Embed Size (px)
Citation preview

IN THE CHANCERY COURT FOR WILLIAMSON COUNTY, TENNESSEE AT FRANKLIN
CITIZENS FOR LIMITED ) GOVERNMENT AND ) CONSITUTIONAL INTEGRITY, INC., ) d/b/a TENNESSEE ST ANDS, et al., )
Plaintiffs, v.
ROGERS C. ANDERSON, in his official capacity as Mayor of Williamson County, Tennessee, and WILLIAMSON COUNTY, TENNESSEE,
Defendants.
) ) ) ) ) ) ) ) ) ) )
Case No. 20CV-49908B Judge Binkley
APPENDIX TO JAMES R. CASCIANO'S DECLARATION OF SCIENTIFIC STUDIES and ARTICLES
APPENDIX TO JAMES R. CASCIANO DECLARATION- 1

TABLE OF CONTENTS
Document Page
Scientific Brief: Community Use of Cloth Masks to Control the Spread ofSARS-CoV-2, Center for Disease Control and Prevention (November 20, 2020) ................................................................................... 5
Mask Facts, Association of American Physicians and Surgeon (September 26, 2020) ............................................................................................................ 15
Mask Use In The Context Of COVID-19, World Health Organization (December 1, 2020) ................................................................. .48
Effectiveness of Adding a Mask Recommendation to Other Public Health Measures to Prevent SARS-Co V-2 Infection in Danish Mask Wearers: A randomized Controlled Trial, ANNALS OF INTERNAL MEDICINE (November 18, 2020) ............................................. 70
Reduction Of Secondary Transmission Of SARS-Cov-2 In Households By Face Mask Use, Disinfection And Social Distancing: A Cohort Study In Beijing, China, BRITISH JOURNAL OF MEDICINE {May 28, 2020) ................................................................... 73
Case-Control Study of Use of Personal Protective Measure and Risk/or SARS-CoV-2 Infection, Thailand, Center for Disease Control and Prevention (November 2020) .............................................. 85
Physical Interventions To Interrupt Or Reduce The Spread Of Respiratory Viruses, Institute For Evidence-Based Healthcare, Bond University (November 20, 2020) ................................................................................. 98
Nonpharmaceutica/ Measures for Pandemic Influenza in Nonhea/thcare Settings - Personal Protective and Environmental Measures, Centers for Disease Control and Prevention (May 2020) ...................................................... 103
A Cluster Randomized Trial Of Cloth Masks Compared With Medical Masks In Healthcare Workers, British Journal Open, (April 2015) ........................................................................................ 110
APPENDIX TO JAMES R. CASCIANO DECLARATION- 2

Household Transmission of SARS-Co V-2, JOURNAL OF AMERICAN MEDICAL ASSOCIATION (December 14, 2020) ............................................................................................................. 128
Post-Lockdown SARS-Cov2 Nucleic Acid Screening In Nearly Ten Million Residents Of Wuhan, China, Nature Communications (November 20, 2020) .................................................................... 160
Guidance on Preparing Workplaces for COVJD-19 U.S. Occupational Safety and Health Administration .......................................................... 186
Rational Use Of Face Masks In The COVJD-19 Pandemic, UK MEDICAL JOURNAL LANCET (March 20, 2020) ............................................................... 221
Double Dutch Face Masks Are 'NOT Necessary' And Could Even Harm The Fight Against Coronavirus, Say Holland's Top Scientists, The Sun (August 2, 2020) ..................................................... 227
Predominant Role of Bacterial Pneumonia as a Cause of Death in Pandemic Influenza: Implications for Pandemic Influenza Preparedness THE JOURNAL OF INFECTIOUS DISEASE (October 2008) ......................................................... 234
When Mask-Wearing Rules in the 1919 Pandemic Faced Resistance, Becky Little (May 6, 2020) ..................................................................... 312
Do Facemasks Limit the Contamination/Spread of Respiratory Viruses? Admin-Spiralab, University of Sao Paulo, Bacterial Genetics Lab (July 27, 2020) ......................................... 319
Rapid Expert Consultation on the Effectiveness of Fabric Masks for the COVID-19 Pandemic, The National Academies of Sciences Engineering Medicine, April 8, 2020) ....................... 326
A Quantitative Assessment of the Total Inward Leakage of NaCl Aerosol Representing Submicron-Size Bioaerosol Through N95Filtering Facepiece Respirators and Surgical Masks, JOURNALOFOCCUPATIONALANDENVIRONMENTALHYGIENE (May 9, 2014) ...................... 342
Mask Use In The Context Of COVID-19, World Health Organization (December 1, 2020) .................................................................. 364
The Psychological Impact Of The COVID-19 Epidemic On College Students
APPENDIX TO JAMES R. CASCIANO DECLARATION- 3

In China, PSYCHIATRY RESEARCH (2020) ............................................................................ 22
Coronavirus Having Major Impact On Young People With Mental Health Needs -New Survey, YoungMinds, March 30, 2020 ...................................................................... 23
APPENDIX TO JAMES R. CASCIANO DECLARATION-4

Scientific Brief: Community Use of Cloth Masks to Control the Spread of SARS-CoV-2 Background
SARS-CoV-2 infection is transmitted predominately by respiratory droplets
generated when people cough, sneeze, sing, talk, or breathe. CDC
recommends community use of masks, specifically non-valved multi-layer
cloth masks, to prevent transmission of SARS-CoV-2. Masks are primarily
intended to reduce the emission of virus-laden droplets ("source control"),
which is especially relevant for asymptomatic or presymptomatic infected
wearers who feel well and may be unaware of their infectiousness to others,
and who are estimated to account for more than 50% of transmissions. 1,2
Masks also help reduce inhalation of these droplets by the wearer
("filtration for personal protection"). The community benefit of masking for
SARS-CoV-2 control is due to the combination of these effects; individual
prevention benefit increases with increasing numbers of people using
masks consistently and correctly.
Source Control to Block Exhaled Virus
Multi-layer cloth masks block release of exhaled respiratory particles into
the environment, 3-6 along with the microorganisms these particles carry.7•8
Cloth masks not only effectively block most large droplets (i.e., 20-30
microns and larger)9 but they can also block the exhalation of fine droplets
and particles (also often referred to as aerosols) smaller than 10 microns
;3,5 which increase in number with the volume of speech 10-12 and specific
types of phonation. 13 Multi-layer cloth masks can both block up to 50-70%
of these fine droplets and particles 3,14 and limit the forward spread of those
that are not captured. 5,6,15,16 Upwards of 80% blockage has been achieved
APPENDIX TO JAMES CASCIANO DECLARATION-5

in human experiments that have measured blocking of all respiratory
droplets, 4 with cloth masks in some studies performing on par with surgical
masks as barriers for source control. 3,9,14
Filtration for Personal Protection
Studies demonstrate that cloth mask materials can also reduce wearers'
exposure to infectious droplets through filtration, including filtration of fine
droplets and particles less than 10 microns. The relative filtration
effectiveness of various masks has varied widely across studies, in large
part due to variation in experimental design and particle sizes analyzed.
Multiple layers of cloth with higher thread counts have demonstrated
superior performance compared to single layers of cloth with lower thread
counts, in some cases filtering nearly 50% of fine particles less than 1
micron .14,17-29 Some materials (e.g., polypropylene) may enhance filtering
effectiveness by generating triboelectric charge {a form of static electricity)
that enhances capture of charged particles 18,30 while others (e.g., silk) may
help repel moist droplets 31 and reduce fabric wetting and thus maintain
breathability and comfort.
Human Studies of Masking and SARS-CoV-2 Transmission
Data regarding the "real-world" effectiveness of community masking are
limited to observational and epidemiological studies.
An investigation of a high-exposure event, in which 2 symptomatically ill hair stylists interacted for an average of 15 minutes with each of 139 clients
during an 8-day period, found that none of the 67 clients who subsequently
consented to an interview and testing developed infection. The stylists and
all clients universally wore masks in the salon as required by local ordinance
and company policy at the time.32
In a study of 124 Beijing households with> 1 laboratory-confirmed case of
APPENDIX TO JAMES CASCIANO DECLARATION-6

SARS-CoV-2 infection, mask use by the index patient and family contacts
before the index patient developed symptoms reduced secondary
transmission within the households by 79%.33
A retrospective case-control study from Thailand documented that, among
more than 1,000 persons interviewed as part of contact tracing
investigations, those who reported having always worn a mask during high
risk exposures experienced a greater than 70% reduced risk of acquiring
infection compared with persons who did not wear masks under these
circumstances. 34
A study of an outbreak aboard the USS Theodore Roosevelt, an
environment notable for congregate living quarters and close working
environments, found that use of face coverings on-board was associated
with a 70% reduced risk. 35
Investigations involving infected passengers aboard flights longer than 10
hours strongly suggest that masking prevented in-flight transmissions, as
demonstrated by the absence of infection developing in other passengers
and crew in the 14 days following exposure.36,37
Seven studies have confirmed the benefit of universal masking in
community level analyses: in a unified hospital system,38 a German city,39 a
U.S. state,40 a panel of 15 U.S. states and Washington, D.C.,41,42 as well as
both Canada43 and the U.S.44 nationally. Each analysis demonstrated that,
following directives from organizational and political leadership for universal
masking, new infections fell significantly. Two of these studies 42,44 and an
additional analysis of data from 200 countries that included the U.S.45 also
demonstrated reductions in mortality. An economic analysis using U.S. data
found that, given these effects, increasing universal masking by 15% could
prevent the need for lockdowns and reduce associated losses of up to $1
trillion or about 5% of gross domestic product. 42
Conclusions
Experimental and epidemiological data support community masking to
APPENDIX TO JAMES CASCIANO DECLARATION-7

reduce the spread of SARS-CoV-2. The prevention benefit of masking is
derived from the combination of source control and personal protection for
the mask wearer. The relationship between source control and personal
protection is likely complementary and possibly synergistic 14, so that
individual benefit increases with increasing community mask use. Further
research is needed to expand the evidence base for the protective effect of
cloth masks and in particular to identify the combinations of materials that
maximize both their blocking and filtering effectiveness, as well as fit,
comfort, durability, and consumer appeal. Adopting universal masking
policies can help avert future lockdowns, especially if combined with other
non-pharmaceutical interventions such as social distancing, hand hygiene,
and adequate ventilation.
References
1 . Moghadas SM, Fitzpatrick MC, Sah P, et al. The implications of silent
transmission for the control of COVID-19 outbreaks. Proc Natl Acad Sci
US A. 2020;117(30):17513-17515.10.1073/pnas.2008373117.
b!1P£.fLwww. ncbi. n Im. n i h .gov LP-LI bmed/.3 26 32012.
2. Johansson MA, Quandelacy TM, Kada S, et al. Controlling COVID-19
requires preventing SARS-CoV-2 transmission from people without
symptoms. submitted. 2020.
3. Lindsley WG, Blachere FM, Law BF, Beezhold DH, Noti JD. Efficacy of
face masks, neck gaiters and face shields for reducing the expulsion of
simulated cough-generated aerosols. medRxiv. 2020.
httQs:/.Ldoi .orgL10.1101L2020.10.05.20207241.
4. Fischer EP, Fischer MC, Grass D, Henrion I, Warren WS, Westman E.
Low-cost measurement of face mask efficacy for filtering expelled
droplets during speech. Sci Adv. 2020;6(36).10.1126/sciadv.abd3083.
b!1P£fLwww.ncbi.nlm.njh,govLP-.ubmed/.32917603. 5. Verma S, Dhanak M, Frankenfield J. Visualizing the effectiveness of
face masks in obstructing respiratory jets. Phys Fluids (1994).
2020;32 ( 6) :061708.10.1063/5.0016018.
APPENDIX TO JAMES CASCIANO DECLARATION-8

http_s:1/.www.ncbi.nlm.nih.govLp_ubmedL32624649.
6. Bahl P, Bhattacharjee S, de Silva C, Chughtai AA, Doolan C, MacIntyre
CR. Face coverings and mask to minimise droplet dispersion and
aerosolisation: a video case study. Thorax. 2020;75(11):1024-
1025.10.1136/thoraxjnl-2020-215748.
http_s:L/.www.ncbi.nlm.nih.gov/.p_ubmed/.32709611.
7. Davies A, Thompson KA, Giri K, Kafatos G, Walker J, Bennett A. Testing
the efficacy of homemade masks: would they protect in an influenza
pandemic? Disaster Med Public Health Prep. 2013;7(4):413-
418.10.1017/dmp.2013.43.
http_s:1/.www.ncbi.nlm.nih.govLp_ubmedL24229526.
8. Leung NHL, Chu DKW, Shiu EYC, et al. Respiratory virus shedding in
exhaled breath and efficacy of face masks. Nature Medicine.
2020;26(5) :676-680.http_s:L/.dx.doi .org/.10.1038/.s41591-020-0843-2.
9. Bandiera L., Pavar G., Pisetta G., et al. Face coverings and respiratory
tract droplet dispersion. medRxiv. 2020.10.1101/2020.08.11.20145086.
https:l/.doi.org/.10.1101/.2020.08.11.20145086.
10. Alsved M, Matamis A, Bohlin R, et al. Exhaled respiratory particles
during singing and talking. Aerosol Sci Technol.
2020.10.1080/02786826.2020.1812502.
11. Asadi S, Wexler AS, Cappa CD, Barreda S, Bouvier NM, Ristenpart WD.
Aerosol emission and superemission during human speech increase
with voice loudness. Sci Rep. 2019;9(1):2348.10.1038/s41598-019-
38808-z. http_s:L/.www.ncbi.nlm.nih.gov/.p_ubmed/.30787335.
12. Morawska L., Johnson GR, Ristovski ZD, et al. Size distribution and
sites of origin of droplets expelled from the human respiratory tract
during expiratory activities. Aerosol Sci. 2009;40(3):256-269.
https:1/.www.sciencedirect.comLscience/.article/.pii/.S002185020800203
6. 13. Abkarian M, Mendez S, Xue N, Yang F, Stone HA. Speech can produce
jet-like transport relevant to asymptomatic spreading of virus. Proc
Natl Acad Sci US A. 2020;117(41):25237-
APPENDIX TO JAMES CASCIANO DECLARATION-9

25245.10.1073/pnas.2012156117.
httgs :L/.www. ncbi. n Im. n i h .gov /.gu bmed/.3 297 8 2 97.
14. Ueki H, Furusawa Y, lwatsuki-Horimoto K, et al. Effectiveness of Face
Masks in Preventing Airborne Transmission of SARS-CoV-2. mSphere.
2020; 5 ( 5) .10.1128/mSphere.00637-20.
httgs:L/.www.ncbi.nlm.nih.gov/.gubmed/.33087517.
15. Rodriguez-Palacios A, Cominelli F, Sasson AR, Pizarro TT, Ilic S. Textile
Masks and Surface Covers-A Spray Simulation Method and a
"Universal Droplet Reduction Model" Against Respiratory Pandemics.
Front Med (Lausanne). 2020;7:260.10.3389/fmed.2020.00260.
httgs:L/.www.ncbi.nlm.nih.gov/.gubmed/.32574342.
16. Viola I.M., Peterson B., Pisetta G., et al. Face coverings, aerosol
dispersion and mitigation of virus transmission risk. 2020.
httgs:L/.arxiv.org/.abs/.2005.10720.
17. Rengasamy S, Eimer B, Shaffer RE. Simple respiratory protection
evaluation of the filtration performance of cloth masks and common
fabric materials against 20-1000 nm size particles. Ann Occup Hyg.
201 0; 54 (7): 789-798.10.1093/annhyg/meq044.
httgs:L/.www.ncbi.nlm.nih.gov/.gubmed/.20584862.
18. Kanda A, Prakash A, Moss GA, Schmoldt M, Grant GD, Guha S. Aerosol
Filtration Efficiency of Common Fabrics Used in Respiratory Cloth
Masks. ACS Nano. 2020;14(5):6339-6347.10.1021/acsnano.0c03252.
httgs:L/.www. ncbi. n Im. n ih .gov /pu bmed/.3 23 2 93 37. 19. Long KD, Woodburn EV, Berg IC, Chen V, Scott WS. Measurement of
filtration efficiencies of healthcare and consumer materials using
modified respirator fit tester setup. PLoS One.
2020;15 (10) :e0240499.10.1371/journal.pone .0240499.
httrJ.s:L/.www. ncbi. nl m. n ih .gov/.P-.U bmed/.33048980. 20. O'Kelly E, Pirog S, Ward J, Clarkson PJ. Ability of fabric face mask
materials to filter ultrafine particles at coughing velocity. BMJ Open.
2020;10 (9) :e039424.10.1136/bmjopen-2020-039424.
httgs:/.Lwww.ncbi.nlm.nih.govLgubmedL32963071.
APPENDIX TO JAMES CASCIANO DECLARATION-10

21. Aydin 0, Emon B, Cheng S, Hong L, Chamorro LP, Saif MTA.
Performance of fabrics for home-made masks against the spread of
COVID-19 through droplets: A quantitative mechanistic study. Extreme
Mech Lett. 2020;40:100924.10.1016/j.eml.2020.100924.
httgs:/./.www.ncbi.nlm.nih.gov/.gubmed/.32835043.
22. Bhattacharjee S, Bahl P, Chughtai AA, MacIntyre CR. Last-resort
strategies during mask shortages: optimal design features of cloth
masks and decontamination of disposable masks during the COVID-19
pandemic. BMJ Open Respir Res. 2020;7(1).10.1136/bmjresp-2020-
000698. httgs:f/.www. ncb i. n Im. n ih .gov /.gu bmed/.3 2 913 00 5.
23. Maurer L, Peris D, Kerl J, Guenther F, Koehler D, Dellweg D. Community
Masks During the SARS-CoV-2 Pandemic: Filtration Efficacy and Air
Resistance. J Aerosol Med Pulm Drug De/iv.
2020.10.1089/jamp.2020.1635.
httgs:/./.www.ncbi.nlm.nih.govLgubmedL32975460.
24. Hill WC, Hull MS, MacCuspie RI. Testing of Commercial Masks and
Respirators and Cotton Mask Insert Materials using SARS-CoV-2
Virion-Sized Particulates: Comparison of Ideal Aerosol Filtration
Efficiency versus Fitted Filtration Efficiency. Nano Lett.
2020; 20 (10): 7642-7647.10.1021/acs. nanolett.0c03182.
httgs:/./.www. ncbi. n Im. n ih .govLgu bmed/.32986441.
25. Whiley H, Keerthirathne TP, Nisar MA, White MAF, Ross KE. Viral
Filtration Efficiency of Fabric Masks Compared with Surgical and N95
Masks. Pathogens. 2020;9 (9) .10.~390/pathogens9090762.
httgs:f/.www.ncbi.nlm.nih.gov/.gubmed/.32957638.
26. Hao W, Parasch A, Williams S, et al. Filtration performances of non
medical materials as candidates for manufacturing facemasks and
respirators. Int J Hyg Environ Health.
2 0 20; 229:11358 2.10.1016/j .ij heh. 2 0 2 0.11358 2.
http_s:f/.www.ncbi.nlm.nih.govLp_ubmedL32917368.
27. van der Sande M, Teunis P, Sabel R. Professional and home-made face
masks reduce exposure to respiratory infections among the general
APPENDIX TO JAMES CASCIANO DECLARA TION-11
population. PLoS One. 2008;3(7):e2618.10.1371/journal.pone.0002618. httgs :/.Lwww. ncbi. n Im. n i h .gov LP-LI bmedL186124 29.
28. Chu DK, Aki EA, Duda S, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet.
2020.10.1016/S0140-6736 ( 20) 31142-9. htt gs :/.L do i .o rgL10 .1016 LSO 14 0-6736 (20)31142-9.
29. Clase CM, Fu EL, Ashur A, et al. Forgotten Technology in the COVID-19 Pandemic: Filtration Properties of Cloth and Cloth Masks-A Narrative Review. Mayo Clin Proc. 2020;95(10):2204-
2 224.10.1016/j. mayocp.2 0 20.07.0 2 0. httgs:/.Lwww. ncbi. n Im. n i h .gov LP-LI bmedL 33012 350.
30. Zhao M, Liao L, Xiao W, et al. Household Materials Selection for
Homemade Cloth Face Coverings and Their Filtration Efficiency Enhancement with Triboelectric Charging. Nano Lett.
2020;20 (7): 5544-5552.10.1021/acs.nanolett.Oc02211. httgs:/.Lwww.ncbi.nlm.nih.govLgLibmedL32484683.
31. Parlin AF, Stratton SM, Culley TM, Guerra PA. A laboratory-based study examining the properties of silk fabric to evaluate its potential as a protective barrier for personal protective equipment and as a functional material for face coverings during the COVID-19 pandemic. PLoS One.
2020;15 (9) :e0239531.10.1371/journal.pone.0239531. httgs :/.Lwww. nc bi. n Im. n i h .gov LP-LI bmedL 3 2 946 5 2 6.
32. Hendrix MJ, Walde C, Findley K, Trotman R. Absence of Apparent Transmission of SARS-CoV-2 from Two Stylists After Exposure at a Hair Salon with a Universal Face Covering Policy - Springfield, Missouri, May 2020. MMWR Morb Mortal Wkly Rep. 2020;69(28):930-932.10.15585/mmwr.mm6928e2. httgs:/.Lwww.ncbi.nlm.nih.govLP-.LibmedL32673300.
33. Wang Y, Tian H, Zhang L, et al. Reduction of secondary transmission of SARS-CoV-2 in households by face mask use, disinfection and social distancing: a cohort study in Beijing, China. BMJ Glob Health.
APPENDIX TO JAMES CASCIANO DECLARATION-12

2020; 5 ( 5) .10.1136/bmjg h-2020-002794. http_s:/.Lwww.ncbi.nlm.nih.govLp_ubmedL32467353.
34. Doung-Ngern P, Suphanchaimat R, Panjangampatthana A, et al. CaseControl Study of Use of Personal Protective Measures and Risk for Severe Acute Respiratory Syndrome Coronavirus 2 Infection, Thailand. Emerg Infect Dis. 2020;26(11).10.3201/eid2611.203003. httgs:/.Lwww.ncbi.nlm.nih.govLgubmedL32931726.
35. Payne DC, Smith-Jeffcoat SE, Nowak G, et al. SARS-CoV-2 Infections and Serologic Responses from a Sample of U.S. Navy Service Members - USS Theodore Roosevelt, April 2020. MMWR Morb Mortal Wkly Rep.
2020;69 (23): 714-721.10.15585/mmwr. mm6923e4. http_s:/.Lwww.ncbi.nlm.nih.govLp_ubmedL32525850.
36. Schwartz KL, Murti M, Finkelstein M, et al. Lack of COVID-19 transmission on an international flight. Cmaj.
2020;192(15):E410.10.1503/cmaj.75015. http_s:/.Lwww.ncbi.nlm.nih.govLgubmedL32392504.
37. Freedman DO, Wilder-Smith A. In-flight Transmission of SARS-CoV-2: a review of the attack rates and available data on the efficacy of face masks. J Travel Med 2020.10.1093/jtm/taaa178. http_s:/.Lwww.ncbi.nlm.nih.govLp_ubmedL32975554.
38. Wang X, Ferro EG, Zhou G, Hashimoto D, Bhatt DL. Association Between Universal Masking in a Health Care System and SARS-CoV-2 Positivity Among Health Care Workers. JAMA.
2020.10.1001/jama.2020.12897. http_s:/.Lwww.ncbi.nlm.nih.govLgubmedL32663246.
39. Mitze T., Kosfeld R., Rode J., Walde K. Face Masks Considerably
Reduce COVID-19 Cases in Germany: A Synthetic Control Method
Approach. IZA - Institute of Labor Economics (Germany);2020.ISSN: 2365-9793, DP No. 13319. httg:L/.ftP-.iza.org/.dg13319.gdf
40. Gallaway MS, Rigler J, Robinson S, et al. Trends in COVID-19 Incidence After Implementation of Mitigation Measures - Arizona, January 22-August 7, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(40):1460-
APPENDIX TO JAMES CASCIANO DECLARATION-13

1463.10.15585/mmwr.mm6940e3.
httgs:fLwww.ncbi.nlm.nih.govLgubmedL33031366.
41. Lyu W, Wehby GL. Community Use Of Face Masks And COVID-19:
Evidence From A Natural Experiment Of State Mandates In The US.
Health Aff (Millwood). 2020;39(8):1419-
1425.10.1377 /hlthaff .2020.00818.
httgs:fLwww.ncbi.nlm.nih.govLgubmedL32543923.
42. Hatzius J, Struyven D, Rosenberg I. Face Masks and GDP. Goldman
Sachs Research httgs:fLwww.goldmansachs.comlinsightsLgagesLface
masks-and-gdg.html. Accessed July 8, 2020.
43. Karaivanov A., Lu S.E., Shigeoka H., Chen C., Pamplona S. Face Masks,
Public Policies And Slowing The Spread Of Covid-19: Evidence from
Canada National Bureau Of Economic Research 2020.Working Paper
27891. httg:fLwww. nber.orglgagerslw27891.
44. Chernozhukov V, Kasahara H, Schrimpf P. Causal Impact of Masks,
Policies, Behavior on Early Covid-19 Pandemic in the U.S. medRxiv.
2020.10.1101/2020.05.27.20115139.
httg:/Lmed rxiv.orgl contentLea rly l20 2 0 LO 5L29 L2 0 2 0.05. 27.2 011513 9 .a bst
ract.
45. Leffler CT, Ing EB, Lykins JD, Hogan MC, McKeown CA, Grzybowski A.
Association of country-wide coronavirus mortality with demographics,
testing, lockdowns, and public wearing of masks (updated August 4,
2020). medRxiv. 2020.10.1101/2020.05.22.20109231.
httg:fLmedrxiv.orgLcontentLearlyL2020L05L25l2020.05.22.20109231.abs
tract.
APPENDIX TO JAMES CASCIANO DECLARATION-14

Mask Facts
curated by Marilyn M. Singleton, M.D., J.D. -
httQ://.marilynsingletonmdjd.com/.
Updated September 26, 2020
Introduction
COVID-19 is as politically-charged as it is infectious. Early in the COVID-19
pandemic, the WHO, the CDC and NIH's Dr. Anthony Fauci discouraged
wearing masks as not useful for non-health care workers. Now they
recommend wearing cloth face coverings in public settings where other
social distancing measures are hard to do (e.g., grocery stores and
pharmacies). The recommendation was published without a single scientific
paper or other information provided to support that cloth masks actually
provide any respiratory protection. Let's look at the data.
The theory behind mask wearing:
APPENDIX TO JAMES CASCIANO DECLARATION-15

• Source control: Cloth mask can trap droplets that come out of a
person's mouth when they cough or sneeze.
• Protection: Personal Protective Equipment (PPE) - only N95 masks
Transmission of SARS-CoV-2
Note: A COVID-19 (SARS-CoV-2) particle is 0.125 micrometers/microns
(µm); influenza virus size is 0.08 - 0.12 µm; a human hair is about 150 µm.
*1 nm = 0.001 micron; 1000 nm = 1 micron; Micrometer (µm) is the
preferred name for micron
*1 meter is = 1,000,000,000 [trillion] nm or 1,000,000 [million] microns
*For a complete dissection and explanation of aerosols and airborne
particles, please see Understanding Particle Size and Aerosol-based
Transmission by Steve Probst. httgs:Uwww.4cconference.comLwg
content/ugloadsL2020L07 LUnderstanding-Particle-Size-and-Aerosol
Based-Transmission.gdf
Droplets
• Virus is transmitted through respiratory droplets produced when an
infected person coughs, sneezes, or talks.
o Larger respiratory droplets (>5 µm) remain in the air for only a
short time and travel only short distances, generally <1 meter.
They fall to the ground
q u ickly.h tt,Qs:/Lwww. the la nee t. com/j_ou rna I s/ja n re sLa rticle/PII S2 213
-2600(.20130245-9jfulltext
o This idea guides the CDC's advice to maintain at least a 6-foot
distance.
• Small ( <5 µm) aerosolized droplets can remain in the air for at least 3
hours and travel long distances (up to 27 ft.). 0 b1t~/Lwww.nejm.org/doiJpdfL10.1056/_NEJMc2004973?
APPENDIX TO JAMES CASCIANO DECLARATION-16

articleTools=true:
o httgs:f/.www.cid rag.um n .ed u/.covid-19 /.god casts-we bi na rs/.sgecia l
eg-masks;
o httgs:f/.www. na g.ed u/.cata log/.2 5769/.ragid-exgert-consu ltation
o n-th e-goss i bi I itY.-of-bi oa e ro so I-s g read-of- sa rs-cov- 2-for -the
cov i d-19- ga n demi c-a g ril-1-2020
Air currents
• In an air conditioned environment these large droplets may travel farther.
• Ventilation. Even the opening of an entrance door and a small window can dilute the number of small droplets to one half after 30 seconds. (This study looked at droplets from uninfected persons). This is clinically relevant because poorly ventilated and populated spaces, like public transport and nursing homes, have high SARS-CoV-2 disease transmission despite physical distancing.
o httQ.s:/Lwww.thelancet.com/j_ourna/s/janresLarticleLPIIS2213-
2600(.20) 30245-9Lfulltext
Humidity
• Since 1961, experiments showed that viral-pathogen-carrying droplets were inactivated within shorter and shorter times as ambient humidity was increased. Dryness drives the small aerosol particles. See e.g., review of studies, httQ.s:/Laagr.orgLarticlesLaagr-20-06-covid-0302
Conclusions
The preponderance of scientific evidence supports that aerosols play a critical role in the transmission of SARS-CoV-2. Years of dose response studies indicate that if anything gets through, you will become infected.
• Thus, any respiratory protection respirator or mask must provide a high
APPENDIX TO JAMES CASCIANO DECLARATION-17

level of filtration and fit to be highly effective in preventing the
transmission of SARS-CoV-2. (Works for Mycobacterium tuberculosis
(3µm)
• Public health authorities define a significant exposure to COVID-19 as
face-to-face contact within 6 feet with a patient with symptomatic
COVID-19 that is sustained for at least a few minutes (and some say
more than 10 minutes or even 30 minutes).
o The chance of catching COVID-19 from a passing interaction in a
public space is therefore minimal.
MASKS
filter EfficieocY-and fit
Data from a University_ of Illinois at Chicago review httQ.s./Lwww. cidraQ.. umn. eduLnews-P-,ersP-,ectiveL2020L04Lcommentant_
masks-al/-covid-19-not-based-sound-data
• HEPA (high efficiency particulate air) filters are 99.97 to 100% efficient.
HEPA filters are tested with particles that are 0.125 µm (the size of
SARS-CoV-2).
• Masks and respirators work by collecting particles through several
physical mechanisms, including diffusion (small particles) and
interception and impaction (large particles).
• Surgical masks are loose-fitting devices that were designed to be worn
by medical personnel to protect accidental contamination of patient
wounds, and to protect the wearer against splashes or sprays of bodily
fluids. They aren't effective at blocking particles smaller than 100 µm.
httP-,s:/Lmultimedia.3m.comLmwsLmediaL957730O/.resP-,irators-andsurgica/-masks-contrast-technica/-bulletin.Q.df
o OSHA/CDC: A surgical mask is not a respirator. It cannot be used
to protect workers who perform or assist with aerosol-generating
procedures, which may create very fine aerosol sprays. A surgical
APPENDIX TO JAMES CASCIANO DECLARATION-18
mask can only be used to protect workers from contact with the large droplets made by patients when they cough, sneeze, talk or breathe. httQ.s://_www.osha.gov/_dtsjguidance/_f/u/_healthcare. html
Laboratory Studies
• N95 filtering facepiece respirators (FFRs) are constructed from electret
(a dielectric material that has a quasi-permanent electric charge.) An
electret generates internal and external electric fields so the filter
material has electrostatic attraction for additional collection of all
particle sizes. As flow increases, particles will be collected less
efficiently.
• A JJmJJJUlY.. fitted N95 will block 95% of tiny air particles down to
0.3 µm from reaching the wearer's face.
o httQ.s://_www.honev_we/1.com/_en-us/_newsroom/_ne ws/_2020/_03/_n95-
masks-ex,:J./ained.
o Problem: no source control. An N95 does not filter exhaled air
passing through the exhaust/exhalation valve (for easier breathing
and less moisture inside the mask).
• Study measuring filter efficiency (2010)
o httQ.s.//_academic. OUQ.. com/_annweh/_artic/e/_54/_7 /_789/_202 7 44:
httQ.s://_www. cidraQ.. umn. edu/_news
QersP-,ective/_2020/_04/_commentarv_-masks-al/-covid-19-not
based-sound-data;
httQ.s://_academic. OUQ.. com/_annweh/_article/_54/_7/_789/_202 7 44
o Filter efficiency was measured across a wide range of small
particle sizes (0.02 to 1 µm) at 33 and 99 L/min.
o All the cloth masks and materials had near zero efficiency at 0.3
µm, a particle size that easily penetrates into the lung (SARS-CoV-
2 is 0.125 µm)
APPENDIX TO JAMES CASCIANO DECLARATION-19

o Efficiency for the entire range of particles
■ T-shirts -10%
■ Scarves -10% to 20%
■ Cloth masks -10% to 30%
■ Sweatshirts - 20% to 40%
■ Towels - 40%
• Study measuring filter efficiency (2014, Korea)
o httg_s:/Laagr. orgLarticlesLaagr-13-06-oa-0201
o Evaluated 44 masks, respirators, and other materials with similar
methods and small aerosols (0.08 and 0.22 µm)
■ N95 FFR filter - >95% efficiency
■ Medical masks - 55% efficiency
■ General {cloth) masks - 38% efficiency
■ Handkerchiefs - 2% {one layer) to 13% (four layers)
efficiency.
• Conclusion: Wearing masks {other than N95) will not be effective at
preventing SARS-CoV-2 transmission, whether worn as source control
or as PPE.
o N95s protect health care workers, but are not recommended for
source control transmission.
o Surgical masks are better than cloth but not very efficient at
preventing emissions from infected patients. Cloth masks must be
3 layers, plus adding static electricity by rubbing with rubber
glove.
o The cloth that serves as the filtration for the mask is meant to trap
particles being breathed in and out. But it also serves as a barrier
to air movement because it forces the air to take the path of least
resistance, resulting in the aerosols going in and out at the sides
of the mask.
o An August 2020 UCSF study suggested that the mask would
decrease the absolute volume of the inoculum. {The
APPENDIX TO JAMES CASCIANO DECLARATION-20

concentrations of bacteria upstream and downstream of the test
devices were measured with an aerodynamic size spectrometer)
htt12.s:/Lucsf. aQQ.. box. comLsLblvo/ kg_Sz0my_dzd82rjks4 wy_leagt036
Human Studies
• Study of correct use of masks (2020, Singapore). 0 btt~//www.medP-agetodav.com/Jnfectiousdiseasef P-ubl ichealth/..8.
6601 0 Overall, data were collected from 714 men and women. Of all ages,
only 90 participants (12.6%) passed the visual mask fit test. About
75% performed strap placement incorrectly, 61% left a "visible gap
between the mask and skin," and about 60% didn't tighten the
nose-clip.
• Study of surgical face mask use in health care workers (2009, Japan).
o httQ.s://.Qubmed.ncbi.nlm.nih.gov/_19216002L
o Masks did not provide benefit in terms of cold symptoms or
getting cold.
• Randomized clinical trial of standard medical/surgical masks in health
care workers (2010, Australia).
o httQs://_onlinelibrartt wilett com/_doi/_eQ.df/_10.1111/j.1750-
2659. 2011.00198.x?fbclid=lwAR3kRYVYDKb0aR-
su9 me9 vY6a8KVR4HZ17J2A B0f fXUABRQdhQ/cBWo.
o Study was spurred by the H1N1 flu. While N95 masks offered
protection against respiratory illness, medical mask wearers and
control group numbers were similar.
• Review of influenza virus and face masks in health care workers
(HCWs) (2010, Hong Kong).
o httQ.s://_www. cam bridge. orgLcore/journalsLeP-.idemio/ogx.-andinfection/_artic/e/jace-masks-to-P-.revent-transmission-of-
APPENDIX TO JAMES CASCIANO DECLARATION-21

influenza-virus-a-sx.stematic
reviewL64D368496EBDE0AFCC6639CCC9DBBC05 0 6 studies of face mask use, both surgical masks and N-95
respirators in HCWs and community settings. The effectiveness of
face masks is probably impacted by compliance issues in both the
healthcare and community setting. Various studies show a lower
level of compliance with face masks or find lower reported
acceptability of face masks compared to hand hygiene behaviors
and other non-pharmaceutical interventions.
• Review of masks against influenza (2012, Europe).
o httg_s:/Lonlinelibrar½wile½CDmLdoiLeg_dfL10.1111/j.1750-
2659.2011. 0030 7. X
o 17 eligible studies. One study had improvement with mask plus
hand sanitizer. None of the studies established a conclusive
relationship between mask/respirator use and protection against
influenza infection.
• *The first randomized controlled trial of cloth masks in health care
workers (2015, Australia).
o httg_s:/Lbmjog_en. bmj. comLcontentL5L4Le0065 77:
httg_s:/Lwww.ncbi.nlm.nih.govfg_mcLarticles/PMC4420971fg_df Lbmj
og_en-2014-006577.g_df
o Penetration of:
■ Cloth masks by particles - 97%
■ Medical masks - 44%,
■ 3M Vflex 9105 N95 - 0.1%
• 3M 9320 N95 - <0.01%
o Cloth masks resulted in significantly higher rates of infection than
medical masks, and also performed worse than the control arm
some of whom may have worn masks.
o The virus may survive on the surface of the face masks
o Self-contamination through repeated use and improper doffing is
APPENDIX TO JAMES CASCIANO DECLARATION-22

possible. A contaminated cloth mask may transfer pathogen from
the mask to the bare hands of the wearer. 0 Moisture retention, reuse of cloth masks, and poor filtration may
result in increased risk of infection.
o Cloth masks should not be recommended for health care workers,
particularly in high-risk situations.
• Review of N95 and surgical masks against respiratory infection (2016).
httg_s:/Lwww. cmaj. caLcontentLcmajL1BBLBL567. f u/1. g_df
o From January 1990 to December 2014. 6 clinical studies: 3
randomized controlled trials (RCTs), 1 cohort study and 2 case-
control studies, and 23 surrogate exposure studies.
o In the meta-analysis of the clinical studies, "no significant
difference between N95 respirators and surgical masks in
associated risk of (a) laboratory-confirmed respiratory infection,
(b) influenza-like illness, or (c) reported work-place absenteeism."
• Review of masks and N95s against respiratory infection (2017,
Singapore).
o httg_s:/Ldoi.orgL10.1093LcidLcix681
o Separate meta-analyses of 6 randomized controlled trials (RCTs)
and 23 observational studies conducted during the 2003 SARS
pandemic.
o Compared to medical masks, N95 respirators provided greater
protection against clinical respiratory illness (CRI) and bacterial
respiratory illness (BRI). These 2 outcomes were common in these
trials (average risks of 8.7% and 7.3%, respectively).
o Compared to masks, N95 respirators conferred superior
protection against clinical respiratory illness and laboratory
confirmed bacterial, but not viral infections or influenza life illness
(ILi).
o Self-reported assessment of clinical outcomes was prone to bias.
o Evidence of a protective effect of masks or respirators against
APPENDIX TO JAMES CASCIANO DECLARATION-23

verified respiratory infection was not statistically significant
(compared to no mask)
• Randomized Controlled Trial: N95s vs medical masks in health care
workers (HCWs) against influenza (2019).
o httg_s://j_amanetwork.com/j_ourna/s/j_amaLfullarticleL2749214
o 2862 randomized participants, 2371 completed the study and
accounted for 5180 HCW-seasons.
o Among outpatient health care personnel, N95 respirators (8.2%)
vs medical masks (7.2%) resulted in no significant difference in the
incidence of laboratory-confirmed influenza. 90% said they wore
the mask all the time.
• Review of N95 respirators versus surgical masks against influenza
(March 2020, China).
o httQ.s:/Ldoi.orgL10.1111/j_ebm.12381
o 6 randomized controlled trials (RCTs) involving 9,171 participants
were included (2015-2020). There were no statistically significant
differences in preventing laboratory-confirmed influenza,
laboratory-confirmed respiratory viral infections, laboratory
confirmed respiratory infection and influenza-like illness using
N95 respirators and surgical masks.
o Meta-analysis indicated a protective effect of N95 respirators
against laboratory-confirmed bacterial colonization.
• CDC Review since 1946 of masks and influenza (May 2020)
o NonQharmaceutical Measures for Pandemic Influenza in
Nonhealthcare Settings-Personal Protective and Environmental
Measures." /J11QS.://wwwnc.cdc.gov/_eid/article/2B/..5/_19-
0994 article o Systematic review. 10 RCTs that reported estimates of the
effectiveness of face masks in reducing laboratory-confirmed
influenza virus infections in the community from literature
APPENDIX TO JAMES CASCIANO DECLARATION-24
published during 1946-July 27, 2018. 0 There is limited evidence for face masks' effectiveness in
preventing laboratory-confirmed influenza virus transmission
either when worn by the infected person for source control or
when worn by uninfected persons to reduce exposure.
o "Proper use of face masks is essential because improper use
might increase the risk for transmission."
• A study of 4 patients (July 2020, South Korea).
o httQ.s:/Lwww. acgjournals. orgLdoiL10. 7326LM20-1342
o Known patients infected with SARS-CoV-2 wore masks and
coughed into a Petrie dish. "Both surgical and cotton masks seem
to be ineffective in preventing the dissemination of SARS-CoV-2
from the coughs of patients with COVID-19 to the environment
and external mask surface."
• Studied different types of face coverings in non-clinical setting (August
2020).
o httg_s:/Ladvances. sciencemag. orgLcontentLearlyL2020L0BL0 7 Lsciad
v.abd3083
o They used a black box, a laser, and a camera. A person wears a
face mask and speaks into the direction of an expanded laser
beam inside a dark enclosure. Droplets that propagate through the
laser beam scatter light, which is recorded with a camera. A
simple computer algorithm then counts the droplets seen in the
video.
o The N95 led to a droplet transmission of below 0.1%.
o Cotton and polypropylene masks, some of which were made from
apron material showed a droplet transmission ranging from 10% to
40%.
o Knitted mask had up to 60% droplet transmission.
o Neck fleece had 110% droplet transmission (10% higher than not
wearing a mask).
APPENDIX TO JAMES CASCIANO DECLARATION-25

o Speaking through some masks (particularly the neck fleece,
bandanas) seemed to disperse the largest droplets into a
multitude of smaller droplets ... which explains the apparent
increase in droplet count relative to no mask in that case.
• See "Positive Effects of Masks" below. A recent study suggested that
the mask would decrease the absolute volume of the inoculum. (The
concentrations of bacteria upstream and downstream of the test
devices were measured with an aerodynamic size spectrometer)
httQ.s:/Lucsf.aQQ..box.comLsLblvolkQ.5zOmx_dzd82rjks4wy_/eagt036
• Austrian observation (August 2020)
o httQ.s./Lcorona-transition.orgLmaskenQ.flicht-brachte-in
osterreich-keinerlei-messbaren-nutzen (in German)
o The introduction, retraction and re-introduction of mandatory face
masks in Austria had no influence at all on the infection rate.
• News reCQ.Ct (August 13, 2020) 0 blt~//sentinelksmo.org/_more-deceP-.tion-kdhe-hid-data-to
justifv_-mask-mandateL
o In Kansas, the 90 counties without mask mandates had lower
coronavirus infection rates than the 15 counties with mask
mandates. To hide this fact, the Kansas health department tried to
manipulate the official statistics and data presentation.
Study from France:
APPENDIX TO JAMES CASCIANO DECLARATION-26

"' ~ "' "' u ~
"' 0
"' :l ... ·;; "' C: 0 ... 0 u ~ > 0 z
10k
7.Sk
Sk
2.Sk
0
-2.Sk
Daily New Cases Cases per Day
Data as of 0:00 GMT +O
bilQ..S..;/.~QLS....Q[g/face-masks-evidence/. (Swiss Policy Research)
Johns Hopkins, 9/21/20
Indoor Mask Mandate
New Confirmed CCVI D-19 Cases per Day, normalized by population
120
100
80
60
40
20
0
)!,
'c3 3 • z
0
I I
httQs ://.twi tter.comLC ovi d 19C rush er /.statu s/.1308013 900 5464 2 8 9 2 8
Negative Effects of Masks
Spain
Look Mum, no mask !
0 '-------~Sweden
Dllys sine• 1 cllse/lm people
APPENDIX TO JAMES CASCIANO DECLARATION-27

Air inside the mask is definitely stale. In filtering particles, the mask makes
it harder to breathe.
Decreased Pa02
• A 2004 observational study of end stage renal disease patients during
dialysis for 4 hours (2004, Taiwan).
o httg_s./jg_ubmed.ncbi.nlm.nih.govL15340662/_;
o httg_s:/Lwww.researchgate.netfg_ublicationL8371248 The g_hy_sio/og
ical_img_act of wearing an N95 mask during hemodialy_sis_as_g_Q
recaution against SAR$ in g_atients with end-stage renal disease
o 39 patients, mean age, 57 years. 70% had decreased PaO2 (from
100 to 92); 19% had hypoxemia (PaO2 <70); all patients had
increased respiratory rate 16 to 18; chest discomfort (3 baseline
patients to 11 patients); respiratory distress (1 baseline patient to
17 patients)
• Stanford engineers estimated that N95 masks cause a 5% to 20%
reduction in 02 intake. This can cause dizziness and lightheadedness.
This can be life-threatening for someone with lung disease or with
respiratory distress. 0 b1..tps:/Lengineering. stanford. edu/_magazine/articleLcovid-19-
promP-,ts-team-engineers-rethink-humble-face-mask
• Study of surgeons in the OR (2008, Turkey).
o httP-.:fLscielo. isciii. esf P-.df LneuroLv19n2L3. P-,df o Scientists looked at 02 levels of surgeons wearing masks while
performing surgery. Found a decrease in the oxygen saturation of
arterial pulsations (peripheral capillary 02 saturation/SpO2) fell
from 98% to 96% and a slight increase in pulse rates compared to
preoperative values in all surgeon groups.
Increased CO2
APPENDIX TO JAMES CASCIANO DECLARATION-28

• This may be merely theoretical. Carbon dioxide molecules freely
diffuse through the masks, allowing normal gas exchange while
breathing.
• CO2 is present in the atmosphere at a level of about 0.04% ·(400ppm).
According to the U.S. Department of Agriculture / OSHA, carbon
dioxide becomes toxic at concentrations above 4 percent
(40,000ppm); symptoms at 5,000-10,000 ppm. 10,000 ppm has been
measured behind mask.
• Experiment (July 2020).
o h ttQ.s://_www.wthr.com/_a rtic/e/_ne ws/_hea I th/_ corona vi rus/_verify_-do
f ace-masks-reduce-oxygen-intake-carbon-di oxide-ex 12.eri men t -
multiQ.le-maskssL531-c00c96cb-9273-4947-949c-
0807f94454a7
o Pulse oximeter and exhaled CO2 (via tube in mask) No change
with mask. (End-tidal capnography or end-tidal CO2 (EtCO2)
monitoring is a non-invasive technique that measures the partial
pressure or maximal concentration of carbon dioxide (CO2) at the
end of an exhaled breath. The normal values are 5-6% CO2, which
is equivalent to 35-45 mmHg.)
• Health care worker study (2005, Scandinavia)
o httQ.s:/f P-.ubmed.ncbi.nlm.nih.gov/_16441251L
o 37.3% reported face-mask-associated headaches, 32.9% reported
headache frequency >6 times per month. 7.6% had taken sick
leave from March 2003 to June 2004 (mean 2 days; range 1-4
days) and 59.5% required use of abortive analgesics because of
headache.
• Health care worker study (2009, Japan) with similar headache results
as Scandinavian study (above).
o htt~/fpubmed.ncbi.nlm.nih.govL19216002L
APPENDIX TO JAMES CASCIANO DECLARATION-29

• While there are some articles reporting OSHA tests, it is not clear they
were proper tests.
• Some people have mistakenly claimed that OSHA standards (e.g., the
Respiratory Protection standard, 29 CFR 1910.134; the Permit-Required
Confined Space standard 29 CFR 1910.146; and the Air Contaminants
standard, 29 CFR 1910.1000) apply to the issue of oxygen or carbon
dioxide levels resulting from the use of medical masks or cloth face
coverings in work settings with normal ambient air (e.g. healthcare
settings, offices, retail settings, construction). These standards do not
apply to the wearing of medical masks or cloth face coverings in work
settings with normal ambient air). These standards would only apply to
work settings where there are known or suspected sources of
chemicals (e.g., manufacturing facilities) or workers are required to
enter a potentially dangerous location (e.g., a large tank or vessel).
httQ.s:/Lwww.osha.gov LSL TCLcovid-19Lcovid-19-fag. html
• It is hard to tell if the headaches experienced by HCWs with N95s is
CO2 or having a strap around the head.
• But when asked should we be worried about CO2, mask proponents
say, "No" because you can exhale around the sides of the mask. This
defeats the purpose. (2006)
httQ.s://.Q.ubmed.ncbi.nlm.nih.govL16441251L
Moisture retention
• Reuse of cloth masks, frequency and effectiveness of cleaning, and
poor filtration may result in increased risk of infection.
• Observations during SARS suggested double-masking and other
practices increased the risk of infection because of moisture, liquid
diffusion.
o httQ.s:/LbmjoQ.en. bmj. comLcontentL5L4Le006577:
APPENDIX TO JAMES CASCIANO DECLARATION-30

httQ.s:/Lwww.ncbi.nlm.nih.govfQ.mcLartic/es/PMC4420971fQ.dfLbmj
og_en-2014-006577.g_df
• Recent study {in German) cultured 82 bacterial colonies & 4 mold
{fungoid) colonies from a child's masks after 8 hours of wear. 0 httg_s:/Ltwitter. comLM MaccruiskeenLstatusL130 726652 766266982
5?s=20
Self-contamination
• Contamination through repeated use and improper doffing is possible.
The virus may survive on the surface of the mask. The pathogen goes
from mask to bare hands.
"Mask mouth"
• Reported by dentists. httg_s:/!JJ.Y.g_ost.comL2020LOBL05Lmask-mouth
is-a-seriouslv_-stinkv_-side-effect-of-wearing-masksL
• Wearing masks increases dryness, which leads to decrease in saliva. It
is the saliva that fights bacteria. Result is decaying teeth, receding gum
lines and seriously sour breath. Gum disease - or periodontal disease
- will eventually lead to strokes and an increased risk of heart
attacks."
World Health Organization {WHO), June 2020
• .bllQ.S.;/.La.p_ps.who. i nt/.iris/.bitstream/.ha nd le/.10665/332293/.WH 0- 2019-nCov-l PC Masks-2020.4-eng.,pdf?sequence=1&isAllowed=y_
• "The likely disadvantages of the use of mask by healthy people in the
general public include:
o potential increased risk of self-contamination due to the
manipulation of a face mask and subsequently touching eyes with
contaminated hands;
o potential self-contamination that can occur if non- medical masks
APPENDIX TO JAMES CASCIANO DECLARATION-31

are not changed when wet or soiled. This can create favourable
conditions for microorganism to amplify;
o potential headache and/or breathing difficulties, depending on
type of mask used;
o potential development of facial skin lesions, irritant dermatitis or
worsening acne, when used frequently for long hours;
o difficulty with communicating clearly;
o potential discomfort;
o a false sense of security, leading to potentially lower adherence to
other critical preventive measures such as physical distancing and
hand hygiene;
o poor compliance with mask wearing, in particular by young
children;
o waste management issues; improper mask disposal leading to
increased litter in public places, risk of contamination to street
cleaners and environment hazard;
o difficulty communicating for deaf persons who rely on lip reading;
o disadvantages for or difficulty wearing them, especially for
children, developmentally challenged persons, those with mental
illness, elderly persons with cognitive impairment, those with
asthma or chronic respiratory or breathing problems, those who
have had facial trauma or recent oral maxillofacial surgery, and
those living in hot and humid environments.
The Hamburg Environmental Institute (July 2020) warned of the inhalation
of chlorine compounds in polyester masks as well as problems in
connection with face mask disposal. httgs:LLswgrs.orgLface-masks
evidenceL; httgs:LLcorona-transition.orgLmaskentragen-noch-ungesunder
als-gedacht (in German)
Psychological Damage in Children (September 11, 2020).
httQ.s:/Lwww.world-todax_-news.com/_70-doctors-in-open-letter-to-ben
wex_ts-abolish-mandatorx_-mouth-mask-at-schoo/-belgiumL
APPENDIX TO JAMES CASCIANO DECLARATION-32

• 70 Belgian doctors begged for cancellation of mask mandate at school.
"In recent months, the general well-being of children and young people
has come under severe pressure. We see in our practices an increasing
number of children and young people with complaints due to the rules
of conduct that have been imposed on them. We diagnose anxiety and
sleep problems, behavioral disorders and fear of contamination. We are
seeing an increase in domestic violence, isolation and deprivation.
Many lack physical and emotional contact; attachment problems and
addiction are obvious. 'The mandatory mouth mask in schools is a major threat to their development. It ignores the essential needs of the growing child. The well-being of children and young people is highly dependent on the emotional connection with others. ( ... ) The aim of education is to create an optimal context so that a maximum
development of young people is possible. The school environment
must be a safe practice field. The mouth mask obligation, on the other hand, makes the school a threatening and unsafe environment, where emotional connection becomes difficult. 'In addition, there is no large-scale evidence that wearing face masks in a non-professional environment has any positive effect on the spread of viruses, let alone on general health.'
Unanswered questions
• Can virions escape an evaporating droplet stuck to a mask fiber?
• What are long-term health effects on HCW, such as headaches, arising
from impeded breathing?
• Are there negative social consequences to a masked society?
• Are there negative psychological consequences to wearing a mask, as
a fear-based behavioral modification?
• What are the environmental consequences of mask manufacturing and
disposal?
Positive Mask Studies
APPENDIX TO JAMES CASCIANO DECLARATION-33
• Some cite a September 2019 study mentioned above
(httg_s:j/jamanetwork.com/journa/s/jamaLfullarticleL2749214J
comparing N95s and surgical masks in preventing flu. BUT there was
no control wearing no mask. The point of the study found that both
types had similar incidence of flu. {N95-8.2% vs 7.2%).
• The main study used is the Missouri hairdressers who were SARS-CoV-
2 infected but asymptomatic and wore a mask; clients did not get
infected.{July 2020)
o httg_s:/Lwww. livescience. comLhair-sty_lists-infected-covid19-face
masks. html:
o httg_s:f Lwww.cdc.gov Lmmwr LvolumesL69Lwr Lmm692 Be 2. htm
o But there is a Chinese report {May [August] 2020) of a COVID
infected asymptomatic person who did not infect 455 persons
with whom he was in contact.
httg_s:ffg_ubmed.ncbi.nlm.nih.govL32513410L
o Asymptomatic people do not cough and sneeze. But one study
showed they shed just as many viruses as symptomatic. {August
2020, Korea)
o h ttg_s:f /ja mane twork. com/j o u rna I s/ja main tern a I med ici neLf u Ila rt i cl eL
2769235
• Review of mask use {March 2020, multi-country)
o httg_s:/Lwww.sciencedirect.comLscienceLarticleLg_iiLS14778939203
02301?via%3Dihub
o 21 studies; 8,686 participants. Mask use by health care workers
{HCWs) and non-HCWs. HCWs had 80% reduction of viral
infections. Non-HCW had 56%. Asian better than Western. Study
stressed that masks were an adjunct to other measures.
o Other factors:
■ Older age of the population, urbanization, obesity, and longer
duration of the outbreak in a country were independently
associated with higher country-wide per-capita coronavirus
APPENDIX TO JAMES CASCIANO DECLARATION-34
mortality.
■ International travel restrictions were associated with lower
per-capita mortality.
■ Other containment measures, testing and tracing polices, and
the amount of viral testing were not statistically significant
predictors of country-wide coronavirus mortality, after
controlling for other predictors.
■ Societal norms and government policies supporting mask
wearing by the public were independently associated with
lower per-capita mortality from COVID-19.
• Review of 8 pre-COVID-19 studies (June 2020, Australia).
o httQ.s:/.Lwww. ncbi. nlm. nih. gov /.Q.mcLarticles/.PMC 732 322 3L?
fbclid=lwAR2Uky_t8GCrK-goc
bgCJhHknW5Q.gy_tBFOfe6txHWI 7eUs9Q.8vsrQ26KIM
o Surgical masks reduced influenza like illnesses (ILi) by 41% and
N95 by 66% (difference was not statistically significant). Save N95
for aerosols.
o No good evidence face masks protect the public against viral
respiratory illnesses
o "Australia and New Zealand currently, the questionable benefits
arguably do not justify health-care staff wearing surgical masks
when treating low-risk patients and may impede the normal caring
relationship between patients, parents and staff."
• Review of masks, physical distancing, eye protection (June 2020,
WHO).
o httQ.s./Lwww. the lancet. com/j_ournalsLJancetLarticle/.PIIS014 0-6736 (.20) 31142-9/julltext
o 172 observational studies across 16 countries and six continents;
MERS, SARS, betacorona, SARS-CoV-2 in health care and non
healthcare settings. N95s better than surgical or 12 layer cotton.
Authors did not rate the certainty of effect as high. Findings were
APPENDIX TO JAMES CASCIANO DECLARATION-35

in accord with those of a cluster randomized trial showing a
potential benefit of continuous N95 respirator use over medical
masks against seasonal viral infections.
• Review of face mask efficacy (July 2020, China).
o httg_s:/Lwww.ncbi.nlm.nih.govfg_mcLarticlesLPMC7253999:
o httg_s:/Lwww.sciencedirect.comLscienceLarticlefg_iiLS14778939203
02301?via%3Dihub
o 21 studies, 8,686 participants: 13 case-control studies, 6 cluster
randomized trials, and 2 cohort studies. 12 studies of health care
workers (HCWs); 8 studies of non-healthcare professional
populations; 1 study of HCWs and relatives of patients. SARS,
H1N1, influenza lab confirmed.
o Masks (N95 and surgical) were generally effective in preventing
the spread of respiratory viruses. After wearing a mask, the risk of
contracting RVls was significantly reduced. Use of masks by
HCWs and non-HCWs can reduce the risk of respiratory virus
infection by 80% and 47% respectively.
o The study they reference regarding "social" masks is footnoted to
a model that assumes complete compliance and universality.
• CDC review of masks and antibody presence in health care workers
(HCWs) (September 2020).
o httg_s:/Lwww.cdc.govLmmwrLvolumesL69LwrLmm6935e2.htm?
~ cid=mm6935e2 w
o 3,248 HCWs observed. 6% had antibodies to SARS-CoV-2; 29%
were asymptomatic; 69% had not had a diagnosis of SARS-Co-V-
2 infection. Prevalence of antibodies was lower (6%) in HCWs who
wore masks that those who did not (9%).
• *Experiment (human) measuring surgical mask efficacy in reducing
virus transmission (April 2020, Hong Kong).
o b.11~//_www.nature.com/_articles/_s41591-020-0843-2
APPENDIX TO JAMES CASCIANO DECLARATION-36

0 246 participants. Infection measured by PCR. Bioaerosol
collecting device, to capture exhaled breath particles. Two size
fractions: < and >5 microns. Surgical masks can efficaciously
reduce the emission of influenza virus particles into the
environment in respiratory droplets, but not in aerosols. Surgical
face masks could be used by ill people to reduce onward
transmission.
• Summer 2020 study with laboratory coughs (Summer 2020)
o httQ.s:fLwww.vumedi.comLvideoLairborne-transmission-face
masks-how-do-different-txQ.es-of-masks-Q.rotect-against
various-ranges-of-ti
Forward motion distance:
■ Handkerchief - 4 feet
■ 3 layer cloth - 1 foot
■ 2 layers sewn cloth-- 2-3 inches
■ Problems:
■ But drops go around the nose and sides of mask.
■ Shields only work for large droplets.
■ Exhalation ports reduce humidity but defeat the purpose
of using the mask.
• A U.S. study of airborne transmission (May 2020)
o httQ.s:fLwww.Q.nas.orgLcontentL117L26L14857
o Study claimed that masks had led to a decrease in infections in
three global hotspots (including New York City). This did not take
into account the natural decrease in infections and other
measures. The study was so flawed that over 40 scientists
recommended that the study be withdrawn.
• A U.S. study comparing states with mask mandates {June 2020).
o btt~/Lwww.healthaffairs.org/doiLfulf/_10.1377/_hlthaff.2020.00818
o Study concluded that mandatory masks had led to a decrease in
APPENDIX TO JAMES CASCIANO DECLARATION-37

infections in 15 states. The study did not take into account that the
incidence of infection was already declining in most states at that
time. A comparison with other states was not made.
• A U.S. study comparing masks, lockdowns in various countries (June
2020).
o httgs:/Lwww.medrxiv.orgLcontentL10.1101L2020.05.22.20109231v3
.fu/1.gdf
o Study concluded that countries with mandatory masks had fewer
deaths than countries without mandatory masks. But the study
compared African, Latin American, Asian and Eastern European
countries with very different infection rates and population
structures.
• * July-August 2020- UCSF - Mask can be a crude "vaccine."
o httgs://jink. SQ.ringer. comLarticleL10.1007 Ls11606-020-06067-8;
o httgs:/Lucsf. aQQ.. box. comLsLblvolkg5z0my_dzd82rjks4 wy_leagt036:
o httgs:/Lwww.neim.orgLdoiLfullL10.1056LNEJMg2026913:
o h ttgs:/Legibiostat. ucsf. eduLnewsLnew-theory_-asks-could-mask
be-crude- 'vaccine';
o httgs:/Lwww. vumedi. comLvideoLcovid-19-mortality_-ugdate-does
masking-reduce-vira/-inoculum-to-which-wearer-is-exgosedL
o Universal masking reduces the "inoculum" or dose of the virus for
the mask-wearer, leading to more mild and asymptomatic infection
manifestations similar to variolation with small pox. CDC estimates
40% asymptomatic. But masked cruise ship folks had 81%
asymptomatic, 95% masked prison folks, food processing plants.
(The concentrations of bacteria upstream and downstream of the
test devices were measured with an aerodynamic size
spectrometer.)
• Many studies ignore the effect of other measures, the natural
development of infection numbers, changes in test activity, or they
APPENDIX TO JAMES CASCIANO DECLARATION-38

compare countries with very different conditions.
Conclusions from Organizations
• The World Health Organization (WHO): (April 6, 2020) o httP-s:LLaQP-S.who.intLirisLbitstreamLhandleL10665L331693LWHO-
2 019-nCov-l PC Masks-20 2 0 .3-eng.!P-df ?seg uence = 1 &i sAI I owed =y_
o "Advice to decision makers on the use of masks for healthy people in community settings:
o The wide use of masks by healthy people in the community setting
is not supported by current evidence and carries uncertainties and
critical risks."
o "Medical masks should be reserved for health care workers. The use of medical masks in the community may create a false
sense of security, with neglect of other essential measures, such
as hand hygiene practices and physical distancing, and may lead
to touching the face under the masks and under the eyes, result in
unnecessary costs, and take masks away from those in health care
who need them most, especially when masks are in short supply."
o "Masks are effective only when used in combination with frequent hand-cleaning with alcohol-based hand rub or soap and water." WHO acknowledges that most people do not use masks properly.
• But in June 8, 2020
o httg_s:/Lagg_s. who. intfjrisLbitstreamLhandleL10665L332293LWHO-
2019-nCov-/ PC Masks-2020.4-eng.pdf?seguence=1&isAl/owed=.Y-
o The World Health Organization has changed its stance on wearing
face masks during the COVID-19 pandemic. People over 60 and
people with underlying medical conditions should wear a medical
grade mask when they're in public and cannot socially distance.
The general public should wear a three-layer fabric mask in those
situations. Admitting that this was despite evidence with
randomized controlled trials. "The use of a mask alone is
APPENDIX TO JAMES CASCIANO DECLARATION-39

insufficient to provide an adequate level of protection or source
control, and other personal and community level measures should
also be adopted to suppress transmission of respiratory viruses." 0 The reasons for recommending masks has little to do with
effectiveness. "The likely advantages of the use of masks by
healthy people in the general public include:
o reduced potential exposure risk from infected persons before they
develop symptoms;
o reduced potential stigmatization of individuals wearing masks to
prevent infecting others (source control) or of people caring for
COVID-19 patients in non-clinical settings;
o making people feel they can play a role in contributing to stopping
spread of the virus;
o reminding people to be compliant with other measures (e.g., hand
hygiene, not touching nose and mouth).
o potential social and economic benefits.
■ Amidst the global shortage of surgical masks and PPE,
encouraging the public to create their own fabric masks may
promote individual enterprise and community integration.
■ the production of non-medical masks may offer a source of
income for those able to manufacture masks within their
communities.
■ Fabric masks can also be a form of cultural expression,
encouraging public acceptance of protection measures in
general.
■ The safe re-use of fabric masks will also reduce costs and
waste and contribute to sustainability."
• Dr. Nancy Messonnier, director of the Center for the National Center
for Immunization and Respiratory Diseases (January 31, 2020):
o httQ.s:fLwww.cdc.gov Lmedia/Je/easesL2020Lt0131-2019-novel
coronavirus. html
o "We don't routinely recommend the use of face masks by the APPENDIX TO JAMES CASCIANO DECLARATION-40

public to prevent respiratory illness .... And we certainly are not
recommending that at this time for this new virus."
• The Centers for Disease Control and Prevention (CDC)
o httg_s:/Lwww.cdc.gov Lf lufQ.rofessiona/sfjnfectioncontro/Lmaskguida
nce.htm
o In March 5, 2019 regarding the flu: "Masks are not usually
recommended in non-healthcare settings; however, this guidance
provides other strategies for limiting the spread of influenza
viruses in the community":
o *Cover their nose and mouth when coughing or sneezing,
o *Use tissues to contain respiratory secretions and, after use, to
dispose of them in the nearest waste receptacle, and
o *Perform hand hygiene (e.g., handwashing with non-antimicrobial
soap and water, and alcohol-based hand rub if soap and water are
not available) after having contact with respiratory secretions and
contaminated objects/materials.
• On August 7, 2020
o Masks are recommended as a simple barrier to help prevent
respiratory droplets from traveling into the air and onto other
people when the person wearing the mask coughs, sneezes, talks,
or raises their voice. This is called source control.
o CDC recommends that people wear masks in public settings and
when around people who don't live in your household, especially
when other social distancing measures are difficult to maintain.
o Masks may help prevent people who have COVID-19 from
spreading the virus to others.
o Masks are most likely to reduce the spread of COVID-19 when
they are widely used by people in public settings.
o Masks should NOT be worn by children under the age of 2 or
anyone who has trouble breathing, is unconscious, incapacitated,
or otherwise unable to remove the mask without assistance.
o Masks with exhalation valves or vents should NOT be worn to help APPENDIX TO JAMES CASCIANO DECLARATION-41

prevent the person wearing the mask from spreading COVID-19 to
others (source control).
• From the New England Journal of Medicine, Universal Masking in the
Covid-19 Era, July 9, 2020;
o httQs:/Lwww.nejm.orgLdoi/jullL10.1056LNEJMQ2006372
o "We know that wearing a mask outside health care facilities offers
little, if any, protection from infection. Public health authorities
define a significant exposure to Covid-19 as face-to-face contact
within 6 feet with a patient with symptomatic Covid-19 that is
sustained for at least a few minutes (and some say more than 10
minutes or even 30 minutes). The chance of catching Covid-19
from a passing interaction in a public space is therefore minimal. In
many cases, the desire for widespread masking is a reflexive
reaction to anxiety over the pandemic." It is also clear that masks
serve symbolic roles. Masks are not only tools, they are also talismans that may help increase health care workers' perceived sense of safety, well-being, and trust in their
hospitals. Although such reactions may not be strictly logical, we
are all subject to fear and anxiety, especially during times of crisis.
One might argue that fear and anxiety are better countered with
data and education than with a marginally beneficial mask.
o But later authors said, "A growing body of research shows that the
risk of SARS-CoV-2 transmission is strongly correlated with the
duration and intensity of contact: the risk of transmission among
household members can be as high as 40%, whereas the risk of
transmission from less intense and less sustained encounters is
below 5%. This finding is also borne out by recent research
associating mask wearing with less transmission of SARS-CoV-2,
particularly in closed settings."
httQ.s:/Lwww.nejm.orgLdoiLfullL10.1056LNEJMc2020836
• Holland's Medical Care Minister Tamara van Ark
APPENDIX TO JAMES CASCIANO DECLARATION-42
0 httgs:fLwww. thesu n .co. u kLnewsL u knewsL12 29 2 8 21 /.face-mas ks
not-necessa ry_-say_-ho I la nd-scienti stsL
o "Despite a global stampede of mask-wearing, data show that 80-
90 percent of people in Finland and Holland say they "never" wear
masks when they go out, a sharp contrast to the 80-90 percent of
people in Spain and Italy who say they "always" wear masks when
they go out. "From a medical point of view, there is no evidence of
a medical effect of wearing face masks, so we decided not to
impose a national obligation."
• Panel, Rational use of face masks in the COVID-19 pandemic (March
2020) o httgs:f/.www.ncbi.nlm.nih.gov/.gmc/articles/.PMC7118603L o Recommendations on face mask use in community settings
• WHO
■ If you are healthy, you only need to wear a mask if you
are taking care of a person with suspected SARS-CoV-2
infection.
■ China
■ People at moderate risk~ of infection: surgical or
disposable mask for medical use.
■ People at low risk~ of infection: disposable mask for
medical use.
■ People at very low risk= of infection: do not have to wear
a mask or can wear non-medical mask (such as cloth
mask).
■ Hong Kong
■ Surgical masks can prevent transmission of respiratory
viruses from people who are ill. It is essential for people
who are symptomatic (even if they have mild symptoms)
to wear a surgical mask.
■ Wear a surgical mask when taking public transport or
staying in crowded places. It is important to wear a mask
APPENDIX TO JAMES CASCIANO DECLARATION-43

properly and practice good hand hygiene before wearing
and after removing a mask.
■ Singapore
■ Wear a mask if you have respiratory symptoms, such as a
cough or runny nose.
■ Japan
■ The effectiveness of wearing a face mask to protect
yourself from contracting viruses is thought to be limited.
If you wear a face mask in confined, badly ventilated
spaces, it might help avoid catching droplets emitted
from others but if you are in an open-air environment, the
use of face mask is not very efficient.
■ USA ■ Centers for Disease Control and Prevention does not
recommend that people who are well wear a face mask
(including respirators) to protect themselves from
respiratory diseases, including COVID-19.
■ US Surgeon General urged people on Twitter to stop
buying face masks
■ UK ■ Face masks play a very important role in places such as
hospitals, but there is very little evidence of widespread
benefit for members of the public.
■ Germany
Final Thoughts
■ There is not enough evidence to prove that wearing a
surgical mask significantly reduces a healthy person's
risk of becoming infected while wearing it. According to
WHO, wearing a mask in situations where it is not
recommended to do so can create a false sense of
security because it might lead to neglecting fundamental
hygiene measures, such as proper hand hygiene.
APPENDIX TO JAMES CASCIANO DECLARATION-44

• Surgical masks are loose fitting. They are designed to protect the
patient from the doctors' respiratory droplets. There wearer is not
protected from others' airborne particles.
• People do not wear masks properly. Many people have the mask under
the nose. The wearer does not have glasses on and the eyes are a
portal of entry. If the virus lands on the conjunctiva, tears will wash it
into the nasopharynx.
• Most studies cannot separate out hand hygiene.
• The designer masks and scarves offer minimal protection. They give a
false sense of security to both the wearer and those around the wearer.
**Not to mention they add a perverse lightheartedness to the situation.
• If you are walking alone, no need for a mask. Avoid other folks; use
common sense.
• Remember: children under 2 years should not wear masks because of
accidental suffocation and difficulty breathing in some.
• Even if a universal mask mandate were imposed, several studies noted
that folks do not use the mask properly and over-report their wearing.
Additionally, how would the mandate be enforced??
• The positive studies are models that assume universality and full
compliance.
• If wearing a mask makes people go out and get Vitamin D - go for it. In
the 1918 flu pandemic people who went outside did better. Early
reports are showing people with COVID-19 with low Vitamin D do
worse than those with normal levels. Perhaps that is why shut-ins do
so poorly.
htt{J.s:/Lwww.medrxiv.orgLcontentL10.1101L2020.04.08.20058578v4
Wash your hands --- If you are sick, stay home!
Objects and surfaces
• Person to person touching
• The CDC's most recent statement regarding contracting COVID-19
APPENDIX TO JAMES CASCIANO DECLARATION-45

from touching surfaces: "Based on data from lab studies on Covid-19
and what we know about similar respiratory diseases, it may be
possible that a person can get Covid-19 by touching a surface or
object that has the virus on it and then touching their own mouth, nose
or possibly their eyes," the agency wrote. "But this isn't thought to be
the main way the virus spreads.
httQs:/Lwww.cdc.gov Lmedia/_releases/_2020/_s0522-cdc-uQ.dates-covid
transmission. html.
• Chinese study with data taken from swabs on surfaces around the
hospital (July 2020)
o httQ.s:/Lwwwnc. cdc. gov LeidLarticleL26/.7L20-088 5 article?
delivery_Name=USCDC 333-DM25707
o The surfaces where tested with the PCR (polymerase chain
reaction) test, which greatly amplifies the viral genetic material if it
is present. That material is detectable when a person is actively
infected. At the time of the study, it was thought to be the most
reliable test. Because of the amplification of the viral material,
there are many false positives. It is not clear that the mere
presence of virus means it is infectious.
■ Computer mouse (ICU 6/8, 75%; General ward (GW) 1/5,
20%)
■ Trash cans {ICU 3/5, 60%; GW 0/8)
■ Sickbed handrails (ICU 6/14, 42.9%; GW 0/12)
■ Doorknobs {GW 1/12, 8.3%)
■ 81.3% of the miscellaneous personal items were positive:
■ Exercise equipment
■ Medical equipment (spirometer, pulse oximeter, nasal
cannula)
■ PC and iPads
■ Reading glasses
■ Cellular phones (83.3% positive for viral RNA)
■ Remote controls for in-room TVs (64.7% percent
APPENDIX TO JAMES CASCIANO DECLARATION-46

positive)
■ Toilets (81.0% positive)
• Room surfaces (80.4% of all sampled)
• Bedside tables and bed rails (75.0%)
■ Window ledges (81.8%)
■ Plastic: up to 2-3 days
■ Stainless Steel: up to 2-3 days
■ Cardboard: up to 1 day
■ Copper: up to 4 hours
■ Floor - gravity causes droplets to fall to the floor. Half of
ICU workers all had virus on the bottoms of their shoes
APPENDIX TO JAMES CASCIANO DECLARATION-47

Mask use in the context of COVID-19
Interim guidance
1 December 2020
This document, which is an update of the guidance published on 5 June 2020, includes new scientific evidence relevant to the use of masks for reducing the spread of SARS-Co V-2, the virus that causes COVID-19, and practical considerations. It contains updated evidence and guidance on the following: • mask management; • SARS-CoV-2 transmission; • masking in health facilities in areas with community,
cluster and sporadic transmission; • mask use by the public in areas with community and
cluster transmission; • alternatives to non-medical masks for the public; • exhalation valves on respirators and non-medical masks; • mask use during vigorous intensity physical activity; • essential parameters to be considered when
manufacturing non-medical masks (Annex).
Key points
• The World Health Organization (WHO) advises the use of masks as part of a comprehensive package of prevention and control measures to limit the spread of SARS-CoV-2, the virus that causes COVID-19. A mask alone, even when it is used correctly, is insufficient to provide adequate protection or source control. Other infection prevention and control (IPC) measures include hand hygiene, physical distancing of at least I metre, avoidance of touching one's face, respiratory etiquette, adequate ventilation in indoor settings, testing, contact tracing, quarantine and isolation. Together these measures are critical to prevent human-to-human transmission of SARS-Co V-2.
• Depending on the type, masks can be used either for protection of healthy persons or to prevent onward transmission (source control).
• WHO continues to advise that anyone suspected or confirmed of having COVID-19 or awaiting viral laboratory test results should wear a medical mask when in the presence of others (this does not apply to those awaiting a test prior to travel).
• For any mask type, appropriate use, storage and cleaning or disposal are essential to ensure that they are as effective as possible and to avoid an increased transmission risk.
Mask use in health care settings • WHO continues to recommend that health workers (1)
providing care to suspected or confirmed COVID-19
1 For adequate ventilation refer to regional or national institutions or heating, refrigerating and air-conditioning societies enacting ventilation requirements. If not available or applicable, a
• World Health Organization
patients wear the following types of mask/respirator in addition to other personal protective equipment that are part of standard, droplet and contact precautions:
- medical mask in the absence of aerosol generating procedures (AGPs)
- respirator, N95 or FFP2 or FFP3 standards, or equivalent in care settings for COVID-19 patients where AGPs are performed; these may be used by health workers when providing care to COVID-19 patients in other settings if they are widely available and if costs is not an issue.
• In areas of known or suspected community or cluster SARS-CoV-2 transmission WHO advises the following:
- universal masking for all persons (staff, patients, visitors, service providers and others) within the health facility (including primary, secondary and tertiary care levels; outpatient care; and long-term care facilities)
- wearing of masks by inpatients when physical distancing of at least 1 metre cannot be maintained or when patients are outside of their care areas.
• In areas of known or suspected sporadic SARS-CoV-2 transmission, health workers working in clinical areas where patients are present should continuously wear a medical mask. This is known as targeted continuous medical masking for health workers in clinical areas;
• Exhalation valves on respirators are discouraged as they bypass the filtration function for exhaled air by the wearer.
Mask use in community settings • Decision makers should apply a risk-based approach
when considering the use of masks for the general public. • In areas of known or suspected community or cluster
SARS-Co V-2 transmission: - WHO advises that the general public should
wear a non-medical mask in indoor ( e.g. shops, shared workplaces, schools - see Table 2 for details) or outdoor settings where physical distancing of at least 1 metre cannot be maintained.
- If indoors, unless ventilation has been be assessed to be adequate 1, WHO advises that the general public should wear a non-medical mask, regardless of whether physical distancing of at least I metre can be maintained.
recommended ventilation rate of IO Vs/person should be met (except healthcare facilities which have specific requirements). For more infonnation consult "Coronavirus (COVID-19) response

- Individuals/people with higher risk of severe complications from COVID-19 (individuals ::::. 60 years old and those with underlying conditions such as cardiovascular disease or diabetes mellitus, chronic lung disease, cancer, cerebrovascular disease or immunosuppression) should wear medical masks when physical distancing of at least 1 metre cannot be maintained.
• In any transmission scenarios: - Caregivers or those sharing living space with
people with suspected or confirmed COVID-19, regardless of symptoms, should wear a medical mask when in the same room.
Mask use in children (2) • Children aged up to five years should not wear masks
for source control. • For children between six and 11 years of age, a risk
based approach should be applied to the decision to use a mask; factors to be considered in the risk-based approach include intensity of SARS-Co V-2 transmission, child's capacity to comply with the appropriate use of masks and availability of appropriate adult supervision, local social and cultural environment, and specific settings such as households with elderly relatives, or schools.
• Mask use in children and adolescents 12 years or older should follow the same principles as for adults.
• Special considerations are required for immunocompromised children or for paediatric patients with cystic fibrosis or certain other diseases (e.g., cancer), as well as for children of any age with developmental disorders, disabilities or other specific health conditions that might interfere with mask wearing.
Manufacturing of non-medical <fabric} masks (Annex} • Homemade fabric masks of three-layer structure (based
on the fabric used) are advised, with each layer providing a function: 1) an innermost layer of a hydrophilic material 2) an outermost layer made of hydrophobic material 3) a middle hydrophobic layer which has been shown to enhance filtration or retain droplets.
• Factory-made fabric masks should meet the minimum thresholds related to three essential parameters: filtration, breathability and fit.
• Exhalation valves are discouraged because they bypass the filtration function of the fabric mask rendering it unserviceable for source control.
Methodology for developing the guidance
Guidance and recommendations included in this document are based on published WHO guidelines (in particular the WHO Guidelines on infection prevention and control of epidemic-and pandemic-prone acute respiratory infections in health care) (2) and ongoing evaluations of all available scientific evidence by the WHO ad hoc COVID-19 Infection Prevention and Control Guidance Development Group (COVID-19 IPC GOG) (see acknowledgement section for list of GOG members). During emergencies WHO publishes interim guidance, the development of which follows a
resources from ASHRAE and others'' https:/ /www .ashrae.org/technical-resources/resources
transparent and robust process of evaluation of the available evidence on benefits and harms. This evidence is evaluated through expedited systematic reviews and expert consensusbuilding through weekly GOG consultations, facilitated by a methodologist and, when necessary, followed up by surveys. This process also considers, as much as possible, potential resource implications, values and preferences, feasibility, equity, and ethics. Draft guidance documents are reviewed by an external review panel of experts prior to publication.
Purpose of the guidance
This document provides guidance for decision makers, public health and IPC professionals, health care managers and health workers in health care settings (including long-term care and residential), for the public and for manufactures of nonmedical masks (Annex). It will be revised as new evidence emerges.
WHO has also developed comprehensive guidance on IPC strategies for health care settings (3), long-term care facilities (LTCF) (4), and home care (5).
Background
The use of masks is part of a comprehensive package of prevention and control measures that can limit the spread of certain respiratory viral diseases, including COVID-19. Masks can be used for protection of healthy persons ( worn to protect oneself when in contact with an infected individual) or for source control ( worn by an infected individual to prevent onward transmission) or both.
However, the use of a mask alone, even when correctly used (see below), is insufficient to provide an adequate level of protection for an uninfected individual or prevent onward transmission from an infected individual (source control). Hand hygiene, physical distancing of at least 1 metre, respiratory etiquette, adequate ventilation in indoor settings, testing, contact tracing, quarantine, isolation and other infection prevention and control (IPC) measures are critical to prevent human-to-human transmission of SARS-CoV-2, whether or not masks are used ( 6).
Mask management
For any type of mask, appropriate use, storage and cleaning, or disposal are essential to ensure that they are as effective as possible and to avoid any increased risk of transmission. Adherence to correct mask management practices varies, reinforcing the need for appropriate messaging (7).
WHO provides the following guidance on the correct use of masks:
• Perform hand hygiene before putting on the mask. • Inspect the mask for tears or holes, and do not use a
damaged mask. • Place the mask carefully, ensuring it covers the mouth
and nose, adjust to the nose bridge and tie it securely to minimize any gaps between the face and the mask. If using ear loops, ensure these do not cross over as this widens the gap between the face and the mask.

• Avoid touching the mask while wearing it. If the mask is accidently touched, perform hand hygiene.
• Remove the mask using the appropriate technique. Do not touch the front of the mask, but rather untie it from behind.
• Replace the mask as soon as it becomes damp with a new clean, dry mask.
• Either discard the mask or place it in a clean plastic resealable bag where it is kept until it can be washed and cleaned. Do not store the mask around the arm or wrist or pull it down to rest around the chin or neck.
• Perform hand hygiene immediately afterward discarding a mask.
• Do not re-use single-use mask. • Discard single-use masks after each use and properly
dispose of them immediately upon removal. • Do not remove the mask to speak. • Do not share your mask with others. • Wash fabric masks in soap or detergent and preferably
hot water (at least 60° Centigrade/140° Fahrenheit) at least once a day. If it is not possible to wash the masks in hot water, then wash the mask in soap/detergent and room temperature water, followed by boiling the mask for 1 minute.
Scientific evidence
Transmission of the SARS-CoV-2 virus
Knowledge about transmission of the SARS-CoV-2 virus is evolving continuously as new evidence accumulates. COVID-19 is primarily a respiratory disease, and the clinical spectrum can range from no symptoms to severe acute respiratory illness, sepsis with organ dysfunction and death.
According to available evidence, SARS-Co V-2 mainly spreads between people when an infected person is in close contact with another person. Transmissibility of the virus depends on the amount of viable virus being shed and expelled by a person, the type of contact they have with others, the setting and what IPC measures are in place. The virus can spread from an infected person's mouth or nose in small liquid particles when the person coughs, sneezes, sings, breathes heavily or talks. These liquid particles are different sizes, ranging from larger 'respiratory droplets' to smaller 'aerosols.' Close-range contact (typically within 1 metre) can result in inhalation of, or inoculation with, the virus through the mouth, nose or eyes (8-13).
There is limited evidence of transmission through fomites ( objects or materials that may be contaminated with viable virus, such as utensils and furniture or in health care settings a stethoscope or thermometer) in the immediate environment around the infected person ( 14-17). Nonetheless, fomite transmission is considered a possible mode of transmission for SARS-Co V-2, given consistent finding of environmental contamination in the vicinity of people infected with SARSCo V-2 and the fact that other coronaviruses and respiratory viruses can be transmitted this way ( 12).
Aerosol transmission can occur in specific situations in which procedures that generate aerosols are performed. The scientific community has been actively researching whether the SARS-CoV-2 virus might also spread through aerosol transmission in the absence of aerosol generating procedures (AGPs) (18, 19). Some studies that performed air sampling in
clinical settings where AGPs were not performed found virus RNA, but others did not. The presence of viral RNA is not the same as replication- and infection-competent (viable) virus that could be transmissible and capable of sufficient inoculum to initiate invasive infection. A limited number of studies have isolated viable SARS-CoV-2 from air samples in the vicinity of COVID-19 patients (20, 21 ).
Outside of medical facilities, in addition to droplet and fomite transmission, aerosol transmission can occur in specific settings and circumstances, particularly in indoor, crowded and inadequately ventilated spaces, where infected persons spend long periods of time with others. Studies have suggested these can include restaurants, choir practices, fitness classes, nightclubs, offices and places of worship (12).
High quality research is required to address the knowledge gaps related to modes of transmission, infectious dose and settings in which transmission can be amplified. Currently, studies are underway to better understand the conditions in which aerosol transmission or superspreading events may occur.
Current evidence suggests that people infected with SARSCo V-2 can transmit the virus whether they have symptoms or not. However, data from viral shedding studies suggest that infected individuals have highest viral loads just before or around the time they develop symptoms and during the first 5-7 days of illness (12). Among symptomatic patients, the duration of infectious virus shedding has been estimated at 8 days from the onset of symptoms (22-24) for patients with mild disease, and longer for severely ill patients ( 12). The period of infectiousness is shorter than the duration of detectable RNA shedding, which can last many weeks ( 17).
The incubation period for COVID-19, which is the time between exposure to the virus and symptom onset, is on average 5-6 days, but can be as long as 14 days (25, 26).
Pre-symptomatic transmission - from people who are infected and shedding virus but have not yet developed symptoms - can occur. Available data suggest that some people who have been exposed to the virus can test positive for SARS-CoV-2 via polymerase chain reaction (PCR) testing 1-3 days before they develop symptoms (27). People who develop symptoms appear to have high viral loads on or just prior to the day of symptom onset, relative to later on in their infection (28).
Asymptomatic transmission - transmission from people infected with SARS-Co V-2 who never develop symptoms -can occur. One systematic review of 79 studies found that 20% (17-25%) of people remained asymptomatic throughout the course of infection. (28). Another systematic review, which included 13 studies considered to be at low risk of bias, estimated that 17% of cases remain asymptomatic (14%-20%) (30). Viable virus has been isolated from specimens of presymptomatic and asymptomatic individuals, suggesting that people who do not have symptoms may be able to transmit the virus to others. (25, 29-37)
Studies suggest that asymptomatically infected individuals are less likely to transmit the virus than those who develop symptoms (29). A systematic review concluded that individuals who are asymptomatic are responsible for transmitting fewer infections than symptomatic and presymptomatic cases (38). One meta-analysis estimated that there is a 42% lower relative risk of asymptomatic transmission compared to symptomatic transmission (30).

Guidance on mask use in health care settings
Masks for use in health care settings
Medical masks are defined as surgical or procedure masks that are flat or pleated. They are affixed to the head with straps that go around the ears or head or both. Their performance characteristics are tested according to a set of standardized test methods (ASTM F2100, EN 14683, or equivalent) that aim to balance high filtration, adequate breathability and optionally, fluid penetration resistance (39, 40).
Filteringfacepiece respirators (FFR), or respirators, offer a balance of filtration and breathability. However, whereas medical masks filter 3 micrometre droplets, respirators must filter more challenging 0.075 micrometre solid particles. European FFRs, according to standard EN 149, at FFP2 performance there is filtration of at least 94% solid NaCl particles and oil droplets. US N95 FFRs, according to NIOSH 42 CFR Part 84, filter at least 95% NaCl particles. Certified FFRs must also ensure unhindered breathing with maximum resistance during inhalation and exhalation. Another important difference between FFRs and other masks is the way filtration is tested. Medical mask filtration tests are performed on a cross-section of the masks, whereas FFRs are tested for filtration across the entire surface. Therefore, the layers of the filtration material and the FFR shape, which ensure the outer edges of the FFR seal around wearer's face, result in guaranteed filtration as claimed. Medical masks, by contrast, have an open shape and potentially leaking structure. Other FFR performance requirements include being within specified parameters for maximum CO2 build up, total inward leakage and tensile strength of straps (41, 42).
A. Guidance on the use of medical masks and respirators to provide care to suspected or confirmed COVID-19 cases
Evidence on the use of mask in health care settings
Systematic reviews have reported that the use of N95/P2 respirators compared with the use of medical masks (see mask definitions, above) is not associated with statistically significant differences for the outcomes of health workers acquiring clinical respiratory illness, influenza-like illness (risk ratio 0.83, 95%CI 0.63-1.08) or laboratory-confirmed influenza (risk ratio 1.02, 95%CI 0. 73-1.43); harms were poorly reported and limited to discom~ort associate~ with lower compliance (43, 44). In many settmgs, preserving the supply of N95 respirators for high-risk, aerosol-generating procedures is an important consideration ( 45).
A systematic review of observational studies ~n the betacoronaviruses that cause severe acute respiratory syndrome (SARS), Middle East respiratory syndrome (MERS) and COVID-19 found that the use of face protection (including respirators and medical masks) is associated with reduced risk of infection among health workers. These studies suggested that N95 or similar respirators might be associated with greater reduction in risk than medical or 12-16-layer cotton masks. However, these studies had important
2 The WHO list of AGPs includes tracheal intubation, non-invasive ventilation, tracheotomy, cardiopulmonary resuscitation, manual
limitations (recall bias, limited information about the situations when respirators were used and limited ability to measure exposures), and very few studies included in the review evaluated the transmission risk of COVID-19 ( 46). Most of the studies were conducted in settings in which AGPs were performed or other high-risk settings ( e.g., intensive care units or where there was exposure to infected patients and health workers were not wearing adequate PPE).
WHO continues to evaluate the evidence on the effectiveness of the use of different masks and their potential harms, risks and disadvantages, as well as their combination with hand hygiene, physical distancing of at least 1 metre and other IPC measures.
Guidance
WHO's guidance on the type of respiratory protection to be worn by health workers providing care to COVID-19 patients is based on 1) WHO recommendations on IPC for epidemicand pandemic-prone acute respiratory infections in health care (47); 2) updated systematic reviews of randomized controlled trials on the effectiveness of medical masks compared to that ofrespirators for reducing the risk of clinical respiratory illness, influenza-like illness (ILi) and laboratoryconfirmed influenza or viral infections. WHO guidance in this area is aligned with guidelines of other professional organizations, including the European Society of Intensive Care Medicine and the Society of Critical Care Medicine, and the Infectious Diseases Society of America ( 48, 49). ·
The WHO COVID-19 IPC GOG considered all available evidence on the modes of transmission of SARS-Co V-2 and on the effectiveness of medical mask versus respirator use to protect health workers from infection and the potential for harms such as skin conditions or breathing difficulties.
Other considerations included availability of medical masks versus respirators, cost and procurement implications and equity of access by health workers across different settings.
The majority (71%) of the GOG members confirmed their support for previous recommendations issued by WHO on 5 June 2020: 1. In the absence of aerosol generating procedures (AGPs) 2,
WHO recommends that health workers providing care to patients with suspected or confirmed COVID-19 should wear a medical mask (in addition to other PPE that are part of droplet and contact precautions).
2. In care settings for COVID-19 patients where AGPs are performed, WHO recommends that health workers should wear a respirator (N95 or FFP2 or FFP3 standard, or equivalent) in ·addition to other PPE that are part of airborne and contact precautions.
In general, health workers have strong preferences about having the highest perceived protection possible to prevent COVID-19 infection and therefore may place high value on the potential benefits of respirators in settings without AGPs. WHO recommends respirators primarily for settings where AGPs are performed; however, if health workers prefer them and they are sufficiently available and cost is not ~ issu~, they could also be used during care for COVID~ 19 pa!1ents m other settings. For additional guidance on PPE, mcludmg PPE
ventilation before intubation, bronchoscopy, sputum induction using nebulized hypertonic saline, and dentistry and autopsy procedures.

beyond mask use by health workers, see WHO IPC guidance during health care when COVID-19 infection is suspected (3) and also WHO guidance on the rational use of PPE ( 45).
Exhalation valves on respirators are discouraged as they bypass the filtration function for exhaled air.
B. Guidance on the use of mask by health workers, caregivers and others based on transmission scenario
Definitions
Universal masking in health facilities is defined as the requirement for all persons (staff, patients, visitors, service providers and others) to wear a mask at all times except for when eating or drinking.
Targeted continuous medical mask use is defined as the practice of wearing a medical mask by all health workers and caregivers working in clinical areas during all routine activities throughout the entire shift.
Health workers are all people primarily engaged in actions with the primary intent of enhancing health. Examples are: nursing and midwifery professionals, doctors, cleaners, other staff who work in health facilities, social workers, and community health workers.
Evidence on universal masking in health care settings
In areas where there is community transmission or large-scale outbreaks of COVID-19, universal masking has been adopted in many hospitals to reduce the potential of transmission by health workers to patients, to other staff and anyone else entering the facility (50).
Two studies found that implementation of a universal masking policy in hospital systems was associated with decreased risk of healthcare-acquired SARS-Co V-2 infection. However, these studies had serious limitations: both were before-after studies describing a single example of a phenomenon before and after an event of interest, with no concurrent control group, and other infection control measures were not controlled for (51, 52). In addition, observed decreases in health worker infections occurred too quickly to be attributable to the universal masking policy.
Guidance
Although more research on universal masking in heath settings is needed, it is the expert opinion of the majority (79%) of WHO COVID-19 IPC ODO members that universal masking is advisable in geographic settings where there is known or suspected community or cluster transmission of the SARS-Co V-2 virus. 1. In areas of known or suspected community or cluster
SARS-Co V-2 transmission, universal masking should be advised in all health facilities (see Table 1 ).
• All health workers, including community health workers and caregivers, should wear a medical mask at all times, for any activity ( care of COVID-19 or nonCOVID-19 patients) and in any common area (e.g., cafeteria, staff rooms).
• Other staff, visitors, outpatients and service providers should also wear a mask (medical or non-medical) at all times
• Inpatients are not required to wear a mask (medical or non-medical) unless physical distancing of at least 1 metre cannot be maintained ( e.g., when being examined or visited at the bedside) or when outside of their care area ( e.g., when being transported).
• Masks should be changed when they become soiled, wet or damaged or if the health worker/caregiver removes the mask ( e.g., for eating or drinking or caring for a patient who requires droplet/contact precautions for reasons other than COVID-19).
2. In the context of known or suspected sporadic SARSCo V-2 virus transmission, WHO provides the following guidance:
• Health workers, including community health workers and caregivers who work in clinical areas, should continuously wear a medical mask during routine activities throughout the entire shift, apart from when eating and drinking and changing their medical masks after caring for a patient who requires droplet/contact precautions for other reasons. In all cases, medical masks must be changed when wet, soiled, or damaged; used medical masks should be properly disposed of at the end of the shift; and new clean ones should be used for the next shift or when medical masks are changed.
• It is particularly important to adopt the continuous use of masks in potentially high transmission risk settings including triage, family physician/general practitioner offices; outpatient departments; emergency rooms; COVID-19 designated units; haematology, oncology and transplant units; and long-term health and residential facilities.
• Staff who do not work in clinical areas ( e.g., administrative staff) do not need to wear a medical mask during routine activities if they have no exposure to patients.
Whether using masks for universal masking within health facilities or targeted continuous medical mask use throughout the entire shift, health workers should ensure the following:
• Medical mask use should be combined with other measures including frequent hand hygiene and physical distancing among health workers in shared and crowded places such as cafeterias, break rooms, and dressing rooms.
• The medical mask should be changed when wet, soiled, or damaged.
• The medical mask should not be touched to adjust it or if displaced from the face for any reason. If this happens, the mask should be safely removed and replaced, and hand hygiene performed.
• The medical mask ( as well as other personal protective equipment) should be discarded and changed after caring for any patient who requires contact/droplet precautions for other pathogens, followed by hand hygiene.
• Under no circumstances should medical masks be shared between health workers or between others wearing them. Masks should be appropriately disposed of whenever removed and not reused.

• A particulate respirator at least as protective as a United States of America (US) National Institute for Occupational Safety and Health-certified N95, N99, US Food and Drug Administration surgical N95, European Union standard FFP2 or FFP3, or equivalent, should be worn in settings for COVID-19 patients where AGPs are performed (see WHO recommendations below). In these settings, this includes continuous use by health workers throughout the entire shift, when this policy is implemented.
Note: Decision makers may consider the transmission intensity in the catchment area of the health facility or community setting and the feasibility of implementing a universal masking policy compared to a policy based on assessed or presumed exposure risk. Decisions need to take into account procurement, sustainability and costs of the policy. When planning masks for all health workers, longterm availability of adequate medical masks ( and when applicable, respirators) for all workers should be ensured, in particular for those providing care for patients with confirmed or suspected COVID-19. Proper use and adequate waste management should be ensured.
The potential harms and risks of mask and respirator use in the health facility setting include:
• contamination of the mask due to its manipulation by contaminated hands (53, 54);
• potential self-contamination that can occur if medical masks are not changed when wet, soiled or damaged; or by frequent touching/adjusting when worn for prolonged periods (55);
• possible development of facial skin lesions, irritant dermatitis or worsening acne, when used frequently for long hours (56-58);
• discomfort, facial temperature changes and headaches from mask wearing (44, 59, 60);
• false sense of security leading potentially to reduced adherence to well recognized preventive measures such as physical distancing and hand hygiene; and risk-taking behaviours ( 61-64 );
• difficulty wearing a mask in hot and humid environments • possible risk of stock depletion due to widespread use in
the context of universal masking and targeted continuous mask use and consequent scarcity or unavailability for health workers caring for COVID 19 patients and during health care interactions with non-COVID-19 patients where medical masks or respirators might be required.
Alternatives to medical masks in health care settings
The WHO's disease commodity package (DCP) for COVID-19 recommends medical masks for health workers to be type II or higher ( 65). Type II medical masks provide a physical barrier to fluids and particulate materials and have bacterial filtration efficiency of ~98% compared to Type I mask, which has bacterial filtration efficiency of ~95% and lower fluid resistance ( 66) In case of stock outs of type II or higher medical masks, health workers should use a type I medical mask as an alternative. Other alternatives such as face shields or fabric masks should be carefully evaluated.
Face shields are designed to provide protection from splashes of biological fluid (particularly respiratory secretions), chemica1 agents and debris ( 67, 68) into the eyes. In the context of protection from SARS-Co V-2 transmission through respiratory droplets, face shields are used by health workers as personal protective equipment (PPE) for eye protection in combination with a medical mask or a respirator (69, 70) While a face shield may confer partial protection of the facial area against respiratory droplets, these and smaller droplets may come into contact with mucous membranes or with the eyes from the open gaps between the visor and the face (71,67).
Fabric masks are not regulated as protective masks or part of the PPE directive. They vary in quality and are not subject to mandatory testing or common standards and as such are not considered an appropriate alternative to medical masks for protection of health workers. One study that evaluated the use of cloth masks in a health care facility found that health care workers using 2 ply cotton cloth masks (a type of fabric mask) were at increased risk of influenza-like illness compared with those who wore medical masks (72).
In the context of severe medical mask shortage, face shields alone or in combination with fabric mask may be considered as a last resort (73). Ensure proper design of face shields to cover the sides of the face and below the chin.
As for other PPE items, if production of fabric masks for use in health care settings is proposed locally in situations of shortage or stock out, a local authority should assess the product according to specific minimum performance standards and required technical specifications (see Annex).
Additional considerations for community care settings
Like other health workers, community health workers should apply standard precautions for all patients at all times, with particular emphasis regarding hand and respiratory hygiene, surface and environmental cleaning and disinfection and the appropriate use of PPE. When a patient is suspected or confirmed of having COVID-19, community health workers should always apply contact and droplet precautions. These include the use of a medical mask, gown, gloves and eye protection (7 4 ).
IPC measures that are needed will depend on the local COVID-19 transmission dynamics and the type of contact required by the health care activity (see Table I). The community health workforce should ensure that patients and workforce members apply precautionary measures such as respiratory hygiene and physical distancing of at least 1 metre (3.3 feet). They also may support set-up and maintenance of hand hygiene stations and community education (74). In the context of known or suspected community or cluster transmission, community health workers should wear a medical mask when providing essential routine services (see Table 1).

Table 1. Mask use in health care settings depending on transmission scenario, target population, setting, activity and type*
Transmission Target population Setting (where) Activity (what) Mask type (which scenario (who) one)*
Known or Health workers and Health facility For any activity in patient-care Medical mask ( or suspected caregivers (including primary, areas (COVID-19 or non- respirator if aerosol community or secondary, tertiary care COVID-19 patients) or in any generating cluster levels, outpatient care, common areas ( e.g., cafeteria, procedures transmission and long-term care staff rooms) performed) ofSARS- Other staff, patients, facilities) For any activity or in any Medical or fabric CoV-2 visitors, service common area mask
suppliers
Inpatients In single or multiple- When physical distance of at bed rooms least 1 metre cannot be
maintained
Health workers and Home visit ( for When in direct contact with a Medical mask caregivers example, for antenatal patient or when a distance of at
or postnatal care, or for least 1 metre cannot be a chronic condition) maintained.
Community Community outreach programmes/essential routine services
Known or Health workers and Health facility In patient care area- irrespective Medical mask suspected caregivers (including primary, of whether patients have sporadic secondary, tertiary care suspected/confirmed COVID-19 transmission Other staff, patients, levels, outpatient care, No routine activities in patient Medical mask not ofSARS- visitors, service and long-term care areas required. Medical CoV-2 cases suppliers and all others facilities) mask should be
worn if in contact or within 1 metre of patients, or according to local risk assessment
Health workers and Home visit ( for When in direct contact or when a Medical mask caregivers example, for antenatal distance of at least 1 metre
or postnatal care, or for cannot be maintained. a chronic condition)
Community Community outreach programs ( e.g., bed net distribution)
No Health workers and Health facility Providing any patient care Medical mask use documented caregivers (including primary, according to SARS-CoV-2 secondary, tertiary care standard and transmission levels, outpatient care, transmission-based
and long-term care precautions facilities)
Community Community outreach programs
Any Health workers Health care facility Performing an AGP on a Respirator (N95 or transmission (including primary, suspected or confirmed COVID- N99 or FFP2 or scenario secondary, tertiary care 19 patient or providing care in a FFP3)
levels, outpatient care, setting where AGPs are in place and long-term care for COVID-19 patients facilities), in settings where aerosol generating procedures (AGP) are performed
• This table refers only to the use of medical masks and respirators. The use of medical masks and respirators may need to be combined with other personal protective equipment and other measures as appropriate, and always with hand hygiene.
Guidance on mask use in community settings
Evidence on the protective effect of mask use in community settings
At present there is only limited and inconsistent scientific evidence to support the effectiveness of masking of healthy people in the community to prevent infection with respiratory viruses, including SARS-CoV-2 (75). A large randomized community-based trial in which 4862 healthy participants were divided into a group wearing medical/surgical masks and a control group found no difference in infection with SARS-CoV-2 (76). A recent systematic review found nine trials ( of which eight were cluster-randomized controlled trials in which clusters of people, versus individuals, were randomized) comparing medical/surgical masks versus no masks to prevent the spread of viral respiratory illness. Two trials were with healthcare workers and seven in the community. The review concluded that wearing a mask may make little or no difference to the prevention of influenza-like illness (ILi) (RR 0.99, 95%CI 0.82 to 1.18) or laboratory confirmed illness (LCI) (RR 0.91, 95%CI 0.66-1.26) (44); the certainty of the evidence was low for ILi, moderate for LCI.
By contrast, a small retrospective cohort study from Beijing found that mask use by entire families before the first family member developed COVID-19 symptoms was 79% effective in reducing transmission (OR 0.21, 0.06-0.79) (77). A casecontrol study from Thailand found that wearing a medical or non-medical mask all the time during contact with a COVID-19 patient was associated with a 77% lower risk of infection (aOR 0.23; 95% CI 0.09-0.60) (78). Several small observational studies with epidemiological data have reported an association between mask use by an infected person and prevention of onward transmission of SARSCo V-2 infection in public settings. (8, 79-81).
A number of studies, some peer reviewed (82-86) but most published as pre-prints (87-104), reported a decline in the COVID-19 cases associated with face mask usage by the public, using country- or region-level data. One study reported an association between community mask wearing policy adoption and increased movement (less time at home, increased visits to commercial locations) (105). These studies differed in setting, data sources and statistical methods and have important limitations to consider (106), notably the lack of information about actual exposure risk among individuals, adherence to mask wearing and the enforcement of other preventive measures (107, 108).
Studies of influenza, influenza-like illness and human coronaviruses (not including COVID-19) provide evidence that the use of a medical mask can prevent the spread of infectious droplets from a symptomatic infected person to someone else and potential contamination of the environment by these droplets (75). There is limited evidence that wearing a medical mask may be beneficial for preventing transmission between healthy individuals sharing households with a sick person or among attendees of mass gatherings (44, 109-114).
3 For adequate ventilation refer to regional or national institutions or heating, refrigerating and air-conditioning societies enacting ventilation requirements. If not available or applicable, a recommended ventilation rate of IO Vs/person should be met (except healthcare facilities which have specific requirements). For more information consult "Coronavirus (COVID-19) response
A meta-analysis of observational studies on infections due to betacoronaviruses, with the intrinsic biases of observational data, showed that the use of either disposable medical masks or reusable 12-16-layer cotton masks was associated with protection of healthy individuals within households and among contacts of cases ( 46). This could be considered to be indirect evidence for the use of masks (medical or other) by healthy individuals in the wider community; however, these studies suggest that such individuals would need to be in close proximity to an infected person in a household or at a mass gathering where physical distancing cannot be achieved to become infected with the virus. Results from cluster randomized controlled trials on the use of masks among young adults living in university residences in the United States of America indicate that face masks may reduce the rate of influenza-like illness but showed no impact on risk of laboratory-confirmed influenza (115, 116).
Guidance
The WHO COVID-19 IPC GOG considered all available evidence on the use of masks by the general public including effectiveness, level of certainty and other potential benefits and harms, with respect to transmission scenarios, indoor versus outdoor settings, physical distancing and ventilation. Despite the limited evidence of protective efficacy of mask wearing in community settings, in addition to all other recommended preventive measures, the GOG advised mask wearing in the following settings:
1. In areas with known or suspected community or cluster transmission of SARS-Co V-2, WHO advises mask use by the public in the following situations (see Table 2):
Indoor settings: - in public indoor settings where ventilation is known to be
poor regardless of physical distancing: limited or no opening of windows and doors for natural ventilation; ventilation system is not properly functioning or maintained; or cannot be assessed;
- in public indoor settings that have adequate3 ventilation if physical distancing of at least 1 metre cannot be maintained;
- in household indoor settings: when there is a visitor who is not a household member and ventilation is known to be poor, with limited opening of windows and doors for natural ventilation, or the ventilation system cannot be assessed or is not properly functioning, regardless of whether physical distancing of at least 1 metre can be maintained;
- in household indoor settings that have adequate ventilation if physical distancing of at least 1 metre cannot be maintained.
resources from ASHRAE and others'' https://wv.·w.ashrae.org/technical-resources/resources

Table 2. Mask use in community settings depending on transmission scenario, setting, target population, purpose and type*
Transmission scenario
Situations/settings (where) Target Population (who)
Known or suspected Indoor settings, where community or ventilation is known to be cluster transmission poor or cannot be assessed or of SARS-Co V-2 the ventilation system is not
General population in public* settings such as shops, shared workplaces, schools, churches, restaurants, gyms, etc. or in enclosed settings such as public transportation. properly maintained,
regardless of whether
physical distancing of at least For households, in indoor settings, when _1 _m_e_t_er_can_b_e_m_a_in_t_a_in_e_d ___ there is a visitor who is not a member of
Indoor settings that have the household adequate 4 ventilation if physical distancing of at least 1 metre cannot be maintained
Outdoor settings where General population in settings such as physical distancing cannot be crowded open-air markets, lining up maintained outside a building, during
demonstrations, etc.
Purpose of mask use
(why)
Potential benefit for source control
Settings where physical Individuals/people with higher risk of Protection
Known or suspected sporadic transmission, or no documented SARSCo V-2 transmission
distancing cannot be severe complications from COVID-19: maintained, and the individual • People aged ~60 years is at increased risk of infection and/or negative outcomes
Risk-based approach
• People with underlying comorbidities, such as cardiovascular disease or diabetes mellitus, chronic lung disease, cancer, cerebrovascular disease, immunosuppression, obesity, asthma
General population Potential benefit for source control and/or protection
Any transmission Any setting in the community Anyone suspected or confirmed of Source scenario having COVID-19, regardless of control
whether they have symptoms or not, or anyone awaiting viral test results, when in the presence of others
• Public indoor setting includes any indoor setting outside of the household
Mask type (which one)
Fabric mask
Medical mask
Depends on purpose (see details in the guidance content)
Medical mask
4 For adequate ventilation refer to regional or national institutions or heating, refrigerating and air-conditioning societies enacting ventilation requirements. Ifnot available or applicable, a recommended ventilation rate of 101/s/person should be met (except healthcare facilities which have specific requirements).). For more information consult "Coronavirus (COVID-19) response resources from ASHRAE and others" https://www.ashrae.org/technical-resources/resources

In outdoor settings: - where physical distancing of at least l metre cannot be
maintained;
individuals/people with higher risk of severe complications from COVID-19 (individuals~ 60 years old and those with underlying conditions such as cardiovascular disease or diabetes mellitus, chronic lung disease, cancer, cerebrovascular disease or immunosuppression) should wear medical masks in any setting where physical distance cannot be maintained.
· 2. In areas with known or suspected sporadic transmission or no documented transmission, as in all transmission scenarios, WHO continues to advise that decision makers should apply a risk-based approach focusing on the following criteria when considering the use of masks for the public: • Purpose of mask use. Is the intention source control
(preventing an infected person from transmitting the virus to others) or protection (preventing a healthy wearer from the infection)?
• Risk of exposure to SARS-Co V-2. Based on the epidemiology and intensity of transmission in the population, is there transmission and limited or no capacity to implement other containment measures such as contact tracing, ability to carry out testing and isolate and care for suspected and confirmed cases? Is there risk to individuals working in close contact with the public ( e.g., social workers, personal support workers, teachers, cashiers)?
• Vulnerability of the mask wearer/population. Is the mask wearer at risk of severe complications from COVID-19? Medical masks should be used by older people (2: 60 years old), immunocompromised patients and people with comorbidities, such as cardiovascular disease or diabetes mellitus, chronic lung disease, cancer and cerebrovascular disease ( 11 7).
• Setting in which the population lives. Is there high population density (such as in refugee camps, camp-like settings, and among people living in cramped conditions) and settings where individuals are unable to keep a physical distance of at least 1 metre (for example, on public transportation)?
• Feasibility. Are masks available at an affordable cost? Do people have access to clean water to wash fabric masks, and can the targeted population tolerate possible adverse effects of wearing a mask?
• Type of mask. Does the use of medical masks in the community divert this critical resource from the health workers and others who need them the most? In settings where medical masks are in short supply, stocks should be prioritized for health workers and at-risk individuals.
The decision of governments and local jurisdictions whether to recommend or make mandatory the use of masks should be based on the above assessment as well as the local context, culture, availability of masks and resources required.
3. In any transmission scenario: • Persons with any symptoms suggestive of COVID-19
should wear a medical mask and (5) additionally: - self-isolate and seek medical advice as soon as they
start to feel unwell with potential symptoms of COVID-19, even if symptoms are mild);
- follow instructions on how to put on, take off, and dispose of medical masks and perform hand hygiene (118);
- follow all additional measures, in particular respiratory hygiene, frequent hand hygiene and maintaining physical distance of at least 1 metre from other persons ( 46). If a medical mask is not available for individuals with suspected or confirmed COVID-19, a fabric mask meeting the specifications in the Annex of this document should be worn by patients as a source control measure, pending access to a medical mask. The use of a nonmedical mask can minimize the projection of respiratory droplets from the user (I I 9, 120).
- Asymptomatic persons who test positive for SARSCo V-2, should wear a medical mask when with others for a period of IO days after testing positive.
Potential benefits/harms
The potential advantages of mask use by healthy people in the general public include: • reduced spread of respiratory droplets containing
infectious viral particles, including from infected persons before they develop symptoms ( 121 );
• reduced potential for stigmatization and greater of acceptance of mask wearing, whether to prevent infecting others or by people caring for COVID-19 patients in non-clinical settings (122);
• making people feel they can play a role in contributing to stopping spread of the virus;
• encouraging concurrent transmission prevention behaviours such as hand hygiene and not touching the eyes, nose and mouth (123-125);
• preventing transmission of other respiratory illnesses like tuberculosis and influenza and reducing the burden of those diseases during the pandemic ( 126).
The potential disadvantages of mask use by healthy people in the general public include: • headache and/or breathing difficulties, depending on
type of mask used (55); • development of facial skin lesions, irritant dermatitis or
worsening acne, when used frequently for long hours (58, 59, 127);
• difficulty with communicating clearly, especially for persons who are deaf or have poor hearing or use lip reading (128, 129);
• discomfort ( 44, 55, 59) • a false sense of security leading to potentially lower
adherence to other critical preventive measures such as physical distancing and hand hygiene ( 105);
• poor compliance with mask wearing, in particular by young children (111, 130-132);
• waste management issues; improper mask disposal leading to increased litter in public places and environmental hazards (133);
• disadvantages for or difficulty wearing masks, especially for children, developmentally challenged persons, those with mental illness, persons with cognitive impairment, those with asthma or chronic respiratory or breathing problems, those who have had facial trauma or recent oral maxillofacial surgery and those living in hot and humid environments (55, 130).

Considerations for implementation
When implementing mask policies for the public, decisionmakers should: • clearly communicate the purpose of wearing a mask,
including when, where, how and what type of mask should be worn; explain what wearing a mask may achieve and what it will not achieve; and communicate clearly that this is one part of a package of measures along with hand hygiene, physical distancing, respiratory etiquette, adequate ventilation in indoor settings and other measures that are all necessary and all reinforce each other;
• inform/train people on when and how to use masks appropriately and safely (see mask management and maintenance sections);
• consider the feasibility of use, supply/access issues ( cleaning, storage), waste management, sustainability, social and psychological acceptance ( of both wearing and not wearing different types of masks in different contexts);
• continue gathering scientific data and evidence on the effectiveness of mask use (including different types of masks) in non-health care settings;
• evaluate the impact (positive, neutral or negative) of using masks in the general population (including behavioural and social sciences) through good quality research.
Mask use during physical activity
Evidence
There are limited studies on the benefits and harms of wearing medical masks, respirators and non-medical masks while exercising. Several studies have demonstrated statistically significant deleterious effects on various cardiopulmonary physiologic parameters during mild to moderate exercise in healthy subjects and in those with underlying respiratory diseases ( 134-140). The most significant impacts have been consistently associated with the use of respirators and in persons with underlying obstructive airway pulmonary diseases such as asthma and chronic obstructive pulmonary disease (COPD), especially when the condition is moderate to severe (136). Facial microclimate changes with increased temperature, humidity and perceptions of dyspnoea were also reported in some studies on the use of masks during exercise ( 134, 141 ). A recent review found negligeable evidence of negative effects of mask use during exercise but noted concern for individuals with severe cardiopulmonary disease (142).
Guidance
WHO advises that people should not wear masks during vigorous intensity physical activity (143) because masks may reduce the ability to breathe comfortably. The most important preventive measure is to maintain physical distancing of at least 1 meter and ensure good ventilation when exercising.
If the activity takes place indoors, adequate ventilation should be ensured at all times through natural ventilation or a properly functioning or maintained ventilation system (144). Particular attention should be paid to cleaning and disinfection of the environment, especially high-touch surfaces. If all the above measures cannot be ensured, consider temporary closure of public indoor exercise facilities ( e.g., gyms).
Face shields for the general public
At present, face shields are considered to provide a level of eye protection only and should not be considered as an equivalent to masks with respect to respiratory droplet protection and/or source control. Current laboratory testing standards only assess face shields for their ability to provide eye protection from chemical splashes ( 145).
In the context of non-availability or difficulties wearing a non-medical mask (in persons with cognitive, respiratory or hearing impairments, for example), face shields may be considered as an alternative, noting that they are inferior to masks with respect to droplet transmission and prevention. If face shields are to be used, ensure proper design to cover the sides of the face and below the chin.
Medical masks for the care of COVID-19 patients at home
WHO provides guidance on how to care for patients with confirmed and suspected COVID-19 at home when care in a health facility or other residential setting is not possible (5).
Persons with suspected COVID-19 or mild COVID-19 symptoms should wear a medical mask as much as possible, especially when there is no alternative to being in the same room with other people. The mask should be changed at least once daily. Persons who cannot tolerate a medical mask should rigorously apply respiratory hygiene (i.e., cover mouth and nose with a disposable paper tissue when coughing or sneezing and dispose of it immediately after use or use a bent elbow procedure and then perform hand hygiene). Caregivers of or those sharing living space with people with suspected COVID-19 or with mild COVID-19 symptoms should wear a medical mask when in the same room as the affected person.
References
1. World Health Organization. The World Health Report 2006 - working together for health. Geneva: World Health Organization; 2006.( https://apps.who.int/iris/handle/10665/43432 accessed 21 November 2020)
2. World Health Organziation. Advice on the use of masks for children in the context ofCOVID-19. Annex to the Advice on the use of masks in the context of COVID-19. Geneva, 2020. (https:/ /apps. who.int/iris/handle/ 10665/3 3 3919 accessed 21 November 2020).
3. World Health Organziation. Infection prevention and control during health care when COVID-19 is suspected: interim guidance. Geneva: World Health Organization; 2020. (https ://apps. who. int/iris/handle/ I 0665/3 3 2879. accessed 21 November 2020).
4. World Health Organziation. Infection prevention and control for long-term care facilities in the context of COVID-19: interim guidance. Geneva: World Health Organization; 2020 (https://apps. who.int/iris/handle/ I 0665/3 315 08 accessed 21 November 2020).

5. World Health Organziation. Home care for patients Host, and Environmental Factors. Ann Intern Med. with suspected or confirmed COVID-19 and 2020;M20-5008. doi: 10. 7326/M20-5008 management of their contacts: interim guidance. 18. Wei J, Li Y. Airborne spread of infectious agents in the Geneva: World Health Organization; 2020 indoor environment. Am J Infect Control. 2016;44(9 (htt12s://a1ws. who.int/iris/handle/ 10665/3 3 3 782. Suppl):S 102-8. accessed 21 November 2020). 19. McCarthy J, McCarthy M. Long range versus short
6. World Health Organziation. Infection prevention and range aerial transmission ofSARS-CoV-2. 2020 control of epidemic-and pandemic prone acute httgs://arxiv.org/gdf/2008.03558.gdf (Accessed 24 respiratory infections in health care. November 2020). (httgs://ai;ms.who.int/iris/bitstream/handle/10665/11265 20. Lednicky JA, Lauzardo M, Fan ZH, et al. Viable 6/9789241507134 eng.ndf?seguence= 1 Accessed 21 SARS-Co V-2 in the air of a hospital room with November 2020). COVID-19 patients. medRxiv.
7. Machida M, Nakamura I, Saito R, Nakaya T, doi:10.l 101/2020.08.03.20167395 Hanibuchi T, Takamiya T, et al. Incorrect Use of Face 21. Ring N, Ritchie K, Mandava L, Jepson R. A guide to Masks during the Current COVID-19 Pandemic among synthesising qualitative research for researchers the General Public in Japan. Int J Environ Res Public undertaking health technology assessments and Health. 2020; 17( 18). systematic reviews. 2011. NHS Quality Improvement
8. Liu J, Liao X, Qian S, Yuan J, Wang F, Liu Y, et al. Scotland (NHS QIS). Community Transmission of Severe Acute Respiratory 22. Wolfel R, Corman VM, Guggemos W, Seilmaier M, Syndrome Coronavirus 2, Shenzhen, China, 2020. Zange S, Muller MA, et al. Virological assessment of Emerg Infect Dis. 2020;26(6):1320-3. hospitalized patients with COVID-2019. Nature.
9. Chan JF, Yuan S, Kok KH, To KK, Chu H, Yang J, et 2020;58 l (7809):465-9. al. A familial cluster of pneumonia associated with the 23. van Kampen J, van de Vijver D, Fraaij P, Haagmans B, 2019 novel coronavirus indicating person-to-person Lamers M, Okba Nea. Shedding of infectious virus in transmission: a study of a family cluster. Lancet. hospitalized patients with coronavirus disease-2019 2020;395( 10223):514-23. (COVID19): duration and key determinants. MedRxiv.
10. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. 2020 doi: 10.1101/2020.06.08.20125310. Clinical features of patients infected with 2019 novel 24. Centers for Disease Control and Prevention. Symptom-coronavirus in Wuhan, China. Lancet. Based Strategy to Discontinue Isolation for Persons 2020;395(10223):497-506. with COVID-19. Atlanta: Centers for Disease Control
11. Burke RM, Midgley CM, Dratch A, Fenstersheib M, and Prevention; Haupt T, Holshue M, et al. Active Monitoring of (htti:2s:/fa,ww.cdc.gov/coronavirus/2019-Persons Exposed to Patients with Confirmed COVID- ncov/communitx/strategx-discontinue-isolation.html, 19 - United States, January-February 2020. MMWR accessed 21 November 2020). Morb Mortal Wkly Rep. 2020;69(9):245-6. 25. Yu P, Zhu J, Zhang Z, Han Y. A Familial Cluster of
12. World Health Organziation. Transmission ofSARS- Infection Associated With the 2019 Novel Coronavirus CoV-2: implications for infection prevention Indicating Possible Person-to-Person Transmission precautions. During the Incubation Period. J Infect Dis. (httns:/ /anns. who.int/iris/handle/ 10665/3 3 3114 2020;221(11):1757-61. E accessed 21 November 2020). 26. Lauer SA, Grantz KH, Bi Q, Jones FK, Zheng Q,
13. World Health Organziation. Coronavirus disease 2019 Meredith HR, et al. The Incubation Period of (COVID-19) Situation Report- 73. Geneva: World Coronavirus Disease 2019 (COVID-19) From Publicly Health Organization; 2020 Reported Confirmed Cases: Estimation and (httns://www.who.int/docs/default- Application. Ann Intern Med. 2020;172(9):577-82. source/coronaviruse/situation-renorts/20200402-sitren- 27. Kimball A, Hatfield KM, Arons M, James A, Taylor J, 73-covid-I 9.Qdf?sfvrsn=5ae25bc7 6, accessed 21 Spicer K, et al. Asymptomatic and Presymptomatic November 2020). SARS-Co V-2 Infections in Residents of a Long-Term
14. Cheng VCC, Wong SC, Chen JHK., Yip CCY, Chuang Care Skilled Nursing Facility- King County, VWM, Tsang OTY, et al. Escalating infection control Washington, March 2020. MMWR Morb Mortal Wkly response to the rapidly evolving epidemiology of the Rep. 2020;69(13):377-81. coronavirus disease 2019 (COVID-19) due to SARS- 28. He X, Lau EHY, Wu P, Deng X, Wang J, Hao X, et al. CoV-2 in Hong Kong. Infect Control Hosp Epidemiol. Temporal dynamics in viral shedding and 2020;4 l ( 5):493-8. transmissibility ofCOVID-19. Nat Med.
15. Ong SWX, Tan YK, Chia PY, Lee TH, Ng OT, Wong 2020;26(5):672-5. MSY, et al. Air, Surface Environmental, and Personal 29. Buitrago-Garcia D, Egli-Gany D, Counotte MJ, Protective Equipment Contamination by Severe Acute Hossmann S, Imeri H, Ipekci AM, et al. Occurrence Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and transmission potential of asymptomatic and From a Symptomatic Patient. JAMA. 2020. presymptomatic SARS-CoV-2 infections: A living 323(16):1610-1612. doi: 10.1001/jama.2020.3227. systematic review and meta-analysis. PLoS Med.
16. van Doremalen N, Bushmaker T, Morris DH, Holbrook 2020; 17(9):e 1003346. MG, Gamble A, Williamson BN, et al. Aerosol and 30. Byambasuren 0, Cardona, M., Bell, K., Clark, J., Surface Stability of SARS-Co V-2 as Compared with Mclaws, M.-L., Glasziou, P. Estimating the extent of SARS-CoV-1. N Engl J Med. 2020;382(16):1564-7. true asymptomatic COVID-19 and its potential for
17. Meyerowitz EA, Richterman A, Gandhi RT, Sax PE. community transmission: systematic review and meta-Transmission ofSARS-CoV-2: A Review of Viral, analysis. JAMMI 2020 doi: 10.3 l 38/jammi-2020-0030
31. Arons MM, Hatfield KM, Reddy SC, Kimball A, James 45. World Health Organziation. Rational use of personal A, Jacobs JR, et al. Presymptomatic SARS-Co V-2 protective equipment for coronavirus disease 2019 Infections and Transmission in a Skilled Nursing (COVID-19). Geneva: World Health Organization; Facility. N Engl J Med. 2020;382(22):2081-90. 2020
32. Hu Z, Song C, Xu C, Jin G, Chen Y, Xu X, et al. (htt:gs://am2s. who.int/iris/rest/bitstreams/ 127 4340/retrie Clinical characteristics of 24 asymptomatic infections ve accessed 21 November 2020). with COVID-19 screened among close contacts in 46. Chu DK, Aki EA, Duda S, Solo K, Y aacoub S, Nanjing, China. Sci China Life Sci. 2020;63(5):706-11. Schunemann HJ, et al. Physical distancing, face masks,
33. Huang R, Xia J, Chen Y, Shan C, Wu C. A family and eye protection to prevent person-to-person cluster of SARS-CoV-2 infection involving 11 patients transmission ofSARS-CoV-2 and COVID-19: a in Nanjing, China. Lancet Infect Dis. 2020;20(5):534-5. systematic review and meta-analysis. Lancet.
34. Pan X, Chen D, Xia Y, Wu X, Li T, Ou X, et al. 2020;395(10242): 1973-87. Asymptomatic cases in a family cluster with SARS- 47. Chan AJ, Islam MK, Rosewall T, Jaffray DA, Easty CoV-2 infection. Lancet Infect Dis. 2020;20(4):410-1. AC, Cafazzo JA. The use of human factors methods to
35. Wang Y, Tong J, Qin Y, Xie T, Li J, Li J, et al. identify and mitigate safety issues in radiation therapy. Characterization of an asymptomatic cohort of SARS- Radiotherapy and Oncology. 2010;97(3):596-600. COV-2 infected individuals outside of Wuhan, China. 48. Brilli RJ, Spevetz A, Branson RD, Campbell GM, Clin Infect Dis. 2020; 71(16):2132-2138. doi: Cohen H, Dasta JF, et al. Critical care delivery in the 10.1093/cid/ciaa629. intensive care unit: defining clinical roles and the best
36. Wei WE, Li Z, Chiew CJ, Yong SE, Toh MP, Lee VJ. practice model. Crit Care Med. 2001;29(10):2007-19. Presymptomatic Transmission of SARS-Co V-2 - 49. Roland D, Mccaffery K, Davies F. Scoring systems in Singapore, January 23-March 16, 2020. MMWR Morb paediatric emergency care: Panacea or paper exercise? Mortal Wkly Rep.2020;69(14):411-5. Journal of paediatrics and child health. 2016;52(2):181-
37. Bae SH, Shin H, Koo HY, Lee SW, Yang JM, Yon 6. DK. Asymptomatic Transmission of SARS-Co V-2 on 50. Klompas M, Morris CA, Sinclair J, Pearson M, Shenoy Evacuation Flight. Emerg Infect Dis. 2020;26( 11 ). ES. Universal Masking in Hospitals in the Covid-19
38. Qiu X, Nergiz I, Maraolo A, Bogoch, Low N, Cevik M. Era. N Engl J Med. 2020;382(2 l ):e63 Defining the role of asymptomatic SARS-Co V-2 51. Seide Iman J, Lewis S, Advani S, Akinboyo I, Epling C, transmission: a living systematic review. MedRxiv. Case M, et al. Universal Masking is an Effective 2020 doi: IO.I 101/2020.09.01.20135194. Strategy to Flatten the SARS-2-Co V Healthcare
39. European Standards. UNE EN 14683:2019+AC:2019. Worker Epidemiologic Curve. Infect Control Hosp Medical Face Masks -Requirements and Test Methods. Epidemiol. 2020:1-5. 2019; (httgs://www .en-standard.eu/une-en-14683- 52. Wang X, Ferro EG, Zhou G, Hashimoto D, Bhatt DL. 2019-ac-2019-medical-face-masks-reguirements-and- Association Between Universal Masking in a Health test-methods/ accessed 21 November 2020) Care System and SARS-CoV-2 Positivity Among
40. ASTM International. F23 Committee. Specification for Health Care Workers. JAMA. 2020; 324(7):703-704. Performance of Materials Used in Medical Face 53. Zamora JE, Murdoch J, Simchison B, Day AG. Masks.(httgs:/ /www .astm.org/Standards/F2100.htm Contamination: a comparison of 2 personal protective accessed 21 November 2020) systems. CMAJ. 2006; 175(3):249-54.
41. National Institute for Occupational Safety and 54. Kwon JH, Burnham CD, Reske KA, Liang SY, Hink T, Health (NIOSH). NIOSH Guide to the Selection and Wallace MA, et al. Assessment of Healthcare Worker Use of Particulate Respirators. Department of Health Protocol Deviations and Self-Contamination During and Human Services (DHHS) NIOSH publication Personal Protective Equipment Donning and Doffing. number 96-101, 1996. Infect Control Hosp Epidemiol. 2017;38(9):1077-83. (httgs://www .cdc.gov/niosh/docs/96-10 I /default.html 55. Bakhit M, Krzyzaniak N, Scott A, Clark J, Glasziou P, accessed 21 November 2020) Del Mar C. Downsides of face masks and possible
42. CEN, E., 2001. 149: 2001 norm: Respiratory protective mitigation strategies: a systematic review and meta-devices-Filtering half masks to protect against analysis. MedRxiv. 2020 doi: particles-Requirements, testing, marking. European IO.I 101/2020.06.16.20133207. Committee for Standardization. 56. Foo CC, Goon AT, Leow YH, Goh CL. Adverse skin (htms://shog.bsigroug.com/ProductDetail?gid=0000000 reactions to personal protective equipment against 00030178264 accessed 21 November 2020). severe acute respiratory syndrome--a descriptive study
43. Long Y, Hu T, Liu L, Chen R, Guo Q, Yang L, et al. in Singapore. Contact Dermatitis. 2006;55(5):291-4. Effectiveness ofN95 respirators versus surgical masks 57. Radonovich LJ, Jr., SimberkoffMS, Bessesen MT, against influenza: A systematic review and meta- Brown AC, Cummings DAT, Gaydos CA, et al. N95 analysis. J Evid Based Med. 2020; 13(2):93-101. Respirators vs Medical Masks for Preventing Influenza
44. Jefferson T DMC, Dooley L, Ferroni E, AI-Ansary LA, Among Health Care Personnel: A Randomized Clinical Bawazeer GA, et al. Physical interventions to interrupt Trial. JAMA. 2019;322(9):824-33. or reduce the spread of respiratory viruses. Cochrane 58. Al Badri F. Surgical mask contact dermatitis and Database of Systematic Reviews 2020;( 11 ):CD006207. epidemiology of contact dermatitis in healthcare doi:10.1002/14651858.CD006207.pub5. 2020. workers. Current Allergy & Clinical Immunology,
2017; 30,3: 183 - 188.

59. Matusiak L, Szepietowska M, Krajewski P, Bialynicki- 73. Centers for Disease Control and Prevention. If You Are Birula R, Szepietowski JC. Inconveniences due to the Immunocompromised, Protect Yourself From COVID-use of face masks during the COVID-19 pandemic: a 19. (httgs://www.cdc.gov/coronavirus/2019-ncov/need-survey study of 876 young people. Dermatol Ther. extra-grecautions/immunocomgromised.html accessed 2020. doi: 10.1111/dth.13567 21 November 2020).
60. MacIntyre CR, Wang Q, Cauchemez S, Seale H, 74. Nielsen J, Landauer TK, editors. A mathematical model Dwyer DE, Yang P, et al. A cluster randomized clinical of the finding of usability problems. Proceedings of the trial comparing fit-tested and non-fit-tested N95 INTERACT'93 and CHI'93 conference on Human respirators to medical masks to prevent respiratory factors in computing systems. ACM. 1993; 206-213. virus infection in health care workers. Influenza Other 75. Chou R, Dana T, Jungbauer R, Weeks C, McDonagh Respir Viruses. 2011;5(3):170-9. MS. Masks for Prevention of Respiratory Virus
61. Morrongiello BA, Major K. Influence of safety gear on Infections, Including SARS-CoV-2, in Health Care and parental perceptions of injury risk and tolerance or Community Settings: A Living Rapid Review. Ann children's risk taking. Inj Prev. 2002;8(1):27-31. Intern Med. 2020; 173(7):542-555. doi: 10.7326/M20-
62. Morrongiello BA, Walpole B, Lasenby J. 3213 Understanding children's injury-risk behavior: wearing 76. Bundgaard H, J. B, Raaschou-Pedersen D, von safety gear can lead to increased risk taking. Accid Buchwald C, Todsen T, Norsk J. Effectiveness of Anal Prev. 2007;39(3):618-23. Adding a Mask Recommendation to Other Public
63. Lasenby-Lessard J, Morrongiello BA. Understanding Health Measures to Prevent SARS-CoV-2 Infection in risk compensation in children: Experience with the Danish Mask Wearers. Ann Intern Med. 2020. doi: activity and level of sensation seeking play a role. 10.7326/M20-6817. Accid Anal Prev. 2011;43(4):1341-7. 77. Wang Y, Tian H, Zhang L, Zhang M, Guo D, Wu W, et
64. DiLillo D, Tremblay G. Maternal and child reports of al. Reduction of secondary transmission of SARS-behavioral compensation in response to safety CoV-2 in households by face mask use, disinfection equipment usage. J Pediatr Psycho I. 2001 ;26(3 ): 175- and social distancing: a cohort study in Beijing, China. 84. BMJ Glob Health. 2020; 5(5): e002794.
65. Thomas EJ, Sexton JB, Helmreich RL. Translating 78. Doung-ngern P, Suphanchaimat R, Panjangampatthana teamwork behaviours from aviation to healthcare: A, Janekrongtham C, Ruampoom D, Daochaeng N. development of behavioural markers for neonatal Associations between mask-wearing, handwashing, and resuscitation. Qual Saf Health Care. 2004 Oct; social distancing practices and risk 2 of COVID-19 13(Suppl 1 ): i57-i64. infection in public: a case-control study in Thailand.
66. Pri-Med Medicinal Products. Mask Protection Emerg Infect Dis. 2020;26(11):2607-2616. Standards & Medical Face Mask Information For Use. 79. Chen J, He H, Cheng W. Potential transmission of (httgs://www.grimed.ca/clinical-resources/astm-mask- SARS-Co V-2 on a flight from Singapore to Hangzhou, grotection- China: An epidemiological investigation. Travel Med standards/#:~:text=Are%20there%20different%20level Infect Dis. 2020; 36: 101816. s%20ot%20grotection%20with%20ASTM- 80. Hendrix MJ, Walde C, Findley K, Trotman R. Absence rated2%20%20160%20%201 %20more%20rows%20 of Apparent Transmission of SARS-Co V-2 from Two accessed 21 November 2020). Stylists After Exposure at a Hair Salon with a
67. Hirschmann MT, Hart A, Henckel J, Sadoghi P, Seil R, Universal Face Covering Policy - Springfield, Mouton C. COVID-19 coronavirus: recommended Missouri, May 2020. MMWR Morb Mortal Wkly Rep. personal protective equipment for the orthopaedic and 2020;69(28):930-2. trauma surgeon. Knee Surg Sports Traumatol Arthrosc. 81. Schwartz KL, Murti M, Finkelstein M, Leis JA, 2020;28( 6): 1690-8. Fitzgerald-Husek A, Bourns L, et al. Lack of COVID-
68. Anon JB, Denne C, Rees D. Patient-Worn Enhanced 19 transmission on an international flight. CMAJ. Protection Face Shield for Flexible Endoscopy. 2020; 192(15):E410. Otolaryngol Head Neck Surg. 2020;163(2):280-3. 82. Chiang CH, Chiang CH, Chiang CH, Chen YC. The
69. McBride ME, Waldrop WB, Fehr JJ, Boulet JR, Practice of Wearing Surgical Masks during the Murray DJ. Simulation in pediatrics: the reliability and COVID-19 Pandemic. Emerg Infect Dis. validity of a multiscenario assessment. Pediatrics. 2020;26(8): 1962. 2011; 128: 335-343. 83. Cheng VC, Wong SC, Chuang VW, So SY, Chen JH,
70. KWtler CJ, Hain R. Fundamental protective Sridhar S, et al. The role of community-wide wearing mechanisms of face masks against droplet infections. J of face mask for control of coronavirus disease 2019 Aerosol Sci. 2020; 148: 105617. (COVID-19) epidemic due to SARS-Co V-2. J Infect.
71. Lindsley WG, Noti JD, Blachere FM, Szalajda N, 2020;81 ( 1):107-14. Beezhold DH. Efficacy of face shields against cough 84. Bo Y, Guo C, Lin C, et al. Effectiveness of non-aerosol droplets from a cough simulator. J Occup pharmaceutical interventions on COVID-19 Environ Hyg. 2014;11(8):509-18. transmission in 190 countries from 23 January to 13
72. MacIntyre CR, Seale H, Dung TC, Hien NT, Nga PT, April 2020. Int J Infect Dis. 2020; 102: 247-253. Chughtai AA, et al. A cluster randomised trial of cloth 85. Lyu W, Wehby GL. Community Use Of Face Masks masks compared with medical masks in healthcare And COVID-19: Evidence From A Natural Experiment workers. BMJ Open. 2015;5(4):e006577. Of State Mandates In The US. Health Aff (Millwood).
2020;39(8): 1419-25.

86. Gallaway MS, Rigler J, Robinson S, Herrick K, Livar E, Komatsu KK, et al. Trends in COVID-19 Incidence After Implementation of Mitigation Measures -Arizona, January 22-August 7, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(40):1460-3.
87. Rader B, White LF, Burns MR, Chen J, Brilliant J, Cohen J, et al. Mask Wearing and Control ofSARSCoV-2 Transmission in the United States. MedRxiv. 2020. doi: 10.l 101/2020.08.23.20078964.
88. Matzinger P, Skinner J. Strong impact of closing schools, closing bars and wearing masks during the Covid-19 pandemic: results from a simple and revealing analysis. MedRxiv. 2020. doi: 10.l 101/2020.09.26.20202457.
89. Kenyon C. Widespread use of face masks in public may slow the spread ofSARS CoV-2: 1 an ecological study. MedRxiv. 2020. doi: 10.l 101/2020.03.31.20048652.
90. Leffler CT, Ing E, Lykins JD, Hogan MC, McKeown CA, Grzybowski A. Association of Country-wide Coronavirus Mortality with Demographics, Testing, Lockdowns, and Public Wearing of Masks. Am J Trop Med Hyg. 2020. doi: 10.4269/ajtmh.20-1015.
91. Lan F-Y, Christophi C, Buley J, Lliaki E, BrunoMurtha L, Sayah A, et al. Effects of universal masking on Massachusetts healthcare workers' COVID-19 incidence. MedRxiv. 2020. doi: 10.l 101/2020.08.09.20171173.
92. Aravindakshan A, Boehnke J, Gholami E, Nayak A. Mask-Wearing During the COVID-19 Pandemic. MedRxiv. 2020. doi: IO.I 101/2020.09.11.20192971.
93. Pletz M, Steiner A, Kesselmeier M, Loeffler B, Trommer S, Weis S, et al. Impact of universal masking in health care and community on SARS-CoV-2 spread. MedRxiv. 2020. doi: 10.1101/2020.09.02.20187021.
94. Fortaleza C, et al. Impact of nonpharmaceutical governmental strategies for prevention and control of COVID-19 in Sao Paulo State, Brazil. MedRxiv. 2020. doi: 10.1101/2020.08.23.20180273.
95. Karaivanov A, Lu SE, Shigeoka H, Chen C, Pamplona S. Face Masks, Public Policies and Slowing the Spread ofCOVID-19: Evidence from Canada. MedRxiv. 2020. doi: IO.I 101/2020.09.24.20201178.
96. Miyazawa D, Kaneko G. Face mask wearing rate predicts country's COVID-19 death rates: with supplementary state-by-state data in the United States. MedRxiv. 2020. doi: 10.l 101/2020.06.22.20137745.
97. Mitze T, Kosfeld R, Rode J, Walde K. Face Masks Considerably Reduce Covid-19 Cases in Germany. MedRxiv. 2020. doi: 10.1101/2020.06.21.20128181.
98. Maloney M, Rhodes N, Y amold P. Mask mandates can limit COVID spread: Quantitative assessment of month-over-month effectiveness of governmental policies in reducing the number of new COVID-19 cases in 3 7 US States and the District of Columbia. MedRxiv. 2020. doi: 10.1101/2020.10.06.20208033.
99. Sruthi C, Biswal M, Saraswat B, Joshi H, Prakash M. How Policies on Restaurants, Bars, Nightclubs, Masks, Schools, and Travel Influenced Swiss COVID-19 Reproduction Ratios. MedRxiv. 2020. doi: I0.1101/2020.10.11.20210641.
100. Lan F, Christophi C, Buley J, Iliaki E, Bruno-Murtha L, Sayah A, et al. Effects of universal masking on Massachusetts healthcare workers' COVID-19 incidence. MedRxiv. 2020. doi: 10.1101/2020.08.09.20171173.
101. Shacham e, Scroggins S, Ellis M, Garza A. Association of County-Wide Mask Ordinances with Reductions in Daily Co VID-19 Incident Case Growth in a Midwestern Region Over 12 Weeks. MedRxiv. 2020. doi: 10.l 101/2020.10.28.20221705.
102. Chernozhukov V, Kasahara H, Schrimpf P. Causal Impact of Masks, Policies, Behavior on Early Covid-19 Pandemic in the U.S. J Econom. 2020. doi: 10.1016/j .jeconom.2020.09 .003.
103. Research GS. Face Masks and GDP. 2020. (https:/ /www .goldmansachs.com/insights/pages/facemasks-and-gdp.htm l accessed 21 November 2020).
104. Scott N, Saul A, Spelman T, Stoove M, Pedrana A, Saeri A. The introduction of a mandatory mask policy was associated with significantly reduced COVID-19 cases in a major metropolitan city. 2020. (Available at SSRN:http://dx.doi.org/10.2139/ssrn.3714648 accessed 29 November 2020).
105. Yan Y, Bayham J, Fenichel E, Richter A. Do Face Masks Create a False Sense of Security? A COVID-19 Dilemma. MedRxiv. 2020. doi: 10.l 101/2020.05.23.20111302.
106. Piantadosi S, Byar DP, Green SB. The ecological fallacy. Am J Epidemiol. 1988;127(5):893-904.
107. Clifford GD, Long WJ, Moody GB, Szolovits P. Robust parameter extraction for decision support using multimodal intensive care data. Philos Trans A Math Phys Eng Sci. 2009 Jan 28; 367(1887): 411-429.
108. Dufault B, Klar N. The quality of modern crosssectional ecologic studies: a bibliometric review. Am J Epidemiol. 2011;174(10):1101-7.
109. Barasheed 0, Alfelali M, Mushta S, Bokhary H, Alshehri J, Attar AA, et al. Uptake and effectiveness of facemask against respiratory infections at mass gatherings: a systematic review. Int J Infect Dis. 2016;47:105-11.
110. Barasheed 0, Almasri N, Badahdah AM, Heron L, Taylor J, McPhee K, et al. Pilot Randomised Controlled Trial to Test Effectiveness ofFacemasks in Preventing Influenza-like Illness Transmission among Australian Hajj Pilgrims in 2011. Infect Disord Drug Targets. 2014;14(2):110-6.
111. Cowling BJ, Chan KH, Fang VJ, Cheng CK, Fung RO, Wai W, et al. Facemasks and hand hygiene to prevent influenza transmission in households: a cluster randomized trial. Ann Intern Med. 2009;151(7):437-46.
112. Lau IT, Tsui H, Lau M, Yang X. SARS transmission, risk factors, and prevention in Hong Kong. Emerg Infect Dis. 2004; 10( 4 ):587-92.
113. Suess T, Remschmidt C, Schink SB, Schweiger B, Nitsche A, Schroeder K, et al. The role of facemasks and hand hygiene in the prevention of influenza transmission in households: results from a cluster randomised trial; Berlin, Germany, 2009-2011. BMC Infect Dis. 2012;12:26.
114. Wu J, Xu F, Zhou W, Feikin DR, Lin CY, He X, et al. Risk factors for SARS among persons without known contact with SARS patients, Beijing, China. Emerg Infect Dis. 2004; 10(2):210-6.

115. Aiello AE, Murray GF, Perez V, Coulbom RM, Davis BM, Uddin M, et al. Mask use, hand hygiene, and seasonal influenza-like illness among young adults: a randomized intervention trial. J Infect Dis. 2010;201(4):491-8.
116. Aiello AE, Perez V, Coulbom RM, Davis BM, Uddin M, Monto AS. Facemasks, hand hygiene, and influenza among young adults: a randomized intervention trial. PLoS One. 2012;7(1):e29744.
117. World Health Organization. Information Note COVID-19 and NCDs. Geneva: World Health Organization. 2020. (https://www.who.int/docs/defaultsource/inaugural-who-partners-forum/covid-19-andncds---final---corr7 .pdr?sfvrsn=9b65e287 I &download=true, accessed 21 November 2020)
118. World Health Organization. Coronavirus disease (COVID-19) advice for the public: When and how to use masks. Geveva: World Health Organization; 2020. (https://www.who.int/emergencies/diseases/novelcoronavirus-2019/advice-for-public/when-and-how-touse-masks, accessed 21 November 2020).
119. Aydin 0, Emon B, Cheng S, Hong L, Chamorro LP, Saif MT A. Performance of fabrics for home-made masks against the spread of COVID-19 through droplets: A quantitative mechanistic study. Extreme Mech Lett. 2020;40:100924.
120. Fischer EP, Fischer MC, Grass D, Henrion I, Warren WS, Westman E. Low-cost measurement of face mask efficacy for filtering expelled droplets during speech. Sci Adv. 2020;6(36).
121. Milton DK, Fabian MP, Cowling BJ, Grantham ML, McDevitt JJ. Influenza virus aerosols in human exhaled breath: particle size, culturability, and effect of surgical masks. PLoS Pathog. 2013;9(3):e1003205.
122. Bion JF, Abrusci T, Hibbert P. Human factors in the management of the critically ill patient. Br J Anaesth. 201O;105(1 ):26-33.
123. Chen YJ, Qin G, Chen J, Xu JL, Feng DY, Wu XY, et al. Comparison of Face-Touching Behaviors Before and During the Coronavirus Disease 2019 Pandemic. JAMA Netw Open. 2020;3(7):e2016924.
124. Shiraly R, Shayan Z, McLaws ML. Face touching in the time of COVID-19 in Shiraz, Iran. Am J Infect Control. 2020. 48(12): 1559-1561.
125. Betsch C, Korn L, Sprengholz P, FelgendreffL, Eitze S, Schmid P, et al. Social and behavioral consequences of mask policies during the COVID-19 pandemic. Proc Natl Acad Sci US A. 2020;117(36):21851-3.
126. Cowling BJ, Ali ST, Ng TWY, Tsang TK, Li JCM, Fong MW, et al. Impact assessment of nonpharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: an observational study. Lancet Public Health. 2020;5( 5):e279-e88.
127. Giacalone S, Minuti A, Spigariolo CB, Passoni E, Nazzaro G. Facial dermatoses in the general population due to wearing of personal protective masks during the COVID-19 pandemic: first observations after lockdown. Clin Exp Dermatol. 2020. doi: 10.1111/ced.14376
128. Hufner K, Hofer A, Spemer-Unterweger B. On the difficulties of building therapeutic relationships when wearing face masks. J Psychosom Res. 2020;138:110226.
129. Crume B. The silence behind the mask: my journey as a deaf pediatric resident amidst a pandemic. Acad Pediatr. 2020. doi: 10.1016/j.acap.2020.10.002.
130. Allison MA, Guest-Warnick G, Nelson D, Pavia AT, Srivastava R, Gesteland PH, et al. Feasibility of elementary school children's use of hand gel and facemasks during influenza season. Influenza Other Respir Viruses. 2010;4(4):223-9.
13 I. Canini L, Andreoletti L, Ferrari P, D'Angelo R, Blanchon T, Lemaitre M, et al. Surgical mask to prevent influenza transmission in households: a cluster randomized trial. PLoS One. 2010;5(1 l):el3998.
132. Uchida M, Kaneko M, Hidaka Y, Yamamoto H, Honda T, Takeuchi S, et al. Effectiveness of vaccination and wearing masks on seasonal influenza in Matsumoto City, Japan, in the 2014/2015 season: An observational study among all elementary schoolchildren. Prev Med Rep. 2017;5:86-91.
133. Zand A, Heir A. Environmental impacts of new Coronavirus outbreak in Iran with an emphasis on waste management sector. J Mater Cycles Waste Manag. 2020 : 1-8.
134. Fikenzer S, Ube T, Lavall D, Rudolph U, Falz R, Busse M, et al. Effects of surgical and FFP2/N95 face masks on cardiopulmonary exercise capacity. Clin Res Cardiol. 2020 Jul 6: 1-9.
135. Harber P, Santiago S, Bansal S, Liu Y, Yun D, Wu S. Respirator physiologic impact in persons with mild respiratory disease. J Occup Environ Med. 2010;52(2): 155-62.
136. Kyung SY, Kim Y, Hwang H, Park JW, Jeong SH. Risks of N95 Face Mask Use in Subjects With COPD. Respir Care. 2020;65(5):658-64.
137. Lee HP, Wang de Y. Objective assessment of increase in breathing resistance of N95 respirators on human subjects. Ann Occup Hyg. 2011;55(8):917-21.
138. Matuschek C, Moll F, Fangerau H, Fischer JC, Zanker K, van Griensven M, et al. Face masks: benefits and risks during the COVID-19 crisis. Eur J Med Res. 2020;25( 1 ):32.
139. Person E, Lemercier C, Royer A, Reychler G. [Effect of a surgical mask on six minute walking distance]. Rev Mal Respir. 2018;35(3):264-8.
140. Wong A Y, Ling SK, Louie LH, Law GY, So RC, Lee DC, et al. Impact of the COVID-19 pandemic on sports and exercise. Asia Pac J Sports Med Arthrosc Rehabil Technol. 2020;22:39-44.
141. Li Y, Tokura H, Guo YP, Wong AS, Wong T, Chung J, et al. Effects of wearing N95 and surgical facemasks on heart rate, thermal stress and subjective sensations. Int Arch Occup Environ Health. 2005;78(6):501-9.
142. Hopkins SR, Dominelli PB, Davis CK, Guenette JA, Luks AM, Molgat-Seon Y, et al. Facemasks and the Cardiorespiratory Response to Physical Activity in Health and Disease. Ann Am Thorac Soc. 2020. doi:10.1513/AnnalsATS.202008-990CME.
143. Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451-62.
144. Yang GZ, Kelley E, Darzi A. Patients' safety for global health. Lancet. 2011; 377(9769): 886-7.
145. Roberge RJ. Face shields for infection control: A review. J Occup Environ Hyg. 2016;13(4):235-42.

146. Jang JY, Kim, S.W. Evaluation of Filtration Performance Efficiency of Commercial Cloth Masks. Journal of Environmental Health Sciences
(~~@7ci~~§f"~Al)2015; 41 (3) 203-215. 147. Jung H, Kim JK, Lee S, Lee J, Kim J, Tsai P, et al.
Comparison of Filtration Efficiency and Pressure Drop in Anti-Yellow Sand Masks, Quarantine Masks, Medical Masks, General Masks, and Handkerchiefs. Aerosol Air Qual. Res. 2014;14, 991-1002.
148. Lustig SR, Biswakarma JJH, Rana D, Tilford SH, Hu W, Su M, et al. Effectiveness of Common Fabrics to Block Aqueous Aerosols of Virus-like Nanoparticles. ACS Nano. 2020;14(6):7651-8.
149. Zangmeister CD, Radney JG, Vicenzi EP, Weaver JL. Filtration Efficiencies of Nanoscale Aerosol by Cloth Mask Materials Used to Slow the Spread of SARSCo V-2. ACS Nano. 2020;14(7):9188-200.
150. Zhao M, Liao L, Xiao W, Yu X, Wang H, Wang Q, et al. Household materials selection for homemade cloth face coverings and their filtration efficiency enhancement with triboelectric charging. Nano Lett. 2020; 20(7):5544-5552.
151. Clase CM, Fu EL, Ashur A, Beale RCL, Clase IA, Dolovich MB, et al. Forgotten Technology in the COVID-19 Pandemic: Filtration Properties of Cloth and Cloth Masks-A Narrative Review. Mayo Clin Proc. 2020;95( 10):2204-24.
152. Jain M, Kim S, Xu C, Li H, Rose G. Efficacy and Use of Cloth Masks: A Scoping Review. Cureus 12(9): e10423. doi:10.7759/cureus.10423
153. Mondal A, Das A, Goswami R. Utility of Cloth Masks in Preventing Respiratory Infections: A Systematic Review. MedRxiv. 2020 doi: 10.l 101/2020.05.07.20093864
154. Roberge RJ, Roberge MR. Cloth face coverings for use as facemasks during the coronavirus (SARS-Cov-2) pandemic: what science and experience have taught us. Disaster Med Public Health Prep. 2020:1-29.
155. Sharma SK, Mishra M, Mudgal SK. Efficacy of cloth face mask in prevention of novel coronavirus infect_ion transmission: A systematic review and meta-analysis. J Educ Health Promot. 2020;9: 192.
156. Taminato M, Mizusaki-Imoto A, Saconato H, Franco E, Puga M, Duarte M, et al. Homemade cloth face masks as a barrier against respiratory droplets -systematic review. Acta Paul Enferm. 2020:eAPE20200103.
157. Bae S, Kim MC, Kim JY, Cha HH, Lim JS, Jung J, et al. Effectiveness of Surgical and Cotton Masks in Blocking SARS-Co V-2: A Controlled Comparison in 4 Patients. Ann Intern Med. 2020;173(1):W22-W3.
158. Ma QX, Shan H, Zhang HL, Li GM, Yang RM, Chen JM. Potential utilities of mask-wearing and instant hand hygiene for fighting SARS-CoV-2. J Med Virol. 2020. doi: 10.1002/jmv.25805.
159. Davies A, Thompson KA, Girl K, Kafatos G, Walker J, Bennett A. Testing the efficacy of homemade masks: would they protect in an influenza pandemic? Disaster Med Public Health Prep. 2013;7(4):413-8.
160. Konda A, Prakash A, Moss GA, Schmoldt M, Grant GD, Guba S. Aerosol Filtration Efficiency of Common Fabrics Used in Respiratory Cloth Masks. ACS Nano. 2020;14(5):6339-47.
161. Neupane BB, Mainali S, Sharma A, Girl B. Optical microscopic study of surface morphology and filtering efficiency of face masks. Peed. 2019;7:e7142.
162. Shakya KM, Noyes A, Kallin R, Peltier RE. Evaluating the efficacy of cloth facemasks in reducing particulate matter exposure. J Expo Sci Environ Epidemiol. 2017;27(3):352-7.
163. Jung H KJ, Lee S, Lee J, Kim J, Tsai P, et al.. Comparison of filtration efficiency and pressure drop in anti-yellow sand masks, quarantine masks, medical masks, general masks, and handkerchiefs. Aerosol Air Qual Res. 2014;14:991-1002.
164. Rengasamy S, Eimer B, Shaffer RE. Simple respiratory protection--evaluation of the filtration performance of cloth masks and common fabric materials against 20-1000 nm size particles. Ann Occup Hyg. 2010;54(7):789-98.
165. Dato VM, Hostler D, Hahn ME. Simple respiratory mask. Emerg Infect Dis. 2006;12(6):1033-4.
166. van der Sande M, Teunis P, Sabel R. Professional and home-made face masks reduce exposure to respiratory infections among the general population. PLoS One. 2008;3(7):e26 l 8.
167. Chughtai AA, Seale H, Dung TC, Hayen A, Rahman B, Raina MacIntyre C. Compliance with the Use of Medical and Cloth Masks Among Healthcare Workers in Vietnam. Ann Occup Hyg. 2016;60(5):619-30.
168. AATCC. AATCC Ml4-2020 Guidance and Considerations for General Purpose Textile Face Coverings: Adult (https://www.aatcc.org/covid/ accessed 28 November 2020)
169. Centers for Disease Control and Prevention. Scientific Brief: Community Use of Cloth Masks to Control the Spread of SARS-CoV-2. https://www .cdc.gov/coronavirus/2019-ncov/more/masking-science-sarscov2.html?tbclid-IwAR28PppCa6x2uxwO8Z2baHM0 KHS4JXx0inzzMOs3zRHV I ggl 0a8mxZfpCw (Accessed 29 November 2020). . . .
170. Swinfen R, Swinfen P. Low-cost telemed1cme m the developing world. J Telemed Telecare. 2002;8(suppl 3):63-5.
171. Lee SA, Hwang DC, Li HY, Tsai CF, Chen CW, ~hen JK. Particle Size-Selective Assessment of Protection of European Standard FFP Respirat~rs and Surgica~ Masks against Particles-Tested with Human SubJects. J Healthc Eng. 2016;2016
Acknowledgments
This document was developed based on advice by the Strategic and Technical Advisory Grou~ for Infecti~us Hazards (STAG-IH), and in consultation with the followmg members of:
1) The WHO Health Emergencies Programme (WHE) Adhoc COVID-19 IPC Guidance Development Group (in alphabetical order):
Jameela Alsalman, Ministry of Health, Bahrain; ~ucha Apisamthanarak, Thammsat University Hospital, Thatland; Baba Aye, Public Services International~ France; Gregory Built, UNICEF, United States of Amenca (USA); Roger Chou, Oregon Health Science University, USA; May Chu,

Colorado School of Public Health, USA; John Conly, Alberta Health Services, Canada; Barry Cookson, University College London, United Kingdom (U.K); Nizam Damani, Southern Health & Social Care Trust, United Kingdom; Dale Fisher, GOARN, Singapore; Joost Hopman, Radboud University Medical Center, The Netherlands; Mushtuq Husain, Institute of Epidemiology, Disease Control & Research, Bangladesh; Kushlani Jayatilleke, Sri Jayewardenapura General Hospital, Sri Lanka; Seto Wing Jong, School of Public Health, Hong Kong SAR, China; Souha Kanj, American University of Beirut Medical Center, Lebanon; Daniele Lantagne, Tufts University, USA; Fernanda Lessa, Centers for Disease Control and Prevention, USA; Anna Levin, University of Sao Paulo, Brazil; Ling Moi Lin, Sing Health, Singapore; Caline Mattar, World Health Professions Alliance, USA; MaryLouise McLaws, University of New South Wales, Australia; Geeta Mehta, Journal of Patient Safety and Infection Control, India; Shaheen Mehtar, Infection Control Africa Network, South Africa; Ziad Memish, Ministry of Health, Saudi Arabia; Babacar Ndoye, Infection Control Africa Network, Senegal; Fernando Otaiza, Ministry of Health, Chile; Diamantis Plachouras, European Centre for Disease Prevention and Control, Sweden; Maria Clara Padoveze, School of Nursing, University of Sao Paulo, Brazil; Mathias Pletz, Jena University, Germany; Marina Salvadori, Public Health Agency of Canada, Canada; Mitchell Schwaber, Ministry of Health, Israel; Nandini Shetty, Public Health England, United Kingdom; Mark Sobsey, University of North Carolina, USA; Paul Ananth Tambyah, National University Hospital, Singapore; Andreas Voss, Canisus-Wilhelmina Ziekenhuis, The Netherlands; Walter Zingg, University of Geneva Hospitals, Switzerland;
2) The WHO Technical Advisory Group of Experts on Personal Protective Equipment (TAG PPE):
Faisal Al Shehri, Saudi Food and Drug Authority, Saudi Arabi; Selcen Ayse, Istanbul University-Cerrahpasa, Turkey; Razan Asally, Saudi Food and Drug Authority, Saudi Arabi; Kelly Catlin, Clinton Health Access Initiative; Patricia Ching, WHO Collaborating Center, The University of Hong Kong, China; Mark Croes, Centexbel, Spring Gombe, United Nations; Emilio Homsey, UK Public Health Rapid Support Team, U.K.; Selcen Kilinc-Balci, United States Centers for
Disease Control and Prevention (CDC), USA; Melissa Leavitt, Clinton Health Access Initiative; John McGhie, International Medical Corps; Claudio Meirovich, Meirovich Consulting; Mike Paddock, UNDP, Trish Perl, University of Texas Southwestern Medical Center, USA; Alain Prat, Global Fund, Ana Maria Rule, Johns Hopkins Bloomberg School of Public Health, U .S.A; Jitendar Sharma, Andra Pradesh MedTEch Zone, India; Alison Syrett, SIGMA, Reiner Voelksen, VOELKSEN Regulatory Affairs, Nasri Yussuf, IPC Kenya.
3) External IPC peer review group:
Paul Hunter, University of East Anglia, U .K; Direk Limmathurotsakul, Mahidol University, Thailand; Mark Loeb, Department of Pathology and Molecular Medicine, McMaster University, Canada; Kalisavar Marimuthu, National Centre for Infectious Diseases, Singapore; Yong Loo Lin School of Medicine, National University of Singapore; Nandi Siegfried, South African Medical Research Council, South Africa.
4) UNICEF observers: Nagwa Hasanin, Sarah Karmin, Raoul Kamadjeu, Jerome Pfaffmann,
WHO Secretariat:
Benedetta Allegranzi, Gertrude Avortri, Mekdim Ayana, Hanan Balkhy, April Baller, Elizabeth Barrera-Cancedda, Anjana Bhushan, Whitney Blanco, Sylvie Briand, Alessandro Cassini, Giorgio Cometto, Ana Paula Coutinho Rehse, Carmem Da Silva, Nino Dal Dayanguirang, Sophie Harriet Dennis, Sergey Eremin, Luca Fontana, Dennis Falzon, Nathan Ford, Nina Gobat, Jonas Gonseth-Garcia, Rebeca Grant, Tom Grein, Ivan Ivanov, Landry Kabego, Catherine Kane, Pierre Claver Kariyo, Ying Ling Lin, Omelia Lincetto, Abdi Mahamud, Madison Moon, Takeshi Nishijima, Kevin Babila Ousman, Pillar Ramon-Pardo, Paul Rogers, Nahoko Shindo, Alice Simniceanu, Valeska Stempliuk, Maha Talaat Ismail, Joao Paulo Toledo, Anthony Twywan, Maria Van Kerkhove, Adriana Velazquez, Vicky Willet, Masahiro Zakoji, Bassim Zayed.
WHO continues to monitor the situation closely for any changes that may affect this interim guidance. Should any factors change, WHO will issue a further update. Otherwise, this interim guidance document will expire 1 year after the date of publication.

Annex: Updated guidance on non-medical (fabric) masks
Background
A non-medical mask, also called fabric mask, community mask or face covering, is neither a medical device nor personal protective equipment. Non-medical masks are aimed at the general population, primarily for protecting others from exhaled virus-containing droplets emitted by the mask wearer. They are not regulated by local health authorities or occupational health associations, nor is it required for manufacturers to comply with guidelines established by standards organizations. Non-medical masks may be homemade or manufactured. The essential performance parameters include good breathability, filtration of droplets originating from the wearer, and a snug fit covering the nose and mouth. Exhalation valves on masks are discouraged as they bypass the filtration function of the mask.
Non-medical masks are made from a variety of woven and nonwoven fabrics, such as woven cotton, cotton/synthetic blends, polyesters and breathable spun bond polypropylene, for example. They may be made of different combinations of fabrics, layering sequences and available in diverse shapes. Currently, more is known about common household fabrics and combinations to make non-medical masks with target filtration efficiency and breathability (119, 146-150). Few of these fabrics and combinations have been systematically evaluated and there is no single design, choice of material, layering or shape among available non-medical masks that are considered optimal. While studies have focussed on single fabrics and combinations, few have looked at the shape and universal fit to the wearer. The unlimited combination of available fabrics and materials results in variable filtration and breathability.
In the context of the global shortage of medical masks and PPE, encouraging the public to create their own fabric masks may promote individual enterprise and community integration. Moreover, the production of non-medical masks may offer a source of income for those able to manufacture masks within their communities. Fabric masks can also be a form of cultural expression, encouraging public acceptance of protection measures in general. The safe re-use of fabric masks will also reduce costs and waste and contribute to sustainability (151-156).
This Annex is destined intended for two types of readers: homemade mask makers and factory-made masks manufacturers. Decision makers and managers (national/subnational level) advising on a type of non-medical mask are also the focus of this guidance and should take into consideration the following features of non-medical masks: breathability, filtration efficiency (FE), or filtration, number and combination of fabric layers material used, shape, coating and maintenance.
Evidence on the effectiveness of non-medical (fabric) masks
A number of reviews have been identified on the effectiveness of non-medical masks ( 151-156). One systematic review (155) identified 12 studies and evaluated study quality. Ten were laboratory studies (157-166), and two reports were from a single randomized trial (72, 167). The majority of studies were conducted before COVID-19 emerged or used laboratory generated particles to assess filtration efficacy. Overall, the reviews concluded that
cloth face masks have limited efficacy in combating viral infection transmission.
Homemade non-medical masks
Homemade non-medical masks made of household fabrics (e.g., cotton, cotton blends and polyesters) should ideally have a three-layer structure, with each layer providing a function (see Figure I) ( 168). It should include:
1. an innermost layer (that will be in contact with the face) of a hydrophilic material ( e.g., cotton or cotton blends of terry cloth towel, quilting cotton and flannel) that is nonirritating against the skin and can contain droplets ( 148)
2. a middle hydrophobic layer of synthetic breathable nonwoven material (spunbond polypropylene, polyester and polyaramid), which may enhance filtration, prevent permeation of droplets or retain droplets ( I 48, 150)
3. an outermost layer made of hydrophobic material (e.g. spunbond polypropylene, polyester or their blends), which may limit external contamination from penetrating through the layers to the wearer's nose and mouth and maintains and prevents water accumulation from blocking the pores of the fabric ( 148).
Although a minimum of three layers is recommended for nonmedical masks for the most common fabric used, single, double or other layer combinations of advanced materials may be used if they meet performance requirements. It is important to note that with more tightly woven materials, breathability may be reduced as the number of layers increases. A quick check may be performed by attempting to breathe, through the mouth, through the multiple layers.
- -----Inner
• Hydrophilic •Cotton or cotton blend
Outer
• Hydrophobic •Polyester
Figure I. Non-medical mask construction using breathable fabrics such as cotton, cotton blends, polyesters, nylon and polypropylene spunbond that are breathable may impart adequate filtration performance when layered. Single- or double-layer combinations of advanced materials may be used if they meet performance requirements (72).
Assumptions regarding homemade masks are that individual makers only have access to common household fabrics and do not have access to test equipment to confirm target performance (filtration and breathability). Figure I illustrates a multi-layer mask construction with examples of fabric options. Very porous materials, such as gauze, even with multiple layers, may provide very low filtration efficiency ( 14 7). Higher thread count fabrics offer improved filtration performance ( 169). Coffee filters, vacuum bags and materials not meant for clothing should be avoided as they may contain injurious content when breathed in. Microporous films such as Gore-Tex are not recommended ( 170).

Factory-made non-medical masks: general considerations for manufacturers
The non-medical mask, including all components and packaging, must be non-haz.ardous, non-toxic and childfriendly (no exposed sharp edges, protruding hardware or rough materials). Factory-made non-medical masks must be made using a process that is certified to a quality management system ( e.g., ISO 900 I). Social accountability standards ( e.g., SAI SA8000) for multiple aspects of fair labour practices, health and safety of the work force and adherence to UNICEF's Children's Rights and Business Principles are strongly encouraged.
Standards organizations' performance criteria
Manufacturers producing masks with consistent standardized performance can adhere to published, freely available guidance from several organiz.ations including those from: the French Standardization Association (AFNOR Group), The European Committee for Standardization (CEN), Swiss National COVID-19 Task Force, the American Association of Textile Chemists and Colorists (AA TCC), the South Korean Ministry of Food and Drug Safety (MFDS), the Italian Standardization Body (UNI) and the Government of Bangladesh.
Essential parameters
The essential parameters presented in this section are the synthesis of the abovementioned regional and national guidance. They include filtration, breathability and fit. Good performance is achieved when the three essential parameters are optimized at the preferred threshold (Figure 2).
Figure 2. mustration of the three essential parameters of filtration, breathability and tit.
The summary of the three essential parameters can be found in Table I and the additional performance considerations in Table 2. The minimum threshold is the minimum acceptable parameter, while the preferred threshold is the optimum.
Filtration and breathability
Filtration depends on the filtration efficiency (in%), the type of challenge particle ( oils, solids, droplets containing bacteria) and the particle size (see Table I). Depending on the fabrics used, filtration and breathability can complement or work against one another. The selection of material for droplet filtration (barrier) is as important as breathability. Filtration is dependent on the tightness of the weave, fibre or thread diameter. Non-woven materials used for disposable masks are manufactured using processes to create polymer fibres that are thinner than natural fibres such as cotton and that are held together by partial melting.
Breathability is the difference in pressure across the mask and is typically reported in millibars (mbar) or Pascals (Pa) or, normalized to the cm2 in mbar/cm2 or Pa/cm2• Acceptable breathability of a medical mask should be below 49 Pa/cm2•
For non-medical masks, an acceptable pressure difference, over the whole mask, should be below 60 Pa/cm2, with lower values indicating better breathability.
Non-medical fabric masks consisting of two layers of polypropylene spunbond and two layers of cotton have been shown to meet the minimum requirements for droplet filtration and breathability of the CEN CWA 17553 guidance. It is preferable not to select elastic material to make masks as the mask material may be stretched over the face, resulting in increased pore size and lower filtration through multiple usage. Additionally, elastic fabrics are sensitive to washing at high temperatures thus may degrade over time.
Coating the fabric with compounds like wax may increase the barrier and render the mask fluid resistant; however, such coatings may inadvertently completely block the pores and make the mask difficult to breathe through. In addition to decreased breathability unfiltered air may more likely escape the sides of the mask on exhalation. Coating is therefore not recommended.
Valves that let unfiltered air escape the mask are discouraged and are an inappropriate feature for masks used for the purpose of preventing transmission.

Table 1. Essential parameters (minimum and preferred thresholds) for manufactured non-medical mask
Essential Minimum threshold Preferred threshold Parameters
1. Filtration* 1.1. filtration
70% @ 3 micron > 70%, without compromising breathability efficiency
1.2. Challenge Solid: sodium chloride (NaCl), Talcum Based on availability particle powder, Holi powder, dolomite, Polystyrene
Latex spheres
Liquid: DEHS Di-Ethyl-Hexyl-Sebacat, paraffin oil
1.3. Particle size Choose either sizes: Range of particle sizes
3 um. 1 um. or smaller
2. Breathability
2.1. Breathing ~60 Pa/cm2 Adult: ~ 40 Pa/cm2
resistance** Paediatric: < 20 Pa/cm2
2.2 Exhalation Not recommended NIA valves
3. Fit
3.1. Coverage Full coverage of nose and mouth, consistent, Same as current requirements snug perimeter fit at the nose bridge, cheeks, chin and lateral sides of the face; adequate surface area to minimize breathing resistance and minimize side leaka2e
3.2 Face seal Not currently required Seal as good as FFR (respirator):
Fit factor of 100 for N95
Maximum Total Inward Leakage of 25% (FFPl requirement)
3.2. Sizing Adult and child Should cover from the bridge of the nose to below the chin and cheeks on either side of the mouth
Sizing for adults and children (3-5. 6-9. 10-12. >12)
3.3Strap strene:th >44.SN
• Smaller particle may result in lower filtration. •• High resistance can cause bypass of the mask. Unfiltered air will leak out the sides or around the nose if that is the easier path.

Fit: shape and sizing
Fit is the third essential parameter, and takes into consideration coverage, seal, sizing, and strap strength. Fit of masks currently is not defined by any standard except for the anthropometric considerations of facia] dimensions (ISO/TS 16976-2) or simplified to height mask (South Korean standard for KF-AD). It is important to ensure that the mask can be held in place comfortably with as little adjustment of the elastic bands or ties as possible.
Mask shapes typically include flat-fold or duckbil1 and are designed to fit closely over the nose, cheeks and chin of the wearer. Snug fitting designs are suggested as they limit leaks of unfiltered air escaping from the mask (148). Ideally the mask should not have contact with the lips, unless hydrophobic fabrics are used in at least one layer of the mask ( 148). Leaks where unfiltered air moves in and out of the mask may be attributed to the size and shape of the mask (171).
Additional considerations
Optional parameters to consider in addition to the essential performance parameters include if reusable, biodegradability for disposal masks, antimicrobial performance where applicable and chemical safety (see Table 2).
Non-medical masks intended to be reusable should include instructions for washing and must be washed a minimum of five cycles, implying initial performance is maintained after each wash cycle.
Advanced fabrics may be biodegradable or compostable at the end of service life, according to a recognized standard process ( e.g., UNI EN 13432, UNI EN 14995 and UNI / PclR 79).
Manufacturers sometimes claim their NM masks have antimicrobial performance. Antimicrobial performance may be due to coatings or additives to the fabric fibres. Treated fabrics must not come into direct contact with mucous membranes; the innermost fabric should not be treated with
antimicrobial additives, only the outermost layer. In addition, antimicrobial fabric standards (e.g., ISO 18184, ISO 20743, AATCC TMl00, AATCC 100) are general1y slow acting. The inhibition on microbial growth may take full effect after 2- or 24-hour contact time depending on the standard. The standards have generally been used for athletic apparel and substantiate claims of odour control performance. These standards are not appropriate for non-medical cloth masks and may provide a false sense of protection from infectious agents. If claims are maid, manufacturers should specify which standard supports antimicrobial performance, the challenge organism and the contact time.
Volatile additives are discouraged as these may pose a health risk when inhaled repeatedly during wear. Certification according to organizations including OEKO-TEX (Europe) or SEK (Japan), and additives complying with REACH (Europe) or the Environmental Protection Agency (EPA, United States of America) indicate that textile additives are safe and added at safe levels.
Table 2. Additional parameters for manufactured nonmedical masks
Additional parameters Minimum thresholds
If reusable, number of wash 5 cycles cvcles
Disposal Reusable
If biodegradable (CFC-BIO), according to UNI EN 13432. UNI EN 14995
Antimicrobial (bacteria, ISO 18184 (virus) virus, fungus) performance
ISO 20743 (bacteria)
ISO 13629 (fungus)
AATCC TMIO0 (bacteria)
Chemical safety Comply with REACH regulation, including inhalation safety
© World Health Organization 2020. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO licence.
WHO reference number: WHO/2019-nCo V /IPC _ Masks/2020.5

Effectiveness of Adding a Mask Recommendation to Other Public Health Measures to Prevent SARSCoV-2 Infection in Danish Mask Wearers : A Randomized Controlled Trial . 2020 Nov 18;M20-6817. doi: 10.7326/M20-6817. Online ahead of print. Henning Bundgaard 1 , Johan Skov Bundgaard 1 , Daniel Emil Tadeusz
Raaschou-Pedersen 1 , Christian von Buchwald 2 , Tobias Todsen 2 , Jakob
Boesgaard Norsk 3 , Mia M Pries-Heje 1 , Christoffer Rasmus Vissing 1
, Pernille B Nielsen 3 , Ulrik C Winsl0w 1 , Kamille Fogh 3 , Rasmus
Hasselbalch 3 , Jonas H Kristensen 3 , Anna Ringgaard 1 , Mikkel Porsborg
Andersen 4 , Nicole Bakkegard Goecke 5 , Ramona Trebbien 6 , Kerstin
Skovgaard 7 , Thomas Benfield 8 , Henrik Ullum 2 , Christian Ton~-Pedersen 4 , KasP-er Iversen 3
Affiliations
PMID: 33205991 PMCID: PMC7707213
DOI: 10.7326LM20-6817
Free PMC article
Background: Observational evidence suggests that mask wearing
mitigates transmission of severe acute respiratory syndrome coronavirus 2
(SARS-CoV-2). It is uncertain if this observed association arises through
protection of uninfected wearers (protective effect), via reduced
APPENDIX TO JAMES CASCIANO DECLARATION-70

transmission from infected mask wearers (source control), or both.
Objective: To assess whether recommending surgical mask use outside the
home reduces wearers' risk for SARS-CoV-2 infection in a setting where
masks were uncommon and not among recommended public health
measures.
Design: Randomized controlled trial (DANMASK-19 [Danish Study to
Assess Face Masks for the Protection Against COVID-19 Infection]).
(ClinicalTrials.gov: NCT04337541).
Setting: Denmark, April and May 2020.
Participants: Adults spending more than 3 hours per day outside the home
without occupational mask use.
Intervention: Encouragement to follow social distancing measures for
coronavirus disease 2019, plus either no mask recommendation or a
recommendation to wear a mask when outside the home among other
persons together with a supply of 50 surgical masks and instructions for
proper use.
Measurements: The primary outcome was SARS-CoV-2 infection in the
mask wearer at 1 month by antibody testing, polymerase chain reaction
(PCR), or hospital diagnosis. The secondary outcome was PCR positivity for
other respiratory viruses.
Results: A total of 3030 participants were randomly assigned to the
recommendation to wear masks, and 2994 were assigned to control; 4862
completed the study. Infection with SARS-CoV-2 occurred in 42
participants recommended masks (1.8%) and 53 control participants (2.1%).
The between-group difference was -0.3 percentage point (95% Cl, -1.2 to
0.4 percentage point; P = 0.38) (odds ratio, 0.82 [Cl, 0.54 to 1.23]; P =
0.33). Multiple imputation accounting for loss to follow-up yielded similar
APPENDIX TO JAMES CASCIANO DECLARATION-71

results. Although the difference observed was not statistically significant,
the 95% Cls are compatible with a 46% reduction to a 23% increase in
infection.
Limitation: Inconclusive results, missing data, variable adherence, patient
reported findings on home tests, no blinding, and no assessment of
whether masks could decrease disease transmission from mask wearers to
others.
Conclusion: The recommendation to wear surgical masks to supplement
other public health measures did not reduce the SARS-CoV-2 infection rate
among wearers by more than 50% in a community with modest infection
rates, some degree of social distancing, and uncommon general mask use.
The data were compatible with lesser degrees of self-protection.
Primary funding source: The Salling Foundations.
APPENDIX TO JAMES CASCIANO DECLARATION-72

Reduction of secondary transmission of SARS-CoV-2 in households by face mask use, disinfection and social distancing: a cohort study in Beijing, China Summary box
What is already known?
• Mitigation of the COVID-19 pandemic depends solely on non
pharmaceutical interventions until drugs or vaccines are available.
Transmission of COVID-19 within families and close contacts accounts
for the majority of epidemic growth. Community mask wearing, hand
washing and social distancing are thought to be effective but the
evidence is not clear.
What are the new findings?
• The overall secondary attack rate in households was 23.0%. Face
masks were 79% effective and disinfection was 77% effective in
preventing transmission, while close frequent contact in the household
increased the risk of transmission 18 times, and diarrhoea in the index
patient increased the risk by four times. The results demonstrate the
importance of the pre-symptomatic infectiousness of COVID-19
patients and shows that wearing masks after illness onset does not
protect.
What do the new findings imply?
• The findings inform universal face mask use and social distancing, not
APPENDIX TO JAMES CASCIANO DECLARATION-73
just in public spaces, but inside the household with members at risk of
getting infected. This further supports universal face mask use, and
also provides guidance on risk reduction for families living with
someone in quarantine or isolation, and families of health workers, who
may face ongoing risk.
Introduction
In the absence of a vaccine for COVID-19, non-pharmaceutical
interventions (NPls) are the only available disease control measures. We
have shown that population level NPls, including travel bans and the
national emergency response, were effective in flattening the COVID-19
epidemic curve in China.1 However, the effect of other NPls, such as mask
use and hygiene practices, have not been well studied in the COVID-19
pandemic.
In the USA, the use of face masks in the community has been
recommended.2 It is thought that universal face mask use (UFMU) may
reduce outward transmission from asymptomatically infected people and
protect well people from becoming infected. However, the World Health
Organization and Public Health England recommend against UFMU on the
grounds that there is little evidence from randomised controlled trials to
support this. Some experts suggest that in a pandemic, the precautionary
principle should be used and UFMU encouraged as it is unlikely to cause
harm and may result in public health gain.3 4 In countries where personal
protective equipment is scarce, people are making their own masks.
In China, over 70% of human-to-human transmission of severe acute
respiratory syndrome coronavirus 2 (SARS-CoV-2) occurred in families.5
6However, data to inform COVID-19 risk reduction in households are
unavailable. Given epidemic growth is dominated by household
transmission,5 6 studying the use of NPls, such as face masks, social
distancing and disinfection in the household setting, may inform community
APPENDIX TO JAMES CASCIANO DECLARATION-74

epidemic control and prevent transmission of COVID-19 in households.
Methods
Study population and design
We conducted a retrospective cohort study involving families of laboratory
confirmed COVID-19 cases in Beijing, China. We defined family members as
those who had lived with primary cases in a house for 4 days before and for
more than 24 hours after the primary cases developed illness related to
COVID-19. As of 21 February 2020, all laboratory confirmed COVID-19
cases reported in Beijing were enrolled in our study and followed-up. The
outcome of interest was secondary transmission in the household. Families
with secondary transmission were defined as those where some or all of the
family members become infected within one incubation period (2 weeks) of
symptom onset of the primary case.
To analyse the predictors of household transmission, we compared families
with and without secondary transmission for various measured risk factors,
preventive interventions and exposures.
Definition of confirmed case
According to national prevention and control guideline (fifth edition),7
confirmed cases were those who met the clinical, epidemiological and
laboratory testing criteria for COVID-19 simultaneously.
Clinical criteria included: (a) fever and/or one or more respiratory
symptoms; (b) radiological evidence of pneumonia; (c) white blood cell
count normal or decreased, and lymphocyte count decreased at the early
stage of illness.
Epidemiological criteria included: (a) visits to/living in Wuhan or cities
around Wuhan or other communities which had already reported COVID-19
APPENDIX TO JAMES CASCIANO DECLARATION-75

cases in the 14 days prior to the onset of symptoms; (b) having contact with
a person known to have infection with SARS-CoV-2 in the 14 days prior to
onset of symptoms; (c) having contact with a person who had fever or
respiratory symptoms and came from Wuhan or adjacent cities or other
communities which had already reported COVID-19 cases in the 14 days
prior to onset of symptoms; (d) being one of the cluster cases.
Suspected cases met one of the epidemiological criteria and ·any two of the
clinical criteria, or met all of the clinical criteria. Confirmed cases were those
suspected cases who met one of the following criteria.: (a) respiratory or
blood specimen tested positive for SARS-CoV-2 by real time reverse
transcriptase-polymerase chain reaction; (b) virus in respiratory or blood
specimen was highly homologous with known SARS-CoV-2 through gene
sequencing.
Data collection
A three part structured questionnaire was developed. The first part included
demographic and clinical information of the primary case. The second part
was mainly focused on the primary case's knowledge about and attitudes
toward COVID-19, and their self-reported practices (mask wearing, social
distancing, living arrangements) and activities in the home. The third part
was about self-reported behaviours of all family members, as well as the
family's accommodation and household hygiene practices from 4 days
before the illness onset to the day the primary case was isolated, including
room ventilation, room cleaning and disinfection. Close contact was defined
as being within 1 m or 3 feet of the primary case, such as eating around a
table or sitting together watching TV. The frequency of contact, disinfection
and ventilation was measured.
After diagnosis, the primary case was hospitalised as per standard practice
in Beijing. Eligible primary cases and their family members were interviewed
between 28 February and 8 March. Data on the primary case were
APPENDIX TO JAMES CASCIANO DECLARATION-76

extracted from epidemiological investigating reports from Beijing Centre for Disease Prevention and Control and supplemented by interview.
The clinical severity of the COVID-19 case was categorised as mild, severe or critical. Mild disease included non-pneumonia and mild pneumonia cases. Severe disease was characterised by dyspnoea, respiratory
frequency ~30/min, blood oxygen saturation s93%, PaO2/FiO2 ratio <300 and/or lung infiltrates >50% within 24-48 hours. Critical cases were those who exhibited respiratory failure, septic shock and/or multiple organ dysfunction/failure.a
Statistical analysis
Risk factors for secondary transmission were analysed by characteristics of the primary case, characteristics of well family members and household hygiene practices. Categorical variables are presented as counts and percentages, and continuous variables as medians (IQR). The x2 test and Fisher exact test were applied to compare difference between groups when necessary. A composite COVID-19 knowledge score and hand hygiene score were created with multiple sub-questions. A multivariable logistic regression model was used to identify risk factors associated with SARSCoV-2 household transmission. Univariable analysis was first performed with all measures and only those variables significant at p<0.1 could be selected in the following multivariable logistic regression analysis. Backward elimination was performed to establish a final model retaining those with p<0.05 in the model. Statistical analyses were performed using SAS software (V.9.4).
Ethics statement
As our study was embedded within the COVID-19 prevention and control practice within public health units, and the telephone interview was a supplementary survey of the epidemiological field investigation, ethics
APPENDIX TO JAMES CASCIANO DECLARATION-77
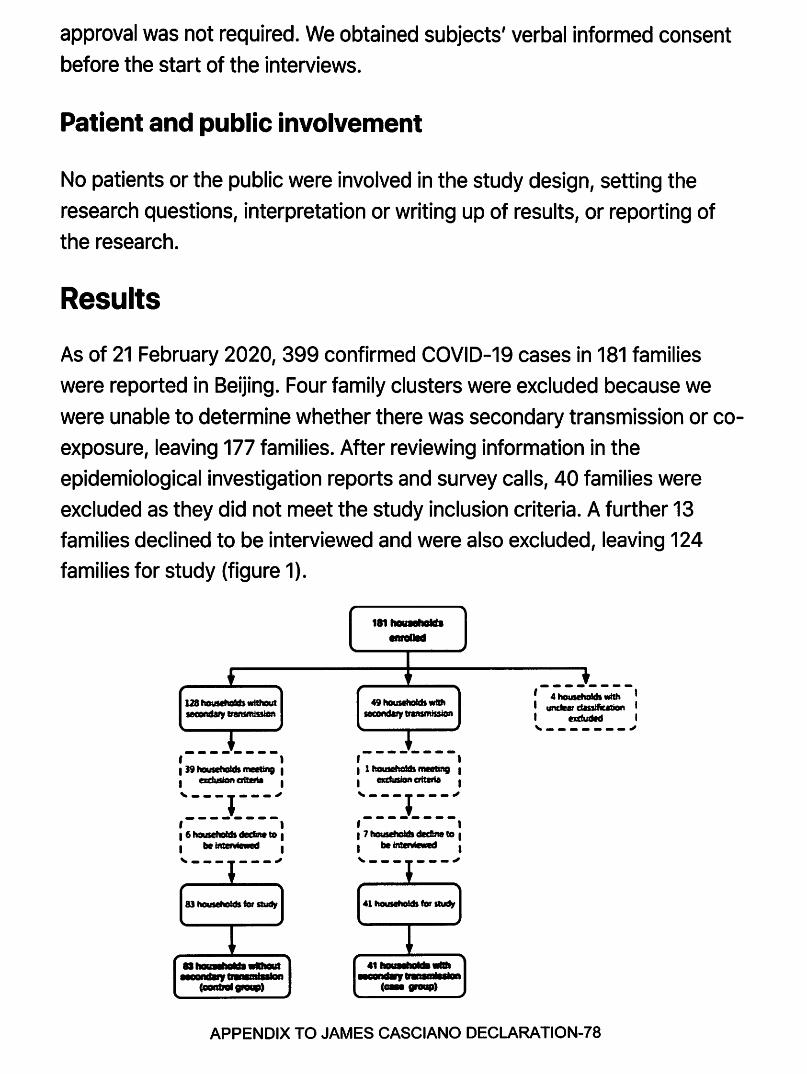
approval was not required. We obtained subjects' verbal informed consent before the start of the interviews.
Patient and public involvement
No patients or the public were involved in the study design, setting the research questions, interpretation or writing up of results, or reporting of the research.
Results
As of 21 February 2020, 399 confirmed COVID-19 cases in 181 families were reported in Beijing. Four family clusters were excluded because we were unable to determine whether there was secondary transmission or coexposure, leaving 177 families. After reviewing information in the epidemiological investigation reports and survey calls, 40 families were excluded as they did not meet the study inclusion criteria. A further 13 families declined to be interviewed and were also excluded, leaving 124 families for study (figure 1).
128tlousltlddswtthcM leCIDftda,y lrlftSffliDlon
,--------, I 39 tlausehatdl meeting I I erdusionaiblta I
'_-_-:_i_-_-_-: I I I 6 househafds ~ to I I be Intel •••d I , ______ .,
83haulellotdsfordudJ
,.,.........,. emallld
49househafdlwftll ~ b'aftSffllssiOn
,--------, I 1 flausetlo!ds meetir'9 I I mcdusion crileril I
'---,---~ ,-.-------, I 7 houlltlaldl dec!fte to I I be lnter1 le ed I ._._ ______ .,
41 tlousetlOlds for~
,-4-~:.;-, I unclear dassific&1ion I I b.'duded I
'-'-------"'
APPENDIX TO JAMES CASCIANO DECLARATION-78

Figure 1
Selection and inclusion of interviewing subjects. Summary of household enrolment, and inclusion and interview response in the analysis of SARS-CoV-2 household transmission in Beijing, China.
Over the 2 weeks of follow-up from onset of the primary case, secondary
transmission occurred in 41/124 families (77 secondary cases), and 83/124
families had no secondary transmission. The overall secondary attack rate
in families was 23.0% (77/335). In the secondary transmission group, 41
primary cases caused 77 secondary cases, with a median secondary case
number in families of 2 (IQR 1-2). In the secondary transmission group, the
secondary attack rate in children <18 years of age was 36.1% (13/36),
compared with 69.6% (64/92) in adults, and the difference between these
two age groups was significant (x2=12.08, p<0.001). The median age of the 13 secondary child cases was 3 years (IQR 2-6), 12/13 were mild and 1/13
was asymptomatic. Of 64 secondary adult cases, 82.8% (53/64) were mild,
10.9% (7/64) were severe, 1.6% (1/64) was critical and 4.7% (3/64) were
asymptomatic. No statistically significant difference was observed in clinical severity between 41 index adult cases (table 1) and 64 secondary adult
cases for the secondary transmission group (p=0.18).
Table 1
Characteristics of primary cases of COVID-19: univariable analysis
Table 2
Characteristics of well family members: univariable analysis
Table3
Characteristics of the residence and household practices: univariable analysis between two family groups
The univariable analysis for association with secondary transmission of
SARS-CoV-2 within families is shown in tables 1-3. Significant associations APPENDIX TO JAMES CASCIANO DECLARATION-79

were:
Characteristics, behaviours and knowledge of the primary case: having
diarrhoea, interval from illness onset to medical isolation >2 days, self
awareness of being infected with SARS-CoV-2 when the primary case
developed the illness, lack of knowledge of their own infectiousness, mask
wearing in the home after illness onset, failing to self-isolate and not eating
separately were associated with transmission (table 1).
Behaviours of family members: having daily close contact with the primary
case at home, and number of family members wearing a mask in the home
before and after the primary case's illness onset date were associated with
transmission (table 2).
Household practices: frequency of using chlorine or ethanol based
disinfectant for household cleaning and household ventilation duration were
protective (table 3).
In multivariable logistic regression model, four factors remained significantly
associated with secondary transmission. The primary case having diarrhoea
in the home and daily close contact with the primary case in the home
increased the risk. Transmission was significantly reduced by frequent use
of chlorine or ethanol based disinfectant in households and family members
(including the primary case) wearing a mask at home before the primary
case developed the illness (table 4).
Table4
Risk factors for SARS-CoV-2 household transmission: multivariable analysis
Discussion
This study confirms that the highest risk of household transmission is prior
to symptom onset, but that precautionary NPls, such as mask use, APPENDIX TO JAMES CASCIANO DECLARATION-SO

disinfection and social distancing in households can prevent COVID-19 transmission during the pandemic. This study is the first to confirm the effectiveness of mask use prior to symptom onset by family members, daily household disinfection and social distancing in the home. This could inform precautionary guidelines for families to reduce intrafamilial transmission in areas where there is high community transmission or other risk factors for COVID-19. Household transmission is a major driver of epidemic growth.5 6 Further, in countries where health system capacity is exhausted, many people with infection are required to self-isolate at home, where their household contacts will be at risk of infection. In our study, the median family size of the 124 families was 4 (range 2-9), usually with children, parents and grandparents, which is similar to the social structure of most Chinese families.9 Therefore, the risk of SARS-CoV-2 household transmission is high if a primary case was introduced and no measure was adopted. We showed that NPls are effective at preventing transmission, even in homes that are crowded and small. UFMU is a low risk intervention with potential public health benefits.3 4 The results suggest that community face mask use is likely to be the most effective inside the household during severe epidemics.
Almost a quarter of family members became infected, and the findings suggest that the risk was highest either before symptom onset or early in the clinical illness, as most primary cases were hospitalised after diagnosis, and interventions were not effective if applied after symptom onset. In the univariate analysis, wearing a mask after illness onset was significant, but in multivariate analysis, only wearing it before symptom onset was effective. Viral load is highest in the 2 days before symptom onset and on the first day of symptoms, and up to 44% of transmission is during the pre-symptomatic period in settings with substantial household clustering.10 11 This supports UFMU, probably by reducing onward transmission from people in the presymptomatic phase of the illness1213 as well as protecting well mask users. Randomised clinical trials of face masks in the household have confirmed protection against other respiratory viruses if compliant, if used
APPENDIX TO JAMES CASCIANO DECLARATION-81

within 36 hours of the primary case symptom onset, and alone or in
combination with hand hygiene.1415 This study now provides specific
evidence for UFMU in settings of high epidemic growth to protect against
COVID-19. In our study, 91.2% (103/113) of primary cases had a high score
on hand hygiene, but it was not effective, confirming the results of previous
randomised clinical trials which showed hand hygiene alone did not protect
against respiratory transmissible viruses, but masks combined with hand
hygiene did have effect.16
As the compliance of UFMU would be poor in the home, there was difficulty
and also no necessity for everyone to wear masks at home. We
recommended that those families with members who were at risk of getting
infected with SARS-CoV-2 (such as ever having contact with a COVID-19
patient, medical workers caring for a COVID-19 patient or having a history
of travelling to high risk areas) should apply UFMU to reduce the risk of
household transmission.
This study showed that social distancing within the home is effective and
having close contact (within 1 m or 3 feet, such as eating around a table or
sitting together watching TV) is a risk factor for transmission. The study
also provides evidence of effectiveness of chlorine or ethanol based
household disinfection in areas with high community transmission, or where
one family member is a health worker, or where there is a risk of COVID-19,
such as during home quarantine, consistent with advice provided by local
health authorities or organisations.17 Diarrhoea as a symptom in the
primary case is also a risk factor for SARS-CoV-2 transmission within
families, which highlights the importance of disinfection of the bathroom
and toilet, as well as closing the toilet lid when flushing to prevent
aerosolisation of the virus.
Our study has limitations. Telephone interview has inherent limitations,
including recall bias. It would take about 20 min to complete an interview,
and 95% (118/124) of interviews were rated as informative by the
APPENDIX TO JAMES CASCIANO DECLARATION-82
interviewers. The evaluation results of mask wearing were reliable, but we
did not collect data on the concentration of disinfectant used by families.
The strengths of the study were that we had complete follow-up data and
were able to accurately ascertain the incidence of secondary transmission
in the cohort.
Conclusions
Household transmission in the pre-symptomatic or early symptomatic
period of COVID-19 is a driver of epidemic growth and any measure aimed
at reducing this can flatten the curve. This study reinforces the high risk of
transmission in households but importantly shows that UFMU and hygiene
measures can significantly reduce the risk of household transmission of
COVID-19, independent of household size or crowding. This is the first
study to show the effectiveness of precautionary mask use, social
distancing and regular disinfection in the household, and can inform
guidelines for prevention of household transmission. The results may also
be informative for families of high risk groups, such as health workers,
quarantined individuals or situations where cases of COVID-19 have to be
managed at home.
Acknowledgments
We thank the staff members in the district and municipal Centres for
Disease Prevention and Control, and medical settings in Beijing for
conducting field investigation, specimen collection, laboratory detection
and case reporting. We also thank all patients and families involved in the
study.
References
1. +J
2. +J
APPENDIX TO JAMES CASCIANO DECLARATION-83

3. +J
4. +J
5. +J
6. +J
7. +J
8. +J
9. +J
10. +J
11. +J
12. +J
13. +J
14. +J
15. +J
16. +J
17. +J
APPENDIX TO JAMES CASCIANO DECLARATION-84

Case-Control Study of Use of Personal Protective Measures and Risk for SARS-CoV 2 Infection, Thailand We evaluated effectiveness of personal protective measures against severe
acute respiratory disease coronavirus 2 (SARS-CoV-2) infection. Our case
control study included 211 cases of coronavirus disease (COVID-19) and
839 controls in Thailand. Cases were defined as asymptomatic contacts of
COVID-19 patients who later tested positive for SARS-CoV-2; controls were
asymptomatic contacts who never tested positive. Wearing masks all the
time during contact was independently associated with lower risk for SARS
CoV-2 infection compared with not wearing masks; wearing a mask
sometimes during contact did not lower infection risk. We found the type of
mask worn was not independently associated with infection and that
contacts who always wore masks were more likely to practice social
distancing. Maintaining >1 m distance from a person with COVID-19, having
close contact for <15 minutes, and frequent handwashing were
independently associated with lower risk for infection. Our findings support
consistent wearing of masks, handwashing, and social distancing to protect
against COVID-19.
Evaluation of the effectiveness of mask-wearing to protect healthy persons
in the general public from infection with severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2), the causative agent of coronavirus disease
(COVID-19), is urgently needed (7,2). On February 27, 2020, during the
early stages of the COVID-19 outbreak, the World Health Organization
(WHO) announced that wearing a mask of any type was not recommended
for asymptomatic persons (3). The rationale at that time was to avoid
unnecessary cost, procurement burden, and a false sense of security (3).
APPENDIX TO JAMES CASCIANO DECLARATION-85

Several systematic reviews found no conclusive evidence to support
widespread use of masks in public settings to protect against respiratory
infectious diseases, such as influenza and severe acute respiratory
syndrome (SARS) (4-6). However, China, South Korea, Japan, Thailand, and
other countries in Asia have recommended the use of face masks among
the general public since early in the COVID-19 pandemic (7). Evidence
suggests that persons with COVID-19 can have a presymptomatic period,
during which they can be contagious and transmit SARS-CoV-2 to others
before symptoms develop (8). These findings led to a change in
recommendations from the US Centers for Disease Control and Prevention
on April 4, 2020, that advised all persons wear a cloth face covering when in
public (9). On April 6 and June 5, 2020, WHO updated its advice on the use
of masks for the general public and encouraged countries that issue the
recommendations to conduct research on this topic (8).
Thailand has been implementing multiple measures against transmission of
SARS-CoV-2 since the beginning of the outbreak (10, 11). The country
established thermal screening at airports on January 3, 2020, and detected
an early case of COVID-19 outside China in a traveler from Wuhan, China,
arriving at Bangkok Suvarnabhumi airport on January 8, 2020 (10). Thailand
uses Surveillance and Rapid Response Teams (SRRTs), together with village
health volunteers, to conduct contact tracing, educate the public about
COVID-19, and monitor close contacts of persons with COVID-19 in
quarantine (11). SRRTs are epidemiologic teams trained to conduct
surveillance, investigations, and initial control of communicable diseases,
such as SARS and influenza (12, 13). More than 1,000 district-, provincial-,
and regional-level SRRTs are working on COVID-19 contact tracing in
Thailand.
By February 2020, public pressure to wear masks in Thailand was high.
However, medical masks became difficult for the public to procure, and the
government categorized medical masks as price-controlled goods. When
the Ministry of Public Health (MoPH) designated COVID-19 a dangerous
APPENDIX TO JAMES CASCIANO DECLARATION-86

communicable disease, according to the Communicable Disease Act of
2015, government officials were empowered to quarantine case-contacts
and close venues (14, 15). On March 3, MoPH recommended public use of
cloth face masks (16). On March 18, schools, universities, bars, nightclubs,
and entertainment venues were closed (17). On March 26, when the country
was reporting »100-150 new COVID-19 cases per day, the government
declared a national state of emergency, prohibited public gatherings, and
enforced wearing of face masks by all persons on public transport (18). On
April 21, MoPH announced 19 new PCR-confirmed COVID-19 cases,
bringing the total number of cases to 2,811 (78). Given the lack of evidence,
we sought to evaluate the effectiveness of mask-wearing, handwashing,
social distancing, and other personal protective measures against SARS
CoV-2 infection in public in Thailand.
Study Design
We conducted a retrospective case-control study by drawing persons with
COVID-19 cases and noninfected controls from a cohort of contact tracing
records of the central SRRT team at the Department of Disease Control
(DDC), MoPH, Thailand. We included contact investigations of 3 large
COVID-19 clusters in nightclubs, boxing stadiums, and a state enterprise
office in Thailand.
Contacts were defined by DDC as persons who had activities with or were
in the same location as a person with confirmed COVID-19 (19,20). The
main aim of contact tracing was to identify and evaluate contacts, perform
reverse transcription PCR (RT-PCR) diagnostic tests, and quarantine high
risk contacts, as defined by the MoPH (AP-.cendix). RT-PCR was performed
at laboratories certified for COVID-19 testing by the National Institute of
Health of Thailand (79,20). Data on risk factors associated with SARS-CoV-
2 infection, such as type of contact and use of mask, were recorded during
contact investigations, but data sometimes were incomplete.
The central SRRT performed contact investigations for clusters of >5 PCRAPPENDIX TO JAMES CASCIANO DECLARATION-87

confirmed COVID-19 cases from the same location within a 1-week period
(79,20). We used these data to identify contacts who were asymptomatic
during March 1-31, 2020. We used all available contact tracing records of
the central SRRT in the study.
We telephoned contacts during April 30-May 27, 2020, and asked details
about their contact with a COVID-19 index patient, such as dates, locations,
duration, and distance of contact. We asked whether contacts wore a mask
during the contact with the index patient, the type of mask, and the
frequency of wearing a mask, which we defined as compliance with mask
wearing. We asked whether and how frequently contacts washed their
hands while with the index patient. We asked whether contacts performed
social distancing and whether they had physical contact with the COVID-19
index patient. If they did not know, or could not remember, contact with the
index patient, we asked whether they had contact with other persons at the
location. We asked whether the contact shared a cup or a cigarette with
other persons in the place they had contact or had highest risk for contact
with the index patient and whether the COVID-19 index patient, if known to
the respondent, had worn a mask {AP-Qendix, Additional Methods). We also
asked, and verified by using DDC records, whether and when the contacts
had symptoms and when COVID-19 was diagnosed.
For our study, we defined cases as asymptomatic contacts who later tested
positive for SARS-CoV-2, on the basis of RT-PCR results available by April
21, 2020. We defined controls as asymptomatic contacts who did not have
positive test results for SARS-CoV-2 by April 21, including those who tested
negative and those who were not tested. We defined asymptomatic
contacts as persons who had contact with or were in the same location as a
symptomatic COVID-19 patient and had no symptoms of COVID-19 on the
first day of contact. We defined index patients as persons identified from
contact tracing data as the potential source of SARS-CoV-2 infection; cases
{as defined above) also could be index patients. We defined primary index
patients as persons whose probable sources of infection were before the
APPENDIX TO JAMES CASCIANO DECLARATION-88

study period, March 1-31; for whom we were not able to identify the source
of infection; or whose probable sources of infection were outside the
contact tracing data included in the study. We defined high-risk exposure
as that which occurred when persons lived in the same household as a
COVID-19 patient; had a direct physical contact with a COVID-19 patient;
were <1 m from a COVID-19 patient for >15 minutes; or were in the same
closed environment, such as a room, nightclub, stadium, or vehicle, <1 m
from a COVID-19 patient for >15 minutes.
We used 21 days after March 31 as a cutoff date based on evidence that
most persons with COVID-19 likely would develop symptoms within 14 days
(27) and that it could take <7 additional days for symptomatic persons
under contact investigation to go to a healthcare facility and be tested for
COVID-19. Our study follows the STROBE guidelines (22).
Statistical Analysis
To include only initially asymptomatic contacts in the study, we excluded
persons who reported having symptoms of COVID-19 at the time of initial
contact with an index patient. Because our study focused on the risk for
infection in the community, we excluded contacts whose contact locations
were healthcare facilities. We also excluded primary index patients if they
were the first to have symptoms at the contact investigation location, had
symptoms since the first day of visiting the location, or were the origin of
infection based on the contact investigation.
We estimated secondary attack rates by using the percentage of new cases
among asymptomatic contacts with high-risk exposure to enable
comparison with other studies. We estimated odds ratios (ORs) and 95%
Cls for associations between developing COVID-19 and factors evaluated.
We used logistic regression with random effects for location and for index
patients nested in the same location. If an asymptomatic contact had
contact with >1 symptomatic COVID-19 index patient, the interviewer
identified the index patient as the symptomatic COVID-19 patient with the APPENDIX TO JAMES CASCIANO DECLARATION-89

closest contact. The percentage of missing values for the variable
indicating whether the index patients wore a mask was 27%; thus, we did
not include this variable in our analyses. For other variables, we assumed
that missing values were missing at random and used imputation by
chained equations (23,24). We created 10 imputed datasets and the
imputation model included the case-control indicator and variables used in
the multivariable models, including sex, age group, contact place, shortest
distance of contact, duration of contact at <1 m, sharing dishes or cups,
sharing cigarettes, handwashing, mask-wearing, and compliance with
mask-wearing. We developed the final multilevel mixed-effect logistic
regression models on the basis of previous knowledge and a purposeful
selection method (25; ApQendix, Additional Analyses). Because of
collinearity between mask use and mask type, we conducted a separate
analysis including mask type in the multilevel mixed-effects logistic
regression model for SARS-CoV-2 infection. We also tested a predefined
interaction between mask type and compliance with mask-wearing
(ApQendix, Additional Analyses).
To clarify patterns of behavior and factors related to compliance with mask
wearing, we used multinomial logistic regression models and the imputed
dataset to estimated OR and 95% Cl for associations between 3 mask
wearing compliance categories, never, sometimes, or all the time; and for
other practices, including handwashing and social distancing during the
contact period. We used logistic regression to estimate p values for
pairwise comparisons.
To estimate the proportional reduction in cases that would occur if
exposure to risk factors was reduced, we estimated the population
attributable fraction by using the imputed dataset and a direct method
based on logistic regression, as described previously (26,27; AQQendix,
Additional Analyses). We performed all analyses by using Stata version 14.2
{StataCorp, httgs:fLwww.stata.com) and R version 4.0.0 {R Foundation for
Statistical Computing, httgs:fLwww.r-groject.org).
APPENDIX TO JAMES CASCIANO DECLARATION-90

Characteristics of the Cohort Data
·,-__,...,wa,.;.;;.;.;.;~-~. -------·----------............ ____ __ ......... -...... .... _...._,_4111119 . ., ...........
-•---•---.. , __ ...,...... ____ ____
• ............... ---=-_,. ______ ....,
• ~ .. -.:-_... .... _ ....... IIM>~J .. ,...#, .. '4
• ___ .. _... __ __
....... t~- .. • .-i:a...,.r
The contact tracing records of the central
SRRT included 1,716 persons who had contact
with or were in the same location as a person
with diagnosed COVID-19 in an investigation
of 3 large clusters (Figure 1). Overall, 18 Figure 1. Flow diagram in case
primary index patients were identified: 11 from control study of severe acute
the nightclub cluster, 5 from the boxing respiratory syndrome coronavirus 2 infections and contacts, Thailand,
stadiums cluster, and 2 from the state March-April 2020. covI0-19,
enterprise office cluster. Timelines of primary coronavirus disease; SARS-cov-2,
index patients from the 3 clusters varied
(AP-Qendix Figures 1-3); we excluded the 18
primary index patients from our analyses.
Characteristics of Cases and Controls
severe acute respiratory syndrome coronavirus 2; SRRT, Surveillance ...
After interviewing each contact by phone and applying the exclusion criteria
(Figure 1), our analysis included 1,050 asymptomatic persons who had
contact with or were in the same location as a symptomatic COVID-19 index
patient during March 1-31, 2020. The median age of persons included was
38 years (IQR 28-51 years); 55% were male, and 45% were female (Table 1).
Most (61%; n = 645) asymptomatic contacts included in the study were
associated with the boxing stadiums cluster, 36% (n = 374) were related to
the nightclub cluster, and 3% (n = 31) were related to the state enterprise
office cluster. Overall, 890 (84.8%) contacts were considered to have high
risk exposure.
Among 1,050 asymptomatic contacts included in our analysis, 211 (20.1%)
tested positive for SARS-CoV-2 by April 21, 2020, and were classified as
cases; 839 (79.9%) never tested positive and were controls. Of the 211
cases, 195 (92.4%) had high-risk exposures and 150 (71.1%) had symptoms
before COVID-19 diagnosis by RT-PCR (AQP-endix). The last date that a
COVID-19 case was detected was April 9, 2020. Among the 839 controls, APPENDIX TO JAMES CASCIANO DECLARATION-91

695 (82.8%) had high-risk exposures and 719 (85.7%) were tested by PCR
at least once.
Among asymptomatic contacts included in the A.:_..:
study, 228 had contact with a COVID-19 index .. ; . :-: · .
patient at nightclubs, 144 at boxing stadiums, · i~'( and 20 at the state enterprise office (Figure 2).
The others had contacts with a COVID-19
index patient at workplaces (n = 277),
households (n = 230), and other places (n =
. ,. ...
8
151). Among 890 asymptomatic contacts with c :-~.-.
high-risk exposures included in the study, the ._., Figure 2. Development and secondary attack rate from boxing stadiums transmission of severe acute
was 86% (111/129), the secondary attack rate respiratory syndrome coronavirus 2
for nightclubs was 18.2% (34/187), the among asymptomatic contacts, Thailand, March-April 2020. Clusters
household secondary attack rate was 16.5% indicate coronavirus disease (COVID(38/230), the workplace secondary attack rate19) contacts from nightclubs (A);
was 4.9% (10/205), and the secondary attack boxing stadiums (B), and the ...
rate at other places was 1.4% (2/139).
Bivariate Analyses
Our analysis showed risk for SARS-CoV-2 infection was negatively
associated with personal protective measures {Table 1). Crude odds ratio
{OR) for infection was 0.08 {95% Cl 0.02-0.31) for those maintaining a
distance of >1 m from a COVID-19 patient; 0.13 (95% Cl 0.04-0.46) for
those whose duration of contact was s15 minutes; 0.41 (95% Cl 0.18-0.91)
for those who performed handwashing sometimes; 0.19 (95% Cl 0.08-0.46)
for those who washed hands often; and 0.16 (95% Cl 0.07-0.36) for those
wearing a mask all the time during contact with a COVID-19 patient. We
noted a higher risk for SARS-CoV-2 infection among persons sharing dishes
or cups {OR 2.71; 95% Cl 1.48-4.94) and sharing cigarettes {OR 6.12; 95%
Cl 2.12-17.72) with other persons in general, not necessarily including a
APPENDIX TO JAMES CASCIANO DECLARATION-92

COVID-19 patient. In the bivariate model, type of mask was associated with
risk for infection (p = 0.003).
Multivariable Analyses
We found a negative association between risk for SARS-CoV-2 infection
and maintaining a distance of >1 m from a COVID-19 patient (adjusted odds
ratio [aOR] 0.15; 95% Cl 0.04-0.63); duration of contact <15 minutes (aOR
0.24; 95% Cl 0.07-0.90); handwashing often (aOR 0.33; 95% Cl 0.13-0.87);
and wearing a mask all the time during contact with a COVID-19 patient
(aOR 0.23; 95% Cl 0.09-0.60) (Table 1). Wearing masks sometimes during
contact with a COVID-19 patient was not statistically significantly
associated with lower risk for infection (aOR 0.87; 95% Cl 0.41-1.84).
Sharing cigarettes with other persons was associated with higher risk for
infection (aOR 3.47; 95% Cl 1.09-11.02).
Compliance with mask-wearing during contact with a COVID-19 patient was
strongly associated with lower risk for infection in the multivariable model.
Because of collinearity with mask-wearing compliance, we did not include
mask type in the final model. We included mask type in a separate
multivariable model and found type of mask was not independently
associated with infection (p = 0.54) (AQgendix Table 1). We found no
evidence of effect modification between mask type and mask-wearing
compliance.
Association Between Mask-Wearing Compliance and Other Social Distancing Practices
Because mask-wearing throughout the contact period was negatively
associated with COVID-19, we further explored characteristics of
participants to ascertain whether wearing a mask produced a potential false
sense of security. We found that during the contact period, 25% of persons
who wore masks all the time reported maintaining >1 m distance from
contacts compared with 18% of persons who did not wear a mask (pairwise
APPENDIX TO JAMES CASCIANO DECLARATION-93

p = 0.03). In addition, persons who wore masks all the time were more likely
to report duration of contact <15 minutes (26% vs. 13% for those who did
not wear a mask; pairwise p<0.001) and washing hands often (79% vs. 26%
for those who did not wear a mask; pairwise p<0.001) (Table 2). We found
that 43% of persons who wore masks sometimes were likely to wash their
hands often compared with those who did not wear masks (26%; pairwise
p<0.001), but they were more likely to have physical contact (50% vs. 42%;
pairwise p = 0.03) and report duration of contact >60 minutes (75% vs.
67%; pairwise p = 0.04) compared with those who did not wear masks.
Our findings provide evidence that mask-wearing, handwashing, and social
distancing are independently associated with lower risk for SARS-CoV-2
infection in the general public in community settings in Thailand. We
observed that wearing masks throughout the period of exposure to
someone infected with SARS-CoV-2 was associated with lower risk for
infection, but wearing masks only sometimes during the period was not.
This evidence supports recommendations to wear masks consistently and
correctly at all times in public (2,7-9).
The effectiveness of mask-wearing we observed is consistent with previous
studies, including a randomized-controlled trial showing that consistent
face mask use reduced risk for influenza-like illness (28), 2 case-control
studies that found that mask-wearing was associated with lower risk for
SARS infection (29,30), and a retrospective cohort study that found that
mask-wearing by index patients or family members at home was associated
with lower risk for SARS-CoV-2 infection (31). Previous studies found use of
surgical masks or similar 12-16-layer cotton reusable masks demonstrated
protection against coronavirus infection in the community (32), but we did
not observe a difference between wearing nonmedical and medical masks
in the general population. Our results suggest that wearing nonmedical
masks in public can potentially reduce transmission of SARS-CoV-2.
Another study found perception of risk of developing COVID-19 can
increase a person's likelihood of wearing a medical mask in nonmedical
APPENDIX TO JAMES CASCIANO DECLARATION-94

settings (T.D. Huynh, unpub. data,
httQs :/ Lwww. med rxiv.orgL contentL10 .1101L20 2 0.0 3. 2 6. 2 0 044388v1).
However, given supply shortages, medical masks should be reserved for
use by healthcare workers.
We found a negative association between risk for SARS-CoV-2 infection
and social distancing, consistent with previous studies that found that >1 m
physical distancing was associated with a large protective effect and
distances of >2 m could be more effective (32). Our findings on
effectiveness of hand hygiene also were consistent with reports in previous
studies (33).
In this study, secondary attack rates at different venues varied widely. The
household secondary attack rate in our study {16.5%) is comparable with
ranges reported previously (11o/o-23%) (34,35), and relatively high
compared with workplaces (4.9%) and other settings {1.4%). Although
quarantine measures can be challenging and sometimes impractical,
household members should immediately separate a person who develops
symptoms of COVID-19; the sick person should stay in a specific room; use
a separate bathroom, if possible; and not share dishes, cups, and other
utensils (36). All household members should wear masks, frequently wash
their hands, and perform social distancing to the extent possible (37).
The high number of COVID-19 cases associated with nightclub exposures
in Bangkok is comparable to a COVID-19 outbreak associated with the
ltaewon nightclub cluster in Seoul, South Korea, during May 2020 (38), in
which persons visited several nightclubs in the same area during a short
period of time. The secondary attack rate in boxing stadiums was high
(86%) but similar to a cluster of COVID-19 cases associated with a football
match in Italy during February 2020 (39). The secondary attack rate of
COVID-19 at a choir practice in the United States was reported to be
53.3o/o-86.7% (40). Secondary attack rates in public gathering places with
high densities of persons shouting anet cheering, such as football and
APPENDIX TO JAMES CASCIANO DECLARATION-95

boxing stadiums, are still uncertain but appear to be high.
Clear and consistent public messaging from policy makers likely can
prevent a false sense of security and promote compliance with social
distancing in Thailand. We found that those who wore masks throughout
the time they were exposed to a COVID-19 patient also were more likely to
wash their hands and perform social distancing. Traditional and social
media outlets can support public health responses by working with
governments to provide consistent, simple, and clear messages (47). In
Thailand, daily briefings from the Centre for COVID-19 Situation
Administration provided clear, consistent messages on social distancing,
how to put on a mask, and how to wash hands, which might have improved
public confidence with the recommendations. Consistent public messages
on how to wear masks correctly also are needed, particularly for those who
wear masks sometimes or incorrectly, such as not covering both nose and
mouth. We found that persons who only intermittently wore masks during
exposure also did not practice social distancing adequately.
Our study has several limitations. First, because our findings were based on
contacts related to 3 major COVID-19 clusters in Thailand during March
2020, they might not be generalizable to all settings. Second, estimated
ORs were conditioned on reported contact with index patients; our study
did not evaluate or consider the probability of having contact with other
infected persons in the community, which could have occurred. Third,
because only 89% of controls were tested, those not tested could have
been infected; therefore, cases might have been missed in persons with
mild or no symptoms or who did not report symptoms or seek care or
testing. Nonetheless, we believe that misclassification likely was minimal
because those who were not tested with RT-PCR were low-risk contacts;
the small number likely would not change our main findings and
recommendations on personal protective measures. Fourth, identifying
every potential contact can be nearly impossible because some persons
might have had contact with >1 COVID-19 patient. Hence, our estimated
APPENDIX TO JAMES CASCIANO DECLARATION-96

secondary attack rates among contacts with high-risk exposure could be
overestimated or underestimated. Fifth, population attributable fraction is
based on several assumptions, including causality, and should be
interpreted with caution (42,43). Finally, findings were subject to common
biases of retrospective case-control studies, including memory bias,
observer bias, and information bias (44). To reduce potential biases, we
used structured interviews in which each participant was asked the same
set of defined questions.
As many countries begin to relax social distancing measures, our findings
provide evidence supporting consistent mask-wearing, handwashing, and
adhering to social distancing recommendations to reduce SARS-CoV-2
transmission in public gatherings. Wearing nonmedical masks in public
could help slow the spread of COVID-19. Complying with all measures could
be highly effective; however, in places with a high population density,
additional measures might be required.
Clear and consistent public messaging on personal protective
recommendations is essential, particularly for targeting those who wear
masks intermittently or incorrectly. Our data showed that no single
protective measure was associated with complete protection from COVID-
19. All measures, including mask-wearing, handwashing, and social
distancing, can increase protection against COVID-19 in public settings.
Dr. Pawinee Doung-ngern is the head of Communicable Disease Unit,
Bureau of Epidemiology, Department of Disease Control, Ministry of Public
Health, Thailand. Her primary research interests include the public health
and epidemiology of communicable diseases.
Top
APPENDIX TO JAMES CASCIANO DECLARATION-97

Physical interventions to interrupt or reduce the spread of respiratory
• viruses BACKGROUND: Viral epidemics or pandemics of acute respiratory
infections (ARls) pose a global threat. Examples are influenza (H1N1)
caused by the H1N1pdm09 virus in 2009, severe acute respiratory
syndrome (SARS) in 2003, and coronavirus disease 2019 (COVID-19)
caused by SARS-CoV-2 in 2019. Antiviral drugs and vaccines may be
insufficient to prevent their spread. This is an update of a Cochrane Review
published in 2007, 2009, 2010, and 2011. The evidence summarised in this
review does not include results from studies from the current COVID-19
pandemic.
OBJECTIVES: To assess the effectiveness of physical interventions to
interrupt or reduce the spread of acute respiratory viruses.
SEARCH METHODS: We searched CENTRAL, PubMed, Embase, CINAHL
on 1 April 2020. We searched ClinicalTrials.gov, and the WHO ICTRP on 16
March 2020. We conducted a backwards and forwards citation analysis on
the newly included studies.
SELECTION CRITERIA: We included randomised controlled trials (RCTs)
and cluster-RCTs of trials investigating physical interventions (screening at
entry ports, isolation, quarantine, physical distancing, personal protection,
hand hygiene, face masks, and gargling) to prevent respiratory virus
transmission. In previous versions of this review we also included
observational studies. However, for this update, there were sufficient RCTs
to address our study aims.
DATA COLLECTION AND ANALYSIS: We used standard methodological
procedures expected by Cochrane. We used GRADE to assess the certainty
APPENDIX TO JAMES CASCIANO DECLARATION-98

of the evidence. Three pairs of review authors independently extracted data
using a standard template applied in previous versions of this review, but
which was revised to reflect our focus on RCTs and cluster-RCTs for this
update. We did not contact trialists for missing data due to the urgency in
completing the review. We extracted data on adverse events (harms)
associated with the interventions.
MAIN RESULTS: We included 44 new RCTs and cluster-RCTs in this
update, bringing the total number of randomised trials to 67. There were no
included studies conducted during the COVID-19 pandemic. Six ongoing
studies were identified, of which three evaluating masks are being
conducted concurrent with the COVID pandemic, and one is completed.
Many studies were conducted during non-epidemic influenza periods, but
several studies were conducted during the global H1 N1 influenza pandemic
in 2009, and others in epidemic influenza seasons up to 2016. Thus, studies
were conducted in the context of lower respiratory viral circulation and
transmission compared to COVID-19. The included studies were conducted
in heterogeneous settings, ranging from suburban schools to hospital
wards in high-income countries; crowded inner city settings in low-income
countries; and an immigrant neighbourhood in a high-income country.
Compliance with interventions was low in many studies. The risk of bias for
the RCTs and cluster-RCTs was mostly high or unclear. Medical/surgical
masks compared to no masks We included nine trials (of which eight were
cluster-RCTs) comparing medical/surgical masks versus no masks to
prevent the spread of viral respiratory illness (two trials with healthcare
workers and seven in the community). There is low certainty evidence from
nine trials (3507 participants) that wearing a mask may make little or no
difference to the outcome of influenza-like illness (ILi) compared to not
wearing a mask (risk ratio (RR) 0.99, 95% confidence interval (Cl) 0.82 to
1.18. There is moderate certainty evidence that wearing a mask probably
makes little or no difference to the outcome of laboratory-confirmed
influenza compared to not wearing a mask (RR 0.91, 95% Cl 0.66 to 1.26; 6
trials; 3005 participants). Harms were rarely measured and poorly reported. APPENDIX TO JAMES CASCIANO DECLARATION-99

Two studies during COVID-19 plan to recruit a total of 72,000 people. One
evaluates medical/surgical masks (N = 6000) (published Annals of Internal
Medicine, 18 Nov 2020), and one evaluates cloth masks (N = 66,000).
N95/P2 respirators compared to medical/surgical masks We pooled trials
comparing N95/P2 respirators with medical/surgical masks (four in
healthcare settings and one in a household setting). There is uncertainty
over the effects of N95/P2 respirators when compared with
medical/surgical masks on the outcomes of clinical respiratory illness (RR
0.70, 95% Cl 0.45 to 1.10; very low-certainty evidence; 3 trials; 7779
participants) and ILi (RR 0.82, 95% Cl 0.66 to 1.03; low-certainty evidence;
5 trials; 8407 participants). The evidence is limited by imprecision and
heterogeneity for these subjective outcomes. The use of a N95/P2
respirator compared to a medical/surgical mask probably makes little or no
difference for the objective and more precise outcome of laboratory
confirmed influenza infection (RR 1.10, 95% Cl 0.90 to 1.34; moderate
certainty evidence; 5 trials; 8407 participants). Restricting the pooling to
healthcare workers made no difference to the overall findings. Harms were
poorly measured and reported, but discomfort wearing medical/surgical
masks or N95/P2 respirators was mentioned in several studies. One
ongoing study recruiting 576 people compares N95/P2 respirators with
medical surgical masks for healthcare workers during COVID-19. Hand
hygiene compared to control Settings included schools, childcare centres,
homes, and offices. In a comparison of hand hygiene interventions with
control (no intervention), there was a 16% relative reduction in the number
of people with ARls in the hand hygiene group (RR 0.84, 95% Cl 0.82 to
0.86; 7 trials; 44,129 participants; moderate-certainty evidence),
suggesting a probable benefit. When considering the more strictly defined
outcomes of ILi and laboratory-confirmed influenza, the estimates of effect
for ILi (RR 0.98, 95% Cl 0.85 to 1.13; 10 trials; 32,641 participants; low
certainty evidence) and laboratory-confirmed influenza (RR 0.91, 95% Cl
0.63 to 1.30; 8 trials; 8332 participants; low-certainty evidence) suggest
the intervention made little or no difference. We pooled all 16 trials (61,372
APPENDIX TO JAMES CASCIANO DECLARATION-100

participants) for the composite outcome of ARI or ILi or influenza, with each
study only contributing once and the most comprehensive outcome
reported. The pooled data showed that hand hygiene may offer a benefit
with an 11% relative reduction of respiratory illness (RR 0.89, 95% Cl 0.84 to
0.95; low-certainty evidence), but with high heterogeneity. Few trials
measured and reported harms. There are two ongoing studies of
handwashing interventions in 395 children outside of COVID-19. We
identified one RCT on quarantine/physical distancing. Company employees
in Japan were asked to stay at home if household members had ILi
symptoms. Overall fewer people in the intervention group contracted
influenza compared with workers in the control group (2.75% versus 3.18%;
hazard ratio 0.80, 95% Cl 0.66 to 0.97). However, those who stayed at
home with their infected family members were 2.17 times more likely to be
infected. We found no RCTs on eye protection, gowns and gloves, or
screening at entry ports.
AUTHORS' CONCLUSIONS: The high risk of bias in the trials, variation in
outcome measurement, and relatively low compliance with the interventions
during the studies hamper drawing firm conclusions and generalising the
findings to the current COVID-19 pandemic. There is uncertainty about the
effects of face masks. The low-moderate certainty of the evidence means
our confidence in the effect estimate is limited, and that the true effect may
be different from the observed estimate of the effect. The pooled results of
randomised trials did not show a clear reduction in respiratory viral infection
with the use of medical/surgical masks during seasonal influenza. There
were no clear differences between the use of medical/surgical masks
compared with N95/P2 respirators in healthcare workers when used in
routine care to reduce respiratory viral infection. Hand hygiene is likely to
modestly reduce the burden of respiratory illness. Harms associated with
physical interventions were under-investigated. There is a need for large,
well-designed RCTs addressing the effectiveness of many of these
interventions in multiple settings and populations, especially in those most
at risk of ARls. APPENDIX TO JAMES CASCIANO DECLARATION-101

Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings-Personal Protective and Environmental Measures Personal Protective Measures
Hand Hygiene
We identified a recent systematic review by ~:.=: ~;-;-;~~~-,---~ Wong et al. on RCTs designed to assess the ::=~~ttt i ~~~ =~ti .. ~-~-..
efficacy of hand hygiene interventions against §:r:: j§7§~~if;~7--transmission of laboratory-confirmed :::.~::~:~-: .~:: ::: : ·:.
-----influenza (8). We used this review as a starting;::.;_~_~~~~~~~~=· . -: point and then searched for additional :::~t-{~ ~ ~ J I~-i ~-: -··-···-j-. -·---··--•. literature published after 2013; we found 3 -----
. . . . . . . Figure 1. Meta-analysis of risk ratios add1t1onal ehg1ble articles pubhshed dunng the for the effect of hand hygiene with or search period of January 1, 2013-August 13, without face mask use on laboratory-2018. In total we identified 12 articles (9-20) confirm~d influenza fro~ 10 .
' ' randomized controlled trials with of which 3 articles were from the updated >11,000 participants. A) Hand search and 9 articles from Wong et al. (8). Twohygiene alone; ...
articles relied on the same underlying dataset (16, 19); therefore, we counted these 2 articles as 1 study, which resulted in 11 RCTs. We further selected 10 studies with >10,000 participants for inclusion in the metaanalysis (Figure 1). We excluded 1 study from the meta-analysis because it provided estimates of infection risks only at the household level, not the individual level (20). We did not generate an overall pooled effect of hand hygiene only or of hand hygiene with or without face mask because of high heterogeneity in individual estimates (12 87 and 82%, respectively). The effect of hand hygiene combined with face masks on laboratory-confirmed
APPENDIX TO JAMES CASCIANO DECLARATION-103

influenza was not statistically significant {RR 0.91, 95% Cl 0.73-1.13; 12 = 35%, p = 0.39). Some studies reported being underpowered because of limited sample size, and low adherence to hand hygiene interventions was observed in some studies.
We further analyzed the effect of hand hygiene by setting because transmission routes might vary in different settings. We found 6 studies in
household settings examining the effect of hand hygiene with or without face masks, but the overall pooled effect was not statistically significant (RR 1.05, 95% Cl 0.86-1.27; /2 = 57%, p = 0.65) (AP-gendix Figure 4) (11-15, 17).
The findings of 2 studies in school settings were different {Aggendix Figure 5). A study conducted in the United States (76) showed no major effect of hand hygiene, whereas a study in Egypt (18) reported that hand hygiene reduced the risk for influenza by >50%. A pooled analysis of 2 studies in university residential halls reported a marginally significant protective effect of a combination of hand hygiene plus face masks worn by all residents {RR 0.48, 95% Cl 0.21-1.08; /2 = 0%, p = 0.08) (AP-gendix Figure 6) (9, 10).
In support of hand hygiene as an effective measure, experimental studies have reported that influenza virus could survive on human hands for a short time and could transmit between hands and contaminated surfaces (2,21).
Some field studies reported that influenza A(H1N1)pdm09 and influenza A{H3N2) virus RNA and viable influenza virus could be detected on the hands of persons with laboratory-confirmed influenza (22,23), supporting the potential of direct and indirect contact transmission to play a role in the spread of influenza. Other experimental studies also demonstrated that hand hygiene could reduce or remove infectious influenza virus from human hands (24,25). However, results from our meta-analysis on RCTs did not provide evidence to support a protective effect of hand hygiene against transmission of laboratory-confirmed influenza. One study did report a major effect, but in this trial of hand hygiene in schools in Egypt, running water had to be installed and soap and hand-drying material had to be introduced into the intervention schools as part of the project (18).
APPENDIX TO JAMES CASCIANO DECLARATION-104

Therefore, the impact of hand hygiene might also be a reflection of the
introduction of soap and running water into primary schools in a lower
income setting. If one considers all of the evidence from RCTs together, it is
useful to note that some studies might have underestimated the true effect
of hand hygiene because of the complexity of implementing these
intervention studies. For instance, the control group would not typically
have zero knowledge or use of hand hygiene, and the intervention group
might not adhere to optimal hand hygiene practices (11, 13, 15).
Hand hygiene is also effective in preventing other infectious diseases,
including diarrheal diseases and some respiratory diseases (8,26). The
need for hand hygiene in disease prevention is well recognized among most
communities. Hand hygiene has been accepted as a personal protective
measure in >50% of national preparedness plans for pandemic influenza
(5). Hand hygiene practice is commonly performed with soap and water,
alcohol-based hand rub, or other waterless hand disinfectants, all of which
are easily accessible, available, affordable, and well accepted in most
communities. However, resource limitations in some areas are a concern
when clean running water or alcohol-based hand rub are not available.
There are few adverse effects of hand hygiene except for skin irritation
caused by some hand hygiene products (27). However, because of certain
social or religious practices, alcohol-based hand sanitizers might not be
permitted in some locations (28). Compliance with proper hand hygiene
practice tends to be low because habitual behaviors are difficult to change
(29). Therefore, hand hygiene promotion programs are needed to advocate
and encourage proper and effective hand hygiene.
Respiratory Etiquette
Respiratory etiquette is defined as covering the nose and mouth with a
tissue or a mask (but not a hand) when coughing or sneezing, followed by
proper disposal of used tissues, and proper hand hygiene after contact with
respiratory secretions (30). Other descriptions of this measure have
APPENDIX TO JAMES CASCIANO DECLARATION-105

included turning the head and covering the mouth when coughing and
coughing or sneezing into a sleeve or elbow, rather than a hand. The
rationale for not coughing into hands is to prevent subsequent
contamination of other surfaces or objects (31). We conducted a search on
November 6, 2018, and identified literature that was available in the
databases during 1946-November 5, 2018. We did not identify any
published research on the effectiveness of respiratory etiquette in reducing
the risk for laboratory-confirmed influenza or ILi. One observational study
reported a similar incidence rate of self-reported respiratory illness (defined
by >1 symptoms: cough, congestion, sore throat, sneezing, or breathing
problems) among US pilgrims with or without practicing respiratory
etiquette during the Hajj (32). The authors did not specify the type of
respiratory etiquette used by participants in the study. A laboratory-based
study reported that common respiratory etiquette, including covering the
mouth by hands, tissue, or sleeve/arm, was fairly ineffective in blocking the
release and dispersion of droplets into the surrounding environment on the
basis of measurement of emitted droplets with a laser diffraction system
(31).
Respiratory etiquette is often listed as a preventive measure for respiratory
infections. However, there is a lack of scientific evidence to support this
measure. Whether respiratory etiquette is an effective nonpharmaceutical
intervention in preventing influenza virus transmission remains
questionable, and worthy of further research.
Face Masks
In our systematic review, we identified 10 RCTs that reported estimates of
the effectiveness of face masks in reducing laboratory-confirmed influenza
virus infections in the community from literature published during 1946-July
27, 2018. In pooled analysis, we found no significant reduction in influenza
transmission with the use of face masks (RR 0.78, 95% Cl 0.51-1.20;
/2 = 30%, p = 0.25) (Figure 2). One study evaluated the use of masks among
APPENDIX TO JAMES CASCIANO DECLARATION-106

pilgrims from Australia during the Hajj A - --- -- --- _ .. _ ----••-. . . . .. ·••-- ~-pilgrimage and reported no major difference in =)f·; ~ : ~j ?~ •·
·--- - .. -- .. - . the risk for laboratory-confirmed influenza a·=-;~ · _______ ::_ ___ ~~
virus infection in the control or mask group
(33). Two studies in university settings
-...... - ......... -····.. . - . - ·- ·-.. . . =:: -~ .· . : = : : :-: ; :: -:: ·~ -·· ... - . . . . - ·-.. . . --- ,.. ---·-·-- . -·-- ··-. c_ .- -------- --
assessed the effectiveness of face masks for ~-:f{: i ~ i ~ ~~ tii { =:L~--= -. : ~ ~ ; ::: :_: ::.: ~'
primary protection by monitoring the incidence:_-_-:_...;:-:~ ·--~ ·· ·· · ;;;.~ · _;_-
of laboratory-confirmed influenza among Figure 2. Meta-analysis of risk ratios • for the effect of face mask use with
student hall residents for 5 months (9, 10). The or without enhanced hand hygiene on
overall reduction in ILi or laboratory-confirmed laboratory-confirmed influenza from
influenza cases in the face mask group was 10 randomized controlled trials with >6,500 participants. A) Face mask ...
not significant in either studies (9, 10). Study
designs in the 7 household studies were slightly different: 1 study provided
face masks and P2 respirators for household contacts only (34), another
study evaluated face mask use as a source control for infected persons only
(35), and the remaining studies provided masks for the infected persons as
well as their close contacts (11-13, 15, 17). None of the household studies
reported a significant reduction in secondary laboratory-confirmed
influenza virus infections in the face mask group (11-13, 15, 17,34,35). Most
studies were underpowered because of limited sample size, and some
studies also reported suboptimal adherence in the face mask group.
Disposable medical masks (also known as surgical masks) are loose-fitting
devices that were designed to be worn by medical personnel to protect
accidental contamination of patient wounds, and to protect the wearer
against splashes or sprays of bodily fluids (36). There is limited evidence
for their effectiveness in preventing influenza virus transmission either when
worn by the infected person for source control or when worn by uninfected
persons to reduce exposure. Our systematic review found no significant
effect of face masks on transmission of laboratory-confirmed influenza.
We did not consider the use of respirators in the community. Respirators are
tight-fitting masks that can protect the wearer from fine particles (37) and
APPENDIX TO JAMES CASCIANO DECLARATION-107

should provide better protection against influenza virus exposures when
properly worn because of higher filtration efficiency. However, respirators,
such as N95 and P2 masks, work best when they are fit-tested, and these
masks will be in limited supply during the next pandemic. These specialist
devices should be reserved for use in healthcare settings or in special
subpopulations such as immunocompromised persons in the community,
first responders, and those performing other critical community functions,
as supplies permit.
In lower-income settings, it is more likely that reusable cloth masks will be
used rather than disposable medical masks because of cost and availability
(38). There are still few uncertainties in the practice of face mask use, such
as who should wear the mask and how long it should be used for. In theory,
transmission should be reduced the most if both infected members and
other contacts wear masks, but compliance in uninfected close contacts
could be a problem (12,34). Proper use of face masks is essential because
improper use might increase the risk for transmission (39). Thus, education
on the proper use and disposal of used face masks, including hand hygiene,
is also needed.
Surface and Object Cleaning
For the search period from 1946 through October 14, 2018, we identified 2
RCTs and 1 observational study about surface and object cleaning
measures for inclusion in our systematic review (4D-42). One RCT
conducted in day care nurseries found that biweekly cleaning and
disinfection of toys and linen reduced the detection of multiple viruses,
including adenovirus, rhinovirus, and respiratory syncytial virus in the
environment, but this intervention was not significant in reducing detection
of influenza virus, and it had no major protective effect on acute respiratory
illness (41). Another RCT found that hand hygiene with hand sanitizer
together with surface disinfection reduced absenteeism related to
gastrointestinal illness in elementary schools, but there was no major
APPENDIX TO JAMES CASCIANO DECLARATION-108

reduction in absenteeism related to respiratory illness (42). A cross
sectional study found that passive contact with bleach was associated with
a major increase in self-reported influenza (40).
Given that influenza virus can survive on some surfaces for prolonged
periods (43), and that cleaning or disinfection procedures can effectively
reduce or inactivate influenza virus from surfaces and objects in
experimental studies (44), there is a theoretical basis to believe that
environmental cleaning could reduce influenza transmission. As an
illustration of this proposal, a modeling study estimated that cleaning of
extensively touched surfaces could reduce influenza A infection by 2% (45).
However, most studies of influenza virus in the environment are based on
detection of virus RNA by PCR, and few studies reported detection of viable
virus.
Although we found no evidence that surface and object cleaning could
reduce influenza transmission, this measure does have an established
impact on prevention of other infectious diseases (42). It should be feasible
to implement this measure in most settings, subject to the availability of
water and cleaning products. Although irritation caused by cleaning
products is limited, safety remains a concern because some cleaning
products can be toxic or cause allergies (40).
APPENDIX TO JAMES CASCIANO DECLARATION-109

A cluster randomised trial of cloth masks compared with medical masks in healthcare workers Strengths and limitations of this study
• The use of cloth masks is widespread around the world, particularly in
countries at high-risk for emerging infections, but there have been no
efficacy studies to underpin their use.
• This study is large, a prospective randomised clinical trial (RCT) and
the first RCT ever conducted of cloth masks.
• The use of cloth masks are not addressed in most guidelines for health
care workers-this study provides data to update guidelines.
• The control arm was 'standard practice: which comprised mask use in
a high proportion of participants. As such (without a no-mask control),
the finding of a much higher rate of infection in the cloth mask arm
could be interpreted as harm caused by cloth masks, efficacy of
medical masks, or most likely a combination of both.
Introduction
The use of facemasks and respirators for the protection of healthcare
workers (HCWs) has received renewed interest following the 2009 influenza
pandemic, 1 and emerging infectious diseases such as avian influenza,2
Middle East respiratory syndrome coronavirus (MERS-coronavirus)3 ,4 and
Ebola virus.5 Historically, various types of cloth/cotton masks (referred to
here after as 'cloth masks') have been used to protect HCWs.6 Disposable
medical/surgical masks (referred to here after as 'medical masks') were
introduced into healthcare in the mid 19th century, followed later by
APPENDIX TO JAMES CASCIANO DECLARATION-110

respirators.7 Compared with other parts of the world, the use of face masks
is more prevalent in Asian countries, such as China and Vietnam.8-11
In high resource settings, disposable medical masks and respirators have
long since replaced the use of cloth masks in hospitals. Yet cloth masks
remain widely used globally, including in Asian countries, which have
historically been affected by emerging infectious diseases, as well as in
West Africa, in the context of shortages of personal protective equipment
(PPE).12 ,13 It has been shown that medical research disproportionately
favours diseases of wealthy countries, and there is a lack of research on the
health needs of poorer countries.14 Further, there is a lack of high-quality
studies around the use of facemasks and respirators in the healthcare
setting, with only four randomised clinical trials (RCTs) to date.15 Despite
widespread use, cloth masks are rarely mentioned in policy documents,16
and have never been tested for efficacy in a RCT. Very few studies have
been conducted around the clinical effectiveness of cloth masks, and most
available studies are observational or in vitro.6 Emerging infectious diseases
are not constrained within geographical borders, so it is important for global
disease control that use of cloth masks be underpinned by evidence. The
aim of this study was to determine the efficacy of cloth masks compared
with medical masks in HCWs working in high-risk hospital wards, against
the prevention of respiratory infections.
Methods
A cluster-randomised trial of medical and cloth mask use for HCWs was
conducted in 14 hospitals in Hanoi, Vietnam. The trial started on the 3
March 2011, with rolling recruitment undertaken between 3 March 2011 and
10 March 2011. Participants were followed during the same calendar time
for 4 weeks of facemasks use and then one additional week for appearance
of symptoms. An invitation letter was sent to 32 hospitals in Hanoi, of which
16 agreed to participate. One hospital did not meet the eligibility criteria;
therefore, 74 wards in 15 hospitals were randomised. Following the
APPENDIX TO JAMES CASCIANO DECLARATION-111

randomisation process, one hospital withdrew from the study because of a
nosocomial outbreak of rubella.
Participants provided written informed consent prior to initiation of the trial.
Randomisation
Seventy-four wards (emergency, infectious/respiratory disease, intensive
care and paediatrics) were selected as high-risk settings for occupational
exposure to respiratory infections. Cluster randomisation was used because
the outcome of interest was respiratory infectious diseases, where
prevention of one infection in an individual can prevent a chain of
subsequent transmission in closed settings.a ,9 Epi info V.6 was used to
generate a randomisation allocation and 74 wards were randomly allocated
to the interventions.
From the eligible wards 1868 HCWs were approached to participate. After
providing informed consent, 1607 participants were randomised by ward to
three arms: (1) medical masks at all times on their work shift; (2) cloth
masks at all times on shift or (3) control arm (standard practice, which may
or may not include mask use). Standard practice was used as control
because the IRB deemed it unethical to ask participants to not wear a mask.
We studied continuous mask use (defined as wearing masks all the time
during a work shift, except while in the toilet or during tea or lunch breaks)
because this reflects current practice in high-risk settings in Asia.a
The laboratory results were blinded and laboratory testing was conducted
in a blinded fashion. As facemask use is a visible intervention, clinical end
points could not be blinded. Figure 1 outlines the recruitment and
randomisation process.
APPENDIX TO JAMES CASCIANO DECLARATION-112

Assessed for eligibility
( I S hospitals)
Didaotmeet J, clip,itity criteria.
Randomised to IP I hmpilal
1607HCWs
I 9
l l Mediml Mask tlothmasks Conqpl
Received allocated Received allocated Followed up
intervention intervention 4S8(HCWs)
SIO(HCWs) S69(HCWs)
1 1 I Analysed An@lysed Analvsed
S80HCWs S69HCWs 4S8HCWs
Figure 1
Consort diagram of recruitment and follow-up (HCWs, healthcare workers).
Primary end points
There were three primary end points for this study, used in our previous
mask RCTs:8 ,9 (1) Clinical respiratory illness (CRI), defined as two or more
respiratory symptoms or one respiratory symptom and a systemic
symptom;17 (2) influenza-like illness (ILi), defined as fever ~38°C plus one
respiratory symptom and (3) laboratory-confirmed viral respiratory
infection. Laboratory confirmation was by nucleic acid detection using
multiplex reverse transcriptase PCR (RT-PCR) for 17 respiratory viruses:
respiratory syncytial virus (RSV) A and B, human metapneumovirus (hMPV),
influenza A (H3N2), (H1N1)pdm09, influenza B, parainfluenza viruses 1-4,
influenza C, rhinoviruses, severe acute respiratory syndrome (SARS)
associated coronavirus (SARS-CoV), coronaviruses 229E, NL63, OC43 and
HKU1, adenoviruses and human bocavirus (hBoV).18-23 Additional end
points included compliance with mask use, defined as using the mask
during the shift for 70% or more of work shift hours.9 HCWs were
APPENDIX TO JAMES CASCIANO DECLARATION-113

categorised as 'compliant' if the average use was equal or more than 70%
of the working time. HCW were categorised as 'non-compliant' if the
average mask use was less than 70% of the working time.
Eligibility
Nurses or doctors aged ~,a years working full-time were eligible. Exclusion
criteria were: (1) Unable or refused to consent; (2) Beards, long moustaches
or long facial hair stubble; (3) Current respiratory illness, rhinitis and/or
allergy.
Intervention
Participants wore the mask on every shift for four consecutive weeks.
Participants in the medical mask arm were supplied with two masks daily for
each 8 h shift, while participants in the cloth mask arm were provided with
five masks in total for the study duration, which they were asked to wash
and rotate over the study period. They were asked to wash cloth masks with
soap and water every day after finishing the shifts. Participants were
supplied with written instructions on how to clean their cloth masks. Masks
used in the study were locally manufactured medical (three layer, made of
non-woven material) or cloth masks (two layer, made of cotton) commonly
used in Vietnamese hospitals. The control group was asked to continue with
their normal practices, which may or may not have included mask wearing.
Mask wearing was measured and documented for all participants, including
the control arm.
Data collection and follow-up
Data on sociodemographic, clinical and other potential confounding factors
were collected at baseline. Participants were followed up daily for 4 weeks
(active intervention period), and for an extra week of standard practice, in
order to document incident infection after incubation. Participants received
APPENDIX TO JAMES CASCIANO DECLARATION-114

a thermometer (traditional glass and mercury) to measure their temperature
daily and at symptom onset. Daily diary cards were provided to record
number of hours worked and mask use, estimated number of patient
contacts (with/without ILi) and number/type of aerosol-generating
procedures (AGPs) conducted, such as suctioning of airways, sputum
induction, endotracheal intubation and bronchoscopy. Participants in the
cloth mask and control group (if they used cloth masks) were also asked to
document the process used to clean their mask after use.
We also monitored compliance with mask use by a previously validated self
reporting mechanism.a Participants were contacted daily to identify
incident cases of respiratory infection. If participants were symptomatic,
swabs of both tonsils and the posterior pharyngeal wall were collected on
the day of reporting.
Sample collection and laboratory testing
Trained collectors used double rayon-tipped, plastic-shafted swabs to
scratch tonsillar areas as well as the posterior pharyngeal wall of
symptomatic participants. Testing was conducted using RT-PCR applying
published methods.19-23 Viral RNA was extracted from each respiratory
specimen using the Viral RNA Mini kit (Qiagen, Germany), following the
manufacturer's instructions. The RNA extraction step was controlled by
amplification of a RNA house-keeping gene (amplify pGEM) using real-time
RT-PCR. Only extracted samples with the house keeping gene detected by
real-time RT-PCR were submitted for multiplex RT-PCR for viruses.
The reverse transcription and PCRs were performed in OneStep (Qiagen,
Germany) to amplify viral target genes, and then in five multiplex RT-PCR:
RSVA/B, influenza A/H3N2, A(H1N1) and B viruses, hMPV (reaction mix 1);
parainfluenza viruses 1-4 (reaction mix 2); rhinoviruses, influenza C virus,
SARS-CoV (reaction mix 3); coronaviruses OC43, 229E, NL63 and HKU1
(reaction mix 4); and adenoviruses and hBoV (reaction mix 5), using a
APPENDIX TO JAMES CASCIANO DECLARATION-115

method published by others.18 All samples with viruses detected by
multiplex RT-PCR were confirmed by virus-specific mono nested or
heminested PCR. Positive controls were prepared by in vitro transcription to
control amplification efficacy and monitor for false negatives, and included
in all runs (except for NL63 and HKU1). Each run always included two
negatives to monitor amplification quality. Specimen processing, RNA
extraction, PCR amplification and PCR product analyses were conducted in
different rooms to avoid cross-contamination.19 ,20
Filtration testing
The filtration performance of the cloth and medical masks was tested
according to the respiratory standard AS/NZS1716.24 The equipment used
was a TSI 8110 Filter tester. To test the filtration performance, the filter is
challenged by a known concentration of sodium chloride particles of a
specified size range and at a defined flow rate. The particle concentration is
measured before and after adding the filter material and the relative
filtration efficiency is calculated. We examined the performance of cloth
masks compared with the performance levels-P1, P2 (=N95) and P3, as
used for assessment of all particulate filters for respiratory protection. The
3M 9320 N95 and 3M Vflex 9105 N95 were used to compare against the
cloth and medical masks.
Sample size calculation
To obtain 80% power at two-sided 5% significance level for detecting a
significant difference of attack rate between medical masks and cloth
masks, and for a rate of infection of 13% for cloth mask wearers compared
with 6% in medical mask wearers, we would need eight clusters per arm
and 530 participants in each arm, and intracluster correlation coefficient
(ICC) 0.027, obtained from our previous study.a The design effect (deft) for
this cluster randomisation trial was 1.65 (deff=1+(m-1)xlCC=1+
(25-1)x0.027=1.65). As such, we aimed to recruit a sample size of 1600
APPENDIX TO JAMES CASCIANO DECLARATION-116
participants from up to 15 hospitals.
Analysis
Descriptive statistics were compared among intervention and control arms.
Primary end points were analysed by intention to treat. We compared the
event rates for the primary outcomes across study arms and calculated p
values from cluster-adjusted x2 tests25 and ICC.25 ,26 We also estimated
relative risk (RR) after adjusting for clustering using a log-binomial model
under generalised estimating equation (GEE) framework.27 We checked for
variables which were unequally distributed across arms, and conducted an
adjusted analysis accordingly. We fitted a multivariable log-binomial model,
using GEE to account for clustering by ward, to estimate RR after adjusting
for potential confounders. In the initial model, we included all the variables
that had p value less than 0.25 in the univariable analysis, along with the
main exposure variable (randomisation arm). A backward elimination
method was used to remove the variables that did not have any
confounding effect.
As most participants in the control arm used a mask during the trial period,
we carried out a post-hoc analysis comparing all participants who used only
a medical mask (from the control arm and the medical mask arm) with all
participants who used only a cloth mask (from the control arm and the cloth
arm). For this analysis, controls who used both types of mask (n=245) or
used N95 respirators (n=3) or did not use any masks (n=2) were excluded.
We fitted a multivariable log-binomial model, to estimate RR after adjusting
for potential confounders. As we pooled data of participants from all three
arms and analysed by mask type, not trial arm, we did not adjust for
clustering here. All statistical analyses were conducted using STATA V.12.28
Owing to a very high level of mask use in the control arm, we were unable to
determine whether the differences between the medical and cloth mask
arms were due to a protective effect of medical masks or a detrimental
APPENDIX TO JAMES CASCIANO DECLARATION-117

effect of cloth masks. To assist in interpreting the data, we compared rates
of infection in the medical mask arm with rates observed in medical mask
arms from two previous RCTs,8 ,9 in which no efficacy of medical masks
could be demonstrated when compared with control or N95 respirators,
recognising that seasonal and geographic variation in virus activity affects
the rates of exposure {and hence rates of infection outcomes) among
HCWs. This analysis was possible because the trial designs were similar
and the same outcomes were measured in all three trials. The analysis was
carried out to determine if the observed results were explained by a
detrimental effect of cloth masks or a protective effect of medical masks.
Results
A total of 1607 HCWs were recruited into the study. The participation rate
was 86% (1607/1868). The average number of participants per ward was 23
and the mean age was 36 years. On average, HCWs were in contact with 36
patients per day during the trial period {range 0-661 patients per day,
median 20 patients per day). The distribution of demographic variables was
generally similar between arms {table 1). Figure 2 shows the primary
outcomes for each of the trial arms. The rates of CRI, ILi and la~oratory
confirmed virus infections were lowest in the medical mask arm, followed by
the control arm, and highest in the cloth mask arm.
Table 1
Demographic and other characteristics by arm of randomisation
APPENDIX TO JAMES CASCIANO DECLARATION-118

7.6
- S.4
3.3
2.3
CRI Virus IU
■ Ooth masks ■ Control ■ Medical mask
Figure 2
0.2
Outcomes in trial arms (CRI, clinical respiratory illness; Ill, influenza-like illness; Virus, laboratory-confirmed viruses).
Table 2 shows the intention-to-treat analysis. The rate of CRI was highest in
the cloth mask arm, followed by the control arm, and lowest in the medical
mask arm. The same trend was seen for ILi and laboratory tests confirmed
viral infections. In intention-to-treat analysis, ILi was significantly higher
among HCWs in the cloth masks group (RR=13.25 and 95% Cl 1.74 to
100.97), compared with the medical masks group. The rate of ILi was also
significantly higher in the cloth masks arm (RR=3.49 and 95% Cl 1.00 to
12.17), compared with the control arm. Other outcomes were not
statistically significant between the three arms.
Table 2
Intention-to-treat analysis
Among the 68 laboratory-confirmed cases, 58 (85%) were due to
rhinoviruses. Other viruses detected were hMPV (7 cases), influenza B (1
case), hMPV/rhinovirus co-infection (1 case) and influenza B/rhinovirus co
infection (1 case) (table 3). No influenza A or RSV infections were detected.
Table 3
Type of virus isolated APPENDIX TO JAMES CASCIANO DECLARATION-119

Compliance was significantly higher in the cloth mask arm (RR=2.41, 95% Cl
2.01 to 2.88) and medical masks arm (RR=2.40, 95% Cl 2.00 to 2.87),
compared with the control arm. Figure 3 shows the percentage of
participants who were compliant in the three arms. A post-hoc analysis
adjusted for compliance and other potential confounders showed that the
rate of ILi was significantly higher in the cloth mask arm (RR=13.00, 95% Cl
1.69 to 100.07), compared with the medical masks arm (table 4). There was
no significant difference between the medical mask and control arms. Hand
washing was significantly protective against laboratory-confirmed viral
infection (RR=0.66, 95% Cl 0.44 to 0.97).
Table 4
Multivariable cluster-adjusted log-binomial model to calculate RR for
study outcomes
70 56.6" 56.8%
(52.5-60.5%) (52.7-60.8")
so
" 111D 40 a 23.6% C
~ 30 (19.9-27.7") -
~
20
10
--,
Medical mask Ooth mask Control
Figure 3
Compliance with the mask wearing-mask wearing more than 70% of working hours.
In the control arm, 170/458 (37%) used medical masks, 38/458 (8%) used
cloth masks, and 245/458 (53%) used a combination of both medical and
cloth masks during the study period. The remaining 1% either reported
using a N95 respirator (n=3) or did not use any masks (n=2).
APPENDIX TO JAMES CASCIANO DECLARATION-120

Table 5 shows an additional analysis comparing all participants who used
only a medical mask (from the control arm and the medical mask arm) with
all participants who used only a cloth mask (from the control arm and the
cloth arm). In the univariate analysis, all outcomes were significantly higher
in the cloth mask group, compared with the medical masks group. After
adjusting for other factors, ILi (RR=6.64, 95% Cl 1.45 to 28.65) and
laboratory-confirmed virus (RR=1.72, 95% Cl 1.01 to 2.94) remained
significantly higher in the cloth masks group compared with the medical masks group.
Table 5
Univariate and adjusted analysis comparing participants who used medical masks and cloth masks*
Table 6 compares the outcomes in the medical mask arm with two
previously published trials.a ,9 This shows that while the rates of CRI were
significantly higher in one of the previously published trials, the rates of
laboratory-confirmed viruses were not significantly different between the
three trials for medical mask use.
Table 6
A comparison of outcome data for the medical mask arm with medical mask outcomes in previously published RCTs
On average, HCWs worked for 25 days during the trial period and washed
their cloth masks for 23/25 (92%) days. The most common approach to
washing cloth masks was self-washing (456/569, 80%), followed by
combined self-washing and hospital laundry (91/569, 16%), and only
hospital laundry (22/569, 4%). Adverse events associated with facemask
use were reported in 40.4% (227/562) of HCWs in the medical mask arm
and 42.6% (242/568) in the cloth mask arm (p value 0.450). General
discomfort (35.1%, 397/1130) and breathing problems (18.3%, 207/1130)
APPENDIX TO JAMES CASCIANO DECLARATION-121

were the most frequently reported adverse events.
Laboratory tests showed the penetration of particles through the cloth
masks to be very high (97%) compared with medical masks (44%) (used in
trial) and 3M 9320 N95 (<0.01%), 3M Vflex 9105 N95 (0.1%).
Discussion
We have provided the first clinical efficacy data of cloth masks, which
suggest HCWs should not use cloth masks as protection against respiratory
infection. Cloth masks resulted in significantly higher rates of infection than
medical masks, and also performed worse than the control arm. The
controls were HCWs who observed standard practice, which involved mask
use in the majority, albeit with lower compliance than in the intervention
arms. The control HCWs also used medical masks more often than cloth
masks. When we analysed all mask-wearers including controls, the higher
risk of cloth masks was seen for laboratory-confirmed respiratory viral
infection.
The trend for all outcomes showed the lowest rates of infection in the
medical mask group and the highest rates in the cloth mask arm. The study
design does not allow us to determine whether medical masks had efficacy
or whether cloth masks were detrimental to HCWs by causing an increase in
infection risk. Either possibility, or a combination of both effects, could
explain our results. It is also unknown whether the rates of infection
observed in the cloth mask arm are the same or higher than in HCWs who
do not wear a mask, as almost all participants in the control arm used a
mask. The physical properties of a cloth mask, reuse, the frequency and
effectiveness of cleaning, and increased moisture retention, may potentially
increase the infection risk for HCWs. The virus may survive on the surface
of the facemasks,29 and modelling studies have quantified the
contamination levels of masks.30 Self-contamination through repeated use
and improper doffing is possible. For example, a contaminated cloth mask
APPENDIX TO JAMES CASCIANO DECLARATION-122
may transfer pathogen from the mask to the bare hands of the wearer. We
also showed that filtration was extremely poor (almost 0%) for the cloth
masks. Observations during SARS suggested double-masking and other
practices increased the risk of infection because of moisture, liquid
diffusion and pathogen retention.31 These effects may be associated with cloth masks.
We have previously shown that N95 respirators provide superior efficacy to
medical masks,8 ,9 but need to be worn continuously in high-risk settings
to protect HCWs.9 Although efficacy for medical masks was not shown,
efficacy of a magnitude that was too small to be detected is possible.a ,9
The magnitude of difference between cloth masks and medical masks in the
current study, if explained by efficacy of medical masks alone, translates to
an efficacy of 92% against ILi, which is possible, but not consistent with the
lack of efficacy in the two previous RCTs.8 ,9 Further, we found no
significant difference in rates of virus isolation in medical mask users
between the three trials, suggesting that the results of this study could be
interpreted as partly being explained by a detrimental effect of cloth masks.
This is further supported by the fact that the rate of virus isolation in the
no-mask control group in the first Chinese RCT was 3.1%, which was not
significantly different to the rates of virus isolation in the medical mask arms
in any of the three trials including this one. Unlike the previous RCTs,
circulating influenza and RSV were almost completely absent during this
study, with rhinoviruses comprising 85% of isolated pathogens, which
means the measured efficacy is against a different range of circulating
respiratory pathogens. Influenza and RSV predominantly transmit through
droplet and contact routes, while Rhinovirus transmits through multiple
routes, including airborne and droplet routes.32 ,33 The data also show
that the clinical case definition of ILi is non-specific, and captures a range
of pathogens other than influenza. The study suggests medical masks may
be protective, but the magnitude of difference raises the possibility that
cloth masks cause an increase in infection risk in HCWs. Further, the
filtration of the medical mask used in this trial was poor, making extremely APPENDIX TO JAMES CASCIANO DECLARATION-123

high efficacy of medical masks unlikely, particularly given the predominant
pathogen was rhinovirus, which spreads by the airborne route. Given the
obligations to HCW occupational health and safety, it is important to
consider the potential risk of using cloth masks.
In many parts of the world, cloth masks and medical masks may be the only
options available for HCWs. Cloth masks have been used in West Africa
during the Ebola outbreak in 2014, due to shortages of PPE, (personal
communication, M Jalloh). The use of cloth masks is recommended by
some health organisations, with caveats.34-36 In light of our study, and the
obligation to ensure occupational health and safety of HCWs, cloth masks
should not be recommended for HCWs, particularly during AGPs and in
high-risk settings such as emergency, infectious/respiratory disease and
intensive care wards. Infection control guidelines need to acknowledge the
widespread real-world practice of cloth masks and should comprehensively
address their use. In addition, other important infection control measure
such as hand hygiene should not be compromised. We confirmed the
protective effects of hand hygiene against laboratory-confirmed viral
infection in this study, but mask type was an independent predictor of
clinical illness, even adjusted for hand hygiene.
A limitation of this study is that we did not measure compliance with hand
hygiene, and the results reflect self-reported compliance, which may be
subject to recall or other types of bias. Another limitation of this study is the
lack of a no-mask control group and the high use of masks in the controls,
which makes interpretation of the results more difficult. In addition, the
quality of paper and cloth masks varies widely around the world, so the
results may not be generalisable to all settings. The lack of influenza and
RSV (or asymptomatic infections) during the study is also a limitation,
although the predominance of rhinovirus is informative about pathogens
transmitted by the droplet and airborne routes in this setting. As in previous
studies, exposure to infection outside the workplace could not be
estimated, but we would assume it to be equally distributed between trial
APPENDIX TO JAMES CASCIANO DECLARATION-124

arms. The major strength of the randomised trial study design is in ensuring
equal distribution of confounders and effect modifiers (such as exposure outside the workplace) between trial arms.
Cloth masks are used in resource-poor settings because of the reduced
cost of a reusable option. Various types of cloth masks (made of cotton,
gauze and other fibres) have been tested in vitro in the past and show lower
filtration capacity compared with disposable masks.7 The protection
afforded by gauze masks increases with the fineness of the cloth and the
number of layers,37 indicating potential to develop a more effective cloth
mask, for example, with finer weave, more layers and a better fit.
Cloth masks are generally retained long term and reused multiple times,
with a variety of cleaning methods and widely different intervals of
cleaning.34 Further studies are required to determine if variations in
frequency and type of cleaning affect the efficacy of cloth masks.
Pandemics and emerging infections are more likely to arise in low-income or
middle-income settings than in wealthy countries. In the interests of global
public health, adequate attention should be paid to cloth mask use in such
settings. The data from this study provide some reassurance about medical
masks, and are the first data to show potential clinical efficacy of medical
masks. Medical masks are used to provide protection against droplet
spread, splash and spray of blood and body fluids. Medical masks or
respirators are recommended by different organisations to prevent
transmission of Ebola virus, yet shortages of PPE may result in HCWs being
forced to use cloth masks.38-40 In the interest of providing safe, low-cost
options in low income countries, there is scope for research into more
effectively designed cloth masks, but until such research is carried out,
cloth masks should not be recommended. We also recommend that
infection control guidelines be updated about cloth mask use to protect the
occupational health and safety of HCWs.
APPENDIX TO JAMES CASCIANO DECLARATION-125

Acknowledgments
The authors would like to thank the staff members from the National
Institute of Hygiene and Epidemiology, Hanoi, Vietnam, who were involved
with the trial. They thank as well to the staff from the Hanoi hospitals who
participated. They also acknowledge the support of 3M for testing of
filtration of the facemasks. 3M was industry partner in the ARC linkage
project grant; however they were not involved in study design, data
collection or analysis. The 3M products were not used in this study.
References
1 . ._J
2. ._J
3. ._J
4. ._J
5. ._J
6. ._J
7. ._J
8. ._J
9. ._J
10. ._J
11 . ._J
12. ._J
13. ._J
14. ._J
15. ._J
16. ._J
17. ._J
18. +J
19. +J
20. +J
21. +J
APPENDIX TO JAMES CASCIANO DECLARATION-126

22 . ._J
23 . ._J
24 . ._J
25 . ._J
26 . ._J
27 . ._J
28. ._J
29. ._J
30. ._J
31 . ._J
32 . ._J
33 . ._J
34 . ._J
35 . ._J
36 . ._J
37 . ._J
38. ._J
39. ._J
40. ._J
APPENDIX TO JAMES CASCIANO DECLARATION-127

Household Transmission of SARSCoV-2 Key Points
Question What is the household secondary attack rate for severe acute
respiratory syndrome coronavirus 2 (SARS-CoV-2)?
Findings In this meta-analysis of 54 studies with 77 758 participants, the
estimated overall household secondary attack rate was 16.6%, higher than
observed secondary attack rates for SARS-CoV and Middle East respiratory
syndrome coronavirus. Controlling for differences across studies,
secondary attack rates were higher in households from symptomatic index
cases than asymptomatic index cases, to adult contacts than to child
contacts, to spouses than to other family contacts, and in households with 1
contact than households with 3 or more contacts.
Meaning These findings suggest that households are and will continue to
be important venues for transmission, even in areas where community
transmission is reduced.
Abstract
Importance Crowded indoor environments, such as households, are high
risk settings for the transmission of severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2).
Objectives To examine evidence for household transmission of SARS-CoV-
2, disaggregated by several covariates, and to compare it with other
coronaviruses.
Data Source PubMed, searched through October 19, 2020. Search terms
included SARS-CoV-2 or COVJD-19 with secondary attack rate, household,
APPENDIX TO JAMES CASCIANO DECLARATION-128

close contacts, contact transmission, contact attack rate, or family transmission.
Study Selection All articles with original data for estimating household
secondary attack rate were included. Case reports focusing on individual
households and studies of close contacts that did not report secondary
attack rates for household members were excluded.
Data Extraction and Synthesis Meta-analyses were done using a
restricted maximum-likelihood estimator model to yield a point estimate and
95% Cl for secondary attack rate for each subgroup analyzed, with a
random effect for each study. To make comparisons across exposure types,
study was treated as a random effect, and exposure type was a fixed
moderator. The Preferred Reporting Items for Systematic Reviews and
Meta-analyses (PRISMA) reporting guideline was followed.
Main Outcomes and Measures Secondary attack rate for SARS-CoV-2,
disaggregated by covariates (ie, household or family contact, index case
symptom status, adult or child contacts, contact sex, relationship to index
case, adult or child index cases, index case sex, number of contacts in
household) and for other coronaviruses.
Results A total of 54 relevant studies with 77 758 participants reporting
household secondary transmission were identified. Estimated household
secondary attack rate was 16.6% (95% Cl, 14.0%-19.3%), higher than
secondary attack rates for SARS-CoV (7.5%; 95% Cl, 4.8%-10.7%) and
MERS-CoV (4.7%; 95% Cl, 0.9%-10.7%). Household secondary attack rates
were increased from symptomatic index cases (18.0%; 95% Cl,
14.2%-22.1%) than from asymptomatic index cases (0.7%; 95% Cl,
0%-4.9%), to adult contacts (28.3%; 95% Cl, 20.2%-37.1%) than to child
contacts (16.8%; 95% Cl, 12.3%-21.7%), to spouses (37.8%; 95% Cl,
25.8%-50.5%) than to other family contacts (17.8%; 95% Cl, 11.7%-24.8%),
and in households with 1 contact (41.5%; 95% Cl, 31.7%-51.7%) than in
households with 3 or more contacts (22.8%; 95% Cl, 13.6%-33.5%). APPENDIX TO JAMES CASCIANO DECLARATION-129
Conclusions and Relevance The findings of this study suggest that given
that individuals with suspected or confirmed infections are being referred to
isolate at home, households will continue to be a significant venue for transmission of SARS-CoV-2.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic is caused by severe
acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which is spread
via direct or indirect contact with infected people via infected respiratory
droplets or saliva, fomites, or aerosols.1,2 Crowded indoor environments
with sustained close contact and conversations, such as households, are a
particularly high-risk setting. 3
The World Health Organization China Joint Mission reported human-to
human transmission in China largely occurred within families, accounting for
78% to 85% of clusters in Guangdong and Sichuan provinces.4 Stay-at
home orders reduced human mobility by 35% to 63% in the United States, 5
63% in the United Kingdom,6 and 54% in Wuhan,7 relative to normal
conditions, which concomitantly increased time at home. Modeling studies
demonstrated that household transmission had a greater relative
contribution to the basic reproductive number after social distancing
(30%-55%) than before social distancing (5%-35%). 8 While current US
Centers for Disease Control and Prevention recommendations are to
maintain 6 feet of distance from a sick household member, this may be
difficult to achieve in practice and not be fully effective. 9
The household secondary attack rate characterizes virus transmissibility.
Studies can collect detailed data on type, timing, and duration of contacts
and identify risk factors associated with infectiousness of index cases and
susceptibility of contacts. Our objective was to estimate the secondary
attack rate of SARS-CoV-2 in households and determine factors that modify
this parameter. We also estimated the proportion of households with index
cases that had any secondary transmission. Furthermore, we compared the APPENDIX TO JAMES CASCIANO DECLARATION-130

SARS-CoV-2 household secondary attack rate with that of other severe
viruses and with that to close contacts for studies that reported the
secondary attack rate for both close and household contacts.
Methods
Definitions
We estimated the transmissibility of SARS-CoV-2 within the household or
family by the empirical secondary attack rate by dividing the number of new
infections among contacts by the total number of contacts. Household
contacts include anyone living in the same residence as the index case.
Family contacts include the family members of index cases, including
individuals who live outside the index case's household. Close contact
definitions varied by study and included physical proximity to an index case,
exceeding a minimum contact time, and/or not wearing effective protection
around index cases before the index case was tested.
Search Strategy
Following Preferred Reporting Items for Systematic Reviews and Meta
analyses (PRISMA) reporting guideline, we searched PubMed using terms
including SARS-CoV-2 or COVID-19 with secondary attack rate, household,
close contacts, contact transmission, contact attack rate, or family
transmission (eTable 1 in the Supplement) with no restrictions on language,
study design, time, or place of publication. The last search was conducted
October 19, 2020.
Eligibility Criteria
Eligibility criteria are described in eAppendix 1 in the Supplement. All
articles with original data for estimating household secondary attack rate
were included. Case reports focusing on individual households and studies
of close contacts that did not report secondary attack rates for household
APPENDIX TO JAMES CASCIANO DECLARATION-131

members were excluded.
Data Extraction
One of us (Z.J.M.) extracted data from each study. Details appear in
eAppendix 2 in the Supplement.
Evaluation of Study Quality and Risk of Bias
To assess the methodological quality and risk of bias of included studies of
SARS-CoV-2, we used the same modified version of the Newcastle-Ottawa
quality assessment scale for observational studies used by Fung et al.10,11
Studies received as many as 9 points based on participant selection (4
points), study comparability (1 point), and outcome of interest (4 points).
Studies were classified as having high (~3 points), moderate (4-6 points),
and low (~7 points) risk of bias. One of us (Z.J.M.) evaluated the study
quality and assigned the quality grades.
Statistical Analysis
Meta-analyses were done using a restricted maximum-likelihood estimator
model to yield Freeman-Tukey double arcsine-transformed point estimates
and 95% Cl for secondary attack rate for each subgroup analyzed, with a
random effect for each study.12 For comparisons across covariates (ie,
household or family, index case symptom status, adult or child contacts,
contact sex, relationship to index case, adult or child index cases, index
case sex, number of household contacts, study location, universal or
symptomatic testing, dates of study) and comparisons with close contacts
and other viruses, study was treated as a random effect, and the covariate
was a fixed moderator. Variables had to have been collected in at least 3
studies to be included in meta-analyses. The Cochran Q test and /2 statistic
are reported as measures of heterogeneity. 12 values of 25%, 50%, and 75%
indicated low, moderate, and high heterogeneity, respectively.13 Stastistical
significance was set at a 2-tailed a= .05. All analyses were done in R version
APPENDIX TO JAMES CASCIANO DECLARATION-132

4.0.2 using the package metafor (R Project for Statistical Computing). 14,15
When at least 10 studies were available, we used funnel plots, Begg
correlation, and Egger test to evaluate publication bias, with significance set
at P < .10.16•17 If we detected publication bias, we used the Duval and
Tweedie trim-and-fill approach for adjustment. 18
Results
We identified 54 relevant published studies that reported household
secondary transmission, with 77 758 participants (eTable 1 in the
Supplement). 19-72 A total of 16 of 54 studies (29.6%) were at high risk of
bias, 27 {50.0%) were moderate, and 11 (20.4%) were low {eTable 2 in the
Supplement). Lower quality was attributed to studies with 1 or fewer test
per contact (35 studies [64.8%]), small sample sizes (31 [57.4%]), and
secondary attack rate not disaggregated by covariates (28 [51.9%]).
A description of index case identification period and methods and symptom
status is provided in eTable 3 in the Supplement. Most studies did not
describe how co-primary index cases were handled or whether secondary
infections could have been acquired from outside the household, both of
which can inflate the empirical secondary attack rate. Testing and
monitoring strategies varied between studies, often reflecting variations in
local testing guidelines implemented as part of contact tracing (eTable 4
and eAppendix 3 in the Supplement).
Figure 1 summarizes secondary attack rates for 44 studies 19-26,28-30,32-
36·38-45,47-57,59,51-53,55-57,59,7o of household contacts and 10 of family
contacts. 26,31,37.45,58,60 ,65 ,68 ,71,72 Estimated mean secondary attack rate for
household contacts was 16.4% (95% Cl, 13.4%-19.6%) and family contacts
was 17.4% (95% Cl, 12.7%-22.5%). One study 40 restricted index cases to
children (age <18 years), resulting in a substantially lower secondary attack
rate of 0.5%. Excluding this outlier, the combined secondary attack rate for
household and family contacts was 17.1% (95%, 14.6%-19.7%). Secondary
APPENDIX TO JAMES CASCIANO DECLARATION-133

attack rates for household and family contacts were more than 3 times
higher than for close contacts (4.8%; 95% Cl, 3.4%-6.5%; P < .001) (eFigure
2 in the Supplement). Significant heterogeneity was found among studies of
household (/2 = 96.9%; P < .001), family (/2 = 93.0%; P < .001), and close (/2 = 97.0%; P < .001) contacts. No significant publication bias was observed for studies of household, family, or close contacts (eFigure 3 in the
Supplement). Secondary attack rates were not significantly different when restricting to 38 studies 19,20,22,23,26-31,34-40,42,44-51,54-57,60,62,63,65,67-69,72
with low or moderate risk of bias (15.6%; 95%, 12.8%-18.5%) (eFigure 4 in
the Supplement). There were no significant differences in secondary attack rates between 21 studies in China22,27,31,36,37,39,45,46,48,58,61-68,70-72 and 33 studies from other countries 19-21,23-26,28-30,32-35,38,40-44,47,49-57,59,60,69
(eFigure 5 in the Supplement), 18 studies that tested symptomatic contacts 19-21,24,25,28,29,33,34,41,47,50,53,56,58,59,61,64 and 33 studies that
reported testing all contacts22,23,26,27,30,31,35-40,42-46,48,49,51,52,54,55,57,60,63,65-67,69-72 (eFigure 6 in the Supplement), and 16
early studies22,23,25,31,37,39,45,58,61,63-66,68,71,72 (January-February) and 20 later studies 19,24,26,29,30,32-35,38,42,44,50,53-56,59,60,69 (March-July) (eFigure
7 in the Supplement).
To study the transmissibility of asymptomatic SARS-CoV-2 index cases, eFigure 8 in the Supplement summarizes 27 studies19-21,23-26,30,32-34,44,45,47,50,52-54,56,59-61,63,64,68,69,72 reporting household secondary
attack rates from symptomatic index cases and 4 studies26,43A4,52 from
asymptomatic or presymptomatic index cases. Estimated mean household
secondary attack rate from symptomatic index cases (18.0%; 95% Cl, 14.2%-22.1%) was significantly higher than from asymptomatic or presymptomatic index cases (0.7%; 95% Cl, 0%-4.9%; P< .001), although there were few studies in the latter group. These findings are consistent with other household studies28,70 reporting asymptomatic index cases as having limited role in household transmission.
There is evidence for clustering of SARS-CoV-2 infections within
APPENDIX TO JAMES CASCIANO DECLARATION-134

households, with some households having many secondary infections while
many others have none.73-75 For example, 1 study 55 reported that 26 of 103
(25.2%) households had all members test positive. This is consistent with
observation of overdispersion in the number of secondary cases per index
case across a range of settings. 3 While most studies reported only the
average number of secondary infections per index case, some also reported
transmission by household. 44,55,56,63,65,69 Figure 2 summarizes the
proportion of households with any secondary transmission. Using an
empirical analysis based on secondary attack rates and mean number of
contacts per household, we found the proportion of households with any
secondary transmission was lower than expected in a setting with no
clustering (eg, most transmission is not characterized by a minority of
infected individuals) (eTable 5 in the Supplement). Ideally, future studies will
assess this formally by fitting a J3 binomial to quantify overdispersion in the
full data.
A number of studies examined factors associated with susceptibility of
household contacts to infection (eTable 6 in the Supplement). Age was the most examined covariate with most studies 20,29,36-39,45,46,48,49,55,63,65,68
I
reporting lower secondary transmission of SARS-CoV-2 to child contacts
than adult contacts. In 5 studies, 2o,3s,39,4s,49 individuals older than 60
years were most susceptible to SARS-CoV-2 infection. Contact age was not
associated with susceptibility in 9 studies, 26,28,32A4A7,58,66,67,70 although
these were typically less powered to detect a difference. Figure 3 summarizes 15 studies22,26,29,37,39,42,44,45,47,49,55,59,60,63,65 reporting
separate secondary attack rates to children and adult contacts. The
estimated mean household secondary attack rate was significantly higher
to adult contacts (28.3%; 95% Cl, 20.2%-37.1%) than to child contacts
(16.8%; 95% Cl, 12.3%-21.7%; P < .001). Significant heterogeneity was found
among studies of adult (/2 = 96.8%; P < .001) and child contacts (/2 = 78.9%;
P < .001). Begg (P = .03) and Egger (P = .03) tests were statistically
significant for studies of adult but not child contacts (eFigure 9 in the
Supplement). One study of adults 63 had a high secondary attack rate in the APPENDIX TO JAMES CASCIANO DECLARATION-135

forest plot. Excluding this study improved the funnel plot symmetry and
resulted in a secondary attack rate to adult contacts of 26.3% (95% Cl, 19.3%-33.2%).
The second most examined factor was sex of exposed contacts, which was not associated with susceptibility for most studies20,22,26,32,36,39,4 4,4s,41-
49,59,65-57,7o except 3.38,46 ,68 eFigure 10 in the Supplement summarizes
results from 11 studies20,39 ,42 ,44 ,45 ,47,49 ,59 ,65 ,57,59 reporting household
secondary attack rates by contact sex. Estimated mean household
secondary attack rate to female contacts (20.7%; 95% Cl, 15.0%-26.9%) was not significantly different than to male contacts (17.7%; 95% Cl, 12.4%-23.8%). Significant heterogeneity was found among studies of
female contacts (12 = 87.4%; P< .001) and male contacts (12 = 87.7%; P
< .001). Moderate asymmetry was observed in the funnel plots, which was significant for studies of female contacts from Egger test (P = .07) but not male contacts (eFigure 11 in the Supplement). However, imputation of an
adjusted effect size using the trim-and-fill method did not significantly change the secondary attack rate to female contacts (19.7%; 95% Cl, 13.9%-25.6%).
Spouse relationship to index case was associated with secondary infection in 4 studies26,45A6,58 of 6 in which this was examined.65,67 Infection risk
was highest for spouses, followed by nonspouse family members and other
relatives, which were all higher than other contacts.46 Figure 4 summarizes results from 7 studies26,44 -46 ,58,65 ,67 reporting household secondary attack
rates by relationship. Estimated mean household secondary attack rate to spouses (37.8%; 95% Cl, 25.8%-50.5%) was significantly higher than to other contacts (17.8%; 95% Cl, 11.7%-24.8%). Significant heterogeneity was
found among studies of spouses (12 = 78.6%; P < .001) and other relationships (12 = 83.5%; P< .001).
Several studies examined factors associated with infectiousness of index cases. Older index case age was associated with increased secondary
APPENDIX TO JAMES CASCIANO DECLARATION-136

infections in 3 studies 20A7,67 of 9 in which this was
examined. 22,36,39,44 ,63,65 eFigure 12 in the Supplement summarizes results
from 3 studies 42,44,51 reporting household secondary attack rates by index
case age. Estimated mean household secondary attack rate from adults
(15.2%; 95% Cl, 6.2%-27.4%) was not significantly different than that from
children (7.9%; 95% Cl, 1.7%-16.8%). Index case sex was associated with
transmission in 3 studies 42A4,67 of 9 in which this was
examined. 20,35,45,47,53,a5 eFigure 13 in the Supplement summarizes results
from 7 studies 20A2A4A5,65,67,69 reporting household secondary attack rates
by index case sex. Estimated mean household secondary attack rate from
female contacts (16.6%; 95% Cl, 11.2%-22.8%) was not significantly
different than from male contacts (16.4%; 95% Cl, 9.0%-25.5%).
Critically severe index case symptoms was associated with higher
infectiousness in 6 studies 20,38,46-48 ,67 of 9 in which this was
examined. 44 ,63,70 Index case cough was associated with infectivity in 2
studies 20,65 of 8 in which this was examined 45-48,63,67 (eAppendix 4 in the
Supplement).
Contact frequency with the index case was associated with higher odds of
infection, specifically at least 5 contacts during 2 days before the index
case was confirmed, 70 at least 4 contacts and 1 to 3 contacts, 63 or frequent
contact within 1 meter.22,67,68 Smaller households were associated with
transmission in 4 studies 20,39,47,49 of 7 in which this was examined. 55,63,65
Figure 5 summarizes results from 6 studies 20,47,49 ,55,s1,65 reporting
household secondary attack rates by number of contacts in the household.
Estimated mean household secondary attack rate for households with 1
contact (41.5%; 95% Cl, 31.7%-51.7%) was significantly higher than
households with at least 3 contacts (22.8%; 95% Cl, 13.6%-33.5%; P< .001)
but not different than households with 2 contacts (38.6%; 95% Cl,
17.9%-61.6%). There was significant heterogeneity in secondary attack
rates between studies with 1 contact (/2 = 52.9%; P = .049), 2 contacts (/2 =
93.6%; P< .001), or 3 or more contacts (/2 = 91.6%; P< .001). Information
APPENDIX TO JAMES CASCIANO DECLARATION-137

was not available on household crowding (eg, number of people per room).
eFigure 14 in the Supplement summarizes 7 studies 76-82 reporting
household secondary attack rates for SARS-CoV, and 7 studies 83-89 for
Middle East respiratory syndrome coronavirus (MERS-CoV). Estimated
mean household secondary attack rate was 7.5% (95% Cl, 4.8%-10.7%) for
SARS-CoV and 4.7% (95% Cl, 0.9%-10.7%) for MERS-CoV (eTable 7 in the
Supplement), both lower than the household secondary attack rate of
16.6% for SARS-CoV-2 in this study (P < .001). The SARS-CoV-2 secondary
attack rate was also higher than secondary attack rates reported for HCoV
NL63 (0-12.6%), HCoV-OC43 (10.6-13.2%), HCoV-229E (7.2-14.9%), and
HCoV-HKU1 (8.6%).90-92 Household secondary attack rates for SARS-CoV-
2 were within the mid-range of household secondary attack rates reported
for influenza, which ranged from 1% to 38% based on polymerase chain
reaction-confirmed infection. 93
Discussion
We synthesized the available evidence on household studies of SARS-CoV-
2. The combined household and family secondary attack rate was 16.6%
(95% Cl, 14.0%-19.3%), although with significant heterogeneity between
studies. This point estimate is higher than previously observed secondary
attack rates for SARS-CoV and MERS-CoV. Households are favorable
environments for transmission. They are what are known as 3Cs
environments, as they are closed spaces, where family members may crowd
and be in close contact with conversation. 94 There may be reduced use of
personal protective equipment relative to other settings.
That secondary attack rates were not significantly different between
household and family contacts may indicate that most family contacts are in
the same household as index cases. Household and family contacts are at
higher risk than other types of close contacts, and risks are not equal within
households. Spouses were at higher risk than other family contacts, which
may explain why the secondary attack rate was higher in households with 1 APPENDIX TO JAMES CASCIANO DECLARATION-138

vs 3 or greater contacts. Spouse relationship to the index case was also a
significant risk factor observed in studies of SARS-CoV and H1N1.82 ,95 This
may reflect intimacy, sleeping in the same room, or longer or more direct
exposure to index cases. Further investigation is required to determine
whether sexual contact is a transmission route. Although not directly
assessed, household crowding (eg, number of people per room) may be
more important for SARS-CoV-2 transmission than the total number of
people per household, as has been demonstrated for influenza. 96-98
The finding that secondary attack rates were higher to adult contacts than
to child contacts is consistent with empirical and modeling studies. 99 ,100
Lower infection rates in children may be attributed to asymptomatic or mild
disease, reduced susceptibility from cross-immunity from other
coronaviruses, 101 and low case ascertainment, 102 but the difference
persisted in studies in which all contacts were tested regardless of
symptoms. Higher transmission rates to adults may be influenced by
spousal transmission. Given the increased risk to spousal contacts, future
studies might compare child contacts and nonspouse adult contacts to
ascertain whether this difference persists. Limited data suggest children
have not played a substantive role in household transmission of SARS-CoV-
2. 40, 103-105 However, a study in South Korea of 10 592 household contacts
noted relatively high transmission from index cases who were aged 10 to 19
years.51 Although children seem to be at reduced risk for symptomatic
disease, it is still unclear whether they shed virus similarly to adults. 106
We did not find associations between household contact or index case sex
and secondary transmission. The World Health Organization reports roughly
even distribution of SARS-CoV-2 infections between women and men
worldwide, with higher mortality in men.107
We found significantly higher secondary attack rates from symptomatic
index cases than asymptomatic or presymptomatic index cases, although
less data were available on the latter. The lack of substantial transmission
APPENDIX TO JAMES CASCIANO DECLARATION-139

from observed asymptomatic index cases is notable. However,
presymptomatic transmission does occur, with some studies reporting the
timing of peak infectiousness at approximately the period of symptom
onset. 108,109 In countries where infected individuals were isolated outside
the home, this could further alter the timing of secondary infections by
limiting contacts after illness onset. 110
Household secondary attack rates were higher for SARS-CoV-2 than SARS
CoV and MERS-CoV, which may be attributed to structural differences in
spike proteins, 111 higher basic reproductive rates, 112 and higher viral loads in
the nose and throat at the time of symptom onset. 113 Symptoms associated
with MERS-CoV and SARS-CoV often require hospitalization, which
increases nosocomial transmission, whereas less severe symptoms of
SARS-CoV-2 facilitate community transmission. 113 Similarly,
presymptomatic transmission was not observed for MERS-CoV or SARSCov.114, 115
Limitations
Our study had several limitations. The most notable is the large amount of
unexplained heterogeneity across studies. This is likely attributable to
variability in study definitions of index cases and household contacts,
frequency and type of testing, sociodemographic factors, household
characteristics (eg, density, air ventilation), and local policies (eg,
centralized isolation). Rates of community transmission also varied across
locations. Given that studies cannot always rule out infections from outside
of the home (eg, nonhousehold contacts), household transmission may be
overestimated. For this reason, we excluded studies that used antibody
tests to diagnose household contacts. Furthermore, many analyses ignored
tertiary transmission within the household, classifying all subsequent cases
as secondary to the index case. Eighteen studies 19-21,24,25,28,29,33,34,41,47,50,53,56,58,59,61,64 involved testing only symptomatic
household contacts, which would miss asymptomatic or subclinical
APPENDIX TO JAMES CASCIANO DECLARATION-140

infections, although secondary attack rate estimates were similar across
studies testing all vs only symptomatic contacts.
Important questions remain regarding household spread of SARS-CoV-2.
Chief among them is the infectiousness of children to their household
contacts and the infectiousness of asymptomatic, mildly ill, and severely ill
index cases. This study did not provide additional elucidation of factors
influencing intergenerational spread. People unable to work at home may
have greater risk of SARS-CoV-2 exposure, which may increase
transmission risk to other household members. There may be
overdispersion in the number of secondary infections per index case, which
could be caused by variations in viral shedding, household ventilation, or
other factors.
Conclusions
The findings of this study suggest that households are and will continue to
be important venues for transmission, even where community transmission
is reduced. Prevention strategies, such as increased mask-wearing at
home, improved ventilation, voluntary isolation at external facilities, and
targeted antiviral prophylaxis, should be further explored.
Back to top
Article Information
Accepted for Publication: November 6, 2020.
Published: December 14, 2020. doi:10.1001/jamanetworkogen.2020.31756
Open Access: This is an open access article distributed under the terms of
the CC-BY License. © 2020 Madewell ZJ et al. JAMA Network Open.
Corresponding Author: Zachary J. Madewell, Department of Biostatistics,
University of Florida, PO Box 117450, Gainesville, FL 32611
APPENDIX TO JAMES CASCIANO DECLARATION-141

Author Contributions: Drs Madewell and Dean had full access to all of the
data in the study and take responsibility for the integrity of the data and the
accuracy of the data analysis.
Concept and design: Madewell, Longini, Dean.
Acquisition, analysis, or interpretation of data: All authors.
Drafting of the manuscript: Madewell, Longini, Dean.
Critical revision of the manuscript for important intellectual content: All
authors.
Statistical analysis: All authors.
Obtained funding: Dean.
Administrative, technical, or material support: Dean.
Supervision: Dean.
Conflict of Interest Disclosures: None reported.
Funding/Support: This work was supported by grant R01-Al139761 from
the National Institutes of Health.
Role of the Funder/Sponsor: The funder had no role in the design and
conduct of the study; collection, management, analysis, and interpretation
of the data; preparation, review, or approval of the manuscript; and decision
to submit the manuscript for publication.
References
1. World Health Organization. Transmission of SARS-CoV-2: implications for
APPENDIX TO JAMES CASCIANO DECLARATION-142

infection prevention precautions. Published July 9, 2020. Accessed
November 11, 2020. httQ£1Lwww.who.intLnews
room/commentariesLdetailLtransmission-of-sars-cov-2-imP-lications-for
infection-P-revention-P-recautions
2. Oran DP, Topal EJ. Prevalence of asymptomatic SARS-CoV-2 infection : a
narrative review. Ann Intern Med. 2020;173(5):362-367. doi:10.7326LM20-
3012PubMedGoogle ScholarCrossref
3. Nishiura H, Oshitani H, Kobayashi T, et al. Closed environments facilitate
secondary transmission of coronavirus disease 2019 {COVID-19).
medRxiv. Preprint published online April 16, 2020.
doi:10.1101/.2020.02.28.20029272Google Scholar
4. World Health Organization. Report of the WHO-China Joint Mission on
Coronavirus Disease 2019 (COVID-19). February 16-24, 2020. Accessed
November 11, 2020. httP-s:lf.www.who.int/.docsLdefault-
sou rceL coronavi ruseLwho-c hi na-joi nt-m i ssi on-on-covi d-19-fi na 1-reQort. Qdf
5. Badr HS, Du H, Marshall M, Dong E, Squire MM, Gardner LM.
Association between mobility patterns and COVID-19 transmission in the
USA: a mathematical modelling study. Lancet Infect Dis.
2020;20(11):1247-1254. doi:10.1016/.S1473-3099(20)30553-
3PubMedGoogle ScholarCrossref
6. Drake TM, Docherty AB, Weiser TG, Yule S, Sheikh A, Harrison EM. The
effects of physical distancing on population mobility during the COVID-19
pandemic in the UK. Lancet Digit Health. 2020;2{8):e385-e387.
doi:10.1016LS2589-7500 (20) 30134-5PubMedGoogle ScholarCrossref
7. Fang H, Wang L, Yang Y. Human mobility restrictions and the spread of
the novel coronavirus (2019-nCoV) in China. National Bureau of Economic
APPENDIX TO JAMES CASCIANO DECLARATION-143
Research. Published March 2020. Accessed November 11, 2020.
http_s:f/.www.nber.org/.p_a p_ers/.w26906
8. Curmei M, llyas A, Evans 0, Steinhardt J. Estimating household
transmission of SARS-CoV-2. medRxiv. Preprint published online June 27,
2020. doi:10.1101/.2020.05.23.20111559Google Scholar
9. US Centers for Disease Control and Prevention. Coronavirus disease 2019
(COVID-19): how to protect yourself and others. Updated November 4,
2020. Accessed November 11, 2020.
http_s:f/.www.cdc.gov/.coronavi rus/.2 019-ncov /.p_revent-getti ng.=
sick/.p_revention. htm I
10.
Wells G. The Newcastle-Ottawa Scale (NOS) for assessing the quality of
nonrandomised studies in meta-analysis. Accessed November 11, 2020.
httg:f/.www.ohri.ca/.p_rograms/.clinical ep_idemiology/.oxford.asg
11.
Fung HF, Martinez L, Alarid-Escudero F, et al; SC-COSMO Modeling
Group. The household secondary attack rate of SARS-CoV-2: a rapid
review. Clin Infect Dis. Published online October 12, 2020:ciaa1558.
doi:10.1093/.cid/.ciaa1558PubMedGoogle Scholar
12. Freeman MF, Tukey JW. Transformations related to the angular and the
square root. Annals Math Stat. 1950;21(4):607-611.
doi:10.1214/.aoms/.1177729756Google ScholarCrossref
13. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring
inconsistency in meta-analyses. BMJ. 2003;327(7414):557-560.
doi:10.1136/.bmj.327. 7 414.557PubMedGoogle ScholarCrossref
14. Viechtbauer W. Conducting meta-analyses in R with the metafor package.
J Stat Software. 2010;36(3):1-48. doi:10.18637/.jss.v036.i03Google
APPENDIX TO JAMES CASCIANO DECLARATION-144

ScholarCrossref
15. R Core Team. R: a language and environment for statistical computing.
Accessed November 13, 2020. httP-s://.www.gbif.org/.tool/.81287/.r-a
language-and-environment-for-statistical-comP-uting
16.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation
test for publication bias. Biometrics. 1994;50(4):1088-1101.
doi:10.2307/.2533446PubMedGoogle ScholarCrossref
17. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis
detected by a simple, graphical test. BMJ. 1997;315(7109):629-634.
doi:10.1136/.bmj.315. 7109.629PubMedGoogle ScholarCrossref
18. Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of
testing and adjusting for publication bias in meta-analysis. Biometrics.
2000;56(2):455-463. doi:10.1111/j.0006-
341 X.2000.00455.xPubMedGoog le ScholarCrossref
19. Adamik B, Bawiec M, Bezborodov V, et al. Bounds on the total number of
SARS-CoV-2 infections: the link between severeness rate, household attack
rate and the number of undetected cases. Published August 15, 2020.
Accessed November 11, 2020. httP-s:/1.docisolation.prod.fire.glass/.?
guid=8579b2af-bdb0-4d1f-f538-bc52f86d984e
20. Arnedo-Pena A, Sabater-Vidal S, Meseguer-Ferrer N, et al. COVID-19
secondary attack rate and risk factors in household contacts in Castellon
(Spain): preliminary report. Enfermedades Emergentes. 2020;19(2):64-70.
Accessed November 11, 2020. https://.docisolation.P-rod.fire.glass/.?
guid=45f61a53-bdcc-40ab-ded8-dd9646aa077cGoogle Scholar
21. Bae S, Kim H, Jung T-Y, et al. Epidemiological characteristics of COVID-
APPENDIX TO JAMES CASCIANO DECLARATION-145

19 outbreak at fitness centers in Cheonan, Korea. J Korean Med Sci.
2020;35(31):e288. doi:10.3346fjkms.2020.35.e288PubMedGoogle Scholar
22. Bi Q, Wu Y, Mei S, et al. Epidemiology and transmission of COVID-19 in
391 cases and 1286 of their close contacts in Shenzhen, China: a
retrospective cohort study. Lancet Infect Dis. 2020;20(8):911-919.
doi:10.1016LS14 73-3099 (20) 30287-5PubMedGoog le ScholarCrossref
23. Bohmer MM, Buchholz U, Corman VM, et al. Investigation of a COVID-19
outbreak in Germany resulting from a single travel-associated primary case:
a case series. Lancet Infect Dis. 2020;20(8):920-928. doi:10.1016LS1473-
3099(20)30314-5PubMedGoogle ScholarCrossref
24. Boscolo-Rizzo P, Borsetto D, Spinato G, et al. New onset of loss of smell
or taste in household contacts of home-isolated SARS-CoV-2-positive
subjects. Eur Arch Otorhinolaryngol. 2020;277(9):2637-2640.
doi:10.1007/.s00405-020-06066-9PubMedGoogle ScholarCrossref
25. Burke RM. Active monitoring of persons exposed to patients with
confirmed COVID-19-United States, January-February 2020. MMWR
Morb Mortal Wkly Rep. 2020;69:245-246.
doi:10.15585Lmmwr. mm6909e1 Google ScholarCrossref
26. Chaw L, Koh WC, Jamaludin SA, Naing L, Alikhan MF, Wong J. SARS
CoV-2 transmission in different settings: analysis of cases and close
contacts from the Tablighi cluster in Brunei Darussalam. Emerg Infect Dis.
2020;26(11):2598-2606. doi:10.3201/.eid2611.202263Google
ScholarCrossref
27. Chen Y, Wang AH, Yi B, et al. [Epidemiological characteristics of
infection in COVID-19 close contacts in Ningbo city]. Zhonghua Liu Xing
Bing Xue Za Zhi. 2020;41(5):667-671. doi:10.3760/.cma.j.cn112338-
APPENDIX TO JAMES CASCIANO DECLARATION-146

20200304-00251 PubMedGoogle Scholar
28.
Cheng HY, Jian SW, Liu DP, Ng TC, Huang WT, Lin HH; Taiwan COVID-
19 Outbreak Investigation Team. Contact tracing assessment of COVID-19
transmission dynamics in Taiwan and risk at different exposure periods
before and after symptom onset. JAMA Intern Med. 2020;180(9):1156-
1163. doi:10.1001/jamainternmed .2020.2020
ArticlePubMedGoogle ScholarCrossref
29. Dattner I, Goldberg Y, Katriel G, et al. The role of children in the spread of
COVID-19: Using household data from Bnei Brak, Israel, to estimate the
relative susceptibility and infectivity of children. medRxiv. Preprint
published online October 11, 2020. doi:10.1101/.2020.06.03.20121145Google
Scholar
30. Dawson P, Rabold EM, Laws RL, et al. Loss of taste and smell as
distinguishing symptoms of COVID-19. Clin Infect Dis. 2020;ciaa799.
doi:10.1093/.cid/.ciaa799PubMedGoogle Scholar
31. Dong XC, Li JM, Bai JY, et al. [Epidemiological characteristics of
confirmed COVID-19 cases in Tianjin]. Zhonghua Liu Xing Bing Xue Za Zhi.
2020;41 (5) :638-641. doi:10.3760/.cma.j .cn112338-20200221-
00146PubMedGoogle Scholar
32. Doung-ngern P, Suphanchaimat R, Panjagampatthana A, et al. Case
control study of use of personal protective measures and risk for SARS-CoV
2 infection, Thailand. Emerg Infect Dis. 2020;26(11):2607-2616.
doi:10.32 01Leid2611. 2 03003 Pu bMedGoog le Sc ho la rCrossref
33. Draper AD, Dempsey KE, Boyd RH, et al. The first 2 months of COVID-19
contact tracing in the Northern Territory of Australia, March-April 2020.
Commun Dis Intel/ (2018). 2020;44:44.PubMedGoogle Scholar
APPENDIX TO JAMES CASCIANO DECLARATION-147

34. Fateh-Moghadam P, Battisti L, Molinaro S, et al. Contact tracing during
phase I of the COVID-19 pandemic in the Province of Trento, Italy: key
findings and recommendations. medRxiv. Preprint published online July
29, 2020. doi:10.1101/.2020.07.16.20127357Google Scholar
35. Han T. Outbreak investigation: transmission of COVID-19 started from a
spa facility in a local community in Korea. Epidemiol Health.
2020;42 ( 0) :e2020056-e2020050.
doi:10.4178/.egih.e2020056PubMedGoogle ScholarCrossref
36. Hu S, Wang W, Wang Y, et al. lnfectivity, susceptibility, and risk factors
associated with SARS-CoV-2 transmission under intensive contact tracing
in Hunan, China. medRxiv. Preprint published online November 3, 2020.
doi:10.1101/.2020.07.23.20160317Google Scholar
37. Hua CZ, Miao ZP, Zheng JS, et al. Epidemiological features and viral
shedding in children with SARS-CoV-2 infection. J Med Viral. Published
online June 15, 2020. doi:10.1002/jmv.26180PubMedGoogle Scholar
38. Islam SS, Noman ASM. Transmission dynamics and contact tracing
assessment of COVID-19 in Chattogram, Bangladesh and potential risk of
close contacts at different exposure settings. Published October 12, 2020.
Accessed November 11, 2020. httgs:f/.gagers.ssrn.com/.sol3/.gagers.cfm?
abstract id=3677863
39. Jing Q-L, Liu M-J, Zhang 28, et al. Household secondary attack rate of
COVID-19 and associated determinants in Guangzhou, China: a
retrospective cohort study. Lancet Infect Dis. 2020;20(10):1141-1150.
doi:10.1016/.S1473-3099 (20) 304 71-0PubMedGoogle ScholarCrossref
40. Kim J, Choe YJ, Lee J, et al. Role of children in household transmission of
APPENDIX TO JAMES CASCIANO DECLARATION-148

COVID-19. Arch Dis Child. 2020;archdischild-2020-319910.
doi:10.1136L archdischild-2020-31991 0PubMedGoogle Scholar
41. COVID-19 National Emergency Response Center, Epidemiology and Case
Management Team, Korea Centers for Disease Control and Prevention.
Coronavirus disease-19: summary of 2,370 contact investigations of the
first 30 cases in the Republic of Korea. Osong Public Health Res Perspect.
2020;11 (2) :81-84. doi:10.24171fj~P-hrP-.2020.11.2.04PubMedGoogle
ScholarCrossref
42. Laxminarayan R, Wahl B, Dudala SR, et al. Epidemiology and
transmission dynamics of COVID-19 in two Indian states. Science.
2020;370(6517):691-697. doi:10.1126Lscience.abd7672PubMedGoogle
ScholarCrossref
43. Lee M, Eun Y, Park K, Heo J, Son H. Follow-up investigation of
asymptomatic COVID-19 cases at diagnosis in Busan, Korea. Epidemiol
Health. 2020;42:e2020046. doi:10.4178L eP-ih.e2020046PubMedGoog le
Scholar
44. Lewis NM, Chu VT, Ye D, et al. Household transmission of SARS-CoV-2
in the United States. Clin Infect Dis. Published online August 16, 2020.
doi:10.1093LcidLciaa1166Google Scholar
45. Li W, Zhang B, Lu J, et al. Characteristics of household transmission of
COVID-19. Clin Infect Dis. 2020;71 (8):1943-1946.
doi:10.1093LcidLciaa450PubMedGoogle ScholarCrossref
46. Liu T, Liang W, Zhong H, et al. Risk factors associated with COVID-19
infection: a retrospective cohort study based on contacts tracing. Emerg
Microbes Infect. 2020;9(1):1546-1553.
doi:10.1080L22221751.2020.1787799PubMedGoogle ScholarCrossref
APPENDIX TO JAMES CASCIANO DECLARATION-149

47. Lopez Bernal J, Panagiotopoulos N, Byers C, et al. Transmission
dynamics of COVID-19 in household and community settings in the United
Kingdom. medRxiv. Preprint published online August 22, 2020.
doi:10.1101/.2020.08.19.20177188Google Scholar
48. Luo L, Liu D, Liao X, et al. Contact settings and risk for transmission in
3410 close contacts of patients with COVID-19 in Guangzhou, China: a
prospective cohort study. Ann Intern Med. Published August 13, 2020.
doi:10. 7326/.M20-2671 PubMedGoogle Scholar
49. Lyngse FP, Kirkeby CT, Halasa T, et al. COVID-19 transmission within
Danish households: a nationwide study from lockdown to reopening.
medRxiv. Preprint published online September 9, 2020.
doi:10.1101/.2020.09.09.20191239Google Scholar
50. Malheiro R, Figueiredo AL, Magalhaes JP, et al. Effectiveness of contact
tracing and quarantine on reducing COVID-19 transmission·: a retrospective
cohort study. Public Health. 2020;189:54-59.
doi:10.1016/L.P-uhe.2020.09.012PubMedGoog le ScholarCrossref
51. Park YJ, Choe YJ, Park 0, et al; COVID-19 National Emergency Response
Center, Epidemiology and Case Management Team. Contact tracing during
coronavirus disease outbreak, South Korea, 2020. Emerg Infect Dis.
2020;26(10) :2465-2468. doi:10.3201/.eid2610.201315PubMedGoogle
ScholarCrossref
52. Park SY, Kim Y-M, Yi S, et al. Coronavirus disease outbreak in call center,
South Korea. Emerg Infect Dis. 2020;26(8):1666-1670.
doi:10.3201/.eid2608.201274PubMedGoogle ScholarCrossref
53. Patel A, Charani E, Ariyanayagam D, et al. New-onset anosmia and
APPENDIX TO JAMES CASCIANO DECLARATION-150
ageusia in adult patients diagnosed with SARS-CoV-2 infection. Clin
Microbiol Infect. Published online June 2 2020.PubMedGoogle Scholar
54. Phiriyasart F, Chantutanon S, Salaeh F, et al. Outbreak investigation of
coronavirus disease (COVID-19) among Islamic missionaries in southern
Thailand, April 2020. Outbreak, Surveillance, Investigation, and Response
(OSIR) Journal. 2020;13(2). Accessed November 11, 2020.
httg ://_www.osi rjourna I. net/.index. P-hP-L osi rL a rticle/_view L19 5
55. Rosenberg ES, Dufort EM, Blog DS, et al; New York State Coronavirus
2019 Response Team. COVID-19 testing, epidemic features, hospital
outcomes, and household prevalence, New York State-March 2020. Clin
Infect Dis. 2020;71 (8):1953-1959. doi:10.1093LcidLciaa549PubMedGoogle
ScholarCrossref
56. Shah K, Desai N, Saxena D, Mavalankar D, Mishra U, Patel GC.
Household secondary attack rate in Gandhinagar district of Gujarat state
from Western India. medRxiv. Preprint published online September 5,
2020. doi:10.1101/.2020.09.03.20187336Google Scholar
57. Son H, Lee H, Lee M, et al. Epidemiological characteristics of and
containment measures for COVID-19 in Busan, South Korea. Epidemiology
and Health. 2020;42:e2020035. doi:10.4178/.egih.e2020035PubMedGoogle
Scholar
58. Sun WW, Ling F, Pan JR, et al. [Epidemiological characteristics of
COVID-19 family clustering in Zhejiang Province]. Zhonghua Yu Fang Yi
Xue Za Zhi. 2020;54(6):625-629. doi:10.3760/_cma.j.cn112150-20200227-
00199PubMedGoogle Scholar
59. Teherani MF, Kao CM, Camacho-Gonzalez A, et al. Burden of illness in
households with SARS-CoV-2 infected children. J Pediatric Infect Dis Soc.
APPENDIX TO JAMES CASCIANO DECLARATION-151

2020;9(5):613-616. doi:10.1093/jRidsLRiaa097PubMedGoogle
ScholarCrossref
60.
van der Hoek W, Backer JA, Bodewes R, et al. [The role of children in the
transmission of SARS-CoV-2]. Ned Tijdschr Geneeskd.
2020;164:D5140.PubMedGoogle Scholar
61.
Wang Z, Ma W, Zheng X, Wu G, Zhang R. Household transmission of
SARS-CoV-2. J Infect. 2020;81 (1):179-182.
doi:10.1016fLjinf.2020.03.040PubMedGoogle ScholarCrossref
62. Wang X, Pan Y, Zhang D, et al. Basic epidemiological parameter values
from data of real-world in mega-cities: the characteristics of COVID-19 in
Beijing, China. BMC Infect Dis. 2020;20(1):526. doi:10.1186/.s12879-020-
05251-9PubMedGoogle ScholarCrossref
63. Wang Y, Tian H, Zhang L, et al. Reduction of secondary transmission of
SARS-CoV-2 in households by face mask use, disinfection and social
distancing: a cohort study in Beijing, China. BMJ Glob Health.
2020;5(5):e002794. doi:10.1136/.bmjgh-2020-002794PubMedGoogle
Scholar
64. Wang X, Zhou Q, He Y, et al. Nosocomial outbreak of COVID-19
pneumonia in Wuhan, China. Eur Respir J. 2020;55(6):2000544.
doi:10.1183/.13993003.00544-2020PubMedGoogle Scholar
65. Wu J, Huang Y, Tu C, et al. Household transmission of SARS-CoV-2,
Zhuhai, China, 2020. Clin Infect Dis. Published online May 11,
2020;ciaa557. doi:10.1093LcidLciaa557PubMedGoogle Scholar
66. Wu Y, Song S, Kao Q, Kong Q, Sun Z, Wang B. Risk of SARS-CoV-2
infection among contacts of individuals with COVID-19 in Hangzhou, China.
APPENDIX TO JAMES CASCIANO DECLARATION-152

Public Health. 2020;185:57-59.
doi:10.1016/L.P-uhe.2020.05.016Pu bMedGoog le ScholarCrossref
67.
Xin H, Jiang F, Xue A, et al. Risk factors associated with occurrence of
COVID-19 among household persons exposed to patients with confirmed
COVID-19 in Qingdao Municipal, China. Transbound Emerg Dis. 2020.
doi:10.1111/.tbed.13743PubMedGoogle Scholar
68. Yu HJ, Hu YF, Liu XX, et al. Household infection: the predominant risk
factor for close contacts of patients with COVID-19. Travel Med Infect Dis. 2020;36:101809. doi:10.1016/j .tmaid .2020.101809PubMedGoog le Scholar
69. Yung CF, Kam KQ, Chong CY, et al. Household transmission of SARS
CoV-2 from adults to children. J Ped. 2020;225:249-251.
doi :10.1016/Lj Reds. 2 0 2 0.07.00 9Goog I e Schola rC rossref
70. Zhang W, Cheng W, Luo L, et al. Secondary transmission of coronavirus
disease from presymptomatic persons, China. Emerg Infect Dis. 2020;26(8) :1924-1926. doi:10.3201/.eid2608.201142Pu bMedGoogle
ScholarCrossref
71. Zhang JZ, Zhou P, Han DB, et al. [Investigation on a cluster epidemic of
COVID-19 in a supermarket in Liaocheng, Shandong province]. Zhonghua Liu Xing Bing Xue Za Zhi. Published April 27, 2020.PubMedGoogle Scholar
72. Zhuang YL, Zhang YT, Li M, et al. [Analysis on the cluster epidemic of
coronavirus disease 2019 in Guangdong Province]. Zhonghua Yu Fang Yi Xue Za Zhi. 2020;54(7):720-725.PubMedGoogle Scholar
73. Stringhini S, Wisniak A, Piumatti G, et al. Seroprevalence of anti-SARS
CoV-2 lgG antibodies in Geneva, Switzerland (SEROCoV-POP): a
population-based study. Lancet. 2020;396(10247):313-319.
APPENDIX TO JAMES CASCIANO DECLARATION-153

doi:10.1016LS0140-6736 ( 2 0) 31304-0 Pub MedGoog I e Schola re rossref
74.
Yang K, Wang L, Li F, et al. Analysis of epidemiological characteristics of
coronavirus 2019 infection and preventive measures in Shenzhen China: a
heavy population city. medRxiv. Preprint published online March 3, 2020.
doi:10.1101L2020.02.28.20028555Google Scholar
75. Fontanet A, Grant R, Tondeur L, et al. SARS-CoV-2 infection in primary
schools in northern France: A retrospective cohort study in an area of high
transmission. medRxiv. Preprint published online June 29, 2020.
doi:10.1101L2020.06.25.20140178Google Scholar
76. Chan LY, Wong JT, Li PK, Lui SF, Fung H, Sung J. Risk of transmission
of severe acute respiratory syndrome to household contacts by infected
health care workers and patients. Am J Med. 2004;116(8):559-560.
doi:10.1016/j .amjmed.2003.11.011 PubMedGoog le ScholarCrossref
77. Goh DL, Lee BW, Chia KS, et al. Secondary household transmission of
SARS, Singapore. Emerg Infect Dis. 2004;10(2):232-234.
doi:10.3201Leid1002.030676PubMedGoogle ScholarCrossref
78. Lau JT, Lau M, Kim JH, Tsui HY, Tsang T, Wong TW. Probable
secondary infections in households of SARS patients in Hong Kong. Emerg
Infect Dis. 2004;10(2):235-243.
doi:10.3201Leid1002.030626Pu bMedGoog le Scholar
79. Wilson-Clark SD, Deeks SL, Gournis E, et al. Household transmission of
SARS, 2003. CMAJ. 2006;175(10):1219-1223.
doi:10.1503/.cmaj.050876PubMedGoogle ScholarCrossref
80. Ou J, Li Q, Zeng G, Dun Z; Centers for Disease Control and Prevention
(CDC). Efficiency of quarantine during an epidemic of severe acute
APPENDIX TO JAMES CASCIANO DECLARATION-154

respiratory syndrome-Beijing, China, 2003. MMWR Morb Mortal Wkly
Rep. 2003;52(43):1037-1040.PubMedGoogle Scholar 81.
Tuan PA, Herby P, Dinh PN, et al; WHO SARS Investigation Team in
Vietnam. SARS transmission in Vietnam outside of the health-care setting.
Epidemiol Infect. 2007;135(3):392-401.
doi:10.1017LS0950268806006996PubMedGoogle ScholarCrossref 82.
Pang X, Zhu Z, Xu F, et al. Evaluation of control measures implemented
in the severe acute respiratory syndrome outbreak in Beijing, 2003. JAMA.
2003;290(24) :3215-3221. doi:10.1001/jama.290.24.3215
ArticlePubMedGoogle ScholarCrossref
83. Al Hosani Fl, Kim L, Khudhair A, et al. Serologic follow-up of Middle East
respiratory syndrome coronavirus cases and contacts-Abu Dhabi, United
Arab Emirates. Clin Infect Dis. 2019;68(3):409-418.
doi:10.1093LcidLciY-503PubMedGoogle ScholarCrossref
84. Arwady MA, Alraddadi B, Basler C, et al. Middle East respiratory
syndrome coronavirus transmission in extended family, Saudi Arabia, 2014.
Emerg Infect Dis. 2016;22(8):1395-1402.
doi:10.3201Leid2208.152015PubMedGoogle ScholarCrossref
85. Assiri A, McGeer A, Perl TM, et al; KSA MERS-CoV Investigation Team.
Hospital outbreak of Middle East respiratory syndrome coronavirus. N
Engl J Med. 2013;369(5):407-416.
doi:10.1056LNEJMoa1306742PubMedGoogle ScholarCrossref
86. Drosten C, Meyer B, Muller MA, et al. Transmission of MERS-coronavirus
in household contacts. N Engl J Med. 2014;371(9):828-835.
doi:10.1056LNEJMoa1405858PubMedGoogle ScholarCrossref
87.
APPENDIX TO JAMES CASCIANO DECLARATION-155

Memish ZA, AI-Tawfiq JA, Alhakeem RF, et al. Middle East respiratory
syndrome coronavirus {MERS-CoV): a cluster analysis with implications for
global management of suspected cases. Travel Med Infect Dis.
2015;13{ 4) :311-314. doi:10.1016/j. tmaid .2015.06.012Pu bMedGoog le
ScholarCrossref
88.
Payne DC, Biggs HM, AI-Abdallat MM, et al. Multihospital outbreak of a
Middle East respiratory syndrome coronavirus deletion variant, Jordan: a
molecular, serologic, and epidemiologic investigation. Open Forum Infect
Dis. 2018;5{5):ofy095. doi:10.1093LofidlofY.095PubMedGoogle Scholar
89. Van Kerkhove MD, Alaswad S, Assiri A, et al. Transmissibility of MERS
CoV infection in closed setting, Riyadh, Saudi Arabia, 2015. Emerg Infect
Dis. 2019;25{10) :1802-1809. doi:10.3201Leid2510.190130PubMedGoogle
ScholarCrossref
90. Esposito S, Basis S, Niesters HG, et al. Impact of human coronavirus
infections in otherwise healthy children who attended an emergency
department. J Med Virol. 2006;78(12):1609-1615.
doi:10.1002/jmv.20745PubMedGoogle ScholarCrossref
91. Manto AS, DeJonge PM, Callear AP, et al. Coronavirus occurrence and
transmission over 8 years in the HIVE cohort of households in Michigan. J
Infect Dis. 2020;222(1):9-16. doi:10.1093linfdisfjiaa161PubMedGoogle
ScholarCrossref
92. Beale S, Lewer D, Aldridge RW, et al. Household transmission of
seasonal coronavirus infections: results from the Flu Watch cohort study.
Wei/come Open Research. 2020;5(145):145. doi:10.12 688LwellcomeoP-en res.160 5 5.1 Google Schola rCrossref
93. Tsang TK, Lau LLH, Cauchemez S, Cowling BJ. Household transmission
APPENDIX TO JAMES CASCIANO DECLARATION-156

of influenza virus. Trends Microbial. 2016;24(2):123-133.
doi:10.1016/j.tim.2015.10.012PubMedGoogle ScholarCrossref 94.
Ministry of Health, Labour, and Welfare. Avoid the "Three Cs"! Accessed
August 5, 2020. httrJs:f.Lwww. mhlw.go.jP-L content/.10900000/.000619576. Rdf 95.
Pang X, Yang P, Li S, et al. Pandemic (H1N1) 2009 among quarantined
close contacts, Beijing, People's Republic of China. Emerg Infect Dis.
2011;17(10):1824-1830. doi:10.3201/.eid1710.101344PubMedGoogle
ScholarCrossref
96.
Tam K, Yousey-Hindes K, Hadler JL. Influenza-related hospitalization of
adults associated with low census tract socioeconomic status and female
sex in New Haven County, Connecticut, 2007-2011. Influenza Other Respir
Viruses. 2014;8(3):274-281. doi:10.1111/.irv.12231 PubMedGoogle
ScholarCrossref
97. Chandrasekhar R, Sloan C, Mitchel E, et al. Social determinants of
influenza hospitalization in the United States. Influenza Other Respir
Viruses. 2017;11(6):479-488. doi:10.1111/.irv.12483PubMedGoogle
ScholarCrossref
98. Sloan C, Chandrasekhar R, Mitchel E, Schaffner W, Lindegren ML.
Socioeconomic disparities and influenza hospitalizations, Tennessee, USA.
Emerg Infect Dis. 2015;21(9):1602-1610.
doi:10.3201/.eid2109.141861 Pu bMedGoogle ScholarCrossref
99. Viner RM, Mytton OT, Benell C, et al. Susceptibility to SARS-CoV-2
infection among children and adolescents compared with adults: a
systematic review and meta-analysis. JAMA Pediatr. Published September
25, 2020. doi:10.1001/jamaP-ediatrics.2020.4573
ArticlePubMedGoogle Scholar
APPENDIX TO JAMES CASCIANO DECLARATION-157

100.
Davies NG, Klepac P, Liu Y, Prem K, Jit M, Eggo RM; CMMID COVID-19
working group. Age-dependent effects in the transmission and control of
COVID-19 epidemics. Nat Med. 2020;26(8):1205-1211.
doi:10.1038/.s41591-020-0962-9PubMedGoog le ScholarCrossref 101.
Huang AT, Garcia-Carreras B, Hitchings MDT, et al. A systematic review
of antibody mediated immunity to coronaviruses: kinetics, correlates of
protection, and association with severity. Nat Commun. 2020;11(1):4704.
doi:10.1038/.s41467-020-18450-4Pu bMedGoog le ScholarCrossref
102. Mehta NS, Mytton OT, Mullins EWS, et al. SARS-CoV-2 (COVID-19): what
do we know about children? a systematic review. Clin Infect Dis. Published
May 11, 2020;ciaa556. doi:10.1093LcidLciaa556PubMedGoogle Scholar
103. Posfay-Barbe KM, Wagner N, Gauthey M, et al. COVID-19 in children and
the dynamics of infection in families. Pediatrics. 2020;146(2):e20201576.
doi:10.1542/.geds.2020-1576Pu bMedGoogle Scholar
104. Lee B, Raszka WV Jr. COVID-19 transmission and children: the child is
not to blame. Pediatrics. 2020;146{2):e2020004879.
doi:10.1542/.geds.2020-004879Pu bMedGoogle Scholar
105. Zhu Y, Bloxham CJ, Hulme KD, et al. Children are unlikely to have been
the primary source of household SARS-CoV-2 infections. medRxiv.
Preprint published online March 30, 2020.
doi:10.1101/.202 0.0 3.2 6. 2 00448 2 6Goog le Scholar
106. L1Huillier AG, Torriani G, Pigny F, Kaiser L, Eckerle I. Culture-competent
SARS-CoV-2 in nasopharynx of symptomatic neonates, children, and
adolescents. Emerg Infect Dis. 2020;26(10):2494-2497.
doi:10.3201Leid2610.202403Google ScholarCrossref
APPENDIX TO JAMES CASCIANO DECLARATION-158

107.
World Health Organization. Gender and COVID-19. Published May 14, 2020. Accessed November 11, 2020.
httgs:fLwww.who.int/pu bl icati onsLWtemLgend er-an d-covi d-19 108.
Walsh KA, Jordan K, Clyne B, et al. SARS-CoV-2 detection, viral load and
infectivity over the course of an infection. J Infect. 2020;81(3):357-371.
doi:10.1016/j_.jinf.2020.06.067PubMedGoogle ScholarCrossref 109.
He X, Lau EHY, Wu P, et al. Temporal dynamics in viral shedding and
transmissibility of COVID-19. Nat Med. 2020;26(5):672-675.
doi:10.1038Ls41591-020-0869-5PubMedGoogle ScholarCrossref
110.
Ali ST, Wang L, Lau EHY, et al. Serial interval of SARS-CoV-2 was
shortened over time by nonpharmaceutical interventions. Science.
2020;369(6507) :1106-1109. doi:10.1126L science.abc9004PubMedGoogle
ScholarCrossref
111.
Rabaan AA, Al-Ahmed SH, Haque S, et al. SARS-CoV-2, SARS-CoV, and
MERS-COV: a comparative overview. lnfez Med. 2020;28(2):174-
184.PubMedGoogle Scholar
112. Petersen E, Koopmans M, Go U, et al. Comparing SARS-CoV-2 with
SARS-CoV and influenza pandemics. Lancet Infect Dis. 2020;20(9):e238-
e244. doi:10.1016LS1473-3099(20)30484-9PubMedGoogle
ScholarCrossref
113. Petrosillo N, Viceconte G, Ergonul 0, Ippolito G, Petersen E. COVID-19,
SARS and MERS: are they closely related? Clin Microbiol Infect.
2020;26(6) :729-734. doi:10.1016/j.cmi.2020.03.026PubMedGoogle
ScholarCrossref
114.
APPENDIX TO JAMES CASCIANO DECLARATION-159

Fraser C, Riley S, Anderson RM, Ferguson NM. Factors that make an
infectious disease outbreak controllable. Proc Natl Acad Sci US A. 2004;101 (16) :6146-6151. doi:10.1073Lgnas.0307 506101 PubMedGoogle
ScholarCrossref
115.
Cowling BJ, Park M, Fang VJ, Wu P, Leung GM, Wu JT. Preliminary
epidemiological assessment of MERS-CoV outbreak in South Korea, May to
June 2015. Euro Survei/1. 2015;20(25):7-13. doi:10.2807/.1560-
7917. ES2015.20.25.21163Pu bMedGoogle ScholarCrossref
APPENDIX TO JAMES CASCIANO DECLARATION-160

Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China , 20 November 2020
Nature Communications 11, Article number: 5917 (2020) Cite this article
1.16m Accesses
2 Citations
19566 Altmetric
Metrics
This article has been updated
Abstract
Stringent COVID-19 control measures were imposed in Wuhan between
January 23 and April 8, 2020. Estimates of the prevalence of infection
following the release of restrictions could inform post-lockdown pandemic
management. Here, we describe a city-wide SARS-CoV-2 nucleic acid
screening programme between May 14 and June 1, 2020 in Wuhan. All city
residents aged six years or older were eligible and 9,899,828 (92.9%)
participated. No new symptomatic cases and 300 asymptomatic cases
(detection rate 0.303/10,000, 95% Cl 0.270-0.339/10,000) were identified.
There were no positive tests amongst 1,174 close contacts of asymptomatic
cases. 107 of 34,424 previously recovered COVID-19 patients tested
positive again (re-positive rate 0.31%, 95% Cl 0.423-0.574%). The
prevalence of SARS-CoV-2 infection in Wuhan was therefore very low five
APPENDIX TO JAMES CASCIANO DECLARATION-161

to eight weeks after the end of lockdown.
Introduction
The Coronavirus Disease 2019 {COVID-19) was first reported in December
2019, and was classified as a pandemic by the World Health Organization
on March 11, 2020 1. Following strict lockdown measures, the COVID-19
epidemic was generally under control in China, and the whole country has
progressed into a post-lockdown phase. In this phase, countries face new
problems and challenges, including how to accurately assess the post
lockdown risk of the COVID-19 epidemic, how to avoid new waves of
COVID-19 outbreaks, and how to facilitate the resumption of economy and
normal social life. As the city most severely affected by COVID-19 in China,
Wuhan had been under lockdown measures from January 23 until April 8,
2020. During the first 2 months after city's reopening, there were only a few
sporadic COVID-19 cases in Wuhan {six newly confirmed cases from April 8
to May 10, 2020 2). However, there was still concern about the risk of
COVID-19 in Wuhan, which seriously affected the resumption of industrial
production and social services, and hampered the normal lives of residents.
In order to ascertain the current status of the COVID-19 epidemic, the city
government of Wuhan carried out a comprehensive citywide nucleic acid
screening of SARS-CoV-2 infection from May 14, 2020 to June 1, 2020.
The citywide screening of SARS-CoV-2 infection in Wuhan is a mass
screening programme in post-lockdown settings, and provided invaluable
experiences or lessons with international relevance as more countries and
cities around the world entering the post-lockdown phase. In this study, we
report the organisation process, detailed technical methods used, and
results of this citywide nucleic acid screening.
Results
There were 10,652,513 eligible people aged :?:6 years in Wuhan (94.1% of
APPENDIX TO JAMES CASCIANO DECLARATION-162

the total population). The nucleic acid screening was completed in 19 days
(from May 14, 2020 to Jun 1, 2020), and tested a total of 9,899,828 persons
from the 10,652,513 eligible people (participation rate, 92.9%). Of the
9899,828 participants, 9,865,404 had no previous diagnosis of COVID-19,
and 34,424 were recovered COVID-19 patients.
The screening of the 9,865,404 participants without a history of COVID-19
found no newly confirmed COVID-19 cases, and identified 300
asymptomatic positive cases with a detection rate of 0.303 (95% Cl 0.270-
0.339)/10,000. The median age-stratified Ct-values of the asymptomatic
cases were shown in Supplementary Table 1. Of the 300 asymptomatic
positive cases, two cases came from one family and another two were from
another family. There were no previously confirmed COVID-19 patients in
these two families. A total of 1174 close contacts of the asymptomatic
positive cases were traced, and they all tested negative for the COVID-19.
There were 34,424 previously recovered COVID-19 cases who participated
in the screening. Of the 34,424 participants with a history of COVID-19, 107
tested positive again, giving a repositive rate of 0.310% (95% Cl 0.423-
0.574%).
Virus cultures were negative for all asymptomatic positive and repositive
cases, indicating no "viable virus" in positive cases detected in this study.
All asymptomatic positive cases, repositive cases and their close contacts
were isolated for at least 2 weeks until the results of nucleic acid testing
were negative. None of detected positive cases or their close contacts
became symptomatic or newly confirmed with COVID-19 during the
isolation period. In this screening programme, single and mixed testing was
performed, respectively, for 76.7% and 23.3% of the collected samples. The
asymptomatic positive rates were 0.321 (95% Cl 0.282-0.364)/10,000 and
0.243 (95% Cl 0.183-0.315)/10,000, respectively.
The 300 asymptomatic positive persons aged from 10 to 89 years, included
132 males (0.256/10,000) and 168 females (0.355/10,000). The APPENDIX TO JAMES CASCIANO DECLARATION-163

asymptomatic positive rate was the lowest in children or adolescents aged
17 and below (0.124/10,000), and the highest among the elderly aged 60
years and above (0.442/10,000) (Table 1). The asymptomatic positive rate in
females (0.355/10,000) was higher than that in males (0.256/10,000).
Table 1 Characteristics of asymptomatic positive individuals.
Full size table
The asymptomatic positive cases were mainly domestic and unemployed
residents (24.3%), retired older adults (21.3%), and public service workers
(11.7%} (Fig.1).
Fig. 1: The occupation distribution of asymptomatic positive cases(%).
2,0.7%
4, 1.3%
■ Housework or unemployment
The emeritus and retirees
Service workers in public place
Industrial labourer
■ Cadres staff
■ Agricultural labourer
■ Student
■ Teacher
■ Medical staff
■ Transportation service personnel
■ Others
Note: Others included the self-employed, military personnel, and so on. (Source data are provided
ass Source Data file.).
Full size imagg
The asymptomatic positive rate in urban districts was on average
0.456/10,000, ranging from 0.317/10,000 in Hongshan to 0.807/10,000 in
Wuchang district. A lower rate of asymptomatic positive cases was found in
suburban districts (0.132/10,000), ranging from 0.047/10,000 in Xinzhou to
0.237/10,000 in Jiangan district (Fig. 2).
APPENDIX TO JAMES CASCIANO DECLARATION-164

Fig. 2: The geographic distribution of the detection rate of asymptomatic positive cases.
,,r
;
Celdlan
0.218
Dollplhu OJll4
Huangpl 0.143
Jiangxla 0.209
., .
• East Lake Hia,Hec:h Development Zone
G.143
Xlnlhou OJM7
0 10Km
Detection rate of asymptomatic patients at District level (per 10.000)
JI{:,:.>--"----...... ;;,r'' "\I"\_ I.
11110.000
0.001--0.100
0.101--0.200
0.201--0.300
0.301--0.400
11110.401--0.600
11110.601--0.750
Note: 1 represents Jianghan district; 2 represents Qiaokou district. (Source data are provided as s
Source Data file.).
Full size imag~
Among the 7280 residential communities in Wuhan, asymptomatic positive
APPENDIX TO JAMES CASCIANO DECLARATION-165

cases were identified in 265 (3.6%) communities (only one case detected in
246 communities), while no asymptomatic positive cases were found in other 96.4% communities.
Testing of antibody against SARS-CoV-2 virus was positive lgG (+) in 190 of
the 300 asymptomatic cases, indicating that 63.3% (95% Cl 57.6-68.8%) of
asymptomatic positive cases were actually infected. The proportion of
asymptomatic positive cases with both lgM (-) and lgG (-) was 36.7% {95%
Cl: 31.2-42.4%; n = 110), indicating the possibility of infection window or
false positive results of the nucleic acid testing (Table 2).
Table 2 Results of the detection of antibody in 300 asymptomatic positive persons.
Full size table
Higher detection rates of asymptomatic infected persons were in Wuchang,
Qingshan and Qiaokou districts, and the prevalence of previously confirmed
COVID-19 cases were 68.243/10,000, 53.767/10,000, and 100.047/10,000,
respectively, in the three districts. Figure .3 shows that districts with a high
detection rate of asymptomatic positive persons generally had a high
prevalence of confirmed COVID-19 cases {rs= 0.729, P = 0.002).
Fig. 3: The prevalence of previously confirmed patients and the detection rate of asymptomatic positive
cases of COVID-19 in each district in Wuhan.
APPENDIX TO JAMES CASCIANO DECLARATION-166

a
I c......, ~8 en o ::Jr-2 ... i& a.~ 'oi GI·-g-GI 8_ cij
~ a.
b
120.000
100.000
80.000
60.000
40.000
20.000
0.900
0.800
.!:! 0.700 'i E-%8 0.600
[~ ~-= 0.500 0 g_ ti o.4oo ~u 0 .E 0300 ~ 5: .
~ 0.200
0.100
100.047
0.807
0.000
a The prevalence of previously confirmed patients of COVID-19 in each district in Wuhan. b The
detection rate of asymptomatic positive cases of COVID-19 in each district in Wuhan. (Source data
are provided ass Source Data file.).
Full size imag~
APPENDIX TO JAMES CASCIANO DECLARATION-167

Discussion
The citywide nucleic acid screening of SARS-CoV-2 infection in Wuhan
recruited nearly 10 million people, and found no newly confirmed cases with
COVID-19. The detection rate of asymptomatic positive cases was very low,
and there was no evidence of transmission from asymptomatic positive
persons to traced close contacts. There were no asymptomatic positive
cases in 96.4% of the residential communities.
Previous studies have shown that asymptomatic individuals infected with
SARS-CoV-2 virus were infectious~, and might subsequently become
symptomatic~. Compared with symptomatic patients, asymptomatic
infected persons generally have low quantity of viral loads and a short
duration of viral shedding, which decrease the transmission risk of SARS
CoV-2'Q.. In the present study, virus culture was carried out on samples from
asymptomatic positive cases, and found no viable SARS-CoV-2 virus. All
close contacts of the asymptomatic positive cases tested negative,
indicating that the asymptomatic positive cases detected in this study were
unlikely to be infectious.
There was a low repositive rate in recovered COVID-19 patients in Wuhan.
Results of virus culturing and contract tracing found no evidence that
repositive cases in recovered COVID-19 patients were infectious, which is
consistent with evidence from other sources. A study in Korea found no
confirmed COVID-19 cases by monitoring 790 contacts of 285 repositive
cases2. The official surveillance of recovered COVID-19 patients in China
also revealed no evidence on the infectiousness of repositive cases2.
Considering the strong force of infection of COVID-198,9,10, it is expected
that the number of confirmed cases is associated with the risk of being
infected in communities. We found that asymptomatic positive rates in
different districts of Wuhan were correlated with the prevalence of
previously confirmed cases. This is in line with the temporal and spatial
evolution (especially the long-tailed characteristic) of infectious diseases11.
APPENDIX TO JAMES CASCIANO DECLARATION-168

Existing laboratory virus culture and genetic studies.9,10 showed that the
virulence of SARS-CoV-2 virus may be weakening over time, and the newly
infected persons were more likely to be asymptomatic and with a lower viral
load than earlier infected cases. With the centralized isolation and
treatment of all COVID-19 cases during the lockdown period in Wuhan, the
risk of residents being infected in the community has been greatly reduced.
When susceptible residents are exposed to a low dose of virus, they may
tend to be asymptomatic as a result of their own immunity. Serological
antibody testing in the current study found that at least 63% of
asymptomatic positive cases were actually infected with SARS-CoV-2 virus.
Nonetheless, it is too early to be complacent, because of the existence of
asymptomatic positive cases and high level of susceptibility in residents in
Wuhan. Public health measures for the prevention and control of COVID-19
epidemic, including wearing masks, keeping safe social distancing in Wuhan
should be sustained. Especially, vulnerable populations with weakened
immunity or co-morbidities, or both, should continue to be appropriately
shielded.
Findings from this study show that COVID-19 was well controlled in Wuhan
at the time of the screening programme. After two months since the
screening programme (by August 9, 2020), there were no newly confirmed
COVID-19 cases in Wuhan. Further testing of SARS-CoV-2 in samples
collected from market environment settings in Wuhan were conducted, and
found no positive results after checking a total of 52,312 samples from 1795
market setting during June 13 to July 2, 2020 12•
This study has several limitations that need to be discussed. First, this was
a cross-sectional screening programme, and we are unable to assess the
changes over time in asymptomatic positive and reoperative results.
Second, although a positive result of nucleic acid testing reveals the
existence of the viral RNAs, some false negative results were likely to have
occurred, in particular due to the relatively low level of virus loads in
asymptomatic infected individuals, inadequate collection of samples, and
APPENDIX TO JAMES CASCIANO DECLARATION-169

limited accuracy of the testing technology 13• Although the screening
programme provided no direct evidence on the sensitivity and specificity of
the testing method used, a meta-analysis reported a pooled sensitivity of
73% (95% Cl 68-78%) for nasopharayngeal and throat swab testing of
COVID-1914• Testing kits used in the screening programme were publicly
purchased by the government and these kits have been widely used in
China and other countries. Multiple measures were taken to possibly
minimise false negative results in the screening programme. For example,
standard training was provided to health works for sample collection to
ensure the sample quality. The experiment procedures, including specimen
collection, extraction, PCR, were according to official guidelines
(Supplementary Note 1). For the real-time RT-PCR assay, two target genes
were simultaneously tested. Even so, false negative results remained
possible, particularly in any mass screening programmes. However, even if
test sensitivity was as low as 50%, then the actual prevalence would be
twice as high as reported in this study, but would still be very low. Around
7.1% of eligible residents did not participate in the citywide nucleic acid
screening and the screening programme did not collect detailed data on
reasons for nonparticipation, which is a limitation of this study. Although
there were no official statistics, a large number of migrant workers and
university students left Wuhan before the lockdown, joining their families in
other cities or provinces for traditional Chinese New Year. Therefore, it is
likely that most nonparticipants were not in Wuhan at the time of the
screening. The main objective of the screening programme was to assess
the risk of COVID-19 epidemic in residents who were actually living in the
post-lockdown Wuhan. Therefore, the estimated positive rates are unlikely
to be materially influenced by nonparticipation of residents who were not in
Wuhan or some residents who did not participate in the screening for other
reasons. Moreover, people who left Wuhan were the target population for
monitoring in other provinces and cities and were required to take nucleic
acid testing. Although there was no official statistics showing the positive
rate of nucleic acid testing in this population, there was no report that
APPENDIX TO JAMES CASCIANO DECLARATION-170

shown a higher positive rate of nucleic acid testing than our findings.
In summary, the detection rate of asymptomatic positive cases in the postlockdown Wuhan was very low (0.303/10,000), and there was no evidence that the identified asymptomatic positive cases were infectious. These findings enabled decision makers to adjust prevention and control strategies in the post-lockdown period. Further studies are required to fully evaluate the impacts and cost-effectiveness of the citywide screening of SARS-CoV-2 infections on population's health, health behaviours, economy, and society.
Methods
Study population and ethical approvals
Wuhan has about 11 million residents in total, with seven urban and eight suburban districts. Residents are living in 7280 residential communities (or residential enclosures, "xiao-qu" in Chinese), and each residential community could be physically isolated from other communities for preventing transmission of COVID-19.
The screening programme recruited residents (including recovered COVID-19 patients) currently living in Wuhan who were aged ~6 years (5,162,960 males, 52.2%). All participants provided written or verbal informed consent after reading a statement that explained the purpose of the testing. For participants who aged 6-17 years old, consent was obtained from their parents or guardians. The study protocol for an evaluation of the programme based on anonymized screening data was approved by the Ethics Committee of the Tongji Medical College Institutional Review Board, Huazhong University of Science and Technology, Wuhan, China (No.
IROG0003571).
Organizational guarantee and community mobilization
APPENDIX TO JAMES CASCIANO DECLARATION-171

A citywide nucleic acid screening group was formed, with specialized task
teams contributing to comprehensive coordination, technical guidance,
quality control, participation invitation, information management,
communication, and supervision of the screening. The city government
invested 900 million yuan (RMB) in the testing programme. From 14 May to
1 June 2020, in the peak time, up to 2907 sample collection sites were
functioning at the same time in Wuhan. Each sample collection site had an
assigned sample collection group, including several health professionals
(staffed according to the number of communities' residents), 2-4 community managers, 1-2 police officers, and 1-2 inspectors. The sampling
sites were set up based on the number and accessibility of local residents.
Local community workers were responsible for a safe and orderly sampling
process to minimise the waiting time. In addition, mobile sampling teams
were formed by primary health care professionals and volunteers to
conduct door-to-door sampling for residents who had physical difficulties
or were unable to walk.
About 50,000 health professionals (mainly doctors and nurses from
community health centers) and more than 280,000 person-times of
community workers and volunteers contributed to sample collection,
transport of equipment and samples collected, arrangement of participation
process, and maintaining order of sampling sites. Public information
communication and participant invitation were implemented through mass
media, mobile messages, WeChat groups, and residential community
broadcasts, so as to increase residents' awareness and the participation.
Acquisition, preservation, and transport of samples
All sampling personnel received standard training for the collection of
oropharyngeal swab samples. To minimise the risk of cross-infection, the
sampling process strictly followed a disinfection process and environmental
ventilation were ensured. The collected samples were stored in a virus
preservation solution or immersed in isotonic saline, tissue culture solution,
APPENDIX TO JAMES CASCIANO DECLARATION-172

or phosphate buffer (Supplementary note 1). Then, all samples were sent to
testing institutions within 4 h using delivery boxes for biological samples
refrigerated with dry ice to guarantee the stability of nucleic acid samples.
Technical methods for laboratory testing of collected samples
A total of 63 nucleic acid testing laboratories, 1451 laboratory workers and
701 testing equipment were involved in the nucleic acid testing. Received
samples were stored at 4 °C and tested within 24 h of collection. Any
samples that could not be tested within 24 h were stored at - 70 °C or below
(Supplementary note 1). In addition to "single testing" (i.e., separate testing
of a single sample), "mixed testing" was also performed for 23% of the
collected samples to increase efficiency, in which five samples were mixed
in equal amounts, and tested in the same test tube. If a mixed testing was
positive for COVID-19, all individual samples were separately retested within
24 h 15•
Details regarding technical methods for sequencing and virus culture were
provided in Supplementary note 1. Real-time reverse transcriptase
polymerase chain reaction (RT-PCR) assay method was used for the nucleic
acid testing. We simultaneously amplified and tested the two target genes:
open reading frame 1ab (ORF1ab) and nucleocapsid protein (N)
(Supplementary Note 1). A cycle threshold value (Ct-value) less than 37
was defined as a positive result, and no Ct-value or a Ct-value of 40 or
more was defined as a negative result. For Ct-values ranging from 37 to 40,
the sample was retested. If the retest result remained less than 40 and the
amplification curve had obvious peak, the sample was classified as positive;
otherwise, it was reported as being negative. These diagnostic criteria were
based on China's official recommendations 16•
For asymptomatic positive cases, virus culture was carried out in biosafety
level-3 laboratories. The colloidal gold antibody test was also performed for
APPENDIX TO JAMES CASCIANO DECLARATION-173

asymptomatic positive cases {Supplementary note 1). All testing results
were double entered into a specifically designed database, and managed by
the Big Data and Investigation Group of the COVID-19 Prevention and
Control Centre in Wuhan, which was established to collect and manage
data relevant to the COVID-19 epidemic.
Participant data collection and management
Before sample collection, residents electronically {using a specifically
designed smartphone application) self-uploaded their personal information,
including ID number, name, sex, age, and place of residence. Then, the
electronic machine system generated a unique personal barcode and stuck
it on the sample tube to ensure the match between the sample and the
participant. Then trained staff interviewed each individual regarding the
history of COVID-19 and previous nucleic acid testing. There was a
database of confirmed COVID-19 cases in Wuhan, which can be used to
validate the self-reported previous COVID-19 infection. All information was
entered into a central database. The testing results were continually
uploaded to the central database by testing institutions. Contact tracing
investigations were conducted on participants who tested positive for
SARS-CoV-2, to track and manage their close contacts. The pre-existing
unique identification code for each resident was used as the programme's
identification number, to ensure information accuracy during the whole
process of screening, from sampling, nucleic acid testing, result reporting,
the isolation of detected positive cases, and tracing of close contacts of
positive cases. All screening information was kept strictly confidential and
was not allowed to be disclosed or used for other purposes other than
clinical and public health management. Personal information of
asymptomatic positive cases was only disclosed to designated medical
institutions and community health centres for the purpose of medical
isolation and identification of close contacts. Researcher was blind to the
study hypothesis during data collection.
APPENDIX TO JAMES CASCIANO DECLARATION-174

Biological security guarantee
Nucleic acid testing was performed in biosafety level-2 (BSL-2)
laboratories, and virus culture was conducted in biosafety level-3
laboratories. Sampling and testing personnel adopted the personal
protective measures according to the standard of biosafety level-3
laboratories. Participating laboratories implemented control measures to
guarantee biological safety in accordance with relevant regulations 17•
Result query and feedback
Two to three days after sample collection, participants could inquire about
their test results using WeChat or Alipay application by their unique ID
numbers. The results included text descriptions of nucleic acid testing and
coloured health codes. A green coloured health code refers to a negative
result, and a red coloured health code indicates a positive result.
Definition and management of identified confirmed cases and close contacts
In this study, all confirmed COVID-19 cases were diagnosed by designated
medical institutions according to National Guidelines for the Prevention and
Control of COVID-19 (Supplementary Note 2). Asymptomatic positive cases
referred to individuals who had a positive result during screening, and they
had neither a history of COVID-19 diagnosis, nor any clinical symptoms at
the time of the nucleic acid testing. Close contacts were individuals who
closely contacted with an asymptomatic positive person since 2 days
before the nucleic acid sampling 16• Repositive cases refer to individuals who
recovered from previously confirmed COVID-19 disease and had a positive
testing again in the screening programme. All repositive cases,
asymptomatic positive persons, and their close contacts were isolated for at
least 2 weeks in designated hotels managed by primary health care
professionals, and they were released from isolation only if two consecutive
APPENDIX TO JAMES CASCIANO DECLARATION-175

nucleic acid tests were negative.
Statistical analysis
Detection rate of asymptomatic positive or repositive cases was calculated
by dividing the number of individuals with a positive result of nucleic acid
testing by the number of participants tested. Because of extremely low
detection rates, we calculated 95% confidence intervals of estimated
proportions using Pearson-Klapper exact method, implemented through R
package "binom" version 1.1-118• SPSS version 22.0 was used for other
statistical analyses. We analyzed the distribution of asymptomatic positive
cases and assessed the Spearman correlation between the asymptomatic
positive rate and the prevalence of previously confirmed COVID-19 cases in
different districts of Wuhan. Differences in asymptomatic positive rates by
sex and age groups were assessed using the x2 test. ArcGIS 10.0 was used
to draw a geographic distribution map of asymptomatic positive cases. A
value of P < 0.05 (two-tailed) was considered statistically significant.
Reporting summary
Further information on research design is available in the Nature Research
ReP-orting Summary linked to this article.
Data availability
Detailed data directly used to generate each figure or table of this study are
available within the article, SupplementarY. Information andsource data are
provided with this paper.
Change history
17 December 2020
The original version of this Article was updated shortl}! after publication,
APPENDIX TO JAMES CASCIANO DECLARATION-176

because the Peer Review file was inadvertently omitted. The error has now
been fixed and the Peer Review file is available to download from the HTML version of the Article.
References
1.
WHO. Coronavirus disease 2019 (COVID-19) Situation Report-51. Data as
reported by national authorities by 10 AM CET 11 March 2020 (WHO, 2020).
2.
Prevention measures taken at Sanmin residential community in Wuhan
Xinhua I English.news.en httg:f/.www.xinhuanet.com/.english/.2020-
05/.11/.c 139048342.htm (2020).
3.
Gandhi, M., Yokoe, D. S. & Havlir, D. V. Asymptomatic transmission, the
Achilles' heel of current strategies to control Covid-19. N. Engl J. Med. 382, 2158-2160 (2020).
CAS Article Google Scholar
4.
He, D. et al. The relative transmissibility of asymptomatic COVID-19
infections among close contacts. Int. J. Infect. Dis. 94, 145-147 (2020).
CAS Article Google Scholar
5.
Arons, M. M. et al. Presymptomatic SARS-CoV-2 infections and
transmission in a skilled nursing facility. N. Engl J. Med. 382, 2081-2090
APPENDIX TO JAMES CASCIANO DECLARATION-177

(2020).
CAS Article Google Scholar
6.
KCDC. Findings from investigation and analysis of re-positive cases
(notice). Division of Risk assessment and International cooperation 2020-
05-19. hllp_s_;/./.www.cdc.go.krLboardLboard.es?
mid=a30402000000&bid=0030 (2020).
7.
National Health Commission. News conference on the prevention and
control of COVID-19. Beijing, 21-04-2020.
httQ:f/.www.nhc.gov.cn/.xcs/.f kdt/.2 02 004/.3e16 b 2 976000411 da 737 c 70 5 23e0
5522.shtml. (2020).
8.
Li, Y. et al. Positive result of Sars-Cov-2 in faeces and sputum from
discharged patient with COVID-19 in Yiwu, China. J. Med Virol.
httP-s:fLdoi.orgL10.1002/jmv.25905 (2020).
9.
Su, Y. C. F. et al. Discovery and Genomic Characterization of a 382-
Nucleotide Deletion in ORF7b and ORF8 during the Early Evolution of SARS
CoV-2. mBio 11, e01610-20 (2020).
CAS PubMed PubMed Central Google Scholar
10.
Lin, Z. Italian scientist: the virulence of SARS-Cov-2 is weakening, the newly
infected person are almost asymptomatic (Chinanews, 2020).
APPENDIX TO JAMES CASCIANO DECLARATION-178

11.
Ajelli, M. et al. Spatiotemporal dynamics of the Ebola epidemic in Guinea
and implications for vaccination and disease elimination: a computational
modeling analysis. BMC Med 14, 130 (2016).
Article Google Scholar
12.
Wuhan Municipal Health Commission. All results were negative by checking
52312 samples from 1795 supermarket and other market environment
setting for 20 days (news).
httQ :/./.wjw.wu ha n .gov.cn/.ztz 1_2.8/.f k/.tzgg/.20 2 007 /.t20 20 070 2 138 93 23. s htm I
. (2020).
13.
Woloshin, S., Patel, N. & Kesselheim, A. S. False negative tests for SARS
CoV-2 infection--challenges and implications. N. Engl. J. Med 383, e38
(2020).
CAS Article Google Scholar
14.
Boger, B. et al. Systematic review with meta-analysis of the accuracy of
diagnostic tests for COVID-19. Am. J. Infect. Control S0196-
6553(20)30693-3. Advance online publication.
httQs:/./.doi .org/.10.1016/.j .ajic. 202 0.07.011 (2020).
15.
Lohse, S. et al. Pooling of samples for testing for SARS-CoV-2 in
asymptomatic people. Lancet Infect. Dis. 20, 1231-1232.
httP-s:fLdoi .org/.10.1016LS14 73-3099 (20) 30362-5 (2020).
APPENDIX TO JAMES CASCIANO DECLARATION-179

CAS Article Google Scholar
16.
National Health Commission of the People's Republic of China. The
prevention and Control Plan of COVID-19 5th edition (National Health
Commission of the People's Republic of China, 2020).
17.
European Centre for Disease Prevention and Control (ECDC). Laboratory
support for COV/D-19 in the EU/EEA. (ECDC, 2020).
18.
Dorai-Raj, S. Package'binom'-Binomial Confidence Intervals For Several
Parameterizations. Version 1.1-1. httgs:fLcran.r
groject.org/.web/.gackages/.binom/.binom.gdf (2014).
Download references
Acknowledgements
We would like to thank all institutions and all citizens in Wuhan for their
support for citywide nucleic acid screening work. We also would like to
thank the Wuhan city government for this citywide nucleic acid testing,
sampling and management, and thank the big data and investigation group
of COVID-19 prevention and control institution in Wuhan (the data and
investigation group of Wuhan Municipal Health Commission) for their efforts
in the data collection. In addition, we would like to thank the National Social
Science Foundation of China (Grant No. 18ZDA085) for supporting the
fund.
Author information
APPENDIX TO JAMES CASCIANO DECLARATION-180

These authors contributed equally: Shiyi Cao, Yong Gan, Chao Wang.
Affiliations
Department of Social Medicine and Health Management, School of Public Health, Tongji Medical College, Huazhong University of Science
and Technology, Wuhan, Hubei, China
Shiyi Cao, Yong Gan, Chao Wang, Yuchai Huang, Tiantian Wang, Yanhong Gong, Hongbin Xu, Xin Shen, Xiaoxv Yin & Zuxun Lu
Norwich Medical School, Faculty of Medicine and Health Science, University of East Anglia, Norwich, UK
Max Bachmann & Fujian Song
Wuhan Municipal Health Commission, Wuhan, Hubei, China
Shanbo Wei
Wuhan Centre for Clinical Laboratory, Wuhan, Hubei, China
Jie Gong
Department of Management Science and Engineering, School of Economics and Management, Jiangxi Science and Technology Normal University, Nanchang, Jiangxi, China
Liqing Li
Tongji Hospital, Huazhong University of Science and Technology, Wuhan, Hubei, China
Kai Lu
Centre for Alcohol Policy Research, School of Psychology and Public
APPENDIX TO JAMES CASCIANO DECLARATION-181

Health, La Trobe University, Melbourne, VIC, Australia
Heng Jiang
Melbourne School of Population and Global Health, University of Melbourne, Melbourne, VIC, Australia
Heng Jiang
School of Public Health, Zhengzhou University, Zhengzhou, Henan, China
Qingfeng Tian
Department of Emergency, Hainan Clinical Research Centre for Acute and Critical Diseases, The Second Affiliated Hospital of Hainan Medical University, Haikou, Hainan, China
Chuanzhu Lv
Contributions
S.Y.C., C.W., X.X.Y., and Z.X.L. conceived the study. C.W., Y.C.H., T.T.W., K.L.,
H.B.X., and X.S. participated in the acquisition of data. S.B.W. and J.G. were
responsible for the on-site specimen collection, laboratory testing quality
evaluation, and control. Y.C.H., T.T.W., and L.Q.L. analyzed the data. H.J.,
Y.H.G., and F.J.S. gave advice on methodology. Q.F.T. and C.Z.L.
investigated the responses to the citywide nucleic acid testing among
residents lived in outside of Wuhan city. S.Y.C., Y.G., C.W., and X.X.Y. drafted
the manuscript, Y.G., M.B., and F.J.S. revised the manuscript, and M.B.,
C.Z.L., and F.J.S. critically commented and edited the manuscript. All
authors read and approved the final manuscript. Z.X.L. is the guarantor of
this study.
Corresponding authors
APPENDIX TO JAMES CASCIANO DECLARATION-182

Correspondence to Chuanzhu Lv or Fujian Song or Xiaoxv Yin or Zuxun Lu.
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Peer review information Nature Communications thanks Junxiong Vincent
Pang and the other, anonymous reviewer(s) for their contribution to the
peer review of this work. Peer review reports are available.
Publisher's note Springer Nature remains neutral with regard to
jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution
4.0 International License, which permits use, sharing, adaptation,
distribution and reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to
the Creative Commons license, and indicate if changes were made. The
images or other third party material in this article are included in the
article's Creative Commons license, unless indicated otherwise in a credit
line to the material. If material is not included in the article's Creative
Commons license and your intended use is not permitted by statutory
regulation or exceeds the permitted use, you will need to obtain permission
directly from the copyright holder. To view a copy of this license, visit
htt g: //_ creat iveco mm on s. o rg/_l ice n ses/_by /_ 4. 0 /..
APPENDIX TO JAMES CASCIANO DECLARATION-183

Regrints and Permissions
About this article
Cite this article
Check for updates
Cao, S., Gan, Y., Wang, C. et al. Post-lockdown SARS-CoV-2 nucleic acid
screening in nearly ten million residents of Wuhan, China. Nat Commun 11,
5917 (2020). https://doi.org/10.1038/s41467-020-19802-w
Download citation
Received18 August 2020
Accepted27 October 2020
Published20 November 2020
DOlhttgs:f.ldoi.org/.10.1038/s41467-020-19802-w
Share this article
Anyone you share the following link with will be able to read this content:
Provided by the Springer Nature Sharedlt content-sharing initiative
Further reading
Comments
By submitting a comment you agree to abide by our Terms and Community:
Guidelines. If you find something abusive or that does not comply with our
APPENDIX TO JAMES CASCIANO DECLARATION-184

Guidance on Preparing Workplaces for COVID-19
OSHA 3990-03 2020
APPENDIX TO JAMES CASCIANO DECLARATION-186

O)~ www.osha.gov
Occupational Safety and Health Act of 1970 11To assure safe and healthful working conditions for working men and women; by authorizing enforcement of the standards developed under the Act; by assisting and encouraging the States in their efforts to assure safe and healthful working conditions; by providing for research1 information, education, and training in the field of occupational safety and health."
This guidance is not a standard or regulation, and it creates no new legal obligations. It contains recommendations as well as descriptions of mandatory safety and health standards. The recommendations are advisory in nature, informational in content, and are intended to assist employers in providing a safe and healthful workplace. The Occupational Safety and Health Act requires employers to comply with safety and health standards and regulations promulgated by OSHA or by a state with an OSHA-approved state plan. In addition, the Act's General Duty Clause, Section 5(a)(1 ), requires employers to provide their employees with a workplace free from recognized hazards likely to cause death or serious physical harm.
Material contained in this publication is in the public domain and may be reproduced, fully or partially, without permission. Source credit is requested but not required.
This information will be made available to sensoryimpaired individuals upon request. Voice phone: (202) 693-1999; teletypewriter (TTY) number: 1-877-889-5627.
APPENDIX TO JAMES CASCIANO DECLARATION-187

Guidance on Preparing Workplaces for COVID-19
U.S. Department of Labor Occupational Safety and Health Administration
OSHA 3990-03 2020
U.S. Department of Labor
APPENDIX TO JAMES CASCIANO DECLARATION-188

Contents
Introduction .......................................... 3
About COVID-19 ....................................... 4
How a COVID-19 Outbreak Could Affect Workplaces ........ 6
Steps All Employers Can Take to Reduce Workers' Risk of Exposure to SARS-CoV-2 ................. 7
Classifying Worker Exposure to SARS-CoV-2 .............. 18
Jobs Classified at Lower Exposure Risk (Caution): What to Do to Protect Workers .......................... 20
Jobs Classified at Medium Exposure Risk: What to Do to Protect Workers .......................... 21
Jobs Classified at High or Very High Exposure Risk: What to Do to Protect Workers .......................... 23
Workers Living Abroad or Travelling Internationally ........ 25
For More Information .................................. 26
OSHA Assistance, Services, and Programs ............... 27
OSHA Regional Offices ................................ 29
How to Contact OSHA ................................. 32
APPENDIX TO JAMES CASCIANO DECLARATION-189

Introduction Coronavirus Disease 2019 (COVID-19) is a respiratory disease caused by the SARS-CoV-2 virus. It has spread from China to many other countries around the world, including the United States. Depending on the severity of COVID-19's international impacts, outbreak conditions-including those rising to the level of a pandemic-can affect all aspects of daily life, including travel, trade, tourism, food supplies, and financial markets.
To reduce the impact of COVID-19 outbreak conditions on businesses, workers, customers, and the public, it is important for all employers to plan now for COVID-19. For employers who have already planned for influenza pandemics, planning for COVID-19 may involve updating plans to address the specific exposure risks, sources of exposure, routes of transmission, and other unique characteristics of SARS-CoV-2 (i.e., compared to pandemic influenza viruses). Employers who have not prepared for pandemic events should prepare themselves and their workers as far in advance as possible of potentially worsening outbreak conditions. Lack of continuity planning can result in a cascade of failures as employers attempt to address challenges of COVID-19 with insufficient resources and workers who might not be adequately trained for jobs they may have to perform under pandemic conditions.
The Occupational Safety and Health Administration (OSHA) developed this COVID-19 planning guidance based on traditional infection prevention and industrial hygiene practices. It focuses on the need for employers to implement engineering, administrative, and work practice controls and personal protective equipment (PPE), as well as considerations for doing so.
This guidance is intended for planning purposes. Employers and workers should use this planning guidance to help identify risk levels in workplace settings and to determine any appropriate control measures to implement. Additional guidance may be needed as COVID-19 outbreak conditions change, including as new information about the virus, its transmission, and impacts, becomes available.
GUIDANCE ON PREPARING WORKPLACES FOR COVID-19
3
APPENDIX TO JAMES CASCIANO DECLARATION-190

The U.S. Department of Health and Human Services' Centers for Disease Control and Prevention (CDC) provides the latest information about COVID-19 and the global outbreak: www.cdc.gov/coronavi rus/2019-ncov.
The OSHA COVID-19 webpage offers information specifically for workers and employers: www.osha.gov/covid-19.
This guidance is advisory in nature and informational in content. It is not a standard or a regulation, and it neither creates new legal obligations nor alters existing obligations created by OSHA standards or the Occupational Safety and Health Act (OSH Act). Pursuant to the OSH Act, employers must comply with safety and health standards and regulations issued and enforced either by OSHA or by an OSHA-approved State Plan. In addition, the OSH Act's General Duty Clause, Section 5(a)(1 ), requires employers to provide their employees with a workplace free from recognized hazards likely to cause death or serious physical harm. OSHA-approved State Plans may have standards, regulations and enforcement policies that are different from, but at least as effective as, OSHA's. Check with your State Plan, as applicable, for more information.
About COVID-19
Symptoms of COVID-19
Infection with SARS-CoV-2, the virus that causes COVID-19, can cause illness ranging from mild to severe and, in some cases, can be fatal. Symptoms typically include fever, cough, and shortness of breath. Some people infected with the virus have reported experiencing other non-respiratory symptoms. Other people, referred to as asymptomatic cases, have experienced no symptoms at all.
According to the CDC, symptoms of COVID-19 may appear in as few as 2 days or as long as 14 days after exposure.
OCCUPATIONAL SAFETY AND HEALTH ADMINISTRATION
4
APPENDIX TO JAMES CASCIANO DECLARATION-191

How COVID-19 Spreads
Although the first human cases of COVID-19 likely resulted from exposure to infected animals, infected people can spread SARS-CoV-2 to other people.
The virus is thought to spread mainly from personto-person, including:
■ Between people who are in close contact with one another (within about 6 feet).
■ Through respiratory
Medium exposure risk jobs include those that require frequent and/or close contact with (i.e., within 6 feet of) other people who may be infected with SARS-CoV-2.
droplets produced when an infected person coughs or sneezes. These droplets can land in the mouths or noses of people who are nearby or possibly be inhaled into the lungs.
It may be possible that a person can get COVID-19 by touching a surface or object that has SARS-CoV-2 on it and then touching their own mouth, nose, or possibly their eyes, but this is not thought to be the primary way the virus spreads.
People are thought to be most contagious when they are most symptomatic (i.e., experiencing fever, cough, and/or shortness of breath). Some spread might be possible before people show symptoms; there have been reports of this type of asymptomatic transmission with this new coronavirus, but this is also not thought to be the main way the virus spreads.
Although the United States has implemented public health measures to limit the spread of the virus, it is likely that some person-to-person transmission will continue to occur.
The CDC website provides the latest information about COVID-19 transmission: www.cdc.gov/coronavirus/2019-ncov/ about/transmission.html.
GUIDANCE ON PREPARING WORKPLACES FOR COVI0-19
5
APPENDIX TO JAMES CASCIANO DECLARATION-192

How a COVID-19 Outbreak Could Affect Workplaces Similar to influenza viruses, SARS-CoV-2, the virus that causes COVID-19, has the potential to cause extensive outbreaks. Under conditions associated with widespread person-toperson spread, multiple areas of the United States and other countries may see impacts at the same time. In the absence of a vaccine, an outbreak may also be an extended event. As a result, workplaces may experience:
■ Absenteeism. Workers could be absent because they are sick; are caregivers for sick family members; are caregivers for children if schools or day care centers are closed; have at-risk people at home, such as immunocompromised family members; or are afraid to come to work because of fear of possible exposure.
■ Change in patterns of commerce. Consumer demand for items related to infection prevention (e.g., respirators) is likely to increase significantly, while consumer interest in other goods may decline. Consumers may also change shopping patterns because of a COVID-19 outbreak. Consumers may try to shop at off-peak hours to reduce contact with other people, show increased interest in home delivery services, or prefer other options, such as drivethrough service, to reduce person-to-person contact.
■ Interrupted supply/delivery. Shipments of items from geographic areas severely affected by COVID-19 may be delayed or cancelled with or without notification.
This illustration, created at the Centers for Disease Control and Prevention {CDC), reveals ultrastructural morphology exhibited by the 2019 Novel Coronavirus (2019-nCoV). Note the spikes that adorn the outer surface of the virus, which impart the look of a corona surrounding the virion, when viewed electron microscopically. This virus was identified as the cause of an outbreak of respiratory illness first detected in Wuhan, China.
Photo: CDC I Alissa Eckert & Dan Higgins
OCCUPATIONAL SAFETY AND HEAL TH ADMINISTRATION
6
APPENDIX TO JAMES CASCIANO DECLARATION-193

Steps All Employers Can Take to Reduce Workers' Risk of Exposure to SARS-CoV-2 This section describes basic steps that every employer can take to reduce the risk of worker exposure to SARS-CoV-2, the virus that causes COVID-19, in their workplace. Later sections of this guidance-including those focusing on jobs classified as having low, medium, high, and very high exposure risksprovide specific recommendations for employers and workers within specific risk categories.
Develop an Infectious Disease Preparedness and Response Plan
If one does not already exist, develop an infectious disease preparedness and response plan that can help guide protective actions against COVID-19.
Stay abreast of guidance from federal, state, local, tribal, and/or territorial health agencies, and consider how to incorporate those recommendations and resources into workplace-specific plans.
Plans should consider and address the level(s) of risk associated with various worksites and job tasks workers perform at those sites. Such considerations may include:
■ Where, how, and to what sources of SARS-CoV-2 might workers be exposed, including:
o The general public, customers, and coworkers; and
o Sick individuals or those at particularly high risk of infection (e.g., international travelers who have visited locations with widespread sustained (ongoing) COVID-19 transmission, healthcare workers who have had unprotected exposures to people known to have, or suspected of having, COVID-19).
■ Non-occupational risk factors at home and in community settings.
GUIDANCE ON PREPARING WORKPLACES FOR COVID-19
7
APPENDIX TO JAMES CASCIANO DECLARATION-194

■ Workers' individual risk factors (e.g., older age; presence of chronic medical conditions, including immunocompromising conditions; pregnancy).
■ Controls necessary to address those risks.
Follow federal and state, local, tribal, and/or territorial (SLTT) recommendations regarding development of contingency plans for situations that may arise as a result of outbreaks, such as:
■ Increased rates of worker absenteeism.
■ The need for social distancing, staggered work shifts, downsizing operations, delivering services remotely, and other exposure-reducing measures.
■ Options for conducting essential operations with a reduced workforce, including cross-training workers across different jobs in order to continue operations or deliver surge services.
■ Interrupted supply chains or delayed deliveries.
Plans should also consider and address the other steps that employers can take to reduce the risk of worker exposure to SARS-CoV-2 in their workplace, described in the sections below.
Prepare to Implement Basic Infection Prevention Measures
For most employers, protecting workers will depend on emphasizing basic infection prevention measures. As appropriate, all employers should implement good hygiene and infection control practices, including:
■ Promote frequent and thorough hand washing, including by providing workers, customers, and worksite visitors with a place to wash their hands. If soap and running water are not immediately available, provide alcohol-based hand rubs containing at least 60% alcohol.
■ Encourage workers to stay home if they are sick.
■ Encourage respiratory etiquette, including covering coughs and sneezes.
OCCUPATIONAL SAFETY AND HEAL TH ADMINISTRATION
8
APPENDIX TO JAMES CASCIANO DECLARATION-195

■ Provide customers and the public with tissues and trash receptacles.
■ Employers should explore whether they can establish policies and practices, such as flexible worksites (e.g., telecommuting) and flexible work hours (e.g., staggered shifts), to increase the physical distance among employees and between employees and others if state and local health authorities recommend the use of social distancing strategies.
■ Discourage workers from using other workers' phones, desks, offices, or other work tools and equipment, when possible.
■ Maintain regular housekeeping practices, including routine cleaning and disinfecting of surfaces, equipment, and other elements of the work environment. When choosing cleaning chemicals, employers should consult information on Environmental Protection Agency (EPA)-approved disinfectant labels with claims against emerging viral pathogens. Products with EPA-approved emerging viral pathogens claims are expected to be effective against SARS-CoV-2 based on data for harder to kill viruses. Follow the manufacturer's instructions for use of all cleaning and disinfection products (e.g., concentration, application method and contact time, PPE).
Develop Policies and Procedures for Prompt Identification and Isolation of Sick People, if Appropriate
■ Prompt identification and isolation of potentially infectious individuals is a critical step in protecting workers, customers, visitors, and others at a worksite.
■ Employers should inform and encourage employees to self-monitor for signs and symptoms of COVID-19 if they suspect possible exposure.
■ Employers should develop policies and procedures for employees to report when they are sick or experiencing symptoms of COVID-19.
GUIDANCE ON PREPARING WORKPLACES FOR COVID-19
9
APPENDIX TO JAMES CASCIANO DECLARATION-196

■ Where appropriate, employers should develop policies and procedures for immediately isolating people who have signs and/or symptoms of COVID-19, and train workers to implement them. Move potentially infectious people to a location away from workers, customers, and other visitors. Although most worksites do not have specific isolation rooms, designated areas with closable doors may serve as isolation rooms until potentially sick people can be removed from the worksite.
■ Take steps to limit spread of the respiratory secretions of a person who may have COVID-19. Provide a face mask, if feasible and available, and ask the person to wear it, if tolerated. Note: A face mask (also called a surgical mask, procedure mask, or other similar terms) on a patient or other sick person should not be confused with PPE for a worker; the mask acts to contain potentially infectious respiratory secretions at the source (i.e., the person's nose and mouth).
■ If possible, isolate people suspected of having COVID-19 separately from those with confirmed cases of the virus to prevent further transmission-particularly in worksites where medical screening, triage, or healthcare activities occur, using either permanent (e.g., wall/different room) or temporary barrier (e.g., plastic sheeting).
■ Restrict the number of personnel entering isolation areas.
■ Protect workers in close contact with (i.e., within 6 feet of) a sick person or who have prolonged/repeated contact with such persons by using additional engineering and administrative controls, safe work practices, and PPE. Workers whose activities involve close or prolonged/ repeated contact with sick people are addressed further in later sections covering workplaces classified at medium and very high or high exposure risk.
OCCUPATIONAL SAFETY AND HEALTH ADMINISTRATION
1 0
APPENDIX TO JAMES CASCIANO DECLARATION-197

Develop, Implement, and Communicate about Workplace Flexibilities and Protections
■ Actively encourage sick employees to stay home.
■ Ensure that sick leave policies are flexible and consistent with public health guidance and that employees are aware of these policies.
■ Talk with companies that provide your business with contract or temporary employees about the importance of sick employees staying home and encourage them to develop non-punitive leave policies.
■ Do not require a healthcare provider's note for employees who are sick with acute respiratory illness to validate their illness or to return to work, as healthcare provider offices and medical facilities may be extremely busy and not able to provide such documentation in a timely way.
■ Maintain flexible policies that permit employees to stay home to care for a sick family member. Employers should be aware that more employees may need to stay at home to care for sick children or other sick family members than is usual.
■ Recognize that workers with ill family members may need to stay home to care for them. See CDC's Interim Guidance for Preventing the Spread of COVID-19 in Homes and Residential Communities: www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-prevent-spread.html.
■ Be aware of workers' concerns about pay, leave, safety, health, and other issues that may arise during infectious disease outbreaks. Provide adequate, usable, and appropriate training, education, and informational material about business-essential job functions and worker health and safety, including proper hygiene practices and the use of any workplace controls (including PPE). Informed workers who feel safe at work are less likely to be unnecessarily absent.
GUIDANCE ON PREPARING WORKPLACES FOR COVID-19
1 1
APPENDIX TO JAMES CASCIANO DECLARATION-198

■ Work with insurance companies (e.g., those providing employee health benefits) and state and local health agencies to provide information to workers and customers about medical care in the event of a COVID-19 outbreak.
Implement Workplace Controls
Occupational safety and health professionals use a framework called the "hierarchy of controls" to select ways of controlling workplace hazards. In other words, the best way to control a hazard is to systematically remove it from the workplace, rather than relying on workers to reduce their exposure. During a COVID-19 outbreak, when it may not be possible to eliminate the hazard, the most effective protection measures are (listed from most effective to least effective): engineering controls, administrative controls, safe work practices (a type of administrative control), and PPE. There are advantages and disadvantages to each type of control measure when considering the ease of implementation, effectiveness, and cost. In most cases, a combination of control measures will be necessary to protect workers from exposure to SARS-CoV-2.
In addition to the types of workplace controls discussed below, CDC guidance for businesses provides employers and workers with recommended SARS-CoV-2 infection prevention strategies to implement in workplaces: www.cdc.gov/coronavirus/2019-ncov/specific-groups/guidance-business-response.html.
Engineering Controls
Engineering controls involve isolating employees from workrelated hazards. In workplaces where they are appropriate, these types of controls reduce exposure to hazards without relying on worker behavior and can be the most cost-effective solution to implement. Engineering controls for SARS-CoV-2 include:
■ Installing high-efficiency air filters.
■ Increasing ventilation rates in the work environment.
■ Installing physical barriers, such as clear plastic sneeze guards.
OCCUPATIONAL SAFETY AND HEAL TH ADMINISTRATION
1 2
APPENDIX TO JAMES CASCIANO DECLARATION-199

■ Installing a drive-through window for customer service.
■ Specialized negative pressure ventilation in some settings, such as for aerosol generating procedures (e.g., airborne infection isolation rooms in healthcare settings and specialized autopsy suites in mortuary settings).
Administrative Controls
Administrative controls require action by the worker or employer. Typically, administrative controls are changes in work policy or procedures to reduce or minimize exposure to a hazard. Examples of administrative controls for SARS-CoV-2 include:
■ Encouraging sick workers to stay at home.
■ Minimizing contact among workers, clients, and customers by replacing face-to-face meetings with virtual communications and implementing telework if feasible.
■ Establishing alternating days or extra shifts that reduce the total number of employees in a facility at a given time, allowing them to maintain distance from one another while maintaining a full onsite work week.
■ Discontinuing nonessential travel to locations with ongoing COVID-19 outbreaks. Regularly check CDC travel warning levels at: www.cdc.gov/coronavirus/2019-ncov/travelers.
■ Developing emergency communications plans, including a forum for answering workers' concerns and internet-based communications, if feasible.
■ Providing workers with up-to-date education and training on COVID-19 risk factors and protective behaviors (e.g., cough etiquette and care of PPE).
■ Training workers who need to use protecting clothing and equipment how to put it on, use/wear it, and take it off correctly, including in the context of their current and potential duties. Training material should be easy to understand and available in the appropriate language and literacy level for all workers.
GUIDANCE ON PREPARING WORKPLACES FOR COVID-19
1 3
APPENDIX TO JAMES CASCIANO DECLARATION-200

Safe Work Practices
Safe work practices are types of administrative controls that include procedures for safe and proper work used to reduce the duration, frequency, or intensity of exposure to a hazard. Examples of safe work practices for SARS-CoV-2 include:
■ Providing resources and a work environment that promotes personal hygiene. For example, provide tissues, no-touch trash cans, hand soap, alcohol-based hand rubs containing at least 60 percent alcohol, disinfectants, and disposable towels for workers to clean their work surfaces.
■ Requiring regular hand washing or using of alcohol-based hand rubs. Workers should always wash hands when they are visibly soiled and after removing any PPE.
■ Post handwashing signs in restrooms.
Personal Protective Equipment (PPE)
While engineering and administrative controls are considered more effective in minimizing exposure to SARS-CoV-2, PPE may also be needed to prevent certain exposures. While correctly using PPE can help prevent some exposures, it should not take the place of other prevention strategies.
Examples of PPE include: gloves, goggles, face shields, face masks, and respiratory protection, when appropriate. During an outbreak of an infectious disease, such as COVID-19, recommendations for PPE specific to occupations or job tasks may change depending on geographic location, updated risk assessments for workers, and information on PPE effectiveness in preventing the spread of COVID-19. Employers should check the OSHA and CDC websites regularly for updates about recommended PPE.
All types of PPE must be:
■ Selected based upon the hazard to the worker.
■ Properly fitted and periodically refitted, as applicable (e.g., respirators).
OCCUPATIONAL SAFETY AND HEAL TH ADMINISTRATION
1 4
APPENDIX TO JAMES CASCIANO DECLARATION-201

■ Consistently and properly worn when required.
■ Regularly inspected, maintained, and replaced, as necessary.
■ Properly removed, cleaned, and stored or disposed of, as applicable, to avoid contamination of self, others, or the environment.
Employers are obligated to provide their workers with PPE needed to keep them safe while performing their jobs. The types of PPE required during a COVID-19 outbreak will be based on the risk of being infected with SARS-CoV-2 while working and job tasks that may lead to exposure.
Workers, including those who work within 6 feet of patients known to be, or suspected of being, infected with SARS-CoV-2 and those performing aerosol-generating procedures, need to use respirators:
■ National Institute for Occupational Safety and Health (NIOSH)-approved, N95 filtering facepiece respirators or better must be used in the context of a comprehensive, written respiratory protection program that includes fit-testing, training, and medical exams. See OSHA's Respiratory Protection standard, 29 CFR 1910.134 at www.osha.gov/laws-regs/regulations/ standardnumber/1910/1910.134.
■ When disposable N95 filtering facepiece respirators are not available, consider using other respirators that provide greater protection and improve worker comfort. Other types of acceptable respirators include: a R/P95, N/R/P99, or N/R/P100 filtering facepiece respirator; an air-purifying elastomeric (e.g., half-face or full-face) respirator with appropriate filters or cartridges; powered air purifying respirator (PAPR) with high-efficiency particulate arrestance (HEPA) filter; or supplied air respirator (SAR). See CDC/ NIOSH guidance for optimizing respirator supplies at: www.cdc.gov/coronavirus/2019-ncov/hcp/respirators-strategy.
GUIDANCE ON PREPARING WORKPLACES FOR COVID-19
1 5
APPENDIX TO JAMES CASCIANO DECLARATION-202

■ Consider using PAPRs or SARs, which are more protective than filtering facepiece respirators, for any work operations or procedures likely to generate aerosols (e.g., cough induction procedures, some dental procedures, invasive specimen collection, blowing out pipettes, shaking or vortexing tubes, filling a syringe, centrifugation).
■ Use a surgical N95 respirator when both respiratory protection and resistance to blood and body fluids is needed.
■ Face shields may also be worn on top of a respirator to prevent bulk contamination of the respirator. Certain respirator designs with forward protrusions (duckbill style) may be difficult to properly wear under a face shield. Ensure that the face shield does not prevent airflow through the respirator.
■ Consider factors such as function, fit, ability to decontaminate, disposal, and cost. OSHA's Respiratory Protection eTool provides basic information on respirators such as medical requirements, maintenance and care, fit testing, written respiratory protection programs, and voluntary use of respirators, which employers may also find beneficial in training workers at: www.osha.gov/SLTC/ etools/respiratory. Also see NIOSH respirator guidance at: www.cdc.gov/niosh/topics/respirators.
■ Respirator training should address selection, use (including donning and doffing), proper disposal or disinfection, inspection for damage, maintenance, and the limitations of respiratory protection equipment. Learn more at: www. osha.gov/SLTC/respiratoryprotection.
■ The appropriate form of respirator will depend on the type of exposure and on the transmission pattern of COVID-19. See the NIOSH "Respirator Selection Logic" at: www.cdc.gov/niosh/docs/2005-100/default.html or the OSHA "Respiratory Protection eTool" at www.osha.gov/ SLTC/etools/respiratory.
OCCUPATIONAL SAFETY AND HEAL TH ADMINISTRATION
1 6
APPENDIX TO JAMES CASCIANO DECLARATION-203

Follow Existing OSHA Standards
Existing OSHA standards may apply to protecting workers from exposure to and infection with SARS-CoV-2.
While there is no specific OSHA standard covering SARSCoV-2 exposure, some OSHA requirements may apply to preventing occupational exposure to SARS-CoV-2. Among the most relevant are:
■ OSHA's Personal Protective Equipment (PPE) standards (in general industry, 29 CFR 1910 Subpart I), which require using gloves, eye and face protection, and respiratory protection. See: www.osha.gov/laws-regs/regulations/ standardnumber/1910#191 0_Su bpart_l.
o When respirators are necessary to protect workers or where employers require respirator use, employers must implement a comprehensive respiratory protection program in accordance with the Respiratory Protection standard (29 CFR 1910.134). See: www.osha.gov/lawsregs/regu lations/standardnum ber/1910/1910.134.
■ The General Duty Clause, Section 5(a)(1) of the Occupational Safety and Health (OSH) Act of 1970, 29 USC 654(a)(1 ), which requires employers to furnish to each worker "employment and a place of employment, which are free from recognized hazards that are causing or are likely to cause death or serious physical harm." See: www.osha.gov/laws-regs/oshact/completeoshact.
OSHA's Bloodborne Pathogens standard (29 CFR 1910.1030) applies to occupational exposure to human blood and other potentially infectious materials that typically do not include respiratory secretions that may transmit SARS-CoV-2. However, the provisions of the standard offer a framework that may help control some sources of the virus, including exposures to body fluids (e.g., respiratory secretions) not covered by the standard. See: www.osha.gov/laws-regs/ regulations/standardnumber/1910/1910.1030.
GUIDANCE ON PREPARING WORKPLACES FOR COVID-19
1 7
APPENDIX TO JAMES CASCIANO DECLARATION-204

The OSHA COVID-19 webpage provides additional information about OSHA standards and requirements, including requirements in states that operate their own OSHA-approved State Plans, recordkeeping requirements and injury/illness recording criteria, and applications of standards related to sanitation and communication of risks related to hazardous chemicals that may be in common sanitizers and sterilizers. See: www.osha.gov/SLTC/covid-19/standards.html.
Classifying Worker Exposure to SARS-CoV-2 Worker risk of occupational exposure to SARS-CoV-2, the virus that causes COVID-19, during an outbreak may vary from very high to high, medium, or lower (caution) risk. The level of risk depends in part on the industry type, need for contact within 6 feet of people known to be, or suspected of being, infected with SARS-CoV-2, or requirement for repeated or extended contact with persons known to be, or suspected of being, infected with SARS-CoV-2. To help employers determine appropriate precautions, OSHA has divided job tasks into four risk exposure levels: very high, high, medium, and lower risk. The Occupational Risk Pyramid shows the four exposure risk levels in the shape of a pyramid to represent probable distribution of risk. Most American workers will likely fall in the lower exposure risk (caution) or medium exposure risk levels.
Occupational Risk Pyramid for COVID-19
OCCUPATIONAL SAFETY AND HEALTH ADMINISTRATION
1 8
APPENDIX TO JAMES CASCIANO DECLARATION-205

Very High Exposure Risk
Very high exposure risk jobs are those with high potential for exposure to known or suspected sources of COVID-19 during specific medical, postmortem, or laboratory procedures. Workers in this category include:
■ Healthcare workers (e.g., doctors, nurses, dentists, paramedics, emergency medical technicians) performing aerosol-generating procedures (e.g., intubation, cough induction procedures, bronchoscopies, some dental procedures and exams, or invasive specimen collection) on known or suspected COVID-19 patients.
■ Healthcare or laboratory personnel collecting or handling specimens from known or suspected COVID-19 patients (e.g., manipulating cultures from known or suspected COVID-19 patients).
■ Morgue workers performing autopsies, which generally involve aerosol-generating procedures, on the bodies of people who are known to have, or suspected of having, COVID-19 at the time of their death.
High Exposure Risk
High exposure risk jobs are those with high potential for exposure to known or suspected sources of COVID-19. Workers in this category include:
■ Healthcare delivery and support staff (e.g., doctors, nurses, and other hospital staff who must enter patients' rooms) exposed to known or suspected COVID-19 patients. (Note: when such workers perform aerosol-generating procedures, their exposure risk level becomes very high.)
■ Medical transport workers (e.g., ambulance vehicle operators) moving known or suspected COVID-19 patients in enclosed vehicles.
■ Mortuary workers involved in preparing (e.g., for burial or cremation) the bodies of people who are known to have, or suspected of having, COVID-19 at the time of their death.
GUIDANCE ON PREPARING WORKPLACES FOR COVID-19 , 9
APPENDIX TO JAMES CASCIANO DECLARATION-206

Medium Exposure Risk
Medium exposure risk jobs include those that require frequent and/or close contact with (i.e., within 6 feet of) people who may be infected with SARS-CoV-2, but who are not known or suspected COVID-19 patients. In areas without ongoing community transmission, workers in this risk group may have frequent contact with travelers who may return from international locations with widespread COVID-19 transmission. In areas where there is ongoing community transmission, workers in this category may have contact with the general public (e.g., schools, high-population-density work environments, some high-volume retail settings).
Lower Exposure Risk (Caution)
Lower exposure risk (caution) jobs are those that do not require contact with people known to be, or suspected of being, infected with SARS-CoV-2 nor frequent close contact with (i.e., within 6 feet of) the general public. Workers in this category have minimal occupational contact with the public and other coworkers.
Jobs Classified at Lower Exposure Risk (Caution): What to Do to Protect Workers For workers who do not have frequent contact with the general public, employers should follow the guidance for "Steps All Employers Can Take to Reduce Workers' Risk of Exposure to SARS-CoV-2," on page 7 of this booklet and implement control measures described in this section.
Engineering Controls
Additional engineering controls are not recommended for workers in the lower exposure risk group. Employers should ensure that engineering controls, if any, used to protect workers from other job hazards continue to function as intended.
OCCUPATIONAL SAFETY AND HEALTH ADMINISTRATION
2 0
APPENDIX TO JAMES CASCIANO DECLARATION-207

Administrative Controls
■ Monitor public health communications about COVID-19 recommendations and ensure that workers have access to that information. Frequently check the CDC COVID-19 website: www.cdc.gov/coronavirus/2019-ncov.
■ Collaborate with workers to designate effective means of communicating important COVID-19 information.
Personal Protective Equipment
Additional PPE is not recommended for workers in the lower exposure risk group. Workers should continue to use the PPE, if any, that they would ordinarily use for other job tasks.
Jobs Classified at Medium Exposure Risk: What to Do to Protect Workers In workplaces where workers have medium exposure risk, employers should follow the guidance for "Steps All Employers Can Take to Reduce Workers' Risk of Exposure to SARS-CoV-2," on page 7 of this booklet and implement control measures described in this section.
Engineering Controls
■ Install physical barriers, such as clear plastic sneeze guards, where feasible.
Administrative Controls
■ Consider offering face masks to ill employees and customers to contain respiratory secretions until they are able leave the workplace (i.e., for medical evaluation/care or to return home). In the event of a shortage of masks, a reusable face shield that can be decontaminated may be an acceptable method of protecting against droplet transmission. See CDC/ NIOSH guidance for optimizing respirator supplies, which discusses the use of surgical masks, at: www.cdc.gov/ coronavirus/2019-ncov/hcp/respirators-strategy.
GUIDANCE ON PREPARING WORKPLACES FOR COVID-19
2 1
APPENDIX TO JAMES CASCIANO DECLARATION-208

■ Keep customers informed about symptoms of COVID-19 and ask sick customers to minimize contact with workers until healthy again, such as by posting signs about COVID-19 in stores where sick customers may visit (e.g., pharmacies) or including COVID-19 information in automated messages sent when prescriptions are ready for pick up.
■ Where appropriate, limit customers' and the public's access to the worksite, or restrict access to only certain workplace areas.
■ Consider strategies to minimize face-to-face contact (e.g., drivethrough windows, phone-based communication, telework).
■ Communicate the availability of medical screening or other worker health resources (e.g., on-site nurse; telemedicine services).
Personal Protective Equipment (PPE)
When selecting PPE, consider factors such as function, fit, decontamination ability, disposal, and cost. Sometimes, when PPE will have to be used repeatedly for a long period of time, a more expensive and durable type of PPE may be less expensive overall than disposable PPE. Each employer should select the combination of PPE that protects workers specific to their workplace.
Workers with medium exposure risk may need to wear some combination of gloves, a gown, a face mask, and/or a face shield or goggles. PPE ensembles for workers in the medium exposure risk category will vary by work task, the results of the employer's hazard assessment, and the types of exposures workers have on the job.
High exposure risk jobs are those with high potential for exposure to known or suspected sources of COVID-19.
Very high exposure risk jobs are those with high potential for exposure to known or suspected sources of COVID-19 during specific medical, postmortem, or laboratory procedures that involve aerosol generation or specimen collection/ handling.
OCCUPATIONAL SAFETY AND HEALTH ADMINISTRATION
2 2
APPENDIX TO JAMES CASCIANO DECLARATION-209

In rare situations that would require workers in this risk category to use respirators, see the PPE section beginning on page 14 of this booklet, which provides more details about respirators. For the most up-to-date information, visit OSHA's COVID-19 webpage: www.osha.gov/covid-19.
Jobs Classified at High or Very High Exposure Risk: What to Do to Protect Workers In workplaces where workers have high or very high exposure risk, employers should follow the guidance for "Steps All Employers Can Take to Reduce Workers' Risk of Exposure to SARS-CoV-2," on page 7 of this booklet and implement control measures described in this section.
Engineering Controls
■ Ensure appropriate air-handling systems are installed and maintained in healthcare facilities. See "Guidelines for Environmental Infection Control in Healthcare Facilities" for more recommendations on air handling systems at: www. cdc.gov/mmwr/preview/mmwrhtml/rr5210a1 .htm.
■ CDC recommends that patients with known or suspected COVID-19 (i.e., person under investigation) should be placed in an airborne infection isolation room (AIIR), if available.
■ Use isolation rooms when available for performing aerosol-generating procedures on patients with known or suspected COVID-19. For postmortem activities, use autopsy suites or other similar isolation facilities when performing aerosol-generating procedures on the bodies of people who are known to have, or suspected of having, COVID-19 at the time of their death. See the CDC postmortem guidance at: www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-postmortem-specimens.html. OSHA also provides guidance for postmortem activities on its COVID-19 webpage: www.osha.gov/covid-19.
GUIDANCE ON PREPARING WORKPLACES FOR COVID-19
2 3
APPENDIX TO JAMES CASCIANO DECLARATION-210

■ Use special precautions associated with Biosafety Level 3 when handling specimens from known or suspected COVID-19 patients. For more information about biosafety levels, consult the U.S. Department of Health and Human Services (HHS) "Biosafety in Microbiological and Biomedical Laboratories" at www.cdc.gov/biosafety/ publications/bmbl5.
Administrative Controls
If working in a healthcare facility, follow existing guidelines and facility standards of practice for identifying and isolating infected individuals and for protecting workers.
■ Develop and implement policies that reduce exposure, such as cohorting (i.e., grouping) COVID-19 patients when single rooms are not available.
■ Post signs requesting patients and family members to immediately report symptoms of respiratory illness on arrival at the healthcare facility and use disposable face masks.
■ Consider offering enhanced medical monitoring of workers during COVID-19 outbreaks.
■ Provide all workers with job-specific education and training on preventing transmission of COVID-19, including initial and routine/refresher training.
■ Ensure that psychological and behavioral support is available to address employee stress.
Safe Work Practices
■ Provide emergency responders and other essential personnel who may be exposed while working away from fixed facilities with alcohol-based hand rubs containing at least 60% alcohol for decontamination in the field.
OCCUPATIONAL SAFETY AND HEALTH ADMINISTRATION
2 4
APPENDIX TO JAMES CASCIANO DECLARATION-211
Personal Protective Equipment (PPE)
Most workers at high or very high exposure risk likely need to wear gloves, a gown, a face shield or goggles, and either a face mask or a respirator, depending on their job tasks and exposure risks.
Those who work closely with (either in contact with or within 6 feet of) patients known to be, or suspected of being, infected with SARS-CoV-2, the virus that causes COVID-19, should wear respirators. In these instances, see the PPE section beginning on page 14 of this booklet, which provides more details about respirators. For the most up-to-date information, also visit OSHA's COVID-19 webpage: www.osha.gov/covid-19.
PPE ensembles may vary, especially for workers in laboratories or morgue/mortuary facilities who may need additional protection against blood, body fluids, chemicals, and other materials to which they may be exposed. Additional PPE may include medical/surgical gowns, fluid-resistant coveralls, aprons, or other disposable or reusable protective clothing. Gowns should be large enough to cover the areas requiring protection. OSHA may also provide updated guidance for PPE use on its website: www.osha.gov/covid-19.
NOTE: Workers who dispose of PPE and other infectious waste must also be trained and provided with appropriate PPE.
The CDC webpage "Healthcare-associated Infections" (www.cdc.gov/hai) provides additional information on infection control in healthcare facilities.
Workers Living Abroad or Travelling Internationally Employers with workers living abroad or traveling on international business should consult the "Business Travelers" section of the OSHA COVID-19 webpage (www.osha.gov/covid-19), which also provides links to the latest:
GUIDANCE ON PREPARING WORKPLACES FOR COVID-19
2 5
APPENDIX TO JAMES CASCIANO DECLARATION-212

■ CDC travel warnings: www.cdc.gov/ coronavirus/2019-ncov/travelers
■ U.S. Department of State (DOS) travel advisories: travel.state.gov
Employers should communicate to workers that the DOS cannot provide Americans traveling or living abroad with medications or supplies, even in the event of a COVID-19 outbreak.
As COVID-19 outbreak conditions change, travel into or out of a country may not be possible, safe, or medically advisable. It is also likely that governments will respond to a COVID-19 outbreak by imposing public health measures that restrict domestic and international movement, further limiting the U.S. government's ability to assist Americans in these countries. It is important that employers and workers plan appropriately, as it is possible that these measures will be implemented very quickly in the event of worsening outbreak conditions in certain areas.
More information on COVID-19 planning for workers living and traveling abroad can be found at: www.cdc.gov/travel.
For More Information Federal, state, and local government agencies are the best source of information in the event of an infectious disease outbreak, such as COVID-19. Staying informed about the latest developments and recommendations is critical, since specific guidance may change based upon evolving outbreak situations.
Below are several recommended websites to access the most current and accurate information:
■ Occupational Safety and Health Administration website: www.osha.gov
■ Centers for Disease Control and Prevention website: www.cdc.gov
■ National Institute for Occupational Safety and Health website: www.cdc.gov/niosh
OCCUPATIONAL SAFETY AND HEALTH ADMINISTRATION
2 6
APPENDIX TO JAMES CASCIANO DECLARATION-213

OSHA Assistance, Services, and Programs OSHA has a great deal of information to assist employers in complying with their responsibilities under OSHA law. Several OSHA programs and services can help employers identify and correct job hazards, as well as improve their safety and health program.
Establishing a Safety and Health Program
Safety and health programs are systems that can substantially reduce the number and severity of workplace injuries and illnesses, while reducing costs to employers.
Visit www.osha.gov/safetymanagement for more information.
Compliance Assistance Specialists
OSHA compliance assistance specialists can provide information to employers and workers about OSHA standards, short educational programs on specific hazards or OSHA rights and responsibilities, and information on additional compliance assistance resources.
Visit www.osha.gov/complianceassistance/cas or call 1-800-321-OSHA (6742) to contact your local OSHA office.
No-Cost On-Site Safety and Health Consultation Services for Small Business
OSHA's On-Site Consultation Program offers no-cost and confidential advice to small and medium-sized businesses in all states, with priority given to high-hazard worksites. On-Site consultation services are separate from enforcement and do not result in penalties or citations.
For more information or to find the local On-Site Consultation office in your state, visit www.osha.gov/consultation, or call 1-800-321-OSHA (6742).
GUIDANCE ON PREPARING WORKPLACES FOR COVID-19
2 7
APPENDIX TO JAMES CASCIANO DECLARATION-214

Under the consultation program, certain exemplary employers may request participation in OSHA's Safety and Health Achievement Recognition Program (SHARP). Worksites that receive SHARP recognition are exempt from programmed inspections during the period that the SHARP certification is valid.
Cooperative Programs
OSHA offers cooperative programs under which businesses, labor groups and other organizations can work cooperatively with OSHA. To find out more about any of the following programs, visit www.osha.gov/cooperativeprograms.
Strategic Partnerships and Alliances
The OSHA Strategic Partnerships (OSP) provide the opportunity for OSHA to partner with employers, workers, professional or trade associations, labor organizations, and/or other interested stakeholders. Through the Alliance Program, OSHA works with groups to develop compliance assistance tools and resources to share with workers and employers, and educate workers and employers about their rights and responsibilities.
Voluntary Protection Programs {VPP}
The VPP recognize employers and workers in the private sector and federal agencies who have implemented effective safety and health programs and maintain injury and illness rates below the national average for their respective industries.
Occupational Safety and Health Training
OSHA partners with 26 OSHA Training Institute Education Centers at 37 locations throughout the United States to deliver courses on OSHA standards and occupational safety and health topics to thousands of students a year. For more information on training courses, visit www.osha.gov/otiec.
OCCUPATIONAL SAFETY AND HEAL TH ADMINISTRATION
2 8
APPENDIX TO JAMES CASCIANO DECLARATION-215

OSHA Educational Materials
OSHA has many types of educational materials to assist employers and workers in finding and preventing workplace hazards.
All OSHA publications are free at www.osha.gov/publications and www.osha.gov/ebooks. You can also call 1-800-321-OSHA (6742) to order publications.
Employers and safety and health professionals can sign-up for QuickTakes, OSHA's free, twice-monthly online newsletter with the latest news about OSHA initiatives and products to assist in finding and preventing workplace hazards. To sign up, visit www.osha.gov/quicktakes.
OSHA Regional Offices Region 1 Boston Regional Office (CT*, ME*, MA, NH, RI, VT*) JFK Federal Building 25 New Sudbury Street, Room E340 Boston, MA 02203 (617) 565-9860 (617) 565-9827 Fax
Region 2 New York Regional Office (NJ*, NY*, PR*, VI*) Federal Building 201 Varick Street, Room 670 New York, NY 10014 (212) 337-2378 (212) 337-2371 Fax
Region 3 Philadelphia Regional Office (DE, DC, MD*, PA, VA*, WV) The Curtis Center 170 S. Independence Mall West, Suite 740 West Philadelphia, PA 19106-3309 (215) 861-4900 (215) 861-4904 Fax
GUIDANCE ON PREPARING WORKPLACES FOR COVID-19
2 9
APPENDIX TO JAMES CASCIANO DECLARATION-216

Region 4 Atlanta Regional Office (AL, FL, GA, KY*, MS, NC*, SC*, TN*) Sam Nunn Atlanta Federal Center 61 Forsyth Street, SW, Room 6T50 Atlanta, GA 30303 (678) 237-0400 (678) 237-0447 Fax
Region 5 Chicago Regional Office {IL*, IN*, Ml*, MN*, OH, WI) John C. Kluczynski Federal Building 230 South Dearborn Street, Room 3244 Chicago, IL 60604 (312) 353-2220 (312) 353-7774 Fax
Region 6 Dallas Regional Office (AR, LA, NM*, OK, TX) A. Maceo Smith Federal Building 525 Griffin Street, Room 602 Dallas, TX 75202 (972) 850-4145 (972) 850-4149 Fax
Region 7 Kansas City Regional Office {IA*, KS, MO, NE) Two Pershing Square Building 2300 Main Street, Suite 1010 Kansas City, MO 64108-2416 (816) 283-8745 (816) 283-0547 Fax
Region 8 Denver Regional Office (CO, MT, ND, SD, UT*, WY*) Cesar Chavez Memorial Building 1244 Speer Boulevard, Suite 551 Denver, CO 80204 (720) 264-6550 (720) 264-6585 Fax
OCCUPATIONAL SAFETY AND HEAL TH ADMINISTRATION
3 0
APPENDIX TO JAMES CASCIANO DECLARATION-217

Region 9 San Francisco Regional Office (AZ*, CA*, HI*, NV*, and American Samoa, Guam and the Northern Mariana Islands) San Francisco Federal Building 90 7th Street, Suite 2650 San Francisco, CA 94103 (415) 625-2547 (415) 625-2534 Fax
Region 10 Seattle Regional Office (AK*, ID, OR*, WA*) Fifth & Yesler Tower 300 Fifth Avenue, Suite 1280 Seattle, WA 98104 (206) 757-6700 (206) 757-6705 Fax
*These states and territories operate their own OSHA-approved job safety and health plans and cover state and local government employees as well as private sector employees. The Connecticut, Illinois, Maine, New Jersey, New York and Virgin Islands programs cover public employees only. (Private sector workers in these states are covered by Federal OSHA). States with approved programs must have standards that are identical to, or at least as effective as, the Federal OSHA standards.
Note: To get contact information for OSHA area offices, OSHA-approved state plans and OSHA consultation projects, please visit us online at www.osha.gov or call us at 1-800-321-OSHA (6742).
GUIDANCE ON PREPARING WORKPLACES FOR COVID-19
3 1
APPENDIX TO JAMES CASCIANO DECLARATION-218

How to Contact OSHA Under the Occupational Safety and Health Act of 1970,
employers are responsible for providing safe and healthful workplaces for their employees. OSHA's role is to help ensure these conditions for America's working men and women by
setting and enforcing standards, and providing training, education and assistance. For more information, visit www.osha.gov or call
OSHA at 1-800-321-OSHA (6742), TTY 1-877-889-5627.
For assistance, contact us. We are OSHA. We can help.
O)SfIX www.osha.gov
OCCUPATIONAL SAFETY AND HEAL TH ADMINISTRATION
32
APPENDIX TO JAMES CASCIANO DECLARATION-219
APPENDIX TO JAMES CASCIANO DE CLARA TION-220

Rational use of face masks in the COVID-19 pandemic Since the outbreak of severe acute respiratory syndrome coronavirus 2
(SARS-CoV-2), the virus that caused coronavirus disease 2019 (COVID-19),
the use of face masks has become ubiquitous in China and other Asian
countries such as South Korea and Japan. Some provinces and
municipalities in China have enforced compulsory face mask policies in
public areas; however, China's national guideline has adopted a risk-based
approach in offering recommendations for using face masks among health
care workers and the general public. We compared face mask use
recommendations by different health authorities (panel ). Despite the
consistency in the recommendation that symptomatic individuals and those
in health-care settings should use face masks, discrepancies were
observed in the general public and community settings. 1, 2, 3, 4 , 5, 6, 7, 8 For
example, the US Surgeon General advised against buying masks for use by
healthy people. One important reason to discourage widespread use of face
masks is to preserve limited supplies for professional use in health-care
settings. Universal face mask use in the community has also been
discouraged with the argument that face masks provide no effective
protection against coronavirus infection.
Panel
Recommendations on face mask use in community settings
WH0 1
• If you are healthy, you only need to wear a mask if you are taking care of a
person with suspected SARS-CoV-2 infection.
China 2
APPENDIX TO JAMES CASCIANO DECLARATION-221

• People at moderate risk* of infection: surgical or disposable mask for
medical use.
• People at low riskt of infection: disposable mask for medical use.
• People at very low risk* of infection: do not have to wear a mask or can
wear non-medical mask (such as cloth mask).
Hong Kong 3
• Surgical masks can prevent transmission of respiratory viruses from
people who are ill. It is essential for people who are symptomatic (even if
they have mild symptoms) to wear a surgical mask.
• Wear a surgical mask when taking public transport or staying in crowded
places. It is important to wear a mask properly and practice good hand
hygiene before wearing and after removing a mask.
Singapore 4
• Wear a mask if you have respiratory symptoms, such as a cough or runny
nose.
Japan 5
• The effectiveness of wearing a face mask to protect yourself from
contracting viruses is thought to be limited. If you wear a face mask in
confined, badly ventilated spaces, it might help avoid catching droplets
emitted from others but if you are in an open-air environment, the use of
face mask is not very efficient.
USA 6
• Centers for Disease Control and Prevention does not recommend that
people who are well wear a face mask (including respirators) to protect
themselves from respiratory diseases, including COVID-19.
• US Surgeon General urged people on Twitter to stop buying face masks.
APPENDIX TO JAMES CASCIANO DECLARATION-222

UK7
• Face masks play a very important role in places such as hospitals, but
there is very little evidence of widespread benefit for members of the
public.
Germany8
• There is not enough evidence to prove that wearing a surgical mask
significantly reduces a healthy person's risk of becoming infected while
wearing it. According to WHO, wearing a mask in situations where it is not
recommended to do so can create a false sense of security because it
might lead to neglecting fundamental hygiene measures, such as proper
hand hygiene.
However, there is an essential distinction between absence of evidence and
evidence of absence. Evidence that face masks can provide effective
protection against respiratory infections in the community is scarce, as
acknowledged in recommendations from the UK and Germany.7, 8 However,
face masks are widely used by medical workers as part of droplet
precautions when caring for patients with respiratory infections. It would be
reasonable to suggest vulnerable individuals avoid crowded areas and use
surgical face masks rationally when exposed to high-risk areas. As evidence
suggests COVID-19 could be transmitted before symptom onset,
community transmission might be reduced if everyone, including people
who have been infected but are asymptomatic and contagious, wear face
masks.
Recommendations on face masks vary across countries and we have seen
that the use of masks increases substantially once local epidemics begin,
including the use of N95 respirators (without any other protective
equipment) in community settings. This increase in use of face masks by
the general public exacerbates the global supply shortage of face masks,
with prices soaring,9 and risks supply constraints to frontline health-care
APPENDIX TO JAMES CASCIANO DECLARATION-223

professionals. As a response, a few countries (eg, Germany and South
Korea) banned exportation of face masks to prioritise local demand. 10 WHO
called for a 40% increase in the production of protective equipment,
including face masks.9 Meanwhile, health authorities should optimise face
mask distribution to prioritise the needs of frontline health-care workers and
the most vulnerable populations in communities who are more susceptible
to infection and mortality if infected, including older adults (particularly
those older than 65 years) and people with underlying health conditions.
People in some regions (eg, Thailand, China, and Japan) opted for
makeshift alternatives or repeated usage of disposable surgical masks.
Notably, improper use of face masks, such as not changing disposable
masks, could jeopardise the protective effect and even increase the risk of
infection.
Consideration should also be given to variations in societal and cultural
paradigms of mask usage. The contrast between face mask use as hygienic
practice (ie, in many Asian countries) or as something only people who are
unwell do (ie, in European and North American countries) has induced
stigmatisation and racial aggravations, for which further public education is
needed. One advantage of universal use of face masks is that it prevents
discrimination of individuals who wear masks when unwell because
everybody is wearing a mask.
It is time for governments and public health agencies to make rational
recommendations on appropriate face mask use to complement their
recommendations on other preventive measures, such as hand hygiene.
WHO currently recommends that people should wear face masks if they
have respiratory symptoms or if they are caring for somebody with
symptoms. Perhaps it would also be rational to recommend that people in
quarantine wear face masks if they need to leave home for any reason, to
prevent potential asymptomatic or presymptomatic transmission. In
addition, vulnerable populations, such as older adults and those with
APPENDIX TO JAMES CASCIANO DECLARATION-224

underlying medical conditions, should wear face masks if available.
Universal use of face masks could be considered if supplies permit. In
parallel, urgent research on the duration of protection of face masks, the
measures to prolong life of disposable masks, and the invention on reusable
masks should be encouraged. Taiwan had the foresight to create a large
stockpile of face masks; other countries or regions might now consider this
as part of future pandemic plans.
Cogyright © 2020 Sputnik/Science Photo Library
Since January 2020 Elsevier has created a COVID-19 resource centre with
free information in English and Mandarin on the novel coronavirus COVID-
19. The COVID-19 resource centre is hosted on Elsevier Connect, the
company's public news and information website. Elsevier hereby grants
permission to make all its COVID-19-related research that is available on the
COVID-19 resource centre - including this research content - immediately
available in PubMed Central and other publicly funded repositories, such as
the WHO COVID database with rights for unrestricted research re-use and
analyses in any form or by any means with acknowledgement of the original
source. These permissions are granted for free by Elsevier for as long as the APPENDIX TO JAMES CASCIANO DE CLARA TION-225

COVID-19 resource centre remains active.
Editorial note: the Lancet Group takes a neutral position with respect to
territorial claims in published maps and institutional affiliations.
APPENDIX TO JAMES CASCIANO DECLARATION-226

Face masks are 1NOT necessary• and could even harm the fight against coronavirus, say Holland 1s top scientists Thomas Burrows 2 Aug 2020,
SCIENTISTS in the Netherlands have said face masks in public places
are "not necessary" and might even have a "negative impact".
The Dutch have not made it compulsory to wear face coverings in public -
despite a rise in coronavirus cases.
4
The Netherlands's top scientists still believe there is no medical evidence to support wearing face
masksCredit: AFP
APPENDIX TO JAMES CASCIANO DECLARATION-227

The nation's top scientists have concluded there is no firm evidence to
make people wear masks.
This is despite the fact the Netherlands has seen an alarming spike in
coronavirus cases since restrictions were eased.
Over the past week, almost 1,400 new coronavirus cases were reported, or
342 more than the week before.
However, the country's top scientists still believe there is no medical
evidence to support wearing face masks - even though 120 countries
across the globe have made them mandatory in public.
4
There has been a spike in coronavirus cases in Netherlands in the last week, as seen across EuropeCredit:
AFP
APPENDIX TO JAMES CASCIANO DE CLARA TION-228

4
Boris Johnson announced that from August 8, Brits will have to wear coverings in cinemas, museums and
galleries Credit: Crown Copyright
Dutch Medical Care Minister Tamara van Ark said: "From a medical point of
view, there is no evidence of a medical effect of wearing face masks, so we
decided not to impose a national obligation."
Coen Berends, spokesman for the National Institute for Public Health and
the Environment, added: "Face masks in public places are not necessary,
based on all the current evidence,
"There is no benefit and there may even be negative impact."
Holland's position is based on assessments by the Outbreak Management
Team, a group of experts advising the government.
It first ruled against masks in May and has re-evaluated the evidence
several times, including again last week.
APPENDIX TO JAMES CASCIANO DECLARATION-229

However Dutch residents must still wear face coverings on public transport.
'EVIDENCE IS CONTRADICTORY'
Christian Hoebe, a professor of infectious diseases in Maastricht and
member of the advisory team, said: 11Face masks should not be seen as a
magic bullet that halts the spread.
"The evidence for them is contradictory. In general, we think you must be
careful with face masks because they can give a false sense of security.
People think they're immune from disease or stop social distancing. That is
very negative."
It puts the Netherlands at odds with most other countries in the world.
Even US President Donald Trump has since done an about-turn and urged
Americans to wear face masks, saying it was "patriotic" to do so (after
previously mocking Joe Biden for wearing one).
In the England, face masks have been compulsory on public transport from
June 15 and in shops and supermarkets from July 24.
From August 8 they: will also be reguired in glaces y:ou come into "contact
with geogle Y.OU do not normallY. meet, such as museums,_galleries, cinemas
and glaces of worshi~.
GRIM TOLL
Covid deaths jump by 1,248 in 24 hours, passing 1 k for third day running
APPENDIX TO JAMES CASCIANO DECLARATION-230

MUTANT SPREAD
Fears Brazilian Covid strain could re-infect those who have fought off virus
TAX BREAK 1SCRAP 1
Rishi Sunak 'refuses to extend stamp duty holiday beyond end of March'
lll'l
MASK ROW
Banker fired after defending 'teen racially abused & kicked in face in bus attack'
SNOWED IN
Snow and ice warning issued for UK this weekend as wintery weather causes chaos
APPENDIX TO JAMES CASCIANO DECLARATION-231

CODE RED
Major incident in Yorkshire after heavy snow leaves ambulance service overwhelmed
The science around wearing a face covering has changed during the
pandemic.
At the outset, the World Health Organisation said healthy people did not
need to wear a mask, unless they were caring for someone who was sick.
Then in April, the WHO said masks could prove useful.
Shortly thereafter, the European Centre for Disease Prevention and Control
issued new recommendations, signalling increased support for masks.
Finally, in June, the WHO said they should be worn in public places where
social distancing is not possible to help stop the spread of coronavirus.
Boris Johnson tells Brits to wear face masks, with police given more powers to enforce as rules extended amid fears of coronavirus second wave
APPENDIX TO JAMES CASCIANO DECLARATION-232

4
US President Donald Trump has done an about-turn and urged Americans to wear face masks, saying it was
"patriotic"Credit: Reuters
APPENDIX TO JAMES CASCIANO DE CLARA TION-233
Predominant Role of Bacterial Pneumonia as a Cause of Death in Pandemic Influenza: Implications for Pandemic Influenza Preparedness Abstract
Background. Despite the availability of published data on 4 pandemics that
have occurred over the past 120 years, there is little modern information on
the causes of death associated with influenza pandemics.
Methods. We examined relevant information from the most recent influenza
pandemic that occurred during the era prior to the use of antibiotics, the
1918-1919 "Spanish flu"; pandemic. We examined lung tissue sections
obtained during 58 autopsies and reviewed pathologic and bacteriologic
data from 109 published autopsy series that described 8398 individual
autopsy investigations.
Results. The postmortem samples we examined from people who died of
influenza during 1918-1919 uniformly exhibited severe changes indicative of
bacterial pneumonia. Bacteriologic and histopathologic results from
published autopsy series clearly and consistently implicated secondary
bacterial pneumonia caused by common upper respiratory-tract bacteria in
most influenza fatalities.
Conclusions. The majority of deaths in the 1918-1919 influenza pandemic
likely resulted directly from secondary bacterial pneumonia caused by
common upper respiratory-tract bacteria. Less substantial data from the
subsequent 1957 and 1968 pandemics are consistent with these findings. If
severe pandemic influenza is largely a problem of viral-bacterial
copathogenesis, pandemic planning needs to go beyond addressing the
APPENDIX TO JAMES CASCIANO DECLARATION-234

,:'.r•,-., '. \· 11 C-i 1
l --. d
'' I
severe pandemic [2].
,,: l:, •.•
....... ,,,.......
--- ' • ~--' ·-✓ • ..... ,' •
r'', ,-. J i -----· ~ ·~ ,'
. 1 r . n 1,... "Ir" ! ' • , • i • l . i ' • ' 111 . d'I o- 8 i ::>, ano nave rev,evveo ep1ae1:--11c;:c>;;:c1 patno1og:ci ar:c
r-nicrobiologic data frorn published repor·ts for 3398 oost1·no1·i:2;Y1
exarninations bearing en this question. VVehave also revievved r-e,b .. d:TL
liJanden1ic influenza virus. investic2tors have !Jec1iun to eJ<2;T·ine vJh\1 it ,i,,,1;s
' 0 ~ .
conclude here that influenza A virus infection in c:onjunction \'/j-: c!c:C[er1a! ·111-:=,, P,. r', ·t ·1· 0 ,·1 1, (=·-ri. ~l-:""'i 1··1~10 C: t. u~-. .-1. ,l'. 1~1' 0 r! .----. ~, i- '1 ·1 ·~ 01 LIi" ·, 1-, ,-., t 1r-· r, 1 r,j,, n 1 ° .,, () 1--1 ri '1..,1 rip,..,. I(-'
- -- '-' ..._,.., \,.j '-' .,, \_, \_,. C 0. L :~ I I I i ':::1 . l t::; I :.:, I C; - .. _, :::_; t-' '-' ~ - ' . ,.. .
APPENDIX TO JAMES CASCIANO DECLARATION-235
Examination of tissue specimens from 1918-1919 influenza fatalities. We reviewed hematoxylin and eosin-stained slides recut from blocks of lung
tissue obtained during autopsy from 58 influenza fatalities in 1918-1919.
These materials, sent during the pandemic from various United States
military bases to the National Tissue Repository of the Armed Forces
Institute of Pathology [8-10], represent all known influenza cases from this
collection for which lung tissue is available.
Pathology and bacteriology research records from the 1918-1919 influenza pandemic. We reviewed the late 19th- and early 20th-century
literature on gross and microscopic influenza pathology and bacteriology,
including evidence from 1918-1919 autopsy series with postmortem
cultures of lung tissue, blood samples (usually heart blood), pleural fluid,
and samples from other compartments. In an effort to obtain all
publications possibly reporting influenza pathology and/or bacteriology in
1918-1919, we searched major bibliographic sources [e.g., 11-17] for papers
in all languages and tables of contents of major journals in English, German,
and French; in addition, we searched all of the papers we identified for
additional citations. From more than 2000 such publications, we carefully
examined the 1539 reports that contained human pathologic and/or
bacteriologic findings (the full bibliographic list available at
httg:LLwww3.niaid.nih.govLtogicsLFluL1918LbibliograghY..htm), 109 of which
provided useful bacteriologic information derived from 173 autopsy series.
These series reported 8398 individual autopsy investigations undertaken in
15 countries, which can be characterized as follows: 96 postmortem lung
tissue culture series, 42 blood culture series, and 35 pleural fluid culture
series. When they were published as parts of an autopsy series, we
included in our analyses antemortem cultures of blood and pleural fluid
samples, which were mostly obtained during the terminal stages of illness.
A priori, we stratified data by military and civilian populations (see
Discussion), and by the quality of lung tissue culture results, considering to
be of "higher quality"; the 68 autopsy series with lung tissue culture results
that reported, for all autopsies, both the presence and absence of negative APPENDIX TO JAMES CASCIANO DECLARATION-236

culture results and the bacterial components of mixed culture results.
Results
Background epidemiologic data on influenza mortality rates in 1918-1919. Although death certificates listing cardiac and other chronic causes
of death increased in number during the time frame of the 1918-1919
pandemic [18], for all age groups death was predominantly associated with
pneumonia and related pulmonary complications [13, 14, 18-20]. The
pandemic caused a "W-shaped"; age-specific mortality curve, which
exhibited peaks in infancy, between about 20-40 years of age, and in
elderly individuals [3, 21]. In all age groups younger than "'65 years, the
influenza mortality rate was elevated beyond what would have been
expected on the basis of data from the previous pandemic of "Russian
influenza"; (1889-1893) [3, 22, 23]. The increased fatality rate in the 3
high-risk age groups was predominantly due to the increased frequency of
bronchopneumonia, not to increased incidence of influenza or an increased
bronchopneumonia case-fatality rate [19]. Because few autopsy reports
and, to our knowledge, no autopsy series addressed conditions other than
predominantly pulmonary complications, nonpulmonary causes of death are
not considered here.
Histologic examination of lung tissue from 1918 victims. The
examination of recut lung tissue sections from 1918-1919 influenza case
material revealed, in virtually all cases, compelling histologic evidence of
severe acute bacterial pneumonia, either as the predominant pathology or
in conjunction with underlying pathologic features now believed to be
associated with influenza virus infection [10, 24] (figure 1). The latter
include necrosis and desquamation of the respiratory epithelium of the
tracheobronchial and bronchiolar tree, dilation of alveolar ducts, hyaline
membranes, and evidence of bronchial and/or bronchiolar epithelial repair
[25, 26]. The majority of the cases examined demonstrated asynchronous
histopathological changes, in which the various stages of development of
APPENDIX TO JAMES CASCIANO DECLARATION-237

the infectious process, from early bronchiolar changes to severe bacterial
parenchymal destruction, were noted in focal areas. The histologic
spectrum observed in the cases corresponded to the characteristic
pathology of bacterial pneumonia, including bronchopneumonia [10,24-33]:
lobar consolidation with pulmonary infiltration by neutrophils in
pneumococcal pneumonia; a bronchopneumonic pattern, edema, and
pleural effusions in streptococcal and sometimes in pneumococcal
pneumonia; and in staphylococcal pneumonia, multiple small abscesses
with a marked neutrophilic infiltration in airways and alveoli [27]. Bacteria
were commonly observed in the sections, often in massive numbers.
Figure 1
Examples of hematoxylin and eosin-stained postmortem lung sections from
4 victims of the 1918-1919 influenza pandemic (see text). A, Typical picture
of severe, widespread bacterial bronchopneumonia with transmural
infiltration of neutrophils in a bronchiole and with neutrophils filling the
airspaces of surrounding alveoli (original magnification, 40x). B, Massive
APPENDIX TO JAMES CASCIANO DE CLARA TION-238

infiltration of neutrophils in the airspaces of alveoli associated with bacterial
bronchopneumonia as in A (original magnification, 200x). C,
Bronchopneumonia with intra-alveolar edema and hemorrhage. Numerous
bacteria are visible both in the edema fluid and in the cytoplasm of
macrophages (original magnification, 400x). D, Bronchopneumonia with
evidence of pulmonary repair. The alveolar epithelium is hyperplastic;
interstitial fibrosis is seen between alveoli (original magnification, 200x).
Published pathologic and/or bacteriologic findings from the 1918-1919 influenza pandemic. Although the cause of influenza was disputed in
1918, there was almost universal agreement among experts [e.g., 20, 27-33] that deaths were virtually never caused by the unidentified etiologic
agent itself, but resulted directly from severe secondary pneumonia caused
by well-known bacterial "pneumopathogens"; that colonized the upper
respiratory tract (predominantly pneumococci, streptococci, and
staphylococci). Without this secondary bacterial pneumonia, experts
generally believed that most patients would have recovered [20]. In type,
pattern, and case-fatality rate, influenza-associated bacterial pneumonia
was typical of pneumonia that was endemic during periods when influenza
was not prevalent [25, 28, 33, 34]. As described above, in cases for which a
single lung pathogen was recovered from culture, the anatomical
pathological type of the pneumonia usually corresponded to what was
expected. Bacteria were commonly observed in cases of pneumonia caused
by each of these pathogens. Such findings reflect the characteristic
pathology of bacterial pneumonia [10, 25, 27].
Surprising aspects of 1918-1919 influenza-associated pneumonia fatalities
included the following: (1) the high incidence of secondary pneumonia
associated with standard bacterial pneumopathogens; (2) the frequency of
pneumonia caused by both mixed pneumopathogens (particularly
pneumococci and streptococci) and by other mixed upper respiratory-tract
bacteria; (3) the aggressiveness of bacterial invasion of the lung, often
resulting in "phenomenal"; [30] numbers of bacteria and poly-
APPENDIX TO JAMES CASCIANO DECLARATION-239

morphonuclear neutrophils, as well as extensive necrosis, vasculitis, and
hemorrhage [20, 32, 33]; and (4) the predominance of bronchopneumonia
and lobular pneumonia, as opposed to lobar pneumonia, consistent with
diffuse predisposing bronchiolar damage [27-33].
Contemporary views of the natural history of severe influenza during
the 1918-1919 influenza pandemic. By examining influenza autopsy
materials from a range of patients in different stages of disease,
pathologists in 1918-1919 identified the primary lesion in early severe
influenza-associated pneumonia as desquamative tracheobronchitis and
bronchiolitis extending diffusely over all or much of the pulmonary tree to
the alveolar ducts and alveoli, associated with sloughing of bronchiolar
epithelial cells to the basal layer, hyaline membrane formation in alveolar
ducts and alveoli, and ductal dilation [20, 24, 27, 29-33].
Primary "panbronchitis"; [35] was thought to reflect rapidly spreading
epithelial cytolytic infection of the entire bronchial tree [32, 35, 36]; this
was thought to have led to the secondary spread of enormous numbers of
bacteria along the denuded bronchial epithelium to every part of the
bronchial tree, following which focal bronchiolar infections broke through
into the lung parenchyma. Secondary bacterial invasion and zones of
vasculitis, capillary thrombosis, and necrosis surrounding areas of
bronchiolar damage were seen in severe cases. As was true for the 58
autopsy cases we reviewed (see above), published autopsies for victims of
the 1918-1919 pandemic generally showed histopathological asynchrony
[20]. Repair, represented by early epithelial regeneration, capillary repair,
and occasionally by fibrosis, was commonly seen in tissues sections from
even the most fulminant fatal cases [20, 27, 32]. Among the i=!=60% of
individuals who survived such severe pneumonia, severe chronic pulmonary
damage was apparently uncommon [37, 38].
Bacteriologic studies in autopsy series during the 1918-1919 influenza pandemic. Negative lung culture results were uncommon in the 96
APPENDIX TO JAMES CASCIANO DECLARATION-240

identified military and civilian autopsy series, which examined 5266
subjects (4.2% of results overall) (table 1; full bibliographic list available at
hll~/./.www3.niaid.njh.gm,/.toP-ics/..Elu/1918/.bibliograP-b.y,htm). In the 68
higher-quality autopsy series, in which the possibility of unreported
negative cultures could be excluded, 92.7% of autopsy lung cultures were
positive for ~1 bacterium (table 1). Of these 96 series, 82 reported
pneumopathogens in ~50% of lungs examined, either alone or in mixed
culture results that included other bacteria (table 1). Outbreaks of
meningococcal pneumonia complicating influenza also were documented
[39]. Despite higher military case-fatality rates, the differences in the
frequency with which specific bacteria were isolated from lung tissue
cultures (table 1) and from culture of blood and pleural or empyema fluids
(data not shown) were minimal. Many of the series were methodologically
rigorous: in one study of approximately 9000 subjects who were followed
from clinical presentation with influenza to resolution or autopsy [40],
researchers obtained, with sterile technique, cultures of either
pneumococci or streptococci from 164 of 167 lung tissue samples. There
were 89 pure cultures of pneumococci; 19 cultures from which only
streptococci were recovered; 34 that yielded mixtures of pneumococci
and/or streptococci; 22 that yielded a mixture of pneumococci,
streptococci, and other organisms (prominently pneumococci and
nonhemolytic streptococci); and 3 that yielded nonhemolytic streptococci
alone. There were no negative lung culture results.
Table 1
APPENDIX TO JAMES CASCIANO DECLARATION-241

,~ •'"41 cl at':urcs trom ~ 0f'9VJsm ~ JCClCh'CfOCJ. bv o,~"Hm
l.)c)o."'t1CC'..S
1~of No c:I ~ s~ ~ r.tr~ ~ ~ ~ ,_,
~sere, ,~, ~ ~t'leln ""1:'I.O ~ ~lt-c)gom ,,~ ... tuct(rd 1,i"Q•MI·
AO~t,, .. 60D 3.515 155CIU) 8151175) l&3(75J a,c, .11 101aon 38701 GI 481(138) 164CUJ A!I ovil,r, ,,. - ~ 1751 380 (11 71 21:11 I 11~ 0, 1GSl'9,ll 1 i••O II mm.7J 131i7 St 3l!)lt94, !,6 1371
AD l'ldlso,y Ol'.:I G¥61nln"'9(1) 6288 mllD.ll 8961170) 417(81) 41 «l.81 110SQ1.0I 619C9SI mnu~ 220'421
All ~- qu,a:,ty m,!,!..-y~
evo.en• ,,. - El:P 307~ 712123 21 s,sJ11ao, lJ:81711 ]1 -0 71 IZICKt, 1.c.4.4 71 lSJ 1!l ~., ]'}; 17 31
Pledoil1w•co ol pnau11iap;s!t11t9:1\!J
noc cordffllCd Ill • 14J 1115 2Wf187J 132111.13) 6164 7) OCOCJ 14021 :none.el CGICll,I) 88(7 7)
NOfl. ~ becter~ 8" L,ied ~ thcu (r)ml'l',c)l'I fWlme!I.., 1018 S~.,:, ~ w;,s CV!tJod ~ (,om,:,1~ ~t'tll!d W!'lh .,-1,x,ra '"'O t~ I
11. rlJ, 111. anl IV.~ IV wa11 oerc,,a:>a· tCIQUd0d M CClt\ta.n,,,g • nurrta of • ~ ~ • S.r~IOCO«ld ~u,Yh::v.i prClOltt\' co,•cr..oanck to St•~«~~, ~"' ~ ~ tno<it otnNwr1 ~'f'9.61N!d St~t ~ ,,om Sr~-w, ~ b.11 111 ~ c,~ otnr,,VOl'I .-.vfld o,-1y • S~ coco.,.· ~ ~ OS1C9J'll0d M ·~""5 • f4 tho ~t ~ o PlfhoQenc Ol'Q,1111'Sm ~"OOCl,S ,nr,.:-~GY" ,ne,ru1g1r,a,., OOf't!"'~ to·"-'-'-'"''"' ~~ ~ "'~#ccrtctspOnds to ~•\A~- Scio~• for~,. .&b>J. tM ·"uod ~~- rel ·at~ l:>.K~Cff.-·
C41e',1:IP~ Mv,,f 'Ofhcf. 0rVJ1":n>3 ¥«iro ~od>J "'11VP(!d ~ or'td W~ 8'Jlo lyptt 1'11S101fM g'c.,l,nt po,oarl-lge
' A hgt'crf qu&Uy terOI ~ dlrllflOd a!! II Ulf'tCI rtl W'\Cfl V'9 l,t:,1,1.a) CU!-J'lt •MU::t:. lc,portl:ld, fo, .0 D,rtopw,s, 1)():1"> t~• P,Moef"Ot ~ ~ of ~•v,,
et.lt'>'O ~ rd tho boct<W"..i ~h <:I m<a<'d c:tJlll'to r~i
Examples of hematoxylin and eosin-stained postmortem lung sections from
4 victims of the 1918-1919 influenza pandemic (see text). A, Typical picture
of severe, widespread bacterial bronchopneumonia with transmural
infiltration of neutrophils in a bronchiole and with neutrophils filling the
airspaces of surrounding alveoli (original magnification, 40x). B, Massive
infiltration of neutrophils in the airspaces of alveoli associated with bacterial
bronchopneumonia as in A (original magnification, 200x). C,
Bronchopneumonia with intra-alveolar edema and hemorrhage. Numerous
bacteria are visible both in the edema fluid and in the cytoplasm of
macrophages (original magnification, 400x). D, Bronchopneumonia with
evidence of pulmonary repair. The alveolar epithelium is hyperplastic;
interstitial fibrosis is seen between alveoli (original magnification, 200x).
In the 14 of 96 autopsy series that did not report the predominance of lung
pneumopathogens [29, 36, 41-53], pneumopathogens accounted
collectively for 37.4% of pneumonia deaths. The rest of the deaths were
associated collectively with either culture of nonpneumopathogenic "other
bacteria,"; such as nonhemolytic and viridans streptococci, "green
producing streptococci"; [54], probably largely corresponding to ahemolytic streptococci, uncharacterized diplostreptococci, Micrococcus
(Moraxella) catarrhs/is, Bacillus (Escherichia) coli, Klebsiella species, and
complex mixed bacteria (36.1% of cultures). Cultures also yielded Bacillus
influenzae (18.8%) and no bacterial growth (7.7%). These findings reflect
APPENDIX TO JAMES CASCIANO DECLARATION-242

rates of bacterial isolation similar to those of the series that reported the
predominance of pneumopathogens (above and table 1), but with higher
isolation rates for "other bacteria"; offsetting the lower isolation rates for
pneumococci, streptococci and staphylococci. It is noteworthy that
pneumococcal typing antisera were unavailable in 11 of these 14 studies,
and that many of the cultured "other"; bacteria were reported as "gram
positive diplococci,"; "streptococci,"; or "diplostreptococci"; (data not
shown), consistent with the possibility that in this early era of bacterial
typing, some of the unidentified organisms in the culture may have been
pneumopathogens.
The predominant coinfecting microorganism in lung tissue cultures
containing ::::1 pneumopathogen was Bacillus inf/uenzae (largely
corresponding to the modern Hemophi/us inf/uenzae), an upper respiratory
tract organism not commonly found in pure culture of samples from any
anatomical compartment [20, 36, 55]. Bacillus influenzae tended to appear
early in symptomatic influenza in association with diffuse bronchitis and/or
bronchiolitis, sometimes infiltrating the bronchiolar submucosa [35]; it
caused seroconversion [56] and was then typically replaced by other
secondary organisms.
Cultures of blood samples in 30 military and 12 civilian series, which
examined a total of 1887 subjects (table 2), had positive results in 70.3% of
cases and typically contained either pneumococci or streptococci in pure
culture. Cultures of pleural or empyema fluid, reported in 23 military and 12
civilian series examining a total of 1245 subjects (table 2), revealed either
streptococci or pneumococci as the most commonly recovered organism in
all but 7 series: in 4 series mixed pneumopathogens predominated, and in 3
series Staphylococcus aureus predominated. Most subjects with positive
culture results in the blood and pleural or empyema fluid series also had ::::1
pneumopathogen cultured in samples from the lungs (data not shown).
Table 2
APPENDIX TO JAMES CASCIANO DECLARATION-243

Blood~
Pkuat~o, ~Ouid ~(,ta 251 41mi'1ary4'1d
Nod ~ ~ ~
1887 !i09Q101
Ho f'J.l d QJ:110 trom W'ld, ~ Wi2S l'00IM70CI by ~'
~ s.~ ~ t'!::-~ Mtt'd S.':l!\A ~ OU't'l4 ~ ~ogr:rn r.'\A,WV ..
311,100, 681361 !,~lt nfll !.• 61 IJ'],
C:trtWl 124~ 163 rJ1 11 511 Ca.J) !.9 t.S 71 CH:> Ol
~ No ~., gn,.,,tt-.
1i'8l14 71 511129.7)
NOTE. fhc, ~ .. ,ro ~~cd by ti-cu o-.nm,or, ~'" ,~,e St•~-cv, ~ -· CU'l•.n>d .vd ,_,..,,..,n1-1 t,'IX'd v.i!h ~- IUl(J ~ I ti ~. 111. 11'112 IV. t)'PO I\' w.is ~,ay ~ ol!I ~~ • nun-w o1 · un~ ~ · Srrc,pflX'Oc'c:\.lj ~'-&'3 probltty corro--...i,ond:110 S:-~,1.11 ~"" mc:it caflCS. mtn1 ~I~ 5~ ~t,o,n S~ ~ b.d <fl~ C4~ ~Y(III raod 0My "Sr~ COCC\4 • ~ wo coteQOtllOd 4S ·...,~ • il !ho~<'•~ ~cd o Plthooc'n< 01Jll'I-~ D~ ~~• menng,r,a., cor.-e~ to -~!IC"'" """""~n6$ ~ ""~"" ODfr~ to ~~ ,r:!~JJC Soo AcMs to, drrt~s ~ tt-o 0
1"Fl,U1d ~~- rd "other t.Kt~.a· ~11:QO!'lftJ Mtt-'f -~. OI~'\ -(I ~fldlr IP!tvii,,d pr,cvn,)1JD0C> .,,_, )I':'~ 8d,j fvt1P ctwf.,QJf~ Q'C41MI po,o-r!...,..
Bacterial culture results in autopsy series involving 96 postmortem cultures
of lung tissue from victims of the 1918-1919 influenza pandemic.
Of 2007 pneumococcal isolates, 874 (43.5%) were serotyped by
agglutination. Type I was isolated from 124 (14.2%) of 874 subjects; type II
from 163 (18.6%); type Ila from 26 (3.0%); type Ill from 184 (21.1%); and
type IV, a category containing diverse and, at the time, untypeable
organisms, from 377 (43.1%).
Pathologic and bacteriologic information obtained from later pandemic and seasonal influenza cases. The viruses that caused the
1957 and 1968 pandemics were descendants of the 1918 virus in which 3
(the 1957 virus) or 2 (the 1968 virus) new avian gene segments had been
acquired by reassortment [21]. Although lower pathogenicity resulted in far
fewer deaths, hence fewer autopsies, most 1957-1958 deaths were
attributable to secondary bacterial pneumonia, as had been the case in
1918. Staphylococcus aureus, a relatively minor cause of the 1918 fatalities,
was predominant in the culture results from 1957-1958 [21, 57-61], and
negative lung tissue cultures were more common, possibly as a result of the
widespread administration of antibiotics [57, 58, 61]. The few relevant data
from the 1968-1969 pandemic (see below) are consistent with information
from the earlier 20th-century pandemics. Human tracheobronchial biopsy
studies performed since the 1957-1958 epidemic characterized the natural
history of influenza virus infection as featuring rapid (within 24 h)
development of bronchial epithelial necrosis, preservation of the basal layer, APPENDIX TO JAMES CASCIANO DECLARATION-244

limited inflammatory response, and evidence of prompt repair [62],
consistent with the observations of pathologists in 1918-1919.
Discussion
In the most recent influenza pandemic that did not involve the use of
antibiotics to suppress bacteria (the 1918-1919 pandemic), histological and
bacteriologic evidence suggests that the vast majority of influenza deaths
resulted from secondary bacterial pneumonia. Compelling evidence for this
conclusion includes the examination of 58 recut and restained autopsy
specimens that showed changes fully consistent with classical descriptions
of extensive bacterial pneumonia [25], culture results from numerous
international autopsy series, and consistent epidemiologic and clinical
findings (table 3).
Table3
MMt &iaoosie5 revealed 5eY8fO bact9fl41 pneumotli8 caused by common upoer •eflPtfatorv o,gan~m,. (20. 27-331
fn l\'PO, p,aftell\ and~ nato. ~ ~ ~ indudlng d'1oft:c lobar pnoumonra. was 1YPice' of Pft8UJTIOllia during periods when inftuonza wan not provatcnt bronchopnoumona essociaied wflh cMfuso -~diam.• p,odcm,,a:od 126. 28. 33. 34)
At iwtcp.sy. ca1ly anci,to, ~tem,vo ,ep.,11 of what aro now thought to be PoffliS1Y v.1B1 changos wcH e-.-cent. ~rQ
~ in pneumonia sun,n,o,s were maumal 120. 30. 32)
Pa2hoP.ogic 1rictUJo of bactoriDf ~ 4S30Ciatod With influonm in 1918-1919 Win~ &imiSar to 1tlo moro tuoM, C4tal mrns'st baaeri3t bf~~ of 1917-1918 l20. 27. 83)
Maced p,,ovmopaihogcn-auocaoted pnoumorua WH moro laial than ~thogcn pr,oumonia (191 Pno1,moma cmo, OJNbl'ted unit~ diffuso and axirm trecheobrond1i%i:9 andfor brondtio!itis. !he MMm!Y of
wflich ~ wiih pneumonia~ &n ctor,too end at'ltofflia1 Cocation 1291 Oemograph:c 4ndt'ot ep;dem~ evidenco
Most inftwnm CQSCS WCSO typal of Cl81I01J GOOtl todlJv: mid.~-and 8IIOCiutod wffll fufJ rocovory 113-171 M011al;fy at an OGM WM associoted wf1fl bxtetiol ~'° rates. not w,th 1nl'!uonza ou.ack rotes 0t P"N!'Umonltl
c,aw-fatohty raioo 119. 211 Ollrdtcft 6-16 Y83I& otct in 1918-1919 IIBd die hig!lest ot1t:d mt.es b1a ma 1owoat fflOltDlnv 1Btes. unmr m raw ma
vocn in 1889-1893 and imfflcdiatct, boforo and Gftor tho 1918-1919 ~ ~ ~ wiih wal wu1ance atone 114. 21,
tnfluonro-olSOQil!Od pnournoru,a inc:rdonco ratos and influenza death rutos Ytero S1Qndll:4tlt)v higher in US mdrta,v camp,, whd\ ~ bec'lef..,, ·coionll.at,on ~a· (631
A-. liino from lnflwnm onso1 co PftOUll'IOllm OMOt in &dtimltofy fotnl cnos c-10 dayiJ) may bo moso consistcn1 with bacteria1 than wal pneumoni3 1291
Troatrncft1 rosoons,o OYldenco The ftB31 tOW81S81 ab9cNation thal Stncl bed rest emt, in die caun!IO of liillCOIJdmted lftfluenm prevented
pneumonb Gftd cto=h is COMistlfflt .il'I an offoct of CICbtion from Cilfflef9 of bbctcrmJ pdioges1t 113. 141
Summary of evidence from the 1918-1919 influenza pandemic consistent
with the conclusion that bacterial pneumonia, rather than primary viral
pneumonia, was the cause of most deaths.
APPENDIX TO JAMES CASCIANO DECLARATION-245

Between 1890 and 1950, most observers believed fatal influenza to be a
polymicrobial infection in which an inciting agent of low pathogenicity
(either a bacterium such as Bacillus influenzae or a "filter passing agent";
most of which have now been identified as viruses) acted synergistically
with known pneumopathogenic bacteria [13, 14, 20, 33, 64-66]. This view
was dramatically supported in 1917-1918 by the measles epidemics in US
Army training camps, in which most deaths resulted from streptococcal
pneumonia or, less commonly, pneumococcal pneumonia [20, 30, 32]. The
pneumonia deaths during the influenza pandemic in 1918 proved so highly
similar, pathologically, to the then-recent pneumonia deaths from the
measles epidemics that noted experts considered them to be the result of
one newly emerging disease: epidemic bacterial pneumonia precipitated by
prevalent respiratory tract agents [20, 33, 63].
The question of whether the pathogenesis of severe influenza-associated
pneumonia was primarily viral (i.e., assumed to be an unknown etiologic
agent in 1918) or a combination of viral and bacterial agents was carefully
considered by pathologists in 1918-1919, without definitive resolution [26,
33]. The issue was addressed anew in the early 1930s when Shope
published a series of experimental studies that involved the just-discovered
swine influenza A virus: severe disease in an animal model resulted only
when the virus and Hemophilus influenzae suis were administered together
[67]. In 1935, Brightman studied combined human influenza and
streptococcal infection in a ferret intranasal inoculation model. Even though
neither agent was pathogenic when administered alone, they were highly
fatal in combination [68]. In rhesus monkeys, human influenza viruses given
intranasally were not pathogenic, but could be made so by nasopharyngeal
instillation of otherwise nonpathogenic bacteria [69]. During the 1940s,
additional studies in ferrets, mice, and rats established that the influenza
virus in combination with any of several pneumopathic bacteria acted
synergistically to produce either a higher incidence of disease, a higher
death rate, or a shortened time to death [70-73]; these effects could be
mitigated or eliminated if antibiotics were given shortly after establishment
APPENDIX TO JAMES CASCIANO DECLARATION-246

of combined infection [73]. More recent data suggest that influenza
vaccination may prevent bacterial disease [74].
As reviewed recently by McCullers [75], a body of experimental research
during the last 3 decades has identified possible mechanisms by which
coinfection with the influenza virus and bacteria might affect pathogenicity.
These include viral neuraminidase (NA)-induced exposure of bacterial
adherence receptors; bacterial NA-induced upregulation of influenza
infection; interleukin 10-induced susceptibility to pneumococci and possibly
staphylococci [76]; interferon type 1 effects [77]; viral PB1-F2 effects, the
proaptotic and mitochondriopathic effects of which are correlated with
enhanced bacterial infection [78]; and virus-induced desensitization to
bacterial Toll-like receptor ligands [79].
We believe that the weight of 90 years of evidence (table 3), including the
exceptional but largely forgotten work of an earlier generation of
pathologists, indicates that the vast majority of pulmonary deaths from
pandemic influenza viruses have resulted from poorly understood
interactions between the infecting virus and secondary infections due to
bacteria that colonize the upper respiratory tract. The data are consistent
with a natural history in which the virus, highly cytopathic to bronchial and
bronchiolar epithelial cells, extends rapidly and diffusely down the
respiratory tree, damages the epithelium sufficiently to break down the
mucociliary barrier to bacterial spread, and if able to gain access to the
distal respiratory tree-perhaps on the basis of receptor affinity [80]-creates
both a direct pathway for secondary bacterial spread and an environment
(cell necrosis and proteinaceous edema fluid) favorable to bacterial growth.
It remains unresolved whether cocolonizing, nonpneumopathic upper
respiratory-tract organisms such as Bacillus (Hemophi/us) influenzae play
an ancillary role, or are merely innocent bystanders. It is uncertain why
Hemophilus influenzae was much less prominent in 1957-1958 and
thereafter, but this phenomenon may relate to antibiotic use and
conceivably, in recent years, to Hemophilus influenzae b vaccination of
APPENDIX TO JAMES CASCIANO DECLARATION-247

children.
The extraordinary severity of the 1918 pandemic remains unexplained. That
the causes of death included so many different bacteria, alone or in
complex combinations, argues against specific virulent bacterial clones.
The pathologic and bacteriologic data appear consistent with copathogenic
properties of the virus itself, perhaps related to viral growth, facility of cell
to-cell spread, cell tropism, or interference with or induction of immune
responses. Certain observers believed that cotransmission of the influenza
agent and of pneumopathogenic bacteria was responsible for many severe
and fatal cases, especially during the October-November 1918 peak of
mortality and case-fatality rates [81]. We speculate that any influenza virus
with an enhanced capacity to spread to and damage bronchial and/or
bronchiolar epithelial cells, even in the presence of an intact rapid
reparative response, could precipitate the appearance of severe and
potentially fatal bacterial pneumonia due to prevalent upper respiratory
tract bacteria.
In the modern era, the widespread use of antibiotics and the establishment
of life-prolonging intensive care unit treatment make it more difficult than it
was in 1918 to document the importance of bacterial lung infection for
influenza-related mortality. Influenza-associated pneumonia patterns may
now be influenced by the administration of pneumococcus, Hemophilus
influenzae b, and meningococcus vaccine, and cases have tended to occur
in elderly individuals, who rarely undergo autopsy. The 1968 influenza
pandemic was mild, and autopsy studies were uncommon [21]. Fatal cases
of influenza-associated viral pneumonia that are considered to be
"primary"; (i.e., with little or no bacterial growth) continue to be identified
[82, 83]; however, their incidence appears to be low, even in pandemic
peaks. The issue of the pathogenesis of fatal influenza-associated
pneumonia remains important; the fact that even severe, virus-induced
tissue damage is normally followed by rapid and extensive repair [20, 26]
suggests that early and aggressive treatment, including antibiotics and
APPENDIX TO JAMES CASCIANO DECLARATION-248

intensive care, could save most patients [84, 85] and also underscores the
importance of prevention and prophylaxis.
The 1918 pandemic and subsequent pandemics differed with respect to the
spectrum and extent of secondary bacterial pneumonia {e.g., the switch in
prevalence during the antibiotic era to predominantly staphylococcal
secondary pneumonia, as opposed to streptococcal, pneumococcal, and
mixed secondary pneumonia; and the greatly decreased involvement of
Bacillus [Hemophilus] influenzae), suggesting that additional factors affect
the level of influenza morbidity and mortality. These might include the use
of antibiotics and antiviral agents, the rate of influenza vaccination and
bacterial vaccination, and demographic and social factors. The aging
population in the United States, the increasing number of persons living in
nursing home facilities, and the number of persons who are
immunosuppressed or affected by cardiac disease, renal disease, and/or
diabetes mellitus all represent potential factors that might change the
profile of morbidity and mortality during a future pandemic. for example,
elderly persons in nursing homes are at risk for pneumonia caused by
enteric organisms and sometimes by drug-resistant nosocomial organisms.
The spread of bacteria such as methicillin-resistant Staphylococcus aureus
and highly pathogenic clones of Streptococcus pyogenes pose more
general risks [86].
The viral etiology of and timing of the next influenza pandemic cannot be
predicted [87]. If, as some fear, a future pandemic is caused by a derivative
of the current highly pathogenic avian H5N1 virus, lessons from previous
pandemics may not be strictly applicable. Although histopathologic
information concerning current human H5N1 infections is sparse [10], its
pathogenic mechanisms may be atypical because the virus is poorly
adapted to humans [88] and because, in certain experimental animal
models [e.g., 89], some strains have induced severe pathology that differs
from the findings associated with circulating human influenza viruses
(which, in these models, cause disease resembling self-limited seasonal
APPENDIX TO JAMES CASCIANO DECLARATION-249

influenza in humans [90]). However, if an H5N1 virus were to fully adapt to
humans, the clinicopathologic spectrum of associated disease could
become more like that of previous pandemics.
If the next pandemic is caused by a human-adapted virus similar to those
recognized since 1918, we believe the infection is likely to behave as it has
in past pandemics, precipitating severe disease associated with prevalent
colonizing bacteria. Recent reviews have discussed the importance of new
and improved influenza antiviral drugs and influenza vaccines in controlling
a pandemic [84, 91, 92]. The present work leads us to conclude that in
addition to these critical efforts, prevention, diagnosis, prophylaxis, and
treatment of bacterial pneumonia, as well as the stockpiling of antibiotics
and bacterial vaccines [84, 85, 93], should be among the highest priorities
in pandemic planning. We are encouraged that such considerations are
already being discussed and implemented by the agencies and individuals
responsible for such plans [94, 95].
Acknowledgments
We thank Betty Murgolo and the staff of the National Institutes of Health
(NIH) Library, for extensive research efforts in locating publications, and the
staff of the History of Medicine Division, National Library of Medicine, NIH,
for additional library research support. Wealso thank Cristina Cassetti, PhD,
and Andrea Scollard, DDS, PhD for translation of Italian language and
Portuguese language papers, respectively; Hillery A. Harvey, PhD, for
scientific assistance; and Gregory K. Folkers, MS, MPH, for helpful
discussion and editorial assistance. John J. McGowan, PhD, and the staff of
the National Institute of Allergy and Infectious Diseases (NIAID) Pandemic
Influenza Digital Archives project provided substantial assistance in
organizing and indexing historical manuscripts.
References
APPENDIX TO JAMES CASCIANO DECLARATION-250

Financial support: Intramural Research Program of the National Institutes of Health; National Institute of Allergy and Infectious Diseases.
Presented in part: 2006 Annual Meeting of the American Epidemiological Society, Berkeley, California, 30 March, 2006; and 2007 Annual Meeting of the American Epidemiological Society, Boston, Massachusetts, 26 March 2007.
© 2008 by the Infectious Diseases Society of America
APPENDIX TO JAMES CASCIANO DECLARATION-311

When Mask-Wearing Rules in the 1918 Pandemic Faced Resistance Most people complied, but some resisted (or poked holes in their masks to smoke).
BeckY. Little May 6, 2020
The influenza P-andemic of 1918 and 1919 was the most deadly flu outbreak in
history, killing up to 50 million people worldwide. In the United States, where it
ultimately killed around 675,000 people, local governments rolled out initiatives
to try to stop its spread. These varied by region, and included closing schools
and places of public amusement, enforcing "no-spitting" ordinances,
encouraging people to use handkerchiefs or disposable tissues and requiring
people to wear masks in public.
Mask-wearing ordinances mainly popped up in the western states, and it
appears most people complied with them. The nation was still fighting in World
War I, and officials framed anti-flu measures as a way to protect the troops from
the deadly outbreak.
WATCH: The Spanish Flu Was Deadlier Than WWI
The first recorded infection was in a U.S. Army private stationed at Fort Riley,
Kansas on March 4, 1918. Although the United States and the other nations at
war initially suppressed news of the flu (neutral Spain freely reported it, hence
the misnomer "Spanish flu"), there was a sense that following these new health
precautions was patriotic.
As one Red Cross PSA put it, "the man or woman or child who will not wear a
mask now is a dangerous slacker." This sense of wartime duty-and the fear of
being seen as a "slacker"-may have motivated those who complied with mask
orders in cities like San Francisco, Seattle, Denver and Phoenix.
Yet even though compliance was high, some complained that the masks were
APPENDIX TO JAMES CASCIANO DECLARATION-312

uncomfortable, ineffective or bad for business. Officials were caught in public
without masks. And after the war ended, and there was no longer a sense that
people should wear masks to keep the troops safe, some dissenters even
formed an "Anti-Mask League" in San Francisco.
WATCH: World War I Documentaries on HISTORY Vault
Masks Were Made of Gauze or Even More Porous Material
Women working for the Red Cross make masks during the pandemic flu in 1918.
Bettmann Archive/Getty Images
In 1918, advanced masks like the N95s that healthcare workers use today were
a long way off. Surgical masks were made of gauze, and many people's flu
masks were made of gauze too. Red Cross volunteers made and distributed
many of these, and newspapers carried instructions for those who may want to make a mask for themselves or donate some to the troops. Still, not everyone
used the standard surgical design or material.
"To entice people to get them to wear them, [cities] were pretty lax in terms of
APPENDIX TO JAMES CASCIANO DECLARATION-313

what people could wear," says J. Alex Navarro, assistant director of the Center
for the History of Medicine at the University of Michigan and one of the editors
in-chief of The American Influenza EP-.idemic of 1918-1919: A Digiral.
EncyQQpedia.
In October 1918, the Seattle Daily Times carried the headline "Influenza Veils
Set New Fashion: Seattle Women Wearing Fine Mesh With Chiffon Border to
Ward Off Malady." These "fashionable" masks and others made from dubious
material probably weren't helping much. Yet there was also debate within the
medical and scientific community about whether multiple-ply gauze masks
were effective either.
For instance, Detroit health commissioner J.W. Inches said gauze masks were
too porous to prevent the spread of the flu among the public. Also, masks are
most effective when worn properly, which wasn't always what happened. In
Phoenix, where most people apparently complied with the city's mask order,
some nonetheless Qoked holes in their masks to smoke-which greatly reduced
their effectiveness.
SEE PHOTOS: The 1918 Flu Camgaigns to Shame Peogle Into Following
New Rules
'Mask Slackers• Faced Enforcement, Punishment
Still, for the small percentage of people who went without a mask entirely,
reports suggest their issue had less to do with the science behind them, and
more to do with personal comfort.
"You read routinely about people not wanting to wear them because they're hot
and stuffy," says NancY. Bristow, chair of the history department at the
University of Puget Sound and author of American Pandemic: The Lost Worlds
of the 1918 Influenza EgJdemic. "Some people argue against them because they
say that they create fear in the public, and that we want to keep people calm;
which I think is really an excuse to critique them because someone doesn't
want to wear them."
APPENDIX TO JAMES CASCIANO DECLARATION-314

PHOTOS: Innovative Ways Peogle Tried to Protect Themselves From the
Flu
Some businesses worried customers would shop less if they had to wear a
mask when they went outside, and some people claimed mask ordinances were
an infringement upon civil liberties. Yet "more important in terms of critiques,"
Bristow says, "is this idea that we've heard today as well that they give people a
false sense of security." As she points out, wearing a mask is less effective
when people don't follow other health guidelines too (and especially if some are
poking holes in their masks to smoke).
Cities that passed masking ordinances in the fall of 1918 struggled to enforce
them among the small portion of people who rebelled. Common punishments
were fines, prison sentences and having your name printed in the paper. In one
horrific incident in San Francisco, a special officer for the board of health shot a
man who refused to wear a mask as well as two bystanders.
This was far different from the treatment San Francisco's leaders received when
they didn't comply. At a boxing match, a police photographer captured images
of several supervisors, a congressman, a justice, a Navy rear-admiral, the city's APPENDIX TO JAMES CASCIANO DECLARATION-315

health officer and even the mayor, all without masks. The health officer paid a
$5 fine and the mayor later paid a $50 fine, but unlike other "mask slackers,~
they received no prison time (not to mention no one shot at them).
Mask-Wearing Declines After the War
A man receives a shave from a barber who wears a mask during the ongoing pandemic in Chicago, Illinois, circa 1918.
Chicago Sun-Times/Chicago Daily News Collection/Chicago History Museum/Getty Images
San Francisco's first masking order began in October and ended in November
after the World War I armistice. In January, when flu cases began to surge again
in San Francisco, the city implemented a second mask order. This time, the
resistance was much more intense. A group of dissenters that included a few
physicians and one member of the Board of Supervisors formed the "Anti-Mask
League," which held a public meeting with over 2,000 attendees.
Navarro speculates the resistance to San Francisco's second mask order may
have been more intense because the country was no longer at war, and some
residents didn't feel the same sense of patriotic duty they had before. In any
case, the city was an outlier. It doesn't appear that there were similar leagues or
protests in other cities.
APPENDIX TO JAMES CASCIANO DECLARATION-316
Nanc~ Tomes, a distinguished professor of history at Stony Brook University
who has written about public health measures during the 1918-1919 flu
pandemic says while there were pockets of resistance to mask-wearing in 1918
and 1919, it was not widespread.
And, unlike handkerchiefs and paper tissues, which Tomes says people began
to use more regularly because of the pandemic, mask-wearing did not catch on
in the United States after the ordinances ended. It's still difficult to say how
effective mask-wearing on its own was in 1918 and 1919. What is clear is that
communities that implemented stronger health measures overall fared better
than those that didn't.
"Today we can look back and see that they flattened the curve and the
communities that did enforce much stricter regulations and for a longer period
of time and began earlier had lower death rates," Bristow says. "But they didn't
have that data tabulated yet, so I think in the aftermath it wasn't as clear that
what they had done had been effective."
Read more:
WhY. the Second Wave of the 1918 Sganish Flu Was So DeadlY.
Sganish Flu - Sv.mgtoms, How It Began & Ended
Amid 1918 Flu Pandemic, America Struggled to Burv. the Dead
WhY. October 1918 Was America's Deadliest Month Ever
Pandemics That Changed History: Iimeline
APPENDIX TO JAMES CASCIANO DECLARATION-317
APPENDIX TO JAMES CASCIANO DECLARATION-318

@ the University of Sao Paulo
DO FACEMASKS LIMIT THE CONTAMINATION/SPREAD OF RESPIRATORY
VIRUSES?
by admin-spiralab July 27, 2020
To limit the spread of respiratory diseases, facemasks can be used by:
- healthy people, avoiding thus contamination by infected individuals
- infected people, limiting the spread of viruses to susceptible individuals
The use of masks is intuitively logical, as it provides a barrier, preventing the spread of droplets
or aerosol containing viral particles. In fact, studies have shown that surgical masks or
respirators are able to retain a large part of the viruses expelled by infected people. Under ideal
conditions, which include the periodic replacement of surgical masks and receiving training for
proper aseptic techniques, masks can be effective in partially containing the transmission of
infectious agents. However, in the real world, where regular people without specific training
must in addition to acquiring an arsenal of surgical masks, remember to thoroughly wash their
hands before wearing a mask, not touching the mask with their hands, not removing it to have a
cup of coffee or enjoy a meal and then put them back on (these masks must be removed and
replaced with new ones), the efficiency of the masks drops tremendously.
The effectiveness of the use of masks as a tool to prevent the spread of respiratory diseases
among regular people (unlike health workers, who receive specific training and have many
masks at their disposal) has been tested in several uclinical trials". Such experiments have been
carried out over the past 15 years, some better conducted than others. A recent study,
published in 2020, compiled the results obtained in the best randomized clinical trials (RCTs) on
this topic (MacIntyre and Chughtai 2020). Randomized means that the individuals who
participated in these studies were divided into subgroups, made up of masked and unmasked
(control group) at random, but balanced in relation to general health condition, sex etc. RCTs
are the golden standard of clinical trials.
APPENDIX TO JAMES CASCIANO DECLARATION-319

Seven studies have been carried out in which healthy individuals in the community wore masks
and another 3 studies in which a mask was worn by infected individuals. Each of these studies
typically involved many tens or even hundreds of people.
It should be noted that in all of these studies, the use of masks took place in the context of
closed places, be they households, student housing or hospitals. In none of these cases the use
of masks in public and open places has been tested. There is a good reason for this, as we will
see later on. Some of these studies tested the effectiveness of masks only, others tested the
effectiveness of masks+ hygiene measures, such as frequent hand washing.
In order to conclude on the effectiveness of masks as able to prevent the spread of respiratory
viruses, there must be a significantly lower number of secondary infections (people who
contract the virus from an infected household member) in the masked group than in the control
group.
In most studies in which masks were used by healthy people with the intention of protecting
them, susceptible individuals, by means of a mask, no statistically significant protective effect
was observed (5 out of 7 studies). That is, in these studies there was no clear difference between
the masked group and the control group. In two studies, a small statistically significant
difference was observed. In one of those (Cowling et al. 2009), there were 3 groups: the control
group, the hands hygiene group and the hands hygiene+ mask group. The hands hygiene group
displayed an odds ratio of 0.46 compared to the control group. This means that the chance of
those wearing masks getting contaminated was 0.46 times lower than that of the control group.
In other words, the chance of the unmasked group to contract the disease was 1 /0.46 = 2.17
times higher. The hand hygiene + masks group showed an odds ratio of 0.33, that is, mask
wearing decreased the risk by 0.13. Therefore, the chance of the hands hygiene+ mask group
for becoming sick was 3 times lower than that of the control group, while the chance of the
hands hygiene group (without masks) to get infected was 2.17 times less than that of the group
control. Clearly, the greatest benefit was frequent hand washing, while mask wearing conferred
a secondary contribution. Furthermore, according to this study, both interventions had a
positive effect if they were applied by the susceptible individuals within the first 36 hours from
the onset of symptoms of the infected individuals with who they were in contact.
APPENDIX TO JAMES CASCIANO DECLARATION-320

Of the 7 studies mentioned above, this is the one that had the most statistically significant
results regarding the use of masks. The other studies displayed either negative results, or
positive outcomes but without statistical significance or other limitations. To see the references
cited in this article and a summary of their results can be found here.
A common, and to some extent correct claim is that facemasks should be worn by everyone in
order to prevent infected individuals (symptomatic, pre-symptomatic or asymptomatic) from
contaminating susceptible individuals. Three studies were carried out that tested this possibility.
One of these studies took place in France (Canini et al. 2010), involving 1 OS infected people. The
authors of this paper concluded that there was no difference between the control group and the
group in which infected people wore masks. In another study carried out in Saudi Arabia
(Barasheed et al. 2014), during the annual Islamic pilgrimage, it was found that the group that
wore masks infected 31 % of the people accommodated in the same tent, while in the control
tent, where the infected did not wear masks, that number rose to 53%. However, these data
were based on reports from the study participants who reported their own symptoms. When
the sick participants were tested for the presence of 5 types of viruses that could potentially
cause these symptoms, the difference between the groups disappeared. Thus, the symptoms
reported by the study participants could have been caused by other factors, other than the
viruses supposedly spread by the infected individuals (with or without masks).
Finally, in a study conducted in China (MacIntyre et al. 2016), 245 infected patients were divided
into 2 groups, with and without facemasks. The number of residents in the same household who
contracted the disease was assessed either by symptoms reporting or laboratory testing.
Infection rates measured by symptom reports showed a downward trend, but not statistically
significant when the facemasks and control groups were compared. However, the advantage of
the masked group was eliminated when the sick individuals were submitted to laboratory tests
to detect the presence of viruses. In this case, there was no difference between the groups.
APPENDIX TO JAMES CASCIANO DECL.ARATION-321

Two caveats must be stressed:
1-AII studies mentioned above involved tests in which individuals wore surgical masks or
respirators. None of them used cloth masks. There is a single RCT that tested the effectiveness
of cloth masks, in a hospital environment - {MacIntyre et al. 2015). Their conclusion is that these
masks should NOT be used in these environments. The group of healthcare workers who wore
cloth masks had a higher risk of contracting respiratory diseases than the control group that did
not wear any masks. ADDENDUM: A new paper {published on 7/21/2020 and not yet peer
reviewed) showed that cloth masks were completely inefficient in containing SARS-CoV-2
particles (Loupa et al. 2020).
2- No study has tested the use of masks in open spaces to limit the spread of respiratory
diseases in the outdoors. The reason for this is simple: the use of masks in open spaces is
unnecessary and defies the laws of microbiology. Viruses expelled by an individual in an open
environment either in the form of aerosol or small droplets are immediately diluted,
considerably reducing what virologists call "infectious dose" (the number of viruses required to
infect a healthy person). Microbiologists working with viruses know that one of the most efficient
ways to stop a viral infection is to dilute the viruses and host cells, which is a good analogy to
what happens in a dynamic open space - viruses spread (dilute) in the air as people walk by. In
addition, in the presence of solar radiation, RNA viruses such as SARS-Cov-2 are inactivated in a
matter of tens of minutes (Lytle and Sagripanti 2005). In other words, for a person to be infected
by viruses expelled by others in an open environment, there must be a great proximity between
them. Unless the infected person sneezes or coughs directly into the susceptible individual's
face, the risk of becoming infected outdoors is very low.
In conclusion, there is little reliable evidence that wearing masks, either by healthy people or by
infected individuals, has any consistent benefit in preventing respiratory disease. The authorities
should take these scientific data into account before decreeing the mandatory use of masks in
public spaces. The use of masks in open places, where there is no agglomeration (minimum
distance of 1 meter between people), as in streets, parks and beaches, defies the basic laws of
microbiology and should not be mandatory. In confined places such as buses, subways and
markets, wearing masks may be recommended.
APPENDIX TO JAMES CASCIANO DECLARATION-322

References
Barasheed 0, Almasri N, Badahdah A-M, et al (2014) Pilot Randomised Controlled Trial to Test
Effectiveness of Facemasks in Preventing Influenza-like Illness Transmission among Australian
Hajj Pilgrims in 2011. Infect Disord Drug Targets 14:110-116.
https://doi.org/10.217/1871526514666141021112855
Bundgaard, H., Bundgaard, J. S., Raaschou-Pedersen, D. E.T., Mariager, AF., Schytte, N., von
Buchwald, C., ... & Benfield, T. (2020). Face masks for the prevention of COVID-19-Rationale and
design of the randomised controlled trial DANMASK-19. Dan Med}, 67, A05200363.
Canini L, Andreoletti L, Ferrari P, et al (2010) Surgical mask to prevent influenza transmission in
households: a cluster randomized trial. PloS One S:e13998.
https://doi.org/10.1371 /journal.pone.0013998
Cowling BJ, Chan K-H, Fang VJ, et al (2009) Facemasks and Hand Hygiene to Prevent Influenza
Transmission in Households. Ann Intern Med 151 :437-446. https://doi.org/10.7326/0003-4819-
151-7-200910060-00142
Glykeria Loupa, Dimitra Karali, SPYRIDON RAPSOMANIKIS. Aerosol filtering efficiency of
respiratory face masks used during the COVID-19 pandemic. medRxiv 2020.07.16.20155119; doi:
https://doi.org/10.1101 /2020.07.16.20155119
Lytle CD, Sagripanti J-L (2005) Predicted Inactivation of Viruses of Relevance to Biodefense by
Solar Radiation. J Virol 79: 14244-14252. https:/ /doi.org/10.1128/JVI. 79.22.14244- 14252.2005
MacIntyre CR, Chughtai AA (2020) A rapid systematic review of the efficacy of face masks and
respirators against coronaviruses and other respiratory transmissible viruses for the
community, healthcare workers and sick patients. Int J Nurs Stud 108:103629.
https://doi.org/10.1016/j.ijnurstu.2020.103629
MacIntyre CR, Seale H, Dung TC, et al (2015} A cluster randomised trial of cloth masks compared
with medical masks in healthcare workers. BMJ Open S:e006577.
https://doi.org/10.1136/bmjopen-2014-006577
MacIntyre CR, Zhang Y, Chughtai AA, et al (2016) Cluster randomised controlled trial to examine
medical mask use as source control for people with respiratory illness. BMJ Open 6:e012330.
https://doi.org/10.1136/bmjopen-2016-012330
APPENDIX TO JAMES CASCIANO DECLARATION-323

Ragid Exgert Consultation on the Eff activeness of Fabric Masks for the C0VID-19 Pandemic (Agril 8, 2020)_ (2020) Consensus Study Report
National Academies of Sciences, Engineering, and Medicine
Contributors
Description
This rapid expert consultation responds to a request from the Office of
Science and Technology Policy (OSTP) concerning the effectiveness of
homemade fabric masks worn by the general public to protect others, as
distinct from protecting the wearer. The request stems from an interest in
reducing transmission within the community by individuals who are
infected, potentially contagious, but symptomatic or presymptomatic.
The National Academies of Sciences, Engineering, and Medicine convened
a standing committee of experts to help inform OSTP on critical science
and policy issues related to emerging infectious diseases and other public
health threats. The standing committee includes members with expertise in
emerging infectious diseases, public health, public health preparedness and
response, biological sciences, clinical care and crisis standards of care, risk
communication, and regulatory issues.
Topics
Health and Medicine - Infectious Disease
Health and Medicine - PolicY., Reviews and Evaluations
APPENDIX TO JAMES CASCIANO DECLARATION-324

Suggested Citation
National Academies of Sciences, Engineering, and Medicine. 2020. Rapid
Expert Consultation on the Effectiveness of Fabric Masks for the COV/D-19
Pandemic (April 8, 2020). Washington, DC: The National Academies Press.
https://doi.org/10.17226/25776.
Import this citation to:
• Bibtex
• EndNote • Reference Manager
Publication Info
8 pages I 8.5 x 11
DO I: htt P-S :/./.do i. o rg/.1 0 .17 2 2 6 /.2 5 7 7 6
APPENDIX TO JAMES CASCIANO DECLARATION-325

A Quantitative Assessment of the Total Inward Leakage of NaCl Aerosol Representing Submicron-Size Bioaerosol Through N95 Filtering Facepiece Respirators and Surgical Masks Respiratory protection provided by a particulate respirator is a function of
particle penetration through filter media and through faceseal leakage.
Faceseal leakage largely contributes to the penetration of particles through
a respirator and compromises protection. When faceseal leaks arise, filter
penetration is assumed to be negligible. The contribution of filter
penetration and faceseal leakage to total inward leakage (TIL) of
submicron-size bioaerosols is not well studied. To address this issue, TIL
values for two N95 filtering facepiece respirator (FFR) models and two
surgical mask (SM) models sealed to a manikin were measured at 8 L and
40 L breathing minute volumes with different artificial leak sizes. TIL values
for different size (20-800 nm, electrical mobility diameter) NaCl particles
representing submicron-size bioaerosols were measured using a scanning
mobility particle sizer. Efficiency of filtering devices was assessed by
measuring the penetration against NaCl aerosol similar to the method used
for NIOSH particulate filter certification. Results showed that the most
penetrating particle size (MPPS) was -45 nm for both N95 FFR models and
one of the two SM models, and -350 nm for the other SM model at sealed
condition with no leaks as well as with different leak sizes. TIL values
increased with increasing leak sizes and breathing minute volumes.
Relatively, higher efficiency N95 and SM models showed lower TIL values.
Filter efficiency of FFRs and SMs influenced the TIL at different flow rates
and leak sizes. Overall, the data indicate that good fitting higher-efficiency
APPENDIX TO JAMES CASCIANO DECLARATION-326

FFRs may offer higher protection against submicron-size bioaerosols.
INTRODUCTION
Influenza and other pandemic infectious diseases cause illness and death
worldwide. The mode of transmission of infection appears to be through
large droplets, aerosols, fomites, or person-to-person contact. O Infected
subjects are known to release a wide size range of particles during
breathing, coughing, sneezing, and talking. The droplets travel some
distance and evaporate to form smaller-size particles. Normal human
subjects and infected individuals release considerable numbers of
submicron diameter particles in the exhaled breath.(-) In one study, exhaled
breath of seven subjects infected with influenza was collected on Teflon
filters and exhaled particle concentrations measured using an optical
particle counter. O Filters were tested for influenza virus by quantitative
polymerase chain reaction (qPCR). Results for four subjects showed
influenza virus particles in exhaled breath and over 87% of particles were
under 1 µm in diameter. Recently, appreciable numbers of influenza
particles were found in the ambient air in different locations. O Submicron
aerosols can remain airborne for prolonged periods because of their low
settling velocity. Infectious aerosol, when inhaled by susceptible persons, is
likely to cause disease.
Respiratory protection is known to reduce the inhalation of infectious
aerosols. The Centers for Disease Control and Prevention (CDC) has
developed recommendations on the use of the National Institute for
Occupational Safety and Health (NIOSH)-approved N95 filtering facepiece
respirators (FFRs) and facemasks for protection against pandemic influenza
virus transmission for home, community, and occupational settings. O SMs
are used as barriers to limit the dissemination of secretions or large droplets
from patient to others. The Food and Drug Administration (FDA) clears the
SMs for sale, based on the test report provided by the manufacturers. SMs
are confused with respirators because both look similar and are worn on the
APPENDIX TO JAMES CASCIANO DECLARATION-327

face. In general, the filter efficiency of N95 FFRs is superior to SMs. (,) Filter
efficiency is enhanced by electrostatic charge on filter media of N95 FFRs.
The most penetrating particle size (MPPS) for N95 FFRs is -50 nm
(electrical mobility diameter). O In the case of SMs, both electrostatic as well
as mechanical (MPPS >100 nm) types are available.0 FFRs are fit-tested
before use in workplaces whereas SMs are not. SMs were used for
respiratory protection in health care facilities when there was a shortage of
respirators during pandemic seasons. 0 Therefore, knowing the
effectiveness of SMs against infectious bioaerosols is of public health
importance.
The effectiveness of N95 FFRs and SMs in health care settings has been
reviewed.(,) One study evaluated the health risk of nurses using respiratory
protection during the severe acute respiratory syndrome (SARS) epidemic
in Canada0 and showed that N95 respirators were more protective than the
SMs. Similarly, N95 respirators and hand washing were found to be
effective in protecting health care workers against SARS transmission. O
Another study reported a dramatic decrease of SARS infection from 52 to 8
among health care staff after implementation of the use of N95 masks,
gloves, and gowns. 0
Recently, the efficacy of N95 FF Rs or SMs against influenza transmission
was evaluated with human subjects exposed to live attenuated influenza
vaccine particles. O Analysis for influenza virus in the nasal washes of test
subjects by reverse transcription-polymerase chain reaction technique
showed that wearing N95 respirators offered a higher level of protection
than SMs. Another study measured the protection factor for SMs and FFRs
on test subjects in a controlled environmental test chamber and showed
that SMs may not be as protective as FFRs. O
Some studies have reported that SMs are as effective as N95 FFRs for
respiratory protection from viral respiratory pathogens.(-) Protection
performance was tested using a fluorescein-KCI aerosol spray onto the
APPENDIX TO JAMES CASCIANO DECLARATION-328

faces of subjects wearing N95 FFRs or SMs and performing intermittent
exercises on a treadmill in a chamber. O Test aerosol size was assumed to be
about 0.1-0.3 µm based on the comparison of the filtration efficiency
obtained for N95 FFRs in their study with the efficiency reported by a
different group. O After the experiment, fluorescent stain on the faces and
KCI concentrations in different layers of FFRs and SMs were analyzed to
calculate the filter efficiency. Results showed that both N95 FFRs and SMs
gave 95% or greater filtration efficiency, and N95 FFRs had about 2%
filtration efficiency higher than the SMs indicating that SMs and N95 FFRs
can provide protection in a relatively low viral aerosol loading environment.
A case-control study in Hong Kong hospitals showed that both SMs and
N95 FFRs were significantly effective in reducing the risk of SARS infection
among staff. O In another study, influenza virus collected during coughing of
patients wearing N95 FFRs or SMs was analyzed by quantitative real time
RT-PCR.o The efficacy of SMs and N95 FFRs was found to be similar in
preventing the spread of influenza virus from patients. Similarly, the use of
SMs compared with N95 FFRs showed a non-inferior rate of laboratory
confirmed influenza. O
Comprehensive information on the relative efficacy of FFRs and SMs for
submicron-size bioaerosols is lacking. To address this issue, the Institute of
Medicine (IOM) recommended further research in key areas including the
effectiveness of facemasks and respirators against infectious particles and
faceseal leakage contributing to the overall total inward leakage (TIL). O TIL
is defined as an inverse function of a protection level offered by a respirator
when the contributions of aerosol penetration through filter media, faceseal
leakage, and leakage through other components are considered. It is known
that FFRs are designed to provide good fitting on the human face unlike the
SMs. Because of the difference in face-fitting characteristics, SMs will have
a larger faceseal leakage than FFRs when used by workers. One way to
compare the performance of FFRs with SMs is to measure the TIL under
controlled leak sizes.
APPENDIX TO JAMES CASCIANO DECLARATION-329
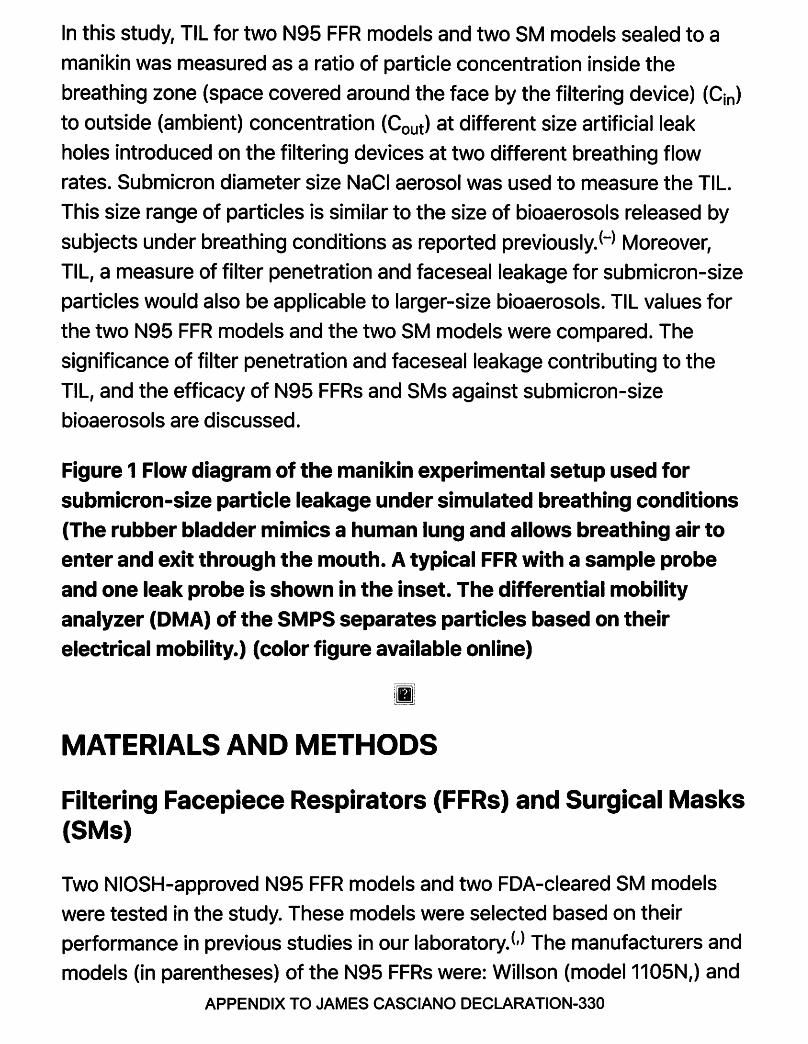
In this study, TIL for two N95 FFR models and two SM models sealed to a
manikin was measured as a ratio of particle concentration inside the
breathing zone (space covered around the face by the filtering device) (Cin)
to outside (ambient) concentration (Cout) at different size artificial leak
holes introduced on the filtering devices at two different breathing flow
rates. Submicron diameter size NaCl aerosol was used to measure the TIL.
This size range of particles is similar to the size of bioaerosols released by
subjects under breathing conditions as reported previously.(-) Moreover,
TIL, a measure of filter penetration and faceseal leakage for submicron-size
particles would also be applicable to larger-size bioaerosols. TIL values for
the two N95 FFR models and the two SM models were compared. The
significance of filter penetration and faceseal leakage contributing to the
TIL, and the efficacy of N95 FFRs and SMs against submicron-size
bioaerosols are discussed.
Figure 1 Flow diagram of the manikin experimental setup used for submicron-size particle leakage under simulated breathing conditions (The rubber bladder mimics a human lung and allows breathing air to enter and exit through the mouth. A typical FFR with a sample probe and one leak probe is shown in the inset. The differential mobility analyzer (DMA) of the SMPS separates particles based on their electrical mobility.) (color figure available online)
Ill
MATERIALS AND METHODS
Filtering Facepiece Respirators (FFRs) and Surgical Masks (SMs)
Two NIOSH-approved N95 FFR models and two FDA-cleared SM models
were tested in the study. These models were selected based on their
performance in previous studies in our laboratory.(,) The manufacturers and
models (in parentheses) of the N95 FFRs were: Willson (model 1105N,) and
APPENDIX TO JAMES CASCIANO DECLARATION-330

San Huei United Company (model 1895N,) labeled as N1 and N2, respectively, and the SM models were: Primed (model PG4-1073,) and 3M (model 1800) labeled as SM1 and SM2, respectively. None of the N95 models tested in the study had exhalation valves.
Filter Efficiency Test
Instantaneous filter penetration of FFRs and SMs was measured to assess their filter efficiency. Penetration of FFRs and SMs was measured using NaCl aerosol (count median diameter (CMD) 75±20 nm) generated by an Automated Filter Tester (AFT) TSI 8130 (TSI Inc., Shorewood, Minn.). O The
AFT measures penetration based on the light scattering of particles that pass through the filter. A Plexiglas test box (L 20 cm x W 20 cm x H 10 cm) with a top and bottom plate containing a hole (2.5 cm diameter) in the center was used for measuring aerosol penetration. O A FFR or SM with its concave side facing down was sealed to a Plexiglas plate (L 20 cm x W 20 cm x H 0.5 cm) using melted wax. A silicone sealant was used to seal the top and bottom plates to make the Plexiglas box airtight. The Plexiglas box containing the FFR or SM was placed between the two filter chucks of the AFT and aligned to keep the top and bottom plate holes facing the upstream and downstream filter chucks, respectively. Penetration was measured for 1 min at 85 L/min constant flow under airtight conditions by closing the filter chucks.
Total Inward Leakage Measurements Using a Manikin Setup
Figure 1 shows a manikin setup employed to evaluate the effect of faceseal leakage on TIL as described previously. O TIL was measured in two general configurations: (1) sealed to the manikin face with no artificial leaks induced through needles; and (2) sealed to the manikin face with artificial leaks induced through needles. A FFR or SM was sealed to a manikin head form using a silicone sealant and placed inside a test chamber (48 x 48 x
APPENDIX TO JAMES CASCIANO DECLARATION-331
48 cm3). The head form was connected to a breathing simulator (Breathing
Simulator Series 1101, Hans Rudolph, Inc., Shawnee, Kans.) through an
isolation chamber consisting of a rubber bladder inside an airtight glass
container. A metal tube (2.5 cm diameter) from the back of the mouth was
connected to an inflatable rubber bladder, which mimics a human lung,
inside the glass container connected to a breathing simulator. The
breathing simulator allows air to go back and forth into the glass container.
In response, ambient air enters the bladder through the FFR sealed to the
manikin head form during inhalation and exits during exhalation. Thus, the
isolation chamber prevented particles created by the breathing simulator
pump from getting inside the breathing zone of the respirator. The
breathing simulator allowed for several parameters to be varied including
tidal volume and breathing rate, which provided simulation of more realistic
breathing conditions.
Table 1 Filter Penetration for the N95 FFR Models and SM Models at 85 L/min Constant Flow {Average of three samples {n = 3), error represents one standard deviation.)
NaCl aerosol used for TIL measurement was different from the aerosol used
for testing filter penetration. Size distribution of NaCl aerosol was obtained
in a manner similar to that described previously. O Briefly, polydisperse NaCl
aerosol was generated using a 1.5% NaCl solution with a constant output
atomizer (TSI 3076) and passed through a dryer, a 85 Kr charge neutralizer
(TSI model 3077A), diluted with 50 L/min of dry air passed through a high
efficiency particulate air filter (HEPA) and then into the test chamber (48 x
48 x 48 cm3; Figure 1). Excess aerosol exited through a hole (1.3 cm
diameter) in the back of the test chamber. A small fan was installed at the
bottom of the chamber to ensure an even distribution of particles
throughout. Aerosol samples from the test chamber were analyzed for
number concentration for different size monodisperse particles (20-
800 nm, electrical mobility diameter) over 240 sec and repeated after a 30
sec interval, using a scanning mobility particle sizer (SMPS) {TSI model APPENDIX TO JAMES CASCIANO DECLARATION-332

3080) with a long differential mobility analyzer (OMA), and an ultra-fine
condensation particle counter (UCPC, TSI 3776). The OMA separates
particles based on their electrical mobility. The count median diameter
(CMO) and mode size (peak size) of the test aerosols were obtained from
the SMPS scans.
The test FFR was equipped with a sample probe to measure aerosol
concentration inside the FFR and two leak probes to introduce artificial
leakage (Figure 1, lnset).O The leak probes (-3 mm diameter and -1 cm
long) were filled with non-hardening putty and increasing leak sizes were
obtained by carefully inserting hypodermic needles (16 and 13 gauge sizes
with inner diameters of 1.18 and 1.80 mm, respectively) through the putty to
provide consistent leak channels through the needles (-2.56 cm long). Care
was taken to ensure the needle was kept open after inserting it into the
putty. The tip of the needle was positioned proximately close to the inner
surface of the respirator. Because the above leak sizes did not produce a
significant difference in the TIL for SMs, larger leak sizes were used.
For comparison, SMs as well as FFRs were fixed with larger leak probes
(-3 mm diameter and -1 cm long). Each leak size was created using two
leak probes, one on each side. TIL was measured with three different leak
sizes (two 3 mm, four 3 mm or six 3 mm). Samples from inside and outside
the FFRs and SMs were withdrawn and analyzed by two SMPS systems
simultaneously. 0 The two SMPS systems scanned the particles in the 20-
800 nm size range three times each three min. Samples were withdrawn
simultaneously during manikin breathing at 8 and 40 L minute volumes with
tidal volumes of 0.5 and 1.5 L, respectively. These tidal volumes
corresponded to 16 and 26.7 breaths per minute, respectively. TIL was
calculated as the ratio of particle concentration inside (Cin) of the FFR or
SM to the outside concentration (Cout) and multiplied by 100%.
RESULTS
APPENDIX TO JAMES CASCIANO DECLARATION-333

Filter Efficiency
NaCl aerosol penetrations for N95 FFR models were lower than the
penetrations for the SM models at 85 L/min flow rate (Table I). In addition,
penetrations for N1 and SM1 were relatively lower than the values obtained
for N2 and SM2, respectively. Based on the penetration values, N1 and SM1
are described as higher-efficiency FFR and SM models, respectively, throughout the article. Table 2
Table 2 Comparison of Total Inward Leakage (TIL) at Two Different Breathing Minute Volumes and Three Leak Sizes (Average of 4 samples (n = 4), error represents one standard deviation.)
Figure 2 Typical TIL values for the two N95 FFR models N1 and N2 at 8 L/min (left column) and 40 L/min (right column) breathing minute volumes (The symbols indicate sealed with no leaks(•), two 1.18 mm leaks (0), and two 1.80 mm leaks(•). The solid vertical line corresponds to the approximate MPPS (45 nm) of the two N95 FFR models. The dashed vertical line corresponds to the mode of the challenge aerosol (75 nm).)
ii]
TIL Measurement Under Breathing Conditions
The size distribution of NaCl aerosol used for TIL measurement showed a
CMD of -82 nm and a mode size (peak size) of -75 nm. Figure 2 shows the
TIL measured at no leak condition and with two small leak sizes at 8 L (left
panels) and at 40 L (right panels) breathing minute volumes for the two
N95 models. TIL for different size particles increased with increasing
breathing minute volumes from 8 to 40 L with no leaks. The most
penetrating particle size (MPPS) was -45 nm for both FFR models which
can be easily seen at 40 L breathing minute volume. With increasing leak APPENDIX TO JAMES CASCIANO DECLARATION-334

sizes (2x1.18 mm and 2x1.80 mm), the TIL for different size particles
increased for the two FFR models at both breathing rates. The MPPS
remained at -45 nm with different leak sizes. The TIL for the MPPS was
higher than the values for the other size particles. Among the two N95
models, N1 showed lower TIL values for different size particles than N2 at
both breathing rates.
Figure 3 shows an increase in the TIL for different size particles with
increasing leak sizes from 3 to 5 (2x3 mm, 4x3 mm, and 6x3 mm,
respectively) for both FFR models, at 8 and 40 L/min. Larger leak holes
(4x3 mm and 6x3 mm) tend to produce similar TIL values for different size
particles. Similar trends in TIL results were obtained for SM1 at different leak
sizes and flow rates (Figure 4, top panels). The MPPS was -45 nm with no
leaks and with a smaller leak size (2x3 mm), which can be seen at 40 L/min.
For SM2, however, TIL values for the various size particles at no leak
condition and with different induced leak sizes showed very little change at
both breathing flow rates (Figure 4, bottom panels). The MPPS for SM2 was
-350 nm at all test conditions. Table II shows the TIL for the two FFR
models and the two SM models at different leak sizes and flow rates.
Models N1, N2 and SM1 showed higher TIL values for 45 nm particles than
for 300 nm size particles at smaller leak sizes as reported previously. (24) For
SM2, however, TIL values were smaller at 45 nm than at 300 nm at all test
conditions.
Figure 3 Typical TIL values for the two N95 FFR models N1 and N2 at 8 L/min (left column) and 40 L/min (right column) breathing minute volumes (The symbols indicate: sealed with no leaks ( •), two 3 mm leaks (0), four 3 mm leaks(•), and six 3 mm leaks (4). The solid vertical line corresponds to the approximate MPPS (45 nm) of the two N95 FFR models. The dashed vertical line corresponds to the mode of the challenge aerosol [75 nm]).
APPENDIX TO JAMES CASCIANO DECLARATION-335

Figure 4 Typical TIL values for the two surgical models SM1 and SM2 at
8 L/min (left column) and 40 L/min (right column) breathing minute volume (The symbols indicate: sealed with no leaks ( •), two 3 mm leaks (0), four 3 mm leaks(•), and six 3 mm leaks (a). The solid vertical line corresponds to the MPPS of ,v45 nm for SM1 and ,v350 nm for SM2 models. The dashed vertical line corresponds to the mode of the challenge aerosol [75 nm]).
DISCUSSION
TIL measured for 20-800 nm diameter size NaCl aerosols for the two N95
FFR models were lower than the values obtained for the two SM models at
the two different breathing flow rates without induced leaks. TIL value
without induced leaks represents penetration through filter media and
agrees with the trend in penetration measured at NIOSH certification test
condition. The inverse relationship between TIL and filter efficiency can also
be seen among the FFR models, N1 (higher efficiency) and N2 (lower
efficiency) as well as between the SM models, SM1 (higher efficiency) and
SM2 (lower efficiency). With increasing leak sizes, TIL for 20-800 nm size
particles increased with increasing breathing flow rates for both FFR models
as well as for the SM1 model. TIL values for the two FFR models were lower
than the values for the SM models at similar flow rates and leak sizes,
indicating the influence of filter efficiency. TIL values for the FFR models
and SM1 did not vary significantly at larger leak sizes where minimum
protection can be expected. However, TIL values between FFRs and SM2
were markedly different. Similar difference in TIL can also be seen between
SM1 and SM2. The results can be explained by the large difference in filter
efficiency between the filtering devices (FFRs and SM1 vs. SM2), and the
inverse relationship between efficiency and TIL.
Results obtained in the present study are consistent with the data for four
different N95 FFR models tested previously. O In that study, two relatively APPENDIX TO JAMES CASCIANO DECLARATION-336

higher-efficiency N95 FFR models showed lower TIL values than two lower
efficiency models with different leak sizes and flow rates. The inverse
relationship between filter efficiency and TIL provides a better explanation
for the higher levels of respiratory protection offered by the N95 FFRs than the SMs reported previously.(,,)
The MPPS was -45 nm for N1, N2, and SM1 models, and -350 nm for SM2
with no faceseal leakage. Similar results were obtained with smaller leak
sizes at different breathing rates. Results from the study indicated that FFRs
producing smaller TIL value at the MPPS may provide relatively higher
protection against submicron virus aerosols. Among the two SM models
tested, SM1 appears to be more effective than SM2 for submicron-size
virus aerosols.
The relative impact of filter penetration is believed to be minimal or
insignificant once leaks are introduced in the facemask. In this study,
artificial leaks introduced in the N95 FFRs and SMs sealed to the manikin
allowed the test aerosols (mode size -75 nm) to enter and exit the
breathing zone (space covered around the face by the filtering device)
during breathing flow conditions. Interestingly, the MPPS values for FFR and
SM models with induced leak sizes were similar to the MPPS obtained with
no leaks. The above phenomenon can be explained by the effect of filter
penetration or filter media characteristic regulating the concentration of
different size particles inside the FFR or SM sealed to the breathing manikin
at different leak sizes. The results are consistent with our previous finding0
that faceseal leakage acts as a gatekeeper and indiscriminately allows the
test aerosols to flow through the leaks and increases the concentration of
all size test aerosol inside the breathing zone, while filter penetration or
filter media characteristic assigns the TIL values for different size particles.
The results obtained in the study indicate that filter penetration potentially
influences the TIL of different size particles. The data provide a better
understanding on the contribution of faceseal leakage and filter penetration
to the overall TIL.
APPENDIX TO JAMES CASCIANO DECLARATION-337

The contributions of filter penetration and faceseal leakage to the TIL
results obtained with the manikin raise the question of how well these
processes are represented when a respirator is worn by a human subject.
Faceseal leakage is known to be a major pathway that contributes to the TIL
of particles.(-) The number of particles penetrating through the faceseal
leakage pathway of the respirators and SMs tested on subjects has been
shown to far exceed the number of particles passing through the filter
medium. O The influence of filter penetration and faceseal leakage on the TIL
measured for test subjects has been described.(,) In one study, the overall
TIL values for Korean half-masks and three different class (top class, 1st
class, and 2nd class) FFR models donned on test subjects were measured.0
Among the FFRs, top class FFRs (~99% efficiency) showed average TIL
values of -5.0%. However, the TIL values for lower-efficiency FFRs ("1st
class'~ ~94% and "2nd class'~ ~80%) were -2 times higher than the TIL
values obtained for "top class" FFRs. Overall, the results indicated lower TIL
values for the higher-efficiency FFRs. This finding is supported by the data
obtained in our recent study on the inter-laboratory comparison of TIL
measurement. O Five different N95 FFR models with different filter
efficiencies were tested on 35 human subjects performing the Occupational
Safety and Health Administration (OSHA) fit-testing exercises in two
different test laboratories. A PortaCount Pro (TSI, Shorewood, Minn.)
measured the Cout /Cin ratio which was then converted to TIL values based
on the inverse relationship between the two parameters. Filter efficiency
was obtained only for four of the five models. Results showed that the
overall TIL values were lower for a relatively higher-efficiency N95 model,
and higher for three lower efficiency models in both laboratories. Moreover,
a good agreement between the two laboratories on the TIL values
measured for different N95 models was obtained, indicating the
measurement was reproducible. Filter efficiency dependence of TIL
obtained for human subjects in the above studies may explain the higher
protection offered by the N95 FFRs compared to the SMS in health care settings.(,,)
APPENDIX TO JAMES CASCIANO DECLARATION-338

Filter efficiency of the N95 FFRs is generally higher than that of SMs
because of the difference in the filter media used for construction. The N95
FFRs are developed to meet more challenging test conditions than are the
SMs. Filter efficiency for N95 FFRs is >95% when tested using charge
neutralized NaCl aerosols with a CMD of 75±20 nm at 85 L/min. The
penetration level does not exceed 5%, up to 200 mg aerosol loading.
However, the performance among SMs may vary widely because of the far
less challenging test methods used for their clearance by the FDA. O
Filtration efficiency of high and moderate barrier SMs is >98% and low
barrier SMs is >95% based on the penetration measured against non
neutralized Staphylococcus aureus bacteria of 3000±300 nm at 28.3 L/min.
Some types of SMs are also tested with 100 nm diameter non-neutralized
polystyrene latex spheres (PSL) at 1 to 25 cm/sec face velocity which may
produce wide differences in their efficiencies. Non-neutralization of test
aerosol may overestimate the filter efficiency and partly contribute to the
enormous difference in the filter performance among SMs. (,) TIL is
dependent on efficiency of the filter device.(,) Because of the higher filter
efficiency, N95 FFRs are expected to show lower TIL values than do SMs as
described previously.(,)
Faceseal leakage is a major pathway for aerosol transport inside the filtering
device.(,) The SMs are not designed to provide a good fitting on a human
face that may allow more aerosol leakage. However, SMs were found to be
as effective as N95 FFRs against aerosol particles similar to the size of
infectious aerosols.(,,) In one study, the transmission of influenza during
routine health care activities by hospital nurses using N95 FFRs and SMs
was assessed. O These authors showed that SMs were equally effective in
preventing influenza virus transmission among health care workers. A
similar conclusion was obtained in other studies.(,) However, the
performance of N95 FFRs may be higher where considerable aerosol
generation can occur during procedures such as intubation or
bronchoscopy. O Other factors, including training and consistency in the use
of the device and concentration of aerosol exposure, can also influence the APPENDIX TO JAMES CASCIANO DECLARATION-339

overall effectiveness of protective devices.
A shortage of respiratory protection devices during pandemic diseases is
possible. To address the issue, the CDC has stockpiled large numbers of
them. Respirators were stockpiled based on several factors, including their
approval for use in health care facilities and availability in the market.
Results obtained in the present study may be important for this stockpiling.
For example, relatively higher efficiency N95 FFRs, as well as SMs, are
expected to produce lower TIL values representing higher protection
against infectious aerosols. This indicates that filter efficiency of respiratory
protection devices should also be considered for stockpiling purposes.
Limitations and Recommendations for Future Studies
The limitations of the current study include the small number of N95 FFR
and SM models tested for TIL measurement. Additional models, including
those equipped with an exhalation valve, need to be tested to obtain
conclusive information on filter efficiency dependence of TIL. Another
limitation of the study is the TIL measurement for particles below 800 nm
size range. TIL study for a wide size range of airborne particles using
additional equipment may provide more realistic information. Nevertheless,
the measurement for 20-800 nm size range provides the underlying
mechanism of regulation of TIL by filter penetration and faceseal leakage
processes. Further studies on TIL, using test subjects, are important to
evaluate the performance of N95 FFRs against submicron-size bioaerosols.
CONCLUSION
Filtration efficiencies of the two N95 FFRs were higher than those of the two
SMs tested in the study against NaCl aerosol. Efficiencies of N1and SM1
were relatively higher than those of N2 and SM2, respectively. TIL for NaCl
aerosol (CMD -82 nm) using a manikin setup showed a MPPS of -45 nm for
N95 FFR models N1 and N2 and SM1 models, and -350 nm for the SM2
APPENDIX TO JAMES CASCIANO DECLARATION-340
model at different flow rates and leak sizes. Leakage of test aerosols
through artificial holes increased the TIL for different size particles while the
MPPS remained at the same sizes obtained at sealed condition with no
artificial leaks, showing that filter penetration regulates TIL. In general,
higher-efficiency N95 and SM models showed lower TIL values than the
lower-efficiency models, indicating the potential influence of filter
efficiency. TIL results obtained in the study indicate that faceseal leakage
allows all the different diameter size test aerosols to enter and exit the
filtering device while filter penetration assigns the TIL for different size
particles. Overall, the data suggest that higher-efficiency N95 FFRs with
good fitting characteristics would provide higher protection against
submicron-size bioaerosols.
ACKNOWLEDGMENTS
The authors acknowledge NIOSH colleagues including Christopher Coffey,
Ray Roberge, and Jay Parker for their useful suggestions and critical review
of the manuscript. This research work was supported by NIOSH funding.
DISCLAIMER
Mention of a commercial product or trade name does not constitute
endorsement by the National Institute for Occupational Safety and Health.
The findings and conclusions of this report are those of the authors and do
not necessarily represent the views of NIOSH. This article not subject to US
copyright law.
APPENDIX TO JAMES CASCIANO DECLARATION-341
Mask use in the context of COVID-19
Interim guidance 1 December 2020
This document, which is an update of the guidance published on 5 June 2020, includes new scientific evidence relevant to the use of masks for reducing the spread of SARS-Co V-2, the virus that causes COVID-19, and practical considerations. It contains updated evidence and guidance on the following: • mask management; • SARS-CoV-2 transmission; • masking in health facilities in areas with community,
cluster and sporadic transmission; • mask use by the public in areas with community and
cluster transmission; • alternatives to non-medical masks for the public; • exhalation valves on respirators and non-medical masks; • mask use during vigorous intensity physical activity; • essential parameters to be considered when
manufacturing non-medical masks (Annex).
Key points
• The World Health Organization (WHO) advises the use of masks as part of a comprehensive package of prevention and control measures to limit the spread of SARS-CoV-2, the virus that causes COVID-19. A mask alone, even when it is used correctly, is insufficient to provide adequate protection or source control. Other infection prevention and control (IPC) measures include hand hygiene, physical distancing of at least I metre, avoidance of touching one's face, respiratory etiquette, adequate ventilation in indoor settings, testing, contact tracing, quarantine and isolation. Together these measures are critical to prevent human-to-human transmission ofSARS-CoV-2.
• Depending on the type, masks can be used either for protection of healthy persons or to prevent onward transmission (source control).
• WHO continues to advise that anyone suspected or confirmed of having COVID-19 or awaiting viral laboratory test results should wear a medical mask when in the presence of others (this does not apply to those awaiting a test prior to travel).
• For any mask type, appropriate use, storage and cleaning or disposal are essential to ensure that they are as effective as possible and to avoid an increased transmission risk.
Mask use in health care settings • WHO continues to recommend that health workers ( 1)
providing care to suspected or confirmed COVID-19
1 For adequate ventilation refer to regional or national institutions or heating, refrigerating and air-conditioning societies enacting ventilation requirements. Ifnot available or applicable, a
• World Heakh I Organization
patients wear the following types of mask/respirator in addition to other personal protective equipment that are part of standard, droplet and contact precautions:
- medical mask in the absence of aerosol generating procedures (AGPs)
- respirator, N95 or FFP2 or FFP3 standards, or equivalent in care settings for COVID-19 patients where AGPs are performed; these may be used by health workers when providing care to COVID-19 patients in other settings if they are widely available and if costs is not an issue.
• In areas of known or suspected community or cluster SARS-Co V-2 transmission WHO advises the following:
- universal masking for all persons ( staff, patients, visitors, service providers and others) within the health facility (including primary, secondary and tertiary care levels; outpatient care; and long-term care facilities)
- wearing of masks by inpatients when physical distancing of at least I metre cannot be maintained or when patients are outside of their care areas.
• In areas of known or suspected sporadic SARS-CoV-2 transmission, health workers working in clinical areas where patients are present should continuously wear a medical mask. This is known as targeted continuous medical masking for health workers in clinical areas;
• Exhalation valves on respirators are discouraged as they bypass the filtration function for exhaled air by the wearer.
Mask use in community settings • Decision makers should apply a risk-based approach
when considering the use of masks for the general public. • In areas of known or suspected community or cluster
SARS-Co V-2 transmission: - WHO advises that the general public should
wear a non-medical mask in indoor ( e.g. shops, shared workplaces, schools - see Table 2 for details) or outdoor settings where physical distancing of at least 1 metre cannot be maintained.
- If indoors, unless ventilation has been be assessed to be adequate 1, WHO advises that the general public should wear a non-medical mask, regardless of whether physical distancing of at least I metre can be maintained.
recommended ventilation rate of 10 1/s/person should be met (except healthcare facilities which have specific requirements). For more information consult "Coronavirus (COVID-19) response

Individuals/people with higher risk of severe complications from COVID-19 (individuals ~ 60 years old and those with underlying conditions such as cardiovascular disease or diabetes mellitus, chronic lung disease, cancer, cerebrovascular disease or immunosuppression) should wear medical masks when physical distancing of at least 1 metre cannot be maintained.
• In any transmission scenarios: - Caregivers or those sharing living space with
people with suspected or confirmed COVID-19, regardless of symptoms, should wear a medical mask when in the same room.
Mask use in children (2) • Children aged up to five years should not wear masks
for source control. • For children between six and 11 years of age, a risk
based approach should be applied to the decision to use a mask; factors to be considered in the risk-based approach include intensity of SARS-Co V-2 transmission, child's capacity to comply with the appropriate use of masks and availability of appropriate adult supervision, local social and cultural environment, and specific settings such as households with elderly relatives, or schools.
• Mask use in children and adolescents 12 years or older should follow the same principles as for adults.
• Special considerations are required for immunocompromised children or for paediatric patients with cystic fibrosis or certain other diseases (e.g., cancer), as well as for children of any age with developmental disorders, disabilities or other specific health conditions that might interfere with mask wearing.
Manufacturing of non-medical (fabric) masks (Annex) • Homemade fabric masks of three-layer structure (based
on the fabric used) are advised, with each layer providing a function: 1) an innermost layer of a hydrophilic material 2) an outermost layer made of hydrophobic material 3) a middle hydrophobic layer which has been shown to enhance filtration or retain droplets.
• Factory-made fabric masks should meet the minimum thresholds related to three essential parameters: filtration, breathability and fit.
• Exhalation valves are discouraged because they bypass the filtration function of the fabric mask rendering it unserviceable for source control.
Methodology for developing the guidance
Guidance and recommendations included in this document are based on published WHO guidelines (in particular the WHO Guidelines on infection prevention and control of epidemic- and pandemic-prone acute respiratory infections in health care) (2) and ongoing evaluations of all available scientific evidence by the WHO ad hoc COVID-19 Infection Prevention and Control Guidance Development Group (COVID-19 IPC GOG) (see acknowledgement section for list of GOG members). During emergencies WHO publishes interim guidance, the development of which follows a
resources from ASHRAE and others'' https://www.ashrae.org/technical-resources/resources
transparent and robust process of evaluation of the available evidence on benefits and harms. This evidence is evaluated through expedited systematic reviews and expert consensusbuilding through weekly GOG consultations, facilitated by a methodologist and, when necessary, followed up by surveys. This process also considers, as much as possible, potential resource implications, values and preferences, feasibility, equity, and ethics. Draft guidance documents are reviewed by an external review panel of experts prior to publication.
Purpose of the guidance
This document provides guidance for decision makers, public health and IPC professionals, health care managers and health workers in health care settings (including long-term care and residential), for the public and for manufactures of nonmedical masks (Annex). It will be revised as new evidence emerges.
WHO has also developed comprehensive guidance on IPC strategies for health care settings (3), long-term care facilities (LTCF) (4), and home care (5).
Background
The use of masks is part of a comprehensive package of prevention and control measures that can limit the spread of certain respiratory viral diseases, including COVID-19. Masks can be used for protection of healthy persons (worn to protect oneself when in contact with an infected individual) or for source control (worn by an infected individual to prevent onward transmission) or both.
However, the use of a mask alone, even when correctly used (see below), is insufficient to provide an adequate level of protection for an uninfected individual or prevent onward transmission from an infected individual (source control). Hand hygiene, physical distancing of at least 1 metre, respiratory etiquette, adequate ventilation in indoor settings, testing, contact tracing, quarantine, isolation and other infection prevention and control (IPC) measures are critical to prevent human-to-human transmission of SARS-Co V-2, whether or not masks are used ( 6).
Mask management
For any type of mask, appropriate use, storage and cleaning, or disposal are essential to ensure that they are as effective as possible and to avoid any increased risk of transmission. Adherence to correct mask management practices varies, reinforcing the need for appropriate messaging (7).
WHO provides the following guidance on the correct use of masks:
• Perform hand hygiene before putting on the mask. • Inspect the mask for tears or holes, and do not use a
damaged mask. • Place the mask carefully, ensuring it covers the mouth
and nose, adjust to the nose bridge and tie it securely to minimize any gaps between the face and the mask. If using ear loops, ensure these do not cross over as this widens the gap between the face and the mask.

• Avoid touching the mask while wearing it. If the mask is accidently touched, perform hand hygiene.
• Remove the mask using the appropriate technique. Do not touch the front of the mask, but rather untie it from behind.
• Replace the mask as soon as it becomes damp with a new clean, dry mask.
• Either discard the mask or place it in a clean plastic resealable bag where it is kept until it can be washed and cleaned. Do not store the mask around the arm or wrist or pull it down to rest around the chin or neck.
• Perform hand hygiene immediately afterward discarding a mask.
• Do not re-use single-use mask. • Discard single-use masks after each use and properly
dispose of them immediately upon removal. • Do not remove the mask to speak. • Do not share your mask with others. • Wash fabric masks in soap or detergent and preferably
hot water (at least 60° Centigrade/140° Fahrenheit) at least once a day. If it is not possible to wash the masks in hot water, then wash the mask in soap/detergent and room temperature water, followed by boiling the mask for 1 minute.
Scientific evidence
Transmission of the SARS-Co V-2 virus
Knowledge about transmission of the SARS-Co V-2 virus is evolving continuously as new evidence accumulates. COVID-19 is primarily a respiratory disease, and the clinical spectrum can range from no symptoms to severe acute respiratory illness, sepsis with organ dysfunction and death.
According to available evidence, SARS-CoV-2 mainly spreads between people when an infected person is in close contact with another person. Transmissibility of the virus depends on the amount of viable virus being shed and expelled by a person, the type of contact they have with others, the setting and what IPC measures are in place. The virus can spread from an infected person's mouth or nose in small liquid particles when the person coughs, sneezes, sings, breathes heavily or talks. These liquid particles are different sizes, ranging from larger 'respiratory droplets' to smaller 'aerosols.' Close-range contact ( typically within 1 metre) can result in inhalation of, or inoculation with, the virus through the mouth, nose or eyes (8-13).
There is limited evidence of transmission through fomites ( objects or materials that may be contaminated with viable virus, such as utensils and furniture or in health care settings a stethoscope or thermometer) in the immediate environment around the infected person (14-17). Nonetheless, fomite transmission is considered a possible mode of transmission for SARS-Co V-2, given consistent finding of environmental contamination in the vicinity of people infected with SARSCo V-2 and the fact that other coronaviruses and respiratory viruses can be transmitted this way (12).
Aerosol transmission can occur in specific situations in which procedures that generate aerosols are performed. The scientific community has been actively researching whether the SARS-CoV-2 virus might also spread through aerosol transmission in the absence of aerosol generating procedures (AGPs) ( 18, 19). Some studies that performed air sampling in
clinical settings where AGPs were not performed found virus RNA, but others did not. The presence of viral RNA is not the same as replication- and infection-competent (viable) virus that could be transmissible and capable of sufficient inoculum to initiate invasive infection. A limited number of studies have isolated viable SARS-Co V-2 from air samples in the vicinity of COVID-19 patients (20, 21 ).
Outside of medical facilities, in addition to droplet and fomite transmission, aerosol transmission can occur in specific settings and circumstances, particularly in indoor, crowded and inadequately ventilated spaces, where infected persons spend long periods of time with others. Studies have suggested these can include restaurants, choir practices, fitness classes, nightclubs, offices and places of worship (12).
High quality research is required to address the knowledge gaps related to modes of transmission, infectious dose and settings in which transmission can be amplified. Currently, studies are underway to better understand the conditions in which aerosol transmission or superspreading events may occur.
Current evidence suggests that people infected with SARSCo V-2 can transmit the virus whether they have symptoms or not. However, data from viral shedding studies suggest that infected individuals have highest viral loads just before or around the time they develop symptoms and during the first 5-7 days of illness ( 12). Among symptomatic patients, the duration of infectious virus shedding has been estimated at 8 days from the onset of symptoms (22-24) for patients with mild disease, and longer for severely ill patients (12). The period of infectiousness is shorter than the duration of detectable RNA shedding, which can last many weeks ( 17).
The incubation period for COVID-19, which is the time between exposure to the virus and symptom onset, is on average 5-6 days, but can be as long as 14 days (25, 26).
Pre-symptomatic transmission - from people who are infected and shedding virus but have not yet developed symptoms - can occur. Available data suggest that some people who have been exposed to the virus can test positive for SARS-CoV-2 via polymerase chain reaction (PCR) testing 1-3 days before they develop symptoms (27). People who develop symptoms appear to have high viral loads on or just prior to the day of symptom onset, relative to later on in their infection (28).
Asymptomatic transmission - transmission from people infected with SARS-CoV-2 who never develop symptoms -can occur. One systematic review of 79 studies found that 20% (17-25%) of people remained asymptomatic throughout the course of infection. (28). Another systematic review, which included 13 studies considered to be at low risk of bias, estimated that 17% of cases remain asymptomatic ( 14%-20%) (30). Viable virus has been isolated from specimens of presymptomatic and asymptomatic individuals, suggesting that people who do not have symptoms may be able to transmit the virus to others. (25, 29-37)
Studies suggest that asymptomatically infected individuals are less likely to transmit the virus than those who develop symptoms (29). A systematic review concluded that individuals who are asymptomatic are responsible for transmitting fewer infections than symptomatic and presymptomatic cases (38). One meta-analysis estimated that there is a 42% lower relative risk of asymptomatic transmission compared to symptomatic transmission (30).

Guidance on mask use in health care settings
Masks for use in health care settings
Medical masks are defined as surgical or procedure masks that are flat or pleated. They are affixed to the head with straps that go around the ears or head or both. Their performance characteristics are tested according to a set of standardized test methods (ASTM F2100, EN 14683, or equivalent) that aim to balance high filtration, adequate breathability and optionally, fluid penetration resistance (39, 40).
Filteringfacepiece respirators (FFR), or respirators, offer a balance of filtration and breathability. However, whereas medical masks filter 3 micrometre droplets, respirators must filter more challenging 0.075 micrometre solid particles. European FFRs, according to standard EN 149, at FFP2 performance there is filtration of at least 94% solid NaCl particles and oil droplets. US N95 FFRs, according to NIOSH 42 CFR Part 84, filter at least 95% NaCl particles. Certified FFRs must also ensure unhindered breathing with maximum resistance during inhalation and exhalation. Another important difference between FFRs and other masks is the way filtration is tested. Medical mask filtration tests are performed on a cross-section of the masks, whereas FFRs are tested for filtration across the entire surface. Therefore, the layers of the filtration material and the FFR shape, which ensure the outer edges of the FFR seal around wearer's face, result in guaranteed filtration as claimed. Medical masks, by contrast, have an open shape and potentially leaking structure. Other FFR performance requirements include being within specified parameters for maximum CO2 build up, total inward leakage and tensile strength of straps ( 41, 42).
A. Guidance on the use of medical masks and respirators to provide care to suspected or confirmed COVID-19 cases
Evidence on the use of mask in health care settings
Systematic reviews have reported that the use of N95/P2 respirators compared with the use of medical masks (see mask definitions, above) is not associated with statistically significant differences for the outcomes of health workers acquiring clinical respiratory illness, influenza-like illness (risk ratio 0.83, 95%CI 0.63-1.08) or laboratory-confirmed influenza (risk ratio 1.02, 95%CI 0.73-1.43); harms were poorly reported and limited to discom~ort associate~ with lower compliance (43, 44). In many settmgs, preservmg the supply of N95 respirators for high-risk, aerosol-generating procedures is an important consideration ( 45).
A systematic review of observational studies on the betacoronaviruses that cause severe acute respiratory syndrome (SARS), Middle East respiratory syndrome (MERS) and COVID-19 found that the use of face protection (including respirators and medical masks) is associated with reduced risk of infection among health workers. These studies suggested that N95 or similar respirators might be associated with greater reduction in risk than medical or 12-16-layer cotton masks. However, these studies had important
2 The WHO list of AGPs includes tracheal intubation, non-invasive ventilation, tracheotomy, cardiopulmonary resuscitation, manual
limitations (recall bias, limited information about the situations when respirators were used and limited ability to measure exposures), and very few studies included in the review evaluated the transmission risk of COVID-19 ( 46). Most of the studies were conducted in settings in which AGPs were performed or other high-risk settings ( e.g., intensive care units or where there was exposure to infected patients and health workers were not wearing adequate PPE).
WHO continues to evaluate the evidence on the effectiveness of the use of different masks and their potential harms, risks and disadvantages, as well as their combination with hand hygiene, physical distancing of at least I metre and other IPC measures.
Guidance
WHO's guidance on the type of respiratory protection to be worn by health workers providing care to COVID-19 patients is based on I) WHO recommendations on IPC for epidemicand pandemic-prone acute respiratory infections in health care (47); 2) updated systematic reviews of randomized controlled trials on the effectiveness of medical masks compared to that of respirators for reducing the risk of clinical respiratory illness, influenza-like illness (ILi) and laboratoryconfirmed influenza or viral infections. WHO guidance in this area is aligned with guidelines of other professional organizations, including the European Society of Intensive Care Medicine and the Society of Critical Care Medicine, and the Infectious Diseases Society of America ( 48, 49). ·
The WHO COVID-19 IPC GOG considered all available evidence on the modes of transmission of SARS-Co V-2 and on the effectiveness of medical mask versus respirator use to protect health workers from infection and the potential for harms such as skin conditions or breathing difficulties.
Other considerations included availability of medical masks versus respirators, cost and procurement implications and equity of access by health workers across different settings.
The majority (71%) of the GOG members confirmed their support for previous recommendations issued by WHO on 5 June 2020: 1. In the absence of aerosol generating procedures (AGPs)2,
WHO recommends that health workers providing care to patients with suspected or confirmed COVID-19 should wear a medical mask (in addition to other PPE that are part of droplet and contact precautions).
2. In care settings for COVID-19 patients where AGPs are performed, WHO recommends that health workers should wear a respirator (N95 or FFP2 or FFP3 standard, or equivalent) in addition to other PPE that are part of airborne and contact precautions.
In general, health workers have strong preferences about having the highest perceived protection possible to prevent COVID-19 infection and therefore may place high value on the potential benefits of respirators in settings without AGPs. WHO recommends respirators primarily for settings where AGPs are performed; however, if health workers prefer them and they are sufficiently available and cost is not ~ issu~, they could also be used during care for COVID-19 patients m other settings. For additional guidance on PPE, including PPE
ventilation before intubation, bronchoscopy, sputum induction using nebulized hypertonic saline, and dentistry and autopsy procedures.

beyond mask use by health workers, see WHO IPC guidance during health care when COVID-19 infection is suspected (3) and also WHO guidance on the rational use of PPE (45).
Exhalation valves on respirators are discouraged as they bypass the filtration function for exhaled air.
B. Guidance on the use of mask by health workers, caregivers and others based on transmission scenario
Definitions
Universal masking in health facilities is defined as the requirement for all persons (staff, patients, visitors, service providers and others) to wear a mask at all times except for when eating or drinking.
Targeted continuous medical mask use is defined as the practice of wearing a medical mask by all health workers and caregivers working in clinical areas during all routine activities throughout the entire shift.
Health workers are all people primarily engaged in actions with the primary intent of enhancing health. Examples are: nursing and midwifery professionals, doctors, cleaners, other staff who work in health facilities, social workers, and community health workers.
Evidence on universal masking in health care settings
In areas where there is community transmission or large-scale outbreaks of COVID-19, universal masking has been adopted in many hospitals to reduce the potential of transmission by health workers to patients, to other staff and anyone else entering the facility (50).
Two studies found that implementation of a universal masking policy in hospital systems was associated with decreased risk of healthcare-acquired SARS-Co V-2 infection. However, these studies had serious limitations: both were before-after studies describing a single example of a phenomenon before and after an event of interest, with no concurrent control group, and other infection control measures were not controlled for (51, 52). In addition, observed decreases in health worker infections occurred too quickly to be attributable to the universal masking policy.
Guidance
Although more research on universal masking in heath settings is needed, it is the expert opinion of the majority (79%) of WHO COVID-19 IPC GOG members that universal masking is advisable in geographic settings where there is known or suspected community or cluster transmission of the SARS-Co V-2 virus. 1. In areas of known or suspected community or cluster
SARS-Co V-2 transmission, universal masking should be advised in all health facilities (see Table 1 ).
• All health workers, including community health workers and caregivers, should wear a medical mask at all times, for any activity ( care of COVID-19 or nonCOVID-19 patients) and in any common area (e.g., cafeteria, staff rooms).
• Other staff, visitors, outpatients and service providers should also wear a mask (medical or non-medical) at all times
• Inpatients are not required to wear a mask (medical or non-medical) unless physical distancing of at least 1 metre cannot be maintained ( e.g., when being examined or visited at the bedside) or when outside of their care area ( e.g., when being transported).
• Masks should be changed when they become soiled, wet or damaged or if the health worker/caregiver removes the mask ( e.g., for eating or drinking or caring for a patient who requires droplet/contact precautions for reasons other than COVID-19).
2. In the context of known or suspected sporadic SARSCo V-2 virus transmission, WHO provides the following guidance:
• Health workers, including community health workers and caregivers who work in clinical areas, should continuously wear a medical mask during routine activities throughout the entire shift, apart from when eating and drinking and changing their medical masks after caring for a patient who requires droplet/contact precautions for other reasons. In all cases, medical masks must be changed when wet, soiled, or damaged; used medical masks should be properly disposed of at the end of the shift; and new clean ones should be used for the next shift or when medical masks are changed.
• It is particularly important to adopt the continuous use of masks in potentially high transmission risk settings including triage, family physician/general practitioner offices; outpatient departments; emergency rooms; COVID-19 designated units; haematology, oncology and transplant units; and long-term health and residential facilities.
• Staff who do not work in clinical areas ( e.g., administrative staff) do not need to wear a medical mask during routine activities if they have no exposure to patients.
Whether using masks for universal masking within health facilities or targeted continuous medical mask use throughout the entire shift, health workers should ensure the following:
• Medical mask use should be combined with other measures including frequent hand hygiene and physical distancing among health workers in shared and crowded places such as cafeterias, break rooms, and dressing rooms.
• The medical mask should be changed when wet, soiled, or damaged.
• The medical mask should not be touched to adjust it or if displaced from the face for any reason. If this happens, the mask should be safely removed and replaced, and hand hygiene performed.
• The medical mask ( as well as other personal protective equipment) should be discarded and changed after caring for any patient who requires contact/droplet precautions for other pathogens, followed by hand hygiene.
• Under no circumstances should medical masks be shared between health workers or between others wearing them. Masks should be appropriately disposed of whenever removed and not reused.

• A particulate respirator at least as protective as a United States of America (US) National Institute for Occupational Safety and Health-certified N95, N99, US Food and Drug Administration surgical N95, European Union standard FFP2 or FFP3, or equivalent, should be worn in settings for COVID-19 patients where AGPs are perfonned (see WHO recommendations below). In these settings, this includes continuous use by health workers throughout the entire shift, when this policy is implemented.
Note: Decision makers may consider the transmission intensity in the catchment area of the health facility or community setting and the feasibility of implementing a universal masking policy compared to a policy based on assessed or presumed exposure risk. Decisions need to take into account procurement, sustainability and costs of the policy. When planning masks for all health workers, longtenn availability of adequate medical masks (and when applicable, respirators) for all workers should be ensured, in particular for those providing care for patients with confinned or suspected COVID-19. Proper use and adequate waste management should be ensured.
The potential harms and risks of mask and respirator use in the health facility setting include:
• contamination of the mask due to its manipulation by contaminated hands (53, 54);
• potential self-contamination that can occur if medical masks are not changed when wet, soiled or damaged; or by frequent touching/adjusting when worn for prolonged periods (55);
• possible development of facial skin lesions, irritant dennatitis or worsening acne, when used frequently for long hours (56-58);
• discomfort, facial temperature changes and headaches from mask wearing (44, 59, 60);
• false sense of security leading potentially to reduced adherence to well recognized preventive measures such as physical distancing and hand hygiene; and risk-taking behaviours ( 61-64 );
• difficulty wearing a mask in hot and humid environments • possible risk of stock depletion due to widespread use in
the context of universal masking and targeted continuous mask use and consequent scarcity or unavailability for health workers caring for COVID 19 patients and during health care interactions with non-COVID-19 patients where medical masks or respirators might be required.
Alternatives to medical masks in health care settings
The WHO's disease commodity package (DCP) for COVID-19 recommends medical masks for health workers to be type II or higher (65). Type II medical masks provide a physical barrier to fluids and particulate materials and have bacterial filtration efficiency of ~8% compared to Type I mask, which has bacterial filtration efficiency of ::::95% and lower fluid resistance ( 66) In case of stock outs of type II or higher medical masks, health workers should use a type I medical mask as an alternative. Other alternatives such as face shields or fabric masks should be carefully evaluated.
Face shields are designed to provide protection from splashes of biological fluid (particularly respiratory secretions), chemical agents and debris (67, 68) into the eyes. In the context of protection from SARS-CoV-2 transmission through respiratory droplets, face shields are used by health workers as personal protective equipment (PPE) for eye protection in combination with a medical mask or a respirator (69, 70) While a face shield may confer partial protection of the facial area against respiratory droplets, these and smaller droplets may come into contact with mucous membranes or with the eyes from the open gaps between the visor and the face (71,67).
Fabric masks are not regulated as protective masks or part of the PPE directive. They vary in quality and are not subject to mandatory testing or common standards and as such are not considered an appropriate alternative to medical masks for protection of health workers. One study that evaluated the use of cloth masks in a health care facility found that health care workers using 2 ply cotton cloth masks (a type of fabric mask) were at increased risk of influenza-like illness compared with those who wore medical masks (72).
In the context of severe medical mask shortage, face shields alone or in combination with fabric mask may be considered as a last resort (73). Ensure proper design of face shields to cover the sides of the face and below the chin.
As for other PPE items, if production of fabric masks for use in health care settings is proposed locally in situations of shortage or stock out, a local authority should assess the product according to specific minimum perfonnance standards and required technical specifications (see Annex).
Additional considerations for community care settings
Like other health workers, community health workers should apply standard precautions for all patients at all times, with particular emphasis regarding hand and respiratory hygiene, surface and environmental cleaning and disinfection and the appropriate use of PPE. When a patient is suspected or confinned of having COVID-19, community health workers should always apply contact and droplet precautions. These include the use of a medical mask, gown, gloves and eye protection (7 4 ).
IPC measures that are needed will depend on the local COVID-19 transmission dynamics and the type of contact required by the health care activity (see Table 1). The community health workforce should ensure that patients and workforce members apply precautionary measures such as respiratory hygiene and physical distancing of at least 1 metre (3.3 feet). They also may support set-up and maintenance of hand hygiene stations and community education (74). In the context of known or suspected community or cluster transmission, community health workers should wear a medical mask when providing essential routine services (see Table 1).

Table 1. Mask use in health care settings depending on transmission scenario, target population, setting, activity and type*
Transmission Target population Setting (where) Activity (what) Mask type (which scenario (who) one)*
Known or Health workers and Health facility For any activity in patient-care Medical mask ( or suspected caregivers (including primary, areas (COVID-19 or non- respirator if aerosol community or secondary, tertiary care COVID-19 patients) or in any generating cluster levels, outpatient care, common areas ( e.g., cafeteria, procedures transmission and long-term care staff rooms) performed) ofSARS- Other staff, patients, facilities) For any activity or in any Medical or fabric CoV-2 visitors, service common area mask
suppliers
Inpatients In single or multiple- When physical distance of at bed rooms least I metre cannot be
maintained
Health workers and Home visit (for When in direct contact with a Medical mask caregivers example, for antenatal patient or when a distance of at
or postnatal care, or for least I metre cannot be a chronic condition) maintained.
Community Community outreach programmes/essential routine services
Known or Health workers and Health facility In patient care area- irrespective Medical mask suspected caregivers (including primary, of whether patients have sporadic secondary, tertiary care suspected/confirmed COVID-19 transmission Other staff, patients, levels, outpatient care, No routine activities in patient Medical mask not ofSARS- visitors, service and long-term care areas required. Medical CoV-2 cases suppliers and all others facilities) mask should be
worn if in contact or within I metre of patients, or according to local risk assessment
Health workers and Home visit ( for When in direct contact or when a Medical mask caregivers example, for antenatal distance of at least I metre
or postnatal care, or for cannot be maintained. a chronic condition)
Community Community outreach programs (e.g., bed net distribution)
No Health workers and Health facility Providing any patient care Medical mask use documented caregivers (including primary, according to SARS-CoV-2 secondary, tertiary care standard and transmission levels, outpatient care, transmission-based
and long-term care precautions facilities)
Community Community outreach programs
Any Health workers Health care facility Performing an AGP on a Respirator (N95 or transmission (including primary, suspected or confirmed COVID- N99 or FFP2 or scenario secondary, tertiary care 19 patient or providing care in a FFP3)
levels, outpatient care, setting where AGPs are in place and long-term care for COVID-19 patients facilities), in settings where aerosol generating procedures (AGP) are performed
• This table refers only to the use of medical masks and respirators. The use of medical masks and respirators may need to be combined with other personal protective equipment and other measures as appropriate, and always with hand hygiene.

Guidance on mask use in community settings
Evidence on the protective effect of mask use in community settings
At present there is only limited and inconsistent scientific evidence to support the effectiveness of masking of healthy people in the community to prevent infection with respiratory viruses, including SARS-CoV-2 (75). A large randomized community-based trial in which 4862 healthy participants were divided into a group wearing medical/surgical masks and a control group found no difference in infection with SARS-CoV-2 (76). A recent systematic review found nine trials ( of which eight were cluster-randomized controlled trials in which clusters of people, versus individuals, were randomized) comparing medical/surgical masks versus no masks to prevent the spread of viral respiratory illness. Two trials were with healthcare workers and seven in the community. The review concluded that wearing a mask may make little or no difference to the prevention of influenza-like illness (ILi) (RR 0.99, 95%CI 0.82 to 1.18) or laboratory confirmed illness (LCI) (RR 0.91, 95%CI 0.66-1.26) (44); the certainty of the evidence was low for ILi, moderate for LCI.
By contrast, a small retrospective cohort study from Beijing found that mask use by entire families before the first family member developed COVID-19 symptoms was 79% effective in reducing transmission (OR 0.21, 0.06-0.79) (77). A casecontrol study from Thailand found that wearing a medical or non-medical mask all the time during contact with a COVID-19 patient was associated with a 77% lower risk of infection (aOR 0.23; 95% CI 0.09-0.60) (78). Several small observational studies with epidemiological data have reported an association between mask use by an infected person and prevention of onward transmission of SARSCo V-2 infection in public settings. (8, 79-81 ).
A number of studies, some peer reviewed (82-86) but most published as pre-prints (87-104), reported a decline in the COVID-19 cases associated with face mask usage by the public, using country- or region-level data. One study reported an association between community mask wearing policy adoption and increased movement (less time at home, increased visits to commercial locations) (105). These studies differed in setting, data sources and statistical methods and have important limitations to consider ( 106), notably the lack of information about actual exposure risk among individuals, adherence to mask wearing and the enforcement of other preventive measures ( I 07, 108).
Studies of influenza, influenza-like illness and human coronaviruses (not including COVID-19) provide evidence that the use of a medical mask can prevent the spread of infectious droplets from a symptomatic infected person to someone else and potential contamination of the environment by these droplets (75). There is limited evidence that wearing a medical mask may be beneficial for preventing transmission between healthy individuals sharing households with a sick person or among attendees of mass gatherings (44, 109-114).
3 For adequate ventilation refer to regional or national institutions or h~ting, refrigerating and air-conditioning societies enacting ventilation requirements. Ifnot available or applicable, a recommended ventilation rate of IO Vs/person should be met (except healthcare facilities which have specific requirements). For more information consult "Coronavirus (COVID-19) response
A meta-analysis of observational studies on infections due to betacoronaviruses, with the intrinsic biases of observational data, showed that the use of either disposable medical masks or reusable 12-16-layer cotton masks was associated with protection of healthy individuals within households and among contacts of cases ( 46). This could be considered to be indirect evidence for the use of masks (medical or other) by healthy individuals in the wider community; however, these studies suggest that such individuals would need to be in close proximity to an infected person in a household or at a mass gathering where physical distancing cannot be achieved to become infected with the virus. Results from cluster randomized controlled trials on the use of masks among young adults living in university residences in the United States of America indicate that face masks may reduce the rate of influenza-like illness but showed no impact on risk of laboratory-confirmed influenza ( 115, 116).
Guidance
The WHO COVID-19 IPC GOG considered all available evidence on the use of masks by the general public including effectiveness, level of certainty and other potential benefits and harms, with respect to transmission scenarios, indoor versus outdoor settings, physical distancing and ventilation. Despite the limited evidence of protective efficacy of mask wearing in community settings, in addition to all other recommended preventive measures, the GOG advised mask wearing in the following settings:
1. In areas with known or suspected community or cluster transmission of SARS-CoV-2, WHO advises mask use by the public in the following situations (see Table 2):
Indoor settings: - in public indoor settings where ventilation is known to be
poor regardless of physical distancing: limited or no opening of windows and doors for natural ventilation; ventilation system is not properly functioning or maintained; or cannot be assessed;
- in public indoor settings that have adequate3 ventilation if physical distancing of at least 1 metre cannot be maintained;
- in household indoor settings: when there is a visitor who is not a household member and ventilation is known to be poor, with limited opening of windows and doors for natural ventilation, or the ventilation system cannot be assessed or is not properly functioning, regardless of whether physical distancing of at least I metre can be maintained;
- in household indoor settings that have adequate ventilation if physical distancing of at least 1 metre cannot be maintained.
resources from ASHRAE and others,, https://www.ashrae.org/technical-resources/resources

Table 2. Mask use in community settings depending on transmission scenario, setting, target population, purpose and type*
Transmission scenario
Situations/settings (where) Target Population (who)
Known or suspected Indoor settings, where community or ventilation is known to be cluster transmission poor or cannot be assessed or of SAR.S-Co V-2 the ventilation system is not
General population in public* settings such as shops, shared workplaces, schools, churches, restaurants, gyms, etc. or in enclosed settings such as public transportation. properly maintained,
regardless of whether
physical distancing of at least For households, in indoor settings, when _1 _m_e_t_er_c_an_b_e_m_a_in_t_a_in_e_d _ ___. there is a visitor who is not a member of
Indoor settings that have the household adequate 4 ventilation if physical distancing of at least 1 metre cannot be maintained
Outdoor settings where General population in settings such as physical distancing cannot be crowded open-air markets, lining up maintained outside a building, during
demonstrations, etc.
Purpose of mask use
(why)
Potential benefit for source control
Settings where physical Individuals/people with higher risk of Protection
Known or suspected sporadic transmission, or no documented SARSCo V-2 transmission
distancing cannot be severe complications from COVID-19: maintained, and the individual • People aged ~60 years is at increased risk of infection and/or negative outcomes
Risk-based approach
• People with underlying comorbidities, such as cardiovascular disease or diabetes mellitus, chronic lung disease, cancer, cerebrovascular disease, immunosuppression, obesity, asthma
General population Potential benefit for source control and/or protection
Any transmission Any setting in the community Anyone suspected or confirmed of Source scenario having COVID-19, regardless of control
whether they have symptoms or not, or anyone awaiting viral test results, when in the presence of others
• Public indoor setting includes any indoor setting outside of the household
Mask type (which one)
Fabric mask
Medical mask
Depends on purpose (see details in the guidance content)
Medical mask
4 For adequate ventilation refer to regional or national institutions or heating, refrigerating and air-conditioning societies enacting ventilation requirements. Ifnot available or applicable, a recommended ventilation rate of 101/s/person should be met (except healthcare facilities which have specific requirements).). For more infonnation consult "Coronavirus (COVID-19) response resources from ASHRAE and others" https://www.ashrae.org/technical-resources/resources

In outdoor settings: - where physical distancing of at least 1 metre cannot be
maintained;
- individuals/people with higher risk of severe complications from COVID-19 (individuals ::: 60 years old and those with underlying conditions such as cardiovascular disease or diabetes mellitus, chronic lung disease, cancer, cerebrovascular disease or immunosuppression) should wear medical masks in any setting where physical distance cannot be maintained.
2. In areas with known or suspected sporadic transmission or no documented transmission, as in all transmission scenarios, WHO continues to advise that decision makers should apply a risk-based approach focusing on the following criteria when considering the use of masks for the public: • Purpose of mask use. Is the intention source control
(preventing an infected person from transmitting the virus to others) or protection (preventing a healthy wearer from the infection)?
• Risk of exposure to SARS-Co V-2. Based on the epidemiology and intensity of transmission in the population, is there transmission and limited or no capacity to implement other containment measmes such as contact tracing, ability to cany out testing and isolate and care for suspected and confinned cases? Is there risk to individuals working in close contact with the public ( e.g., social workers, personal support workers, teachers, cashiers)?
• Vulnerability of the mask wearer/population. Is the mask wearer at risk of severe complications from COVID-19? Medical masks should be used by older people (2: 60 years old), immunocompromised patients and people with comorbidities, such as cardiovascular disease or diabetes mellitus, chronic lung disease, cancer and cerebrovascular disease ( 117).
• Setting in which the population lives. Is there high population density (such as in refugee camps, camp-like settings, and among people living in cramped conditions) and settings where individuals are unable to keep a physical distance of at least 1 metre (for example, on public transportation)?
• Feasibility. Are masks available at an affordable cost? Do people have access to clean water to wash fabric masks, and can the targeted population tolerate possible adverse effects of wearing a mask?
• Type of mask. Does the use of medical masks in the community divert this critical resource from the health workers and others who need them the most? In settings where medical masks are in short supply, stocks should be prioritized for health workers and at-risk individuals.
The decision of governments and local jurisdictions whether to recommend or make mandatory the use of masks should be based on the above assessment as well as the local context, culture, availability of masks and resources required.
3. In any transmission scenario: • Persons with any symptoms suggestive of COVID-19
should wear a medical mask and ( S) additionally: - self-isolate and seek medical advice as soon as they
start to feel unwell with potential symptoms of COVID-19, even if symptoms are mild);
- follow instructions on how to put on, take off, and dispose of medical masks and perform hand hygiene (118);
- follow all additional measures, in particular respiratory hygiene, frequent hand hygiene and maintaining physical distance of at least I metre from other persons ( 46). If a medical mask is not available for individuals with suspected or confirmed COVID-19, a fabric mask meeting the specifications in the Annex of this document should be worn by patients as a source control measure, pending access to a medical mask. The use of a nonmedical mask can minimize the projection of respiratory droplets from the user (119, 120).
- Asymptomatic persons who test positive for SARSCo V-2, should wear a medical mask when with others for a period of 10 days after testing positive.
Potential benefits/harms
The potential advantages of mask use by healthy people in the general public include: • reduced spread of respiratory droplets containing
infectious viral particles, including from infected persons before they develop symptoms ( 121 );
• reduced potential for stigmatization and greater of acceptance of mask wearing, whether to prevent infecting others or by people caring for COVID-19 patients in non-clinical settings (122);
• making people feel they can play a role in contributing to stopping spread of the virus;
• encouraging concurrent transmission prevention behaviours such as hand hygiene and not touching the eyes, nose and mouth (123-125);
• preventing transmission of other respiratory illnesses like tuberculosis and influenza and reducing the burden of those diseases during the pandemic (126).
The potential disadvantages of mask use by healthy people in the general public include: • headache and/or breathing difficulties, depending on
type of mask used (55); • development of facial skin lesions, irritant dermatitis or
worsening acne, when used frequently for long hours (58, 59, 127);
• difficulty with communicating clearly, especially for persons who are deaf or have poor hearing or use lip reading ( 128, 129);
• discomfort (44, 55, 59) • a false sense of security leading to potentially lower
adherence to other critical preventive measures such as physical distancing and hand hygiene ( 105);
• poor compliance with mask wearing, in particular by young children (111, 130-132);
• waste management issues; improper mask disposal leading to increased litter in public places and environmental hazards (133);
• disadvantages for or difficulty wearing masks, especially for children, developmentally challenged persons, those with mental illness, persons with cognitive impairment, those with asthma or chronic respiratory or breathing problems, those who have had facial trauma or recent oral maxillofacial surgery and those living in hot and humid environments (55, 130).

Considerations for implementation
When implementing mask policies for the public, decisionmakers should: • clearly communicate the purpose of wearing a mask,
including when, where, how and what type of mask should be worn; explain what wearing a mask may achieve and what it will not achieve; and communicate clearly that this is one part of a package of measures along with hand hygiene, physical distancing, respiratory etiquette, adequate ventilation in indoor settings and other measures that are all necessary and all reinforce each other;
• inform/train people on when and how to use masks appropriately and safely (see mask management and maintenance sections);
• consider the feasibility of use, supply/access issues ( cleaning, storage), waste management, sustainability, social and psychological acceptance ( of both wearing and not wearing different types of masks in different contexts);
• continue gathering scientific data and evidence on the effectiveness of mask use (including different types of masks) in non-health care settings;
• evaluate the impact (positive, neutral or negative) of using masks in the general population (including behavioural and social sciences) through good quality research.
Mask use during physical activity
Evidence
There are limited studies on the benefits and harms of wearing medical masks, respirators and non-medical masks while exercising. Several studies have demonstrated statistically significant deleterious effects on various cardiopulmonary physiologic parameters during mild to moderate exercise in healthy subjects and in those with underlying respiratory diseases ( 134-140). The most significant impacts have been consistently associated with the use of respirators and in persons with underlying obstructive airway pulmonary diseases such as asthma and chronic obstructive pulmonary disease (COPD), especially when the condition is moderate to severe (136). Facial microclimate changes with increased temperature, humidity and perceptions of dyspnoea were also reported in some studies on the use of masks during exercise (134, 141). A recent review found negligeable evidence of negative effects of mask use during exercise but noted concern for individuals with severe cardiopulmonary disease (142).
Guidance
WHO advises that people should not wear masks during vigorous intensity physical activity (143) because masks may reduce the ability to breathe comfortably. The most important preventive measure is to maintain physical distancing of at least 1 meter and ensure good ventilation when exercising.
If the activity takes place indoors, adequate ventilation should be ensured at all times through natural ventilation or a properly functioning or maintained ventilation system ( 144 ). Particular attention should be paid to cleaning and disinfection of the environment, especially high-touch surfaces. If all the above measures cannot be ensured, consider temporary closure of public indoor exercise facilities ( e.g., gyms).
Face shields for the general public
At present, face shields are considered to provide a level of eye protection only and should not be considered as an equivalent to masks with respect to respiratory droplet protection and/or source control. Current laboratory testing standards only assess face shields for their ability to provide eye protection from chemical splashes (145).
In the context of non-availability or difficulties wearing a non-medical mask (in persons with cognitive, respiratory or hearing impairments, for example), face shields may be considered as an alternative, noting that they are inferior to masks with respect to droplet transmission and prevention. If face shields are to be used, ensure proper design to cover the sides of the face and below the chin.
Medical masks for the care of COVID-19 patients at home
WHO provides guidance on how to care for patients with confirmed and suspected COVID-19 at home when care in a health facility or other residential setting is not possible (5).
Persons with suspected COVID-19 or mild COVID-19 symptoms should wear a medical mask as much as possible, especially when there is no alternative to being in the same room with other people. The mask should be changed at least once daily. Persons who cannot tolerate a medical mask should rigorously apply respiratory hygiene (i.e., cover mouth and nose with a disposable paper tissue when coughing or sneezing and dispose of it immediately after use or use a bent elbow procedure and then perform hand hygiene). Caregivers of or those sharing living space with people with suspected COVID-19 or with mild COVID-19 symptoms should wear a medical mask when in the same room as the affected person.
References
1. World Health Organization. The World Health Report 2006 - working together for health. Geneva: World Health Organization; 2006.( https://apps. who.int/iris/handle/ 10665/43432 accessed 21 November 2020)
2. World Health Organziation. Advice on the use of masks for children in the context ofCOVID-19. Annex to the Advice on the use of masks in the context of COVID-19. Geneva, 2020. (https:/ /apps. who. int/iris/handle/ I 0665/3 3 3919 accessed 21 November 2020).
3. World Health Organziation. Infection prevention and control during health care when COVID-19 is suspected: interim guidance. Geneva: World Health Organization; 2020. (https://apps. who. int/iris/handle/ 10665/3 3 2879. accessed 21 November 2020).
4. World Health Organziation. Infection prevention and control for long-term care facilities in the context of COVID-19: interim guidance. Geneva: World Health Organization; 2020 (https://apps.who.int/iris/handle/10665/331508 accessed 21 November 2020).

5. World Health Organziation. Home care for patients Host, and Environmental Factors. Ann Intern Med. with suspected or confirmed COVID-19 and 2020;M20-5008. doi: 10. 7326/M20-5008 management of their contacts: interim guidance. 18. Wei J, Li Y. Airborne spread of infectious agents in the Geneva: World Health Organization; 2020 indoor environment. Am J Infect Control. 2016;44(9 (httgs://a1ms. who.int/iris/handle/ 10665/3 3 3 782. Suppl):S 102-8. accessed 21 November 2020). 19. McCarthy J, McCarthy M. Long range versus short
6. World Health Organziation. Infection prevention and range aerial transmission of SARS-Co V-2. 2020 control of epidemic-and pandemic prone acute httgs:/ /arxiv .org/Qdf/2008 .03 5 5 8.gdf (Accessed 24 respiratory infections in health care. November 2020). (httgs://aggs. who.int/iris/bitstream/handle/10665/11265 20. Lednicky JA, Lauzardo M, Fan ZH, et al. Viable 6/9789241507134 eng.gdf?seguence=l Accessed 21 SARS-Co V-2 in the air of a hospital room with November 2020). COVID-19 patients. medRxiv.
7. Machida M, Nakamura I, Saito R, Nakaya T, doi: 10.1101/2020.08.03.20167395 Hanibuchi T, Takamiya T, et al. Incorrect Use of Face 21. Ring N, Ritchie K, Mandava L, Jepson R. A guide to Masks during the Current COVID-19 Pandemic among synthesising qualitative research for researchers the General Public in Japan. Int J Environ Res Public undertaking health technology assessments and Health. 2020;17(18). systematic reviews. 2011. NHS Quality Improvement
8. Liu J, Liao X, Qian S, Yuan J, Wang F, Liu Y, et al. Scotland (NHS QIS). Community Transmission of Severe Acute Respiratory 22. Wolfel R, Corman VM, Guggemos W, Seilmaier M, Syndrome Coronavirus 2, Shenzhen, China, 2020. Zange S, Muller MA, et al. Virological assessment of Emerg Infect Dis. 2020;26(6):1320-3. hospitalized patients with COVID-2019. Nature.
9. Chan JF, Yuan S, Kok KH, To KK, Chu H, Yang J, et 2020;581 (7809):465-9. al. A familial cluster of pneumonia associated with the 23. van Kampen J, van de Vijver D, Fraaij P, Haagmans B, 2019 novel coronavirus indicating person-to-person Lamers M, Okba Nea. Shedding of infectious virus in transmission: a study of a family cluster. Lancet. hospitalized patients with coronavirus disease-2019 2020;395(10223):514-23. (COVID19): duration and key determinants. MedRxiv.
10. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. 2020 doi:10.1101/2020.06.08.20125310. Clinical features of patients infected with 2019 novel 24. Centers for Disease Control and Prevention. Symptom-coronavirus in Wuhan, China. Lancet. Based Strategy to Discontinue Isolation for Persons 2020;395(10223 ):497-506. with COVID-19. Atlanta: Centers for Disease Control
11. Burke RM, Midgley CM, Dratch A, Fenstersheib M, and Prevention; Haupt T, Holshue M, et al. Active Monitoring of (httgs://www.cdc.gov/coronavirus/2019-Persons Exposed to Patients with Confirmed COVID- ncov/communit)'./strateg)'.-discontinue-isolation.html, 19 - United States, January-February 2020. MMWR accessed 21 November 2020). Morb Mortal Wkly Rep. 2020;69(9):245-6. 25. Yu P, Zhu J, Zhang Z, Han Y. A Familial Cluster of
12. World Health Organziation. Transmission ofSARS- Infection Associated With the 2019 Novel Coronavirus CoV-2: implications for infection prevention Indicating Possible Person-to-Person Transmission precautions. During the Incubation Period. J Infect Dis. (htt12s://a1212s.who.int/iris/handle/l 0665/333114 2020;221(11):1757-61. E accessed 21 November 2020). 26. Lauer SA, Grantz KH, Bi Q, Jones FK, Zheng Q,
13. World Health Organziation. Coronavirus disease 2019 Meredith HR, et al. The Incubation Period of (COVID-19) Situation Report-73. Geneva: World Coronavirus Disease 2019 (COVID-19) From Publicly Health Organization; 2020 Reported Confirmed Cases: Estimation and (httns://www.who.int/docs/default- Application. Ann Intern Med. 2020;172(9):577-82. source/ coronaviruse/situation-renorts/20200402-sitre{!- 27. Kimball A, Hatfield KM, Arons M, James A, Taylor J, 73-covid-19.gdf?sfvrsn=5ae25bc7 6, accessed 21 Spicer K, et al. Asymptomatic and Presymptomatic November 2020). SARS-Co V-2 Infections in Residents of a Long-Tenn
14. Cheng VCC, Wong SC, Chen JHK, Yip CCY, Chuang Care Skilled Nursing Facility- King County, VWM, Tsang OTY, et al. Escalating infection control Washington, March 2020. MMWR Morb Mortal Wkly response to the rapidly evolving epidemiology of the Rep. 2020;69(13):377-81. coronavirus disease 2019 (COVID-19) due to SARS- 28. He X, Lau EHY, Wu P, Deng X, Wang J, Hao X, et al. CoV-2 in Hong Kong. Infect Control Hosp Epidemiol. Temporal dynamics in viral shedding and 2020;41 ( 5):493-8. transmissibility ofCOVID-19. Nat Med.
15. Ong SWX, Tan YK, Chia PY, Lee TH, Ng OT, Wong 2020;26( 5):672-5. MSY, et al. Air, Surface Environmental, and Personal 29. Buitrago-Garcia D, Egli-Gany D, Counotte MJ, Protective Equipment Contamination by Severe Acute Hossmann S, Imeri H, Ipekci AM, et al. Occurrence Respiratory Syndrome Coronavirus 2 (SARS-Co V-2) and transmission potential of asymptomatic and From a Symptomatic Patient. JAMA. 2020. presymptomatic SARS-Co V-2 infections: A living 323(16):1610-1612. doi: 10.1001/jama.2020.3227. systematic review and meta-analysis. PLoS Med.
16. van Doremalen N, Bushmaker T, Morris DH, Holbrook 2020;17(9):e1003346. MG, Gamble A, Williamson BN, et al. Aerosol and 30. Byambasuren 0, Cardona, M., Bell, K., Clark, J., Surface Stability of SARS-CoV-2 as Compared with McLaws, M.-L., Glasziou, P. Estimating the extent of SARS-CoV-1. N Engl J Med. 2020;382(16):1564-7. true asymptomatic COVID-19 and its potential for
17. Meyerowitz EA, Richtennan A, Gandhi RT, Sax PE. community transmission: systematic review and meta-Transmission ofSARS-CoV-2: A Review of Viral, analysis. JAMMI 2020 doi: 10.3138/jammi-2020-0030

31. Arons MM, Hatfield KM, Reddy SC, Kimball A, James 45. World Health Organziation. Rational use of personal A, Jacobs JR, et al. Presymptomatic SARS-CoV-2 protective equipment for coronavirus disease 2019 Infections and Transmission in a Skilled Nursing (COVID-19). Geneva: World Health Organization; Facility. N Engl J Med. 2020;382(22):2081-90. 2020
32. Hu Z, Song C, Xu C, Jin G, Chen Y, Xu X, et al. (htt12s://a1212s. who.int/iris/rest/bitstreams/ 12 74340/retrie Clinical characteristics of 24 asymptomatic infections ve accessed 21 November 2020). with COVID-19 screened among close contacts in 46. Chu DK, Akl EA, Duda S, Solo K, Y aacoub S, Nanjing, China. Sci China Life Sci. 2020;63(5):706-11. Schunemann HJ, et al. Physical distancing, face masks,
33. Huang R, Xia J, Chen Y, Shan C, Wu C. A family and eye protection to prevent person-to-person cluster of SARS-Co V-2 infection involving 11 patients transmission of SARS-Co V-2 and COVID-19: a in Nanjing, China. Lancet Infect Dis. 2020;20(5):534-5. systematic review and meta-analysis. Lancet.
34. Pan X, Chen D, Xia Y, Wu X, Li T, Ou X, et al. 2020;395( 10242): 1973-87. Asymptomatic cases in a family cluster with SARS- 47. Chan AJ, Islam MK, Rosewall T, Jaffray DA, Easty CoV-2 infection. Lancet Infect Dis. 2020;20(4):410-1. AC, Cafazzo JA. The use of human factors methods to
35. Wang Y, Tong J, Qin Y, Xie T, Li J, Li J, et al. identify and mitigate safety issues in radiation therapy. Characterization of an asymptomatic cohort of SARS- Radiotherapy and Oncology. 2010;97(3):596-600. COV-2 infected individuals outside of Wuhan, China. 48. Brilli RJ, Spevetz A, Branson RD, Campbell GM, Clin Infect Dis. 2020; 71(16):2132-2138. doi: Cohen H, Dasta JF, et al. Critical care delivery in the 10.1093/cid/ciaa629. intensive care unit: defining clinical roles and the best
36. Wei WE, Li Z, Chiew CJ, Yong SE, Toh MP, Lee VJ. practice model. Crit Care Med. 2001;29(10):2007-19. Presymptomatic Transmission of SARS-Co V-2 - 49. Roland D, McCaffery K, Davies F. Scoring systems in Singapore, January 23-March 16, 2020. MMWR Morb paediatric emergency care: Panacea or paper exercise? Mortal Wkly Rep. 2020;69(14):411-5. Journal of paediatrics and child health. 20 l 6;52(2): 181-
37. Bae SH, Shin H, Koo HY, Lee SW, Yang JM, Yon 6. DK. Asymptomatic Transmission ofSARS-CoV-2 on 50. Klompas M, Morris CA, Sinclair J, Pearson M, Shenoy Evacuation Flight. Emerg Infect Dis. 2020;26( 11 ). ES. Universal Masking in Hospitals in the Covid-19
38. Qiu X, Nergiz I, Maraolo A, Bogoch, Low N, Cevik M. Era. N Engl J Med. 2020;382(2 l ):e63 Defining the role of asymptomatic SARS-CoV-2 51. Seidelman J, Lewis S, Advani S, Akinboyo I, Epling C, transmission: a living systematic review. MedRxiv. Case M, et al. Universal Masking is an Effective 2020 doi: 10.l 101/2020.09.01.20135194. Strategy to Flatten the SARS-2-Co V Healthcare
39. European Standards. UNE EN 14683:2019+AC:2019. Worker Epidemiologic Curve. Infect Control Hosp Medical Face Masks-Requirements and Test Methods. Epidemiol. 2020:1-5. 2019; (httns:/ /www .en-standard.eu/une-en-14683- 52. Wang X, Ferro EG, Zhou G, Hashimoto D, Bhatt DL. 2019-ac-2019-medical-face-masks-reguirements-and- Association Between Universal Masking in a Health test-methods/ accessed 21 November 2020) Care System and SARS-CoV-2 Positivity Among
40. ASTM International. F23 Committee. Specification for Health Care Workers. JAMA. 2020; 324(7):703-704. Performance of Materials Used in Medical Face 53. Zamora JE, Murdoch J, Simchison B, Day AG. Masks.(htms://www.astm.orgl'.Standards/F2 l 00.htm Contamination: a comparison of 2 personal protective accessed 21 November 2020) systems. CMAJ. 2006;175(3):249-54.
41. National Institute for Occupational Safety and 54. Kwon JH, Burnham CD, Reske KA, Liang SY, Hink T, Health (NIOSH). NIOSH Guide to the Selection and Wallace MA, et al. Assessment of Healthcare Worker Use of Particulate Respirators. Deparbnent of Health Protocol Deviations and Self-Contamination During and Human Services (DHHS) NIOSH publication Personal Protective Equipment Donning and Doffing. number96-101, 1996. Infect Control Hosp Epidemiol. 2017 ;3 8(9): 1077-83. (httns://www .cdc.gov/niosh/docs/96-10 I /default.html 55. Bakhit M, Krzyzaniak N, Scott A, Clark J, Glasziou P, accessed 21 November 2020) Del Mar C. Downsides of face masks and possible
42. CEN, E., 2001. 149: 2001 norm: Respiratory protective mitigation strategies: a systematic review and meta-devices-Filtering half masks to protect against analysis. MedRxiv. 2020 doi: particles-Requirements, testing, marking. European 10.1101/2020.06.16.20133207. Committee for Standardization. 56. Foo CC, Goon AT, Leow YH, Goh CL. Adverse skin (htt12s://sho12.bsigroug.com/ProductDetail?gid=0000000 reactions to personal protective equipment against 00030178264 accessed 21 November 2020). severe acute respiratory syndrome--a descriptive study
43. Long Y, Hu T, Liu L, Chen R, Guo Q, Yang L, et al. in Singapore. Contact Dermatitis. 2006;55(5):291-4. Effectiveness of N95 respirators versus surgical masks 57. Radonovich LJ, Jr., SimberkoffMS, Bessesen MT, against influenza: A systematic review and meta- Brown AC, Cummings DAT, Gaydos CA, et al. N95 analysis. J Evid Based Med. 2020;13(2):93-101. Respirators vs Medical Masks for Preventing Influenza
44. Jefferson T DMC, Dooley L, Ferroni E, Al-Ansary LA, Among Health Care Personnel: A Randomized Clinical Bawazeer GA, et al. Physical interventions to interrupt Trial. JAMA. 2019;322(9):824-33. or reduce the spread of respiratory viruses. Cochrane 58. Al Badri F. Surgical mask contact dermatitis and Database of Systematic Reviews 2020;( 11 ):CD006207. epidemiology of contact dermatitis in healthcare doi: 10.1002/14651858.CD006207 .pubS. 2020. workers. Current Allergy & Clinical Immunology,
2017; 30,3: 183 - 188.

59. Matusiak L, Szepietowska M, Krajewski P, Bialynicki- 73. Centers for Disease Control and Prevention. If You Are Birula R, Szepietowski JC. Inconveniences due to the Immunocompromised, Protect Yourself From COVID-use of face masks during the COVID-19 pandemic: a 19.(htt12s://www.cdc.gov/coronavirus/2019-ncov/need-survey study of 876 young people. Dermatol Tuer. extra-12recautions/imm unocom12romised.htm I accessed 2020. doi: 10.1 l 1 l/dth.13567 21 November 2020).
60. MacIntyre CR, Wang Q, Cauchemez S, Seale H, 74. Nielsen J, Landauer Tl(, editors. A mathematical model Dwyer DE, Yang P, et al. A cluster randomized clinical of the finding of usability problems. Proceedings of the trial comparing fit-tested and non-fit-tested N95 INTERACT'93 and CHI'93 conference on Human respirators to medical masks to prevent respiratory factors in computing systems. ACM. 1993; 206-213. virus infection in health care workers. Influenza Other 75. Chou R, Dana T, Jungbauer R, Weeks C, McDonagh Respir Viruses. 2011;5(3):170-9. MS. Masks for Prevention of Respiratory Virus
61. Morrongiello BA, Major K. Influence of safety gear on Infections, Including SARS-Co V-2, in Health Care and parental perceptions of injury risk and tolerance or Community Settings: A Living Rapid Review. Ann children's risk taking. Inj Prev. 2002;8(1):27-31. Intern Med. 2020;173(7):542-555. doi:10.7326/M20-
62. Morrongiello BA, Walpole B, Lasenby J. 3213 Understanding children's injury-risk behavior: wearing 76. Bundgaard H, J. B, Raaschou-Pedersen D, von safety gear can lead to increased risk taking. Accid Buchwald C, Todsen T, Norsk J. Effectiveness of Anal Prev. 2007;39(3):618-23. Adding a Mask Recommendation to Other Public
63. Lasenby-Lessard J, Morrongiello BA. Understanding Health Measures to Prevent SARS-CoV-2 Infection in risk compensation in children: Experience with the Danish Mask Wearers. Ann Intern Med. 2020. doi: activity and level of sensation seeking play a role. 10.7326/M20-6817. Accid Anal Prev. 2011;43(4):1341-7. 77. Wang Y, Tian H, Zhang L, Zhang M, Guo D, Wu W, et
64. DiLillo D, Tremblay G. Maternal and child reports of al. Reduction of secondary transmission of SARS-behavioral compensation in response to safety CoV-2 in households by face mask use, disinfection equipment usage. J Pediatr Psychol. 2001;26(3):175- and social distancing: a cohort study in Beijing, China. 84. BMJ Glob Health. 2020; 5(5): e002794.
65. Thomas EJ, Sexton JB, Helmreich RL. Translating 78. Doung-ngern P, Suphanchaimat R, Panjangampatthana teamwork behaviours from aviation to healthcare: A, Janekrongtham C, Ruampoom D, Daochaeng N. development of behavioural markers for neonatal Associations between mask-wearing, handwashing, and resuscitation. Qual Saf Health Care. 2004 Oct; social distancing practices and risk 2 of COVID-19 13(Suppl 1 ): i57-i64. infection in public: a case-control study in Thailand.
66. Pri-Med Medicinal Products. Mask Protection Emerg Infect Dis. 2020;26(11):2607-2616. Standards & Medical Face Mask Information For Use. 79. Chen J, He H, Cheng W. Potential transmission of (htt12s://www.12rimed.ca/clinical-resources/astm-mask- SARS-CoV-2 on a flight from Singapore to Hangzhou, 12rotection- China: An epidemiological investigation. Travel Med standards/#:~:text=Are%20there%20different%20level Infect Dis. 2020; 36: 101816. s%20of1>/o20Qrotection%20with%20ASTM- 80. Hendrix MJ, Walde C, Findley K, Trotman R. Absence rated3%20%20160%20%201 %20more%20rows%20 of Apparent Transmission of SARS-Co V-2 from Two accessed 21 November 2020). Stylists After Exposure at a Hair Salon with a
67. Hirschmann MT, Hart A, Henckel J, Sadoghi P, Seil R, Universal Face Covering Policy - Springfield, Mouton C. COVID-19 coronavirus: recommended Missouri, May 2020. MMWR Morb Mortal Wkly Rep. personal protective equipment for the orthopaedic and 2020;69(28):930-2. trauma surgeon. Knee Surg Sports Traumatol Arthrosc. 81. Schwartz KL, Murti M, Finkelstein M, Leis JA, 2020;28( 6): 1690-8. Fitzgerald-Rusek A, Bourns L, et al. Lack of COVID-
68. Anon JB, Denne C, Rees D. Patient-Worn Enhanced 19 transmission on an international flight. CMAJ. Protection Face Shield for Flexible Endoscopy. 2020; 192( 15):E410. Otolaryngol Head Neck Surg. 2020;163(2):280-3. 82. Chiang CH, Chiang CH, Chiang CH, Chen YC. The
69. McBride ME, Waldrop WB, Fehr JJ, Boulet JR, Practice of Wearing Surgical Masks during the Murray DJ. Simulation in pediatrics: the reliability and COVID-19 Pandemic. Emerg Infect Dis. validity of a multiscenario assessment. Pediatrics. 2020;26(8): 1962. 2011; 128: 335-343. 83. Cheng VC, Wong SC, Chuang VW, So SY, Chen JH,
70. Kllhler CJ, Hain R. Fundamental protective Sridhar S, et al. The role of community-wide wearing mechanisms of face masks against droplet infections. J of face mask for control of coronavirus disease 2019 Aerosol Sci. 2020; 148: 105617. (COVID-19) epidemic due to SARS-Co V-2. J Infect.
71. Lindsley WO, Noti JD, Blachere FM, Szalajda N, 2020;81(1):l 07-14. Beezhold DH. Efficacy of face shields against cough 84. Bo Y, Guo C, Lin C, et al. Effectiveness of non-aerosol droplets from a cough simulator. J Occup pharmaceutical interventions on COVID-19 Environ Hyg. 2014;11(8):509-18. transmission in 190 countries from 23 January to 13
72. MacIntyre CR, Seale H, Dung TC, Hien NT, Nga PT, April 2020. Int J Infect Dis. 2020; 102: 247-253. Chughtai AA, et al. A cluster randomised trial of cloth 85. Lyu W, Wehby GL. Community Use Of Face Masks masks compared with medical masks in healthcare And COVID-19: Evidence From A Natural Experiment workers. BMJ Open. 2015;5(4):e006577. Of State Mandates In The US. Health Aff (Millwood).
2020;39(8): 1419-25.

86. Gallaway MS, Rigler J, Robinson S, Herrick K, Livar E, Komatsu KK, et al. Trends in COVID-19 Incidence After Implementation of Mitigation Measures -Arizona, January 22-August 7, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(40):1460-3.
87. Rader B, White LF, Burns MR, Chen J, Brilliant J, Cohen J, et al. Mask Wearing and Control of SARSCoV-2 Transmission in the United States. MedRxiv. 2020. doi: 10.1101/2020.08.23.20078964.
88. Matzinger P, Skinner J. Strong impact of closing schools, closing bars and wearing masks during the Covid-19 pandemic: results from a simple and revealing analysis. MedRxiv. 2020. doi: IO.I 101/2020.09.26.20202457.
89. Kenyon C. Widespread use of face masks in public may slow the spread ofSARS CoV-2: 1 an ecological study. MedRxiv. 2020. doi: 10.1101/2020.03.31.20048652.
90. Leffler CT, Ing E, Lykins JD, Hogan MC, McKeown CA, Grzybowski A. Association of Country-wide Coronavirus Mortality with Demographics, Testing, Lockdowns, and Public Wearing of Masks. Am J Trop Med Hyg. 2020. doi: 10.4269/ajtmh.20-1015.
91. Lan F-Y, Christophi C, Buley J, Lliaki E, BrunoMurtha L, Sayah A, et al. Effects of universal masking on Massachusetts healthcare workers' COVID-19 incidence. MedRxiv. 2020. doi: 10.1101/2020.08.09.20171 l 73.
92. Aravindakshan A, Boehnke J, Gholami E, Nayak A. Mask-Wearing During the COVID-19 Pandemic. MedRxiv. 2020. doi: 10.1101/2020.09.1 l.20192971.
93. Pletz M, Steiner A, Kesselmeier M, Loeffler B, Trommer S, Weis S, et al. Impact of universal masking in health care and community on SARS-Co V-2 spread. MedRxiv. 2020. doi: IO.I 101/2020.09.02.20187021.
94. Fortaleza C, et al. Impact ofnonpharmaceutical governmental strategies for prevention and control of COVID-19 in Sao Paulo State, Brazil. MedRxiv. 2020. doi: 10.1101/2020.08.23.20180273.
95. Karaivanov A, Lu SE, Shigeoka H, Chen C, Pamplona S. Face Masks, Public Policies and Slowing the Spread ofCOVID-19: Evidence from Canada. MedRxiv. 2020. doi: 10.l 101/2020.09.24.20201 l 78.
96. Miyazawa D, Kaneko G. Face mask wearing rate predicts country's COVID-19 death rates: with supplementary state-by-state data in the United States. MedRxiv. 2020. doi: 10.1101/2020.06.22.20137745.
97. Mitze T, Kosfeld R, Rode J, Walde K. Face Masks Considerably Reduce Covid-19 Cases in Germany. MedRxiv. 2020. doi: IO.I 101/2020.06.21.20128181.
98. Maloney M, Rhodes N, Yamold P. Mask mandates can limit COVID spread: Quantitative assessment of month-over-month effectiveness of governmental policies in reducing the number of new COVID-19 cases in 3 7 US States and the District of Columbia. MedRxiv. 2020. doi: IO.I 101/2020.10.06.20208033.
99. Sruthi C, Biswal M, Saraswat B, Joshi H, Prakash M. How Policies on Restaurants, Bars, Nightclubs, Masks, Schools, and Travel Influenced Swiss COVID-19 Reproduction Ratios. MedRxiv. 2020. doi: 10.1101/2020.10.11.20210641.
100. Lan F, Christophi C, Buley J, Iliaki E, Bruno-Murtha L, Sayah A, et al. Effects of universal masking on Massachusetts healthcare workers' COVID-19 incidence. MedRxiv. 2020. doi: 10.1101/2020.08.09.20171173.
101. Shacham e, Scroggins S, Ellis M, Garza A. Association of County-Wide Mask Ordinances with Reductions in Daily Co VID-19 Incident Case Growth in a Midwestern Region Over 12 Weeks. MedRxiv. 2020. doi: 10.1101/2020.10.28.20221705.
102. Chemozhukov V, Kasahara H, Schrimpf P. Causal Impact ofMasks, Policies, Behavior on Early Covid-19 Pandemic in the U.S. J Econom. 2020. doi: 10.1016/j.jeconom.2020.09.003.
103. Research GS. Face Masks and GDP. 2020. (https://www.goldmansachs.com/insights/pages/facemasks-and-gdp.html accessed 21 November 2020).
104. Scott N, Saul A, Spelman T, Stoove M, Pedrana A, Saeri A. The introduction of a mandatory mask policy was associated with significantly reduced COVID-19 cases in a major metropolitan city. 2020. (Available at SSRN :http://dx.doi.org/l 0.2139/ssm.3 714648 accessed 29 November 2020).
105. Yan Y, Bayham J, Fenichel E, Richter A. Do Face Masks Create a False Sense of Security? A COVID-19 Dilemma. MedRxiv. 2020. doi: 10.1101/2020.05.23.20111302.
106. Piantadosi S, Byar DP, Green SB. The ecological fallacy. Am J Epidemiol. 1988;127(5):893-904.
107. Clifford GD, Long WJ, Moody GB, Szolovits P. Robust parameter extraction for decision support using multimodal intensive care data. Philos Trans A Math Phys Eng Sci. 2009 Jan 28; 367(1887): 411-429.
108. Dufault B, Klar N. The quality of modem crosssectional ecologic studies: a bibliometric review. Am J Epidemiol. 2011;174(10):1101-7.
109. Barasheed 0, Alfelali M, Mushta S, Bokhary H, Alshehri J, Attar AA, et al. Uptake and effectiveness of facemask against respiratory infections at mass gatherings: a systematic review. Int J Infect Dis. 2016;47:105-11.
110. Barasheed 0, Almasri N, Badahdah AM, Heron L, Taylor J, McPhee K, et al. Pilot Randomised Controlled Trial to Test Effectiveness ofFacemasks in Preventing Influenza-like Illness Transmission among Australian Hajj Pilgrims in 2011. Infect Disord Drug Targets. 2014;14(2):110-6.
111. Cowling BJ, Chan KH, Fang VJ, Cheng CK, Fung RO, Wai W, et al. Facemasks and hand hygiene to prevent influenza transmission in households: a cluster randomized trial. Ann Intern Med. 2009;151(7):437-46.
112. Lau IT, Tsui H, Lau M, Yang X. SARS transmission, risk factors, and prevention in Hong Kong. Emerg Infect Dis. 2004;10(4):587-92.
113. Suess T, Remschmidt C, Schink SB, Schweiger B, Nitsche A, Schroeder K, et al. The role of facemasks and hand hygiene in the prevention of influenza transmission in households: results from a cluster randomised trial; Berlin, Gennany, 2009-2011. BMC Infect Dis. 2012;12:26.
114. Wu J, Xu F, Zhou W, Feikin DR, Lin CY, He X, et al. Risk factors for SARS among persons without known contact with SARS patients, Beijing, China. Emerg Infect Dis. 2004; 10(2):210-6.
115. Aiello AE, Murray GF, Perez V, Coulborn RM, Davis BM, Uddin M, et al. Mask use, hand hygiene, and seasonal influenza-like illness among young adults: a randomized intervention trial. J Infect Dis. 2010;201 ( 4 ):491-8.
116. Aiello AE, Perez V, Coulborn RM, Davis BM, Uddin M, Monto AS. Facemasks, hand hygiene, and influenza among young adults: a randomized intervention trial. PLoS One. 2012;7(1):e29744.
117. World Health Organization. Information Note COVID-19 and NCDs. Geneva: World Health Organization. 2020. (https://www.who.int/docs/defaultsource/inaugural-who-partners-forum/covid-19-andncds---final---corr7 .pdf?sfvrsn=9b65e287 1 &download=true, accessed 21 November 2020)
118. World Health Organization. Coronavirus disease (COVID-19) advice for the public: When and how to use masks. Geveva: World Health Organization; 2020. (https:/lwww.who.int/emergencies/diseases/novelcoronavirus-2019/advice-for-public/when-and-how-touse-masks. accessed 21 November 2020).
119. Aydin 0, Emon B, Cheng S, Hong L, Chamorro LP, Saif MT A. Performance of fabrics for home-made masks against the spread of COVID-19 through droplets: A quantitative mechanistic study. Extreme Mech Lett. 2020;40: 100924.
120. Fischer EP, Fischer MC, Grass D. Henrion I, Warren WS, Westman E. Low-cost measurement of face mask efficacy for filtering expelled droplets during speech. Sci Adv. 2020;6(36).
121. Milton DK, Fabian MP, Cowling BJ, Grantham ML, McDevitt JJ. Influenza virus aerosols in human exhaled breath: particle size, culturability, and effect of surgical masks. PLoS Pathog. 2013;9(3):el003205.
122. Bion JF, Abrusci T, Hibbert P. Human factors in the management of the critically ill patient. Br J Anaesth. 2010;105(1):26-33.
123. Chen YJ, Qin G, Chen J, Xu JL, Feng DY, Wu XY, et al. Comparison of Face-Touching Behaviors Before and During the Coronavirus Disease 2019 Pandemic. JAMA Netw Open. 2020;3(7):e2016924.
124. Shiraly R, Shayan Z, Mclaws ML. Face touching in the time of COVID-19 in Shiraz, Iran. Am J Infect Control. 2020. 48(12): 1559--1561.
125. Betsch C, Korn L, Sprengholz P, FelgendreffL, Eitze S, Schmid P. et al. Social and behavioral consequences of mask policies during the COVID-19 pandemic. Proc Natl Acad Sci US A. 2020;117(36):21851-3.
126. Cowling BJ, Ali ST, Ng TWY. Tsang TK, Li JCM, Fong MW. et al. Impact assessment ofnonpharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: an observational study. Lancet Public Health. 2020;5( 5):e279-e88.
127. Giacalone S, Minuti A. Spigariolo CB, Passoni E, Nazzaro G. Facial dermatoses in the general population due to wearing of personal protective masks during the COVID-19 pandemic: first observations after lockdown. Clin Exp Dermatol. 2020. doi: 10.1111/ced.14376
128. Hufher K, Hofer A. Sperner-Unterweger B. On the difficulties of building therapeutic relationships when wearing face masks. J Psychosom Res. 2020;138:l 10226.
129. Crume B. The silence behind the mask: my journey as a deaf pediatric resident amidst a pandemic. Acad Pediatr. 2020. doi: 10.1016/j.acap.2020.10.002.
130. Allison MA. Guest-Warnick G, Nelson D, Pavia AT, Srivastava R, Gesteland PH, et al. Feasibility of elementary school children's use of hand gel and facemasks during influenza season. Influenza Other Respir Viruses. 2010;4(4):223-9.
131. Canini L, Andreoletti L, Ferrari P, D'Angelo R, Blanchon T, Lemaitre M, et al. Surgical mask to prevent influenza transmission in households: a cluster randomized trial. PLoS One. 2010;5(1 l):el3998.
132. Uchida M, Kaneko M, Hidaka Y, Yamamoto H, Honda T, Takeuchi S, et al. Effectiveness of vaccination and wearing masks on seasonal influenza in Matsumoto City, Japan, in the 2014/2015 season: An observational study among all elementary schoolchildren. Prev Med Rep. 2017;5:86-91.
133. Zand A, Heir A. Environmental impacts of new Coronavirus outbreak in Iran with an emphasis on waste management sector. J Mater Cycles Waste Manag. 2020 : 1-8.
134. Fikenzer S, Ube T, Lavall D, Rudolph U, Falz R, Busse M, et al. Effects of surgical and FFP2/N95 face masks on cardiopulmonary exercise capacity. Clin Res Cardiol. 2020 Jul 6: 1-9.
135. Harber P, Santiago S, Bansal S, Liu Y, Yun D, Wu S. Respirator physiologic impact in persons with mild respiratory disease. J Occup Environ Med. 2010;52(2): 155-62.
136. Kyung SY, Kim Y, Hwang H, Park JW, Jeong SH. Risks ofN95 Face Mask Use in Subjects With COPD. Respir Care. 2020;65(5):658-64.
137. Lee HP, Wang de Y. Objective assessment of increase in breathing resistance of N95 respirators on human subjects. Ann Occup Hyg. 2011;55(8):917-21.
138. Matuschek C, Moll F, Fangerau H, Fischer JC, Zanker K, van Griensven M, et al. Face masks: benefits and risks during the COVID-19 crisis. Eur J Med Res. 2020;25(1 ):32.
139. Person E, Lemercier C, Royer A, Reychler G. [Effect of a surgical mask on six minute walking distance]. Rev Mal Respir. 2018;35(3):264-8.
140. Wong A Y, Ling SK, Louie LH, Law GY, So RC, Lee DC, et al. Impact of the COVID-19 pandemic on sports and exercise. Asia Pac J Sports Med Arthrosc Rehabil Technol. 2020;22:39-44.
141. Li Y, Tokura H. Guo YP, Wong AS, Wong T, Chung J, et al. Effects of wearing N95 and surgical facemasks on heart rate, thermal stress and subjective sensations. Int Arch Occup Environ Health. 2005;78(6):501-9.
142. Hopkins SR, Dominelli PB, Davis CK, Guenette JA, Luks AM, Molgat-Seon Y, et al. Facemasks and the Cardiorespiratory Response to Physical Activity in Health and Disease. Ann Am Thorac Soc. 2020. doi: 10.1513/ AnnalsATS.202008-990CME.
143. Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24): 1451-62.
144. Yang GZ, Kelley E, Darzi A. Patients' safety for global health. Lancet. 2011; 377(9769): 886-7.
145. Roberge RJ. Face shields for infection control: A review. J Occup Environ Hyg. 2016;13(4):235-42.

146. Jang JY, Kim, S.W. Evaluation of Filtration Performance Efficiency of Commercial Cloth Masks. Journal of Environmental Health Sciences
(~~~~.!i!.-c!§l'~IJ=l>2015; 41 (3) 203-215. 147. Jung H, Kim JK, Lee S, Lee J, Kim J, Tsai P, et al.
Comparison of Filtration Efficiency and Pressure Drop in Anti-Yellow Sand Masks, Quarantine Masks, Medical Masks, General Masks, and Handkerchiefs. Aerosol Air Qual. Res. 2014;14, 991-1002.
148. Lustig SR, Biswakarma JJH, Rana D, Tilford S:8, Hu W, Su M, et al. Effectiveness of Common Fabncs to Block Aqueous Aerosols of Virus-like Nanoparticles. ACS Nano. 2020;14(6):7651-8.
149. Zangmeister CD, Radney JG, Vicenzi EP, Weaver JL. Filtration Efficiencies ofNanoscale Aerosol by Cloth Mask Materials Used to Slow the Spread of SARSCo V-2. ACS Nano. 2020;14(7):9188-200.
150. Zhao M, Liao L, Xiao W, Yu X, Wang H, Wang Q, et al. Household materials selection for homemade cloth face coverings and their filtration efficiency enhancement with triboelectric charging. Nano Lett. 2020; 20(7):5544-5552.
151. Clase CM, Fu EL, Ashur A, Beale RCL, Clase IA, Dolovich MB, et al. Forgotten Technology in the COVID-19 Pandemic: Filtration Properties of Cloth and Cloth Masks-A Narrative Review. Mayo Clin Proc. 2020;95( 10):2204-24.
152. Jain M, Kim S, Xu C, Li H, Rose G. Efficacy and Use of Cloth Masks: A Scoping Review. Cureus 12(9): el0423. doi:10.7759/cureus.10423
153. Mondal A, Das A, Goswami R. Utility of Cloth Masks in Preventing Respiratory Infections: A Systematic Review. MedRxiv. 2020 doi: 10.l 101/2020.05.07.20093864
154. Roberge RJ, Roberge MR. Cloth face coverings for use as facemasks during the coronavirus (SARS-Cov-2) pandemic: what science and experience have taught us. Disaster Med Public Health Prep. 2020:1-29.
155. Sharma SK, Mishra M, Mudgal SK. Efficacy of cloth face mask in prevention of novel coronavirus infect~on transmission: A systematic review and meta-analysis. J Educ Health Promot. 2020;9: 192.
156. Taminato M, Mizusaki-Imoto A, Saconato H, Franco E, Puga M, Duarte M, et al. Homemade cloth face masks as a barrier against respiratory droplets -systematic review. Acta Paul Enferm. 2020:eAPE20200103.
157. Bae S, Kim MC, Kim JY, Cha HH, Lim JS, Jung J, et al. Effectiveness of Surgical and Cotton Masks in Blocking SARS-Co V-2: A Controlled Comparison in 4 Patients. Ann Intern Med. 2020;173(1):W22-W3.
158. Ma QX, Shan H, Zhang HL, Li GM: Yang~' Chen JM. Potential utilities of mask-weanng and mstant hand hygiene for fighting SARS-Co V-2. J Med Virol. 2020. doi: 10.1002/jmv.25805.
159. Davies A, Thompson KA, Girl K., Kafatos G, Walker J, Bennett A. Testing the efficacy of homemade masks: would they protect in an influenza pandemic? Disaster Med Public Health Prep. 2013;7(4):413-8.
160. Konda A, Prakash A, Moss GA, Schmoldt M, Grant GD, Guha S. Aerosol Filtration Efficiency of Common Fabrics Used in Respiratory Cloth Masks. ACS Nano. 2020;14(5):6339-47.
161. Neupane BB, Mainali S, Sharma A, Girl B. Optical_ microscopic study of surface morphology and filtenng efficiency offace masks. PeerJ. 2019;7:e7142.
162. Shakya KM, Noyes A, Kallin R, Peltier RE. Evaluating the efficacy of cloth facemasks in reducing particulate matter exposure. J Expo Sci Environ Epidemiol. 2017;27(3):352-7.
163. Jung H KJ, Lee S, Lee J, Kim J, Tsai P, et al.. . Comparison of filtration efficiency and pressure drop m anti-yellow sand masks, quarantine masks, medical masks, general masks, and handkerchiefs. Aerosol Air Qual Res. 2014;14:991-1002.
164. Rengasamy S, Eimer B, Shaffer RE. Simple respiratory protection--evaluation of the filtration performance of cloth masks and common fabric materials against 20-1000 nm size particles. Ann Occup Hyg. 2010;54(7):789-98.
165. Dato VM, Hostler D, Hahn ME. Simple respiratory mask. Emerg Infect Dis. 2006;12(6):1033-4.
166. van der Sande M, Teunis P, Sabel R. Professional and home-made face masks reduce exposure to respiratory infections among the general population. PLoS One. 2008;3(7):e26 l 8.
167. Chughtai AA, Seale H, Dung TC, Hayen A, Rahman B, Raina MacIntyre C. Compliance with the Use of Medical and Cloth Masks Among Healthcare Workers in Vietnam. Ann Occup Hyg. 2016;60(5):619-30.
168. AATCC. AATCC Ml4-2020 Guidance and Considerations for General Purpose Textile Face Coverings: Adult (https://www .aatcc.org/covid/ accessed 28 November 2020)
169. Centers for Disease Control and Prevention. Scientific Brief: Community Use of Cloth Masks to Control the Spread ofSARS-CoV-2. https://www .cdc.gov/coronavirus/2019-ncov/more/masking-science-sarscov2.html?tbclid-IwAR28PppCa6x2uxwO8Z2baHM0 KHS4JXx0inzzMOs3zRHV I ggl 0a8mxZfpCw (Accessed 29 November 2020). . . .
170. Swinfen R, Swinfen P. Low-cost telemed1cme m the developing world. J Telemed Telecare. 2002;8(suppl 3):63-5.
171. Lee SA, Hwang DC, Li HY, Tsai CF, Chen CW, Chen JK. Particle Size-Selective Assessment of Protection of European Standard FFP Respirat~rs and Surgica~ Masks against Particles-Tested with Human SubJects. J Healthc Eng. 2016;2016
Acknowledgments
This document was developed based on advice by the Strategic and Technical Advisory Grou~ for Infecti~us Hazards (STAG-IH), and in consultation with the followmg members of:
1) The WHO Health Emergencies Programme (WHE) A?hoc COVID-19 IPC Guidance Development Group (m alphabetical order):
Jameela Alsalman, Ministry of Health, Bahrain; ~ucha Apisamthanarak, Thammsat University Hospital, Thailand; Baba Aye, Public Services International~ France; Gregory Built, UNICEF, United States of Amenca (USA); Roger Chou, Oregon Health Science University, USA; May Chu,

Colorado School of Public Health, USA; John Conly, Alberta Health Services, Canada; Barry Cookson, University College London, United Kingdom (U.K); Nizam Damani, Southern Health & Social Care Trust, United Kingdom; Dale Fisher, GOARN, Singapore; Joost Hopman, Radboud University Medical Center, The Netherlands; Mushtuq Husain, Institute of Epidemiology, Disease Control & Research, Bangladesh; Kushlani Jayatilleke, Sri Jayewardenapura General Hospital, Sri Lanka; Seto Wing Jong, School of Public Health, Hong Kong SAR, China; Souha Kanj, American University of Beirut Medical Center, Lebanon; Daniele Lantagne, Tufts University, USA; Fernanda Lessa, Centers for Disease Control and Prevention, USA; Anna Levin, University of Sao Paulo, Brazil; Ling Moi Lin, Sing Health, Singapore; Caline Mattar, World Health Professions Alliance, USA; MaryLouise Mclaws, University of New South Wales, Australia; Geeta Mehta, Journal of Patient Safety and Infection Control, India; Shaheen Mehtar, Infection Control Africa Network, South Africa; Ziad Memish, Ministry of Health, Saudi Arabia; Babacar Ndoye, Infection Control Africa Network, Senegal; Fernando Otaiza, Ministry of Health, Chile; Diamantis Plachouras, European Centre for Disease Prevention and Control, Sweden; Maria Clara Padoveze, School of Nursing, University of Sao Paulo, Brazil; Mathias Pletz, Jena University, Germany; Marina Salvadori, Public Health Agency of Canada, Canada; Mitchell Schwaber, Ministry of Health, Israel; Nandini Shetty, Public Health England, United Kingdom; Mark Sobsey, University ofNorth Carolina, USA; Paul Ananth Tambyah, National University Hospital, Singapore; Andreas Voss, Canisus-Wilhelmina Ziekenhuis, The Netherlands; Walter Zingg, University of Geneva Hospitals, Switzerland;
2) The WHO Technical Advisory Group of Experts on Personal Protective Equipment (TAG PPE):
Faisal Al Shehri, Saudi Food and Drug Authority, Saudi Arabi; Selcen Ayse, Istanbul University-Cerrahpasa, Turkey; Razan Asally, Saudi Food and Drug Authority, Saudi Arabi; Kelly Catlin, Clinton Health Access Initiative; Patricia Ching, WHO Collaborating Center, The University of Hong Kong, China; Mark Croes, Centexbel, Spring Gombe, United Nations; Emilio Homsey, UK Public Health Rapid Support Team, U.K.; Selcen Kilinc-Balci, United States Centers for
Disease Control and Prevention (CDC), USA; Melissa Leavitt, Clinton Health Access Initiative; John McGhie, International Medical Corps; Claudio Meirovich, Meirovich Consulting; Mike Paddock, UNDP, Trish Perl, University of Texas Southwestern Medical Center, USA; Alain Prat, Global Fund, Ana Maria Rule, Johns Hopkins Bloomberg School of Public Health, U .S.A; Jitendar Sharma, Andra Pradesh MedTEch Zone, India; Alison Syrett, SIGMA, Reiner Voelksen, VOELKSEN Regulatory Affairs, Nasri Yussuf, IPC Kenya.
3) External IPC peer review group:
Paul Hunter, University of East Anglia, U.K; Direk Limmathurotsakul, Mahidol University, Thailand; Mark Loeb, Department of Pathology and Molecular Medicine, McMaster University, Canada; Kalisavar Marimuthu, National Centre for Infectious Diseases, Singapore; Yong Loo Lin School of Medicine, National University of Singapore; Nandi Siegfried, South African Medical Research Council, South Africa.
4) UNICEF observers: Nagwa Hasanin, Sarah Karmin, Raoul Kamadjeu, Jerome Pfaffinann,
WHO Secretariat:
Benedetta Allegranzi, Gertrude Avortri, Mekdim Ayana, Hanan Balkhy, April Baller, Elizabeth Barrera-Cancedda, Anjana Bhushan, Whitney Blanco, Sylvie Briand, Alessandro Cassini, Giorgio Cometto, Ana Paula Coutinho Rehse, Carmem Da Silva, Nino Dal Dayanguirang, Sophie Harriet Dennis, Sergey Eremin, Luca Fontana, Dennis Falzon, Nathan Ford, Nina Gobat, Jonas Gonseth-Garcia, Rebeca Grant, Tom Grein, Ivan Ivanov, Landry Kabego, Catherine Kane, Pierre Claver Kariyo, Ying Ling Lin, Omelia Lincetto, Abdi Mahamud, Madison Moon, Takeshi Nishijima, Kevin Babila Ousman, Pillar Ramon-Pardo, Paul Rogers, Nahoko Shindo, Alice Simniceanu, Valeska Stempliuk, Maha Talaat Ismail, Joao Paulo Toledo, Anthony Twywan, Maria Van Kerkhove, Adriana Velazquez, Vicky Willet, Masahiro Zakoji, Bassim Zayed.
WHO continues to monitor the situation closely for any changes that may affect this interim guidance. Should any factors change, WHO will issue a further update. Otherwise, this interim guidance document will expire I year after the date of publication.

Annex: Updated guidance on non-medical (fabric) masks
Background
A non-medical mask, also called fabric mask, community mask or face covering, is neither a medical device nor personal protective equipment. Non-medical masks are aimed at the general population, primarily for protecting others from exhaled virus-containing droplets emitted by the mask wearer. They are not regulated by local health authorities or occupational health associations, nor is it required for manufacturers to comply with guidelines established by standards organizations. Non-medical masks may be homemade or manufactured. The essential performance parameters include good breathability, filtration of droplets originating from the wearer, and a snug fit covering the nose and mouth. Exhalation valves on masks are discouraged as they bypass the filtration function of the mask.
Non-medical masks are made from a variety of woven and nonwoven fabrics, such as woven cotton, cotton/synthetic blends, polyesters and breathable spunbond polypropylene, for example. They may be made of different combinations of fabrics, layering sequences and available in diverse shapes. Currently, more is known about common household fabrics and combinations to make non-medical masks with target filtration efficiency and breathability (119, 146-150). Few of these fabrics and combinations have been systematically evaluated and there is no single design, choice of material, layering or shape among available non-medical masks that are considered optimal. While studies have focussed on single fabrics and combinations, few have looked at the shape and universal fit to the wearer. The unlimited combination of available fabrics and materials results in variable filtration and breathability.
In the context of the global shortage of medical masks and PPE, encouraging the public to create their own fabric masks may promote individual enterprise and community integration. Moreover, the production of non-medical masks may offer a source of income for those able to manufacture masks within their communities. Fabric masks can also be a form of cultural expression, encouraging public acceptance of protection measures in general. The safe re-use of fabric masks will also reduce costs and waste and contribute to sustainability ( 151-156).
This Annex is destined intended for two types of readers: homemade mask makers and factory-made masks manufacturers. Decision makers and managers (national/subnational level) advising on a type of non-medical mask are also the focus of this guidance and should take into consideration the following features of non-medical masks: breathability, filtration efficiency (FE), or filtration, number and combination of fabric layers material used, shape, coating and maintenance.
Evidence on the effectiveness of non-medical (fabric) masks
A number of reviews have been identified on the effectiveness of non-medical masks ( 151-156). One systematic review ( 155) identified 12 studies and evaluated study quality. Ten were laboratory studies (157-166), and two reports were from a single randomized trial (72, 167). The majority of studies were conducted before COVID-19 emerged or used laboratory generated particles to assess filtration efficacy. Overall, the reviews concluded that
cloth face masks have limited efficacy in combating viral infection transmission.
Homemade non-medical masks
Homemade non-medical masks made of household fabrics (e.g., cotton, cotton blends and polyesters) should ideally have a three-layer structure, with each layer providing a function (see Figure I) ( 168). It should include:
1. an innermost layer (that will be in contact with the face) of a hydrophilic material ( e.g., cotton or cotton blends of terry cloth towel, quilting cotton and flannel) that is nonirritating against the skin and can contain droplets ( 148)
2. a middle hydrophobic layer of synthetic breathable nonwoven material (spunbond polypropylene, polyester and polyaramid), which may enhance filtration, prevent permeation of droplets or retain droplets ( 148, 150)
3. an outermost layer made of hydrophobic material (e.g. spunbond polypropylene, polyester or their blends), which may limit external contamination from penetrating through the layers to the wearer's nose and mouth and maintains and prevents water accumulation from blocking the pores of the fabric ( 148).
Although a minimum of three layers is recommended for nonmedical masks for the most common fabric used, single, double or other layer combinations of advanced materials may be used if they meet performance requirements. It is important to note that with more tightly woven materials, breathability may be reduced as the number of layers increases. A quick check may be performed by attempting to breathe, through the mouth, through the multiple layers.
Inner
• Hydrophilic •Cotton or cotton blend
Outer
• Hydrophobic •Polyester
Figure I. Non-medical mask construction using breathable fabrics such as cotton, cotton blends, polyesters, nylon and polypropylene spunbond that are breathable may impart adequate filtration performance when layered. Single- or double-layer combinations of advanced materials may be used if they meet performance requirements (72).
Assumptions regarding homemade masks are that individual makers only have access to common household fabrics and do not have access to test equipment to confirm target performance (filtration and breathability). Figure 1 illustrates a multi-layer mask construction with examples of fabric options. Very porous materials, such as gauze, even with multiple layers, may provide very low filtration efficiency ( 14 7). Higher thread count fabrics offer improved filtration performance ( 169). Coffee filters, vacuum bags and materials not meant for clothing should be avoided as they may contain injurious content when breathed in. Microporous films such as Gore-Tex are not recommended ( 170).

Factory-made non-medical masks: general considerations for manufacturers
The non-medical mask, including all components and packaging, must be non-hazardous, non-toxic and childfriendly (no exposed sharp edges, protruding hardware or rough materials). Factory-made non-medical masks must be made using a process that is certified to a quality management system ( e.g., ISO 9001 ). Social accountability standards ( e.g., SAi SA8000) for multiple aspects of fair labour practices, health and safety of the work force and adherence to UNICEF's Children's Rights and Business Principles are strongly encouraged.
Standards organizations' performance criteria
Manufacturers producing masks with consistent standardized performance can adhere to published, freely available guidance from several organizations including those from: the French Standardization Association (AFNOR Group), The European Committee for Standardization (CEN), Swiss National COVID-19 Task Force, the American Association of Textile Chemists and Colorists (AA TCC), the South Korean Ministry of Food and Drug Safety (MFDS), the Italian Standardization Body (UNI) and the Government of Bangladesh.
Essential parameters
The essential parameters presented in this section are the synthesis of the abovementioned regional and national guidance. They include filtration, breathability and fit. Good performance is achieved when the three essential parameters are optimized at the preferred threshold (Figure 2).
Figure 2. Illustration of the three essential parameters of fdtration, breatbability and fit.
The summary of the three essential parameters can be found in Table 1 and the additional performance considerations in Table 2. The minimum threshold is the minimum acceptable parameter, while the preferred threshold is the optimum.
Filtration and breathability
Filtration depends on the filtration efficiency (in%), the type of challenge particle ( oils, solids, droplets containing bacteria) and the particle size (see Table 1 ). Depending on the fabrics used, filtration and breathability can complement or work against one another. The selection of material for droplet filtration (barrier) is as important as breathability. Filtration is dependent on the tightness of the weave, fibre or thread diameter. Non-woven materials used for disposable masks are manufactured using processes to create polymer fibres that are thinner than natural fibres such as cotton and that are held together by partial melting.
Breathability is the difference in pressure across the mask and is typically reported in millibars (mbar) or Pascals (Pa) or, normalized to the cm2 in mbar/cm2 or Pa/cm2• Acceptable breathability of a medical mask should be below 49 Pa/cm2•
For non-medical masks, an acceptable pressure difference, over the whole mask, should be below 60 Pa/cm2, with lower values indicating better breathability.
Non-medical fabric masks consisting of two layers of polypropylene spunbond and two layers of cotton have been shown to meet the minimum requirements for droplet filtration and breathability of the CEN CWA 17553 guidance. It is preferable not to select elastic material to make masks as the mask material may be stretched over the face, resulting in increased pore size and lower filtration through multiple usage. Additionally, elastic fabrics are sensitive to washing at high temperatures thus may degrade over time.
Coating the fabric with compounds like wax may increase the barrier and render the mask fluid resistant; however, such coatings may inadvertently completely block the pores and make the mask difficult to breathe through. In addition to decreased breathability unfiltered air may more likely escape the sides of the mask on exhalation. Coating is therefore not recommended.
Valves that let unfiltered air escape the mask are discouraged and are an inappropriate feature for masks used for the purpose of preventing transmission.

Table 1. Essential parameters (minimum and preferred thresholds) for manufactured non-medical mask
Essential Minimum threshold Preferred threshold Parameters
1. Filtration* 1.1. filtration
70% @ 3 micron > 70%, without compromising breathability efficiency
1.2. Challenge Solid: sodium chloride (NaCl), Talcum Based on availability particle powder, Holi powder, dolomite, Polystyrene
Latex spheres
Liquid: DEHS Di-Ethyl-Hexyl-Sebacat, paraffin oil
1.3. Particle size Choose either sizes: Range of particle sizes
3 um. 1 um. or smaller
2. Breathability
2.1. Breathing S60 Pa/cm2 Adult: S 40 Pa/cm2
resistance** Paediatric: < 20 Pa/cm2
2.2 Exhalation Not recommended NIA valves
3. Fit
3.1. Coverage Full coverage of nose and mouth, consistent, Same as current requirements snug perimeter fit at the nose bridge, cheeks, chin and lateral sides of the face; adequate surface area to minimize breathing resistance and minimize side leakruze
3.2 Face seal Not currently required Seal as good as FFR (respirator):
Fit factor of 100 for N95
Maximum Total Inward Leakage of 25% (FFPl requirement)
3.2. Sizing Adult and child Should cover from the bridge of the nose to below the chin and cheeks on either side of the mouth
Sizing for adults and children (3-5, 6-9, 10-12, >12)
3.3Strap stren2th >44.SN
• Smaller particle may result in lower filtration. •• High resistance can cause bypass of the mask. Unfiltered air will leak out the sides or around the nose if that is the easier path.

Fit: shape and sizing
Fit is the third essential parameter, and takes into consideration coverage, seal, sizing, and strap strength. Fit of masks currently is not defined by any standard except for the anthropometric considerations of facial dimensions (ISO/TS 16976-2) or simplified to height mask (South Korean standard for KF-AD). It is important to ensure that the mask can be held in place comfortably with as little adjustment of the elastic bands or ties as possible.
Mask shapes typically include flat-fold or duckbill and are designed to fit closely over the nose, cheeks and chin of the wearer. Snug fitting designs are suggested as they limit leaks of unfiltered air escaping from the mask ( 148). Ideally the mask should not have contact with the lips, unless hydrophobic fabrics are used in at least one layer of the mask ( 148). Leaks where unfiltered air moves in and out of the mask may be attributed to the size and shape of the mask (171).
Additional considerations
Optional parameters to consider in addition to the essential performance parameters include if reusable, biodegradability for disposal masks, antimicrobial performance where applicable and chemical safety (see Table 2).
Non-medical masks intended to be reusable should include instructions for washing and must be washed a minimum of five cycles, implying initial performance is maintained after each wash cycle.
Advanced fabrics may be biodegradable or compostable at the end of service life, according to a recognized standard process (e.g., UNI EN 13432, UNI EN 14995 and UNI/ PdR 79).
Manufacturers sometimes claim their NM masks have antimicrobial performance. Antimicrobial performance may be due to coatings or additives to the fabric fibres. Treated fabrics must not come into direct contact with mucous membranes; the innermost fabric should not be treated with
antimicrobial additives, only the outermost layer. In addition, antimicrobial fabric standards (e.g., ISO 18184, ISO 20743, AATCC TMIO0, AATCC 100) are generally slow acting. The inhibition on microbial growth may take full effect after 2- or 24-hour contact time depending on the standard. The standards have generally been used for athletic apparel and substantiate claims of odour control performance. These standards are not appropriate for non-medical cloth masks and may provide a false sense of protection from infectious agents. If claims are maid, manufacturers should specify which standard supports antimicrobial performance, the challenge organism and the contact time.
Volatile additives are discouraged as these may pose a health risk when inhaled repeatedly during wear. Certification according to organizations including OEKO-TEX (Europe) or SEK (Japan), and additives complying with REACH (Europe) or the Environmental Protection Agency (EPA, United States of America) indicate that textile additives are safe and added at safe levels.
Table 2. Additional parameters for manufactured nonmedical masks
Additional parameters Minimum thresholds
If reusable, number of wash 5 cycles cycles
Disposal Reusable
If biodegradable (CFC-BIO), according to UNI EN 13432. UNI EN 14995
Antimicrobial (bacteria, ISO 18184 (virus) virus, fungus) performance
ISO 20743 (bacteria)
ISO 13629 (fungus)
AA TCC TM 100 (bacteria)
Chemical safety Comply with REACH regulation, including inhalation safety
© World Health Organization 2020. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO licence.
WHO reference number: WHO/2019-nCo V /IPC _Masks/2020.5
GLOBAL INFLUENZA PROGRAMME
Non-pharmaceutical public health measures for mitigating the risk and impact of epidemic and pandemic influenza
(mt?.~\ World Health ~~ti Organization ~
APPENDIX TO JAMES CASCIANO DECLARATION-364

ISBN 978-92-4-151683-9 e World Health Organization 2019
Some rights reserved. This work is available under the Creative Commons AttributionNonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; http,;/ /cr,:,ativernrnrnons org/ i icen ses/bv nc-sa/3 .0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation:"This translation was not created by the World Health Organization (WHO}. WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition~
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization.
Suggested dtation. Non-pharmaceutical public health measures for mitigating the risk and impact of epidemic and pandemic influenza; 2019. Licence: CC BY-NC-SA 3 O IGO.
Cataloguing-In-Publication (CIP) data. CIP data are available at http/ /anns.who.int/:ris Sales, rights and licensing. To purchase WHO publications, see l:tt:):/ /J:)ps.v,,.ho.1nt/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/ rlhout/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers' products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.
Iii NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-365

Cont nts Non-pharmaceutical public health measures for mitigating the risk and impact of epidemic and pandemic influenza
Acknowledgements
Abbreviations and acronyms
Glossary
Executive summary
1. Introduction
1.1. Introduction
1.1.1. Human influenza virus transmission
1.1.2. Public health importance
1.1.3. History of the guidelines for NPls in influenza pandemics
1.2. Scope, purpose and target audience
1.3. International Health Regulations
1.4. Pandemic influenza severity assessment framework
1.5. Guideline development process
1.5.1. Contributors to the process
1.5.2. Guideline development steps
2. Summary of recommendations
3. Communication for behavioural impact
4. Personal protective measures
4.1. Hand hygiene
4.2. Respiratory etiquette
4.3. Face masks
5. Environmental measures
5.1. Surface and object cleaning
5.2. Other environmental measures
5.2.1. Ultraviolet light
5.2.2. Increased ventilation
5.2.3. Modifying humidity
6. Social distancing measures
6.1. Contact tracing
6.2. Isolation of sick individuals
6.3. Quarantine of exposed individuals
6.4. School measures and closures
6.5. Workplace measures and closures
6.6. Avoiding crowding
7. Travel-related measures
7.1. Travel advice
7.2. Entry and exit screening
7.3. Internal travel restrictions
7.4. Border closure
References
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-366
iv
V
vi
5
5
5
5
9
9
10
10
10
10
11
13
19
20
20
24
26
28
28
31
31
33
35
37
37
40
44
48
53
57
79
60
62
64
67
70

Acknowledgements
This document is the product of collaboration between the World Health Organization (WHO) Global Influenza Programme and the WHO Collaborating Centre for Infectious Disease Epidemiology and Control, School of Public Health, The University of Hong Kong.
The University of Hong Kong team was led by Benjamin Cowling, and included Jessica Wong, Sukhyun Ryu, Huizhi Gao, Eunice Shiu, Jingyi Xiao and Min Whui Fong. The team's contributions to carrying out the systematic reviews and developing this document are gratefully acknowledged.
WHO appreciates the contributions of the following experts before, during and after the Technical Consultation on Non-pharmaceutical Public Health Measures for Mitigating the Risk and Impact of Epidemic and Pandemic Influenza, which was held from 26 to 28 March 2019 in Hong Kong Special Administrative Region (SAR), China:
Allison Aiello, Alanoud Aljifri, Gemma Arellano, Gina Charos, Francisco de Paula Junior, Aleksander Deptula, Narangerel Dorj, Hind Ezzine, Rosaura Gutierrez-Vargas, Anand Krishnan, Vernon Lee, Svenn-Erik Mamelund, Punam Mangtani, Jeffrey McFarland, Armelle Viviane Ngomba, Jonathan Nguyen Van-Tam, Hitoshi Oshitani, Pasi Penttinen, Carrie Reed, Amra Uzicanin and Dayan Wang.
WHO also wishes to extend its appreciation to all who reviewed and commented on the earlier version of this document during the public comment period. The following individuals identified themselves but are not among the lists above:
Faruque Ahmed, Salah Al Awaidy, Kossi Badziklou, Aleksander Deptula, Luzhao Feng, Gary Lamont, Raina Nikiforova, Junxiong Vincent Pang, Trinehessevik Paulsen and Osvaldo Uez.
The following WHO staff and consultants are acknowledged for their contributions to the development and review of this document:
Abdinasir Abubakar, Isabelle Bergeri, Sylvie Briand, Caroline S. Brown, Amgad A. Elkholy, Julia Fitzner, Philip Gould, Aspen Hammond, Michala Hegermann-Lindencrone, Belinda L Herring, Masaya Kato, Jaya Lamichhane, Ann Moen, Sonja Olsen, Soatiana C. Rajatonirina, Gina Samaan, Magdi Samaan, Bhagawan D. Shrestha, Katelijn A.H. Vandemaele, Andrea Vicari, Wenqing Zhang and Weigong Zhou.
The technical editing of this document was performed by Hilary Cadman and the Cadman Editing Services team.
m NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-367

Abbreviations and acronyms
ACH air changes per hour
Cl confidence interval
COMBI communication for behavioural impact
GDP gross domestic product
GRADE Grading of Recommendations Assessment, Development and Evaluation
IHR International Health Regulations
NPI non-pharmaceutical intervention
OR odds ratio
PISA pandemic influenza severity assessment
RCT randomized controlled trial
RNA ribonucleic acid
RR rate ratio
SAR Special Administrative Region
USA United States of America
UV ultraviolet
WHO World Health Organization
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-368

Glossary
Contact tracing
Closure
Entry and exit screening
Isolation
Movement restridion
Identification and follow-up of persons who may have come into contact with an infected person.
Halting the operation of an institution or business.
Screening travellers for influenza virus infection at their arrival in and departure from border crossings, ports and airports.
Separation or confinement of a person who has or is suspected of having influenza virus infection, to prevent further infections.
Limitation on the movements of a person who has or is suspected of having influenza virus infection.
Personal protective measures Measures to reduce personal risk of infection, such as hand washing and face masks.
Quarantine
Respiratory etiquette
Symptomatic influenza
Travel Advice
Separation or restriction of the movement of persons who may be infected, based either on exposure to other infected people or on a history of travel to affected areas.
Basic reproductive number, a measure of transmissibility. This number represents the average number of people infected by one infectious case in a completely susceptible population.
Simple hygiene practices taken by people who are coughing or sneezing to prevent person-to-person transmission of respiratory infections.
Influenza virus infection causing an acute illness, most commonly with rapid onset of fever and other respiratory symptoms, although a proportion of illnesses are afebrile.
Health advice to travellers provided by national or international health agencies to help travellers understand the risks involved during the travel and take the necessary preventive measures or precautions to protect their health while travelling.
m NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-369
EXECUTIVE SUMMARY Introduction Influenza pandemics occur at unpredictable intervals, and cause considerable morbidity and mortality. Influenza virus is readily transmissible from person to person, mainly during close contact, and is challenging to control. In the early stage of influenza epidemics and pandemics, there may be delay in the availability of specific vaccines and limited supply of antiviral drugs. Non-pharmaceutical interventions (NPls) are the only set of pandemic countermeasures that are readily available at all times and in all countries. The potential impacts of NPls on an influenza epidemic or pandemic are to delay the introduction of the pandemic virus into a population; delay the height and peak of the epidemic if the epidemic has started; reduce transmission by personal protective or environmental measures; and reduce the total number of infections and hence the total number of severe cases.
Scope and purpose This document provides recommendations for the use of NPls in future influenza epidemics and pandemics based on existing guidance documents and the latest scientific literature. The specific recommendations are based on a systematic review of the evidence on the effectiveness of NPls, including personal protective measures, environmental measures, social distancing measures and travel-related measures. The information provided here will be useful for national authorities that are developing or updating their plans for mitigating the impact of influenza epidemics and pandemics.
Target audience This guideline is intended to support the development and updating of national plans for mitigating influenza epidemics and pandemics in community settings. The recommendations included in this guideline will also be of interest to individuals, organizations, institutions and local health authorities.
Methods The guideline development process included the following stages:
1. Identify a list of NPls that have the potential to contribute to pandemic mitigation for further review and evaluation.
2. Identify and evaluate existing systematic reviews of the NPls listed in Step 1, and perform new systematic reviews for each NPI if recently published reviews were not available.
3. Assess the body of evidence on the effectiveness of each of the NPls.
4. Determine the direction and strength of recommendations.
S. Draft the guideline document based on evidence and planning for strategy implementation.
The guideline development process included the formation of four main groups: a World Health Organization (WHO) guideline steering group, a systematic review team from the University of Hong Kong, a guideline development group and an external review group. The primary responsibilities of these four groups are, respectively, to oversee the process of the guideline development, to review the evidence base for each NPI, to formulate recommendations based on scientific evidence and other considerations, and to review the guidelines.
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-370

Available evidence The evidence base for this guideline included systematic reviews of 18 NPls, covering:
personal protective measures (e.g. hand hygiene, respiratory etiquette and face masks);
environmental measures (e.g. surface and object cleaning, and other environmental measures);
social distancing measures (e.g. contact tracing, isolation of sick individuals, quarantine of exposed individuals, school measures and closures, workplace measures and closures, and avoiding crowding); and
• travel-related measures (e.g. travel advice, entry and exit screening, internal travel restrictions and border closure).
The evidence base on the effectiveness of NPls in community settings is limited, and the overall quality of evidence was very low for most interventions. There have been a number of highquality randomized controlled trials (RCTs) demonstrating that personal protective measures such as hand hygiene and face masks have, at best, a small effect on influenza transmission, although higher compliance in a severe pandemic might improve effectiveness. However, there are few RCTs for other NPls, and much of the evidence base is from observational studies and computer simulations. School closures can reduce influenza transmission but would need to be carefully timed in order to achieve mitigation objectives. Travel-related measures are unlikely to be successful in most locations because current screening tools such as thermal scanners cannot identify pre-symptomatic infections and afebrile infections, and travel restrictions and travel bans are likely to have prohibitive economic consequences.
Recommendations Eighteen recommendations are provided in this guideline (Table 1 ). The recommendations take into account the quality of the supporting evidence, the strength of each recommendation and other considerations. In taking decisions on interventions, each WHO Member State and each local area will need to take into account the feasibility and acceptability of proposed interventions, in addition to their anticipated effectiveness and impact. This guideline provides an overview of relevant considerations.
D NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-371

Table 1. Recommendations on the use of NPls by severity level
SEVERITY
Any
Moderate
High
Extraordinary
Not recommended in any circumstances
PANDEMIC•
Hand hygiene Respiratory etiquette Face masks for symptomatic individuals Surface and object cleaning Increased ventilation Isolation of sick individuals Travel advice
As above, plus Avoiding crowding
As above, plus Face masks for public School measures and closures
As above, plus Workplace measures and closures Internal travel restrictions
UV light Modifying humidity Contact tracing Quarantine of exposed individuals Entry and exit screening Border closure
NPI: non-pharmaceutical intervention; UV: ultraviolet.
• A pandemic is defined as a global epidemic caused by a new influenza virus to which there is little or no pre-existing immunity in the human population ( 7).
EPIDEMIC
Hand hygiene Respiratory etiquette Face masks for symptomatic individuals Surface and object cleaning Increased ventilation Isolation of sick individuals Travel advice
As above, plus Avoiding crowding
As above, plus Face masks for public School measures and closures
As above, plus Workplace measures and closures
UV light Modifying humidity Contact tracing Quarantine of exposed individuals Entry and exit screening Internal travel restrictions Border closure
------------------------" WORLD HEALTH ORGANIZATION 1:.1
APPENDIX TO JAMES CASCIANO DECLARATION-372

The most effective strategy to mitigate the impact of a pandemic is to reduce contacts between infected and uninfected persons, thereby reducing the spread of infection, the peak demand for hospital beds, and the total number of infections, hospitalizations and deaths. However, social distancing measures (e.g. contact tracing, isolation, quarantine, school and workplace measures and closures, and avoiding crowding) can be highly disruptive, and the cost of these measures must be weighed against their potential impact. Early assessments of the severity and likely impact of the pandemic strain will help public health authorities to determine the strength of intervention. In all influenza epidemics and pandemics, recommending that those who are ill isolate themselves at home should reduce transmission. Facilitating this should be a particular priority. In more severe pandemics, measures to increase social distancing in schools, workplaces and public areas would further reduce transmission.
Experimental studies suggest that hand hygiene can reduce virus on the hands. However, there is insufficient scientific evidence from RCTs to support the efficacy of hand hygiene alone to reduce influenza transmission in influenza epidemics and pandemics. Hand hygiene is an important intervention to reduce the risk of other common infectious diseases; therefore, it should be recommended at all times, regardless of the lack of efficacy against confirmed influenza reported in a number of RCTs. There is also a lack of evidence for the effectiveness of improved respiratory etiquette and the use of face masks in community settings during influenza epidemics and pandemics. Nevertheless, these NPls may be conditionally recommended for ill persons because of other considerations (e.g. the high cost of face masks), and they are generally feasible and acceptable. It is likely that these personal interventions could be effective if implemented in combination.
There is sufficient evidence on the lack of effectiveness of entry and exit screening to justify not recommending these measures in influenza pandemics and epidemics. There is weak evidence, mainly from simulation studies, that travel restrictions may only delay the introduction of infections for a short period, and this measure may affect mitigation programmes, be disruptive of supply chains or be unacceptable to communities for various reasons. There is no evidence on the effectiveness of travel advice; however, given the potential benefits. it is recommended that health authorities provide advice for travellers. Border closures may be considered only by small island nations in severe pandemics and epidemics, but must be weighed against potentially serious economic consequences.
This document will serve as a core component of WHO's influenza prevention and control programme in community settings. The successful implementation of this guideline depends on the inclusion of NPls as a robust strategic plan at national and local levels, as well as the appropriate application of its recommendations.
D NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-373

INTRODUCTION 1.1. Introduction
1.1.1. Human influenza virus transmission Influenza virus infection causes acute respiratory illness that is usually self-limiting but can be severe in some cases. Influenza virus infects the upper and lower respiratory tract, and spreads between people, mainly during close contact. The routes of transmission are often categorized into three specific modes - contact, aerosols and (large) respiratory droplets (2) - as outlined below.
Contact transmission Contact transmission is either direct or indirect. Transmission via direct physical contact can occur between an infected individual and a susceptible individual (e.g. through kissing or shaking hands). Transmission via indirect contact occurs through an intermediate object (e.g. touching contaminated surfaces or objects, and then touching nose or eyes) (2). Several studies have shown that influenza virus can survive for prolonged periods on certain types of surfaces, and can survive on hands for a short time (3).
Aerosol transmission Influenza virus can be detected in fine particle aerosols with an aerodynamic diameter of less than 5 µm, emitted by infected individuals in exhalations, coughs and sneezes (4). These tiny particles ( <5 µm) can reach the membrane surfaces of the upper respiratory tract and the epithelial cells of the lower respiratory tract (2). Although most aerosol transmission is likely to occur at close range because of dilution and inactivation over distance and time, these particles can remain suspended in the air for extended periods and may be responsible for higher rates of transmission, particularly in crowded areas (5).
Respiratory droplet transmission Droplet transmission is typically defined as transmission via droplets that follow a ballistic trajectory after emission and do not remain airborne; these particles have an aerodynamic diameter of 5-1 O µm (6). Virus-laden droplets are expelled into the environment by breathing, coughing and sneezing. These droplets generally travel short distances (1-2 m from the source) (5). Respiratory droplets are often thought to be the most common route of influenza transmission, although there is limited evidence to support this view.
Impacts of modes of transmission The various modes of transmission have implications for the effectiveness of personal protective measures against influenza transmission. Also, uncertainty over the specific role of contact and aerosol transmission has hindered the optimization of control strategies. In settings where multiple exposures occur, removing one mode of transmission (e.g. by intense hand hygiene) may not be sufficient to reduce overall transmission en. Isolating infected individuals - that is, keeping them away from others - is likely to reduce transmission by all modes.
1.1.2. Public health importance Influenza epidemics cause considerable impact each year, and influenza pandemics occur from time to time with potentially devastating health and economic effects. Because of the delay in the availability of specific vaccines and the limited stockpiles of antiviral drugs, non-pharmaceutical interventions (NPls) are often the only available intervention when a new pandemic influenza virus emerges and begins to spread (8). The implementation of community mitigation measures may help to reduce the impact of influenza epidemics and pandemics.
------------------------0 WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-374

Seasonal and pandemic influenza Seasonal epidemics of human influenza A and B virus infections occur in the winter months almost every year in temperate locations (9), leading to the commonly used term "seasonal" influenza. In tropical and subtropical locations, influenza A and B epidemics occur with weaker seasonality (10) or with year-round circulation (71).
Influenza viruses rapidly evolve to escape the immunity that results from prior infections, allowing continued circulation. The virus strains included in influenza vaccines are reviewed twice each year and are updated if necessary, to maintain higher effectiveness against prevalent circulating strains. Segments of the population at higher risk of severe outcomes from seasonal influenza infections include young children, older adults, adults with underlying medical conditions and pregnant women (9).
Influenza pandemics occur when a new influenza A virus emerges to which the population has little or no immunity. Before the 2009-2010 pandemic, it was believed that pandemics occurred when new influenza A subtypes emerged in the human population and replaced the previously circulating subtypes, as occurred in 1918-1919 with A(Hl Nl ), in 1957-1958 with A(H2N2) and in 1968-1969 with A(H3N2). When influenza A(H 1 N 1) re-emerged in 1977 after a 20-year absence ( 7 2), and co-circulated with A(H3N2) rather than replacing it, the re-emergence was not declared a pandemic. However, when the A(Hl N1 )pdm09 strain emerged in 2009, it was declared a pandemic after it spread globally, demonstrating that pandemic strains do not need to be a new subtype, but with shifted antigenicity from same sub type of seasonal influenza viruses circulating previously.( 7 3). Influenza pandemics are associated with higher attack rates because of the lack of population immunity, and they can have a substantial health impact. Some of the differences between seasonal and pandemic influenza are shown in Table 2 (9, 74-76).
Table 2. Comparison of lnterpandemic ("seasonar) influenza epidemics and pandemic influenza
INTERPANDEMIC INFLUENZA
Frequency Common: every year or almost every year
Viruses Involved Influenza A and 81
Antigenic Relatively small antigenic changes every characteristics year
Immunity Some population immunity from previous infections and from vaccination
Vaccines Specific vaccines available, with strains reviewed twice per year and updated as appropriate
Antivirals Antiviral drugs available in some locations, and used for the treatment of severe influenza or as clinically appropriate
b Influenza C virus Infections are sporadically detected, but this type has not been linked to large epidemics or major disease burden.
PANDEMIC INFLUENZA
Irregular: perhaps a few times each century
Influenza A
Major antigenic change in surface proteins
Low levels of population immunity
Specific vaccines may not be available for the first 6 months
Large stockpiles of antiviral drugs available in some
1 locations
i
D NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-375

Vulnerable population
lmpad
INTERPANDEMIC INFLUENZA
Groups with weaker immunity at highest risk of severe disease (e.g. young children, older adults, adults with underlying medical conditions and pregnant women)
Perhaps 500 000 respiratory deaths on average each year
PANDEMIC INFLUENZA
Attack rates may be highest in children and young adults; pregnant women are often at higher risk, as documented in several previous pandemics; the population segments at highest risk of severe influenza are unpredictable
Potentially millions of deaths
There were three major pandemics in the 20th century, commonly referred to as theuSpanish flu" in 1918-1919, the uAsian flu" in 1957-1958 and the "Hong Kong flu" in 1968-1969 (Table 3). The most serious of these was the pandemic caused by the A(Hl Nl) virus in 1918-1919, which resulted in 20-50 million deaths, and had a particularly notable impact on mortality in young adults (77). The A(H2N2) pandemic in 1957-1958 and the A(H3N2) pandemic in 1968-1969 each caused around 1 million deaths worldwide, with the greatest impact on mortality being in older adults (78).
The first influenza pandemic in the 21st century, which occurred in 2009-2010, was caused by a new strain of influenza A(Hl Nl) virus that was antigenically shifted from the seasonal influenza A(Hl Nl) strains circulating at the time, but antigenically similar to A(Hl Nl) strains that had circulated before 1950 ( 19). The virus is thought to have emerged in central America shortly before it was first detected in North America in April 2009, and subsequently spread rapidly to other parts of the world (20). Because of the similarity with older A(Hl Nl) viruses, older adults had some immunity, reducing the impact of A(Hl Nl )pdm09 in this age group (21). Globally, the pandemic was estimated to have caused 123 000-203 000 respiratory deaths in 2009 (22).
1918-1919°Spanlsh flu"
1957-1958°Aslan flu"
1968-1969"HongKongflu"
2009-2010 H1N1pdm09
H1N1 20-50 million deaths ( 7 7)
H2N2 1.1 million deaths (23)
H3N2 1 million deaths (23) -----------+----------------
H1N1 123 000-203 000 respiratory deaths (22)
Influenza pandemics typically occur in epidemic waves. For example, in 2009 the United States of America (USA) experienced a spring epidemic of A(H 1 N 1 )pdm09 that had a limited impact; the spring epidemic was followed by a much larger autumn epidemic that had a major health impact (24). Subsequent epidemics of A(Hl Nl )pdm09 have occurred every 2-3 years since 2009, with similar epidemiological characteristics to other seasonal influenza epidemics.
----------------0 WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-376

The origin of pandemics A much greater range of influenza A subtypes of viruses circulates in animals, particularly in wild aquatic birds. Although human infections with avian influenza A subtypes are sporadic, there is a risk that these viruses will develop the capacity for effective transmission among humans, leading to the next pandemic. The emergence of highly pathogenic A(HSN 1) in 1997 raised the significant concern because of the severity of laboratory-confirmed human infections (25). More than 1000 laboratory-confirmed human infections with avian influenza A(H7N9) virus occurred in China in the period 2013-2018 (26), with no sustained human-to-human transmission (27). Several other avian influenza A subtypes (e.g. H9N2, H6N 1 and H7N7) have caused sporadic human infections (28). As demonstrated in 2009, influenza pandemics can also emerge from swine influenza viruses.
Non-pharmaceutical interventions NPls (also known as non-pharmacological interventions) include all measures or actions, other than the use of vaccines or medicines, that can be implemented to slow the spread of influenza in a population. In the early stage of influenza epidemics and pandemics, NPls are often the most accessible interventions, because of the time it takes to make specific vaccines available and because most locations do not have large stockpiles of antiviral drugs (8). Therefore, these mitigation measures will play a major role in reducing transmission in community settings. There are several objectives of NPls in an epidemic that is the first wave or subsequent wave of a pandemic or a seasonal influenza epidemic (29, 30).
Some NPls may be able to delay the start of an epidemic, which could be particularly important if the resulting delay is long enough to allow specific vaccines to be distributed and reduce the impact of the epidemic. Once an epidemic has started, NPls may also be used to delay the peak of the epidemic, again allowing time for vaccines to be distributed, or for health care providers to better prepare for a surge in cases.
By reducing transmission in the community, the epidemic may be spread out over a longer period, with a reduced epidemic peak. This can be particularly important if the health system has limited resources or capacity {e.g. in terms of hospital beds and ventilators). Also, overall morbidity and mortality can be reduced even if the total number of infections across the epidemic is not reduced.
Some interventions may aim to reduce the total number of infections, and therefore also reduce the total number of severe cases, hospitalizations and deaths.
Each of these consequences should contribute to reducing the overall impact of the epidemic or pandemic. NPls outside of health care settings usually focus on reducing transmission by personal protective or environmental measures {e.g. hand hygiene); reducing the spread in the community {e.g. isolating and treating patients, closing schools and cancelling mass gatherings); limiting the international spread (e.g. traveller screening); and improving risk communication with the public (31).
a NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-377
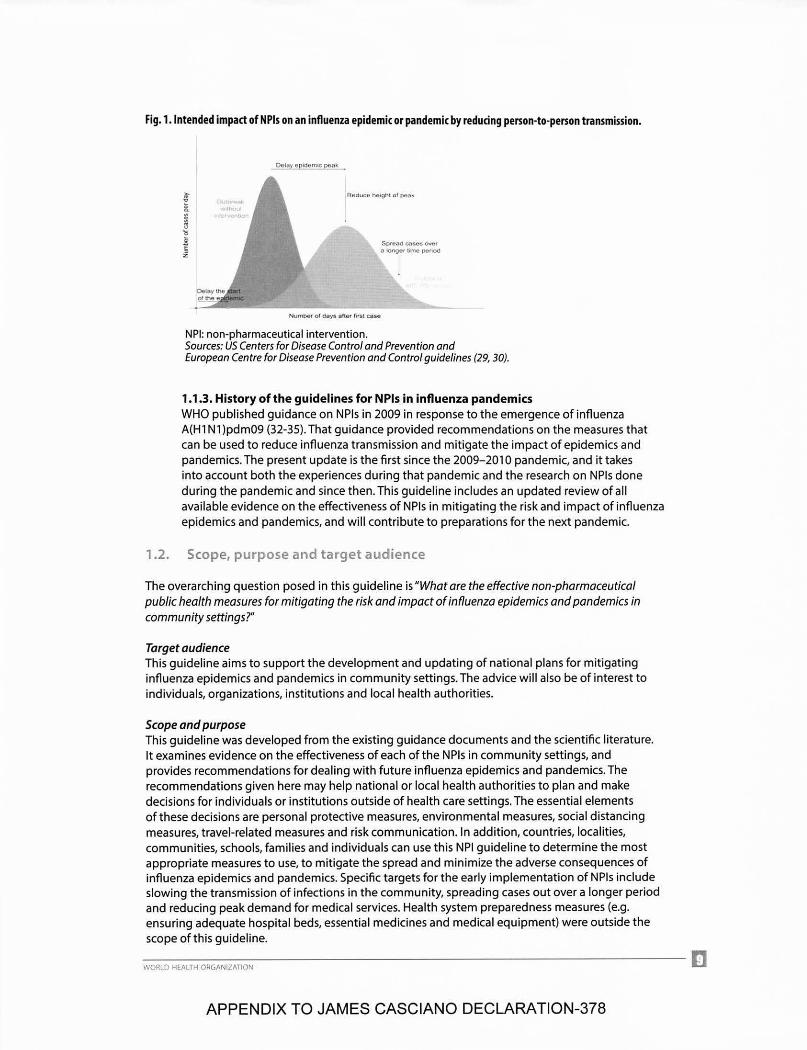
Fig. 1. Intended impact of NPls on an influenza epidemic or pandemic by reducing person-to-person transmission.
Spreacs cnses °""' a longor tlrne penod
Numoer of Clays aher first case
NPI: non-pharmaceutical intervention. Sources: US Centers for Disease Control and Prevention and European Centre for Disease Prevention and Control guidelines (29, 30).
1.1.3. History of the guidelines for NPls in influenza pandemics WHO published guidance on NPls in 2009 in response to the emergence of influenza A(Hl Nl)pdm09 (32-35). That guidance provided recommendations on the measures that can be used to reduce influenza transmission and mitigate the impact of epidemics and pandemics. The present update is the first since the 2009-2010 pandemic, and it takes into account both the experiences during that pandemic and the research on NPls done during the pandemic and since then. This guideline includes an updated review of all available evidence on the effectiveness of NPls in mitigating the risk and impact of influenza epidemics and pandemics, and will contribute to preparations for the next pandemic.
1.2. Scope, purpose and target audience
The overarching question posed in this guideline is "What are the effective non-pharmaceutical public health measures for mitigating the risk and impact of influenza epidemics and pandemics in community settings?"
Target audience This guideline aims to support the development and updating of national plans for mitigating influenza epidemics and pandemics in community settings. The advice will also be of interest to individuals, organizations, institutions and local health authorities.
Scope and purpose This guideline was developed from the existing guidance documents and the scientific literature. It examines evidence on the effectiveness of each of the NPls in community settings, and provides recommendations for dealing with future influenza epidemics and pandemics. The recommendations given here may help national or local health authorities to plan and make decisions for individuals or institutions outside of health care settings. The essential elements of these decisions are personal protective measures, environmental measures, social distancing measures, travel-related measures and risk communication. In addition, countries, localities, communities, schools, families and individuals can use this NPI guideline to determine the most appropriate measures to use, to mitigate the spread and minimize the adverse consequences of influenza epidemics and pandemics. Specific targets for the early implementation of NPls include slowing the transmission of infections in the community, spreading cases out over a longer period and reducing peak demand for medical services. Health system preparedness measures (e.g. ensuring adequate hospital beds, essential medicines and medical equipment) were outside the scope of this guideline. _______________________ ...
WORLD HEALTH ORGANIZATION a:J
APPENDIX TO JAMES CASCIANO DECLARATION-378

The systematic review had some limitations, including publication bias and difficulties in addressing generalisability owing to the countries and regions where the studies selected were performed. Social and cultural differences between different countries and regions will influence the overall effectiveness of the NPI in different countries, and this needs to be emphasized, to moderate expectations. Implementation of NPls should be flexible depending on the local or national situation (or both).
1.3. International Health Regulations
The International Health Regulations (IHR) (2005) (36) entered into force in 2007 and have two overarching objectives (Article 2):
• to set out obligations and mechanisms for"a public health response to the international spread of disease in ways that are commensurate with and restricted to public health risks, and which avoid unnecessary interference with international traffic and trade"; and
• to strengthen the preparedness and capacities of countries so they can proactively detect, assess, report and address acute public health threats early.
The IHR (2005) seek to balance the sovereignty of individual States Parties with the common good of the international community, and take account of economic and social interests as well as the protection of health. Under the IHR (2005), governments are entitled to implement public health measures to protect the health of their populations during public health events respecting three golden rules, which are that such measures must be based on scientific principles, respect human rights, and not be more onerous or intrusive than reasonably available alternatives. When measures exceed these parameters, countries are obliged to provide the public health rationale to WHO within 48 hours of implementation, and to rescind the measures if they are deemed unjustified.
1.4. Pandemic influenza severity assessment framework
The pandemic influenza severity assessment (PISA) framework was introduced by WHO in 2017 (37). The severity of an influenza epidemic or pandemic is evaluated and monitored through three specific indicators: transmissibility (referring to incidence}, seriousness of disease, and impact on health care system and society. The severity is categorized into five levels: no activity or below seasonal threshold, low, moderate, high or extraordinary (37). The PISA framework is being tested and improved during seasonal influenza epidemics; the aim is to help public health authorities to monitor and assess the severity of influenza, and to inform appropriate decisions and recommendations on interventions. Of particular relevance to these guidelines on NPI use, the PISA evaluation of severity may inform the choice of which interventions to use and when to use them (e.g. some interventions may only be recommended in severe epidemics or pandemics).
1.5. Guideline development process
1.s.1. Contributors to the process This guidance document was developed with contributions from the systematic review team, guideline development and review groups and WHO Secretariat (the steering group} in accordance with the requirements of the WHO handbook for guideline development (38). The details of the contributors can be found in the Acknowledgements.
II!] NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-379

1.5.2. Guideline development steps
Systematic review Following the process outlined in the WHO handbook for guideline development (38), evidence was identified, synthesized and presented in a comprehensive and unbiased manner. Based on the list of specific NPls provided by the steering group, a systematic review was conducted for each NPI using four databases {MEDLINE, PubMed, EMBASE and Cochrane Library) and the Cochrane Central Register of Controlled Trials {CENTRAL).
The review steps were as follows: 1. Developing research questions, and inclusion or exclusion criteria. 2. Searching for any systematic review published within 5 years {i.e. since January 2014),
and updating that existing review if a recently published review was found. 3. Conducting a full systematic review if a recent review could not be identified. 4. Selecting articles and extracting data. Two independent reviewers screened all
titles and abstracts of the potentially relevant studies; if the studies described the effectiveness of NPls in reducing influenza virus transmission, the reviewers read the full-length text and extracted relevant data.
No language restriction was applied in the search. The specific search terms and criteria can be found in the Annex. Two reviewers independently screened titles, abstracts and full texts, and two reviewers independently conducted the data extraction for each study. If a consensus could not be reached, further discussion was held or an opinion was obtained from a third independent reviewer.
The systematic review explored the evidence base on the effectiveness of each NPI. The specific targets of the evidence included reducing transmission, delaying the start of the epidemic, delaying the peak of the epidemic, spreading out infections over a longer period, and reducing the total number of infections.
Evaluation of the evidence For each included study the risk of bias was assessed as part of the quality of evidence evaluation. In general, randomized controlled trials (RCTs) provided the strongest evidence, followed by observational studies and then computer simulations. The strength of individual studies could also be modified based on the risk of bias. The main types of bias in the systematic review of interventions are discussed below (39).
Potential limitations in RCTs include: lack of allocation concealment; lack of blinding; loss to follow-up and failure to adhere to the intention-to-treat principle; reporting bias; and lack of generalizability due to strict inclusion criteria.
Potential limitations in observational studies include: failure to describe the eligibility criteria; flaws in the measurement of exposure or outcome {or both); potential for bias due to confounding; and incomplete or inadequate follow-up.
----------------~ WORLD HEALTH ORGANIZATION LIJll
APPENDIX TO JAMES CASCIANO DECLARATION-380

The Grading of Recommendations Assessment, Development and Evaluation {GRADE) (40) approach was used to rate the quality of evidence for each NPI, based on the question of whether NPls can reduce influenza transmission in the community. The quality of evidence was ranked as high, moderate, low or very low, based on each study's risk of bias {including publication bias), consistency, directness and precision of results (40). Two reviewers independently assessed the risk of bias and the quality of evidence. Disagreements were resolved by a third reviewer if consensus could not be reached.
Development of recommendations A technical consultation meeting for the development of this guidance was held in Hong Kong Special Administrative Region {SAR), China, on 26-28 March 2019. The systematic review team presented the outcomes of the systematic review. Recommendations were formulated by the guideline development group to determine the direction and strength of a recommendation by six indicators according to the WHO handbook for guideline development (38); the indicators are quality of the evidence, values and preferences, balance of benefits and harms, resource implications, acceptability and feasibility. In addition, ethical issues were taken into consideration. The strength of recommendations expressed the confidence of the guideline development group members in balancing desirable and undesirable consequences, which were classified as:
"recommendedn - the group is confident that the desirable effects outweigh the undesirable results;
"conditionally recommendedn - the group believes that the balance between benefits and harms is uncertain, and some conditions should apply when implementing the recommendation; or
"not recommended" - the group is confident that the disadvantages outweigh the advantages.
m NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-381
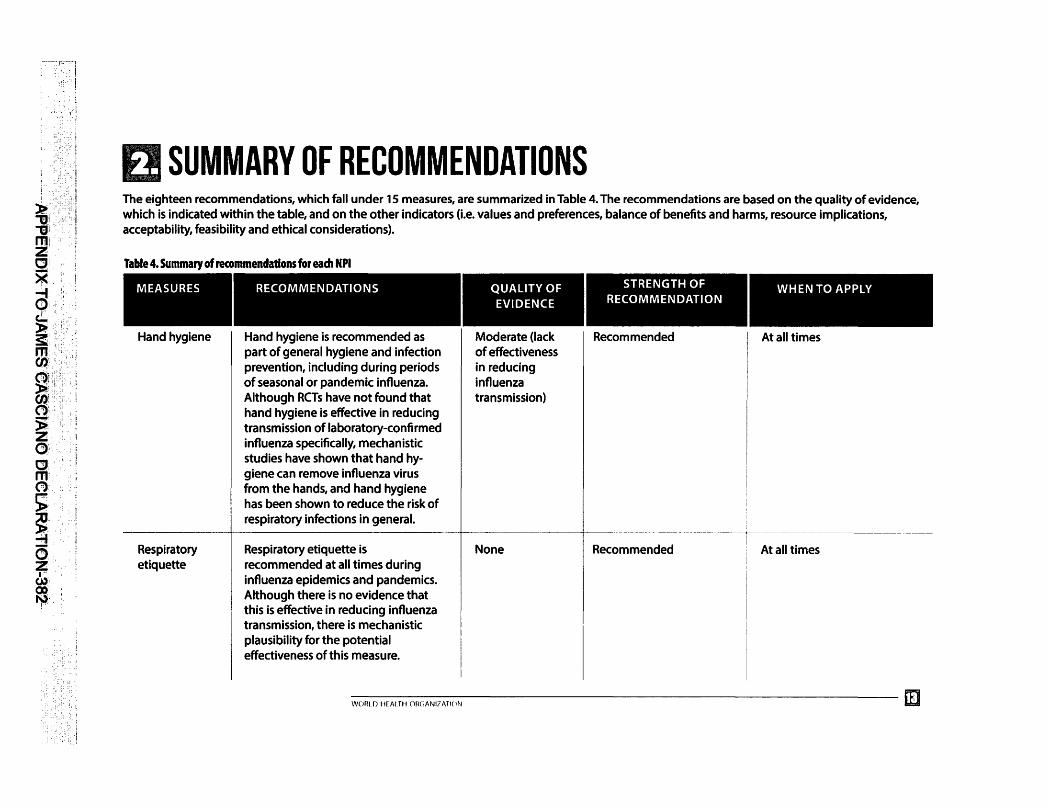
EJ SUMMARY OF RECOMMENDATIONS The eighteen recommendations, which fall under 15 measures, are summarized in Table 4. The recommendations are based on the quality of evidence, which is indicated within the table, and on the other indicators (i.e. values and preferences, balance of benefits and harms, resource implications, acceptability, feasibility and ethical considerations).
Table 4. Summary of recommendations for each NPI
MEASURES
Hand hygiene
Respiratory etiquette
RECOMMENDATIONS
Hand hygiene is recommended as part of general hygiene and infection prevention, including during periods of seasonal or pandemic influenza. Although RCTs have not found that hand hygiene is effective in reducing transmission of laboratory-confirmed influenza specifically, mechanistic studies have shown that hand hygiene can remove influenza virus from the hands, and hand hygiene has been shown to reduce the risk of respiratory infections in general.
Respiratory etiquette is recommended at all times during influenza epidemics and pandemics. Although there is no evidence that this is effective in reducing influenza transmission, there is mechanistic plausibility for the potential effectiveness of this measure.
QUALITY OF EVIDENCE
Moderate (lack of effectiveness in reducing influenza transmission)
None
STRENGTH OF RECOMMENDATION
Recommended
Recommended
I
I
WHEN TO APPLY
At all times
At all times
----------------~ WORIIJ HEALTH OW,I\Nl71\Tl(IN L&;,i
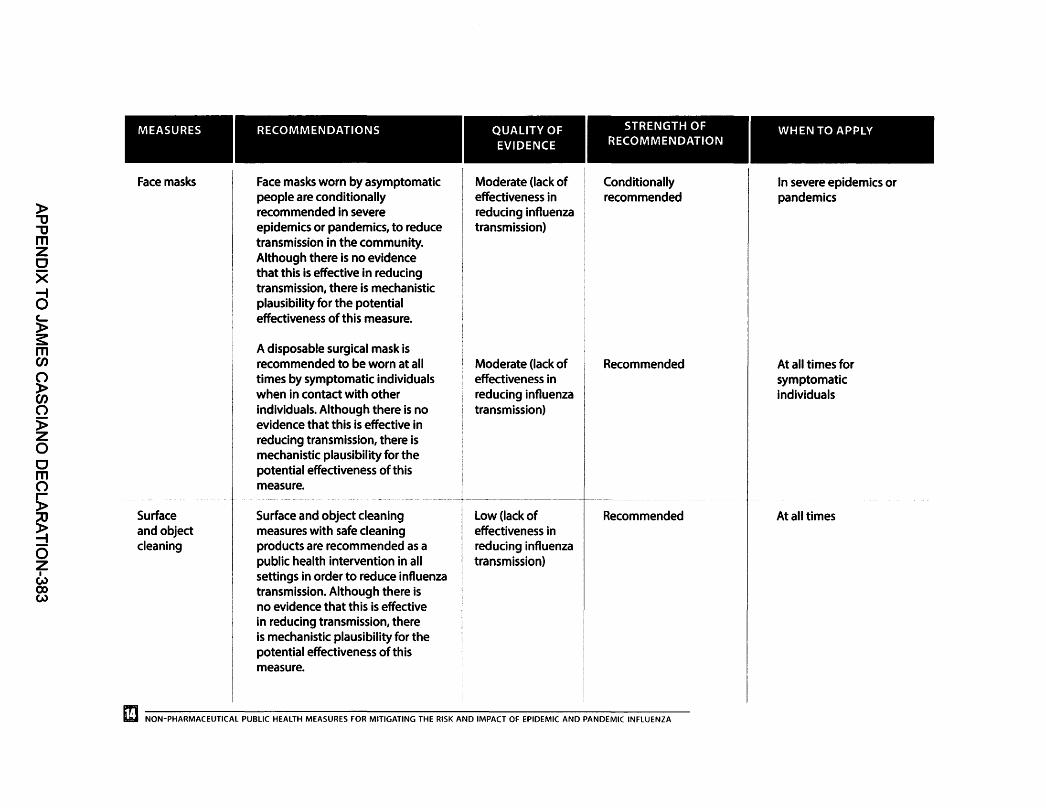
)> "'tJ "'tJ m z CJ X -I 0 c.... )> s: m "' () )>
"' ()
)> z 0 CJ m ()
s; ! 0 z I w
0) w
MEASURES RECOMMENDATIONS
Face masks Face masks worn by asymptomatic people are conditionally recommended in severe epidemics or pandemics, to reduce transmission in the community. Although there is no evidence that this is effective in reducing transmission, there is mechanistic plausibility for the potential effectiveness of this measure.
A disposable surgical mask is recommended to be worn at all times by symptomatic individuals when in contact with other individuals. Although there is no evidence that this is effective in reducing transmission, there is mechanistic plausibility for the potential effectiveness of this measure.
Surface Surface and object cleaning and object measures with safe cleaning cleaning products are recommended as a
public health intervention in all settings in order to reduce influenza transmission. Although there is no evidence that this is effective in reducing transmission, there is mechanistic plausibility for the potential effectiveness of this measure.
QUALITY OF EVIDENCE
Moderate (lack of effectiveness in reducing influenza transmission)
Moderate (lack of effectiveness in reducing influenza transmission)
Low (lack of effectiveness in reducing influenza transmission)
STRENGTH OF RECOMMENDATION
Conditionally recommended
Recommended
Recommended
m NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
WHEN TO APPLY
In severe epidemics or pandemics
At all times for symptomatic individuals
At all times

I
MEASURES RECOMMENDATIONS
Other Installing UV light in enclosed and environmental crowded places (e.g. educational
)> measures institutions and workplaces) is "'O "'O not recommended for reasons of m feasibility and safety. z 0
Increasing ventilation is X ~ recommended in all settings to 0 reduce the transmission of influenza c.... virus. Although there is no evidence )> that this is effective in reducing s:: m transmission, there is mechanistic en plausibility for the potential () effectiveness of this measure. )> en () There is no evidence that modifying )> humidity (either increasing humidity z in dry climates, or reducing humidity 0 in hot and humid climates) is an 0 effective intervention, and this is not m () recommended because of concerns s;: about cost, feasibility and safety.
! Contact tracing Active contact tracing is not
0 recommended in general because
z there is no obvious rationale for it in I most Member States. This intervention (.-)
CX> could be considered in some ~
locations and circumstances to collect information on the characteristics of the disease and to identify cases, or to delay widespread transmission in the very early stages of a pandemic in isolated communities.
WORI [) Hf Al TH OR(JANl?ATION
QUALITY OF EVIDENCE
None
Very low (effective)
None
Very low (unknown)
STRENGTH OF RECOMMENDATION
Not recommended
Recommended
Not recommended
Not recommended
I
WHEN TO APPLY
N/A
At all times
N/A
N/A

)> "lJ "lJ m z CJ X
d c... )> s: m en
i 0 )> z 0 CJ m 0 s;: ! 0 z I
u) 0) 01
MEASURES
Isolation of sick individuals
Quarantine of exposed individuals
School measures and closures
RECOMMENDATIONS
Voluntary isolation at home of sick individuals with uncomplicated illness is recommended during all influenza epidemics and pandemics, with the exception of the individuals who need to seek medical attention. The duration of isolation depends on the severity of illness (usually 5-7 days) until major symptoms disappear.
Home quarantine of exposed individuals to reduce transmission is not recommended because there is no obvious rationale for this measure, and there would be considerable difficulties in implementing it.
School measures (e.g. stricter exclusion policies for ill children, increasing desk spacing, reducing mixing between classes, and staggering recesses and lunchbreaks) are conditionally recommended, with gradation of interventions based on severity. Coordinated proactive school closures or class dismissals are suggested during a severe epidemic or pandemic. In such cases, the adverse effects on the community should be fully considered (e.g. family burden and economic considerations), and the timing and duration should be limited to a period that is judged to be optimal.
QUALITY OF EVIDENCE
Very low (effective)
Very low (variable effectiveness)
Very low (variable effectiveness)
STRENGTH OF RECOMMENDATION
Recommended
Not recommended
Conditionally recommended
II] NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
WHEN TO APPLY
At all times
N/A
Gradation of interventions based on severity; school closure can be considered in severe epidemics and pandemics

MEASURES RECOMMENDATIONS
Workplace Workplace measures (e.g. measures and encouraging teleworking from home,
)> closures staggering shifts, and loosening '1J policies for sick leave and paid leave) '1J are conditionally recommended, with m z gradation of interventions based on CJ severity. Extreme measures such as X workplace closures can be considered -I in extraordinarily severe pandemics in 0 c.... order to reduce transmission. )> s: Avoiding Avoiding crowding during moderate m crowding and severe epidemics and pandemics en C') is conditionally recommended, with )> gradation of strategies linked with en severity in order to increase the C')
)> distance and reduce the density
z among populations. 0 CJ Travel advice Travel advice is recommended for m citizens before their travel as a public C')
s; health intervention in order to avoid potential exposure to influenza and
! to reduce the spread of influenza.
0 Entry and exit Entry and exit screening for z screening infection in travellers is not I w recommended, because of 0) a, the lack of sensitivity of these
measures in identifying infected but asymptomatic (i.e. pre-symptomatic) travellers.
WORi D HF Al TH ORC,ANI? ATION
QUALITY OF EVIDENCE
Very low (effective)
Very low (unknown)
None
Very low (lack of effectiveness in reducing influenza transmission)
STRENGTH OF RECOMMENDATION
Conditionally recommended
------ ----·----·-·· -- - ·-
Conditionally recommended
Recommended
Not Recommended
WHEN TO APPLY
Gradation of interventions based on severity; workplace closure should be a last step only considered in extraordi-narily severe epidemics and pandemics
Moderate and severe epidem-ics and pandemics
Early phase of pandemics
N/A
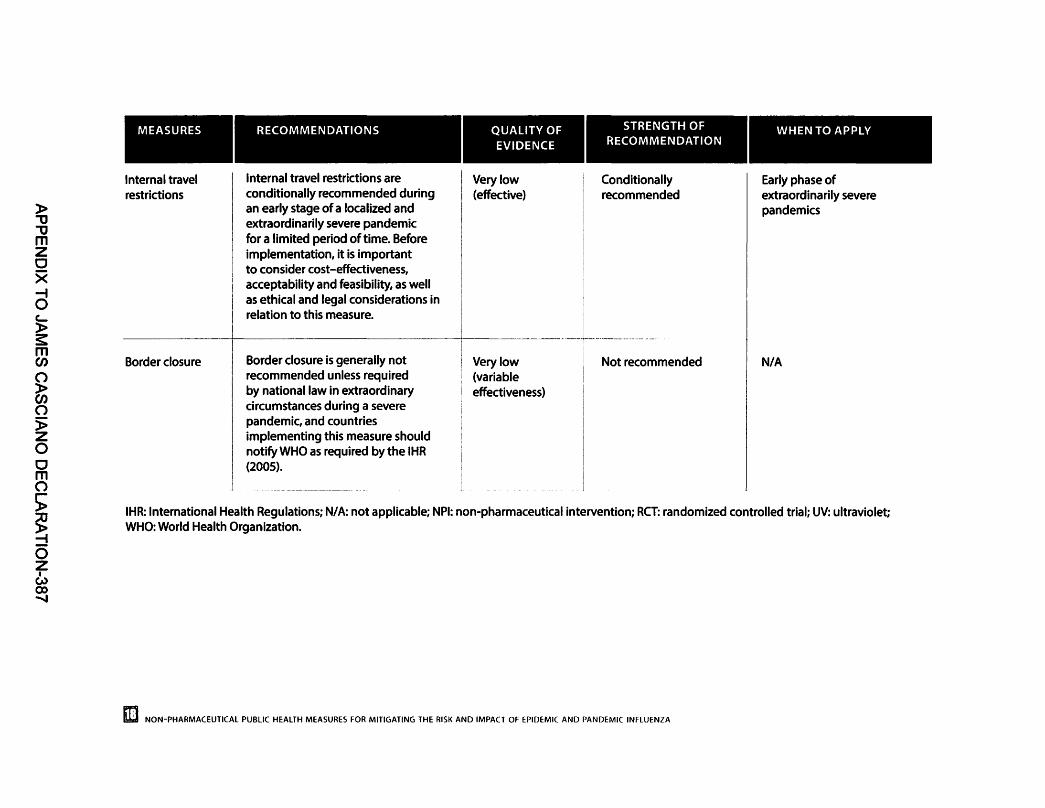
)> "lJ "lJ m z 0 X --i 0 ~ )> s:: m en
~ (") )> z 0 0 m (")
> ! 0 z I w
CX> .......
I MEASURES
Internal travel restrictions
Border closure
RECOMMENDATIONS
Internal travel restrictions are conditionally recommended during an early stage of a localized and extraordinarily severe pandemic for a limited period of time. Before implementation, it is important to consider cost-effectiveness, acceptability and feasibility, as well as ethical and legal considerations in relation to this measure.
Border closure is generally not recommended unless required by national law in extraordinary circumstances during a severe pandemic, and countries implementing this measure should notify WHO as required by the IHR (2005).
QUALITY OF EVIDENCE
Very low (effective}
Very low (variable effectiveness}
STRENGTH OF RECOMMENDATION
Conditionally recommended
Not recommended
WHEN TO APPLY
Early phase of extraordinarily severe pandemics
N/A
IHR: International Health Regulations; N/A: not applicable; NPI: non-pharmaceutical intervention; RCT: randomized controlled trial; UV: ultraviolet; WHO: World Health Organization.
II] NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA

COMMUNICATION FOR BEHAVIOURAL IMPACT
Communication for behavioural impact (COMBI) (4 7) is a planning framework and an implementation method for using communication strategically to achieve positive behavioural and social results. It involves health education, health literacy, health promotion, risk communication and social mobilization, and it plays a critical role in the implementation of the NPI measures by modifying behaviour. COMBI identifies the barriers and constraints that prevent people from choosing to adopt healthy behaviour, and ensures that communication is appropriately applied and can contribute to achieving expected behavioural impact.
In the implementation of the recommended NPI measures, COMBI should be used to: • share the rationale; • encourage active engagement; • empower people with information; • adapt recommendations to the local context; and • quickly develop effective communication strategies, messages and materials, using existing
resources and partnerships.
The rest of this section discusses each of these points.
Share the rationale This involves explaining to people why certain behaviour is important. Transparency in sharing information and its rationale helps to build trust and increases the likelihood of cooperation.
Encourage active engagement This involves: • encouraging people to seek information from credible sources; and • ensuring that neighbours, communities and networks receive and understand accurate
information, report possible influenza cases and help communities in managing ill people.
In this approach, people are viewed as "partners in prevention~ rather than simply as recipients of information. The approach is therefore likely to create ownership, resulting in better adoption of recommended behaviours and more proactive communities. Such partners in prevention are also more likely to find creative ways to mobilize community resources and help build capacity that might be useful in the future.
Empower people with information People and communities will take their own decisions on the basis of the balance of forces of their own circumstances. The communication approach should emphasize information sharing and community problem solving as ways of helping people to find a set of doable actions, so that they ask"How can we effectively prevent infection and protect ourselves, our families and our community?0
Adapt recommendations to the local context It is important to take into account people's capacity to act on the advice being given. The recommended behaviour must be doable and be adapted to people's lifestyle; otherwise, it will not be widely adopted. For example, there is a need to ensure that marginalized groups (e.g. those living in inadequate or overcrowded housing, religious minorities and people beyond the reach of
________________ m WORLD HEALTH ORGANIZATION W
APPENDIX TO JAMES CASCIANO DECLARATION-388

the mass media) are also engaged in prevention and protection, have access to information and have the capacity to act upon it.
Use existing resources and partnerships to quickly develop effective communication strategies, messages and materials Working through existing communication and coordination bodies makes it easier to harmonize messages, approaches and use of channels. It is important to invest resources in understanding the current knowledge, attitude and practices on the implementation of NPls - this can help to reduce the impact of pandemic and thus craft policy and workflow to more effectively manage the public's concerns, compliance and expectations. In turn, this may help Member States to achieve a higher effectiveness for these NPls. Training on crisis communication for selected community leaders and key national stakeholders as part of pandemic preparedness is also important.
PERSONAL PROTECTIVE MEASURES This section covers three types of personal protective measures: hand hygiene, respiratory etiquette and face masks.
4.1. Hand hygiene
Summary of evidence Twelve articles describing 11 RCTs (two studies were the same project during the same period but studied different questions) of hand hygiene were included in a systematic review, and a metaanalysis was undertaken of 1 0 studies including more than 11 000 participants in total (42-53). It was not possible to make a pooled estimate of the effectiveness of hand hygiene with or without face masks because of the high heterogeneity (see Annex). In the pooled analysis of six studies that examined hand hygiene together with face masks, there was no statistically significant protective effect when all settings outside of health care were combined (rate ratio [RR]: 0.91, 95% confidence interval [Cl]: 0.73-1.13, P=0.39, 12=35%) (42-47). Two studies were conducted in an elementary school setting but had very different findings: one study conducted in the USA found no significant effect of hand hygiene, with a precise estimate of the risk ratio close to 1; in contrast, a large trial in Egypt reported a statistically significant reduction of more than 50% in laboratoryconfirmed influenza cases in the intervention group (RR: 0.47, 95% Cl: 0.39-0.56, P<0.01) (48, 49). Two studies in university halls of residence found no statistically significant effect of hand hygiene with face masks (RR: 0.48, 95% Cl: 0.21-1.08, P=0.08, 12=0%) (42, 43). In addition, in household settings the efficacy of hand hygiene with or without a face mask was not significant (RR: 1.05, 95% Cl=0.86-1.27, P=0.65, 12=57%) (44-47, 50, 57). Several trials reported that poor adherence to hand hygiene may contribute to the low efficacy observed (44-46).
Influenza virus can survive for a short time on human hands and transmit from contaminated surfaces to hands, supporting the potential for contact transmission to occur (54-56). Hand hygiene is effective to inactivate or reduce viable influenza virus on human hands (57-59). In theory, hand hygiene could prevent indirect contact transmission of influenza; however, hand hygiene adherence is often suboptimal, even in intervention studies.
Testing the efficacy of hand hygiene in RCTs is complicated by the fact that the comparison groups cannot be asked to stop washing their hands. Thus, evidence from RCTs is typically based on either an increase in the quantity of hand hygiene episodes or non-inferiority trials focusing on certain products (e.g. hand sanitizer in combination with hand washing versus hand washing alone), making it difficult to estimate the efficacy of hand hygiene alone. Within this context, existing
EilJ NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-389

hand hygiene studies are of a moderate overall quality, and they do not provide strong evidence that increased hand hygiene or different hand hygiene modalities are highly effective at reducing influenza. However, there are several experimental studies (57-60) that provide evidence that hand hygiene can inactivate or remove influenza and therefore reduce transmission.
OVERALL RESULT OF EVIDENCE ON HAND HYGIENE
1. Eleven RCTs were included in this review. Although hand hygiene was not effective against laboratory-confirmed influenza in a meta-analysis in community settings and university halls, it was effective in one of two trials conducted in schools.
2. Although compliance with optimal (intense) hand hygiene practices was imperfect in these RCTs, compliance with proper hand hygiene might not be substantially higher in community settings, even in severe influenza epidemics and pandemics.
3. Experimental studies suggested that hand hygiene could effectively inactivate or reduce influenza virus on hands; hence, theoretically, hand hygiene could prevent influenza transmission.
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence There is a moderate overall quality of evidence that hand hygiene does not have a substantial effect on transmission of laboratory-confirmed influenza.
Values and preferences It is well-established that hand hygiene can substantially reduce many important infectious diseases, particularly diarrhoeal diseases, and there is good evidence that hand hygiene can also reduce respiratory illnesses, although not laboratory-confirmed influenza. Hand hygiene is most often performed with water and soap; alcohol-based hand sanitizers are another option for waterless hand disinfection in some locations. Most communities would understand the importance and effectiveness of hand hygiene in preventing common infections, and would agree with the concept of encouraging hand hygiene to prevent infection, although education campaigns might be needed in some communities.
Balance of benefits and harms Hand hygiene had no significant effect on transmission of laboratory-confirmed influenza, other than in the RCT in schools in Egypt. The guideline development group concluded that, in general, the evidence from controlled trials indicates that hand hygiene is not effective in preventing laboratory-confirmed influenza, but it is possible that a major change in hand hygiene from a very low level to a very high level might reduce influenza transmission. Hand hygiene does prevent transmission of other infections, including diarrhoeal and respiratory diseases, and can substantially improve public health (61 ). There are no adverse effects of hand hygiene, other than possible soap or alcohol allergies (62).
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-390

Resource implications Hand hygiene is one of the most cost-effective measures for preventing infections in health care settings (63). It is an important component of general hygiene campaigns in communities, and can reduce the incidence of a variety of infections and associated morbidity and mortality. Clean running water is not available in some communities and would be a barrier. Alcohol hand-rub may be too expensive in some settings.
Ethical considerations There are no major ethical issues regarding hand hygiene with soap and water. Alcohol-based hand-rub might not be permitted in some locations due to religious objections (64).
Acceptability More than half of published national pandemic plans have included hand hygiene as a prevention measure (65). Given the low cost and broad impact on infections, it is a very acceptable intervention. However, the guideline development group considered that compliance and adherence is low (especially compliance to proper hand hygiene practice) because it is hard to make substantial behavioural changes.
Feasibility Many countries have already conducted public hand hygiene campaigns to reduce communicable diseases (65). This intervention is considered to be very feasible.
RECOMMENDATION:
Hand hygiene is recommended as part of general hygiene and infection prevention, including during periods of seasonal or pandemic influenza. Although RCTs have not found that hand hygiene is effective in reducing transmission of laboratory-confirmed influenza specifically, mechanistic studies have shown that hand hygiene can remove influenza virus from the hands, and hand hygiene has been shown to reduce the risk of respiratory infections in general.
Population: General public
When to apply: At all times
FACTORS ASSESSMENT RATIONALE
Quality of evidence
Values and preferences
Moderate (lack of effectiveness in reducing influenza transmission)
Favourable Favourable
Moderate quality of evidence from 1 O RCTs in a meta-analysis involving > 11 000 participants that hand hygiene is ineffective in reducing influenza transmission in the community, although experimental studies suggested that hand hygiene could theoretically prevent influenza transmission.
Hand hygiene has an established effect on common diarrhoeal infections and can also reduce some respiratory infections and other infections.
EE NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-391

FACTORS ASSESSMENT RATIONALE
Balance of benefits and harms
Resource implications
Ethical considerations
Acceptability
Feasibility
Overall strength of recommendation
Favourable
Favourable
Conditional
Favourable
Favourable
Recommended
No important adverse effects of hand hygiene with water and soap, other than possible soap or alcohol allergies.
Hand hygiene with soap and water is generally very cost-effective given the reduction in common infections and no additional equipment is needed.
No major ethical issues. There may be religious objections to alcohol hand-rub.
No major concerns with acceptability, but the compliance and adherence of this intervention may be difficult to change substantially.
Very feasible because it is normal practice.
Although hand hygiene does not have proven efficacy against laboratoryconfirmed influenza in RCTs, it is recommended because it has been shown to deadivate or remove influenza virus from the hands in experimental studies, and can reduce the burden of those other infedions on the health system during influenza epidemics and pandemics.
Knowledge gaps: There are important gaps in our knowledge of the mechanisms of personto-person transmission of influenza, including the importance of direct and indirect contact, the degree of viral contamination on hands and various types of surfaces in different settings, and the potential for contact transmission to occur in different locations and under different environmental conditions. Additional research on increasing hand hygiene compliance would also be valuable. There is little information on whether greater reductions in transmission could be possible with combinations of personal interventions (e.g. isolation away from family members as much as possible, plus using face masks and enhancing hand hygiene).
RCT: randomized controlled trial.
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-392

4.2. Respiratory etiquette
Summary of evidence Respiratory etiquette refers to the actions used when people cough or sneeze (66); it is a simple hygiene practice to prevent person-to-person transmission of respiratory infections. Measures include (6n covering the mouth and nose with a hand, sleeve or tissue when coughing or sneezing; finding the nearest waste basket to dispose of the used tissue immediately; and washing hands after touching respiratory secretions or contaminated objects (or both). A total of 80 articles were retrieved from four electronic databases, and no scientific studies were identified for inclusion in this review.
Respiratory etiquette is a common and acceptable practice in relation to personal hygiene; however, there is no research on the effectiveness of respiratory etiquette on the reduction of laboratory-confirmed influenza virus infection.
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence The quality of evidence could not be judged because no study was identified.
Values and preferences Respiratory etiquette and hygiene is recognized as important in many communities. Improvements in respiratory etiquette in communities could prevent the spread of a variety of infections.
Balance of benefits and harms There are no anticipated harms of improved respiratory etiquette.
Resource implications Efforts to improve respiratory etiquette in communities would not be expensive and could be included as part of broader public health campaigns.
Ethical considerations There are no major ethical considerations in relation to respiratory etiquette. Cultural contexts may be considered when recommending specific actions such as covering coughs with hands or tissues.
Acceptability Improved respiratory etiquette should be acceptable in most locations.
Feasibility This is a feasible intervention, and respiratory etiquette campaigns have been successful for acute respiratory infections (66). Furthermore, 32 Member States have included respiratory etiquette in their national pandemic preparedness plans (65).
EIJ NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-393

r
RECOMMENDATION:
Respiratory etiquette is recommended at all times during influenza epidemics and pandemics. Although there is no evidence that this is effective in reducing influenza transmission, there is mechanistic plausibility for the potential effectiveness of this measure.
Population: General public
When to apply: At all times
FACTORS ASSESSMENT RATIONALE
Quality of evidence
Values and preferences
Balance of benefits and harms
Resource implications
Ethical considerations
Acceptability
Feasibility
Overall strength of recommendation
None
Conditional
Favourable
Favourable
Favourable
Favourable
Favourable
Recommended
No scientific evidence on the effectiveness of respiratory etiquette.
Respiratory etiquette is a simple personal protective measure to prevent infection, but may not always be recognized as important in some cultures and locations.
No anticipated harms.
No significant costs for the general public.
There are no major ethical considerations. Cultural contexts and norms may be considered when recommending specific actions such as covering coughs with hands or tissues.
No major concerns with acceptability.
Highly feasible.
Although there is no research on the impad of respiratory etiquette on laboratory-confirmed influenza lnfedlon, this is a simple, feasible and acceptable intervention that may reduce transmission and reduce the impad of epidemics and pandemics.
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-394

Knowledge gaps: There is still no evidence about the quantitative effectiveness of respiratory etiquette against influenza virus. RCTs of interventions to improve respiratory etiquette would be valuable.
RCT: randomized controlled trial.
4.3. Face masks
Summary of evidence Ten relevant RCTs were identified for this review and meta-analysis to quantify the efficacy of community-based use of face masks, including more than 6000 participants in total (42-47, 50, 68-70). Most trials combined face masks with improved hand hygiene, and examined the use of face masks in infected individuals (source control) and in susceptible individuals. In the pooled analysis, although the point estimates suggested a relative risk reduction in laboratory-confirmed influenza of 22% (RR: 0.78, 95% Cl: 0.51-1.20, 12=30%, P=0.25) in the face mask group, and a reduction of 8% in the face mask group regardless of whether or not hand hygiene was also enhanced (RR: 0.92, 95% Cl=0.75-1.12, 12=30%, P=0.40), the evidence was insufficient to exclude chance as an explanation for the reduced risk of transmission. Some studies reported that low compliance in face mask use could reduce their effectiveness. A study suggested that surgical and N95 (respirator) masks were effective in preventing the spread of influenza (77).
r OVERALL RESULT OF EVIDENCE ON FACE MASKS
1. Ten RCTs were included in the meta-analysis, and there was no evidence that face masks are effective in reducing transmission of laboratory-confirmed influenza.
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence There is a moderate overall quality of evidence that face masks do not have a substantial effect on transmission of influenza.
Values and preferences Face mask use is common to prevent transmission of infections in health care settings around the world, and a widely used measure in some communities, particularly in South-East Asia.
Balance of benefits and harms There are no major adverse effects of face mask use. There might be issues with allergies in some individuals, and prolonged use of face masks can be uncomfortable or inconvenient.
Resource implications Reusable cloth face masks are not recommended. Medical face masks are generally not reusable, and an adequate supply would be essential if the use of face masks was recommended. If worn by a symptomatic case, that person might require multiple masks per day for multiple days of illness.
m NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-395

Ethical considerations There are no major ethical considerations in the use of face masks. Masks may be more culturally acceptable in some locations, and other health behaviours may affect compliance (72).
Acceptability Face masks are widely used in health care settings to prevent transmission of infections, and are used in the community in some parts of the world (65). They are likely to be acceptable if recommended, particularly in more severe epidemics and pandemics. However, face masks are not appropriate under some circumstances (e.g. during sleep). The guideline development group also considered that compliance may not be high in some areas and populations.
Feasibility Twenty-eight Member States have included the use of face masks in their national influenza preparedness plan (65). Feasibility can be enhanced by education campaigns to improve usage and compliance. The guideline development group believed that this intervention is feasible, especially for symptomatic individuals.
RECOMMENDATION:
Face masks worn by asymptomatic people are conditionally recommended in severe epidemics or pandemics, to reduce transmission in the community. Disposable, surgical masks are recommended to be worn at all times by symptomatic individuals when in contact with other individuals. Although there is no evidence that this is effective in reducing transmission, there is mechanistic plausibility for the potential effectiveness of this measure.
Population: Population with symptomatic individuals; and general public for protection
When to apply: At all times for symptomatic individuals (disposable surgical mask), and in severe epidemics or pandemics for public protection (face masks)
FACTORS ASSESSMENT RATIONALE
Quality of Moderate (lack of According to the GRADE approach, evidence effectiveness in there was moderate quality of evidence
reducing influenza involving >6000 participants that face transmission) masks are ineffective in reducing influenza
transmission in the community. -~--·--~----~-
Values and Favourable Masks can be worn by symptomatic or preferences exposed persons to reduce transmission
(source control), or by uninfected persons in the community to reduce their risk of infection.
Balance of Favourable No significant harms anticipated. benefits and harms
Resource Conditional Costly in some settings, and supplies may implications be limited.
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-396

FACTORS ASSESSMENT RATIONALE
Ethical considerations
Acceptability
Feasibility
Favourable
Conditional
Conditional ------r
No major ethical considerations.
Likely to be acceptable, but not appropriate in some circumstances and the adherence and compliance is low.
Dependent on availability, but more feasible for symptomatic individuals.
r Overall strength of recommendation
Recommended for symptomatic individuals, and conditionally recommended for public protection
Given the costs and the uncertain effectiveness, face masks are conditionally recommended only in severe influenza epidemics or pandemics for the protection of the general population, but are recommended for symptomatic individuals at all times .
... r
Knowledge gaps: There are important gaps in our knowledge of the mechanisms of personto-person transmission of influenza, including the importance of transmission through droplets of different sizes including small particle aerosols, and the potential for droplet and aerosol transmission to occur in different locations and with different environmental conditions. Additional high-quality RCTs of the efficacy of face masks against laboratoryconfirmed influenza would be valuable.
GRADE: Grading of Recommendations Assessment, Development and Evaluation; RCT: randomized controlled trial.
(J ENVIRONMENTAL MEASURES 5.1. Surface and object cleaning
Summary of evidence Three studies were included in the systematic review to study the effectiveness of surface and object cleaning in reducing influenza transmission (73-75). An RCT with disinfection of toys and linen in day care facilities found a reduction in the detection of viruses in the environment, but no significant effect on laboratory-confirmed influenza or acute respiratory illnesses among children (74). Another RCT conducted in elementary schools reported that surface disinfection combined with hand hygiene could reduce absenteeism due to gastrointestinal illness, but not absenteeism due to respiratory illness (75). A cross-sectional study showed that passive contact with sodium hypochlorite (bleach) in households was significantly associated with an increase in the rate of self-reported influenza, which the authors of the article hypothesized had occurred due to the immunosuppressive properties of bleach (73).
m NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-397

Influenza virus can survive on surfaces and objects for a few hours and up to 1 week (54, 55, 76-78). Influenza virus RNA has been detected in various settings outside of health care settings, but little of the RNA was found to be viable (74, 79-83). Surface and object cleaning is effective at inactivating or reducing viable influenza virus on surfaces (84-86). In theory, surface and object cleaning could prevent indirect contact transmission of influenza.
r OVERALL RESULT OF EVIDENCE ON SURFACE AND OBJECT CLEANING
1. Two RCTs and one cross-sectional study were included in the systematic review.
2. There was evidence that surface and object cleaning could reduce detections of virus in the environment, but there was no evidence of effectiveness against laboratory-confirmed influenza virus infection.
3. Experimental studies suggested that surface and object cleaning could effectively inactivate or reduce viable influenza virus on surfaces; theoretically, this intervention could prevent influenza transmission.
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence There is a low overall quality of evidence that cleaning of surfaces and objects does not have a substantial effect on transmission of respiratory disease.
Values and preferences A telephone survey in Europe found that most (8296) participants believed that cleaning or disinfecting objects might reduce the risk of influenza (87). Environmental cleaning is a common strategy to reduce a variety of infections.
Balance of benefits and harms Cleaning using detergent-based cleaners or bleach can inactivate or remove influenza viruses from surfaces and objects, and in theory could reduce influenza transmission. However, most disinfectants (e.g. bleach} require a pre-cleaning step before the disinfectant is applied, and it is not safe to add water to chlorine solutions (88, 89). Incorrect use of disinfectants and poor ventilation when using the disinfectant can be harmful (29).
Resource implications The implementation of surface and object cleaning would involve relatively minor resources. The cost of disinfectants is relatively low.
Ethical considerations Cleaning product selection is a major issue. Some disinfectants are irritants and may lead to adverse effects in sensitive populations (73); also, they may not be applicable in some countries or regions due to the prohibition of alcohol (64). However, most countries have no legislation restricting the use of alcohol in household cleaning agents, and even in Muslim tradition, alcohol is permitted as a cleansing ingredient (64). In addition, the safety of cleaning personnel should also be considered.
-W-OR-LD_H_E-AL-TH-0-RG_A_N_IZA-TI-ON-1
---------------------------- ~
APPENDIX TO JAMES CASCIANO DECLARATION-398

Acceptability This intervention is highly accepted by policy-makers and health workers worldwide. However, the acceptability may vary among different countries.
Feasibility This intervention is highly feasible. Disinfectants are available from a variety of sources, such as general supermarkets or convenience stores.
RECOMMENDATION:
Surface and object cleaning measures with safe cleaning products are recommended as a public health intervention in all settings in order to reduce influenza transmission. Although there is no evidence that this is effective in reducing transmission, there is mechanistic plausibility for the potential effectiveness of this measure.
Population: General population
When to apply: At all times
FACTORS ASSESSMENT RATIONALE
Quality of evidence
Values and preferences
Balance of benefits and harms
Resource implications
Ethical considerations
Acceptability
Feasibility
Low (lack of effectiveness in reducing influenza transmission)
Favourable
Conditional
Favourable
Conditional
Favourable
Favourable
i
I
:
!
i
Very limited evidence on the effectiveness or lack of effectiveness of environmental cleaning. Surface and object cleaning is ineffective in reducing respiratory disease transmission in the community, although experimental studies suggest that theoretically surface and object cleaning could prevent influenza transmission.
Likely to be perceived as a simple but important measure, if recommended.
Safety concerns with some cleaning products.
The cost of disinfectants is low.
In some locations, cleaning with alcohol may not be allowed, but other chemicals can be used.
-------~~---
Likely to be acceptable if recommended.
Disinfectants can be obtained from various sources.
---
EE NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-399

r
Overall strength of recommendation
Recommended There are no major disadvantages of surface and object cleaning, so this measure Is recommended despite the lack of evidence on effectiveness.
Knowledge gaps: Only three studies were included in our systematic review and only two of them were RCTs. More trials are needed to study the effect of surface and object cleaning on influenza prevention. The best evidence of pandemic preparedness would be provided by studies in which the outcome is laboratory-confirmed influenza, rather than acute respiratory infections. Studies are needed in various settings (e.g. household, school, workplace and public place). The effectiveness of different cleaning products in preventing influenza transmission - in terms of cleaning frequency, cleaning dosage, cleaning time point, and cleaning targeted surface and object material - remains unknown.
RCT: randomized controlled trial.
5.2. Other environmental measures
5.2.1. Ultraviolet light Summary of evidence The systematic review did not identify any studies that quantified the effectiveness of ultraviolet (UV) light in reducing influenza transmission. UV light is a means of disinfection; it breaks down microorganisms and can be used to prevent the spread of certain infectious diseases (90).
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence The quality of evidence could not be judged because no study was identified.
Values and preferences The guideline development group noted that UV light intervention would not be useful if the surface is covered, and would probably have a limited impact on transmission given the likely modes of influenza transmission.
Balance of benefits and harms The effectiveness of UV light against influenza transmission is uncertain. Exposure to UV light may increase the risk of skin cancers and eye problems (91 ). The guideline development group considered UV light intervention to be harmful in some circumstances.
Resource Implications Installing and maintaining UV light fixtures is expensive. However, the guideline development group believed that costs in settings with a large number of people (e.g. public transport) may be reasonable given the potential impact.
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-400

r
Ethical considerations No major ethical concerns were identified in relation to the use of UV light.
Acceptability The use of UV light to reduce influenza transmission by disinfection of the environment is likely to have limited acceptability, because of the costs and complexity of installation and maintenance. The guideline development group believed it would be unlikely that these fixtures could be installed at short notice, such as in the early stages of an influenza pandemic.
Feasibility The use of UV disinfection is hindered by safety concerns.
RECOMMENDATION:
Installing UV light in enclosed and crowded places (e.g. educational institutions and workplaces) is not recommended for reasons of feasibility and safety.
Population: People exposed to risk in closed and crowded places
When to apply: N/ A
FACTORS ASSESSMENT RATIONALE
Quality of None No study was identified in the review. evidence
Values and Conditional Uncertain. preferences
Balance of Conditional Safety concerns. benefits and harms
Resource Conditional Substantial costs associated with installing implications and maintaining UV light fixtures.
Ethical Conditional No major ethical concerns. considerations
Acceptability Conditional Uncertain acceptability given costs and complexity of installation and maintenance.
--
Feasibility Conditional UV light may not be feasible because of high costs and safety concerns.
EE NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-401

r
r
Overall strength of recommendation
Not Recommended The use of UV light is hindered by feasibility and safety concerns.
Knowledge gaps: The effectiveness of UV light in reducing influenza transmission still requires more evidence. Potential safety issues are also an important consideration and more scientific evidence is needed to confirm effectiveness and feasibility as a community mitigation measure for influenza epidemics and pandemics.
N/ A: not applicable; UV: ultraviolet.
5.2.2. Increased ventilation Summary of evidence A simulation study predicted a reduction of transmission among kindergarten students by enhancing the air changes per hour (ACH) (92). Two simulation studies evaluated the effectiveness of increasing ventilation in reducing influenza transmission in community settings (93, 94). One of these two studies suggested a reduction of daily peak infections by increasing ACH under the baseline scenario (93), and the other predicted that the peak infection rate could be reduced by more than 60% by doubling or tripling the ventilation rate (94).
OVERALL RESULT OF EVIDENCE ON INCREASED VENTILATION
1. In simulation studies, increasing the ventilation rate reduced influenza transmission.
2. There is mechanistic plausibility for increased ventilation to reduce transmission - specifically aerosol transmission and perhaps to a lesser extent large respiratory droplet transmission or indirect contact transmission.
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence There is a very low overall quality of evidence that increasing ventilation has an effect on transmission of influenza.
Values and preferences Increasing ventilation is a common practice in many locations, for a multitude of reasons.
Balance of benefits and harms There is no major harm associated with increased ventilation. Airflow pattern and flow direction are important considerations (95). If the outdoor temperature is very low, thermal comfort may be an issue. Exposure to air pollution and allergens may trigger asthmatic attacks.
----------------~ WORLD HEALTH ORGANIZATION ~
APPENDIX TO JAMES CASCIANO DECLARATION-402

Resource implications The cost of opening windows is likely to be low. There may be costs associated with increasing ventilation for buildings or homes with mechanical ventilation (e.g. increased electricity costs). In cold climates, increased natural or mechanical ventilation could also increase heating costs.
Ethical considerations There are no major ethical considerations associated with the use of increased ventilation.
Acceptability The acceptability of increased ventilation is likely to be high.
Feasibility Increased ventilation is likely to be feasible in most settings.
RECOMMENDATION:
Increasing ventilation is recommended in all settings to reduce the transmission of influenza virus. Although there is no evidence that this is effective in reducing transmission, there is mechanistic plausibility for the potential effectiveness of this measure.
Population: General Population
When to apply: At all times
Values and Favourable preferences
Balance of Conditional benefits and harms
Resource Conditional implications
Ethical Favourable considerations
Acceptability Favourable
Feasibility Conditional
The only evidence was provided by simulation studies. In those studies, increased ventilation was predicted to be effective in reducing influenza transmission in the community.
Commonly used intervention.
Exposure to air pollution and allergens may trigger asthmatic attacks.
May lead to increased heating costs or increased electricity costs.
No major ethical considerations.
Increased ventilation is highly accepted.
Increased ventilation is feasible in most locations.
EIJ NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-403

Overall strength of recommendation
Recommended Effectiveness is uncertain, but Increased ventilation Is simple and feasible in most locations.
Knowledge gaps: Simulation models provide a weak level of evidence. RCTs would provide more compelling evidence on the efficacy of increasing ventilation in reducing influenza transmission.
RCT: randomized controlled trial.
5.2.3. Modifying humidity Summary of evidence Increased humidity has been correlated with reduced influenza transmission in cold and dry climates (96, 97), and very high humidity has been associated with increased transmission in hot and humid climates ( 7 7). Nevertheless, no study was identified in the review that quantified the effectiveness of modifying humidity (as an intervention) in reducing influenza transmission.
Elevated humidification (absolute humidity at 9 millibars) was shown to reduce influenza A virus detections in the air and on fomite (markers and wooden toys) in a preschool classroom (97). A simulation study also predicted a 17.5-31.6% reduction of influenza virus survival in rooms with a humidifier operating in a residential setting (98). Another simulation study predicted that nearly five times more influenza virus from stimulated coughs would remain infectious at 7-23% relative humidity (RH) than at an RH of more than 43% in a 1-hour collection (99).
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence The quality of evidence cannot be judged because no study was identified in the review.
Values and preferences Uncertain.
Balance of benefits and harms Humidification may increase the growth of mould and mildew, harming health ( 700). According to WHO, indoor dampness or mould creates a considerable health burden (e.g. asthma) in children (707).
Resource implications Humidifiers are expensive to purchase and maintain.
Ethical considerations There are no major ethical considerations in relation to modifying humidity.
________________ ffi WORLD HEALTH ORGANIZATION ~
APPENDIX TO JAMES CASCIANO DECLARATION-404

r
\...
r
Acceptability Modifying humidity is likely to be acceptable.
Feasibility There may be insufficient availability of humidifiers at short notice, and it may not be feasible to humidify buildings across a community.
RECOMMENDATION:
There is no evidence that modifying humidity (either increasing humidity in dry climates, or reducing humidity in hot and humid climates) is an effective intervention, and this is not recommended because of concerns about cost, feasibility and safety.
Population: N/ A
When to apply: N/ A
FACTORS ASSESSMENT RATIONALE
Quality of evidence
Values and preferences
Balance of benefits and harms
Resource implications
Ethical considerations
Acceptability -----~ --
Feasibility
Overall strength of recommendation
None
Conditional
Conditional
Conditional
Favourable
Favourable
Conditional
Not Recommended
No study was identified in the review.
Uncertain.
Higher humidity may increase the growth of mould and mildew, causing harm.
Costly to purchase and maintain.
There are no major ethical considerations.
Likely to be acceptable.
Humidity may not be feasible as a population-level intervention.
The use of mechanical humidity is hindered by feaslblllty and safety reasons.
Knowledge gaps: The exact biological mechanism of how humidity affects the survival of the influenza virus is unclear (96, 97). Many studies have looked at the effect under laboratory conditions, but very few have tested these effects in natural settings. It would be informative to conduct RCTs of humidification as an intervention to reduce influenza transmission.
N/ A: not applicable; RCT: randomized controlled trial.
~ NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-405

SOCIAL DISTANCING MEASURES 6. 1. Contact tracing
Summary of evidence Four simulation studies were included in the systematic review (102-105), none of which studied contact tracing as a single intervention. Contact tracing was studied in combination with other interventions such as quarantine, isolation and provision of antiviral drugs. Evidence for the overall effectiveness of contact tracing varied. A simulation model with RO= 1.8 reported that the combination of contact tracing, quarantine, isolation and antiviral drugs could reduce the infection attack rate by 40% ( 7 02), while another study predicted that it would be difficult to control influenza even with 90% contact tracing and quarantine because of the presumed high level of pre-symptomatic or asymptomatic transmission ( 104). A combination of isolation, treatment of cases, contact tracing, quarantine and post-exposure prophylaxis was estimated to delay the epidemic peak for 6 weeks, assuming a case detection rate of 30% ( 7 05). In addition, the combination of contact tracing with quarantine has been suggested to be more effective than when combined with symptom monitoring (703).
OVERALL RESULT OF EVIDENCE ON CONTACT TRACING
1. Evidence for overall effectiveness of contact tracing was limited. All included studies were simulation models.
2. Only one study reported on the effect of adding contact tracing to isolation and quarantine. Such addition was estimated to provide at most a modest benefit, but at the same time would increase considerably the number of quarantined individuals.
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence There is a very low overall quality of evidence that contact tracing has an unknown effect on the transmission of influenza.
Values and preferences There is uncertainty about the values and preferences of contact tracing among the community for control of influenza. Mandatory contact tracing may cause concerns and uneasiness to some cases and their contacts; however, voluntary reporting of contacts can prevent such concerns.
Balance of benefits and harms Contact tracing allows the rapid identification of at-risk individuals once a case has been detected. This intervention reduces the delay between symptom onset and treatment, as well as implementation of preventive measures for onward transmission ( 7 06). The guideline development group considered contact tracing to be a potentially important measure in reducing cross-border transmission. However, contact tracing on a large scale can lead to ethical issues such as leakage of information, and inefficient usage of resources, including human resources ( 10n.
-----------------------ED WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-406

Resource implications Following up contacts of an infected individual who may have been exposed often has low costeffectiveness in the control of influenza, resulting in high direct costs. Considerable amounts of human resources are also needed for contact tracing.
Ethical considerations There are a few ethical issues surrounding the implementation of contact tracing as an intervention. Also, contact identification of infected individuals brings about privacy concerns (707). Some individuals may perceive stigma and refuse to be contact traced. Nevertheless, contact tracing may be justified, given that it allows the identification of persons at risk, and the timely provision of treatment and care (706, 707). There may be more ethical concerns when contact tracing is coupled with measures such as household quarantine. Contact tracing can substantially increase the proportion of people quarantined, but may not offer much additional benefit to existing interventions (702). In addition, contact tracing may not be an equitable intervention, because its successful implementation relies on availability of resources and technology.
Acceptability The evidence is limited and the acceptability of contact tracing among the public is uncertain.
Feasibility Contact tracing requires a large amount of trained personnel and resources (e.g. telecommunications); hence, it may be less feasible in low- to middle-income countries where resources are limited. In addition, the implementation and effectiveness of contact tracing rely on the capacity to detect cases, and contact tracing efforts are likely to be hampered by the short incubation and infectious periods of influenza (704). The triggers to activate and de-activate contact tracing for optimal effect in controlling influenza remain unknown.
,
\..
RECOMMENDATION:
Active contact tracing is not recommended in general because there is no obvious rationale for it in most Member States. This intervention could be considered in some locations and circumstances to collect information on the characteristics of the disease and to identify cases, or to delay widespread transmission in the very early stages of a pandemic in isolated communities.
Population: Individuals who have come into contact with an infected person
When to apply: N/ A
FACTORS ASSESSMENT RATIONALE
Quality of evidence
Values and preferences
Very low (unknown)
Conditional
All included articles are simulation models and the inherent limitations lead to a very low quality of evidence. Contact tracing combined with other interventions is effective in reducing influenza transmission in the community, but the effect of contact tracing alone is unknown.
There is uncertainty or variability in the values and preferences among different interest groups.
EI: NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-407

FACTORS ASSESSMENT RATIONALE
Balance of benefits and harms
Resource implications
Ethical considerations
Acceptability
Feasibility
Overall strength of recommendation
! Conditional
Conditional
Conditional
Conditional
Conditional
Not Recommended
Contact tracing can reduce onward transmission; however, the relevant ethical issues and inefficient usage of resources mean that the balance of benefits and harms is uncertain.
Contact tracing requires a large amount of resources, including human resources.
Privacy and equity concerns may exist for the implementation of contact tracing.
The acceptability of contact tracing among stakeholders is uncertain because of limited evidence.
Feasibility of contact tracing may be low when resources are limited; also, it is affected by the short incubation period of influenza.
There Is no obvious rationale in most Member States.
Knowledge gaps: There are few studies on the effectiveness of contact tracing on influenza in the community, and none that have studied contact tracing as a single intervention. Some epidemiological studies have documented contact tracing of air passengers and crew; however, the risk for influenza transmission onboard aircraft is still uncertain (708). Therefore, the effectiveness of contact tracing cannot be assessed from these studies. Moreover, currently available studies for community settings are all simulation studies - evidence of greater strength is needed to provide a more robust understanding of the effectiveness and value of contact tracing. Still unclear are the impacts of different intensities of contact tracing, and the optimal time frame, feasibility and cost-benefit.
N/ A: not applicable.
----------------~ WORLD HEALTH ORGANIZATION ~
APPENDIX TO JAMES CASCIANO DECLARATION-408

6.2. Isolation of sick individuals
Summary of evidence Terms relevant to isolation are defined below (Table 5).
Table S. Definition of terms relevant to isolation
TERM
Isolation
Case isolation
Patient isolation
Home isolation
Voluntary isolation
Self-isolation
DEFINITION
Separation or restriction of movement of ill persons with an infectious disease to prevent transmission to others ( 7 09).
Separation or restriction of movement of ill persons with an infectious disease at home or in a health care facility, to prevent transmission to others (29, 109).
Isolation of ill persons with an infectious disease in a health care facility, to prevent transmission to others (29).
Home confinement of ill persons with an infectious disease (often not needing hospitalization), to prevent transmission to others (29, 709).
Voluntary separation or restriction of movement of ill persons in a designated room to prevent transmission to others. This is usually in their own homes, but could be elsewhere (709).
See 'Voluntary isolation'.
The systematic review identified four epidemiological studies (110-113) and 11 simulation studies that were eligible for inclusion in our review (702, 104, 114-122).
Among the four epidemiological studies, a reduction in the cumulative incidence of infections and reproduction number due to an isolation policy was recorded during an influenza A(H 1 N 1 )pdm09 outbreak on a navy ship ( 7 7 0). Two studies suggested a reduction in attack rate in a physical training camp and a residential home for older adults ( 110, 7 7 7). In the 1918-1919 pandemic, excess death rates due to pneumonia and influenza decreased in New York City and Denver after isolation and quarantine were implemented ( 7 7 3).
Eleven simulation studies were conducted based on a wide range of assumptions, studying isolation as a single intervention or combined with other interventions. Six of the 11 studies predicted that implementation of case isolation would decrease the number of infections ( 7 02, 114-117, 119). In contrast, one study showed the difficulty in controlling influenza because of a potentially high proportion of asymptomatic transmission ( 7 04). Some studies predicted that isolation of sick individuals could delay the peak of an epidemic (116-118). One study predicted that isolation of 40% of cases would delay the epidemic peak by 83 days ( 116), while another predicted a similar effect, in which isolation of a reasonable proportion of cases would delay the arrival of the pandemic in countries globally (7 78). Although isolation alone was suggested to have a greater impact than other interventions, a combination of isolation and other interventions could further improve the effectiveness (102, 115, 117, 119).
cm -NO_N ___ PH-A-RM_A_C_EU_T_IC-AL_P_U_BL-IC_H_E_A-LT-H -M-EA-S-UR_E_S -FO_R_M-IT-IG-AT-IN_G_T_H_E -RI-SK_A_N_D_IM-P-AC_T_O_F_EP-ID_E_M_IC_A_N_D _PA_N_D_EM-IC_I_N-FL-UE_N_ZA--
APPENDIX TO JAMES CASCIANO DECLARATION-409

OVERALL RESULT OF EVIDENCE ON ISOLATION OF SICK INDIVIDUALS
1. Epidemiological and simulation studies suggested that isolation of sick individuals could reduce transmission in epidemics and pandemics. There is mechanistic plausibility for this intervention to be effective in reducing transmission.
2. The overall effectiveness of isolation is moderate, and combination with other interventions may improve the effectiveness.
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence There is a very low overall quality of evidence that isolation of sick individuals has a substantial effect on transmission of influenza except in closed settings.
Values and preferences There could be variability in values and preferences among groups of people assigned to undergo isolation. Isolation can cause distress through fear and risk perceptions, especially when people face unclear information and communication during a disease outbreak (723). Many staff and contacts related to isolated patients may report social stigma and emotional strain due to loss of anonymity ( 124). Those who are not intimate with the patients, however, could consider isolation to be an effective intervention in reducing their own chances of being infected ( 123).
Balance of benefits and harms The objective of case isolation is to reduce transmission by reducing contact between ill persons and those who are susceptible (109). The overall effectiveness of isolation is moderate, and is greater when combined with other NPls. However, individuals who share a room with an isolated case (e.g. a family member or roommate) may be at a higher risk of infection, owing to increased contact ( 125).
Resource Implications The evidence for cost-benefit and cost-effectiveness of case isolation is limited across settings and all evaluation was qualitative rather than quantitative. A stochastic simulation model showed that encouraging voluntary isolation of patients is a more effective strategy than school closure. Case isolation is also relatively inexpensive compared with school closure ( 126). A model based on the population of Canada reported high cost-effectiveness with a combination of communitycontact reduction measures including personal protective measures, voluntary isolation and antiviral therapy ( 117). However, the cost-effectiveness of isolation alone was unclear. Direct costs might have a disproportionate impact on low-income groups, although the impact was considered moderate, and was mainly related to employment losses through people staying at home for 7-10 days ( 125, 7 27). Isolating patients may also increase the workload of health care workers or family members. The Implementation of case Isolation would Involve a relatively large amount of resources.
________________ r,n) WORLD HEALTH ORGANIZATION ~
APPENDIX TO JAMES CASCIANO DECLARATION-410

Ethical considerations Implementation of isolation in general does not bring about many ethical concerns, because home isolation is often adopted voluntarily by individuals who do not feel well enough to work or engage in other daily activities ( 116, 119). Some ethical concerns may arise when isolation interventions are mandatory; the main concerns being freedom of movement ( 7 28) and social stigma ( 124). Although isolation is an important intervention, some individuals may face economic pressure to go to work rather than stay at home ( 7 29). Home isolation may also bring about increased risks of infection among household members. Older adults who live alone may not receive sufficient care and support when home isolation is implemented (88). Finally, although the evidence related to equity is limited, isolation could reduce the rate of infection in areas with poor sanitation and vulnerability, thereby increasing equity.
Acceptability Isolation of sick individuals is generally widely accepted by policy-makers and health workers, whereas the acceptability and compliance of case isolation among the public varies. A survey conducted among university students in the USA showed that at least 75% of people would like to isolate themselves from others when they are ill (130); however, only 6.4% of the cases remained at home (home isolation) ( 7 31). In a review, five studies reported that 50-96% of respondents intend to stay home rather than go to work when they are symptomatic; however, in another six studies the values reported were significantly lower (1-26%) ( 7 32). Family structure or the presumed infection status of family members can affect whether people accept isolation plans ( 702); for example, young children are less likely to be isolated alone at any stage of an epidemic ( 7 02).
Feasibility Isolation of sick individuals may not be feasible in certain circumstances, and there are some obstacles to isolation. Infected individuals who do not know of their infection status (e.g. pre-symptomatic or asymptomatic) could perpetuate transmission in the community (29). The effectiveness of case isolation is sensitive to the timing of response; however, such delay may be inevitable in some situations and will greatly reduce the effectiveness of this measure (7 78). In addition, ethical and social issues related to case isolation may contribute to the variable acceptability and compliance among the community.
r RECOMMENDATION:
Voluntary isolation at home of sick individuals with uncomplicated illness is recommended during all influenza epidemics and pandemics, with the exception of the individuals who need to seek medical attention. The duration of isolation depends on the severity of illness (usually 5-7 days) until major symptoms disappear.
Population: Infected cases
When to apply: At all times
FACTORS ASSESSMENT RATIONALE
Quality of evidence
Very low (effective)
Most evidence was from simulation studies; four epidemiological studies are all considered as providing very low quality evidence. There is theoretical plausibility for isolation to be effective in reducing influenza transmission in the community.
CE NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DE CLARA TION-411

FACTORS ASSESSMENT RATIONALE
Values and preferences
Balance of benefits and harms
Resource implications
Ethical considerations
Acceptability
Feasibility
Conditional
Conditional
Conditional
Conditional
Favourable
Conditional
Overall Recommended strength of recommendation
Values and preferences vary substantially among the community. Fear and social stigma are commonly experienced by patients and health care workers, while individuals who are not related to the isolated patients may consider case isolation to be an effective intervention in reducing their chances of being infected.
Home isolation could increase the risk of infection among family members.
Home isolation should not incur resources from the public sector but may be costly at a societal level. Isolation outside the home could be very costly.
Some ethical concerns arise when isolation measures are mandated, such as restriction of freedom of movement, lack of support for older adults who do not have a carer and economic pressure from work absenteeism.
Acceptability and compliance of isolation are variable, but generally at a moderate level.
This intervention may not be feasible because of many obstacles.
Home isolation of ill individuals is simple, feasible and likely to be acceptable in all influenza epidemics and pandemics. Isolation of ill individuals outside the home is unlikely to be feasible In most locations
Knowledge gaps: Most currently available studies on the effectiveness of isolation are simulation studies, which have a low strength of evidence. Available epidemiological studies looked at isolation combined with other interventions, or did not use laboratory-confirmed influenza as the outcome of interest. Although it is difficult to study isolation using RCTs, such studies would be very valuable. Understanding of transmission dynamics is incomplete, including the importance of pre-symptomatic contagiousness ( 7 33) and the fraction of infections that are asymptomatic ( 7 34). The optimum strategy for symptomatic persons is still uncertain.
RCT: randomized controlled trial.
________________ f,c:'1 WORLD HEALTH ORGANIZATION ~
APPENDIX TO JAMES CASCIANO DECLARATION-412

6.3. Quarantine of exposed individuals
Summary of evidence Terms relevant to isolation are defined below (Table 6).
Table 6. Definhion of terms relevant to quarantine
TERM DEFINITION
Quarantine Imposed separation or restriction of movement of persons who are exposed, who may or may not be infected but are not ill, and who may become infectious to others (709).
Household quarantine Confinement (commonly at home) of non-ill household contacts of a person with proven or suspected influenza (29, 709).
Home quarantine Home confinement of non-ill contacts of a person with proven or suspected influenza.
Self-quarantine Voluntary confinement of non-ill contacts of a person with proven or suspected influenza.
Work quarantine 1) Measures taken by workers who have been exposed and who
Maritime quarantine
Onboard quarantine
work in a setting where the disease is especially likely to transmit (or where there are people at higher risk from infection); for example, people working in homes for the elderly, and nurses in high-risk units (709).
2) Measures taken by health care workers who choose to stay away from their families when off duty, to avoid carrying the infection home (709).
Monitoring of all ship's passengers and crew for a defined period before permission is given to disembark( 7 35).
Monitoring of all flight's passengers and crew for a defined period before permission is given to disembark ( 7 36); this is also known as "airport quarantine" ( 7 36).
Six epidemiological studies (112, 135-139) and 10 simulation studies (702, 105, 114, 115, 117, 140-144) were eligible for inclusion in the review. Quarantine measures studied included household quarantine, border quarantine and maritime quarantine. Quarantine was studied as a single intervention or in combination with other interventions, generally with isolation and antiviral prophylaxis.
A quasi-RCT in Japan illustrated that voluntary waiting at home reduced risk of infection and number of infections (137). When a combination of isolation and quarantine was implemented in 1918-1919, excess death rates due to pneumonia and influenza were shown to decrease in New York City and Denver (112). Mandatory quarantine has also been shown to reduce the number of cases at the peak of epidemic fivefold, and it delayed the epidemic peak during the pandemic (H 1 N 1) 2009 in Beijing ( 139). Maritime quarantine in small island nations was reported to have delayed or prevented the arrival of the 1918-1919 pandemic, indirectly reducing mortality in the region (135). One study assessed onboard quarantine inspection and found a minimal
OJ NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-413

impact in detecting and preventing the entry of cases; however, following up with passengers thereafter was found to be effective in preventing secondary infection from travellers ( 7 36). An epidemiological study in Australia in 2009 found that the odds of a household contact who was currently quarantined with the index case-patient becoming a secondary case-patient increased for each additional day (adjusted odds ratio [OR]: 1.25, 95% Cl: 1.06-1.47) ( 7 38).
Among the simulation studies reviewed, four studies predicted a reduction in attack rate and cumulated incidence when quarantine of exposed individuals is implemented ( 7 02, 114, 115, 117). Combining quarantine with other interventions (e.g. household isolation with prophylaxis, school closure and workplace distancing) was suggested to further reduce influenza transmission (102, 114, 115). In addition, household quarantine has been suggested to be highly effective in reducing peak size and the total number of cases in a pandemic ( 7 44), whereas border quarantine had a minimal impact on reducing the number of cases (143). Three studies reported the effectiveness of household quarantine and border quarantine in delaying the epidemic peak ( 7 05, 117, 143). The combination with other interventions further improved the effectiveness of quarantine in delaying the epidemic peak ( 7 7 7).
If quarantine were to be implemented, a reasonable period of time would be 4 days after exposure, which covers two incubation periods of seasonal influenza. If data were available on the incubation period of a new pandemic strain, then the quarantine period could be adjusted accordingly.
r OVERALL RESULT OF EVIDENCE ON QUARANTINE OF EXPOSED INDIVIDUALS
1. The review identified six epidemiological studies and 10 simulation studies eligible for inclusion.
2. Quarantine is generally effective in reducing burden of disease and transmissibility, and in delaying the peak of the epidemic.
3. Some studies suggested a significant improvement in effectiveness of quarantine when combined with other interventions such as case isolation, antiviral prophylaxis or school closure.
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence
_,J
There is a very low overall quality of evidence that quarantine of exposed individuals has an effect on transmission of influenza; the studies identified in the review reported or predicted variable effectiveness.
Values and preferences Values and preferences among quarantined populations are uncertain and variable. A survey in Turkey showed that a moderate percentage of students (69.4%) believed that quarantine was an effective intervention in reducing the transmission of influenza (145). The public expressed serious concerns for the potential outcomes of mandatory quarantine, such as overcrowding, exposure to infection, and inability to work, shop or contact family members (146, 147). Fear and a sense of
------------------------CE WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-414

shame were also experienced by a proportion of the community, and many thought it impolite to maintain a distance from a sick acquaintance or relative ( 7 48). Health care workers were adversely affected due to the fear of acquiring infection ( 123). However, a study reported that 86.9% of the respondents held an optimistic attitude towards the effectiveness of quarantine ( 7 49).
Balance of benefits and harms The overall effectiveness of quarantine in reducing the burden of disease and delaying the peak of an epidemic is moderate. Quarantine may be particularly useful when antiviral drug resources are limited (725). However, the location of quarantine is an important factor in deciding whether the intervention will bring about any harm. During the influenza A(H 1 N 1 )pdm09 pandemic, a study from China reported that university students who were quarantined in the room with a confirmed case were at higher risk of illness ( 7 50). A quasi-cluster RCT reported similar results, finding that more home-quarantined individuals fell ill when there was a sick family member ( 7 37). The likelihood of a household contact who is concurrently quarantined with an isolated individual becoming a second case has been estimated to increase with each day of quarantine ( 7 38). Thus, family members who share the same room or facilities with the infected case may have an increased risk of acquiring influenza.
Resource implications Large-scale quarantine could be resource intensive. Household quarantine may be more costeffective in locations with limited capacity; however, enforcing quarantine or monitoring compliance could still be a challenge because of resource constraints.
Ethical considerations As with isolation, the main ethical concern of quarantine is freedom of movement of individuals ( 7 39). However, such concern is more significant for quarantine, because current evidence on the effectiveness of quarantine varies, and the measure involves restriction of movement of asymptomatic and mostly uninfected individuals. Mandatory quarantine increases such ethical concern considerably compared with voluntary quarantine ( 7 28). In addition, household quarantine can increase the risks of household members becoming infected ( 114, 137, 138). It has been suggested that a combined policy of household quarantine with antiviral prophylaxis can alleviate such concerns ( 7 7 4), but large stockpiles of antiviral drugs may not always be available for prophylactic use. Maritime quarantine and border quarantine are subject to similar concerns. On the other hand, onboard quarantine involves a shorter duration of restriction of movement, but current evidence suggests that this intervention has low cost-effectiveness and minimal impact on influenza control.
Acceptability Acceptability and compliance of quarantine are variable, but are generally at a moderate level ( 725). In a telephone survey conducted in Australia, more than 90% of respondents reported being willing to stay at home, especially after being given brief information about pandemic influenza (94.1% before and 97.5% after) (151). Two other studies had a similar conclusion, with 94% (752) and 92.8% ( 7 49) of respondents reported to adhere to a quarantine recommendation. However, a cross-sectional survey in Australia reported different results, with only 53% of households being fully compliant with quarantine. The compliance was better among individuals who had more understanding about quarantine (OR: 2.27) ( 7 53). Similar to the isolation of sick individuals, family structure or infection status of family members affects an individual's decision about whether to accept quarantine plans (702).
m NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-415

Feasibility There are some barriers and obstacles to the successful implementation of quarantine of exposed individuals. Home quarantine with infected cases can significantly increase the risk of acquiring infection ( 725). In addition, because the incubation period of a novel pandemic influenza strain may be uncertain, home quarantine may at times be implemented for an extended period, which will cause financial burden on families due to work absenteeism ( 154). There have been programmes of quarantine in 61 % of national pandemic plans, but detailed strategies of quarantine implementation were not provided and existing infrastructure may vary by country (65).
r RECOMMENDATION:
Home quarantine of exposed individuals to reduce transmission is not recommended because there is no obvious rationale for this measure, and there would be considerable difficulties in implementing it.
Population: People who have had contact with infected cases
When to apply: N/A
FACTORS ASSESSMENT RATIONALE
Quality of Very low The quality of evidence across all evidence {variable effectiveness) included articles, with the exception
of a quasi-cluster RCT, is very low. The effect of quarantine in reducing influenza transmission varied.
Values and Conditional There are likely to be concerns about preferences issues such as overcrowding, exposure to
infection and inability to contact family members when quarantine measures are implemented. However, most people should consider quarantine as a justifiable intervention.
Balance of Conditional The overall effectiveness in control of benefits and influenza is moderate; however, individuals harms subjected to quarantine with an infected
case could be at higher risk of acquiring infection.
Resource Conditional The evidence of cost-benefit or cost-implications effectiveness of quarantine measures is
limited, but the guideline development group believed that resources could be better used in other mitigation measures.
Ethical Conditional Individual freedom of movement and considerations the increased risk of infection among
individuals subjected to home quarantine with an infected case are essential ethical issues.
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-416
Cl

FACTORS ASSESSMENT RATIONALE
Acceptability
Feasibility
Overall strength of recommendation
Favourable
Conditional
Not Recommended
Acceptability and compliance of quarantine varies, but are generally at a moderate level.
The feasibility of quarantine measures may not be high owing to the possible increase in secondary cases, and the financial burden due to work absenteeism.
Not recommended due to feasibility concerns with very low quality of evidence.
r ~
Knowledge gaps: Most of the currently available evidence on the effectiveness of quarantine on influenza control was drawn from simulation studies, which have a low strength of evidence. Available epidemiological studies did not rely fully on laboratory-confirmed influenza as the outcome of interest. Although it is difficult to study quarantine using RCTs, robust data from experimental studies would be valuable. In addition, as part of simulation studies, assumptions have been made in various aspects of model construction, many of which still require more robust evidence; for example, the asymptomatic fraction among all infections, the possibility of "superspreaders" and the nature of compliance behaviour (102, 141). There was limited information in the literature on the ideal or optimum timing of quarantine.
~ ~
N/A: not applicable; RCT: randomized controlled trial.
6.4. School measures and closures
Summary of evidence School-age children are particularly important in influenza transmission in the community, and attack rates are typically highest in this age group in epidemics and pandemics. School measures to reduce influenza transmission vary in scope from very simple measures (e.g. increasing distancing between desks) through to drastic measures (e.g. completely closing all schools). The systematic review team focused on school closures because this is the most well-studied measure; the team also examined evidence on other measures.
One published review examined school measures other than school closures, including increasing desk distance between students, cancelling or postponing after-school activities, restricting access to common areas, staggering the school schedule, reducing mixing during transport to and from school, dividing classes into smaller groups, and cancelling classes that bring students together from multiple classrooms (155). Another potentially important measure could be increasing attention to influenza-like symptoms in children, and either ensuring that ill children do not attend school or segregating them from other students.
cm NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-4-17
These measures could promote social distancing and decrease density among students, but there was limited evidence on the effectiveness of these measures ( 7 55).
Closure of schools can be reactive or proactive (Table 7) ( 7 56). Reactive closures occur when schools are closed after the occurrence of influenza outbreaks in those schools. Proactive closures occur when schools or groups of schools are closed as a deliberate measure to reduce transmission in the community, whether or not there have been influenza outbreaks in those schools. Class dismissal refers to the scenario where schools remain open but classes are not held; this can serve the purpose of continuing to provide school meals and childcare to some children (e.g. those from lower income families).
Table 7. Definition of terms relevant to school dosures
TERM
School closure
Class dismissal
Reactive closure or dismissal
Proactive closure or dismissal
Ill: influenza-like illness.
DEFINITION
School is closed to all children and staff.
School campus remains open with administrative staff, but most children stay home.
School is closed after a substantial incidence of Ill is reported among children or staff (or both) in that school.
School is closed before a substantial transmission among children and staff is reported.
A systematic review published in 2013 identified 79 epidemiological studies on school closures, and summarized the evidence as demonstrating that this intervention could reduce the transmission of pandemic and seasonal influenza among school children; however, the optimum strategy (e.g. length of closure, and whether it should be reactive or proactive) remained unclear, owing to heterogeneity of the data ( 157). The current systematic review updated the 2013 review, identifying 22 additional epidemiological studies that met the inclusion criteria, giving a total evidence base of 101 studies (Annex).
Included studies fell into a number of types. The first type of study involved the analysis of proactive school closures implemented in seasonal epidemics or in pandemics. A comprehensive analysis of interventions conducted in the USA in the 1918-1919 pandemic estimated that early and sustained interventions, including school closures, reduced overall mortality by up to 25% in some cities (758). Two other studies examined NPls in the 1918-1919 pandemic, and reported that the combined use of NPls (including school closures) was able to delay the time to peak mortality, and to reduce peak mortality and overall mortality ( 112, 159). Two studies conducted in Hong Kong SAR during the 2009 pandemic reported that a proactive 4-week school closure followed by scheduled school summer holidays reduced transmission in the community ( 160, 161), with one study estimating that the reproductive number was reduced from 1.7 to 1.5 during the proactive closures, and to 1.1 during the rest of the summer holidays ( 7 6 7). A study of school closures in Mongolia estimated a reduction in the overall attack rate by 1.1 % and a delay in the epidemic peak by more than 1 week ( 7 62).
A second group of studies investigated reactive school closures. One detailed study of transmission in a school in Pennsylvania identified no effect of the reactive closure that was implemented when 27% of students already had symptoms (763). Two studies conducted in Japan estimated reductions in the epidemic peak and overall attack rate by about 24% and 20% ( 164, 165). A study of reactive school closures in London in 2009 estimated that the closures reduced the reproductive number ________________ r,r,, WORLD HEALTH ORGANIZATION ~
APPENDIX TO JAMES CASCIANO DECLARATION-418
from 1.33 (95% Cl: 1.11-1.56) to 0.43 (95% Cl: 0.35-0.52) (166). A study in the USA suggested that absenteeism could be reduced by about 2-3% after the reopening of school that had been closed due to outbreaks (167), and another study estimated that outbreak duration decreased by 4.98 days for a 2-day closure (768). However, other studies did not show a beneficial effect in reactive school closures in terms of reducing the overall attack rate and influenza duration ( 169, 7 70).
A third group of studies investigated the impact of regular school holidays. A study in France estimated that routine school holidays prevented 18% of seasonal influenza cases (18-21% in children) ( 177). Analysis of data from London from the 2009 pandemic suggested that transmission was substantially lower in the summer holidays of 2009, but resurged after schools reopened ( 7 72). An epidemiological analysis in Peru also reported that the number of infected cases declined throughout a school closure period (7 73). One study in the USA found an unchanged pattern in school-age children, but increasing influenza incidence among adults and children aged under 5 years during planned winter holidays (774). In addition, a cohort study in the USA indicated no difference in post-break absenteeism in schools on holidays compared with schools that remained open at the same time (RR: 1.07, 95% Cl: 0.96-1.20) ( 175). More recently, planned school holidays, including winter or summer holidays with the addition of some public holidays, were estimated to reduce influenza transmission ( 176-185) in terms of reducing transmission by 10-40% ( 176, 179-181, 185) and delaying the peak for more than 1 week ( 183, 184).
, OVERALL RESULT OF EVIDENCE ON SCHOOL MEASURES AND CLOSURES
1. The effect of reactive school closure in reducing influenza transmission varied but was generally limited. Proactive closures and planned school holidays had a moderate impact on transmission.
2. Although school closures alone might have an impact, combination with other interventions improved the effectiveness.
3. If schools remain open during a pandemic or epidemic, school measures can be considered in order to reduce transmission
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence There is a very low overall quality of evidence, and the studies that have been published reported or predicted that school measures and closures have a variable effect on transmission of influenza.
Values and preferences There was little variability in the importance that populations assign to school closures; for example, in a survey in the USA, 92% of caregivers and 89% of teachers reported that they believed school closures were somewhat effective in reducing Influenza cases among school-age children (786). School closures affect families with children.
EE NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-419

Balance of benefits and harms School closures can reduce influenza transmission, but the timing and duration is critical, and mistimed closures could lack impact. On the other hand, closures could have a major impact on the safety, health and nutrition of children in lower income families ( 7 87); for example, missing work to take care of children can affect income ( 7 25), and access to free school meals could be an additional concern for low-income families (788). School measures would reduce density and contact rates among students, and these interventions may cause mild disruption to schools and communities.
Resource Implications School closure is one of the measures that is found to be potentially not cost-effective ( 7 89). A review suggested that the cost of proactive closure can be significant, at £0.2 billion -£1.2 billion per week in the United Kingdom of Great Britain and Northern Ireland (which equates to 0.2-1 % of the United Kingdom's gross domestic product [GDP]), with similar results found in Australia ( 7 25). Proactive closure in the USA for 4 weeks could cost US$ 10-47 billion (0.1-0.3% of GDP) ( 7 90). Another study in the USA also estimated a $21 billion (> 3% GDP) loss for an 8-week reactive school closure ( 797). A simulation study predicted that school closures could reduce influenza transmission, but at increased cost to society ( 7 92). School measures could have some resource implications.
Ethical considerations School closures raise major ethical issues for families and communities ( 125, 188). Closures can have a substantial social impact because they may require parents to make other arrangements for care or supervision of their children, which can be particularly challenging for some families, especially if closures are prolonged. Social equity concerns might be exacerbated when closing schools, because children from lower income families may receive subsidized free food at school ( 7 88). Students' educational advancement could be jeopardized if they miss important exams or class work, and do not have alternative learning strategies (32). Moreover, media reporting of school closures may increase pandemic-related fears and concerns among the local community (32). Extending the school holidays might increase travel and thus lead to the temporary loss of health care workers from the health care system. Moreover, the availability of parents or caregivers would need to be taken into account when excluding ill children from school; segregation of ill children at school might be an alternative to exclusion in some locations.
Acceptability Two studies in the USA and Australia suggested that most families {more than 90%) agree to the implementation of school closure as a potential intervention to reduce influenza transmission ( 151, 193). To accommodate the closure period, the school may be required to extend the school year or offer alternative learning programmes (e.g. online learning), which may require extensive discussions with local authorities, given that extra costs may be incurred in extending the school year. There are also practical difficulties in communicating needs at different levels (national, local, school and individual), particularly in situations where uncertainty and risk assessments may change rapidly (194, 195). Such measures will probably only be acceptable to most stakeholders when the benefits clearly outweigh the negative consequences. According to a review of state government planning documents in the USA, in their published influenza preparedness for schools, 42% of the states mentioned that school measures could promote social distancing ( 7 55). The acceptability of school measures at a national level is likely to be high.
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-420

r
Feasibility The feasibility of school closure is questionable. Reactive school closures, rather than proactive school closures, are often implemented for operational reasons ( 794). Proactive school closures have been implemented during seasonal epidemics in some locations ( 7 94). School closures are most effective if children stay at home rather than engaging in extracurricular activities, although this may be difficult to control ( 196, 197). Most (61 %) national pandemic influenza preparedness implementation plans give recommendations about school closures but lack further detail (65). There may be considerable variation in social structures and legal frameworks relating to school closures in different Member States (198, 799). The guideline development group suggested that a class dismissal intervention could still include a provision for children of low-income families or essential workers to attend school, and this could be a more flexible measure than complete school closure.
RECOMMENDATION:
School measures (e.g. stricter exclusion policies for ill children, increasing desk spacing, reducing mixing between classes, and staggering recesses and lunchbreaks) are conditionally recommended, with gradation of interventions based on severity. Coordinated proactive school closures or class dismissals are suggested during a severe epidemic or pandemic. In such cases, the adverse effects on the community should be fully considered (e.g. family burden and economic considerations), and the timing and duration should be limited to a period that is judged to be optimal.
Population: Students and staff in childcare facilities and schools
When to apply: Gradation of interventions based on severity; school closure can be considered in severe epidemics and pandemics
FACTORS ASSESSMENT RATIONALE
Quality of Very low No RCTs were identified, and the quality of evidence (variable evidence is very low. The effect of school
1 effectiveness) measures and closures in reducing influenza transmission was variable.
~-·· - ·-~-~--~
Values and Favourable There was little variability in the importance preferences that populations assign to school closures.
Balance of benefits Conditional The balance between benefits and harms and harms is uncertain for school closures, which may
cause the loss of work or salary.
Resource Conditional School closures were associated with implications moderate costs but were less cost-effective
than stockpiling antiviral drugs or pre-pandemic vaccines.
Ethical I Conditional School closure has ethical repercussions considerations on families and communities, such as the
loss of subsidies for lower income families, and increasing fear and concern in the community (which may be exacerbated by heightened media attention).
~ NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-421

FACTORS ASSESSMENT RATIONALE
Acceptability
Feasibility
Overall strength of recommendation
Conditional
Conditional
Conditionally recommended
Most families would accept the class dismissal decision, but the decisionmaking authority to close schools in different jurisdictions varies widely. School authorities may fear incurring extra costs by extending the school year. School measures are likely to be highly acceptable at a national level.
Because of the uncertainty and variability of influenza transmission, it is difficult to predict whether it will develop into a severe epidemic or pandemic.
School measures are likely to be feasible in any epidemic or pandemic. The balance between the advantages and disadvantages of school closures is less certain, but closure may be considered in more severe scenarios.
Knowledge gaps: More research is needed on the best triggers to close and reopen schools, and on the optimal timing and duration of school closures in order to maximize the impact of this disruptive intervention. The difference in compliance between individuals of different social status is still uncertain. There was little research on the impact of school measures on transmission.
RCT: randomized controlled trial.
6.5. Workplace measures and closures
Summary of evidence The systematic review identified 12 simulation studies and three epidemiological studies from the systematic review published by Ahmed et al. (200), and four additional studies from the updated search ( 117, 137,201,202). Workplace measures included paid-leave policy, telework from home, staggered shifts (e.g. having different activity and meal times, and times of entry and exit from the workplace), reduced contact and weekend extension. The epidemiological and simulation studies included in the review by Ahmed et al. suggested that these measures could reduce the overall number of influenza cases. In addition, the implementation of a workplace measure alone was associated with a median 23% reduction in the cumulative incidence of infections to a reproductive number of 1.9 or less (200). Simulation studies also showed a delay and reduction in the peak influenza attack rate; however, the effectiveness was estimated to decline with a higher basic reproductive number or a delay in implementation of the intervention (200).
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-422

Among the four most recent articles since the review by Ahmed et al., a quasi-cluster RCT in Japan showed that paid sick leave policy in the workplace reduced the overall risk of influenza A (Hl Nl) by about 20% in one influenza season ( 7 37). The other two epidemiological studies in the USA illustrated that providing paid sick leave could help to reduce transmission in workplaces resulting in an overall decrease of influenza-related absenteeism (207,202). Workplace measures combined with other interventions (e.g. school closures, personal protective measures and antiviral drugs) showed greater effectiveness ( 7 7 7).
Evidence on the effectiveness of workplace closure is limited; six simulation studies were identified (114, 142, 203-206). The simulation suggested that large-scale workplace closures could delay the time of peak occurrence for 5-10 days, but such closures were less effective than other interventions (e.g. school closures) (204,205). Closing all schools and closing 10% of workplaces could only delay the peak time by around 4% (206). Some studies predicted that workplace closures combined with school closures would be effective in reducing the spread of influenza by decreasing the overall attack rate by about 15-45% and decreasing the height of the epidemic peak by up to 40% (114,203,206). One simulation study predicted that the single strategy of workplace closure would have little impact; however, the combination of workplace closure, school closure, home isolation and a modest level of antiviral drug coverage would be effective in mitigating the impact of an epidemic ( 142).
OVERALL RESULT OF EVIDENCE ON WORKPLACE MEASURES AND CLOSURES
1. The included studies indicated that workplace measures (e.g. telework from home, staggered shifts, weekend extension and paid-leave policy) could reduce both the overall and the peak number of influenza cases, as well as delaying the occurrence ofthepeak.
2. The overall effectiveness and feasibility of workplace measures is modest, but combination with other interventions can improve its effectiveness.
3. The strength of evidence on workplace closure is very low because the identified studies are all simulation studies. Large-scale workplace closures could delay the epidemic peak for more than 1 week, and small-scale closures may have a modest impact on attack rate or peak number.
~ ~
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence There is a very low overall quality of evidence that workplace measures and closures reduce influenza transmission.
Values and preferences There was uncertainty and variability in the importance that populations assign to workplace measures to reduce influenza transmission. A study in the Netherlands reported that 30% of respondents believed that staying home from work is an efficacious means of reducing influenza transmission (207); in another study, 93% of New York State residents believed that staying home is effective in preventing influenza transmission (208). A study in the USA showed that 28% of
mJ NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-423

employed respondents reported that they might lose their jobs or businesses as a result of having to stay home from work for 7-1 O days in the event of a pandemic influenza outbreak ( 127). This would also cause severe personal economic crises among some members of the public, but less so for those who received pay while they worked remotely ( 127).
Limited studies showed the values and perceptions among the population on the potential consequences of workplace closures. One study mentioned that large-scale workplace closures might raise the public's concern about the potential economic and financial consequences (209). Although there is limited evidence, it may be reasonable to expect increased levels of distress among employers and employees in the event of a workplace closure, because of possible operational and financial impacts (270).
Balance of benefits and harms Workplace measures could potentially reduce transmission by about 20-30%, based on the included studies. A review illustrated that telecommuting without pay would be inequitable, and would impact particularly on self-employed people or low-income families, because they have a higher risk of suffering from severe financial problems as a result of workplace measures ( 125). Large-scale workplace closures are likely to have substantial economic consequences. However, if school closures are also implemented, workplace closures may avoid the need for some working parents to make other childcare arrangements.
Resource implications The guideline development group believed that workplace measures and closures might be an economic burden on the government. Telecommuting was found to be modestly effective in reducing influenza transmission, but also likely to be economically disruptive ( 125). The most costly strategy considered in a simulation study was that of a continuous school closure together with a continuous 50% workplace non-attendance; this scenario has the highest overall cost (US$ 103 million) and the highest cost per prevented case (US$ 9894 per case) (211). Workplace closures can also be economically disruptive ( 125), and the cost of full workplace closures for any period of time will have significant economic impact (88).
Ethical considerations Workplace measures and closures could affect the economy and productivity of a society. A survey in the USA found that self-employed individuals and those unable to work from home might not be able to comply with recommended workplace measures because of job insecurity and financial considerations ( 125, 127). Social equity concerns may be exacerbated by workplace closure due to the lack of income to pay for necessities in lower income families.
Acceptability Workplace measures may be acceptable if they are well-planned in selected workplaces. Most stakeholders are unlikely to find workplace closures acceptable. The guideline development group encouraged giving isolated and quarantined individuals the opportunity to telework. Employees will accept workplace closures only if there is no anxiety regarding job security and income replacement (88). In addition, companies and authorities will not accept this intervention because of high operational costs.
Feasibility Telework, paid-leave policy and staggered-shift measures are unlikely to be feasible in most circumstances. Workplace closure is also likely to have a number of feasibility issues; for example, many companies provide essential services to the community or facilitate off-site working, and thus cannot be closed. Overall, the guideline development group believed that mandated workplace closure is unlikely to be feasible.
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-424

r
RECOMMENDATION:
Recommendation: Workplace measures (e.g. encouraging teleworking from home, staggering shifts, and loosening policies for sick leave and paid leave) are conditionally recommended, with gradation of interventions based on severity. Extreme measures such as workplace closures can be considered in extraordinarily severe pandemics in order to reduce transmission.
Population: Selected workplaces
When to apply: Gradation of interventions based on severity. Workplace closure should be a last step that is only considered in extraordinarily severe epidemics and pandemics
FACTORS ASSESSMENT RATIONALE
Quality of evidence
Values and preferences
Balance of benefits and harms
Resource implications
Ethical considerations
Acceptability
Feasibility
Very Low (effective)
Conditional
Conditional
Conditional
Conditional
Conditional
Conditional
One quasi-cluster RCT is on workplace measures, and the quality of the rest of the evidence is very low. All identified studies of workplace closure are simulation studies, which provide very low quality of evidence. Workplace measures and closures are effective in reducing influenza transmission in the community.
There is significant uncertainty surrounding people's values and preferences on workplace measures and closures.
Potentially effective in reducing influenza transmission, but may have economic harms.
Workplace measures and closures can be economically disruptive.
Workplace measures and closures may have adverse impacts on the economy and productivity of a society.
Unlikely to be acceptable in all but the most severe pandemics.
Many workplaces cannot be closed (e.g. those that provide essential services). Workplace closures may have limited feasibility.
m NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECL.ARA TION-425

Overall strength of recommendation
Conditionally recommended
The balance between the advantages and disadvantages of implementing workplace measures and closures is uncertain. Some measures may be relatively feasible and may contribute to reduced transmission in the community. Workplace closures may only be warranted as an extreme social distancing measure In an extraordinarily severe pandemic.
Knowledge gaps: As with school closures, more research is needed on the best trigger factors, timing and duration of workplace closures in order to maximize the impact of this highly disruptive intervention. There is a need for a comprehensive review of the ethical issues of workplace measures, as well as a comparison of the benefits and costs of implementing the measures. Other potential workplace measures have not been studied in depth, such as providing segregated working areas for people with mild symptoms. In addition, studies are needed on feasibility and scope of implementation of workplace measures, and the potential impact on families and the public.
RCT: randomized controlled trial.
6.6. Avoiding crowding
Summary of evidence Three epidemiological journal articles were included in our systematic review (112, 159, 212). One of those studies concerned World Youth Day 2008 pilgrims; it found that sleeping in a small group reduced the transmission of influenza compared with sleeping in one large hall (212). Another two articles were based on the 1918-1919 pandemic; both articles found that timely bans on public gatherings and closure of public places appeared to reduce the excess death rate (Spearman p=0.31 and 0.46) (112, 159). However, it is impossible to determine the individual effects of measures to avoid crowding in these studies.
r OVERALL RESULT OF EVIDENCE ON AVOIDING CROWDING
1. The effect of measures to avoid crowding alone in reducing transmission is uncertain.
2. Timely and sustained application of measures to avoid crowding may reduce influenza transmission, although the quality of evidence of its effectiveness is very low.
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-426

Quality of evidence There is a very low overall quality of evidence on whether avoiding crowding can reduce transmission of influenza.
Values and preferences There was uncertainty or variability in the importance that populations assign to avoiding crowding to reduce influenza transmission. A survey in Thailand reported that 54% of respondents believed that avoiding gatherings of five or more people could reduce the spread of diseases during an outbreak (2 7 3). Surveys in the United Kingdom and the Netherlands also showed a similar result: half of the respondents believed that this intervention would reduce the risk of getting infected with the influenza virus (87, 207).
There are differences in perception of expected outcomes from avoiding crowding among different populations. Some participants in a survey in the USA argued that they would approve of avoiding religious activities if it could reduce influenza transmission (209); however, other people believed that avoiding gatherings might prevent them from receiving support (e.g. worshipping and praying together) from their religious community during the crisis (209).
Balance of benefits and harms Avoiding crowding, in combination with other social distancing measures, may reduce influenza transmission, but there is no conclusive evidence to determine its effect (214). Modification, postponement or cancellation of mass gatherings may have cultural or religious implications, and may incur considerable costs (88, 209).
Resource implications The financial fragility of religious organizations was a concern, and mandatory closure may be seen as a financial hardship for many institutions (209). Governments might face legal liabilities for financial losses associated with workplace measures or closures.
Ethical considerations Avoiding crowding may have cultural or religious implications (209). Gatherings are important places to share information during influenza, which can comfort people and reduce fear. The abolition of religious gatherings may violate the devout faith of the participants and make them feel morally guilty. The guideline development group suggested that it would not be possible to cancel some events (e.g. the Hajj).
Acceptability The acceptability of avoiding crowding among the public may depend on the type and importance of the gathering ( 125). In a survey in Australia in 2007, 94.2% of participants were reported as being willing to avoid public events (757), and a polling study in five countries (Argentina, Japan, Mexico, United Kingdom and the USA) in 201 O showed that 11-69% of respondents would like to avoid places where many people gather (e.g. shopping centres or sporting events) during a pandemic (215). However, some participants might oppose the mandatory cancellation of religious gatherings during a pandemic (209). During a WHO consultation of influenza A(H 1 N 1 )pdm09, most reporting countries stated they had not instituted restrictions on mass gatherings, and were taking a wait-and-see approach for any upcoming events in their countries (216).
Feasibility There have been recommendations for the prohibition of mass gatherings but without further details in most (66%) national pandemic influenza preparedness implementation plans (65). However, it is still uncertain whether measures to avoid crowding alone would have a large effect.
~ NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK ANO IMPACT OF EPIDEMIC ANO PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-427

r
\.
RECOMMENDATION:
Avoiding crowding during moderate and severe epidemics and pandemics is conditionally recommended, with gradation of strategies linked with severity in order to increase the distance and reduce the density among populations.
Population: People who gather in crowded areas (e.g. large meetings, religious pilgrimages, national events and transportation hub locations).
When to apply: Moderate and severe epidemics and pandemics.
FACTORS ASSESSMENT RATIONALE
Quality of evidence
Values and preferences
Balance of benefits and harms
Resource implications
Very Low (unknown)
Conditional
Conditional
Conditional
Ethical ----~j Conditional consider~ions
Acceptability Conditional
Feasibility Conditional
No RCTs were found and the quality of evidence across all reviewed articles is very low. The effect of measures to avoid crowding alone is unknown.
Some people believe that the outcome of this intervention is conducive to reducing the risk of viral transmission, but others may view it as a barrier to accessing group support and personal freedom.
The effect of measures to avoid crowding alone is uncertain, and this intervention may have cultural or religious implications.
There might be cost considerations among organizers, attendees and employees.
There may be cultural or religious issues.
Likely to be acceptable in severe pandemics.
The programmatic considerations and existing infrastructure may hinder the implementation of avoiding crowding.
Overall Conditionally recommended
The balance between the advantages and disadvantages of avoiding crowding is less certain, but may be justifiable in severe pandemics.
strength of recommendation
Knowledge gaps: There are still major gaps in our understanding of person-to-person transmission dynamics. The reduction of mass gatherings is likely to reduce transmission in the community, but its potential effects are difficult to predict with accuracy. Large-scale RCTs
\. are unlikely to be feasible.
RCT: randomized controlled trial.
------------------------~ WORLD HEALTH ORGANIZATION ~
APPENDIX TO JAMES CASCIANO DECLARATION-428

E! TRAVEL-RELATED MEASURES 7 .1. Travel advice
Summary of evidence There is no evidence measuring the effect of travel advice on influenza transmission.
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence The quality of evidence cannot be judged because no study was identified.
Values and preferences Travel advice helps the public make informed decisions when travelling, and offers them an objective assessment of the risks involved in travelling during an epidemic or pandemic (217). Travel advice increases travellers' awareness of travel risk in affected regions. No literature on the values and preferences of travel advice was identified in the systematic review.
Balance of benefits and harms Travel advice can potentially reduce travellers' exposure to influenza viruses and limit the spread by deterring travel to regions affected by epidemics or pandemics (278). However, travel advice that recommends public avoidance of travel or trade may have financial consequences to the local and global economy (279). The systematic review did not identify any literature that demonstrated benefits and harms related to travel advice.
Resource implications The resource implications of providing information to individuals depend on the approach used to disseminate travel advice. However, the overall resource implications of providing travel advice are uncertain.
Ethical considerations Strategies to maintain public trust and increase compliance with the travel advice should be carefully considered (279).
Acceptability Public health authorities have generally included public awareness campaigns as part of their ongoing strategy to increase travellers' awareness of infectious disease risks, including influenza, during travel. Issues with acceptability of travel advice are unlikely, but cultural issues and potential economic consequences should be considered.
Feasibility Member States routinely provide travel advice for infectious diseases (e.g. dengue, malaria and Middle East respiratory syndrome), and they did provide advice in the early stages of the 2009 Hl Nl pandemic.
[l[ -N-ON---PH_A_R_M-AC_E_U_TI_CA_L_P_U_BL_IC_H_E_A_LT_H_M-EA_S_U-RE_S_F_OR_M_IT-IG-AT-IN_G_T_H_E-RI-SK_A_N_D_I_M_PA_CT_O_F -EP-1D_E_M_IC_A_N_D_PA_N_D_EM-IC-IN_F_LU-E-NZ_A __
APPENDIX TO JAMES CASCIANO DE CLARA TION-429

I
r
r
\..
RECOMMENDATION:
Travel advice is recommended for citizens before their travel as a public health intervention in order to avoid potential exposure to influenza and to reduce the spread of influenza.
Population: Citizens before travelling
When to apply: Early phase of pandemics
FACTORS ASSESSMENT RATIONALE
Quality of None No scientific evidence identified in the evidence systematic review.
i
Values and Favourable Travel advice can increase travellers' preferences awareness of travel risk in areas where they
may be exposed to circulating influenza viruses.
Balance of Favourable Although travel advice may contribute to benefits and the reduction of potential exposure and harms onward transmission of infections, there
may be economic consequences of reduced travel.
Resource Favourable Uncertain. May have consequences for implications countries affected early if travel advisories
are issued against those countries.
Ethical Favourable No major ethical issues. considerations
Acceptability Favourable Travel advice is likely to be acceptable in most settings.
Feasibility Favourable Travel advice is already used for other infections and in previous pandemics; there are no anticipated feasibility issues.
Overall Recommended No scientific evidence was Identified for strength of the effediveness of travel advice against-recommendation pandemic influenza; however, providing
information to travellers is simple, feasible and acceptable.
Knowledge gaps: Studies measuring the effect of travel advice on influenza transmission would be welcome.
~
I ~
----------------F;fl WORLD HEALTH ORGANIZATION W
APPENDIX TO JAMES CASCIANO DECLARATION-430

7 .2. Entry and exit screening
Summary of evidence Ten articles related to entry and exit screening were included in this review (785, 220-228). Observational studies conducted at airports estimated that the sensitivity of entry screening was low (226-228). Among arriving international travellers, half of the influenza cases were identified more than a day after arrival (through passive case finding and contact tracing in the community), although 37% of the influenza cases were screened while passing through the border entry site (185). Simulation studies estimated that screening international travellers may help to delay the epidemic by less than 2 weeks (0-12 days) (220-222).
OVERALL RESULT OF EVIDENCE ON ENTRY AND EXIT SCREENING
1. Ten studies were included in this review. 2. Considering the asymptomatic period of infected patients and
the sensitivity of screening devices, the effectiveness of screening travellers is likely to be very limited.
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence There is a very low overall quality of evidence that entry and exit screening can delay the introduction of infection to a country and local transmission.
Values and preferences The sensitivity of screening can have an impact on the effectiveness of traveller screening at entry and exit points. Screening measures included health declarations, visual inspections and thermography to detect disease symptoms (229). One of the major criteria for screening travellers for influenza infections is fever, and screening sensitivity is largely reliant on detecting fever by available instruments. Infrared thermometers are used at some borders due to the instantaneous and non-invasive nature of their use. A study conducted in Japan during the influenza pandemic A(H1 N1 )pdm09 in 2009 reported that the sensitivity of infrared thermometers was 50.8-70.4% and the specificity 63.6-81.7% (224). A study conducted in New Zealand reported that the sensitivity of infrared thermal image scanners was 84-86% and the specificity 31-71 % (225). It is possible that some travellers with fever might opt to take antipyretics to reduce their symptoms before travel, to avoid detection of their fever by thermal scanners or thermometers.
Molecular diagnostics such as polymerase chain reaction {PCR) can be used at ports of entry, but these are generally more cost and resource intensive, and are unlikely to be applied to a large number of travellers (223). Point-of-care antigen detection tests might be more feasible but would also be costly (223).
Balance of benefits and harms The systematic review identified no literature on the harm of screening travellers. Influenza cases may remain asymptomatic for a few days {up to 2 days for seasonal influenza) { 7 85), symptom presentation varies and screening methods are imperfect (230); therefore, traveller screening for symptoms of influenza virus infection has major limitations in preventing the introduction of influenza into a location, and reducing the overall attack rate and duration of an epidemic (228).
DE NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-431

Resource implications Substantial public health resources would be required, including adequate numbers of trained staff, screening devices and laboratory resources, and adequate infrastructure to conduct effective screening of travellers (228).
Ethical considerations Involuntary screening needs to be considered and implemented with care to respect the privacy of travellers (219).
Acceptability Screening travellers using infrared thermometers continues to be used in some ports of entry and is generally accepted by policy-makers as a uvisible" public health measure. Exit screening was not implemented in the 2009 influenza pandemic, and its acceptability for preventing or delaying the introduction of influenza infections to a location is uncertain.
Feaslblllty Entry screening is used in some ports of entry and has been shown to be feasible.
RECOMMENDATION:
Entry and exit screening for infection in travellers is not recommended, because of the lack of sensitivity of these measures in identifying infected but asymptomatic (i.e. presymptomatic) travellers.a
Population: N/ A
When to apply: N/ A
FACTORS ASSESSMENT RATIONALE
Quality of evidence
Values and preferences
Balance of benefits and harms
Resource implications
Very low (lack of effectiveness in reducing influenza transmission)
Conditional
Conditional
Conditional
The overall quality of available evidence was very low, and the overall effectiveness of entry and exit screening on influenza pandemics is ineffective due to the sensitivity of screening measures and asymptomatic period of infected patients.
One of the major criteria used in the screening of travellers for influenza infections is fever. Thus, screening sensitivity is largely reliant on the detection of fever.
There was no literature on the benefits and harms of traveller screening.
Substantial public health resources are required, which may be better used elsewhere.
_,J
11 Some locations routinely monitor the temperature of Incoming travellers; for example, In an effort to Identify Incoming travellers with symptoms of Ebola virus disease, avian influenza, Middle East respiratory syndrome or some other emerging Infectious disease. The recommendation here to not Implement entry or exit screening Is specific to seasonal and pandemic Influenza.
----------------F;rl WORLD HEALTH ORGANIZATION ~
APPENDIX TO JAMES CASCIANO DECLARATION-432

\..
FACTORS ASSESSMENT RATIONALE
Ethical Conditional considerations
Acceptability Favourable
Feasibility Favourable
Overall Not Recommended strength of recommendation
Involuntary screening may have ethical or legal implications.
Screening is likely to be acceptable in general.
Feasibility has been demonstrated for several infectious diseases.
Not recommended due to the overall ineffectiveness in reducing the introdudion of infection and delaying local transmission.
Knowledge gaps: There were no high-quality studies on the effectiveness of entry and exit screening. Studies on the best approaches to screening travellers at different times, with different measures and for different pathogens are required to understand the potential advantages of screening travellers (230).
N/ A: not applicable.
7 .3. Internal travel restrictions This section covers internal travel restrictions only- international travel restrictions are not covered in this document1•
Summary of evidence One epidemiological study (23 7) and four simulation studies ( 114, 162, 232, 233) related to internal travel restrictions were included in this review. A time-series analysis study conducted in the USA showed that frequency of domestic airline travel is temporally associated with the rate of influenza spread, and following the September 11 attacks in 2001, a reduction in such travel delayed the epidemic peak by 13 days compared with the average for other years (23 7). A simulation study predicted that implementation of a strict travel restriction (95% travel restriction, enforced for 4 weeks) could reduce the epidemic peak by 12%, and a moderate restriction (50% travel restriction, enforced for 2-4 weeks) could delay the pandemic peak by 1-1.5 weeks (162). Another simulation study predicted that an internal travel restriction of more than 80% could be beneficial (232). A strict internal travel restriction (90%) was also consistently found to delay the epidemic peak by 2 weeks in the United Kingdom, and by less than 1 week in the USA (114). However, a 75% restriction had almost no effect ( 7 74).
r OVERALL RESULT OF EVIDENCE ON INTERNAL TRAVEL RESTRICTIONS
1. Five studies were included, four of which were simulation studies. 2. The effectiveness of internal travel restrictions depends on the level of
restriction - only very strict restrictions would be expected to have an impact on influenza transmission.
1 The WHO IHR secretariat Is In the process of developing a guidance on the effectiveness of travel and trade restrictions to prevent, delay or control international spread of diseases, lndudlng pandemic Influenza.
~ NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-433

Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence There is a very low overall quality of evidence that internal travel restrictions can reduce influenza transmission.
Values and preferences Values and preferences related to internal travel restrictions are uncertain.
Balance of benefits and harms Legal and ethical issues surrounding restrictions on freedom of movement of persons (2 7 9) and economic consequences are potential harms that may result from internal travel restrictions (234).
Resource implications Restricting internal travel would require a large amount of public resources, including the provision of public advice and a large number of staff. Furthermore, there would be consequences for the supply chains of food and essential medicines due to the disruption of movement.
Ethical considerations The human right to freedom of movement should be considered (279), as should potential adverse economic impacts, particularly in vulnerable populations such as migrant workers and individuals who need to travel to seek medical attention (219).
Acceptability There is limited evidence for the effectiveness of internal travel restrictions, and it has legal, ethical and economic implications. Although 37% of national pandemic preparedness plans of Member States have travel restriction plans as a component of NPls (65), the acceptability is still undetermined.
Feasibility Some countries have already included travel restriction plans in their national pandemic preparedness plans. However, some countries cannot implement those plans because of their own laws. Therefore, travel restriction plans may be challenging to implement because of legal, ethical, economic and resource implications.
r
RECOMMENDATION:
Internal travel restrictions are conditionally recommended during an early stage of a localized and extraordinarily severe pandemic for a limited period of time. Before implementation, it is important to consider cost-effectiveness, acceptability and feasibility, as well as ethical and legal considerations in relation to this measure.
Population: General public
When to apply: Early phase of extraordinarily severe pandemics
----------------l:E WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-434

FACTORS
Quality of evidence
Values and preferences
Balance of benefits and harms
Resource implications
Ethical considerations
Acceptability
Feasibility
Overall strength of recommendation
ASSESSMENT
Very low (effective)
Conditional
Conditional
Conditional
Conditional
Conditional
Conditional
Conditionally recommended
i
!
RATIONALE
The overall quality of the evidence was very low for the effectiveness of internal travel restrictions in an influenza epidemic or pandemic. Very strict internal travel restrictions are effective in reducing influenza transmission in the community.
Uncertain.
Internal travel restrictions can have important economic consequences. There is no published evidence of potential benefits, but theoretically transmission would be reduced.
Substantial implementation cost may be incurred.
The human rights of free movement should be considered, as should the adverse economic effects, particularly in vulnerable populations such as migrant workers and individuals who need to travel to access medical care.
Uncertain. . ---- -·--·-- . ·-~
Some countries already have travel restriction plans in place in the event of an epidemic or pandemic; however, some countries cannot implement these because of their own laws.
This measure can be conditionally recommended during the early stage of a localized extraordinarily severe pandemic for a limited period of time.
Knowledge gaps: No high-quality studies for the effectiveness of internal travel restrictions were identified. Studies to assess the effectiveness of internal travel restrictions and the costeffectiveness of this measure would be valuable to inform decisions on its use and to identify potential barriers to its implementation.
--~-·
m -N-ON---PH_A_R-MA_C_EU_TI_C_A_L P-U-B-LIC_H_E_A_LT_H_M-EA-S-UR_E_S _FO_R_M_IT-IG-A-JI-NG_T_H_E_RI-SK_A_N_D_IM_P_A_CT_O_F_E-PID_E_M_IC_A_N_D_PA_N_D_EM_I_C -,N-FL-U-EN_Z_A --
APPENDIX TO JAMES CASCIANO DECLARA TION-435

7 .4. Border closure
Summary of evidence Eleven articles related to border closure were included in the systematic review ( 7 7 4, 135, 204, 231, 235-239). Two were epidemiological studies (735,237) and nine were simulation studies (774,204, 234-240). An epidemiological study suggested an important influence of international air travel on the timing of influenza introduction (237). Another historical analysis of the 1918-1919 pandemic suggested that strict border control was a successful method for delaying and preventing influenza from arriving in South Pacific islands ( 7 35).
A simulation study predicted that 99% restriction of cross-border travel between Hong Kong SAR and mainland China may delay the epidemic peak by about 3.5 weeks compared with non-travel restriction (235). Another simulation study conducted in Italy predicted that international air travel restriction would delay the peak of epidemic by about 1-3 weeks, depending on the transmission rate and the level of restriction (204). However, the attack rate was not significantly affected (204). Furthermore, simulation studies based on a global scale model also predicted that international travel restriction would delay epidemics by about 2-3 weeks (236) and significantly delay its global spread (5-133 days) (23n. Strict border control of 99.9% may be effective in delaying the epidemic peak by 6 weeks, while 90% and 99% border control would delay the epidemic peak by 1.5 and 3 weeks, respectively ( 7 7 4). International travel restriction is estimated to slow the importation of infections (234,238), but would not reduce the epidemic duration (238). Because the supply of essential items to a population, such as food and medical supplies, often relies on importation, strict border closures need to be carefully considered before implementation in island countries and territories (239).
r OVERALL RESULT OF EVIDENCE ON BORDER CLOSURE
1. Eleven studies were Included in this review. 2. Generally, only strict border closures are expected to be effective
within small island nations. 3. For island nations, border closure should be carefully considered
because it may affect the supply of essential items to the population.
Summary of considerations of members of the guideline development group for determining the direction and strength of the recommendations The guideline development group, with the support of the steering group, formulated recommendations that were informed by the evidence presented and took into account quality of evidence, values and preferences, balance of benefits and harms, resource implications, ethical considerations, acceptability and feasibility, as outlined below.
Quality of evidence There is a very low overall quality of evidence that border closure has an effect on transmission of influenza, and studies in the literature reported or predicted variable effectiveness.
Values and preferences Values and preferences related to border closure are uncertain.
Balance of benefits and harms No scientific evidence of the harm of border closure for individuals was identified. However, it is reasonable to expect that strict border control could affect daily life and have serious economic consequences.
_,J
----------------~ WORLD HEALTH ORGANIZATION lt:,,l.t
APPENDIX TO JAMES CASCIANO DECLARATION-436

Resource implications No costing studies on border closure were identified; however, the cost will be prohibitive in most countries because of the closure of borders (air, land and sea). Substantial public resources would be needed, including the provision of public advice and large numbers of staff to restrict crossborder travel. Furthermore, there would be consequences for the supply chain for food and essential medicines, as well as broader economic consequences.
Ethical considerations The right to free movement of persons should be considered (2 7 9). As with internal travel restrictions, border closure applied by nations should be done voluntarily as much as possible, and compulsory intervention should be involved as a last resort (219). Furthermore, the stigmatization and discrimination of individuals from affected areas and economic impacts of border closures should also be carefully considered (279,247).
Acceptability There is limited evidence for the effectiveness of border closures, and it has legal, ethical and economic implications.
Feasibility Border closure in severe pandemics is technically feasible, and it may be most effective if implemented in the very early phase of a pandemic. However, the above-mentioned ethical, economic and resource implications affect its feasibility.
RECOMMENDATION:
Border closure is generally not recommended unless required by national law in extraordinary circumstances during a severe pandemic, and countries implementing this measure should notify WHO as required by the IHR (2005).
Population: General Public
When to apply: N/ A
FACTORS ASSESSMENT RATIONALE
Quality of evidence Very low The overall quality of evidence for the (variable effectiveness of border closure was very effectiveness) low. The effect of border closure in reducing
influenza transmission is varied. I
Values and Conditional Uncertain. preferences
Balance of benefits Conditional May be effective in delaying importation of and harms new cases but at major economic cost.
·-
Resource Conditional A large amount of public resources would implications be needed and there would be considerable
economic consequences.
Ethical Conditional Ethical issues relating to restrictions of free considerations movement should be carefully considered.
--
m: NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-437

FACTORS ASSESSMENT RATIONALE
Acceptability Conditional
Feasibility Conditional
Overall Not Recommended strength of recommendation
There is limited evidence for the effectiveness of border closure, and it has legal, ethical and economic consequences. However, the acceptability is still unclear.
Likely not to be feasible in most locations.
Overall, border closure is not recommended unless required by national law or in extraordinary circumstances during a severe pandemic, and countries should notify WHO as required by IHR. This is due to the very low quality of evidence, economic consequences, resource Implications and ethical implications.
Knowledge gaps: Due to the lack of high-quality evidence, the benefit of border closure is still uncertain (237). Cost-benefit studies to assess the advantages and disadvantages of border closure are needed.
IHR: International Health Regulations; N/ A: not applicable; WHO: World Health Organization.
----------------~ WORLD HEALTH ORGANIZATION ~
APPENDIX TO JAMES CASCIANO DECLARATION-438
REFERENCES
World Health Organization (WHO). Pandemic influenza [website]. 2019 (http://www.euro. who.int/en/health-topics/communicable-diseases/influenza/pandemic-influenza, accessed 28 May 2019).
2 Killingley B, Nguyen-Van-Tam J. Routes of influenza transmission. Influenza Other Respir Viruses. 2013;7(Suppl 2):42-51 (https://www.ncbi.nlm.nih.gov/pubmed/24034483, accessed 26 June 2019).
3 Pandemic Influenza Preparedness Team. Routes of transmission of the influenza virus: scientific evidence base review. London: Department of Health; 2011 (https://assets.publish ing.service.gov.uk/government/uploads/system/u pleads/attachment data/file/21 566 7 I dh 125332.pdf, accessed 26 June 2019).
4 Yan J, Grantham M, Pantelic J, Bueno de Mesquita PJ, Albert B, Liu Fetal. Infectious virus in exhaled breath of symptomatic seasonal influenza cases from a college community. Proc Natl Acad Sci USA. 2018;115(5):1081-6.
5 Gralton J, Tovey E, Mclaws M-L, Rawlinson WD. The role of particle size in aerosolised pathogen transmission: a review. J Infect. 2011 ;62(1 ):1-13 (https://www.sciencedirect.com/ science/article/pii/50163445310003476, accessed 26 June 2019).
6 Tellier R. Aerosol transmission of influenza A virus: a review of new studies.JR Soc Interface. 2009;6(Suppl 6):5783-590 (https://www.ncbi.nlm.nih.gov/pubmed/l 9773292, accessed 26 June 2019).
7 Cowling BJ, Ip DKM, Fang VJ, Suntarattiwong P, Olsen SJ, Levy Jet al. Aerosol transmission is an important mode of influenza A virus spread. Nat Commun. 2013;4:1935 (https://doi. org/10.1038/ncomms2922, accessed 26 June 2019).
8 Aledort JE, Lurie N, Wasserman J, Bozzette SA. Non-pharmaceutical public health interventions for pandemic influenza: an evaluation of the evidence base. BMC Public Health. 2007;7(1 ):208 (https://doi.org/1 O. l l 86/l 471-2458-7-208, accessed 26 June 2019).
9 World Health Organization (WHO). Influenza (seasonal) [website]. 2018 (https://www.who. int/news-room/fact-sheets/detail/influenza-(seasonall, accessed 2 July 2019).
10 Bloom-Feshbach K, Alonso WJ, Charu V, Tamerius J, Simonsen L, Miller MA et al. Latitudinal variations in seasonal activity of influenza and respiratory syncytial virus (RSV): a global comparative review. PLoS One. 2013;8(2):e54445.
11 Tamerius JD, Shaman J, Alonso WJ, Bloom-Feshbach K, Uejio CK, Comrie A et al. Environmental predictors of seasonal influenza epidemics across temperate and tropical climates. PLoS Pathog. 2013;9(3):e1003194 (https://www.ncbi.nlm.nih.gov/ pubmed/23505366, accessed 26 June 2019).
12 Rozo M, Gronvall GK. The reemergent 1977 Hl Nl strain and the gain-of-function debate. MBio. 2015;6(4).
13 Gatherer D. The 2009 Hl Nl influenza outbreak in its historical context. J Clin Virol. 2009;45(3): 17 4-8.
14 US Centers for Disease Control and Prevention. How is pandemic flu different from seasonal flu? [website]. 2015 (https://www.cdc.gov/flu/pandemic-resources/basics/about.html. accessed 2 July 2019).
IZll NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-439

15 Saunders-Hastings PR, Krewski D. Reviewing the history of pandemic influenza: understanding patterns of emergence and transmission. Pathogens. 2016;5(4):66 (https://www.ncbi.nl m. nih.gov/pubmed/27929449, accessed 26 June 2019).
16 Mento AS, Comanor L, Shay DK, Thompson WW. Epidemiology of Pandemic Influenza: Use of Surveillance and Modeling for Pandemic Preparedness. J Infect Dis. 2006;194 (Supplement_2):S92-S7 (http://dx.doi.org/10.1086/507559. accessed.
17 World Health Organization (WHO). Past pandemics [website]. 2019 (https://www.euro.who. int/en/health-topics/communicable-diseases/influenza/pandemic-influenza/past-pandem~ accessed 25 June 2019).
18 Simonsen L, Clarke MJ, Schonberger LB, Arden NH, Cox NJ, Fukuda K. Pandemic versus epidemic influenza mortality: A pattern of changing age distribution. J Infect Dis. 1998;178(1 ):53-60 (https:/ /dx.doi.org/10. 1086/515616, accessed 26 June 2019).
19 Skountzou I, Koutsonanos DG, Kim JH, Powers R, Satyabhama L, Masseoud F et al. Immunity to pre-1950 Hl Nl influenza viruses confers cross-protection against the pandemic swineorigin 2009 A (Hl Nl) influenza virus. J lmmunol. 2010;185(3):1642-9 (https://www.ncbi.nl m. nih.gov/pubmed/20585035, accessed 26 June 2019).
20 Trifonov V, Khiabanian H, Rabadan R. Geographic dependence, surveillance, and origins of the 2009 influenza A (H 1 N 1) virus. N Engl J Med. 2009;361 (2):115-9.
21 World Health Organization (WHO). What is the pandemic (Hl Nl) 2009 virus? [website]. 201 O (https://www.who.int/csr/disease/swineflu/freguently asked questions/about disease/en/. accessed 25 June 2019).
22 Simonsen L, Spreeuwenberg P, Lustig R, Taylor RJ, Fleming OM, Kroneman M et al. Global mortality estimates for the 2009 influenza pandemic from the GLaMOR project: A modeling study. PLoS Med. 2013;10(11):e1001558 (https://doi.org/10.1371 /journal.pmed.1001558, accessed 26 June 2019).
23 US Centers for Disease Control and Prevention. Past pandemics [website]. 2018 (https:// www.cdc.gov/flu/pandemic-resources/basics/past-pandemics.html. accessed 2 July 2019).
24 Gog JR, Ballesteros S, Viboud C, Simonsen L, Bjornstad ON, Shaman J et al. Spatial transmission of 2009 pandemic influenza in the US. PLoS Com put Biol. 2014;10(6):e 1003635-e (https:llwww.ncbi.nIm.ni h.gov /pu bmed/24921923. accessed 26 June 2019).
25 Lai S. Qin Y, Cowling BJ, Ren X, Wardrop NA, Gilbert M et al. Global epidemiology of avian influenza A H5N1 virus infection in humans. 1997-2015: a systematic review of individual case data. Lancet Infect Dis. 2016;16(7):el 08-el 8.
26 Wang X, Jiang H, Wu P, Uyeki TM, Feng L, Lai Set al. Epidemiology of avian influenza A H7N9 virus in human beings across five epidemics in mainland China. 2013-17: an epidemiological study of laboratory-confirmed case series. Lancet Infect Dis. 2017;17(8):822-32.
27 Wang X, Wu P, Pei Y. Tsang TK, Gu D. Wang Wet al. Assessment of human-to-human transmissibility of avian influenza A(H7N9) virus across 5 waves by analyzing clusters of case patients in mainland China, 2013-2017. Clin Infect Dis. 2019;68(4):623-31.
28 Neumann G, Kawaoka Y. Transmission of influenza A viruses. Virology. 2015;479-480:234-46 (https://www.sciencedirect.com/science/article/pi i/S004268221 5001452. accessed 26 June 2019).
29 Qualls N, Levitt A. Kanade N, Wright-Jegede N, Dopson S, Biggerstaff Met al. Community mitigation guidelines to prevent pandemic influenza - United States, 2017. MMWR Recomm Rep. 2017;66(1 ):1-34 (https://www.ncbi.nlm.nih.gov/pubmed/28426646. accessed 26 June 2019).
30 Literature review on the effectiveness of non-pharmaceutical countermeasures against pandemic influenza. Stockholm: European Centre for Disease Prevention and Control; 2018.
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-440

31 World Health Organization Writing Group, Bell D, Nicoll A, Fukuda K, Horby P, Monto A et al. Non-pharmaceutical interventions for pandemic influenza, international measures. Em erg Infect Dis. 2006;12( 1 ):81-7 (https://www.ncbi.nIm.ni h.gov /pu bmed/16494 722, accessed 26 June 2019).
32 World Health Organization (WHO). Reducing transmission of pandemic (H 1 N 1) 2009 in school settings. Geneva: WHO; 2009 (https://www.who.int/csr/resources/publications/swineflu/reducing transmission h 1 n 1 2009/en/, accessed 26 June 2019).
33 World Health Organization (WHO). Public health measures during the influenza A(Hl Nl )2009 pandemic. Geneva: WHO; 2011 (https:/ /www.who.int/influenza/preparedness/ measures/en/. accessed 26 June 2019).
34 World Health Organization (WHO). Interim planning considerations for mass gatherings in the context of pandemic (H 1 N 1) 2009 influenza. Geneva: WHO; 2009 (https://www.who.int/ csr/resources/publications/swineflu/h 1 n 1 mass gatherings/en/. accessed 26 June 2019).
35 World Health Organization (WHO). Public health for mass gatherings: key considerations Geneva: WHO; 2015 (https://www.who.int/ihr/publications/WHO HSE GCR 2015.5/en/. accessed 26 June 2019).
36 World Health Organization (WHO). International Health Regulations (2005), second edition. Geneva: WHO; 2005 (https://www.who.int/ihr/9789241596664/en/, accessed 26 June 2019).
37 World Health Organization (WHO). Pandemic influenza severity assessment (PISA): a WHO guide to assess the severity of influenza in seasonal epidemics & pandemics. Geneva: WHO; 2017 (https://apps.who.int/iris/bitstream/handle/10665/259392/WHO-WHE-IHM-GIP-2017.2-eng.pdf:jsessionid=357DD06249B82A8C475F71 DAC88071 AE?sequence=1, accessed 26 June 2019).
38 World Health Organization (WHO). WHO handbook for guideline development, 2nd ed. Geneva: WHO; 2014 (https://www.who.int/iris/handle/10665/145714, accessed 26 June 2019).
39 Guyatt GH, Oxman AD, Vist G, Kunz R, Brozek J, Alonso-Coello Pet al. GRADE guidelines: 4. Rating the quality of evidence - study limitations (risk of bias). J Clin Epidemiol. 2011;64(4):407-15.
40 Guyatt G, Oxman AD, Aki EA, Kunz R, Vist G, Brozek J et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011 ;64(4):383-94 (https://www.sciencedirect.com/science/article/pii/S0895435610003306. accessed 26 June 2019).
41 World Health Organization (WHO). Communication for behavioural impact (COMBI). Geneva: WHO; 2012 (https://www.who.int/ihr/publications/combi toolkit outbreaks/en/ accessed 26 June2019).
42 Aiello AE, Murray GF, Perez V, Coulborn RM, Davis BM, Uddin M et al. Mask use, hand hygiene, and seasonal influenza-like illness among young adults: a randomized intervention trial. J Infect Dis. 2010;201 (4):491-8.
43 Aiello AE, Perez V, Coulborn RM, Davis BM, Uddin M, Monto AS. Facemasks, hand hygiene, and influenza among young adults: a randomized intervention trial. PLoS One. 2012;7(1 ):e29744.
44 Cowling BJ, Chan K-H, Fang VJ, Cheng CK, Fung RO, Wai W et al. Facemasks and hand hygiene to prevent influenza transmission in households: a cluster randomized trial. Ann Intern Med. 2009;151 (7):437-46.
45 Larson EL, Ferng Y-H, Wong-Mcloughlin J, Wang S, Haber M, Morse SS. Impact of nonpharmaceutical interventions on URls and influenza in crowded, urban households. Public Health Rep. 2010;125(2):178-91.
m NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-441

46 Simmerman JM, Suntarattiwong P, Levy J, Jarman RG, Kaewchana S, Gibbons RV et al. Findings from a household randomized controlled trial of hand washing and face masks to reduce influenza transmission in Bangkok, Thailand. Influenza Other RespirViruses. 2011;5(4):256-67.
47 Suess T, Remschmidt C, Schink SB, Schweiger B, Nitsche A, Schroeder Ket al. The role of facemasks and hand hygiene in the prevention of influenza transmission in households: results from a cluster randomised trial; Berlin, Germany, 2009-2011. BMC Infect Dis. 2012;12{1 ):26.
48 Stebbins S, Cummings DA, Stark JH, Vukotich C, Mitruka K, Thompson Wet al. Reduction in the incidence of influenza A but not influenza B associated with use of hand sanitizer and cough hygiene in schools: a randomized controlled trial. Pediatr Infect Dis J. 2011;30(11):921.
49 Talaat M, Afifi S, Dueger E, EI-Ashry N, Marfin A, Kandeel A et al. Effects of hand hygiene campaigns on incidence of laboratory-confirmed influenza and absenteeism in schoolchildren, Cairo, Egypt Emerg Infect Dis. 2011 ;17(4):619.
50 Cowling BJ, Fung RO, Cheng CK, Fang VJ, Chan KH, Seto WH et al. Preliminary findings of a randomized trial of non-pharmaceutical interventions to prevent influenza transmission in households. PLoS One. 2008;3(5):e2101.
51 Ram PK, DiVita MA, Khatun-e-Jannat K, Islam M, Krytus K, Cercone E et al. Impact of intensive handwashing promotion on secondary household influenza-like illness in rural Bangladesh: findings from a randomized controlled trial. PLoS One. 2015;10(6):eOl 25200.
52 Azman AS, Stark JH, Althouse BM, Vukotich Jr CJ, Stebbins S, Burke OS et al. Household transmission of influenza A and B in a school-based study of non-pharmaceutical interventions. Epidemics. 2013;5(4): 181-6.
53 Levy JW, Suntarattiwong P, Simmerman JM, Jarman RG, Johnson K, Olsen SJ et al. Increased hand washing reduces influenza virus surface contamination in Bangkok households, 2009-2010. Influenza Other RespirViruses. 2014;8(1):13-6.
54 Bean B, Moore BM, Sterner B, Peterson LR, Gerding ON, Balfour HH, Jr. Survival of influenza viruses on environmental surfaces.J Infect Dis. 1982;146(1):47-51 {https://www.ncbi.nlm. nih.gov/pubmed/6282993, accessed 26 June 2019).
55 Mukherjee DV, Cohen B, Bovina ME, Desai S, Whittier S, Larson EL. Survival of influenza virus on hands and fomites in community and laboratory settings. Am J Infect Control. 2012;40(7):590-4 (https://www.ncbi.nlm.nih.gov/pubmed/22264744, accessed 26 June 2019).
56 Thomas Y, Boquete-Suter P, Koch D, Pittet D, Kaiser L. Survival of influenza virus on human fingers. Clin Microbiol Infect. 2014;20(1):058-64 (https://www.ncbi.nlm.nih.gov/ pubmed/23927722, accessed 26 June 2019).
57 Grayson ML, Melvani S, Druce J, Barr IG, Ballard SA, Johnson PD et al. Efficacy of soap and water and alcohol-based hand-rub preparations against live Hl Nl influenza virus on the hands of human volunteers. Clin Infect Dis. 2009;48(3):285-91 (https://www.ncbi.nlm.nih. gov/pubmed/19115974, accessed 26 June 2019).
58 Larson EL, Cohen B, Baxter KA. Analysis of alcohol-based hand sanitizer delivery systems: efficacy of foam, gel, and wipes against influenza A {Hl Nl) virus on hands. Am J Infect Control. 2012;40(9):806-9 {https://www.ncbi.nlm.nih.gov/pubmed/22325728, accessed 26 June 2019).
59 Tuladhar E, Hazeleger WC, Koopmans M, Zwietering MH, Duizer E, Beumer RR. Reducing viral contamination from finger pads: Handwashing is more effective than alcohol-based hand disinfectants. J Hosp Infect 2015;90(3):226-34 {https://www.ncbi.nlm.nih.gov/ pubmed/25936671, accessed 26 June 2019).
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-442

60 Chabrelie A, Mitchell J, Rose J, Charbonneau D, Ishida Y. Evaluation of the influenza risk reduction from antimicrobial spray application on porous surfaces. Risk Anal. 2018;38(7):1502-17 (https://www.ncbi.nlm.nih.gov/pubmed/29278668, accessed 26 June 2019).
61 Wong VW, Cowling BJ, Aiello AE. Hand hygiene and risk of influenza virus infections in the community: a systematic review and meta-analysis. Epidemiol Infect. 2014;142(5):922-32.
62 Loffler H, Kampf G. Hand disinfection: How irritant are alcohols? J Hosp Infect. 2008;70 (Suppl 1 ):44-8 (https://www.ncbi.nlm.nih.gov/pubmed/18994681, accessed 26 June 2019).
63 World Health Organization (WHO). WHO guidelines on hand hygiene in health care: first global patient safety challenge clean care is safer care. Geneva: WHO; 2009 Chttps://www. ncbi.nlm.nih.gov/books/NBK 143995/, accessed 26 June 2019).
64 Ahmed QA, Memish ZA, Allegranzi B, Pittet D. Muslim health-care workers and alcohol-based handrubs. Lancet. 2006;367(9515):1025-7.
65 World Health Organization (WHO). Comparative analysis of national pandemic influenza preparedness plans. Geneva:WHO; 2011 (https://www.who.int/influenza/resources/ documents/comparative analysis php 2011 en.pdf?ua=1, accessed 26 June 2019).
66 Zayas G, Chiang MC, Wong E, MacDonald F, Lange CF, Senthilselvan A et al. Effectiveness of cough etiquette maneuvers in disrupting the chain of transmission of infectious respiratory diseases. BMC Public Health. 2013;13:811 (https://www.ncbi.nlm.nih.gov/pubmed/24010919, accessed 26 June 2019).
67 US Centers for Disease Control and Prevention. Respiratory hygiene/cough etiquette in healthcare settings [website]. Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases (NCIRD); 2012 (https:/ /www.cdc.gov/flu/professionals/infectioncontrol/resphygiene.htm. accessed 25 June 2019).
68 Barasheed 0, Almasri N, Badahdah AM, Heron L, Taylor J, McPhee K et al. Pilot randomised controlled trial to test effectiveness of facemasks in preventing influenza-like illness transmission among Australian hajj pilgrims in 2011. Infect Disord Drug Targets. 2014;14(2):110-6.
69 MacIntyre CR, Cauchemez S, Dwyer DE, Seale H, Cheung P, Browne G et al. Face mask use and control of respiratory virus transmission in households. Emerg Infect Dis. 2009;15(2):233-41.
70 MacIntyre CR, Zhang Y, Chughtai AA, Seale H, Zhang D, Chu Yet al. Cluster randomised controlled trial to examine medical mask use as source control for people with respiratory illness. BMJ Open. 2016;6(12):e0l 2330.
71 Johnson OF, Druce JD, Birch C, Grayson ML. A quantitative assessment of the efficacy of surgical and N95 masks to filter influenza virus in patients with acute influenza infection. Clin Infect Dis. 2009;49(2):275-7 (https://www.ncbi.nlm.nih.gov/pubmed/19522650, accessed 26 June 2019).
72 Wada K, Oka-Ezoe K, Smith DR. Wearing face masks in public during the influenza season may reflect other positive hygiene practices in Japan. BMC Public Health. 2012;12:1065 (https://www.ncbi.nlm.nih.gov/pubmed/23227885, accessed 26 June 2019).
73 Casas L, Espinosa A, Borras-Santos A, Jacobs J, Krop E, Heederik D et al. Domestic use of bleach and infections in children: a multicentre cross-sectional study. Occup Environ Med. 2015;72(8):602-4.
74 lbfeltT, Engelund EH, Schultz AC, Andersen LP. Effect of cleaning and disinfection of toys on infectious diseases and micro-organisms in daycare nurseries. J Hosp Infect. 2015;89(2):109-15.
75 Sandora TJ, Shih MC, Goldmann DA. Reducing absenteeism from gastrointestinal and respiratory illness in elementary school students: a randomized, controlled trial of an infection-control intervention. Pediatrics. 2008;121 (6):el 555-62.
m NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-443

76 Greatorex JS, Diga rd P, Curran MD, Moynihan R, Wensley H, Wreghitt T et al. Survival of influenza A(Hl Nl) on materials found in households: Implications for infection control. PloS One. 2011;6(11):e27932 (https://www.ncbi.nlm.nih.gov/pubmed/22132172, accessed 26 June 2019).
77 Oxford J, Berezin EN, Courvalin P, Dwyer DE, Exner M, Jana LA et al. The survival of influenza A(Hl Nl)pdm09 virus on 4 household surfaces. Am J Infect Control. 2014;42(4):423-5 (https://www.ncbi.nlm.nih.gov/pubmed/24679569. accessed 26 June 2019).
78 Thomas Y, Vogel G, Wunderli W, Suter P, Witschi M, Koch D et al. Survival of influenza virus on banknotes. Appl Environ Microbial. 2008;74(10):3002-7 (https://www.ncbi.nlm.nih.gov/ pubmed/18359825. accessed 26 June 2019).
79 Boone SA, Gerba CP. The occurrence of influenza A virus on household and day care center fomites. J Infect. 2005;51 (2):103-9 (https://www.ncbi.nlm.nih.gov/pubmed/16038759. accessed 26 June 2019).
80 Bright KR. Boone SA. Gerba CP. Occurrence of bacteria and viruses on elementary classroom surfaces and the potential role of classroom hygiene in the spread of infectious diseases. J Sch Nurs. 2010;26(1):33-41.
81 lkonen N, Savolainen-Kopra C. Enstone JE. Kulmala I, Pasanen P, Salmela A et al. Deposition of respiratory virus pathogens on frequently touched surfaces at airports. BMC Infect Dis. 2018;18( 1 ):437 (https://www.ncbi.n I m.n i h.gov /pu bmed/30157776. accessed 26 June 2019).
82 Killingley B. Greatorex J, Digard P, Wise H. Garcia F, Varsani H et al. The environmental deposition of influenza virus from patients infected with influenza A(Hl Nl )pdm09: Implications for infection prevention and control. J Infect Public Health. 2016;9(3):278-88 (https://www.ncbi.nlm.nih.gov/pubmed/26653976. accessed 26 June 2019).
83 Simmerman JM, Suntarattiwong P, Levy J. Gibbons RV, Cruz C, Shaman Jet al. Influenza virus contamination of common household surfaces during the 2009 influenza A (Hl Nl) pandemic in Bangkok, Thailand: Implications for contact transmission. Clin Infect Dis. 2010;51(9):1053-61 (https://www.ncbi.nlm.nih.gov/pubmed/20879867, accessed 26 June 2019).
84 Jeong EK. Bae JE, Kim IS. Inactivation of influenza A virus Hl Nl by disinfection process. Am J Infect Control. 2010;38(5):354-60 (https://www.ncbi.nlm.nih.gov/pubmed/20430477, accessed 26 June 2019).
85 Tuladhar E, Hazeleger WC, Koopmans M, Zwietering MH, Beumer RR, Duizer E. Residual viral and bacterial contamination of surfaces after cleaning and disinfection. Appl Environ Microbial. 2012;78(21 ):7769-75 {https://www.ncbi.n I m.n i h.gov /pu bmed/22941071. accessed 26 June 2019).
86 Verhaelen K, Bouwknegt M, Rutjes S, de Roda Husman AM, Duizer E. Wipes coated with a singlet-oxygen-producing photosensitizer are effective against human influenza virus but not against norovirus. Appl Environ Microbial. 2014;80(14):4391-7 (https://www.ncbi.nlm. nih.gov/pubmed/24814795. accessed 26June 2019).
87 Rubin GJ. Amiot R, Page L, Wessely S. Public perceptions, anxiety, and behaviour change in relation to the swine flu outbreak: cross sectional telephone survey. BMJ. 2009;339:b2651 (https://www.bmj.com/content/bmj/339/bmj.b2651.full.pdf. accessed 26 June 2019).
88 European Centre for Disease Prevention and Control (ECDC). Expert opinion on the scientific evidence-base for effectiveness of non-pharmaceutical countermeasures against pandemic influenza. Stockholm: ECDC; 2019.
89 Communicable Diseases Network Australia (CDNA). Guidelines for the prevention. control and public health management of influenza outbreaks in residential care facilities in Australia. Australia: CDNA; 2017 (https://www.health.gov.au/internet/main/publishing.nsf / Content/27BE697 A7FBFSABSCA257BF0001 D3AC8/SFile/RCF Guidelines.pdf. accessed 26 June 2019).
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-444

90 Reed NG. The history of ultraviolet germicidal irradiation for air disinfection. Public Health Rep. 2010;125(1 ):15-27 (https://www.ncbi.nlm.nih.gov/pubmed/20402193. accessed 26 June 2019).
91 American Cancer Society. What is ultraviolet (UV) radiation? [website]. 2017 (https://www. cancer.org/cancer/skin-cancer/prevention-and-early-detection/what-is-uv-radiation.html. accessed 25 June 2019).
92 Chen SC. Liao CM. Modelling control measures to reduce the impact of pandemic influenza among schoolchildren. Epidemiol Infect. 2008;136(8):1035-45 (https://www.ncbi.nlm.nih. gov/pubmed/17850689. accessed 26 June 2019).
93 Gao X. Li Y. Leung GM. Ventilation control of indoor transmission of airborne diseases in an urban community. Indoor Built Environ. 2009;18(3):205-18 (https://doi. org/10.1177 /1420326X09104141. accessed 26 June 2019).
94 Gao X. Wei J, Cowling BJ, Li Y. Potential impact of a ventilation intervention for influenza in the context of a dense indoor contact network in Hong Kong. Sci Total Environ. 2016;569-570:373-81 (https://www.sciencedirect.com/science/article/pii/S0048969716313535. accessed 26 June 2019).
95 Qian H. Zheng XJJoTD. Ventilation control for airborne transmission of human exhaled bio-aerosols in buildings. J Thorac Dis. 2018:S2295-S304 (http://jtd.amegroups.com/article/ view/18723. accessed 26 June 2019).
96 Lowen AC. Steel J. Roles of humidity and temperature in shaping influenza seasonality. J Virol. 2014;88(14):7692-5 (https://www.ncbi.nlm.nih.gov/pubmed/24 789791. accessed 26 June 2019).
97 Reiman JM, Das B, Sindberg GM, Urban MD, Hammerlund MEM, Lee HB et al. Humidity as a non-pharmaceutical intervention for influenza A. PLoS One. 2018;13(9):e0204337 (https://www.ncbi.nlm.nih.gov/pubmed/30252890. accessed 26 June 2019).
98 Myatt TA, Kaufman MH, Allen JG, MacIntosh DL, Fabian MP, McDevitt JJ. Modeling the airborne survival of influenza virus in a residential setting: the impacts of home humidification. Environ Health. 2010;9:55 (https://www.ncbi.nlm.nih.gov/ pubmed/20815876. accessed 26 June 2019).
99 Noti JD. Blachere FM. McMillen CM, Lindsley WG, Kashon ML. Slaughter DR et al. High humidity leads to loss of infectious influenza virus from simulated coughs. PLoS One. 2013;8(2):e57 485 (https://www.ncbi.nl m.n ih.gov /pu bmed/23460865. accessed 26 June 2019).
100 Institute of Medicine. Damp indoor spaces and health. Washington, DC: The National Academies Press; 2004 (https:/ /www.nap.edu/catalog/11011 /damp-indoor-spaces-andhealth. accessed 26 June 2019).
101 World Health Organization (WHO). WHO guidelines for indoor air quality: Dampness and mould. Geneva: WHO; 2009 (https://apps.who.int/iris/bitstream/handle/10665/164348/ E92645.pdf:jsessionid=SBCDB7732AFBA2068207F8771576F0DA?seguence=1. accessed 26 June 2019).
102 Wu JT, Riley S, Fraser C, Leung GM. Reducing the impact of the next influenza pandemic using household-based public health interventions. PLoS Med. 2006;3(9):e361 (https://www.ncbi.nlm.ni h.gov /pmc/a rticles/PMC 1526 768/pdf /pmed.0030361.pdf. accessed 26 June 2019).
103 Peak CM, Childs LM. Grad YH, Buckee CO. Comparing nonpharmaceutical interventions for containing emerging epidemics. Proc Natl Acad Sci USA. 2017;114(15):4023-8.
104 Fraser C, Riley S. Anderson RM, Ferguson NM. Factors that make an infectious disease outbreak controllable. Proc Natl Acad Sci USA. 2004;101(16):6146-51.
U3 NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-445

105 An der Heiden M, Buchholz U, Krause G, Kirchner G, Claus H, Haas WH. Breaking the waves: modelling the potential impact of public health measures to defer the epidemic peak of novel influenza A/H 1 N 1. PLoS One. 2009;4(12):e8356.
106 Eames KT, Webb C, Thomas K, Smith J, Salmon R, Temple JM. Assessing the role of contact tracing in a suspected H7N2 influenza A outbreak in humans in Wales. BMC Infect Dis. 2010;10:141.
107 Torda A. Ethical issues in pandemic planning. Med J Aust. 2006;185(Suppl 10):573-6.
108 European Centre for Disease Prevention and Control (ECDC). Risk assessment guidelines for infectious diseases transmitted on aircraft (RAGIDA): influenza. Stockholm: ECDC; 2014 (https:llecdc.europa.eu/sites/portal/files/media/en/publications/Publications/influenza-RAGIDA-2014.pdf. accessed 26 June 2019).
109 European Centre for Disease Prevention and Control (ECDC). Guide to public health measures to reduce the impact of influenza pandemics in Europe: 'The ECDC menu'. Stockholm: ECDC; 2009.
110 Chu CY, de Silva UC, Guo JP, Wang Y, Wen L, Lee VJ et al. Combined interventions for mitigation of an influenza A (H 1 N 1) 2009 outbreak in a physical training camp in Beijing, China. Int J Infect Dis. 2017;60:77-82 (https://www.ncbi.nlm.ni h.gov /pu bmed/28483 722. accessed 26 June 2019).
111 Gaillat J, Dennetiere G, Raffin-Bru E, Valette M, Blanc MC. Summer influenza outbreak in a home for the elderly: application of preventive measures. J Hosp Infect. 2008;70(3):272-7.
112 Markel H, Lipman HB, Navarro JA, Sloan A, Michalsen JR, Stern AM et al. Nonpharmaceutical interventions implemented by US cities during the 1918-1919 influenza pandemic. JAMA. 2007;298(6):644-54 (https://jamanetwork.com/journals/jama/articlepdf /208354/ joc70085 644 654.pdf. accessed 26 June 2019).
113 Vera OM, Hora RA, Murillo A, Wong JF, Torre AJ, Wang D et al. Assessing the impact of public health interventions on the transmission of pandemic H1 Nl influenza a virus aboard a Peruvian navy ship. Influenza Other RespirViruses. 2014;8(3):353-9 (https://www.ncbi.nlm. nih.gov/pmc/articles/PMC4181484/pdf /irv0008-0353.pdf. accessed 26 June 2019).
114 Ferguson NM, Cummings DA, Fraser C, Cajka JC, Cooley PC, Burke OS. Strategies for mitigating an influenza pandemic. Nature. 2006;442(7101):448-52 (https://www.nature.com/ articles/nature04795, accessed 26 June 2019).
115 Halloran ME, Ferguson NM, Eubank S, Longini IM, Jr., Cummings DA, Lewis B et al. Modeling targeted layered containment of an influenza pandemic in the United States. Proc Natl Acad Sci USA. 2008;105(12):4639-44 (https://www.pnas.org/content/pnas/105/12/4639.full.pdf, accessed 26 June 2019).
116 Flahault A, Vergu E, Coudeville L, Grais RF. Strategies for containing a global influenza pandemic. Vaccine. 2006;24(44-46):6751-5 {https://www.sciencedirect.com/science/article/ pii/50264410X06006311 ?via%3Dihub, accessed 26 June 2019).
117 Saunders-Hastings P, Quinn Hayes B, Smith R, Krewski D. Modelling community-control strategies to protect hospital resources during an influenza pandemic in Ottawa, Canada. PLoS One. 2017;12(6):eOl 79315 (https://doi.org/10. 1371/journal.pone.0179315. accessed 26 June2019).
118 Wang L, Zhang Y, Huang T, Li X. Estimating the value of containment strategies in delaying the arrival time of an influenza pandemic: A case study of travel restriction and patient isolation. Phys Rev E Stat Nonlin Soft Matter Phys. 2012;86(3 Pt 1):032901 (https://journals. aps.org/pre/abstract/10.1103/PhysRevE.86.032901, accessed 26 June 2019).
WORLD HEALTH ORGANIZATION
APPENDIX TO JAMES CASCIANO DECLARATION-446

119 Kelso JK, Milne GJ, Kelly H. Simulation suggests that rapid activation of social distancing can arrest epidemic development due to a novel strain of influenza. BMC Public Health. 2009;9:117 (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2680828/pdf/1471-2458-9-117. ruH, accessed 26 June 2019).
120 Zhang Q Wang D. Antiviral prophylaxis and isolation for the control of pandemic influenza. Int J Environ Res Public Health. 2014;11 (8):7690-712 (https://www.ncbi.n I m.n i h.gov /pmc/ articles/PMC4143827 /. accessed 26 June 2019).
121 Zhang Q Wang D. Assessing the role of voluntary self-isolation in the control of pandemic influenza using a household epidemic model. Int J Environ Res Public Health. 2015;12(8):9750-67 (https:Uwww.ncbi.nlm.nih.gov/pubmed/26295248. accessed 26 June 2019).
122 Yasuda H SK. Measures against transmission of pandemic Hl Nl influenza in Japan in 2009: simulation model. Euro Surveill. 2009;14(44).
123 Johal SS. Psychosocial impacts of quarantine during disease outbreaks and interventions that may help to relieve strain.NZ Med J. 2009;122(1296):47-52.
124 Teasdale E, Santer M, Geraghty AWA, Little P, Yardley L. Public perceptions of nonpharmaceutical interventions for reducing transmission of respiratory infection: systematic review and synthesis of qualitative studies. BMC Public Health. 2014;14(1 ):589 (https://doi. org/10.1186/1471-2458-14-589, accessed 26 June 2019).
125 Rashid H, Ridda I, King C, Begun M, Tekin H, Wood JG et al. Evidence compendium and advice on social distancing and other related measures for response to an influenza pandemic. Paediatr Respir Rev. 2015;16(2):119-26.
126 Haber MJ, Shay DK, Davis XM, Patel R, Jin X, Weintraub E et al. Effectiveness of interventions to reduce contact rates during a simulated influenza pandemic. Emerg Infect Dis. 2007;13(4):581-9 (https:Uwww.ncbi.nlm.nih.gov/pubmed/17553273. accessed 26 June 2019).
127 Blake KO, Blendon RJ. Viswanath K. Employment and compliance with pandemic influenza mitigation recommendations. Emerg Infect Dis. 2010;16(2):212-8 (https://www.ncbi.nlm.nih. gov/pubmed/20113549. accessed 26 June 2019).
128 Gostin L, Berkman B. Pandemic influenza: Ethics, law. and the public's health. Admin. L. Rev. 2007;59:121 (https:Uscholarship.law.georgetown.edu/facpub/449/. accessed 26 June 2019).
129 Gray L. MacDonald C. Mackie B, Paton D, Johnston D, Baker MG. Community responses to communication campaigns for influenza A (Hl Nl): a focus group study. BMC Public Health. 2012;12(1):205 (https://doi.org/10.1186/1471-2458-12-205, accessed 26 June 2019).
130 Loustalot F, Silk BJ, Gaither A, Shim T, Lamias M, Dawood Fetal. Household transmission of 2009 pandemic influenza A CH 1 N 1) and nonpharmaceutical interventions among households of high school students in San Antonio, Texas. Clin Infect Dis. 2011 ;52 (Suppl 1):5146-553 {https:Udx.doi.org/10.1093/cid/ciq057, accessed 26 June 2019).
131 Mitchell T, Dee DL, Phares CR, Lipman HB, Gould LH, Kutty Pet al. Non-pharmaceutical interventions during an outbreak of 2009 pandemic influenza A (Hl Nl) virus infection at a large public university, April-May 2009. Clin Infect Dis. 2011;52(suppl_l):S138-S45 (https:U dx.doi.org/10.1093/cid/ciq056. accessed 26 June 2019).
132 Tooher R, Collins JE, Street JM, Braunack-Mayer A, Marshall H. Community knowledge, behaviours and attitudes about the 2009 Hl Nl Influenza pandemic: a systematic review. Influenza Other Respir Viruses. 2013;7(6):1316-27.
133 Patrozou E, Mermel LA. Does influenza transmission occur from asymptomatic infection or prior to symptom onset? Public Health Rep. 2009;124(2):193-6.
llil NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-447

134 Leung NH, Xu C, Ip DK, Cowling BJ. Review article: The fraction of influenza virus infections that are asymptomatic: a systematic review and meta-analysis. Epidemiology. 2015;26(6):862-72.
135 Mcleod MA, Baker M, Wilson N, Kelly H, Kiedrzynski T, Kool JL. Protective effect of maritime quarantine in South Pacific jurisdictions, 1918-19 influenza pandemic. Emerg Infect Dis. 2008;14(3):468-70 (https:/ /www.ncbi .n lm.n i h.gov /pmc/articles/PMC25 70822/pdf /07-0927 finalD.pdf. accessed 26 June 2019).
136 Fujita M, Sato H, Kaku K, Tokuno S, Kanatani Y, Suzuki Set al. Airport quarantine inspection, follow-up observation, and the prevention of pandemic influenza. Aviat Space Environ Med. 2011 ;82(8):782-9.
137 Miyaki K, Sakurazawa H, Mikurube H, Nishizaka M, Ando H, Song Yet al. An effective quarantine measure reduced the total incidence of influenza A H 1 N 1 in the workplace: another way to control the H1 N1 flu pandemic. J Occup Health. 2011 ;53(4):287-92.
138 van Gernert C, Hellard M, McBryde ES, Fielding J, Spelman T, Higgins Net al. lntrahousehold transmission of pandemic (Hl N1) 2009 virus, Victoria, Australia. Emerg Infect Dis. 2011;17(9):1599-607.
139 Li X, Geng W, Tian H, Lai D. Was mandatory quarantine necessary in China for controlling the 2009 H1N1 pandemic? lntJ Environ Res Public Health. 2013;10(10):4690-700 (https://res. mdpi.com/ijerph/ijerph-10-04690/article deploy/ijerph-10-04690.pdf?filename=&attachment= 1, accessed 26 June 2019).
140 Longini IM, Jr., Nizam A, Xu S, Ungchusak K, Hanshaoworakul W, Cummings DA et al. Containing pandemic influenza at the source. Science. 2005;309(5737):1083-7 Ul1mill science.sciencemag.org/content/309/5737 /1083.long, accessed 26 June 2019).
141 Nishiura H, Wilson N, Baker MG. Quarantine for pandemic influenza control at the borders of small island nations. BMC Infect Dis. 2009;9:27 (https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC2670846/pdf/1471-2334-9-27.pdf, accessed 26June 2019).
142 Roberts MG, Baker M, Jennings LC. Sertsou G, Wilson N. A model for the spread and control of pandemic influenza in an isolated geographical region. J R Soc Interface. 2007;4(13):325-30 (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2359860/pdf/rsif20060176.pdf. accessed 26 June 2019).
143 Sato H, Nakada H, Yamaguchi R, Imoto S, Miyano S, Kami M. When should we intervene to control the 2009 influenza A(H1 N1) pandemic? Euro Surveill. 2010;15(1 ).
144 Yang Y, Atkinson PM, Ettema D. Analysis of CDC social control measures using an agent-based simulation of an influenza epidemic in a city. BMC Infect Dis. 2011 ;11 :199 (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3151229/pdf/1471-2334-11-199.pdf. accessed 26 June 2019).
145 Akan H, Gural Y, lzbirak G, Ozdath S, Yilmaz G, Vitrine! A et al. Knowledge and attitudes of university students toward pandemic influenza: a cross-sectional study from Turkey. BMC Public Health. 2010;10(1):413 (https://doi.org/10.1186/1471-2458-10-413. accessed 26 June 2019).
146 Gostin L. Public health strategies for pandemic influenza: Ethics and the law. JAMA. 2006;295(14):1700-4 (https://dx.doi.org/10.1001 /jama.295.14.1700. accessed 26 June 2019).
147 Blendon RJ, DesRoches CM, Cetron MS, Benson JM, Meinhardt T, Pollard W. Attitudes toward the use of quarantine in a public health emergency in four countries. Health Aff (Millwood). 2006;25(2):wl 5-25.
148 Seale H, MakJPI, Razee H, MacIntyre CR. Examining the knowledge, attitudes and practices of domestic and international university students towards seasonal and pandemic influenza. BMC Public Health. 2012;12:307-(https://www.ncbi.nlm.nih.gov/pubmed/22537252, accessed 26 June 2019).
________________ i.-r.,
WORLD HEALTH ORGANIZATION (..&ii
APPENDIX TO JAMES CASCIANO DECLARATION-448

149 Teh B, Olsen K, Black J, Cheng AC, Aboltins C, Bull Ket al. Impact of swine influenza and quarantine measures on patients and households during the Hl Nl/09 pandemic. Scand J Infect Dis. 2012;44(4):289-96.
150 Chu C-Y, Li C-Y, Zhang H, Wang Y, Huo DH, Wen Let al. Quarantine methods and prevention of secondary outbreak of pandemic (H 1 Nl) 2009. Emerg Infect Dis. 2010;16(8):1300-2 (https://www.ncbi.nlm.nih.gov/pubmed/20678330. accessed 26 June 2019).
151 Eastwood K, Durrheim D, Francis JL, d'Espaignet ET, Duncan S, Islam Fetal. Knowledge about pandemic influenza and compliance with containment measures among Australians. Bull World Health Organ. 2009;87(8):588-94 {https:Uwww.ncbi.nlm.nih.gov/pubmed/19705008. accessed 26 June 2019).
152 McVernon J, Mason K, Petrony S, Nathan P, LaMontagne AD, Bentley R et al. Recommendations for and compliance with social restrictions during implementation of school closures in the early phase of the influenza A (Hl Nl) 2009 outbreak in Melbourne, Australia. BMC Infect Dis. 2011 ;11 :257- (https://www.ncbi.nlm.nih.gov/pubmed/21958428, accessed 26 June 2019).
153 Kavanagh AM, Bentley RJ, Mason KE, McVernon J, Petrony S, Fielding Jet al. Sources, perceived usefulness and understanding of information disseminated to families who entered home quarantine during the Hl Nl pandemic in Victoria, Australia: a cross-sectional study. BMC Infect Dis. 2011;11:2.
154 Rothstein MA, Talbott MK. Encouraging compliance with quarantine: A proposal to provide job security and income replacement. Am J Public Health. 2007;97(Suppl 1 ):S49-S56 (https://www.ncbi.nlm.nih.gov/pubmed/17413059. accessed 26 June 2019).
155 Uscher-Pines L, Schwartz HL, Ahmed F, Zheteyeva Y, Meza E, Baker G et al. School practices to promote social distancing in K-12 schools: Review of influenza pandemic policies and practices. BMC Public Health. 2018;18(1 ):406 (https://doi.org/10.1186/s 12889-018-5302-3. accessed 26 June 2019).
156 Cauchemez S, Ferguson NM, Wachtel C, Tegnell A, Saour G, Duncan Bet al. Closure of schools during an influenza pandemic. Lancet Infect Dis. 2009;9(8):473-81 (https://www.ncbi.nl rn. nih.gov/pubmed/19628172. accessed 26 June 2019).
157 Jackson C, Vynnycky E, Hawker J, Olowokure B, Mangtani P. School closures and influenza: systematic review of epidemiological studies. BMJ Open. 2013;3(2).
158 Bootsma MC, Ferguson NM. The effect of public health measures on the 1918 influenza pandemic in U.S. cities. Proc Natl Acad Sci USA. 2007;104(18):7588-93.
159 Hatchett RJ, Mecher CE, Lipsitch M. Public health interventions and epidemic intensity during the 1918 influenza pandemic. Proc Natl Acad Sci USA. 2007;104(18):7582-7 {https://www.ncbi.nlm.nih.gov/pubmed/17416679. accessed 26 June 2019).
160 Cowling BJ, Lau MS, Ho LM, Chuang SK, Tsang T, Liu SH et al. The effective reproduction number of pandemic influenza: prospective estimation. Epidemiology. 2010;21 (6):842-6.
161 Wu JT, Cowling BJ, Lau EH, Ip DK, Ho LM, Tsang T et al. School closure and mitigation of pandemic (Hl Nl) 2009, Hong Kong. Emerg Infect Dis. 2010;16(3):538-41.
162 Bolton KJ, McCaw JM, Moss R, Morris RS, Wang S, Burma A et al. Likely effectiveness of pharmaceutical and non-pharmaceutical interventions for mitigating influenza virus transmission in Mongolia. Bull World Health Organ. 2012;90(4):264-71.
163 Cauchemez S, Bhattarai A, Marchbanks TL, Fagan RP, Ostroff S, Ferguson NM et al. Role of social networks in shaping disease transmission during a community outbreak of 2009 Hl Nl pandemic influenza. Proc Natl Acad Sci USA. 2011;108(7):2825-30.
164 Kawano S, Kakehashi M. Substantial Impact of School Closure on the Transmission Dynamics during the Pandemic Flu Hl Nl-2009 in Oita,Japan. PloS One. 2015;10(12):e0144839.
[E -NO_N ___ PH-A-RM_A_C_EU-TI-CA_L_P-UB_L_IC-H-EA-LT_H_M-EA_S_U-RE-S-FO_R_M_IT-IG-AT-IN_G_T_H_E R-1S_K_A-ND-IM-PA_C_T _OF_E_P_ID-EM-IC_A_N_D_PA_N_D_EM-IC-IN-FL-UE_N_ZA--
APPENDIX TO JAMES CASCIANO DECLARATION-449

165 Sato T, Akita T, Tanaka J. Evaluation of strategies for control and prevention of pandemic influenza (Hl Nl pdm) in Japanese children attending school in a rural town. Simulation using mathematical models. Nihon Koshu Eisei Zasshi. 2013;60(4):204-11.
166 Hens N, Calatayud L, Kurkela S, Tamme T, Wallinga J. Robust reconstruction and analysis ofoutbreak data: influenza A(Hl Nl)v transmission in a school-based population. Am J Epidemiol. 2012;176(3):196-203.
167 Russell ES, Zheteyeva Y, Gao H, Shi J, Rainey JJ, Thoroughman D et al. Reactive school closure during increased influenza-like illness (Ill) activity in western Kentucky, 2013: A field evaluation of effect on iii incidence and economic and social consequences for families. Open Forum Infect Dis. 2016;3(3):ofwl 13.
168 Sugisaki K, Seki N, Tanabe N, Saito R, Sasaki A, Sasaki S et al. Effective school actions for mitigating seasonal influenza outbreaks in Niigata, Japan. PLoS One. 2013;8(9):e74716.
169 Chen T, Huang Y, Liu R, Xie Z, Chen S, Hu G. Evaluating the effects of common control measures for influenza A (Hl Nl) outbreak at school in China: a modeling study. PLoS One. 2017;12(5):e0l 77672.
170 Chen T, Zhao B, Liu R, Zhang X, Xie Z, Chen S. Simulation of key interventions for seasonal influenza outbreak control at school in Changsha, China. J Int Med Res. 2018:300060518764268.
171 Cauchemez S, Valleron AJ, Boelle PY, Flahault A, Ferguson NM. Estimating the impact of school closure on influenza transmission from sentinel data. Nature. 2008;452(7188):750-4.
172 Birrell PJ, Ketsetzis G, Gay NJ, Cooper BS, Presanis AM, Harris RJ et al. Bayesian modeling to unmask and predict influenza A/Hl Nl pdm dynamics in London. Proc Natl Acad Sci USA. 2011;108(45):18238-43.
173 Chowen G, Viboud C, Munayco CV, Gomez J, Simonsen L, Miller MA et al. Spatial and temporal characteristics of the 2009 A/H 1 N 1 influenza pandemic in Peru. PloS One. 2011;6(6):e21287.
174 Wheeler CC, Erhart LM, Jehn ML Effect of school closure on the incidence of influenza among school-age children in Arizona. Public Health Rep. 2010;125(6):851-9.
175 Rodriguez CV, Rietberg K, Baer A, Kwan-Gett T, Duch in J. Association between school closure and subsequent absenteeism during a seasonal influenza epidemic. Epidemiology. 2009;20(6):787-92.
176 Ali ST, Kadi AS, Ferguson NM. Transmission dynamics of the 2009 influenza A (H 1 N 1) pandemic in India: the impact of holiday-related school closure. Epidemics. 2013;5(4):157-63.
177 Chowen G, Towers S, Viboud C, Fuentes R, Sotomayor V. Rates of influenza-like illness and winter school breaks, Chile, 2004-2010. Emerg Infect Dis. 2014;20(7):1203-7.
178 Chu Y, Wu Z, Ji J, Sun J, Sun X, Qin G et al. Effects of school breaks on influenza-like illness incidence in a temperate Chinese region: an ecological study from 2008 to 2015. BMJ Open. 2017;7(3):e0l 3159.
179 Eames KT, Tilston NL, Brooks-Pollock E, Edmunds WJ. Measured dynamic social contact patterns explain the spread of H 1 N 1 v influenza. PloS Com put Biol. 2012;8{3):e 1002425.
180 Earn DJ, He D, Loeb MB, Fonseca K, Lee BE, Dushoff J. Effects of school closure on incidence of pandemic influenza in Alberta, Canada. Ann Intern Med. 2012;156(3):173-81.
181 Ewing A, Lee EC, Viboud C, Bansal S. Contact, travel, and transmission: the impact of winter holidays on influenza dynamics in the United States. J Infect Dis. 2017;215(5):732-9.
182 Garza RC, Basurto-Davila R, Ortega-Sanchez IR, Carlino LO, Meltzer Ml, Albalak R et al. Effect of winter school breaks on influenza-like illness, Argentina, 2005-2008. Emerg Infect Dis. 2013;19(6):938-44.
-W-OR-LD-H-EA-LT_H_OR-G-AN-IZ-AT-IO_N __________________________ CD
APPENDIX TO JAMES CASCIANO DECLARATION-450

183 Luca G, Kerckhove KV, Coletti P, Poletto C, Bossuyt N, Hens N et al. The impact of regular school closure on seasonal influenza epidemics: a data-driven spatial transmission model for Belgium. BMC Infect Dis. 2018;18(1 ):29.
184 Te Beest DE, Birrell PJ, Wallinga J, De Angelis D, van Boven M. Joint modelling of serological and hospitalization data reveals that high levels of pre-existing immunity and school holidays shaped the influenza A pandemic of 2009 in the Netherlands. J R Soc Interface. 2015;12(103).
185 Yu H, Cauchemez S, Donnelly CA, Zhou L, Feng L, Xiang N et al. Transmission dynamics, border entry screening, and school holidays during the 2009 influenza A (Hl Nl) pandemic, China. Emerg Infect Dis. 2012;18(5):758-66 (https://www.ncbi.nlm.nih.gov/ pubmed/22515989. accessed 26 June 2019).
186 Shi J, Njai R, Wells E, Collins J, Wilkins M, Dooyema C et al. Knowledge, attitudes, and practices of nonpharmaceutical interventions following school dismissals during the 2009 Influenza A H1 N1 pandemic in Michigan, United States. PloS One. 2014;9(4):e94290-e (https://www. ncbi.nlm.nih.gov/pubmed/24747300, accessed 26 June 2019).
187 Berkman BE. Mitigating pandemic influenza: the ethics of implementing a school closure policy. J Public Health Manag Pract. 2008;14(4):372-8.
188 Jarquin VG, Callahan DB, Cohen NJ, Balaban V, Wang R, Beato R et al. Effect of school closure from pandemic CH1 N1) 2009, Chicago, Illinois, USA. Emerg Infect Dis. 2011;17(4):751-3 (https://www.ncbi.nlm.nih.gov/pubmed/21470482. accessed 26June 2019).
189 Pasquini-Descamps H, BrenderN, Maradan D. Value for money in Hl Nl influenza: A systematic review of the cost-effectiveness of pandemic interventions. Value Health. 2017;20(6):819-27 (https:/ /www.sciencedirect.com/science/article/pii/S 1098301516304922. accessed 26 June 2019).
190 Lempel H, Epstein JM, Hammond RA. Economic cost and health care workforce effects of school closures in the U.S. PloS Curr. 2009;1:RRN1051-RRN (https://www.ncbi.nlm.nih.gov/ pubmed/20025205. accessed 26 June 2019).
191 Brown ST, Tai JH, Bailey RR, Cooley PC, Wheaton WD, Potter MA et al. Would school closure for the 2009 Hl Nl influenza epidemic have been worth the cost?: a computational simulation of Pennsylvania. BMC Public Health. 2011 ;11 :353.
192 Sander B, Nizam A, Garrison LP, Jr., Postma MJ, Halloran ME, Longini IM, Jr. Economic evaluation of influenza pandemic mitigation strategies in the United States using a stochastic microsimulation transmission model. Value Health. 2009;12(2):226-33 (https:llwww.ncbi.nlm.nih.gov/pubmed/18671770. accessed 26 June 2019).
193 Parental attitudes and experiences during school dismissals related to 2009 influenza A (Hl Nl) - United States, 2009. MMWR Morb Mortal Wkly Rep. 2010;59(35):1131-4.
194 Cauchemez S, Van Kerkhove MD, Archer BN, Cetron M, Cowling BJ, Grove P et al. School closures during the 2009 influenza pandemic: national and local experiences. BMC Infect Dis. 2014;14(1):207 (https://doi.org/10.1186/1471-2334-14-207, accessed 26June 2019).
195 Klaiman T, Kraemer JD, Stoto MA. Variability in school closure decisions in response to 2009 H 1 N 1: a qualitative systems improvement analysis. BMC Public Health. 2011 ;11 (1 ):73 (https:/ /doi.org/10.1186/1471-2458-11-73. accessed 26 June 2019).
196 Chen WC, Huang AS, Chuang JH, Chiu CC, Kuo HS. Social and economic impact of school closure resulting from pandemic influenza NHl Nl. J Infect. 2011;62(3):200-3.
197 Horney JA, Moore Z, Davis M, MacDonald PDM. Intent to receive pandemic influenza A (Hl Nl) vaccine, compliance with social distancing and sources of information in NC, 2009. PLoS One. 2010;5(6):e 11226 (https:/ /doi.org/10.13 71 /jou rnal.pone.0011226, accessed 26 June2019).
m NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-451
198 Stern AM, Cetron MS, Markel H. Closing the schools: lessons from the 1918-19 U.S. influenza pandemic. Health Aff (Millwood). 2009;28{6):wl 066-78.
199 Zhang T, Fu X, Ma S, Xiao G, Wong L, Kwoh CK et al. Evaluating temporal factors in combined interventions of workforce shift and school closure for mitigating the spread of influenza. PLoS One. 2012;7{3):e32203 (https://doi.org/10.1371 /journal.pone.0032203, accessed 26 June2019).
200 Ahmed F, Zviedrite N, Uzicanin A. Effectiveness of workplace social distancing measures in reducing influenza transmission: a systematic review. BMC Public Health. 2018;18(1):518 (https:/ /doi.org/10.1186/s 12889-018-5446-1, accessed 26 June 2019).
201 Asfaw A, Rosa R, Pana-Cryan R. Potential economic benefits of paid sick leave in reducing absenteeism related to the spread of influenza-like illness. J Occup Environ Med. 2017;59(9):822-9.
202 Piper K, Youk A, James AE, Ill, Kumar S. Paid sick days and stay-at-home behavior for influenza. PLoS One. 2017;12{2):e0l 70698 {https://doi.org/10.1371/journal.pone.0170698, accessed 26 June2019).
203 Carrat F, Luong J, Lao H, Salle A-V, Lajaunie C, Wackernagel H. A 'small-world-like' model for comparing interventions aimed at preventing and controlling influenza pandemics. BMC Medicine. 2006;4{1 ):26 (https:/ /doi.org/10.1186/17 41-7015-4-26, accessed 26 June 2019).
204 Ciofi degli Atti ML, Merler S, Rizzo C, Ajelli M, Massari M, Manfredi Pet al. Mitigation measures for pandemic influenza in Italy: Aan individual based model considering different scenarios. PLoS One. 2008;3(3):el 790 {https:/ /doi.org/10.1371 /journal.pone.ODO 1790. accessed 26 June 2019).
205 Xia H, Nagaraj K, Chen J, Marathe MV. Synthesis of a high resolution social contact network for Delhi with application to pandemic planning. Artif lntell Med. 2015;65(2):113-30.
206 Mao L. Evaluating the combined effectiveness of influenza control strategies and human preventive behavior. PLoS One. 2011;6(10):e24706.
207 Bults M, Beaujean DJ, de Zwart O, Kok G, van Empelen P, van Steenbergen JE et al. Perceived risk, anxiety, and behavioural responses of the general public during the early phase of the Influenza A (Hl Nl) pandemic in the Netherlands: results of three consecutive online surveys. BMC Public Health. 2011;11:2-{https://www.ncbi.nlm.nih.gov/pubmed/21199571. accessed 26 June 2019).
208 Kiviniemi MT, Ram PK, Kozlowski LT, Smith KM. Perceptions of and willingness to engage in public health precautions to prevent 2009 Hl Nl influenza transmission. BMC Public Health. 2011;11(1):152 {https://doi.org/10.1186/1471-2458-11-152. accessed 26 June 2019).
209 Baum NM, Jacobson PD, Goold SD. nlisten to the peoplen: public deliberation about social distancing measures in a pandemic. Am J Bioeth. 2009;9( 11 ):4-14.
21 0 Institute of Medicine Forum on Microbial Threats. The National Academies Collection: reports funded by National Institutes of Health, Ethical and legal considerations in mitigating pandemic disease: workshop summary, Washington (DC), National Academies Press (US) National Academy of Sciences. 2007.
211 Halder N, Kelso JK, Milne GJ. Cost-effective strategies for mitigating a future influenza pandemic with Hl Nl 2009 characteristics. PLoS One. 2011 ;6(7):e22087 (https:lldoi.org/10.1371/journal.pone.0022087. accessed 26 June 2019).
212 Staff M, Torres Ml. An influenza outbreak among pilgrims sleeping at a school without purpose built overnight accommodation facilities. Commun Dis lntell Q Rep. 2011;35(1):10-5.
213 Hickey J, Gagnon AJ, Jitthai N. Pandemic preparedness: perceptions of vulnerable migrants in Thailand towards WHO-recommended non-pharmaceutical interventions: a cross-sectional study. BMC Public Health. 2014;14(1):665 (https://doi.org/10.1186/1471-2458-14-665. accessed 26 June 2019).
________________ r;r, WORLD HEALTH ORGANIZATION ~
APPENDIX TO JAMES CASCIANO DECLARATION-452

214 lshola DA, Phin N. Could influenza transmission be reduced by restricting mass gatherings? Towards an evidence-based policy framework. J Epidemiol Glob Health. 2011 ;1 (1 ):33-60.
215 SteelFisher GK, Blendon RJ, Ward JRM, Rapoport R, Kahn EB, Kohl KS. Public response to the 2009 influenza A Hl Nl pandemic: a polling study in five countries. Lancet Infect Dis. 2012;12(11):845-50 (https://doi.org/10.1016/S 1473-3099(12)70206-2. accessed 26 June 2019).
216 World Health Organization (WHO). WHO consultation on suspension of classes and restriction of mass gatherings to mitigate the impact of epidemics caused by the new influenza A (H 1 N 1 ). Geneva: WHO; 2009 (https://www.who.int/ csr /resou rces/pu bl ications/ swineflu/who consultation 20090624 en.pdf?ua= 1. accessed 26 June 2019).
217 Government of Canada. Travel advice and advisories [website]. 2019 (https://travel.gc.ca/travelling/advisories. accessed 16 January 2018).
218 Goeijenbier M, van Genderen P, Ward BJ, Wilder-Smith A, Steffen R, Osterhaus AD. Travellers and influenza: Risks and prevention. J Travel Med. 2017;24(1 )(https://www.ncbi.nlm.nih.gov/ pubmed/28077609. accessed 26 June 2019).
219 World Health Organization (WHO). Ethical considerations in developing a public health response to pandemic influenza. Geneva: WHO; 2007 (https://www.who.int/csr/resources/ publications/WHO CDS EPR GIP 2007 2/en/. accessed 26 June 2019).
220 Caley P, Becker NG, Philp DJ. The waiting time for inter-country spread of pandemic influenza. PLoS One. 2007;2(1):e143 (https://www.ncbi.nlm.nih.gov/pubmed/17206278, accessed 26 June 2019).
221 Cowling BJ, Lau LL, Wu P, Wong HW, Fang VJ. Riley Set al. Entry screening to delay local transmission of 2009 pandemic influenza A (Hl Nl ). BMC Infect Dis. 2010;10:82 (https://www.ncbi.nlm.nih.gov/pubmed/20353566. accessed 26 June 2019).
222 Malone JD, Brigantic R, Muller GA, Gadgil A, Delp W, McMahon BH et al. U.S. airport entry screening in response to pandemic influenza: Modeling and analysis. Travel Med Infect Dis. 2009;7(4):181-91 (https://www.ncbi.nl m.n ih.gov /pu bmed/19717097. accessed 26 June 2019).
223 Chen J, Yang K, Zhang M, Shen C, Chen J, Wang G et al. Rapid identification of imported influenza viruses at Xiamen International Airport via an active surveillance program. Clin Microbiol Infect. 2018;24(3):289-94 (https://www.ncbi.nlm.nih.gov/pubmed/28587905. accessed 26 June 2019).
224 Nishiura H, Kamiya K. Fever screening during the influenza CH 1 N 1-2009) pandemic at Narita International Airport, Japan. BMC Infect Dis. 2011;11:111 (https://www.ncbi.nlm.nih.gov/ pubmed/21539735. accessed 26 June 2019).
225 Priest PC, Duncan AR, Jennings LC, Baker MG. Thermal image scanning for influenza border screening: Results of an airport screening study. PLoS One. 2011;6(1):e14490 (https://www.ncbi.nlm.nih.gov/pubmed/21245928. accessed 26 June 2019).
226 Hale MJ, Hoskins RS, Baker MG. Screening for influenza ACH 1 N 1 )pdm09, Auckland International Airport, New Zealand. Emerg Infect Dis. 2012;18(5):866-8 (https://www.ncbi.nlm.nih.gov/pubmed/225161 OS, accessed 26 June 2019).
227 Sakaguchi H, Tsunoda M, Wada K, Ohta H, Kawashima M, Yoshino Yet al. Assessment of border control measures and community containment measures used in Japan during the early stages of Pandemic CH 1 N 1) 2009. PLoS One. 2012;7(2):e31289 (https://www.ncbi.n Im. nih.gov/pubmed/22355354, accessed 26 June 2019).
228 Priest PC, Jennings LC, Duncan AR, Brunton CR, Baker MG. Effectiveness of border screening for detecting influenza in arriving airline travelers. Am J Public Health. 2013;103(8):1412-8 (https://www.ncbi.nlm.nih.gov/pubmed/23237174. accessed 26 June 2019).
[IJ NON-PHARMACEUTICAL PUBLIC HEALTH MEASURES FOR MITIGATING THE RISK AND IMPACT OF EPIDEMIC AND PANDEMIC INFLUENZA
APPENDIX TO JAMES CASCIANO DECLARATION-453

229 Read JM, Diggle PJ, Chirombo J, Solomon T, Baylis M. Effectiveness of screening for Ebola at airports. Lancet. 2015;385(9962):23-4 (https://www.ncbi.n I m.n i h.gov /pu bmed/2546 7590. accessed 26 June 2019).
230 Gostic KM, Kucharski AJ, Lloyd-Smith JO. Effectiveness of traveller screening for emerging pathogens is shaped by epidemiology and natural history of infection. Elife. 2015;4 (https://www.ncbi.nlm.nih.gov/pubmed/25695520. accessed 26 June 2019).
231 Brownstein JS, Wolfe CJ. Mandi KO. Empirical evidence for the effect of airline travel on inter-regional influenza spread in the United States. PloS Med. 2006;3(1 0):e401 (https://www.ncbi.nlm.nih.gov/pubmed/169681 15. accessed 26 June 2019).
232 Wood JG, Zamani N, MacIntyre CR, Beckert NG. Effects of internal border control on spread of pandemic influenza. Emerg Infect Dis. 2007;13(7):1038-45 (https://www.ncbi.nlm.nih.gov/ pubmed/18214176. accessed 26 June 2019).
233 Germann TC, Kadau K, Longini IM. Jr., Macken CA. Mitigation strategies for pandemic influenza in the United States. Proc Natl Acad Sci USA. 2006;103(15):5935-40 (https://www.ncbi.nlm.nih.gov/pubmed/16585506, accessed 26 June 2019).
234 Lam EH, Cowling BJ, Cook AR, Wong JV, Lau MS, Nishiura H. The feasibility of age-specific travel restrictions during influenza pandemics. Theor Biol Med Model. 2011 ;8:44 (https://www.ncbi.nlm.nih.gov/pubmed/22078655, accessed 26 June 2019).
235 Chong KC, Ying Zee BC. Modeling the impact of air, sea. and land travel restrictions supplemented by other interventions on the emergence of a new influenza pandemic virus. BMC Infect Dis. 2012;12:309(https://www.ncbi.nlm.nih.gov/pubmed/23157818. accessed 26 June 2019).
236 Epstein JM. Goedecke OM, Yu F, Morris RJ, Wagener DK. Bobashev GV. Controlling pandemic flu: the value of international air travel restrictions. PloS One. 2007;2(5):e401 (https:/ /www. ncbi.nlm.nih.gov/pubmed/17476323. accessed 26 June 2019).
237 Cooper BS, Pitman RJ, Edmunds WJ, Gay NJ. Delaying the international spread of pandemic influenza. PloS Med. 2006;3(6):e212 (https://www.ncbi.nlm.nih.gov/pubmed/16640458. accessed 26 June 2019).
238 Hollingsworth TD, Ferguson NM, Anderson RM. Will travel restrictions control the international spread of pandemic influenza? Nat Med. 2006;12(5):497-9 (https://www.ncbi. nlm.nih.gov/pubmed/16675989. accessed 26 June 2019).
239 Eichner M, Schwehm M. Wilson N, Baker MG. Small islands and pandemic influenza: potential benefits and limitations of travel volume reduction as a border control measure. BMC Infect Dis. 2009;9:160 (https://www.ncbi.nlm.nih.gov/pubmed/19788751. accessed 26 June 2019).
240 Bajardi P, Poletto C, Ramasco JJ. Tizzoni M, Colizza V, Vespignani A. Human mobility networks, travel restrictions, and the global spread of 2009 H1 N1 pandemic. PLoS One. 2011 ;6(1 ):el 6591 (https://www.ncbi.nlm.nih.gov/pubmed/21304943. accessed 26 June 2019).
241 World Health Organization (WHO). Guidance for managing ethical issues in infectious disease outbreaks. Geneva: WHO; 2016 (https://www.who.int/blueprint/what/researchdevelopment/guidance for managing ethical issues.pdf?ua=1. accessed 26 June 2019).
-W-OR-LD-H-EA-LT_H_O_RG-AN-IZ-AT-IO_N ___________________________ rn
APPENDIX TO JAMES CASCIANO DECLARATION-454





























