Embed Size (px)
Citation preview
Atypical adenomatous hyperplasia of lung:its incidence and analysis of clinical,glycohistochemical and structural featuresincluding newly defined growth regulators andvascularization
Klaus Kaysera,*, Johnson Obiefune Nwoyea, Zdravko Kosjerinab,Thorsten Goldmannc, Ekkehard Vollmerc, Herbert Kaltnerd,Sabine Andred, Hans-Joachim Gabiusd
a UICC-TPCC, Institute of Pathology, Charite, Humboldt University, Schumannstr. 20-23, D-10117 Berlin,Germanyb Institute of Pathology, University Novi Sad, Novi Sad, Serbia, Yugoslaviac Institute of Pathology, Forschungszentrum Borstel, Borstel, Germanyd Institute of Physiological Chemistry, Faculty of Veterinary Medicine, Ludwig-Maximilians-University,Munich, Germany
Received 3 February 2003; received in revised form 15 May 2003; accepted 19 May 2003
KEYWORDS
Atypical adenomatous
hyperplasia;
Frequency;
Syntactic structure
analysis;
Lectin;
Vascularization
Summary Background: Adenomatous hyperplasia of the peripheral lung has beensuggested to be a preneoplastic lesion leading to peripherally localized lungcarcinomas. The paucity of data about cellular and vascular characteristics of thislesion in comparison to normal lung prompted this investigation. Material andmethods : We describe results of two investigations comprising 75 cases and 70 cases,respectively, with atypical adenomatous hyperplasia (AAH) of the lung, respectively:(a) a prospective study part with thorough analysis of surgical lung specimens (lobesand lungs) for light microscopical detection of the lesion; and (b) a retrospectivestudy part with immuno- and lectin histochemical analysis of AAH and non-neoplasticlung parenchyma monitoring expression of growth-related markers and changes invascularization patterns. Sections of the individual cases were examined by an image-analyzing system including automated measurement of staining intensities andstructure analysis. Results : The prospective study part revealed an incidence ofAAH in 2/31 cases with squamous cell carcinoma and in 5/32 cases with adenocarci-nomas. No relation to pT- or pN stages was detectable, high grade AAHs were seen tobe close to the tumor lesions (B/2 cm distance) and those with low grade at greaterdistances. Statistically significantly increased levels of expression of anti-apoptoticbcl-2, macrophage migration inhibitory factor (MIF) capable to suppress p53activities, heparin-binding lectin, interleukin-2, galectin-1 and of binding sites for
*Corresponding author. Tel.: �/49-6221-41-3827; fax: �/49-6221-45-1570.E-mail address: [email protected] (K. Kayser).
Lung Cancer (2003) 42, 171�/182
www.elsevier.com/locate/lungcan
0169-5002/03/$ - see front matter – 2003 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/S0169-5002(03)00289-7
the endogenous lectins galectins-1, -3 and -7 were determined. In addition, alveolar-lining cells, which express these markers, formed spatial clusters, which harbordifferent levels of structural entropy. AAH displayed an increased level of vascular-ization characterized by regular size and increased number of newly formed vessels.Interpretation : The prospective and retrospective study parts point to a closeassociation of AAH with peripherally localized adenocarcinoma of the lung. AAH ischaracterized by pronounced alteration of expression of several growth-relatedmarkers and probably non-reversible changes in vascularization.– 2003 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
The status of knowledge on development ofphenotypic features of centrally localized bron-chial carcinomas has matured over the last dec-ades. Originating from major bronchi, thesecarcinoma types appear to follow a distinct se-quence of events starting with hyperplasia with orwithout squamous cell metaplasia and variousdegrees of cellular atypia, finally reaching thestatus of a carcinoma in situ with further malignantspread [1,2]. This concept can explain the highfrequency of centrally localized squamous, largecell, and small cell carcinomas. As epidemiologicand hospital-based studies indicate, there is acurrent shift in tumor incidence. The constant oreven declining incidence of centrally localized(squamous cell) carcinomas is counterbalanced byan increasing incidence of (often peripherallylocalized) adenocarcinomas prompting the ques-tion on the analysis of peripherally localized pre-cancerous lesions [3]. One of the candidatespotentially figuring as a precursor of adenocarci-nomas is the so-called atypical adenomatous hy-perplasia (AAH). As defined by the WHO, it is afocal lesion, in which the involved alveoli andrespiratory bronchi are lined by monotonous,slightly atypical cuboidal to low columnar epithe-lial cells with dense nuclear chromatin. This lesionof the peripheral lung, which can already bedetected by high-resolution CT-techniques [4],has striking similarities with well-differentiatedadenocarcinomas of the bronchiolo-alveolar typeand is characterized as follows:
a) It is a focal lesion measuring about 5 mm inmaximum diameter.
b) It possesses well-defined boundaries.c) It displays atypical bronchioloalveolar cuboidal
cells, which proliferate along the inter-alveolarsepta.
d) The inter-alveolar septa are slightly thickened.e) Atypical cells of AAH exhibit different degrees
of nuclear atypia (commonly graded 1�/3).
f) Bronchiolar metaplasia may be present.g) The lesions are often observed at the boundary
of adenocarcinomas of the lung [5,6].
The frequency of these lesions has been reportedto range from 5 to 25% in resected lung specimens[7�/9]. Cytometric studies supported by profiling ofgrowth-related markers showed that AAH is oftencharacterized by non-diploid cellular proliferationwhich can even be of monoclonal origin [10,11].Prompted by the initial glycohistochemical ana-lyses delineating the correlation of histoblood-group-epitope binding and survival in lung cancera down-regulation of this parameter indicated thatthe system of protein (lectin)�/carbohydrate inter-actions could also be perturbed in preneoplasia[12,13]. Given the assumed significance of thehyperplasia for carcinoma development, we nowreport the findings of a prospective study under-taken to contribute further data to assessment offrequency and association with the main lesion ofsurgical lung specimens (lungs and lobes), and thenof a retrospective analysis to evaluate the expres-sion and binding capacities of a panel of immuno/glycohistochemical markers with emphasis on en-dogenous lectins. In detail, the markers wereselected to offer an insight into the relationshipof AAH to changes in immune factors with rele-vance of p53-dependent growth regulation (macro-phage migration inhibitory factor (MIF),interleukin-2 (IL-2)), in the expression of endogen-ous lectins with relevance for growth control andcell adhesion/migration (galectin-1 (Gal-1), galec-tin-3 (Gal-3), galectin-7 (Gal-7), heparin-bindinglectin (HBL)), in the arrangement of vasculariza-tion (CD34), in proliferation (Ki-67 (MIB-1)) and inexpression of an apoptosis-associated protein (bcl-2). We also measured the structuralarrangements of alveolar lining cells inrelation to expression/abundance of binding sitesof applied substances in search for a detailedevaluation of AAH in comparison to normal lungparenchyma.
172 K. Kayser et al.
2. Material and methods
2.1. Patients
This study comprises the results of two differentinvestigations on atypical alveolar hyperplasia(AAH), namely a prospective study (I) on 75surgical specimens (lobes and lungs containingmalignant or benign lesions) with detailed macro-scopic evaluation of the lesion-free lung parench-yma and a retrospective study with assessment ofclinical data (including survival of patients) focus-ing on characterization of cellular features. Aero-genous intrapulmonary spread of adenocarcinomawas carefully excluded by thorough application ofdefinition of AAH, as defined by the WHO. Con-tiguous lesions with the edge of a carcinoma wereonly considered as AAH if they displayed a stillrecognizable individual lesion, and, in addition,characteristic nuclear and cellular features, whichcould unambiguous be differentiated from those ofthe carcinoma cells. The material has been col-lected from the files of the Institute of Pathology,Forschungszentrum Borstel, Borstel, Germany(study I) and of the Department of Pathology,Thoraxklinik, Heidelberg, Germany (study II). Thecharacteristics of the patients are given in Table 1.Male patients constituted the majority of thepatient group. The number of included patientsand the thorough analysis of the lung tissue allowedto test previous observations whether AAH is morefrequently seen in women than in men [14,15].
2.2. Tissue material, markers and stainingtechnique
The obtained surgical specimens were expandedby air inflation via the main bronchi and immedi-ately fixed with buffered formalin in both studies.The specimens of study I were cut in serial sectionsmeasuring 6 mm in thickness. The entire surfacewas thoroughly examined by visual inspection witha hand-held magnifying glass. A complete cross-section of the tumor in the section with themaximum tumor area was embedded as was alsodone for tissue regions suspicious for AAH (yellow-ish-white tissue parts mimicking fibrosis). In addi-tion, a minimum of four tissue pieces was takeneach at a distance 20, 40, 60, and 80 mm,measured from the tumor boundary. The minimumnumber of blocks per case obtained from theperipheral lung (not including the main lesion)was 16. The tissue blocks were embedded inparaffin, the histological sections were stainedwith hematoxilin/eosin, carefully examined micro-scopically, and their profiles documented by use ofa digital camera (Nikon Coolpix 95). The diagnosisof AAH was independently reached by three ob-servers (EV, KK, SK) and based upon the followingcriteria:
a) Circumscribed, well-defined lesion with atypi-cal alveolar lining cells arranged in a ‘chain-like’ structure along the inter-alveolar septula.
b) Hyperplasia of these cells with various degreesof nuclear atypia.
Table 1 Synopsis of material
Feature Study I (no AAH) Study I (with AAH) Study I total Study II
Men 56 8 64 42Women 10 1 11 28Men (age; years) 619/9 659/11 629/9 639/11Women (age; years) 559/13 50 599/12 589/15
Tumor stagesLung carcinoma 58 8 66 46pT1 10 1 11 23pT2 28 7 35 14pT3/T4 20 0 20 9pN0 22 5 27 18pN1 18 3 21 15pN2/pN3 18 0 18 13
Cell typeSquamous 29 2 31 11Adeno 27 5 32 34Large cell 2 1 3 1Others/metastasis 2 0 2 14Benign/no tumor 6 1 7 10
Atypical adenomatous hyperplasia of lung 173

c) Thickened inter-alveolar septula with mild tomoderate mononuclear inflammatory infil-trates.
A characteristic micrograph of these lesions isshown in Fig. 1.
The 70 cases of study II were selected from thefiles of the Department of Pathology, Thoraxklinik,Heidelberg, Germany. Histological sections of thecorresponding blocks were immuno/glycohisto-chemically stained with the following commerciallyavailable markers: anti-bcl-2 (Dako, Hamburg,Germany), anti-Ki-67 (MIB1, Clone 7B11, ZymedLaboratories, San Francisco, USA), anti-thyroidtranscription factor-1 (TTF1, DAKO, Hamburg,Germany) and anti-interleukin-2 (IL-2, DAKO, Ham-burg, Germany). In addition, polyclonal antibodiesagainst macrophage migration inhibitory factor(MIF), calcyclin (CAL; S100A6), heparin-bindinglectin (HBL) and members of the galectin familyof endogenous lectins, i.e. galectins-1, -3 and -7,were used. The production of these markersincluding rigorous specificity controls to excludecross-reactivity to related proteins from a family,e.g. S100-related proteins and galectins, has beenreported previously [16�/21]. Moreover, to furtherprobe the expression profile of ligands for growth-regulatory mediators we also tested labeled galec-tins completing the study of expression of thelectins and their binding sites. The purification,labeling protocol and specificity controls havebeen described elsewhere [22]. The probes wereapplied to deparaffinated and rehydrated sections
according to protocols recommended by the man-ufacturers or optimized previously using the com-mon peroxidase�/antiperoxidase (PAP) the avidin�/
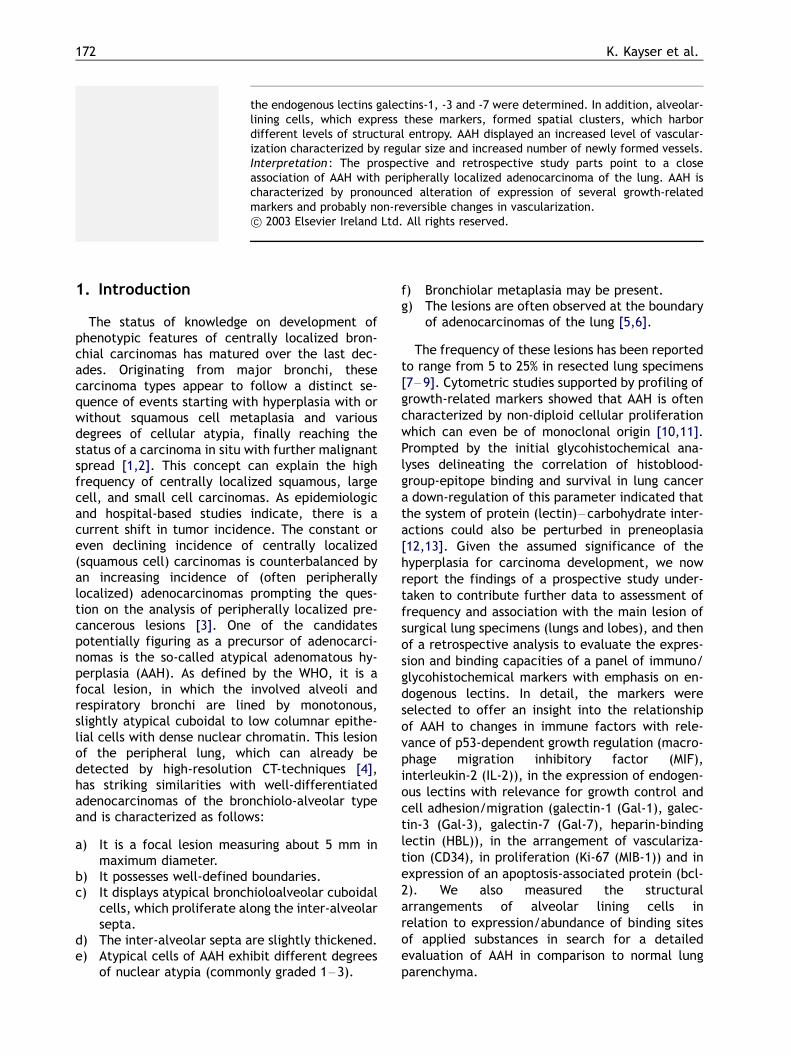
biotin (ABC) techniques with commercially ABC kitreagents (Camon, Wiesbaden, Germany). The la-beled galectins were applied at a concentration of20 mm/ml. Specific binding of probes was visua-lized by the chromogenic substrates diaminobenzi-dine/H2O2. Control experiments includedcompetitive inhibition with excess of free ligand/antigen and omission of the primary marker tovisualize marker-independent staining, e.g. bybinding of reagents to endogenous biotin or tomannose-binding sites. A characteristic result ofobtained staining is given in Fig. 2.
2.3. Image analysis and grading of stainingreactivity
All immuno/lectin histochemically stained slideswere subjected to a two-step semi-automated /automated image analysis as follows: the areas ofinterest (AAH and non-AAH lung parenchyma) wereinteractively selected from the tumor boundaryand digitized by a digital camera (Leica CD100)mounted on a Leica microscope (OrthoLux, objec-tive �/40, aperture 0.75) into a 512�/512 pixelmatrix. The images digitized in the red�/green�/
blue (rgb) color space were stored and subjectedto automated gray value normalization in order toobtain a fixed gray value threshold independentfrom the individual staining intensity and sectionthickness. For segmentation the (rgb)*/color
Fig. 1 Microphotograph of atypical alveolar hyperplasia: note the cuboidal alveolar lining cells with dense nuclearchromatin, and the moderate to severe atypia of the alveolar lining cells. HE, �/20.
174 K. Kayser et al.
space was then transformed into a singular gray-value space (sgv) by the principal componentanalysis, and for evaluating the immuno/ligandreaction color (brown) into the hue-saturation-intensity (hsi)*/color space. Based upon a fixedsegmentation threshold chosen according to thetechnique of Otsu a segmentation of the alveolarlining cells in the (sgv)*/space and their stainingintensity in the (hsi)*/color space was automati-cally performed by self-written programs basedupon a commercially available image analysissystem (DIAS, University of Jena, Jena, Germany).After segmentation, the staining intensity of thesegmented cells in the selected color space wasgraded into the following four levels: negative,weak, moderate, and strong. Cases harboring B/
10% of moderately to strongly stained cells weregrouped as negative, the others as positive. Aminimum of 300 cells and 50 vessels per case wasprocessed. The obtained images were subjected tostereological analysis (volume fraction, numericaldensity in case of MIB- and bcl-2-stained nuclei orCD34-stained vessels) as well as computationsbased upon syntactic structure analysis. The latterincludes the calculation of distances betweennearest neighboring cells, the formation of spatialclusters in terms of their average radius, the meannumber of included epithelial cells and the com-putation of the structural entropy E(MST) accord-ing to the equation:
E(MST)�c�X
fii=im)2�(di=dm)2g;
with the following abbreviations: E(MST), struc-tural entropy; ii, difference in staining intensity ofan individual cell and its nearest neighbor; im,
mean of difference of staining intensity of all cells;di, distance between the individual cell and itsnearest neighbor; dm, mean distance between allnearest neighboring cells.
The technical procedure and the theoretic back-ground were described in detail elsewhere [23�/
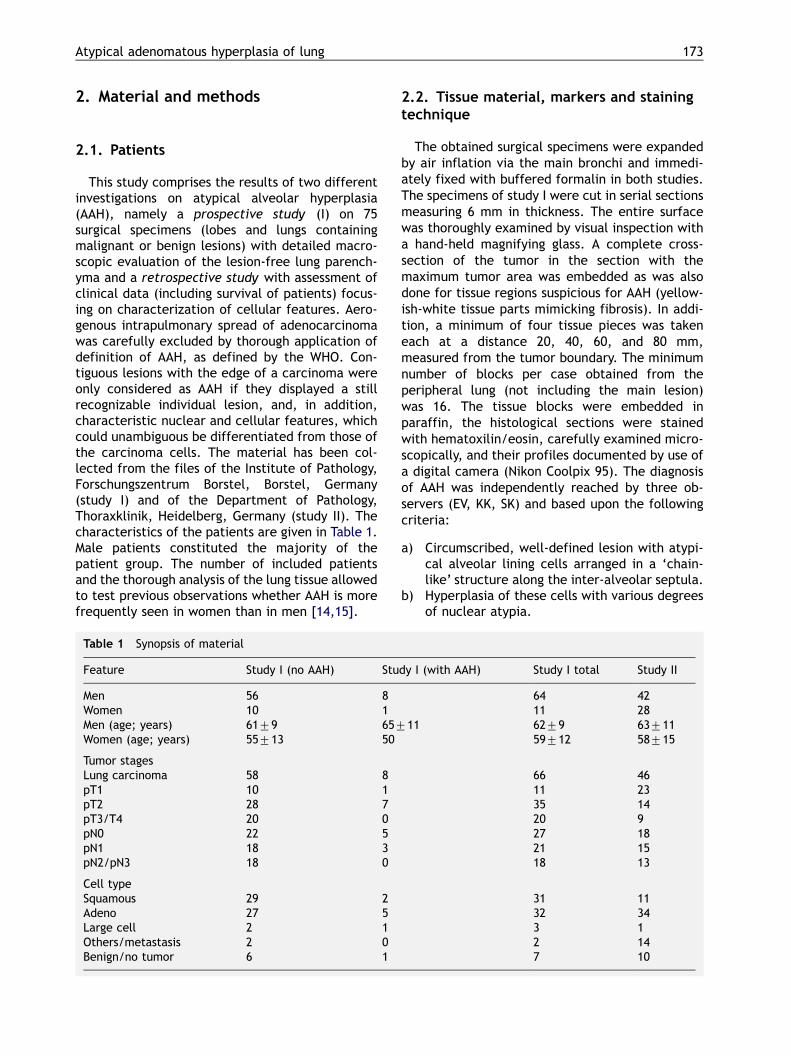
25]. A characteristic result of obtained distributionof structural entropy in AAH is shown in Fig. 3. Thestatistical analysis was performed with a commer-cially available program package (NumberCruncher Statistical System, NCSS, Kaysville,Utah, USA) and included x2 test, multivariatediscriminant analysis, factor analysis and K-meansclustering.
Fig. 2 Microphotograph of AAH, visualization of accessible sites for galectin-3, ABC, �/20.
Fig. 3 Distribution of E(MST) in AAH (GAL-1). Asindicated by the graph (lines) a still preserved lung tissuestructure can be seen; however, the irregularly stainingintensity combined with greater distances betweenneighbouring alveolar lining cells reflects to highE(MST) values, especially at the endpoints of the graph(dark or black disks).
Atypical adenomatous hyperplasia of lung 175
3. Results
The obtained frequency in AAH is shown in Table1. It was 12% in all cases and 15.6% in cases withadenocarcinoma. In our study, patients with AAHwere more likely men than women and slightlyolder compared to patients without detectableAAH. This gender distribution cannot be readilyreconciled with previous observations, which partlyreported a higher frequency of AAH in womencompared to men or an equal sex distribution[2,8,15]. The obvious close association of AAHwith adenocarcinomas (Table 1) is in agreementwith previous reports [15]. In the retrospectivestudy, only one singular AAH lesion per case, in theprospective study only one case with two lesionswas noted. All lesions were small, and measuredbetween 2 and 6 mm in maximum diameter.Regarding pT/pN-status of excised lung carcinomasno statistically significant correlation to AAH in-cidence was apparent (Table 1). The degree ofcellular atypia in AAH is closely associated with itsdistance from the tumor boundary (Table 2). Thepercentage of smokers and the inhaled amount ofcigarette smoke is similar for both genders (Table3) and, notably, comparable to the distributionseen in patients with lung carcinomas [26]. A non-negligible number of patients with AAH harbor anincreased amount of asbestos fibers in their lungspecimens, especially in men (Table 3). Followingthis addition of AAH incidence in relation to clinicalparameters and risk factors to the literature weproceeded to perform immuno- and lectin histo-chemistry. The applied set of probes revealedstatistically significant differences in staining in-tensities of AAH lesions compared to non-neoplas-tic lung parenchyma of the same patient (Table 4).In detail, the anti-apoptotic protein bcl-2 and MIF,which is capable to bypass the tumor suppressoractivity of p53, were detected in a higher percen-tage of AAH than normal lung parts of the patientsamples. The same tendency holds true for IL-2,the heparin-binding lectin, galectin-1 (but not
galectins-3 and -7), galectin-binding sites and theexpression of the proliferation marker. Followingthis evaluation we performed a detailed imageanalysis and processing of the resulting data toobtain measures of the distribution of cells and theinherent level of entropy of cell arrangement. Thecalculation of this parameter has been introducedto integrate marker expression in cells with theirtopological arrangement [24,25].
The respective data are presented in Table 5. Ingeneral, the calculated level of structural entropyis rather low compared to results obtained fromprimary and secondary lung malignancies, whichranges between 150 and 200 [26]. As illustrated inFig. 3, only limited area sections harbored markedaberrations in cellular arrangement visualized byblack coloring. The application of syntactic struc-ture analysis revealed a nearly preserved texture ofthe lung parenchyma, as indicated by the graph.However, there is an increased variation of dis-tances and staining intensities between neighbor-ing cells, which is shown by size and dark to blackcoloring of the disks. The bigger and darker thedisks, the greater are the obtained differences.The significantly increased numerical extent ofheterogeneity was reflected in staining for exam-ple for MIF presence, revealing a significant differ-ence between AAH and non-neoplasticparenchyma. Multivariate analysis, especially clus-ter analysis, afforded information on potentialcluster formation of structural features betweenthe applied probes and respective differencesbetween AAH and non-neoplastic lung. Thus, thisanalysis can assist to pinpoint additive/synergisticeffector pathways of tested markers. The results ofthe calculations are presented in Table 6, whichshows a network of obtained correlations betweenexpression/binding capacities of ligands and struc-tural features. For example, if the structuralentropy (staining heterogeneity) of Gal-7b in-creases, that of Gal-7, Gal-3 increases too, andonly that of Gal-1b and Gal-3b is not affected. Inmost of the clusters, the structural entropy andcluster radius of expression and binding capacitiesof galectin-1 and -3 were associated to each otherwith high correlation coefficients. The spatialheterogeneity of an AAH lesion can be obtainedby measuring the staining intensities of its epithe-lial cells. Cells with identical (strong) stainingintensity often form spatial clusters. The size ofthese cellular clusters assigned to different sub-stances was positively correlated to each other forthe majority of applied substances (Table 6). Forexample, the larger the cell cluster for bcl-2, thelarger were those for MIF, IL-2, HBL, Gal-1, Gal-3,Gal-1b, Gal-3b, with the exception of that for MIB-
Table 2 Distance of AAH from tumor boundary(study I)
Distance (cm) Number of cases
High grade Low grade
1�/3 3 �/
3�/5 2 �/
5�/7 2 �/
7�/9 �/ 1Mean distance 2.6 cm 7.1 cm
176 K. Kayser et al.
1, which is negatively correlated, i.e. decreases.These data intimate concerted spatial correlationsin situ, which also emerged in similar data on meandistance of neighboring cells and structural entropyE(MST) (Table 6).
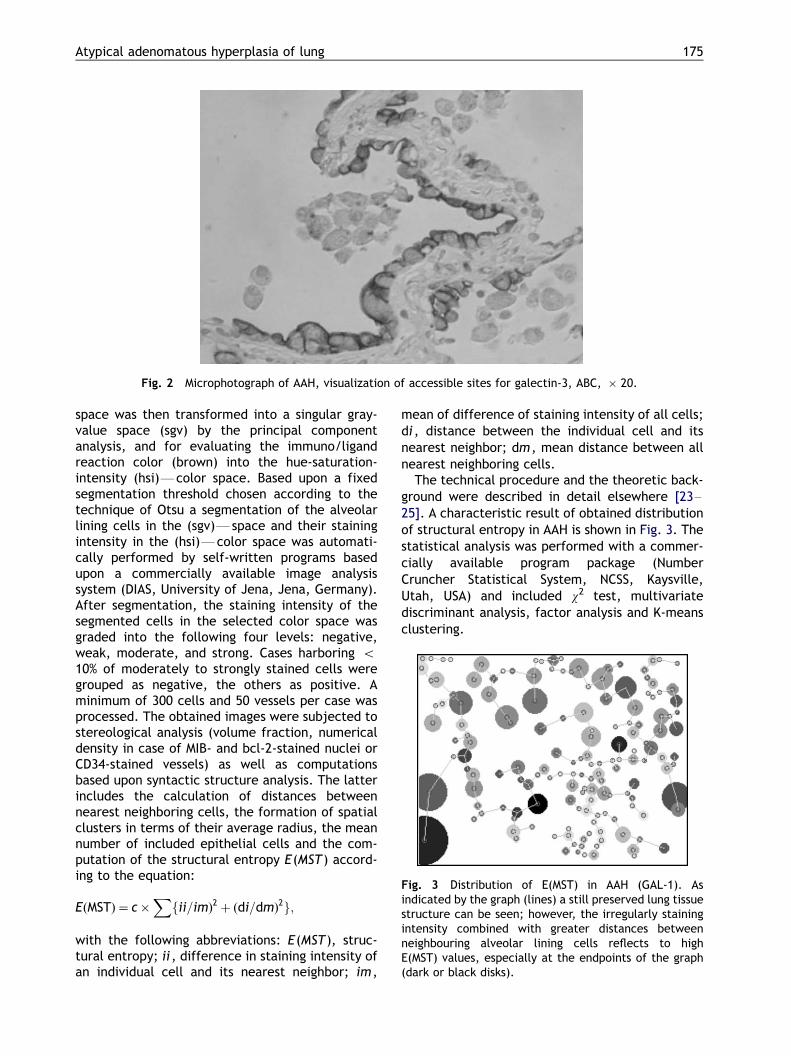
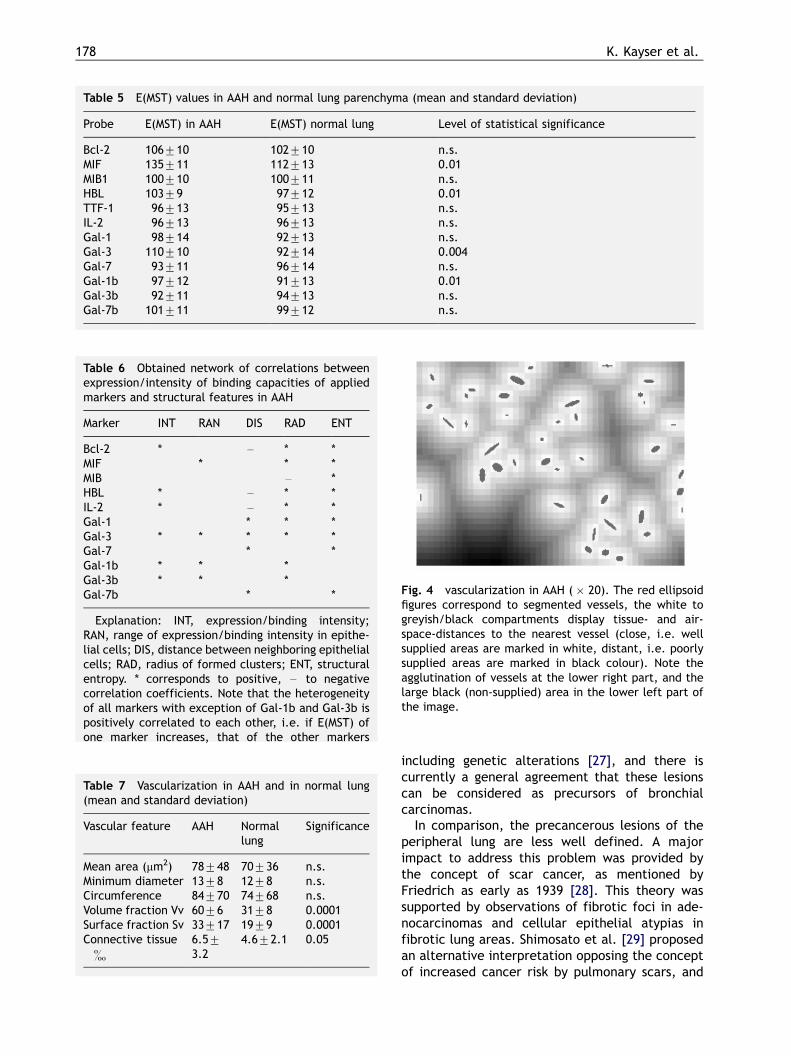
A further parameter of potential relevance forthe progression of the disease is vascularization.The determined parameters in vascularization ofAAH are quantitatively compiled in Table 7. Inter-estingly, parameters measured in absolute valuesof the vessels (minimum diameter, circumference,etc.) remained unchanged. In contrast, stereologi-cal features such as volume- and surface-fraction,were increased in AAH. As exemplarily shown inFig. 4, there was a focal density increase of smallvessels in AAH, as delineated by the measure-ments. These observations suggested that thenumber of vessels was increased in AAH, while
they maintained their size in both AAH and normallung parenchyma.
4. Discussion
4.1. Frequency and clinical data
Precancerous lesions of the lower respiratorytract exhibit changes of the phenotype, whichinclude alterations of the epithelium of the air-conducting and air-exchanging system. The altera-tions of the bronchial epithelium are characterizedby squamous metaplasia with various degrees ofnuclear and cellular atypia, finally progressing intoa carcinoma in situ [1,2]. Histochemical analysis ofcentrally localized lesions revealed aberrations ofthe expression profile of suppressor activities
Table 3 Clinical features and occupational/lifestyle risk factors of patients with AAH (study II, mean and standarddeviation)
Feature Men (N�/42) Women (N�/28) Total (N�/70)
Heart disease 18 10 28Diabetes mellitus 1 1 2COPD* 22 13 35Number of smokers (packyears) 28 (399/19) 14 (429/22) 42 (409/20)Asbestos burden (fibers/g wet tissue) 479/20 159/12 349/19Patients with asbestos�/threshold** 26 6 32Patients with toxic exposure 29 0 29
* COPD: chronic obstructive lung disease.** Threshold of asbestos burden: number of asbestos fibers/g wet tissue �/15 (f/g).
Table 4 Relative frequency of marker positivity in AAH and normal lung parenchyma
Probe Positivity in AAH(percent, N�/70)
Positivity in normal lung(percent, N�/70)
Level of statisticalsignificance
Bcl-2 71.4 35.7 0.0001MIF 67.1 40.0 0.004HBL 72.9 32.9 0.0001TTF-1 54.3 55.7 n.s.IL-2 81.4 45.7 0.0001Gal-1 64.3 22.9 0.00001Gal-3 55.7 50.0 n.s.Gal-7 34.3 37.1 n.s.Gal-1b 48.4 25.7 0.002Gal-3b 30.1 8.6 0.004Gal-7b 64.3 41.4 0.006MIB (Nv in %)* 4.59/2.9 2.39/1.2 0.05
* Mean and standard deviation.
Atypical adenomatous hyperplasia of lung 177
including genetic alterations [27], and there iscurrently a general agreement that these lesionscan be considered as precursors of bronchialcarcinomas.
In comparison, the precancerous lesions of theperipheral lung are less well defined. A majorimpact to address this problem was provided bythe concept of scar cancer, as mentioned byFriedrich as early as 1939 [28]. This theory wassupported by observations of fibrotic foci in ade-nocarcinomas and cellular epithelial atypias infibrotic lung areas. Shimosato et al. [29] proposedan alternative interpretation opposing the conceptof increased cancer risk by pulmonary scars, and
Table 5 E(MST) values in AAH and normal lung parenchyma (mean and standard deviation)
Probe E(MST) in AAH E(MST) normal lung Level of statistical significance
Bcl-2 1069/10 1029/10 n.s.MIF 1359/11 1129/13 0.01MIB1 1009/10 1009/11 n.s.HBL 1039/9 979/12 0.01TTF-1 969/13 959/13 n.s.IL-2 969/13 969/13 n.s.Gal-1 989/14 929/13 n.s.Gal-3 1109/10 929/14 0.004Gal-7 939/11 969/14 n.s.Gal-1b 979/12 919/13 0.01Gal-3b 929/11 949/13 n.s.Gal-7b 1019/11 999/12 n.s.
Table 6 Obtained network of correlations betweenexpression/intensity of binding capacities of appliedmarkers and structural features in AAH
Marker INT RAN DIS RAD ENT
Bcl-2 * �/ * *MIF * * *MIB �/ *HBL * �/ * *IL-2 * �/ * *Gal-1 * * *Gal-3 * * * * *Gal-7 * *Gal-1b * * *Gal-3b * * *Gal-7b * *
Explanation: INT, expression/binding intensity;RAN, range of expression/binding intensity in epithe-lial cells; DIS, distance between neighboring epithelialcells; RAD, radius of formed clusters; ENT, structuralentropy. * corresponds to positive, �/ to negativecorrelation coefficients. Note that the heterogeneityof all markers with exception of Gal-1b and Gal-3b ispositively correlated to each other, i.e. if E(MST) ofone marker increases, that of the other markers
Table 7 Vascularization in AAH and in normal lung(mean and standard deviation)
Vascular feature AAH Normallung
Significance
Mean area (mm2) 789/48 709/36 n.s.Minimum diameter 139/8 129/8 n.s.Circumference 849/70 749/68 n.s.Volume fraction Vv 609/6 319/8 0.0001Surface fraction Sv 339/17 199/9 0.0001Connective tissue�
6.59/
3.24.69/2.1 0.05
Fig. 4 vascularization in AAH (�/20). The red ellipsoidfigures correspond to segmented vessels, the white togreyish/black compartments display tissue- and air-space-distances to the nearest vessel (close, i.e. wellsupplied areas are marked in white, distant, i.e. poorlysupplied areas are marked in black colour). Note theagglutination of vessels at the lower right part, and thelarge black (non-supplied) area in the lower left part ofthe image.
178 K. Kayser et al.
assuming that fibrous tissue of adenocarcinomahad been originated by the malignancy itself.
Morphologically, a typical alveolar hyperplasiapresents characteristics, which justify the use ofthe term ‘preneoplasia’ [2,13,15]. In fact, cases ofAAH are often hard to distinguish from well-differentiated adenocarcinomas such as bronch-iolo-alveolar carcinomas: they contain hyperplasticalveolar lining cells with various degrees of cellularand nuclear atypia, they might be associated withgoblet cell metaplasia, and they are well circum-scribed and of small size [2,7,13,27]. Rigorousdefinition of their incidence is difficult, as thisassessment mainly depends on investigations withrather small sizes. To our knowledge, epidemiolo-gic studies on the incidence of AAH have not yetbeen published. Hospital-based reports on fre-quency of these lesions ranges from 1.2 to 23.2%[7,14,15,27,30]. Its occurrence was more fre-quently observed in surgical specimens with ade-nocarcinomas than in specimens resected due tonon-malignant lesions [7,15]. Our data are ingeneral agreement with the frequency describedin these reports: AAH lesions could be detected in9/75 resected lobes and lungs, and also in speci-mens with adenocarcinomas (15.6%), while theywere less often seen in lobes with squamous cellcarcinomas (6.5%). However, the gender distribu-tion was different questioning the impact of thisfactor on AAH development. No association of AAHwith tumor stage or lymph node involvement orextent of smoking could be delineated. Our data inthis respect are in complete agreement with thoseof the study of Nakahara et al. [7]. Interestingly,patients with AAH were significantly older thanthose without detectable AAH in our cohorts, afinding which lends support to the theory of aprecursor lesion. Multiple AAHs were*/again inagreement with the literature*/rare [31�/33] andobserved in only one case of our prospective study.
According to our clinical data, the majority ofpatients with AAH were heavy smokers with anaverage cigarette consumption of 40 packyears. Nodifferences in smoking habits could be observedbetween men and women at a statistically signifi-cant level, a finding concurrent with the literature[7,15,34]. In close association with extensivesmoking numerous patients developed a chronicobstructive lung disease (Table 3). In addition, theasbestos burden of lungs with AAH was high. Insum, importance of occupational and lifestyle riskfactors for disease development could be deli-neated from the patient’s data, arguing in favorof an assumed precursor relation. The morphologi-cal monitoring included the assessment of a further
parameter, i.e. the occurrence of AAH in relationto that of cancer, if present.
4.2. Cellular atypia of AAH
Most of the lesions were obtained in closevicinity of malignancy of the peripheral lung.Nearly all of these lesions displayed marked tosevere cellular and nuclear atypia, which is inaccordance with data a previous report [13]. Thelesion in our panel with only mild atypia wasdetected at a large distance from a contemporaryadenocarcinoma. Based on these data, there ap-pears to be an indication for a non-negligibleassociation between the distance of the lesionsfrom the primary malignancy of the lungs and thelevel of cellular atypia. No association with the sizeof the lesions and the distance or differentiationcould be delineated. The proposed separation ofAAH from bronchiolo-alveolar carcinoma by ab-sence of high cellularity, papillary structures ormeasuring the size of nuclei and of lesion (B/5 mmin maximum diameter) [35] cannot strictly berecommended by our data. Regarding correspond-ing data obtained from squamous cell metaplasiaand cellular atypias in relation to bronchial squa-mous cell carcinoma [1,2], however, our data setappears to be analogous.
4.3. Immuno/lectin histochemical stainingand syntactic structure analysis
Having thus completed the analysis of clinicaland morphological data, we selected a panel ofmarkers for immuno/lectin histochemical analysisto put the concept of AAH being a malignancyprecursor to a further test. Explicitly, it would thenbe likely that apoptosis markers in AAH are reducedand p53 functionality impaired.
In the first step, we set up the method for datacollection. To rely on a reproducible classificationof cases into positive or negative free of observer-dependent bias, an automated image analysismonitoring also grades of staining properties wasperformed. Cases with more than 90% of negativealveolar lining cells were classified as negative inboth AAH and non-neoplastic lung tissue. Thedetails of the procedure for syntactic structureanalysis which had been developed to routineapplication and applied to various lung tumorclasses are described elsewhere [18,20,23�/25].With this technique we observed a series ofdifferences between AAH and normal alveolarlining cells.
Atypical adenomatous hyperplasia of lung 179
As compiled in Table 4, the anti-apoptoticprotein bcl-2 showed an increased frequency inAAH compared to normal cases. An interestingenhancement of presence was also seen for MIF.Originally defined as lymphokine, this protein isnow known to be able to partially suppress p53-dependent growth-regulatory activities, therebyopening the way for sustained cell growth[36,37]. Its expression was found to be up-regu-lated in adenocarcinoma relative to bronchial andalveolar epithelium [38]. Intriguingly, MIF has alsobeen implied in promoting neo-vascularization instudies in vitro and in vivo [39]. The significant up-regulation in frequency of occurrence thus fits wellwith the tumor expression profile and a role enroute to tumor development. A general trend foran up-regulation also concerns binding sites for afamily of growth-regulatory/adhesion-mediatingendogenous lectins, i.e. galectins [40�/43]. Metho-dologically, the introduction of tissue lectins intohistochemical analysis advances the elucidation ofthe role of glycan/protein receptors, establishingan in situ information transfer system relative tothe common use of plant lectins [40]. The resultsclearly revealed that regulation for the differentfamily members in a cell, the inherent networkcomplexity having been recently mapped by RT-PCR analysis [44], was non-uniform and thatgalectin-1 expression is up-regulated. This lectinis crucial for an in vitro system of cell transforma-tion by its capacity for correct targeting ofoncogenic H-ras to its final membrane sites andto redirect Ras signaling [45]. Following activation,it also triggers cell-type-specific modulation of cellgrowth and migration in tumor cells and hasimmunomodulatory properties [21,46,47], under-scoring the emerging relevance to monitor lectinexpression by snythetic probes and antibodies [48].Interestingly, the frequency of galectin expressionrevealed similarities to that of adenocarcinomas(not shown).
Proceeding from the assessment of marker ex-pression the relative topology of cell positioningand staining was monitored. In principle, galectin-dependent staining in AAH displayed a more pro-nounced level of heterogeneity in intensity anddistance between centers of neighboring cells thanthat of non-neoplastic cells. When computing thestructural entropy as a measure of a deviation froma regular pattern, staining for MIF and anti-apop-totic galectin-3 showed up in the group of signifi-cant differences in AAH. In absolute values, theextent of measured E(MST) was still low comparedto that of primary or secondary lung malignanttumors, which is about 150�/200 [24,25,44]. How-
ever, markers indicative of potential for furtherprogress were detectable.
A correlation between the detected parameterchanges could provide valuable information onmechanisms for development of such lesions andtheir progression toward malignant growth. Profilechanges can readily be set into relation to topolo-gical presentation such as cluster formation, dis-tance between neighboring cells, or intercellularheterogeneity (structural entropy). Intensity ofbinding to endogenous ligands and its range weremainly associated between Gal-1 and Gal-3, incontrast to cluster radius of strongly stained cellsand E(MST), which displayed a close correlationbetween galectin binding/expression and the ex-pression of MIF and bcl-2. These findings indicatedthe formation of ‘spatially well-grouped cellularsociologies’ in AAH: for example, the larger thespatial size of an individual group of cells harboringa high expression/binding capacity of Gal-3, thelarger was the associated cluster of cells stronglyexpressing IL-2 or MIF, and the smaller was that ofproliferating cells (i.e. expressing MIB-1). In otherwords, the interaction of epithelial cells withpresence/expression of galectins (Gal-1, Gal-3,Gal-7), bcl-2, IL-2 and MIF might enhance theintercellular heterogeneity and further modulatethe*/already slightly accelerated-proliferation.
As indicated above, enhanced MIF expressioncould have notable ramifications for vasculariza-tion, prompting the discussion of respective data inthis context. The absolute features including themean vascular area of a vessel, the minimumdiameter and the mean circumference were nearlyidentical in both AAH and non-neoplastic lungparenchyma. The stereologic features, however,differed, and the volume and surface fraction Vvand Sv of AAH exceeded those of normal lung by afactor 2. The results thus indicate that the size ofvessels in AAH remained nearly unchanged, butthat the density of vascularization was remarkablyincreased. In addition, a focal aggregation ofvessels could be noted in AAH, as exemplarilydemonstrated in Fig. 4. The spatial agglutinationof vessels which are segmented and demonstratedby the red ellipsoid figures induces irregularities inblood supply of lung parenchyma, which is indi-cated by white (good supply) to black (poor supply)spaces. The same phenomenon had been reportedfor primary lung carcinomas [49,50]. A functionalcorrelation to MIF presence is a likely process onthe level of biochemical effectors. Growth regula-tion by reduction in apoptosis and stimulation oftransformation in which galectin-1 could play a rolemight be reflected in the proliferation rate ofatypical cells in AAH which measured about 4.5%.
180 K. Kayser et al.
It was slightly increased when compared to non-neoplastic lung parenchyma. Thus, our markeranalysis extends the panel of molecules, whichcould play important roles in establishment of thelesion and the assumed transition to the malignantphenotype.
Acknowledgements
The financial support by the Wilhelm Sander-Stiftung (Munich), the Verein zur Forderung desbiologisch-technologischen Fortschritts in der Med-izin e.V., and the International Association for theStudy of Lung Cancer (IASLC) is gratefully acknowl-edged.
References
[1] Carter D. Squamous cell carcinoma of the lung: an update.Semin Diag Pathol 1985;2:226�/34.
[2] Kayser K. Analytical lung pathology. Heidelberg, New York:Springer Verlag, 1995.
[3] Kayser K, Altiner M, Dienemann H, Gabius H-J. Changesduring the last decade in clinical parameters of operatedlung carcinoma patients of a center for thoracic surgeryand the prognostic significance of TNM, morphometric,cytometric, and glycohistochemical properties. ThoracCardiovasc Surg 1997;45:196�/9.
[4] Kawakami S, Sone S, Takashima S, et al. Atypical adeno-matous hyperplasia of the lung: correlation between high-resolution CT findings and histopathologic features. EurRadiol 2001;11:811�/4.
[5] Shimosato Y, Matsuno MN. Adenocarcinoma of the lung: itsdevelopment and malignant progression. Lung Cancer1993;9:99�/108.
[6] Carey FA, Fergusson RJ, Kerr KM, Lamb D. Alveolar atypicalhyperplasia in association with primary pulmonary adeno-carcinoma: a study of 10 cases. Thorax 1992;47:1041�/3.
[7] Nakahara R, Yokose T, Nagai K, et al. Atypical adenomatoushyperplasia of the lung: a clinicopathological study of 118cases including cases with multiple atypical adenomatoushyperplasia. Thorax 2001;56:302�/5.
[8] Weng S, Tsuchiya E, Kasuga T, Sugano H. Incidence ofatypical bronchioalveolar cell hyperplasia of the lung:relation to histological subtypes of lung cancer. VirchowsArch Pathol Anatom 1992;420:463�/71.
[9] Kosjerina Z, Goldmann T, Kayser K. Frequency in surgicalspecimens and morphology of atypical alveolar hyperplasiaof the lung, Elec. J. Pathol. Histol. 2002;8: 023-04.
[10] Yokozaki M, Kodama T, Yokose T, et al. Differentiation ofatypical adenomatous hyperplasia and adenocarcinoma ofthe lung by use of DNA ploidy and morphometric analysis.Mod Pathol 1996;9:1156�/64.
[11] Niho S, Yokose T, Suzuki K, et al. Monoclonality of atypicaladenomatous hyperplasia of the lung. Am J Pathol1999;154:249�/54.
[12] Kayser K, Bovin NV, Korchagina EY, et al. Correlation ofexpression of binding sites for synthetic blood group A-, B-and H-trisaccharides and for sarcolectin with survival ofpatients with bronchial carcinoma. Eur J Cancer1994;30A:653�/7.
[13] Kayser K, Andre S, Bovin NV, et al. Preneoplasia-associatedexpression of calcyclin and of binding sites for syntheticblood group A/H trisaccharide*/exposing neoglycoconju-gates in human lung. Cancer Biochem Biophys1997;15:235�/43.
[14] Chapman AD, Kerr KM. The association between atypicaladenomatous hyperplasia and primary lung cancer. Br JCancer 2000;83:632�/6.
[15] Mori M, Rao SK, Popper HH, et al. Atypical adenomatoushyperplasia of the lung: a probable forerunner in thedevelopment of adenocarcinoma of the lung. Mod Pathol2001;14:72�/84.
[16] Gabius H-J, Kohnke-Godt B, Leichsenring M, Bardosi A.Heparin-binding lectin of human placenta as a tool forhistochemical ligand localization and ligand isolation. JHistochem Cytochem 1991;39:1249�/56.
[17] Zeng F-Y, Gabius H-J. Carbohydrate-binding specificity ofcalcyclin and its expression in human tissues and leukemiccells. Arch Biochem Biophys 1991;289:137�/44.
[18] Andre S, Kojima S, Yamazaki N, et al. Galectins-1 and -3and their ligands in tumor biology. J Cancer Res Clin Oncol1999;125:461�/74.
[19] Kayser K, Zink S, Andre S, et al. Primary colorectalcarcinomas and their intrapulmonary metastases: clinical,glyco-, immuno- and lectin histochemical, nuclear andsyntactic structure analysis with emphasis on correlationwith period of occurrence of metastases and survival.Apmis 2002;110:435�/46.
[20] Rorive S, Eddafali B, Fernandez S, et al. Changes ingalectin-7 and cytokeratin-19 expression during the pro-gression of malignancy in thyroid tumors: diagnostic andbiological implication. Mod Pathol 2002;15:1294�/301.
[21] Wollina U, Graefe T, Feldrappe S, et al. Galectin finger-printing by immuno- and lectin histochemistry in cutaneouslymphoma. J Cancer Res Clin Oncol 2002;128:103�/10.
[22] Andre S, Pieters RJ, Vrasidas I, et al. Wedgelike glycoden-drimers as inhibitors of binding of mammalian galectins toglycoproteins, lactose maxiclusters and cell surface glyco-conjugates. ChemBioChem 2001;2:822�/30.
[23] Kayser K, Kayser G, Bovin NV, et al. Quantitative evaluationof ligandohistochemistry with cytoplasmic markers: pro-gram structure and application to lung carcinomas. Elec JPathol Histol 1995;1:954�/1002.
[24] Kayser K, Gabius H-J. The application of thermodynamicprinciples to histochemical and morphometric tissue re-search: principles and practical outline with focus on theglycosciences. Cell Tissue Res 1999;296:443�/55.
[25] Kayser K, Gabius H-J. Graph theory and the entropyconcept in histochemistry. Theoretical considerations,application in histopathology and the combination withreceptor-specific approaches. Prog Histochem Cytochem1997;32:1�/106.
[26] Kayser K, Kayser G, Eichhorn S, et al. Association ofprognosis in surgically treated lung cancer patients withcytometric, histometric and ligand histochemical proper-ties: with an emphasis on structural entropy. Anal QuantCytol Histol 1998;20:313�/20.
[27] Colby TV, Wistuba II, Gazdar A. Precursors to pulmonaryneoplasia, Adv. Anat. Pathol. 1998;5: 205�/215.
[28] Friedrich G. Periphere Lungenkrebse auf dem Bodenpleuranaher Narben. Virchows Arch Pathol Anat1939;304:230�/47.
[29] Shimosato Y, Kodoma T, Kameya Y. Morphogenesis ofperipheral type adenocarcinoma of the lung. In: ShimosatoY, editor. Morphogenesis of lung cancer wall. Boca Raton,FL: CRC Press, 1982:65�/89.
Atypical adenomatous hyperplasia of lung 181
[30] Miller R. Bronchioloalveolar cell adenomas. Am J SurgPathol 1990;14:904�/12.
[31] Yokose T, Doi M, Tanno K, et al. Atypical adenomatoushyperplasia of the lung in autopsy cases. Lung Cancer2001;33:155�/61.
[32] Weng S, Tsuchiya E, Satoh Y, et al. Multiple atypicaladenomatous hyperplasia of type II pneumonocytes andbronchiolo-alveolar carcinoma. Histopathology1990;16:101�/3.
[33] Nomori H, Horio H, Naruke T, et al. A case of multipleatypical adenomatous hyperplasia of the lung detected bycomputed tomography. Jpn J Clin Oncol 2001;31:514�/6.
[34] Kitamura H, Kameda Y, Ito T, Hayashi H. Atypical adeno-matous hyperplasia of the lung. Implications for thepathogenesis of peripheral lung adenocarcinoma. Am JClin Pathol 1999;111:610�/22.
[35] Kitamura H, Kameda Y, Nakamura N, et al. Atypicaladenomatous hyperplasia and bronchoalveolar lung carci-noma. Analysis by morphometry and the expressions of p53and carcinoembryonic antigen. Am J Surg Pathol1996;20:553�/62.
[36] Mitchell RA, et al. Macrophage migration inhibitory factor(MIF) sustains macrophage porinflammatory function byinhibiting p53: regulatory role in the innate immuneresponse. Proc Natl Acad Sci USA 2002;99:345�/50.
[37] Hudson JD, et al. A proinflammatory cytokine inhibits p53tumor suppressor activity. J Exp Med 1999;190:1375�/82.
[38] Kamimura A, et al. Intracellular distribution of macrophagemigration inhibitory factor predicts the prognosis ofpatients with adenocarcinoma of the lung. Cancer2000;89:334�/41.
[39] Ogawa H, et al. An antibody for macrophage migrationinhibitory factor suppresses tumor growth and inhibitstumor-associated angiogenesis. Cytokine 2000;12:309�/14.
[40] Gabius H-J. Concepts of tumor lectinology. Cancer Invest1997;15:454�/64.
[41] Danguy A, Camby I, Kiss R. Galectins and cancer. Biochim
Biophys Acta 2002;1572:285�/93.[42] Gabius H-J, Andre S, Kaltner H, Siebert H-C. The sugar
code: functional lectinomics. Biochim Biophys Acta
2002;1572:165�/77.[43] Rabinovich GA, Rubinstein N, Toscano M. Role of galectins
in inflammatory and immunomodulatory processes. Bio-
chim Biophys Acta 2002;1572:274�/84.[44] Lahm H, Andre S, Hoflich A, et al. Comprehensive galectin
fingerprinting in a panel of 61 human tumor cell lines by RT-
PCR and its implications for diagnostic and therapeutic
procedures. J Cancer Res Clin Oncol 2001;127:375�/86.[45] Elad-Sfadia G, Haklai R, Ballan E, et al. Galectin-1
augments Ras activation and diverts Ras signals to Raf-1
at the expense of phosphoinositide 3-kinase. J Biol Chem
2002;277:37 169�/75.[46] Gabius H-J. Probing the cons and pros of lectin-induced
immuno-modulation. Biochimie 2001;83:659�/66.[47] Kopitz J, von Reitzenstein C, Andre S, et al. Negative
regulation of neuroblastoma cell growth by carbohydrate-
dependent surface binding of galectin-1 and functional
divergence from galectin-3. J Biol Chem 2001;276:35 917�/
23.[48] Gabius H-J. Glycohistochemistry: the why and how of
detection and localization of endogenous lectins. Anat
Histol Embryol 2001;30:3�/31.[49] Kayser K, Berthold S, Eichhorn S, et al. Application of
attributed graphs in diagnostic pathology. Anal Quant Cytol
Histol 1996;18:286�/92.[50] Kayser K, Richter B, Stryciak R, et al. Positive and negative
correlations between vascularization and parameters de-
rived from integrated nuclear fluorescence and syntactic
structure analysis in human lung carcinomas. Anal Cell
Pathol 1997;15:73�/83.
182 K. Kayser et al.





























