for criteria to perform a SBT (at least twice daily in two centers)
- SBT performed with T-piece or minimal PS support (between 7 and 12 cmH2O, the latter if HME
was used), with criteria of success or failure. The duration of SBT was 30 to 120 minutes
- Standardized extubation criteria were used in all study patients: after succeeding a spontaneous
breathing trial, the following criteria had to be present in both groups:
1. Ratio of partial pressure of arterial oxygen over fraction of inspired oxygen higher than 200 mm
Hg
2. Positive end-expiratory no greater than 5 cm of water
3. In patients with abundant airway secretions, efficient cough as assessed with specific scores
recommended
4. Epinephrine or norepinephrine infusion rate no greater than 0.5 mg per hour
5. Glasgow Coma Scale score greater than 8
6. Little or no sedation
Clinical criteria required for extubation (in all centers)
The following recommendations about clinical criteria for extubation were used by all study
centers:
1-Respiratory requirements
- PaO2/FiO2 >200 and with PEEP < 5cmH2O
- In the computer-driven weaning group: extubation when recommended by the
computer-driven system.
- In the control group: extubation when a spontaneous breathing test is successful.

36
In both groups, in case of abundant secretions, preserved coughing that is clearly audible
(spontaneously or during suctioning) is required (E1, E2).
2-Hemodynamic requirements:
- In both groups, hemodynamic stability with epinephrine and norepinephrine
requirements no greater than 0.5 mg/h
3-Neurological requirements:
- in both groups, the Glasgow Coma Scale must be > 8
- sedation must be stopped or minimal; analgesics can be maintained as needed to keep
the patient comfortable
4-Other
No procedure necessitating sedation (transesophageal echocardiography, gastrointestinal
endoscopy) or surgery is planned.
Dialysis, body temperature between 36 °C and 39 °C, and anemia in the absence of active
bleeding do not contraindicate extubation.
In case of respiratory failure after extubation, noninvasive ventilation could be used if deemed
appropriate by the physician. In patients who required reintubation, the usual weaning protocol
was used subsequently.
In the control group, ventilatory settings were chosen by the physician in charge of the patient, and
no recommendations were made regarding the type of ventilator nor the ventilatory mode except
that closed-loop modalities were not allowed. Tracheostomy was possible when required but in
both groups was to be performed no sooner than 10 days after admission to the intensive care unit.

37
In both groups, sedation was at the discretion of the physician. No changes in usual sedation
procedures were introduced during this study.
Follow-up
The patients were followed until discharged home from the hospital. Patient characteristics
recorded for the study included the Simplified Acute Physiologic Score II (E3), the Logistic Organ
Dysfunction score (E4), and the McCabe score (E5). At inclusion, the following data were
recorded: ventilatory parameters and arterial blood gases, duration of invasive mechanical
ventilation before inclusion, presence of comorbidities, hemodynamic parameters, body
temperature. The following were recorded every day: ventilatory mode; maximal and minimal
level of pressure support, positive end-expiratory pressure, and oxygen fraction; date of extubation;
and intensive care unit complications including infections and pneumonia, thromboembolic
disease, gastro-intestinal tract diseases, ischemic heart disease, and weaning complications (failure
being defined as reintubation within 72 hours, self-extubation, and laryngeal dyspnea with stridor).
Use of noninvasive ventilation after extubation and tracheostomy were also noted.
Amounts of sedative agents, neuromuscular blockers, and corticosteroids used in each patient were
recorded before and after inclusion until the first extubation. Drugs used for sedation and analgesia
were midazolam, fentanyl, propofol, and morphine. The daily dosage of each drug was collected
from the intubation day to the day of first extubation, and the mean daily dosages of each drug in
each patient before and after inclusion were calculated. For the statistical analysis we converted
mean propofol and morphine daily dosages to midazolam and fentanyl equivalents. We considered
that 1 mg of midazolam was equivalent to 42 mg of propofol (according to Higgings et al. who
achieved similar degrees of sedation with 0.3±0.002 µg/kg/min of midazolam and 12.6±1.45

38
µg/kg/min in patients recovering from scheduled cardiac surgery (E6)). For opioids, 20 µg of
fentanyl was considered equivalent to 1 mg of morphine (E7).
All interruptions of the computer-driven weaning system were recorded, as well as technical
problems.
End-points
The primary end-points were the time to successful extubation, defined as the time from inclusion
until successful extubation (followed by 72 hours without ventilator support) and the total duration
of mechanical ventilation.
In patients with tracheostomy, the first day of full separation from the ventilator followed by 72
hours of spontaneous unassisted breathing was taken as the day of successful separation (i.e., the
time of decannulation was not considered).
Secondary end-points were the time to first extubation, the total duration of ventilatory support,
length of intensive care unit and hospital length of stay, number of intensive care unit
complications, number of nosocomial pneumonia episodes, complications of extubation, intensive
care unit mortality, and hospital mortality.
Principles of the computer-driven ventilation
The working principles of the computer-driven ventilation have been explained elsewhere (E8-
E12). In brief, a knowledge-based system is embedded into a ventilator set on pressure-support
ventilation and adapts the level of pressure support based on a continuous evaluation of the
patient’s respiratory needs, in order to keep the patient within a so-called “comfort zone”. Comfort
was defined primarily as a respiratory rate between 15 and 30 breaths per minute (up to 34 in
patients with neurological disease), a tidal volume above a minimum threshold (250 ml if weight is

39
less than 55 kilograms and 300 ml otherwise), and end-tidal CO2 level below a maximum threshold
(55 mm Hg, and 65 mm Hg in patients with chronic obstructive pulmonary disease). To reach
these targets, the level of inspiratory assistance in pressure-support ventilation is intermittently
adapted by the system (E8, E11) by steps of 2 to 4 cm of water, taking into account the previous
breathing-pattern history since the patient was connected to the system. In addition, the system
automatically tries to reduce the pressure support down to a minimal level. At this point, tolerance
to spontaneous breathing with a low pressure support level is assessed. If the patient successfully
passes this test, a message recommending separation from the ventilator is displayed on the screen.
Several complementary rules allow the system to manage transient instabilities, suctioning, or
hazardous situations.
The fraction of inspired oxygen and the level of positive end-expiratory pressure are not managed
by the system. The physician in charge of the patient had to set these parameters and could also
modify the level of pressure support at any time by changing the ventilator settings.
Statistical analysis
To calculate the number of patients to be included, we reviewed previous studies looking at
weaning from mechanical ventilation. The median duration of weaning varied across studies from
3.5 to 3.9 days (E13), 3 to 4 days (E14), and 5.7, 3.7 to 9.3 days (E15). The present study aimed at
enrolling patients at an early stage, before they met usual criteria for weaning initiation, and at
excluding patients who needed ventilation for less than 24 hours. Therefore, the duration of the so-
called “weaning time” was expected to range from 5 to 8 days. To show a reduction in the weaning
time by two days (from 7 to 5 days, 30 percent) with an expected standard deviation of 5 days, a
power of 0.80, and an α risk of 0.05, 75 patients were needed in each arm. No interim analysis was
planned.

40
The analysis was performed in the two groups as treated. Results are given as medians
(25th-75th interquartile ranges). Proportions and rates were compared using the chi-square test or
the Fisher exact test when required. The Mann-Whitney U test was used to analyze mechanical
ventilation durations or length of stay. The cumulative probability of remaining on mechanical
ventilation was analysed by the Kaplan-Meier method and a log-rank test was used to assess
differences between groups. For this purpose, we considered that patients were successfully
extubated if they were able to remain on spontaneous breathing for at least 72 hours without being
reintubated. P values smaller than 0.05 were considered significant. All the P values were two-
sided. Statistical analysis was performed with SPSS software, version 9.0.0.

41
Supplementary results
Results of the main end point expressed as mean ± SD (Computer-driven weaning vs Usual
weaning):
Weaning time: 4.4 ± 4.7 vs 8.3 ± 15.4 days
Duration of mechanical ventilation: 8.7 ± 7.6 vs 14.0 ± 18.9 days
ICU length of stay: 17.5 ± 18.6 vs 24.3 ± 21.2 days
Results concerning the compliance to the weaning guidelines in the control group:
The compliance to weaning guidelines can be estimated indirectly from:
- The high compliance to the modes of ventilation recommended during weaning (Table E2)
- We also tried to estimate the proportion of SBTs conducted divided by SBT Eligible Days
as follows:
Performed SBT: 121 episodes of SBTs performed on T-piece were performed in the control group;
unfortunately this does not include other SBT techniques (PSV+/-CPAP.....)
SBT eligible days: We hypothesized that an indication to perform SBT existed in patients
ventilated with a “weaning” mode (PSV or SIMV), apart from day 1 (where patients were
supposed to be included at an early stage) and except when FiO2 was at or above 50%.
In the control group, weaning modes (PSV and SIMV) were used during 414 days (392+22).
Subtracting day 1 and days at or above 50% or FiO2, we could estimate that T-piece trials were
performed 51% of the days of ventilation with PSV or SIMV at FiO2 below 50%.This could
indicate that weaning was suboptimal if one assumes that other screening criteria were present.
However, because only the SBTs performed with T-piece were recorded, this ratio may be
underestimated.
42
Results concerning tracheostomy:
Tracheostomy was delayed in both groups as recommended by protocol: the median time of
tracheostomy (intubation to tracheostomy) was 16 (25-75 percentiles: 10-21) in the automatic
weaning group and 23 (25-75 percentiles: 18-43) in the control group.

43
Information on the computer-driven ventilation
The computer-driven ventilation (E8-E12, E16-E19)
This is a closed-loop knowledge-based system used for ventilator management in the
intensive care unit and specifically designed to improve the weaning process. It is dedicated at
managing pressure-support ventilation (PSV), with or without positive end-expiratory pressure
(PEEP). The knowledge corpus used to develop this computer-driven ventilation came mainly
from the scientific literature and from a group of intensivists, physiologists, and scientists at the
Henri Mondor Teaching Hospital (Créteil, France) (E8-E11). In the present study, the system was
used to drive an Evita 4 ventilator (Dräger, Lübeck, Germany).
The knowledge-based system interprets clinical data in real-time and controls the
mechanical assistance provided to the patient with a 24-hour per day management,. The system
develops a therapeutic strategy that gradually reduces the level of assistance, at a pace depending
on the patient’s tolerance, and evaluates the patient’s ability to breathe without mechanical
assistance.
The system uses three main parameters acquired from the ventilator: respiratory rate (RR),
which is the main driver of the ventilation, tidal volume (Vt), and end-tidal partial pressure of CO2
(PETCO2). It controls the level of pressure above PEEP during ventilation in PSV mode. The
knowledge-based system has two main functions: 1) automatic adaptation of the assistance and 2)
development and application of a weaning strategy. The system implemented on a commercial
ventilator works through the same principles and rules than in the most recent studies (E9-E11).
The new rules introduced in the system are based on recent published data concerning the effect of
humidification devices during assisted mechanical ventilation and the results of a pilot study
(E19):

44
- Rules concerning the lower pressure support level according to the humidification device (20-
24): to compensate for HME dead space the level of pressure support has to be increased in
comparison with heated humidifiers. The estimated increased need varied among the studies from
5 to 10 cmH2O.
- Another rule was introduced following clinical evaluation: the possibility for the system to
decrease the level of minimum pressure support below the predefined value, down to 5 cmH2O. In
some cases (patients with near normal respiratory mechanics), the predefined minimum PS was too
high, leading to overassistance of the patient and a “ventilatory diagnosis” of “hyperventilation”
(respiratory rate below 15/min and ETCO2 below 55 mmHg) which prevented the system from
doing the automatic spontaneous breathing test. Indeed, this test can be performed only if the
patient has a ventilatory diagnosis of “normal ventilation”.
1) Automatic adaptation of assistance
The general strategy used is as follows: 1) The knowledge-based system tries to keep the
patient in a situation of “comfort” defined as follows. The system allows the patient breathing
freely with a respiratory rate between 15 (RRmin) and 30 breaths per minute (34 in case of
neurological disease) (RRmax), a tidal volume above a minimum threshold (VtMin=250 ml if
weight is less than 55 kg and VtMin=300 ml otherwise) and a PETCO2 below a maximum
threshold (max PETCO2=55 mmHg, or max PETCO2=65 mmHg in patients with chronic
obstructive pulmonary disease). When these criteria are met, the knowledge-based system
diagnoses Normal ventilation; 2) To reach the above-defined targets, the level of pressure in PSV
is periodically adapted by the computer-driven ventilation, being increased in case of RR above
RRmax and lowered in case of RR below RRmin and below PETCO2 thresholds.

45
The algorithm is based on a “ventilatory diagnosis” defined from values of respiratory rate, tidal
volume and end-tidal CO2 averaged every 2 to 5 minutes. The pace of display for this ventilatory
diagnosis (2 to 5 minutes), the magnitude of the pressure changes and the duration of the
spontaneous breathing trial depends on previous breathing pattern history since the patient was
connected to the system: contingent on the first level of pressure support used (higher or lower
than 15 cmH2O) at the time of connection, the duration of the spontaneous breathing trials lasts
from 30 minutes to 2 hours. The magnitude of the pressure decrement (2 or 4 cmH2O) is also based
on the previous breathing-pattern history. The required duration of stability before assistance is
decreased depends on the level of pressure delivered to the patient, which reflects disease severity.
The system tolerates transient instabilities.
2) Automatic weaning strategy
In addition to the above-mentioned strategy designed to maintain the patient in a situation
of comfort, the system tries to reduce the pressure level automatically by steps of 2 to 4 cm H2O,
taking into account the breathing pattern history. When a minimal level of PSV is reached, an
observation period is carried out: if tolerance is good, a recommendation for separation from
the ventilator is displayed on the computer screen. This process is equivalent to a “spontaneous
breathing trial” with results given to the clinician.
When the computer-driven ventilation recommends separation (the patient is “ready for
separation”), extubation can be envisaged. If extubation is delayed for any reason, however, there
are several options, the ventilator will continue monitoring and ventilatory adaptation according on
pre-defined rules.
The minimum level of pressure support to be used during the “spontaneous breathing trial”
has been determined from previous physiological studies (E23, E25). Moreover, to compensate for

46
Heat and Moisture Exchanger (HME) dead space the level of pressure support has to be increased
again for 5 to 10 cmH2O in comparison with Heated Humidifier (HH). This was based on recent
studies comparing effects of humidification device use on breathing pattern and work of breathing
(E20-E24).
The minimum levels threshold also depends on the tracheal access (tracheostomy versus oral or
nasal intubation). These conditions must be entered in the system by the clinician before starting a
session. Other pieces of information are necessary to start the session: presence of specific clinical
condition (chronic obstructive pulmonary disease, central neurological disease), weight of the
patient.
The minimal levels used for the test are as follows:
Tracheostomy + HH =5 cmH2O
Tracheostomy + HME =9 cmH2O
Endotracheal intubation + HH =7 cmH2O
Endotracheal intubation + HME =12 cmH2O
To avoid overassistance, the level of pressure support could be decreased down to a minimum of 5
cmH2O in case of hyperventilation with such levels of pressure support.
As soon as the patient reaches the minimum level of pressure support with a “ventilatory
diagnosis” of “normal ventilation”, the “spontaneous breathing trial” begins automatically and is
called by the system “observation period”: its duration varies from 30 minutes to 2 hours according
to previous breathing pattern history. If the patient remains stable (i.e., if the level of pressure
support remains stable at the minimum level, with a “normal ventilation”) during all the
observational period, the following message is displayed on the screen: “the patient does not need
ventilatory support”, and the clinician has to check other weaning and extubation criteria
(haemodynamic, neurology, ability to protect upper airway…).

47
If the patient is not stable, the pressure support increased according to the ventilatory diagnosis
(example: increase of the level of pressure support of 2 cmH2O in case of diagnosis of
“tachypnea”, or of 4 cmH2O in case of “severe tachypnea” with thresholds defining upon patient
category: COPD, neurological disorder or none of these factors). If the pressure support is
increased by the system, the observation period (spontaneous breathing trial) ends. Then, if the
pressure support goes back to the minimal value, an observational period occurs again, till the
patient complete this period with normal ventilation.
The level of PEEP must be lower or equal to 5 cmH2O to start the observational period (the
spontaneous breathing trial). This rule avoids weaning patients needing high levels of PEEP.
3) What is needed before starting?
To ventilate the patient correctly, the computer needs information, which must be entered
by the user before starting ventilation with the computer-driven ventilation.
This information includes body weight, whether the patient has chronic CO2 retention
and/or COPD, the route of tracheal intubation (endotracheal intubation or tracheotomy) and
whether a heat-and-moisture exchanger (“artificial nose”) is used for humidification. The first two
questions are used to set the limits for Vt and PETCO2, whereas the other two serve to determine
the minimal level of pressure used in the final step of the weaning strategy (spontaneous breathing
trial).
4) What can be modified during the ventilation phase?
At any time and for any reason, the user can take control of the ventilator by switching back
to a conventional mode. This erases the ventilation history recorded by the system.
During ventilation with the computer-driven ventilation, all settings are available to the
user (FiO2, trigger, PEEP and alarm limits). All ventilator alarms remain available throughout the

48
period of automatic control. Specific knowledge is introduced to manage alarming situations such
as apnea and disconnection.
Endotracheal suctioning can be performed as often as required without any special
maneuver on the computer. Several rules allow the system to recognize disconnection and
suctioning. This recognition induces several actions.
Last, the clinician can modify the level of pressure support during ventilation by the system
but this resets ventilation with this new level.
Examples of rules used to manage the level of pressure:
When the respiratory rate is above 30 breaths/min (RRMax) (34 in case of neurological
disease) and PETCO2 and tidal volume are acceptable, the knowledge-based system diagnoses
Tachypnea and increases the assistance by 2 cm H2O. When the respiratory rate exceeds 36
breaths/min, the knowledge-based system diagnoses Severe Tachypnea and increases the pressure
support by 4 cm H2O. When the respiratory rate is less than 15 breaths/min (RRMin), with no
increase in PETCO2, Hyperventilation is diagnosed and pressure support is decreased by 4 cm
H2O. When tidal volume or PETCO2 are outside the defined range (Insufficient Ventilation),
pressure support is increased by 2 cm H2O.
Examples of special actions:
Often, suctioning is performed in response to the presence of secretions that may have
increased the pressure needs. If assistance was increased prior to disconnection, the system
recognizing disconnection replaces the low level of assistance immediately after reconnection.

49
REFERENCES
E1. Coplin, W. M., Pierson, D. J., Cooley, K. D., Newell, D. W., and Rubenfeld, G. D.
Implications of extubation delay in brain-injured patients meeting standard weaning criteria. Am J
Respir Crit Care Med 2000 161:1530-6.
E2. Khamiees, M., Raju, P., DeGirolamo, A., Amoateng-Adjepong, Y., and Manthous, C. A.
Predictors of extubation outcome in patients who have successfully completed a spontaneous
breathing trial. Chest 2001 120:1262-70.
E3. Le Gall, J. R., Lemeshow, S., and Saulnier, F. A new Simplified Acute Physiology Score
(SAPS II) based on a European/North American multicenter study. Jama 1993 270:2957-63.
E4. Le Gall, J. R., Klar, J., Lemeshow, S., Saulnier, F., Alberti, C., Artigas, A., and Teres, D.
The Logistic Organ Dysfunction system. A new way to assess organ dysfunction in the intensive
care unit. ICU Scoring Group. Jama 1996 276:802-10.
E5. McCabe, W. R., and Jackson, G. G. Gram-negative bacteriemia: I.Etiology and ecology.
Archives of Internal Medicine 1962 110:847-855.
E6. Higgins, T. L., Yared, J. P., Estafanous, F. G., Coyle, J. P., Ko, H. K., and Goodale, D. B.
Propofol versus midazolam for intensive care unit sedation after coronary artery bypass grafting.
Crit Care Med 1994 22:1415-23.
E7. Jacobi, J., Fraser, G. L., Coursin, D. B., Riker, R. R., Fontaine, D., Wittbrodt, E. T.,
Chalfin, D. B., Masica, M. F., Bjerke, H. S., Coplin, W. M., et al. Clinical practice guidelines for
the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med 2002 30:119-
41.
E8. Dojat, M., Brochard, L., Lemaire, F., and Harf, A. A knowledge-based system for assisted
ventilation of patients in intensive care units. Int J Clin Monit Comput 1992 9:239-50.

50
E9. Dojat, M., Harf, A., Touchard, D., Laforest, M., Lemaire, F., and Brochard, L. Evaluation
of a knowledge-based system providing ventilatory management and decision for extubation. Am J
Respir Crit Care Med 1996 153:997-1004.
E10. Dojat, M., Pachet, F., Guessoum, Z., Touchard, D., Harf, A., and Brochard, L. NeoGanesh:
a working system for the automated control of assisted ventilation in ICUs. Artif Intell Med 1997
11:97-117.
E11. Dojat, M., Harf, A., Touchard, D., Lemaire, F., and Brochard, L. Clinical evaluation of a
computer-controlled pressure support mode. Am J Respir Crit Care Med 2000 161:1161-6.
E12. Dojat, M., and Brochard, L. Knowledge-based systems for automatic ventilatory
management. Respir Care Clin N Am 2001 7:379-96, viii.
E13. Saura, P., Blanch, L., Mestre, J., Valles, J., Artigas, A., and Fernandez, R. Clinical
consequences of the implementation of a weaning protocol. Intensive Care Med 1996 22:1052-6.
E14. Esteban, A., Frutos, F., Tobin, M. J., Alia, I., Solsona, J. F., Valverdu, I., Fernandez, R., de
la Cal, M. A., Benito, S., Tomas, R., et al. A comparison of four methods of weaning patients from
mechanical ventilation. Spanish Lung Failure Collaborative Group. N Engl J Med 1995 332:345-
50.
E15. Brochard, L., Rauss, A., Benito, S., Conti, G., Mancebo, J., Rekik, N., Gasparetto, A., and
Lemaire, F. Comparison of three methods of gradual withdrawal from ventilatory support during
weaning from mechanical ventilation. Am J Respir Crit Care Med 1994 150:896-903.
E16. Dojat, M., and Pachet, F. Effective domain-dependent reuse in medical knowledge bases.
Computer and Biomedical Research 1995 28:403-432.
E17. Dojat, M., and Sayettat, C. A realistic model for temporal reasoning in real-time patient
monitoring. Applied Artificial Intelligence 1996:121-143.

51
E18. Chittaro, L., and Dojat, M. Using a general theory of time and change in patient
monitoring: experiment and evaluation. Comput Biol Med 1997 27:435-452.
E19. Bouadma, L., Lellouche, F., Cabello, B., Porta, V., Deye, N., Levy, S., Mancebo, J., and
Brochard, L. Use of an automated control system to adapt the level of pressure support and manage
weaning. Intensive Care Med 2002 28:S23.
E20. Pelosi, P., Solca, M., Ravagnan, I., Tubiolo, D., Ferrario, L., and Gattinoni, L. Effects of
heat and moisture exchangers on minute ventilation, ventilatory drive, and work of breathing
during pressure-support ventilation in acute respiratory failure. Crit Care Med 1996 24:1184-8.
E21. Iotti, G. A., Olivei, M. C., and Braschi, A. Mechanical effects of heat-moisture exchangers
in ventilated patients. Crit Care 1999 3:R77-82.
E22. Campbell, R. S., Davis, K., Jr., Johannigman, J. A., and Branson, R. D. The effects of
passive humidifier dead space on respiratory variables in paralyzed and spontaneously breathing
patients. Respir Care 2000 45:306-12.
E23. Brochard, L., Rua, F., Lorino, H., Lemaire, F., and Harf, A. Inspiratory pressure support
compensates for the additional work of breathing caused by the endotracheal tube. Anesthesiology
1991 75:739-45.
E24. Girault, C., Breton, L., Richard, J. C., Tamion, F., Vandelet, P., Aboab, J., Leroy, J., and
Bonmarchand, G. Mechanical effects of airway humidification devices in difficult to wean
patients. Crit Care Med 2003 31:1306-11.
E25. Diehl, J. L., El Atrous, S., Touchard, D., Lemaire, F., and Brochard, L. Changes in the
work of breathing induced by tracheotomy in ventilator-dependent patients. Am J Respir Crit Care
Med 1999 159:383-8.
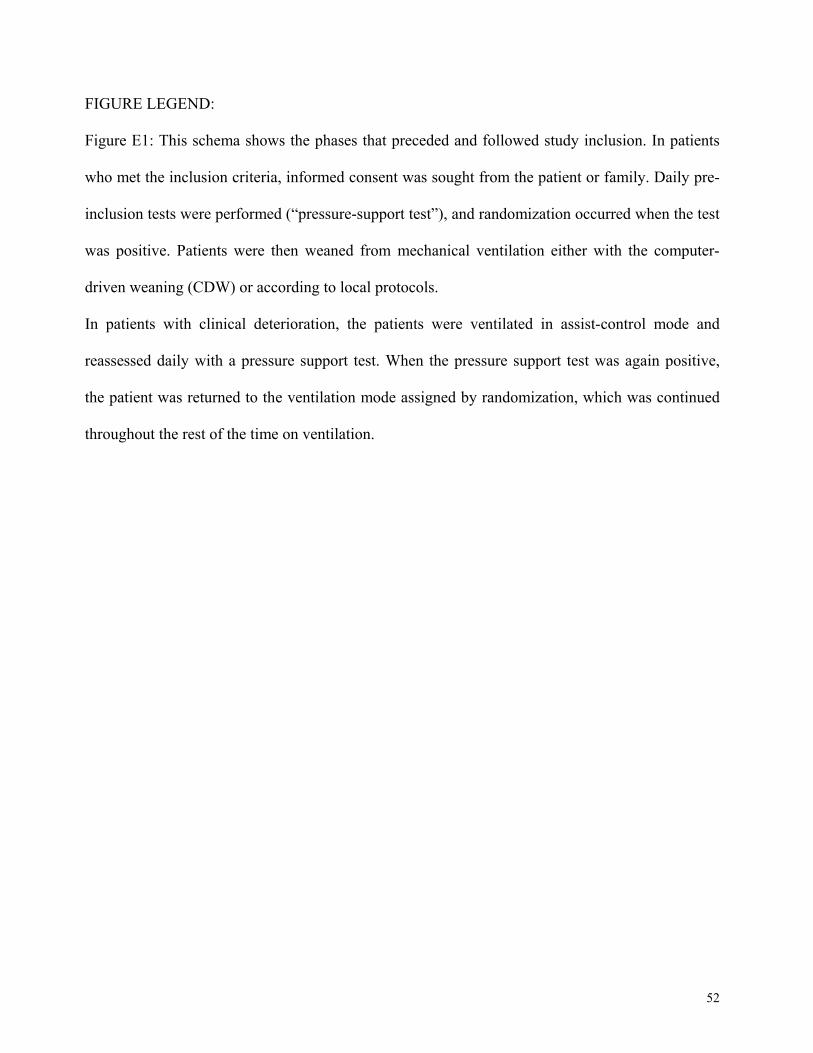
52
FIGURE LEGEND:
Figure E1: This schema shows the phases that preceded and followed study inclusion. In patients
who met the inclusion criteria, informed consent was sought from the patient or family. Daily pre-
inclusion tests were performed (“pressure-support test”), and randomization occurred when the test
was positive. Patients were then weaned from mechanical ventilation either with the computer-
driven weaning (CDW) or according to local protocols.
In patients with clinical deterioration, the patients were ventilated in assist-control mode and
reassessed daily with a pressure support test. When the pressure support test was again positive,
the patient was returned to the ventilation mode assigned by randomization, which was continued
throughout the rest of the time on ventilation.

53
Table E1 Comparisons of outcomes for ICU survivors in the two groups
CDW denotes computer-driven weaning. †The time to first extubation is the time from study
inclusion (first positive pressure-support test) to first extubation. *The time to successful
extubation is the time from study inclusion (first positive pressure-support test) to last successful
extubation. Duration of mechanical ventilation is the time from intubation to first or last successful
extubation (total). Data are expressed as medians (25th-75th interquartile range).
OUTCOME median no. of days
(interquartile ranges) CDW
groupUsual weaning
group P
Value Survived(N=58)
Survived (N=54)
Time to first extubation † 2.00 (1.00-5.00)
3.00 (2.00-8.00) 0.005
First period of mechanical ventilation duration † 5.00 (3.00-10.00)
7.00 (5.00-13.00) 0.01
Time to successful extubation * 2.00
(1.00-6.00) 4.00
(2.00-9.00) 0.009
Duration of mechanical ventilation * 6.00
(3.00-14.00)10.00
(6.00-20.00) 0.006
Table E1 COMPARISON OF OUTCOMES FOR ICU SURVIVORS IN THE TWO GROUPS

54
Table E2. This table shows the modes of ventilation (expressed in days of ventilation and in
percentage of the total days of ventilation after inclusion) used after study inclusion in each study
group. The number of T-piece trials performed in each group is also displayed.
CDW denotes computer-driven weaning, PSV pressure support ventilation, ACV assist controlled
ventilation, SIMV synchronized intermittent mandatory ventilation
VENTILATION MODES USEDAFTER INCLUSION
P Value
Days on PSV (%) 0.001 Days on ACV (%) Days on SIMV (%)
number of T-tube trials
22 (4.0)
Usual weaning group
(N = 70)
12
CDW group
(N = 74)
293 (75.5)64 (16.5)
398 (71.5)134 (24.5)
124
31 (8.0)
TABLE E2 VENTILATION MODES USED.*

55
Table E3 This table shows the average daily doses of sedatives and opioids according to prescription preferences in each centers. Only Brussels used propofol as main sedative, the other centers used midazolam. Creteil, Geneva and Paris used fentanyl as opioid, Barcelona used morphine and Brussels used sufentanyl.
TABLE E3: AVERAGE DAILY DOSE OF SEDATIVES AND OPIOIDS
SEDATIVES CDW group Usual weaning group P value Creteil, Barcelona, Geneva and Paris (n=45) (n=45) Midazolam (mg/day)
Before inclusion After inclusion
Propofol (mg/day) Before inclusion After inclusion
31 (0-61) 0 (0-3)
0 (0-95) 0 (0-2)
34 (5-55) 0 (0-0)
0 (0-341) 0 (0-5)
0.79 0.20
0.77 0.45
Brussels
(n=22)
(n=18)
Midazolam (mg/day) Before inclusion After inclusion
Propofol (mg/day) Before inclusion After inclusion
Drug not used
1804 (1280-2167) 0 (0-65)
Drug not used
1583 (1037-3240) 121 (0-363)
0.90 0.04
OPIOIDS
Barcelona (n=18) (n=14) Morphine (mg/day)
Before inclusion After inclusion
Fentanyl (µg/day) Before inclusion After inclusion
Sufentanyl (µg/day) Before inclusion After inclusion
12 (2-19) 1 (0-6)
Drug not used
Drug not used
6.5 (1-15)
2 (0-5)
Drug not used
Drug not used
0.22 0.59
Creteil, Geneva and Paris
(n=27)
(n=31)
Morphine (mg/day) Before inclusion After inclusion
Fentanyl (µg/day) Before inclusion After inclusion
Sufentanyl (µg/day) Before inclusion After inclusion
Drug not used
530 (0-1080) 0 (0-150)
Drug not used
Drug not used
961 (44-1695) 0 (0-400)
Drug not used
0.20 0.28
Brussels
(n=22)
(n=18)
Morphine (mg/day) Before inclusion
Drug not used
Drug not used

56
After inclusion Fentanyl (µg/day)
Before inclusion After inclusion
Sufentanyl (µg/day) Before inclusion After inclusion
Drug not used
0 (0-0) 0 (0-0)
Drug not used
0 (0-185) 0 (0-0)
0.39 0.74
CDW denotes computer-driven weaning
“Drug not used” means that in the specific center the sedative/analgesic is not used or very
unfrequently used.

57
Figure E1:
= PRE-INCLUSION PHASE
_
+
= INCLUSION PHASE
RANDOMIZATION
+ +
INCLUSION
Wea
ning
Tim
e
+/- NIV
Ventilatory support stopped for 72 h
Clin
ical
wor
seni
ng, s
edat
ion
>24h
→
Ass
ist-
Con
trol
Ven
tilat
ion
Informed consent signed
EXTUBATION (or SB in case of tracheostomy)
CDW Usual Weaning
Daily
Pressure-support test

58
APPENDIX 1
Weaning guidelines (control group)
Usual weaning guidelines used in the participating centers. No change was made for the study.
1) Créteil, Henri Mondor Teaching Hospital
Steps Criteria Action
1) Daily screening test • PEEP ≤5cmH2O, FiO2 ≤
50%
• No vasopressor
• Sepsis under control
• No sedation or Ramsay
score 2-3
• Cough
2) Spontaneous breathing test if
screening criteria met The followings are not contraindication to
the spontaneous breathing :anemia, T°<
39 °C, dobutamine, need for dialysis,
etc.
• PSV 7 (No HME) or 12 cm
H2O (With HME)
• or T-piece
• 30 minutes to 2 hours
(depending on pre-test
probability)
• no PEEP
Daily
To be repeated when
negative:
Extubation if well
tolerated (RR< 35/min,
hemodynamics and SpO2
satisfactory and stable,
consciousness satisfactory,
pH>7.35). ABG when
doubtful
3) Ventilation during the weaning
period
Pressure-support ventilation
RR 25-35/min and comfortable
Never use SIMV
The PSV level is also a “guide” • If ≤15 cm H2O=> SB test
4) Weaning tests:
No routine tests (maximal inspiratory
or expiratory pressure, f/Vt)
If probability uncertain or
patient failed the SB test
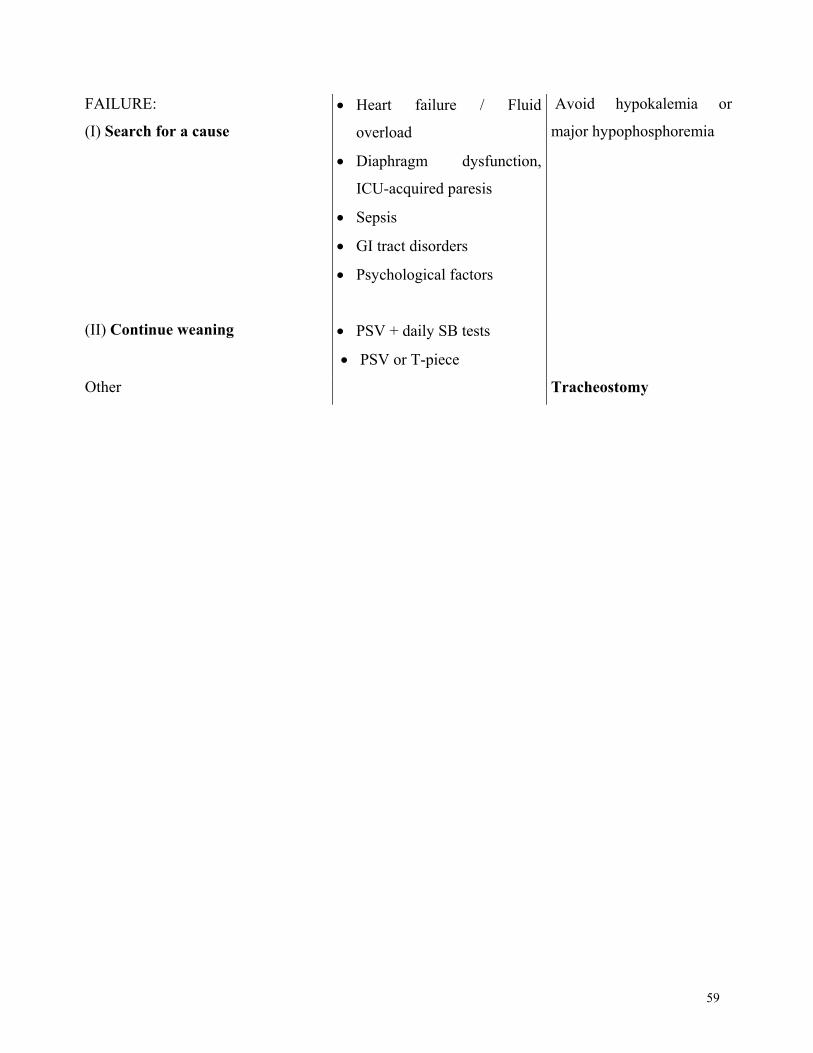
59
FAILURE:
(I) Search for a cause
• Heart failure / Fluid
overload
• Diaphragm dysfunction,
ICU-acquired paresis
• Sepsis
• GI tract disorders
• Psychological factors
Avoid hypokalemia or
major hypophosphoremia
(II) Continue weaning
• PSV + daily SB tests
• PSV or T-piece
Other Tracheostomy

60
2) Geneva:
NO
Mechanical ventilation Question asked at least twice a day:
Weaning possible ?
YES
NO
YES
YES NO
YES
NO
Initiation of weaning • Stop or decrease sedation • Level of Pressure Support: 20 cmH2O
Question asked at least twice a day: Spontaneous breathing test feasible ?
PS level 20 cmH2O above PEEP > 60 minutes?
- Level of consciousness good - Efficient swallowing - Efficient cough
Spontaneous breathing test during 30' First choice: Pressure support 10 cmH2O, ± PEEP 5 cmH2O Other choices: - T-piece trial
- CPAP, flow 30 l/min. PEEP ≤ 5 cmH2O
Extubation criteria present?
Adaptation
of PS
and/or
PEEP level
Spontaneous breathing test feasible if after 60' with PS 20 cmH2O, PEEP ≤ 5 cmH2O (all must be present): - Respiratory rate ≤ 30/' - Tidal volume ≥ 6 ml/kg - No hemodynamic instability - SpO2 ≥ 90% and FIO2 ≤ 0.40 - No other contraindication
Weaning possible if all criteria below present: - Improvement of condition that led to intubation - No uncontrolled severe infection - Metabolic disorders corrected - Hemoglobin level adequate - No hemodynamic instability - PaO2 > 8.5 kPa with FIO2 ≤ 0.40 and PEEP ≤ 5 cmH2O
Extubation possible?
YES NO
EXTUBATION Patient weaned but extubation not possible
Extubation criteria (all must be present) - Respiratory rate ≤ 30/' - Pulse < 120/' - Syst. ABP < 180 and > 90 mmHg - No hemodynamic instability - PaO2 ≥ 8.5 kPa and FIO2 ≤ 0.40 - pH > 7.30

61
3) Sant Pau Hospital Weaning process can begin if:
• The cause of the respiratory failure is partially or completely controlled, including
SpO2 ≥ 90% with FiO2 ≤ 0.5 and PEEP ≤ 5 cm H2O
• Hemodynamic stability (systolic blood pressure between 90 and 160 mm Hg + heart
rate between 60 and 125 beats per minute + absence of uncontrolled arrhythmias)
• Temperature < 39 °C
• Hemoglobin ≥ 8 g/dL
• Absence of significant water or electrolyte abnormalities
• Patients can follow simple orders and there is no need for high-dose sedatives
• For patients with neurological disorders:
Glasgow Coma Scale > 8, intracranial pressure < 20 mm Hg, cerebral perfusion
pressure > 60 mmHg
Patients who meet these criteria undergo a spontaneous breathing test (2 hours on a T-tube or
pressure support ventilation with 7 cm H2O of pressure support and PEEP ≤ 5 cm H2O). The
following indicate an inability to tolerate spontaneous breathing:
• Respiratory rate >35 per minute + clinical manifestations*
• Hypoxemia (PaO2 <60 mmHg under O2 flow ≥4 L/min)
• Acidosis (pH ≤7.3)
* Clinical manifestations: systolic blood pressure ≥ 160 mmHg or ≤ 90 mmHg, heart rate ≥
140 bpm or increase by 25% or more over baseline, new arrhythmia, worse level of
consciousness, sweating, or agitation.
1. Patients are extubated if they successfully complete the 2-hour spontaneous breathing
trial and can cough effectively.
2. For patients who cannot tolerate the spontaneous breathing test, weaning is continued
on pressure-support ventilation. Pressure support is adjusted to achieve a respiratory
frequency of 25-30 per minute and good clinical adaptation. Pressure support is
diminished as soon as possible according to tolerance by the patient. Extubation is
performed when the patient can tolerate low pressure support levels (near 10 cm H2O)

62
with low PEEP levels (≤ 5 cm H2O), provided clinical tolerance and cough are
adequate.
3. Daily spontaneous breathing trials are performed in patients who are not weaned in
pressure support mode (Item 1).
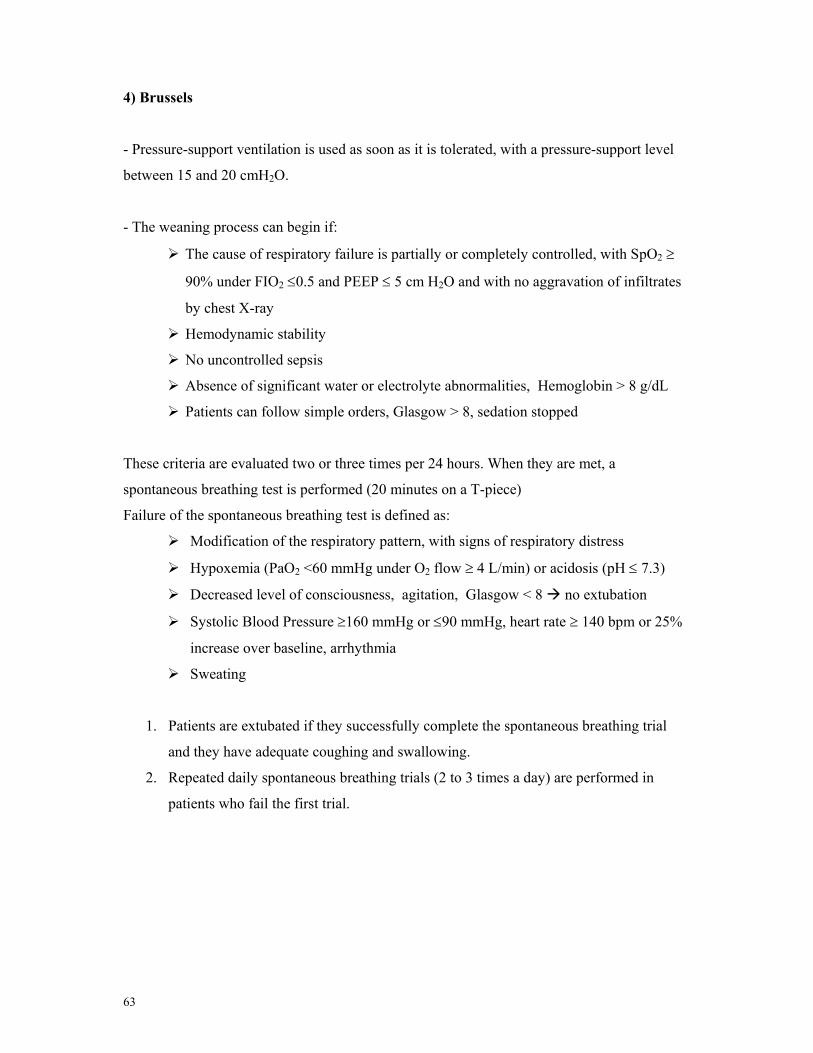
63
4) Brussels
- Pressure-support ventilation is used as soon as it is tolerated, with a pressure-support level
between 15 and 20 cmH2O.
- The weaning process can begin if:
The cause of respiratory failure is partially or completely controlled, with SpO2 ≥
90% under FIO2 ≤0.5 and PEEP ≤ 5 cm H2O and with no aggravation of infiltrates
by chest X-ray
Hemodynamic stability
No uncontrolled sepsis
Absence of significant water or electrolyte abnormalities, Hemoglobin > 8 g/dL
Patients can follow simple orders, Glasgow > 8, sedation stopped
These criteria are evaluated two or three times per 24 hours. When they are met, a
spontaneous breathing test is performed (20 minutes on a T-piece)
Failure of the spontaneous breathing test is defined as:
Modification of the respiratory pattern, with signs of respiratory distress
Hypoxemia (PaO2 <60 mmHg under O2 flow ≥ 4 L/min) or acidosis (pH ≤ 7.3)
Decreased level of consciousness, agitation, Glasgow < 8 no extubation
Systolic Blood Pressure ≥160 mmHg or ≤90 mmHg, heart rate ≥ 140 bpm or 25%
increase over baseline, arrhythmia
Sweating
1. Patients are extubated if they successfully complete the spontaneous breathing trial
and they have adequate coughing and swallowing.
2. Repeated daily spontaneous breathing trials (2 to 3 times a day) are performed in
patients who fail the first trial.





























