Embed Size (px)
Citation preview

c© 2008 Wiley Periodicals, Inc. 565
CASE REPORTS
Off-Pump Total CavopulmonaryConnection in a Patient withHypoplastic Right PulmonaryArtery and Right LungSecondary to Kyphoscoliosis
Murat Ugurlucan, M.D.,∗ Kemal Nisli,
M.D.,† Emin Tireli, M.D.,∗ and Enver
Dayioglu, M.D.∗
∗Department of Cardiovascular Surgery, and†Department of Pediatric Cardiology,Istanbul, Turkey
ABSTRACT The last-stage palliation of patients with
single ventricle physiology hearts is Fontan proce-
dure and its modifications that can be performed
with or without cardiopulmonary bypass in the cur-
rent era. Pulmonary vasculature and status of the
lungs are critically important for the success of the
operation. In this report, we present a 10-year-old
patient with single ventricle heart and severely hy-
poplastic unilateral pulmonary artery and respec-
tive lung due to kyphoscoliosis who underwent
extracardiac Fontan procedure without cardiopul-
monary bypass, successfully. doi: 10.1111/j.1540-8191.2007.00541.x (J Card Surg 2008;23:565-568)
Fontan operation and its modifications are the last-stage palliation of patients with single ventricle. It re-quires well-preserved ventricular functions and maybe, moreover, suitable pulmonary vasculature and pul-monary bed for the best outcome.1 Review of theliterature reveals a very rare group of single ventriclepatients of Fontan candidates who posses only onesuitable lung and pulmonary artery for the systemic ve-nous anastomosis2–6 and even presence of a singlelung is not accepted as a contraindication for the oper-ation. However, compromise or absence of the unilat-eral lung and the pulmonary artery requires deliberateplanning and careful design during the operation.
In this report, we present our experience of extracar-diac Fontan operation without cardiopulmonary bypass(CPB) in a 10-year-old patient with hypoplastic right pul-monary artery and right lung that developed due to se-vere kyphoscoliosis.
Address for correspondence: Murat Ugurlucan, MD, Istanbul Univer-sity, Istanbul Medical Faculty, Department of Cardiovascular Surgery,34390 Capa, Fatih, Istanbul, Turkey. Fax: +90-212-534-22-32; e-mail:[email protected] [email protected]
CASE REPORT
The patient was a 10-year-old girl who had previ-ously undergone a central shunt operation through me-dian sternotomy with a 5 mm polytetrafluoroethilen(PTFE, Goretex, W.L. Gore & Associates, Inc., Nework,Denmark) graft for transposition of great arteries (TGA),ventricular septal defect (VSD) and hypoplastic pul-monary arteries when she was first admitted to theclinic one year ago due to severe cyanosis. She hadbeen cyanotic since birth; however, she had not under-gone any palliative procedures for the relief of cyanosisuntil nine years of age. She had severe kyphoscoliosis(Fig. 1); chest X-ray showing compression of the rightlung and situs totalis inversus (Fig. 2). Abdominal siturwas also inverted. Her room air arterial saturation andhematocrit level were 73% and 59%, respectively. Shewas considered for end-stage palliation of single ven-tricle. Echocardiography of the patient showed devel-opment of left pulmonary artery and the hypoplasticright pulmonary artery (5–6 mm in diameter). Angiog-raphy confirmed the echocardiography findings (Fig. 3)and indicated a mean 10 mmHg pressure in the left pul-monary artery, while right pulmonary artery could hardlybe visualized. Pulmonary function tests indicated de-creased forced vital capacity and peak expiratory flowbut relatively preserved vital capacity.
The operation was performed through standard me-dian sternotomy. The ascending aorta, pulmonary ar-teries, and superior (SVC) and inferior (IVC) vena cavaeand the previous central shunt were dissected free andcontrolled. Diameters of the left pulmonary artery andthe right pulmonary artery were measured as 18 mmand 6 mm, respectively. Systemic anticoagulation wasachieved with intravenous heparin (100 units/kg). Ve-nous cannulae were placed in the right atrium and theSVC, and a transient external shunt was constructedbetween the SVC and the right atrium by connectingthese two venous cannulae with a Y-connector. TheSVC was clamped below the cannula and transectedfrom cavoatrial junction.7 The atrial end was oversewn.The left pulmonary artery was partially clamped with alateral Castenada clamp allowing shunt flow to the bothpulmonary arteries. An arteriotomy was performed onthe anterosuperior aspect of the left pulmonary artery.SVC was anastomosed to this region of the left pul-monary artery with two running 7.0 polypropylene su-tures. Then the clamps on SVC and left pulmonaryartery were removed. The aortopulmonary shunt wasligated and dissected. The pulmonary artery bifurcationwas clamped proximal to the bidirectional Glenn shuntallowing the blood flow to the left pulmonary artery.Pulmonary bifurcation and right pulmonary artery wererestored and enlarged with a pericardial patch. Thenthe clamp on the pulmonary bifurcation was removedto mediate the SVC flow to both of the pulmonaryarteries. The cranial end of a 20 mm diameter PTFE

566 UGURLUCAN, ET AL.COMPROMISED LUNG OFF-PUMP FONTAN
J CARD SURG2008;23:565-589
Figure 1. Kyphoscoliosis of the patient leading to severechest deformity.
tube graft was anastomozed to the arteriotomy per-formed on the inferior aspect of the left pulmonaryartery with a continuous 6.0 polypropylene suture. Thegraft was clamped at its mid-portion. Venous cannulaewere placed in the right atrium and IVC through previ-ously placed purse-string sutures, and then connectedwith a Y-connector.7 In order to minimize hemodynamicdeterioration during IVC-graft anastomosis, low-dosedopamine infusion (5µgr/kg/min) was started. After theestablishment of transient external shunt between theIVC and the right atrium, the IVC was clamped andpartially transected leaving a 3–4 mm continuous seg-ment at the cavoatrial junction. The caudal end of thegraft was anastomosed to the IVC with a running 6.0polypropylene suture. Following deaeration the clampsand then the IVC-right atrium bypass cannulae wereremoved. The cardiac end of the IVC was oversewn.
Figure 2. Preoperative chest X-ray showing compression ofthe right lung, situs totalis inversus.
Fontan pressure was measured to be 18 mmHg andfenestration between the PTFE tube graft and the rightatrial free wall was constructed with a 4 mm PTFE graft.
Postoperative course was complicated mainly withpulmonary complications. She was extubated six hourspostoperatively but reentubated due to increase inpCO2. At the intensive care unit, two other extubation
Figure 3. Angiography showing well-developed left pul-monary artery; (LPA) however, right pulmonary artery is hardlyvisualized.

J CARD SURG2008;23:565-589
UGURLUCAN, ET AL.COMPROMISED LUNG OFF-PUMP FONTAN
567
Figure 4. Postoperative chest X-ray.
trials failed due to the same reason. One last trial beforea tracheostomy could be successful on the sixth post-operative day; however, the patient required intensivechest physiotherapy (Fig. 4). Intensive care unit staywas 13 days and she was discharged without any com-plications on the 18th postoperative day with room sat-uration above 91%. A control computed tomographyangiography showed patent flow of both vena cavaeflow mostly to the left pulmonary artery as well as tothe reconstructed right pulmonary artery (Fig. 5A, B).
DISCUSSION
Fontan operation and its modifications are acceptedas the last-stage modern treatment for the patientswith single ventricle physiology. The operation results
Figure 5. Postoperative computed tomography angiography showing flow of both vena cavae to the left pulmonary artery (LPA)(A), and to the reconstructed right pulmonary artery (RPA) (B). MPA = main pulmonary artery.( Acknowledgment: Images wereprinted as mirror images due to misunderstanding by the computed tomography laboratory personelle)
in the loss of antegrade pulsatile flow to the pulmonarycirculation; passive venous flow is directed to the pul-monary bed. Thus, the status of the proximal pul-monary anatomy and the distal vasculature are amongcritical determinants of the Fontan procedure.3,4
Today, most of the patients are generally redo caseswith a history of a band or a shunt operation that maylead to deterioration of the pulmonary arteries. In orderto minimize the effects of previous operations on theresistance to the passive systemic venous flow, thedistorted segments of the pulmonary tree should bereconstructed carefully.8
On the other hand, there is a rare group of single ven-tricle patients who have only one functional lung. Thismay result from pulmonary arterial stretch and steno-sis, which is a very well-known long-term complicationof shunt operations due to the short graft size that maytotally obstruct one side pulmonary artery.8 Physiologi-cally, if one of the lungs is somehow lost or decreasesin volume, as a compensatory mechanism, the remain-ing lung expands its capacity to a certain degree. How-ever, the increase in the capacity of the unilateral lungcan never make up for the volume of double lungs.9
In pulmonary function tests, forced vital capacity andpeak expiratory flow are negatively affected whereasvital capacity, which may slightly decrease, is usuallypreserved in these patients; hence, it is encouragingfor surgeons especially for the early postoperative out-come of the Fontan operation. There are a few reportsin the literature presenting the results of Fontan oper-ation and its modifications in single lung, single ventri-cle patients. The pathology has been studied mostly byTchervenkov, MD.3,4 The first successful operation hasbeen published by Sade and Gillette in 1989.2 Zacharyet al.5 and Jacobs et al.6 presented their experiencesin relatively larger series of patients (seven and 12 pa-tients, respectively). Zachary et al. indicated a loweroxygen saturation (87% vs 91%) in the end in singlelung patients undergoing Fontan procedure when com-pared with the functional double lung cases.5 Al-Khaldiet al. present their successful single lung Fontan oper-ation in an adult case.4 However, all the authors unitein the utmost importance of the status of pulmonarycirculation for the success of the Fontan procedure. Itis accepted that pulmonary artery distortion, hypopla-sia of the total pulmonary vascular bed, and elevated

568 UGURLUCAN, ET AL.COMPROMISED LUNG OFF-PUMP FONTAN
J CARD SURG2008;23:565-589
pulmonary vascular resistance are all risk factors foradverse outcome after Fontan operations.2-6,10
Today, two main factors such as pulmonary arterypressure and ejection fraction of the single ventricleare accepted as the predictors of Fontan operation.1
Pulmonary vascular resistance has a higher importanceif one of the lungs is compromised. Thus, the postop-erative course may be complicated more commonlywith pulmonary problems in these patients. Specialprecautions should be undertaken to minimize thesepossible problems. There are various attempts to mini-mize the pulmonary effects of the cardiopulmonary by-pass in patients undergoing total cavopulmonary con-nection. Kawahira et al. in their 38 patients seriesdetected that inflammatory reactions were attenuatedwhen the Fontan procedure was employed in an off-pump fashion compared with the usual procedure onbypass.11 Pertosssian et al. concluded that the extrac-ardiac Fontan operation with minimal use of cardiopul-monary bypass was associated with favorable intraop-erative hemodynamics, low fenestration rate, minimalrisk of thrombosis or stenosis, and minimal early- andlate-rhythm disturbance.12 At our institution, our strat-egy is to perform all Fontan procedures in an off-pumpmanner in order to prevent the side effects of cardiopul-monary bypass.7 However, the operation requires ex-perience and especially during IVC-conduit anastomo-sis, any mistake may be life threatening. The majortechnical difficulty of the off-pump Fontan procedureis during the IVC-conduit anastomosis. The field is notwide and the exposure may not be perfect. These havebeen the main reasons why many authors have not pre-ferred the off-pump technique. Since our first casesbetween 1999 and 2002,7 we have modified our tech-nique and do not completely transsect the IVC from thecavoatrial junction. We leave a 3–4 mm undivised seg-ment between the IVC and right atrium until the com-pletion of the conduit anastomosis. It is obviously safer.In our modest series we executed off-pump extracar-diac Fontan procedure safely. Since our last patient hadsevere kyphoscoliosis and hypoplastic right pulmonaryartery, we were more eager on performing the opera-tion in an off-pump fashion. As a result, we can proposethat off-pump technique should not be accepted as acontraindication in cases with hypoplastic right and leftpulmonary arteries and that requires patchplasty to pul-monary artery branches.
Another issue for our patient was whether to per-form a staged operation (i.e., Glenn shunt followed byFontan completion in the other surgical stage) or to-tal cavopulmonary connection in a single stage. Ourchoice had been single stage operation with the ideato prevent further intubation, extubation, and periopera-tive complications of the following surgical procedureswith good postoperative intensive care unit treatment.Moreover, physiologically in the very early periods oflife, SVC carries 40% to 50% of whole body venousreturn to the heart. However, with the growth of thechild the IVC begins to dominate in the systemic ve-nous return and ratio of blood from the SVC to IVC be-comes 40 of 60.4,13 A preliminary Glenn shunt would
not be sufficient to increase the oxygen levels in a 10-year-old child, neither would increase exercise capacity;thus, this was another reason to perform total cavopul-monary anastomosis in our patient.
In conclusion, the status of the pulmonary circula-tion is crucial for the success of the Fontan proce-dure. Although it is very rare and carries increasedrisks, compromised lung and hypoplastic pulmonaryartery should not be accepted as contraindications forthe total cavopulmonary connection in single ventricle.However, the operation should be planned strategicallyand in experienced hands off-pump extracardiac Fontanseems to be an attractive alternative especially for thisparticular patient group.
REFERENCES
1. Hosein RB, Clarke AJ, McGuirk SP, et al: Factors influ-encing early and late outcome following the Fontan pro-cedure in the current era. The ‘Two Commandments’?Eur J Cardiothorac Surg 2007;31(3):344-353.
2. Sade RM, Gillette PC: Fontan operation in a case of sin-gle functional pulmonary artery. J Thorac Cardiovasc Surg1989;98(1):153-154.
3. Tchervenkov CI, Chedrawy EG, Korkola SJ: Fontan op-eration for patients with severe distal pulmonary arterystenosis, atresia, or a single lung. Semin Thorac Cardio-vasc Surg Pediatr Card Surg Annu 2002;5:68-75.
4. Al-Khaldi A, Chedrawy EG, Tchervenkov CI, et al: Suc-cessful single-lung fontan operation in an adult: 5-yearfollow-up. Ann Thorac Surg 2005;79(3):1042-1044.
5. Zachary CH, Jacobs ML, Apostolopoulou S, et al: One-lung Fontan operation: Hemodynamics and surgical out-come. Ann Thorac Surg 1998;65(1):171-175.
6. Jacobs ML, Schneider DJ, Pourmoghadam KK, et al: To-tal cavopulmonary connection to one lung. Semin ThoracCardiovasc Surg Pediatr Card Surg Annu 2004;7:72-79.
7. Tireli E, Ugurlucan M, Basaran M, et al: ExtracardiacFontan operation without cardiopulmonary bypass. J Car-diovasc Surg (Torino) 2006;47(6):699-704.
8. Ugurlucan M, Surmen B, Sayin OA, et al: Systemic to pul-monary artery shunt in single ventricle. Eur J CardiothoracSurg 2006;29(5):864.
9. Hsia CC, Herazo LF, Fryder-Doffey F, et al: Compensatorylung growth occurs in adult dogs after right pneumonec-tomy. J Clin Invest 1994;94(1):405-412.
10. Levy M, Danel C, Tamisier D, et al: Histomorpho-metric analysis of pulmonary vessels in single ven-tricle for better selection of patients for the Fontanoperation. J Thorac Cardiovasc Surg 2002;123(2):263-270.
11. Kawahira Y, Uemura H, Yagihara T: Impact of the off-pump Fontan procedure on complement activation andcytokine generation. Ann Thorac Surg 2006;81(2):685-689.
12. Petrossian E, Reddy VM, Collins KK, et al: The extrac-ardiac conduit Fontan operation using minimal approachextracorporeal circulation: Early and midterm outcomes.Thorac Cardiovasc Surg 2006;132(5):1054-1063.
13. Zellner JL, Sade MR: Paliative shunt procedures in cyan-otic congenital heart disease, In Baue AE, Geha AS, Ham-mond LG, Laks H, Naunheim KS, (eds): Glenn’s Thoracicand Cardiovascular Surgery, 6th ed. Pretince-Hall Publish-ing, US, 1996,pp. 1073-1083.

J CARD SURG2008;23:565-589
SHAKER, ET AL.ACUTE TYPE A AORTIC DISSECTION
569
Acute Type A Aortic Dissectionat Seven Weeks of Gestationin a Marfan Patient: Case Report
Walid H. Shaker, M.D.,∗ Amal A. Refaat,
M.D.,† Mohammed A. Hakamei, M.S.,∗
and Mohamed F. Ibrahim, F.R.C.S. (C/Th)∗
∗Prince Salman Heart Center – King FahadMedical City, Riyadh, KSA; †King’s CollegeHospital, London, UK
ABSTRACT A 34-year-old Marfan patient at the sev-
enth week of pregnancy presented with acute type
A aortic dissection and severe aortic regurgita-
tion. The aortic valve and ascending aorta were
replaced successfully using circulatory arrest and
deep hypothermia. At 35 weeks of gestation, the
patient underwent a cesarean section and deliv-
ered a healthy baby. To our knowledge, this case
is the first to report a favorable fetal outcome fol-
lowing surgical repair of acute dissection in the
first trimester of pregnancy. doi: 10.1111/j.1540-8191.2007.00551.x (J Card Surg 2008;23:569-570)
Marfan syndrome is an autosomal dominant geneticdisorder resulting in a diminished strength of connec-tive tissue. Principal complications of the disease areaortic dilatation and the risk of acute dissection, whichcan be fatal to both the mother and the fetus.
CASE REPORT
A 34-year-old Marfan patient at seven weeks of ges-tation was presented to our emergency room withacute tearing chest pain, radiating to the back. Hermother died from acute dissection during labor. Her ob-stetric history included two normal vaginal deliveriesand two early abortions. Her cardiac enzymes, bloodgases, and electrocardiogram were all normal. ChestX-ray showed widened mediastinum. The transtho-racic echocardiography (TTE) and the transesophagealechocardiography (TEE) confirmed the presence ofacute aortic dissection with a spiral flap just abovethe sinotubular junction and severe aortic regurgitation(Fig. 1). The dissection was verified by a computed to-mography (CT) scan (Fig. 2). Obstetric consultation con-firmed positive fetal viability.
A full discussion with the patient and her family in-cluded the need for an emergency open-heart surgerywith cardiopulmonary bypass, the need for systemicanticoagulation, and the poor fetal outcome. Despiteher age and possible future pregnancies, she electedto have a mechanical valve. An emergency Bental oper-ation surgery was performed replacing the aortic valve
Address for correspondence: Dr. Mohamed Ibrahim, Head Car-diac Surgery Center, King Fahad Medical City, P.O. Box 59046,Riyadh 11525 MBN 30105, KSA. Fax: 0099662889999-1112; e-mail:[email protected]
Figure 1. TTE showing spiral flap of aortic dissection abovethe sinotubular junction.
and the ascending aorta. Sevoflurane, midazolam, andfentanyl were given for anesthesia. Cardiopulmonarybypass was initiated using femoral-right atrial cannula-tion. Aortic surgery was conducted with a brief periodof circulatory arrest and deep hypothermia (11 minutes,18 oC). A 25-mm ATS Aortic Valve Graft (ATS Medical,Minneapolis, MN, USA) was implanted, with reimplan-tation of the coronary Ostia. The cross-clamp time was159 minutes. Total circulatory arrest time was 11 min-utes. There were no intraoperative complications. Thepatient was transferred to intensive care unit in stablecondition. The fetal viability was positive immediatelyafter surgery. Vasoconstrictor drugs were avoided dur-ing postoperative course. Postoperative medicationsconsisted of B-blockers, heparin, and diuretics. The pa-tient was extubated after eight hours and transferredto the ward after 48 hours. At the seventh postoper-ative day, she was transferred to the Maternity Hos-pital to continue her pregnancy care and continue herintravenous heparin till the end of the first trimester.Fetal viability and growth were monitored closely and
Figure 2. CT scan confirmed the spiral flap in the ascendingaorta.

570 FURUKAWA, ET AL.TREATMENT OF FULMINANT MYOCARDITIS
J CARD SURG2008;23:565-589
were good. She was discharged home after completingthree-month gestation. Subsequent anticoagulation un-til cesarean section was achieved with Warfarin main-taining an international normalized ratio (INR) 2 to 3.
In week 35 of gestation, the patient gave birthto a healthy boy through cesarean section (weight1700 grams, 41 cm; Apgar score, 8). Subsequent clin-ical examinations and TTE of the mother showed noabnormalities. After consultation, the patient decidedto have a tubal ligation.
COMMENT
Acute aortic dissection occurring during pregnancy isa rare but recognized phenomenon. About half of dis-sections seen in women aged less than 40 years oc-cur during pregnancy.1 Most reported cases are associ-ated with connective tissue disease (e.g., Marfan’s syn-drome), systemic hypertension, and congenital heartdisease, including coarctation and bicuspid aortic valve.
The most common site of pregnancy-associated dis-section is the proximal aorta, and aortic rupture usuallyoccurs during the third trimester or first stage of labor.2
Published data are limited regarding aortic dissec-tion in Marfan pregnant women. Most of these pa-tients experienced dissection during labor and had Ben-tal operation after cesarean section. To our knowledge,only three reports of pregnant Marfan patients under-going aortic surgery before labor and birth have beenpublished.3-5 Sakaguchi and colleagues3 reported fourMarfan pregnant women. Three underwent cesareansection, followed by Bental operation with favorableoutcome. One patient had surgery while fetus in uterowith miscarriage just after cardiac surgery. In the casereported by Naito and colleagues,4 a pregnant Marfanpatient with acute aortic dissection underwent a Ben-tal operation at 24 weeks of gestation and delivered ahealthy baby by cesarean section in week 33. In the re-cent case reported by Seeburger and his colleagues,5
a pregnant Marfan patient at 17 weeks of gestationhad acute type A aortic dissection. She underwent aor-tic valve and arch replacement and delivered a healthybaby by cesarean section at 34 weeks of gestation. Ourpatient is considered the first published case of a preg-nant Marfan who experienced acute aortic dissectionduring the first trimester and had a surgical correctionwith favorable outcome to mother and baby. Aortic rootdilatation that exceeds 4 cm or an increase of aortic sizeduring pregnancy is an identified risk factor for the oc-currence of type A dissection in Marfan patients.6 Thisunderlines the importance of counseling of all Marfanpatients during pregnancy to avoid the feared complica-tion of aortic dissection. Acute aortic dissection duringpregnancy can be serious for both mother and fetuswith a reported mortality of 1% per hour if untreated.2
This time-related mortality rate imposes the need forhigh degree of suspicion and reliable diagnostic tools.The bedside TTE is used for initial diagnosis with sen-sitivity and specificity of 75% and 90%, respectively.2
The TEE has sensitivity and specificity as high as 99%and 98%, respectively.2 The close relation betweenthe aortic dissection and pregnancy initiated Zeebregts
and colleagues7 to follow these cases over 12 years.They suggested a guideline for management accord-ing to the gestational age aiming to save two lives.Before 28 weeks of gestation, as in our case, aorticsurgery with the fetus kept in uterus is recommended.After 32 weeks of gestation, primary cesarean sectionfollowed by aortic repair at the same operation is themanagement of choice. The use of cardiopulmonary by-pass (CPB) is associated with maternal mortality of 3%and a fetal mortality of 20%.8 Hypothermia has beendescribed to reduce placental blood flow and increaseuterine contraction.8 In our case, deep hypothermia andshort circulatory arrest (11 minutes) were used withfavorable outcome. In the postoperative period, vaso-constrictor drugs should be avoided because of theireffects on uterine vessels.
REFERENCES
1. Ergin MA, Lansman SL, Griepp RB: Dissections of aorta.In Baue AE, Geha AS, Hammond GL, et al. (eds): Glenn’sThoracic and Cardiovascular Surgery. 5th ed. Norwalk, CT,Appelton & Lange, 1991, pp. 1955-1961.
2. Khan AK, Nair CK: Clinical, diagnostic and management per-spectives of aortic dissection. Chest 2002;122:311-328.
3. Sakaguchi M, Kitahara H, Seto T, et al: Surgery for acutetype A aortic dissection in pregnant patients with Marfansyndrome. Eur J Cardiothorac Surg 2005;28:280-285.
4. Naito H, Naito H, Tada K: Open heart operation for a preg-nant patient with Marfan syndrome. Masui 2005;54:525-529.
5. Seeburger J, Mohr FW, Falk V: Acute type A dissection at17 weeks of gestation in a Marfan patient. Ann Thorac Surg2007;83(2):674-676.
6. Rossiter JP, Repke JT, Morales AJ, et al: A prospective lon-gitudinal evaluation of pregnancy in the Marfan syndrome.Am J Obstet Gynecol 1995;173:1599-1606.
7. Zeebregts CJ, Schepens MA, Hameeteman TM, et al:Acute aortic dissection complicating pregnancy. Ann Tho-rac Surg 1997;64:1345-1348.
8. Pomini F, Mercogliano D, Cavalletti C, et al: Car-diopulmonary bypass in pregnancy. Ann Thorac Surg1996;61:259-268.
Successful Treatment ofFulminant Myocarditis withMechanical Circulatory Support
Nobuyuki Furukawa, M.D., Mitsumasa
Hata, M.D., Akira Sezai, M.D., Tetsuya
Niino, M.D., Masataka Yoda, M.D.,
Satoshi Unosawa, M.D., and Kazutomo
Minami, M.D.
Department of Cardiovascular Surgery,Nihon University School of Medicine, Tokyo,Japan
ABSTRACT A 66-year-old man with acute fulminant
myocarditis was supported by a left ventricular

J CARD SURG2008;23:565-589
FURUKAWA, ET AL.TREATMENT OF FULMINANT MYOCARDITIS
571
assist device (LVAD) for 22 days, and successfully
recovered from severe heart failure. Prior to this, he
was treated using percutaneous cardiopulmonary
support (PCPS) for five days. However, cardiac
function was not recovered, so we conducted
implantation of the LVAD. It is essential to make an
immediate decision regarding LVAD implantation
to save patients with fulminant myocarditis. doi:10.1111/j.1540-8191.2007.00556.x (J Card Surg2008;23:570-572)
Acute fulminant myocarditis is uncommon but canbe the cause of rapid cardiac decompensation, whichis associated with high mortality. However, if the pa-tient survives the acute inflammatory phase, recoveryoccurs in about one-half of the patients.1,2 Here, wereport the case in which a 66-year-old man with acutefulminant myocarditis, supported by a left ventricularassist device for 22 days as a bridge to recovery, withthe review of literatures. It is essential to make an im-mediate decision regarding LVAD implantation to savepatients with fulminant myocarditis.
CASE REPORT
A previously healthy 66-year-old man with a fewdays’ history of malaise, appetite loss, fever (103 F),and dyspnea was admitted to his local clinic. On arrival,his blood pressure was 98/60 and an electrocardiogramrevealed sinus tachycardia at 160 beats/min with dif-fuse ST-segment elevation. Transthoracic echocardiog-raphy showed global severe left ventricular dysfunctionand an ejection fraction of 15%; so intra-aortic balloonpump (IABP) was inserted. The patient was then re-ferred to our institution for consideration of mechanicalcirculatory support.
A laboratory examination showed the following data:white blood cell count 7800 × 109/L, C-reactive pro-tein (CRP) 10.7 mg/dL, creatinin phosphokinase (CPK)758U/L, troponin I 33.5 ng/dL, myoglobin 227 ng/mL,lactate dehydrogenase (LDH) 819U/L. The chest X-rayfilm showed bilateral pulmonary congestion (Fig. 1).The patient was in a state of shock upon arrival at ourhospital. He was admitted to the circulatory care unitand immediately intubated and percutanous cardiopul-monary support (PCPS) was introduced. We used in-travenous gamma globulin and a broad spectrum ofantibiotics, but his condition did not improve. The bloodculture was negative, but an assay of the viral antibodytiter identified the origin of this case to be Type B in-fluenza virus.
PCPS was applied for five days, but the patient’shemodynamic condition continued to worsen. Therewas no improvement in echocardiographic or hemo-dynamic parameters, and pulmonary congestion in thechest X-ray films had deteriorated. The right leg wherethe PCPS was cannulated showed ischemic change,and hematuria and hemolysis were persistently
Address for correspondence: Dr. Nobuyuki Furukawa, Department ofCardiovascular Surgery, Nihon University School of Medicine, 30-1Oyaguchi-kamimachi, Itabashi-ku Tokyo, 173-8610, Japan. Fax: 81-3-3955-9818; e-mail: [email protected]
Figure 1. Chest radiograph on admission showing bilateralpulmonary congestion and cardiac enlargement.
present. It was deemed difficult to continue use of thePCPS until respiratory and circulatory conditions wouldrecover, so we decided to implant a left ventricularassist device (LVAD) (Toyobo Co., Ltd., Japan) (Fig. 2).Blood was drained from the left atrium and perfusedto the ascending aorta, and the IABP and PCPSremoved during the operation. Intraoperatively, wefound that the heart was poorly contractile and mildlyenlarged. After surgery, the cardiac function graduallyrecovered, the cardiac index came up from 2.5 to4.0 L/min/m2 and the mean pulmonary wedge pressure(PCWP) came down from 25 to 17 mmHg, with LVADflow of 4.2 L/min adjusted to fixed-rate mode. Sincepostoperative bleeding decreased, heparin-based
Figure 2. Postoperative chest radiograph.

572 FURUKAWA, ET AL.TREATMENT OF FULMINANT MYOCARDITIS
J CARD SURG2008;23:565-589
Figure 3. Chest radiograph after removed the LVAD.
anticoagulation treatment was resumed, controlledwithin 150∼200 sec of activated coagulation time(ACT). Pulmonary congestion observed in X-raysgradually improved. An echocardiogram was per-formed once a week after the operation revealingimprovement in cardiac function, eventually the LVADwas successfully removed on POD27 (Fig. 3). Theejection fraction came up to 55% on POD34. Physicalrehabilitation was started and he became sufficientlymobile. He was discharged from the hospital onPOD46, and continues to do well.
DISCUSSION
Acute fulminant myocarditis is an uncommon condi-tion. Clinical presentation can range from a minor viralsyndrome to rapid and fatal circulatory collapse, whichis resistant to high-dose inotropic agents, steroids, andimmunosuppressive therapy. However, spontaneousrecession of the inflammatory process can occur in upto one-half of such patients.1,2 McCarthy et al. notedthat, if a patient with fulminant myocarditis does notdie during acute phase, the long-term prognosis wouldbe good, avoiding both death and transplantation.3
Mechanical circulatory support (MCS) such as PCPSand VADs could serve as a bridge for myocardial recov-ery. Reiss et al. reported that the hemodynamic criteriafor implantation of a support system are: cardiac in-dex <2.0L/min/m2, central venous pressure (CVP) orleft atrial pressure (LAP) >20 mmHg, and urine output<20 mL/hour, despite maximal pharmacological ther-apy.4 Aoyama et al. reported that 30 of 52 patients(57.7%) with myocarditis assisted by PCPS survivedand returned to social life. Significant factors concern-ing the prognosis were the severity of cardiac and renaldysfunction, and prevention of circulatory disturbancesof the legs and multiple organ failure directly associ-
ated to the use of PCPS.5 Maejima et al. reported thatsix of eight patients (75%) with fulminant myocarditisand low left ventricular ejection fraction were treatedusing PCPS and survived.6 Good results have beenreported, particularly for children with fulminant my-ocarditis treated using ECMO, however, it does not al-ways allow adequate output to be reached when usedfor adults.7
We usually first use a PCPS for cardiogenic shockbecause it is more easily and quickly introduced thanVADs. PCPS is a highly effective form of hemodynamicsupport for acute phases of cardiogenic shock due tofulminant myocarditis. But a PCPS cannot be used forlong time because of its several profound complica-tions such as bleeding, hemolysis, hematuria, ischemicchange of the lower limb. It is necessary to make animmediate decision regarding the implantation of VADwhich is more powerful, durable, and biocompatiblethan PCPS, if there is no sign of improvement of my-ocardial function.
We describe the case of a patient with acute ful-minant myocarditis who was treated using a PCPSfor five days but could not recover, so immediatelyunderwent LVAD implantation and was successfullybridged to recovery. It is important to switch fromPCPS to LVAD immediately for surviving acute phasesof fulminant myocarditis when the cardiac function re-covery is not sufficient and longer support would benecessary.
REFERENCES
1. Maybaum S, Stockwell P, Naka Y, et al: Assessment of my-ocardial recovery in a patient with acute myocarditis sup-ported with a left ventricular assist device. J Heart LungTransplant 2003;22:202-209.
2. Davies JE, Kirklin JK, Pearce FB, et al: Mechanical circula-tory support for myocarditis: How much recovery shouldoccur before device removal? J Heart Lung Transplant2002;21:1246-1249.
3. McCarthy 3rd RE, Boehmer JP, Hruban RH, et al: Long-termoutcome of fulminant myocarditis as compared with acute(nonfulminant) myocarditis. N Engl J Med 2000;342:690-695.
4. Reiss N, el-Banayosy A, Posival H, et al: Management ofacute fulminant myocarditis using circulatory support sys-tems. Artif Organs 1996;20:964-970.
5. Aoyama N, Izumi T, Hiramori K, et al: National surveyof fulminant myocarditis in Japan: Theraputic guidelinesand long-term prognosis of using percutaneous cardiopul-monary support for fulminant myocarditis (special re-port from a scientific committee). Circ J 2002;66:133-144.
6. Maejima Y, Yasu T, Kubo N, et al: Long-term progno-sis of fulminant myocarditis rescued by percutaneouscardiopulmonary support device. Circ J 2004;68:829-833.
7. Leprince P, Combes A, Bonnet N, et al: Circulatory sup-port for fulminant myocarditis: Consideration for implan-tation, weaning and explantation. Eur J Cardiothorac Surg2003;24;399-403.

J CARD SURG2008;23:565-589
HENAINE, ET AL.CARDIAC HYDATID CYST
573
Coronary Artery Bypassin Myocardial Ischemia of theYoung Due to Hydatid Cyst
Roland Henaine, M.D., Jean Louis
Mathevet, M.D., Hugues Rouviere, M.D.,
Sylvie Di-Filippo, M.D., Ph.D., Maxime
Cannesson, M.D., Jean-Francois Obadia,
M.D., Ph.D., and Jean Ninet, M.D., Ph.D.
Cardiac Surgery C Department, CardiologicHospital Louis Pradel, Lyon, France
ABSTRACT Cardiac hydatid cyst is an uncommon
disease, especially in France. It is rarely responsi-
ble for myocardial ischemia, and even more rarely
in the young. We report the clinical features and
imaging of a 24-year-old Tunisian woman with hy-
datid cyst of the free wall of the left ventricle re-
sponsible for myocardial ischemia, associated with
a hepatic hydatid cyst. Management consisted of a
combination of surgery with cystopericystectomy
and coronary artery bypass graft and prolonged
medical treatment as for treatment of hepatic hy-
datid cyst. Three-year follow-up revealed no recur-
rence. This case illustrates two interesting points:
the rare clinical presentation of cardiac hydatid cyst
with a coronary syndrome in a young 24-year-old
woman related to compression of the left ante-
rior descending artery by the cyst with a need for
coronary artery bypass graft after resection of the
cyst, and the value of medical treatment of hy-
datid disease, even for cardiac localization. doi:10.1111/j.1540-8191.2008.00626.x (J Card Surg2008;23:573-575)
Cardiac hydatid cyst (HC) is a rare site of Echinococ-cus granulosus parasitic infection and has a variableclinical presentation: an asymptomatic cyst may be dis-covered incidentally, or discovered following a compli-cation.1,2 The ultrasound appearance is highly sugges-tive of the diagnosis, which must always be confirmedby serology, and treatment is mainly surgical.
The authors report the exceptional case of an unsta-ble angina in a 24-year-old woman related to a com-pressive HC, whose medical and surgical treatment,including a coronary revascularization, was effective.
CASE REPORT
Ms. M, 23 years old, born in Tunisia and living inFrance since one year, was hospitalized for investiga-tion of crushing, retrosternal chest pain, occurring onincreasingly less intense effort, associated with palpi-tations. Clinical examination was normal, electrocardio-
Address for correspondence: Roland Henaine, M.D., Department ofCardiac Surgery C, Cardiologic Hospital Louis Pradel, Avenue duDoyen Lepine , 69394 Lyon, France. Fax: +33-4-72-34-18-53; e-mail:[email protected]
gram revealed ischemic signs in the superior lateral ter-ritory, and chest X-ray showed marked enlargementof the left and right heart border. Cardiac morphol-ogy was investigated by transesophageal echocardio-graphy demonstrating a large (66 × 55 mm) homoge-neous cystic mass with irregular margins, arising fromthe lateral wall of the left ventricle. Computed tomog-raphy and magnetic resonance imaging confirmed thecystic nature and intramyocardial position of the lesion(Fig. 1A). Coronary disorders were analyzed by stresstest revealing ischemia of the lateral territory. Coro-nary angiography showed a dilated right coronary arteryensuring retrograde revascularization of all of the leftcoronary network, a long left common coronary artery,stretched by an underlying mass under and reduced toa thin line (Fig. 1B), and left ventriculography showedmarked intracavitary vaulting of the anteroinferior wall.The diagnosis was then confirmed by positive E. gran-ulosus serology and the general work-up revealed apolycystic lesion in the liver.
RESULTS
Therapeutic management consisted of surgery. Af-ter midline sternotomy and opening of the pericardium,the diagnosis was confirmed by the presence of a cystlaminating the myocardium from the left atrioventricu-lar groove to the middle segment of the left anterior de-scending (LAD) artery. Cardiopulmonary bypass (CPB)was established. After aortic clamping and cardiople-gia in the aortic root, compresses soaked in hypertonicsaline were placed on the posterior surface of the cystand around the heart to prevent dissemination of para-sites. Needle aspiration of the cyst evacuated 120 mLof crystal clear fluid and was completed by intracysticlavage with hypertonic saline. Finally, there was incisionof the dome and easy one-piece exclusion of the cystmembrane, which floated freely inside the cyst cavity(Fig. 2). After that, there was progressive weaning ofCPB. The aortic cross clamping time was 65 minutes.However, CPB had to be resumed due to signs of STsegment elevation in the inferior territory. LAD stenosisinduced by the cyst clearly persisted after resection ofthe cyst and it was decided to perform coronary arterybypass graft between the left internal mammary arteryand the LAD. CPB was then easily weaned with no is-chemic recurrence, and without inotropic support. Ef-fective chemotherapy of hydatid disease using alben-dazole was started intraoperatively. The postoperativecourse was uneventful: extubation at the sixth post-operative hour and return to the ward the followingday. The patient remained asymptomatic and was dis-charged 10 days after the operation. The hepatic HCwas operated on three months later. The postoperativecourse was also uneventful. Follow-up at three yearsremained normal.
CONCLUSIONS
Cardiac echinococcosis is rare, even in endemiccountries, representing only 0.5% to 2% of all sites.It is more frequent in the 30 to 40-year age group, witha male predominance. In France, it is almost exclusivelyan imported disease.

574 HENAINE, ET AL.CARDIAC HYDATID CYST
J CARD SURG2008;23:565-589
Figure 1. (A) Magnetic resonance imaging showing the site of the hydatid cyst compressing the left ventricle. (B) Coronary andleft ventricular angiography showing compression of the left coronary trunk by the hydatid cyst.
Although infestation of the heart by the hexacanthembryo mainly occurs via the intravenous or lymphaticroute, the cyst is situated in the left heart three timesmore frequently than in the right heart. This affinity ofthe parasite, especially for the left ventricle, was clar-ified by the studies by James,3 emphasizing the im-portance of the ventricular muscle mass and its bloodsupply, allowing implantation of the parasite. The car-diac site is always primary, but can be the starting pointfor other sites, especially hepatic as in our case. Someseries have reported associated visceral lesions in asmany as 40% of cases.4
Clinical manifestations are initially limited, due to theslow growth of the cyst, and the diagnosis is often es-tablished in asymptomatic patients. However, the cystcan progress to fissure or even intracardiac or extrac-ardiac rupture, with allergic reaction and secondary le-
Figure 2. Operative view after opening the cyst, showing itsintimate relations with the left anterior descending artery.
sions involving the brain in 55% of cases.5 The sec-ond mechanism of discovery involves the mechanicalrepercussions of the cyst, with nonspecific signs: mi-tral or tricuspid valve disease,6 conduction disorders,or arrhythmias for septal cysts1; and extrinsic coronarycompression for cysts in the free wall.6 The presentcase perfectly illustrates this complication: this is a veryrare form of coronary syndrome in a young woman, re-lated to the compression of the left anterior descend-ing artery by the cyst. Very few similar cases have beenin the literature, even in endemic countries, as thesefeatures are usually observed in the case of pericardialrather than intramural cysts, and more often in olderpeople, after a long history of HC.7 Such cysts haveonly exceptionally required coronary revascularizationby bypass graft.8
The diagnostic approach is essentially based ontwo types of examination: Echinococcus serology andechocardiography. Treatment consists of surgery.
Current guidelines for the management of hepaticHC indicate that surgery must be combined with neoad-juvant and adjuvant medical treatment with albenda-zole,9 which allows preoperative sterilization of the cystand therefore a lower risk of intraoperative dissemina-tion, and some authors have suggested that postopera-tive treatment also allows a reduction of recurrences.10
However, this efficacy is difficult to evaluate due to thevery low incidence of recurrences (never described forcardiac HC). In our case, treatment was started im-mediately postoperatively and was continued for sixmonths. The absence of recurrence at three years con-firms the value of this treatment in the management ofhydatid disease. However, in comparison with hepaticHC, clinical examination, ultrasound, and immunologi-cal surveillance are required.

J CARD SURG2008;23:565-589
MORIMOTO, ET AL.ASCENDING AORTA WITH AORTIC DISSECTION
575
REFERENCES
1. Kammoun S, Frikha I, Fourati K, et al: Hydatid cyst ofthe heart located in interventricular septum. Can J Cardiol2000;56:41-44.
2. Kardaras F, Kardara D, Tselikos D, et al: Fifteen yearsurveillance of echinococcal heart disease from a refer-ral hospital in Greece. Eur Heart J 1996;17:1265-1270.
3. James TN: Anatomy of the coronary arteries in health anddisease. Circulation 1958;32:1020.
4. Trigano JA, Mourot F, Talmoudi T, et al: Symptomatologyof hydatid cyst of the heart. Study of a continuous series of13 cases and value of X-ray computed tomography. ArchMal Cr 1985;78:1895-1899.
5. Elhattaoui M, Charei N, Bennis A, et al: Kyste hydatiquedu cr, propos de 10cas. Arch Mal Cr 2006;99:19-25.
6. Oliver JM, Sotillo JF, Dominguez FJ, et al: Two-dimensional echocardiographic features of echinococco-sis of the heart and great blood vessels. Clinical and sur-gical implications. Circulation 1988;17:327-337.
7. Kosar F, Aksoy Y, Sahin I, et al: Pericardial hydatid cystmimicking acute coronary syndrome. Tex Heart Inst J2005;32(4):570-572.
8. Yilik L, Ergunes K, Yetkin U, et al: Coronary revasculariza-tion and cysthydatid operation Heart Lung 2004;33(1):42-45.
9. Gil-Grande LA, Rodriguez-Caabeiro F, Prieto JG, et al: Ran-domised controlled trial of efficacity of albendazole in intraabdominal hydatid disease. Lancet 1993;342:1269-1272.
10. Eroglu A, Kurkcuoglu C, Karaoglanoglu N, et al: Primaryhydatid cysts of the medistinum. Eur J Cardiothorac Surg2002;22:599-601.
Unusual False Aneurysm of theAscending Aorta Associatedwith Ruptured Acute Type AAortic Dissection
Hironobu Morimoto, M.D., Koji Tsuchiya,
M.D., Masato Nakajima, M.D.,
and Okihiko Akashi, M.D.
Department of Cardiovascular Surgery,Yamanashi Central Hospital, Yamanashi,Japan
ABSTRACT False aneurysm of the thoracic aorta un-
related to trauma, or to previous aortic or cardiac
surgery, is extremely rare. We encountered a case
of ascending aortic false aneurysm formation as-
sociated with ruptured acute type A aortic dissec-
tion. The false aneurysm, which was contained by
thin connective tissue surrounding the aortic wall,
was located beside the false lumen of the dissected
ascending aorta, expanding toward the transverse
sinus. We immediately decided to perform an emer-
gency operation. We noted the large entry site at
the anterior wall of the dissected ascending aorta
after resection of the flap. We identified the false
aneurysm arising from a small tear of the false lu-
men. Graft replacement of the ascending aorta us-
ing a tube graft was performed. The postoperative
course was satisfactory. This pathology was be-
lieved to be not only a consequence of hemostasis,
but also a process of re-rupture of the dissected
aorta. doi: 10.1111/j.1540-8191.2008.00677.x (JCard Surg 2008;23:575-576)
CLINICAL SUMMARY
An 84-year-old woman with a history of hyper-tension was admitted to another hospital, present-ing with chest pain and nausea. Although her symp-toms resolved after admission, chest pain recurred onthe fifth day. Chest computed tomography (CT) re-vealed acute type A aortic dissection, and she wasreferred to our hospital for surgery. On arrival, herhemodynamic status was stable. Echocardiographydemonstrated pericardial effusion and mild aortic re-gurgitation (AR). We examined the CT films fromthe referring hospital and recognized dissection ofthe aorta (De Bakey type II) with a dilatation of5 cm in diameter, a small amount of pericardial effusion,and ascending aortic false aneurysm—arising from thefalse lumen of the dissected ascending aorta, towardthe transverse sinus space (Fig. 1). Preoperatively, weinterpreted this as a coronary artery aneurysm or mal-position of the left auricular appendage, because wehad never previously recognized a false aneurysm ofthis kind.
We immediately decided to perform an emergencyoperation. Commencing a median sternotomy, the peri-cardial cavity was found to be filled with old blood. Stan-dard cardiopulmonary bypass was instituted with rightatrial drainage and left femoral arterial return, and withright upper pulmonary venous venting. After antegrade
Address for correspondence: Hironobu Morimoto, M.D., Depart-ment of Cardiovascular Surgery, The Heart Institute of Japan, TokyoWomen’s Medical University, 8-1 Kawada-cho, Shinjuku-ku. Tokyo 162-8666, Japan. Fax: 81-3-3356-0441; e-mail: [email protected]
Figure 1. Preoperative CT demonstrating the false aneurysmarising from the false lumen of the dissected ascending aorta(white arrow). LA = left atrium; PA = pulmonary artery.

576 SUN, ET AL.PFO CLOSURE FAILURE WITH AMPLATZER
J CARD SURG2008;23:565-589
Figure 2. (A) Surgical view showing a small tear of the adventitia of the dissected aorta (black arrow). (B) The schema.
cold blood cardioplegia was selectively administered(with topical hypothermia), cardiac arrest was obtained.We noted the large entry site at the anterior wall ofthe dissected ascending aorta (2 cm above the sino-tubular junction) after resection of the flap. We identi-fied the false aneurysm arising from a small tear of thefalse lumen, which was surrounded by connective tis-sue and hematoma (Fig. 2).
Graft replacement of the ascending aorta usinga tube graft was performed under deep hypother-mic circulatory arrest. The postoperative course wassatisfactory.
DISCUSSION
Mediastinal false aneurysm is recognized as a rarebut life-threatening complication after thoracic aor-tic surgery. Various predisposing factors—includinginfection, suture dehiscence or loosening, and tis-sue necrosis—have been reported.1,2 However, falseaneurysm of the thoracic aorta unrelated either totrauma or to previous aortic or cardiac surgery is ex-tremely rare.
In the present case, the false aneurysm was associ-ated with rupture of an acute aortic dissection. Thereare few reports in the literature about the occurrenceof false aneurysm associated with acute aortic dis-section. The rupture of a dissected ascending aortamost frequently induces cardiac tamponade, with en-suing hemodynamic instability. This is the most com-mon cause of death in patients with acute type A aorticdissection.3 Clinically, we often experience rapid de-terioration of hemodynamics in patients with cardiactamponade caused by acute aortic dissection duringstand-by surgery. It was believed that re-rupture ofthe dissected aorta could be a major causative fac-tor in such cases. In the present case, the false lu-men of the dissected ascending aorta penetrated tothe pericardial cavity and was contained by thin con-nective tissue within the transverse sinus space, re-sulting in the formation of a false aneurysm and stablehemodynamics.
We were unable to find any reference to a simi-lar case in the literature. However, we conjecture that
when the adventitia of the dissected aorta developeda small tear, the blood pressure fell suddenly and tem-porarily, resulting in the formation of a false aneurysmcontained by thin connective tissue surrounding the as-cending aorta. Furthermore, we considered this to benot only a result of hemostasis, but also a process ofre-rupture of the dissected aorta.
We acknowledge the fine illustration, which Dr. FuminagaSuetsugu drew.
REFERENCES
1. Albuquerque FC, Krasna MJ, McLaughlin JS. Chronic, trau-matic pseudoaneurysm of the ascending aorta. Ann ThoracSurg 1992;54:980-982.
2. Katsumta T, Moorjani N, Vaccari G, Westaby S. Mediastinalfalse aneurysm after thoracic aortic surgery. Ann ThoracSurg 2000;70:547-552.
3. Crawford ES. The diagnosis and management of aortic dis-section. JAMA 1990;264:2537-2541.
PFO Closure Failure WithAmplatzer: A Patient WithConcomitant Multiple StrokeRisk Factors
Xiumei Sun, M.D., Jennifer Ellis, M.D.,
Lowell Satler, M.D., and Peter C. Hill,
M.D.
Section of Cardiac Surgery, Department ofSurgery, Washington Hospital Center,Washington, D.C
doi: 10.1111/j.1540-8191.2008.00588.x (J CardSurg 2008;23:576-578)

J CARD SURG2008;23:565-589
SUN, ET AL.PFO CLOSURE FAILURE WITH AMPLATZER
577
Figure 1. Amplatzer device with septal remnant in place.
Patent foramen ovale (PFO)-associated stroke is ex-tensively recognized, but more than one PFO alongwith multiple risk factors of stroke is rarely reported.In this study, we present the case of a 57-year-old manwith multiple large PFOs, right-to-left shunting, resid-ual shunting, and continuing strokes after closure of thePFO with an Amplatzer device. This case shows the dif-ficulty in identifying a middle-age patient with multiplestroke risk factors and the complexity of how to definethe benefit from device closure of a PFO.
In July 2005, a 57-year-old white male presented tohospital complaining of slurred speech, right-arm weak-ness, and chest pain lasting for three days. Before thisadmission, he had multiple admissions to other clinicfacilities with diagnoses of coronary disease (CAD),hypertension, hypertension crisis, cerebrovascular dis-ease, heart failure, hypercholesterolemia, and human
Address for correspondence: Jennifer Ellis, M.D., Section of CardiacSurgery, Department of Surgery, Washington Hospital Center, 110 Irv-ing Street, N.W., Suite 1E3, Washington, D.C. 20010-2975. Fax: 202-291-1436; e-mail: [email protected]
Figure 2. Uncorrected PFOs.
immunodeficiency virus (HIV) carrier and disease. Hisblood pressure is 192/123 mmHg; hemoglobin level is16.4g/dL, platelet count of 324,000/mm3, and CD4 cellcount of 475. Prior to a complete evaluation, he signedout against medical advice when his speech and armweakness improved. Approximately one month later,he was readmitted with the same complaints. His med-ical evaluation at that time included magnetic reso-nance imaging (MRI) of the brain, carotid Doppler ultra-sounds, bilateral lower-extremity Dopplers, chest V/Qscan, magnetic resonance angiogram of the brain, andcardiac echocardiography. He was diagnosed as hav-ing acute left internal capsule lacunar infarcts with righthemiparesis, pulmonary thromboembolism, hyperten-sion, hypercholesterolemia, CAD with 70% stenosis ofleft anterior descending artery (LAD), and one PFO, andno evidence for deep vein thrombosis (DVT). The cardi-ologist noted that the patient had 70% LAD stenosis,but there were no acute EKG abnormalities presentat that time. After review of the patient’s multiplemedical problems by his primary physician and cardi-ologist, he underwent implantation of an Amplatzerdevice and was prescribed warfarin, ACE inhibitors,aspirin, clopidogrel, metoprolol, amlodipine, atorvas-tatin, and anti-HIV drugs. The immediate postproce-dure echo showed no flow across the foramen ovale.He was recommended re-evaluation after four to sixweeks for percutaneous coronary intervention.
The patient was not compliant with his medicationsand, in June 2006, was readmitted with acute blurredvision, generalized weakness, left facial numbness, andunsteady gait. A MRI indicated acute cerebral vas-cular accidents (CVAs) involving both cerebral hemi-spheres. Duplex of the legs was negative for DVT.Transesophageal echocardiogram (TEE) revealed no ev-idence of left atrial thrombus, but did reveal two 2-mmPFOs near his closure device, a right-to-left shunt, anda residual shunt around the device. He had moderateconcentric left ventricular hypertrophy and an ejectionfraction of 55%. His CD4 cell count was 225, plateletcount of 176,000/mm3. His coagulopathy work-up re-vealed a hypercoagulable state with a decreased factorS level of 37%. Serum C-reactive protein, antithrombinIII, factor V, and lupus anticoagulant and homocysteinelevels were normal. He was restarted on beta blocker,ACE inhibitor, Ca2+ channel blocker, antiplatelet ther-apy, anticoagulation, and anti-HIV treatment.
One month later, the patient was readmitted withacute onset of right-sided numbness and weaknessalong with aphasia and dysarthria. His International Nor-malized Ratio (INR) was 1.2. Repeated MRI showedmultiple new infarcts in the right basal ganglia and leftthalamus that were not present one month prior. Thepatient also had new caudad and other periventricu-lar white matter infarcts in both cerebral hemispheres.There were multiple old lacunar infarcts present on thethalamus, basal ganglia, and cerebellum. Because ofhis ongoing strokes in the presence of incompletelyclosed PFOs, his known CAD, and his history of non-compliance to anticoagulation medications, the patientunderwent a coronary artery bypass graft (CABG) withleft internal mammary artery bypass grafting of the LADcoronary artery (LIMA-LAD), excision of the Amplatzer

578 YEREBAKAN, ET AL.RIGHT VENTRICULAR SUPPORT AFTER HEART TRANSPLANTATION
J CARD SURG2008;23:565-589
Figure 3. Amplatzer device at one year with tissue ingrowth.
device, closure of PFOs, and closure of the intra-arterialseptum in July 2006. We present this case report toshow the size of the persistent openings, the level ofendothelization after one year of implantation, and thecomplexity of multiple PFOs with multiple risk factors.
COMMENT
According to National Heart/Stroke Associationguidelines, this patient had multiple risk factors forstroke. His risks were hypertension, atherosclerosis,obesity, PFOs, hypercoagulable state, and acquired im-munodeficiency syndrome (AIDS). PFO is present inup to 27% of general population and has been in-creasingly recognized as a source of paradoxical em-bolism associated with cerebrovascular events. Theprevalence of a PFO with cryptogenic stroke in patientsyounger than 55 years of age is 46%.1 TranscatheterPFO closure has proved to be a safe, effective alter-native to medical therapy or to surgical closure for sec-ondary prevention of cerebrovascular events; however,recurrent stroke in the presence of incomplete clo-sure with residual shunting remains a major adverseevent.2,3 The reported one-year incidence of recurrentstroke for patients treated with transcatheter closure is0.0% to 4.9%, compared with 3.8% to 12.0% in medi-cally treated patients.4 Older patients and patients withother cardiovascular risk factors can have more than a50% recurrent stroke or other neurologic event rate.2,3
A large PFO size (>2 mm) or an associated atrial sep-tal aneurysm is the morphologic characteristic of thePFO that can account for an additional risk of stroke re-currence.5 Whether a residual shunt is associated withan increased risk for events is controversial2,3 due todiffering shunt morphology/anatomy.
Our patient presented multiple PFOs, residual shunt,and multiple additional risk factors for stroke. The sub-sequent incomplete closure of the PFOs along withthe incomplete epithelization of the closure device wasconsistent with a compromised prognosis.
REFERENCES
1. Lamy C, Giannesini C, Zuber M, et al: Clinical and imag-ing finding in cryptogenic stroke patients with and without
patent foramen ovale: The PFO-ASA study: Atrial septalaneurysm. Stroke 2002;33:706-711.
2. Hung J, Landzberg MJ, Jenkins KJ, et al: Closure ofpatent foramen ovale for paradoxical emboli: Intermediate-term risk of recurrent neurological events followingtranscatheter device placement. J Am Coll Cardiol2000;35:1311-1316.
3. Braun M, Gliech V, Boscheri A, et al: Transcatheter closureof patent foramen ovale (PFO) in patients with paradoxicalembolism. Periprocedural safety and mid-term follow-up re-sults of three different device occluder systems. Eur HeartJ 2004;25:424-430.
4. Khairy P, O’Donnell CP, Landzberg MJ. Transcatheter clo-sure versus medical therapy of patent foramen ovale andpresumed paradoxical thromboemboli: A systematic re-view. Ann Intern Med 2003;139:753-760.
5. Mas JL, Arquizan C, Lamy C, et al: Patent ForamenOvale and Atrial Septal Aneurysm Study Group. Recurrentcerebrovascular events associated with patent foramenovale, atrial septal aneurysm, or both. New Engl J Med2001;345:1740-1746.
Right Ventricular FailureFollowing HeartTransplantation-Recovery AfterExtended Mechanical Support
Can Yerebakan, M.D., Semih Buz, M.D.,
Michael Huebler, M.D., Yug Weng, M.D.,
Ph.D., Hans Lehmkuhl, M.D., Ph.D., and
Roland Hetzer, M.D., Ph.D.
Department of Thoracic and CardiovascularSurgery, German Heart Institute Berlin,Berlin, Germany
ABSTRACT Early graft failure, particularly right ven-
tricular dysfunction, remains a significant determi-
nant of early morbidity and mortality in heart trans-
plant recipients. If conservative medical manage-
ment fails to help recover cardiac allograft func-
tion, mechanical circulatory support either bridg-
ing to recovery or retransplantation remains the
last option. We report on a 16-year-old patient with
hypertropic nonobstructive cardiomyopathy who
was weaned successfully from a right ventricu-
lar assist device (RVAD) after extended right ven-
tricular mechanical support for three months fol-
lowing heart transplantation. doi: 10.1111/j.1540-8191.2008.00698.x (J Card Surg 2008;23:578-580)
Right ventricular failure after orthotopic heart trans-plantation is a life-threatening complication. In suchcases, refractory to medical management, mechani-cal circulatory assistance is an inevitable option. How-
Address for correspondence: Can Yerebakan, M.D., PatriotischerWeg 82, 18057, Rostock, Germany. Fax: 0049-381-494-6109; e-mail:[email protected]

J CARD SURG2008;23:565-589
YEREBAKAN, ET AL.RIGHT VENTRICULAR SUPPORT AFTER HEART
TRANSPLANTATION579
ever, the prognosis of early graft or right heart failureis still poor even with temporary mechanical circulatorysupport.1,2
A 16-year-old female with hypertropic nonobstruc-tive cardiomyopathy was transferred to our institutionin May 2005 for heart transplantation. Preoperatively,she had twice undergone cardiopulmonary resusci-tation secondary to ventricular fibrillation. The recipi-ent’s preoperative hemodynamic evaluation revealedpulmonary artery pressures (PAP) of 40/15/25 mmHg,a transpulmonary gradient (TPG) of 4 to 6 mmHg, andpulmonary vascular resistance (PVR) of 1.5 Wood units.A donor heart from a 39-year-old female (160 cm,50 kg), who had suffered from a cerebral glioblas-toma, was transplanted to the patient (158 cm, 47 kg)orthotopically. After an uncomplicated technical pro-cedure and cessation of cardiopulmonary bypass,unfortunately, severe right ventricular dysfunctionensued unexpectedly with the need for high-dosecatecholamine support in the immediate postoper-ative period. Despite comprehensive pharmacologi-cal support with epinephrine, dobutamine, iloprost,nitroglycerin, nitric oxide, and PDE-inhibitors intraop-eratively, it was not possible to stabilize the right ven-tricular function. We decided to implant a nonpulsatileflow assist system for short-term support (Biomedicus,Eden Prairie, MN, USA) and the patient was transferredto our intensive care unit. During the first postoperativeweek, attempts were made to reduce the pump flowguided by echocardiographic monitoring of the rightventricular function. Despite full medical and mechani-cal support, no recovery was seen; so, an implantationof a long-term paracorporal right ventricular assist de-vice (RVAD; Berlin Heart Excor, Berlin, Germany) wasperformed on the fifth postoperative day. Serial pump-stop echocardiographic evaluations were employed inorder to monitor right ventricular function closely, aim-ing to determine the explantability of the RVAD.
The first echocardiogram on the tenth postopera-tive day (under maximal medical therapy) showed awell-preserved left ventricular function (left ventricu-lar ejection fraction (LVEF) 70%, enddiastolic diameter(LVEDD) 35 mm) with no ejection from the right ven-tricle and RVEDD of 23 mm. The second scan on thetwelfth postoperative day was performed two minutesafter pump stop showed LVEF 70%, LVEDD 33 mm,and RVEF 15%, RVEDD 35 mm. Results of the secondoff-pump scan, performed one week later were: LVEF80%, LVEDD 26 mm, and RVEF 20%, RVEDD 15 mm.The patient was reregistered for high-urgency heart-lung transplantation because of the lack of recovery ofthe right ventricular function. Meanwhile she had devel-oped systemic infection, and respiratory and acute re-nal insufficiencies. Therefore, her status was changedto “nontransplantable” in the fifth postoperative weekuntil such time as her infection might resolve.
In the eighth postoperative week, echocardiographicanalysis of the right ventricle during pump stop showednormal diameter time and ejection fractions of bothventricles so that weaning from the RVAD seemedto be possible at once (LVEF 70%, LVEDD 46 mm,and RVEF 65%, RVEDD 26 mm). As a precaution,
medical preconditioning with iloprost and sildenafil forone week was carried out. The RVAD was removedafter 80 days of mechanical circulatory support with-out any operative or postoperative complications. Af-ter explantation of the assist device, we observed fullyrecovered right ventricular function following a shortperiod of medical support (epinephrine, nitric oxide, ilo-prost, milrinone, and nitroglycerin), which was reducedand then terminated within one week. The patient wastransferred to our normal transplant ward two monthsafter explantation of the RVAD and was discharged forrehabilitation following intensive physiotherapy threemonths later.
CONCLUSIONS
Early right-sided circulatory failure following hearttransplantation remains a challenge for physicians andhas dismal prognosis.3 Therapeutic options are limitedif right ventricular failure is resistant to conservativetreatment. Mechanical circulatory support with the aimof either for bridging to recovery or retransplantationhas been practiced for many years, producing mod-est results in this setting.2,4,5,6 In other preliminaryexperimental studies, it has been reported that lessinvasive mechanical circulatory support may be morefavorable.7
In this case, treatment of early severe right ventric-ular failure after orthotopic heart transplantation in a16-year-old girl was successful using extended me-chanical circulatory support of the right ventricle.
Initial evaluation of right ventricular function duringmaximal mechanical and medical support was followedby weekly off-pump tests in order to guide fluid and in-otropic therapy. Additionally, pharmacological, ventila-tory, and mechanical support for the right ventricle wasmaximized in order to optimize right ventricular functionby controlling preload, decreasing afterload, and provid-ing inotropic support for both ventricles. Finally, afterthe point of “full recovery,” removal of the RVAD wasreached, and full pharmacological support was againapplied for preconditioning. Serial pump-stop echocar-diographic evaluations of right ventricular function arehelpful in determining the suitable time point of RVADremoval.
In most cases, the exact reason for isolated rightventricular dysfunction after heart transplantation is un-clear. The risk factors for early right ventricular dysfunc-tion have been postulated as an elevated PAP, PVR, orTPG in the recipient; extended ischemic time; marginalgraft function; insufficient graft protection; difference inbody size between donor and recipient or right ventric-ular ischemia by means of spasm of the right coronaryartery; and air or particulate embolism. These risk fac-tors, however, have also been discussed having con-troversial significance regarding the development ofpostoperative right ventricular dysfunction by many au-thors.
In this case, the reason for early right ventricular fail-ure is not clear. Since there was a slightly elevatedPAP as a result of left ventricular dysfunction, a nor-mal PVR and TPG, no body size mismatch between

580 CICEKCIOGLU, ET AL.PMI-VSD REPAIR WITH THORACOTOMY
J CARD SURG2008;23:565-589
donor and recipient, no differing, long-practiced surgicaltechniques and strategies for myocardial protection inour center, and a good donor heart function, these riskfactors would be excluded as reasons for right ventricu-lar failure. Furthermore, perioperatively, there were nosigns for myocardial ischemia in clinical and laboratoryfindings.
The most interesting feature of this case is the recov-ery of right heart function following extended mechan-ical right ventricular support of 80 days. This may indi-cate an adaptation of the right ventricle although therehas been no clear difference in the pulmonary circula-tion between the donor and recipient except a slightlyelevated PAP in the recipient. If only an elevated PAPwould be sufficient to cause such a severe right ventric-ular compromise remains unclear whereas it is knownthat in other cases patients with even higher PVR andTPG can be transplanted successfully. The question,whether a retransplantation or an extended mechani-cal support would lead to a better outcome for suchpatients, cannot be yet answered. Extended mechan-ical circulatory support is known to be marked with ahigh rate of thromboembolic, hemorrhagic, and device-related complications and infections, but the institutionof less invasive and safer assist systems in future mayovercome some of these complications.
In conclusion, right ventricular dysfunction followingheart transplantation remains in most cases an unpre-dictable cause of early morbidity and mortality. Thechoice of the suitable mechanical support (type of as-sist device, mode of support) should be made individ-ually in every case according to overall hemodynamicsand center-experience. Isolated right ventricular failurehas been considered as a temporary entity and is likelyto allow weaning from the assist device.5 Extendedmechanical circulatory support may restore right ven-tricular dysfunction even after months. Serial pump-stop echocardiographies may be helpful to determinethe time point of the explantability of the RVAD andprotect the right ventricle from further jeopardy in thissetting.
Acknowledgments: I gratefully acknowledge the support byMichael Jurmann, M.D., Ph.D., and Christoph Knosalla, M.D.,Ph.D., and from the German Heart Institute Berlin, and thankAnne Gale, editor in Life Sciences, for editorial assistance.
REFERENCES
1. Nakatani T, Radovancevic B, Frazier OH: Right heart as-sist for acute right ventricular failure after orthotopic hearttransplantation. ASAIO Trans 1987;33:695-698.
2. Karavana MN, Sinha P, Eng M, et al: Mechanical supportfor the failing cardiac allograft: A single center experience.J Heart Lung Transplant 2003;22:542-547.
3. Klima U, Ringes-Lichtenberg S, Warnecke G, et al: Severeright heart failure after heart transplantation. A single centerexperience. Transplant Int 2005;18(3):326-332.
4. Chen JM, Lewin HR, Rose EA, et al: Experience with rightventricular assist devices for perioperative right-sided cir-culatory failure. Ann Thorac Surg 1996;61(1):305-310.
5. Jurmann MJ, Haverich A, Schafers HJ, et al: Early graft fail-ure after heart transplantation: Circulatory assist versus re-
transplantation. In: Akutsu T (ed.): Artificial Heart 3. SpringerVerlag, Tokyo, Japan, 1991; pp. 275-284.
6. Jurmann MJ, Wahlers T, Coppola R, et al: Early graft fail-ure following cardiac transplantation: Management by ex-tracorporeal circulatory assist and retransplantation. J HeartTransplant 1989;8:474-478.
7. Martin J, Benk C, Yerebakan C, et al: The new “Impella”intracardiac microaxial pump for treatment of right heart fail-ure after orthotopic heart transplantation. Transplant Proc2001;33(7 and 8):3549-3550.
Residual PostmyocardialInfarction Ventricular SeptalDefect Repair through RightAtrium with Right Thoracotomyon Beating Heart Technique
Ferit Cicekcioglu, M.D.,∗ Ufuk Tutun,
M.D.,∗ Ali Ihsan Parlar, M.D.,∗ Kerem Yay,
M.D.,∗ Yesim Guray, M.D.,† and Salih
Fehmi Katircioglu, M.D.∗
∗Cardiovascular Surgery Clinic, and†Cardiology Clinic, Turkiye Yuksek IhtisasHospital, Ankara, Turkey
ABSTRACT Background and Aim: The incidence of
residual opening after repair of postmyocardial in-
farction ventricular septal defect (VSD) was re-
ported to be 10% to 25%. Redo surgery with re-
median sternotomy is more complex than primary
surgery and is consequently associated with higher
mortality and morbidity due to the myocardial
and patent coronary grafts injury during pericar-
dial dissection. Methods: A 59-year-old female pa-
tient had coronary artery bypass grafting and clo-
sure of post myocardial infarction ventricular sep-
tal defect with patch 10 months earlier in a differ-
ent cardiac center. She was admitted to the hospi-
tal for severe congestive heart failure. Results: She
was operated because of the residual opening af-
ter repair of post myocardial infarction ventricular
septal defect. Post myocardial infarction ventricu-
lar septal defect closure was performed through
the right atrium by on-pump beating heart tech-
nique via the right thoracotomy. Conclusions: Clo-
sure of post myocardial infarction ventricular sep-
tal defect with this technique offers an alternative
and safe approach to repair of the residual VSD
when the coronary bypass grafts are patent. doi:10.1111/j.1540-8191.2007.00543.x (J Card Surg2008;23:580-583)
Address for correspondence: Salih Fehmi Katircioglu, M.D., Cardiovas-cular Surgery Clinic, Turkiye Yuksek Ihtisas Hospital, 06100, Sihhiye,Ankara, Turkey. Fax: +90-312-229-58-68; e-mail: [email protected]
J CARD SURG2008;23:565-589
CICEKCIOGLU, ET AL.PMI-VSD REPAIR WITH THORACOTOMY
581
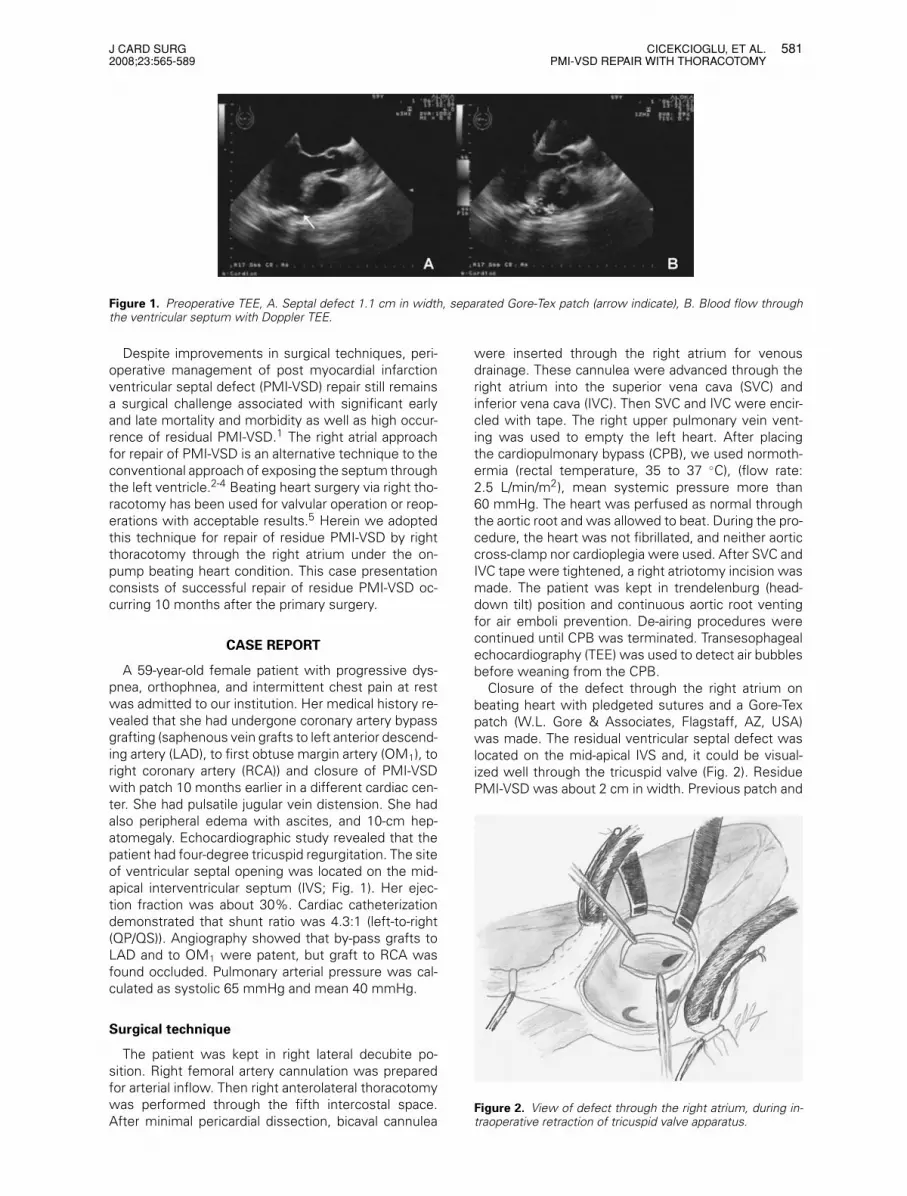
Figure 1. Preoperative TEE, A. Septal defect 1.1 cm in width, separated Gore-Tex patch (arrow indicate), B. Blood flow throughthe ventricular septum with Doppler TEE.
Despite improvements in surgical techniques, peri-operative management of post myocardial infarctionventricular septal defect (PMI-VSD) repair still remainsa surgical challenge associated with significant earlyand late mortality and morbidity as well as high occur-rence of residual PMI-VSD.1 The right atrial approachfor repair of PMI-VSD is an alternative technique to theconventional approach of exposing the septum throughthe left ventricle.2-4 Beating heart surgery via right tho-racotomy has been used for valvular operation or reop-erations with acceptable results.5 Herein we adoptedthis technique for repair of residue PMI-VSD by rightthoracotomy through the right atrium under the on-pump beating heart condition. This case presentationconsists of successful repair of residue PMI-VSD oc-curring 10 months after the primary surgery.
CASE REPORT
A 59-year-old female patient with progressive dys-pnea, orthophnea, and intermittent chest pain at restwas admitted to our institution. Her medical history re-vealed that she had undergone coronary artery bypassgrafting (saphenous vein grafts to left anterior descend-ing artery (LAD), to first obtuse margin artery (OM1), toright coronary artery (RCA)) and closure of PMI-VSDwith patch 10 months earlier in a different cardiac cen-ter. She had pulsatile jugular vein distension. She hadalso peripheral edema with ascites, and 10-cm hep-atomegaly. Echocardiographic study revealed that thepatient had four-degree tricuspid regurgitation. The siteof ventricular septal opening was located on the mid-apical interventricular septum (IVS; Fig. 1). Her ejec-tion fraction was about 30%. Cardiac catheterizationdemonstrated that shunt ratio was 4.3:1 (left-to-right(QP/QS)). Angiography showed that by-pass grafts toLAD and to OM1 were patent, but graft to RCA wasfound occluded. Pulmonary arterial pressure was cal-culated as systolic 65 mmHg and mean 40 mmHg.
Surgical technique
The patient was kept in right lateral decubite po-sition. Right femoral artery cannulation was preparedfor arterial inflow. Then right anterolateral thoracotomywas performed through the fifth intercostal space.After minimal pericardial dissection, bicaval cannulea
were inserted through the right atrium for venousdrainage. These cannulea were advanced through theright atrium into the superior vena cava (SVC) andinferior vena cava (IVC). Then SVC and IVC were encir-cled with tape. The right upper pulmonary vein vent-ing was used to empty the left heart. After placingthe cardiopulmonary bypass (CPB), we used normoth-ermia (rectal temperature, 35 to 37 ◦C), (flow rate:2.5 L/min/m2), mean systemic pressure more than60 mmHg. The heart was perfused as normal throughthe aortic root and was allowed to beat. During the pro-cedure, the heart was not fibrillated, and neither aorticcross-clamp nor cardioplegia were used. After SVC andIVC tape were tightened, a right atriotomy incision wasmade. The patient was kept in trendelenburg (head-down tilt) position and continuous aortic root ventingfor air emboli prevention. De-airing procedures werecontinued until CPB was terminated. Transesophagealechocardiography (TEE) was used to detect air bubblesbefore weaning from the CPB.
Closure of the defect through the right atrium onbeating heart with pledgeted sutures and a Gore-Texpatch (W.L. Gore & Associates, Flagstaff, AZ, USA)was made. The residual ventricular septal defect waslocated on the mid-apical IVS and, it could be visual-ized well through the tricuspid valve (Fig. 2). ResiduePMI-VSD was about 2 cm in width. Previous patch and
Figure 2. View of defect through the right atrium, during in-traoperative retraction of tricuspid valve apparatus.

582 CICEKCIOGLU, ET AL.PMI-VSD REPAIR WITH THORACOTOMY
J CARD SURG2008;23:565-589
Figure 3. View of Gore-Tex patch through the right atriumafter repair, during intraoperative retraction of tricuspid valveapparatus.
sutures were not effective and excised. Additionally,annular dilatation, valvular fibrosis, and retraction wereobserved in the tricuspid valve.
PMI-VSD closure was performed with polypropylenesutures with Teflon pledgets, which passed throughthe healthy tissue and an appropriate-sized Gore-Texpatch in a horizontal mattress fashion (Fig. 3). Visualiza-tion for the suture placement was good. Because tri-cuspid valve was not suitable for repair, tricuspid valvereplacement was carried out with 29-mm bioprosthe-sis. The CPB time was 120 minutes without cross-clamp. The patient was weaned from CPB withoutany difficulty and no rhythm disturbance was observed.The postoperative period was uneventful. Echocardio-graphy performed prior to discharge revealed a resid-ual small 1.2:1 left-to-right shunt, with reduction ofpulmonary artery pressure from preoperative systolic65 mmHg to postoperative 35 mmHg systolic pressure(Fig. 4). The patient was discharged from the hospitalon the sixth postoperative day with New York HeartAssociation functional classification class II. She wasin good condition two months after the operation.
Figure 4. Postoperative TTE view; arrow indicates residualventricular septal defect.
DISCUSSION
PMI-VSD is a rare condition which occurred in 1%to 3% of cases before pharmacological and mechan-ical reperfusion therapy.6 Nowadays, the incidence isapproximately 0.2% of all cases with acute myocardialinfarction.6 Septal rupture may occur within 10 to 14days after the infarction, but this period may be as shortas a few hours or as long as two weeks or one month.5
PMI-VSD is most commonly located in the anteroapicalseptum (in approximately 60% of cases). These septalruptures are caused by anteroseptal myocardial infarc-tion following occlusion of the left anterior descendingartery. Inferoposterior septal defects are less commonthan anterior and apical defects (in approximately 20%to 40% of cases), and occur following inferoseptal in-farction, which is usually due to occlusion of a dominantright coronary artery or, less frequently, a dominant cir-cumflex artery.6,7
Despite improvements in surgical techniques, PMI-VSD remains a surgical challenge associated withsignificant morbidity and early and late mortality.1,8,9
Conservative treatment is not recommended becausemost patients develop congestive heart failure and car-diogenic shock and finally die. Mortality in only medi-cal treatment is extremely high, above 90%, whereasmortality after surgical treatment varies between 19%and 60% in different studies.1,6,8,9 Surgery should beperformed soon after the diagnosis is made in mostpatients. Conventional repair of a PMI-VSD has beenperformed by ventriculotomy through the infarct zone.However, this approach carries a significant risk due tohemorrhage, extension of infarction, or further progres-sion of ventricular dysfunction.
Frassani et al. reported that the incidence of resid-ual defect after traditional operative repair was 10%to 25%.10 Remedian sternotomy is a potentially riskytechnique for reoperations, especially for patients hav-ing patent bypass grafts and scar tissue on the ven-tricular muscle. Reoperation is more complex than pri-mary surgery.11 Myocardial and patent coronary bypassgrafts injury, excessive bleeding, and poor myocardialprotection during operation are some of the factorsincreasing the risk of mortality and morbidity duringthe reoperation.12 In addition, the evidence from US(Society of Thoracic Surgeons) and UK (Society of Car-diothoracic Surgeons) national databases would sup-port the view that revisional heart surgery carried atwo-fold to three-fold increase in mortality. Right lateralthoracotomy approach has been used previously in mi-tral valve reoperations with acceptable results.13 It hasbeen suggested that this approach saves time, is saferfor emergency procedures, and is helpful in situationsin which difficult dissection of the heart, such as patentinternal mammary artery or saphenous vein grafts, arepresent. Our group adopted a technique of reoperationfor revisional mitral valve surgery via right thoracotomyduring normothermic CPB without cross-clamping theproximal aorta. This technique is simple, eliminates my-ocardial ischemia during cardioplegic arrest and needof hypothermia, shortens CPB time, and does not in-crease the risk of central nervous system (CNS) injury.

J CARD SURG2008;23:565-589
KORKMAZ, ET AL.AIR EMBOLISM BY BLOWER-MISTER
583
Thompson et al. used this technique for mitral valvereoperations, and demonstrated that overall CNS in-jury rate was only 1.6%.5 It is also clearly demon-strated that the operative technique offers a guaranteeagainst air embolism. Normothermic perfusion also re-duces the risks of induced hypothermic coagulopathyand blood loss, and enhances physiologic condition formyocardium. We believe that allowing the myocardiumto beat at normothermia with maintenance of normalcoronary perfusion offers optimal myocardial protec-tion by better preservation of myocardial blood flowdistribution. This is particularly important in patientshaving impaired left ventricle function and in reoper-ations. In this case report, we adopted this techniquefor transatrial closure of residual PMI-VSD with perfectresults. This technique offers a simple, effective, andsafe alternative to the conventional techniques. Hypo-thetically, the increase in the risk of air embolism wasnot observed, because competent aortic valve (like aor-tic cross-clamp) was offered a guarantee against airembolism. Furthermore, this technique is likely to beadvantageous especially in elderly patients who havecalcified aorta. The only drawback of this technique isthe presence of aortic incompetency.
The reason why we switched to the right thoraco-tomy and the right atrial incision was based on our initialexperiment regarding PMI-VSD repair via the right atri-atomy. This operation was performed with mediastinalsplit and conventional cardioplegia technique.4 We ob-serve that the right atrial approach gives us sufficientexposure without incising the ventricular muscle. Thisexperience encourages us to approach the right atriumvia the right thoracotomy to repair the PMI-VSD. Thistechnique is especially important if the patient has un-dergone the operations previously.
Repair of residual PMI-VSD through the right atriumby on-pump beating heart technique via the right tho-racotomy approach offers an alternative method forrepair of midmuscular or posterior ventricular septaldefects. In the present case, a successful repair ofresidual PMI-VSD through right atrium on beating heartwithout cross clamping the aorta via right thoracotomyis presented. The simplicity of this operation and thepatient’s rapid recovery are remarkable.
In conclusion, closure of PMI-VSD through the rightatrium by on-pump beating heart technique via the rightthoracotomy offers an alternative approach to repair ofthe residual VSD. This technique is especially usefulwhen the coronary bypass grafts are patent. This tech-nique abolishes the additional damage to the ventricleand to the patent grafts; therefore, it enhances the effi-ciency of myocardial protection, and reduces the risksof the postoperative complication rates, resulting in in-creased survival.
REFERENCES
1. Blanche C, Khan SS, Chaux A, et al: Postinfarction ven-tricular septal defect in elderly: Analysis and results. AnnThorac Surg 1994;57:1244-1247.
2. Filgueira JL, Battistessa SA, Estable H, et al: Delayed re-pair of an acquired posterior septal defect through a rightatrial approach. Ann Thorac Surg 1986;42:208-209.
3. Rousou JA, Engelman RM, Breyer RH, et al: Transatrialrepair of postinfarction posterior ventricular septal defect.Ann Thorac Surg 1987;43:665-666.
4. Cicekcioglu F, Tutun U, Demirtas E, et al: Repair of postin-farction ventricular septal defect through the right atrium.Thorac Cardiovasc Surg 2006;54:426-428.
5. Thompson MJ, Behranwala A, Campanella C, et al: Imme-diate and long-term results of mitral prosthetic replace-ment using a right thoracotomy beating heart technique.Eur J Cardiothorac Surg 2003;24:47-51.
6. Crenshaw BS, Granger CB, Birnbaum Y, et al: Risk fac-tors, angiographic patterns, and outcomes in patients withventricular septal defect complicating acute myocardial in-farction. GUSTO-I (Global Utilization of Streptokinase andTPA for Occluded Coronary Arteries) Trial Investigators.Circulation 2000;101:27-32.
7. Mann JM, Roberts WC: Acquired ventricular septal defectduring acute myocardial infarction: Analysis of 38 unop-erated necropsy patients and comparison with 50 unop-erated necropsy patients without rupture. Am J Cardiol1988;62:8-19.
8. Deja MA, Szostek J, Widenka K, et al: Post infarction ven-tricular septal defect – can we do better? Eur J Cardiotho-rac Surg 2000;18:194-201.
9. Cerin G, Di Donato M, Dimulescu D, et al: Surgical treat-ment of ventricular septal defect complicating acute my-ocardial infarction. Experience of a north Italian referralhospital. Cardiovasc Surg 2003;11:149-154.
10. Frassani R, Gelsomino S: A right atrial approach in redopostinfarction ventricular septal defect. Cardiovasc Surg1999;7;656-658.
11. Antunes MJ: Techniques of valvular reoperation. Eur J Car-diothorac Surg 1992;6:S54-S57.
12. Hannan EL, Kilburn H Jr, O’Donnell JF, et al: Adult openheart surgery in New York state. An analysis of riskfactors and hospital mortality rates. J Am Med Assoc1990;264:2768-2774.
13. Praeger PI, Pooley RW, Moggio RA, et al: Simplifiedmethod for reoperation on the mitral valve. Ann ThoracSurg 1989;48:835-837.
Coronary Air Embolism inOff-Pump Surgery Caused byBlower-Mister Device
Askin Ali Korkmaz, M.D.,∗ Mustafa
Guden, M.D.,∗ Feride Korkmaz, M.D.,†and Murat Yuce, M.D.‡∗Department of Cardiovascular Surgery,†Department of Anaesthesiology, and‡Department of Cardiology, Sema Hospital,Istanbul, Turkey
ABSTRACT Gaseous emboli caused by the blower-
mister result in air locks within coronary ves-
sels. We describe the case of a coronary air em-
bolism caused by a blower-mister device on off-
pump surgery. The tip of the device unexpectedly
entered the coronary artery through arteriotomy

584 KORKMAZ, ET AL.AIR EMBOLISM BY BLOWER-MISTER
J CARD SURG2008;23:565-589
and caused the air emboli. Air locks in the coro-
nary circulation led to hemodynamic deterioration,
and cardiopulmonary bypass was started following
the emergency cannulation. doi: 10.1111/j.1540-8191.2008.00614.x (J Card Surg 2008;23:583-585)
A special surgical technique is required to perform ananastomosis on a coronary artery under beating heartprocedures without cardiopulmonary bypass (CPB).The anastomotic site must be cleared of blood to facili-tate the performance of the distal anastomoses. How-ever, coronary blood flow frequently compromises aclear view of the opened coronary vessels. A blower-mister system is used liberally in off-pump coronaryoperations to maintain a bloodless field for accuratesuturing. The system helps provide excellent visual-ization by delivering a controllable column of humidi-fied air, thereby pushing the blood gently away fromthe anastomosis site. Reported significant side ef-fects of this method are rare. We will consider a caseof coronary air embolism causing an acute coronarysyndrome.
A 65-year-old male patient with a diagnosis ofthree-vessel coronary artery disease had comorbidi-ties, namely chronic obstructive pulmonary disorder(COPD) and peripheral vascular disease. The left ven-tricular ejection fraction was 40% while the cardiotho-racic index was 55%. Consequently, coronary arterybypass graft (CABG) with beating heart technique wasplanned. After median sternotomy, first right descend-ing posterior (RDP) distal anastomosis was performeddue to totally occluded right coronary artery (RCA).Medtronic Starfish (Medtronic Inc., Minneapolis, MN,USA) was used for heart positioning. Medtronic Oc-topus 4 was applied for vessel stabilization with sideclamping of the aorta proximal anastomosis. Afterward,left internal mammary artery-left anterior descending(LIMA-LAD) anastomosis was completed. The saphe-nous vein graft, the proximal anastomosis of whichwas already performed, was utilized for OM1 distalanastomosis. Lastly, the graft was used for sequentialanastomosis on the OM2 coronary arteries. After posi-tioning the heart, when making the toe of the anosto-mosis on the obtuse marginal, the blower-mister wasaccidentally inserted in the coronary artery, which ledto gaseous emboli in the coronary artery. Right afterthis incident a couple of normal beats were observed;however, severe arrhythmias occurred. Hemodynamicinstability developed due to compromised left ventri-cle (LV) contractility. We performed the now necessaryemergency CPB. Cardiac arrest was achieved with an-tegrade and retrograde blood cardioplegia. Retrogradecardioplegia was applied to discharge the gaseous em-boli in the coronary arteries. The OM2 sequential anas-tomosis was completed. The patient was weaned fromCPB with medium dosage inotropic and intraaortic bal-loon bump (IABP) support. The duration of his intensive
Address for correspondence: Askin Ali Korkmaz, M.D., Sema Hospital,Kalp Damar Cerrahisi Sahil yolu sk. No: 16, Dragos 34844, Maltepe Is-tanbul, Turkey. Fax: +90-216-3528359; e-mail: [email protected]
care unit stay was three days. He was discharged onthe seventh postoperative day.
COMMENT
With technological developments beating heartCABG has regained popularity. This technique is pre-ferred especially in high-risk patients with comorbidi-ties.1
In order to obtain a clear view during coronary anasto-mosis both the distal and proximal sides of the coronaryartery can be occluded with elastic loops. However,as this technique is likely to jeopardize the endothe-lium of the coronary artery, only the proximal occlu-sion is preferred. But in case of proximal occlusion,the backflow from the coronary artery hinders a del-icate anastomosis. An alternative method to obtain aclear view is to use blower-mister or saline infusionwith humidified air blowing.2 A blower-mister providesa clearer view. High velocity air jets may cause irre-versible endothelial damage.3 Another instrument thatmay be used is an intracoronary shunt to maintain thecoronary blood flow while providing a clear view for theanastomosis. On the other hand, it is reported that in-tracoronary shunts may jeopardize the endothelium ofthe coronary artery; thus, patency rates of the graftsare decreased.4 Due to this negative effect, the useof this shunt is not recommended when not obliga-tory. Even though the blower-mister may be seen tobe preferable, one should bear in mind that this instru-ment may lead to complications like gaseous emboliin coronary arteries. The hemodynamic instability de-veloped due to gaseous emboli may make it neces-sary to switch to CABG on pump. When this is thecase, both the morbidity and mortality rates increasesignificantly.5
Coronary artery air embolism can severely compli-cate the preoperative course for patients undergoingoff-pump CABG, leading to myocardial ischemia orinfarction, life-threatening arrhythmias, persistent hy-potension and even cardiac arrest. Early awareness anddiagnosis of coronary air with the establishment of ap-propriate management strategies may prevent its po-tentially lethal consequences.
We advocate the following precautions to preventthe development of gaseous emboli during the use ofblower-mister.
(1) CO2 must be used instead of O2 or room air(2) The air flow must be kept at the minimal level,
and should not be increased unless it is neces-sary for a clear view.
(3) The blower-mister must be kept as far as possi-ble from the coronary artery.
REFERENCES
1. Meharwal ZS, Mishra YK, Kohli V, et al: Off-pump multi-vessel coronary artery surgery in high-risk patients. AnnThorac Surg 2002;74(4):S1353-S1357.

J CARD SURG2008;23:565-589
WEBER, ET AL.ASCENDING AORTIC DISSECTION
585
2. Wippermann J, Albes JM, Liebing K, et al: Simple on-site assembled blower-mister device provides sufficienthumidification and visualization in off-pump surgery. AnnThorac Surg 2006;82(3):1134-1136.
3. Okazaki Y, Takarabe K, Murayama J, et al: Coronaryendothelial damage during off-pump CABG related tocoronary-clamping and gas insufflation. Eur J CardiothoracSurg 2001;19(6):834-839.
4. Dygert JH, Thatte HS, Kumbhani DJ, et al: Intracoronaryshunt-induced endothelial cell damage in porcine heart.Surg Res 2006;131(2):168-174, Epub 2006 Jan 18.
5. Jin R, Hiratzka LF, Grunkemeier GL, et al: Aborted off-pump coronary artery bypass patients have much worseoutcomes than on-pump or successful off-pump patients.Circulation 2005;112(9 Suppl):I332-I337.
Ascending Aortic DissectionAfter Proximal BypassAnastomotic Device
Alberto Weber, M.D., Reza Tavakoli,
M.D., P.h.D., and Michele Genoni, M.D.
Department for Cardiovascular Surgery,University Hospital, Zurich, Switzerland
ABSTRACT Ascending aortic dissection is a known
complication of cardiac surgery. Different type of
devices allowing performance of proximal bypass
anastomoses without aortic side-clamping are sup-
posed to reduce the risk for aortic dissection. We
report a case in which ascending aortic dissec-
tion occurred six months after off-pump coronary
artery bypass surgery, with the entry tear arising
directly from a proximal anastomosis performed
with the Heartstring hemostatic seal system. doi:10.1111/j.1540-8191.2007.00561.x (J Card Surg2008;23:585-586)
Aortic dissection is a rare but well-known compli-cation after manipulation of the ascending aorta duringopen heart surgery, and it is associated with a high mor-tality rate.1,2 To maintain the quality of care in off-pumpcoronary artery bypass (OPCAB) patients, a no-touchtechnique of the ascending aorta is important and/or ifnot possible, to perform the proximal anastomoses onthe aorta with a no-clamp technique.3
CASE REPORT
A 79-year-old man with unstable angina (CCS-IV andNYHA-IV) was referred to our center for coronary an-giography. The patient’s vascular risk factors includednicotine abuse, dyslipidemia, arterial hypertension, anddiabetes. He presented also with peripheral arterial
Address for correspondence: Alberto Weber, M.D., Department forCardiovascular Surgery, University Hospital, Raemistrasse 100, 8091-Zurich, Switzerland. Fax: +41-44-2554446; e-mail: [email protected]
vascular disease with a known aneurysm of the de-scending thoracic aorta. Additionally, an aorto-bifemoralgraft and a femoro-popliteal bypass were implanted fiveyears before to treat an infra-renal abdominal aneurysmand a persistent claudication. In the preoperative CTscan, the ascending aorta showed a maximal diame-ter of 3.9 cm and arteriosclerotic plaques over the aor-tic arch. Cardiac catheterization revealed three-vesseldisease with severe coronary sclerosis. Preoperativetransesophageal echocardiography (TEE) showed a re-duced left ventricular function with an ejection fractionof 25%. The standard Euroscore was 11. The left ra-dial artery and both internal mammary arteries wereprepared. Complete OPCAB revascularization was per-formed. The quality of the anastomoses was con-trolled using transient time flow measurement (Medis-tim, Norway). The left mammary artery was grafted tothe left anterior descending coronary artery. The radialartery was anastomosed sequentially to the diagonalbranch and the circumflex artery. The right mammaryartery was completely harvested and grafted as a sidebranch off the radial artery to the posterior descend-ing. The left mammary artery presented a small caliberand was not considered for T/Y-graft anastomosis be-cause of mismatch with the radial artery. Therefore, theradial artery was implanted into the ascending aorta us-ing the Heartstring device after all distal anastomoseswere done.
The intraoperative and postoperative course was un-eventful. Postoperative TEE was unchanged comparedto the preoperative examination. Eight days postoper-atively, the patient was discharged. On discharge, rou-tine blood analysis was normal. Blood pressure was123/75 mmHg with amlodipine 5 mg daily, ramiprile2.5 mg daily, and sotalolhydrochlorid (beta-blockade)40 mg three times a day.
Six months later, the asymptomatic patient was re-ferred to our institution as scheduled to perform afollow-up CT scan of the aneurysm of the descend-ing aorta, which showed no change compared to theprior one. Surprisingly, the ascending aorta showed adiameter increase up to 6.6 cm and a dissection mem-brane that extended from above the right coronary si-nus to the brachiocephalic trunk (Fig. 1A). Becauseof the high risk of spontaneous rupture, surgical re-pair of the dissection was undertaken in this otherwiseasymptomatic patient.
The preoperative TEE showed an impaired left ven-tricular function with an ejection fraction of 20% and aminimal aortic valve insufficiency. The right subclavianartery and the right femoral vein were cannulated. Theentry of the dissection originated from the proximal ra-dial artery anastomosis on the anterior ascending aorta(Fig. 1B) and the neo-hole on the aorta showed a veryirregular shape. The ascending aorta was replaced bya 26-mm Dacron graft. The proximal radial artery graftwas reimplanted into the graft. Unfortunately, the pa-tient developed massive ST elevations on the ECG andeven with maximal inotropic drugs support (no intra-aortic balloon pump due to the descending aorta find-ings) it was not possible to wean the extracorporealcardiopulmonary circulation and the patient died in theoperation theater.

586 FIORANI, ET AL.ANTERIOR CHEST CLOSURE ONLY WITH OMENTAL FLAP
J CARD SURG2008;23:565-589
Figure 1. (A) Aortic dissection (CT scan 6 months postoperative) with entry arising from proximal bypass anastomosis. (B) Intra-operative finding: the metal probe shows the immediate connection between the proximal anastomosis of the radial artery andthe entry tear of the dissection.
COMMENT
In a recent study, acute ascending aortic dissec-tion was found to have an incidence of 0.97% afterOPCAB.4 That might be, at least in part, due to thefact that in OPCAB, aortic side-clamping for perform-ing the proximal anastomoses is done under normalblood pressure and pulsatile conditions that might adda potential distress to the direct laceration, torsion, ormechanical compression of the ascending aorta.
The method of choice to minimize aortic manipula-tion is the use of arterial conduits for in situ or T-graftarterial configurations.
Furthermore, to avoid this potential complication, ef-forts have been made to develop mechanical devicesthat allow performing the proximal anastomoses with-out aortic side-clamping. Since the beginning of 2003,we exclusively use the Heartstring device (Guidant,IN, USA) to construct all proximal anastomoses on theaorta. Using this device, we have been able to reduceneurological complications (Table 1). This device selec-tively addresses the question of clampless revascu-larization without adding new problems derived fromthe anastomosis technique, which seems to be thedrawback of several automatic proximal anastomosisdevices currently in development.5
In conclusion, the present report underlines furtherthe need for long-term follow-up of patients in whomnew devices for proximal anastomoses are used, tocheck for the potential development of late aortic dis-section. Besides, it emphasizes the importance of iden-tifying predisposing factors that might help select ap-propriate patients for the application of such devices.
TABLE 1
Neurological Outcome in Patients Undergoing
OPCAB by Using Heart String (Guidant, IN, USA)
for Construction of the Proximal Aortic
Anastomoses
03-12/2003 01-12/2004N of N of
patients = 189 patients = 256
Proximal anastomoses, n 333 451Neurological events 1% 0%
REFERENCES
1. Stanger O, Oberwalder P, Dacar D, et al: Late dissec-tion of the ascending aorta after previous cardiac surgery:Risk, presentation and outcome. Eur J Cardiothorac Surg2002;21:453-458.
2. Boruchow IB, Iyengar R, Jude JR: Injury to asdending aortaby partial-occlusion clamp during aorta-coronary bypass. JThorac Cardiovasc Surg 1977;73:303-305.
3. Tavakoli R, Reuthebuch O, Hofer Ch, et al: Off-pump coro-nary bypass grafting: The Zurich experience. Heart SurgForum 2005;(4):1113-1118.
4. Chavanon O, Carrier M, Cartier R, et al: Increased incidenceof acute ascending aortic dissection with off-pump aorto-coronary bypass surgery? Ann Thorac Surg 2001;71:117-121.
5. Reuthebuch O, Kadner A, Lachat M, et al: Early bypassocclusion after deployment of Nitinol connector devices. JThorac Cardiovasc Surg 2004;127(4):1-6.
A Rare Case of Anterior ChestClosure Only with Omental FlapAfter Devastating Mediastinitis:Case Report
Vinicio Fiorani, M.D., Sabjan Memishaj,
M.D., Andrea Nocchi, M.D.,
Ernesto Tappainer, M.D., Nicola
Pederzolli, M.D., Jacopo Manfredi, M.D.,
and Mario Zogno, M.D.
Cardiac Surgery Department, Hospital“Carlo Poma”, Mantova, Italy
ABSTRACT We describe a case of 73-year-old pa-
tient who has been operated in emergency on triple
coronary artery bypass graft (CABG), which was
complicated with respiratory insufficiency and dev-
astating mediastinitis. The anterior mediastinum
was closed with an omental flap that was allowed
to epitelize spontaneously. The patient was dis-
charged after 110 days. Despite the large number of
cases with mediastinitis described in the literature,

J CARD SURG2008;23:565-589
FIORANI, ET AL.ANTERIOR CHEST CLOSURE ONLY WITH OMENTAL FLAP
587
the chest closure with only an omental flap without
closure of subcutaneous tissue and skin is rare. doi:10.1111/j.1540-8191.2008.00575.x (J Card Surg2008;23:586-589)
Although the frequency of developing mediastinitisafter cardiac surgery is not high, it is still a seriouscomplication. In particular methicillin resistant Staphy-lococcus aureus (MRSA) induced mediastinitis is re-sistant to drugs and with high-frequency wound ster-nal necrosis and destruction affect the prognosis. Wereport a patient with MRSA induced mediastinitis af-ter coronary artery bypass graft (CABG), with sternalwound necrosis and destruction exposing anterior me-diastinum, who was treated with omental flap pediclewithout subcutaneous tissue and skin closure. To date,the patient is alive.
CASE REPORT
The patient was a 73-year-old man with middlebronco pulmonary chronic obstruction (BPCO) and withinsulin dependent diabetes who was admitted with un-stable angina. On-pomp CABG, left internal mammaryartery (LIMA) to left anterior descending artery (LAD),great saphena vein (GVS) to obtuse marginal artery(OM), and right descending posterior artery (RDP) wasperformed. The time of aortic cross-clamp was 55 min-utes. Intravenous administration of cefazolin (1g, thricedaily) was given on the day of surgery. Severe cough-ing, that could not be controlled by any drugs, occurredafter surgery. Sternal instability and serous with pyo-genic discharge from the wound were noted on day11 after surgery (this was associated with necrotic tis-sue) and a fever of 39◦C developed. Immediately, thesteel wire was removed, mediastinum debridement,and the wound cleaned with povidone iodine (PI) with-out chest closure. Routinely, we close the sternum onlywhen the infection is eradicated. Simultaneously, van-comycin hidrochloride was administered intravenously.The respiratory condition was unstable and he wasreintubated. Respiratory insufficiency was caused bythe absence of the sternum with consequent wors-ening of mechanical ventilation and pulmonary infec-tion. In the wound discharge, MRSA and Pseudomonasaeruginosa were detected. We also decided to usemeropenem (1g, thrice daily) for Gram negative.
After 13 days of antibiotic therapy and PI cleansingin the absence of complete regression of the infec-tion, we decided to close the anterior chest with anomental flap and change the drugs with intravenousadministration of linezolid (600 mg, twice daily) andcontinuing to use meropenem. Isolation and prepara-tion of omentum with his vascular pedicle were per-formed. Wide debridement of the necrotic and destruc-ted tissue of sternal, ribs, and cutaneous soft tissuewas performed with resection of two-thirds of the an-terior chest wall (50 cm2). We achieved the closure
All authors contributed equally to this case presentation.Address for correspondence: Vinicio Fiorani, M.D., Cardiac SurgeryDepartment, Hospital “Carlo Poma”, Via Albertoni-1, 46100 Mantova,Italy. Fax: 0376-201267; e-mail: [email protected]
of the mediastinal cavity with an omental flap pedi-cle, which was fixed with single sutures around thewound. Drains for continuous cleansing were placedin the left thoracic cavity of the anterior and poste-rior mediastinum. The large mediastinal cavity createdwas closed only with an omental flap without subcu-taneus tissue and skin closure (Fig. 1). For continu-ous cleansing, 500 mL of physiological saline supple-mented with 2 mL of 10% PI was used at 40 mL/hevery six hours. Drains for drainage were continuouslyaspirated with negative pressure and the volumes ofcleansing and drainage were strictly managed. In addi-tion, the absence of accumulation of cleansing solutionin the mediastinum and thoracic cavity was confirmedat any time by chest X-ray examination. A large serumdischarge from omental flap was observed during thefirst days, because of that frequent gauze changing wasperformed with immediate recovery of liquids and pro-teins. One hundred and fifty milliliters of physiologicalsaline containing 600 mg of linezolid was administeredto the local site via the cleansing drain for 25 minutes,twice a day, and drain was clamped for 40 minutes af-ter administration. On day 35, the thoracic cavity drainwas obstructed and the drain was removed. MRSA wasnot detected by culture of discharges from mediasti-nal drain. Intravenous administration of linezolid wascontinued. Linezolin (600 mg, twice daily) was admin-istered intravenously for 15 days after removal of drain.Thyroid function was normal. Creatinine level was in-creased to 1.7 mg/dL during linezolid and meropenemadministration; white blood cell (WCB) and c-reactiveprotein (CRP) decreased and epithelization of omen-tal flap was mostly performed continuing from periph-ery to the center of the wound. The meropenem wassuspended after 43 days. The epithelization of omen-tal flap was facilitated using platelets gel, which waschanged every two days, and with the help of pro-tease modulating matrix (promogram Johnson & John-son wound management Ltd, Gargrave, Skipton, U.K.)a sterile absorbent product is made from collagen andoxidized regenerated cellulose. The tracheotomy res-piratory tube was disconnected on day 85 and thetracheotomy wound was closed. The patient was dis-charged on day 110, after second surgery resuming ev-ery day life without recurrence of inflammation (Fig. 2).
DISCUSSION
Mediastinitis is an infrequent yet potentially devas-tating complication following cardiac surgery (incidence1% to 3%, mortality 10% to 20%). Previous studieshave identified risk factors. One of the main problemsin case of mediastinitis is the devastating ability of theinfection to destroy the involved tissue.1-3
In our case, sternal wound infection was caused byMRSA, which recently increased due to overuse ofβ-lactams. A vancomycin resistant Enterococcus withlow sensitivity has been reported in recent years.4
Therapy for mediastinitis includes continuous cleansingand pedicle flap with the omentum and pectoral mus-cle; as the omentum is rich in blood vessels and lymph

588 FIORANI, ET AL.ANTERIOR CHEST CLOSURE ONLY WITH OMENTAL FLAP
J CARD SURG2008;23:565-589
Figure 1. Omental flap during epithelization.
vessels, an omental flap is very effective for infectedlesions. However, the omental flap is selected only forintractable cases in our institution, because the inflam-mation may disseminate to the abdominal region. Inour case, the omentum has been harvested as usual.Care has been taken to obtain as much length as pos-
Figure 2. Complete epithelization of omental flap.
sible. It was thinned and praped along the right ventri-cle and used to fill the superior mediastinum. Funda-mental, it was also the contemporary, appropriate, andunusual antibiotic therapy with meropenem and line-zolid. Cleansing with antibiotics and iodine solutionsaugment the antibacterial effect of therapy for omen-tal flap. The gel platelet and the promogram were ex-tremely useful to accelerate epithelization of omentalflap. The wound-healing process is a complex processin which a multitude of cellular and humoral compo-nents interact to restore a wound defect. Platelets andtheir released cytokines and growth factors are piv-otal in the modulation of this entire process. Plateletgels, that we have used, have a high concentration ofplatelets that release the bioactive proteins and growthfactors necessary to initiate and accelerate tissue re-pair and regeneration. In creating a platelet gel, autol-ogous blood is centrifuged to produce a concentratehigh in both platelets and plasma. This concentratecan be applied to wounds, providing hemostasis, adhe-sion, and enhanced wound healing. Platelet gels haveglobal applications in surgery.5 We also used the pro-mogram (Johnson & Johnson), able to rebalance andmodulate the pathological wound environment in allchronic wounds. Excess proteases are inactivated inan irreversible way, whilst endogenous growth factorsare simultaneously protected. On absorption of promo-gram into the wound, the proteases remain inactivatedand the growth factors are released active back intothe wound.6 In conclusion, it is important to emphasizethat in devastating mediastinitis with large destructionof costal, cutaneous, and subcutaneous tissue, with dif-ficult control of infection, omental flap represents theonly choice for patient treatment. The pectoral mus-cle flap represents the best way to close the ante-rior thoracic cavity, but when this thing is impossible,as in our case, because of devastating destruction of

J CARD SURG2008;23:565-589
FIORANI, ET AL.ANTERIOR CHEST CLOSURE ONLY WITH OMENTAL FLAP
589
tissue caused by infection (MRSA), the omental flapcan be used without any alternative cover. This casealso shows the importance of early appropriate antibi-otic therapy and finally, it is important to use tools thatimprove the epithelization process of omental flap, likeplatelets gel and promogram.
REFERENCES
1. Eklund AM, Lyytikainen O, Klemets P, et al: Mediastinitisafter more than 10,000 cardiac surgical procedures. AnnThorac Surg 2006;82(5):1784-1789.
2. Francel TJ, Kouchoukos NT: A rational approach to wounddifficulties after sternotomy: Reconstruction and long termresults. Ann Thorac Surg 2001;72:1419-1429.
3. Milano CA, Georgiade G, Muhlbaier LH, et al: Comparisonof omental and pectoralis flaps for poststernotomy medi-astinitis. Ann Thorac Surg 1999;67(2):377-380; discussion380-381.
4. Sezai A, Shiomo M, Inoue T: Efficacy of continous cleansingwith teicoplanin on POST-CABG meticilin-resistant Staphy-lococcus aureus (MRSA) mediastinitis. Ann Thoracic Car-diovasc Surg 2004;10:191-194.
5. Eppley BL, Pietrzak WS, Blanton M: Platelet-rich plasma: Areview of biology and applications in plastic surgery. PlastReconstr Surg 2006;118(6):147e-159e.
6. Veves A, Sheehan P, Pham HT: A randomized, controlledtrial of promogran (a collagen/oxidized regenerated cellu-lose dressing) vs standard treatment in the managementof diabetic foot ulcers. Arch Surg 2002;137(7):822-827.





























