Embed Size (px)
Citation preview

Anti-inflammatory Effect of Rosmarinic Acid and an Extract ofRosmarinus officinalis in Rat Models of Local and Systemic
InflammationJoao Rocha1, Maria Eduardo-Figueira1, Andreia Barateiro1, Adelaide Fernandes1, Dora Brites1, Rosario Bronze2, Catarina MM Duarte2,
Ana Teresa Serra2, Rui Pinto1, Marisa Freitas3, Eduarda Fernandes3, Beatriz Silva-Lima1, Helder Mota-Filipe1 and Bruno Sepodes1
1iMed.ULisboa, Faculty of Pharmacy - University of Lisbon, Lisboa, Portugal, 2ITQB/IBET, Quinta do Marques Estac�~ao Agron�omica Nacional,Oeiras, Portugal and 3REQUIMTE, Laboratory of Applied Chemistry, Department of Chemical Sciences, Faculty of Pharmacy, University of Porto,
Porto, Portugal
(Received 14 July 2014; Accepted 25 September 2014)
Abstract: Rosmarinic acid is a polyphenolic compound and main constituent of Rosmarinus officinalis and has been shown topossess antioxidant and anti-inflammatory properties. We aimed to evaluate the anti-inflammatory properties of rosmarinic acidand of an extract of R. officinalis in local inflammation (carrageenin-induced paw oedema model in the rat), and further evaluatethe protective effect of rosmarinic acid in rat models of systemic inflammation: liver ischaemia–reperfusion (I/R) and thermalinjury models. In the local inflammation model, rosmarinic acid was administered at 10, 25 and 50 mg/kg (p.o.), and the extractwas administered at 10 and 25 mg/kg (equivalent doses to rosmarinic acid groups) to male Wistar rats. Administration of ros-marinic acid and extract at the dose of 25 mg/kg reduced paw oedema at 6 hr by over 60%, exhibiting a dose–response effect,suggesting that rosmarinic was the main contributor to the anti-inflammatory effect. In the liver I/R model, rosmarinic acid wasadministered at 25 mg/kg (i.v.) 30 min. prior to the induction of ischaemia and led to the significant reduction in the serum con-centration of transaminases (AST and ALT) and LDH. In the thermal injury model, rosmarinic acid was administered at 25 mg/kg (i.v.) 5 min. prior to the induction of injury and significantly reduced multi-organ dysfunction markers (liver, kidney, lung)by modulating NF-jB and metalloproteinase-9. For the first time, the anti-inflammatory potential of rosmarinic acid has beenidentified, as it causes a substantial reduction in inflammation, and we speculate that it might be useful in the pharmacologicalmodulation of injuries associated to inflammation.
Rosmarinus officinalis L., popularly named rosemary, hasbeen used in folk medicine with several pharmacologicaleffects being associated to its consumption, including its anti-inflammatory effects [1,2], and rosmarinic acid (RA) is one ofits main phenolic compounds [3].Two studies have evaluated the kinetics of rosmarinic
acid when administered orally to rats [4,5]. These studiesshowed that rosmarinic acid was readily absorbed in thegastrointestinal tract (according to Konishi and Kobayashi[6], it crosses intestinal epithelium by passive diffusion) andreaches the peak plasma concentration at 0.5 hr post-admin-istration. Metabolites formed are a result of glucuronidation,sulphation and methylation of rosmarinic acid and are theneliminated in the urine. The effect of R. officinalis and ros-marinic acid on metabolizing enzymes was also studied inWistar rats [7]. This study demonstrated that the extract ofR. officinalis was able to induce the enzymes CYP1A1,CYP2B1/2, CYP2E1, glutathione S-transferase and UDP-glu-curonosyl transferase, but this effect was not observedwhen rosmarinic acid was administered alone. The authorshave attributed this effect to the presence of flavones andmonoterpenes.
It has been widely recognized for many years that certaintypes of inflammatory tissue injury are mediated by reactiveoxygen metabolites and that in addition to promoting directtoxicity, they may also initiate and/or amplify inflammationvia the up-regulation of several genes involved in the inflam-matory response [8].A vast amount of circumstantial evidence implicates oxy-
gen-derived free radicals and high-energy oxidants as media-tors of inflammation, shock and ischaemia/reperfusion injury[9]. Antioxidant effects of extracts of R. officinalis have beenreported in in vitro studies, exhibiting scavenging of superox-ide anion, peroxynitrite and nitric oxide [10–13].Also, reactive oxygen species play a major role in the organ
injury of many inflammatory-mediated events, including sys-temic inflammation and ischaemia–reperfusion [9], particularlyof the liver [14]. Hepatic ischaemia–reperfusion is a majorcomponent of injury in vascular occlusion both during liversurgery and during liver transplantation. The pathophysiologyof hepatic ischaemia–reperfusion includes several mechanismsthat contribute to various degrees of the overall organ damage,and formation of reactive oxygen species (ROS) and oxidantstress are the most invoked disease mechanisms in ischaemia–reperfusion injury [15].Generation of reactive oxygen species during the reperfu-
sion process can be prevented or attenuated, and that has beenshown to reduce liver injury in experimental models of ischae-
Author for correspondence: Bruno Sepodes, Faculty of Pharmacy,University of Lisbon, Avenida Prof. Gama Pinto, 1649-003 Lisbon,Portugal (fax +351 217946470, e-mail [email protected]).
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
Basic & Clinical Pharmacology & Toxicology Doi: 10.1111/bcpt.12335

mia–reperfusion [9,16]. Therefore, given the potential antioxi-dant and anti-inflammatory effects of R. officinalis and ros-marinic acid, they might have protective effects in the injurysustained by the liver subjected to ischaemia–reperfusion.Lungs represent the first frontier between oxygen entry into
the organism and delivery to the mitochondria and are there-fore exposed to higher concentrations of oxygen and reactiveoxygen species [17], leading to the amplification of inflamma-tory processes [18]. A disruption of oxidative balance wasfound to be important in the pathogenesis of lung inflamma-tory diseases, such as acute lung injury (ALI) and acute respi-ratory distress syndrome (ARDS) [19], pneumonia, burn,chronic obstructive pulmonary disease and lung ischaemia–reperfusion [20–22].Our aim was to determine the in vitro antioxidant activity
of a R. officinalis extract and rosmarinic acid and to evaluateand compare their in vivo anti-inflammatory effect on a localmodel of inflammation – the carrageenin-induced paw oedemain the rat. We further evaluated the protective effect of ros-marinic acid administration in a hepatic ischaemia–reperfusionmodel and in a thermal injury model in the rat, taking intoaccount the previously described role of oxidative stress inthese systemic inflammatory injuries.
Materials and Methods
Chemicals. Rosmarinic acid was obtained from Sigma-AldrichQu�ımica SA (Sintra, Portugal). Dried leaves of R. officinalis wereobtained from Ervital – Plantas Arom�aticas e Medicinais, Lda. (Mezio,Portugal). Apyrogenic saline (0.9% NaCl) was obtained from B. BraunMedical Lda. (Queluz, Portugal). Unless otherwise stated, all othercompounds were obtained from Sigma-Aldrich Qu�ımica SA (fig. 1).
Production of the R. officinalis extract. A methanolic extract wasprepared with the dried leaves of R. officinalis and performed with acontinuous Soxhlet extractor equipment (Soxtherm Automatic;Gerhardt Bonn, Germany). The extraction was performed boiling 7 gof R. officinalis dried leaves, with 50 mL of methanol resulting in anextract of 20 mL.
Characterization of the chemical profile of the R. officinalis extract.
High-performance liquid chromatography (HPLC-UV). Acetonitrileand methanol were acquired from Lab-Scan (Dublin, Ireland), andphosphoric acid was acquired from Riedel-deHaen (Seelze,Germany). Deionized water (conductivity of 0.050) was obtained bya Milli-Q system (Millipore, Molsheim, France). A Surveyorequipment from Thermo Finnigan with a diode array detector(Thermo Finnigan Surveyor, San Jose, CA, USA), a fluorescence
detector (Shimadzu, RF-535 Kyoto, Japan) and an electrochemicaldetector (Dionex, ED40 Bannockburn IL, USA) with a vitreouscarbon electrode were used. Separations were performed at 35°Cwith a LiChrospher C18 (5 lm, 250 mm 9 4 mm i.d.) column fromMerck Darmstadt, Germany with a guard column of the same type.The samples were injected using a 20-lL loop. The separationswere carried out with a flow rate of 700 lL/min., and the mobilephase consisted of a gradient mixture of eluent A (phosphoric acid0.1%) and eluent B (phosphoric acid–acetonitrile–water 5:400:595,v/v/v). The following gradient of eluents was used: 0–15 min. from0 until 20% eluent B; 10 min. with 20% eluent B; 25–70 min. from20 until 70% eluent B; 70–75 min. with 70% eluent B; 75–85 min.from 70 until 100% eluent B; 85–90 min. with 100% eluent B.Diode array detection (DAD) was performed between 200 and800 nm. Electrochemical detection was programmed for a linearvariation of �1.0 V at 1.0 V in 1.00 sec. (detection by integratedvoltammetry using a cyclic variation of the potential). The dataacquisition systems were ChromQuest version 4.0 (Thermo FinniganSurveyor) for the diode array detector and software 4880 (UnicamLinda-a-Velha, Portugal) for the electrochemical and fluorescencedetectors. A standard solution of rosmarinic acid was prepared(180 p.p.m.), and the peaks of both the standard solution andsample solution (diluted 1:40) were compared.
Liquid chromatography with mass spectrometry (LC-MS). A WatersHPLC equipment (Waters 2695) with a DAD detector (Waters 2996Milford, USA) and a Micromass MS equipment (Micromass,Quattro micro API) were used. Separations were performed with aWaters dC18 column (5 lm, 2.1 9 150 mm). The samples wereinjected using a loop of 20 lL. The separations were carried outwith a flow rate of 700 lL/min., and the mobile phase consisted ofa gradient mixture of eluent A (formic acid 0.5%) and eluent B(acetonitrile). The following gradient of eluents was used: 0–60 min. from 5 until 20% eluent B; 60–80 min. from 20 to 28%eluent B; 80–82 min. from 28 until 30% eluent B; 82–87 min. with30% eluent B; 87–95 min. from 30 until 5% eluent B; 95–100 min. with 0% eluent B. Diode detection was performedbetween 210 and 600 nm.
Characterization of the antioxidant capacity.
Total phenolic content. The total concentrations of phenoliccompounds present in the natural extracts were determined accordingto the Folin–Ciocalteu colorimetric method [23]. Briefly, theappropriate diluted solutions of extracts were oxidized with a Folin–Ciocalteu reagent (Panreac, Barcelona Spain), and the reaction wasneutralized with sodium carbonate. The absorbance of the sampleswas measured at 765 nm on a spectrophotometer (GenesysTM 10UVThermoScientific, Waltham MA, USA) after 30 min. at 40°C. Gallicacid (Fluka, Seelze, Germany) was used as standard, and the resultwas expressed as means of three replicates (mg of gallic acid equiv/Lof extract – mg GAE/L) [20].
Oxygen radical absorbance capacity (ORAC). ORAC assay was usedto evaluate the antioxidant capacity of the samples towards peroxylradicals. The assay was carried out using the method described bySerra et al. [24], which measures the ability of the antioxidant speciespresent in the sample to inhibit the oxidation of FL catalysed byAAPH-generated peroxyl radicals (ROO˙). The composition of thereaction mixture was 6.3 9 10�8 M FL, 1.28 9 10�2 M AAPH(prepared in 75 mM PBS, pH 7.4) and the appropriate diluted sample,making up a total volume of 1.8 mL. The reaction was started by theaddition of AAPH to the mixture placed in a 10-mm-widefluorescence cuvette at 37°C. Fluorescence emitted by the reducedform of FL was measured and recorded every 1 min. at the emissionwavelength of 515 nm and excitation wavelength of 493 nmFig. 1. Chemical structure of rosmarinic acid.
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
2 JOAO ROCHA ET AL.

(fluorescence spectrophotometer with thermostatic bath, model CaryEclipse; Varian Santa Clara CA, USA) for a period of 30 min.Phosphate buffer (PBS) was used as a blank, and 1, 5, 12.5, 25 and50 lM Trolox solutions were used as control standards. All samples,including the blank and the controls, were analysed in triplicate. FinalORAC values were calculated using a regression equation between theTrolox concentration and the net area under the FL decay curve. Dataare expressed as millimolar of Trolox equivalent antioxidant capacity(TEAC), and the experiment was performed in triplicate [24].
Hydroxyl radical absorbance capacity (HORAC). The HORAC assaywas based on a previously reported method [24,25], modified for theFL800 microplate fluorescence reader (Bio-Tek Instruments, Isaza,Portugal). The FL800 microplate fluorescence reader was used withfluorescence filters for an excitation wavelength of 485 � 20 nm andan emission wavelength of 530 � 25 nm, and the plate reader wascontrolled by software Gen5 (Biotek, Winnoski VT, USA. Caffeicacid was used as the standard as it provides a wider linear range ascompared to gallic acid. Data were expressed as mM of caffeic acidequivalents (CAE). All samples were analysed as triplicates.
Neutrophil oxidative burst. Isolation of human neutrophils.Following informed consent, venous blood was collected from healthyvolunteers by antecubital venipuncture, into K3EDTA vacuum tubes.The isolation of human neutrophils was performed by the gradientdensity, as previously reported [26,27].
Evaluation of neutrophils’ oxidative burst. The chemiluminescentprobe luminol has been thoroughly studied and used for monitoring theproduction of reactive species by neutrophils, namely the superoxideanion radical (O2˙
�), hydrogen peroxide (H2O2), hydroxyl radical(HO˙), hypochlorous acid (HOCl), nitric oxide (˙NO) and peroxynitriteanion (ONOO�) [28]. The measurement of neutrophils’ oxidative burstwas undertaken by chemiluminescence, by monitoring ROS-inducedoxidation of luminol, according to a previously described procedure[29]. The reaction mixtures contained neutrophils (1 9 106 cells/mL)and the following reagents at the indicated final concentrations (in afinal volume of 250 lL): tested compounds at various concentrations,luminol (500 lM) and phorbol myristate acetate (PMA) (160 nM).Cells were pre-incubated with luminol and the tested compounds for5 min. before the addition of PMA, and the measurements were carriedout at 37°C, under continuous soft shaking. Kinetic readings wereinitiated immediately after cell stimulation. Measurements were taken atthe peak of the curve. This peak was observed at around 10 min. Effectsare expressed as the per cent inhibition of luminol oxidation. Each studycorresponds to, at least, four individual experiments, performed intriplicate in each experiment.
In vivo anti-inflammatory activity.
Experimental methods. Experiments were conducted according to theHome Office Guidance in the Operation of Animals (ScientificProcedures) Act 1986, published by Her Majesty’s Stationary Office,London, UK, and the Institutional Animal Research Committee Guidefor the Care and Use of Laboratory Animals published by the USNational Institutes of Health (NIH Publication No. 85-23, revised1996), as well as to the currently adopted EC regulations. Finally, thestudies are in compliance with the ARRIVE Guidelines for ReportingAnimal Research summarized at www.nc3rs.org.uk. Paw oedemastudies were carried out using male Wistar rats weighing 100–150 g(Harlan Ib�erica, Barcelona, Spain). Hepatic ischaemia–reperfusionstudies were carried out using male Wistar rats weighing 250–300 g(Harlan Ib�erica). Thermal injury studies were carried out using maleWistar rats weighing 320–380 g. All animals received a standard dietand water ad libitum.
Carrageenin-induced paw oedema. The carrageenin-induced pawoedema of the rat hind paw is a suitable model to study acute localinflammation and widely considered to be one of the most usefulmodels in the evaluation of anti-inflammatory activity ofinvestigational compounds [30,31].Paw oedema was induced by a single subplantar injection into the
rat left hind paw of 0.1 mL of a 1% k-carrageenin sterile saline solu-tion. Paw volume was measured by means of a volume displacementmethod using a plethysmometer (Digital Plethysmometer LE7500; Le-tica Scientific Instruments (Reagente 5, Porto, Portugal)). Paw volumewas measured immediately after the injection of carrageenin (V0 orbasal volume) and 6 hr later (V6 hr).Paw oedema was expressed as percentage of increase in paw vol-
ume 6 hr after carrageenin injection relative to the basal valuesaccording to the equation: % = (V6 hr � V0)/V0 9 100.The rats were randomly allocated into eight experimental groups as
described:1 Control Group: animals were subjected to subplantar injection into
the rat left hind paw of 0.1 mL sterile saline and administeredwith vehicle dimethyl sulfoxide – DMSO 10% (1 mL/kg, p.o.)(n = 6);
2 Carrageenin Group: animals subjected to paw oedema inductionby injection into the rat left hind paw of 0.1 mL of k-carrageenin(1%) and administered with vehicle (1 mL/kg, p.o.) (n = 10);
3 RA10 Group: animals subjected to paw oedema induction andpre-treated with rosmarinic acid (10 mg/kg, p.o.) 30 min. beforek-carrageenin injection (n = 8);
4 RA25 Group: animals subjected to paw oedema induction andpre-treated with rosmarinic acid (25 mg/kg, p.o.) 30 min. beforek-carrageenin injection (n = 8);
5 RA50 Group: animals subjected to paw oedema induction andpre-treated with rosmarinic acid (50 mg/kg, p.o.) 30 min. beforek-carrageenin injection (n = 8);
6 E10 Group: animals subjected to paw oedema induction and pre-treated with R. officinalis extract (10 mg/kg, p.o.) 30 min. beforek-carrageenin injection (n = 8);
7 E50 Group: animals subjected to paw oedema induction and pre-treated with R. officinalis extract (50 mg/kg, p.o.) 30 min. beforek-carrageenin injection (n = 8);
8 Indomethacin Group: animals subjected to paw oedema inductionand pre-treated with indomethacin (10 mg/kg, p.o.) 30 min. beforek-carrageenin injection (n = 8).
Hepatic ischaemia–reperfusion. The rats were randomly allocated intofive experimental groups as described:1 Control Group: the data were obtained from non-manipulated ani-
mals, that is rats that were not subjected to any surgical procedure(n = 6).
2 Sham Group: rats that were subjected to the surgical proceduresdescribed below except for liver I/R. Rats were administered vehi-cle (saline with 10% DMSO, 1 mL/kg i.v.) 30 min. prior to liverI/R (n = 4);
3 I/R Group: rats that were subjected to the surgical proceduresdescribed below and underwent liver ischaemia for 45 min. fol-lowed by reperfusion for 2 hr (n = 8);
4 RA + I/R Group: rats that were administered with RA (25 mg/kgi.v.) 30 min. prior to liver I/R (n = 8);
5 RA Sham Groups: rats that were administered with (25 mg/kgi.v.) and that were subjected to the surgical procedures describedbelow except for liver I/R (n = 4).
Hepatic ischaemia–reperfusion model was performed as previouslydescribed [16,32]. Briefly, anaesthetized rats were placed onto a ther-mostatically controlled heating mat (Harvard Apparatus Ltd, Kent,
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
EFFECT OF ROSMARINIC ACID IN INFLAMMATION 3

UK), and body temperature maintained at 37 � 0.5°C by means of arectal probe attached to a homoeothermic blanket. A tracheotomy wasperformed to maintain airway patency and to facilitate spontaneousrespiration. The jugular vein was cannulated (PP25, internal diameter0.40 mm; Portex, Hythe, Kent, UK) for the administration of saline oranaesthesia as required. A midline laparotomy was performed to care-fully expose the liver. For the liver I/R surgical procedures, ligamentattachments connecting the liver, diaphragm, abdominal wall andneighbouring organs were divided. The liver hilus was exposed to findthe common hepatic artery and the portal vein. A vascular microclampwas used to interrupt the portal venous and arterial hepatic blood sup-ply to the three cephalic lobes of the liver during 45 min. The threecaudal lobes retained an intact portal inflow and venous out-flow, pre-venting the intestinal venous congestion and possible leakage of bacte-ria or bacterial products to the circulation. Reperfusion commencedonce the vascular clip was removed, and was allowed to proceed for2 hr. Occlusion was verified visually by the change in the colour ofthe liver to a paler shade, and reperfusion by a blush. Other rats weresubjected to sham operation (sham operated), which underwent surgi-cal procedures similar to the I/R group rats but did not undergo I/R ofthe liver clamping and were maintained under anaesthesia for the dur-ing the experiment. For these experiments, all rats were anaesthetizedwith sodium pentobarbital (60 mg/kg i.p., Eutasil; Sanofi VeterinariaPorto Salvo, Portugal), and anaesthesia was maintained by supplemen-tary i.p. boli. At the end of all experiments, rats were killed by anoverdose of anaesthetic.At the end of the reperfusion period for the liver I/R experiments
and whenever appropriate regarding other experiments, blood was col-lected from the catheter placed in the right carotid artery into a serumSST gel and clot activator tube (Becton, Dickinson and CompanyFranklin Lakes NJ, USA) and was centrifuged (2000 g for 10 min. at4°C) to separate the serum. The serum was analysed within 24 hr (Co-bas c111 benchtop analyzer; Roche Sistemas de Diagn�osticos, Lda.Amadora, Portugal), and liver injury was assessed by measuring therise in the serum levels of alanine aminotransferase (ALT, a specificmarker for hepatic parenchymal injury), aspartate aminotransferase(AST, a non-specific marker for hepatic injury) and lactate dehydroge-nase (LDH, a marker of non-specific cellular injury).
Thermal injury. The rats were randomly allocated into 4 experimentalgroups as described:1 Sham Group: rats that were subjected to the surgical procedures
described below except for thermal injury. Rats were administeredvehicle (saline with 10% DMSO, 1 mL/kg i.v.) 5 min. prior tothermal injury (n = 9);
2 Thermal Injury Group: rats that were subjected to the surgical pro-cedures described below and underwent thermal injury (n = 14);
3 RA+Thermal Injury Group: rats that were administered with RA(25 mg/kg i.v.) 5 min. prior to thermal injury (n = 14);
4 RA Sham Group: rats that were administered with (25 mg/kg i.v.)and that were subjected to the surgical procedures described belowexcept for thermal injury (n = 6).
Briefly, anaesthetized rats were placed onto a thermostatically con-trolled heating mat (Harvard Apparatus Ltd), and body temperaturemaintained at 37 � 0.5°C by means of a rectal probe attached to a ho-moeothermic blanket. A tracheotomy was performed to maintain airwaypatency, facilitate spontaneous respiration and removal of secretions.The jugular vein was cannulated for the administration of saline or anaes-thesia as required, and the carotid artery was cannulated (PP50, I.D.0.58 mm; Portex Kent, UK) for haemodynamic monitoring by a pressuretransducer (MLT0380 BP Transducer; AD Instruments Oxford, UK) andblood collection at the end of the experiment. A 30% third-degree skinburn was induced by immersing dorsal-shaved skin into 99°C water for10 sec. using a synthetic foam template after surgical procedure. Thesham control groups were submitted to identical procedures as the other
groups except that room temperature water was used instead of heatedwater. After-burn animals were dried and placed over the heating mat for6 hr. For these experiments, all rats were anaesthetized with sodium pen-tobarbital (60 mg/kg i.p., Eutasil; Sanofi Veterinaria), and anaesthesiawas maintained by supplementary boli. At the end of all experiments,rats were killed by an overdose of anaesthetic.At the of the experiment, blood was collected from the catheter
placed in the right carotid artery into a serum SST gel and clot activa-tor tube and was centrifuged (3000 r.p.m. for 10 min. at 4°C) to sepa-rate the serum. The serum was analysed within 24 hr, and liver injurywas assessed by measurement of the rise in the serum levels of alanineaminotransferase (ALT, a specific marker for hepatic parenchymalinjury), aspartate aminotransferase (AST, a non-specific marker forhepatic injury) and lactate dehydrogenase (LDH, a marker of non-spe-cific cellular injury), and kidney injury was assessed by measurementof the rise in the serum levels of creatinine and urea. Measurements ofthe serum levels of pro-inflammatory cytokines (TNF-a, IL-1b, IL-6)were also taken by ELISAs (Quantikine� Rat TNF-a/TNFSF1AImmunoassay, Quantikine� Rat IL-1b/IL-1F2 Immunoassay,Quantikine� IL-6 Immunoassay from R&D Systems Inc., Citomed,Lda, Lisboa, Portugal).
Assessment of lung injury. At the end of the experiments,bronchoalveolar lavage fluid was collected into 15-mL Falcon tubes.Collection was performed by instillation of 10 mL of saline at 4°Cthrough the trachea cannula. The samples were centrifuged (3000r.p.m., 10 min., 4°C), the supernatant was divided into aliquots todetermine albumin and cytokine levels (TNF-a, IL-1b, IL-6), and thesediment was reconstituted in saline for the polymorphonuclear cellcount. Albumin levels were measured in a Cobas c111 benchtopanalyzer (Roche Sistemas de Diagn�osticos, Lda.). Polymorphonuclearcell count was performed on an Automated Hematology System(ADVIA 2120; Siemens Munich, Germany) following May–Grunwald–Giemsa coloration.Lung tissue samples were obtained at the end of the 6-hr period
after thermal injury and were fixed in 4% paraformaldehyde in PBSfor 72 hr at room temperature, dehydrated through a graded ethanolseries and embedded in paraffin (n = 3 per group). Haematoxylin andeosin (H&E) staining was performed as previously described [33], andimages were acquired using a brightfield Axioskop microscope (Zeiss,G€ottingen, Germany).For Western blot analysis of Akt and glycogen synthase kinase 3-
beta (GSK-3b) expression, frozen tissue sample cells were lysed inRIPA buffer containing Tris 50 mM (pH 8.0), 5 mM EDTA (pH8.0), 150 mM NaCl, 1% NP-40, 10% glycerol and 0.1% SDS, andsonicated for 20 sec. The lysate was centrifuged at 14,000 9 g for10 min. at 4°C, and the supernatants were collected and stored at�80°C. Protein concentrations were determined using Nanodrop ND-1000 (ThermoScientific, Wilmington DE, USA. Cell extracts contain-ing equal amounts of protein (100–150 lg) were separated onsodium dodecyl sulphate–polyacrylamide gel electrophoresis andtransferred to a nitrocellulose membrane. The membranes wereblocked with 5% non-fat milk, incubated with the primary antibodyovernight at 4°C rabbit anti-p-Akt [1:1000 (#12178; Cell Signalling,Beverly, MA, USA)], rabbit anti-Akt [(1:1000) (#4691; Cell Signal-ling)], goat anti-p-GSK-3b [(1:200) (#sc-11757; Santa Cruz, CA,USA)], mouse anti-GSK-3b [(1:1000) (#9832; Cell Signalling)] andthen with a horseradish peroxidase-labelled secondary antibody for1 hr at room temperature. After extensive washes, immunoreactivebands were detected by LumiGLO� (Cell Signalling) and visualizedby autoradiography with Hyperfilm ECL. Phosphorylation levels ofAkt and GSK-3b were analysed by the ratio of the phosphorylatedform to total enzyme levels and expressed as fold change.
Evaluation of factor nuclear kappa B (NF-kB) activity. Nuclearextracts were prepared according to the rapid Dignam method [34].
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
4 JOAO ROCHA ET AL.

Briefly, at the end of the incubation, cells were resuspended in400 lL ice-cold buffer [10 mM HEPES (pH 7.9), 10 mM KCl,0.1 mM EDTA, 0.1 mM EGTA, 1 mM dithiothreitol (DTT) and0.5 mM phenylmethylsulphonyl fluoride (PMSF)] for 20 min. on iceand vortexed vigorously for 5 sec. after the addition of 25 lL NonidetP40 (10%). Cell lysates were centrifuged at 10,000 9 g for 30 sec. at4°C, and the pelleted nuclei were lysed with 50 lL ice-cold buffer[10 mM HEPES (pH 7.9), 0.4 M NaCl, 10 mM EDTA, 10 mMEGTA, 1 mM DTT, 1 mM PMSF] for 20 min. at 4°C. Nuclearlysates were centrifuged at 14,000 9 g for 10 min. at 4°C, and thenuclear proteins recovered in the supernatants were stored at �80°C.After protein determination using the protein assay kit (Bio-Rad,Hercules, CA, USA), the p65 NF-jB subunit expression in eachcompartment was analysed by Western blot as previously described[35]. Extracts containing equal amounts of protein (50 lg) wereseparated on sodium dodecyl sulphate–polyacrylamide gelelectrophoresis and transferred to a nitrocellulose membrane. Themembranes were blocked with 5% non-fat milk, incubated with theprimary antibody overnight at 4°C [rabbit anti-p65 NF-jB subunit(1:1000) (SC-372; SantaCruz Biotechology)] and then with ahorseradish peroxidase-labelled secondary antibody for 1 hr at roomtemperature. After extensive washes, immunoreactive bands weredetected by LumiGLO� (Cell Signalling) and visualized byautoradiography with Hyperfilm ECL. Results were normalized tototal protein lane content measured following Amido Black staining.
Evaluation of cell death. Cell death was evaluated by caspase-3activation as previously described [36]. The activity of caspase-3 wasdetermined in tissue homogenates by enzymatic cleavage ofchromophore p-nitroanilide (pNA) from the substrate Ac-DEVD-pNAfor caspase-3, according to manufacturer’s instructions. The proteolyticreaction was carried out in protease assay buffer [50 mM HEPES (pH7.4); 100 mM NaCl; 0.1% (w/v) CHAPS; 10 mM DTT; 0.1 mMEDTA; 10% (v/v) glycerol], containing 2 mM specific substrate. Afterthe incubation of the reaction mixtures for 1–2 hr at 37°C, the formationof pNA was measured in a microplate reader (PR 2100; BioRadLaboratories, Inc.) at k=405 nm with a reference filter at 620 nm.Readings were normalized to total protein content determined using aprotein assay kit (Bio-Rad) according to the manufacturer’sspecification, and expressed as fold change of respective control.
Gelatin zymography (Metalloproteinases assay). Activity of matrixmetalloproteinase (MMP-9) was assessed by gelatin zymography asdescribed before [37]. Aliquots of tissue homogenates were analysedby SDS-PAGE zymography in 0.1% gelatine–10% acrylamide gels
under non-reducing conditions. After electrophoresis, gels werewashed for 1 hr with 2.5% Triton X-100 (in 50 mM Tris pH 7.4;5 mM CaCl2; 1 lM ZnCl2) to remove SDS and renature the matrixmetalloproteinases (MMP) species in the gel. Then, the gels wereincubated in the developing buffer (50 mM Tris pH 7.4; 5 mMCaCl2; 1 lM ZnCl2) overnight to induce gelatine lysis. For enzymeactivity analysis, the gels were stained with 0.5% CoomassieBrilliant Blue R-250 (Sigma-Aldrich Quimica SA, Sintra Portugal)and destained in 30% ethanol/10% acetic acid/H2O. Gelatinaseactivity, detected as a white band on a blue background, wasquantified by computerized image analysis and normalized with totalcellular protein. MMP-9 was detected as the band with 92 kDa.
Statistical analysis. The results were expressed as the mean � S.E.M.and were compared using a one-factorial ANOVA test, followed by aBonferroni’s post hoc test performed with a GraphPad PrismStatistical Package (version 5.0 GraphPad Software, La Jolla CA,USA)). A p-value less than 0.05 was considered to be statisticallysignificant.
Results
Characterization of the chemical profile of the R. officinalisextract.Chemical characterization of the extract by HPLC-UV andHPLC-MS revealed a high concentration of rosmarinic acid(4684 p.p.m., corresponding to 1.34 g of rosmarinic acid per100 g dried leaves) as demonstrated by the chromatographicprofile of a 280-nm HPL-UV (fig. 2), indicating that theextraction procedure had optimal conditions for the preferen-tial extraction of rosmarinic acid. Chemical profiling of theextract also revealed the presence of other phenolic com-pounds, although in minor concentrations (caffeic acid, p-coumaric acid, chlorogenic acid, ellagic acid, ferulic acid,rosmanol, rutin, luteolin, methoxyluteolin, nepitin).
Characterization of the antioxidant capacity.The antioxidant capacity assays demonstrated that both ros-marinic acid and R. officinalis extract have high antioxidantcapacities (table 1), although R. officinalis extract presented amuch higher activity.
Rosmarinic acid
Fig. 2. Chromatogram profile (1:10) of the Rosmarinus officinalis extract on wavelength 280 nm.
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
EFFECT OF ROSMARINIC ACID IN INFLAMMATION 5

Neutrophil oxidative burst.Pre-incubation of the neutrophils with rosmarinic acid resultedin an inhibition of luminol oxidation, induced by neutrophilactivation by phorbol myristate acetate (PMA) (fig. 3). Thereduction was statistically significant compared with controlneutrophils (incubation with PMA only) and exhibits a con-centration–response relation. The inhibitory concentration 50%(IC50) was 1.2 � 0.3 lM.
Carrageenin-induced paw oedema.As expected, intraplantar injection of carrageenin in rats led toan increase in paw volume after 6 hr (114 � 11.2%) whencompared with the control group. This increase was signifi-cantly reduced in a dose-dependent manner by pre-treatmentwith rosmarinic acid and R. officinalis extract, with the mostsignificant effect observed at the doses 25 and 50 mg/kg(increase in paw volume of 45.3 � 12.8% and 44.4 � 13%,respectively) (fig. 4).A comparison of the effect of a single administration of ros-
marinic acid (25 mg/kg) with the effect of lycopene (50 mg/kg), tempol (30 mg/kg), Trolox (30 mg/kg) and indomethacin(10 mg/kg), known antioxidant and anti-inflammatory sub-stances, showed that rosmarinic acid administration reducedoedema formation at the same magnitude as those substances(fig. 5).
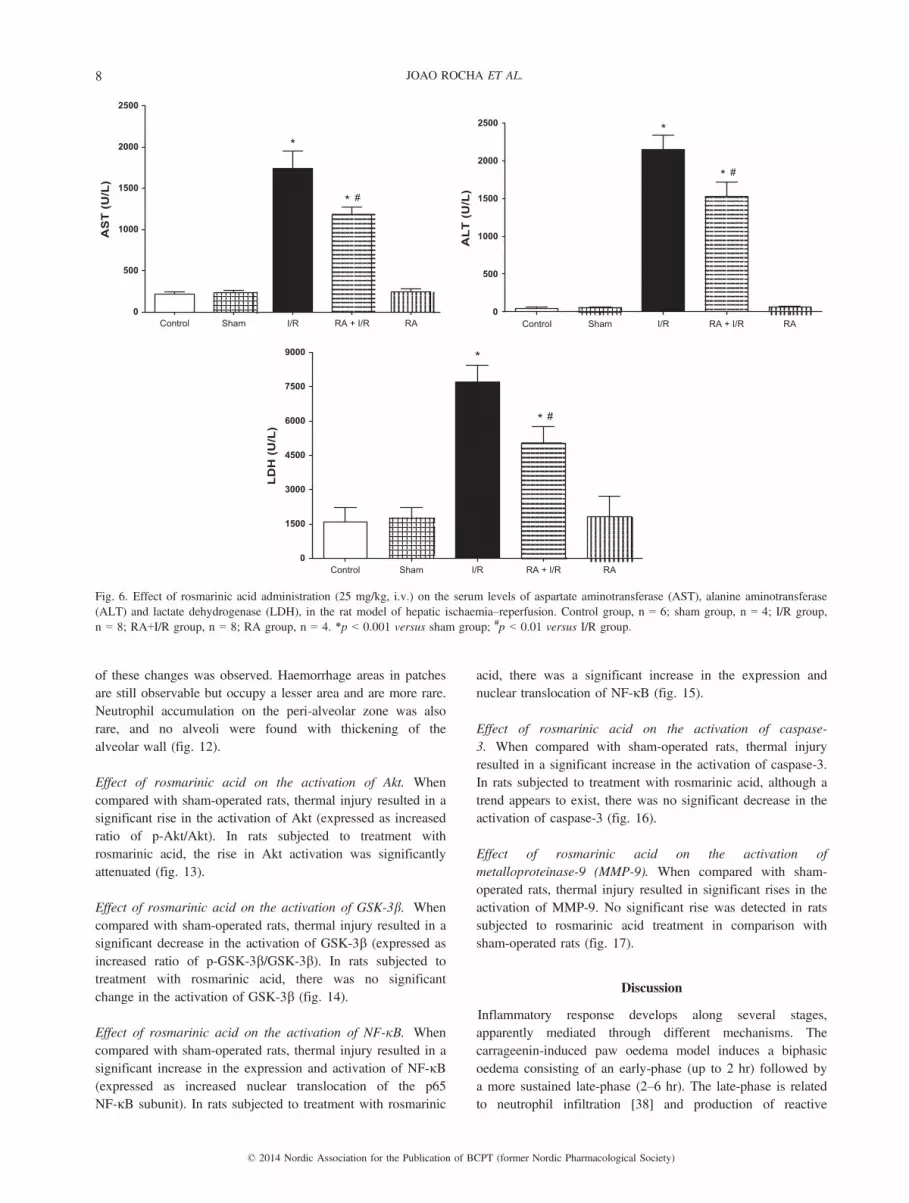
Hepatic ischaemia–reperfusion.In sham-operated rats, the surgical procedure did not producea significant change in serum levels of AST, ALT or LDHwhen compared with the control group. When compared withsham-operated rats, I/R of the liver resulted in significant risesin the serum levels of the marker enzymes AST, ALT andLDH, demonstrating the development of hepatocellular injury.In rats subjected to I/R pre-treated with rosmarinic acid, theserum rise in AST, ALT and LDH was significantly reducedby 35%, 35% and 45%, respectively. Rosmarinic acid byitself, when administered to rats not subjected to I/R injury,had no significant effect on AST, ALT and LDH serum levels(fig. 6).
Thermal injury model.
Effect of rosmarinic acid on liver and kidney injury. Whencompared with sham-operated rats, thermal injury resulted insignificant rises in the serum levels of the marker enzymes ASTand ALT, demonstrating the development of hepatocellularinjury. No significant rise was detected in rats subjected torosmarinic acid treatment in comparison with sham-operatedrats, indicating that rosmarinic acid administration prevented thedevelopment of hepatocellular injury. Termal injury also led toa significant rise in creatinine and urea serum levels indicatingthe development of kidney injury or dysfunction. In ratssubjected to treatment with rosmarinic acid, the rise increatinine serum level was significantly attenuated, althoughurea levels were not statistically different from rats subjectedonly to thermal injury. Rats subjected to thermal injury alsoexhibited a rise in serum levels of LDH, a non-specific markerof cell injury. No significant rise in LDH levels was detected inrats subjected to rosmarinic acid treatment in comparison withsham-operated rats (fig. 7).
Effect of rosmarinic acid on cytokine serum levels. Whencompared with sham-operated rats, thermal injury resulted insignificant rises in the serum levels of pro-inflammatory
Table 1.Characterization of the antioxidant capacity of rosmarinic acid andRosmarinus officinalis extract.
Total phenoliccontent ORAC HORAC
Rosmarinicacid
– 112 mM TEAC 66 mM CAE
R. officinalisextract
62.5 mM GAE 1384 mM TEAC 1516 mM CAE
GAE, gallic acid equivalents; CAE, caffeic acid equivalents; TEAC,Trolox equivalent antioxidant capacity.
***
0.2 0.5 0.9 1.9 3.8 7.50
25
50
75
100
******
**
μM
Lum
inol
oxi
datio
n by
act
ivat
ed n
eutr
ophi
ls (%
inhi
bitio
n)
Fig. 3. Inhibitory effect of rosmarinic acid (0.2–7.5 lM) on human neutrophils’ oxidative burst stimulated with PMA. **p < 0.01 and***p < 0.001 compared with the control assay (PMA alone). The values are given as the mean � S.E.M. (n ≥ 4).
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
6 JOAO ROCHA ET AL.

cytokines (TNF-a, Il-1b and IL-6). No significant rise wasdetected in rats subjected to rosmarinic acid treatment incomparison with sham-operated rats (fig. 8).
Effect of rosmarinic acid on cytokine bronchoalveolar lavagefluid (BALF) levels. When compared with sham-operatedrats, thermal injury resulted in significant rises in the BALFlevels of pro-inflammatory cytokines (TNF-a, IL-1b and IL-6). No significant rise in the BALF levels of TNF-a andIL-6 was detected in rats subjected to rosmarinic acidtreatment in comparison with sham-operated rats, and therise in the BALF levels of IL-1b was significantly reduced(fig. 9).
Effect of rosmarinic acid on albumin concentration onbronchoalveolar lavage fluid (BALF). When compared withsham-operated rats, thermal injury resulted in significant risesin the BALF levels of albumin demonstrating the disruptionof the alveolo-capillary membrane. No significant rise was
detected in rats subjected to rosmarinic acid treatment incomparison with sham-operated rats (fig. 10).
Effect of rosmarinic acid on the polymorphonuclear (PMN)cell presence on bronchoalveolar lavage fluid (BALF). Whencompared with sham-operated rats, thermal injury resulted insignificant rises in the leucocyte and neutrophil number inBALF and also an increase in neutrophil percentage. Nosignificant rise was detected in these parameters in ratssubjected to rosmarinic acid treatment in comparison withsham-operated rats (fig. 11).
Effect of rosmarinic acid on lung histology. When comparedwith sham-operated rats, thermal injury resulted in structuralchanges that indicate lung tissue injury, namely neutrophilaccumulation on the peri-alveolar zone, hyaline membraneformation with thickening of the alveolar wall and intra-alveolar (clots) and tissue haemorrhage (patchy formation). Inrats subjected to rosmarinic acid treatment, a marked reduction
Fig. 4. Effect of Rosmarinus officinalis extract and rosmarinic acid administration on the rat paw oedema development elicited by carrageenin 6 hrafter oedema induction. Effect of a single administration of R. officinalis extract (E10 mg/kg, n = 8; and E25 mg/kg, n = 8, p.o.) in comparisonwith the effect of a single administration of rosmarinic acid (RA10 mg/kg, n = 8; RA25 mg/kg, n = 8; RA50 mg/kg, n = 8, p.o.) and indometha-cin (10 mg/kg, p.o., n = 8). The data are presented as means with their standard errors. *p < 0.001 versus control group; ‡p < 0.01 versus controlgroup; #p < 0.01 versus carrageenin group.
Control Carrageenan RA 25 Lycopene Tempol Trolox Indomethacin–100
102030405060708090
100110120130
% p
aw v
olum
e in
crea
se
*
##
## #
Fig. 5. Comparison of the anti-inflammatory effect of rosmarinic acid with known antioxidant and anti-inflammatory substances. Effect of a singleadministration of rosmarinic acid (RA25 mg/kg, n = 8; p.o.), lycopene (50 mg/kg, n = 8; p.o.), tempol (30 mg/kg, n = 8; p.o.), Trolox (30 mg/kg,n = 8; p.o.) and indomethacin (10 mg/kg, p.o., n = 8). The data are presented as means with their standard errors. *p < 0.001 versus control group;#p < 0.01 versus carrageenin group (Bignotto et al., 2009).
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
EFFECT OF ROSMARINIC ACID IN INFLAMMATION 7
of these changes was observed. Haemorrhage areas in patchesare still observable but occupy a lesser area and are more rare.Neutrophil accumulation on the peri-alveolar zone was alsorare, and no alveoli were found with thickening of thealveolar wall (fig. 12).
Effect of rosmarinic acid on the activation of Akt. Whencompared with sham-operated rats, thermal injury resulted in asignificant rise in the activation of Akt (expressed as increasedratio of p-Akt/Akt). In rats subjected to treatment withrosmarinic acid, the rise in Akt activation was significantlyattenuated (fig. 13).
Effect of rosmarinic acid on the activation of GSK-3b. Whencompared with sham-operated rats, thermal injury resulted in asignificant decrease in the activation of GSK-3b (expressed asincreased ratio of p-GSK-3b/GSK-3b). In rats subjected totreatment with rosmarinic acid, there was no significantchange in the activation of GSK-3b (fig. 14).
Effect of rosmarinic acid on the activation of NF-jB. Whencompared with sham-operated rats, thermal injury resulted in asignificant increase in the expression and activation of NF-jB(expressed as increased nuclear translocation of the p65NF-jB subunit). In rats subjected to treatment with rosmarinic
acid, there was a significant increase in the expression andnuclear translocation of NF-jB (fig. 15).
Effect of rosmarinic acid on the activation of caspase-3. When compared with sham-operated rats, thermal injuryresulted in a significant increase in the activation of caspase-3.In rats subjected to treatment with rosmarinic acid, although atrend appears to exist, there was no significant decrease in theactivation of caspase-3 (fig. 16).
Effect of rosmarinic acid on the activation ofmetalloproteinase-9 (MMP-9). When compared with sham-operated rats, thermal injury resulted in significant rises in theactivation of MMP-9. No significant rise was detected in ratssubjected to rosmarinic acid treatment in comparison withsham-operated rats (fig. 17).
Discussion
Inflammatory response develops along several stages,apparently mediated through different mechanisms. Thecarrageenin-induced paw oedema model induces a biphasicoedema consisting of an early-phase (up to 2 hr) followed bya more sustained late-phase (2–6 hr). The late-phase is relatedto neutrophil infiltration [38] and production of reactive
Control I/R RA + I/R0
500
1000
1500
2000
2500
*
#*
AS
T (
U/L
)
Control I/R RA + I/RRA RA0
500
1000
1500
2000
2500 *
#*
AL
T (
U/L
)
Control
Sham Sham
Sham I/R RA + I/R RA0
1500
3000
4500
6000
7500
9000 *
#*
LD
H (
U/L
)
Fig. 6. Effect of rosmarinic acid administration (25 mg/kg, i.v.) on the serum levels of aspartate aminotransferase (AST), alanine aminotransferase(ALT) and lactate dehydrogenase (LDH), in the rat model of hepatic ischaemia–reperfusion. Control group, n = 6; sham group, n = 4; I/R group,n = 8; RA+I/R group, n = 8; RA group, n = 4. *p < 0.001 versus sham group; #p < 0.01 versus I/R group.
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
8 JOAO ROCHA ET AL.

Control Sham I/R RA + I/R RA Control Sham I/R RA + I/R RA
Control Sham I/R RA + I/R RA
0
500
1000
1500
2000
2500
*
#*
AST
(U/L
)
0
500
1000
1500
2000
2500 *
#*
ALT
(U/L
)
0
1500
3000
4500
6000
7500
9000 *
#*
LDH
(U/L
)
Fig. 7. Effect of rosmarinic acid administration (25 mg/kg, i.v.) on the serum levels of aspartate aminotransferase (AST), alanine aminotransferase(ALT), lactate dehydrogenase (LDH), creatinine and urea, in the rat model of thermal injury. Sham group, n = 9; thermal injury (TI) group,n = 14; RA + TI group, n = 14; RA group, n = 6. *p < 0.05 versus sham group; #p < 0.05 versus TI group.
RA + TITISham0
50
100
150
200
250*
#
IL-6
(pg/
mL)
RA + TITISham0
100
200
300
400
500 *
#
IL-1
β (p
g/m
L)
RA + TITISham0
25
50
75
100
125
150
175 *
#
TNF-
α (p
g/m
L)
Fig. 8. Effect of rosmarinic acid administration (25 mg/kg, i.v.) on the serum levels of TNF-a, IL-1b and IL-6, in the rat model of thermal injury. Shamgroup, n = 9; thermal injury (TI) group, n = 14; RA + TI group, n = 14; RA group, n = 6. *p < 0.05 versus sham group; #p < 0.05 versus TI group.
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
EFFECT OF ROSMARINIC ACID IN INFLAMMATION 9

species such as hydrogen peroxide, superoxide radical, perox-ynitrite [39] and pro-inflammatory prostanoids [40]. Thismodel has been used greatly in research and has become themainstay in the elucidation of pharmacodynamic properties inthe support of non-clinical development of most of the non-steroidal anti-inflammatory drugs [30].Several in vitro and in vivo studies have shown that reactive
oxygen species play a central role in the physiopathology of
the inflammatory process [41,42] and contribute greatly to tis-sue injury caused by inflammation [43]. In fact, reactive oxy-gen species are already considered as a valid therapeutic targetin the development of new drugs for the treatment of diseaseswith a strong inflammatory component [44,45], and severalplant-derived products are already in a late stage for drugdevelopment aiming for therapeutic indications where oxida-tive stress and inflammation might play a significant role [46].The high concentration of phenolic acids in extracts of R. offi-cinalis has been considered to be related to its antioxidantcapacity [47,48], anti-inflammatory [12] and antibacterialactivity [47]. Given the central role of oxidation and reactiveoxygen species in inflammation and the known antioxidanteffects of rosmarinic acid and R. officinalis, we aimed to eval-uate their effect in this model of acute local inflammation.Our results suggest that pre-treatment with rosmarinic acid orR. officinalis extract significantly reduces the increase in pawvolume by inhibiting the inflammatory processes associatedwith oedema formation.Administration of an extract of R. officinalis and rosmarinic
acid led to an anti-inflammatory effect as demonstrated by a60% reduction in paw oedema volume in comparison withcontrol animals. Administration of the extract, in a dose equiv-alent to 25 mg/kg of rosmarinic acid, exhibited the same mag-nitude of effect, suggesting that it was RA that mainlycontributed to the anti-inflammatory effect observed. Giventhe naturally higher antioxidant capacity of the extract in rela-tion to rosmarinic acid alone, it is possible to assume that the
AcR + QQSham0
50
100
150
200
250 *
#
IL-6
(pg/
mL)
AcR + QQSham0
50
100
150
200
250
300
350
400
450 *
#
IL-1
β (p
g/m
L)
AcR + QQSham0
5
10
15
20
25 *
#
TNF-
α (p
g/m
L)
Fig. 9. Effect of rosmarinic acid administration (25 mg/kg, i.v.) on the bronchoalveolar lavage fluid levels of TNF-a, IL-1b and IL-6, in the ratmodel of thermal injury. Sham group, n = 9; thermal injury (TI) group, n = 14; RA + TI group, n = 14; RA group, n = 6. *p < 0.05 versus shamgroup; #p < 0.05 versus TI group.
Sham TI RA + TI RA0
1
2
3
4
*
#
#
Albu
min
con
cent
ratio
n on
BAL
F (m
g/dL
)
Fig. 10. Effect of rosmarinic acid administration (25 mg/kg, i.v.) onthe bronchoalveolar lavage fluid levels of albumin, in the rat model ofthermal injury. Sham group, n = 9; thermal injury (TI) group, n = 14;RA + TI group, n = 14; RA group, n = 6. *p < 0.05 versus shamgroup; #p < 0.05 versus TI group.
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
10 JOAO ROCHA ET AL.

anti-inflammatory effect exhibited in this model of acuteinflammation might not be solely related to the antioxidantcapacity, but also to other mechanisms that may need furtherinvestigation. The same magnitude of effect exhibited by ros-marinic acid compared with other known and extensively stud-ied antioxidant and anti-inflammatory substances (tempol,Trolox, lycopene and indomethacin) suggests that rosmarinicacid may have the potential to reduce inflammatory-inducedtissue injury in other inflammation models and through differ-ent mechanisms of action.Most interestingly, rosmarinic acid was also able to inhi-
bit the inflammatory process associated with hepatic ischae-mia–reperfusion, thereby reducing liver injury sustained afterreperfusion. Liver injury caused by ischaemia–reperfusionconsists of an interruption of blood supply to the liver fol-lowed by reperfusion. When the blood supply is restored,the organs are usually subjected to a further insult, aggra-vating the injury created within the ischaemic period [32].This reperfusion insult is a direct consequence of a complexinterplay between different mechanisms. The initial phase(until 2 hr after reperfusion) is characterized by oxidativestress. The destructive effects of ischaemia–reperfusion resultfrom the acute generation of ROS subsequent to reoxygen-ation. These ROS inflict direct tissue damage and initiate acascade of deleterious cellular responses leading to inflam-mation, cell death and organ failure [49]. A previous work
has also demonstrated the protective effect of rosmarinicacid on liver injury. Administration of rosmarinic acid(135 mg/kg, p.o.) reduced lipopolysaccharide-induced liverinjury in D-galactosamine-sensitized mice, and the liver pro-tection exhibited by RA was related to the scavenging orreducing activities of superoxide and peroxynitrite [50].Osakabe et al. also observed that the magnitude of rosmari-nic effect was similar to that of administration of an extractof Perilla frutescens with an equivalent dose of RA, attrib-uting the protective effect of the extract to its main constit-uent, rosmarinic acid.Thermal injury has a very severe clinical prognosis and lim-
ited therapeutic options. Severe thermal injury leads frequentlyto systemic inflammatory response syndrome with subsequentmulti-organ dysfunction syndrome and a potentially fatal out-come, being the main cause of death in burned patients [51].Acute lung injury (ALI) and acute respiratory distresssyndrome (ARDS) are at the top of the list of early complica-tions in burned patients and associated with a high mortality[52–54].Several physiopathological events are considered the main
contributors in the development of acute lung injury, includ-ing systemic release of inflammatory mediators (cytokines),chemotaxis and activation of neutrophils (oxidative burst)and activation of cellular pathways involved in cell death[55].
Fig. 11. Effect of rosmarinic acid administration (25 mg/kg, i.v.) on the bronchoalveolar lavage fluid number and percentage of polymorphonuclearcells, in the rat model of thermal injury. Sham group, n = 9; thermal injury (TI) group, n = 14; RA + TI group, n = 14; RA group, n = 6.*p < 0.05 versus sham group; #p < 0.05 versus TI group.
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
EFFECT OF ROSMARINIC ACID IN INFLAMMATION 11

The scalding burn model used in this model is widely citedin the literature [56–58], and we were able to prove that itleads to the internationally acknowledged main features of anexperimental model of ALI/ARDS [59].We demonstrated that administration of rosmarinic acid was
able to reduce systemic release of pro-inflammatory cytokinesand also attenuated the multi-organ injury (liver, kidney andlung) induced by scald. Specifically on the lung, the histologi-cal analysis of the lung showed that there was a markedreduction in the histological signs of lung tissue injury withan appearance closer to sham-operated rats, not subjected tothermal injury.Along with the formation of ROS, the infiltration and accu-
mulation of polymorphonuclear leucocytes within the tissueshas been considered a hallmark of the acute inflammatoryresponse, including local inflammation [34] hepatic ischae-mia–reperfusion [14,60], acute lung injury [61,62] and sys-temic inflammation [63,64]. A prominent feature of acuteinflammation is enhanced vascular permeability resulting inoedema formation. Such changes in vascular permeability havebeen known to be dependent upon polymorphonuclear leuco-cyte interactions with the vascular endothelium [63]. Our
results revealed inhibition of the neutrophils’ oxidative burstby rosmarinic acid in a dose-dependent manner suggesting thatits anti-inflammatory effect might be related, at least in part,by inhibition of neutrophil activation.Mechanistic studies performed on the lung tissue in the
thermal injury model revealed that the beneficial effectexhibited by rosmarinic acid might not be related to modu-lation of the PI3K-Akt-GSK-3b pathway but rather throughactivation of the NF-jB pathway and inhibition of MMP-9activation. MMP-9 has been shown to regulate the activa-tion of pro-apoptotic factors such as the Fas/FasL complex[65], and direct inhibition of MMP-9 or its gene transcrip-tion has been shown to be beneficial in several lung injuryexperimental models [66–68]. Given the importance of theNF-jB pathway on cell survival [69] and its role in thecrosstalk with several other pathways related to apoptosis,cell fate and inflammation [70,71], we might speculate thatrosmarinic acid might exhibit pleiotropic mechanisms andact through the modulation of NF-jB closely related path-ways.Given that the inflammatory process is a multi-factorial
network of different mediators and that oxidative stress and
A B
C D
E F
Fig. 12. Effect of rosmarinic acid administration (25 mg/kg, i.v.) on the lung tissue histological features, in the rat model of thermal injury. (A)Sham group (1009); (B) sham group (4009); (C) thermal injury group (1009); (D) thermal injury group (4009); (E) rosmarinic acid + thermalinjury group (1009); and (F) rosmarinic acid + thermal injury group (4009). Images are representative of at least 4 experiments performed on dif-ferent days.
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
12 JOAO ROCHA ET AL.

neutrophil oxidative burst play an important role in bothmodels of inflammation used in this work, it is possible tospeculate that rosmarinic acid might be exhibiting ananti-inflammatory activity by a net effect, which includes itsantioxidant properties, inhibition of neutrophil activity, inhi-bition of MMP-9 activity and modulation of the NF-jBpathway.Therefore, rosmarinic acid administration might be useful in
the management of inflammatory processes, and furtherresearch on anti-inflammatory effects of rosmarinic acid andR. officinalis might lead to the discovery of new pharmacolog-ical tools in the treatment of inflammatory diseases. Given therecognized role of inflammation and oxidative stress in neuro-degenerative diseases [72], cardiovascular diseases [73],
P-GSK3β - - 46 kDa
- 46 kDaGSK3β total -
Sham TI RA + TI
Sham TI
RA + TI
0.0
0.5
1.0
1.5
2.0
2.5
pGSK
/GSK
pro
tein
exp
ress
ion
(fold
cha
nge)
#
Fig. 14. Effect of rosmarinic acid administration (25 mg/kg, i.v.) onthe lung tissue GSK-3b activation, in the rat model of thermal injury.Sham group, n = 9; thermal injury (TI) group, n = 14; RA + TIgroup, n = 14; RA group, n = 6. *p < 0.05 versus sham group;#p < 0.05 versus TI group.
Sham TI RA + TI
NF-κB- - 65 kDa
C N C N C N
Sham TI RA + TI0
5
10
15
20 CytoplasmNucleus
NF-
κB p
rote
in e
xpre
ssio
n(fo
ld c
hang
e)
*
#
Fig. 15. Effect of rosmarinic acid administration (25 mg/kg, i.v.) onthe lung tissue NF-jB activation, in the rat model of thermal injury.Sham group, n = 9; thermal injury (TI) group, n = 14; RA + TIgroup, n = 14; RA group, n = 6. *p < 0.05 versus sham group;#p < 0.05 versus TI group.
Fig. 16. Effect of rosmarinic acid administration (25 mg/kg, i.v.) onthe lung tissue caspase-3 activation, in the rat model of thermal injury.Sham group, n = 9; thermal injury (TI) group, n = 14; RA + TIgroup, n = 14; RA group, n = 6. *p < 0.05 versus sham group;#p < 0.05 versus TI group.
Sham TI RA + TI
P-AKT - - 60 kDa
AKT total - - 60 kDa
#
*
Sham TI
RA + TI
0.0
0.5
1.0
1.5
2.0
2.5
pAK
T/A
KT
prot
ein
expr
essi
on(fo
ld c
hang
e)
Fig. 13. Effect of rosmarinic acid administration (25 mg/kg, i.v.) onthe lung tissue Akt activation, in the rat model of thermal injury.Sham group, n = 9; thermal injury (TI) group, n = 14; RA + TIgroup, n = 14; RA group, n = 6. *p < 0.05 versus sham group;#p < 0.05 versus TI group.
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
EFFECT OF ROSMARINIC ACID IN INFLAMMATION 13

respiratory diseases [74] and cancer [75], these promisingresults might unveil a potential research field for rosmarinicacid and its clinical applications.
AcknowledgementsJoao Rocha was supported by FCT under a Doctoral Grant
(SFRH/BD/64180/2009). Marisa Freitas acknowledges thefinancial support by FCT for the Pos-doc grant (SFRH/BPD/76909/2011), in the scope of ‘QREN e POPH e Tipologia 4.1e Formacao Avancada’, cosponsored by FSE and by NationalFunds of MCTES.
References
1 Gonzalez-Trujano ME, Pena EI, Martinez AL, Moreno J,Guevara-Fefer P, Deciga-Campos M et al. Evaluation of theantinociceptive effect of Rosmarinus officinalis L. using three dif-ferent experimental models in rodents. J Ethnopharmacol2007;111:476–82.
2 Takaki I, Bersani-Amado LE, Vendruscolo A, Sartoretto SM, DinizSP, Bersani-Amado CA et al. Anti-inflammatory and antinocicep-tive effects of Rosmarinus officinalis L. essential oil in experimen-tal animal models. J Med Food 2008;11:741–6.
3 del Ba~no MJ, Lorente J, Castillo J, Benavente-Garc�ıa O, del R�ıoJA, Ortu~no A et al. Phenolic diterpenes, flavones, and rosmarinicacid distribution during the development of leaves, flowers, stems,and roots of Rosmarinus officinalis. Antioxidant activity. J AgricFood Chem 2003;51:4247–53.
4 Nakazawa T, Ohsawa K. Metabolism of rosmarinic acid in rats. JNat Prod 1998;61:993–6.
5 Baba S, Osakabe N, Natsume M, Terao J. Orally administered ros-marinic acid is present as the conjugated and/or methylated formsin plasma, and is degraded and metabolized to conjugated forms ofcaffeic acid, ferulic acid and m-coumaric acid. Life Sci2004;75:165–78.
6 Konishi Y, Kobayashi S. Transepithelial transport of rosmarinicacid in intestinal Caco-2 cell monolayers. Biosci Biotechnol Bio-chem 2005;69:583–91.
7 Debersac P, Vernevaut MF, Amiot MJ, Suschetet M, Siess MH.Effects of a water-soluble extract of rosemary and its purified com-ponent rosmarinic acid on xenobiotic-metabolizing enzymes in ratliver. Food Chem Toxicol 2001;39:109–17.
8 Conner EM, Grisham MB. Inflammation, free radicals, and antioxi-dants. Nutrition 1996;4:274–7.
9 Cuzzocrea S, Riley DP, Caputi AP, Salvemini D. Antioxidant ther-apy: a new pharmacological approach in shock, inflammation, andischemia/reperfusion injury. Pharmacol Rev 2001;53:135–59.
10 Choi HR, Choi JS, Han YN, Bae SJ, Chung HY. Peroxynitritescavenging activity of herb extracts. Phytother Res 2002;4:364–7.
11 Nakamura Y, Ohto Y, Murakami A, Ohigashi H. Superoxide scav-enging activity of rosmarinic acid from Perilla frutescens BrittonVar. acuta f. viridis. J Agric Food Chem 1998;46:4545–50.
12 Peng CH, Su JD, Chyau CC, Sung TY, Ho SS, Peng CC et al.Supercritical fluid extracts of rosemary leaves exhibit potent anti-inflammation and anti-tumor effects. Biosci Biotechnol Biochem2007;71:2223–32.
13 Qiao S, Li W, Tsubouchi R, Haneda M, Murakami K, Takeuchi Fet al. Rosmarinic acid inhibits the formation of reactive oxygenand nitrogen species in RAW264.7 macrophages. Free Radic Res2005;39:995–1003.
14 Jaeschke H. Mechanisms of liver injury. II. Mechanisms of neutro-phil-induced liver cell injury during hepatic ischemia-reperfusionand other acute inflammatory conditions. Am J Physiol Gastroin-test Liver Physiol 2006;6:G1083–8.
15 Jaeschke H, Woolbright BL. Current strategies to minimize hepaticischemia-reperfusion injury by targeting reactive oxygen species.Transplant Rev (Orlando) 2012;2:103–14.
16 Sepodes B, Maio R, Pinto R, Marques C, Mendes-do-Vale J,McDonald MC et al. Tempol, an intracelullar free radical scaven-ger, reduces liver injury in hepatic ischemia-reperfusion in the rat.Transplant Proc 2004;36:849–53.
17 Ward PA. Oxidative stress: acute and progressive lung injury. AnnN Y Acad Sci 2010;1203:53–9.
18 Zimmerman JJ. Oxidant stress in acute lung injury. In: Wong HR,Shanley T (eds). Molecular Biology of Acute Lung Injury, 1st edn.Springer, Berlin, Germany, 2001;83–99.
19 Crimi E, Sica V, Slutsky AS, Zhang H, Williams-Ignarro S,Ignarro LJ et al. Role of oxidative stress in experimental sepsisand multisystem organ dysfunction. Free Radic Res2006;40:665–72.
20 Bowler RP, Crapo JD. Oxidative stress in allergic respiratory dis-eases. J Allergy Clin Immunol 2002;110:349–56.
21 Crapo JD. Oxidative stress as an initiator of cytokine release andcell damage. Eur Respir J 2003;44:4s–6s.
22 Rahman I, Kelly F. Biomarkers in breath condensate: a promisingnew non-invasive technique in free radical research. Free RadicRes 2003;37:1253–66.
23 Singleton VL, Rossi JA. Colorimetry of total phenolics with phos-phomolybdic-phosphotungstic acid reagents. Am J Enol Vitic1965;16:144–58.
24 Serra AT, Rocha J, Sepodes B, Matias AA, Feliciano RP, de Carv-alho A et al. Evaluation of cardiovascular protective effect of dif-ferent apple varieties - Correlation of response with composition.Food Chem 2012;135:2378–86.
25 Ou B, Hampsch-Woodill M, Flanagan J, Deemer EK, Prior RL,Huang D. Novel fluorometric assay for hydroxyl radical preventioncapacity using fluorescein as the probe. J Agric Food Chem2002;50:2772–7.
26 Freitas M, Porto G, Lima JL, Fernandes E. Isolation and activationof human neutrophils in vitro: the importance of the anticoagulantused during blood collection. Clin Biochem 2008;41:570–5.
27 Freitas M, Porto G, Lima JL, Fernandes E. Optimization of experi-mental settings for the analysis of human neutrophils oxidativeburst in vitro. Talanta 2009;78:1476–83.
28 Freitas M, Lima JL, Fernandes E. Optical probes for detection andquantification of neutrophils’ oxidative burst: a review. Anal ChimActa 2009;649:8–23.
29 Fernandes E, Costa D, Marques AP, Reis RL, Lima JLFC. Inhibi-tion of human neutrophil oxidative burst by pyrazolone derivatives.Free Radic Biol Med 2006;40:632–40.
Fig. 17. Effect of rosmarinic acid administration (25 mg/kg, i.v.) onthe lung tissue metalloproteinase-9 (MMP-9) activation, in the ratmodel of thermal injury. Sham group, n = 9; thermal injury (TI)group, n = 14; RA + TI group, n = 14; RA group, n = 6. *p < 0.05versus sham group; #p < 0.05 versus TI group.
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
14 JOAO ROCHA ET AL.

30 Vogel HG. Drug Discovery and Evaluation: PharmacologicalAssays. Springer-Verlag and Heidelberg GmbH & Co., Berlin,Germany, 2002;751–72.
31 Bignotto L, Rocha J, Sepodes B, Eduardo-Figueira M, Pinto R,Chaud M et al. Anti-inflammatory effect of lycopene on carra-geenan-induced paw oedema and hepatic ischaemia-reperfusion inthe rat. Br J Nutr 2009;102:126–33.
32 Sepodes B, Maio R, Pinto R, Sharples E, Oliveira P, McDonald Met al. Recombinant human erythropoietin protects the liver fromhepatic ischemia-reperfusion injury in the rat. Transpl Int2006;19:919–26.
33 Fischer AE, Jacobson KA, Rose J, Zeller R. Hematoxylin andeosin staining of tissue and cell sections. CSH Protoc 2008;2008:pdb.prot4986.
34 Schreiber E, Matthias P, M€uller MM, Schaffner W. Rapid detec-tion of octamer binding proteins with ‘mini-extracts’, preparedfrom a small number of cells. Nucleic Acids Res 1989;17:6419.
35 Fernandes A, Falc~ao AS, Silva RF, Gordo AC, Gama MJ, Brito MAet al. Inflammatory signalling pathways involved in astroglial activa-tion by unconjugated bilirubin. J Neurochem 2008;96:1667–79.
36 Barateiro A, Vaz AR, Silva SL, Fernandes A, Brites D. ER stress,mitochondrial dysfunction and calpain/JNK activation are involvedin oligodendrocyte precursor cell death by unconjugated bilirubin.Neuromolecular Med 2012;14:285–302.
37 Silva SL, Vaz AR, Barateiro A, Falc~ao AS, Fernandes A, BritoMA et al. Features of bilirubin-induced reactive microglia: fromphagocytosis to inflammation. Neurobiol Dis 2010;40:663–75.
38 Di Rosa M, Giroud JP, Willoughby DA. Studies on the mediatorsof the acute inflammatory response induced in rats in different sitesby carrageenan and turpentine. J Pathol 1971;104:15–29.
39 Khattab MM. Tempol, a membrane-permeable radical scavenger,attenuates peroxynitrite- and superoxide anion-enhanced carra-geenan-induced paw edema and hyperalgesia: a key role for super-oxide anion. Eur J Pharmacol 2006;548:167–73.
40 Cuzzocrea S, Zingarelli B, Hake P, Salzman AL, Szab�o C. Antiin-flammatory effects of mercaptoethylguanidine, a combined inhibi-tor of nitric oxide synthase and peroxynitrite scavenger, incarrageenan-induced models of inflammation. Free Radic Biol Med1998;24:450–9.
41 Landino LM, Crews BC, Timmons MD, Morrow JD, Marnett LJ.Peroxynitrite, the coupling product of nitric oxide and superoxide,activates prostaglandin biosynthesis. Proc Natl Acad Sci USA1996;93:15069–74.
42 D’Acquisto F, May MJ, Ghosh S. Inhibition of nuclear factorkappa B (NF-B): an emerging theme in anti-Inflammatory thera-pies. Mol Interv 2002;2:22–35.
43 Thiemermann C, McDonald MC, Cuzzocrea S. The stable nitrox-ide, tempol, attenuates the effects of peroxynitrite and oxygen-derived free radicals. Crit Care Med 2001;29:223–4.
44 Cuzzocrea S, Thiemermann C, Salvemini D. Potential therapeuticeffect of antioxidant therapy in shock and inflammation. Curr MedChem 2004;11:1147–62.
45 Naito Y, Takano H, Yoshikawa T. Oxidative stress-related mole-cules as a therapeutic target for inflammatory and allergic diseases.Curr Drug Targets Inflamm Allergy 2005;4:511–5.
46 Kaplan M, Mutlu EA, Benson M, Fields JZ, Banan A, Keshavarz-ian A. Use of herbal preparations in the treatment of oxidant-medi-ated inflammatory disorders. Complement Ther Med 2007;15:207–16.
47 Moreno S, Scheyer T, Romano CS, Vojnov AA. Antioxidant andantimicrobial activities of rosemary extracts linked to their poly-phenol composition. Free Radic Res 2006;40:223–31.
48 Erkan N, Ayranci G, Ayranci E. Antioxidant activities of rosemary(Rosmarinus officinalis L.) extract, blackseed (Nigella sativa L.)essential oil, carnosic acid, rosmarinic acid and sesamol. FoodChem 2008;110:76–82.
49 Elias-Mir�o M, Jim�enez-Castro MB, Rod�es J, Peralta C. Currentknowledge on oxidative stress in hepatic ischemia/reperfusion. FreeRadic Res 2013;8:555–68.
50 Osakabe N, Yasuda A, Natsume M, Sanbongi C, Kato Y, OsawaT et al. Rosmarinic acid, a major polyphenolic component of Peri-lla frutescens, reduces lipopolysaccharide (LPS)-induced liverinjury in D-galactosamine (D-GalN)-sensitized mice. Free RadicBiol Med 2002;33:798–806.
51 Dahiya P. Burns as a model of SIRS. Front Biosci (Landmark Ed)2009;1:4962–7.
52 Dancey DR, Hayes J, Gomez M, Schouten D, Fish J, Peters Wet al. ARDS in patients with thermal injury. Intensive Care Med1999;25:1231–6.
53 Herridge MS, Cheung AM, Tansey CM, Matte-Martyn A, Diaz-Granados N, Al-Saidi F et al. One-year outcomes in survivors ofthe acute respiratory distress syndrome. N Engl J Med2003;348:683–93.
54 Rodriguez JL, Miller CG, Garner WL, Till GO, Guerrero P, MooreNP et al. Correlation of the local and systemic cytokine responsewith clinical outcome following thermal injury. J Trauma1993;34:684–95.
55 Ipaktchi K, Mattar A, Niederbichler AD, Hoesel LM, Vollmann-shauser S, Hemmila MR et al. Attenuating burn wound inflamma-tory signaling reduces systemic inflammation and acute lunginjury. J Immunol 2006;177:8065–71.
56 Abdullahi A, Amini-Nik S, Jeschke MG. Animal models in burnresearch. Cell Mol Life Sci 2014;71(17):3241–55 (in press).
57 Brachkova MI, Marques P, Rocha J, Sepodes B, Duarte MA, PintoJF. Alginate films containing Lactobacillus plantarum as wounddressing for prevention of burn infection. J Hosp Infect2011;79:375–7.
58 Jeschke MG, Einspanier R, Klein D, Jauch KW. Insulin attenuatesthe systemic inflammatory response to thermal trauma. Mol Med2002;8:443–50.
59 Matute-Bello G, Downey G, Moore BB, Groshong SD, MatthayMA, Slutsky AS et al. An official American Thoracic Societyworkshop report: features and measurements of experimentalacute lung injury in animals. Am J Respir Cell Mol Biol2011;44:725–38.
60 Datta G, Fuller BJ, Davidson BR. Molecular mechanisms of liverischemia reperfusion injury: insights from transgenic knockoutmodels. World J Gastroenterol 2013;11:1683–98.
61 Grommes J, Soehnlein O. Contribution of neutrophils to acute lunginjury. Mol Med 2011;17:293–307.
62 Lee WL, Downey GP. Neutrophil activation and acute lung injury.Curr Opin Crit Care 2001;7:1–7.
63 Edens HA, Parkos CA. Neutrophil transendothelial migration andalteration in vascular permeability: focus on neutrophil-derivedazurocidin. Curr Opin Hematol 2003;10:25–30.
64 Fry DE. Sepsis, systemic inflammatory response, andmultiple organ dysfunction: the mystery continues. Am Surg2012;78:1–8.
65 Parks WC, Wilson CL, Lopez-Boado YS. Matrix metalloproteinas-es as modulators of inflammation and innate immunity. Nat RevImmunol 2004;4:617–29.
66 Davey A, McAuley DF, O’Kane CM. Matrix metalloproteinases inacute lung injury: mediators of injury and drivers of repair. EurRespir J 2011;38:959–70.
67 Qiu Z, Hu J, Van den Steen PE, Opdenakker G. Targeting matrixmetalloproteinases in acute inflammatory shock syndromes. CombChem High Throughput Screen 2012;15:555–70.
68 Vandenbroucke RE, Dejonckheere E, Libert C. A therapeutic rolefor matrix metalloproteinase inhibitors in lung diseases? Eur RespirJ 2011;38:1200–14.
69 Baud V, Karin M. Is NF-kappaB a good target for cancer therapy?Hopes and pitfalls. Nat Rev Drug Discov 2012;8:33–40.
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
EFFECT OF ROSMARINIC ACID IN INFLAMMATION 15

70 Ghosh S, Hayden MS. New regulators of NF-kappaB in inflamma-tion. Nat Rev Immunol 2008;8:837–48.
71 Oeckinghaus A, Hayden MS, Ghosh S. Crosstalk in NF-jB signal-ing pathways. Nat Immunol 2011;12:695–708.
72 Minghetti L. Role of inflammation in neurodegenerative diseases.Curr Opin Neurol 2005;18:315–21.
73 Lin CP, Lin FY, Huang PH, Chen YL, Chen WC, Chen HY et al.Endothelial progenitor cell dysfunction in cardiovascular diseases:
role of reactive oxygen species and inflammation. Biomed Res Int2013;2013:845037.
74 Rosanna DP, Salvatore C. Reactive oxygen species,inflammation, and lung diseases. Curr Pharm Des 2012;18:3889–900.
75 Reuter S, Gupta SC, Chaturvedi MM, Aggarwal BB. Oxidativestress, inflammation, and cancer: how are they linked? Free RadicBiol Med 2010;49:1603–16.
© 2014 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)
16 JOAO ROCHA ET AL.





























