Embed Size (px)
Citation preview

Additional Value of Myocardial Perfusion Imaging DuringDobutamine Stress Magnetic Resonance for the Assessment
of Coronary Artery DiseaseRolf Gebker, MD; Cosima Jahnke, MD; Robert Manka, MD; Ashraf Hamdan, MD;
Bernhard Schnackenburg, PhD; Eckart Fleck, MD; Ingo Paetsch, MD
Background—Dobutamine stress magnetic resonance (DSMR) imaging has emerged as a valuable tool for the detectionof inducible wall motion abnormalities. The role of perfusion imaging during DSMR is not well defined. We examinedwhether the addition of myocardial perfusion imaging during DSMR provides incremental benefit for the evaluation ofcoronary artery disease.
Methods and Results—DSMR was combined with perfusion imaging in 455 consecutive patients who were scheduled forclinically indicated invasive coronary angiography. Perfusion images were acquired in 3 standard short-views at rest andduring maximum dobutamine-atropine stress. Wall motion and perfusion images were interpreted sequentially, blindedto other data. Significant (�70%) stenoses were present in 285 patients on invasive coronary angiography. The use ofDSMR combined with perfusion imaging versus DSMR increased sensitivity (91% versus 85%, P�0.001), but notspecificity (70% versus 82%, P�0.001), resulting in identical overall diagnostic accuracy (84% versus 84%, P�NS;Youden index 0.61 versus 0.67). DSMR combined with perfusion imaging enabled the correct diagnosis of coronaryartery disease in an additional 13% of DSMR-negative patients at the cost of 11% more false-positive cases.
Conclusion—The addition of perfusion imaging during DSMR improves sensitivity for the diagnosis of coronary arterydisease but does not enhance overall diagnostic accuracy because of a concomitant decrease in specificity. (CircCardiovasc Imaging. 2008;1:122-130.)
Key Words: magnetic resonance imaging � coronary disease � myocardium � perfusion � dobutamine � ischemia
Dobutamine stress magnetic resonance (DSMR) wallmotion imaging is an established clinical method with
high diagnostic and prognostic value for the evaluation ofcoronary artery disease (CAD).1–4 Because of a high intrinsiccontrast between intracavitary blood and the endocardiumDSMR allows an accurate delineation of the endocardialborder and thus compares favorably with stress echocardiog-raphy.5,6 Nevertheless, wall motion studies during dobuta-mine have a number of inherent limitations, eg, interobservervariability of qualitative wall motion scoring.7 In addition, thepresence of left ventricular hypertrophy (LVH)8 and restingwall motion abnormalities (WMAs)9 are known to reducediagnostic accuracy and may impair the ability of DSMR todetect CAD.
The capability of cardiovascular magnetic resonance(CMR) to evaluate myocardial perfusion has been demon-strated in several studies as well.10–12 Although vasodilatorssuch as adenosine are usually applied to perform perfusionstudies, dobutamine may cause enough myocardial bloodflow heterogeneity to detect perfusion deficits in myocardialterritories supplied by a coronary artery with a critical
stenosis.13,14 In nuclear and echocardiographic studies,15,16
dobutamine proved to be a useful stress agent for theinduction of myocardial perfusion deficits. Recent advancesin magnetic resonance gradient performance and innovativepulse sequence design led to a substantial increase in acqui-sition speed of CMR first pass perfusion imaging therebyallowing multislice imaging at higher heart rates.17
Editorial see p 92Clinical Perspective see p 130
Thus, we sought to determine whether CMR perfusionimaging during high-dose dobutamine stress (DSMRP) addsadditional diagnostic value to DSMR for the detection ofischemia in patients with known and suspected CAD, asdefined by invasive coronary angiography.
Materials and MethodsPatient populationThe study was conducted in accordance with the standards of theCharite Ethics Committee. Written informed consent was given byall patients. DSMRP was performed prospectively in 455 consecu-
Received March 14, 2008; accepted July 22, 2008.From the German Heart Institute Berlin, Germany.The online-only Data Supplement can be found at http://circimaging.ahajournals.org/cgi/content/full/CIRCIMAGING.108.779108/DC1.Correspondence to Rolf Gebker, Deutsches Herzzentrum Berlin, Augustenburger Platz 1, 13353 Berlin, Germany. E-mail [email protected]© 2008 American Heart Association, Inc.
Circ Cardiovasc Imaging is available at http://circimaging.ahajournals.org DOI: 10.1161/CIRCIMAGING.108.779108
122 by guest on July 4, 2015http://circimaging.ahajournals.org/Downloaded from
tive patients who were scheduled for a clinically indicated coronaryangiography with suspected and known CAD. Patients with contra-indications to either magnetic resonance imaging (noncompatiblebiometallic implants or claustrophobia) or dobutamine (acute coro-nary syndrome, severe hypertension, significant aortic stenosis,myocarditis, endocarditis, pericarditis), and patients with arrhythmiawere not considered for study inclusion. All patients were instructedto refrain from any �-blockers or nitrates 24 hours before the MRI.
Magnetic Resonance Imaging
Imaging ProtocolMRI was performed with the patient in supine position with a 1.5-TMR scanner (Philips Intera CV, Best, The Netherlands) equippedwith a Nova gradient system (33 mT/m; 160 mT/m/ms) based onPhilips release 11. A 5-element cardiac synergy coil was used forsignal reception. Cardiac synchronization was performed by using 4electrodes placed on the left anterior hemithorax (vector electrocar-diography), and scans were triggered on the R wave of the ECG.
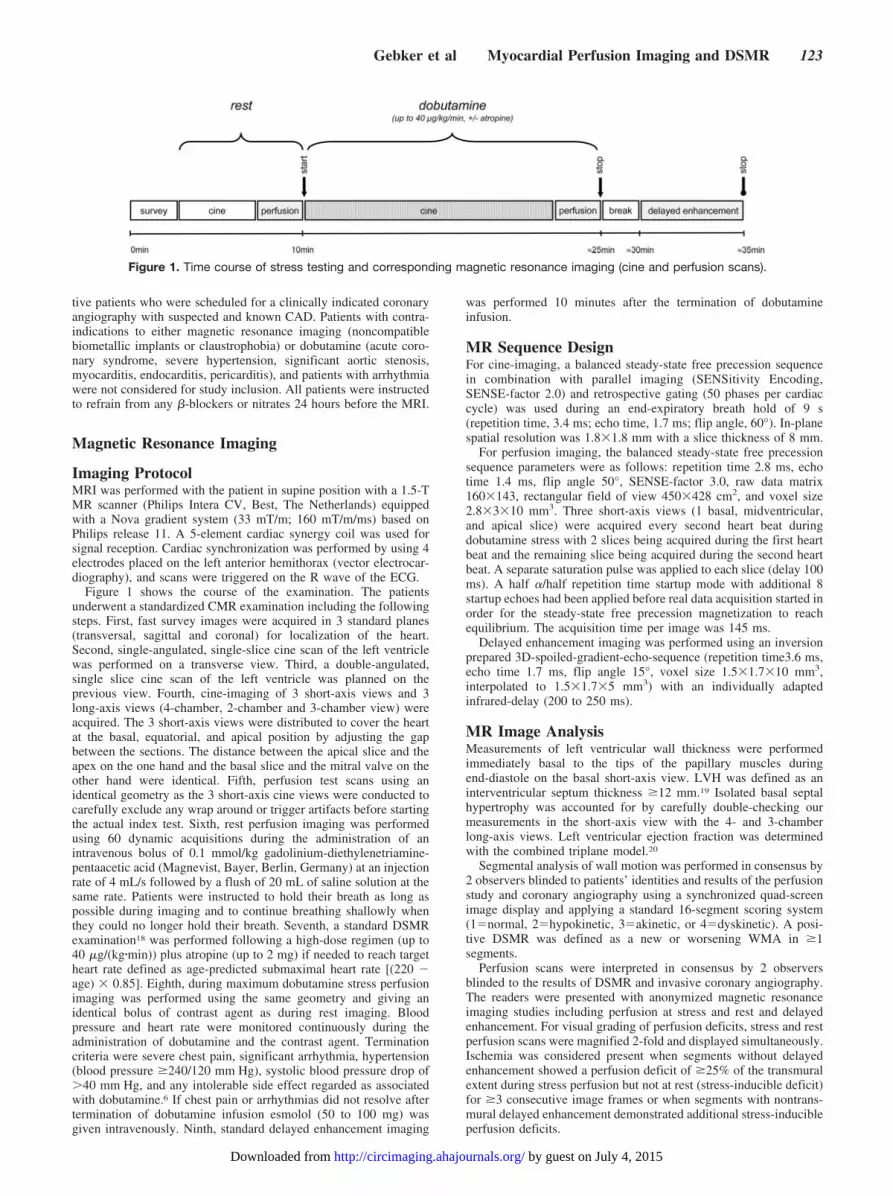
Figure 1 shows the course of the examination. The patientsunderwent a standardized CMR examination including the followingsteps. First, fast survey images were acquired in 3 standard planes(transversal, sagittal and coronal) for localization of the heart.Second, single-angulated, single-slice cine scan of the left ventriclewas performed on a transverse view. Third, a double-angulated,single slice cine scan of the left ventricle was planned on theprevious view. Fourth, cine-imaging of 3 short-axis views and 3long-axis views (4-chamber, 2-chamber and 3-chamber view) wereacquired. The 3 short-axis views were distributed to cover the heartat the basal, equatorial, and apical position by adjusting the gapbetween the sections. The distance between the apical slice and theapex on the one hand and the basal slice and the mitral valve on theother hand were identical. Fifth, perfusion test scans using anidentical geometry as the 3 short-axis cine views were conducted tocarefully exclude any wrap around or trigger artifacts before startingthe actual index test. Sixth, rest perfusion imaging was performedusing 60 dynamic acquisitions during the administration of anintravenous bolus of 0.1 mmol/kg gadolinium-diethylenetriamine-pentaacetic acid (Magnevist, Bayer, Berlin, Germany) at an injectionrate of 4 mL/s followed by a flush of 20 mL of saline solution at thesame rate. Patients were instructed to hold their breath as long aspossible during imaging and to continue breathing shallowly whenthey could no longer hold their breath. Seventh, a standard DSMRexamination18 was performed following a high-dose regimen (up to40 �g/(kg�min)) plus atropine (up to 2 mg) if needed to reach targetheart rate defined as age-predicted submaximal heart rate [(220 �age) � 0.85]. Eighth, during maximum dobutamine stress perfusionimaging was performed using the same geometry and giving anidentical bolus of contrast agent as during rest imaging. Bloodpressure and heart rate were monitored continuously during theadministration of dobutamine and the contrast agent. Terminationcriteria were severe chest pain, significant arrhythmia, hypertension(blood pressure �240/120 mm Hg), systolic blood pressure drop of�40 mm Hg, and any intolerable side effect regarded as associatedwith dobutamine.6 If chest pain or arrhythmias did not resolve aftertermination of dobutamine infusion esmolol (50 to 100 mg) wasgiven intravenously. Ninth, standard delayed enhancement imaging
was performed 10 minutes after the termination of dobutamineinfusion.
MR Sequence DesignFor cine-imaging, a balanced steady-state free precession sequencein combination with parallel imaging (SENSitivity Encoding,SENSE-factor 2.0) and retrospective gating (50 phases per cardiaccycle) was used during an end-expiratory breath hold of 9 s(repetition time, 3.4 ms; echo time, 1.7 ms; flip angle, 60°). In-planespatial resolution was 1.8�1.8 mm with a slice thickness of 8 mm.
For perfusion imaging, the balanced steady-state free precessionsequence parameters were as follows: repetition time 2.8 ms, echotime 1.4 ms, flip angle 50°, SENSE-factor 3.0, raw data matrix160�143, rectangular field of view 450�428 cm2, and voxel size2.8�3�10 mm3. Three short-axis views (1 basal, midventricular,and apical slice) were acquired every second heart beat duringdobutamine stress with 2 slices being acquired during the first heartbeat and the remaining slice being acquired during the second heartbeat. A separate saturation pulse was applied to each slice (delay 100ms). A half �/half repetition time startup mode with additional 8startup echoes had been applied before real data acquisition started inorder for the steady-state free precession magnetization to reachequilibrium. The acquisition time per image was 145 ms.
Delayed enhancement imaging was performed using an inversionprepared 3D-spoiled-gradient-echo-sequence (repetition time3.6 ms,echo time 1.7 ms, flip angle 15°, voxel size 1.5�1.7�10 mm3,interpolated to 1.5�1.7�5 mm3) with an individually adaptedinfrared-delay (200 to 250 ms).
MR Image AnalysisMeasurements of left ventricular wall thickness were performedimmediately basal to the tips of the papillary muscles duringend-diastole on the basal short-axis view. LVH was defined as aninterventricular septum thickness �12 mm.19 Isolated basal septalhypertrophy was accounted for by carefully double-checking ourmeasurements in the short-axis view with the 4- and 3-chamberlong-axis views. Left ventricular ejection fraction was determinedwith the combined triplane model.20
Segmental analysis of wall motion was performed in consensus by2 observers blinded to patients’ identities and results of the perfusionstudy and coronary angiography using a synchronized quad-screenimage display and applying a standard 16-segment scoring system(1�normal, 2�hypokinetic, 3�akinetic, or 4�dyskinetic). A posi-tive DSMR was defined as a new or worsening WMA in �1segments.
Perfusion scans were interpreted in consensus by 2 observersblinded to the results of DSMR and invasive coronary angiography.The readers were presented with anonymized magnetic resonanceimaging studies including perfusion at stress and rest and delayedenhancement. For visual grading of perfusion deficits, stress and restperfusion scans were magnified 2-fold and displayed simultaneously.Ischemia was considered present when segments without delayedenhancement showed a perfusion deficit of �25% of the transmuralextent during stress perfusion but not at rest (stress-inducible deficit)for �3 consecutive image frames or when segments with nontrans-mural delayed enhancement demonstrated additional stress-inducibleperfusion deficits.
Figure 1. Time course of stress testing and corresponding magnetic resonance imaging (cine and perfusion scans).
Gebker et al Myocardial Perfusion Imaging and DSMR 123
by guest on July 4, 2015http://circimaging.ahajournals.org/Downloaded from

For the overall assessment, patients were judged to have CAD ifinducible WMAs or inducible perfusion deficits were evident. Theseoverall results were compared with those from DSMR assessment.
To assess interobserver variability for interpretation of DSMRP, 2independent observers scored perfusion imaging qualitatively basedon the reading criteria mentioned earlier in a randomly selectedsample of 50 studies. The interobserver agreement in our laboratoryis 91% for DSMR.21
Coronary angiographyAll 455 patients underwent coronary x-ray angiography within 1month after magnetic resonance imaging. Conventional coronaryx-ray angiography was performed using the transfemoral Judkinsapproach with selective catheterization of the left and right coronaryartery system in multiple projections. The classification of patientsinto those with and without obstructive CAD was based on theircurrent coronary status as assessed by invasive angiography. Theangiograms were evaluated visually for the presence of significantstenoses (ie, �50% and �70% luminal diameter reduction) in majorepicardial coronary arteries and their branches (vessel diameter�2.0 mm) by highly experienced interventionalists; all readers wereblinded to the MR data. In patients with bypass grafts, significantarterial or vein graft stenoses were assigned to the recipient nativecoronary vessel. The angiographic results were then classified as 1-,2- and 3-vessel disease or exclusion of significant obstructive CAD.
Statistical AnalysisStatistical analysis was performed using the SPSS software packagerelease 15.0.1 (Chicago, Ill). For all continuous parameters, mean �standard deviation is given. Comparisons were made with 2 samplet tests for continuous data and �2 tests for discrete. McNemar’s testwas used to compare the diagnostic accuracy of techniques. Sensi-tivity, specificity, and diagnostic accuracy were calculated accordingto standard definitions. The Youden index, defined as sensitivity plusspecificity minus 1, was also applied to compare the 2 tests.22 TheWilcoxon test was applied to paired samples. Agreement betweenthe 2 methods and between observers was assessed with � statis-tics.23 Statistical tests were two-tailed; significance was considered ifP�0.05.
ResultsDobutamine Stress TestAssessment of wall motion at rest was feasible in all patients.Table 1 summarizes the reasons for nondiagnostic tests.Technical difficulties like poor ECG-triggering and insuffi-cient image quality during stress precluded interpretation ofwall motion and perfusion images in 12 (3%) patients. In 29(6%) patients, target heart rate was not achieved eitherbecause of a maximum infusion of dobutamine-atropine (13patients) without reaching target heart rate or because of earlytermination of the examination as a result of limiting sideeffects (16 patients); thus, DSMRP was feasible in 414patients (91%). The clinical data of the final population of thestudy are presented in Table 2.
The mean dosages of dobutamine and atropine given were34�7.4 �g/(kg�min) and 0.3�0.4 mg, respectively. Atropinewas administered in 217 (52%) patients. Table 3 summarizesthe hemodynamic data. Most patients (62%) experienced sideeffects during the infusion like chest pain (54%) or dyspnea(32%). One patient had self-limiting ventricular tachycardiaduring dobutamine infusion. No death, myocardical infrac-tion, or ventricular fibrillation occurred. Target heart rate wasachieved in 388 (94%) patients and 26 patients (6%) devel-
oped new WMAs before reaching target heart rate; in thesecases, stress perfusion imaging was performed at this stresslevel and the dobutamine infusion was terminated.
Table 1. Reasons for Nondiagnostic Tests
Reasons for Nondiagnostic Tests n (%)
Nondiagnostic tests 41 (9)
Technical reasons (insufficient ECG-triggering) 5 (1)
Insufficient image quality 7 (2)
Maximum infusion in submaximal negative 13 (3)
Limiting side effects 16 (3)
Patient request 2
Severe chest pain 4
Severe dyspnea 3
Severe increase in blood pressure(�240/120 mm Hg)
2
Paroxysmal atrial fibrillation 4
Ventricular tachycardia (self-limiting) 1
Values are n (%) unless otherwise noted
Values are n (%) unless otherwise noted.
Table 2. Patient Demographics
Patient Characteristics
Age, yr 63�9
Range 32–85
Gender, M/F 297/117
BMI, kg/m2 27�4
Risk factors and patient history, n (%)
Hypertension 290 (70)
Hypercholesterolemia 276 (67)
Smoking 121 (29)
Diabetes mellitus 114 (28)
Family history 94 (23)
LVEF, % 56�8
Patients with LVH 126 (30)
Resting wall motion abnormalities 190 (46)
Prior CAD 267 (64)
Prior Myocardial infarction 197 (48)
Prior PCI 232 (56)
Prior CABG 92 (22)
Serum creatinine, mg/dL 0.99�0.25
GFR, mL/min 89�27
Vessel disease (coronary stenosis�70%), n (%)
1-CAD 167 (40)
2-CAD 99 (24)
3-CAD 19 (5)
BMI indicates body mass index; LVEF, left ventricular ejection fraction; LVH,left ventricular hypertrophy (septum �12 mm); CABG, coronary artery bypassgraft surgery; GFR, glomerular filtration rate estimated using Cockroft equation;Values are n (%) unless otherwise noted and expressed as mean�SD.
124 Circ Cardiovasc Imaging September 2008
by guest on July 4, 2015http://circimaging.ahajournals.org/Downloaded from

Coronary AngiographyCAD (�70% stenosis) was present in 285 (69%) patients.Among these patients, 167 (59%) had single-vessel, 99 (35%)had 2-vessel, and 19 (7%) had 3-vessel CAD. The remaining129 (31%) patients had no significant CAD.
Results of DSMR and DSMRPNew or worsening WMAs occurred in 264 (64%) patients.DSMR had a sensitivity of 85% for the detection of CAD, asdefined by �70% stenosis by coronary angiography and aspecificity of 82%. Stress-inducible perfusion deficits weredetected in 269 (65%) patients. A stress-inducible WMA orperfusion deficit occurred in 299 patients (72%). Perfusiondeficits occurred in the presence of inducible WMAs in 234of 264 patients (89%) and in the absence of inducible WMAsin 35 of 150 patients (13%).
The use of DSMRP versus DSMR to detect CAD asdefined by �70% luminal narrowing increased sensitivity(91% versus 85%, P�0.001, Table 4), whereas specificitydecreased (70% versus 82%, P�0.001) resulting in identicaloverall diagnostic accuracy (84% versus 84%, P n.s.). Whendefining CAD as �50% luminal narrowing, diagnostic accu-racy increased significantly for DSMR versus DSMRP from82% to 85%, respectively (P�0.001). The Youden indexsuggested that DSMRP did not provide a measurable diag-nostic advantage in the overall study cohort (Table 4).However, in those 150 patients without inducible WMAs, wefound that adding DSMRP enabled the correct diagnosis in anadditional 13% (19/150, �70% stenosis) or 15% (23/150, for�50% stenosis) of patients. In 68% (13/19) of these patients,the number of ischemic segments was �3; 42% (8/19) hadmultivessel CAD (ie, 2- or 3-vessel CAD). This advantage insensitivity came at the cost of 11% (16/150, �70% stenosis)or 8% (12/150, for �50% stenosis) more false-positive cases.
Subgroup AnalysisDSMRP led to a significant increase in sensitivity anddiagnostic accuracy in patients with LVH from 79% to 91%(P�0.001) and from 80% to 87% (P�0.001, Table 4),respectively, without significant reduction in specificity from85% to 74% (P�0.25). The Youden index was similar forDSMRP versus DSMR (0.65 versus 0.64) when definingCAD as �70% stenosis. With DSMR alone, sensitivitydecreased in patients with LVH versus patients without LVH(79% versus 88%, P�0.52), whereas specificity increased(85% versus 81%, P�0.63).
In patients with resting WMAs, the use of DSMRPcompared with DSMR also led to a significant increment in
sensitivity from 82% to 89% (P�0.002) with a nonsignificantreduction in specificity from 73% to 61% (P�0.125) and asignificant increase in diagnostic accuracy from 80% to 84%(P�0.001). However, the Youden index implied that DSMRwas superior to DSMRP in patients with resting WMAs (seeTable 4). With DSMR alone sensitivity and specificitydecreased for patients with resting WMAs versus patientswithout resting WMAs (82% versus 88%, P�0.53; and 73%versus 85%, P�0.001, respectively). The results for using�50% luminal narrowing for the definition of CAD can befound in Table 4. Representative imaging examples are givenin Figures 2 and 3.
In patients with prior CAD the use of DSMRP led to asignificant increment in sensitivity from 83% to 90%(P�0.001) with a significant decline in specificity from 75%to 65% (P�0.03) and a significant increase in diagnosticaccuracy from 82% to 85% (P�0.001). In patients withoutprior CAD DSMRP was associated with a significant increasein sensitivity from 87% to 95% (P�0.001) as well. However,the decrease in specificity from 88% to 74% (P�0.001) led toa decrease in overall diagnostic accuracy from 87% to 84%compared with DSMR alone when CAD was defined as�70% luminal narrowing.
In patients with single-vessel CAD, the use of DSMRPsignificantly improved sensitivity from 84% to 91%(P�0.001).
In patients with no LVH, no resting WMAs, no prior CAD,and no single-vessel CAD, the use of DSMRP compared withDSMR led to a nonsignificant increase in sensitivity from88% to 94% (P�0.125) and a significant decrease in speci-ficity from 87% to 72% (P�0.02) resulting in a significantdecrease in diagnostic accuracy from 87% to 78% (P�0.008,Table 4).
The application of the Youden index suggested thatDSMRP was not associated with a measurable diagnosticadvantage in most patient subgroups (Table 4).
Segmental AnalysisThe number of segments exhibiting inducible WMAs in theabsence of perfusion deficits was 318 (4.8%). The number ofsegments experiencing perfusion deficits in the absence ofinducible WMAs was 516 (7.8%). The total number of mis-matched segments was thus 12.6%. In 132 patients, perfusiondeficits involved more segments; in 83 patients, less segmentswere involved than WMAs; and in 84 patients, the number ofischemic segments was identical. The mean number of ischemicsegments in patients with perfusion deficits versus patients withinducible WMAs was 3.6�1.9 versus 2.9�1.5 (P�0.001),respectively.
Delayed enhancement was present in 197 patients with amean number of 3.1�1.8 segments. In 162 of these 197patients, perfusion deficits or inducible WMAs were present.In 64 patients, perfusion deficits were more extensive thanWMAs, in 60 patients WMAs were less extensive thanperfusion deficits, and in 38 patients identical. The meannumber of ischemic segments in patients with perfusiondeficits versus patients with inducible WMAs was 3.1�2.1versus 2.8�1.5, P�0.12.
Table 3. Hemodynamic Data
Rest Stress
Heart rate, bpm 72�14 137�15*
Systolic blood pressure, mm Hg 132�23 142�31*
Diastolic blood pressure, mm Hg 71�12 70�15
Pulse pressure product, bpm�mm Hg 9539�2773 19463�4737*
Values are expressed as mean�SD.*P�0.001.
Gebker et al Myocardial Perfusion Imaging and DSMR 125
by guest on July 4, 2015http://circimaging.ahajournals.org/Downloaded from

Tabl
e4.
Diag
nost
icPe
rfor
man
ceof
DSM
RPan
dDS
MR
Sens
itivi
tySp
ecifi
city
Accu
racy
Youd
en-In
dex
DSM
RDS
MRP
PDS
MR
DSM
RPP
DSM
RDS
MRP
PDS
MR
DSM
RP
Coro
nary
Sten
osis
�70
%
Allp
atie
nts
241/
285
(85)
260/
285
(91)
0.00
110
6/12
9(8
2)90
/129
(70)
0.00
134
7/41
4(8
4)35
0/41
4(8
4)n.
s.0.
670.
61
Patie
nts
with
LVH*
78/9
9(7
9)90
/99
(91)
�0.
001
23/2
7(8
5)20
/27
(74)
0.25
101/
126
(80)
110/
126
(87)
�0.
001
0.64
0.65
Rest
ing
WM
As12
8/15
7(8
2)13
9/15
7(8
9)0.
001
24/3
3(7
3)20
/33
(61)
0.12
515
2/19
0(8
0)15
9/19
0(8
4)�
0.00
10.
550.
5
Prio
rCA
D17
6/21
0(8
3)18
9/21
0(9
0)�
0.00
143
/57
(75)
37/5
7(6
5)0.
0321
9/26
7(8
2)22
6/26
7(8
5)�
0.00
10.
580.
55
Nopr
ior
CAD
65/7
5(8
7)71
/75
(95)
�0.
001
63/7
2(8
8)53
/72
(74)
�0.
001
128/
147
(87)
124/
147
(84)
�0.
001
0.75
0.69
Sing
le-v
esse
lCAD
141/
167
(84)
152/
167
(91)
0.00
1
NoLV
H,no
rest
ing
WM
As,
nopr
ior
CAD,
nosi
ngle
-ves
selC
AD14
/16
(88)
15/1
6(9
4)0.
125
41/4
7(8
7)34
/47
(72)
0.02
55/6
3(8
7)49
/63
(78)
0.00
80.
750.
66
Coro
nary
Sten
osis
�50
%
Allp
atie
nts
252/
315
(80)
275/
315
(87)
�0.
001
87/9
9(8
8)75
/99
(76)
�0.
001
339/
414
(82)
350/
414
(85)
�0.
001
0.68
0.63
Patie
nts
with
LVH*
80/1
06(7
6)92
/106
(87)
�0.
001
18/2
0(9
0)15
/20
(75)
0.05
98/1
26(7
8)10
7/12
6(8
5)�
0.00
10.
660.
62
Rest
ing
WM
As13
4/17
0(7
9)14
6/17
0(8
6)�
0.00
117
/20
(85)
14/2
0(7
0)0.
018
151/
190
(79)
160/
190
(84)
�0.
001
0.64
0.56
Prio
rCA
D18
4/23
4(7
9)19
9/23
4(8
5)�
0.00
127
/33
(82)
23/3
3(7
0)�
0.00
121
1/26
7(7
9)22
2/26
7(8
3)�
0.00
10.
610.
55
Nopr
ior
CAD
68/8
1(8
4)76
/81
(94)
0.00
860
/66
(91)
52/6
6(7
9)0.
008
128/
147
(87)
128/
147
(87)
n.s.
0.75
0.73
Sing
le-v
esse
lCAD
100/
126
(79)
106/
126
(84)
0.03
NoLV
H,no
rest
ing
WM
As,
nopr
ior
CAD,
nosi
ngle
-ves
selC
AD15
/21
(71)
18/2
1(8
6)0.
0237
/42
(88)
32/4
2(7
6)�
0.00
152
/63
(83)
50/6
3(7
9)0.
008
0.59
0.62
Valu
esar
en
(%)
unle
ssot
herw
ise
note
dab
brev
iatio
nsar
eas
defin
edin
text
.*E
nd-d
iast
olic
wal
l-thi
ckne
ssof
inte
rven
tricu
lar
sept
um�
12m
m.
126 Circ Cardiovasc Imaging September 2008
by guest on July 4, 2015http://circimaging.ahajournals.org/Downloaded from

Interobserver AgreementIn 50 randomly selected patients from the study population,the interobserver agreement (ie, agreement on test positivityor negativity) of DSMRP was 88% (��0.67).
DiscussionWe found that DSMRP provided good diagnostic accuracyfor the detection of CAD. However, though DSMRP im-proved sensitivity compared with DSMR, no gain in overalldiagnostic accuracy was detectable because of a concomitantdecrease in specificity for the overall population and allsubgroups.
Cardiac Stress Testing With CMRCMR has been shown to be a clinically useful and versatiletechnique for the detection of myocardial ischemia.24 Both
the detection of stress-inducible WMAs as well as thedepiction of inducible perfusion deficits have been estab-lished as independent techniques to diagnose myocardialischemia.6,11 However, the clinical usefulness of combinedwall motion and perfusion assessment during application ofdobutamine is less well defined, and it is unknown whetherhigh-dose dobutamine-atropine perfusion imaging providesincremental diagnostic information. Several clinical studiesapplying echocardiography16 or nuclear imaging techniques25
provided evidence that dobutamine can effectively induceperfusion deficits. The induction of myocardial ischemiaduring dobutamine stress testing is largely attributed to anincrease in myocardial oxygen demand with subsequentworsening of left ventricular wall motion in areas subtendedby coronary arteries with relevant stenoses. Besides anincrease in contractility and rate-pressure product, dobuta-mine may also exert a direct vasodilatative effect on coronaryvessels.14,26 Recent studies have shown that the extent ofhyperemia with standard dobutamine-atropine stress testing isnot less than that observed with dipyridamole.27
CMR is regarded the standard of reference for the assess-ment of left ventricular function and regional wall motion atrest.24 Compared with echocardiography, CMR has beenshown to be diagnostically superior for the detection ofWMAs because of a consistently high endocardial borderdelineation.5,6 Although additional diagnostic value was as-cribed to dobutamine perfusion imaging with echocardiogra-phy,28 it is unclear whether the same applies to CMR.Furthermore, diagnostic accuracy of dobutamine stress wallmotion studies for the detection of CAD is impaired inpatients with LVH8 and resting WMAs.9
Delayed enhancement imaging has been demonstrated tobe a highly sensitive and specific technique to diagnosemyocardial scar tissue and has become part of a routine CMRexamination today. Because the administration of an extra-cellular contrast agent is mandatory for delayed enhancement,total examination duration with additional perfusion imagingduring dobutamine stress is only marginally prolonged (�3minutes).
Diagnostic Accuracy of DSMRPDSMRP yielded a high number of diagnostic examinations,as 91% were either positive for ischemia or negative afterreaching target heart rate. Main reasons for early terminationof the examination were insufficient hemodynamic responseto dobutamine-atropine administration or limiting cardiacside effects such as chest pain, dyspnea, hypertension, andatrial fibrillation and were comparable to studies usingdobutamine stress perfusion scintigraphy29 and echocardiog-raphy.30 Noncardiac side effects such as nausea, headache,and anxiety were not uncommon but usually well toleratedwithout the need to terminate the examination. Only aminority of patients had to be excluded because of insuffi-cient image quality or technical failure of DSMRP. Inaddition, the interobserver agreement for DSMRP is gooddespite the heterogeneity of our patient population.
Our study showed that inducible myocardial perfusiondeficits could be detected by DSMRP. Furthermore, DSMRPis significantly more sensitive than DSMR for the detection
Figure 2. False-negative DSMR but true-positive results forDSMRP in a patient with multiple stenoses of LAD, LCX anddistal occlusion of RCA. DSMR: inferior hypokinesia at rest withno improvement during low dose dobutamine and no stress-inducible WMA during maximum dobutamine stress (blackarrows); DSMRP: small inferior subendocardial perfusion deficitat rest (white arrow) and stress-inducible perfusion deficit duringmaximum dobutamine stress (white arrows).
Figure 3. False-negative DSMR but true-positive DSMRP inpatient with LVH, proximal occlusion of the RCA and retrogradefilling by collaterals from LAD. DSMRP clearly demonstrates astress-inducible perfusion deficit of the apical inferior wall.
Gebker et al Myocardial Perfusion Imaging and DSMR 127
by guest on July 4, 2015http://circimaging.ahajournals.org/Downloaded from

of CAD in the overall population of our study. This finding isin line with the ischemic cascade theory, which states thatperfusion deficits precede WMAs and electrocardiographicchanges.31 Our study also showed that the sensitivity inidentifying patients with single-vessel CAD is significantlyhigher for DSMRP compared with DSMR, which furthersupports the aforementioned theory. Animal studies haveconfirmed this phenomenon by demonstrating that dobuta-mine causes a reduction in coronary flow distal to a noncrit-ical coronary stenosis whereas wall thickening remains nor-mal.32 Our results regarding diagnostic accuracy of DSMRwere within the range of previously published data,3,6,7
thereby reflecting its reliability in detecting significant CAD.However, the observed increase in sensitivity for DSMRP inour study did not translate into an improved diagnosticaccuracy because of a significant decrease in specificity.Other studies using dobutamine perfusion imaging havereported lower values for specificity either.28,33 This might beexplained by several factors. Half of the patients responsiblefor false-positives during DSMRP were diabetic, and 75% ofthem had arterial hypertension. Both of these risk factors areknown to cause impaired coronary vasoreactivity even in theabsence of a significant epicardial coronary arterial narrow-ing.34,35 In addition, the decline in specificity of DSMRPmight be attributed to CMR specific artifacts (mainly suscep-tibility), which arise from gadolinium bolus administration,motion, or limited spatial resolution, and are known to reducespecificity in CMR perfusion studies.36
Our study showed that DSMRP exhibited a higher sensi-tivity for the detection of CAD in patients with LVH. Apossible explanation for this might be inherent to the perfu-sion imaging approach, because it depicts inducible regionalinhomogeneities of myocardial blood flow rather than theirfunctional consequences. Moreover, in patients with LVH leftventricular obliteration during dobutamine stress and diastol-ic dysfunction associated with increased myocardial stiffnessare known phenomena, which can interfere with the identifi-cation of WMAs.37,38 However, the recognition of a perfusiondeficit in a largely obliterated left ventricle should be lessdemanding and might further serve as an explanation as towhy DSMRP might be a better test than DSMR to detectischemia in patients with LVH. The fact that in our study thedifferences in specificity did not reach statistical significancein patients with LVH was somewhat surprising taking intoaccount that patients with hypertrophy have a high probabil-ity of microvascular coronary disease and impaired coronaryflow reserve39 and was most likely because of the smallnumber of patients with negative invasive angiograms.
In patients with prior CAD the use of DSMRP also led toa significant increase in sensitivity. Conversely, in patientswith no LVH, no resting WMAs, no prior CAD, and nosingle-vessel CAD, DSMRP was associated with a lowerdiagnostic accuracy because of a significant decrease inspecificity. Thus, our results indicate that DSMRP is notnecessarily justified in all patients but may be advantageousin those in whom a high sensitivity is desirable.
The Youden index gives equal weight to sensitivity andspecificity without reflecting CAD prevalence. Although it isgenerally desirable to choose a test that has high values for
both, sensitivity and specificity may not be equally importantin clinical practice. Patients who are at high risk for futurecardiac events may benefit from a test with high sensitivity.In the present study, DSMRP enabled the correct diagnosis inan additional 13% of DSMR-negative patients: 68% (13/19)demonstrated ischemia in �3 segments with multivesselCAD in 42% (8/19), and thus, these patients are at consider-able risk for future cardiac events.2,40 In addition, moreaccurate detection of disease extent with DSRMP mayfacilitate better risk stratification.
Study LimitationsCatheterization results were based on visual analysis andnot on quantitative coronary angiography. A commonproblem in validating noninvasive techniques for thedetection of myocardial ischemia is the lack of an optimalstandard of reference.41 The present study documents thediagnostic accuracy of DSMRP in patient populationtypically referred to a tertiary care hospital, and manypatients had prior CAD and myocardial infarctions. Thus,our results may be applicable only to a similar clinicalsetting. Multicenter studies are required before the clinicalrole of DSMRP for the assessment of myocardial perfusioncan be determined. The perfusion sequence, contrast agent(gadolinium-diethylenetriaminepentaacetic acid), and itsdosage were optimized for visual evaluation of MR perfu-sion. Previous publications reporting on (semi)quantitativeanalysis mainly used lower doses of gadolinium-diethylenetriaminepentaacetic acid because quantification,but not visual assessment, suffers from nonlinearity betweencontrast agent concentration and signal intensity. Thus, thepresent data set does not allow for quantification, and wecannot assure whether it would produce similar results.
Summary and ConclusionsDSMRP is a safe noninvasive stress modality and is useful toassess patients with suspected and known CAD. Comparedwith DSMR the addition of perfusion imaging during high-dose dobutamine stress is associated with a significant in-crease in sensitivity which is offset by a decrease in speci-ficity for the overall population and the subgroups of ourstudy. In patients with a negative DSMR result, DSMRPenabled the correct diagnosis of CAD in an additional 13%(�70% stenosis) of patients at the cost of 11% more false-positive cases. The findings of our study suggest that DSMRPmight be helpful in identifying patients in whom the benefitof very high sensitivity outweighs the disadvantage of lowerspecificity. Future studies are needed to determine whetherDSMRP may provide incremental prognostic value.
DisclosuresNone.
References1. Hundley WG, Morgan TM, Neagle CM, Hamilton CA, Rerkpattanapipat
P, Link KM. Magnetic resonance imaging determination of cardiacprognosis. Circulation. 2002;106:2328–2333.
2. Jahnke C, Nagel E, Gebker R, Kokocinski T, Kelle S, Manka R, Fleck E,Paetsch I. Prognostic value of cardiac magnetic resonance stress tests:
128 Circ Cardiovasc Imaging September 2008
by guest on July 4, 2015http://circimaging.ahajournals.org/Downloaded from
adenosine stress perfusion and dobutamine stress wall motion imaging.Circulation. 2007;115:1769–1776.
3. Paetsch I, Jahnke C, Wahl A, Gebker R, Neuss M, Fleck E, Nagel E.Comparison of dobutamine stress magnetic resonance, adenosine stressmagnetic resonance, and adenosine stress magnetic resonance perfusion.Circulation. 2004;110:835–842.
4. Wahl A, Paetsch I, Gollesch A, Roethemeyer S, Foell D, Gebker R,Langreck H, Klein C, Fleck E, Nagel E. Safety and feasibility ofhigh-dose dobutamine-atropine stress cardiovascular magnetic resonancefor diagnosis of myocardial ischaemia: experience in 1000 consecutivecases. Eur Heart J. 2004;25:1230–1236.
5. Hundley WG, Hamilton CA, Thomas MS, Herrington DM, Salido TB,Kitzman DW, Little WC, Link KM. Utility of fast cine magnetic res-onance imaging and display for the detection of myocardial ischemia inpatients not well suited for second harmonic stress echocardiography.Circulation. 1999;100:1697–1702.
6. Nagel E, Lehmkuhl HB, Bocksch W, Klein C, Vogel U, Frantz E, EllmerA, Dreysse S, Fleck E. Noninvasive diagnosis of ischemia-induced wallmotion abnormalities with the use of high-dose dobutamine stress MRI:comparison with dobutamine stress echocardiography. Circulation. 1999;99:763–770.
7. Paetsch I, Jahnke C, Ferrari VA, Rademakers FE, Pellikka PA, HundleyWG, Poldermans D, Bax JJ, Wegscheider K, Fleck E, Nagel E. Deter-mination of interobserver variability for identifying inducible left ven-tricular wall motion abnormalities during dobutamine stress magneticresonance imaging. Eur Heart J. 2006;27:1459–1464.
8. Smart SC, Knickelbine T, Malik F, Sagar KB. Dobutamine-atropinestress echocardiography for the detection of coronary artery disease inpatients with left ventricular hypertrophy. Importance of chamber sizeand systolic wall stress. Circulation. 2000;101:258–263.
9. Hoffmann R, Lethen H, Marwick T, Arnese M, Fioretti P, Pingitore A,Picano E, Buck T, Erbel R, Flachskampf FA, Hanrath P. Analysis ofinterinstitutional observer agreement in interpretation of dobutaminestress echocardiograms. J Am Coll Cardiol. 1996;27:330–336.
10. Nagel E, Klein C, Paetsch I, Hettwer S, Schnackenburg B, WegscheiderK, Fleck E. Magnetic resonance perfusion measurements for the nonin-vasive detection of coronary artery disease. Circulation. 2003;108:432–437.
11. Schwitter J, Nanz D, Kneifel S, Bertschinger K, Buchi M, Knusel PR,Marincek B, Luscher TF, von Schulthess GK. Assessment of myocardialperfusion in coronary artery disease by magnetic resonance: a comparisonwith positron emission tomography and coronary angiography. Circu-lation. 2001;103:2230–2235.
12. Wolff SD, Schwitter J, Coulden R, Friedrich MG, Bluemke DA,Biederman RW, Martin ET, Lansky AJ, Kashanian F, Foo TK, Licato PE,Comeau CR. Myocardial first-pass perfusion magnetic resonanceimaging: a multicenter dose-ranging study. Circulation. 2004;110:732–737.
13. Fung AY, Gallagher KP, Buda AJ. The physiologic basis of dobutamineas compared with dipyridamole stress interventions in the assessment ofcritical coronary stenosis. Circulation. 1987;76:943–951.
14. Krivokapich J, Huang SC, Schelbert HR. Assessment of the effects ofdobutamine on myocardial blood flow and oxidative metabolism innormal human subjects using nitrogen-13 ammonia and carbon-11acetate. Am J Cardiol. 1993;71:1351–1356.
15. Elhendy A, Sozzi FB, Valkema R, van Domburg RT, Bax JJ, RoelandtJR. Dobutamine technetium-99m tetrofosmin SPECT imaging for thediagnosis of coronary artery disease in patients with limited exercisecapacity. J Nucl Cardiol. 2000;7:649–654.
16. Porter TR, Xie F, Silver M, Kricsfeld D, Oleary E. Real-time perfusionimaging with low mechanical index pulse inversion Doppler imaging.J Am Coll Cardiol. 2001;37:748–753.
17. Plein S, Radjenovic A, Ridgway JP, Barmby D, Greenwood JP, Ball SG,Sivananthan MU. Coronary artery disease: myocardial perfusion MRimaging with sensitivity encoding versus conventional angiography.Radiology. 2005;235:423–430.
18. Paetsch I, Jahnke C, Fleck E, Nagel E. Current clinical applications ofstress wall motion analysis with cardiac magnetic resonance imaging. EurJ Echocardiogr. 2005;6:317–326.
19. Salton CJ, Chuang ML, O’Donnell CJ, Kupka MJ, Larson MG, KissingerKV, Edelman RR, Levy D, Manning WJ. Gender differences and normalleft ventricular anatomy in an adult population free of hypertension. Acardiovascular magnetic resonance study of the Framingham Heart StudyOffspring cohort. J Am Coll Cardiol. 2002;39:1055–1060.
20. Thiele H, Paetsch I, Schnackenburg B, Bornstedt A, Grebe O, WellnhoferE, Schuler G, Fleck E, Nagel E. Improved accuracy of quantitativeassessment of left ventricular volume and ejection fraction by geometricmodels with steady-state free precession. J Cardiovasc Magn Reson.2002;4:327–339.
21. Jahnke C, Nagel E, Gebker R, Kokocinski T, Kelle S, Manka R, Fleck E,Paetsch I. Prognostic value of cardiac magnetic resonance stress tests:adenosine stress perfusion and dobutamine stress wall motion imaging.Circulation. 2007;115:1769–1776.
22. Perkins NJ, Schisterman EF. The inconsistency of “optimal” cutpointsobtained using two criteria based on the receiver operating characteristiccurve. Am J Epidemiol. 2006;163:670–675.
23. Kramer MS, Feinstein AR. Clinical biostatistics. LIV. The biostatistics ofconcordance. Clin Pharmacol Ther. 1981;29:111–123.
24. Pennell DJ, Sechtem UP, Higgins CB, Manning WJ, Pohost GM, Rade-makers FE, van Rossum AC, Shaw LJ, Yucel EK. Clinical indications forcardiovascular magnetic resonance (CMR): Consensus Panel report.J Cardiovasc Magn Reson. 2004;6:727–765.
25. Dijkmans PA, Senior R, Becher H, Porter TR, Wei K, Visser CA,Kamp O. Myocardial contrast echocardiography evolving as a clin-ically feasible technique for accurate, rapid, and safe assessment ofmyocardial perfusion: the evidence so far. J Am Coll Cardiol. 2006;48:2168 –2177.
26. Bartunek J, Wijns W, Heyndrickx GR, de Bruyne B. Effects of dobuta-mine on coronary stenosis physiology and morphology: comparison withintracoronary adenosine. Circulation. 1999;100:243–249.
27. Tadamura E, Iida H, Matsumoto K, Mamede M, Kubo S, Toyoda H,Shiozaki T, Mukai T, Magata Y, Konishi J. Comparison of myocardialblood flow during dobutamine-atropine infusion with that after dipyri-damole administration in normal men. J Am Coll Cardiol. 2001;37:130–136.
28. Moir S, Haluska BA, Jenkins C, Fathi R, Marwick TH. Incrementalbenefit of myocardial contrast to combined dipyridamole-exercise stressechocardiography for the assessment of coronary artery disease. Circu-lation. 2004;110:1108–1113.
29. Elhendy A, Valkema R, van Domburg RT, Bax JJ, Nierop PR, Cornel JH,Geleijnse ML, Reijs AE, Krenning EP, Roelandt JR. Safety of dobuta-mine-atropine stress myocardial perfusion scintigraphy. J Nucl Med.1998;39:1662–1666.
30. Tsutsui JM, Elhendy A, Anderson JR, Xie F, McGrain AC, Porter TR.Prognostic value of dobutamine stress myocardial contrast perfusionechocardiography. Circulation. 2005;112:1444–1450.
31. Nesto RW, Kowalchuk GJ. The ischemic cascade: temporal sequence ofhemodynamic, electrocardiographic and symptomatic expressions of is-chemia. Am J Cardiol. 1987;59:23C–30C.
32. Bin JP, Le DE, Jayaweera AR, Coggins MP, Wei K, Kaul S. Directeffects of dobutamine on the coronary microcirculation: comparison withadenosine using myocardial contrast echocardiography. J Am Soc Echo-cardiogr. 2003;16:871–879.
33. Elhendy A, O’Leary EL, Xie F, McGrain AC, Anderson JR, Porter TR.Comparative accuracy of real-time myocardial contrast perfusion imagingand wall motion analysis during dobutamine stress echocardiography forthe diagnosis of coronary artery disease. J Am Coll Cardiol. 2004;44:2185–2191.
34. Di Carli MF, Janisse J, Grunberger G, Ager J. Role of chronic hyper-glycemia in the pathogenesis of coronary microvascular dysfunction indiabetes. J Am Coll Cardiol. 2003;41:1387–1393.
35. Wang L, Jerosch-Herold M, Jacobs DR, Jr, Shahar E, Folsom AR.Coronary risk factors and myocardial perfusion in asymptomatic adults:the Multi-Ethnic Study of Atherosclerosis (MESA). J Am Coll Cardiol.2006;47:565–572.
36. Di Bella EV, Parker DL, Sinusas AJ. On the dark rim artifact in dynamiccontrast-enhanced MRI myocardial perfusion studies. Magn Reson Med.2005;54:1295–1299.
37. Miyamoto MI, Rose GA, Weissman NJ, Guerrero JL, Semigran MJ,Picard MH. Abnormal global left ventricular relaxation occurs earlyduring the development of pharmacologically induced ischemia. J Am SocEchocardiogr. 1999;12:113–120.
38. Tanimoto M, Pai RG, Jintapakorn W. Normal changes in left ventricularfilling and hemodynamics during dobutamine stress echocardiography.J Am Soc Echocardiogr. 1995;8:488–493.
39. Pichard AD, Gorlin R, Smith H, Ambrose J, Meller J. Coronary flowstudies in patients with left ventricular hypertrophy of the hypertensivetype. Evidence for an impaired coronary vascular reserve. Am J Cardiol.1981;47:547–554.
Gebker et al Myocardial Perfusion Imaging and DSMR 129
by guest on July 4, 2015http://circimaging.ahajournals.org/Downloaded from

40. Hachamovitch R, Berman DS, Shaw LJ, Kiat H, Cohen I, Cabico JA,Friedman J, Diamond GA. Incremental prognostic value of myocardialperfusion single photon emission computed tomography for the pre-diction of cardiac death: differential stratification for risk of cardiac deathand myocardial infarction. Circulation. 1998;97:535–543.
41. Bartunek J, Marwick TH, Rodrigues AC, Vincent M, VanSchuerbeeck E, Sys SU, de Bruyne B. Dobutamine-induced wallmotion abnormalities: correlations with myocardial fractional flowreserve and quantitative coronary angiography. J Am Coll Cardiol.1996;27:1429 –1436.
CLINICAL PERSPECTIVEThe assessment of regional wall motion during dobutamine stress magnetic resonance (DSMR) is an established clinicalmethod with high diagnostic and prognostic value for the evaluation of coronary artery disease (CAD); however, the roleof dobutamine stress MR perfusion imaging (DSMRP) is unclear. Thus, the present study assessed the diagnosticinformation derived from additional perfusion imaging during high-dose dobutamine-atropine stress in a large referralpopulation. Compared with DSMR alone, DSMRP generally resulted in an increase in sensitivity and a decrease inspecificity for the detection of significant CAD. Overall DSMRP enabled the correct diagnosis of CAD in an additional13% of DSMR negative patients at the cost of 11% more false-positive studies. DSMRP might be considered a usefuldiagnostic test for CAD detection in patients in whom the benefit of very high sensitivity outweighs the disadvantage oflower specificity.
130 Circ Cardiovasc Imaging September 2008
by guest on July 4, 2015http://circimaging.ahajournals.org/Downloaded from

Fleck and Ingo PaetschRolf Gebker, Cosima Jahnke, Robert Manka, Ashraf Hamdan, Bernhard Schnackenburg, Eckart
Resonance for the Assessment of Coronary Artery DiseaseAdditional Value of Myocardial Perfusion Imaging During Dobutamine Stress Magnetic
Print ISSN: 1941-9651. Online ISSN: 1942-0080 Copyright © 2008 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Cardiovascular Imaging
doi: 10.1161/CIRCIMAGING.108.7791082008;1:122-130; originally published online July 30, 2008;Circ Cardiovasc Imaging.
http://circimaging.ahajournals.org/content/1/2/122World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circimaging.ahajournals.org/content/suppl/2008/10/14/CIRCIMAGING.108.779108.DC1.htmlData Supplement (unedited) at:
http://circimaging.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Imaging Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Cardiovascular Imagingin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 4, 2015http://circimaging.ahajournals.org/Downloaded from





























