Embed Size (px)
Citation preview
M A R C H 5 - 9 , 2 0 0 6 • S N O W M A S S , C O L O R A D O
2006
Aspen RetinalDetachment Society
Meeting Notes
ARDS
34thAnnual
MEDICAL CONFERENCE PLANNERS, INC.
1251Post Road, Scarsdale, NY10583
914-722-0664 phone
914-722-0465 fax
www.medconfs.com
The ARDS wishes to acknowledge
Genentech, Inc., whose generous gift
made the publication of
this book possible.
Aspen R
etinal Detachm
ent Society Meeting N
otes 2006
Dear Aspen Retinal Detachment Society Participant,
This year we are delighted to offer you this booklet of notes, supplemented
by the majority of slide presentations (edited), from our recent meeting.
The notes were taken and assembled by two young, talented, rising retinal
stars – Drs. Paul Chan and Andrew Moshfeghi – who attended every talk
and captured the essence of the vigorous post-talk discussion, for which the
ARDS is deservedly famous.
This work was made possible by an educational grant graciously provided
by Genentech, Inc. which supported not only the production costs of the
booklet, but also provided a stipend so that these two young physicians might
attend and participate in this exciting meeting.
We are grateful to Genentech, to Drs. Chan and Moshfeghi, and to all of you
for contributing to the intellectual vibrancy of ARDS. We hope you will find
this booklet interesting, and also of value to you in the care of your patients.
Please join us March 4-8, 2007 for the 35th Annual ARDS Meeting.
Sincerely,
Donald J. D’Amico, MD William O. Edward, MD Timothy G. Murray, MD
34thAnnual
Aspen RetinalDetachment Society
Meeting
JOINTLY SPONSORED BY THE ASPEN RETINAL DETACHMENT SOCIETY AND THE SPOKANE COUNTY MEDICAL SOCIETY
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO
35thAnnual
Aspen RetinalDetachment Society
Meeting
March 4-8, 2007Snowmass Conference
Center
MEDICAL CONFERENCE PLANNERS, INC.1251 Post Road, Scarsdale, NY10583
914-722-0664
www.medconfs.com
For Information
2007Save the
Date
34th Annual Meeting Program . . . . . . . . . . . . . . . . . . . . . . . 2
MONDAY, MARCH 6
I. Vitreoretinal Surgery with 25-Gauge Instruments: The Wills Experience . . . . . . . . . . . . . . 4PowerPoint Presentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . A.2
Carl D. Regillo, MD
II. Advances in 25-Gauge Vitrectomy Indications and Techniques . . . . . . . . . . . . . . . . . . . . . . 5Carl C. Awh, MD
III. Neuro-ophthalmic Insights for the Retina Specialist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7William F. Hoyt, MD
IV. Avastin Experience . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Robert Avery, MD
V. Vitrectomy for Diabetic Macular Edema: One Year Results of the VIDE Study . . . . . . . . . . . 10PowerPoint Presentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . A.4
Giacomo Panozzo, MD
VI. Failure of Lamina Puncture and Radial Optic Neurotomy for CRVO . . . . . . . . . . . . 12PowerPoint Presentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . A.8
Donald J. D’Amico, MD
TUESDAY, MARCH 7
I. Changing Concepts in the Treatment of Primary Rhegmatogenous Retinal Detachment . . 13PowerPoint Presentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . A.11
Periklis D. Brazitikos, MD
II. Anti-VEGF Therapy for Age-related Macular Degeneration . . . . . . . . . . . . . . 15PowerPoint Presentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . A.18
Allen C. Ho, MD
III. Macugen Therapy for Exudative Macular Degeneration and Diabetic Retinopathy . . . . . . . . . 17PowerPoint Presentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . A.26
Gregg T. Kokame, MD, MMM
IV. Current Status of Photodynamic Therapy for Age-related Macular Degeneration . . . . . . . . . . 18PowerPoint Presentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . A.38
Carl D. Regillo, MD
V. Pneumatic Displacement of Subretinal Hemorrhage in Age-related Macular Degeneration . . . . . . . . . . . . . . 19Mark W. Johnson, MD
VI. Case Presentations on AMD Management . . . . . . 20Moderator: Allen C. Ho, MD
Contents
WEDNESDAY, MARCH 8
I. 25-Gauge Vitrectomy: Evolution and Surgical Pearls . . . . . . . . . . . . . . . . . . . 22PowerPoint Presentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . A.45
Allen C. Ho, MD
II. New Devices for Vitreoretinal Surgery . . . . . . . . . 23Carl C. Awh, MD
III. A Sober Reappraisal of Intravitreal Triamcinolone for Retinal Indications . . . . . . . . . . 24PowerPoint Presentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . A.50
Donald J. D’Amico, MD
IV. Dislocated Posterior Chamber IOLs: New Presentations and New Techniques in Management . . . . . . . . . . . . . . . 25PowerPoint Presentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . A.55
Gregg T. Kokame, MD, MMM
V. THE TAYLOR SMITH LECTURE: Pseudomelanomas of Choroid and Ciliary Body . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26PowerPoint Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . A.62
PowerPoint Presentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . A.63
Jerry A. Shields, MD
THURSDAY, MARCH 9
I. Systemic Drugs in the Treatment of Uveitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Presentation Outline . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A.74
Janet L. Davis, MD
II. Infectious Complications of Intravitreal Steroids. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Mark W. Johnson, MD
III. Myopic Traction Maculopathy: A Slowly Progressive and Treatable Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29PowerPoint Presentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . A.78
Giacomo Panozzo, MD
IV. Diagnosis and Managementof Intraocular Lymphoma . . . . . . . . . . . . . . . . . . . . . . . 31Presentation Outline . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A.84
Janet L. Davis, MD
V. OCT-Guided Macular Surgery . . . . . . . . . . . . . . . . . . 32PowerPoint Presentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . A.87
Periklis D. Brazitikos, MD
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . .
34th Annual Meeting Program
Sunday, March 56:00 pm-9:00 pmMeeting RegistrationNASTAR Ski Race & Picnic Lunch RegistrationWelcome Dinner
Snowmass Conference CenterHoaglund Room
Monday, March 63:15-3:55 pmExhibits/Après ski refreshments
3:55-4:00Opening Remarks
4:00-4:25Vitreoretinal Surgery with 25-GaugeInstruments: The Wills ExperienceCarl D. Regillo, MD
4:25-4:50Advances in 25-Gauge VitrectomyIndications and TechniquesCarl C. Awh, MD
4:50-5:10Discussion of previous two papers
5:10-5:35Neuro-ophthalmic Insights for the Retina SpecialistWilliam F. Hoyt, MD
5:35-6:05Break
6:05-6:40Vitrectomy for Diabetic Macular Edema: One Year Results of the VIDE StudyGiacomo Panozzo, MD
6:40-6:55Discussion
6:55-7:20Failure of Lamina Puncture andRadial Optic Neurotomy for CRVODonald J. D’Amico, MD
7:20-7:30Discussion
Tuesday, March 73:15-4:00 pm
Exhibits/Après ski refreshments
4:00-4:25
Changing Concepts in theTreatment of PrimaryRhegmatogenous RetinalDetachmentPeriklis D. Brazitikos, MD
4:25-4:35
Discussion
4:35-5:00
Anti-VEGF Therapy for Age-related Macular DegenerationAllen C. Ho, MD
5:00-5:15
Discussion
5:15-5:40
Macugen Therapy for Exudative Macular Degeneration and Diabetic RetinopathyGregg T. Kokame, MD, MMM
5:40-5:55
Discussion
5:55-6:25
Break
6:25-6:50
Current Status of PhotodynamicTherapy for Age-related Macular DegenerationCarl D. Regillo, MD
6:50-7:00
Discussion
7:00-7:20
Pneumatic Displacement ofSubretinal Hemorrhage in Age-related Macular DegenerationMark W. Johnson, MD
7:20-7:30
Discussion
Wednesday, March 812:00 noon
NASTAR race at the Spider SabichRace Arena followed by lunch at theSpider Sabich Picnic Cabin. Racersand non-racers are invited. Picnicwill be held if races are cancelled.Check for location of picnic in caseof race cancellation.
3:15-4:00 pm
Exhibits/Après ski refreshments
4:00-4:20
A Sober Reappraisal of Intravitreal Triamcinolone forRetinal IndicationsDonald D’Amico, MD
4:20-4:30
Discussion
4:30-4:50
New Devices for Vitreoretinal SurgeryCarl C. Awh, MD
4:50-5:00
Discussion
5:00-5:20
Dislocated IOLs: New Presentationsand New Techniques in ManagementGregg T. Kokame, MD, MMM
5:20-5:35
Discussion
5:35-6:00
Improved Wide Angle and BimanualIllumination for Vitreous SurgeryAllen C. Ho, MD
6:00-6:10
Discussion
6:10-6:40
Break
6:40-7:15
THE TAYLOR SMITH LECTURE: Pseudomelanomas of Choroid and Ciliary BodyJerry A. Shields, MD
7:15-7:30
Discussion
2 ASPEN RETINAL DETACHMENT SOCIETY MEETING
7:30
Van departure from SnowmassConference Center to L’Hosteria
8:00
Closing Dinner at L’HosteriaRistorante with presentation ofNASTAR ski prizes and taping ofThe Jerry Bovino Show
Thursday, March 93:15-4:00 pm
Exhibits/Après ski refreshments
4:00-4:25
Essentials of ImmunosuppressiveMedicationsJanet L. Davis, MD
4:25-4:35
Discussion
4:35-5:00
Infectious Complications ofIntravitreal SteroidsMark W. Johnson, MD
5:00-5:15
Discussion
5:15-5:40
Myopic Traction Maculopathy:A Slowly Progressive and Treatable ConditionGiacomo Panozzo, MD
5:40-5:50
Discussion
5:50-6:15
Intraocular Lymphoma: Advances in Diagnosis and ManagementJanet L. Davis, MD
6:15-6:25
Discussion
6:25-6:55
Break
6:55-7:20
OCT Guidance in Macular SurgeryPeriklis D. Brazitikos, MD
7:20-7:30
Discussion
7:30
Meeting Adjourns
Speakers
Carl C. Awh, MDRetina-Vitreous AssociatesNashville, TN
Periklis D. Brazitikos, MDAssistant Professor of OphthalmologyAristotle University of ThessalonikiThessaloniki, Greece
Donald J. D’Amico, MDProfessor of OphthalmologyHarvard Medical SchoolMassachusetts Eye & Ear InfirmaryBoston, MA
Janet L. Davis, MDProfessor of OphthalmologyBascom Palmer Eye InstituteMiami, FL
Allen C. Ho, MDProfessor of OphthalmologyThomas Jefferson UniversityPhiladelphia, PA
William F. Hoyt, MD Professor, Neuro-ophthalmology Unit, Dept. of NeurosurgeryUniversity of California, San FranciscoSan Francisco, CA
Mark W. Johnson, MDProfessor of Ophthalmology and Visual SciencesKellogg Eye CenterUniversity of MichiganAnn Arbor, MI
Gregg T. Kokame, MD, MMM Clinical Professor of OphthalmologyDepartment of SurgeryUniversity of Hawaii School of MedicineHonolulu, HI
Giacomo Panozzo, MDTheia Fondazione per l’OftalmologiaVerona, Italy
Carl D. Regillo, MDProfessor of OphthalmologyWills Eye HospitalThomas Jefferson UniversityPhiladelphia, PA
Jerry A. Shields, MDDirector, Oncology ServiceWills Eye HospitalProfessor of Ophthalmology Thomas Jefferson UniversityPhiladelphia, PA
Corporate Support
The Aspen Retinal DetachmentSociety gratefully acknowledges thefollowing companies for their support.
BLACK DIAMOND LEVEL
Genentech, Inc.
PLATINUM LEVEL
Alcon Laboratories, Inc.Bausch & LombNovartis OphthalmicsOptiMedica Corporation(OSI) Eyetech/Pfizer Ophthalmics
GOLD LEVEL
Carl Zeiss MeditecDutch Ophthalmic, USAInnovative Imaging, Inc.Insight Instruments, Inc.MedOne Surgical, Inc.Synergetics, Inc.
SILVER LEVEL
VisionCare OphthalmicTechnologies
CME CreditThis activity has been planned andimplemented in accordance with the Essentials and Standards of theWashington State Medical Associa-tion (WSMA) CME AccreditationCommittee through the partnershipof the Spokane County MedicalSociety (SCMS) and the AspenRetinal Detachment Society. TheSCMS, a WSMA accredited sponsor,designates this educational activityfor a maximum number of 14 hours(14.0) of Category I to satisfy therelicensure requirements of theWashington State Medical QualityAssurance Commission and theAmerican Medical AssociationPhysician’s Recognition Award. Eachphysician should claim only thosehours of credit that he/she actuallyspent in the educational activity.
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO 3
Monday, March 6
I. Vitreoretinal Surgery with 25-Gauge Instruments: The Wills ExperienceCarl D. Regillo, MD
NOTES 1
Dr. Regillo presented an overview of the published litera-ture on and his experience with 25-gauge instrumentationfor vitreoretinal surgery. He noted there was a paucity ofpeer-reviewed literature on the subject and what waspublished was retrospective studies that were primarilybased on early experience with the technology (mainlywith the Bausch and Lomb system). Dr. Regillo presenteddata outlining his experience with the Alcon Accurus25g system used on 70 patients at the Wills Eye Hospital.
There are two commercially available systems: one fromBausch and Lomb (TSV-25) and one from Alcon, thelatter being more widely-used. To be certain, 25gvitrectomy has become very popular among vitreoretinalsurgeons, and an informal poll of the audience revealedthat the majority of ARDS participants were using 25gtechniques on many of their cases.
The advantages of 25g over 20g vitrectomy include: fastersurgical time, less iatrogenic cataract, and possibly lessfinancial burden. (Although 25g surgical packs are moreexpensive, it may be actually cheaper overall due to thefact that the surgeon is not using sutures, diathermy.)Disadvantages include postoperative wound leak andassociated transient hypotony, decreased surgical manipu-lation capabilities due to instrument flex, and theoreticallyincreased risks of endophthalmitis and retinal detachmentdue to vitreous incarceration in the sutureless wound.
Case selection is felt to be important when planning touse 25g vitrectomy. “Ideal” 25g vitrectomy indicationsinclude: epiretinal membrane, macular hole, non-clearing vitreous hemorrhage, endophthalmitis, andvitrectomy for eyes with previous glaucoma filteringblebs (to avoid disruption of the conjunctiva). Non-complex retinal detachment and retained lens fragmentswere considered “good” indications, while “less-ideal”indications included retinal detachment with PVR and“bad” diabetic traction retinal detachment. Improvedillumination with the Xenon light source and chandeliersystems as well as a host of new and improved instru-ments with increased stiffness are increasing the use of25g vitrectomy by vitreoretinal surgeons. This hasresulted in greater surgeon comfort, but a learning curvestill exists for those transitioning to 25g cases.
NOTES 2
The advantages of 25-gauge vitrectomy include shorteroperating times, faster post-operative healing, greaterpost-operative comfort, less surgical trauma, and possiblylower cost and lower rates of cataract formation. Oper-ating times may vary depending on the case, but macularcases are generally faster with the use of 25-gauge. Withrespect to cost, although 25-gauge vitrectomy packs aremore expensive than 20-gauge packs, given that operatingtimes may be shorter with 25-gauge vitrectomy, theoverall cost of surgery may be less.
The disadvantages of 25-gauge vitrectomy may includepost-operative wound leaks, post-operative hypotony,decreased intraocular capabilities due to limitations withinstrumentation, and increased vitreous incarcerationwhich may subsequently lead to increased rates of post-operative endophthalmitis and retinal tears/detachments. Limitations secondary to instrumentationare becoming much less of a problem as the developmentof new instruments has facilitated surgery with 25-gauge systems.
Variable rates of complications have been noted andcurrently there has been limited data published on 25-gauge vitrectomy. To date, there have only been twoseries published with 50 or more cases.
In a retrospective study by Dr. Regillo’s group looking atoutcomes of 25-gauge vitrectomy, high rates of anatomicand visual success were demonstrated. Sclerotomy sutureswere required in 5 eyes (7.1%) and sclerotomy-relatedretinal tears occurred in 2 eyes (2.8%). Overall, transientpost-operative hypotony was not clinically significant inthis series of 70 eyes and the only statistically significantdecline in IOP was seen in the fluid filled eyes.Regardless, in 4 fluid filled eyes (6.2%) resolution ofhypotony occurred by 1 week without intervention. Oneweek intraocular pressures were shown to be identical tothe final IOP and on average the mean post-operativepressure did not change over time.
This study also suggested that cataract progression asmeasured by any increase of cataract in the post-operative period is most likely not significantly less in25-gauge vitrectomy as compared to 20-gauge vitrectomy.
In a companion study of 347 eyes with macular puckersor holes, low rates of intra- and post-operative retinaltears and detachments were seen when comparing 25-gauge to 20-gauge vitrectomy. The results of this studywere not, however, statistically significant, but they didshow an interesting trend which suggests that withrespect to iatrogenic retinal tears or detachments thereare no increased problems with 25-gauge compared to20-gauge.
4 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Case selection is also important when deciding to use 25-gauge. Ideal cases may include macular pucker,macular hole, non-clearing vitreous hemorrhage,endophthalmitis, and eyes requiring preservation of the conjunctiva for filtering surgery.
In summary, 25-gauge may be ideal for select cases suchas macular pucker and macular holes, and the need formore published data is needed to demonstrate safety of25-gauge versus 20-gauge vitrectomy.
See Regillo PowerPoint presentation, A.2.
II. Advances in 25-Gauge VitrectomyIndications and TechniquesCarl C. Awh, MD
NOTES 1
Dr. Awh discussed his extensive experience with theBausch and Lomb TSV-25 25g vitrectomy system. Heechoed Dr. Regillo’s comments on what constituted idealindications for 25g vitrectomy as well as the advantagesand disadvantages of the transconjunctival suturelessvitrectomy approach as compared to conventional 20gvitrectomy. He discussed adjuvant use of intravitrealkenalog to aid in visualization of the vitreous, especiallyanterior vitreous and mentioned that the trocars can alsobe used through the clear cornea to address anteriorsegment pathology more directly.
In fact, the latest generation trocars are reportedly much sharper than the previous iteration and as a resultdo not cause disruption of sutureless clear cornealwounds made by cataract surgeons. This is ideal insofaras 25g vitrectomy can be used more routinely to addressposterior segment complications of anterior segmentsurgery (e.g., retained lens fragments, endophthalmitis).The Bausch and Lomb 25g vitrectomy port is larger thanthe Alcon port, which he felt eased removal of smallretained lens fragments.
Dr. Awh presented an overview of the technical basis of25g vitrectomy efficacy as well as a comparison of electric-(Bausch and Lomb) versus pneumatic- (Alcon) drivenvitrectomy handpieces. Mention was made of 23g suture-less vitrectomy instrumentation, though Dr. Awh admittedhe had not used this approach. Both Drs. Regillo andAwh fielded several questions from the audience.
NOTES 2
With the advent of newer instrumentation and moreexperience by surgeons, 25-gauge vitrectomy may havenow reached a point where it is the preferred techniquefor select cases. Such cases include:
1. Vitrectomy in patients with filtering blebs2. Macular pucker surgery after previous vitrectomy
or scleral buckling3. Dropped lens fragment4. Vitreous incarceration with retained lens5. Vitrectomy with submacular tPA6. Diabetic membrane dissection
Vitrectomy in patients with filtering blebs
Dr. Awh presented 9 cases of 25-gauge vitrectomy inpatients with filtering blebs where because of 25-gaugevitrectomy, the conjunctiva in these patients waspreserved very nicely.
Macular pucker surgery after previous vitrectomy
or scleral buckling
Patients who develop macular pucker after previousvitrectomy or scleral buckling may also benefit from 25-gauge as this technique spares the need for difficultconjunctival openings. And even though surgery maytake longer to peel larger membranes with 25-gaugeinstruments, time lost may be made up with the ease of opening and closing these cases.
Dropped lens fragments
Since the newer generation trocar is sharper thanprevious models, you are less likely to disrupt a clearcornea wound with trocar placement. In addition, with a larger port designed by Bausch and Lomb, the cuttercan handle material better.
Diabetic membrane dissection
The small tip of the 25-gauge cutter may actually make itmuch easier to dissect these membranes. And with theChandelier, you have the option of doing your dissectionbimanually.
Technical advances in 25-gauge vitrectomy includestiffer light pipes, stiffer laser probes, and the creation ofa 25-gauge MVR blade. The Xenon light source is alsomuch better than older 25-gauge lighting systems andprovides more uniform lighting.
Regardless, 25-gauge vitrectomy does have some limita-tions. For example, there may be limitations associatedwith a smaller wound, and if you have a taut posteriorhyaloid, it may be necessary to convert to 20-gauge. Incases such as intraocular foreign body reomovals whereyou may need bigger instruments, 20-gauge would also be the preferred technique.
23-gauge vitrectomy may be a good option in the future.However there are early concerns in that the sclerotomiesrequire an oblique incision, which may subsequently leadto more scleral issues during reoperations.
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO 5
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Discussion of presentations by Drs. Regillo and Awh
DISCUSSION 1
Q: Is beveling or angling the trocars a helpful technique?
A: Both reported that they were not doing it and didn’tfeel it was necessary, although several vitreoretinalsurgeons report using this approach in an attempt todecrease hypotony postoperatively.
Q: Isn’t there a theoretical concern about a higher rateof endophthalmitis due to the fact that the eye is notcompletely closed at the end of the case?
A: The concern is there, but there appears to be nosafety signal yet. Only a few cases of endophthalmitishave been reported. Conjunctival displacement andprobable plugging of the sclerotomies with peripheralvitreous also likely reduce the risk. A thorough iodineprep is key.
Q: Don’t we expect a higher rate of retinal tears/detachment due vitreous incarceration?
A: Thankfully that has not borne out to be the case.David Williams has one series that had an abnormallyhigh detachment rate after 25g vitrectomy for floaters.Perhaps those patients also had abnormal vitreous thatpredisposed them to retinal detachment?
Q: Do you perform a fluid-air exchange at the end ofcases routinely? Do you use subconjunctival antibioticsfor these 25g cases?
A: In general, they were reporting use of routine fluid-airexchange at the conclusion of 25g cases. Dr. Regillooccasionally will inject air for someone he has performed a very complete vitrectomy or who might have a greaterrisk for choroidals (e.g., myopes, glaucoma patients).Most injecting cephalorsporin antibiotics subconjunc-tivally, avoiding direct exposure of aminoglycosideantibiotics to the sclerotomy site.
Q: When it does occur, when does postoperativehypotony resolve?
A: Hypotony typically occurs in 6% of cases andgenerally resolves within 2 weeks.
DISCUSSION 2
Q: Neither Dr. Regillo or Dr. Awh showed the use ofbeveled incisions when inserting the trocar. Do youthink that using a beveled incision is helpful?
A: From my experience I haven’t had problems withhypotony. But if I did, I would think about using abeveled incision.
A: A beveled incision is not easy to make and I don’tthink that it is necessary.
Q: I have some concerns about the safety of 25-gauge.One would intuitively think that in a wound that is notclosed with a suture, you essentially have an openedwound. Therefore you would think that you will have an increased rate of endophthalmitis and retinal detach-ment (if there is less vitreous removal and increasedvitreous incarceration).
Although your group has not shown this to be the case,David Williams has shown an increased rate of retinaldetachment with 25-gauge vitrectomy and MikePeterson has concerns about a higher rate of endoph-thalmitis. I am surprised about the low rate of hypotonybeing 6%. Did you include those patients with anintraocular pressure of 7-10 mmHg?
A: I’m happy to see that our results did not indicate anincreased rate of retinal detachment. I would guess thatwith the trocar you will have less intraoperative retinalbreaks, but with the possibility of increased vitreousincarceration in 25-gauge cases you would have anincreased rate of retinal detachment post-operatively.Overall, I don’t think that 25-gauge vitrectomy is moredangerous than 20-gauge vitrectomy.
A: I agree that there is an increased risk of endoph-thalmitis and I’ve spoken with David Williams about the possibility of increased endophthalmitis. I think thatpatients with vitreous floaters may have an increased risk of retinal detachment after vitrectomy. This may be because these patients have an unusual vitreoretinalinterface.
Q: Do you both inject air into the vitreous cavity in all your cases?
A: In this study I was putting gas and not air into theeye. I was not doing what Steve Charles did, which wasput air in. In the myopic eye or glaucoma patients I putair in to minimize chances of post-operative hypotony,thinking that these eyes may have an increased risk of choroidals.
Q: Did you compare hypotony rates in air versus fluid filled eyes?
A: Yes
Q: (to the audience) How many eyes that arehypotonous day one or two will result in long termhypotony? How many resolve within one week? Andwhat would happen if you leave these people alone?
6 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
A: We had a few eyes that had low pressures on thesame day of surgery, but by a week everyone had nohypotony. We also performed UBM on some patientswhich showed vitreous incarceration. Therefore wegenerally put a little antibiotic right over the sclerotomysite. You may also consider putting a little bleb ofantibiotic subconjunctivally.
The key point though is that the hypotony most oftenjust goes away.
Q: Beveled question. Even though you think that thearchitecture is different with a beveled incision, I thinkthat an angled incision may be useful and may even helpprevent post-operative endophthalmitis.
A: With regard to vitreous incarceration it’s not only in25-gauge and also occurs in 20-gauge, but I agree that itoccurs a little more often with 25-gauge. I think it wouldbe nice to compare beveled versus nonbeveled incisionswith 25-gauge.
A: Post-operative hypotony is not benign. I’ve had patients who have had choroidals on post-operative day one.
A: There is an ophthalmologist in Italy who did a UBM study that showed vitreous incarceration to belimited with the use a beveled incision. I bevel all my incisions.
Q: (to the audience) How many of you have done 25-gauge? I now do a fair percentage of cases 25-gauge. I think a big issue for us is the cost of the packs.
Q: I have not seen a significant amount of hypotony.Wound management. Should you manipulate the eye?
A: David Chow performed all the different techniquesand the average post-operative intraocular pressure was the same. I don’t think it makes a difference whetheror not you manipulate the eye when removing thetrocars. I think that the introduction of the instrumentsmakes a difference in determining whether or not youget post-operative hypotony. If you move the eye aroundtoo much you may even get more post-operativehypotony.
Q: The infusion port is just as likely to leak. I think that transient hypotony is a problem.
A: Our hypotony rate is not much different fromprevious reports.
III. Neuro-ophthalmic Insights for the Retina SpecialistWilliam F. Hoyt, MD
NOTES 1
Dr. Hoyt presented several fascinating neuroophthal-mologic cases. The first case was a 26 year old forestryworker who sustained an arrow injury to the rightorbit/globe, impressively depicted on an external photo-graph and CT scan of the orbit and brain. The patienthad the arrow removed and underwent neurosurgicalintervention. He survived, but had a contralateral lefthemianopia and loss of the right globe.
The second case started with a fundus photograph of apatient with a pale optic nerve and peripapillary fibrosisin the setting of central retinal artery occlusion. It turnedout this patient had Hollenhorst syndrome due to headshift and prolonged orbital compression during a surgicalprocedure on his spine. This characteristically demon-strates enlarged muscle bellies on a coronal T1-weightedMRI scan and muscle bellies with black centers withperipheral edema on a coronal T2-weighted MRI scan.
The third set of cases dealt with a condition ofanomalous central retinal vein architecture in which the entire retina drains into a vein circumferentiallyarranged at the edge of the optic disc, typically nasally.This was first described by a Czech named Kraupa in1915 while working in Prague. It was later similarlydescribed by a host of individuals elsewhere (including:Oxilia, Coats, Czernmak, Hoyt, and Ronne amongothers). Kraupa coined the term “Optikusrandvenen,”which is German for “edge vein.” All central retinalveins do not drain down the center of the optic nerve,instead some drain directly into choroidal veins, some go to the retrobulbar soft tissue in the intraconal space.These edge veins often times take the place of a properlylocated central retinal vein and at other times may occurin combination with a normal central retinal vein. Thisis sometimes referred to as a “disko vacio” or “emptydisk” to the lack of a CRV at the papilla.
“Nettleship collaterals” were also discussed. These areunusual collateral vessels bridging the choroid and centralretinal artery which is often totally obstructed. These areoften called “junk collaterals” and they often originatefrom the choroid and anastomose with filling braches ofthe central retinal artery. These were first described byNettleship in his 1891 FESTSCHRIFT for Helmoltz.Gonin and Hayreh later described similar cases. To getjunk collaterals, occlusion of the central retinal arterymust occur right near the lamina. This often occurs withcalcium emboli from the heart, due to its sticky edges.
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO 7
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
NOTES 2
Case 1: A 26 year old forestry worker referred for evalu-ation of an intraorbital and intracranial foreign body. InMay 1993 the patient was initiated into club “mountainmen anonymous.” The initiation ritual involved a bowand arrow, and a beer can. There was a misfire and thepatient was referred for treatment after the arrow enteredthe right orbit.
CT scan showed an arrow perforating the skull.
The arrow missed the carotid artery and was seen onimaging to be violating the occipital tip.
The patient survived but was left with a complete lefthomonymous hemianopia.
Case 2 (Hollenhorst Syndrome): Hollenhorst syndrome:neurosurgical headrest syndrome. Orbital and ocularcompression by a headrest during cervical surgery.Pressure on the brow and the muscles swell.
MRI with gadolinium may show necrosis in the centralmuscle belly of the rectus muscles.
T2 weighted images show high water content in thesurrounding portion of the rectus muscles and this mayappear days after a compression accident in the neuro-surgery theater.
Case 3 (Edge Vein): There have been several reportsdescribing an edge vein:1. Czermak: 18882. Kraupa (Prague): 1915 & 19243. v. herrenschwand: 19164. Oxilia: 1949
An edge vein represents a large venous channel draininginto the edge of the optic disc. All central veins don’tdrain to the center of the disc and into the intraconalspace. Some drain into the choroidal veins.
Dr. Hoyt has a website that you can access by going to:http://medlib.med.utah.edu/NOVEL/Hoyt/. You canaccess over 800 optic disc photos in this collection of 35-40 years.
Case 4 (Nettleship Collaterals): In order to get good junkcollaterals you need to occlude the artery. Calcium has a lot of sticky edges and can really stick and jam theartery closed. Where does the calcium come from?Microvegetation. And if you see Nettleship collateralsyou should look for a cardiac source.
Discussion of presentation by Dr. Hoyt
Q: Do you ever see Nettleship collaterals in an eye with preserved vision?
A: I have not.
IV: Avastin ExperienceRobert Avery, MD
NOTES 1
Bob Avery from Santa Barbara discussed his experiencetreating patients with retinovascular disease with intra-vitreal Avastin. Dr. Avery was an early adopter ofintravitreal Avastin use, after seeing the early resultsshown by Phil Rosenfeld. Initially there was a belief thatintravitreally delivered Avastin – which is a humanizedversion of a mouse monoclonal antibody to VEGF-A –would be too large to penetrate the retina. However, theearly experience showing clinical response to intravitrealAvastin debunked that theory.
This was further reinforced by collaborative research byDr. Avery and Anat Lowenstein that demonstrated full-thickness retinal penetration of Avastin in rabbit eyes.This was in accordance with a previous publication byDennis Han that also demonstrated full thickness retinalpenetration of a human IgG. Because both bevacizumab(Avastin) and ranibizumab (Lucentis) both bind allbiologically active isoforms of VEGF-A, it is notsurprising that Avastin appears to have (though as yetunproven) similar clinical efficacy to that seen withLucentis.
In his early experience with intravitreal Avastin, heexcluded patients with systemic risk factors (stroke,recent heart attack, thromboembolic disease history) and utilized the 1.25 mg dose. Most patients had failedeither Macugen or PDT or both, but later he begantreating patients primarily with Avastin.
Dr. Avery shared the results of his recently publishedarticle in Ophthalmology outlining his experience withintravitreal Avastin for patients with neovascular AMD.He also alluded to the several articles that were justpublished in the March issue of Retina on intravitrealAvastin for varied indications. Dr. Avery showed severalclinical examples of intravitreal Avastin for the treat-ment of subfoveal CNV due to AMD. In addition, hegave several examples of patients treated with intra-vitreal Avastin for PDR, DME, CRVO, and NVG. He feels preoperative intravitreal Avastin in diabeticpatients with traction retinal detachment with or with-out vitreous hemorrhage cuts down on intraoperativehemorrhage and can even facilitate clearing of hemor-rhage in non-operated patients.
8 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
For PDR in particular, he tested varying dilutions ofAvastin. In the paper describing the maximally tolerateddose of Lucentis by Rosenfeld et al, the greatest efficacywas seen with the lowest dose. So this suggested thatperhaps a lower dose of Avastin might be more effica-cious. Dr. Avery did not find that lower doses of Avastinfor neovascular AMD were useful, but in diabeticsinstead of giving his usual dose of 1.25 mg in 0.05 ml, he tested concentrations that were 1/10th, 1/20th,1/100th, and 1/200th the original strength withpersistent – albeit diminished – efficacy. Dr. Averycommented that although a clinical effect was still seenat the most dilute concentrations, the efficacy did notappear to be as great with that seen with the full-strength formulation.
He also showed a case of a patient who was treated withintravitreal Avastin for rubeosis iridis in one eye whodeveloped contralateral regression of rubeosis iridis. Thissuggested that systemic circulating levels of Avastin arehigh enough to have a biologic effect outside of thetreated eye. This may indicate a potential safety concern,but the risk is unknown. He had one patient whopresented with a red painful eye and a mild anteriorchamber reaction three weeks after her fourth intra-vitreal Avastin injection. She was treated with topicalsteroids and cycloplegia with resolution of her symptoms.
In summary, intravitreal Avastin appears to be efficaciousfor the treatment of neovascular AMD, thoughcontrolled data are lacking. Most feel that Lucentis willreplace Avastin once it is approved for AMD, but thatperhaps Avastin will continued to be used in severalsettings: for indigent patients who cannot access Lucentis,for non-reimbursed non-AMD non-FDA approvedindications of Lucentis (DME, CME for CRVO etc), andperhaps to a great extent outside of the USA due to thefinancial advantage of Avastin over Lucentis.
NOTES 2
Phil Rosenthal pioneered the use of Avastin for wetmacular degeneration.
The typical dose used is 1.25 mg (0.05mL) and is mostcommonly given to patients who have failed Macugen or photodynamic therapy.
The first patient that was treated with Avastin by Dr. Avery was seen to flatten within one week aftertreatment. This patient remained flat for about threemonths and within six months the patient’s subretinalfluid recurred again. The patient’s fellow eye had thesame disease process and was treated showing similarresults. ICG angiogram showed a slight increase inplaque formation as the subretinal fluid resolved.
Patients with retinal pigment epithelial detachments(PED) may also show flattening of the PED aftertreatment with Avastin. In one patient, the PED did notflatten initially but after reinjection at one month, thePED resolved. ICG in this case also showed a slightincrease in plaque formation as the elevation flattened.
RAP lesions have also been reported to respond toAvastin injection.
Publication in Ophthalmology:
Intravitreal bevacizumab (Avastin) for neovascular age-related maculardegeneration. Avery RL, Pieramici DJ, Rabena MD, Castellarin AA,Nasir MA, Giust MJ. Ophthalmology. 2006 Mar;113(3):363-372.e5.Epub 2006 Feb 3.
Pre treatment OCT and post treatment OCT werecompared. The visions, however, were not ETDRSvisions but instead were Snellen visual acuities.Regardless, the results showed a trend of improved visualacuity for every patient in the study.
There are nine papers in Retina regarding Avastin:
1. Intravitreal bevacizumab (Avastin) for refractory pseudophakiccystoid macular edema. Mason JO 3rd, Albert MA Jr, Vail R.Retina. 2006 Mar;26(3):356-7.
2. Rapid improvement of rubeosis iridis from a single bevacizumab(Avastin) injection. Davidorf FH, Mouser JG, Derick RJ. Retina.2006 Mar;26(3):354-6.
3. Regression of retinal and iris neovascularization after intravitrealbevacizumab (Avastin) treatment. Avery RL. Retina. 2006Mar;26(3):352-4.
4. Intravitreal bevacizumab (Avastin) treatment of macular edema incentral retinal vein occlusion: a short-term study. Iturralde D,Spaide RF, Meyerle CB, Klancnik JM, Yannuzzi LA, Fisher YL,Sorenson J, Slakter JS, Freund KB, Cooney M, Fine HF Retina.2006 Mar;26(3):279-84.
5. Intravitreal bevacizumab (Avastin) treatment of proliferativediabetic retinopathy complicated by vitreous hemorrhage. SpaideRF, Fisher YL. Retina. 2006 Mar;26(3):275-8.
6. Electrophysiologic findings after intravitreal bevacizumab (Avastin)treatment. Maturi RK, Bleau LA, Wilson DL. Retina. 2006Mar;26(3):270-4.
7. Electrophysiologic and retinal penetration studies following intra-vitreal injection of bevacizumab (Avastin). Shahar J, Avery RL,Heilweil G, Barak A, Zemel E, Lewis GP, Johnson PT, Fisher SK,Perlman I, Loewenstein A. Retina. 2006 Mar;26(3):262-9.
8. Electrophysiologic and retinal penetration studies following intrav-itreal injection of bevacizumab (Avastin). Shahar J, Avery RL,Heilweil G, Barak A, Zemel E, Lewis GP, Johnson PT, Fisher SK,Perlman I, Loewenstein A. Retina. 2006 Mar;26(3):262-9.
9. Testing intravitreal toxicity of bevacizumab (Avastin). Manzano RP,Peyman GA, Khan P, Kivilcim M. Retina. 2006 Mar;26(3):257-61.
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO 9
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .

ERG studies show no toxicity and VEP show nodifference after intravitreal Avastin injection. IntenseILM staining with Avastin has been shown in rabbiteyes, and Avastin has also been shown to go into theINL and rod outer segments.
13 years ago Tony Adamis showed that diabetic eyeshave high levels of VEGF and that retinal neovasculari-zation regressed after Avastin injection for PDR.
Targeting angiogenesis, the underlying disorder in neovascular age-related macular degeneration. Ng EW, Adamis AP. Can J Ophthalmol.2005 Jun;40(3):352-68.
Injection of Avastin in one eye may also show an effectin the fellow eye. There have been unpublished reportsciting regression of retinal neovascularization in thefellow after Avastin injection.
There is a biologic effect with lower doses of Avastin, but this effect is not as robust. At 1/10th the usual dose avery robust response is seen and a good response is seenat 1/20th the dose. At 1/100th the dose there is someresponse but it has been noticed that some retinalneovascularization does not respond as well. 1/200th wasalso tried, and there was only a partial response to thisconcentration.
Surgery for diabetic tractional retinal detachments maybenefit from preoperative Avastin injection. One weekafter injection of Avastin, abnormal vessels have beenshown to shrink dramatically on fluorescein angiogramand color photographs. This potentially can make asignificant difference when operating on these eyes as itmay speed up surgery and enable the surgeon to peelmembranes more safely.
One side effect, however, that has been attributed toAvastin is uveitis. A case was presented where 3 weekspost injection a patient developed uveitis. The uveitisresponded to pred forte and experienced no change invision secondary to the uveitis.
Overall, the future for Avastin looks promising for thetreatment of AMD and retinal vascular disease.
V. Vitrectomy for Diabetic Macular Edema: One Year Results of the VIDE StudyGiacomo Panozzo, MD
NOTES 1
Dr. Panozzo joined us from Verona, Italy and discussedthe 12 month results of the VIDE study of vitrectomy fordiabetic macular edema. As background, he discussedthat although focal/grid laser for DME was found to bebeneficial in the ETDRS, we all have patients withdiffuse diabetic macular edema that cannot be effectivelymanaged with laser and the use of intravitreal kenalog isassociated with its own host of problems.
Lewis and others in the early 1990s suggested thatpatients with a taut and thickened posterior hyaloid andDME benefited from vitrectomy. Many of these earlystudies, however, were short case-series that were uncon-trolled and used varying approaches with each patient.What is lacking is a study evaluating a standardizedsurgical approach to patients with diffuse DME.
The only prospective and randomized study evaluatingvitrectomy for diffuse DME was by Stolba et al in 2005who concluded that vitrectomy with membrane peelingwas superior to observation. However, this studyinvolved ILM peeling, allowed previous laser treatmentwithin 4 months, included patients taut hyaloid andERM, and had short follow-up (6 months). So, the lackof a standardized data for the surgical treatment of diffuseDME patients was the basis for the vitrectomy versusnatural history for non-tractional DME study (VIDEstudy; VIDE means “seen” in Italian).
Dr. Panozzo discussed the study design, methods, andresults from the VIDE study and these are outlined in the attached Powerpoint outline. Of note, ICG dye andintravitreal kenalog were not allowed. At the 3 studysites, enrollment was completed in December 2005 with107 eyes enrolled.
In the natural history cohort, there were no statisticallysignificant differences in visual acuity, retinal thickness,and retinal volume between baseline, 6 months, and 12 months. For the natural history cohort, patients withhigh HgA1C levels had worse VA, higher macularvolume measurements, and slightly higher retinalthickness levels.
10 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Conversely, tighter HgA1C levels had more favorable in indices. For the vitrectomy cohort, there were nostatistically significant improvements seen with VA,retinal thickness, and retinal volume between baseline, 6 months, and 12 months. Similarly there was notbenefit between vitrectomy and natural history for eachof these indices at each timepoint. These are preliminarydata, only. More robust data analysis is expected withevaluation of 2 year outcomes as well.
NOTES 2
Dr. Panozzo has been pursuing an organized approach todiabetic macular edema (DME) and has been working ona classification system for DME. He has been workingwith THEIA, which is a foundation whose goals are toprovide support for clinical research, information, andteaching in the vitreoretinal field. The foundation is alsointerested in establishing a fellowship of 18 months totrain vitreoretinal specialists.
The aim of the VIDE study is to compare vitrectomyversus natural history for non tractional diabetic macularedema. Laser is generally less effective for the treatmentof diffuse diabetic macular edema (DDME), therefore itis important to search for new therapies. One approachthat has been suggested is to perform vitrectomy fordiffuse DME. Early reports have been favorable, showingthat vitrectomy may be better than treating with laser orintravitreal steroid injection.
Stolba reported the first prospective randomized studylooking at vitrectomy for diffuse diabetic macular edema.The study, however, was not conclusive since theyenrolled patients who had laser treatment four monthsprior to enrollment. Follow-up in this study was alsolimited.
Vitrectomy for persistent diffuse diabetic macular edema. Stolba U,Binder S, Gruber D, Krebs I, Aggermann T, Neumaier B. Am JOphthalmol. 2005 Aug;140(2):295-301.
Therefore, looking at the insufficient data available forthis matter, Dr. Panozzo has developed a study that aimsto tell us more about the natural history of diffusediabetic macular edema and determine whether or notvitrectomy is effective for treating this type of edema.
Included in the study:1. Patients with DDME without traction2. A control group to determine the natural history of
DDME without traction3. Data on glycemic control and kidney function4. One year minimum follow-up
The study also looked to define DDME on OCT. OCT was performed on each patient.
DDME was defined on OCT as:1. Diffuse retinal thickening in at least 75% of the
macular area2. Volume > 8mm3
3. Absence of traction on OCT
Exclusion criteria included:1. Type 1 diabetes2. Previous treatment within 8 months3. Previous vitrectomy in both eyes4. Focal macular edema5. Presence of traction6. Severe foveal hard exudates
There were 107 eyes that fulfilled the criteria for enroll-ment into the study. The results showed that diffuseDME is fairly stable at one year. Glycemic control alsohad a correlation with DME. If the HgbA1c was low orintermediate then there was no correlation between theHgbA1c and visual acuity. However, if the HgbA1c wasgreater than 9, then the visual acuity was low and theretinal thickness as measured by OCT was higher.
In the 13 eyes (12 eyes recruited at baseline and 1 eyerecruited for worsening of vision during follow-up) thatunderwent vitrectomy and had a minimum of 6 monthsfollow-up, vitrectomy showed no difference at 6 monthswhen compared to the natural history group, and at 1year the natural history group showed better results thanthe vitrectomy group. In addition, there were no differ-ences with regard to retinal thickness and volume.
Regardless of this preliminary data, a larger vitrectomygroup and longer follow-up is needed in order to see ifthere really is any difference between vitrectomy andnatural history.
See Panozzo PowerPoint presentation, A.4.
Discussion of presentation by Dr. Panozzo
DISCUSSION 1
Q: Did cataract affect your results?
A: This was evaluated and cataract did not affect theVA results.
Q: Did the intensity of involvement of the internalmedicine doctors have an influence on patients HgA1C levels?
A: Overall, patients were relatively tightly controlledthroughout the study with similar levels of internistinvolvement in the patient care.
Q: Did you also evaluate blood pressure effects?
A: We did, and this is something we are still analyzing.
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO 11
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
An informal poll of the audience suggested many areperforming PPV for diffuse DME. Some reported goodresults, but there is a feeling that ILM peeling is neededand some report using ICG as well.
DISCUSSION 2
Q: With regard to the hemoglobin A1c, did all thepatients have the same effort to lower their levels or didthey remain stable? So even though they were in thestudy, you didn’t see any drop?
A: They remained stable.
Q: Did you look into systemic hypertension?
A: Yes
Q: (to the audience) How many of you are doingvitrectomy for DME?
A: I am still pretty conservative in respecting theETDRS results. I will still use intravitreal steroids andlaser first. And if that’s failed, then I’ll go ahead and do avitrectomy even if the OCT does not show a tractionalcomponent. Often I still find a taught ILM and I’ve hadgood results with those cases, and these patients remainstable for many months.
I have had some good results with vitrectomy and Ialways use ICG when peeling ILM.
Q: Was cataract an issue? Was the vision decreasesecondary to cataract?
A: Cataract was not an issue.
VI. Failure of Lamina Puncture and Radial Optic Neurotomy for CRVODonald J. D’Amico, MD
NOTES 1
Dr. D’Amico evaluated his experience with laminapuncture (LP) and the data reported by Mitch Opremcakfor radial optic neurotomy (RON) to treat CRVO.Alternative treatment strategies for CRVO and CRVO-associated CME were reviewed (pegaptanib, ranibizumab,bevacizumab, anticoagulation, and triamcinoloneacetonide).
Dr. D’Amico reviewed the pathophysiology of CRVO.We know from Dick Green’s classic study, that there is aprelaminar clot in the optic nerve head in CRVO. Itmakes sense, therefore, that creating a potential spacewithin the nerve head would give the CRV room todilate and perhaps allow the clot to dislodge.
We know from the Central Vein Occlusion Study(CVOS) that initial VA is predictive of final VA. So65% of those who had an initial VA of 20/40 or betterhad a final VA of 20/40 or better, but conversely 79% ofthose with an initial VA worse than 20/200 had a finalVA worse than 20/200.
Therefore, based on the preclinical data andOpremcack’s promising early results, a trial was designedto evaluate the efficacy of LP in patients with a poorprognosis (initial VA worse than 20/200). Twentypatients, aged 65 years and older, with a CRVOdiagnosed within one year and a presenting VA of lessthan 20/200 were recruited into the pilot study. Based onCVOS natural history data, we would expect that only3.5 patients would have improved VA and what we sawwas that 3 patients had improved VA.
If we apply that same math to Opremcak’s RON results,we would expect that 2.5 of 11 patients would haveimproved VA. What we saw with his data was insteadthat 7 of 11 patients had improved VA. Perhaps due tothe presence of baseline vitreous hemorrhage in theRON series, an accurate diagnosis of CRVO was notestablished? If these patients had only a vitreous hemor-rhage without a CRVO, it would not be surprising to getsuch good visual results with the RON approach. Thesame math holds true for a larger analysis of 65 eyestreated with RON.
With these data and the known extensive complicationsof these aggressive surgical procedures in mind, Dr.D’Amico no longer advocates the use of the LP to treat CRVO. In addition, he issues the same caveat for RON.
NOTES 2
Transvitreal optic disc surgery for the treatment ofCRVO remains controversial and for the most part, theoutcomes of surgery parallel the natural history ofCRVO. The studies concerning radial optic neurotomy(RON) and lamina puncture for CRVO are pilot studies.The results with lamina puncture do not differ signifi-cantly from the natural history reported in the CVOS,and the procedure has been abandoned.
12 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .

Similarly, the RON data available in published series to date do not show significant benefit. The RON datapresented by Opremcak is also biased in that some of thepatients included in the study had retinal and vitreoushemorrhage, and these patients may have had bettervision if not for the hazy media. In summary, meta-analysis does not support any beneficial effect for RONsurgery either.
See D’Amico PowerPoint presentation, A.8.
Discussion of presentation by Dr. D’Amico
DISCUSSION 1
Q: What does Dr. Hayreh think of LP/RON?
A: He seems pleased with Dr. D’Amico’s analysis as hewas not a believer in this surgical approach.
Dr. Edwards discussed his experience with aggressiveanticoagulation (with Coumadin) for CRVO patients.He felt this approach was safe with internist involve-ment, but that the jury is out on efficacy. It is difficult torecruit patients and he has only 20 or so patients aftermany years.
DISCUSSION 2
Q: How many patients (with CRVO) showed a signifi-cant improvement after they had been stable after 6month, because in my experience they improve only inthe first 6 months.
A: Hayreh has a study showing that many initiallyaffected patients may have substantially better visualacuity at one and two years. The situation for carefulcomparison has become further clouded, because now inthe RON world we are seeing surgeons combining RONwith other modalities such as ILM peel and IVK.
Comment: We got the idea of using anticoagulation forCRVO from the cardiologists who observed that whenthey had patients with thrombi and they increased theINR to 3.5, that clots go away. In Hayreh’s study wenever got the INR up. It’s not the coumadin that islysing the clot, you are just freezing the size of themigration of the clot. All you need is a good liver tofibrolyse the clot.
Comment: I think that further study for the treatment of CRVO has to be randomized. Whatever we try withCRVO needs to be controlled because of the naturalhistory of this condition.
Tuesday, March 7
I. Changing Concepts in theTreatment of PrimaryRhegmatogenous Retinal DetachmentPeriklis D. Brazitikos, MD
NOTES 1
Dr. Brazitikos from Greece discussed the use ofvitrectomy without scleral buckling for primaryrhegmatogenous retinal detachment (RD). The idealsurgical approach to retinal detachment repair would beone with a high rate of surgical reattachment (over90%), preservation of visual acuity, and an absence ofsignificant complications. The complications of scleralbuckling were discussed (e.g., drainage of subretinal fluid complications, diplopia, pain) as well as the factthat the retina is not completely flat at the conclusion of the case and persistent subfoveal fluid can prolongvisual recovery.
He also added that due to changing trends, there is not universally good training in the lost art of scleralbuckling. As a result, few people have good training inthis approach, which does not have a truly standardizedapproach (many intraoperative decisions: size and extentof element, drainage/no drainage, air/gas/no tamponade).
Pars plana vitrectomy (PPV) instrumentation hasimproved greatly over the years, especially with regard to high-speed instrumentation, improved illuminationwith wide-angle viewing, as well as surgical adjuvants(e.g., endolaser, perfluorocarbon liquids). These advanceshave turned the tables on the preferred surgical approachto primary RD. In the 1970s, 99% of surgeons utilizedscleral buckling while a recent survey in 1999 showedthat only 37% chose scleral buckling compared to 63% choosing PPV.
Vitrectomy has several advantages over scleral buckling:better visualization, less anesthesia required, direct reliefof vitreoretinal traction, intraoperative reattachment,and less postoperative pain and discomfort. Cataract isan expected consequence, postoperative positioning andflying restriction is an inconvenience, and perhaps PPVis “too much surgery” for many presentations of RD.
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO 13
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Dr. Brazitikos reviewed the published literature on this topic in an analytic fashion. The lecture outlineincludes this extensive review as well as a review of hisrandomized clinical trial of PPV versus scleral buckle forthe treatment of pseudophakic RD. His trial used astandardized surgical approach with 20g PPV, retinalattachment with PFO or endodrainage, cryopexy ofbreaks, fluid air exchange, and 20% SF6. No use ofexoplants was allowed with PPV. The standardizedapproach to SB included the use of a circumferentiallyplaced 240 style buckling element, 15mm tightening ofthe band, no air/gas unless absolutely necessary, andtransscleral endodrainage when indicated.
He concluded that of the 3 randomized trials evaluatingpseudophakic RD, 2 favored PPV. For the randomizedtrial evaluating surgical approaches to phakic RD, nodifference was found between SB and PPV. It is unlikelythat definitive trials will be performed to answer thequestion what surgical approach is better for patientswith phakic RD and physicians will have to take thecharacteristics of each to determine what is best for their patient. Nevertheless, it is true that there is anexpanding spectrum of indications for PPV in themanagement of primary RD (phakic and pseudophakic).
NOTES 2
The severity and complexity of primary retinal detach-ments (RD) may vary between distinct types of RD, andthe ideal surgical technique to repair these detachmentsshould have a high rate of repair (> 90%) after a singlesurgery and have a low rate of complications.
Over the years scleral buckling (SB) has essentiallybecome a lost art as many are turning to pars planavitrectomy (PPV) as the initial procedure for RD repair.
Advantages of PPV without SB include:1. Most cases can be managed with local anesthesia2. Better visualization of breaks (wide angle systems)3. Vitreoretinal traction is permanently eliminated4. Intraoperative reattachment5. Clear media after surgery6. No astigmatism, strabismus, refractive changes7. Minimal post-operative discomfort and pain
(25-gauge)
Complications of PPV:1. Increased costs2. Gas: positioning, air travel, etc3. Low vision till absorption of gas (3 to 10 weeks)4. More post-operative visits5. Nuclear sclerosis – cataract > 90%6. Better to be avoided in eyes with functioning
accommodation
So to compare which procedure (SB vs. PPV) might bebest for surgical success in pseudophakic retinal detach-ments, the following study was performed:
Primary pars plana vitrectomy versus scleral bucklesurgery for the treatment of pseudophakic retinaldetachment: a randomized clinical trial. Brazitikos PD,Androudi S, Christen WG, Stangos NT. Retina. 2005Dec;25(8):957-64.
The study concluded that PPV may offer advantages overSB in reattachment of pseudophakic retinal detachment.
Currently, a German study looking at SB vs PPV inrhegmatogenous RD “SPR Study” is under way. The SPRstudy is a prospective, randomized, multicenter study, andto date, unpublished data from this study suggests thatPPV shows better success and less reoperations.
Overall, however, it is unlikely that a single type ofvitreoretinal surgery will be perfect for every retinaldetachment and it is important to have evidence baseddecision making to determine which type of surgeryworks best for a particular situation.
With regard to post-operative failure, what causes failurepostoperatively?
Wilkinson noted that buckle failures are more likely dueto preoperative PVR In 1993, however, Hakin reportedthat initial failure after PPV was most commonly due tomissed breaks and then to PVR. (Primary vitrectomy forrhegmatogenous retinal detachment. Hakin KN, LavinMJ, Leaver PK. Graefes Arch Clin Exp Ophthalmol.1993 Jun;231(6):344-6.)
See Brazitikos PowerPoint presentation, A.11.
Discusion of presentation by Dr. Brazitikos
DISCUSSION 1
Q: What is your indication for pneumatic retinopexy?
A: I do not perform pneumatic retinopexy inpseudophakes.
14 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Q: Did your PPV failures have inferior breaks?
A: No, PVR was the major cause and there was asclerotomy break.
Q: Do you use anything besides a 240 band? We use a 42 band at our institution, because it is easier to placewith broader ability to imbricate.
A: We standardized the technique, but the 240 is theelement we chose.
Q: Perhaps your SB success rate is a testimony to poorteaching. I think fellowships should still teach SB.
A: I agree, we need to do a better job teaching people to do SB.
DISCUSSION 2
Q: What is your indication for doing pneumaticretinopexy?
A: I never do pneumatic retinopexy in pseudophakiccases and I will perform pneumatic retinopexy in phakiceyes with small superior breaks with a small amount ofsubretinal fluid.
Q: Have you looked back at the cases that failed to seeif they had an inferior break?
A: One case had a new break at the sclerotomy site.Others had new breaks secondary to PVR. I think thatPVR is probably more aggressive after PPV than SB.
Q: Have you used any other element other than a 240 band?
A: In this study we had to standardize the techniques so this was a concern.
Q: Do you do 360 laser?
A: From what I have seen, there is no higherreattachment rate using buckle after PPV. And Ipersonally don’t do 360 laser.
Comment: I want to emphasize the importance ofcategorizing detachments. When you talk about a failurerate of 30% after SB, I don’t think that makes sense.Maybe this is an effect of training. I’m very confidentthat buckling will remain in our armamentarium.
Comment: Younger surgeons don’t know how to buckle.
II. Anti-VEGF Therapy for Age-related Macular DegenerationAllen C. Ho, MD
NOTES 1
Dr. Ho reviewed the available data on the available and forthcoming anti-VEGF therapies for neovascularAMD. He discussed the anti-VEGF aptamer pegaptanib(Macugen) and the 1 and 2 year results of the VISIONtrial. He emphasized that patients do better withMacugen than with usual care, but that patientscontinued to lose vision. A recent analysis of thosetreated with Macugen with early disease and smalllesions tend to do better than those who have moreadvanced disease.
He also discussed the monoclonal antibody fragment to VEGF ranibizumab (Lucentis) and the results to theFOCUS (Phase II), MARINA (Phase III, minimallyclassic and occult lesions), and the ANCHOR studies(Phase III, predominantly classic). The efficacy ofLucentis appears to be independent of lesion type, withnearly 40% of patients having 20/40 or better vision atone year, 95% of patients losing less than 15 letters ofVA, and approximately 1/3 of patients gaining 3 or morelines of VA at one year. In all the Lucentis studies, the mean change in VA from baseline to one year was a gain in VA.
So, clearly, Lucentis sets a new standard for AMDtreatment efficacy, but is it safe? We know that Macugenhas proven to be a very safe drug, both from an ocularand a systemic standpoint. Lucentis, too, appears to have a low incidence of ocular adverse events. Numerically,there were more non-fatal serious systemic AE’s in the0.5 mg Lucentis group compared to the 0.3 mg group andcontrol group, but no clear systemic safety signal hasbeen identified.
The PIER study (Phase III, altered dosing strategy) andthe SAILOR study (Phase III, safety and enhancedaccess) are ongoing and will provide additional safetydata. FDA approval is pending, with a decision expectedin late June. The VEGF-Trap, small interfering RNAmolecules (siRNA), and anecortave acetate(RETAANE) were also briefly discussed as potentiallymarketable AMD drugs several years down the road.
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO 15
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
The CATT trial was also discussed. This is a trialsponsored by the NEI that proposes a comparison head-to-head of Lucentis versus intravitreal Avastin andpotentially PDT and/or RETAANE. This study is not yetfunded, but the U-10 grant has been submitted. DanMartin from Emory would be the PI and an enrollmentof 1,230 patients is anticipated at multiple sites. So, insummary, multiple anti-VEGF strategies exist. Macugenushered in the anti-VEGF era and Avastin and Lucentisare exciting new treatment modalities.
NOTES 2
VEGF is a homodimeric glycoprotein and is secreted bymany cells in response to stress. It induces angiogenesisand vascular permeability. VEGF is a family of multipleisoforms. We focus on VEGF A, which binds to tworeceptor sites because it is a homodimeric compound.
In the anti-VEGF wars there are different ways ofinhibiting VEGF:1. Kinase inhibitors2. siRNA3. VEGF trap4. Aptamer (Macugen)5. Squalamine6. Anti-VEGF (Avastin, Lucentis)
Macugen: Inhibits soluble isoform of VEGF 165 and isthe first improved anti-VEGF for AMD. Its lowesteffective dose is 300 ug and it can be used for all forms ofexudative AMD.
Classification scale of classic vs. occult seems lessimportant these days as Macugen has come into thepicture.
Macugen has shown a benefit in stabilizing visual acuityat one and two years and has shown a slight increase invisual acuity from 11 to 17 percent to greater than 2 line gainers from one to two years. However, the mostimportant contribution of the VISION trial is the safetyprofile which showed no evidence of systemic compli-cations, no evidence of thromboembolis events, and low rates of endophthalmitis, traumatic cataract, andretinal detachment.
Lucentis: Lucentis is another anti-VEGF moleculewhich is affinity matured to create a specific moleculethat attacks all VEGF isotypes.
Two studies looking at Lucentis for AMD are MARINAand ANCHOR; MARINA looking at Lucentis forminimally classic/occult lesions and ANCHOR lookingat Lucentis vs. PDT for predominantly classic lesions.
MARINA:
Conclusions at 1 Year:
• 95% of Ranibizumab subjects lost fewer than 15 lettersvs 62% of sham
• 25-34% of Ranibizumab subjects improved 15 or moreletters vs 5% of sham
• All other vision outcomes also favored Ranibizumab
• Low rate of ocular serious adverse events
• Presumed Endophthalmitis (0.6%), Uveitis (0.6%)
• No apparent systemic safety concerns; continue to monitor
Conculsions at 2 Years:
• 90% of Ranibizumab subjects lost fewer than 15 lettersvs 53% of sham; continued benefit through year 2.
• Low rate of ocular serious adverse events
• Thromboembolic events– Sham 3%– 300 ug 4.6%– 500 ug 4.2%
Patients treated with Lucentis showed a very rapidresponse with a significant reduction in edema. Overall,the ocular side effects are all less than 1%, howeverthromboembolic events, even though not statisticallysignificant in the 500 ug group, displayed a numericaldifference that we have to be aware of.
ANCHOR:
Conclusions (12 month vision outcomes):
Clinically and statistically significant benefit vs PDT inpredominantly classic CNV
• ~95% lost fewer than 15 letters
• 8.5-11.3 letter improvement in mean VA
• 36-40% improved 15 or more letters
• 6-12% improved 30 or more letters
Conclusions (12 month safety):
• Low rate of ocular serious adverse events
• No imbalance of non-ocular adverse events overall,except APTC arterial thromboembolic events only in 0.5 mg dose– PDT: 3 subjects (2.1%)– 0.3 ranibizumab: 3 subjects (2.2%)– 0.5 ranibizumab: 6 subjects (4.3%)
16 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .

Similar to MARINA, thromboembolic events werenumerically higher but not statistically significant in the 500 ug group.
So as a result of the VISION, ANCHOR, and MARINAstudies, our future will really launch from Lucentis as abenchmark for efficacy and Macugen as a benchmark for safety. Combination trials are ultimately what we will be doing.
See Ho PowerPoint presentation, A.18.
Discussion of the presentation by Dr. Ho
DISCUSSION 1
Q: Describe the impact of the CATT trial.
A: Avastin is optimally given PRN, but we have no data to support that approach. So a study is needed. The Lucentis OCT guided treatment study (Pronto) isokay, but it is only 40 pts and we cannot draw PRNtreatment conclusions from that. The PIER study is non-comparative (dose vs dose) and it’s a small trial (184pts). Therefore we need a bigger study to evaluate thebest drug and the best dosing strategy. Avastin, ifeffective, could potentially save Medicare 4.2 billiondollars annually.
DISCUSSION 2
Comment: We designed a trial using combinationtherapies using Avastin or Lucentis. But we want to look at what the best monotherapy is. Our experiencewith Avastin is that we would much rather use it on aPRN basis. We have no good data to support usingAvastin on a PRN basis. PRONTO is limited still withfew patients enrolled. We have designed a study withover 1,000 patients.
Comment: I think the crux of the issue is what we do in the absence of clinical trials data and not what we dowith the clinical trials data. Don’t we need to wait forclinical trials data? Don’t we have a responsibility to our patients to wait? I think the controversy is that ifAvastin is covered and Lucentis is available, where do we stand in terms of the decision process of how to treat wet AMD?
III. Macugen Therapy for Exudative Macular Degeneration and Diabetic RetinopathyGregg T. Kokame, MD
NOTES 1
Dr. Kokame reiterated the results of the VISION trial ofpegaptanib (Macugen) for subfoveal CNV due to AMD.He stressed the safety of multiple injections of intra-vitreal Macugen not only in the trial but also in thepost-marketing surveillance period. Post-marketingadverse events were minimal with over 75,000 injectionsperformed. There was no evidence of alterations of theretinal or choroidal vasculature noted nor signs of severe inflammation.
The two-year efficacy and safety results were thenreviewed, showing a continuing benefit with ongoingtherapy. He reiterated the fact that subgroup analysis ofthe VISION trial patients showed that earlier lesionstend to fare better, with a greater proportion of patientswith early lesions gaining 3 lines compared to all-comers.
Dr. Kokame also reviewed the ongoing studies ofMacugen for DME. The patients in one of the phase 2trials underwent 3 mandatory injections every 6 weeksfollowed by 3 injections at the investigator’s discretion.Three doses (0.3, 1, and 3 mg) were tested. In the 0.3 mggroup, 18% of patients experience at 3 line gain and asignificant OCT central retinal thickness decrease. Thehigher dose groups had less of a clinical effect. Based onthese Phase II results, a Phase III trial is being organized.
Macugen has also been shown to have an “on/off” effect on neovacularization in PDR patients. In addition,a trial is underway to determine the efficacy of Macugenfor CRVO.
NOTES 2
How are we going to use Macugen in clinical practice?Will we use Macugen as monotherapy? Will combinedtherapy be better? Pharmacotherapy in general may bevery important in early disease, and patients with earlymanifestations of neovascular AMD may benefit morefrom Macugen monotherapy. With regard to combi-nation therapy, trials looking at PDT and Macugen usedtogether are underway. The biologic rationale for PDTand Macugen is that after PDT there is an upregulationof VEGF, and phase 1 data using Macugen and PDTshows a 60% gain of 3 lines of vision which supports theuse of combination therapy.
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO 17
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Another alternative to combination therapy is to induce therapy with one drug and then maintain with a different agent. For example, consider intravitrealKenalog (IVK) followed by Macugen maintenance oreven intravitreal Avastin followed by Macugenmaintenance.
Trials are also being performed looking at Macugen fordiabetic retinopathy. To date, the results have beenpromising, showing regression of neovascularization aswell as showing an a decrease in retinal thickness in the0.3mg group. The absolute amount of thickness thatchanged was about 64 microns and there were lesspatients requiring focal/grid laser in the treatment group.
In summary, Macugen is the first to validate the use ofanti-VEGF therapy in ocular disease. It has a favorablesafety profile locally and systemically throughout thetrials and in post-marketing survey. Macugen may also bemore effective in early lesions and promising in retinalvascular diseases.
See Kokame PowerPoint presentation, A.26.
IV. Current Status of Photodynamic Therapy for Age-related Macular DegenerationCarl D. Regillo, MD
NOTES 1
Dr. Regillo discussed the history of AMD therapies (laser, PDT) and the relevant studies that supportedthese approaches (MPS, TAP, VIP, VIO, and VIMstudies). Standard fluence PDT probably works well forminimally classic CNV, and reduced fluence probablyworks better, but good data on this point are lacking.VIO evaluated PDT for occult CNV and served toconfirm the results of the VIP trial. There is goodevidence for the use of verteporfin PDT for predomi-nantly classic CNV, while less impressive evidence exists for other lesion subtypes. However, even PDT for predominantly classic CNV leads to continued loss of vision.
Now ranibizumab (Lucentis) has been demonstrated inthe ANCHOR and MARINA trials to have phenomenalefficacy this appears to be a paradigm shift in terms ofredefining AMD treatment efficacy. Despite the efficacyof Lucentis, there is still the problem of too frequentdosing. Perhaps PDT has a role in combination withLucentis and other agents to improve on PDT efficacy?
A rationale for combination therapy exists insofar asPDT is known to upregulate VEGF and is transientlyproinflammatory. So, combining a steroid with PDTwould seem to be beneficial. There is precedence forcombination therapy with PDT. PDT has been combinedwith intravitreal triamcinolone (Kenalog) to treatneovascular AMD. Spaide demonstrated the efficacy ofthis approach in his early, small case-series. SubsquentPDT and Kenalog papers have shown similar efficacy inretrospective studies.
There are 4 prospective clinical trials underway todetermine the efficacy and safety of combination therapy with PDT (VisTA, RETINA, VERTACL, andVERITAS). PDT is being evaluated in conjunction with Macugen in a trial with 360 patients (enrollmentcompleted in January 2004). Patients with predomi-nantly classic CNV are randomized 2:1 to receivebaseline PDT (and as needed every 3 months thereafter) andMacugen every 6 weeks – or – Sham PDT and Macugenevery 6 weeks.
In addition, Ursula Schmidt-Erfurth is studying thecombination of Lucentis with PDT in the PROTECTstudy: initially, patients receive baseline PDT and 3monthly doses of Lucentis for predominantly classic andsmall occult lesions. This is then followed by PDT every3 months only if the investigator feels it is indicated. We expect to see results of the PROTECT study atARVO 2005.
In summary, there is a limited role for PDT monotherapyin the future. If combination trials with PDT and anti-VEGF and other anti-permeability agents prove fruitfulat providing synergy or reduced treatment intervals, PDT may serve as a useful adjunctive therapy. PDTmonotherapy will still play a role in the management ofCNV from non-AMD sources, for central serous chorio-retinopathy, and choroidal hemangioma.
NOTES 2
An overview of the trials looking at photodynamictherapy for the treatment of CNV as well as the trialslooking at combination therapy was discussed. The trialsreviewed included:
• TAP: Treatment of Age-Related Macular Degenerationwith Photodynamic Therapy
• VIP: Verteporfin in Photodynamic Therapy
• VIM: Verteporfin in Minimally Classic CNV
• VIO: Verteporfin in Occult CNV
18 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Combination Treatment:
• PROTECT: Lucentis and PDT
• VERITAS: PDT and Macugen v. PDT andTriamcinolone v. PDT
• EOP1012: PDT and Macugen
• VisTA (Visudyne and triamcinolone)– 120 patients; predominantly occult CNV– 0, 1 or 4 mg TA + verteporfin therapy
• RETINA (Canada)– 120 patients; predominantly classic CNV– 0 or 4 mg TA + verteporfin therapy
• VERTACL (NEI/QLT)– 300 patients; all CNV types– 0, 1 or 4 mg TA + verteporfin therapy
Conclusions: CNV is a chronic multifactorial disease,and targeting different pathways may lead to a synergisticeffect with better outcomes. In the future, monotherapywill have a limited role, and effective treatment willmost likely involve combination therapy. With regard toPDT, combination therapy has the potential to reducethe need for retreatment and follow-up, decrease therisks of adverse events due to fewer treatments, anddefine a finite course of treatment.
See Regillo PowerPoint presentation, A.38.
V. Pneumatic Displacement of Subretinal Hemorrhage in Age-related Macular DegenerationMark W. Johnson, MD
NOTES 1
The natural history of moderate to large submacularhemorrhages due to neovascular AMD is poor.Submacular hemorrhage has been shown to be toxic tothe photoreceptors experimentally. As a result, VA rarelyimproves beyond 20/200 left untreated. The submacularsurgery trials in 2004 showed no visual benefit forextraction of blood and CNV. Visual acuity greater than20/80 is typically seen in only 16% of patients.
Pneumatic displacement of subretinal hemorrhage withintraocular gas and intravitreal tissue plasminogenactivator (tPA) was first proposed by Heriot in 1996.This was later demonstrated in a paper by Hassan et al in 1999. This is a low-cost and simple office-basedprocedure. Used in selective cases, good outcomes arepossible. I use the following criteria:
• Recent hemorrhage (less than 3 weeks, but longer than 3 days)
• Reading vision prior to the hemorrhage
• Thick blood under the fovea
• Absent subRPE hemorrhage subfoveally
• Not a massive hemorrhage
Some people feel pneumatic displacement for thinsubfoveal hemorrhage is indicated to facilitate diagnosisand treatment (angiography, then PDT or laser), but inthe age of anti-VEGF therapy this is probably no longerindicated. Especially because thin subretinal hemorrhagesoften resolve without much sequelae and probably nottoxic in the way that larger subretinal hemorrhages can be.
Dr. Johnson reviewed the literature on the topic and this can be found in the attached outline. It should benoted that the efficacy of the procedure does not appearto be related to the amount of tPA used. However, thereis a dose-limiting toxicity of tPA given intraocularly.Intravitreal tPA at dosages of 50 micrograms in 0.1ml are retinotoxic in rabbit and cat eyes and the l-argininevehicle is known to be toxic. Severe toxicity is seen indoses of 100, 50, and as low as 30 micrograms. Therefore,it is recommended to avoid doses greater than 25 micro-grams for intravitreal injection and 10-20 micrograms for subretinal injection.
Asked how he would treat his mom? If she had moderateSRH, he would avoid a fresh clot less than 3 days, inject0.3 to 0.5 cc of SF6 with 2 days prone positioning. If nothelpful, he would then inject 25 micrograms of tPA andposition for an additional 2-3 days. For a larger SRH, hewould use PPV, subretinal TPA, and gas.
NOTES 2
There are no definitive answers on how to best treatsubmacular hemorrhage. And because of the significantvariability in the clinical course of these patients it isdifficult to determine the visual prognosis in patientswith submacular hemorrhage. Poor prognostic factorsinclude thick blood under the fovea and the presence ofAMD, with these patients rarely having visual outcomesbetter than 20/200.
The use of tPA has improved outcomes in selectedpatients, but historically surgical outcomes have beendisappointing. The submacular surgery trials in 2004demonstrated no visual benefit from removal of bloodand CNVM vs. natural history.
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO 19
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Pneumatic displacement has been suggested as an alter-native. Heriot was the first to inject a gas bubble and usetPA. Advantages of this procedure are that it may besimple and minimally invasive, have a lower cost and isoffice based, and may be less traumatic to the RPE. Inthe current literature 60-100% of eyes show improve-ment with gas and tPA. These results, however, mirrorthose for just gas alone.
So is there a role for adjunctive tPA? For several reasons,it would be difficult to perform a trial looking at this.
1. Efficacy doesn’t appear to vary with the dose of tPA used.
2. We know that gas alone is effective in many cases.
3. tPA doesn’t cross the rabbit retina.
A study of the ability of tissue plasminogen activator to diffuse into the subretinal space after intravitreal injection in rabbits. Kamei M,Misono K, Lewis H. Am J Ophthalmol. 1999 Dec;128(6):739-46
Several studies have looked at treatment of submacularhemorrhage with PPV with subretinal tPA and air-fluidexchange:
Pars plana vitrectomy, subretinal injection of tissue plasminogenactivator, and fluid-gas exchange for displacement of thick submacularhemorrhage in age-related macular degeneration. Haupert CL, McCuenBW 2nd, Jaffe GJ, Steuer ER, Cox TA, Toth CA, Fekrat S, Postel EA.Am J Ophthalmol. 2001 Feb;131(2):208-15.
It is believed that with this approach you may getsuperior tPA delivery to the subretinal space with lessmanipulation of the clot. You may also be able to avoidpossible photoreceptor damage that may occur duringdisplacement of a fresh clot. This procedure is, however,more expensive relative to pneumatic displacementalone and outcomes may not be any better thanintraocular gas injection.
One must also be careful of tPA toxicity. In humans,severe toxicity has occurred with 100ug/0.1mL.
Reduced ERGs and diffuse RPE changes with 2successive doses of 50 ug/0.1mL has been observed, andpigmentary changes may be seen in concentrations aslow as 30 ug/0.1ml. Concentrations greater than 20ug/0.1ml are not recommended, and greater than25ug/0.1mL should be avoided. Other potential compli-cations of tPA injection include break through vitreoushemorrhage, endophthalmitis, and retinal break/detachment.
Guidelines for treatment of submacular hemorrhage
Moderate Hemorrhage:• Avoid fresh clot (<3 days)• Inject 0.3 to 0.5 cc SF6• Position prone for 2 days• If displacement inadequate, inject tPA 25 ug• Position for additional 2-3 days (after diffusion)
Lagger Heme (>5mm)• Pars plana vitrectomy, subretinal tPA, and gas
Discussion of the presentation by Dr. Johnson
DISCUSSION 1
Q: How much does tPA cost and is it okay to use morethan 1 dose per vial?
A: The safest option is to use one dose from a commer-cially available 2 mg vial of TPA ($80) used separatelyfor each procedure. Definitely avoid use of frozenaliquots.
DISCUSSION 2
Q: What is the cost of the 2mg vial of tPA?
A: About $80.
VI. Case Presentations on AMD ManagementModerated by Dr. Ho, with Panelists Drs. Avery, Johnson, Kokame, and Regillo
CASE PRESENTATIONS 1:
Case 1 (Ho): How would you treat a juxta/subfoveal
small classic CNV lesion with VA 20/80?
Regillo: PDT and Kenalog 1st. Would consider Avastinor Macugen. Let patient decide.
Avery: The patient would likely do well with the above3 therapies. If one fails, I would go to the others. If thepatient is comfortable with off-label therapy, I wouldconsider Avastin despite the fact that this would be using an off-label drug as primary therapy. I wouldn’t give Macugen, despite good subgroup analysis on small lesions.
Kokame: This is a case with a good prognosis. I wouldfirst offer the patient SAILOR trial enrollment. I alsoagree with previous speakers’ choice of the above 3 treatments.
20 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Johnson: I do use Avastin and it is tempting based onANCHOR data to try Avastin (due to Lucentissimilarity). My tendency is to go straight to SAILORtrial enrollment, but failing that, I would use PDT plusKenalog. For my mom, I would give Avastin. Avastin isthe most powerful drug besides Lucentis that I’ve seen. I don’t like using Macugen first. I usually go straight to Avastin.
Ho: I will try Macugen first for several doses. Then I willconsider switching to Avastin, generally speaking.
Case 2 (Ho): How would you treat a 70 year-old with
new VA loss to 20/100 due to a subfoveal RAP lesion?
Avery: Avastin. SANA study (intravenous Avastinstudy) showed a good response of intravenous Avastin for RAP lesions.
Regillo: PDT and Kenalog not okay for these lesions.PDT alone not so good. I would be inclined to use pureanti-VEGF treatments for this type of lesion.
Johnson: Avastin, if not amenable to laser photocoagu-lation (no RPE elevation on ICG and extrafoveal) lasergoes just to the intraretinal component RAP.
Kokame: Let patient decide after discussing options.Would consider PDT with Avastin.
Ho: Poll of audience: Only 1 pt not an Avastin user.
Case 3 (Ho): How would you treat a huge SRH with
VA HM and some subretinal fibrosis evident?
Johnson: PPV plus subretinal TPA and gas.
Case 4 (Ho): How would you treat a case of
juxtafoveal CNV?
Johnson: Thermal laser with some overlap (50 microns)is first option. If it’s too close, I would enroll the patientin the SAILOR trial, or else use PDT and Kenalog.
Kokame: Small lesion, good prognosis. Macugen wouldwork well, Avastin or PDT alone.
Regillo: PDT and Kenalog.
Q: Is there a role for PDT alone?
A1: I would consider PDT alone for a juxtafoveal lesionif no intraretinal edema, otherwise I would stick withcombination therapy.
A2: I wouldn’t use PDT alone for hardly anything unless there was a steroid response glaucoma. For thejuxtafoveal lesion, I would use Avastin.
Q: With MPS style laser photocoagulation, there is 50% recurrence rate. I can’t justify photocoagulation atall. Is there still a role for thermal laser?
A: Admittedly the recurrence rate with MPS laser ishigh, but if you take the 50 percent that didn’t recur,that’s a great save (no series of intravitreal injectionsneeded if it is controlled).
CASE PRESENTATIONS 2:
Case 1
Comment: Barely subfoveal and farely small classiclesion. I’ve gotten good results from PDT with IVK. The newer Macugen results are good as well. I would beinclined to do PDT and IVK. Avastin is an option. I would also like to see if there was thickening.
Comment: I tend to agree. I think this will do well withany of these treatments. I would discuss the options withthe patient, but PDT with IVK works well.
Q: What’s your sense of liability when you offer Avastinright out of the box?
Comment: The risk is higher but your benefit is higher aswell. I would tend to not do Macugen, but you havemore liability with Avastin.
Comment: I agree that this scenario has one of the bestprognosis given the size of the lesion. I would have tooffer this patient the SAILOR trial. What everybody elsesaid is true in that this would fit into all of the therapies.
Comment: I do use Avastin. And it’s tempting based onthe ANCHOR data to discard PDT and say that Avastinand Lucentis are better. My tendency is to want to usePDT with IVK in this patient. I would also considerputting the patient in the SAILOR trial, but if it weremy mother I would go straight to Avastin.
Comment: I would try Macugen in a patient like thisfirst. And then putting in a variety of input, the patient’sknowledge of Avastin etc., I would switch to Avastin.
Case 2: RAP lesion. 70 year old with new loss
of vision to 20/100.
Comment: RAP seems to respond to PDT/IVK but it alsoresponds to Avastin. I think Kenalog alone may helpwith these eyes. For my own eye I would put myself inthe SAILOR trial.
Comment: My experience with these lesions is mixed. I’m not so sure that PDT/IVK works so well all the time.I’d be more inclined to use pure anti-VEGF treatment for these.
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO 21
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Comment: So far this seems to be the best responder toAvastin. But my hope is that I could treat with laserphotocoagulation. I would do an ICG angiogram and anOCT, and if there is no RPE elevation then I would usethermal laser on this lesion.
Comment: Blankenship says you have to treat the patientand not the eye. We don’t have any good studiescomparing PDT/IVK and Avastin. I would consider PDT plus Avastin on the same day.
Case 3: Visual Acuity: HM; Large subretinal
hemorrhage and subretinal fibrosis
Comment: If this was a fresh hemorrhage, I would do aPPV/tPA/Pneumatic Displacement
Comment: I would do the same. With tPA I place tPA in several areas and one at the inferior border of thehemorrhage.
Q: Do you have a picture of a juxtafoveal CNVM? How would you treat this?
Comment: I would laser safely with some overlap, 50micron overlap, and still be outside the foveal center. I would talk to the patient about PDT/IVK and Avastinand the SAILOR study.
Comment: This is a relatively small lesion. Macugenwould work well. Avastin or PDT alone would beoptions.
Comment: Spaide reported PDT and IVK for nonsubfoveal lesions with very good results.
Q: Does this audience believe that there is a role forPDT alone? I don’t think we have good data.
Comment: I would consider PDT alone for this lesion,especially if there was no intraretinal edema.
Comment: I personally think that I wouldn’t use PDTalone for anything unless they have steroid responsiveglaucoma. I would probably use Avastin.
Comment: To me in all the MPS trials it recurred in over 50% of cases. I find it hard to justify photo-coagulation at all because it has too high a recurrencerate. I think that it is terrific that we are playing withthese pharmaceuticals.
Comment: To throw off thermal laser is a bit premature.Admittedly it has a high recurrence rate, but to take the50% who don’t recur, that to me is a great save. Andwith regard to spreading of the scar, we still have patientswho are 5 years post laser who are 20/20. And if theyrecur then we still have other treatments we can use.
Wednesday, March 8
I. 25-Gauge Vitrectomy: Evolution and Surgical PearlsAllen C Ho, MD
NOTES 1
Dr. Ho reviewed his experiences with new light sourcesfor vitreoretinal surgery. The new Xenon light sourcesare felt to be indispensable. There is a wider cone ofillumination with brighter imagery. Dr. Ho also discussedchandelier systems for conventional and 25g vitrectomyapproaches. The Tornambe torpedo is one chandeliersystem that can be placed transconjunctivally at the 6:00 position, but he only recommends its use in pseudo-phakes or aphakes (doesn’t feel that conjunctivaldisplacement is necessary for torpedo placement).
With regard to 25g instrumentation, he also agrees thatthe newest generation instruments are stiffer and better.More important than the stiffness of the instrument,however, is the need for good patient head positioning(retroflexion) at the start of the case. This latter pointcould not be overemphasized. He especially likes the 25g DSP forceps from Grieshaber. Endophthalmitis is aconcern with transconjunctival sutureless vitrectomy and this is something everyone is paying attention to,but hypotony doesn’t seem to be a big problem.
A comparison of the new 23g and 25g systems was made. One advantage of the new 23g system is that thecutting aperture is even more distal on the handpiece tipthan the 25g (which is more distally located than the20g system).
NOTES 2
The advantages of 25 gauge vitrectomy include lesstrauma, less pain, less inflammation, highly controlledfluidics, rapid post operative recovery, increased patientsatisfaction, and increased O.R. efficiencies.
Disadvantages include poor illumination, fewer ancillaryinstruments, post operative hypotony/wound leak, andthe instruments have been too flexible. These concerns,however, have all been addressed and improved on. Thesmaller gauge instruments are now less rigid and newlighting systems provide better visualization. First gener-ation light pipes had narrower illumination. Now, newergeneration light pipes give broader lighting. And withthe Xenon light source, which may even be consideredmandatory when performing 25 gauge vitrectomy, even
22 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
better lighting is provided with no documented issues oftoxicity. The Chandelier lighting system has also beenproven to be very useful in both 20 and 25 gaugevitrectomy. It’s more difficult to see the vitreous as well,but with the Chandelier it is possible to performbimanual surgery.
With regard to instrumentation the Alcon DSP forcepsfor 25-gauge are very good, but the curved scissor andilluminated forceps are poor. Hypotony is not a bigconcern, but the possibility of endophthalmitis is realand subconjunctival antibiotics are recommended.
Therefore, with the development of new instrumentationand lighting systems, the role of 25-gauge vitrectomy is expanding.
25-gauge pearls:• Retroflex head position• Wide angle viewing system, BIOM• Superior Access-Rotate Infusion Cannula
See Ho PowerPoint presentation, A.45.
Discussion of presentation by Dr. Ho
DISCUSSION 1:
Q: What setting do you use the endoilluminator (re: concern for phototoxicity)?
A: For the Accurus light source, I keep it at 3 all thetime. For the Xenon light source, I use in the middlerange and adjust as necessary. We worry about photo-toxicity more often when we use illuminated picks in the macula.
Q: What antibiotic do you use postoperatively?
A: I use Ancef subconjunctivally for all my 25g cases.
DISCUSSION 2:
Q: At what setting do you put the Xenon illuminator?
A: If using the Accurus I put the light source on High 3.I put the Xenon box in the middle range at 50 and then adjust it accordingly. I’m always concerned aboutphototoxicitiy. We used to see toxicity the most with an illuminated pick, so it’s good to move the light source around.
Q: Have you tried putting the sclerotomies at 3 and 9?
A: Head position is really important to drive the eye.
Q: What do you use for subconjunctival injection? Idon’t think it’s necessary and you run the risk of toxicity.
A: Ancef.
II. New Devices for Vitreoretinal SurgeryCarl C. Awh, MD
NOTES 1
Dr. Awh shared his clinical experience with several newdevices and illumination systems for vitreoretinal surgery.He showed the Synergetics Silicone Lens Ring for 25gcases, which has no sutures and does not require anassistant. It simply balances off the pre-placed 25gtrocars. Similarly, the Volk SSV Mini Quad lens wasdescribed as a very stable lens that achieves a good wide-angle view and is autoclaveable.
With regard to light sources, the Photon 25g chandelierfrom Synergetics was shown with its green malleablefiber optic tubing that allows the retina surgeon to bendthe cable so as to follow contour of the patient’s face tomake it unobtrusive during surgery. This device also usesa calibrated marker for proper transscleral passage andlocalization. The assistant then hands the surgeon thechandelier device with heavy forceps and the surgeonthen inserts it transsclerally. For the 25g cannula-chandelier, one needs a 4th cannula. It uses the samecannula inserter, then plug the chandelier into this.
Dr. Awh described his favorite light source: the Photon,which he prefers over the Xenon light source. He feelsthis is the brightest and safest light source based on afavorable “hazard curve.” He described a variety of Photonilluminated 20g and 25g products (picks, infusion lights,scissors, and laser probes). These were compared andcontrasted with the available Alcon counterparts.
In addition, he discussed other surgical adjuncts forvisualization such as ICG dye. Because of the concern for retinal toxicity, he likes to deliver a specific amount.He is currently testing a Precision MicroinjectorPrototype (to be available from Bausch and Lomb) thatallows Tb syringe loaded with ICG dye to be depressedwith automated delivery of a very precise amount ofICG. While only a small amount of dye is delivered withthis approach, it is typically enough to at least get theILM peel started. After that, one can find the rest of themembrane/ILM without much difficulty.
The new Bausch and Lomb electric cutter (vitrectomyhandpiece) was described as being lighter, shorter, andmore front-heavy. This variety is also less likely tophysically interfere with the BIOM wide-field imagingapparatus. New valved cannulas that prevent backflowwhen empty (without instruments occluding theapertures) were shown. These are not available yet, butshould be available for both 20g and 25g in the nearfuture (one year).
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO 23
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
NOTES 2
Illumination and visualization in 25-gauge vitrectomy ismuch improved. New lenses have also been developed toaccommodate 25-gauge surgery. For example, the VolkSSV Mini-Quad Lens which is a fairly stable lens and isautoclavable between cases.
New lighting systems include:
Photon 25-Gauge ChandelierThe Chandelier enables the surgeon to use two instru-ments at the same time. The tubing is malleable and canbend to fit the contours of the patient’s face.
Photon XenonThe Photon Xenon light source is the brightest andsafest for 25 gauge and allows us to develop devices thataren’t available with other light sources. It also has thesafest ranking of all the light sources available.
Safety RankingPhoton Xenon > Alcon Halogen > B L Metal Halide >Alcon Xenon > DORC Metal Halide
ICG is another useful tool, but a problem with ICG isthat many surgeons use it excessively and simply pour iton the macula. Therefore, a precision microinjector hasbeen developed. Currently only a prototype is availablethat enables the surgeon to deliver any measured amountof fluid into the eye and in using ICG it is recommendedthat the macula is touched in several places and not inthe center. Air-fluid exchange is not required.
Other improvements made for 25 gauge surgery includethe new handle for the Bausch and Lomb cutter and thenew electric cutter which provides 50% higher flow at50% cut rate. Valved cannulas are also an improvementas they reduce the amount of fluid leaving the eye. These cannulas are not yet commercially available.
Discussion of presentation by Dr. Awh
Q: How often do you use the Chandelier?
A: I don’t use it routinely. It’s not necessary for maculapuckers or holes. I use for diabetic retinal detachmentsand any situation we use PRP, any case you want to workwith two instruments.
Q: Do you use intravitreal Kenalog for 25-gauge?
A: It does help to see the vitreous if the only light youhave on the eye is the Chandelier.
Q: In terms of speed of removal, many people were usingenzymes; does the vitreous need to be liquefied to easeremoval?
A: I think it would be great. But now with this newelectric cutter I think we are good.
Q: I’d like your advice on 2 problems:1. Cases that are difficult and require multiple
instrument exchanges2. Cases with a lot of bleeding
A: I think that for the diabetics, Bob Avery gave us agood trick in giving Avastin prior to surgery. I have goodcontrol of bleeding because the flow around the instru-ments is so limited, and with the Chandelier or with theilluminated infusion it allows me to have diathermy inone hand and the soft tip in the other. Now we can dosurgery bimanually.
With regard to the cannulas going in and out, that canhappen, but it happens more often especially when thefellows are operating. Before you didn’t have to worry somuch about the angle of insertion, but now with thecannulas you do.
III. A Sober Reappraisal of Intravitreal Triamcinolone for Retinal IndicationsDonald J. D’Amico, MD
NOTES 1
Dr. D’Amico reviewed the history and published liter-ature on the use of intraocular corticosteroids. We are allfamiliar with the known contemporary indications ofintravitreal corticosteroids (AMD, CME of all causes). In the Archives in 1944, Von Sallmann demonstrated theefficacy of intravitreal penicillin in the management of arabbit model of experimental endophthalmitis.
In the 1950s Maylath, and then Graham and Peymanand Diamond in the 1970s explored the use of intra-vitreal steroids for the treatment of endophthalmitis, butno toxicity studies were carried out. Several accidentalcases of intravitreal steroid injections have beendescribed; some resulted in unexpected efficacy whileanother resulted in a $127.6 million lawsuit against thesteroid manufacturer!
In an often published paper by Brooks McCuen in 1981,no toxicity was seen with intravitreal triamcinolone.However, it was suggested that this study did not go farenough. Rather, they should have pushed higher andhigher doses until toxic levels were detected. Scholes, in1985, described how visible white collections of intra-vitreal kenalog are observed for as long as 23 days, butthe half-life measured only 1.6 days. So, the visibleamount of intraocular whitish material did not correlatewith vitreous drug levels.
24 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .

Dr. D’Amico reviewed the results of an animal study by Rodney Bucher and Mark Johnson et al from theUniversity of Michigan. This study involved an experi-mental model of endophthalmitis. What was found wasthat intravitreal triamcinolone acetonide lowers thethreshold number of bacteria (S. epidermidis) requiredfor the development of culture-positive endophthalmitis.It also delays the onset of endophthalmitis-associatedvitritis (however, the vitritis is more pronounced), butdoes not affect the efficacy of vancomycin therapy.
He also reviewed the results of his toxicity study ofintravitreal triamcinolone in Dutch-belted rabbits. Thisstudy demonstrated histopathologic evidence of photo-receptor and RPE damage at doses of 4 and 20 mg.Interesting, the benzyl alcohol drug vehicle caused noapparent retinal damage. This is in line with cell culturedata recently presented by Barry Kupperman.
He concluded that intravitreal triamcinolone canproduce a rapid and substantial decrease in retinalthickness with an improvement in visual acuity. Whilethe mechanism of this effect is unknown, in most condi-tions (except perhaps CRVO) the improvement istemporary. He noted that randomized studies of longterm benefit are lacking. Cataract and glaucoma arecommon, and most studies do not fully account for thisco-morbidity. Toxicity appears linked to drug, not to thevehicle. Further research is needed, and will result inmore sophisticated drugs for treatment of macular edema
NOTES 2
Intravitreal steroids have become ubiquitous in ourtreatment of diabetic macular edema, branch retinal veinocclusion, central retinal vein occlusion, postsurgicalcystoid macular edema, and age-related macular degener-ation. Intravitreal triamcinolone can produce a rapid and substantial decrease in retinal thickness with animprovement in visual acuity. The mechanism of thiseffect, however, is unknown.
In most conditions (except perhaps CRVO) theimprovement is temporary, and randomized studies oflong term benefit are lacking for other conditions. Sideeffects such as cataract and glaucoma are common, andmost studies have not fully accounted for this co-morbidity. And although many believe it is the vehiclethat may cause toxicity, studies have shown that it isactually the drug that is responsible for toxicity.
Further research is needed to look at the effectivenessand safety of intravitreal steroids.
See D’Amico PowerPoint presentation, A.50.
Discusion of the presentation by Dr. D’Amico
Q: (to audience) Do people here still believe thatPDT/IVK is still good?
Q: What do you think about Posurdex and long actingagents?
A: I think it’s an amazingly good direction to go.However, I am concerned about the development ofglaucoma. Also, I’m not sure about cost benefit. But I’mlooking forward to these devices.
Q: What about toxicity?
A: In low doses you can probably avoid it.
Comment: At the recent angiogenesis meeting in Miami,Kupperman presented some data presenting toxicity onretinal culture cells and cell death, and this has lead himto stop using it as a surgical adjuvant.
Comment: It has been revolutionary in my practice to use PDT/IVK.
Comment: To address the retinal toxicitiy issue I used toput Kenalog in after my membrane peels and some of mypatients had macular pigmentary changes that may bedue to triamcinolone.
Comment: Using Decadron in the eye may be a greatidea. There may be less toxicity. Kupperman’s workshows that triamcinolone is toxic.
IV. Dislocated Posterior ChamberIOLs: New Presentations and New Techniques in ManagementGregg T. Kokame, MD
NOTES
The problem of how to mangage dislocated IOLs stillremains a challenging one to resolve. There is no clearanswer as to how to manage dislocated IOLs and as IOL designs have changed, new approaches to surgicalcorrection of dislocation need to be developed. It isimportant to individualize the surgical approach todifferent presentations and be prepared for all surgicaloptions e.g. if one plans to reposition and this is notpossible then one should be prepared to exchange orremove the IOL. Externalization techniques have beenproven to be a more stable and secure way to accomplishscleral fixation, and clear corneal incision externalizationis a stable and controlled technique without the need fora large incision to exchange or remove the IOL.
See Kokame PowerPoint presentation, A.55.
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO 25
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Discussion of the presentation by Dr. Kokame
Comment: One other technique is that of suturing theIOL to the iris.
Response: That’s true. I find it useful in small pupil casesand in the last one I did, the patient did well.
Comment: I hardly ever do scleral fixation cases. If youwant to remove the IOL, make a slit in the anteriorcapsule. With the acrylic IOL you can fold them andremove them through a small incision. I’m going toprophesize that people are going to move away fromscleral fixation.
Comment: A lot of implants in the bag have shorthaptics so they are unstable in the sulcus.
Comment: I’ve had problems with scleral fixation where10 to 15 years after surgery, the haptics erode throughthe sclera and the lens falls back.
Comment: I completely agree with Tim. In secondaryIOLs I never permit the Anterior segment surgeon to gobehind the iris. In the anterior segment world an AClens is considered as a marked failure. I think that thereis often a lot residual cortex and capsule which ismistakenly left in the eye in the name of maintainingextra support for the IOL. Using an ACIOL is a good option.
V. Taylor R. Smith Lecture:Pseudomelanomas of Choroid and Ciliary BodyIntroduction by Dr. Donald J. D’AmicoLecture by Dr. Jerry A Shields
NOTES 1
Dr. Shields presented an outstanding series of fundusphotographs depicting lesions simulating posterior uveal malignant melanoma. Several common simulatinglesions were presented as well as even more examples of rare simulating lesions (pseudomelanomas). Heconcluded that there are several lesions that maysimulate uveal melanoma, but that most can bedifferentiated clinically. While some are more difficult,ancillary studies are helpful. As always, clinicalexperience is important.
NOTES 2
Several lesions may simulate uveal melanoma andinability to recognize pseudomelanomas may lead toerroneous diagnosis and enucleation. Specific pseudo-melanomas include:1. Choroidal nevus2. PEHCR “Peripheral Disciform”3. CHRPE4. Idiopathic Hemorrhagic PED5. Choroidal hemangioma6. CEHCR (“wet” AMD)7. RPE hyperplasia8. Melanocytoma9. Choroidal metastasis10. Hemorrhagic chorooidal detachment11. Vasoproliferative tumor12. Rhegmatogenous RD13. Serous choroidal detachment14. Uveal effusion syndrome15. Granuloma16. Adenoma of the RPE or CPE17. Sclerochoroidal calcification18. Cataract19. Retinal capillary hemangioma20. Adenoma of the nonpigmented ciliary epithelium21. Leiomyoma of the ciliary body22. Degenerative retinoschisis23. Retinal cavernous hemangioma24. Vortex vein varix25. Vitreouis hemorrhage26. Choroidal osteoma27. Posterior scleritis28. Combined hamartoma29. Choridal schwannoma30. Choroidal hemorrhage31. Globe compression
Most pseudomelanomas may be differentiated from uvealmelanoma based on clinical features and even thoughsome lesions may be more difficult to recognize thanothers, ancillary studies may be very helpful when thediagnosis is unclear. Overall, clinical experience isextremely important.
See Shields PowerPoint introduction, A.62.
See Shields PowerPoint presentation, A.63.
26 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .

Thursday, March 9
I. Systemic Drugs in the Treatment of UveitisJanet L. Davis, MD
NOTES 1
Dr. Davis outlined an evidence-based approach to theuse of immunosuppressive agents for the treatment ofuveitis. Unfortunately, randomized clinical trials in thisfield are largely lacking.
Case-series and expert opinions are the predominantform of evidence. The risks of these drugs are not trivial(sterility, malignancy) and their benefits are not alwaysclear. Her outline reviews the available evidence for the use of oral/intravenous corticosteroids and steroid-sparing immunosuppressive agents for the managementof uveitis.
For the oral/intravenous corticosteroids class, severalpoints deserve special mention. She outlined her“General Rules of Use of Corticosteroids,” whichincludes concomitant use of Calcium (1500 IU per day),stress the use of weight-bearing exercise, and avoid aheavy diet. In addition, she described 3 useful cortico-steroid regimens: 1) the 14 day no taper, 2) the 6 weektaper to zero, and 3) the 3 month taper. One mustmonitor blood pressure, glycemic status, and body weightthroughout the course of prolonged therapy.
More specifically, Regimen 1 is good for acute anterioruveitis and consists of: 3 days of hourly Pred Forte, thenoral prednisone 20 mg PO TID with meals for 14 days,then stop cold turkey with no refills, then taper topicalPred Forte.
Regimen 2 is indicated for severe scleritis or badpanuveitis (Behcets) and consists of: 3 days IVSolumedrol 500 mg to 1gm daily for 3 days.
Regimen 3a consists of an 8wk course of oral prednisoneat starting dose of 60 mg daily which is then followed by20% reductions at intervals 3 days to 3 weeks (usuallytakes 8 weeks to taper completely). Regimen 3b is the 3month approach with a trial taper. This is similar toregimen 3a except a trial of steroid-sparing agents isattempted at week 4 with concomitant steroid taper.With regard to the “Medrol Dose-Pak,” Dr. Davis feelsthis is not proportionate in strength or duration for anyknown form of uveitis and should be banned.
A detailed review of the steroid-sparing agents (anti-metabolites, macrolide antibiotics, biologics, andcytotoxics) was then presented. Within each class, shechose a “best in class” drug. Her review also includedmechanism of action, proposed indications, knowncomplications, and cost of therapy. The reader is referredto the attached outline for details. In conclusion, Dr.Davis noted that we use systemic agents in the manage-ment of uveitis in the absence of substantial evidence. It is therefore imperative to rely upon good clinicaljudgment when making treatment decisions. Closemonitoring for side-effects and complications of therapy is crucial.
NOTES 2
Oral or intravenous steroids and steroid sparing agentsare frequently used to control uveitis if drops or injec-tions have failed. However, randomized controlledclinical trials looking at the effectiveness and safety ofthese drugs are essentially lacking. To date, uncontrolledobservational case series dominate the literature, andsystemic drugs are prescribed and dosed without adequateevidence supporting their use. Therefore, clinicaljudgment is critical with careful selection of the agentand expert monitoring for toxicity. Ultimately we needbetter data supporting the use of systemic steroids andsteroid sparing agents, and need consensus guidelines tohelp justify therapy.
Select publications cited:
Guidelines for the use of immunosuppressive drugs in patients withocular inflammatory disorders: recommendations of an expert panel.Jabs DA, Rosenbaum JT, Foster CS, Holland GN, Jaffe GJ, Louie JS,Nussenblatt RB, Stiehm ER, Tessler H, Van Gelder RN, Whitcup SM,Yocum D. Am J Ophthalmol. 2000 Oct;130(4):492-513
Systemic drug toxicity trends in immunosuppressive therapy of immuneand inflammatory ocular disease. Tamesis RR, Rodriguez A, ChristenWG, Akova YA, Messmer E, Foster CS. Ophthalmology. 1996May;103(5):768-75.
Mycophenolate mofetil. A useful immunosuppressive in inflammatoryeye disease. Larkin G, Lightman S. Ophthalmology. 1999Feb;106(2):370-4.
Methotrexate treatment for sarcoid-associated panuveitis. Dev S,McCallum RM, Jaffe GJ. Ophthalmology. 1999 Jan;106(1):111-8.
Methotrexate therapy for chronic noninfectious uveitis: analysis of acase series of 160 patients. Samson CM, Waheed N, Baltatzis S, FosterCS. Ophthalmology. 2001 Jun;108(6):1134-9.
A controlled trial of azathioprine in Behcet’s syndrome. Yazici H,Pazarli H, Barnes CG, Tuzun Y, Ozyazgan Y, Silman A, Serdaroglu S,Oguz V, Yurdakul S, Lovatt GE, et al. N Engl J Med. 1990 Feb1;322(5):281-5.
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO 27
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
A clinical trial of FK506 in refractory uveitis. Mochizuki M, Masuda K,Sakane T, Ito K, Kogure M, Sugino N, Usui M, Mizushima Y, Ohno S,Inaba G, et al. Am J Ophthalmol. 1993 Jun 15;115(6):763-9.
Cyclosporine vs tacrolimus therapy for posterior and intermediateuveitis. Murphy CC, Greiner K, Plskova J, Duncan L, Frost NA,Forrester JV, Dick AD. Arch Ophthalmol. 2005 May;123(5):634-41.
Long-term follow-up of patients treated with short-term high-dosechlorambucil for sight-threatening ocular inflammation. Goldstein DA,Fontanilla FA, Kaul S, Sahin O, Tessler HH. Ophthalmology. 2002Feb;109(2):370-7.
Humanized anti-interleukin-2 (IL-2) receptor alpha therapy: long-termresults in uveitis patients and preliminary safety and activity data forestablishing parameters for subcutaneous administration. NussenblattRB, Thompson DJ, Li Z, Chan CC, Peterson JS, Robinson RR, ShamesRS, Nagarajan S, Tang MT, Mailman M, Velez G, Roy C, Levy-ClarkeGA, Suhler EB, Djalilian A, Sen HN, Al-Khatib S, Ursea R, SrivastavaS, Bamji A, Mellow S, Sran P, Waldmann TA, Buggage RR. JAutoimmun. 2003 Nov;21(3):283-93.
Decreased incidence of anterior uveitis in patients with ankylosingspondylitis treated with the anti-tumor necrosis factor agents infliximaband etanercept. Braun J, Baraliakos X, Listing J, Sieper J. ArthritisRheum. 2005 Aug;52(8):2447-51.
Etanercept therapy in children with treatment-resistant uveitis. ReiffA, Takei S, Sadeghi S, Stout A, Shaham B, Bernstein B, Gallagher K,Stout T. Arthritis Rheum. 2001 Jun;44(6):1411-5.
The use of interferon alpha in Behcet disease: review of the literature.Kotter I, Gunaydin I, Zierhut M, Stubiger N. Semin Arthritis Rheum.2004 Apr;33(5):320-35.
See Davis presentation outline, A.74.
Discussion of the presentation by Dr. Davis
Q: How do you dose your oral prednisone? When do youuse subtenons and periocular steroids?
A: Prednisone works better in divided doses and there’sonly so much that the gut can absorb.
You’re not gong to get adrenal suppression before 3 weeksso you can stop cold turkey, but if you are keeping aperson on it long term, you should have AM only dosingand at 30 to 40 mg. It depends on what your goals are.But I like TID dosing.
If there’s posterior segment disease, macular edema, andvitritis and you’re not ready to go to oral steroids orsteroid sparing agents then I go to periocular first andthen go to intravitreal injection if CME is still present.
Q: What’s your take on long term steroid implants?
A: I think they’re very effective. The NEI is trying to do a randomized clinical trial to compare Retisert tosystemic steroids. I think this is very difficult to dobecause one is a surgical procedure and the other is systemic.
I think that if you need an intense treatment, theRetisert is a good option.
Q: What about the complications?
A: Everybody gets a cataract and a third of the patientsget glaucoma, but none of the patients ever complainedbecause they were aware of the complications.
II. Infectious Complications of Intravitreal SteroidsMark W. Johnson, MD
NOTES 1
This presentation gelled nicely with Dr. D’Amico’s“Sober reappraisal of intravitreal steroids” presentation.Dr. Johnson reviewed the evidence that steroids cause or at least increase the susceptibility to endophthalmitis.In addition, endophthalmitis prevention strategies werereviewed. Endophthalmitis associated with intravitrealkenalog use presents with less pain and a delayed onsetof symptoms (median 10 days) compared to endoph-thalmitis not associated with intravitreal kenalog use.
He also reviewed the relatively high rate ofendophthalmitis (2.4%) associated with the sustainedintraocular steroid delivery device RETISERT. Themajority of RETISERT patients were noted to havewound-related problems (exposed sutures, vitreous wick, wound leak). Dr. Johnson suggested avoiding the use of multi-dose vials of any drug, but especiallycorticosteroids.
Similar to Dr. D’Amico’s talk, he reviewed his animalstudy on the apparent increased susceptibility toendophthalmitis for eyes pretreated with intravitrealkenalog. Dr. Johnson also reviewed concensus expertopinions with regard to intravitreal injections including:avoiding blepharitis eyes, iodine prep of surface and lids,eyelid speculum use, single-use vials, and avoidance of paracentesis.
Prudent, but not-concensus opinions with regard tointravitreal kenalog include: pre- and post-injectiontopical antibiotics, the use of sterile gloves and adhesivedrape, and displacement of the conjunctiva to avoidexternalized vitreous wick. He recommended avoidanceof intravitreal kenalog at the end of or prior to intra-ocular surgery, despite the popularity of this approach.Causing use of IVTA in tx of established endoph-thalmitis before sensitivities.
28 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX 29
NOTES 2
Intravitreal Dexamthasone was the first steroid to beused as an adjunct to the treatment of endophthalmitis.Now there is triamcinolone, fluocinolone (Retisert), and Posurdex.
There are lingering questions, however, about the rate of infectious endophthalmitis after intravitreal injectionof steroids, and many cases are still presumed sterileinflammatory reactions to the vehicle, endotoxin orother contaminants. Review of the literature suggeststhat intravitreal steroids are associated with a higherincidence of infectious endophthalmitis.
Retrospective prevalence estimates from 0.5% to 1%with the prevalence seen to be higher with triamci-nolone than with other medications.
Unpublished data concerning Retisert has cited theincidence of infectious endophthalmitis to be 2.4%compared to 0.5% with the ganciclovir implant. Thesecases are not typically occurring soon after the surgerybut with a median time to occurrence of 37 weeks. Only9% (2/22 cases) occurred within 2 weeks of implantationand 18% (4/22) occurred with intercurrent procedures(filtering procedure, caract surgery, triamcinoloneinjection). The majority of these patients who developedendophthalmitis had wound problems e.g. exposedsutures, wound leak, and an extruding implant.
This increased risk of endophthalmitis after steroidinjection or Retisert implant may be secondary tomultiple issues, which include:
1. Wound problems:
• Vitreous wick upon needle withdrawal
• Steroid associated inhibition of wound helingfollowing Retisert implantation
• Exposed sutures following Retisert implantation
2. Multi dose vials may be susceptible to contamination.
3. Susceptibility to endophthalmitis increased by corti-costeroid induced ocular immunosuppression.
It has been demonstrated that eyes with injection ofboth triamcinolone acetonide and bacteria were 12.2times more likely to develop culture positive endoph-thalmitis than eyes with the same dose of bacteria alone.The presence of triamcinolone acetonide may thereforeturn a subthreshold inoculum into a threshold inolculumresulting in endophthalmitis.
For this reason, it may be recommended to avoidinjection of intravitreal Kenalog at the end of or prior tointraocular surgery as bacteria is commonly introducedinto the eye during surgery, and this may be even morecommon with sutureless techniques.
Select publications cited:
Microbiologic studies of multiple-dose containers of triamcinoloneacetonide and lidocaine hydrochloride. Bucher RS, Johnson MW.Retina. 2005 Apr-May;25(3):269-71.
Effect of intravitreal triamcinolone acetonide on susceptibility toexperimental bacterial endophthalmitis and subsequent response totreatment. Bucher RS, Hall E, Reed DM, Richards JE, Johnson MW,Zacks DN. Arch Ophthalmol. 2005 May;123(5):649-53.
Acute endophthalmitis incidence: intravitreal triamcinolone. WestfallAC, Osborn A, Kuhl D, Benz MS, Mieler WF, Holz ER. ArchOphthalmol. 2005 Aug;123(8):1075-7.
Intravitreal triamcinolone acetonide Complication of infectious andsterile endophthalmitis. Kreissig I, Degenring RF, Jonas JB.Ophthalmologe. 2006 Jan;103(1):30-4.
III. Myopic Traction Maculopathy: A Slowly Progressive and Treatable DiseaseGiacomo Panozzo, MD
NOTES 1
Myopic traction maculopathy (MTM) can be seen in upto 50% of eyes even without symptoms. There are manysources of VA loss in high myopia, and MTM appears tobe an underrecognized source of VA loss. There is arelationship between MTM and staphyloma. VA is oftennot correlated with OCT picture and often there is verygood VA despite horrific-appearing OCT images. Thenatural history is stable when the MTM involves focaland more concave areas of the staphyloma and is moreslowly progressive when involving or threatening the fovea.
The pathogenesis likely involves 2 factors: externaltraction (progressive bulb elongation, staphyloma, lowelasticity of vessels/internal limiting membrane) andinternal traction (tangengial traction due to epiretinalmembrane and anteroposterior vitreoretinal traction).There is almost always a vitreal membrane or a series ofvitreal membranes inserting posteriorly. Often onedoesn’t see this vitreoretinal traction on OCT because itis out of the field of view of the standard OCT scan. Butif you look eccentrically and peripherally and defocus theOCT scan, you can often find the offending vitrealmembrane (scan 360 degrees).
MTM can also present as a shallow foveal detachmentwith foveoschisis. Perhaps macular detachment precedesfull-thickness macular hole development in highlymyopic eyes. Retinal foveoschisis can be thought of as astage 1 macular hole with a progressive shallow detach-ment and later hole formation. These traction-freemacular holes typically remain stable over time and don’tneed surgery. They generally do not progress to frankretinal detachment.
NOTES 2
Myopic traction maculopathy (MTM) is an anamolousinteraction between the posterior retina and the vitreous,and can present with many small zones of retinoschisis inthe deepest places of a stpahyloma. Sometimes schisis islimited to the most concave areas and sometimes it isassociated with a shallow retinal detachment.
There is no relationship between MTM and posteriorvitreous detachment (PVD), but there is a relationshipbetween MTM and posterior staphyloma. Many featurescan confound our findings when it comes to assessingvisual acuity in these patients. Often, patients with highmyopia may be amblyopic or have significant chori-oretinal atrophy as to affect visual acuity.
MTM is generally stable when involving one or moreconcave areas of the staphyloma, but in most cases it isslowly progressive when involving or threatening the fovea.
The pathogenesis of MTM depends both on external and internal traction. External traction is determined bythe progressive elongation of the staphyloma and lowelasticity of the vessels/ILM. Internal traction, which isthe pivotal factor, involves tangential traction (e.g.ERM) and anteroposterior vitreal traction.
In the current study by Dr. Panozzo, surgery for MTMwas investigated and it was found that surgery with notamponade leads to good anatomical and functionalrecovery. From a functional point of view the resultsfollowed the anatomical data with surgery leading todecreased metamorphopsia and reduced central scotoma.Previous published series used gas tamponade, howeverthis study found that gas was not necessary.
Select publications cited:
Foveal retinoschisis and retinal detachment in severely myopic eyeswith posterior staphyloma. Takano M, Kishi S. Am J Ophthalmol. 1999Oct;128(4):472-6.
Prevalence and characteristics of foveal retinal detachment withoutmacular hole in high myopia. Baba T, Ohno-Matsui K, Futagami S,Yoshida T, Yasuzumi K, Kojima A, Tokoro T, Mochizuki M. Am JOphthalmol. 2003 Mar;135(3):338-42.
Optical coherence tomography findings in myopic tractionmaculopathy. Panozzo G, Mercanti A. Arch Ophthalmol. 2004Oct;122(10):1455-60.
Vitrectomy and gas tamponade without internal limiting membranepeeling for myopic foveoschisis. Kwok AK, Lai TY, Yip WW. Br JOphthalmol. 2005 Sep;89(9):1180-3.
See Panozzo PowerPoint presentation, A.78.
Discussion of the presentation by Dr. Panozzo
DISCUSSION 1
Q: Are you sure it’s schisis? Because usually schisis-related retinal detachments or patients with juvenilex-linked retinoschisis who flatten with surgery, do notnote VA improvement and will still have an absolutescotoma. It is probably best to call it a schisis-like cavity.
A: I agree.
DISCUSSION 2
Q: Do you have any suggestions in where we canpurchase instruments that are long enough?
A: DORC made something long enough for these eyes.
Q: Is anyone in Italy doing scleral reinforcement forStaphyloma?
A: Ratiglia has done it in Milan. I think this is adangerous procedure
Q: Do you think that the ILM itself is a tractional factor in this entity?
A: No. I don’t.
Q: Given your observation of the slow resolution andthose cases with macular hole formation, would you usegas tamponade?
A: I think that whatever you do, a macular hole willdevelop as the retina is flattening. I think that if youforce the retina flat too much, this force could create ahole. I use it only when I see a macular hole.
Q: Is this really schisis? Do you have any additional data on high resolution OCT that shows that this isreally schisis?
A: There are some clues that help you with this. So Ithink it is.
Comment: It is analogous to optic pit maculopathy andeven on our current generation OCTs I think it’sprobably not accurate to call it true schisis. I think it isschisis-like.
30 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
IV. Diagnosis and Managementof Intraocular Lymphoma Janet L. Davis, MD
NOTES 1
Primary intraocular lymphoma is the main subject of thistalk and represents ocular disease only, however, a largepercentage develop brain lymphoma. Another source ofintraocular lymphoma is via metastasis from systemiclymphoma (more rare). Both types look the same and thelymphoma grows along Bruchs membrane, appearing assolid RPE detachments (pathognomic). Subretinal andexudative growth patterns are also seen.
The diagnosis of suspected lymphoma can be long:unfortunately, it typically takes 1 to 2 years for a patientto get a definitive primary intraocular lymphomadiagnosis. This appears as solid sub-RPE infiltrates,homogeneous vitreous infiltrates, in a white eye withoutother signs of inflammation (no synechiae or CME).Fluorescein angiography reveals a characteristic leopardspot appearance and retinal vessel staining.
Non-ocular diagnosis. If an MRI diagnosis is made orbrain biopsy specimen is in hand, then a separate ocularbiopsy is not needed. A lumbar puncture with normalMRI is unlikely to be positive. Available ocular testing is really improving: cytology, gene rearrangement, andflow cytometry. Also there is avaible testing towardinfection, vitreous culture, PCR, and intraocularantibody assays.
If a vitrectomy is carried out, what one does with thevitreous cells is most important (cytology studies arelacking, but it is prudent to send for flow cytometry insearch of a uveitic or lympomatous pattern, PCR for gene rearrangements to look for clonality as a surrogatemarker for lymphoma, and intracellular DNA for infec-tious cases).
Cytology is the gold standard and is enhanced by cyto-centcentrifugation, supported by immunohistochemistryor flow cytometry. Immunohistochemistry and surveil-lance for disease-specific T-and B- lymphocyte markersare other approaches. Activation markers and cell-lineage markers are helpful to confirm whether thediagnosis is lymphoma or uveitis. PCR amplicificationcan help confirm B- or T-cell lymphoma diagnosis. Some like to evaluate the ratio of IL-10 to IL-6, but I don’t use this approach. It is only useful to diagnose B-cell lymphomas.
A retinal or chorioretinal biopsy is good for when thereisn’t much vitreous inflammation or when your previousvitrectomy biopsy specimen was negative but you havediscrete retinal, choroidal, or sub-RPE lesions that can be aspirated easily. This isn’t mandatory, but if you havesub-RPE infiltrates without significant vitreitis, it is good to check for lymphoma or fungus. The diagnosticvitreous yield for suspected lymphoma ranges from 38 to 62%, while that for known lymphoma ranges from 46% to 77%.
Treatment previously consisted of a knee jerk reaction toimmediate ocular irradiation with brain and neural axisirradiation in certain cases too. However, ocular irradi-ation does not treat cerebral disease and vice-versa.Newer treatment protocols are also utilizing intrathecalchemotherapy. Systemic chemotherapy is also utilized(rituximab and temazolamide for b cell lympomas).There is also a role for intravitreal methotrexate asprimary therapy. The ophthalmologist should be awarethat oncologists view this disease differently.
The prednisone challenge theory for diagnosis oflymphoma is fallacious because many patients withlymphoma will note improvement in their symptoms.
It is unknown what the meaning of lymphoma celllocalization is: are vitreous cells more aggressive thansub-RPE cells? We can hopefully answer these questionswith larger numbers of patients studied and we are coor-dinating studies with the NEI. For non-sight threateningdisease, it is okay to observe temporarily if the diagnosisis uncertain. But, not everyone agrees with this.Oncologists view this as a sanctuary disease. Dr. Davisnever pushes patients with vitreous-only involvement to undergo full chemotherapy.
NOTES 2
Ocular lymphoma comes in two forms, primaryintraocular lymphoma and ocular metastasis fromsystemic lymphoma. Lymphoma grows along Bruch’smembrane and clinically, there is pebbling of the RPEwith solid RPE detachments which are characteristic ofocular lymphoma. Angiographic changes include leopardspots and staining of the retinal vessels. MRI of the brainis also essential in the workup for ocular lymphoma asprimary intraocular lymphoma is often associated withbrain involvement.
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO 31
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Cytology, gene rearrangement, and flow cytometry areimportant in confirming the diagnosis, and chorioretinalbiopsy may even be considered. Treatment may consist ofocular irradiation, intrathecal chemotherapy, high dosemethotrexate, intravitreal methotrexate, and Rituximaband Temazolamide.
See Davis presentation outline, A.84.
Discussion of the presentation by Dr. Davis
Comment: I think it’s better to proceed to a diagnosticvitrectomy if you have the support in pathology/cytologyto do so.
Q: The sensitivity of the subretinal aspirate: I had 2cases where I was sure the patient had lymphoma and Idid a subretinal biopsy. I slipped a bent 25 gauge needleinto the subretinal space and the cells were easilyaspirated with excellent results.
Comment: If it’s a non-sight threatening disease, then itmight be okay to just watch it. I never push people withvitreous only involvement to go ahead and take fullchemotherapy.
Q: Are there any cells that you cannot aspiratesubretinally?
A: If you see a yellow bump, you can aspirate thosethings definitely, but if you see just speckling you mightnot be able to. Sometimes I let these areas grow a bit so I can get a good sample.
V. OCT-Guided Macular SurgeryPeriklis D. Brazitikos, MD
NOTES 1
Dr. Brazitikos discussed the utility of OCT in surgicalapproach to patients with vitreomacular tracition,impending macular hole, full-thickness macular hole,myopic traction maculopathy, and patients with diabeticmacular edema. He showed several interesting clinicalexamples of each, including pre- and post-operativevignettes. He presented a case with an optic-disc pit andmacular detachment in which OCT demonstrated a focalouter retinal/RPE defect that underwent macularbuckling surgery.
In conclusion, he described how OCT has become themost common means to assess the macula easilyovertaking fluorescein angiography (CNV excepted). He also noted that combining fundus photos with OCTgives almost as much information as the face to faceexamination of the macula, and that OCT contributes toaccurate diagnosis of previously surgical misdiagnosedmaculopathies (vitreomacular traction, partial thicknessmacular hole).
NOTES 2
OCT has helped us substantially in our analysis of thevitreomacular interface, measurement of macularthickness, and visualization of macular histologic alter-ations. Combining fundus photographs with OCT givesus almost as much information as the face to face exami-nation of the macula. OCT has contributed to theaccurate diagnosis of previously misdiagnosedmaculopathies, and overall, OCT has changed the waywe manage patients, providing visual evidence as to whysurgical treatment is needed, and may also assist inproviding a prognosis for post-operative visual acuity.
See Brazitikos PowerPoint presentation, A.87.
32 ASPEN RETINAL DETACHMENT SOCIETY MEETING NOTES
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
APPENDIX
PowerPoint presentations
from the 34th Annual
Aspen Retinal Detachment
Society Meeting
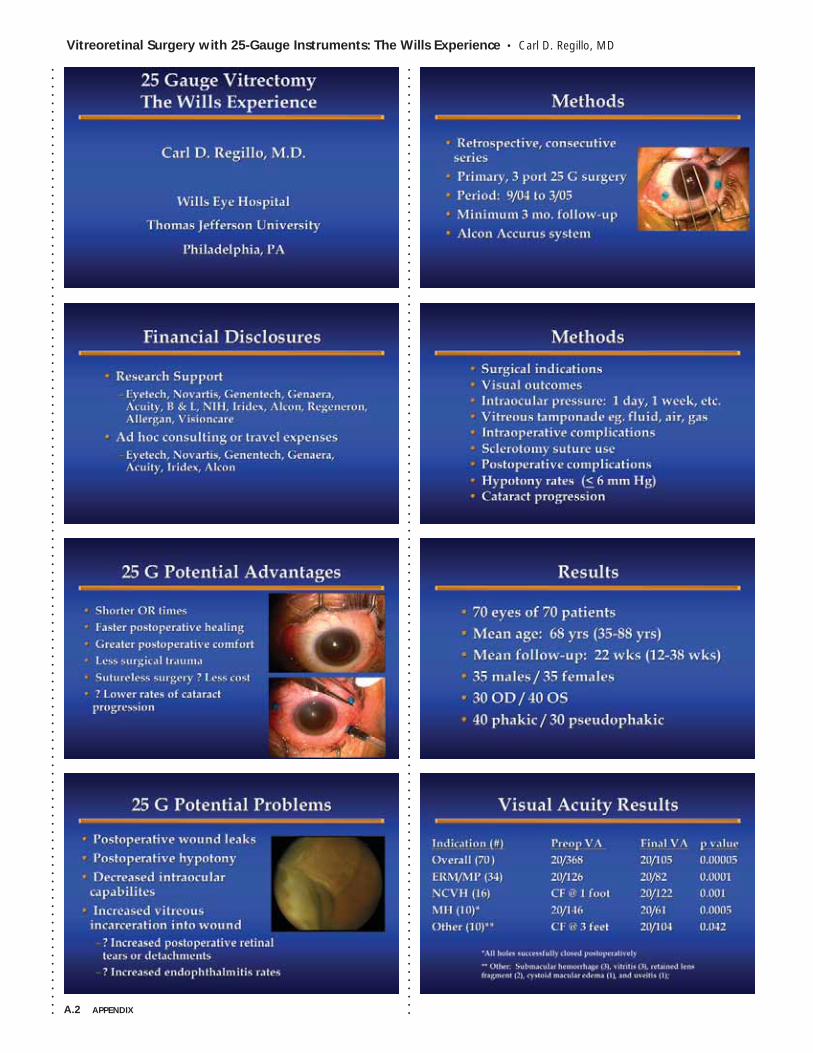
A.2 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Vitreoretinal Surgery with 25-Gauge Instruments: The Wills Experience • Carl D. Regillo, MD
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Vitreoretinal Surgery with 25-Gauge Instruments: The Wills Experience • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.3
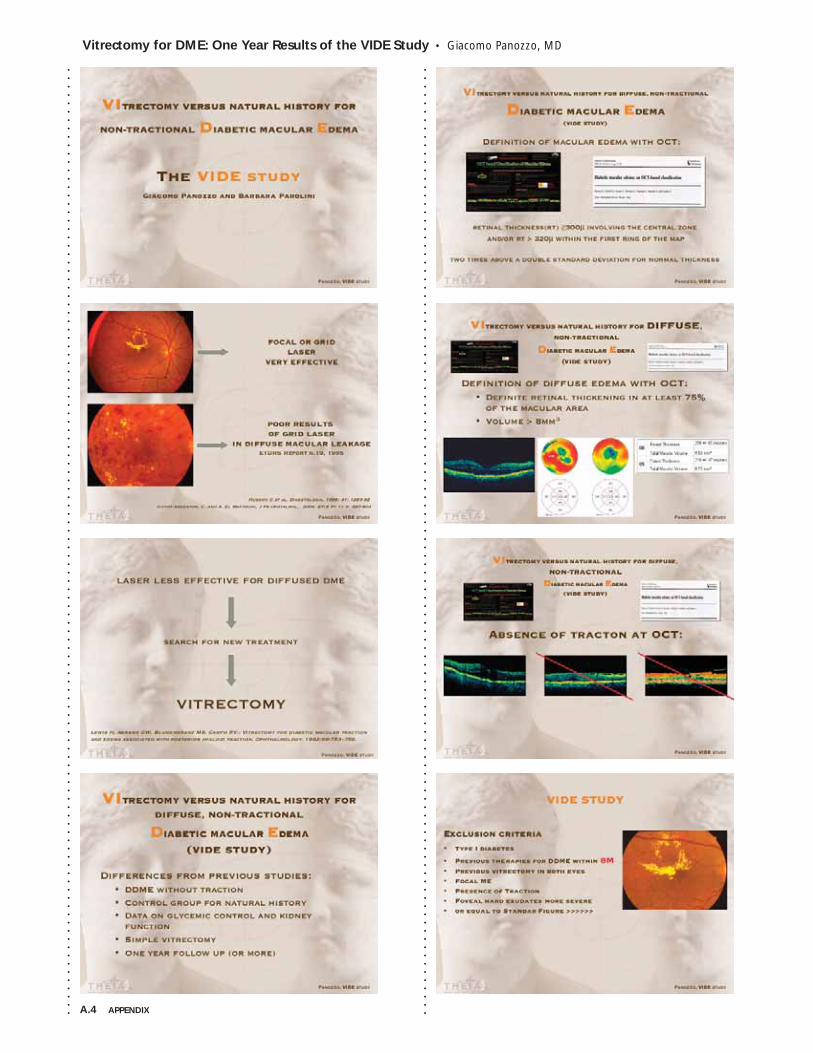
A.4 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Vitrectomy for DME: One Year Results of the VIDE Study • Giacomo Panozzo, MD
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
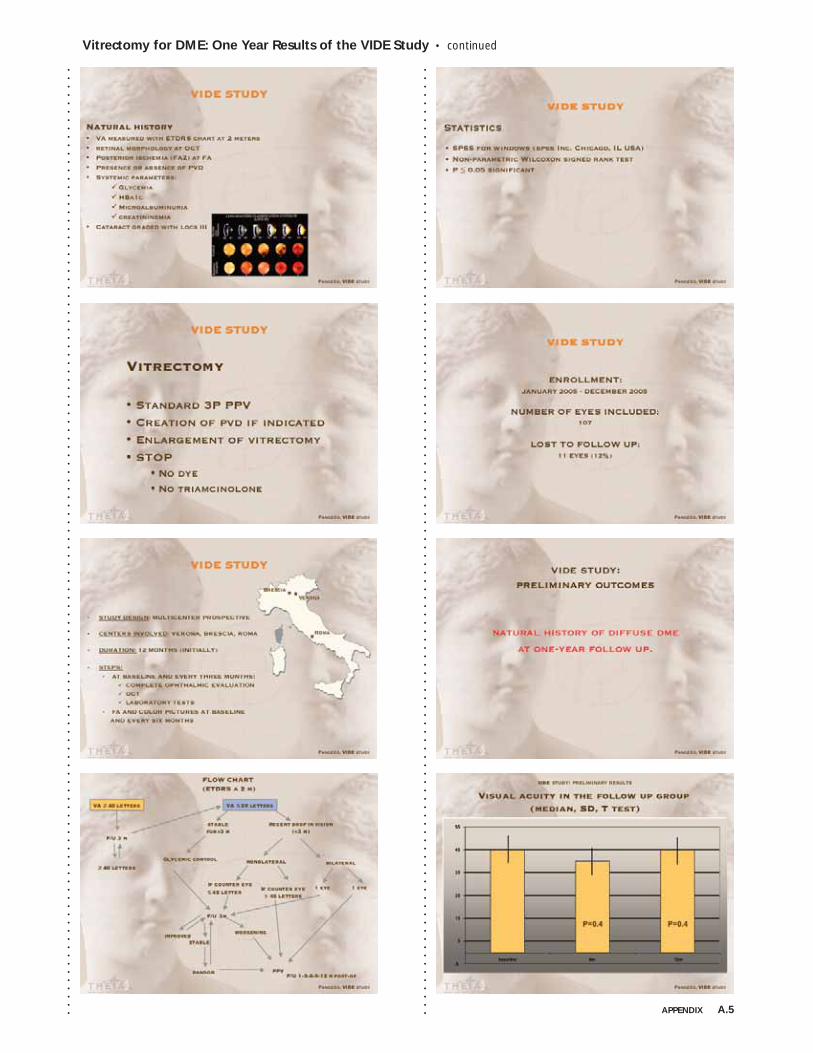
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Vitrectomy for DME: One Year Results of the VIDE Study • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.5
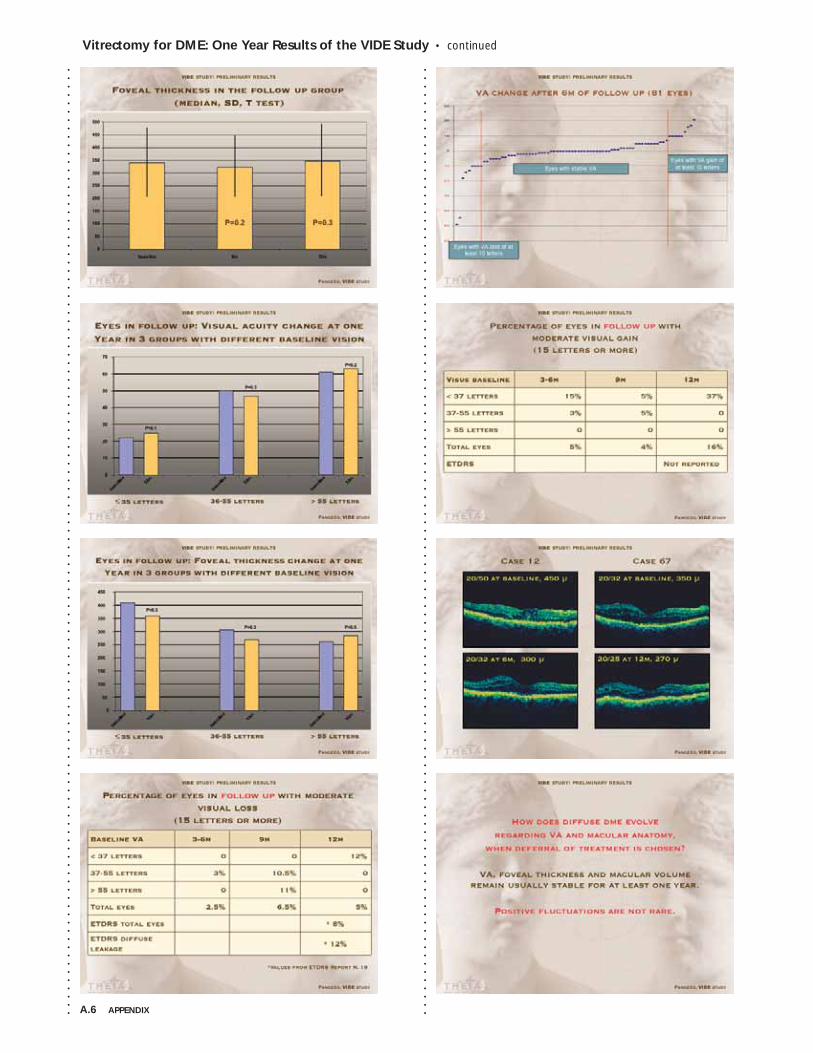
A.6 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Vitrectomy for DME: One Year Results of the VIDE Study • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
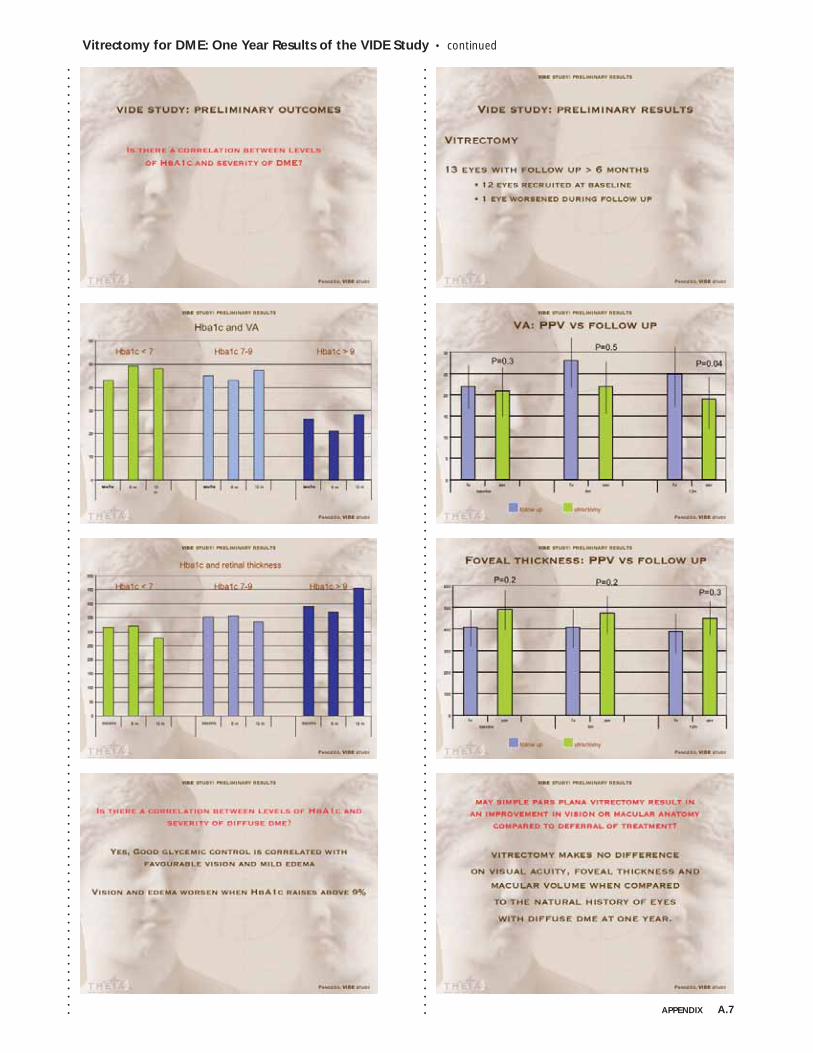
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Vitrectomy for DME: One Year Results of the VIDE Study • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.7
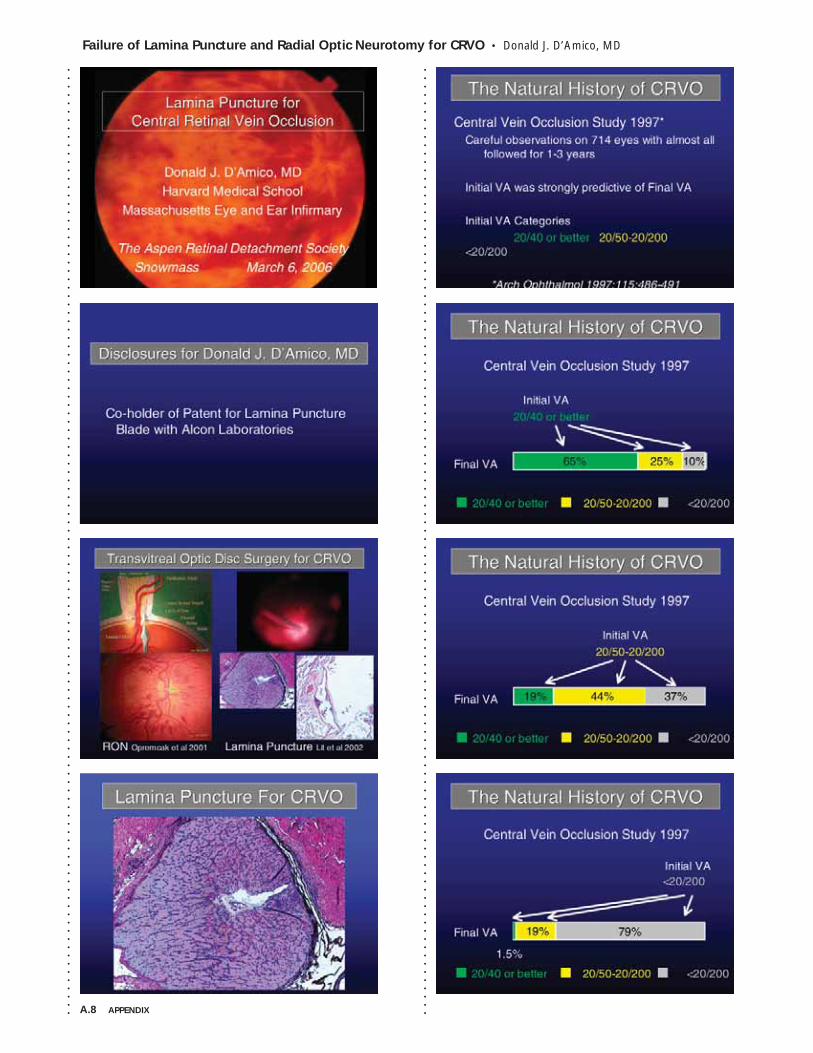
A.8 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Failure of Lamina Puncture and Radial Optic Neurotomy for CRVO • Donald J. D’Amico, MD
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
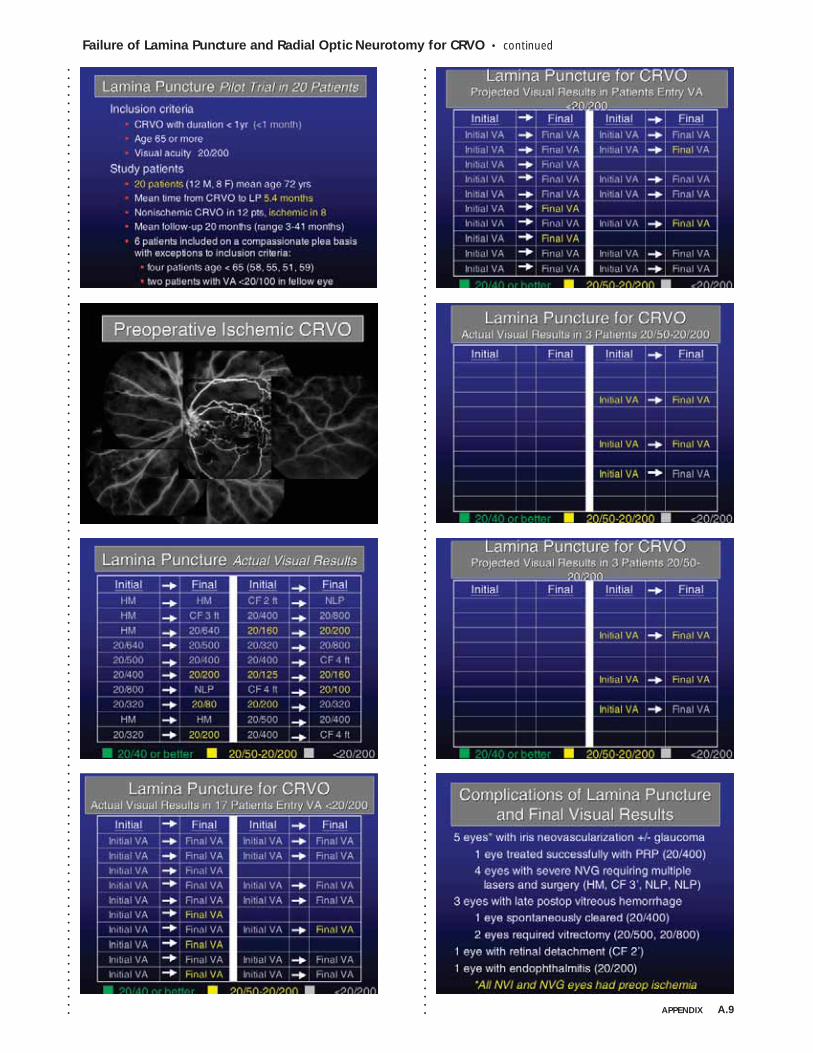
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Failure of Lamina Puncture and Radial Optic Neurotomy for CRVO • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.9
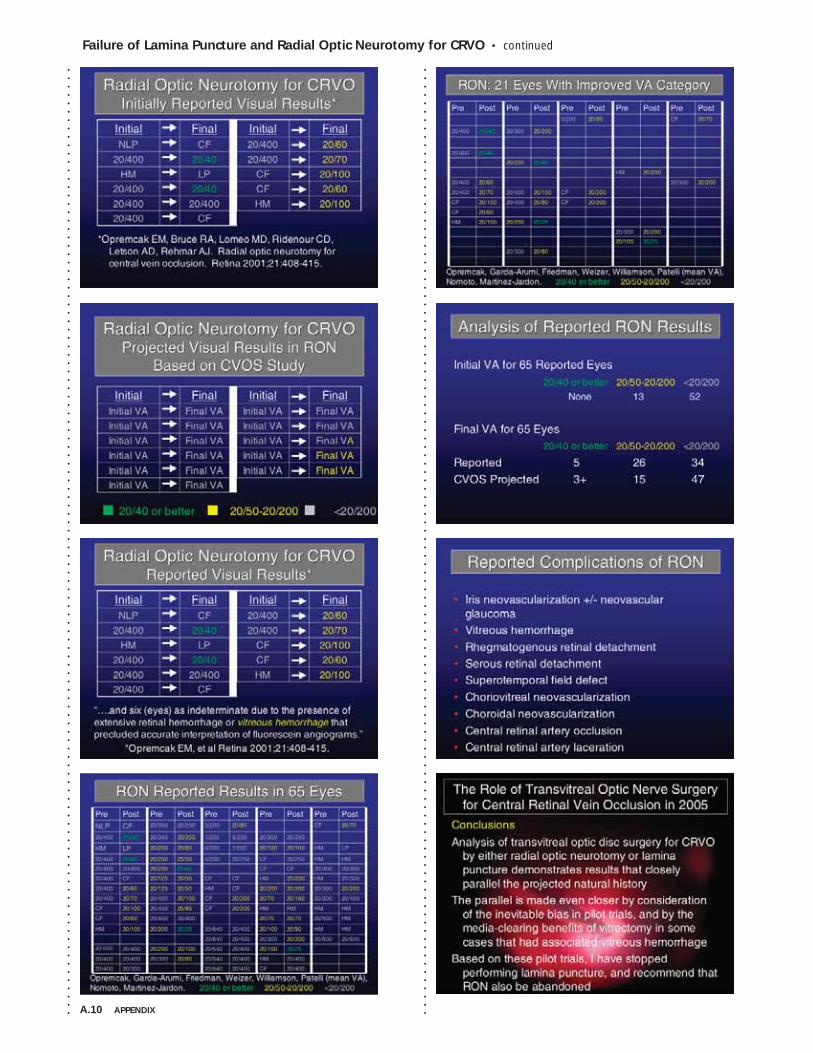
A.10 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Failure of Lamina Puncture and Radial Optic Neurotomy for CRVO • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
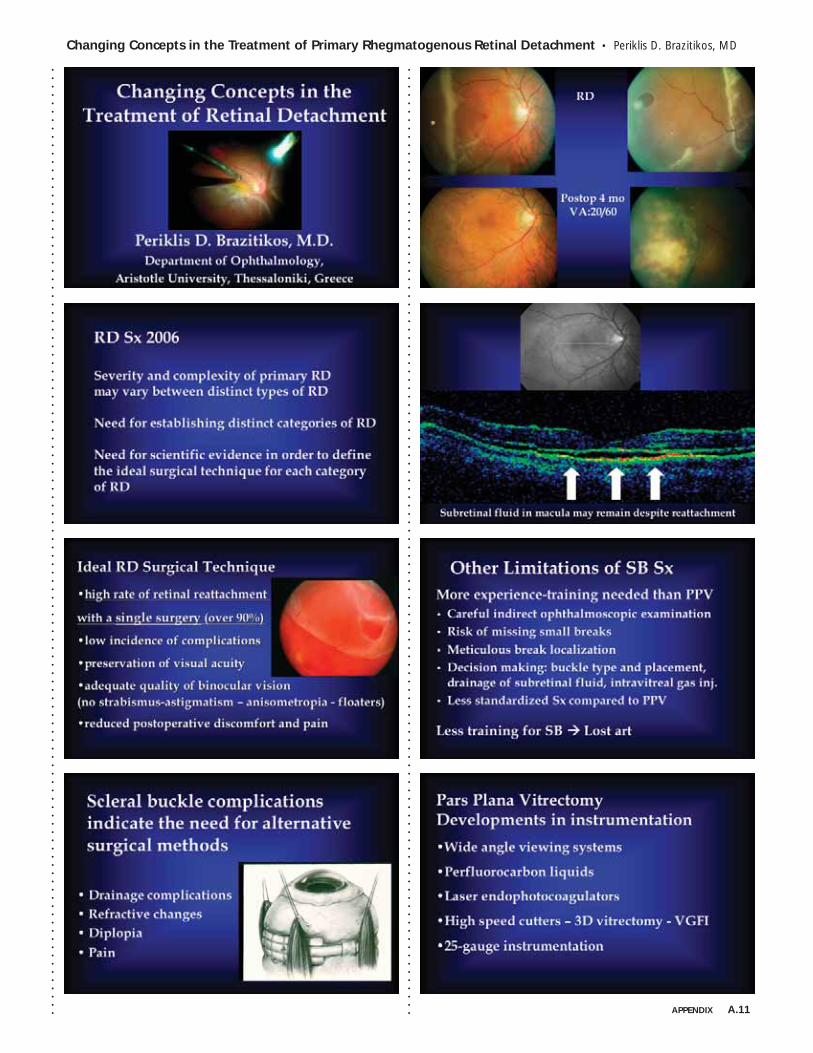
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Changing Concepts in the Treatment of Primary Rhegmatogenous Retinal Detachment • Periklis D. Brazitikos, MD
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.11
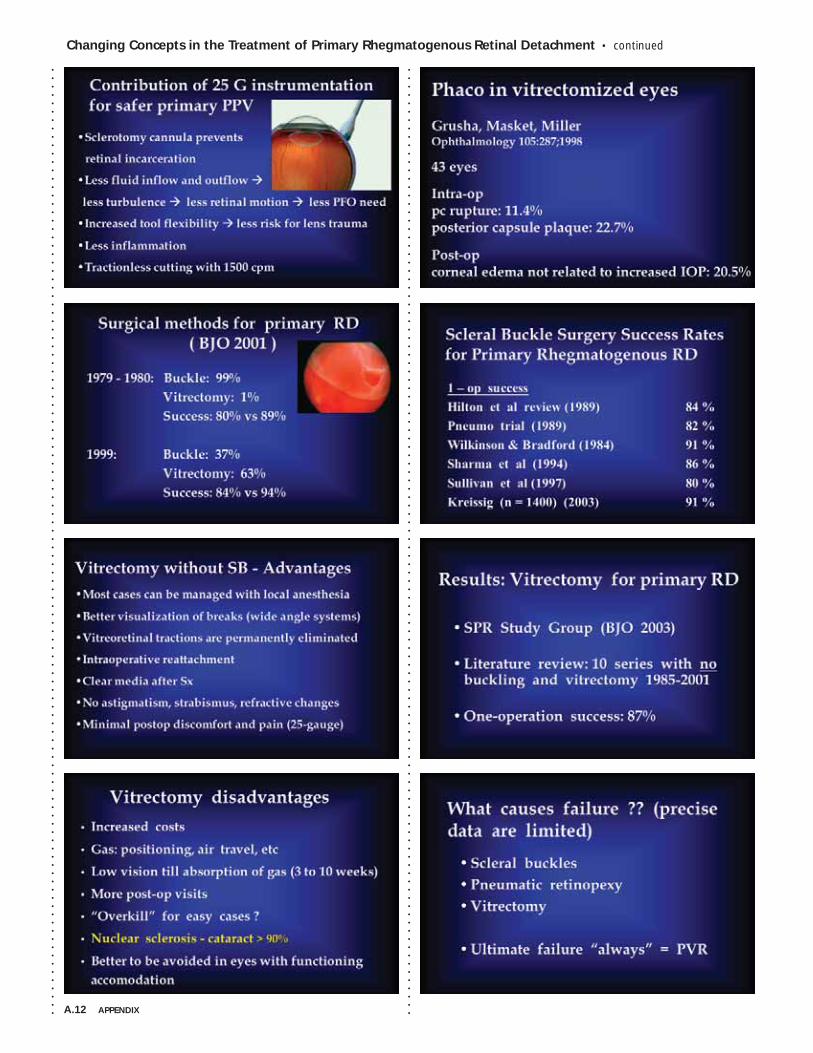
A.12 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Changing Concepts in the Treatment of Primary Rhegmatogenous Retinal Detachment • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
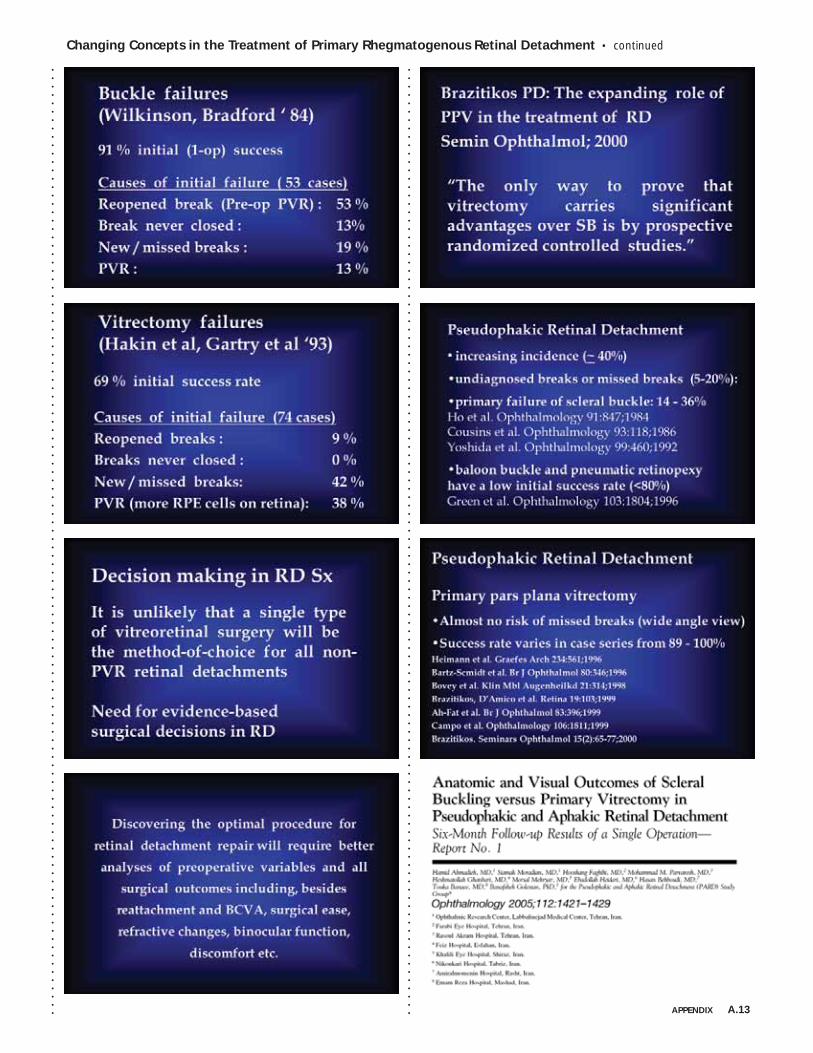
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Changing Concepts in the Treatment of Primary Rhegmatogenous Retinal Detachment • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.13
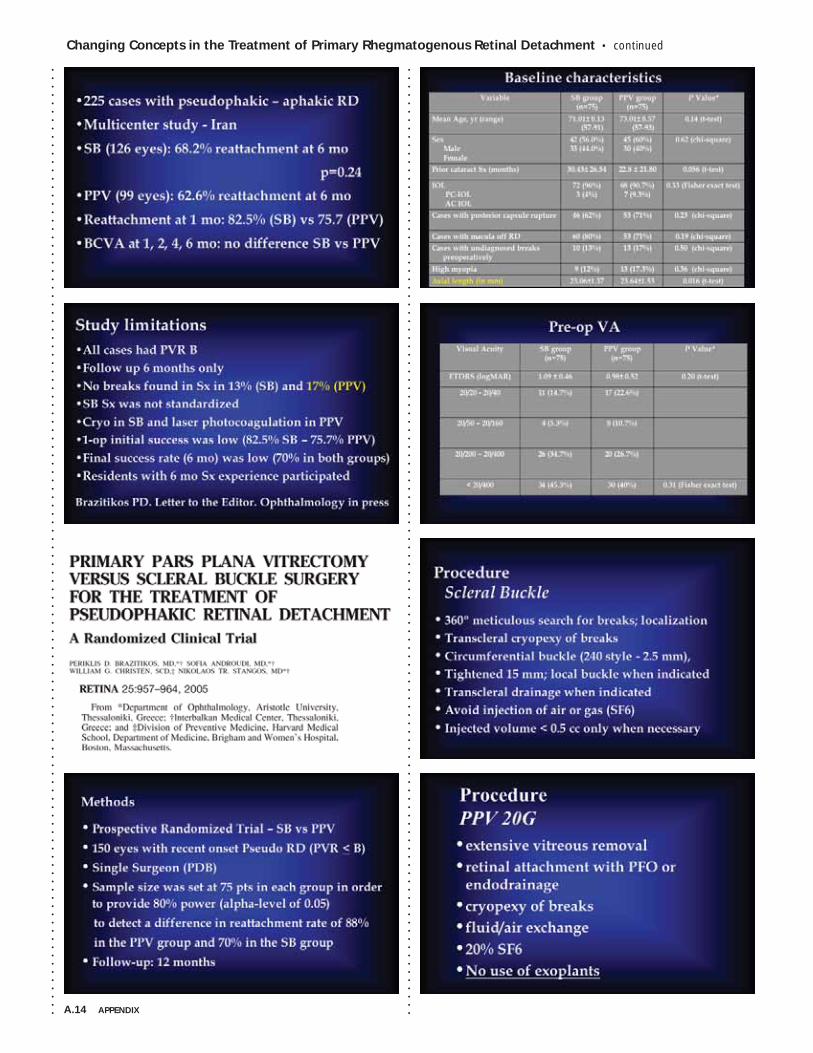
A.14 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Changing Concepts in the Treatment of Primary Rhegmatogenous Retinal Detachment • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
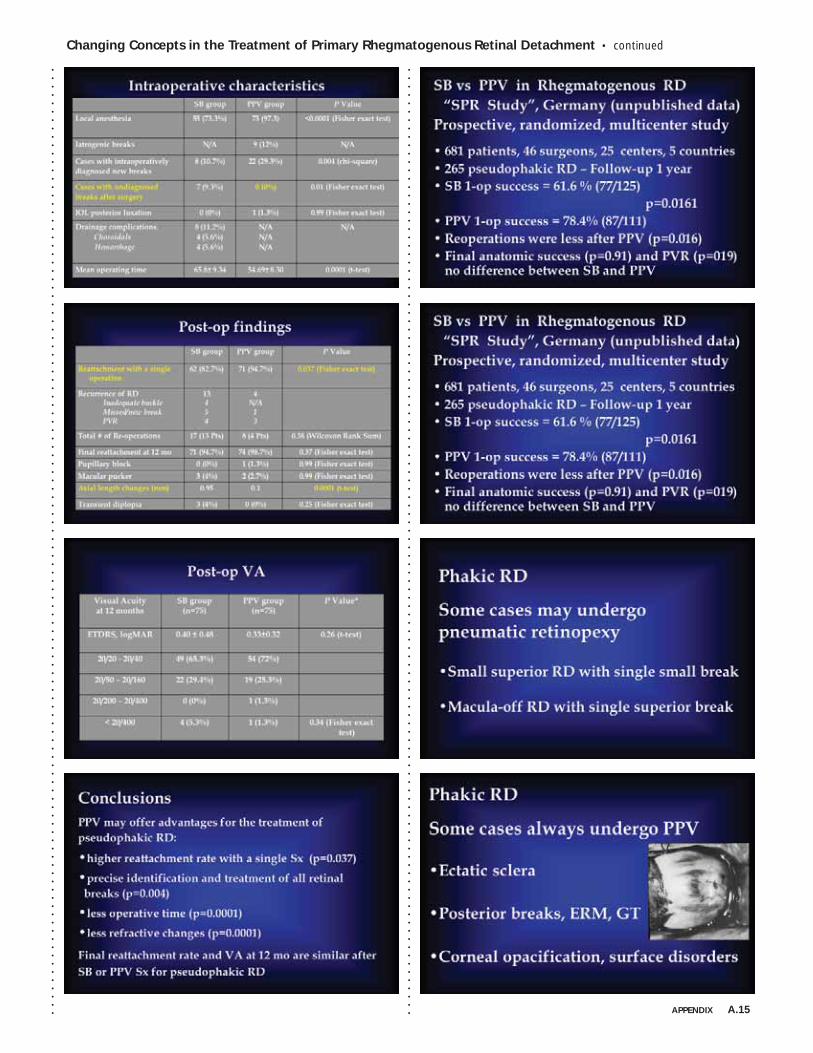
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Changing Concepts in the Treatment of Primary Rhegmatogenous Retinal Detachment • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.15
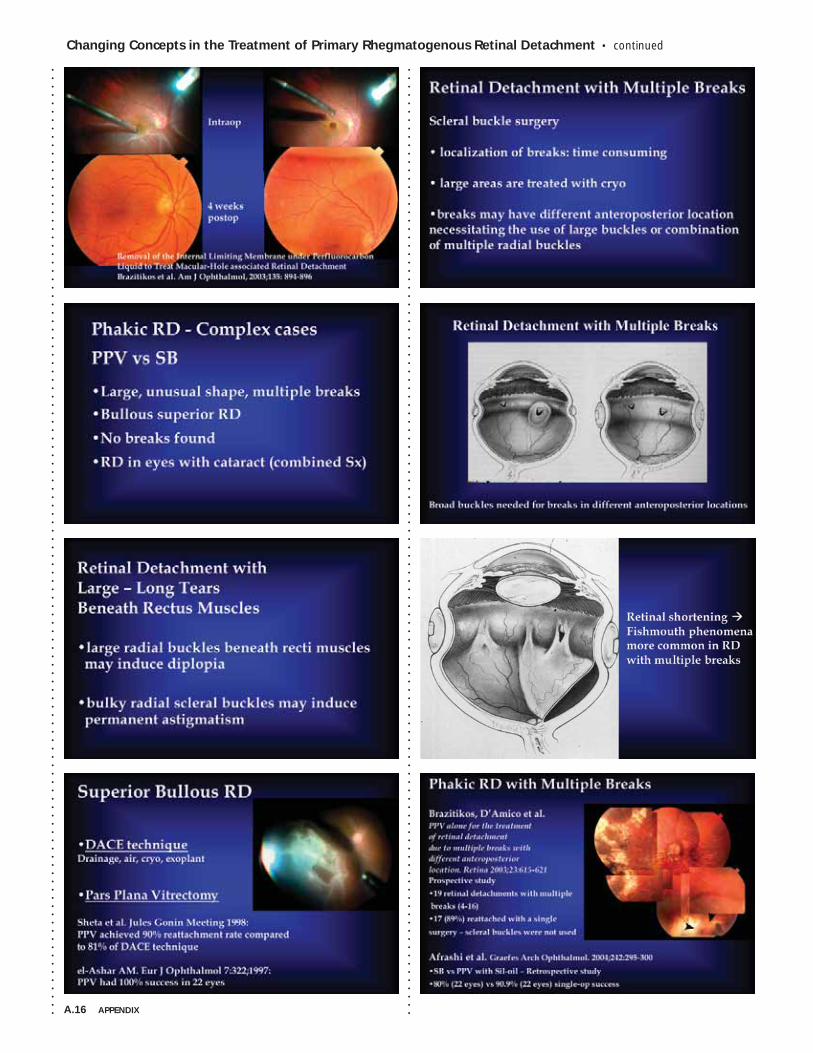
A.16 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Changing Concepts in the Treatment of Primary Rhegmatogenous Retinal Detachment • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Changing Concepts in the Treatment of Primary Rhegmatogenous Retinal Detachment • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.17
A.18 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Anti-VEGF Therapy for AMD • Allen C. Ho, MD
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
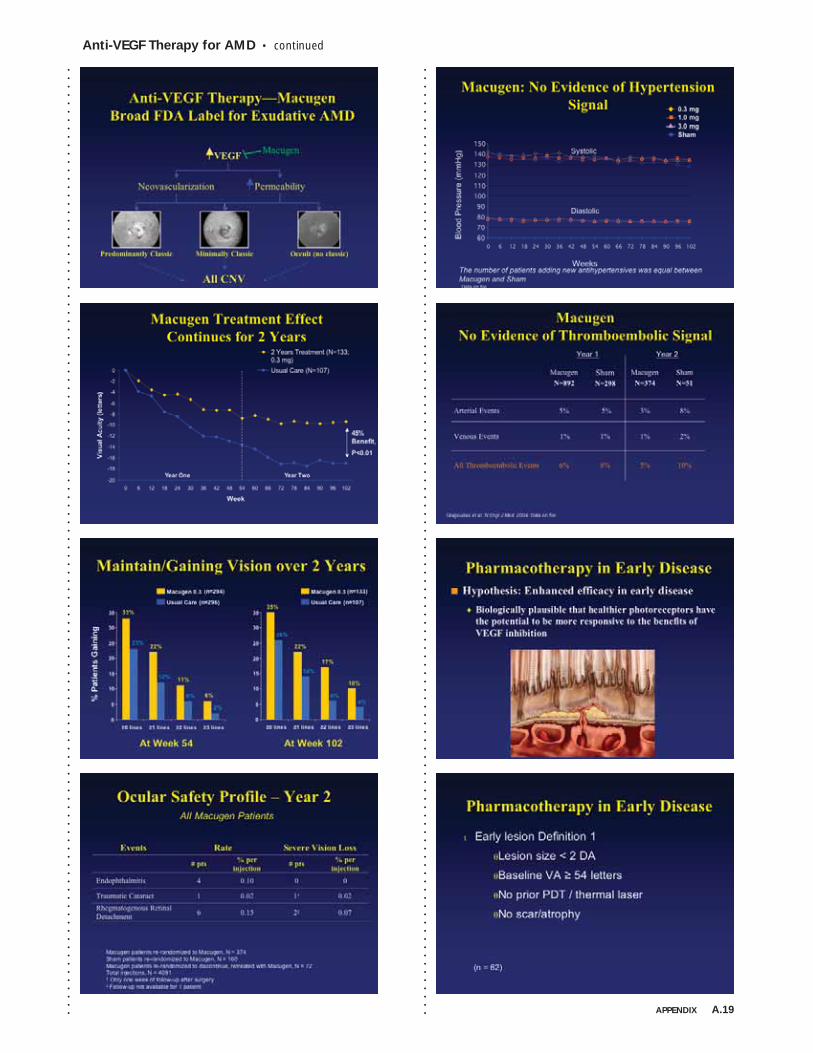
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Anti-VEGF Therapy for AMD • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.19
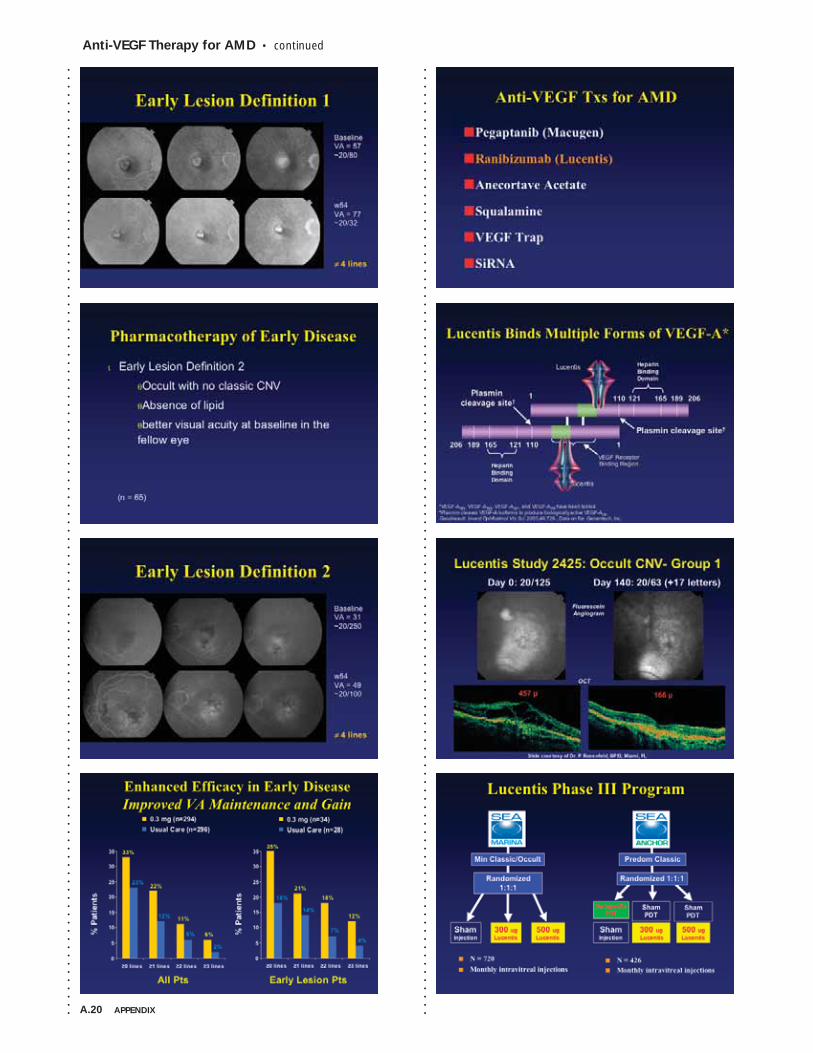
A.20 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Anti-VEGF Therapy for AMD • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
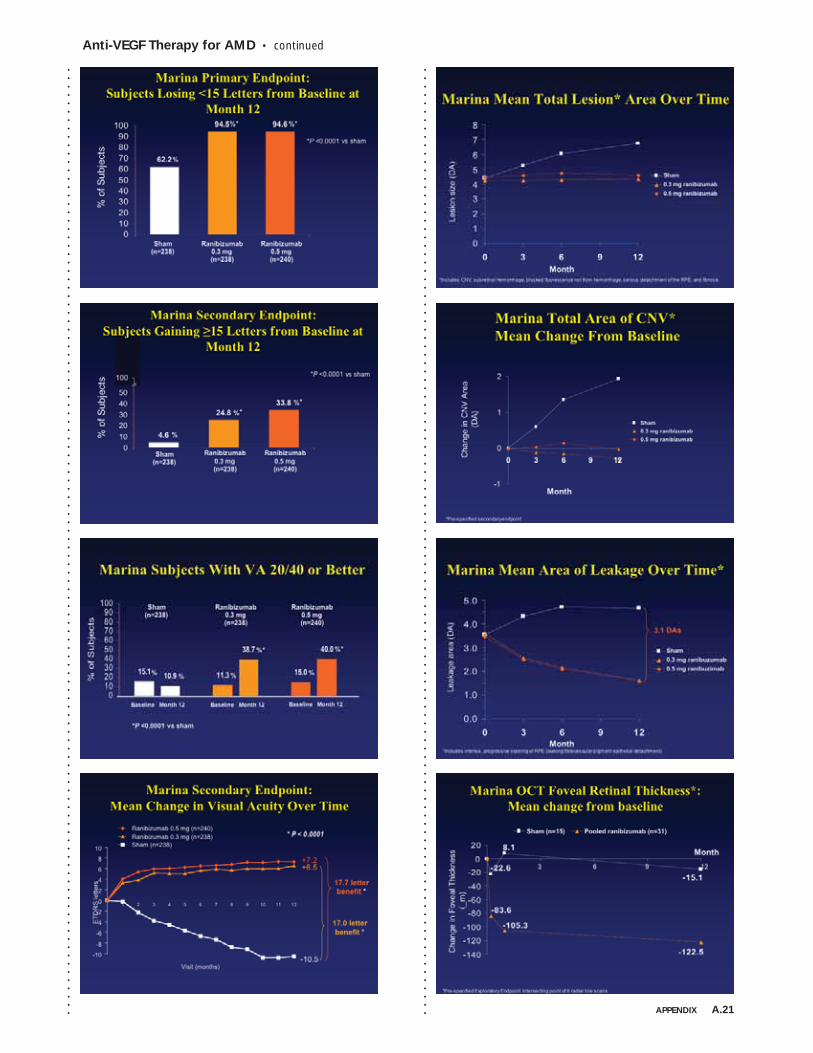
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Anti-VEGF Therapy for AMD • continued
APPENDIX A.21
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
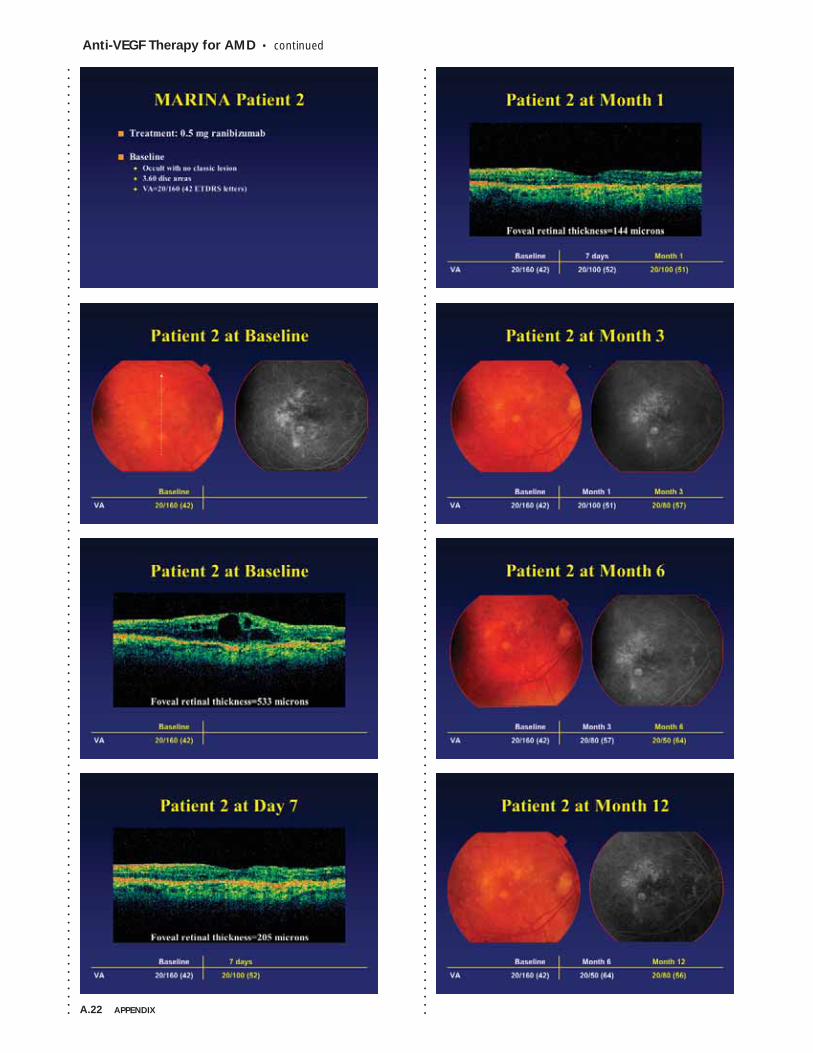
A.22 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Anti-VEGF Therapy for AMD • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
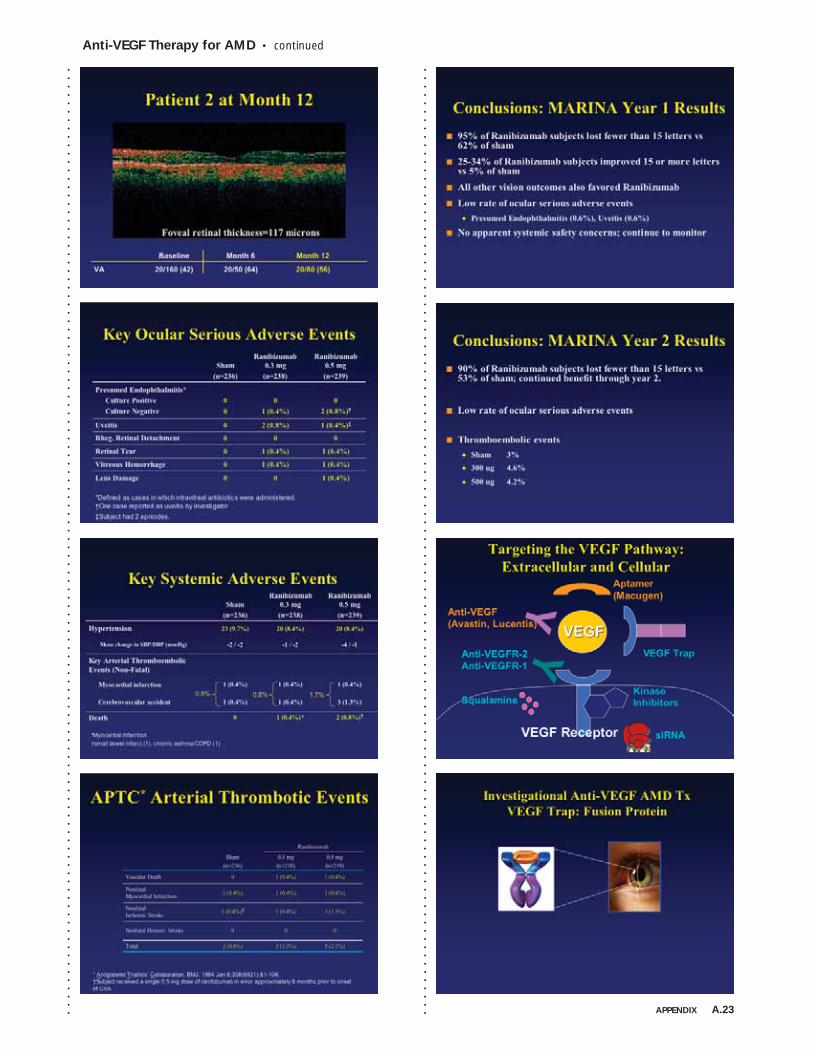
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Anti-VEGF Therapy for AMD • continued
APPENDIX A.23
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
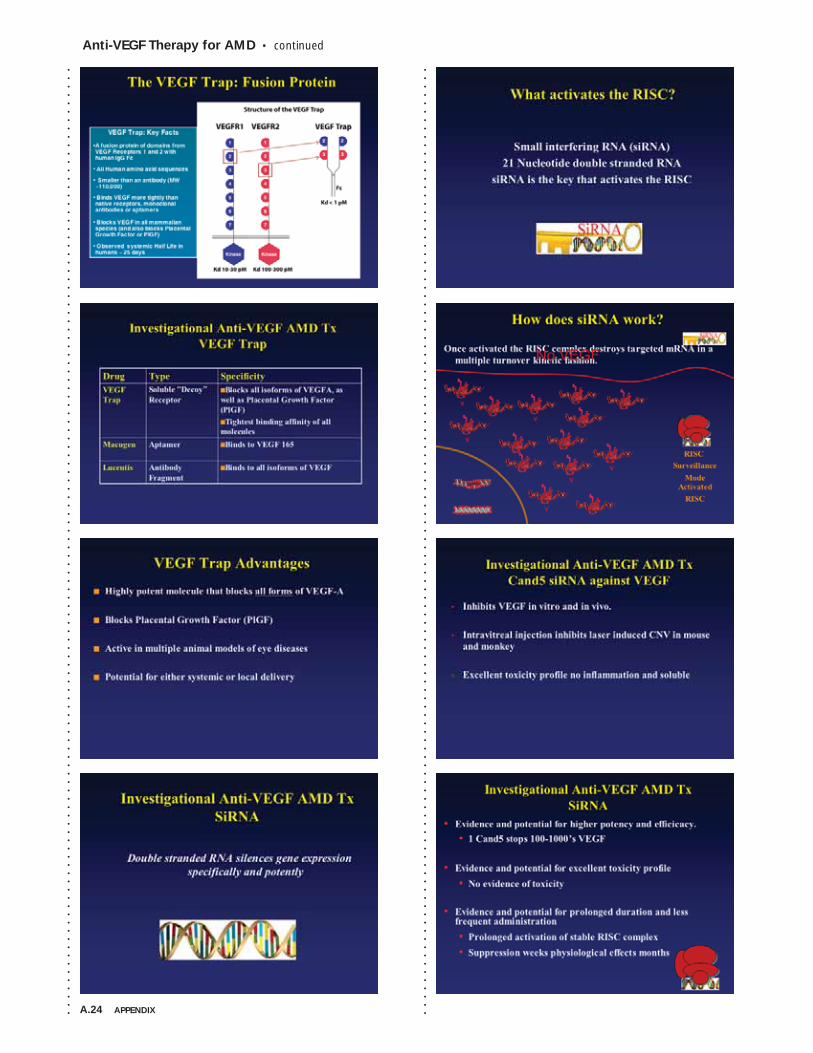
A.24 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Anti-VEGF Therapy for AMD • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
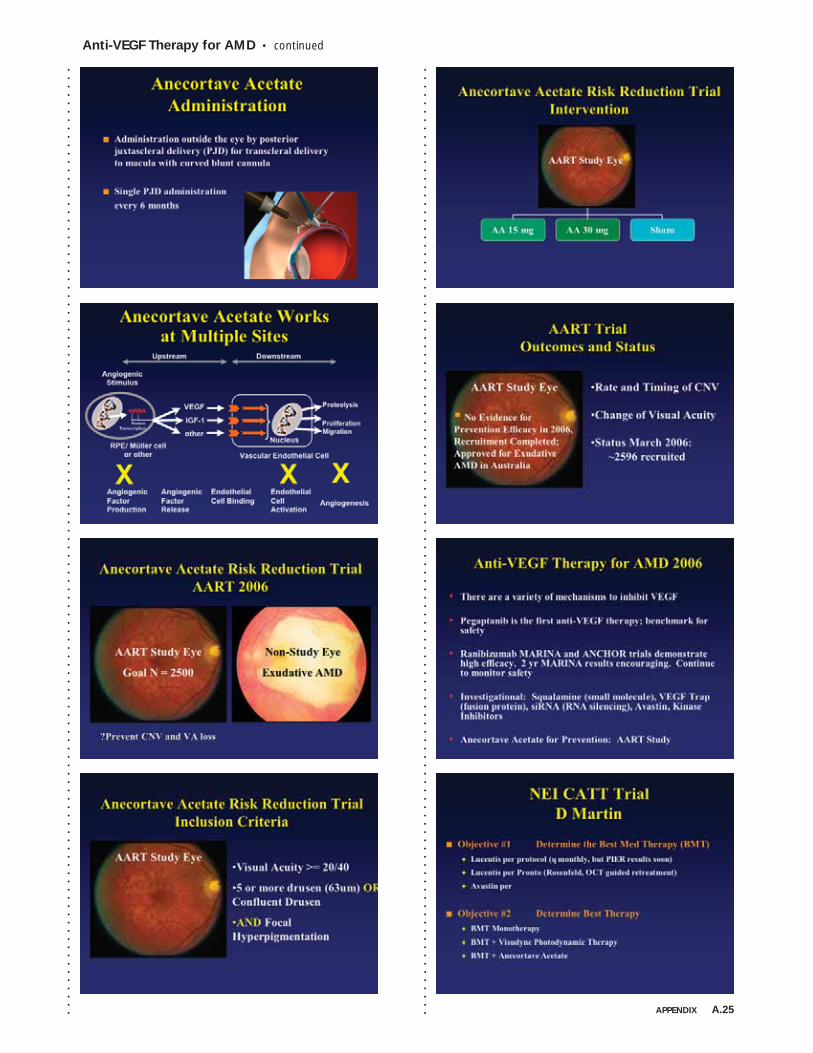
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Anti-VEGF Therapy for AMD • continued
APPENDIX A.25
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .

A.26 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Macugen Therapy for Exudative Macular Degeneration and Diabetic Retinopathy • Gregg T. Kokame, MD, MMM
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
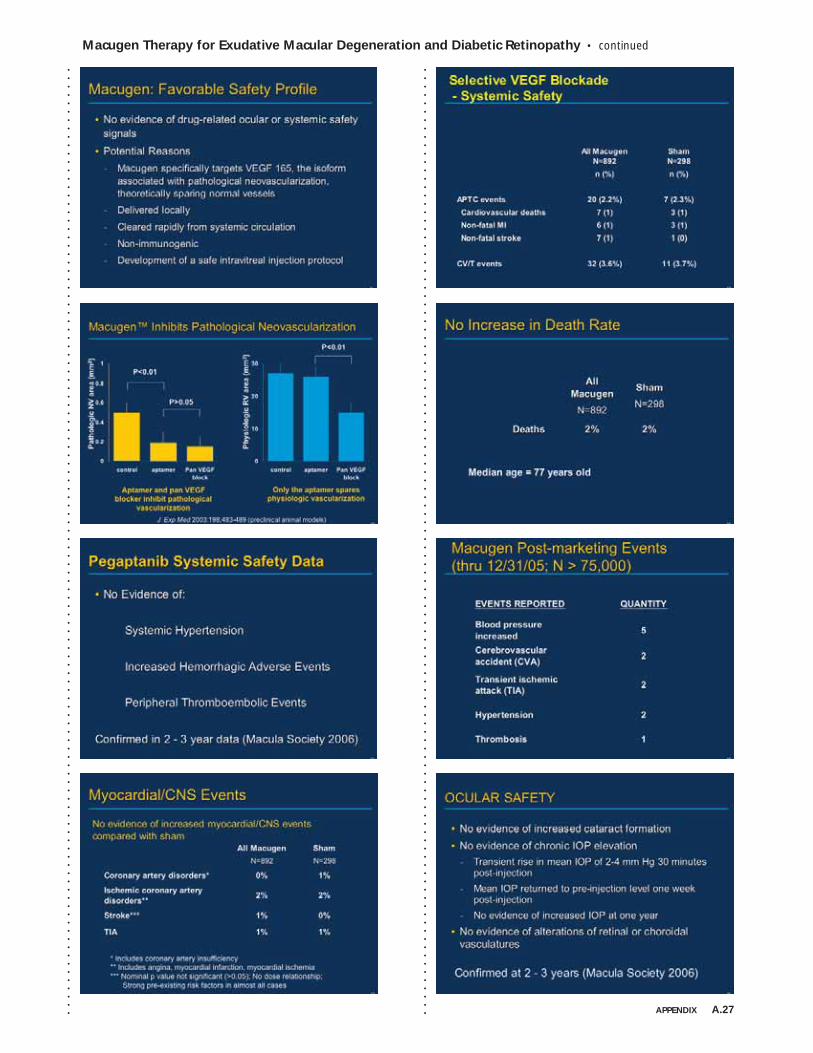
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Macugen Therapy for Exudative Macular Degeneration and Diabetic Retinopathy • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.27
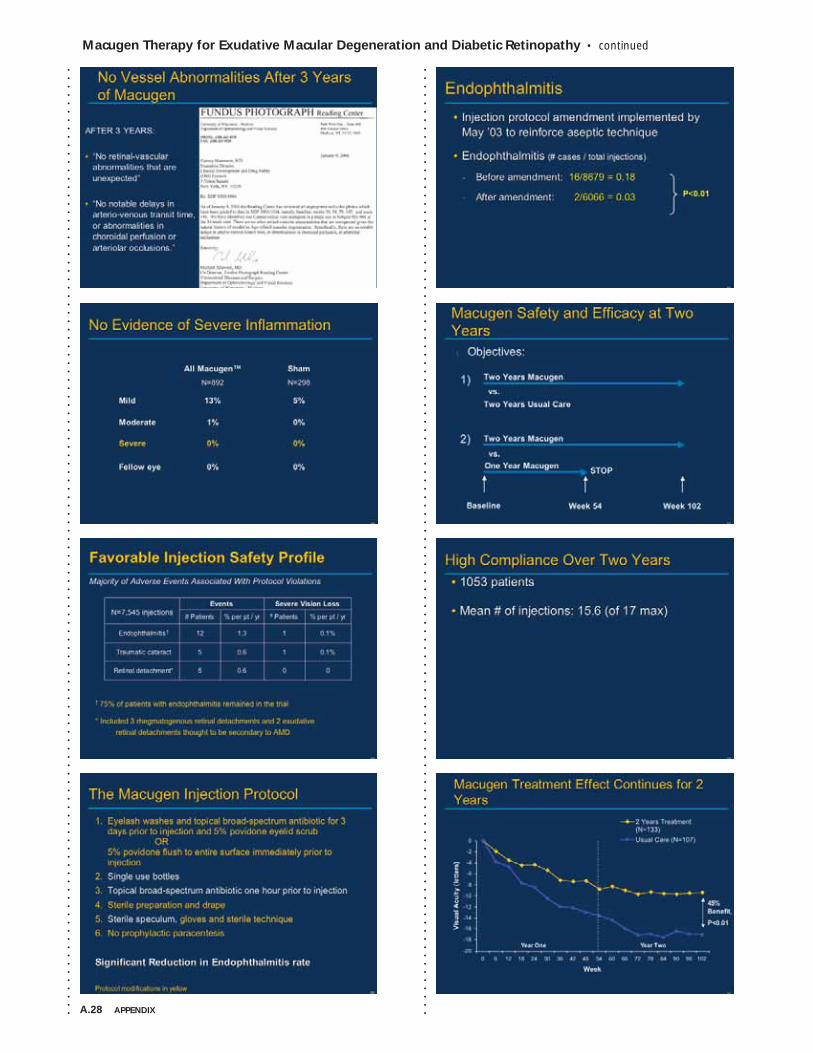
A.28 APPENDIX
Macugen Therapy for Exudative Macular Degeneration and Diabetic Retinopathy • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
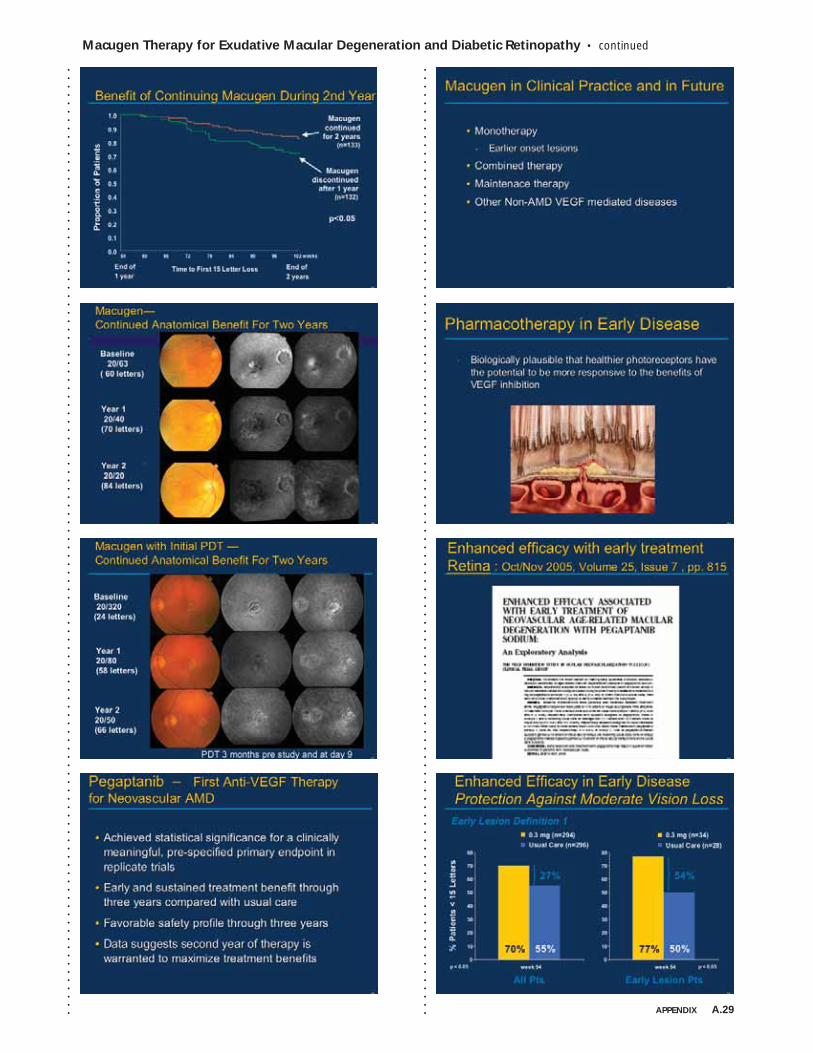
Macugen Therapy for Exudative Macular Degeneration and Diabetic Retinopathy • continued
APPENDIX A.29
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
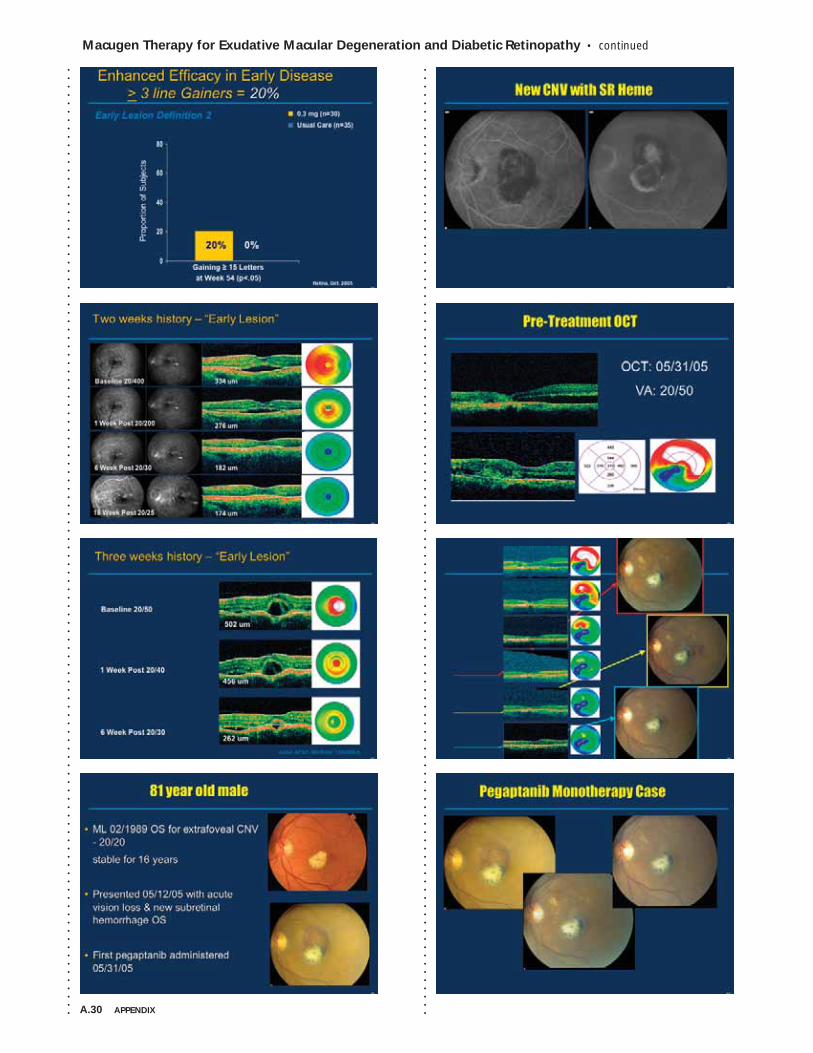
A.30 APPENDIX
Macugen Therapy for Exudative Macular Degeneration and Diabetic Retinopathy • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
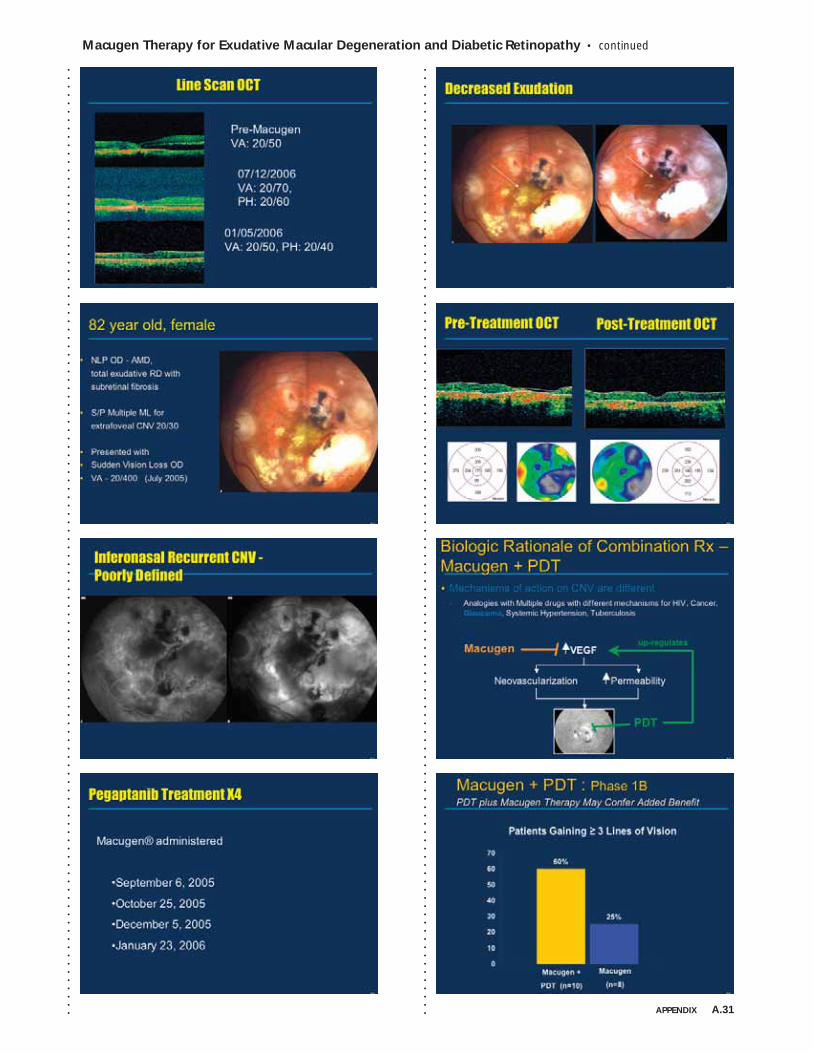
Macugen Therapy for Exudative Macular Degeneration and Diabetic Retinopathy • continued
APPENDIX A.31
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
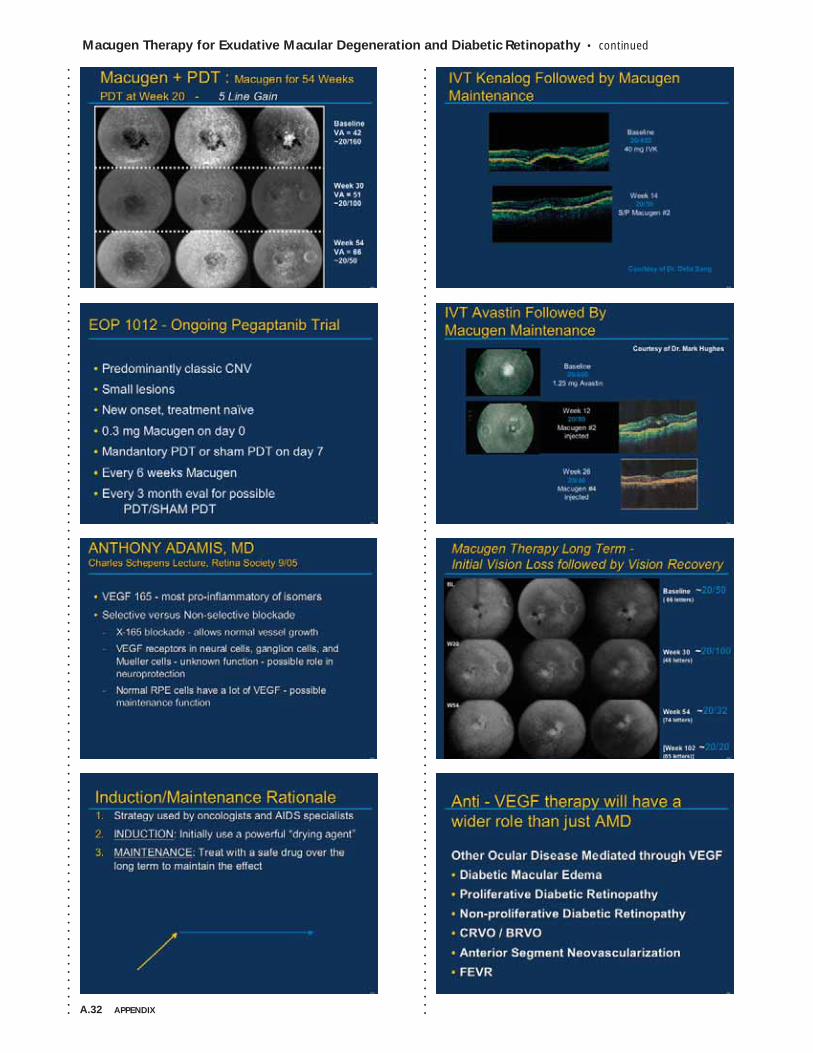
A.32 APPENDIX
Macugen Therapy for Exudative Macular Degeneration and Diabetic Retinopathy • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
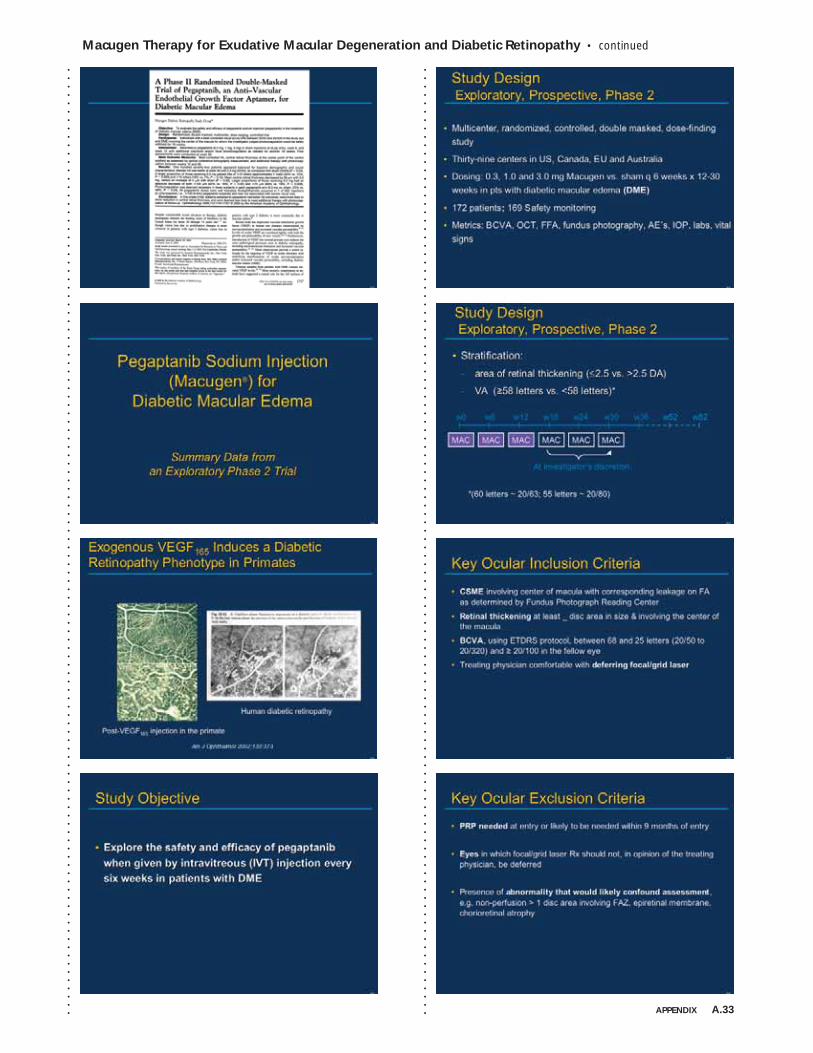
Macugen Therapy for Exudative Macular Degeneration and Diabetic Retinopathy • continued
APPENDIX A.33
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
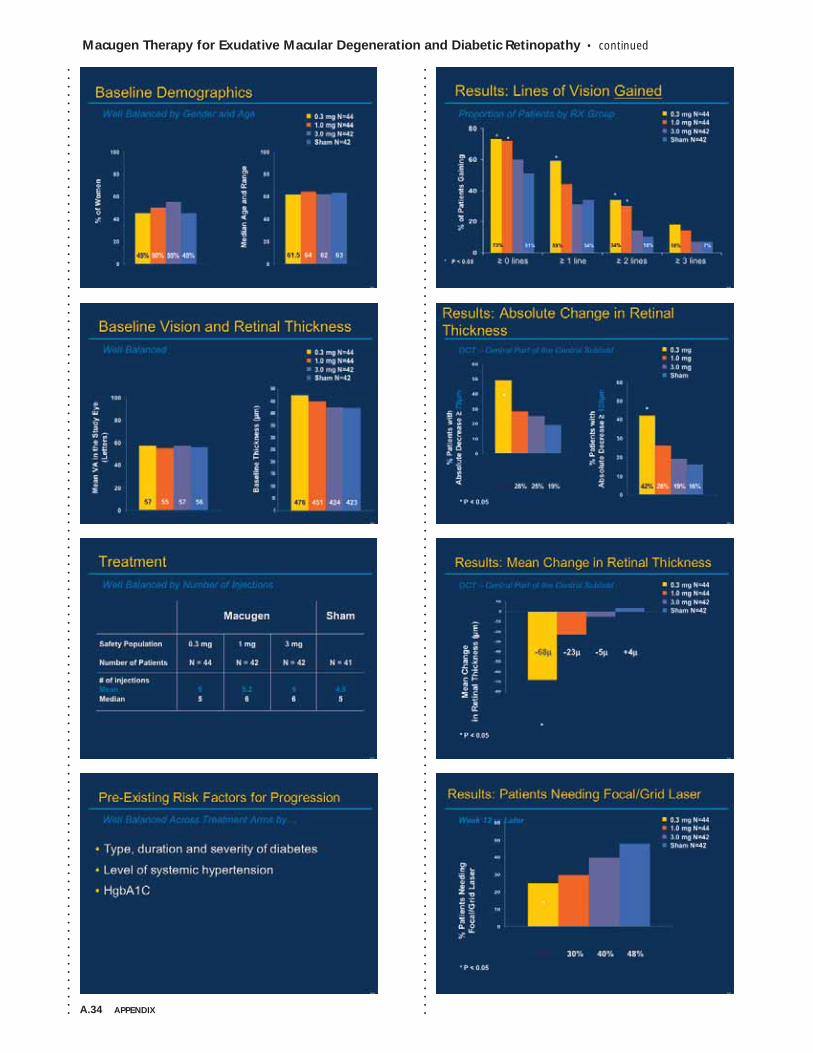
A.34 APPENDIX
Macugen Therapy for Exudative Macular Degeneration and Diabetic Retinopathy • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
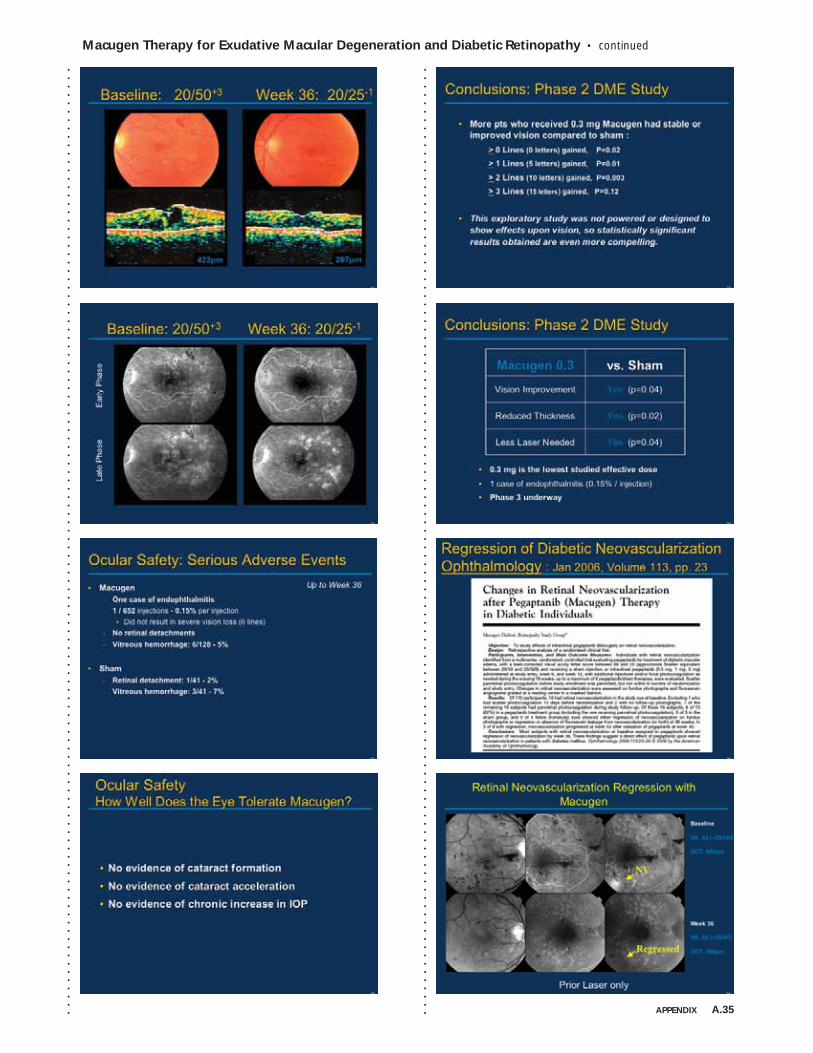
Macugen Therapy for Exudative Macular Degeneration and Diabetic Retinopathy • continued
APPENDIX A.35
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .

A.36 APPENDIX
Macugen Therapy for Exudative Macular Degeneration and Diabetic Retinopathy • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
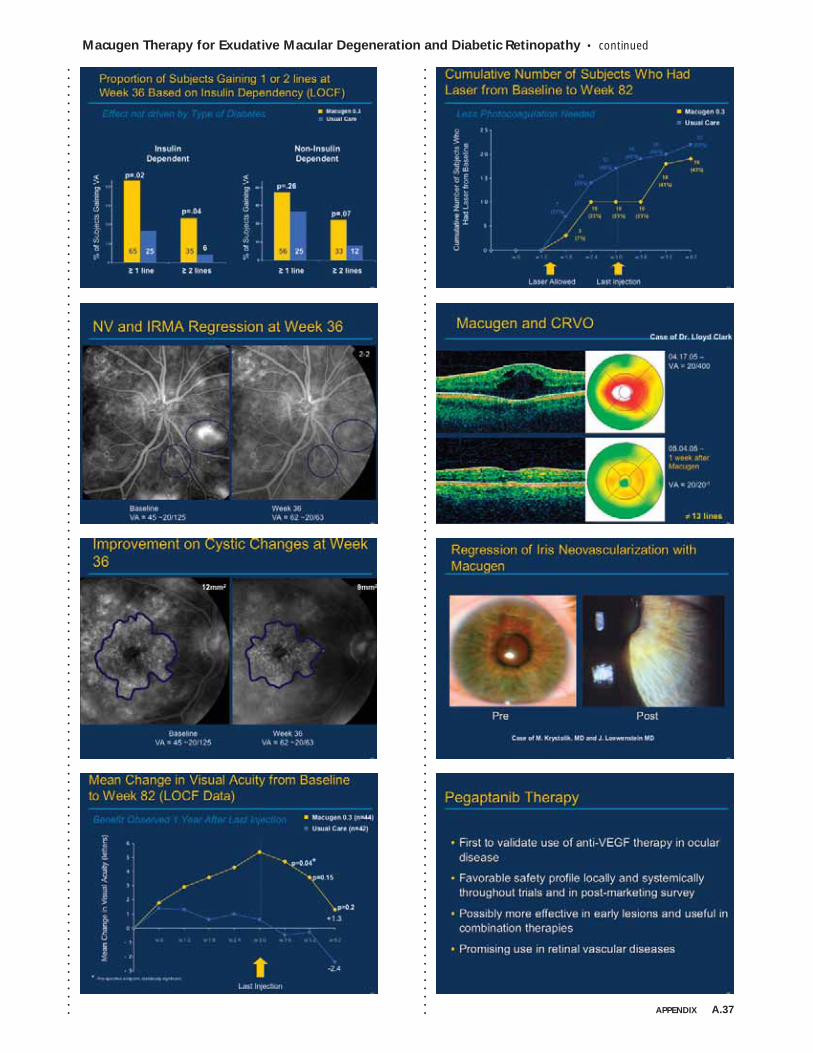
Macugen Therapy for Exudative Macular Degeneration and Diabetic Retinopathy • continued
APPENDIX A.37
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
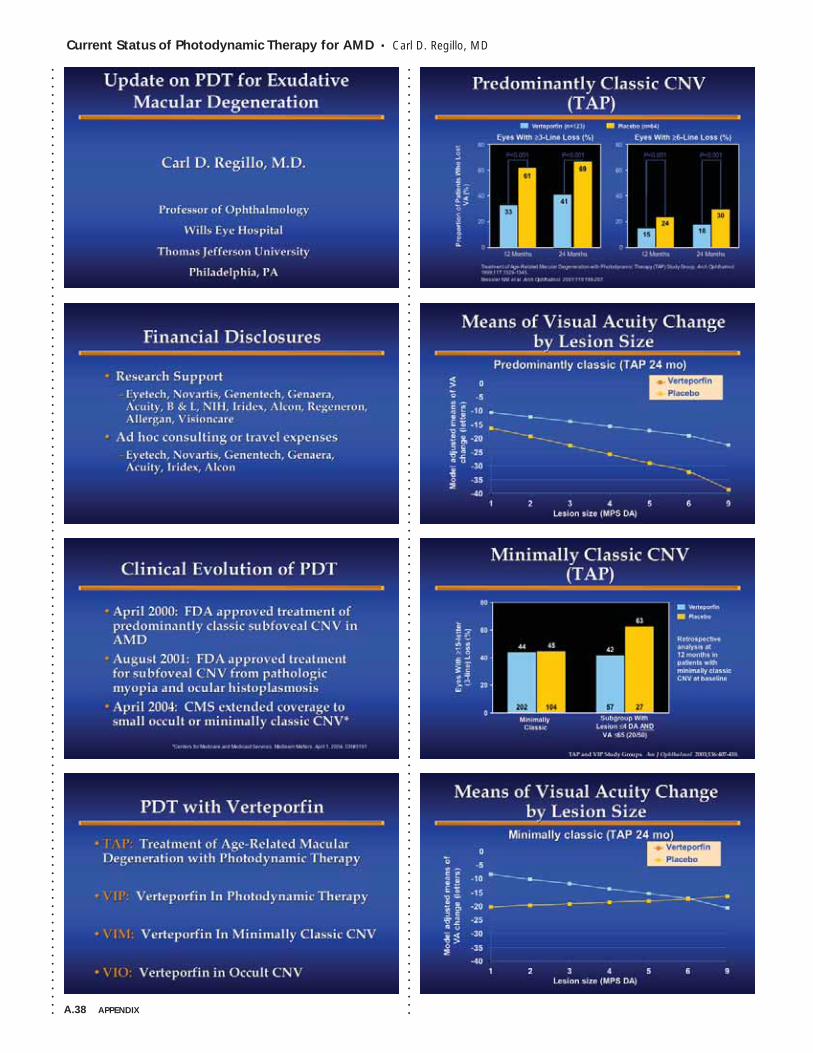
A.38 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Current Status of Photodynamic Therapy for AMD • Carl D. Regillo, MD
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
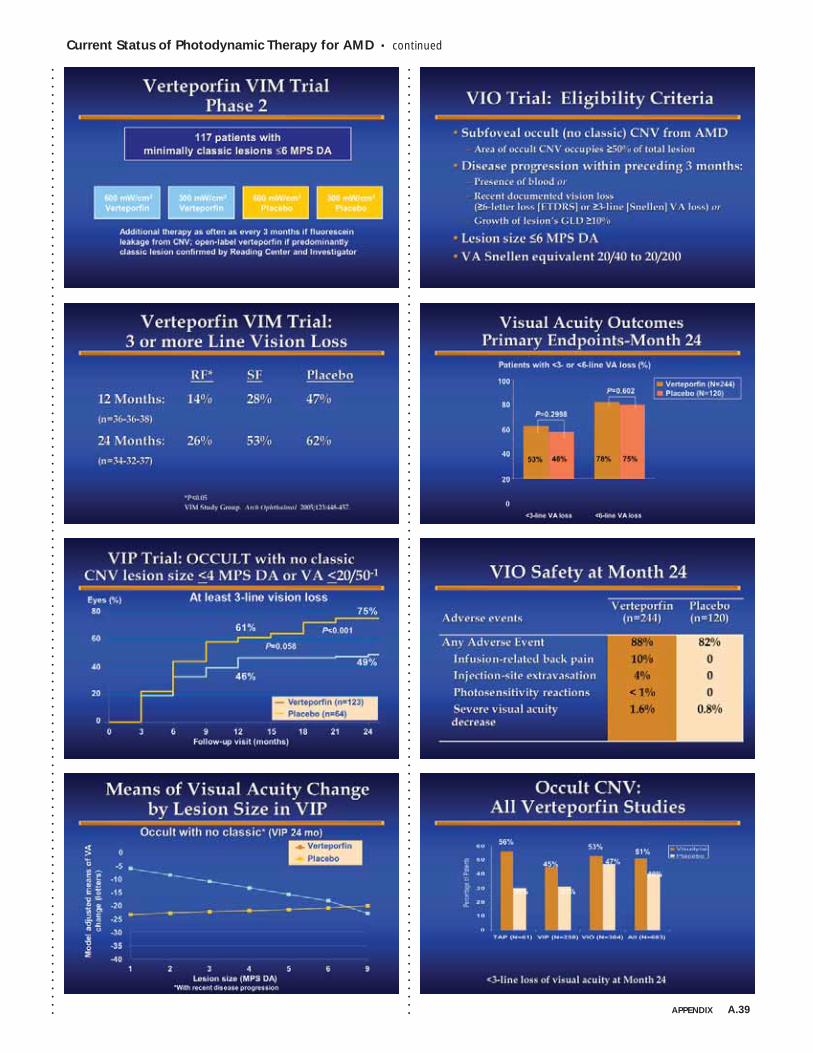
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Current Status of Photodynamic Therapy for AMD • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.39
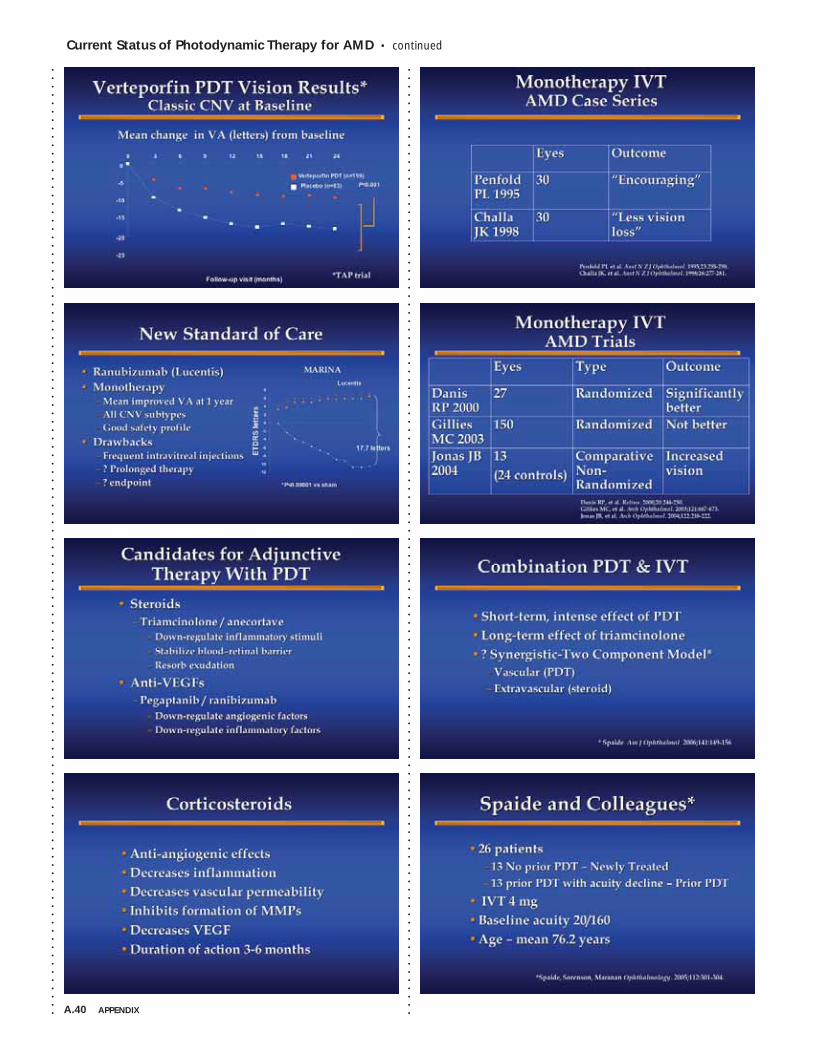
A.40 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Current Status of Photodynamic Therapy for AMD • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
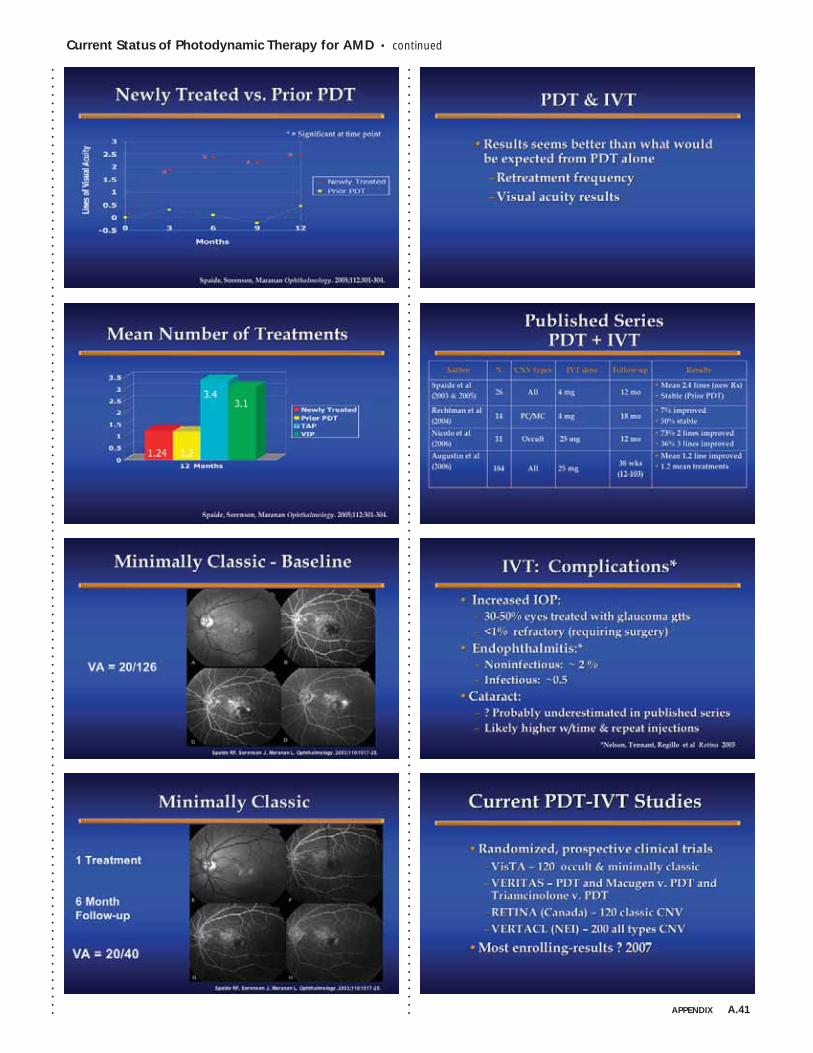
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Current Status of Photodynamic Therapy for AMD • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.41
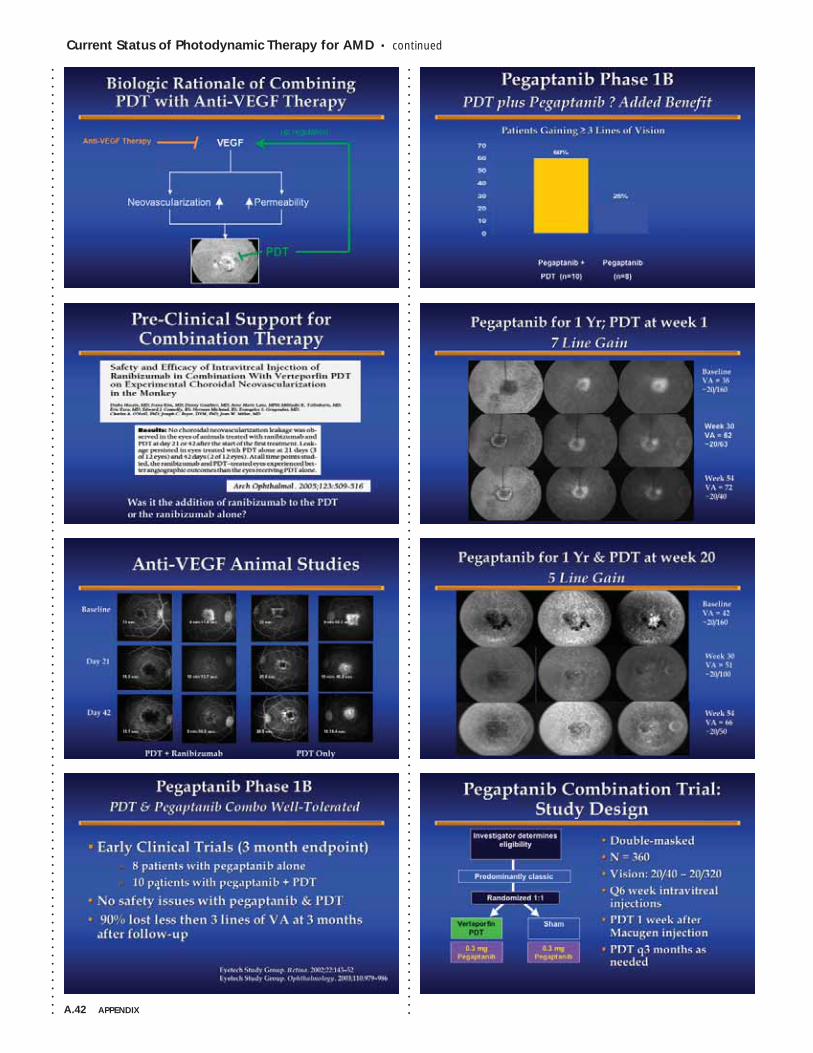
A.42 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Current Status of Photodynamic Therapy for AMD • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
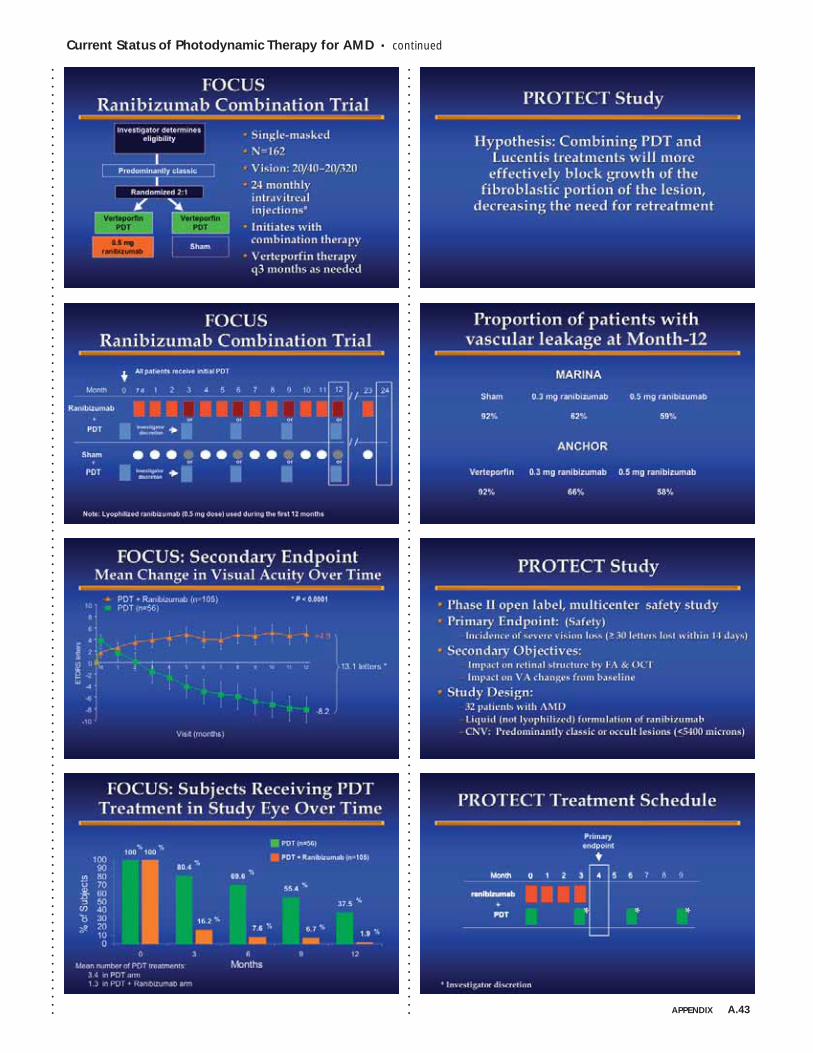
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Current Status of Photodynamic Therapy for AMD • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.43
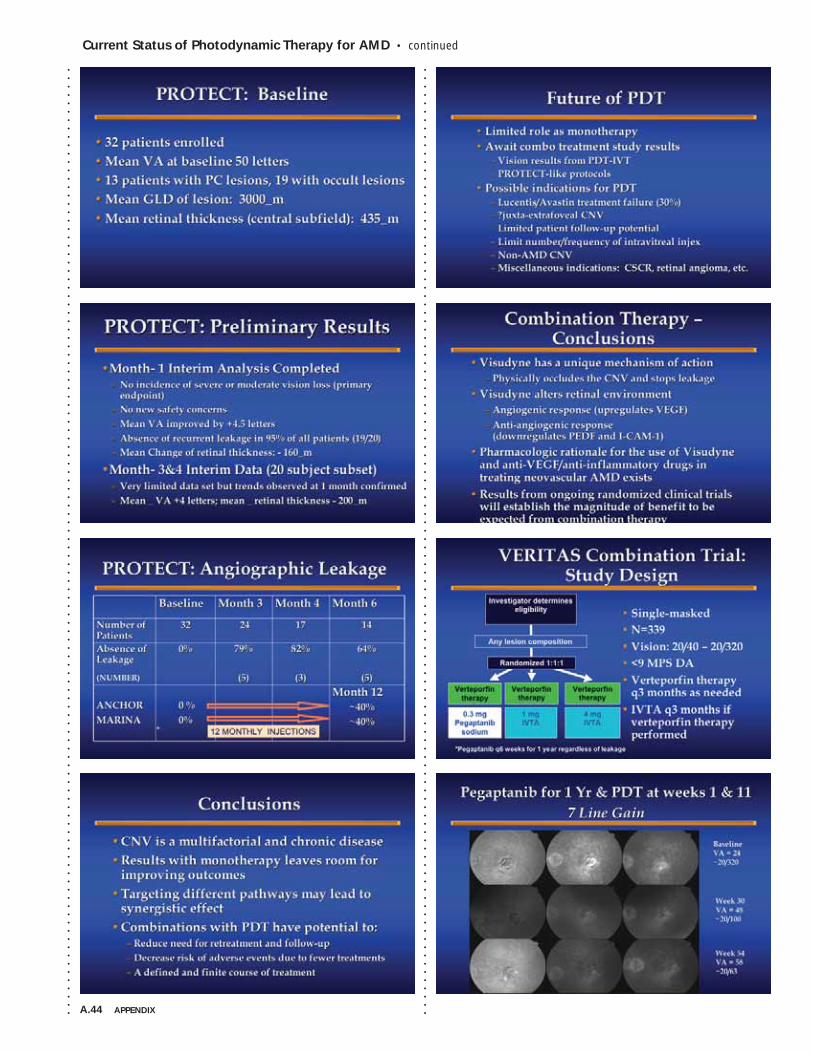
A.44 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Current Status of Photodynamic Therapy for AMD • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
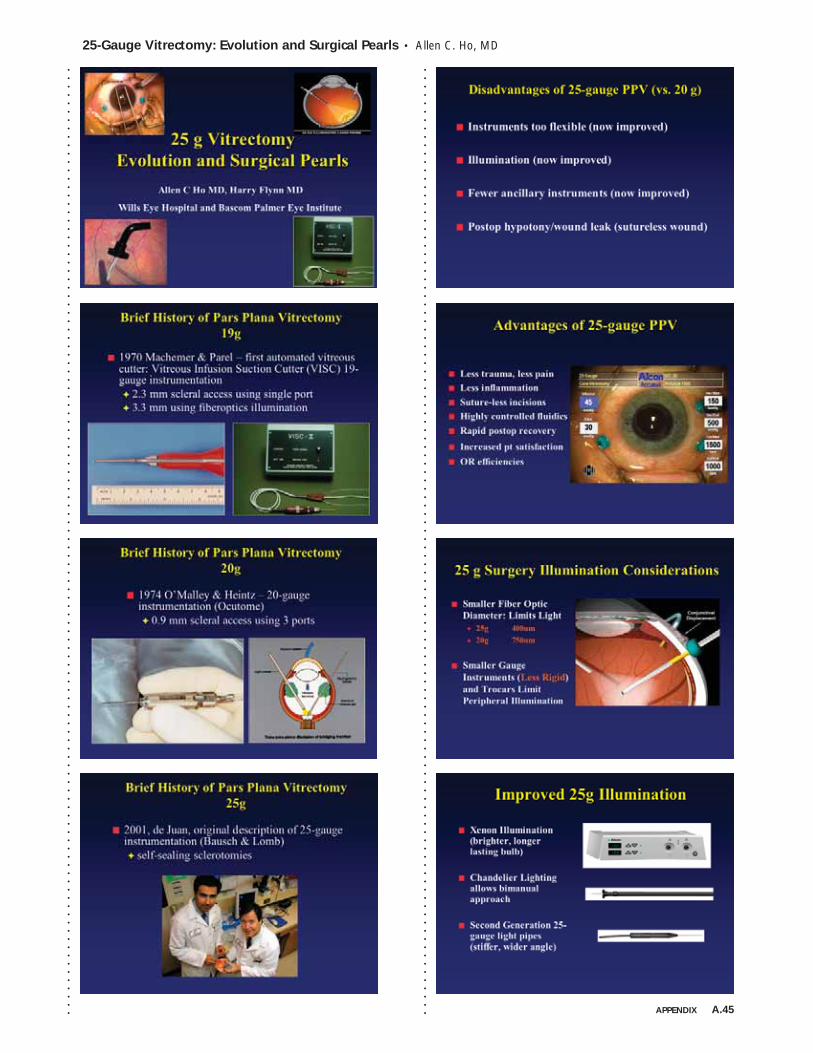
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
25-Gauge Vitrectomy: Evolution and Surgical Pearls • Allen C. Ho, MD
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.45
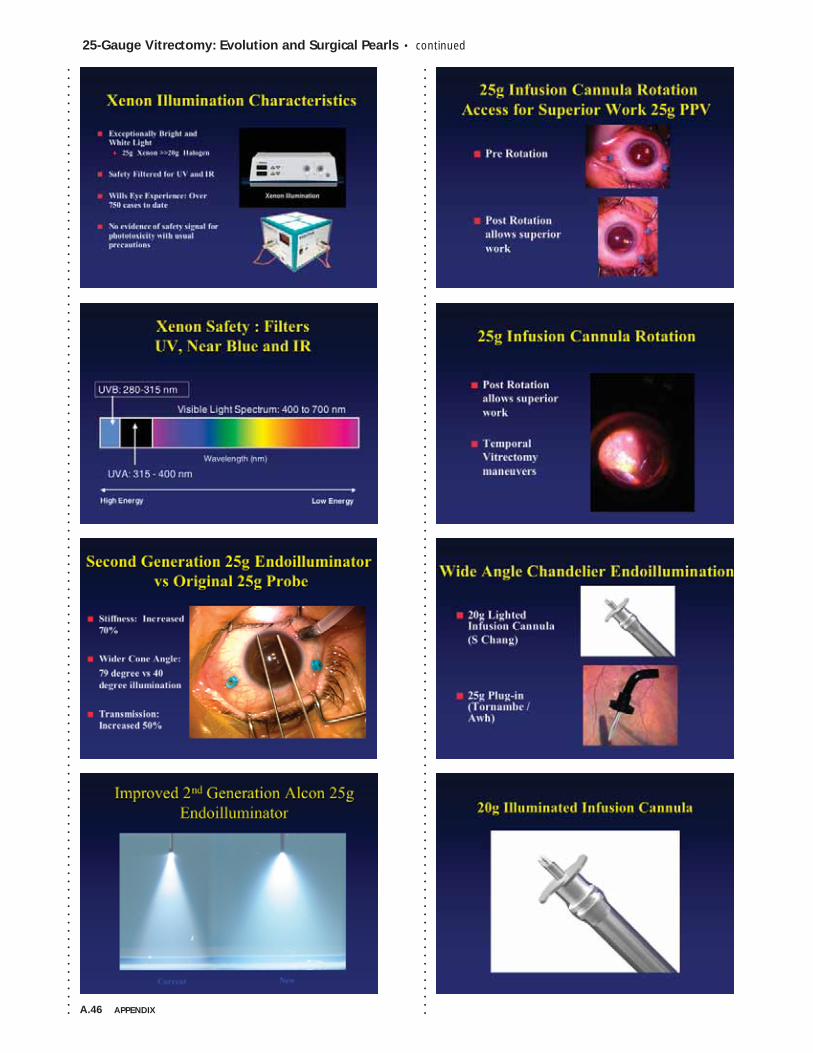
A.46 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
25-Gauge Vitrectomy: Evolution and Surgical Pearls • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
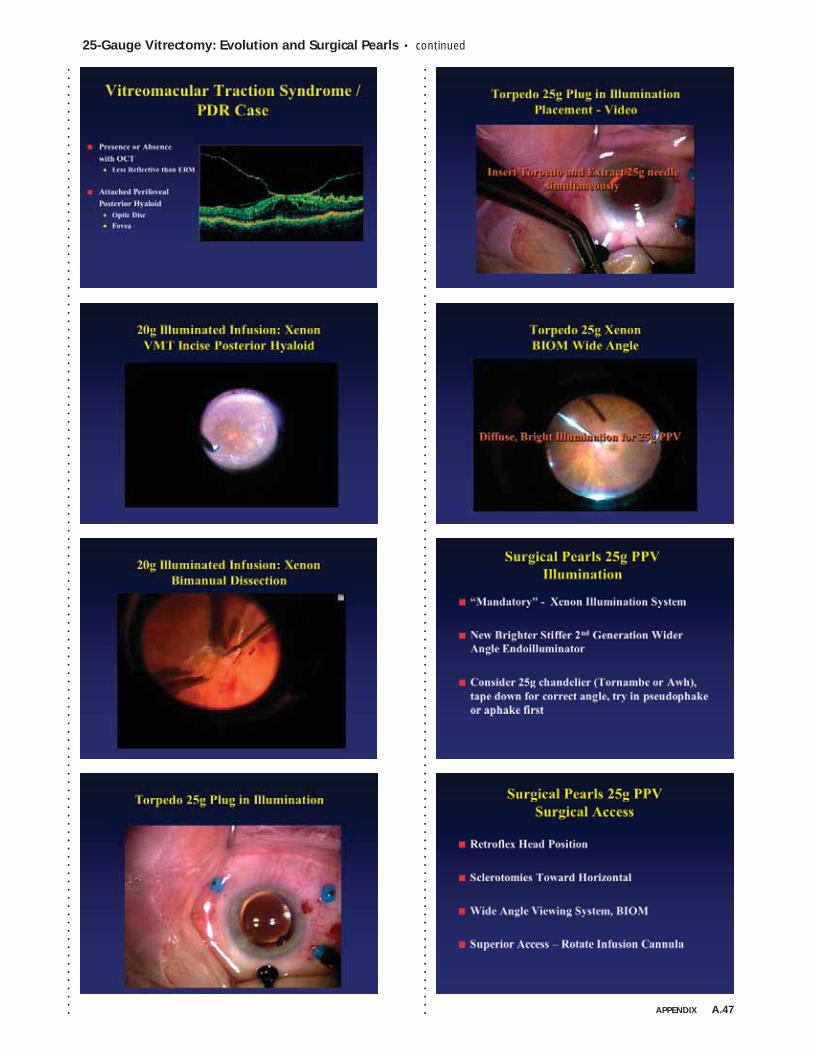
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
25-Gauge Vitrectomy: Evolution and Surgical Pearls • continued
APPENDIX A.47
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
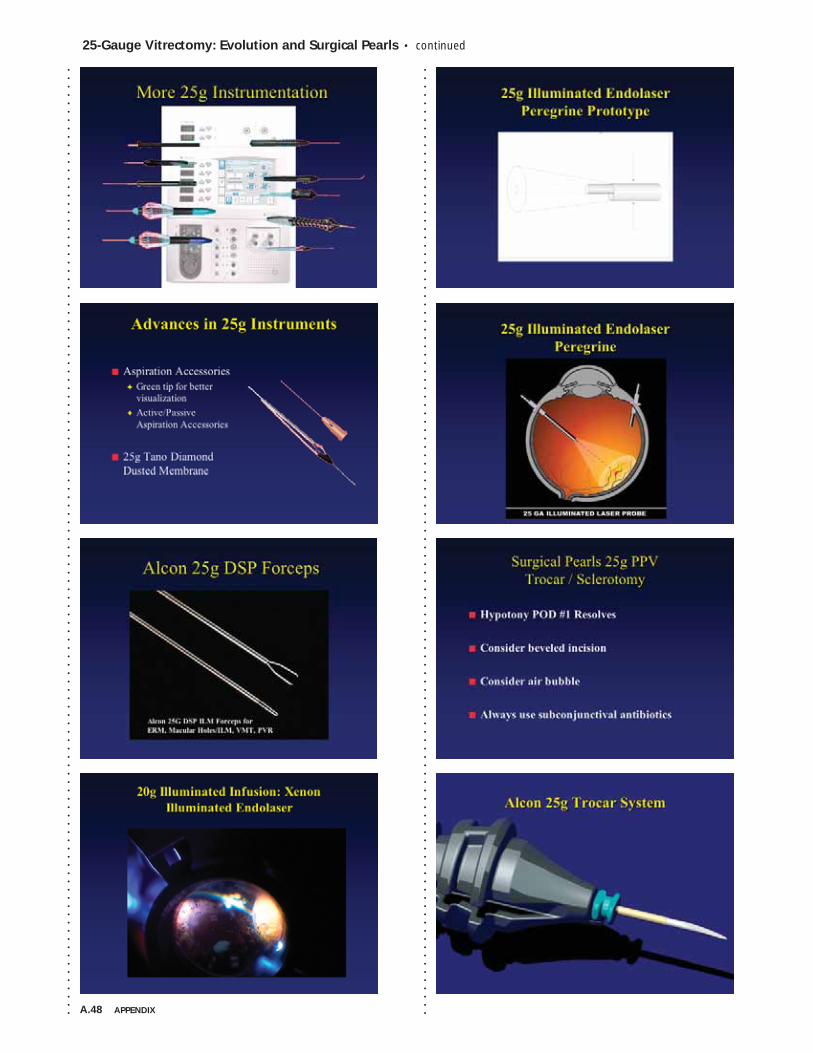
A.48 APPENDIX
25-Gauge Vitrectomy: Evolution and Surgical Pearls • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
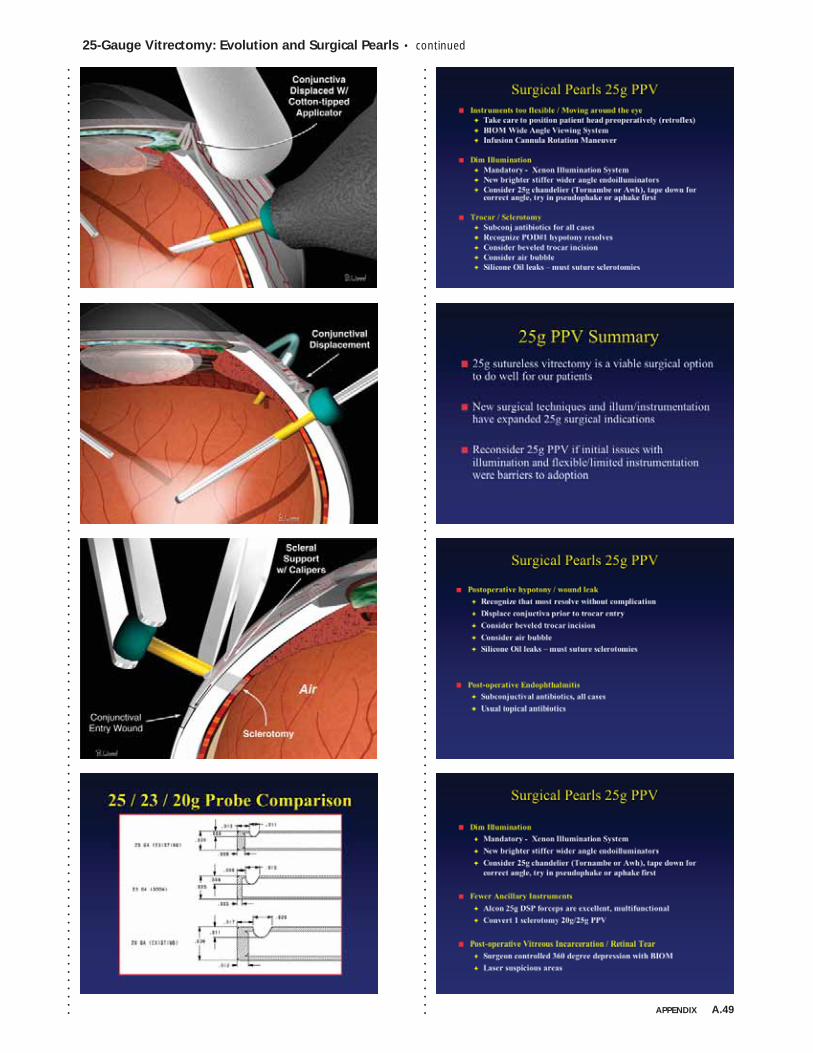
25-Gauge Vitrectomy: Evolution and Surgical Pearls • continued
APPENDIX A.49
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
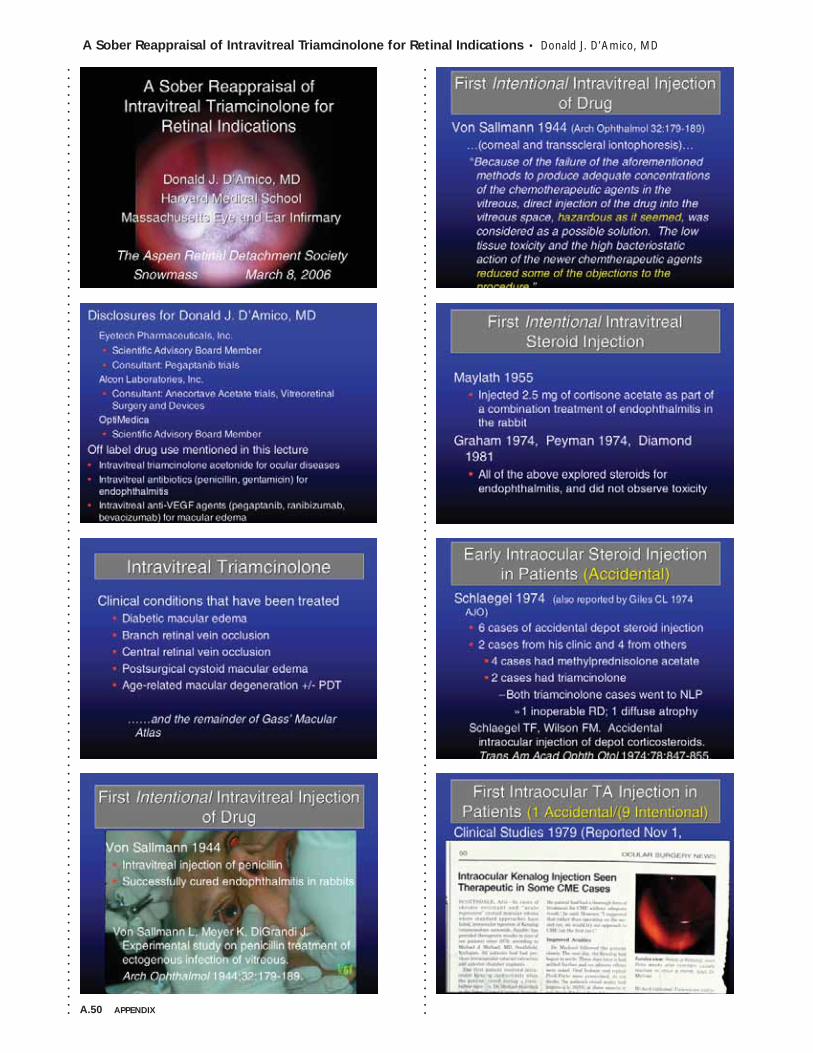
A.50 APPENDIX
A Sober Reappraisal of Intravitreal Triamcinolone for Retinal Indications • Donald J. D’Amico, MD
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
A Sober Reappraisal of Intravitreal Triamcinolone for Retinal Indications • continued
APPENDIX A.51
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
A.52 APPENDIX
A Sober Reappraisal of Intravitreal Triamcinolone for Retinal Indications • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
A Sober Reappraisal of Intravitreal Triamcinolone for Retinal Indications • continued
APPENDIX A.53
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
A.54 APPENDIX
A Sober Reappraisal of Intravitreal Triamcinolone for Retinal Indications • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
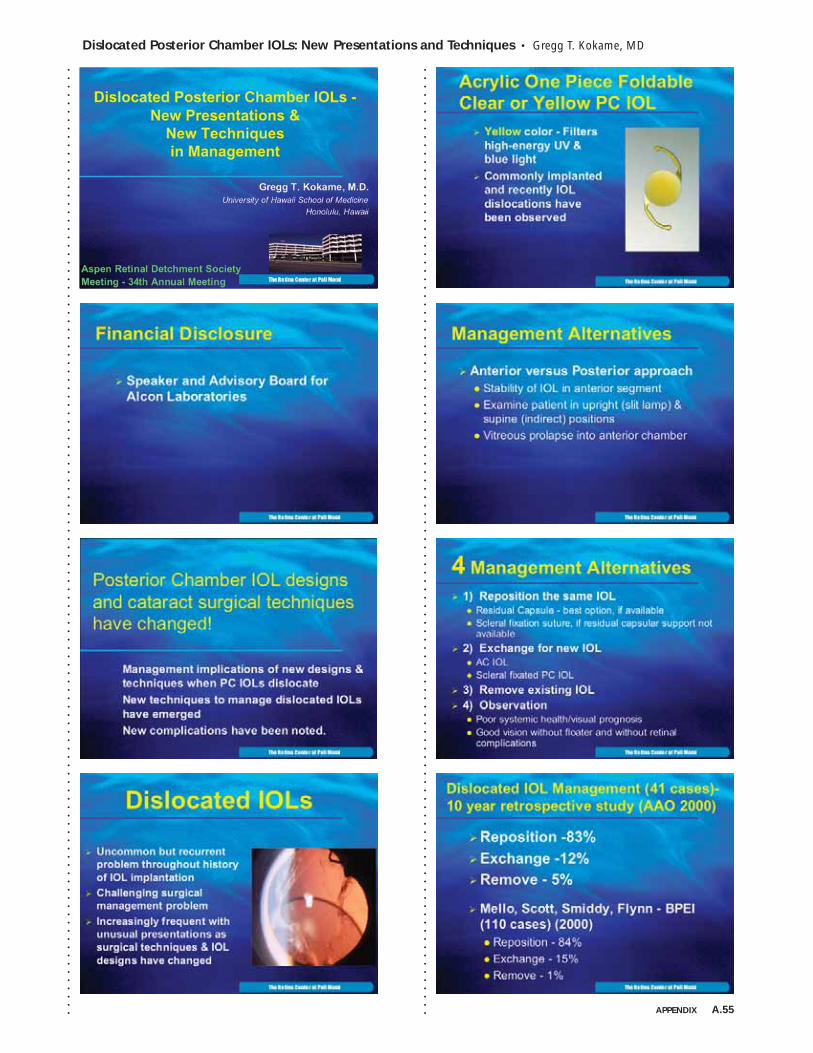
Dislocated Posterior Chamber IOLs: New Presentations and Techniques • Gregg T. Kokame, MD
APPENDIX A.55
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
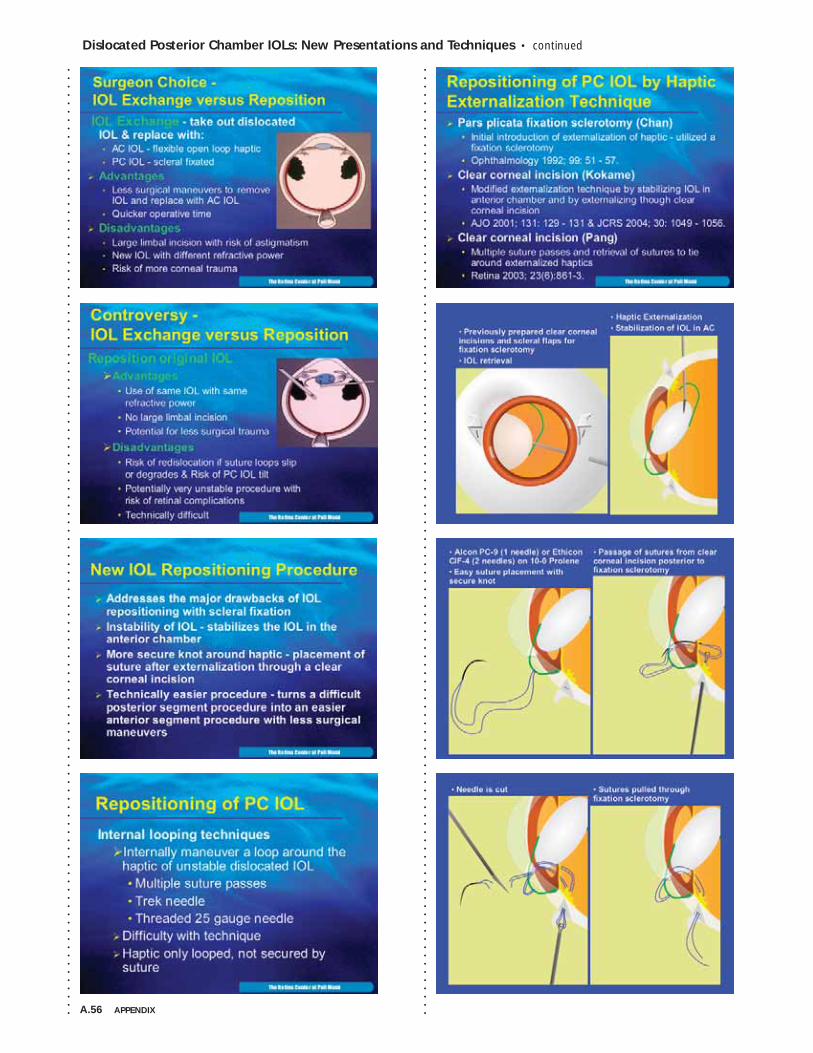
A.56 APPENDIX
Dislocated Posterior Chamber IOLs: New Presentations and Techniques • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
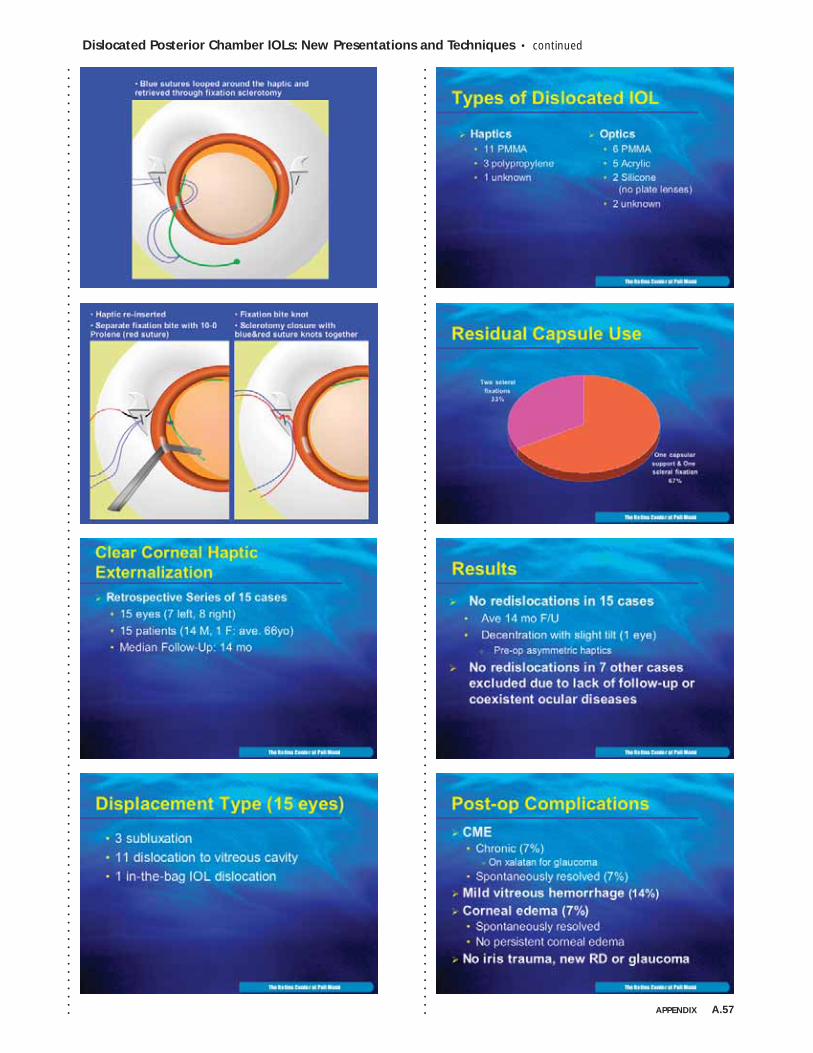
Dislocated Posterior Chamber IOLs: New Presentations and Techniques • continued
APPENDIX A.57
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
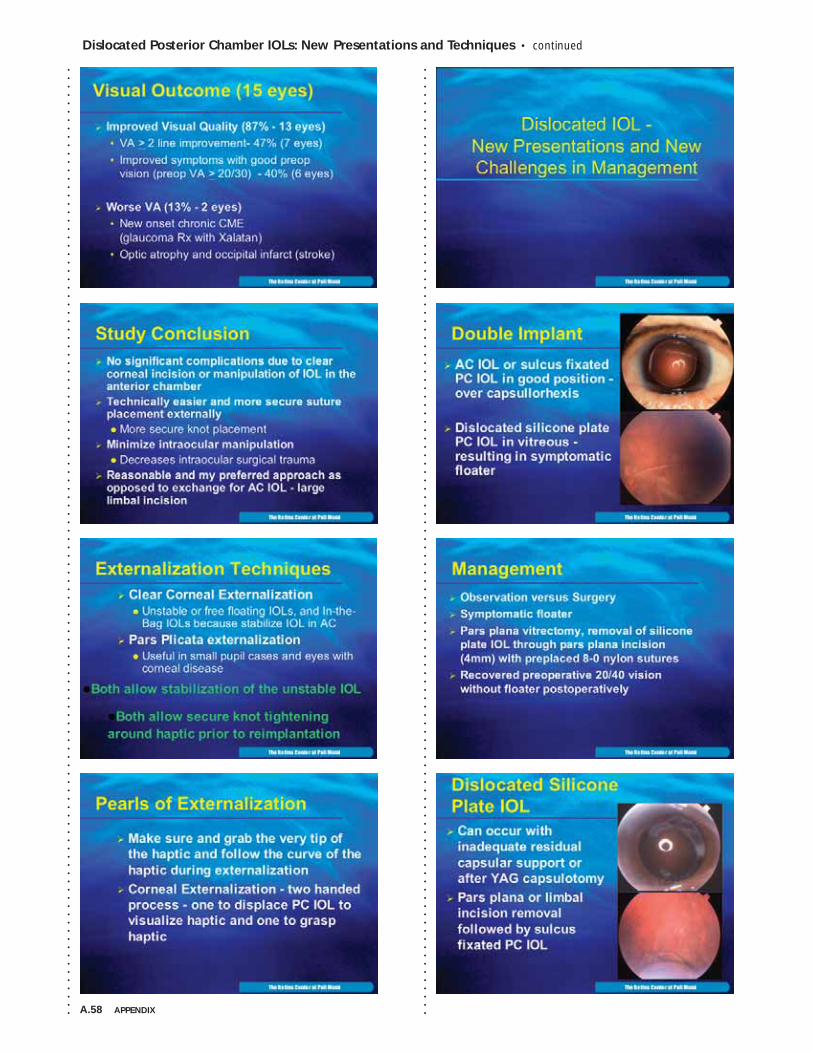
A.58 APPENDIX
Dislocated Posterior Chamber IOLs: New Presentations and Techniques • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Dislocated Posterior Chamber IOLs: New Presentations and Techniques • continued
APPENDIX A.59
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
A.60 APPENDIX
Dislocated Posterior Chamber IOLs: New Presentations and Techniques • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Dislocated Posterior Chamber IOLs: New Presentations and Techniques • continued
APPENDIX A.61
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
A.62 APPENDIX
The Taylor Smith Lecture • Introduction by Donald J. D’Amico, MD
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
The Taylor Smith Lecture: Pseudomelanomas of Choroid and Ciliary Body • Jerry A. Shields, MD
APPENDIX A.63
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
A.64 APPENDIX
The Taylor Smith Lecture: Pseudomelanomas of Choroid and Ciliary Body • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
The Taylor Smith Lecture: Pseudomelanomas of Choroid and Ciliary Body • continued
APPENDIX A.65
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
A.66 APPENDIX
The Taylor Smith Lecture: Pseudomelanomas of Choroid and Ciliary Body • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
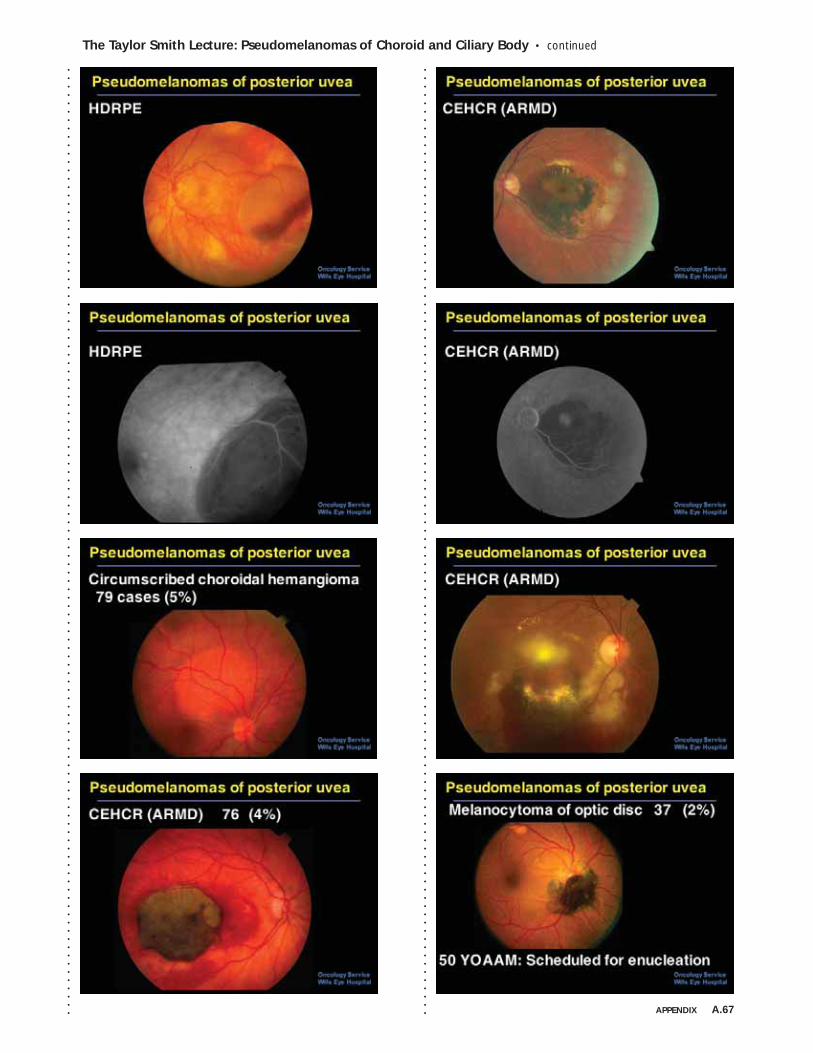
The Taylor Smith Lecture: Pseudomelanomas of Choroid and Ciliary Body • continued
APPENDIX A.67
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
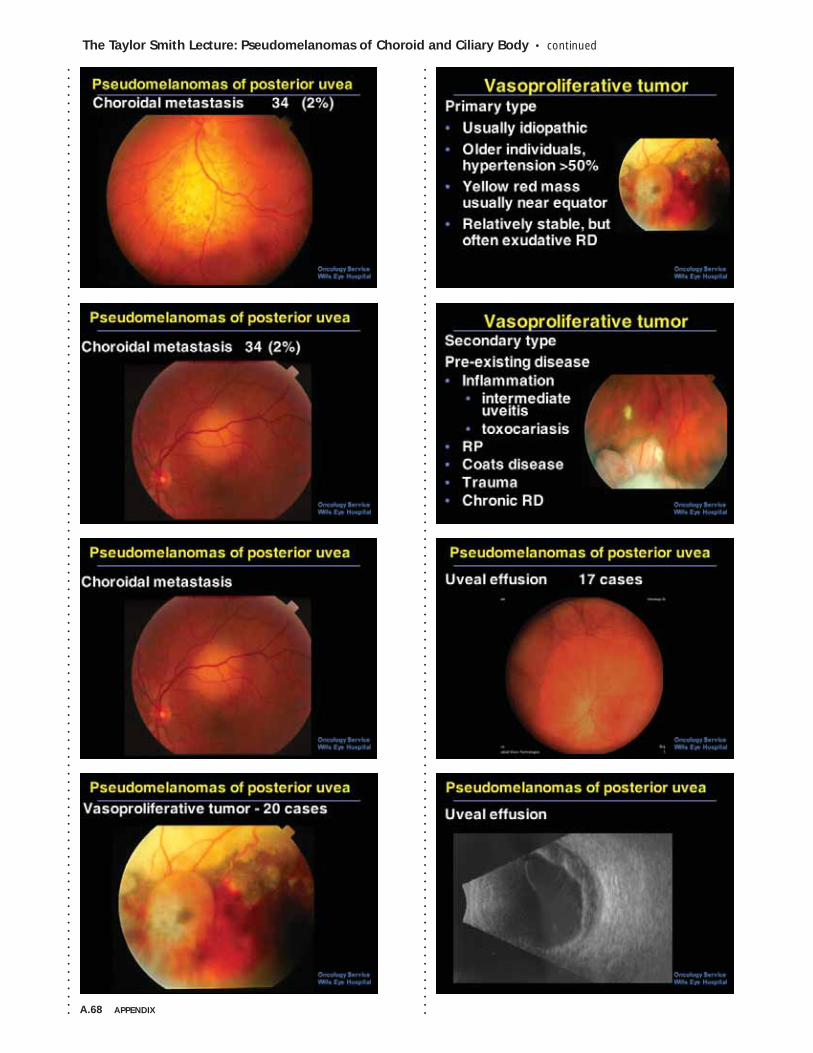
A.68 APPENDIX
The Taylor Smith Lecture: Pseudomelanomas of Choroid and Ciliary Body • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
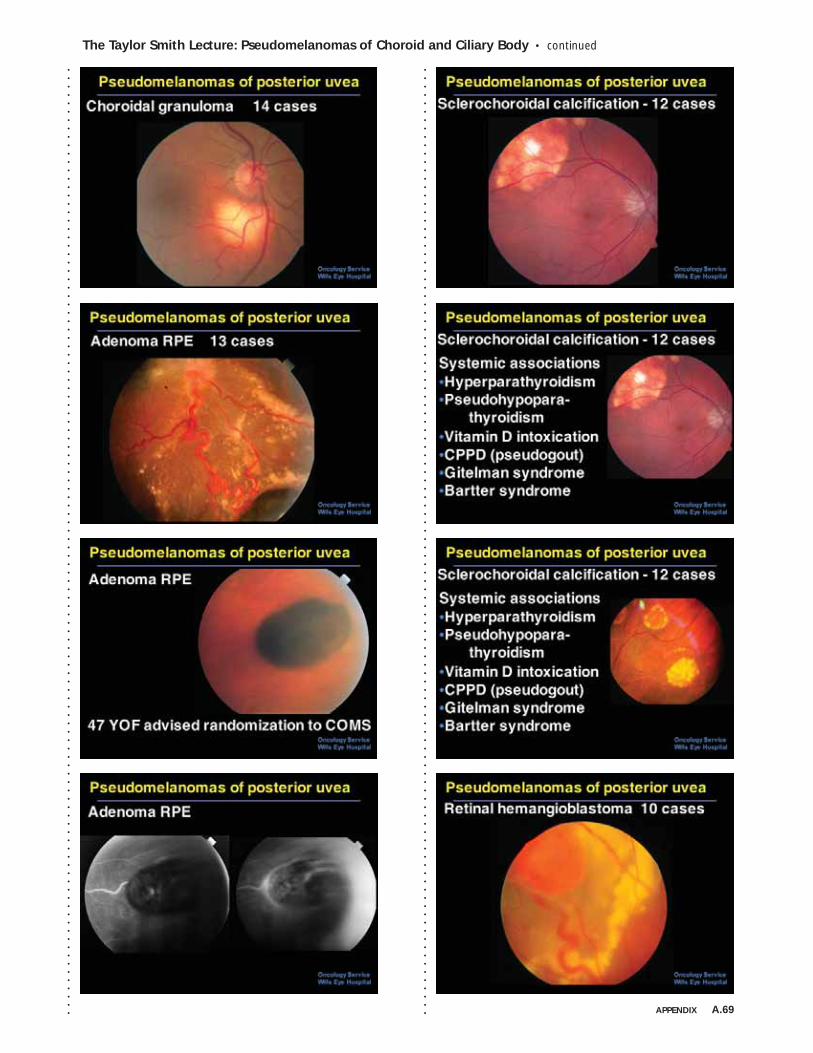
The Taylor Smith Lecture: Pseudomelanomas of Choroid and Ciliary Body • continued
APPENDIX A.69
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
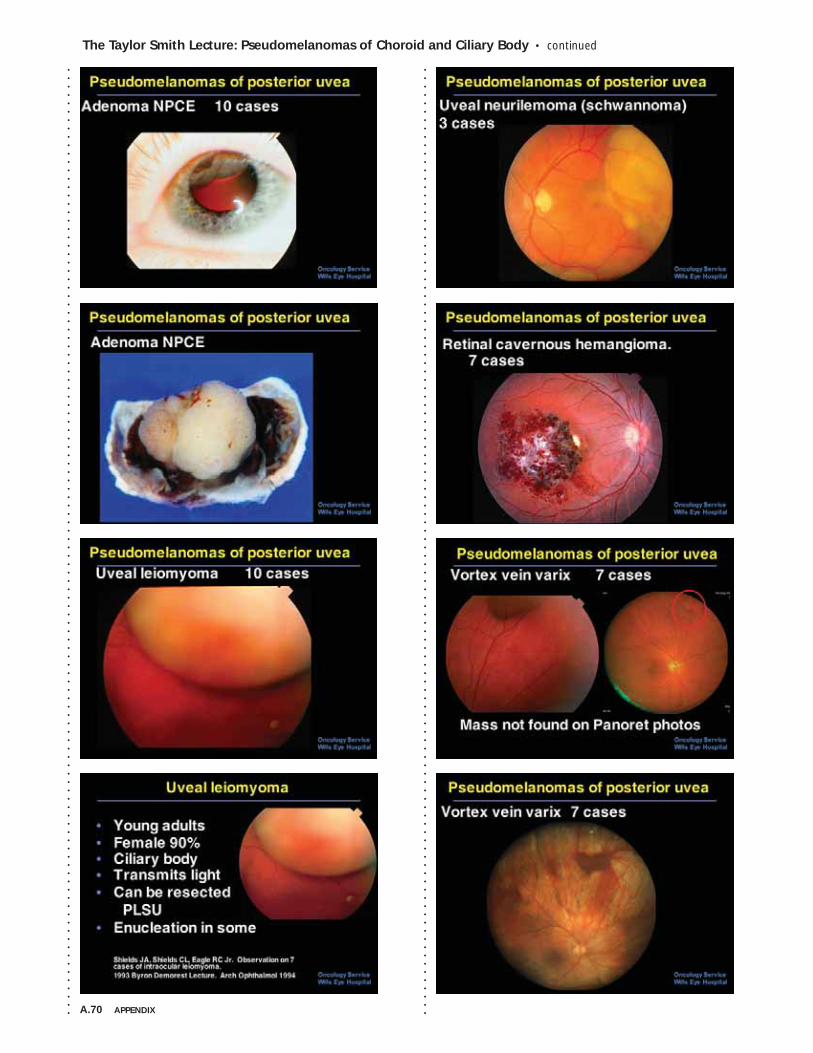
A.70 APPENDIX
The Taylor Smith Lecture: Pseudomelanomas of Choroid and Ciliary Body • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
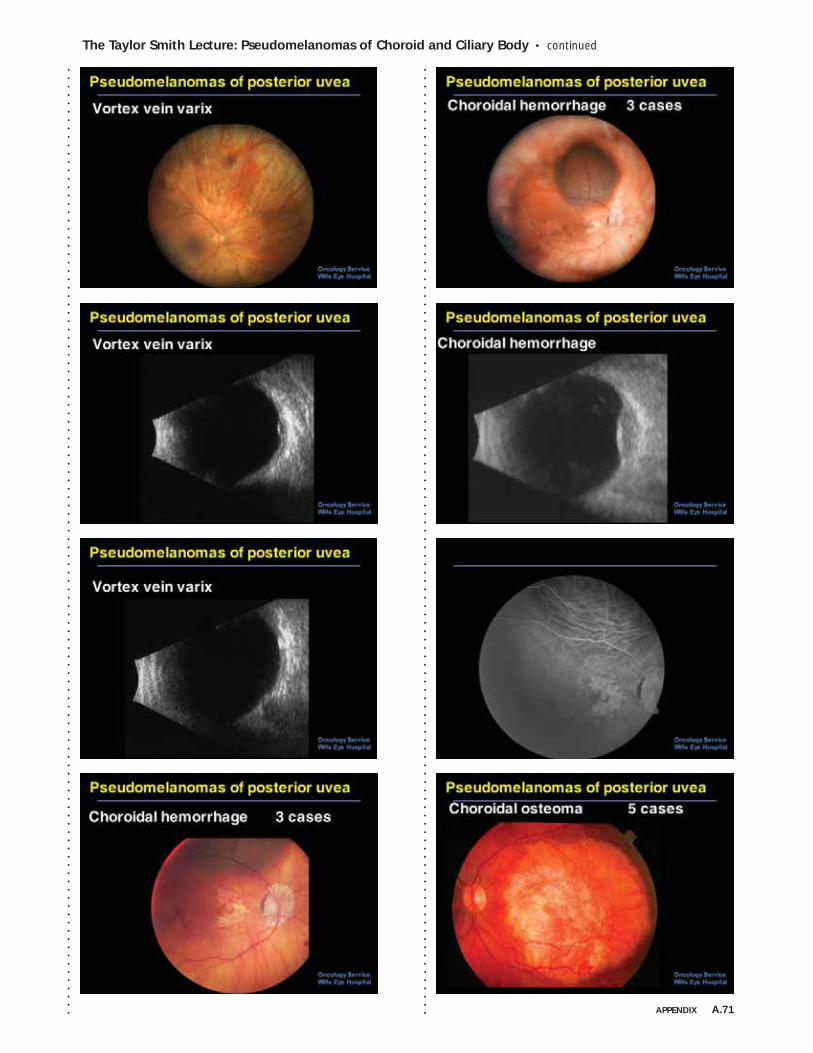
The Taylor Smith Lecture: Pseudomelanomas of Choroid and Ciliary Body • continued
APPENDIX A.71
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
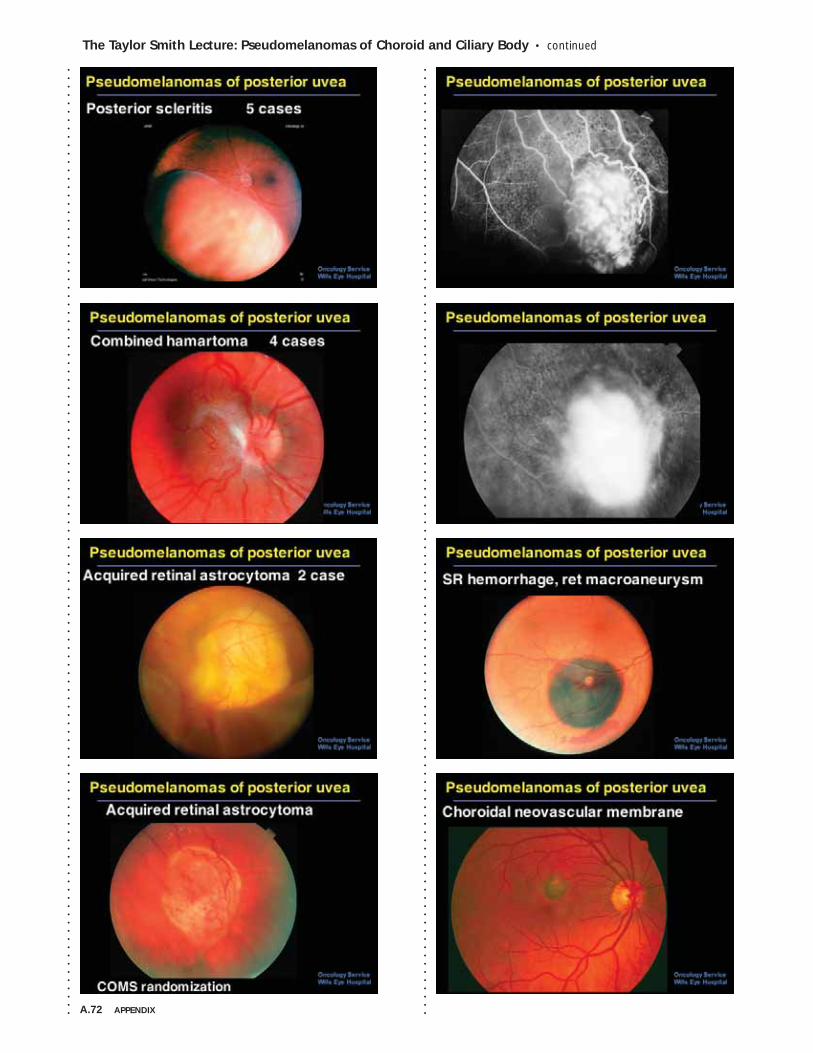
A.72 APPENDIX
The Taylor Smith Lecture: Pseudomelanomas of Choroid and Ciliary Body • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
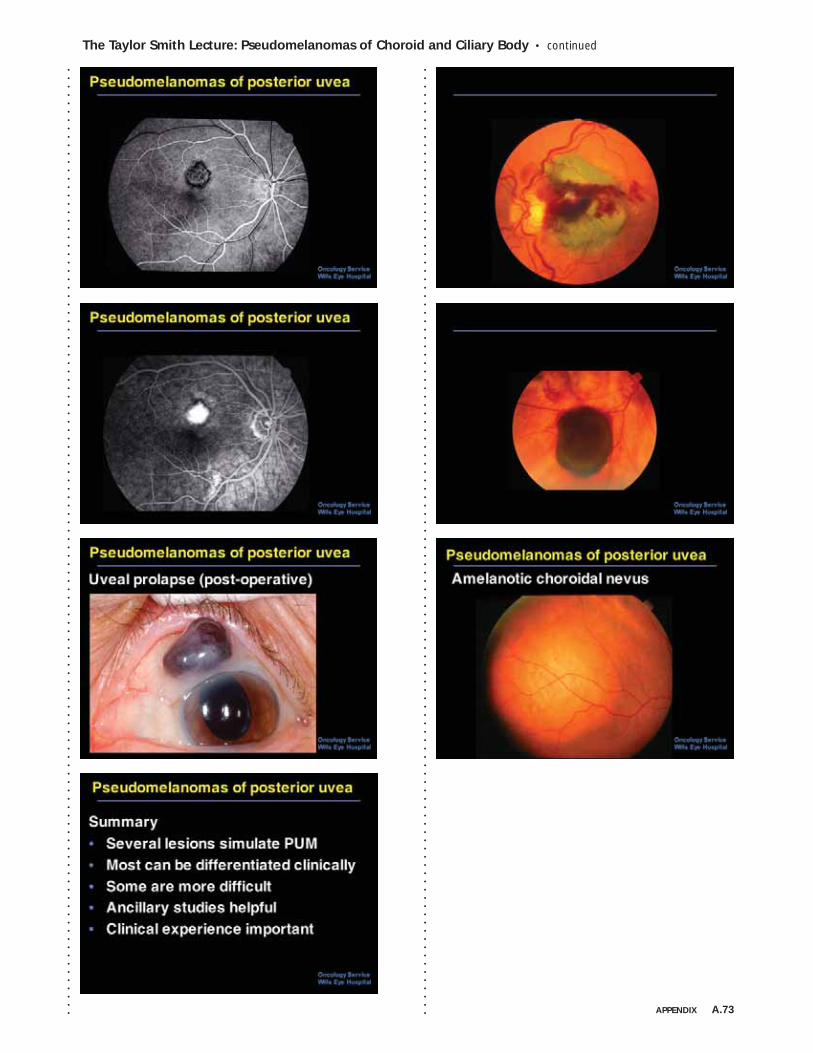
The Taylor Smith Lecture: Pseudomelanomas of Choroid and Ciliary Body • continued
APPENDIX A.73
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
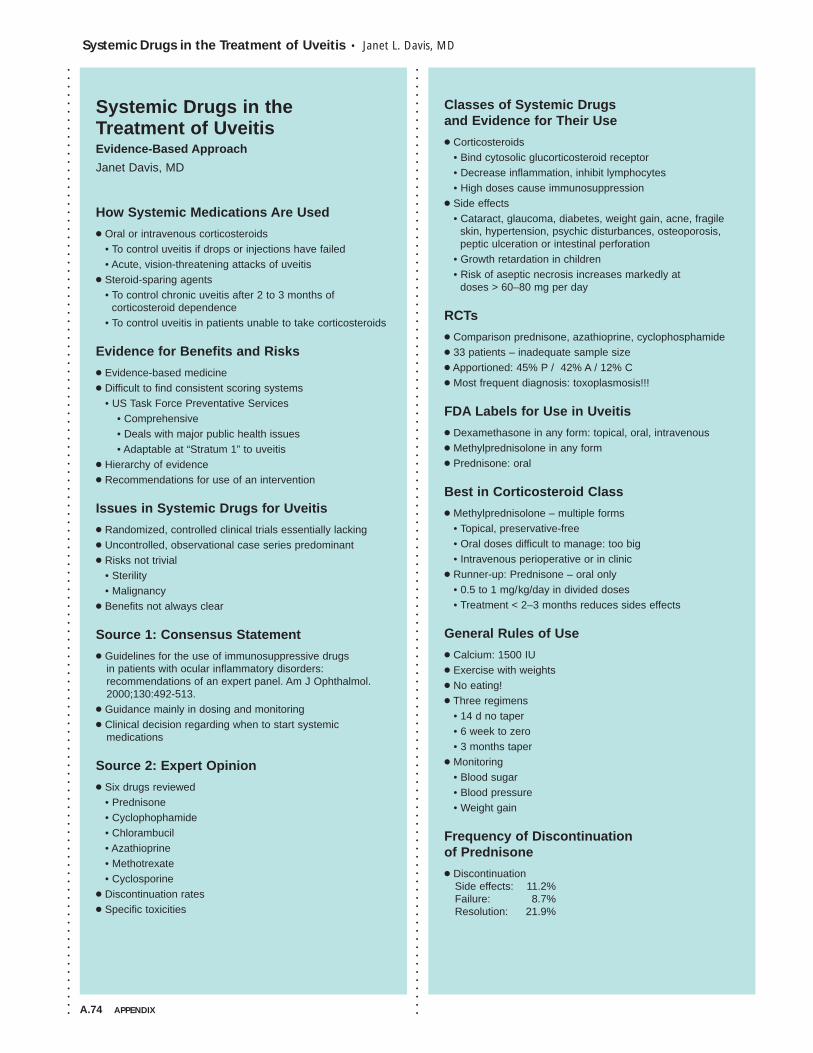
A.74 APPENDIX
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Systemic Drugs in the Treatment of Uveitis • Janet L. Davis, MD
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Systemic Drugs in the Treatment of UveitisEvidence-Based Approach
Janet Davis, MD
How Systemic Medications Are Used
● Oral or intravenous corticosteroids • To control uveitis if drops or injections have failed• Acute, vision-threatening attacks of uveitis
● Steroid-sparing agents• To control chronic uveitis after 2 to 3 months of
corticosteroid dependence• To control uveitis in patients unable to take corticosteroids
Evidence for Benefits and Risks
● Evidence-based medicine ● Difficult to find consistent scoring systems
• US Task Force Preventative Services• Comprehensive • Deals with major public health issues• Adaptable at “Stratum 1” to uveitis
● Hierarchy of evidence● Recommendations for use of an intervention
Issues in Systemic Drugs for Uveitis
● Randomized, controlled clinical trials essentially lacking● Uncontrolled, observational case series predominant● Risks not trivial
• Sterility• Malignancy
● Benefits not always clear
Source 1: Consensus Statement
● Guidelines for the use of immunosuppressive drugs in patients with ocular inflammatory disorders: recommendations of an expert panel. Am J Ophthalmol.2000;130:492-513.
● Guidance mainly in dosing and monitoring ● Clinical decision regarding when to start systemic
medications
Source 2: Expert Opinion
● Six drugs reviewed• Prednisone• Cyclophophamide• Chlorambucil• Azathioprine• Methotrexate• Cyclosporine
● Discontinuation rates● Specific toxicities
Classes of Systemic Drugs and Evidence for Their Use
● Corticosteroids• Bind cytosolic glucorticosteroid receptor• Decrease inflammation, inhibit lymphocytes• High doses cause immunosuppression
● Side effects • Cataract, glaucoma, diabetes, weight gain, acne, fragile
skin, hypertension, psychic disturbances, osteoporosis,peptic ulceration or intestinal perforation
• Growth retardation in children • Risk of aseptic necrosis increases markedly at
doses > 60–80 mg per day
RCTs
● Comparison prednisone, azathioprine, cyclophosphamide● 33 patients – inadequate sample size● Apportioned: 45% P / 42% A / 12% C● Most frequent diagnosis: toxoplasmosis!!!
FDA Labels for Use in Uveitis
● Dexamethasone in any form: topical, oral, intravenous● Methylprednisolone in any form● Prednisone: oral
Best in Corticosteroid Class
● Methylprednisolone – multiple forms• Topical, preservative-free• Oral doses difficult to manage: too big• Intravenous perioperative or in clinic
● Runner-up: Prednisone – oral only• 0.5 to 1 mg/kg/day in divided doses• Treatment < 2–3 months reduces sides effects
General Rules of Use
● Calcium: 1500 IU● Exercise with weights● No eating!● Three regimens
• 14 d no taper• 6 week to zero• 3 months taper
● Monitoring• Blood sugar• Blood pressure• Weight gain
Frequency of Discontinuation of Prednisone
● DiscontinuationSide effects: 11.2%Failure: 8.7%Resolution: 21.9%
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Systemic Drugs in the Treatment of Uveitis • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . APPENDIX A.75
Regimen 1: Two Week High Dose No TaperRegimen 2: Three Day Intravenous
● 500 mg to 1 gram IV daily for 3 days● Failure of orals to control or initial panic● Evidence
• Uveitis: small case series from Australia• Optic neuritis: RCT demonstrating safety in outpatient
use in ophthalmologists’ office
Regimen 3a: Eight Week CourseRegimen 3b: Three Month with Trial TaperBan the Medrol Dose-PakAnti-Metabolites
● Methotrexate• Inhibits dihydrofolate reductase, DNA replication
● Azathioprine• Purine nucleoside analog
● Mycophenolate mofetil• Interferes with T and B lymphocyte production
Example: JRA Uveitis
● Trend toward liberal use of methotrexate in children with uveitis
● Most JRA uveitis is probably mild• No visual loss in the Olmstead County, Minnesota• 97% > = 20/40 in Finland in population-based study• 50% not treated in Australian rheumatology clinic
● BUT, JRA causes disproportionate amount of severe uveitis in referral clinics and terrifies uveitis experts
JRA Complications from 1 Yr to 3 YrCase Series
● Methotrexate: Retrospective, noncomparative • 11 patients
• 8 with sarcoidosis• 3 with presumed sarcoidosis
• Decrease in corticosteroid use• Preserved or improved vision in 90%
● Methotrexate: Retrospective, noncomparative• 160 patients• Steroid-sparing in 56%• Preserved or improved vision in 90%
● Methotrexate: Retrospective• 43 children with JRA
RCTs of Azathioprine
● Azathioprine studied in iridocyclitis 1969● Azathioprine for Behçet uveitis – placebo controlled
• Less new uveitis in 25 patients without uveitis at baseline• Less second eye involvement in 14 patients• Fewer episodes of hypopyon uveitis in 48 patients
with uveitis at baseline
Uncontrolled Clinical Trials
● Mycophenolate mofetil• Larkin G. Ophthalmology. 1999;106:370.
• Open-label, prospective, uncontrolled pilot study. • 11 patients; 10 of 11 “favorable” response• Few side effects
● Kilmartin D. Lancet. 1998;352:35.• Open-label, uncontrolled• 9 patients; 1 of 9 had worsened vision• Mild side effects
Discontinuation FrequencyBest in Anti-Metabolite Class
● Mycophenolate mofetil $$$• Appears well tolerated• Effective in higher doses
• Range is 1 to 3 grams per day in 2 doses• Monitor CBC
• Can be used in children and adults● Azathioprine $: strong clinical trials data● Methotrexate $: track record in children
Macrolide Antibiotics
Functional Effects of CSAand FK506 After Binding
● Inhibition of calcineurin-mediated dephosphorylation• Prevents transfer of NFAT* into nucleus• Blocks JNK and p38 signaling pathways
• Triggered by antigen recognition• Interferes with lymphocyte proliferation• Reduces IL-2 production
• Predicted synergy with IL-2 antagonists such as daclizumab and basiliximab
Functional Effects of Sirolimus
● Inhibits kinase linked to cell growth control• mTOR (mammalian target of rapamycin)• Downstream effector of Protein Kinase B pathway
• G1 phase arrest• Constitutively expressed in leukemias• VEGF mediates activity through mTOR
● Interferes with signal transduction for T-cell proliferation• Signal 2: CD-28• Signal 3: IL-2
● SRL-FKBP12 does not inhibit IL-2 production● Reduces cellular proliferation
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .A.76 APPENDIX
Systemic Drugs in the Treatment of Uveitis • continued
Adverse Effects
● Drug interactions – Same for all• Antifungals• Erythromycin• St John’s Wort• Grapefruit• HIV protease inhibitors• Calcium blockers
● Cyclosporine• Renal toxicity – HTN• Neurologic toxicity• Gingival hyperplasia• Increased hair
● Tacrolimus• Renal toxicity – HTN• Peripheral neuropathy• Diabetes
● Sirolimus• Myelosuppression• Non-specific side effects
Cyclosporine in Uveitis
● Japanese study comparing CSA to colchicine in Behçet disease RCT
● Treatment endpoints met in 46% of patients randomized to either cyclosporine or prednisolone RCT
● Cyclosporine in 15 children with uveitis
Case Series
● Cyclosporine• Pediatric uveitis: 29 children• Behçet uveitis
• 19 patients USA• 12 patients Turkey
• Noninfectious uveitis• 50 patients USA• 13 patients UK
Clinical Trials with Tacrolimus
● Open label study in Japan 1993• 53 pts – 41 with Behçet uveitis• 0.1 to 0.15 mg/kg/day• Target trough 15–25 µg/l
Tacrolimus vs. Cyclosporine
● Tacrolimus in uveitis patients failing CSA• Start < 0.1 mg/kg/day in two doses• Maintain 0.06 mg/kg/day in two doses• 9/11 eyes with reduced inflammation*• Mean trough 8 µg/l
● Tacrolimus in uveitis patients failing CSA• Improvement in 5/6 patients **• Target trough range 1–15 µg/l
● Randomized trial of Tacrolimus vs. CSA***• 37 patients• Two-thirds of each group responded to treatment
with improvement in uveitis• Higher blood pressure and cholesterol in
cyclosporine group
RCTs of Cyclosporine
● Japanese study comparing to colchicine 1989● Met treatment endpoints in 46% of patients randomized
to either cyclosporine or prednisolone● More renal side effects and hypertension than tacrolimus
Other Clinical Trials
● Cyclosporine• Cyclosporine + ketoconazole vs. cyclosporine
• Antifungal drugs permit reduction in dose• Cyclosporine renal toxicity and hypertension*
• Renal biopsies indicating interstitial fibrosis• Lowering dose to < 3 mg/kg/day mitigates toxicity
Uncontrolled Clinical Trials
● Cyclosporine• Cyclosporine + ketoconazole vs. cyclosporine• Cyclosporine A vs. cyclosporine G• Cyclosporine renal toxicity
Biologics
● Cytokines and cytokine inhibitors• Interferon alpha-2a – antiviral, anti-inflammatory• TNF-inhibitors
• Etanercept – receptor analog that binds TNF• Infliximab – antibody binds to receptor
● Antibodies• Daclizumab – binds to IL-2 receptor• Intravenous immunoglobulin – unknown
Daclizumab
● Controlled clinical trial NIH• 10 patients subcutaneous vs. IV• No discontinuation for side effects• Reduction in other systemic meds
● Retrospective uncontrolled series• 14 patients MEEI • 59% improved
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Systemic Drugs in the Treatment of Uveitis • continued
APPENDIX A.77
TNF-Inhibitors
● Etanercept• Small case series
• Improvement in 10/13 pts with JRA• Underpowered RCT in JRA
• 12 patients at NIH• No reduction in recurrences as methotrexate tapered
• RCT in ankylosing spondylitis• Placebo-controlled• Infliximab arm as well• Reduction in AAU attacks by 50%
Infliximab
● Case series• 6 of 7 patients with AAU and spondyloarthropathy
responded to one dose● RCT in ankylosing spondylitis
• Placebo-controlled• Etanercept arm as well• Reduction in AAU attacks by 80%
EtanerceptBinding of TNF-Inhibitors to TNF
Interferon Alpha-2a
● Recent review article summarizing 33 clinical case series in use of IFN alpha in Behcet uveitis• Evidence level II-3 (multiple time series)• Systematic review meeting criteria for fair evidence
(individual papers not meeting criteria for good evidence)• Excellent clinical reference
Risks of Biologics
● Daclizumab: no discontinuations noted● Interferon: side effects of lymphopenia, depression, thyroid
disease, few discontinuations● TNF-inhibitors: severe infections, reactivation of tuberculosis,
onset of multiple sclerosis (especially infliximab), death• Effects may be more severe in uveitis as levels of TNF in
blood low compared to systemic disease• Work-up for TB before starting. MRI brain in IU.
Best in Biologics Class
● Infliximab• Clearly superior to etanercept• Subcutaneous monoclonal antibody being studied
(adalimumab)• Risk profile tolerable• $$$$
● Runner-up: Interferon alpha-2a• Surprising effects such as elimination of CME• Increasing use beyond Behcet disease
Cytotoxics
● Cyclophosphamide• Alkylating agent• Decreases activated T and B lymphocytes• Suppresses helper T cells• Bone marrow suppression, infection, sterility, secondary
malignancy, cystitis, alopecia, nausea vomiting. Bladdercancer 5% > 8 y
• More potent in oral form• Less toxic in pulse intravenous form
● Chlorambucil• The Magic Bullet• Remission with short-term high dose therapy• Incremental daily dosing – 2 mg more each week• Treat until WBC <3,000 or platelets <100,000
• Mean maximum dose 20 mg• Mean total dose 1429 mg• Mean duration of treatment 16 weeks
• Wait for recovery• 53 patients at the University of Chicago• No malignancies in average 4 years of follow-up
Discontinuation FrequencyBest in Cytotoxics Class
● Cyclophosphamide• Nearly as efficacious as chlorambucil• Risk of bladder cancer more monitorable than risk
of leukemia• Works fast as steroid sparing agent
Conclusion
● Systemic drugs are prescribed and dosed without adequate evidence supporting use
● Clinical judgment critical• Expert monitoring for toxicity• Selection of agent
• Intensity of inflammation• Patient-specific factors
● Consensus guidelines help justify therapy● Historically, patients did much worse, but long-term
effects not known
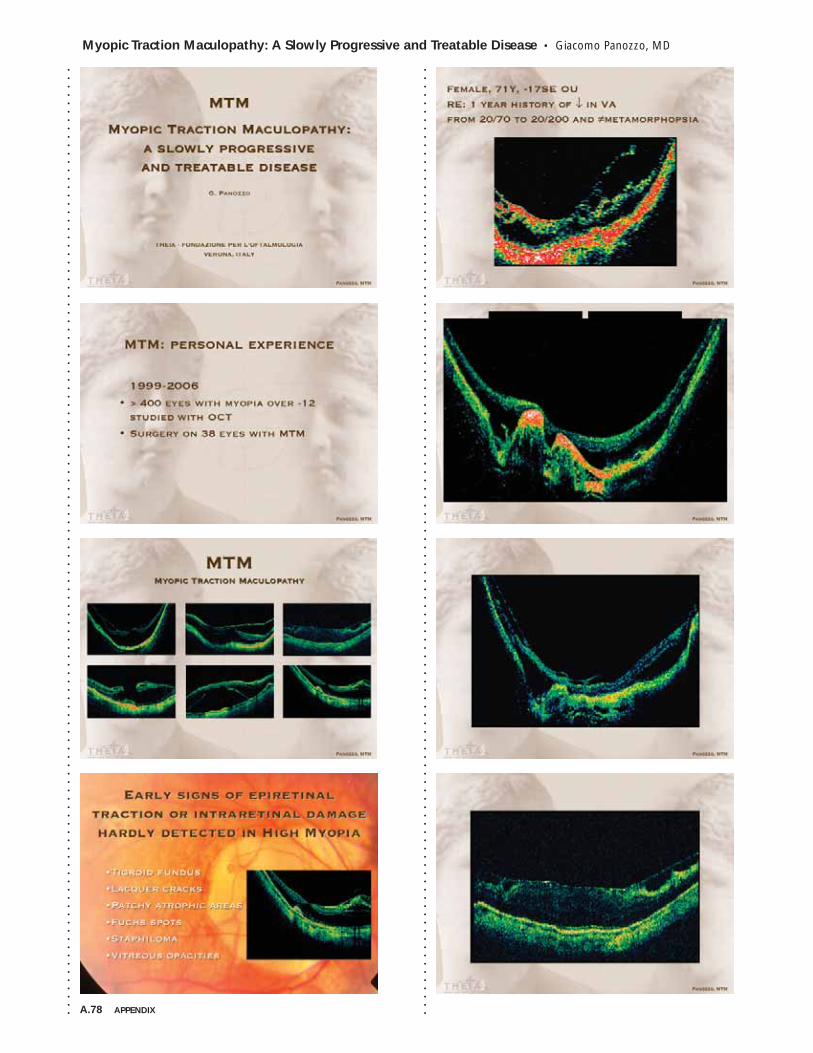
A.78 APPENDIX
Myopic Traction Maculopathy: A Slowly Progressive and Treatable Disease • Giacomo Panozzo, MD
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
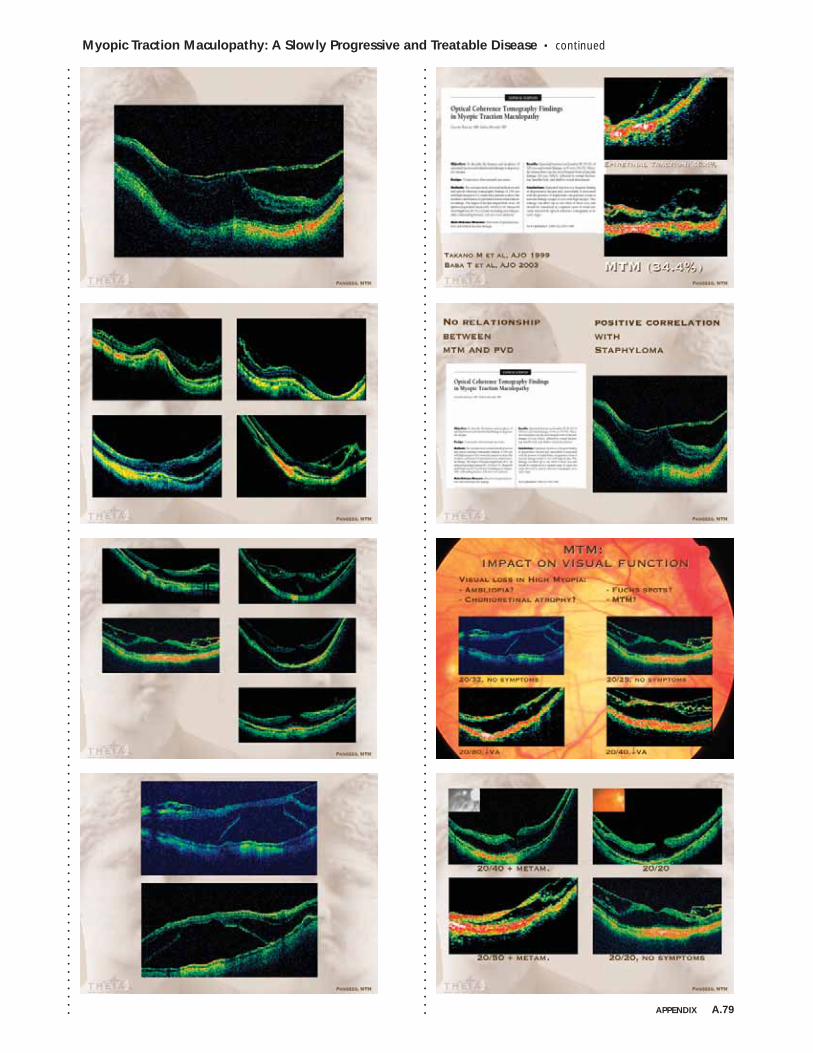
Myopic Traction Maculopathy: A Slowly Progressive and Treatable Disease • continued
APPENDIX A.79
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
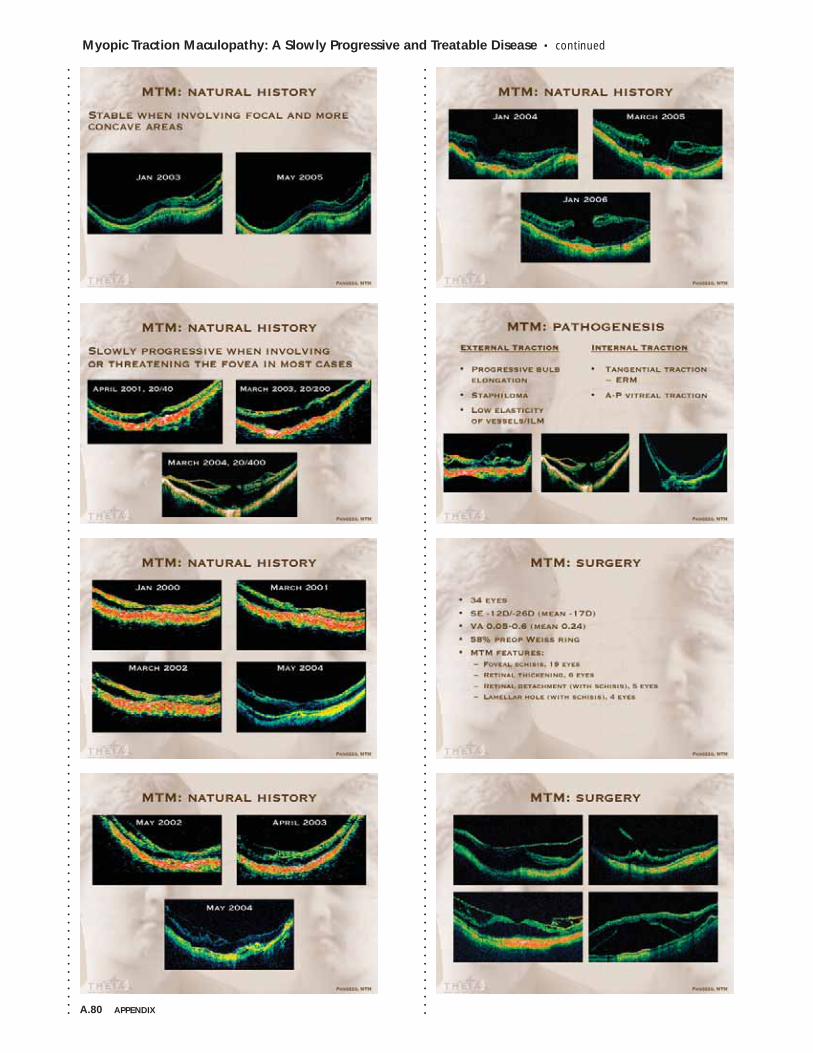
A.80 APPENDIX
Myopic Traction Maculopathy: A Slowly Progressive and Treatable Disease • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
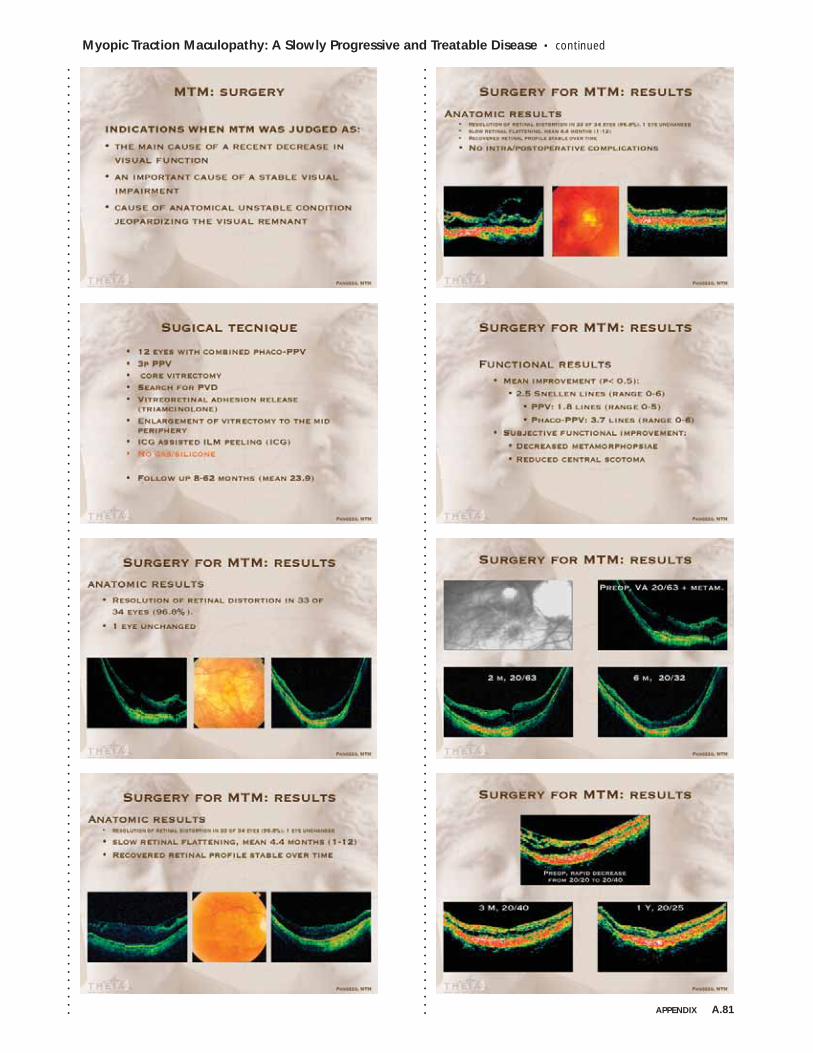
Myopic Traction Maculopathy: A Slowly Progressive and Treatable Disease • continued
APPENDIX A.81
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
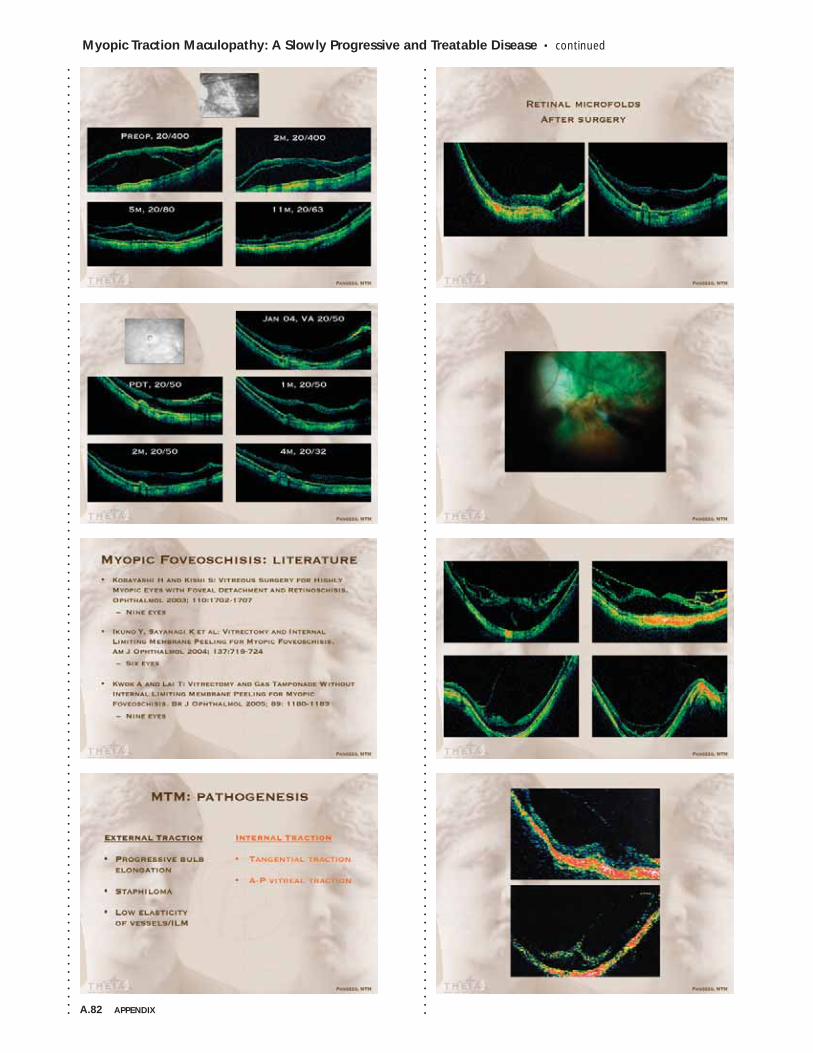
A.82 APPENDIX
Myopic Traction Maculopathy: A Slowly Progressive and Treatable Disease • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
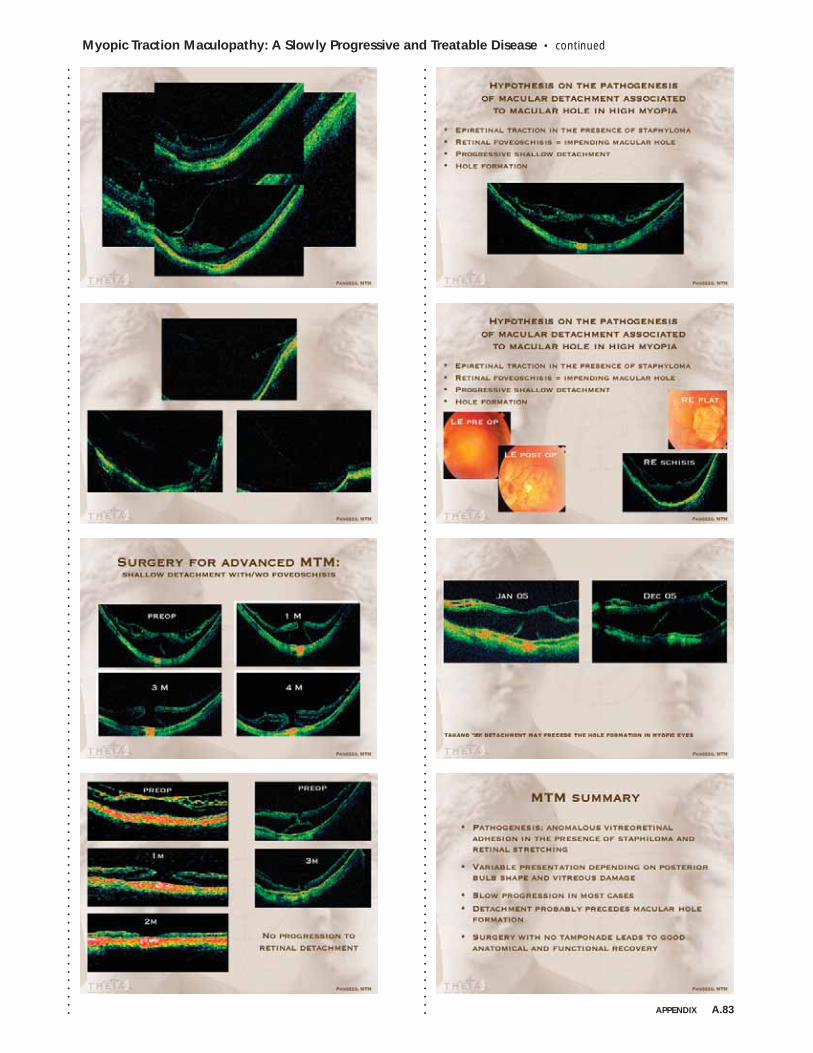
Myopic Traction Maculopathy: A Slowly Progressive and Treatable Disease • continued
APPENDIX A.83
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
A.84 APPENDIX
Diagnosis and Management of Intraocular Lymphoma • Janet L. Davis, MD
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Diagnosis and Management of Intraocular LymphomaJanet Davis, MD
Intraocular Lymphoma
● Primary intraocular lymphoma• Ocular disease only• Large percentage develop brain lyphoma• Multicentric? Metastatic? Passage through visual pathways?
● Metastatic from systemic lymphoma
Solid RPE DetachmentsSubretinal and Exudative
Clinical Diagnosis: Suspected Lymphoma
● Solid sub-RPE infiltrates● Homogeneous vitreous infiltrates
• White eye, no posterior synechiae• +/- CME • Angiographic changes
• Leopard spot• Retinal vessel staining
Non-Ocular Diagnosis
● MRI of brain and brain biopsy• Separate ocular biopsy not needed
● MRI of brain and lumbar puncture• Lumbar puncture with normal MRI unlikely to be positive
Available Ocular Testing
● Testing directed toward malignancy• Cytology, gene rearrangement, and flow cytometry
● Testing directed toward infection• Vitreous culture• PCR amplification • Intraocular antibodies
● Chorioretinal biopsy
Use of Intraocular Fluid
● Vitreous humor• Culture
• Bacterial, fungal, viral, toxoplasmosis• PCR
• Detection of foreign DNA• Detection of mutated DNA (lymphoma)
• Cytokines• IL-10 to IL-6 ratio
● Aqueous humor • Cytokines (IL-10)• PCR (viral DNA)
Use of Vitreous Cells
● Cytology – studies small• Lymphoma diagnosed in 7 of 12 pts (58%)
• Improved to 10/12 after 2 biopsies (83%) – NIH• Earliest studies only about one-third
● Flow cytometry• Uveitic and lymphomatous patterns
● Polymerase chain reaction • Gene rearrangements (clonality)• Intracellular DNA of virus or microorganism
Diagnosing Lymphoma
● Cytology is gold standard• Enhanced by preparation with cytocentrifugation• Supported by immunohistochemistry or flow cytometry
Benefits of Immunohistochemistry
● Cell-surface staining• B-cell lymphoma: kappa or lambda restriction,
reduced T cells• T-cell lymphoma: aberrant markers, reduced B cells
Cell Surface MarkersT-Lymphocyte MarkersB-Lymphocyte MarkersActivation MarkersCell Lineage MarkersPredictive Value Flow Cytometry
Molecular Biologic Approach
● B-cell lymphomas• PCR amplification of the variable region of the heavy
immunoglobulin chain• Gene rearrangement implies clonality• Kappa and lambda gene rearrangements
● T-cell lymphomas• PCR amplification of T-cell receptor gamma gene• Gene rearrangement implies clonality
Microdissection of Specimens
● Laser guided microdissection or manual method● PCR on selected cells with abnormal appearance● Possibility of diagnosis of clonality because of
small number of cells
Interleukin-10
● Interleukin-10 to Interleukin-6 ratio● Both made by B-cells
• IL-10 anti-inflammatory• IL-6 pro-inflammatory
● Extremely high levels of IL-10 reported in cases in intraocular lymphoma
● Exceptions also reported in the literature● Aqueous or vitreous humor
Diagnosis and Management of Intraocular Lymphoma • continued
APPENDIX A.85
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Retinal or Chorioretinal Biopsy
● Sub-RPE infiltrates with insignificant vitreitis• Lymphoma• Nocardia• Fungus
● Retinal infiltrates
Lymphoma without VitreitisSubretinal AspirationSub-RPE DepositsSubretinal AbscessesMaximizing Biopsy Material
● Complete unknown● Histopathology or cytology
• Infective organisms visible by microscopy • Virus visible by electron microscopy
• But may see cytopathic effect on histology• Correlates infection with host response• Detects granulomatous inflammation or other
key features
Maximizing Biopsy Material
● Infection strongly suspected● Culture
• Full culture requires selective media• Minimal array: Thioglycolate broth and MRC-5 cell line
• May miss fungi, anaerobes, tuberculosis
Maximizing Biopsy Material
● Infection strongly suspected● PCR or in situ hybridization or immunohistopathology
• Organisms stipulated before test• Efficient, but impossible to test everything• Some global testing strategies
• 16S ribosome (pan bacterial)• Pan fungal strategies
Expected ResultsPublished Series
● Verbraeken 1996: 25 patients• 8 pts (32%) diagnosable • 3 infections, 5 malignancy• 4 other with visible characteristic lesions
● Green 1995: 405 consecutive cases• 53% for suspected endophthalmiitis• + cytology in 48.3% of 87 patients suspected of
intraocular lymphoma
Published Series
● Mruthyunjaya Ophthalmology 2002• 87 patients, 90 eyes over 10 years• 71 eyes had indication of possible malignancy
• 83% cytopathology• 43% microbiologic culture, 14% T. Canis antibody• 36% PCR
• Specific cause determined in 35 eyes (39%)• 42% of those with indication of infection• 10% of those with indication of possible lymphoma
(7 of 71)● Davis AJO 2005● 48 of 78 (61.5%) confirmed by PPV● Distribution of final diagnoses
• 23% lymphoma• 19% chronic endophthalmitis• 14% atypical chorioretinitis• 15% chronic post-op infection• 28% immunologically mediated uveitis
● 13 of 28 patients operated for suspected lymphomadiagnosed by vitreous testing (46%)
● 13 of 17 patients with a final diagnosis of lymphomadiagnosed by vitreous testing (77%)
Case Series: Diagnostic Vitrectomy
● Performed to detect lymphoma or chronic intraocular infection masquerading as an immunologically mediated uveitis
● Prior case series:• Palexas and Green, 112+ pts, 1995 63%• Verbraeken, 26 pts, 1996 32%• Akpek and Foster, 26 pts, 1999 42%• Mruthyunjaya and Jaffe, 87 pts, 2002 39%• Davis, Miller, Ruiz, 78 pts, 2005 62%
Yields for Lymphoma Diagnosis
● Number of positive diagnoses/number operated for suspected lymphoma• Palexas and Green, 87 pts, 1995 48%• Mruthyunjaya, 71 pts, 2002 10%• Davis, 2005
• 28 pts suspected of lymphoma 46%• 17 pts known to have lymphoma 77%
Treatment
● Previous treatment consisted of knee-jerk ocular irradiation• In some cases, brain and neuro-axis as well
● Ocular irradiation does not modify course of diseaseregarding brain involvement
● Brain irradiation an insufficient treatment for primary CNS lymphoma
A.86 APPENDIX
Diagnosis and Management of Intraocular Lymphoma • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
More Current Treatment
● Modified lymphoma protocols with intrathecal chemo• Poor penetration into CNS
● High dose methotrexate• Better tolerability than most chemo• Use of high dose pushes drug into the CNS
Treatment
● Rituximab and temazolamide● Mannitol to open blood brain barrier with intraarterial
ARA-C and methotrexate• Not used for treatment of eyes• Combined with intravitreal methotrexate injection
● Intravitreal injection of methotrexate as primary therapy
Conclusions: Different Viewpoints
● Ophthalmologist• PIOL is lymphoma• Brain will eventually be involved: treat it• LP unlikely to be positive if MRI is normal• Vision needs to be considered• I can evaluate but not treat
● Oncologist• PIOL might be lymphoma• If brain not involved, irradiate the eyes• Of course you need a lumbar puncture• Only treatment of malignancy important• I can treat but not evaluate
Conclusions: Diagnosis
● Cytology is gold standard● T-cell, B-cell, kappa, lambda only● Molecular tests experimental● Negative MRI means no brain involvement● Cytology conclusive in only 30%-80%● Full panel flow cytometry● Molecular tests may be new gold standard● MRIs don’t show diffuse infiltrates
Conclusions: Treatment
● Ocular irradiation is effective● No chemotherapy for PIOL without brain involvement● Modified CHOP or methotrexate only● Ocular irradiation works temporarily● Chemotherapy for PIOL may kill non-imageable CNS cells● Innovative regimens may have a place
An Illustrative Case
● 64 yo male with floaters in the left eye for one year• Previously treated with oral and intravitreal steroids.
Now beginning to see floaters in right eye.• No cell in anterior chambers
Blurred Vision Left EyeDiagnostic Vitrectomy
● Cytology negative● 2:1 kappa:lambda ratio (3:1 diagnostic for B cell
lymphoma)● Gene rearrangements in T-cell receptor region and
B-cell IgH region● Treatment with high dose methotrexate requested.
Oncologist agreed. Patient refused.
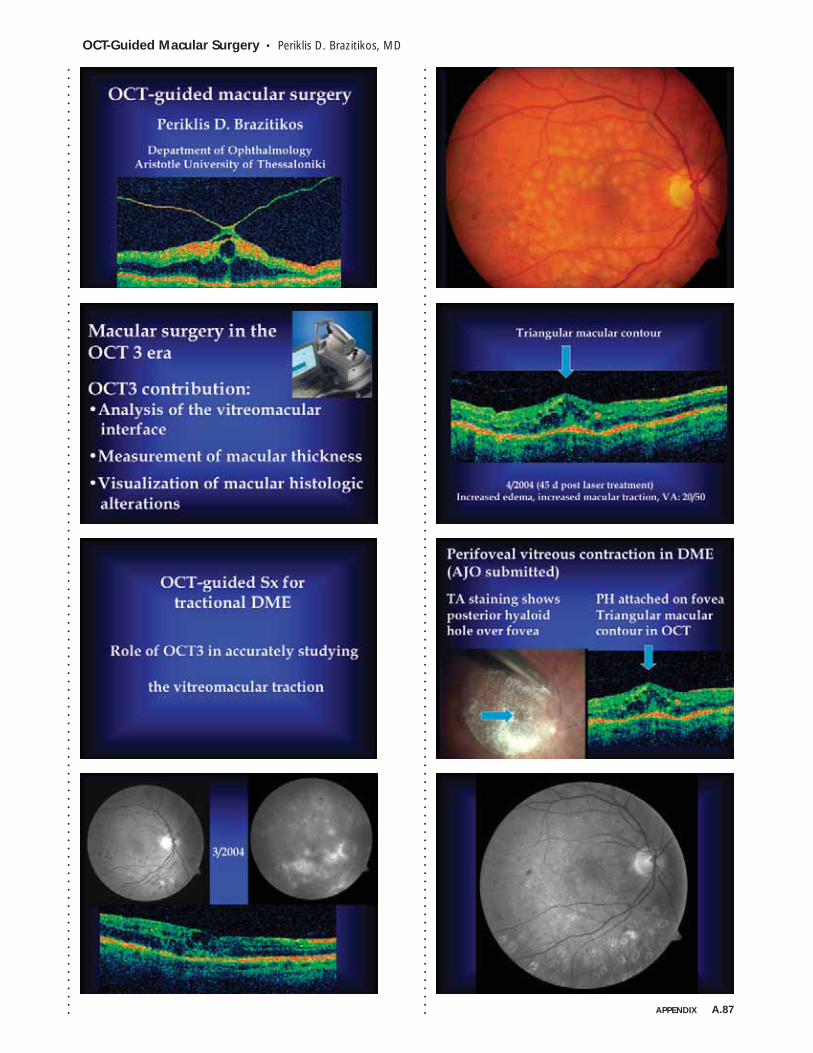
OCT-Guided Macular Surgery • Periklis D. Brazitikos, MD
APPENDIX A.87
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
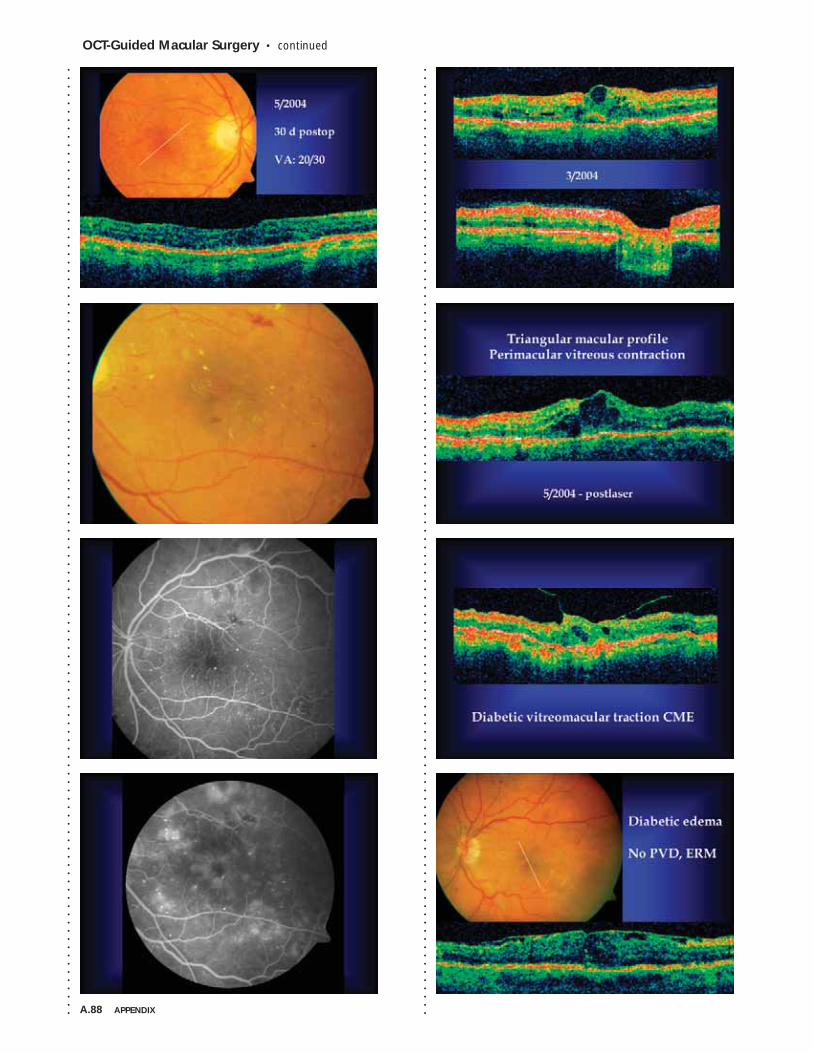
A.88 APPENDIX
OCT-Guided Macular Surgery • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
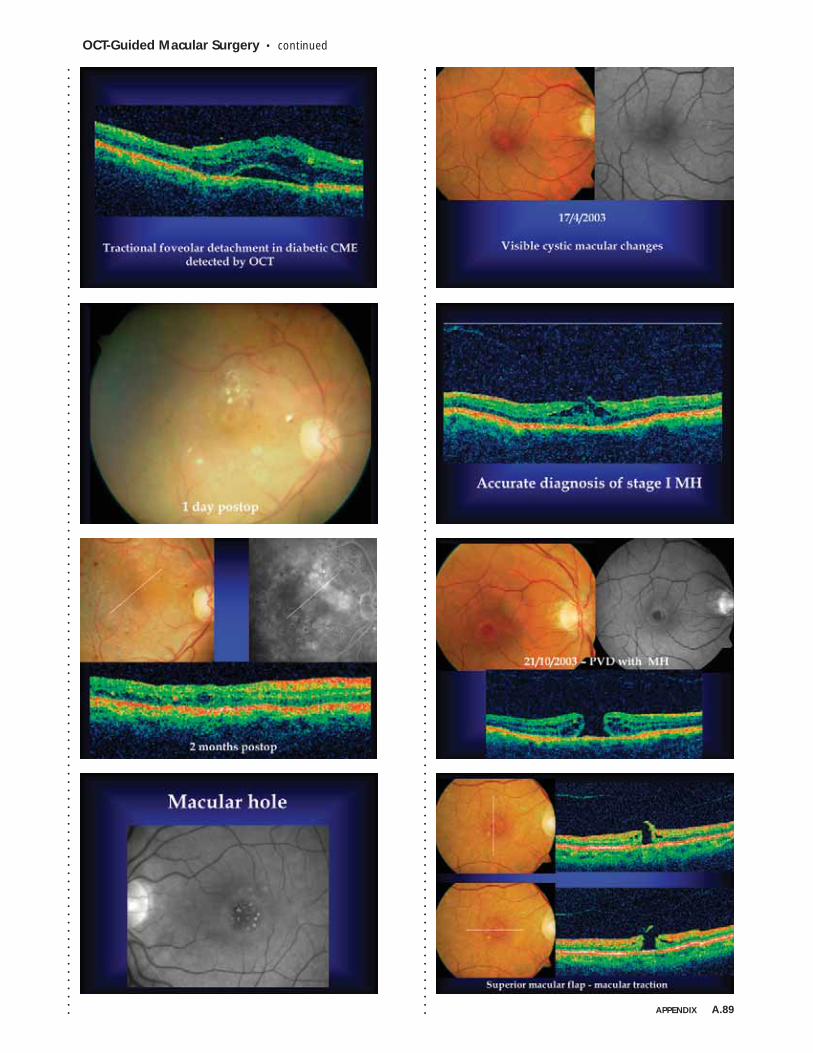
OCT-Guided Macular Surgery • continued
APPENDIX A.89
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
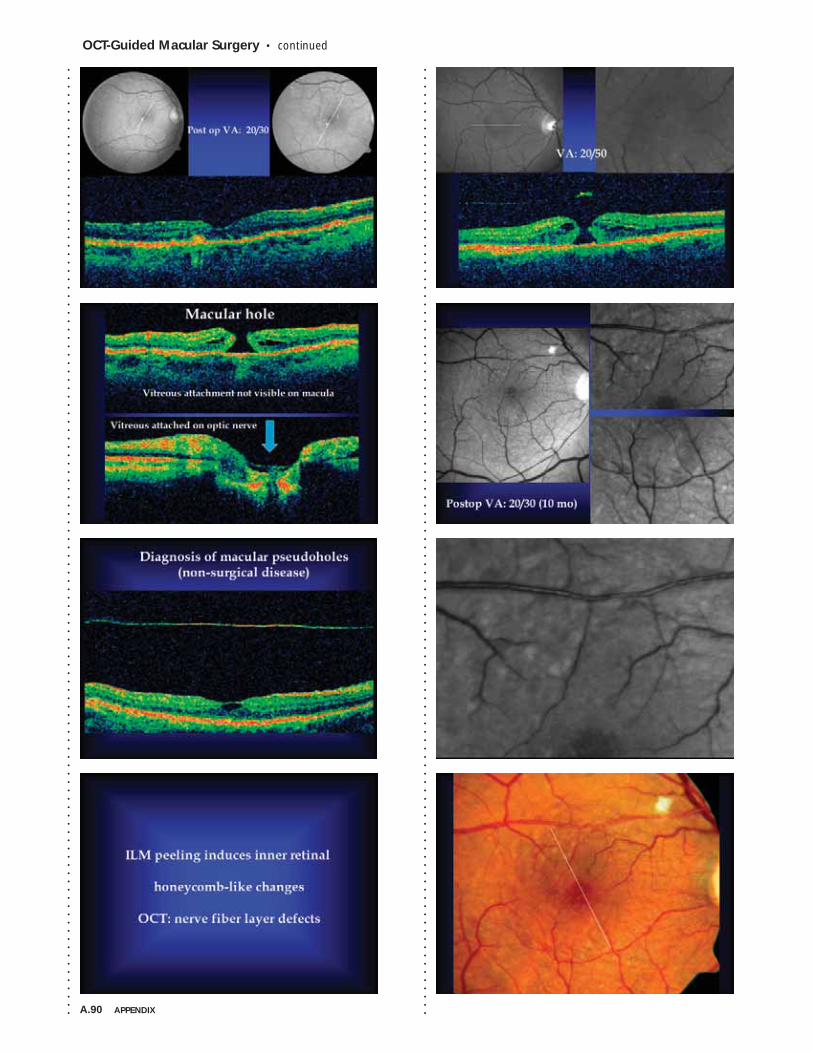
A.90 APPENDIX
OCT-Guided Macular Surgery • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
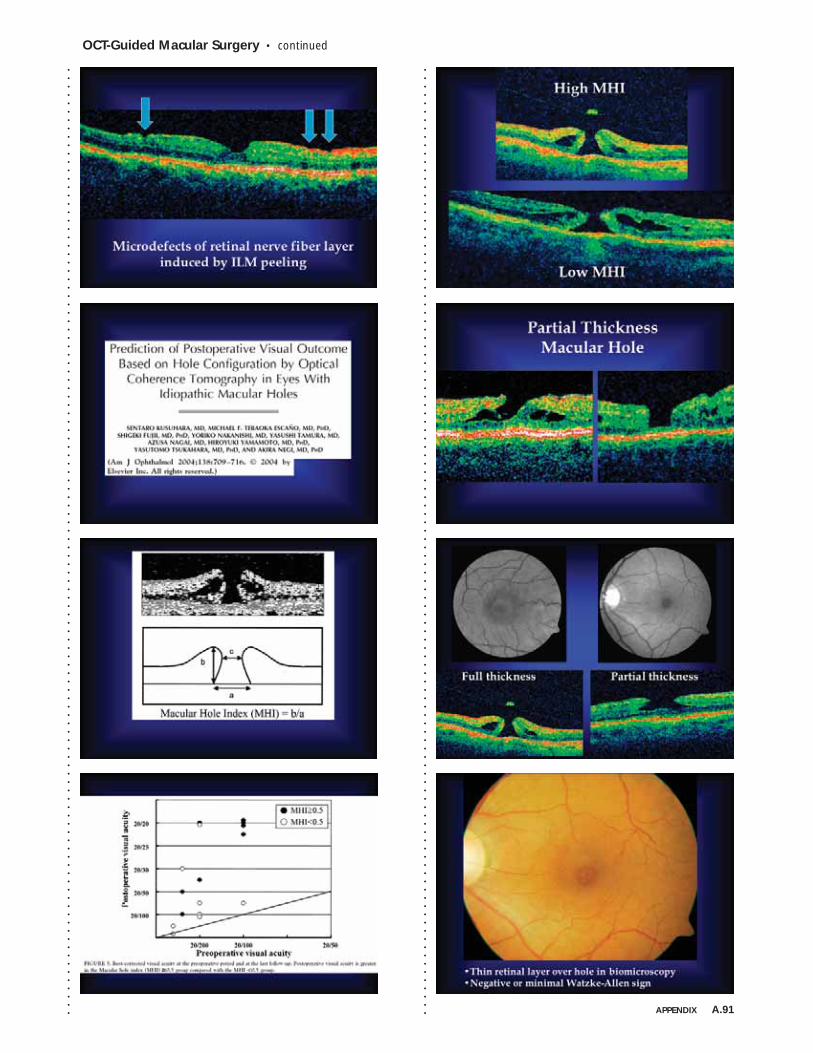
OCT-Guided Macular Surgery • continued
APPENDIX A.91
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
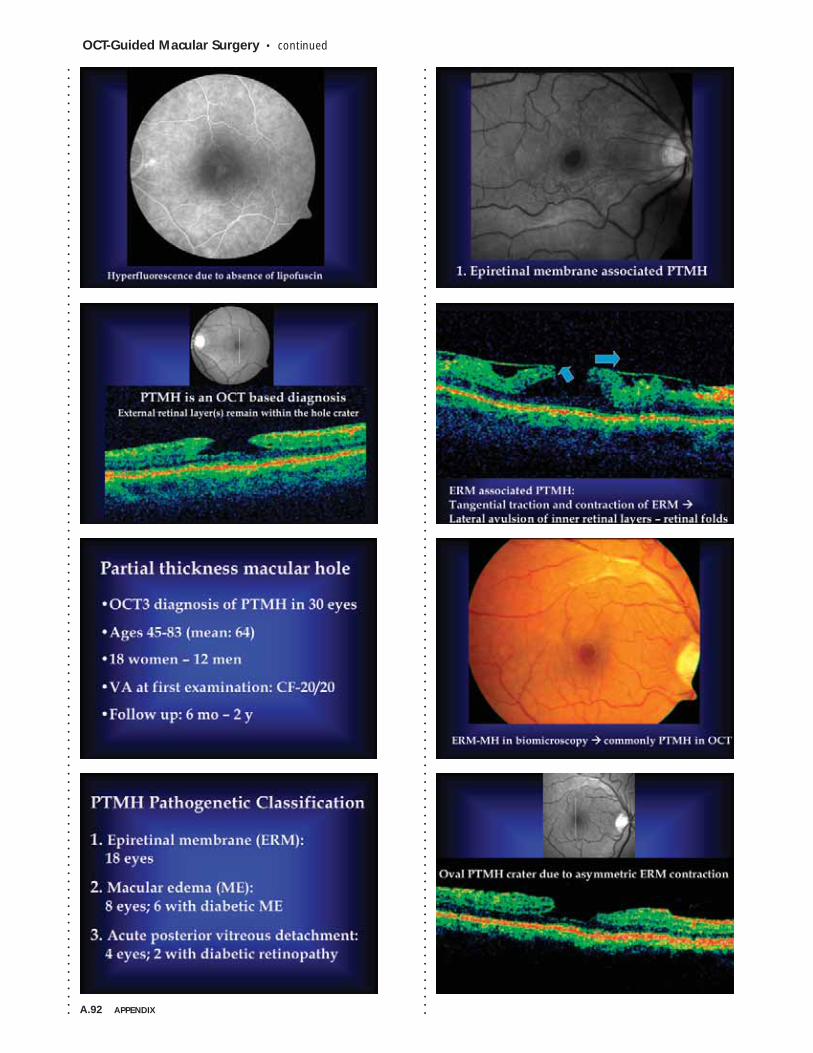
A.92 APPENDIX
OCT-Guided Macular Surgery • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
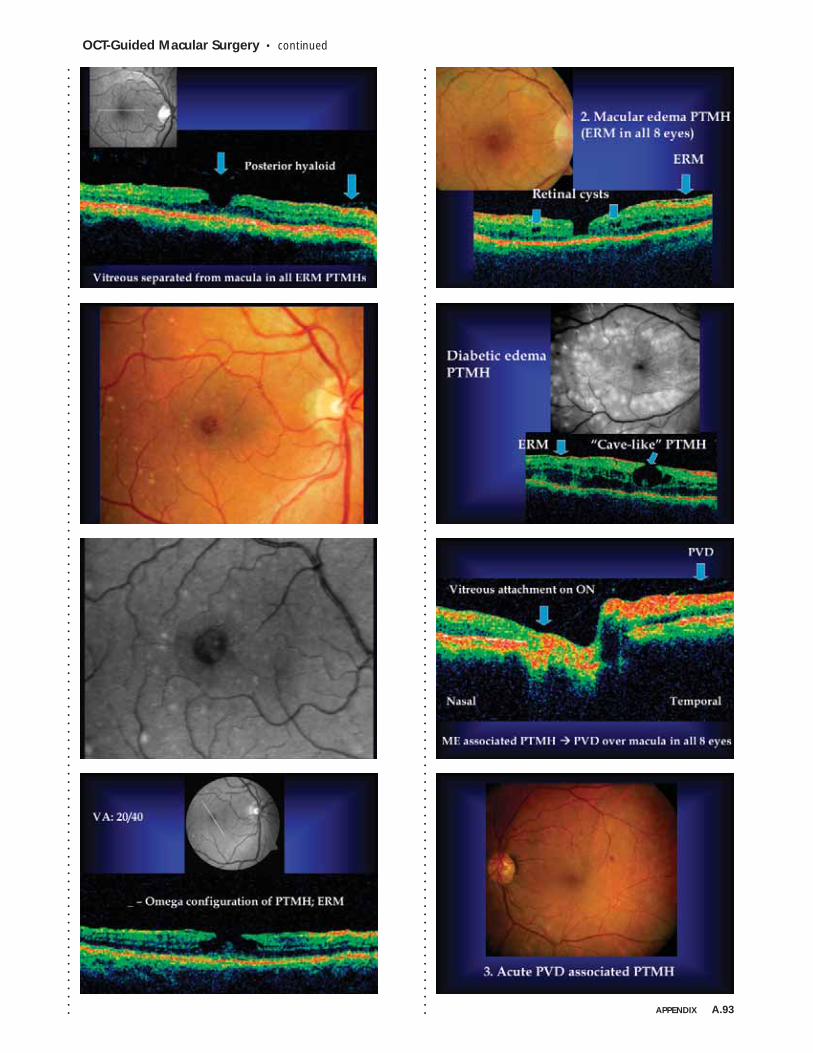
OCT-Guided Macular Surgery • continued
APPENDIX A.93
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
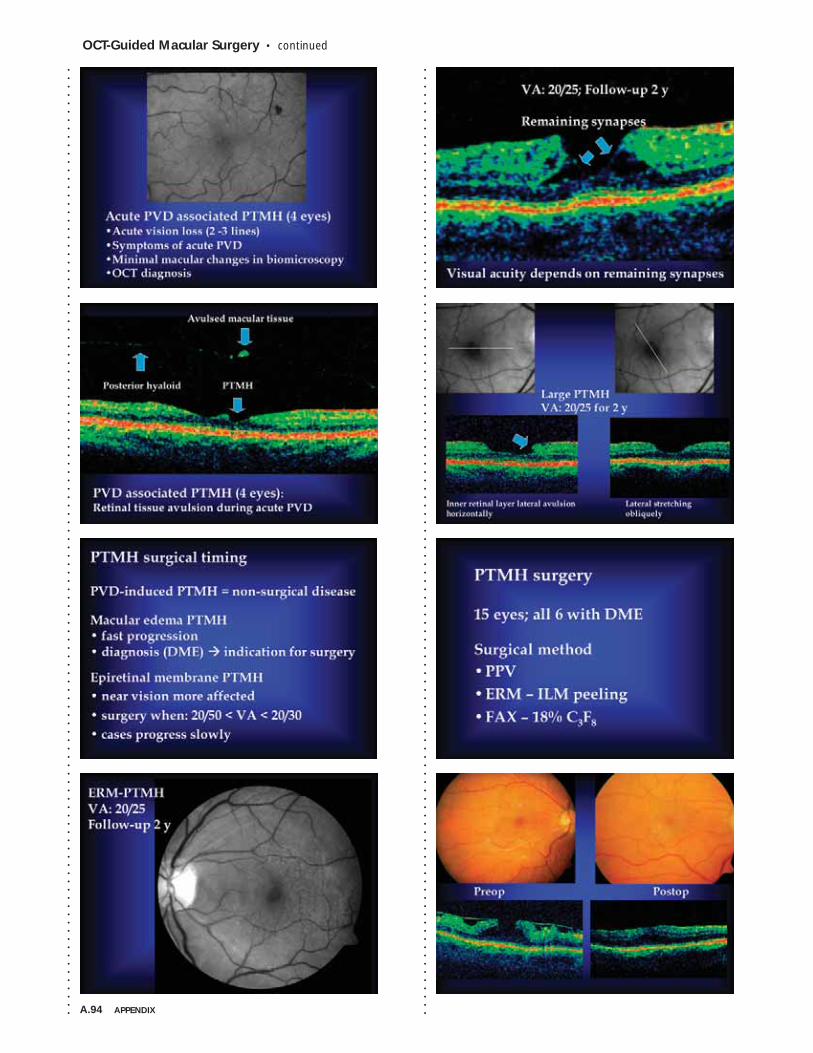
A.94 APPENDIX
OCT-Guided Macular Surgery • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
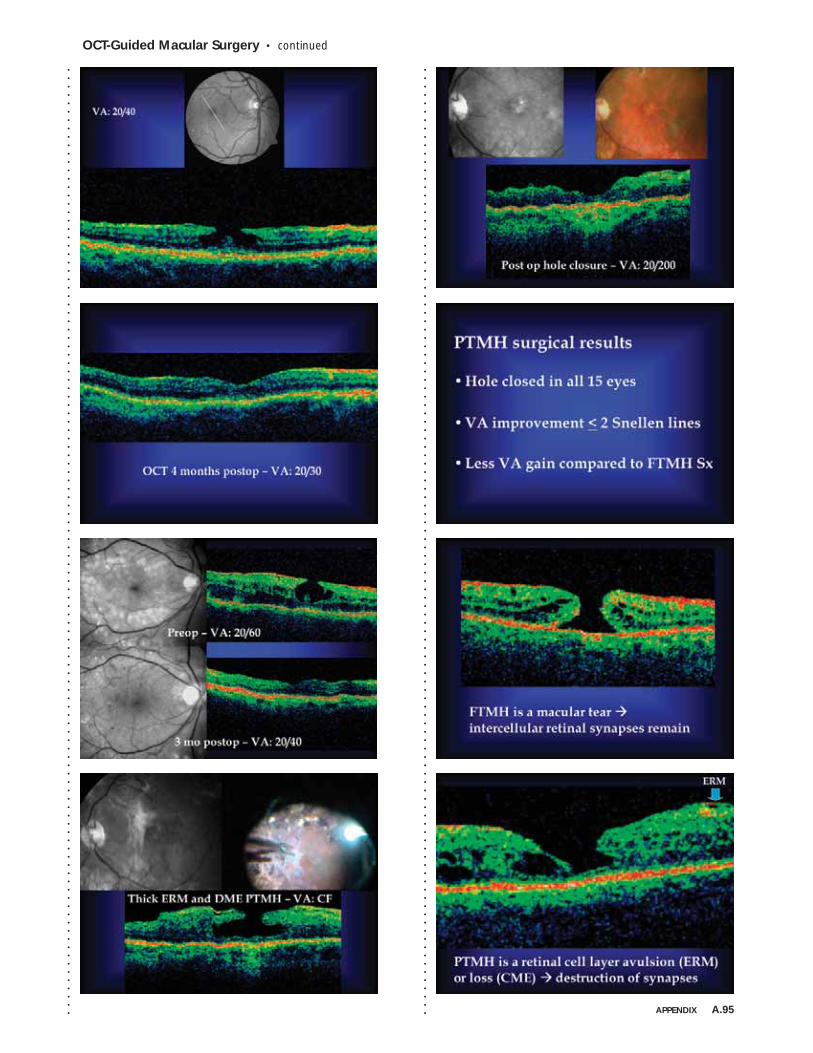
OCT-Guided Macular Surgery • continued
APPENDIX A.95
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
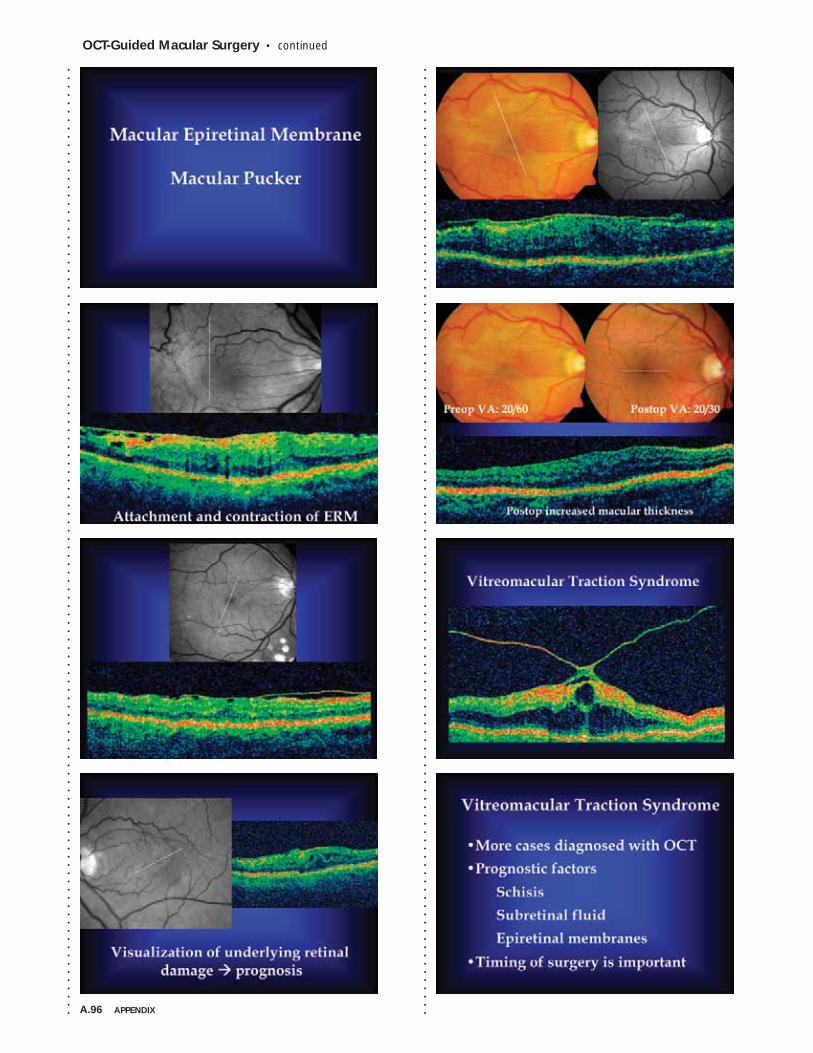
A.96 APPENDIX
OCT-Guided Macular Surgery • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
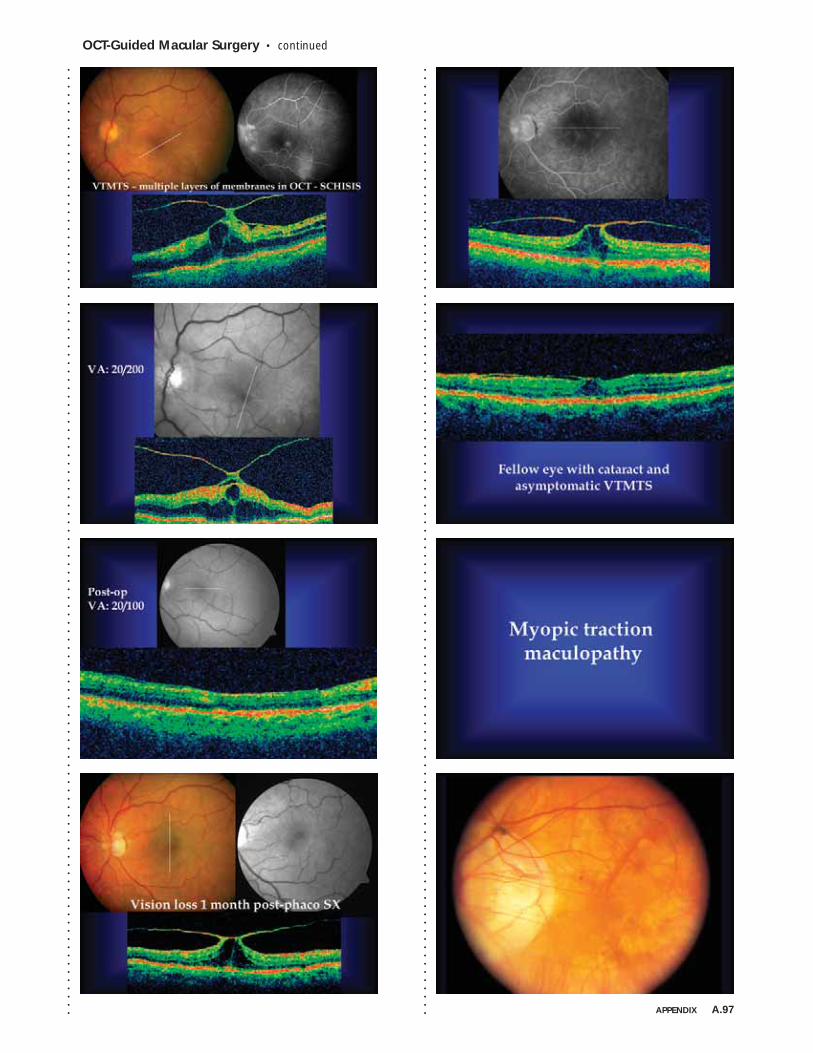
OCT-Guided Macular Surgery • continued
APPENDIX A.97
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
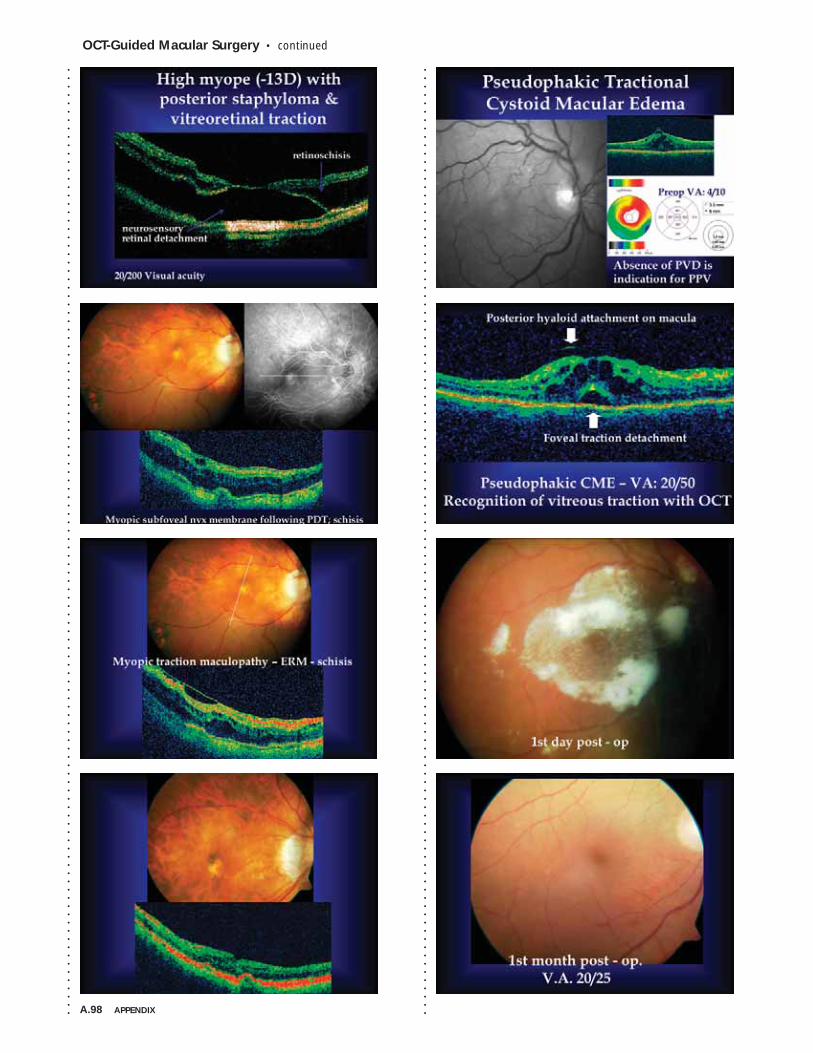
A.98 APPENDIX
OCT-Guided Macular Surgery • continued
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
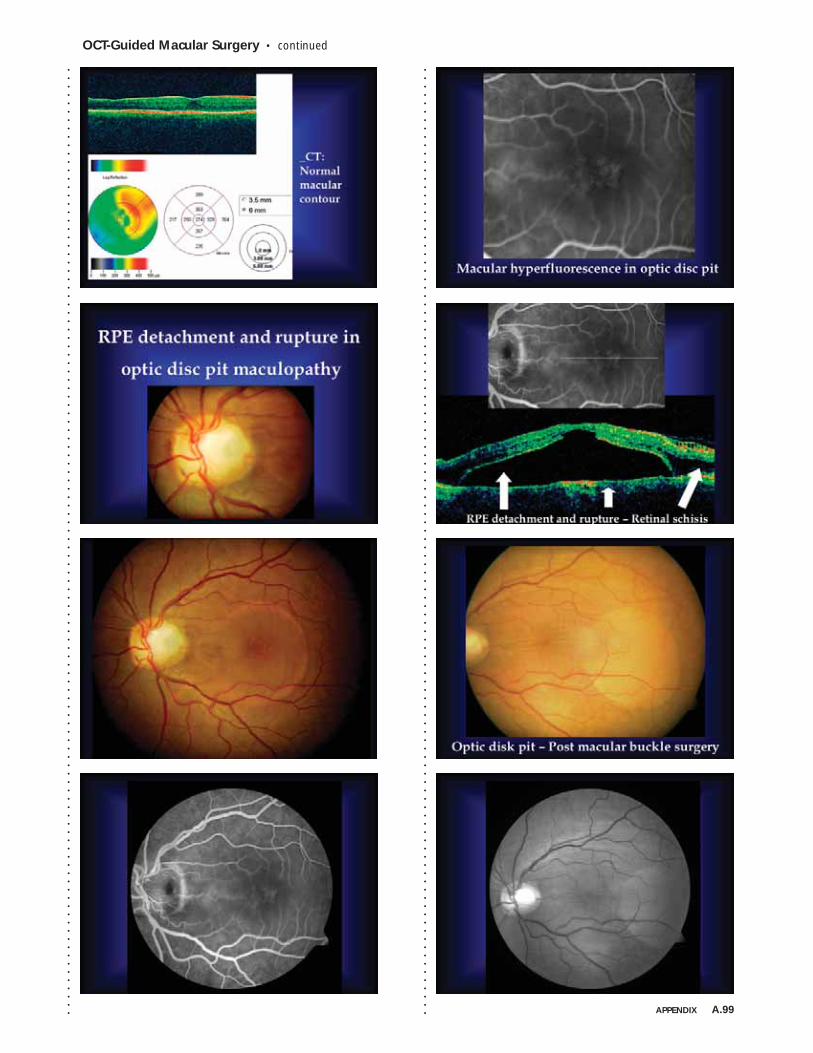
OCT-Guided Macular Surgery • continued
APPENDIX A.99
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
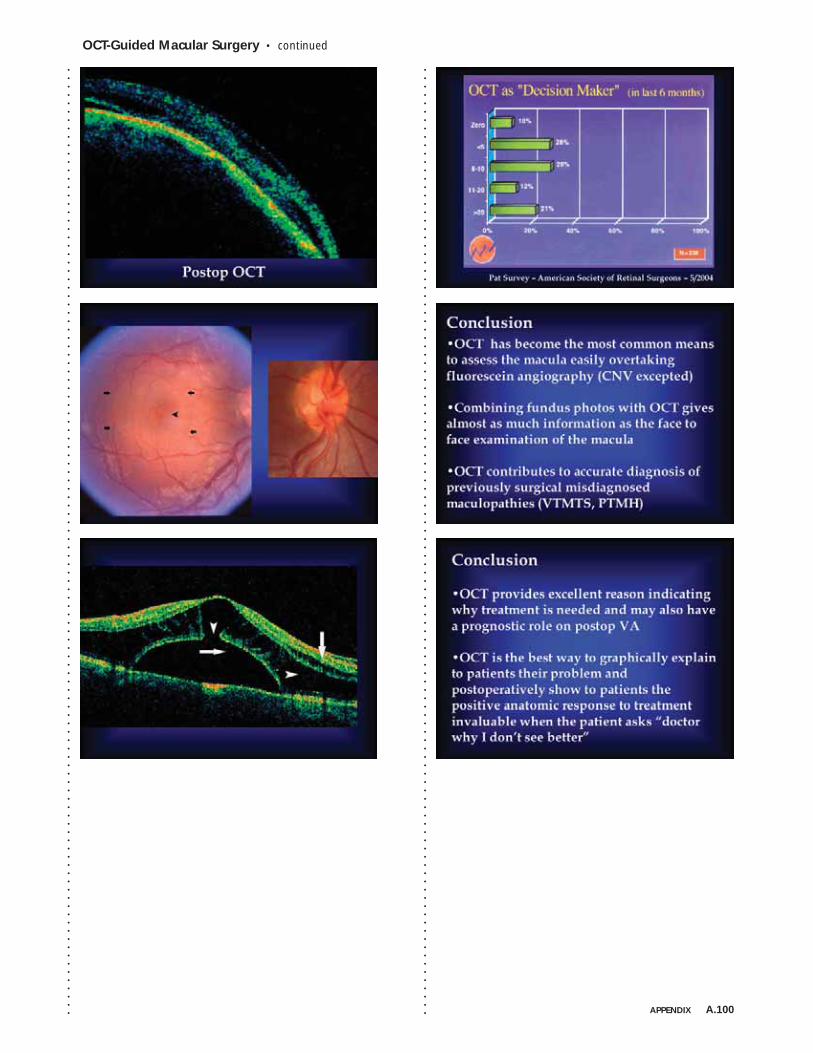
OCT-Guided Macular Surgery • continued
APPENDIX A.100
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . .
Dear Aspen Retinal Detachment Society Participant,
This year we are delighted to offer you this booklet of notes, supplemented
by the majority of slide presentations (edited), from our recent meeting.
The notes were taken and assembled by two young, talented, rising retinal
stars – Drs. Paul Chan and Andrew Moshfeghi – who attended every talk
and captured the essence of the vigorous post-talk discussion, for which the
ARDS is deservedly famous.
This work was made possible by an educational grant graciously provided
by Genentech, Inc. which supported not only the production costs of the
booklet, but also provided a stipend so that these two young physicians might
attend and participate in this exciting meeting.
We are grateful to Genentech, to Drs. Chan and Moshfeghi, and to all of you
for contributing to the intellectual vibrancy of ARDS. We hope you will find
this booklet interesting, and also of value to you in the care of your patients.
Please join us March 4-8, 2007 for the 35th Annual ARDS Meeting.
Sincerely,
Donald J. D’Amico, MD William O. Edward, MD Timothy G. Murray, MD
34thAnnual
Aspen RetinalDetachment Society
Meeting
JOINTLY SPONSORED BY THE ASPEN RETINAL DETACHMENT SOCIETY AND THE SPOKANE COUNTY MEDICAL SOCIETY
MARCH 5–9, 2006 • SNOWMASS VILLAGE, COLORADO
35thAnnual
Aspen RetinalDetachment Society
Meeting
March 4-8, 2007Snowmass Conference
Center
MEDICAL CONFERENCE PLANNERS, INC.1251 Post Road, Scarsdale, NY10583
914-722-0664
www.medconfs.com
For Information
2007Save the
Date
M A R C H 5 - 9 , 2 0 0 6 • S N O W M A S S , C O L O R A D O
2006
Aspen RetinalDetachment Society
Meeting Notes
ARDS
34thAnnual
MEDICAL CONFERENCE PLANNERS, INC.
1251Post Road, Scarsdale, NY10583
914-722-0664 phone
914-722-0465 fax
www.medconfs.com
The ARDS wishes to acknowledge
Genentech, Inc., whose generous gift
made the publication of
this book possible.
Aspen R
etinal Detachm
ent Society Meeting N
otes 2006





























