Embed Size (px)
Citation preview

An Intelligent Decision Support System forPersonalized Cancer Treatment
M.A. Al-Mamun, Nabila Kazmi, A. Hossain, P.Vickers and Yang Jiang
Computational Intelligence Research GroupSchool of Computing, Engineering, and Information Sciences (CEIS), Northumbria University
Newcastle upon Tyne, NE1 8ST, UKEmail: mohammed.al-mamun; nabila.kazmi;alamgir.hosasin;paul.vickers and yang.jiang {@northumbria.ac.uk}
Abstract— Cancer is one of the biggest killers in the westernworld; every two minutes someone is diagnosed with cancer inthe UK. Personalized treatment of cancer, which simply meansselecting a treatment best suited to an individual involving theintegration and translation of several new technologies in clinicalcare of patients. Conventional cancer treatments include surgery,radiotherapy and chemotherapy. Among these, therapeuticallytreatment requires optimal control of radiation/drug to minimizetoxic effect and in turn to minimize side effect. We propose ahybrid prediction model consist of avascular tumour growthmodel from a tumour image and intelligent drug schedulingschema for drug penetration. Our main aim is to develop anintelligent decision support system which helps to analyze thetumour microenvironment constraints like cell-cell adhesion, cellmovement, extra-cellular matrix (ECM) and optimal solutions ofdrug scheduling problem. Hypoxia and drug resistance are alsoincorporated in the model to achieve the predictive results forevery patient as both of them considered as the main reason forchemotherapy and radiotherapy treatment failure. Finally, ourgoal is to provide a dynamic and effective personalized cancertreatment model to support the oncologist for making rightdecisions to the right patient at the right time.
Keywords—Artificial intelligence, Tumour growth,Personalized cancer treatment and Extracellular matrix (ECM)
I. INTRODUCTION
Cancer is known as a big public health plight in the UKand many other countries of the world. Cancer related deathshave been escalating meteorically, according to the WorldHealth Organization 7.6 million people worldwide died ofcancer in 2008. According to the statistical analysis of WorldCancer Report, cancer rates might further rise by 50% to 15million new cases in 2020 [1] [2]. The exact number of cancercases is still not known due to incomplete registration ofcancer cases in some parts of the world. Despite the pace ofrecent discoveries in cancer research, cancer specialists arestill not able to treat all cancers successfully. Understandingthe complexity of the cellular processes that are dys-regulatedin cancer progression provides a significant challenge whenstudying the disease and considering treatment options. A
comprehensive study is required to understand tumourdevelopment and what drugs will target the pathways vital fortumour survival. New strategies are required that could turnwhat is currently an obstruction into a considerable advantagefor cancer therapy.
Cancer is an abnormal growth of cells caused by multiplechanges in gene expression leading to dys-regulated balanceof cell proliferation and cell death, and ultimately into apopulation of cells that can invade tissues and metastasize todistant sites. Cancer refers to a set of disease where normalcells of the body lose their mechanisms which are responsiblefor controlling their growth and motility. Cancer cellstypically proliferate in an exponential fashion, the size of thecancerous mass is measured experimentally as a volume,though this mass is often referred to in terms of the number ofcells 109 [3].
This paper presents an investigation into the developmentof an intelligent decision support system for predicting thetoxicity and required drug concentration prior or during thechemotherapy or radiotherapy. We propose a hybrid predictionmodel consist of avascular tumour growth model from atumour image and intelligent drug scheduling schema for drugpenetration. Our main aim is to develop an intelligent decisionsupport system which allows analyzing the tumourmicroenvironment constraints like cell-cell adhesion, cellmovement, extra-cellular matrix (ECM) and optimal solutionsof drug scheduling problem. Finally, our goal is to provide adynamic personalized cancer treatment model to support theOncologist.
II. PROBLEM BACKGROUND
The main treatment of cancer includes surgery,radiotherapy, chemotherapy, hormone therapy,bisphosphonates, bone marrow and stem cell transplants, andbiological, therapies. Chemotherapy is one of the essential andcommon treatment methods for cancer dealing with differentchemo drugs (i.e. treatment with cell killing (cytotoxic)drugs). Patients may have just one chemotherapy drug or acombination of different chemotherapy drugs. There are manydifferent drugs currently available and new ones are beingdeveloped all the time. These drugs are often used as part of
multimodality therapy that is along with surgery and/orradiotherapy to achieve and maintain remission. Inradiotherapy, radiation is used to destroy cells in the region oftreatment. Normal cells rapidly repair this damage but cancercells are not able to do this [4]. Chemotherapy can beadministered through a vein, injected into a body cavity, ordelivered orally in the form of a pill. Chemotherapy isdifferent from surgery or radiation in a context that itcirculates in the blood, reaches to parts of body where thecancer might have spread and then ultimately kills the cells[5]. Radiotherapy kills cell by damaging their DNA, whileoxygen molecules keep this damage permanent resulting intocell death Siim et al. [6]. Normal cells are less sensitive toradiotherapy. Hypoxic cells are generally resistant towardschemotherapy and radiotherapy, and are considered as one ofthe major cause of treatment failure [7]. Hypoxia is recognizedas a factor that helps tumour cells survive by giving them amore aggressive phenotype. The majority of tumours greaterthan 1mm3 in size have hypoxic regions because of irregularblood vessel structure and increased distance from bloodvessels. Poor drug penetration due to the deformed capillaryvessels of tumours and the increased distance of tumour cellsfrom blood vessels [8].
Inefficient drug diffusion to the most severe hypoxicregions of solid tumours causes a failure of chemotherapy tokill all cancer cells and results into tumour recurrence. AgainRadiotherapy and chemotherapy mainly target aerobic fractionof cells and their action could be enhanced using bioreductivedrugs. Our model has been prepared to remove the hypoxicregion from a tumour prior to or during treatment.Bioreductive drugs such as Tirapazamine (TPZ) andBanoxantrone (AQ4N) have been experimented on and putinto clinical trials [9]. TPZ is in clinical phase II and III trialswith radiotherapy and the anti-cancer drug cisplatinrespectively. In this investigation, firstly we reconstruct thetumour growth model according to the patient’s tumour image(can be either CT image or mammogram) and biological data.The most challenging problems like drug resistance andhypoxia problem are related with tumour complex behaviourand drug penetration. For these we construct the twoequivalent growth model both in tissue and cellular level.
III. METHODOLOGY
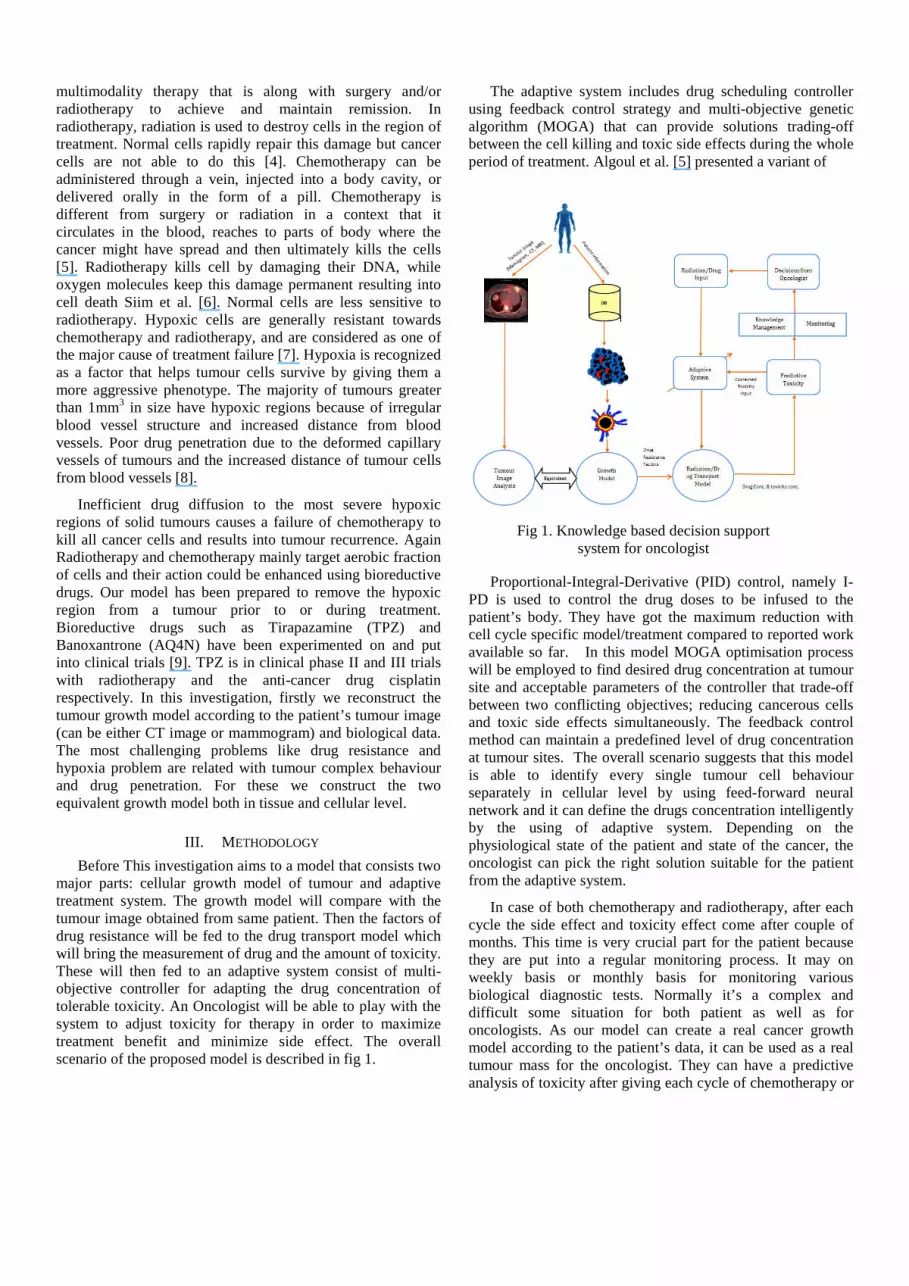
Before This investigation aims to a model that consists twomajor parts: cellular growth model of tumour and adaptivetreatment system. The growth model will compare with thetumour image obtained from same patient. Then the factors ofdrug resistance will be fed to the drug transport model whichwill bring the measurement of drug and the amount of toxicity.These will then fed to an adaptive system consist of multi-objective controller for adapting the drug concentration oftolerable toxicity. An Oncologist will be able to play with thesystem to adjust toxicity for therapy in order to maximizetreatment benefit and minimize side effect. The overallscenario of the proposed model is described in fig 1.
The adaptive system includes drug scheduling controllerusing feedback control strategy and multi-objective geneticalgorithm (MOGA) that can provide solutions trading-offbetween the cell killing and toxic side effects during the wholeperiod of treatment. Algoul et al. [5] presented a variant of
Proportional-Integral-Derivative (PID) control, namely I-PD is used to control the drug doses to be infused to thepatient’s body. They have got the maximum reduction withcell cycle specific model/treatment compared to reported workavailable so far. In this model MOGA optimisation processwill be employed to find desired drug concentration at tumoursite and acceptable parameters of the controller that trade-offbetween two conflicting objectives; reducing cancerous cellsand toxic side effects simultaneously. The feedback controlmethod can maintain a predefined level of drug concentrationat tumour sites. The overall scenario suggests that this modelis able to identify every single tumour cell behaviourseparately in cellular level by using feed-forward neuralnetwork and it can define the drugs concentration intelligentlyby the using of adaptive system. Depending on thephysiological state of the patient and state of the cancer, theoncologist can pick the right solution suitable for the patientfrom the adaptive system.
In case of both chemotherapy and radiotherapy, after eachcycle the side effect and toxicity effect come after couple ofmonths. This time is very crucial part for the patient becausethey are put into a regular monitoring process. It may onweekly basis or monthly basis for monitoring variousbiological diagnostic tests. Normally it’s a complex anddifficult some situation for both patient as well as foroncologists. As our model can create a real cancer growthmodel according to the patient’s data, it can be used as a realtumour mass for the oncologist. They can have a predictiveanalysis of toxicity after giving each cycle of chemotherapy or
Fig 1. Knowledge based decision supportsystem for oncologist

radiotherapy. Our main objective is to develop an intelligentpersonalized treatment model for cancer with intelligentdecision support system for supporting the oncologist. Wehave developed two avascular tumour growth models both intissue and cellular level.
According to Martin’s model tumour cell population maybe calculated from tumour volume measurements, since thereis an approximately linear relationship between tumourvolume and cell number [3]. Previously there are three growthmodels used to simulate and predict different type of tumourgrowth by Martin, these include Gompertz, Logistic andExponential model. For all three models the initial tumourburden is taken 1010 cells and the initial tumour populationdoubling time is 4 weeks. It is shown in fig 2.
0 100 200 300 400 500 6000
200
400
600
800
1000
1200
time(days)
ce
lls
Exponential
Logistic
Gompertz
Fig 2. Different models of calculating the cell populations
In our case, as we are constructing our own tumour growthmodel from a tumour image, we took our own growth patternand cell number after specific intervals.We have followed theSherratt and Chaplain [10] model for tissue level model withmodification in solving the partial differential equations. Ourcellular level model is designed according to Nabila et al. [11].It includes extracellular matrix (ECM) and cell-cell adhesionwhich are the most important constraints for drug resistance.An artificial neural network (ANN) based scheme wasimplemented to define cellular behavior based on theenvironmental variables. We found that the tumourmicroenvironment strongly influenced tumour morphologyand growth rates. The results of the growth model werevalidated by the use of in vitro experiments using multicellulartumour spheroids. We have developed a hybrid model tomeasure tumour response to an anticancer drug TPZ. Thismodel can calculate tumour mass with the consideration ofoxygen, glucose, extracellular matrix (ECM), cell-celladhesion and cell movement as key microenvironmentalparameters.
The proposed feed-forward neural network's structure isdivided into three layers; an input layer I, a hidden layer H andan output layer O. The number of specific cell's neighbors n(x,t), it’s local chemical concentrations; oxygen O2(x, t), glucoseG(x, t) and hydrogen ions produced by the cell H(x, t) are fedas input to the network. The connections between the input
and the hidden layer w and then the hidden and the outputlayer W are established using some weight matrices. Theconnection wij defines the link between node j of the inputlayer and node i of the hidden layer and Wij is a connectionbetween node j of the hidden and node i of the output layer
whilei andj are the thresholds for node I in the hidden layerand node j in the output layer respectively. The inputparameters are transferred to the hidden layer and this layerdoes its processing using standard transfer function T(x) (4)
(defined below), weight matrix w and threshold vector. Thehidden layer then passes the calculated values to the outputlayer that performs its calculation using T(x) as a transfer
function, W matrix and threshold.
(4)
(5)
(6)
w =
W =
The network produces the phenotype of the cell at theoutput layer. The nodes at the output layer are divided intoproliferation, quiescent, apoptosis and movement phenotypes.The model checks the values at first three output nodes andselects the greatest one as the life cycle phenotype for the cell.Fig 3 shows the neural network view.
Previously, many researchers have attempted to usecellular automata for tumour growth modeling. The very firstone was done by Düchting and Vogelsaenger [12], where themodel used to investigate the effects of radiotherapy. Someattempts have been made to model the impact of tumourmicroenvironments on tumour growth via cellular automata

(CA) modeling approach [13][14]. Literature shows that cell-cell adhesion, cell movement due to cell's attraction and therole of extra cellular matrix (ECM) on tumour growth activityare the important factors during tumour growth process.Nabila et al. considered these factors [11]. Previously Gerleeand Anderson did not consider this factor at all in their model[15].
In reality, it’s often difficult to maintain optimumchemotherapy doses that can maximize the abnormal cellkilling as well as reducing side effects. The mostchemotherapy drugs used in cancer treatment are toxic agentsand usually have narrow therapeutic indices. To make thechemotherapeutic treatment effective, optimum drugscheduling is required to balance between the beneficial andtoxic side effects of the cancer drugs. Conventional clinical
Fig 3. The basic structure of the neural network that modelsthe response of each tumour cells due to the impact of tumour
microenvironments.
methods very often fail to find drug doses that balancebetween these two due to their inherent conflicting nature. Inthis investigation, mathematical models for cancerchemotherapy are used to predict the number of tumour cellsand control the tumour growth during treatment. A feedbackcontrol method will be used so as to maintain certain level ofdrug concentrations at the tumour sites according to Algoul etal. [5]. As our growth model can identify each and every cell’sbehaviour by differentiating them into three categoriesproliferating, quiescent and necrotic cells, we will take the twocompartment model [16].
Fig 4, shows a two compartment model where P(Proliferating) presents the combination of the first four stagesof the cell cycle as mentioned earlier G1,S,G2, M and Q
Proliferation
cells
Quiescent cells
Dead cells
a
nn
b
m
Fig 4. Two compartments functional within tumour tissue
(Quiescent cells) indicates stage . The parameters m and bexpress the immigrants between the proliferating cells andquiescent cells respectively. Here a is indicates to the growthrate of cycling cells and n is the natural decay of the cyclingcells.
Many Mathematical models have been developedpreviously to describe the growth and control of tumours[3][17][18]. Hassani et al. [19] presented an optimal controlproblem of chemotherapy drug scheduling doses for patientswith progressive cancer. Two mathematical models ofefficient cancer chemotherapy were compared by Dua et al.[16]. One model treated the whole cancer as a unique entity:the cell cycle non- specific one and the second one was cellcycle specific which divided the cancer into twocompartments: cyclic and non-cyclic. Algoul et al. [5]presented a computational model that calculated the rate ofchange of cancer cell number with respect to time, single drugconcentration and drug toxicity. They successfully minimizedthe toxic effects of the drugs especially with the use of arepeated pattern employing a genetic algorithm (GA)technique computing optimal inputs for the developedproportional, integral and derivative (PID) controller andusing the Martin mathematical model of drug concentration.
IV. REUSLTS AND DISCUSSION
Our main objective of this investigation is to provide anintelligent model which can allow the oncologist to take theright decision to the right patient at the right time that called aspersonalized treatment in brief. For reconstructing the modelfrom image and biological data we developed tissue levelmodel as well as cellular level model. The tissue level modelsucceeds in providing a more realistic description of avasculartumour growth process according to [20]. Here we have giventhe tumour growth pattern in image form in tissue level.

Fig 5.Snapshots of simulated tumour growth at t=2,4,....16 intissue level model
The graphical output presented in fig 5 shows thedifferences in the evolution of the tumour sub-populations ofproliferating, quiescent and necrotic cells. We solved theprevious Sherratt and Chaplain [10] model by using finitedifference scheme and previously this model was calibrated byusing experimental data obtained from Nirmala [20][21].
For cellular level model we have developed a hybridcellular automaton model which investigated the effects ofsome important constraints including oxygen, glucoseconsumption, hydrogen ion production, the ECM, cell-celladhesion and cell movement as key environmental parameters.The approach developed a neural network that described thebehaviour of each abnormal cell based on various tumourmicroenvironments. The main aim was to observe the changesin tumour morphology and growth rate of tumour with boththe evolution of time and the inclusion of various growthconstraints. Interesting results were obtained that haveresemblance to the “real world” scenarios especially in thecase of tumour morphology and its growth curve pattern. Theresults divide benign tumours into an outer lining ofproliferating cells and the inner area filled with the quiescentand dead cells (the necrotic core which is due to the lack ofnutrients), which is quite similar to the in vitro data. Themodel predicts the survival conditions for abnormal cells andshows that the diffusion limited supply of nutrients is one ofthe major causes of cell death. Cell-ECM and cell-celladhesion, as well as cell movement show an extreme influenceon the tumour growth rates. The ECM slowed down tumourgrowth but paradoxically, cell movement speeded up the cellsgrowth rate by allowing cells space to accommodate daughtercells. Fig 6 shows the tumour growth after 20 days and 25days simultaneously.
Subsequently, the growth model was validated with theresults of experiments conducted on multicellular tumourspheroids at cancer research institute at Bradford. Forvalidation purposes the HT-29 human colon carcinoma celllines was used. The results showed a good resemblance interms of tumour growth. It is worth mentioning that the modelrealistically calculates the growth rates of spheroid in variousenvironmental factors and it also suggests the tumourmicroenvironment as a major predictor of cell behaviour.
2700 2800 2900 3000 3100 3200 3300
2700
2800
2900
3000
3100
3200
3300
µm
µm
2700 2800 2900 3000 3100 3200 3300
2700
2800
2900
3000
3100
3200
3300
µm
µm
Fig 6. Solid tumour morphology at different stages of growth(a) shows tumour mass after 20 days, (b) after 25 days (Theblue region represents dead cells, red represents quiescent
cells and the green proliferating cells)
Another important conclusion can be drawn from ourinvestigation that our proposed cellular model can provide thetumour growth according to the monolayer cell lines. Asmentioned earlier that all the three previous growth modelstake 1010 cells as an initial burden and initial tumourpopulation doubling time is 4 weeks, but our model gives thethe real tumour growth morphology from one cell at the centreof grid. Fig 7 shows the growth curves of the tumour upto 100days. For the tissue level model it is earlier mentioned inanother work that, he experimental total cell count is 7015 att=1[20]. So, the both tumour growth model can allow theoncologists to work with a piece of tumour mass which hasgrown exactly from the real tumour mass. This will feed to therest of the part of the model for the prediction of the toxicityand required drug concentration prior any treatment or duringthe treatment of the patient for either chemotherapy orradiotherapy.
Fig 7. This shows a model of the growth of abnormal cellsincluding proliferating, stationary and dead cells with (•) andwithout (+) cell movement, while ECM was absent in both
cases

As intensity-modulated radiotherapy (IMRT) is a newermethod of delivering radiation to target structures, it needs thepredictive results for the patients. IMRT used for the treatmentof head, neck and prostate cancer which optimizes the deliveryof irradiation to irregularly-shaped volumes and can generateconcave dose distributions and dose gradients with narrowermargins. The recent work shows that high-dose radiotherapyfor prostate cancer using IMRT and IGRT resulted in lowrates of acute toxicity and preliminary results of late toxicityare promising [22][23]. Our model can open a new dimensionfor IMRT, as it needs the predictive results about patient’stumour status. Our model can be feed to IMRT for predictingtoxicity and side effect for every patient.
V. CONCLUSION AND FUTURE WORKS
This investigation presents a complete personalized cancertreatment schema which contains its own tumour growth model(tissue and cellular level model) for tumour mass generationand an optimization drug scheduling mechanism for predictionof toxicity and drug concentration prior or during the treatment.Our growth model is a unique one to identify each and everytumour cell behavior based on the tumour microenvironmentconstraints like cell-cell adhesion, cell movement and (ECM).The major contribution of this work is the prediction of toxicityand drug concentration based on tumour microenvironmentfactors and efficient drug penetration and drug scheduling,which may reduce the number of chemotherapy or radiotherapycycle and provide the right dose to the patient according totheir tumour profile. Our next target is to develop the adaptivesystem for calculating the drug concentration and side-effectsand also trained the neural network by an appropriate data set.We are optimistic this model can provide the best personalizedcancer regime for the patients with cellular level datavalidation. This work could inform various futureinvestigations, including the exploration of angiogenesis andepithelial-to-mesenchymal-transition (EMT) to update thetumour growth model. Our future work will be implement thedrug scheduling controller with TPZ and developing a drugtransport model. This will give us an opportunity to build thismodel to study the pharmacokinetic and pharmacodynamicproperties of TPZ, to predict the response of cellular proteins toTPZ inside the hypoxic regions of tumours.
REFERENCES
[1] World Health Organizations,Available at:http://www.who.int/cancer/en/ (Accessed: 02 February 2012).
[2] WorldHealth Organizations, Available at: http://www.who.int/mediacentre/news/releases/2003/pr27/en/ (Accessed: 02 February2012).
[3] R. Martin, and K. Teo, “Optimal control of drug administration inchemotherapy tumour Growth”, 1 ed. World Scientific, 1994, pp.95-111.
[4] J. Tepper, J.K. Mark, N. Donna, H. Donna, E.R. Carolyn, G.Richard, K. Krystyna, W. Christopher, S. David and M. Robert,“Phase III trial of trimodality therapy with cisplatin, fluorouracil,radiotherapy, and surgery compared with surgery alone foresophageal cancer: CALGB 9781”, Journal of Clinical Oncology,26 (7), 2008 , pp. 1086-1092.
[5] S. Alam, S. Algoul, M.A. Hossain, and M.A. Majumder, “Multi-objective particle swarm optimisation for phase specific cancerdrug scheduling”, Communications in Computer and InformationScience CSBio Conference, 2010 ,pp. 180-192.
[6] B.G. Siim, D.R. Menke, M.J. Dorie, and J.M. Brown,“Tirapazamine-induced cytotoxicity and DNA damage intransplanted tumours: relationship to tumour hypoxia”, CancerResearch, 57, 1997, pp. 2922-2928.
[7] A.M. Shannon, D.J. Bouchier-Hayes, C.M. Condron, and D.Toomey, “Tumour hypoxia, chemotherapeutic resistance andhypoxia-related therapies”, Cancer Treatment Reviews, 29 (4),2003, pp. 297-307.
[8] L. Marcu, and I. Olver, , “Tirapazamine: from bench to clinicaltrials‟, Current Clinical Pharmacology”, 1, 2006, pp. 71-79.
[9] L.H. Patterson, and S.R. Mckeown, “AQ4N: a new approach tohypoxia-activated cancer chemotherapy”, British Journal ofCancer, 83 (12), 2000, pp. 1589-1593.
[10] J.A. Sherratt, and M.A.J. Chaplain, “A new mathematical modelfor avascular tumour growth”, Journal of Mathematical Biology,43, 2001, pp. 291-312.
[11] N. Kazmi, M.A. Hossain, and R. Phillips, “Intelligent modellingfor benign tumour growth with cell-cell and cell-matrix adhesionand movement”, 10th IEEE International Conference onComputer and Information Technology (CIT), 2010 ,(Nominatedfor best paper award: was at top 10 out of 524 papers).
[12] W. Düchting, T. Vogelsaenger, “Analysis, forecasting and controlof three-dimensional tumour growth and treatment”, J. Med. Syst.8, 1984, 461–475.
[13] A.R.A. Anderson, A.M. Weaver, P.T. Cummings and V.Quaranta, Tumour morphology and phenotypic evolution drivenby selective pressure from the microenvironment, Cell 127(2006), 905–915.
[14] K. Smallbone, R.A. Gaten by, R.J. Gillies, P.K. Maini and D.J.Gavaghan, Metabolic changes during carcinogenesis: Potentialimpact on invasiveness, Journal of Theoretical Biology 244 2007,703–713.
[15] P. Gerlee, and A.R.A. Anderson, “An evolutionary hybrid cellularautomaton model of solid tumour growth”, Journal of TheoreticalBiology, 246 (4), 2007, pp. 583-603.
[16] P. Dua, V. Dua, and N. Pistikopoulos, “Optimal delivery ofchemotherapeutic agents In cancer”, Computer and ChemicalEngineering, vol. 32, 2008, pp. 99-107.
[17] J. McCall, A. Petrovski, and A. Shakya, “EvolutionaryAlgorithms for Cancer Chemotherapy Optimization”,Computational Intelligence in Bioinformatics: 2008, pp. 265-296.
[18] J. Westman, B. Fabijonas, D. Kern, and F. Hanson,“Compartmental Model for Cancer Evolution: Chemotherapy andDrug Resistance”, 2001, Citeulke: 2693574
[19] Hassani and Naghihi, “Reinforcement Learning Based Control ofTumour Growth with Chemotherapy”, International Conferenceon System Science and Engineering, 2010, 185-189.
[20] K.C. Ang , “Analysis of a Tumour Growth Model withMATLAB”, (invited paper) Proceedings of the 14th AsianTechnology Conference in Mathematics, Beijing, China, 2009.
[21] C. Nirmala, J.A. Rao, A.C. Ruifrok, L.A. Langford and M.Obeyesekere, “Growth characteristics of glioblastoma spheroids”,International Journal of Oncology, 2001, 19, 1109-1115.
[22] M. Guckenberger, S. Ok, B Polat, Reinhart A. Sweeney, MFlentje, “Toxicity after Intensity-Modulated, Image-GuidedRadiotherapy for Prostate Cancer”, Strahlenther Onkol,2010;186:535–43.
[23] A. Al-Mamgani, WD. Heemsbergen, STH. Peeters and JV.Lebesque, “Role of intensity-modulated radiotherapy in reducingtoxicity in dose escalation for localized prostate cancer”, Int JRadiat Oncol Biol Phys. 2009;73(3):685-91.





























