Embed Size (px)
Citation preview

R
Ai
LSa
b
c
d
e
a
ARRA
KAACSEBSMCHL
C
obaNe
0h
Neuroscience and Biobehavioral Reviews 36 (2012) 1897–1919
Contents lists available at SciVerse ScienceDirect
Neuroscience and Biobehavioral Reviews
jou rna l h omepa ge: www.elsev ier .com/ locate /neubiorev
eview
ltered circadian profiles in attention-deficit/hyperactivity disorder: Anntegrative review and theoretical framework for future studies
indita Imeraja,∗, Edmund Sonuga-Barkeb,c, Inge Antropa, Herbert Roeyersc, Roeljan Wiersemac,arah Bala, Dirk Debouttea,d,e
Ghent University Hospital, Department of Psychiatry and Medical Psychology, Child and Adolescent Psychiatry Research Unit, 0K12F, De Pintelaan 185, 9000 Ghent, BelgiumSouthampton University, School of Psychology, Shackleton Building (B44), Highfield Campus, Southampton SO17 1BJ, United KingdomGhent University, Department of Experimental-Clinical and Health Psychology, Henri Dunantlaan 2, 9000 Ghent, BelgiumAntwerp University, Collaborate Antwerp Psychiatry Research, Universiteitsplein 1, 2610 Antwerp, BelgiumUniversity Centre Child and Adolescent Psychiatry, Lindendreef 1, 2020 Antwerp, Belgium
r t i c l e i n f o
rticle history:eceived 19 February 2011eceived in revised form 20 April 2012ccepted 23 April 2012
eywords:DHDrousalircadianuprachiasmatic nucleus
a b s t r a c t
Disruptions in the sleep–wake cycle and the circadian system have been found in a wide range of psychi-atric disorders and are generally correlated with clinical severity and diminished quality of life. Emergingevidence suggests similar disturbances may be found in attention-deficit/hyperactivity disorder (ADHD).Here we review the available literature on across the day fluctuations in ADHD-related processes interms of; (i) time of day effects on behavior and activity; (ii) morningness–eveningness chronotypology;(iii) sleep/wake rhythms; and (iv) rhythmicity in neuroendocrine and neurophysiological responsive-ness. On this basis, we propose a neurobiological framework to guide future study, which sees circadianeffects in ADHD, along with other aspects of ADHD arousal-related deficits (e.g., cognitive energeticdeficits), as being the result of dysregulated locus coeruleus function. Based on this perspective specific
veningnessehaviorleepelatonin
ortisoleart rateocus coeruleus
recommendations for future research are presented.© 2012 Elsevier Ltd. All rights reserved.
ontents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18982. Review of circadian profiles in ADHD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1899
2.1. Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18992.2. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1899
2.2.1. Chronotypology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18992.2.2. Diurnal variations in behavior and performance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1899
2.2.3. Sleep–wake rhythms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.2.4. Circadian effects on neuroendocrine and neurophysiolog2.2.5. Summary of findings, limitations and clinical implicationAbbreviations: APA, American Psychiatric Association; ADHD, attention-deficit hyperutput cycles kaput gene; LC, locus coeruleus; MSLT, multiple sleep latency test; PSG, polysehavior checklist; MEQ, morningness–eveningness questionnaire; SOI, sleep onset insomxis; CRF, corticotropin releasing factor; RAS, reticular activation system; DMH, dorsomE, noradrenaline; PFC, prefrontal cortex; DRD-4 gene, dopamine receptor D4 gene; fMRI,lectroencephalogram; ERP, event related potential.∗ Corresponding author. Tel.: +32 9 332 48 74; fax: +32 9 332 27 58.
E-mail address: [email protected] (L. Imeraj).
149-7634/$ – see front matter © 2012 Elsevier Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.neubiorev.2012.04.007
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1901ical processes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1905s of research to date. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1908
activity disorder; SCN, suprachiasmatic nucleus; CLOCK gene, circadian locomotoromnography; ODD, oppositional defiant disorder; CD, conduct disorder; CBCL, child
nia; DLMO, dim light melatonin onset; HPA axis, hypothalamic-pituitary-adrenaledial hypothalamic nucleus; VLPO area, sleep-related ventrolateral preoptic area;
functional magnetic resonance imaging; PET, positron emission tomography; EEG,

1898 L. Imeraj et al. / Neuroscience and Biobehavioral Reviews 36 (2012) 1897–1919
3. LC-mediated arousal dysfunction in ADHD – a working hypothesis linking context-driven, cognitive energetic, and context-independentcircadian-based alterations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19093.1. The role of locus coeruleus in arousal and circadian effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19093.2. ADHD, arousal and deficient state regulation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19093.3. Existing evidence implicating LC-related noradrenergic function in ADHD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19103.4. A working hypothesis: circadian effects as a special case of LC/arousal dysfunction in ADHD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1911
4. Proposals for future study of circadian effects in ADHD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19124.1. Prediction 1: ADHD is associated with LC-mediated circadian rhythm alterations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1912
4.1.1. LC tonic hyperactivity in ADHD is more expressed at specific times of day than others. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19124.1.2. There is a disruption in the circadian rhythms of LC-noradrenergic mediated arousal in ADHD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19124.1.3. Subjects with ADHD show specific alterations in behavioral and peripheral physiological measures of arousal as a
function of time of day . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19134.1.4. Circadian disruptions in different arousal-related measures (LC, arousal, and behavioral/physiological measures)
will be highly correlated in ADHD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19134.2. Prediction 2: there is an interaction of time of day effects and specific environmental stimuli suggesting a ‘shared LC state
regulation pathway deficit’ in ADHD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19134.3. Prediction 3: the association with circadian rhythm is only valid for a subgroup of ADHD and may overlap with
other psychiatric conditions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19145. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1914
Financial disclosures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1914Acknowledgment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1914
. . . . . .
1
rcapdAmTtae(sitAcAppds
ebrP2punct2hypii
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. Introduction
There is mounting evidence to support the notion that circadianhythms are altered in a wide range of psychiatric diseases, espe-ially affective disorders (see for reviews: Boivin, 2000; Germainnd Kupfer, 2008; McClung, 2007; Wirz-Justice, 2006). For exam-le, impaired sleep and daytime fatigue are included in theiagnostic criteria for depressive disorders (American Psychiatricssociation, APA, 2000) where diurnal variations in symptoms (e.g.,ood and psychomotor activity) have frequently been reported.
hese fluctuations are reflected in physiological measures suchhat, compared to a control population, depressive patients showlterations in circadian rhythms of melatonin and (Pacchierottit al., 2001) cortisol levels (Deuschle et al., 1997); body temperatureDaimon et al., 1992); and heart rate (Stampfer, 1998). Moreover,ome interventions that change the timing of the biological clockn the brain (e.g., sleep deprivation, light therapy) have efficacy asreatments for these conditions (Wehr et al., 1979). For instance,gomelatine, a new antidepressive agent with phase advancingharacteristics has become available (Fornaro et al., 2010; San andrranz, 2008) and appears to be effective in at least a subgroup ofatients (Duke, 2008). Diurnal variations in symptoms and alteredrofiles of circadian markers are also found in seasonal depressiveisorder (Lewy et al., 2006), bipolar disorder (Harvey, 2008), andchizophrenia (Rao et al., 1994).
In attention-deficit/hyperactivity disorder (ADHD) it is well-stablished that behavioral symptoms and performance fluctuateoth spontaneously over time and in response to changing envi-onmental contexts (Antrop et al., 2005a; Luman et al., 2005;ower, 1992; Sonuga-Barke et al., 1996; Toplak and Tannock,005; Wiersema et al., 2006b; Zentall and Zentall, 1976). In clinicalractice, sleep–wake problems are frequently reported by individ-als with ADHD or their parents, even though these problems areot currently included in the diagnostic criteria. As disruptions ofircadian rhythms and sleep–wake cycles are generally expectedo have a significant impact on symptom severity (Fallone et al.,001), daytime functioning (Bearpark and Michie, 1987), andealth outcomes (Gangwisch, 2009; Scheer et al., 2009), in recentears, researchers have become increasingly interested in the
ossibility that such effects are implicated in ADHD pathophys-ology. Gathering knowledge on diurnal variations in ADHD ismportant as these results may improve educational guidelines
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1914
(such as optimal timing of academic lessons) and diagnostic andtherapeutic assessments. For example, knowledge of time of dayeffects could lead to the adjustment of dosing and timing of ADHDmedication to optimally observe and treat problematic behaviorat a particular time of day. Furthermore, if findings on disruptedcircadian rhythms are confirmed in ADHD, they may point to thevalue of circadian-based therapies in ADHD such as melatonintreatment and light therapy. To the best of our knowledge, thereis no review that assesses findings on circadian effects in ADHD.
To date, the underlying mechanisms of circadian rhythm alter-ations in psychiatric disorders in general, or in some of theseconditions specifically, are still unknown. The suprachiasmaticnucleus (SCN) in the ventral hypothalamus (Weaver, 1998) isthought to drive these 24-h fluctuations in both physiological (e.g.,body temperature, heart rate, hormone secretion) and psycholog-ical (cognitive performance, personality and behavior) functions(Carrier and Monk, 2000; Haus, 2007; Hofstra and de Weerd, 2008;Tankova et al., 1994; Young, 2006). This biological clock has anendogenous nature – rhythms persist even in the absence of exter-nal, environmental information. However, exogenous cues, alsocalled zeitgebers (e.g., light, but also sleep deprivation and socialcues), tune this clock to a specific rhythm. The SCN is responsiblefor the functional time synchronization of all peripheral oscillatorsfound in cells, tissues, and organs. Communication to peripheralstructures takes place through both neural and endocrine factors,and enhances synchronized functioning of different human sys-tems, including the central nervous system, the autonomic nervoussystem, and the endocrine tissues (Haus, 2007). The sleep–wakecycle is also regulated by the SCN. However, this circadian pro-cess (process C) interacts with a homeostatic process (process S)to maintain wakefulness (which we further refer to as arousal; aphysiological and psychological state of being awake, aware, andalert) during the day and to consolidate sleep at night. Whereasthe process C is particularly important in the timing of sleep andarousal states, the process S regulates the duration and structureof sleep (Borbély, 1982). When considering the available evidence,disruptions in circadian rhythms and sleep–wake cycles have usu-ally been related to changes in the timing of the biological clock(though alternative hypotheses have been provided; e.g., social
zeitgeber theory, process S deficiency; Boivin, 2000; Grandin et al.,2006). Alterations in biological clock timing have been seen asa consequence of changes in neurotransmitter activity related to
behav
ti(
pimo(CoraAdl
2
cbishhtda(B2haSht
2
Sc“cwoiw1lgfiosgPtre
AsiH
L. Imeraj et al. / Neuroscience and Bio
he condition (Maurizi, 1984; Pacchierotti et al., 2001), but theres emerging research on circadian locomotor output cycles kaputCLOCK) genes as an etiological factor (Barnard and Nolan, 2008).
The current paper has two aims. First, to systematically reviewublished data on across the day fluctuations in ADHD behav-
or, performance and physiological functioning in terms of; (i)orningness–eveningness chronotypology; (ii) time of day effects
f behavior and activity; (iii) sleep/wake rhythm problems; andiv) rhythmicity in neuroendocrine and neurophysiological factors.linical implications of these (putative) effects will also be drawnut. Second, to develop a neurobiological framework to guide futureesearch into circadian disruptions in ADHD. At the heart of thisccount is the hypothesis that disrupted circadian rhythms inDHD, along with other arousal-related processes thought to beeficient in ADHD such as cognitive energetic problems, are due to
ocus coeruleus (LC) dysfunction.
. Review of circadian profiles in ADHD
ADHD is one of the most prevalent psychiatric disorders inhildren and adolescents (Spencer et al., 2007), characterizedy persistent problems in attention, hyperactivity and impulsiv-
ty (APA, 2000). Based on the symptomatology, different ADHDubtypes can be distinguished namely the inattentive type, theyperactive-impulsive type, and the combined (inattentive andyperactive-impulsive) type. Although pervasiveness and persis-ence of symptoms and impairment are important criteria for theiagnosis of ADHD (APA, 2000), time- and context-dependent vari-bility in behavioral symptoms and performance has been reportedAntrop et al., 2005a; Luman et al., 2005; Power, 1992; Sonuga-arke et al., 1996; Toplak and Tannock, 2005; Wiersema et al.,006b; Zentall and Zentall, 1976). Fluctuations in ADHD behaviorave typically been explained in terms of either context-dependentcute changes in arousal state (both hypo- and hyperarousal; seeections 3.2 and 3.3 for more detailed information), which in turnave been thought to display spontaneous circadian effects acrosshe day (see Sections 3.1 and 3.4 for more detailed information).
.1. Method
An electronic literature search was performed using Web ofcience and Pubmed (Medline) databases. Search terms were “cir-adian” or “diurnal” or “time of day” intersected with “ADHD” orhyperactivity”. Based on the results of these strings, a more spe-ific search was conducted using all combinations of previous termsith “eveningness” or “physical activity” or “sleep” or “melatonin”
r “cortisol” or “heart rate”. A search through the references of orig-nal and related articles resulted in additional citations. Searches
ere restricted to papers in the English language published from967 to the present and included all studies with children, ado-
escents, and adults as participants. Since the “sleep” search stringenerated a lot of original articles and reviews, this paper focuses onndings with high relevance to the sleep–wake ‘rhythm’, i.e. resultsn sleep duration, sleep latency, and sleep efficiency as obtained byubjective and objective evaluations. The latter comprises investi-ations using either actigraph or multiple sleep latency test (MSTL).olysomnography (PSG) research mainly focusing on sleep ‘archi-ecture’, e.g. REM and non-REM, and ADHD has been thoroughlyeviewed elsewhere (Cohen-Zion and Ancoli-Israel, 2004; Corteset al., 2009, 2006; Sadeh et al., 2006) and is not reviewed again here.
Because the literature directly related to circadian measures and
DHD is limited, studies using a single or short-term basal mea-urement of a circadian endocrine or autonomic variable were alsoncluded, even if they did not examine complete circadian patterns.owever, studies including a basal pre-test measurement in theioral Reviews 36 (2012) 1897–1919 1899
context of an experimental task were deemed to be less relevantfor this review: these measurements could be influenced by antic-ipatory stress and have therefore only limited value in circadianevaluations. Time of day effects reported in behavioral studies werealso considered, even if these primarily focused on contextual fac-tors and not on 24-h fluctuations. In addition, studies in patientswith ADHD and comorbid disorders such as insomnia or disruptivebehavioral disorders (i.e., oppositional defiant disorder (ODD) orconduct disorder (CD)) were reviewed although it is often difficultto disentangle the effects of the comorbid disorders from ADHDitself.
2.2. Results
The searches yielded studies using both subjective (e.g., ques-tionnaires on chronotypology and sleep) and objective (e.g.,endocrine measures, activity, and physiological registration)dependent measures. The majority of studies evaluated circadianrhythms in a naturalistic setting.
2.2.1. ChronotypologyChronotypology refers to a continuum on which individuals
can be rated from high morning to high evening types (Cavalleraand Giudici, 2008; Kerkhof, 1985; Tankova et al., 1994). Themorningness–eveningness paradigm correlates highly with circa-dian rhythms and physiological measures of arousal (Baehr et al.,2000; Jankowski and Ciarkowska, 2008). We identified one paper ina general population of children and three papers in a clinical sam-ple of adults with ADHD addressing this issue. In a healthy childpopulation aged 8–13, Susman et al. (2007) described an associa-tion between ADHD symptoms and distinctive patterns of circadianpreference. The authors reported eveningness to be associated withhigher scores on both attention problems and rule-breaking behav-ior in boys as measured by the Child Behavior Checklist (CBCL;Achenbach, 2001). In a clinical population of adults with ADHD,Rybak et al. (2007) found a circadian phase delay during thefall/winter period in adults with ADHD: they reported evening-ness, as measured by the morningness–eveningness questionnaire(MEQ) (Horne and Ostberg, 1976), to correlate with both subjec-tive (Brown Adult Attention-Deficit Disorder Scale; Brown, 1996)and objective (Conners’ Continuous Performance Test; Conners,2000) measures of attention deficits in ADHD. The associationbetween eveningness and ADHD appeared to be independent ofcomorbid seasonal affective disorder. Caci et al. (2009) confirmedthis relationship in adults suspected of having ADHD. Althoughinattention symptoms were strongly related to eveningness intheir study, impulsivity and hyperactivity were not. Therefore, theauthors suggested that eveningness may constitute an endopheno-type of the predominantly inattentive subtype of ADHD. Also Baeet al. (2010) supported the idea that eveningness may be stronglyassociated with inattention problems in adult ADHD. Consider-ing hyperactivity and impulsivity, they reported an associationwith eveningness in male subjects only. The link between ADHDand a later time of day preference (i.e., eveningness) is thoughtto reflect a delayed timing of optimal arousal levels. One pos-sibility is that this differential across the day arousal pattern inADHD is due to an altered 24-h rhythmic control of the biologicalclock.
2.2.2. Diurnal variations in behavior and performanceBehavioral observational research has provided overwhelm-
ing evidence for significant group differences between ADHD
and controls in terms of mean levels of attention and activ-ity measured across long periods of time. Although fluc-tuations in ADHD symptomatology and performance havebeen well studied in relation to changing environmental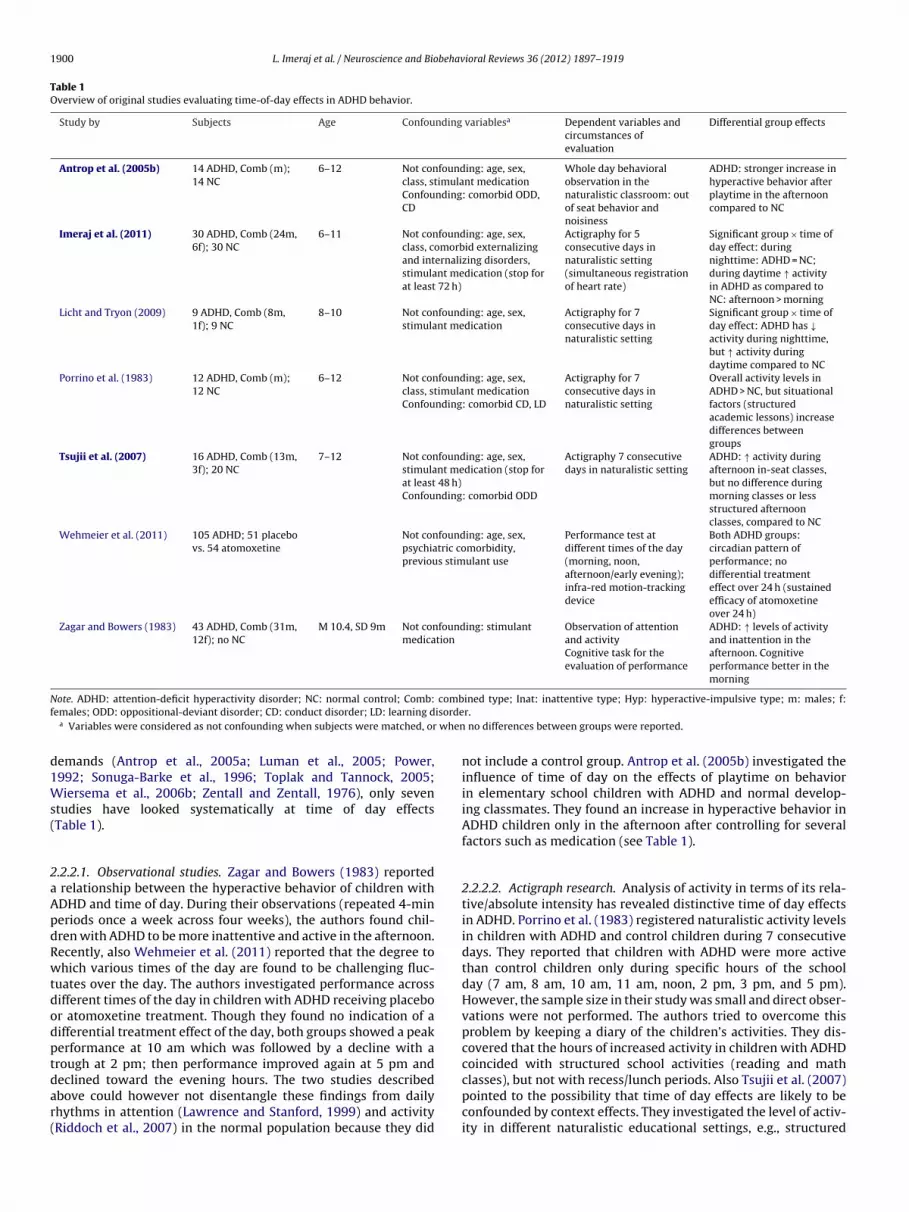
1900 L. Imeraj et al. / Neuroscience and Biobehavioral Reviews 36 (2012) 1897–1919
Table 1Overview of original studies evaluating time-of-day effects in ADHD behavior.
Study by Subjects Age Confounding variablesa Dependent variables andcircumstances ofevaluation
Differential group effects
Antrop et al. (2005b) 14 ADHD, Comb (m);14 NC
6–12 Not confounding: age, sex,class, stimulant medicationConfounding: comorbid ODD,CD
Whole day behavioralobservation in thenaturalistic classroom: outof seat behavior andnoisiness
ADHD: stronger increase inhyperactive behavior afterplaytime in the afternooncompared to NC
Imeraj et al. (2011) 30 ADHD, Comb (24m,6f); 30 NC
6–11 Not confounding: age, sex,class, comorbid externalizingand internalizing disorders,stimulant medication (stop forat least 72 h)
Actigraphy for 5consecutive days innaturalistic setting(simultaneous registrationof heart rate)
Significant group × time ofday effect: duringnighttime: ADHD = NC;during daytime ↑ activityin ADHD as compared toNC: afternoon > morning
Licht and Tryon (2009) 9 ADHD, Comb (8m,1f); 9 NC
8–10 Not confounding: age, sex,stimulant medication
Actigraphy for 7consecutive days innaturalistic setting
Significant group × time ofday effect: ADHD has ↓activity during nighttime,but ↑ activity duringdaytime compared to NC
Porrino et al. (1983) 12 ADHD, Comb (m);12 NC
6–12 Not confounding: age, sex,class, stimulant medicationConfounding: comorbid CD, LD
Actigraphy for 7consecutive days innaturalistic setting
Overall activity levels inADHD > NC, but situationalfactors (structuredacademic lessons) increasedifferences betweengroups
Tsujii et al. (2007) 16 ADHD, Comb (13m,3f); 20 NC
7–12 Not confounding: age, sex,stimulant medication (stop forat least 48 h)Confounding: comorbid ODD
Actigraphy 7 consecutivedays in naturalistic setting
ADHD: ↑ activity duringafternoon in-seat classes,but no difference duringmorning classes or lessstructured afternoonclasses, compared to NC
Wehmeier et al. (2011) 105 ADHD; 51 placebovs. 54 atomoxetine
Not confounding: age, sex,psychiatric comorbidity,previous stimulant use
Performance test atdifferent times of the day(morning, noon,afternoon/early evening);infra-red motion-trackingdevice
Both ADHD groups:circadian pattern ofperformance; nodifferential treatmenteffect over 24 h (sustainedefficacy of atomoxetineover 24 h)
Zagar and Bowers (1983) 43 ADHD, Comb (31m,12f); no NC
M 10.4, SD 9m Not confounding: stimulantmedication
Observation of attentionand activityCognitive task for theevaluation of performance
ADHD: ↑ levels of activityand inattention in theafternoon. Cognitiveperformance better in themorning
N combf isorde
when
d1Ws(
2aApdRwtdodptdar(
ote. ADHD: attention-deficit hyperactivity disorder; NC: normal control; Comb:emales; ODD: oppositional-deviant disorder; CD: conduct disorder; LD: learning d
a Variables were considered as not confounding when subjects were matched, or
emands (Antrop et al., 2005a; Luman et al., 2005; Power,992; Sonuga-Barke et al., 1996; Toplak and Tannock, 2005;iersema et al., 2006b; Zentall and Zentall, 1976), only seven
tudies have looked systematically at time of day effectsTable 1).
.2.2.1. Observational studies. Zagar and Bowers (1983) reported relationship between the hyperactive behavior of children withDHD and time of day. During their observations (repeated 4-mineriods once a week across four weeks), the authors found chil-ren with ADHD to be more inattentive and active in the afternoon.ecently, also Wehmeier et al. (2011) reported that the degree tohich various times of the day are found to be challenging fluc-
uates over the day. The authors investigated performance acrossifferent times of the day in children with ADHD receiving placebor atomoxetine treatment. Though they found no indication of aifferential treatment effect of the day, both groups showed a peakerformance at 10 am which was followed by a decline with arough at 2 pm; then performance improved again at 5 pm and
eclined toward the evening hours. The two studies describedbove could however not disentangle these findings from dailyhythms in attention (Lawrence and Stanford, 1999) and activityRiddoch et al., 2007) in the normal population because they didined type; Inat: inattentive type; Hyp: hyperactive-impulsive type; m: males; f:r.
no differences between groups were reported.
not include a control group. Antrop et al. (2005b) investigated theinfluence of time of day on the effects of playtime on behaviorin elementary school children with ADHD and normal develop-ing classmates. They found an increase in hyperactive behavior inADHD children only in the afternoon after controlling for severalfactors such as medication (see Table 1).
2.2.2.2. Actigraph research. Analysis of activity in terms of its rela-tive/absolute intensity has revealed distinctive time of day effectsin ADHD. Porrino et al. (1983) registered naturalistic activity levelsin children with ADHD and control children during 7 consecutivedays. They reported that children with ADHD were more activethan control children only during specific hours of the schoolday (7 am, 8 am, 10 am, 11 am, noon, 2 pm, 3 pm, and 5 pm).However, the sample size in their study was small and direct obser-vations were not performed. The authors tried to overcome thisproblem by keeping a diary of the children’s activities. They dis-covered that the hours of increased activity in children with ADHDcoincided with structured school activities (reading and math
classes), but not with recess/lunch periods. Also Tsujii et al. (2007)pointed to the possibility that time of day effects are likely to beconfounded by context effects. They investigated the level of activ-ity in different naturalistic educational settings, e.g., structured
behav
iCddmnsAgptaba–eb
2
hC2ehsMtssc2a2ca2wmdsfttatmotsicawao
2rdaldnet
L. Imeraj et al. / Neuroscience and Bio
n-seat classes and non-structured classes at different times of day.hildren with ADHD were significantly more active than controlsuring structured in-seat lessons in the afternoon, but no groupifferences were found during non-structured classes, or duringorning classes. More recently, Licht and Tryon (2009) found a sig-
ificant group × time of day interaction effect in their naturalistictudy investigating activity levels in a small group of children withDHD and controls during 1 week. As hyperactivity in the ADHDroup was only obvious during daytime and not during nighttimeeriods, the authors suggested that – along with contextual fac-ors – circadian rhythms might play a role in these differentialctivity patterns. Similar findings were obtained in a larger sampley Imeraj et al. (2011). Moreover, their finding of higher daytimectivity levels – especially during noon and early afternoon hours
confirmed an important role for time of day effects in addition tonvironmental conditions in the expression of (afternoon) problemehavior in ADHD.
.2.3. Sleep–wake rhythmsTen reviews on sleep patterns and ADHD in children and adults
ave already been published (Cohen-Zion and Ancoli-Israel, 2004;ortese et al., 2009, 2006; Gruber, 2009; Owens et al., 2009; Owens,005; Philipsen et al., 2006; Sadeh et al., 2006; Van der Heijdent al., 2005a; Walters et al., 2008). In general, sleep studies in ADHDave given mixed results on both subjective (i.e., clinical history,leep diaries, and rating scales) and objective (i.e., actigraphy, andSTL) sleep measures. The presence of different confounding fac-
ors in different studies have been suggested to be responsible forome of these discrepancies, e.g., age and sex (Boonstra et al., 2007),easonal effects (Boonstra et al., 2007), temporal changes in DSMlassification (Cortese et al., 2006), ADHD subtype (Wiggs et al.,005), medication status (Corkum et al., 1999; Cortese et al., 2006),nd psychiatric comorbidity (Corkum et al., 1999; Cortese et al.,006). The relation between ADHD and sleep becomes even moreomplex as sleep-related disorders such as restless leg syndromend sleep apnea can present alongside ADHD (Van der Heijden et al.,005a). Primary sleep disorders may be a true comorbid conditionith idiopathic ADHD, but some children may actually have a pri-ary sleep disorder, misdiagnosed as ADHD, due to the fact that
iurnal manifestations of primary sleep disorders can mimic ADHDymptoms (Chervin et al., 2002; Cortese et al., 2005). As this reviewocuses on the effect of circadian rhythms in ADHD, we concen-rate here on circadian characteristics of the sleep–wake cycle, i.e.,ime of falling asleep, time of awakening, disturbed sleep phases,nd daytime sleepiness, in children and adults with ADHD. As theiming of the sleep–wake cycle is controlled by the circadian pace-
aker (i.e., the process C; Borbély, 1982), alterations in the timingf sleep and awakening could reflect an underlying circadian shift ofhe biological clock. Such disruption can cause significant daytimeleepiness, which is hypothesized to be more pronounced earliern the day. However, daytime sleepiness and nighttime awakeningould also reflect problems in the arousal-sleep “flip-flop” mech-nism pointing to instability of the transition between sleep andake, not necessarily related to specific times of day (Schwartz
nd Roth, 2008). For an overview of the 26 subjective and objectiveriginal papers included, see Table 2 .
.2.3.1. Subjective evaluations. Nighttime parameters with highelevance to the sleep–wake rhythm include sleep onset, sleepuration, nighttime awakenings and difficulties with morningwakenings. Considering sleep onset difficulties and sleep onsetatency, some studies report that children with ADHD show more
ifficulties initiating sleep or have longer sleep onset latency thanormal controls (Hvolby et al., 2009; O’Brien et al., 2003a,b; Owenst al., 2000), whereas other studies report sleep onset problemso be associated with ODD comorbidity and stimulant medicationioral Reviews 36 (2012) 1897–1919 1901
rather than ADHD itself (Corkum et al., 1999; Mick et al., 2000).Higher bedtime resistance in an ADHD population with ODD mayexacerbate sleep complaints. However, an added effect of comor-bid ODD on problematic behavior scores around bedtime was notconfirmed by the study of Hvolby et al. (2009). As Owens et al.(2000) included unmedicated children with ADHD, stimulant med-ication could not be responsible for sleep onset latency problemsreported in their study. With respect to total sleep duration, someauthors reported no differences in sleep duration considering clin-ical samples of children with ADHD and normal controls (Hvolbyet al., 2009; Marcotte et al., 1998; Mick et al., 2000), in contrast toother authors who reported both longer (Corkum et al., 2001) andshorter (Owens et al., 2000) sleep duration in ADHD. Several recentstudies in larger population samples confirmed that short sleepduration is associated with problems related to attentional con-trol and hyperactivity/impulsivity (Paavonen et al., 2009; Pesonenet al., 2010; Touchette et al., 2009). In terms of sleep efficiency,some studies reported more nighttime awakenings in children withADHD compared to normal controls (O’Brien et al., 2003a), whereasothers found no differences (Hvolby et al., 2009; Mick et al., 2000).Although some authors described more difficulties with morningawakenings (Chiang et al., 2010; Corkum et al., 2001; Owens et al.,2009), others found no support for this (Corkum et al., 1999; Micket al., 2000; O’Brien et al., 2003a). With regard to daytime param-eters, excessive daytime sleepiness has consistently been foundto be more common in children with ADHD compared to normalcontrols (Chiang et al., 2010; Cortese et al., 2009; O’Brien et al.,2003a,b; Owens et al., 2009, 2000). To date, there are few stud-ies of adolescents and adults. In adolescence, subjective severity ofsleep problems was related to stimulant medication and comorbiddepressive symptoms (Stein et al., 2002), whereas in adults withADHD, sleep problems such as sleep onset problems, difficultieswith morning awakenings, and daytime sleepiness were reportedto occur independent of stimulant medication and comorbidity(Schredl et al., 2007; Surman et al., 2009).
2.2.3.2. Objective evaluations. Actigraphy is a practical and accu-rate method to assess circadian rhythm disorders as actigraphicdata can also be analyzed in terms of more general patterns of activ-ity and rest as indicative of the sleep–wake cycle (Morgenthaleret al., 2007). Actigraphic studies in ADHD show mixed results(Cohen-Zion and Ancoli-Israel, 2004). Crabtree et al. (2003) found adelayed sleep onset in a group of children with ADHD referred to asleep center. As the authors included both medication treated andunmedicated children, results may be confounded by medicationstatus. However, in unmedicated samples of children with ADHD(children discontinued medication or were medication naïve),shorter sleep duration (Owens et al., 2009) and longer sleep onsetlatency (Hvolby et al., 2008) have been confirmed as comparedto controls. Nevertheless, sleep onset latencies have been shownto increase following stimulant medication in multiple (placebo-controlled) studies (Corkum et al., 2008; Ironside et al., 2010;Schwartz et al., 2004). For example, Barkley et al. (1990) found15% of their subjects with ADHD experiencing insomnia during theplacebo condition and more than 50% in the methylphenidate con-dition. Beneficial effects of medication on some aspects of sleepsuch as nighttime awakenings and parasomnias have also beenreported (Kim et al., 2010).
Not all studies using objective measures have found differen-tiating sleep–wake results in ADHD (Corkum et al., 2001; Daganet al., 1997; Gruber et al., 2000). One explanation for this inconsis-tency is that higher night-to-night variability accounts for similar
mean sleep estimates in ADHD and control groups, despite the factthat standard deviations are significantly different between groups(Crabtree et al., 2003; Gruber et al., 2000; Van der Heijden et al.,2005a). Another possibility is that sleep/wake findings are only
1902 L. Imeraj et al. / Neuroscience and Biobehavioral Reviews 36 (2012) 1897–1919
Table 2Overview of original studies evaluating sleep–wake rhythms with sleep questionnaires and actigraphy in ADHD.
Study by Subjects Age Confounding variablesa Dependent variables andcircumstances ofevaluation
Differential group effects
Boonstra et al. (2007) 33 ADHD, 32 Comb and1 Hyp (16m, 17f); 39NC
ADHD: M 37.9,SD 10.3
Not confounding: age, sex,stimulant medication (notmedicated)Possibly confounding:comorbid depression andanxiety
Actigraphy for 7 nights(placebo condition prior toparticipation in medicationtrial)
Daytime activity:ADHD > NC; nighttimeactivity: ADHD = NCADHD: ↑ sleep onsetlatency, ↓ sleep efficiency,and shorter within-nightperiods of uninterruptedsleep compared to NC
Chiang et al. (2010) 325 ADHD, 174 Comb,130 Inat, 21 Hyp(265m, 60f); 257 NC
10–17 Possibly confounding: sex,age, subtype, psychiatriccomorbidity, stimulantmedication
Psychiatric interview fordiagnosis of ADHD, otherpsychiatric disorders, andsleep problems ordisorders
After controlling forconfounders: all ADHDsubtypes: ↑ insomnia, ↑daytime napping, difficultymorning awakenings, ↑sleep duration comparedto NC; ↑ circadian rhythmproblems in ADHD-Comband ↑ hypersomnia inADHD-Inat
Corkum et al. (1999) 79 unmedicatedADHD; 22 medicatedADHD; 35 clinicalcomparison; 36 NC
6–12 Not confounding: age, sexConfounding: IQ, ADHDsubtype, stimulantmedication, comorbid LD,ODD, CD, anxiety disorder
Sleep questionnaires ADHD: ↑ prevalence ofdyssomnias related tocomorbid ODD andstimulant medication
Corkum et al. (2001) 25 ADHD, 5 Hyp, 6 Inat,14 comb (20m, 5f); 25NC
7–11 Not confounding: age, sex,comorbid ODD and anxietyConfounding: IQ, ADHDsubtype, comorbid CD anddepressive disorder
Sleep questionnaire anddiaryActigraphy for 7consecutive nights
Subjective longer sleepduration, ↑ sleep onset,difficulty morningawakenings, ↑ bedtimeresistance, but noactigraphic differences inADHD compared to NC
Crabtree et al. (2003) 97 ADHD (75m, 22f) ofwhom 16 hadactigraphy and 69 PSGevaluation; no NC
3–18 Confounding: age, sex,stimulant medication,comorbid mood andanxiety disorders
Sleep questionnaireActigraphy for thevaluation of sleep during14 days (+PSG)
Subjective: ↑ prevalence ofsleep complaints (e.g.,difficulties initiating andmaintaining sleep, snoring,enuresis, restless sleep,daytime sleepiness)Objective: ↑ night-to-nightvariability, delayed sleeponset
Dagan et al. (1997) 12 ADHD; 12 NC (m) 6–12 Not confounding: sex,comorbid disordersConfounding: age,stimulant medication
Sleep questionnaireSleep unstructuredinterviewActigraphy for 3 nights
Subjective: ADHD = NCObjective: ↓ sleepefficiency and ↑ nighttimeactivity levels in ADHD, butno difference in sleep onsetor sleep durationcompared to NC
Golan et al. (2004) 34 ADHD (26m, 8f); 32NC (21m, 11d)
ADHD: M 12.4,SD 4.6
Not confounding: age, sex,stimulant medication (stop3 days before assessment)Confounding: BMI
MSTL (+PSG) ADHD: ↑ daytimesleepiness
Gruber et al. (2000) 38 ADHD, 14 Inat, 4Hyp, 20 Comb (m); 64NC (m)
6–14 Not confounding: age, sex,stimulant medication,comorbid ODD/CD
Actigraphy for 5consecutive nightsSleep logs
ADHD: ↑ night-to-nightvariability in sleepestimates
Hvolby et al. (2008) 45 ADHD, 64 otherpsychiatric disorder, 97NC (total: 153m, 53f)
5–11 Not confounding:stimulant medicationPossibly confounding: age,sexConfounding: comorbidODD, CD, emotionaldisorders
Actigraphy for at least 5consecutive nights
ADHD: ↑ sleep onsetlatency and more irregularsleep pattern thanpsychiatric control and NCgroup. No effect ofcomorbid ODD
Hvolby et al. (2009) 45 ADHD, 64 otherpsychiatric disorders,212 NC
5–11 Not confounding:stimulant medicationConfounding: age, sex,comorbid disorder ODD,CD, emotional disorders
Sleep questionnaire ADHD: ↑ sleep onsetlatency, but no differenceregarding numbers ofawakenings per night andtotal sleep time per night.No added effect ofcomorbid ODD
Lecendreux et al. (2000) 30 ADHD (m); 22controls with LD
5–10 Not confounding: age, sex,pubertal stage, stimulanttherapy, comorbidpsychiatric disorders
MSTL ADHD: ↑ daytimesleepiness

L. Imeraj et al. / Neuroscience and Biobehavioral Reviews 36 (2012) 1897–1919 1903
Table 2 (Continued)
Study by Subjects Age Confounding variablesa Dependent variables andcircumstances ofevaluation
Differential group effects
Marcotte et al. (1998) 43 ADHD; 11 LD; 25ADHD/LD; 86 NC
6–12 Not confounding: age, sex,stimulant medication
Sleep questionnaire ↑ sleep and breathingproblems and ↑ sleepinessin ADHD, LD, and ADHD/LDcompared to NC, but nodifferences betweenclinical groups
Mick et al. (2000) 122 ADHD; 105 NC 12–17 Not confounding: agePossibly confounding: sexConfounding: comorbidity,stimulant medication
Sleep questionnaire ↑ subjective sleepproblems in ADHD (e.g.difficulty falling asleep,nighttime awakenings, anddifficulty waking up), butfrequently accounted forcomorbidity and stimulantmedication
O’Brien et al. (2003a) 44 severe ADHDsymptoms; 27 mildADHD symptoms; 39NC, all from generalpopulation
5–7 Not confounding:comorbid psychiatricsymptomsPossibly confounding: age,sex, stimulant medication
Behavioral assessmentsSleep questionnaire (+PSG)
ADHD symptoms ∼ morenighttime awakenings,difficulty initiating sleep,and daytime sleepiness
O’Brien et al. (2003b) 53stimulant-medicatedADHD; 34non-medicated ADHD;53 NC
5–7 Not confounding: ageConfounding: sex,comorbid disorders
Sleep habits questionnaire(+PSG)
Both medicated andnon-medicated childrenwith ADHD: ↑ nightmares,↑ enuresis, but nosignificant difference indaytime sleepiness. Nosignificant effect of MPH
Owens et al. (2000) 46 ADHD; 46 NC 5–10 Not confounding: age, sex,stimulant medication (nocurrent use), comorbiddepression and anxietydisorderConfounding: comorbidODD/CD, and LD
Sleep questionnaire ADHD: ↑ sleepdisturbances reported byparents (e.g., ↓ sleepduration, ↑ sleep onsetlatency, daytimesleepiness) and children (↑bedtime resistance)
Owens et al. (2009) 80 ADHD; 45 NC 6–14 Not confounding: age, BMI,stimulant medication (nocurrent use)Confounding: sex, ADHDsubtype, comorbid ODD
Diary on sleep and daytimebehaviorActigraphy for at least 5consecutive days
Subjective: more daytimesleepiness and difficultygetting up on child-report;difficulty falling asleep anddifficulty getting up onparent-reportObjective: shorter actualsleep time, fewer sleepinterruptions, but moretotal interrupted sleep inADHD
Paavonen et al. (2009) 280 children fromgeneral population(146f, 134m) weredivided in short,average, and longsleepers (based onsleep questionnaire)
7–8 ActigraphSleep questionnaireADHD rating scale
Behavioral symptoms ofADHD ∼ ↓ sleep duration
Pesonen et al. (2010) General population(145f, 135m)
8 Behavioral assessments(Child Behavior Checklist)Actigraph for 7 nights(range: 3–14)
Short sleepduration ∼ problems inattentional control andexternalizing behaviors;irregularity in sleepduration ∼ internalizingproblems
Schredl et al. (2007) 120 ADHD (64f, 56m)(31 Inat, 87 Comb, 2Hyp) from whom 61without comorbidity,current substanceabuse, and medicationintake; 444 NC
18–62 Possibly confounding: age,sex, subtype, stimulantmedication,antidepressants, comorbiddepression, anxietydisorder, tic disorder, OCD,substance abuse
Sleep questionnaires ADHD without comorbidityand without medicationintake: ↑ sleep problems(e.g., feeling unrefreshed inthe morning); comorbidityand depressivesymptoms ∼ insomnia. Noeffect of medication
Stein et al. (2002) 32 non-medicatedADHD (m); 35medicated ADHD; 77NC (m)
13–16 Not confounding: sex, age,comorbid sever behavioralproblems, internalizingdisorders, and drug abuseConfounding: medication,internalizing symptoms
Sleep questionnaire Severity of sleepdisturbance:non-medicatedADHD = NC < medicatedADHD with an added effectof depressive symptoms

1904 L. Imeraj et al. / Neuroscience and Biobehavioral Reviews 36 (2012) 1897–1919
Table 2 (Continued)
Study by Subjects Age Confounding variablesa Dependent variables andcircumstances ofevaluation
Differential group effects
Surman et al. (2009) 182 ADHD; 117 NC 18–55 Not confounding: sexPossibly confounding: age,comorbid internalizingdisorders, stimulantmedication
Sleep questionnaire ADHD: later bedtimes, ↑sleep onset latency,difficulty going to bed andwaking in the morning, ↑daytime sleepiness,independent of stimulanttherapy and comorbidity
Touchette et al. (2009) 2057 children from thegeneral population
1.5–5 Questionnaire to assessdevelopmental trajectoriesof nighttime sleep durationand hyperactivity
Hyperactivity ∼ nighttimesleep duration
Van der Heijden et al. (2005b) 87 ADHD with SOI, 33ADHD without SOI
6–12 Not confounding:stimulant medication(naïve)Possibly confounding: age,sex, comorbid ODD,anxiety disorder, affectivedisorder
Actigraphy for 7consecutive daysDLMO (hourly from 6 pmto 10 pm)
ADHD with SOI: delayedsleep phase and delayedDLMO, compared to ADHDwithout SOI
Van Veen et al. (2010) 40 ADHD (21m, 19f) ofwhom 31 reported SOI;38 NC
18–55 Not confounding: age, sex,stimulant medication,melatonin,antidepressants,antipsychotics (free for atleast 1 month)Possibly confounding:ADHD subtype, comorbiddepression and anxiety,nicotine
Actigraphy for 7 daysDim light melatonin onsetduring 1 night at hourlyintervals between 9 pm to1 am
Both groups of ADHD: ↑sleep onset latency and ↓sleep efficiency comparedto NCADHD with SOI: delayedstart and end of their sleepperiod and a delayedmelatonin onset comparedwith ADHD without SOIand NC
Wiggs et al. (2005) 71 ADHD (63m, 8f); 23NC
3–15 Not confounding: age, sex,stimulant medication(non-medicated)
Sleep diaryClinical historyActigraphy for 5 nights
Subjective sleepdisturbances (e.g., sleepinitiation problems) inADHDNo objective groupdifferences in sleeppatterns
Note. Both clinical and general population studies are considered. Medication intervention studies were not included in this table. ADHD: attention-deficit hyperactivityd hyperC : poly
when
adasiotliord2fs(lnIscsuc
dtT
isorder; NC: normal control; Comb: combined type; Inat: inattentive type; Hyp:
D: conduct disorder; LD: learning disorder; MSTL: multiple sleep latency test; PSGa Variables were considered as not confounding when subjects were matched, or
pplicable to a specific subgroup of children with ADHD as Vaner Heijden et al. (2005b) reported different findings in ADHD with
comorbid sleep disorder and ADHD without sleep problems. Aubgroup of children with ADHD and comorbid chronic sleep onsetnsomnia (SOI) disorder, compared to children with ADHD with-ut sleep problems, showed a delayed sleep onset (on actigraphy)ogether with a delayed onset of the nocturnal melatonin peak (dimight melatonin onset, DLMO). As no control group was includedn this study, one cannot be certain to what extent ADHD withr without SOI would differ from controls. Parallel findings haveecently been obtained in adults with ADHD and SOI (significantifferences between ADHD with and without SOI; Van Veen et al.,010). However, the authors also included a normal control grouprom which both ADHD with SOI and ADHD without SOI differed inleep onset latency and sleep efficiency. Similarly, Boonstra et al.2007) reported that adults with ADHD (irrespective of SOI) takeonger to fall asleep, have lower sleep efficiency, and shorter within-ight periods of uninterrupted sleep compared to normal controls.
t is possible that the biological clock influencing the timing ofleep–wake cycles is set to a later time in children with ADHD asompared to controls. The DLMO additionally reflects this delayedleep timing. The use of melatonin as a marker for circadian eval-ation and the effect of melatonin treatment to reset the circadianlock in ADHD are discussed below.
Two studies using the MSLT reported significantly moreaytime sleepiness in children and adolescents with ADHDhan in controls (Golan et al., 2004; Lecendreux et al., 2000).his means that subjects with ADHD have shorter sleep onset
active-impulsive type; m: males; f: females; ODD: oppositional-deviant disorder;somnography; DLMO: dim light melatonin onset; SOI: sleep onset insomnia.
no differences between groups were reported.
latency during one or more daytime naps. Although childrenwith ADHD were more sleepy throughout the day, Golan et al.(2004) observed the most severe sleepiness was in the morn-ing (8 am). This finding is consistent with a delayed circadianrhythm in ADHD. In a driving simulation experiment, similarresults were obtained in adult drivers with ADHD: they weremore susceptible to fatigue earlier in the day (Reimer et al.,2007).
Altogether, a majority of studies on sleep–wake rhythms sup-port a delayed sleep phase syndrome, suggestive of a disruption ofthe 24-h sleep/arousal control, in (at least a subgroup of) subjectswith ADHD. Several factors may have confounded these results(see Table 2 for more detailed study-specific information). How-ever, a recent meta-analysis by Cortese et al. (2009), controlling formedication status and comorbidity, confirmed more sleep onsetdifficulties, night awakenings, difficulties with morning awaken-ings, higher sleep onset latency and lower sleep efficiency inchildren with ADHD (irrespective of comorbid SOI diagnosis). Thesecharacteristics provide additional support for the hypothesis ofa delayed sleep phase syndrome in ADHD. As this meta-analysisdid not consider other confounding factors (e.g., comorbid anxi-ety or depression, stress, difficulty settling down), it needs to befurther determined to what extent these problems are specificto ADHD (or at least to a subgroup of ADHD). To address these
issues a transdiagnostic approach has been proposed in the treat-ment of insomnia across a variety of psychiatry disorders (Harveyet al., 2011). This approach could be especially useful in relation toADHD given that SOI problems occur in up to 54% of ADHD cases
behav
a2
2n
rli
2ucstdaceBaa
aK2aAiTndawoiHflsDAwAn
tac2iSasaccieole
2aw
L. Imeraj et al. / Neuroscience and Bio
ffecting daily functioning and quality of life (Tjon Pian Gi et al.,003).
.2.4. Circadian effects on neuroendocrine andeurophysiological processes
To date, research using neuroendocrine (e.g., cortisol) and neu-ophysiological (e.g., heart rate) measures in ADHD is mainlyaboratory-based. However some data from more naturalistic stud-es measuring across the day changes is available.
.2.4.1. Melatonin. Melatonin is an interesting hormonal markersed in the evaluation of circadian rhythms which affects the cir-adian regulation of different biological functions, including theleep–wake cycle. Melatonin production by the pineal gland andhe retina occurs at night such that concentrations are very lowuring daytime, increase at nightfall (DLMO) and peak around 3–4m (Haus, 2007). DLMO production is the most reliable marker ofircadian phase position (Hofstra and de Weerd, 2008; Klermant al., 2002; Van der Heijden et al., 2005b; see also Macchi andruce (2004), Claustrat et al. (2005), and Benloucif et al. (2008) for
more detailed description of melatonin regulation, secretion, andnalysis).
Deviant melatonin levels have been related to several psychi-tric disorders including depression, mania (Crasson et al., 2004;ennedy et al., 1996), and seasonal affective disorder (Lewy et al.,006). Very recently, Chaste et al. (2011) provided the first geneticscertainment of defects in the melatonin pathway of patients withDHD. Two studies have examined endogenous melatonin rhythms
n children with ADHD and there is one study in adults (see alsoable 2). Compared to control subjects, Nováková et al. (2011) didot report different 24-h melatonin profiles in their group of chil-ren with ADHD (6–12 y). However, when considering youngernd older subgroups separately, subtle developmental differencesere revealed: i.e., in the oldest children with ADHD (10–12 y)
nly the onset, but not the offset, phase delayed with increas-ng age. In their group of children with ADHD (6–12 y), Van dereijden et al. (2005b) reported that 73% of subjects met the criteria
or sleep onset insomnia. Based on the measurements of activityevels and DLMO, they found evidence for a delayed sleep phaseyndrome, i.e. longer sleep onset, later wake-up time, and delayedLMO (Nagtegaal et al., 1998), in their subgroup of children withDHD and comorbid chronic SOI compared to the group with ADHDithout sleep problems. This has been confirmed in adults withDHD with SOI compared to adults with ADHD without SOI andormal controls (Van Veen et al., 2010).
The therapeutic use of exogenous melatonin (5 mg melatonin inhe evening), used to reset the timing function of the SCN, is associ-ted with advanced sleep onset and DLMO compared to placebo inhildren with idiopathic chronic sleep onset insomnia (Smits et al.,001, 2003). Also in children with ADHD, melatonin administration
s considered to be an effective treatment of initial SOI (Bendz andcates, 2010). Significant improvement in sleep parameters suchs sleep onset and sleep onset latency were described in both non-timulant treated (Hoebert et al., 2009; Van der Heijden et al., 2007)nd stimulant treated (Tjon Pian Gi et al., 2003; Weiss et al., 2006)hildren with ADHD and insomnia. Although melatonin resets theircadian timing system, no effect of melatonin on daytime behav-or symptoms could be observed in the study of Van der Heijdent al. (2007). In contrast, parents stated that melatonin was notnly effective for sleep onset insomnia, but also for behavior prob-ems in the 3-year follow-up assessment of this sample (Hoebertt al., 2009).
.2.4.2. Cortisol. The hypothalamic-pituitary-adrenal (HPA) axis islso sensitive to time information from the SCN (Haus, 2007),hich is reflected in a typical diurnal cortisol pattern with a
ioral Reviews 36 (2012) 1897–1919 1905
trough (the nadir) around midnight. In normal subjects, cortisolconcentrations gradually increase 2–3 h after bedtime, with apeak (the acrophase) 30–45 min after awakening, i.e., the cortisolawakening response. Levels then decrease gradually to nighttimeconcentrations (Buckley and Schatzberg, 2005; Edwards et al.,2001). Cortisol level in saliva is a reliable peripheral measure ofarousal (see also Levine et al. (2007) for a review on the analysis ofcortisol).
With respect to ADHD, cortisol levels have mostly been mea-sured in response to stress (Hong et al., 2003; Randazzo et al.,2008; Shin and Lee, 2007; Snoek et al., 2004; van West et al., 2009),although a few attempts have been made to evaluate the influenceof time of day. Although most of the stress response studies alsodescribe basal cortisol levels on a single pre-stress measurement,results on this measure are inconsistent and have only limited valuein the evaluation of diurnal cortisol patterns. Intra- and inter-dayvariability in individual cortisol patterns requires an evaluationusing repeated cortisol measures across several days (Bartels et al.,2003; Edwards et al., 2001; Houtveen and de Geus, 2009; Schulzet al., 1997). To our knowledge, such an ‘ideal’ investigation has onlybeen applied in one study (Imeraj et al., 2012). We therefore includestudies with multiple measurements across 1 day (combined morn-ing and basal sampling), but also studies including awakening orbasal samples only. For an overview of the 13 studies considered,see Table 3 .
Most studies of diurnal patterns of cortisol have found a rela-tionship between ADHD symptoms and altered circadian cortisolpatterns. Results are inconsistent however showing both hypo-and hyperarousal deviations at different time points. Consideringstudies with repeated measurements across 1 day, Kaneko et al.(1993) originally found a normal diurnal cortisol pattern in only43.3% of the children with ADHD, suggesting a dysregulation of theHPA axis in the majority of children. Though Pesonen et al. (2011)could not find an association beween ADHD symptoms and diurnalcortisol profile in 8-year-old children from the general population,other authors did. In a slightly older population sample, Susmanet al. (2007) reported a small morning-to-afternoon cortisol ratioin boys – but not girls – with attention problems, which suggestsan atypical circadian rhythm. Also Sondeijker et al. (2007) reportedADHD problems to be associated with higher basal evening cortisollevels in a general child population sample. However, they reportedthe opposite effect of sex of child compared to Susman et al. (2007)with high rates of ADHD problems being associated with higherawakening cortisol levels in boys, but not in girls. Studies con-sidering only awakening values also suggested a dysregulation ofthe HPA axis in ADHD, although findings were inconsistent. Someauthors found a lower cortisol awakening response in a group ofchildren with ADHD compared to a group of controls (Blomqvistet al., 2007; Ma et al., 2011), whereas Hatzinger et al. (2007)found higher morning peak levels in a much younger populationsample of boys with hyperactivity symptoms. In contrast to pre-vious findings, two recent studies failed to find any difference onmorning cortisol between children with ADHD (without comorbiddisorders) and control children (Freitag et al., 2009; Wang et al.,2011). Only one study has examined this in adults which reportedno effect of ADHD diagnosis (Hirvikoski et al., 2009): both theoverall cortisol levels and the typical diurnal cortisol rhythm,including the awakening response, were normal in ADHD.
Considering the high comorbidity rates of ODD in ADHD, incon-sistent results may be explained by confounding effects of ODD.According to the hypo-arousal theory (Quay, 1965; Raine, 1996),disruptive disorders such as ODD and CD are linked to lower basal
cortisol levels and lower stress responses (McBurnett et al., 2000;Moss et al., 1995; van Goozen et al., 2000, 1998), but also to lowermorning values (Pajer et al., 2001; Shirtcliff et al., 2005). Resultsrelating to ADHD with comorbid ODD/CD are inconsistent. Some
1906 L. Imeraj et al. / Neuroscience and Biobehavioral Reviews 36 (2012) 1897–1919
Table 3Overview of original studies evaluating circadian cortisol rhythms in children and adults with ADHD.
Study by Subjects Age Confounding variablesa Dependent variables andcircumstances ofevaluation
Differential group effects
Blomqvist et al. (2007) 18 ADHD, 13 Comb (15m, 3f); 71 NC (47m, 24f)
13 Not confounding: age,glucocorticoïd medicationConfounding: stimulantmedication, sex, ADHDsubtype
Saliva cortisol: collected ona school day: one uponawakening and one 30 minlater
ADHD: ↓ cortisol levels30 min after awakeningthan NC
Freitag et al. (2009) 123 ADHD; 69 NC 6–12 Not confounding: ageConfounding: sex, ADHDsubtype stimulantmedication, comorbidODD, CD, anxiety disorder
Saliva cortisol: collected on2 consecutive weekenddays: immediately afterawakening, and 30, 45, and60 min thereafter
Cortisol awakeningresponse: ADHD withODD < ADHD withoutODD/CD = NC
Hastings et al. (2009) 170 ADHD, 59 Inat, 25 Hyp,86 Comb (m); no NC
6–11 Not confounding:stimulant medicationConfounding: ADHDsubtype and comorbiddisorders
Saliva cortisol: one samplecollected within 15 min ofwaking
No association betweenwaking cortisol levels andcomorbid diagnoses orproblems in children withADHD
Hatzinger et al. (2007) 102 pre-schoolers from thegeneral population
5 Behavioral emotionalassessmentSaliva cortisol samples:collected at 0, 10, 20, and30 min after awakeningduring one regularweekday
Hyperactivity/impulsivitysymptoms in boys ∼ ↑ HPAaxis activity
Hirvikoski et al. (2009) 28 ADHD, 24 Comb, 4 Inat;28 NC
19–54 Not confounding: age, sexConfounding: comorbiddepression and anxietydisorder
Saliva cortisol: collectedduring a separateweekday: after awakening,30 min after awakening,between 5 pm and 6 pm,and at bedtime, or, at thelatest, at 11 pm
Overall cortisol levels anddiurnal cortisol rhythm:ADHD = NC
Imeraj et al. (2011) 31 ADHD (all Comb; 22with and 11 without ODD);31 NC
6–12 Not confounding: age, sex,comorbid ODD andinternalizing disorders,stimulant medication
Saliva cortisol: collected atfive times a day(awakening, 30 min afterawakening, noon, 4 pm, 8pm) across 5 consecutivedays
Cortisol awakeningresponse: ADHD = NCDiurnal cortisol profilesacross the day: significantgroup × time effectassociated with thepresence of absence ofODD comorbidity (ADHD:flatter slope with relativemorning hypo-arousal andevening hyperarousal;ADHD with ODD: steeperslope with relativemorning hyperarousal andevening hypo-arousal)
Kaneko et al. (1993) 30 ADHD (25m; 5f); 30controls with ASS
ADHD: M 8.6SD 3.3
Not confounding: age, sex,comorbid depressivedisorderPossibly confounding:comorbid ODD, stimulantmedication
Saliva cortisol: collected at8 am, 10 am, noon, 4 pm, 8pm, and 10 pm, and anextra morning sample onsecond day
ADHD: majority had nonormal diurnal cortisolrhythm
Ma et al. (2011) 128 ADHD (44 Inat, 52Comb, 32 Hyp); 30 NC
6–14 y Not confounding: age, sex,psychiatric comorbidity,ADHD subtypePossibly confounding:intelligence, stimulantmedication
Plasma cortisol (and ACTH)collected at 8 am
ADHD: ↓ morning cortisollevels than NCHyp: ↓ morning cortisollevels than Inat and CombADHD
Pesonen et al. (2011) General population (143m;129f)
8 Behavioral assessment(ADHD rating scale andChild Behavior Checklist)Saliva cortisol: collected atawakening, 15 min afterawakening, 30 min afterawakening, 10:30 am,noon, 5 pm, bedtime
No association betweenADHD symptoms anddiurnal cortisol pattern
Schulz et al. (1997) 23 aggressive boys withADHD; 27 nonaggressiveboys with ADHD
7–11 Not confounding: age, sex;IQ, medication (free for atleast 4 weeks), comorbiddepression or anxietydisorderConfounding: CD
Plasma cortisol: collectedat 9:45 am and 9:55 am
Cortisol levels: aggressiveADHD = nonaggressiveADHD

L. Imeraj et al. / Neuroscience and Biobehavioral Reviews 36 (2012) 1897–1919 1907
Table 3 (Continued)
Study by Subjects Age Confounding variablesa Dependent variables andcircumstances ofevaluation
Differential group effects
Sondeijker et al. (2007) 1768 children from thegeneral population
10–12 Behavioral questionnairesSaliva cortisol: collected ona normal day, shortly afterwaking up, half an hourlater, and at 8 pm
ADHD problems ∼ ↑cortisol levels at 8 pm
Susman et al. (2007) 111 children from thegeneral population
8–13 (CMEP)Saliva cortisol: collected ona nonschool day:immediately afterawakening, 20 minpostwake time, 40 minpostwake time, at noon, at4 pm, and at bedtime
Attention problems ∼ ↓ amto pm cortisol ratio in boysonly
Wang et al. (2011) 50 ADHD; 50 NC 6–12 y Not confounding: age, sex,psychiatric comorbidity,stimulant medication
Saliva cortisol (and DHEA)was collected at 8 AM
Morning cortisol:ADHD = NC
Note. ADHD: attention-deficit hyperactivity disorder; NC: normal control; Comb: combined type; Inat: inattentive type; Hyp: hyperactive-impulsive type; m: males; f:f isorde
when
awvaldasrVbIfi8iosrtm
2nblebMofkcabe
c(22CtaH
emales; ODD: oppositional-deviant disorder; CD: conduct disorder; LD: learning da Variables were considered as not confounding when subjects were matched, or
uthors confirmed a hypo-arousal pattern in children with ADHDith ODD measuring both awakening (Freitag et al., 2009) and basal
alues (Kariyawasam et al., 2002) while other authors failed to findny robust association between waking levels and comorbid prob-ems in ADHD (Hastings et al., 2009). In line with these findings, noifferences in basal levels between ADHD children with aggressionnd without aggression have been reported (Schulz et al., 1997),uggesting the possibility that certain characteristics of ADHD,ather than aggression, could be associated with cortisol levels.ery recently, this complex relation between ADHD/ODD comor-idity and diurnal cortisol profiles has become a focus of interest.
n the study of Imeraj et al. (2012), salivary cortisol was sampledve times a day (awakening, 30 min after awakening, noon, 4 pm,
pm). Their findings supported time-related arousal disruptionsn children with ADHD associated with the presence or absencef ODD comorbidity. More specifically, it seemed that the ADHDubgroup without ODD comorbidity showed a flatter slope withelative morning hypo-arousal and evening hyperarousal, whereashe ADHD with ODD subgroup showed a steeper slope with relative
orning hyperarousal and evening hypo-arousal.
.2.4.3. Heart rate. As arousal involves activation of the autonomicervous system, physiological dysregulation of this system coulde related to several psychiatric disorders involving arousal prob-
ems (Dietrich et al., 2007; Lorber, 2004; Ortiz and Raine, 2004). Forxample, a relation between low basal heart rate and disruptiveehaviors has been established by several authors (Lorber, 2004;ezzacappa et al., 1997; Ortiz and Raine, 2004). However, results
n autonomic functioning in ADHD are less clear. Moreover, studiesocusing on full circadian patterns are still limited despite the well-nown time of day effects in heart rate. Recently, normal intrinsicircadian rhythms have been described (Waterhouse et al., 2007):n average day–night difference in resting heart rate of 6.5 bpm haseen replicated by several authors (Burgess et al., 1997; Kerkhoft al., 1998; Scheer et al., 2003).
Research in relation to ADHD has mainly focused on spe-ific laboratory conditions such as stress inducing performanceLackschewitz et al., 2008), peer provocation (Waschbusch et al.,002), performance (Borger and van der Meere, 2000; Crone et al.,003), and reward (Beauchaine et al., 2001; Crone et al., 2003;
rowell et al., 2006; Iaboni et al., 1997; Luman et al., 2007). Pre-est heart rate usually did not differ between subjects with ADHDnd normal controls (Iaboni et al., 1997; Lackschewitz et al., 2008).owever, these levels may be influenced by anticipatory stress andr; CMEP: child morningness–eveningness preference scale no differences between groups were reported.
studies have tended not to investigate time of day fluctuations inADHD. Only recently, a study on 24-h heart rate patterns in ADHDhas been completed (Imeraj et al., 2011).
Crowell et al. (2006) reported lower basal heart rate (pre-testvalue) in children with ADHD with ODD. Herpertz et al. (2001)compared ADHD groups with and without comorbid CD – theyreported lower autonomic responses in the comorbid but not inthe ADHD-only group, relative to controls. Although non-specificskin conductance responses were significantly different betweengroups in this study, this was not the case for resting heart ratelevels. In contrast, van Lang et al. (2007) reported a higher meanbasal heart rate (measured between 1 pm and 5 pm) in a group ofchildren with high scores on ADHD with CD/ODD compared to agroup with ADHD without comorbidity. These results suggest thatdifferences in basal heart rate and autonomic functioning could bedue to confounding effects of comorbidity, medication, and time ofday.
Recently, Tonhajzerova et al. (2009) found that unmedicatedchildren with ADHD without comorbid disorders were more likelyto display tachycardia compared to normal controls during a short-term evaluation (three intervals of 5 min) in both supine positionand orthostasis. These measurements were conducted between 8am and noon. Although this study was limited by a small sampleand possible confounding effects of stress in a laboratory setting,spectral analysis of these results indicated changes in the cardiacautonomic regulation, i.e., decreased cardiac vagal modulation insupine position and altered ability of dynamic activation of theautonomic nervous system in response to orthostasis. It has beenhypothesized that such an autonomic imbalance – low parasympa-thetic activity and a relative sympathetic dominance – reflects lowheart rate variability, a marker for prefrontal hypo-activity (Thayerand Sternberg, 2006) as seen in ADHD (Arnsten, 1998; Halperinand Schulz, 2006; Himelstein et al., 2000; Valera et al., 2007). Veryrecently, the finding of higher heart rate levels in non-medicatedchildren with ADHD was confirmed during a 5-day heart rate regis-tration study (Imeraj et al., 2011). Additional analyses revealed thatgroup effects were larger at specific times of the day, namely after-noon and nighttime hours; a finding independent of activity andcomorbid psychiatric disorders. The authors suggested that time ofday may be an important contributor to alter heart rate patterns
in ADHD. Especially the increase in nighttime levels, i.e., restingheart rate, seems important as this measure refers to a lower vagaltone which is associated with cardiovascular disease and mortality(Thayer and Lane, 2007).
1 behav
2o
paliatwltsgm
edwdAbnrcs
sssscutawmidirte
ttbPlshcis2e
etaoabtaa
in unmedicated children with ADHD, this might question the use
908 L. Imeraj et al. / Neuroscience and Bio
.2.5. Summary of findings, limitations and clinical implicationsf research to date
Although patchy and inconsistent, this review found initial sup-ort for disrupted circadian rhythms in ADHD with respect to eachrea reviewed. First, a circadian phase delay was suggested in (ateast a subgroup of) subjects with ADHD. This evidence was clearestn relation to chronotypology and sleep–wake rhythms, pointing ton association of ADHD with self-reported optimal arousal later inhe day (i.e., eveningness) and with later sleep times, difficultiesith morning awakenings, and excessive daytime sleepiness ear-
ier in the day. The idea that the biological clock is responsible forhis delayed timing of sleep-arousal states in ADHD was furtherupported by melatonin studies showing a delayed DLMO in a sub-roup of subjects with ADHD and chronic SOI, which improved afterelatonin treatment.Second, on the behavioral level, studies supported time of day
ffects in attention, performance, and activity. However, groupifferences were particularly expressed during afternoon hours,hich runs counter to the previously hypothesized circadian phaseelay. One possibility is that optimal arousal levels in children withDHD are set at later times of the day as compared to controls,ut both still occur in the morning/noon rather than the after-oon. Alternatively, more overt problematic behavior could be theesult of a complex interaction between specific times of day (espe-ially afternoon) and contextual conditions (e.g., high cognitive,elf-regulatory demands).
Finally, published data on across the day fluctuations in corti-ol and heart rate, although inconsistent, provide some additionalupport for this point of view. With respect to cortisol, most dataupport differential diurnal cortisol patterns in ADHD, but thepecific time points (awakening vs. evening) responsible for thisircadian effect could not been established. Very recently, the eval-ation of diurnal cortisol patterns during multiple days revealedhat ADHD with or without ODD subgroups may be hypo- vs. hyper-roused at different times of the day (Imeraj et al., 2012). Despiteell-established across the day fluctuations in heart rate in nor-al populations, in ADHD, this measure has mostly been examined
n relation to stress without taking into account possible time ofay effects. There is only one longer-term evaluation of heart rate
n ADHD. In this study, children with ADHD showed higher heartate levels which were particularly expressed during the night andhe afternoon, suggesting that circadian effects are important inxplaining autonomic dysfunction in ADHD (Imeraj et al., 2011).
These results must be interpreted in the light of study limita-ions. First, most of the studies were not designed to investigateime of day effects in ADHD and so the results may be confoundedy factors that influence the endogenous biological clock function.otential confounders include; (i) environmental factors such asight, climate and latitude; (ii) developmental factors such as age,ex, pubertal stage, menstrual cycle stage; (iii) factors related toealth status (including tobacco use, caffeine intake, and alcoholonsumption) and disease characteristics (including ADHD sever-ty, subtype, comorbidity, and medication status); and (iv) factors astress, digestion, motivation, and physical exercise (Atkinson et al.,007; Blatter and Cajochen, 2007; Carskadon et al., 1993; Corteset al., 2006; Portaluppi et al., 2008).
Second, studies have typically used a small number of measuresvaluated during relative short observation periods. This limitshe interpretability and generalizability of results across biologicalnd psychological systems. In circadian research, combinationsf measures have been suggested to be important as interactionsnd common pathways between several circadian markers haveeen described. For example, there is a mutual link between
he autonomic nervous system and the HPA axis: sympatheticctivation results in higher production of CRF and therefore,lso of cortisol; inversely, corticotropin releasing factor (CRF)ioral Reviews 36 (2012) 1897–1919
stimulates noradrenergic neurons (Chrousos and Gold, 1998;Sondeijker et al., 2007). Also interactions between melatonin andcardiovascular function (Scheer et al., 2003; Zawilska et al., 2009),between melatonin and body temperature (Zawilska et al., 2009)and between HPA axis functioning and sleep patterns have beenreported (Buckley and Schatzberg, 2005; Edwards et al., 2001).High inter- and intra-day variability in these circadian measureswarrants longer-term evaluations (Bartels et al., 2003; Edwardset al., 2001; Houtveen and de Geus, 2009; Schulz et al., 1997).
Finally, previous research does not assess which mechanismsmay underpin the association of disrupted circadian rhythms andADHD and does not allow inferences to be drawn about the causalrole of such circadian effects. On the one hand, a delayed timing ofsleep-arousal states by the SCN seems to be important in subjectswith ADHD. Though this finding could probably not be generalizedto all subjects, considering the heterogeneous nature of ADHD, adisrupted circadian regulation of arousal could aggravate ADHDsymptoms or could even represent a specific developmental path-way in at least some cases. On the other hand, in general, arousaldysregulation in ADHD seems to be associated with a more com-plex pattern of behavioral problems throughout the day, whichare even more expressed in interaction with environmental andstress-related events.
Despite inconsistencies in studies and methodological limita-tions the emerging evidence for circadian effects may eventuallyhave practical value. For example, children with ADHD and comor-bid insomnia (aged 6–14) were reported to benefit from exogenousmelatonin administration – with or without combined stimulantmedication treatment. It may therefore be valuable to routinelyevaluate sleep problems in ADHD to detect this subgroup andimprove their outcomes. Although light therapy seems effective inadults with ADHD and a delayed sleep phase (Rybak et al., 2004), sofar, no melatonin medication studies in this population are avail-able. Well-designed studies to establish optimal dosing regimensfor different age groups and long-term safety are needed (Bendzand Scates, 2010).
Identifying the afternoon as a period of risk for ADHD (espe-cially when there is an overlap with high environmental demands)may encourage further educational adaptations considering thetiming of academic lessons. Relatedly, adjustment of dosing andtiming of ADHD medication to optimally observe and treat prob-lematic behavior considering its fluctuating expression shouldbe considered. Although some studies have already attemptedto adapt medication dose-release methodology to behaviouralneeds throughout the day (Chavez et al., 2009; Pelham et al.,2001; Sonuga-Barke et al., 2004; Swanson et al., 2004), treatmentresponse curves across the day are still insufficiently documented(Sonuga-Barke et al., 2008b) and systematic methods of assessmentof time of day effects for clinical purposes need to be further devel-oped. Though the specific mechanisms that may underpin time ofday effects in arousal dysregulation are still unknown, such knowl-edge may guide specific therapeutic choices for individual patientsas arousal levels are often the target of focus for interventions. Forexample, according to Stadler et al. (2008), children with a lowerbasal heart rate, i.e., lower autonomic arousal, profit less from psy-chotherapy than children with higher basal heart rate. In contrast,stimulant medication increases arousal, and it may therefore beespecially useful at times of underarousal (Hermens et al., 2007;but see Section 3.3 for more detailed information on action mecha-nisms). Such adaptations in the timing of arousal-based treatmentsmay be particularly relevant in different ADHD subgroups (e.g.,with or without ODD). As nighttime tachycardia has been reported
of stimulant medication that could further increase heart rate lev-els (Daniels, 2009; Hammerness et al., 2011). Though Vitiello et al.(2012) concluded that stimulant treatment in ADHD probably does

behav
npbreact2
3hc
etetletAhoiAwibecomFieaptit(rtAfr
3
saaita2Lacar
L. Imeraj et al. / Neuroscience and Bio
ot increase the risk for hypertension over a 10-year period, theersistent adrenergic effect on heart rate during treatment maye an important issue especially for adult’s with ADHD who are atisk due to higher rates of adult obesity and tobacco use (Cohent al., 1999; Young and Bray, 2007). As in normal populations,n association of circadian misalignment with obesity and otherardiovascular risk factors has been reported, this could even fur-her increase health risks in ADHD (Gangwisch, 2009; Scheer et al.,009).
. LC-mediated arousal dysfunction in ADHD – a workingypothesis linking context-driven, cognitive energetic, andontext-independent circadian-based alterations
Studies to date provide a fragmented pattern of circumstantialvidence linking ADHD to altered circadian rhythms. A more sys-ematic approach to studying the relationship between time of dayffects and ADHD needs to be established and this in turn needso be built on a platform underpinned by biologically and psycho-ogically plausible models. Here we describe one such frameworkstablished on a working hypothesis of the biological basis of puta-ive circadian disruptions in ADHD, their links to other aspects ofDHD function, and their biological and psychological roots. In thisypothesis we postulate that circadian disruptions are one aspectf a more general arousal regulation problem that has already beendentified as the basis for a range of cognitive energetic deficits inDHD (Sergeant and Van der Meere, 1988, 1990). More specifically,e suggest an extension of models of altered arousal mechanisms
n ADHD (Sergeant and Van der Meere, 1988, 1990) encompassingoth cognitive energetic effects due to alter responses to changes innvironmental context and disrupted patterns of spontaneous cir-adian activity across the day. Therefore in addition to the patternf findings relating to circadian effects in ADHD reported above thisodel is built on two areas of well-established existing evidence.
irst, that LC function, as a key locus in noradrenergic pathwaysn the brain is implicated in arousal more generally and circadianffects specifically. Second, the evidence that arousal mechanismsre altered in ADHD leading to general difficulties in regulatinghysiological state in response to changing conditions. These pat-erns of evidence highlight the potential role of the LC disruptionn ADHD as a biological mediator of both context-specific cogni-ive energetic effects and context-independent circadian effectsthis model is represented in Fig. 1). In the following section, weeview the literature linking LC function (and noradrenergic func-ion more generally) to (i) arousal and circadian processes and (ii)DHD pathophysiology more generally. We then identify areas for
uture research exploring the role of LC dysfunction specifically inelation to circadian effects in ADHD (see Section 4).
.1. The role of locus coeruleus in arousal and circadian effects
The LC, the main noradrenergic nucleus in the brain, is respon-ible for the regulation of cortical arousal which can be describeds a physiological and psychological state of being awake, awarend alert (Aston-Jones, 2005; Samuels and Szabadi, 2008). Arousalnvolves the activation of the reticular activation system (RAS) inhe brain stem, the autonomic nervous system and – if induced orccompanied by stress – the endocrine system (Pfaff and Banavar,007; Pfaff et al., 2007; Schwartz and Roth, 2008; Silver andeSauter, 2008). Next to arousal-influencing effects of factors such
s hormonal stress reactivity, emotions, temperament, and psy-hopharmacotherapy, it is assumed that arousal state regulation islso driven by circadian rhythms (Silver and LeSauter, 2008). A cor-ect timing of the circadian clock (SCN) is important to orchestrateioral Reviews 36 (2012) 1897–1919 1909
neural activity, regulate sleep–wake states, and control emotionand cognition functions (Vicentic et al., 2009).
The hypothesis that the LC shows fluctuations in diurnal activ-ity has been supported in animals. Aston-Jones (2005) describedan indirect projection from the SCN, the circadian pacemaker, tothe LC with the dorsomedial hypothalamic nucleus (DMH) as arelay from the SCN to the LC. The DMH plays a major role in cir-cadian rhythms of corticosteroid and other endocrine secretion,locomotor activity, and sleep (Chou et al., 2003; Germain andKupfer, 2008). In this SCN–DMH–LC circuit, wakefulness is inducedby hypocretin/orexin neuropeptides activating the arousal-relatedLC (Ivanov and Aston-Jones, 2000), and inversely, suppressingthe sleep-related ventrolateral preoptic areas (VLPO) (Winsky-Sommerer et al., 2003).
When noradrenaline (NE) is released from the LC, it exertsunique and additive wake-promoting actions through binding onnoradrenergic receptor subtypes �1 and � (please see Berridge andWaterhouse (2003) for a more detailed review). Such noradrener-gic release in the cortex may produce a prolonged depolarizationof cortical neurons that would increase their responsiveness toother inputs, for example dopaminergic prefrontal cortex (PFC)circuits (Gorelova et al., 2002). In contrast to �1 and � recep-tors that are thought to exist at postsynaptic sites primarily, �2receptors can be found both pre- and postsynaptically. Binding ofNE on the �2 receptor has sedative effects. Pre-synaptic receptorsprovide a local feedback mechanism for counteracting excessiverelease of NE (please see Berridge and Waterhouse (2003) for amore detailed review). Though clonidine, an �2 noradrenergic ago-nist, decreases LC firing (thus suppresses NE release), it enhancescognitive performance through binding on postsynaptic recep-tors in PFC (Berridge and Devilbiss, 2011). This way, the LC-NEsystem has been reported to be involved not only in (i) initia-tion of behavioral and neuronal activity ready to collect sensoryinformation (e.g., waking), but also in (ii) modulation of sensoryinformation processing, attention, and memory within the wakingstate (Berridge and Waterhouse, 2003). These behavioral processeshave been associated with different discharge modes of LC: thetonic noradrenergic release (i.e., spontaneous, baseline activity ofthe nucleus; which shows a circadian rhythm with an increase fromsleep to waking) and the phasic discharge (i.e., brief, rapid increasesin response to environmental stimuli when awake). In the lattercase, phasic activation takes place in response to the processingof task-relevant stimuli and optimalizes task performance (onlypossible when tonic discharge levels are moderately increased),whereas in the tonic mode (high levels of ongoing tonic activity),the LC fails to respond phasically to task demands an effect associ-ated with poor focused attention and exploration (Aston-Jones andCohen, 2005). Parallel to the Yerkes–Dodson relationship betweenarousal and performance, the authors proposed a theory statingthat optimal performance is associated with moderate LC tonicactivity and prominent phasic LC activation and that poor per-formance is associated with both low levels (inattentive, drowsy,sleepy) and high levels (distractible) of tonic activity, with smallor even absent LC phasic responses. As the LC is associated withboth circadian regulation and cognitive performance, Aston-Joneset al. (2001) hypothesized that circadian changes in LC activitymay be reflected in complex task behavior, such as a circadianfluctuation in cognitive ability, next to alterations in sleep–wakecycles.
3.2. ADHD, arousal and deficient state regulation
In ADHD the best evidence of arousal-related dysregulationcomes from studies of the impact of changing environmental con-text on information processes. These have usually been interpretedin the light of state regulation deficits using cognitive energetic

1910 L. Imeraj et al. / Neuroscience and Biobehavioral Reviews 36 (2012) 1897–1919
ontex
mVsdrtraB
dvIofptiifdrrhsd(drl
Fig. 1. Working hypothesis on LC-mediated arousal dysfunction in ADHD linking c
odels (Sergeant and Van der Meere, 1988, 1990). Sergeant andan der Meere (1988, 1990) first interpreted the non-optimaltate of arousal as due to failures to appropriately allocate efforturing information processing. In this model state dysregulationefers to an imbalance between three, closely linked, energetic sys-ems, namely effort, arousal and activation. Difficulties in stateegulation in ADHD are predicted to arise not only from underrousal/activation but also due to over arousal/activation (Sonuga-arke et al., 2010; Van der Meere, 2005).
To date, taken from this perspective, the focus of the primaryeficit in ADHD relates to the response preparation-related acti-ation processes which are associated with response organization.n their review, Sonuga-Barke et al. (2010) point to investigationf cognitive performance in ADHD children during tasks with dif-erent event rates (the key probe of activation processes) whichrovide support for environmental influences on state regula-ion, the importance of ‘optimal’ stimulation and relevance of thenverted U-curve (parallel to the Yerkes–Dodson relationship) link-ng event rate to performance via arousal/activation levels: duringast event rate, ADHD children responded fast and inaccurate, whileuring slow event rate, they are expected to show slow-inaccurateesponding. Although there is currently little research on the neu-obiological correlates of this deficit, a role for LC dysfunctionas been suggested (Sonuga-Barke et al., 2010). This suggestionhifts the primary focus of interest from dopaminergic to nora-renergic deficits in ADHD. For a long time, the dopamine theory
Levy, 1991) has been the leading dogma, suggesting an inhibitoryopaminergic effect at prefrontal/striatal level in ADHD, which hasepeatedly been supported by neuroimaging, genetic and stimu-ant medication studies (Faraone and Biederman, 1998; Faraonet-driven cognitive energetic and context-independent circadian-based alterations.
and Khan, 2005; Levy and Swanson, 2001; Solanto, 1984). Morerecent data, however, suggest an important modulating role of theLC and noradrenergic arousal pathways on dopaminergic PFC func-tion.
3.3. Existing evidence implicating LC-related noradrenergicfunction in ADHD
The cognitive energetic models described above hypothesizethat state regulation deficits are in part related to LC dysfunction(Sergeant and Van der Meere, 1988, 1990). Tonic activity of theLC system, located in the RAS, is associated with the regulationof arousal and several state-dependent processes, such as sensoryinformation processing, attention, working memory, and motorprocesses (Arnsten and Dudley, 2005; Devilbiss and Waterhouse,2004; Sonuga-Barke et al., 2010). Below we hypothesize that thepathophysiology of ADHD involves an ‘overdrive’ of the LC, withexcessive noradrenergic tonic release leading to reduce capac-ity of the PFC to respond to phasic stimuli (Mefford and Potter,1989; Pliszka et al., 1996; Sonuga-Barke et al., 2010). More specif-ically, the increase in tonic discharge above a certain level hasbeen associated with less robust phasic discharge and decreasein focused attention and increase in impulsivity (Aston-Jones andCohen, 2005). Reciprocal connections between the PFC and theLC have been hypothesized by Arnsten et al. (1996), pointing tothe role of noradrenergic in concert with dopaminergic systems
in explaining prefrontal dysregulation (Levy and Swanson, 2001).Studies showed that NE may enhance “signal/noise” processing inthe PFC via actions at �2 receptors (increase signal) and impairits function via �1 and � receptors; these processes coincide with
behav
oDtsd
�iacsOiBoodBtdbsbastiptigmtierrmmbawAdca
3L
sbwtd1ter
cae(i
L. Imeraj et al. / Neuroscience and Bio
ptimal dopamine (D1) stimulation (decrease noise) and excessive1 stimulation respectively (see review Arnsten, 2006). Therefore,
he authors suggest that catecholamines may act as a chemicalwitch: turning on PFC during normal waking and turning it offuring drowsiness or stress.
With respect to ADHD, monkey models with blockade of the2 receptors of the PFC created symptoms of ADHD (hyperactivity,
mpulsivity, and impaired working memory), whereas clonidine,n �2 noradrenergic agonist used in the treatment of ADHD, hasognitive-enhancing effects due to its ability to activate post-ynaptic �2 receptors (see review Berridge and Devilbiss, 2011).ther treatment modalities in ADHD support (modulatory) deficits
n noradrenergic pathways (see Berridge and Devilbiss, 2011;iederman and Spencer, 1999; del Campo et al., 2011 for reviewsn this topic). For example, beneficial arousal-promoting effectsf psychostimulants are due not only to extracellular increases inopamine but also in NE concentrations in the PFC (Devilbiss anderridge, 2008). Looking more closely at electrotonic coupling, onhe level of the LC, low-dose administrated stimulants moderatelyecreased the tonic discharge (which is however overcompensatedy drug-induced elevations in extracellular NE), but largely pre-erved phasic signaling which is important in the regulation ofehavioral actions (Berridge and Devilbiss, 2011). Also modafinil,n analeptic drug used in the treatment of narcolepsy and exces-ive daytime sleepiness, has been suggested to shift the LC to lowonic, high phasic activity which potentially enhances PFC functionn ADHD (del Campo et al., 2011). Additionally, tricyclic antide-ressants (noradrenergic reuptake inhibitors) have been describedo be effective in the treatment of ADHD symptoms through anncrease of extracellular NE in the PFC by blocking noradrener-ic reuptake (Biederman and Spencer, 1999). Finally, the idea thatodulation of noradrenergic circuits may improve ADHD symp-
oms is supported by the newer ADHD agent atomoxetine, whichs also a selective inhibitor of noradrenergic transporters. Swansont al. (2006) showed that atomoxetine increases NE in several brainegions including the PFC and dopamine in the PFC (not in otheregions such as striatum and nucleus accumbens). Therefore, ato-oxetine is assumed to have less abuse potential as compared toethylphenidate. The clinical use of atomoxetine has moreover
een promoted in terms of its 24-h treatment of inattention, hyper-ctivity/impulsivity. Though it needs to be further investigated tohat extent this drug modulates circadian rhythm in humans withDHD, recent data suggest that atomoxetine may reset the circa-ian clock in mice (O’Keeffe et al., 2012). Finally, atomoxetine isonsidered to be a first-line treatment in patients with comorbidnxiety or tics (Garnock-Jones and Keating, 2009).
.4. A working hypothesis: circadian effects as a special case ofC/arousal dysfunction in ADHD
Based on the above review we postulate that in this casetate regulation problems and altered circadian effects in ADHDoth arise from shared origins in dysfunctional SCN–DMH–LC path-ays (see Fig. 1). This hypothesis is based specifically on the idea
hat (i) ADHD is associated with tonic hyperactivity of the LC (asescribed above in the state regulation model; Mefford and Potter,989; Pliszka et al., 1996; Sonuga-Barke et al., 2010), and (ii) thathe LC itself is integrally involved in the regulation of circadianffects generated by the SCN (Aston-Jones et al., 2007), next to itsole in behavioral states and cognitive performance.
Direct evidence for the functionality of the SCN–DMH–LC cir-uit comes from patients with a lesioned SCN who fail to modulate
ttention, dysregulating the timing of the attention focus (Cohent al., 1997). Also with respect to hyperactivity, Sylvester et al.2002) described a modulating role of SCN as suggested in stud-es with rats (Stephan and Zucker, 1972). Though little techniquesioral Reviews 36 (2012) 1897–1919 1911
are available yet to detect dysfunctions of the SCN (Sylvester et al.,2002), clock gene polymorphisms are expected to alter the tim-ing of the circadian pacemaker (Rosenwasser, 2010). With respectto ADHD, Levitan et al. (2004) suggested a link between polymor-phisms of the 7-repeat allele of the dopamine receptor D4 gene(DRD-4), ADHD and circadian rhythm problems. Other authorshave recently established a more direct link between ADHD andgenetic circadian dysregulation by describing a significant associ-ation between polymorphisms of the 3′-untranslated region of theCLOCK gene – a gene previously linked to both sleep disturbancesand evening preference – and ADHD (Kissling et al., 2008; Xu et al.,2010). Also Brookes et al. (2006) detected associations between twogenes in the circadian rhythm system and ADHD. Very recently,Yan et al. (2011) pointed to additional evidence linking disrup-tion in circadian rhythms with ADHD. In their NK1 receptor lackingmice, resembling abnormalities in ADHD, performance varied as afunction of time of day and for some measures of response con-trol an interaction between NK1 function and circadian rhythmswas observed. The authors mention that this is not surprising asNK1R are prevalent in regions responsible for circadian control (e.g.,SCN) and antagonist agents have been reported to cause daytimefatigue, insomnia, and disruptions of circadian motor activity. Onthe level of DMH, lesions have also been reported to reduce circa-dian rhythms of wakefulness, locomotor activity, and cortisol levels(Chou et al., 2003). On the level of the LC, there is evidence for acircadian rhythm in its impulse activity and its role in producingtransitions between sleep–waking cycles; after lesions of the LC, adecrease in the amplitude of the circadian rhythms in sleep–wakecycles was noted as described in reviewed work of Aston-Jones et al.(2007). In their experiments, they additionally showed that lightdeprivation caused substantial decreases in noradrenergic neuro-transmission in the rat’s frontal cortex.
Despite the role of the LC in circadian regulation, it is currentlynot known whether an overdrive of this nucleus is specificallyassociated with a circadian phase delay. However, this hypothesisis highly plausible; Aston-Jones et al. hypothesized that upreg-ulated noradrenergic release may contribute to both sleep (e.g.,sleep onset insomnia) and behavioral symptomatology (e.g., day-time hyperactivity and inattention) in ADHD, as they observedthese specific ADHD types of behavior during the tonic mode ofactivity in monkey LC. Though we assume that sleep onset prob-lems may subsequently lead to difficulties with awakening anddaytime sleepiness, these problems may also relate more directlyto hyperactive tonic discharge of the LC. With respect to morningawakening, an increase in tonic activity is needed for transitionfrom sleep to wake. High baseline levels are however associatedwith less variability (Phillips et al., 2000) (see Section 4.1.2; pupildiameter), which may hypothetically impede such transitions. Dur-ing wake, changes in the tonic and subsequently phasic activity ofthe LC have been associated with fluctuations in alertness underspecific conditions (Aston-Jones, 2005). As in our review above itwas noted that ADHD behavior becomes more overt at specifictimes of day, it is reasonable to hypothesize that the two func-tions of the LC – its role in both state control and performance– interact and that ‘baseline LC hyperarousal’ in ADHD leads toa complex profile of circadian-regulated and context-dependentbehavioral dysregulation. It still needs to be determined thoughhow time of day effects would interact with the expression of thetonic/phasic mode of LC activity – or transitions between them –to affect prefrontal functioning.
Though highlighting the link between circadian alterations andADHD may allow us to identify novel processes for study in ADHD,
the complexity of the working hypothesis presented above must berecognized (see Fig. 1). First, neurotransmitter systems do not oper-ate independently, and the interaction between NE, dopamine, andserotonin is probably important in psychopathology (Harvey et al.,
1 behav
2dcst2vblNubrsuhr(aamsdt2
4
cabtl(ia
irAtmaobtsAaw
4r
4s
awshlwt
912 L. Imeraj et al. / Neuroscience and Bio
011). In addition to the noradrenergic circuitry described above,opaminergic and serotonergic dysfunctions may additionally linkircadian alterations to ADHD as these neurotransmitters are them-elves influenced by the circadian rhythm system and consideredo be pathophysiologically involved in ADHD (Faraone and Khan,005; Levy, 2009; Paclt et al., 2005; Pattij and Vanderschuren, 2008;an der Kooij and Glennon, 2007). Second, complex interactionsetween neurotransmitters, clock genes, and circadian neurobio-
ogical structures have been described. For example, Barnard andolan (2008) refer to the fact that clock gene expression is mod-lated by neurotransmitter effects. The circadian clock has alsoeen described to be influenced by an ‘overdrive’ of the LC andelated increase in noradrenergic activity (Maurizi, 1984) such aseen in ADHD. This could be due to inadequate noradrenergic stim-lation of the pineal gland, altering the concentrations of its mainormonal product melatonin, which in turn is important in theegulation of the circadian clock containing melatonin receptorsPacchierotti et al., 2001). Finally, the idea that circadian alterationsre an expression of ADHD-related arousal-based problems is prob-bly only valid for a specific subsample of subjects with ADHD, anday also be present in other psychiatric disorders. This hypothe-
is is in line with for example findings that executive functioningeficits and delay aversion are implicated in ADHD, though that nei-her is necessary for ADHD nor specific too it (Sonuga-Barke et al.,008a).
. Proposals for future study of circadian effects in ADHD
In this section we discuss future directions for research indi-ated by the LC-based model of circadian effects described abovend described in Fig. 1. Multilevel interdisciplinary research wille necessary to address the current gaps in this research area. Athis point, there is evidence for a link between ADHD, dysregu-ated arousal and LC, and a link between LC and circadian rhythmsdescribed above). More systematic research however is needed tonvestigate circadian-related effects in ADHD to confirm currentlyvailable findings presented in the review.
Based on the model proposed above, we formulate the follow-ng predictions: (i) ADHD is associated with LC-mediated circadianhythm alterations; subpredictions are: (a) LC tonic hyperactivity inDHD is more expressed at specific times of day than others; (b)
here is a disruption in the circadian rhythms of LC-noradrenergicediated arousal in ADHD; (c) subjects with ADHD show specific
lterations in behavioral and physiological measures as a functionf time of day; (d) circadian disruptions in LC activity, arousal, andehavioral/physiological measures will be correlated in ADHD; (ii)here is an interaction of time of day effects and specific environmentaltimuli suggesting a ‘shared LC state regulation pathway deficit’ inDHD; and (iii) the theory of disrupted circadian rhythms is prob-bly only valid for a subgroup of cases with ADHD and may overlapith other psychiatric conditions.
.1. Prediction 1: ADHD is associated with LC-mediated circadianhythm alterations
.1.1. LC tonic hyperactivity in ADHD is more expressed atpecific times of day than others
ADHD has been associated with an ‘overdrive’ of the LC (Meffordnd Potter, 1989; Pliszka et al., 1996; Sonuga-Barke et al., 2010),hich is in turn involved in the circadian regulation of arousal and
leep–wake states (Aston-Jones et al., 2007). These findings rely
eavily on animal studies, but it is reasonable – though still chal-enging – to investigate the LC in humans with ADHD and to detecthether the LC dysfunction in ADHD is circadian sensitive. One way
o do so is the use of neuroimaging methods, such as functional
ioral Reviews 36 (2012) 1897–1919
magnetic resonance imaging (fMRI) and positron emission tomog-raphy (PET). To address this question imaging procedures need tobe repeated across a 24-h period. During daytime hours, this hasbeen done before not only for visualization of circadian activity inthe LC but also in the SCN (Schmidt et al., 2009), when subjectswere exposed to different environmental stimulus/task conditionsat different times of day. Scanning during sleep will be cumber-some but is theoretically feasible. However, practical problems mayarise as it is difficult to fall asleep during scanning procedures. APET protocol to study sleep in a naturalistic setting has been pro-vided, though with decreased temporal resolution (Nofzinger et al.,1998). In this regard, less invasive, peripheral arousal measures andelectroencephalogram (EEG) (as described in the second and thirdsubprediction) may be interesting to (additionally) study sleep inhumans.
Pharmacological studies also allow investigation of the LC func-tion and activity. For example, studies with clonidine used forADHD or as an anesthetic have provided in-depth knowledge onsleep–wake and cognition regulatory functions through the studyof binding on pre- and postsynaptic �2 adrenergic receptors (seefor reviews: Arnsten et al., 1996; Berridge and Devilbiss, 2011).Another example relates to disruption of circadian rhythms indopaminergic concentration and receptor activity which have beenlinked to circadian symptomatology in drug addiction (Falcon andMcClung, 2009; Naber et al., 1980; Sleipness et al., 2007). In theirreview, Manev and Uz (2009) reported time-dependent behav-ioral actions of both cocaine and amphetamines. In relation tonoradrenergic receptors, circadian rhythms are thought to be mod-ified by tricyclic antidepressants (Wirz-Justice et al., 1980) andatomoxetine (O’Keeffe et al., 2012). It will be valuable to exploretime-dependent effects on ADHD drugs’ working mechanisms con-sidering both dopaminergic and noradrenergic pathways. Suchknowledge could guide more systematic effect-evaluation studiestaking into account time of day effects of different drug-releasingmodalities for ADHD (Swanson et al., 2004) to treat time-specificarousal problems in this population (see prediction 2).
4.1.2. There is a disruption in the circadian rhythms ofLC-noradrenergic mediated arousal in ADHD
In recent research, the utility of two candidate psychophysio-logical markers of LC-noradrenergic activity has been investigated:the P3-event related potential (ERP) and pupil diameter (Murphyet al., 2011). The P3 is an ERP component peaking 300–600 ms aftera task-relevant stimulus, which has been argued to represent acortical electrophysiological correlate of the phasic LC responseand the noradrenergic potentiation of information processing(Nieuwenhuis et al., 2005). A second index is pupil diameter, anautonomic measure involving both sympathetic and parasympa-thetic activity, which has been hypothesized to reflect both tonicand phasic aspects of LC activity. More specifically, upregulationof tonic noradrenergic activity has been associated with increasesin baseline pupil diameter and decrease in pupillary variability,while pupil dilatory response occurs to a wide range of task-relatedstimuli (Phillips et al., 2000).
To confirm the circadian-related prediction above, it would benecessary to assess baseline pupil diameter at different times ofthe day in both cases with and without ADHD. Because of theclose relation between tonic/phasic LC activity in daytime cognitiveperformance it is important to detect whether ADHD-associatedincreases in tonic activity (and therefore larger pupil diameter base-line) are more expressed at different times of the day. With respectto the P3, which is assumed to reflect phasic activity, amplitudes
have often been found to be smaller in ADHD as compared to con-trols (Barry et al., 2003b). There is evidence that P3 differences inADHD are related to arousal states: for example, in their event ratestudy, Wiersema et al. (2006a,b) found altered P3 components in
behav
tadc
subpadteaflr1tdiri
dca�ctEtw
4at
vetpoTtrfma2cvemGloja‘2snbcHh
L. Imeraj et al. / Neuroscience and Bio
he ADHD as compared to a control group only when in under-roused state. However, as of yet, no study has evaluated time ofay effect on P3 deviation in ADHD. Suggestions to investigate theircadian-environmental overlap are discussed in prediction 2.
Though pupillometry is often used in research on daytimeleepiness (decreased pupil size due to parasympathetic influence)nder both light and darkness conditions, measurements cannote made “during” sleep. With respect to P3, small or even absentotentials are expected during sleep as low tonic firing rate does notllow phasic discharge. Though studies analyzing auditory inputuring sleep observed a sleep P3, it is uncertain to what extenthis potential is equivalent to waking P3 (Bastuji et al., 2002). Nev-rtheless, further investigation of the role of the LC in regulatingutonomic nervous system and sleep–wake cycles is important asuctuations in a variety of measures of “arousal state” (e.g., heartate) have been reported to affect P3 morphology (Polich and Kok,995). Such peripheral measures may provide an excellent alterna-ive to monitor arousal states during both night and day (see alsoescription in prediction 1c): Nieuwenhuis et al. (2011) described
n their review that changes in LC activity are not only highly cor-elated with changes in P3 component and pupil diameter, but alson skin conductance level and heart rate.
Alternatively, EEG is very suitable for this purpose as it is airect index of the electrical activity of the brain. More specifi-ally, the �/ ratio and power in the EEG signal have been useds a marker of central nervous system arousal. In ADHD, higher/ and deviances have been argued as an indication of corti-al underarousal (see Barry et al. (2003a) for a review). As of yet,here are no studies that evaluated time of day effects for theseEG deviances. MSTL represents another option for the evalua-ion of daytime sleepiness and PSG for more micro-evaluation ofake–sleep transitions and nighttime awakenings.
.1.3. Subjects with ADHD show specific alterations in behavioralnd peripheral physiological measures of arousal as a function ofime of day
Though behavioral and physiological measures of arousal havealue in the evaluation of 24-h patterns, studies evaluating theseffects in ADHD have mostly been confounded so far. Sugges-ions to address the issue of sample heterogeneity are discussed inrediction 3. To control for environmental confounding effects, lab-ratory protocols have been developed for circadian evaluations.he constant routine protocol controls for possible exogenous fac-ors in order to avoid their masking influences on the endogenoushythm of the measured variables. In this protocol, both contextualactors, such as light, feeding and activity, and circadian measure-
ent conditions are strictly regulated (Atkinson et al., 2007; Baileynd Heitkemper, 2001; Blatter and Cajochen, 2007; Scheer et al.,003). However, this methodology not only raises financial, practi-al and ethical issues, especially in children, but also the ecologicalalidity of such procedure is questionable. Therefore, longer-termvaluations in naturalistic settings, including multiple ‘combined’easurements across several days, are required (Houtveen and deeus, 2009). As an extension to previous research, we propose a
onger-term ‘combined’ approach that may include the assessmentf environmental information (e.g., lights out, daily activities), sub-ective and objective sleep/wake assessments during several daysnd nights (e.g., actigraphy, DLMO, MSLT, PSG), in addition to a
full’ circadian cortisol investigation (several measurements a day),4-h registration of heart rate (with simultaneous ‘control’ mea-urement of activity), and alternative measures which so far haveot been carried out in ADHD. Useful alternative measures could
e for example blood pressure (Houtveen and de Geus, 2009), skinonductance (Hot et al., 1999) and body temperature (Bailey andeitkemper, 2001; Hofstra and de Weerd, 2008). It must be notedowever that some measures, for example of body temperature, areioral Reviews 36 (2012) 1897–1919 1913
probably not feasible in children as it is a relatively invasive pro-cedure. Finally, heart rate variability and spectral analysis of thismeasure are today one of the best methods to follow the activityof autonomic nervous system and its differential influences of theortho- and parasympathetic branches during night.
4.1.4. Circadian disruptions in different arousal-related measures(LC, arousal, and behavioral/physiological measures) will behighly correlated in ADHD
Based on our working hypothesis, we expect that circadianeffects on different arousal-related measures will be highly cor-related within participants with ADHD. However, if circadiandiscrepancies between measures exist, this may reveal subtledifferences in underlying neural processes. For example, whenstudying the circadian SCN–DMH–LC circuit, DMH lesions appearto eliminate circadian rhythms of corticosteroids but not melatonin(Chou et al., 2003). These authors hypothesize that a ‘combined’ dis-ruption of cortisol and melatonin rhythm may be originated in theSCN – which is highly sensitive to melatonin input – rather thanthe DMH as other studies lesioning DMH and regions outside theDMH found circadian alterations in both measures.
Examination of the correlation between peripheral and morefundamental measures is also warranted. Schmidt et al. (2009)studied the influence of circadian and homeostatic processeson cognitive performance in different chronotypes (morning vs.evening) by imaging the LC and SCN (fMRI) during performance-related tasks (reaction times) at two test sessions (morningvs. evening). Participants were also monitored by PSG at theirpreferred bedtimes during two consecutive nights; combinedwith assessments of subjective sleepiness, objective vigilance,and hourly collected saliva samples for assessment of melatoninphase starting 7 h prior to habitual sleep time. Such a proto-col might be adapted (oddball performance tasks) and extendedwith, for example, P3-ERP evaluation or pupil diameter responseas these measures have been associated with information pro-cessing, reflecting phasic activity of the LC-noradrenergic system(Nieuwenhuis et al., 2005).
In our literature review some studies suggested a circadianphase delay in ADHD. Normally, during sleep and drowsiness thereis low tonic activity, whereas tonic activity is increased when oneis alert (Aston-Jones and Cohen, 2005). If a circadian delay is trulypresent in ADHD, following this reasoning this would mean rel-atively low tonic LC activity in the morning and relatively hightonic LC activity in evening. These deviations would both lead tonon-optimal performance: in the morning reflected by inattentive,drowsiness and being non-alert, in the evening by distractibility(see model Aston-Jones, p. 406 in Aston-Jones and Cohen, 2005). Atthis point, it is difficult to say what phasic indices of LC will do, asduring both (too) low and high tonic LC activity, phasic responseswill be diminished (as can be measured by P3 component, pupildiameter response). In terms of baseline tonic LC activity, a smallerpupil diameter in the morning, but larger in the evening would bepredicted.
4.2. Prediction 2: there is an interaction of time of day effects andspecific environmental stimuli suggesting a ‘shared LC stateregulation pathway deficit’ in ADHD
From a more theoretical perspective, current task protocolscould be used at different times of the day to investigate the influ-ence of arousing environmental stimuli on state regulation deficitsin ADHD to see whether these results fluctuate across the day. In his
study with NK1R-lacking mice, Yan et al. (2011) explicitly includedthe time of day during which mice were trained and tested. Basedon their findings, the authors suggested that “time of day might bea key variable in studies of ADHD patients and that the effect of an
1 behav
icabdaqe
tqrstscidbp(S
rumtaatTtuss
4vp
easrpsaw(mpucA(tdtt(
5
l
914 L. Imeraj et al. / Neuroscience and Bio
nteraction between NK1R function and circadian rhythms on responseontrol merits further investigation.” A concrete test of the inter-ction of time of day and environmental effects of arousal coulde performed using event rate effects during different times ofay, for example morning vs. afternoon. Therefore, we addition-lly recommend longer-term evaluations of ADHD behavior (bothuantitative and qualitative) in different contexts or under differentnvironmental conditions.
One context of interest would refer to the lab school protocolhat is used in medication effect-evaluation studies so far. Thisuasi-experimental naturalistic setting allows for the combinedegistration of behavior and additional measures (e.g., heart rate,aliva sampling) under different context conditions (e.g., academicasks, free play) controlling for possible time of day effects. Thoughuch protocols typically include ADHD children during summeramps, comparison with typically developing children would benteresting to detect during which specific situations and times ofay group differences become more overt. This information woulde very useful in the further evaluation of medication effects to treatroblematic behavior especially at times when it is more expressedChavez et al., 2009; Pelham et al., 2001; Sonuga-Barke et al., 2004;wanson et al., 2004).
Another context of relevance is stress. Though arousal is closelyelated to stress, Pfaff et al. (2007) provided a framework tonderstand the asymmetric relation between stress and arousalechanisms, suggesting that stimuli causing stress are theorized
o cause arousal, but inversely, that not all stimuli causing arousalre stressful. Whereas autonomic responses (e.g., heart rate) arectivated in both stressful and non-stressful arousal conditions,he HPA axis (e.g., cortisol) is only activated in stressful conditions.herefore, the combined diurnal assessment of heart rate and cor-isol in diurnal evaluations could further explore to what extentnderlying hypotheses relating time of day effects in arousal arepecific for ADHD or whether they are the product of a more generaltress-related dysregulation.
.3. Prediction 3: the association with circadian rhythm is onlyalid for a subgroup of ADHD and may overlap with othersychiatric conditions
Considering the heterogeneous nature of ADHD, it seems nec-ssary to determine whether alterations in peripheral measuresnd underlying pathways, if confirmed in ADHD, are specific forome cases with the disorder or to what extent sleep–wake dis-uptions reflect a transdiagnostic phenomenon relevant acrosssychiatric disorders. Therefore, we suggest that future researchhould account for confounding effects related to age and sex char-cteristics, but also to ADHD subtype, ADHD severity, comorbidityith externalizing disorders (ODD, CD), internalizing disorders
anxiety, depression), or sleep disorders, and use of (stimulant)edication. One could aim to study homogeneous clinical sam-
les, but – what may be even more fascinating – would be these of a large-scale heterogeneous sample and a search for spe-ific subgroups of patients with circadian dysregulation. Cases withDHD and sleep–wake problems and cases with executive function
state regulation) deficit problems would be especially interestingo study. ADHD subgroups may be differentially affected by time ofay effects; however, some may show eveningness chronotypologyo inattention problems (Caci et al., 2009), whereas others reportedhe combined group to be more vulnerable for circadian problemsChiang et al., 2010).
. Conclusion
In line with evidence in other psychiatric disorders, the currentiterature provides some initial evidence of at least a subgroup of
ioral Reviews 36 (2012) 1897–1919
children with ADHD with circadian problems. Considering the het-erogeneous nature of the disorder, it is plausible that anomaliesrelated to one or more circadian measures reflect a distinct sub-group. Though it is not clear to what extent these problems arespecific for ADHD at this stage, available evidence suggests that thecircadian rhythm disruptions can at least modify severity and out-come, and may in some cases play a more etiological role. Althoughpathophysiological theories on ADHD so far largely ignored cir-cadian effects on arousal and ADHD symptomatology, developingknowledge in several circadian domains, including underlying neu-robiological mechanisms, led us to propose a working hypothesisthat could serve as a framework for further research. In this puta-tive model ADHD-related disruption of circadian processes andcontext-specific effects on arousal-related processes such as cog-nitive energetic deficits are hypothesized to be the result of LCdysfunction. Here we review the potential implications of thismodel for clinical practice and future research.
Financial disclosures
Lindita Imeraj: no disclosures or conflicts of interest to report.Edmund Sonuga-Barke:
Recent speaker board: Shire, UCB PharmaCurrent & recent consultancy: UCB Pharma, ShireCurrent & recent research support: Janssen Cilag, Shire, Qbtech,Flynn PharmaAdvisory Board: Shire, Flynn Pharma, UCB Pharma, Astra ZenecaConference support: Shire
Inge Antrop: no disclosures or conflicts of interest to report.Herbert Roeyers:
Concultancy: ShireResearch support: Shire, LillyConference support: Lilly
Roeljan Wiersema: no disclosures or conflicts of interest toreport.
Sarah Bal: no disclosures or conflicts of interest to report.Dirk Deboutte: no disclosures or conflicts of interest to report.
Acknowledgment
This work was financially supported by the Fund for ScientificResearch, Flanders, Belgium (3G032607).
References
Achenbach, T.M., 2001. Child Behavior Checklist for Ages 4-18 (CBCL/4-18). Univer-sity of Vermont, Burlington.
Antrop, I., Buysse, A., Roeyers, H., Van Oost, P., 2005a. Activity in children with ADHDduring waiting situations in the classroom: a pilot study. The British Journal ofEducational Psychology 75, 51–69.
Antrop, I., Roeyers, H., De Baecke, L., 2005b. Effects of time of day on classroombehaviour in children with ADHD. School Psychology International 26, 29–43.
American Psychiatric Association (APA), 2000. Diagnostic and Statistical Manual ofMental Disorders, fourth ed. American Psychiatric Press, Washington, D.C.
Arnsten, A.F., 2006. Fundamentals of attention-deficit/hyperactivity disorder: cir-cuits and pathways. The Journal of Clinical Psychiatry 67, 7–12.
Arnsten, A.F., Dudley, A.G., 2005. Methylphenidate improves prefrontal corticalcognitive function through alpha2 adrenoceptor and dopamine D1 receptoractions: relevance to therapeutic effects in attention deficit hyperactivity disor-der. Behavioural Brain Function 1, 2.
Arnsten, A.F., Steere, J.C., Hunt, R.D., 1996. The contribution of alpha 2-noradrenergic
mechanisms of prefrontal cortical cognitive function. Potential significancefor attention-deficit hyperactivity disorder. Archives of General Psychiatry 53,448–455.Arnsten, A.F.T., 1998. Catecholamine modulation of prefrontal cortical cognitivefunction. Trends in Cognitive Sciences 2, 436–447.

behav
A
A
A
A
A
B
B
B
B
B
B
B
B
B
B
B
B
B
B
B
B
B
B
B
B
B
B
B
L. Imeraj et al. / Neuroscience and Bio
ston-Jones, G., 2005. Brain structures and receptors involved in alertness. SleepMedicine 6, S3–S7.
ston-Jones, G., Chen, S., Zhu, Y., Oshinsky, M.L., 2001. A neural circuit for circadianregulation of arousal. Nature Neuroscience 4, 732–738.
ston-Jones, G., Cohen, J.D., 2005. An integrative theory of locus coeruleus-norepinephrine function: adaptive gain and optimal performance. AnnualReview of Neuroscience 28, 403–450.
ston-Jones, G., Gonzalez, M., Doran, S., 2007. Role of the locus coeruleus-norepinephrine system in arousal and circadian regulation of the sleep–wakecycle. In: Ordway, G.A., Schwartz, M.A., Frazer, A. (Eds.), Brain Norepinephrine:Neurobiology and Therapeutics. Cambridge University Press, Cambridge, pp.157–195.
tkinson, G., Edwards, B., Reilly, T., Waterhouse, J., 2007. Exercise as a synchroniserof human circadian rhythms: an update and discussion of the methodologicalproblems. European Journal of Applied Physiology 99, 331–341.
ae, S.M., Park, J.E., Lee, Y.J., Cho, I.H., Kim, J.H., Koh, S.H., Kim, S.J., Cho, S.J., 2010.Gender difference in the association between adult attention deficit hyperactiv-ity disorder symptoms and morningness-eveningness. Psychiatry and ClinicalNeuroscience 64, 649–651.
aehr, E.K., Revelle, W., Eastman, C.I., 2000. Individual differences in the phase andamplitude of the human circadian temperature rhythm: with an emphasis onmorningness-eveningness. Journal of Sleep Research 9, 117–127.
ailey, S.L., Heitkemper, M.M., 2001. Circadian rhythmicity of cortisol and body tem-perature: morningness-eveningness effects. Chronobiology International 18,249–261.
arkley, R.A., McMurray, M.B., Edelbrock, C.S., Robbins, K., 1990. Side-effects ofmethylphenidate in children with attention-deficit hyperactivity disorder – asystematic, placebo-controlled evaluation. Pediatrics 86, 184–192.
arnard, A.R., Nolan, P.M., 2008. When clocks go bad: neurobehavioural conse-quences of disrupted circadian timing. PLoS Genetics 4, e1000040.
arry, R.J., Clarke, A.R., Johnstone, S.J., 2003a. A review of electrophysiology inattention-deficit/hyperactivity disorder: I. Qualitative and quantitative elec-troencephalography. Clinical Neurophysiology 114, 171–183.
arry, R.J., Johnstone, S.J., Clarke, A.R., 2003b. A review of electrophysiology inattention-deficit/hyperactivity disorder: II. Event-related potentials. ClinicalNeurophysiology 114, 184–198.
artels, M., de Geus, E.J.C., Kirschbaum, C., Sluyter, F., Boomsma, D.I., 2003. Heritabil-ity of daytime cortisol levels in children. Behavior Genetics 33, 421–433.
astuji, H., Perrin, F., Garcia-Larrea, L., 2002. Semantic analysis of auditory inputduring sleep: studies with event related potentials. International Journal of Psy-chophysiology 46, 243–255.
earpark, H.M., Michie, P.T., 1987. Changes in morningness-eveningness scoresduring adolescence and their relationship to sleep/wake disturbances. Chrono-biologia 14, 151.
eauchaine, T.P., Katkin, E.S., Strassberg, Z., Snarr, J., 2001. Disinhibitorypsychopathology in male adolescents: discriminating conduct disorderfrom attention-deficit/hyperactivity disorder through concurrent assess-ment of multiple autonomic states. Journal of Abnormal Psychology 110,610–624.
endz, L.M., Scates, A.C., 2010. Melatonin treatment for insomnia in pediatricpatients with attention-deficit/hyperactivity disorder. The Annals of Pharma-cotherapy 44, 185–191.
enloucif, S., Burgess, H.J., Klerman, E.B., Lewy, A.J., Middleton, B., Murphy, P.J., Parry,B.L., Revell, V.L., 2008. Measuring melatonin in humans. Journal of Clinical SleepMedicine 4, 66–69.
erridge, C.W., Devilbiss, D.M., 2011. Psychostimulants as cognitive enhancers: theprefrontal cortex, catecholamines, and attention-deficit/hyperactivity disorder.Biological Psychiatry 69, e101–e111.
erridge, C.W., Waterhouse, B.D., 2003. The locus coeruleus-noradrenergic system:modulation of behavioral state and state-dependent cognitive processes. BrainResearch Reviews 42, 33–84.
iederman, J., Spencer, T., 1999. Attention-deficit/hyperactivity disorder (ADHD) asa noradrenergic disorder. Biological Psychiatry 46, 1234–1242.
latter, K., Cajochen, C., 2007. Circadian rhythms in cognitive performance,methodological constraints, protocols, theoretical underpinnings. Physiology &Behavior 90, 196–208.
lomqvist, M., Holmberg, K., Lindblad, F., Fernell, E., Ek, U., Dahllof, G., 2007. Salivarycortisol levels and dental anxiety in children with attention deficit hyperactivitydisorder. European Journal of Oral Sciences 115, 1–6.
oivin, D.B., 2000. Influence of sleep-wake and circadian rhythm disturbances inpsychiatric disorders. Journal of Psychiatry & Neuroscience 25, 446–458.
oonstra, A.M., Kooij, J.J.S., Oosterlaan, J., Sergeant, J.A., Buitelaar, J.K., Van Someren,E.J.W., 2007. Hyperactive night and day? Actigraphy studies in adult ADHD: abaseline comparison and the effect of methylphenidate. Sleep 30, 433–442.
orbély, A.A., 1982. A two process model of sleep regulation. Human Neurobiology1, 195–204.
orger, N., van der Meere, J., 2000. Motor control and state regulation in childrenwith ADHD: a cardiac response study. Biological Psychology 51, 247–267.
rookes, K., Xu, X., Chen, W., Zhou, K., Neale, B., Lowe, N., Anney, R., Franke, B., Gill,M., Ebstein, R., Buitelaar, J., Sham, P., Campbell, D., Knight, J., Andreou, P., Altink,M., Arnold, R., Boer, F., Buschgens, C., Butler, L., Christiansen, H., Feldman, L.,
Fleischman, K., Fliers, E., Howe-Forbes, R., Goldfarb, A., Heise, A., Gabriels, I.,Korn-Lubetzki, I., Johansson, L., Marco, R., Medad, S., Minderaa, R., Mulas, F.,Muller, U., Mulligan, A., Rabin, K., Rommelse, N., Sethna, V., Sorohan, J., Uebel,H., Psychogiou, L., Weeks, A., Barrett, R., Craig, I., Banaschewski, T., Sonuga-Barke, E., Eisenberg, J., Kuntsi, J., Manor, I., McGuffin, P., Miranda, A., Oades,ioral Reviews 36 (2012) 1897–1919 1915
R.D., Plomin, R., Roeyers, H., Rothenberger, A., Sergeant, J., Steinhausen, H.C.,Taylor, E., Thompson, M., Faraone, S.V., Asherson, P., 2006. The analysis of 51genes in DSM-IV combined type attention deficit hyperactivity disorder: asso-ciation signals in DRD4, DAT1 and 16 other genes. Molecular Psychiatry 11,934–953.
Brown, T.E., 1996. Manual for Brown Attention Deficit Disorder Scales. The Psycho-logical Corporation, San Antonio (Texas).
Buckley, T.M., Schatzberg, A.F., 2005. Review: on the interactions of thehypothalamic-pituitary-adrenal (HPA) axis and sleep: normal HPA axis activ-ity and circadian rhythm, exemplary sleep disorders. The Journal of ClinicalEndocrinology and Metabolism 90, 3106–3114.
Burgess, H.J., Trinder, J., Kim, Y., Luke, D., 1997. Sleep and circadian influences on car-diac autonomic nervous system activity. American Journal of Physiology. Heartand Circulatory Physiology 273, H1761–H1768.
Caci, H., Bouchez, J., Bayle, F.J., 2009. Inattentive symptoms of ADHD are related toevening orientation. Journal of Attention Disorders 13, 36–41.
Carrier, J., Monk, T.H., 2000. Circadian rhythms of performance: new trends. Chrono-biology International 17, 719–732.
Carskadon, M.A., Vieira, C., Acebo, C., 1993. Association between puberty and delayedphase preference. Sleep 16, 258–262.
Cavallera, G.M., Giudici, S., 2008. Morningness and eveningness personality. A surveyin literature from 1995 up till 2006. Personality and Individual Differences 44,3–21.
Chaste, P., Clement, N., Botros, H.G., Guillaume, J.L., Konyukh, M., Pagan, C., Scheid,I., Nygren, G., Anckarsäter, H., Rastam, M., Ståhlberg, O., Gillberg, I.C., Melke,J., Delorme, R., Leblond, C., Toro, R., Huguet, G., Fauchereau, F., Durand, C.,Boudarene, L., Serrano, E., Lemière, N., Launay, J.M., Leboyer, M., Jockers, R.,Gillberg, C., Bourgeron, T., 2011. Genetic variations of the melatonin pathwayin patients with attention-deficit and hyperactivity disorders. Journal of PinealResearch 51, 394–399.
Chavez, B., Sopko Jr., M.A., Ehret, M.J., Paulino, R.E., Goldberg, K.R., Angstadt, K., Bog-art, G.T., 2009. An update on central nervous system stimulant formulationsin children and adolescents with attention-deficit/hyperactivity disorder. TheAnnals of Pharmacotherapy 43, 1084–1095.
Chervin, R.D., Archbold, K.H., Dillon, J.E., Panahi, P., Pituch, K.J., Dahl, R.E., Guillem-inault, C., 2002. Inattention, hyperactivity, and symptoms of sleep-disorderedbreathing. Pediatrics 109, 449–456.
Chiang, H.L., Gau, S.S.F., Ni, H.C., Chiu, Y.N., Shang, C.Y., Wu, Y.Y., Lin, L.Y., Tai, Y.M.,Soong, W.T., 2010. Association between symptoms and subtypes of attention-deficit hyperactivity disorder and sleep problems/disorders. Journal of SleepResearch 19, 535–545.
Chou, T.C., Scammell, T.E., Gooley, J.J., Gaus, S.E., Saper, C.B., Lu, J., 2003. Critical roleof dorsomedial hypothalamic nucleus in a wide range of behavioral circadianrhythms. Journal of Neurosciene 23, 10691–10702.
Chrousos, G.P., Gold, P.W., 1998. A healthy body in a healthy mind – and vice versa –the damaging power of uncontrollable stress. The Journal of Clinical Endocrinol-ogy and Metabolism 83, 1842–1845.
Claustrat, B., Brun, J., Chazot, G., 2005. The basic physiology and pathophysiology ofmelatonin. Sleep Medicine Reviews 9, 11–24.
Cohen-Zion, M., Ancoli-Israel, S., 2004. Sleep in children with attention-deficithyperactivity disorder (ADHD): a review of naturalistic and stimulant interven-tion studies. Sleep Medicine Reviews 8, 379–402.
Cohen, H., Matar, M.A., Kaplan, Z., Kotler, M., 1999. Power spectral analysis of heartrate variability in psychiatry. Psychotherapy and Psychosomatics 68, 59–66.
Cohen, R.A., Barnes, H.J., Jenkins, M., Albers, H.E., 1997. Disruption of short-durationtiming associated with damage to the suprachiasmatic region of the hypothala-mus. Neurology 48, 1533–1539.
Conners, C.K., 2000. Conners’ Continuous Performance Test. Multi-Health SystemsInc., North Tonawanda (New York).
Corkum, P., Moldofsky, H., Hogg-Johnson, S., Humphries, T., Tannock, R., 1999.Sleep problems in children with attention-deficit/hyperactivity disorder: impactof subtype, comorbidity, and stimulant medication. Journal of the AmericanAcademy of Child and Adolescent Psychiatry 38, 1285–1293.
Corkum, P., Panton, R., Ironside, S., MacPherson, M., Williams, T., 2008. Acute impactof immediate release methylphenidate administered three times a day on sleepin children with attention-deficit/hyperactivity disorder. Journal of PediatricPsychology 33, 368–379.
Corkum, P., Tannock, R., Moldofsky, H., Hogg-Johnson, S., Humphries, T., 2001.Actigraphy and parental ratings of sleep in children with attention-deficit-hyperactivity disorder (ADHD). Sleep 24, 303–312.
Cortese, S., Faraone, S.V., Konofal, E., Lecendreux, M., 2009. Sleep in childrenwith attention-deficit/hyperactivity disorder: meta-analysis of subjective andobjective studies. Journal of the American Academy of Child and AdolescentPsychiatry 48, 894–908.
Cortese, S., Konofal, E., Lecendreux, M., Arnulf, I., Mouren, M.C., Darra, F., Bernardina,B.D., 2005. Restless legs syndrome and attention-deficit/hyperactivity disorder:a review of the literature. Sleep 28, 1007–1013.
Cortese, S., Mid, E.K., Yateman, N., Mouren, M.C., Lecendreux, M., 2006. Sleep andalertness in children with attention-deficit/hyperactivity disorder: a systematicreview of the literature. Sleep 29, 504–511.
Crabtree, V.M., Ivanenko, A., Gozal, D., 2003. Clinical and parental assessment of sleep
in children with attention-deficit/hyperactivity disorder referred to a pediatricsleep medicine center. Clinical Pediatrics 42, 807–813.Crasson, M., Kjiri, S., Colin, A., Kjiri, K., L’Hermite-Baleriaux, M., Ansseau, M., Legros,J.J., 2004. Serum melatonin and urinary 6-sulfatoxymelatonin in major depres-sion. Psychoneuroendocrinology 29, 1–12.

1 behav
C
C
D
D
D
d
D
D
D
D
D
E
F
F
F
F
F
F
G
G
G
G
G
G
G
G
H
H
916 L. Imeraj et al. / Neuroscience and Bio
rone, E.A., Jennings, J.R., van der Molen, M.W., 2003. Sensitivity to interferenceand response contingencies in attention-deficit/hyperactivity disorder. Journalof Child Psychology and Psychiatry 44, 214–226.
rowell, S.E., Beauchaine, T.P., Gatzke-Kopp, L., Sylvers, P., Mead, H., Chipman-Chacon, J., 2006. Autonomic correlates of attention-deficit/hyperactivitydisorder and oppositional defiant disorder in preschool children. Journal ofAbnormal Psychology 115, 174–178.
agan, Y., Zeevi-Luria, S., Sever, Y., Hallis, D., Yovel, I., Sadeh, A., Dolev, E., 1997. Sleepquality in children with attention deficit hyperactivity disorder: an actigraphicstudy. Psychiatry and Clinical Neurosciences 51, 383–386.
aimon, K., Yamada, N., Tsujimoto, T., Takahashi, S., 1992. Circadian rhythm abnor-malities of deep body temperature in depressive disorders. Journal of AffectiveDisorders 26, 191–198.
aniels, S.R., 2009. Cardiovascular effects of methylphenidate. The Journal of Pedi-atrics 155, 84–89.
el Campo, N., Chamberlain, S.R., Sahakian, B.J., Robbins, T.W., 2011. The rolesof dopamine and noradrenaline in the pathophysiology and treatment ofattention-deficit/hyperactivity disorder. Biological Psychiatry 69, E145–E157.
euschle, M., Schweiger, U., Weber, B., Gotthardt, U., Korner, A., Schmider, J., Stand-hardt, H., Lammers, C.H., Heuser, I., 1997. Diurnal activity and pulsatility of thehypothalamus-pituitary-adrenal system in male depressed patients and healthycontrols. The Journal of Clinical Endocrinology and Metabolism 82, 234–238.
evilbiss, D.M., Berridge, C.W., 2008. Cognition-enhancing doses ofmethylphenidate preferentially increase prefrontal cortex neuronalresponsiveness. Biological Psychiatry 64 (7), 626–635.
evilbiss, D.M., Waterhouse, B.D., 2004. The effects of tonic locus ceruleus out-put on sensory-evoked responses of ventral posterior medial thalamic andbarrel field cortical neurons in the awake rat. Journal of Neuroscience 24,10773–10785.
ietrich, A., Riese, H., Sondeijker, F., Greaves-Lord, K., Van Roon, A.M., Ormel, J.,Neeleman, J., Rosmalen, J.G.M., 2007. Externalizing and internalizing problemsin relation to autonomic function: a population-based study in preadoles-cents. Journal of the American Academy of Child and Adolescent Psychiatry 46,378–386.
uke, B.J., 2008. Pathogenic effects of central nervous system hyperarousal. MedicalHypotheses 71, 212–217.
dwards, S., Evans, P., Hucklebridge, F., Clow, A., 2001. Association between time ofawakening and diurnal cortisol secretory activity. Psychoneuroendocrinology26, 613–622.
alcon, E., McClung, C.A., 2009. A role for the circadian genes in drug addiction.Neuropharmacology 56, 91–96.
allone, G., Acebo, C., Arnedt, J.T., Seifer, R., Carskadon, M.A., 2001. Effects of acutesleep restriction on behavior, sustained attention, and response inhibition inchildren. Perceptual and Motor Skills 93, 213–229.
araone, S.V., Biederman, J., 1998. Neurobiology of attention-deficit hyperactivitydisorder. Biological Psychiatry 44, 951–958.
araone, S.V., Khan, S.A., 2005. Candidate gene studies of attention-deficit/hyperactivity disorder. In: Teleconference on New Developmentsin the Treatment of Attention-Deficit/Hyperactivity Disorder. PhysiciansPostgraduate Press, Electr Network, pp. 13–20.
ornaro, M., Prestia, D., Colicchio, S., Perugi, G., 2010. A systematic, updated reviewon the antidepressant agomelatine focusing on its melatonergic modulation.Current Neuropharmacology 8, 287–304.
reitag, C.M., Hanig, S., Palmason, H., Meyer, J., Wust, S., Seitz, C., 2009. Cortisolawakening response in healthy children and children with ADHD: impact ofcomorbid disorders and psychosocial risk factors. Psychoneuroendocrinology34, 1019–1028.
angwisch, J.E., 2009. Epidemiological evidence for the links between sleep, circa-dian rhythms and metabolism. Obesity Reviews 10 (Suppl. 2), 37–45.
arnock-Jones, K.P., Keating, G.M., 2009. Atomoxetine: a review of its use inattention-deficit hyperactivity disorder in children and adolescents. PaediatricDrugs 11 (3), 203–226.
ermain, A., Kupfer, D.J., 2008. Circadian rhythm disturbances in depression. HumanPsychopharmacology: Clinical and Experimental 23, 571–585.
olan, N., Shahar, E., Ravid, S., Pillar, G., 2004. Sleep disorders and daytimesleepiness in children with attention-deficit/hyperactive disorder. Sleep 27,261–266.
orelova, N., Seamans, J.K., Yang, C.R., 2002. Mechanisms of dopamine activation offast-spiking interneurons that exert inhibition in rat prefrontal cortex. Journalof Neurophysiology 88, 3150–3166.
randin, L.D., Alloy, L.B., Abramson, L.Y., 2006. The social zeitgeber theory, circa-dian rhythms, and mood disorders: review and evaluation. Clinical PsychologyReview 26, 679–694.
ruber, R., 2009. Sleep characteristics of children and adolescents with attentiondeficit-hyperactivity disorder. Child and Adolescent Psychiatric Clinics of NorthAmerica 18, 863–876.
ruber, R., Sadeh, A., Raviv, A., 2000. Instability of sleep patterns in children withattention-deficit/hyperactivity disorder. Journal of the American Academy ofChild and Adolescent Psychiatry 39, 495–501.
alperin, J.M., Schulz, K.P., 2006. Revisiting the role of the prefrontal cortex in thepathophysiology of attention-deficit/hyperactivity disorder. Psychological Bul-
letin 132, 560–581.ammerness, P.G., Perrin, J.M., Shelley-Abrahamson, R., Wilens, T.E., 2011. Cardio-vascular risk of stimulant treatment in pediatric attention-deficit/hyperactivitydisorder: update and clinical recommendations. Journal of the AmericanAcademy of Child and Adolescent Psychiatry 50, 978–990.
ioral Reviews 36 (2012) 1897–1919
Harvey, A.G., 2008. Sleep and circadian rhythms in bipolar disorder: seeking syn-chrony, harmony, and regulation. The American Journal of Psychiatry 165,820–829.
Harvey, A.G., Murray, G., Chandler, R.A., Soehner, A., 2011. Sleep disturbance as trans-diagnostic: consideration of neurobiological mechanisms. Clinical PsychologyReview 31, 225–235.
Hastings, P.D., Fortier, I., Utendale, W.T., Simard, L.R., Robaey, P., 2009. Adrenocorti-cal functioning in boys with attention-deficit/hyperactivity disorder: examiningsubtypes of ADHD and associated comorbid conditions. Journal of AbnormalChild Psychology 37, 565–578.
Hatzinger, M., Brand, S., Perren, S., von Wyl, A., von Klitzing, K., Holsboer-Trachsler,E., 2007. Hypothalamic-pituitary-adrenocortical (HPA) activity in kindergartenchildren: importance of gender and associations with behavioral/emotional dif-ficulties. Journal of Psychiatric Research 41, 861–870.
Haus, E., 2007. Chronobiology in the endocrine system. Advanced Drug DeliveryReviews 59, 985–1014.
Hermens, D.F., Cooper, N.J., Clark, C.R., Debrota, D., Clarke, S.D., Williams, L.M., 2007.An integrative approach to determine the best behavioral and biological markersof methylphenidate. Journal of Integrative Neuroscience 6 (1), 105–140.
Herpertz, S.C., Wenning, B., Mueller, B., Qunaibi, M., Sass, H., Herpertz-Dahlmann,B., 2001. Psychophysiological responses in ADHD boys with and without con-duct disorder: implications for adult antisocial behavior. Journal of the AmericanAcademy of Child and Adolescent Psychiatry 40, 1222–1230.
Himelstein, J., Newcorn, J.H., Halperin, J.M., 2000. The neurobiology of attention-deficit hyperactivity disorder. Frontiers in Bioscience: a Journal and VirtualLibrary 5, 461–478.
Hirvikoski, T., Lindholm, T., Nordenstrom, A., Nordstrom, A.L., Lajic, S., 2009. Highself-perceived stress and many stressors, but normal diurnal cortisol rhythm,in adults with ADHD (attention-deficit/hyperactivity disorder). Hormones andBehavior 55, 418–424.
Hoebert, M., Van der Heijden, K.B., van Geijlswijk, I.M., Smits, M.G., 2009. Long-term follow-up of melatonin treatment in children with ADHD and chronic sleeponset insomnia. Journal of Pineal Research 47, 1–7.
Hofstra, W.A., de Weerd, A.W., 2008. How to assess circadian rhythm in humans: areview of literature. Epilepsy & Behavior 13, 438–444.
Hong, H.J., Shin, D.W., Lee, E.H., Oh, Y.H., Noh, K.S., 2003. Hypothalamic-pituitary-adrenal reactivity in boys with attention deficit hyperactivity disorder. YonseiMedical Journal 44, 608–614.
Horne, J.A., Ostberg, O., 1976. A self-assessment questionnaire to determinemorningness-eveningness in human circadian rhythms. International Journalof Chronobiology 4, 97–110.
Hot, P., Naveteur, J., Leconte, P., Sequeira, H., 1999. Diurnal variations oftonic electrodermal activity. International Journal of Psychophysiology 33,223–230.
Houtveen, J.H., de Geus, E.J.C., 2009. Noninvasive psychophysiological ambulatoryrecordings study design and data analysis strategies. European Psychologist 14,132–141.
Hvolby, A., Jorgensen, J., Bilenberg, N., 2008. Actigraphic and parental reports of sleepdifficulties in children with attention-deficit/hyperactivity disorder. Archives ofPediatrics & Adolescent Medicine 162, 323–329.
Hvolby, A., Jorgensen, J., Bilenberg, N., 2009. Parental rating of sleep in children withattention deficit/hyperactivity disorder. European Child & Adolescent Psychiatry18, 429–438.
Iaboni, F., Douglas, V.I., Ditto, B., 1997. Psychophysiological response of ADHD chil-dren to reward and extinction. Psychophysiology 34, 116–123.
Imeraj, L., Antrop, I., Roeyers, H., Deschepper, E., Bal, S., Deboutte, D., 2011. Diurnalvariations in arousal: a naturalistic heart rate study in children with ADHD.European Child & Adolescent Psychiatry 20, 381–392.
Imeraj, L., Antrop, I., Roeyers, H., Swanson, J., Deschepper, E., Bal, S., Deboutte,D., 2012. Time-of-day effects in arousal: disrupted diurnal cortisol pro-files in children with ADHD. Journal of Child Psychology and Psychiatry,http://dx.doi.org/10.1111/j.1469-7610.2012.02526.x.
Ironside, S., Davidson, F., Corkum, P., 2010. Circadian motor activity affected bystimulant medication in children with attention-deficit/hyperactivity disorder.Journal of Sleep Research 19, 546–551.
Ivanov, A., Aston-Jones, G., 2000. Hypocretin/orexin depolarizes and decreasespotassium conductance in locus coeruleus neurons. Neuroreport 11, 1755–1758.
Jankowski, K.S., Ciarkowska, W., 2008. Diurnal variation in energetic arousal, tensearousal, and hedonic tone in extreme morning and evening types. ChronobiologyInternational 25, 577–595.
Kaneko, M., Hoshino, Y., Hashimoto, S., Okano, T., Kumashiro, H., 1993. Hypothalamicpituary-adrenal axis function in children with attention-deficit hyperactivitydisorder. Journal of Autism and Developmental Disorders 23, 59–65.
Kariyawasam, S.H., Zaw, F., Handley, S.L., 2002. Reduced salivary cortisol in childrenwith comorbid Attention deficit hyperactivity disorder and oppositional defiantdisorder. Neuroendocrinology Letters 23, 45–48.
Kennedy, S.H., Kutcher, S.P., Ralevski, E., Brown, G.M., 1996. Nocturnal melatoninand 24-hour 6-sulphatoxymelatonin levels in various phases of bipolar affectivedisorder. Psychiatry Research 63, 219–222.
Kerkhof, G.A., 1985. Inter-individual differences in the human circadian system – areview. Biological Psychology 20, 83–112.
Kerkhof, G.A., Van Dongen, H.P.A., Bobbert, A.C., 1998. Absence of endogenous cir-cadian rhythmicity in blood pressure? American Journal of Hypertension 11,373–377.
Kim, H.W., Yoon, I.Y., Cho, S.C., Kim, B.N., Chung, S., Lee, H., Kim, C.W., Park, S.K., Yoo,H.J., 2010. The effect of OROS methylphenidate on the sleep of children with

behav
K
K
L
L
L
L
L
L
L
L
L
L
L
L
L
M
M
M
M
M
M
M
M
M
M
M
M
M
N
N
L. Imeraj et al. / Neuroscience and Bio
attention-deficit/hyperactivity disorder. International Clinical Psychopharma-cology 25, 107–115.
issling, C., Retz, W., Wiemann, S., Coogan, A.N., Clement, R.M., Hunnerkopf, R.,Conner, A.C., Freitag, C.M., Rosler, M., Thome, J., 2008. A polymorphism at the3′-untranslated region of the CLOCK gene is associated with adult attention-deficit hyperactivity disorder. American Journal of Medical Genetics Part B:Neuropsychiatric Genetics 147B, 333–338.
lerman, E.B., Gershengorn, H.B., Duffy, J.F., Kronauer, R.E., 2002. Comparisons ofthe variability of three markers of the human circadian pacemaker. Journal ofBiological Rhythms 17, 181–193.
ackschewitz, H., Huther, G., Kroner-Herwig, B., 2008. Physiological and psycho-logical stress responses in adults with attention-deficit/hyperactivity disorder(ADHD). Psychoneuroendocrinology 33, 612–624.
awrence, J.B., Stanford, M.S., 1999. Impulsivity and time of day: effects on perfor-mance and cognitive tempo. Personality and Individual Differences 26, 199–207.
ecendreux, M., Konofal, E., Bouvard, M., Falissard, B., Mouren-Simeoni, M.C., 2000.Sleep and alertness in children with ADHD. Journal of Child Psychology andPsychiatry 41, 803–812.
evine, A., Zagoory-Sharon, O., Feldman, R., Lewis, J.G., Weller, A., 2007. Measuringcortisol in human psychobiological studies. Physiology & Behavior 90, 43–53.
evitan, R.D., Masellis, M., Lam, R.W., Muglia, P., Basile, V.S., Jain, U., Kaplan, A.S.,Tharmalingam, S., Kennedy, S.H., Kennedy, J.L., 2004. Childhood inattention anddysphoria and adult obesity associated with the dopamine D4 receptor gene inovereating women with seasonal affective disorder. Neuropsychopharmacology29, 179–186.
evy, F., 1991. The dopamine theory of attention-deficit hyperactivity disorder(ADHD). The Australian and New Zealand Journal of Psychiatry 25, 277–283.
evy, F., 2009. Dopamine vs noradrenaline: inverted-U effects and ADHD theories.The Australian and New Zealand Journal of Psychiatry 43, 101–108.
evy, F., Swanson, J.M., 2001. Timing, space and ADHD: the dopamine theory revis-ited. The Australian and New Zealand Journal of Psychiatry 35, 504–511.
ewy, A.J., Lefler, B.J., Emens, J.S., Bauer, V.K., 2006. The circadian basis of winterdepression. Proceedings of the National Academy of Sciences of the United Statesof America 103, 7414–7419.
icht, C.A., Tryon, W.W., 2009. Are children diagnosed with the combined form ofADHD pervasively hyperactive? Behavior Modification 33, 655–681.
orber, M.F., 2004. Psychophysiology of aggression, psychopathy, and conduct prob-lems: a meta-analysis. Psychological Bulletin 130, 531–552.
uman, M., Oosterlaan, J., Hyde, C., van Meel, C.S., Sergeant, J.A., 2007. Heart rate andreinforcement sensitivity in ADHD. Journal of Child Psychology and Psychiatry48, 890–898.
uman, M., Oosterlaan, J., Sergeant, J.A., 2005. The impact of reinforcement con-tingencies on AD/HD: a review and theoretical appraisal. Clinical PsychologyReview 25, 183–213.
a, L., Chen, Y.H., Chen, H., Liu, Y.Y., Wang, Y.X., 2011. The function of thehypothalamus-pituitary-adrenal axis in children with ADHD. Brain Research1368, 159–162.
acchi, M.M., Bruce, J.N., 2004. Human pineal physiology and functional significanceof melatonin. Frontiers in Neuroendocrinology 25, 177–195.
anev, H., Uz, T., 2009. Dosing time-dependent actions of psychostimulants. Inter-national Review of Neurobiology 88, 25–41.
arcotte, A.C., Thacher, P.V., Butters, M., Bortz, J., Acebo, C., Carskadon, M.A., 1998.Parental report of sleep problems in children with attentional and learningdisorders. Journal of Developmental and Behavioral Pediatrics 19, 178–186.
aurizi, C.P., 1984. A mechanism of mania and the chemistry of dreams: a hypoth-esis. Southern Medical Journal 77, 1491.
cBurnett, K., Lahey, B.B., Rathouz, P.J., Loeber, R., 2000. Low salivary cortisol andpersistent aggression in boys referred for disruptive behavior. Archives of Gen-eral Psychiatry 57, 38–43.
cClung, C.A., 2007. Circadian genes, rhythms and the biology of mood disorders.Pharmacology & Therapeutics 114, 222–232.
efford, I.N., Potter, W.Z., 1989. A neuroanatomical and biochemical basis for atten-tion deficit disorder with hyperactivity in children: a defect in tonic adrenalinemediated inhibition of locus coeruleus stimulation. Medical Hypotheses 29,33–42.
ezzacappa, E., Tremblay, R.E., Kindlon, D., Saul, J.P., Arseneault, L., Seguin, J., Pihl,R.O., Earls, F., 1997. Anxiety, antisocial behavior, and heart rate regulation inadolescent males. Journal of Child Psychology and Psychiatry 38, 457–469.
ick, E., Biederman, J., Jetton, J., Faraone, S.V., 2000. Sleep disturbances associ-ated with attention deficit hyperactivity disorder: the impact of psychiatriccomorbidity and pharmacotherapy. Journal of Child and Adolescent Psychophar-macology 10, 223–231.
orgenthaler, T., Alessi, C., Friedman, L., Owens, J., Kapur, V., Boehlecke, B., Brown,T., Chesson, A., Coleman, J., Lee-Chiong, T., Pancer, J., Swick, T.J., 2007. Prac-tice parameters for the use of actigraphy in the assessment of sleep and sleepdisorders: an update for 2007. Sleep 30, 519–529.
oss, H.B., Vanyukov, M.M., Martin, C.S., 1995. Salivary cortisol responses and riskfor substance-abuse in prepubertal boys. Biological Psychiatry 38, 547–555.
urphy, P.R., Robertson, I.H., Balsters, J.H., O’Connell, R.G., 2011. Pupillometry andP3 index the locus coeruleus–noradrenergic arousal function in humans. Psy-chophysiology, http://dx.doi.org/10.1111/j.1469-8986.2011.01226.x.
aber, D., Wirzjustice, A., Kafka, M.S., Wehr, T.A., 1980. Dopamine receptor-bindingin rat striatum – ultradian rhythm and its modification by chronic imipramine.Psychopharmacology 68, 1–5.
agtegaal, J.E., Kerkhof, G.A., Smits, M.G., Swart, A.C.W., Van der Meer, Y.G., 1998.Delayed sleep phase syndrome: a placebo-controlled cross-over study on the
ioral Reviews 36 (2012) 1897–1919 1917
effects of melatonin administered five hours before the individual dim lightmelatonin onset. Journal of Sleep Research 7, 135–143.
Nieuwenhuis, S., Aston-Jones, G., Cohen, J.D., 2005. Decision making, the P3,and the locus coeruleus–norepinephrine system. Psychological Bulletin 131,510–532.
Nieuwenhuis, S., De Geus, E.J., Aston-Jones, G., 2011. The anatomical and func-tional relationship between the P3 and autonomic components of the orientingresponse. Psychophysiology 48, 162–175.
Nofzinger, E.A., Mintun, M.A., Price, J., Meltzer, C.C., Townsend, D., Buysse, D.J.,Reynolds Iii, C.F., Dachille, M., Matzzie, J., Kupfer, D.J., 1998. A method for theassessment of the functional neuroanatomy of human sleep using FDG PET. BrainResearch Protocols 2, 191–198.
Nováková, M., Paclt, I., Ptácek, R., Kuzelová, H., Hájek, I., Sumová, A., 2011. Sali-vary melatonin rhythm as a marker of the circadian system in healthy childrenand those with attention-deficit/hyperactivity disorder. Chronobiology Interna-tional 28, 630–637.
O’Brien, L.M., Holbrook, C.R., Mervis, C.B., Klaus, C.J., Bruner, J.L., Raffield, T.J., Ruther-ford, J., Mehl, R.C., Wang, M., Tuell, A., Hume, B.C., Gozal, D., 2003a. Sleepand neurobehavioral characteristics of 5-to 7-year-old children with parentallyreported symptoms of attention-deficit/hyperactivity disorder. Pediatrics 111,554–563.
O’Brien, L.M., Ivanenko, A., Crabtree, V.M., Holbrook, C.R., Bruner, J.L., Klaus, C.J.,Gozal, D., 2003b. Sleep disturbances in children with attention deficit hyperac-tivity disorder. Pediatric Research 54, 237–243.
O’Keeffe, S.M., Thome, J., Coogan, A.N., 2012. The noradrenaline reuptake inhibitoratomoxetine phase-shifts the circadian clock in mice. Neuroscience 201,219–230.
Ortiz, J., Raine, A., 2004. Heart rate level and antisocial behavior in children andadolescents: a meta-analysis. Journal of the American Academy of Child andAdolescent Psychiatry 43, 154–162.
Owens, J., Sangal, R.B., Sutton, V.K., Bakken, R., Allen, A.J., Kelsey, D., 2009. Subjectiveand objective measures of sleep in children with attention-deficit/hyperactivitydisorder. Sleep Medicine 10, 446–456.
Owens, J.A., 2005. The ADHD and sleep conundrum: a review. Journal of Develop-mental and Behavioral Pediatrics 26, 312–322.
Owens, J.A., Maxim, R., Nobile, C., McGuinn, M., Msall, M., 2000. Parental andself-report of sleep in children with attention-deficit/hyperactivity disorder.Archives of Pediatrics & Adolescent Medicine 154, 549–555.
Paavonen, E.J., Raikkonen, K., Lahti, J., Komsi, N., Heinonen, K., Pesonen, A.K., Jar-venpaa, A.L., Strandberg, T., Kajantie, E., Porkka-Heiskanen, T., 2009. Short sleepduration and behavioral symptoms of attention-deficit/hyperactivity disorderin healthy 7-to 8-year-old children. Pediatrics 123, E857–E864.
Pacchierotti, C., Iapichino, S., Bossini, L., Pieraccini, F., Castrogiovanni, P., 2001.Melatonin in psychiatric disorders: a review on the melatonin involvement inpsychiatry. Frontiers in Neuroendocrinology 22, 18–32.
Paclt, I., Koudelova, J., Krepelova, A., Uhlikova, P., Gazdikova, M., Bauer, P., 2005.Biochemical markers and genetic research of ADHD. Neuroendocrinology Letters26, 423–430.
Pajer, K., Gardner, W., Rubin, R.T., Perel, J., Neal, S., 2001. Decreased cortisol levelsin adolescent girls with conduct disorder. Archives of General Psychiatry 58,297–302.
Pattij, T., Vanderschuren, L., 2008. The neuropharmacology of impulsive behaviour.Trends in Pharmacological Sciences 29, 192–199.
Pelham, W.E., Gnagy, E.M., Burrows-Maclean, L., Williams, A., Fabiano, G.A., Morrisey,S.M., Chronis, A.M., Forehand, G.L., Nguyen, C.A., Hoffman, M.T., Lock, T.M., Fiel-belkorn, K., Coles, E.K., Panahon, C.J., Steiner, R.L., Meichenbaum, D.L., Onyango,A.N., Morse, G.D., 2001. Once-a-day concerta methylphenidate versus three-times-daily methylphenidate in laboratory and natural settings. Pediatrics 107,E105.
Pesonen, A.K., Kajantie, E., Jones, A., Pyhälä, R., Lahti, J., Heinonen, K., Eriksson, J.G.,Strandberg, T.E., Räikkönen, K., 2011. Symptoms of attention deficit hyperactiv-ity disorder in children are associated with cortisol responses to psychosocialstress but not with daily cortisol levels. Journal of Psychiatric Research 45,1471–1476.
Pesonen, A.K., Raikkonen, K., Paavonen, E.J., Heinonen, K., Komsi, N., Lahti, J., Kajantie,E., Jarvenpaa, A.L., Strandberg, T., 2010. Sleep duration and regularity are asso-ciated with behavioral problems in 8-year-old children. International Journal ofBehavioral Medicine 17, 298–305.
Pfaff, D., Banavar, J.R., 2007. A theoretical framework for CNS arousal. Bioessays 29,803–810.
Pfaff, D.W., Martin, E.M., Ribeiro, A.C., 2007. Relations between mechanisms of CNSarousal and mechanisms of stress. Stress 10, 316–325.
Philipsen, A., Hornyak, M., Riemann, D., 2006. Sleep and sleep disorders in adultswith attention deficit/hyperactivity disorder. Sleep Medicine Reviews 10,399–405.
Phillips, M.A., Szabadi, E., Bradshaw, C.M., 2000. Comparison of the effects of cloni-dine and yohimbine on spontaneous pupillary fluctuations in healthy humanvolunteers. Psychopharmacology 150, 85–89.
Pliszka, S.R., McCracken, J.T., Maas, J.W., 1996. Catecholamines in attention-deficithyperactivity disorder: current perspectives. Journal of the American Academyof Child and Adolescent Psychiatry 35, 264–272.
Polich, J., Kok, A., 1995. Cognitive and biological determinants of P300: an integrativereview. Biological Psychology 41, 103–146.
Porrino, L.J., Rapoport, J.L., Behar, D., Sceery, W., Ismond, D.R., Bunney, W.E., 1983. Anaturalistic assessment of the motor-activity of hyperactive boys. 1. Comparisonwith normal controls. Archives of General Psychiatry 40, 681–687.

1 behav
P
P
Q
R
R
R
R
R
R
R
R
S
S
S
S
S
S
S
S
S
S
S
S
S
S
S
S
S
S
918 L. Imeraj et al. / Neuroscience and Bio
ortaluppi, F., Touitou, Y., Smolensky, M., 2008. Ethical and methodological stan-dards for laboratory and medical biological rhythm research. ChronobiologyInternational 25, 999–1016.
ower, T.J., 1992. Contextual factors in vigilance testing of children with ADHD.Journal of Abnormal Child Psychology 20, 579–593.
uay, H.C., 1965. Psychopathic personality as pathological stimulation-seeking. TheAmerican Journal of Psychiatry 122, 180–183.
aine, A., 1996. Autonomic nervous system factors underlying disinhibited, antiso-cial, and violent behavior – biosocial perspectives and treatment implications.Annals of the New York Academy of Sciences 794, 46–59.
andazzo, W.T., Dockray, S., Susman, E.J., 2008. The stress response in adolescentswith inattentive type ADHD symptoms. Child Psychiatry and Human Develop-ment 39, 27–38.
ao, M.L., Gross, G., Strebel, B., Halaris, A., 1994. Circadian rhythm of tryptophan,serotonin, melatonin, and pituitary hormones in schizophrenia. Biological Psy-chiatry 35, 151–163.
eimer, B., D’Ambrosio, L.A., Coughlin, J.F., Fried, R., Biederman, J., 2007.Task-induced fatigue and collisions in adult drivers with attention deficit hyper-activity disorder. Traffic Injury Prevention 8, 290–299.
iddoch, C.J., Mattocks, C., Deere, K., Saunders, J., Kirkby, J., Tilling, K., Leary, S.D.,Blair, S.N., Ness, A.R., 2007. Objective measurement of levels and patterns ofphysical activity. Archives of Disease in Childhood 92, 963–969.
osenwasser, A.M., 2010. Circadian clock genes: non-circadian roles in sleep, addic-tion, and psychiatric disorders? Neuroscience and Biobehavioral Reviews 34,1249–1255.
ybak, Y.E., McNeely, H.E., Mackenzie, B.E., Jain, U.R., Levitan, R.D., 2004. Anopen trial of light therapy in adult attention-deficit/hyperactivity disorder.In: 16th Annual Conference of the Society-for-Light-Treatment-and-Biological-Rhythms, Toronto, pp. 1527–1535.
ybak, Y.E., McNeely, H.E., Mackenzie, B.E., Jain, U.R., Levitan, R.D., 2007. Seasonalityand circadian preference in adult attention-deficit/hyperactivity disorder: clin-ical and neuropsychological correlates. Comprehensive Psychiatry 48, 562–571.
adeh, A., Pergamin, L., Bar-Haim, Y., 2006. Sleep in children with attention-deficithyperactivity disorder: a meta-analysis of polysomnographic studies. SleepMedicine Reviews 10, 381–398.
amuels, E.R., Szabadi, E., 2008. Functional neuroanatomy of the noradrenergic locuscoeruleus: its roles in the regulation of arousal and autonomic function part I:principles of functional organisation. Current Neuropharmacology 6, 235–253.
an, L., Arranz, B., 2008. Agomelatine: a novel mechanism of antidepressant actioninvolving the melatonergic and the serotonergic system. European Psychiatry23, 396–402.
cheer, F., Kalsbeek, A., Buijs, R.M., 2003. Cardiovascular control by the suprachi-asmatic nucleus: neural and neuroendocrine mechanisms in human and rat.Biological Chemistry 384, 697–709.
cheer, F.A., Hilton, M.F., Mantzoros, C.S., Shea, S.A., 2009. Adverse metabolicand cardiovascular consequences of circadian misalignment. Proceedings ofthe National Academy of Sciences of the United States of America 106,4453–4458.
chmidt, C., Collette, F., Leclercq, Y., Sterpenich, V., Vandewalle, G., Berthomier, P.,Berthomier, C., Phillips, C., Tinguely, G., Darsaud, A., 2009. Homeostatic sleeppressure and responses to sustained attention in the suprachiasmatic area. Sci-ence 324, 516–519.
chredl, M., Alm, B., Sobanski, E., 2007. Sleep quality in adult patients with atten-tion deficit hyperactivity disorder (ADHD). European Archives of Psychiatry andClinical Neuroscience 257, 164–168.
chulz, K.P., Halperin, J.M., Newcorn, J.H., Sharma, V., Gabriel, S., 1997. Plasma cor-tisol and aggression in boys with ADHD. Journal of the American Academy ofChild and Adolescent Psychiatry 36, 605–609.
chwartz, G., Ben Amor, L., Grizenko, N., Lageix, P., Baron, C., Boivin, D.B., Joober,R., 2004. Actigraphic monitoring during sleep of children with ADHD onmethylphenidate and placebo. Journal of the American Academy of Child andAdolescent Psychiatry 43, 1276–1282.
chwartz, J.R., Roth, T., 2008. Neurophysiology of sleep and wakefulness: basic sci-ence and clinical implications. Current Neuropharmacology 6, 367–378.
ergeant, J., Van der Meere, J., 1988. What happens after a hyperactive child commitsan error? Psychiatry Research 24, 157–164.
ergeant, J., Van der Meere, J., 1990. Convergence of approaches in localizing thehyperactivity deficit. In: Lahey, B.B., Kazdin, A.E. (Eds.), Advances in Clinical ChildPsychology. Plenum, New York, pp. 207–246.
hin, D.W., Lee, S.H., 2007. Blunted hypothalamo-pituitary-adrenal axis reactivity isassociated with the poor intelligence performance in children with attention-deficit/hyperactivity disorder. Neuropediatrics 38, 298–303.
hirtcliff, E.A., Granger, D.A., Booth, A., Johnson, D., 2005. Low salivary cortisol levelsand externalizing behavior problems in youth. Development and Psychopathol-ogy 17, 167–184.
ilver, R., LeSauter, J., 2008. Circadian and homeostatic factors in arousal. Annals ofthe New York Academy of Sciences 1129, 263–274.
leipness, E.P., Sorg, B.A., Jansen, H.T., 2007. Contribution of the suprachiasmaticnucleus to day: night variation in cocaine-seeking behavior. Physiology & Behav-ior 91, 523–530.
mits, M.G., Nagtegaal, E.E., Van der Heijden, J., Coenen, A.M.L., Kerkhof, G.A., 2001.
Melatonin for chronic sleep onset insomnia in children: a randomized placebo-controlled trial. Journal of Child Neurology 16, 86–92.mits, M.G., van Stel, H.F., Van der Heijden, K., Meijer, A.M., Coenen, A.M.L., Kerkhof,G.A., 2003. Melatonin improves health status and sleep in children with idio-pathic chronic sleep-onset insomnia: a randomized placebo-controlled trial.
ioral Reviews 36 (2012) 1897–1919
Journal of the American Academy of Child and Adolescent Psychiatry 42,1286–1293.
Snoek, H., Van Goozen, S.H.M., Matthys, W., Buitelaar, J.K., Van Engeland, H., 2004.Stress responsivity in children with externalizing behavior disorders. Develop-ment and Psychopathology 16, 389–406.
Solanto, M.V., 1984. Neuropharmacological basis of stimulant drug action in atten-tion deficit disorder with hyperactivity: a review and synthesis. PsychologicalBulletin 95, 387–409.
Sondeijker, F., Ferdinand, R.F., Oldehinkel, A.J., Veenstra, R., Tiemeier, H., Ormel, J.,Verhulst, F.C., 2007. Disruptive behaviors and HPA-axis activity in young adoles-cent boys and girls from the general population. Journal of Psychiatric Research41, 570–578.
Sonuga-Barke, E.J., Swanson, J.M., Coghill, D., DeCory, H.H., Hatch, S.J., 2004. Efficacyof two once-daily methylphenidate formulations compared across dose levelsat different times of the day: preliminary indications from a secondary analysisof the COMACS study data. BMC Psychiatry 4, 28.
Sonuga-Barke, E.J.S., Sergeant, J.A., Nigg, J., Willcutt, E., 2008a. Executive dysfunc-tion and delay aversion in attention deficit hyperactivity disorder: nosologicand diagnostic implications. Child and Adolescent Psychiatric Clinics of NorthAmerica 17, 367–384.
Sonuga-Barke, E.J., Van Lier, P., Swanson, J.M., Coghill, D., Wigal, S., Vandenberghe,M., Hatch, S., 2008b. Heterogeneity in the pharmacodynamics of two long-actingmethylphenidate formulations for children with attention deficit/hyperactivitydisorder. European Child and Adolescent Psychiatry 4, 245–254.
Sonuga-Barke, E.J.S., Wiersema, J.R., van der Meere, J.J., Roeyers, H., 2010. Context-dependent dynamic processes in attention deficit/hyperactivity disorder:differentiating common and unique effects of state regulation deficits and delayaversion. Neuropsychology Review 20, 86–102.
Sonuga-Barke, E.J.S., Williams, E., Hall, M., Saxton, T., 1996. Hyperactivity and delayaversion. 3. The effect on cognitive style of imposing delay after errors. Journalof Child Psychology and Psychiatry 37, 189–194.
Spencer, T.J., Biederman, J., Mick, E., 2007. Attention-deficit/hyperactivity disor-der: diagnosis, lifespan, comorbidities, and neurobiology. Journal of PediatricPsychology 32, 631–642.
Stadler, C., Grasmann, D., Fegert, J.H., Holtmann, H., Poustka, F., Schmeck, K., 2008.Heart rate and treatment effect in children with disruptive behavior disorders.Child Psychiatry and Human Development 39, 299–309.
Stampfer, H.G., 1998. The relationship between psychiatric illness and the circadianpattern of heart rate. The Australian and New Zealand Journal of Psychiatry 32,187–198.
Stein, D., Pat-Horenczyk, R., Blank, S., Dagan, Y., Barak, Y., Gumpel, T.P., 2002. Sleepdisturbances in adolescents with symptoms of attention-deficit/hyperactivitydisorder. Journal of Learning Disabilities 35, 268–275.
Stephan, F.K., Zucker, I., 1972. Circadian rhythms in drinking behavior and locomo-tor activity of rats are eliminated by hypothalamic lesions. Proceedings of theNational Academy of Sciences of the United States of America 69, 1583–1586.
Surman, C.B.H., Adamson, J.J., Petty, C., Biederman, J., Kenealy, D.C., Levine, M., Mick,E., Faraone, S.V., 2009. Association between attention-deficit/hyperactivity dis-order and sleep impairment in adulthood: evidence from a large controlledstudy. The Journal of Clinical Psychiatry 70, 1523–1529.
Susman, E.J., Dockray, S., Schiefelbein, V.L., Herwehe, S., Heaton, J.A., Dorn,L.D., 2007. Morningness/eveningness, morning-to-afternoon cortisol ratio, andantisocial behavior problems during puberty. Developmental Psychology 43,811–822.
Swanson, C.J., Perry, K.W., Koch-Krueger, S., Katner, J., Svensson, K.A., Bymaster, F.P.,2006. Effect of the attention deficit/hyperactivity disorder drug atomoxetine onextracellular concentrations of norepinephrine and dopamine in several brainregions of the rat. Neuropharmacology 50, 755–760.
Swanson, J.M., Wigal, S.B., Wigal, T., Sonuga-Barke, E., Greenhill, L.L., Biederman,J., Kollins, S., Nguyen, A.S., DeCory, H.H., Dirksen, S.J.H., Hatch, S.J., 2004. Acomparison of once-daily extended-release methylphenidate formulations inchildren with attention-deficit/hyperactivity disorder in the laboratory school(The COMACS study). Pediatrics 113, E206–E216.
Sylvester, C.M., Krout, K.E., Loewy, A.D., 2002. Suprachiasmatic nucleus projection tothe medial prefrontal cortex. A viral transneuronal tracing study. Neuroscience114, 1071–1080.
Tankova, I., Adan, A., Buelacasal, G., 1994. Circadian typology and individual differ-ences – a review. Personality and Individual Differences 16, 671–684.
Thayer, J.F., Lane, R.D., 2007. The role of vagal function in the risk for cardiovasculardisease and mortality. Biological Psychology 74, 224–242.
Thayer, J.F., Sternberg, E., 2006. Beyond heart rate variability – vagal regulation ofallostatic systems. Annals of the New York Academy of Sciences 1088, 361–372.
Tjon Pian Gi, Cecil V., Broeren, Joris P.A., Sander Starreveld, J., Versteegh, Florens G.A.,2003. Melatonin for treatment of sleeping disorders in children with attentiondeficit/hyperactivity disorder: a preliminary open label study. European Journalof Pediatrics 162, 554–555.
Tonhajzerova, I., Ondrejka, I., Adamik, P., Hruby, R., Javorka, M., Trunkvalterova, Z.,Mokra, D., Javorka, K., 2009. Changes in the cardiac autonomic regulation inchildren with attention deficit hyperactivity disorder (ADHD). Indian Journal ofMedical Research 130, 44–50.
Toplak, M., Tannock, R., 2005. Time perception: modality and duration effects in
attention-deficit/hyperactivity disorder (ADHD). Journal of Abnormal Child Psy-chology 33, 639–654.Touchette, E., Cote, S.M., Petit, D., Liu, X.C., Boivin, M., Falissard, B., Tremblay, R.E.,Montplaisir, J.Y., 2009. Short nighttime sleep-duration and hyperactivity trajec-tories in early childhood. Pediatrics 124, E985–E993.

behav
T
V
V
V
V
v
V
v
v
v
V
v
V
V
W
W
L. Imeraj et al. / Neuroscience and Bio
sujii, N., Okada, A., Kaku, R., Kuriki, N., Hanada, K., Matsuo, J., Kusube, T., Hitomi,K., 2007. Association between activity level and situational factors in childrenwith attention deficit/hyperactivity disorder in elementary school. Psychiatryand Clinical Neurosciences 61, 181–185.
alera, E.M., Faraone, S.V., Murray, K.E., Seidman, L.J., 2007. Meta-analysis of struc-tural imaging findings in attention-deficit/hyperactivity disorder. BiologicalPsychiatry 61, 1361–1369.
an der Heijden, K.B., Smits, M.G., Gunning, W.B., 2005a. Sleep-related disorders inADHD: a review. Clinical Pediatrics 44, 201–210.
an der Heijden, K.B., Smits, M.G., Van Someren, E.J.W., Gunning, W.B., 2005b. Idio-pathic chronic sleep onset insomnia in attention-deficit/hyperactivity disorder:a circadian rhythm sleep disorder. Chronobiology International 22, 559–570.
an der Heijden, K.B., Smits, M.G., Van Someren, E.J.W., Ridderinkhof, K.R., Gunning,W.B., 2007. Effect of melatonin on sleep, behavior, and cognition in ADHD andchronic sleep-onset insomnia. Journal of the American Academy of Child andAdolescent Psychiatry 46, 233–241.
an der Kooij, M.A., Glennon, J.C., 2007. Animal models concerning the role ofdopamine in attention-deficit hyperactivity disorder. Neuroscience and Biobe-havioral Reviews 31, 597–618.
an der Meere, J.J., 2005. State-regulation and ADHD. In: Gozal, D., Molfese, D.L.(Eds.), Attention Deficit Hyperactivity Disorder: from Genes to Animal Modelsto Patients. Humana, Totawa, NJ, pp. 413–433.
an Goozen, S.H.M., Matthys, W., Cohen-Kettenis, P.T., Buitelaar, J.K., van Engeland,H., 2000. Hypothalamic-pituitary-adrenal axis and autonomic nervous systemactivity in disruptive children and matched controls. Journal of the AmericanAcademy of Child and Adolescent Psychiatry 39, 1438–1445.
an Goozen, S.H.M., Matthys, W., Cohen-Kettenis, P.T., Gispen-de Wied, C., Wiegant,V.M., van Engeland, H., 1998. Salivary cortisol and cardiovascular activity dur-ing stress in oppositional-defiant disorder boys and normal controls. BiologicalPsychiatry 43, 531–539.
an Lang, N.D.J., Tulen, J.H.M., Kallen, V.L., Rosbergen, B., Dieleman, G., Ferdinand,R.F., 2007. Autonomic reactivity in clinically referred children attention-deficit/hyperactivity disorder versus anxiety disorder. European Child &Adolescent Psychiatry 16, 71–78.
an Veen, M.M., Kooij, J.J., Boonstra, A.M., Gordijn, M., Van Someren, E.J.W., 2010.Delayed circadian rhythm in adults with attention-deficit/hyperactivitydisorder and chronic sleep-onset insomnia. Biological Psychiatry 67,1091–1096.
an West, D., Claes, S., Deboutte, D., 2009. Differences in hypothalamic-pituitary-adrenal axis functioning among children with ADHD predominantly inattentiveand combined types. European Child & Adolescent Psychiatry 18, 543–553.
icentic, A., Benca, R., Duncan, M.J., Frank, E., McClung, C., Nelson, R.J., 2009. Bio-logical rhythms, higher brain function, and behavior: gaps, opportunities, andchallenges. Brain Research Reviews 62, 57–70.
itiello, B., Elliott, G.R., Swanson, J.M., Arnold, L.E., Hechtman, L., Abikoff, H., Molina,B.S., Wells, K., Wigal, T., Jensen, P.S., Greenhill, L.L., Kaltman, J.R., Severe, J.B.,Odbert, C., Hur, K., Gibbons, R., 2012. Blood pressure and heart rate over 10years in the Multimodal Treatment Study of children with ADHD. The AmericanJournal of Psychiatry 169, 167–177.
alters, A.S., Silvestri, R., Zucconi, M., Chandrashekariah, R., Konofal, E., 2008.Review of the possible relationship and hypothetical links between attentiondeficit hyperactivity disorder (ADHD) and the simple sleep related movement
disorders, parasomnias, hypersomnias, and circadian rhythm disorders. Journalof Clinical Sleep Medicine 4, 591–600.ang, L.J., Huang, Y.S., Hsiao, C.C., Chiang, Y.L., Wu, C.C., Shang, Z.Y., Chen, C.K., 2011.Salivary dehydroepiandrosterone, but not cortisol, is associated with attentiondeficit hyperactivity disorder. World Journal of Biological Psychiatry 12, 99–109.
ioral Reviews 36 (2012) 1897–1919 1919
Waschbusch, D.A., Pelham, W.E., Jennings, J.R., Greiner, A.R., Tarter, R.E., Moss, H.B.,2002. Reactive aggression in boys with disruptive behavior disorders: behavior,physiology, and affect. Journal of Abnormal Child Psychology 30, 641–656.
Waterhouse, J., Atkinson, G., Reilly, T., Jones, H., Edwards, B., 2007. Chronophysiologyof the cardiovascular system. Biological Rhythm Research 38, 181–194.
Weaver, D.R., 1998. The suprachiasmatic nucleus: a 25-year retrospective. Journalof Biological Rhythms 13, 100–112.
Wehmeier, P.M., Schacht, A., Wolff, C., Otto, W.R., Dittmann, R.W., Banaschewski,T., 2011. Neuropsychological outcomes across the day in children withattention-deficit/hyperactivity disorder treated with atomoxetine: results froma placebo-controlled study using a computer-based continuous performancetest combined with an infra-red motion tracking device. Journal of Child andAdolescent Psychopharmacology 21, 433–444.
Wehr, T.A., Wirz-Justice, A., Goodwin, F.K., Duncan, W., Gillin, J.C., 1979. Phaseadvance of the circadian sleep-wake cycle as an antidepressant. Science 206,710–713.
Weiss, M.D., Wasdell, M.B., Bomben, M.M., Rea, K.J., Freeman, R.D., 2006. Sleephygiene and melatonin treatment for children and adolescents with ADHD andinitial insomnia. Journal of the American Academy of Child and Adolescent Psy-chiatry 45, 512–519.
Wiersema, R., Van Der Meere, J., Antrop, I., Roeyers, H., 2006a. State regulation inadult ADHD: an event-related potential study. Journal of Clinical and Experi-mental Neuropsychology 28, 1113–1126.
Wiersema, R., van der Meere, J., Roeyers, H., Van Coster, R., Baeyens, D., 2006b.Event rate and event-related potentials in ADHD. Journal of Child Psychologyand Psychiatry 47, 560–567.
Wiggs, L., Montgomery, P., Stores, G., 2005. Actigraphic and parent reports of sleeppatterns and sleep disorders in children with subtypes of attention-deficithyperactivity disorder. Sleep 28, 1437–1445.
Winsky-Sommerer, R., Boutrel, B., de Lecea, L., 2003. The role of the hypcretinergicsystem in the integration of networks that dictate the states of arousal. DrugNews & Perspectives 16, 504–512.
Wirz-Justice, A., 2006. Biological rhythm disturbances in mood disorders. Interna-tional Clinical Psychopharmacology 21, S11–S15.
Wirz-Justice, A., Kafka, M.S., Naber, D., Wehr, T.A., 1980. Circadian rhythms in ratbrain alpha-and beta-adrenergic receptors are modified by chronic imipramine.Life Science 27, 341–347.
Xu, X.H., Breen, G., Chen, C.K., Huang, Y.S., Wu, Y.Y., Asherson, P., 2010. Associationstudy between a polymorphism at the 3′-untranslated region of CLOCK gene andattention deficit hyperactivity disorder. Behavioural Brain Function 6, 48.
Yan, T.C., Dudley, J.A., Weir, R.K., Grabowska, E.M., Pena-Oliver, Y., Ripley, T.L.,Hunt, S.P., Stephens, D.N., Stanford, S.C., 2011. Performance deficits of NK1receptor knockout mice in the 5-choice serial reaction-time task: effects ofd-amphetamine, stress and time of day. PLoS One 6, e17586.
Young, M.E., 2006. The circadian clock within the heart: potential influence onmyocardial gene expression, metabolism, and function. American Journal ofPhysiology. Heart and Circulatory Physiology 290, H1–H16.
Young, M.E., Bray, M.S., 2007. Potential role for peripheral circadian clock dyssyn-chrony in the pathogenesis of cardiovascular dysfunction. Sleep Medicine 8,656–667.
Zagar, R., Bowers, N.D., 1983. The effect of time of day on problem-solving andclassroom-behavior. Psychology in the Schools 20, 337–345.
Zawilska, J.B., Skene, D.J., Arendt, J., 2009. Physiology and pharmacology of melatoninin relation to biological rhythms. Pharmacological Reports 61, 383–410.
Zentall, S.S., Zentall, T.R., 1976. Activity and task-performance of hyperactive-children as a function of environmental stimulation. Journal of Consulting andClinical Psychology 44, 693–697.





























