Embed Size (px)
Citation preview
A Post Hoc Analysis of the Impact on Hostility and Agitation of Quetiapine and Haloperidol Among Patients with Schizophrenia
K.N. Roy Chengappa, MD, 1,2 Jeffrey M. Goldstein, PhD, 3 Mike Greenwood, BS, 4 Vineeth John, MDJ and Joseph Levine, MD 1,5 J Western Psychiatric Institute and Clinic, University of Pittsburgh School of Medicine, Pittsburgh, 2Special Studies Center at Mayview State Hospital, Bridgeville, Pennsylvania, 3AstraZeneca, Wilmington, Delaware, 4AstraZeneca, Macclesfield, United Kingdom, and 5Ber Sheva Mental Health Center, Ben Gurion University of the Negev, Bet Sheva, Israel
A B S T R A C T
Background: Quetiapine, a drug with a broad pharmacologic profile (similar to that of clozapine), may show benefits for agitation in patients with psychoses. Also, quetiapine may be superior to placebo and either equal or superior to halo- peridol in treating this symptom. Available data for other second-generation anti- psychotic agents show that quetiapine may have better efficacy in improving agi- tation compared with haloperidol.
Objective: This reanalysis of a previously reported pivotal clinical trial assessed whether quetiapine or haloperidol has benefits for the treatment of hostility and agitation among patients experiencing an acute exacerbation of schizophrenia.
Methods: Patients aged 18 to 65 years of either sex and any ethnicity who had a diagnosis of schizophrenia based on the Diagnostic and Statistical Manual of Men- tal Disorders, Revised Third Edition criteria and who were experiencing an acute ex- acerbation were recruited into the study. A priori, data from patients assigned to 4 therapeutically effective quetiapine treatment groups (150, 300, 600, and 750 mg) in a previously reported &week, double-blind, placebo-controlled clinical trial were combined and compared with data from patients given haloperidol 12 mg or placebo on an agitation measure derived from the Brief Psychiatric Rating Scale (BPRS). Patients who received at least 2 weeks of treatment who had a base- line assessment and at least 1 postbaseline assessment after the 2 weeks of treat- ment were included. An analysis of variance with the baseline hostility score and
Accepted for publication November 15, 2002. Printed in the USA. Reproduction in whole or part is not permitted. 0149-2918/03/$ 19.00
5 3 0 Copyright © 2003 Excerpta Medica, Inc.
K.N.R. Chengappa et al.
center as covariates was used to assess treatment effects of quetiapine or haloper- idol versus placebo for changes in agitation scores. A path analysis was used to separate the direct from the indirect effects (via improvements in psychoses and/or overall psychopathology) on agitation scores of quetiapine relative to haloperidol.
Results: A total of 257 patients (193 men, 64 women) were studied. The com- bined quettapine groups comprised 175 patients; the haloperidol group, 42 pa- tients; and the placebo group, 40 patients. Quetiapine treatment reduced agita- tion scores significantly among patients with acute psychoses compared with placebo. A slight reduction in agitation scores was found when haloperidol treat- ment was compared with placebo, but this difference was not statistically signif- icant. Compared with haloperidol, quetiapine treatment had a direct and signifi- cant effect on agitation that was independent of the improvement in psychotic symptoms.
Conclusions: The data in this study suggest that quetiapine treatment has ben- efits for hostility and agitation among patients experiencing an acute exacerbation of schizophrenia. Furthermore, the path analysis indicated that, relative to halo- peridol, quetiapine appeared to have direct effects on agitation that were inde- pendent of improvements in psychoses or overall psychopathology, as assessed by the BPRS. (Clin Ther. 2003;25:530-541) Copyright © 2003 Excerpta Medica, Inc.
Key words: quetiapine, hostility, aggression, agitation, schizophrenia, antipsy- chotic, psychosis.
I N T R O D U C T I O N
Since the introduction of clozapine in 1990, studies have suggested benefits of this agent in the treatment of clinical domains in psychiatric patients beyond the tra- ditional positive and negative symptoms and disorganized features of schizophre- nia. For instance, in several studies, 1-4 clozapine reduced hostile and aggressive behavior in psychiatric patients. Another study 5 suggested a similar reduction in aggression in risperidone-treated patients (P = 0.010). However, these data have limitations because of the open or mirror-image study designs, the lack of com- parators, and the absence of randomized assignment, parallel groups, and con- trolled data. Hostility and violence present serious management issues in the treat- ment of patients with psychoses. Also, it is difficult to conduct controlled studies involving informed consent in imminently violent patients. Therefore, if indirect data from rigorously controlled studies can be used to confirm the results of open studies with regard to improvements in hostility, then the second-generation an- tipsychotic agents will have been demonstrated to provide benefits beyond the tra- ditional clinical domains in the treatment of patients with psychoses. Reanalysis of data from a previously reported large, multicenter, pivotal study 6 of quetiapine for
531
CLINICAL THERAPEUTICS ®
the treatment of acute exacerbation of schizophrenia provided the opportunity to assess this important clinical question. Although these data did not specifically address hostility, measures of hostility were available from psychopathology scales.
In a double-blind, placebo-controlled study 6 conducted in 26 centers in North America, 5 fixed oral doses of quetiapine were compared with 12 mg/d of halo- peridol in patients with schizophrenia. The details about traditional measures of efficacy in the treatment of psychosis have been reported previously6; further- more, those data were used in obtaining regulatory approval of quetiapine for the treatment of schizophrenia. Two additional questions were posited of this study. First, was the efficacy of a therapeutically effective dose (150-750 mg/d) of que- tiapine superior or comparable to the efficacy of either haloperidol or placebo on measures of agitation? Second, what were the contributions of the direct versus indirect (ie, through indirect improvements in overall psychopathology and/or positive symptoms) effects of quetiapine compared with those of haloperidol on measures of agitation? We hypothesized that: (1) quetiapine, a drug with a broad pharmacologic profile (similar to that of clozapine), would show benefits for agi- tation in patients with psychoses and (2) the efficacy of quetiapine would be su- perior to placebo and either equal or superior to haloperidol. Furthermore, based on available data for other second-generation antipsychotic agents, we hypothe- sized that quetiapine would show better efficacy in improving agitation compared with haloperidol.
PATIENTS A N D M E T H O D S
Patients The original 6-week study 6 was a multicenter, double-blind, randomized,
placebo-controlled, parallel-group design comparing 5 fixed doses of quetiapine* with 12 mg/d haloperidol. That trial was approved by center-designated institu- tional review boards, and written informed consent was obtained from all partic- ipants after they had been given a complete description of the study.
In brief, patients aged 18 to 65 years of either sex and any ethnicity who had a diagnosis of schizophrenia based on the Diagnostic and Statistical Manual of Men- tal Disorders, Revised Third Edition 7 (DSM-III-R) criteria and who were experienc- ing an acute exacerbation were recruited into the study. In addition, eligible pa- tients scored >27 on the 18-item Brief Psychiatric Rating Scale 8 (BPRS), on which each item is scored from 0 to 6 (0 = not present, 1 = very mild, 2 = mild, 3 = moderate, 4 = moderately severe, 5 = severe, 6 = very severe). They also were re- quired to score 3 or higher (moderate) on >2 items from the BPRS positive symp-
"Trademark: Seroquel ® (AstraZeneca Pharmaceuticals LE Wilmington, Delaware).
532
K.N.R. Chengappa et al.
tom cluster (conceptual disorganization, suspiciousness, hallucinatory behavior, unusual thought content) and a score of 4 or higher (moderately ill) on the 7- item Clinical Global Impression (CGI) scale 9 Severity of Illness subscale (0 = normal, 1 = minimal, 2 = mild, 3 = moderate, 4 = moderately severe, 5 = severe, 6 = among the most extreme). Patients using depot antipsychotic medications were excluded within 1 dosing interval. Patients were medically stable at study entry
In addition to laboratory measures, tolerability was assessed clinically and us- ing 2 rating scales: the Simpson-Angus Scale, 1° modified to include akathisia, and the Abnormal Involuntary Movement Scale. 9 During the prerandomization phase of up to 7 days, patients discontinued previous psychotropic agents and received single-blind placebo tablets. Placebo responders (ie, those with >20% decrease in BPRS total scores or >l-point decrease in CGI Severity of Illness subscale) were withdrawn from the study. All patients were assessed at baseline (day 0) using BPR5 and other efficacy and tolerability measures. Patients then were randomized to receive 1 of 5 fixed oral daily doses (75, 150, 300, 600, or 750 mg, given in 3 divided doses per day) of quetiapine or 12 mg of haloperidol or placebo for 6 weeks. As noted in the original study, 6 the selected haloperidol dose was consid- ered a midrange effective dose on the basis of earlier haloperidol literature and comparator studies with other atypical antipsychotic agents. Each patient's dose was titrated to their randomized dose assignment over a period of up to 2 weeks, followed by fixed and stable daily doses of medication up to week 6. Allowed concomitant medications were chloral hydrate for insomnia and lorazepam for agitation. Following baseline measurements, BPRS and other assessments were scheduled for weeks 1, 2, 3, 4, 5, and 6, and were not done within 6 and 12 hours, respectively, of either chloral hydrate or lorazepam administration.
In addition to the entry criteria for the parent study, patients included in this re- analysis had received the drug for at least 2 weeks (to ensure that their target as- signment dose of study medication was reached) and had a baseline assessment and at least 1 postbaseline assessment after the minimum 2 weeks of treatment. Also, the 150-, 300-, 600-, and 750-mg quetiapine treatment groups were combined because these doses were therapeutically effective against placebo, 6 unlike the 75-mg queti- apine group, which was excluded for purposes of this analysis. The reanalysis of the previously reported trial was approved by the University of Pittsburgh institutional review board as an exempt-from-consent study The authors had provided a proposal to assess the impact on hostility and agitation in the different treatment arms of the study The deidentified data were provided to the authors to review as analyzed data.
Variables The measure of hostility (behavioral agitation score [BAS]) derived from the BPRS
was calculated as the mean of the following 5 itemsli: hostility, anxiety, tension, un- cooperativeness, and excitement. The BPR5 positive symptom cluster score (PSCS) is
533

CLINICAL THERAPEUTICS ®
defined as the mean of the previously mentioned 4 items in the BPRS symptom clus- ter: conceptual disorganization, suspiciousness, hallucinatory behavior, and unusual thought content. The BPRS total (BPRS-Total) score is a standard measure to repre- sent overall psychopathology. An alternative BPRS (A-BPRS) score was derived from the sum of the remaining 9 BPRS items (ie, items not in either the BAS or PSCS): grandiosity, blunted affect, emotional withdrawal, somatic concern, guilt feeling, mannerism and posturing, depression, motor retardation, and disorientation.
Statistical Analysis A statistical software package, SAS version 6.12 (SAS Institute Inc., Cary, North
Carolina), was used to perform all statistical analyses, For the BAS, the mean (SD) value and number of patients were tabulated for each visit. First, an analysis of co- variance was performed using only patients who had at least 2 weeks of treatment and a baseline and at least 1 postbaseline BPRS assessment after the minimum 2 weeks of treatment. This model fitted baseline BASs and center as covariates in the analyses. This analysis addressed the first hypothesis. Four quetiapine-treated groups (150, 300,600, and 750 mg) were combined and the least squares mean was com- pared with placebo. Haloperidol treatment was similarly compared with placebo.
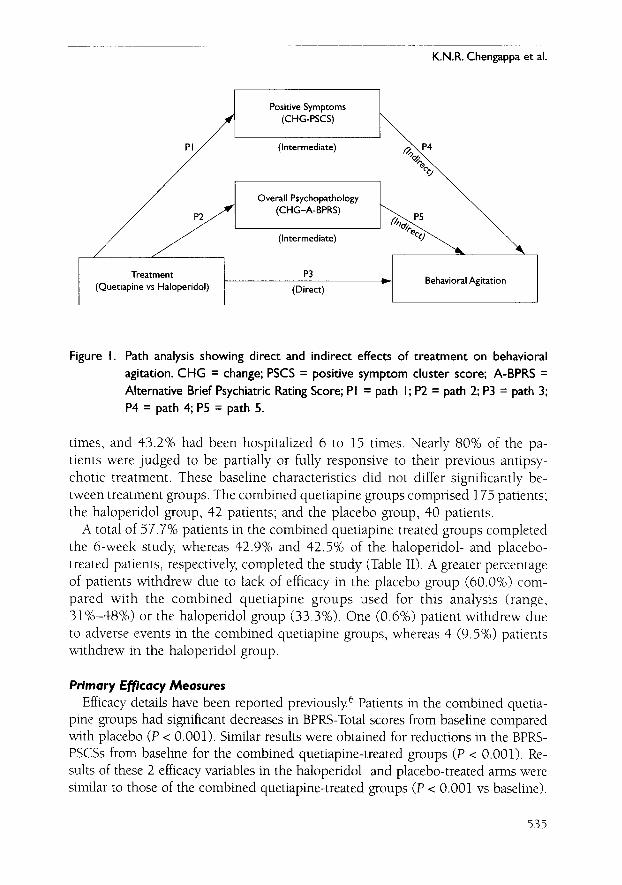
The path analytic statistical method was used to assess the second hypothesis. A path analysis for the measure of agitation and hostility was carried out using the BAS as the terminal variable in the path analysis (ie, hostility) and the SAS- derived change scores for the BPRS-PSCS and the A-BPRS as the potential inter- mediate variables (Figure 1).
Consequently, the total effect of treatment on BASs of quetiapine relative to halo- peridol was calculated from the path (P) diagram as (P1 × P4 + P2 × P5 + P3), and this was compared with the direct effect (P3).
The path analysis was designed so that any positive coefficients implied a better (ie, larger difference in change scores from baseline) result with quetiapine compared with haloperidol. Statistical significance was set at P < 0.05. All tests were 2 sided.
RESULTS
Overall Population and Disposition Details of efficacy for psychoses among patients with acute exacerbations of
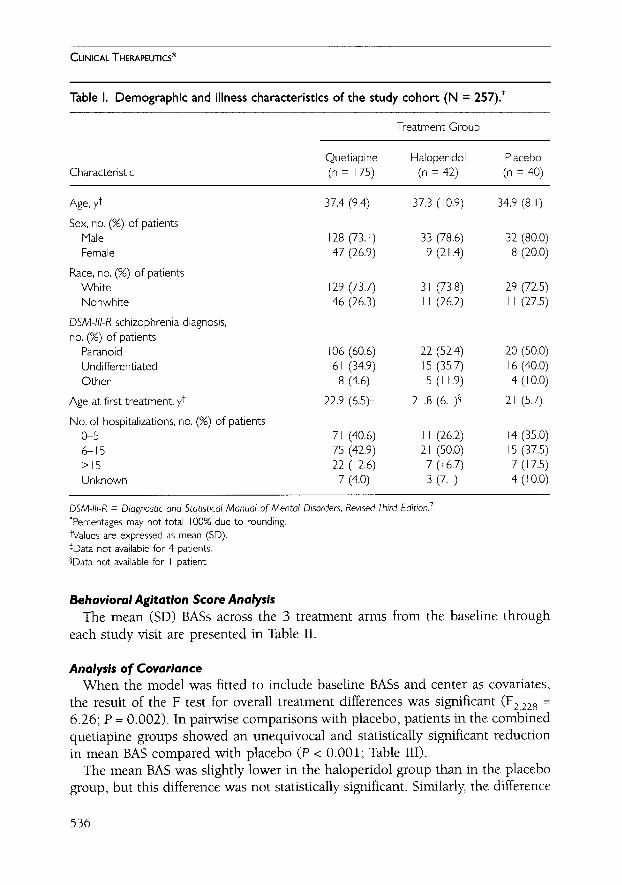
schizophrenia have been reported in detail previously. 6 For the purposes of the present analysis, the demographic and illness characteristics of the patients are presented in Table I. In brief, 257 adult patients (193 men, 64 women) were stud- ied. Of these patients, 73.5% were white. The mean duration of illness was 15.0 years; 57.6% and 35.8% of patients were classified as having chronic paranoid schizophrenia and chronic undifferentiated schizophrenia, respectively. Further- more, 37.4% of the enrolled patients had been previously hospitalized 0 to 5
534
K.N.R. Chengappa et al.
PI
Treatment (Quetiapine vs Haloperidol)
Positive Symptoms ~~o~.. p4 (CHG-PSCS) (Intermediate)
Overall Psychopathology ~ N (CHG-A-BPRS) (Intermediate)
P3 I~ Behavioral Agitation (Direct)
Figure I. Path analysis showing direct and indirect effects of t reatment on behavioral agitation. CHG = change; PSCS = positive symptom cluster score; A-BPRS = Alternative Brief Psychiatric Rating Score; PI = path I; P2 = path 2; P3 = path 3; P4 = path 4; P5 = path 5.
times, and 43.2% had been hospitalized 6 to 15 times. Nearly 80% of the pa- tients were judged to be partially or fully responsive to their previous antipsy- chotic treatment. These baseline characteristics did not differ significantly be- tween treatment groups. The combined quetiapine groups comprised 175 patients; the haloperidol group, 42 patients; and the placebo group, 40 patients.
A total of 57.7% patients in the combined quetiapine-treated groups completed the 6-week study, whereas 42.9% and 42.5% of the haloperidol- and placebo- treated patients, respectively, completed the study (Table II). A greater percentage of patients withdrew due to lack of efficacy in the placebo group (60.0%) com- pared with the combined quetiapine groups used for this analysis (range, 31%-48 %) or the haloperidol group (33.3 %). One (0.6 %) patient withdrew due to adverse events in the combined quetiapine groups, whereas 4 (9.5%) patients withdrew in the haloperidol group.
Primary Eff icacy Measures Efficacy details have been reported previously. 6 Patients in the combined quetia-
pine groups had significant decreases in BPRS-Total scores from baseline compared with placebo (P < 0.001). Similar results were obtained for reductions in the BPRS- PSCSs from baseline for the combined quetiapine-treated groups (P < 0.001). Re- suits of these 2 efficacy variables in the haloperidol- and placebo-treated arms were similar to those of the combined quetiapine-treated groups (P < 0.001 vs baseline).
535
CLINICAL THERAPEUTICS@
Table I. Demographic and illness characteristics of the study cohort (N = 257).*
Treatment Group
Characteristic
Quetiapine Haloperidol
(n = 175) (n = 42)
Placebo
(n = 40)
Age, yt 37.4 (9.4) 37.3 (I 0.9)
Sex, no. (%) of patients
Male I28 (73. I) 33 (78.6)
Female 47 (26.9) 9 (2 I .4)
Race, no. (%) of patients
White 129 (73.7) 3 I (73.8)
Nonwhite 46 (26.3) I I (26.2)
DSM-III-R schizophrenia diagnosis,
no. (%) of patients
Paranoid IO6 (60.6) 22 (52.4)
Undifferentiated 6 I (34.9) I5 (35.7)
Other 8 (4.6) 5 (I I .9)
Age at first treatment, yt 22.9 (6.5)* 21.8 (6.1)5
No. of hospitalizations, no. (%) of patients
o-5 71 (40.6) I I (26.2)
6-15 75 (42.9) 21 (50.0)
>I5 22 ( 12.6) 7 (16.7)
Unknown 7 (4.0) 3 (7. I )
DSM-III-R = Diagnostic and Statistrcol Manual of Mental Disorders, Revised Third Edltjon.7
*Percentages may not total 100% due to rounding.
tValues are expressed as mean (SD).
*Data not available for 4 patients.
§Data not available for I patient.
34.9 (8.1)
32 (80.0)
8 (20.0)
29 (72.5)
I I (27.5)
20 (50.0)
I6 (40.0)
4 ( 10.0)
21 (5.7)
I4 (35.0)
I5 (37.5)
7 ( 17.5)
4 (I 0.0)
Behavioral Agitation Score Analysis
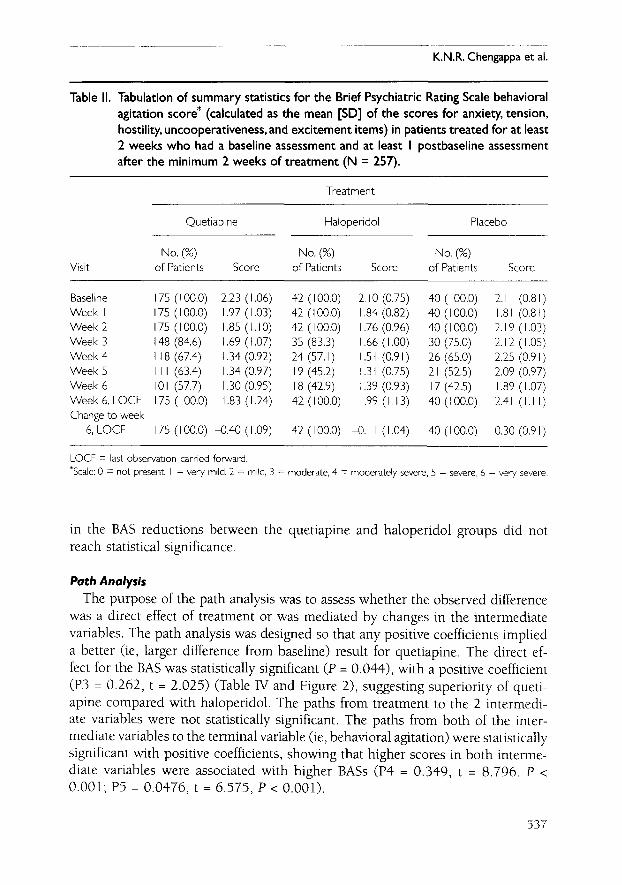
The mean (SD) BASS across the 3 treatment arms from the baseline through each study visit are presented in Table II.
Analysis of Covariance When the model was fitted to include baseline BASS and center as covariates,
the result of the F test for overall treatment differences was significant (Fz 228 = 6.26; P = 0.002). In pairwise comparisons with placebo, patients in the combined quetiapine groups showed an unequivocal and statistically significant reduction in mean BAS compared with placebo (P < 0.001; Table III).
The mean BAS was slightly lower in the haloperidol group than in the placebo group, but this difference was not statistically significant. Similarly, the difference
536
K.N.R. Chengappa et al.
Table II. Tabulation of summary statistics for the Brief Psychiatric Rating Scale behavioral agitation score* (calculated as the mean [SD] of the scores for anxiety, tension, hostility, uncooperativeness, and excitement items) in patients treated for at least 2 weeks who had a baseline assessment and at least I postbaseline assessment after the minimum 2 weeks of treatment (N = 257).
Treatment
Quetiapine Haloperidol Placebo
No. (%) No. (To) No. (%)
Visit o f Patients Score of Patients Score of Patients Score
Baseline Week l Week 2 Week 3 Week 4 Week 5
Week 6 Week 6, LOCF
Change to week 6, LOCF
75 (I 00.0) 75 (I 00.0) 75 (I 00.0) 48 (84.6) 18 (67.4) I I (63.4) 01 (57.7)
175 (100.0)
2.23 (1.06) .97 (1.03) .85 (I,10) .69 (I ,07) .34 (0.92) .34 (0.97) .30 (0.95) .83 (I .24)
42 (I 00.0) 2.10 (0.75) 40 (I 00.0) 2. I I (0.81) 42 (I 00.0) 1.84 (0.82) 40 (I 00.0) 1.81 (0.8 t) 42 (I 00.0) 1.76 (0.96) 40 (I 00.0) 2.19 (I .03) 35 (83.3) 1.66 (I .00) 30 (75.0) 2.12 (I .05) 24 (57. I) 1.51 (0.91) 26 (65.0) 2.25 (0.9 I) 19 (45.2) 1.31 (0.75) 21 (52.5) 2.09 (0.97) 18 (42.9) 1.39 (0.93) 17 (42.5) 1.89 (I.07) 42 (100.0) 1.99 (I. 13) 40 (100.0) 2.41 (I. I I)
175 (100.0) -0.40 (I.09) 42 (100.0) ~).11 (I.04) 40 (100.0) 0.30 (0.91)
LOCF = last observation carried forward, *Scale: 0 = not present, I = very mild, 2 = mild, 3 = moderate, 4 = moderately severe, 5 = severe, 6 = very severe,
in the BAS reduct ions be tween the quet iapine and haloper idol groups did not reach statistical significance.
Path Analysis The purpose of the pa th analysis was to assess whe ther the observed difference
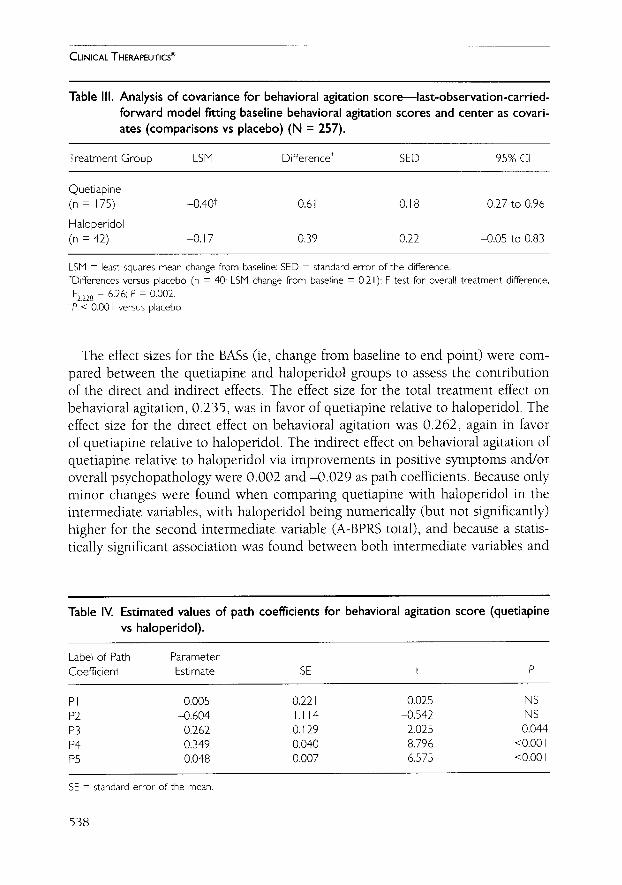
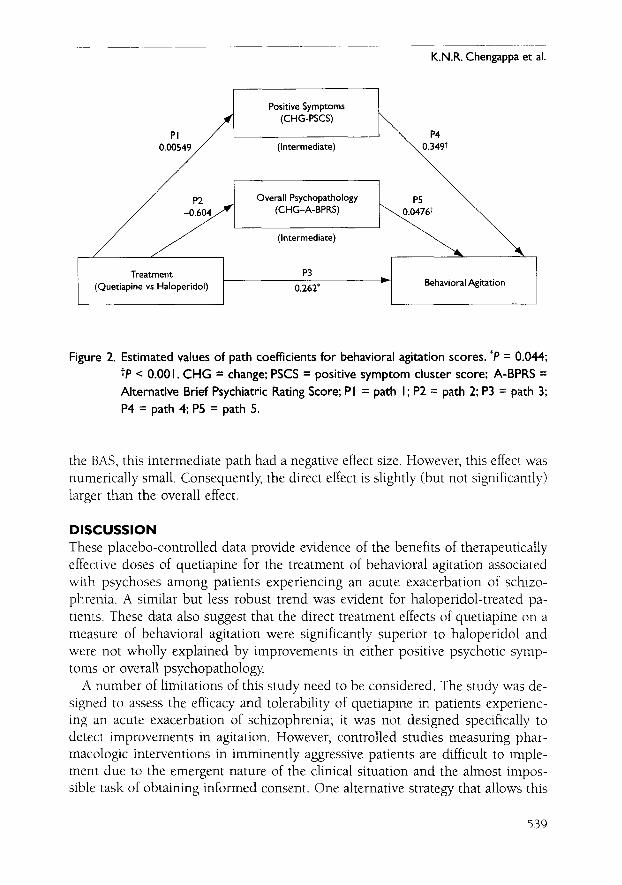
was a direct effect of t rea tment or was media ted by changes in the intermediate variables. The pa th analysis was designed so that any positive coefficients implied a better (ie, larger difference from baseline) result for quetiapine. The direct ef- fect for the BAS was statistically significant (P = 0.044), wi th a positive coefficient (P3 = 0.262, t = 2.025) (Table IV and Figure 2), suggesting superiori ty of queti- apine compared wi th haloperidol. The paths from t rea tment to the 2 intermedi- ate variables were not statistically significant. The paths from both of the inter- mediate variables to the terminal variable (ie, behavioral agitation) were statistically significant wi th positive coefficients, showing that higher scores in bo th interme- diate variables were associated wi th h igher BASs (P4 = 0.349, t = 8.796, P < 0.001; P5 = 0.0476, t = 6.575, P < 0.001).
537
CLINICAL THERAPEUTICS @
Table III. Analysis of covariance for behavioral agitation score last-observation-carried- forward model fitting baseline behavioral agitation scores and center as covari- ates (comparisons vs placebo) (N = 257).
T r e a t m e n t G r o u p LSM Di f fe rence ~ SED 95% CI
Quetiapine (n = 175) -0.40f 0.61 0.18 0,27 to 0.96
Haloperidol (n = 42) -0.17 0,39 0.22 -0.05 to 0.83
LSM = least squares mean change from baseline; SED = standard error o f the difference.
*Differences versus placebo (n = 40; LSM change from baseline = 0.21); F test for overall t reatment difference,
F2,228 - 6.26; P = 0.002. Ip < 0.001 versus placebo.
The effect sizes for the BASs (ie, change from baseline to end point) were com- pared between the quetiapine and haloperidol groups to assess the contribution of the direct and indirect effects. The effect size for the total treatment effect on behavioral agitation, 0.235, was in favor of quetiapine relative to haloperidol. The effect size for the direct effect on behavioral agitation was 0.262, again in favor of quetiapine relative to haloperidol. The indirect effect on behavioral agitation of quetiapine relative to haloperidol via improvements in positive symptoms and/or overall psychopathology were 0.002 and -0.029 as path coefficients. Because only minor changes were found when comparing quetiapine with haloperidol in the intermediate variables, with haloperidol being numerically (but not significantly) higher for the second intermediate variable (A-BPRS total), and because a statis- tically significant association was found between both intermediate variables and
Table IV. Estimated values of path coefficients for behavioral agitation score (quetiapine vs haloperidol).
Label of P a t h Parameter Coefficient Estimate SE t P
P I 0.005 0.221 0.025 NS P2 q).604 I. I 14 0.542 NS P3 0.262 0.129 2.025 0.044 P4 0.349 0.040 8.796 <0.001 P5 0.048 0.007 6.575 <0.001
SE = standard error o f the mean.
538
K.N.R. Chengappa et al.
Treatment (Quetiapine vs Haloperidol)
Positive Symptoms (CHG-PSCS)
(Intermediate)
Overall Psychopathology (CHG-A-BPRS)
(Intermediate)
P3 Behavioral Agitation 0.262*
Figure 2. Estimated values of path coefficients for behavioral agitation scores. *P = 0.044; tp < 0.001. CHG = change; PSCS = positive symptom cluster score; A-BPRS =
Alternative Brief Psychiatric Rating Score; PI = path I; P2 = path 2; P3 = path 3; P4 = path 4; P5 = path 5.
the BAS, this intermediate path had a negative effect size. However, this effect was numerically small. Consequently, the direct effect is slightly (but not significantly) larger than the overall effect.
D I S C U S S I O N
These placebo-controlled data provide evidence of the benefits of therapeutically effective doses of quetiapine for the treatment of behavioral agitation associated with psychoses among patients experiencing an acute exacerbation of schizo- phrenia. A similar but less robust trend was evident for haloperidol-treated pa- tients. These data also suggest that the direct treatment effects of quetiapine on a measure of behavioral agitation were significantly superior to haloperidol and were not wholly explained by improvements in either positive psychotic symp- toms or overall psychopathology.
A number of limitations of this study need to be considered. The study was de- signed to assess the efficacy and tolerability of quetiapine in patients experienc- ing an acute exacerbation of schizophrenia; it was not designed specifically to detect improvements in agitation. However, controlled studies measuring phar- macologic interventions in imminently aggressive patients are difficult to imple- ment due to the emergent nature of the clinical situation and the almost impos- sible task of obtaining informed consent. One alternative strategy that allows this
539
CLINICAL THERAPEUTICS ®
important clinical question to be addressed is to use available data sets from con- trolled efficacy studies, as was done in the present study.
In addition, a number of caveats need to be applied to the path analysis used. Specifically, with this multiple-regression method, the analysis assumes that any relationships between the variables are solely in the direction described by the path analysis, such that variable X may affect variable Y,, but variable Y does not affect variable X (ie, causal order), and that the covariance between any 2 vari- ables in the model is due solely to the direct causal relationships described by the path analysis (ie, causal closure). Consequently, if a variable or a relationship among variables is missing from the model, then the model itself may be incor- rect or inadequate to test a given hypothesis. In the present study, the model as- sumed that treatment (quetiapine vs haloperidol) had effects on agitation that were either direct or indirect (ie, were mediated by improvements in positive psy- chotic symptoms and overall psychopathology). However, this path analysis did include the relevant baseline scores to adjust for any possible differences between the 2 active comparators, and yet quetiapine achieved superiority over haloperi- dol on the total and direct effects of the agitation measure.
In a study using linear regression, Rabinowitz et a112 assessed clozapine for aggressive patients and, confirming earlier work by Volavka et al, 2 noted that a substantial proportion of the variance in the overall improvement was in fact ex- plained by a reduction in hostility scores rather than a reduction in psychosis scores.
Another criticism may be that the model used in the present study might not include all of the possible variables that could influence hostility. For instance, akathisia has been associated with violence among psychiatric patients treated with the older neuroleptic agents. 13 In the previous study, 6 only 15% of the haloperidol-treated group experienced akathisia, whereas this rate ranged from 0% to 8% in the placebo- and quetiapine-treated groups. Thus, it is unlikely that akathisia accounts for much of the improvement in hostility with quetiapine rel- ative to haloperidol in the present data.
Although it could be argued that initial improvements in hostility and agitation are related to excessive sedation associated with these new agents, the incidence of sedation (6%-10%) in the previous study 6 was comparable and also relatively low among all treatment groups.
C O N C L U S I O N S This post hoc analysis of a previously conducted pivotal clinical trial suggests that effective doses of quetiapine have therapeutic effects on hostility and behavioral agitation among patients experiencing an acute exacerbation of schizophrenia. Furthermore, unlike haloperidol, quetiapine appears to have direct effects on agi- tation relatively independent of its benefits for positive symptoms.
540
K.N.R. Chengappa et al.
A C K N O W L E D G M E N T S The authors acknowledge the editorial assistance of Ms. Tracy Anderson and CHC Communications in Pennsylvania for preparation of the figures and the submis- sion packet to the journal.
R E F E R E N C E S 1. Mallya AR, Roos PD, Roebuck-Colgan K. Restraint, seclusion, and clozapine..] Clin
Psychiatry. 1992;53:395-397. 2. Volavka J, Zito JM, Vitrai J, Czobar P. Clozapine effects on hostility and aggression in
schizophrenia. J Clin Psychopharmacol. 1993;13:287-289. 3. Chiles JA, Davidson E McBride D. Effects of clozapine on use of seclusion and re-
straint at a state hospital. Hosp Community Psychiatry. 1994;45:269-271. 4. Chengappa KN, Ebeling "17, Kang JS, et al. Clozapine reduces severe self-mutilation
and aggression in psychotic patients with borderline personality disorder. J Clin Psy- chiatry. 1999;60:477-484.
5. Chengappa KN, Levine J, Ulrich R, et al. Impact of risperidone on seclusion and re- straint at a state psychiatric hospital. Can,] Psychiatry. 2000;45:827-832.
6. Arvanitis LA, Miller BG. Multiple fixed doses of "Seroquel" (quetiapine) in patients with acute exacerbation of schizophrenia: A comparison with haloperidol and placebo. The Seroquel Trial 13 Study Group. Biol Psychiatry. 1997;42:233-246.
7. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Revised Third Edition. Washington, DC: American Psychiatric Association; 1987.
8. Overall JE, Gorham DR. The brief psychiatric rating scale. Psychological Report. 1962; 10:799-812.
9. Guy W,, ed. ECDEUAssessment Manual for Psychopharmacology. Rev ed. Bethesda, Md: US Department of Health, Education and Welfare; 1976. Publication ADM-76-338.
10. Simpson GM, Angus JW A rating scale for extrapyramidal side effects. Aeta Psychiatr Stand Suppl. 1970;212:11-19.
11. Kinon BJ, Roychowdhury SM, Milton DR, Hill AL. Effective resolution with olanza- pine of acute presentation of behavioral agitation and positive psychotic symptoms in schizophrenia. J Clin Psychiatry. 2001 ;62(Suppl 2): 17-21.
12. Rabinowitz J, Avnon M, Rosenberg V. Effect of clozapine on physical and verbal ag- gression. 5chizophr Res. 1996;22:249-255.
13. Herrera JN, Sramek JJ, Costa JEet al. High potency neuroleptics and violence in schizophrenics. J Nerv Ment Dis. 1988;176:558-561.
Address correspondence to: K.N. Roy Chengappa, MD, FRCPC, Western Psychiatric Institute and Clinic, Special Studies Center at Mayview State Hospital, University of Pittsburgh Medical Center, 3811 O'Hara Street, Pittsburgh, PA 15213-2593. E-mail: [email protected]
541





























