Embed Size (px)
Citation preview

Autism Spectrum Disorder: Forensic Aspects and Sentencing
Considerations
By
Caitlin Eve Robertson
BPsych(Hons)
Submitted in partial fulfilment of the requirements for the degree of
Doctor of Psychology (Forensic)
Deakin University
February 2017
iv
Acknowledgements
A well-known proverb advises that it takes a village to raise a child. It appears
that it similarly takes a community to complete a thesis. To my primary supervisor
Jane McGillivray, I have enjoyed working with you on my thesis, through frustrations
and successes. Your guidance, patience and pragmatism have been greatly
appreciated and your support has been a critical component to my success. Many
thanks are also owed to other staff within Deakin University for their support and
advice in addressing speed bumps, in particular Clint Gurtman, George Yousef and
Steve Bowe.
Many others have been pulled into and along on this journey with me. It is my
great fortune that my supporters are too numerous to mention individually, however
the willingness of these individuals to act as my financers, companions, sympathisers
and cheerleaders is all the more remarkable given my often singular focus,
intermittent irritability and limited availability. Although many deserve thanks,
particular recognition is owed for my parents, whom I expect never considered that
their daughter would continue to be so dependent on them, practically, emotionally
and financially, into adulthood. Thank you.
v
Table of Contents
Acknowledgements ..................................................................................................... iv
List of Tables ............................................................................................................. xiv
List of Figures ............................................................................................................ xv
List of Appendices .................................................................................................... xvi
List of Common Abbreviations .............................................................................. xvii
Abstract .................................................................................................................. xviii
Chapter 1. Introduction and Overview of Thesis ..................................................... 1
1.1. Clarification of Assumptions and Scope of the Current Thesis .............. 3
1.2. Overview of Thesis Chapters .................................................................. 6
1.2.1. Chapter 2. ........................................................................................ 6
1.2.2. Chapter 3. ........................................................................................ 6
1.2.3. Chapter 4. ........................................................................................ 7
1.2.4. Chapter 5. ........................................................................................ 8
1.2.5. Chapter 6. ........................................................................................ 8
1.2.6. Chapter 7. ........................................................................................ 8
1.2.7. Chapter 8. ........................................................................................ 9
1.2.8. Chapter 9. ........................................................................................ 9
Chapter 2. Introduction to Autism Spectrum Disorder .......................................... 1
2.1. Diagnostic Features of Autism Spectrum Disorder ................................. 2
2.1.1. Deficits in social communication and social interaction. ................ 2
2.1.2. Restricted, repetitive patterns of behavior, interests, or activities. . 3
2.1.3. Clinical specifiers. ........................................................................... 3
vi
2.2. Changing definitions: Asperger, The Autism Spectrum and Diagnostic
Modifications ................................................................................................ 4
2.2.1. Is Asperger’s syndrome a discrete condition? ................................. 5
2.2.2. Changes to diagnostic criteria and diagnostic continuity. ............... 7
2.3. The Epidemiology of Autism Spectrum Disorder ................................. 11
2.3.1. Gender variances in prevalence. .................................................... 14
2.3.1.1. Gender differences in presentation. ........................................ 14
2.3.1.2. The extreme male brain theory. .............................................. 15
2.3.2. Upward trend in prevalence over time. ......................................... 15
2.3.3. Variation in prevalence according to age. ..................................... 17
2.3.3.1. Difficulties with diagnosis in adulthood. ............................... 17
2.3.3.2. Confounding factors and changing diagnostic definitions. .... 19
2.3.3.3. Remittance of autistic symptomatology. ................................ 19
2.4. Psychosocial Outcomes in Adulthood and Adolescence ....................... 21
2.4.1. Lack of community-based support services for adults with ASD. 23
2.4.2. Potential areas of difficulty for adults with ASD. ......................... 23
2.4.2.1. Low levels of social participation. ......................................... 24
2.4.2.2. Loneliness and social dissatisfaction. ..................................... 24
2.4.2.3. Low academic and vocational achievement. .......................... 26
2.4.2.4. Challenging Behaviours and Forensic issues. ........................ 27
2.5. Summary of Chapter .............................................................................. 28
Chapter 3. Autism Spectrum Disorder and Offending Behaviour ....................... 30
3.1. Case Reports of Offending Perpetrated by Individuals with Autism
Spectrum Disorder ...................................................................................... 30
vii
3.2. Prevalence of Offending Behaviour Amongst Individuals with Autism
Spectrum Disorder ...................................................................................... 32
3.2.1. Research regarding prevalence of ASD amongst offending
populations. ............................................................................................. 33
3.2.2. Research regarding prevalence of offending amongst ASD
populations. ............................................................................................. 46
3.2.3. The Contribution of Co-Morbid Conditions. ................................ 54
3.2.3.1. Co-morbid Intellectual Disability and offending. .................. 54
3.2.3.2. Psychiatric co-morbidity and offending. ................................ 55
3.2.3.3. A double hit? ASD, offending behaviour and psychopathy. .. 57
3.2.4. Summary of research findings regarding prevalence of offending
and ASD. ................................................................................................. 59
3.3. Features of ASD Potentially Associated with Offending Behaviour .... 62
3.3.1. Socio-communicative impairments. .............................................. 63
3.3.1.1. ‘Zero Degrees’ of empathy. ................................................... 63
3.3.1.2. Social naïveté and vulnerability to exploitation. .................... 66
3.3.1.3. Lack of understanding or misinterpretation of social cues and
norms. .................................................................................................. 67
3.3.1.4. Asynchronous development: Inconsistency between socio-
communicative (psychosexual) and sexual development. ................... 68
3.3.2. Restricted or repetitive patterns of behaviour, interests or activities.
................................................................................................................. 70
3.3.2.1. Rigidity applying learned social norms. ................................. 70
3.3.2.2. Escalation associated with the disruption of routines. ........... 71
3.3.2.3. Preoccupation with special interests. ..................................... 72
viii
3.3.2.4. Interpersonal fixations. ........................................................... 73
3.3.2.5. Escalation associated with sensory hypersensitivity. ............. 74
3.3.2.6. Retaliation for perceived victimization. ................................. 75
3.3.3. Summary regarding the potential relevance of ASD traits to
offending behaviour ................................................................................ 77
3.4. The Nature of Offending Behaviour Perpetrated by Individuals with
ASD ............................................................................................................ 78
3.5. Summary of Chapter .............................................................................. 81
Chapter 4. Study 1: Self-Report of Offending and the Autistic Phenotype ......... 85
4.1. Rationale ................................................................................................ 85
4.1.1. Defining and measuring “offending behaviour”: Official data vs.
self-report. ............................................................................................... 86
4.1.2 The Present Study ........................................................................... 88
4.2. Method ................................................................................................... 89
4.2.1. Participants. ................................................................................... 90
4.2.2. Measures. ....................................................................................... 90
4.2.2.1. Demographic information. ..................................................... 91
4.2.2.2. Psychopathic traits. ................................................................. 91
4.2.2.3. Autistic traits. ......................................................................... 91
4.2.2.4. Engagement in offending behaviour. ..................................... 93
4.3. Results ................................................................................................... 95
4.3.1. Missing Data. ................................................................................ 95
4.3.2. Annual Engagement in Offending and Other Delinquent
Behaviours. .............................................................................................. 95
ix
4.3.2.1. Overall annual frequency and variety of engagement in
offending and other delinquent behaviours. ........................................ 96
4.3.2.2. Offence-types endorsed. ......................................................... 97
4.3.3. Adjudication and dispositional outcomes. .................................... 97
4.3.3.1. Lifetime frequency of charges and arrests. ............................ 99
4.3.3.2. Lifetime disposition and application of discretionary and
diversionary alternatives. ..................................................................... 99
4.4. Discussion .............................................................................................. 99
4.4.1. Self-reported engagement in offending behaviour. ..................... 100
4.4.2. Offence typologies across the autistic phenotype. ...................... 100
4.4.3. Forensic response to delinquent behaviour. ................................ 102
4.4.4. Limitations. ................................................................................. 103
4.4.5. Implications and directions for future research. .......................... 106
Chapter 5. The Legal Response: Legal Considerations and CJS Awareness Regarding ASD .......................................................................................... 108
5.1. Legislation and Common Law Regarding Defendants with Mental
Disorders ................................................................................................... 108
5.1.1. Fitness to stand trial. .................................................................... 109
5.1.2. The Mental Impairment defence. ................................................ 110
5.1.3. Mental disorder as a mitigating factor during sentencing. .......... 112
5.2. The Legal Status of Defendants with Autism Spectrum Disorder ...... 117
5.2.1. Legislative considerations: Fitness to Stand Trial and the Mental
Impairment Defence .............................................................................. 117
5.2.1.1 Fitness to stand trial. .............................................................. 118
5.2.1.2. The Mental Impairment defence. ......................................... 121
x
5.2.1.3. Theory in practice: The practical relevance of Fitness and
mental Impairment legislation to ASD. ............................................. 123
5.2.2. ASD as a mitigating factor during sentencing: The relevance of
Verdins’ principles. ............................................................................... 125
5.3. Judicial Awareness and Perceptions of ASD ...................................... 127
5.4. Chapter Summary ................................................................................ 130
Chapter 6. Study 2: A Preliminary Assessment of Knowledge and Perceptions of Autism Spectrum Disorder in Australian Magistrate’s Courts. ........... 133
6.1. Rationale .............................................................................................. 133
6.1.1. How do judges decide? ............................................................... 134
6.1.2. Forensic Decision-Making and ASD. ......................................... 136
6.2. Method ................................................................................................. 137
6.2.1. Aim. ............................................................................................. 137
6.2.2. Participants. ................................................................................. 137
6.2.3. Materials. ..................................................................................... 138
6.3. Results ................................................................................................. 138
6.3.1. Response Rates. ........................................................................... 138
6.3.2. Magistrates’ understanding of ASD. ........................................... 138
6.3.3. Magistrates self-assessed competence with regards to ASD in the
CJS. ....................................................................................................... 140
6.3.4. Perceived propensity towards offending and victimization. ....... 140
6.3.5. Magistrates’ perceptions of the potential forensic relevance of
ASD. ...................................................................................................... 140
6.3.5.1. Enhancing communication and understanding. ................... 141
6.3.5.2. Likely response to dispositional alternatives. ...................... 142
xi
6.3.5.3. Consideration of the legal status of offenders with ASD. .... 143
6.3.6. Importance of the court being made aware of ASD. ................... 143
6.3.6.1. ASD Training Amongst Australian Magistrates. ................. 144
6.3.6.2. The role of forensic psychologists in informing courts
regarding ASD. .................................................................................. 145
6.4. Discussion ............................................................................................ 146
6.4.1. A coherent and consistent approach? .......................................... 148
6.4.2. The role of psychologists in assisting courts. .............................. 151
6.4.3. Limitations of the current study. ................................................. 152
6.4.4. Implications of findings and directions future research. ............. 154
Chapter 7. Questions of Morality Amongst Individuals with ASD .................... 158
7.1. The Moral/Conventional Distinction ................................................... 159
7.2. Studies Investigating Moral Processing amongst Individuals with ASD
.................................................................................................................. 160
7.3. True Moral Processing or Rule Following for Rule Following’s Sake?
.................................................................................................................. 165
7.4. The Breadth of the Moral Domain ...................................................... 168
7.5. Moral Foundations Theory .................................................................. 169
7.5.1. Care/Harm. .................................................................................. 170
7.5.2. Fairness/Cheating. ....................................................................... 170
7.5.3. Loyalty/Betrayal. ......................................................................... 171
7.5.4. Authority/Subversion. ................................................................. 171
7.5.5. Sanctity/Degradation. .................................................................. 171
7.5.6 What can Moral Foundations Theory reveal about moral reasoning
in ASD? ................................................................................................. 172
xii
Chapter 8. Study 3: Disparities in moral intuitions and the autistic phenotype175
8.1. Rationale .............................................................................................. 175
8.2. Aims and Hypotheses .......................................................................... 177
8.2.1. Care/Harm. .................................................................................. 177
8.2.2. Fairness/Cheating. ....................................................................... 178
8.2.3. Loyalty/Betrayal. ......................................................................... 179
8.2.4. Authority/Subversion. ................................................................. 180
8.2.5. Sanctity/Degradation. .................................................................. 181
8.3. Method ................................................................................................. 182
8.3.1. Participants. ................................................................................. 182
8.3.2. Materials. ..................................................................................... 183
8.3.2.1. Demographic information. ................................................... 183
8.3.2.2. Psychopathic traits. ............................................................... 184
8.3.2.3. Autistic traits. ....................................................................... 185
8.3.2.4. Moral intuitions. ................................................................... 186
8.4. Results ................................................................................................. 187
8.4.1. Missing data. ............................................................................... 188
8.4.2. Contribution of demographic variables. ...................................... 188
8.4.3. Assumption testing. ..................................................................... 189
8.4.3.1. Sample size. .......................................................................... 189
8.4.3.2. Outlying data. ....................................................................... 190
8.4.3.3. Normality of residuals. ......................................................... 190
8.4.3.4. Multicollinearity/Singularity. ............................................... 190
8.4.3.5. Independence of residuals. ................................................... 193
8.4.3.6. Homoscedasticity. ................................................................ 193
xiii
8.4.4. Regression Analyses: AQ scores and foundation endorsement. . 193
8.5. Discussion ............................................................................................ 195
Chapter 9. Discussion of thesis and limitations. ................................................... 199
9.1. Limitations of the Current Thesis ........................................................ 201
9.2. Nexus Between ASD, Moral Reasoning and Engagement in Offending
Behaviour .................................................................................................. 203
References ................................................................................................................ 208
Appendices ............................................................................................................... 282
xiv
List of Tables
Table 1. DSM-IV-TR and DSM-5 Criteria for Autism Spectrum Disorder ................ 8
Table 2. Prevalence of ASD within Offending Populations ..................................... 36
Table 3. Prevalence of Offending Behaviour Amongst Individuals with ASD ......... 47
Table 4. Annual frequency and nature of offence-like behaviours amongst
respondents reporting engagement in delinquent acts .................................. 98
Table 5. Moral reasoning stages as defined by the Japanese Human External Action
and Internal Reasoning Type (HEART) ..................................................... 163
Table 6. Participant responses on learning disability screening items ...................... 184
Table 7. Example items for each MFQ domain* ...................................................... 187
Table 8. Means, alpha reliability coefficients, and zero-order Pearson correlations
reflecting the associations between AQ scores, LSRP scores, Age, learning
disability composite scores and MFQ foundations (n = 153) ..................... 192

xv
List of Figures
Figure 1. ASD prevalence estimates by age group for data collected in the SDAC
2009 and SDAC 2012. ........................................................................................ 17
Figure 2. Linear relationship between AQ scores and mean ratings on each of the five
moral foundations. ............................................................................................. 194
xvi
List of Appendices
Appendix A DSM-5 Criteria for Autism Spectrum Disorder
Appendix B Gillberg Diagnostic Criteria for Asperger’s Syndrome
Appendix C List of Locations Contacted for Participant Recruitment
Appendix D Levenson Self-Report Psychopathy Scale
Appendix E Self-Report of Offending Behaviour
Appendix F Crimes Statistics Agency Offence Classification (2015)
Appendix G Autism Spectrum Disorder and the Courts: Lawyer
Response (n = 1)
Appendix H Autism Spectrum Disorder and the Courts: Survey
Distributed to Magistrates
Appendix I Moral Foundations Questionnaire
Appendix J Regression Statistics for Hierarchical Regression
Analyses Predicting Moral Foundations from AQ
Scores
Appendix K Breusch-Pagan and Koenker Test Macro
Appendix L Heteroskedasticity Adjusted Standard Errors Macro
xvii
List of Common Abbreviations
APA American Psychiatric Association
ASD Autism Spectrum Disorder
CJS Criminal Justice System
CMIA Crimes (Mental Impairment and Unfitness to be Tried) Act
1997 (Vic)
DSM Diagnostic and Statistical Manual of Mental Disorders
DSM-IV-TR Diagnostic and Statistical Manual of Mental Disorders,
fourth edition, text review
DSM-5 Diagnostic and Statistical Manual of Mental Disorders, fifth
edition
HFA High Functioning Autism
ICD International Classification of Disease and Health Related
Problems
ID Intellectual Disability
IQ Intelligence Quotient
MFQ Moral Foundations Questionnaire
MFT Moral Foundations Theory
PDD Pervasive Developmental Disorder
WHO World Health Organisation
xviii
Abstract
Amid increasing public and academic interest, a growing body of literature has
explored offending behaviour perpetrated by individuals with Autism Spectrum
Disorder (ASD). On balance, the extant literature indicates that while most
individuals with ASD are law-abiding, a subset engage in offending behaviour with
consequent involvement of the criminal justice system (CJS). It has been argued that
the expression of features characteristic of ASD may be a major contributory factor to
offending behavior observed amongst this population and may additionally cause
difficulties for individuals with ASD in navigating the demands of the CJS. Such
observations raise questions regarding the legal status of individuals with ASD and
the appropriate CJS response to offending behaviour amongst this population. This
thesis presents three studies exploring forensic aspects of ASD. First, typologies of
offending across the ASD phenotype are examined via an internet-based survey
amongst a community sample (n = 109). Results indicated no significant differences
in self-reported frequency or variety of offending and few differences in offence
typologies according to ASD trait severity, as measured by the Autism Quotient. The
views of the Australian magistracy (n = 21) are explored in the second study, with
results confirming prior academic conjecture that disparity exists amongst the
judiciary in regards to knowledge and attitudes regarding ASD. Finally, the relevance
of ASD to moral culpability and mitigation is considered through an online survey
exploring the potential link between ASD symptomatology and morality according to
a contemporary theoretical model (n = 106). Findings revealed that ASD trait severity
predicted differential endorsement of factors considered morally relevant. The
discussion includes the limitations and practical implications arising from these
studies and directions for future research.
1
Chapter 1. Introduction and Overview of Thesis
Autism Spectrum Disorder (ASD) is a life-long neurodevelopmental disorder
that affects the way that an individual communicates with and relates to other people
(American Psychiatric Association; APA, 2013). More specifically, ASD is defined
by the presence of impairments in communication, social interaction and imagination,
alongside repetitive and restricted patterns of thought and behaviour (APA, 2013).
Substantial variation is evident in the behavioural phenotype of ASD, dependent on a
number of factors, including the severity of autistic symptomatology, the age of the
affected individual and the presence (or absence) of co-morbid conditions (APA,
2013). Accordingly, presentation, degree of impairment and support needs differ
significantly between individuals with ASD diagnoses. While academic efforts have
resulted in significant advances in our understanding of biological and clinical
perspectives of ASD, a historical emphasis of ASD as a disorder of childhood has
meant that research efforts have largely centred on the lives of children with ASD
(Woodbury-Smith, 2014).
The knowledge base regarding ASD in adulthood remains relatively limited
(Fombonne, 2012; Howlin & Moss, 2012; Ketelaars et al., 2007); however,
researchers have increasingly explored issues pertinent to understanding the
presentation and support needs of adults with ASD. The results of long-term follow-
up studies indicate wide variation in psychosocial outcomes for this population
(Howlin, 1997, 2000; Palermo, 2004); while some individuals achieve positive
outcomes in adulthood, a significant proportion of adults with ASD face
disadvantages in a range of domains including, but not limited to, occupational
engagement, social functioning and quality of life (Howlin, 1997, 2000). Of
particular interest to the current thesis is the small but significant number of
2
individuals among those with greater overall disadvantage who were documented to
have engaged in illegal behaviours, with consequent forensic involvement (Howard &
O'Brien, 2009; King & Murphy, 2014; Raggi, Xenitidis, Moisan, Deeley, &
Robertson, 2013; Woodbury-Smith, 2014).
The involvement of individuals with ASD in the Criminal Justice System
(CJS) raises important questions in regards to the legal status and the appropriate
legal response to offending behaviour amongst such individuals (Fazio, Pietz, &
Denney, 2012). Such considerations have resulted in increasing academic interest
regarding the forensic aspects of ASD as well as the implications the diagnosis carries
as an individual progresses through legal proceedings (Browning & Caulfield, 2011;
Fazio et al., 2012). A growing number of researchers, policy makers and practitioners
have called for increased exploration of these forensic aspects of ASD in order to
inform policy and practice regarding disposition, management and the provision of
intervention services that respond to or aim to circumvent offending behaviour
amongst the ASD population (Allen et al., 2008; Browning & Caulfield, 2011; Fazio
et al., 2012; Hayes, 2006, 2007; Lerner, Haque, Northrup, Lawer, & Bursztajn, 2012;
Lindsay & Taylor, 2005). Despite the increased interest in this area, the state of
knowledge regarding the forensic implications of ASD remains in its infancy
(Barkham, Gunasekaran, & Lovelock, 2013; King & Murphy, 2014).
The aim of the current thesis is to address some of the legal considerations
that may be pertinent when individuals with ASD come into contact with the CJS as
the result of their offending behaviour. Several issues arising from the literature and
from practice require further attention:
1. Inconsistencies in the literature base regarding the prevalence and nature
of offending amongst individuals with ASD.
3
2. Inconsistency in academic and forensic practitioner opinions regarding the
forensic relevance of ASD.
3. Indications of a significant level of unawareness of ASD amongst CJS
workers, including amongst the judiciary.
4. The presence of significant challenges faced by mental health
professionals in advising and educating courts regarding the relevant
aspects of ASD.
These issues are investigated in the current thesis, with particular attention
dedicated to the association between ASD trait severity and the nature of reported
offending behaviours, judicial perceptions regarding ASD and issues of morality (a
factor often important in forensic decision-making).
1.1. Clarification of Assumptions and Scope of the Current Thesis
On July 20, 2012, James Holmes attended a midnight screening of the new
Batman movie sequel “The Dark Night Rises” in the town of Aurora, Colorado.
Shortly after the movie commenced, he shot and killed 12 individuals, injuring 70
others. In the aftermath of the shooting, Joe Scarborough, a popular American news
anchor on the show ‘Morning Joe’ commented that “more often than not”, offences of
this nature were perpetrated by individuals that are “somewhere, I believe, on the
Autism scale” (Alvarez, 2012). As in this instance, the presence of ASD has been
reported by the media and within academic sources for a number of high-profile cases
involving the commission of serious crimes, including for individuals such as Jeffrey
Dahmer (Allely, Minnis, Thompson, Wilson, & Gillberg, 2014; Silva, Ferrari, &
Leong, 2002); Ted Kaczynski (Allely et al., 2014; Silva, Ferrari, & Leong, 2003);
Joel Rifkin (Silva, Leong, Smith, Hawes, & Ferrari, 2005); Adam Lanza (Im, 2016);
Martin Bryant (Wooley, 2011); and Anders Brevik (Allely et al., 2014). Widespread
4
reporting that linked ASD with such lurid cases of offending behaviour appears to
have contributed to public alarm and conjecture of a causal link between ASD and
serious criminal behaviour, despite a lack of persuasive empirical evidence
supporting this conclusion (Lerner et al., 2012).
It is understandable that observers seek causative explanations when faced
with behaviour that significantly deviates from social norms, particularly where such
violations result in significant harm to others (Brewer & Young, 2015). Given that
ASD is frequently associated with unusual behaviour that violates social norms, it is
perhaps unsurprising that ASD has been raised as one such potentially causative
factor (Brewer & Young, 2015). However, the preparedness of media and academic
sources to evoke ASD (often speculatively and/or posthumously) in their attempts to
explain criminal behaviour risks contributing to a perception of adults with ASD as
“socially undesirable individuals with a propensity for committing violent or other
serious crimes” (Brewer & Young, 2015, p. 14).
The negative impacts on public perceptions regarding individuals with
psychiatric diagnoses in cases where the condition has been portrayed as a
precipitating factor for offending behaviour has been demonstrated (Angermeyer &
Matschinger, 2005; Corrigan & Watson, 2002; Hatwell, 2004; Lamb, Weinberger, &
Gross, 2004; West, Vayshenker, Rotter, & Yanos, 2015). Anecdotal evidence
suggests that this holds true for the ASD population. For example, a public post on
the Facebook group “Families Against Autistic Shooters” (no longer an active page)
was reported to have described individuals with ASD as “cold calculating killing
machines with no regard for human life” following a mass-shooting in Oregon, U.S.A
(Solomon, 2015). The stigma elicited from such media portrayals appears likely to
have negative implications for assimilation and integration within community settings
5
and may be prejudicial in the context of interactions with the CJS (Brewer & Young,
2015). To be clear from the outset, it is not argued in the current thesis that
individuals with ASD necessarily possess an elevated risk for engagement in
offending behaviour; indeed, it will become evident in later chapters that, at present,
the extant literature does not support a direct association between ASD and
criminality.
Notwithstanding the observation that the majority of individuals with ASD
appear to be law-abiding, it is evident that some will come into contact with the CJS
due to engagement in offending behaviour and will thus require forensic disposition.
Failure by the CJS to respond effectively in such instances (for example, due to a
failure to take into account the presence of an ASD diagnosis during forensic
decision-making) may lead to inappropriate assessments and disposition, an
inefficient use of resources in an already under-resourced area of practice and
potential deleterious consequences for community safety. The purpose of this thesis is
to thus inform policy and practice regarding the appropriate management of offending
behaviour where it is perpetrated by an individual with ASD, on the basis that such
individuals are likely to present with unique precipitants, support needs and
challenges for habilitation and community integration1.
1 Integration and habilitation, rather than reintegration and rehabilitation, in
recognition that many incarcerated individuals, particularly those with developmental
disorders, do not possess a history of stable and adaptive functioning within the
community. Accordingly, the emphasis on a return to a productive and prosocial
lifestyle espoused by the concepts of habilitation and integration may not be
applicable to this population.
6
1.2. Overview of Thesis Chapters
Following this introductory chapter, the thesis is comprised of four chapters
providing critical reviews and analyses of relevant literature (Chapters 2, 3, 5 and 7),
and the presentation of three novel empirical studies exploring patterns of delinquent
behaviour (Chapter 4), judicial perceptions (Chapter 6), and issues of morality
(Chapter 8) according to the presence of ASD symptomatology. The final chapter
consists of an overall discussion in which limitations and implications of the
presented research are outlined and suggestions are provided on directions for further
research to facilitate a deeper and more integrated knowledgebase concerning the
forensic aspects of ASD (Chapter 9).
1.2.1. Chapter 2. Prior to focus on the forensically relevant aspects of ASD, it
is useful to provide a more general overview of issues related to identification,
presentation and the psychosocial impact of ASD. In Chapter 2, these issues are
explored, with particular attention given to issues pertaining to psychosocial
outcomes observed amongst adults with ASD, including the challenges faced by
those who evidence poorer outcomes in adulthood. Given that the majority of
individuals with ASD are law-abiding, it is considered unlikely that any of the factors
explored in Chapter 2 would, in isolation, explain engagement in offending
behaviour. However, exploration of the phenotypical, psychosocial and
epidemiological aspects of ASD provides a crucial context for the complex forensic
issues discussed in later chapters.
1.2.2. Chapter 3. A critical review of the available empirical evidence
regarding the involvement of individuals with ASD in offending behaviour is
provided in Chapter 3. This chapter includes an overview of the cognitive and
behavioural processes associated with ASD that have been proposed to contribute to
7
engagement in offending behaviour amongst this population. It is argued that the
inconsistent results presented in the literature are insufficient to provide a detailed
understanding of prevalence and typology of offending perpetrated by individuals
with ASD. It is further argued that continued attempts to determine the actual
prevalence of offending amongst the ASD population may be a fruitless endeavour
that diverts attention and resources from other important issues related to the care and
treatment of these individuals within the CJS. In contrast, it is suggested that the
systematic exploration of offence-typologies amongst people with symptoms of ASD
may provide more opportunities to accurately inform practice and policy in regards to
offending amongst individuals with ASD.
1.2.3. Chapter 4. Chapter 4 presents empirical data, drawn from an internet-
based survey, which systematically investigated self-reported characteristics of and
forensic response to delinquent behaviours amongst a community-based sample of
individuals displaying varying degrees of ASD – consistent symptomatology. The
rationale for the study design is explained within this chapter, along with a
description of the methodology and the results. The chapter concludes with a
discussion of the results in relation to the available literature and potential directions
for future academic exploration in this area. The results of the study suggest that
dispositional, diversionary and discretionary provisions are equivalently applied to
individuals with ASD as to their neurotpyical peers. Whilst this result appears to
indicate that individuals with ASD are not disadvantaged in the context of forensic
disposition, it is argued that the determination of the appropriate treatment of
individuals with ASD within the CJS must be considered in the context of the
intended function and underlying philosophy of legislation and legal practice
regarding forensic disposition.
8
1.2.4. Chapter 5. Chapter 5 explores the treatment of offenders with ASD
within the CJS within the context of current sentencing legislation and practice in
Australia. Potential difficulties faced by individuals with ASD in understanding the
nature of their illegal conduct and in navigating the demands of the CJS are discussed
with reference to legislation and legal precedent concerning the disposition of cases
where defendants possess a mental impairment. Significant variation in the forensic
response to offenders with ASD is identified in the literature reviewed in Chapter 5,
suggesting a lack of awareness regarding the nature and presentation of ASD amongst
judicial officers. It is argued that misinformed impressions about individuals with
ASD amongst the judiciary, either pre-existing or formed during the course of court
proceedings, may be prejudicial to forensic outcomes where individuals with ASD
are charged with a criminal offence.
1.2.5. Chapter 6. The knowledge and understanding of ASD among
magistrates sitting within Australian jurisdictions is explored in the second empirical
study of the thesis. Specifically, an explorative study in the form of a free-response
pencil-and-paper questionnaire was conducted in order to map the perceptions and
attitudes held by members of the Australian magistracy in regard to persons with
ASD who appear in their courts. Chapter 6 outlines the reasoning and design for the
study, the methodology of the study is described, and the results are presented. The
chapter concludes with a discussion of the results in relation to the literature and
current operation of the CJS, and the potential role for forensic psychology in regard
to offenders with ASD.
1.2.6. Chapter 7. As outlined in prior chapters, forensic psychology
represents a key ally to the courts in determining the applicability of various legal
principles to particular legal cases. In order to better inform the courts on such
9
matters, research that explores issues pertinent to legal decision-making is an
important endeavour. As described in Chapter 6, the issue of moral understanding is
pertinent to the sentencing of defendants with ASD. A critical review of existing
literature exploring moral functioning amongst individuals with ASD is provided in
Chapter 7, and it is suggested that the methodological approach adopted in prior
research may have resulted in only a partial understanding of this critical issue in law.
A contemporary model of morality, Moral Foundations Theory, is introduced and the
potential contribution of such to the state of knowledge regarding morality and ASD
is explored in order to provide some background to the study presented in Chapter 8.
1.2.7. Chapter 8. Chapter 8 comprises a study of moral processing across the
autistic phenotype. Specifically, the association between ASD trait severity and
responses on a questionnaire regarding moral intuitions is empirically investigated.
The rationale for the study design is explained, along with a description of the
methodology and presentation of results. Critically, in contrast to prior research in
this area, this study demonstrated that the severity of reported ASD traits predicted
differential endorsement on a range of potential areas of moral concern. Chapter 8
concludes with a discussion of these results in the context of the available literature
and current practice in relation to the disposition of cases involving a defendant with
ASD.
1.2.8. Chapter 9. The final chapter consists of an overall discussion that
provides a review of the key findings and implications of the research undertaken
within this dissertation. Specifically, the theoretical and clinical implications
emerging from previous chapters are drawn together, the limitations of the empirical
studies are discussed and some brief recommendations for future research and
practice are provided.
1
Chapter 2. Introduction to Autism Spectrum Disorder
In 1943, child psychiatrist Leo Kanner produced detailed descriptions of
eleven children who were admitted under his care. According to Kanner, these eight
boys and three girls displayed a unique “combination of extreme autism2,
obsessiveness, stereotypy and echolalia” (p. 248). On the basis of his observations,
Kanner suggested the delineation of a previously unrecognised disorder, which is
today known as Autism Spectrum Disorder (ASD). In the decades following
Kanner’s initial descriptions, the ‘autistic’ phenotype has received significant
academic attention and substantial gains have been made in the identification,
treatment and management of individuals with ASD.
ASD is a life-long neurodevelopmental disorder that affects the way that an
individual communicates with and relates to other people. The behavioural phenotype
is remarkably heterogeneous, aptly summarized by the assertion that “If you have met
one person with autism, you’ve met one person with autism” (Advancing Futures for
Adults with Autism, 2010, pg. 1). For example, while delayed language is common
amongst individuals with ASD, linguistic skills vary significantly with some
individuals remaining mute while others are voluble and display grammatically
correct (although often idiosyncratic) use of language (APA, 2013; Tager-Flusberg,
Paul, & Lord, 2005). Similarly, some individuals present with co-occurring
intellectual disability (ID) or psychiatric disorder that may complicate the course and
presentation of ASD and impact on adaptive functioning (La Malfa, Lassi, Bertelli,
Salvini, & Placidi, 2004; Mazzone, Ruta, & Reale, 2012; Moseley, Tonge, Brereton, 2 The term “autism” was adopted by Kanner from Eugen Bleuler’s (1911)
monograph regarding schizophrenia (Kanner, 1973). Bleuler (1911) used the term to
denote a “detachment from reality, together with the relative and absolute
predominance of the inner life” observed amongst patients with schizophrenia (p. 63).
2
& Einfeld, 2011). Throughout the literature, a number of clinical descriptions and
operational definitions for ASD exist. However, the dominant and most recently
updated approach for diagnosis is according to criteria outlined in the Diagnostic and
Statistical Manual of Mental Disorders of the American Psychological Association.
2.1. Diagnostic Features of Autism Spectrum Disorder
ASD is diagnosed according to a dyad of observable impairments in socio-
communicative and behavioural domains defined within the current edition of the
Diagnostic and Statistical Manual of Mental Disorders (DSM-5; APA, 2013).
Specific manifestations of such deficits may vary according to a number of factors
including the developmental level of the individual, their language ability and their
access to intervention and ongoing sources of support. The observed impairments
must, however, be present from early childhood (i.e. sustained) and limit or impair
functioning across a range of contexts (i.e. pervasive) (APA, 2013).
2.1.1. Deficits in social communication and social interaction. Socio-
communicative deficits amongst individuals with ASD may be evident in
abnormalities or deficiencies in speech, non-verbal communication, social-emotional
reciprocity and/or understanding of social cues required to initiate and maintain social
relationships (APA, 2013). Spontaneous nonverbal communicative behaviour (e.g.
eye-contact, gestures, facial expression, speech intonation) may be reduced or
altogether absent and incongruities in verbal and nonverbal communication are
common (Stefanatos, 2012; Tager-Flusberg et al., 2005). Those individuals who
develop speech often display pedantic and repetitious use of language and difficulties
with pragmatics, syntax and other subtleties involved in verbal and non-verbal
communication (Stefanatos, 2012; Tager-Flusberg et al., 2005). Verbal
communication is typically one-sided and individuals with ASD may appear asocial;
3
however, social relationships are frequently desired, often in the absence of a
complete understanding of what such relationships entail (APA, 2013; Attwood,
2007; Locke, Ishijima, Kasari, & London, 2010; Mazurek, 2014).
2.1.2. Restricted, repetitive patterns of behavior, interests, or activities.
As with socio-communicative deficits, significant variations in the manifestation of
restrictive and repetitive behaviours are evident amongst individuals with ASD
(APA, 2013; Leekam, Uljarevic, & Prior, 2011). Individuals may display motor
stereotypies such as hand-flapping or rocking, atypical object use and echolalic or
otherwise repetitious speech processes (Goldman et al., 2009; Leekam et al., 2011;
van Santen, Sproat, & Presmanes Hill, 2013). Sensory abnormalities are often present
and impact on behavioural restriction; with hyper- and hypo- reactivity associated
with atypical responses to sensory stimuli including attraction or aversion to
particular sensations, including those associated with food aversions or apparent
indifference to pain (Billstedt, Gillberg, & Gillberg, 2005; Leekam, Nieto, Libby,
Wing, & Gould, 2007; Zachor & Ben-Itzchak, 2014). Behavioural and psychological
inflexibility may also be associated with a resistance towards change, resulting in
engagement in ritualized patterns of thought and behaviour (APA, 2013; Leekam et
al., 2011).
2.1.3. Clinical specifiers. ASD diagnoses are adapted to the individual by
inclusion of specifiers detailing the severity of autistic symptoms and the presence of
commonly observed clinical features and comorbidities (APA, 2013). Specifically,
the DSM-5 requires diagnosing clincians to specify the level of support required to
manage the severity of impairment displayed by an individual across each of the two
diagnostic domains, from those ‘requiring support’ to those ‘requiring very
substantial support’. In addition, the identification of co-morbid ID, catatonia or
4
language disorder is emphasized through the presence of specifiers regarding these
areas of functioning. Assessors should also specify whether the ASD diagnosis is
associated with a known medical, genetic or environmental condition or where co-
morbid neurodevelopmental, mental or behavioural disorder is evident (see Appendix
A for the full DSM-5 diagnostic criteria).
2.2. Changing definitions: Asperger, The Autism Spectrum and Diagnostic
Modifications
Around the same time as Kanner’s (1943) descriptions of his autistic patients
in America, Asperger (1944) published a series of case studies of children in Vienna
who presented with socio-communicative deficits and an obsessive pursuit of
idiosyncratic interests. Although Kanner and Asperger were (at least initially)
unaware of each other’s work, the core impairments described by each author were
markedly similar. In particular, both authors identified the social detachment
observed amongst their patients as a central feature of their psychopathology and
accordingly, both adopted the term ‘autistic’ to describe and classify the phenotype.
In contrast to Kanner’s case reports, which rapidly came to the attention of the
international academic and medical community, Asperger’s contributions received
little attention outside of the German literature until 1981 when Lorna Wing
published an English translation of his observations, augmented with clinical
illustrations from her own practice. Although Wing (1981a) emphasized that the
phenotypes described by Kanner and Asperger were “more alike than unalike” (p.
122), she asserted that the term ‘Asperger’s syndrome’ possessed clinical utility to
classify individuals who were higher functioning and who presented with less severe
manifestations of autistic symptomatology. Wing (2000) later reiterated she had not
intended for the term “Asperger’s syndrome” to denote a diagnostic entity that was
5
mutually exclusive from other autistic disorders. Whatever Wing’s (1981a) original
intentions, many readers of her work considered Asperger’s syndrome to represent a
technically and diagnostically distinct entity and the classification was included as a
discrete condition in diagnostic manuals from the 1990s (APA, 1995; World Health
Organization, WHO, 1992).
2.2.1. Is Asperger’s syndrome a discrete condition? Prior to the publication
of the DSM-5 in May 2013, both major diagnostic systems (i.e. the previous edition
of the DSM [DSM-IV-TR, APA, 2000] and the International Classification of
Diseases (10th Ed) of the World Health Organization [ICD-10, 2004]) shared common
diagnostic criteria that conceptualized Asperger’s syndrome as a unique diagnostic
entity. In contrast to those with Kanner’s autism (known variously within diagnostic
systems as autism, autistic disorder or childhood autism), individuals with Asperger’s
syndrome were considered to possess at least average IQ, age-appropriate (although
often idiosyncratic) language and an absence of gross impairments in adaptive
behaviour (APA, 2000; Howlin & Moss, 2012; WHO, 2004). However, there was
considerable debate regarding the validity of the differential diagnosis of these
disorders, with the accumulated evidence suggesting that these diagnostic entities
were synonymous (Macintosh & Dissanayake, 2004).
Research has revealed a great deal of overlap and few qualitative differences
in presentation between Asperger’s syndrome and other autistic phenotypes
(Freeman, Cronin, & Candelam, 2002; Macintosh & Dissanayake, 2004; Szatmari,
Bartolucci, & Bremner, 1989). Neuropsychological testing has neither identified a
distinct cognitive profile that consistently discriminated between such diagnoses, nor
demonstrated different aetiology or developmental courses (Freeman et al., 2002;
Ghaziuddin & Mountain-Kimchi, 2004; Miller & Ozonoff, 2000). In addition, reports
6
from both parents and clinicians have suggested that individuals diagnosed with
Asperger’s syndrome often displayed impairments in adaptive behaviour skills that
diagnostic criteria indicated should be preserved (Attwood, 2006). Further, studies
involving independent review of existing diagnoses have indicated that Asperger’s
syndrome can rarely be confirmed on the basis of strict diagnostic criteria (Mayes,
Calhoun, & Crites, 2001; Miller & Ozonoff, 1997; Tyron, Mayes, Rhodes, & Waldo,
2006). Specifically, such research has found that many, if not all, individuals
diagnosed with Asperger’s syndrome met criteria for Autistic Disorder, suggestive of
a failure of assessors to apply hierarchical exclusionary criteria as required by
diagnostic manuals (Howlin, 2004; Mayes et al., 2001; Miller & Ozonoff, 1997;
Tyron et al., 2006).
On the basis of the empirical evidence, it appears that dissimilarities observed
between Asperger’s Syndrome and other autistic disorders were quantitative
variations in the severity of impairments rather than qualitative differences between
disorders (Macintosh & Dissanayake, 2004). In support of such, several studies have
indicated that the expression of autistic traits occurs along a continuum that is
approximately normally distributed, ranging from those who are severely impaired at
one extreme, to those with less severe manifestations and few adaptive impairments
and shading into ‘eccentric normality’ in the general population (Broadbent & Stokes,
2013; Hoekstra, Bartels, Verweij, & Boomsma, 2007; Wing, 1991). Such
observations are in line with the view that the autistic phenotype exists along a
spectrum, whereby individuals vary in presentation according to the number and
severity of traits expressed (Freeman et al., 2002; Tyron et al., 2006; Wing, 1991).
The consensus that autistic traits occur along an ‘autism spectrum’ resulted in a
reconceptualization of the way in which autistic disorders are defined and identified.
7
2.2.2. Changes to diagnostic criteria and diagnostic continuity. The
previous edition of the Diagnostic and Statistical Manual (APA, 2000) listed a
number of discrete disorders associated with the characteristic traits of ASD, under
the diagnostic category of ‘pervasive developmental disorders’ (PDDs). With the
publication of the DSM-5 came a number of changes to the diagnostic criteria for
disorders associated with the autism spectrum, reflecting the current state of
knowledge regarding autistic traits and the nature of impairments observed amongst
diagnosed individuals (summarized in Table 1).
At present, the International Classification of Diseases (WHO, 2004)
continues to classify disorders on the autism spectrum as PDDs and differentiates
Asperger’s syndrome from other disorders within this category3; however, the
uncertain nosological status and striking similarities in presentation between
Asperger’s syndrome and other autistic phenotypes are explicitly acknowledged
within the ICD-10 diagnostic criteria. Further, at the time of writing, the beta draft for
the upcoming edition of the ICD (ICD-11, anticipated for publication in 2017)
indicated that the diagnostic criteria regarding disorders on the autism spectrum are
likely to be modified to correspond with the DSM-5 nomenclature (WHO, 2015).
3 Childhood autism, Atypical autism, Rett syndrome, Other childhood
disintegrative disorder, Overactive disorder associated with mental retardation and
stereotyped movements, Pervasive developmental disorder, unspecified.
8
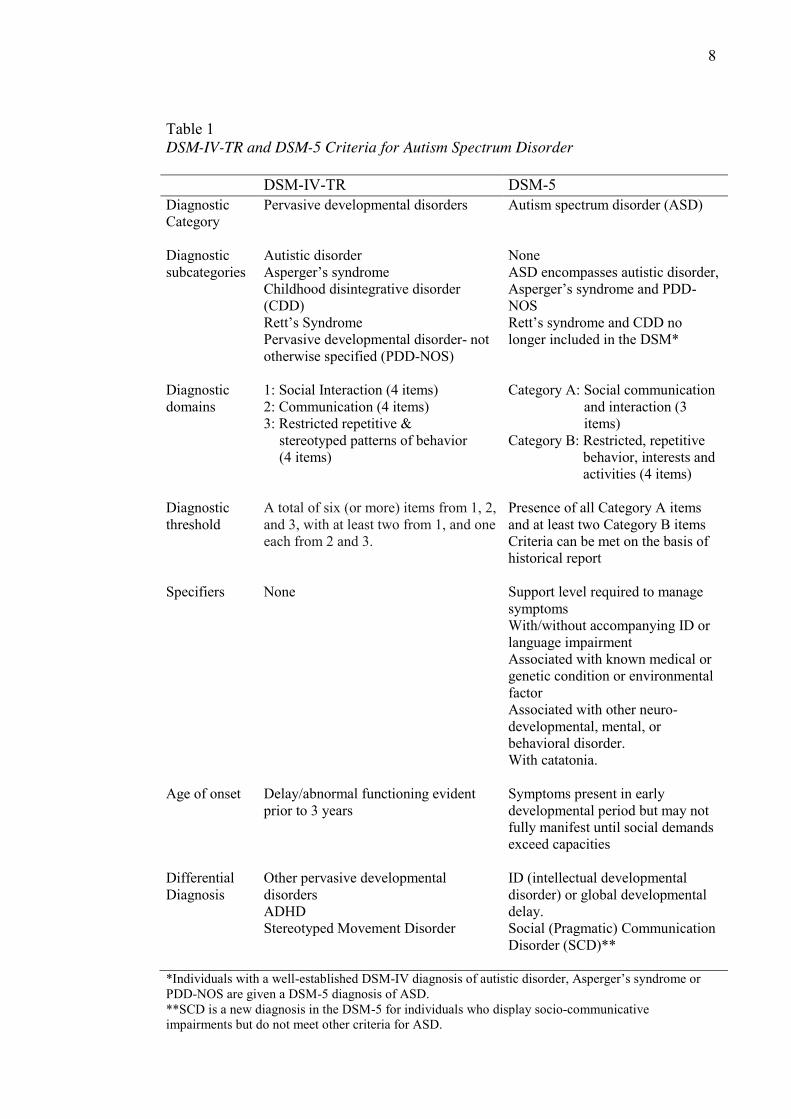
Table 1 DSM-IV-TR and DSM-5 Criteria for Autism Spectrum Disorder DSM-IV-TR DSM-5 Diagnostic Category
Pervasive developmental disorders Autism spectrum disorder (ASD)
Diagnostic subcategories
Autistic disorder Asperger’s syndrome Childhood disintegrative disorder (CDD) Rett’s Syndrome Pervasive developmental disorder- not otherwise specified (PDD-NOS)
None ASD encompasses autistic disorder, Asperger’s syndrome and PDD-NOS Rett’s syndrome and CDD no longer included in the DSM*
Diagnostic domains
1: Social Interaction (4 items) 2: Communication (4 items) 3: Restricted repetitive & 3::stereotyped patterns of behavior 3::(4 items)
Category A: Social communication Category A: and interaction (3 Category A: items) Category B: Restricted, repetitive Category C: behavior, interests and Category C: activities (4 items)
Diagnostic threshold
A total of six (or more) items from 1, 2, and 3, with at least two from 1, and one each from 2 and 3.
Presence of all Category A items and at least two Category B items Criteria can be met on the basis of historical report
Specifiers None Support level required to manage symptoms With/without accompanying ID or language impairment Associated with known medical or genetic condition or environmental factor Associated with other neuro-developmental, mental, or behavioral disorder. With catatonia.
Age of onset Delay/abnormal functioning evident prior to 3 years
Symptoms present in early developmental period but may not fully manifest until social demands exceed capacities
Differential Diagnosis
Other pervasive developmental disorders ADHD Stereotyped Movement Disorder
ID (intellectual developmental disorder) or global developmental delay. Social (Pragmatic) Communication Disorder (SCD)**
*Individuals with a well-established DSM-IV diagnosis of autistic disorder, Asperger’s syndrome or PDD-NOS are given a DSM-5 diagnosis of ASD. **SCD is a new diagnosis in the DSM-5 for individuals who display socio-communicative impairments but do not meet other criteria for ASD.
9
A comprehensive and critical review of the recent and upcoming
modifications to the diagnostic criteria for ASD and related disorders is beyond the
scope of the current thesis, and has been discussed in detail elsewhere (APA, 2012;
Hyman, 2013; Lauritsen, 2013; Lord & Jones, 2012; Mandy, Charman, & Skuse,
2012; Miller, 2014; Nemeroff et al., 2013; Skuse, 2012; Volkmar & Reichow, 2013;
Wing, Gould, & Gillberg, 2010). However, it is important to note that the diagnostic
modifications have not occurred without some controversy, with several authors
expressing concerns regarding the impact of the changes in clinical and academic
spheres (e.g. Nemeroff et al., 2013; Volkmar & Reichow, 2013). A limited number of
studies exist that have considered the impact of the revision to diagnostic criteria on
the validity and continuity of diagnosis, many of which were conducted prior to the
publication of the DSM-5, using draft versions of the criteria. The results of pre-
publication studies were inconsistent, with some authors demonstrating general
continuity in diagnosis according to the two editions of the DSM (Mazefsky,
McPartland, Gastgeb, & Minshew, 2013), while others considered the DSM-5 criteria
to represent an unwarranted narrowing of the spectrum (Barton, Robins, Jashar,
Brennan, & Fein, 2013; Frazier et al., 2012; Gibbs, Aldridge, Chandler, Witzlsperger,
& Smith, 2012; Mattila et al., 2011; McPartland, Reichow, & Volkmar, 2012). Some
of these studies have suggested that the DSM-5 criteria are biased towards more
impaired individuals in terms of intellectual functioning (Mattila et al., 2011;
McPartland et al., 2012) or engagement in challenging behaviours (Beighley et al.,
2013).
More recently, Kim et al. (2014) compared the prevalence of ASD according
to the published DSM-5 and DSM-IV-TR criteria in an epidemiologic sample of
South Korean children (n = 55, 266) and concluded that most individuals with DSM-
10
IV-TR diagnoses of autistic disorder (99%) and Asperger’s syndrome (92%)
continued to meet DSM-5 criteria for ASD. However, a significant minority of
individuals with DSM-IV-TR diagnoses of PDD-NOS (37%) did not meet DSM-5
criteria for ASD4. Similarly, Young and Rodi (2014) found that individuals who met
DSM-IV-TR criteria for PDD-NOS were disproportionately unlikely to meet DSM-5
criteria for ASD amongst individuals referred for assessment to an autism-specialist
psychological practice in Adelaide, Australia (n = 233). Of concern, none of the 20
individuals who met diagnostic criteria for PDD-NOS within Young and Rodi’s
sample were considered to meet DSM-5 criteria for ASD. Further, only 56% of
individuals who met diagnostic criteria for Asperger’s syndrome met DSM-5 criteria
for ASD.
In response to concerns regarding the continuity of diagnosis and the related
issues of identity, advocacy and the provision of services for individuals with existing
diagnoses (see for example, Spillers, Sensui, & Linton, 2014), the DSM-5 criteria
includes a ‘grandfather clause’ which indicates that a diagnosis of ASD should be
extended to any individual with a pre-existing and well-established DSM-IV-TR
diagnosis of Asperger’s syndrome or PDD-NOS. However, uncertainty remains
regarding the validity and applicability of prior research, which has included
participants identified according to earlier diagnostic criteria (Volkmar & Reichow,
2013; Wing et al., 2010). The current thesis adopts the term ASD, in line with the
DSM-5 (APA, 2013) nomenclature as it is considered that this most closely reflects
the current state of knowledge supported by the research. However, due to the relative
4 While 37% of children who met DSM-IV-TR criteria for PDD-NOS did not
meet DSM-5 criteria for ASD, 32% of those individuals met criteria for SCD (Kim et
al., 2014).
11
recency of the changes to the diagnostic criteria, it is noted that prior research has not
always adopted this definition. Indeed, while the concept of the autism spectrum was
widely accepted in both empirical and lay-literature prior to inclusion of ASD in the
DSM-5, much of the extant research cited within this volume is focused specifically
on individuals diagnosed with Asperger’s syndrome. In recognition of this limitation,
the original terminology (e.g. Asperger’s syndrome, infantile autism, autistic
disorder, Pervasive Developmental Disorders) has been retained when describing the
contributions of other authors throughout this volume.
2.3. The Epidemiology of Autism Spectrum Disorder
An accurate prevalence for ASD within the international population is yet to
be established. The DSM-5 (APA, 2013) indicates a prevalence rate of around 1% for
ASD; however, significant variation exists between research findings (Williams,
Higgings, & Brayne, Saracino, Noseworthy, Steiman, Reisinger, & Fombonne, 2010;
2006). In a review of 133 epidemiological studies published between 1966 and 2013,
Tsai (2014) reported prevalence estimates for autistic disorder (and the equivalent
diagnosis ‘infantile autism’) that ranged from 0.7 (Treffert, 1970) to 190
(Ghanizadhe, 2008) per 10,000 individuals. Similarly, Tsai (2014) found marked
variation in prevalence estimates for the broader autistic phenotype (defined as ASD
and/or PDD) with estimated prevalence rates ranging from 1.4 (Al-Farsi et al., 2010)
to 264 (Kim et al., 2011) individuals per 10, 000. It is generally agreed that variations
in prevalence estimates across studies are primarily artefactual in nature and most
significantly influenced by methodological variables (Zaroff & Uhm, 2012).
Specifically, differences in diagnostic criteria, methods of case identification and
evaluation, variations in target population size and characteristics, geographical
residence of participants and other methodological disparities between studies appear
12
likely to have contributed to the vast discrepancies in estimated prevalence rates
observed within the extant literature (Elsabbagh et al., 2012; Tsai, 2014; Williams et
al., 2006; Williams, Mellis & Peat, 2005).
In Australia, prevalence estimates for ASD have been similarly variable.
Williams, MacDermott, Ridley, Glasson and Wray (2008) collected ASD prevalence
data for children under 16 years from education, welfare and public health agencies
across Australia in 2003/4 and found significant variation in rates reported in each
state/territory and between agencies surveyed within the same regions. For example,
the reported prevalence of ASD amongst children aged 6-12 years varied from 9.6 to
40.8 individuals per 10,000 with similar discrepancies observed across the 0-5 and
13-16 year age groups. Other research conducted within Australian populations have
variously reported estimated ASD prevalence rates per 10,000 individuals of 39.2 in a
region of Victoria (Icasiano, Hewson, Machet, Cooper, & Marshall, 2004), 51 in
children born between 1994 and 1999 in Western Australia (Parner et al., 2011) and
340 in a youth mental health service in Melbourne, Victoria (Fraser et al., 2011).
In 2014, the Australian Bureau of Statistics (ABS) published ‘Autism in
Australia’; an overview of the epidemiology of ASD in Australia with data drawn
from the 2012 Survey of Disability, Ageing and Carers (SDAC 2012). The SDAC
2012 was a nation-wide investigation of the self-reported prevalence, etiology and
impact of disability with the primary purpose of informing policy and service
provision for individuals living with a disability, older individuals (those aged 65
years and over), and their carers. A similar survey was conducted in previous years
(1981, 1988, 1993, 1998, 2003 and 2009) and the data-collection for the 2012 survey
occurred between 5 August 2012 and 2 March 2013 across approximately 27,400
private dwellings, 500 non-private dwellings, and 1,000 health establishments (ABS,
13
2013). According to the data collected, an estimated 115, 400 Australians (0.5% of
the general population) were diagnosed with ASD. However, there are several
methodological limitations that reduce confidence in the prevalence rate reported for
ASD in the ABS (2014) report.
The SDAC 2012 was not a diagnostic survey and relied upon a self-report
methodology whereby disability was identified according to a catalogue of 15 areas
of adaptive functioning (e.g. speech impairment, learning difficulties). Respondents
were asked to indicate whether such impairments were personally relevant and
subsequent questioning identified any diagnosed conditions that resulted in the
difficulties that were reported (ABS, 2014). Efforts were not made to confirm the
validity of reported diagnoses nor whether an individual met diagnostic criteria for a
condition on the basis of reported symptoms (ABS, 2014). In addition, the 15 areas of
functioning on which respondents were queried did not include impairments in social
interaction, a key aspect and diagnostic feature of the autistic phenotype (ABS, 2014).
Accordingly, the survey design may have resulted in limited opportunities for the
identification of ASD and self-diagnosed or misdiagnosed conditions may have been
included within the prevalence data.
Further, although the SDAC 2012 was a large-scale survey with wide scope,
the sample excluded those living in very remote areas, households in some
indigenous communities, individuals living in boarding schools, those incarcerated in
custodial settings and individuals living with homelessness (ABS, 2014). It is unclear
how each of these exclusions may have impacted on prevalence estimates, however
given that there is some (equivocal) international evidence of an overrepresentation of
ASD amongst those living with homelessness (Evans, 2011) and within secure
settings (see Chapter 3) it appears possible that the data may underestimate the
14
overall prevalence of ASD in Australia. Conversely, the estimated prevalence for
ASD reported by the ABS (2014) may be inflated by the inclusion of individuals who
would not meet current diagnostic criteria for ASD. As the data collection period for
the SDAC 2012 pre-dated the recent DSM update, the adopted definition of ASD was
equivalent to the DSM-IV-TR diagnostic category of PDD. Accordingly, individuals
who reported a diagnosis of CDD and Rett’s syndrome (both of which are no longer
understood to exist on the autism spectrum) were included in analyses regarding
ASD. Although the above methodological limitations reduce confidence in the
accuracy of the prevalence estimate provided by the ABS (2014), the report provides
useful information regarding epidemiological trends for ASD in Australia.
2.3.1. Gender variances in prevalence. Consistent with the results of
international research (e.g. Briugha et al., 2009; Centre for Disease Control and
Prevention, 2014; Kim et al., 2011), the SDAC 2012 data indicated that ASD
diagnoses in Australia were vastly more common amongst males than females (ABS,
2014). Specifically, the SDAC 2012 data demonstrated estimated prevalence rates for
ASD amongst males (0.8%) that were 4 times in excess of that reported for females
(0.2%). At present, the observed overrepresentation of ASD amongst males is not
completely understood, however several authors have hypothesized explanations for
this disparity.
2.3.1.1. Gender differences in presentation. Some authors (e.g. Attwood,
2006; Ehlers & Gillberg, 1993; Gould & Ashton-Smith, 2011; Lai et al., 2011) have
speculated that the male predominance in ASD prevalence occurs as an artefact of
difficulties regarding case identification amongst females. For example, Attwood
(2007) suggests a reduced prominence of characteristic impairments associated with
Asperger’s syndrome amongst females as a result of a greater ability to mimic others’
15
behaviour as a means of masking such difficulties. The gender differences in the
presentation of ASD may result in fewer females being referred for diagnosis or
higher rates of missed or misdiagnosis amongst those females that are referred.
Indeed, Dworzynski, Ronald, Bolton, and Happe (2012) found that, in the absence of
concomitant intellectual or behavioural problems, girls with equivalent levels of
autistic traits were less likely than their male counterparts to be diagnosed with ASD.
Such observations may indicate that diagnostic criteria and assessment procedures for
ASD are biased towards male presentations (Dworzynski et al., 2012; Gould &
Ashton-Smith, 2011).
2.3.1.2. The extreme male brain theory. In contrast, some authors have
asserted that exaggerations of personality differences that naturally exist between
typically developing males and females may be directly related to the aetiology of
ASD, resulting in a true gender disparity in prevalence (Baron-Cohen, 2002; Lawson,
Baron-Cohen, & Wheelwright, 2004; Wing, 1981b). This hypothesis, often referred
to as the extreme male brain theory of autism (Baron-Cohen, 2002), holds that
typically developing males possess a spontaneous preference for systemizing (i.e.
mathematical/spatial reasoning and detail-oriented processing), while females are
predisposed towards empathizing (i.e. recognising, comprehending and responding to
the emotional state of others). On this view, individuals with ASD are considered to
be hyper-systemizers and more males meet the diagnostic threshold due to the higher
likelihood of such characteristics occurring amongst even typically developing males
(Baron-Cohen, 2002).
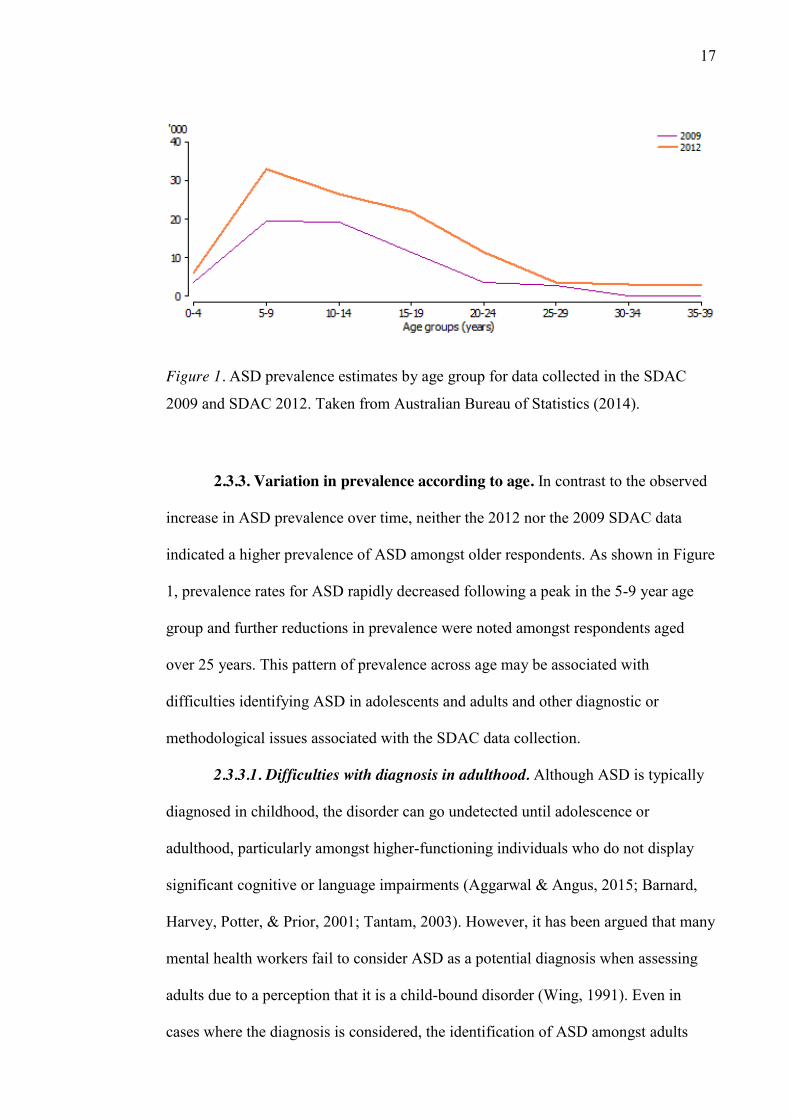
2.3.2. Upward trend in prevalence over time. Comparison between the
SDAC 2012 and the results of earlier SDAC surveys revealed an upward trend in
ASD prevalence across time (see Figure 1). Specifically, an estimated 79% increase
16
in prevalence was noted by the ABS (2014) when comparing current data to that from
the 2009 SDAC, which identified a diagnosis of ASD in an estimated 64,400 people
(ABS, 2010). This finding is consistent with the results of international research
(Isaksen, Diseth, Schjølberg, & Skeldal, 2013; Kim et al., 2014; Matson &
Kozlowski, 2011; Reber, 2012; Saracino et al., 2010; Tsai, 2014), in which higher
prevalence rates have been observed in more recent studies.
An adequate explanation for the progressive increase in prevalence has not
been delineated to date, and it is not possible to rule out the possibility of an actual
increase in the incidence of ASD; however, it is generally accepted that the rise in
prevalence is at least in part artefactual (Matson & Kozlowski, 2011; McLeer &
McNeils; Williams et al., 2014). Specifically, it has been argued that changes in
diagnostic criteria, individual-level diagnostic substitutions (i.e. individuals receiving
contemporary diagnoses of ASD who had been previously (mis)diagnosed with other
disorders), better methods of detection and increased awareness amongst
professionals and the general community may be implicated in the apparent increase
of prevalence over time (Isaksen et al., 2013; King & Bearman, 2009; Matson &
Kozlowski, 2011; Wazana, Bresnahan, & Kline, 2007; Williams et al., 2014).
17
Figure 1. ASD prevalence estimates by age group for data collected in the SDAC
2009 and SDAC 2012. Taken from Australian Bureau of Statistics (2014).
2.3.3. Variation in prevalence according to age. In contrast to the observed
increase in ASD prevalence over time, neither the 2012 nor the 2009 SDAC data
indicated a higher prevalence of ASD amongst older respondents. As shown in Figure
1, prevalence rates for ASD rapidly decreased following a peak in the 5-9 year age
group and further reductions in prevalence were noted amongst respondents aged
over 25 years. This pattern of prevalence across age may be associated with
difficulties identifying ASD in adolescents and adults and other diagnostic or
methodological issues associated with the SDAC data collection.
2.3.3.1. Difficulties with diagnosis in adulthood. Although ASD is typically
diagnosed in childhood, the disorder can go undetected until adolescence or
adulthood, particularly amongst higher-functioning individuals who do not display
significant cognitive or language impairments (Aggarwal & Angus, 2015; Barnard,
Harvey, Potter, & Prior, 2001; Tantam, 2003). However, it has been argued that many
mental health workers fail to consider ASD as a potential diagnosis when assessing
adults due to a perception that it is a child-bound disorder (Wing, 1991). Even in
cases where the diagnosis is considered, the identification of ASD amongst adults
18
presents some unique challenges, which may result in missed diagnosis or
misdiagnosis of such individuals.
The diagnosis of ASD requires careful consideration of current
symptomatology and developmental history; however, many adults with ASD display
limited insight regarding their functioning, poor language skills and specific reporting
impairments that impact on their ability to provide an accurate and sufficiently
detailed developmental history (Fombonne, 2012; Lombardo, Barnes, Wheelwright,
& Baron-Cohen, 2007). Accordingly, accurate diagnosis frequently relies on
corroborative evidence regarding socio-developmental impairments (Royal College
of Psychiatrists, 2006). However, appropriate informants may be unavailable at the
time that an adult presents for assessment and medical or educational records are
frequently absent, contradictory or insufficient for such purposes (Fombonne, 2012;
Tantam, 2003; Royal College of Psychiatrists, 2006)5. In addition, individuals with
ASD frequently develop compensatory strategies as they age which may suppress
behavioural manifestations of the characteristic impairments associated with ASD
(Frith, 1991).
The presence of comorbid psychiatric disorders in adulthood may further
complicate the course or presentation of ASD, resulting in a lack of clarity regarding
the symptomatic profile of the presenting individual or the aetiology of observable
traits (Frith, 1991; APA, 2013; Royal College of Psychiatrists, 2006; Mazzone, et al.,
2012). In such cases, deficits may become more apparent in novel contexts, during
periods of developmental crisis or in complex social environments where situational 5 As a reflection of such difficulties, the DSM-5 (APA, 2013) allows for a
diagnosis of ASD in the absence of detailed developmental information on the basis
of presentation in adulthood providing that no evidence exists that suggests good
social communicative skills in childhood.
19
demands exceed the individual’s adaptive skill level (Royal College of Psychiatrists,
2006; Tantam, 2003).
2.3.3.2. Confounding factors and changing diagnostic definitions. In
addition to difficulties regarding the identification of ASD in adulthood, age-group
variations in prevalence may be associated with confounding factors or specific
methodological issues with the design of the SDAC 2012. For example, it is possible
that the variation in prevalence across age groups observed in the SDAC data may be
associated with an individual’s contact with the educational system. The ABS (2014)
note that 85% of individuals reporting a diagnosis of ASD in the SDAC 2012 were
identified on the basis of the presence of learning difficulties. The peak in prevalence
within the 5-9 year age group coincides with the time that formal education
commences in Australia, at which time learning impairments may become more
evident. Conversely, as individuals age out of the education system, learning is no
longer a daily focus and learning impairments become less apparent, resulting in a
lower likelihood of identification according to the SDAC 2012 methodology (ABS,
2014). Changes to diagnostic criteria for ASD over time accompanied by a reluctance
of respondents to report ASD in older individuals due to the stigma of such
conditions may also partially account for the variations in ASD prevalence observed
across age groups (ABS, 2014).
2.3.3.3. Remittance of autistic symptomatology. The age-group variation in
prevalence observed in the SDAC 2012 data may also be a reflection of a tendency
towards improvement in autistic symptomatology and subsequent increases in
adaptive behaviour as an individual ages, such that they no longer meet the threshold
for diagnosis (McLeer & McNeils; Tantam, 2003; Williams et al., 2006). In support
of such, several studies indicate a modest abatement in autistic symptomatology
20
(Gray et al., 2012; Schall & McDonough, 2010; Seltzer, Shattuck, Abbeduto, &
Greenberg, 2004; Shattuck et al., 2007), decreases in maladaptive behaviours
(Anderson, May, & Lord, 2011) and improvements on measures of adaptive
functioning (Gillespie-Lynch et al., 2012; McGovern & Sigman, 2005) across the
life-span, particularly amongst those with less severe manifestations of ASD. Despite
evidence of a general trend towards symptomatic and functional improvement, a
worsening of symptoms may occur for a subset of individuals with ASD (Gray et al.,
2012), and others experience periods of regression in adaptive functioning,
particularly in times of developmental crisis (Kobayashi, Murata, & Yoshinaga,
1992; Périsse et al., 2010; Seltzer et al., 2004; Tantam, 2003).
Although the developmental trajectory for adults and adolescents with ASD is
not homogenous, evidence from research suggests that the majority of individuals
diagnosed with ASD will continue to meet diagnostic criteria into adulthood
(Billstedt et al., 2005; Billstedt, Gillberg, & Gillberg, 2007; Cederlund, Hagberg,
Billstedt, Gillberg, & Gillberg, 2008; Howlin, Goode, Hutton, & Rutter, 2004; Lotter,
1978; McGovern & Sigman, 2005). Even in cases where individuals experience
improvements in symptom severity and general adaptive functioning, adults with
ASD often present with ongoing impairments or difficulties coping with the
increasing social demands of adulthood (Anderson et al., 2011; Ballaban-Gil, Rapin,
Tuchman, & Shinnar, 1996; Billstedt et al., 2007; Gray et al., 2012; Holwerda, van
der Klink, Groothoff, & Brouwer, 2012; Howlin, 2000; Howlin, Mawhood, & Rutter,
2000; Seltzer et al., 2004; Shattuck et al., 2007). These ongoing deficits appear likely
to contribute to functional impairment and may consequently impact on psychosocial
outcomes for adults with ASD (Seltzer et al., 2004). Indeed, perhaps paradoxically,
21
psychosocial difficulties may increase with age as an individual’s expected and
perceived competence increases (Howlin, 2004).
2.4. Psychosocial Outcomes in Adulthood and Adolescence
Much of what we know about ASD after childhood is anecdotal. Indeed, the
personal accounts of diagnosed individuals (e.g. Carpenter, 1992; Fleischmann &
Fleischmann, 2012; Grandin, 1992, 2006, 2011; Grandin & Panek, 2013; Lissner,
1992; Sinclair, 1992) and their families (e.g. Akerley, 1992; Dewey, 1992;
Fleischmann & Fleischmann, 2012; Happe, 1991; Park, 1992; Sullivan, 1992;
Turnbull, 2010) have provided valuable insights into the experiences of adults and
adolescents with disorders on the autism spectrum. However, in recent years,
increasing academic interest regarding the impact of ASD throughout the life-course
has resulted in a proliferation of clinical case reports, longitudinal follow-up studies
and cross-sectional research focused on psychosocial outcomes and quality of life in
adolescence and adulthood (e.g. Ballaban-Gil et al., 1996; Barnard et al., 2001;
Barneveld, Swaab, Fagel, van Engeland, & de Sonneville, 2014; Billstedt et al., 2005;
Billstedt et al., 2007; Billstedt, Gillberg, & Gillberg, 2011; Cederlund et al., 2008;
Eaves & Ho, 2008; Farley et al., 2009; Green, Gilchrist, Burton, & Cox, 2000;
Howlin et al., 2004; Howlin et al., 2000; Marriage, Wolverton, & Marriage, 2009;
Orsmond, Shattuck, Cooper, Sterzing, & Anderson, 2013; von Knorring & Hågglof,
1993; Whitehouse, Watt, Line, & Bishop, 2009).
Recent reviews of the available literature (Henninger & Taylor, 2013; Howlin
& Moss, 2012; Levy & Perry, 2011; Magiati, Tay, & Howlin, 2014; Seltzer et al.,
2004; Tobin, Drager, & Richardson, 2014; Wright, Brooks, D'Astous, & Grandin,
2013) reveal a wide variability in psychosocial outcomes amongst adults with ASD.
While case reports and cross-sectional research show that some individuals with ASD
22
can have positive outcomes in adulthood, including engaging in paid employment and
effectively integrating within society (Howlin, 2000), longitudinal follow-up studies
have frequently indicated that many are significantly disadvantaged in a range of
domains (Barneveld et al., 2014; Billstedt et al., 2007; Gray et al., 2014; Howlin et
al., 2004; Howlin et al., 2000; Orsmond et al., 2013; Whitehouse, Watt, et al., 2009).
Kanner’s (1973) follow-up study of individuals who were diagnosed with autism in
childhood (n = 96) demonstrates the wide range of potential outcomes for this
population. As adults, some of these individuals were employed, lived in their own
homes and pursued opportunities for social engagement (e.g. membership to social
groups or clubs). However, significant numbers did not have close reciprocal
relationships and the majority remained highly dependent and resided with parents or
in institutions.
Today, more people with ASD are living within the community due to the
deinstitutionalisation approach of the 1980s and 1990s, involving moving individuals
with mental illness and disabilities out of large state institutions into community-
based accommodation (Mayes & Koegel, 2003). The deinstitutionalization of these
populations is intended to provide a more enriched life experience and protect
individuals from abuse, maltreatment and isolation within institutions (Chowdhury &
Benson, 2011; Howard & O'Brien, 2009). However, some argue that
deinstitutionalization does not meet these aims due to a lack of appropriate supports
for vulnerable individuals within the community (Howard & O'Brien, 2009). As a
result, many individuals, including those with ASDs, are now living in the
community with inadequate support for successful social integration (Pasterfield,
2009).

23
2.4.1. Lack of community-based support services for adults with ASD. For
many individuals with ASD, adulthood heralds the loss of access to essential
resources as they ‘age-out’ of childhood support and intervention services and enter
the adult system, where they frequently fall through the gap between existing mental
health and disability services (Barkham et al., 2013; Barnard et al., 2001; Berney,
2007; McLeer & McNeils, 2012; Shattuck et al., 2012). Despite increasing
availability and accessibility of services for children with ASD, the provision of
support for adults remains an underdeveloped area of research and practice (Berney,
2007; Howlin & Moss, 2012; Kuangparichat, 2010; Pasterfield, 2009; Shattuck et al.,
2012). The available research indicates that support needs amongst adults with ASD
are heterogeneous; some require daily support whereas others only require occasional
assistance in specific areas of functioning (Barkham et al., 2013; Wright et al., 2013).
However, few options for formal support exist within the community and the support
needs of adults with ASD and their families are largely unmet, particularly amongst
those who do not possess psychiatric comorbidities or cognitive impairment (APA,
2014; Barkham et al., 2013; Berney, 2007; Kuangparichat, 2010; Magiati et al., 2014;
McLeer & McNeils, 2012; Pasterfield, 2009; Shattuck et al., 2012). In the absence of
appropriate support and intervention opportunities, families frequently face
challenges assisting their relatives with ASD to navigate the social transitions and
increasing demands throughout adolescence and adulthood (Howlin & Moss, 2012).
2.4.2. Potential areas of difficulty for adults with ASD. Many adults with
ASD, including higher-functioning individuals with intelligence in the average range,
experience ongoing challenges across multiple domains associated with the socio-
communicative deficits, sensory sensitivities and behavioural and cognitive rigidity
that are characteristic of ASD (Billstedt et al., 2007; Howlin et al., 2004; Howlin &
24
Moss, 2012; Levy & Perry, 2011; Marriage et al., 2009; Mazurek, 2014; Tobin et al.,
2014). Few adults with ASD live independently, social participation is typically
restricted and low academic and vocational achievement are common amongst the
adult ASD population (Billstedt et al., 2005; Cederlund et al., 2008; Eaves & Ho,
2008; Gray et al., 2014; Holwerda et al., 2012; Howlin et al., 2004; Howlin et al.,
2000; Marriage et al., 2009). Further, the characteristic features of ASD have been
argued to precipitate engagement in socially unacceptable or destructive conduct that,
in the absence of appropriate supports, may place adolescents and adults with ASD at
greater risk of becoming involved in the CJS (Barry-Walsh & Mullen, 2004;
Mouridsen, 2012).
2.4.2.1. Low levels of social participation. International research has
consistently indicated that fewer than half of adults with ASD regularly participate in
community-based social events or recreational activities that would provide
opportunities to establish and maintain positive social relationships (Barnard et al.,
2001; Billstedt et al., 2007; Eaves & Ho, 2008; Liptak, Kennedy, & Dosa, 2011).
Barnard et al. (2001) found that approximately a third (31%) of adults with autism or
Asperger’s syndrome did not participate in any social activities whatsoever. Further,
studies comparing social functioning amongst similar-aged peers suggest that adults
with ASD are more socially isolated than those with non-spectrum developmental
disabilities, learning disorders and emotional disturbances (Anderson et al., 2011;
Orsmond et al., 2013).
2.4.2.2. Loneliness and social dissatisfaction. Given that desired levels of
social participation may vary substantially between individuals, it is important to
consider the subjective experiences of adults with ASD regarding this domain of
functioning (Henninger & Taylor, 2013; Tobin et al., 2014). While it is evident that
25
low levels of social participation are common amongst adults with ASD, the impact
of such on the wellbeing and quality of life of this population appears to be variable.
The extant research suggests that feelings of loneliness are common amongst
adolescents and adults with ASD (Jobe & Williams White, 2007; Mazurek, 2014;
Müller, Schuler, & Yates, 2008; Whitehouse, Durkin, Jaquet, & Ziatas, 2009) and
depressive and anxious symptomatology in the context of low social connectedness
have been reported amongst this population (Mazurek, 2014; Müller et al., 2008).
Increasing dissatisfaction and distress have been reported by some individuals with
ASD throughout adolescence and adulthood as they become increasingly cognizant of
their socio-communicative difficulties and social isolation (Müller et al., 2008).
Conversely, some adults with ASD appear indifferent or may embrace their social
isolation, for example by identifying as a “lone wolf” (Müller et al., 2008, p. 179).
While the research suggests that some adults with ASD experience loneliness
and emotional disturbance in response to social isolation, there are others for whom
low levels of social connectedness and participation do not appear to cause distress.
For example, in an investigation of social outcomes amongst a group of men (n = 19)
who were diagnosed with ASD in childhood, little or no sense of loneliness was
reported by informants in a majority of cases (63%) despite an observed lack of
friendships amongst these individuals (Howlin et al., 2000). It has been argued that
individuals with ASD may be protected from the ill-effects of poor social functioning
where they gain a sense of identify and self-worth through achievement in other
domains (Attwood, 2007). For example, Temple Grandin, a high-functioning woman
with a diagnosis of ASD, reports that her sense of achievement in employment has
reduced the impact of her social isolation, stating that:
26
I know that things are missing in my life but I have an exciting career that
occupies my every waking hour. Keeping myself busy keeps my mind off
what I may be missing. Sometimes parents and professionals worry too much
about the social life of an adult with autism (Grandin, 2006, p. 160).
Having a fulfilling and meaningful work-life may therefore protect some
individuals from experiencing psychological distress in response to challenges in
social functioning (Attwood, 2007). Unfortunately, the available evidence indicates
that adults with ASD frequently face challenges associated with educational
engagement and workforce participation.
2.4.2.3. Low academic and vocational achievement. Low levels of
educational attainment, alongside inflated rates of unemployment and
underemployment have been reported to occur amongst the ASD population (ABS,
2014; Barnard et al., 2001; Eaves & Ho, 2008; Gray et al., 2014; Holwerda et al.,
2012; Howlin et al., 2004; Pasterfield, 2009; Tobin et al., 2014). In a UK study of
social outcomes amongst more than 400 individuals, employment was identified by
more able adults with ASD as the most significant barrier they faced (Barnard et al.,
2001). Despite a wide range of general and specific marketable skills amongst adults
with ASD, it is estimated that approximately half of this population neither engages
in employment nor educational pursuits (Barnard et al., 2001; Eaves & Ho, 2008;
Howlin & Moss, 2012; Tobin et al., 2014). As little as 2% of individuals with more
severe manifestations of ASD are in any kind of paid employment (Barnard et al.,
2001) and those adults who are employed frequently work in menial positions with
poor pay rates (Eaves & Ho, 2008). Consequently, individuals with ASD frequently
lack the financial resources to support independent living (ABS, 2014; Howlin et al.,
2004). Further, given that unemployment is associated with psychological distress in
27
the general population (Paul & Moser, 2009), it is unlikely that economic instability
will be the only significant impact of low vocational engagement amongst adults with
ASD.
Vocational and educational disengagement results in fewer opportunities for
social integration and interaction alongside a lack of purpose and structured routine
within daily life (Paul & Moser, 2009). The loss of these aspects of employment may
be of particular concern for individuals with ASD due to difficulties experienced in
the social domain, proneness to emotional disturbance and a tendency towards
defining self-identity according to vocational achievements (Attwood, 2007).
Consequently, the low levels of academic and vocational engagement observed
amongst adults with ASD are likely to impact perceptions of self-worth and ability to
cope with life stressors amongst this population (Attwood, 2007; ABS, 2014). When
coupled with the socio-communicative and behavioural impairments characteristic of
ASD, feelings of low self-worth and poor coping skills may increase the likelihood of
engagement in self-injurious or disruptive behaviours.
2.4.2.4. Challenging Behaviours and Forensic issues. It is not uncommon
for adults with ASD to display a range of challenging behaviours, including self-
injurious behaviours as well as aggressive and disruptive behaviour directed towards
others (Billstedt et al., 2005; Matson & Adams, 2014; McClintock, Hall, & Oliver,
2003; McNeils & McLeer, 2012; Périsse et al., 2010; Tantam, 2003). Such
behaviours appear to occur amongst adults with ASD with high frequency and
chronicity and have been cited as one of the most common precursors to
psychopharmacological and other specialist intervention throughout the ASD
population (Billstedt et al., 2005; Murphy et al., 2005). For example, a meta-analysis
regarding challenging behaviours amongst individuals with ID demonstrated that
28
aggression, property damage and self-injurious behaviours are more prevalent
amongst individuals with primary diagnoses of ASD than amongst peers without
ASD diagnoses (McClintock et al., 2003). Inappropriate sexual behaviours have also
been noted to occur amongst the ASD population (Haracopos & Pedersen, 1992;
Ruble & Dalrymple, 1993). Such behaviours may at times result in substantial harm
to the self or others and in some circumstances may result in forensic ramifications
(King & Murphy, 2014; Raggi et al., 2013).
2.5. Summary of Chapter
Individuals with ASD are a diverse population with marked heterogeneity in
socio-communicative and behavioural abilities and idiosyncrasies. The preceding
chapter provided an overview of the epidemiology of ASD, with a particular focus on
issues related to presentation, support needs and difficulties experienced in adulthood.
Although the academic literature regarding ASD in adulthood remains limited, it is
clear that significant variations in psychosocial outcomes exist amongst this
population. Specifically, while the extant research indicates that most individuals
with ASD integrate successfully into the community, some are evidently less
successful in doing so and poor outcomes across several important domains are not
uncommon. Of particular interest, challenging behaviours are evident amongst those
with poorer outcomes, which on some occasions may result in forensic consequences.
Although this does not mean that all or most people with ASD will engage in
offending behaviours in adulthood, it is important to consider the extent to which
offending behaviour may occur amongst the ASD population, and the appropriate
forensic response where such behaviours do occur. Offending behaviours and the
forensic issues that arise when offending behaviour is perpetrated by adults with ASD

29
form the primary focus of the current thesis, and are considered in more detail in the
following chapters.
30
Chapter 3. Autism Spectrum Disorder and Offending Behaviour
Discussed in Chapter 1, in recent years, a concerning trend has arisen whereby
individuals who have committed heinous crimes have been reported as being “on the
spectrum” within media reports and the academic literature. Such assumptions appear
to have led to the perception that individuals with ASD diagnoses are dangerous and
possess an elevated propensity towards the perpetration of serious violent offences. In
an attempt to address such perceptions, and to provide some context regarding the
scope of the forensic relevance of ASD, the current chapter explores the extant
academic literature regarding the prevalence and nature of offending behaviour
observed amongst the ASD population.
3.1. Case Reports of Offending Perpetrated by Individuals with Autism
Spectrum Disorder
Instances of offending behaviour perpetrated by individuals with ASD have
been described in case reports throughout the academic literature. Asperger (1944)
himself commented on physical aggression and perceived violent tendencies amongst
the children he examined; however, Mawson, Grounds, and Tantam (1985) appear to
have been the first to explicitly argue the presence of a direct association between an
ASD diagnosis and offending behaviour. Mawson et al. (1985) described a 44-year-
old man who met diagnostic criteria for Asperger’s syndrome and who possessed an
extensive history of engagement in violent behaviours, with ostensibly unusual
motivations. For example, it was reported that this individual assaulted, or attempted
to assault, several women (including stabbing two with a screwdriver) due to his
disapproval of their attire or dislike of women drivers and, on more than one
occasion, engaged in assaultive behaviour in attempts to silence noisy pets or crying
infants and children. It was further noted that he disclosed a series of obsessive
31
violent cognitions while incarcerated, for example, an interest in the effects of
poisons and fantasies regarding the dissection of infants. On the basis of this single
case study, Mawson et al. (1985) speculated that the “association between Asperger’s
syndrome and violent behavior is more common than has been recognized and that
more such individuals are to be found in long-term care institutions” (p. 569).
A proliferation of case reports describing offending behaviour amongst
individuals with autism and Asperger’s syndrome has since corroborated Mawson et
al.’s (1985) initial study. Such reports involve adjudicated and non-adjudicated
instances of stealing, fire-setting, sexual offending and non-sexualized violent
behaviour (including homicide), as well as harm caused to others as a consequence of
specialised interests (e.g. with medical experimentation, the mechanisms of
paedophilia or the flickering of flames) or poor social decision-making (e.g.
Chesterman & Rutter, 1993; Everall & Lecouteur, 1990; Griffin-Shelley, 2010;
Haskins & Silva, 2006; Katz & Zemishlany, 2006; Kelbrick & Radley, 2013;
Kristiansson & Sorman, 2008; Radley & Shaherbano, 2011; Raja & Azzoni, 2001;
Ray, Marks, & Bray-Garretson, 2010; Schwartz-Watts, 2005). However, despite
increasing availability, it is not clear that academic case reports describing instances
of offending are representative of the larger population of individuals with ASD.
Indeed, two large-scale literature reviews exist that provide a challenge to the
proposition of a systematic association between ASD and offending behaviour.
Ghaziuddin, Tsai and Ghaziuddin (1991) reviewed 21 studies (primarily case
reports) regarding the clinical features of Asperger’s syndrome published between
1944 and 1990 for evidence of violent behaviour amongst the included individuals (n
= 132). On the basis of this review, the authors concluded that there was no clear
evidence of an association between Asperger’s syndrome and violent crime. More
32
recently, Mouridsen (2012) provided a narrative review that included 23 empirical
studies and case reports regarding the hypothesized relationship between ASD and
offending and similarly concluded that there was no clear evidence that individuals
with ASD are any more likely than the general population to engage in offending
behaviour. However, the methodology employed in these reviews may have skewed
results and impacted generalizability of their stated conclusions. For example, narrow
inclusion criteria adopted by Ghaziuddin et al. (1991) resulted in the exclusion of a
number of studies (e.g. Tantam, 1988) that, if included, would have increased the
incidence of violent behaviours within their sample. Mouridsen (2012) did not
provide an account of their adopted search strategy nor exclusion criteria, thus
limiting the opportunity to evaluate the likely inclusiveness of their review. What
follows is an updated overview of the empirical literature that has investigated the
prevalence and characteristics of offending behaviour amongst individuals with ASD.
3.2. Prevalence of Offending Behaviour Amongst Individuals with Autism
Spectrum Disorder
In order to provide an updated review of the empirical evidence regarding the
rate of offending amongst individuals with ASD, a systematic literature search with
no date parameters was conducted. Published research that explored the intersect
between ASD and offending behaviour was identified by means of a four-stage
search process: (1) literature databases (PsycINFO, PubMed, PsycEXTRA) and other
online search engines (e.g. Google) were used to identify studies that considered ASD
and offending; (2) backwards citation searches were undertaken with literature
identified in the first stage of the search process; (3) hand-search of journals likely to
include relevant papers (e.g. Journal of Intellectual Disabilities and Offending Special
Issue: Autism Spectrum Conditions and Offending); and (4) citation searches of
33
unpublished theses and online articles on the topic of ASD and crime. Search terms
were Autis*, Asperger*, ASD, pervasive developmental disorder,
neurodevelopmental and offend*, crim*, violen*, forensic. Each of the ASD-relevant
search terms was entered alongside each of the offending-relevant search terms. A
full-text copy of one conference paper (Hawes, 2003) identified in stage two of the
search procedure was unable to be sourced via online databases and was consequently
requested and provided via email by the editor of the conference proceedings.
Inclusion criteria were deliberately wide to allow a more comprehensive
overview than previous reviews: all original studies that discussed prevalence or
frequency of ASD among offending populations and/or offending behaviour among
individuals with a diagnosis or traits of ASD were included for analysis. Articles
were excluded if they were descriptive case reports, they were concerned with
witnesses or victims with ASD, rather than suspects or offenders, they were focused
on treatment or characteristics of offending and did not provide information regarding
prevalence or they were literature reviews.
A total of 33 original studies that met inclusion criteria were identified; these
comprised research of two kinds: that which investigated the presence of ASD within
offending populations (represented in Table 2) and that which considered the rate of
offending amongst ASD populations (represented in Table 3). The identified studies
lacked consistency in their adopted diagnostic approach, consideration of
confounding factors and definitions of offending behaviour. As a consequence of the
vast methodological variation between studies, a meta-analysis was not undertaken
and the current review was limited to a descriptive synthesis and analysis of results.
3.2.1. Research regarding prevalence of ASD amongst offending
populations. As seen in Table 2, prevalence estimates for ASD in forensic settings
34
varied significantly across the literature, ranging from 0.2% for Asperger’s syndrome
in a consecutive series of patients admitted to a secure psychiatric intensive care unit
in Italy (Raja & Azzoni, 2001) to 30% for ASD amongst those admitted to an English
inpatient forensic intellectual disability service over a 6-year period (Esan, Chester,
Gunaratna, Hoare, & Alexander, 2015). Such variation in prevalence estimates may
be artefactual, reflecting differences in methodology and sample characteristics
between studies. Comparison groups have not been employed consistently across all
studies of this nature and without understanding the characteristics of the highly
selected and specialized study samples, questions remain regarding the
appropriateness of those comparisons that have been made. For example, concerns
have been raised regarding the appropriateness of comparison between the prevalence
of ASD in secure facilities and the prevalence of ASD reported by Ehlers and
Gillberg (1993) amongst school-aged children in mainstream Swedish schools (Hall
& Bernal, 1995).
The observed variation in prevalence estimates may also reflect true
differences in prevalence rates for ASD across different jurisdictions due to the
availability of diversion options or support services and differences in sentencing
policies and practices within each jurisdiction. Similarly, differences may exist
between settings within the same jurisdiction as a function of the stage of disposition
and disparities in the identification and accommodation of psychological disorder.
For example, inflated rates of ASD observed within secure psychiatric facilities may,
at least in part, be due to the recognition and subsequent diversion of such individuals
from prison environments (Robinson et al., 2012). Relatedly, for some of the secure
settings surveyed by researchers, admissions were occasionally made on the basis of
unmanageable behaviour in less secure settings, rather than for offending behaviour
35
per se (e.g. Scragg & Shah, 1994). Nonetheless, when compared to the prevalence
rate of 1% for ASD in the general population reported by the DSM-5 (APA, 2013),
the cumulative results of the included studies are suggestive of an overrepresentation
of ASD within forensic settings (King & Murphy, 2014).
Of note, an overrepresentation of ASD amongst offending populations may
not necessarily be reflective of a higher risk of offending amongst individuals with
ASD. In contrast, any inflation in ASD rates observed in forensic settings could occur
due to systematic vulnerabilities within the CJS, resulting in an increased likelihood
that individuals with ASD are detected and/or convicted for involvement in offending
behaviours (Mouridsen, 2012). Studies suggest that individuals with ASD are often
misinterpreted during police questioning, have a tendency to be overly compliant, are
quick to admit guilt and frequently stick rigidly to an account once it has been put
forward (Allen et al., 2008; de la Cuesta, 2010; Murrie et al., 2002; North, Russell, &
Gudjonsson, 2008) Additionally, due to deficits in understanding social cues, a
tendency to be poor historians and difficulty differentiating their actions from those
of others, individuals with ASD may not present as credible suspects in court (Hare,
Gould, Mills, & Wing, Freckelton & List, 2009; 1999). In light of these
considerations, some authors have suggested that the inflated prevalence rates
reported in studies that identify ASD in offending populations represent an over-
estimation of the true rate of offending amongst individuals with ASD.
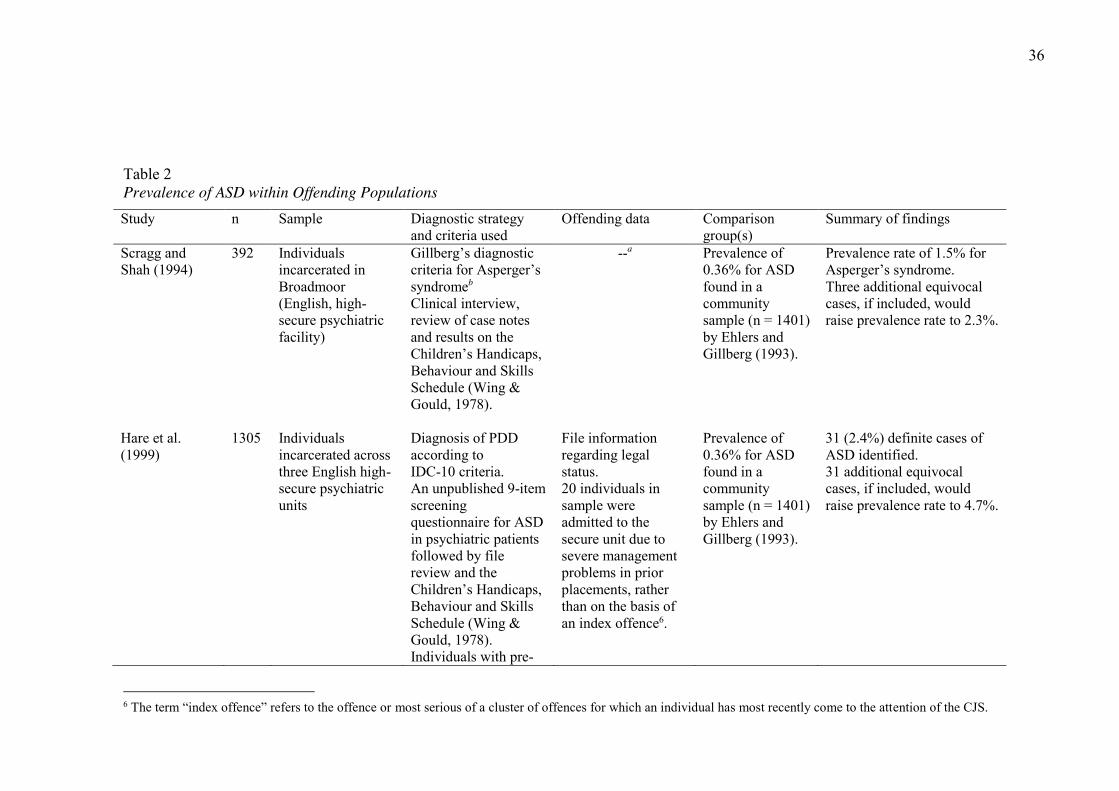
36
Table 2 Prevalence of ASD within Offending Populations Study
n Sample Diagnostic strategy and criteria used
Offending data Comparison group(s)
Summary of findings
Scragg and Shah (1994)
392 Individuals incarcerated in Broadmoor (English, high-secure psychiatric facility)
Gillberg’s diagnostic criteria for Asperger’s syndromeb Clinical interview, review of case notes and results on the Children’s Handicaps, Behaviour and Skills Schedule (Wing & Gould, 1978).
--a Prevalence of 0.36% for ASD found in a community sample (n = 1401) by Ehlers and Gillberg (1993).
Prevalence rate of 1.5% for Asperger’s syndrome. Three additional equivocal cases, if included, would raise prevalence rate to 2.3%.
Hare et al. (1999)
1305 Individuals incarcerated across three English high-secure psychiatric units
Diagnosis of PDD according to IDC-10 criteria. An unpublished 9-item screening questionnaire for ASD in psychiatric patients followed by file review and the Children’s Handicaps, Behaviour and Skills Schedule (Wing & Gould, 1978). Individuals with pre-
File information regarding legal status. 20 individuals in sample were admitted to the secure unit due to severe management problems in prior placements, rather than on the basis of an index offence6.
Prevalence of 0.36% for ASD found in a community sample (n = 1401) by Ehlers and Gillberg (1993).
31 (2.4%) definite cases of ASD identified. 31 additional equivocal cases, if included, would raise prevalence rate to 4.7%.
6 The term “index offence” refers to the offence or most serious of a cluster of offences for which an individual has most recently come to the attention of the CJS.
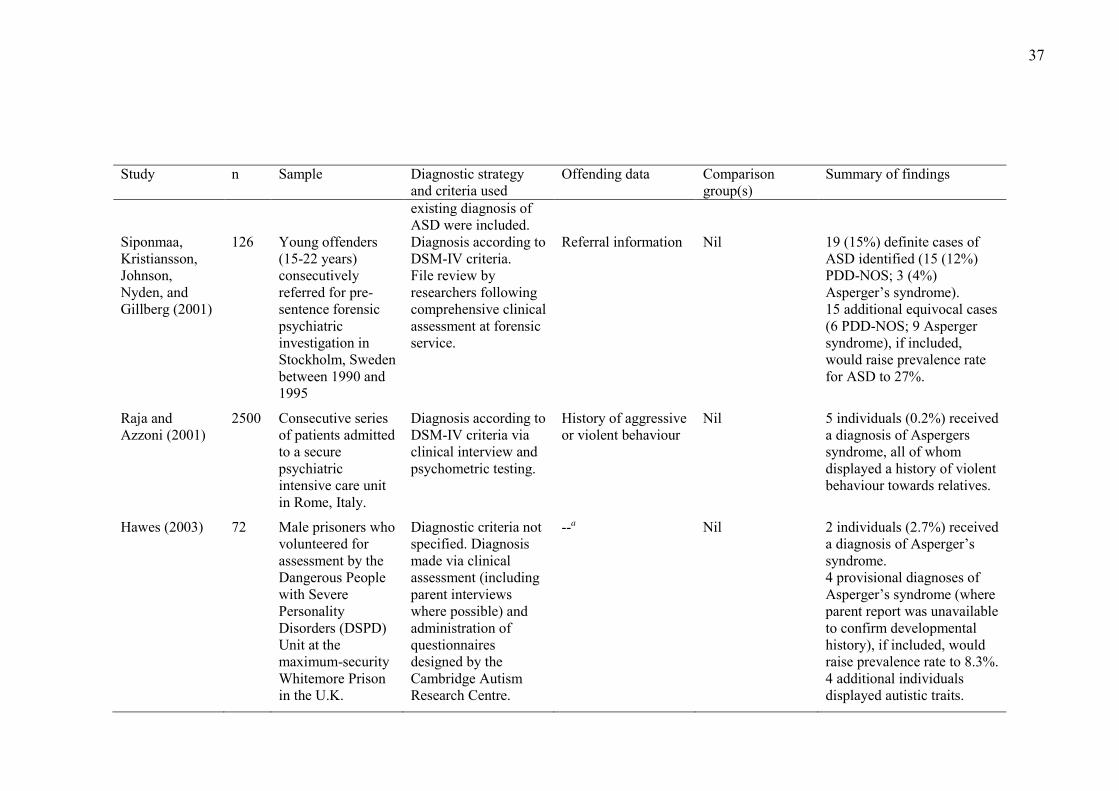
37
Study
n Sample Diagnostic strategy and criteria used
Offending data Comparison group(s)
Summary of findings
existing diagnosis of ASD were included.
Siponmaa, Kristiansson, Johnson, Nyden, and Gillberg (2001)
126 Young offenders (15-22 years) consecutively referred for pre-sentence forensic psychiatric investigation in Stockholm, Sweden between 1990 and 1995
Diagnosis according to DSM-IV criteria. File review by researchers following comprehensive clinical assessment at forensic service.
Referral information Nil 19 (15%) definite cases of ASD identified (15 (12%) PDD-NOS; 3 (4%) Asperger’s syndrome). 15 additional equivocal cases (6 PDD-NOS; 9 Asperger syndrome), if included, would raise prevalence rate for ASD to 27%.
Raja and Azzoni (2001)
2500 Consecutive series of patients admitted to a secure psychiatric intensive care unit in Rome, Italy.
Diagnosis according to DSM-IV criteria via clinical interview and psychometric testing.
History of aggressive or violent behaviour
Nil 5 individuals (0.2%) received a diagnosis of Aspergers syndrome, all of whom displayed a history of violent behaviour towards relatives.
Hawes (2003) 72 Male prisoners who volunteered for assessment by the Dangerous People with Severe Personality Disorders (DSPD) Unit at the maximum-security Whitemore Prison in the U.K.
Diagnostic criteria not specified. Diagnosis made via clinical assessment (including parent interviews where possible) and administration of questionnaires designed by the Cambridge Autism Research Centre.
--a Nil 2 individuals (2.7%) received a diagnosis of Asperger’s syndrome. 4 provisional diagnoses of Asperger’s syndrome (where parent report was unavailable to confirm developmental history), if included, would raise prevalence rate to 8.3%. 4 additional individuals displayed autistic traits.
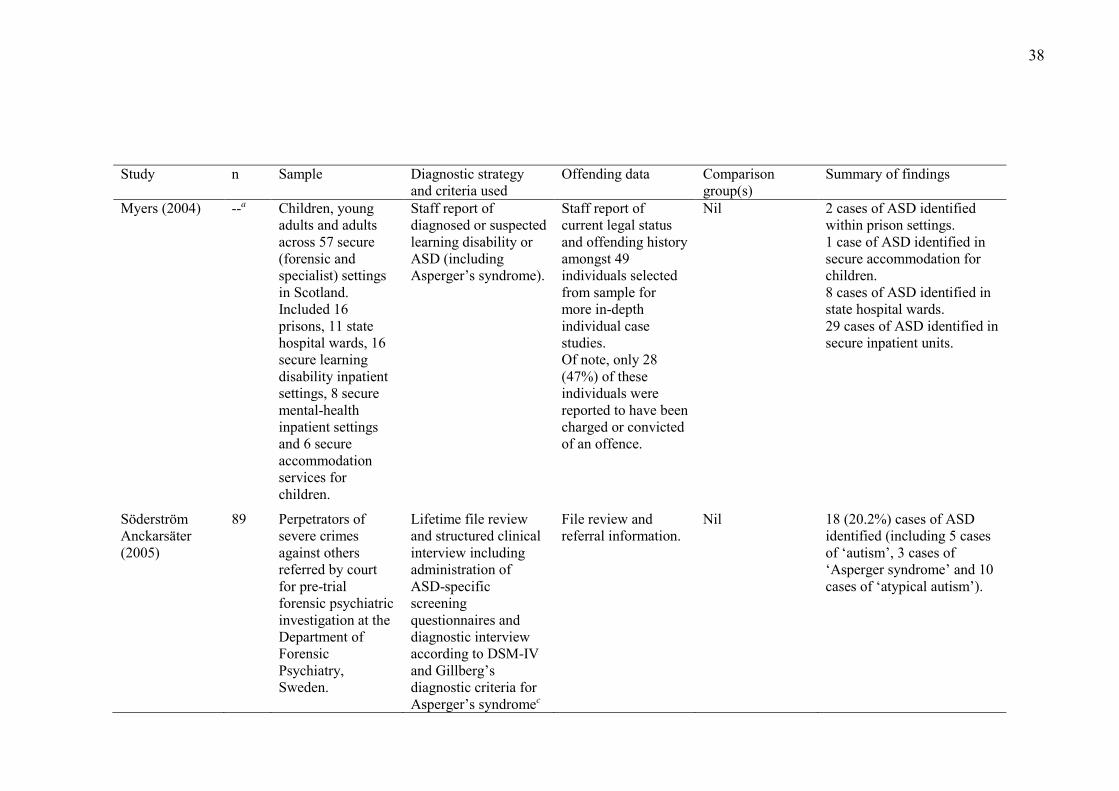
38
Study
n Sample Diagnostic strategy and criteria used
Offending data Comparison group(s)
Summary of findings
Myers (2004) --a Children, young adults and adults across 57 secure (forensic and specialist) settings in Scotland. Included 16 prisons, 11 state hospital wards, 16 secure learning disability inpatient settings, 8 secure mental-health inpatient settings and 6 secure accommodation services for children.
Staff report of diagnosed or suspected learning disability or ASD (including Asperger’s syndrome).
Staff report of current legal status and offending history amongst 49 individuals selected from sample for more in-depth individual case studies. Of note, only 28 (47%) of these individuals were reported to have been charged or convicted of an offence.
Nil 2 cases of ASD identified within prison settings. 1 case of ASD identified in secure accommodation for children. 8 cases of ASD identified in state hospital wards. 29 cases of ASD identified in secure inpatient units.
Söderström Anckarsäter (2005)
89 Perpetrators of severe crimes against others referred by court for pre-trial forensic psychiatric investigation at the Department of Forensic Psychiatry, Sweden.
Lifetime file review and structured clinical interview including administration of ASD-specific screening questionnaires and diagnostic interview according to DSM-IV and Gillberg’s diagnostic criteria for Asperger’s syndromec
File review and referral information.
Nil 18 (20.2%) cases of ASD identified (including 5 cases of ‘autism’, 3 cases of ‘Asperger syndrome’ and 10 cases of ‘atypical autism’).
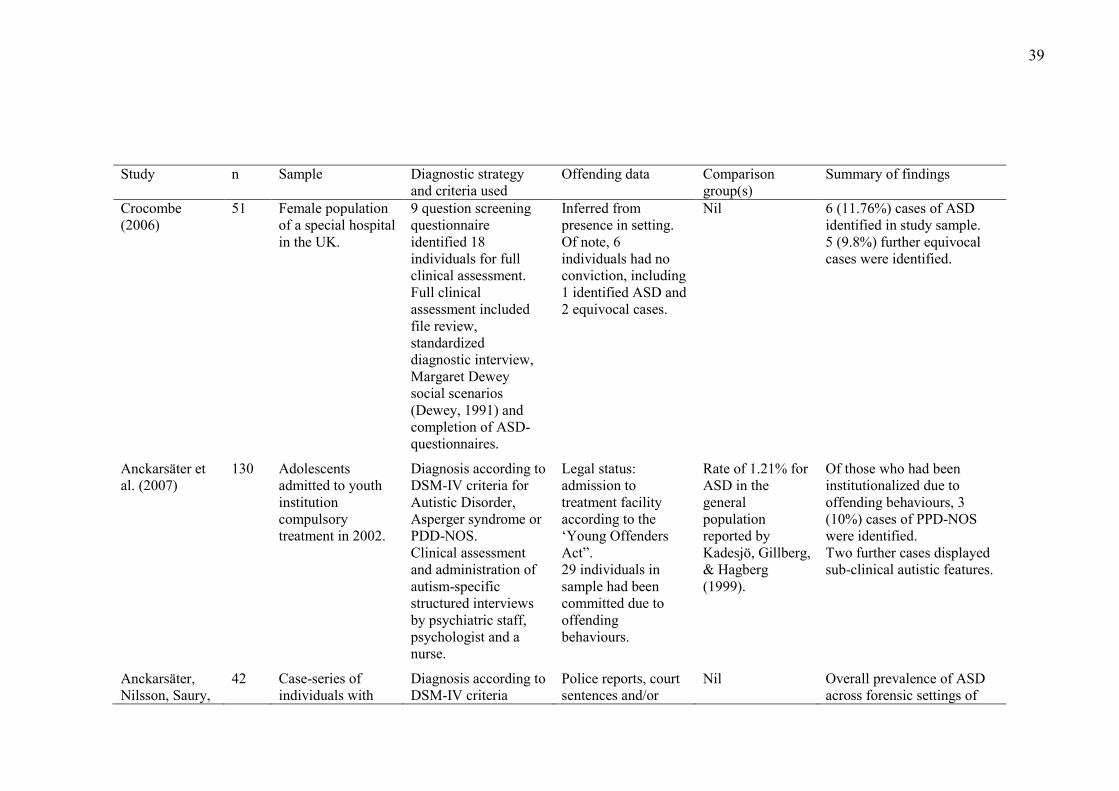
39
Study
n Sample Diagnostic strategy and criteria used
Offending data Comparison group(s)
Summary of findings
Crocombe (2006)
51 Female population of a special hospital in the UK.
9 question screening questionnaire identified 18 individuals for full clinical assessment. Full clinical assessment included file review, standardized diagnostic interview, Margaret Dewey social scenarios (Dewey, 1991) and completion of ASD- questionnaires.
Inferred from presence in setting. Of note, 6 individuals had no conviction, including 1 identified ASD and 2 equivocal cases.
Nil 6 (11.76%) cases of ASD identified in study sample. 5 (9.8%) further equivocal cases were identified.
Anckarsäter et al. (2007)
130 Adolescents admitted to youth institution compulsory treatment in 2002.
Diagnosis according to DSM-IV criteria for Autistic Disorder, Asperger syndrome or PDD-NOS. Clinical assessment and administration of autism-specific structured interviews by psychiatric staff, psychologist and a nurse.
Legal status: admission to treatment facility according to the ‘Young Offenders Act”. 29 individuals in sample had been committed due to offending behaviours.
Rate of 1.21% for ASD in the general population reported by Kadesjö, Gillberg, & Hagberg (1999).
Of those who had been institutionalized due to offending behaviours, 3 (10%) cases of PPD-NOS were identified. Two further cases displayed sub-clinical autistic features.
Anckarsäter, Nilsson, Saury,
42 Case-series of individuals with
Diagnosis according to DSM-IV criteria
Police reports, court sentences and/or
Nil Overall prevalence of ASD across forensic settings of
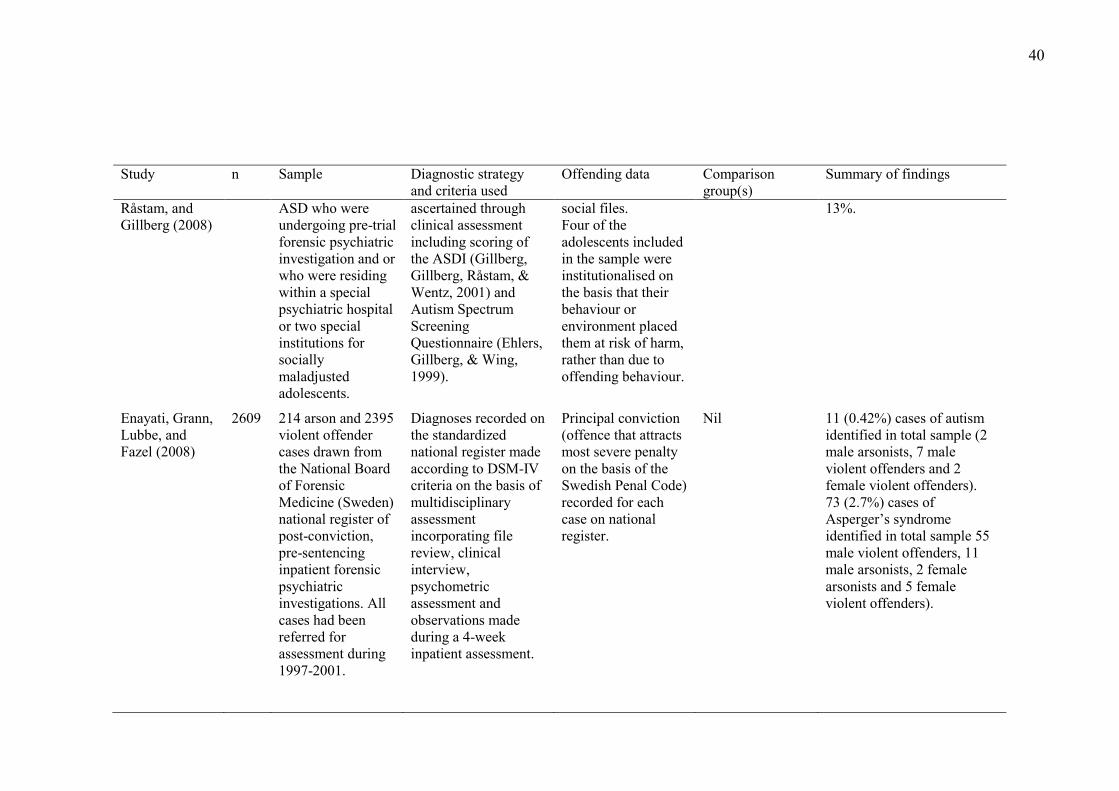
40
Study
n Sample Diagnostic strategy and criteria used
Offending data Comparison group(s)
Summary of findings
Råstam, and Gillberg (2008)
ASD who were undergoing pre-trial forensic psychiatric investigation and or who were residing within a special psychiatric hospital or two special institutions for socially maladjusted adolescents.
ascertained through clinical assessment including scoring of the ASDI (Gillberg, Gillberg, Råstam, & Wentz, 2001) and Autism Spectrum Screening Questionnaire (Ehlers, Gillberg, & Wing, 1999).
social files. Four of the adolescents included in the sample were institutionalised on the basis that their behaviour or environment placed them at risk of harm, rather than due to offending behaviour.
13%.
Enayati, Grann, Lubbe, and Fazel (2008)
2609 214 arson and 2395 violent offender cases drawn from the National Board of Forensic Medicine (Sweden) national register of post-conviction, pre-sentencing inpatient forensic psychiatric investigations. All cases had been referred for assessment during 1997-2001.
Diagnoses recorded on the standardized national register made according to DSM-IV criteria on the basis of multidisciplinary assessment incorporating file review, clinical interview, psychometric assessment and observations made during a 4-week inpatient assessment.
Principal conviction (offence that attracts most severe penalty on the basis of the Swedish Penal Code) recorded for each case on national register.
Nil 11 (0.42%) cases of autism identified in total sample (2 male arsonists, 7 male violent offenders and 2 female violent offenders). 73 (2.7%) cases of Asperger’s syndrome identified in total sample 55 male violent offenders, 11 male arsonists, 2 female arsonists and 5 female violent offenders).
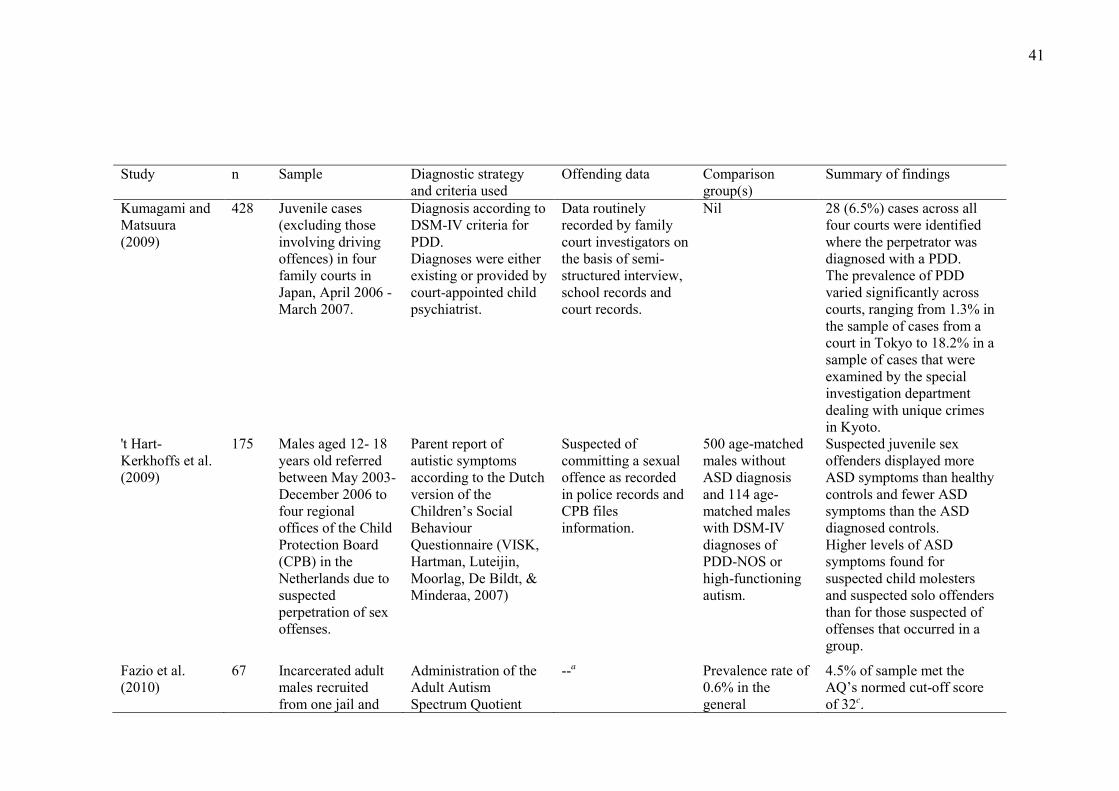
41
Study
n Sample Diagnostic strategy and criteria used
Offending data Comparison group(s)
Summary of findings
Kumagami and Matsuura (2009)
428 Juvenile cases (excluding those involving driving offences) in four family courts in Japan, April 2006 - March 2007.
Diagnosis according to DSM-IV criteria for PDD. Diagnoses were either existing or provided by court-appointed child psychiatrist.
Data routinely recorded by family court investigators on the basis of semi-structured interview, school records and court records.
Nil 28 (6.5%) cases across all four courts were identified where the perpetrator was diagnosed with a PDD. The prevalence of PDD varied significantly across courts, ranging from 1.3% in the sample of cases from a court in Tokyo to 18.2% in a sample of cases that were examined by the special investigation department dealing with unique crimes in Kyoto.
't Hart-Kerkhoffs et al. (2009)
175 Males aged 12- 18 years old referred between May 2003- December 2006 to four regional offices of the Child Protection Board (CPB) in the Netherlands due to suspected perpetration of sex offenses.
Parent report of autistic symptoms according to the Dutch version of the Children’s Social Behaviour Questionnaire (VISK, Hartman, Luteijin, Moorlag, De Bildt, & Minderaa, 2007)
Suspected of committing a sexual offence as recorded in police records and CPB files information.
500 age-matched males without ASD diagnosis and 114 age-matched males with DSM-IV diagnoses of PDD-NOS or high-functioning autism.
Suspected juvenile sex offenders displayed more ASD symptoms than healthy controls and fewer ASD symptoms than the ASD diagnosed controls. Higher levels of ASD symptoms found for suspected child molesters and suspected solo offenders than for those suspected of offenses that occurred in a group.
Fazio et al. (2010)
67 Incarcerated adult males recruited from one jail and
Administration of the Adult Autism Spectrum Quotient
--a Prevalence rate of 0.6% in the general
4.5% of sample met the AQ’s normed cut-off score of 32c.
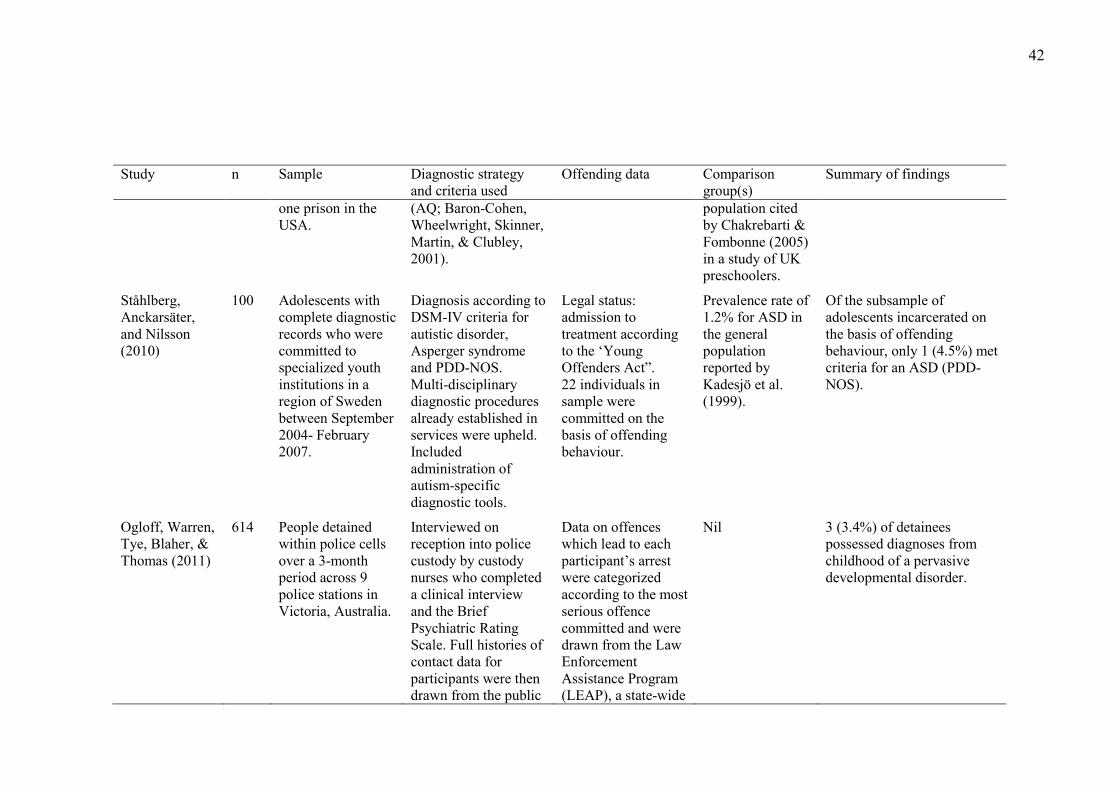
42
Study
n Sample Diagnostic strategy and criteria used
Offending data Comparison group(s)
Summary of findings
one prison in the USA.
(AQ; Baron-Cohen, Wheelwright, Skinner, Martin, & Clubley, 2001).
population cited by Chakrebarti & Fombonne (2005) in a study of UK preschoolers.
Ståhlberg, Anckarsäter, and Nilsson (2010)
100 Adolescents with complete diagnostic records who were committed to specialized youth institutions in a region of Sweden between September 2004- February 2007.
Diagnosis according to DSM-IV criteria for autistic disorder, Asperger syndrome and PDD-NOS. Multi-disciplinary diagnostic procedures already established in services were upheld. Included administration of autism-specific diagnostic tools.
Legal status: admission to treatment according to the ‘Young Offenders Act”. 22 individuals in sample were committed on the basis of offending behaviour.
Prevalence rate of 1.2% for ASD in the general population reported by Kadesjö et al. (1999).
Of the subsample of adolescents incarcerated on the basis of offending behaviour, only 1 (4.5%) met criteria for an ASD (PDD-NOS).
Ogloff, Warren, Tye, Blaher, & Thomas (2011)
614 People detained within police cells over a 3-month period across 9 police stations in Victoria, Australia.
Interviewed on reception into police custody by custody nurses who completed a clinical interview and the Brief Psychiatric Rating Scale. Full histories of contact data for participants were then drawn from the public
Data on offences which lead to each participant’s arrest were categorized according to the most serious offence committed and were drawn from the Law Enforcement Assistance Program (LEAP), a state-wide
Nil 3 (3.4%) of detainees possessed diagnoses from childhood of a pervasive developmental disorder.
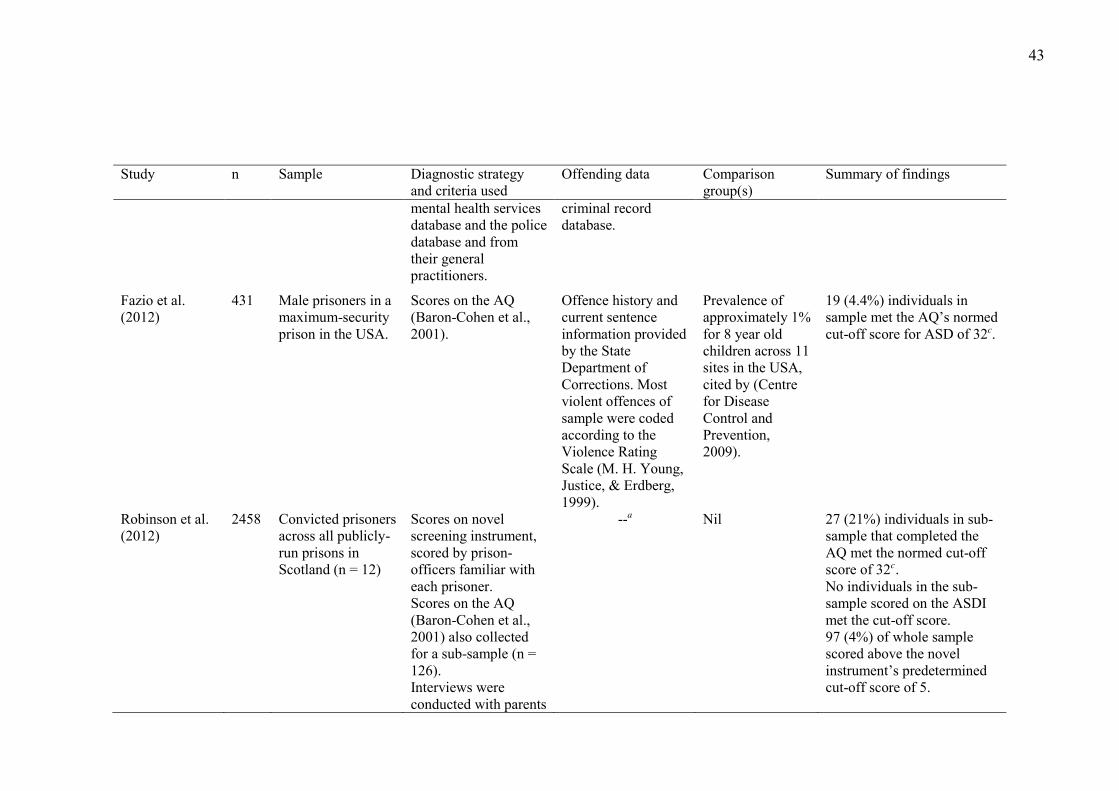
43
Study
n Sample Diagnostic strategy and criteria used
Offending data Comparison group(s)
Summary of findings
mental health services database and the police database and from their general practitioners.
criminal record database.
Fazio et al. (2012)
431 Male prisoners in a maximum-security prison in the USA.
Scores on the AQ (Baron-Cohen et al., 2001).
Offence history and current sentence information provided by the State Department of Corrections. Most violent offences of sample were coded according to the Violence Rating Scale (M. H. Young, Justice, & Erdberg, 1999).
Prevalence of approximately 1% for 8 year old children across 11 sites in the USA, cited by (Centre for Disease Control and Prevention, 2009).
19 (4.4%) individuals in sample met the AQ’s normed cut-off score for ASD of 32c.
Robinson et al. (2012)
2458 Convicted prisoners across all publicly-run prisons in Scotland (n = 12)
Scores on novel screening instrument, scored by prison-officers familiar with each prisoner. Scores on the AQ (Baron-Cohen et al., 2001) also collected for a sub-sample (n = 126). Interviews were conducted with parents
--a Nil 27 (21%) individuals in sub-sample that completed the AQ met the normed cut-off score of 32c. No individuals in the sub-sample scored on the ASDI met the cut-off score. 97 (4%) of whole sample scored above the novel instrument’s predetermined cut-off score of 5.
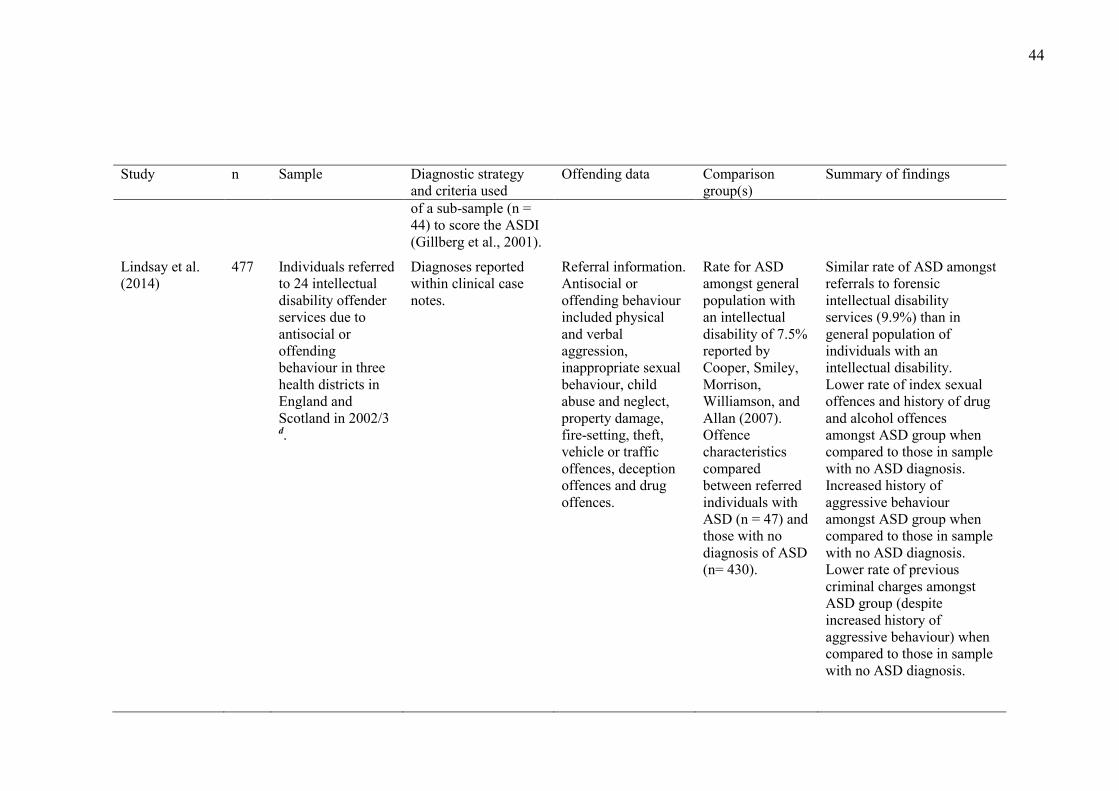
44
Study
n Sample Diagnostic strategy and criteria used
Offending data Comparison group(s)
Summary of findings
of a sub-sample (n = 44) to score the ASDI (Gillberg et al., 2001).
Lindsay et al. (2014)
477 Individuals referred to 24 intellectual disability offender services due to antisocial or offending behaviour in three health districts in England and Scotland in 2002/3
d.
Diagnoses reported within clinical case notes.
Referral information. Antisocial or offending behaviour included physical and verbal aggression, inappropriate sexual behaviour, child abuse and neglect, property damage, fire-setting, theft, vehicle or traffic offences, deception offences and drug offences.
Rate for ASD amongst general population with an intellectual disability of 7.5% reported by Cooper, Smiley, Morrison, Williamson, and Allan (2007). Offence characteristics compared between referred individuals with ASD (n = 47) and those with no diagnosis of ASD (n= 430).
Similar rate of ASD amongst referrals to forensic intellectual disability services (9.9%) than in general population of individuals with an intellectual disability. Lower rate of index sexual offences and history of drug and alcohol offences amongst ASD group when compared to those in sample with no ASD diagnosis. Increased history of aggressive behaviour amongst ASD group when compared to those in sample with no ASD diagnosis. Lower rate of previous criminal charges amongst ASD group (despite increased history of aggressive behaviour) when compared to those in sample with no ASD diagnosis.
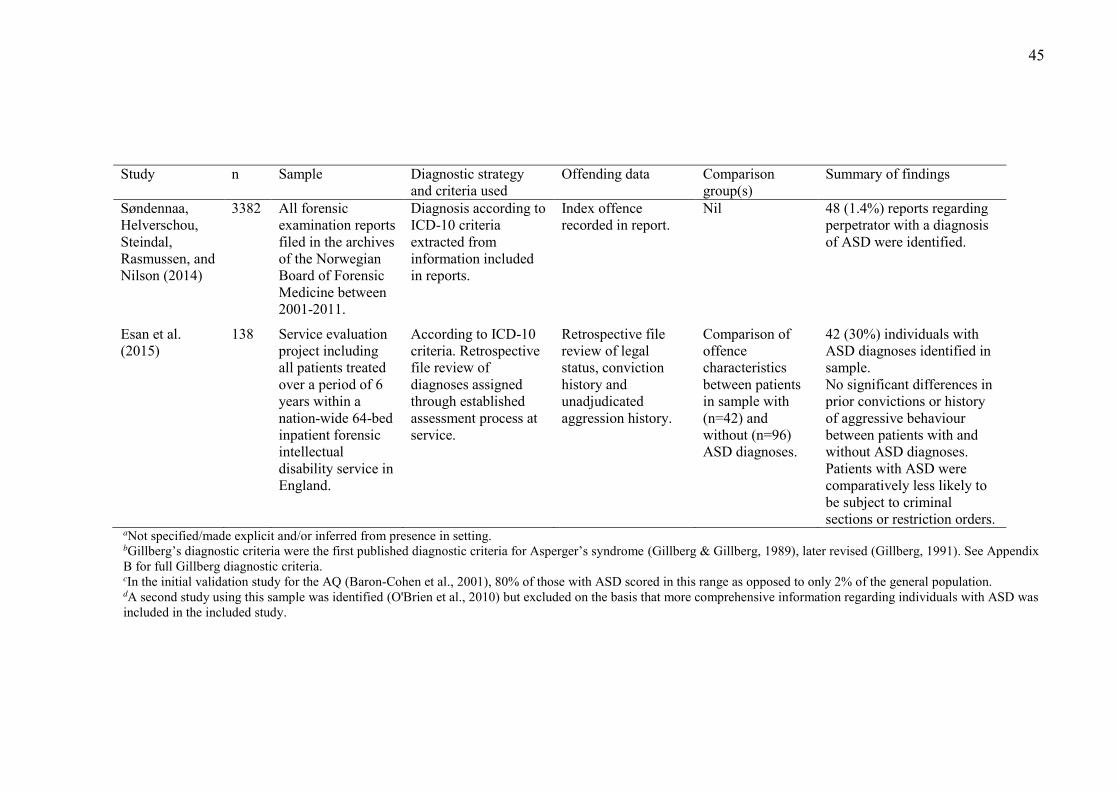
45
Study
n Sample Diagnostic strategy and criteria used
Offending data Comparison group(s)
Summary of findings
Søndennaa, Helverschou, Steindal, Rasmussen, and Nilson (2014)
3382 All forensic examination reports filed in the archives of the Norwegian Board of Forensic Medicine between 2001-2011.
Diagnosis according to ICD-10 criteria extracted from information included in reports.
Index offence recorded in report.
Nil 48 (1.4%) reports regarding perpetrator with a diagnosis of ASD were identified.
Esan et al. (2015)
138 Service evaluation project including all patients treated over a period of 6 years within a nation-wide 64-bed inpatient forensic intellectual disability service in England.
According to ICD-10 criteria. Retrospective file review of diagnoses assigned through established assessment process at service.
Retrospective file review of legal status, conviction history and unadjudicated aggression history.
Comparison of offence characteristics between patients in sample with (n=42) and without (n=96) ASD diagnoses.
42 (30%) individuals with ASD diagnoses identified in sample. No significant differences in prior convictions or history of aggressive behaviour between patients with and without ASD diagnoses. Patients with ASD were comparatively less likely to be subject to criminal sections or restriction orders.
aNot specified/made explicit and/or inferred from presence in setting. bGillberg’s diagnostic criteria were the first published diagnostic criteria for Asperger’s syndrome (Gillberg & Gillberg, 1989), later revised (Gillberg, 1991). See Appendix B for full Gillberg diagnostic criteria. cIn the initial validation study for the AQ (Baron-Cohen et al., 2001), 80% of those with ASD scored in this range as opposed to only 2% of the general population. dA second study using this sample was identified (O'Brien et al., 2010) but excluded on the basis that more comprehensive information regarding individuals with ASD was included in the included study.
46
3.2.2. Research regarding prevalence of offending amongst ASD
populations. Similar to research regarding ASD amongst offending populations,
considerable diversity exists in the methodology and results of studies that have
explored offending behaviours amongst those with ASD. As shown in Table 3,
prevalence estimates ranged from 0.5% for sexual convictions amongst individuals
with ASD admitted to Swedish hospitals (Langstrom, Grann, Ruchkin, Sjostedt, &
Fazel, 2009) to 48% for self-reported offending amongst a community-based sample
of adults with ASD in the UK (Woodbury-Smith, Clare, Holland, & Kearns, 2006)
and 52% for public masturbation amongst residents of (non-forensic) supported
accommodation services in Denmark (Haracopos & Pedersen, 1992). The method by
which studies defined and measured offending behaviour appeared to provide a
partial explanation for the variation in reported prevalence estimates. Unsurprisingly,
lower prevalence estimates were associated with studies limited to conviction data
(e.g. Hippler, Viding, Klicpera, & Happé, 2010; Langstrom et al., 2009) than those
where wider contact with the CJS was considered (e.g. Brookman-Frazee et al., 2009;
Cheely et al., 2012). Those studies that took into consideration the self-report or
observation of inappropriate, antisocial or offending behaviours (Haracopos &
Pedersen, 1992; Tantam, 1988; Woodbury-Smith et al., 2006) yielded the highest
prevalence rates.
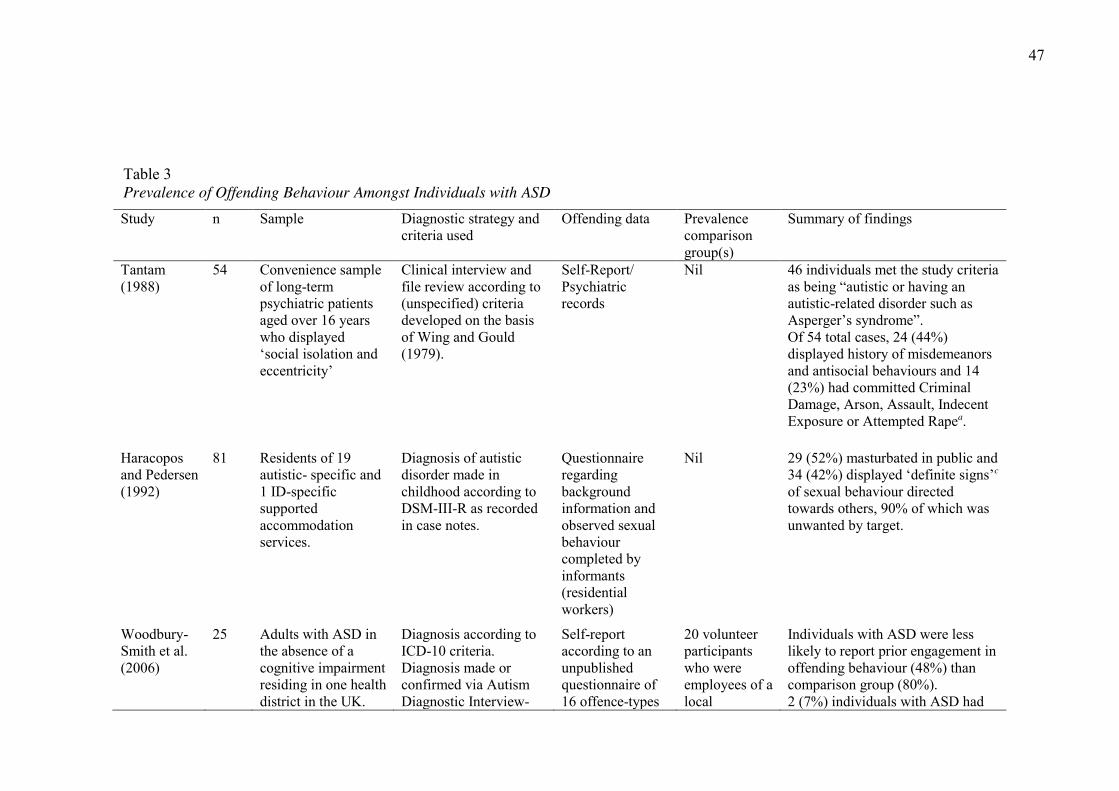
47
Table 3 Prevalence of Offending Behaviour Amongst Individuals with ASD Study n Sample Diagnostic strategy and
criteria used Offending data Prevalence
comparison group(s)
Summary of findings
Tantam (1988)
54 Convenience sample of long-term psychiatric patients aged over 16 years who displayed ‘social isolation and eccentricity’
Clinical interview and file review according to (unspecified) criteria developed on the basis of Wing and Gould (1979).
Self-Report/ Psychiatric records
Nil 46 individuals met the study criteria as being “autistic or having an autistic-related disorder such as Asperger’s syndrome”. Of 54 total cases, 24 (44%) displayed history of misdemeanors and antisocial behaviours and 14 (23%) had committed Criminal Damage, Arson, Assault, Indecent Exposure or Attempted Rapea.
Haracopos and Pedersen (1992)
81 Residents of 19 autistic- specific and 1 ID-specific supported accommodation services.
Diagnosis of autistic disorder made in childhood according to DSM-III-R as recorded in case notes.
Questionnaire regarding background information and observed sexual behaviour completed by informants (residential workers)
Nil 29 (52%) masturbated in public and 34 (42%) displayed ‘definite signs’c
of sexual behaviour directed towards others, 90% of which was unwanted by target.
Woodbury-Smith et al. (2006)
25 Adults with ASD in the absence of a cognitive impairment residing in one health district in the UK.
Diagnosis according to ICD-10 criteria. Diagnosis made or confirmed via Autism Diagnostic Interview-
Self-report according to an unpublished questionnaire of 16 offence-types
20 volunteer participants who were employees of a local
Individuals with ASD were less likely to report prior engagement in offending behaviour (48%) than comparison group (80%). 2 (7%) individuals with ASD had
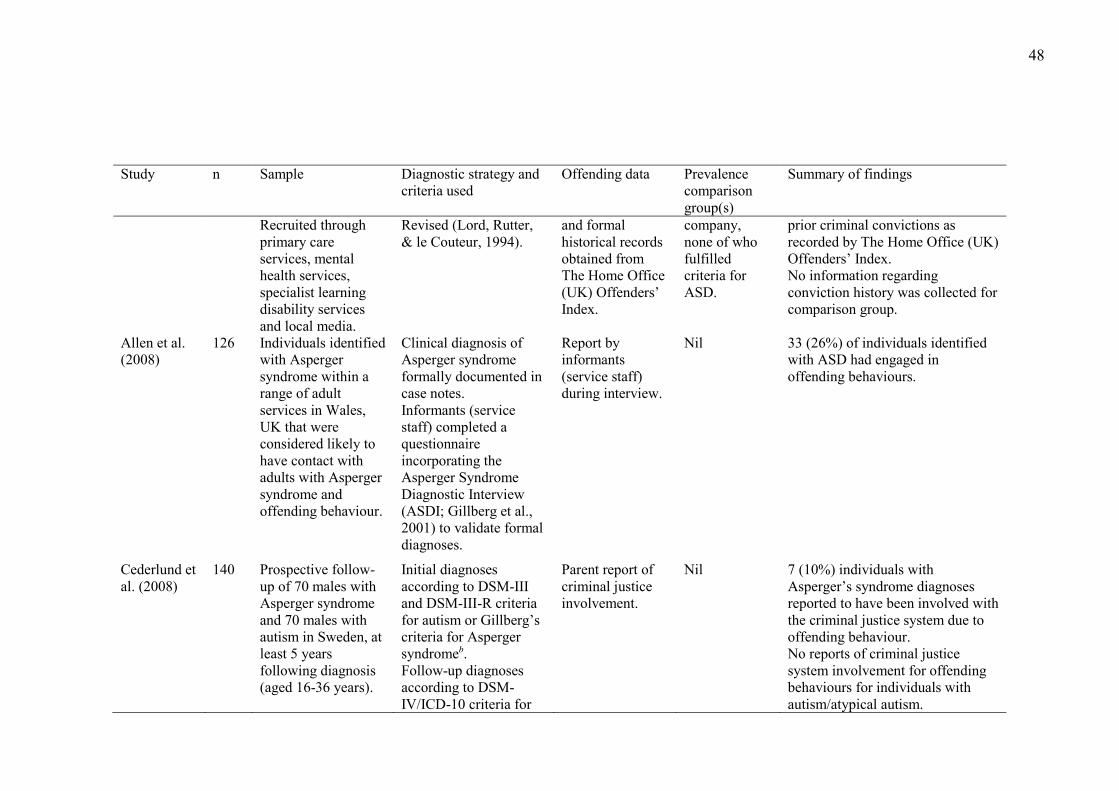
48
Study n Sample Diagnostic strategy and criteria used
Offending data Prevalence comparison group(s)
Summary of findings
Recruited through primary care services, mental health services, specialist learning disability services and local media.
Revised (Lord, Rutter, & le Couteur, 1994).
and formal historical records obtained from The Home Office (UK) Offenders’ Index.
company, none of who fulfilled criteria for ASD.
prior criminal convictions as recorded by The Home Office (UK) Offenders’ Index. No information regarding conviction history was collected for comparison group.
Allen et al. (2008)
126 Individuals identified with Asperger syndrome within a range of adult services in Wales, UK that were considered likely to have contact with adults with Asperger syndrome and offending behaviour.
Clinical diagnosis of Asperger syndrome formally documented in case notes. Informants (service staff) completed a questionnaire incorporating the Asperger Syndrome Diagnostic Interview (ASDI; Gillberg et al., 2001) to validate formal diagnoses.
Report by informants (service staff) during interview.
Nil 33 (26%) of individuals identified with ASD had engaged in offending behaviours.
Cederlund et al. (2008)
140 Prospective follow-up of 70 males with Asperger syndrome and 70 males with autism in Sweden, at least 5 years following diagnosis (aged 16-36 years).
Initial diagnoses according to DSM-III and DSM-III-R criteria for autism or Gillberg’s criteria for Asperger syndromeb. Follow-up diagnoses according to DSM-IV/ICD-10 criteria for
Parent report of criminal justice involvement.
Nil 7 (10%) individuals with Asperger’s syndrome diagnoses reported to have been involved with the criminal justice system due to offending behaviour. No reports of criminal justice system involvement for offending behaviours for individuals with autism/atypical autism.
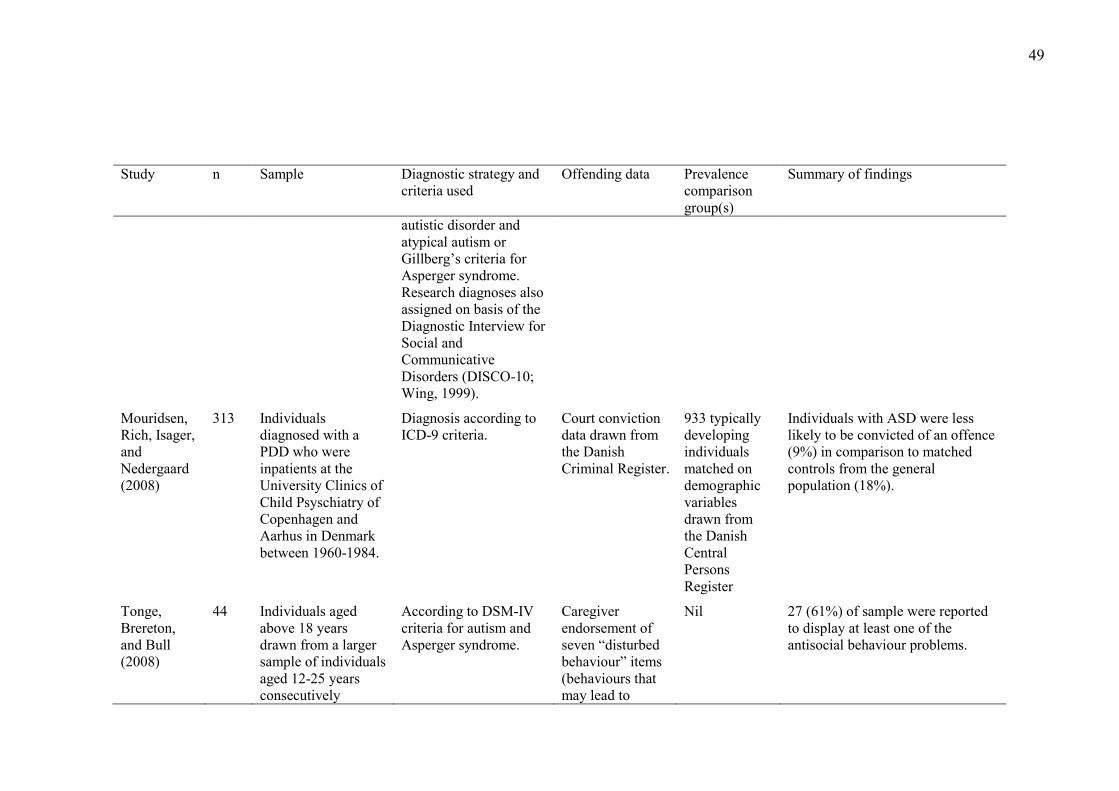
49
Study n Sample Diagnostic strategy and criteria used
Offending data Prevalence comparison group(s)
Summary of findings
autistic disorder and atypical autism or Gillberg’s criteria for Asperger syndrome. Research diagnoses also assigned on basis of the Diagnostic Interview for Social and Communicative Disorders (DISCO-10; Wing, 1999).
Mouridsen, Rich, Isager, and Nedergaard (2008)
313 Individuals diagnosed with a PDD who were inpatients at the University Clinics of Child Psyschiatry of Copenhagen and Aarhus in Denmark between 1960-1984.
Diagnosis according to ICD-9 criteria.
Court conviction data drawn from the Danish Criminal Register.
933 typically developing individuals matched on demographic variables drawn from the Danish Central Persons Register
Individuals with ASD were less likely to be convicted of an offence (9%) in comparison to matched controls from the general population (18%).
Tonge, Brereton, and Bull (2008)
44 Individuals aged above 18 years drawn from a larger sample of individuals aged 12-25 years consecutively
According to DSM-IV criteria for autism and Asperger syndrome.
Caregiver endorsement of seven “disturbed behaviour” items (behaviours that may lead to
Nil 27 (61%) of sample were reported to display at least one of the antisocial behaviour problems.
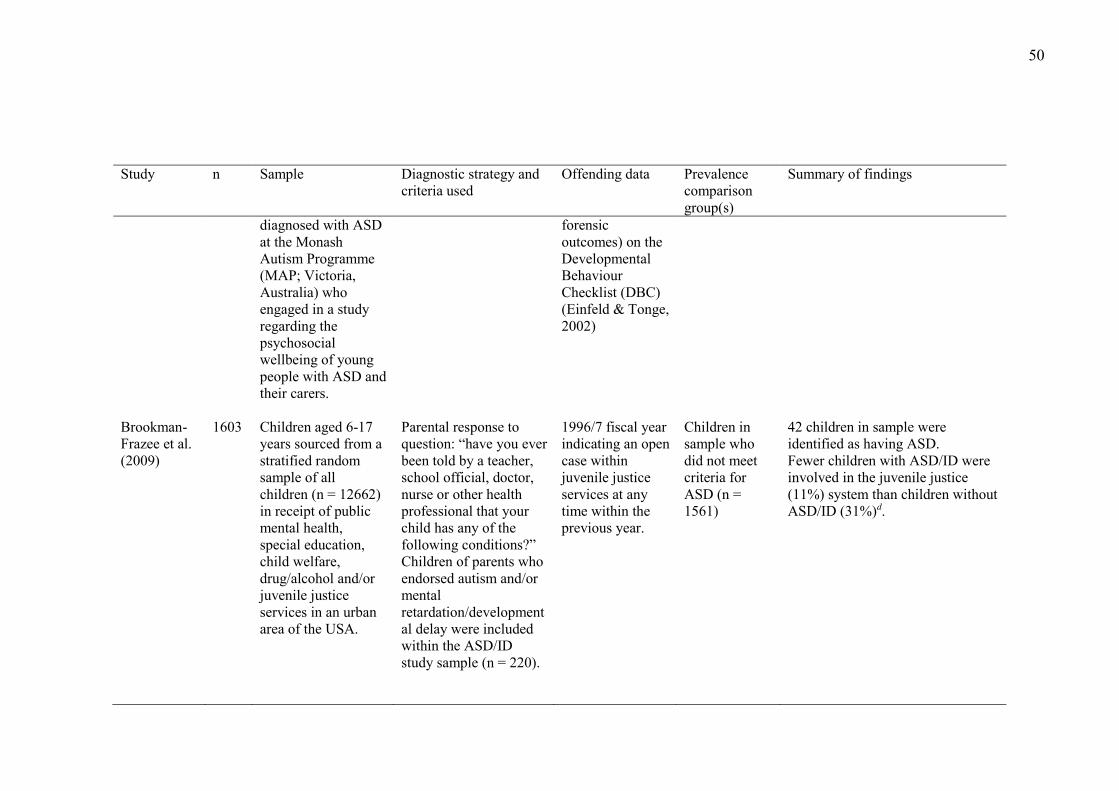
50
Study n Sample Diagnostic strategy and criteria used
Offending data Prevalence comparison group(s)
Summary of findings
diagnosed with ASD at the Monash Autism Programme (MAP; Victoria, Australia) who engaged in a study regarding the psychosocial wellbeing of young people with ASD and their carers.
forensic outcomes) on the Developmental Behaviour Checklist (DBC) (Einfeld & Tonge, 2002)
Brookman-Frazee et al. (2009)
1603 Children aged 6-17 years sourced from a stratified random sample of all children (n = 12662) in receipt of public mental health, special education, child welfare, drug/alcohol and/or juvenile justice services in an urban area of the USA.
Parental response to question: “have you ever been told by a teacher, school official, doctor, nurse or other health professional that your child has any of the following conditions?” Children of parents who endorsed autism and/or mental retardation/developmental delay were included within the ASD/ID study sample (n = 220).
1996/7 fiscal year indicating an open case within juvenile justice services at any time within the previous year.
Children in sample who did not meet criteria for ASD (n = 1561)
42 children in sample were identified as having ASD. Fewer children with ASD/ID were involved in the juvenile justice (11%) system than children without ASD/ID (31%)d.
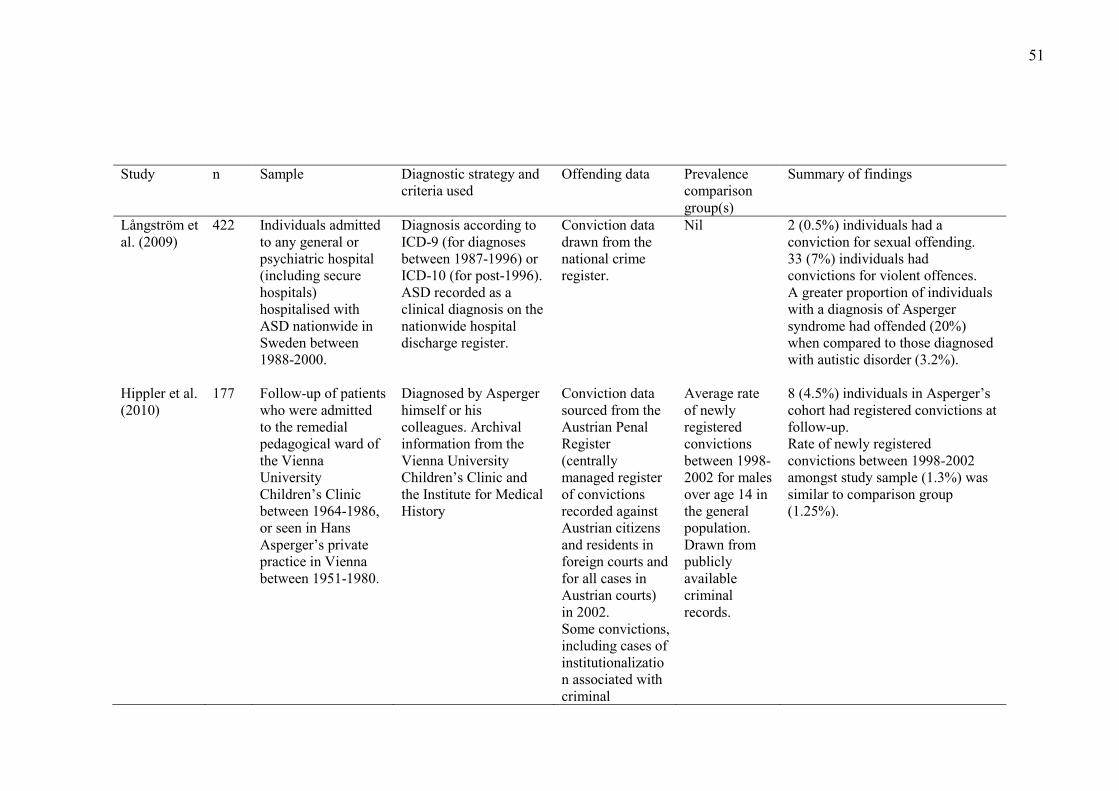
51
Study n Sample Diagnostic strategy and criteria used
Offending data Prevalence comparison group(s)
Summary of findings
Langstrom et al. (2009)
422 Individuals admitted to any general or psychiatric hospital (including secure hospitals) hospitalised with ASD nationwide in Sweden between 1988-2000.
Diagnosis according to ICD-9 (for diagnoses between 1987-1996) or ICD-10 (for post-1996). ASD recorded as a clinical diagnosis on the nationwide hospital discharge register.
Conviction data drawn from the national crime register.
Nil 2 (0.5%) individuals had a conviction for sexual offending. 33 (7%) individuals had convictions for violent offences. A greater proportion of individuals with a diagnosis of Asperger syndrome had offended (20%) when compared to those diagnosed with autistic disorder (3.2%).
Hippler et al. (2010)
177 Follow-up of patients who were admitted to the remedial pedagogical ward of the Vienna University Children’s Clinic between 1964-1986, or seen in Hans Asperger’s private practice in Vienna between 1951-1980.
Diagnosed by Asperger himself or his colleagues. Archival information from the Vienna University Children’s Clinic and the Institute for Medical History
Conviction data sourced from the Austrian Penal Register (centrally managed register of convictions recorded against Austrian citizens and residents in foreign courts and for all cases in Austrian courts) in 2002. Some convictions, including cases of institutionalization associated with criminal
Average rate of newly registered convictions between 1998-2002 for males over age 14 in the general population. Drawn from publicly available criminal records.
8 (4.5%) individuals in Asperger’s cohort had registered convictions at follow-up. Rate of newly registered convictions between 1998-2002 amongst study sample (1.3%) was similar to comparison group (1.25%).
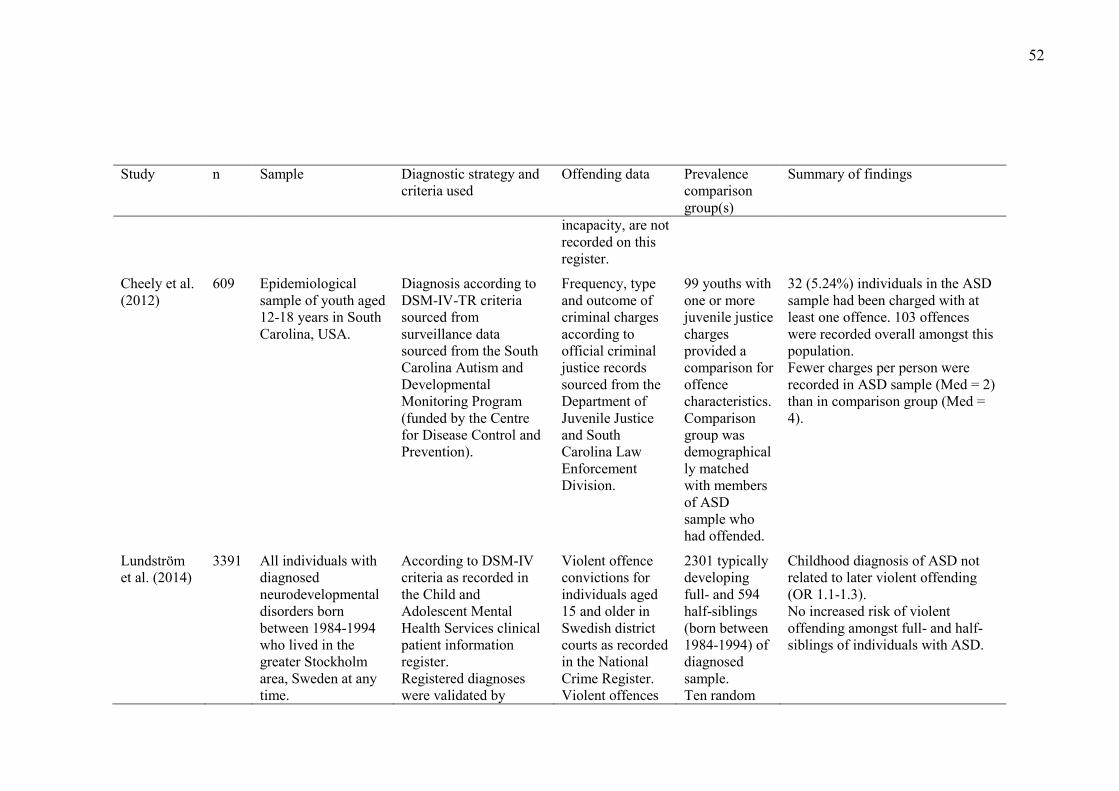
52
Study n Sample Diagnostic strategy and criteria used
Offending data Prevalence comparison group(s)
Summary of findings
incapacity, are not recorded on this register.
Cheely et al. (2012)
609 Epidemiological sample of youth aged 12-18 years in South Carolina, USA.
Diagnosis according to DSM-IV-TR criteria sourced from surveillance data sourced from the South Carolina Autism and Developmental Monitoring Program (funded by the Centre for Disease Control and Prevention).
Frequency, type and outcome of criminal charges according to official criminal justice records sourced from the Department of Juvenile Justice and South Carolina Law Enforcement Division.
99 youths with one or more juvenile justice charges provided a comparison for offence characteristics. Comparison group was demographically matched with members of ASD sample who had offended.
32 (5.24%) individuals in the ASD sample had been charged with at least one offence. 103 offences were recorded overall amongst this population. Fewer charges per person were recorded in ASD sample (Med = 2) than in comparison group (Med = 4).
Lundström et al. (2014)
3391 All individuals with diagnosed neurodevelopmental disorders born between 1984-1994 who lived in the greater Stockholm area, Sweden at any time.
According to DSM-IV criteria as recorded in the Child and Adolescent Mental Health Services clinical patient information register. Registered diagnoses were validated by
Violent offence convictions for individuals aged 15 and older in Swedish district courts as recorded in the National Crime Register. Violent offences
2301 typically developing full- and 594 half-siblings (born between 1984-1994) of diagnosed sample. Ten random
Childhood diagnosis of ASD not related to later violent offending (OR 1.1-1.3). No increased risk of violent offending amongst full- and half- siblings of individuals with ASD.
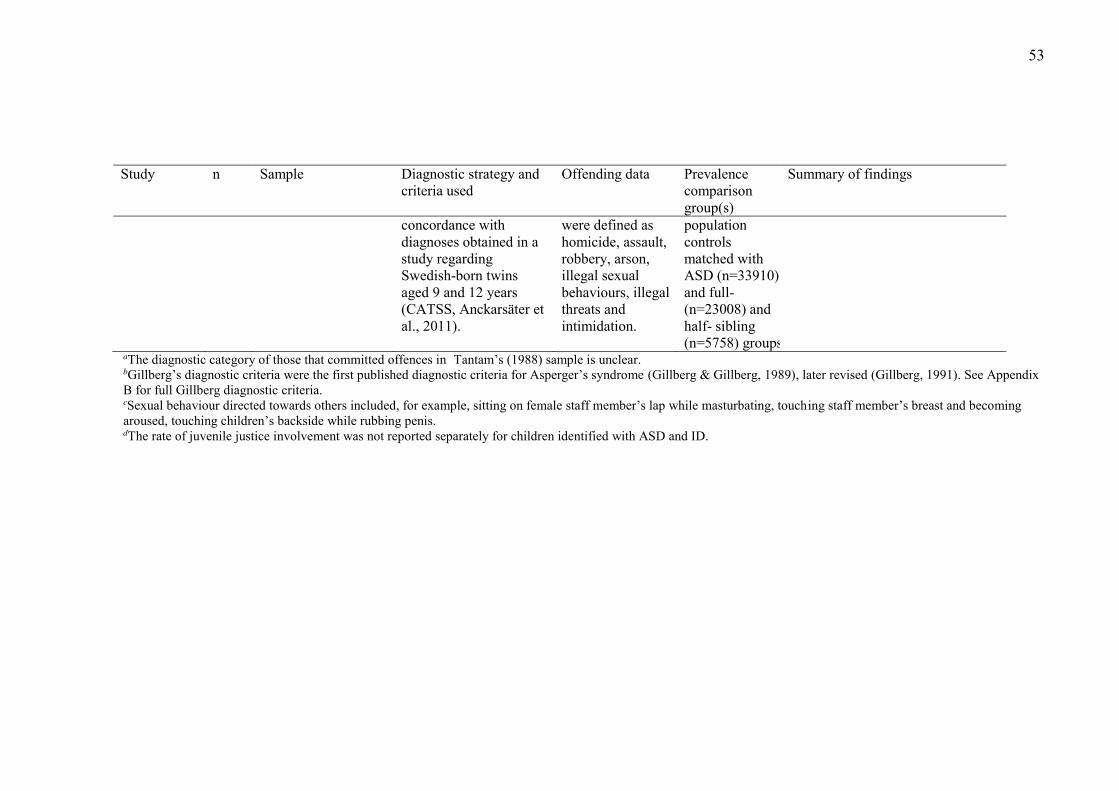
53
Study n Sample Diagnostic strategy and criteria used
Offending data Prevalence comparison group(s)
Summary of findings
concordance with diagnoses obtained in a study regarding Swedish-born twins aged 9 and 12 years (CATSS, Anckarsäter et al., 2011).
were defined as homicide, assault, robbery, arson, illegal sexual behaviours, illegal threats and intimidation.
population controls matched with ASD (n=33910) and full- (n=23008) and half- sibling (n=5758) groups
aThe diagnostic category of those that committed offences in Tantam’s (1988) sample is unclear. bGillberg’s diagnostic criteria were the first published diagnostic criteria for Asperger’s syndrome (Gillberg & Gillberg, 1989), later revised (Gillberg, 1991). See Appendix B for full Gillberg diagnostic criteria. cSexual behaviour directed towards others included, for example, sitting on female staff member’s lap while masturbating, touching staff member’s breast and becoming aroused, touching children’s backside while rubbing penis. dThe rate of juvenile justice involvement was not reported separately for children identified with ASD and ID.
54
Despite the substantial variation in methodology and reported results across
the included studies, it is noteworthy that where a comparison group was employed,
rates of offending behaviour amongst individuals with ASD were equivalent or lower
than that of non-ASD participants (Brookman-Frazee et al., 2009; Cheely et al., 2012;
Hippler et al., 2010; Langstrom et al., 2009; Mouridsen et al., 2008; Woodbury-Smith
et al., 2006). Such observations suggest that individuals with ASD are not at
increased risk of engagement in offending behaviour and may, in fact, be less likely
to offend than those in the general population.
3.2.3. The Contribution of Co-Morbid Conditions. One criticism of the
extant literature regarding ASD and offending regards the failure of the research to
consider or control for the impact of conditions that co-exist with ASD and which are
known to be associated with engagement in offending behaviour. Co-morbidity is
common amongst the ASD population (APA, 2013; WHO, 2004) and a number of
studies have demonstrated that co-morbid conditions are similarly common among
offenders with ASD (Anckarsäter et al., 2008; Newman & Ghaziuddin, 2008).
Accordingly, it is important to consider the potential contribution of co-morbid
conditions to the numbers of individuals with ASD that have been reported to engage
in offending behaviour (Brewer & Young, 2015).
3.2.3.1. Co-morbid Intellectual Disability and offending. Intellectual
disability (ID) frequently co-occurs with ASD and is characterized by substantial
limitations or deficits in cognitive and adaptive functioning, both of which must be
present in the developmental period (APA, 2013; WHO, 2004). Individuals with an
ID frequently experience disadvantage on socio-environmental factors known to
increase vulnerability for engagement in offending behaviours (e.g. Dickson,
Emerson, & Hatton, 2005). It is generally accepted that individuals with ID are over-
55
represented within the CJS, although there is some debate as to the extent of this
over–representation (Hayes, 2006; Howard & O'Brien, 2009; Talbot, 2010). In
contrast, offending behaviours appear less common amongst individuals with co-
morbid ID within the ASD population, with prior research demonstrating no
relationship between IQ and conviction rates, or higher conviction rates amongst
individuals with higher intellectual functioning (Hare et al., 1999; Langstrom et al.,
2009; Mouridsen et al., 2008). Such findings may reflect a greater opportunity and
capability to engage in offending behaviour amongst higher-functioning ASD
individuals (Holland, Clare, & Mukhopadhyay, 2002; Langstrom et al., 2009), or a
reluctance of others to report “challenging behaviours” exhibited by lower
functioning individuals that may otherwise have been considered to constitute
offending behaviour (see Raggi et al., 2013). They may also result from the
application of legal defenses (e.g. mental impairment or fitness to stand trial) in the
adjudication of cases where an individual has a comorbid ID (Freckelton & List,
2009).
3.2.3.2. Psychiatric co-morbidity and offending. As with ID, comorbid
psychiatric disorder (i.e. mood disorders, behavioural disorders and psychosis) is
common amongst the ASD population, with some studies suggesting that up to 84%
of adults with ASD possess a co-occurring mental illness (Hofvander et al., 2009;
Howlin & Moss, 2012; Tantam, 2000). Internationally, research has indicated the
presence of an association between psychiatric disorders, particularly psychotic and
substance abuse disorders, and engagement in offending in the general offending
population (Arseneault, Moffitt, Caspi, Taylor, & Silva, 2000; Ogloff, Talevski,
Lemphers, Wood, & Simmons, 2015; Tiihonen, Isohanni, Räsänen, Koiranen, &
Moring, 1997; Volavka, 2013). Some authors have thus argued that problematic
56
antisocial behaviours observed amongst some individuals with ASD may occur
primarily in the context of such comorbid psychiatric diagnoses (Haskins & Silva,
2006; Mazzone et al., 2012; Newman & Ghaziuddin, 2008; Palermo, 2004; Wachtel
& Shorter, 2013; Woodbury-Smith et al., 2005).
In their review of 37 case studies of violent offending amongst individuals
with Asperger’s syndrome, Newman and Ghaziuddin (2008) identified diagnosable or
‘probable’ co-morbid psychiatric disorder in the majority (83.8%) of cases. Similarly,
Bleil Walters et al. (2013) found that adjudicated adolescent sexual offenders with
ASD (n = 27) self-reported a significantly higher degree of depressive symptoms than
their non-ASD counterparts (n = 16). In contrast, there is evidence that offending
observed amongst the ASD population is less likely to be associated with substance
use disorders. Specifically, the research has indicated that drug offences, substance
abuse histories and intoxication at the time of offending are all less common amongst
offenders with ASD when compared with the general offending population (de la
Cuesta, 2010; Dein & Woodbury-Smith, 2010; Hippler et al., 2010; Murphy, 2003,
2013; Wahlund & Kristiansson, 2006; Woodbury-Smith et al., 2006). These results
have been challenged however by Langstrom et al. (2009) who found that both
psychotic disorder and substance use disorder were risk factors for engagement in
violent offending amongst individuals hospitalized with ASD in Sweden between
1988 and 2000 (n = 422).
It appears likely that the results of studies in which inflated rates of
psychiatric comorbidity amongst ASD offenders have been demonstrated may have
been confounded by the settings in which such research was undertaken. Specifically,
the majority of such studies have been conducted within mental health settings, which
may be more likely than other dispositional alternatives to accommodate any offender
57
with a psychiatric diagnosis (King & Murphy, 2014). Further, psychiatric
comorbidity does not appear to provide a comprehensive explanation for offending
behaviours amongst the whole offending ASD population. As noted by Newman and
Ghaziuddin (2008), although many violent offenders with ASD may possess a
comorbid diagnosis, there are also a number of individuals who have displayed
offending behaviours in the absence of psychiatric disorder. Similarly, in an
investigation of risk assessment amongst violent offenders with ASD (n = 20),
Murphy (2013) found that historical or active major mental illness and substance
abuse histories were not significant risk factors for more than half of the sample.
While it is noted that the influence of co-occurring conditions may increase
risk for offending in some individuals with ASD, psychiatric comorbidity does not
provide a complete explanation for offences perpetrated by individuals with ASD. A
full exploration of the complex interaction between ASD traits, co-occurring
symptomatology and offending is beyond the scope of the current thesis, and is
available elsewhere (e.g. Brewer & Young, 2015).
3.2.3.3. A double hit? ASD, offending behaviour and psychopathy.
Psychopathy is considered to be a developmental disorder in which an individual
manifests antisocial personality traits and behavioural patterns including
manipulativeness, callousness, a lack of remorse, extreme egocentricity, and an
inability to form meaningful relationships (Aharoni, Antonenko, & Kiehl, 2011;
Blair, 2008; Mullen, 1992). Given this psychological and behavioural profile, it is
unsurprising that research has consistently demonstrated a strong association between
psychopathy and offending behaviour (Anckarsäter, 2005; Glenn, Iyer, Graham,
Koleva, & Haidt, 2009; Shoemaker, 2011). Although psychopathy has a prevalence
58
rate of only 1% in the general population, Hare, Hart, and Harpur (1991) report that
the prevalence rate in forensic settings may exceed 20%.
Anecdotal accounts have highlighted a potential overlap in aspects of the
clinical presentation of psychopathy and ASD; for example, apparent egocentricity
and deficits for some aspects of empathic concern have been described for both
conditions (Bjørkly, 2009; Fitzgerald, 2003; Murphy, 2007; Murrie et al., 2002).
Accordingly, it has been argued that the seemingly callous behaviour observed in
some individuals with ASD is due to co-morbid psychopathy (Damm, 2010; Mazzone
et al., 2012; Rogers, Viding, Blair, Frith, & Happe, 2006). As such, Rogers et al.
(2006) contend “reports and concerns about ‘chilling’ nasty behaviour in a young
person with ASD should not be dismissed as ‘just part of the autism/Asperger
syndrome’…” but that co-morbid psychopathy should be considered in such cases (p.
1797).
Review of case reports, however, suggests that some individuals with ASD
may offend independently of psychopathic status. For example, psychopathy was not
indicated in Murphy’s (2010) case study of “AB”, who stabbed to death his employer
in response to being made redundant. AB was diagnosed with an ASD but scored a
low overall profile of behaviours and traits associated with psychopathy (≈ 9) on the
gold standard measure of psychopathy in adults, the Hare Psychopathy Checklist
Revised (PCL-R; Hare, 2003). Similarly, in a study investigating the PCL-R profiles
of 13 inpatients with Asperger’s syndrome in Broadmoor psychiatric hospital, none
reached established cut-off scores for psychopathy (Murphy, 2007). These authors
suggest that individuals with ASD may display a lack of awareness of wrongdoing in
the absence of psychopathy. For example, despite his low overall score on the PCL-
R, AB still scored highly on items that indicate a lack of remorse or guilt, shallow
59
affect, lack of empathy and a failure to accept responsibility for his actions (Murphy,
2010).
Case reports suggest that the profiles of offenders with ASD differ from those
of offenders with elevated levels of psychopathic traits in terms of motivation for
offending and the way in which they view their offences. In offences committed by
those high in psychopathy, excessive displays of planned and goal-directed violence
are common (Bjørkly, 2009). The psychopath is motivated by self-interest and
offending behaviour is contingent on positive reinforcement (Freckelton & List,
2009). In contrast, offending behaviour observed amongst individuals with ASD
appears better characterized as compulsive, ritualistic or reactive attempts to avoid
uncomfortable affective experiences, described in more detail below (Bjørkly, 2009;
Freckelton & List, 2009; Murrie et al., 2002). Further, while psychopaths tend to
deny accounts of violent acts, individuals with ASD typically immediately confess to
illegal acts, despite maintaining that their actions were justified (Bjørkly, 2009). Due
to such differences between the profiles of individuals with ASD who offend and
offenders with high levels of psychopathy, together with the observation that
offending behaviour can occur amongst individuals with ASD who do not exhibit
high levels of psychopathy, co-morbid psychopathy is not considered a sufficient
explanation for offending behaviour seen amongst some individuals with ASD.
3.2.4. Summary of research findings regarding prevalence of offending
and ASD. Whilst there is an emerging literature base investigating a hypothesized
association between ASD and engagement in offending behaviour, prevalence
estimates remain equivocal, both in regards to unlawful behaviour in this population
and the presence of ASD amongst individuals within forensic settings. Studies on this
topic differ in their intended aims, adopted diagnostic criteria, consideration of
60
confounding factors and definitions of offending behaviour; consequently, the results
are difficult to compare and may be unreliable (Anckarsäter et al., 2008; de la Cuesta,
2010). Efforts to establish an accurate prevalence rate for offending behaviour
amongst individuals with ASD are further hampered by a lack of agreement regarding
the prevalence of ASD within the general population (Browning & Caulfield, 2011)
and the frequent use of small, highly selective, and therefore potentially biased study
samples, raising the possibility that findings are not representative of the whole ASD
population (Im, 2016; King & Murphy, 2014).
Recent reviews of the extant literature in this area argue that the nature of
forensic involvement amongst the ASD population may be influenced by factors
external to those associated with engagement in offending behaviours (Brewer &
Young, 2015; King & Murphy, 2014). For example, prevalence estimates may be
inflated by systematic vulnerabilities faced by individuals with ASD within the
context of the CJS, which may result in an increased likelihood that a person with
ASD will admit involvement in illegal acts, be prosecuted for perpetrating a crime, be
referred for forensic evaluation or actually receive a conviction. Others have argued
that current prevalence estimates derived from official CJS data represent an under-
estimation of the true prevalence because they do not account for the numbers of
individuals who may offend without detection, are subject to diversion, or are not
formally charged (King & Murphy, 2014). In support of this contention, it has been
suggested that unlawful behaviour amongst individuals with ASD may not always
lead to contact with the CJS, particularly where such behaviours are interpreted in the
context of ‘challenging behaviour’ rather than as constituting a criminal offense
(Raggi et al., 2013). For example, in a study of offending behaviour amongst adults
with Asperger’s syndrome, Allen et al. (2008) found that a substantial minority (44%)
61
of participants did not receive a CJS disposal (i.e. where an incident results in CJS
involvement and is resolved through legal proceedings) following engagement in
unlawful behaviour. Thus, for many individuals with ASD, disruptive behaviours
need to be severe or repeated, and perpetuated in the absence of mitigating
circumstances, in order for a conviction to be received for their engagement in
behaviours that could otherwise be interpreted as criminal offending.
In sum, the extant research regarding the frequency with which individuals
with ASD engage in offending behaviour consists of studies conducted in specialized
settings across different jurisdictions, with variations in methodology and criteria for
identifying both ASD-status and offending behaviour, and which generally fail to
systematically consider the impact of factors unrelated to engagement in offending
behaviour that may artificially inflate or suppress commonly used indices of
offending. Comparison groups, where they are employed, often appear questionable
in their suitability and confounding factors are considered infrequently and
inconsistently. In this context, the wide variation in reported prevalence is
unsurprising and any conclusions drawn on the basis of the existing literature
regarding criminal propensity within the ASD population thus remain tentative. On
face value, existing prevalence studies appear to suggest an over-representation of
individuals with ASD within offending populations; however, when the
methodological flaws of such studies are examined, it is evident that such data are
inconclusive. Critically, the majority of the more robust studies in this area have
found that individuals with ASD are no more likely to commit offences (Ghaziuddin
et al., 1991; Hippler et al., 2010) or in fact, may be less likely to offend (Mouridsen et
al., 2008; Woodbury-Smith et al., 2006) when compared to offending rates within the
general population. Accordingly, at present, the available literature does not support
62
the conclusion that individuals with ASD offend at a rate that is disproportionate to
that in the general population (King & Murphy, 2014).
Notwithstanding methodological weaknesses, prior research in this area has
demonstrated that at least some individuals with ASD engage in offending behaviour
and, as a result of such behaviour, are made subject to restrictions imposed through
the CJS. Even if the true prevalence of offending behaviour amongst individuals with
ASD is equivalent, or indeed, lower than that in the general population, a more
important question is whether, and the extent to which, the core features of ASD may
drive offending behaviour in this population (Woodbury-Smith & Dein, 2014). This
question is critical to considerations at every level of criminal justice involvement,
ranging from informing early intervention and prevention efforts and assisting police
to appropriately apprehend and interview individuals with ASD in relation to
offending behaviours, the application of legislative provisions by the judiciary in the
disposition of a guilty defendant, through to determining the most effective and
humane options for punishment and rehabilitation of an offender with ASD. Although
the available evidence is not supportive of an inevitable link between ASD and
criminal behaviours, case reports suggest that some of the characteristic features of
ASD may contribute, independently or in concert with other factors, to the
engagement in offending behaviour by some individuals with ASD.
3.3. Features of ASD Potentially Associated with Offending Behaviour
While the weight of the current literature indicates that individuals with ASD
are largely law abiding, it is suggested from other empirical literature that specific
socio-communicative and behavioural deficits inherent to ASD may, under particular
provocative circumstances, precipitate offending behaviours (Allen et al., 2008;
Barry-Walsh & Mullen, 2004; Browning & Caulfield, 2011; Howlin, 2000; Lerner et
63
al., 2012). Indeed, a growing number of case studies describe offending behaviours
that appear to have occurred in the context of diagnostically relevant features of the
disorder (e.g. Barry-Walsh & Mullen, 2004; Kohn, Fahum, Ratzoni, & Apter, 1998;
Murrie et al., 2002; Schwartz-Watts, 2005). For example, it has been proposed that
socio-communicative deficits associated with ASD may result in maladaptive
behaviours due to social naivety, difficulties understanding and responding
appropriately to social norms and increased vulnerability to victimization and
exploitation by antisocial peers. Simultaneously, the cognitive and behavioural
rigidity common amongst individuals with ASD may precipitate offending in the
context of the obsessive pursuit of specialized interests, maladaptive responses to
sensory overloading, or distress arising from disrupted routines.
Of note, the available literature regarding the nexus between ASD
symptomatology and engagement in offending behaviour is limited by the low base
rate of such behaviour. Accordingly, the issues discussed below are predominantly
drawn from anecdotal data or case reports. Whilst these methods of investigation are
vulnerable to bias and limit the extent to which conclusions can be generalised, they
nonetheless provide some insight and direction for future empirical exploration.
3.3.1. Socio-communicative impairments. Impairments in social interaction
associated with difficulties interpreting and responding to social cues have been
described as some of the most significant and enduring features of ASD (Shattuck et
al., 2007). As a result of these impairments (e.g. social naivety and deficits in socio-
emotional reciprocity), individuals with ASD may experience difficulties interpreting
and responding to social situations appropriately, which may precipitate engagement
in offending behaviour. An overview of the empirical evidence regarding such factors
is provided below.
64
3.3.1.1. ‘Zero Degrees’ of empathy. Baron-Cohen (2011) coined the phrase
“zero degrees of empathy” to describe individuals who lack the ability to demonstrate
empathic concern for others. Individuals with ASD are amongst those described as
possessing ‘zero degrees’ of empathy, evidenced by “no awareness of how you come
across to others, how to interact with others, or how to anticipate their feelings or
reactions” (Baron-Cohen, 2011, p. 45). Indeed, individuals with ASD have been
shown to commonly demonstrate difficulties identifying others’ mental states,
recognizing offending-relevant emotional expressions (e.g. fear or distress), and
responding appropriately to the affective cues of others (e.g. Ashwin, Chapman,
Colle, & Baron-Cohen, 2006; Harms, Martin & Wallace, 2010; Humphreys,
Minshew, Leonard, & Behrmann, 2007). As a consequence of insensitivity to the
intentions or emotional state of others, some individuals with ASD may present with
an egocentric orientation, associated with a tendency to treat others as objects and
occasionally resulting in inappropriate, aggressive or otherwise maladaptive
behaviours.
Empathy deficits have been reported to precipitate some instances of
offending behaviour perpetrated by individuals with ASD, including violence (Baron-
Cohen, 1988; Tantam, 1991; Wing, 1981a); stalking (Stokes, Newton, & Kaur, 2007)
and sexual offending (Murrie et al., 2002). According to Mahoney (2009), empathy
and perspective-taking deficits may be critical contributing factors to engagement in
offences related to child exploitation material amongst individuals with ASD.
Specifically, Mahoney (2009) argues that, while the general population may readily
understand that the production of child pornographic images involves the abuse of a
child, this may not be the case for an individual with Asperger’s syndrome due to
impairments in recognizing and processing nonverbal cues:
65
He cannot detect the abuse – he assumes the child is in the picture because the
child desires to be there. But even if he detected the abuse or unhappiness of
the depicted child, the individual with AS may not understand why he, a mere
observer, should be held responsible for someone else’s abuse of a child.
After all, he is simply receiving the images, not producing or further
distributing them. And he has probably received them for free, so he has not
materially assisted the producer. Not only does the AS individual have
difficulty recognizing child sexual abuse and coercion, but he also has
difficulty understanding that the law views receiving an already existing
image of child abuse as the perpetuation of abuse (Mahoney, 2009, p. 44).
Such was the case for Nick Dubbin, a man with ASD who was convicted of
offences relating to child pornography (Attwood, Hénault, & Dubin, 2014). Nick
reported that he came across child exploitation materials while using online
pornography to explore his sexual identity in the context of uncertainty regarding his
sexual preferences. A lack of awareness of the full implications of accessing such
materials is evident in Nick’s reflections on these events:
At the time, I didn’t understand that downloading free images on my
computer in the privacy of my residence could lead to the severe legal
consequences I later experienced. I also didn’t understand at the time that the
children in the images had been victimized in the process of creating those
images. I honestly had no idea that I was causing harm to anyone. It is very
embarrassing to admit that I needed to have this information spelled out for
me, as I wasn’t able to make that connection on my own. After my arrest, Dr.
Green spent considerable time explaining the issue of victim awareness to me.
66
I was horrified to learn that these minors had been mistreated and that I had
not been able to see that (Attwood et al., 2014, p. 99).
The association between empathy and autism appears to be more complicated
than previously believed; it would be inaccurate to suggest that individuals with ASD
categorically lack the ability to empathise with others (Blair, 2008). To the contrary,
in many cases when individuals with ASD are made aware of the distress of others,
they demonstrate empathic concern (Baron-Cohen, 2011; Higgs & Carter, 2015).
Simultaneously, although a substantial body of evidence supports an association
between low levels of empathy and engagement in offending behaviour (Barnett &
Mann, 2013; Barriga, Sullivan-Cosetti, & Gibbs, 2009; Burke, 2001; Geer,
Estupinan, & Maguno-Mire, 2000; Jolliffe & Farrington, 2004, 2007), Baron-Cohen
(2011) argues that empathy deficits are necessary but insufficient to precipitate
engagement in harmful behaviours. Accordingly, “low empathy merely sets the scene
for cruelty” (Baron-Cohen, 2011, p.15).
3.3.1.2. Social naïveté and vulnerability to exploitation. The socio-
communicative impairments associated with ASD appear frequently to result in a
naïve or superficial understanding of social dynamics and difficulties recognising the
intentions of others (Hudson & Nijboer, 2012; Murrie et al., 2002). Such difficulties,
alongside strong desires to build friendships in the absence of a sound understanding
of what friendship entails, may result in difficulties recognizing malicious motives
and place individuals with ASD at risk of exploitation by others (Howlin, 2004).
Accordingly, it has been maintained that some individuals with ASD may be directed
or convinced by others to commit offenses or act as an accomplice in criminal acts
(Bishop, 2008; Howlin, 2000). Individuals with ASD may engage in directed
unlawful behaviour unwittingly (Howlin, 2000); alternatively, some may volunteer to
67
do so, egged on by peers, in attempts to gain or maintain their membership in an
antisocial peer-group (Tantam, 2003).
Howlin (2004) cites the example of “Berty,” who was picked up by police
after stolen goods were spotted lined up neatly in the window of his front room. It
later transpired that a local gang had frequently used Berty as a drug-runner and to
store items they had stolen. Similarly, “Darren” was arrested when he was stopped for
a vehicle roadworthiness check in a getaway car that was filled with stolen goods
from a robbery perpetrated by a local gang; the others had by this time fled the scene
(Howlin, 2004).
3.3.1.3. Lack of understanding or misinterpretation of social cues and
norms. As a result of poor perspective taking skills and insensitivity to environmental
and social cues, individuals with ASD may be “unable to predict or understand other
people’s actions” (Strock, 2007, p.7). This may render them unaware of or unable to
interpret many of the social rules that most people take for granted (e.g. not looking
in windows, not touching other people’s possessions and respecting personal space),
resulting in inappropriate social approaches in their interactions with others (Kennedy
& Adolphs, 2014; Sinclair, 1992; Travers et al., 2013). For example, they may
divulge personal information in inappropriate social settings or stand too close to
others (Kennedy & Adolphs, 2014; Travers et al., 2013). Another potential
consequence of difficulties understanding social cues may be mistaking social
niceties as representative of interpersonal intimacy (Howlin, 2004). For example,
polite engagement with a friendly tone may occasionally be interpreted by an
individual with ASD as indicative of an enduring friendship or romantic relationship
(Howlin, 2004).
68
Generally, such social faux pas do not cause significant harm, however, cases
of offending have been documented amongst individuals with ASD in the context of
misunderstanding social norms. An example of such is described in Haskins and
Silva’s (2006) case study of “Mr B” - a teacher who was charged with multiple
instances of ‘child annoyance’ after he inappropriately touched the shoulders of a
number of his female adolescent students. Of note, Mr B’s inappropriate behaviour
did not appear driven by sexual motives; in contrast, most instances occurred in the
full view of others, suggesting that his behaviour resulted from a lack of appreciation
that such interactions were socially unacceptable.
3.3.1.4. Asynchronous development: Inconsistency between socio-
communicative (psychosexual) and sexual development. Incongruent developmental
profiles are common amongst individuals with ASD, such that an individual may be
significantly impaired in one area of functioning whilst displaying age-appropriate
development in others (Attwood et al., 2014). Of particular relevance, disparities in
socio-communicative and physical sexual development are frequently evident,
whereby an individual may possess age-appropriate sexual interest and urges
alongside limited sexual knowledge and difficulties performing the complex social
skills required to initiate and maintain intimate relationships (Brown-Lavoie, Viecili,
& Weiss, 2014; Chappell, 2011; Howlin, 2004; Mahoney, 2009; Ray et al., 2010;
Sevlever, Roth, & Gillis, 2013). Such asynchronous development may place some
individuals with ASD at risk of sexual offending (Gougeon, 2010; Howlin, 2004;
Murrie et al., 2002; Ray et al., 2010).
In a review of research regarding sexuality and ASD, Gougeon (2010)
concluded that “individuals with autism are sexual; they are interested in sexuality,
have sexual needs, and oftentimes want to develop relationships with others” (p.348).
69
Unfortunately, characteristic deficits in communication and social skills are
commonly significant barriers to successful romantic functioning (Post, Hayes,
Storey, Loughrey, & Campbell, 2014; Stokes et al., 2007). Consequently, the
attempts of individuals with ASD to acquire sexual partners may be inappropriate,
and at times unlawful (Howlin, 2004; Murrie et al., 2002; Stokes et al., 2007). Due to
difficulties with perspective-taking, for example, individuals with ASD may fail to
recognise when others are not romantically interested and pursue an intimate
relationship when it is inappropriate to do so (Post, Hayes, et al., 2014). This was
evident in the case of “Mr. Parish”, who was charged with four counts of indecent
and unlawful assault after rubbing an unknown woman’s legs, back and buttocks as
his way of “trying to get to know her, to see if something would come out of it; a
relationship or something” (Freckelton & List, 2009, p. 26).
Previous research has suggested that in comparison to neurotypical peers,
individuals with ASD possess incomplete sexual knowledge (Ruble & Dalrymple,
1993; Stokes & Kaur, 2005) and have fewer opportunities to access informal learning
opportunities afforded to neurotypical peers through adolescent relationships or peer
interactions (Attwood, 2007; Hénault, 2005). In the absence of a peer reference
group, some individuals with ASD may restrict or suppress their sexuality (Grandin,
2006); others may develop unusual (and potentially deviant) sexual interests (Tantam,
2003) or seek to explore their sexuality through alternative sources, such as online
pornography (Attwood et al., 2014). In this context, some individuals with ASD,
possessing a limited understanding of consent and failing to appropriately assimilate
contextual cues, may possess an elevated risk for engagement in child sexual offences
(Murrie et al., 2002), including accessing child exploitation materials (Attwood,
2007; Attwood et al., 2014).
70
Difficulties establishing appropriate sexual relationships may also increase
risk for sexual offending related to the selection of inappropriate targets for sexual
activities. Murrie and colleague’s (2002) case study of “CD” an adult male with
Asperger’s syndrome, provides a clear example of sexual offending perpetrated
against an underage boy in the context of difficulties initiating relationships with age-
appropriate individuals. CD’s attempts at eliciting sex from age-appropriate
individuals were passive and naïve, including standing in close proximity to women
“until sex happened” (p. 62). While these approaches were generally unsuccessful,
CD experienced more success eliciting sexual relationships with male partners, in
exchange for accommodation and financial support. CD came to the attention of the
CJS following repeated sexual encounters with a teenage boy over the period of
several days until CD refused to continue providing financial support for the boy.
Notably, CD was arrested for sexual assault of a minor only after he attended a police
station to report his stereo stolen by the youth.
3.3.2. Restricted or repetitive patterns of behaviour, interests or activities.
As with socio-communicative deficits, the restrictive and repetitive behaviours,
interests and activities associated with ASD appear to have been implicated in some
instances of offending behaviour. Specifically, it has been argued that characteristic
preoccupation with specialized interests, resistance to change and sensory
abnormalities may, in some cases, lead to offending behaviours.
3.3.2.1. Rigidity applying learned social norms. While individuals with ASD
can learn and reason according to social rules when these are made explicit, it has
been suggested that they may fail to generalize and apply such knowledge to their
own behaviour in real life situations (Wing, 1997; Zalla, Machery, & Leboyer, 2008).
Alternatively, once a rule is acquired, it may be applied rigidly and inflexibly,
71
regardless of the social context (Howlin, 2004). Consistent with such, Wing (1997)
reports that individuals with ASD can be “literal and pedantic” in their adherence to
the law and may reprimand others, even strangers, out of concern that such rules be
followed (p. 254). Somewhat paradoxically, this pedantic focus on rules may
inadvertently trigger problem behaviour due to frustration when others break the
rules. For example, The National Autistic Society (2005) present the case of a man
who caused criminal damage to parked cars due to his frustration that the owners of
the cars were ignoring parking regulations.
3.3.2.2. Escalation associated with the disruption of routines. A preference
for repetition and consistency is a common characteristic amongst individuals with
ASD. As a result, they often behave in a ritualized manner, carrying out the same
routines every day or for each activity; for example, following planned travel routes
and routines in food preparation or personal hygiene (Howlin, 2004). Such tendencies
appear related to attempts to reduce anxiety by enhancing predictability often not
afforded to individuals with ASD due to their difficulties interpreting the social world
(Gunasekaran, 2012). They commonly face difficulties cognitively integrating
unexpected changes to routines (e.g. a train running late), potentially leading to
heightened levels of anxiety and distress (Gunasekaran, 2012). In such instances,
some individuals with ASD have been reported to react with aggressive outbursts.
For example, Baron-Cohen (1988) described the case of 21-year-old “John”, who
attacked others, including his 71-year-old “girlfriend”, when his routines were
disturbed.
The tendency to engage in fixed, repetitive routines may also cause problems
when individuals repeatedly engage in activities where inappropriate to do so, and
often, despite warnings to cease. For example, Haskins and Silva (2006) describe “Mr
72
C”, who enjoyed going to computer labs at a local university. As he was not a student
at the university, he was informed that he was trespassing and warned on several
occasions to discontinue his visits. However, Mr C persisted and was consequently
formally charged on two occasions. Similarly, in a case described by Howlin (2004),
a young man with ASD, “Joey”, came into contact with the CJS after being found
sitting in the middle of a kitchen floor of the house of an elderly pensioner, watching
their washing machine in action. Apparently, Joey had started entering the houses of
unknown neighbours following the closure of a local Laundromat he had previously
attended daily to watch the machines. Further forensic concerns were raised when
Joey punched one of the police officers who escorted him back to the home he shared
with his parents, apparently outraged at being accused of breaking the law.
3.3.2.3. Preoccupation with special interests. Individuals with ASD often
have areas of specialized interest. These interests differ from the interests or hobbies
of the general population in their content and by the intensity with which they are
pursued (Woodbury-Smith et al., 2010). Individuals with ASD often pursue their
specialized interests in such an intense, single-minded manner that they are unaware
that their actions may place themselves or others at risk of harm (Chen et al., 2003;
The National Autistic Society, 2005; Woodbury-Smith et al., 2010). Additionally,
individuals may be driven to engage in criminal acts, such as theft or trespass, in
pursuit of their special interests (Archer & Hurley, 2013; Chen et al., 2003;
Woodbury-Smith et al., 2010).
Haskins and Silva (2006) present the case of “Mr. A.” a young man with a
specialized interest in fire, which appeared to precipitate his engagement in offending
behaviour. At the time of his offending behaviour, Mr. A. was a volunteer fireman.
After stealing a colleague’s credit card, he purchased and stored fire-fighting
73
equipment in his apartment where he later lit a fire that caused the death of his young
daughter. Barry-Walsh and Mullen (2004) similarly describe a case where an
individual with Asperger’s syndrome perpetrated an arson offence that appeared
related to his specialized interest. Specifically, the young man demonstrated an
enduring interest in fire, deriving enjoyment from watching the flickering of flames,
including watching the pilot light of his furnace for hours. His offence occurred when
he lit a fire to watch the flickering.
Palermo (2013) argues that the specialized interests of some individuals with
ASD may result in a vulnerability to radicalization, citing as an example, the case of a
13-year old boy with Asperger’s syndrome who possessed a preoccupation with the
autobiographies of historical authoritarian dictators (e.g. Adolf Hitler, Chairman
Mao). This intense interest apparently fostered admiration for contemporary
authoritarian leaders and identification with extreme right-wing views, resulting in
the publication of a personal manifesto where authoritarian regimes, including Nazi
Germany, were idealized.
A preoccupation with weapons, the effects of poisons, witchcraft,
dismemberment, sexual fantasies and death or the act of killing have also been
documented as direct precipitants of offending behaviours amongst the offending
ASD population (Murrie et al., 2002; Radley & Shaherbano, 2011; Wing, 1997).
3.3.2.4. Interpersonal fixations. At times, the social advances of an individual
with ASD may become focused on one person and result in stalking behaviour (Post,
Hayes, et al., 2014; Post, Storey, Haymes, Campbell, & Loughrey, 2014). Stalking is
defined as “focused, repetitive, and persistent following that is unsolicited and
unwanted by the person who becomes the object of attention” (Haskins & Silva,
2006, pg. 381). Among the ASD population, such behaviour may occur as the result
74
of sexual desire or desire to build an intimate relationship (Stokes et al., 2007),
however, stalking behaviours may also occur as a result of or a desire for friendship
more generally and a misunderstanding of what friendship entails (Howlin, 2004).
Such was evident in the case of “Susie,” who became intrusive in her attempts to
establish a friendship with another young woman who regularly greeted Susie during
her morning commute to school (Howlin, 2004). Over time, Susie sourced this
woman’s phone number and address and would wait for her to return from work and
follow her home. While the target of Susie’s attention became increasingly distressed,
Susie showed little appreciation of the impact of her behaviour and insisted that this
woman was her friend (Howlin, 2004).
Occasionally, an individual with an ASD may develop a sense of entitlement
over the person that is the target of their focused attention and feel rejected when the
attention is not reciprocated (Beardon, 2008; Haskins & Silva, 2006). These feelings
of rejection can lead to aggravation and aggressive outbursts (Haskins & Silva, 2006).
For example, Katz and Zemishlany (2006) described a man who became fixated on a
woman who had interviewed him for a job and subsequently engaged in aggressive
stalking behaviour. He made repeated phone calls to the woman and began showing
up at her workplace to stare at her. The woman did not reciprocate his approaches and
the man had several angry outbursts in relation to this, including making threats to
kill the woman. Other cases of reported stalking behaviour amongst those with ASD
have included instances of kidnapping, imprisonment, and attempted murder
(Haskins & Silva, 2006).
3.3.2.5. Escalation associated with sensory hypersensitivity. Difficulties
integrating and modulating sensory stimuli is common amongst individuals with ASD
(Grandin, 1992; Grandin & Panek, 2013; Leekam et al., 2007; Zachor & Ben-Itzchak,
75
2014). Because ASD impacts the manner in which an individual processes sensory
information, some people have an atypical response to stimuli, such as cold or pain.
Such sensory oversensitivity can be distressing and even painful for the individual.
For example, in describing her own hypersensitivities, Grandin (1992) indicates that
“Sudden loud noises hurt my ears like a dentist’s drill hitting a nerve” (p. 107) and
“Stimuli that were insignificant to most people were like Chinese water torture” (p.
108). Thus, it has been hypothesized that even seemingly insignificant environmental
features may trigger a state of heightened arousal amongst individuals with ASD,
resulting in abnormal behaviours, including absconding to familiar places as a way to
reduce the presence of unprocessed sensory information or violent outbursts in the
context of an acute stress response (Chown, 2010; Health and Social Care Overview
and Scrutiny Committee, 2012).
Schwartz-Watts (2005) describes two cases where sensory hypersensitivity
was considered relevant in court proceedings related to murder charges perpetrated by
individuals with ASD. The first case involved a 22-year-old man who shot an 8-year-
old boy after the victim ran over his foot with a bicycle. Post-offence neurological
assessment of the offender revealed that he experienced tactile hypersensitivity and as
a result, he received a life prison sentence instead of the death penalty. In the second
case, a 35 -year- old man was acquitted of shooting his neighbour who had struck him
on the face, glasses and head during an altercation after the court heard that he
experienced oversensitivity associated with his glasses and head.
3.3.2.6. Retaliation for perceived victimization. The social deficits and
idiosyncrasies exhibited by individuals with ASD place them at higher risk of
victimization through bullying and social rejection (Attwood et al., 2014; Bishop,
2008; Cappadocia, Weiss, & Pepler, 2012; Rieffe, Camodeca, Pouw, Lange, &
76
Stockmann, 2012; Schroeder, Cappadocia, Bebko, Pepler, & Weiss, 2014).
Additionally, due to their difficulty reading others’ intentions, individuals with ASD
may perceive innocuous acts as intentional or threatening (Freckelton & List, 2009;
Wing, 1997). Perceived victimization may result in a profound sense of alienation
from others and intense feelings of having been wronged (Murphy, 2013). In the
absence of effective communication, conflict resolution and adaptive coping skills,
such experiences may lead to frustration, embarrassment, anger or fear, and
ultimately an assault on the perceived perpetrator (Murphy, 2013; Wing, 1997).
Further, given that individuals with ASD tend to ruminate over perceived
victimization and may displace feelings of resentment and aggression, such
victimization may result in seemingly unprovoked assaults on innocent people (Hare,
Freckelton & List, 2009; 1999; Murrie et al., 2002; Tantam, 2003; Wing, 1997).
Such a reaction to perceived victimization is evident in Murrie et al.’s (2002)
description of “AB”, a 31-year-old man with ASD who was convicted for arson. In
the year leading up to his offences, AB engaged in rumination about his childhood, in
particular, about perceived mistreatment by schoolmates:
… AB described the year prior to his offense as a period in which he became
increasingly preoccupied with those who had wronged him and increasingly
convinced that he needed to avenge himself. He reportedly considered
burglary for revenge, but later began to fantasize about fire setting. When AB
saw an arson report on the news, he decided that fire setting was the best way
to solve his problems (Murrie et al., 2002, p. 62).
AB was charged with 11 counts of arson to houses in his neighbourhood
during a two-month period. Of note, the victims had no connection to those AB had
77
set out to punish other than small similarities between the targeted houses and the
childhood homes of those that he perceived had mistreated him. Further, AB was
unable to appreciate that the acts of arson had not impacted those that he had intended
to punish and maintained that his actions were justified.
Like AB, many others with ASD may feel that offending behaviour is a
defensible reaction to perceived mistreatment by others. There are a number of
reports of individuals with ASD who justified their offending behaviour as self-
defence or justified revenge. Such reports include a man who vandalized seats on a
bus because he believed that the bus driver had deliberately failed to stop when he
hailed it the day before (Woodbury-Smith et al., 2006) and a man who stabbed to
death his boss because he thought she was to blame for his redundancy (Murphy,
2010). When queried, both of these men asserted that their behaviour was a
reasonable reaction to the situation.
3.3.3. Summary regarding the potential relevance of ASD traits to
offending behaviour. Following the above discussion regarding the potential
relevance of ASD traits to offending behaviour, it is pertinent to reiterate that overall,
there is no indication of an increased propensity towards criminality among this
population. It cannot be automatically assumed that a causal relationship exists
between ASD symptomatology and an individuals’ offending behaviour, because
precipitating factors identified in the general criminological literature (e.g. poor
educational achievement, pro-violent attitudes) are also likely to be relevant to
offenders with ASD (Alexander et al., 2016; Woodbury-Smith et al., 2005).
Nevertheless, the described literature suggests that diagnostically-relevant traits of
ASD may be implicated in some instances of offending. In some instances, such
factors appear only peripherally related, as one of multiple interacting causal factors,
78
while other descriptions highlight traits associated with a diagnosis of ASD as the
primary precipitants to offending behaviour (Brewer & Young, 2015). Critically, the
conclusions described above represent academic conjecture drawn from descriptive
analyses of a small number of cases. In the absence of systematic exploration with
larger samples, any attempt to generalise motives and triggers for offending
behaviour from the academic literature requires caution (Schwartz-Watts, 2005).
Gaining an understanding of any potential links between the features of ASD
and criminality is an essential task, both descriptively and legally, to ensure
consistency and integrity in determinations regarding the legal status and forensic
response for those individuals amongst this population who engage in offending
behaviour (Lerner et al., 2012). While the above-described considerations may assist
to guide thinking in these areas, they clearly do not provide a complete picture.
Indeed, exponential increases would be expected in offending rates amongst the ASD
population if such diagnostically relevant traits provided a sufficient and exhaustive
explanation for engagement offending behaviours (Lerner et al., 2012). Inversely,
estimates of the prevalence of individuals with ASD who engage in offending
behaviour remain relatively low. Accordingly, consideration of other factors that may
contribute to engagement in offending behaviour, or which may impact legal
implications for such behaviour amongst the ASD population will be necessary to
inform service provision and promote effective forensic outcomes.
3.4. The Nature of Offending Behaviour Perpetrated by Individuals with ASD
Brewer and Young (2015) propose that a better understanding of offending
behaviour perpetrated by individuals with ASD may be gained through examination
of the characteristics of offences perpetrated by this population. Several authors have
argued that individuals with ASD demonstrate an elevated propensity towards the
79
commission of certain types of offending, for example, arson (Enayati et al., 2008;
Hare et al., 1999; Mouridsen et al., 2008; Siponmaa et al., 2001; Woodbury-Smith et
al., 2010), property damage (Hippler et al., 2010; Woodbury-Smith et al., 2006;
Woodbury-Smith & Dein, 2014), stalking (Haskins & Silva, 2006; Post, Hayes, et al.,
2014; Post, Storey, et al., 2014; Stokes et al., 2007), interpersonal violence (Gook,
2014; Schwartz-Watts, 2005; Wachtel & Shorter, 2013; Woodbury-Smith et al.,
2006), sexual offences (Gook, 2014; Kumagami & Matsuura, 2009; Murrie et al.,
2002), or computer-related crime (Seigfried, O'Quinn, & Treadway, 2015). However,
the evidence is inconsistent and at times contradictory. For example, while
Mouridsen et al. (2008) found a significantly elevated rate of arson offences amongst
29 offenders with a diagnosis of PDD when compared to matched controls from the
general population, Kumagami and Matsuura (2009) demonstrated no differences in
the frequency of arson perpetration between offenders with PDD (n = 28) and without
PDD (n = 289) within juvenile courts in Japan. Hippler et al. (2010) found no
significant differences when comparing convictions for individuals in Hans
Asperger’s original cohort (n = 177) to patterns of offending in the general
population.
A more consistent (although not undisputed) finding is that offending amongst
individuals with ASD more likely consists of crimes against the person7 than other
offence-types and in comparison to offenders who do not display evidence of ASD
(Anckarsäter et al., 2008; Cheely et al., 2012; Gook, 2014; Kumagami & Matsuura,
2009; Woodbury-Smith et al., 2006). For example, in an unpublished thesis in which 7 Crimes against the person are offences that involve harm or attempted harm
towards a specific person(s) (e.g. murder, assault or offences of a sexual nature) as
opposed to more general harm caused to an entire community or organization (Pink,
2011).
80
the presence of ASD traits amongst a prison population in Victoria, Australia was
investigated, Gook (2014) reported that individuals with a clinically significant
degree of ASD traits were more likely to have an index offence of an interpersonal
nature (n = 9; 88.9%) when compared with those who did not display evidence of
ASD traits (n = 76; 57.9%). Similarly, in a prevalence study of criminal justice
system involvement among young Americans with ASD (12-18 years) between 2000
and 2006 (n = 609), Cheely et al. (2012) found higher rates of interpersonal offending
amongst individuals with ASD than matched controls. Specifically, of those who had
been charged with an offence (32.5%), crimes against the person were perpetrated
significantly more frequently amongst the ASD youth (n = 40; 38.8%) than in their
non-ASD counterparts (n = 122; 19.8%). Further, youths with ASD were more likely
to have been charged with crimes against the person than crimes against property
(20.4%), drug law violations (3.9%), offences against public order (30.1%) or status
offences (behaviours that are only considered a criminal offence when committed by
minors, e.g. truancy; 5.8%).
In contrast, a large, well-controlled study by Lundström et al. (2014) indicated
that individuals with a diagnosis of ASD do not possess a particular propensity
towards interpersonal offending. Specifically, Lundström et al. (2014) examined
convictions for violent crimes, encompassing actual and attempted homicide, assault,
arson, robbery, sexual offending, and threat- and intimidation-related offending,
amongst a birth-cohort (1994-2005) of individuals diagnosed with various
neurodevelopmental disorders by child and adolescent mental health services in
Sweden (n = 3,391). The conviction rates of probands were compared to those of
comparisons, including full- (n = 2301) and half-siblings (n = 594) as well as ten
(non-related) matched control groups (n = 33,910), and after adjustments for the
81
impact of potential confounders (parental income and education status) and mediators
(for example, drug use, psychotic disorder, alcohol abuse). In contrast to other
neurodevelopmental disorders (e.g. ADHD), there was no evidence of an increased
propensity for violent criminal behaviour amongst those with a diagnosis of ASD (n
= 954).
In sum, similar to research regarding prevalence of offending, the limited
body of evidence regarding the propensity for individuals with ASD towards the
commission of particular offence types is both inconsistent and inconclusive, and
marred by methodological limitations (King & Murphy, 2014). Comparisons in this
area are further complicated by the small sample sizes that are frequently yielded
when data are split by offence type (Brewer & Young, 2015). A number of studies
suggest an increased propensity towards interpersonal offending amongst the ASD
population, however this has been refuted by others, most notably a large, well-
controlled study by Lundström et al. (2014) that suggested no increased prevalence of
interpersonally violent offending amongst individuals with ASD. Accordingly,
conclusions are limited regarding the typology of offending amongst individuals with
ASD.
3.5. Summary of Chapter
This chapter provided an overview of research investigating the frequency and
nature of offending behaviours amongst individuals with ASD. While population
studies and case reports have highlighted such offending behaviour, the exact
frequency and nature of offending amongst this population remains unknown.
Despite rapid growth in recent years, empirical research regarding ASD and
offending behaviour remains relatively scant. The available findings are both limited
and inconsistent, being principally comprised of retrospective case reports and
82
examinations of narrow populations within secure psychiatric settings. As a result,
there is some controversy over whether research to date accurately reflects the
prevalence of ASD within the criminal justice system.
On face value, studies revealing an over-representation of ASD in forensic
settings alongside several case reports describing criminal behaviour perpetrated by
individuals with ASD appear to support the proposition of an association between
ASD and offending behaviour (e.g. Allen et al., 2008; Hare et al., 1999; Scragg &
Shah, 1994; Siponmaa et al., 2001). Others, however, provide evidence that
individuals with ASD are no more likely to offend and may, in fact, be more law-
abiding than the general population (Ghaziuddin et al., 1991; e.g. Howlin, 2000;
McGeer, 2008b; Wing, 1997). On balance, the available literature base does not
provide compelling evidence of an association between ASD and offending
behaviour.
Agreement regarding the exact prevalence of offending behaviour amongst
the ASD population may never be reached; not only because of methodological flaws
within the extant research, but also because prevalence rates are likely to vary
throughout the CJS. Specifically, the availability of early intervention and prevention
services, legal mandates and diversionary practices are likely to vary between
jurisdictions and prevalence rates of ‘special populations’ (such as those with ASD)
may differ as research progresses through the different stages of the CJS (Hayes,
2006, 2007). For example, it seems likely that more individuals with ASD may be
held in remand settings than in sentenced prisons, due to failures to identify the
presence of developmental disorders at this early stage, while individuals may be
diverted out of the CJS following diagnosis. For such reasons, Hayes (2006) argued
that the issue of prevalence of offending amongst intellectually disabled individuals
83
is a “red herring” that distracts researchers and policy-makers from considering the
real issues faced by the CJS in responding to such individuals. This is undoubtedly
also the case amongst other potentially vulnerable groups, such as those with ASD.
Methodological failings aside, the available research confirms that at least
some individuals with ASD engage in unlawful behaviours. Even if the prevalence of
individuals with ASD engaging in offending behaviour is the same as the prevalence
of ASD in the community (approximately 0.5% in Australia, according to the
Australian Bureau of Statistics, 2014), a substantial number of cases of offending
behaviour would involve individuals with ASD over the course of a year. In
Magistrates Courts in Australia, with a turnover of 588,167 finalised defendants per
annum (2015-16; Australian Bureau of Statistics, 2016), a prevalence rate of 0.5%
would equate to some 2941 cases involving defendants with an ASD diagnosis. This
number does not include those individuals who may experience a clinically
significant degree of ASD traits, but who have not yet been diagnosed, or those who
display sub-clinical ASD traits. The critical issue in regards to individuals with ASD
who come into contact with the CJS is the provision of effective services to protect
this potentially vulnerable population and to enhance community safety, for example,
by addressing factors associated with engagement in offending behaviours. An
understanding of the nature and characteristics of offending behaviours perpetrated
by individuals with ASD will be vital to inform legal policy and ensure that services
are appropriately targeted to aid the management and rehabilitation of those who do
appear as defendants within the CJS (Brewer & Young, 2015; Lerner et al., 2012).
Although not unanimously supported, several authors have argued that
individuals with ASD may be proportionally more likely than neurotypical peers to
engage in interpersonal offending, including sexual and non-sexual violence (Cheely
84
et al., 2012; Gook, 2014; Kumagami & Matsuura, 2009; Woodbury-Smith et al.,
2006). Despite widespread discussion, to date a systematic investigation of the
characteristics of offences committed by persons with ASD has not, to the author’s
knowledge, been undertaken. Accordingly, much of what is known about the nature
and precipitants of offending amongst individuals with ASD is anecdotal or
theoretical in nature. Such limited evidence is insufficient to identify the true scale of
this issue or inform policy and practice in this area (Woodbury-Smith & Dein, 2014).
Consequently, there is scope for further research in this area to inform the prevention,
early intervention and management of offending behaviour amongst the ASD
population, thus reducing the potential for inappropriate or ineffective distribution of
resources within the CJS; an already under-resourced system. In this context, the
following chapter describes a study in which the characteristics of self-reported
offending according to ASD symptom severity are explored.
85
Chapter 4. Study 1: Self-Report of Offending and the Autistic Phenotype
4.1. Rationale
Ongoing debate regarding a potential association between ASD and
engagement in offending behaviours has resulted in a growing body of academic
literature concerning the forensic aspects of ASD. Despite such, our understanding of
issues related to prevention, early intervention and forensic responses to offending
behaviours perpetrated by individuals with ASD remains limited. Research findings
have been inconsistent, primarily drawn from case reports or prevalence studies
within narrow and specialized population samples. Whilst highlighting the presence
and potential scope of offending behaviours amongst individuals with ASD, these
findings have provided little guidance in regards to early intervention, management
and rehabilitation of individuals with ASD within the CJS. Thus, there is a need for
systematic research exploring issues that directly inform and enhance early
intervention, rehabilitation and ultimately, forensic outcomes for individuals with
ASD who engage in offending behaviour.
According to Freckelton (2013a), investigating the characteristics of offending
behaviour where it occurs within the ASD population, including the identification of
any offence typologies and CJS responses to offending and other delinquent
behaviour, is a “modest but useful start” to inform policy and provide focus for future
academic attention and efforts to address problematic behaviour (p. 431). Such data
may assist to direct research and practice in a more targeted manner, ensuring that
resources are allocated appropriately to foster positive forensic outcomes for such
individuals. For example, should individuals with ASD be found to possess an
elevated propensity towards violent crime, with less likelihood of involvement in
drug-related offending, this would support the use of resources to explore and
86
intervene on potential predisposing, precipitating, perpetuating and protective factors
in regards to violent offences, and a reduced focus on drug and alcohol related
intervention for this population.
As described in Chapter 3, the literature exploring the nature of offending
behaviour amongst the ASD population is limited in both quality and quantity;
primarily derived from case studies or prevalence studies, that utilise formal indices
of offending, and which frequently consider only particular offence-types (Bjørkly,
2009; Haskins & Silva, 2006; Murrie et al., 2002; Woodbury-Smith et al., 2006). The
findings from this research have been inconsistent, and at times contradictory. The
current study seeks to explore self-reported offence characteristics amongst a sample
of individuals living within the community with a view to determining whether the
offence patterns of those individuals who report characteristics of ASD differ from
those of their neurotypical peers. Specifically, this study aims to identify and explore
offending profiles, and the consequent forensic response to such behaviours, as
reported by individuals with higher degree of ASD-consistent traits and compared
with those with a lower degree of such traits. It is anticipated that the results of this
study will provide a broad overview of criminality as it relates to the ASD phenotype
and assist to inform future research efforts in this area.
4.1.1. Defining and measuring “offending behaviour”: Official data vs.
self-report. Consistent with criminological research more generally, much of the
prior research that concerns offending amongst individuals with ASD has relied on
formal indices of offending (e.g. conviction data, contact with the CJS, presence
within forensic settings) obtained from official statistics to guide conclusions
regarding the frequency and nature of offences perpetrated by individuals with ASD
(Woodbury-Smith et al., 2006). This is problematic because much illegal behaviour is
87
undetected and unreported (Theobald, Farrington, Loeber, Pardini, & Piquero, 2014),
and the proportion of detected criminal behaviour that results in a criminal conviction
following criminal proceedings may be similarly small (Holland et al., 2002;
Langdon, Clare, & Murphy, 2011). Additionally, much of the available research has
considered a restricted range of offence-types with vague or narrow definitions (e.g.
“violence”) and within specialized settings (e.g. secure psychiatric wards). As
described in Chapter 3, concerns have been raised regarding the validity and
generalisability of such methodological approaches in determining the pattern and
nature of offending amongst the ASD population. In this context, Woodbury-Smith et
al. (2006) argue a need for more research conducted outside of forensic settings that
considers a wide range of ‘commonplace’ offences and which does not rely on
criminal convictions to properly explore offending behaviour amongst individuals
with ASD.
Critically, the correlation between engagement in illegal behaviours and
indices reliant on contact with the CJS is not perfect, with conviction data thought to
represent the “tip of the iceberg” of offending behaviours (Farrington, 2001, p. 2).
Further, such data may be vulnerable to systematic biases associated with failures to
report or detect some offending behaviours, and differences in the operation of legal
principles designed to divert vulnerable individuals from the CJS (Junger-Tas &
Marshall, 1999; Thornberry & Krohn, 2000). Accordingly, the focus on official
indices of criminal involvement in prior research raises concerns regarding the
accuracy and generalizability of findings, particularly within special populations,
such as those with ASD (Farrington, 2001; Huizinga & Elliott, 1986; Thornberry &
Krohn, 2000; Woodbury-Smith et al., 2006). Further, the self-report methodology
provides the opportunity for further exploration regarding the characteristics of
88
reported offending behaviours, through the consideration of details unlikely to be
recorded by formal indices of offending (e.g. whether the offence was planned, and/or
the nature and seriousness of unadjudicated delinquent behaviour). In this context, it
has been argued that self-reports of offending may provide a more complete picture
of criminal involvement than is provided by data derived from official statistics
related to contact with the CJS (Farrington, 2001; Junger-Tas & Marshall, 1999;
Thornberry & Krohn, 2000).
Acceptable levels of test-retest reliability and content, construct and criterion
validity have been consistently demonstrated within recent studies and reviews of
self-report approaches to exploring offending behaviours (Dubow, Huesmann, Boxer,
& Smith, 2014; Farrington, 2001; Jolliffe et al., 2003; Junger-Tas & Marshall, 1999;
Thornberry & Krohn, 2000). Despite such, doubts have been raised regarding the
validity of self-reported data, due to concerns that some individuals may conceal,
exaggerate or have difficulties accurately recalling their criminal involvement
(Farrington, 2001; Huizinga & Elliott, 1986). Further, lower levels of reliability and
validity have been found for ethnically or gender diverse populations (Hindelang,
Hirschi, & Weis, 1981; Knight, Little, Losoya, & Mulvey, 2004), suggesting that
there may be some samples for whom such methodology should be used only with
caution (Thornberry & Krohn, 2000). Nonetheless, while self-report methods have
potential limitations, it has been argued that this is true of all measures used to
explore social behaviour and such measures have become an accepted methodology
for cross-sectional research in this field (Farrington, 2001; Junger-Tas & Marshall,
1999).
4.1.2 The Present Study. Using a self-report internet-based survey
methodology, the current study explored the nature of offending and other delinquent
89
behaviour across the autistic phenotype within a community-based sample, recruited
with advertisements targeted to agencies likely to have contact with the ASD
population. A self-report methodology was chosen in order to address concerns
regarding potential biases in official statistics of offending behaviour amongst the
ASD population. The primary aim of this study was to investigate whether
differences existed in offence-types reported according to the presence of ASD traits
amongst a non-clinical community-based sample. On the basis of previous research
regarding offending behaviour among individuals with ASD (reviewed in Chapter 3),
it was hypothesized that individuals who endorse a clinically significant degree of
characteristics indicative of ASD would report a higher frequency of interpersonal
offences when compared to respondents who did not display characteristics of ASD.
Contact with the CJS, associated with reported offending, was also considered
to determine whether dispositional outcomes may apply differentially for cases of
offending behaviour involving individuals displaying ASD traits. Specifically, the
current study sought information on whether illegal behaviours attracted the attention
of police, whether police contact resulted in forensic sanctions and the nature of any
sanctions previously received by respondents. Theoretical and academic conjecture
regarding the forensic response to offending behaviour by individuals with ASD has
been inconsistent and variously argued in terms of an inflated or reduced risk for
detection, conviction and forensic disposition than neurotypical peers (see Chapter 3;
also Chapter 5). Accordingly, specific hypotheses were not delineated regarding
forensic contact.
4.2. Method
An internet-based cross-sectional survey design was utilised to explore any
extant relationships between ASD-trait severity and self-reported offending
90
characteristics amongst a self-selected community-based sample. Data were analysed
using SPSS Statistics 23.0.
4.2.1. Participants. A targeted sampling approach was adopted to promote a
broad distribution of ASD trait severity such that both individuals with a high degree
of ASD traits and those with few traits would be represented within the study sample.
The sample self-selected for participation via advertisements on social media, and
targeted advertisement through organizations likely to be in contact with adults with
ASD (see Appendix C for a full list of locations contacted by the researcher for the
purposes of participant recruitment). Data were provided on an online survey by 172
respondents. The majority of respondents were female (65.7%) and approximately
one third were male (32.4%); 2 respondents (1.9%) indicated that they identified as
androgynous or did not provide this information. Reported age ranged from 18 to 64
years. Most were Australian (56.5%) or North American (19.4%), with the remainder
of respondents reporting British (9.3%), European (5.6%), New Zealand (2.8%),
Asian (2.8%), Canadian (1.9%), South American (0.9%), or African (0.9%) heritage.
4.2.2. Measures. Respondents completed an online survey that included
measures for autistic symptomatology, self-reported engagement in offending
behaviour and a range of demographic variables thought likely to be differentially
associated with offending rates (e.g. gender, age). This study was granted approval
from the University Human Ethics Committee and participants were informed
through a plain-language statement presented prior to commencing the survey that
participation was voluntary and that they could chose to withdraw at any time prior to
survey submission. Consent was inferred through submission of survey responses,
which occurred by participants clicking on a “submit” button on the last page of the
survey.
91
4.2.2.1. Demographic information. A wide variety of socio-environmental
factors have been identified within the criminological, sociological and psychological
literature as contributing to offending behaviour within the general population
(Farrington, 2003; Langdon, Clare, et al., 2011; Morizot & Kazemian, 2014;
Thornberry & Krohn, 2003). Such socio-demographic factors almost certainly also
contribute to engagement in criminal behaviour either alone, or in combination with
other factors, amongst individuals with ASD. Coverage of the vast array of potential
influences on engagement in offending behaviour was beyond the scope of this thesis.
However, a subset of factors considered likely to contribute to criminal involvement
was measured through the collection of data for demographic factors, including
respondents’ age, gender and formal educational attainment. In addition, responses
provided by respondents on four dichotomous (yes/no) response items were collected,
for the purposes of screening for the presence of potential learning disabilities (i.e.
Have you ever received a pension or benefit for a disability? Have you ever been in a
special class or school for students with a learning disability? Do you think you are a
slow learner? Do you have a learning disability?).
4.2.2.2. Psychopathic traits.The presence of psychopathic traits was measured
according to the Levenson Self Report of Psychopathy (LSRP; Levenson, Kiehl, &
Fitzpatrick, 1995, see Appendix D) to determine whether such traits may bias results.
The LSRP is a well-validated 26-item self-report screening measure designed to
assess psychopathic traits, attitudes and beliefs in non-incarcerated populations.
Descriptive and reliability (Cronbach’s alpha) data for the LSRP in the present
sample were as follows: M = 57.51, SD = 12.516, α = .844.
4.2.2.3. Autistic traits. The diagnosis of ASD in adulthood is often
challenging due to the heterogeneity of presentation and difficulties gaining
92
information regarding developmental histories and symptom patterns (Allison,
Auyeung, & Baron-Cohen, 2012; Fombonne, 2012). However, a number of brief
standardized screening tools exist that have been developed to aid the identification
of ASD in adults. For the current study, the presence of autistic traits was measured
according to the most commonly used screening measure for ASD, the Autism
Quotient (AQ; Baron-Cohen et al., 2001).
The AQ is a well validated measure that quantitatively assesses the degree to
which adults exhibit autistic traits according to 50 items across five theoretically
based sub-scales: Social Skill, Communication, Imagination, Attention to Detail and
Attention Switching). Items on the AQ are counterbalanced such that for half, a
positive response indicates an autistic-like trait, whereas for the other half, a negative
response is indicative. Higher scores indicate the presence of characteristics more
similar to those indicated by a diagnosis of ASD. Although not diagnostic, the AQ is
well validated and scores have been shown to correlate with validated biological
markers for ASD (e.g. testosterone levels and brain activity) and the tool’s
psychometric properties have been validated cross-culturally (Allison et al., 2012;
Baron-Cohen et al., 2001; Wouters & Spek, 2011). Prior research has demonstrated
that scores on the AQ reliably differentiate between adults with a diagnosis of autism
and their neurotypical counterparts (Allison et al., 2012; Baron-Cohen et al., 2001;
Wouters & Spek, 2011), as well as those with psychiatric conditions, such as
schizophrenia (Wouters & Spek, 2011). In the current study, the Cronbach alpha
coefficient was high (α = 0.934), suggesting excellent internal reliability.
Baron-Cohen and colleagues (2001) have recommended a cut-off score of 32
as providing a good indicator of the likelihood that an individual would meet the
diagnostic criteria for ASD, with 80% of adults with ASD and only 2% of those
93
without ASD recording a score at or above this cut-off. However, there is evidence of
some variation in cut-off scores dependent on population samples. For example, in a
validation study of the AQ in an Australian sample, Broadbent and Stokes (2013)
reported that a cut-off score of 29 on the AQ most reliably differentiated individuals
with a diagnosis of ASD from neurotypical peers (1% false-positive rate). Given the
suggestion from prior research that cut-off scores may vary according to population,
and the high number of respondents in the current study who reported Australian
heritage (n = 60; 55%), a median-split was utilized to allocate respondents to
comparison groups on the basis of their total AQ scores (High vs. Low).
4.2.2.4. Engagement in offending behaviour. An adapted version of The
Self-Report of Offending Questionnaire (SRO; Huizinga, Esbenson, & Weihar, 1991)
was used in the current study to elicit self-report of involvement in antisocial or
criminal behaviour (See Appendix E for the adapted SRO survey completed by
participants in the current study). The SRO was designed for use amongst community
samples of individuals aged 7 years to adulthood and asks respondents to indicate
whether they have engaged in 24 delinquent and criminal behaviours (i.e. behaviours
which could lead to arrest by the police, prosecution and conviction by a court) in the
past year. For each item endorsed by a respondent, a set of follow-up questions were
asked to elicit further information regarding the self-reported behaviour (e.g.
“Thinking of the last time you did this, were you alone or with others?”). Due to an
insufficient sample size and the low frequency of self-reported engagement in
delinquent behaviours amongst the current sample, comparisons at this level were not
undertaken.
According to standard reporting procedures in criminology, self-reported
offending can be explored in two ways: a variety score (the number of different types
94
of criminal acts in which the person engages) and frequency scores (the total number
of unique criminal acts committed, regardless of type). Variety and frequency scores
are generally very highly correlated and have been used interchangeably for analysis
throughout the criminological literature (Hindelang et al., 1981). Offending variety
scores are considered to overcome several potential difficulties that may arise where
frequency scores are used (Brame, Paternoster, & Bushway, 2004; Monahan &
Piquero, 2009). Specifically, variety scores ensure that criminality is not
overestimated due to the impact of multiple instances of minor delinquent behaviours,
are more likely than frequency scores to possess properties better suited for analysis
(i.e. more likely to conform to an approximately normal distribution) and may be
more accurate and reliable than frequency scores due to the increased likelihood of
inaccuracies in recall and count processes for repeated events (Moffitt, Caspi, Rutter,
& Silva, 2001; Monahan & Piquero, 2009; Schwarz, 2005). For the current study,
both frequency and variety scores were utilized to explore self-reported delinquency
within the study sample. An annual offending variety score was created and was the
number of discrete delinquent acts endorsed on the SRO as occurring within the
previous year. Frequency of offending was calculated for the last year by summing
responses to the question “How many times have you done this in the past 12
months?” for each delinquent act endorsed.
Delinquent behaviours on the SRO were grouped into offence-type categories
for further analysis of typologies of offending amongst the study sample. Categories
were defined according to the Crimes Statistics Agency Offence Classification
(Crime Statistics Agency, 2015), with offences represented across five categories
included within the classification system (Crimes Against The Person; Property
Offences, Public Order and Security Offences, Disorderly and Offensive Conduct,
95
Traffic and Vehicle Offences and Drug Selling Offences; see Appendix F for full list
of offence categories within the Offence Classification).
4.3. Results
4.3.1. Missing Data. Initial inspection of the data revealed that missing data
points constituted 1.07% of the data overall. A non-significant Little’s MCAR test,
χ2(14046) = 7630.83, p = 1.0, provided evidence that the data were missing
completely at random (Little, 1988). Given that missing data were minimal and
appeared to be missing at random, it was considered that a complete case analysis
strategy was unlikely to introduce unjustified bias to the data. Missing data were
present for 64 respondents; only complete cases were included for subsequent
analyses. Thus, the sample for the current study’s analysis was reduced to 108.
4.3.2. Annual Engagement in Offending and Other Delinquent
Behaviours. Of the 108 respondents to the survey, 37 reported engagement in one or
more delinquent behaviours included on the SRO within the previous year. The
number of delinquent behaviours endorsed ranged from 1 to 9, with a mean of 1.95
(SD = 1.60) delinquent behaviours reported per respondent (median = 1). The
subsample of respondents who endorsed committing delinquent acts in the past year
did not differ from those who reported no past-year delinquency in regards to
demographic variables, including age, gender and indicators of potential learning
disabilities. Further, total AQ scores did not differ significantly between individuals
who reported delinquency (n = 37, M = 28.41, SD = 11.38) and those that denied
engagement in delinquent acts included on the SRO (n = 71, M = 28.83, SD = 11.69)
within the last year, t(106) = .181, p = .857. LSRP scores were higher amongst
respondents who reported engagement in one or more delinquent acts within the past
year (M = 61.97, SD = 15.54) when compared to respondents who did not report
96
engagement in delinquent acts according to the SRO (M = 55.15, SD = 10.06),
Welch’s t(52.18) = -2.42, p = .019. This difference was consistent with prior research
that has demonstrated an association between psychopathy and engagement in
antisocial behaviours (see Chapter 3).
Within the subsample of 37 respondents who reported past-year engagement
in delinquent behaviours, total AQ scores ranged from 8 to 46, with a mean of 28.41
(SD = 11.38) and a median of 31. Skewness and kurtosis statistics for total AQ scores
within this sample did not fall outside of the acceptable ranges of ±2 and ±7
respectively, indicating that data approximated a. normal distribution (Tabachnick &
Fidell, 2013). Participants scoring less than the median AQ score (31) were allocated
to the ‘Low AQ’ group (n = 17, M = 17.41, SD = 5.39), while those scoring 31 or
above were allocated to the ‘High AQ’ group (n = 20, M = 37.75, SD = 4.59).
Demographic variables, including age, gender and responses on the learning
disability items, did not differ significantly between respondents within the High vs.
Low AQ groups. However, LSRP scores were significantly higher amongst
respondents within the High AQ group (M = 66.95, SD = 12.14) when compared to
LSRP scores within the Low AQ group (M = 56.12, SD = 17.35), indicating a higher
degree of self-reported psychopathic traits amongst those within the delinquent
subsample who reported a higher degree of ASD traits, t(35) = 2.23, p = .033.
4.3.2.1. Overall annual frequency and variety of engagement in offending
and other delinquent behaviours. Annual offence variety scores did not differ
between respondents within the High AQ group (n = 20, M = 1.9, SD = 1.21) and
those within the Low AQ group (n = 17, M = 2.0, SD = 2.0), t(35) = -.187, p = .853.
Similar to variety scores, the reported annual frequency of engagement in any
delinquent behaviour did not vary significantly between respondents within the High
97
AQ group (M= 20.9, SD = 55.4) and those within the Low AQ group (M = 7, SD =
9.26), Welch’s t(20.24) = 1.104, p = .283.
4.3.2.2. Offence-types endorsed. Table 4 provides details regarding the
proportion of respondents who endorsed past-year engagement in offence-like
behaviour and the reported frequency with which such behaviours were committed,
according to offence categories defined within the Crimes Statistics Agency Offence
Classification (2015). A greater proportion of respondents within the Low AQ group
reported engagement in traffic-and-driving-related offences within the last year, when
compared with those within the High AQ group, χ2(1) = 7.619, p = .006. No other
significant differences were found between respondents within the High vs. Low AQ
groups for endorsement or self-reported frequency of engagement in delinquent
behaviour types included for analysis.
4.3.3. Adjudication and dispositional outcomes. Self-report of the lifetime
frequency of contact with the CJS and adjudication outcomes were explored amongst
respondents to determine the extent to which AQ scores predicted the applicability of
discretionary and diversionary legal provisions. Within the total sample (n = 108),
AQ scores ranged from 7 to 47, with a mean of 28.69 (SD = 11.53) and a median of
31.5. Participants scoring less than the median AQ score (31.5) were allocated to the
‘Low AQ’ group (n = 54, M = 18.5, SD = 6.31), while those scoring 31.5 or above
were allocated to the ‘High AQ’ group (n = 54, M = 38.87, SD = 4.16).
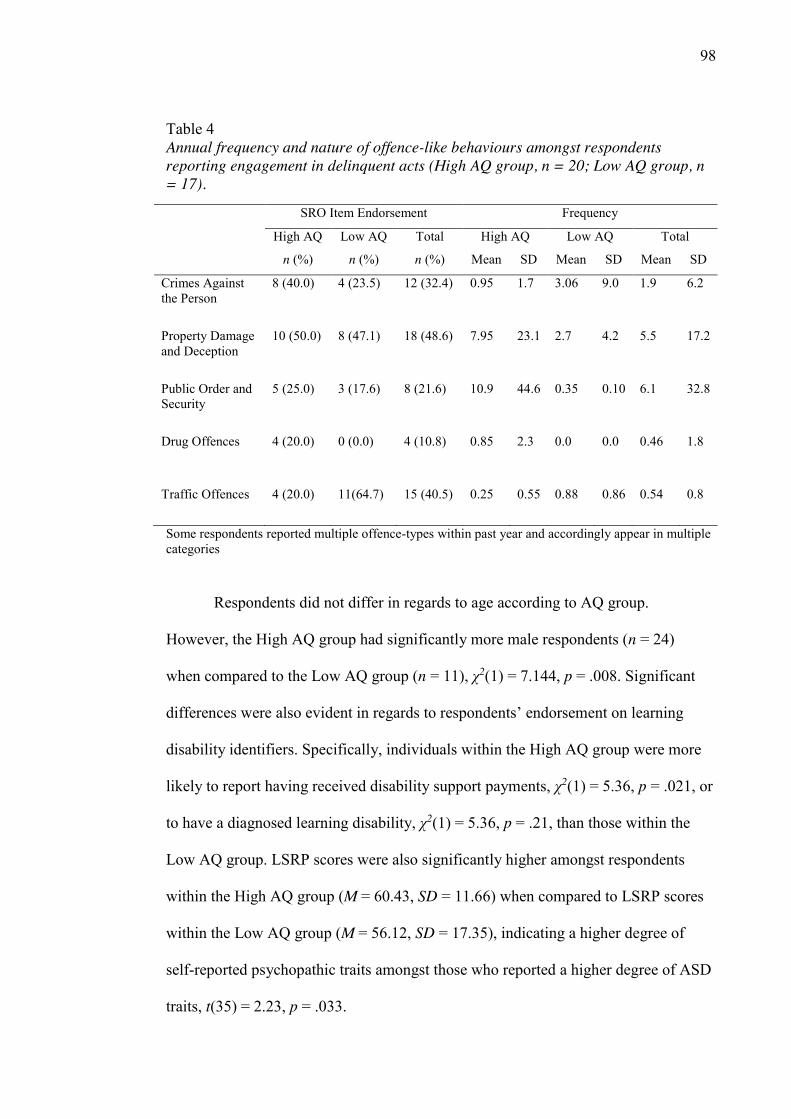
98
Table 4 Annual frequency and nature of offence-like behaviours amongst respondents reporting engagement in delinquent acts (High AQ group, n = 20; Low AQ group, n = 17).
Some respondents reported multiple offence-types within past year and accordingly appear in multiple categories
Respondents did not differ in regards to age according to AQ group.
However, the High AQ group had significantly more male respondents (n = 24)
when compared to the Low AQ group (n = 11), χ2(1) = 7.144, p = .008. Significant
differences were also evident in regards to respondents’ endorsement on learning
disability identifiers. Specifically, individuals within the High AQ group were more
likely to report having received disability support payments, χ2(1) = 5.36, p = .021, or
to have a diagnosed learning disability, χ2(1) = 5.36, p = .21, than those within the
Low AQ group. LSRP scores were also significantly higher amongst respondents
within the High AQ group (M = 60.43, SD = 11.66) when compared to LSRP scores
within the Low AQ group (M = 56.12, SD = 17.35), indicating a higher degree of
self-reported psychopathic traits amongst those who reported a higher degree of ASD
traits, t(35) = 2.23, p = .033.
SRO Item Endorsement Frequency
High AQ Low AQ Total High AQ Low AQ Total
n (%) n (%) n (%) Mean SD Mean SD Mean SD
Crimes Against the Person
8 (40.0) 4 (23.5) 12 (32.4) 0.95 1.7 3.06 9.0 1.9 6.2
Property Damage and Deception
10 (50.0) 8 (47.1) 18 (48.6) 7.95 23.1 2.7 4.2 5.5 17.2
Public Order and Security
5 (25.0) 3 (17.6) 8 (21.6) 10.9 44.6 0.35 0.10 6.1 32.8
Drug Offences 4 (20.0) 0 (0.0) 4 (10.8) 0.85 2.3 0.0 0.0 0.46 1.8
Traffic Offences 4 (20.0) 11(64.7) 15 (40.5) 0.25 0.55 0.88 0.86 0.54 0.8
99
4.3.3.1. Lifetime frequency of charges and arrests. No significant differences
were found in the number of self-reported lifetime charges or arrests between
respondents in the High AQ group (M = .19, SD = .48) when compared to the
responses of the Low AQ group (M = .07, SD = .33), Welch’s t(93.78) = -1.407, p =
.163.
4.3.3.2. Lifetime disposition and application of discretionary and
diversionary alternatives. Respondents’ self-report of the application of various
diversionary and dispositional outcomes following police contact (lifetime) also did
not differ on the basis of AQ group. Specifically, no significant differences were
found in the proportion of respondents reporting that prior police contact had resulted
in being warned and released, χ2(1) = 1.93, p = .165, held in jail, Fisher’s χ2(1) =
4.86, p = .06, mandated to participate in a treatment program, χ2(1) = 4.86, p = .06,
referred for counselling, Fisher’s χ2(1) = .21, p = .65, court appearances, χ2(1) = .787,
p = .375, probation, Fisher’s χ2(1) = ,343, p = .558, the imposition of fines, χ2(1) =
2.42, p = .120, restitution payments, Fisher’s χ2(1) = .343, p = 1.0, community
service, Fisher’s χ2(1) = 2.16, p = .27, and incarceration in a secure hospital or
correctional facility, Fisher’s χ2(1) = 2.04, p = .495.
4.4. Discussion
The overarching aim of this study was to explore the nature of offending and
other delinquent behaviour, and the CJS response to such, across the breadth of the
ASD phenotype. Specifically, data drawn from a self-report survey regarding
delinquency were analysed to determine whether offence typologies and the legal
response to delinquent behaviours differ according to ASD trait severity within a self-
selected community sample. These aims represent a departure from the
preponderance of previous academic literature regarding ASD and offending
100
behaviour, which has primarily aimed to identify ASD within forensic samples or
determine the prevalence of offending behaviour amongst the ASD population. It is
hoped that the results of the current study may go some way to directing future
research efforts to inform the provision of services to enhance forensic outcomes for
individuals with ASD.
4.4.1. Self-reported engagement in offending behaviour. The current study
was not designed to estimate prevalence of offending amongst individuals with ASD
and several aspects of the study design presented as barriers for accurate estimates of
such (e.g. the study sample did not consist of a whole population or cohort, and
efforts were not made to ensure that the sample was wholly representative of such).
Despite this caveat, it was noted that, within the sample, the self-reported annual
frequency of engagement in delinquent behaviours did not significantly vary
according to ASD trait severity. Similarly, the frequency of lifetime charges or arrests
for offending behaviour did not vary according to the degree of ASD consistent traits
reported by respondents, suggesting that propensity towards engagement in offending
behaviour amongst the ASD population does not differ from that in the general
population.
4.4.2. Offence typologies across the autistic phenotype. Contrary to the
hypothesis, the suggestion that individuals with ASD possess an increased propensity
towards engagement in offences resulting in interpersonal harm was not supported.
Specifically, there were no differences between respondents with higher ASD trait
severity and those reporting few or no ASD traits in past-year engagement in
behaviours causing interpersonal harm. Indeed, within the current sample, no
differences were revealed in regards to reported engagement and frequency of
engagement in delinquent behaviours that constituted crimes against the person,
101
property damage and deception, public order and security, and drug-related
offending. Similarly, the reported annual variety of delinquent behaviours did not
differ on the basis of AQ group (High vs. Low), suggesting that offence diversity
does not vary according to the autistic phenotype.
Traffic offences constituted the only offence-type that significantly differed
between respondents within the high AQ and low AQ comparison groups.
Specifically, individuals endorsing a clinically significant degree of ASD consistent
traits were less likely to report engagement in traffic and driving related offences than
those reporting fewer ASD traits. Such results may suggest that individuals with ASD
are more likely to adhere to legal requirements associated with being a road-user.
However, it should be considered whether this result is artefactual; it may be the case
that the lower rate of past-year driving violations amongst those with more ASD traits
occurred as an artefact of a lower base-rate and reduced frequency of driving amongst
those respondents.
Given that the current study did not measure and control for respondents’
driving status, it is not possible to determine whether differences in the frequency
with which respondents drove may explain the lower rate of reported traffic
violations amongst respondents with higher ASD traits; however, it appears likely
that this may be the case. Prior research has demonstrated that individuals with ASD
experience significant difficulties learning to drive, are delayed in comparison to
neurotypical peers in obtaining a drivers’ license and, once licensed, drive less
frequently than non-ASD drivers (Chee et al., 2015; Cox, Reeve, Cox, & Cox, 2012;
Daly, Nicholls, Patrick, Brinckman, & Schultheis, 2014; Falkmer et al., 2015). For
example, in a recent Australian study regarding the viewpoints of individuals with
ASD in regards to driving, a significantly smaller proportion of participants with
102
ASD (n = 50) reported possessing a drivers’ license (34%) when compared with non-
ASD counterparts (68%; n = 57) (Chee et al., 2015). Further, in a recent study of
driving behaviours amongst ASD drivers (where only those who hold a driver’s
license were included in the sample) ASD drivers were significantly more likely to
report problem driving behaviours, including intentional violations, mistakes, and
lapses in concentration, within a 2 year period, when compared to neurotypical peers
(Daly et al., 2014). Future research could examine this relationship further, including
exploration of factors likely to assist individuals with ASD to drive within the bounds
of legislative requirements if it is established that traffic violations are more common
amongst this population once driving status is taken into consideration.
4.4.3. Forensic response to delinquent behaviour. A second aim of the
current study was to explore whether differences existed in the application of
dispositional alternatives according to ASD trait severity. Results demonstrated that
those with clinically significant degrees of ASD symptoms had been made subject to
a similar range of diversionary and dispositional alternatives as the result of police
contact as those who reported few, or no, ASD traits. On face value, such results
suggested that individuals with ASD are not systemically disadvantaged in regards to
the forensic response to delinquent behaviour. However, a narrow focus on the
equality of forensic outcome (in regards to, for example, the application of
diversionary and dispositional outcomes) may overlook the different needs of diverse
cohorts (Glanfield, 1999). Accordingly, equal application of dispositional and
diversionary alternatives is not necessarily indicative of equity within the context of
criminal law.
Although the results of the current study indicated equality in regards to the
application of diversionary and dispositional alternatives across the autistic
103
phenotype, it is unclear whether equivalence in regards to the application of such
alternatives constitutes equitable treatment in regards to the legal process. In
determining whether such results reflect equitable application of legal protections
related to mental impairment, consideration must be given to the legal status of
individuals with ASD. Later chapters will explore the legal status of individuals with
ASD in further detail; for now, it will suffice to alert the reader that a body of
academic literature exists that argues the relevance and potential significance of ASD
traits to forensic decision-making related to the disposition of cases involving
delinquent behaviours perpetrated by individuals with ASD (e.g. Archer & Hurley,
2013; Barry-Walsh & Mullen, 2004; Brewer & Young, 2015; Freckelton, 2011,
2012b, 2013b; Freckelton & List, 2009).
4.4.4. Limitations. The current study possessed several limitations. First, the
small sample size prevented a comprehensive statistical analysis of the data. Larger
samples would be required to model data to determine the manner in which specific
factors of ASD may contribute to offending behaviour. Further, the use of a targeted
sampling approach within the current study, including convenience and targeted
recruitment techniques, raise the likelihood that the sample may not be representative
of the general population. Thus, while it is possible that individuals with ASD offend
with similar frequency and offence-variation than those who do not present with
ASD, this result may be artefactual; occurring as the result of methodological
weaknesses, including sample biases, systematic differences in recall or
idiosyncrasies in responding on the SRO.
Nonetheless, the sampling methods employed in the current sample ensured
that both individuals with very few ASD traits and those who would be likely to
display clinically significant severity of ASD symptomatology self-selected for
104
participation. Indeed, half of the study sample (n=108) possessed AQ scores above
32; the cut-off recommended by the authors of the screening tool. It should be noted
that respondents were assigned to the Low or High AQ group on the basis of their AQ
score, relative to the scores of the rest of the sample. Accordingly, the recommended
cut-off scores on the AQ were not employed to differentiate those reporting a
clinically significant degree of ASD traits. Nonetheless, 18 respondents in the High
AQ group for annual delinquency analyses (n = 20; 90%), and 54 respondents in the
High AQ group for lifetime analyses (n = 54; 100%) scored in the range of clinical
levels for traits associated with ASD, according to the cut-off score of 32
recommended by the authors of the AQ (Baron-Cohen et al., 2001).
Critically, the AQ is not diagnostic and independent verification of ASD
diagnoses was not undertaken in the current study, thus AQ scores can only be taken
to identify ‘the degree to which an adult has autistic traits’ (Baron-Cohen et al. 2001,
p.6) for respondents within the current sample. Thus, although individuals within the
“High AQ” group reported ASD trait severity within the range considered clinically
significant, it is unclear which, if any, respondents would meet formal diagnostic
criteria for ASD. Moreover, given that the current study did not query the presence or
impact of potential comorbid psychiatric or medical conditions, it is not possible to
determine whether features of these conditions confounded self-reports regarding
delinquency and the forensic response to such amongst respondents.
The self-report methodology of the current study also presents potential
concerns regarding the validity of results. While the limitations of using official
indices of offending (e.g. criminal convictions) are well known, support for the use of
self-report measures, such as the SRO Questionnaire utilized in this study, is also far
from universal. Critically, the SRO does not represent an exhaustive list of delinquent
105
behaviours, is skewed towards less serious delinquent behaviours and, given the
international sample of the current study, it is possible that the delinquent behaviours
included may not constitute criminal behaviours across each jurisdiction represented
within the sample. Further, the cross-sectional nature of the study resulted in data that
only provides ‘snapshots’ of offending behaviour, which is unable to explore the full
trajectory of onset, career length and progression, escalation, offence switching or
changes in specialization and desistance. Given that patterns of offending behaviour
have been shown to change across criminal careers (e.g. Gilman et al., 2014), this
may not provide a full picture of offending behaviour amongst individuals with ASD.
The use of a self-report methodology may be particularly problematic when
considering the intended population sample of individuals with ASD. Of note, the
SRO has not been validated for use with the ASD population and there is some
evidence of systematic biases in regards to the manner in which individuals with
ASD interpret and respond to survey items (Daly et al., 2014; Howlin et al., 2015;
Williams, 2010). Such biases, if present, would have the potential to significantly
impact the results of the current study. For example, an increased tendency towards
admission of delinquency amongst individuals with ASD (Allen et al., 2008; de la
Cuesta, 2010; Murrie et al., 2002; North et al., 2008) may have resulted in a lower
threshold amongst individuals with higher degrees of ASD traits to endorse items on
the SRO. In this context, it is possible that the results of the current study were
inflated and individuals with ASD are in fact less likely to engage in offending
behaviour than their neurotypical peers. Conversely, it may be the case that literal and
pedantic interpretations of SRO items may have masked an increased frequency of
delinquent behaviours amongst individuals with ASD (e.g. failing to endorse the item
“In the last 12 months have you hit someone you lived with, with the idea of hurting
106
them?” due to a perception that their actions constituted a “punch” or “smack” rather
than a “hit”). Further, given that the survey from which the data were drawn was only
available for completion online, only individuals who were computer literate and had
access to an Internet connection could participate. It is noteworthy, however, that
issues with generalizability are prevalent throughout the literature involving adults
with ASD (Howlin et al., 2015). Specifically, the voluntary nature of research
participation, alongside the likelihood that individuals with certain ASD-consistent
traits may be unwilling to take part in unfamiliar activities are considered to reduce
the external validity of research involving adults with ASD (Falkmer et al., 2015;
Howlin et al., 2015). As a result of such limitations, conclusions regarding
delinquency amongst individuals with ASD drawn from the current study remain
tentative.
4.4.5. Implications and directions for future research. Whether individuals
with ASD possess a particular propensity towards particular offending behaviours has
been vigorously debated. In light of the growing prevalence of ASD within the
community, it is imperative that researchers explore such issues in attempts to
identify and address potential vulnerabilities in regards to the involvement by some
people with ASD in antisocial behaviours. Such efforts are vital to inform efforts
directed towards prevention and early intervention for delinquent behaviours amongst
the ASD population. Methodological limitations aside, the current study is one of the
first, to the authors’ knowledge, that set out to systematically investigate these issues.
Given the preliminary nature of the results, this is an area that most certainly
warrants additional empirical investigation. Future research in this area should be
directed towards examining the nature of offending behaviours amongst a larger,
more representative sample of the ASD population. Another potential direction for
107
future research is to investigate whether specific neurocognitive impairments
associated with ASD are associated with vulnerabilities in regards to engagement in
particular offence types. Ultimately, this type of research will assist to inform the
nature of supports and interventions geared to prevent and respond to offending
behaviours amongst the ASD population.
Questions of prevalence and propensity towards particular offence-types need
not be resolved, however, in order to address issues related to responding to
offending behaviours amongst the ASD population or the management of such
individuals within the CJS. At present, there are no clear dispositional pathways for
individuals with ASD who are convicted of a criminal offence (Freckelton, 2013b;
Murrie et al., 2002). As demonstrated by the responses provided in the current study,
individuals with ASD may variously be made subject to a community disposal or
attract the application of diversionary alternatives (such as referral for a treatment
program or admission to a secure psychiatric facility), whist others find themselves
sentenced to a term of incarceration within a prison. This variation in forensic
outcome may be appropriate, given that a similar variation was noted for neurotypical
peers. A critical question is whether the presence and impact of an ASD diagnosis are
appropriately considered in the disposition of cases involving defendants with ASD
(Woodbury-Smith & Dein, 2014). This issue is explored in further detail in
succeeding chapters.
108
Chapter 5. The Legal Response: Legal Considerations and CJS
Awareness Regarding ASD
As emphasised in earlier chapters, the vast majority of individuals with ASD
are law abiding; however, at least some may come into contact with the CJS due to
engagement in criminal behaviours. Such individuals raise challenges for the CJS in
determining and enacting an appropriate forensic response. Specifically, the presence
of individuals with ASD within the CJS raises questions regarding criminal
responsibility and competence and, relatedly, the application of legal provisions in the
disposition of such cases. Despite the potential for significant negative ramifications
following inappropriate forensic responses to offending behaviour (miscarriages of
justice and reduced community safety, for example), little research exists that has
systematically explored issues related to the disposition of cases involving defendants
with ASD. In this chapter, the limited extant literature regarding such issues is
examined, with a particular emphasis on the applicability to individuals with ASD of
legislation and case law that guides judicial decision-making regarding the
disposition of mentally disordered defendants. To provide context for such a
discussion, the chapter commences with a description of the legal frameworks in
Australia regarding mentally disordered offenders, with special reference to the
legislative landscape in the state of Victoria.
5.1. Legislation and Common Law Regarding Defendants with Mental Disorders
Legal provisions exist in most jurisdictions internationally, to moderate
punishment for individuals who lacked the mental capacity to fully appreciate the
nature or moral quality of their criminal behaviour (Loughnan, 2012). Such
provisions exist in recognition that punishment is not an appropriate response to
criminal behaviours amongst individuals without the mental capacity to understand
109
the immoral nature or legal ramifications of their actions (Victorian Law Reform
Commission, 2013). Substantively, a defendant’s mental functioning bares relevance
to the determination of their fitness to stand trial, the applicability of defences related
to their criminal responsibility and the nature and severity of the sentence imposed in
response to the offending behaviour. Legislation and common law principles exist in
most jurisdictions internationally that explicitly outline the conditions by which
fitness and culpability are determined, with minor variations existing between
Australian jurisdictions. As a means by which to anchor later comments regarding the
disposition of offenders with ASD, the relevant law in Victoria, Australia, is briefly
outlined below.
5.1.1. Fitness to stand trial. The issue of fitness to stand trial pertains to the
ability of an accused person to understand and effectively participate in a legal trail
(Loughnan, 2012). Fitness is defined similarly across Australian jurisdictions; in
Victoria the conditions applicable to fitness are codified in section 6 of the Crimes
(Mental Impairment and Unfitness to be Tried) Act 1997 (Vic) (CMIA), as follows:
1) A person is unfit to stand trial for an offence if, because the person’s
mental processes are disordered or impaired, the person is or, at some
time during the trial will be-
a. unable to understand the nature of the charge; or
b. unable to enter a plea to the charge and to exercise the right to
challenge jurors or the jury; or
c. unable to understand the nature of the trial (namely that it is an
inquiry as to whether the person committed the offence); or
d. unable to follow the course of the trial; or
110
e. unable to understand the substantial effect of any evidence that
may be given in support of the prosecution; or
f. unable to give instructions to his or her legal practitioner.
2) A person is not unfit to stand trial only because he or she is suffering
from memory loss. (s6, CMIA).
An accused person who is deemed by a jury to meet any of the criteria
outlined above may be found unfit to stand trial (s7(1), CMIA). If a defendant is
found not capable to stand trial, the trial may be postponed until such time that the
person is deemed fit, however, if the person is unlikely to become fit to stand trial in
the foreseeable future or remains unfit after a period of adjournment, a special
hearing is conducted to resolve the criminal case. The special hearing is heard before
a jury and adopts a modified criminal procedure that takes into account the inability
of the defendant to participate fully in the trial with three possible outcomes: the
defendant may be found criminally responsible for committing the offence (or
another relevant offence), charges may be dropped, or the defendant found not guilty
by reason of mental impairment (Victorian Law Reform Commission, 2013).
5.1.2. The Mental Impairment defence. The defence of Mental Impairment
generally serves to excuse an accused offender from criminal responsibility due to an
inability to understand that their conduct was wrong. In order to establish criminal
responsibility for an act (i.e. guilt), two aspects must be proven: actus reus and mens
rea (Denney, 2012; Erickson & Felthous, 2009; Ferguson & Ogloff, 2011; Morse,
1999). Actus reus refers to the commission of the prohibited act while mens rea refers
to a state of mind when committing the act, that is, the intent to commit the act
(Denney, 2012; Ferguson & Ogloff, 2011). In law, a person is held criminally
responsible for their offenses if it can be proved that they committed an offence
111
(actus reus) and that they did so intentionally (mens rea) (Morse, 1999). In contrast,
if, due to mental disorder or disability, an individual does not have the capacity to
form intent, they may be excused from criminal responsibility on the grounds of
mental impairment (Ferguson & Ogloff, 2011; Levy, 2011; Morse, 1999).
Central to the Mental Impairment defence is the assumption that punishment
is not an appropriate response in cases where an individual cannot understand the
legal ramifications of their behaviour, because they cannot be deterred or influenced
by mere punishment from repeating such behaviours (Victorian Law Reform
Commission, 2013). Simultaneously, the courts are charged with the responsibility to
protect the community from those who pose an unacceptable risk of harm to
themselves, or others (Victorian Law Reform Commission, 2013). Thus, the Mental
Impairment defence serves to protect a potentially vulnerable group of individuals
(i.e. the “mentally impaired”) from undue punishment, while still recognising that
measures may be required to mitigate the risk such individuals may pose to the
community (Victorian Law Reform Commission, 2013).
As with the legislation regarding fitness to stand trial, the precise standards by
which Mental Impairment is determined vary across Australian jurisdictions. In
Victoria, the conditions required to establish the defence of mental impairment are
codified in section 20 of the CMIA as follows:
1) The defence of mental impairment is established for a person charged with an
offence if, at the time of engaging in conduct constituting the offence, the
person was suffering from a mental impairment that had the effect that—
a. he or she did not know the nature and quality of the conduct; or
b. he or she did not know that the conduct was wrong (that is, he or she
could not reason with a moderate degree of sense and composure
112
about whether the conduct, as perceived by reasonable people, was
wrong).
2) If the defence of mental impairment is established, the person must be found
not guilty because of mental impairment (s20, CMIA)
The critical issue in determining the applicability of the Mental Impairment
defence is in regards to the cognitive, moral and volitional capacities of the offender
in question. Essentially, if, as the result of a diagnosable mental condition, an
individual does not possess an understanding that they were ‘wrong’ in engaging in
the offending behaviour, was unable to control their behaviour, or held a false belief
that their behaviour was appropriate, they could be deemed ‘not guilty because of
mental impairment, and will not be considered criminally culpable for their
behaviour. Defendants found ‘not guilty because of mental impairment’ become
subject to the special powers of the court, under which they may be released
unconditionally, under supervision, or detained for appropriate treatment (Victorian
Law Reform Commission, 2013).
5.1.3. Mental disorder as a mitigating factor during sentencing. The
sentencing of an offender found to be guilty is frequently described as the most
demanding task faced by the judiciary; requiring judicial officers to weigh issues
related to community safety against mitigating factors, such as an offender’s
perceived moral blameworthiness and the likely impact of any punishment imposed
(Edgely, 2009; Edney & Bagaric, 2007; Freckelton, 2007; Potas, 1981; Walvisch,
2010). Over the last 20 years, provisions have been enacted to govern the sentencing
process and in most Australian jurisdictions dedicated sentencing legislation exists
(Edney & Bagaric, 2007; Mackenzie, Stobbs, & O'Leary, 2010). In Victoria, the
purposes of sentencing, the hierarchy of sentencing courts and a range of aggravating
113
and mitigating factors to which sentencing judges may turn their mind are codified in
the Sentencing Act 1991 (Vic). However, Australian legislation provides little
guidance in regards to the practical application of such factors, including which ought
to take precedence where competing principles are evident in a single case (Edgely,
2009; Ritchie, Hudson, Kenny, & Darby, 2016). Nor does the legislation specifically
address the issue of sentencing offenders with impaired mental functioning (Edney &
Bagaric, 2007; Freiberg, 2010; Mackenzie et al., 2010). Thus, in Australia, the act of
sentencing, and particularly the sentencing of mentally disordered offenders, is
largely driven by judicial discretion.
It is nonetheless expected that sentencing decisions adhere to common law
mandates, set out in previous court decisions (Potas, 1981). In most jurisdictions in
Australia, deliberations regarding the sentencing of offenders with a mental
impairment are primarily guided by the consideration of a range of mitigating factors
set out in the Victorian Court of Appeal’s decision in R v Verdins, Buckly and Vo
(2007) (Freckelton, 2007, 2012a; Walvisch, 2010). The Verdins’ decision, described
by Freckelton (2007) as “Australia’s most sophisticated and subtle analysis of the
relationship between impaired mental functioning and sentencing” (p. 1), expanded
on previous court decisions (in particular, Tsiaras v The Queen [1996]), in
considering whether ‘mental impairments’ possessed by an offender would impact
their response to dispositional alternatives such that the purposes of sentencing –
namely general and specific deterrence, just punishment and denunciation – would
not be served by imposing such a sentence.
The Verdins decision set out a (non-exhaustive) list of six ways in which the
mental functioning of an offender may render it appropriate to moderate moral
culpability, and accordingly, the type and severity of punishment imposed during
114
sentencing. Specifically, the Court of Appeal held that the following factors ought to
be taken into account when imposing a sentence for any offender “…shown to have
been suffering at the time of the offence (and/or to be suffering at the time of
sentencing) from a mental disorder or abnormality or an impairment of the mental
function.” (R v Verdins [n 7] 271):
1) The condition may reduce the moral culpability of the offending conduct, as
distinct from the offender’s legal responsibility. Where that is so, the
condition affects the punishment that is just in all the circumstances; and
denunciation is less likely to be a relevant sentencing objective.
2) The condition may have a bearing on the kind of sentence that is imposed
and the conditions in which it should be served.
3) Whether general deterrence should be moderated or eliminated as a
sentencing consideration depends upon the nature and severity of the
symptoms exhibited by the offender, and the effect of the condition on the
mental capacity of the offender, whether at the time of the offending or at the
date of sentence or both.
4) Whether specific deterrence should be moderated or eliminated as a
sentencing consideration likewise depends upon the nature and severity of the
symptoms of the condition as exhibited by the offender, and the effect of the
condition on the mental capacity of the offender, whether at the time of the
offending or at the date of the sentence or both.
5) The existence of the condition at the date of sentencing (or its foreseeable
recurrence) may mean that a given sentence will weigh more heavily on the
offender than it would on a person in normal health.
115
6) Where there is a serious risk of imprisonment having a significant adverse
effect on the offender’s mental health, this will be a factor tending to mitigate
punishment” (R v Verdins (2007) 16 VR 269 at 32).
A thorough analysis of the practical application of these factors is beyond the
scope of this thesis, and is available elsewhere (e.g. Freckelton, 2007; Gee & Ogloff,
2014; Walvisch, 2010). Critically, the considerations delineated in R v Verdins,
Buckly and Vo (2007) pertain to the moral culpability of an offender, rather than legal
responsibility. This distinction is important; in contrast to dichotomous
determinations of the impact of mental impairment according to the abovementioned
legislation (i.e. an offender is either fit- or unfit-; criminally responsible or not
criminally responsible), moral culpability can be conceptualised as a “continuum of
blameworthiness” informed by the “extent to which the background and
circumstances of the defendant influenced, predisposed, or diminished the
defendant’s moral sensibilities and the exercise of volition or free will”
(Cunningham, 2012, p.108). It follows that any sanction imposed on an offender
should similarly be moderated in line with the nature and severity of any extant
symptomatology; such that offenders with mental impairments are not punished as
harshly as other (non-impaired) offenders (Cunningham, 2012; Walvisch, 2010).
Thus, in regards to the application of Verdins’ principles, the pertinent consideration
is the degree to which a mental impairment may have influenced a defendant’s moral
understanding at the time of offending, or would be likely to impact on their
experience of the available dispositional alternatives (Walvisch, 2010).
The court is explicit that the application of the principles delineated in R v
Verdins, Buckly and Vo (2007) may apply “whether or not the condition in question
would properly be described as a (serious) mental illness” (Verdins [n 7] 271,
116
emphasis added), and is therefore not restricted to cases of severe psychiatric illness.
This definition for ‘mental impairment’ is deliberately broad; more so than in the
Crimes (Mental Impairment and Unfitness to be Tried) Act 1996 and prior court
decisions concerning mental impairment (e.g. Veen v The Queen [No.1] (1979) 143
CLR 458). Thus, the impact of impaired mental functioning can now be considered
amongst a vastly wider group of offenders than was permitted in legislation or
common law preceding the Verdins’ decision. However, it is clear that the
considerations raised in R v Verdins, Buckley and Vo (2007) are not intended to act as
a form of automatic leniency for offenders with such impairments (Freckelton, 2007).
As Justice Cavanough iterated in R v Oznek [2007] VSC 192 at [22]:
There is a need for identification in the evidence of the type of mental
impairment from which it is asserted that the offender was suffering at the
time; and secondly (and more importantly), there is a need for clear evidence
that any such condition had any of the effects which tend to reduce moral
culpability.
Thus, where an offender is identified as possessing a mental impairment, as
defined by Verdins, this represents only the beginning of the sentencing court’s
enquiry to determine whether this impairment ought to be considered as mitigating
for the purposes of sentencing. Specifically, the court must determine how the
particular impairment may have impacted the offender’s mental state and behavioural
control in the context of the precipitating circumstances to their offending, at the time
of the offending, or how it is likely to impact functioning in the future (Freckelton,
2007).
117
5.2. The Legal Status of Defendants with Autism Spectrum Disorder
Criminal responsibility and criminal culpability among offenders with ASD
began to receive attention in Australia following the finding that Martin Bryant, who
in 1996 murdered 37 people at Port Arthur in Tasmania, had a diagnosis of Asperger
Syndrome8 (Freckelton, 2011; Mullen, 1996). Since that time, ASD diagnoses have
been raised with increasing frequency during criminal proceedings in international
and Australian jurisdictions (Freckelton, 2011, 2013a, 2013b). These cases raise a
complex set of issues for the judiciary, who are required to make decisions related to
criminal intent, legal responsibility and the likely impact of any legal sanctions
imposed in responding to illegal behaviours (Baron-Cohen, et al., 2001; Freckelton,
2011; Hare et al., 1999; Royal College of Psychiatrists, 2006).
5.2.1. Legislative considerations: Fitness to Stand Trial and the Mental
Impairment Defence. Notably, the mere presence of a diagnosable condition does
not automatically provide grounds for the operation of legislative provisions designed
to protect vulnerable individuals from unduly harsh outcomes within the CJS
(Walvisch, 2010). While establishing the presence of an impairment, through a DSM-
5 diagnosis or otherwise, is a necessary initial task for the operation of such legal
provisions, the diagnosis of a mental disorder is not, on its own, sufficient to call into
operation the protections for mentally disorder defendants. Establishing the nexus
between any extant condition and the defendant’s engagement in offending behaviour
(and, in the case of sentencing, the likely impact of punishment) is the primary
consideration (Freckelton & List, 2009; Lerner et al., 2012; Walvisch, 2010). While
such determinations take place on a case-by-case basis, a reasonable place to start
such deliberations is in the consideration of the nexus between the characteristic
8 This finding was later disputed and regarded a misdiagnosis (Mullen, 1996).
118
symptomatology of a particular condition and the affected individual’s mental state
and behaviour at the time of offending.
5.2.1.1 Fitness to stand trial. Several of the core features of ASD could be
expected to complicate participation in the legal process, potentially impacting on
comprehension and giving rise to communication problems within the context of
criminal proceedings (Allen et al., 2008; Freckelton, 2013b; Hall, Godwin, Wright, &
Abramson, 2007; Taylor, Mesibov, & Debbaudt, 2009). For example, literalness and
rigidity in thought and difficulties integrating verbal information may result in
difficulties for defendants with ASD in interpreting the meaning and implications of
questions put to them by legal representatives during examinations (Hall, Godwin,
Wright, & Abramson, 2007; Taylor et al., 2009). Further, a tendency towards
detailed-oriented processing and strong preference for routine and familiarity may
evoke confusion and agitation amongst individuals with ASD, increasing their
vulnerability to decompensation in the unfamiliar environment of the courtroom
(Health and Social Care Overview and Scrutiny Committee, 2012).
In such circumstances, a defendant with ASD may be reluctant to
communicate and may engage in maladaptive coping behaviours, thus impacting their
ability to appropriately and meaningfully participate in court processes or instruct
their lawyer on relevant matters (Health and Social Care Overview and Scrutiny
Committee, 2012). Consistent with such, in a study by Allen and colleagues (2008)
regarding the experiences of defendants with Asperger’s syndrome, participants self-
reported a range of specific difficulties experienced during court proceedings,
including problems with comprehending the court processes and difficulties
communicating with legal representation (e.g. “My barrister made things really
119
confusing. He wasn’t telling me what was going on or what was gonna happen next
[…] I was just really confused and annoyed”; p. 754).
In a recent study in which the impact of ASD on fitness to stand trial was
systematically investigated, Brewer, Davies, and Blackwood (2016) revealed a
significantly poorer understanding of concepts related to competency amongst adult
offenders with a diagnosis of ASD (n = 15) when compared to (non-offender) adults
with no diagnosis of ASD (n = 15). Specifically, participants viewed portions of a 15-
minute filmed vignette of typical court proceedings and then responded to items
relevant to the excerpt on a novel measure designed to assess fitness to stand trial
according to the legislation in England and Wales9. Whilst no differences were
revealed in overall scores on the fitness to stand trial measure, the responses of
individuals with ASD indicated a poorer understanding of issues related to
understanding the evidence and case presented in the vignette, the process and
implications of entering a plea, and in regards to the roles of CJS personnel and
courtroom processes represented in the fitness to stand trial measure. Thus, it was
evident that under certain circumstances, defendants with ASD may be negatively
impacted in regards to their ability to understand and follow the judicial process and
the nature of the charges brought against them.
Of note, despite their poorer understanding of a range of concepts vital to
understanding court processes, participants with ASD in Brewer and colleagues’
(2016) study considered themselves to be more familiar with courtroom procedures
than the control group of non-ASD non-offenders. In this context, Brewer et al. 9 Although this measure was designed for use in England and Wales, a great
deal of overlap exists between the legal criteria to assess fitness to stand trial in
Australia. Thus, while some caution is required in generalising the results of Brewer
et al.’s (2016) study, the results of such may inform issues in Australian jurisdictions.
120
cautioned that both individuals with ASD and CJS professionals alike may
overestimate competency amongst offenders with ASD, resulting in the inadequate
provision of support, and potentially, unjust forensic outcomes. Indeed, several
authors have agreed that the difficulties that individuals with ASD face in navigating
the demands of the courtroom are often overlooked, particularly amongst those with
normative or above-average intellectual functioning, because they may not
immediately present with clear evidence of impairment (Allen et al., 2008; Brewer et
al., 2016; Freckelton, 2013b; Hare et al., 1999). Despite such, studies that have
reviewed court outcomes involving such defendants suggest that most are considered
fit to stand trial. For example, in five cases of offenders with Asperger’s syndrome
reviewed by Barry-Walsh and Mullen (2004) the individuals were found fit to stand
trial in all cases. Similarly, all but one of Allen et al.’s (2008) participants that had
been processed through the CJS were deemed fit to plea (n = 9).
It has been argued that the majority of individuals with ASD can be
appropriately accommodated within court proceedings through the provision of
relatively modest special measures, such as familiarizing the defendant with the
courtroom setting prior to appearing, removal of formal attire such as wigs and
gowns, simplifying language used during questioning, or the presence of an
intermediary during examinations (Cutler, 2014; Health and Social Care Overview
and Scrutiny Committee, 2012; Talbot, 2012). Of note, despite describing various
difficulties with participation in court proceedings, two of the participants in Allen et
al.’s (2008) study reported that their awareness and comprehension of the trial was
aided by effective communication with support persons and legal representatives (e.g.
“I had a good barrister…he explained the court process to me, and the other couple
of guys who saw me…they explained everything to me”; Allen et al., 2008, p. 755).
121
Consistent with such reports, Brewer et al. (2016) found no differences between
individuals with ASD and the control group in regards to their understanding of
instructing legal representatives. This suggests that, in some cases, the
aforementioned difficulties faced by individuals with ASD when appearing in court
may be ameliorated through appropriate support and effective communication.
5.2.1.2. The Mental Impairment defence. As outlined in Chapter 3, a range of
diagnostically-relevant features of ASD (e.g. narrowed focus, cognitive rigidity,
limited perspective-taking capacities and deficits in consequential thinking) have
been argued, under certain circumstances, to contribute causatively to engagement
offending behaviour. These features result in difficulties for individuals with ASD in
interpreting and understanding the behaviour of others, and in predicting and
appreciating the impact of their own behaviour on others (Freckelton, 2011). Taylor
et al. (2009) argues that by virtue of such socio-communicative impairments,
individuals with ASD may unwittingly become involved in offending behaviours,
bringing the Mental Impairment defence into consideration:
Persons with ASD often get into trouble without even realizing that they have
committed an offense. Offenses such as making threatening statements;
personal, telephone, or internet stalking; inappropriate sexual advances;
downloading child pornography; accomplice crime with false friends; and
making physical outbursts at school or in the community, would certainly
strike most of society as offenses which demand some sort of punishment.
This assumption, though valid at face value, may not take into account the
particular issues that challenge the ASD individual […] what appears as anti-
122
social behaviour to the “regular” world is often simply the manifestation of
the ASD person’s misunderstandings (Taylor et al., 2009, p.3).
Indeed, in many cases of offending behaviour amongst individuals with ASD
described in the academic literature, there was a demonstrable nexus between the
offending behaviour and symptomatology of ASD, such that the Mental Impairment
defence could be argued to apply (e.g. Barry-Walsh & Mullen, 2004; Beardon, 2008).
Further, a number of case reports have highlighted offenders with ASD who maintain
a view that their offending behaviour was justified, and refute others’ suggestions to
the contrary with great indignation (Wing, 1997). Other reports suggest that by virtue
of socio-communicative or cognitive/behavioural eccentricities, individuals with
ASD may be unable to appreciate that such conduct is ‘wrong’ (Freckelton, 2013a;
Freckelton & List, 2009; Katz & Zemishlany, 2006; Mayes & Koegel, 2003). Such
appears relevant to the case of “M”, a man who was arrested following a “high degree
of violence towards another person/persons” (undisclosed details; Beardon, 2008,
p.72). M reportedly demonstrated awareness that others viewed his offending
behaviour to be “bad”, however he refuted such by stating that his behaviour was
simply an “unfortunate event” (Beardon, 2008, p. 70).
The socio-communicative and behavioural impairments associated with ASD
may also increase propensity towards provocation amongst the ASD population
which, in the context of behavioural rigidity and underdeveloped emotional
regulation skills, may lead to maladaptive responses, including the perpetration of
violence. For example, Schwartz-Watts (2005) detail a case where a defendant shot
and killed a neighbour who had struck his face, and knocked his glasses, following an
argument. The defendant reportedly retrieved two guns from his bedroom, shooting
123
the victim repeatedly until death. Such violence was formulated in the context of the
defendant’s hypersensitivity to having his glasses touched, thus resulting in a
perception of greater harm than was caused physically during the altercation. Of
particular relevance to Mental Impairment determinations, the defendant reportedly
“was unable to appreciate the “overkill” of his victim”, due to his misperception
(gleaned from watching “America’s Most Wanted” and horror movies) that people
are able to continue attacking after being shot (p. 392).
In summary, at least some individuals with ASD may engage in offending
behaviour in the absence of volitional control or appreciation of the moral
implications of their actions, raising questions in regards to whether such individuals
ought to be considered criminally responsible for their offending behaviour (Barry-
Walsh & Mullen, 2004; de la Cuesta, 2010; Freckelton, 2011; Freckelton & List,
2009; Hall et al., 2007; Murrie et al., 2002). Nonetheless, in many cases, exculpatory
defences are not pursued in such cases, raising questions as to the practical relevance
of such defences to criminal proceedings with offenders with ASD.
5.2.1.3. Theory in practice: The practical relevance of Fitness and mental
Impairment legislation to ASD. A critical issue to the operation of legislative
provisions for offenders with mental disorders is the determination of which
conditions ought to be specified as constituting a ‘mental impairment' for the
purposes of such processes (Robertson, 2013). The term is not explicitly defined in
the legislation in Victoria, Australia and adopted definitions vary across other
Australian jurisdictions (White, Day, & Hackett, 2007). Accordingly, the debate
continues across Australian jurisdictions regarding the conditions that ought to attract
such special consideration (see, for example, Robertson, 2013). Similarly, opinion
varies as to the relevance of such legislation to defendants with ASD.
124
Of note, the available research suggests that where offending behaviour
occurs amongst the ASD population, this is more commonly perpetrated by higher-
functioning individuals whose ASD symptomatology may be less severe
(Gunasekaran & Chaplin, 2012). Conversely, the threshold for determining an
offender as ‘mentally impaired’ as defined in the Australian legislation is high
(Freckelton & Selby, 2013; Victorian Law Reform Commission, 2013). Thus, in most
cases, the impairments displayed amongst defendants with ASD may not be deemed
sufficiently severe as to evoke the operation of such legislative protections. Further,
even in cases where it appears that an offender with ASD would meet threshold
requirements of severity, legal representatives may be reluctant to pursue such
defences.
It should be noted that being found ‘unfit to stand trial’ or ‘not guilty because
of mental impairment’ does not result in the automatic release of an offender. Indeed,
in such cases, offenders may be ordered to supervision or detainment for compulsory
treatment within a secure facility until their symptomatology has dissipated
sufficiently to satisfy the courts that they no longer pose an unacceptable risk to the
community. Because ASD is a neurodevelopmental disorder with core
symptomatology that is relatively resistant to intervention, offenders with ASD who
are deemed ‘unfit to plea’ or ‘not guilty because of mental impairment’ are likely to
face substantial difficulties in satisfying the courts that they have sufficiently
addressed the precipitants of their offending behaviour and may be subject to court-
ordered restrictions for lengthier periods than would be imposed if they are held fully
criminally responsible (Freckelton, 2011). Indeed, given that ASD is a lifelong
disorder, it is feasible that in some cases, such restrictions may apply on an
effectively indefinite basis. Thus, legal representatives may be reticent to raise the
125
legislative protections afforded for mentally disordered offenders, particularly where
charges are not serious (Freckelton, 2011).
Due to the likelihood that many defendants with ASD will not meet severity
thresholds to be deemed ‘mentally impaired’, and the potential for somewhat
draconian consequences should Fitness to Stand Trial or Mental Impairment
legislation be enacted, such legislation appears of limited practical relevance in most
cases of offending behaviour amongst the ASD population (Woodbury-Smith &
Dein, 2014). Nonetheless, any impairments that impact a defendant’s moral or
volitional capacities ought to be taken into account when dealing with offending
behaviour, such that the forensic response is measured and effective. As described
above, the Verdins’ principles adopt a deliberately broad conceptualisation of ‘mental
impairment’ in consideration of the moral culpability of a guilty offender.
Accordingly, thresholds for the applicability of such considerations are lower and
more likely to bear relevance to offenders with ASD when compared to the operation
of the legislative provisions described above. As a result, a diagnosis of ASD may be
of greater relevance during the sentencing of a guilty offender (Attwood, 2007).
5.2.2. ASD as a mitigating factor during sentencing: The relevance of
Verdins’ principles. In recent years, ASD diagnoses have most frequently been
raised in Australian jurisdictions at the sentencing stage of criminal proceedings, with
diagnostically-relevant features of ASD argued to both mitigate the moral
blameworthiness of an offender and/or increase the burden of incarceration for such
individuals (Freckelton, 2013a; Freckelton & List, 2009).
Issues related to moral processing amongst individuals with ASD are explored
in greater detail in later chapters (see Chapter 7 and 8); however, it is pertinent to note
at this stage that case reports suggest that whilst many individuals with ASD will
126
recognise that their offending behaviour was ‘wrong’, they may nonetheless lack a
complete understanding of what ‘wrong’ entails in regards to the social and emotional
implications of their behaviour (Hare et al., 1999; Wing, 1997). This lack of socio-
emotional understanding of ‘wrongness’ is evident in a case study by Beardon (2008)
of “E”, a woman who was arrested after letters she wrote to her college tutors over a
period of several months (initially in search of friendship) became threatening.
Beardon (2008) notes that E clearly demonstrated a lack of perspective-taking in her
persistent attempts to establish friendships despite a lack of interest from her tutors
and several cautions from police. Although E reportedly demonstrated an
appreciation that her behaviour was ‘wrong’, such that she knew not to repeat this
behaviour, her reports indicated that her motivation to desist was in relation to her
fear of future police contact, rather than in any appreciation of the impact of her
behaviour on the victims (her tutors). Thus, individuals with ASD may have a basic
understanding that a behaviour is unacceptable with reference to learned socio-
conventional ‘rules’ or legal implications, without having an appreciation of the
socio-emotional impact of such behaviour on victims.
Also of relevance to Verdins’ principles, it has been increasingly argued that
individuals with ASD may face particular difficulties in a prison environment that
render incarceration more burdensome than for prisoners without ASD (Freckelton,
2013a). The socio-communicative difficulties associated with ASD have been argued
to result in increased vulnerability to victimisation, manipulation, exploitation or
retribution within the prison setting; for example, due to misinterpreting, failing to
recognise or disregarding the somewhat rigid and paradoxical nature of the unwritten
rules for co-existing with other prisoners (Cashin & Newman, 2009; English & Heil,
2005; Mbuba, 2012). A thorough examination of potential difficulties faced by
127
individuals with ASD within a custodial environment is beyond the scope of the
current thesis, however, the author has published a recent review on this topic during
the course of the current doctoral candidature (Robertson & McGillivray, 2015).
Recent examination of court decisions in cases involving defendants with
ASD has revealed a lack of coherence in the way in which judicial officers have
applied Verdins’ principles during sentencing and “something of a backlash” in ASD
being considered significantly mitigating in recent years (Freckelton, 2013a). In the
context of such observations, Freckelton (2013a) argued that “there is a significant
forensic distance to travel and many challenges […] before courts are enabled
meaningfully to appreciate for any given defendant the impact likely to have been
exercised on offending behaviour by an ASD” (p.1). One such challenge to
overcome pertains to unawareness and misunderstandings of ASD held amongst CJS
workers, including judicial officers (Freckelton, 2013a).
5.3. Judicial Awareness and Perceptions of ASD
Freckelton (2013a) argues that the marked inconsistency in Australian court
decisions involving defendants with ASD exposes a significant degree of
unawareness and misunderstanding amongst judicial officers as to the forensic
significance of ASD. If true, the potential nexus between features of ASD and an
individual’s engagement in offending behaviour and prospects for rehabilitation may
be overlooked during the disposition of a case, impacting the effective management
of such individuals within the CJS (Barry-Walsh & Mullen, 2004; Browning &
Caulfield, 2011; Katz & Zemishlany, 2006; Murrie et al., 2002; Woodbury-Smith &
Dein, 2014). Further, in the absence of an adequate understanding of ASD, any
unusual or maladaptive behaviours demonstrated by a defendant with ASD may be
misinterpreted by the judiciary, with the potential to unfairly impact dispositional
128
outcomes (Freckelton, 2013a; Murrie et al., 2002). For example, the socio-
communicative impairments displayed by some defendants with ASD (e.g. reduced
eye contact, a tendency to misinterpret questioning, difficulties with temporal
relationships, slowed verbal processing, echolalia, and other unusual mannerisms)
may be misinterpreted as indicative of dishonesty or contempt, or as demonstrative of
guilt and a lack of remorse (Freckelton, 2013b; Haskins & Silva, 2006; Health and
Social Care Overview and Scrutiny Committee, 2012; Ingram, Lyons, Lee, &
Bowron, 2012; Mahoney, 2009; Murrie et al., 2002; Taylor et al., 2009). In this
context, misinformed impressions regarding ASD amongst the judiciary may be
highly prejudicial where such individuals are being tried for a criminal offence (Allen
et al., 2008; Freckelton, 2013b).
Despite the potential impact on issues of justice, human rights and community
safety, judicial awareness of ASD is an issue that has received limited academic
attention. The only published research that has empirically explored judicial attitudes
regarding the sentencing of individuals with ASD is described in a series of papers by
Berryessa (2014a, 2014b, 2016a, 2016b). Utilising a mixed-methods approach,
Berryessa surveyed and interviewed 21 Californian Superior Court judges to ascertain
their views on a range of issues pertinent to forensic decision-making involving
individuals with High Functioning Autism (HFA), including their personal
experiences and perceptions on media portrayals. Of note, all 21 judges reported
some prior exposure to ASD, and 18 indicated personal experiences with individuals
with the disorder (e.g. friends or family members who had a diagnosis of ASD)
(Berryessa, 2014b). In this context, it is thus highly likely that participating judges
possessed a greater understanding of ASD, when compared with other members of
the judiciary.
129
Overall, the judges viewed HFA as relevant to criminal proceedings and
reported a recognition of the potential stigmatising effect of misperceptions regarding
the disorder, particularly in regards to negative portrayals in the media (Berryessa,
2014a, 2016a, 2016b). However, inconsistencies were noted in regards to their
understanding of the particular impact of HFA on sentencing and participants
expressed uncertainty in regards to the disposition of cases where offenders possessed
a diagnosis. According to Berryessa (2016a), whilst some of the interviewed judges
did not view HFA as relevant to the sentencing process, the majority (n = 15)
reported that an awareness of a defendant’s diagnosis would be relevant to assist the
judiciary in determining whether the offending behaviour was a consequence of
symptomatology associated with the disorder (Berryessa, 2016a).
Twelve of the 21 judges specifically referred to the mitigating or aggravating
effect of a HFA diagnosis when sentencing a guilty offender (Berryessa, 2016a).
Specifically, nine judges viewed HFA as a potential mitigating factor in sentencing,
with a reported majority of these indicating the particular relevance to the issue of
Mens Rea; that is, the extent to which an offender with HFA could be considered to
have wilfully and intentionally committed the offence in question (Berryessa, 2014b).
In contrast, three judges described HFA as a potentially aggravating, because of a
view that a diagnosed individual may pose a significant risk to personal and public
safety. For example, one judge was reported to opine, “I think it would be a detriment
to [offenders] in future cases. Judges are going to be concerned because they’re more
likely to re-offend” (Berryessa, 2016a; p. 2772).
In regards to selecting appropriate sanctions for offenders with HFA,
Berryessa (2016a) reported a prevailing view amongst participating judges that they
were responsible for ensuring that individuals with HFA are provided opportunities to
130
receive the support and intervention required to assist them to establish and maintain
an offence-free lifestyle. It was reported that the majority of participants viewed the
imposition of a custodial sentence as ineffective for such objectives, and potentially
damaging for an offender with HFA, with discontent expressed at the lack of suitable
dispositional alternatives (Berryessa, 2016a). One participating judge reported “[…]
When they’re placed in a jail or a prison cell, they’re basically being warehoused
because we don’t have a better way of dealing with it…My concern is that we don’t
have an effective way…” (Berryessa, 2016a; p. 2772).
Of note, the judges who participated in Berryessa’s (2014a, 2014b, 2016a,
2016b) study expressed differing views as to the way in which HFA may impact
sentencing deliberations. As noted by Berryessa (2016a), the divergent views
expressed by judges suggest that offenders with ASD may receive differential
treatment within the course of criminal proceedings, and particularly during
sentencing, dependant on the particular views and opinions of the presiding judge.
Such observations are consistent with prior academic literature that identified
substantial inconsistencies in the way in which ASD has been considered in recent
court decisions (Freckelton, 2011, 2013a, 2013b; Freckelton & List, 2009).
5.4. Chapter Summary
While much of the current literature refutes a direct causal relationship
between ASD and engagement offending behaviour, several authors have argued that
in many cases where an individual with ASD has perpetrated an offence, they have
done so in the context of ASD traits and symptomatology. Although there is no
agreement in regards to the prevalence of offending behaviour within the ASD
population, there is a general consensus that offending behaviour occurs more
frequently amongst higher functioning individuals and that amongst such individuals,
131
ASD symptomatology may contribute to a complex constellation of environmental,
situational, and personality factors to precipitate offending behaviour. Thus, in the
absence of comorbid conditions, the legislated criminal defences for mentally
disordered offenders (e.g. Fitness to Stand Trial, Mental Impairment), whilst
theoretically applicable, may bear little practical relevance to defendants with ASD.
However, the recognition of ASD as a contributory factor to offending behaviour
raises the relevance of such to mitigation during sentencing, as seen in Australian
courts (Freckelton, 2013a).
Despite the increasing frequency with which such issues are raised in criminal
proceedings, the sentencing of offenders with mental illnesses, including those with
ASD, remains an underdeveloped topic of study (Goodman-Delahunty, Forsterlee, &
Forsterlee, 2005; Walvisch, 2010). The limited research regarding the sentencing of
offenders with ASD suggests that judges experience uncertainty in determining the
forensic relevance and impact of ASD and that this contributes to variability in
regards to the imposition of sanctions in response to offending behaviour amongst
this population (Berryessa, 2014a, 2014b, 2016a; Freckelton, 2011, 2013a, 2013b;
Freckelton & List, 2009). Such concerns are paired with calls for better training on
ASD for all CJS personnel (Browning & Caulfield, 2011), and for increased
availability of accurate, effective and unbiased expert evidence to guide the judiciary
in their deliberations during the course of criminal proceedings (Berryessa, 2016a;
Freckelton & List, 2009). Given that sentencing impacts on the freedom, future and
treatment of individuals found guilty of an offence, it is important that such issues are
examined further.
Strong recommendations have been made for additional research into the
characteristics and needs of individuals with ASD within the CJS (Bleil Walters et
132
al., 2013; Cheely et al., 2012; Dein & Woodbury-Smith, 2010; Woodbury-Smith et
al., 2006). The aim of succeeding chapters is to contribute to the evidence base
through an investigation of the views and perceptions of the judiciary in an Australian
context, and the potential impact of ASD traits on moral processing (relevant to
criminal responsibility and moral culpability). Specifically, preliminary evidence
regarding judicial awareness and perceptions of ASD amongst an Australian sample
of judicial officers is presented in Chapter 6, the question of morality amongst
individuals with ASD is explored in Chapter 7, with new data presented in Chapter 8
from a self-report survey exploring the relationship between ASD- consistent traits
and domains of moral concern.
133
Chapter 6. Study 2: A Preliminary Assessment of Knowledge and
Perceptions of Autism Spectrum Disorder in Australian Magistrate’s Courts.
6.1. Rationale
In recent years, the presence of ASD has been raised in the context of court
proceedings with increasing frequency and the available academic literature has
highlighted the potential relevance of ASD at all stages of CJS involvement (Allen et
al., 2008; Freckelton, 2011, 2013b; Hall et al., 2007). Individuals with ASD may
present with unique precipitants to their offending behaviour, associated with
divergent risk profiles and forensic needs, requiring specialized support to enable
them to successfully navigate and benefit from forensic intervention (Allen et al.,
2008; Browning & Caulfield, 2011). Due to the potential prejudicial impact of such
difficulties, the identification and awareness of the potential impact of ASD amongst
CJS personnel is critical to promote fair and effective responses to offending
behaviour amongst this population (Allen et al., 2008; Browning & Caulfield, 2011).
Much of the literature is critical of the criminal justice response to offenders
with ASD, with several authors expressing concerns regarding the potential
deleterious impact of interactions between individuals with ASD and CJS personnel
who are uninformed or misinformed regarding the nature and potential forensic
significance of the disorder (e.g. Allen et al., 2008; Archer & Hurley, 2013;
Browning & Caulfield, 2011; Debbaudt & Rothman, 2001; Haskins & Silva, 2006;
Mayes & Koegel, 2003; McAdam, 2012; Murrie et al., 2002; Teagardin, Dixon,
Smith, & Granpeesheh, 2012). Given the substantial legal and social consequences
inherent in court decisions, concerns regarding the prejudicial impact of ASD may be
particularly pertinent when considering interactions with the judiciary. The aim of the
study reported in this chapter is to augment the findings from Berryessa’s study
134
through an investigation of the manner in which members of the Australian judiciary
understand and perceive ASD and how this may impact on decision-making, and in
particular the imposition of sanctions during the disposition of cases where a
defendant possesses an ASD diagnosis.
6.1.1. How do judges decide? In their role as legal adjudicators, judicial
officers play a crucial role in the administration of justice and imposition of the legal
response to offending behaviour (Attwood et al., 2014; Vidmar, 2011). Judges act as
the sole fact-finder and ultimate decision-maker in the vast majority of criminal and
civil proceedings (Guthrie, Rachlinski, & Wistrich, 2001) and are charged with a
responsibility of ensuring that forensic responses to offending behaviour are
sufficient to protect and punish, but not overly punative or otherwise detrimental to
the offender, victims of crime or the wider community. Even in cases where juries are
involved, judicial officers preside; acting as both gatekeepers for testimony admitted
into evidence and advisors, instructing jury members on relevant legal matters
(Gatowski et al., 2001). Consequently, in the course of a single case a judge may
make numerous important decisions related to the interpretation of legislation or
application of legal precedents and principles established under common law.
In making such decisions, judicial officers are expected to put aside their own
attitudes and dispassionately consider only the information brought before them that
is relevant to the interpretation of the facts of a case and application of relevant
legislation and principles derived from case law (Wrightsman, 1999). However,
decision-making is a highly complex psychological process and a substantial body of
literature drawn from decades of lay-person research has demonstrated that
extraneous variables, including schemas associated with labels, alongside other
personal attitudes, values and beliefs, may impact interpretation of facts and produce
135
systematic errors in judgment and legal decision-making (e.g. Guthrie et al., 2001;
MacCoun, 1989; Wrightsman, 1999). Legal realists assert that decisions made by
members of the judiciary are similarly influenced by socio-political factors, personal
attitudes, moods and perceptions10 held in regards to those who appear before them
(Danziger et al., 2011; Frank, 1930, 1931; Wistrich, Rachlinski, & Guthrie, 2015).
Prior research has confirmed that judicial decisions may indeed be influenced
by a range of extra-legal factors, providing support to the view that members of the
judiciary are vulnerable to psychological biases despite their experience and training
in adjudicating legal matters (Cappon & Laenen, 2013; Cunliffe, 2014; Curry &
Miller, 2015; Danziger et al., 2011; Korkman, Svanbäck, Finnilä, & Santtila, 2014;
Redding & Brooke Hensl, 2011; Vidmar, 2011; Wistrich et al., 2015; Zaykowski,
Kleinstuber, & McDonough, 2014). In a study of the role of emotions in judicial
decision-making, Wistrich et al. (2015) demonstrated that the decisions of North
American federal trial judges (n = 1800) more frequently favoured parties who
elicited positive affective responses, when compared to those to whom they were
unsympathetic, across a range of hypothetical cases where the legal facts did not
differ. Other research has specifically demonstrated that judicial knowledge and
perceptions regarding mental illness and disability can impact deliberation and
disposition in cases involving individuals possessing such conditions (Parry, 2005;
Perlin & Gould, 1995; Wrightsman, 1999). Anecdotal evidence suggests that the
same is true in Australian jurisdictions; for example Freiberg (2010) reported that
“[…] from years of using hypothetical sentencing scenarios with judicial officers as
part of a training exercise, my personal experience is that judges differ substantially
10 Humorously characterised by the trope “what the judge ate for breakfast”
(Danziger, Levav, & Avnaim-Pesso, 2011).
136
when considering exactly the same facts” (p. 206). Together, such findings suggest
that personal views and attitudes held by the judiciary, including feelings of enmity
or empathy, may unduly influence the disposition of cases and, correspondingly,
forensic outcomes for defendants (Wistrich et al., 2015).
6.1.2. Forensic Decision-Making and ASD. As described in the previous
chapter, the extant research regarding judicial awareness of ASD has demonstrated
limited ASD knowledge and awareness amongst judicial officers internationally
(Freckelton, 2011; Freckelton & List, 2009). The basis of claims of incomplete ASD
knowledge in judicial officers, however, is largely extrapolated from inconsistencies
in court decisions (e.g. Freckelton, 2013b; Freckelton & List, 2009), with relatively
little empirical attention given to the reported views of judicial officers regarding
defendants with ASD. The current study was undertaken to specifically explore the
knowledge base and underlying perceptions of members of the Australian judiciary
regarding the forensic relevance and appropriate management of ASD within the CJS.
Although some cases, including serious indictable offences may be heard in
higher courts, the majority of criminal cases heard across Australian jurisdictions
commence and are finalised in the Magistrate’s Court (93% in 2014/15; Australian
Bureau of Statistics, 2015). Due to the large volume of cases heard and evidence that
individuals with ASD were more likely to engage in minor offences, it was expected
that judicial decision-makers sitting within Australian Magistrates’ Courts were likely
to encounter defendants with ASD more frequently than judges sitting within other
courts. Accordingly, the current study focused on the views of the magistracy. In
view of the incomplete knowledge base demonstrated by other key personnel within
the Australian CJS (Gook, 2014) and the inconsistencies noted in Australian court
decisions regarding defendants with ASD (Freckelton, 2013b), it was expected that
137
the responses from participating magistrates would demonstrate some inconsistencies
in ASD knowledge and awareness.
In recognition that it is often the legal representatives who will first raise a
defendant’s mental impairment in Australian jurisdictions, efforts were made to
include the views of lawyers by distribution of a similar survey amongst legal firms
in Australia. Legal firms were located within each jurisdiction where Magistrates
were surveyed through publicly available search engines (i.e. Google). Hard-copy
surveys were sent to the identified firms, with the number sent being equivalent to the
number of lawyers advertised within the firm and the number of magistrates surveyed
within the jurisdiction. Only one response was received and accordingly, the
perceptions of lawyers have not been included in the current chapter. The responses
of the single respondent from this group are included in Appendix G.
6.2. Method
6.2.1. Aim. The aim of the current study was to investigate the knowledge and
understanding of ASD among magistrates sitting within Australian jurisdictions, in
order to gain a better understanding of the way in which legislation and case law may
be applied for individuals with ASD when facing legal ramifications for offending
behaviours. Also explored were magistrates perceptions and attitudes of the role of
psychologists in informing legal decisions involving persons with ASD with the hope
that this may inform future efforts of psychological science to assist the legal
response to offending behaviour amongst the ASD population.
6.2.2. Participants. Participants were Magistrates presiding in Australian
courts in 2014. Initial contact was made via the Chief Magistrate or their
administrative staff in each Australian jurisdiction via publicly available contact
details, seeking their support for the research to proceed within their jurisdiction. A
138
total of 221 surveys were distributed to magistrates in hard copy with assistance of
the office of the Chief Magistrate or other administrative assistants in those
jurisdictions where in principle support was provided.
6.2.3. Materials. A free-response pencil-and-paper questionnaire was
conducted in order to map the perceptions and attitudes held by members of the
Australian magistracy in regard to persons with ASD who appear in their courts.
Review of the literature identified two prior survey studies exploring the
understanding of ASD and other disabilities amongst police services in the United
States (Roach Anleu & Mack, 2007) and the United Kingdom (Modell & Mak, 2008).
The question set included in the survey for the current study was adapted from those
used in these earlier studies to be applicable to the judiciary. In addition, an item was
added to elicit judicial perceptions regarding the role of forensic psychologists in
advising courts on the forensic significance of an ASD diagnosis. The full survey is
provided in Appendix H.
6.3. Results
6.3.1. Response Rates. A total of 21 responses were received out of 221
surveys mailed to magistrates, a response rate of 10.5%. Low response rates are not
unusual for surveys targeted at the judiciary; a cohort that has been traditionally
characterized as a difficult population to engage in social science research (Dobbin et
al., 2001). The nature of the data and the small sample size precluded tests of
statistical significance and formal qualitative analysis; nonetheless, the responses
summarized descriptively below provide a preliminary insight of judicial perceptions,
attitudes and decision-making involving defendants with ASD.
6.3.2. Magistrates’ understanding of ASD. Respondents’ understanding of
the nature of ASD was evaluated by the question: What does the term Autism
139
Spectrum Disorder mean to you? In analysing the accuracy and completeness of
responses to the question, ASD was defined as a life-long developmental disorder,
existing along a spectrum of severity and characterized by impairments in socio-
communicative and behavioural domains.
Responses to this item revealed significant variability in the understanding of
the nature of ASD amongst Australian magistrates. The majority of respondents
demonstrated some insight regarding the nature of ASD; five respondents referenced
socio-communicative deficits; nine recognized that individuals with a diagnosis of
ASD may relate to others or the environment in impaired or unusual ways and nine
respondents referred to a range in severity of symptomatology in their response. One
respondent expressed concern regarding the validity and potential over-diagnosis of
the disorder, viewing ASD as “A vague imprecise term resorted to by psychologists
and widely over-diagnosed by them to explain any aberrant behaviour” (Participant;
P15). Two respondents (incorrectly) described ASD to be defined according to
intellectual ability (“a form of intellectual disability” [P2] or “an intellectual and
behavioral disorder” [P9]).
Responses to a second question, What difference do you see, if any, between
Autism Spectrum Disorder and intellectual disability?, confirmed that inconsistencies
existed amongst members of the Australian magistracy in regards to recognizing
ASD as distinct from ID, suggesting a potential lack of awareness of high-functioning
ASD presentations. Specifically, while the majority of respondents identified that
intellectual disability and ASD were distinct disorders (66%), four reported that they
were unsure of any differences and three respondents (incorrectly) viewed that there
was no difference between ASD and ID.
140
6.3.3. Magistrates self-assessed competence with regards to ASD in the
CJS. Magistrates reported a moderate level of understanding in regards to issues
relating to ASD within the CJS. The average self-assessment competency rating (1 =
least competent; 5 = most competent) was approximately 2.5 (n = 20), however there
was significant variation in competency ratings across respondents. One respondent
(whose response was excluded in calculating the self-assessed competency average)
rated their level of understanding as “-10” (P8). The self-assessed competence ratings
provided by respondents appeared generally consistent with the level of reported
personal experience with ASD and the understanding demonstrated by respondents in
their responses to other items on the survey.
6.3.4. Perceived propensity towards offending and victimization. The
majority of respondents were either unsure/unable to respond or of the opinion that
individuals with ASD were no more likely to be perpetrators or victims of offending
behaviour (61.9%). Of those who responded, however, a greater proportion viewed
individuals with ASD as more likely to be perpetrators of crime than victims (23%
and 14.3% respectively).
6.3.5. Magistrates’ perceptions of the potential forensic relevance of ASD.
Three questions assessed magistrates’ perceptions of the potential forensic relevance
of ASD; “Why do you think it could be important to understand Autism Spectrum
Disorder to allow you to do your job effectively?”, “During sentencing, would a
diagnosis of Autism Spectrum Disorder be an important consideration? Why/Why
not?”, and “In your opinion, should individuals with Autism Spectrum Disorder
receive different treatment in the CJS?”
Responses to the latter of these questions suggested that participating
magistrates generally viewed that the impact of ASD could be appropriately
141
accounted for under existing discretionary powers available to the judiciary. For
example, one magistrate responded “Only in the sense that anyone with a recognized
condition is treated differently- i.e. that condition is taken into account” (P10).
Similarly, another respondent remarked, “No. All are equal before the law however,
those with special needs can be catered for within discretion” (P13).
The majority (n= 16) of respondents indicated a willingness to utilize
diversionary options or otherwise moderate sentences imposed for defendants with
ASD (e.g. “…Deterrence, particularly general deterrence which I think is a concept of
little/no relevance to an ASD offender […] If pleading guilty an ASD offender should
be diverted to a mental health court (where available)” [P20]). In contrast, one
respondent expressed concern that differential treatment of individuals with ASD
within the CJS may lead to inflated levels of ASD diagnosis: “All should be equal
before the law. Favouring people with alleged ASD would only lead to ridiculous
levels of diagnosis, as is already the case with PTSD” (P15).
Only one respondent indicated that they did not view an understanding of
ASD to be relevant to their work as a judicial officer. Overall, respondents’ views on
the ways in which an ASD diagnosis may be forensically relevant fell into three main
themes: enhancing communication and understanding, determining the likely
response to dispositional alternatives, and to inform considerations related to the legal
status of offenders with ASD.
6.3.5.1. Enhancing communication and understanding. The importance of
enhancing effective communication and understanding of court processes for
defendants with ASD was highlighted by a number of respondents. For example, one
noted “ASD affects a range of ways in which people present and communicate-
essential elements of court process e.g. getting their/my point across…” (P7). It was
142
noteworthy that one magistrate specifically addressed the potentially prejudicial
impact of atypical courtroom responses for those with higher functioning
manifestations of ASD, specifying that an understanding of ASD was important
“Particularly with those having a mild condition [such that] the court can properly
assess responses given to determine the impact of demeanour in weighing evidence”
(P13).
6.3.5.2. Likely response to dispositional alternatives. Several respondents (n
= 12) referenced the importance of considering whether the features of ASD may
decrease the likelihood that the individual will be able to comply with and benefit
from rehabilitative efforts (e.g. [P1]; “…it may affect such matters as suspension of
sentence or not and/or conditions in a bond” [P18]). In order to inform such
decisions, it was highlighted that “…I need to know how they may respond to,
particularly to imprisonment, or community service or a bond or supervision and
counselling” (P14). In this context, responses emphasized that the court should be
certain that any order imposed in response to offending behaviour “…is not setting up
the accused to fail” (P13). Respondents also referred specifically to concerns
regarding the ability of an offender to adhere to the conditions of community orders
(e.g. “as a magistrate I need to understand the extent to which a person with ASD is
able to comply with any orders that I make” [P3]; “…Important consideration in
terms of whether offender could comply with a community order or similar” [P9]); or
the likely response to rehabilitative efforts (“…it may explain a reason for offending
and have relevance to issues of rehabilitation” [P21]; “…An understanding may
inform treatment and rehabilitation options” [P17]); and whether imprisonment may
be more burdensome for the individual (“…Imprisonment may be more difficult for
them” [P5]).
143
6.3.5.3. Consideration of the legal status of offenders with ASD. A number
(n = 10) of respondents indicated that an ASD diagnosis was relevant to
considerations regarding the application of legislation and case law relevant to
criminal responsibility and culpability. One respondent aptly summarized these issues
(in response to the question Why do you think it could be important to understand
Autism Spectrum Disorder to allow you to do your job effectively?) as follows: “In
assessing guilt and innocence there is a mental element and so you need to understand
how the mind of an accused function. In sentencing this understanding helps assess
the criminality of the offence and the appropriate sentence” (P10).
Three respondents indicated that an ASD diagnosis was likely to impact an
individual’s criminal responsibility (e.g. “Understanding offenders’ perceptions and
ability to control their behaviour is important when assessing levels of responsibility”
[P18]). A greater number of respondents (n= 8) identified ASD as particularly
relevant to sentencing, with two specifically referring to the invocation of Verdins
principles in sentencing decisions involving offenders with ASD (e.g. “…would lead
to consideration of Verdins’ factors in sentencing” [P8]).
6.3.6. Importance of the court being made aware of ASD. The participating
Magistrates’ responses emphasized the importance of the court being appropriately
informed of the presence and likely impact of ASD for an offender, such that
discretionary powers could be employed during decision-making. Several examples
of such responses are presented below:
“…The personal characteristics e.g. drug addiction, mental health condition,
intellectual disability, etc. are always considered (if known)” (P17).
144
“…If their particular qualities are made known to the court then I consider the
“system” has the capacity to take them into account in an appropriate way”
(P7).
“…I stress this is an uninformed answer. I need to know more about ASD and
its effects” (P14).
To further explore magistrates’ perceptions regarding available sources of
information, respondents’ views were sought regarding the provision of ASD-specific
treatment and the role of forensic psychologists in informing courts on such issues.
6.3.6.1. ASD Training Amongst Australian Magistrates. Participation in
specific ASD training was seldom reported among respondents. None of the
respondents had undertaken formalized training in the context of their roles within the
magistracy, although two reported seeking information regarding ASD via requests
for psychological or psychiatric court reports. Two respondents indicated that they
had obtained an understanding of ASD through working in mental health or specialist
courts where information was readily available and one respondent indicated that they
had benefitted from education in dealing with defendants with ASD through
consultation with a court psychiatric liaison officer. Other reported sources of
information about ASD included personal experience with close family members (n =
2) and personal reading (n=2).
All but one respondent expressed current interest in undertaking professional
training related to ASD; the participant without current interest (P15) indicated
“doubt if training would be of benefit”, although they expressed a willingness to
consider participation in training in the instance that they were advised by a
psychiatrist that this could be of use (“None from a psychologist. Might be
worthwhile if psychiatrists say training required”).
145
Amongst those who expressed interest in professional training, specific areas
of interest included: basic information regarding characteristic features and the
impact on behaviour (particularly in regards to offending behaviour); strategies to
enhance effective communication and management within court; and advice
regarding the likely response to various sentence-types (including the likely impact of
incarceration and treatment within the prison system). Other respondents were
broader in their expressed training interests, indicating that they would be interested
in attending “whatever is available” (P12) or “Training which would improve
understanding of criminal justice issues as they relate to people with ASD” (P1). It
was suggested by respondents that presentations could occur at annual training days
or conferences provided by the magistracy and that the effectiveness would be
enhanced if such training were delivered by “an expert who also understands the
court system.” (P10).
6.3.6.2. The role of forensic psychologists in informing courts regarding
ASD. The views of participating magistrates on the value of forensic psychologists in
informing the court regarding ASD were diverse. Specifically, responses to the
question, “What role do you see for forensic psychologists in informing the court
regarding Autism Spectrum Disorder?” varied from indications that such evidence
was “Highly relevant. I would have significant regard to any such report” (P5) to the
significantly less favourable “Nil role. Psychiatric opinion should be the only mental
health evidence allowed.” (P15).
The majority of participating magistrates (n=19) expressed in principle
support for the admission of psychological reports to inform courts regarding ASD,
however, the importance of the report writer’s expertise was emphasised (e.g. “They
need to be an expert…” [P17]). Respondents reported that the relevant issues on
146
which psychologists may inform the court were primarily associated with
considerations relevant to understanding the nexus between the features of the
disorder and offending behaviour (e.g. “Explaining nature of the disorder and whether
there is any connection between the condition and criminal offending” [P8]), or the
likely response of an individual with ASD to dispositional alternatives (e.g. “To make
the person’s particular qualities (given the range of impacts) known to a court and
identify issues going to the tailoring of outcomes thereby enhancing rehabilitative and
other outcomes” [P7]). One participant’s response on this item revealed
dissatisfaction with the dispositional alternatives available to courts when considering
offenders with ASD: “…none of this is much use when there seems to be no funded
support for these people” (P16).
6.4. Discussion
At present, there is a dearth of research exploring issues relating to the
sentencing of offenders with ASD. The current study aimed to contribute to this
underdeveloped area, with an empirical focus on views and perceptions amongst the
Australian magistracy regarding ASD, and the pertinent issues associated with
sentencing offenders from this population. The (limited) prior literature in this area
has been largely speculative, inferred from past legal decisions (e.g. Freckelton,
2013b), or has been undertaken in international jurisdictions (e.g. Berryessa, 2014b),
where the legal provisions for mentally impaired offenders may differ from
Australian contexts. Such research has revealed unawareness and uncertainty
regarding ASD amongst the judiciary, raising concerns that judicial officers may not
adequately consider the unique habilitative needs of offenders with ASD when
enacting a forensic response to their offending behaviours. If judges fail to consider
147
such factors, the forensic response may be ineffective at best, or, at worst highly
detrimental to both the offender and the future safety of the community.
A second reason to emphasise the forensic response to ASD is that there is no
clear dispositional pathway for offenders with this disorder (Murrie et al., 2002). As
identified by a respondent in the current study, there is little in the way of targeted
programs or funding for the forensic ASD population, and it is unclear whether the
available service alternatives have sufficient expertise to support and (re)habilitate
such individuals (Woodbury-Smith & Dein, 2014). It is hoped that research into
current dispositional pathways for offenders with ASD, such as provided in the
current study, may act as an impetus for further research and for action in regards to
service provision to assist such individuals to establish and maintain a pro-social
lifestyle.
The findings of the current study confirm the speculation made in previous
literature that a gap exists in the knowledge and views of the judiciary regarding
ASD, and that such disparity may result in differential treatment in cases where an
individual with ASD faces legal disposition due to offending behaviour. Overall,
participating magistrates demonstrated a general awareness of the presentation and
symptomatology of ASD; however, responses evidenced significant variation in
regards to views of the forensic relevance of such. Further, one magistrate expressed
a strong view that there was a risk that ASD would be over-diagnosed in an attempt
to excuse criminal behaviour, and thus would not be considered relevant during
criminal proceedings over which they presided.
It is important to recognize that respondents self-selected for participation in
this study, thus rendering it likely that they would generally possess greater interest,
and a corresponding greater awareness of ASD than would be expected for the wider
148
cohort of Australian judicial officers. Consistent with such, three respondents
indicated personal experience with an individual with a diagnosis of ASD and a
further three indicated that they had presided over mental health courts or worked in
close consultation with a mental health professional with whom they consulted on
cases where an individual may possess a psychological disorder. In this context, the
self-reported knowledge and competence ratings of participating magistrates are
considered likely to be an over-estimation of the knowledge base within the broader
judiciary. As such, it would appear that there may well be considerable room for
improvement in awareness and understanding of ASD amongst the Australian
magistracy more generally.
6.4.1. A coherent and consistent approach? The major finding of the
current study was that significant variation exists across Australian magistrates in
regard to their understanding of and attitudes toward ASD, and in particular the
forensic relevance of ASD. This variation, alongside prior research indicating that
extraneous factors can impact on decisions made by judicial officers, raises concerns
regarding the consistency with which offenders with ASD are processed and managed
within Australian Magistrates’ courts.
Consistency in sentencing is a fundamental tenet of Australian law, and is
crucial to promote equal access to justice within the CJS (Freiberg, 2014; Krasnostein
& Freiberg, 2013; Mackenzie, 2002). Essentially, Australian legal principles hold that
all legally relevant factors remaining stable, cases with similar facts ought to attract
similar dispositional outcomes (Krasnostein & Freiberg, 2013). The critical
consideration is consistency in the approach with which a judicial officer considers a
case, rather than consistency in the particular sanction(s) imposed (Freiberg, 2010;
Krasnostein & Freiberg, 2013; Ritchie et al., 2016). Indeed, disparity in sanctions
149
imposed may well be justified, on the grounds of the seriousness of the offending
behaviour, or the personal history and vulnerabilities of the offender, and other
situational factors relevant to the legal facts of a case (Krasnostein & Freiberg, 2013;
Mackenzie, 2002). Disparity in sentencing is justifiable where this occurs as the result
of legally relevant factors, but is unjustifiable when such disparity occurs due to
extraneous variables, for example, differences between judges (Krasnostein &
Freiberg, 2013). Unjustifiable disparity presents as a legitimate concern for the
promotion of a fair and just CJS, impacting on both the human and legal rights of
offenders and public confidence in the administration of justice (Krasnostein &
Freiberg, 2013).
Australian courts have recognised the potential deleterious impact that
unjustifiable disparity poses for the administration of justice. Specifically, in Lowe v
The Queen (1984) 154 CLR 606, at 610, it was held that:
Just as consistency in punishment — a reflection of the notion of equal justice
— is a fundamental element in any rational and fair system of criminal justice,
so inconsistency in punishment, because it is regarded as a badge of
unfairness and unequal treatment under the law, is calculated to lead to an
erosion of public confidence in the integrity of the administration of justice. It
is for this reason that the avoidance and elimination of unjustifiable
discrepancy in sentencing is a matter of abiding importance to the
administration of justice and to the community.
Despite this recognition, Field (2012) describes criminal sentencing in
Australia as a “geographical lottery”, whereby “[…] punishment actually received for
any given crime in Australia is as much the product of the precise geographical
150
location in which it is committed as it is the mood of the judicial officer passing
sentence” (p. 1). While all unwarranted sentencing disparities are cause for alarm,
evidence of disparities disadvantaging a potentially vulnerable population, such as
those with ASD, may be especially troubling. In this context, the responses provided
in the current study were both encouraging and alarming. It was encouraging that the
majority of magistrates were able to identify key characteristics of ASD, but alarming
that their attitudes regarding the proper allowances and considerations during
sentencing differed so markedly.
Whilst there are some early signs of progress towards increased awareness
and understanding of ASD within Australian courts, inconsistencies appear to remain
in the knowledgebase and attitudes of judicial officers. The incomplete
knowledgebase and disparity in attitudes regarding the relevance of ASD to criminal
proceedings identified amongst the Australian magistracy raises concerns that judicial
officers may not be sufficiently informed and prepared to engage meaningfully in
deliberation of the potential impacts of a diagnosis of ASD on an individuals’
behaviour and support needs. Consequently, offenders with ASD may be subject to
differential treatment during the course of criminal proceedings in Australian courts,
not on the basis of legally relevant factors (i.e. the nature of their offence or the
manner in which their disorder impacted on their offending or capacity to cope with
disposal options), but due to the attitudes of the presiding magistrate. In this context,
expert advice and testimony from mental health professionals, including forensic
psychologists, appear invaluable to assist the court to understand the features of ASD,
and to integrate such information to inform their decision-making during sentencing
(Freckelton & List, 2009).
151
6.4.2. The role of psychologists in assisting courts. Freckelton (2011, 2013a,
2013b) proposed that mental health professionals are critical allies to the courts in
informing of the potential forensic significance of ASD and correcting
misperceptions that may otherwise lead to unjust and ineffective responses to
criminal behaviour amongst the ASD population. Indeed, it is becoming increasingly
common for mental health professionals (namely psychiatrists and psychologists) to
be called by courts to provide evidence to assist in deliberations as to the disposition
of cases involving individuals with ASD (Freckelton, 2013a). Forensic psychologists,
who possess expertise in both psychological disorders and the psychological
determinants of offending behaviour, appear well-placed to enact this role; however,
given that judicial officers act as gatekeepers regarding the expert testimony that is
allowed in court proceedings, the extent to which psychologists provide evidence
may be determined by the judiciaries’ perceptions of psychologists’ role and expertise
in regards to ASD and the law.
In contrast to such views, the findings of the current study identified some
uncertainty in regards to the expertise of forensic psychologists amongst the
Australian magistracy. On the whole, magistrates who responded to the current study
expressed favourable opinions regarding the role of forensic psychologists in advising
courts on such matters. However, one magistrate indicated their view that only
psychiatric evidence ought to be admitted in regards to mental impairment. This
respondent went further to report a disinterest in attending any training or workshops
regarding ASD, unless a psychiatrist recommended this. In the context of a historical
preference towards psychiatric testimony for matters related to mental state (see for
example, R v MacKenny, 1981) and uncertainty regarding the expertise of
psychologists amongst the Australian judiciary (see Day et al., 2000), these views
152
may reflect a continued attitude within the Australian magistracy that psychologists
may not be as qualified or knowledgeable as psychiatrists on matters relevant to legal
decision-making.
6.4.3. Limitations of the current study. The conclusions that can be drawn
from this study are limited by concerns regarding the generalizability of results to
real-world legal decision-making by magistrates across Australia. Specifically, the
findings are based on the responses of a small sample of Magistrates, and the extent
to which they are representative of the entire Australian magistracy is unclear. Efforts
were made to maximise participation rates, through seeking in principle support from
the Chief Magistrate in each jurisdiction and communicating this to potential
participants in the Plain Language Statement provided with the survey. Further, the
survey was designed to be brief, requiring minimum effort to complete and return
(i.e. did not require the use of technology, was printed on a single, double-sided sheet
of paper, and accompanied by an addressed, postage-paid envelope for returning the
survey to the researchers). It is recognized, however, that judicial officers are a
difficult cohort to engage in social research and low response rates to surveys appear
to be the norm (e.g. Berryessa, 2014a, 2014b; Dobbin et al., 2001; Robinson, 2012).
Although the sample size concords with that obtained in other studies with similar
scope and methodology, the low response rate and potential bias necessitates caution
in interpreting results.
In some Australian jurisdictions there are specialised liaison, dispositional and
diversionary options, including specialised mental health courts, to which individuals
with mental impairments may be referred (Davidson, 2015; Richardson & McSherry,
2010). However, the diversionary and dispositional alternatives available are largely
dependent on funding, and availability of such services differs substantially across
153
jurisdictions (Richardson & McSherry, 2010). Participants in the current study
referred to their past involvement with such services and it appeared likely that such
experiences and the availability of alternative dispositional options might impact on
attitudes and decision-making for cases where offenders were displaying traits
indicative of ASD. In order to conserve the brevity of the survey and protect
anonymity amongst respondents, demographic and other contextual data were not
collected for the current study. It is thus unknown whether participants sat in
jurisdictions where such specialist services, or other diversionary options, are
available. Furthermore, due to the high level of personal experience and interest in the
subject matter amongst the study participants, the opinions stated in response to the
current survey may differ to that of the larger population of magistrates in Australia,
who chose not to participate. As such, caution is warranted in any attempts to
generalise the findings of the current study to the knowledge and attitudes of the
Australian magistracy more generally. It appears likely, however, that a wider
sample, particularly one that included magistrates with less personal experience
and/or interest in ASD would result in further deviation in views expressed.
Perhaps a greater concern regarding the generalizability of results is in
relation to the limited ecological validity of the current study. Specifically,
participants were not asked to make a legal determination in relation to a real or even
hypothetical case involving an individual with ASD. Further, the survey provided no
information regarding ASD to magistrates, in contrast to usual court proceedings,
whereby magistrates are provided with information by legal representatives and aided
by experts in the field to determine any aspects of an offender’s situation that may
bear relevance to their decision-making. Thus, although past research has
demonstrated that preconceived notions can impact judicial decision-making
154
regarding offenders with serious mental illness, the current study cannot definitively
answer the question of whether the same results would be found in regards to
offenders with ASD in real-world situations in Australian jurisdictions.
Despite the above-described limitations, the findings of the current study are
significant in that they identify substantial diversity in judicial awareness and
personal attitudes regarding ASD, as well as the forensic relevance of ASD across
Australian jurisdictions. These findings thus enable recommendations regarding
direction of future research in the field.
6.4.4. Implications of findings and directions future research. The results
of the present study provide a preliminary assessment of the beliefs held by judges
about ASD, however, further research is clearly needed. Indeed, the lack of research
regarding the legal response to offending behaviour amongst the ASD population in
Australia makes the area ripe for further study. Examples of topics for further
research in this area include: more detailed and formalised exploration of knowledge
and perceptions of ASD amongst the judiciary, perhaps utilising validated
questionnaires (e.g. the AKQ and PANQ-F; Gook, 2014); investigating how judges
assess defendants with ASD in real cases, particularly whether disparity in knowledge
and attitudes do in fact precipitate inconsistencies in the approach to disposal;
exploration of the knowledge and management of offenders with ASD in other
branches of the CJS; and research on the availability and use of diversionary options
suitable to this population, including comparison of the impact of different
dispositional and diversionary options on forensic outcomes, including the offenders’
wellbeing and recidivism rates. Future research efforts could also investigate the
reasons behind the apparent reluctance of some judicial officers to utilise expert
testimony from psychologists and drivers for attitudinal change, both in regards to the
155
potential forensic relevance of ASD, and the role of forensic psychologists in
assisting courts to make decisions in regards to offenders with ASD.
Findings from the current study strongly suggest that a greater understanding
of potentially relevant aspects of ASD is needed to assist the judiciary to respond
consistently and effectively to offending behaviour amongst this population.
Magistrates do not need to be experts in ASD. In fact, as long as the relevant legal
facts are identified and accurately communicated by legal representatives and expert
witnesses (if allowed by the presiding judicial officer), the nature of the legal
response will in most cases be self-evident (Richardson, 1991). In some cases,
however, it is clear that divergent responses are possible; and this appears to be the
case in regards to judicial understanding of whether and how legal principles ought to
apply to offenders with ASD. Thus, a basic understanding of communication needs
and social problem-solving capacities amongst individuals with ASD, alongside
exploration of other factors relevant to sentencing appears likely to enhance the
consistency and effectiveness of the forensic response to defendants with ASD in
Australia. In this regard, it was promising that the majority of magistrates who
participated in the current study expressed a willingness to attend professional
training designed to inform them of the potential forensic significance of ASD.
The nature and availability of professional development programs varies
across jurisdictions, however most Australian magistrates have regular opportunities
to participate in formalised training (Roper, 2006). As suggested by the magistrates
who participated in the current study, an efficient and effective means of
mainstreaming ASD awareness training for the judiciary would be to embed such
training within existing professional development and training days, rather than
developing and delivering stand-alone courses. The views provided by respondents in
156
the current study may go some way towards assisting practitioners who design and
deliver judicial professional development programmes to identify pertinent
information to include in training curricula. Consultation with existing judicial
training providers and judicial representatives will be critical to ensure that training
objectives do not overextend to inappropriate topics (e.g. comments of legal
culpability in individual cases), thus impacting on judicial independence.
In addition, there is a need for effective and unbiased testimony from experts
on ASD to assist to inform courts on relevant matters during criminal proceedings
(Freckelton, 2013a; Freckelton & List, 2009). However, there are indications arising
from court decisions that mental health experts in the forensic area have not
consistently demonstrated sufficient knowledge and awareness of forensically-
relevant aspects of ASD to ensure that the courts are adequately supported to make
informed and fair decisions in regards to procedural and dispositional issues in cases
involving defendants with ASD (Freckelton, 2013b). It is vital that psychologists
seeking to provide expert evidence regarding offending behaviour amongst the ASD
population are sufficiently prepared to comment accurately and meaningfully on
matters identified by legal practitioners as relevant to criminal deliberation and
disposition. The findings of the current study can assist experts, such as forensic
psychologists, to identify the areas in which magistrates require information to
disabuse them of misperceptions and thus better prepare testimony for cases
involving individuals with ASD. Simultaneously, there is a need for additional
research into the characteristics and needs of individuals with ASD within the CJS to
inform practice, including the provision of expert testimony, with the aim to enhance
forensic outcomes for this population (Cheely et al., 2012; Dein & Woodbury-Smith,
2010; Freckelton, 2013a, 2013b; Woodbury-Smith et al., 2006).
157
One issue that was identified by the magistrates in the current study as
relevant to sentencing offenders with ASD was the extent to which such individuals
possess a moral understanding of their offending behaviour. This issue is explored in
detail in the chapters that follow.
158
Chapter 7. Questions of Morality Amongst Individuals with ASD
As described in Chapter 5, case reports suggest that individuals with ASD
who come into contact with the CJS due to engagement in offending behaviour often
do not recognise that their offending behaviour was morally wrong (Barry-Walsh &
Mullen, 2004). This suggests that divergent moral reasoning may constitute an
underlying factor for offending in some people with ASD, bearing relevance to
judicial deliberations and decision-making, in particular regarding criminal
responsibility and proportionate sentencing (Lerner et al., 2012). Any evidence of
impaired or unusual moral reasoning amongst offenders with ASD also provides a
potential direction for the development of early intervention and treatment programs
for this population. Information on the way in which individuals with ASD
understand and make moral judgments is thus essential to inform policy and practice
in regards to the prevention of future offending by people with ASD, as well as the
appropriate management and intervention for those who do offend.
The growing and increasingly complex field of philosophical and
psychological exploration of human morality is beyond the scope of this thesis, and is
described elsewhere (e.g. Baril & Wright, 2012; Haidt, 2007, 2008; Haidt & Kesebir,
2010; Jaarsma, 2013; Kagan, 2008; Palmer, 2003). Importantly, it has been
demonstrated that moral reasoning ability is closely associated with socio-cognitive
and socio-affective skills, particularly those associated with emotion recognition,
perspective-taking and empathy (Bzdok et al., 2012; Cushman, Young, & Greene,
2010; Kretschmer, Lampmann, & Altgassen, 2014). Consequently, it has been argued
that individuals who possess mental disorders involving deficits in these areas are
likely to display associated impairments in moral decision-making (Schneider et al.,
2013).
159
Critically, individuals with ASD have been reported to possess difficulties in
recognising and regulating emotions (e.g. Ashwin, Chapman, Colle, & Baron-Cohen,
2006; Bird & Cook, 2013; Hill, Berthoz, & Frith, 2004; Ketelaars, 2016; Rieffe et al.,
2012), understanding the perspectives and mental states of others (e.g. Baron-Cohen,
1995; Kretschmer et al., 2014), and empathizing (e.g. Blair, 2008; Golan & Baron-
Cohen, 2006; Lombardo et al., 2007). These related deficits suggest that impairments
in morality may also be prevalent amongst individuals with ASD. Because ASD is
characterised by problems with reciprocal social interaction, impaired
communication, repetitive behaviours/narrow interests and impairments in the very
aspects of social cognition and emotional processing held necessary for moral
reasoning, a growing body of work has focused on moral reasoning in individuals
with ASD. Although these studies have involved a range of methodologies and
assessment tools, many have assessed morality according to a classical moral
reasoning task - the moral/conventional distinction task.
7.1. The Moral/Conventional Distinction
The moral/conventional distinction is generally regarded as a major
breakthrough in the study of morality (Shoemaker, 2011). Originally developed in
1978 by Larry Nucci and Elliot Turiel, the moral/conventional task asks participants
to distinguish transgressions that are of a moral nature from those that are merely
conventional. The ability to distinguish between these domains is generally
considered to be representative of an intact moral sense. In the literature concerning
the moral/conventional distinction, moral transgressions are defined as acts that result
in harm or injustices to others, while conventional transgressions are defined by their
consequences for social order (Blair, 1996). Prototypical examples of moral
transgressions include stealing, breaking promises and killing or injuring other
160
people, while prototypical examples of conventional transgressions include wearing
gender- or context- inappropriate clothing (e.g. men wearing dresses or wearing
pyjamas to school), or licking the plate at the dinner table (Kelly, Stich, Haley, Eng,
& Fessler, 2007).
The distinction between moral and conventional transgressions is measured
according to participants’ judgments across three dimensions; permissibility (Was it
right or wrong for X to do Y?), seriousness (On a scale of one to ten, how right [or
wrong, depending on the first answer] was it for X to do Y?) and contingency on
authority consent (Would it be OK for X to Y if the teacher says X can?) (Blair, 1995).
Studies have shown that children as young as 39 months, across different cultures and
nationalities, systematically differentiate moral and conventional transgressions
according to these dimensions (Lisciandra, Postma, & Colombo, 2012; Smetana,
1993; Vignemont & Frith, 2008).
Generally, moral transgressions are judged to be more serious and less
permissible than conventional transgressions (Smetana, 1993). Additionally, the
permissibility of conventional transgressions is judged to be contingent on the
prohibition of the act by an authority figure while moral transgressions are judged as
non-permissible even when there is no explicit rule prohibiting the act (Blair, 1996;
Smetana, 1993). This pattern has been observed in many populations, and has also
been argued to hold true amongst individuals with ASD (Blair, 1996; Grant, Boucher,
Riggs, & Grayson, 2005; Shulman, Guberman, Shilling, & Bauminger, 2012; Zalla,
Barlassina, Buon, & Leboyer, 2011).
7.2. Studies Investigating Moral Processing amongst Individuals with ASD
Blair (1996) was the first to investigate moral processing amongst children
with autism using the moral/conventional distinction task. Blair compared
161
performance on the task between children with autism (n = 20), children with
learning disabilities (n = 10) and typically developing children (n = 10). The children
were able to distinguish between moral and conventional transgressions equally,
leading to the conclusion that moral processing abilities amongst individuals with
autism remain intact.
Subsequent research has confirmed Blair’s original finding that children with
ASD can distinguish between conventional rule violations and immoral acts along a
range of dimensions (Grant et al., 2005; Kretschmer et al., 2014; Leslie, Mallon, &
DiCorcia, 2006; Li, Zhu, & Gummerum, 2014; Shulman et al., 2012). For example,
Grant et al. (2005) demonstrated that children with autism or Asperger’s syndrome (n
= 19) were as likely as both children with learning disabilities (n = 17) and typically
developing children (n = 20) to base their judgments of the “naughtiness” of
characters in vignettes involving harmful behaviours on the character’s motive
(accidental vs. deliberate). They also viewed harm to people as more serious than
damage to property. Similarly, Leslie et al. (2006) found that both typically
developing pre-schoolers (n = 15) and same-aged children with a diagnosis of autism
or PDD (NOS) (n=17) were able to distinguish “good” acts (e.g. sharing) from “bad”
acts (e.g. hitting) described in moral stories. Further, the children with
autism/PDD(NOS) demonstrated intact ability to distinguish between the distress of a
victim of a moral transgression (e.g. a child pulling their hair) and that of a “cry-
baby”, whose distress was not related to another’s transgression (e.g. a child who
became upset because he was not permitted to eat both his and another child’s
cookie). These previous studies thus indicate that children with ASD are generally
able to distinguish between moral violations (that involve a suffering victim whose
personal rights are violated, e.g. hitting others) and conventional transgressions
162
(characterised by infraction of normative prohibitions but with no consequence for
others’ welfare; e.g. talking out of turn), according to the dimensions of
permissibility, seriousness and authority dependence.
In contrast, however, Takeda, Kasai, and Kato (2007) found that children with
high functioning Pervasive Developmental Disorder (HF PDD; n = 23) scored
significantly lower than typically developing peers (n = 23) on the Japanese Human
External Action and Internal Reasoning Type (HEART), a standardized test for
evaluating moral judgement in school children. The HEART presents a moral
dilemma through a short story and a cartoon, and asks participants to endorse one of
four responses corresponding to a 4-stage hierarchy of moral reasoning (i.e. from
“amoral”, to “pre-conventional”, “conventional”, and “autonomous”; see Table 5).
According to Takeda et al. while both children with HF PDD and typically
developing children demonstrated moral reasoning at the “conventional” level, more
of the typically developing children demonstrated “autonomous” moral reasoning. On
the basis of an assumption that morality develops in a hierarchical, stage-like manner
(as defined by Takeda et al., 2007), these results were interpreted as suggesting that
children with HF ASD possess less advanced moral reasoning than same age peers.
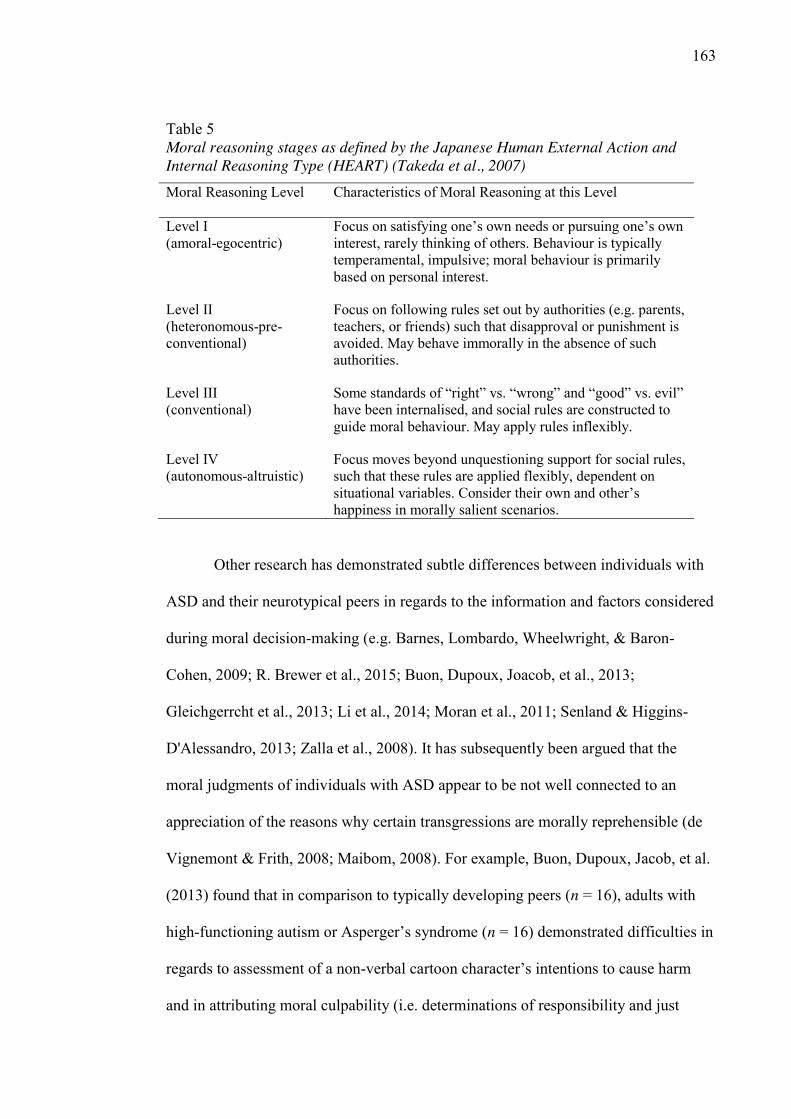
163
Table 5 Moral reasoning stages as defined by the Japanese Human External Action and Internal Reasoning Type (HEART) (Takeda et al., 2007) Moral Reasoning Level Characteristics of Moral Reasoning at this Level
Level I (amoral-egocentric)
Focus on satisfying one’s own needs or pursuing one’s own interest, rarely thinking of others. Behaviour is typically temperamental, impulsive; moral behaviour is primarily based on personal interest.
Level II (heteronomous-pre-conventional)
Focus on following rules set out by authorities (e.g. parents, teachers, or friends) such that disapproval or punishment is avoided. May behave immorally in the absence of such authorities.
Level III (conventional)
Some standards of “right” vs. “wrong” and “good” vs. evil” have been internalised, and social rules are constructed to guide moral behaviour. May apply rules inflexibly.
Level IV (autonomous-altruistic)
Focus moves beyond unquestioning support for social rules, such that these rules are applied flexibly, dependent on situational variables. Consider their own and other’s happiness in morally salient scenarios.
Other research has demonstrated subtle differences between individuals with
ASD and their neurotypical peers in regards to the information and factors considered
during moral decision-making (e.g. Barnes, Lombardo, Wheelwright, & Baron-
Cohen, 2009; R. Brewer et al., 2015; Buon, Dupoux, Joacob, et al., 2013;
Gleichgerrcht et al., 2013; Li et al., 2014; Moran et al., 2011; Senland & Higgins-
D'Alessandro, 2013; Zalla et al., 2008). It has subsequently been argued that the
moral judgments of individuals with ASD appear to be not well connected to an
appreciation of the reasons why certain transgressions are morally reprehensible (de
Vignemont & Frith, 2008; Maibom, 2008). For example, Buon, Dupoux, Jacob, et al.
(2013) found that in comparison to typically developing peers (n = 16), adults with
high-functioning autism or Asperger’s syndrome (n = 16) demonstrated difficulties in
regards to assessment of a non-verbal cartoon character’s intentions to cause harm
and in attributing moral culpability (i.e. determinations of responsibility and just
164
punishment) on the basis of this information. Specifically, participants with HFA/AS
deemed accidental acts of harm and harm that was merely coincidental to the actions
of the protagonist as more intentional, when compared to the responses of a
neurotypical control group. Further, in comparison to neurotypical peers, participants
with HFA/AS attributed a higher degree of moral responsibility for the victim’s
suffering to the protagonist when such harm was accidental or where the actions of
the protagonist were coincidental to the harm caused. Relatedly, participants with
HFA/AS deemed the protagonist as deserving greater punishment for accidental acts
of harm, than did the neurotypical control group. Moran et al. (2011) similarly
concluded: “In judging accidental harms, ASD participants appeared to show an
under-reliance on information about a person’s innocent intention and, as a direct
result, an overreliance on the action’s negative outcome” (p. 2688).
In addition to an apparent insensitivity to issues of intentionality in moral
reasoning, it has been argued that individuals with ASD tend to present with
difficulties translating morally salient emotional cues (i.e. feelings of empathy) into
their moral judgements (Brewer et al., 2015; Fan, Chen, Chen, Decety, & Cheng,
2014; Patil, Melsbach, Henning-Fast, & Silani, 2016; Senland & Higgins-
D'Alessandro, 2013; Zalla et al., 2011). For example, Zalla et al. (2011) asked
participants to distinguish between two moral transgressions (a child hitting another
child/pulling another child’s hair), two conventional transgressions (child wearing
pyjamas to school/adult drinking tomato soup straight out of the bowl) and two
conventional transgressions that were intended to invoke disgust (child puts her
finger in her nose/person spits in their drink before consuming it). The results showed
that participants with high-functioning autism or Asperger’s syndrome (n=20) judged
conventional and conventional-disgust transgressions to be significantly more serious
165
when compared with their neurotypical counterparts (n = 33) and failed to distinguish
between conventional-disgust transgressions and moral transgressions in terms of
seriousness. Similarly, adolescents with ASD in a study by Senland and Higgins-
D'Alessandro (2013) self-reported difficulties integrating empathic responses to
support their daily behavioural choices in morally salient interpersonal interactions (n
= 32). A neuroimaging study by Schneider et al. (2013) confirmed that, compared to
non-clinical samples, individuals with ASD (n=28) demonstrate significantly reduced
activation of empathy-related regions in the brain when engaging in reasoning about
moral dilemma scenarios. In the context of such evidence and with regards to moral
processing, it has been argued that “individuals with ASD may rely on learnt social
norms rather than emotional information” (Brewer et al., 2015, p.593).
7.3. True Moral Processing or Rule Following for Rule Following’s Sake?
Typical adult moral development allows for flexibility in applying moralistic
rules; in contrast, anecdotal evidence suggests that individuals with ASD may apply
rigid social rules to navigate their interpersonal interactions (Howlin, 2004; Jaarsma,
2013). Further, on the basis of the previous literature, it appears that the moral
judgments of individuals with ASD may be not well connected to an appreciation of
the reasons why certain transgressions are morally reprehensible (Maibom, 2008). To
what extent then do the actions that have been identified as manifesting an intact
moral processing ability amongst individuals with ASD represent a genuine moral
sense as opposed to simple rule following?
McGeer (2008b) hypothesised that individuals with ASD are highly motivated
to follow rules and deeply concerned that others do so too, not out of a genuine sense
of morality, but stemming from strong logical reasoning skills, alongside a need for
predictability in the order of the social world. Due to the difficulties individuals with
166
ASD have in understanding and responding to social cues, other people’s behaviour
can be seen to be wholly unpredictable and overwhelming, producing anxiety and
fear (McGeer, 2008b). Rules and routines may help to keep things the same, making
the world more predictable and more approachable.
Consistent with this idea, there is evidence that individuals with ASD
demonstrate a tendency to justify moral judgements according to the concrete
application of rules, or the expected negative reactions of authority figures. For
example, when children in Grant’s (2005) study were asked to explain their
judgments of culpability (‘Why do you think X was naughtier?’), the justifications
offered by children with autism or Asperger’s syndrome were deemed to be of poorer
quality (often just reiterations of the storyline) than those provided by typically
developing children. Similarly, in a study by Shulman et al. (2012), preadolescents
and adolescents with ASD provided poor justifications for (generally accurate)
moral/conventional distinctions. Specifically, individuals with ASD (n = 18) tended
to provide justifications that included more extraneous information than those of
typically developing counterparts (n = 18). Additionally, the justifications offered by
individuals with ASD typically aligned to simplistic and concrete rules (e.g. “”that’s
bad” or “you can’t do that”) or on the expectation of negative appraisals of authority
figures (e.g. “the teacher will get mad”). They were also less able to apply these rules
flexibly in different contexts. Research investigating moral processing amongst adult
participants with ASD has similarly uncovered a tendency towards rule-based
approaches to moral reasoning tasks. For example, in a study by Zalla et al. (2011),
participants with high-functioning autism or Asperger’s syndrome (n=20) were most
likely to justify decisions about moral culpability on a moral/conventional distinction
167
task according to the contravention of “rules” while neurotypical peers (n = 20) were
most likely to appeal to others’ welfare.
The view that individuals with ASD rigidly follow learned rules to guide their
behaviour is reflected in the personal accounts of high functioning individuals with
ASD. For example:
…I had a strict moral upbringing, and I learned as a child that stealing, lying
and hurting other people were wrong. As I grew older I observed that it was
alright to break certain rules but not others. I constructed a decision-making
program for whether rules could be broken by classifying wrongdoing into
three categories: “really bad,” “sins of the system,” and “illegal but not bad.”
Rules classified as really bad must never be broken. Stealing, destroying
property, and injuring other people are in this category, and they were easy to
understand. The “illegal but not bad” rules can often be broken with little
consequence. Examples would be slight speeding on the freeway and illegal
parking. The “sins of the system” category covers rules that have very stiff
penalties for seemingly illogical reasons.” (Grandin, 2006, pp. 108-109).
Further research using measures that investigate the factors or rules that are
salient for individuals when making moral judgments (rather than those that simply
measure the moral judgments made) are needed to gain a better understanding of
moral processing amongst individuals with ASD. Simultaneously, it is necessary to
consider whether the extant literature in this area has investigated a sufficiently broad
range of concerns on which to base conclusions regarding issues of morality amongst
individuals with ASD.
168
7.4. The Breadth of the Moral Domain
Researchers in moral psychology have typically adopted a definition of
morality that pertains to matters of harm, rights and justice (Haidt & Graham, 2007).
Consequently, the prior research regarding morality amongst individuals with ASD
centers on a definition of morality that centers on concerns of justice or the
prevention of harm. According to a justice/care concept of morality adopted in the
moral/conventional distinction literature, it is the presence of a person that suffers (a
victim) that distinguishes moral from conventional transgressions (Blair, 1996). This
view has some empirical support. Specifically, it has been shown that whether an
individual considers abortion to be a moral or conventional transgression may be
determined by whether they judge the act to involve a victim or not (Smetana, 1982).
Further, Smetana (1985) showed that unknown transgressions (represented by
nonsense words) are considered immoral if they are associated with the suffering of
another.
However, recent investigations suggest that the moral domain should not be
limited to concerns about the welfare of others (Haidt, 2001, 2007). Harm to another
is neither a necessary nor sufficient quality for a transgression to be considered moral
rather than merely conventional (Aharoni et al., 2011; Haidt, 2001). Consider, for
example, a hypothetical situation proposed by Haidt (2001) involving a brother and
sister who privately and willingly consent to having sex with each other and take
proper precautions in terms of birth control. Individuals tend to have a very strong
intuition that it is wrong for the siblings to have sex, despite the fact that there is not
an identifiable victim (Haidt, 2001). Having sex with a dead chicken, wiping a toilet
with a national flag and cannibalism of a dead person who has agreed to be a tissue
donor are examples of other acts that tend to be judged as morally wrong, despite
169
difficulty in determining a victim (Haidt, 2001). Similarly, not all instances of harm
are considered a moral violation (Nichols, 2002). Indeed, many acts that cause
suffering to identifiable ‘victims’, for example, visits to the dentist or natural
disasters, are not typically considered to be morally wrong (Aharoni et al., 2011). If
some acts that cause suffering in others are not immoral, and other acts that do not
cause suffering to others are considered immoral, there must be concerns other than
concerns about others’ welfare that are morally relevant (McGeer, 2008a).
To more fully describe such nuances in moral reasoning, recent work in moral
psychology has defined models of morality according to a broader domain, including
but not limited to concerns regarding harm and welfare of others (Graham et al.,
2011; Haidt & Graham, 2007, 2009; Haidt & Joseph, 2008; Rozin, Lowery, Imada, &
Haidt, 1999). One theory that encompasses the multi-faceted nature of morality is
Haidt and colleagues’ Moral Foundations Theory (Graham et al., 2011; Haidt, 2012;
Haidt & Graham, 2009).
7.5. Moral Foundations Theory
Haidt, Graham, and their colleagues developed Moral Foundations Theory
(MFT) on the basis of anthropological, sociological, and evolutionary evidence that
the moral domain is broader than issues of harm, rights and justice (Graham, Haidt, &
Nosek, 2009; Graham et al., 2011; Haidt, 2008, 2012; Haidt & Graham, 2007; Haidt,
Graham, & Joseph, 2009). According to MFT, morality is driven by intuition,
accomplished by rapid, automatic and unconscious psychological processes, and
organized according to five universal moral “foundations”, each with their own
evolutionary and cultural explanations (Graham et al., 2009; Graham et al., 2011;
Haidt, 2012; Haidt & Joseph, 2004). Consistent with earlier theoretical perspectives
(Gibbs, 1979; Kohlberg, 1969; Turiel, 1983), the moral foundations identified
170
included concerns regarding the wellbeing of others (“Care/Harm” and
“Fairness/Cheating”); however, MFT argues that human moral reasoning is not
limited to these concerns, identifying three additional areas of moral concern:
“Loyalty/Betrayal”, “Authority/Subversion” and “Sanctity/Degradation” (Haidt,
2012):
7.5.1. Care/Harm. MFT, consistent with more traditional models of morality,
recognises concerns regarding the minimisation of harm and suffering as a central
component of morality. Humans, like other mammals, have developed a sensitivity to
the distress of others in response to the evolutionary need to protect and care for the
young, vulnerable or injured (Haidt & Graham, 2007; Haidt & Joseph, 2008). As
such, we feel approval for compassion and kindness and other acts that reduce
distress in others and view acts that lead to suffering as immoral (Haidt & Graham,
2007). According to MFT, however, cultures vary in the degree to which the
prevention of harm, and related virtues (such as kindness and compassion) are valued,
dependent on the relative prioritization of other moral foundations (Haidt & Graham,
2007).
7.5.2. Fairness/Cheating. Co-operation with ‘non-kin’ others and reciprocal
altruism have held many evolutionary benefits for human cultures throughout history
(Haidt & Joseph, 2008). As such, humans are primed towards collaboration and to
value ideas that support alliances, including fairness and justice, with a corresponding
sensitivity to signs of cheating and deception in others (Haidt & Graham, 2007; Haidt
& Joseph, 2004). Simultaneously, some cultures have identified autonomy, equality
and respect for individual rights as virtuous in response to participation in reciprocal
interactions within such alliances (Haidt & Graham, 2007).
171
7.5.3. Loyalty/Betrayal. Belonging to a group has several evolutionary
benefits, particularly in regards to identity formation, co-operation and physical
protection (Haidt & Joseph, 2008). Humans thus possess a long evolutionary history
of living in groups, resulting in the development of specialised socio-cognitive and
socio-affective systems that support cooperation with in-group members, and
preparing for, recognising and responding to threats to group cohesion, particularly
those from external sources (Haidt & Graham, 2007). Consequently, loyalty and
patriotism have become regarded as virtues, whilst acts that threaten the in-group,
such as treason and cowardice, can be seen as immoral (Haidt & Joseph, 2008).
7.5.4. Authority/Subversion. Historically, the groups that have formed
amongst humans have been hierarchically structured, whereby certain members assert
dominance (Haidt & Graham, 2007; Haidt & Joseph, 2008). As a result,
psychological systems have evolved that allow humans to expertly navigate and
benefit from coexistence within hierarchical communities (Haidt & Graham, 2007).
While many psychological accounts of hierarchies indicate that all forms of
inequality involve oppression, Haidt and Joseph (2008) hold that the development
and maintenance of stable hierarchies can have evolutionary merit. While
subordinates must show respect and defer to superiors, they can expect in return to be
protected from disorder within the group and external threats (Haidt & Joseph, 2008).
As such, according to MFT, subversion or the disrespect of authority figures may be
seen as immoral.
7.5.5. Sanctity/Degradation. The foundation of purity/sanctity is based on
the emotion of disgust (Haidt & Graham, 2007). In evolutionary terms, disgust
protects the body from contamination from bacteria and other harmful contagions;
however, in many cultures disgust has generalised to the social realm and extends to
172
judgements of potential (physical or social) contamination by others on the basis of
appearance, social standing, or other individual differences (Haidt & Graham, 2007).
In many cultures, the concept of moral disgust has generalised further, particularly in
regards to religious practices, and includes promotion or condemnation of activities,
for example, chastity and piousness or hedonism and carnal gratification (Haidt &
Graham, 2007).
7.5.6. What can Moral Foundations Theory reveal about moral reasoning
in ASD? The results of prior research investigating moral reasoning amongst
individuals with ASD have been somewhat mixed. Overall, it appears that, when
compared to typically developing peers, individuals with ASD do not possess gross
impairments in recognising and distinguishing moral harms from transgressions that
are merely conventional. However, there do appear to be some discrepancies in the
manner in which at least some individuals with ASD approach moral judgements,
including difficulties in integrating salient information such as intentionality and
morally salient emotional responses. Such characteristics could lead to difficulties for
ASD individuals in navigating morally salient interpersonal interactions in everyday
life (Moran et al., 2011). Of note, however, the investigations of moral reasoning
amongst individuals with ASD from which such conclusions are drawn have typically
adopted a definition of morality limited to considerations of justice and harm, which
MFT holds as only a subset of human morality.
According to MFT, the five moral foundations can be used to describe
differences in mature moral ideologies cross-culturally and between groups within
larger cultures (Haidt & Joseph, 2004). That is, all humans possess the same innate
array of moral intuitions, whilst these are endorsed and expressed differentially,
dependent on individual differences (i.e. cultural, political, developmental, or
173
temperamental factors; Haidt & Graham, 2007). For example, individuals with liberal
political orientations typically present with moral concerns based upon issues of
Care/Harm and Fairness/Cheating only, whilst politically conservative individuals
rely upon all five moral foundations in their assessment and navigation of morally
salient situations (Haidt & Graham, 2007). MFT thus provides a conceptual
organization for measuring and describing differences in moral concerns across
individuals, social groups, and cultures (Graham et al., 2011).
With reference to differences in moral foundation endorsement between
political and religious liberals and conservatives, Haidt and Graham (2007) describe
how a failure to recognise that moral concern can extend past issues related to justice,
equality and victimisation may result in difficulties understanding the views of others
who hold differing moral foundations to one’s own. Specifically, Haidt and Graham
argue that conservatives hold a range of moral concerns, some of which individuals
with more liberal political orientations do not consider relevant, resulting in an
“invisible wall separating liberal and conservative moralities” (p. 111). This “wall”
renders it difficult, if not impossible, for religious and political liberals to understand
why their conservative peers might hold views they perceive as unjust (e.g. views
against marriage equality). Haidt and Graham (2007) further hold that recognising the
broader range of moral foundations as moral concerns, rather than amoral, immoral or
otherwise abnormal, may provide “a doorway through the wall”, allowing individuals
with liberal orientations to “step (briefly) beyond their moral comfort zone and see
issues from the perspective of others” (p.111).
It follows that the narrow definition of morality adopted in the evidence base
regarding moral reasoning amongst individuals with ASD may similarly impact our
understanding and conclusions in regards to the moral agency of individuals within
174
the ASD population. For example, on the basis of the failure of individuals with ASD
to prioritise scenarios involving harm from those involving disgust, Zalla et al. (2011)
concluded that such individuals present with impairments in moral reasoning.
However, the categorisation of scenarios evoking disgust as moral does not present a
challenge to the conceptualisation of the moral domain according to MFT. Thus,
exploring the innate moral concerns of individuals with ASD may be a modest, but
informative start to understanding morality amongst this population. In this light, the
next chapter describes a study undertaken to explore the association between ASD
trait severity and moral foundation endorsement according to MFT.
175
Chapter 8. Study 3: Disparities in moral intuitions and the autistic
phenotype
8.1. Rationale
Throughout the literature, case examples of peculiar moral sensibilities
amongst individuals with ASD are prevalent. In contrast, a review of the empirical
literature revealed that individuals with ASD perform similarly to neurotypical peers
on some measures of moral reasoning, suggesting that such abilities are largely intact
amongst the ASD population. Questions remain, however, regarding the validity and
applicability of such conclusions, given that prior research in this area has
predominantly relied on the performance of children on a traditional moral
recognition task that adopts a unitary definition of morality according to the presence
(or absence) of harm. As described in the previous chapter, recent theoretical and
empirical contributions challenge such unitary conceptualizations, suggesting that the
moral domain should not be limited to concerns regarding the welfare of others
(Haidt, 2001, 2007).
Contemporary models of morality have been developed which consider harm
and welfare as only one of multiple morally relevant domains. Such theoretical
models provide an opportunity to explore inconsistencies in moral judgments that
have been observed amongst individuals with ASD. Haidt’s (2012) MFT is one such
contemporary model of morality that delineates five empirically substantiated
domains of human moral concern (care/harm, fairness/cheating, loyalty/betrayal,
sanctity/degradation and authority/subversion11), originally drawn from
anthropological and evolutionary evidence. The current chapter describes a study that 11 MFT and each of the five moral domains were described in more detail in
the preceding chapter.
176
investigates whether the presence of autistic traits impacts on morality according to
MFT.
Describing MFT as “a valuable analysis of morality”, Baron-Cohen (2013)
argued that individuals with ASD often display behaviours consistent with each of the
five moral domains (p. 212). Specifically, Baron-Cohen asserted that individuals with
ASD have been observed to provide care for their aging parents, pets and children
(care/harm domain), are politically engaged in campaigns for social justice
(fairness/cheating domain), are loyal employees and group members (loyalty/betrayal
domain), are keenly aware of social hierarchies, demanding consistency, honesty and
ethical behaviour from leaders (authority/subversion domain), and are “as picky as
anyone” regarding purity of body and mind (sanctity/degradation domain) (p. 213).
Of note, Baron-Cohen’s argument is theoretical in nature, relying largely on
anecdotal behavioural observations of individuals with ASD. The current study aims
to test these claims using Graham, Haidt, and Nosek’s (2008) Moral Foundations
Questionnaire (MFQ); a self-report tool developed to provide a quantitative measure
of moral intuitions as per MFT.
It should be emphasized at the outset that MFT is descriptive in nature,
providing a model by which disparities in moral thought and behaviour can be
explored and understood (Graham et al., 2013). Relatedly, the MFQ only aims to
measure respondents’ subjective intuitions regarding moral matters and does not
speak to objective abilities (Aharoni et al., 2011). In this context, the current study
does not attempt to make inferences regarding moral deficits nor superiorities and
aims only to describe disparities in moral concerns, if any, that exist dependent on
reported ASD traits.
177
8.2. Aims and Hypotheses
Adopting a dimensional approach to the construct of ASD (in line with the
conceptualisation of the autistic phenotype existing along a continuum), the aim of
the current study was to investigate how MFT may apply to individuals with higher
levels of autistic traits, and whether there is differentiation between the responses of
individuals with differing levels of autistic traits. Specifically, the question
investigated was whether moral intuitions, as measured on the 30-item MFQ, differ
across the ASD phenotype (i.e. whether high levels of ASD traits experience or
process morality differently to those with lower levels, who are therefore less likely
to meet the diagnostic criteria for ASD).
In contrast to Baron-Cohen (2013), it was predicted on the basis of empirical
and anecdotal evidence that moral foundation endorsement would vary according to
the degree of self-reported autistic traits. Separate hypotheses were made regarding
endorsement of each MFQ domain, as presented below:
8.2.1. Care/Harm. As discussed in Chapter 7, children with ASD have been
shown to perform similarly to neurotypical peers on moral recognition tasks that
emphasise a harm/welfare conceptualization of morality (Blair, 1999; Grant et al.,
2005). Indeed, research has suggested that individuals with ASD consider harm
caused to others as immoral and worthy of punishment, even in circumstances where
the harm caused was recognised as unintentional (Buon, Dupoux, Jacob, et al., 2013;
Koster-Hale, Saxe, Dungan, & Young, 2013; Moran et al., 2011). Further, Li, Zhu
and Gummerum (2014) demonstrated that when making moral judgments of a
protagonist’s behaviour in social stories, children with high-functioning autism
appeared more sensitive to harm caused to others, judging acts resulting in harm as
less permissible than their neurotypical peers. With respect to Haidt’s taxonomy,
178
these results suggest that the care/harm moral foundation is well developed amongst
individuals with ASD. Accordingly, it was hypothesised that individuals with higher
degrees of traits consistent with ASD would exhibit higher endorsement for the
care/harm foundation than individuals with lower levels of such traits.
8.2.2. Fairness/Cheating. Results of research relevant to the endorsement of
the fairness/cheating moral foundation amongst individuals with ASD are mixed. In
Sally and Hill’s (2006) study of children’s behaviour during participation in an
economic cooperation game, children with ASD were more likely than typically
developing counterparts to refuse fair proposals or accept (unfair) low initial offers,
suggesting a poor understanding or low sensitivity to unfair treatment. In contrast,
Rutherford and Ray (2009) found that adults with ASD demonstrated preserved
abilities to detect and distinguish cheaters from those who committed social faux pas
on the basis of an honest mistake.
More recently, Schmitz, Banerjee, Pouw, Stockmann, and Rieffe (2015)
revealed that, in comparison to typically developing peers, children with ASD
displayed lower prioritization of equality in situations where no obvious harm is
caused (to the self or another) during participation in an economic social decision-
making game. Specifically, compared to neurotypical peers, children with ASD were
less likely to favour an equal distribution of coins during a computerised allocation
task (adapted from Fehr, Bernhard, & Rockenbach, 2008) in cases where the
distribution represented a relative gain (albeit unequal) for both players (i.e. one
participant received two coins while the other received one) but not where explicit
harm could be identified (i.e. one participant gets no coins). If egalitarianism is taken
to represent a more general orientation to concerns of fairness, these results suggest
that cooperative behaviour observed amongst individuals with ASD may be aligned
179
with the care/harm moral foundation, rather than motivated by concerns of fairness.
On this basis, it was hypothesized for the current study that individuals with a higher
degree of traits indicative of ASD would be less likely to endorse the
Fairness/Cheating moral foundation when compared to respondents who displayed
fewer autistic traits.
8.2.3. Loyalty/Betrayal. There is little research available that directly informs
hypotheses regarding the importance of the Loyalty/Betrayal foundation amongst the
ASD population. The available research suggests that individuals with ASD often
experience poor quality relationships, resulting in low levels of social connectedness
and a significant degree of social isolation (Liptak et al., 2011; Müller et al., 2008;
Orsmond et al., 2013). A significant majority of the adult ASD population do not
experience close reciprocal friendships (Eaves & Ho, 2008; Howlin et al., 2004;
Liptak et al., 2011; Whitehouse, Durkin, et al., 2009) and report a lack of skills
required to initiate such relationships (Müller et al., 2008). Conclusions regarding the
longevity of established friendships amongst the ASD population are mixed, with
some prior research suggesting that friendships are shorter than those of typically
developing peers (Bauminger & Shulman, 2003), whilst others have described
relationships of significant duration, suggesting a degree of commitment to such
relationships (Potter, 2014; Rosetti, 2011).
Despite inconsistent findings in regards to the nature of in-group relationships
amongst the ASD population, individuals with ASD have been characterised as
exceedingly honest and loyal within the context of their employment (The National
Autistic Society, 2013) and personal relationships (Chappell, 2011). Co-operative
behaviour is also evident amongst individuals with ASD, with Downs and Smith
(2004) reporting no differences in cooperative behaviour between children with
180
autism and typically developing children during participation in a social decision-
making game. There is some evidence that children with ASD may prioritise co-
operative behaviour to a greater degree than typically developing children in their
interactions with others. Specifically, Li et al. (2014) found that 6-12 year old
children with High-Functioning Autism (n =38) demonstrated a similar degree of
cooperative behaviour when playing a moral dilemma game with “morally nice”,
“morally naughty” or stranger opponents, whilst typically developing children (n =
31) showed higher co-operation when interacting with “morally nice” children than
with “morally naughty” opponents or strangers.
Although there is some experimental evidence for cooperative play among
children with ASD, case studies suggest that intense attachments experienced by
individuals with ASD may result in problematic behaviours such as stalking or
antisocial acts perpetrated at the directive of those that they consider as friends (see
Chapter 3). These instances suggest that individuals with ASD may experience
“friendship” differently to the typically developing population, and it is unclear to
what extent such ‘loyal’ or co-operative behaviours observed amongst individuals
with ASD are motivated by moral concern as opposed to reflecting socio-
communicative impairments (e.g. social naivety) or behavioural rigidity (i.e. a
preference against change in social circumstances). Accordingly, insufficient
evidence exists regarding the Loyalty/Betrayal moral foundation to inform
predictions about the impact of autistic traits in either direction.
8.2.4. Authority/Subversion. As discussed in Chapter 7, evidence exists that
individuals with ASD may base their moral judgments on learned rules and
expectations, or the expected negative reactions of authority figures (Shulman et al.,
2012; Takeda et al., 2007). For example, on discussing his engagement in antisocial
181
behaviours, a young man with Asperger’s syndrome was reported by Beardon (2008)
to remark, “I know what’s right and wrong because Mum and Dad have taught me”
(p. 137). As noted by Beardon (2008), this statement suggests that the young man’s
moral understanding derived from his parent’s instruction, rather than his own moral
intuition. Similarly, Takeda et al. (2007) argued that when children with high-
functioning pervasive developmental disorder approached a test of moral judgment
they appeared to “choose the answer that is closest to what they have been taught (by
their parents or teachers) in previous similar conditions” (p. 412). On the basis of
such evidence, it was hypothesised for the current study that individuals with higher
degrees of ASD traits would exhibit higher endorsement for the authority/subversion
foundation than individuals with lower levels of such traits.
8.2.5. Sanctity/Degradation. As explained in the previous chapter, the
sanctity/degradation foundation encompasses concerns regarding social and religious
practices and stems from the affective experience of disgust. Although prior research
suggests that individuals with ASD are unlikely to subscribe to religious beliefs
(Caldwell-Harris, Murphy, Velazquez, & McNamara, 2011), there is some evidence
that disgust constitutes a salient moral cue amongst the ASD population. Specifically,
Zalla et al. (2011) found that, in contrast to typically-developing peers, adults with
ASD did not differentiate between disgust-invoking transgressions and transgressions
resulting in harm to another in terms of perceived seriousness. Accordingly, for the
current study, it was expected that individuals with higher levels of traits consistent
with ASD would indicate higher endorsement of the sanctity/degradation foundation
when compared to those reporting lower levels of such traits.
182
8.3. Method
The current study utilised an online questionnaire to explore relationships
between self-reported ASD trait severity and moral foundation endorsement,
controlling for psychopathic trait severity, amongst a community-based sample who
self-selected for participation.
8.3.1. Participants. Respondents consisted of 172 individuals (aged 18-77
years) who self-selected for participation in an online survey study. Respondents
were recruited via online advertisements on social media, research-related webpages
and through organisations thought likely to be in contact with adults with ASD (see
Appendix C for a full list of advertisement locations). This study was granted
approval from the University Human Ethics Committee and participants were
informed through a plain-language statement presented prior to commencing the
survey that participation was voluntary and that they could chose to withdraw at any
time prior to survey submission. Consent was inferred through submission of survey
responses, which occurred by participants clicking on a “submit” button on the last
page of the survey.
The majority of participants were female (68%), while 4 (2.3%) participants
identified as androgynous or chose not to respond to this item. A majority of
respondents reported Australian/New Zealander (57%), Northern American/Canadian
(19.8%), British (11.6%) or European (7.6%) heritage. The remaining respondents
(4.1%) reported other non-Western cultural backgrounds (i.e. South American,
African or Asian). The majority of respondents had completed secondary education
(30.2%) or some degree of tertiary study, including those who had completed an
undergraduate university degree or diploma (32.6%), a postgraduate degree (23.8%)
or an apprenticeship or trade qualification (3.5%). The remaining respondents (9.9%)
183
had not completed secondary education. Cases with more than 10% missing data
were considered incomplete and excluded from subsequent analyses (n = 4).
8.3.2. Materials. Respondents completed an online survey that included
measures for autistic symptomatology, psychopathy, moral foundation endorsement
and a range of demographic variables likely to influence responses on the MFQ.
8.3.2.1. Demographic information. Data were collected for a range of
demographic factors, specifically, age, formal educational attainment and nationality.
In addition, participants’ responses on four dichotomous (yes = 2/no = 1) response
items were collected, for the purposes of screening for the presence of an identified or
potential learning disability (i.e. Have you ever received a pension or benefit for a
disability? Have you ever been in a special class or school for students with a
learning disability? Do you think you are a slow learner? Do you have a learning
disability?). These four items were coded as dichotomous variables (yes = 1; no = 2;
see Table 6 for a summary of participants’ responses on these items) and summed to
create a composite score for analysis, with higher scores indicating greater likelihood
that the respondent possessed a learning disability or cognitive impairment.
Cronbach’s Alpha for the composite score was low (0.56), indicating low internal
reliability.
Reliability analyses indicated that removal of the item “Have you ever
received a pension or benefit for a disability?” would improve the internal reliability
of the learning disability composite score. Given that disability pensions and benefits
can be provided for a range of physical, psychological and cognitive impairments, it
was considered that this item measured a broader range of impairment than was
intended for the current purposes and this item was removed from the composite
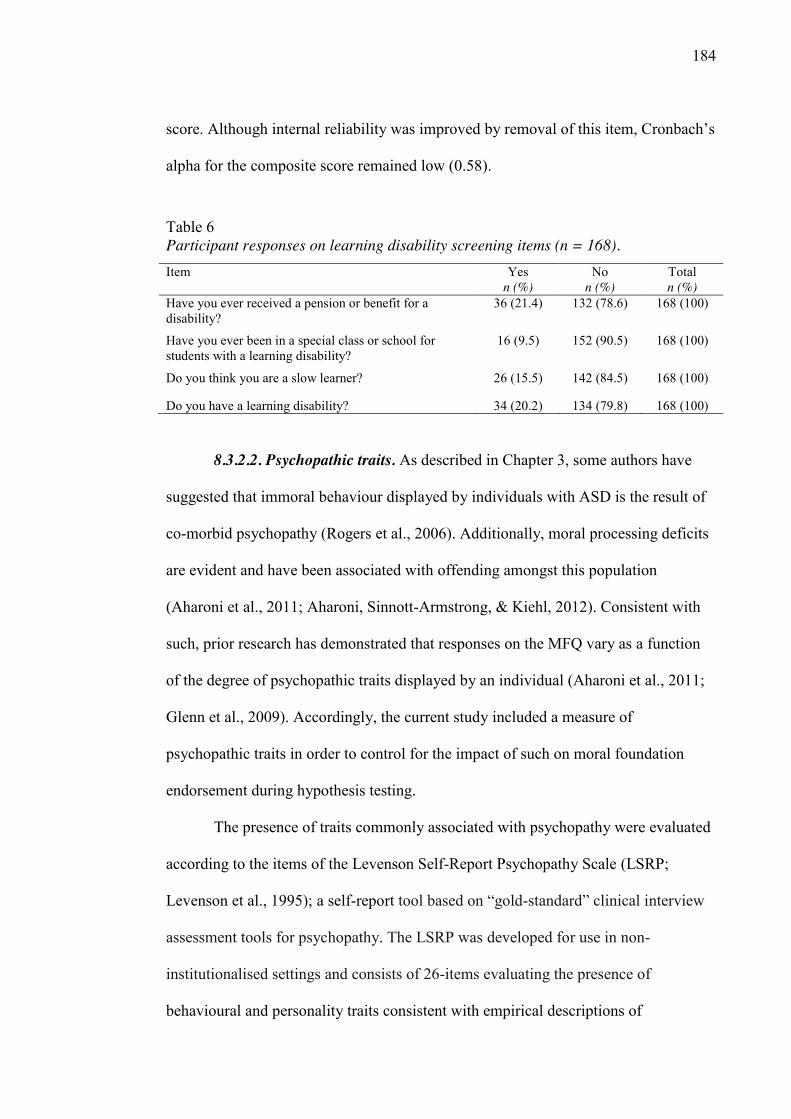
184
score. Although internal reliability was improved by removal of this item, Cronbach’s
alpha for the composite score remained low (0.58).
Table 6 Participant responses on learning disability screening items (n = 168).
Item Yes n (%)
No n (%)
Total n (%)
Have you ever received a pension or benefit for a disability?
36 (21.4) 132 (78.6) 168 (100)
Have you ever been in a special class or school for students with a learning disability?
16 (9.5) 152 (90.5) 168 (100)
Do you think you are a slow learner? 26 (15.5) 142 (84.5) 168 (100)
Do you have a learning disability? 34 (20.2) 134 (79.8) 168 (100)
8.3.2.2. Psychopathic traits. As described in Chapter 3, some authors have
suggested that immoral behaviour displayed by individuals with ASD is the result of
co-morbid psychopathy (Rogers et al., 2006). Additionally, moral processing deficits
are evident and have been associated with offending amongst this population
(Aharoni et al., 2011; Aharoni, Sinnott-Armstrong, & Kiehl, 2012). Consistent with
such, prior research has demonstrated that responses on the MFQ vary as a function
of the degree of psychopathic traits displayed by an individual (Aharoni et al., 2011;
Glenn et al., 2009). Accordingly, the current study included a measure of
psychopathic traits in order to control for the impact of such on moral foundation
endorsement during hypothesis testing.
The presence of traits commonly associated with psychopathy were evaluated
according to the items of the Levenson Self-Report Psychopathy Scale (LSRP;
Levenson et al., 1995); a self-report tool based on “gold-standard” clinical interview
assessment tools for psychopathy. The LSRP was developed for use in non-
institutionalised settings and consists of 26-items evaluating the presence of
behavioural and personality traits consistent with empirical descriptions of
185
psychopathy. Participants indicated endorsement for each of the 26 items of the
LSRP according to a 5-point likert-like scale (“disagree strongly”, “disagree”,
“neither agree nor disagree”, “agree”, “agree strongly”). Following reverse scoring
for 7 negatively weighted items, item responses were summed to create a continuous
total LSRP score. Internal reliability for the LSRP was assessed using Cronbach’s
alpha with results suggesting good internal reliability (α = 0.86).
8.3.2.3. Autistic traits. The presence of autistic traits was measured according
to the Autism Quotient (AQ; Baron-Cohen et al., 2001). The AQ is an empirically
based self-report questionnaire developed to assess the presence of traits associated
with a diagnosis of ASD amongst adults with normal intelligence (Baron-Cohen et
al., 2001). The AQ has been used to explore relationships between ASD
symptomatology and a wide range of psychological constructs relevant to morality,
including personality characteristics, affective processing and empathy (Austin, 2005;
Lassalle & Itier, 2014; Lombardo et al., 2007; Wheelwright et al., 2006) and the
tool’s psychometric properties have been validated cross-culturally (Allison et al.,
2012; Baron-Cohen et al., 2001; Wakabayashi, Baron-Cohen, Wheelwright, & Tojo,
2006; Wouters & Spek, 2011). In the current study, the Cronbach alpha coefficient
was high (α = 0.95), suggesting excellent internal reliability.
Each item of the AQ describes a characteristic associated with the ASD
phenotype and the extent to which respondents agree with the item is measured
according to a four-point likert-like scale: “definitely agree”, “slightly agree”,”
slightly disagree” and “definitely disagree”). According to the original scoring system
delineated by Baron-Cohen et al. (2001), total AQ scores are determined by summing
item responses according to a dichotomous scale, where ‘autistic’ responses are
scored as one and ‘non-autistic’ responses are scored a zero. The current study
186
preserved the four-point response scale in scoring; combining each item response to
determine total AQ scores, reverse keying where necessary. Higher AQ total scores
represented the presence of a greater degree of ASD-like traits, with the minimum
score (50) indicating an absence of such traits and the maximum score (200) full
endorsement of all autistic traits measured on the AQ. This scoring approach has been
adopted in other recent research utilizing the AQ and allows for greater
differentiation among responses, retaining valuable information regarding the degree
of respondent endorsement for traits consistent with ASD (Austin, 2005; Auyeung,
Baron-Cohen, Wheelwright, & Allison, 2008; Hoekstra et al., 2007; Jobe & Williams
White, 2007).
8.3.2.4. Moral intuitions. Moral intuitions were measured according to the
30-item Moral Foundations Questionnaire (MFQ; Graham et al., 2008). The MFQ is
a self-report measure that consists of two sections rated on a 6-point scale (zero to
five), with 16 items evaluating the extent to which participants endorse statements as
relevant to decision-making regarding “right or wrong”, and 16 items regarding the
extent of participants’ agreement with “moral rules” related to each of five moral
domains outlined by MFT (see Table 7 for example of MFQ items). Scoring of the
MFQ was facilitated by SPSS syntax made available by the authors at
www.moralfoundations.org.
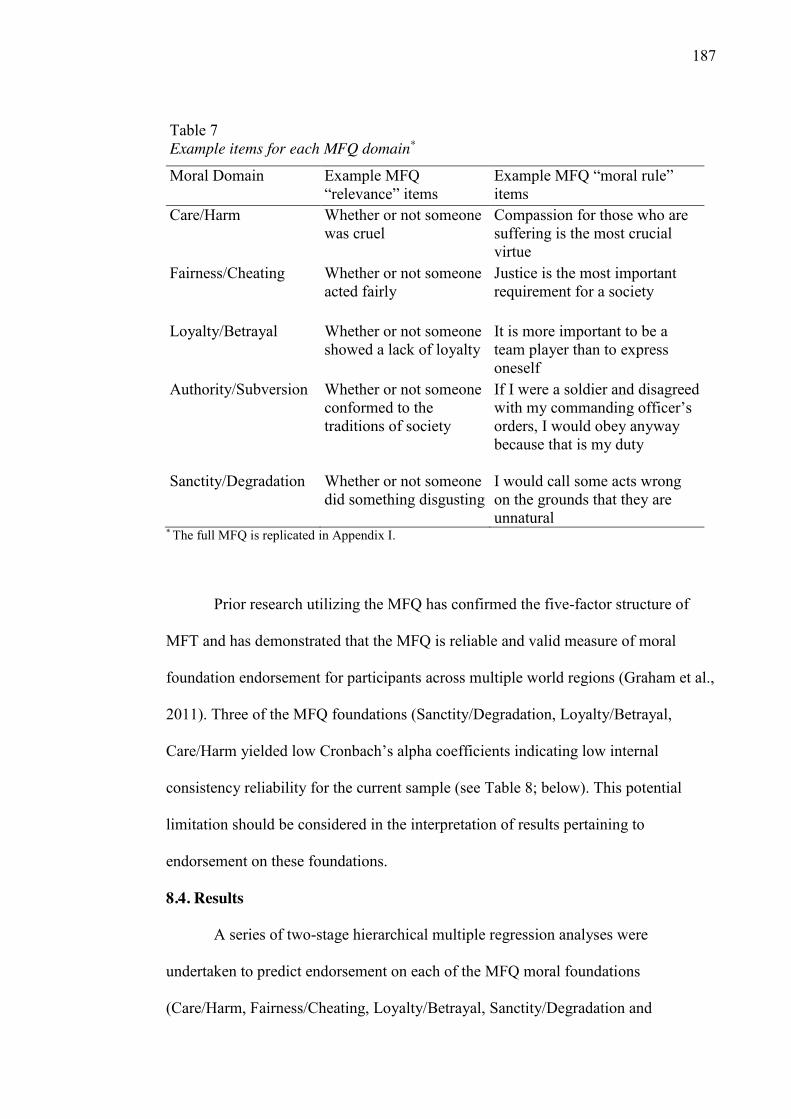
187
* The full MFQ is replicated in Appendix I.
Prior research utilizing the MFQ has confirmed the five-factor structure of
MFT and has demonstrated that the MFQ is reliable and valid measure of moral
foundation endorsement for participants across multiple world regions (Graham et al.,
2011). Three of the MFQ foundations (Sanctity/Degradation, Loyalty/Betrayal,
Care/Harm yielded low Cronbach’s alpha coefficients indicating low internal
consistency reliability for the current sample (see Table 8; below). This potential
limitation should be considered in the interpretation of results pertaining to
endorsement on these foundations.
8.4. Results
A series of two-stage hierarchical multiple regression analyses were
undertaken to predict endorsement on each of the MFQ moral foundations
(Care/Harm, Fairness/Cheating, Loyalty/Betrayal, Sanctity/Degradation and
Table 7 Example items for each MFQ domain*
Moral Domain Example MFQ “relevance” items
Example MFQ “moral rule” items
Care/Harm
Whether or not someone was cruel
Compassion for those who are suffering is the most crucial virtue
Fairness/Cheating
Whether or not someone acted fairly
Justice is the most important requirement for a society
Loyalty/Betrayal
Whether or not someone showed a lack of loyalty
It is more important to be a team player than to express oneself
Authority/Subversion
Whether or not someone conformed to the traditions of society
If I were a soldier and disagreed with my commanding officer’s orders, I would obey anyway because that is my duty
Sanctity/Degradation Whether or not someone did something disgusting
I would call some acts wrong on the grounds that they are unnatural
188
Authority/Subversion) according to AQ scores. Demographic data and total LSRP
scores were entered at stage one of the regression to control for the impact of such
variables on foundation endorsement. AQ scores were entered at the second step.
8.4.1. Missing data. Following exclusion of incomplete responses (n = 4),
missing data points constituted 0.27% of the data overall. A non-significant Little’s
MCAR test, χ2(4433) = 4472.93, p = .334, provided evidence that the data were
missing completely at random (Little, 1988). Missing data were replaced at the item
level for each scale separately using expectation maximization based imputation.
8.4.2. Contribution of demographic variables. Demographic variables (i.e.
age, gender, nationality, formal educational attainment and learning disability
indicator composite score) were differentially related to scores on the AQ and the
MFQ. AQ scores did not differ systematically according to the age or highest level of
formal educational attainment reported by participants. The learning disability
composite score was significantly correlated to AQ scores, r = .301, p < .001, but was
not significantly related to endorsement for any of the moral foundations.
Accordingly, age, formal educational attainment and learning disability composite
scores were not included as covariates and were excluded from subsequent analyses.
An analysis of variance (ANOVA) indicated that a significant relationship
existed between AQ scores and nationality, F(4, 163) = 6.748, p < .001. Similarly,
AQ scores were significantly related to respondents’ reported gender, F(2, 165) =
6.881, p = .001. Consistent with prior research (Graham et al., 2011), significant
gender and cultural/regional differences existed in moral foundation endorsement.
Specifically, in the current study, nationality was significantly related to endorsement
of the Authority/Subversion, F(4, 163) = 3.520, p = .009, and Sanctity/Degradation,
189
F(4, 163) = 3.413, p =.01, moral foundations and gender was significantly related to
endorsement of the Care/Harm domain on the MFQ, F (2, 165) = 4.805, p = .009.
No a priori predictions were made regarding the effect of demographic
variables on the relationship between AQ scores and moral foundation endorsement;
accordingly, gender and nationality were entered as covariates during hypothesis
testing. Nationality was represented in the regression analyses as four dummy
variables with Australian/New Zealander respondents serving as the reference group.
Given the small number of individuals who indicated androgyny or chose not to
respond to the “gender” item of the survey (n = 4), the responses of these individuals
were excluded pairwise from further analyses, and gender was entered as a
dichotomous variable (i.e. male/female).
8.4.3. Assumption testing. Prior to hypothesis testing, the relevant
assumptions for hierarchical multiple regression were assessed.
8.4.3.1. Sample size. Tabachnick and Fidell (2013) provide a formula for
calculating sample size requirements for multiple regression, taking into account the
number of variables that you wish to use: N > 50 + 8m (where m = number of
independent variables). According to this formula, a sample size of 106 was deemed
adequate, given seven independent variables12 entered for regression analysis.
Following exclusion of cases due to incomplete responses, the sample size for
the current study was 164. Data screening revealed a further 14 respondents who
responded to one or both consistency check items on the MFQ in a manner suggestive
of a response set. These cases were excluded from subsequent analyses, resulting in a
12 Independent variables entered: gender, four nationality dummy variables, LSRP
total score, and AQ total score.
190
total included sample of 150 respondents. Accordingly, the sample size for the
current study was considered sufficient.
8.4.3.2. Outlying data. Scans of the complete data after scale scoring revealed
three univariate outliers13 using a z-score criterion of ±3.29 (Tabachnick & Fidell,
2013). Univariate outliers were winzorised to reduce bias due to extreme values
during analysis. No multivariate outliers were identified following screening using
Mahalanobis distance scores; (p < 0.001).
8.4.3.3. Normality of residuals. To confirm that the assumption of normality
was met, the standardized residuals for each regression analysis were assessed
according to the Sharipo-Wilk statistic and absolute skew and kurtosis scores. The
Sharipo-Wilk statistic was non-significant for standardized residuals associated with
the analyses predicting endorsement of the purity (p = .226), in-group (p = .526) and
authority (p = .384) foundations, providing evidence that the assumption of normality
was satisfied for these analyses. A significant Sharipo-Wilk statistic was obtained for
the standardized residuals associated with the prediction of endorsement of the
Care/Harm (p = .001) and Fairness/Cheating (p = .009) foundations, indicating a
distribution that deviated from normality. Despite this, skewness and kurtosis
statistics did not fall outside of the acceptable ranges of ±2 and ±7 respectively
(Curran, West, & Finch, 1996). Accordingly, whilst the residuals on these analyses
appeared to depart from a strict Gaussian distribution, this departure was not extreme
and transformations were not undertaken to correct the distribution.
8.4.3.4. Multicollinearity/Singularity. An examination of correlations
revealed that no independent variables were highly correlated, indicating that
13 Variables for which univariate outliers were identified were age (x1) and LSRP
total score (x2).
191
assumptions of singularity and multicollinearity were not violated (see Table 8).
Further, the collinearity statistics (i.e. tolerance and VIF) for each regression analysis
were examined and all fell within accepted limits (Hair, Anderson, Tatham, & Black,
1995; Menard, 1995). Accordingly, the assumption of multicollinearity was deemed
to have been met.
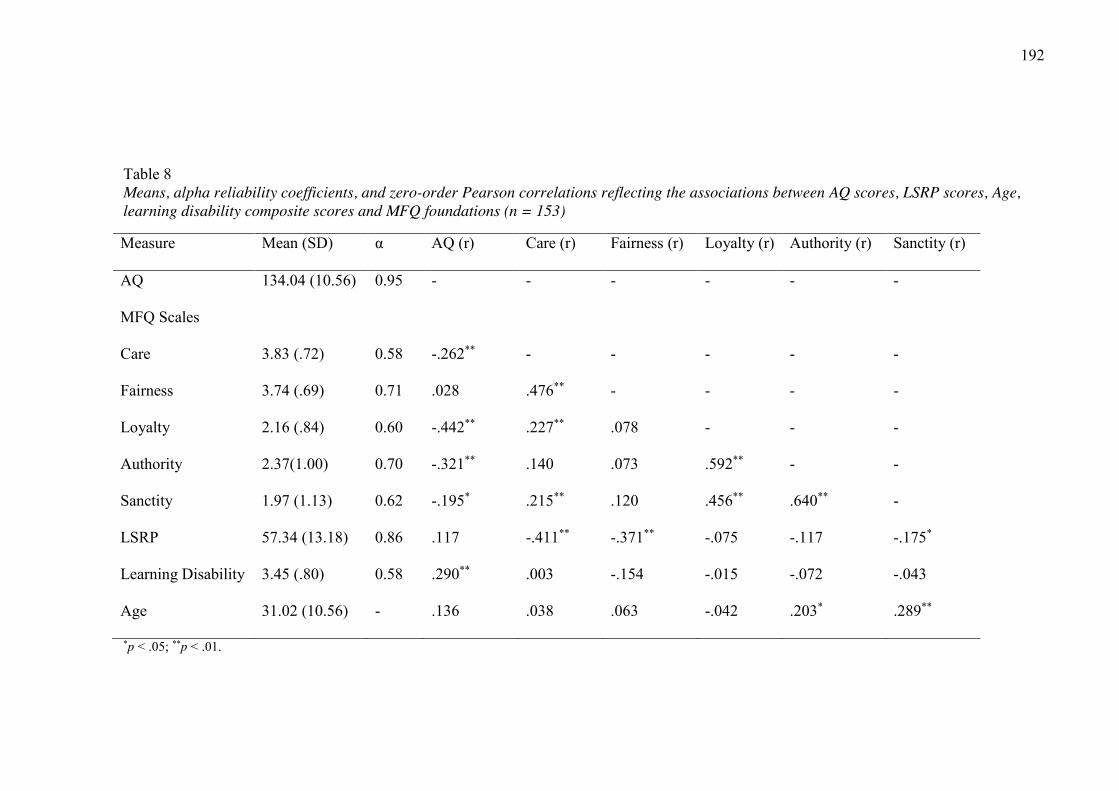
192
Table 8 Means, alpha reliability coefficients, and zero-order Pearson correlations reflecting the associations between AQ scores, LSRP scores, Age, learning disability composite scores and MFQ foundations (n = 153)
Measure Mean (SD) α AQ (r) Care (r) Fairness (r) Loyalty (r) Authority (r) Sanctity (r)
AQ 134.04 (10.56) 0.95 - - - - - -
MFQ Scales
Care 3.83 (.72) 0.58 -.262** - - - - -
Fairness 3.74 (.69) 0.71 .028 .476** - - - -
Loyalty 2.16 (.84) 0.60 -.442** .227** .078 - - -
Authority 2.37(1.00) 0.70 -.321** .140 .073 .592** - -
Sanctity 1.97 (1.13) 0.62 -.195* .215** .120 .456** .640** -
LSRP 57.34 (13.18) 0.86 .117 -.411** -.371** -.075 -.117 -.175*
Learning Disability 3.45 (.80) 0.58 .290** .003 -.154 -.015 -.072 -.043
Age 31.02 (10.56) - .136 .038 .063 -.042 .203* .289**
*p < .05; **p < .01.
193
8.4.3.5. Independence of residuals. The Durbin-Watson statistics
for each of the regression analyses were used to test for autocorrelation. The Durbin-
Watson statistics for the regression analyses ranged from 1.654 and 1.855, which
were considered within the acceptable range of 1.5 – 2.5.
8.4.3.6. Homoscedasticity. The Breusch-Pagan (1979) and Koenker (1981)
tests for heteroscedasticity were used to statistically evaluate the assumption of
homoscedasticity of residuals for each hierarchical regression undertaken during
hypothesis testing.14 The more robust Koenker test was used where the Sharipo-Wilks
statistic had revealed deviations from normality. These tests were significant for
analyses pertaining to the Fairness/Cheating, Loyalty/Betrayal, Sanctity/Degradation
and Authority/Subversion foundations, indicating evidence of heteroscedasticity for
these regression analyses. A robust (heteroscedasticity-consistent) standard error
estimator15 was employed to estimate accurate standard errors and p-values for
regression analyses where the assumption of homoscedasticity was violated. The
HC3 method was adopted, as recommended by Long and Ervin (2000) for sample
sizes less than 250.
8.4.4. Regression Analyses: AQ scores and foundation endorsement. To
test the hypotheses, the extent to which total AQ score predicted endorsement on each
of the five moral foundations was assessed, controlling for gender, nationality and 14 SPSS syntax macro by Marta Garcia-Granero for the Breusch-Pagan and
Koenker test was downloaded from http://spsstools.net/de/syntax/442/. The syntax
was edited to allow for missing data and is presented in Appendix K. 15 Use of the robust (heteroscedasticity-consistent) estimator of standard
errors was facilitated by SPSS macro and syntax taken from Hayes and Cai (2007).
This macro, presented in Appendix L, includes an optional “setwise test” that tests
the effect of a chosen variable (or set of variables) after controlling for all other
variables entered into the macro.
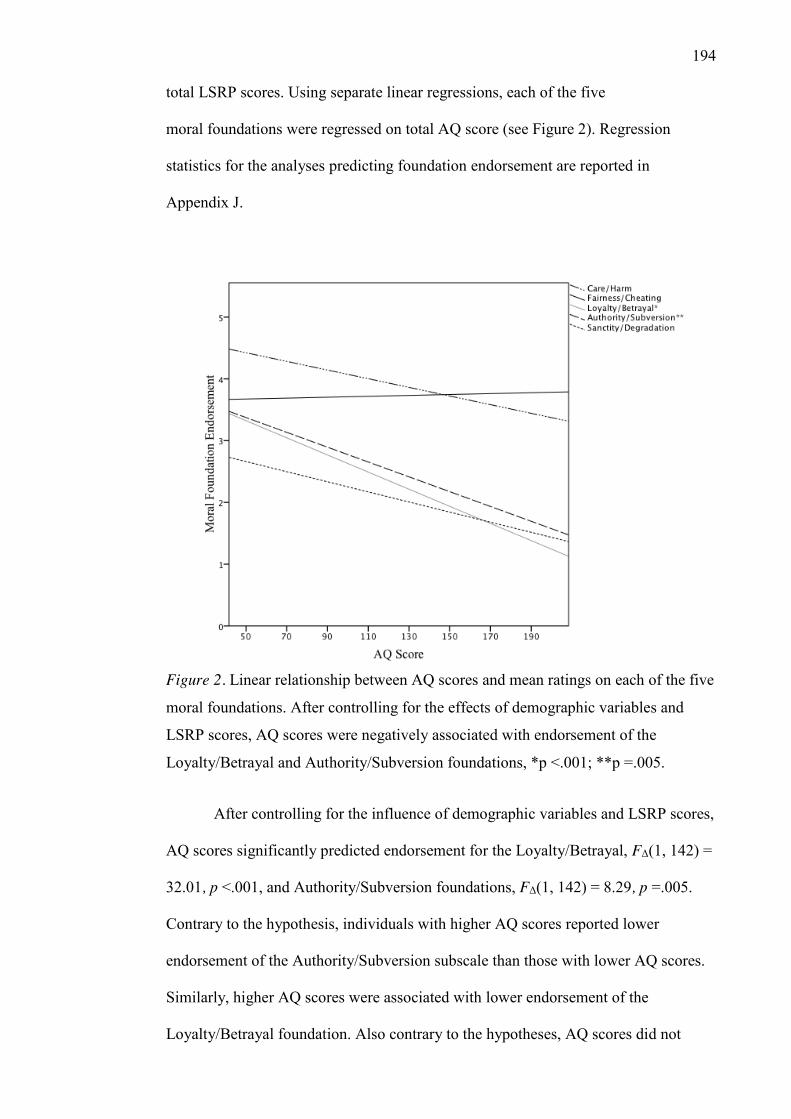
194
total LSRP scores. Using separate linear regressions, each of the five
moral foundations were regressed on total AQ score (see Figure 2). Regression
statistics for the analyses predicting foundation endorsement are reported in
Appendix J.
Figure 2. Linear relationship between AQ scores and mean ratings on each of the five
moral foundations. After controlling for the effects of demographic variables and
LSRP scores, AQ scores were negatively associated with endorsement of the
Loyalty/Betrayal and Authority/Subversion foundations, *p <.001; **p =.005.
After controlling for the influence of demographic variables and LSRP scores,
AQ scores significantly predicted endorsement for the Loyalty/Betrayal, FΔ(1, 142) =
32.01, p <.001, and Authority/Subversion foundations, FΔ(1, 142) = 8.29, p =.005.
Contrary to the hypothesis, individuals with higher AQ scores reported lower
endorsement of the Authority/Subversion subscale than those with lower AQ scores.
Similarly, higher AQ scores were associated with lower endorsement of the
Loyalty/Betrayal foundation. Also contrary to the hypotheses, AQ scores did not
195
significantly predict endorsement of the Care/Harm, FΔ(1, 142) = 3.565, p
=.061, Fairness/Cheating, FΔ(1, 142) = 0.392, p =.5321, or Sanctity/Degradation,
FΔ(1, 142) = 1.02, p = .3135, moral foundations, after controlling for demographic
variables and LSRP scores.
8.5. Discussion
The current study examines morality and ASD traits through the lens of MFT
in an attempt to better understand anecdotal reports of peculiar moral concerns
amongst the ASD population. Specifically, it aimed to explore any extant associations
between moral foundation endorsement and ASD-trait severity, as measured by AQ
scores, amongst a sample of 164 individuals who self-selected for participation
following targeted advertising for recruitment of both neurotypical individuals and
persons likely to possess a diagnosis of ASD. As hypothesised, ASD trait severity (as
measured by scores on the AQ) predicted differential moral foundation endorsement
on the MFQ. Specifically, individuals with higher degrees of ASD-consistent traits
demonstrated a narrower range of moral concerns; individuals reporting experiencing
a higher degree of ASD consistent traits were significantly less likely to consider
moral principles of Authority/Subversion and Loyalty/Betrayal when making moral
judgements in their daily lives. Contrary to the hypotheses, increased ASD trait
severity was did not predict with endorsement of the Care/Harm, Fairness/Cheating
or Sanctity/Degradation moral foundations, however, there was a trend towards lower
endorsement of the Harm/Care foundations as AQ scores increased.
The Authority/Subversion and Loyalty/Betrayal foundations, along with the
Sanctity/Degradation foundation, have been labelled as “binding” foundations;
hypothesised to promote moral behaviour by binding individuals into pro-social roles
and duties within groups and institutions, thus limiting selfish, hedonistic and
anarchical tendencies (Graham et al., 2013). In contrast, the “individualising”
196
foundations of Care/Harm and Fairness/Cheating emphasise respect for
the rights of others above all other considerations (Graham et al., 2013). Impairments
in social interaction is a diagnostic feature of ASD, resulting in difficulties navigating
social groups and institutions, and low levels of social engagement amongst adults
with ASD (see Chapter 2). In this context, it is unsurprising that individuals who
reported greater ASD trait severity would be less likely to prioritise the binding
foundations, which emphasise community participation and social interaction; that is,
due to the neurocognitive impairments and behavioural tendencies characteristic of
ASD, the psychological systems underpinning moral intuitions in the “binding”
sphere may not fully develop. Alternatively, individuals with ASD may possess
moral intuitions for binding foundations, but be unable to effectively process such,
due to their socio-cognitive and affective difficulties.
Of note, research with non-ASD populations (Wright & Baril, 2011), has
found that cognitively taxing participants, using cognitive load and ego depletion
tasks, results in reduced endorsement of the binding moral foundations. Given that
ASD appears to be associated with cognitive inflexibility and reduced information
processing efficiency, individuals who possess a greater degree of ASD traits appear
likely to be particularly vulnerable to the effects of an increased cognitive load (see
for example, Mackie & Fan, 2016). Thus, the negative association between self-
reported ASD trait severity and endorsement of the Authority/Subversion and
Loyalty/Betrayal foundations may be reflective of an increased cognitive load and/or
difficulties with self-regulation amongst individuals with a higher levels of self-
reported ASD traits, due to a mismatch between their socio-cognitive and socio-
affective abilities and the highly complex social skills required for moral reasoning.
This view would be consistent with the self-report of adolescents with ASD, who
considered they possessed intact empathic responses, but difficulties integrating such
197
into moral decision-making during challenging social interactions
(Senland & Higgins-D'Alessandro, 2013). Alternatively, participation in the current
study may have been more cognitively taxing on respondents with higher degrees of
ASD traits, resulting in a temporary deprioritisation of the “binding” foundations. A
temporary deprioritisation would explain the lack of an association between ASD trait
severity and endorsement of the Sanctity/Degradation foundation in the current study,
despite prior research indicating that individuals with ASD, unlike neurotypical
counterparts, judge disgust-evoking acts as similar to harmful acts in regard to
seriousness and moral culpability (Zalla et al., 2011).
While the MFQ has been extensively validated (Graham et al., 2013; Graham
et al., 2011), the psychometric properties have not been established in regards to use
with the ASD population. Critically, completing the MFQ relies on both an
individual’s linguistic skills and their ability to engage in metacognition. Of note, the
ability of individuals with ASD to engage in self-reflection regarding their own
mental states has been questioned, with Williams (2010) arguing that individuals with
ASD are “at least as impaired at recognising their own mental states as at recognising
mental states in other people” (p.474). Further, because the MFQ involves
respondents’ rating of abstract principles, rather than judgment of concrete scenarios,
it is unclear to what extent foundation endorsement translate to moral judgement or
behaviour (Clifford, Iyengar, Cabeza, & Sinnott-Armstrong, 2015). Future research
could seek to validate the MFQ with the ASD population or, alternatively, explore
moral foundations amongst this population through alternative methodology. For
example, future research could explore morality amongst individuals with ASD
utilising one of a growing number of MFT assessment measures have been recently
developed (Graham et al., 2013). Given the likely difficulties for individuals with
ASD in hypothesising about their own moral intuitions with reference to somewhat
198
abstract concepts (as in the MFQ), the use of a measure that includes more
concrete examples of moral foundations may be a substantial improvement to the
current study. One option of this nature is the Moral Foundations Vignettes, a
measure recently developed by Clifford et al. (2015) to assess moral judgment
according to a standardised set of carefully constructed and diverse scenarios that
represent concrete moral violations according to MFT.
Other methodological limitations are also present for the current study. It
should be noted that the study sample was relatively small and self-selected from a
non-clinical population for participation in the internet-based study. Whilst a targeted
advertising approach was utilised to increase the likelihood of recruiting individuals
with a diagnosis of ASD, such diagnoses were not confirmed, and consequently, the
current study relies on AQ scores to provide an indication of ASD trait severity. It
remains unknown whether individuals who meet the formal diagnostic criteria for
ASD would judge the moral scenarios in the same manner as the individuals who
participated in the current study. Further, the current study was unable to take into
account the full range of factors that may be related to the development and
maintenance of moral intuitions, which may include personality factors, social
experiences, and critically, political orientation.
Notwithstanding these limitations, this study provides some initial evidence
that ASD trait severity may predict the moral intuitions as defined by MFT.
Specifically the results demonstrated some disparity in moral foundation endorsement
on the MFQ, associated with self-reported ASD trait severity. These results expand
on previous research in the area of morality and ASD, which has been limited to
considerations of issues of justice and harm, by considering a broader moral domain.
Ongoing work will be required to confirm the findings of this preliminary study with
a larger, more representative sample and more stringent methodology.
199
Chapter 9. Discussion of thesis and limitations.
In the introductory chapter of this thesis, several forensic issues pertaining to
individuals ASD were identified as requiring further investigation, including those
related to the prevalence and nature of offending behaviour perpetrated by this
population, awareness of ASD amongst key stakeholders within the CJS, and the
relevance of ASD to legal issues involved in the forensic response to offending
behaviours. These issues have formed the focus of the current thesis, with particular
attention dedicated to exploring the prevalence and nature of offending behaviour
amongst the ASD population, perceptions regarding ASD amongst the Australian
magistracy and the association between ASD trait severity and issues of morality (a
factor often important to forensic decision-making during the disposition of a case).
While a growing number of studies have investigated forensic issues in this
population (reviewed in Chapter 3), significant methodological flaws limit the
conclusions that can be drawn from such research. While the literature does not
support the presence of an increased risk of engaging in offending behaviour for
individuals with ASD, it is nonetheless apparent that some individuals with ASD do
engage in offending behaviour, with resulting contact with the CJS. Indeed, a novel
empirical study described in Chapter 4 suggested that individuals with ASD may
come into contact with the CJS at a similar rate, and for a similar range of offending
behaviours, as the neurotypical population. While the growing literature base
regarding prevalence of offending amongst the ASD population provides some
information regarding the scale and nature of this issue, it has not addressed
important questions pertaining to the disposition of cases involving offenders with
ASD, the provision of intervention services and their overall management within the
CJS.
200
In some cases, it appears likely that an offender’s diagnosis of
ASD will not bear direct relevance to criminal proceedings; clearly, some individuals
with ASD may engage in offending behaviour for reasons quite beyond the specific
characteristics of ASD. However, for others, impairments associated with a diagnosis
of ASD will bear relevance to their ability to participate in criminal proceedings, their
moral culpability, or likely response to sanctions, with direct implications for the
imposition of a proportionate sentence (see Chapter 5). Accordingly, a sound
understating of the nature, and potential forensic implications of ASD, is essential
amongst CJS personnel, and particularly judicial officers, to promote consistent and
effective responses for offending behaviour amongst this population. Novel research
presented in Chapter 6 revealed significant variation in awareness and perceptions
regarding the forensic relevance of ASD amongst Australian magistrates, with such
variation likely to precipitate inconsistencies in the consideration of ASD during
criminal proceedings.
Mental health workers, including forensic psychologists, may assist to address
such inconsistencies, through the development and delivery of training for judicial
officers, and the provision of expert testimony. The extent to which such educative
efforts are helpful, however, will depend on the accuracy and relevance of
information provided therein. To that end, Chapter 7 explored the extant literature in
regards to moral reasoning amongst individuals with ASD, a factor that was
identified in preceding chapters as bearing significant relevance to proportionate
sentencing and other legal decision-making involving defendants with ASD. It
became clear that the extant research in this area has thus far failed to provide a full
account of morality amongst the ASD population, due to a narrowed focus on the
subset of moral concern associated with the prevention of harm and promotion of
justice. Chapter 8 presented an original study that explored the association between
201
ASD trait severity and MFT, a contemporary model of morality that
considers a wider moral domain. The findings of this study suggested that some
subtle differences may exist in regards to the factors individuals with ASD consider
morally relevant, when compared with neurotypical peers. Further research with
larger sample sizes and more stringent methodology is required to confirm these
findings.
9.1. Limitations of the Current Thesis
As with the preceding evidence base regarding ASD and offending behaviour,
the studies presented in this thesis have several limitations that require
acknowledgement. Many of these limitations have been discussed in the preceding
chapters, however, some apply across the whole of this thesis, and thus warrant
further comment. First, the quantitative data presented within this thesis is
correlational, limiting discussion of causal direction. Further, ASD diagnoses were
not confirmed amongst participants in these studies, thus, conclusions are limited to
discussions of individuals with elevated levels of self-reported ASD-consistent traits.
Such factors are present for much of the literature concerning the forensic aspects of
ASD, and are likely to be difficult (although not impossible) to address, given ethical
considerations and the low base rate of offending behaviour amongst the ASD
population, as well as the general population as a whole.
A more immediate concern for the generalizability of the findings is that the
impact of co-morbid conditions on offending and morality was not sufficiently
accounted for in the studies presented within this thesis. It is well documented that
forensic populations have higher rates of mental illness when compared to individuals
in the community (e.g. Dudeck et al., 2011; Hatwell, 2004; Lamb et al., 2004;
Morrison, 1991; Mullen, 2001; Ogloff et al., 2015; Ogloff et al., 2011; Skeem,
Manchak, & Peterson, 2011). Similarly, psychiatric co-morbidity is common for
202
individuals with ASD (see Chapter 2). It has thus been suggested that co-
morbid psychiatric conditions may contribute causatively to offending behaviour
among individuals with ASD (Chown, 2010; Newman & Ghaziuddin, 2008).
Similarly, it is feasible that co-morbid psychiatric conditions, particularly those that
may interfere with emotional or cognitive processing, may impact on moral
sensitivity and agency. Given the particular relevance of psychopathy for both
morality and engagement in offending behaviour, a measure of psychopathic traits
was included in the studies within this thesis; however, other conditions which may
influence moral foundation endorsement and/or risk of offending for individuals with
ASD were not considered. Further investigation into the role and effects of co-
existing conditions, including mental illness, ID and personality traits among this
population is clearly needed.
An additional limitation is that the data reported in this thesis consists entirely
of self-report measurements of traits, attributes, behaviours, and judgments. It has
been argued that the use of self-report measures may be particularly problematic with
individuals with ASD, because they may present with different response patterns to
neurotypical peers (Daly et al., 2014; Schwarz, 2005). For example, the responses of
individuals with higher degrees of ASD traits may be impacted by limitations in self-
awareness (Williams, 2010). Findings from prior research regarding the use of self-
report measures with the ASD population are mixed, with some studies suggesting
that individuals with ASD provide accurate reports of their internal experiences and
behaviour, for example emotional disturbance (Ozsivadjian, Hibberd, & Hollocks,
2013), and eating behaviours (Karlsson, Råstam, & Wentz, 2013), while other
research has suggested a trend towards underreporting on measures of symptom
severity (Bishop & Seltzer, 2012; Mazefsky et al., 2013). Other than the AQ, the
measures utilised in this thesis have not been validated for use with the ASD
203
population. Future research is needed to confirm the psychometric
properties of such measures when used with individuals with ASD.
9.2. Nexus Between ASD, Moral Reasoning and Engagement in Offending
Behaviour
Whilst the research presented in this thesis suggests that a diagnosis of ASD
may be relevant to issues of competence and moral responsibility, the mere presence
of a diagnosis, on its own, is not sufficient to exculpate, or even moderate
responsibility for offending behaviours (Lerner et al., 2012; Mayes & Koegel, 2003).
As described in Chapter 2, there is significant variation in presentation amongst
individuals with ASD, with this variability arguably more pronounced in regards to
symptomatology, behavioural adaptation, and overall functioning amongst adults
with ASD. The enormous variation in the ASD phenotype creates some uncertainty
regarding the generalizability of the research regarding forensic issues, and
recommendations as to the applicability of legislation and case law related to the
disposition of offending behaviour perpetrated by an individual with ASD. A
defendant’s diagnosis of ASD can thus be highly exculpatory, or largely irrelevant
during criminal proceedings; as with all mental impairments, the crucial issue is the
determination of a nexus between the disorder and their engagement in offending
behaviour.
The relevance of a diagnosis of ASD to the legal status of an offender was
discussed in Chapter 5. Here it was argued that while the presence of a diagnosis may
be relevant to the application of both legislative and common law provisions, in
practice, ASD is primarily relevant during the sentencing stage of criminal
proceedings. In regards to proportionate sentencing for this population, the critical
issue is the impact of an ASD diagnosis in legally relevant areas. Should it be
considered that a defendant’s offending behaviour occurred in the context of traits
204
associated with an ASD diagnosis (i.e. the ASD traits played a causal or
contributory role in the offending, or the defendant’s moral appreciation of the
offending), or that the presence of ASD would be likely to render sanctions more
burdensome than would be the case in the absence of such, the extent to which the
offender ought to be considered morally responsible for his behaviour should be
considered and dealt with appropriately during disposition. In contrast, in cases where
an offender’s impairment is not shown to impact in legally relevant ways (i.e.
significantly impacting their ability to comprehend legal processes, precipitating their
engagement in offending behaviour, or have bearing in regards to their management
and rehabilitation), the offender will be held fully culpable for their conduct,
irrespective of the severity of the diagnosed condition (Walvisch, 2010). Thus, in any
case involving an offender with ASD, the nexus between symptomatology associated
with the disorder and the offender’s cognitive, moral or volitional capacities, and
likely experience of available sanctions requires consideration. The current thesis
aimed to provide some initial insights regarding such nexus, with a particular focus
on issues of morality amongst individuals with ASD.
Despite speculation in the literature, there is no definitive evidence that
suggests that moral reasoning is related to behavioural problems, such as offending
behaviour, for individuals with ASD. Within the psychological literature there is a
substantial body of work that considers the relationship between moral reasoning and
engagement in offending behaviours (e.g. Barriga et al., 2009; Brooks, Bock, &
Nrvaez, 2013; Erickson & Felthous, 2009; Langdon, Clare, et al., 2011; Langdon,
Murphy, Clare, Steverson, & Palmer, 2011; Palmer, 2003; Palmer & Hollin, 1999;
Raine & Yang, 2006). Meta-analytic studies have demonstrated a robust relationship
between moral reasoning and engagement in offending behaviour amongst juveniles,
such that immature moral reasoning was associated with offending within juvenile
205
populations (Blasi, 1980; Nelson, Smoth, & Dodd, 1990; Stams et al.,
2006). The results of studies investigating moral reasoning amongst adult offender
populations are mixed, with some suggesting no significant deficits in moral
orientation and reasoning abilities between convicted offenders and the non-offending
population (Griffore & Samuels, 1978), whilst others have found significantly lower
level socio-moral reasoning amongst adult convicted offenders when compared with
non-offenders (Stevenson, Hall, & Innes, 2003; Thornton & Reid, 1982; Valliant,
Gauthier, Pottier, & Kosmyna, 2000). Somewhat counter-intuitively, evidence
regarding moral competency and engagement in offending behaviour amongst
offenders with an ID has suggested that offenders with ID may present with more
mature moral reasoning, when compared to non-offenders with an ID (Langdon,
Clare, et al., 2011; Langdon, Murphy, et al., 2011; McDermott & Langdon, 2016).
This finding underlies the complexity of the relationship between morality and
engagement in offending behaviour, warranting exploration of this relationship in
other clinical groups, including individuals with ASD.
Of note, similar to the literature regarding morality amongst individuals with
ASD, much of the literature that investigates the relationship between moral
reasoning and engagement in offending behaviours does not include adult samples
and relies on traditional conceptualisations of morality, those which emphasise a
moral domain centered on issues of victimization and harm. Consideration of a
broader moral domain is warranted, given that legal principles may not always be
based on issues of victimization. Consider again Haidt’s (2001) hypothetical scenario
regarding consensual sexual contact between siblings. There are laws prohibiting
Incest (i.e. penetrative sexual contact between a person and their direct lineal family
member) in every Australian jurisdiction, and consent is not considered a defence for
such behaviour in any Australian state or territory (Crimes Act 1900s 78A [NSW];
206
Crimes Act 1958 s 44 [Vic]; Criminal Code s 222 [Qld]; Criminal Law
Consolidation Act 1935 s 72 [SA]; Criminal Code s 329 [WA]; Criminal Code s 133
[Tas]; Crimes Act 1900 s 62 [ACT]; Criminal Code s134 [NT]). Accordingly, certain
behaviours may be considered both immoral and illegal, even in cases where no
obvious transgressor/victim dyad can be identified.
Recent research has begun to investigate the relationship between the moral
foundations in MFT and engagement in offending behaviour. For example, Vecina
(2014) revealed that, after controlling for gender and political orientation,
endorsement of the Authority/Subversion and Sanctity/Degradation foundations
significantly discriminated between non-offenders (n = 260) and convicted domestic
violence offenders (n = 317). The relationship between moral foundation
endorsement and psychopathy has also been explored, with results suggesting that the
moral deficits that drive much of the offending behaviour observed in psychopathy
are concentrated to the domains of Care/Harm and Fairness/Cheating, whilst other
moral intuitions remain intact (Aharoni et al., 2011; Glenn et al., 2009). What such
findings mean in regards to the legal status of such individuals remains unclear.
The findings discussed within this thesis provide an initial insight that ASD
trait severity may be related to disparities in moral foundation endorsement,
according to the MFQ. The problem remains however, that there is little evidence that
moral reasoning is predictive of moral behaviour among individuals with ASD. Thus,
further research is needed to a) confirm whether disparities exist in the moral
foundations of individuals with a formal diagnosis of ASD, b) explore whether
disparities in moral foundations are related to behavioural outcomes within the ASD
population and c) notwithstanding the results of these prior investigations, determine
whether disparities in moral foundations may discriminate between offenders and
non-offenders with ASD. Later, longitudinal research that examines changes in an

207
individual’s moral foundations following educational interventions, the
imposition of sanctions and relocation (for example, to a secure setting) may provide
evidence for whether moral foundation alteration may present as a potential target for
prevention, early intervention and habilitation with the ASD population.
208
References
't Hart-Kerkhoffs, L. A., Jansen, L. M., Doreleijers, T. A., Vermeiren, R., Minderaa, R.,
& Hartman, C. A. (2009). Autism spectrum disorder symptoms in juvenile
suspects of sex offenses. Journal of Clinical Psychiatry, 70(2), 266-272.
doi:10.4088/JCP.08m04635
Advancing Futures for Adults with Autism. (2010). National Town Hall Executive
Summary. Retrieved from http://www.afaa-
us.org/storage/documents/AFAA_National_Town_Hall_Executive_Summary.pdf
Aggarwal, S., & Angus, B. (2015). Misdiagnosis versus missed diagnosis: diagnosing
autism spectrum disorder in adolescents. Australasian Psychiatry, 23(2), 120-
123. doi:10.1177/1039856214568214
Aharoni, E., Antonenko, O., & Kiehl, K. A. (2011). Disparities in the moral intuitions of
criminal offenders: The role of psychopathy. Journal of Research in Personality,
45, 322-327. doi:10.1016/j.jrp.2011.02.005
Aharoni, E., Sinnott-Armstrong, W., & Kiehl, K. A. (2012). Can psychopathic offenders
discern moral wrongs? A new look at the moral/conventional distinction. Journal
of Abnormal Psychology, 121(2), 484-497. doi:10.1037/a0024796
Akerley, M. S. (1992). The last bird. In E. Schopler & G. B. Mesibov (Eds.), High-
Functioning Individuals With Autism. New york: Plenum Press.
Al-Farsi, Y. M., Al-Sharbati, M. M., Al-Farsi, O. A., Al-Shafee, M. S., Brooks, D. R., &
Waly, M. I. (2010). Brief report: Prevalence of autistic spectrum disoders in the
Sultanate of Oman. Journal of Autism & Developmental Disorders, 41(6), 821-
825. doi:10.1007/s10803-010-1094-8
209
Alexander, R. T., Langdon, P. E., Chester, V., Barnoux, M. F. L., Gunaratna,
I. J., & Hoare, S. (2016). Heterogeneity within autism spectrum disorder in
forensic mental health: The introduction of typologies. Advances in Autism, 2(4),
-. doi:10.1108/AIA-08-2016-0021
Allely, C. S., Minnis, H., Thompson, L., Wilson, P., & Gillberg, C. (2014).
Neurodevelopmental and psychosocial risk factors in serial killers and mass
murderers. Aggression and Violent Behavior, 19, 288-301.
doi:10.1016/j.avb.2014.04.004
Allen, D., Evans, C., Hider, A., Hawkins, S., Peckett, H., & Morgan, H. (2008).
Offending behaviour in adults with Asperger syndrome. Journal of Autism and
Developmental Disorders, 38, 748-758. doi:DOI 10.1007/s10803-007-0442-9
Allison, C., Auyeung, B., & Baron-Cohen, S. (2012). Toward brief "red flags" for autism
screening: The short autism spectrum quotient and the short quantitative checklist
in 1,000 cases and 3,000 controls. Journal of the American Academy of Child and
Adolescent Psychiatry, 51(2), 202-212.
Alvarez, A. (Producer). (2012, 26 March, 2016). Joe Scarborough: People Like James
Holmes May Be 'Somewhere On The Autism Scale'. Mediaite. Retrieved from
http://www.mediaite.com/tv/joe-scarborough-people-like-james-holmes-may-be-
somewhere-on-the-autism-scale/
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental
disorders, 4th ed., text revision (4th ed., text revision ed.). Washington, DC:
Author.
American Psychiatric Association. (2012). DSM-5 development. Retrieved from
http://www.dsm5.org
210
American Psychiatric Association. (2013). Diagnostic and statistical manual
of mental disorders, 5th ed. Washington, DC: Author.
Anckarsäter, H. (2005). Clinical neuropsychiatric symptoms in perpetrators of severe
crimes against persons. Nordic Journal of Psychiatry, 59(4), 246-252.
doi:10.1080/08039480500213709
Anckarsäter, H., Lundstrom, S., L., K., Kerekes, N., Palm, C., Carlström, E., . . .
Lichtenstein, P. (2011). The child and adolescent twin study in Sweden (CATSS).
Twin Research and Human Genetics: The Official Journal of the International
Society for Twin Studies, 14(6), 495-508. doi:10.1375/twin.14.6.495
Anckarsäter, H., Nilsson, T., Saury, J.-M., Råstam, M., & Gillberg, C. (2008). Autism
spectrum disorders in institutionalized subjects. Nordic Journal of Psychiatry,
62(2), 160-167.
Anckarsäter, H., Nilsson, T., Ståhlberg, O., Gustafson, M., Saury, J.-M., Råstam, M., &
Gillberg, C. (2007). Prevalences and configurations of mental disorders among
institutionalised adolescents. Developmental Neurorehabilitation, 10(1), 57-65.
doi:10.1080/13638490600864157
Anderson, D. K., May, M. P., & Lord, C. (2011). Changes in maladaptive behaviours
from midchildhood to young adulthood in autism spectrum disorder. American
Journal on Intellectual & Developmental Disabilities, 116(5), 381-397.
doi:10.1352/1944-7558-116.5.381
Angermeyer, M. C., & Matschinger, H. (2005). Labelling - stereotype - dicrimination:
An investigation of the stigma process. Social Psychiatry & Psychiatric
Epidemiology, 40, 391 - 395. doi:10.1007/s00127-005-0903-4
211
Archer, N., & Hurley, E. A. (2013). A justice system failing the autistic
community. Journal of Intellectual Disabilities and Offending Behaviour, 4(1/2),
53-59.
Armytage, L. (2015). Educating Judges: Towards Improving Justice. A Survey of Global
Practice. (Vol. 4). The Netherlands.: Koninklijke Brill NV.
Arseneault, L., Moffitt, T. E., Caspi, A., Taylor, P. J., & Silva, P. A. (2000). Mental
disorders and violence in a total birth cohort. Archives of General Psychiatry,
57(10), 979-986. doi:10.1001/archpsyc.57.10.979
Ashwin, C., Chapman, E., Colle, L., & Baron-Cohen, S. (2006). Impaired recognition of
negative basic emotions in autism: A test of the amygdala theory. Social
Neuroscience, 1(3-4), 349-363. doi:10.1080/17470910601040772
Asperger, H. (1944). 'Autistic psychopathy' in childhood. Translated and annotated by. In
U. Frith (Ed.), Autism and Apserger syndrome. (1991). Cambridge: Cambridge
University Press.
Attwood, T. (2006). Asperger's syndrome. Tizard Learning Disability Review, 11(4), 3-
11.
Attwood, T. (2007). The Complete Guide to Asperger's Syndrome. London, UK: Jessica
Kingsley Publishers.
Attwood, T., Hénault, I., & Dubin, N. (2014). The Autism Spectrum, Sexuality and the
Law. London: Jessica Kingsley Publishers.
Austin, E. J. (2005). Personality correlates of the broader autism phenotype as assessed
by the Autism Spectrum Quotient (AQ). Personality and individual differences,
38(2), 451-460. doi:10.1016/j.paid.2004.04.022
212
Australian Bureau of Statistics. (2010). Disability, Ageing and Carers,
Australia: Summary of Findings, 2009. Canberra: Author. Retrieved from
http://www.abs.gov.au/AUSSTATS/[email protected]/Lookup/4430.0Main+Features120
09?OpenDocument
Australian Bureau of Statistics. (2014). Autism in Australia, 2012. Canberra: Author.
Retrieved from
http://www.abs.gov.au/AUSSTATS/[email protected]/Latestproducts/4428.0Main
Features12012?opendocument&tabname=Summary&prodno=4428.0&issue=201
2&num=&view=
Australian Bureau of Statistics. (2015). Criminal Courts, Australia 2013-14. Cat. No.
4513.0. Canberra: Author.
Australian Bureau of Statistics (2016). Criminal Courts, Australia 2014-15. Cat. No.
4513.0. Canberra: Author.
Auyeung, B., Baron-Cohen, S., Wheelwright, S., & Allison, C. (2008). The autism
spectrum quotient: Children's version (AQ-Child). Journal of Autism and
Developmental Disorders, 38, 1230-1240. doi:10.1007/s10803-007-0504-z
Ballaban-Gil, K., Rapin, I., Tuchman, R., & Shinnar, S. (1996). Longitudinal
examination of the behavioural, language and social hanges in a population of
adolescents and young adults with autistic disorder. Pediatric Neurology, 15(3),
217-223.
Baril, G. L., & Wright, J. C. (2012). Different types of moral cognition: Moral stages
versus moral foundations. Personality and individual differences, 53, 468-473.
doi:10.1016/j.paid.2012.04.018
213
Barkham, E., Gunasekaran, S., & Lovelock, C. (2013). Medium and secure
care: forensic aspects of autism and Asperger's syndrome. Journal of Intellectual
Disabilities and Offending Behaviour, 4(1/2), 9-16. doi:10.1108/JIDOB-02-2013-
0005
Barnard, J., Harvey, V., Potter, D., & Prior, A. (2001). Ignored or ineligible? The reality
for adults with autism spectrum disorders. London: The National Autistic
Society.
Barnes, J. L., Lombardo, M. V., Wheelwright, S., & Baron-Cohen, S. (2009). Moral
dilemmas film task: A study of spontaneous narratives by individuals with autism
spectrum conditions. Autism Research, 2, 148-156.
Barnett, G., & Mann, R. E. (2013). Empathy deficits and sexual offending: A model of
obstacles to empathy. Aggression and Violent Behavior, 18, 228-239.
doi:10.1016/j.avb.2012.11.010
Barneveld, P. S., Swaab, H., Fagel, S., van Engeland, H., & de Sonneville, L. M. J.
(2014). Quality of life: A case-controlled long-term follow-up study, comparing
young high-functioning adults with autism spectrum disorders with adults with
other psychiatric disorders diagnosed in childhood. Comprehensive Psychiatry,
55, 302-310. doi:10.1016/j.comppsych.2013.08.001
Baron-Cohen, S. (1988). An assessment of violence in a young man with Asperger's
syndrome. Journal Of Child Psychology And Psychiatry, And Allied Disciplines,
29(3), 351-360.
Baron-Cohen, S. (1995). Mindblindedness: An essay on autism and theory of mind.
Cambridge, Mass.: MIT Press.
214
Baron-Cohen, S. (2002). The extreme male brain theory of autism. Trends in
Cognitive Sciences, 6(6), 248-254.
Baron-Cohen, S. (2011). The Science of Evil: On Empathy and The Origins of Cruelty.
New York: Basic Books.
Baron-Cohen, S. (2013). Empathy deficits in autism and psychopaths: Mirror opposites?
In M. R. Nabaji & S. A. Gelman (Eds.), Navigating the Social World. New York:
Oxford University Press.
Baron-Cohen, S., Wheelwright, S., Skinner, R., Martin, J., & Clubley, E. (2001). The
autism-spectrum quotient (AQ): Evidence from Asperger syndrome/high-
functioning autism, males and females, scientists and mathematicians. Journal of
Autism and Developmental Disorders, 31, 5-17.
Barriga, A. Q., Sullivan-Cosetti, M., & Gibbs, J. C. (2009). Moral cognitive correlates of
empathy in juvenile delinquents. Criminal Behaviour and Mental Health, 19,
253-264. doi:10.1002/cbm.740
Barry-Walsh, J. B., & Mullen, P. E. (2004). Forensic aspects of Asperger's syndrome.
Journal of Forensic Psychiatry and Psychology, 15(1), 96-107.
Barton, M. L., Robins, D. L., Jashar, D., Brennan, L., & Fein, D. (2013). Sensitivity and
specificity of proposed DSM-5 criteria for autism spectrum disorder in toddlers.
Journal of Autism & Developmental Disorders, 43, 1184-1195.
doi:10.1007/s10803-013-1817-8
Bauminger, N., & Shulman, C. (2003). The deveopment and maintenence of friendship
in high-functioning children with autism. Autism, 7(1), 81-97.
doi:10.1177/1362361303007001007
215
Beardon, L. (2008). Asperger Syndrome and Perceived Offending Conduct: A
Qulitative Study. Sheffield Hallam University.
Beighley, J. S., Matson, J. L., Rieske, R. D., Jang, J., Cervantes, P. E., & Goldin, R. L.
(2013). Comparing challenging behaviour in children diagnosed with autism
spectrum disorders according to the DSM-IV-TR and the proposed DSM-5.
Developmental Neurorehabilitation, 16(6), 375-381.
doi:10.3109/17518423.2012.760119
Berney, T. (2007). Services for adults with autism spectrum disorders. Advances in
Mental Health and Learning Disabilities, 1(2), 45-47.
Berryessa, C. M. (2014a). Judicial perceptions of media portrayals of offenders with high
functioning autistic spectrum disorders. International Journal of Criminology and
Sociology, 3, 46-60. doi:http://dx.doi.org/10.6000/1929-4409.2014.03.04
Berryessa, C. M. (2014b). Judiciary views on criminal behaviour and intention of
offenders with high-functioning autism. Journal of Intellectual Disabilities and
Offending Behaviour, 5(2), 97-106. doi:10.1108?JDOB-02-2014-0002
Berryessa, C. M. (2016a). Brief report: Judicial attitudes regarding the sentencing of
offenders with High Functioning Autism. Journal of Autism & Developmental
Disorders, 46(8), 2770-2773. doi:10.1007/s10803-016-2798-1
Berryessa, C. M. (2016b). Judges' views on evidence of genetic contriutions to mental
disorders in court. The Journal of Forensic Psychiatry and Psychology, 27(4),
586-600. doi:10.1080/14789949.2016.1173718
Billstedt, E., Gillberg, C., & Gillberg, C. (2005). Autism after adolescence: population-
based 13- to 22-year follow-up study of 120 individuals with autism diagnosed in
216
childhood. Journal of Autism & Developmental Disorders, 35(3), 351-
360. doi:10.1007/s10803-005-3302-5
Billstedt, E., Gillberg, I. C., & Gillberg, C. (2007). Autism in adults: symptom patterns
and early childhood predictors. Use of the DISCO in a community sample
followed from childhood. Journal of Child Psychology & Psychiatry, 48(11),
1102-1110. doi:10.1111/j.1469-7610.2007.01774.x
Billstedt, E., Gillberg, I. C., & Gillberg, C. (2011). Aspects of quality of life in adults
diagnosed with autism in childhood. Autism, 15(1), 17-20.
doi:10.1177/1362361309346066
Bird, G., & Cook, R. (2013). Mixed emotions: The contribution of alexithymia to the
emotional symptoms of autism. Translational Psychiatry, 3, e285.
doi:10.1038/tp.2013.61
Bishop, D. (2008). An Examination of the links between Autistic Spectrum Disorders
and offending behaviour in young People. Internet Journal of Criminology, 1-32.
Bishop, D., & Seltzer, M. M. (2012). Self-reported autism symptoms in adults with
autism spectrum disorders. Journal of Autism & Developmental Disorders,
42(11), 2354-2363. doi:10.1007/s10803-012-1483-2.
Bjørkly, S. (2009). Risk and dynamics of violence in Asperger's syndrome: A systematic
review of the literature. Aggression and Violent Behavior, 14(5), 306-312.
doi:10.1016/j.avb.2009.04.003
Blair, R. J. R. (1995). A cognitive developmental approach to morality: investigating the
psychopath. Cognition, 57, 1-29. doi:10.1016/0010-0277(95)00676-P
Blair, R. J. R. (1996). Brief Report: Morality in the autistic child. Journal of Autism and
Developmental Disorders, 26(5), 571-579. doi:10.1007/BF02172277
217
Blair, R. J. R. (1999). Psychophysiological responsiveness to the distress of
others in children with autism. Personality and individual differences, 26, 477-
485.
Blair, R. J. R. (2008). Fine cuts of empathy and the amygdala: Dissociable deficits in
psychopathy and autism. Quarterly Journal of Experimental Psychology, 61(1),
157-170. doi:10.1080/17470210701508855
Blasi, A. (1980). Bridging moral cognition and moral action: A critical review of the
literature. Psychological Bulletin, 88(1), 1-45. doi:10.1037/0033-2909.88.1.1
Bleil Walters, J., Hughes, T. L., Sutton, L. R., Marshall, S. N., Crothers, L. M., Lehman,
C., Huang, A. (2013). Maltreatment and depression in adolescent sexual
offenders with an autism spectrum disorder. Journal of Child Sexual Abuse:
Research, Treatment, & Program Innovations for Victims, Survivors, &
Offenders, 22(1), 72-89. doi:10.1080/10538712.2013.735357
Bleuler, E. (1911). Dementia Praecox or the Group of Schizophrenias. (J. Z. (1950),
Trans.). New York.: International Universities Press.
Brame, R., Paternoster, R., & Bushway, S. D. (2004). Criminal offending frequency and
offense switching Journal of Contemporary Criminal Justice, 20(2), 201-214.
doi:10.1177/1043986204263779
Breusch, T. S., & Pagan, A. R. (1979). A simple test for heteroscedasticity and random
coefficient variation. Econometrica, 47(5). doi:10.2307/1911963
Brewer, N., & Young, R. L. (2015). Crime and Autism Spectrum Disorder. London,
U.K.: Jessica Kingsley Publishers.
Brewer, R., Marsh, A. A., Catmur, C., Cardinale, E. M., Stoycos, S., & Cook, R. (2015).
The impact of autism spectrum disorder and alexithymia on judgments of moral
218
acceptability. Journal of Abnormal Psychology, 124(3), 589-595.
doi:10.1037/abn0000076
Brewer, R. J., Davies, G. M., & Blackwood, N. J. (2016). Fitness to plead: The impact of
autism spectrum disorder. Journal of Forensic Psychology Practice, 16(3), 182-
197. doi:10.1080/15228932.2016.1177285
Briugha, T., McManus, S., Meltzer, H., Smith, J., Scott, F. J., Purdon, S., Bankart, J.
(2009). Autism spectrum disorders in adults living in households throughout
England: Report from the Adult Psychiatric Morbidity Survey 2007. Retrieved
from UK: http://www.ic.nhs.uk/asdpsychiatricmorbidity07
Broadbent, J., & Stokes, M. A. (2013). Validation of autism spectrum quotient adult
version in an Australian sample. Autism Research and Treatment, 1-7.
doi:10.1155/2013/984205
Brookman-Frazee, L., Baker-Ericzén, M., Stahmer, A., Mandell, D., Haine, R. A., &
Hough, R. L. (2009). Involvement of youths with autism spectrum disorders or
intellectual disabilities in multiple public service systems. Journal of Mental
Health Research in Intellectual Disabilities, 2, 201-219.
doi:10.1080/19315860902741542
Brooks, J., Bock, T., & Nrvaez, D. (2013). Moral motivation, moral judgement and
antisocial behaviour. Journal of Research in Character Education, 9(2), 149-165.
Brown-Lavoie, S. M., Viecili, M. A., & Weiss, J. A. (2014). Sexual knowledge and
victimization in adults with autism spectrum disorders. Journal of Autism &
Developmental Disorders, 44, 2185-2196. doi:10.1007/s10803-014-2093-y
219
Browning, A., & Caulfield, L. (2011). The prevalence and treatment of people
with Asperger's syndrome in the criminal justice system. Criminology and
Criminal Justice, 11, 165-180. doi:DOI: 10.1177/1748895811398455
Buon, M., Dupoux, E., Jacob, P., Chaste, P., Leboyer, M., & Zalla, T. (2013). The role of
causal and intentional judgements in moral reasoning in individuals with high
functioning autism. Journal of Autism & Developmental Disorders, 43, 458-470.
doi:10.1007/s10803-012-1588-7
Buon, M., Dupoux, E., Joacob, P., Chaste, P., Leboyer, M., & Zalla, T. (2013). The role
of causal and intentional judgments in moral reasoning in individuals with high
functioning autism. Journal of Autism & Developmental Disorders, 43, 458-470.
doi:10.1007/s10803-012-1588-7
Burke, D. M. (2001). Empathy in sexually offending and nonoffending adolescent males.
Journal of Interpersonal Violence, 16(3), 222-233.
doi:10.1177/088626001016003003
Bzdok, D., Schilbacj, L., Vogeley, K., Schneider, K., Laird, A. R., Langer, R., &
Eickhoff, S. B. (2012). Parsing the neural correlates of moral cognition: ALE
meta-analysis on morality, theory of mind, and empathy. Brain Structure and
Function, 217, 783-796. doi:10.1007/s00429-012-0380-y
Caldwell-Harris, C., Murphy, C. F., Velazquez, T., & McNamara, P. (2011). Religious
belief systems of persons with high functinoing autism. Paper presented at the
Annual Meeting of the Cognitive Science Society, Boston, MA.
Cappadocia, M. C., Weiss, J. A., & Pepler, D. J. (2012). Bullying experiences among
children and youth with Austiam Spectrum Disorders. Journal of Autism &
Developmental Disorders, 42(2), 266-277. doi:10.1007/s10803-011-1241-x
220
Cappon, L., & Laenen, F. V. (2013). Mental health in juvenile judges'
decision-making: Review of literature. International Journal of Law and
Psychiatry, 36, 65-72. doi:10.1016/j.ijlp.2012.11.010
Carpenter, A. (1992). Autistic adulthood: A challenging journey. In E. Schopler & G. B.
Mesibov (Eds.), High-Functioning Individuals With Autism. New York: Plenum
Press.
Cashin, A., & Newman, C. (2009). Autism in the criminal justice detention system: a
review of the literature. Journal of Forensic Nursing, 5(2), 70-75.
doi:10.1111/j.1939-3938.2009.01037.x
Cederlund, M., Hagberg, B., Billstedt, E., Gillberg, I. C., & Gillberg, C. (2008). Asperger
syndrome and autism: A comparative longitudinal follow-up study more than 5
years after original diagnosis. Journal of Autism & Developmental Disorders, 38,
72-85. doi:10.1007/s10803-007-0364-6
Centre for Disease Control and Prevention. (2009). Prevalence of autism spectrum
disorders - Autism and developmental disabilities monitoring network, United
States, 2006. Morbidity and Mortality Weekly Report: Surveillance Summaries,
58(SS10), 1-20.
Centre for Disease Control and Prevention. (2014). Prevalence of autism spectrum
disorder among children aged 8 years- Autism and developmental disabilities
monitoring network, 11 sites, United States, 2010. Morbidity and Mortality
Weekly Report: Surveillance Summaries, 63(SS2).
Chakrebarti, S., & Fombonne, E. (2005). Pervasive developmental disorders in preschool
children: Confirmation of high prevalence. American Journal of Psychiatry,
162(6), 1133-1141. doi:10.1176/appi.ajp.162.6.1133
221
Chappell, S. (2011). Friendship and intimate relationships in people on the
autism spectrum. (Doctorate in Clinical Psychology), University of Warwick, The
Univeristy of Warwick Institutional Repository. Retrieved from
http://go.warwick.ac.uk/wrap/56667
Chee, D. Y., Lee, H. C., Falkmer, M., Barnett, T., Falkmer, O., Siljehav, J., & Falkmer,
T. (2015). Viewpoints on driving of individuals with and without autism
spectrum disorder. Developmental Neurorehabilitation, 18(1), 26-36.
doi:10.3109/17518423.2014.964377
Cheely, C., Carpenter, L., Letourneau, E., Nicholas, J., J., C., & King, L. (2012). The
prevalence of youth with autism spectrum disorder in the criminal justice system.
Journal of Autism & Developmental Disorders, 42, 1856-1862.
doi:10.1007/s10803-011-1427-2
Chen, P. S., Chen, S. J., Yang, Y. K., Yeh, T. L., Chen, C. C., & Lo, H. Y. (2003).
Asperger's disorder: a case report of repeated stealing and the collecting
behaviours of an adolescent patient. Acta Psychiatrica Scandinavica, 107(1), 73-
76. doi:10.1034/j.1600-0447.2003.01354.x
Chesterman, P., & Rutter, S. (1993). Case report: Asperger's syndrome and sexual
offending. The Journal of Forensic Psychiatry, 4(3), 555-562.
doi:10.1080/09585189308408222
Chowdhury, M., & Benson, B. (2011). Deinstitutionalization and quality of life of
individuals with intellectual disability: A review of the international literature.
Journal of Policy and Practice in Intellectual Disabilities, 8(4), 256-265.
Chown, N. (2010). 'Do you have any difficulties that I may not be aware of?' A study of
autism awareness and understanding in the UK police service. International
222
Journal of Police Science and Mangagement, 12(2), 256-273.
doi:10.1350/ijps.2010.12.2.174
Clifford, S., Iyengar, V., Cabeza, R., & Sinnott-Armstrong, W. (2015). Moral
foundations vignettes: a standardized stimulus database of scenarios based on
moral foundations theory. Behaviour Research Methods, 1-21.
doi:10.3758/s13428-014-0551-2
Cooper, S. A., Smiley, E., Morrison, J., Williamson, A., & Allan, L. (2007). Mental ill-
health in adults with intellectual disabilities: prevalence and associated factors.
British Journal of Psychiatry, 190, 27-35. doi:10.1192/bjp.bp.106.022483
Corrigan, P. W., & Watson, A. C. (2002). Understanding the impact of stigma on people
with mental illness. World Psychiatry, 1(1), 16-20.
Cox, N. B., Reeve, R. E., Cox, S. M., & Cox, D. J. (2012). Brief report: Driving and
young adults with ASD: Parents' experiences. Journal of Autism &
Developmental Disorders, 42, 2257-2262. doi:10.1007/s10803-012-1470-7
Crimes Act 1900 (ACT). Available from:
http://www.austlii.edu.au/au/legis/act/consol_act/ca190082/
Crimes Act 1900 (NSW). Available from:
http://www.austlii.edu.au/au/legis/nsw/consol_act/ca190082/
Crimes Act 1958 (Vic), Available from:
http://www.austlii.edu.au/au/legis/vic/consol_act/ca195882/
Criminal Code 1899 (Qld). Available from:
http://www.austlii.edu.au/au/legis/qld/consol_act/cc189994
Criminal Code Act (NT). Available from:
http://www.austlii.edu.au/au/legis/nt/consol_act/cca115/
223
Criminal Code 1924 (Tas). Available from:
http://www.austlii.edu.au/au/legis/tas/consol_act/cca1924115/
Criminal Code 1913 (WA). Available from:
http://www.austlii.edu.au/au/legis/wa/consol_act/ccaca1913252/notes.html#appe
ndixb
Criminal Law Consolidation Act 1935 (SA). Available from
http://www.austlii.edu.au/au/legis/sa/consol_act/clca1935262/
Crime Statistics Agency. (2015). CSA Offence Classification. Available from:
http://www.crimestatistics.vic.gov.au/home/about+the+data/classifications/offenc
e+classification
Crocombe, J. (2006). The Prevalence of Autistic Spectrum Condition Amongst the
Female Population of One Special Hospital. Keele University.
Cunliffe, E. (2014). Judging, fast and slow: using decision-making theory to explore
judicial fact determination The international Journal of Evidence & Proof, 18,
139-180. doi:10.1350/ijep.2014.18.2.447
Cunningham, M. D. (2012). Evaluation for Capital Sentencing. In R. Roesch & P. A.
Zapf (Eds.), Forensic Assessments in Criminal and Civil Law: A Handbook for
Lawyers. New York, U.S.A: Oxford Univeristy Press.
Curran, P. J., West, S. G., & Finch, J. F. (1996). The robustness of test statistics to
nonnormality and specification error in confirmatory factor analysis.
Psychological Methods, 1(1), 16 - 29. doi:10.1037/1082-989X.1.1.16
Curry, B., & Miller, B. (2015). Judicial specialization and ideological decision making in
the US courts of appeals. Law & Social Inquiry, 40(1), 29-50.
doi:10.1111/lsi.12051
224
Cushman, F., Young, L., & Greene, J. (2010). Our multi-system moral
psychology: Towards a consensus view. In J. Doris, G. Harman, S. Nichols, J.
Prinz, W. Sinnott-Armstrong, & S. Stich (Eds.), The Oxford handbook of moral
psychology (pp. 47-71). Oxford, United Kingdom: Oxford University Press.
Cutler, J. (2014). Supporting witnesses and defendants with Autistic Spectrum Disorder.
Intermediaries for Justice.
Daly, B. P., Nicholls, E. G., Patrick, K. E., Brinckman, D. D., & Schultheis, M. T.
(2014). Driving behaviours in adults with Autism Spectrum Disorders. Journal of
Autism & Developmental Disorders, 44, 3119-3128. doi:10.1007/s10803-014-
2166-y
Damm, L. (2010). Emotions and moral agency. Philosophical Explorations, 13(3), 275-
292. doi:10.1080/13869795.2010.501898
Danziger, S., Levav, J., & Avnaim-Pesso, L. (2011). Extraneous factors in judicial
decisions. PNAS, 108(17), 6889-6892. doi:10.1073/pnas.1018033108
Davidson, F. (2015). Court Liason Services and Mental Health Court Programs in
Australia. Retrieved from https://offenderhealth.net.au/sites/default/files/Mental
Health and Diversion National Report.pdf
Day, A., White, J., Howells, K., Whitford, H., O'Brien, K., & Chartres, D. (2000). The
uses of court-ordered psychiatric and psychological reports in South Australian
magistrates' courts. Psychiatry, Psychology & Law, 7(2), 254-263.
doi:10.1080/13218710009524992
de la Cuesta, G. (2010). A selective review of offending behaviour in individuals with
autism spectrum disorders. Journal of Learning Disabilities & Offending
Behaviour, 1(2), 47-58.
225
de Vignemont, F., & Frith, U. (2008). Autism, Morality and Empathy. In W.
Sinnott-Armstrong (Ed.), Moral Psychology (Vol. 3: The Neuroscience of
Morality: Emotions, Brain Disorders and Development). Massachusetts:
Massachusetts Institute of Technology.
Debbaudt, D., & Rothman, D. (2001). Contact with individuals with autism: Effective
resolutions. FBI Law Enforcement Bulletin, 20-24.
Dein, K., & Woodbury-Smith, M. R. (2010). Asperger sundrome and criminal behaviour.
Advances in Psychiatric Treatment, 16, 37-43. doi:10.1192/apt.bp.107.005082
Denney, R. L. (2012). Criminal responsibility and other criminal forensic issues. In G. J.
Larrabee (Ed.), Forensic Neuropsychology: A Scientific Approach (pp. 473-500).
New York: 2nd Edition.
Dewey, M. (1991). Living with Asperger's syndrome. In U. Frith (Ed.), Autism and
Asperger Syndrome. Cambridge, UK: Cambridge University Press.
Dewey, M. (1992). Autistic eccentricity. In E. Schopler & G. B. Mesibov (Eds.), High-
Functioning Individuals With Autism. New York: Plenum Press.
Dickson, K., Emerson, E., & Hatton, C. (2005). Self-reported antisocial behaviour:
prevalence and risk factors amongst adolescents with and without intellectual
disability. Journal of Intellectual Disability Research, 49(11), 820-826.
doi:10.1111/j.1365-2788.2005.00727.x
Dobbin, S. A., Gatowski, S. I., Ginsberg, G. P., Merlino, M. L., Dahir, V., & Richardson,
J. T. (2001). Surveying difficult populations: Lessons learned from a national
survey of state trial court judges. The Justice System Journal, 22(3), 287-314.
226
Downs, A., & Smith, T. (2004). Emotional understanding, cooperation, and
social behaviour in hihg-functinoing children with autism. Journal of Autism &
Developmental Disorders, 34(6), 625-635. doi:10.1007/s10803-004-5284-0
Dowsett, J. A. (1991). Judicial Education: Where are the Emporor's New Clothes? Paper
presented at the Supreme and Federal Court Judge's Conference, Auckland, NZ.
Doyle, J. (2004, Tuesday 11 May 2004). Investing in the Judiciary. Paper presented at
the Sir Richard Blackburn Lecture Australian National University.
Dubow, E. F., Huesmann, L. R., Boxer, P., & Smith, C. (2014). Childhood predictors and
age 48 outcomes of self-reports and official records of offending. Criminal
Behaviour and Mental Health, 24, 291-304. doi:10.1002/cbm.1929
Dudeck, M., Drenkhahn, K., Spitzer, C., Barnow, S., Kopp, D., Kuwert, P., . . . Dünkel,
F. (2011). Traumatization and mental distress in long-term prisoners in Europe.
Punishment and Society, 13(4), 403-423. doi:10.1177/1462474511414782
Dworzynski, K., Ronald, A., Bolton, P., & Happe, F. (2012). How different are girls and
boys above and below the diagnostic threshold for autism spectrum disorders?
Journal of the American Academy of Child and Adolescent Psychiatry, 51(8).
doi:10.1016/j.jaac.2012.05.018.
Eaves, L. C., & Ho, H. H. (2008). Young adult outcome of autism spectrum disorders.
Journal of Autism & Developmental Disorders, 38, 379-747.
doi:10.1007/s10803-007-0441-x
Edgely, M. (2009). Common law sentencing of mentally impaired offenders in
Australian courts: A call for coherence and consistency. Psychiatry , Psychology
and Law, 16(2), 240-261. doi:10.1080/13218710802242037
227
Edney, R., & Bagaric, M. (2007). Australian Sentencing: Principles and
Practice. Port Melbourne, Australia: Cambridge University Press.
Ehlers, S., & Gillberg, C. (1993). The epidemiology of Asperger syndrome. A total
population study. Journal Of Child Psychology And Psychiatry, And Allied
Disciplines, 34(8), 1327-1350.
Ehlers, S., Gillberg, C., & Wing, L. (1999). A screening questionnaire for Asperger
syndrome and other high-functioning autism spectrum disorders in school age
children. Journal of Autism & Developmental Disorders, 29(2), 129-141.
Einfeld, S. L., & Tonge, B. J. (2002). Manual for the Developmental Behaviour
Checklist: Primary Carer Version (DBC-P) & Teacher Version (DBC-T) (2nd.
ed. ed.). Clayton, Melbourne: Monash University Centre for Developmental
Psychiatry and Psychology.
Elsabbagh, M., Divan, G., Koh, Y. J., Kim, Y. S., Kauchali, S., Marcín, C., . . .
Fombonne, E. (2012). Global prevalence of autism and other pervasive
developmental disorders. Autism Research, 5(3), 160-179. doi:10.1002/aur.239
Enayati, J., Grann, M., Lubbe, S., & Fazel, S. (2008). Psychiatric morbidity in arsonists
referred for forensic psychiatric assessment in Sweden. The Journal of Forensic
Psychiatry and Psychology, 19(2), 139-147. doi:10.1080/14789940701789500
English, K., & Heil, P. (2005). Prison rape: What we know today. Corrections
Compendium, 30(5), 1-5; 42-44.
Erickson, S. K., & Felthous, A. R. (2009). Introduction to this Issue: The neuroscience
and psychology of moral decision making and the law. Behavioral Sciences & the
Law, 27(2), 119-121. doi:10.1002/bsl.858
228
Esan, F., Chester, V., Gunaratna, I. J., Hoare, S., & Alexander, R. T. (2015).
The clinical forensic and treatment outcome factors of patients with autism
spectrum disorder treated in a forensic intellectual disability service. Journal of
Applied Research in Intellectual Disabilities, 28, 193-200. doi:10.1111/jar.12121
Evans, R. (2011). The life we choose: shaping autism services in Wales: The National
Autistic Society Cymru.
Everall, I. P., & Lecouteur, A. (1990). Firesetting in an adolescent boy with Asperger's
syndrome. British Journal of Psychiatry, 157, 284-287.
Falkmer, M., Barnett, T., Horlin, C., Falkmer, O., Siljehav, J., Fristedt, S., . . . Falkmer,
T. (2015). Viewpoints of adults with and without Autism Spectrum Disorders on
public transport. Transportation Research Part A, 80, 163-183.
doi:10.1016/j.tra.2015.07.019
Fan, Y., Chen, C., Chen, S., Decety, J., & Cheng, Y. (2014). Empathic arousal and social
understnaing in individuals with autism: evidence from fMRI and ERP
measurements. Social Cognitive and Affective Neuroscience, 9, 1203-1213.
doi:10.1093/scan/nst101
Farley, M. A., McMahon, W. M., Fombonne, E., Jenson, W. R., Miller, J., Gardner, M., .
. . Coon, H. (2009). Twenty-year outcome for individuals with autism and
average or near-average cognitive abilities. Autism Research, 2, 109-118.
doi:10.1002/aur.69
Farrington, D. P. (2001). What has been learned from self-reports about criminal careers
and the causes of offending? Retrieved from Cambridge:
229
Farrington, D. P. (2003). Developmental and life-course criminology: Key
theoretical and empirical issues - The 2002 Sutherland Aware address.
Criminology, 41(2), 221 - 256. doi:10.1111/j.1745-9125.2003.tb00987.x
Fazio, R. L., Pietz, C. A., Burton-Madden, M., Henry, L., Maxey, M., & Ivey, M. (2010,
2010). Prevalence of Autism Spectrum Disorders in Incarcerated Males: Legal
Implications. Paper presented at the APA 118th Annual Convention, San Diego,
California.
Fazio, R. L., Pietz, C. A., & Denney, R. L. (2012). An estimate of the prevalence of
autism-spectrum disorders in an incarcerated population. Open Access Journal of
Forensic Psychology, 4, 69-80.
Fehr, E., Bernhard, H., & Rockenbach, B. (2008). Egalitarianism in young children.
Nature, 454, 1079 - 1084. doi:10.1038/nature07155
Ferguson, M., & Ogloff, J. R. P. (2011). Criminal responsibility evaluations: Role of
psychologists in assessment. Psychiatry, Psychology & Law, 18(1), 79-94.
doi:10.1080/13218719.2010.482952
Field, D. (2012). Criminal sentencing : the geographical lottery. Precedent(112).
Fitzgerald, M. (2003). Callous unemotional traits and Asperger's syndrome? Journal of
the American Academy of Child and Adolescent Psychiatry, 42(9), 1011.
Fleischmann, A., & Fleischmann, C. (2012). Carly's Voice. New York: Touchstone.
Fombonne, E. (2012). Autism in adult life. The Canadian Journal of Psychiatry, 57(5),
273-274.
Frank, J. (1930). Law and the Modern Mind. New Brunswick, U.S.A.: Transaction
Publishers.
230
Frank, J. (1931). Are judges human? Part one: The effect on legal thinking of
the assumption that judges behave like human beings. University of Pennsylvania
Law Review, 80, 17-53.
Fraser, R., Angus, B., Cotton, S., Gentle, E., Allott, K., & Thompson, A. (2011).
Prevalence of autism spectrum conditions in a youth mental health service.
Australian and New Zealand Journal of Psychiatry, 45(5), 426-426.
doi:10.3109/00048674.2011.563731
Frazier, T. W., Youngstrom, E. A., Speer, L., Embacher, R., Hardan, A., & Eng, C.
(2012). Validation of proposed DSM-5 criteria for autism spectrum disorder.
Journal of the American Academy of Child and Adolescent Psychiatry, 51(1), 28-
40.
Freckelton, I. (2007). Sentencing offenders with impaired mental functioning R v
Verdins, Buckley and Vo [2007] VSCA 102; (2007) 169 A Crim R 581 Maxwell
P, Vincent and Buchanan JJ. Psychiatry , Psychology and Law, 14(2), 359-363.
Freckelton, I. (2011). Autism spectrum disorders and the criminal law. In M.
Mohammadi (Ed.), A Comprehensive Book on Autism Spectrum Disorders:
InTech. Retrieved from http://www.intechopen.com/books/a-comprehensive-
book-on-autism-spectrum-disorders/autism-spectrum-disorders-and-the-criminal-
law.
Freckelton, I. (2012a). Expert evidence by mental health professionals: The
communication challenge posed by evidence about autism spectrum disorder,
brain injuries and Huntington's disease. International Journal of Law and
Psychiatry, 35, 372-379. doi:10.1016/j.ijlp.2012.09.008
231
Freckelton, I. (2012b). Expert evidence by mental health professionals: The
communication challenge posed by evidence about Autism Spectrum Disorder,
brain injuries, and Huntington's Disease. International Journal of Law and
Psychiatry, 35, 372-379. doi:10.1016/j.ijlp.2012.09.008
Freckelton, I. (2013a). Autism spectrum disorder: Forensic issues and challenges for
mental health professionals and courts. Journal of Applied Research in
Intellectual Disabilities, 26, 420-434. doi:10.1111/jar.12036
Freckelton, I. (2013b). Forensic issues in autism spectrum disorder: Learning from court
decisions. In M. Fitzgerald (Ed.), Recent Advances in Autism Spectrum Disorders
(Vol. II).
Freckelton, I., & List, D. (2009). Asperger's disorder, criminal responsibility and
criminal culpability. Psychiatry, Psychology & Law, 16(1), 16-40.
doi:10.1080/13218710902887483
Freckelton, I., & Selby, H. (2013). Expert Evidence: Law, Practice, Procedure and
Advocacy (5th ed.). Pyrmont, N.S.W.: Lawbook Co./Thomson Reuters.
Freeman, B. J., Cronin, P., & Candelam, P. (2002). Asperger syndrome or autistic
disorder? The diagnostic dilemma. Focus on Autism and Other Developmental
Disabilities, 17, 145-151.
Freiberg, A. (2010). Australia: exercising discretion in sentencing policy and practice.
Federal Sentencing Reporter, 22(4), 204-212. doi: 10.1525/fsr.2010.22.4.204.
Freiberg, A. (2014). Fox and Freiberg's Sentencing: State and Federal Law in Victoria
(3rd ed. ed.). Australia: Lawbook Co.
Frith, U. (1991). Autism and Asperger Syndrome. Cambridge, UK: Cambridge University
Press.
232
Gatowski, S. I., Dobbin, S. A., Richardson, J. T., Ginsburg, G. P., Merlino,
M. L., & Dahir, V. (2001). Asking the gatekeepers: A national survey of judges
on judging expert evidence in a post-daubert world. Law and Human Behavior,
25(5), 433-458. doi:10.1023/A:1012899030937
Gbadebo-Goyea, E. A., Akpudo, H., Jackson, C. D., Wassef, T., Barker, N. C.,
Cunningham-Burley, R., Bailey, R. K. (2012). Collaboration: The paradigm of
practice approach between the forensic psychiatrist and the forensic psychologist.
Frontiers in Psychiatry, 3, 1-6. doi:10.3389/fpsyt.2012.00089
Gee, D. G., & Ogloff, J. R. P. (2014). Sentencing offenders with impaired mental
functioning: R v Verdins, Buckley and Vo [2007] at the clinical coalface.
Psychiatry, Psychology & Law, 21(1), 46-66.
doi:10.1080/13218719.2013.774682
Geer, J. H., Estupinan, L. A., & Maguno-Mire, G. M. (2000). Empathy, social skills, and
other relevant cognitive processes in rapists and child molesters. Agression and
Violent Behaviour, 5(1), 99-126. doi:10.1016/S1359-1789(98)00011-1
Ghanizadhe, A. (2008). A preliminary study on screening prevalence of pervasive
developmental disorder in schoolchildren in Iran. Journal of Autism &
Developmental Disorders, 38, 759-763. doi:10.1007/s10803-007-0445-6
Ghaziuddin, M., & Mountain-Kimchi, K. (2004). Defining the intellectual profile of
Asperger syndrome: Comparison with high-functioning autism. Journal of Autism
and Developmental Disorders, 34(3), 279-284.
Ghaziuddin, M., Tsai, L., & Ghaziuddin, N. (1991). Brief report: Violence in Asperger
syndrome, a critique. Journal of Autism & Developmental Disorders, 21(3), 349-
354.
233
Gibbs, J. C. (1979). Kohlberg's moral stage theory. A Piagetian revision.
Human Development, 22, 89-112.
Gibbs, V., Aldridge, F., Chandler, F., Witzlsperger, E., & Smith, K. (2012). Brief report:
An exploratory study comparing diagnostic outcomes for autism spectrum
disorders under DSM-IV-TR with the proposed DSM-5 revision. Journal of
Autism and Developmental Disorders, 42, 1750-1756. doi:10.1007/s10803-012-
1560-6
Gillberg, C. (1991). Clinical and neurobiological aspects of Asperger syndrome in six
family studies. In U. Frith (Ed.), Autism and Asperger Syndrome. Cambridge,
UK: Cambrdge University Press.
Gillberg, C., & Gillberg, C. (1989). Asperger syndrome - some epidemiological
considerations: A research note. Journal of Child Psychology & Psychiatry,
30(4), 631-638.
Gillberg, C., Gillberg, C., Råstam, M., & Wentz, E. (2001). The Asperger syndrome (and
high-functioning autism) diagnostic interview (ASDI): a preliminary study of a
new structured clinical interview. Autism, 5(1), 57-66. doi:
10.1177/1362361301005001006
Gillespie-Lynch, K., Sepeta, L., Wang, Y., Marshall, S. N., Gomez, L., Sigman, M., &
Hutman, T. (2012). Early childhood predictors of the social competence of adults
with autism. Journal of Autism & Developmental Disorders, 42, 161-174.
doi:10.1007/s10803-011-1222-0
Gilman, A. B., Hill, K. G., Kim, B. K. E., Nevell, A., Hawkins, J. D., & Farrington, D. P.
(2014). Understanding the relationship bewteen self-reported offending and
234
official criminal charges across early adulthood. Criminal Behaviour
and Mental Health, 24, 229-240. doi:10.1002/cbm.1934
Glanfield, L. (1999). Boundaries and challenges within criminal justice. Paper presented
at the National Outlook Symposium on Crime in Australia, Mapping the
Boundaries of Australia's Criminal Justice System, Canberra.
Gleichgerrcht, E., Torralva, T., Rattazzi, A., Marenco, V., Roca, M., & Manes, F. (2013).
Selective impairment of cognitive empathy for moral judgement in adults with
high functioning autism. Social Cognitive and Affective Neuroscience, 8, 780-
788. doi:10.1093/scan/nss067
Glenn, A. L., Iyer, R., Graham, J., Koleva, S., & Haidt, J. (2009). Are all types of
morality compromised in psychopathy? Journal of Personality Disorders, 23(4).
Golan, O., & Baron-Cohen, S. (2006). Systemising empathy: Teaching adults with
Asperger syndrome or high-functioning autism to recognise complex emotions
using interactive multimedia. Development and Psychopathology, 18, 591-617.
doi:10.10170S0954579406060305
Goldman, S., Wang, C., Salgado, M., Greene, P., Kim, M., & Rapin, I. (2009). Motor
sterotypies in children with autism and other developmental disorders.
Developmental Medicine and Child Neurology, 51, 30-38. doi:10.1111/j.1469-
8749.2008.03178.x
Goodman-Delahunty, J., Forsterlee, L., & Forsterlee, R. (2005). Dealing with the guilty
offender. In N. Brewer & K. D. Williams (Eds.), Psychology and Law: An
Empirical Perspective. New York: The Guilford Press.
Gook, L. (2014). Offenders with Autism Spectrum Disorder: Screening, Characteristics
and Staff Awareness. DPsych(Forensic), Deakin University.
235
Gougeon, N. A. (2010). Sexuality and autism: A critical review of selected
literature using a social-relational model of disability. American Journal of
Sexuality Education, 5, 328-361. doi:10.1080/15546128.2010.527237
Gould, J., & Ashton-Smith, J. (2011). Missed diagnosis or misdiagnosis? Girls and
women on the autism spectrum. Good Autism Practice, 12(1), 34-41.
Graham, J., Haidt, J., Koleva, S., Motyl, M., Iyer, R., Wokci, S. P., & Ditto, P. H. (2013).
Moral Foundations Theory: The pragmatic validity of moral pluralism. Advances
in Experimental Social Psychology, 47, 55-130. doi:10.1016/B978-0-12-407236-
7.00002-4
Graham, J., Haidt, J., & Nosek, B. A. (2008). The Moral Foundations Questionnaire (full
version, July 2008).
Graham, J., Haidt, J., & Nosek, B. A. (2009). Liberals and conservatives rely on different
sets of moral foundations. Journal of Personality and Social Psychology, 96(5),
1029-1046. doi:10.1037/a0015141
Graham, J., Nosek, B. A., Haidt, J., Iyer, R., Koleva, S., & Ditto, P. H. (2011). Mapping
the Moral Domain. Journal of Personality and Social Psychology, 101(2), 366-
385.
Grandin, T. (1992). An inside view of autism. In E. Schopler & G. B. Mesibov (Eds.),
High-Functioning Individuals With Autism. New York: Plenum Press.
Grandin, T. (2006). Thinking In Pictures: My Life With Autism (2nd edition). New York:
Vintage Books.
Grandin, T. (2011). The Way I See It: A Personal Look at Autism and Asperger's (2nd
Edition ed.). Arlington, Texas: Future Horizons, Inc.
236
Grandin, T., & Panek, R. (2013). The Autistic Brain. USA: Houghton Mifflin
Harcourt Publishing Company.
Grant, C. M., Boucher, J., Riggs, K. J., & Grayson, A. (2005). Moral understanding in
children with autism. Autism, 9, 317-331. doi:10.1177/1362361305055418
Gray, K., Keating, C., Taffe, J., Brereton, A. V., Einfeld, S. L., Reardon, T. C., & Tonge,
B. J. (2014). Adult outcomes in autism: Community inclusion and living skills.
Journal of Autism & Developmental Disorders, 44, 3006-3015.
doi:10.1007/s10803-014-2159-x
Gray, K., Keating, C., Taffe, J., Brereton, A. V., Einfeld, S. L., & Tonge, B. J. (2012).
Trajectory of behaviour and emotional problems in autism. American Journal on
Intellectual and Developmental Disabilities, 117(2), 121-133. doi:10.1352/1944-
7588-117-2.121
Green, J., Gilchrist, A., Burton, D., & Cox, A. (2000). Social and psychiatric functioning
in adolescents with Asperger syndrome compared with conduct disorder. Journal
of Autism & Developmental Disorders, 30(4), 279.
Griffin-Shelley, E. (2010). An Asperger's adoloscent sex addict, sex offender: A case
study. Sexual Addiction and Compulsivity, 17, 46-64.
doi:10.1080/10720161003646450
Griffore, R. J., & Samuels, D. D. (1978). Moral judgement of residents of a maximum
security correctional facility. The Journal of Psychology, 100(1), 3-7.
doi:10.1080/00223980.1978.9923462
Gunasekaran, S. (2012). Assessment and management of risk in autism. Advances in
Mental Health and Intellectual Disabilities, 6(6), 314-320.
doi:10.1108/20441281211285964
237
Gunasekaran, S., & Chaplin, E. (2012). Autism spectrum disorders and
offending. Advances in Mental Health and Intellectual Disabilities, 6(6), 308-
313. doi:10.1108/20441281211285955
Guthrie, C., Rachlinski, J. J., & Wistrich, A. J. (2001). Inside the judicial mind. Cornell
Law Review, 86(4), 777-830.
Haidt, J. (2001). The emotional dog and its rational tail: A social intuitionist approach to
moral judgment. Psychological Review, 108(4), 814-834. doi:10.1037/0033-
295x.108.4.814
Haidt, J. (2007). The new synthesis in moral psychology. Science, 316, 998-1002.
doi:10.1126/science.1137651
Haidt, J. (2008). Morality. Perpectives on Psychological Science, 3(1), 65-72.
Haidt, J. (2012). The Righteous Mind. Why Good People Are Divided by Politics and
Religion. USA: Pantheon Books.
Haidt, J., & Graham, J. (2007). When morality opposes justice: Conservatives have
moral intuitions that librals may not recognise. Social Justice Research.
Haidt, J., & Graham, J. (2009). Planet of the Durkheimians, where community, authority,
and sacredness are foundations of morality. In J. Jost, A. C. Kay, & H.
Thorisdottir (Eds.), Social and Psychological Bases of Ideology and System
Justification (pp. 371-401). New York, NY: Oxford.
Haidt, J., Graham, J., & Joseph, C. (2009). Above and below left-right: Ideological
narrative and moral foundations. Psychological Inquiry, 20, 110-119.
doi:10.1080/10478400903028573
Haidt, J., & Joseph, C. (2004). Intuitive ethics: how innately prepared intuitions generate
culturally variable virtues. Daedalus, Fall, 55-66.
238
Haidt, J., & Joseph, C. (2008). The Moral Mind. In P. Carruthers, S.
Laurence, & S. Stich (Eds.), The Innate Mind (Vol. 3: Foundations and the
Future): Oxford Scholarship Online.
doi:10.1093/acprof:oso/9780195332834.001.0001
Haidt, J., & Kesebir, S. (2010). Morality. In S. Friske, D. Gilbert, & G. Lindzey (Eds.),
Handbook of Social Psychology (pp. 797-832). Hoebeken, NJ: Wiley.
Hair, J. F. J., Anderson, R. E., Tatham, R. L., & Black, W. C. (1995). Multivariate Data
Analysis New York: Macmillan.
Hall, A., Godwin, M., Wright, H., & Abramson, R. (2007). Criminal justice issues and
autistic disorder. In R. Gabriels & D. Hill (Eds.), Growing Up with Autism:
Working with School-age Children and Adolescents. New York: The Guildford
Press.
Hall, I., & Bernal, J. (1995). Correspondence: Asperger's syndrome and violence. British
Journal of Psychiatry, 166, 262.
Happe, F. (1991). The autobiographical writings of three Asperger syndrome adults:
problems of interpretation and implications for theory. In U. Frith (Ed.), Autism
and Asperger Syndrome. Cambridge, UK: Cambridge University Press.
Haracopos, D., & Pedersen, L. (1992). Sexuality and autism: Danish report. Retrieved
from http://www.autismuk.com/?page_id=1293
Hare, D. J., Gould, J., Mills, R., & Wing, L. (1999). A preliminary study of individuals
with autistic spectrum disorders in three special hospitals in England. London:
National Autistic Society.
Hare, R. D. (2003). Manual for the Hare Psychopathy Checklist - Revised. Toronto, ON.:
Multi-Health Systems Inc.
239
Hare, R. D., Hart, S. D., & Harpur, T. J. (1991). Psychopathy and the DSM-
IV criteria for antisocial personality disorder. Journal of Abnormal Psychology,
100(3), 391-398.
Harms, M. B., Martin, A., & Wallace, G. L. (2010). Facial emotion recognition in autism
spectrum disorders: A review of behavioural and neuroimaging studies.
Neuropsychological Review, 20, 290-322. doi: 10.1007/s11065-010-9138-6
Hartman, C. A., Luteijin, E., Moorlag, A., De Bildt, A., & Minderaa, R. (2007).
Vragenlijst voor Inventarisatie van Sociaal gedrag van Kinderen (VISK):
Herziene handleiding. Amsterdam, the Netherlands: Harcourt Test Publishers.
Haskins, B. G., & Silva, J. A. (2006). Asperger's disorder and criminal behaviour:
Forensic-psychiatric considerations. The Journal of the American Academy of
Psychiatry and the Law, 34, 374-384.
Hatwell, S. (2004). Triple stigma: Persons with mental illness and substance abuse
problems in the criminal justice system. Criminal Justice Policy Review, 15(1),
84-99. doi:10.1177/0887403403255064
Hawes, V. (2003). Developmental disorders in prisoners volunteering for DSPD
assessment. Paper presented at the Proceedings of the 2nd International
Conference on the Care and Treatment of Offenders with a Learning Disability,
Preston, U.K.
Hayes, S. (2006). People with Intellectual Disabilities in the Criminal Justice System-
when is Disability a Crime? Paper presented at the Lock 'them' up? Disability and
mental illness aren't crimes, Brisbane, Australia.
Hayes, S. (2007). Missing out: Offenders with learning disabilities and the criminal
justice system. British Journal of Learning Disabilities, 35(146-153).
240
Health and Social Care Overview and Scrutiny Committee. (2012). Adults
with autism and the criminal justice system. Retrieved from Birmingham, U. K.:
Hénault, I. (2005). Asperger's Syndrome and Sexuality: From Adolescence Through
Adulthood. London, UK: Jessica Kingsley Publishers.
Henninger, N. A., & Taylor, J. L. (2013). Outcomes in adults with autism spectrum
disorders: a historical perspective. Autism, 17(1), 103-116.
doi:10.1177/1362361312441266
Higgs, T., & Carter, A. J. (2015). Autism spectrum disorder and sexual offending:
Responsivity in forensic interventions. Agression and Violent Behaviour.
doi:10.1016/j.avb.2015.04.003
Hill, E., Berthoz, S., & Frith, U. (2004). Brief Report: Cognitive processing of own
emotions in individuals with Autistic Spectrum Disorder and in their relatives.
Journal of Autism & Developmental Disorders, 34(2), 229–235. .
doi:10.1023/B:JADD.0000022613.41399.14
Hindelang, M. J., Hirschi, T., & Weis, J. G. (1981). Measuring Delinquency. Berverly
Hills, U.S.A: Sage Publications.
Hippler, K., Viding, E., Klicpera, C., & Happé, F. (2010). Brief report: No increase in
criminal convictions in Hans Asperger’s original cohort. Journal of Autism &
Developmental Disorders, 40(6), 774-780. doi:10.1007/s10803-009-0917-y
Hoekstra, R. A., Bartels, D. M., Verweij, C. J. H., & Boomsma, D. I. (2007). Heritability
of autistic traits in the general population. Arch of Pediatr Adolesc Med, 161,
372-377.
Hofvander, B., Delorme, R., Chaste, P., Nyden, A., Wentz, E., Ståhlberg, O., Leboyer,
M. (2009). Psychiatric and psychosocial problems in adults with normal-
241
intelligence autism spectrum disorders. BMC Psychitary, 9.
doi:10.1186/1471-244X-9-35
Holland, T., Clare, I. C. H., & Mukhopadhyay, T. (2002). Prevalence of 'criminal
offending' by men and women with intellectual disability and the characteristics
of 'offenders': implications for research and service development. . Journal of
Intellectual Disability Research, 46(1), 6-20. doi:10.1046/j.1365-
2788.2002.00001.x
Holwerda, A., van der Klink, J., Groothoff, J., & Brouwer, S. (2012). Predictors for work
participation in individuals with an autism spectrum disorder: A systematic
review. Journal of Occupational Rehabilitation, 22, 333-352.
doi:10.1007/s10926-011-9347-8
Howard, M., & O'Brien, J. (2009). Criminal injustice for vulnerable people. Paper
presented at the Social Inclusion: The Future of Ageing, Disability and
Substituted Decision-Making, Brisbane, Australia.
Howlin, P. (1997). Prognosis in autism: Do specialist treatments affect long-term
outcome? European Child & Adolescent Psychiatry, 6(2), 55-72.
doi:10.1007/bf00566668
Howlin, P. (2000). Outcome in adult life for more able individuals with autism or
asperger syndrome. Autism, 4, 63-83. doi:10.1177/1362361300004001005
Howlin, P. (2004). Autism and Asperger Syndrome (second edition ed.). London, UK:
Routledge.
Howlin, P., Arciuli, J., Begeer, S., Brock, J., Clarke, K., Costley, D., . . . Einfeld, S. L.
(2015). Research on adults with autism spectrum disorder: Rountable report.
242
Journal of Intellectual and Developmental Disability, 40(4), 388-393.
doi:10.3109/13668250.2015.1064343
Howlin, P., Goode, S., Hutton, J., & Rutter, M. (2004). Adult outcome for children with
autism. Journal of Child Psychology & Psychiatry, 45(2), 212-229.
Howlin, P., Mawhood, L., & Rutter, M. (2000). Autism and developmental receptive
langague disorder- a follow-up comparison in early adult life. II: Social,
behavioural, and psychitric outcomes. Journal of Child Psychology & Psychiatry,
41(5), 561-578.
Howlin, P., & Moss, P. (2012). Adults with autism spectrum disorders. The Canadian
Journal of Psychiatry, 57(5), 275-283.
Hudson, M., & Nijboer, T. C. W. (2012). Implicit social learning in relation to autistic-
like traits. Journal of Autism & Developmental Disorders, 42(12), 2534-2545.
doi:10.1007/s10803-012-1510-3
Huizinga, D., & Elliott, D. S. (1986). Reassessing the reliability and validity of self-
report delinquency measures. Journal of Quantitatvie Criminology, 2(4), 293-
327.
Huizinga, D., Esbenson, F., & Weihar, A. (1991). Are there multiple paths to
delinquency? The Journal of Criminal Law and Criminology, 82, 83-188.
Humphreys, K., Minshew, N., Leonard, G. L., & Behrmann, M. (2007). A fine-grained
analysis of facial expression processing in high-functioning adults with autism.
Neuropsychologia, 45(4), 685-695. doi: 10.1016/j.neuropsychologia.2006.08.003
Hyman, S. L. (2013). New DSM-5 includes changes to autism criteria. AAP News.
doi:10.1542/aapnews.20130604-1
243
Icasiano, F., Hewson, P., Machet, P., Cooper, C., & Marshall, A. (2004).
Childhood autism spectrum disorder in the Barwon region: A community based
study. Journal of Paediatrics and Child Health, 40(12), 696-701.
doi:10.1111/j.1440-1754.2004.00513.x
Im, D. S. (2016). Template to perpetrate: An update on violence in autism spectrum
disorder. Harvard Review of Psychiatry, 24(1), 14-35.
doi:10.1097/HRP.0000000000000087
Ingram, R., Lyons, B., Lee, J., & Bowron, R. (2012). Autism and the criminal justice
system: Incompatible differences. International Journal of Social Health
Information Management, 5(12), 28.
Isaksen, J., Diseth, T., Schjølberg, S., & Skeldal, O. H. (2013). Autism spectrum
disorders- Are they really epidemic? European Journal of Paediatric Neurology,
17, 327-333. doi:10.1016/j.ejpn.2013.03.003
Jaarsma, P. (2013). Cultivation of empathy in individuals with high-functioning autism
spectrum disorder. Ethic and Education, 8(3), 290-300.
doi:10.1080/17449642.2013.878514
Jobe, L. E., & Williams White, S. (2007). Loneliness, social relationships, and a broader
autism phenotype in college students. Personality and individual differences, 42,
1479-1489. doi:10.1016/j.paid.2006.10.021
Jolliffe, D., & Farrington, D. P. (2004). Empathy and offending: A systematic review and
meta-anlysis. Aggression and Violent Behavior, 9, 441-476.
doi:10.1016/j.avb.2003.03.001
244
Jolliffe, D., & Farrington, D. P. (2007). Examining the relationship between
low empathy and self-reported offending. Legal & Criminological Psychology,
12(2), 265-286. doi:10.1348/135532506x147413
Jolliffe, D., Farrington, D. P., Hawkins, J. D., Catalao, R., F., Hill, K., G. , & Kosterman,
R. (2003). Predictive, concurrent, prospective and reterospective validaity of self-
reported delinquency. Criminal Behaviour and Mental Health, 13(3), 179-197.
doi:10.1002/cbm.541
Junger-Tas, J., & Marshall, I. H. (1999). The self-report methodology in crime research.
Crime and Justice, 25, 291-367.
Kadesjö, B., Gillberg, C., & Hagberg, B. (1999). Brief report: Autism and Asperger
syndrome in seven-year-old children: A total population study. Journal of Autism
& Developmental Disorders, 29(4), 327-331. doi:10.1023/A:1022115520317
Kagan, J. (2008). Morality and Its Development. In W. Sinnott-Armstrong (Ed.), Moral
Psychology (Vol. 3: The Neuroscience of Morality: Emotion, Brain Disorders,
and Development). Massachusetts: Massachusetts Institute of Technology Press.
Kanner, L. (1943). Autistic disturbances of affective contact. Nervous Child, 2, 217-250.
Kanner, L. (1973). Childhood Psychosis: Initial Studies and New Insights. Washington,
D. C.: V. H. Winston & Sons.
Karlsson, L., Råstam, M., & Wentz, E. (2013). The SWedish Eating Assessment for
autism spectrum disorders (SWEAA) - Validation of a self-report questionnaire
targeting eating disturbances within the autism spectrum. Research in
Developmental Disabilities, 34(7), 2224-2233. doi:10.1016/j.ridd.2013.03.035.
Katz, N., & Zemishlany, Z. (2006). Criminal responsibility in Asperger's syndrome. The
Israel Journal of Psychiatry and Related Sciences, 43(3), 166-173.
245
Kelbrick, M., & Radley, J. (2013). Forensic rehabilitation in Asperger
syndrome: a case report. Journal of Intellectual Disabilities and Offending
Behaviour, 4(1/2), 60-64.
Kelly, D., Stich, S., Haley, K., Eng, S., & Fessler, D. (2007). Harm, affect, and the
moral/conventional distinction. Mind and Language, 22(2), 117-131.
Kennedy, D. P., & Adolphs, R. (2014). Violations of personal space by individuals with
Autism Spectrum Disorder. PLoS ONE, 9(8), e103369. doi:10.1371/journal.
pone.0103369
Ketelaars, C. (2016). Emotion recognition and alexitymia in high functioning females
with autism spectrum disorder. Research in Autism Spectrum Disorders, 21, 51-
60. doi:10.1016/j.rasd.2015.09.006
Ketelaars, C., Horwitz, E., Sytema, S., Bos, J., Wiersma, D., Minderaa, R., & Hartman,
C. A. (2007). Brief report: Adults with mild autism spectrum disorders (ASD):
Scores on the Autism Spectrum Quotient (AQ) and Comorbid Psychopathology.
Journal of Autism and Developmental Disorders, 38, 176-180.
doi:10.1007/s10803-007-0358-4
Kim, Y. S., Fombonne, E., Koh, Y., Kim, S., Cheon, K., & Leventhal, B. L. (2014). A
comparison of DSM-IV pervasive developmental disorder and DSM-5 autism
spectrum disorder prevalence in an epidemiologic sample. Journal of the
American Academy of Child and Adolescent Psychiatry, 53(5), 500-508.
Kim, Y. S., Leventhal, B. L., Koh, Y., Fombonne, E., Laska, E., Lim, E., Grinker, R.
(2011). Prevalence of autism spectrum disorders in a total population sample.
American Journal of Psychiatry, 168(9), 904-912.
246
King, C., & Murphy, G. H. (2014). A systematic review of people with
Autism Spectrum Disorder and the criminal justice system. Journal of Autism &
Developmental Disorders, 44, 2717-2733. doi:10.1007/s10803-014-2046-5
King, M., & Bearman, P. (2009). Diagnostic change and the increased prevalence of
autism. International Journal of Epidemiology, 38, 1224-1234.
doi:10.1093/ije/dyp261
Knight, G. P., Little, M., Losoya, S. H., & Mulvey, E. P. (2004). The self-report of
offending among serious juvenile offenders: Cross-gender, cross-ethnic/race
measurement equivalence. Youth Violence and Juvenile Justice, 2(3), 273-295.
doi:10.1177/1541204004265878
Kobayashi, R., Murata, T., & Yoshinaga, K. (1992). A follow up study of 201 children
with autism in Kyushu and Yamaguchi areas, Japan. Journal of Autism &
Developmental Disorders, 22(3), 395-411. doi:10.1007/BF01048242
Koenker, R. (1981). A note on studentizing a test for heteroscedasticity. Journal of
Econometrics, 17(1), 107-112. doi:10.1016/0304-4076(81)90062-2
Kohlberg, L. (1969). Stages and sequences: The cognitive development approach to
socialization. In D. A. Goslin (Ed.), Handbook of Socialization Theory of
Research (pp. 347-480). Chicago, IL: Rand McNally.
Kohn, Y., Fahum, T., Ratzoni, G., & Apter, A. (1998). Agression and sexual offense in
Asperger's syndrome. Israel Journal of Psychiatry and Related Sciences, 35(4),
293-299.
Korkman, J., Svanbäck, S., Finnilä, K., & Santtila, P. (2014). Judges'views of child
sexual abuse: Evaluating beliefs against research findings in a Finnish sample.
Scandanavian Journal of Psychology, 55, 497-504. doi:10.1111/sjop.12147
247
Koster-Hale, J., Saxe, R., Dungan, J., & Young, L. L. (2013). Decoding moral
judgments from neural representations of intentions. Proc Natl Acad Sci USA,
110(14), 5648 - 5653. doi:10.1073/pnas.1207992110
Krasnostein, S., & Freiberg, A. (2013). Pursuing consistency in an individualistic
sentencing framework: If you know where you're going, how do you know when
you've got there? Law and Contemporary Problems, 76(1), 265-288.
Kretschmer, A., Lampmann, S., & Altgassen, M. (2014). Relations between moral
reasoning, theory of mind and executive functions in children with autism
spectrum disorders. International Journal of Developmental Disabilities, 60(3),
174-183. doi:10.1179/2047387714Y.0000000045
Kristiansson, M., & Sorman, K. (2008). Autism spectrum disorders - legal and forensic
psychiatric aspects and reflections. Clinical Neuropsychiatry, 5(1), 55-61.
Kuangparichat, M. (2010). Legal rights of young adults with autim: Transitioning into
mainstream adulthood. Widener Law Review, 16(1), 175-196.
Kumagami, T.., & Matsuura, N. (2009). Prevalence of pervasive developmental disorder
in juvenile court cases in Japan. Journal of Forensic Psychiatry & Psychology,
20(6), 974-987. doi:10.1080/14789940903174170
La Malfa, G., Lassi, S., Bertelli, M., Salvini, R., & Placidi, G. F. (2004). Autism and
intellectual disability: a study of prevalence on a smaple of the Italian population.
Journal of Intellectual Disability Research, 48(3), 262-267. doi:10.1111/j.1365-
2788.2003.00567.x
Lai, M., Lombardo, M. V., Pasco, G., Ruigrok, A. N. V., Wheelwright, S. J., Sadek, S.
A., Baron-Cohen, S. (2011). A behavioural comparison of male and female adults
248
with high functioning autism spectrum conditions. PLoS ONE, 6(6),
e20835. doi:10.1371/journal.pone.0020835
Lamb, H. R., Weinberger, L. E., & Gross, B. H. (2004). Mentally ill persons in the
criminal justice system: Some perspectives. Psychiatric Quarterly, 75(2), 107 -
126.
Langdon, P. E., Clare, I. C. H., & Murphy, G. H. (2011). Moral reasoning theory and
illegal behaviour by adults with intellectual disabilities. Psychology, Crime &
Law, 17(2), 101-115. doi:10.1080/10683160903392384
Langdon, P. E., Murphy, G. H., Clare, I. C. H., Steverson, T., & Palmer, E. J. (2011).
Relationships among moral reasoning, empathy, and distorted cognitions in men
with intellectual disabilities and a history of criminal offending. American
Journal of Intellectual and Developmental Disabilities, 116(6), 438 - 456.
doi:10.1352/1944-7558-116.6.438
Langstrom, N., Grann, M., Ruchkin, V., Sjostedt, G., & Fazel, S. (2009). Risk factors for
violent offending in autism spectrum disorder: A national study of hospitalized
individuals. Journal of Interpersonal Violence, 10, 1358-1370.
doi:10.1177/0886260508322195
Lassalle, A., & Itier, R. J. (2014). Autistic traits influence gaze-oriented attention to
happy but not fearful faces. Social Neuroscience, 10(1), 70-88.
doi:10.1080/17470919.2014.958616
Lauritsen, M. B. (2013). Autism spectrum disorders. European Child & Adolescent
Psychiatry, 22(Suppl 1), S37-S42. doi:10.1007/s00787-012-0359-5
249
Lawson, J., Baron-Cohen, S., & Wheelwright, S. (2004). Empathising and
systemising in adults with and without Asperger syndrome. Journal of Autism &
Developmental Disorders, 34(3), 301-310.
doi:10.1023/B:JADD.0000029552.42724.1b
Leekam, S. R., Nieto, C., Libby, S. J., Wing, L., & Gould, J. (2007). Describing the
sensory abnormalities of children and adults with autism. Journal of Autism and
Developmental Disorders, 37(5), 894-910.
Leekam, S. R., Uljarevic, M., & Prior, M. R. (2011). Restricted and repetitive behaviours
in autism spectrum disorders: A review of research in the last decade.
Psychological Bulletin, 137(4), 562-593. doi:10.1037/a0023341
Lerner, M. D., Haque, O. S., Northrup, J. D., Lawer, L., & Bursztajn, H. J. (2012).
Emerging perspectives on adolescents and young adults with High-Functioning
Autism Spectrum Disorders, violence, and criminal law. The Journal of the
American Academy od Psychiatry and the Law, 40(2), 177-190.
Leslie, A. M., Mallon, R., & DiCorcia, J. A. (2006). Transgressors, victims, and cry
babies: Is basic moral judgement spared in autism? Social Neuroscience, 1(3-4),
270-283. doi:10.1080/17470910600992197
Levenson, M. R., Kiehl, K. A., & Fitzpatrick, C. M. (1995). Assessing psychopathic
attributes in a noninstitutionalized population. Journal of Personality and Social
Psychology, 68(1), 151-158. doi:10.1037/0022-3514.68.1.151
Levy, A., & Perry, A. (2011). Outcomes in adolescents and adults with autism: A review
of the literature. Research in Autism Spectrum Disorders, 5, 1271-1282.
doi:10.1016/j.rasd.2011.01.023
250
Levy, K. (2011). Dangerous psychopaths: Criminally responsible but not
morally responsible, subject to criminal punishment and to preventive detention.
San Diego Law Review, 48(4), 1299-1395.
Li, J., Zhu, L., & Gummerum, M. (2014). The relationship between moral judgment and
cooperation in children with high-functioning autism. Scientific Reports, 4, 1-6.
doi:10.1038/srep04314
Lindsay, W. R., Carson, D., O'Brien, G., Holland, A. J., Taylor, J. L., Wheeler, J., &
Steptoe, L. (2014). A comparison of referrals with and without autism spectrum
disorder to forensic intellectual disability services. Psychiatry , Psychology and
Law, 21(6), 947-954. doi:10.1080/13218719.2014.918081
Lindsay, W. R., & Taylor, J. L. (2005). A selective review of research on offenders with
developmental disabilities: Assessment and treatment. Clinical Psychology and
Psychotherapy, 12, 201-214. doi:10.1002/cpp.450
Liptak, G. S., Kennedy, J. A., & Dosa, N. P. (2011). Social participation in a nationally
representative sample of older youth and young adults with autism. Journal of
Developmental and Behavioural Pediatrics, 32(4), 277-283.
doi:10.1097/DBP.0b013e31820b49fc
Lisciandra, C., Postma-Nilsenová, M., & Colombo, M. (2013). Conformorality: Group
conditioning of normative judgment. Review of Philosophy and Psychology, 4(4),
751-764. doi: 10.1007/s13164-013-0161-4
Lissner, K. (1992). insider's point of view. In E. Schopler & G. B. Mesibov (Eds.), High-
Functioning Individuals With Autism. New York: Plenum Press.
251
Little, R. J. A. (1988). A test of missing completely at random for
multivariate data with missing values. Journal of the American Statistical
Association, 83(404), 1198-1202. doi:10.1080/01621459.1988.10478722
Locke, J., Ishijima, E. H., Kasari, C., & London, N. (2010). Loneliness, friendship
quality and the social networks of adolescents with high-functioning autism in an
inclusive school setting. Journal of Research in Special Educational Needs,
10(2), 74-81. doi:10.1111/j.1471-3802.2010.01148.x
Lombardo, M. V., Barnes, J. L., Wheelwright, S., & Baron-Cohen, S. (2007). Self-
referential cognition and empathy in autism. PLoS ONE, 2(9), e883.
doi:10.1371/journal.pone.0000883
Long, J. S., & Ervin, L. H. (2000). Using heteroscedasticity consistent standard errors in
the linear regression model. The American Statistician, 54(3), 217 - 224.
doi:10.1080/00031305.2000.10474549
Lord, C., & Jones, R. M. (2012). Annual research review: Re-thinking the classification
of autism spectrum disorders. Journal of child psychology and psychiatry, 53(5),
490-509. doi:10.111/j.1469-7610.2012.02547.x
Lord, C., Rutter, M., & le Couteur, A. (1994). Autism diagnostic interview-revised: A
revised version of a diagnostic interview for caregivers of individuals with
possible pervasive developmental disorders. Journal of Autism & Developmental
Disorders, 24(5), 659-685. doi:10.1007/BF02172145
Lotter, V. (1978). Follow-up studies. In M. Rutter & E. Schopler (Eds.), Autism. A
Reappraisal of Concpets and Treatment (pp. 475-495). New York: Plenum Press.
Loughnan, A. (2012). Manifest Madness: Mental Incapacity in Criminal Law. Oxford,
U.K.: Oxford University Press.
252
Lowe v R (1984) 154 CLR 606.
Lundström, S., Forsman, M., Larsson, H., Kerekes, N., Serlachius, E., Langstrom, N., &
Lichtenstein, P. (2014). Childhood neurodevelopmental disorders and violent
criminality: A sibling control study. Journal of Autism & Developmental
Disorders, 44, 2707-2716. doi:10.1007/s10803-013-1873-0
MacCoun, R. J. (1989). Experimental research on jury decision-making. Science, 244,
1046-1050.
Macintosh, K. E., & Dissanayake, C. (2004). Annotation: The similarities and
differences between autistic disorder and Asperger's disorder: a review of the
epirical evidence. Journal of child psychology and psychiatry, 45(421-434).
Mackenzie, G. (2002). Achieving consistency in sentencing: Moving to best practice?
University of Queensland Law Journal, 22(1), 74 - 90.
Mackenzie, G., Stobbs, N., & O'Leary, J. (2010). Principles of Sentencing. Sydney,
Australia: The Federation Press.
Mackie, M., & Fan, J. (2016). Reduced efficiency and capacity of cognitive control in
Autism Spectrum Disorder. Autism Research, 9, 403-414. doi:10.1002/aur.1517
Magiati, I., Tay, X. W., & Howlin, P. (2014). Cognitive, language, social and
behavioural outcomes in adults with autism spectrum disorders: A systematic
review of longitudinal follow-up studies in adulthood. Clinical Psychology
Review, 34, 73-86. doi:10.1016/j.cpr.2013.11.002
Mahoney, M. J. (2009). Asperger's Syndrome and the Criminal Law: The Special Case of
Child Pornography. Retrieved from http://www.harringtonmahoney.com
253
Maibom, H. (2008). The Will to Conform. In W. Sinnott-Armstrong (Ed.),
Moral Psychology (Vol. 3: The Neuroscience of Morality: Emotion, Braun
Disorders, and Development). Massachusetts: Massachusetts Institute of
Technology Press.
Mandy, W., Charman, T., & Skuse, D. H. (2012). Testing the construct validity of
proposed criteria for DSM-5 autism spectrum disorder. Journal of the American
Academy of Child and Adolescent Psychiatry, 51(1), 41-50.
Marriage, S., Wolverton, A., & Marriage, K. (2009). Autism spectrum disorder grown
up: A chart review of adult functioning. J Can Acad Child Adolesc Psychiatry,
18(4), 322-328.
Matson, J. L., & Adams, H. L. (2014). Characteristics of agression among persons with
autism spectrum disorders. Research in Autism Spectrum Disorders, 8, 1578 -
1584. doi:10.1016/j.rasd.2014.08.004
Matson, J. L., & Kozlowski, A. M. (2011). The increasing prevalence of autism spectrum
disorders. Research in Autism Spectrum Disorders, 5, 418-425.
doi:10.1016/j.rasd.2010.06.004
Mattila, M., Kielinen, M., Linna, S., Jussila, K., Ebeling, H., Bloigu, R., Moilanen, I.
(2011). Autism spectrum disorders according to DSM-IV-TR and comparison
with DSM-5 draft criteria: An epidemiological study. Journal of the American
Academy of Child and Adolescent Psychiatry, 50(6), 583-592.
doi:10.1016/j.jaac.2011.04.001
Mawson, D., Grounds, A., & Tantam, D. (1985). Violence and Asperger's syndrome: A
case study. British Journal of Psychiatry, 147, 566-569.
doi:10.1192/bjp.147.5.566
254
Mayes, S. D., Calhoun, S. L., & Crites, D. L. (2001). Does DSM-IV
Asperger's Disorder Exist? Journal of Abnormal Child Psychology(3).
Mayes, T. A., & Koegel, R. L. (2003). Persons with autism and criminal justice: Core
concepts and leading cases. Journal of Positive Behavior Interventions, 5(2), 92-
100. doi:10.1177/10983007030050020401
Mazefsky, C., McPartland, J., Gastgeb, H., & Minshew, N. (2013). Brief report:
Comparability of DSM-IV and DSM-5 ASD research samples. Journal of Autism
& Developmental Disorders, 43, 1236-1242. doi:10.1007/s10803-012-1665-y
Mazurek, M. O. (2014). Loneliness, friendship, and well-being in adults with autism
spectrum disorders. Autism, 18(3), 223-232. doi:10.1177/1362361312474121
Mazzone, L., Ruta, L., & Reale, L. (2012). Psychiatric comorbidities in asperger
syndrome and high functioning autism: diagnostic challenges. Annals of General
Psychiatry, 11(1), 16-28. doi:10.1186/1744-859x-11-16
Mbuba, J. (2012). Lethal rejection: Recounting offenders' experience in prison and
societal reaction post release. The Prison Journal, 92(2), 231-252.
doi:10.1177/0032885512439009
McAdam, P. (2012). Knowledge and understanding of the autism spectrum amongst
prison staff. Prison Service Journal, 202.
McClintock, K., Hall, S., & Oliver, C. (2003). Risk markers associaed with challenging
behaviours in people with intellectual disabilities: a meta-analytic study. Journal
of Intelectual Disability Research, 47(6), 405-416. doi:10.1046/j.1365-
2788.2003.00517.x
McDermott, E., & Langdon, P. E. (2016). The moral reasoning abilities of men and
women with intellectual disabilities who have a history of criminal offending
255
behaviour. Legal and Criminological Psychology, 21(1), 25-40.
doi:10.1111/lcrp.12051
McGeer, V. (2008a). The Makings of a Moral Sensibility: Replies to Commentaries. In
W. Sinnott-Armstrong (Ed.), Moral Psychology (Vol. 3: The Neuroscience of
Morality: Emotions, Brain Disorders, and Development). Massachusetts:
Massachsetts Institute of Technology Press.
McGeer, V. (2008b). Varieties of Moral Agency: Lessons from Autism. In W. Sinnott-
Armstrong (Ed.), Moral Psychology (Vol. 3: The Neuroscience of Morality:
Emotion, Brain Disorders, and Development). Massachusetts: Massachusetts
Institute of Technology Press.
McGovern, C. W., & Sigman, M. (2005). Continuity and change from early childhood to
adolescence in autism. Journal of Child Psychology & Psychiatry, 46(4), 401-
408. doi:10.1111/j.1469-7610.2004.00361.x
McLeer, S. V., & McNeils, D. N. (2012). Diagnosis and assessment of adults with ASDs.
In M. Reber (Ed.), The Autism Spectrum: Scientific Foundations and Treatment.
New York, USA: Cambridge University Press.
McNeils, D. N., & McLeer, S. V. (2012). Service and treatment planning for adults with
ASDs. In M. Reber (Ed.), The Autism Spectrum: Scientific Foundations and
Treatment. New York, USA: Cambridge University Press.
McPartland, J., Reichow, B., & Volkmar, F. R. (2012). Sensitivity and specificity of
proposed DSM-5 diagnostic criteria for autism spectrum disorder. Journal of the
American Academy of Child and Adolescent Psychiatry, 51(4), 368-383.
256
Menard, S. (1995). Applied Logistic Regression Analysis: Sage University
Series on Quantitative Applications in the Social Sciences. Thousand Oaks,
California: Sage.
Miller, J. (2014). DSM-5 and autism spectrum disorders: The changes you haven't heard
about yet. Journal of Clinical Psychiatry, 75(11), 1326-1327.
Miller, J., & Ozonoff, S. (1997). Did Asperger's cases have Asperger disorder? A
research note. Child Psychology & Psychiatry & Allied Disciplines, 38(2), 247-
251. doi:10.1111/j.1469-7610.1997.tb02354.x
Miller, J., & Ozonoff, S. (2000). The external validity of Asperger disorder: Lack of
evidence from the domain of neuropsychology. . Journal of Abnormal
Psychology, 109(2), 227-238.
Modell, S. J., & Mak, S. M. (2008). A preliminary assessment of police officers'
knowledge and perceptions of persons with disabilities. Intellectual and
Developmental Disabilities, 46(3), 183-189. doi:10.1352/2008.46:183–189
Moffitt, T. E., Caspi, A., Rutter, M., & Silva, J. A. (2001). Sex Differences in Antisocial
Behaviour: Conduct Disorder, Delinquency and Violence in the Dunedin
Longitudinal Study. Cambridge, U.K.: Cambridge University Press.
Monahan, K. C., & Piquero, A. R. (2009). Investigating the longitudinal relation between
offending frequency and offending variety. Criminal Justice and Behavior, 36(7),
653-673. doi:10.1177/0093854809335527
Moran, J. M., Young, L. L., Saxe, R., Lee, S. M., O'Young, D., Mavros, P. L., &
Gabrieli, J. D. (2011). Impaired theory of mind for moral judgment in high-
functioning autism. PNAS, 108(7), 2688-2692. doi:10.1073/pnas.1011734108
257
Morizot, J., & Kazemian, L. (2014). The Development of Criminal and
Antisocial Behaviour: Theory, Research and Practival Applications. New York:
Springer International Publishing.
Morrison, E. F. (1991). Victimization in prison: Implications for the mentally ill inmate
and for health professionals. Archives of Psychiatric Nursing, 5(1), 17-24.
Morse, S. J. (1999). Craziness and criminal responsibility. Behavioral Sciences & the
Law, 17(2), 147-164.
Moseley, D. S., Tonge, B. J., Brereton, A. V., & Einfeld, S. L. (2011). Psychiatric
comorbidity in adolescents and young adults with autism. Journal of Mental
Health Research in Intellectual Disabilities, 4, 229-243.
doi:10.1080/19315864.2011.595535
Mouridsen, S. E. (2012). Current status of research on autism spectrum disorders and
offending. Research in Autism Spectrum Disorders, 6, 79-86.
doi:10.1016/j.rasd.2011.09.003
Mouridsen, S. E., Rich, B., Isager, T., & Nedergaard, N. J. (2008). Pervaisive
developmental disorders and criminal behaviour: A case control study.
international Journal of Offender Therapy and Comparitive Criminology, 52(2),
196-205. doi:10.1177/0306624X07302056
Mullen, P. (1992). Psychopathy: a developmental disorder of ethical action. Criminal
Behaviour and Mental Health, 2(2), 234–244. doi: 10.1002/cbm.1992.2.2.234
Mullen, P. (1996). Psychiatric Report: Martin Bryant, Date of Birth 7/5/66. Retrieved
from http://kildall.apana.org.au/autism/articles/bryant.html
Mullen, P. (2001). A Review of the Relationship Between Mental Disorders and
Offending Behaviours and on the Management of Mentally Anormal Offenders in
258
the Health and Criminal Justice Services. Retrieved from
http://www.aic.gov.au/crc/reports/mullen.html
Müller, E., Schuler, A., & Yates, G. B. (2008). Social challenges and supports from the
perspective of individuals with Asperger syndrome and other autism spectrum
disabilities. Autism, 12(2), 173-190. doi:10.1177/1361307086664
Murphy, D. (2003). Admission and cognitive details of male patients diagnosed with
Asperger's syndrome detained in a special hospital: comparison with a
schizophrenia and personality disorder sample. The Journal of Forensic
Psychiatry and Psychology, 14(3), 506-542. doi:10.1080/1478994031000152736
Murphy, D. (2007). Hare Psychopathy Checklist Revised profiles of male patients with
Asperger's syndrome detained in high security psychiatric care. The Journal of
Forensic Psychiatry and Psychology, 18(1), 120-126.
doi:10.1080/14789940601014777
Murphy, D. (2010). Extreme violence in a man with an autistic spectrum disorder:
assessment and treatment within high-security psychiatric care. Journal of
Forensic Psychiatry & Psychology, 21(3), 462-477.
doi:10.1080/14789940903426885
Murphy, D. (2013). Risk assessment of offenders with an autism spectrum disorder.
Journal of Intellectual Disabilities and Offending Behaviour, 4(1/2), 33-41.
doi:10.1108/JIDOB-02-2013-0004
Murphy, G. H., Beadle-Brown, J., Wing, L., Gould, J., Shah, A., & Holmes, N. (2005).
Chronicity of challenging behaviours in people with severe intellecutal
disabilities and/or autism: A total population sample. Journal of Autism &
Developmental Disorders, 35(4), 405-418. doi:10.1007/s10803-005-5030-2
259
Murrie, D. C., Warren, J. I., Kristiansson, M., & Dietz, P. E. (2002).
Asperger's syndrome in forensic settings. International Journal of Forensic
Mental Health, 1(1), 59-70. doi:10.1080/14999013.2002.10471161
Myers, F. (2004). On the Borderline? People with Learning Disabilities and/or Autistic
Spectrum Disorders in Secure, Forensic and Other Specialist Settings.
Edinburgh: Scottish Development Centre for Mental Health.
Nelson, J. R., Smoth, D. J., & Dodd, J. (1990). The moral reasoning of juvenile
delinquents: A meta-analysis. Journal of Abnormal Child Psychology, 18(3), 231-
239. doi:10.1007/BF00916562
Nemeroff, C. B., Weinberger, D., Rutter, M., MacMillan, H. L., Bryant, R. A., Wesslet,
S., Lysaker, P. (2013). DSM-5: a collection of psychiatrist views on the changes,
controversies, and future directions. BioMed Central Medicine, 11(202).
doi:10.1186/1741-7015-11-202
Newman, S. S., & Ghaziuddin, M. (2008). Violent crime in Asperger syndrome: The role
of psychiatric comorbidity. Journal of Autism and Developmental Disorders, 38,
1848-1852. doi:10.1007/s10803-008-0580-8
Nichols, S. (2002). Norms with feeling: towards a psychological account of moral
judgment. Cognition, 84, 221-236. doi:10.1016/S0010-0277(02)00048-3
North, A. S., Russell, A. J., & Gudjonsson, G. H. (2008). High functioning autism
spectrum disorders: An investigation of psychological vulnerabilities during
interrogative interview. Journal of Forensic Psychiatry and Psychology, 19(3),
323-334.
260
Nucci, L. P., Turiel, E. (1978). Social interactions and the development of
social concepts in preschool children. Child Development, 49(2), 400-407. doi:
10.2307/1128704.
O'Brien, G., Taylor, J. L., Lindsay, W. R., Holland, A. J., Carson, D., Steptoe, L.,
Wheeler, J. (2010). A multi-centre study of adults with learning disabilities
referred to services for antisocial or offending behaviour: demographic,
individual, offending and service characteristics. Journal of Learning Disabilities
& Offending Behaviour, 1(2), 5-15.
Ogloff, J. R. P., Talevski, D., Lemphers, A., Wood, M., & Simmons, M. (2015). Co-
occurring mental illness. substance use disorders, and antisocial personality
disorder among clients of forensic mental health services. Psychiatric
Rehabilitation Journal, 38(1), 16-23. doi:10.1037/prj0000088
Ogloff, J. R. P., Warren, L., Tye, C., Blaher, F., & Thomas, S. (2011). Psychiatric
symptoms and histories among people detained in police cells. Social Psychiatry
& Psychiatric Epidemiology, 46(9), 871-880. doi:10.1007/s00127-010-0256-5
Orsmond, G. I., Shattuck, P. T., Cooper, B. P., Sterzing, P. R., & Anderson, K. A.
(2013). Social participation among adults with an autism spectrum disorder.
Journal of Autism & Developmental Disorders, 43, 2710-2719.
doi:10.1007/s10803-013-1833-8
Ozsivadjian, A., Hibberd, C., & Hollocks, M. J. (2013). Brief report: The use of self-
report measures in young people with Autism Spectrum Disorder to access
symptoms of anxiety, depression and negative thoughts. Journal of Autism &
Developmental Disorders, 44(4), 969-974. doi: 10.1007/s10803-013-1937-1
261
Palermo, M. T. (2004). Pervasive developmental disorders, psychiatric
comorbidities, and the law. international Journal of Offender Therapy and
Comparitive Criminology, 48(1), 40-48. doi:10.1177/0306624X03257713
Palermo, M. T. (2013). Developmental disorders and political extremism: A case study
of Asperger syndrome and the neo-nazi subculture. Journal of Forensic
Psychology Practice, 13, 341-354. doi:10.1080/15228932.2013.817890
Palmer, E. J. (2003). An overview of the relationship between moral reasoning and
offending. Australian Psychologist, 38(3), 165-174.
Palmer, E. J., & Hollin, C. R. (1999). Social competence and sociomoral reasoning in
young offenders. Applied Cognitive Psychology, 13, 79-87.
Park, C. (1992). Autism into art: a handicap transfigured. In E. Schopler & G. B.
Mesibov (Eds.), High-Functioning Individuals With Autism. New York: Plenum
Press.
Parner, E. T., Thorsen, P., Dixon, G., de Klerk, N., Leonard, H., Nassar, N., . . . Glasson,
E. J. (2011). A comparison of autism prevalence trends in Denmark and Western
Australia. Journal of Autism and Developmental Disorders, 41(12), 1601-1608.
doi:10.1007/s10803-011-1186-0
Parry, J. W. (2005). The death penalty and persons with mental disabilities: A lethal dose
of stigma, sanism, fear of violence, and faulty predictions of dangerousness.
Mental and Physical Disability Law Reporter, 29(5), 667 - 669.
Pasterfield, R. (2009). A strategy for adults with an autism spectrum disorder iving in
wokingham borough. Retrieved from Wokingham, U.K. :
262
Patil, I., Melsbach, J., Henning-Fast, K., & Silani, G. (2016). Divergent roles
of autistic and alexithymic traits in utilitarian moral judgements in adults with
autism. Scientific Reports, 6(23637). doi:10.1038/srep23637
Paul, K. I., & Moser, K. (2009). Unemployment impairs mental health: Meta-analyses.
journal of Vocational Behaviour, 74, 264-282. doi:10.1016/j.jvb.2009.01.001
Périsse, D., Amiet, C., Consoli, A., Thorel, M., Gorfinkel-An, I., Bodeau, N., . . . Cohen,
D. (2010). Risk factors of acute behavioural regression in psychiatrically
hospitalized adolescents with autism. Journal of the Canadian Academy of Child
and Adolescent Psychiatry, 19(2), 100-108.
Perlin, M., & Gould, K. (1995). Rashomon and the criminal law: Mental disability and
the federal sentencing guidelines. American Journal of Criminal Law, 22(431),
431-460.
Pink, B. (2011). Australian and New Zealand standard offence classification. .Retrieved
from:
http://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/1234.02011?Open
Post, M., Hayes, S., Storey, K., Loughrey, T., & Campbell, C. (2014). Understanding
stalking behaviours by individuals with Autism Spectrum Disorders and
recommended prevention strategies for school settings. Journal of Autism &
Developmental Disorders, 44, 2698-2706. doi:10.1007/s10803-012-1712-8
Post, M., Storey, K., Haymes, L., Campbell, C., & Loughrey, T. (2014). Stalking
behaviours by individuals with Autism Spectrum Disorders in employment
settings: Understanding stalking behaviour and developing appropriate supports.
Education and Training in Autism and Developmental Disabilities, 49(1), 102-
110.
263
Potas, I. (1981). Sentencing the mentally disordered offender in Australia.
International Journal of Law and Psychiatry, 4, 107-122.
Potter, C. (2014). I didn't used to have much friends': exploring the friendship concepts
and capabilities of a boy with autism and severe learning disabilities. British
Journal of Learning Disabilities, 43, 208-218. doi:10.1111/bld.12098
Radley, J., & Shaherbano, Z. (2011). Asperger syndrome and arson: A case study.
Advances in Mental Health and Intellectual Disabilities, 5(6), 32-36.
doi:10.1108/20441281111187171
Raggi, C., Xenitidis, K., Moisan, M., Deeley, Q., & Robertson, D. (2013). Adults with
autism spectrum disorder and learning disability presenting with challenging
behaviour: how tolerant should we be? Journal of Intellectual Disabilities and
Offending Behaviour, 4(1/2), 42-52.
Raine, A., & Yang, Y. (2006). Neural foundations to moral reasoning and antisocial
behaviour. Social Cognitive and Affective Neuroscience, 13, 203-213.
Raja, M., & Azzoni, A. (2001). Asperger's disorder in the emergency psychiatric setting.
General Hospital Psychiatry, 23(5), 285-293. doi:10.1016/s0163-8343(01)00155-
4
Ray, F., Marks, C., & Bray-Garretson, H. (2010). Challenges to treating adolescents with
Asperger's syndrome who are sexually abusive. Sexual Addiction and
Compulsivity: The journal of Treatment and Prevention, 11(4), 265-285.
doi:10.1080/10720160490900614
Reber, M. (2012). Epidemiology of autism. In M. Reber (Ed.), The Autism Spectrum:
Scientific Foundations and Treatment. New York, USA: Cambridge University
Press.
264
Redding, R. E., & Brooke Hensl, K. (2011). Knowledgeable judges make a
difference: Judicial beliefs affect juvenile court transfer decisions. Juvenile and
Family Court Journal, 62(3), 15-24.
Richardson, E., & McSherry, B. (2010). Diversion down under — Programs for
offenders with mental illnesses in Australia. International Journal of Law and
Psychiatry, 33, 249-257. doi:10.1016/j.ijlp.2010.06.007
Richardson, I. (1991). Changing Needs for Judicial Decision Making. Paper presented at
the Supreme and Federal Court Judges' Conference, Auckland, NZ.
Rieffe, C., Camodeca, M., Pouw, L. B. C., Lange, A. M. C., & Stockmann, L. (2012).
Don't anger me! Bullying, victimization, and emotion dysregulation in young
adolescents with ASD. European Journal of Developmental Psychology, 9(3),
351-370. doi:10.1080/17405629.2012.680302
Ritchie, D., Hudson, N., Kenny, A., & Darby, P. (2016). Sentencing Guidance in
Victoria Report. Retrieved from Melbourne, Victoria:
Roach Anleu, S. R., & Mack, K. (2007). Magistrates, Magistrates Courts, and social
change. Law & Policy, 29(2).
Robertson, C. E. (2013). The Operation of the Mental Impairment Defence in South
Australia: Submission from the Australian Psychological Society's College of
Forensic Psychology (SA Section). Retrieved from Report prepared on behalf of
the Australian Psychological Society's College of Forensic Psychology for
submission to the Sentencing Advisory Council:
Robertson, C. E., & McGillivray, J. A. (2015). Autism behind bars: a review of the
research literature and discussion of key issues. Journal of Forensic Psychiatry &
Psychology, 26(6), 719-736. doi:10.1080/14789949.2015.1062994.
265
Robinson, L., Spencer, M. D., Thomson, L. D. G., Stanfield, A. C., Owens, D.
G. C., Hall, J., & Johnstone, E. C. (2012). Evaluation of a screening instrument
for autism spectrum disorders in prisoners. PLoS ONE, 7(5), 1-8.
doi:10.1371/journal.pone.0036078
Robinson, P. (2012). An empirical study of settlement conference nuts and bolts:
Settlement judges facilitating commuication, compromise and fear. Harvard
Negotiation Law Review, 17(97), 97-150.
Rogers, J., Viding, E., Blair, R. J., Frith, U., & Happe, F. (2006). Autism spectrum
disorder and psychopathy: shared cognitive underpinnings or double hit?
Psychological Medicine, 36, 1789-1798. doi:10.1017/S0033291706008853
Roper, C. (2006). A national standard for professional development for Australian
judicial officers. Retrieved from: https://njca.com.au/wp-
content/uploads/2013/01/A-National-Standard-for-Professional-Development.pdf
Rosetti, Z. S. (2011). "That's how we do it": Friendship work bewteen high school
students with and without autism or developmental disability. Research and
Practice for Persons with Severe Disabilities, 36(1-2), 23-33. doi:
10.2511/rpsd.36.1-2.23
Rozin, P., Lowery, L., Imada, S., & Haidt, J. (1999). The CAD triad hypothesis: A
mapping between three moral emotions (contempt, anger, disgust) and three
moral codes (commuity, autonomy, divinity). Journal of Personality and Social
Psychology, 76(4), 574 - 586.
Ruble, L. A., & Dalrymple, N. J. (1993). Social/sexual awareness of persons with autism:
A parental perspective. Archives of Sexual Behaviour, 22(3), 229-240.
doi:10.1007/BF01541768
266
Rutherford, M. D., & Ray, D. (2009). Cheater detection is preserved in autism
spectrum disorders. Journal of Social, Evolutionary, and Cultural Psychology,
3(2), 105-117. doi:10.1037/h0099327
R v MacKenny (1981) 72 Cr App R 78.
R v Oznek [2007] VSC 192.
R v Verdins, Buckley and Vo [2007] VSCA 104; (2007) 169 A Crim R 581.
Sally, D., & Hill, E. (2006). The development of interpersonal strategy: Autism, theory
of mind, cooperation and fairness. Journal of Economic Psychology, 27, 73-97.
doi:10.1016/j.joep.2005.06.015
Saracino, J., Noseworthy, J., Steiman, M., Reisinger, L., & Fombonne, E. (2010).
Diagnostic and assessment issues in autism surveillance and prevalence. J Dev
Phys Disabil, 22, 317-330. doi:10.1007/s10882-010-9205-1
Schall, C. M., & McDonough, T. (2010). Autism spectrum disorders in adolescence and
early adulthood: Characteristics and issues. Journal of Vocational Rehabilitation,
32, 81-88. doi:10.3233/JVR-2010-0503
Schmitz, E. A., Banerjee, R., Pouw, L. B., Stockmann, L., & Rieffe, C. (2015). Better to
be equal? Challenges to equality for cognitively able children with autism
spectrum disorders in a social decision game. Autism, 19(2), 178-186.
doi:10.1177/1362361313516547
Schneider, K., Pauly, K. D., Gossen, A., Mevissen, L., Michel, T. M., Gur, R. C., . . .
Habel, U. (2013). Neural correlates of moral reasoning in autism spectrum
disorder. Social Cognitive and Affective Neuroscience, 8, 702-710.
doi:10.1093/scan/nss051
267
Schroeder, J. H., Cappadocia, M. C., Bebko, J. M., Pepler, D. J., & Weiss, J.
A. (2014). Shedding light on a pervaisive problem: A review of research on
bullying experiences amongst children with Autism Spectrum Disorders. Journal
of Autism & Developmental Disorders, 44(7), 1520-1534. doi:10.1007/s10803-
013-2011-8
Schwartz-Watts, D. M. (2005). Asperger's disorder and murder. The Journal of the
American Academy of Psychiatry and the Law, 33, 390-393.
Schwarz, N. (2005). Cognition, aging and self-reports. In D. Park & N. Schwarz (Eds.),
Cognitive Aging -- A Primer (2nd ed.). Philiadelphia, PA: Psychology Press.
Scragg, P., & Shah, A. (1994). Prevalence of Asperger's syndrome in a secure hospital.
British Journal of Psychiatry, 165, 679-682.
Seigfried, -. S., K. C., O'Quinn, C. L., & Treadway, K. N. (2015). Assessing the
relationship bewteen autistic traits and cyberdeviancy in a sample of college
students Behaviour and Information Technology, 34(5), 533-542.
doi:10.1080/0144929X.2014.978377
Seltzer, M. M., Shattuck, P. T., Abbeduto, L., & Greenberg, J. S. (2004). Trajectory of
development in adolescents and adults with autism. Mental Retardation and
Developmental Disabilities, 10, 234-247. doi:10.1002/mrdd.20038
Senland, A. K., & Higgins-D'Alessandro. (2013). Moral reasoning and empathy in
adolescents with autism specrum disorder: implications for moral education.
Journal of Moral Education, 42(2), 209-223. doi:10.1080/03057240.2012.752721
Sentencing Act 1991 (Vic). Retrieved from:
http://www.austlii.edu.au/au/legis/vic/consol_act/sa1991121/
268
Sevlever, M., Roth, M. E., & Gillis, J. M. (2013). Sexual abuse and offending
in adutism spectrum disorders. Sexuality & Disability, 31, 189-200.
doi:10.1007/s11195-013-9286-8
Shattuck, P. T., Roux, A. M., Hudson, L. E., Lounds Taylor, J., Maenner, M. J., & Trani,
J. F. (2012). Services for adults with an autism spectrum disorder. The Canadian
Journal of Psychiatry, 57(5), 284-291.
Shattuck, P. T., Seltzer, M. M., Greenberg, J. S., Orsmond, G. I., Bolt, D., Kring, S., . . .
Lord, C. (2007). Change in autism symptoms and maladaptive behaviours in
adolescents and adults with an autism spectrum disorder. Journal of Autism &
Developmental Disorders, 37, 1735-1747. doi:10.1007/s10803-006-0307-7
Shoemaker, D. W. (2011). Psychopathy, responsibility, and the moral/conventional
distinction. Southern Journal of Philosophy, 49, 99-124. doi:10.1111/j.2041-
6962.2011.00060.x
Shulman, C., Guberman, A., Shilling, N., & Bauminger, N. (2012). Moral and social
reasoning in autism spectrum disorders. Journal of Autism and Developmental
Disorders, 42, 1364-1376. doi:10.1007/s10803-011-1369-8
Silva, J. A., Ferrari, M. M., & Leong, G. B. (2002). The case of Jeffery Dahmer: Sexual
serial homocide from a neuropsychiatric developmental perspective. Journal of
Forensic Sciences, 47(6), 1-13.
Silva, J. A., Ferrari, M. M., & Leong, G. B. (2003). Asperger's disorder and the origins of
the unabomber. American Journal of Forensic Psychiatry, 24(2), 5-43.
Silva, J. A., Leong, G. B., Smith, R., Hawes, E., & Ferrari, M. M. (2005). Analysis of
serial homicide in the case of Joel Rifkin using the neuropsychiatric
developmental model. American Journal of Forensic Psychiatry, 26(4), 25-55.
269
Sinclair, J. (1992). Bridging the gaps: an inside-out view of autism (or, do you
know what I don't know?). In E. Schopler & G. B. Mesibov (Eds.), High-
Functioning Individuals With Autism. New York: Plenum Press.
Siponmaa, L., Kristiansson, M., Johnson, C., Nyden, A., & Gillberg, C. (2001). Juvenile
and young adult mentally disordered offenders: The role of child neuropsychiatric
disorders. . Journal of the American Academy of Psychiatry and the Law, 29(4),
420-426.
Skeem, J. L., Manchak, S., & Peterson, J. (2011). Correctional policy for offenders with
mental illness: Creating a new paradigm for recidivism reduction. Law and
human Behaviour, 35, 110-126. doi:10.1007/s10979-010-9223-7
Skuse, D. H. (2012). DSM-5's conceptualisation of autistic disorders. Journal of the
American Academy of Child and Adolescent Psychiatry, 51(4), 344-346.
doi:10.1016/j.jaac.2012.02.009
Smetana, J. G. (1982). Concepts of Self and Morality: Women's Reasoning About
Abortion. California, U.S.A.: Praeger Publishers Inc.
Smetana, J. G. (1985). Preschool children's conceptions of transgressions: Effects of
varying moral and conventional domain-related attributes. Developmental
Psychology, 21(1), 18-29. doi:10.1037/0012-1649.21.1.18
Smetana, J. G. (1993). Understanding of social rules. In M. Bennett (Ed.), The
Development of Social Cognition. New York: The Guildford Press.
Solomon, A. (2015, October 12). The Myth of the 'Autistic Shooter'. The New York
Times. Available at: http://www.nytimes.com/2015/10/12/opinion/the-myth-of-
the-autistic-shooter.html?emc=edit_ty_20151012&nl=opinion&nlid=59439727&
_r=2
270
Söderström Anckarsäter, H. (2005). Clinical neuropsychiatric symptoms in
perpetrators of severe crimes against persons. Nordic Journal of Psychiatry,
59(4), 246-252. doi:10.1080/08039480500213709
Søndennaa, E., Helverschou, S. B., Steindal, K., Rasmussen, K., & Nilson, B. (2014).
Violence and sexual offending behaviour in people with autism spectrum disorder
who have undergone a psychiatric forensic examination. Psychological Reports,
115(1), 32-34. doi:10.2466/16.15.PR0.115c16z5
Spillers, J. L. H., Sensui, L. M., & Linton, K. F. (2014). Concerns abut identifiy and
services among people with autism and Asperger's regarding DSM-5 changes.
Journal of Social Work in Disability and Rehabilitation, 13(3), 247-260.
doi:10.1080/1536710X.2014.912186
Ståhlberg, O., Anckarsäter, H., & Nilsson, T. (2010). Mental health problems in youths
committed to juvenile institutions: prevalences and treatment needs. European
Child & Adolescent Psychiatry, 19, 893-903. doi:10.1007/s00787-010-0137-1
Stams, G. J., Brugman, D., Deković, M., van Rosmalen, L., van der Laan, P., & Gibbs, J.
C. (2006). The moral judgement of juvenile delinquents: A meta-anlaysis.
Journal of Abnormal Child Psychology, 34(5), 692-708. doi:10.1007/s10802-006-
9056-5
Stefanatos, G. A. (2012). Developmental neuropsychology of autism. In M. Reber (Ed.),
The Autism Spectrum: Scientific Foundations and Treatment. Cambridge:
Cambridge University Press.
Stevenson, S. F., Hall, G., & Innes, J. M. (2003). Sociomoral reasoning and criminal
sentiments in Australian men and women violent offenders and non-offenders.
International Journal of Forensic Psychology, 1(1), 111-119.
271
Stokes, M. A., & Kaur, A. (2005). High-functioning autism and sexuality: A
parental perpective. Autism, 9(3), 266-289. doi:10.1177/1362361305053258
Stokes, M. A., Newton, N., & Kaur, A. (2007). Stalking, and social and romantic
functioning among adolescents and adults with autism spectrum disorder. Journal
of Autism & Developmental Disorders, 37, 1969-1986. doi:10.1007/s10803-006-
0344-2
Strock, M. (2007). Autism spectrum disorders: Pervasive developmental disorders. With
Addendum. . Maryland, U.S.A.: National Institute of Mental Health.
Sullivan, R. (1992). Parent Essays: Rain Man and Joseph. In E. Schopler & G. B.
Mesibov (Eds.), High-Functioning Individuals With Autism. New York: Plenum
Press.
Szatmari, P., Bartolucci, G., & Bremner, R. (1989). Asperger's syndrome and autism:
Comparison of early history and outcome. Developmental Medicine and Child
Neurology, 31, 709-720.
Tabachnick, B. G., & Fidell, L. S. (2013). Using Multivariate Statistics. New Jersey,
U.S.A: Pearson.
Tager-Flusberg, H., Paul, R., & Lord, C. (2005). Language and communication in
autism. . Handbook of autism and pervasive developmental disorders, 1, 335-364.
Takeda, T., Kasai, K., & Kato, N. (2007). Moral judgement in high-functioning
pervasive developmental disorders. Psychiatry and clinical neuroscience, 61,
407-414. doi:10.1111/j.1440-1819.2007.01678.x
Talbot, J. (2010). Prisoners' voices: experiences of the criminal justice system by
prisoners with learning disabilities. Tizard Learning Disability Review, 15(3).
doi:10.5042/tldr.2010.0403
272
Talbot, J. (2012). Fair Access to Justice? Support for vulnerable defendants
in the criminal courts. Retrieved from London, U.K. :
Tantam, D. (1988). Lifelong eccentricity and social isolation: I. Psychiatric, social and
forensic aspects. British Journal of Psychiatry, 153, 777-782.
Tantam, D. (1991). Asperer syndrome in adulthood. In U. Frith (Ed.), Autism and
Apsergers Syndrome. Cambridge, UK: Cambridge University Press.
Tantam, D. (2000). Adolescence and adulthood of individuals with Asperger syndrome.
In A. Klin, F. R. Volkmar, & S. S. Sparrow (Eds.), Asperger Syndrome. New
York: The Guilford Press.
Tantam, D. (2003). The challenge of adolescents and adults with Asperger syndrome.
Child and Adolescent Psychiatric Clinics, 12, 143-163.
Taylor, K., Mesibov, G. B., & Debbaudt, D. (2009). Autism in the criminal justice
system. Retrieved from
http://www.humeautismcop.com/uploads/2/1/6/8/21682656/autism_criminal_just
ice.pdf
Teagardin, J., Dixon, D. R., Smith, M. N., & Granpeesheh, D. (2012). Randomized trial
of law enforcement training on autism spectrum disorders. Research in Autism
Spectrum Disorders, 6(3), 1113-1118. doi:10.1016/j.rasd.2012.02.002
The National Autistic Society. (2005). Autism: a guide for criminal justice professionals.
London: The National Autistic Society.
The National Autistic Society. (2013). Untapped Talent: A Guide to Employing People
With Autism. Retrieved from
http://www.hao2.eu/sites/default/files/Untapped_Talent_-_English.pdf
273
Theobald, D., Farrington, D. P., Loeber, R., Pardini, D. A., & Piquero, A. R.
(2014). Scaling up from convictions to self-reported offending. Criminal
Behaviour and Mental Health, 24, 265-276. doi:10.1002/cbm.1928
Thornberry, T. P., & Krohn, M. D. (2000). The self-report method for measuring
deliquency and crime Measurement and Analysis of Crime and Justice (Vol. 4,
pp. 33-83). Washington, D. C.: U.S. National Institute of Justice.
Thornberry, T. P., & Krohn, M. D. (2003). Taking Stock of Delinquency: An Overview of
Findings From Contemporary Longitudinal Studies. New York: Kluwer
Academic/Plenum Publishers.
Thornton, D., & Reid, R. L. (1982). Moral reasoning and type of criminal offence.
British Journal of Social Psychology, 21(3), 231-238. doi:10.1111/j.2044-
8309.1982.tb00544.x
Tiihonen, J., Isohanni, M., Räsänen, P., Koiranen, M., & Moring, J. (1997). Specific
major mental disorders and criminality: A 26-year prospective study of the 1966
Northern Finland birth cohort. American Journal of Psychiatry, 154(6), 840-845.
doi:10.1176/ajp.154.6.840
Tobin, M. C., Drager, K. D. R., & Richardson, L. F. (2014). A systematic review of
social participation for adults with autism spectrum disorders: Support, social
functioning and quality of life. Research in Autism Spectrum Disorders, 8, 214-
229. doi:10.1016/j.rasd.2013.12.002
Tonge, B. J., Brereton, A. V., & Bull, K. (2008). Life transition problems: Young people
wih autism spectrum disorders. Retrieved from Victoria, Australia:
Travers, B. G., Powell, P. S., Mussey, J. L., Klinger, L. G., Crisler, M. E., & Klinger, M.
R. (2013). Spatial and identity cues differentially affect implicit contextual cueing
274
in adulescents and adults with Autism Spectrum Disorder. Journal of
Autism & Developmental Disorders, 43(6), 2393 -2404. doi:10.1007/s10803-013-
1787-x
Treffert, D. A. (1970). Epidemiology of infantile autism. Archives of General Psychiatry,
22(5). doi:10.1001/archpsyc.1970.01740290047006
Tsai, L. (2014). Impact of DSM-5 on epidemiology of autism spectrum disorder.
Research in Autism Spectrum Disorders, 8, 1454-1470.
doi:10.1016/j.rasd.2014.07.016
Tsiaras v R [1996] 1 VR 398.
Turiel, E. (1983). The Development of Social Knowledge: Morality and Convention. New
York, NY: Cambridge University Press.
Turnbull, A. (2010, November 4, 2010). Transitioning to Enviable Lives for Adults with
Autism. Paper presented at the Geneva Centre International Symposium on
Autism Toronto, Canada.
Tyron, P. A., Mayes, S. D., Rhodes, R. L., & Waldo, M. (2006). Can Asperger's disorder
be differentiated from autism using DSM-IV criteria? Focus on Autism and Other
Developmental Disabilities, 21, 2-6.
Valliant, P. M., Gauthier, T., Pottier, D., & Kosmyna, R. (2000). Moral reasoning,
interpersonal skills, and cognition of rapists, child molesters, and incest
offenders. Psychological Reports, 86, 67-75.
van Santen, J. P. H., Sproat, R. W., & Presmanes Hill, A. (2013). Quantifying repetitive
speech in autism spectrum disorders and language impairment. Autism Research,
6, 372-383. doi:10.1002/aur.1301
275
Vecina, M. L. (2014). The five moral foundations sacredness scale in men in
court-mandated treatment for violently abusing their partners. Personality and
individual differences, 64, 46-51. doi:10.1016/.j.paid.2014.02.021
Veen v R [No.1] (1979) 143 CLR 458
Victorian Law Reform Commission. (2013). Review of the Crimes (Mental Impairment
and Unfitness to be Tried) Act 1997: Consultation Paper. Retrieved from
Melbourne, Victoria: http://www.lawreform.vic.gov.au/sites/default/files/Crimes
Mental Impairment consultation paper.pdf
Vidmar, N. (2011). The psychology of trial judging. Current Directions in Psychological
Science, 20(1), 58-62. doi:10.1177/0963721410397283
Vignemont, F., & Frith, U. (2008). Autism, morality and empathy. In W. Sinnott-
Armstrong (Ed.), Moral Psychology (Vol. 3: The neuroscince of morality:
emotion, brain disorders, and development, pp. 273-280). Massachusetts:
Massachusetts Institute of Technology.
Viljoen, J., Roesch, R., Ogloff, J. R. P., & Zapf, P. A. (2003). The role of Canadian
psychologists in comducting fitness and criminal responsibility evaluations.
Canadian Psychology, 44(4), 369-381.
Volavka, J. (2013). Violence in schizophrenia and bipolar disorder. Psychiatria
Danubina, 25(1), 24-33.
Volkmar, F. R., & Reichow, B. (2013). Autism in DSM-5: progress and challenges.
Molecular Autism, 4(13). doi:10.1186/2040-2392-4-13
von Knorring, A., & Hågglof, B. (1993). Autism in Northern Sweden. A population
based follow-up study: Psychopathology. European Child and Adulescent
Psychiatry, 2(2), 91-97.
276
Wachtel, L. E., & Shorter, E. (2013). Autism plus psychosis: A 'one-two
punch' risk for tragic violence? Medical Hypotheses, 81.
doi:10.1016/j.mehy.2013.05.032
Wahlund, K., & Kristiansson, M. (2006). Offender characteristics in lethal violence with
special reference to antisocial and autistic personality traits. Journal of
Interpersonal Violence, 21(8), 1081-1091. doi:10.1177/0886260506290289
Wakabayashi, A., Baron-Cohen, S., Wheelwright, S., & Tojo, Y. (2006). The Autism-
Spectrum Quotient (AQ) in Japan: A cross-cultural comparison. Journal of
Autism & Developmental Disorders, 36(2), 263-270. doi:10.1007/s10803-005-
0061-2
Walvisch, J. (2010). Sentencing offenders with impaired mental funtioning: Developing
Australia's "most sophisticted and subtle" analysis. Psychiatry , Psychology and
Law, 17(2).
Wazana, A., Bresnahan, M., & Kline, J. (2007). The autism epidemic: Fact or artefact?
Journal of the American Academy of Child and Adolescent Psychiatry, 46(6),
721-730.
West, M. L., Vayshenker, B., Rotter, M., & Yanos, P. T. (2015). The influence of mental
illness and criminality self-stigmas and racial self-concept on outcomes in a
forensic psychiatric sample. Psychatric Rehabilitation Journal, 38(2), 150-157.
doi:10.1037/prj0000133
Wheelwright, S., Baron-Cohen, S., Goldenfeld, N., Delaney, J., Fine, D., Smith, R.,
.Wakabayashi, A. (2006). Predicting autism spectrum quotient (AQ) from the
systemizing quotient-revised (SQ-R) and empathy quotient (EQ). Brain
Research, 1079(1), 47-56. doi:10.1016/j.brainres.2006.01.012
277
Whitbread v R (1995) 78 A Crim R 452.
White, J., Day, A., & Hackett, L. (2007). Writing Reports for Court. QLD, Australia:
Australian Academic Press.
Whitehouse, A. J., Durkin, K., Jaquet, E., & Ziatas, K. (2009). Friendship, loneliness and
depression in adolescents with Asperger's syndrome. Journal of Adolescence, 32,
309-322. doi:10.1016/j.adolescence.2008.03.004
Whitehouse, A. J., Watt, H. J., Line, E., & Bishop, D. (2009). Adult psychosocial
outcomes of children with specific language impairment, pragmatic langauge
impairment and autism. International Journal of Language and Communication
Disorders, 44(4), 511-528.
Williams, D. (2010). Theory of own mind in autism: Evidence of a specific deficit in
self-awareness? Autism, 14(5), 474-494. doi:10.1177/1362361310366314
Williams, J. G., Higgings, J. P. T., & Brayne, C. E. G. (2006). Systematic review of
prevalence studies of autism spectrum disoders. Archives of Disease in
Childhood, 91, 8-15. doi:10.1136/adc.2004.062083
Williams, K., MacDermott, S., Ridley, G., Glasson, E. J., & Wray, J. A. (2008). The
prevalence of autism in Australia. Can it be established from existing data?
Journal of Paediatrics and Child Health, 44(9), 504-510. doi:10.1111/j.1440-
1754.2008.01331.x
Williams, K., Mellis, C., & Peat, J. K. (2005). Incidence and prevalence of autism.
Advances in Speech Language Pathology, 7(1), 31-40.
doi:10.1080/14417040500055227
278
Williams, K., Woolfenden, S., Roberts, J., Rodger, S., Bartak, L., & Prior, M.
(2014). Autism in context 1: Classification, counting and causes. Journal of
Paediatrics and Child Health, 50, 335-340. doi:10.1111/jpc.12451
Wing, L. (1981a). Asperger's syndrome: a clinical account. Psychological Medicine,
11(1), 115-129. doi:10.1017/S0033291700053332
Wing, L. (1981b). Sex ratios in early childhood autism and related conditions. Psychiatry
Research, 5, 129-137. doi:10.1016/0165-1781(81)90043-3
Wing, L. (1991). The relationship between Asperger's syndrome and Kanner's autism. In
U. Frith (Ed.), Autism and Asperger Syndrome. Cambridge, UK: Cambridge
University Press.
Wing, L. (1997). Asperger's syndrome: Management requires diagnosis. Journal of
Forensic Psychiatry, 8(2), 253-257. doi:10.1080/09585189708412008
Wing, L. (1999). Diagnostic interview for social and communication disroders. Manual.
Bromley, U.K.: Ventre for Social and Communication Disorders.
Wing, L. (2000). Past and future of research on Asperger syndrome. In A. Klin, F. R.
Volkmar, & S. S. Sparrow (Eds.), Asperger Syndrome. New York: Guilford
Press.
Wing, L., & Gould, J. (1978). Systematic recording of behaviours and skills of retarded
and psychotic children. Journal of Autism & Developmental Disorders, 8(1), 79-
97. doi:1007/BF01550280
Wing, L., & Gould, J. (1979). Severe impairments of social interaction and associated
abnormalities in children: Epidemiology and classification. Journal of Autism &
Developmental Disorders, 9(1), 11-29. doi:10.1007/BF01531288
279
Wing, L., Gould, J., & Gillberg, C. (2010). Autism spectrum disorder in the
DSM-V: Better or worse than the DSM-IV? Research in Developmental
Disabilities, 32, 768-773. doi:10.1016/j.ridd.2010.11.003
Wistrich, A. J., Rachlinski, J. J., & Guthrie, C. (2015). Heart versus head: Do judges
follow the law or follow their feelings? Texas Law Review, 93(4), 855-923.
Woodbury-Smith, M. R. (2014). Editorial: ASD and illegal behaviours. Journal of
Autism & Developmental Disorders, 44, 2679-2681. doi:10.1007/s10803-014-
2237-0
Woodbury-Smith, M. R., Clare, I., Holland, A. J., Watson, P. C., Bambrick, M., Kearns,
A., & Staufenberg, E. (2010). Circumscribed interests and 'offenders' with autism
spectrum disorders: a case-control study. Journal of Forensic Psychiatry &
Psychology, 21(3), 366-377. doi:10.1080/14789940903426877
Woodbury-Smith, M. R., Clare, I. C. H., Holland, A. J., & Kearns, A. (2006). High
functioning autistic spectrum disorders, offending and other law-breaking:
findings from a community sample. Journal of Forensic Psychiatry &
Psychology, 17(1), 108-120. doi:10.1080/14789940600589464
Woodbury-Smith, M. R., Clare, I. C. H., Holland, A. J., Kearns, A., Staufenberg, E., &
Watson, P. (2005). A case-control study of offenders with high functioning
autistic spectrum disorders. Journal of Forensic Psychiatry & Psychology, 16(4),
747-763. doi:10.1080/14789940500302554
Woodbury-Smith, M. R., & Dein, K. (2014). Autism spectrum disorder (ASD) and
unlawful behaviour: Where do we go from here? Journal of Autism and
Developmental Disorders, 44, 2734-2741. doi:10.1007/s10803-014-2216-5
Wooley, C. (Writer). (2011). A Mother's Burden. In D. Keens (Producer): 60 Minutes.
280
World Health Organisation. (2015). ICD-11 Beta Draft (Joint Linearization
for Mortality and Morbidity Statistics). Retrieved from
http://apps.who.int/classifications/icd11/browse/l-m/en -
/http%3a%2f%2fid.who.int%2ficd%2fentity%2f437815624
World Health Organization. (2004). ICD-10: international statistical classification of
dieases and related health problems, tenth edition, fourth version (2nd ed.).
Geneva: World Health Organization.
Wouters, S. G. M., & Spek, A. A. (2011). The use of the Autism-spectrum Quotient in
differntiating high-functioning adults with autism, adults with schizophrenia and
a neurotypical adult control group. Research in Autism Spectrum Disorders, 5,
1169-1175. doi:10.1016/j.rasd.2011.01.002
Wright, J. C., & Baril, G. L. (2011). The role of cognitive resources in determining our
moral intuitions: Are we all liberals at heart? Journal of Experimental Social
Psychology, 47, 1007-1012. doi:10.1016/j.jesp.2011.03.014
Wright, S. D., Brooks, D. E., D'Astous, V., & Grandin, T. (2013). The challenge and
promise of autism spectrum disorders in adulthood and aging: A systematic
review of the literature (1990-2013). Autism Insights, 5, 21-73.
doi:10.4137/AUI.S11072
Wrightsman, L. S. (1999). Judicial Decision Making: Is Psychology Relevant? New
York: Kluwer Academic/Plenum Publishers.
Young, M. H., Justice, J., & Erdberg, P. (1999). Risk factors for ciolent behaviour among
incarcerated male psychiatric patients: A multimethod approach. Assessment,
6(3), 243-258. doi:10.1177/107319119900600305
281
Young, P. W. (1993). Current Topics: Sex Education for Judges. The
Australian Law Journal, 67, 323 - 327.
Young, R. L., & Rodi, M. L. (2014). Redefining autism spectrum disorder using DSM-5:
The implications of the proposed DSM-5 criteria for autism spectrum disorders.
Journal of Autism & Developmental Disorders, 44, 758-765.
doi:10.1007/s10803-013-1927-3
Zachor, D. A., & Ben-Itzchak, E. (2014). The relationship between clinical presentation
and unusual sensory interests in autism spectrum disorders: A preliminary
investigation. Journal of Autism & Developmental Disorders, 44, 229-235.
doi:10.1007/s10803-013-1867-y
Zalla, T., Barlassina, L., Buon, M., & Leboyer, M. (2011). Moral judgment in adults with
autism spectrum disorders. Cognition, 121(1), 115-126.
doi:10.1016/j.cognition.2011.06.004
Zalla, T., Machery, E., & Leboyer, M. (2008). Intentional action and moral judgment in
asperger syndrome and high-functioning autism.
Zaroff, C. M., & Uhm, S. Y. (2012). Prevalence of autism spectrum disorders and
influence of country of measurement and ethnicity. Social Psychiatry &
Psychiatric Epidemiology, 47, 395 - 398. doi:10.1007/s00127-011-0350-3
Zaykowski, H., Kleinstuber, R., & McDonough, C. (2014). Judicial narratives of ideal
and deviant victims in judges'capital sentencing decisions. American Journal of
Criminal Justice, 39, 716-731. doi:10.1007/s12103-014-9257-3

282
Appendices
283
APPENDIX A
DSM-5 Diagnostic Criteria for Autism Spectrum Disorder
A. Persistent deficits in social communication and social interaction across multiple contexts, as manifested by the following, currently or by history (examples are illustrative, not exhaustive): 1. Deficits in social-emotional reciprocity, ranging, for example, from abnormal
social approach and failure of normal back-and-forth conversation; to reduced sharing of interests, emotions, or affect; to failure to initiate or respond to social interactions.
2. Deficits in nonverbal communicative behaviors used for social interaction, ranging, for example, from poorly integrated verbal and nonverbal communication; to abnormalities in eye contact and body language or deficits in understanding and use of gestures: to a total lack of facial expressions and nonverbal communication.
3. Deficits in developing, maintaining, and understanding relationships, ranging, for example, from difficulties adjusting behavior to suit various social contexts; to difficulties in sharing imaginative play or in making friends; to absence of interest in peers.
Specify current severity:
Severity is based on social communication impairments and restricted, repetitive patterns of behavior (see Table below).
B. Restricted, repetitive patterns of behavior, interests, or activities, as manifested by at least two of the following, currently or by history (examples are illustrative, not exhaustive): 1. Stereotyped or repetitive motor movements, use of objects, or speech (e.g.,
simple motor stereotypies, lining up toys or flipping objects, echolalia, idiosyncratic phrases).
2. Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, need to take same route or eat same food every day).
3. Highly restricted, fixated interests that are abnormal in intensity or focus (e.g., strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interests).
4. Hyper- or hyporeactivity to sensory input or unusual interest in sensory aspects of the environment (e.g., apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement).
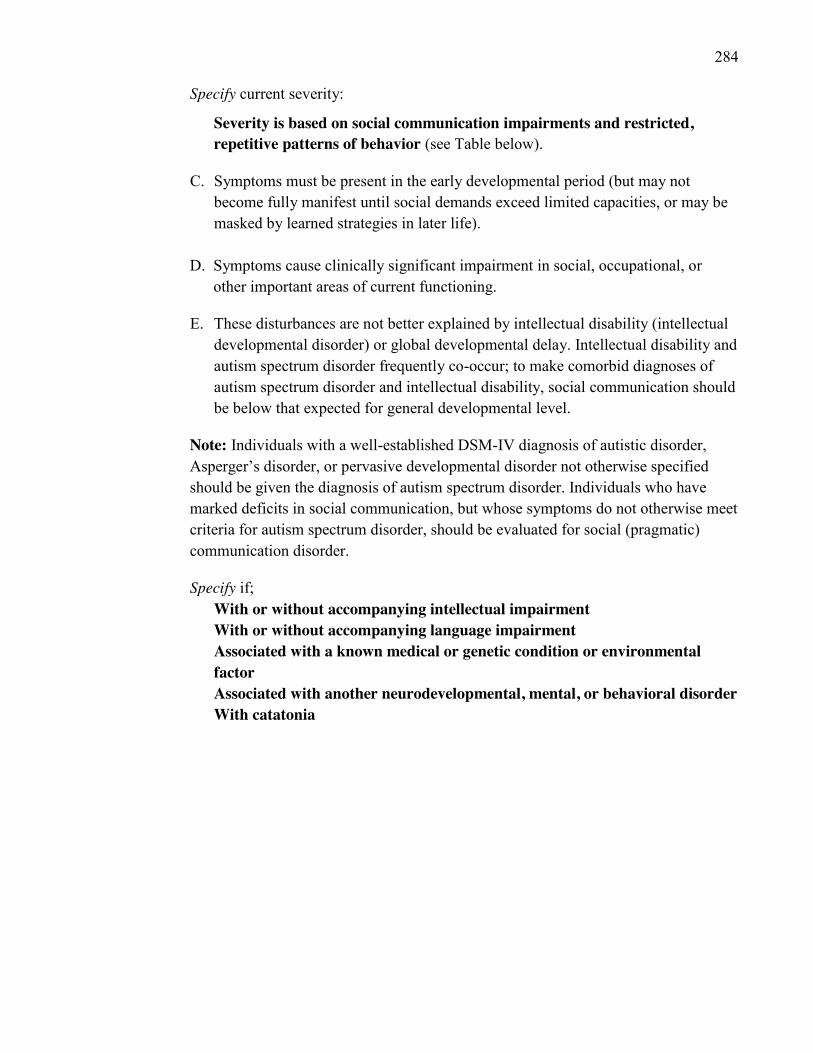
284
Specify current severity:
Severity is based on social communication impairments and restricted, repetitive patterns of behavior (see Table below).
C. Symptoms must be present in the early developmental period (but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life).
D. Symptoms cause clinically significant impairment in social, occupational, or
other important areas of current functioning.
E. These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay. Intellectual disability and autism spectrum disorder frequently co-occur; to make comorbid diagnoses of autism spectrum disorder and intellectual disability, social communication should be below that expected for general developmental level.
Note: Individuals with a well-established DSM-IV diagnosis of autistic disorder, Asperger’s disorder, or pervasive developmental disorder not otherwise specified should be given the diagnosis of autism spectrum disorder. Individuals who have marked deficits in social communication, but whose symptoms do not otherwise meet criteria for autism spectrum disorder, should be evaluated for social (pragmatic) communication disorder.
Specify if; With or without accompanying intellectual impairment With or without accompanying language impairment Associated with a known medical or genetic condition or environmental factor Associated with another neurodevelopmental, mental, or behavioral disorder With catatonia
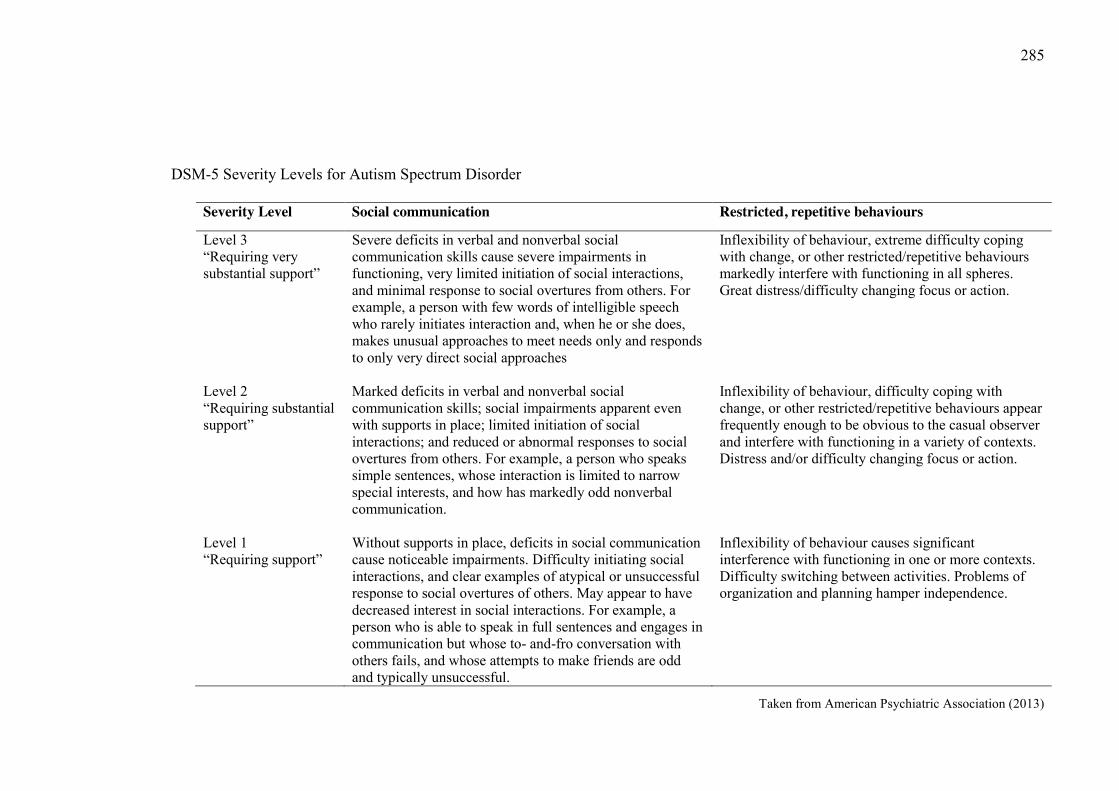
285
DSM-5 Severity Levels for Autism Spectrum Disorder
Taken from American Psychiatric Association (2013)
Severity Level Social communication Restricted, repetitive behaviours
Level 3 “Requiring very substantial support”
Severe deficits in verbal and nonverbal social communication skills cause severe impairments in functioning, very limited initiation of social interactions, and minimal response to social overtures from others. For example, a person with few words of intelligible speech who rarely initiates interaction and, when he or she does, makes unusual approaches to meet needs only and responds to only very direct social approaches
Inflexibility of behaviour, extreme difficulty coping with change, or other restricted/repetitive behaviours markedly interfere with functioning in all spheres. Great distress/difficulty changing focus or action.
Level 2 “Requiring substantial support”
Marked deficits in verbal and nonverbal social communication skills; social impairments apparent even with supports in place; limited initiation of social interactions; and reduced or abnormal responses to social overtures from others. For example, a person who speaks simple sentences, whose interaction is limited to narrow special interests, and how has markedly odd nonverbal communication.
Inflexibility of behaviour, difficulty coping with change, or other restricted/repetitive behaviours appear frequently enough to be obvious to the casual observer and interfere with functioning in a variety of contexts. Distress and/or difficulty changing focus or action.
Level 1 “Requiring support”
Without supports in place, deficits in social communication cause noticeable impairments. Difficulty initiating social interactions, and clear examples of atypical or unsuccessful response to social overtures of others. May appear to have decreased interest in social interactions. For example, a person who is able to speak in full sentences and engages in communication but whose to- and-fro conversation with others fails, and whose attempts to make friends are odd and typically unsuccessful.
Inflexibility of behaviour causes significant interference with functioning in one or more contexts. Difficulty switching between activities. Problems of organization and planning hamper independence.
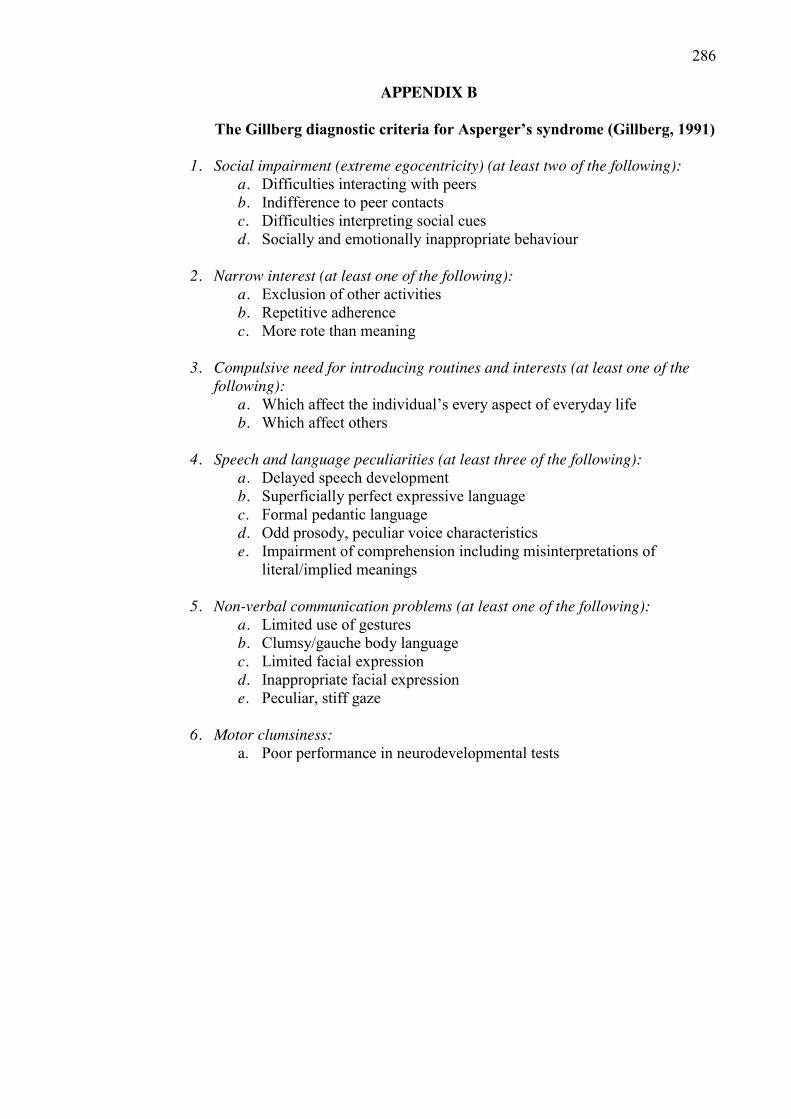
286
APPENDIX B
The Gillberg diagnostic criteria for Asperger’s syndrome (Gillberg, 1991)
1. Social impairment (extreme egocentricity) (at least two of the following): a. Difficulties interacting with peers b. Indifference to peer contacts c. Difficulties interpreting social cues d. Socially and emotionally inappropriate behaviour
2. Narrow interest (at least one of the following):
a. Exclusion of other activities b. Repetitive adherence c. More rote than meaning
3. Compulsive need for introducing routines and interests (at least one of the
following): a. Which affect the individual’s every aspect of everyday life b. Which affect others
4. Speech and language peculiarities (at least three of the following):
a. Delayed speech development b. Superficially perfect expressive language c. Formal pedantic language d. Odd prosody, peculiar voice characteristics e. Impairment of comprehension including misinterpretations of
literal/implied meanings
5. Non-verbal communication problems (at least one of the following): a. Limited use of gestures b. Clumsy/gauche body language c. Limited facial expression d. Inappropriate facial expression e. Peculiar, stiff gaze
6. Motor clumsiness:
a. Poor performance in neurodevelopmental tests
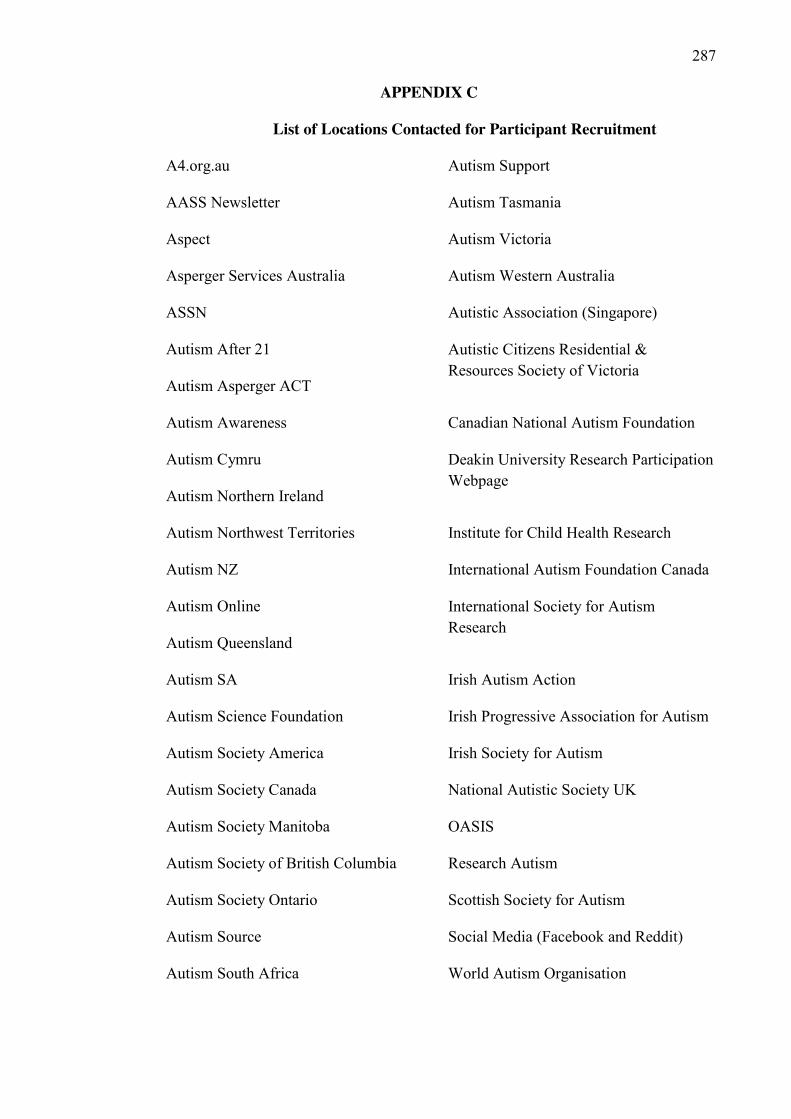
287
APPENDIX C
List of Locations Contacted for Participant Recruitment
A4.org.au Autism Support
AASS Newsletter Autism Tasmania
Aspect Autism Victoria
Asperger Services Australia Autism Western Australia
ASSN Autistic Association (Singapore)
Autism After 21
Autism Asperger ACT
Autistic Citizens Residential & Resources Society of Victoria
Autism Awareness Canadian National Autism Foundation
Autism Cymru
Autism Northern Ireland
Deakin University Research Participation Webpage
Autism Northwest Territories Institute for Child Health Research
Autism NZ International Autism Foundation Canada
Autism Online
Autism Queensland
International Society for Autism Research
Autism SA Irish Autism Action
Autism Science Foundation Irish Progressive Association for Autism
Autism Society America Irish Society for Autism
Autism Society Canada National Autistic Society UK
Autism Society Manitoba OASIS
Autism Society of British Columbia Research Autism
Autism Society Ontario Scottish Society for Autism
Autism Source Social Media (Facebook and Reddit)
Autism South Africa World Autism Organisation
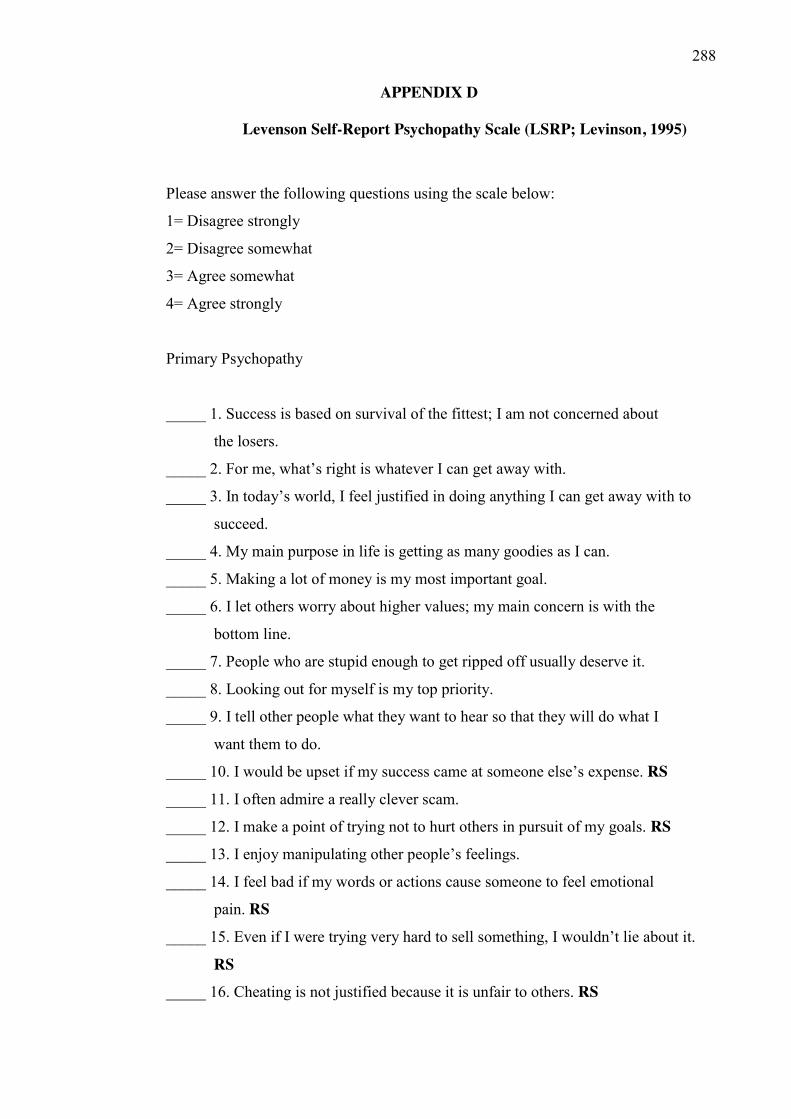
288
APPENDIX D
Levenson Self-Report Psychopathy Scale (LSRP; Levinson, 1995)
Please answer the following questions using the scale below:
1= Disagree strongly
2= Disagree somewhat
3= Agree somewhat
4= Agree strongly
Primary Psychopathy
_____ 1. Success is based on survival of the fittest; I am not concerned about
the losers.
_____ 2. For me, what’s right is whatever I can get away with.
_____ 3. In today’s world, I feel justified in doing anything I can get away with to
succeed.
_____ 4. My main purpose in life is getting as many goodies as I can.
_____ 5. Making a lot of money is my most important goal.
_____ 6. I let others worry about higher values; my main concern is with the
bottom line.
_____ 7. People who are stupid enough to get ripped off usually deserve it.
_____ 8. Looking out for myself is my top priority.
_____ 9. I tell other people what they want to hear so that they will do what I
want them to do.
_____ 10. I would be upset if my success came at someone else’s expense. RS _____ 11. I often admire a really clever scam.
_____ 12. I make a point of trying not to hurt others in pursuit of my goals. RS
_____ 13. I enjoy manipulating other people’s feelings.
_____ 14. I feel bad if my words or actions cause someone to feel emotional
pain. RS
_____ 15. Even if I were trying very hard to sell something, I wouldn’t lie about it.
RS
_____ 16. Cheating is not justified because it is unfair to others. RS
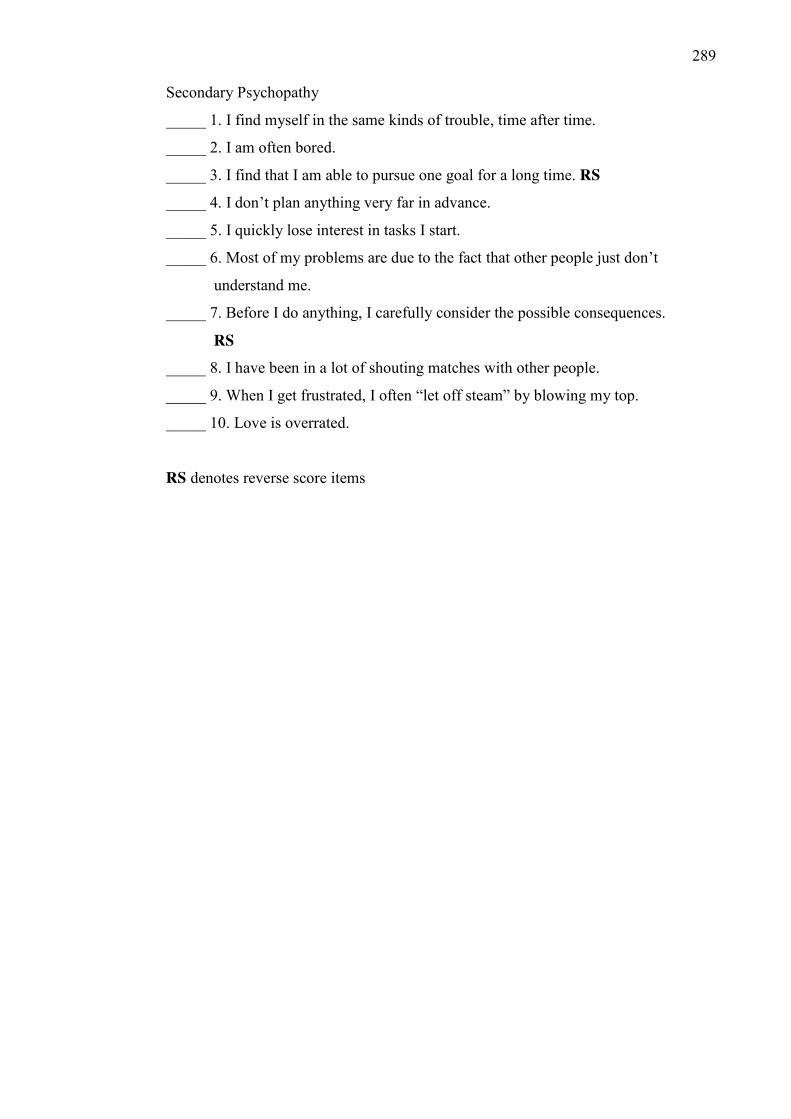
289
Secondary Psychopathy
_____ 1. I find myself in the same kinds of trouble, time after time.
_____ 2. I am often bored.
_____ 3. I find that I am able to pursue one goal for a long time. RS
_____ 4. I don’t plan anything very far in advance.
_____ 5. I quickly lose interest in tasks I start.
_____ 6. Most of my problems are due to the fact that other people just don’t
understand me.
_____ 7. Before I do anything, I carefully consider the possible consequences.
RS
_____ 8. I have been in a lot of shouting matches with other people.
_____ 9. When I get frustrated, I often “let off steam” by blowing my top.
_____ 10. Love is overrated.
RS denotes reverse score items
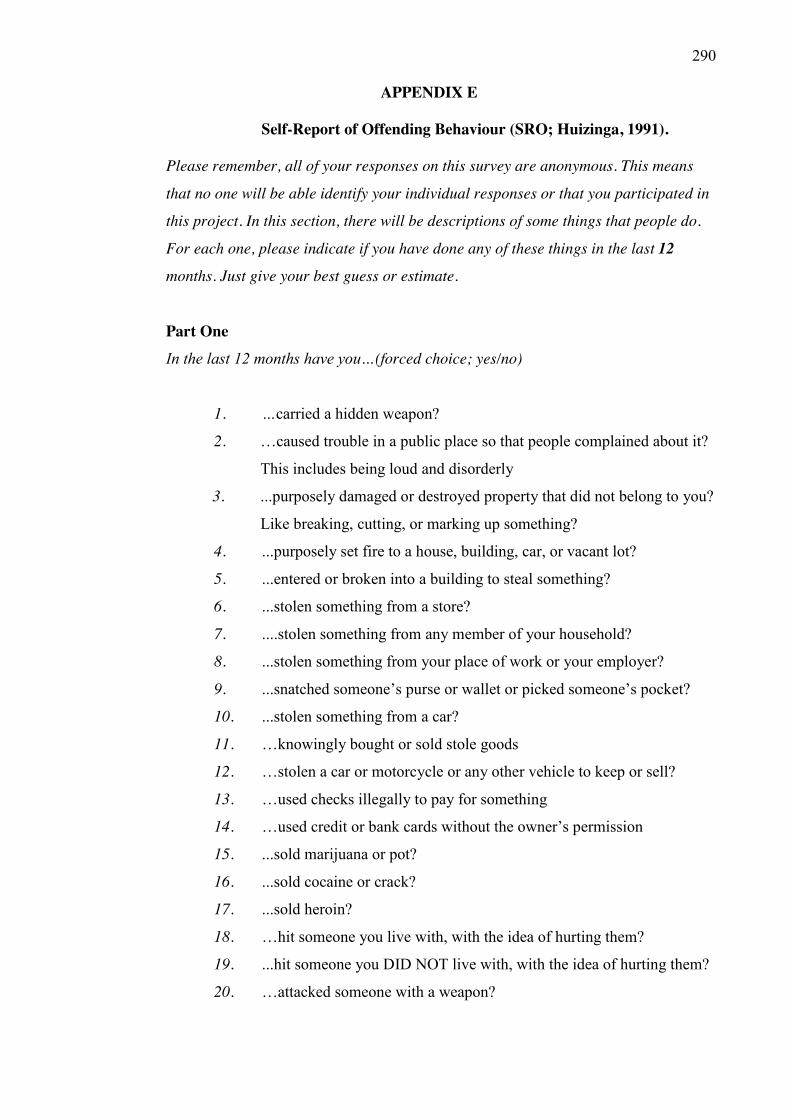
290
APPENDIX E
Self-Report of Offending Behaviour (SRO; Huizinga, 1991).
Please remember, all of your responses on this survey are anonymous. This means
that no one will be able identify your individual responses or that you participated in
this project. In this section, there will be descriptions of some things that people do.
For each one, please indicate if you have done any of these things in the last 12
months. Just give your best guess or estimate.
Part One In the last 12 months have you…(forced choice; yes/no)
1. …carried a hidden weapon?
2. …caused trouble in a public place so that people complained about it?
This includes being loud and disorderly
3. ...purposely damaged or destroyed property that did not belong to you?
Like breaking, cutting, or marking up something?
4. ...purposely set fire to a house, building, car, or vacant lot?
5. ...entered or broken into a building to steal something?
6. ...stolen something from a store?
7. ....stolen something from any member of your household?
8. ...stolen something from your place of work or your employer?
9. ...snatched someone’s purse or wallet or picked someone’s pocket?
10. ...stolen something from a car?
11. …knowingly bought or sold stole goods
12. …stolen a car or motorcycle or any other vehicle to keep or sell?
13. …used checks illegally to pay for something
14. …used credit or bank cards without the owner’s permission
15. ...sold marijuana or pot?
16. ...sold cocaine or crack?
17. ...sold heroin?
18. …hit someone you live with, with the idea of hurting them?
19. ...hit someone you DID NOT live with, with the idea of hurting them?
20. …attacked someone with a weapon?
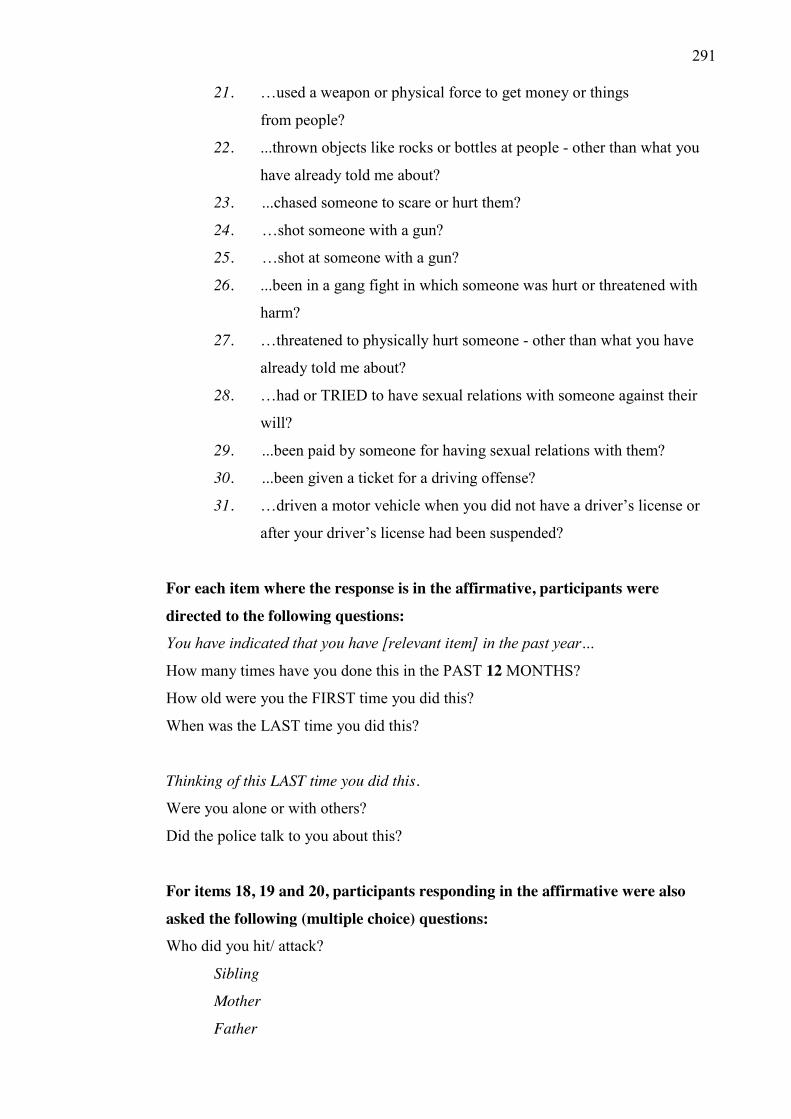
291
21. …used a weapon or physical force to get money or things
from people?
22. ...thrown objects like rocks or bottles at people - other than what you
have already told me about?
23. ...chased someone to scare or hurt them?
24. …shot someone with a gun?
25. …shot at someone with a gun?
26. ...been in a gang fight in which someone was hurt or threatened with
harm?
27. …threatened to physically hurt someone - other than what you have
already told me about?
28. …had or TRIED to have sexual relations with someone against their
will?
29. ...been paid by someone for having sexual relations with them?
30. ...been given a ticket for a driving offense?
31. …driven a motor vehicle when you did not have a driver’s license or
after your driver’s license had been suspended?
For each item where the response is in the affirmative, participants were directed to the following questions: You have indicated that you have [relevant item] in the past year…
How many times have you done this in the PAST 12 MONTHS?
How old were you the FIRST time you did this?
When was the LAST time you did this?
Thinking of this LAST time you did this.
Were you alone or with others?
Did the police talk to you about this?
For items 18, 19 and 20, participants responding in the affirmative were also asked the following (multiple choice) questions: Who did you hit/ attack?
Sibling
Mother
Father
292
Friend
Partner
Partner’s child
Roommate
Neighbour
Acquaintance
Stranger
Other
Was anyone you hit hurt seriously enough to see a doctor?
For item 21, participants responding in the affirmative were also asked: Where did this happen?
School
Playground
Street
Business
Bar
Car
Other (please specify)
For item 28, participants responding in the affirmative were also asked: Did you know this person?
Was the person the opposite or same sex?
Did you physically harm or threaten to hurt this person to get them to have sex with
you?
Part Two. I would now like you to think about any time that you have had contact with the
police. As a result of contact with the police, have any of the following things
happened?
Forced Choice (yes/no)
Were you warned and released?
Were you held in jail for some time?
Were you sent to a treatment program?
293
Were you referred for counselling?
Have you gone to court for something you have done?
Have you been on probation?
Have you been fined money?
Have you had to make restitution or pay someone back?
Have you had to do community service?
Have you been sent to live in a secure hospital or correctional facility?
Have you been arrested or charge with an offense?
String Variable
How many times have you ever been arrested or charged with an offence?
294
APPENDIX F
Crimes Statistics Agency Offence Classification (2015).
Division A - Crimes against the person
A10 Homicide and related offences A11 Murder A12 Attempted murder A13 Accessory or conspiracy to murder A14 Manslaughter A15 Driving causing death A20 Assault and related offences A21 Serious assault A22 Assault police, emergency services or other authorised officer A23 Common assault A30 Sexual offences A31 Rape A32 Indecent assault A33 Incest A34 Sexual offences against children A39 Other sexual offences A40 Abduction and related offences A41 Abduction A42 False imprisonment A43 Slavery and sexual servitude offences A50 Robbery A51 Aggravated robbery A52 Non-Aggravated robbery A60 Blackmail and extortion A61 Blackmail A62 Extortion A70 Stalking, harassment and threatening behaviour A71 Stalking A72 Harassment & private nuisance A73 Threatening behaviour A80 Dangerous and negligent acts endangering people A81 Dangerous driving A82 Neglect or ill treatment of people A83 Throw or discharge object endangering people A89 Other dangerous or negligent acts endangering people
295
Division B - Property and deception offences
B10 Arson B11 Cause damage by fire B12 Cause a bushfire B19 Other fire related offences B20 Property damage B21 Criminal damage B22 Graffiti B29 Other property damage offences B30 Burglary/Break and enter B31 Aggravated burglary B32 Non-aggravated burglary B40 Theft B41 Motor vehicle theft B42 Steal from a motor vehicle B43 Steal from a retail store B44 Theft of a bicycle B45 Receiving or handling stolen goods B46 Fare evasion B49 Other theft B50 Deception B51 Forgery and counterfeiting B52 Possess equipment to make false instrument B53 Obtain benefit by deception B54 State false information B55 Deceptive business practices B56 Professional malpractice and misrepresentation B59 Other deception offences B60 Bribery B61 Bribery of officials
Division C - Drug offences
C10 Drug dealing and trafficking C11 Drug dealing C12 Drug trafficking C20 Cultivate or manufacture drugs C21 Cultivate drugs C22 Manufacture drugs C23 Possess drug manufacturing equipment or precursor
296
C30 Drug use and possession C31 Drug use C32 Drug possession C90 Other drug offences C99 Other drug offences
Division D - Public order and security offences
D10 Weapons and explosives offences D11 Firearms offences D12 Prohibited and controlled weapons offences D13 Explosives offences D20 Disorderly and offensive conduct D21 Riot and affray D22 Drunk and disorderly in public D23 Offensive conduct D24 Offensive language D25 Criminal intent D26 Disorderly conduct D30 Public nuisance offences D31 Privacy offences D32 Hoaxes D33 Begging D34 Defamation and libel D35 Improper movement on public or private space D36 Other public nuisance offences D40 Public security offences D41 Immigration offences D42 Sabotage D43 Hacking D44 Terrorism offences
D49 Other public security offences
Division E - Justice procedures offences E10 Justice procedures E11 Escape custody E12 Fail to appear E13 Resist or hinder officer E14 Pervert the course of justice or commit perjury E15 Prison regulation offences
297
E19 Other justice procedures offences E20 Breaches of orders E21 Breach family violence order E22 Breach intervention order E23 Breach bail conditions E29 Breach of other orders
Division F - Other offences
F10 Regulatory driving offences F11 Drink driving F12 Drug driving F13 Speeding offences F14 Parking offences F15 Licensing offences F16 Registration and roadworthiness offences F19 Other regulatory driving offences F20 Transport regulation offences F21 Public transport F22 Aviation regulations offences F23 Maritime regulations offences F24 Pedestrian offences F29 Other transport regulation offences F30 Other government regulatory offences F31 Betting and gaming offences F32 Commercial regulation offences F33 Liquor & tobacco licensing offences F34 Pornography and censorship offences F35 Intellectual property F36 Prostitution offences F39 Other government regulatory offences F90 Miscellaneous offences F91 Environmental offences F92 Public health and safety offences F93 Cruelty to animals F94 Dangerous substance offences F99 Other miscellaneous offences

298
APPENDIX G
Autism Spectrum Disorder and the Courts Lawyer Response (n = 1).
299
AUTISM SPECTRUM DISORDER AND THE COURTS Should you wish to participate in this research, please provide your responses in the space provided below. If you require more space for your responses, please attach additional pages.
1. What does the term Autism Spectrum Disorder mean to you?
2. What difference do you see, if any, between Autism Spectrum Disorder and intellectual disability?
3. Why do you think it could be important to understand Autism Spectrum Disorder to allow you to do your job effectively?
4. On a scale of 1 to 5 (with 5 being the most competent) how do you perceive your understanding of issues relating to criminal justice and individuals with ASD?
5. What training on Autism Spectrum Disorder have you received/would you like to receive?
That a person has difficulty with emotional communication and understanding social
cues.
3
To give us insight into offending behaviour and relating to clients.
Plenty. ASD is in my understanding related to emotional intelligence rather than
cognitive function.
None but would be welcomed.
300
6. How would you determine whether Autism Spectrum Disorder might be an important consideration for a particular client?
7. In your experience, are persons with Autism Spectrum Disorder more often victims of crimes or perpetrators of crimes?
8. At what stage and for what purpose might you raise a diagnosis of Autism Spectrum Disorder in the context of a criminal trial?
9. In your opinion, should individuals with an Autism Spectrum Disorder receive different treatment in the Criminal Justice System? Why/Why not?
10. What role do you see for forensic psychologists in informing the court regarding Autism Spectrum Disorder?
Thankyou for your participation. Please return your completed survey via the included reply-paid envelope as soon as possible and by 30 May 2014. If you require further information concerning this project you can contact the researchers responsible at ([email protected]) or ([email protected]; or by phone on (03) 92446426).
Very important. Reports are crucial to the court’s understanding of the individual.
Yes. The court must/should take into consideration a person’s needs to ensure the process is fair.
Early on; to explore whether or not the person had an understanding of right/wrong. So, the relationship w/ legal culpability.
Outside of my experience to say.
Specialist neuropsych report.

301
APPENDIX H
Autism Spectrum Disorder and the Courts: Survey Distributed to
Magistrates.
302
AUTISM SPECTRUM DISORDER AND THE COURTS Should you wish to participate in this research, please provide your responses in the space provided below. If you require more space for your responses, please attach additional pages.
1. What does the term Autism Spectrum Disorder mean to you?
2. What difference do you see, if any, between Autism Spectrum Disorder and intellectual disability?
3. Why do you think it could be important to understand Autism Spectrum Disorder to allow you to do your job effectively?
4. On a scale of 1 to 5 (with 5 being the most competent) how do you perceive your understanding of issues relating to criminal justice and individuals with ASD?
5. What training have you received on dealing with people with Autism Spectrum Disorder?
303
6. What training on dealing with people with Autism Spectrum Disorder would you like to receive?
7. In your experience, are persons with Autism Spectrum Disorder more often victims of crimes, or perpetrators of crimes?
8. During sentencing, would a diagnosis of Autism Spectrum Disorder be an important consideration? Why/Why not?
9. In your opinion, should individuals with an Autism Spectrum Disorder receive different treatment in the Criminal Justice System? Why/Why not?
10. What role do you see for forensic psychologists in informing the court regarding Autism Spectrum Disorder?
Thankyou for your participation. Please return your completed survey via the included reply-paid envelope as soon as possible and by 30 May 2014. If you require further information concerning this project you can contact the researchers responsible at ([email protected]) or ([email protected]; or by phone on (03) 92446426).
304
APPENDIX I
Moral Foundations Questionnaire (MFQ; Graham, Haidt & Nosek,
2008).
Part 1.
When you decide whether something is right or wrong, to what extent are the
following considerations relevant to your thinking? Please rate each statement using
this scale:
[0] = not at all relevant (This consideration has nothing to do with my ]
judgments of right and wrong)
[1] = not very relevant
[2] = slightly relevant
[3] = somewhat relevant
[4] = very relevant
[5] = extremely relevant (This is one of the most important factors when I
judge right and wrong)
______Whether or not someone suffered emotionally
______Whether or not some people were treated differently than others
______Whether or not someone’s action showed love for his or her country
______Whether or not someone showed a lack of respect for authority
______Whether or not someone violated standards of purity and decency
______Whether or not someone was good at math
______Whether or not someone cared for someone weak or vulnerable
______Whether or not someone acted unfairly
______Whether or not someone did something to betray his or her group
______Whether or not someone conformed to the traditions of society
______Whether or not someone did something disgusting
305
______Whether or not someone was cruel
______Whether or not someone was denied his or her rights
______Whether or not someone showed a lack of loyalty
______Whether or not an action caused chaos or disorder
______Whether or not someone acted in a way that God would approve of
Part 2.
Please read the following sentences and indicate your agreement or disagreement:
[0] [1] [2] [3] [4] [5]
Strongly Moderately Slightly Slightly Moderately Strongly disagree disagree disagree agree agree agree
______Compassion for those who are suffering is the most crucial virtue.
______When the government makes laws, the number one principle should be
ensuring that everyone is treated fairly.
______I am proud of my country’s history.
______Respect for authority is something all children need to learn.
______People should not do things that are disgusting, even if no one is harmed.
______It is better to do good than to do bad.
______One of the worst things a person could do is hurt a defenseless animal.
______Justice is the most important requirement for a society.
______People should be loyal to their family members, even when they have done
something wrong.
______Men and women each have different roles to play in society.
______I would call some acts wrong on the grounds that they are unnatural.
______It can never be right to kill a human being.
306
______ I think it’s morally wrong that rich children inherit a lot of money
while poor children inherit nothing.
______ It is more important to be a team player than to express oneself.
______ If I were a soldier and disagreed with my commanding officer’s orders, I
would obey anyway because that is my duty.
______ Chastity is an important and valuable virtue.
The Moral Foundations Questionnaire (full version, July 2008) by Jesse Graham, Jonathan Haidt, and Brian Nosek. For more information about Moral Foundations Theory and scoring this form, see: www.MoralFoundations.org
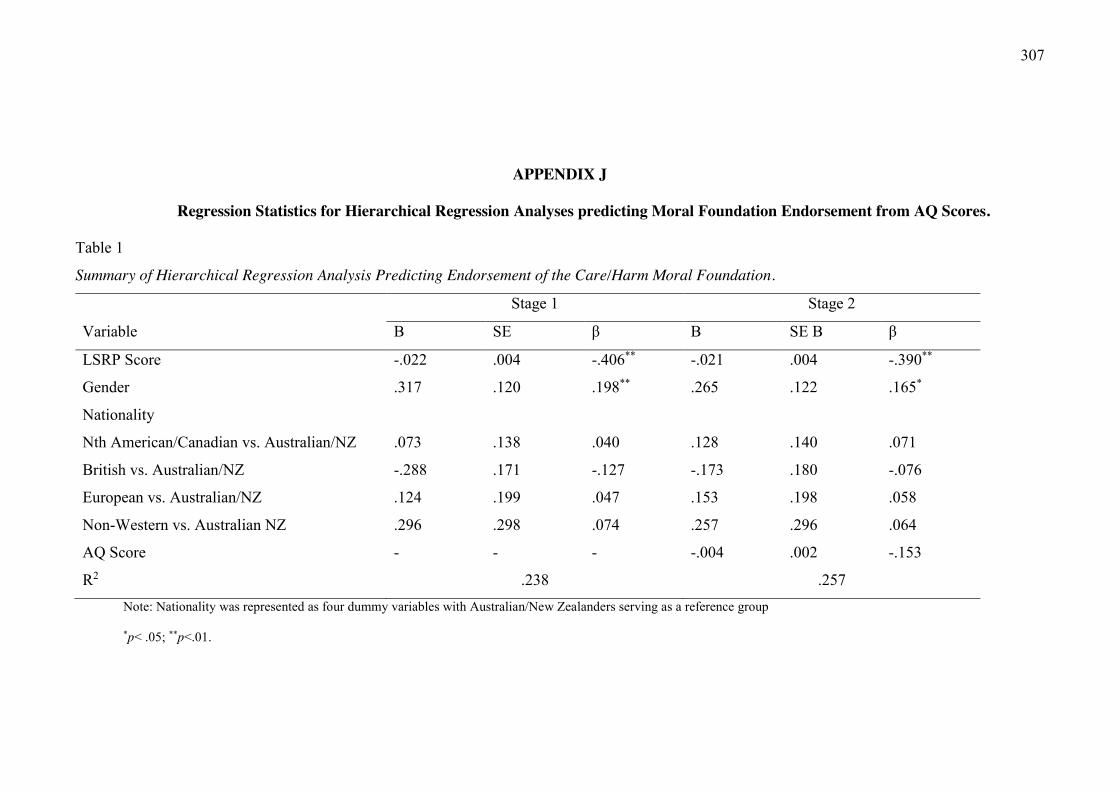
307
APPENDIX J
Regression Statistics for Hierarchical Regression Analyses predicting Moral Foundation Endorsement from AQ Scores.
Table 1
Summary of Hierarchical Regression Analysis Predicting Endorsement of the Care/Harm Moral Foundation.
Stage 1 Stage 2
Variable B SE β B SE B β
LSRP Score -.022 .004 -.406** -.021 .004 -.390**
Gender .317 .120 .198** .265 .122 .165*
Nationality
Nth American/Canadian vs. Australian/NZ .073 .138 .040 .128 .140 .071
British vs. Australian/NZ -.288 .171 -.127 -.173 .180 -.076
European vs. Australian/NZ .124 .199 .047 .153 .198 .058
Non-Western vs. Australian NZ .296 .298 .074 .257 .296 .064
AQ Score - - - -.004 .002 -.153
R2 .238 .257 Note: Nationality was represented as four dummy variables with Australian/New Zealanders serving as a reference group
*p< .05; **p<.01.
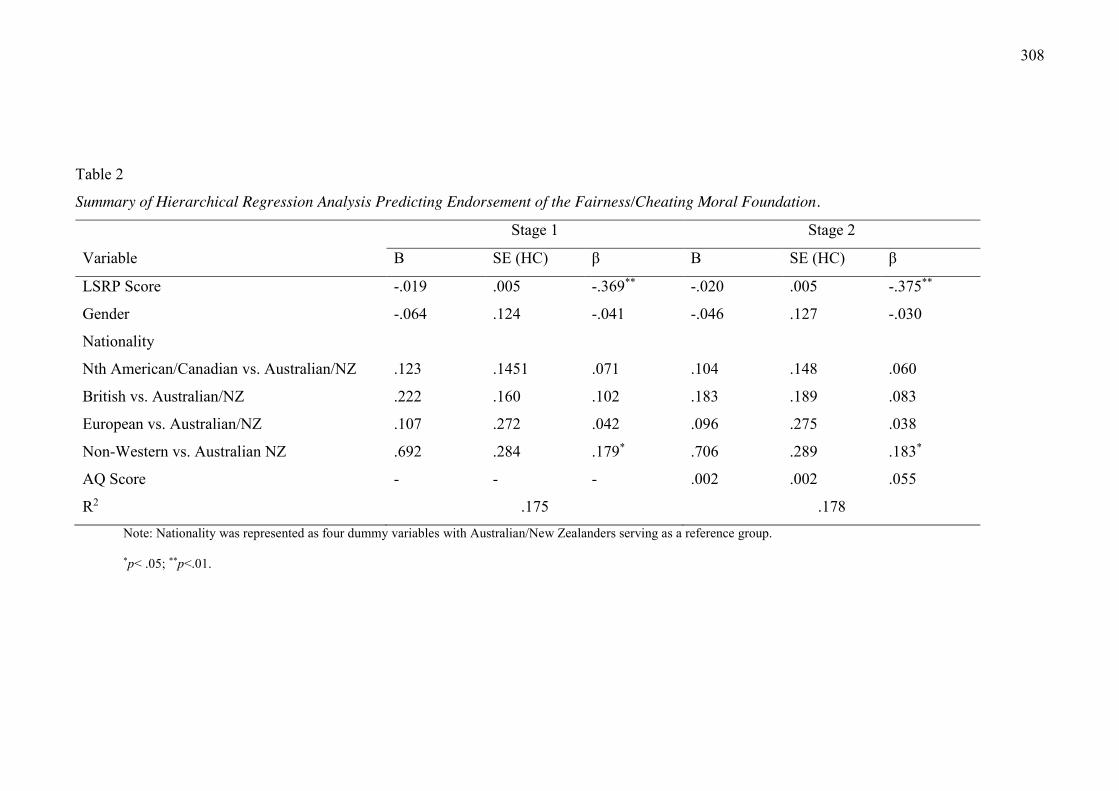
308
Table 2
Summary of Hierarchical Regression Analysis Predicting Endorsement of the Fairness/Cheating Moral Foundation.
Stage 1 Stage 2
Variable B SE (HC) β B SE (HC) β
LSRP Score -.019 .005 -.369** -.020 .005 -.375**
Gender -.064 .124 -.041 -.046 .127 -.030
Nationality
Nth American/Canadian vs. Australian/NZ .123 .1451 .071 .104 .148 .060
British vs. Australian/NZ .222 .160 .102 .183 .189 .083
European vs. Australian/NZ .107 .272 .042 .096 .275 .038
Non-Western vs. Australian NZ .692 .284 .179* .706 .289 .183*
AQ Score - - - .002 .002 .055
R2 .175 .178 Note: Nationality was represented as four dummy variables with Australian/New Zealanders serving as a reference group.
*p< .05; **p<.01.
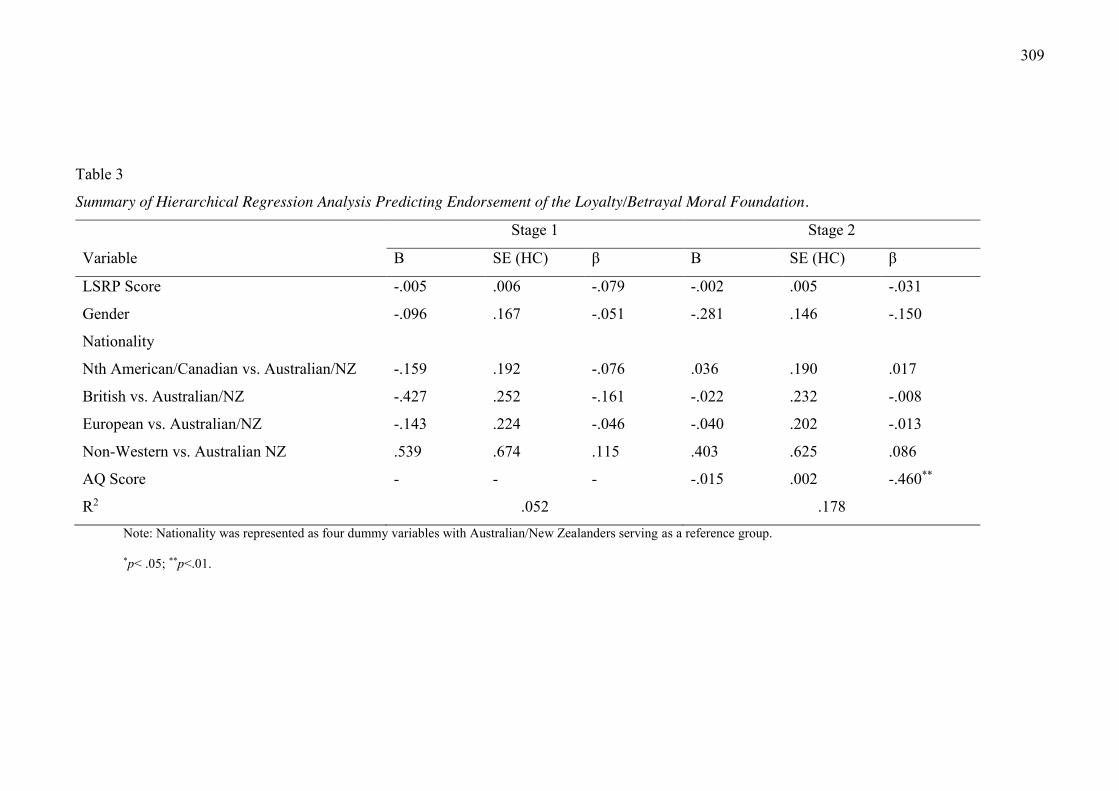
309
Table 3
Summary of Hierarchical Regression Analysis Predicting Endorsement of the Loyalty/Betrayal Moral Foundation.
Stage 1 Stage 2
Variable B SE (HC) β B SE (HC) β
LSRP Score -.005 .006 -.079 -.002 .005 -.031
Gender -.096 .167 -.051 -.281 .146 -.150
Nationality
Nth American/Canadian vs. Australian/NZ -.159 .192 -.076 .036 .190 .017
British vs. Australian/NZ -.427 .252 -.161 -.022 .232 -.008
European vs. Australian/NZ -.143 .224 -.046 -.040 .202 -.013
Non-Western vs. Australian NZ .539 .674 .115 .403 .625 .086
AQ Score - - - -.015 .002 -.460**
R2 .052 .178 Note: Nationality was represented as four dummy variables with Australian/New Zealanders serving as a reference group.
*p< .05; **p<.01.
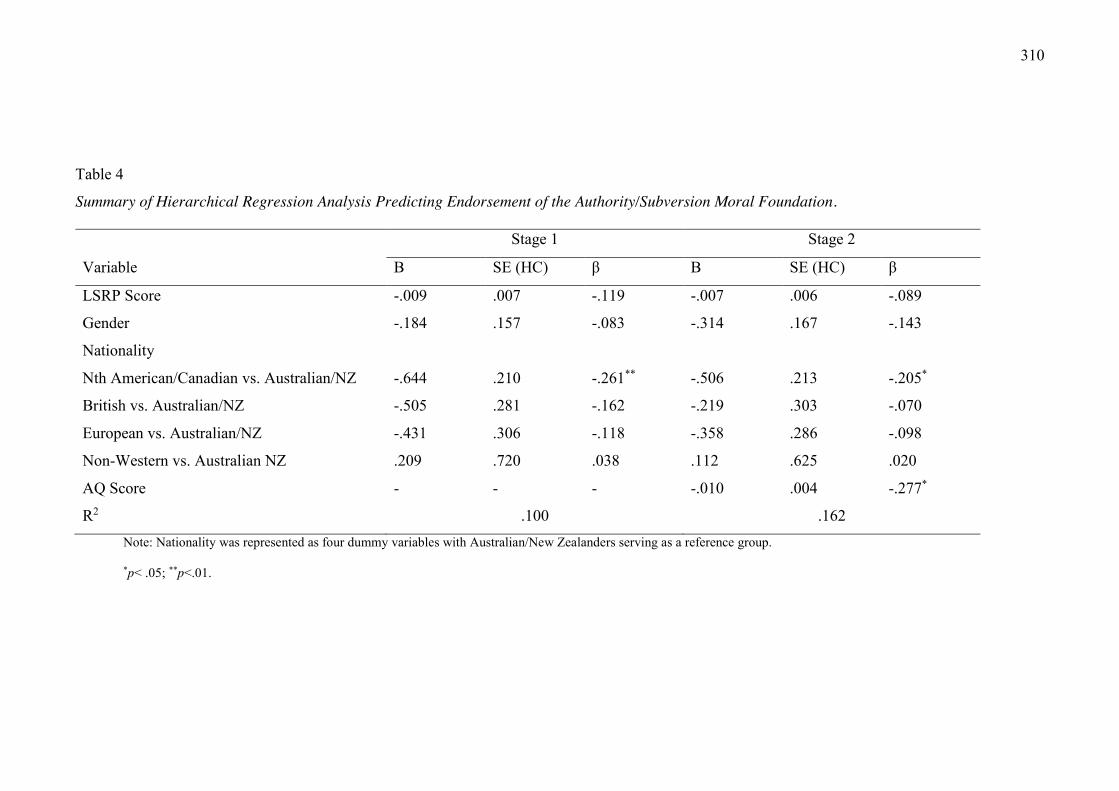
310
Table 4
Summary of Hierarchical Regression Analysis Predicting Endorsement of the Authority/Subversion Moral Foundation.
Stage 1 Stage 2
Variable B SE (HC) β B SE (HC) β
LSRP Score -.009 .007 -.119 -.007 .006 -.089
Gender -.184 .157 -.083 -.314 .167 -.143
Nationality
Nth American/Canadian vs. Australian/NZ -.644 .210 -.261** -.506 .213 -.205*
British vs. Australian/NZ -.505 .281 -.162 -.219 .303 -.070
European vs. Australian/NZ -.431 .306 -.118 -.358 .286 -.098
Non-Western vs. Australian NZ .209 .720 .038 .112 .625 .020
AQ Score - - - -.010 .004 -.277*
R2 .100 .162 Note: Nationality was represented as four dummy variables with Australian/New Zealanders serving as a reference group.
*p< .05; **p<.01.
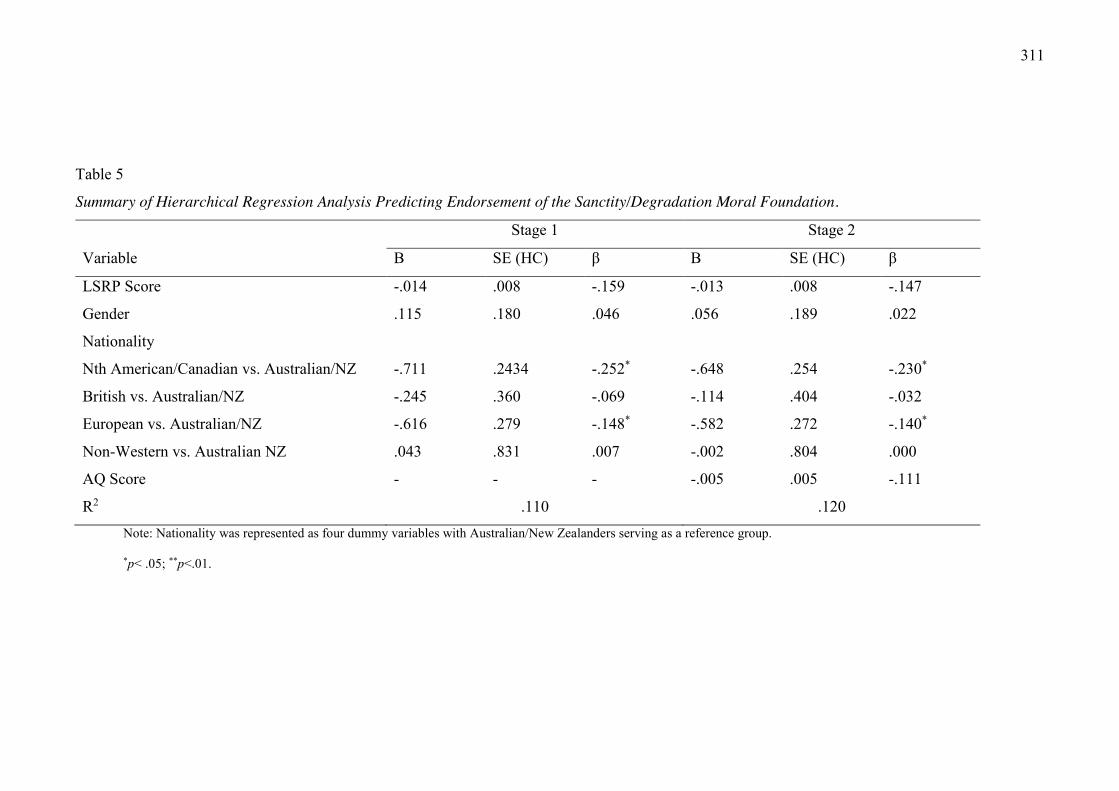
311
Table 5
Summary of Hierarchical Regression Analysis Predicting Endorsement of the Sanctity/Degradation Moral Foundation.
Stage 1 Stage 2
Variable B SE (HC) β B SE (HC) β
LSRP Score -.014 .008 -.159 -.013 .008 -.147
Gender .115 .180 .046 .056 .189 .022
Nationality
Nth American/Canadian vs. Australian/NZ -.711 .2434 -.252* -.648 .254 -.230*
British vs. Australian/NZ -.245 .360 -.069 -.114 .404 -.032
European vs. Australian/NZ -.616 .279 -.148* -.582 .272 -.140*
Non-Western vs. Australian NZ .043 .831 .007 -.002 .804 .000
AQ Score - - - -.005 .005 -.111
R2 .110 .120 Note: Nationality was represented as four dummy variables with Australian/New Zealanders serving as a reference group.
*p< .05; **p<.01.
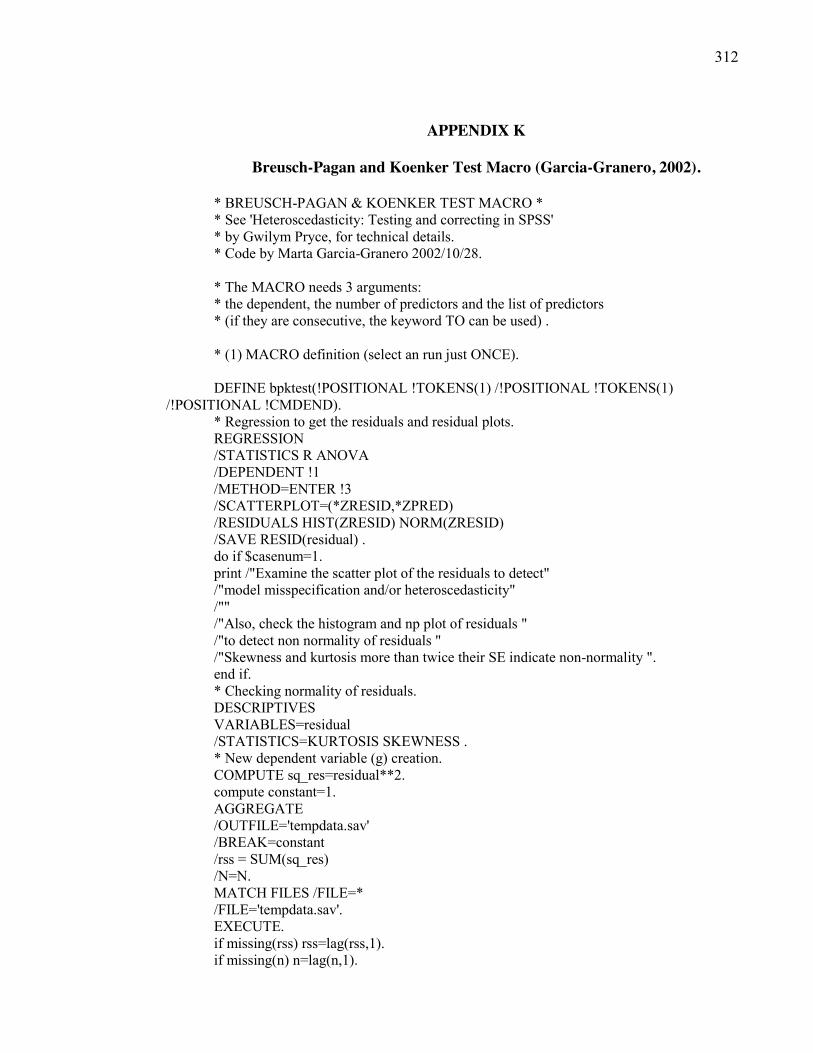
312
APPENDIX K
Breusch-Pagan and Koenker Test Macro (Garcia-Granero, 2002).
* BREUSCH-PAGAN & KOENKER TEST MACRO * * See 'Heteroscedasticity: Testing and correcting in SPSS' * by Gwilym Pryce, for technical details. * Code by Marta Garcia-Granero 2002/10/28. * The MACRO needs 3 arguments: * the dependent, the number of predictors and the list of predictors * (if they are consecutive, the keyword TO can be used) . * (1) MACRO definition (select an run just ONCE). DEFINE bpktest(!POSITIONAL !TOKENS(1) /!POSITIONAL !TOKENS(1)
/!POSITIONAL !CMDEND). * Regression to get the residuals and residual plots. REGRESSION /STATISTICS R ANOVA /DEPENDENT !1 /METHOD=ENTER !3 /SCATTERPLOT=(*ZRESID,*ZPRED) /RESIDUALS HIST(ZRESID) NORM(ZRESID) /SAVE RESID(residual) . do if $casenum=1. print /"Examine the scatter plot of the residuals to detect" /"model misspecification and/or heteroscedasticity" /"" /"Also, check the histogram and np plot of residuals " /"to detect non normality of residuals " /"Skewness and kurtosis more than twice their SE indicate non-normality ". end if. * Checking normality of residuals. DESCRIPTIVES VARIABLES=residual /STATISTICS=KURTOSIS SKEWNESS . * New dependent variable (g) creation. COMPUTE sq_res=residual**2. compute constant=1. AGGREGATE /OUTFILE='tempdata.sav' /BREAK=constant /rss = SUM(sq_res) /N=N. MATCH FILES /FILE=* /FILE='tempdata.sav'. EXECUTE. if missing(rss) rss=lag(rss,1). if missing(n) n=lag(n,1).
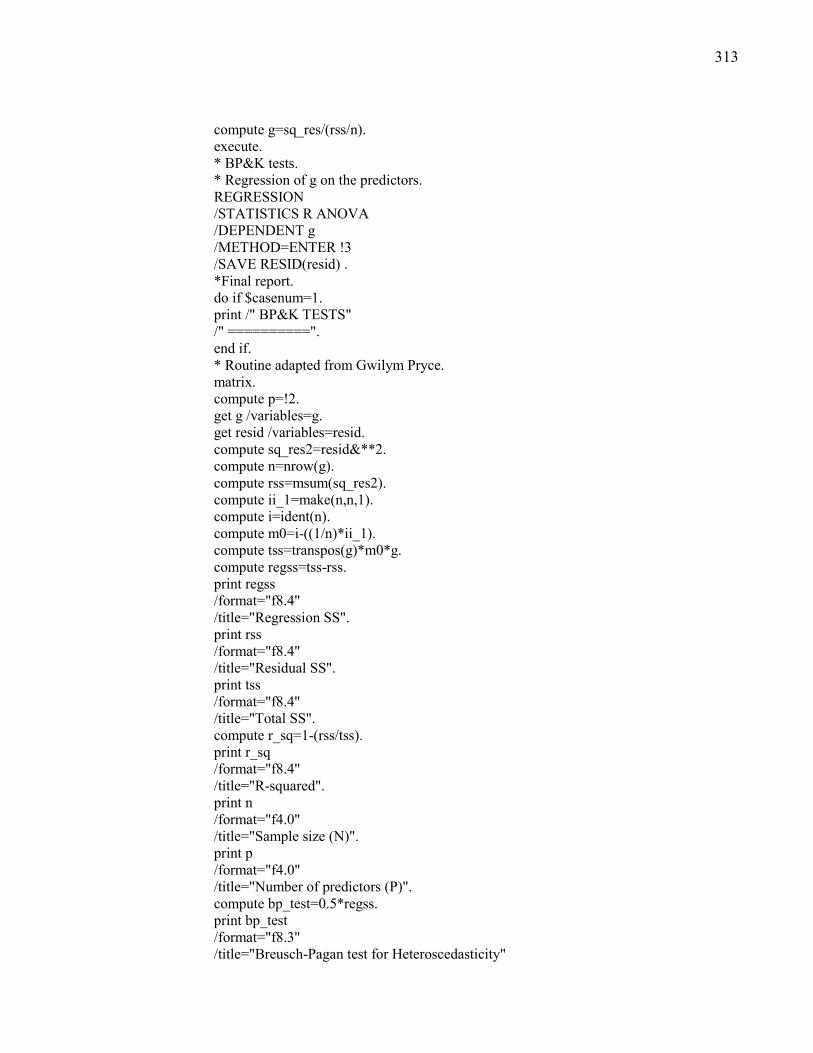
313
compute g=sq_res/(rss/n). execute. * BP&K tests. * Regression of g on the predictors. REGRESSION /STATISTICS R ANOVA /DEPENDENT g /METHOD=ENTER !3 /SAVE RESID(resid) . *Final report. do if $casenum=1. print /" BP&K TESTS" /" ==========". end if. * Routine adapted from Gwilym Pryce. matrix. compute p=!2. get g /variables=g. get resid /variables=resid. compute sq_res2=resid&**2. compute n=nrow(g). compute rss=msum(sq_res2). compute ii_1=make(n,n,1). compute i=ident(n). compute m0=i-((1/n)*ii_1). compute tss=transpos(g)*m0*g. compute regss=tss-rss. print regss /format="f8.4" /title="Regression SS". print rss /format="f8.4" /title="Residual SS". print tss /format="f8.4" /title="Total SS". compute r_sq=1-(rss/tss). print r_sq /format="f8.4" /title="R-squared". print n /format="f4.0" /title="Sample size (N)". print p /format="f4.0" /title="Number of predictors (P)". compute bp_test=0.5*regss. print bp_test /format="f8.3" /title="Breusch-Pagan test for Heteroscedasticity"
314
+ " (CHI-SQUARE df=P)". compute sig=1-chicdf(bp_test,p). print sig /format="f8.4" /title="Significance level of Chi-square df=P (H0:" + "homoscedasticity)". compute k_test=n*r_sq. print k_test /format="f8.3" /title="Koenker test for Heteroscedasticity" + " (CHI-SQUARE df=P)". compute sig=1-chicdf(k_test,p). print sig /format="f8.4" /title="Significance level of Chi-square df=P (H0:" + "homoscedasticity)". end matrix. !ENDDEFINE. * (2) Sample data (replace by your own)*. INPUT PROGRAM. - VECTOR x(20). - LOOP #I = 1 TO 50. - LOOP #J = 1 TO 20. - COMPUTE x(#J) = NORMAL(1). - END LOOP. - END CASE. - END LOOP. - END FILE. END INPUT PROGRAM. execute. * x1 is the dependent and x2 TO x20 the predictors. * (3) MACRO CALL (select and run). COUNT WMTMiss = x1 TO x20 (missing). TEMPORARY. SELECT IF WMTMiss=0. BPKTEST x1 19 x2 TO x19.
315
APPENDIX L
Heteroskedasticity Adjusted Standard Errors Macro (Hayes and Cai, 2007).
DEFINE hcreg (dv =!charend ('/')/iv =!charend ('/') /test = !charend('/') !default (0) /const = !charend('/') !default(1) /method = !charend ('/') !default (3) /covmat = !charend('/') !default(0)). PRESERVE. set length = none. SET MXLOOP = 100000000. MATRIX. GET x/file = */variables = !dv !iv/names = dv/missing = omit. compute y=x(:,1). compute x=x(:,2:ncol(x)). compute iv5 = x. compute pr = ncol(x). compute n = nrow(x). compute L = ident(pr). compute tss=cssq(y)-(((csum(y)&**2)/n)*(!const <> 0)). do if (!const = 0). compute iv = t(dv(1,2:ncol(dv))). compute df2 = n-pr. else. compute iv = t({"Constant", dv(1,2:ncol(dv))}). compute con = make(n,1,1). compute x={con,x}. compute df2 = n-pr-1. compute L1 = make(1,pr,0). compute L = {L1;L}. end if. compute dv=dv(1,1). compute b = inv(t(x)*x)*t(x)*y). compute k = nrow(b). compute invXtX = inv(t(x)*x). compute h = x(:,1). loop i=1 to n. compute h(i,1)= x(i,:)*invXtX*t(x(i,:)). end loop. compute resid = (y-(x*b)). compute mse = csum(resid&**2)/(n-ncol(x)). compute pred = x*b. compute ess= cssq(resid). do if (!method = 2 or !method = 3). loop i=1 to k. compute x(:,i) = (resid&/(1-h)&**(1/(4-!method)))&*x(:,i). end loop. end if. do if (!method = 0 or !method = 1). loop i=1 to k. compute x(:,i) = resid&*x(:,i). end loop. end if. do if (!method = 5). loop i=1 to k. compute x(:,i) = sqrt(mse)&*x(:,i). end loop. end if. do if (!method = 4). compute mn = make(n,2,4). compute pr3 = n-df2. compute mn(:,2) = (n*h)/pr3. compute ex=rmin(mn). loop i=1 to k. compute x(:,i) = (resid&/(1-h)&**(ex/2))&*x(:,i). end loop. end if. compute hc = invXtX*t(x)*x*invXtX. do if (!method = 1). compute hc = (n/(n-k))&*hc. end if. compute F = (t(t(L)*b)*inv(t(L)*hc*L)*((t(L)*b)))/pr). compute pf = 1-fcdf(f,pr,df2). compute r2 = (tss-ess)/tss. compute pf = {r2,f,pr,df2,pf}. do if (!method <> 5). print !method/title = "HC Method"/format F1.0. end if. print dv/title = "Criterion Variable"/format A8. print pf/title = "Model Fit:"/clabels = "R-sq" "F" "df1" "df2" "p"/format F10.4. compute sebhc = sqrt(diag(hc)). compute te = b&/sebhc. compute p = 2*(1-tcdf(abs(te), n-nrow(b))). compute oput = {b,sebhc, te, p}. do if (!method <> 5). print oput/title = 'Heteroscedasticity-Consistent Regression Results'/clabels = "Coeff" "SE(HC)" "t" "P>|t|"/rnames = iv/format f10.4. else if (!method = 5). print oput/title = 'OLS Regression Results Assuming Homoscedasticity'/clabels = "Coeff" "SE" "t" "P>|t|"/rnames = iv/format f10.4. end if. compute iv2 = t(iv). do if (!covmat = 1). print hc/title = 'Covariance Matrix of Parameter Estimates'/cnames = iv/rnames = iv2/format f10.4. end if. do if (!test > 0 and !test < pr). compute L2 = make(pr-!test+!const,!test,0). compute L = {L2;L((pr+1-!test+!const):(pr+!const),(pr-!test+1):(pr))}. compute F = (t(t(L)*b)*inv(t(L)*hc*L)*((t(L)*b)))/!test). compute pf = 1-fcdf(f,!test,df2). compute pf = {f,!test,df2,pf}. print pf/title = "Setwise Hypothesis Test" /clabels = "F" "df1" "df2" "p"/format F10.4. compute iv = t(iv((pr+1-!test+!const):(pr+!const),1)). print iv/title = "Variables in Set:"/format A8. end if. END MATRIX. RESTORE. !END DEFINE. HCREG dv = "variable_name" /iv = "variable_name1" "variable_name2", etc. /const = 1 /method = 3 /covmat = 1 /test = 1





























