Embed Size (px)
Citation preview

HUMAN GENE THERAPY 13:65–100 (January 1, 2002)Mary Ann Liebert, Inc.
Analysis of Risk Factors for Local Delivery of Low- andIntermediate-Dose Adenovirus Gene Transfer Vectors to
Individuals with a Spectrum of Comorbid Conditions
RONALD G. CRYSTAL,1,2 BEN-GARY HARVEY,2 JUAN P. WISNIVESKY,2 KELLEY A. O’DONOGHUE,2
KAREN W. CHU,3 JAMAN MARONI,2 JOLENE C. MUSCAT,2 ALLISON L. PIPPO,2
CONNIE E. WRIGHT,2 ROBERT J. KANER,2 PHILIP L. LEOPOLD,2 PAUL D. KESSLER,3
HENRIK S. RASMUSSEN,3 TODD K. ROSENGART,4 and CHARLEEN HOLLMANN2
ABSTRACT
In this study we analyze the adverse events and abnormal laboratory parameters following local administra-tion of low (,109 particle units) and intermediate (109–1011 particle units) single and repetitive doses (140 to-tal) of E12E32 adenovirus (Ad) gene transfer vectors administered to the respiratory epithelium, solid tu-mors, skin, myocardium, and skeletal muscle in eight gene transfer trials since April 1993. In the accompanyingpaper by Harvey et al., (Hum. Gene Ther. 2002; 13:15–63), we conclude that for the total group, no deathswere attributable to the Ad vectors per se, and the incidence of major adverse events likely caused by an Advector was 0.7%. The present study analyzes the trials as a group to evaluate risk factors for the adverseevents, abnormal values among laboratory parameters, and known deaths. Ten putative risk factors were as-sessed, including “patient-related” (age, sex, comorbid index and pretherapy anti-Ad antibodies), “vector-re-lated” (dose, route, transgene, and number of vector administrations), and “trial-related” (trial in which theindividual was enrolled, and whether surgery was part of the trial). While assessment of each factor individ-ually suggested several possible associations with adverse events, abnormal laboratory parameters, or deaths,multivariate analysis identified only age, comorbid index, and surgery (comorbid index for death; age andsurgery for nondeath adverse events) as variables significantly associated with increased risk for a major(severity scale 3–4 of 4) adverse event for individuals enrolled in these gene transfer trials. Importantly, mul-tivariate analysis suggested that vector-related parameters, including dose, route, transgene, or number ofvector administrations at the doses and routes evaluated in these studies, do not appear to be significant riskfactors for a major adverse event. With the caveat that these are phase I, uncontrolled trials, we concludethat (1) there is no definitive risk factor that will clearly predict a major adverse outcome resulting from lo-cal administration of low and intermediate doses of Ad gene transfer vectors; and (2) major adverse eventsin these gene transfer trials are associated primarily with the study population and/or trial procedures, notthe Ad vectors themselves. This assessment is consistent with the concept that local administration of low andintermediate doses of Ad gene transfer vectors appears to be well tolerated.
65
1Institute of Genetic Medicine, Weill Medical College of Cornell University, New York, NY 10021.2Division of Pulmonary and Critical Care Medicine, Weill Medical College of Cornell University, New York, NY 10021.3GenVec, Inc., Gaithersburg, MD 20878.4Division of Cardiothoracic Surgery, Evanston Northwestern Healthcare, Evanston, IL 60201.

OVERVIEW SUMMARY
This study analyzes risk factors for the development of ad-verse events, abnormal laboratory parameters, and deathsamong 90 individuals with a variety of comorbid conditionsreceiving 140 local administrations of low (,109 particleunits) and intermediate doses (109–1011 particle units) of ad-enovirus gene transfer vectors to six different sites in eighttrials. The major adverse outcomes were linked primarilyto the age and underlying disorder of the participant andthe inclusion of surgery in the trial, not to other patient-,vector-, or trial-related risk factors. Within the constraintsof the design of these phase I trials, these observations areconsistent with the concept that local administration of lowand intermediate doses of adenovirus gene transfer vectorsis well tolerated.
INTRODUCTION
IN VIVO ADMINISTRATION of adenovirus (Ad) gene transfer vec-tors to most organs of experimental animals results in robust
gene transfer and transgene expression, with variable persis-tence of expression of the recombinant transgene depending onthe route, dose, transgene, species, and/or strain of the experi-mental animal (Engelhardt et al., 1994; Kass-Eisler et al., 1994;Barr et al., 1995; Crystal, et al., 1995; Wilson, 1996; Kaplanand Smith, 1997; Anderson, 1998). On the basis of studiesdemonstrating safety and efficacy in experimental animals, wehave administered E12E32 recombinant Ad vectors to 90 in-dividuals with a variety of comorbid conditions in 8 phase I hu-man studies since April 1993 (Crystal et al., 1994, 1997, 1998;Hay et al., 1995; Crystal et al., 1995b; Crystal, 1998; Harveyet al., 1999a–d; Rosengart et al., 1999a,b). Among those par-ticipating were individuals with cystic fibrosis, colon cancermetastatic to the liver, normal individuals, and individuals withcardiovascular disease, including coronary artery disease or pe-ripheral vascular disease. These studies included a total of 140doses (ranging from 1 single dose to 7 repetitive doses) of Advectors encoding 3 different transgenes (human cystic fibrosistransmembrane conductance regulator [CFTR] cDNA, Esche-richia coli cytosine deaminase [CD] gene, and human vascularendothelial growth factor [VEGF] 121 cDNA). The doses ofvectors were in the low (,109 particle units [PU]), and inter-mediate range (109 to 1011 PU). All were administered in a lo-cal fashion directly to a specific site, including the nasal ep-ithelium, bronchial epithelium, solid tumor, skin, myocardium,and skeletal muscle.
In an accompanying paper (Harvey et al., 2002), we describethe trials, the long-term follow-up of the study population, thelaboratory values over time, the adverse events identified, as-sessment of shedding of the vector and/or wild-type virus, theneoplasms identified during the trials, and details regarding allknown deaths in the study population. In this paper, we ana-lyze the adverse events and abnormal laboratory parameters inthe overall study population to identify possible risk factors re-lated to the study population, the vectors per se, or the trial pro-cedures. Finally, we assess the various risk factors to determinewhether the deaths and other major adverse events observed inthese studies might be predicted in future trials.
MATERIALS AND METHODS
Adenovirus vectors
All vectors used in the trials are E12E32 replication-defi-cient Ad based on serotype 5 (Crystal et al., 1994; Harvey etal., 1999b). AdCFTR and AdGVCFTR.10 express the humanCFTR cDNA, AdGVCD.10 the E. coli CD gene, andAdGVVEGF121.10 the human VEGF 121 (VEGF121) cDNA(Crystal et al., 1994; Harvey et al., 1999b). Details regardingthe construction, production, purification, and characterizationof these vectors can be found in the accompanying paper (Har-vey et al., 2002).
Regulatory issues and study design
All studies were approved by the local Institutional ReviewBoards and Biosafety Committees and the Food and Drug Ad-ministration, Center for Biologics Evaluation and Research(FDA, CBER), and reviewed by the National Institutes ofHealth Recombinant DNA Advisory Committee (NIH-RAC).The results of these studies, including all adverse events, havebeen reported appropriately under federal regulations. Informedconsents were obtained from all study participants.
All studies included an assessment of a variety of generaland organ-specific safety parameters, and host defense param-eters relevant to Ad vectors. The “cystic fibrosis bolus” trial(RAC # 9212-034; FDA BB-IND 4855) was designed to assessCFTR gene expression in the nasal and bronchial epitheliumafter single administration of the AdCFTR vector administeredby slow bolus to the nose and bronchi of individuals with cys-tic fibrosis (Crystal et al., 1994, 1995; Hay et al., 1995; McEl-vaney and Crystal, 1995). The “cystic fibrosis spray” study(RAC # 9409-085; FDA BB-IND 5702) was designed to eval-uate the expression of CFTR mRNA in airway epithelial cellsafter single and repetitive administration of the AdGVCFTR.10vector to the airway epithelium of individuals with CF (Crys-tal et al., 1995a; Harvey et al., 1999b). The “colon cancer met-astatic to liver” trial (RAC # 9509-125; FDA BB-IND 6442)was designed as a prodrug study to examine the histologic, im-munohistochemical, and apoptosis-related parameters in tumorsremoved at hepatic resection after the direct administration ofthe AdGVCD.10 vector to hepatic metastases of biopsy-provencolorectal carcinoma with concomitant oral administration ofthe prodrug 5-fluorocytosine (Crystal et al., 1997). The “nor-mal, intradermal” study (RAC # 9701-171; FDA BB-IND 6950)was designed to assess the host responses to single or repeti-tive intradermal administration of the AdGVCD.10 vector to nor-mal individuals (Harvey et al., 1999a). The “normal, intra-bronchial” trial (RAC # 9708-209; FDA BB-IND 6950) wasdesigned to evaluate local and systemic host responses and per-sistence of the vector genome in the airway epithelium after in-trabronchial spray administration of the AdGVCD.10 vector tonormal individuals (Harvey et al., 1999c,d,e). The “cardiac, ad-junct to coronary artery bypass graft (CABG), intramyocardial”study (RAC # 9711-221; FDA BB-IND 7381) was designed toevaluate myocardial angiogenesis induced by direct myocardialadministration of the AdGVVEGF121.10 vector to individualswith severe coronary artery disease undergoing CABG and car-diopulmonary bypass. The study individuals were assessed witha variety of cardiac-related parameters before and at various
CRYSTAL ET AL.66

times after vector administration (Rosengart et al., 1999a,b).The “cardiac, minimally invasive surgery (MIS), sole therapy,intramyocardial” trial (RAC # 9806-258; FDA BB-IND 7381)was similar to the “cardiac, adjunct to CABG” study, exceptthat it was carried out with a small thoracotomy or thora-coscopy, and administration of the AdGVVEGF121.10 vectorwas the only therapy (Rosengart et al., 1999a,b). The “periph-eral vascular disease (PVD), skeletal muscle” study (RAC #9804-243; FDA BB-IND 7630) was designed to assess lowerextremity angiogenesis in individuals with intermittent claudi-cation or limb-threatening ischemia after direct intramuscularadministration of the AdGVVEGF121.10 vector to the affectedlimb. The study individuals were evaluated with parameters re-lated to lower limb perfusion before and after vector adminis-tration. This study group included control individuals that re-ceived placebo. In addition to the groups described above, a“cardiac, CABG” control group, receiving routine CABG withcardiopulmonary bypass but no vector, was assessed for a num-ber of safety-related blood values after surgery.
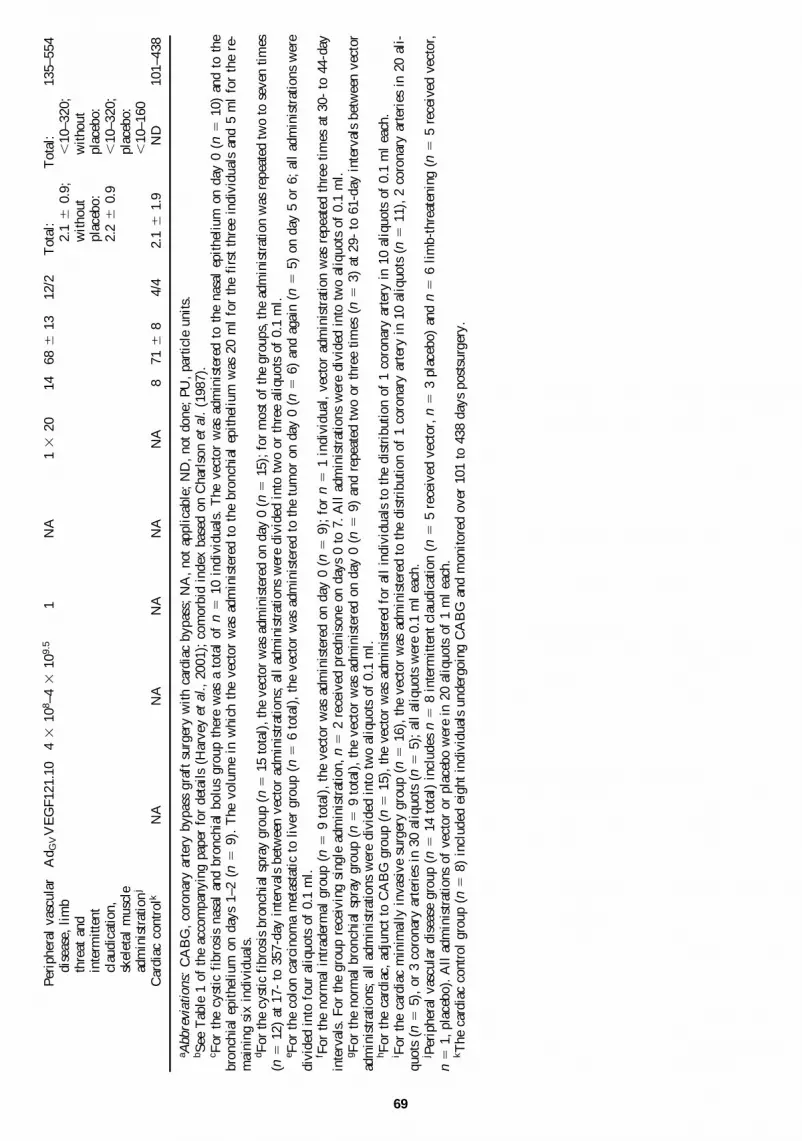
An overview of the parameters relating to the vector andstudy individuals can be found in Table 1. Further details re-garding each study and all participants can be found in the ac-companying paper (Harvey et al., 2002), previous publications(Crystal et al., 1994, 1997; Hay et al., 1995; Harvey et al.,1999a–c; Rosengart et al., 1999a,b), and copies of the proto-cols on file with the National Institutes of Health RecombinantDNA Advisory Committee, Suite 323, 6006 Executive Boule-vard, MSC 7052, Bethesda, MD 20892-7052).
Laboratory parameters
As described in the accompanying paper (Harvey et al.,2001), among the variety of safety parameters assessed in alltrials at baseline and at numerous time points after vector ad-ministration, we chose 14 variables relevant to laboratory ab-normalities observed in experimental animals receiving highdoses of Ad vectors (Simon et al., 1993; Brody et al., 1994;Cichon et al., 1999; Friedmann, 1999a; Lozier et al., 1999,Nunes et al., 1999), as well as parameters relevant to blood he-molysis and coagulation dysfunction observed in some experi-mental animals, and associated with the recent death of a genetherapy patient at the University of Pennsylvania (Batshaw etal., 1999). The 14 parameters are in five groups: (1) systemic(systolic blood pressure, temperature, white blood count[WBC]); (2) coagulation (prothrombin time [PT], partial throm-boplastin time [PTT], platelets, fibrinogen); (3) liver (alkalinephosphatase, aspartate aminotransferase [AST], alanine amino-transferase [ALT]); (4) hemolysis (indirect bilirubin, lactate de-hydrogenase [LDH], hemoglobin); and (5) renal (creatinine).Each of these parameters was assessed in three time periods af-ter vector administration (early [0–7 days], intermediate [8–30days], and late [.30 days]), with the maximum abnormal value(temperature, WBC, alkaline phosphatase, AST, ALT, PT, PTT,indirect bilirubin, LDH, creatinine) or minimum abnormal value(systolic blood pressure, platelets, fibrinogen, hemoglobin)recorded for each time period. To assess the frequency of ab-normal values for each parameter, the value postvector was plot-ted in relation to the value prevector; this was done for eachtime period. With the normal range superimposed on each plot,each parameter (for each time period) could be assessed for
high, normal, or low values postvector versus high, normal, orlow values prevector. From this assessment, the relevant fre-quency of abnormal values was determined, for example, forAST in the early time period, the percentages of all values thatwere in the low or normal range pretherapy that became highin the early period postvector were considered to be abnormal.
Deaths
Among the 90 individuals receiving Ad vectors, there were13 deaths in the total follow-up period of 130.4 patient-years(see Tables 1 and 8 and Fig. 1 in the accompanying paper byHarvey et al., 2002). In the control groups, there was 1 deathover the 12.9-patient-year follow-up period. For the purposesof analysis relevant to risk factors, the deaths were divided intothree time periods: (1) acute—death in hospital after vector ad-ministration; (2) postdischarge from the hospitalization inwhich the vector was administered to 1 year; and (3) .1 yearfrom the last administration of vector. For the one death in theCABG control group, the acute, postdischarge to 1 year, and.1-year periods relate to the time of surgery.
Adverse events
The adverse events (AEs) were modeled after the NationalCancer Institute (NCI) Common Toxicity Criteria (NCI,Bethesda, MD) as described in the accompanying paper (Har-vey et al., 2002). For each organ system (hematologic, coagu-lation, hepatic, renal, gastrointestinal, neurologic, systemic,cardiovascular, pulmonary, and “other” [e.g., dermatologic]),the AEs were recorded in the three time periods defined above(early, intermediate, and late), using a 1–4 scale: grade 1, min-imal; grade 2, moderate; grade 3, severe; grade 4, intolerable.For discussion purposes, grades 1 and 2 were considered “mi-nor AEs” and grades 3 and 4 “major AEs.” Overall, there were319 AEs observed in the 102 individuals in the study popula-tion (see Tables 2–6 in the accompanying paper by Harvey etal., 2002). Of these, 276 AEs were in the 90 individuals re-ceiving Ad vectors, and 43 were among the controls.
Analysis
For purposes of analysis, the putative “risk factors” for AEs,abnormal laboratory parameters, or death were grouped as (1)“patient related” (age, sex, comorbid index, and pretherapy anti-Ad neutralizing antibodies); (2) “vector related” (dose, route,transgene, and number of vector administrations); and (3) “trialrelated” (trial in which the individual was enrolled, and whetheror not surgery was part of the trial).
For the “patient-related” factors, the ages in the combinedstudies ranged from 16 to 88 years. There were 78% males and22% females. To provide a basis for assessing the risk of deathof individuals participating in the various gene transfer trials,each participant was assigned a comorbid index based on theclassification of Charlson et al. (1987). This classification wasoriginally developed to provide a prognostic taxonomy for co-morbid conditions that singly or in combination might alter therisk of short-term mortality for patients enrolled in longitudi-nal studies. Pretherapy anti-Ad neutralizing antibodies weremeasured in the serum just prior to vector administration (Har-
ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 67

TA
BL
E1.
In V
ivo
HU
MA
NG
EN
ET
RA
NS
FE
RST
UD
IES
US
ING
LO
CA
LA
DM
INIS
TR
AT
ION
OF
LO
W-
AN
DIN
TE
RM
ED
IAT
E-D
OS
EA
DE
NO
VIR
US
VE
CT
OR
Sa,
b
Vec
tors
Stud
y in
divi
dual
s
Inte
rval
(da
ys)
No.
of
betw
een
firs
tad
min
is-
and
last
Vol
ume
Com
orbi
dA
nti-
Ad
Day
sD
ose
rang
etr
atio
nsA
d ve
ctor
adm
inis
-A
geSe
xin
dex
tite
rfo
llow
-up
Stud
yG
roup
Vec
tor
(PU
)(r
ange
)ad
min
istr
atio
nte
red
(ml)
n(y
ears
)(M
/F)
(mea
n 6
SD)
(ran
ge)b
(ran
ge)
Cys
tic
Nas
al a
ndA
dCF
TR
4 3
106 –
1 3
1010
11–
20.
210
276
50
6/4
16
0,
10–2
083
–241
0fi
bros
isbr
onch
ial
bolu
sc(n
asal
)4
310
7 –4
310
101
20,
5(b
ronc
hial
)B
ronc
hial
spr
ayd
Ad G
VC
FT
R.1
02
310
7 –2
310
101–
717
–357
0.1
32,
1528
6 9
013
/21.
16
0.4
,10
–320
60–1
742
0.1
33
Col
onP
ercu
tane
ous
Ad G
VC
D.1
04
310
8 –4
310
91–
25–
60.
1 3
46
656
80
5/1
6.7
6 0
.8,
10–8
024
–109
1ca
rcin
oma
adm
inis
trat
ion
met
asta
tic
to t
umor
e
to l
iver
Nor
mal
Intr
ader
mal
fA
d GV
CD
.10
7 3
107 –
7 3
109
1–3
30–4
40.
1 3
209
326
90
8/1
06
0,
10–3
205–
951
Bro
nchi
al s
pray
gA
d GV
CD
.10
7 3
108 –
7 3
1010
1–3
29–6
10.
1 3
209
316
70
8/1
06
0,
10–1
6027
–497
Car
dio-
Car
diac
, ad
junc
tA
d GV
VE
GF1
21.1
04
310
8 –4
310
101
NA
0.1
310
1560
6 1
011
/42.
96
2.1
,10
–320
5–69
9va
scul
arto
CA
BG
,m
yoca
rdia
lad
min
istr
atio
nh
Car
diac
, m
inim
ally
Ad G
VV
EG
F121
.10
4 3
109 –
4 3
1010
1N
A0.
1 3
10–3
016
606
11
11/5
3.1
6 1
.4,
10–3
2032
–481
inva
sive
sur
gery
,so
le t
hera
py,
myo
card
ial
adm
inis
trat
ioni
68
Per
iphe
ral
vasc
ular
Ad G
VV
EG
F121
.10
4 3
108 –
4 3
109.
51
NA
1 3
2014
686
13
12/2
Tot
al:
Tot
al:
135–
554
dise
ase,
lim
b2.
16
0.9
;,
10–3
20;
thre
at a
ndw
itho
utw
itho
utin
term
itten
tpl
aceb
o:pl
aceb
o:cl
audi
catio
n,2.
26
0.9
,10
–320
;sk
elet
al m
uscl
epl
aceb
o:ad
min
istr
atio
nj
,10
–160
Car
diac
con
trol
kN
AN
AN
AN
AN
A8
716
80
4/4
2.1
6 1
.9N
D10
1–43
8
a Abb
revi
atio
ns:
CA
BG
, co
rona
ry a
rter
y by
pass
gra
ft s
urge
ry w
ith
card
iac
bypa
ss;
NA
, no
t ap
plic
able
; N
D,
not
done
; PU
, pa
rtic
le u
nits
.b S
ee T
able
1 o
f th
e ac
com
pany
ing
pape
r fo
r de
tail
s (H
arve
y et
al. ,
200
1);
com
orbi
d in
dex
base
d on
Cha
rlso
n et
al.
(198
7).
c For
the
cys
tic
fibr
osis
nas
al a
nd b
ronc
hial
bol
us g
roup
the
re w
as a
tot
al o
f n
510
ind
ivid
uals
. T
he v
ecto
r w
as a
dmin
iste
red
to t
he n
asal
epi
thel
ium
on
day
0 (n
510
) an
d to
the
bron
chia
l ep
ithe
lium
on
days
1–2
(n
59)
. T
he v
olum
e in
whi
ch t
he v
ecto
r w
as a
dmin
iste
red
to t
he b
ronc
hial
epi
thel
ium
was
20
ml
for
the
firs
t th
ree
indi
vidu
als
and
5 m
l fo
r th
e re
-m
aini
ng s
ix i
ndiv
idua
ls.
d For
the
cys
tic
fibr
osis
bro
nchi
al s
pray
gro
up (
n5
15 t
otal
), t
he v
ecto
r w
as a
dmin
iste
red
on d
ay 0
(n
515
); f
or m
ost
of t
he g
roup
s, t
he a
dmin
istr
atio
n w
as r
epea
ted
two
to s
even
tim
es(n
512
) at
17-
to
357-
day
inte
rval
s be
twee
n ve
ctor
adm
inis
trat
ions
; al
l ad
min
istr
atio
ns w
ere
divi
ded
into
tw
o or
thr
ee a
liqu
ots
of 0
.1 m
l.e F
or t
he c
olon
car
cino
ma
met
asta
tic
to l
iver
gro
up (
n5
6 to
tal)
, th
e ve
ctor
was
adm
inis
tere
d to
the
tum
or o
n da
y 0
(n5
6) a
nd a
gain
(n
55)
on
day
5 or
6;
all
adm
inis
trat
ions
wer
edi
vide
d in
to f
our
aliq
uots
of
0.1
ml.
f For
the
nor
mal
int
rade
rmal
gro
up (
n5
9 to
tal)
, th
e ve
ctor
was
adm
inis
tere
d on
day
0 (
n5
9);
for
n5
1 in
divi
dual
, ve
ctor
adm
inis
trat
ion
was
rep
eate
d th
ree
tim
es a
t 30
- to
44-
day
inte
rval
s. F
or t
he g
roup
rec
eivi
ng s
ingl
e ad
min
istr
atio
n, n
52
rece
ived
pre
dnis
one
on d
ays
0 to
7.
All
adm
inis
trat
ions
wer
e di
vide
d in
to t
wo
aliq
uots
of
0.1
ml.
g For
the
nor
mal
bro
nchi
al s
pray
gro
up (
n5
9 to
tal)
, th
e ve
ctor
was
adm
inis
tere
d on
day
0 (
n5
9) a
nd r
epea
ted
two
or t
hree
tim
es (
n5
3) a
t 29
- to
61-
day
inte
rval
s be
twee
n ve
ctor
adm
inis
trat
ions
; al
l ad
min
istr
atio
ns w
ere
divi
ded
into
tw
o al
iquo
ts o
f 0.
1 m
l.h F
or t
he c
ardi
ac,
adju
nct
to C
AB
G g
roup
(n
515
), t
he v
ecto
r w
as a
dmin
iste
red
for
all
indi
vidu
als
to t
he d
istr
ibut
ion
of 1
cor
onar
y ar
tery
in
10 a
liqu
ots
of 0
.1 m
l ea
ch.
i For
the
car
diac
min
imal
ly i
nvas
ive
surg
ery
grou
p (n
516
), t
he v
ecto
r w
as a
dmin
iste
red
to t
he d
istr
ibut
ion
of 1
cor
onar
y ar
tery
in
10 a
liqu
ots
(n5
11),
2 c
oron
ary
arte
ries
in
20 a
li-
quot
s (n
55)
, or
3 c
oron
ary
arte
ries
in
30 a
liqu
ots
(n5
5);
all
aliq
uots
wer
e 0.
1 m
l ea
ch.
j Per
iphe
ral
vasc
ular
dis
ease
gro
up (
n5
14 t
otal
) in
clud
es n
58
inte
rmit
tent
cla
udic
atio
n (n
55
rece
ived
vec
tor,
n5
3 pl
aceb
o) a
nd n
56
lim
b-th
reat
enin
g (n
55
rece
ived
vec
tor,
n5
1, p
lace
bo).
All
adm
inis
trat
ions
of
vect
or o
r pl
aceb
o w
ere
in 2
0 al
iquo
ts o
f 1
ml
each
.k T
he c
ardi
ac c
ontr
ol g
roup
(n
58)
inc
lude
d ei
ght
indi
vidu
als
unde
rgoi
ng C
AB
G a
nd m
onit
ored
ove
r 10
1 to
438
day
s po
stsu
rger
y.
69

vey et al., 1999b). For those individuals receiving more thanone administration of an Ad vector, the serum anti-Ad neutral-izing antibody titers were reevaluated prior to each vector ad-ministration and considered as an independent value. Anti-Adneutralizing antibody titers ranged from undetectable (,10) to320 titer units.
The doses of Ad vectors ranged from 4 3 106 to 7 3 1010
PU. Five routes were assessed as risk factors: respiratory ep-ithelium, percutaneous to solid tumors, intradermal, epicardialadministration to the myocardium, and skeletal muscle. In thecystic fibrosis bolus study, the vector was administered to twosites in the respiratory tract, the nasal epithelium and thebronchial epithelium. Since no AEs observed were localized tothe nasal epithelium, it was excluded from further analysis, butparameters relevant to other organ systems were assessed forpossible abnormalities after nasal administration. Three trans-genes were examined: CFTR, CD, and VEGF121. For the num-ber of vector administrations, the various parameters weregrouped as single administration, two administrations, and threeor more administrations.
For the trial design-related assessment, each trial was con-sidered separately, including the trials requiring no surgery con-comitantly with the administration of vector (normal skin, CFbolus, CF spray, normal bronchial spray, PVD, and PVD con-trol) and the trials requiring surgery (colon cancer, cardiac ad-junct to CABG, cardiac MIS sole therapy, and cardiac control).The individuals in the colon cancer trial underwent hepatic re-section on days 3 to 10 after the last (second) administration ofvector; for analysis purposes the 0–7 days after the second vec-tor was considered to be an “early” period postvector.
For purposes of discussion of the data, the term “adverseevents” is used to refer to any AEs independent of severity scale(see Tables 2–6 in the accompanying paper by Harvey et al.,2001), “abnormal laboratory parameter” is used to refer to theparameters falling into the two sectors (of the nine sector lab-oratory value versus pretherapy value plots) described above(see Results). The term “deaths” refers to death occurring atany time period unless otherwise specified. Finally, the term“major adverse event” refers to grade 3–4 on the toxicity scale,and includes deaths (graded as 4) and nondeaths (graded as 3or 4). For the purposes of analysis, for those individuals whodied, if there were grade 3 or 4 AEs for a given individual inthe same time period (early, intermediate, or late) as the indi-vidual’s death, then it was considered as a single, serious AE,and considered as a “death.” Major adverse events not associ-ated with a death in the same time period were considered asa single major adverse event if they were clearly linked to asingle grade 3–4 event (e.g., congestive heart failure, arrhyth-mia, and renal failure all linked to a myocardial infarction).
Single-parameter assessment. The adverse events were eval-uated for each risk factor in three categories: (1) frequency ofAEs per number of administrations of vector; (2) average sever-ity of AE; and (3) type of AE. The abnormal laboratory pa-rameters were assessed for each risk factor in two categories:(1) frequency of abnormal laboratory parameters per number ofadministrations of vector; and (2) type of abnormal laboratoryparameters. The deaths at the different time periods followingvector administration were assessed for each risk factor. In ad-dition, the actual 1-year mortality was compared with the 1-
year mortality predicted by the comorbid index (Charlson et al.,1987).
Multivariate analysis. To further analyze all major adverseevents (the 13 deaths in the vector trials plus the 1 death amongthe controls, as well as other major adverse events not associ-ated with death [severity scale 3 or 4]; see Tables 2–6 and 8 inthe accompanying article by Harvey et al., 2001), multivariateanalysis was performed to identify variables independently as-sociated with a major adverse event. Variables analyzed in-cluded age, sex, comorbid index, pretherapy anti-Ad neutraliz-ing titer, vector dose (highest dose administered to theindividual), route of administration, type of vector, type of trial,and the presence or absence of surgical treatment. The multi-variate analysis was carried out separately for deaths and ma-jor adverse events not associated with death.
In regard to multivariate analysis of death, there were 13known deaths occurring in the study population receiving Advectors over a 130.4-patient-year follow-up period and 1 deathamong the control groups over a 12.9-patient-year follow-upperiod. In the accompanying paper (Harvey et al., 2002), thesedeaths were assessed individually regarding links to the Ad vec-tor per se (none [0 of 13] were judged as possibly linked) or tothe procedure used to administer the Ad vector (1 of 13 werejudged as possibly linked). In the present study, the 13 deathsin the vector trials and 1 death among the controls were furtheranalyzed using the proportional-hazards model to identify vari-ables independently associated with the likelihood of death af-ter controlling for all 10 baseline risk factors (Rosner, 1995b).All 10 potential risk factors were included in the proportional-hazards model and significance values were computed for eachvariable. The model was then refined by excluding those vari-ables without any explanatory power in the model (as indicatedby a high p value). In regard to multivariate analysis for majorAEs other than death, logistic regression analysis was used(Ross, 1976; Rosner, 1995b). The risk factors evaluated, andthe analysis methodology, were similar to those described formultivariate analysis of death.
Other statistical analysis
All data are presented as means 6 standard deviation. Othercomparisons are specifically indicated in the text. All analyseswere performed with the SPSS statistical program (SPSS,Chicago, IL).
RESULTS
The 8 trials included 90 individuals receiving 140 adminis-trations of Ad vectors expressing 3 different transgenes to 6 dif-ferent sites (Table 1). In the accompanying paper (Harvey etal., 2002), the adverse events, laboratory parameters, and deathsare assessed in the context of each of the eight trials. With thatapproach to the data, we concluded that there was a low risk(incidence of 0.7%) for a major adverse event after local ad-ministration of low and intermediate doses of an Ad vector thatwas attributable to the Ad vector per se. In the present study,the total data set is evaluated to determine whether there arerisk factors that might predict the safety of local administration
CRYSTAL ET AL.70

of low and intermediate doses of Ad vectors to individuals witha broad spectrum of comorbid conditions.
Characteristics of the study population
To put the relationships among risk factors, adverse events,and abnormal laboratory parameters in context, it is useful firstto assess the distribution of these parameters among the studypopulation (Figs. 1–4).
Distribution of risk factors. The average age of the overallpopulation receiving Ad vector was 47 6 20 years. The studyparticipants receiving vector were in two general groups: ayounger group including those with cystic fibrosis and normalindividuals (mean ages of 27 and 32 years, respectively) andan older group including those with colon cancer, coronaryartery disease, and peripheral vascular disease (mean ages,60–70 years; Fig. 1A). On average, those with PVD were theoldest (mean age, 70 years) and those in the CF bolus groupthe youngest (mean age, 27 years). For individuals receivingvectors, males dominated, from 60% in the CF bolus group to89% in the normal individual groups (Fig. 1B). For the 90 in-dividuals receiving Ad vectors, there were 78% males and 22%females.
As a group, the total population receiving Ad vectors had anaverage comorbid index of 2.0 6 2.0, with a range from 0 (nor-mals) to 8 (colon cancer metastatic to liver). Unlike the othertrials that had a narrow range of comorbid indices among theparticipants, the individuals with cardiovascular disease (car-diac adjunct to CABG, MIS with sole therapy, PVD) had co-morbid indices with a broad range, from 0 to 6, with an aver-age of 2.8 (Fig. 1C). The pretherapy anti-Ad neutralizingantibodies among individuals receiving Ad vectors includedtiters from undetectable (,10) to 320 (Fig. 1D). The range ofpretherapy titers was indistinguishable among the groups.
The doses of Ad vectors administered ranged from 4 3 106
to 7 3 1010 PU. Most groups received doses in the low and in-termediate ranges, with the individuals with cardiac diseasetending to receive amounts of vector mostly in the intermedi-ate dose category (Fig. 1E). On the basis of the trial design, in-dividuals in the CF bolus study and in all of the cardiovascu-lar trials received a single administration of vector (CF bolusreceived administration to two sites, nasal and bronchial, 1–2days apart; for analysis purposes, this was considered one timepoint), whereas those in the CF spray, colon cancer, normalskin, and normal bronchi trials received from one to seven ad-ministrations of vector, with an average of 1.2 vector adminis-trations per individual (in the normal skin trial) to 2.9 admin-istrations per individual (in the CF spray trial; Fig. 1F).Approximately one-half (55%) of all vector administrationswere directed toward the respiratory epithelium (n 5 34 indi-viduals received vectors via the respiratory epithelial route, andmost of the repetitive administrations of vectors were via thatroute; Fig. 1G). The myocardium was the next most frequentsite of vector administration (22%, representing 31 individualsreceiving single administration of vector), followed by tumor,skin, and skeletal muscle administration (each 7–8% of all vec-tor administrations). Among the three transgenes used, theCFTR cDNA was used most commonly (45% of all vector ad-
ministrations), followed by the VEGF121 cDNA (29%) and theCD gene (26%; Fig. 1H).
The relative proportion of all study individuals within eachtrial was similar among the trials, with the lowest in the coloncancer trial (6%, the trial with the smallest number of study in-dividuals) to 18% (the cardiac MIS, sole therapy trial; Fig. 1I).A large number (44%) of the total study population had a ma-jor surgical procedure (CABG with cardiopulmonary bypass orthoracotomy/thoracoscopy in the cardiac trials, or hepatic re-section in the colon cancer trial), while 56% had no surgery(CF, normal, and PVD trials; Fig. 1J). Among the no-surgerygroups, there were some invasive procedures used to adminis-ter the vectors, from bronchoscopy (CF trials, normal bronchialtrial), multiple percutaneous injections into skeletal muscle(PVD trial), or least invasive, by intradermal administration(normal skin trial). Bronchoscopy was also used to collect bi-ologic samples in the CF and normal individual trials.
Distribution of adverse events. Among the 319 adverseevents (276 in individuals receiving vectors, 43 in controls),52% were in the early time period (0–7 days), 20% were in theintermediate period (8–30 days), and 28% were in the late pe-riod (.30 days) after vector administration. The most commontype of AE (normalized to the number of vector administra-tions) was cardiovascular or systemic. Pulmonary, hematologic,gastrointestinal, hepatic, and renal were next, with coagulation,neurologic, and a mixed group of “other” the least common(Fig. 2A). The average severity of AE was similar among thecategories (Fig. 2B). The average severity was highest in thecardiovascular (average severity of 2.4 on a 1-to-4 scale) andrenal (2.3) categories, and lowest in the “other” (1.3) and hema-tologic (1.3) categories, with all other categories in the 1.5 to2.0 range (Fig. 2B).
Distribution of abnormal laboratory parameters. Of the.40,000 individual laboratory parameters measured in thestudy population before and after administration of Ad vectors,.20,000 were assessed in the accompanying (Harvey et al.,2002) and present papers, representing 14 specific parametersrelevant to putative risks of administering Ad vectors. As de-scribed in Materials and Methods, the highest (or lowest, de-pending on variable) value in the early (0–7 days), intermedi-ate (8–30 days), or late (.30 days) time periods was assessedin the context of pretherapy values for that parameter. For ex-ample, among the systemic laboratory parameters, WBCs pro-vided an assessment of inflammation, a parameter relevant tothe host responses observed in experimental animals after ad-ministration of high doses of Ad vectors (Simon et al., 1993;Brody et al., 1994; Cichon et al., 1999; Friedmann, 1999a;Lozier et al., 1999; Nunes et al., 1999). In the early period,31% of WBC measurements were abnormal (e.g., high whenthe pretherapy values were in the low or normal range; Fig.3A). However, by the intermediate period after vector admin-istration, the proportion of abnormal WBC values was down to8% (Fig. 3B), and by the late period, it was 6% (Fig. 3C). Inthe early period, the abnormal WBCs were dominated by theindividuals undergoing surgery (54% of the early abnormal val-ues) or bronchoscopy (41% of the early abnormal values).
Other examples of abnormal laboratory parameters that arerelevant to the course of the individual who died at the Uni-
ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 71

versity of Pennsylvania include parameters relevant to hemoly-sis (indirect bilirubin), coagulation (platelets, fibrinogen), andliver function (ALT) (Fig. 3D–L). In the early period, only 12%of the indirect bilirubin values were abnormally high (almostentirely in the colon cancer/hepatic resection group), and thiswas even lower (4%) in the intermediate period (Fig. 3D andE), that is, hemolysis appeared to be uncommon after local ad-ministration of low and intermediate doses of Ad vectors. Inregard to abnormal coagulation parameters relevant to earlysigns of disseminated intravascular coagulation, 19% of plateletvalues were abnormally low in the early period, but this wasalmost entirely an acute response in individuals undergoing sur-gery. By the intermediate time period, only 1% of platelet val-ues were abnormally low (Fig. 3F and G). Fibrinogen levelswere rarely abnormally low in the early or intermediate peri-ods (2 and 1% respectively; Fig. 3H and I). As an example, rel-evant to liver function, the ALT values were abnormally highin 13% of values in the early period, representing almost en-tirely the individuals undergoing hepatic resection (Fig. 3J). Bythe intermediate and late time periods, this was reduced to 6and 7%, respectively (Fig. 3K and L).
For all studies combined, the most common abnormal labo-ratory parameters were a low hemoglobin (13.7% of all abnor-mal laboratory parameters within each group of parameters) andelevated WBC (12.8%), both occurring mostly in associationwith surgery (Fig. 4). Next most common were reduced levelsof platelets (7.2%), and elevated PTT (5.5%), indirect bilirubin(4.9%), ALT (4.8%), AP (4.3%), and temperature (3.8%). Rel-atively infrequent were increased levels of LDH (2.9%), PT(2.2%), AST (1.6%), and creatinine (0.7%), and decreased lev-els of systolic blood pressure (1.9%) or fibrinogen (0.8%). Ex-cept for the uncommon examples of renal dysfunction distrib-uted throughout the early, intermediate, and late time periods,the majority of all other abnormal laboratory tests occurred inthe early period after vector administration, ranging from 35%(alkaline phosphatase) to 100% (fibrinogen).
Single-variable assessment of risk factors for adverseevents and abnormal laboratory parameters
For all 90 individuals receiving a total number of 140 Advector administrations in the gene transfer trials, there was an
average frequency of 2.0 adverse events per administration ofvector (see Table 2 in Harvey et al., 2002). Approximately one-half (51%) were in the early period after vector administration,with 19% in the intermediate period and 30% in the late pe-riod. Overall, these AEs had an average severity of 1.9, with amean severity of 1.6 in the early period, 2.0 in the intermedi-ate period, and 2.3 in the late period (including the severity rankof 4 for each of the 13 deaths occurring 5 to 1788 days aftervector administration).
Parameters related to the study individuals as risk factors.Other than data relating to variability among murine strains,there are few data in the experimental animal literature relatingto the potential toxicity of Ad vectors relevant to age and sex,inherited or experimentally induced comorbid conditions, orprevious immunization against Ad (Simon et al., 1993; Brodyet al., 1994; Yang et al., 1995a,b; Wilmott, 1996; Cichon et al.,1999; Friedmann, 1999a; Lozier et al., 1999; Nunes et al.,1999). In this context, it is of interest to assess these risk fac-tors related to the individuals in the study population, includ-ing age, sex, comorbid index, and pretherapy anti-Ad neutral-izing antibody titer (Figs. 5–8). With the important caveat thatseveral of these risk factors overlap (e.g., the cancer and car-diovascular groups include older populations and the samegroups have the highest comorbid indices), individual assess-ment of these putative risk factors leads to interesting observa-tions.
The frequency of AEs per vector administration appeared toincrease with increasing age, with an average of 5.4 AEs in the$70-year group compared with 0.3 AE in the 20- to 29-yeargroup (Fig. 5A). For almost all age groups, the majority of AEswere in the early time period. Interestingly, despite the trendtoward increased frequency of AEs with age, the average sever-ity of AEs was no different, ranging from 1.4 (1 to 4 scale) to2.0 (Fig. 5B). Among the specific types of AE, systemic, car-diovascular, pulmonary, gastrointestinal (GI), hepatic, andhematologic AEs were most prevalent (Fig. 5C). There were noobvious relationships among the specific type of AE and age,except for the ,30-year age groups having fewer cardiovascu-lar AEs (as might be expected from the individuals with car-diovascular disease being in the older age groups). The fre-
CRYSTAL ET AL.72
FIG. 1. Distribution of risk factors among the study populations. (A) Age of individuals in the different trials; the number aboveeach column represents the mean 6 SD. (B) Sex (percent males) of individuals in the different trials; the number above each col-umn represents the mean percentage for each group; the dashed line indicates equal distribution among sexes. (C) Comorbid in-dices among individuals in the different trials. (D) Pretherapy anti-Ad neutralizing antibodies in the different trials. (E) Dose ofAd vectors administered in the different trials. The doses below the lower horizontal dashed line represent “low” doses; thosebetween the two dashed lines represent “intermediate” doses. For (C–E), each symbol represents a different individual. For (D):For those with .1 vector administration, the highest anti-Ad titer for each individual is shown. For (E) only: (s � ) CF, bolus trial,dose to nasal epithelium; ( s ) CF, bolus trial, dose to bronchial epithelium. For (C–E): A plus (1) next to symbols indicatesdeaths; #, malignancy. For (D): ND, not done. (F) Relative number of vector administrations among the different trials as a per-centage of all vector administrations (n 5 140 total). The numbers above the columns represent the percentage of all vector ad-ministrations in all trials represented by that specific trial, and the numbers within the columns represent the average number ofvectors administered per individual for that trial. (G) Route of administration of Ad vectors used in the various trials. (H) Rela-tive proportion of different transgenes in the expression cassette of Ad vectors used in the various trials. (I) Relative proportionof individuals receiving Ad vectors participating in each trial. For (G–I): Numbers above each column represents the mean per-cent for each group. (J) Relative proportion of study individuals who underwent major surgery as part of the study. The surgeryincluded hepatic resection (colon cancer trial), median sternotomy with cardiopulmonary bypass (cardiac adjunct group), or smallthoracotomy or thoracoscopy (cardiac minimally invasive surgery, sole therapy group).

ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 73

CRYSTAL ET AL.74
FIG. 1. Continued.

quency of abnormal laboratory parameters seemed to be muchhigher in age groups $50 years, in contrast to the apparentlymore gradual age-dependent increasing frequency of abnormallaboratory parameters for adverse events (compare Fig. 5A andD). Most abnormal laboratory parameters at all age groups wereobserved in the early time periods. Assessment of the types ofabnormal laboratory parameters suggested no striking differ-ences with age (Fig. 5E).
Interestingly, although all trials enrolled predominantlymales (Fig. 1B) and the total number of AEs were much greaterin males (Fig. 6C), the frequency of AEs per vector adminis-tration appeared to be higher in females (males, 1.9; females,2.4; Fig. 6A). Among the AEs in females, most (77%) were inthe early period compared with males, in whom the AEs weremore evenly distributed in time. However, the severity of AEswas no different among the sexes (Fig. 6B), nor were the typesof AE, with systemic and cardiovascular AEs dominating inboth groups (Fig. 6C). There were many more total number of
abnormal laboratory values observed in males (Fig. 6E), and aslightly higher frequency of abnormal laboratory parameters pervector administration among females (Fig. 6D). In females, ab-normal hemolysis parameters dominated, with systemic and co-agulation laboratory parameters also frequently abnormal. Aroughly similar pattern was observed in males. Renal functionabnormalities were uncommon in both sexes.
The comorbid index, a parameter developed empirically byCharlson et al. (1987) to help predict the mortality of individ-uals admitted to hospitals, appeared to roughly predict the fre-quency of AEs per vector administration, with comorbid indicesof 3–4 associated with 5.5 AEs per administration and indices$5 associated with 3.8 AEs per administration (Fig. 7A). Incontrast, comorbid indices of 0 and 1–2 were associated withfar fewer AEs (frequency per administration of 1.0 and 1.2, re-spectively). The comorbid index did not appear to be linked tothe severity of AEs (Fig. 7B), or to the specific type of AE (Fig.7C). Like the frequency of AEs, the higher comorbid indices
ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 75
FIG. 1. Continued.

CRYSTAL ET AL.76
FIG. 2. Relationships among frequency and severity of specific categories of adverse events among the entire study popula-tion receiving Ad vectors. (A) Mean frequency of specific types of AE (AEs per administration of an Ad vector). The numbersabove the columns represent the mean for each group. (B) Mean severity of specific types of AE. The numbers above the columnsrepresent the mean for each group; the error estimates represent the mean 6 SD. For both panels, the sections within each col-umn represent the proportion (percent; shown as a number within each section) of AEs that occurred in the early (hatched sec-tion), intermediate (open section), or late (solid section) time periods within each category. The height of each section should notbe read off the ordinate. Abbreviations: heme, hematologic; coag, coagulation; GI, gastrointestinal; neuro, neurological; CV, car-diovascular; pulm, pulmonary.

appeared to be associated with a higher frequency of laboratoryabnormalities per vector administration (Fig. 7D), but not withthe type of laboratory abnormality (Fig. 7E).
Unlike age, sex, and comorbid index, pretherapy anti-Adneutralizing antibody titer did not appear to be associated withany aspect of AE or abnormal laboratory parameter. This in-cluded frequency, severity or type of AE per vector adminis-tration, and frequency or type of abnormal laboratory parame-ter per vector administration (Fig. 8A–E).
Relevant to the observations regarding study individual-re-lated risk factors in the individuals receiving Ad vectors, withthe caution that the PVD and CABG “control” groups are lim-ited in number, it is of interest to assess the patient-related riskfactors relevant to adverse events and abnormal laboratory pa-rameters in these control individuals. This was not possible inthose categories where the data were normalized to vector ad-ministration (i.e., frequency of AEs and abnormal laboratoryparameters [panels A and D, respectively, in Figs. 5–8]), butwas possible for severity of adverse events, types of adverseevents, and types of abnormal laboratory parameters (panels B,C, and E in Figs. 5–8). In regard to age for the two controlgroups, AEs were observed only in individuals .50 years. Theaverage severity of AEs ranged from 1.6 to 2.1, similar to thatin those individuals receiving vector (Fig. 5A). The type of AEsin the controls showed no obvious trends with age, nor did thetypes of abnormal laboratory parameters (not shown). With re-gard to sex, the severity of AEs in the control groups (1.7, males;2.4, females) was in the same range as for those receiving vec-tor (Fig. 6B). There were no major differences among controlsand those receiving vector regarding the types of AE or ab-normal laboratory parameters (not shown). In reference to co-morbid index, the control groups had a gradual increase inseverity of AEs with increasing index value (severity 1.8 forindices 1–2, 1.9 for indices 3–4, and 2.5 for indices $5), incontrast to those receiving vector, where there were no differ-ences in AE severity with the different indices (Fig. 7B). Likethe other patient-related parameters, the control groups had nomarked differences in types of AE or abnormal laboratory pa-rameters with increasing comorbid indices (not shown). In re-gard to anti-Ad titer, insufficient data were available in the con-trol groups to assess this parameter.
Parameters related to the Ad vectors as risk factors. It hasbeen well documented that high doses (.1011 PU total dose)of Ad vectors induce a variety of adverse events and abnormallaboratory parameters in experimental animals, although the fre-quency, severity, and type of abnormalities are dependent on amultitude of factors, including species, strain, transgene in theexpression cassette, and route of vector administration (Simonet al., 1993; Brody et al., 1994, Cichon et al., 1999; Friedmann,1999a; Lozier et al., 1999; Nunes et al., 1999). In the contextof these observations with high doses of Ad vectors in experi-mental animals, it is of interest to examine whether the risk fac-tors associated with the vectors appear to correlate with the de-velopment of AEs or abnormal laboratory parameters inindividuals receiving local administration of low and interme-diate doses of Ad vectors (Figs. 9–11).
For purposes of analysis, the doses were grouped as 107, 108,109, and 1010 PU, with a given “dose” representing all doseswithin that log range, for example, 108 PU represents doses
from 108 to ,109 PU. There were limited numbers of doses inthe 107-PU range (Fig. 1E), so only three dose ranges were con-sidered as risk factors: 108, 109, and 1010 PU. The frequencyof AEs per vector administration appeared to be higher (3.1AEs per vector administration) at the 1010-PU dose comparedwith 109-PU (1.8 AEs per administration) and 108-PU (2.0 AEsper administration) doses (Fig. 9A). For the highest (1010-PU)dose group, more AEs were in the intermediate time period(54%), whereas at the 108- and 109-PU doses, the timing of theAEs was more spread out. Despite this increase in frequencyof AEs at the 1010-PU dose range, there was no apparent asso-ciation of increased severity of AEs with increasing dose, al-though there appeared to be relatively more intermediate AEsat the highest dose (Fig. 9B). There was no clear specificity inthe type of AE experienced with increasing dose (Fig. 9C).There was a moderate increase in the frequency of abnormallaboratory values as the dose increased (Fig. 9D). Interestingly,although there were no AEs in the 107-PU dose range, therewere abnormal laboratory values with the 107-PU dose (1.6 AEsper administration), increasing to 2.0 at 108 PU, 2.1 at 109 PU,and 2.5 at 1010 PU. The majority (60–69%) of abnormal labo-ratory values were observed in the early period at all doses.Like the lack of apparent association of dose dependency tospecific types of AE, there was no apparent dose dependencywith the categories of abnormal laboratory values (Fig. 9E).
Two routes of vector administration were rarely associatedwith AEs (skin, 0 AE per administration; bronchi, 0.4 AE peradministration), one route had an intermediate frequency of AEs(tumor, 2.4 AEs per administration), and two routes had a highfrequency of AE (myocardium, 5.2 AEs per administration;skeletal muscle, 6.1 AEs per administration; Fig. 10A). Inter-estingly, most AEs following myocardial administration wereearly (57%), while for skeletal muscle, most AEs occurred inthe late time period after vector administration (64%; Fig. 10A).Severity of AEs showed no trend relating to route of vector ad-ministration (Fig. 10B). The distribution of types of AE wassimilar for administration to the myocardium and skeletal mus-cle, with the highest proportion associated with cardiovascularAEs (29 and 38%, respectively), likely reflecting the underly-ing cardiovascular disease. In contrast, for the bronchi and tu-mor routes, systemic AEs were the most common (45 and 31%,respectively; Fig. 10C). As with the AEs, the frequency of lab-oratory abnormalities was lowest in the skin and bronchi groups.The highest frequency of abnormal laboratory findings was inthe colon cancer group (6.3 per administration), with the myo-cardial route next most frequent (4.5 per administration), fol-lowed by the skeletal muscle group (2.0 per administration; Fig.10D). Most abnormal laboratory values linked to specific routeswere in the early time periods. The distribution of specific typesof laboratory abnormalities was broadly similar among the dif-ferent routes of vector administration, except for administrationto the skin, where the relatively few abnormal values were as-sociated only with coagulation or systemic parameters. Liverfunction test abnormalities were relatively common in the coloncancer group, as expected given that these individuals under-went hepatic resection (Fig. 10E).
When the transgene in the expression cassette was assessedas a single variable, the VEGF transgene was the most fre-quently associated with AEs per administration (5.4 AEs peradministration compared with only 0.8 for the CD transgene
ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 77

and 0.4 for the CFTR transgene [Fig. 11A]). All transgenestended to have AEs more frequently in the early period. Therewere no differences in the severity of AE associated with dif-ferent transgenes (Fig. 11B). Consistent with the use of VEGFtransgene being associated with the highest frequency of AEsper administration, the most common type of AE associatedwith the VEGF transgene was cardiovascular (32%; Fig. 11C).In contrast, systemic AEs dominated the use of the CFTR (40%of all AEs) and CD (37%) transgenes, with cardiovascular AEsuncommon (,10%) in association with the use of either trans-gene. Like the frequency of AEs, the frequency of abnormallaboratory parameters was more common with the VEGF trans-gene (3.8 abnormal laboratory parameters per administration),but the differences with the other transgenes were not as greatas the differences among the AEs (CD, 2.3 abnormal labora-tory parameters per administration; CFTR, 0.9; Fig. 11D). Thetypes of abnormal laboratory parameters were similar for thedifferent transgenes (Fig. 11E).
There was an impressive inverse relationship in the fre-quency of AEs per administration with the number of admin-istrations of Ad vectors (Fig. 12A). The majority of the AEs inall groups were early. The severity of AEs was no different withone, two, or three or more vector administrations (Fig. 12B),and the types of AE were roughly similar, although the pro-portions of systemic AEs were almost twofold higher with twoadministrations compared with one administration (the numbersof AEs was so low at three or more vector administrations thatit was difficult to assess; Fig. 12C). Like the frequency of AEs,the frequency of abnormal laboratory parameters also decreasedwith increased number of administrations of vector (Fig. 12D).The distribution among the types of laboratory abnormalitiesshowed no clear pattern with increasing numbers of adminis-trations (Fig. 12E).
Parameters related to trial design as risk factors. The eighttrials described in this study included procedures to the studyindividual that ranged from almost innocuous (e.g., intradermalin the normal skin trial), to the more invasive, involving seda-tion but not surgery (e.g., fiberoptic bronchoscopy in both theCF trials and the normal individual trials, or multiple intra-muscular administrations in the PVD trial), to those involvingvarious degrees of major surgery (e.g., CABG with cardiopul-monary bypass in the cardiac adjunct trial, thoracotomy/thora-coscopy in the MIS sole therapy cardiac trial, or hepatic resec-
tion in the colon cancer trial). Therefore, it is not surprising thatthere appeared to be an association of adverse events and ab-normal laboratory parameters with trial design.
There was a markedly higher frequency of AEs per vectoradministration in the cardiac adjunct to CABG (6.1 AEs per ad-ministration), cardiac MIS (4.2), and cancer trials (2.4) com-pared with the normal skin (0), CF bolus (0.7), CF spray (0.2),and normal bronchi (0.3) trials (Fig. 13A). In the context thatthe PVD trial did not involve major surgery, it was a surprisethat there was such a high frequency of AEs per administrationin this trial (6.1). Comparison of the timing of AEs among thedifferent trials with a high frequency of AEs demonstrated thatthe PVD trial had a much higher frequency in the late period(64%, with only 30% in the early period), compared with theother trials with a high frequency of AEs per administration(cardiac adjunct to CABG, 59% early, 18% late; cardiac MIS,54% early, 28% late; and colon cancer, 54% early, 19% late).Despite the obvious differences among the trials in terms of fre-quency of AEs per vector administration, the average severityof AE was similar among the trials (except for the normal skintrial, for which there were no AEs; Fig. 13B). The type of AEvaried considerably among the various trials, dominated mostlyby systemic and cardiovascular AEs, appearing to vary with theprimary disorder, for example, the cardiovascular trials had ahigher frequency of cardiovascular AEs, and the CF and nor-mal trials had few cardiovascular AEs (Fig. 13C). The fre-quency of abnormal laboratory values also showed noticeabledifferences among the trials (Fig. 13D). However, while thecardiac adjunct (5.6 per vector administration) MIS (3.4), andcolon cancer (6.3) trials showed a high frequency of abnormallaboratory parameters per vector administration, the PVD trialhad far fewer abnormal laboratory parameters per vector ad-ministration (2.0) than might be expected for a trial with highAEs per administration (Fig. 13D). Further, whereas the AEs as-sociated with PVD were dominated by late-period AEs, the ab-normal laboratory parameters associated with PVD were morecommon in the early time period, as were the abnormal labora-tory parameters associated with the cardiac and cancer trials.Like the AEs, there was no specific pattern of types of abnor-mal laboratory parameters associated with the different trials.
Aside from the striking increased frequency of AEs associ-ated with the PVD trial, the trials with the highest frequency ofAEs were those involving surgery (Fig. 13A). In that context,considering “surgery” versus “no surgery” as a risk factor, there
CRYSTAL ET AL.78
FIG. 3. Examples of assessment of laboratory parameters at various time periods after Ad vector administration related to thepretherapy baseline values for each individual. For each time period (early, 0–7 days after vector administration; intermediate,8–30 days; late, .30 days), a single value represents the maximum or minimum value for each time period (maximum valuesfor white blood cell [WBC], indirect bilirubin, alanine aminotransferase [ALT]; minimum value for platelets and fibrinogen). Thediagonal line represents the line of identity for the value at that time period and the pretherapy value. (A) WBC early period; (B)WBC intermediate; (C) WBC late; (D) indirect bilirubin early; (E) indirect bilirubin intermediate; (F) platelets early; (G) plateletsintermediate; (H) fibrinogen early; (I) fibrinogen intermediate; (J) ALT early; (K) ALT intermediate; (L) ALT late. In all pan-els, the horizontal and vertical lines delineate the normal range for each value. For the analysis of “abnormal” laboratory pa-rameters, two sectors from each graph were examined. For example, for WBC, indirect bilirubin, and ALT, the upper middle(normal pretherapy, high posttherapy) represents the abnormal parameters; for platelets and fibrinogen, the lower middle (nor-mal pre, low post) represents abnormal parameters. Symbols for all panels are as follows: ( s ) CF bolus; ( s � ) CF spray; (e ) can-cer; ( u ) normal skin; ( u � ) normal bronchi; (n ) cardiac adjunct; ( , ) cardiac MIS sole therapy; ( x ) PVD limb threatening; (n � )PVD limb threatening placebo; ( v ) PVD intermittent claudication; ( , � ) PVD intermittent claudication placebo; (m ) cardiac con-trols.

ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 79

CRYSTAL ET AL.80
FIG. 3. Continued.

was an apparent difference in the frequency of AEs per ad-ministration for the surgery group (4.4 AEs per administration)compared with the no-surgery group (0.9; Fig. 14A). The rela-tive timing of the AEs among the two groups was similar. Therewas no difference in the severity of AEs among the surgery andno-surgery groups (Fig. 14B) and no obvious differences in thetypes of AE among the two groups (Fig. 14C). Like the fre-quency of AEs, those undergoing surgery had a noticeablyhigher frequency of abnormal laboratory parameters (4.9 AEsper administration) compared with the nonsurgery group (0.9;Fig. 14D). The timing of the abnormal laboratory parameterswas similar among the surgery and nonsurgery groups, as werethe classes of abnormal laboratory parameters (Fig. 14E).
Risk factors for death and other major adverse events
The major adverse events were examined in two groups:deaths and major adverse events other than death. Both cate-
gories of major AE were evaluated first in the context of indi-vidual risk factors and then by multivariate analysis.
Individual risk factors and risk for death. In regard to deaths,most occurred in the colon cancer and cardiovascular groups(Table 2). As assessed in the accompanying paper (Harvey etal., 2002), the 1-year mortality for each of these trials was wellwithin that expected for each of these groups. The deaths thatwere acute (within the period of hospitalization after vector ad-ministration) and postdischarge to 1 year tended to be in theolder age groups (Fig. 5F). The deaths occurring $1 year aftervector administration were distributed among all age groups(Fig. 5F). Among the deaths there were more males, consistentwith there being more males enrolled in the trials (Fig. 6F).
The deaths at the acute and postdischarge to 1-year time pe-riod tended to be in the individuals with higher comorbid in-dices, and the deaths at .1 year mostly in those with lower in-
ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 81
FIG. 4. Frequency of abnormalities of specific types of laboratory tests in the study population. The data are presented as fre-quency of abnormal laboratory parameters relative to all laboratory tests for that parameter. The data are based on the type ofgraphic analysis shown in Fig. 3 (see Fig. 3 legend and Materials and Methods for a definition of “abnormal” for each time pe-riod). The number above each column represents the mean percentage for each parameter. For each parameter, each column issubdivided as to the proportion (percentage) of events occurring in the early (hatched section), intermediate (open section), andlate (solid reaction) time periods. The height of each section should not be read off the ordinate. BP, Blood pressure; Temp, tem-perature; Plat, platelets; AP, alkaline phosphatase; Ind bili, indirect bilirubin; Hb, hemoglobin; Creat, creatinine.

dices prior to entering the study (Fig. 7F). Interestingly, in allcases, the actual 1-year mortality of the individuals receivingAd vectors was less than the 1-year mortality predicted by thecomorbid index (Fig. 15). With the caveat that the comorbidindex likely overestimates the 1-year mortality for some groups(e.g., normals), in some cases, the differences were quite strik-ing, including the 85% predicted 1-year mortality for the coloncancer group compared with the actual 33% 1-year mortality,26% predicted compared with the actual 0% for the CF groups,and the predicted 52% compared with 13% for the two cardiacgroups combined. Other than the PVD and cardiac CABG con-trol groups, where the comorbid index provided a reasonable(#2-fold difference) predictor of 1-year mortality, the individ-uals receiving an Ad gene transfer vector invariably had .2-fold lower 1-year mortality than that predicted by the comor-bid instrument.
There did not appear to be any relationship among thepretherapy anti-Ad neutralizing antibody titers as a risk factorfor death, and there were no deaths in individuals with titers.90 (Fig. 8F). In regard to dose, deaths were observed at alldoses other than the 107-PU range. There was no apparent re-lationship of death with dose, other than that the two acutedeaths were both in the $109-PU dose range (Fig. 9F). Deathsoccurred in trials using all different routes of vector adminis-
tration except intradermal (Fig. 10F). Deaths were observedwith all transgenes, although the only acute deaths occurred af-ter administration of the vector with the VEGF and CD trans-genes (Fig. 11F). Interestingly, most deaths occurred with onlyone vector administration (n 5 8), whereas there was only onedeath in the group receiving three or more vector administra-tions (Fig. 12F). Deaths occurred in all of the trials except forthose involving normal individuals and the PVD controls, al-though the majority of deaths were in the cancer and cardio-vascular trials (Fig. 13F). Nine of the 14 deaths occurring af-ter vector administration were in trials involving surgery, andall but 3 occurred after discharge from the hospitalization dur-ing which the vector was administered (Fig. 14F).
Individual risk factors and risk for nondeath major adverseevents. In regard to major AEs other than death, there were atotal of 62 such events among 90 individuals receiving vector,and 11 events among 12 controls (Table 2; also see Tables 3–6in the accompanying paper by Harvey et al., 2002). The moststriking observation was that, other than the one major non-death AE in the CF bolus trial (see Table 3 in the accompany-ing paper by Harvey et al., 2002), all other major AEs not as-sociated with death occurred in the cardiovascular groups,including the cardiac adjunct to CABG trial (31 events, 2.1 per
CRYSTAL ET AL.82
FIG. 5. Age of the study population as a risk factor for development of adverse events, abnormal laboratory parameters, ordeath after administration of an Ad gene transfer vector. The entire study population of 90 individuals receiving 140 adminis-trations of Ad vectors in 8 different trials was graphed by age as indicated. For (A–E), the sections within each column repre-sent the proportion (percentage) of AEs that occurred within the categories defined in the legends for each panel. The height ofeach section should not be read off the ordinate. (A) Frequency of adverse events (AEs per administration of an Ad vector). Num-bers at the top of each column represent the mean for each group. For the 20- to 29-year category, the numbers to the right ofthe column represent (bottom to top) the early, intermediate, and late period. (B) Severity of adverse events (among all positiveAEs). Numbers above each column represent the mean for each group. Error estimates represent the mean 6 SD for each group.Numbers within each column represent the percentages within each group that occur in the early, intermediate, or late time pe-riod. (C) Type of adverse events (percentage of each type within each category). The number at the top of each column repre-sents the percentage of all positive AEs associated with each category. Numbers within each column refer to the relative per-centage of each type of AE for each category. Categories of AE include the following: (a) other, e.g., skin; (b) pulm, pulmonary;(c) CV, cardiovascular; (d) syst, systemic; (e) neuro, neurological; (f) GI, gastrointestinal; (g) renal; (h) hepatic; (i) coag, coag-ulation; (j) heme, hematologic. (D) Frequency of abnormal laboratory parameters (number per administration of an Ad vector).Numbers above each column represent the mean for each group. The numbers within each column represent the percentageswithin each group that occur in the early, intermediate, or late time period. (E) Type of abnormal laboratory parameter (amongall abnormal laboratory tests). Numbers at the top of each column represent the percentages of all abnormal laboratory parame-ters associated with each category. Numbers within each column refer to the relative percentage of each type of AE for each cat-egory. Each column is subdivided into types of abnormal laboratory parameter: (k) renal 5 creatinine; (l) hemolysis 5 indirectbilirubin, LDH, hemoglobin; (m) hepatic 5 AP, AST, ALT; (n) coagulation 5 PT, PTT, platelets, fibrinogen; (o) systemic 5 BP,temperature, WBC; see Materials and Methods. (F) Deaths occurring in the acute period, postdischarge to 1 year, or .1 year.The symbols are identical as those for Fig. 1C; note that there were n 5 13 deaths in the vector administration groups, and n 51 death in a control group (CABG control, indicated by r ). For definitions of groupings, see Materials and Methods. N, No datain this category.
FIG. 6. Sex of the study population as a risk factor. (A) Frequency of AEs; (B) severity of AEs; (C) type of AE; (D) frequencyof abnormal laboratory parameters; (E) type of abnormal laboratory parameters; (F) deaths. See legend to Fig. 5 for details.
FIG. 7. Comorbid indices of the study population pretherapy as a risk factor. (A) Frequency of specific types of AE; (B) sever-ity of specific types of AE; (C) type of AE; (D) frequency of abnormal laboratory parameters; (E) type of abnormal laboratoryparameters; (F) deaths. See legend to Fig. 5 for details.
FIG. 8. Pretherapy serum anti-Ad neutralizing antibodies as a risk factor. (A) Frequency of specific types of AE; (B) severityof specific types of AE; (C) type of AE; (D) frequency of abnormal laboratory parameters; (E) type of abnormal laboratory pa-rameters. (F) deaths (for some individuals, the anti-Ad titers were not determined; see accompanying paper by Harvey et al.,2001). See legend to Fig. 5 for details.

ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 83
FIG
. 5

CRYSTAL ET AL.84
FIG
. 6

ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 85
FIG
. 7

CRYSTAL ET AL.86
FIG
. 8

individual), the cardiac MIS/sole therapy trial (16 events, 1.0per individual), the PVD trial (14 events, 1.4 per individual),the PVD controls (2 events, 0.5 per individual), and cardiaccontrols (9 events, 1.1 per individual; Table 2). The individu-als with most nondeath major AEs were in the older age groups(63 6 13 years), mostly male (74%), had a higher comorbid in-dex pretherapy (2.7 6 1.5), had a broad range of pretherapyanti-Ad antibodies (,10–320), received doses in the 108- to1010-PU range, all had single administration of vectors via themyocardial (n 5 18) or skeletal muscle route (n 5 8), and most(n 5 15) had major surgery (CABG with cardiopulmonary by-pass n 5 8, thoracotomy/thoracoscopy).
The observation of higher incidence of nondeath major AEsin the PVD trial compared with the cardiac MIS/sole therapytrial is of interest, because the identical vector(AdGVVEGF121.10) was used and the average doses werehigher in the cardiac MIS/sole therapy trial (by more than 10-fold; Fig. 1E). Further, the cardiac MIS/sole therapy trial in-volved surgery (thoracotomy or thoracoscopy) whereas in thePVD trial, the vector was administered via multiple injectionsto skeletal muscle under mild sedation. One clue as to the dif-ferences among these trials can be found in the timing of thenondeath major AEs. Whereas the timing of many of the car-diac MIS/sole therapy events was early (38%, 6 of 16) or in-termediate (56%, 9 of 16), all of the PVD events occurred inthe intermediate period (100%, 14 of 14). Assessment of thetypes of nondeath AE also provides a clue: many of those as-sociated with the cardiac MIS/sole therapy trial were linked tothe surgical procedure (e.g., hemothorax, myocardial infarction,renal insufficiency, respiratory failure), or were associated withthe underlying disorder (angina, requirement for other majortherapeutic interventions); all of the nondeath AEs linked to thePVD trial were associated with the severity of the underlyingdisorder (e.g., requirement of a major therapeutic intervention,thrombosis, claudication, angina, amputation).
Multivariate analysis of risk factors and risk for death. Mul-tivariate analysis demonstrated that only the pretherapy co-morbid index was significantly associated with the risk of deathafter adjusting for other potential risk factors (p 5 0.03). Thus,subjects with higher comorbid indices at study entry had an in-creased risk of dying over the follow-up period. This is not anunexpected finding, since the comorbid index is an empiric in-strument designed to predict 1-year mortality of individualswith comorbid conditions being admitted to a hospital (Charl-son et al., 1987). More importantly, the results of the multi-variate analysis suggest that, in this group of individuals re-ceiving local administration of low and intermediate doses ofAd vectors, none of the vector-related risk factors were signif-icantly associated with the risk of death. These observations areconsistent with the conclusion in the accompanying paper (Har-vey et al., 2002) that, when considered individually, no deathin these gene transfer trials appeared to be linked to the vectorper se.
Multivariate analysis of risk factors and risk for nondeathmajor AEs. Multivariate analysis of risk factors for nondeathmajor AEs in the early or intermediate period (grouped to-gether) revealed that only increasing age (p 5 0.04) and sur-gery (p 5 0.01) were independently associated with the pres-
ence of a nondeath major adverse event after controlling for theeffect of other risk factors. Importantly, despite the apparentlink (to various degrees) of sex, comorbid index, dose, route ofadministration, transgene, and number of administrations (in-versely) with the frequency of AEs per administration, none ofthese factors proved to be significantly associated with the riskof developing a nondeath major AE in these groups of indi-viduals after other risk factors were taken into account.
DISCUSSION
The present study analyzes the adverse events, abnormal lab-oratory parameters, and deaths observed in 8 trials involving atotal of 140 local administrations of low and intermediate dosesof adenovirus gene transfer vectors to 6 sites in 90 individuals.In the accompanying paper (Harvey et al., 2002), in which weassess each trial individually, we concluded that no deaths werelinked to the Ad vectors per se, and that the incidence of ma-jor (severity rank 3–4 out of 4) adverse events likely caused byan Ad vector was 0.7%. In the present study, we grouped thetotal experience from the 8 trials to determine whether 10 pu-tative risk factors associated with the individual (age, sex, co-morbid index, or pretherapy anti-Ad antibody titer), adenovi-rus vector (dose, route of administration, transgene in theexpression cassette, or number of vector administrations), orthe gene transfer trial (trial design or involvement of major sur-gery in the trial) could be predictive of the safety of similar de-signed trials.
Although individual analysis of each of these putative riskfactors suggested interesting associations with the deaths, otheradverse events, and abnormal laboratory parameters observedin these trials, assessment of the major (death and nondeath)adverse events by multivariate analysis to account for all riskfactors demonstrated that only the comorbid index predicteddeath. It was also determined that age and whether surgery waspart of the trial design predicted the development of major ad-verse events other than death. There is an insufficient numberof study participants in these combined phase I studies to ab-solutely rule out local administration of low- or intermediate-dose Ad vectors as a cause of the major adverse events ob-served in these in vivo gene transfer trials. In addition, the resultsof the analysis may be limited because of significant differencesin the baseline characteristics of the individuals in the proto-cols included in the study. Although several variables were in-cluded in the multivariate analysis to adjust for factors knownto influence the risk of developing a major adverse events ordeath (e.g., age, sex, and comorbidity), we could not adjust forunrecognized risk factors. A comorbidity index was used to ad-just for the presence of other comorbid conditions, an impor-tant risk factor for death and major adverse events, the two out-comes evaluated in this analysis. This index was not specificallydeveloped or tested in gene therapy patients and, thus, this in-strument needs to be further assessed in regard to predictingoutcome in this group of study participants. However, in thecontext that comorbid conditions, age, and major surgery areexpected risk factors for major adverse events in this study pop-ulation independent of gene transfer, and the fact that multi-variate analysis demonstrated no significant association of vec-tor-related factors with major adverse events, the data suggest
ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 87

that local administration of these doses of Ad vectors appearsto be well tolerated and that initiation of phase II studies is war-ranted.
Risk factors associated with the study individual
The risk factors associated with the study individual thatwere evaluated included age, sex, comorbid index, and prether-apy anti-Ad neutralizing antibody titer. Of these, only the co-morbid index was linked to the outcome of death and only agewas predictive of the development of nondeath major adverseevents.
It would be expected that the comorbid index might predictmortality, since the index was empirically developed to predictmortality of individuals with various comorbid conditions whowere hospitalized (Charlson et al., 1987). Interestingly, the ac-tual 1-year mortality of the study population in each of the tri-als was lower than that predicted by the comorbid index. Shouldthis observation hold up in additional trials, survival might bea useful parameter for some adenovirus-mediated in vivo genetransfer phase II–III trials that include the appropriate controlgroups.
Little information has been published that provides insightas to whether there is an additive or synergistic risk to usinglocal administration of low and intermediate doses of Ad vec-tors in experimental animals with hereditary or induced co-morbid conditions, and the data that are available suggest thereis no increased risk. For example, in a porcine model of coro-nary artery disease, myocardial administration of intermediatedoses of an Ad vector was not associated with increased mor-tality and did not induce significant amounts of myocardial in-flammation or necrosis, results similar to the same doses in nor-mal animals (Patel et al., 1999).
In regard to humans, with the caveats that the “control” PVDand cardiac CABG/bypass groups are limited in terms of num-ber of study individuals, and are not matched to the entire studypopulation, it is of interest that (1) the 1-year mortality of theCABG group was comparable to that of the cardiac gene trans-fer groups (see accompanying paper by Harvey et al., 2002);and (2) on average, the frequency (per individual) of adverseevents and abnormal laboratory parameters in the two control
groups were in the same range as that of the comparable genetransfer groups.
The simplest explanation for age as a risk factor for increasedfrequency for major adverse events other than death is that therisk for adverse events naturally increases with this parameter,particularly in the context that a large proportion of the studypopulation (46%) was $50 years old when entering the study.There are no experimental animal studies that directly examineage as a risk factor for the development of adverse events af-ter administration of Ad vectors. However, intracerebral ad-ministration of replication-deficient Ad vectors at 106 PFU toaged rats did not result in any additional adverse events (Cas-tel-Barthe et al., 1996).
No other putative risk factors associated with the study in-dividual correlated significantly with major adverse events. Al-though assessment of sex by itself suggested that the frequencyof AEs per vector administration might be higher in females,sex did not appear to be important when other factors weretaken into account. Finally, the extent of pretherapy anti-Ad an-tibodies bore no significant relationship to death or the devel-opment of other major AE in these groups of patients, that is,while prior exposure to adenovirus may play a role in limitingthe efficacy of gene transfer (Mastrangeli et al., 1996; Mack etal., 1997), preexisting immunity against the same serotype Addoes not appear to be a safety concern with local administra-tion of these doses of Ad vectors to humans.
Risk factors associated with the adenovirus vectors
One of the striking observations in the multivariate analysisis that no vector-related factors, including dose, route of ad-ministration, transgene in the expression cassette, or number oftimes the vector was administered, appear to be risk factors inthis study population for death or nondeath major adverseevents when other factors are taken into account.
The lack of correlation with dose is of particular interest sincethere are extensive data with experimental animals demon-strating that high doses of Ad vectors are associated with an in-creased incidence of major adverse events, although many fac-tors modify this response, including purity of the vector,species, strain, transgene, and route (Simon et al., 1993; Brody
CRYSTAL ET AL.88
FIG. 9. Dose of administered Ad vector as a risk factor. (A) Frequency of specific types of AE; (B) severity of specific typesof AE; (C) type of AE; (D) Frequency of abnormal laboratory parameters; (E) type of abnormal laboratory parameters; (F) deaths.See legend to Fig. 5 for details.
FIG. 10. Route of administration of the Ad vector as a risk factor. (A) Frequency of specific types of AE; (B) severity of spe-cific types of AE; (C) type of AE; (D) frequency of abnormal laboratory parameters; (E) type of abnormal laboratory parame-ters; (F) deaths. See legend to Fig. 5 for details. For (A) numbers to right of “bronchi” refer (bottom to top) to early, intermedi-ate, and late time periods; for (D), same for “skin.”
FIG. 11. Transgene in the expression cassette of the Ad vector as a risk factor. (A) Frequency of specific types of AE; (B)severity of specific types of AE; (C) type of AE; (D) frequency of abnormal laboratory parameters; (E) type of abnormal labo-ratory parameters; (F) deaths. See legend to Fig. 5 for details. For (A), numbers to right of “CFTR” refer (bottom to top) to early,intermediate, and late time periods.
FIG. 12. Number of vector administrations of an Ad vector to the study individual as a risk factor. (A) Frequency of specifictypes of AE; (B) severity of specific types of AE; (C) type of AE; (D) frequency of abnormal laboratory parameters; (E) typeof abnormal laboratory parameters; (F) deaths. See legend to Fig. 5 for details. For (A), numbers to right of “$3” refer (bottomto top) to early, intermediate, and late time periods.

ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 89
FIG
. 9

CRYSTAL ET AL.90
FIG
. 10

ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 91
FIG
. 11

CRYSTAL ET AL.92
FIG
. 12

1994; Cichon et al., 1999; Friedmann, 1999a; Lozier et al.,1999; Nunes et al., 1999). There are several differences fromthese experimental animal studies and the human Ad vector tri-als analyzed in the present study that might explain the appar-ent lack of association of vector dose with major adverse eventsin humans. First, most studies demonstrating major “toxicity”of Ad vectors in experimental animals use doses 102- to 103-fold greater per kilogram body weight than the doses used inthe trials analyzed in the present study (Simon et al., 1993;
Brody et al., 1994; Cichon et al., 1999; Friedmann, 1999a;Lozier et al., 1999; Nunes et al., 1999). The highest dose usedin the present study was approximately 109 PU/kg, a level lowerthan the doses typically associated with major adverse eventsin experimental animals (Cichon et al., 1999; Lozier et al.,1999; Morral et al., 1999; Nunes et al., 1999). Second, all ofthe routes used in the present study were local, whereas mostexperimental animal studies demonstrating major adverseevents in association with Ad vectors use systemic (intravas-
ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 93
FIG. 13. Type of Ad vector gene transfer trial as a risk factor. (A) Frequency of specific types of AE; (B) Severity of specifictypes of AE; (C) type of AE; (D) frequency of abnormal laboratory parameters; (E) type of abnormal laboratory parameters; (F)deaths. See legend to Fig. 5 for details. The trials involving no surgery are grouped on the left and the trials involving surgeryare grouped on the right.

cular) administration of the vector (Cichon et al., 1999; Lozieret al., 1999; Morral et al., 1999; Nunes et al., 1999). Third,there is increasing evidence that the pharmacokinetics of Advectors may be different in at least some large experimental an-imals compared with the more commonly used rodent models(Worgall et al., 1997; Hackett et al., 1999). It is unknownwhether the response of humans to Ad vectors is closer to thatof large experimental animals such as the pig, where systemicadministration of an Ad vector results in most of the vector lo-calizing to lung (Hackett et al., 1999), or to that of rodents,where systemic administration results in predominantly hepaticlocalization (Worgall et al., 1997). Fourth, all of the humanstudies described in this study utilized Ad vector preparationscontaining ,1 replication-competent adenovirus (RCA) per to-tal dose administered (Crystal et al., 1994, 1998; Hay et al.,1995; Crystal, 1998; Harvey et al., 1999a–d; Rosengart et al.,1999a,b). In the context that testing for RCA is cumbersome,time consuming, and expensive, most Ad vector preparationsused in studies with experimental animals utilize RCA tests thatare simpler, but have a lower sensitivity than the RCA testsused to evaluate preparations of clinical-grade Ad vectors(Crystal et al., 1994). In this regard, some of the toxicity at-tributed to Ad vectors in experimental animal studies may beassociated with RCA contaminating the vector preparations(Nunes et al., 1999). Finally, Ad vectors may interact with bloodelements of humans differently from that of at least some ex-perimental animals (Hackett et al., 1999). This observation, andthe knowledge that there are marked differences in the inflam-
matory responses of different murine strains to Ad vectors, maybe relevant to the death at the University of Pennsylvania, wherehemolysis was one of the earliest events associated with in-travascular administration of 4 3 1013 PU of an Ad vector, thatis, the hemolysis may have resulted from high dose, the in-travascular route, or possibly specific characteristics of thestudy individual. Whatever the mechanism, there was no evi-dence of significant hemolysis linked to the local administra-tion of low or intermediate doses of Ad vectors in the presentstudy, nor was there evidence of disseminated intravascular co-agulation, another abnormality in the University of Pennsylva-nia case (Food and Drug Administration, 1999).
When considered as an individual risk factor, it appeared thatuse of the VEGF transgene was associated with an increasedfrequency of adverse events. However, after controlling forother risk factors, multivariate analysis did not identify trans-gene as a specific risk factor. The apparent link of the VEGFtransgene to adverse events in the individual assessment waslikely because the vector containing this transgene was usedonly in the cardiovascular studies, all of which involved indi-viduals who were older, with average high comorbid indicesand who underwent a major surgical procedure as part of thetrial.
One interesting observation of the multivariate analysis re-lated to vectors was that repetitive administration of Ad vec-tors was not associated with an increase in the frequency of ma-jor adverse events. In fact, when examined as a single variable,there appeared to be an inverse relationship of increasing num-
CRYSTAL ET AL.94
FIG. 13. Continued.
FIG. 14. Surgery as part of the study design as a risk factor. (A) Frequency of specific types of AE; (B) severity of specifictypes of AE; (C) type of AE; (D) frequency of abnormal laboratory parameters; (E) type of abnormal laboratory parameters; (F)deaths. See legend to Fig. 5 for details.

ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 95

TA
BL
E2.
MA
JOR
AD
VE
RS
EE
VE
NT
SA
FT
ER
AD
MIN
IST
RA
TIO
NO
FA
DE
NO
VIR
US
VE
CT
OR
Sa
Dea
ths
(num
ber)
bM
ajor
AE
oth
er t
han
deat
h (n
umbe
r)c
Per
Per
Per
Per
Per
Per
Tri
ald
grou
pin
divi
dual
adm
inis
trat
ion
Acu
ted/
c to
1 y
r.
1 yr
grou
pin
divi
dual
adm
inis
trat
ion
Ear
lyIn
term
edia
teL
ate
CF
bol
use
20.
20.
10
02
10.
10.
11
00
CF
spr
ay1
0.1
0.0
00
10
0.0
0.0
00
0C
olon
can
cer
30.
50.
30
21
00.
00.
00
00
Nor
mal
ski
n0
0.0
0.0
00
00
0.0
0.0
00
0N
orm
al b
ronc
hial
00.
00.
00
00
00.
00.
00
00
Car
diac
adj
unct
40.
30.
32
11
312.
12.
126
50
Car
diac
MIS
10.
10.
10
10
161.
01.
06
91
PV
D2
0.2
0.2
02
014
1.4
1.4
014
0P
VD
con
trol
00.
0N
A0
00
20.
5N
Af
02
0C
ardi
ac c
ontr
ol1
0.1
NA
10
09
1.1
NA
81
0T
otal
:14
0.1
0.1
36
573
0.7
0.5
4131
1G
roup
rec
eivi
ng13
0.1
0.1
26
562
0.7
0.4
3328
1ve
ctor
Con
trol
gro
up1
0.1
NA
10
011
0.9
NA
83
0
a "M
ajor
" ad
vers
e ev
ent
(AE
) de
fine
d as
sev
erit
y ca
tego
ry 3
or
4 (s
ee T
able
s 2–
6 in
the
acc
ompa
nyin
g pa
per
by H
arve
y et
al.,
2002
).b D
eath
s ar
e ca
tego
rize
d pe
r gr
oup,
per
ind
ivid
ual,
per
adm
inis
trat
ion,
and
in
thre
e ti
me
peri
ods:
acu
te,
duri
ng t
he h
ospi
tali
zati
on f
or v
ecto
r ad
min
istr
atio
n (o
r ho
spit
aliz
atio
n du
ring
cont
rol
peri
od);
d/c
to
1 yr
, di
scha
rge
from
hos
pita
liza
tion
to
1 yr
; an
d .
1 yr
.c M
ajor
AE
s ot
her
than
dea
th a
re c
ateg
oriz
ed i
n a
sim
ilar
fas
hion
as
deat
hs,
exce
pt t
he t
ime
peri
ods
of e
arly
(0–
7 da
ys),
int
erm
edia
te (
8–30
day
s),
and
late
(.
30 d
ays)
cor
resp
ond
toth
e cl
assi
fica
tion
of
AE
s as
des
crib
ed i
n M
ater
ials
and
Met
hods
.d C
F, C
ysti
c fi
bros
is;
MIS
, m
inim
ally
inv
asiv
e su
rger
y; P
VD
, pe
riph
eral
vas
cula
r di
seas
e.e I
n th
e C
F b
olus
stu
dy t
here
was
one
AE
in
the
firs
t hu
man
tri
al u
sing
an
aden
ovir
us g
ene
tran
sfer
vec
tor
that
ind
uced
a s
yste
mic
and
pul
mon
ary
synd
rom
e cl
earl
y re
late
d to
the
vec
-to
r. A
lthou
gh e
ach
of t
he i
ndiv
idua
l A
Es
was
cla
ssif
ied
as 1
–2 s
ever
ity
(i.e
., “m
inor
”),
toge
ther
the
syn
drom
e w
as c
onsi
dere
d m
ajor
and
thu
s it
is
incl
uded
in
this
ana
lysi
s; s
ee a
ccom
-pa
nyin
g pa
per
by H
arve
y et
al.,
(200
2) a
nd r
efer
ence
s (C
ryst
al e
t al
.,19
94;
McE
lvan
ey a
nd C
ryst
al,
1995
) fo
r de
tail
s.f N
A,
Not
app
lica
ble.
96

bers of administrations and the number of adverse events. Thereasons for this are likely complex, but may be related to thefollowing: (1) except for the cancer trial, the trials involvingolder individuals with higher comorbid indices utilized only oneadministration of the vector (i.e., the cardiovascular trials),whereas the repetitive administrations were in trials utilizingindividuals who were younger and with low comorbid indices(i.e., the normal and cystic fibrosis trials); and (2) whereas therewas no apparent association of anti-Ad neutralizing antibodieswith adverse events, repetitive administration of Ad vectorsmay enhance systemic anti-Ad titers in some individuals (Har-vey et al., 1999b; Nunes et al., 1999), resulting in preventionof the next administration of Ad vector reaching tissues, thusserving as a “protection” against Ad-induced toxicity (Nunes etal., 1999).
It is also of interest that the multivariate analysis demon-strated that route was not a risk factor for the development ofmajor adverse events. This does not mean that local adminis-tration to all organs/routes of administration of Ad vectors willbe risk free, but at least for low and intermediate doses of Advectors administered by the routes used in the present study
(nasal epithelium, bronchial epithelium, intradermal, percuta-neous to solid tumors, epicardial administration to the myo-cardium, and percutaneous to skeletal muscle), route does notappear to be a significant risk factor. Importantly, all of the vec-tor administrations in the present study were done in a localfashion, directly to a specific organ. In experimental animals,systemic “spillover” from local administration of Ad vectors isusually minimal, although the extent of spillover depends onthe target tissue, dose, and the volume in which the vector isadministered (Kass-Eisler et al., 1994; Goldman et al., 1995;Huard et al., 1995). This is different from intravascular ad-ministration, in which systemic spread is much more likely(Kass-Eisler et al., 1994; Oualikene et al., 1994; Huard et al.,1995; Cichon et al., 1999; Lozier et al., 1999; Nunes et al.,1999). In view of the death at the University of Pennsylvania,in which the intravascular route was used, attention in futurestudies should continue to focus on the risk for adverse eventsassociated with the intravascular route.
Host responses to the low level of Ad gene expression fromthe adenovirus genome after vector administration are thoughtto be responsible for the majority of the adverse events in stud-
ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 97
FIG. 15. Comparison of actual 1-year mortality with the 1-year mortality predicted by the comorbid index. For each group oftrials (normal, cystic fibrosis [CF], colon cancer [Ca], cardiac and peripheral vascular disease [PVD], PVD control and cardiaccontrols), the 1-year mortality predicted by the comorbid index (indicated by d ) is compared with the actual 1-year mortality forthe group ( s ). For details, see Tables 1 and 2 and Fig. 1C–E, and see Tables 1 and 8 and Fig. 1 in the accompanying paper byHarvey et al. (2001).

ies of experimental animals (Yang et al., 1995a). For this rea-son, there has been considerable effort in the gene therapy fieldto develop advanced forms of Ad vectors in which various genesor all genes have been deleted, with the goal of diminishingvector-induced host responses (Engelhardt et al., 1994; Amal-fitano and Chamberlain, 1997; Armentano et al., 1997; Harrodet al., 1998; Friedmann, 1999b). It is of interest, therefore, thatall of the Ad vectors in the present study were so-called “first-generation” E12E32 Ad vectors, that is, collectively, the pres-ent study provides evidence that local administration of low andintermediate doses of these first-generation vectors does not ap-pear to pose a significant risk to a study population with a va-riety of comorbid conditions as well as normals.
Risk factors associated with study design
It is not surprising that multivariate analysis showed that sur-gery as part of the trial design would be linked to increased fre-quency of nondeath major adverse events. However, one un-expected observation in the present study was the apparent highnumber of adverse events observed in the peripheral vasculardisease trial, particularly late adverse events. Although the smallnumbers of study participants obviates definitive conclusionsregarding the reasons for this, it is unlikely linked to the singleadministration of the VEGF vector, as the identical vector inhigher doses was administered directly to the myocardium inthe two cardiac trials. A more likely explanation is that pe-ripheral vascular disease is associated with a high comorbid in-dex in an older population, with a constellation of disorders(typically severe atherosclerosis and/or diabetes) that frequentlyleads to adverse events as part of the natural history of the dis-order (Violi et al., 1996; Strano et al., 1996; Killewich et al.,1998; Nicoloff et al., 1998; Rihal et al., 1999).
Can major adverse events be predicted in Ad vectorgene transfer trials?
Multivariate analysis is the preferred methodology to ana-lyze the association of variables after adjustment for potentialconfounding factors. The main limitation of the analysis in ourstudy is the inability to completely capture the baseline differ-ences of the study participants with the variables included inthe regression model. For example, although a comorbidity in-dex was used to adjust for the presence of other comorbid con-ditions, this index was not specifically developed for individu-als receiving gene therapy. In addition, significant correlationamong some variables included in the regression model couldhave prevented adequate explorations of interactions amongthese factors.
Despite these limitations, the results of the analysis are im-portant given the limited data currently available addressing thesafety of gene therapy. The results of these studies should bereevaluated as information from large studies including morehomogeneous populations becomes available.
Analysis of the 90 individuals in all 8 trials individually (seeaccompanying paper by Harvey et al., 2002), and in the pres-ent study, considering the 8 trials together in the context of 10putative risk factors, has led to the conclusion that local ad-ministration of low and intermediate doses of Ad vectors ap-pear to be associated with a low incidence of major adverseevents attributable to the vector. While age, comorbid index,
and the inclusion of surgery in the trial design are risk factorsthat may have specific relevance to participating in an Ad vec-tor gene transfer trial, these are common sense risk factors forany clinical trial, that is, independent of participation in a genetransfer trial, there is an increase in the frequency of major ad-verse events as individuals age, develop comorbid conditions,and undergo surgery. With the caveat that this analysis focuseson phase I studies of heterogeneous design and with limitednumber of study individuals, and considering that there may beother, unknown factors that may play a role in theincidence/severity of adverse events after Ad vector adminis-tration, we conclude that there is no definitive risk factor thatwill clearly predict a major adverse outcome resulting directlyfrom local administration of low and intermediate doses of Advectors. Together, the evidence suggests that the major adverseevents in these gene transfer trials are associated primarily withthe study population and/or trial design, not the Ad vectorsthemselves. These observations are consistent with the conceptthat local administration of low or intermediate doses of Advectors appears to be well tolerated.
ACKNOWLEDGMENTS
We thank S. Papps for help with the data analysis, R. Za-laznick for helpful discussions, and N. Mohamed for help inpreparing this manuscript. These studies were supported, inpart, by NIH P01 HL51746-06A1, R21 CA75153, R01 HL57318, and General Clinical Research Centers ProgramM01RR00047 and M01RR00102; the Will Rogers MemorialFund, Los Angeles, CA; the Cystic Fibrosis Foundation,Bethesda, MD; the Jeffry M. and Barbara Picower Foundation,Palm Beach, FL; GenVec, Inc., Gaithersburg, MD; and Parke-Davis/Warner-Lambert, Ann Arbor, MI. R.G.C. and T.K.R. areconsultants to, and hold equity in, GenVec, Inc.
REFERENCES
AMALFITANO, A., and CHAMBERLAIN, J.S. (1997). Isolation andcharacterization of packaging cell lines that coexpress the adenovi-rus E1, DNA polymerase, and preterminal proteins: Implications forgene therapy. Gene Ther. 4, 258–263.
ANDERSON, W.F. (1998). Human gene therapy. Nature 392, 25–30.ARMENTANO, D., ZABNER, J., SACKS, C., SOOKDEO, C.C.,
SMITH, M.P., ST. GEORGE, J.A., WADSWORTH, S.C., SMITH,A.E., and GREGORY, R.J. (1997). Effect of the E4 region on thepersistence of transgene expression from adenovirus vectors. J. Vi-rol. 71, 2408–2416.
BARR, D., TUBB, J., FERGUSON, D., SCARIA, A., LIEBER, A.,WILSON, C., PERKINS, J., and KAY, M.A. (1995). Strain relatedvariations in adenovirally mediated transgene expression from mousehepatocytes in vivo: Comparisons between immunocompetent andimmunodeficient inbred strains. Gene Ther. 2, 151–155.
BATSHAW, M.L., RAPER, S.E., and WILSON, J.M. (1999). Study ofadenoviral vector-mediated gene transfer in liver in adults with par-tial ornithine transcarbamylase deficiency (IND 6624): Review ofdata. Presented at the RAC meeting December 8–10, 1999, Wash-ington, D.C.
BRODY, S.L., METZGER, M., DANEL, C., ROSENFELD, M.A., andCRYSTAL, R.G. (1994). Acute responses of non-human primates toairway delivery of an adenovirus vector containing the human cys-
CRYSTAL ET AL.98
tic fibrosis transmembrane conductance regulator cDNA. Hum. GeneTher. 5, 821–836.
CASTEL-BARTHE, M.N., JAZAT-POINDESSOUS, F., BAR-NEOUD, P., VIGNE, E., REVAH, F., MALLET, J., and LAMOUR,Y. (1996). Direct intracerebral nerve growth factor gene transfer us-ing a combinant adenovirus: Effect on basal forebrain cholinergicneurons during aging. Neurobiol. Dis. 3, 76–86.
CHARLSON, M.E., POMPEI, P., ALES, K.L., and MACKENZIE,C.R. (1987). A new method of classifying prognostic comorbidity inlongitudinal studies: Development and validation. J. Chronic Dis. 40,373–383.
CICHON, G., SCHMIDT, H.H., BENHIDJEB, T., LOSER, P.,ZIEMER, S., HAAS, R., GREWE, N., SCHNIEDERS, F., HEEREN,J., MANNS, M.P., SCHLAG, P.M., and STRAUSS, M. (1999). In-travenous administration of recombinant adenoviruses causes throm-bocytopenia anemia and erythroblastosis in rabbits. J. Gene Med. 1,360–371.
CRYSTAL, R.G. (1995). Transfer of genes to humans: Early lessonsand obstacles to success. Science 270, 404–410.
CRYSTAL, R.G. (1998). Phase I study of direct administration of areplication deficient adenovirus vector (AdGVVEGF121.10) contain-ing the VEGF cDNA to the ischemic myocardium of individuals withdiffuse coronary artery disease via minimally invasive surgery. RAC#9806-258. Office of Recombinant DNA Activities, National Insti-tutes of Health, Suite 323, 6006 Executive Boulevard, MSC 7052,Bethesda, MD 20892-7052.
CRYSTAL, R.G., MCELVANEY, N.G., ROSENFELD, M.A., CHU,C.S., MASTRANGELI, A., HAY, J.G., BRODY, S.L., JAFFE, H.A.,EISSA, N.T., and DANEL, C. (1994). Administration of an adeno-virus containing the human CFTR cDNA to the respiratory tract ofindividuals with cystic fibrosis. Nat. Genet. 8, 42–51.
CRYSTAL, R.G., JAFFE, A., BRODY, S., MASTRANGELI, A.,MCELVANEY, N.G., ROSENFELD, M., CHU, C.S., DANEL, C.,HAY, J., and EISSA, T. (1995a). A phase 1 study, in cystic fibrosispatients, of the safety, toxicity, and biological efficacy of a singleadministration of a replication deficient, recombinant adenovirus car-rying the cDNA of the normal cystic fibrosis transmembrane con-ductance regulator gene in the lung. Hum. Gene Ther. 6, 643–666.
CRYSTAL, R.G., MASTRANGELI, A., SANDERS, A., COOKE, J.,KING, T., GILBERT, F., HENSCHKE, C., PASCAL, W., HERENA,J., HARVEY, B.G., HIRSCHOWITZ, E., DIAZ, D., RUSSI, T.,PACHECO, F., SIKAND, V., and BRION, P. (1995b). Evaluationof repeat administration of a replication deficient, recombinant ade-novirus containing the normal cystic fibrosis transmembrane con-ductance regulator cDNA to the airways of individuals with cysticfibrosis. Hum. Gene Ther. 6, 667–703.
CRYSTAL, R.G., HIRSCHOWITZ, E., LIEBERMAN, M., DALY, J.,KAZAM, E., HENSCHKE, C., YANKELEVITZ, D., KEMENY, N.,SILVERSTEIN, R., OHWADA, A., RUSSI, T., MASTRANGELI,A., SANDERS, A., COOKE, J., and HARVEY, B.G. (1997). PhaseI study of direct administration of a replication deficient adenovirusvector containing the E. coli cytosine deaminase gene to metastaticcolon carcinoma of the liver in association with the oral administra-tion of the pro-drug 5-fluorocytosine. Hum. Gene Ther. 8, 985–1001.
CRYSTAL, R.G., ROSENGART, T.K., ISOM, O.W., et al. (1998).Phase I study of direct administration of a replication deficient ade-novirus vector (AdGVVEGF121.10) containing the VEGF121 cDNAto the ischemic myocardium of individuals with life threatening dif-fuse coronary artery disease. RAC Report # 9711221. Office of Re-combinant DNA Activities, National Institutes of Health, Suite 323,6006 Executive Boulevard, MSC 7052, Bethesda, MD 20892-7052.
ENGELHARDT, J.F., LITZKY, L., and WILSON, J.M. (1994). Pro-longed transgene expression in cotton rat lung with recombinant ade-noviruses defective in E2a. Hum. Gene Ther. 5, 1217–1229.
FOOD AND DRUG ADMINISTRATION. (1999). Debra Knorr, Ex-ecutive Secretary, Recombinant Advisory Committee (RAC). Letter
to Members, NIH RAC, September 21, 1999. Immediate Notifica-tion—Serious Adverse Events. Bethesda, MD 20892.
FRIEDMANN, T. (1999a). Structure and genetic organization of ade-novirus vectors; adenovirus vectors; strategies to adapt adenoviralvectors for gene therapy applications: Targeting and integration. InThe Development of Human Gene Therapy. (Cold Spring HarborLaboratory Press, Cold Spring Harbor, NY) pp. 61–130.
FRIEDMANN, T. (1999b). The origins, evolution, and directions ofhuman gene therapy. In The Development of Human Gene Therapy.(Cold Spring Harbor Laboratory Press, Cold Spring Harbor, NY) pp.1–20.
GOLDMAN, M.J., LITZKY, L.A., ENGELHARDT, J.F., and WIL-SON, J.M. (1995). Transfer of the CFTR gene to the lung of non-human primates with E1-deleted, E2a-defective recombinant adeno-viruses: A preclinical toxicology study. Hum. Gene Ther. 6, 839–851.
HACKETT, N.R., LEE, L.Y., SILVA, I., EL-SAWY, T., POLCE, D.R.,ROSENGART, T.K., and CRYSTAL, R.G. (1999). Biodistributionof adenovirus gene therapy vectors in pigs following myocardial ad-ministration by various routes. American Society of Gene Therapy,Program of the 2nd Annual Meeting, Washington, D.C., June 9–13,1999, p. 33a.
HARROD, K.S., HERMISTON, T.W., TRAPNELL, B.C., WOLD,W.S., and WHITSETT, J.A. (1998). Lung-specific expression of adenovirus E3-14.7K in transgenic mice attenuates adenoviral vec-tor-mediated lung inflammation and enhances transgene expression.Hum. Gene Ther. 9, 1885–1898.
HARVEY, B.-G., WORGALL, S., ELY, S., LEOPOLD, P.L., andCRYSTAL, R.G. (1999a). Cellular immune responses of healthy in-dividuals to intradermal administration of an E12E32 adenovirusgene transfer vector. Hum. Gene Ther. 10, 2817–2823.
HARVEY, B.G., HACKETT, N.R., EL-SAWY, T., ROSENGART,T.K., HIRSCHOWITZ, E.A., LIEBERMAN, M.D., LESSER, M.L.,and CRYSTAL, R.G. (1999b). Variability of human systemic hu-moral immune responses to adenovirus gene transfer vectors admin-istered to different organs. J. Virol. 73, 6729–6742.
HARVEY, B.G., LEOPOLD, P.L., HACKETT, N.R., GRASSO, T.M.,WILLIAMS, P.M., TUCKER, A.L., KANER, R.J., FERRIS, B.,GONDA, I., SWEENEY, T.D., RAMALINGAM, R., KOVESDI, I.,SHAK, S., and CRYSTAL, R.G. (1999c). Airway epithelial CFTRmRNA expression in cystic fibrosis patients after repetitive admin-istration of a recombinant adenovirus. J. Clin. Invest. 104,1245–1255.
HARVEY, B.-G., HACKETT, N.R., SCOTT, E., and CRYSTAL, R.G.(1999d). Administration of an E12E32 adenovirus vector to airwayepithelial cells of normal individuals elicits minimal local host re-sponses. American Society of Gene Therapy, Program of the 2ndAnnual Meeting, Washington, D.C., June 9–13, 1999, p. 155a.
HARVEY, B.-G., HACKETT, N.R., and CRYSTAL, R.G. (1999e).Persistence of the vector genome in bronchial epithelial cells of nor-mal individuals following airway spray administration of an E12E32
adenovirus vector. Pediatr. Pulmonol. Suppl. 19, 225.HARVEY, B.-G., MARONI, J., O’DONOGHUE, K.A., CHU, K.W.,
MUSCAT, J.C., PIPPO, A.L., WRIGHT, C.E., HOLLMANN, C.,WISNIVESKY, J.P., KESSLER, P., RASMUSSEN, H., ROSEN-GART, T.K., and CRYSTAL, R.G. (2002). Safety of local deliveryof low and intermediate dose adenovirus gene transfer vectors to in-dividuals with a spectrum of comorbid conditions. Hum. Gene Ther.13, 15–63.
HAY, J.G., MCELVANEY, N.G., HERENA, J., and CRYSTAL, R.G.(1995). Modification of nasal epithelial potential differences of in-dividuals with cystic fibrosis consequent to local administration of anormal CFTR cDNA adenovirus gene transfer vector. Hum. GeneTher. 6, 1487–1496.
HUARD, J., LOCHMULLER, H., ACSADI, G., JANI, A., MASSIE,B., and KARPATI, G. (1995). The route of administration is a ma-
ANALYSIS OF RISK FACTORS FOR ADENOVIRUS GENE TRANSFER 99

jor determinant of the transduction efficiency of rat tissues by ade-noviral recombinants. Gene Ther. 2, 107–115.
KAPLAN, J.M., and SMITH, A.E. (1997). Characterization of factorsinvolved in modulating. Hum. Gene Ther. 8, 45–56.
KASS-EISLER, A., FALCK-PEDERSEN, E., ELFENBEIN, D.H.,ALVIRA, M., BUTTRICK, P.M., and LEINWAND, L.A. (1994).The impact of developmental stage, route of administration and theimmune system on adenovirus-mediated gene transfer. Gene Ther.1, 395–402.
KILLEWICH, L.A., GARDNER, A.W., MACKO, R.F., HANNA, D.J.,GOLDBERG, A.P., COX, D.K., and FLINN, W.R. (1998). Progres-sive intermittent claudication is associated with impaired fibrinoly-sis. J. Vasc. Surg. 27, 645–650.
LOZIER, J.N., METZGER, M.E., DONAHUE, R.E., and MORGAN,R.A. (1999). Adenovirus-mediated expression of human coagulationfactor IX in the rhesus macaque is associated with dose-limiting tox-icity. Blood 94, 3968–3975.
MACK, C.A., SONG, W.R., CARPENTER, H., WICKHAM, T.J.,KOVESDI, I., HARVEY, B.G., MAGOVERN, C.J., ISOM, O.W.,ROSENGART, T., FALCK-PEDERSEN, E., HACKETT, N.R.,CRYSTAL, R.G., and MASTRANGELI, A. (1997). Circumventionof anti-adenovirus neutralizing immunity by administration of an ad-enoviral vector of an alternate serotype. Hum. Gene Ther. 8, 99–109.
MASTRANGELI, A., HARVEY, B.G., YAO, J., WOLFF, G.,KOVESDI, I., CRYSTAL, R.G., and FALCK-PEDERSEN, E.(1996). “Sero-switch” adenovirus-mediated in vivo gene transfer:Circumvention of anti-adenovirus humoral immune defenses againstrepeat adenovirus vector administration by changing the adenovirusserotype. Hum. Gene Ther. 7, 79–87.
MCELVANEY, N.G., and CRYSTAL, R.G. (1995). IL-6 release andairway administration of human CFTR cDNA adenovirus vector. Nat.Med. 1, 182–184.
MORRAL, N., O’NEAL, W., RICE, K., LELAND, M., KAPLAN, J.,PIEDRA, P.A., ZHOU, H., PARKS, R.J., VELJI, R., AGUILAR-CORDOVA, E., WADSWORTH, S., GRAHAM, F.L.,KOCHANEK, S., CAREY, K.D., and BEAUDET, A.L. (1999). Ad-ministration of helper-dependent adenoviral vectors and sequentialdelivery of different vector serotype for long-term liver-directed genetransfer in baboons. Proc. Natl. Acad. Sci. U.S.A. 96, 12816–12821.
NICOLOFF, A.D., TAYLOR, L.M.J., MCCLAFFERTY, R.B., MON-ETA, G.L., and PORTER, J.M. (1998). Patient recovery after in-frainguinal bypass grafting for limb salvage. J. Vasc. Surg. 27, 256–263.
NUNES, F.A., FURTH, E.E., WILSON, J.M., and RAPER, S.E. (1999).Gene transfer into the liver of nonhuman primates with E1-deletedrecombinant adenoviral vectors: Safety of readministration. Hum.Gene Ther. 10, 2515–2526.
OUALIKENE, W., GONIN, P., and ELOIT, M. (1994). Short and longterm dissemination of deletion mutants of adenovirus in permissive(cotton rat) and non-permissive (mouse) species. J. Gen. Virol. 75,2765–2768.
PATEL, S.R., LEE, L.Y., MACK, C.A., POLCE, D.R., EL-SAWY, T.,HACKETT, N.R., ILERCIL, A., JONES, E.C., HAHN, R.T., ISOM,O.W., ROSENGART, T.K., and CRYSTAL, R.G. (1999). Safety ofdirect myocardial administration of an adenovirus vector encodingvascular endothelial growth factor 121. Hum. Gene Ther. 10,1331–1348.
RIHAL, C.S., SUTTON-TYRRELL, K., GUO, P., KELLER, N.M.,JANDOVA, R., SELLERS, M.A., SCHAFF, H.V., and HOLMES,D.R.J. (1999). Increased incidence of periprocedural complicationsamong patients with peripheral vascular disease undergoing myo-cardial revascularization in the bypass angioplasty revascularizationinvestigation. Circulation 100, 171–177.
ROSENGART, T.K., LEE, L.Y., PATEL, S.R., KLIGFIELD, P.D.,OKIN, P.M., HACKETT, N.R., ISOM, O.W., and CRYSTAL, R.G.(1999a). Six-month assessment of a phase I trial of angiogenic genetherapy for the treatment of coronary artery disease using direct in-
tramyocardial administration of an adenovirus vector expressing theVEGF121 cDNA. Ann. Surg. 230, 466–470.
ROSENGART, T.K., LEE, L.Y., PATEL, S.R., SANBORN, T.A.,PARIKH, M., BERGMAN, G.W., HACHAMOVITCH, R., SZULC,M., KLIGFIELD, P.D., OKIN, P.M., HAHN, R.T., DEVEREUX,R.B., POST, M.R., HACKETT, N.R., FOSTER, T., GRASSO, T.M.,LESSER, M.L., ISOM, O.W., and CRYSTAL, R.G. (1999b). An-giogenesis gene therapy: Phase I assessment of direct intramyocar-dial administration of an adenovirus vector expressing VEGF121cDNA to individuals with clinically significant severe coronary arterydisease. Circulation 100, 468–474.
ROSNER, B. (1995a). Hypothesis testing: Present-time data. In Fun-damentals in Biostatistics. (Wadsworth Publishing, Belmont, CA)pp. 585–631.
ROSNER, B. (1995b). Regression and correlation methods. In Funda-mentals in Biostatistics. (Wadsworth Publishing, Belmont, CA) pp.443–549.
ROSS, P. (1976). Use of the logistic model in retrospective studies.Biometrics 32, 599–606.
SIMON, R.H., ENGELHARDT, J.F., YANG, Y., ZEPEDA, M., WE-BER-PENDLETON, S., GROSSMAN, M., and WILSON, J.M.(1993). Adenovirus-mediated transfer of the CFTR gene to lung ofnonhuman primates: Toxicity study. Hum. Gene Ther. 4, 771–780.
STRANO, A., HOPPENSTEADT, D., WALENGA, J.M., FAREED,J., SABBA, C., BERARDI, E., ALLEGRA, C., CARLIZZA, A., BI-NAGHI, F., FRONTEDDU, F., DEL GUERCIO, R., DEL GUER-CIO, M., PINTO, A., ALLETTO, G., NAZZARI, M., and FERRARI,P.A. (1996). Plasma levels of the molecular markers of coagulationand fibrinolysis in patients with peripheral arterial disease. Semin.Thromb. Hemost. 22(Suppl.1), 35–40.
VIOLI, F., CRIQUI, M., LONGONI, A., and CASTIGLIONI, C.(1996). Relation between risk factors and cardiovascular complica-tions in patients with peripheral vascular disease. Results from theA.D.E.P. study. Atherosclerosis 120, 25–35.
WILMOTT, R.W., AMIN, R.S., PEREZ, C.R., WERT, S.E., KELLER,G., BOIVIN, G.P., HIRSCH, R., DE INOCENCIO, J., LU, P., REIS-ING, S.F., YEI, S., WHITSETT, J.A., and TRAPNELL, B.C. (1996).Safety of adenovirus-mediated transfer of the human cystic fibrosistransmembrane conductance regulator cDNA to the lungs of nonhu-man primates. Hum. Gene Ther. 7, 301–318.
WILSON, J.M. (1996). Adenoviruses as gene-delivery vehicles. N.Engl. J. Med. 334, 1185–1187.
WORGALL, S., WOLFF, G., FALCK-PEDERSEN, E., and CRYS-TAL, R.G. (1997). Innate immune mechanisms dominate elimina-tion of adenoviral vectors following in vivo administration. Hum.Gene Ther. 8, 37–44.
YANG, Y., LI, Q., ERTL, H.C., and WILSON, J.M. (1995a). Cellularand humoral immune responses to viral antigens create barriers tolung-directed gene therapy with recombinant adenoviruses. J. Virol.69, 2004–2015.
YANG, Y., XIANG, Z., ERTL, H.C., and WILSON, J.M. (1995b). Up-regulation of class I major histocompatibility complex antigens byinterferon gamma is necessary for T-cell-mediated elimination of re-combinant adenovirus-infected hepatocytes in vivo. Proc. Natl. Acad.Sci. U.S.A. 92, 7257–7261.
Address reprint requests to:Dr. Ronald G. Crystal
Institute of Genetic MedicineWeill Medical College of Cornell University—
New York Presbyterian Hospital515 East 71 Street, Suite 1000
New York, NY 10021
E-mail: [email protected]
Published online: December 21, 2001.
CRYSTAL ET AL.100

This article has been cited by:
1. Crystal Ronald G.. 2014. Adenovirus: The First Effective In Vivo Gene Delivery Vector. Human GeneTherapy 25:1, 3-11. [Citation] [Full Text HTML] [Full Text PDF] [Full Text PDF with Links][Supplemental Material]
2. Stephen M. Kaminsky, Todd K. Rosengart, Jonathan Rosenberg, Maria J. Chiuchiolo, Benjamin Van deGraaf, Dolan Sondhi, Ronald G. Crystal. 2013. Gene Therapy to Stimulate Angiogenesis to Treat DiffuseCoronary Artery Disease. Human Gene Therapy 24:11, 948-963. [Abstract] [Full Text HTML] [Full TextPDF] [Full Text PDF with Links]
3. Krista M. Honkonen, Mikko T. Visuri, Tomi V. Tervala, Paavo J. Halonen, Mari Koivisto, MarkkuT. Lähteenvuo, Kari K. Alitalo, Seppo Ylä-Herttuala, Anne M. Saaristo. 2013. Lymph Node Transferand Perinodal Lymphatic Growth Factor Treatment for Lymphedema. Annals of Surgery 257:5, 961-967.[CrossRef]
4. Stephen M. Kaminsky, Lucy Quach, Stacey Chen, Lorraine Pierre-Destine, Benjamin Van de Graaf,Sébastien Monette, Jonathan B. Rosenberg, Bishnu P. De, Dolan Sondhi, Neil R. Hackett, Jason G. Mezey,Todd K. Rosengart, Ronald G. Crystal. 2013. Safety of Direct Cardiac Administration of AdVEGF-All6A+,a Replication-Deficient Adenovirus Vector cDNA/Genomic Hybrid Expressing All Three Major Isoformsof Human Vascular Endothelial Growth Factor, to the Ischemic Myocardium of Rats. Human Gene TherapyClinical Development 24:1, 38-46. [Abstract] [Full Text HTML] [Full Text PDF] [Full Text PDF withLinks] [Supplemental Material]
5. Todd K. Rosengart, Muath M. Bishawi, Michael S. Halbreiner, Mathew Fakhoury, Eileen Finnin, CharleenHollmann, Annie Laurie Shroyer, Ronald G. Crystal. 2013. Long-Term Follow-Up Assessment of a Phase1 Trial of Angiogenic Gene Therapy Using Direct Intramyocardial Administration of an Adenoviral VectorExpressing the VEGF121 cDNA for the Treatment of Diffuse Coronary Artery Disease. Human GeneTherapy 24:2, 203-208. [Abstract] [Full Text HTML] [Full Text PDF] [Full Text PDF with Links]
6. B. J. Baum, I. Alevizos, C. Zheng, A. P. Cotrim, S. Liu, L. McCullagh, C. M. Goldsmith, P. D. Burbelo,D. E. Citrin, J. B. Mitchell, L. K. Nottingham, S. F. Rudy, C. Van Waes, M. A. Whatley, J. S. Brahim,J. A. Chiorini, S. Danielides, R. J. Turner, N. J. Patronas, C. C. Chen, N. P. Nikolov, G. G. Illei. 2012.Early responses to adenoviral-mediated transfer of the aquaporin-1 cDNA for radiation-induced salivaryhypofunction. Proceedings of the National Academy of Sciences 109:47, 19403-19407. [CrossRef]
7. Ronald G. Crystal, Stephen M. Kaminsky, Neil R. Hackett, Todd K. Rosengart. 2012. Double-Blinded,Placebo-Controlled, Randomized Gene Therapy Using Surgery for Vector Delivery. Human Gene Therapy23:5, 438-441. [Citation] [Full Text HTML] [Full Text PDF] [Full Text PDF with Links]
8. Cuong Q Nguyen, Hongen Yin, Byung Ha Lee, John A Chiorini, Ammon B Peck. 2011. IL17: potentialtherapeutic target in Sjögren's syndrome using adenovirus-mediated gene transfer. Laboratory Investigation91:1, 54-62. [CrossRef]
9. James Devaney, Maya Contreras, John G Laffey. 2011. Clinical Review: Gene-based therapies for ALI/ARDS: where are we now?. Critical Care 15:3, 224. [CrossRef]
10. Dmitry M Shayakhmetov, Nelson C Di Paolo, Karen L Mossman. 2010. Recognition of Virus Infectionand Innate Host Responses to Viral Gene Therapy Vectors. Molecular Therapy 18:8, 1422-1429. [CrossRef]
11. Julie L. Boyer, Carolina Sofer-Podesta, John Ang, Neil R. Hackett, Maria J. Chiuchiolo, Svetlana Senina,David Perlin, Ronald G. Crystal. 2010. Protective Immunity Against a Lethal Respiratory Yersinia pestisChallenge Induced by V Antigen or the F1 Capsular Antigen Incorporated into Adenovirus Capsid. HumanGene Therapy 21:7, 891-901. [Abstract] [Full Text HTML] [Full Text PDF] [Full Text PDF with Links]
12. Bruce J. Baum, Changyu Zheng, Ilias Alevizos, Ana P. Cotrim, Shuying Liu, Linda McCullagh, Corinne M.Goldsmith, Nancy McDermott, John A. Chiorini, Nikolay P. Nikolov, Gabor G. Illei. 2010. Developmentof a gene transfer-based treatment for radiation-induced salivary hypofunction. Oral Oncology 46:1, 4-8.[CrossRef]

13. Dmitry M. Shayakhmetov. 2010. Virus Infection Recognition and Early Innate Responses to Non-Enveloped Viral Vectors. Viruses 2:1, 244-261. [CrossRef]
14. I SPRINGER, P NIEHOFF, Y ACIL, M MARGET, A LANGE, P WARNKE, H PIELENZ, J ROLDAN,J WILTFANG. 2008. BMP-2 and bFGF in an irradiated bone model. Journal of Cranio-MaxillofacialSurgery 36:4, 210-217. [CrossRef]
15. Shadi Ghali, Marlese P. Dempsey, Deirdre M. Jones, Raymond H. Grogan, Peter E. Butler, Geoffrey C.Gurtner. 2008. Plastic Surgical Delivery Systems for Targeted Gene Therapy. Annals of Plastic Surgery 60:3,323-332. [CrossRef]
16. Q Zhu, C W Thomson, K L Rosenthal, M R McDermott, S M Collins, J Gauldie. 2008. Immunization withadenovirus at the large intestinal mucosa as an effective vaccination strategy against sexually transmittedviral infection. Mucosal Immunology 1:1, 78-88. [CrossRef]
17. Ingo N.G. Springer, Patrick H. Warnke, Hendrik Terheyden, Yahya Açil, Anne Bülhoff, SolveigKuchenbecker, Hendrik Bolte, Paul A.J. Russo, Eleftherios G. Vairaktaris, Jörg Wiltfang. 2007.Craniectomy and noggin application in an infant model. Journal of Cranio-Maxillofacial Surgery 35:3,177-184. [CrossRef]
18. Bi-Jun Huang, Ran-Yi Liu, Jia-Ling Huang, Zhi-Hui Liang, George Fu Gao, Jiang-Xue Wu, WenlinHuang. 2007. Long-Term Toxicity Studies in Canine of E10A, An Adenoviral Vector for HumanEndostatin Gene. Human Gene Therapy 18:3, 207-221. [Abstract] [Full Text PDF] [Full Text PDF withLinks]
19. Bruce J. Baum, Changyu Zheng, Ana P. Cotrim, Corinne M. Goldsmith, Jane C. Atkinson, Jaime S.Brahim, John A. Chiorini, Antonis Voutetakis, Rose Anne Leakan, Carter Van Waes, James B. Mitchell,Christine Delporte, Songlin Wang, Stephen M. Kaminsky, Gabor G. Illei. 2006. Transfer of the AQP1cDNA for the correction of radiation-induced salivary hypofunction. Biochimica et Biophysica Acta (BBA)- Biomembranes 1758:8, 1071-1077. [CrossRef]
20. Timothy P. O'Connor, Ronald G. Crystal. 2006. Genetic medicines: treatment strategies for hereditarydisorders. Nature Reviews Genetics 7:4, 261-276. [CrossRef]
21. C Zheng, A Voutetakis, MR Kok, CM Goldsmith, GBJ Smith, S Elmore, A Nyska, M Vallant, RD Irwin,BJ Baum. 2006. Toxicity and biodistribution of a first-generation recombinant adenoviral vector, in thepresence of hydroxychloroquine, following retroductal delivery to a single rat submandibular gland. OralDiseases 12:2, 137-144. [CrossRef]
22. Dolan Sondhi, Neil R. Hackett, Stephen M. Kaminsky, Mark M. Souweidane, Michael G. Kaplitt, RonaldG. CrystalGene Therapy for the Late Infantile Form of Batten Disease 317-333. [CrossRef]
23. Robert G. Pergolizzi, Rachel Dragos, Alexander E. Ropper, André Menez, Ronald G. Crystal. 2005.Protective Immunity Against α-Cobratoxin Following a Single Administration of a Genetic VaccineEncoding a Non-Toxic Cobratoxin Variant. Human Gene Therapy 16:3, 292-298. [Abstract] [Full TextPDF] [Full Text PDF with Links]
24. Julie L. Boyer, Gary Kobinger, James M. Wilson, Dr. Ronald G. Crystal. 2005. Adenovirus-Based GeneticVaccines for Biodefense. Human Gene Therapy 16:2, 157-168. [Abstract] [Full Text PDF] [Full Text PDFwith Links]
25. Huibi Cao, David R. Koehler, Dr. Jim Hu. 2004. Adenoviral Vectors for Gene Replacement Therapy. ViralImmunology 17:3, 327-333. [Abstract] [Full Text PDF] [Full Text PDF with Links]
26. Joseph W Szokol, Glenn S Murphy, Jeffery S Vender, Martin Nitsun. 2004. Gene therapy in heart and lungdisease. Current Opinion in Anaesthesiology 17:1, 13-20. [CrossRef]
27. Mia Jullig, Wei V. Zhang, N. Susan Stott. 2004. Gene therapy in orthopaedic surgery: the current status.ANZ Journal of Surgery 74:1-2, 46-54. [CrossRef]
28. B Baum. 2003. Advances in vector-mediated gene transfer. Immunology Letters 90:2-3, 145-149. [CrossRef]29. Yadi Tan, Neil R. Hackett, Julie L. Boyer, Ronald G. Crystal. 2003. Protective Immunity Evoked Against
Anthrax Lethal Toxin After a Single Intramuscular Administration of an Adenovirus-Based Vaccine

Encoding Humanized Protective Antigen. Human Gene Therapy 14:17, 1673-1682. [Abstract] [Full TextPDF] [Full Text PDF with Links]
30. Saul Benedict Freedman. 2002. Clinical trials of gene therapy for atherosclerotic cardiovascular disease.Current Opinion in Lipidology 13:6, 653-661. [CrossRef]
31. Ben-Gary Harvey, Jaman Maroni, Kelley A. O'Donoghue, Karen W. Chu, Jolene C. Muscat, Allison L.Pippo, Connie E. Wright, Charleen Hollmann, Juan P. Wisnivesky, Paul D. Kessler, Henrik S. Rasmussen,Todd K. Rosengart, Ronald G. Crystal. 2002. Safety of Local Delivery of Low- and Intermediate-DoseAdenovirus Gene Transfer Vectors to Individuals with a Spectrum of Morbid Conditions. Human GeneTherapy 13:1, 15-63. [Abstract] [Full Text PDF] [Full Text PDF with Links]





























