Embed Size (px)
Citation preview
Advanced implantable drug delivery technologies: transforming the clinical landscape of therapeutics for chronic diseases
Fernanda P. Pons-Faudoa1,2, Andrea Ballerini1,3, Jason Sakamoto1, Alessandro Grattoni1,4,5
1Department of Nanomedicine, Houston Methodist Research Institute, 6670 Bertner Avenue, Houston, TX 77030, USA
2School of Medicine and Health Sciences, Tecnologico de Monterrey, Avenida Eugenio Garza Sada 2501, 64849 Monterrey, NL, Mexico
3Department of Oncology and Onco-Hematology, University of Milan, Via Festa del Perdono 7, 20122 Milan, Italy
4Department of Surgery, Houston Methodist Hospital, 6550 Fannin Street, Houston, TX 77030, USA
5Department of Radiation Oncology, Houston Methodist Hospital, 6550 Fannin Street, Houston, TX 77030, USA
Abstract
Chronic diseases account for the majority of all deaths worldwide, and their prevalence is expected
to escalate in the next 10 years. Because chronic disorders require long-term therapy, the
healthcare system must address the needs of an increasing number of patients. The use of new
drug administration routes, specifically implantable drug delivery devices, has the potential to
reduce treatment-monitoring clinical visits and follow-ups with healthcare providers. Also,
implantable drug delivery devices can be designed to maintain drug concentrations in the
therapeutic window to achieve controlled, continuous release of therapeutics over extended
periods, eliminating the risk of patient non-compliance to oral treatment. A higher local drug
concentration can be achieved if the device is implanted in the affected tissue, reducing systemic
adverse side effects and decreasing the challenges and discomfort of parenteral treatment.
Although implantable drug delivery devices have existed for some time, interest in their
therapeutic potential is growing, with a global market expected to reach over $12 billion USD by
2018. This review discusses implantable drug delivery technologies in an advanced stage of
development or in clinical use and focuses on the state-of-the-art of reservoir-based implants
including pumps, electromechanical systems, and polymers, sites of implantation and side effects,
and deployment in developing countries.
Alessandro Grattoni, [email protected].
Compliance with ethical standards J.S and A.G. disclose a financial interest in NanoMedical systems, Inc. F.P.P. and A.B. disclose no competing financial interest.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
HHS Public AccessAuthor manuscriptBiomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Published in final edited form as:Biomed Microdevices. ; 21(2): 47. doi:10.1007/s10544-019-0389-6.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Keywords
MEMS; NEMS; Non-biodegradable polymers; Long-acting formulations; Implants
1. Introduction
Chronic disease can be defined as a disease that continues or reoccurs over a long period of
time. Chronic diseases encompass cardiovascular diseases, diabetes, respiratory diseases,
and other disorders that affect a large number of people, are costly to manage, and increase
disability-adjusted life years (DALYs) (Bernell and Howard 2016). With one DALY
equaling a year loss of disease-free life, DALYs are a measure of the burden of disease
across the population (World Health Organization n.d.). Some chronic health disorders are
manageable with appropriate treatment. However, the prevalence of chronic diseases such as
cardiovascular diseases, diabetes, cancers, respiratory diseases, and human
immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) is steadily
increasing and expected to affect 157 million people in the US by 2020 (Comlossy 2013).
The global burden of chronic conditions also continues to rise (Fig. 1) and is projected to
account for 69% of all deaths worldwide, of which 80% will be in developing countries, by
2030 (Alwan et al. 2010; Samb et al. 2010). As the global economic impact of chronic
diseases is estimated to reach $47 trillion in the next two decades, concerted efforts are
focused on relieving this burden (World Economic Forum and Harvard School of Public
Health 2011).
Traditional intervention via oral or intravenous administration of therapeutics has several
limitations. Some drugs have poor bioavailability and require multiple doses, augmenting
the risk of resistance and side effects as well as the potential for drug abuse. Additionally,
poor patient adherence has direct effects on medication efficacy. Non-adherence is a major
concern, 30 to 50% of adults with chronic conditions in the US do not take their medications
as prescribed and this has been correlated with 125,000 deaths and 10% of hospitalizations
annually. This results in an annual economic burden of $100 billion USD in health care
services (Cutler et al. 2018; Kini and Ho 2018; Pagès-Puigdemont et al. 2016; Oung et al.
2017). Social and technological efforts such as patient education services, health care
provider interventions, reminder tools, and electronic monitoring devices have tried to tackle
with medication non-adherence with no significant success (Kini and Ho 2018; Pagès-
Puigdemont et al. 2016; Oung et al. 2017; World Health Organization 2003). Because of the
correlation between increased non-adherence and higher illness prevalence there is an
obvious need to find a solution for medication non-adherence (Atinga et al. 2018; Pagès-
Puigdemont et al. 2016).
Compared with traditional systemic delivery, implantable drug delivery devices offer many
advantages. Site-specific implantation can bypass the absorption and distribution phase of
oral and peripheral regimens, resulting in higher drug concentrations in targeted areas
(Danckwerts and Fassihi 1991). Thus, drug levels can be maintained in the therapeutic
window by virtue of controlled, continuous release of therapeutics. Importantly, as this
technology can be used over extended periods, it eliminates the possibility of poor patient
Pons-Faudoa et al. Page 2
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
compliance and decreases the discomfort of parenteral treatment (Park 2014). Therefore
implantable drug delivery technologies provide site-specificity and deal with medication
non-adherence, transforming the clinical landscape of therapeutics for chronic diseases.
Controlled drug delivery technologies have progressed over the last six decades to third-
generation modulated delivery systems, with increasing interest in long-term delivery
systems (Farina et al. 2017; Meng and Hoang 2012a; Park 2014; Yun et al. 2015).
Accordingly, the global market for implantable drug delivery is growing—valued at $9.05
billion USD in 2013 and expected to be $12.42 billion by the end of 2018. Newer, more
easily applicable machineries improve the scalability of implantable drug delivery devices.
Companies and small start-ups find implantable devices profitable because they are cost-
effective and lower overall treatment cost (Kumar and Pillai 2018), and there is high demand
to file patents on versatile implantable drug delivery devices that can be tailored for multiple
drugs (Coherent Market Insights 2017; Yang and Pierstorff 2012). Another potential benefit
is the opportunity for pharmaceutical companies to exploit medications coming off patent, as
patent expirations can be extended by creating new products that combine patented
medications and implantable devices (Beall et al. 2016). Implantable drug delivery devices
can also be advantageous for less prevalent chronic diseases such as drug abuse, pain
management, and neurological disorders. Furthermore, telemedicine can allow physicians to
remotely control drug release rate from the implant or maximize treatment effectiveness
through the use of artificial intelligence and machine learning algorithms (Ross et al. 2017).
In this article, we highlight current technologies for long-term drug delivery in advanced
stages of development or in clinical use, with a brief discussion of the use, mechanism of
function, advantages, and limitations of each system. This review will demonstrate how
advanced implantable drug delivery technologies can transform the clinical landscape of
therapeutics for chronic illnesses. The drug delivery systems covered include reservoir-based
polymer systems, pumps, and electromechanical systems, excluding polymeric fully
degradable systems and long-term delivery devices that are not completely implanted, which
are thoroughly revised elsewhere (Kamaly et al. 2016; Majeed and Thabit 2018). We further
present a clinical perspective on sites of implantation and potential strategies to improve
device development associated with patient acceptance, and device deployment in the
developing world.
2. Reservoir-based polymer systems
Reservoir-based polymer systems are passive implants with a simple design consisting of a
drug core surrounded by a non-degradable polymeric film (Fig. 2a). Drug release rate is
controlled by polymeric coating properties, such as polymer configuration, molecular
weight, and coating thickness, as well as physicochemical properties of the drug, such as
solubility, particle size, and molecular weight. Historically, polymeric systems have been
employed for site-specific mid–/long-term systemic drug administration after subcutaneous
implantation. However, most polymeric systems suffer from an initial drug release burst,
which can potentially reach toxic levels and endanger the patient. After this burst, drug core
concentrations decrease, possibly to below their therapeutic window (Kumar and Pillai
2018; Yang and Pierstorff 2012).
Pons-Faudoa et al. Page 3
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Polymer systems require constant drug concentration within the drug core to achieve zero-
order kinetic drug release. These implants often employ the polymers silicone, polyvinyl
alcohol (PVA), and ethylene vinyl acetate (EVA). By contrast, biodegradable implants use
naturally occurring polymers (e.g., human serum albumin, collagen, gelatin) or synthetic
polymers (e.g., polylactic acid, polyglycolic acid, polylactic-co-glycolic acid copolymer)
(Kumar and Pillai 2018; Yang and Pierstorff 2012).
Son et al. (2017) developed a 3D-printed porous cylindrical device called Biocage that can
be filled with a drug. The Biocage is small enough to fit inside a 22-gauge needle for direct
delivery and robust enough to be implanted directly into the target issue. The Biocage has
the following dimensions: 300-μm hollow inner diameter, 20-μm outer wall, 40-μm solid
base, 900-μm height, and 5-μm-diameter pores (Fig. 2b). The creators demonstrated
fluorescent microsphere release from the implant but did not determine the drug release rate.
They also confirmed that the Biocage can be used for local drug delivery within the brain
and explain how 3D printing offers structural and material versatility to the device. However,
although the materials are biocompatible and biodegradable, they are not yet approved by
the US Food and Drug Administration (FDA). Nevertheless, this technological platform
shows much promise, as it offers drug versatility, has high drug loading efficiency, and can
be implanted within the target organ.
In 2006, the FDA approved a similar reservoir-based polymer system, Implanon® (Merck,
Kenilworth, NJ, USA), a 4 cm × 22 mm non-biodegradable implant, as a female hormone-
based contraceptive. An EVA copolymer rod encompasses 68 mg etonogestrel, which
controls the daily release of progestin for up to 3 years. However, the release rate decreases
over time, from 60 to 70 μg/day in first couple of weeks to 35–45, 30–40, and 25–30 μg/day
at the end of the first, second, and third year, respectively (FDA Reference IDs: 3080389,
4,100,681) (Allen et al. 2016; Huber 1998). However, another study extending its use to 5
years indicated an efficacy of 100% (Ali et al. 2016), suggesting that if the device is still
effective after 5 years, patients have likely received supraoptimal doses. Therefore, this
implant should be further improved to deliver at a constant rate for 3–5 years. In some cases,
the Implanon® was incorrectly inserted, making its localization for removal difficult for
healthcare professionals. This led to the design of Nexplanon®, a second-generation device
with the addition of the radiopaque ingredient barium sulfate, which entered the US market
in 2011 (FDA Reference IDs: 3080389, 4,100,681) (Allen et al. 2016; Huber 1998).
The Hydron® implant (Endo Pharmaceuticals Solutions Inc., Malvern, PA, USA) consists of
a hydrogel polymeric reservoir called MedLaunch™ that is spun-cast into a 3.5 cm × 3 mm
tube (Stevenson et al. 2012). Two of these non-biodegradable reservoir-based polymeric
system implants are already on the market: Vantas® and SUPPRELIN® LA. The drug core
contains 50 mg histrelin acetate in both implants, but the drug delivery rate is modified for
the treatment of two different diseases (Fig. 2c). The Vantas® implant delivers 50μg/day for
12 months to relieve symptoms of prostate cancer, whereas the SUPPRELIN® LA implant
releases 65 μg/day for 12 months to treat children with central precocious puberty (FDA
Reference IDs: 4099967, 2,887,911). Currently, there are no reports of decreasing drug
release rates from these implants, which could be attributed to their shorter treatment
periods. The Hydron® implant technology was also adapted to deliver 84 mg octreotride, a
Pons-Faudoa et al. Page 4
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
somatostatin analog, for up to 6 months to treat acromegaly. However, the phase 3 clinical
trial was terminated for business reasons (NCT01295060) (Endo Pharmaceuticals n.d.;
Stevenson et al. 2012).
ProNeura™ (Titan Pharmaceuticals Inc., San Francisco, CA, USA) is a non-biodegradable
rod composed of an EVA matrix and a drug formulation. The Probuphine® implant,
ProNeura™ with buprenorphine, was FDA-approved in 2016 for the maintenance treatment
of opioid dependence. Four 26 × 2.5 mm implants are needed to maintain therapeutic drug
levels (Fig. 2d). Each device contains 80 mg buprenorphine hydrochloride, a partial opioid
agonist, delivered at a controlled rate for up to 6 months (FDA Reference ID: 4215185).
Probuphine® has proved more cost-effective than sublingual buprenorphine, as it minimizes
fluctuations in plasma concentrations and reduces clinic and pharmacy visits by eliminating
the need for daily supervision (Barnwal et al. 2017; Carter et al. 2017). Currently, preclinical
studies are testing the use of ProNeura™ to deliver a dopamine agonist(ropinirole)andT3for
the treatment of Parkinson’s disease and hypothyroidism, respectively (Titan
Pharmaceuticals n.d.).
All above-mentioned reservoir-based polymer systems are subcutaneously implanted in the
inner arm, as they require systemic therapeutic levels. However, two non-biodegradable
implants are FDA-approved for intravitreal management of ophthalmology-related diseases:
Retisert® (Bausch & Lomb, Rochester, NY, USA) and ILUVIEN® (Alimera Sciences Inc.,
Alpharetta, GA, USA). Because ocular diseases affecting the posterior chamber require
constant drug exposure, both devices take advantage of the higher viscosity in the vitreous
humor, which increases drug half-life. Retisert® treats chronic noninfectious uveitis and can
achieve drug release for 30 months but must then be removed (FDA Reference ID: 2955048)
(Borkar et al. 2017; Haghjou et al. 2011; Logan et al. 2016; Yasin et al. 2014). ILUVIEN®
can maintain therapeutic levels in the vitreous humor for up to 36 months for the treatment
of diabetic macular edema (DME) in vitrectomized and non-vitrectomized eyes (Carle et al.
2014; Hawrami et al. 2016; Kumar et al. 2016; Meireles et al. 2017; Pessoa et al. 2018).
After 36 months, a new implant can be inserted without removing the previous implant, as
no side effects have been reported from having multiple implants in the eye (FDA Reference
ID: 3635981) (Borkar et al. 2017; Hawrami et al. 2016; Logan et al. 2016; Wang et al. 2013;
Yasin et al. 2014).
Retisert® consists of a drug formulation tablet enclosed in a silicone elastomer cup with an
outlet consisting of a PVA membrane (Fig. 2e). The tablet contains 0.59 mg fluocinolone
acetonide (FA), a corticosteroid, and the following inactive ingredients: microcrystalline
cellulose, PVA, and magnesium stearate. Retisert® passively delivers FA into the vitreous
humor for the treatment of chronic noninfectious uveitis affecting the posterior chamber
(FDA Reference ID: 2955048) (Borkar et al. 2017; Haghjou et al. 2011; Logan et al. 2016;
Yasin et al. 2014). ILUVIEN® is a 3.5 × 0.37 mm rod made of polyimide with a non-
permeable cap on one end and a permeable PVA membrane on the other end. The inside of
the rod is composed of a PVA matrix with 0.19 mg FA (Fig. 2f). This implant is not the first
line of therapy but is only approved for DME eyes that did not respond to laser therapy and
anti-VEGF therapy (Elaraoud et al. 2016a; Figueira et al. 2017; Massin et al. 2016). Real-
world results indicate the efficacy of ILUVIEN®, demonstrating improved best corrected
Pons-Faudoa et al. Page 5
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
visual acuity and central foveal thickness (Alfaqawi et al. 2017; Amoaku et al. 2015; Bailey
et al. 2017; Bertelmann et al. 2013; Bertelmann and Schulze 2015; Cunha-Vaz et al. 2014;
Elaraoud et al. 2016b, c; El-Ghrably et al. 2017; Fusi-Rubiano et al. 2018; Gonçalves et al.
2017; Mourtzoukos 2017; Quhill and Quhill 2016; Saedon et al. 2017; Schmit-Eilenberger
2015; Syed 2017; Veritti et al. 2017; Yang et al. 2015). Another implant, Vetrisert®, was
FDA-approved for the treatment of cytomegalovirus retinitis but was later discontinued. A
pellet of 4.5 mg ganciclovir was enclosed between PVA and EVA and was found to relieve
symptoms for up to 8 months (Yasin et al. 2014). Vetrisert® was also effective in treating
cytomegalovirus retinitis in AIDS patients, extending the progression of retinitis from 15 to
226 days (Martin 1994).
In summary, reservoir-based polymer systems are the type of implant that has received the
most FDA approval and has been on the market the longest. All use the same mechanism of
release: drug diffusion through non-biodegradable polymer film. A comparison of their
advantages and limitations is shown in Table 1.
3. Pumps
3.1 Osmotic pumps
Osmotic pumps were developed in the 1950s by Rose and Nelson for drug delivery in
animals. Since then, numerous designs have found clinical use for the treatment of human
diseases (Keraliya et al. 2012; Santus and Baker 1995). Implantable osmotic pumps are drug
delivery devices developed for the sustained administration of therapeutics over extended
periods of time ranging from months to years. Osmotic pumps are conventionally composed
of a hollow cylinder containing a drug reservoir and an osmotic engine separated by a
movable piston. The drug reservoir is directly connected to the outside through micro-holes,
and the osmotic engine is separated from the outside by means of a semipermeable
membrane.
The mechanism of osmotic pump-driven drug release occurs after the pump is implanted.
The osmotic engine, which contains high concentration of osmolytes (i.e., salts), drives an
osmotic flow of interstitial fluid through the semipermeable membrane. The inward H2O
flow increases hydrostatic pressure in the osmotic reservoir, which exerts force on the piston
(Fig. 3a). The piston is pushed toward the drug reservoir and causes injection of the drug
solution in an equivalent amount to the volume of drug solution displaced. Ideally, this
process is continuous and terminates when the piston has displaced the entire amount of
drug solution and has reached the extreme end of the drug reservoir. Other osmotic pumps
have a different design in which the osmotic engine surrounds the drug reservoir (Fig. 3b).
In these pumps, a high salt concentration in the osmotic engine displaces the drug out
through the micro-orifice at a controlled rate by compressing the drug reservoir (Cobo et al.
2015; Herrlich et al. 2012; Kumar and Pillai 2018; McConville 2011).
Viadur® (Bayer Healthcare Pharmaceuticals, Berlin, Germany) was a non-biodegradable
titanium osmotic implant that utilized a DUROS® controlled release pump to administer
leuprolide acetate, a gonadotropin-releasing hormone analog, for 12 months for the
palliative treatment of advanced prostate cancer (FDA Reference ID: 2888026) (Rohloff et
Pons-Faudoa et al. Page 6
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
al. 2008).Despite successful clinical trials and FDA approval, Viadur® was removed from
the market in 2007 due to its lack of cost-effectiveness and limited long-term market
viability. In general, the fabrication and assembly procedures as well as the quality control of
osmotic implants may ultimately be too expensive to justify their clinical use as an
alternative to conventional drug administration approaches.
The Medici Drug Delivery System™ (Intarcia Therapeutics Inc., Boston, MA, USA) is an
osmotic mini-pump tailored to hold a certain drug volume over different dosing intervals
(Intarcia Therapeutics n.d.-a). ITCA 650 utilizes the Medici Drug Delivery System™ to
achieve continuous delivery of exenatide, a glucagon-like peptide-1 receptor agonist, for the
treatment of type 2 diabetes. The pump maintains exenatide release for 6 months and is
undergoing further development for a 1-year dose (Intarcia Therapeutics n.d.-c). A challenge
to delivering a 1-year dose is the necessity of maintaining a constant concentration of
osmolyte in the osmotic engine over the entire duration of the treatment to achieve constant
drug elution. As such, the osmolyte must be included in a supersaturated form to maintain its
constant concentration despite the inward flow of H2O. When a substantial amount of drug
has been released, release rate may decline as a result of reduced osmotic flow.
ITCA 650 has completed its phase 3 clinical trial, called FREEDOM. However, the FDA
issued a Complete Response Letter regarding manufacturing aspects, and the device is
currently on an FDA clinical hold (Genetic Engineering and Biotechnology News 2018).
Titanium osmotic pump manufacturing can be very expensive, as these pumps require
extremely tight dimensional and geometrical tolerances as well as lathe machining for
minimal surface roughness in the inner implant cavity. Intarcia is currently resolving these
issues, and the Medici Drug Delivery System™ will be adapted for the continuous delivery
of HIV pre-exposure prophylaxis (PrEP) (Intarcia Therapeutics n.d.-b).
Osmotic pumps have been further developed to improve intravesical drug delivery using
osmotic flow of H2O from urine instead of interstitial fluid. GemRIS™ and lidocaine-
releasing intravesical system (LiRIS®) (TARIS Biomedical®, Lexington, MA, USA), which
utilize the TARIS® System, are elastomeric tubular osmotic intravesical implants that
deliver gemcitabine and lidocaine, respectively, to treat bladder diseases. The TARIS®
System is a dual-lumen silicone tube containing an osmotic engine encompassing the solid
drug core in one lumen and nitinol wireform in the other (Fig. 3c). The permeability of
silicone permits H2O from the urine to diffuse through the osmotic engine into the drug core
and dissolve the drug. This creates an osmotic pressure in the osmotic engine that forces
drug solution out through the orifice (Fig. 3b).
Intravesical osmotic pumps are currently undergoing clinical trials. GemRIS™ completed a
phase 1b clinical trial to assess its safety and tolerability in muscle-invasive bladder cancer
patients (NCT02722538) (Taris Biomedical LLC n.d.-a). GemRIS™ will also undergo a
phase 1b clinical trial with Opdivo® (nivolumab) in the same patient population as well as
two other clinical trials for non-muscle-invasive bladder cancer (NCT02720367) and
muscle-invasive bladder cancer unfit for radical cystectomy (NCT03404791) (Taris
Biomedical LLC n.d.-b; Taris Biomedical LLC n.d.-c).
Pons-Faudoa et al. Page 7
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
An advantage of the TARIS® System is that the drug is loaded in solid form, which
augments its loading efficiency. Also, the implant does not have moving components,
decreasing the risk of potential failure and reducing fabrication costs. The device can
achieve local sustained release of drug, minimizing side effects and frequent drug catheter
injections to the bladder. These implants have received positive feedback from people who
suffer from bladder diseases seeking a new drug administration strategy (Cima et al. 2014;
Herrlich et al. 2012; Matheson 2014; Nickel et al. 2012; Taris Biomedical LLC n.d.-d).
Nonetheless, accidental rupture of the implant can cause drug overdose from the dissolving
solid drug core, and the device may be difficult to efficiently remove from the body without
cystoscopy.
3.2 Peristaltic pumps
Peristaltic pumps have been used clinically for many years. In 1881, Eugene Allen was the
first to patent the peristaltic pump in the US for blood transfusions (US249285A) (Allen
1881; INTEGRA Biosciences n.d.). Years later, cardiothoracic surgeon Dr. Michael
DeBakey created the DeBakey pump that was used in the Gibbon heart-lung machine in
1953 (Winters 2015). Positive displacement is the driving force for pumping fluids contained
in a tube inside the peristaltic pump. Rollers attached to the external circumference of a rotor
compress the flexible tube, trapping liquid drug doses between rollers. As the rotor rotates,
the rollers displace the drug in the tube and the tube returns to its natural state after passage
of the drug, a process known as peristalsis (Fig. 4a). This peristalsis transports the drug
toward the pump outlet and into a catheter for delivery to the target site.
This technology has been applied to create an implantable peristaltic pump capable of
chronically administering therapeutics at the target site (Berg and Dallas 2013). However,
the implant is relatively large to accommodate the mechanical components, battery, and
drug. As such, the volumetric loading efficiency, defined as the ratio of drug reservoir
volume to implant volume, is greatly limited to 22–30% (Medtronic 2011). A disadvantage
of this pump is that its size restricts the implantation site, requiring a catheter to administer
the drug at the target site. This technological platform is already on the market as the
SynchroMed™ II pump (Medtronic, Fridley, MN, USA), an implantable FDA-approved
system composed of a pump reservoir, reservoir fill port, reservoir valve, pump tubing,
check valve, catheter port, and implanted catheter (Fig. 4b) (Kosturakis and Gebhardt 2012;
Pope and Deer 2015). Drug is percutaneously loaded in the reservoir fill port and passes
through the reservoir valve into the pump reservoir. The design of the pump reservoir
involves pressurized gas stored below the reservoir. Thus, at normal body temperature, the
gas expands and displaces the drug in the pump reservoir into the pump tubing. The
SynchroMed™ II pump then transports the drug in a peristaltic motion through the pump
tube, check valve, catheter port, and implanted catheter, where it is released at the target site
(Bolash et al. 2015; Christo and Bottros 2014; Meng and Hoang 2012b; Pope and Deer
2015).
This pump is FDA-approved for the chronic delivery of treprostinil, morphine sulfate, and
ziconotide. Intravenous treprostinil, epidural/intrathecal morphine sulfate, and intrathecal
ziconotide are delivered for the treatment of pulmonary arterial hypertension, chronic
Pons-Faudoa et al. Page 8
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
intractable pain, and severe chronic pain management, respectively (Bourge et al. 2016;
Medtronic 2017). In Sweden, the SynchroMed™ II pump is administering
intracerebroventricular PDFG-BB in Parkinson’s disease patients in a phase 1/2a study
evaluating its safety and tolerability (NCT00866502) (Newron Sweden AB n.d.; Paul et al.
2015).
Chronic drug delivery requires careful dose monitoring by a healthcare professional to
maintain adequate therapeutic levels. The SynchroMed™ II pump can be programmed by
telemetry to deliver a wide range of therapeutic flow rates, thus personalizing the drug dose
for each patient (Li et al. 2012; Medtronic 2017). Likewise, pain tolerance differs between
patients, so an advantage of this pump is that the patient can self-administer an additional
dose through a personal therapy manager (PTM), a handheld accessory with a lockout
system ensuring that the patient does not administer more drug than is approved by the
doctor (Bhatia et al. 2014). Currently, the PTM is undergoing a phase 4 clinical trial for
patient-controlled intrathecal analgesia with bupivacaine for chronic low back pain
(NCT02886286) (Ilias et al. 2008; Salim M Hayek and University Hospitals Cleveland
Medical Center n.d.).
Because these pumps require a battery, their lifespan is limited to 4–7 years. Also, their low
volumetric loading efficiency of 22–30% requires a large pump and limits the size of the
reservoir compared with the volume of the device. Consequently, patients must go to a
healthcare professional to refill the pump every 3–4 months, which affects patient
acceptability (Bolash et al. 2015; Christo and Bottros 2014; Meng and Hoang 2012b; Pope
and Deer 2015). Another setback is reports that magnetic resonance imaging (MRI)
temporarily stops the pump motor rotor. As a result, all patients must undergo assessment of
pump motor function after an MRI (Kosturakis and Gebhardt 2012; Pope and Deer 2015).
Peristaltic systems are also costly to manufacture (Rajgor et al. 2011).
3.3 Infusion pumps
Infusion pumps utilize a chlorofluorocarbon propellant, whose change from liquid to gas at
body temperature serves as the driving force to deliver a drug. This implantable mechanical
system is divided into two chambers: propellant and drug. The drug chamber is a collapsible
bellow that compresses as gas expands from the propellant chamber. This forces the drug out
through an exit port into the pump catheter (Fig. 5). Because body temperature is constant,
the drug is delivered at a steady rate and is tunable by changing the drug concentration in the
drug reservoir. An advantage of infusion pumps is that no battery is required for drug
administration, avoiding the need for replacement (Rajgor et al. 2011).
The Codman® 3000 pump (Codman & Shurtleff, Inc., Raynham, MA, USA) is an infusion
pump FDA-approved for intrathecal delivery of morphine sulfate for pain management and
hepatic arterial infusion of chemotherapy to the tumor site. The pump achieves a constant
flow rate by maintaining a pump drive pressure of approximately 0.6 bar at body
temperature. There are different titanium Codman® 3000 pump drug reservoir sizes: 16, 30,
or 50 ml. Thus, the Codman® 3000 pump size depends on the model and can measure 6.12–
8.64 × 3.20–3.74 cm and weigh 98–173 g. As a result, a disadvantage of the pump is its low
volumetric loading efficiency of 14–29%. However, the pump can be transcutaneously
Pons-Faudoa et al. Page 9
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
refilled every 4–8 weeks through a self-sealing silicone central port (Baert et al. 2008;
Codman and Shurtleff 2003; Codman & Shurtleff n.d.).
In a study evaluating baclofen delivery for severe spasticity treatment, the Codman® 3000
pump demonstrated an accuracy higher than 90% (Ethans et al. 2005). Although this
accuracy is similar to that of peristaltic pumps, the infusion pump has a lifetime warranty
advantage as it omits the battery. Furthermore, a pilot study of the delivery of darunavir via
the caudal vena cava by the Codman® 3000 pump for HIV PrEP confirmed a steady-state
plasma drug concentration with an average of 40 ng/ml in two dogs. This study also
highlights the versatility of the pump and catheter through its adaption to deliver viscous
solutions (Baert et al. 2008). Although the Codman® 3000 pump is highly acceptable by
patients, especially for hepatic arterial infusion for chemotherapy, its production stopped in
April 2018. This halt was likely due to low profitability, with pumps costing from $7000 to
$11,000 USD, and low demand, with only 300 sales per year in the US (Grady and Kaplan
2018).
Another dynamic implant that relies on a positive driving force to modulate drug dosing is
the Prometra® pump (Flowonix Medical Inc., Mt. Olive, NJ, USA). This FDA-approved
chronic pain management pump delivers morphine intrathecally and uses the same positive
pressure gas expansion actuation design as the Codman® 3000 pump but with battery-
powered valves for flow regulation (Fig. 4) (Christo and Bottros 2014; Cobo et al. 2015;
Kumar and Pillai 2018; Wilkes 2014). The titanium device is relatively large to
accommodate the electrical components that permit remotely controlled drug release,
measuring 7.1 × 2 cm with an unfilled weight of 150 g and drug reservoir volume of 20 ml.
Programmable dose changes are a big advance for implants, as they give patients the ability
to self-administer drug from an implant as they would with oral pills. The FDA-approved
patient therapy controller (PTC™) offers patients flexibility to manage their pain (Deer and
Pope 2015; Flowonix Medical n.d.). Also, external control of dosing is a requirement for
pain management because dosing throughout the day is variable (Kumar and Pillai 2018).
In a study of 110 patients with chronic pain, Prometra® pumps had higher dosing accuracy
when administering morphine sulfate compared with SynchroMed™ II pumps (Christo and
Bottros 2014; Rauck et al. 2010). This could be attributed to the Prometra® pump valves
delivering more precise drug doses due to their employment of simple open-and-close
mechanisms. By contrast, SynchroMed™ II pumps have a fixed drug dose between rollers
that cannot be finely tuned. Furthermore, the accuracy, efficacy, and safety of Prometra®
pumps were demonstrated in patients for up to 12 months (Kalyvas et al. 2014; Rauck et al.
2010, 2013).
A major disadvantage of Prometra® pumps is the need to completely remove medication
prior to MRI, as magnetic fields may open the valves and empty the drug reservoir, causing
drug overdose (Christo and Bottros 2014; Pope and Deer 2015). To avoid this procedure and
achieve an MRI compatible implant, a flow-activated safety valve (FAV™) was incorporated
in the new pump model, Prometra® II. However, the pump was recalled in 2017 due to a
failure of the FAV™ during an MRI scan, resulting in a patient receiving a fatal dose (U.S.
Food and Drug Administration 2018). Although Prometra® II was designed to prevent the
Pons-Faudoa et al. Page 10
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
need for pre-MRI medication removal, the recall mandates emptying the drug reservoirs in
Prometra® and Prometra® II pumps before an MRI scan (Flowonix Medical 2018).
However, as physicians and healthcare workers are aware of this necessity, this is not a
restrictive problem with careful monitoring.
In summary, pumps with different mechanisms of action can be chosen depending on the
patient’s disease, drug release longevity, and site of implantation. Larger peristaltic and
infusion pumps can possibly be used to treat chronic diseases due to their larger drug
reservoir and refill feature, whereas smaller osmotic pumps maintain constant drug release
for systemic or site-specific effects (Kumar and Pillai 2018). A comparison of advantages
and limitations of peristaltic, osmotic, and infusion pumps is shown in Table 2.
4. Microfabricated systems
In the biomedical field, electromechanical systems offer distinctive solutions for drug release
related to precision dosing. There is much interest in implants that incorporate this
technology and are fabricated in the micro- and nanometer range (Kumar and Pillai 2018).
Microscopic and nanoscopic devices with features in the microscale and nanoscale array are
termed microelectromechanical systems (MEMS) and nanoelectromechanical systems
(NEMS), respectively.
When these implants are scaled down, the driving forces of drug release change with respect
to the decrease in area and volume; forces such as adhesion and surface tension have a
greater effect on molecules, which is convenient for controlled drug delivery (Bhushan
2007). Given the incredible variety of technologies proposed, in this section we will review
some representative MEMS and NEMS undergoing preclinical research or clinical
development.
4.1 Mems
Fluidic MEMS show potential for drug delivery applications and can be integrated with
electronic components to allow remote control over drug administration. Santini et al. (1999)
developed one of the first microfluidic devices capable of pulsatile release. It consists of a
microfabricated silicon wafer containing an array of drug reservoirs capped by gold
membranes (Fig. 6a, b) (Maloney et al. 2005). The device allows the selective opening of
single reservoirs by applying an electrical potential to the gold membranes. An
electrochemical reaction causes the complete dissolution of the membrane, allowing drug
release (Fig. 6c). This technology was adapted for leuprolide release by Microchips Biotech,
Inc. (Bedford, MA, USA).
Micro-CHIP allows the remote control of drug delivery. This system utilizes electronic
circuitry for radio-frequency communication with the remote control unit for triggering
dissolution of capping reservoir membranes. This system is complex and requires a power
source consisting of a battery (Fig. 6d), which occupies ~40% of the implant volume due to
the significant power consumption of the device. Micro-CHIP has arrays of drug reservoirs
of 300–600 nl each that can be individually opened over time, creating a pulsatile delivery
profile (Farra et al. 2012; Grayson et al. 2004). To mimic constant delivery, the reservoirs
Pons-Faudoa et al. Page 11
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
should be opened at frequent time points. The rate of release from each reservoir can be
controlled by modification of the dissolving capping layer (Santini et al. 2000).
Micro-CHIP devices have been developed for different experimental applications. One of the
most relevant applications is the delivery of leuprolide in a canine model (Prescott et al.
2006). For this purpose, the implant contains 100 drug reservoirs providing a total reservoir
volume of 30 μl, corresponding to 2.5 mg leuprolide acetate powder (Grayson et al. 2004).
The device, with approximate dimensions of 4.5 × 5.5 × 1 cm3, has a volume of
approximately 30 ml, meaning that its nominal loading efficiency is 0.1%. More recently, a
different version of Micro-CHIP was tested in a clinical trial (Farra et al. 2012). This implant
delivers teriparatide, synthetic human parathyroid hormone fragments [hPTH(1–34)], which
is the only treatment approved for anabolic osteoporosis and requires daily injection (Watson
2012). The device, with approximate dimensions of 5.4 × 3.1 × 1.1 cm3, contains 20
reservoirs containing 40 μg teriparatide each, providing a total reservoir volume of 12 μl.
This Micro-CHIP has a volume of approximately 15 ml and a nominal loading efficiency of
0.08%. However, Farra et al. (2012) report that the drug loading procedure does not allow
complete yield of all drug reservoirs, which reduces the effective loading efficiency to below
0.08%.
These implants have the benefit of being made of components that can be microfabricated
with conventional semiconductor technologies. The shell can be machined or injection-
molded for the low-cost parallel fabrication of a large number of parts. Nonetheless, the
assembly, loading, and sterilization of the device is expensive. Additionally, the extremely
low loading efficiency significantly limits its applicability for long-term sustained delivery
of therapeutics. However, the Micro-CHIP will be tested with a variety of chronic drug
therapies since Teva Pharmaceuticals partnered with Microchips Biotech Inc. in 2015
(Microchips Biotech 2015).
Humayun et al. developed prototypes of one of the first ocular MEMS pumps for the
treatment of DME and noninfectious uveitis. The Posterior MicroPump Delivery System
(PMP) is implanted on the sclera beneath the conjunctiva and delivers micro- and nanodoses
intravitreally. The PMP can be wirelessly programmed with The Eye™. The device is 13 ×
16 × 5 mm in size and is custom-contoured for a reduced front height to fit on the outer
surface of the eye. The PMP has a drug reservoir with a refill port, battery, electronics,
electrolysis chamber, and cannula (Fig. 7a). When the device is turned on, an electrical
potential electrolyzes H2O into H2 and O2, which returns to H2O when turned off. The gases
generate pressure on the drug reservoir and force the drug into the cannula at a desired dose
(Fig. 7b) (Cobo et al. 2015; Gutiérrez-Hernández et al. 2014; Humayun et al. 2014; Yasin et
al. 2014). Use of the PMP for delivering ranibizumab, an angiogenic inhibitor, for 90 days
was demonstrated to be safe. However, four of the eleven patients received a lower than
target dose (Humayun et al. 2014). PMP safety was previously assessed in a 1-year canine
study (Gutiérrez-Hernández et al. 2014). Humayun et al. patented the technology and
created the company Replenish Inc. (Pasadena, CA, USA), which produces Replenish
MicroPumps.
Pons-Faudoa et al. Page 12
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
4.2 NEMS
4.2.1 NEMS for constant delivery—At the nanoscale, the properties of fluids under
confinement can be beneficially leveraged. Nanochannels constitute highly precise and
accurate delivery vehicles for the delivery of therapeutics in a controllable manner. When the
size of the channels shrinks to the size of the diffusing analytes, wall-to-molecule
interactions play a dominant role in molecular release, causing constrained and saturated
diffusion (Ziemys et al. 2011; Ziemys et al. 2010). Therefore, nanochannels can passively
control the release of molecules through concentration-driven transport as long as the drug
reservoir is supersaturated (Bruno et al. 2018). Taking advantage of these nanoscale effects,
constant, sustained release of drugs can be achieved by judiciously tailoring the size and
surface chemistry of nanochannels. This nanochannel approach was developed by various
groups, with pioneering studies of silicon nanochannels conducted by Ferrari et al. and
Desai et al. in the 1990s (Chu et al. 1997; Desai et al. 1999; Ferrari et al. 1995; Grattoni et
al. 2009; Chu et al. 1999).
Nanochannel membranes can easily be mounted on a drug reservoir to achieve constant rate,
zero-order kinetic drug release from the reservoir. These implants are still in the preclinical
phase but have a high market acceptability due to low manufacturing costs. The titanium
oxide nanotube membrane, NanoPortal Membrane (Nano Precision Medical, Emeryville,
CA, USA), is attached to a small, rice grain-sized cylindrical implant (Fig. 8a). This implant
was designed to be subcutaneously implanted through an in-office procedure. Currently, this
technology is in preclinical development to release glucagon-like peptide-1 agonists for 3
months to up to 1 year (Nano Precision Medical n.d.-a; Nano Precision Medical n.d.-b;
Nano Precision Medical n.d.-c). A larger cylindrical titanium device measuring 4 cm × 4
mm has two membranes with NANOPOR™ (Delpor Inc., San Francisco, CA, USA)
technology fixed at each end (Fig. 8b) (Delpor n.d.-a; Delpor n.d.-f). DLP-202 and DLP-414
can release hGH for 3 months and exenatide for 3–6 months, respectively (Delpor n.d.-d;
Delpor n.d.-e). To maintain constant release, drugs must be soluble to form supersaturated
solutions within the drug reservoir to saturate the nanochannels. Insoluble drugs cannot
saturate nanochannels and thus do not have zero-order kinetics. Prozor™ (Delpor Inc., San
Francisco, CA, USA) technology enables release of insoluble drugs by maintaining an acidic
pH in the drug reservoir (Delpor n.d.-g). DLP-114 and DLP-119 are a 6–12-month
formulation of risperidone and 3-month formulation of olanzapine, respectively. Both are
antipsychotic drugs, with risperidone used to treat schizophrenia and olanzapine used to treat
bipolar disorder (Delpor n.d.-b; Delpor n.d.-c).
The nanochannel Delivery System (nDS) has nanochannels as small as 2.5 nm with tight
tolerances on size, geometry, and surface properties. It was further developed by Grattoni et
al. and is currently in clinical translation (Grattoni et al. 2009, 2011a c). The nDS
membrane, a 5 × 20 × 12.3 mm or 43 × 28.5 × 8.7 mm silicon chip, represents the core of
the nDS implantable technology (Fig. 9a). The membrane exploits the previously mentioned
nanoscale phenomena to passively control the constant release of drugs, biological
molecules, and nanoparticles without requiring movable components or actuation (Fig. 9b)
(Fine et al. 2010; Grattoni et al. 2011a). The implant contains the nDS membrane, a
mechanically robust shell, and loading ports with sealing components. This simple
Pons-Faudoa et al. Page 13
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
architecture allows for high effective loading efficiency, which, depending on the size and
shape of the implant, may range from 60 to 90% (Fig. 9c). This technology is suitable for
the use of drugs in liquid, suspension, solid, and powder forms in water, organic solvent, or
lipid-based formulations. This offers flexibility in terms of its employment for a broad
spectrum of therapeutic applications, enabling the delivery of drugs in their most stable
formulation for long-term treatment. Transcutaneous refilling allows the treatment of
chronic pathologies over several years without need for explantation and replacement.
The nDS technology was validated in vitro and in vivo in rodents, dogs, pigs, and non-
human primates with a constant, sustained release of drug molecules and nanoparticles over
a broad range of molecular sizes at release rates relevant for medical applications (Di Trani
et al. 2019; Ferrati et al. 2013 2015; Filgueira et al. 2016; Fine et al. 2010; Grattoni et al.
2011c; Sih et al. 2013). The nDS can sustain release of HIV PrEP antiretroviral drugs,
tenofovir alafenamide fumarate, and emtricitabine for 83 days in non-human primates and
allow transcutaneous drug refilling (Chua et al. 2018b). Grattoni et al. developed a
cylindrical intratumoral device approximately 3.5 mm long with a silicone cap at one end
and a smaller nDS on the other end (Fig. 9d). This device, termed the nanofluidic-based drug
eluting seed (NDES), has a reservoir capacity of 3.3–5 μl and is percutaneously delivered
intratumorally via minimally invasive insertion with a trocar. The authors demonstrated that
the intratumoral sustained release of CD40 and OX40 from the NDES increases immune cell
infiltration. Thus, the nDS nanochannel platform has the potential to expand available
clinical options for intratumoral immunotherapy delivery (Chua et al. 2018a; Di Trani et al.
2017; Hood et al. 2016).
4.2.2. NEMS for tunable delivery—Some diseases require a variable rather than a
constant drug delivery dose. The passively controlled nDS membrane can be accompanied
by electrodes to adjust the delivery rate of drugs, allowing for programmable dose
modulation, remote titration, and responses to sensor feedback (Fine et al. 2011; Grattoni et
al. 2011b). After applying a 1 .5V direct current electrical field across the membrane, ionic
species redistribute across the nanochannels, causing ionic concentration polarization that
can be modified to tune drug release rate (Bruno et al. 2015, 2016; Di Trani et al. 2017;
Grattoni et al. 2011a). The dynamically controlled nDS membrane can be mounted on a
drug reservoir remotely controlled via Bluetooth Low Energy communication (Fig. 9e). This
technology has been validated in vitro, demonstrating changes in methotrexate release when
transmembrane potential is applied. A disadvantage of this device is that its volumetric
loading efficiency is low (22%) due to the volume of the circuitry chamber. However, this
implant is an adaptable research tool for drug development and pharmacological studies (Di
Trani et al. 2017).
To summarize, MEMS and NEMS take advantage of micro- and nanoscale transport
properties for drug delivery. Nanofluidics enables zero-order drug release kinetics for
months with no potentially dangerous initial burst release. Although most are not yet FDA-
approved, there is great potential to make small implants that can treat a wide variety of
diseases. Table 3 shows a comparison of advantages and limitations of MEMS and NEMS.
Pons-Faudoa et al. Page 14
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
5. Sites of implantation
Although implants offer refined and efficacious means for controlled drug delivery, they all
require placement by a healthcare professional. Surgical procedures vary based on the site of
implantation and are associated with potential challenges and adverse effects. Although side
effects are usually mild, they can be significant in some cases. Here, we describe various
insertion procedures and provide an overview of their most common challenges to provide
insight that can aid in the development of the next generation of drug delivery implants.
Figure 10 illustrates the different sites of implantation for implants.
5.1 Intraocular placement
In addition to drug loading efficiency, the implantation procedure of a device is also of great
importance when designing an implant. The end goal is the use of a minimally invasive in-
office procedure by a trained healthcare professional that does not require post-operative
care. Both ILUVIEN® and Retisert® posterior chamber implantations are performed in a
doctor’s office, as they require aseptic conditions and anesthesia. ILUVIEN® is minimally
invasive, whereas Retisert® is invasive due to its shape. The small cylindrical shape of
ILUVIEN® fits inside a needle and permits intravitreal injection (Fig. 11a). A benefit is that
there is no need for stitches as the sclera can self-heal from the needle wound, reducing
complications (Borkar et al. 2017; Logan et al. 2016). By contrast, Retisert® requires
sclerotomy along with blood vessel cauterization to insert the irregularly shaped device and
sutures to anchor it within the posterior chamber (Fig. 11b). The sclerotomy incision also
requires subconjunctival antibiotics and a steroid injection (Bausch & Lomb n.d.; Yasin et al.
2014). The incision must be re-opened for removal, but the implant can be replaced using
the same anchoring suture in the sclera. However, some ophthalmologists prefer to insert a
new Retisert® at another incision site, leaving the old implant in place. If the patient
requires a third implant, ophthalmologists will replace the first implant (Nicholson et al.
2012). Retisert® limitations could be addressed by changing the implant shape to a cylinder
to allow a non-invasive procedure. The irregularly shaped Retisert® device contains 0.59 mg
FA compared with 0.19 mg in the smaller, cylinder-shaped ILUVIEN®. Accordingly,
multiple smaller cylinder implants could be injected into the vitreous humor to maintain the
therapeutic dose for DME treatment.
Even though implantable devices offer the obvious and needed advantages of site-specific
therapeutic delivery, there are some limitations and challenges directly related to the
physical presence of an object in the eye. Patients must be monitored for the most common
complications, intraocular pressure elevation and endophthalmitis, after implantation,
because a foreign device is introduced into a pressure-regulated chamber (FDA Reference
IDs: 2955048; 3635981) (Alfaqawi et al. 2017; Bausch & Lomb n.d.; Borkar et al. 2017;
Logan et al. 2016; Parrish et al. 2016; Wright and Hall 2016; Yasin et al. 2014). Although
ILUVIEN® has the convenience of a suture-less procedure, there are reports of implant
migration into the anterior chamber, blocking the visual axis, and dislodgement into the
infusion cannula during vitrectomy (Andreatta et al. 2017; El-Ghrably et al. 2015; Moisseiev
and Morse 2016; Papastavrou et al. 2017). Reported Retisert® adverse effects are mostly
sclerotomy-related: hypotony, temporary decrease in visual acuity, cataract formation,
Pons-Faudoa et al. Page 15
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
choroidal detachment, retinal detachment, vitreous hemorrhage, wound dehiscence, implant
dislocation, and scleral melt (FDA Reference ID: 2955048) (Almeida et al. 2015; Chang et
al. 2015; Freitas-Neto et al. 2015; Petrou et al. 2014; Yasin et al. 2014). For these reasons,
the doctor performs indirect ophthalmoscopy to verify correct placement of the implant,
adequate central retinal artery perfusion, and absence of complications (FDA Reference IDs:
2955048; 3635981) (Bausch & Lomb n.d.; Yasin et al. 2014). Nonetheless, as previously
mentioned, the benefits of both of these implants outweigh the few complication reports.
An approach to avoiding placement of foreign devices in the vitreous humor is to anchor an
implant episclerally and deliver drugs into the posterior chamber through a cannula, like the
Replenish MicroPump. The PMP reservoir and intraocular cannula are sutured episclerally
between the superior and lateral rectus muscles to impede movement (Fig. 11c). A
sclerotomy is required, but the incision is small as only the cannula must be inserted into the
posterior chamber, followed by suturing of the conjunctiva (Humayun et al. 2014). An
advantage of the PMP is its ease of access and the possibility of refilling the drug reservoir,
eliminating future device removal or replacement (Yasin et al. 2014). A major limitation of
the PMP is that it has not undergone clinical trials, so although it has a refill feature, its
safety and efficacy have yet to be established.
5.2 Upper inner arm subcutaneous placement
The subcutaneous tissue is advantageous for drug delivery because the gastrointestinal tract
is bypassed, thus improving drug bioavailability for systemic administration (Kumar and
Pillai 2018). Also, the implantation site should be discrete but readily accessible for a quick
in-office procedure and not uncomfortable to the patient. Thus, the most widely used
implantation site in the clinic is the upper inner arm, for which implants are cylindrical and
have a personalized applicator device that facilitates their insertion. Implant placement is an
in-office procedure performed by a trained healthcare provider that takes approximately 10
min. Implanon®, Nexplanon®, SUPPRELIN® LA, and Vantas® are inserted in the inner
side of the non-dominant upper arm approximately 8–10 cm above the medial epicondyle of
the humerus after injection of local anesthesia (Fig. 11d) (FDA Reference IDs: 2887911;
3080389; 4099967; 4100681).Probuphine® implants are inserted at the same site but require
a minor incision followed by insertion of four implants. These are positioned in a close fan-
shaped distribution 4–6 mm apart with the fan opening toward the shoulder (Fig. 11e) (FDA
Reference ID: 4215185) (Itzoe and Guarnieri 2017; Smith et al. 2017). Interestingly,
different subcutaneous implantation sites have been adapted to meet the patient’s needs.
Nexplanon® was inserted in the scapular region in patients at risk of self-removal of the
implant (Pragout et al. 2018). In elderly patients, Vantas® is subcutaneously inserted in the
abdominal region due to patient-limited arm mobility (Woolen et al. 2014).
When inserting implants into the upper arm, it is important to avoid the sulcus between the
biceps and triceps muscles and the neurovascular bundle that lies deeper in the subcutaneous
tissue to avoid complications such as peripheral nerve injury and paresthesia (Laumonerie et
al. 2018). Equally important, the presence of the device must always be verified immediately
after insertion to circumvent implant migration. There are reports of difficulty removing
Implanon®/Nexplanon® devices associated with peripheral nerve injury and implant
Pons-Faudoa et al. Page 16
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
migration (Barlow-Evans et al. 2017; Chevreau et al. 2018; Chung et al. 2017; Diego et al.
2017; Guiahi et al. 2014; Laumonerie et al. 2018; Odom et al. 2017). Regardless, the
benefits are indisputable given the high efficacy rate and that most common adverse effects
reported for these implants include erythema, hematoma, application site pain, and edema
are quick to resolve (FDA Reference IDs: 2887911; 3080389; 4099967; 4100681; 4215185)
(Davis et al. 2014; Donnelly et al. 2015; Eugster 2015; Fisher et al. 2014; Itzoe and
Guarnieri 2017; Pedroso et al. 2015; Serati et al. 2015; Shumer et al. 2016; Silverman et al.
2015; Simon et al. 2016; Smith et al. 2017).
5.3 Abdominal subcutaneous placement
The size of peristaltic and infusion pumps necessitates catheters for site-specific drug
delivery and restricts them to a subcutaneous abdominal implantation site. SynchroMed™ II,
Codman® 3000, and Prometra® pumps require surgery under general anesthesia, resulting
in a significantly higher costs, as this procedure take 1–3 h in an operating room due to the
requirement for fluoroscopy for intrathecal catheter placement and verification (Flowonix
Medical Inc. 2017; Medtronic 2017). At this implantation site, 27% of reported
complications of intrathecal delivery are related to surgical procedures (Stetkarova et al.
2010). A surgeon implants a filled pump subcutaneously in the abdomen in a pump pocket
no more than 2.5 cm from the surface of the skin and connects the intracatheter (Fig. 11f).
The pump pocket and the spinal incision site are irrigated, sutured, and covered in dressing
to avoid infection (Flowonix Medical Inc. 2017; Medtronic 2017). For intravenous
treprostinil administration, a catheter is inserted into the superior vena cava via a subclavian,
cephalic, jugular, or axillary puncture, anchored to the venotomy site, and connected to the
abdominal pump pocket (Fig. 11g) (Bourge et al. 2016).
A benefit of these pumps is transcutaneous drug refill, allowing longer treatment durations.
However, potential severe complications from erroneous subcutaneous injection of drug
during device refilling have been reported (Maino et al. 2014; Perruchoud et al. 2012; Ruan
et al. 2010). With this in mind, ultrasound-guided pump refill is a feasible and simple
technique that reduces the probability of refill-related complications (Gofeld and McQueen
2011; Saulino and Gofeld 2014). Common minor adverse effects reported for
SynchroMed™ II, Codman® 3000, and Prometra® pumps are implant site pain, edema, and
hematoma (Codman & Shurtleff; Ethans et al. 2005; Pope and Deer 2017; Rauck et al.
2013). As previously mentioned, these pumps have movable components that control drug
delivery, increasing the risk of device malfunctions. There are reports of cases in which the
pump had to be explanted due to pump failures (Kalyvas et al. 2014; Riordan and Murphy
2015; Sgouros et al. 2010). These discoidal pumps are limited by their size and therefore
necessitate catheters to deliver the drug to the site of interest. Given that most complications
are attributable to catheter malfunctions, implants should be redesigned to omit the need for
catheters (Ethans et al. 2005; Kalyvas et al. 2014; Miracle et al. 2011; Stetkarova et al.
2010). Even though abdominal subcutaneous placement of pumps clearly has limitations and
challenges, the devices have had a positive impact on improving patient health and living
conditions, outweighing the complications and reported adverse effects.
Pons-Faudoa et al. Page 17
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
5.4 Intravesical placement
Other implants that have a drug release rate dependent on the targeted organ are GemRIS
and LiRIS. Both of these site-specific devices are placed in the bladder as an in office
procedure that does not require an operating room. Insertion of the implant was a priority in
their design, as it changes shape after it is implanted in the bladder. At first, it is shaped as a
long tube positioned in a catheter-like tool that enables easy insertion into the bladder (Fig.
11h). After delivery, the implant wire restructures the implant into a pretzel-like shape that
impedes expulsion of the device through the urethra. After the treatment period, the implant
is removed via cystoscopy (Matheson 2014; Nickel et al. 2012). Possible complications are
yet to be reported, as these implants are currently in clinical trials.
5.5 Next generation of implantable drug delivery systems
The complexity and limitations of surgical procedures for implantation and explantation
have significant effects on patient acceptability of the technology. As such, future device
designs should employ minimally invasive approaches, smaller implant volumes, and fewer
insertion-explantation procedures to fully leverage their potential. Cylindrical devices, such
as the polymeric implants Implanon®/Nexplanon®, SUPPRELIN® LA, Vantas, and
ILUVIEN® and the osmotic pumps GemRIS, LiRIS, and Viadur®, have minimally invasive
insertion procedures. Yet, their major disadvantage is the need for implant replacement if the
patient wishes to continue the medication. For this reason, implants intended to be inserted
subcutaneously in the inner arm need to incorporate a drug refill feature, like pumps. As
previously mentioned, the discoidal subcutaneous abdominal pumps SynchroMed™ II,
Codman® 3000, and Prometra® II have this feature, but the pump size is a key limitation, as
it requires surgery for implantation-explantation. If implants are to become a mainstream
drug administration route, implants should be carefully designed with a small volume for
minimally invasive implantation and chronically sustained drug delivery eluding insertion-
explantation with drug refillability.
Even if new implants are designed with these considerations, patient counseling will be
crucial to increase acceptability. Implantation procedures lower patient acceptance because
all procedures guarantee pain and discomfort, even if only from the local anesthetic.
Therefore, patients will require counseling to show the potential cumulative benefits of
prolonged compliance-free therapy, with optimized drug delivery far outweighing potential
risks and immediate discomfort (Danckwerts and Fassihi 1991; Kumar and Pillai 2018;
Rajgor et al. 2011). Also, data demonstrating the value of using implants over conventional
treatment could drive insurance companies to cover the costs. Insurance companies may be
more willing to pay for less expensive conventional therapy than to reimburse an outpatient
procedure to insert the implant as well as cover the costs associated with the implant (i.e.
refilling, removal, etc.).
6. Deployment in the developing world
The burden of chronic diseases in developing countries is rapidly increasing and has
unfavorable social, economic, and health consequences (Alwan et al. 2010). Often, these
countries have unreliable healthcare services that incite poor health practices, medication
Pons-Faudoa et al. Page 18
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
non-adherence and subsequently increase mortality rates. An important cause of non-
adherence in developing countries is the high cost of therapeutics and paucity of health
resources, which results in waste and underutilization of already limited resources. Also,
healthcare center visits are linked to patient compliance since these trips are time-consuming
and expensive. To ensure that all countries receive quality healthcare, national and
international agencies must invest in developing countries (Atinga et al. 2018; Fullman et al.
2017; Pagès-Puigdemont et al. 2016; World Health Organization 2003). A proposal to
resolve medication non-adherence due to lack of health resources and healthcare centers are
long-term drug delivery devices. The Bill and Melinda Gates Foundation, among others,
strive to resolve this issue by supporting different companies for the development of long-
term sustained release implants that can be administered in developing countries.
Pregnancy is not a chronic disease but does require sustained prenatal care to ensure that
both the baby and mother are healthy. Sustainable Development Goals call for a reduction in
maternal deaths to fewer than 70 per 100,000 by 2030 (Kassebaum et al. 2016). Moreover,
Millennium Development Goals call for universal access to reproductive healthcare,
specifically contraceptives. Providing free contraception implants to girls and women in
developing countries could benefit 120 million women and help prevent approximately 30
million unintended pregnancies, which in turn would reduce infant and maternal mortality
by 280,000 and 30,000 deaths, respectively (Bill & Melinda Gates Foundation n.d.).
The Bill and Melinda Gates Foundation invested in Microchips Biotech to develop a
microchip that releases levonorgestrel, a progestin, for 16 years and can be stopped at any
time with a wireless controller (Lee 2014). Jadelle® (Bayer, Leverkusen, Germany) is a
polymer-based levonorgestrel-releasing implant similar to Implanon®. Jadelle® was
prequalified by the World Health Organization in 2009, and the Jadelle Access Program was
launched by the Bill and Melinda Gates Foundation and Bayer in 2013. The goal of this
program is to deliver 27 million implants in 6 years. Bayer will supply the Jadelle®
implants, and the Foundation will cover default risk. Although Jadelle® is approved in the
US, it was not sold as of 2015 (Bayer AG Pharmaceuticals n.d.).
The Bill and Melinda Gates Foundation has also taken interest in the prevention of HIV and
supported the research of Intarcia Therapeutics, Inc. to develop a pump that can store
enough drug doses for 6–12 months, enabling people in developing countries to have HIV
protection (Intarcia Therapeutics Inc n.d.-b). Although the Bill and Melinda Gates
Foundation has taken a big step toward investing in drug delivery implants in developing
countries, more efforts are needed.
The feasibility of deploying implants in developing countries largely depends on cost,
simplicity in device implantation, and patient acceptance. The cost of devices can certainly
represent a barrier for their deployment. In principle, the implant cost should be close to the
cost of the drug itself. Complex electromechanical systems and pumps may be too expensive
to achieve ample utilization. Due to the limited health care resources, deployment in
developing countries may be exclusively limited to implants which require minimally
invasive procedures such as subcutaneous placement in the inner arm. In this case, the
surgical technique and expertise needed is nominal and can be easily taught ad hoc. As
Pons-Faudoa et al. Page 19
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
previously discussed, larger systems for either subcutaneous or deeper implantation would
not be as attainable because of the invasive surgery required and the needs for follow-ups
and longer recovery periods. Refillable implants could be very relevant in the context of
preventive therapies for infectious diseases or for chronic treatments. Transcutaneous
refilling can extend the life span of an implant while avoiding repeated surgical removal and
replacement procedures. However, as it has been shown for SynchroMed™ pump-like
systems, refilling requires specilized training to avoid failures that could be catastrophic with
drug leakage in the surrounding tissues. Patient acceptability is key for the success of
implantable systems. In cases such as the treatment and prevention of HIV, the use of
implants is faced with the issue of ‘stigma’ associated with the disease. In these
circumstances, the implantation site is determinant as patients may be concerned about the
visibility of the device underneath the skin. Other factors, such as religion and spiritual
beliefs also play an important role: studies revealed one of the reasons for medication non-
adherence is that patients usually prefer spiritual or divine healing causations beyond
medical treatment, as a result of low trust in new medication technologies, their efficacy and
fear of side effects (Atinga et al. 2018; Pagès-Puigdemont et al. 2016).
On a different note, implants have the potential of addressing one key problem in deliverying
medical treatments. Implants can minimize the frequency with which patients have to visit
the health care centers, avoiding multiple lengthy travels and thus improving adherence to
treatment. Ideally, tunable implants where clinicians can remotely adjust medication regimes
and monitor patients through telemedicine could be advantageous. However, these systems
may in turn be more expensive and therefore not implementable.
7. Conclusions
The treatment of chronic diseases will shift from oral dosing to implantable drug delivery
devices as they obviate patient non-adherence and potentially limit side effects. Different
passive and dynamic drug delivery technologies have received FDA approval, are in clinical
trials, or are in an advanced stage of development. Consideration of current implantation
procedures can further improve implant designs and thereby increase patient acceptability.
Long-term delivery devices for chronic illness treatment with minimally invasive approaches
for implantation should be employed for use in developing countries and to reduce DALYs.
In conclusion, advanced implantable drug delivery devices hold promise as more effective
treatment tools, transforming the clinical landscape of therapeutics given the growing
incidence of chronic diseases.
Acknowledgements
We thank Virginia Facciotto ([email protected]) for the design of graphics and figures. Funding support from The Nancy Owens Breast Cancer Foundation, Center for the Advancement of Science in Space (CASIS) GA-2013-118, CASIS GA2014-145, NIH NIAID R01 AI120749-01A1, NIH NIGMS R01 GM 127558.
References
Alfaqawi F, Lip PL, Elsherbiny S, Chavan R, Mitra A, Mushtaq B, Eye 31, 650 (2017) [PubMed: 28106887]
Pons-Faudoa et al. Page 20
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Ali M, Akin A, Bahamondes L, Brache V, Habib N, Landoulsi S, Hubacher D, Hum. Reprod 31, 2491 (2016) [PubMed: 27671673]
Allen EE, Instrument for transfusion of blood with patent 249,285. 8 11 1881.
Allen RH, Kaunitz AM, Hickey M, in Williams Textb. Endocrinol, 13th edn, ed. by Melmed S, Polonsky KS, Larsen PR, Kronenberg HM. (Elsevier, Philadelphia, 2016), pp. 664–693
Almeida DRP, Chin EK, Mears K, Russell SR, Mahajan VB, Retin. Cases Brief Rep 9, 142 (2015) [PubMed: 25411930]
Alwan A, MacLean DR, Riley LM, d’Espaignet ET, Mathers CD, Stevens GA, Bettcher D, Lancet 376, 1861 (2010) [PubMed: 21074258]
Amoaku WMK, Saker S, Stewart EA, Eye 29, 1115 (2015) [PubMed: 26113500]
Andreatta W, Elaraoud I, Mitra A, Retin. Cases Brief Rep, 1 (2017) [PubMed: 26705236]
Atinga RA, Yarney L, Gavu NM, PLoS One 13, e0193995 (2018) [PubMed: 29590156]
Baert L, Schueller L, Tardy Y, Macbride D, van’t Klooster G, Borghys H, Clessens E, Van Den Mooter G, Van Gyseghem E, Van Remoortere P, Int. J. Pharm 355, 38 (2008) [PubMed: 18337029]
Bailey C, Chakravarthy U, Lotery A, Menon G, Talks J, Bailey C, Kamal A, Ghanchi F, Khan C, Johnston R, McKibbin M, Varma A, Mustaq B, Brand C, Talks J, Glover N, Eye 31, 1707 (2017) [PubMed: 28737758]
Barlow-Evans R, Jaffer K, Balogun M, BMJ Case Rep. bcr (2017)
Barnwal P, Das S, Mondal S, Ramasamy A, Maiti T, Saha A, Ther. Adv. Psychopharmacol 7, 119 (2017) [PubMed: 28348732]
Bausch & Lomb, Retisert®: Surgical Procedure For Implantation (n.d.), http://www.bauschretinarx.com/Portals/50/files/baus3920-retisert-surgical-Instructions-rgb-p6.pdf.Accessed 5 Mar 2018
Bayer AG Pharmaceuticals, Bayer AG Pharmaceuticals: Implant Initiative Family Planning Choices in secure long-term contraception (n.d.), http://pharma.bayer.com/en/commitment-responsibility/family-planning/implant-initiative/.Accessed 25 Feb 2018
Beall RF, Nickerson JW, Kaplan WA, Attaran A, PLoS One 11, e0148939 (2016) [PubMed: 26910128]
Berg JM, Dallas T, in Encycl. Microfluid. Nanofluidics, ed. by Li D. (Springer US, Boston, 2013), pp. 1–12
Bernell S, Howard SW, Front. Public Health 4, (2016)
Bertelmann T, Schulze S, Ophthalmol. Ther 4, 51 (2015) [PubMed: 25672501]
Bertelmann T, Senior Physician A Messerschmidt-Roth, and Study Coordinator, Department of Ophthalmology, Philipps University, Marburg, Germany, Eur. Ophthalmic Rev 07, 122 (2013)
Bertolote JM, World Health Organization: Neurological Disorders Affect Millions Globally WHO Report (2005). http://www.who.int/mediacentre/news/releases/2007/pr04/en/.Accessed 18 June 2018
Bhatia G, Lau ME, Koury KM, Gulur P, F1000Research (2014)
Bhushan B, Microelectron. Eng 84, 387 (2007)
Bill & Melinda Gates Foundation, Bill & Melinda Gates Foundation: What We Do Family Planning Strategy Overview (n.d.). https://www.gatesfoundation.org/What-We-Do/Global-Development/Family-Planning.Accessed 25 Feb 2018
Bolash R, Udeh B, Saweris Y, Guirguis M, Dalton JE, Makarova N, Mekhail N, Neuromodulation Technol. Neural Interface 18, 150(2015)
Borkar DS, Ung C, Sobrin L, Int. Ophthalmol. Clin 57, 193 (2017) [PubMed: 28885257]
Bourge RC, Waxman AB, Gomberg-Maitland M, Shapiro SM, Tarver JH, Zwicke DL, Feldman JP, Chakinala MM, Frantz RP, Torres F, Cerkvenik J, Morris M, Thalin M, Peterson L, Rubin LJ, Chest 150, 27 (2016) [PubMed: 27396777]
Bruno G, Geninatti T, Hood RL, Fine D, Scorrano G, Schmulen J, Hosali S, Ferrari M, Grattoni A, Nanoscale 7, 5240 (2015) [PubMed: 25707848]
Bruno G, Canavese G, Liu X, Filgueira CS, Sacco A, Demarchi D, Ferrari M, Grattoni A, Nanoscale 8, 18718 (2016) [PubMed: 27787528]
Pons-Faudoa et al. Page 21
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Bruno G, Di Trani N, Hood RL, Zabre E, Filgueira CS, Canavese G, Jain P, Smith Z, Demarchi D, Hosali S, Pimpinelli A, Ferrari M, Grattoni A, Nat. Commun 9, 1682 (2018) [PubMed: 29703954]
Carle MV, Chu TG, Boyer DS, Expert Rev. Ophthalmol 9, 81 (2014)
Carter JA, Dammerman R, Frost M, J. Med. Econ 20, 893 (2017) [PubMed: 28604141]
Chang PY, Kresch Z, Samson CM, Gentile RC, Ocul. Immunol. Inflamm 23, 453 (2015)
Chevreau J, Krief D, Abou Arab O, Zitoun M, Foulon A, Sergent F, Gondry J, Eur. J. Obstet. Gynecol. Reprod. Biol 224, 81 (2018) [PubMed: 29554605]
Christo P, Bottros M, J. Pain Res, 615 (2014)
Chu WH, Huen T, Tu JK, Ferrari M, in edited by Gourley PL (1997), pp. 111–122
Chu W-H,Chin R, Huen T,Ferrari M, J. Microelectromechanical Syst 8, 34 (1999)
Chua CYX, Jain P, Susnjar A, Rhudy J, Folci M, Ballerini A, Gilbert A, Singh S, Bruno G, S. F. C, Yee C, Butler EB, Grattoni A, (2018a) Nanofluidic drug-eluting seed for sustained intratumoral immunotherapy in triple negative breast cancer. Journal of Controlled Release 285:23–34 [PubMed: 30008369]
Chua CYX, Jain P, Ballerini A, Bruno G, Hood RL, Gupte Manas, Gao S, Trani ND, Susnjar A, Shelton K, Bushman LR, Folci M, Filgueira CS, Marzinke MA, Anderson PL, Hu M, Nehete P, Arduino RC, Sastry JK, Grattoni A.o, (2018b) Transcutaneously refillable nanofluidic implant achieves sustained level of tenofovir diphosphate for HIV pre-exposure prophylaxis. Journal of Controlled Release 286315–325 [PubMed: 30092254]
Chung M, Loudill C, Wieler M, Farnam J, Ahn SH, J. Vasc. Interv.Radiol 28, 466 (2017) [PubMed: 28231925]
Cima MJ, Lee H, Daniel K, Tanenbaum LM, Mantzavinou A, Spencer KC, Ong Q, Sy JC, Santini J, Schoellhammer CM, Blankschtein D, Langer RS, J. Controlled Release 190, 157 (2014)
Cobo A, Sheybani R, Meng E, Adv. Healthc. Mater 4, 969 (2015) [PubMed: 25703045]
Codman & Shurtleff, Patient Information Booklet for Pain Management Therapy CODMAN 3000 Implantable Constant-Flow Infusion Pump (2003).
Codman & Shurtleff, CODMAN 3000 Implantable Constant-Flow Infusion Pump: Prescribing Information (n.d.). http://www.codmanpumps.com/Products_pumps_epi.asp.Accessed 23 Apr 2018.
Coherent Market Insights, Global Implantable Drug Delivery Devices Market, by Product Type (Drug Infusion Pumps, Intraocular Drug Delivery Devices, Contraceptive Drug Delivery Devices and Stents), by Technology (Biodegradable Implants and Non Bio Degradable Implants), by Application (Ophthalmology, Cardiovascular, Birth Control/Contraception and Others) and by Region - Trends and Forecast till 2025 (Coherent Market Insights, 2017), p. 144.
Comlossy M, Chronic Disease Prevention and Management (2013).
Cunha-Vaz J, Ashton P, Iezzi R,Campochiaro P, Dugel PU,Holz FG, Weber M, Danis RP, Kuppermann BD, Bailey C, Billman K, Kapik B, Kane F, Green K, Ophthalmology 121, 1892 (2014) [PubMed: 24935282]
Cutler RL, Fernandez-Llimos F, Frommer M, Benrimoj C, GarciaCardenas V, BMJ Open 8, e016982 (2018)
Danckwerts M, Fassihi A, Drug Dev. Ind. Pharm 17, 1465 (1991)
Davis JS, Alkhoury F, Burnweit C, J. Pediatr. Surg 49, 807 (2014) [PubMed: 24851775]
Deer TR, Pope JE, Expert Rev. Clin. Pharmacol 8, 507 (2015) [PubMed: 26294072]
Delpor, Delpor Delivering the Future of Medicine: Delpor’s Device Device (n.d.-a). https://www.delpor.com/delpors-device/ Accessed 24 Feb 2018.
Delpor, Delpor Delivering the Future of Medicine: Products DLP-114 (n.d.-b), https://www.delpor.com/products/dlp-114/. Accessed 24 Feb 2018.
Delpor, Delpor Delivering the Future of Medicine: Products DLP-119 (n.d.-c), https://www.delpor.com/products/dlp-119/. Accessed 24 February 2018
Delpor, Delpor Delivering the Future of Medicine: Products DLP-202 (n.d.-d). https://www.delpor.com/products/dlp-202/. Accessed 24 February 2018
Delpor, Delpor Delivering the Future of Medicine: Products DLP-414 (n.d.-e), https://www.delpor.com/products/dlp-414/. Accessed 24 February 2018
Pons-Faudoa et al. Page 22
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Delpor, Delpor Delivering the Future of Medicine: Technologies NANOPOR (n.d.-f). https://www.delpor.com/technologies/nanopor/ Accessed 24 February 2018
Delpor, Delpor Delivering the Future of Medicine: Technologies PROZOR (n.d.-g), https://www.delpor.com/technologies/prozor/. Accessed 24 February 2018
Desai TA, Hansford DJ, Kulinsky L, Nashat AH, Rasi G, Tu J, Wang Y, Zhang M, Ferrari M, Biomed Microdevices 2, 11 (1999)
Di Trani N, Grattoni A, Ferrari M, in (IEEE, 2017), pp. 40.6.1–40.6.4.
Di Trani N, Jain P, Chua CYX, Ho JS, Bruno G, Susnjar A, Pons-Faudoa FP, Sizovs A, Hood RL, Smith ZW, Ballerini A, Filgueira CS, Grattoni A, Nanomedicine 16, 1 (2019) [PubMed: 30468870]
Diego D, Tappy E, Carugno J, Contraception 95, 218 (2017) [PubMed: 27865875]
Donnelly S, Shuriff D, Stylianos S, Zitsman J, J. Pediatr. Surg. Case Rep 3, 523 (2015)
Elaraoud I, Andreatta W, Kidess A, Bhatnagar A, Tsaloumas M, Quhill F, Yang Y, BMC Ophthalmol 16 (2016a)
Elaraoud I, Attawan A, Quhill F, Ophthalmol. Ther 5, 95 (2016b) [PubMed: 26885863]
Elaraoud H Quhill F. Quhill, Ophthalmol. Ther 5, 105 (2016c) [PubMed: 27116231]
El-Ghrably IA, Saad A, Dinah C, Ophthalmol. Ther 4, 129 (2015) [PubMed: 26199036]
El-Ghrably I, Steel DHW, Habib M, Vaideanu-Collins D, Manvikar S, Hillier RJ, Eur. J. Ophthalmol 27, 357 (2017) [PubMed: 28165610]
Endo Pharmaceuticals, ClinincalTrials.gov Identifier NCT01295060 (n.d.). https://clinicaltrials.gov/ct2/show/NCT01295060. Accessed 21 Sept 2018.
Ethans KD, Schryvers OI, Nance PW, Casey AR, Spinal Cord 43, 214 (2005) [PubMed: 15545981]
Eugster EA, in Endocr. Dev, edited by Cappa M, Cianfarani S, Ghizzoni L,Loche S, and Maghnie M (S.KargerAG,2015), pp. 54–59.
Farina M, Ballerini A, Torchio G, Rizzo G, Demarchi D, Thekkedath U, Grattoni A, Biomed. Microdevices 19, 42 (2017) [PubMed: 28484917]
Farra R, Sheppard NF, McCabe L, Neer RM, Anderson JM, Santini JT, Cima MJ, Langer R, Sci. Transl. Med 4, 122ra21 (2012)
Ferkol T, Schraufnagel D, Ann. Am. Thorac. Soc 11, 404 (2014) [PubMed: 24673696]
Ferrari M,Chu I, Desai I, Hansford D,Mazzoni G,Huen T, Zhang M, MRS Proc 414 (1995)
Ferrati S, Fine D, You J, De Rosa E, Hudson L, Zabre E, Hosali S, Zhang L, Hickman C, Bansal SS, et al., J. Control. Release 172, 1011 (2013) [PubMed: 24095805]
Ferrati S, Nicolov E, Zabre E, Geninatti T, Shirkey BA, Hudson L, Hosali S, Crawley M, Khera M, Palapattu G, Grattoni A, J. Sex. Med 12, 1375 (2015) [PubMed: 25930087]
Figueira J, Henriques J, Amaro M, Rosas V, Alves D, Cunha-Vaz J, Ophthalmic Res 57, 166 (2017) [PubMed: 28178701]
Filgueira CS, Nicolov E, Hood RL, Ballerini A, Garcia-Huidobro J, Lin JZ, Fraga D, Webb P, Sabek OM, Gaber AO, Phillips KJ, Grattoni A, Int. J. Obes 40, 1776 (2016)
Fine D, Grattoni A, Hosali S, Ziemys A, Rosa ED, Gill J, Medema R, Hudson L, Kojic M, Milosevic M, Iii LB, Goodall R, Ferrari M, Liu X, Lab. Chip 10, 3074 (2010) [PubMed: 20697650]
Fine D, Grattoni A, Zabre E, Hussein F, Ferrari M, Liu X, Lab. Chip 11, 2526 (2011) [PubMed: 21677944]
Fisher MM, Lemay D, Eugster EA, J. Pediatr 164, 912 (2014) [PubMed: 24433825]
Flowonix Medical, Flowonix: Healthcare provider MRI information (2018), http://www.flowonix.com/healthcare-provider/mri-information Accessed 18 Sept 2018
Flowonix Medical Inc., Prometra® II Programmable Pump (REF 13827) For Use with Intrathecal Catheter (2017)
Flowonix Medical, PR Newswire: Flowonix Medical, Inc. Announces First Use of Its Patient Therapy Controller (PTC™) (n.d.). https://www.prnewswire.com/news-releases/flowonix-medical-inc-announces-first-use-of-its-patient-therapy-controller-ptc-300134985.html. Accessed 23 Apr 2018
Freitas-Neto CA, Maghsoudlou A, Dhanireddy S, Payal A, Boonsopon S, Ratwatte MD, Foster CS, Ocul. Immunol. Inflamm 23, 425 (2015) [PubMed: 25541739]
Pons-Faudoa et al. Page 23
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Fullman N et al., The Lancet 390, 1423 (2017)
Fusi-Rubiano W, Mukherjee C, Lane M, Tsaloumas MD, Glover N, Kidess A, Denniston AK, Palmer HE, Manna A, Morjaria R, BMC Ophthalmol 18 (2018)
Genetic Engineering & Biotechnology News, Genetic Engineering & Biotechnology News: Intarcia Axes 60, Halts Studies after FDA Clinical Hold (2018), https://www.genengnews.com/gen-news-highlights/intarcia-axes-60-halts-studies-after-fda-clinical-hold/81255457. Accessed 23 Apr 2018
Gofeld M, McQueen CK, Pain Med 12, 607 (2011) [PubMed: 21481161]
Goldberg DS, McGee SJ, BMC Public Health 11 (2011)
Gonçalves RS,Teixeira C,Coelho P,CaseRep.Ophthalmol8, 465(2017)
Grady D, Kaplan S, New York Times: A lifesaving pump for cancer patients is being phased out (2018), https://www.nytimes.com/2018/04/25/health/liver-pump-cancer-medical-device.html. 13 Sept 2018
Grattoni A, De Rosa E, Ferrati S, Wang Z, Gianesini A, Liu X, Hussain F, Goodall R, Ferrari M, J. Micromech. Microeng 19(115), 018 (2009)
Grattoni A, Fine D, Zabre E, Ziemys A, Gill J, Mackeyev Y, Cheney MA, Danila DC, Hosali S, Wilson LJ, et al., ACS Nano 5, 9382 (2011a) [PubMed: 22032773]
Grattoni A, Parazynski S, Hussain F, Mech. Eng. Mag. Sel. Artic 133, 23 (2011b)
Grattoni A, Shen H, Fine D, Ziemys A, Gill JS, Hudson L, Hosali S, Goodall R, Liu X, Ferrari M, Pharm. Res 28, 292 (2011c) [PubMed: 20593302]
Grayson ACR, Shawgo RS, Johnson AM, Flynn NT, Li Y, Cima MJ, Langer R, Proc. IEEE 92, 6 (2004)
Guiahi M, Tocce K, Teal S, Green T, Rochon P, Contraception 90, 606 (2014) [PubMed: 25081861]
Gutiérrez-Hernández J-C, Caffey S, Abdallah W, Calvillo P, González R, Shih J, Brennan J, Zimmerman J, MartínezCamarillo J-C, Rodriguez AR, Varma R, Santos A, Sánchez G, Humayun M, Transl. Vis. Sci. Technol 3, 8 (2014)
Haghjou M, Soheilian M, Abdekhodaie MJ, J Ophthalmic Vis Res 6, 317 (2011) [PubMed: 22454753]
Hawrami A, Laviers H, Patra S, Zambarakji H, Acta Ophthalmol. (Copenh.) 94 (2016)
Hayek Salim M and University Hospitals Cleveland Medical Center, ClinicalTrials.gov Identifier NCT02886286 (n.d.). https://clinicaltrials.gov/ct2/show/NCT02886286 Accessed 21 September 2018.
Herrlich S, Spieth S, Messner S, Zengerle R, Adv. Drug Deliv. Rev 64, 1617 (2012) [PubMed: 22370615]
Hood RL, Bruno G, Jain P, Anderson J, Wolfe T, Quini C, Schmulen J, Li XC, Butler EB, Krishnan S, Grattoni A, J. Biomed. Nanotechnol 12, 1907 (2016) [PubMed: 29360309]
Huber J, Contraception 58, 85S (1998) [PubMed: 10095978]
Humayun M, Santos A, Altamirano JC, Ribeiro R, Gonzalez R, de la Rosa A, Shih J, Pang C, Jiang F, Calvillo P, Huculak J, Zimmerman J, Caffey S, Transl. Vis. Sci. Technol 3, 5 (2014)
Ilias W, le Polain B, Buchser E, Demartini L, the oPTiMa study group, Pain Pract 8, 164 (2008) [PubMed: 18384501]
Intarcia Therapeutics Inc., Intarcia Therapeutics: Investors & Media Press Releases(n.d.). http://www.intarcia.com/media/press-releases/2016-dec-29-intarcia-equity-financing-gates-foundation.html Accessed 25 February 2018.
Intarcia Therapeutics, Intarcia Therapeutics: Pipeline & Technology (n.d.-a). http://www.intarcia.com/pipeline-technology/Accessed 24 February 2018
Intarcia Therapeutics, Intarcia Therapeutics: Pipeline & Technology HIV Prevention (n.d.-b). http://www.intarcia.com/pipeline-technology/hiv-prevention.html Accessed 24 February 2018
Intarcia Therapeutics, Intarcia Therapeutics: Pipeline & Technology Pipeline (n.d.-c). http://www.intarcia.com/pipeline-technology/pipeline.html Accessed 24 February 2018
INTEGRA Biosciences, INTEGRA: Peristaltic Pump - How It Works (n.d.). https://www.integra-biosciences.com/united-states/en/news/peristaltic-pump-how-it-works Accessed 18 June 2018.
Itzoe M, Guarnieri M, Drug Des. Devel. Ther 11, 1429 (2017)
Pons-Faudoa et al. Page 24
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Kalyvas AV, Themistocleous MS, Mpoutos N, Themistoklis K, Korfias S, and Sakas D, in Conf. Congr. Eur. Soc. Ster. Funct. Neurosurg (2014).
Kamaly N et al., The Lancet 388, 1775 (2016)
Kassebaum NJ et al., The Lancet 388, 1775(2016)
Keraliya RA, Patel C, Patel P, Keraliya V, Soni TG, Patel RC, Patel MM, ISRN Pharm 2012, 1 (2012)
Kini V, Ho PM, JAMA 320, 2461 (2018) [PubMed: 30561486]
Kosturakis A, Gebhardt R, Pain Physician 15, 475 (2012) [PubMed: 23159963]
Kumar A and Pillai J, In Nanostructures Eng. Cells Tissues Organs (Elsevier, 2018), pp. 473–511.
Kumar A, Alfahad Q, Mitra A, Elsherbiny S, Lip PL, Eye 30, 763 (2016) [PubMed: 26795414]
Laumonerie P, Blasco L, Tibbo ME, Leclair O, Kerezoudis P, Chantalat E, Mansat P, World Neurosurg 111, 317 (2018) [PubMed: 29309985]
Lee D, BBC News: ‘Remote control’ contraceptive chip available ‘by 2018’ (2014). http://www.bbc.com/news/technology-28193720 Accessed 22 February 2018.
Li T, Evans AT, Chiravuri S, Gianchandani RY, Gianchandani YB, Adv. Drug Deliv. Rev 64, 1639 (2012) [PubMed: 22580183]
Logan SA, Weng CY, Carvounis PE, Int. Ophthalmol. Clin 56, 127 (2016)
Maino P, Koetsier E, Perez RSGM, Anesth R, Pain Med 39, 434 (2014)
Majeed W, Thabit H, Expert Rev. Med. Devices 15, 579 (2018) [PubMed: 30027775]
Maloney JM, Uhland SA, Polito BF, Sheppard NF, Pelta CM, Santini JT, J. Controlled Release 109, 244 (2005)
Martin DF, Arch. Ophthalmol 112, 1531 (1994) [PubMed: 7993207]
Massin P, Erginay A, Dupas B, Couturier A, Tadayoni R, Clin. Ophthalmol 10, 1257 (2016) [PubMed: 27468222]
Matheson R, MIT News: Big step in battling bladder disease (2014). http://news.mit.edu/2014/startups-bladder-disease-medical-device-acquired-1016 Accessed 18 June 2018.
McConville C, 30, 764 (2011).
Medtronic, Medtronic SYNCHROMED® II Programmable Pumps Implant Manual (2011).
Medtronic, Medtronic: Healthcare Professionals SynchroMed II Drug Infusion Pump (2017). http://www.medtronic.com/us-en/healthcare-professionals/products/neurological/intrathecal-baclofen-therapy-systems/synchromed-ii.html Accessed 24 February 2018.
Meireles A, Goldsmith C, El-Ghrably I, Erginay A, Habib M, Pessoa B, Coelho J, Patel T, Tadayoni R, Massin P, Atorf J, Augustin AJ, Eye 31, 684 (2017) [PubMed: 28085139]
Meng E, Hoang T, Ther. Deliv 3, 1457 (2012a) [PubMed: 23323562]
Meng E, Hoang T, Adv. Drug Deliv. Rev 64, 1628 (2012b) [PubMed: 22926321]
Microchips Biotech, Microchips Biotech: Teva and Microchips Biotech Announce Partnership toEnhance PatientOutcomes throughDigital Drug Delivery Technology (2015). http://microchipsbiotech.com/news-pr-item.php?news=10 Accessed 24 February 2018.
Miracle AC, Fox MA, Ayyangar RN, Vyas A, Mukherji SK, Quint DJ, Am. J. Neuroradiol 32, 1158 (2011) [PubMed: 21030478]
Moisseiev E, Morse LS, JAMA Ophthalmol 134, 1067 (2016) [PubMed: 27367921]
Mourtzoukos S, Expert Rev. Ophthalmol 12, 95 (2017)
Nano Precision Medical, Nano Precision Medical Technology: The Goldilocks Effect (n.d.-a). http://www.nanoprecisionmedical.com/technology/the-goldilocks-effect Accessed 24 February 2018.
Nano Precision Medical, Nano Precision Medical Technology: NanoPortal Technology (n.d.-b). http://www.nanoprecisionmedical.com/technology/nanoportal-technology Accessed 24 February 2018.
Nano Precision Medical, Nano Precision Medical Technology: NanoPortal Capsule (n.d.-c). http://www.nanoprecisionmedical.com/technology/nanoportal-capsule Accessed 24 February 2018.
Newron Sweden AB, ClinicalTrials.gov Identifier NCT00866502 (n.d.). https://clinicaltrials.gov/ct2/show/NCT00866502 Accessed 21 September 2018.
Nicholson BP, Singh RP, Sears JE, Lowder CY, Kaiser PK, Am. J. Ophthalmol 154, 969 (2012) [PubMed: 22981365]
Pons-Faudoa et al. Page 25
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Nickel JC, Jain P, Shore N, Anderson J, Giesing D, Lee H, Kim G, Daniel K, White S, Larrivee-Elkins C, Lekstrom-Himes J, Cima M, Sci. Transl. Med 4, 143ra100 (2012)
Odom EB, Eisenberg DL, Fox IK, Contraception 96, 89 (2017) [PubMed: 28583591]
Oung AB, Kosirog E, Chavez B, Brunner J, Saseen JJ, Ther. Adv. Chronic. Dis 8, 113 (2017) [PubMed: 28815008]
Pagès-Puigdemont N, Mangues MA, Masip M, et al., Adv. Ther 33, 1740 (2016) [PubMed: 27503082]
Papastavrou VT, Zambarakji H, Dooley I, Eleftheriadis H, Jackson TL, Retin. Cases Brief Rep 11, 44 (2017) [PubMed: 26909535]
Park K, J. Controlled Release 190, 3 (2014)
Parrish RK, Campochiaro PA, Pearson PA, Green K, Traverso CE, FAME Study Group, Ophthalmic Surg. Lasers Imaging Retina 47, 426(2016) [PubMed: 27183546]
Paul G, Zachrisson O, Varrone A, Almqvist P, Jerling M, Lind G, Rehncrona S, Linderoth B, Bjartmarz H, Shafer LL, Coffey R, Svensson M,Mercer KJ, Forsberg A,Halldin C, Svenningsson P, Widner H, Frisén J, Pålhagen S, Haegerstrand A, J. Clin. Invest 125, 1339 (2015) [PubMed: 25689258]
Pedroso C, Martins I, Palma F, and Machado AI, Case Rep 2015, bcr2014206256 (2015).
Perruchoud C, Bovy M, Durrer A, Rosato M, Rutschmann B, Mustaki J-P, Buchser E, Neuromodulation Technol. Neural Interface 15, 31 (2012)
Pessoa B, Coelho J, Correia N, Ferreira N, Beirão M, Meireles A, Ophthalmic Res 59, 68 (2018) [PubMed: 29248913]
Petrou P, Koutsandrea C, Papaconstantinou D, Mpouritis D, Georgalas I, Drug Des. Devel. Ther, 2373 (2014)
Pope JE, Deer TR, Pain Manag 5, 175 (2015) [PubMed: 25971641]
Pope JE and Deer TR, in Treat. Chronic Pain Cond, ed. By Pope JE and Deer TR (Springer New York, New York, NY, 2017), pp. 191–193.
Pragout D, Darrouzain F, Marret H, Eur. J. Obstet. Gynecol. Reprod. Biol (2018)
Prescott JH, Lipka S, Baldwin S, Sheppard NF, Maloney JM, Coppeta J, Yomtov B, Staples MA, Santini JT, Nat. Biotechnol 24, 437 (2006) [PubMed: 16531991]
Quhill H, Quhill F, Case Rep. Ophthalmol 7, 301 (2016) [PubMed: 28203186]
Rajgor N, Bhaskar V, Patel M, Syst. Rev. Pharm 2, 91 (2011)
Rauck R, Deer T, Rosen S, Padda G, Barsa J, Dunbar E, Dwarakanath G, Neuromodulation Technol. Neural Interface 13, 102 (2010)
Rauck R, Deer T, Rosen S, Padda G, Barsa J, Dunbar E, Dwarakanath G, Neuromodulation Technol. Neural Interface 16, 163 (2013)
Riordan J, Murphy P, Neuromodulation Technol. Neural Interface 18, 433 (2015)
Rohloff CM, Alessi TR, Yang B,Dahms J, Carr JP, Lautenbach SD, J. Diabetes Sci. Technol 2, 461 (2008) [PubMed: 19885211]
Ross JS, Bates J, Parzynski C, Akar J, Curtis J, Desai N, Freeman J, Gamble G, Kuntz R, Li S-X, Marinac-Dabic D,Masoudi F,Normand S-L, Ranasinghe I, Shaw R, Krumholz H, Med. Devices Evid. Res 10, 165 (2017)
Ruan X, Couch P, Liu H, Shah RV, Wang F, Chiravuri S, Pain Physician 13, 337 (2010) [PubMed: 20648202]
Rudlang T, Brasso K, Austin J Urol 3, 1045 (2016)
Saedon H, Anand A, Yang Y, Clin. Ophthalmol 11, 583 (2017) [PubMed: 28392675]
Samb B, Desai N, Nishtar S, Mendis S, Bekedam H, Wright A,Hsu J, Martiniuk A, Celletti F, Patel K, Adshead F, McKee M, Evans T, Alwan A, Etienne C, The Lancet 376, 1785 (2010)
Santini JT, Cima MJ, Langer R, Nature 397, 335 (1999) [PubMed: 9988626]
Santini JJ, Richards A, Scheidt R, Cima M, Langer R, Angewandte Chemie International Edition 39, 2396 (2000) [PubMed: 10941095]
Santus G, Baker RW, J. Controlled Release 35, 1 (1995)
Saulino M, Gofeld M, Neuromodulation Technol. Neural Interface 17, 696 (2014)
Schmit-Eilenberger V, Clin. Ophthalmol, 801 (2015) [PubMed: 25999689]
Pons-Faudoa et al. Page 26
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Serati M, Bogani G, Kumar S, Cromi A, Ghezzi F, Contraception 91, 91 (2015) [PubMed: 25284356]
Sgouros S, Charalambides C, Matsota P, Tsangaris I, Kostopanagiotou G, Pediatr. Neurosurg 46, 62 (2010) [PubMed: 20516743]
Shumer DE, Nokoff NJ, Spack NP, Adv. Pediatr 63, 79 (2016) [PubMed: 27426896]
Sih J, Bansal SS, Filipini S, Ferrati S, Raghuwansi K, Zabre E, Nicolov E, Fine D, Ferrari M, Palapattu G, Grattoni A, Anal. Bioanal. Chem 405, 1547 (2013) [PubMed: 23090650]
Silverman LA, Neely EK,Kletter GB, Lewis K, Chitra S,Terleckyj O, Eugster EA, J. Clin. Endocrinol. Metab 100, 2354 (2015) [PubMed: 25803268]
Simon C, Agier MS, Béné J, Muller C, Vrignaud L, Marret H, Jonville-Bera AP, Gynécologie Obstétrique J, Biol. Reprod 45, 1074 (2016)
Smith L, Mosley J, Johnson J, and Nasri M, 42, 505 (2017).
Son AI, Opfermann JD, McCue C, Ziobro J, Abrahams JH, Jones K, Morton PD, Ishii S, Oluigbo C, Krieger A, Liu JS, Hashimoto-Torii K, Torii M, Sci. Rep 7 (2017)
Steel Z, Marnane C, Iranpour C, Chey T, Jackson JW, Patel V, Silove D, Int. J. Epidemiol 43, 476 (2014) [PubMed: 24648481]
Stetkarova I, Yablon SA, Kofler M, Stokic DS, Neurorehabil. Neural Repair 24, 609 (2010) [PubMed: 20233964]
Stevenson CL, Santini JT, Langer R, Adv. Drug Deliv. Rev 64, 1590 (2012) [PubMed: 22465783]
Syed YY, Drugs 77, 575 (2017) [PubMed: 28283896]
Taris Biomedical LLC, ClinicalTrials.gov Identifier NCT02722538 (n.d.-a). https://clinicaltrials.gov/ct2/show/NCT02722538 Accessed 21 September 2018.
Taris Biomedical LLC, ClinicalTrials.gov Identifier NCT02720367 (n.d.-b). https://clinicaltrials.gov/ct2/show/NCT02720367 Accessed 21 September 2018.
Taris Biomedical LLC, ClinicalTrials.gov Identifier NCT03404791 (n.d.-c). https://clinicaltrials.gov/ct2/show/NCT03404791 Accessed 21 September 2018.
Taris Biomedical LLC, Taris Biomedical: Taris Advantage (n.d.-d). http://www.tarisbiomedical.com/taris-advantage.php Accessed 24 February 2018.
The Global Cancer Observatory, International Agency for Research on Cancer: All cancers fact sheet (2018). http://gco.iarc.fr/today/data/factsheets/cancers/39-All-cancers-fact-sheet.pdf Accessed 26 October 2018.
Titan Pharmaceuticals, Titan Pharmaceuticals: Pipeline (n.d.). https://www.titanpharm.com/pipeline/overview Accessed 25 February 2018.
U.S. Food and Drug Administration, U.S. Food and Drug Administration: Class 2 Device Recall Prometra II Programmable Infusion PumpPump (2018). https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfRES/res.cfm?id=156065 Accessed 23 April 2018.
Veritti D, Sarao V, Diplotti L, Samassa F, Lanzetta P, Expert Opin. Pharmacother 18, 1507 (2017) [PubMed: 28764565]
Vos T et al., The Lancet 386, 743 (2015)
Wang J, Jiang A, Joshi M, Christoforidis J, Hindawi Publ. Corp 2013, 1 (2013)
Watson JT, Sci. Transl. Med 4, 122ed1 (2012)
Wilkes D, J. Pain Res, 571 (2014) [PubMed: 25336986]
Winters WL, Methodist DeBakey Cardiovasc. J 11, 5 (2015) [PubMed: 26635916]
Woolen S, Holzmeyer C, Nesbitt E, Siami PF, Prostate Cancer 2014, 1 (2014)
World Economic Forum and Harvard School of Public Health, Methodological Appendix: The Global Economic Burden of Non-Communicable Diseases (2011).
World Health Organization, Adherence to Long-Term Therapies: Evidence for Action (2003).
World Health Organization, Global Report on Diabetes (WHO Press, World Health Organization, Geneva, 2016)
World Health Organization, World Health Organization Metrics: DisabilityAdjusted Life Year (DALY) (n.d.). http://www.who.int/healthinfo/global_burden_disease/metrics_daly/en/ Accessed 18 September 2018.
Wright C, Hall J, Drug Des. Devel. Ther, 1543 (2016)
Pons-Faudoa et al. Page 27
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Yang W-W, Pierstorff E, J. Lab. Autom 17, 50 (2012) [PubMed: 22357608]
Yang Y, Bailey C, Holz FG, Eter N, Weber M, Baker C, Kiss S, Menchini U, RuizMoreno JM, Dugel P, Lotery A, Eye 29,1173(2015) [PubMed: 26113503]
Yasin MN, Svirskis D, Seyfoddin A, Rupenthal ID, J. Controlled Release 196, 208 (2014)
Yun YH, Lee BK, Park K, J. Controlled Release 219, 2 (2015)
Ziemys A, Grattoni A, Fine D, Hussain F, Ferrari M, J. Phys. Chem. B 114(11), 117 (2010)
Ziemys A, Kojic M, Milosevic M, Kojic N, Hussain F, Ferrari M, Grattoni A, J. Comput. Phys 230, 5722 (2011)
Pons-Faudoa et al. Page 28
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
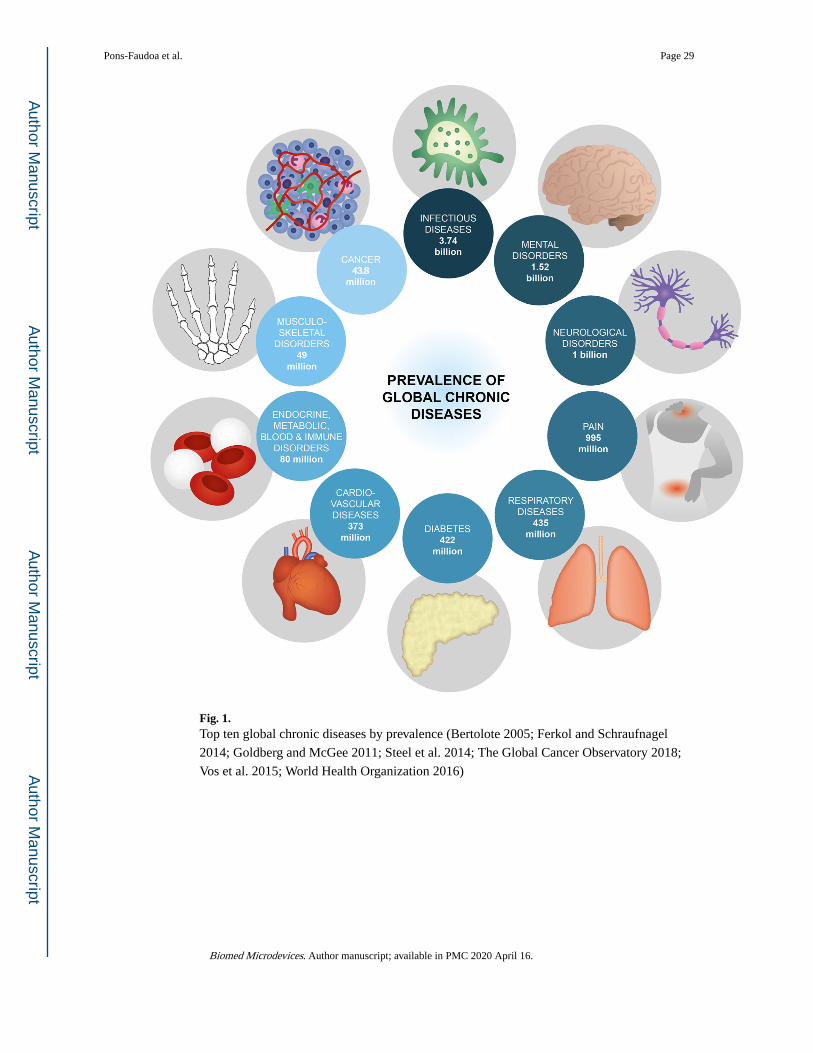
Fig. 1. Top ten global chronic diseases by prevalence (Bertolote 2005; Ferkol and Schraufnagel
2014; Goldberg and McGee 2011; Steel et al. 2014; The Global Cancer Observatory 2018;
Vos et al. 2015; World Health Organization 2016)
Pons-Faudoa et al. Page 29
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
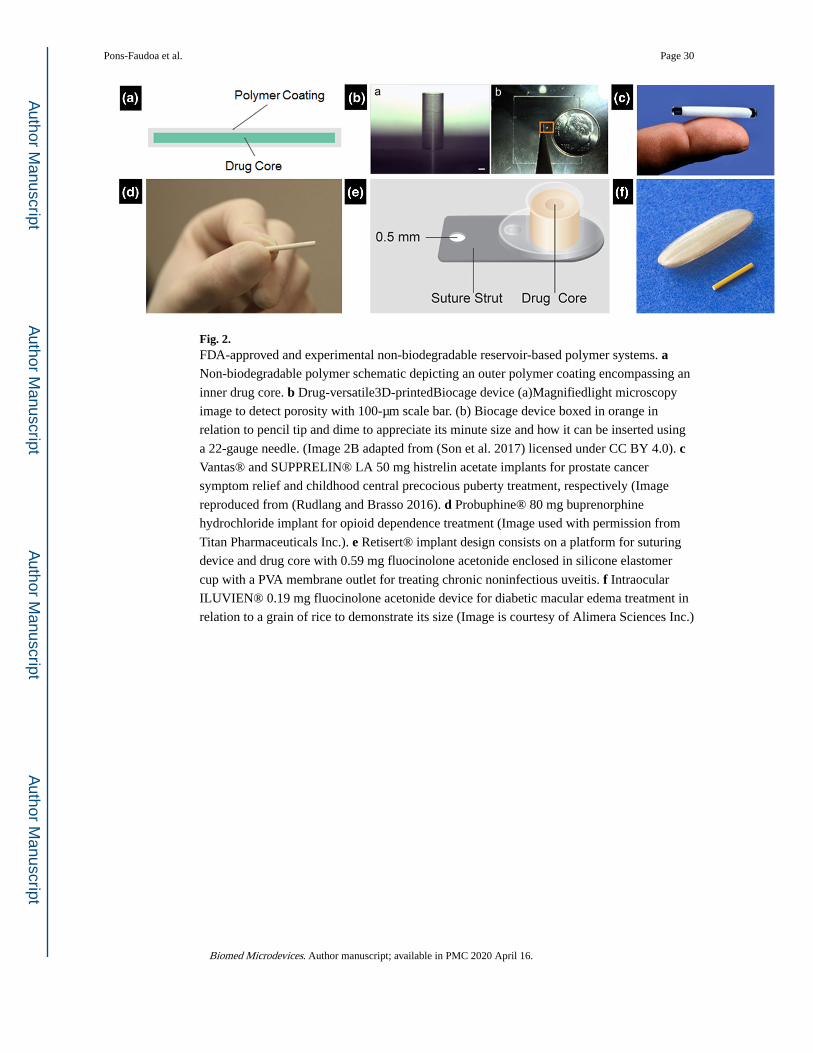
Fig. 2. FDA-approved and experimental non-biodegradable reservoir-based polymer systems. a Non-biodegradable polymer schematic depicting an outer polymer coating encompassing an
inner drug core. b Drug-versatile3D-printedBiocage device (a)Magnifiedlight microscopy
image to detect porosity with 100-μm scale bar. (b) Biocage device boxed in orange in
relation to pencil tip and dime to appreciate its minute size and how it can be inserted using
a 22-gauge needle. (Image 2B adapted from (Son et al. 2017) licensed under CC BY 4.0). c Vantas® and SUPPRELIN® LA 50 mg histrelin acetate implants for prostate cancer
symptom relief and childhood central precocious puberty treatment, respectively (Image
reproduced from (Rudlang and Brasso 2016). d Probuphine® 80 mg buprenorphine
hydrochloride implant for opioid dependence treatment (Image used with permission from
Titan Pharmaceuticals Inc.). e Retisert® implant design consists on a platform for suturing
device and drug core with 0.59 mg fluocinolone acetonide enclosed in silicone elastomer
cup with a PVA membrane outlet for treating chronic noninfectious uveitis. f Intraocular
ILUVIEN® 0.19 mg fluocinolone acetonide device for diabetic macular edema treatment in
relation to a grain of rice to demonstrate its size (Image is courtesy of Alimera Sciences Inc.)
Pons-Faudoa et al. Page 30
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
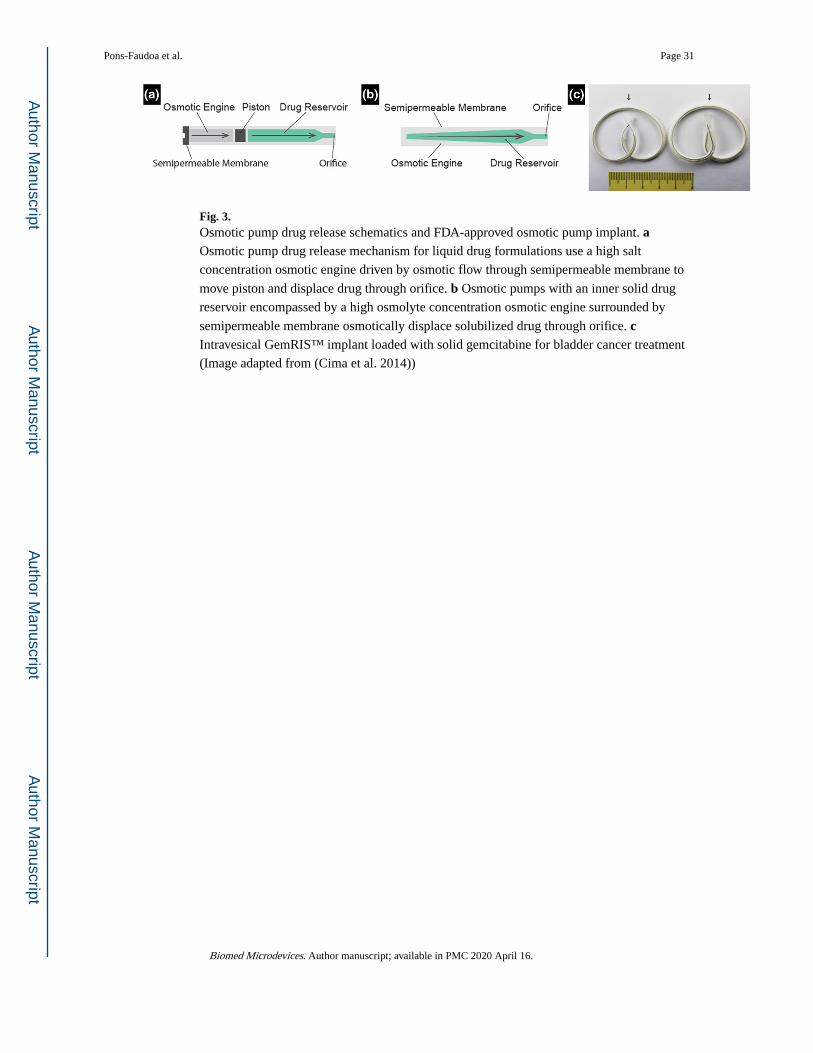
Fig. 3. Osmotic pump drug release schematics and FDA-approved osmotic pump implant. a Osmotic pump drug release mechanism for liquid drug formulations use a high salt
concentration osmotic engine driven by osmotic flow through semipermeable membrane to
move piston and displace drug through orifice. b Osmotic pumps with an inner solid drug
reservoir encompassed by a high osmolyte concentration osmotic engine surrounded by
semipermeable membrane osmotically displace solubilized drug through orifice. c Intravesical GemRIS™ implant loaded with solid gemcitabine for bladder cancer treatment
(Image adapted from (Cima et al. 2014))
Pons-Faudoa et al. Page 31
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
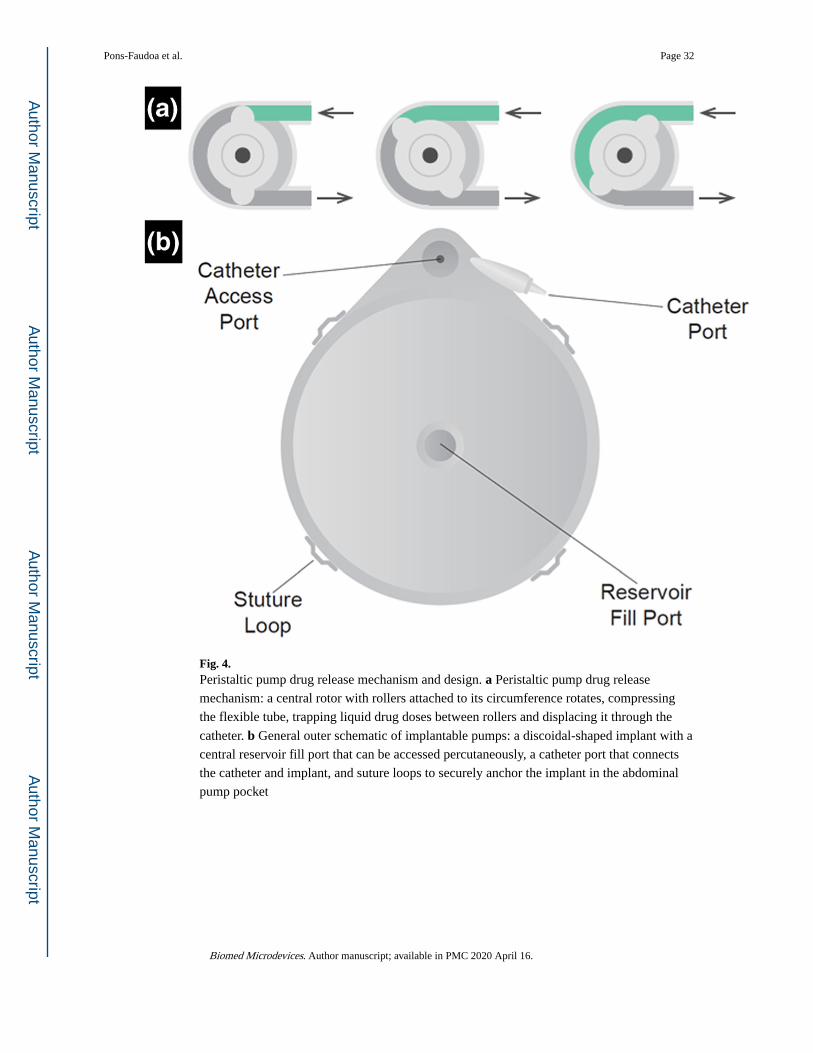
Fig. 4. Peristaltic pump drug release mechanism and design. a Peristaltic pump drug release
mechanism: a central rotor with rollers attached to its circumference rotates, compressing
the flexible tube, trapping liquid drug doses between rollers and displacing it through the
catheter. b General outer schematic of implantable pumps: a discoidal-shaped implant with a
central reservoir fill port that can be accessed percutaneously, a catheter port that connects
the catheter and implant, and suture loops to securely anchor the implant in the abdominal
pump pocket
Pons-Faudoa et al. Page 32
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
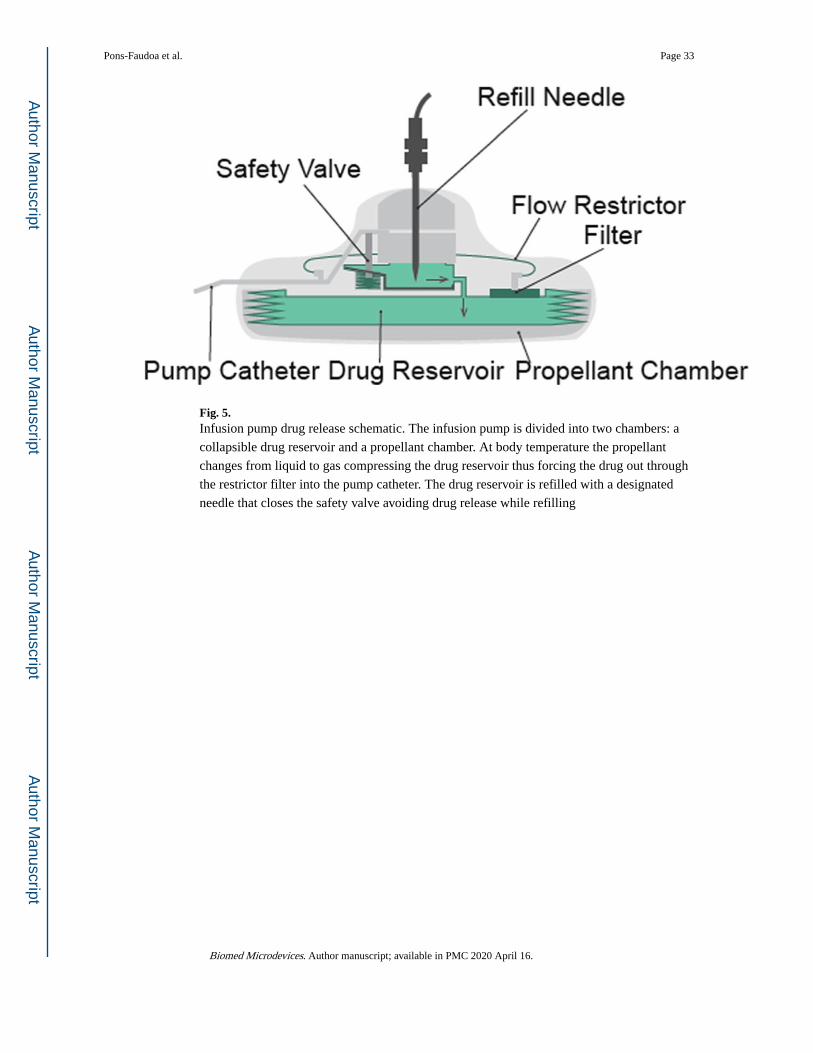
Fig. 5. Infusion pump drug release schematic. The infusion pump is divided into two chambers: a
collapsible drug reservoir and a propellant chamber. At body temperature the propellant
changes from liquid to gas compressing the drug reservoir thus forcing the drug out through
the restrictor filter into the pump catheter. The drug reservoir is refilled with a designated
needle that closes the safety valve avoiding drug release while refilling
Pons-Faudoa et al. Page 33
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
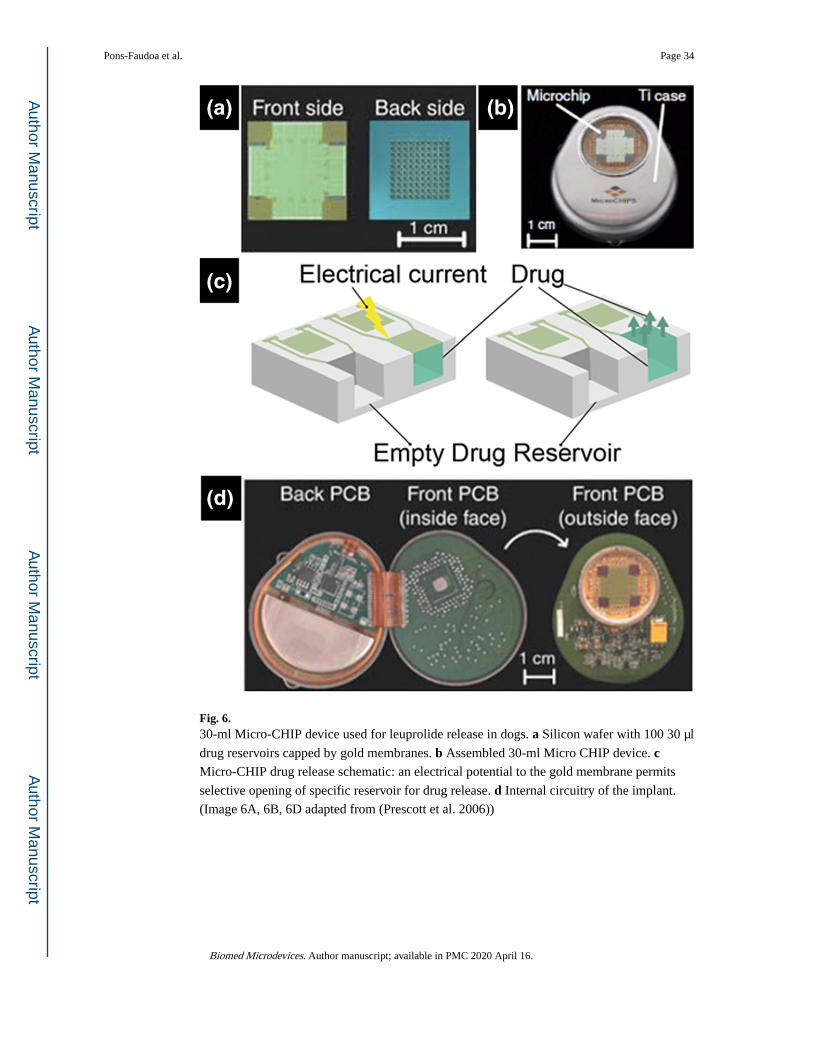
Fig. 6. 30-ml Micro-CHIP device used for leuprolide release in dogs. a Silicon wafer with 100 30 μl
drug reservoirs capped by gold membranes. b Assembled 30-ml Micro CHIP device. c Micro-CHIP drug release schematic: an electrical potential to the gold membrane permits
selective opening of specific reservoir for drug release. d Internal circuitry of the implant.
(Image 6A, 6B, 6D adapted from (Prescott et al. 2006))
Pons-Faudoa et al. Page 34
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
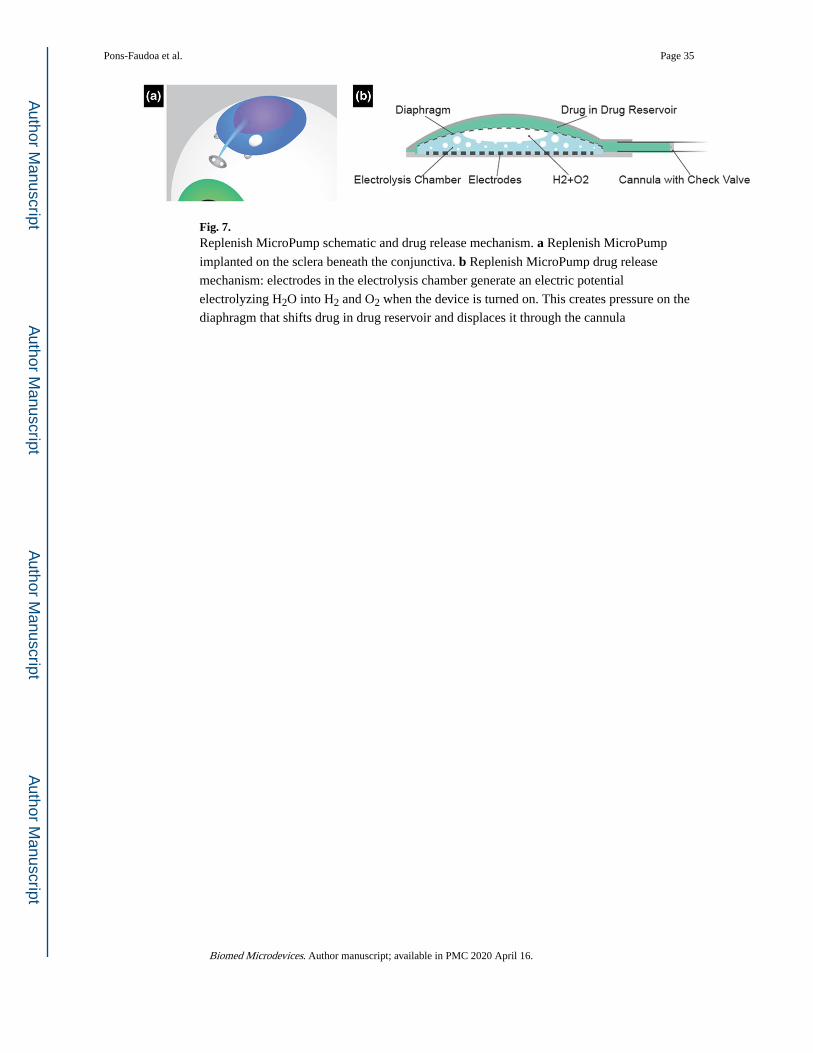
Fig. 7. Replenish MicroPump schematic and drug release mechanism. a Replenish MicroPump
implanted on the sclera beneath the conjunctiva. b Replenish MicroPump drug release
mechanism: electrodes in the electrolysis chamber generate an electric potential
electrolyzing H2O into H2 and O2 when the device is turned on. This creates pressure on the
diaphragm that shifts drug in drug reservoir and displaces it through the cannula
Pons-Faudoa et al. Page 35
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
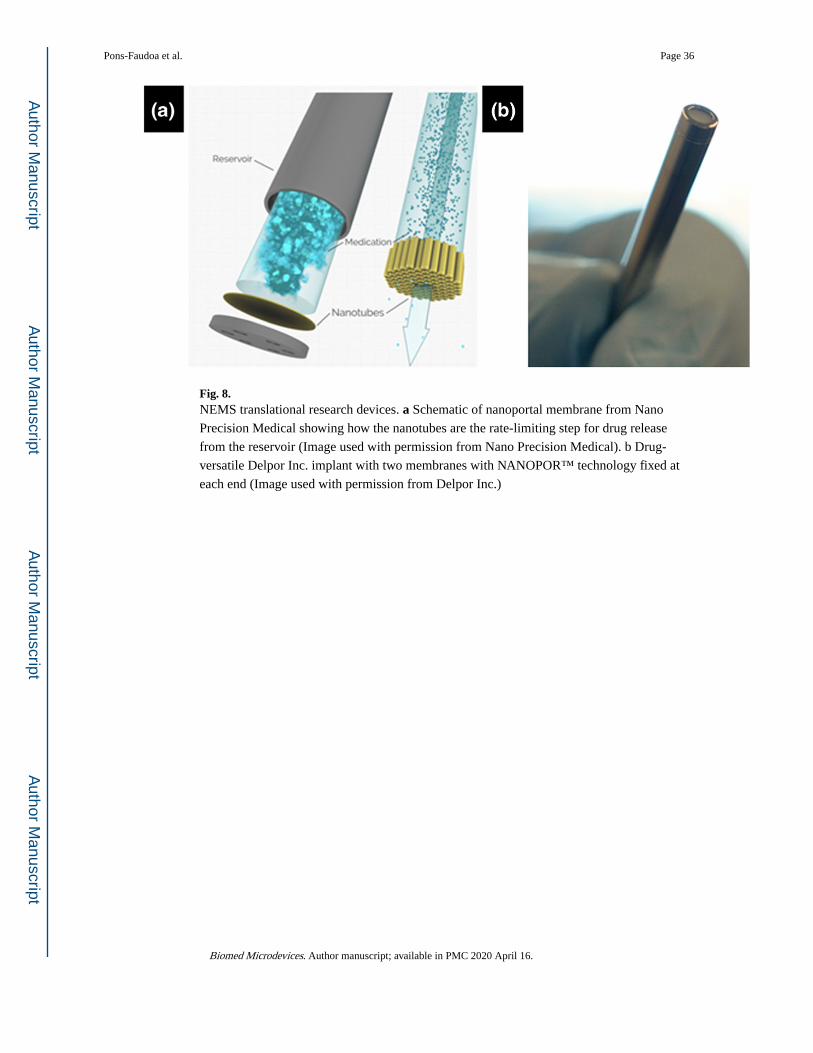
Fig. 8. NEMS translational research devices. a Schematic of nanoportal membrane from Nano
Precision Medical showing how the nanotubes are the rate-limiting step for drug release
from the reservoir (Image used with permission from Nano Precision Medical). b Drug-
versatile Delpor Inc. implant with two membranes with NANOPOR™ technology fixed at
each end (Image used with permission from Delpor Inc.)
Pons-Faudoa et al. Page 36
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
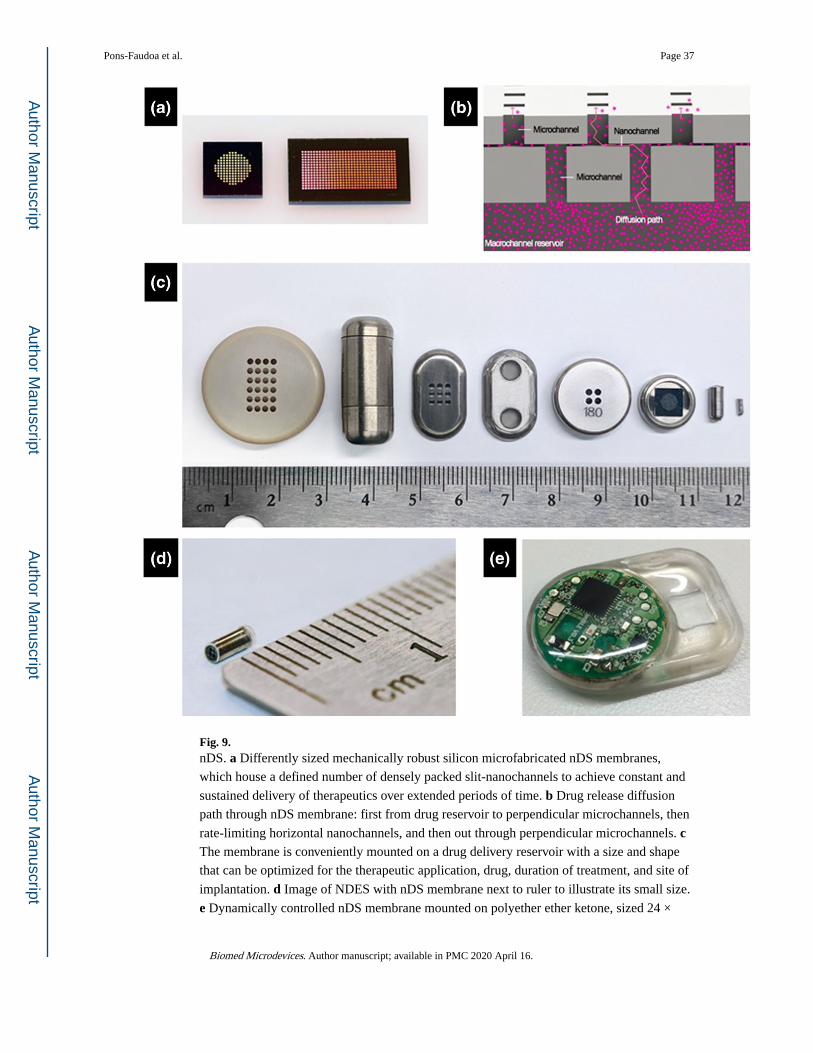
Fig. 9. nDS. a Differently sized mechanically robust silicon microfabricated nDS membranes,
which house a defined number of densely packed slit-nanochannels to achieve constant and
sustained delivery of therapeutics over extended periods of time. b Drug release diffusion
path through nDS membrane: first from drug reservoir to perpendicular microchannels, then
rate-limiting horizontal nanochannels, and then out through perpendicular microchannels. c The membrane is conveniently mounted on a drug delivery reservoir with a size and shape
that can be optimized for the therapeutic application, drug, duration of treatment, and site of
implantation. d Image of NDES with nDS membrane next to ruler to illustrate its small size.
e Dynamically controlled nDS membrane mounted on polyether ether ketone, sized 24 ×
Pons-Faudoa et al. Page 37
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
34× 4.5 mm3, with an 800-μl drug reservoir chamber and a circuitry chamber with the
electronics and battery
Pons-Faudoa et al. Page 38
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
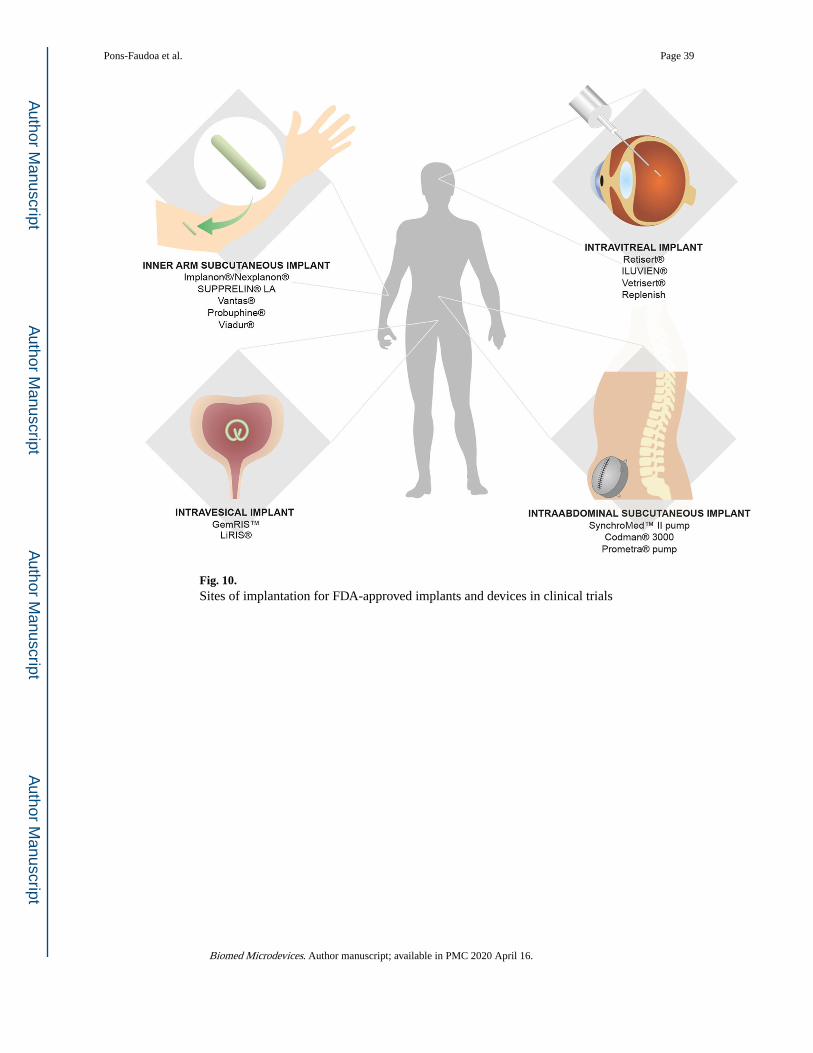
Fig. 10. Sites of implantation for FDA-approved implants and devices in clinical trials
Pons-Faudoa et al. Page 39
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
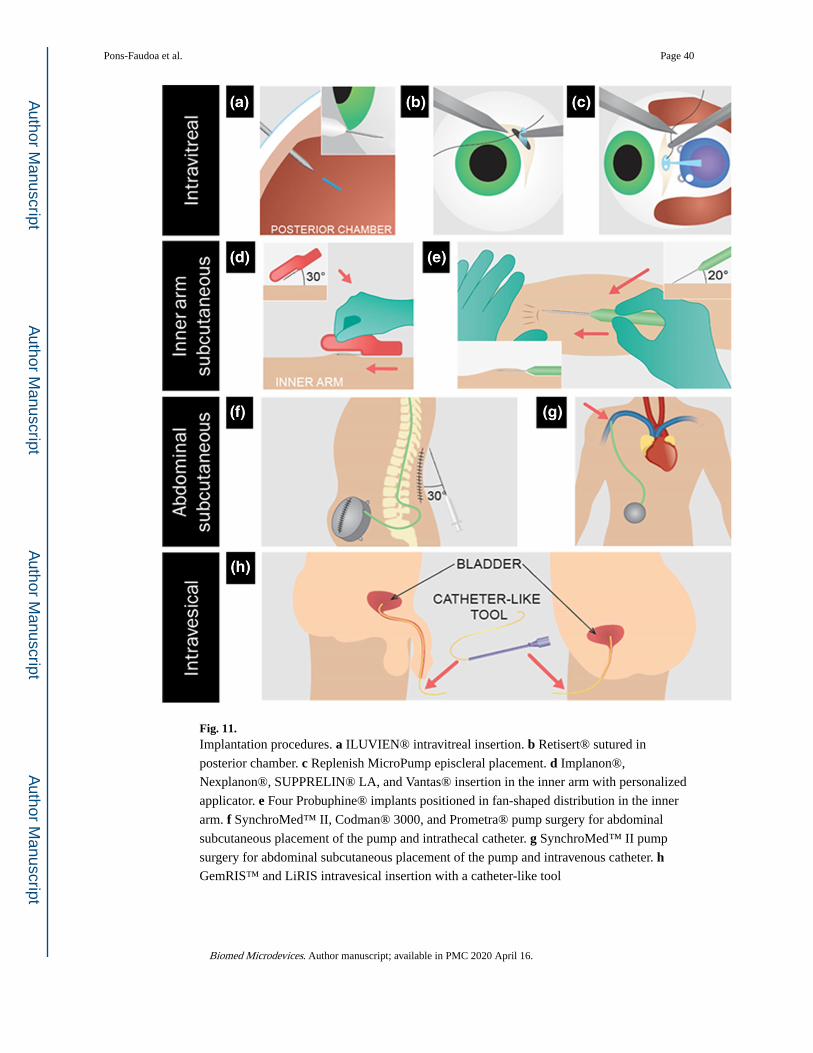
Fig. 11. Implantation procedures. a ILUVIEN® intravitreal insertion. b Retisert® sutured in
posterior chamber. c Replenish MicroPump episcleral placement. d Implanon®,
Nexplanon®, SUPPRELIN® LA, and Vantas® insertion in the inner arm with personalized
applicator. e Four Probuphine® implants positioned in fan-shaped distribution in the inner
arm. f SynchroMed™ II, Codman® 3000, and Prometra® pump surgery for abdominal
subcutaneous placement of the pump and intrathecal catheter. g SynchroMed™ II pump
surgery for abdominal subcutaneous placement of the pump and intravenous catheter. h GemRIS™ and LiRIS intravesical insertion with a catheter-like tool
Pons-Faudoa et al. Page 40
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
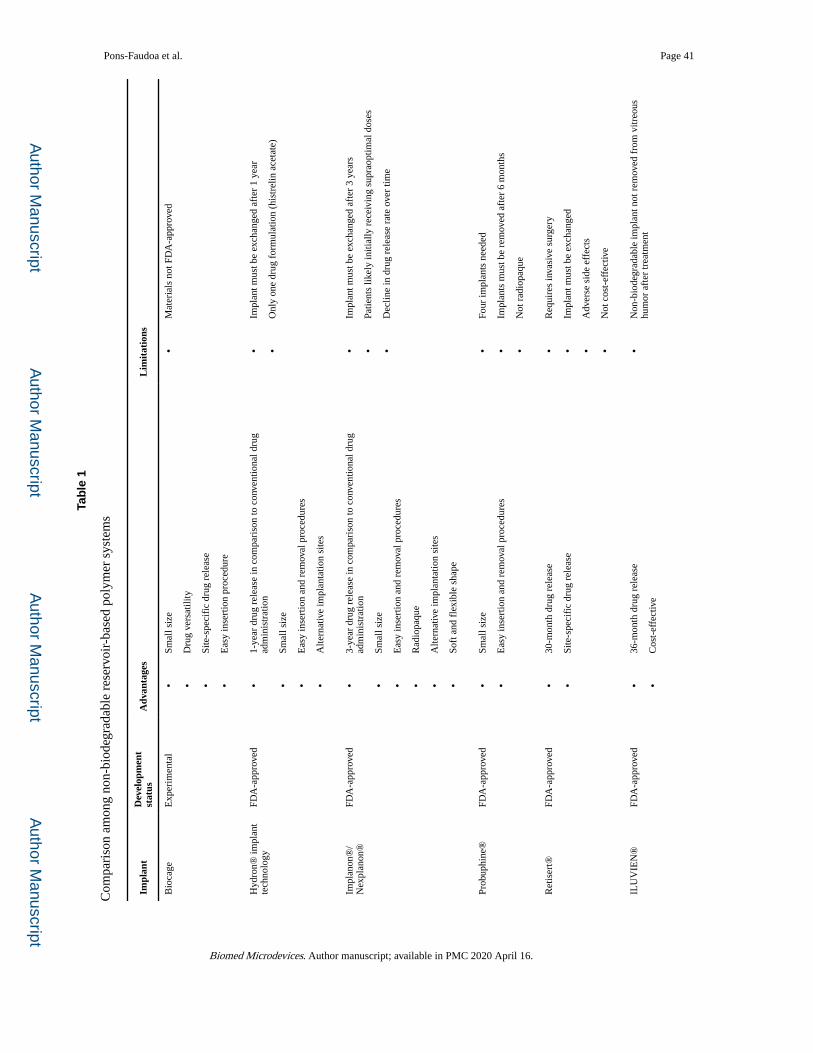
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Pons-Faudoa et al. Page 41
Tab
le 1
Com
pari
son
amon
g no
n-bi
odeg
rada
ble
rese
rvoi
r-ba
sed
poly
mer
sys
tem
s
Impl
ant
Dev
elop
men
t st
atus
Adv
anta
ges
Lim
itat
ions
Bio
cage
Exp
erim
enta
l•
Smal
l siz
e
•D
rug
vers
atili
ty
•Si
te-s
peci
fic
drug
rel
ease
•E
asy
inse
rtio
n pr
oced
ure
•M
ater
ials
not
FD
A-a
ppro
ved
Hyd
ron®
impl
ant
tech
nolo
gyFD
A-a
ppro
ved
•1-
year
dru
g re
leas
e in
com
pari
son
to c
onve
ntio
nal d
rug
adm
inis
trat
ion
•Sm
all s
ize
•E
asy
inse
rtio
n an
d re
mov
al p
roce
dure
s
•A
ltern
ativ
e im
plan
tatio
n si
tes
•Im
plan
t mus
t be
exch
ange
d af
ter
1 ye
ar
•O
nly
one
drug
for
mul
atio
n (h
istr
elin
ace
tate
)
Impl
anon
®/
Nex
plan
on®
FDA
-app
rove
d•
3-ye
ar d
rug
rele
ase
in c
ompa
riso
n to
con
vent
iona
l dru
g ad
min
istr
atio
n
•Sm
all s
ize
•E
asy
inse
rtio
n an
d re
mov
al p
roce
dure
s
•R
adio
paqu
e
•A
ltern
ativ
e im
plan
tatio
n si
tes
•So
ft a
nd f
lexi
ble
shap
e
•Im
plan
t mus
t be
exch
ange
d af
ter
3 ye
ars
•Pa
tient
s lik
ely
initi
ally
rec
eivi
ng s
upra
optim
al d
oses
•D
eclin
e in
dru
g re
leas
e ra
te o
ver
time
Prob
uphi
ne®
FDA
-app
rove
d•
Smal
l siz
e
•E
asy
inse
rtio
n an
d re
mov
al p
roce
dure
s
•Fo
ur im
plan
ts n
eede
d
•Im
plan
ts m
ust b
e re
mov
ed a
fter
6 m
onth
s
•N
ot r
adio
paqu
e
Ret
iser
t®FD
A-a
ppro
ved
•30
-mon
th d
rug
rele
ase
•Si
te-s
peci
fic
drug
rel
ease
•R
equi
res
inva
sive
sur
gery
•Im
plan
t mus
t be
exch
ange
d
•A
dver
se s
ide
effe
cts
•N
ot c
ost-
effe
ctiv
e
ILU
VIE
N®
FDA
-app
rove
d•
36-m
onth
dru
g re
leas
e
•C
ost-
effe
ctiv
e
•N
on-b
iode
grad
able
impl
ant n
ot r
emov
ed f
rom
vitr
eous
hu
mor
aft
er tr
eatm
ent
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Pons-Faudoa et al. Page 42
Impl
ant
Dev
elop
men
t st
atus
Adv
anta
ges
Lim
itat
ions
•Si
te-s
peci
fic
drug
rel
ease
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
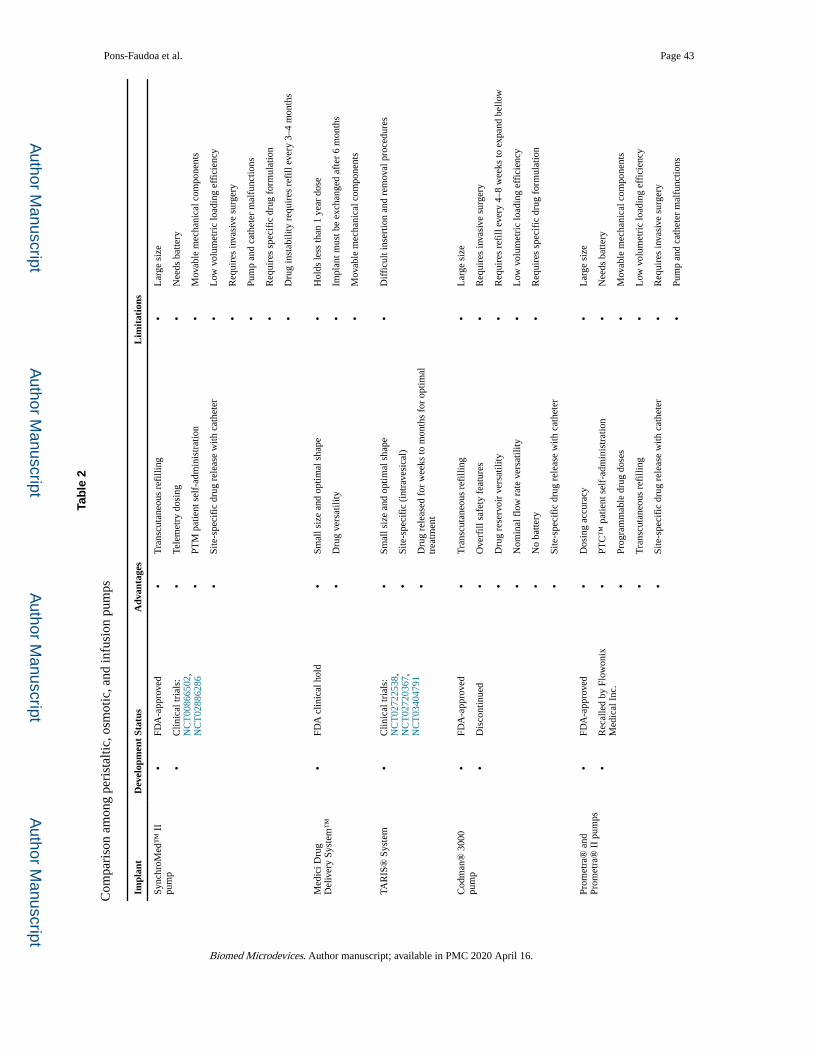
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Pons-Faudoa et al. Page 43
Tab
le 2
Com
pari
son
amon
g pe
rist
altic
, osm
otic
, and
infu
sion
pum
ps
Impl
ant
Dev
elop
men
t St
atus
Adv
anta
ges
Lim
itat
ions
Sync
hroM
ed™
II
pum
p•
FDA
-app
rove
d
•C
linic
al tr
ials
: N
CT
0086
6502
, N
CT
0288
6286
•T
rans
cuta
neou
s re
filli
ng
•Te
lem
etry
dos
ing
•PT
M p
atie
nt s
elf-
adm
inis
trat
ion
•Si
te-s
peci
fic
drug
rel
ease
with
cat
hete
r
•L
arge
siz
e
•N
eeds
bat
tery
•M
ovab
le m
echa
nica
l com
pone
nts
•L
ow v
olum
etri
c lo
adin
g ef
fici
ency
•R
equi
res
inva
sive
sur
gery
•Pu
mp
and
cath
eter
mal
func
tions
•R
equi
res
spec
ific
dru
g fo
rmul
atio
n
•D
rug
inst
abili
ty r
equi
res
refi
ll ev
ery
3–4
mon
ths
Med
ici D
rug
Del
iver
y Sy
stem
™•
FDA
clin
ical
hol
d•
Smal
l siz
e an
d op
timal
sha
pe
•D
rug
vers
atili
ty
•H
olds
less
than
1 y
ear
dose
•Im
plan
t mus
t be
exch
ange
d af
ter
6 m
onth
s
•M
ovab
le m
echa
nica
l com
pone
nts
TAR
IS®
Sys
tem
•C
linic
al tr
ials
: N
CT
0272
2538
, N
CT
0272
0367
, N
CT
0340
4791
•Sm
all s
ize
and
optim
al s
hape
•Si
te-s
peci
fic
(int
rave
sica
l)
•D
rug
rele
ased
for
wee
ks to
mon
ths
for
optim
al
trea
tmen
t
•D
iffi
cult
inse
rtio
n an
d re
mov
al p
roce
dure
s
Cod
man
® 3
000
pum
p•
FDA
-app
rove
d
•D
isco
ntin
ued
•T
rans
cuta
neou
s re
filli
ng
•O
verf
ill s
afet
y fe
atur
es
•D
rug
rese
rvoi
r ve
rsat
ility
•N
omin
al f
low
rat
e ve
rsat
ility
•N
o ba
ttery
•Si
te-s
peci
fic
drug
rel
ease
with
cat
hete
r
•L
arge
siz
e
•R
equi
res
inva
sive
sur
gery
•R
equi
res
refi
ll ev
ery
4–8
wee
ks to
exp
and
bello
w
•L
ow v
olum
etri
c lo
adin
g ef
fici
ency
•R
equi
res
spec
ific
dru
g fo
rmul
atio
n
Prom
etra
® a
nd
Prom
etra
® I
I pu
mps
•FD
A-a
ppro
ved
•R
ecal
led
by F
low
onix
M
edic
al I
nc.
•D
osin
g ac
cura
cy
•PT
C™
pat
ient
sel
f-ad
min
istr
atio
n
•Pr
ogra
mm
able
dru
g do
ses
•T
rans
cuta
neou
s re
filli
ng
•Si
te-s
peci
fic
drug
rel
ease
with
cat
hete
r
•L
arge
siz
e
•N
eeds
bat
tery
•M
ovab
le m
echa
nica
l com
pone
nts
•L
ow v
olum
etri
c lo
adin
g ef
fici
ency
•R
equi
res
inva
sive
sur
gery
•Pu
mp
and
cath
eter
mal
func
tions
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
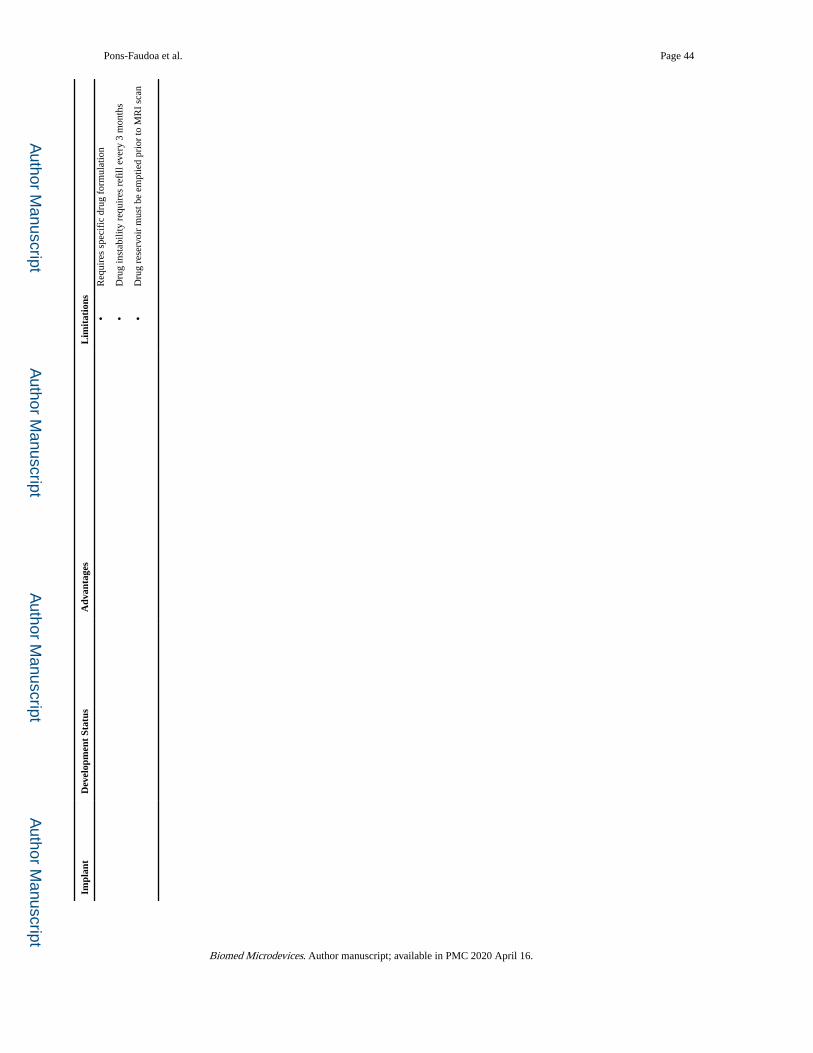
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Pons-Faudoa et al. Page 44
Impl
ant
Dev
elop
men
t St
atus
Adv
anta
ges
Lim
itat
ions
•R
equi
res
spec
ific
dru
g fo
rmul
atio
n
•D
rug
inst
abili
ty r
equi
res
refi
ll ev
ery
3 m
onth
s
•D
rug
rese
rvoi
r m
ust b
e em
ptie
d pr
ior
to M
RI
scan
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
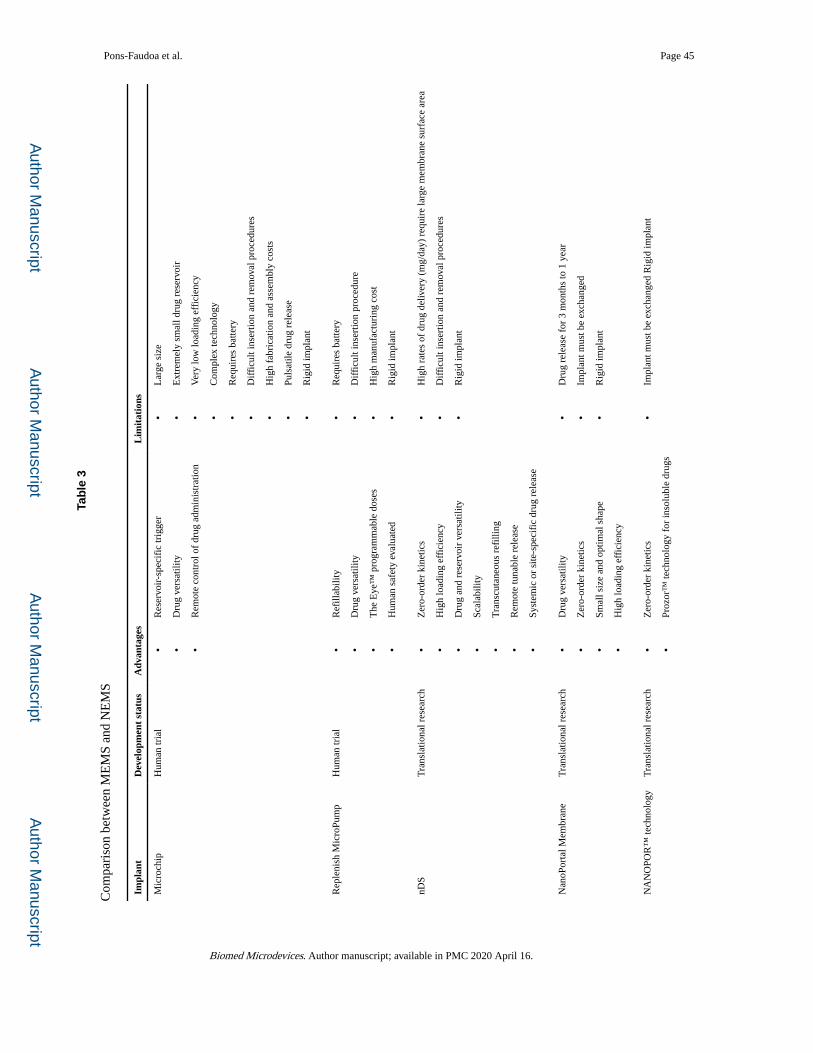
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Pons-Faudoa et al. Page 45
Tab
le 3
Com
pari
son
betw
een
ME
MS
and
NE
MS
Impl
ant
Dev
elop
men
t st
atus
Adv
anta
ges
Lim
itat
ions
Mic
roch
ipH
uman
tria
l•
Res
ervo
ir-s
peci
fic
trig
ger
•D
rug
vers
atili
ty
•R
emot
e co
ntro
l of
drug
adm
inis
trat
ion
•L
arge
siz
e
•E
xtre
mel
y sm
all d
rug
rese
rvoi
r
•V
ery
low
load
ing
effi
cien
cy
•C
ompl
ex te
chno
logy
•R
equi
res
batte
ry
•D
iffi
cult
inse
rtio
n an
d re
mov
al p
roce
dure
s
•H
igh
fabr
icat
ion
and
asse
mbl
y co
sts
•Pu
lsat
ile d
rug
rele
ase
•R
igid
impl
ant
Rep
leni
sh M
icro
Pum
pH
uman
tria
l•
Ref
illab
ility
•D
rug
vers
atili
ty
•T
he E
ye™
pro
gram
mab
le d
oses
•H
uman
saf
ety
eval
uate
d
•R
equi
res
batte
ry
•D
iffi
cult
inse
rtio
n pr
oced
ure
•H
igh
man
ufac
turi
ng c
ost
•R
igid
impl
ant
nDS
Tra
nsla
tiona
l res
earc
h•
Zer
o-or
der
kine
tics
•H
igh
load
ing
effi
cien
cy
•D
rug
and
rese
rvoi
r ve
rsat
ility
•Sc
alab
ility
•T
rans
cuta
neou
s re
filli
ng
•R
emot
e tu
nabl
e re
leas
e
•Sy
stem
ic o
r si
te-s
peci
fic
drug
rel
ease
•H
igh
rate
s of
dru
g de
liver
y (m
g/da
y) r
equi
re la
rge
mem
bran
e su
rfac
e ar
ea
•D
iffi
cult
inse
rtio
n an
d re
mov
al p
roce
dure
s
•R
igid
impl
ant
Nan
oPor
tal M
embr
ane
Tra
nsla
tiona
l res
earc
h•
Dru
g ve
rsat
ility
•Z
ero-
orde
r ki
netic
s
•Sm
all s
ize
and
optim
al s
hape
•H
igh
load
ing
effi
cien
cy
•D
rug
rele
ase
for
3 m
onth
s to
1 y
ear
•Im
plan
t mus
t be
exch
ange
d
•R
igid
impl
ant
NA
NO
POR
™ te
chno
logy
Tra
nsla
tiona
l res
earc
h•
Zer
o-or
der
kine
tics
•Pr
ozor
™ te
chno
logy
for
inso
lubl
e dr
ugs
•Im
plan
t mus
t be
exch
ange
d R
igid
impl
ant
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.
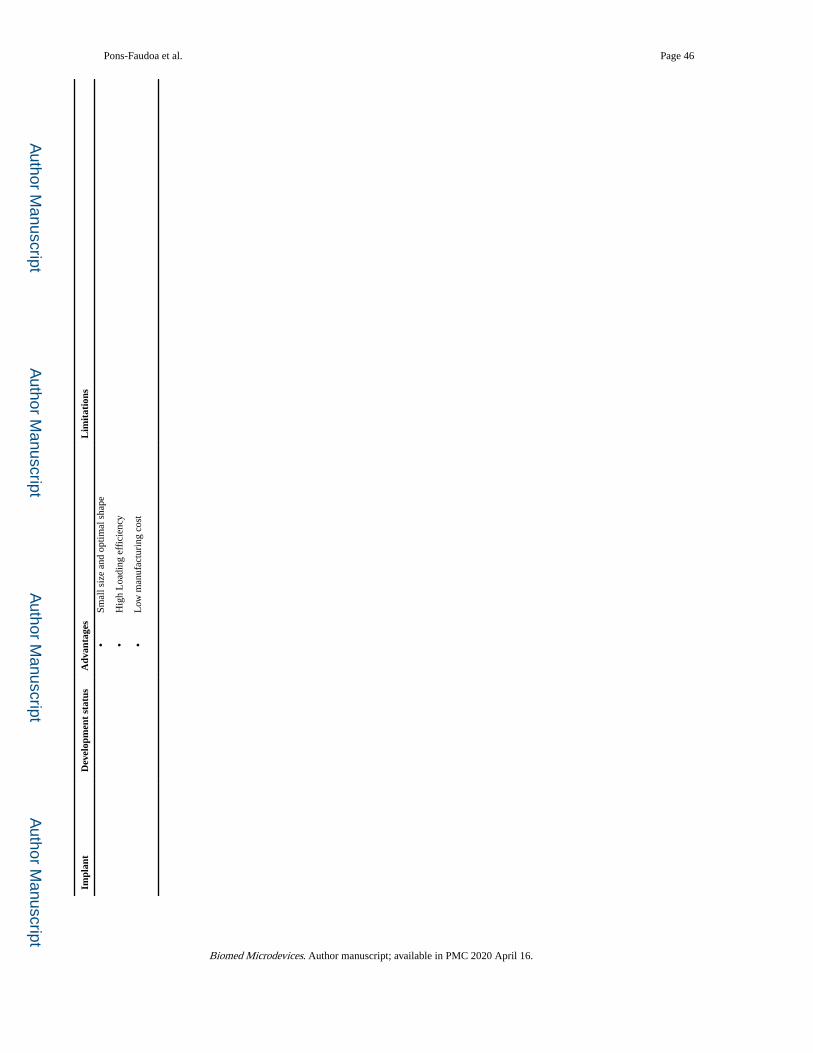
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Pons-Faudoa et al. Page 46
Impl
ant
Dev
elop
men
t st
atus
Adv
anta
ges
Lim
itat
ions
•Sm
all s
ize
and
optim
al s
hape
•H
igh
Loa
ding
eff
icie
ncy
•L
ow m
anuf
actu
ring
cos
t
Biomed Microdevices. Author manuscript; available in PMC 2020 April 16.





























