Embed Size (px)
Citation preview

Analgesia for relief of pain due to uterine cramping/involution
after birth (Review)
Deussen AR, Ashwood P, Martis R
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2011, Issue 5
http://www.thecochranelibrary.com
Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
16DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
17AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
18ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
18REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
22CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
47DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 NSAID versus placebo, Outcome 1 Pain Reduction (SPID). . . . . . . . . . . 52
Analysis 1.2. Comparison 1 NSAID versus placebo, Outcome 2 Pain reduction (pain intensity 6 hours). . . . . . 53
Analysis 1.3. Comparison 1 NSAID versus placebo, Outcome 3 Summed Relief Score. . . . . . . . . . . . 54
Analysis 1.4. Comparison 1 NSAID versus placebo, Outcome 4 Pain analogue score compared with baseline. . . . 55
Analysis 1.5. Comparison 1 NSAID versus placebo, Outcome 5 Global rating. . . . . . . . . . . . . . 56
Analysis 1.6. Comparison 1 NSAID versus placebo, Outcome 6 Pain reduction > 50%. . . . . . . . . . . 57
Analysis 1.7. Comparison 1 NSAID versus placebo, Outcome 7 VAS 1-4 at 30 minutes. . . . . . . . . . . 57
Analysis 1.8. Comparison 1 NSAID versus placebo, Outcome 8 No pain relief. . . . . . . . . . . . . . 58
Analysis 1.9. Comparison 1 NSAID versus placebo, Outcome 9 Adverse effects. . . . . . . . . . . . . . 59
Analysis 2.1. Comparison 2 NSAID versus opioid, Outcome 1 Pain reduction (SPID). . . . . . . . . . . . 60
Analysis 2.2. Comparison 2 NSAID versus opioid, Outcome 2 Pain reduction (pain intensity 6 hours). . . . . . 60
Analysis 2.3. Comparison 2 NSAID versus opioid, Outcome 3 Pain reduction (summed pain relief ). . . . . . . 61
Analysis 2.4. Comparison 2 NSAID versus opioid, Outcome 4 No pain relief. . . . . . . . . . . . . . . 62
Analysis 2.5. Comparison 2 NSAID versus opioid, Outcome 5 Adverse effects. . . . . . . . . . . . . . 63
Analysis 3.1. Comparison 3 Opioid versus placebo, Outcome 1 Pain reduction (SPID). . . . . . . . . . . 63
Analysis 3.2. Comparison 3 Opioid versus placebo, Outcome 2 Pain reduction (pain intensity 6 hours). . . . . . 64
Analysis 3.3. Comparison 3 Opioid versus placebo, Outcome 3 Pain reduction (summed relief score). . . . . . 64
Analysis 3.4. Comparison 3 Opioid versus placebo, Outcome 4 No pain relief. . . . . . . . . . . . . . 65
Analysis 3.5. Comparison 3 Opioid versus placebo, Outcome 5 Adverse effects. . . . . . . . . . . . . . 65
Analysis 4.1. Comparison 4 Flurbiprofen versus aspirin, Outcome 1 Pain reduction (pain intensity 6 hours). . . . 66
Analysis 4.2. Comparison 4 Flurbiprofen versus aspirin, Outcome 2 No pain relief. . . . . . . . . . . . . 66
Analysis 5.1. Comparison 5 Ketorolac versus aspirin, Outcome 1 Pain reduction (SPID). . . . . . . . . . . 67
Analysis 5.2. Comparison 5 Ketorolac versus aspirin, Outcome 2 Pain reduction (summed relief score). . . . . . 68
Analysis 5.3. Comparison 5 Ketorolac versus aspirin, Outcome 3 Global rating. . . . . . . . . . . . . . 69
Analysis 6.1. Comparison 6 Ketorolac: different doses, Outcome 1 Pain reduction (SPID). . . . . . . . . . 69
Analysis 6.2. Comparison 6 Ketorolac: different doses, Outcome 2 Pain reduction (summed relief score). . . . . 70
Analysis 6.3. Comparison 6 Ketorolac: different doses, Outcome 3 Global rating. . . . . . . . . . . . . . 70
Analysis 7.1. Comparison 7 Codeine: different doses, Outcome 1 Pain reduction (pain intensity 6 hours). . . . . 71
Analysis 7.2. Comparison 7 Codeine: different doses, Outcome 2 No pain relief. . . . . . . . . . . . . . 71
Analysis 8.1. Comparison 8 Nalbuphine versus codeine, Outcome 1 No pain relief. . . . . . . . . . . . . 72
Analysis 9.1. Comparison 9 Paracetamol versus placebo, Outcome 1 Pain reduction (pain intensity 6 hours). . . . 72
Analysis 9.2. Comparison 9 Paracetamol versus placebo, Outcome 2 Adverse effects. . . . . . . . . . . . . 73
Analysis 10.1. Comparison 10 Paracetamol versus aspirin, Outcome 1 Pain reduction (pain intensity 6 hours). . . 73
Analysis 10.2. Comparison 10 Paracetamol versus aspirin, Outcome 2 Adverse effects. . . . . . . . . . . . 74
Analysis 11.1. Comparison 11 TENS versus placebo, Outcome 1 VAS 1-4 at 30 minutes. . . . . . . . . . . 74
Analysis 12.1. Comparison 12 TENS plus Metamizol versus placebo, Outcome 1 VAS 1-4 at 30 minutes. . . . . 75
iAnalgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 13.1. Comparison 13 TENS plus Metamizol versus TENS, Outcome 1 VAS 1-4 at 30 minutes. . . . . 75
Analysis 14.1. Comparison 14 TENS plus Metamizol versus Metamizol, Outcome 1 VAS 1-4 at 30 minutes. . . . 76
Analysis 15.1. Comparison 15 TENS versus Metamizol, Outcome 1 VAS 1-4 at 30 minutes. . . . . . . . . . 76
76HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
76CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
77DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
77SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
77DIFFERENCES BETWEEN PROTOCOL AND REVIEW . . . . . . . . . . . . . . . . . . . . .
77INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iiAnalgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Analgesia for relief of pain due to uterine cramping/involutionafter birth
Andrea R Deussen1, Pat Ashwood1, Ruth Martis2
1Discipline of Obstetrics and Gynaecology, The University of Adelaide, North Adelaide, Australia. 2Faculty of Applied Sciences and
Allied Health, School of Midwifery, Christchurch Polytechnic Institute of Technology (CPIT), Christchurch, New Zealand
Contact address: Andrea R Deussen, Discipline of Obstetrics and Gynaecology, The University of Adelaide, Women’s and Children’s
Hospital, Level 1 QVB, 72 King William Street, North Adelaide, South Australia, 5006, Australia. [email protected].
Editorial group: Cochrane Pregnancy and Childbirth Group.
Publication status and date: New, published in Issue 5, 2011.
Review content assessed as up-to-date: 6 April 2011.
Citation: Deussen AR, Ashwood P, Martis R. Analgesia for relief of pain due to uterine cramping/involution after birth. CochraneDatabase of Systematic Reviews 2011, Issue 5. Art. No.: CD004908. DOI: 10.1002/14651858.CD004908.pub2.
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Women may experience differing types of pain and discomfort following birth, including cramping after birth pains associated with
uterine involution.
Objectives
To assess the effectiveness and safety of analgesia for relief of after birth pains following vaginal birth.
Search strategy
We searched the Cochrane Pregnancy and Childbirth Group’s Trials Register (31 December 2010) and the reference lists of trials and
review articles.
Selection criteria
All identified published and unpublished randomised controlled trials comparing two different types of analgesia or analgesia with
placebo or analgesia with no treatment, for the relief of after birth pains following vaginal birth. Types of analgesia included pharma-
cological and non-pharmacological.
Data collection and analysis
Two review authors assessed trial quality and extracted data independently.
Main results
We have included 18 studies (involving 1498 women) in this review. However, only nine of the included studies (with 750 women)
reported 24 comparisons of analgesia with other analgesia or placebo and had data that could be included in our meta-analyses. The
majority of studies investigated pharmacological analgesics and these were grouped into classes for this review. Non-steroidal anti-
inflammatory drugs (NSAIDs) were significantly better than placebo at relieving pain from uterine involution as assessed by their
summed pain intensity differences (SPID) (mean difference (MD) 4.34; 95% confidence interval (CI) 2.87 to 5.82; three studies, 204
women) and summed pain relief scores (MD 5.94; 95% CI 3.83 to 8.01; three studies, 204 women). NSAIDS were compared with
opioids in one small study of 23 women reporting SPID and summed pain relief and found no difference. A larger study of 127 women
1Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

found NSAIDs to be significantly better than opioids at reducing pain intensity six hours following study intervention (MD -0.70;
95% CI -1.04 to -0.35). Opioids were compared with placebo in three studies that could be included in meta-analyses; one small study
of 23 women reporting SPID and summed pain relief and found no difference. One study of 95 women found no difference in pain
intensity six hours following the study intervention. A third study of 108 women found significantly more women in the placebo group
reported no pain relief than women in the opioid group (risk ratio 0.10; 95% CI 0.04 to 0.23). Aspirin was significantly better than
paracetamol when pain intensity score was assessed six hours after study intervention (MD 0.85; 95% CI 0.29 to 1.41; one study 48
women) at relieving pain from uterine involution. Paracetamol was not better than placebo when pain intensity was assessed six hours
after the study intervention in one study of 48 women.
Authors’ conclusions
Non-steroidal anti-inflammatory drugs (NSAID) including aspirin were better than placebo at relieving pain from uterine cramping/
involution following vaginal birth. NSAIDs were better than paracetamol and paracetamol was not better than placebo, though numbers
of participants for these comparisons were small. Data for opioids compared with NSAIDs and opioids compared with placebo were
conflicting, with some measures showing similar effect and others indicating NSAIDs were better than opioids and opioids were not
better than placebo. There were insufficient data to make conclusions regarding the effectiveness of opioids at relieving pain from
uterine cramping/involution.
The median year of publication of included studies was 1981; therefore more research is needed to assess the effectiveness of current
pharmacological and non-pharmacological analgesia at relieving pain from uterine cramping/involution following vaginal birth.
P L A I N L A N G U A G E S U M M A R Y
Pain relief for after pains (uterine cramping/involution) after the baby’s birth
Women may experience cramping pain and discomfort following the birth of their baby as the uterus contracts and returns to its pre-
pregnancy size. These after pains are caused by involutionary contractions and usually last for two to three days after childbirth. They
are more evident for women who have previously had a baby. Breastfeeding stimulates the uterus to contract and increases the severity
of after birth pains. This review is about pain relief for after pains experienced by women following vaginal birth.
Types of analgesia used to relieve the pain include paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs) included aspirin and
naproxen, opioids including codeine and non-pharmacological methods such as transcutaneous electrical nerve stimulation (TENS).
The results from 18 randomised controlled trials involving 1498 women, of which nine (750 women) had data that could be included
in the review meta-analyses, indicated that aspirin and other NSAIDs including naproxen were more effective at relieving uterine
cramping pain than paracetamol or a placebo. NSAIDs included naproxen, aspirin, ketorolac and flurbiprofen. Only naproxen is still
used in women who are breastfeeding. Aspirin is not recommended for use by breastfeeding women as there is concern that it will be
passed to the baby in the breast milk. Codeine was not always more effective than a placebo or NSAIDs in the included studies and can
sedate breastfed babies. Women offered codeine for pain relief should be informed about the potential for adverse effects for their babies.
Codeine should only be prescribed for breastfeeding women with after birth pain if there is no alternative and their breastfed infants
should be closely monitored for sedation and signs of codeine toxicity. Information about the safety of the NSAIDs for breastfeeding
women and their babies was limited.
The majority of analyses in this review included only one study with small numbers of participants. The average year of the included
studies is 1981 and therefore further research is recommended comparing NSAIDs currently available and known to be safe for women
who are breastfeeding and their babies.
B A C K G R O U N D
Description of the condition
Women may experience differing types of pain and discomfort
2Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

following the birth of their baby. This may include incisional pain
after a caesarean section, perineal pain following perineal trauma
or episiotomy during vaginal birth, nipple pain from breastfeed-
ing and cramping after birth pains associated with involution of
the uterus. Following birth, the uterus returns to its normal size
through involution, a process of intermittent uterine contractions.
These involutionary contractions may be painful and are com-
monly felt for two or three days after birth (Ladewig 1990).
The incidence and severity of after birth pains is not widely re-
ported. However, multiparous women usually experience more
pain as the lost tone of the uterus of the multiparous woman
contracts and relaxes alternately. This is also true of a uterus that
is greatly distended as in a multiple pregnancy or polyhydram-
nios (Ladewig 1990). It has been further hypothesised that child-
birth can induce central neural changes that increase predisposi-
tion for pain during the postpartum period suggesting multiparous
women’s perception of uterine cramp pain is increased through a
process of central sensitisation of nociceptive neurons (Holdroft
2003). Endogenous oxytocin released during breastfeeding stim-
ulates the uterus to contract and increases the severity of after
birth pains felt by the mother. Thus after birth pains may hinder
successful breastfeeding, reducing the mother’s ability to care for
her new baby and may impair the establishment of good-quality
mother-baby interactions as has been shown with perineal pain
(Sleep 1991). In contrast, the uterus of the primiparous woman re-
mains contracted after birth (Ladewig 1990), hence these women
do not commonly experience after birth pains. It has been docu-
mented that some women consider their after birth pains to be a
major burden requiring powerful analgesia (Mander 1998).
A number of randomised trials comparing the safety and effective-
ness of various analgesics have been published. After birth pains
and perineal tissue injury after vaginal birth are established clini-
cal pain models for the investigation of efficacy of new analgesic
agents (Bloomfield 1998; Windle 1989).
Description of the intervention
Analgesia is any agent used to relieve pain. Analgesia includes phar-
macological and non-pharmacological interventions. Pharmaco-
logical analgesia can be further classified: simple analgesics (in-
cluding paracetamol and non-steroidal anti-inflammatory drugs
(NSAID) like aspirin and naproxen) and opioid analgesics (in-
cluding codeine and morphine) (MIMS 2008).
Paracetamol and codeine are commonly used analgesics following
childbirth. Paracetamol is secreted in small amounts into breast-
milk and not considered hazardous (Berlin 1980; Bitzen 1981;
Hale 2010; Notorianni 1987). Codeine is considered moderately
safe in breastfeeding women (Hale 2010). However, it has been
suggested in the literature that babies may become sedated by
maternal intake of codeine (Davis 1985; Findlay 1981), and one
case of a baby succumbing to codeine toxicity has been described
(Koren 2006). Women offered codeine for pain relief should be
informed about the potential for adverse effects. Codeine should
only be prescribed for breastfeeding women with after birth pain if
there is no alternative and their breastfed infants should be closely
monitored for sedation and signs of codeine toxicity (Koren 2006).
Hale 2010 in Medications and Mothers’ Milk does not recom-
mend aspirin use in breastfeeding women, although there is evi-
dence that only extremely small amounts of salicylic acid are se-
creted into breastmilk (Erickson 1979; Findlay 1981).
Non-pharmacological analgesia may include massage, heat packs,
cold packs, hypnotherapy, acupuncture and transcutaneous elec-
trical nerve stimulation (TENS).
How the intervention might work
Analgesia can decrease pain or perception of pain in several ways.
Systemic analgesic drugs can be categorised into different classes.
Simple analgesics like paracetamol inhibit central nervous system
prostaglandin synthesis (Rang 2007). NSAIDs including aspirin
and naproxen have an anti-inflammatory action (Rang 2007). Nar-
cotic analgesics including codeine and morphine reduce percep-
tion of pain by inhibiting pain-transmission neurons and reducing
the psychological response to pain (Rang 2007).
Non-pharmacological analgesia may work through a number of
mechanisms; TENS is thought to inhibit nociception (Olsen
2007).
Why it is important to do this review
Women may experience pain after birth from several sources, in-
cluding uterine involution and perineal trauma. Management of
pain after birth is important and can impact on a woman’s return
to normal activities and caring for her baby.
There is very little in the literature to guide women and clinicians
in the management of pain from uterine cramping/involution.
The aim of this review is to systematically assess what is known
about the effectiveness and safety of analgesia for relief pain from
uterine cramping/involution.
The Cochrane Library now has a generic protocol for meta-anal-
yses of interventional studies for perineal trauma (Chou 2010).
The first review using this protocol assessing paracetamol (ac-
etaminophen) has been published (Chou 2010a). This review will
contribute to what is known about the management of postpar-
tum pain.
O B J E C T I V E S
To assess the effectiveness and safety of analgesia for relief of after
birth pains following vaginal birth.
3Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
M E T H O D S
Criteria for considering studies for this review
Types of studies
All identified published and unpublished randomised controlled
trials comparing two different types of analgesia or analgesia with
placebo or analgesia with no treatment, for the relief of after birth
pains following vaginal birth. We have included studies that met
the inclusion criteria that were reported in abstract form only. We
have not included quasi-randomised studies in this review.
Types of participants
Women who have given birth vaginally, who may require analgesia
for after birth pains.
Types of interventions
Randomised controlled trials comparing any type of analgesia (ex-
cluding pharmacological analgesics that are no longer available or
that are not approved for use in this population) for after birth
pains following vaginal birth with:
• any other type of analgesia;
• placebo;
• no treatment.
Analgesic intervention may be administered once as a single dose
or dosage repeated at therapeutic intervals.
Types of outcome measures
Primary outcomes
(1) Pain, however measured by the authors, at the following time
periods or as close as possible to:
• up to six hours after birth;
• up to 12 hours after birth;
• up to 18 hours after birth;
• up to 24 hours after birth;
• up to 48 hours after birth;
• up to 72 hours after birth;
• up to seven days after birth.
(2) Number of women breastfeeding at discharge.
(3) Number of women breastfeeding around six weeks post dis-
charge.
(4) Neonatal side effects in those breastfeeding.
(5) Maternal side effects of treatment (including nausea, vomiting,
dizziness, drowsiness, pruritis, uterine atony, vaginal blood loss).
(6) Maternal satisfaction with treatment.
Outcomes need to be reported separately for pain from uterine
involution.
Secondary outcomes
(1) Need for additional analgesia.
(2) Length of hospital stay.
(3) Need for readmission.
(4) Additional health service access in regard to after birth pains.
(5) Mother-baby interactions.
(6) Cost of analgesic treatment.
Outcomes need to be reported separately for uterine cramps.
Search methods for identification of studies
Electronic searches
We searched the Cochrane Pregnancy and Childbirth Group’s Tri-
als Register by contacting the Trials Search Co-ordinator (31 De-
cember 2010).
The Cochrane Pregnancy and Childbirth Group’s Trials Register
is maintained by the Trials Search Co-ordinator and contains trials
identified from:
1. quarterly searches of the Cochrane Central Register of
Controlled Trials (CENTRAL);
2. weekly searches of MEDLINE;
3. weekly searches of EMBASE;
4. handsearches of 30 journals and the proceedings of major
conferences;
5. weekly current awareness alerts for a further 44 journals
plus monthly BioMed Central email alerts.
Details of the search strategies for CENTRAL, MEDLINE and
EMBASE, the list of handsearched journals and conference pro-
ceedings, and the list of journals reviewed via the current aware-
ness service can be found in the ‘Specialized Register’ section
within the editorial information about the Cochrane Pregnancy
and Childbirth Group.
Trials identified through the searching activities described above
are each assigned to a review topic (or topics). The Trials Search
Co-ordinator searches the register for each review using the topic
list rather than keywords.
Searching other resources
We tried to contact the original trial authors for clarification or
additional data (this is identified in the tables under included or
excluded studies), and searched the reference lists of trials and
review articles.
We did not apply any language restrictions.
4Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Data collection and analysis
Selection of studies
Two review authors evaluated trials under consideration for inclu-
sion without consideration of their results (Andrea Deussen (AD)
and Ruth Martis (RM); Pat Ashwood (PA) and AD. We also in-
dependently assessed the risk of bias in each individual trial. We
resolved differences of opinion by discussion. There was no blind-
ing of authorship. We processed included trial data as described
in the Cochrane Handbook for Systematic Reviews of Interventions(Higgins 2009).
Data extraction and management
We designed a form to extract data. For eligible studies, at least
two review authors extracted the data using the agreed form. We
resolved discrepancies through discussion and entered the data
into Review Manager software (RevMan 2008) and checked for
accuracy.
We contacted a number of authors of the original reports to provide
us with further details. However, the response rate was low and
is identified in the tables of included and excluded studies (seeCharacteristics of included studies and Characteristics of excluded
studies).
Assessment of risk of bias in included studies
Two review authors independently assessed risk of bias for each
study using the criteria outlined in the Cochrane Handbook forSystematic Reviews of Interventions (Higgins 2009). We resolved
any disagreement by discussion or by involving a third assessor.
(1) Random sequence generation (checking for possible
selection bias)
We described for each included study the method used to generate
the allocation sequence in sufficient detail to allow an assessment
of whether it should produce comparable groups.
We assessed the method as:
• low risk of bias (any truly random process, e.g. random
number table; computer random number generator),
• high risk of bias (any non-random process, e.g. odd or even
date of birth; hospital or clinic record number) or,
• unclear risk of bias.
(2) Allocation concealment (checking for possible selection
bias)
We described for each included study the method used to conceal
allocation to interventions prior to assignment and assess whether
intervention allocation could have been foreseen in advance of, or
during recruitment, or changed after assignment.
We assessed the methods as:
• low risk of bias (e.g. telephone or central randomisation;
consecutively numbered sealed opaque envelopes);
• high risk of bias (open random allocation; unsealed or non-
opaque envelopes, alternation; date of birth);
• unclear risk of bias.
(3) Blinding (checking for possible performance bias)
We described for each included study the methods used, if any, to
blind study participants and personnel from knowledge of which
intervention a participant received. We judged studies at low risk
of bias if they were blinded, or if we judged the lack of blinding
could not have affected the results. We assessed blinding separately
for different outcomes or classes of outcomes.
We assessed the methods as:
• low, high or unclear risk of bias for participants;
• low, high or unclear risk of bias for personnel;
• low, high or unclear risk of bias for outcome assessors.
(4) Incomplete outcome data (checking for possible attrition
bias due to the amount, nature and handling of incomplete
outcome data)
We described for each included study, and for each outcome or
class of outcomes, the completeness of data including attrition and
exclusions from the analysis. We state whether attrition and exclu-
sions were reported and the numbers included in the analysis at
each stage (compared with the total randomised participants), rea-
sons for attrition or exclusion where reported, and whether miss-
ing data were balanced across groups or were related to outcomes.
Where sufficient information is reported, or was supplied by the
trial authors, we re-include missing data in the analyses which we
undertook.
We assessed methods as:
• low risk of bias (e.g. no missing outcome data; missing
outcome data balanced across groups);
• high risk of bias (e.g. numbers or reasons for missing data
imbalanced across groups; ‘as treated’ analysis done with
substantial departure of intervention received from that assigned
at randomization);
• unclear risk of bias.
(5) Selective reporting (checking for reporting bias)
We described for each included study how we investigated the
possibility of selective outcome reporting bias and what we found.
We assessed the methods as:
• low risk of bias (where it is clear that all of the study’s pre-
specified outcomes and all expected outcomes of interest to the
review have been reported);
• high risk of bias (where not all the study’s pre-specified
outcomes have been reported; one or more reported primary
5Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

outcomes were not pre-specified; outcomes of interest are
reported incompletely and so cannot be used; study fails to
include results of a key outcome that would have been expected
to have been reported);
• unclear risk of bias.
(6) Other bias (checking for bias due to problems not
covered by 1 to 5 above)
We described for each included study any important concerns we
have about other possible sources of bias.
We assessed whether each study was free of other problems that
could put it at risk of bias:
• low risk of other bias;
• high risk of other bias;
• unclear whether there is risk of other bias.
(7) Overall risk of bias
We made explicit judgements about whether studies are at high risk
of bias, according to the criteria given in the Handbook (Higgins
2009). With reference to (1) to (6) above, we will assess the likely
magnitude and direction of the bias and whether we consider it
is likely to impact on the findings. We will explore the impact
of the level of bias through undertaking sensitivity analyses - see’Sensitivity analysis’.
Measures of treatment effect
Dichotomous data
For dichotomous data, we presented the results as summary risk
ratio (RR) with 95% confidence intervals (CI).
Continuous data
For continuous data, we used the mean difference if outcomes
were measured in the same way between trials. We used the stan-
dardised mean difference to combine trials that measured the same
outcome, but used different methods.
Unit of analysis issues
Crossover trials
We identified crossover trials as not being appropriate for this
intervention.
Dealing with missing data
For included studies, we noted the levels of attrition. We explored
the impact of including studies with high levels of missing data
in the overall assessment of treatment effect by using sensitivity
analysis.
We carried out the outcomes analyses, as far as possible, on an in-
tention-to-treat basis, i.e. we attempted to include all participants
randomised to each group in the analyses, regardless of whether
or not they received the allocated intervention. The denominator
for each outcome in each trial was the number randomised minus
any participants whose outcomes are known to be missing.
Assessment of heterogeneity
We assessed statistical heterogeneity in each meta-analysis using
the T², I² and Chi² statistics. We regarded heterogeneity as sub-
stantial if I² was greater than 30% and either T² was greater than
zero, or there was a low P value (less than 0.10) in the Chi² test
for heterogeneity.
We were unable to explore substantial heterogeneity by subgroup
analysis as the range of analgesia was so wide that subgroup com-
parison was not possible. We had intended to explore the data with
a subgroup analysis for caesarean section, but it was too difficult to
differentiate between incisional pain and uterine cramping; hence
we excluded these data from the review.
Assessment of reporting biases
In future updates of this review, if there are 10 or more studies
in the meta-analysis we will investigate reporting biases (such as
publication bias) using funnel plots. We will assess funnel plot
asymmetry visually, and use formal tests for funnel plot asymmetry.
For continuous outcomes we will use the test proposed by Egger
1997, and for dichotomous outcomes we will use the test proposed
by Harbord 2006. If we detect asymmetry in any of these tests
or by a visual assessment, we will perform exploratory analyses to
investigate it.
Data synthesis
We carried out statistical analysis using the Review Manager soft-
ware (RevMan 2008). We used fixed-effect meta-analysis for com-
bining data where it was reasonable to assume that studies were
estimating the same underlying treatment effect: i.e. where trials
were examining the same intervention, and the trials’ populations
and methods were judged sufficiently similar. If there was clinical
heterogeneity sufficient to expect that the underlying treatment ef-
fects differed between trials, or if we detected substantial statistical
heterogeneity, we used random-effects meta-analysis to produce
an overall summary if we considered an average treatment effect
across trials clinically meaningful. We treated the random-effects
summary as the average range of possible treatment effects, and
6Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

we discussed the clinical implications of treatment effects differing
between trials. If the average treatment effect was not clinically
meaningful, we did not combine trials.
If we have used random-effects analyses, we have presented the
results as the average treatment effect with its 95% confidence
interval, and the estimates of T² and I².
Subgroup analysis and investigation of heterogeneity
We intended to explore possible sources of heterogeneity using
subgroup analyses. However, this was not possible with the in-
cluded trials. The range of analgesia, the timing of observations
and the types of observations were too varied.
In future updates of this review, as more data become available,
we plan to carry out the following subgroup analyses:
• nulliparous versus primiparous;
• up to six hours after birth versus more than six hours; up to
12 hours after birth versus more than 12 hours; up to 18 hours
after birth verus more than 18 hours; up to 24 hours after birth
verus more than 24 hours; up to 48 hours after birth verus more
than 48 hours; up to 72 hours after birth versus more than 72
hours;
• type of anaesthesia during birth (for example epidural
anaesthesia versus no anaesthesia).
We will restrict subgroup analyses to the primary outcomes.
For fixed-effect inverse variance meta-analyses, we will assess dif-
ferences between subgroups by interaction tests. For random-ef-
fects and fixed-effect meta-analyses using methods other than in-
verse variance, we will assess differences between subgroups by in-
spection of the subgroups’ confidence intervals; non-overlapping
confidence intervals indicate a statistically significant difference in
treatment effect between the subgroups.
Sensitivity analysis
We intended to conduct sensitivity analyses by comparing the
outcomes before and after exclusion of the trials with high risk of
bias or unclear risk of bias for sequence generation or allocation
concealment; however, included trials and their outcomes were
too varied.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies.
See Characteristics of included studies and Characteristics of
excluded studies.
Results of the search
The search strategy identified 54 studies, of which we have in-
cluded 18 studies with 1498 postpartum women in the review
(Bettigole 1981; Bloomfield 1977 Study 1; Bloomfield 1977
Study 2; Bloomfield 1978; Bloomfield 1981; Bloomfield 1986a;
Bloomfield 1986b; Bloomfield 1987; Jain 1978; Kantor 1984b;
Laska 1981 Study 1; Laska 1981 Study 2; Mehlhorn 2005; Okun
1982; Olsen 2007; Pan 1993; Skovlund 1991; Skovlund 1991a).
We have excluded 36 (Azpiroz 1971; Baptisti 1971; Beaver 1980;
Benson 1963; Bloomfield 1988; Bloomfield 1983; Bloomfield
1986c; Bloomfield 1988a; Bonica 1957; Bruni 1965; Finch 1957;
Gindhart 1971; Goodman 2005; Gruber 1962; Gruber 1963;
Gruber 1971a; Gruber 1971b; Gruber 1979; Hartemann 1968;
Kantor 1984a; Laska 1983; Linder 1997; Mehlhorn 2006; Nunlee
2000; Olson 1984; Prockop 1960; Ray 1993; Redick 1980; Rubin
1984; Smith 1973; Sunshine 1983; Sunshine 1985; Sunshine
1986; Sunshine 1989; van Wering 1972; von Pein 1974).
We have undertaken to have four studies translated. Azpiroz 1971
(Spanish, excluded study); Hartemann 1968 (French, excluded
study), Mehlhorn 2005 (German, included study) and Mehlhorn
2006 (German, excluded study).
Included studies
Nine of the included studies with 750 women reported 24 compar-
isons of analgesia with other analgesia or placebo and had data that
could be included in meta-analyses (Bettigole 1981; Bloomfield
1978; Bloomfield 1981; Bloomfield 1986a; Bloomfield 1986b;
Bloomfield 1987; Jain 1978; Kantor 1984b; Mehlhorn 2005).
The remaining nine studies with 581 women reported 14 com-
parisons of analgesia with other analgesia or placebo, but did not
present data that could be meta-analysed (Bloomfield 1977 Study
1; Bloomfield 1977 Study 2; Laska 1981 Study 1; Laska 1981
Study 2; Okun 1982; Olsen 2007; Pan 1993; Skovlund 1991;
Skovlund 1991a).
Outcome measures in the included studies varied.
Pain intensity (x hours)
Pain intensity is a simple assessment of pain intensity at a time
point, typically measured at baseline before the study interven-
tion and again at various time points after the study intervention.
Women were asked to rate their pain using a four- or five-point
scale with zero representing no pain and three or four representing
the worst pain. We calculated mean and standard deviation for all
observations at a single time point and compared between study
groups.
Summed pain intensity difference (SPID)
A commonly used measure was the summed pain intensity differ-
ence. Typically, women were asked before the study intervention
7Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

to rate their pain intensity using a four- or five-point scale with
zero representing no pain and three or four representing the worst
pain. Following administration of the study intervention, women
were again asked to rate the intensity of their pain using the same
scale. The difference between the two measurements was calcu-
lated, the post-study intervention observation pain intensity was
subtracted from the baseline observation pain intensity, giving a
pain intensity difference. This was repeated at intervals following
administration of the study intervention, and the calculated pain
intensity differences for each time point were summed, giving one
numeric value (SPID) for each participant. High SPID values in-
dicate greater pain relief. Mean and standard deviation of the SPID
values were calculated and compared between study groups.
Summed pain relief score
Women were asked to grade their pain relief at various time points
after the study intervention using a four- or five-point scale with
zero representing no pain relief and three or four representing com-
plete pain relief. These observations were repeated a set number
of times after the study intervention and summed giving a single
summed pain relief score for each participant, mean and standard
deviation were calculated for each study group.
Global rating
Typically women were asked at the final observation to rate the
effect of the study intervention on a numeric scale, often zero to
10, with zero representing the worst pain relief they have ever had
and 10 being the best. The score was summed for each study group
and mean and standard deviations calculated.
Pain reduction greater than 50%
Women were asked to grade their pain relief at various time points
after the study intervention using a four- or five-point scale with
zero representing no pain relief and three or four representing com-
plete pain relief. These observations were repeated a set number
of times after the study intervention. Pain reduction greater than
50% was determined by the presence or absence of a fall of greater
than 50% in the level of pre-study intervention pain intensity at
any time during the first three hours after study intervention. Risk
ratios (RR) and 95% confidence intervals (CI) were calculated.
Visual analogue scale one to four at 30 minutes
Women were asked to rate their pain 30 minutes after the study
intervention using a visual analogue scale numbered one to ten
with one representing no pain and ten representing the worst
pain.Their scores were dichotomised to scores of one to four in-
clusive or scores of five to ten inclusive. RR and 95% CIs were
calculated.
Pain analogue score
A single measure on a visual scale of zero to 10 with the lowest
value representing the least pain.
Pain analogue score compared with baseline
A 20 cm line marked zero (no pain) and 100 (worst pain ever ex-
perienced) was used; women marked this visual analogue scale to
represent their pain intensity before the study intervention and at
intervals after the study intervention. Observations at four hours
post-intervention were obtained and a percentage change from
baseline was calculated; ie the first baseline observation was 100%
pain intensity, subsequent measurements were measured as a per-
centage of the baseline measurement.
Visual analogue scale difference
Women rated the pain on a 100 mm visual analogue scale, with
0 mm representing ’no pain’ and 100 mm representing ’pain as
bad as it could be’. Assessment was repeated at two and four hours
after the study intervention and subtracted form baseline giving a
pain intensity difference.
No pain relief
The number of women who did not experience any pain relief
after the study intervention was reported and RR and 95% CIs
were calculated.
Excluded studies
We excluded 24 studies because they included participants with
other sources of postpartum pain, including pain from perineal
trauma, and did not distinguish between pain source in the analy-
ses (Azpiroz 1971; Beaver 1980; Benson 1963; Bonica 1957; Bruni
1965; Finch 1957; Goodman 2005; Gruber 1962; Gruber 1963;
Gruber 1979; Hartemann 1968; Kantor 1984a; Nunlee 2000;
Olson 1984; Ray 1993; Redick 1980; Rubin 1984; Smith 1973;
Sunshine 1983; Sunshine 1985; Sunshine 1986; Sunshine 1989;
van Wering 1972; von Pein 1974).
We excluded three studies because the methods were unclear or not
well enough described to include (Gruber 1971a; Gruber 1971b;
Laska 1983). Two studies were quasi-randomised and therefore
excluded (Baptisti 1971; Prockop 1960).
Two of the identified studies were conference proceedings that
did not include enough detail for inclusion (Bloomfield 1983;
Bloomfield 1986c) and one study was an abstract with insufficient
inclusion details and confirmed by the author as not completed
(Mehlhorn 2006). Another two studies were registered with the
Oxford Perinatal Trials Register but not published (personal com-
munications to the Oxford Register from the first author confirms
that the studies were not published and not likely to be published)
(Bloomfield 1988; Bloomfield 1988a).
8Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Risk of bias in included studies
We assessed included studies for methodological quality on the
basis of selection bias (allocation concealment and sequence gen-
eration), performance bias (blinding), attrition bias (incomplete
outcome data), and selective reporting bias (see Methods above
and Figure 1 and Figure 2). The median year of publication of the
18 included studies is 1982; at this period, trial methodology was
often not well reported making assessment of risk of bias difficult.
Figure 1. Methodological quality graph: review authors’ judgements about each methodological quality
item presented as percentages across all included studies.
9Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 2. Methodological quality summary: review authors’ judgements about each methodological quality
item for each included study.
10Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Allocation
Twelve of the 18 included studies had adequate sequence gener-
ation and were rated as being at low risk of bias: Bettigole 1981;
Bloomfield 1977 Study 1; Bloomfield 1977 Study 2; Bloomfield
1978; Bloomfield 1981; Bloomfield 1986a; Bloomfield 1986b;
Bloomfield 1987; Laska 1981 Study 1; Laska 1981 Study 2;
Mehlhorn 2005; Olsen 2007. The remaining six studies did not
report sufficient detail to assess sequence generation and were rated
as having ’unclear’ risk of bias. Eight studies had low risk of bias
for allocation concealment: Bloomfield 1977 Study 1; Bloomfield
1977 Study 2; Bloomfield 1978; Bloomfield 1981; Bloomfield
1986a; Bloomfield 1986b; Bloomfield 1987; Olsen 2007. The re-
maining 10 studies were rated unclear risk of bias for allocation
concealment. See also Figure 2.
Blinding
We assessed blinding as adequate (low risk of bias) in 15 of
the included studies: Bettigole 1981; Bloomfield 1977 Study 1;
Bloomfield 1977 Study 2; Bloomfield 1978; Bloomfield 1981;
Bloomfield 1986a; Bloomfield 1986b; Bloomfield 1987; Laska
1981 Study 1; Laska 1981 Study 2; Mehlhorn 2005; Okun 1982;
Olsen 2007; Pan 1993; Skovlund 1991. We assessed the remain-
ing three studies as being unclear risk of bias. See also Figure 2.
Incomplete outcome data
We assessed 14 of the included studies as having addressed incom-
plete data for reporting (low risk of bias).
We assessed one study as unclear risk of bias (Bettigole 1981) and
three studies did not address incomplete outcome data and were
assessed as high risk of bias (Kantor 1984b; Olsen 2007; Skovlund
1991a). See also Figure 2 and Characteristics of included studies.
Selective reporting
All but one of the included studies reported outcomes described
in their methods and were assessed as being low risk of bias. The
exception was Pan 1993, which was an abstract only and was
assessed as unclear risk of bias. See also Figure 2.
Other potential sources of bias
Several studies investigated codeine as an analgesic for after pains
(Bettigole 1981; Bloomfield 1986a; Kantor 1984b; Laska 1981
Study 1;Laska 1981 Study 2). Codeine may be formulated with
phosphate or sulfate. The authors of this review have combined re-
sults for codeine regardless of formulation as the active ingredient.
Codeine has similar efficacy regardless of formulation (Martindale
2010).
We assessed all but one study as unclear for other potential sources
of bias as none of the studies published potential sources of bias or
had available protocols. Olsen 2007 was the exception, with dis-
crepancies found in the reported number of subjects randomised
and number of subjects with outcome data, and was therefore
rated as a definite for sources of bias. See also Figure 2.
Effects of interventions
NSAID versus placebo
Ten studies (Bettigole 1981; Bloomfield 1978; Bloomfield 1981;
Bloomfield 1986a; Bloomfield 1986b; Bloomfield 1987; Jain
1978; Laska 1981 Study 1; Laska 1981 Study 2; Okun 1982)
compared NSAIDs with placebo, seven of which reported data
suitable for meta-analysis.
Primary outcomes
Summed pain intensity difference (SPID)
Summed pain intensity difference was reported in three stud-
ies comparing aspirin 650 mg , fenoprofen 200 mg, ketorolac 5
mg, ketorolac 10 mg and naproxen 550 mg with placebo. These
data were pooled to measure the effect of this class of drug com-
pared with placebo. NSAIDs were significantly better than placebo
(mean difference (MD) 4.34; 95% CI 2.87 to 5.82; three studies,
204 women) (Analysis 1.1).
Laska 1981 Study 1 of 143 women reported mean SPIDs compar-
ing fenoprofen 50 mg, 100 mg, 200 mg and 300 mg (means 8.1,
8.1, 9.0 and 7.9 respectively) with placebo (mean 2.2) and found
all doses of fenoprofen to be significantly better than placebo. The
effect size in this study was approximately four times greater for
all doses of fenoprofen than placebo. Laska 1981 Study 2 of 161
women reported mean summed pain intensity difference scores of
fenoprofen 12.5 mg, 25 mg, 50 mg, 100 mg and 200 mg (means
5.3, 6.4, 5.7, 6.9 and 6.2 respectively) approximately double that
of placebo (mean 3.1) and this was significant.
Both study 1 and 2 have used the same number of observations
over the same time period to calculate mean SPIDs and mean total
pain relief scores. It is not clear why the results show an effect size
of three times in study one and two times in study 2. These studies
reported means but no standard deviations or P values.
Okun 1982 reported aspirin to be significantly better at relieving
uterine cramp pain than placebo as measured by mean SPIDs (one
study, 63 women, no useable data).
11Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Pain reduction (pain intensity six hours)
Pain intensity at six hours was reported for aspirin 650 mg (two
studies) and flurbiprofen 50 mg (one study) with placebo. NSAIDs
were significantly better than placebo (MD -0.80; 95% CI -1.12
to -0.47; three studies, 148 women) (Analysis 1.2).
Summed pain relief score
Summed relief score was reported in three studies comparing as-
pirin 650 mg, fenoprofen 200 mg, ketorolac 5 mg, ketorolac 10
mg and naproxen 550 mg with placebo. NSAIDs were signifi-
cantly better than placebo (MD 5.94; 95% CI 3.86 to 8.01; three
studies, 204 women) (Analysis 1.3).
The mean total pain relief score was approximately four times
greater for fenoprofen 50 mg, 100 mg, 200 mg and 300 mg (means
12.0, 12.2, 13.2 and 11.8 respectively) than placebo (mean 3.6)
in Laska 1981 Study 1 (one study 143 women) and approximately
two times greater for fenoprofen 12.5 mg, 25 mg, 50 mg, 100
mg and 200 mg (means 8.1,9.6, 8.6, 10.6 and 9.6 respectively)
than placebo (mean 4.9) in Laska 1981 Study 2 (one study, 161
women).
Pain analogue score compared with baseline
One study compared aspirin 650 mg and aspirin 800 mg with
caffeine 64 mg with placebo and reported a pain analogue score as
a percentage of reported baseline pain. NSAIDs were significantly
better than placebo (MD -43.57; 95% CI -81.07 to -6.07; one
study, 23 women) (Analysis 1.4).
Global rating
A global rating of the analgesic intervention was reported by two
studies comparing aspirin 650 mg, ketorolac 5mg, ketorolac 10
mg and naproxen 550 mg. NSAIDs were significantly better than
placebo (MD 1.88; 95% CI 1.00 to 2.77; three studies, 180
women) (Analysis 1.5).
Pain reduction greater than 50%
One study comparing aspirin 650 mg with placebo reported the
number of people experiencing greater than 50% pain reduction
from baseline at any time during the first three hours after treat-
ment (RR 1.27; 95% CI 0.96 to 1.66; one study, 40 women)
(Analysis 1.6).
Visual analogue scale (VAS) one to four at 30 minutes
One study comparing metamizol 625 mg with placebo reported
the number of women indicating mild pain using a VAS at 30
minutes after the study intervention and found no difference (RR
1.06; 95% CI 0.31 to 3.57; one study, 61 women) (Analysis 1.7).
No pain relief
One study comparing aspirin 650 mg and flurbiprofen 50 mg with
placebo, significantly less women in the NSAID group reported
that they did not experience pain relief (RR 0.12; 95% CI 0.03 to
0.45; two studies, 96 women) (Analysis 1.8).
Adverse effects
Adverse effects reported on three studies comparing aspirin 650 mg
and fenoprofen 200 mg with placebo were similar in the NSAID
and placebo groups (RR 1.12; 95% CI 0.60 to 2.08; two studies,
116 women).
NSAID versus opioid
A NSAID and opioid were compared in five studies (Bettigole
1981; Bloomfield 1986a; Kantor 1984b; Laska 1981 Study 1;
Laska 1981 Study 2); three studies reported data that could be
included in a meta-analysis.
Primary outcomes
Summed pain intensity difference (SPID)
One study reported SPID comparing fenoprofen 200 mg with
codeine 60 mg and they were similar (MD 2.28; 95% CI -2.85 to
7.41; one study, 23 women) (Analysis 2.1).
Laska 1981 Study 1 of 144 women reported mean SPIDs com-
paring fenoprofen 50 mg, 100 mg, 200 mg and 300 mg (means
8.1, 8.1, 9.0 and 7.9 respectively) with codeine phosphate 60 mg
(mean 4.5) and found all doses of fenoprofen to be significantly
better than codeine phosphate 60 mg. The effect size was approx-
imately two times greater for all doses of fenoprofen than codeine
phosphate 60 mg. Laska 1981 Study 2 of 161 women reported
mean SPIDs for fenoprofen 12.5 mg, 25 mg, 50 mg, 100 mg and
200 mg (means 5.3, 6.4, 5.7, 6.9 and 6.2 respectively) and codeine
phosphate (mean 6.1) and they were not significantly different.
Both study 1 and 2 have used the same number of observations
over the same time period to calculate mean SPID scores and mean
total pain relief scores. It is not clear why the results show an effect
size of two times in study one and no difference in study 2. These
studies reported means but no standard deviations or P values.
Pain reduction (pain intensity six hours)
One study reported pain intensity at six hours following study
intervention for the following comparisons: fenoprofen 200 mg
with codeine 60 mg; aspirin 650 mg with codeine 60 mg; aspirin
650 mg with codeine 120 mg; flurbiprofen 50 mg with codeine
60 mg and flurbiprofen 50 mg with codeine 120 mg. NSAIDs
were significantly better than opioids (MD -0.70; 95% CI -1.04,
-0.35; one study, 127 women) (Analysis 2.2).
12Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Summed pain relief score
One study reported summed pain relief score and found no dif-
ference (MD 3.35; 95% CI -3.57 to 10.27; one study, 23 women)
(Analysis 2.3) between NSAID (fenoprofen 200 mg) and NSAID
(codeine 60 mg).
One study of 144 women with no data suitable for meta-analysis
reported the mean total pain relief score was almost two times
greater for fenoprofen 50 mg, 100 mg, 200 mg and 300 mg (means
12.0, 12.2, 13.2 and 11.8 respectively) than codeine phosphate
60 mg (mean 7.26) in Laska 1981 Study 1. A second study of 161
women reported mean SPIDs for fenoprofen 12.5 mg, 25 mg,
50 mg, 100 mg and 200 mg (means 8.1, 9.6, 8.6, 10.6 and 9.6
respectively) and they were not significantly different to the mean
SPID for codeine phosphate 60 mg (mean 9.4), in Laska 1981
Study 2.
No pain relief
Two studies reported the numbers of women who did not experi-
ence pain relief comparing the following NSAIDS with opioids:
aspirin 650 mg with codeine 60 mg; aspirin 650 mg with codeine
120 mg; flurbiprofen 50 mg with codeine 60 mg; flurbiprofen 50
mg with codeine 60 mg and nalbuphine 15 mg with codeine 60
mg. The numbers of women who did not experience pain relief
was not different for NSAIDs and opioids (RR 0.87; 95% CI 0.32
to 2.35; two studies, 199 women) (Analysis 2.4).
Adverse effects
One study comparing fenoprofen 200 mg with codeine 60 mg
found no differences in the number of reported adverse effects
(RR 1.67; 95% CI 0.50 to 5.56; one study, 33 women) (Analysis
2.5).
Opioid versus placebo
An opioid was compared with placebo in five studies (Bettigole
1981; Bloomfield 1986a; Kantor 1984b; Laska 1981 Study 1;
Laska 1981 Study 2); three studies reported data that could be
included in a meta-analysis.
Primary outcomes
Summed pain intensity difference (SPID)
One study comparing codeine 60 mg with placebo found no sig-
nificant difference in SPID (MD 0.42; 95% CI -0.41 to 1.25; one
study, 23 women) (Analysis 3.1).
Two studies (Laska 1981 Study 1; Laska 1981 Study 2) compared
codeine phosphate 60 mg with placebo and reported mean SPIDs
and found codeine sulfate 60 mg to be significantly better (two
studies, 112 women, no data).
Pain reduction (pain intensity six hours)
Pain intensity at six hours was reported in one study comparing
codeine 60 mg and codeine 120 mg with placebo and found that
these opioids were not better than placebo (MD 0.06; 95% CI -
0.40 to 0.52; one study, 95 women) (Analysis 3.2).
Summed pain relief score
One study comparing codeine 60mg with placebo found no sig-
nificant difference in summed pain relief score (MD 0.50; 95%
CI -0.34 to 1.33; one study, 23 women) (Analysis 3.3).
Laska 1981 Study 1 and Laska 1981 Study 2 reported summed
relief scores for 60 mg codeine phosphate to be significantly better
than placebo (two studies, 112 women, no useable data).
No pain relief
One study reported the number of women who did not experience
pain relief comparing nalbuphine 15 mg and codeine 60 mg with
placebo and found opioids to be significantly better at relieving
pain than placebo (RR 0.10; 95% CI 0.04 to 0.23; one study, 108
women) (Analysis 3.4).
Adverse effects
One study reported adverse effects and those reported for codeine
60 mg were not different to the number of adverse effects reported
for placebo (RR 0.65; 95% CI 0.20 to 2.12; one study, 23 women)
(Analysis 3.5).
Aspirin 650 mg versus aspirin 800 mg plus caffeine 64
mg
Primary outcomes
Pain analogue score compared with baseline
Jain 1978reported a percentage change from baseline on a 100-
point analogue scale and found no significant difference between
aspirin 650 mg and aspirin 800 mg plus caffeine 64 mg (one trial,
15 women, no data).
Fenoprofen: different doses
Primary outcomes
Summed pain intensity difference (SPID)
Laska 1981 Study 1 of 115 women found that the mean SPIDs
for fenoprofen 50 mg, 100 mg, 200 mg and 300 mg (means 8.1,
13Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

8.1, 9.0 and 7.9 respectively) were similar to Laska 1981 Study
2 of 134 women, which found the mean SPIDs were similar for
fenoprofen 12.5 mg, 25 mg, 50 mg, 100 mg and 200 mg (means
5.3, 6.4, 5.7, 6.9 and 6.2 respectively). Both study 1 and 2 have
used the same number of observations over the same time period
to calculate SPID. It is not clear why the results of the two studies
differ greatly or why very similar results are reported across a large
range of doses of fenoprofen. The lack of reporting of standard
deviations makes interpretation of these results difficult. It was not
possible to meta-analyse.
Summed pain relief score
Laska 1981 Study 1 of 115 women found the mean total pain relief
scores for fenoprofen 50 mg, 100 mg, 200 mg and 300 mg (means
12.0, 12.2, 13.2 and 11.8 respectively). Laska 1981 Study 2 of
134 women found similar total pain relief scores for fenoprofen
12.5 mg, 25 mg, 50 mg, 100 mg and 200 mg (means 8.1, 9.6, 8.6,
10.6 and 9.6 respectively). Both study 1 and 2 have used the same
number of observations over the same time period to calculate
mean pain relief scores. It is not clear why the results of the two
studies differ greatly or why very similar results are reported across
a large range of doses of fenoprofen. The lack of reporting of
standard deviations makes interpretation of these results difficult.
It was not possible to meta-analyse.
Flurbiprofen 50 mg versus aspirin 650 mg
Primary outcomes
Summed pain intensity difference (SPID)
In one study of 64 women (Bloomfield 1986b), the SPIDs over the
six hours of observation showed flurbiprofen 50 mg to be similar
to aspirin 650 mg, however no standard deviations were reported.
Summed pain relief score
The summed pain relief scores over the six hours of observation
showed flurbiprofen 50 mg to be similar to aspirin 650 mg; how-
ever, no standard deviations were reported (one study, 64 women).
Pain reduction (pain intensity six hours)
Flurbiprofen 50 mg was not significantly different to aspirin 650
mg for pain intensity six hours after the intervention (MD -0.32;
95% CI -0.81 to 0.17; one study, 64 women) (Analysis 4.1).
No pain relief
The number of people reporting no pain relief was similar (RR
0.23; 95% CI 0.01 to 4.52; one study, 64 women) (Analysis 4.2).
Ketorolac 5 mg or 10 mg versus aspirin 650 mg
Primary outcomes
Summed pain intensity difference (SPID)
In one study of 90 women (Bloomfield 1986b), mean SPIDs were
not significantly different for Ketorolac 5 mg or 10 mg compared
with aspirin 650 mg (MD 0.23; 95% CI -1.68 to 2.15) (Analysis
5.1).
Summed pain relief score
Mean total pain relief score indicated ketorolac 5 mg and ketorolac
10mg was not better than aspirin 650 mg (MD 1.17; 95% CI -
1.27 to 3.61; one study, 90 women) (Analysis 5.2).
Global rating
The global rating score was not significantly different for ketorolac
5 mg or ketorolac 10 mg compared with aspirin 650 mg (MD -
0.15; 95% CI -1.08 to 0.79; one study, 90 women) (Analysis 5.3).
Ketorolac: different doses
Primary outcomes
Summed pain intensity difference (SPID)
In one study of 60 women (Bloomfield 1986b), the mean summed
pain intensity difference score was not significantly different (MD
2.11; 95% CI -0.24 to 4.46) (Analysis 6.1).
Summed pain relief score
When ketorolac 5 mg was compared with ketorolac 10 mg, the
mean summed pain relief score showed ketorolac 10 mg to be
significantly better (MD 3.40; 95% CI 0.46 to 6.34; one study,
60 women) (Analysis 6.2).
Global rating
Global rating was not significantly different for ketorolac 5 mg
compared with ketorolac 10mg (MD 1.16; 95% CI -0.09 to 2.41;
one study, 60 women) (Analysis 6.3).
14Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Codeine: different doses
Primary outcomes
Pain reduction (pain intensity six hours)
Codeine sulfate 60 mg was compared with codeine sulfate 120 mg
in one study of 63 women (Bloomfield 1986a), finding that the
different doses were not significantly different (MD 0.07; 95% CI
-0.42 to 0.56) (Analysis 7.1) for pain intensity scores at six hours
following intervention.
No pain relief
The number of people who did not experience pain relief was
similar for codeine 60 mg and codeine sulfate 120 mg (RR 1.03;
95% CI 0.07 to 15.79; one study, 63 women) (Analysis 7.2).
Morphine (epidural) 2 mg versus oxycodone 5 mg and
paracetamol 325 mg
Primary outcomes
Pain analogue score
Pan 1993 in one study of 31 women compared morphine (epidu-
ral) 2 mg with oxycodone 5 mg and paracetamol 325 mg. They
reported that the analogue pain score for uterine cramp pain (zero
to 10) was significantly less (P < 0.05) for women receiving mor-
phine (epidural) 2 mg. The average pain score in the morphine
(epidural) 2 mg group was 1.31 and in the oxycodone 5 mg and
paracetamol 325 mg group was 4.43 (no standard deviations).
Nalbuphine 15 mg versus codeine 60 mg
Primary outcomes
No pain relief
Kantor 1984b found the number of women reporting no pain
relief was similar for nalbuphine 15 mg and codeine (formulation
not specified) 60 mg (RR 0.70; 95% CI 0.13 to 3.97; one study,
72 women) (Analysis 8.1).
Paracetamol different doses versus placebo
Primary outcomes
Summed pain intensity difference (SPID)
One study reported SPID for paracetamol compared with placebo
and found no significant difference between paracetamol 1000 mg
and placebo, though standard deviations were not reported.
Pain reduction (pain intensity six hours)
Bloomfield 1981 in one study of 48 women found paracetamol
650 mg was not significantly better than placebo at relieving pain
from uterine cramps when measuring mean pain intensity at six
hours post dose (MD -0.12; 95% CI -0.71 to 0.47; one study, 48
women) (Analysis 9.1).
Adverse effects
Adverse effects were similar for paracetamol 1000 mg and placebo
(RR 2.36; 95% CI 0.95 to 5.88; one study, 48 women) (Analysis
9.2).
VAS difference
Skovlund 1991 using a sequential trial design of 45 women found
paracetamol 1000 mg was significantly better than placebo at two
hours post medication; however, we were unable to include the
data in this review. (The median difference in effect was 13.5 mm
(95% CI 3.24) and 13 mm (95% CI 2 to 24) at four hours post
treatment.
Paracetamol 650 mg versus aspirin 650 mg
Primary outcomes
Pain reduction (pain intensity six hours)
Paracetamol 650 mg was compared with aspirin 650 mg in one
study (Bloomfield 1981) which found that the pain intensity six
hours after the intervention was significantly less in the aspirin
650 mg group (MD 0.85; 95% CI 0.29 to 1.41; one study, 48
women) (Analysis 10.1).
Adverse effects
There were no differences in adverse effects (RR 1.31; 95% CI
0.65 to 2.64; one study, 48 women) (Analysis 10.2).
15Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

TENS 100 Hz versus placebo
Primary outcomes
VAS one to four at 30 minutes
TENS 100 Hz was compared with placebo by Mehlhorn 2005.
There was a trend toward more women reporting “good pain re-
lief ” 30 minutes after treatment in the TENS 100 Hz group com-
pared with the placebo group (RR 1.04; 95% CI 0.29 to 3.73;
one study, 55 women) (Analysis 11.1).
TENS 100 Hz and metamizol 625 mg versus placebo
Primary outcomes
VAS one to four at 30 minutes
TENS 100 Hz plus metamizol 625 mg was compared with placebo
by Mehlhorn 2005. There was a trend toward more women re-
porting “good pain relief ” 30 minutes after treatment in the TENS
100 Hz plus metamizol 625 mg group compared with the placebo
group (RR 2.57; 95% CI 0.92 to 7.13; one study, 58 women)
(Analysis 12.1).
TENS 100 Hz and metamizol 625 mg versus TENS
100 Hz
Primary outcomes
VAS one to four at 30 minutes
Mehlhorn 2005 compared TENS 100 Hz plus metamizol 625 mg
with TENS 100 Hz alone as part of a four-arm randomised con-
trolled trial. The number of women reporting “good pain relief ”
(VAS between one and four) at 30 minutes after treatment was
not significantly different in either group (RR 2.48; 95% CI 0.89
to 6.86; one study, 57 women) (Analysis 13.1). There was a trend
toward greater pain relief in the TENS plus metamizol group.
TENS 100 Hz and metamizol 625 mg versus
metamizol 625 mg
Primary outcomes
VAS one to four at 30 minutes
TENS 100 Hz plus metamizol 625 mg was compared with
metamizol 625 mg alone by Mehlhorn 2005. There was a trend
toward more women reporting “good pain relief ” 30 minutes after
treatment in the TENS 100 Hz plus metamizol 625 mg group
compared with the metamizol 625 mg group (RR 2.42; 95% CI
0.95 to 6.16; one study, 63 women) (Analysis 14.1).
TENS 100 Hz versus metamizol 625 mg
Primary outcomes
VAS one to four at 30 minutes
Mehlhorn 2005 compared TENS 100 Hz with metamizol 625
mg and found no significant difference in the number of women
reporting “good pain relief ” (RR 0.98; 95% CI 0.29 to 3.29; one
study, 60 women) (Analysis 15.1).
TENS high (50 mA) versus low intensity (10-15 mA)
Primary outcomes
VAS one to four at 30 minutes
Olsen 2007 compared high intensity (HI) TENS 50 mA with low
intensity (LI)TENS 10-15 mA in a small study of 21 women.
The authors concluded HI TENS to be better than LI TENS;
however, these results have a high risk of bias. There is a clear
baseline imbalance - numbers in abstract differ from those given
in CONSORT. There is no account given for the discrepancy of
the numbers. Therefore we could not include these data.
D I S C U S S I O N
Summary of main results
This review has found non-steroidal ant-inflammatory drugs
(NSAIDs) including aspirin, to be better than placebo for reliev-
ing pain due to uterine cramping/involution after vaginal birth.
NSAIDs including aspirin were better than placebo at relieving
pain from uterine cramping/involution following vaginal birth.
NSAIDs were better than paracetamol and paracetamol was not
better than placebo though numbers of participants for these com-
parisons were small. Data for opioids compared with NSAIDs
and opioids compared with placebo were conflicting, with some
16Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

measures showing similar effect and others indicating NSAIDs
were better than opioids and opioids were not better than placebo.
There were insufficient data to make conclusions regarding the
effectiveness of opioids at relieving pain from uterine cramping/
involution.
There is little evidence regarding the effectiveness of paracetamol.
There was a trend towards paracetamol being less effective than
aspirin and naproxen and not better than placebo. Finding parac-
etamol to be less effective than NSAIDs is consistent with find-
ings of a review of NSAIDs for primary dysmenorrhoea or uter-
ine cramping pain associated with menstruation (Marjoribanks
2010). Codeine was better than placebo but not better than as-
pirin.
The included studies reported little, if any, information on the
safety of the various forms of analgesia for use by women who were
breastfeeding.
There is limited information about the safety of the NSAIDs for
breastfeeding women and their babies. The following NSAIDs
have been included in this review; aspirin, fenoprofen, flurbipro-
fen, ketorolac, metamizole and naproxen.
The World Health Organization working group on drugs in lacta-
tion determined that aspirin is not safe for use during breastfeeding
(Bennett 1988). Although extremely small amounts of aspirin are
secreted in breastmilk, it has been implicated in Reye Syndrome
and should be avoided (Hale 2010).
Fenoprofen, flurbiprofen and ketorolac have been studied in a
limited number of women; they are difficult to detect in breast-
milk following recommended dosages, and are considered safe for
breastfeeding women (Hale 2010).
Metamizol has been removed from sale in many countries due
to serious adverse effects including agranulocytosis and aplastic
anaemia. It has been studied in a very small number of breastfeed-
ing women and detected in small amounts in their breastmilk.
Metamizole is generally not recommended, as safer alternatives are
available (Hale 2010).
Naproxen is considered moderately safe for breastfeeding women
in short-term use. It has a longer half-life and one case has been
documented of an infant with prolonged bleeding, haemorrhage
and acute anaemia. Long-term use of naproxen in breastfeeding
women may be hazardous (Hale 2010).
Safety of other classes of drugs included in this review
Paracetamol, a simple analgesic, has been well researched in breast-
feeding women; amounts passed into breastmilk are considered
too small to be hazardous and in recommended doses it is consid-
ered safe (Hale 2010).
Codeine, a mild opiate, can be detected in small amounts in breast-
milk; infant apnoea has been reported (Davis 1985) and there has
been one infant death linked to codeine usage (Koren 2006). De-
spite this, codeine is considered safe in moderation (Hale 2010).
Hereditary polymorphisms of the drug-metabolising enzyme cy-
tochrome P450 2D6 (CYP2D6) mean that some individuals lack-
ing this enzyme will find codeine ineffective (Cascorbi 2003). Be-
tween one and three percent of middle-Europeans and up to 29%
of Ethiopians display CYP2D6 gene duplications and are ultra-
rapid metabolisers of codeine to morphine (Cascorbi 2003); be-
cause of this, they may pass potentially fatal concentrations of
morphine to their infants through breastmilk. One such infant
death has been reported (Koren 2006). Codeine may cause consti-
pation (Hale 2010). Women should be informed of the risks and
the infants of breastfeeding women who take codeine preparations
observed for signs of sedation and codeine toxicity.
Morphine has not been well studied in breastfeeding women; how-
ever, it is thought to be the opiate of choice in lactating women.
The limited information available suggests that the amount de-
tected in breastmilk of women receiving morphine via patient con-
trolled analgesia pumps is unlikely to be clinically relevant in sta-
ble breastfeeding infants (Hale 2010). Morphine taken orally is
poorly absorbed (approximately 26% of the dose), therefore in-
fants would absorb approximately one-quarter of the small amount
of morphine found in breastmilk of women using morphine for
pain relief. It is possible that sedation of newborn infants and res-
piratory problems may occur with higher doses of morphine.
Nalbuphine is a potent synthetic narcotic similar in potency to
morphine. In a study of 20 women, less than 0.02% of the adult
dose was detected in breastmilk and no known complications have
been reported regarding infant ingestion of breastmilk of women
given nalbuphine (Hale 2010).
Paracetamol and oxycodone: oxycodone is an opioid analgesic de-
rived from opium. This combined analgesic is considered moder-
ately safe for breastfeeding women and their infants (Hale 2010).
Overall completeness and applicability ofevidence
The average year of the included studies is 1981; the majority
of analyses in this review are based on single studies with small
numbers of participants, and drugs in common use today such as
ibuprofen have not been tested for this condition. As previously
stated, many of the randomised controlled studies included in this
review were intended to investigate the drugs in use and postpar-
tum women were a convenient sample to test. Outcomes impor-
tant to women, their infants and adverse impact on breastfeeding
have not been assessed.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
There is little information or evidence regarding currently avail-
able analgesia to treat postpartum women experiencing pain from
uterine cramping and involution after vaginal birth.
17Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

This review cannot make any recommendation for clinical prac-
tice.
Implications for research
Further research is required, including a survey of postpartum
women to describe appropriately their experience of uterine
cramping and involution.
The median year of publication of included studies was 1981;
more research is needed to include current pharmacological and
non-pharmacological analgesics.
The review authors believe there is sufficient information regarding
pharmacological analgesia versus placebo. A well controlled study
should compare drugs in current use known to be safe in this
population.
There is insufficient information regarding non-pharmacological
analgesia and these should be assessed in well designed controlled
randomised studies.
Studies should report all outcomes of relevance to women and
their babies and healthcare providers.
A C K N O W L E D G E M E N T S
Sheree Agett was a contributing author for the protocol, but unable
to continue with the review process. We thank her for her input.
A special thank you to Ms Philippa Middleton from The Univer-
sity of Adelaide for her guidance and support.
We would like to acknowledge and thank Professor Caroline
Crowther from The University of Adelaide (Director of ARCH)
for the guidance she provided with the interpretation of the re-
sults.
Mr Neil Hotham, Senior Specialist Drug Information Pharmacist,
Women’s and Children’s Hospital, Adelaide, Australia has been
invaluable in assisting with the understanding of the wide range
of pharmaceuticals that were presented in the studies.
As part of the pre-publication editorial process, this review has
been commented on by three peers (an editor and two referees
who are external to the editorial team), a member of the Pregnancy
and Childbirth Group’s international panel of consumers and the
Group’s Statistical Adviser.
R E F E R E N C E S
References to studies included in this review
Bettigole 1981 {published data only}
Bettigole JB. A double-blind comparison of placebo,
codeine, and fenoprofen in patients with postpartum pain.
Current Therapeutic Research 1981;29:778–84.
Bloomfield 1977 Study 1 {published data only}
Bloomfield SS, Barden TP, Mitchell J. Aspirin and codeine
in two postpartum pain models. Clinical Pharmacology and
Therapeutics 1976;20(4):499–503.∗ Bloomfield SS, Barden TP, Mitchell J. Naproxen,
aspirin, and codeine in postpartum uterine pain. ClinicalPharmacology and Therapeutics 1977;21(4):414–21.
Bloomfield 1977 Study 2 {published data only}
Bloomfield SS, Barden TP, Mitchell J. Aspirin and codeine
in two postpartum pain models. Clinical Pharmacology and
Therapeutics 1976;20(4):499–503.∗ Bloomfield SS, Barden TP, Mitchell J. Naproxen,
aspirin, and codeine in postpartum uterine pain. ClinicalPharmacology and Therapeutics 1977;21(4):414–21.
Bloomfield 1978 {published data only}
Bloomfield SS, Barden TP, Mitchell J. Fendosal and aspirin
in postpartum uterine pain. Clinical Pharmacology andTherapeutics 1978;23(4):390–6.
Bloomfield 1981 {published data only}
Bloomfield SS, Barden TP, Mitchell J. A comparison
of pirprofen, aspirin, acetaminophen and placebo in
postpartum uterine cramp pain. Current Therapeutic
Research 1981;30:S139–S145.
Bloomfield 1986a {published data only}
Bloomfield SS, Barden TP, Mitchell J, Bichlmeier G.
Flurbiprofen, aspirin, and codeine in postpartum uterine
pain. Clinical Pharmacology and Therapeutics 1981;29:
234–5.
Bloomfield SS, Barden TP, Mitchell J, Bichlmeir G.
A comparison of flurbiprofen, aspirin and placebo in
postpartum uterine pain. Current Therapeutic Research1981;30:670–9.
Bloomfield SS, Cissell GB, Mitchell J, Barden TP. Codeine
and aspirin analgesia in postpartum uterine cramps:
qualitative aspects of quantitative assessments. ClinicalPharmacology and Therapeutics 1983;34:488–95.∗ Bloomfield SS, Mitchell J, Cissell G, Barden TP.
Flurbiprofen, aspirin, codeine, and placebo for postpartum
uterine pain. American Journal of Medicine 1986;80:65–70.
Bloomfield 1986b {published data only}
Bloomfield SS, Mitchell J, Cissell, G, Peters N, Nelson ED,
Barden TP. Keterolac vs aspirin with or without codeine
for postpartum or postoperative pain. Proceedings of
10th International Congress of Pharmacology; 1987 Aug;
Sydney, Australia. 1987:P590.
Bloomfield SS, Mitchell J, Cissell G, Barden TP. RS-
37619 and aspirin analgesia for postpartum uterine cramps.
Clinical Pharmacology and Therapeutics 1984;35(2):228.∗ Bloomfield SS, Mitchell J, Cissell GB, Barden TP, Yee
JP. Keterolac versus aspirin for postpartum uterine pain.
Pharmacotherapy 1986;6:247–52.
18Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bloomfield 1987 {published data only}∗ Bloomfield SS, Cissell GB, Nancy NM, Mitchell J, Nelson
ED, Bardon TP. Anirolac vs Naproxen for postpartum
uterine pain. Clinical Pharmacology and Therapeutics 1987;
42(1):89–95.
Bloomfield SS, Nelson ED, Mitchell J, Cissel GB, Peters N,
Barden TP. Anirolac and naproxen analgesia for postpartum
uterine cramp pain. Clinical Pharmacology and Therapeutics1986;39(2):181.
Jain 1978 {published data only}∗ Jain AK, McMahon FG, Ryan JR, Unger D, Richard
V. Aspirin and aspirin-caffeine in postpartum pain relief.
Clinical Pharmacology and Therapeutics 1978;24:69–75.
Jain AK, McMahon FG, Ryan JR, Unger D, Richard W. A
comparison of aspirin-caffeine versus aspirin: results of two
double-blind placebo controlled studies in postpartum pain.
Clinical Pharnacology and Therapeutics 1978;23(1):116.
Kantor 1984b {published data only}
Kantor T, Hopper M. Oral nalbuphine in postpartum pain.
Clinical Pharmacology and Therapeutics 1984;35(1):46–9.
Laska 1981 Study 1 {published data only}∗ Laska EM, Sunshine A. Fenoprofen and codeine analgesia.
Clinical Pharmacology and Therapeutics 1981;29(5):606–16.
Offen WW, Gruber CM. Dose response to fenoprofen
calcium using placebo and codeine as controls. Journal ofMedicine 1985;16(4):439–52.
Sunshine A, Laska E, Zighelboim I, Desenne J. A
comparison of the analgesic responses of fenoprofen,
codeine, and placebo in postpartum and postoperative pain.
Current Therapeutic Research 1981;29(5):771–7.
Laska 1981 Study 2 {published data only}∗ Laska EM, Sunshine A. Fenoprofen and codeine analgesia.
Clinical Pharmacology and Therapeutics 1981;29(5):606–16.
Offen WW, Gruber CM. Dose response to fenoprofen
calcium using placebo and codeine as controls. Journal ofMedicine 1985;16(4):439–52.
Sunshine A, Laska E, Zighelboim I, Desenne J. A
comparison of the analgesic responses of fenoprofen,
codeine, and placebo in postpartum and postoperative pain.
Current Therapeutic Research 1981;29(5):771–7.
Mehlhorn 2005 {published data only}
Mehlhorn G, Beckmann MW, Schild RL, Binder
H. Analgesia of afterpains with transcutaneous nerve
stimulation (TENS) vs. metamizole. A prospective,
randomized placebo controlled double blind study
[Analgesie von schmerzhaften Nachwehen mittels
transkutaner elektrischer Nervenstimulation (TENS) vs.
Metamizol]. Geburtshilfe und Frauenheilkunde 2005;65:
266–71.
Okun 1982 {published data only}
Okun R. Evaluation of the analgesic effect of fendosal in
patients with postpartum uterine cramp or episiotomy pain.
Current Therapeutic Research, Clinical and Experimental
1982;32(1):65–73.
Olsen 2007 {published data only}
Olsen MF, Elden H, Janson ED, Litjer H, Stener-Victorin
E. A comparison of high- verus low-intensity, high-
frequency transcutaneous electric nerve stimulation for
painful postpartum uterine contractions. Acta Obstetrica et
Gynecologica Scandinavica 2007;86(3):310–4.
Pan 1993 {published data only}
Pan PH, Moore C, Blass N. Low dose epidural morphine
provides better analgesia than oral percocet for post vaginal
delivery. Regional Anesthesia 1993;18(2S):15.
Skovlund 1991 {published data only}
Skovlund E, Fyllingen G, Landre H, Nesheim BL.
Comparison of postpartum pain treatments using a
sequential trial design. I. Paracetamol versus placebo.
European Journal of Clinical Pharmacology 1991;40(4):
343–7.
Skovlund 1991a {published data only}
Skovlund E, Fyllingen G, Landre H, Nesheim BL.
Comparison of postpartum pain treatments using a
sequential trial design. II. Naproxen verus paracetamol.
European Journal of Clinical Pharmacology 1991;40:539–42.
References to studies excluded from this review
Azpiroz 1971 {published data only}
Azpiroz P, Garcia G. Clinical trial of a new analgesic CI-
473 Parke Davis, in puerperal pain. [Ensayo clinico de un
nuevo analgesico, CI–473 Parke Davis, en los entuertos
puerperales]. Toko-Ginecologia Practica 1971;30:135–59.
Baptisti 1971 {published data only}
Baptisti A, Gruber CM, Santos EL. The effectiveness and
side-effect liability of propoxyphene hydrochloride and
propoxyphene napsylate in patients with postpartum uterine
cramping. Toxicology and Applied Pharmacology 1971;19:
519–27.
Beaver 1980 {published data only}
Beaver WT, McMillan D. Methodological considerations in
the evaluation of analgesic combinations: acetaminophen
(paracetamol) and hydrocodone in postpartum women.
British Journal of Clinical Pharmacology 1980;10:
215S–223S.
Benson 1963 {published data only}
Benson RC. Double blind evaluation of analgesic agents in
the postpartum patient. Western Journal of Surgery 1963;71:
167–9.
Bloomfield 1988 {published data only (unpublished sought but not
used)}
Bloomfield SS. The comparative efficacy of Voltaren
(diclofenac), naproxen sodium and placebo in the treatment
of postpartum uterine cramp pain. Personal communication
1988.
Bloomfield 1983 {published data only}
Bloomfield SS, Mitchell J, Bichlmeir LPN, Barden TP. Low
dose ibuprofen and aspirin analgesia for postpartum uterine
cramps. American Society for Clinical Pharmacology and
Therapeutics 1983;33:194.
19Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bloomfield 1986c {published data only}
Bloomfield SS, Kantor TG, Hopper M, Mitchell J. Aspirin
(S) and acetaminophen (C), regular vs extra-strength, for
postpartum uterine cramps. Clinical Pharmacology andTherapeutics 1986;38:181.
Bloomfield 1988a {published data only (unpublished sought but not
used)}
Bloomfield SS. A double-blind placebo-controlled parallel
evaluation of the comparative analgesic efficacy between
intramuscularly administered lysine acetylsalicylate (LAS)
and oral aspirin (ASA) in postpartum uterine cramp pain.
Personal Communication 1988.
Bonica 1957 {published data only}
Bonica JJ, Hadfield D, Bennett B. The management of
postpartum pain with dihydrohydroxycodeinone (percodan)
evaluation with codeine and placebo. Western Journal of
Surgery 1957;2:84–8.
Bruni 1965 {published data only}
Bruni JR, Holt RE. Controlled double-blind evaluation
of three analgesic medications for postpartum discomfort.
Obstetrics and Gynecology 1065;25:76–81.
Finch 1957 {published data only}
Finch JS, DeKornfeld TJ. Clonixin: a clinical evaluation of
a new oral analgesic. Journal of Clinical Pharmacology 1971;
11(5):371–7.
Gindhart 1971 {published data only}
Gindhart JD. A rationale for studying analgesia. A double
blind study in postpartum patients. Current Therapeutic
Research 1971;13:240–50.
Goodman 2005 {published data only}
Goodman SR, Drachenberg AM, Johnson S, Kim-Lo SH,
Smiley RM. Decreased use of oral pain medication after
vaginal delivery with a single dose of epidural morphine
(abstract). Anesthesiology 2001;95(Suppl):A1029.
Goodman SR, Drachenberg AM, Johnson SA, Kim-
Loo SH, Smiley RM. Decreased postpartum use of oral
pain medication after a single dose of epidural morphine.
Anesthesiology 2001;94(1A):A83.∗ Goodman SR, Drachenberg AM, Johnson SA, Negron
MA, Kim-Lo SH, Smiley RM. Decreased postpartum use
of oral pain medication after a single dose of epidural
morphine. Regional Anesthesia and Pain Medicine 2005;30
(2):134–9.
Gruber 1962 {published data only}
Gruber CM, Baptisti A, Chernish SM. Comparitive
evaluation of analgesic agents in postpartum patients: oral
dextropropoxyphene, codeine and meperidine. Anesthesia
and Analgesia 1962;1(5):538–44.
Gruber 1963 {published data only}
Gruber CM, Baptisti A. Estimating the acceptability of
morphine and noracymethadol in postpartum patients.
Clinical Pharmacology and Therapeutics 1963;4(2):172–81.
Gruber 1971a {published data only}
Gruber CM, Wolen RL, Baptisti A. Analgesia scores as timed
responses following oral administration of propoxyphene to
postpartum patients. Toxicology and Applied Pharmacology
1971;19:504–11.
Gruber 1971b {published data only}
Gruber CM, Baptisti A, Kiplinger GF. Relief of postpartum
uterine cramping with propoxyphene and aspirin. Toxicology
and Applied Pharmacology 1971;19:546–53.
Gruber 1979 {published data only}
Gruber CM, Bauer RO, Bettigole JB, Lash AF, McDonald
JS. A multicenter study for analgesia involving fenoprofen,
propoxyphene (alone or in combination) with placebo and
aspirin controls in postpartum pain. Journal of Medicine
1979;10(1-2):65–98.
Hartemann 1968 {published data only}
Hartemann J, Landes P, Bertrand P. Results of treatment of
post-partum pain with C.B. 3697 [Resultats du traitement
des tranches du post–partum par le C.B. 3697]. Bulletin de
la Societe Nationale de Gynecologie et d’Obstetrique de France1968;20(2):176–8.
Kantor 1984a {published data only}∗ Kantor T, Cavalier MB, Hopper RN, Roepke MS. A
double-blind comparison of ketoprofen codeine, and
placebo in patients with moderate to severe postpartum
pain. Journal of Clinical Pharmacology 1984;24:228–34.
Kantor TG, Hopper M. Oral ketoprofen as an analgesic on a
post-partum model. Clinical Pharmacology and Therapeutics1983;33:196.
Laska 1983 {published data only}
Laska EM, Sunshine A, Zighelboim I, Roure C, Marrero
I, Wanderling J, et al.Effect of caffeine on acetaminophen
analgesia. Clinical Pharmacology and Therapeutics 1983;33
(4):498–509.
Linder 1997 {published data only}
Linder N, German B, Bessant D, Sirota L, Zylber-Katz
E, Martin O, et al.The pharmacological effect on term
neonates of analgesic drugs ingested through maternal milk.
Canadian Journal of Clinical Pharmacology 1997;4:112–4.
Mehlhorn 2006 {published data only}
Mehlhorn G, Esche C, Fashing PA, Lux MP, Goecke
T, Binder H, et al.Analgesia for afterpains by means
of transcutaneous electrical nerve stimulation (TENS)
vs, placebo TENS. A prospective randomised placebo
controlled trial [Analgesie von schmerzhaften Nachwehen
mittels transkutane elektrische Nervenstimmulation
(TENS) vs. Placebo–TENS. Eine randomisierte
placebokontrollierte Doppelblindstudie]. Geburtshilfe and
Frauenheilkunde 2006;66 Suppl:S108.
Nunlee 2000 {published data only}
Nunlee WY, Perry PM, Lawal AH, Ivankovich AD. Does a
single dose of epidural morphine provide extended analgesia
after vaginal delivery. Anesthesiology 2000;93(3A):A1060.
Olson 1984 {published data only}
Olson N, Sunshine A, Roure C, Colon A, Laska EM,
Santiago H, et al.Analgesic efficacy of suprofen, codeine and
placebo. Pain 1984;2 Suppl:238.
20Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Prockop 1960 {published data only}
Prockop LD, Eckenhoff JE, McElroy RC. Evaluation
of dextropropoxyphene, codeine, and acetylsalicylic
compound. Obstetrics & Gynecology 1960;16:113–8.
Ray 1993 {published data only}
Ray S, Swami A, Kadim M, Morgan B. Efficacy of
diclofenac in a single prophylactic dose in post partum pain.
International Journal of Obstetric Anesthesia 1993;2:58.
Redick 1980 {published data only}
Redick LF, Bromage PR. Postpartum epidural narcotic
analgesia. Anesthesiology 1980;53:S297.
Rubin 1984 {published data only}
Rubin A, Winter L. A double-blind randomized study of
an aspirin/caffeine combination versus acetaminophen/
aspirin combination versus acetaminophen versus placebo in
patients with moderate to severe post-partum pain. Journal
of International Medical Research 1984;12:338–44.
Smith 1973 {published data only}
Smith GM, Coletta CG, McBride S, McPeek B. Use of
subjective responses to evaluate efficacy of mild analgesic-
sedative combinations. Clinical Pharmacology andTherapeutics 1973;15:118–29.
Sunshine 1983 {published data only}
Sunshine A, Zighelboim I, De Sarrazin C, De Castro A,
Olson NZ, Laska E. A study of the analgesic efficacy of
nalbuphine hydrochloride in patients with postpartum
pain. Current Therapeutic Research 1983;33(1):108–14.
Sunshine 1985 {published data only}
Sunshine A, Zighelboim I, Olson NZ, De Sarrazin C,
Laska E. A comparative oral analgesic study of indoprofen,
aspirin, and placebo in postpartum pain. Journal of ClinicalPharmacology 1985;25:374–80.
Sunshine 1986 {published data only}
Sunshine A, Olson NZ, Siegel C, Laska E. Oral analgesic
study of ketoprofen, aspirin and placebo in post-partum
pain. Clinical Pharmacology and Therapeutics 1983;33:154.∗ Sunshine A, Zighelboim I, Laska E, Siegel C, Olson
NZ, De Castro A. A double-blind, parallel comparison
of ketoprofen, aspirin, and placebo in patients with post-
partum pain. Journal of Clinical Pharmacology 1986;26:
706–11.
Sunshine 1989 {published data only}
Sunshine A, Laska E, Siegel C, Zighelboim I, De Castro A,
Sorrentino J, Smith D, Bartizek R. Analgesic adjuvancy
of caffeine with ibuprofen in three different postpartum
pain populations. Clinical Pharmacology and Therapeutics.
1989; Vol. 45:174.
van Wering 1972 {published data only}
van Wering RF, Bleker OP. Oral analgesia in post-
partum pain: a comparison of ibuprofen (’Brufen’) and
dextropropoxyphene. Current Medical Research and Opinion
1972;1(1):49–52.
von Pein 1974 {published data only}
von Pein W. Double blind study using benzydamine in
the puerperium [Doppelblindstudie mit Benzydamine im
Wochenbett]. Gynakologische Rundschau 1974;14:327–8.
Additional references
Bennett 1988
Bennett PN. Drugs and Human Lactation. Amsterdam:
Elsevier, 1988.
Berlin 1980
Berlin CM Jr, Yaffe, SJ, Ragni M. Disposition of
acetaminophen in milk, saliva and plasma of lactating
women. Pediatric Pharmacology 1980;1(2):135–41.
Bitzen 1981
Bitzen PO, Gustafsson B, Jostell KG, Melander Q, Wahlin-
Boll E. Excretion of paracetamol in human breast milk.
European Journal of Clinical Pharmacology 1981;20(2):
123–5.
Bloomfield 1998
Bloomfield SS, Mitchell J, Cissell G, Barden TP. Analgesic
sensitivity of two post-partum models. Pain 1986;27(2):
171–9.
Cascorbi 2003
Cascorbi I. Pharmacogenetics of cytochrome P4502D6:
genetics background and clinical implications. EurpoeanJournal of Clinical Investigation 2003;33(Suppl 2):17–22.
Chou 2010
Chou D, Abalos E, Gyte GML, Gülmezoglu AM.
Drugs for perineal pain in the early postpartum period:
generic protocol (Protocol). Cochrane Database ofSystematic Reviews 2009, Issue 3. [DOI: 10.1002/
14651858.CD007734.pub2]
Chou 2010a
Chou D, Abalos E, Gyte GML, Gülmezoglu AM.
Paracetamol/acetaminophen (single administration) for
perineal pain in the early postpartum period. CochraneDatabase of Systematic Reviews 2010, Issue 3. [DOI:
10.1002/14651858.CD008407]
Davis 1985
Davis JM, Bhutari VK. Neonatal apnea and maternal
codeine use. Pediatric Research 1985;19(4):170A.
Egger 1997
Egger M, Smith GD, Schneider M, Minder C. Bias in
meta-analysis detected by a simple, graphical test. BMJ1997;315:629–34.
Erickson 1979
Erickson SH, Oppenheim GL. Aspirin in breast milk.
Journal of Family Practice 1979;8(1):189–90.
Findlay 1981
Findlay JW, DeAngelis RL, Kearney MF, Welch RM,
Findlay JM. Analgesic drugs in breast milk and plasma.
Clinical Pharmacology Therapy 1981;29(5):625–33.
21Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Hale 2010
Hale TW. Medications and mother’s milk: a manual oflactational pharmacology. 14th Edition. Amarillo: Hale
Publishing LP, 2010.
Harbord 2006
Harbord RM, Egger M, Sterne JA. A modified test for
small-study effects in meta-analyses of controlled trials with
binary endpoints. Statistics in Medicine 2006;25:3443–57.
Higgins 2009
Higgins JPT, Green S, editors. Cochrane Handbook for
Systematic Reviews of Interventions Version 5.0.2 [updated
September 2009]. The Cochrane Collaboration, 2009.
Available from www.cochrane-handbook.org.
Holdroft 2003
Holdrocft A, Snivdongs S, Cason A, Dore C, Berkely K.
Pain and uterine contractions during breast feeding in the
immediate post-partum period increase with parity. Pain
2003;104:589–96.
Koren 2006
Koren G, Cairns J, Chitayat D, Gaedigk A, Leeder SJ.
Pharmacogenetics of morphine poisoning in a breastfed
neonate of a codeine-prescribed mother. The Lancet 2006;
368:704.
Ladewig 1990
Ladewig PA, London ML, Olds SB. Essentials of maternal-newborn nursing. 2nd Edition. Redwood City: Addison-
Wesley, 1990.
Mander 1998
Mander R. Pain in childbearing and its control. Oxford:
Blackwell Science, 1998.
Marjoribanks 2010
Marjoribanks J, Proctor M, Farquhar C, Derks RS.
Nonsteroidal anti-inflammatory drugs for dysmenorrhoea.
Cochrane Database of Systematic Reviews 2010, Issue 1.
[DOI: 10.1002/14651858.CD001751.pub2]
Martindale 2010
Sweetman S (Ed). Martindale: The Complete Drug
Reference [Online]. http://www.medicinescomplete.com.
Pharmaceutical Press, Accessed 24th Novemeber 2010.
MIMS 2008
MIMS. MIMS Annual 2008. St Leonards NSW: CMP
Medica, 2008.
Notorianni 1987
Notorianni LJ, Oldham HG, Bennett PN. Passage of
paracetamol in breast milk and its subsequent metabolism
by the neonate. British Journal of Clinical Pharmacology
1987;24(1):63–7.
Rang 2007
Rang HP, Dale MM, Ritter JM, Flower RJ. Rang and Dale’s
Pharmacology. Philadelphia: Churchill Livingstone Elsevier,
2007.
RevMan 2008
The Nordic Cochrane Centre, The Cochrane Collaboration.
Review Manager (RevMan) Version 5.0 for Windows.
Copenhagen: The Nordic Cochrane Centre, The Cochrane
Collaboration, 2008.
Sleep 1991
Sleep J. Perineal care: a series of five randomised trials. In:
Robinson S, Thompson AM editor(s). Midwives, research
and childbirth. Vol. 2, Chapman & Hall, 1991:199–251.
Windle 1989
Windle ML, Booker LA, Rayburn WF. Postpartum pain
after vaginal delivery. A review of comparative analgesic
trials. Journal of Reproductive Medicine 1989;34(11):891–5.∗ Indicates the major publication for the study
22Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Bettigole 1981
Methods Randomised controlled trial.
Sample size calculation not discussed.
Paper does not state how many women were randomised.
Participants No information about where the women participated or time frame of study.
Included: 35 postpartum women aged 46 years or less with acute uterine cramp pain,
review authors have assumed women had vaginal delivery. Women gave informed con-
sent.
Excluded: women who had received analgesics in the preceding 4 hours.
Interventions Following initial pain assessment women were randomly allocated to 1 of 3 treatment
groups.
• Treatment group 1 received 2 doses of placebo 4 hours apart, each dose was 1
capsule and its composition is not stated (N = 12).
• Treatment group 2 received 2 doses of codeine sulfate 60 mg 4 hours apart, each
dose was 1 capsule (N = 11).
• Treatment group 3 received 2 doses of fenoprofen 200 mg 4 hours apart, each
dose was 1 capsule (N = 12).
Outcomes Pain assessed by an observer before the first dose and at hourly intervals for 8 hours
asking women to rate pain intensity on a 5-point scale; no pain (0), a little (1), some (2)
, a lot (3), terrible (4) and pain relief on 5-point scale; no relief (0), a little (1), some (2)
, a lot (3), complete relief (4).
Pain intensity difference was calculated for each observation and summed and pain relief
scores were summed. Mean pain intensity difference and mean pain relief score for each
hourly observation and summed pain intensity difference mean and mean total relief as
assessed by the observer.
After the final pain observation at 8 hours women were asked to report on adverse drug
reactions from a checklist which included; drowsiness, dizziness, asthenia, headache,
abdominal discomfort, hidrosis, nausea, vomiting, tinnitus, tremor, tachycardia, blurred
vision, hypertension, nervousness, itching/rash, edema, dry mouth.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Study medications were “prescribed in ran-
dom order”.
Allocation concealment (selection bias) Unclear risk Insufficient information to permit judge-
ment.
23Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bettigole 1981 (Continued)
Blinding (performance bias and detection
bias)
All outcomes
Low risk Study medication was presented as “cap-
sules of identical appearance”.
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk The number of women who were ran-
domised is not given. Includes only partic-
ipants for whom complete data were avail-
able.
Selective reporting (reporting bias) Low risk Outcomes stated in the methods have been
reported. No protocol available.
Other bias Unclear risk No protocol available. Limited informa-
tion on important baseline characteristics
of participants; age, parity and initial pain
assessment.
Bloomfield 1977 Study 1
Methods STUDY 1.
Randomised controlled trial.
Sample size calculation not discussed.
Participants Single centre study at Cincinnati General Hospital - time frame not given.
Included: 140 women with moderate or severe postpartum uterine cramp pain within
48 hours of an uncomplicated birth.
Excluded: women experiencing episiotomy pain greater than their uterine cramp pain;
unmarried women less than 18 years of age; women with history of aspirin or codeine
allergy; women given analgesics, sedatives or other psychotropic within previous 6 hours;
women breastfeeding their babies.
Interventions Following initial pain assessment women were randomly allocated to 1 of 3 treatment
groups, stratified by initial pain intensity, moderate or severe, and given a single dose of
study medication.
• Naproxen 300 mg (3 capsules of naproxen 100 mg) (N = 35).
• Naproxen 600 mg (3 capsules of naproxen 200 mg) (N = 35).
• Codeine sulfate 60 mg (1 capsule codeine sulfate 60 mg and 2 lactose placebo) (N
= 35).
• Lactose placebo (3 capsules; lactose placebo) (N = 35).
Outcomes Women were interviewed before drug administration and 1/2 hour post drug admin-
istration, then hourly for 7 hours. They were asked to rate pain intensity on a 4-point
ordinal scale of no pain (0), mild pain (1), moderate pain (2) or severe pain (3). Pain
relief was estimated by calculating pain intensity difference scores from the pain intensity
scores. Women were asked to report side effects. Vital signs were observed and recorded
at 1, 2 and 6 hours post drug administration.
Mean pain intensity scores at each time interval, SPID scores, body temperature at each
time interval and side effects.
24Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bloomfield 1977 Study 1 (Continued)
Women were asked about side effects with minimal use of leading questions and without
use of a checklist at the final interview. Vital signs including arterial pressure, pulse and
respiratory rates and oral temperature were obtained before and 1, 2 and 6 hours after
drug administration.
Notes Doses of 300 mg and 600 mg of naproxen were more effective than codeine in relieving
postpartum uterine cramp pain, although there is a longer latency and peak analgesia
time than codeine. No differences in vital signs except significant reduction in body
temperature with both doses of naproxen. No differences in side effects. No data for
meta-analyses.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Women were randomised using a “prede-
termined balanced schedule”.
Allocation concealment (selection bias) Low risk Study medications were “pre-packaged in
individual dose vials”.
Blinding (performance bias and detection
bias)
All outcomes
Low risk “Double blind” study. “All capsules were
identical in appearance and taste.”
Incomplete outcome data (attrition bias)
All outcomes
Low risk Data from all women randomised were in-
cluded in analyses.
Selective reporting (reporting bias) Low risk Outcomes stated in methods were re-
ported. No protocol available.
Other bias Unclear risk No protocol available.
Bloomfield 1977 Study 2
Methods STUDY 2.
Randomised controlled trial.
Sample size calculation not discussed.
Participants Single centre study at Cincinnati General Hospital - time frame not given.
Included: 90 women with severe or moderate postpartum uterine cramp pain within 48
hours of an uncomplicated birth.
Excluded: women experiencing episiotomy pain greater than their uterine cramp pain;
unmarried women less than 18 years of age; women with history of aspirin or codeine
allergy; women given analgesics, sedatives or other psychotropic within previous 6 hours;
women breastfeeding their babies.
25Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bloomfield 1977 Study 2 (Continued)
Interventions Following initial pain assessment women were randomly allocated to 1 of 3 treatment
groups, stratified by initial pain intensity, moderate or severe, and given a single dose of
study medication.
• Naproxen sodium 275 mg (1 tablet of naproxen sodium 275 mg, 1 table placebo)
(N = 30).
• Aspirin 650 mg (2 tablets of aspirin 325mg) (N = 30).
• Lactose placebo (2 tablets lactose placebo) (N = 30).
Outcomes Women were interviewed before drug administration and 1/2 hour post drug admin-
istration then hourly for 7 hours. They were asked to rate pain intensity on a on a 4-
point ordinal scale of no pain (0), mild pain (1), moderate pain (2) or severe pain (3)
. Pain relief was estimated by calculating pain intensity difference scores from the pain
intensity scores.
Pain intensity difference scores were calculated by subtracting baseline pain intensity
scores from pain intensity scores at observed time points. Women were asked to rate pain
relief at the third hour as greater than 50% or not.
Women were asked about side effects with minimal use of leading questions and without
use of a checklist at the final interview. Vital signs including arterial pressure, pulse and
respiratory rates and oral temperature were obtained before and 1, 2 and 6 hours after
drug administration.
Notes 275 mg naproxen sodium was as effective as aspirin 650 mg in relieving postpartum uter-
ine cramp pain. However, naproxen sodium has a longer latency and time to peak anal-
gesia than aspirin. Body temperature was significantly lowered in the naproxen sodium
women and there were no differences in reported side effects.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Women were randomised using a “prede-
termined balanced schedule”.
Allocation concealment (selection bias) Low risk Study medications were “pre-packaged in
individual dose vials”.
Blinding (performance bias and detection
bias)
All outcomes
Low risk “Double blind” study. “All tablets were
identical in appearance and taste.”
Incomplete outcome data (attrition bias)
All outcomes
Low risk Data from all women randomised were in-
cluded in analyses.
Selective reporting (reporting bias) Low risk Outcomes stated in methods were re-
ported. No protocol available.
Other bias Unclear risk No protocol available.
26Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bloomfield 1978
Methods Randomised controlled trial.
Sample size calculation not stated.
Participants Single centre study at Cincinnati General Hospital - time frame not given.
Included: 40 postpartum women, within 48 hours of birth, with moderate or severe
uterine cramp pain as assessed by the woman. Women were 18 years or older.
Excluded: women experiencing episiotomy pain greater than their uterine cramp pain;
unmarried women less than 18 years of age; women with history of aspirin allergy;
women given analgesics, sedatives or other psychotropic within previous 6 hours; women
breastfeeding their babies.
Interventions Following initial pain assessment women were randomly allocated to 1 of 3 treatment
groups, stratified by initial pain intensity, moderate or severe, and given 1 of 3 study
medications on demand.
• Aspirin 650 mg (2 capsules aspirin 325 mg) (N = 20).
• Placebo (2 capsules -unknown composition) (N = 20).
Outcomes Pain was assessed at 1/2 hour post study medication then hourly for 7 hours. All interviews
were conducted by the same trained nurse observer.
Pain intensity measured on an ordinal scale from no pain (0), mild pain (1), medium
pain (2) or severe pain (3). Pain intensity difference scores were calculated by subtracting
baseline pain intensity scores from pain intensity scores at observed time points. Women
were asked to rate pain relief at the third hour as greater than 50% or not.
Women were asked about side effects with minimal use of leading question and without
use of a checklist at the final interview. Vital signs including arterial pressure, pulse and
respiratory rates and oral temperature were obtained before and 1, 2 and 7 hours after
drug administration.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Randomly assigned using a “pre-deter-
mined balanced schedule”.
Allocation concealment (selection bias) Low risk Medications presented in “pre-packed code
numbered vials”.
Blinding (performance bias and detection
bias)
All outcomes
Low risk The study was “double blind”. “All capsules
were identical in taste and appearance.”
Incomplete outcome data (attrition bias)
All outcomes
Low risk Data from all women randomised were in-
cluded in analyses.
Selective reporting (reporting bias) Low risk All outcomes in methods were reported. No
protocol available.
27Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bloomfield 1978 (Continued)
Other bias Unclear risk No protocol available.
Bloomfield 1981
Methods Randomised controlled trial.
Sample size calculation not stated.
Participants Single centre study at Cincinatti General Hospital - time frame not given.
Included: 74 women with moderate or severe postpartum uterine cramp pain within 48
hours of an uncomplicated birth.
Excluded: women given analgesics or other central nervous system drugs within previous
6 hours; women with a known allergy to aspirin or paracetamol (acetaminophen); women
breastfeeding their babies.
Interventions Women were randomly allocated to 1 of 3 treatment groups, stratified by initial pain
intensity, moderate or severe, and given a single oral dose (2 capsules) of 1 of the following:
• Aspirin 650 mg (N = 26).
• Paracetamol (Acetaminophen) 650 mg (N = 22).
• Placebo (N = 26).
Outcomes Women were interviewed by a trained nurse observer at baseline, 1/2 hour post treatment
and hourly for 6 hours.
Pain intensity measured and scored on a 4-point ordinal scale, no pain (0), mild (1),
moderate (2) or severe (3). Pain intensity difference scores were calculated by subtracting
baseline pain intensity scores from pain intensity scores at observed time points. Women
were asked to rate pain relief at the third hour as greater than 50% or not.
Women were asked about side effects with minimal use of leading questions and without
use of a checklist at the final interview.
Notes (PID at 6 hours used.)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk “Within each of the 2 pain strata there was
a separate, balanced randomisation of pa-
tients...”
Allocation concealment (selection bias) Low risk Use of “coded capsules”.
Blinding (performance bias and detection
bias)
All outcomes
Low risk Use of “identical coded capsules”.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Data on all women randomised were re-
ported.
28Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bloomfield 1981 (Continued)
Selective reporting (reporting bias) Low risk All outcomes in methods were reported. No
protocol available.
Other bias Unclear risk No protocol available. Limited description
of baseline characteristics of participants.
Bloomfield 1986a
Methods Randomised controlled trial.
Sample size calculation not stated.
Participants Single centre study at Cincinnati General Hospital - time frame not given.
Included: 159 hospitalised postpartum women, 18 years or older with an uncomplicated
birth and moderate or severe uterine cramps.
Excluded: women who experienced episiotomy pain greater than their uterine cramp
pain; women with history of hypersensitivity to aspirin or codeine; women given anal-
gesics, sedatives or other psychotropic within previous 6 hours; known drug dependence;
women breastfeeding their babies.
Interventions Women were randomly allocated to 1 of 5 treatment groups, stratified by initial pain
intensity, moderate or severe, and given a single oral dose (2 capsules) of 1 of the following:
• Flurbiprofen 50 mg (2 capsules flurbiprofen 25 mg) (N = 30).
• Aspirin 650 mg (2 capsules aspirin 325 mg) (N = 34).
• Codeine sulfate 60 mg (1 capsule codeine sulfate 60 mg, 1 capsule placebo) (N =
32).
• Codeine sulfate 120 mg (2 capsules codeine sulfate 60 mg) (N = 31).
• Placebo (2 capsules placebo of unknown composition) (N = 32).
Outcomes Pain assessed by an observer before the first dose and at half hour or hourly intervals for
6 hours asking women to rate pain intensity and pain relief on a 4-point scale; none (0)
, slight (1), moderate (2), severe or complete relief (3). From the initial observation the
pain intensity difference and sum of pain intensity difference and sum of pain relief were
calculated.
At the final observation women verbally rated the global effect of the drug with “0” the
worst and “10” the best pain reliever ever taken. Side effects elicited were graded on a 4-
point verbal ordinal rating scale of severity with minimal use of leading questions.
Notes Same data reported in Bloomfield 1981 (paper); Bloomfield 1981 (conference proceed-
ing); Bloomfield 1983 (paper).
“The pain intensity score for each unperformed interview was adjusted to the pretreat-
ment value, and the adjusted scores were analysed.”
Standard deviations were calculated from the reported standard errors.
Risk of bias
Bias Authors’ judgement Support for judgement
29Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bloomfield 1986a (Continued)
Random sequence generation (selection
bias)
Low risk Women were “randomly assigned”.
Allocation concealment (selection bias) Low risk Medications were “pre packed, code num-
bered”.
Blinding (performance bias and detection
bias)
All outcomes
Low risk The study was double blind, the patient
and the caregiver. The medications were
’identical in taste and appearance’.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Data on all women randomised have been
reported. Including appropriately imputed
data for the 9 women who withdrew.
Selective reporting (reporting bias) Low risk All outcomes stated in the methods were
reported. No protocol available.
Other bias Unclear risk No protocol available.
Bloomfield 1986b
Methods Randomised controlled trial.
Sample size calculation not stated.
Participants Single centre study at Cincinnati General Hospital - time frame not given.
Included: 120 hospitalised women with moderate or severe uterine cramp pain within
48 hours of an uncomplicated vaginal birth.
Excluded: women who experienced episiotomy pain greater than their uterine cramp
pain; unmarried women less than 18 years of age; women with history of hypersensitivity
to aspirin or other non-steroidal anti-inflammatory drugs; women given analgesics, seda-
tives or other psychotropic within previous 4 hours; known drug dependence; women
breastfeeding their babies.
Interventions Following initial pain assessment women were randomly allocated to 1 of 4 treatment
groups and given appropriate study medication on demand. Randomisation was stratified
by initial pain intensity and by 1 of 2 nurse observers.
• Ketorolac 5 mg (1 capsule 5 mg keterolac and 1 placebo) (N = 30).
• Ketorolac 10 mg (1 capsule 10mg keterolac and 1 placebo) (N = 30).
• Aspirin 650 mg (2 capsules 325 mg aspirin) (N = 30).
• Placebo (2 capsules placebo) (N = 30).
Outcomes Women were interviewed before drug administration and 1/2 hour post treatment and
then hourly for 6 hours. Pain intensity was measured on a 4-point ordinal scale and
pain relief on a 5-point ordinal scale (not described). Women were asked to give a global
rating of the medication at the final interview on a scale of 0 (worst) to 10 (best pain
reliever ever taken).
Pain intensity difference, summed pain intensity difference, mean total pain relief scores,
mean global rating.
30Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bloomfield 1986b (Continued)
Women were questioned about side effects at the final interview with minimal leading
questions and without a checklist.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Women were assigned using a “predeter-
mined balanced randomization schedule”.
Allocation concealment (selection bias) Low risk Study medications were “packaged in indi-
vidual code numbered containers”.
Blinding (performance bias and detection
bias)
All outcomes
Low risk “Capsules were identical in taste and ap-
pearance.”
Incomplete outcome data (attrition bias)
All outcomes
Low risk Data on all women randomised have been
reported. Including appropriately imputed
data for the 10 women who withdrew.
Selective reporting (reporting bias) Low risk All outcomes stated in methods are re-
ported. No protocol available.
Other bias Unclear risk No protocol available.
Bloomfield 1987
Methods Randomised controlled trial.
Sample size calculation not stated.
Participants Single centre study at Cincinnati General Hospital - time frame not given.
Included: 60 hospitalised women with moderate of severe uterine cramp pain within 48
hours of an uncomplicated vaginal birth.
Excluded: women were excluded with known hypersensitivity to aspirin or non-steroidal
anti-inflammatory drugs, if they had been given other analgesia or were breastfeeding
their babies.
Interventions Following initial pain assessment women were randomly allocated to 1 of 2 treatment
groups and given appropriate study medication on demand. Randomisation was stratified
by initial pain intensity and by 1 of 2 nurse observers.
• Naproxen sodium 550 mg (2 capsules 275 mg naproxen sodium) (N = 30).
• Placebo (2 capsules placebo) (N = 30).
Outcomes Women were interviewed before drug administration and 1/2 hour post treatment and
then hourly for 6 hours. Pain intensity was measured on a 4-point ordinal scale and
pain relief on a 5-point ordinal scale (not described). Women were asked to give a global
31Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bloomfield 1987 (Continued)
rating of the medication at the final interview on a scale of 0 (worst) to 10 (best pain
reliever ever taken).
Pain intensity difference, summed pain intensity difference, mean total pain relief scores,
mean global rating.
Women were questioned about side effects at each interview without a checklist or
leading questions.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Women were assigned using a “predeter-
mined balanced randomized schedule”.
Allocation concealment (selection bias) Low risk Study medications were “packaged in code-
numbered individual dose containers”.
Blinding (performance bias and detection
bias)
All outcomes
Low risk “All capsules identical in taste and appear-
ance.”
Incomplete outcome data (attrition bias)
All outcomes
Low risk Data on all women randomised have been
reported.
Selective reporting (reporting bias) Low risk All outcomes stated in methods are re-
ported. No protocol available.
Other bias Unclear risk No protocol available.
Jain 1978
Methods Randomised controlled trial.
Sample size calculation not stated.
Participants Location and time of study not stated.
Included: 23 postpartum women who had an uncomplicated vaginal birth with moderate
or severe uterine cramp pain (self rated pain score of 60% or more). The women were
aged between 16 and 35 years of age.
Excluded: women dependent on analgesics or tranquillizers or hypersensitive to salicylates
or caffeine. Women with gastrointestinal, hepatic or renal disease or history psychiatric
illness.
Interventions Following initial pain assessment participants were allocated to 1 of 3 treatment groups
and given 1 dose of study medication.
• Aspirin 650 mg (N = 7).
• Aspirin 800 mg plus caffeine 64 mg (N = 8).
32Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Jain 1978 (Continued)
• Placebo (N = 8).
Outcomes Pain intensity was assessed at trial entry, 1, 2, 3 and 4 hours following the intervention
using an ordinal scale 0 (no pain), 2 (slight), 4 (moderate), 6 (severe)and 8 (very severe).
Pain relief was assessed using an ordinal scale 0 (worse), 2 (unchanged), 4 (less than half
gone) and 8 (complete relief ).
At the last interview women were asked about side effects.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Methods state “patients were separated at
random”.
Allocation concealment (selection bias) Unclear risk Insufficient information to permit judge-
ment.
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Insufficient information to permit judge-
ment although methods state ’double
blind’.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Data on all women randomised are re-
ported.
Selective reporting (reporting bias) Low risk All outcomes stated in methods were re-
ported. No protocol available.
Other bias Unclear risk No protocol available. Recruitment and
randomisation included women with epi-
siotomy pain, yet study not stratified by
source of pain. Outcomes reported sepa-
rately according to source of pain.
Kantor 1984b
Methods Randomised controlled trial.
Sample size calculation not stated.
Participants Single centre study, Bellevue Hospital. Time not given.
Included: 121 postpartum women who complained of moderate or severe uterine cramp
pain (review authors have assumed vaginal birth).
Excluded: women breastfeeding; previous severe adverse reactions to narcotics; treated
with other analgesia or sedative-tranquillisers; severe renal, hepatic, cardiac or neurolog-
ical deficits; history of drug abuse.
33Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Kantor 1984b (Continued)
Interventions Women were randomly allocated to 1 of 3 treatment groups and given 1 dose of study
medication followed by observations at 30 minutes and hourly for 6 hours.
• Single dose of oral nalbuphine 15 mg (N) (N = 35).
• Codeine 60 mg (C) (N = 37).
• Placebo (P) (N = 36).
Outcomes Pain intensity measured using an ordinal scale, none (1), slight (2), moderate (3) or
severe (4). Pain relief measured using an ordinal scale, none (1), slight (2), moderate (3)
, marked (4) or complete (5). Women were also questioned about side effects. Number
of women who dropped out or required additional analgesia were recorded.
Notes The formulation of codeine (phosphate or sulfate) is not stated.
121 women randomised (N = 39, C = 42, P = 40), 3 post randomisation exclusions (1
from each group). Women with episiotomy pain were included and most of the analyses
included all women. There were 3 episiotomy women in N, 4 in C and 3 in P.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Insufficient information to make a judge-
ment. Study described as “randomized”.
Allocation concealment (selection bias) Unclear risk Insufficient information to make a judge-
ment.
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Insufficient information to make a judge-
ment. Study described as “double blind”.
Incomplete outcome data (attrition bias)
All outcomes
High risk 3 of the women randomised were excluded
from analyses because of “administrative
deviations from protocol”.
Selective reporting (reporting bias) Low risk All outcomes stated in methods are re-
ported. No protocol available.
Other bias Unclear risk No protocol available. Insufficient infor-
mation on baseline characteristics of study
participants.
34Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
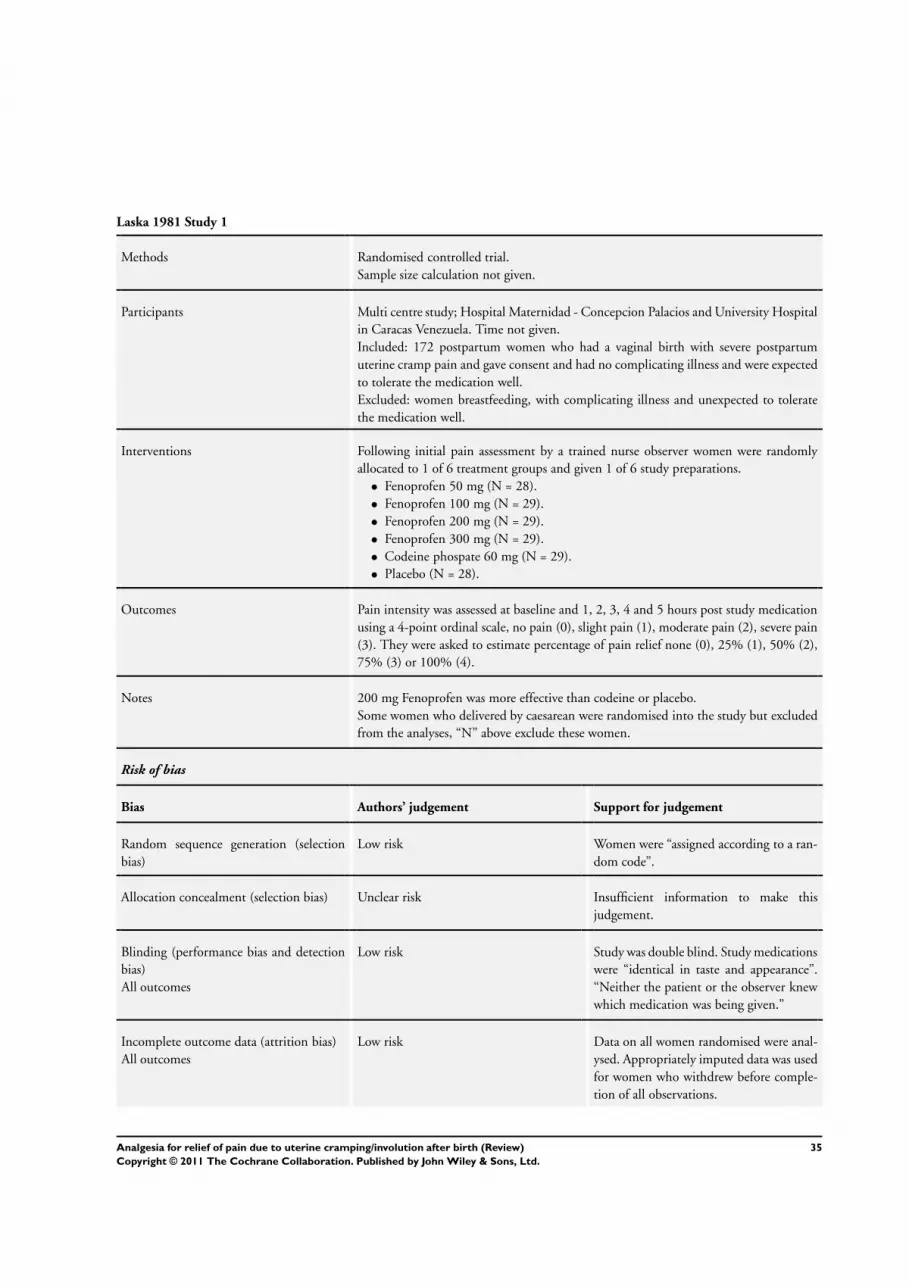
Laska 1981 Study 1
Methods Randomised controlled trial.
Sample size calculation not given.
Participants Multi centre study; Hospital Maternidad - Concepcion Palacios and University Hospital
in Caracas Venezuela. Time not given.
Included: 172 postpartum women who had a vaginal birth with severe postpartum
uterine cramp pain and gave consent and had no complicating illness and were expected
to tolerate the medication well.
Excluded: women breastfeeding, with complicating illness and unexpected to tolerate
the medication well.
Interventions Following initial pain assessment by a trained nurse observer women were randomly
allocated to 1 of 6 treatment groups and given 1 of 6 study preparations.
• Fenoprofen 50 mg (N = 28).
• Fenoprofen 100 mg (N = 29).
• Fenoprofen 200 mg (N = 29).
• Fenoprofen 300 mg (N = 29).
• Codeine phospate 60 mg (N = 29).
• Placebo (N = 28).
Outcomes Pain intensity was assessed at baseline and 1, 2, 3, 4 and 5 hours post study medication
using a 4-point ordinal scale, no pain (0), slight pain (1), moderate pain (2), severe pain
(3). They were asked to estimate percentage of pain relief none (0), 25% (1), 50% (2),
75% (3) or 100% (4).
Notes 200 mg Fenoprofen was more effective than codeine or placebo.
Some women who delivered by caesarean were randomised into the study but excluded
from the analyses, “N” above exclude these women.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Women were “assigned according to a ran-
dom code”.
Allocation concealment (selection bias) Unclear risk Insufficient information to make this
judgement.
Blinding (performance bias and detection
bias)
All outcomes
Low risk Study was double blind. Study medications
were “identical in taste and appearance”.
“Neither the patient or the observer knew
which medication was being given.”
Incomplete outcome data (attrition bias)
All outcomes
Low risk Data on all women randomised were anal-
ysed. Appropriately imputed data was used
for women who withdrew before comple-
tion of all observations.
35Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Laska 1981 Study 1 (Continued)
Selective reporting (reporting bias) Low risk All outcomes stated in methods were re-
ported. No protocol available.
Other bias Unclear risk No protocol available. Women who gave
birth by caesarean were randomised but ex-
cluded from the analyses. Unclear if ran-
domisation was stratified by source of pain;
uterine cramp or episiotomy although data
analysed separately.
Laska 1981 Study 2
Methods Randomised controlled trial.
Sample size calculation not given.
Participants Multi centre study; Hospital Maternidad - Concepcion Palacios and University Hospital
in Caracas Venezuela. Time not given.
Included: 188 postpartum women, who had a vaginal birth with severe postpartum
uterine cramp pain and gave consent and had no complicating illness and were expected
to tolerate the medication well.
Excluded: women breastfeeding, with complicating illness and unexpected to tolerate
the medication well.
Interventions Following initial pain assessment by a trained nurse observer women were randomly
allocated to 1 of 7 treatment groups and given 1 of 7 study preparations.
• Fenoprofen 12.5 mg (N = 27).
• Fenoprofen 25 mg (N = 27).
• Fenoprofen 50 mg (N = 26).
• Fenoprofen 100 mg (N = 27).
• Fenoprofen 200 mg (N = 27).
• Codeine phosphate 60 mg (N = 27).
• Placebo (N = 27).
Outcomes Pain intensity was assessed at baseline and 1, 2, 3, 4 and 5 hours post study medication
using a 4-point ordinal scale, no pain (0), slight pain (1), moderate pain (2), severe pain
(3). They were asked to estimate percentage of pain relief none (0), 25% (1), 50% (2),
75% (3) or 100% (4).
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Women were “assigned according to a ran-
dom code”.
36Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Laska 1981 Study 2 (Continued)
Allocation concealment (selection bias) Unclear risk Insufficient information to make this
judgement.
Blinding (performance bias and detection
bias)
All outcomes
Low risk Study was double blind. Study medications
were “identical in taste and appearance”.
“Neither the patient or the observer knew
which medication was being given.”
Incomplete outcome data (attrition bias)
All outcomes
Low risk Data on all women randomised were anal-
ysed. Appropriately imputed data were
used for women who withdrew before com-
pletion of all observations.
Selective reporting (reporting bias) Low risk All outcomes stated in methods were re-
ported. No protocol available.
Other bias Unclear risk No protocol available. Women who gave
birth by caesarean were randomised but ex-
cluded from the analyses. Unclear if ran-
domisation was stratified by source of pain;
uterine cramp or episiotomy although data
analysed separately.
Mehlhorn 2005
Methods Randomised controlled trial.
Sample size calculation not given.
Participants Single centre study at Frauenklinik Friedrich-Alexander Universitat Erlangen, Erlangen,
Germany. (Time not stated)
541 multiparous women randomised into 4 groups but 423 women excluded due to
minimal involutionary pain.
118 multiparous women remained in trial
Time and place not stated.
Interventions • Group 1: TENS (fixed 100 Hz) and 625 mg metamizole (as 25 drops) (N = 30).
• Group 2: TENS (fixed 100 Hz) and placebo (as 25 drops looking and tasting
similar to metamizole) (N = 27).
• Group 3: placebo-TENS (dial fixed on 100 Hz but not working) and 625 mg
metamizole (as 25 drops) (N = 33).
• Group 4: placebo-TENS (dial fixed on 100 Hz but not working) and placebo (as
25 drops looking and tasting similar to metamizole) (N = 28).
Maximum dose was 4 x 25 Metamizole drops (625 mg) in 24 hours (total of 2500 mg).
Pain score obtained with VAS; scaled 1 - 10.
Outcomes Women rated their pain using a visual analogue pain scale - VAS scaled 0-10. Number
of women rating their pain 0-4 on VAS was reported.
Pain assessment documented at 2 min, 10 min, 20 min and 30 min intervals.
37Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Mehlhorn 2005 (Continued)
Notes RM emailed first author (Dec 2009 and Jan 2010) and corresponded to ascertain in-
formation re randomisation, adequate sequence generation, allocation concealment and
blinding. All correspondence in German.
RM emailed first author Nov 2010 to determine time and place of study - no response.
Abstract in German and English. The 2005 paper translated by Ruth Martis.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Multiparous women were assigned to 1 of
4 groups. Randomised via computer gen-
erated allocation.
Allocation concealment (selection bias) Low risk Corresponding random number was on
TENS devices and trial medication bottles.
Blinding (performance bias and detection
bias)
All outcomes
Low risk Double blinded - placebo medication
(drops) and placebo TENS were used. The
women, administrators and trial coordina-
tor were blinded.
Incomplete outcome data (attrition bias)
All outcomes
Low risk 541 women were randomised, however,
423 reported minimal pain and did not re-
quire pain relief therefore did not partic-
ipate further in the study. Data from the
remaining 118 women who did participate
in the intervention were included.
Selective reporting (reporting bias) Low risk All outcomes stated in the methods were
reported. No protocol cited but available
from first author on request.
Other bias Low risk None of the included women had used
TENS before.
Okun 1982
Methods Randomised controlled trial.
Participants Location and time not stated.
Included: 157 postpartum women, within 48 hours of delivery, with moderate or severe
uterine cramp pain as assessed by the woman. The women ranged in age from 18 years
to 42 years.
Excluded: women who were breastfeeding and/or using other analgesia or psychotropic
drugs.
38Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Okun 1982 (Continued)
Interventions Following initial pain assessment women were randomly allocated to 1 of 5 groups,
stratified by initial pain intensity, moderate, severe or very severe. They were given a dose
of 1 of the 5 study preparations in the form of 2 identical capsules.
• Fendosal 100 mg (2 capsules Fendosal 50 mg) (N = 31).
• Fendosal 200 mg (2 capsules Fendosal 100 mg) (N = 32).
• Fendosal 400 mg (2 capsules Fendosal 200 mg) (N = 31).
• Aspirin 650 mg (2 capsules aspirin 325 mg) (N = 32).
• Placebo (2 capsules - composition not specified) (N = 31).
Outcomes The same nurse assessed their pain intensity at 1, 2, 3, 4, 5, 6, and 7 hours after the
initial dose.
Pain intensity was assessed as no pain (1), mild pain (2), moderate pain (3), severe pain
(4), very severe pain (5). At 1 and 2 hours the women were asked if the relief from pain
was greater than 50%.
Side effects were reported by women.
Notes No data for meta-analyses.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk “Assignment to treatment was randomized between
groups.”
Allocation concealment (selection bias) Unclear risk Insufficient information to make this judgement.
Blinding (performance bias and detection
bias)
All outcomes
Low risk The study was “double-blind”. Study medications “were
administered as identical-looking capsules”.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Data on all women randomised were reported.
Selective reporting (reporting bias) Low risk All outcomes in methods were reported.
Other bias Unclear risk No protocol available. Unclear if randomisation was
stratified by source of pain; uterine cramp or episiotomy
although data analysed separately.
Olsen 2007
Methods Randomised controlled trial.
Participants Single centre study at the Sahlgrenska University Hospital, Gothenburg, Sweden during
2004.
Included: 22 women following uncomplicated vaginal birth and painful postpartum
uterine contractions requiring pain relief.
39Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Olsen 2007 (Continued)
Excluded: women with systemic disorders; abnormal pregnancy; operative delivery and
receiving analgesic treatment for other pain. Swedish as second language.
Interventions Women were randomly allocated to 1 of 2 treatment groups.
• HI TENS (50 mA for 1 minute, repeated up to 2 times if pain not relieved) (N =
13).
• LI TENS (10-15 mA, repeated up to 2 times if pain not relieved) (N = 8).
In both groups the TENS electrodes were placed over the lower part of the abdomen
bilaterally over the uterus.
Outcomes Women were asked to estimate their pain intensity using a 100 mm VAS ranging from
no pain to worst possible pain, before and after treatment.
Women in both groups rated the discomfort of treatment using a 5-point verbal scale
from no discomfort to worst possible discomfort. To clarify the difference between
the 2 components, women were informed that they should rate both how painful the
postpartum uterine contractions were and how unpleasant they thought the contractions
were.
All possible adverse events were recorded.
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Women were randomised using a “computer generated
random table”.
Allocation concealment (selection bias) Low risk “Groups coded and transferred to pre-sealed opaque en-
velopes.”
Blinding (performance bias and detection
bias)
All outcomes
Low risk “Single-blind” study. Double blind not appropriate for
this intervention. Assume women were blind.
Incomplete outcome data (attrition bias)
All outcomes
High risk The data from 1 of 13 women in 1 of the intervention
groups were excluded because she withdrew after expe-
riencing discomfort.
Selective reporting (reporting bias) Low risk All outcomes stated in methods were reported. No pro-
tocol available.
Other bias High risk Baseline imbalance - numbers in abstract differ from
those given in CONSORT.
40Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Pan 1993
Methods Randomised controlled trial.
Participants Location and time of study not stated.
Included: 31 women, 24-48 hours following normal vaginal birth, who had an epidural
catheter in place.
Excluded: not stated.
Interventions Women were randomly allocated to 1 of 2 treatment groups.
• Group I: Morphine - epidural (Durmorph) 2 mg (4 mL) with normal saline (6
mL) epidurally after the birth of the baby, then oral placebo 1-2 tablets every 3-4 hrs as
requested for 24 hours.
• Group II: normal saline 10 mL epidurally after the birth of the baby, then 1-2
tablets of percocet (oxycodone 5 mg and acetaminophen 325 mg) every 3-4 hrs as
requested for 24 hours.
Outcomes Overall analogue pain score. Pain score associated with uterine cramps, backaches, som-
nolence score and respiratory rate were recorded every 2 hours and when women re-
quested pain medication for 24 hours after their birth.
Total number of requests for analgesia.
Adverse effects.
Notes AD emailed author for expansion of data but had no reply. Therefore unable to meta-
analyse data.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk States women were “randomized”.
Allocation concealment (selection bias) Unclear risk Insufficient information to make this judgement.
Blinding (performance bias and detection
bias)
All outcomes
Low risk The study was double-blinded such that the women,
the nurse and the person evaluating the patient did not
know the treatment allocation.
Incomplete outcome data (attrition bias)
All outcomes
Low risk Data on all women randomised are reported.
Selective reporting (reporting bias) Unclear risk Poster abstract only. Insufficient information to make
judgement. No protocol available.
Other bias Unclear risk Poster abstract only. Insufficient information to make
judgement. No protocol available.
41Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Skovlund 1991
Methods Randomised controlled trial.
Participants Location and time of study not stated.
Included: 78 postpartum women with uterine cramps and possible concomitant epi-
siotomy pain after vaginal birth requesting analgesia.
Excluded: women allergic to paracetamol.
Interventions Women were randomly allocated to 1 of 2 groups.
• Paracetamol 1000 mg (2 tablets paracetamol 500 mg) (N = 21).
• Placebo (2 tablets) (N = 24).
The medications were identical in appearance.
Outcomes Women were asked to rate their pain on a VAS measuring 100 mm at trial entry and
again at 2 and 4 hours post medication. Uterine cramp pain and episiotomy pain were
recorded separately.
Uterine pain intensity and uterine pain intensity difference.
Women were asked if they experienced any adverse effects, none were suggested to them.
Notes Paracetamol was significantly better than placebo at 2 hours post medication. The median
difference in effect was 13.5 mm (95% CI 3.24).
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Insufficient information to make a judgement. States
“the randomization was unconstrained”.
Allocation concealment (selection bias) Unclear risk Not stated.
Blinding (performance bias and detection
bias)
All outcomes
Low risk Double blind. “Identical appearing tablets.”
Incomplete outcome data (attrition bias)
All outcomes
Low risk 1 woman (placebo group) excluded as she had received
analgesia 1 hour prior to inclusion. Results included for 1
woman in placebo group who was under study when trial
stopped. 2 women withdrew after 2 hours observation,
no 4-hour data included. Appropriately imputed data
were used for women who withdrew before 2 hours.
Selective reporting (reporting bias) Low risk All outcomes stated in methods were reported. No pro-
tocol available.
Other bias Unclear risk No protocol available.
42Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Skovlund 1991a
Methods Randomised controlled trial.
Participants Location and time of study not stated.
Included: 64 postpartum women with uterine cramps and possible concomitant epi-
siotomy pain after vaginal birth requesting analgesia.
Women allergic to paracetamol or naproxen were excluded.
Interventions Women were randomly allocated to 1 of 2 groups.
• Paracetamol 1000 mg (2 tablets paracetamol 500 mg, 1 tablet placebo) (N = 30).
• Naproxen 500 mg (1 tablet naproxen 500 mg and 2 tablets placebo) (N = 26).
The medications were Identical in appearance.
Outcomes Women were asked to rate their pain on a VAS measuring 100 mm at trial entry and
again at 2 and 4 hours post medication.
Uterine pain intensity (mm on VAS) and uterine pain intensity difference (mm) at 2
and 4 hours after medication.
Women were asked if they experienced any adverse effects, none were suggested to them.
Notes No difference in uterine pain intensity at 2 hours between the 2 treatment groups
Sequential design.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Insufficient information to make a judgement. Study
described as ’tablets were made, randomized and packed’.
Allocation concealment (selection bias) Unclear risk Not stated.
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk States “double dummy technique used to make the study
double blind”. No information about appearance of
tablets.
Incomplete outcome data (attrition bias)
All outcomes
High risk 3 women excluded as misunderstood administration of
medication (2 in paracetamol group, 1 in naproxen
group). 1 excluded from paracetamol group as expe-
rienced only episiotomy pain. Results included for 4
women in paracetamol group who were under study
when trial stopped.
Selective reporting (reporting bias) Low risk All outcomes stated in methods were reported. No pro-
tocol available.
Other bias Unclear risk No protocol available. Unclear if randomisation was
stratified by source of pain; uterine cramp or episiotomy
although data analysed separately.
VAS: visual analogue scale
43Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Azpiroz 1971 Women with any postpartum pain included without differentiation between origin of pain.
Translated from Spanish to English by Ruth Martis with the assistance of a translation software.
Baptisti 1971 Inappropriate study design for this review. Insufficient detail on who participated and how pain scores were
derived and analysed.
Beaver 1980 Women with episiotomy pain and uterine cramp pain included and analysed together. Separate n for pain
subgroups not available.
Benson 1963 Includes women with any postpartum pain - no subgroup analyses.
Bloomfield 1988 Trial registered with Oxford Perinatal Trials Database - never reported. Confirmed by author.
Bloomfield 1983 Conference proceeding only - insufficient information.
Bloomfield 1986c Conference proceeding only - insufficient information.
Bloomfield 1988a Trial registered with Oxford Perinatal Trials Database - never reported. Confirmed by author.
Bonica 1957 Results combine perineal pain and uterine cramp pain.
Bruni 1965 Source of postpartum pain not specified or separated for analyses.
Finch 1957 Type of pain not separated. Not a suitable study design for inclusion.
Gindhart 1971 The medications tested are no longer available for use as it was associated with severe adverse effects.
Goodman 2005 Data not separated into source of pain. Confirmation from author.
Gruber 1962 Results for pain intensity and change in pain intensity; do not separate uterine cramp pain from incisional
(episiotomy) pain. No useable data.
Gruber 1963 Results for pain intensity and change in pain intensity do not separate uterine cramp pain from incisional
(episiotomy) pain.
Gruber 1971a Participants may have participated on more than 1 day and therefore included as 2 participants. No suitable
data could be extracted.
Gruber 1971b Participants may have participated on more than 1 day and therefore included as 2 participants. No suitable
data could be extracted.
Gruber 1979 No useful data - conclusions based on data pooled from both sources of pain - uterine cramp and episiotomy.
Paper focus is on methods of analyses.
44Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Hartemann 1968 Does not differentiate between postpartum pains. Overall only gives ’good and bad results’.
Translated from French to English with the assistance of Philippa Middleton and by Ruth Martis with the
assistance of a translation software.
Kantor 1984a Results for pain intensity and change in pain intensity do not separate uterine cramp pain from incisional
(episiotomy) pain.
Laska 1983 Not a suitable study design for this review. Some analyses of source of pain but does not separate the various
doses of the medications being tested.
Linder 1997 Women were not randomized. They were selected by a nurse who attempted to match baseline chrarateristics.
Mehlhorn 2006 Abstract only in supplement of journal. Data analysis not completed, as confirmed by email with author.
Translated into English by Ruth Martis.
Nunlee 2000 Abstract of conference proceedings only. Results do not separate uterine cramp pain from incisional (episiotomy
pain). Attempts to contact author unsuccessful, (Internet, email and mail).
Olson 1984 Abstract from conference presentation only available. Results for pain intensity and change in pain intensity do
not separate uterine cramp pain from incisional (episiotomy) pain.
Prockop 1960 Study method not suitable for inclusion. Randomisation was by ward, analyses by individual. 1 of the medications
tested (ASA compound) is no longer in use.
Ray 1993 Abstract only. Does not differentiate between types of pain. Attempts to contact author unsuccessful.
Redick 1980 Conference abstract only. This study was done on analgesia for postpartum women with no description of the
source of the pain.
Rubin 1984 Study done on postpartum women with episiotomies. No description of type of pain other than this. Not certain
uterine cramp pain included.
Smith 1973 No definition of postpartum pain. Paper about analgesic-sedative effect of drug combination. Analyses include
post surgical men and women.
Sunshine 1983 Analyses do not separate pain from uterine cramping and pain from episiotomies.
Sunshine 1985 Inlcudes episiotomy, CS and uterine cramps. Episiotomy and CS pain analyses together. Uterine pain was not
analysed alone as the numbers were too small.
Sunshine 1986 Analyses does not separate type of pain.
Sunshine 1989 Conference abstract only. Insufficient detail.
van Wering 1972 Includes any source of postpartum pain analyses does not separate type of pain.
von Pein 1974 Abstract only. Does not describe source of pain in puerperium.
45Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

CS: caesarean section
46Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
Comparison 1. NSAID versus placebo
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Pain Reduction (SPID) 3 204 Mean Difference (IV, Fixed, 95% CI) 4.34 [2.87, 5.82]
1.1 Aspirin 650 mg 1 40 Mean Difference (IV, Fixed, 95% CI) 2.76 [-0.83, 6.35]
1.2 Fenoprofen 200 mg 1 24 Mean Difference (IV, Fixed, 95% CI) 4.92 [1.43, 8.41]
1.3 Ketorolac 5 mg 1 40 Mean Difference (IV, Fixed, 95% CI) 1.99 [-1.62, 5.60]
1.4 Ketorolac 10 mg 1 40 Mean Difference (IV, Fixed, 95% CI) 4.10 [0.39, 7.81]
1.5 Naproxen 550 mg 1 60 Mean Difference (IV, Fixed, 95% CI) 6.16 [3.58, 8.74]
2 Pain reduction (pain intensity 6
hours)
2 148 Mean Difference (IV, Fixed, 95% CI) -0.80 [-1.12, -0.47]
2.1 Aspirin 650 mg 2 102 Mean Difference (IV, Fixed, 95% CI) -0.81 [-1.18, -0.43]
2.2 Flurbiprofen 50 mg 1 46 Mean Difference (IV, Fixed, 95% CI) -0.78 [-1.42, -0.14]
3 Summed Relief Score 3 204 Mean Difference (IV, Fixed, 95% CI) 5.94 [3.86, 8.01]
3.1 Aspirin 650 mg 1 40 Mean Difference (IV, Fixed, 95% CI) 3.4 [-1.43, 8.23]
3.2 Fenoprofen 200 mg 1 24 Mean Difference (IV, Fixed, 95% CI) 6.91 [0.95, 12.87]
3.3 Ketorolac 5 mg 1 40 Mean Difference (IV, Fixed, 95% CI) 2.70 [-2.30, 7.70]
3.4 Ketorolac 10 mg 1 40 Mean Difference (IV, Fixed, 95% CI) 6.1 [1.35, 10.85]
3.5 Naproxen 550 mg 1 60 Mean Difference (IV, Fixed, 95% CI) 8.57 [4.97, 12.17]
4 Pain analogue score compared
with baseline
1 23 Mean Difference (IV, Fixed, 95% CI) -43.57 [-81.07, -
6.07]
4.1 Aspirin 650 mg 1 12 Mean Difference (IV, Fixed, 95% CI) -42.3 [-92.35, 7.75]
4.2 Aspirin 800 mg with
Caffeine 64 mg
1 11 Mean Difference (IV, Fixed, 95% CI) -45.20 [-101.83,
11.43]
5 Global rating 2 180 Mean Difference (IV, Fixed, 95% CI) 1.88 [1.00, 2.77]
5.1 Aspirin 650 mg 1 40 Mean Difference (IV, Fixed, 95% CI) 1.36 [-0.67, 3.39]
5.2 Ketorolac 5 mg 1 40 Mean Difference (IV, Fixed, 95% CI) 0.60 [-1.52, 2.72]
5.3 Ketorolac 10 mg 1 40 Mean Difference (IV, Fixed, 95% CI) 1.76 [-0.31, 3.83]
5.4 Naproxen 550 mg 1 60 Mean Difference (IV, Fixed, 95% CI) 2.64 [1.33, 3.95]
6 Pain reduction > 50% 1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
6.1 Aspirin 650 mg 1 Risk Ratio (M-H, Fixed, 95% CI) 0.0 [0.0, 0.0]
7 VAS 1-4 at 30 minutes 1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
7.1 Metamizol 625 mg 1 Risk Ratio (M-H, Fixed, 95% CI) 0.0 [0.0, 0.0]
8 No pain relief 1 96 Risk Ratio (M-H, Fixed, 95% CI) 0.12 [0.03, 0.45]
8.1 Aspirin 650 mg 1 50 Risk Ratio (M-H, Fixed, 95% CI) 0.19 [0.04, 0.87]
8.2 Flurbiprofen 50 mg 1 46 Risk Ratio (M-H, Fixed, 95% CI) 0.05 [0.00, 0.85]
9 Adverse effects 3 116 Risk Ratio (M-H, Random, 95% CI) 1.12 [0.60, 2.08]
9.1 Aspirin 650 mg 2 92 Risk Ratio (M-H, Random, 95% CI) 1.04 [0.34, 3.20]
9.2 Fenoprofen 200 mg 1 24 Risk Ratio (M-H, Random, 95% CI) 1.2 [0.50, 2.88]
47Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Comparison 2. NSAID versus opioid
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Pain reduction (SPID) 1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
1.1 Fenoprofen 200 mg vs
codeine 60 mg
1 Mean Difference (IV, Fixed, 95% CI) 0.0 [0.0, 0.0]
2 Pain reduction (pain intensity 6
hours)
1 127 Mean Difference (IV, Fixed, 95% CI) -0.70 [-1.04, -0.35]
2.1 Aspirin 650 mg v codeine
60 mg
1 33 Mean Difference (IV, Fixed, 95% CI) -0.49 [-1.18, 0.20]
2.2 Aspirin 650 mg v codeine
120 mg
1 32 Mean Difference (IV, Fixed, 95% CI) -0.56 [-1.31, 0.19]
2.3 Flurbiprofen 50 mg v
codeine 60 mg
1 31 Mean Difference (IV, Fixed, 95% CI) -0.81 [-1.44, -0.18]
2.4 Flurbiprofen 50 mg v
codeine 120 mg
1 31 Mean Difference (IV, Fixed, 95% CI) -0.88 [-1.56, -0.20]
3 Pain reduction (summed pain
relief )
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
3.1 Fenoprofen 200 mg vs
codeine 60 mg
1 Mean Difference (IV, Fixed, 95% CI) 0.0 [0.0, 0.0]
4 No pain relief 2 199 Risk Ratio (M-H, Fixed, 95% CI) 0.87 [0.32, 2.35]
4.1 Aspirin 650 mg v codeine
60 mg
1 33 Risk Ratio (M-H, Fixed, 95% CI) 1.88 [0.19, 18.80]
4.2 Aspirin 650 mg v codeine
120 mg
1 32 Risk Ratio (M-H, Fixed, 95% CI) 1.76 [0.18, 17.56]
4.3 Flurbiprofen 50 mg v
codeine 60 mg
1 31 Risk Ratio (M-H, Fixed, 95% CI) 0.35 [0.02, 8.08]
4.4 Flurbiprofen 50 mg v
codeine 120 mg
1 31 Risk Ratio (M-H, Fixed, 95% CI) 0.35 [0.02, 8.08]
4.5 Nalbuphine 15 mg vs
codeine 60 mg
1 72 Risk Ratio (M-H, Fixed, 95% CI) 0.70 [0.13, 3.97]
5 Adverse effects 1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
5.1 Fenoprofen 200 mg vs
codeine 60 mg
1 Risk Ratio (M-H, Fixed, 95% CI) 0.0 [0.0, 0.0]
Comparison 3. Opioid versus placebo
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Pain reduction (SPID) 1 Std. Mean Difference (IV, Fixed, 95% CI) Totals not selected
1.1 Codeine 60 mg 1 Std. Mean Difference (IV, Fixed, 95% CI) 0.0 [0.0, 0.0]
2 Pain reduction (pain intensity 6
hours)
1 95 Mean Difference (IV, Fixed, 95% CI) 0.06 [-0.40, 0.52]
2.1 Codeine 60 mg 1 48 Mean Difference (IV, Fixed, 95% CI) 0.03 [-0.61, 0.67]
2.2 Codeine 120 mg 1 47 Mean Difference (IV, Fixed, 95% CI) 0.10 [-0.57, 0.77]
48Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
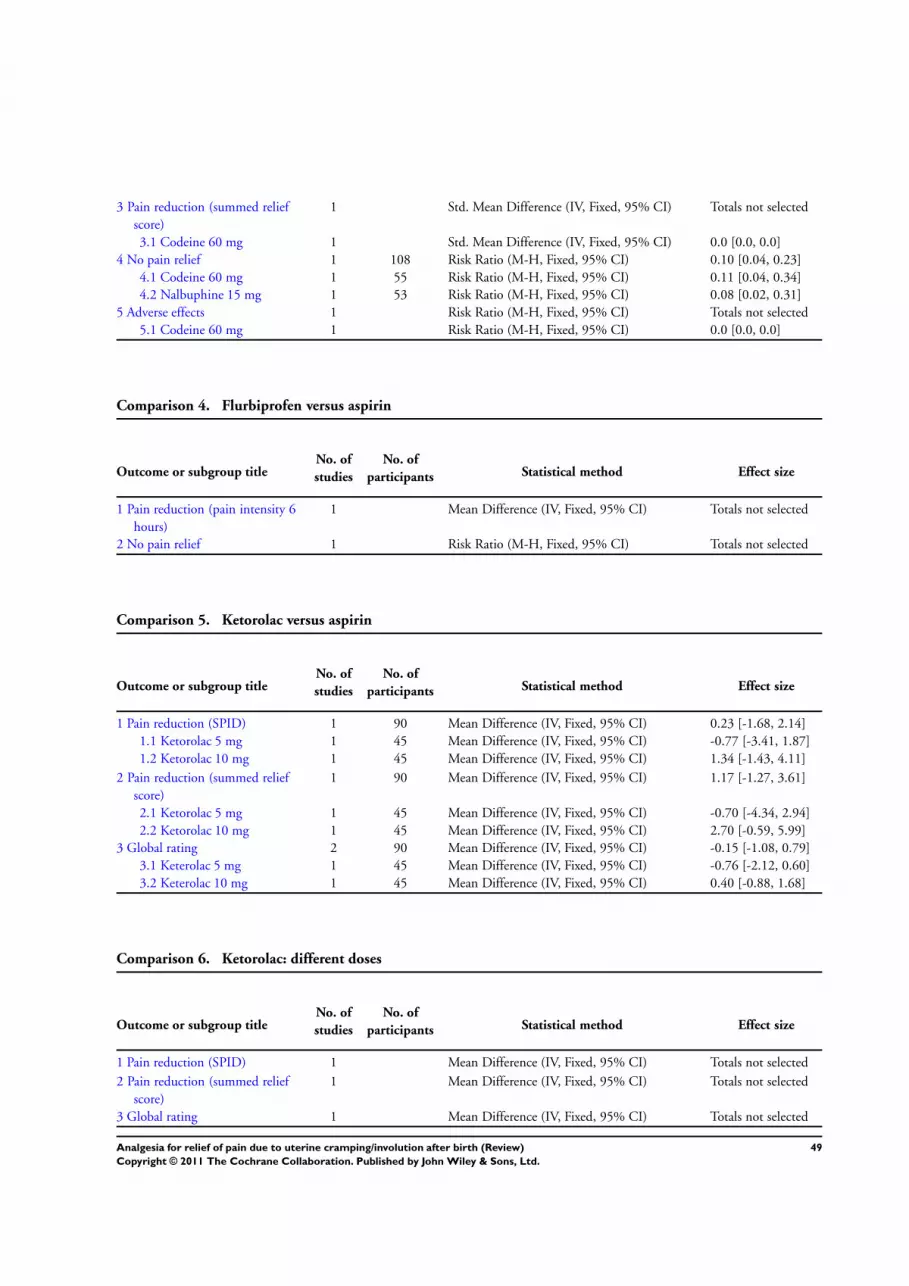
3 Pain reduction (summed relief
score)
1 Std. Mean Difference (IV, Fixed, 95% CI) Totals not selected
3.1 Codeine 60 mg 1 Std. Mean Difference (IV, Fixed, 95% CI) 0.0 [0.0, 0.0]
4 No pain relief 1 108 Risk Ratio (M-H, Fixed, 95% CI) 0.10 [0.04, 0.23]
4.1 Codeine 60 mg 1 55 Risk Ratio (M-H, Fixed, 95% CI) 0.11 [0.04, 0.34]
4.2 Nalbuphine 15 mg 1 53 Risk Ratio (M-H, Fixed, 95% CI) 0.08 [0.02, 0.31]
5 Adverse effects 1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
5.1 Codeine 60 mg 1 Risk Ratio (M-H, Fixed, 95% CI) 0.0 [0.0, 0.0]
Comparison 4. Flurbiprofen versus aspirin
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Pain reduction (pain intensity 6
hours)
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
2 No pain relief 1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
Comparison 5. Ketorolac versus aspirin
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Pain reduction (SPID) 1 90 Mean Difference (IV, Fixed, 95% CI) 0.23 [-1.68, 2.14]
1.1 Ketorolac 5 mg 1 45 Mean Difference (IV, Fixed, 95% CI) -0.77 [-3.41, 1.87]
1.2 Ketorolac 10 mg 1 45 Mean Difference (IV, Fixed, 95% CI) 1.34 [-1.43, 4.11]
2 Pain reduction (summed relief
score)
1 90 Mean Difference (IV, Fixed, 95% CI) 1.17 [-1.27, 3.61]
2.1 Ketorolac 5 mg 1 45 Mean Difference (IV, Fixed, 95% CI) -0.70 [-4.34, 2.94]
2.2 Ketorolac 10 mg 1 45 Mean Difference (IV, Fixed, 95% CI) 2.70 [-0.59, 5.99]
3 Global rating 2 90 Mean Difference (IV, Fixed, 95% CI) -0.15 [-1.08, 0.79]
3.1 Keterolac 5 mg 1 45 Mean Difference (IV, Fixed, 95% CI) -0.76 [-2.12, 0.60]
3.2 Keterolac 10 mg 1 45 Mean Difference (IV, Fixed, 95% CI) 0.40 [-0.88, 1.68]
Comparison 6. Ketorolac: different doses
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Pain reduction (SPID) 1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
2 Pain reduction (summed relief
score)
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
3 Global rating 1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
49Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Comparison 7. Codeine: different doses
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Pain reduction (pain intensity 6
hours)
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
2 No pain relief 1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
Comparison 8. Nalbuphine versus codeine
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 No pain relief 1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
Comparison 9. Paracetamol versus placebo
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Pain reduction (pain intensity 6
hours)
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
2 Adverse effects 1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
Comparison 10. Paracetamol versus aspirin
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Pain reduction (pain intensity 6
hours)
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
2 Adverse effects 1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
50Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Comparison 11. TENS versus placebo
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 VAS 1-4 at 30 minutes 1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
Comparison 12. TENS plus Metamizol versus placebo
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 VAS 1-4 at 30 minutes 1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
Comparison 13. TENS plus Metamizol versus TENS
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 VAS 1-4 at 30 minutes 1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
Comparison 14. TENS plus Metamizol versus Metamizol
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 VAS 1-4 at 30 minutes 1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
Comparison 15. TENS versus Metamizol
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 VAS 1-4 at 30 minutes 1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
51Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.1. Comparison 1 NSAID versus placebo, Outcome 1 Pain Reduction (SPID).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 1 NSAID versus placebo
Outcome: 1 Pain Reduction (SPID)
Study or subgroup NSAID Placebo Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Aspirin 650 mg
Bloomfield 1986b 30 10.05 (4.22) 10 7.29 (5.26) 16.9 % 2.76 [ -0.83, 6.35 ]
Subtotal (95% CI) 30 10 16.9 % 2.76 [ -0.83, 6.35 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.51 (P = 0.13)
2 Fenoprofen 200 mg
Bettigole 1981 12 8.92 (4.42) 12 4 (4.31) 17.8 % 4.92 [ 1.43, 8.41 ]
Subtotal (95% CI) 12 12 17.8 % 4.92 [ 1.43, 8.41 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.76 (P = 0.0058)
3 Ketorolac 5 mg
Bloomfield 1986b 30 9.28 (4.33) 10 7.29 (5.26) 16.7 % 1.99 [ -1.62, 5.60 ]
Subtotal (95% CI) 30 10 16.7 % 1.99 [ -1.62, 5.60 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.08 (P = 0.28)
4 Ketorolac 10 mg
Bloomfield 1986b 30 11.39 (4.93) 10 7.29 (5.26) 15.8 % 4.10 [ 0.39, 7.81 ]
Subtotal (95% CI) 30 10 15.8 % 4.10 [ 0.39, 7.81 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.17 (P = 0.030)
5 Naproxen 550 mg
Bloomfield 1987 30 12.23 (5.15) 30 6.07 (5.04) 32.7 % 6.16 [ 3.58, 8.74 ]
Subtotal (95% CI) 30 30 32.7 % 6.16 [ 3.58, 8.74 ]
Heterogeneity: not applicable
Test for overall effect: Z = 4.68 (P < 0.00001)
Total (95% CI) 132 72 100.0 % 4.34 [ 2.87, 5.82 ]
Heterogeneity: Chi2 = 4.41, df = 4 (P = 0.35); I2 =9%
Test for overall effect: Z = 5.77 (P < 0.00001)
Test for subgroup differences: Chi2 = 4.41, df = 4 (P = 0.35), I2 =9%
-10 -5 0 5 10
Favours Placebo Favours NSAID
52Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.2. Comparison 1 NSAID versus placebo, Outcome 2 Pain reduction (pain intensity 6 hours).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 1 NSAID versus placebo
Outcome: 2 Pain reduction (pain intensity 6 hours)
Study or subgroup NSAID Placebo Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Aspirin 650 mg
Bloomfield 1981 26 0.42 (0.77) 26 1.39 (0.92) 50.0 % -0.97 [ -1.43, -0.51 ]
Bloomfield 1986a 34 0.79 (1.11) 16 1.25 (1.13) 23.8 % -0.46 [ -1.13, 0.21 ]
Subtotal (95% CI) 60 42 73.8 % -0.81 [ -1.18, -0.43 ]
Heterogeneity: Chi2 = 1.52, df = 1 (P = 0.22); I2 =34%
Test for overall effect: Z = 4.16 (P = 0.000032)
2 Flurbiprofen 50 mg
Bloomfield 1986a 30 0.47 (0.88) 16 1.25 (1.13) 26.2 % -0.78 [ -1.42, -0.14 ]
Subtotal (95% CI) 30 16 26.2 % -0.78 [ -1.42, -0.14 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.40 (P = 0.016)
Total (95% CI) 90 58 100.0 % -0.80 [ -1.12, -0.47 ]
Heterogeneity: Chi2 = 1.52, df = 2 (P = 0.47); I2 =0.0%
Test for overall effect: Z = 4.80 (P < 0.00001)
Test for subgroup differences: Chi2 = 0.00, df = 1 (P = 0.95), I2 =0.0%
-4 -2 0 2 4
Favours NSAID Favours Placebo
53Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.3. Comparison 1 NSAID versus placebo, Outcome 3 Summed Relief Score.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 1 NSAID versus placebo
Outcome: 3 Summed Relief Score
Study or subgroup NSAID Placebo Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Aspirin 650 mg
Bloomfield 1986b 30 15.5 (5.48) 10 12.1 (7.12) 18.4 % 3.40 [ -1.43, 8.23 ]
Subtotal (95% CI) 30 10 18.4 % 3.40 [ -1.43, 8.23 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.38 (P = 0.17)
2 Fenoprofen 200 mg
Bettigole 1981 12 12.08 (8.89) 12 5.17 (5.65) 12.1 % 6.91 [ 0.95, 12.87 ]
Subtotal (95% CI) 12 12 12.1 % 6.91 [ 0.95, 12.87 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.27 (P = 0.023)
3 Ketorolac 5 mg
Bloomfield 1986b 30 14.8 (6.57) 10 12.1 (7.12) 17.2 % 2.70 [ -2.30, 7.70 ]
Subtotal (95% CI) 30 10 17.2 % 2.70 [ -2.30, 7.70 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.06 (P = 0.29)
4 Ketorolac 10 mg
Bloomfield 1986b 30 18.2 (4.93) 10 12.1 (7.12) 19.0 % 6.10 [ 1.35, 10.85 ]
Subtotal (95% CI) 30 10 19.0 % 6.10 [ 1.35, 10.85 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.52 (P = 0.012)
5 Naproxen 550 mg
Bloomfield 1987 30 20 (6.57) 30 11.43 (7.61) 33.2 % 8.57 [ 4.97, 12.17 ]
Subtotal (95% CI) 30 30 33.2 % 8.57 [ 4.97, 12.17 ]
Heterogeneity: not applicable
Test for overall effect: Z = 4.67 (P < 0.00001)
Total (95% CI) 132 72 100.0 % 5.94 [ 3.86, 8.01 ]
Heterogeneity: Chi2 = 4.83, df = 4 (P = 0.30); I2 =17%
Test for overall effect: Z = 5.61 (P < 0.00001)
Test for subgroup differences: Chi2 = 4.83, df = 4 (P = 0.30), I2 =17%
-20 -10 0 10 20
Favours Placebo Favours NSAID
54Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.4. Comparison 1 NSAID versus placebo, Outcome 4 Pain analogue score compared with baseline.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 1 NSAID versus placebo
Outcome: 4 Pain analogue score compared with baseline
Study or subgroup NSAID Placebo Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Aspirin 650 mg
Jain 1978 8 33.3 (41.7) 4 75.6 (41.7) 56.1 % -42.30 [ -92.35, 7.75 ]
Subtotal (95% CI) 8 4 56.1 % -42.30 [ -92.35, 7.75 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.66 (P = 0.098)
2 Aspirin 800 mg with Caffeine 64 mg
Jain 1978 7 30.4 (46.1) 4 75.6 (46.1) 43.9 % -45.20 [ -101.83, 11.43 ]
Subtotal (95% CI) 7 4 43.9 % -45.20 [ -101.83, 11.43 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.56 (P = 0.12)
Total (95% CI) 15 8 100.0 % -43.57 [ -81.07, -6.07 ]
Heterogeneity: Chi2 = 0.01, df = 1 (P = 0.94); I2 =0.0%
Test for overall effect: Z = 2.28 (P = 0.023)
Test for subgroup differences: Chi2 = 0.01, df = 1 (P = 0.94), I2 =0.0%
-100 -50 0 50 100
Favours NSAID Favours Placebo
55Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.5. Comparison 1 NSAID versus placebo, Outcome 5 Global rating.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 1 NSAID versus placebo
Outcome: 5 Global rating
Study or subgroup NSAID Placebo Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Aspirin 650 mg
Bloomfield 1986b 30 8.13 (1.94) 10 6.77 (3.07) 19.0 % 1.36 [ -0.67, 3.39 ]
Subtotal (95% CI) 30 10 19.0 % 1.36 [ -0.67, 3.39 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.32 (P = 0.19)
2 Ketorolac 5 mg
Bloomfield 1986b 30 7.37 (2.63) 10 6.77 (3.07) 17.3 % 0.60 [ -1.52, 2.72 ]
Subtotal (95% CI) 30 10 17.3 % 0.60 [ -1.52, 2.72 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.55 (P = 0.58)
3 Ketorolac 10 mg
Bloomfield 1986b 30 8.53 (2.3) 10 6.77 (3.07) 18.2 % 1.76 [ -0.31, 3.83 ]
Subtotal (95% CI) 30 10 18.2 % 1.76 [ -0.31, 3.83 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.66 (P = 0.096)
4 Naproxen 550 mg
Bloomfield 1987 30 8.37 (2.08) 30 5.73 (3.01) 45.5 % 2.64 [ 1.33, 3.95 ]
Subtotal (95% CI) 30 30 45.5 % 2.64 [ 1.33, 3.95 ]
Heterogeneity: not applicable
Test for overall effect: Z = 3.95 (P = 0.000077)
Total (95% CI) 120 60 100.0 % 1.88 [ 1.00, 2.77 ]
Heterogeneity: Chi2 = 2.96, df = 3 (P = 0.40); I2 =0.0%
Test for overall effect: Z = 4.18 (P = 0.000029)
Test for subgroup differences: Chi2 = 2.96, df = 3 (P = 0.40), I2 =0.0%
-4 -2 0 2 4
Favours Placebo Favours NSAID
56Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.6. Comparison 1 NSAID versus placebo, Outcome 6 Pain reduction > 50%.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 1 NSAID versus placebo
Outcome: 6 Pain reduction > 50%
Study or subgroup NSAID Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Aspirin 650 mg
Bloomfield 1978 19/20 15/20 1.27 [ 0.96, 1.66 ]
0.2 0.5 1 2 5
Favours Placebo Favours NSAID
Analysis 1.7. Comparison 1 NSAID versus placebo, Outcome 7 VAS 1-4 at 30 minutes.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 1 NSAID versus placebo
Outcome: 7 VAS 1-4 at 30 minutes
Study or subgroup NSAID Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Metamizol 625 mg
Mehlhorn 2005 5/33 4/28 1.06 [ 0.31, 3.57 ]
0.01 0.1 1 10 100
Favours Placebo Favours NSAID
57Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.8. Comparison 1 NSAID versus placebo, Outcome 8 No pain relief.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 1 NSAID versus placebo
Outcome: 8 No pain relief
Study or subgroup NSAID Placebo Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Aspirin 650 mg
Bloomfield 1986a 2/34 5/16 48.9 % 0.19 [ 0.04, 0.87 ]
Subtotal (95% CI) 34 16 48.9 % 0.19 [ 0.04, 0.87 ]
Total events: 2 (NSAID), 5 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 2.14 (P = 0.032)
2 Flurbiprofen 50 mg
Bloomfield 1986a 0/30 5/16 51.1 % 0.05 [ 0.00, 0.85 ]
Subtotal (95% CI) 30 16 51.1 % 0.05 [ 0.00, 0.85 ]
Total events: 0 (NSAID), 5 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 2.07 (P = 0.038)
Total (95% CI) 64 32 100.0 % 0.12 [ 0.03, 0.45 ]
Total events: 2 (NSAID), 10 (Placebo)
Heterogeneity: Chi2 = 0.72, df = 1 (P = 0.40); I2 =0.0%
Test for overall effect: Z = 3.14 (P = 0.0017)
Test for subgroup differences: Chi2 = 0.65, df = 1 (P = 0.42), I2 =0.0%
0.005 0.1 1 10 200
Favours NSAID Favours Placebo
58Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.9. Comparison 1 NSAID versus placebo, Outcome 9 Adverse effects.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 1 NSAID versus placebo
Outcome: 9 Adverse effects
Study or subgroup NSAID Placebo Risk Ratio Weight Risk Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
1 Aspirin 650 mg
Bloomfield 1978 4/20 7/20 28.2 % 0.57 [ 0.20, 1.65 ]
Bloomfield 1981 9/26 5/26 33.7 % 1.80 [ 0.70, 4.65 ]
Subtotal (95% CI) 46 46 61.9 % 1.04 [ 0.34, 3.20 ]
Total events: 13 (NSAID), 12 (Placebo)
Heterogeneity: Tau2 = 0.39; Chi2 = 2.50, df = 1 (P = 0.11); I2 =60%
Test for overall effect: Z = 0.07 (P = 0.94)
2 Fenoprofen 200 mg
Bettigole 1981 6/12 5/12 38.1 % 1.20 [ 0.50, 2.88 ]
Subtotal (95% CI) 12 12 38.1 % 1.20 [ 0.50, 2.88 ]
Total events: 6 (NSAID), 5 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 0.41 (P = 0.68)
Total (95% CI) 58 58 100.0 % 1.12 [ 0.60, 2.08 ]
Total events: 19 (NSAID), 17 (Placebo)
Heterogeneity: Tau2 = 0.06; Chi2 = 2.53, df = 2 (P = 0.28); I2 =21%
Test for overall effect: Z = 0.35 (P = 0.73)
Test for subgroup differences: Chi2 = 0.04, df = 1 (P = 0.84), I2 =0.0%
0.01 0.1 1 10 100
Favours NSAID Favours Placebo
59Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.1. Comparison 2 NSAID versus opioid, Outcome 1 Pain reduction (SPID).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 2 NSAID versus opioid
Outcome: 1 Pain reduction (SPID)
Study or subgroup NSAID Opioid Mean Difference Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Fenoprofen 200 mg vs codeine 60 mg
Bettigole 1981 12 8.92 (4.42) 11 6.64 (7.57) 2.28 [ -2.85, 7.41 ]
-20 -10 0 10 20
Favours Opioid Favours NSAID
Analysis 2.2. Comparison 2 NSAID versus opioid, Outcome 2 Pain reduction (pain intensity 6 hours).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 2 NSAID versus opioid
Outcome: 2 Pain reduction (pain intensity 6 hours)
Study or subgroup NSAID Opioid Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Aspirin 650 mg v codeine 60 mg
Bloomfield 1986a 17 0.79 (1.11) 16 1.28 (0.91) 24.6 % -0.49 [ -1.18, 0.20 ]
Subtotal (95% CI) 17 16 24.6 % -0.49 [ -1.18, 0.20 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.39 (P = 0.16)
2 Aspirin 650 mg v codeine 120 mg
Bloomfield 1986a 17 0.79 (1.11) 15 1.35 (1.06) 20.7 % -0.56 [ -1.31, 0.19 ]
Subtotal (95% CI) 17 15 20.7 % -0.56 [ -1.31, 0.19 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.46 (P = 0.14)
3 Flurbiprofen 50 mg v codeine 60 mg
Bloomfield 1986a 15 0.47 (0.88) 16 1.28 (0.91) 29.6 % -0.81 [ -1.44, -0.18 ]
Subtotal (95% CI) 15 16 29.6 % -0.81 [ -1.44, -0.18 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.52 (P = 0.012)
-2 -1 0 1 2
Favours NSAID Favours Opioid
(Continued . . . )
60Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup NSAID Opioid Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
4 Flurbiprofen 50 mg v codeine 120 mg
Bloomfield 1986a 15 0.47 (0.88) 16 1.35 (1.06) 25.1 % -0.88 [ -1.56, -0.20 ]
Subtotal (95% CI) 15 16 25.1 % -0.88 [ -1.56, -0.20 ]
Heterogeneity: not applicable
Test for overall effect: Z = 2.52 (P = 0.012)
Total (95% CI) 64 63 100.0 % -0.70 [ -1.04, -0.35 ]
Heterogeneity: Chi2 = 0.87, df = 3 (P = 0.83); I2 =0.0%
Test for overall effect: Z = 3.99 (P = 0.000067)
Test for subgroup differences: Chi2 = 0.87, df = 3 (P = 0.83), I2 =0.0%
-2 -1 0 1 2
Favours NSAID Favours Opioid
Analysis 2.3. Comparison 2 NSAID versus opioid, Outcome 3 Pain reduction (summed pain relief).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 2 NSAID versus opioid
Outcome: 3 Pain reduction (summed pain relief)
Study or subgroup NSAID Opioid Mean Difference Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Fenoprofen 200 mg vs codeine 60 mg
Bettigole 1981 12 12.08 (8.89) 11 8.73 (8.05) 3.35 [ -3.57, 10.27 ]
-20 -10 0 10 20
Favours Opioid Favours NSAID
61Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.4. Comparison 2 NSAID versus opioid, Outcome 4 No pain relief.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 2 NSAID versus opioid
Outcome: 4 No pain relief
Study or subgroup NSAID Opioid Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Aspirin 650 mg v codeine 60 mg
Bloomfield 1986a 2/17 1/16 13.0 % 1.88 [ 0.19, 18.80 ]
Subtotal (95% CI) 17 16 13.0 % 1.88 [ 0.19, 18.80 ]
Total events: 2 (NSAID), 1 (Opioid)
Heterogeneity: not applicable
Test for overall effect: Z = 0.54 (P = 0.59)
2 Aspirin 650 mg v codeine 120 mg
Bloomfield 1986a 2/17 1/15 13.4 % 1.76 [ 0.18, 17.56 ]
Subtotal (95% CI) 17 15 13.4 % 1.76 [ 0.18, 17.56 ]
Total events: 2 (NSAID), 1 (Opioid)
Heterogeneity: not applicable
Test for overall effect: Z = 0.48 (P = 0.63)
3 Flurbiprofen 50 mg v codeine 60 mg
Bloomfield 1986a 0/15 1/16 18.4 % 0.35 [ 0.02, 8.08 ]
Subtotal (95% CI) 15 16 18.4 % 0.35 [ 0.02, 8.08 ]
Total events: 0 (NSAID), 1 (Opioid)
Heterogeneity: not applicable
Test for overall effect: Z = 0.65 (P = 0.52)
4 Flurbiprofen 50 mg v codeine 120 mg
Bloomfield 1986a 0/15 1/16 18.4 % 0.35 [ 0.02, 8.08 ]
Subtotal (95% CI) 15 16 18.4 % 0.35 [ 0.02, 8.08 ]
Total events: 0 (NSAID), 1 (Opioid)
Heterogeneity: not applicable
Test for overall effect: Z = 0.65 (P = 0.52)
5 Nalbuphine 15 mg vs codeine 60 mg
Kantor 1984b 2/35 3/37 36.8 % 0.70 [ 0.13, 3.97 ]
Subtotal (95% CI) 35 37 36.8 % 0.70 [ 0.13, 3.97 ]
Total events: 2 (NSAID), 3 (Opioid)
Heterogeneity: not applicable
Test for overall effect: Z = 0.40 (P = 0.69)
Total (95% CI) 99 100 100.0 % 0.87 [ 0.32, 2.35 ]
Total events: 6 (NSAID), 7 (Opioid)
Heterogeneity: Chi2 = 1.49, df = 4 (P = 0.83); I2 =0.0%
Test for overall effect: Z = 0.27 (P = 0.79)
Test for subgroup differences: Chi2 = 1.48, df = 4 (P = 0.83), I2 =0.0%
0.01 0.1 1 10 100
Favours NSAID Favours Opioid
62Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.5. Comparison 2 NSAID versus opioid, Outcome 5 Adverse effects.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 2 NSAID versus opioid
Outcome: 5 Adverse effects
Study or subgroup NSAID Opioid Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Fenoprofen 200 mg vs codeine 60 mg
Bettigole 1981 6/18 3/15 1.67 [ 0.50, 5.56 ]
0.01 0.1 1 10 100
Favours NSAID Favours Opioid
Analysis 3.1. Comparison 3 Opioid versus placebo, Outcome 1 Pain reduction (SPID).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 3 Opioid versus placebo
Outcome: 1 Pain reduction (SPID)
Study or subgroup Opioid Placebo Std. Mean Difference Std. Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Codeine 60 mg
Bettigole 1981 11 6.64 (7.57) 12 4 (4.31) 0.42 [ -0.41, 1.25 ]
-4 -2 0 2 4
Favours Placebo Favours Opioid
63Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.2. Comparison 3 Opioid versus placebo, Outcome 2 Pain reduction (pain intensity 6 hours).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 3 Opioid versus placebo
Outcome: 2 Pain reduction (pain intensity 6 hours)
Study or subgroup Opioid Placebo Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Codeine 60 mg
Bloomfield 1986a 32 1.28 (0.91) 16 1.25 (1.13) 52.3 % 0.03 [ -0.61, 0.67 ]
Subtotal (95% CI) 32 16 52.3 % 0.03 [ -0.61, 0.67 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.09 (P = 0.93)
2 Codeine 120 mg
Bloomfield 1986a 31 1.35 (1.06) 16 1.25 (1.13) 47.7 % 0.10 [ -0.57, 0.77 ]
Subtotal (95% CI) 31 16 47.7 % 0.10 [ -0.57, 0.77 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.29 (P = 0.77)
Total (95% CI) 63 32 100.0 % 0.06 [ -0.40, 0.52 ]
Heterogeneity: Chi2 = 0.02, df = 1 (P = 0.88); I2 =0.0%
Test for overall effect: Z = 0.27 (P = 0.79)
Test for subgroup differences: Chi2 = 0.02, df = 1 (P = 0.88), I2 =0.0%
-1 -0.5 0 0.5 1
Favours Placebo Favours Opioid
Analysis 3.3. Comparison 3 Opioid versus placebo, Outcome 3 Pain reduction (summed relief score).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 3 Opioid versus placebo
Outcome: 3 Pain reduction (summed relief score)
Study or subgroup Opioid Placebo Std. Mean Difference Std. Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Codeine 60 mg
Bettigole 1981 11 8.73 (8.05) 12 5.17 (5.65) 0.50 [ -0.34, 1.33 ]
-10 -5 0 5 10
Favours Placebo Favours Opioid
64Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.4. Comparison 3 Opioid versus placebo, Outcome 4 No pain relief.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 3 Opioid versus placebo
Outcome: 4 No pain relief
Study or subgroup Opioid Placebo Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Codeine 60 mg
Kantor 1984b 3/37 13/18 50.5 % 0.11 [ 0.04, 0.34 ]
Subtotal (95% CI) 37 18 50.5 % 0.11 [ 0.04, 0.34 ]
Total events: 3 (Opioid), 13 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 3.82 (P = 0.00013)
2 Nalbuphine 15 mg
Kantor 1984b 2/35 13/18 49.5 % 0.08 [ 0.02, 0.31 ]
Subtotal (95% CI) 35 18 49.5 % 0.08 [ 0.02, 0.31 ]
Total events: 2 (Opioid), 13 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 3.61 (P = 0.00030)
Total (95% CI) 72 36 100.0 % 0.10 [ 0.04, 0.23 ]
Total events: 5 (Opioid), 26 (Placebo)
Heterogeneity: Chi2 = 0.15, df = 1 (P = 0.70); I2 =0.0%
Test for overall effect: Z = 5.28 (P < 0.00001)
Test for subgroup differences: Chi2 = 0.15, df = 1 (P = 0.70), I2 =0.0%
0.01 0.1 1 10 100
Favours Opioid Favours Placebo
Analysis 3.5. Comparison 3 Opioid versus placebo, Outcome 5 Adverse effects.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 3 Opioid versus placebo
Outcome: 5 Adverse effects
Study or subgroup Opioid Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 Codeine 60 mg
Bettigole 1981 3/11 5/12 0.65 [ 0.20, 2.12 ]
0.005 0.1 1 10 200
Favours Opioid Favours Placebo
65Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.1. Comparison 4 Flurbiprofen versus aspirin, Outcome 1 Pain reduction (pain intensity 6 hours).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 4 Flurbiprofen versus aspirin
Outcome: 1 Pain reduction (pain intensity 6 hours)
Study or subgroup Flurbiprofen 50mg Aspirin 650mg Mean Difference Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Bloomfield 1986a 30 0.47 (0.88) 34 0.79 (1.11) -0.32 [ -0.81, 0.17 ]
-1 -0.5 0 0.5 1
Favours Flurbiprofen 50mg Favours Aspirin 650mg
Analysis 4.2. Comparison 4 Flurbiprofen versus aspirin, Outcome 2 No pain relief.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 4 Flurbiprofen versus aspirin
Outcome: 2 No pain relief
Study or subgroup Flurbiprofen 50mg Aspirin 650mg Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Bloomfield 1986a 0/30 2/34 0.23 [ 0.01, 4.52 ]
0.01 0.1 1 10 100
Favours Flurbiprofen Favours Aspirin 650mg
66Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
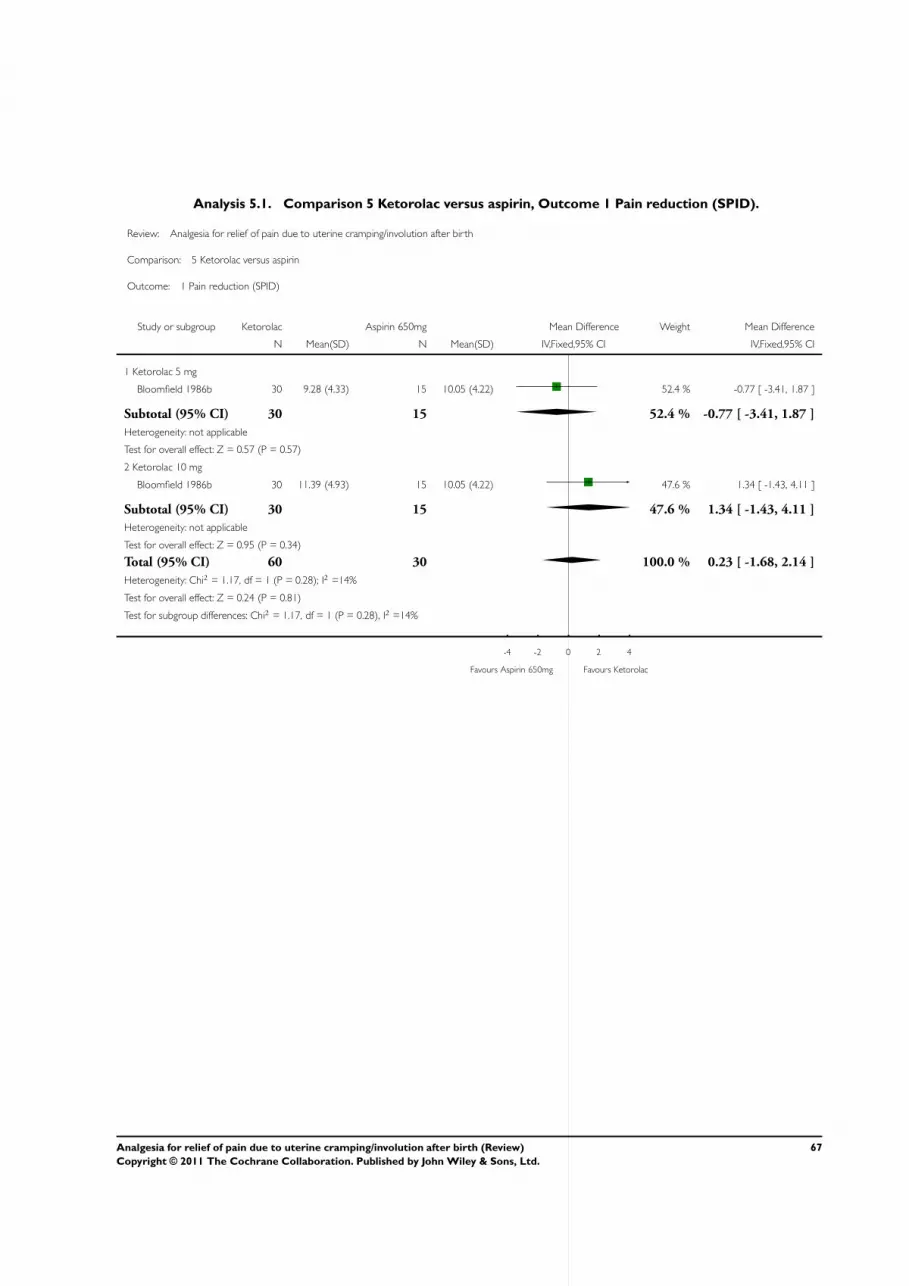
Analysis 5.1. Comparison 5 Ketorolac versus aspirin, Outcome 1 Pain reduction (SPID).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 5 Ketorolac versus aspirin
Outcome: 1 Pain reduction (SPID)
Study or subgroup Ketorolac Aspirin 650mg Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Ketorolac 5 mg
Bloomfield 1986b 30 9.28 (4.33) 15 10.05 (4.22) 52.4 % -0.77 [ -3.41, 1.87 ]
Subtotal (95% CI) 30 15 52.4 % -0.77 [ -3.41, 1.87 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.57 (P = 0.57)
2 Ketorolac 10 mg
Bloomfield 1986b 30 11.39 (4.93) 15 10.05 (4.22) 47.6 % 1.34 [ -1.43, 4.11 ]
Subtotal (95% CI) 30 15 47.6 % 1.34 [ -1.43, 4.11 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.95 (P = 0.34)
Total (95% CI) 60 30 100.0 % 0.23 [ -1.68, 2.14 ]
Heterogeneity: Chi2 = 1.17, df = 1 (P = 0.28); I2 =14%
Test for overall effect: Z = 0.24 (P = 0.81)
Test for subgroup differences: Chi2 = 1.17, df = 1 (P = 0.28), I2 =14%
-4 -2 0 2 4
Favours Aspirin 650mg Favours Ketorolac
67Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
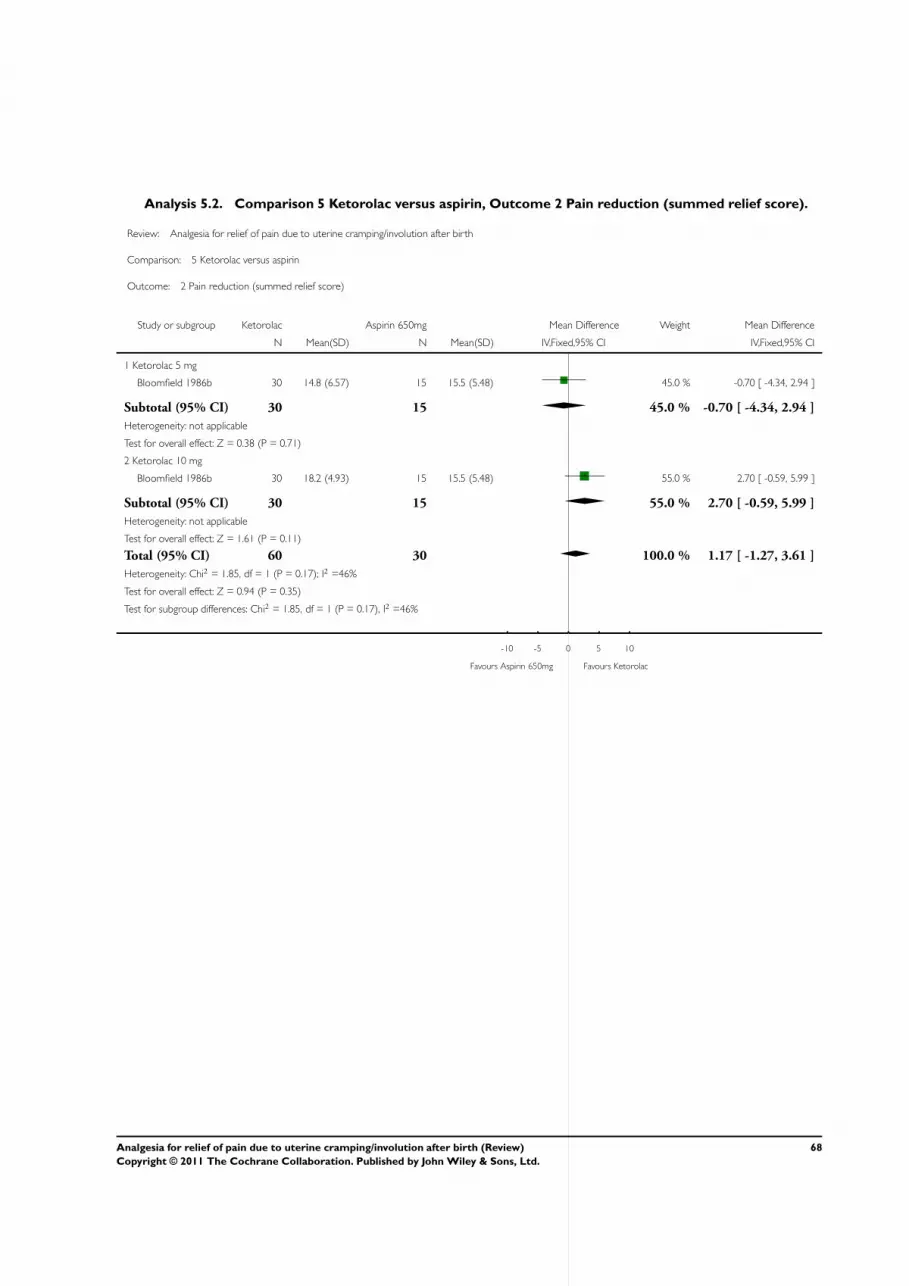
Analysis 5.2. Comparison 5 Ketorolac versus aspirin, Outcome 2 Pain reduction (summed relief score).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 5 Ketorolac versus aspirin
Outcome: 2 Pain reduction (summed relief score)
Study or subgroup Ketorolac Aspirin 650mg Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Ketorolac 5 mg
Bloomfield 1986b 30 14.8 (6.57) 15 15.5 (5.48) 45.0 % -0.70 [ -4.34, 2.94 ]
Subtotal (95% CI) 30 15 45.0 % -0.70 [ -4.34, 2.94 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.38 (P = 0.71)
2 Ketorolac 10 mg
Bloomfield 1986b 30 18.2 (4.93) 15 15.5 (5.48) 55.0 % 2.70 [ -0.59, 5.99 ]
Subtotal (95% CI) 30 15 55.0 % 2.70 [ -0.59, 5.99 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.61 (P = 0.11)
Total (95% CI) 60 30 100.0 % 1.17 [ -1.27, 3.61 ]
Heterogeneity: Chi2 = 1.85, df = 1 (P = 0.17); I2 =46%
Test for overall effect: Z = 0.94 (P = 0.35)
Test for subgroup differences: Chi2 = 1.85, df = 1 (P = 0.17), I2 =46%
-10 -5 0 5 10
Favours Aspirin 650mg Favours Ketorolac
68Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.3. Comparison 5 Ketorolac versus aspirin, Outcome 3 Global rating.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 5 Ketorolac versus aspirin
Outcome: 3 Global rating
Study or subgroup Keterolac Aspirin 650mg Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Keterolac 5 mg
Bloomfield 1987 30 7.37 (2.63) 15 8.13 (1.94) 47.0 % -0.76 [ -2.12, 0.60 ]
Subtotal (95% CI) 30 15 47.0 % -0.76 [ -2.12, 0.60 ]
Heterogeneity: not applicable
Test for overall effect: Z = 1.10 (P = 0.27)
2 Keterolac 10 mg
Bloomfield 1986b 30 8.53 (2.3) 15 8.13 (1.94) 53.0 % 0.40 [ -0.88, 1.68 ]
Subtotal (95% CI) 30 15 53.0 % 0.40 [ -0.88, 1.68 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.61 (P = 0.54)
Total (95% CI) 60 30 100.0 % -0.15 [ -1.08, 0.79 ]
Heterogeneity: Chi2 = 1.48, df = 1 (P = 0.22); I2 =32%
Test for overall effect: Z = 0.31 (P = 0.76)
Test for subgroup differences: Chi2 = 1.48, df = 1 (P = 0.22), I2 =32%
-4 -2 0 2 4
Favours Aspirin 650mg Favours Keterolac
Analysis 6.1. Comparison 6 Ketorolac: different doses, Outcome 1 Pain reduction (SPID).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 6 Ketorolac: different doses
Outcome: 1 Pain reduction (SPID)
Study or subgroup Keterolac 10mg Keterolac 5mg Mean Difference Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Bloomfield 1986b 30 11.39 (4.93) 30 9.28 (4.33) 2.11 [ -0.24, 4.46 ]
-4 -2 0 2 4
Favours Keterolac 5mg Favours Keterolac 10mg
69Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.2. Comparison 6 Ketorolac: different doses, Outcome 2 Pain reduction (summed relief score).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 6 Ketorolac: different doses
Outcome: 2 Pain reduction (summed relief score)
Study or subgroup Ketorolac 10mg Ketorolac 5mg Mean Difference Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Bloomfield 1986b 30 18.2 (4.93) 30 14.8 (6.57) 3.40 [ 0.46, 6.34 ]
-4 -2 0 2 4
Favours Ketorolac 5mg Favours Ketorolac 10mg
Analysis 6.3. Comparison 6 Ketorolac: different doses, Outcome 3 Global rating.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 6 Ketorolac: different doses
Outcome: 3 Global rating
Study or subgroup Ketorolac 10mg Ketorolac 5mg Mean Difference Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Bloomfield 1986b 30 8.53 (2.3) 30 7.37 (2.63) 1.16 [ -0.09, 2.41 ]
-2 -1 0 1 2
Favours Ketorolac 5mg Favours Ketorolac 10mg
70Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
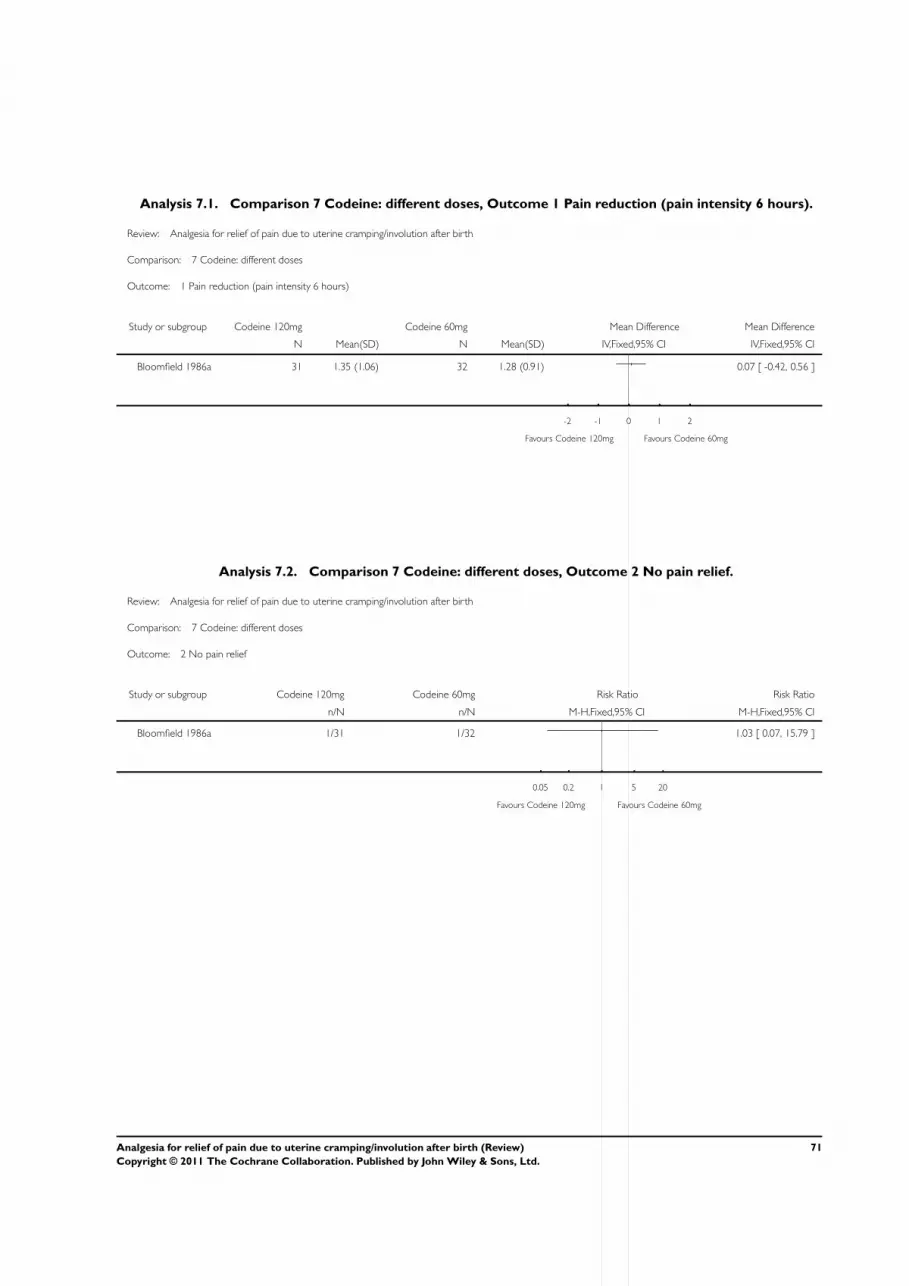
Analysis 7.1. Comparison 7 Codeine: different doses, Outcome 1 Pain reduction (pain intensity 6 hours).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 7 Codeine: different doses
Outcome: 1 Pain reduction (pain intensity 6 hours)
Study or subgroup Codeine 120mg Codeine 60mg Mean Difference Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Bloomfield 1986a 31 1.35 (1.06) 32 1.28 (0.91) 0.07 [ -0.42, 0.56 ]
-2 -1 0 1 2
Favours Codeine 120mg Favours Codeine 60mg
Analysis 7.2. Comparison 7 Codeine: different doses, Outcome 2 No pain relief.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 7 Codeine: different doses
Outcome: 2 No pain relief
Study or subgroup Codeine 120mg Codeine 60mg Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Bloomfield 1986a 1/31 1/32 1.03 [ 0.07, 15.79 ]
0.05 0.2 1 5 20
Favours Codeine 120mg Favours Codeine 60mg
71Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 8.1. Comparison 8 Nalbuphine versus codeine, Outcome 1 No pain relief.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 8 Nalbuphine versus codeine
Outcome: 1 No pain relief
Study or subgroup Nalbuphine Codeine Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Kantor 1984b 2/35 3/37 0.70 [ 0.13, 3.97 ]
0.01 0.1 1 10 100
Favours Nalbuphine Favours Codeine
Analysis 9.1. Comparison 9 Paracetamol versus placebo, Outcome 1 Pain reduction (pain intensity 6 hours).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 9 Paracetamol versus placebo
Outcome: 1 Pain reduction (pain intensity 6 hours)
Study or subgroup Paracetamol 650mg Placebo Mean Difference Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Bloomfield 1981 22 1.27 (1.13) 26 1.39 (0.92) -0.12 [ -0.71, 0.47 ]
-1 -0.5 0 0.5 1
Favours Paracetamol 650 Favours Placebo
72Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 9.2. Comparison 9 Paracetamol versus placebo, Outcome 2 Adverse effects.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 9 Paracetamol versus placebo
Outcome: 2 Adverse effects
Study or subgroup Paracetamol 650mg Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Bloomfield 1981 10/22 5/26 2.36 [ 0.95, 5.88 ]
0.01 0.1 1 10 100
Favours Paracetamol Favours Placebo
Analysis 10.1. Comparison 10 Paracetamol versus aspirin, Outcome 1 Pain reduction (pain intensity 6
hours).
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 10 Paracetamol versus aspirin
Outcome: 1 Pain reduction (pain intensity 6 hours)
Study or subgroup Paracetamol 650mg Aspirin 650mg Mean Difference Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Bloomfield 1981 22 1.27 (1.13) 26 0.42 (0.77) 0.85 [ 0.29, 1.41 ]
-4 -2 0 2 4
Favours Paracetamol Favours Aspirin 650mg
73Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 10.2. Comparison 10 Paracetamol versus aspirin, Outcome 2 Adverse effects.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 10 Paracetamol versus aspirin
Outcome: 2 Adverse effects
Study or subgroup Paracetamol 650mg Aspirin 650mg Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Bloomfield 1981 10/22 9/26 1.31 [ 0.65, 2.64 ]
0.01 0.1 1 10 100
Favours Paracetamol Favours Aspirin 650mg
Analysis 11.1. Comparison 11 TENS versus placebo, Outcome 1 VAS 1-4 at 30 minutes.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 11 TENS versus placebo
Outcome: 1 VAS 1-4 at 30 minutes
Study or subgroup TENS Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Mehlhorn 2005 4/27 4/28 1.04 [ 0.29, 3.73 ]
0.01 0.1 1 10 100
Favours Placebo Favours TENS
74Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 12.1. Comparison 12 TENS plus Metamizol versus placebo, Outcome 1 VAS 1-4 at 30 minutes.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 12 TENS plus Metamizol versus placebo
Outcome: 1 VAS 1-4 at 30 minutes
Study or subgroup TENS + Metamizol Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Mehlhorn 2005 11/30 4/28 2.57 [ 0.92, 7.13 ]
0.01 0.1 1 10 100
Favours Placebo Favours TENS + Metamizol
Analysis 13.1. Comparison 13 TENS plus Metamizol versus TENS, Outcome 1 VAS 1-4 at 30 minutes.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 13 TENS plus Metamizol versus TENS
Outcome: 1 VAS 1-4 at 30 minutes
Study or subgroup TENS + Metamizol TENS Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Mehlhorn 2005 11/30 4/27 2.48 [ 0.89, 6.86 ]
0.01 0.1 1 10 100
Favours TENS Favours TENS + Metamizol
75Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 14.1. Comparison 14 TENS plus Metamizol versus Metamizol, Outcome 1 VAS 1-4 at 30 minutes.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 14 TENS plus Metamizol versus Metamizol
Outcome: 1 VAS 1-4 at 30 minutes
Study or subgroup TENS + Metamizol Metamizol Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Mehlhorn 2005 11/30 5/33 2.42 [ 0.95, 6.16 ]
0.01 0.1 1 10 100
Favours Metamizol Favours TENS + Metamizol
Analysis 15.1. Comparison 15 TENS versus Metamizol, Outcome 1 VAS 1-4 at 30 minutes.
Review: Analgesia for relief of pain due to uterine cramping/involution after birth
Comparison: 15 TENS versus Metamizol
Outcome: 1 VAS 1-4 at 30 minutes
Study or subgroup TENS Metamizol Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Mehlhorn 2005 4/27 5/33 0.98 [ 0.29, 3.29 ]
0.01 0.1 1 10 100
Favours Metamizol Favours TENS
H I S T O R Y
Protocol first published: Issue 3, 2004
Review first published: Issue 5, 2011
76Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C O N T R I B U T I O N S O F A U T H O R S
Pat Ashwood (PA), Andrea Deussen (AD) and Sheree Agett (SA) wrote the protocol. Ruth Martis (RM), AD and PA discussed the
scope of the review and reviewed all possible trials for inclusion and exclusion and extracted data. AD entered data into RevMan and
PA checked data entry. AD drafted the results and AD, PA and RM discussed and agreed on the interpretation.
D E C L A R A T I O N S O F I N T E R E S T
None known.
S O U R C E S O F S U P P O R T
Internal sources
• The University of Adelaide - Australian Research Centre for Health of Women and Babies (ARCH), Australia.
Release time for attending a 1 week dedicated work-in for data analyses.
External sources
• Australasian Cochrane Centre, Monash University, Melbourne, Australia.
One week on-site guidance and support for progressing with review.
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
Protocol changed to exclude studies reporting after birth pain in women following caesarean birth.
Protocol changed to exclude meta-analyses on drugs no longer in use or contraindicated in lactation.
The methods have been updated to reflect the latest Cochrane Handbook and the Cochrane Pregnancy and Childbirth Group’s
methodological guidelines.
Sheree Agett is no longer an author on this review. Ruth Martis has now joined the review team.
We did not carry out the additional searching (EMBASE, CINAHL AND MIDIRS) specified in the protocol.
I N D E X T E R M S
Medical Subject Headings (MeSH)
Analgesia, Obstetrical [∗methods]; Analgesics, Opioid [therapeutic use]; Anti-Inflammatory Agents, Non-Steroidal [therapeutic use];
Muscle Cramp [∗complications]; Pain [∗drug therapy]; Randomized Controlled Trials as Topic; Uterine Contraction [∗physiology];
Uterine Diseases [∗drug therapy]
77Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

MeSH check words
Female; Humans; Pregnancy
78Analgesia for relief of pain due to uterine cramping/involution after birth (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.





























