Embed Size (px)
Citation preview
ABELOFF’S CLINICAL ONCOLOGY
FIFTH EDITION
JOHN E. NIEDERHUBER, MDExecutive Vice President, Inova Health SystemCEO and Director, Inova Comprehensive Cancer and Research InstituteCEO, Inova Translational Medicine InstituteFalls Church, Virginia;Professor, Oncology and SurgeryThe Johns Hopkins University School of MedicineDeputy DirectorJohns Hopkins Clinical Research NetworkBaltimore, Maryland
James O. Armitage, MDJoe Shapiro Professor of MedicineUniversity of Nebraska Medical CenterOmaha, Nebraska
James H. Doroshow, MDBethesda, Maryland
Michael B. Kastan, MD, PhDExecutive Director, Duke Cancer InstituteWilliam W. Shingleton Professor, Pharmacology and Cancer BiologyDuke University Medical CenterDurham, North Carolina
Joel E. Tepper, MDHector MacLean Distinguished Professor of Cancer ResearchDepartment of Radiation OncologyUNC Lineberger Comprehensive Cancer CenterUniversity of North Carolina School of MedicineChapel Hill, North Carolina
1600 John F. Kennedy Blvd.Ste. 1800Philadelphia, PA 19103-2899
ABELOFF’S CLINICAL ONCOLOGY, FIFTH EDITION ISBN: 978-1-4557-2865-7
Copyright © 2014 by Churchill Livingstone, an imprint of Elsevier Inc.
No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions.
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Notices
Knowledge and best practice in this field are constantly changing. As new research and experience broaden our understanding, changes in research methods, professional practices, or medical treatment may become necessary.
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds, or experiments described herein. In using such information or methods they should be mindful of their own safety and the safety of others, including parties for whom they have a professional responsibility.
With respect to any drug or pharmaceutical products identified, readers are advised to check the most current information provided (i) on procedures featured or (ii) by the manufacturer of each product to be administered, to verify the recommended dose or formula, the method and duration of administration, and contraindications. It is the responsibility of practitioners, relying on their own experience and knowledge of their patients, to make diagnoses, to determine dosages and the best treatment for each individual patient, and to take all appropriate safety precautions.
To the fullest extent of the law, neither the Publisher nor the authors, contributors, or editors, assume any liability for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
Previous editions copyrighted 2008, 2004, 2000, 1995
ISBN: 978-1-4557-2865-7
Content Strategy Director: Mary GatschSenior Content Strategist: Kate DimockSenior Content Development Specialist: Taylor BallPublishing Services Manager: Patricia TannianSenior Project Manager: John CaseyDesigner: Lou Forgione
Printed in China
Last digit is the print number: 9 8 7 6 5 4 3 2 1
219
• The World Health Organization (WHO) classification of hematologic neoplasms includes tumors of lymphoid, myeloid, histiocytic, and dendritic cell lineages.
• Each disease is defined as a distinct entity based on a constellation of morphologic, clinical, and biological features.
• The cell of origin is the starting point of disease definition.
• Some lymphomas and leukemias can be identified by routine morphologic approaches. However, for many diseases, knowledge of the immunophenotype and molecular genetics/cytogenetics plays an important role in the differential diagnosis.
• The sites of presentation and involvement are an important clue to underlying biological distinctions. Extranodal lymphomas differ in many respects from their nodal counterparts.
• Many lymphoma entities display a range in cytologic grade and clinical aggressiveness, making it difficult to stratify lymphomas according to clinical behavior. A number of prognostic factors influence clinical outcome, including stage, international prognostic index, cytologic grade, gene expression profile, secondary genetic events, and the host environment.
• The WHO classification includes five major categories of myeloid
diseases, all of which are clonal stem cell disorders exhibiting variable maturation in the affected lineages and either effective or ineffective hematopoiesis:Ⴜ Myeloproliferative neoplasmsႼ Myeloid (and lymphoid) neoplasms
with eosinophilia and abnormalities of PDGFRA, PDGFRB, or FGFR1
Ⴜ Myelodysplastic/myeloproliferative neoplasms
Ⴜ Myelodysplastic syndromesႼ Acute myeloid leukemia
• Among myeloid neoplasms, genetic features predict behavior better than morphology alone, necessitating genetic studies for accurate diagnosis.
S U M M A R Y O F K E Y P O I N T S
16 WHO Classification of Hematologic Malignancies
Elaine S. Jaffe and James Vardiman
INTRODUCTIONIn recent years, the discipline of hematopathology has emphasized the integration of morphology and biological markers for diagnosis. In this respect, the approaches used in hematologic diagnosis often have served as a model for other areas of pathology. For example, in the early 1980s, detection of rearrangements of the antigen recep-tor genes in lymphoid cells was used to indicate both clonality and cell lineage, long before molecular diagnostic techniques became commonplace in pathology. Biological approaches such as immuno-histochemistry, cytogenetics, and molecular biology enhance diagnos-tic accuracy and play a critical role in the definition of disease entities.1
Classification approaches for both lymphoid and myeloid neo-plasms have undergone significant reappraisal during the past 40 years. These changes have resulted from insights gained through the application of immunologic and molecular techniques, as well a better understanding of the clinical aspects of lymphoma and leuke-mia through advances in diagnosis, staging, and treatment.
HISTORICAL BACKGROUNDThe approach to classification of hematologic malignancies has evolved from descriptive approaches based on either cytologic or clinical features to a modern approach to taxonomy incorporating
cutting-edge technologies. The methods range from immunopheno-typic approaches, which characterize the surface molecules and func-tional attributes of the neoplastic cells, to genomic approaches, which decipher genetic changes associated with neoplastic transformation. Most of these changes have taken place during the past 40 years. However, the pace of new knowledge is likely to change dramatically with the capacity for whole genome sequencing.
The earliest classification schemes for lymphomas—those pro-posed by Gall and Mallory2 and Rappaport3—were based on cyto-logic and architectural features. However, insights into the complexities of the normal immune system led to attempts to relate the lympho-mas to their normal cellular counterparts. In the 1970s, efforts to establish an immunologically based classification were led largely by Karl Lennert and colleagues in Europe and by Lukes and Collins in the United States.1 Several European and American groups pub-lished proposals for the classification of lymphoma, and competing classification systems in use in clinical studies made it difficult to compare outcome data from different treatment centers.4-7 The inability of the pathologists to develop consensus and agree on a common approach led to the development of a working formula-tion for the non-Hodgkin lymphomas, after a National Cancer Institute–directed study was conducted to evaluate the six published schemes.8
The working formulation tried to stratify lymphomas according to clinical outcome based on clinical trials conducted in the 1970s.8

Part I: Science of Clinical Oncology220
a rare disease for which highly effective forms of therapy have been developed.16 However, the purine analogues 2′ deoxycoformycin and 2′-chlorodeoxyadenosine have not been similarly effective in treating other B-cell leukemias and lymphomas.
The REAL classification was the first to emphasize the importance of molecular oncology in defining disease entities. Cancer is increas-ingly recognized as a genetic disease.17 For many lymphomas, a good correlation exists between the molecular pathogenesis and routine histologic and immunophenotypic features. For example, the t(14;18) translocation involving the BCL2 and IGH@ genes is highly associ-ated with follicular lymphoma diagnosed by routine methods. In addition, the recognition of some molecular phenotypes can be rec-ognized by immunohistochemistry, such as cyclin D1 overexpression in the diagnosis of mantle cell lymphoma, or anaplastic lymphoma kinase (ALK) expression in anaplastic large cell lymphoma. Variations in the genetic complexity score also have been shown to influence clinical outcome, with pediatric lymphomas generally having many fewer genetic anomalies than adult lymphomas.18,19
However, for many lymphoma subtypes, particularly the mature T-cell malignancies, the molecular pathogenesis is not known. The REAL/WHO classifications recognized limitations in our knowledge and created “generic groupings” for the broad categories of disease that could not be resolved with existing data; these categories include diffuse large B-cell lymphomas (DLBCL) and peripheral T-cell lym-phomas, unspecified. Although a number of morphologic variants had been described, evidence that these variants delineated distinct biological or clinical entities was lacking.
Subsequent studies affirmed the principles of the REAL classifica-tion.20 The use of precise disease definitions enhanced diagnostic accuracy and reduced inter-observer variability. The significance of identifying individual disease entities was confirmed by overall sur-vival and failure-free survival data.
Precise disease definitions have also facilitated the discovery of the molecular pathogenesis of lymphomas and leukemias. Many patho-genetic insights have followed on the heels of the identification of a disease along clinical lines (Table 16-1). Moreover, advances in therapy are best achieved when studies are conducted on a homoge-neous disease entity. For example, the approaches to therapy of extra-nodal marginal B-cell lymphoma of mucosal-associated lymphoid tissues type differ from those of more systemic small B-cell malignan-cies. The ultimate goal in this model is molecularly targeted therapy, directed at the genomic alterations specific to the tumor.
In 2001 the International Agency for Research on Cancer, under the auspices of the WHO, published a unified and internationally accepted classification scheme for all lymphoid, myeloid, histiocytic,
Its proponents believed that attempts to relate tumors to the normal immune system were premature, and in essence it was a morphologi-cally based scheme, differing in only minor ways from the Rappaport classification, which had been in widespread use in the United States. A similar paradigm developed in the classification of acute myeloid and lymphoid leukemias. Earlier classification systems emphasized morphologic approaches, although the French–American–British (FAB) classification did use enzyme cytochemistry to identify cellular lineage and degree of maturation, at least within the myeloid and monocytic neoplasms.9 The categories of acute lymphoblastic leukemia—L1, L2, and L3—included both mature and immature lymphoid malignancies, because L3 was largely composed of mature blastic B cells similar to the cells of Burkitt lymphoma (BL). Although L1 and L2 were both of lymphoblastic origin, they correlated poorly with precursor T- or B-cell lineage.
Modern immunophenotypic and molecular approaches for char-acterizing lymphoid and myeloid cells are now readily available. The use of these new biological approaches has transformed our under-standing of hematologic neoplasia. Immunophenotypic, cytogenetic, and genotypic studies have permitted an impartial analysis of ques-tions that were unresolved when addressed with only routinely stained sections or smears and have allowed the incorporation of objective criteria into the definition and diagnostic criteria for hematologic malignancies. Indeed, a broad international consensus has emerged on many topics. This consensus was embodied in the Revised European-American Classification of Lymphoid Neoplasms (REAL classification) published by the International Lymphoma Study Group in 199410 and was broadened to include myeloid and histio-cytic neoplasms in the World Health Organization (WHO) classification.11
THE NEXT STEPS FOR LYMPHOMA: REAL TO WHOThe REAL classification10 and its successor the WHO classification11 represented a new paradigm in the classification of lymphoid neo-plasms. The focus was on the identification of “real” diseases, rather than a global theoretical framework, such as survival (working for-mulation), or cellular differentiation (Kiel classification). The REAL classification was based on the building of consensus and recognized that a comprehensive classification system was beyond the experience of any one individual. The WHO classification effort, which involved input from multiple experts, maintained this approach.
The REAL classification departed from traditional schemes by emphasizing that each disease was a distinct entity defined by a con-stellation of laboratory and clinical features—that is, morphology, immunophenotype, genetic features, clinical presentation, and course. The inclusion of clinical criteria was one of the more novel aspects of the International Lymphoma Study Group approach. The REAL classification recognized that the site of presentation is often a signpost for underlying biological distinctions, as in extranodal lymphomas of the mucosal-associated lymphoid tissues12 or many forms of T-cell lymphoma.13 Accurate diagnosis requires knowledge of the clinical history, because biologically distinct entities may appear cytologically similar.
Moreover, within a given disease entity, a number of prognostic factors influence the clinical outcome. Cytologic grade is one type of prognostic factor and is used in the stratification of follicular lym-phoma. Clinical features, such as the stage or international prognostic index, also markedly affect survival and response to treatment.14,15 For these reasons, it is not possible to stratify lymphoma subtypes accord-ing to clinical grade. Moreover, clinical groupings for either protocol treatment or routine clinical practice are generally not feasible. In evaluating new therapies, the data for each disease must be evaluated individually. Indeed, treatment approaches for one type of lymphoid malignancy are not necessarily applicable to other diseases, even of the same cell lineage. This point is exemplified by hairy cell leukemia,
Table 16-1 Representative Pathogenetic Insights Based on a Disease-Oriented Approach to Lymphoma Classification
Disease PathogenesisAdult T-cell leukemia/lymphoma HTLV-I
Extranodal NK/T-cell lymphoma, nasal type
EBV, genetics
Anaplastic large cell lymphoma ALK
Mantle cell lymphoma CCND1
Follicular lymphoma BCL2
MALT lymphoma Helicobacter, MALT1
Burkitt lymphoma MYC
Primary effusion lymphoma HHV-8/KSHV
EBV, Epstein-Barr virus; HHV, human herpesvirus; HTLV-1, human T-cell leukemia virus I; KSHV, Kaposi sarcoma–associated herpesvirus; MALT, mucosal-associated lymphoid tissues; NK, natural killer.
221WHO Classification of Hematologic Malignancies • CHAPTER 16
and dendritic cell neoplasms.11 The WHO monograph was part of a series encompassing all human neoplasms, with the goal to integrate pathology diagnosis with genetics to arrive at biologically relevant classification systems. The WHO adopted the approach of the REAL classification for the lymphoid malignancies, because this approach had been validated, and in turn applied the same principles to tumors of other hematopoietic lineages, mainly myeloid and histiocytic tumors.
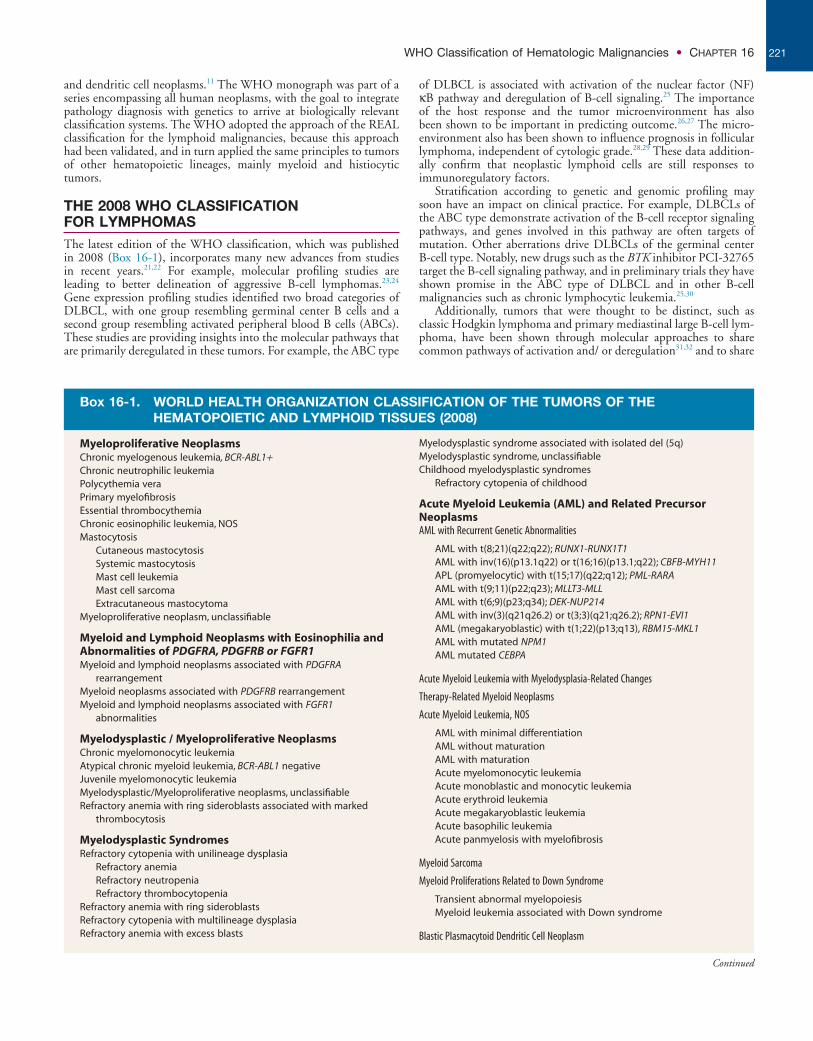
THE 2008 WHO CLASSIFICATION FOR LYMPHOMASThe latest edition of the WHO classification, which was published in 2008 (Box 16-1), incorporates many new advances from studies in recent years.21,22 For example, molecular profiling studies are leading to better delineation of aggressive B-cell lymphomas.23,24 Gene expression profiling studies identified two broad categories of DLBCL, with one group resembling germinal center B cells and a second group resembling activated peripheral blood B cells (ABCs). These studies are providing insights into the molecular pathways that are primarily deregulated in these tumors. For example, the ABC type
of DLBCL is associated with activation of the nuclear factor (NF) κB pathway and deregulation of B-cell signaling.25 The importance of the host response and the tumor microenvironment has also been shown to be important in predicting outcome.26,27 The micro-environment also has been shown to influence prognosis in follicular lymphoma, independent of cytologic grade.28,29 These data addition-ally confirm that neoplastic lymphoid cells are still responses to immunoregulatory factors.
Stratification according to genetic and genomic profiling may soon have an impact on clinical practice. For example, DLBCLs of the ABC type demonstrate activation of the B-cell receptor signaling pathways, and genes involved in this pathway are often targets of mutation. Other aberrations drive DLBCLs of the germinal center B-cell type. Notably, new drugs such as the BTK inhibitor PCI-32765 target the B-cell signaling pathway, and in preliminary trials they have shown promise in the ABC type of DLBCL and in other B-cell malignancies such as chronic lymphocytic leukemia.25,30
Additionally, tumors that were thought to be distinct, such as classic Hodgkin lymphoma and primary mediastinal large B-cell lym-phoma, have been shown through molecular approaches to share common pathways of activation and/ or deregulation31,32 and to share
Box 16-1. WORLD HEALTH ORGANIZATION CLASSIFICATION OF THE TUMORS OF THE HEMATOPOIETIC AND LYMPHOID TISSUES (2008)
Myeloproliferative NeoplasmsChronic myelogenous leukemia, BCR-ABL1+Chronic neutrophilic leukemiaPolycythemia veraPrimary myelofibrosisEssential thrombocythemiaChronic eosinophilic leukemia, NOSMastocytosis
Cutaneous mastocytosisSystemic mastocytosisMast cell leukemiaMast cell sarcomaExtracutaneous mastocytoma
Myeloproliferative neoplasm, unclassifiable
Myeloid and Lymphoid Neoplasms with Eosinophilia and Abnormalities of PDGFRA, PDGFRB or FGFR1Myeloid and lymphoid neoplasms associated with PDGFRA
rearrangementMyeloid neoplasms associated with PDGFRB rearrangementMyeloid and lymphoid neoplasms associated with FGFR1
abnormalities
Myelodysplastic / Myeloproliferative NeoplasmsChronic myelomonocytic leukemiaAtypical chronic myeloid leukemia, BCR-ABL1 negativeJuvenile myelomonocytic leukemiaMyelodysplastic/Myeloproliferative neoplasms, unclassifiableRefractory anemia with ring sideroblasts associated with marked
thrombocytosis
Myelodysplastic SyndromesRefractory cytopenia with unilineage dysplasia
Refractory anemiaRefractory neutropeniaRefractory thrombocytopenia
Refractory anemia with ring sideroblastsRefractory cytopenia with multilineage dysplasiaRefractory anemia with excess blasts
Myelodysplastic syndrome associated with isolated del (5q)Myelodysplastic syndrome, unclassifiableChildhood myelodysplastic syndromes
Refractory cytopenia of childhood
Acute Myeloid Leukemia (AML) and Related Precursor NeoplasmsAML with Recurrent Genetic Abnormalities
AML with t(8;21)(q22;q22); RUNX1-RUNX1T1AML with inv(16)(p13.1q22) or t(16;16)(p13.1;q22); CBFB-MYH11APL (promyelocytic) with t(15;17)(q22;q12); PML-RARAAML with t(9;11)(p22;q23); MLLT3-MLLAML with t(6;9)(p23;q34); DEK-NUP214AML with inv(3)(q21q26.2) or t(3;3)(q21;q26.2); RPN1-EVI1AML (megakaryoblastic) with t(1;22)(p13;q13), RBM15-MKL1AML with mutated NPM1AML mutated CEBPA
Acute Myeloid Leukemia with Myelodysplasia-Related Changes
Therapy-Related Myeloid Neoplasms
Acute Myeloid Leukemia, NOS
AML with minimal differentiationAML without maturationAML with maturationAcute myelomonocytic leukemiaAcute monoblastic and monocytic leukemiaAcute erythroid leukemiaAcute megakaryoblastic leukemiaAcute basophilic leukemiaAcute panmyelosis with myelofibrosis
Myeloid Sarcoma
Myeloid Proliferations Related to Down Syndrome
Transient abnormal myelopoiesisMyeloid leukemia associated with Down syndrome
Blastic Plasmacytoid Dendritic Cell Neoplasm
Continued
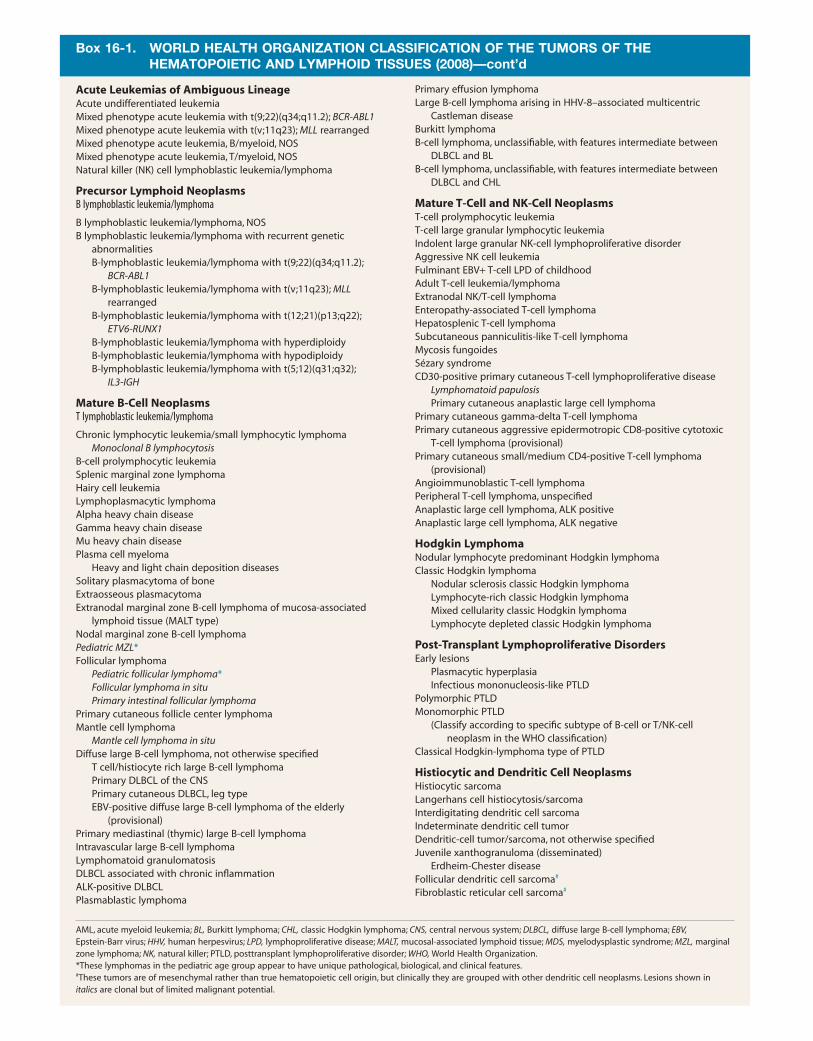
Box 16-1. WORLD HEALTH ORGANIZATION CLASSIFICATION OF THE TUMORS OF THE HEMATOPOIETIC AND LYMPHOID TISSUES (2008)—cont’d
Acute Leukemias of Ambiguous LineageAcute undifferentiated leukemiaMixed phenotype acute leukemia with t(9;22)(q34;q11.2); BCR-ABL1Mixed phenotype acute leukemia with t(v;11q23); MLL rearrangedMixed phenotype acute leukemia, B/myeloid, NOSMixed phenotype acute leukemia, T/myeloid, NOSNatural killer (NK) cell lymphoblastic leukemia/lymphoma
Precursor Lymphoid NeoplasmsB lymphoblastic leukemia/lymphoma
B lymphoblastic leukemia/lymphoma, NOSB lymphoblastic leukemia/lymphoma with recurrent genetic
abnormalitiesB-lymphoblastic leukemia/lymphoma with t(9;22)(q34;q11.2);
BCR-ABL1B-lymphoblastic leukemia/lymphoma with t(v;11q23); MLL
rearrangedB-lymphoblastic leukemia/lymphoma with t(12;21)(p13;q22);
ETV6-RUNX1B-lymphoblastic leukemia/lymphoma with hyperdiploidyB-lymphoblastic leukemia/lymphoma with hypodiploidyB-lymphoblastic leukemia/lymphoma with t(5;12)(q31;q32);
IL3-IGH
Mature B-Cell NeoplasmsT lymphoblastic leukemia/lymphoma
Chronic lymphocytic leukemia/small lymphocytic lymphomaMonoclonal B lymphocytosis
B-cell prolymphocytic leukemiaSplenic marginal zone lymphomaHairy cell leukemiaLymphoplasmacytic lymphomaAlpha heavy chain diseaseGamma heavy chain diseaseMu heavy chain diseasePlasma cell myeloma
Heavy and light chain deposition diseasesSolitary plasmacytoma of boneExtraosseous plasmacytomaExtranodal marginal zone B-cell lymphoma of mucosa-associated
lymphoid tissue (MALT type)Nodal marginal zone B-cell lymphomaPediatric MZL*Follicular lymphoma
Pediatric follicular lymphoma*Follicular lymphoma in situPrimary intestinal follicular lymphoma
Primary cutaneous follicle center lymphomaMantle cell lymphoma
Mantle cell lymphoma in situDiffuse large B-cell lymphoma, not otherwise specified
T cell/histiocyte rich large B-cell lymphomaPrimary DLBCL of the CNSPrimary cutaneous DLBCL, leg typeEBV-positive diffuse large B-cell lymphoma of the elderly
(provisional)Primary mediastinal (thymic) large B-cell lymphomaIntravascular large B-cell lymphomaLymphomatoid granulomatosisDLBCL associated with chronic inflammationALK-positive DLBCLPlasmablastic lymphoma
Primary effusion lymphomaLarge B-cell lymphoma arising in HHV-8–associated multicentric
Castleman diseaseBurkitt lymphomaB-cell lymphoma, unclassifiable, with features intermediate between
DLBCL and BLB-cell lymphoma, unclassifiable, with features intermediate between
DLBCL and CHL
Mature T-Cell and NK-Cell NeoplasmsT-cell prolymphocytic leukemiaT-cell large granular lymphocytic leukemiaIndolent large granular NK-cell lymphoproliferative disorderAggressive NK cell leukemiaFulminant EBV+ T-cell LPD of childhoodAdult T-cell leukemia/lymphomaExtranodal NK/T-cell lymphomaEnteropathy-associated T-cell lymphomaHepatosplenic T-cell lymphomaSubcutaneous panniculitis-like T-cell lymphomaMycosis fungoidesSézary syndromeCD30-positive primary cutaneous T-cell lymphoproliferative disease
Lymphomatoid papulosisPrimary cutaneous anaplastic large cell lymphoma
Primary cutaneous gamma-delta T-cell lymphomaPrimary cutaneous aggressive epidermotropic CD8-positive cytotoxic
T-cell lymphoma (provisional)Primary cutaneous small/medium CD4-positive T-cell lymphoma
(provisional)Angioimmunoblastic T-cell lymphomaPeripheral T-cell lymphoma, unspecifiedAnaplastic large cell lymphoma, ALK positiveAnaplastic large cell lymphoma, ALK negative
Hodgkin LymphomaNodular lymphocyte predominant Hodgkin lymphomaClassic Hodgkin lymphoma
Nodular sclerosis classic Hodgkin lymphomaLymphocyte-rich classic Hodgkin lymphomaMixed cellularity classic Hodgkin lymphomaLymphocyte depleted classic Hodgkin lymphoma
Post-Transplant Lymphoproliferative DisordersEarly lesions
Plasmacytic hyperplasiaInfectious mononucleosis-like PTLD
Polymorphic PTLDMonomorphic PTLD
(Classify according to specific subtype of B-cell or T/NK-cell neoplasm in the WHO classification)
Classical Hodgkin-lymphoma type of PTLD
Histiocytic and Dendritic Cell NeoplasmsHistiocytic sarcomaLangerhans cell histiocytosis/sarcomaInterdigitating dendritic cell sarcomaIndeterminate dendritic cell tumorDendritic-cell tumor/sarcoma, not otherwise specifiedJuvenile xanthogranuloma (disseminated)
Erdheim-Chester diseaseFollicular dendritic cell sarcoma#
Fibroblastic reticular cell sarcoma#
*These lymphomas in the pediatric age group appear to have unique pathological, biological, and clinical features.#These tumors are of mesenchymal rather than true hematopoietic cell origin, but clinically they are grouped with other dendritic cell neoplasms. Lesions shown in italics are clonal but of limited malignant potential.
AML, acute myeloid leukemia; BL, Burkitt lymphoma; CHL, classic Hodgkin lymphoma; CNS, central nervous system; DLBCL, diffuse large B-cell lymphoma; EBV, Epstein-Barr virus; HHV, human herpesvirus; LPD, lymphoproliferative disease; MALT, mucosal-associated lymphoid tissue; MDS, myelodysplastic syndrome; MZL, marginal zone lymphoma; NK, natural killer; PTLD, posttransplant lymphoproliferative disorder; WHO, World Health Organization.

223WHO Classification of Hematologic Malignancies • CHAPTER 16
THE MYELOID NEOPLASMS: FROM FAB TO WHOTo some extent, the evolution of the classification of myeloid neo-plasms has paralleled advances in the methodology used to study them, and in the past few years the focus of most studies has been on their genetic infrastructure. These investigations have led to the concept that myeloid neoplasms are acquired clonal stem cell disor-ders that arise through aberrations of multiple genes that control the proliferation, survival, and maturation of normal hematopoietic cells and that successful therapy will likely depend on targeting the genetic abnormalities or cellular pathways they affect. When coupled with morphologic, clinical, and phenotypic data, the genetic information has extended the ability to recognize and define distinct disease entities.
In the current WHO classification (Summary Box), the myeloid neoplasms are stratified into leukemias comprising precursor cells (blasts) with minimal if any maturation, acute myeloid leukemia (AML), and neoplasms with proliferation and maturation in one or more of the myeloid lineages that is effective (myeloproliferative neoplasms; MPNs), ineffective (myelodysplastic syndrome; MDS), or effective in some lineages but not in others (MDS/MPN). An additional category, myeloid and lymphoid neoplasms with eosino-philia and abnormalities of PDGFRA, PDGFRB, or FRGR1, identi-fies a unique group of stem cell neoplasms in which the genetic lesion leads to a constitutively activated receptor tyrosine kinase (TK) that drives the proliferation and in which the neoplastic cells may show differentiation toward lymphoid or myeloid lineages with prominent eosinophilia in the blood, marrow, and/or other tissues.52-54 Because the neoplasms with PDGFRA and PDGFRB rearrangements respond to imatinib therapy, this category illustrates an example for which the classification may define an entity and molecularly directed therapy as well.
The FAB proposals provided uniform classification criteria for AML and MDS based on a disciplined approach to their morphol-ogy,9,55 and remnants of the FAB persist even in the most recent WHO classification of AML and MDS. The introduction of the FAB schemes coincided with advances in cytogenetic techniques and inquiry into the genetic nature of leukemic cells, and a number of correlations were soon found between some FAB subgroups and specific cytogenetic abnormalities. Furthermore, it became apparent that recurring cytogenetic abnormalities often provide better prog-nostic information than morphologic classification alone.56-58 It was not surprising therefore that the Clinical Advisory Committee for the third edition of the WHO classification recommended incorporation of cytogenetic abnormalities of proven clinical significance into the classification of myeloid malignancies. Thus genetically defined sub-groups of AML—mainly chromosomal translocations involving tran-scription factors associated with characteristic morphologic and clinical features—were introduced into the WHO classification.59
In the years between the third and fourth editions of the WHO classification, it was realized that multiple genetic lesions—not only microscopically detectable chromosomal abnormalities but also gene mutations—cooperate to establish the leukemic process.60 Impor-tantly, some mutations, such as those involving NPM1 and CEBPA, were identified in cytogenetically normal AML (CN-AML), whereas others, such as mutated FLT3, were found not only in association with CN-AML but also with well-defined cytogenetic abnormali-ties.58,61-63 The detection of mutations in CN-AML opened a new avenue of inquiry into the pathogenesis and diverse outcomes of this large group of patients with AML. Additionally, some of the gene mutations, such as mutated NPM1 and CEBPA, are associated with consistent morphologic and phenotypic abnormalities and thus con-tribute to the recognition of specific new disease entities.
Currently, nearly 50% of all cases of AML are in part “genetically defined” in the WHO classification. More recent studies using full-genome evaluation techniques in AML have revealed an increasing
many genetic aberrations in common.33 These genomic insights have also helped elucidate the nature of lymphomas that appear to bridge the gap between classic Hodgkin lymphoma and mediastinal lym-phoma, the so-called “grey zone lymphomas,” which also are termed “B-cell lymphoma with features intermediate between DLBCL and classic Hodgkin lymphoma” in the WHO classification.34,35 Indeed, composite, sequential, and grey zone lymphomas are observed with some regularity.36
Another “intermediate” category introduced into the WHO system is “B-cell lymphoma with features intermediate between DLBCL and BL.”37,38 Historically it has been difficult for pathologists to distinguish some DLBCL with a very high growth fraction from BL with atypical cytology. In addition, some cases have a molecular gene expression profile of BL but carry additional cytogenetic abnor-malities, most often involving BCL2 or BCL6. These double-hit and triple-hit lymphomas have a very aggressive clinical course.39 This borderline category was introduced to recognize and delineate these cases. Although it is likely that this group of cases will be defined at the genetic level, the impact of an isolated MYC translocation in DLBCL has not been resolved.
The 2008 WHO classification includes other new areas of emphasis. The 2001 classification recognized two clonal lymphoid proliferations of indeterminate malignant potential, lymphomatoid granulomatosis (a B-cell–derived Epstein-Barr virus–driven process), and lymphomatoid papulosis (a usually clonal but indolent T-cell lymphoproliferative disease). In the past few years we have gained a much greater awareness of the multistep nature of lymphomagenesis, and a number of clonal lymphoid proliferations have been identified that, while carrying early genetic changes of malignancy, have a very limited capacity for progression. These proliferations include mono-clonal B-cell lymphocytosis, which carries many of the molecular alterations of chronic lymphocytic leukemia40; follicular lymphoma in situ,41 which carries the BCL2/IGH@ translocation; and mantle cell lymphoma in situ,42 which carries the CCND1/IGH@ transloca-tion. Each of these clonal proliferations may be detected in the patient using sensitive immunophenotypic or molecular methods but may not progress to clinically significant disease requiring therapeutic intervention. The fact that these alterations represent only an incipi-ent step in the pathway to malignancy is underscored by the fact that cells carrying the BCL2 and CCND1 translocations can be found in healthy individuals.43 The likelihood of identifying the translocation increases with age. When recognized in tissues, the cells of these in situ lesions occupy the microanatomic compartment of the relevant cell type. Thus we see follicular lymphoma in situ within otherwise reactive-appearing germinal centers, or the cells of mantle cell lym-phoma in situ occupying the mantle cell cuff. Examples of incipient lesions derived from T cells include seroma-associated anaplastic large cell lymphoma associated with breast implants44 and certain very indolent cutaneous T-cell lymphoproliferative “lymphomas,” such as primary cutaneous CD4+ small/medium-sized T-cell lymphoprolif-erative disease.45-47
Another new aspect of the WHO classification is the recognition of certain lymphoproliferative lesions that are preferentially associated with certain age groups. These lesions include the pediatric types of follicular lymphoma and marginal zone lymphoma, which occur mainly in children but also occur sporadically in older patients.48,49 At the other end of the spectrum, Epstein-Barr virus–positive DLBCL of the “elderly” is mainly seen in older individuals and is thought to be a result of a failure in immune surveillance.50,51 Although these tumors are most common past the age of 60 years, as with the “pedi-atric type” of lymphoma, they also occur sporadically in younger patients. The age distribution of these lesions may provide clues to pathogenesis and also aid in diagnosis. For example, it has been shown that DLBCLs occurring in children carry many fewer genetic aberrations than do morphologically similar tumors in adults.18,19 This fact may in part explain the excellent prognosis associated with most pediatric lymphomas.

Part I: Science of Clinical Oncology224
of patients with different survival times and disease complications.85,86 Whether this controversy will be resolved as more experience is devel-oped with the WHO criteria for PMF and ET and as the criteria are more stringently refined remains to be determined.
Most cases of systemic mastocytosis (SM) are associated with the gain-of-function mutation, KIT D816V.87 This mutation results in the activation of the TK receptor KIT, which, along with the myeloproliferative-like features of SM, argued for the inclusion of SM under the MPN umbrella. Some cases of SM are associated with prominent eosinophilia, in which case a PDGFRA abnormality may be present that is mutually exclusive of the KIT D816V. Cases of SM with PDGFRA rearrangement should be classified according to the genetic defect.88
Since the discovery of the JAK2 V617F in 2005, array-based technologies and candidate gene sequencing have revealed numerous additional mutations in the MPNs, often coexisting with mutated JAK2 and/or with each other. The genes involved include modifiers of the JAK-STAT pathway such as CBL and SH2B3 (also known as LNK), as well as genes that affect epigenetic modifiers, such as TET2, DNMT3A, ASXL1, and EZH2, among others.89-91 The role of these genes in MPN is not yet clarified, and whether they will have any impact on diagnosis or classification is not clear.
MDSs remain among the most diagnostically challenging of the myeloid neoplasms. The current WHO classification of MDS resem-bles the initial FAB scheme except that chronic myelomonocytic leukemia was relocated to a different category, MDS/MPN, in rec-ognition that it has both myelodysplastic and myeloproliferative fea-tures, and the category of refractory anemia with excess blasts in transformation was eliminated.92 Refinements made in the third and fourth editions of the WHO classification have improved the prognostic value of the various subgroups of MDS.93-96 However, a significant issue is the identification of early-stage MDS, when mor-phologic findings are inconclusive for the diagnosis yet the patient has an unexplained refractory anemia, thrombocytopenia, and/or neutropenia. This problem was identified as the most pressing MDS issue at the Clinical Advisory Committee meeting for the fourth edition of the WHO classification. In response to this issue, diagnostic criteria were changed to allow a presumptive diagnosis of MDS if the morphologic features are not conclusive but specific myelodysplastic-related cytogenetic abnormalities are present. The detection of certain phenotypic abnormalities by flow cytometry, particularly the asynchronous expression of maturation-associated antigens, is also accepted as at least suggestive of MDS in the appro-priate clinical context, although a more standardized and rigorous approach to flow cytometry analysis of such cases is needed.97 Whether molecular studies using directed or whole-genome sequencing may be helpful in determining the clonality of such cases is unknown. Somatic point mutations of one or more genes have been reported in 50% or more of patients with well-defined MDS, but their fre-quency is low in patients with fewer than 5% blasts and/or low International Prognostic Scoring System scores, and such studies may not be rewarding in early MDS.98,99 Thus the search for the minimal diagnostic criteria of MDS may not be easily resolved.
The foregoing paragraphs have focused on some of the major changes and issues in the diagnosis and classification of the myeloid neoplasms. It is reasonable to assume that as our knowledge evolves, molecular and genetic data will continue to be incorporated into diagnostic algorithms and classification nomenclature. Indeed, an integrated genomic approach to the assessment of neoplasms may reveal characteristic genomic profiles that can be used to tailor indi-vidual therapy, and genomic profiling of patients’ germline DNA may identify loci that predispose to myeloid neoplasms—a particularly important point for patients who are exposed to cytotoxic therapy.66 However, the number of recently described genetic abnormalities that are specific for a disease is relatively few, and the genetic data need to be put in the context of a disease entity to be appropriately under-stood and used.
number of mutations in genes encoding transcription factors, signaling proteins, and epigenetic regulators.64-66 How should these mutations be integrated into the WHO classification? Currently, all of the genetically defined AML entities have characteristic if not specific morphologic, phenotypic, and/or clinical features. Many of the recently reported mutations have an impact on prognosis but do not seem to define a distinct entity.67,68 For example, in CN-AML, mutated FLT3 confers a poor prognosis, yet it can be found in the core-binding factor AMLs and even in acute promyelocytic leukemia, as well as in cytogenetically normal patients.69 It is an important prognostic factor but does not define an entity. Recently, an interna-tional expert panel has proposed a scheme that integrates the WHO classification of genetically defined AML with genetic abnormalities that are mainly prognostic factors into a “standardized risk reporting scheme” that is useful for choosing therapy and that may serve as a model to integrate prognostic information with the classification.69
The 50% of cases of AML that do not fall into a “genetically defined” category illustrate how different features play a role in defin-ing a disease entity. In the subgroups of AML with myelodysplastic-related changes, equal importance is given to morphology, clinical history, and cytogenetics in defining the entity, although admittedly, controversy exists about whether the myelodysplastic-related genetic abnormalities best define this group.70,71 In therapy-related AML, the history of exposure to cytotoxic therapy is the ultimate factor for inclusion. The subgroup “AML, not otherwise specified,” which lacks any distinct clinical, immunophenotypic, or genetic characteristics, remains defined largely by morphologic criteria similar to those in the initial FAB classification. This group will likely diminish as new knowledge accumulates.
The most recent WHO classification also emphasizes two AML-related but distinct categories, the unique myeloid proliferations related to Down syndrome and a recently recognized disorder, blastic plasmacytic dendritic cell neoplasm. This latter disorder includes most cases previously classified as blastic natural killer–cell lymphoma/leukemia or agranular CD4+ CD56+ hematodermic neoplasm and is an aggressive disorder derived from a precursor of plasmacytoid dendritic cells, cells that are part of the innate immune system.72-74 Although leukemic involvement is common, many cases manifest with cutaneous disease.
Another group of myeloid neoplasms that is partially genetically defined is the MPNs. The detection of the BCR-ABL1 fusion gene has been used for years to confirm the diagnosis of chronic myeloid leukemia. The more recent discovery of activating mutations of genes that encode TKs involved in signal transduction pathways has revo-lutionized the diagnostic assessment of the BCR-ABL1–negative MPNs. The principle mutation, JAK2 V617F, is found in almost all cases of polycythemia vera (PV) and in about 50% of cases of essential thrombocythemia (ET) and primary myelofibrosis (PMF). A few cases of PV carry a similar mutation of JAK2 exon 12, and up to 10% of patients with ET and PMF have mutations of MPL.75-79 However, none of these mutations is specific for any single MPN. Furthermore, because 40% to 50% of cases of ET and PMF lack the JAK2 V617F or mutated MPL, additional criteria are required to diagnose them. The WHO classification combines genetic information with histo-pathologic and clinical criteria to distinguish PV, ET, and PMF from each other and from reactive marrow proliferations that may mimic them.80 An early “prefibrotic” form of PMF that has no or minimal fibrosis is also recognized. It is associated with thrombocytosis that often mimics ET, and many persons would be diagnosed as having ET according to the previous Polycythemia Vera Study Group crite-ria.81 The histologic features that define prefibrotic PMF and distin-guish it from ET have become a point of controversy for the WHO classification. Some authors have disputed the existence or importance of the prefibrotic phase and claim that the WHO criteria for its rec-ognition are not reproducible.82-84 However, other investigators have published articles stating that the application of the WHO criteria to patients with marked thrombocytosis defines two distinct populations
225WHO Classification of Hematologic Malignancies • CHAPTER 16
is a milestone, because it is the first classification system for lympho-mas and leukemias that is universally accepted and in use on a worldwide basis. It is also a roadmap for future scientific and clinical investigations. The use of common diagnostic criteria will facilitate collaboration and synthesis of data generated from such studies.
CONCLUSIONThe WHO classification is based on the integration of traditional morphologic observations with biological data related to the patho-genesis of disease. Although the ultimate goal might be a genetically defined classification system in which the molecular pathogenesis of every neoplasm is known, this aim is undoubtedly some years away. However, the recognition of carefully defined disease entities should facilitate the investigation of pathogenetic mechanisms and the devel-opment of molecularly targeted therapies. The WHO classification
The complete reference list is available online at www.expertconsult.com.
R E F E R E N C E S1. Jaffe ES, Harris NL, Stein H, Isaacson PG. Classi-
fication of lymphoid neoplasms: the microscope as a tool for disease discovery. Blood 2008;112(12): 4384–99.
10. Harris NL, Jaffe ES, Stein H, et al. A revised European-American classification of lymphoid neo-plasms: a proposal from the International Lym-phoma Study Group. Blood 1994;84(5):1361–92.
19. Deffenbacher KE, Iqbal J, Sanger W, et al. Molecu-lar distinctions between pediatric and adult mature B-cell non-Hodgkin lymphomas identified through genomic profiling. Blood 2012;28:28.
20. A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin’s lym-phoma. The Non-Hodgkin’s Lymphoma Classifica-tion Project. Blood 1997;89(11):3909–18.
21. Campo E, Swerdlow SH, Harris NL, et al. The 2008 WHO classification of lymphoid neoplasms and beyond: evolving concepts and practical applica-tions. Blood 2011;117(19):5019–32.
22. Swerdlow SH, Campo E, Harris NL, et al. WHO classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. Lyon, France: International Agency for Research on Cancer; 2008.
23. Rosenwald A, Wright G, Chan WC, et al. The use of molecular profiling to predict survival after chemotherapy for diffuse large-B-cell lymphoma. The New England Journal of Medicine 2002; 346(25):1937–47.
26. Lenz G, Wright G, Dave SS, et al. Stromal gene signatures in large-B-cell lymphomas. The New England Journal of Medicine 2008;359(22): 2313–23.
28. Dave SS, Wright G, Tan B, et al. Prediction of survival in follicular lymphoma based on molecular features of tumor-infiltrating immune cells. The New England Journal of Medicine 2004;351(21): 2159–69.
31. Savage KJ, Monti S, Kutok JL, et al. The molecular signature of mediastinal large B-cell lymphoma differs from that of other diffuse large B-cell lym-phomas and shares features with classical Hodgkin lymphoma. Blood 2003;102(12):3871–9.
32. Rosenwald A, Wright G, Leroy K, et al. Molecular diagnosis of primary mediastinal B cell lymphoma identifies a clinically favorable subgroup of diffuse large B cell lymphoma related to Hodgkin lym-phoma. The Journal of Experimental Medicine 2003;198(6):851–62.
34. Traverse-Glehen A, Pittaluga S, Gaulard P, et al. Mediastinal Gray Zone Lymphoma: The Missing Link Between Classic Hodgkin’s Lymphoma and Mediastinal Large B-Cell Lymphoma. The Ameri-can Journal of Surgical Pathology 2005;29(11): 1411–21.
37. Jaffe ES, Pittaluga S. Aggressive B-Cell Lymphomas: A Review of New and Old Entities in the WHO Classification. Hematology Am Soc Hematol Educ Program 2011;2011:506–14.
38. Salaverria I, Siebert R. The Gray Zone Between Burkitt’s Lymphoma and Diffuse Large B-Cell Lym-phoma From a Genetics Perspective. J Clin Oncol 2011;29(14):1835–43.
39. Aukema SM, Siebert R, Schuuring E, et al. Double-hit B-cell lymphomas. Blood 2011;117(8):2319– 31.
40. Shanafelt TD, Ghia P, Lanasa MC, et al. Monoclo-nal B-cell lymphocytosis (MBL): biology, natural history and clinical management. Leukemia 2010; 24(3):512–20.
41. Jegalian AG, Eberle FC, Pack SD, et al. Follicular lymphoma in situ: clinical implications and com-parisons with partial involvement by follicular lym-phoma. Blood 2011;118(11):2976–84.
42. Carvajal-Cuenca A, Sua LF, Silva NM, et al. In situ mantle cell lymphoma: clinical implications of an incidental finding with indolent clinical behavior. Haematologica 2011;4:4.
43. Roulland S, Faroudi M, Mamessier E, et al. Early steps of follicular lymphoma pathogenesis. Adv Immunol 2011;111:1–46.
50. Dojcinov SD, Venkataraman G, Pittaluga S, et al. Age-related EBV-associated lymphoproliferative dis-orders in the Western population: a spectrum of reactive lymphoid hyperplasia and lymphoma. Blood 2011;117(18):4726–35.
51. Oyama T, Yamamoto K, Asano N, et al. Age-related EBV-associated B-cell lymphoproliferative disorders constitute a distinct clinicopathologic group: a study of 96 patients. Clin Cancer Res 2007;13(17): 5124–32.
52. Cools J, DeAngelo DJ, Gotlib J, et al. A tyrosine kinase created by fusion of the PDGFRA and FIP1L1 genes as a therapeutic target of imatinib in idiopathic hypereosinophilic syndrome. N Engl J Med 2003;348(13):1201–14.
56. Grimwade D, Walker H, Oliver F, et al. The impor-tance of diagnostic cytogenetics on outcome in AML: analysis of 1,612 patients entered into the MRC AML 10 trial. The Medical Research Council Adult and Children’s Leukaemia Working Parties. Blood 1998;92(7):2322–33.
57. Bacher U, Kern W, Schnittger S, et al. Further cor-relations of morphology according to FAB and WHO classification to cytogenetics in de novo acute myeloid leukemia: a study on 2,235 patients. Ann Hematol 2005;84(12):785–91.
58. Mrozek K, Bloomfield CD. Chromosome aberra-tions, gene mutations and expression changes, and prognosis in adult acute myeloid leukemia. Hematology Am Soc Hematol Educ Program 2006:169–77.
59. Vardiman JW, Thiele J, Arber DA, et al. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leuke-mia: rationale and important changes. Blood 2009;114(5):937–51.
62. Falini B, Mecucci C, Tiacci E, et al. Cytoplasmic nucleophosmin in acute myelogenous leukemia
with a normal karyotype. N Engl J Med 2005;352(3):254–66.
64. Dohner H, Gaidzik VI. Impact of genetic features on treatment decisions in AML. Hematology Am Soc Hematol Educ Program 2011;2011:36– 42.
66. Godley LA, Cunningham J, Dolan ME, et al. An integrated genomic approach to the assessment and treatment of acute myeloid leukemia. Semin Oncol 2011;38(2):215–24.
69. Dohner H, Estey EH, Amadori S, et al. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European Leukemi-aNet. Blood 2010;115(3):453–74.
85. Barbui T, Thiele J, Passamonti F, et al. Survival and disease progression in essential thrombocythemia are significantly influenced by accurate morphologic diagnosis: an international study. J Clin Oncol 2011;29(23):3179–84.
87. Pardanani A. Systemic mastocytosis in adults: 2011 update on diagnosis, risk stratification, and manage-ment. Am J Hematol 2011;86(4):362–71.
88. Tefferi A, Levine RL, Lim KH, et al. Frequent TET2 mutations in systemic mastocytosis: clinical, KITD816V and FIP1L1-PDGFRA correlates. Leu-kemia 2009;23(5):900–4.
89. Tefferi A. Mutations galore in myeloproliferative neoplasms: would the real Spartacus please stand up? Leukemia 2011;25(7):1059–63.
90. Cross NC. Genetic and epigenetic complexity in myeloproliferative neoplasms. Hematology Am Soc Hematol Educ Program 2011;2011:208– 14.
91. Vannucchi AM, Biamonte F. Epigenetics and mutations in chronic myeloproliferative neoplasms. Haematologica 2011;96(10):1398–402.
94. Bernasconi P, Klersy C, Boni M, et al. World Health Organization classification in combination with cytogenetic markers improves the prognostic stratification of patients with de novo primary myelodysplastic syndromes. Br J Haematol 2007;137(3):193–205.
96. Cazzola M, Della Porta MG, Travaglino E, Malcovati L. Classification and prognostic evalua-tion of myelodysplastic syndromes. Semin Oncol 2011;38(5):627–34.
97. Porwit A. Role of flow cytometry in diagnostics of myelodysplastic syndromes—beyond the WHO 2008 classification. Semin Diagn Pathol 2011; 28(4):273–82.
98. Bacher U, Haferlach T, Kern W, et al. A comparative study of molecular mutations in 381 patients with myelodysplastic syndrome and in 4130 patients with acute myeloid leukemia. Haematologica 2007;92(6):744–52.
99. Bejar R, Stevenson K, Abdel-Wahab O, et al. Clini-cal effect of point mutations in myelodysplastic syndromes. N Engl J Med 2011;364(26):2496– 506.
225.e1WHO Classification of Hematologic Malignancies • CHAPTER 16
R E F E R E N C E S1. Jaffe ES, Harris NL, Stein H, Isaacson PG.
Classification of lymphoid neoplasms: the micro-scope as a tool for disease discovery. Blood 2008; 112(12):4384–99.
2. Gall EA, Mallory TB. Malignant lymphoma: a clinico-pathologic survey of 618 cases. Am J Pathol 1942;18:381–429.
3. Rappaport H. Tumors of the hematopoietic system. Atlas of Tumor Pathology. Vol Section III. Series I ed. Washington, DC: Armed Forces Institute of Pathol-ogy; 1966.
4. Lukes R, Collins R. Immunologic characterization of human malignant lymphomas. Cancer 1974;34: 1488–503.
5. Gerard-Marchant R, Hamlin I, Lennert K, et al. Classification of non-Hodgkin’s lymphomas. Lancet 1974;ii:406–8.
6. Bennett MH, Farrer-Brown G, Henry K, Jeliffe AM. Classification of non-Hodgkin’s lymphomas. Lancet 1974;2:405–6.
7. Dorfman RF. Letter: Classification of non-Hodgkin’s lymphomas. Lancet 1974;2(7886):961–2.
8. Non-Hodgkin’s lymphoma pathologic classification project. National Cancer Institute sponsored study of classifications of non-Hodgkin’s lymphomas: summary and description of a Working Formulation for clinical usage. Cancer 1982;49:2112–35.
9. Bennett JM, Catovsky D, Daniel MT, et al. Propos-als for the classification of the acute leukaemias. French–American–British (FAB) co-operative group. Br J Haematol 1976;33(4):451–8.
10. Harris NL, Jaffe ES, Stein H, et al. A revised European-American classification of lymphoid neo-plasms: a proposal from the International Lym-phoma Study Group. Blood 1994;84(5):1361–92.
11. Jaffe ES, Harris NL, Stein H, Vardiman J. Pathology and Genetics of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC Press; 2001.
12. Isaacson PG. Mucosa-associated lymphoid tissue lymphoma. Seminars in hematology 1999;36(2): 139–47.
13. Jaffe ES. Pathobiology of peripheral T-cell lympho-mas. Hematology Am Soc Hematol Educ Program 2006:317–22.
14. Johnston A, Salles G. Prognostic systems for lym-phomas. Hematology/Oncology Clinics of North America 2008;22(5):839–61, viii.
15. Armitage JO. The aggressive peripheral T-cell lym-phomas: 2012 update on diagnosis, risk stratifica-tion, and management. Am J Hematol 2012;87(5): 511–9.
16. Grever MR. Hairy cell leukemia: a successful model for experimental therapeutics—pentostatin and new ideas. Leukemia & Lymphoma 2011;52(Suppl 2):25–8.
17. Buetow KH, Klausner RD, Fine H, et al. Cancer Molecular Analysis Project: weaving a rich cancer research tapestry. Cancer Cell 2002;1(4):315–8.
18. Klapper W, Kreuz M, Kohler CW, et al. Patient age at diagnosis is associated with the molecular charac-teristics of diffuse large B-cell lymphoma. Blood 2012;119(8):1882–7.
19. Deffenbacher KE, Iqbal J, Sanger W, et al. Molecu-lar distinctions between pediatric and adult mature B-cell non-Hodgkin lymphomas identified through genomic profiling. Blood 2012;28:28.
20. A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin’s lym-phoma. The Non-Hodgkin’s Lymphoma Classifica-tion Project. Blood 1997;89(11):3909–18.
21. Campo E, Swerdlow SH, Harris NL, et al. The 2008 WHO classification of lymphoid neoplasms and beyond: evolving concepts and practical appli-cations. Blood 2011;117(19):5019–32.
22. Swerdlow SH, Campo E, Harris NL, et al. WHO classification of Tumours of Haematopoietic and
Lymphoid Tissues. 4th ed. Lyon, France: Interna-tional Agency for Research on Cancer; 2008.
23. Rosenwald A, Wright G, Chan WC, et al. The use of molecular profiling to predict survival after che-motherapy for diffuse large-B-cell lymphoma. The New England Journal of Medicine 2002;346(25): 1937–47.
24. Shipp MA, Ross KN, Tamayo P, et al. Diffuse large B-cell lymphoma outcome prediction by gene-expression profiling and supervised machine learn-ing. Nat Med 2002;8(1):68–74.
25. Yang Y, Shaffer AL 3rd, Emre NC, et al. Exploiting Synthetic Lethality for the Therapy of ABC Diffuse Large B Cell Lymphoma. Cancer Cell 2012;21(6): 723–37.
26. Lenz G, Wright G, Dave SS, et al. Stromal gene signatures in large-B-cell lymphomas. The New England Journal of Medicine 2008;359(22): 2313–23.
27. Monti S, Savage KJ, Kutok JL, et al. Molecular profiling of diffuse large B-cell lymphoma identifies robust subtypes including one characterized by host inflammatory response. Blood 2005;105(5): 1851–61.
28. Dave SS, Wright G, Tan B, et al. Prediction of survival in follicular lymphoma based on molecular features of tumor-infiltrating immune cells. The New England Journal of Medicine 2004;351(21): 2159–69.
29. Relander T, Johnson NA, Farinha P, et al. Prognostic factors in follicular lymphoma. J Clin Oncol 2010;28(17):2902–13.
30. Kenkre VP, Kahl BS. The Future of B-Cell Lym-phoma Therapy: The B-Cell Receptor and its Downstream Pathways. Curr Hematol Malig Rep 2012;7(3):216–20.
31. Savage KJ, Monti S, Kutok JL, et al. The molecular signature of mediastinal large B-cell lymphoma differs from that of other diffuse large B-cell lym-phomas and shares features with classical Hodgkin lymphoma. Blood 2003;102(12):3871–9.
32. Rosenwald A, Wright G, Leroy K, et al. Molecular diagnosis of primary mediastinal B cell lymphoma identifies a clinically favorable subgroup of diffuse large B cell lymphoma related to Hodgkin lym-phoma. The Journal of Experimental Medicine 2003;198(6):851–62.
33. Steidl C, Shah SP, Woolcock BW, et al. MHC class II transactivator CIITA is a recurrent gene fusion partner in lymphoid cancers. Nature 2011; 471(7338):377–81.
34. Traverse-Glehen A, Pittaluga S, Gaulard P, et al. Mediastinal Gray Zone Lymphoma: The Missing Link Between Classic Hodgkin’s Lymphoma and Mediastinal Large B-Cell Lymphoma. The Ameri-can Journal of Surgical Pathology 2005;29(11): 1411–21.
35. Eberle FC, Salaverria I, Steidl C, et al. Gray zone lymphoma: chromosomal aberrations with immu-nophenotypic and clinical correlations. Mod Pathol 2011;24(12):1586–97.
36. Jaffe ES, Wilson WH. Gray zone, synchronous, and metachronous lymphomas: Diseases at the interface of non-Hodgkin’s lymphomas and Hodgkin’s Lym-phoma. In: Mauch PM, Armitage JO, Coiffier B, et al, editors. Non-Hodgkin’s Lymphoma. Philadel-phia, PA: Lippincott, Williams, and Wilkins; 2004. p. 69–80.
37. Jaffe ES, Pittaluga S. Aggressive B-Cell Lymphomas: A Review of New and Old Entities in the WHO Classification. Hematology Am Soc Hematol Educ Program 2011;2011:506–14.
38. Salaverria I, Siebert R. The Gray Zone Between Burkitt’s Lymphoma and Diffuse Large B-Cell Lym-phoma From a Genetics Perspective. J Clin Oncol 2011;29(14):1835–43.
39. Aukema SM, Siebert R, Schuuring E, et al. Double-hit B-cell lymphomas. Blood 2011;117(8): 2319–31.
40. Shanafelt TD, Ghia P, Lanasa MC, et al. Monoclo-nal B-cell lymphocytosis (MBL): biology, natural history and clinical management. Leukemia 2010; 24(3):512–20.
41. Jegalian AG, Eberle FC, Pack SD, et al. Follicular lymphoma in situ: clinical implications and com-parisons with partial involvement by follicular lym-phoma. Blood 2011;118(11):2976–84.
42. Carvajal-Cuenca A, Sua LF, Silva NM, et al. In situ mantle cell lymphoma: clinical implications of an incidental finding with indolent clinical behavior. Haematologica 2011;4:4.
43. Roulland S, Faroudi M, Mamessier E, et al. Early steps of follicular lymphoma pathogenesis. Adv Immunol 2011;111:1–46.
44. Roden AC, Macon WR, Keeney GL, et al. Seroma-associated primary anaplastic large-cell lymphoma adjacent to breast implants: an indolent T-cell lym-phoproliferative disorder. Mod Pathol 2008;21(4): 455–63.
45. Rodriguez Pinilla SM, Roncador G, Rodriguez-Peralto JL, et al. Primary cutaneous CD4+ small/medium-sized pleomorphic T-cell lymphoma expresses follicular T-cell markers. The American Journal of Surgical Pathology 2009;33(1):81–90.
46. Grogg KL, Jung S, Erickson LA, et al. Primary cutaneous CD4-positive small/medium-sized pleo-morphic T-cell lymphoma: a clonal T-cell lympho-proliferative disorder with indolent behavior. Mod Pathol 2008;21(6):708–15.
47. Beltraminelli H, Leinweber B, Kerl H, Cerroni L. Primary cutaneous CD4+ small-/medium-sized pleomorphic T-cell lymphoma: a cutaneous nodular proliferation of pleomorphic T lymphocytes of undetermined significance? A study of 136 cases. The American Journal of Dermatopathology 2009;31(4):317–22.
48. Taddesse-Heath L, Pittaluga S, Sorbara L, et al. Marginal zone B-cell lymphoma in children and young adults. The American Journal of Surgical Pathology 2003;27(4):522–31.
49. Oschlies I, Salaverria I, Mahn F, et al. Pediatric fol-licular lymphoma—a clinico-pathological study of a population-based series of patients treated within the Non-Hodgkin’s Lymphoma—Berlin-Frankfurt-Munster (NHL-BFM) multicenter trials. Haemato-logica 2010;95(2):253–9.
50. Dojcinov SD, Venkataraman G, Pittaluga S, et al. Age-related EBV-associated lymphoproliferative dis-orders in the Western population: a spectrum of reactive lymphoid hyperplasia and lymphoma. Blood 2011;117(18):4726–35.
51. Oyama T, Yamamoto K, Asano N, et al. Age-related EBV-associated B-cell lymphoproliferative disorders constitute a distinct clinicopathologic group: a study of 96 patients. Clin Cancer Res 2007;13(17): 5124–32.
52. Cools J, DeAngelo DJ, Gotlib J, et al. A tyrosine kinase created by fusion of the PDGFRA and FIP1L1 genes as a therapeutic target of imatinib in idiopathic hypereosinophilic syndrome. N Engl J Med 2003;348(13):1201–14.
53. Metzgeroth G, Walz C, Score J, et al. Recurrent finding of the FIP1L1-PDGFRA fusion gene in eosinophilia-associated acute myeloid leukemia and lymphoblastic T-cell lymphoma. Leukemia 2007;21(6):1183–8.
54. Gotlib J. Eosinophilic myeloid disorders: new clas-sification and novel therapeutic strategies. Curr Opin Hematol 2010;17(2):117–24.
55. Bennett JM, Catovsky D, Daniel MT, et al. Propos-als for the classification of the myelodysplastic syn-dromes. Br J Haematol 1982;51(2):189–99.
Part I: Science of Clinical Oncology225.e2
56. Grimwade D, Walker H, Oliver F, et al. The impor-tance of diagnostic cytogenetics on outcome in AML: analysis of 1,612 patients entered into the MRC AML 10 trial. The Medical Research Council Adult and Children’s Leukaemia Working Parties. Blood 1998;92(7):2322–33.
57. Bacher U, Kern W, Schnittger S, et al. Further cor-relations of morphology according to FAB and WHO classification to cytogenetics in de novo acute myeloid leukemia: a study on 2,235 patients. Ann Hematol 2005;84(12):785–91.
58. Mrozek K, Bloomfield CD. Chromosome aberra-tions, gene mutations and expression changes, and prognosis in adult acute myeloid leukemia. Hematology Am Soc Hematol Educ Program 2006:169–77.
59. Vardiman JW, Thiele J, Arber DA, et al. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leuke-mia: rationale and important changes. Blood 2009;114(5):937–51.
60. Kelly LM, Gilliland DG. Genetics of myeloid leu-kemias. Annu Rev Genomics Hum Genet 2002;3: 179–98.
61. Frohling S, Schlenk RF, Stolze I, et al. CEBPA mutations in younger adults with acute myeloid leukemia and normal cytogenetics: prognostic rele-vance and analysis of cooperating mutations. J Clin Oncol 2004;22(4):624–33.
62. Falini B, Mecucci C, Tiacci E, et al. Cytoplasmic nucleophosmin in acute myelogenous leukemia with a normal karyotype. N Engl J Med 2005; 352(3):254–66.
63. Mrozek K, Marcucci G, Paschka P, et al. Clinical relevance of mutations and gene-expression changes in adult acute myeloid leukemia with normal cyto-genetics: are we ready for a prognostically prioritized molecular classification? Blood 2007;109(2):431– 48.
64. Dohner H, Gaidzik VI. Impact of genetic features on treatment decisions in AML. Hematology Am Soc Hematol Educ Program 2011;2011:36–42.
65. Rocquain J, Carbuccia N, Trouplin V, et al. Com-bined mutations of ASXL1, CBL, FLT3, IDH1, IDH2, JAK2, KRAS, NPM1, NRAS, RUNX1, TET2 and WT1 genes in myelodysplastic syn-dromes and acute myeloid leukemias. BMC Cancer 2010;10:401.
66. Godley LA, Cunningham J, Dolan ME, et al. An integrated genomic approach to the assessment and treatment of acute myeloid leukemia. Semin Oncol 2011;38(2):215–24.
67. Marcucci G, Haferlach T, Dohner H. Molecular genetics of adult acute myeloid leukemia: prognostic and therapeutic implications. J Clin Oncol 2011; 29(5):475–86.
68. Rollig C, Bornhauser M, Thiede C, et al. Long-term prognosis of acute myeloid leukemia according to the new genetic risk classification of the European LeukemiaNet recommendations: evaluation of the proposed reporting system. J Clin Oncol 2011; 29(20):2758–65.
69. Dohner H, Estey EH, Amadori S, et al. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European Leukemi-aNet. Blood 2010;115(3):453–74.
70. Weinberg OK, Seetharam M, Ren L, et al. Clinical characterization of acute myeloid leukemia with myelodysplasia-related changes as defined by the 2008 WHO classification system. Blood 2009; 113(9):1906–8.
71. Miesner M, Haferlach C, Bacher U, et al. Multilin-eage dysplasia (MLD) in acute myeloid leukemia (AML) correlates with MDS-related cytogenetic abnormalities and a prior history of MDS or MDS/MPN but has no independent prognostic relevance: a comparison of 408 cases classified as “AML not otherwise specified” (AML-NOS) or “AML with myelodysplasia-related changes” (AML-MRC). Blood 2010;116(15):2742–51.
72. Chaperot L, Bendriss N, Manches O, et al. Identi-fication of a leukemic counterpart of the plasmacy-toid dendritic cells. Blood 2001;97(10):3210–7.
73. Facchetti F, Vermi W, Mason D, Colonna M. The plasmacytoid monocyte/interferon producing cells. Virchows Arch 2003;443(6):703–17.
74. Jegalian AG, Facchetti F, Jaffe ES. Plasmacytoid den-dritic cells: physiologic roles and pathologic states. Adv Anat Pathol 2009;16(6):392–404.
75. James C, Ugo V, Le Couedic JP, et al. A unique clonal JAK2 mutation leading to constitutive signal-ling causes polycythaemia vera. Nature 2005; 434(7037):1144–8.
76. Kralovics R, Passamonti F, Buser AS, et al. A gain-of-function mutation of JAK2 in myeloproliferative disorders. N Engl J Med 2005;352(17):1779–90.
77. Levine RL, Wadleigh M, Cools J, et al. Activating mutation in the tyrosine kinase JAK2 in polycythe-mia vera, essential thrombocythemia, and myeloid metaplasia with myelofibrosis. Cancer Cell 2005; 7(4):387–97.
78. Baxter EJ, Scott LM, Campbell PJ, et al. Acquired mutation of the tyrosine kinase JAK2 in human myeloproliferative disorders. Lancet 2005;365(9464):1054–61.
79. Tefferi A, Thiele J, Vardiman JW. The 2008 World Health Organization classification system for myelo-proliferative neoplasms: order out of chaos. Cancer 2009;115(17):3842–7.
80. Thiele J, Kvasnicka HM, Orazi A, et al. Essential thrombocythaemia. In: Swerdlow SH, Campo E, Harris NL, et al, editors. WHO classification of tumours of haematopoietic and lymphoid tissues. 4th ed. Lyon, France: International Agency for Research on Cancer; 2008, p. 48–50.
81. Thiele J, Kvasnicka HM. Chronic myeloprolifera-tive disorders with thrombocythemia: a comparative study of two classification systems (PVSG, WHO) on 839 patients. Ann Hematol 2003;82(3):148– 52.
82. Wilkins BS, Erber WN, Bareford D, et al. Bone marrow pathology in essential thrombocythemia: interobserver reliability and utility for identifying disease subtypes. Blood 2008;111(1):60–70.
83. Campbell PJ, Bareford D, Erber WN, et al. Reticu-lin accumulation in essential thrombocythemia: prognostic significance and relationship to therapy. J Clin Oncol 2009;27(18):2991–9.
84. Buhr T, Hebeda K, Kaloutsi V, et al. European Bone Marrow Working Group trial on reproducibility of World Health Organization criteria to discriminate essential thrombocythemia from prefibrotic primary myelofibrosis. Haematologica 2012;97(3):360–5.
85. Barbui T, Thiele J, Passamonti F, et al. Survival and disease progression in essential thrombocythemia are significantly influenced by accurate morphologic diagnosis: an international study. J Clin Oncol 2011;29(23):3179–84.
86. Finazzi G, Carobbio A, Thiele J, et al. Incidence and risk factors for bleeding in 1104 patients with essen-tial thrombocythemia or prefibrotic myelofibrosis diagnosed according to the 2008 WHO criteria. Leukemia 2011;26(4):716–9.
87. Pardanani A. Systemic mastocytosis in adults: 2011 update on diagnosis, risk stratification, and manage-ment. Am J Hematol 2011;86(4):362–71.
88. Tefferi A, Levine RL, Lim KH, et al. Frequent TET2 mutations in systemic mastocytosis: clinical, KITD816V and FIP1L1-PDGFRA correlates. Leu-kemia 2009;23(5):900–4.
89. Tefferi A. Mutations galore in myeloproliferative neoplasms: would the real Spartacus please stand up? Leukemia 2011;25(7):1059–63.
90. Cross NC. Genetic and epigenetic complexity in myeloproliferative neoplasms. Hematology Am Soc Hematol Educ Program 2011;2011:208–14.
91. Vannucchi AM, Biamonte F. Epigenetics and muta-tions in chronic myeloproliferative neoplasms. Hae-matologica 2011;96(10):1398–402.
92. Vardiman J, Brunning RD, Arber DA, et al. Intro-duction and overview of the classification of the myeloid neoplasms. In: Swerdlow SH, Campo E, Harris NL, et al, editors. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Lyon: IARC; 2008. p. 18–30.
93. Germing U, Gattermann N, Strupp C, et al. Validation of the WHO proposals for a new classi-fication of primary myelodysplastic syndromes: a retrospective analysis of 1600 patients. Leuk Res 2000;24(12):983–92.
94. Bernasconi P, Klersy C, Boni M, et al. World Health Organization classification in combination with cytogenetic markers improves the prognostic strati-fication of patients with de novo primary myelodys-plastic syndromes. Br J Haematol 2007;137(3): 193–205.
95. Komrokji RS, Zhang L, Bennett JM. Myelodysplas-tic syndromes classification and risk stratification. Hematol Oncol Clin North Am 2010;24(2): 443–57.
96. Cazzola M, Della Porta MG, Travaglino E, Malcovati L. Classification and prognostic evalua-tion of myelodysplastic syndromes. Semin Oncol 2011;38(5):627–34.
97. Porwit A. Role of flow cytometry in diagnostics of myelodysplastic syndromes—beyond the WHO 2008 classification. Semin Diagn Pathol 2011;28(4): 273–82.
98. Bacher U, Haferlach T, Kern W, et al. A comparative study of molecular mutations in 381 patients with myelodysplastic syndrome and in 4130 patients with acute myeloid leukemia. Haematologica 2007;92(6):744–52.
99. Bejar R, Stevenson K, Abdel-Wahab O, et al. Clini-cal effect of point mutations in myelodysplastic syndromes. N Engl J Med 2011;364(26):2496– 506.

225.e3WHO Classification of Hematologic Malignancies • CHAPTER 16
SELF-ASSESSMENT QUESTIONS1. The Revised European-American Classification of Lymphoid
Neoplasms (REAL)/World Health Organization (WHO) classifi-cation includes which of the following features in the definition of a lymphoma?A. ImmunophenotypeB. Clinical featuresC. GeneticsD. All of above
1. Answer: D. The REAL classification departed from traditional schemes by emphasizing that each disease was a distinct entity, defined by a constellation of laboratory and clinical features—that is, morphology, immunophenotype, genetic features, clinical presenta-tion, and course. The same approach was adopted by the WHO classification, first published in 2001.
2. Follicular lymphoma, one of the most common subtypes of lym-phoma in adults, is characterized by translocations involving which of the following genes?A. MYCB. CCND1C. BCL2D. BCL6
2. Answer: C. The BCL2/IGH@ translocation is identified in approximately 85% to 90% of adult follicular lymphomas, but is adult in the pediatric variant of follicular lymphoma. The transloca-tion can also be found by sensitive PCR-based techniques in a pro-portion of healthy adults, a number that increases with age.
3. Which of the following myeloid proliferations is a clonal disorder?A. Chronic myelogenous leukemiaB. Refractory anemia with ring sideroblastsC. Systemic mastocytosisD. All of above
3. Answer: D. All myelodysplastic and myeloproliferative neo-plasms are clonal stem cell disorders that arise through aberrations of multiple genes that control the proliferation, survival, and maturation of normal hematopoietic cells. They show differences in the degree of maturation and differentiation, but nevertheless, all are derived from a clonal stem cell.
4. The peripheral blood cells of a 70-year-old woman with leukocy-tosis are reported to carry the JAK2 V617F mutation. This finding proves:A. The patient does have polycythemia vera.B. The patient does not have chronic myelomonocytic
leukemia.C. The patient does not have primary myelofibrosis.D. The patient has a clonal hematopoietic neoplasm.
4. Answer: D. The finding of the JAK2 mutation indicates that there is a clonal proliferation present, but by itself it is not diagnostic of any single disease. It is found in almost 95% of cases of polycy-themia vera and 50% to 60% of cases of essential thrombocythemia and primary myelofibrosis. It is also found in about 5% to 10% of cases of chronic myelomonocytic leukemia and even in rare cases of acute myeloid leukemia (AML). As with virtually all other mutations in hematopoietic neoplasms, its diagnostic significance must be con-sidered in the context of the clinical and morphologic findings.
5. In cytogenetically normal AML, the most significant prognostic information is likely to be:A. The French–American–British classification as “M5b.”B. The WHO classification as “AML, not otherwise specified.”C. The presence or absence of mutations of NPM1, FLT3, or
CEBPA.D. The height of the white blood cell count.
5. Answer: C. A number of genetic mutations clearly affect the prognosis of cytogenetically normal AML. Usually, mutated NPM1 and CEBPA are associated with a favorable outcome if they occur as the sole abnormality, whereas the FLT3 ITD mutation infers a worse prognosis, even when it occurs in the presence of other mutations that by themselves carry a good outcome. In general in persons with AML, genetic findings usually outweigh morphologic classification as prognostic factors.





























