Embed Size (px)
Citation preview

Cardiovascular & Haematological Disorders-Drug Targets, 2008, 8, 99-117 99
1871-529X/08 $55.00+.00 © 2008 Bentham Science Publishers Ltd.
Beyond Hemostasis: The Role of Platelets in Inflammation, Malignancy and Infection
Archibald McNicol1,2 and Sara J. Israels3,4,*
1Departments of Oral Biology, 2Pharmacology & Therapeutics, 3Pediatrics & Child Health and 4the Manitoba Institute of Cell Biology, University of Manitoba, Winnipeg, Manitoba
Abstract: Platelets play a complex role in hemostasis and thrombosis. The expression of multiple membrane receptors, both constitutive and activation-dependent, mediates platelet adhesion and aggregation at sites of vascular lesion. Platelet
activation leads to exocytosis of granular constituents, release of newly synthesized mediators, and discharge of mem-
brane-bound transcellular signaling molecules. Many of the same mechanisms that play a role in hemostasis and thrombo-
sis facilitate platelet participation in other physiological or pathological processes including inflammation, malignancy
and the immune response. Platelet receptors such as GPIb/IX/V, P-selectin, P-selectin glycoprotein ligand 1, CD40 and
the IIbß3 integrin, crucial to hemostasis, have been implicated in the progression of such inflammatory conditions as
atherosclerosis, rheumatoid arthritis and inflammatory bowel disease, in the progression and metastatic spread of malig-nancies, and in the immune response to bacterial challenge. The release of platelet granular contents, including adhesive
proteins, growth factors and chemokines/cytokines, that serve to facilitate hemostasis and wound repair, also function in
acute and chronic inflammatory disease and in tumor cell activation and growth. Platelets contribute to host defence as
they recognise bacteria, recruit traditional immune cells to the site of infection and secrete bactericidal mediators. The
primary focus of this review is the “non-haemostatic” functions of platelets in physiological and pathological states.
Key Words: Platelets, inflammation, metastasis, angiogenesis, immunity.
INTRODUCTION
Platelets are the smallest cells in circulating blood, have a biconvex disc structure with an equatorial diameter of 2-3
m, and are anucleate. They are derived from progenitor megakaryocytes in the bone marrow. Following their normal life-span of 8-10 days they are removed from the circulation during passage through the spleen. The role of platelets in hemostasis was recognised very early [1]; their role in thrombosis sometime later [2]. The consequences of platelet dysfunction, and the potential of the platelet as a therapeutic target, have been realized and exploited [3].
In invertebrates the functions of host defence and hemo-stasis are shared by a single cell type. The best-characterized examples of this are the nucleated amebocytes of the horse-shoe crab--these aggregate and release their granule contents in response to such stimuli as exposure to foreign surfaces or bacterial endotoxin [4]. Non-mammalian vertebrate throm-bocytes and mammalian platelets have retained non-hemo-static roles in host defence and inflammation. During the last decade, advances in functional analyses, knock-out models, microscopy and characterization of the platelet proteome have dramatically expanded our understanding of the role of platelets in a variety of patho-physiological states, including inflammatory disorders, tumor progression and infection.
PLATELETS IN HEMOSTASIS AND THROMBOSIS
The dynamics of blood flow dictate that circulating plate-lets are found primarily along the vessel wall, well posi-
*Address correspondence to this author at the Manitoba Institute of Cell Biology, Rm. ON2021A, 675 McDermot Ave. Winnipeg, Manitoba, Canada, R3E 0V9; Tel: (204) 787-4141; Fax: (204) 786-0195; E-mail: [email protected]
tioned for rapid response at sites of endothelial lesions. The platelet response to vessel wall injury with exposure of sub-endothelial collagen is characterized by the phases of adhe-sion, amplification and stabilization. This response is medi-ated by a variety of cell surface receptors, some of which are constitutively present in an active conformation, some of which require structural rearrangement to gain functional integrity, and others that translocate to the platelet surface following platelet activation [5].
The platelet glycoprotein (GP) Ib/IX/V complex acts as an initial adhesive receptor at the endothelial lesion by bind-ing to collagen-associated von Willebrand Factor (vWF). Under low shear conditions, collagen binds to platelets via
the 2ß1 integrin (GPIa/IIa); GPVI and CD36 also bind to collagen. Interestingly, both GPIb/IX/V and CD36 are plate-let receptors for thrombospondin-1, an alternative to vWF in mediating platelet adhesion under defined conditions. Sev-eral other platelet surface integrins function as adhesive re-ceptors, notably IIbß3 (immobilized fibrinogen), 5ß1 (fi-
bronectin), Vß3 (vitronectin) and 6ß1 (laminin) [5].
Following adhesion, a number of soluble mediators en-gage specific receptors that result in platelet activation and amplification of the initial response as additional platelets are attracted to the site. Thrombin, a product of the coagulation cascade, is a powerful platelet agonist, mediated by the pro-tease-activated receptors (PAR) 1 and 4, and by GPIb/ IX/V. Activated platelets release ADP and thromboxane (Tx) A2,both of which promote positive feedback stimuli via P2Y1
and P2Y12, and via TP and TPß receptors, respectively. In addition, platelets express receptors for epinephrine, platelet activating factor (PAF), serotonin, vasopressin and immuno-

100 Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 McNicol and Israels
globulin G (IgG), each contributing to, and enhancing, plate-let activation [5].
Additional platelets are recruited to the site of injury through two specific processes: First the release, by exocyto-sis from platelet dense granules, of serotonin and of a non-metabolic pool of ADP- the latter, in particular, is an impor-tant secondary mediator of platelet activation [6]. Second the synthesis and release of TxA2 a pro-aggregatory mediator critical to the full haemostatic function of the platelet [5]. TxA2 is generated by the sequential actions of phospholipase A2, which liberates arachidonic acid from membrane phos-pholipids, cyclooxygenase-1, which converts arachidonic acid to prostaglandin endoperoxides (PGG2/PGH2), then thromboxane synthetase for the final synthesis of TxA2. At-tenuation of either of these amplification pathways inhibits
platelet function and significantly prolongs bleeding invivo. Therapeutic ADP receptor antagonists, such as clopi-dogrel, and the cyclooxygenase inhibitor aspirin are effective anti-thrombotic agents.
Additional platelets recruited by ADP- or TxA2-mediated mechanisms combine with the fragile layer of adherent plate-lets at the site of injury to form a consolidated hemostatic plug, or aggregate. This is facilitated by an activation-mediated conformational change in the IIbß3 integrin, lead-ing to the expression of its adhesive protein binding domain. Fibrinogen is the major physiological ligand for this domain- a bivalent molecule, fibrinogen binds to IIbß3 molecules on adjacent platelets, establishing firm cross-linking to form a stable plug [5].
In addition to the release of dense granule constituents, two other exocytotic processes occur during platelet activa-tion: the release of alpha granules and of lysosomal granules. Alpha granules contain a large number of proteins of diverse function, including adhesive proteins, chemokines, cytoki-nes, coagulation factors and protease inhibitors (Table 1;note that this table provides the definitions for all alpha granule protein abbreviations that appear in the text) [7,8]. Lysosomal granules contain a variety of acid proteases, acid glycosidases, acid phosphatases and aryl sulfatases [5].
During the process of exocytosis, granular membranes fuse with the plasma membrane, resulting in the translocation of granular membrane proteins onto the platelet surface. In this way, increased numbers of constitutively-expressed proteins, and novel proteins, appear on the platelet surface. Proteins up-regulated on the platelet surface in this manner include the IIbß3 integrin, P-selectin (CD62P), CD63, and the CD40 ligand (CD40L; CD154) [5].
The phospholipid component of platelet plasma mem-branes is significantly altered following activation. The in-crease in expression of phosphatidylserine on the external leaflet of the plasma membrane provides a larger surface area for the assembly of coagulation factor complexes and generation of thrombin. Two populations of small membrane vesicles, microparticles and exosomes, are released from activated platelets [9]. Microparticles have a similar phos-phatidylserine-enriched composition to that of the plasma
membrane of activated platelets and serve to significantly increase the surface area available for thrombin generation. Thrombin activates additional platelets and cleaves fibrino-gen to fibrin; polymerized fibrin stabilizes the platelet plug. Exosomes are smaller membrane vesicles released from acti-vated platelets following fusion of multivesicular bodies and alpha granules with the plasma membrane [9]. Although exosomes do not have procoagulant function, they do ex-press CD63 and prion protein, and have been implicated in the inter-cellular transfer of information.
PLATELETS AND INFLAMMATION
Atherosclerosis
The first suggestion that platelets have a role in inflam-mation came, not surprisingly, from a pair of observations related to atherosclerosis [10,11]: that atherosclerosis was an inflammatory lesion, and that platelets were not merely pas-sive constituents trapped in the atherosclerotic plaque. The etiology of atherosclerosis is highly complex [12,13] and a detailed description is beyond the scope of this review. Briefly, increased levels of circulating low density lipoprotein (LDL) diffuse through endothelial cell junctions into the sub-endothelial matrix. The trapped LDL undergoes a variety of structural modifications, including lipid oxidation, resulting in the formation, and trapping, of minimally oxidized LDL. The accumulation of minimally oxidized LDL triggers the activation of the overlying endothelial cells. This activation is characterized by a loss of vascular integrity, cytokine pro-duction, and the expression and shedding of leukocyte adhe-sive molecules [14], leading to the recruitment and binding of monocytes and lymphocytes. These leukocytes “roll” along the endothelium and pass through endothelial cell junctions in a classic inflammatory response. The intensity of the re-sponse is regulated by multiple factors, including genetic fac-tors, elevated levels of free radicals generated by smoking, hypertension or diabetes mellitus, elevated levels of homo-cysteine, sex hormones and infections (e.g. herpes virus, Chlamydophila pneumoniae). Sub-endothelial monocytes proliferate and differentiate into macrophages that engulf highly oxidized LDL to form foam cells - accumulation of these cells appear as fatty streaks; they release extracellular lipids to form a necrotic core. Under the influence of cytoki-nes and growth factors a mature atherosclerotic fibrous plaque is formed as the necrotic core enlarges, becomes cal-cified and is infiltrated by smooth muscle cells [12,13].
Although it has been long appreciated that platelets are incorporated into the thrombus that forms at the site of ma-ture plaque, their role in the early stages of atherosclerosis has been recognised more recently [15; Fig. (1)]. The charac-terization of the platelet releasate has identified a large num-ber of proteins with significant pro-inflammatory properties, including PF4, interleukin (IL)-1ß and RANTES [8]. Studies using a variety of murine knockout models established that quiescent platelets adhere to, and roll on, stimulated endothe-lial cells and demonstrated that there was a delay in the pro-gression of the disease when certain adhesive proteins were absent [16].

Beyond Hemostasis Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 101
The process underlying the adhesion of quiescent plate-lets to activated endothelial cells has been the subject of con-
siderable study. In vitro studies using activated human um-bilical cord endothelial cells (HUVECs) demonstrated that antibodies to either vWF or IIbß3 attenuate platelet adhe-sion, supporting the role of these proteins in the process [17]. Furthermore, blocking antibodies to the primary platelet vWF receptor GPIb/IX/V inhibited atherosclerotic plaque formation in an apoE-/- murine model, establishing vWF as a
mediator of platelet adhesion to dysfunctional (i.e. where endothelial cell-dependent vasodilation is impaired [14]), and to activated endothelial cells [16,18].
P-Selectin
P-selectin has been implicated as a factor in the platelet-related development of atherosclerosis. P-selectin is expressed only on the surface of activated platelets and, similarly, is ex-pressed following activation of endothelial cells. Intravital microscopy studies in mice have demonstrated that quiescent platelets initially bind loosely to, and then roll on, endothe-
lial cells; these processes are mediated by the expression of P-selectin on endothelial cells, but not on the platelets [16,17,19]. P-selectin glycoprotein ligand 1 (PSGL-1; CD15) and GPIb/IX/V have both been implicated as P-selectin counter-receptors on the platelet surface. Both PSGL-1 and GPIb/IX/V are constitutively expressed on the surface of quiescent platelets and probably function in tandem to medi-ate the initial interaction of platelets with endothelial cell P-selectin [16,17,19]. Regardless of the counter-receptor(s) involved, the P-selectin-mediated adhesion is fragile and reversible (Fig. (1b)).
During the adhesion process, activation of platelets initi-ates a number of events with important pro-inflammatory implications. Activated platelets express several integrins in their “open” conformation, of which IIbß3 is the most im-
portant [16,17,19]. The IIbß3 binds adhesive proteins such as fibrinogen, vWF and fibronectin which tether the platelets to ICAM-1 and Vß2 on activated endothelial cells, thereby consolidating platelet adhesion (Fig. (1c)). Studies in an apoE/ IIb double-deficient murine model showed signifi-
Table 1. Platelet Alpha Granule Constituents
Adhesive Proteins Chemokines Other
Fibrinogen chain
Fibrinogen chain
Fibrinogen chain
Fibronectin
Thrombospondin 1
Vitronectin
Von Willebrand Factor (vWF)
Connective Tissue-Activating Peptide (CTAPIII; CXCL7)
Epithelial Neutrophil Activating Peptide (ENA-78; CXCL5)
GRO- (CXCL1)
I-309 (CCL1)
Interleukin-8 (IL-8; CXCL8)
Macrophage Inflammatory Protein 1 (MIP-1 ; CCL3)
Monocyte Chemoattractant Protein-1 (MCP-1; CCL2)
Monocyte Chemoattractant Protein-3 (MCP-3; CCL7)
Neutrophil-Activating Peptide-2 (NAP-2; CXCL7)
Platelet Basic Protein (CXCL7)
Platelet Factor (PF4; CXCL4)
Platelet Factor 4 variant 1 (PF4alt; CXCL4L1)
Regulated upon Activation, Normal T-cell Expressed, and Se-
creted (RANTES; CCL5)
Stromal Cell-Derived Factor (SDF-1; CXCL12)
Thymus and Activation-Regulated Chemokine (TARC; CCL17)
-Thromboglobulin ( -TG; CXCL7)
Cytokines Growth Factors
Interleukin-1 (IL-1 )
High Mobility Group Box
Chromosomal Protein-1
(HMGB1)
Basic fibroblast growth factor (bFGF)
Epidermal growth factor (EGF)
Hepatocyte growth factor (HGF)
Insulin-like growth factor-1 (IGF-1)
Insulin-like growth factor-2 (IGF-2)
Platelet-derived endothelial cell growth factor (PD-ECGF)
Platelet-derived growth factor (PDGF)
Transforming growth factor (TGF- )
Vascular endothelial growth factor A (VEGF-A)
Vascular endothelial growth factor C (VEGF-C)
Albumin
Amyloid -A4 protein
Angiopoietin-1
Angiostatin
Clusterin
Endostatin
Factor V
Factor XI
Factor XIII
High-molecular weight kininogen (HMWK)
Matrix metalloproteinase-2 (MMP-2)
Metalloproteinase inhibitor-1
Multimerin
Osteonectin
Plasminogen
Plasminogen activator inhibitor (PAI-1)
Protein C inhibitor
Protein S
Secretory granule proteoglycan core protein
(SGPCP)
Thrombocidin-1 (TC-1)
Thrombocidin-2 (TC-2)
Thymosin -4
Tissue inhibitor of metalloproteinase (TIMP-4)
von Willebrand antigen-II
2 macroglobulin
2-antiplasmin
-actinin 1
-actinin 2
-actinin 4
Protein and peptide contents of alpha granules that are released upon platelet activation, in response to a variety of stimuli. From Harrison and Cramer [7] and Coppinger et al. [8].
102 Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 McNicol and Israels
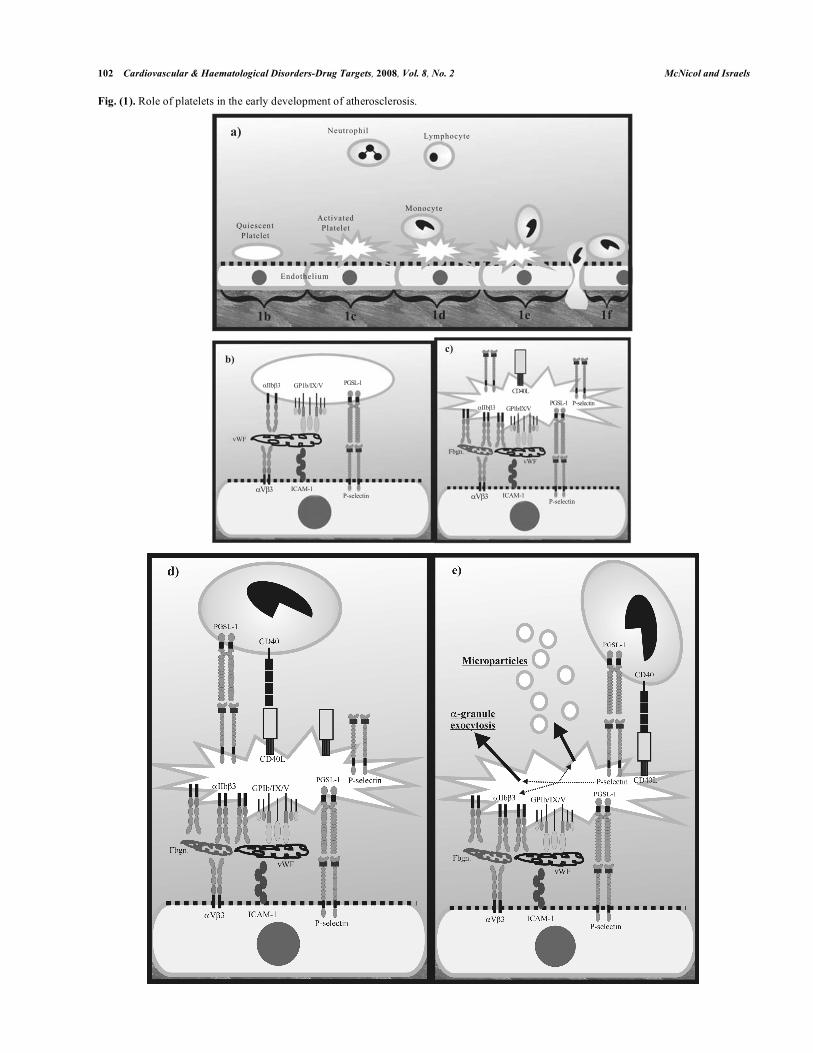
Fig. (1). Role of platelets in the early development of atherosclerosis.
!"
!"#$%&
'()*
'()*$
# ++,-*. /0&12+324!"#$%+ !%567689:;
## ## #$% $ $
<1=;>
?@<
415>A +'>BC%D!%587689:; !%587689:;
##& '(('
#()*+,
-
!++1". "!&12+E24!"#$%&
'()*$
'()*
!"#$%&
!./0-+12**3456748%8
9%504:-07%52*8
*"

Beyond Hemostasis Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 103
(Fig. 1. Contd….)
Fig. (1 a). The progression of platelet involvement during the early stages of atherosclerosis. Quiescent, discoid platelets bind to the dysfunc-tional endothelium (broken line) and become activated, losing their discoid appearance and extending filopodia. Monocytes bind to, then roll
on, the activated platelets and finally migrate through the endothelial layer. Platelet-derived transcellular mediators stimulate changes in the
endothelial cells facilitating the direct binding and rolling of monocytes on the luminal surface. This progression is seen in more detail in fig-
ures 1b-1f.
Fig. (1b). Platelet receptors (GPIb/IX/V, IIb 3, PSGL-1), endothelial cell receptors/counter receptors (ICAM-1, V 3, P-selectin), and
adhesive proteins (vWF) mediate the binding of quiescent platelets to dysfunctional endothelial cells.
Fig. (1c). The platelet is activated, the IIb 3 integrin is in an open, fibrinogen binding conformation, and the platelets express P-selectin and
CD40L.
Fig. (1d). Monocytes, via PSGL-1 and CD40, bind to the adherent, activated platelet
Fig. (1e). Monocytes roll along the adherent platelets to an endothelial cell junction. Concomitantly, platelets release microparticles and se-
crete -granule contents. Microparticles serve to deliver multiple transcellular mediators to the endothelial cell including RANTES.
Fig. (1f). RANTES binds to its serpentine receptor (CCR1/CCR5) leading to an upregulation of the luminal expression of monocyte-binding
adhesive receptors.
cantly reduced atherosclerotic plaque development [17,20]. As outlined above, activated platelets also express P-selectin on their surface, which serves multiple pro-inflammatory roles [16,17,19,21,22]. First, P-selectin mediates the adhesion and rolling of PSGL-1-expressing immune cells (monocytes, neutrophils, lymphocytes) on the adherent platelets (Fig. (1d)). Second, P-selectin-mediated signaling leads to the clustering of IIbß3 on the platelet surface, enhancing the anchoring capacity of the integrin and facilitating firm plate-let adhesion to the endothelium (Fig. (1c,d)). Third, the en-gagement of P-selectin appears critical in the exocytosis of platelet alpha granule-derived chemokines (Fig. (1e); Table 1) some of which have been shown to participate in the de-velopment of the atherosclerotic lesion. Fourth, P-selectin
facilitates the delivery of platelet-derived chemokines, nota-bly RANTES (see below), to the endothelium (Fig. (1e)).
CD40/CD40 Ligand
Platelet adhesion/activation is associated with the upregu-lation of CD40L, a member of the TNF family, which is also found on activated T lymphocytes, monocytes, endothe-lial cells and vascular smooth muscle cells [16,19,23,24,25]. The CD40L receptor is CD40, an integral membrane protein expressed on a variety of cells including B cells, monocytes, endothelial cells, fibroblasts, vascular smooth muscle cells and platelets. A proportion of CD40L is shed from activated platelets in a soluble form (sCD40L); it has been estimated that 95% of circulating sCD40L is platelet-derived [24]. The
C:8FGHIF9:8765
JB30,#
!"#$%&
!%567689:;''J+2''JK
*

104 Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 McNicol and Israels
plasma level of sCD40L is regarded as predictive of recur-rent cardiovascular disorders, such as myocardial infarction and stroke, but not of the development of atherosclerosis [25].
In atherosclerosis, membrane-bound CD40L, but not sCD40L, interacts with endothelial cells and induces the ex-
pression of leukocyte adhesive molecules (e.g. VCAM,
ICAM, E - selectin), pro-inflammatory cytokines (e.g. IL-6, IL-8, MCP-1) and matrix metalloproteinases [24,25]. In ad-dition monocytes and macrophages are activated to release a range of pro-inflammatory mediators. However, the associa-tion between platelet-derived CD40L and the early stages of atherosclerosis is less well defined than, for example, the role played by T lymphocyte-derived CD40L. In contrast, both platelet membrane-bound CD40L and platelet-derived sCD40L play important roles in the later stages of athero-thrombosis where they induce tissue factor expression on endothelial cells and monocytes, and bind directly to IIbß3to stabilize thrombi [23,24,25]. The engagement of platelet CD40 by either sCD40L or CD40L-expressing T-cells leads to the activation of platelets and the exocytosis of RANTES which, as outlined below, appears to be an important pro-inflammatory mediator [26].
Studies using either CD40L-deficient mice or anti-CD40L blocking antibodies showed both decreased overall athero-sclerotic plaque development and a more stable, collagen-rich, macrophage- and T lymphocyte-poor plaque structure [23]. Thus the CD40/CD40L system is implicated in athero-sclerosis, and in a number of other inflammatory disorders
(e.g. arthritis, psoriasis, multiple sclerosis, Crohn’s disease).
Chemokines/Cytokines
Interestingly, platelets also express receptors for a variety of chemokines, notably for MCP-1 (CCR2), IL-8 (CXCR2), fractalkine (CX3CR1), RANTES (CCR1/CCR5), SDF-1 (CXCR4), and TARC and MDC (both CCR4) [19]. Platelet activation has been reported to occur in response to SDF-1 and fractalkine [27]; murine platelets lacking the fractalkine receptor CX3CR1 display a decreased atherosclerotic pheno-type [28]. In contrast, the engagement of CXCR4 or CCR4 by their respective chemokine, although not leading to plate-let activation per se, significantly enhances the effect of low levels of platelet agonists, such as thrombin or ADP [19]. Thus, these chemokines may play a role in the post-adhesion platelet activation early in the development of the atheroscle-rotic lesion. These platelet receptors may also serve to accu-mulate chemokines at the lesion, as has been postulated for CCR2. CCR2 is a low affinity MCP-1 receptor on platelets; the engagement of CCR2 by MCP-1, however, has no effect on platelet function. Platelets transport MCP-1 to the lesion where it dissociates from CCR2 and accumulates at that site [22].
RANTES is a major contributing factor to the vascular inflammation associated with atherosclerosis. It is stored in platelet alpha granules and released following activation as a component of microparticles [19]. The microparticles pro-vide an efficient, localised transfer mechanism, depositing
the RANTES onto the activated endothelium (Fig. (1f)). The binding of RANTES to the endothelium enhances monocyte recruitment and activates monocytic integrins, consolidating their attachment and rolling at the atherosclerotic lesion [29].
PF4 was the first member of the chemokine family iden-tified in platelets. It is released from activated platelets in a P-selectin-dependent manner and, depending on the presence of individual co-stimuli, plays multiple pro-inflammatory roles [19]. In the presence of tumor necrosis factor- (TNF-
), platelet-derived PF4 stimulates both neutrophil exocyto-sis and firm adhesion to the endothelium. It also facilitates RANTES-induced adhesion of monocytes to the endothe-lium. The presence of PF4 and RANTES together is associ-ated with the progression of atherosclerosis, and conversely antagonism of RANTES receptors significantly decreases the size of atherosclerotic lesions. The effects of PF4 are not limited to direct interactions with leukocytes. PF4 has been shown to inhibit the degradation of the LDL receptor, thereby limiting lipoprotein removal with associated pro-atherogenic consequences [17]. PF4 also enhances the uptake of oxidized LDL by macrophages-it is found associated with macrophages in early, and with foam cells in late, atherosclerotic lesions [17].
Platelets store and, upon activation, release a number of other chemokines including MIP-1 , MCP-3, TARC, GRO-
and ENA-78 (Table 1; Fig. (1e)). In addition, ß-TG is a precursor of CTAPIII, PBP and NAP-2. These molecules are likely to have an impact on the recruitment and activation of leukocytes during the progression of atherosclerosis [19,22].
Several cytokines are secreted by activated platelets [17,19], of which IL-1 has been the most widely studied. Platelets store IL-1ß in its precursor pro-IL-1ß form [17,19]. Platelet activation leads to the rapid release of active IL-1ß in both a soluble form and in association with microparticles [19] (Fig. (1e)). Although both forms enhance endothelial cell adhesiveness for neutrophils, microparticle-associated IL-1ß is significantly more effective, possibly because of the presence of additional pro-inflammatory factors, such as P-selectin, on microparticles [30]. The conversion of pro-IL-1ß to IL-1ß, and subsequent release of IL-1ß from platelets, oc-
curs in a ß3 integrin-mediated process and, as demonstrated in vitro, continues for several hours [30]. This suggests that platelets play a significant role in the chronic inflammatory response.
Growth Factors
Several other atherogenic mediators are released by acti-vated platelets that may have a role in the chronic stages of atherosclerosis, although in most cases the evidence is cur-rently circumstantial. PDGF and TGF-ß, both secreted from
-granules, lead to smooth muscle cell proliferation and bio-synthesis respectively [31]. Consequently, both are likely to be involved during the stages of plaque development where smooth muscle cells proliferate and infiltrate the plaque [17].
The contribution of platelets to inflammation associated with other disorders is less well delineated, however platelets have been implicated in the etiology of conditions such as

Beyond Hemostasis Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 105
inflammatory bowel disease (IBD), rheumatoid arthritis, systemic lupus erythematosus, psoriasis and migraine [32].
Inflammatory Bowel Disease
Several lines of evidence support a role for platelets in ulcerative colitis and Crohn’s disease, the two most common forms of IBD [24]. The platelets of individuals with both conditions express significantly elevated levels of activation markers, such as P-selectin and CD40L, in combination with elevated levels of plasma ß-TG, PF4, and sCD40L, consis-tent with platelet activation [24]. Interestingly, the P-selectin expression on platelets has been reported to be found primar-ily in mesenteric rather than in peripheral venous blood. Histopathological examination of rectal mucosal capillaries from patients with IBD showed the presence of mi-crothrombi, although their presence is unrelated to the sever-ity of inflammation. Platelets readily adhere to human intes-
tinal microvascular endothelial cells (HIMECs) incubated in vitro with IL-1ß. The accompanying expression of platelet CD40L serves to facilitate platelet binding to the endothelial cells. CD40L stimulates endothelial cells to upregulate sur-face levels of VCAM-1 and ICAM-1, two primary leukocyte receptors, and to release the neutrophil chemoattractant IL-8 [33]. Platelet-derived sCD40L also stimulates intestinal cells to increase adhesive receptor expression and chemokine re-lease. The platelets of individuals with IBD also release
RANTES, which in in vitro studies, has been shown to be highly bound to HIMECs [24].
Based on these studies, Danese and colleagues have sug-gested a sequence of events whereby platelets adhere to in-testinal microvascular endothelial cells activated by IBD. The platelets release sCD40L, RANTES and potentially other chemokines, which are localized to the endothelium. This results in the increased expression of adhesive receptors, leukocyte adhesion and migration into the interstitium where inflammation occurs [24].
Rheumatoid Arthritis
It is well-documented that platelets accumulate in the synovial fluid of individuals with rheumatoid arthritis, al-though the significance is not well understood. The platelets from individuals with rheumatoid arthritis express increased levels of IIbß3 and form increased numbers of complexes with monocytes, neutrophils and lymphocytes. However, their platelets do not express more P-selectin, nor does their plasma have elevated levels of TGF-ß [34]. Studies using an animal model of arthritis have shown that platelets adhere to, and roll on, arthritic endothelium [35]. Thus it is unclear whether platelets contribute to the disease progression or respond to the pathological setting of rheumatoid arthritis. For example, platelets are responsive to both platelet activat-ing factor and IgG, both of which are elevated in rheumatoid arthritis.
Psoriasis
It has been recognized for 30 years that psoriasis is a risk factor for thrombosis. The circulating blood of patients with psoriasis has significantly more platelet microaggregates and
elevated ß-TG levels, when compared to blood of control individuals [36]. The platelets of individuals with psoriasis are hypersensitive to soluble agonists such as ADP, collagen and arachidonic acid due, at least partly, to enhanced cy-clooxygenase activity [37]. It was suggested that platelet hy-peractivity led to the release of mitogenic and inflammatory mediators that contributed to the psoriasis [36]. More recent studies in a murine model demonstrated that activated plate-lets could roll on skin venules in a P-selectin- and IIbß3 -mediated manner [38]. Furthermore platelet P-selectin ex-pression is increased in individuals with psoriasis [38]. Al-though many platelet-associated inflammatory mediators are
implicated in the progression of psoriasis (e.g. CD40, CD40L, fractalkine) the role, if any, that platelets play in the development of the disease remains conjecture.
Migraines
For several decades platelets have been implicated as one of the principle etiological factors underlying migraine head-ache [3 9,40]. This was based largely on the hypothesis that migraine was considered to be a disorder of vascular tone, that serotonin was the major contributing factor, and that the platelets of these patients abnormally handled serotonin [40]. There is now evidence that migraine can be considered as an inflammatory disorder specifically within cephalic tissue. It is proposed that the release of inflammatory mediators acti-vates peripheral nocioceptors associated with sensory fibres innervating the meninges [41]. A variety of contributing me-diators have been proposed, including protons, free radicals, complement, prostaglandins, kinins and cytokines [41], in-cluding several platelet-derived cytokines (e.g. IL-1, ß-TG).
Although there is no conclusive evidence linking the exocytosis of cytokines from platelets with the onset or pro-gression of migraines, it is interesting to note that platelet hyperactivity has long been recognized as a hallmark of this condition; indeed there is a small, but significant, increase in the incidence of stroke associated with migraines. Thus it is plausible that enhanced platelet release may provide inflam-matory mediators that synergize with other mediators of mi-graine. Furthermore, in common with other inflammatory conditions, there is now evidence that patients experiencing migraine without aura, in contrast to either those with aura or controls, have significantly increased formation of platelet-leukocyte complexes [42]. The identity of the receptors in-volved has not been determined.
Inflammatory Pulmonary Disease
Finally, a role for platelets in various pulmonary condi-tions has been postulated. The platelets of individuals with asthma have higher than control levels of expressed P-selectin [43], and platelet-derived P-selectin functions to re-cruit leukocytes to their lungs [44]. Studies in human ex vivo asthma models demonstrated that antibodies to P-selectin attenuate platelet-leukocyte complex formation and subse-quent pulmonary recruitment [45].
O’Sullivan and Michelson have summarized reports of an intrinsic platelet dysfunction underpinning cystic fibrosis

106 Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 McNicol and Israels
[46]. The platelets from these individuals appear hyperactive with increased production of both TxA2 and sCD40L. The relationship between platelets and the progression of cystic fibrosis remains to be fully addressed [46].
A role for platelet-derived P-selectin in the development of inflammatory lung disease has been recently postulated [47]. In a murine model of acute lung injury, P-selectin-mediated platelet-neutrophil interactions were critical to dis-ease progression, and pulmonary inflammation was attenu-ated by blocking P-selectin. Furthermore antagonism of the platelet TxA2 receptor significantly inhibited platelet-neutro-phil interactions and subsequent neutrophil adhesion to, and activation of, endothelial cells. Thus, it appears the platelet cyclooxygenase pathway modulates the progression of in-flammatory lung disease.
Therapeutic Implications for Inflammation
Anti-platelet drugs (i.e. those agents which affect platelet function) play a well-defined role in the primary and secon-dary prevention of arterial thrombotic disorders. Inhibition of cyclooxygenase-1 by aspirin with resultant decreased TxA2
generation, and antagonism of the ADP receptor by clopi-dogrel or ticlopidine attenuate the amplification pathways of platelet activation. In addition, the blockade of the active site of IIbß3 by humanized antibodies such as abciximab sig-nificantly reduces thrombotic complications associated with percutaneous coronary intervention. The development of safe, effective, orally active IIbß3 antagonists as anti-thrombotics has proved to be more challenging [48].
The multiple effects of platelets in inflammatory diseases suggest that anti-platelet therapy may produce clinical bene-fit in these disorders. Aspirin is well accepted as an anti-inflammatory agent, however its anti-platelet actions are observed at doses (81-325 mg/day), significantly lower than those required for traditional anti-inflammatory effects (1500 mg/day). Some of the beneficial effects of aspirin in cardio-vascular disease, including atherosclerosis, are clearly not a result of an anti-platelet action. For example, aspirin inhibits reactive oxygen formation, increases nitric oxide synthase and reduces C-reactive protein levels, each of which is cardiopro-tective but platelet-independent. Thus the complexity of the situation in atherosclerosis makes it difficult to assign specific benefit to the anti-platelet actions of aspirin in early stages of atherosclerosis. In contrast, platelet inhibition is of funda-mental importance to aspirin’s actions in athero-throm-bosis.
Few studies have addressed traditional anti-platelet drugs in non-atherosclerotic inflammatory conditions. At present, there is little evidence to support a specific anti-platelet action of aspirin in inflammatory disorders.
Interestingly, a number of drugs in addition to traditional
anti-platelet agents (e.g. aspirin, ticlopidine, clopidogrel, abciximab) have been shown to decrease the release of mi-croparticles specifically from platelets, including: pravas-tatin, eprosartan, nifedipine, digoxin, iloprost and vitamin K [49]. Although microparticles have been implicated in a
number of inflammatory conditions, the specific beneficial anti-microparticle effects of these drugs have not been ad-dressed.
PLATELETS AND MALIGNANCY
Platelets play a significant role in the pathogenesis of malignancy. There is now evidence for the contribution of platelets to tumor cell proliferation, metastasis, and tumor angiogenesis, in animal models, and in a variety of tumors types including carcinomas of breast, colon, lung, ovary and melanoma. The association between malignancy and throm-bosis was first recognized in 1865 by the French clinician Armand Trousseau who made the observation that migratory thrombophlebitis could be an indicator of occult malignancy; he subsequently diagnosed his own fatal pancreatic carcinoma by this sign [50,51]. Trousseau’s syndrome, the clinical manifestation of the hypercoagulable state, seen particularly with advanced carcinomas, is the result of a complex interac-tion among tumor cells, inflammatory cells, endothelium and platelets. A decade later, the German surgeon Theodor Bill-roth described tumor thrombi within the blood vessels of patients with cancer, and surmised that tumor emboli played a role in the development of metastatic disease [52].
The interaction of platelets and tumor cells is bidirec-tional, with tumor cell-expressed proteins activating plate-lets, and activated platelets promoting tumor survival and progression by a number of different mechanisms discussed below. The clinical importance of understanding the details of these interactions is to determine whether it is possible to use targeted therapy that prevent the contribution of platelets or their releasates without incurring significant bleeding. Some of these potential targets are common to inflammation and malignancy; inhibiting those targets could abrogate the contribution of platelets in both settings.
The role of platelets in the development of experimental pulmonary metastases was originally recognized by Gasic and colleagues in the 1960s. Thrombocytopenic mice were protected from development of pulmonary metastases fol-lowing tail vein injection of tumor cells [53]; this benefit was reversed by platelet transfusion [54]. Subsequent studies have confirmed a role for platelets in the development of metastases, the formation of tumor emboli and the arrest of tumor cells at sites on the vessel wall [55].
Tumor Cell-Platelet Aggregate Formation
The formation of platelet-tumor aggregates confers a survival advantage to malignant cells by protecting them from immune surveillance [56,57], allowing their persistence in the vascular compartment and enhancing metastatic poten-tial [53,54,58,59]. Platelets facilitate the adhesion of tumor cells to vessel wall and release growth factors that may en-hance tumor cell growth and angiogenesis at sites of ex-travasation (Fig. (2)).
Activation of platelets is the result of multiple mecha-nisms available to tumor cells. Thrombin, cancer procoagu-lant or cathepsin B, and matrix metalloproteinase-2 released
Beyond Hemostasis Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 107
from cancer cells can all activate platelets. Tumor-generated thrombin also has an autocrine effect on tumor cells, and stimulates heterotypic aggregate formation. A second mecha-nism depends on the constitutive expression of tissue factor on the surface of some tumor cells leading to activation of the coagulation cascade and thrombin generation on the pro-coagulant platelet surface. The potential to activate platelets varies among tumor cell lines, but the capacity of tumor cell lines to induce platelet aggregates in vitro correlates with in-creased in vivo thrombosis and metastases [55,60].
Platelet-tumor cell aggregates result from the cross-linking
of platelet integrins, primarily IIb 3, with integrins ex-
pressed on tumor cells, such as v 3 [61], by adhesive
ligands such as fibrinogen, fibronectin and vWF. In some tumor cell lines, including breast, prostate, colon and mela-noma, ectopic expression of megakaryocytic genes results in
the expression of functional IIb 3 [62-65]. Expression of
IIb 3 on tumor cells also may result from its transfer by
microvesicles, released from activated platelets, to the sur-face of malignant cells [66,67]. GPIb/IX/V is involved, and blocking of its interaction with vWF reduces platelet-tumor cell interactions [68-70]. Participation by other receptors
( 3 1, 5 1) and adhesive proteins (laminin, vitronectin, thrombospondin, and collagen) also has been identified [71]. Tumor cell-platelet adhesion mimics that of inflammatory cells, with initial tethering and rolling mediated by P-selectin
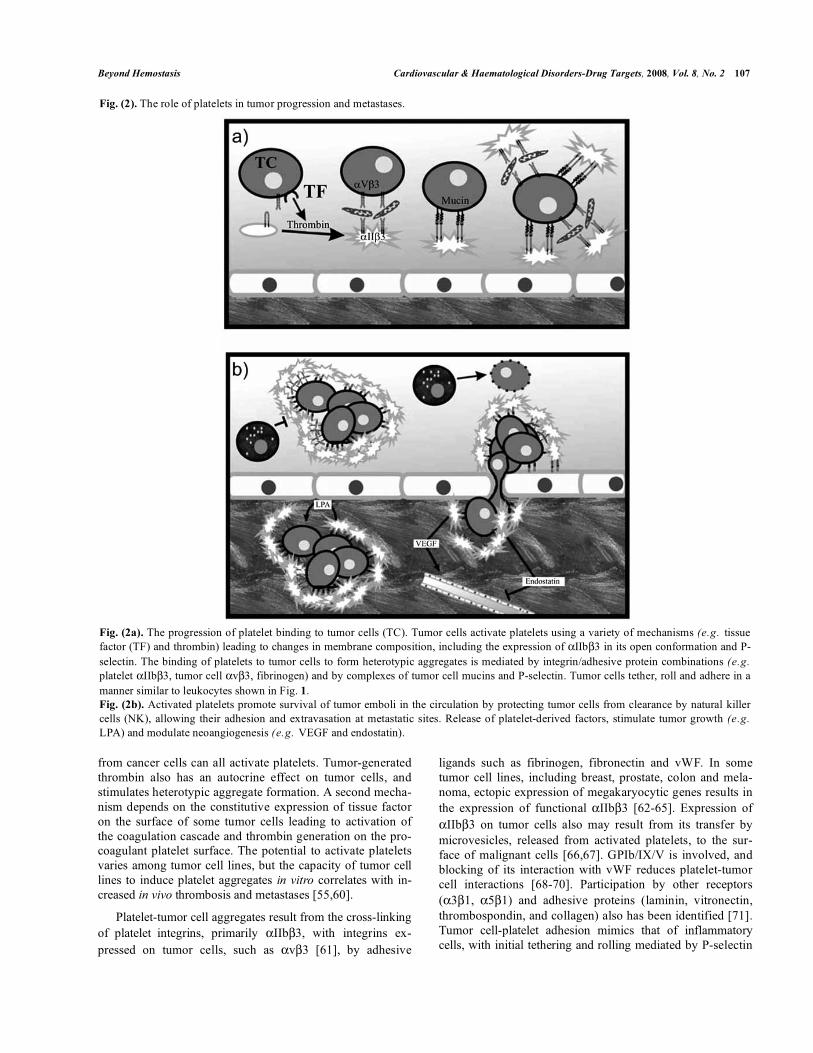
Fig. (2). The role of platelets in tumor progression and metastases.
Fig. (2a). The progression of platelet binding to tumor cells (TC). Tumor cells activate platelets using a variety of mechanisms (e.g. tissue
factor (TF) and thrombin) leading to changes in membrane composition, including the expression of IIb 3 in its open conformation and P-
selectin. The binding of platelets to tumor cells to form heterotypic aggregates is mediated by integrin/adhesive protein combinations (e.g.
platelet IIb 3, tumor cell v 3, fibrinogen) and by complexes of tumor cell mucins and P-selectin. Tumor cells tether, roll and adhere in a
manner similar to leukocytes shown in Fig. 1.Fig. (2b). Activated platelets promote survival of tumor emboli in the circulation by protecting tumor cells from clearance by natural killer
cells (NK), allowing their adhesion and extravasation at metastatic sites. Release of platelet-derived factors, stimulate tumor growth (e.g.
LPA) and modulate neoangiogenesis (e.g. VEGF and endostatin).

108 Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 McNicol and Israels
followed by firm adhesion to 3 integrins by fibrinogen and
vWF [72](Fig. (2a)).
P-selectin, which plays a critical role in the interaction of platelets with inflammatory cells, is also emerging as a piv-otal receptor in platelet-tumor cell interaction and the forma-tion of platelet-tumor cell aggregates. The binding of P-selectin to carcinoma mucins mediates this interaction. Al-though some tumor cells, such as HL-60, express PSGL-1 [21], in most cases, the selectins recognize aberrantly glyco-sylated mucins [73-75] or the GPI-linked surface mucin CD24 [76], which carry sialylated, fucosylated and sulfated carbohydrates [77,78]. Specific cleavage of these mucins blocked platelet binding to the tumor cells [77]. Heparan sulfate-like proteoglycans expressed on some tumors can also function as P-selectin ligands [77,79], and this finding has prompted the investigation of heparin therapy targeted at the selectin-ligand association (see below).
Platelets and Tumor Metastases
The role of platelets in promoting experimental metasta-ses in mouse models has been demonstrated using a variety of techniques to produce thrombocytopenia. More recently, NF-E2 mice with marked thrombocytopenia have been shown to be relatively protected from pulmonary metastases follow-ing tail vein injection of melanoma cells [80]. Fibrinogen deficiency also is protective [80,81]. Platelets play an active role in these models as inhibition of platelet activation or
aggregation abrogates metastatic potential. Inhibition of I-
Ib 3-mediated fibrinogen binding by monoclonal antibodies,
pharmacological inhibitors or by the genetic loss of integrin
3 decreases metastases [82,83,84]. Inhibition of platelet
activation by prostacyclin blocks tumor-induced platelet ac-tivation and experimental metastases [85]. Genetic altera-tions resulting in thrombin receptor PAR-4 deficiency [80]
or G protein G q deficiency [86], give rise to mice with sig-
nificant defects in agonist-induced platelet aggregation and thrombus formation despite normal platelet counts, and pro-tection from hematogenous metastases in comparison to wild-type mice. Similar protection is observed in P-selectin-deficient mice when injected with mucin-producing carci-nomas [87].
The contribution of activated platelets to metastatic po-tential is likely multifactorial (Fig. (2b)). The mechanisms by which platelets contribute to metastases include: (1) The arrest of tumor cells at sites of vascular damage by tethering and rolling on adherent platelet and or endothelial cell ex-pressed P-selectin, followed by integrin-mediated stable adhe-sion [72,88]. The interaction of platelets and tumor cells at the vessel wall bears many similarities to the interaction of platelet/leukocyte responses to inflammation. (2) The provi-sion of a physical barrier protects tumor cells from elimina-tion by the immune surveillance of natural killer cells. Common to several of the knock-out murine models de-scribed above, was the observation that impaired platelet function did not alter the initial localization of tumor cells in the lungs, but did affect the survival and growth of the tumor
emboli [86,87]. In the G q -/- mice this survival advantage
was lost following depletion of NK cells using anti-asialo GM1 antibodies [86], suggesting that activated platelets may prevent the direct cell-cell contact required for NK cell-mediated tumor lysis [56,57,89].
Platelets and Tumor Growth
Activated platelets also contribute directly to tumor cell proliferation and survival at both primary and metastatic sites, by contributing to thrombin generation, release of soluble mediators, and the generation of microparticles and exososmes that transfer other growth mediators to adjacent tumor cells.
Thrombin has been demonstrated to promote tumor growth and metastases in murine models of spontaneously metastasizing breast cancer. Pretreatment of mice with hi-rudin decreased tumor growth by ten-fold, and metastases more significantly [90]. Endogenous thrombin generation results from the expression of tissue factor on the surface of tumor cells activating coagulation factors on the procoagu-lant surface of activated platelets. Ectopic expression of the thrombin receptor PAR-1 on tumor cells and its activation by thrombin enhances tumor cell growth and metastases [71]. This cycle of tumor-induced thrombin generation by platelets and thrombin-induced tumor cell activation and growth can be
interrupted in vitro by either direct thrombin inhibitors [71] or PAR-1 inhibitors [91].
Lysophosphatidic acid (LPA) is a bioactive water-soluble phospholipid that has recently been shown to have a signifi-cant role in cancer cell proliferation, migration and metasta-ses. LPA interacts with G - protein-coupled LPA receptors that feed into multiple effector pathways by activating three G proteins, Gq, Gi and G12/13. In tumor cells these pathways enhance a variety of biological activities including cell pro-liferation, survival, migration, invasion, and the inhibition of differentiation [92,93]. There appear to be several sources for the LPA found in the tumor milieu, including generation of LPA by a tumor cell ecto-enzyme autotaxin, a lysophos-pholipase that cleaves lysophosphatidylcholine. LPA also is generated and released by platelets, the product of phosphol-ipase A2 cleavage of phosphatidic acid. Activation of plate-lets by tumor cells stimulates LPA production and release, which then binds to tumor cell LPA receptors (Fig. (2b)).Using a breast cancer cell line that over-expressed the LPA receptor, tumor cells could be stimulated by the supernatant from activated platelets, and this effect was abolished by treatment of the supernatant with LPA degradation enzymes [94]. In this model, platelet LPA also stimulated tumor cell release of IL-6 and -8, enhancing osteoclast activity and bone resorption at sites of bony metastases [94].
Platelets release growth factors, adhesive proteins and chemokines that stimulate tumor activity directly, or recruit inflammatory cells that release soluble mediators such as
TNF that inhibits tumor cell apoptosis [95], promoting tu-mor cell survival. A potent source of mediators that can in-fluence tumor cell growth is platelet microvesicles, both sur-face-derived microparticles and exosomes, which have been shown to increase the growth and invasive potential of lung

Beyond Hemostasis Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 109
and breast cancer cells. The effects of isolated platelet mi-
crovesicles on tumor cells in vitro included activation of proliferative signaling pathways, and enhanced proliferation and survival of cells in serum-free cultures [66,67]. In-creased numbers of circulating peripheral blood microvesi-cles have been correlated with poorer prognosis in patients with gastric carcinoma [96].
Tumor Angiogenesis
Platelet granules contain both pro-angiogenic and anti-angiogenic factors (Table 2). These factors are released fol-lowing platelet activation and secretion (Fig. (2b)); the bal-ance appears to favour platelets providing a pro-angiogenic stimulus in the context of malignancy [97,98]. Recent evi-dence suggests that pro- and anti-angiogenic mediators may be packaged in distinct subsets of alpha granules [99], and released by specific stimulation of one proteinase-activated receptor, (PAR-1 induces release of VEGF) versus another (PAR-4 induces release of endostatin) [100].
Table 2. Angiogenic Factors in Platelet Alpha Granules
Pro-Angiogenic Mediators Anti-Angiogenic Mediators
VEGF-A and VEGF-C
bFGF
HGF
IGF-1 and -2
EGF
PDGF
PD-ECGF
Angiopoietin- 1
MMP-2
PF4 (CXCL4)
Thrombospondin- 1
Angiostatin
Endostatin
TGF-
PAI-1
TIMP-4
The most significant link between platelets and tumor an-giogenesis may be VEGF. Platelets provide a large reservoir of VEGF that is released following tumor cell-induced acti-vation. The concentration of platelet-derived VEGF is a bet-ter predictor of tumor progression than serum concentrations of VEGF [101]. In vitro studies have shown that platelets stimulate endothelial cell proliferation and tube formation
[102,103], and inhibitors of IIb 3 such as abciximab block
tumor cell-induced platelet VEGF secretion and sprouting of endothelial cells [104]. VEGF stimulates the endothelial cell expression of tissue factor and release of vWF, enhancing platelet adhesion to tumor vessel wall. The abnormal tumor vasculature and resultant turbulent flow also may contribute to platelet adhesion, degranulation and increased release of angiogenic factors within the tumor [105].
The release of platelet-derived microparticles under these conditions also may play a role in angiogenesis; platelet mi-croparticles stimulate tumor cell expression of angiogenic factors including IL-8, VEGF and HGF and membrane met-alloproteinases involved in degradation of extracellular ma-trix and remodeling of the basement membrane [66].
Therapeutic Implications for Malignancies
The complex interaction of platelets with tumor cells makes the platelet and platelet-generated effector molecules apt targets. Despite in vitro studies showing inhibition of tu-mor-cell -induced platelet aggregation, aspirin, ticlopidine and prostacyclin failed to affect experimental metastases in mouse models [54,68]. More success was seen in experimen-tal models with agents such as the chimeric antibody abcixi-mab and the peptide epifibatide that block integrin binding to adhesive proteins. Integrin blockade has been shown to in-hibit platelet-tumor cell adhesion, experimental metastases and platelet-induced sprouting of endothelial cells [68,82, 106]. Inhibitors of thrombin generation, including coumar-ins, heparins, and direct thrombin inhibitors such as hirudin, also decreased experimental metastases [55,71,107].
At present, the most promising therapeutic agent is hepa-rin. Clinical trials have demonstrated a survival advantage for unfractionated and low molecular weight heparins over placebo in subgroups of cancer patients without thrombosis [108,109], and over warfarin in cancer patients with venous thrombosis [110]. The advantage of heparin may be that its effects on tumor growth and metastases are multiple, includ-ing inhibition of thrombin generation, fibrin formation, tumor cell stimulation through PAR-1 receptors, and platelet acti-vation (Table 3). Heparin also blocks binding of tumor cell glyscosaminoglycans to selectins on platelets and endothelial cells, inhibiting formation of heterotypic aggregates and their adhesion to the blood vessel wall [77,111].
Table 3. Anti-Malignant Properties of Heparin
Inhibition of thrombin and fibrin formation
Inhibition of tumor cell adhesion to platelets and endothelial cells
Interference with selectin binding to tumor cell glycosaminoglycans
Inhibition of angiogenesis
Stimulation of apoptosis
Immune system modulation
The ideal therapeutic agent(s) will be one that inhibits platelet adhesion and release without increasing the risk of bleeding beyond a tolerable range. We know little about the optimal timing or duration for these agents to be effective in preventing tumor progression and metastases, as most ex-perimental models are not true reproductions of clinical tu-mor progression.
PLATELETS AND IMMUNITY
The potential association of infections, both bacterial and viral, with the development of cardiovascular disease has long been suspected. The best characterized is infective en-docarditis [112], although a variety of infectious agents also have been implicated in the etiology of conditions such as atherosclerosis [113], myocardial infarction [114] and stroke [115]. Only recently have mechanistic relationships been

110 Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 McNicol and Israels
partially elucidated, and platelets have been implicated as major contributors to the development and progression of infection-associated cardiovascular disease. It is becoming clear, however, that in addition to contributing to adverse out-comes, platelets play a host-defence role against bacterial pathogens in particular [19].
Platelets and Bacteria
The interaction between platelets and bacteria has re-cently been extensively reviewed [116]. Bacterial species cause platelet aggregation utilizing a variety of the mecha-nisms; even within individual species there may be strain-specific mechanisms of platelet activation. For example Staphylococcus aureus, the most frequent causative pathogen responsible for infective endocarditis [117], activates plate-lets by differing mechanisms depending on the presence of specific proteins on the bacterial cell wall. S. aureus can stimulate platelets via mechanisms involving: IgG and its associate platelet receptor Fc RIIA, fibrinogen and its recep-tor IIbß3, vWF and its receptor GPIb/IX/V, and comple-ment [116]. Indeed, the specific process invoked by individ-ual strains of S. aureus likely dictates the speed of the plate-let activation response [116]. A number of other pathogens implicated in infective endocarditis, including species of the Staphylococcus (S. epidermidis, S. capitis) and Streptococ-cus (S. sanguis, S. agalactiae, S. pyogenes, S. gordonii, S. pneumoniae, S. mitis) genii, as well as Neisseria gonnor-rhoeae and Pseudomonas aeruginosa, have been shown to activate platelets using similar strategies to those utilized by S. aureus [116].
The relationship between bacterial infections and coro-nary artery disease is less clear and somewhat controversial. Individuals with active infections are at a higher risk and those who have received antibiotics in the previous year are at lower risk for acute cardiovascular events [116]. Ott and colleagues identified the presence of DNA from a number of different bacterial species in atherosclerotic plaques [113]. Consequently, it has been suggested that coronary artery diseases, such as atherosclerosis [113] and myocardial in-farction [114], are not associated with any single pathogen but rather with the cumulative effects of multiple organisms- the concept of total pathogenic burden [113,114,116].
Helicobacter pylori, coincidentally first reported by Gi-ulio Bizzozero [118] who also shares credit for the original identification of platelets [2], is now accepted as the causa-tive organism of many gastric disorders, and may also in-crease the risk of myocardial infarction and atherosclerosis [119]. Similarly, Chlamydophila pneumoniae (previously known as Chlamydia pneumoniae) has been reported to in-crease the risk of myocardial infarction, although prophylac-tic antibiotic therapy failed to prevent acute events in a high-risk population group [120-122].
Transient bacteremias with normal orally-derived bacte-ria are common, not only after dental procedures (extraction, endodontic treatment, periodontal surgery, root scaling) [123,124] but following regular “non-invasive” procedures such as brushing [125] (notably with the use of electronic
toothbrushes [126]), and in individuals with periodontal dis-ease [127]. Such transient bacteremias, which involve both anaerobes, such as Porphyromonas gingivalis, and aerobes, such as S. sanguis, would contribute significantly and regu-larly to total pathogenic burden. P. gingivalis and S. sanguis have both been isolated from atherosclerotic plaque [128], although only P. gingivalis is a perio-pathogen [129]. Con-sequently there has been considerable interest in the relation-ship between oral disease, primarily periodontal disease, and cardiovascular disease.
A systematic review completed in 2003 suggests an overall moderate association between periodontal disease and athero-thrombosis, including coronary artery disease, stroke and peripheral vascular disease [130]. Furthermore, studies in pigs and in mice have shown that infection with P. gingivalis is as effective as a high cholesterol diet at inducing athero-sclerosis [131,132]. Invasive, perio-pathogenic strains of P. gingivalis have been shown to upregulate the expression of adhesive receptors on [133], and the release of chemoattrac-tants from, cultured endothelial cells [134]. This provides a potential mechanism for the genesis of atherosclerotic le-sions, including the adhesion of platelets to the activated endothelial cells, as outlined above. Interestingly an invasive strain of P. gingivalis enhances tissue factor expression and activity, but attenuates tissue factor pathway inhibitor levels [135], suggesting multiple targets in addition to platelets.
Individual strains of H. pylori, S. sanguis and P. gin-givalis have been shown to activate platelets in vitro [116]. In each case, the presence of IgG and its platelet receptor Fc RIIA and probably, vWF and its platelet receptor GPIb/IX/V, are essential for activation to occur. Fitzgerald and colleagues have proposed a general scheme by which platelet activation can be stimulated by bacterial pathogens (Fig. (3a)). This involves the initial adhesion of the bacte-rium to the platelet - this may involve either the direct inter-action of a bacterial wall or membrane protein (e.g. clumping factors A and B, fibronectin binding proteins A and B, ser-ine-rich protein, serine-aspartate repeat protein), with a plate-let receptor (e.g. GPIb/IX/V, IIbß3) or via an intervening plasma protein (e.g. vWF, fibrinogen). Subsequently, circu-lating antibodies to proteins on the bacterial surface activate the adherent platelets by engaging Fc RIIA [116]. Initial activation includes the synthesis and release of TxA2 (most bacteria-induced platelet aggregation is aspirin-sensitive), and the subsequent expression and occupation of fibrinogen binding sites on IIbß3 for full aggregation to take place. It should be noted that a role for factors excreted by bacteria in platelet activation cannot be excluded [116] (Fig. (3)).
Platelets and Innate Immunity
The response to infection comprises a rapid, antigen-independent innate response and a delayed, prolonged anti-gen-specific adaptive response. The innate response to bacte-rial infections is multi-factorial and has been reviewed for several specific invading organisms [136,137]. In general, bacteria secrete and/or express ligands (e.g. gram negative bacteria-derived LPS, gram positive-derived lipoteichoic ac-
Beyond Hemostasis Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 111
ids, bacterial cell wall peptidoglycans) for the toll-like recep-tor (TLR) family of membrane proteins [138,139]. To date 12 TLRs have been described in humans and have been lo-calized primarily to phagocytic cells (e.g. monocytes, macrophages), epithelial cells and, as discussed below, plate-lets. Several of the TLRs, including TLR-1, TLR-2, TLR-4 and TLR-6 are expressed on the cell surface. TLR-2 forms heterodimeric complexes with TLR-1 or TLR-6 and binds lipoproteins and lipoteichoic acids, whereas TLR-4 recog-nises a variety of ligands, although LPS and viral proteins appear to be its primary agonists. In contrast, some TLRs such as TLR-8 and TLR-9 are located intracellularly and serve as receptors for single stranded RNA and DNA, re-spectively [138,139]. Engagement of TLR-expressing cells leads to cell-specific release of transcellular mediators, pri-
marily chemokines and cytokines that mediate the immune response to invading organisms [138,139].
Interestingly platelets have been shown to express several TLRs, including TLR-1, TLR-2, TLR-4, TLR-6, TLR-8 and TLR-9 [140,141] with increased surface expression of TLR-2 and TLR-9 following activation [141]. The role of platelet TLRs remains unclear. Studies in mice demonstrated that engagement of TLR-4 by LPS stimulated an IIbß3-medi-ated binding of platelets to fibrinogen in the absence of P-selectin expression [142]. Furthermore LPS binding to TLR-4 caused thrombocytopenia in mice and, in the presence of anti-platelet antibodies, was associated with decreased TNFproduction [143]. Recently Semple and colleagues demon-strated that platelet-bound LPS, presumably via TLR-4, syn-
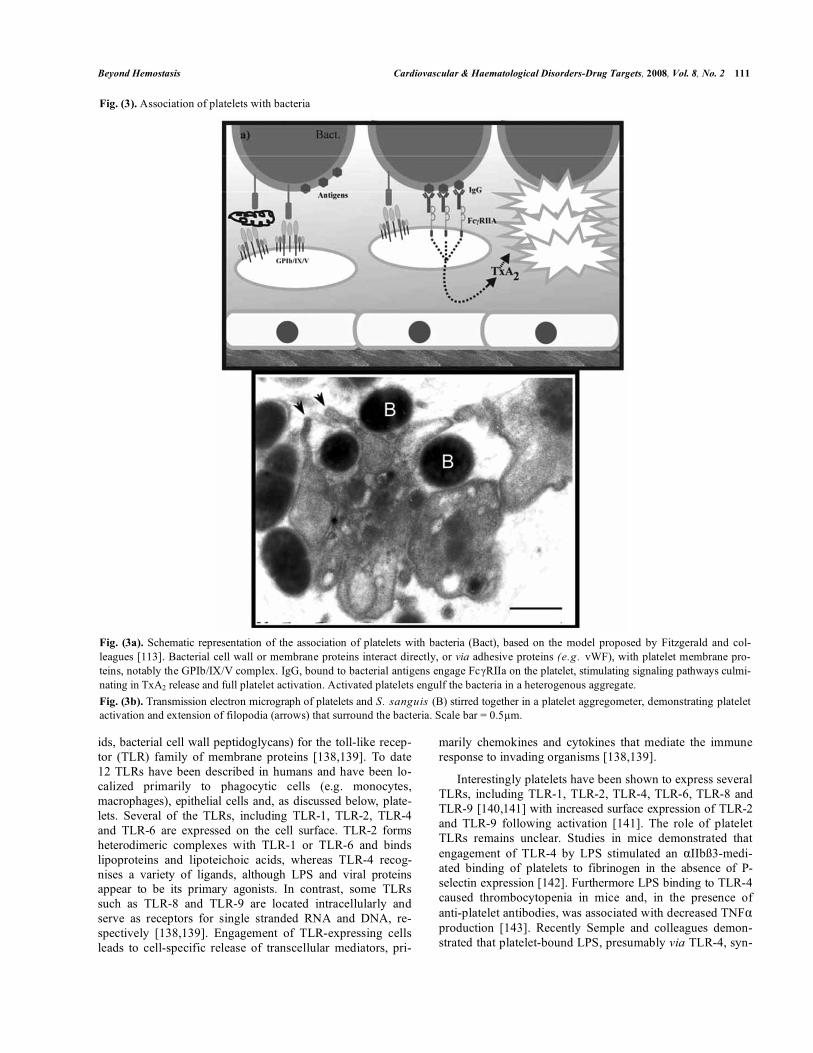
Fig. (3). Association of platelets with bacteria
Fig. (3a). Schematic representation of the association of platelets with bacteria (Bact), based on the model proposed by Fitzgerald and col-
leagues [113]. Bacterial cell wall or membrane proteins interact directly, or via adhesive proteins (e.g. vWF), with platelet membrane pro-
teins, notably the GPIb/IX/V complex. IgG, bound to bacterial antigens engage Fc RIIa on the platelet, stimulating signaling pathways culmi-
nating in TxA2 release and full platelet activation. Activated platelets engulf the bacteria in a heterogenous aggregate.
Fig. (3b). Transmission electron micrograph of platelets and S. sanguis (B) stirred together in a platelet aggregometer, demonstrating platelet activation and extension of filopodia (arrows) that surround the bacteria. Scale bar = 0.5 m.

112 Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 McNicol and Israels
ergizes with anti-platelet antibodies thereby enhancing Fc-receptor-mediated phagocytosis [144].
The effects of LPS on IIbß3-mediated fibrinogen binding may suggest a role for TLRs in platelet activation. The LPS-induced release of sCD40L from platelets was attenuated by blockade of TLR-4 but not of TLR-2 or TLR-9 [145], consis-tent with the elevated levels of sCD40L observed in the plasma of patients with meningococcal sepsis [146]. In con-trast, Ward and colleagues were unable to show an effect of ligands for TLR-2 or TLR-4 on cytosolic calcium mobilisa-tion, P-selectin expression or aggregation, either alone or in combination with traditional platelet agonists such as platelet activating factor, epinephrine or ADP[147].
Anti-Bacterial Efects of Platelets
Intriguingly platelets may serve an anti-bacterial function. It has been proposed that, as platelets rapidly accumulate at sites of injury/infection, they may play similar “surveillance” roles to that of traditional immune cells such as macro-phages, mast cells and dendritic cells [148]. The upregula-tion of CD40L on the platelets surface (in response to vascu-lar damage, soluble agonists or bacteria) has effects on adap-tive immunity, including accelerating dendritic cell matura-tion, stimulating IgG production by B cells and enhancing T cell activity [149]. Bacteria-induced platelet activation re-sults in the secretion of granular contents, including various chemokines that, as outlined above for inflammation, serve to attract immune cells (monocytes, basophils, NK cells, macrophages) to the site of infection [148]. Finally, platelets adhering to and aggregating around bacteria may promote bacterial clearance [148]; indeed activated platelets may in-ternalize bacteria thereby removing them from the circula-tion [19].
Platelet alpha granules also contain thrombocidins, mem-bers of a family of anti-bacterial proteins that are found pri-marily in neutrophils and play a central role in the innate immune system [19]. Two thrombocidins have been charac-terized, TC-1 and TC-2, which are variants of neutrophil-activating peptide-2 (NAP-2) and connective tissue-acti-vating peptide-III (CTAP-3) respectively. TC-1 and TC-2, but not the parent molecules, are bactericidal for several organ-isms including E. coli and S. aureus, and are fungicidal for Cryptococcus neoformans [150]. Studies in rabbits have shown thrombocidins to be important for host defence against Streptococci-induced endocarditis [151]. Further-more, the thymosin- 4, PBP, RANTES and PF-4 released from activated platelets have been reported to have bacterio-
cidal effects against E. coli and S. aureus when tested in vitro [152].
Platelets and Viruses
Associations between platelets and several viral infections have been proposed. The hepatitis B virus (HBV) will bind to GPVI on the platelet membrane which, it has been sug-gested, may serve to facilitate viral transport and promote viral survival [153]. Studies, primarily in animal models of HBV infection, have demonstrated that platelets facilitate the
accumulation of cytotoxic T lymphocytes in intrahepatic sites of necrosis and inflammation It is unclear whether this is the result of the interaction of platelets with HBV particles or platelet participation in the inflammatory response as out-lined above.
Platelets have been shown to engulf viruses, most notably human immunodeficiency virus type 1 (HIV-1); a significant proportion of circulating HIV-1 is associated with platelets. The adhesion of HIV-1 to platelets is mediated by two plate-let membrane proteins, dendritic cell-specific intercellular adhesion molecule 3-grabbing non-integrin (DC-SIGN), and C-type lectin-like receptor 2 (CLEC-2) [156]. DC-SIGN facilitates the endocytosis of HIV-1 by platelets [157], whereas CLEC-2 is linked to Src kinase/phospholipase C 2pathways and is unlikely to be involved in HIV-1 uptake [156]. The importance of these platelet receptors, viral up-take and intracellular signaling to the progression of HIV-1 disease is unknown.
Platelets and Prions
The transmissible spongiform encephalopathies (TSE) are a family of neurodegenerative disorders that include bo-vine spongiform encephalopathy in cattle, scrapie in sheep, and Creutzfeldt-Jakob Disease and Gerstmann-Straussler-Schienker syndrome in humans. Infectious forms of TSE are due to a variant protease-resistant form (PrPres) of a normal cellular protein, prion protein (PrP) [158]. PrP is a gly-cophosphatidylinositol-linked membrane protein of unknown function. However, its conversion to PrPres renders the pro-tein highly infectious, affecting health care and agricultural policies worldwide. PrP is present on the membrane of plate-let alpha granules [159] and is released on exosomes following platelet activation [160]. The presence of PrPres in platelets has not been reported, however its sequestration, and subse-quent exosomal release, could have significant implications for TSE disease transmission, notably by blood transfusions [161].
Therapeutic Implications for Infections
The therapeutic implications of manipulating interactions between platelets and bacteria have not been widely ad-dressed, although several antibiotics, notably penicillin, may have anti-platelet side-effects. The increased understanding of the role of both bacterial pathogens and platelets in the development of atherosclerosis has led to the identification
of specific potential targets. The IgG receptor Fc RIIA is a
common mediator of platelet responses to multiple bacterial species. Antagonism of this receptor represents a logical strat-egy [116], particularly in keeping with the concept of total
pathogenic burden. Furthermore, Fc RIIA antagonists are
unlikely to compromise the hemostatic function of platelets, avoiding the bleeding risks associated with traditional anti-platelet drugs. The anti-bacterial potential of platelets could be utilized by selectively releasing, or mimicking, thrombo-cidins.
The role of platelet interactions with T lymphocytes in the progression of hepatic necrosis and inflammation caused by

Beyond Hemostasis Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 113
HBV, has raised the possibility that anti-platelet drugs may reduce the severity of chronic liver disease in HBV infected individuals [154] Studies are currently underway to deter-mine the beneficial effects of aspirin and clopidogrel in HBV-induced liver disease.
CONCLUSION
Platelets have retained many of the functions of the primitive multi-functional hemocyte. The predominant func-tion of platelets is considered to be hemostasis, where they play a complex role integrated with other soluble and cellular participants. Platelets adhere to the exposed sub-endothelial collagen of a damaged vessel wall, are activated, up-regulate additional adhesive receptors and secrete transcellular me-diators, contributing to the formation of a stable platelet ag-gregate. Defective activation of platelets compromises he-mostasis and can result in excessive clinical bleeding. In contrast inappropriate platelet activation is associated with arterial thrombotic conditions such as myocardial infarction and stroke. Platelets are a primary target for the prevention of recurrent cardiovascular thrombosis.
It is now clear that platelets have a wider repertoire of physiological roles and therefore are implicated in more pathological conditions than thrombosis; they are active par-ticipants in the immune response and host-defence. In these situations, platelets function like traditional immune cells such as macrophages and mast cells, binding to bacteria, secreting chemokines, and clearing invading organisms from the circulation. Many of the underlying mechanisms used by platelets in their immune response are identical to, or exten-sions of, the hemostatic processes. Their contributions to pathological lesions in inflammatory disorders, and to tumor progression, are the result of these responses at the wrong place and time.
The challenge for therapeutic intervention in these dis-eases will be to identify drugs that preferentially block spe-cific targets involved in the complex contribution of platelets to inflammation or tumor progression, while leaving their hemostatic function at least partially intact.
ACKNOWLEDGEMENTS
The authors would like to thank Dr. E. D. Israels for helpful suggestions during the preparation of this manuscript and E.M. McMillan-Ward for preparation of Fig. (3b). SJI is funded by a grant from Cancer Care Manitoba and AM by a grant from the Heat and Stroke Foundation of Canada.
REFERENCES
[1] Schultze, M. Ein heizbarer Objecttisch und seine Verwendung bei Untersuchungen des Blutes. Archiv für mikroscopische Anatomie, 1865, 1, 1-42.
[2] Bizzozero, G. Su di un nuovo elemento morfologico del sangue dei mammiferi e sulla sua importanza nella trombosi e nella coagulazi-one. Osservatore Gazetta delle Cliniche, 1881, 17, 785-787.
[3] Meadows, T.A.; Bhatt, D.L. Clinical aspects of platelet inhibitors and thrombus formation. Circ. Res., 2007, 100, 1261-1275.
[4] Levin, J. In: Platelets, (Michelson, A.D., Ed.). Academic Press: Burlington, 2007, 2nd Edit, pp., 3-22.
[5] Jackson, S.P. The growing complexity of platelet aggregation. Blood, 2007, 109, 5087-5095.
[6] McNicol, A., Israels, S.J. Platelet dense granules: structure, func-tion and implications for haemostasis. Thromb. Res., 1999, 95, 1-18.
[7] Harrison, P.; Cramer, E.M. Platelet alpha-granules. Blood Rev., 1993, 7, 52-62.
[8] Coppinger, J.A.; Cagney, G.; Toomey, S.; Kislinger, T.; Belton, O.; McRedmond, J.P.; Cahill, D.J.; Emili, A.; Fitzgerald, D.J.; Ma-guire, P.B. Characterization of the proteins released from activated platelets leads to localization of novel platelet proteins in human atherosclerotic lesions. Blood, 2004, 103, 2096-2104.
[9] Heijnen, H.F.; Schiel, A.E.; Fijnheer, R.; Geuze, H.J.; Sixma, J.J. Activated platelets release two types of membrane vesicles: mi-crovesicles by surface shedding and exosomes derived from exocy-tosis of multivesicular bodies and alpha-granules. Blood, 1999, 94,3791-3799.
[10] Ross R. The arterial wall and atherosclerosis. Annu. Rev. Med., 1979, 30, 1-15.
[11] Ross, R. The pathogenesis of atherosclerosis: a perspective for the 1990s. Nature, 1993, 362, 801-809.
[12] Ross, R. Atherosclerosis--an inflammatory disease. N. Engl. J. Med., 1999, 340, 115-126.
[13] Lusis, A.J. Atherosclerosis. Nature, 2000, 407, 233-241. [14] Bijl, M. Endothelial activation, endothelial dysfunction and prema-
ture atherosclerosis in systemic autoimmune diseases. Neth. J. Med., 2003, 61, 273-277
[15] Steinhubl, S.R.; Moliterno, D.J. The role of the platelet in the pathogenesis of atherothrombosis. Am. J. Cardiovasc. Drugs, 2005,5, 339-408.
[16] Wagner, D.D.; Burger, P.C. Platelets in inflammation and thrombo-sis. Arterioscler. Thromb. Vasc. Biol., 2003, 23, 2131-2137.
[17] Gawaz, M.; Langer, H.; May, A.E. Platelets in inflammation and atherogenesis. J. Clin. Invest., 2005, 115, 3378-3384.
[18] Massberg, S.; Brand, K.; Gruner, S.; Page, S.; Muller, E.; Muller, I.; Bergmeier, W.; Richter, T.; Lorenz, M.; Konrad, I.; Nieswandt, B.; Gawaz, M. A critical role of platelet adhesion in the initiation of atherosclerotic lesion formation. J. Exp. Med., 2002, 196, 887-896.
[19] von Hundelshausen, P.; Weber, C. Platelets as immune cells: Bridging inflammation and cardiovascular disease. Circ. Res., 2007, 100, 27-40.
[20] Massberg, S.; Schurzinger, K.; Lorenz, M.; Konrad, I.; Schulz, C.; Plesnila, N.; Kennerknecht, E.; Rudelius, M.; Sauer, S.; Braun, S.; Kremmer, E.; Emambokus, N.R.; Frampton, J.; Gawaz, M. Platelet adhesion via glycoprotein IIb integrin is critical for atheroprogres-sion and focal cerebral ischemia: an in vivo study in mice lacking glycoprotein IIb. Circulation, 2005, 112, 1180-1188.
[21] Chen, M.; Geng, J. P-selectin mediates adhesion of leukocytes, platelets, and cancer cells in inflammation, thrombosis, and cancer growth and metastasis. Arch. Immunol. Ther. Exp., 2006, 54, 75-84.
[22] Weber, C. Platelets and chemokines in atherosclerosis: Partners in crime. Circ. Res., 2005, 96, 612-616.
[23] Prasad, K.S.; Andre, P.; Yan, Y.; Phillips, D.R. The platelet CD40L/GPIIb-IIIa axis in atherothrombotic disease. Curr. Opin. Hematol., 2003, 10, 356-361.
[24] Danese, S.; Fiocchi, C. Platelet activation and the CD40/CD40 ligand pathway: mechanisms and implications for human disease. Crit. Rev. Immunol., 2005, 25, 103-121.
[25] Lutgens, E.; Lievens, D.; Beckers, L.; Donners, M.; Daemen, M. CD40 and its ligand in atherosclerosis. Trends Cardiovasc. Med., 2007, 17, 118-123.
[26] Danese, S.; de la Motte, C.; Reyes, B.M.; Sans, M.; Levine, A.D.; Fiocchi, C. T cells trigger CD40-dependent platelet activation and granular RANTES release: a novel pathway for immune response amplification. J. Immunol., 2004, 172, 2011-2015.
[27] Schafer, A.; Schulz, C.; Eigenthaler, M.; Fraccarollo, D.; Kobsar, A.; Gawaz, M.; Ertl, G.; Walter, U.; Bauersachs, J. Novel role of the membrane-bound chemokine fractalkine in platelet activation and adhesion. Blood, 2004, 103, 407-4 12.
[28] Lesnik, P.; Haskell, C.A.; Charo, I.F. Decreased atherosclerosis in CX3CR1-/- mice reveals a role for fractalkine in atherogenesis. J. Clin. Invest., 2003, 111, 333-140.
[29] Mause, S.F.; von Hundelshausen, P.; Zernecke, A.; Koenen, R.R.; Weber, C. Platelet microparticles: A transcellular delivery system
114 Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 McNicol and Israels
for RANTES promoting monocyte recruitment on endothelium. Ar-terioscler. Thromb. Vasc. Biol., 2005, 25, 1512-1518.
[30] Lindemann, S.; Tolley, N.D.; Dixon, D.A.; McIntyre, T.M.; Prescott, S.M.; Zimmerman, G.A.; Weyrich, A.S. Activated plate-lets mediate inflammatory signaling by regulated interleukin 1ß synthesis. J. Cell Biol., 2001, 154, 485-490.
[31] Steinhubl, S.R.; Newby, L.K.; Sabatine, M.; Uchiyama, S.; Connor, M.; Endres, M.; Avezum, A.; Wahlberg, E. Platelets and atherothrombosis: An essential role for inflammation in vascular disease - a review. Int. J. Angiol., 2005, 14, 211-217.
[32] Steinhubl, S.R. Platelets as mediators of inflammation. Haematol. Oncol. Clin. N. Am., 2007, 21, 115-121.
[33] Danese, S.; de la Motte, C.; Sturm, A.; Vogel, J.D.; West, G.A.; Strong, S.A.; Katz, J.A.; Fiocchi, C. Platelets trigger a CD40-dependent inflammatory response in the microvasculature of in-flammatory bowel disease patients. Gastroenterology, 2003, 124,1249-1264.
[34] Bunescu, A.; Seideman, P.; Lenkei, R.; Levin, K.; Egberg, N. En-hanced Fcgamma receptor I, alphaMbeta2 integrin receptor expres-sion by monocytes and neutrophils in rheumatoid arthritis: interac-tion with platelets J. Rheumatol., 2004, 31, 2347-2355.
[35] Schmitt-Sody, M.; Klose, A.; Gottschalk, O.; Metz, P.; Gebhard, H.; Zysk, S.; Eichhorn, M.E.; Hernandez-Richter, T.M.; Jansson, V.; Veihelmann, A. Platelet-endothelial cell interactions in murine antigen-induced arthritis. Rheumatology (Oxford), 2005, 44, 885-889.
[36] Berrettini, M.; Parise, P.; Constantini, V.; Grasselli, S.; Nenci, G.G. Platelet activation in psoriasis. Thromb. Haemost., 1985, 53, 195-197.
[37] Vila, L.; Cullare, C.; Sola, J., Puig, L.; de Castellarnau, C.; de Mor-agas, J.M. Cyclooxygenase activity is increased in platelets from pso-riatic patients. J. Invest. Dermatol., 1991, 97, 922-926.
[38] Ludwig, R.J.; Schultz, J.E.; Boehncke, W.; Podda, M.; Tandi, C.; Krombach, F.; Baatz, H.; Kaufmann, R.; von Adrian, U.H.; Zoll-ner, T.M. Activated, not resting, platelets increase leukocyte rolling in murine skin utilizing a distinct set of adhesion molecules. J. In-vest. Dermatol., 2004, 122, 830-836.
[39] Ferrari, M.D.; Saxena, P.R. On serotonin and migraine: a clinical and pharmacological review. Cephalalgia., 1993, 13, 151-165.
[40] Hanington, E. Migraine: A blood disorder? Lancet, 1978, 2(8088), 501-503.
[41] Waeber, C.; Moskowitz, M.A. Migraine as an inflammatory disor-der. Neurology, 2005, 64, S9-S 15.
[42] Zeller, J.A.; Lindner, V.; Frahm, K.; Baron, R.; Deuschl, G. Plate-let activation and platelet-leucocyte interaction in patients with mi-graine. Subtype differences and influence of triptans. Cephalalgia, 2005, 25, 536-541.
[43] Moritani, C.; Ishioka, S.; Haruta, Y.; Kambe, M.; Yamakido, M. Activation of platelets in bronchial asthma. Chest, 1998, 113, 452-458.
[44] Pitchford, S.C.; Momi, S.; Giannini, S.; Casali, L.; Spina, D.; Page, C.P.; Gresele, P. Platelet P-selectin is required for pulmonary eosi-nophil and lymphocyte recruitment in a murine model of allergic inflammation. Blood, 2005, 105, 2074-2081.
[45] Ulfman, L.H.; Joosten, D.P.; van Aalst, C.W.; Lammers, J.W.; van de Graaf, E.A.; Koenderman, L.; Zwaginga, J.J. Platelets promote eosinophil adhesion of patients with asthma to endothelium under flow conditions. Am. J. Respir. Cell. Mol. Biol., 2003, 28, 512-519.
[46] O'Sullivan, B.P.; Michelson, A.D. The inflammatory role of plate-lets in cystic fibrosis. Am. J. Respir. Crit. Care Med., 2006, 173,483-490.
[47] Kuebler, W.M. Selectins revisited: the emerging role of platelets in inflammatory lung disease. J. Clin. Invest., 2006, 116, 3106-3108.
[48] Meadows, T.A.; Bhatt, D.L. Clinical aspects of platelet inhibitors and thrombus formation. Circ. Res., 2007, 100, 1261-1275
[49] Morel O.; Toti F.; Hugel B.; Bakouboula B.; Camoin-Jau L.; Dig-nat-George F.; Freyssinet J.M. Procoagulant microparticles: dis-rupting the vascular homeostasis equation? Arterioscler. Thromb. Vasc. Biol., 2006, 26, 2594-2604.
[50] Trousseau, A. Phlegmasia alba dolens. Clinique Medicale de L’ Hotel-Dieu Paris. New Syndenham Society: London, 1865; pp., 94-96.
[51] Rickles, F.R.; Falanga, A. Molecular basis for the relationship be-tween thrombosis and cancer. Thromb. Res., 2001, 102, V215-V224.
[52] Billroth, T. Lectures on surgical pathology and therapeutics: a handbook for students and practitioners. New Syndenham Society: London, 1878; Vol. II, p., 355.
[53] Gasic, G.J.; Gasic, T.B.; Stewart, C.C. Antimetastatic effects asso-ciated with platelet reduction. Proc. Natl. Acad. Sci. USA, 1968, 61,46-52.
[54] Karpatkin, S.; Ambrogio, C.; Pearlstein, E. Lack of effect of in vivo prostacyclin on the development of pulmonary metastases in mice following intravenous injection of CT26 colon carcinoma, Lewis lung carcinoma, or B16 amelanotic melanoma cells. Cancer Res., 1984, 44, 3880-3883.
[55] Nash, G.F.; Turner, L.F.; Scully, M.F.; Kakkar, A.K. Platelets and cancer. Lancet Oncol., 2002, 3, 425-430.
[56] Philippe, C.; Philippe, B.; Fouquery, B.; Periz, J.; Lebret, M.; Baud, L. Protection from tumor necrosis factor-mediated cytolysis by platelets. Am. J. Pathol., 1993, 143, 1713-1723.
[57] Shau, H.; Roth, M.D.; Golub, S.H. Regulation of natural killer function by nonlymphoid cells. Nat. Immunol., 1993, 12, 235-249.
[58] Pearlstein, E.; Ambrogio, C.; Karpatkin, S. Effect of anti-platelet antibody on the development of pulmonary metastases following injection of CT26 colon adencarcinoma, Lewis lung carcinoma and B16 amelanotic melanoma tumor cells in mice. Cancer Res., 1984,44, 3884-3887.
[59] Juarez, P.; Alonso-Escolano, D.; Radomski, M.W. Platelet-cancer interactions: mechanisms and pharmacology of tumour cell-induced platelet aggregation. Br. J. Pharmacol., 2004, 143, 819-826.
[60] Pearlstein, E.; Salk, P.L.; Yogeeswaran, G.; Karpatkin, S. Correla-tion between spontaneous metastatic potential, platelet-aggregating activity of cell surface extracts, and cell surface sialylation in 10 metastatic-variant derivatives of a rat renal sarcoma cell line. Proc. Natl. Acad. Sci. USA, 1980, 77, 4336-4339.
[61] Felding-Habermann, B.; O’Toole, T.E.; Smith, J.W.; Fransvea, E.; Ruggeri, Z.M.; Ginsberg, M.H.; Hughes, P.E.; Pampori, N.; Shattil, S.J.; Saven, A.; Mueller, B.M. Integrin activation controls metasta-sis in human breast cancer. Proc. Natl. Acad. Sci. USA, 2001, 98,1853-1858.
[62] McGregor, B.C.; McGregor, J.L.; Weiss, L.M.; Wood, J.S.; Hu, C.H.; Boukerche, H.; Warnke, R.A. Presence of cytoadhesins on human metastatic melanomas but not on benign melanocytes. Am. J. Clin. Pathol., 1989, 92, 495-499.
[63] Chiang, H-S.; Peng, H-C.; Huang, T-F. Characterization of integrin expression and regulation on SW-480 human colon adenocarcinoma cells and the effect of rhodamine on basal and up-regulated tumor cell adhesion. Biochim. Biophys. Acta, 1994, 1224, 506-516.
[64] Trikha, M.; Timar, J.; Lundy, S.K. ; Szkeres, K.; Tang, K.; Grignon, D.; Porter, A.T.; Honn, K.V. Human prostate carcinoma cells express functional IIb 3 integrin. Cancer Res., 1996, 56,5071-5078.
[65] Chen, Y.Q.; Trikha, M.; Gao, X.; Bazaz, R.; Porter, A.T.; Timar, J.; Honn, K.V. Ectopic expression of platelet integrin IIb 3 in tumor cells from various species and the histological origin. Int. J. Can-cer, 1997, 72, 642-648.
[66] Janowska-Wieczorek, A.; Wysoczynski, M.; Kijowski, J.; Mar-quez-Curtis, L.; Machalinski, B.; Ratajckak, J.; Ratajczak, M.Z. Microvesicles derived from activated platelets induce metastasis and angiogenesis in lung cancer. Int. J. Cancer, 2005,113,752-760.
[67] Janowska-Wieczorek, A.; Marquez-Curtis, L.A.; Wysoczynski, M.; Ratajczak, M.Z. Enhancing effect of platelet-derived microvesicles on the invasive potential of breast cancer cells. Transfusion, 2006,46, 1199-1209.
[68] Karpatkin, S.; Pearlstein, E.; Ambroglio, C.; Coller, B. Role of adhesive proteins in platelet tumor interaction in vitro and metasta-sis formation in vivo. J. Clin. Invest., 1988, 81, 1012-1019.
[69] Clezardin, P.; Drouin, J.; Morel-Kopp, M.C.; Hanss, M.; Kehrel, B.; Serre, C.M.; Kaplan, C.; Delmas, P.D. Role of platelet mem-brane glycoproteins Ib/IX and IIb/IIIa, and of platelet alpha-granule proteins in platelet aggregation induced by human osteosarcoma cells. Cancer Res., 1993, 53, 4695-4700.
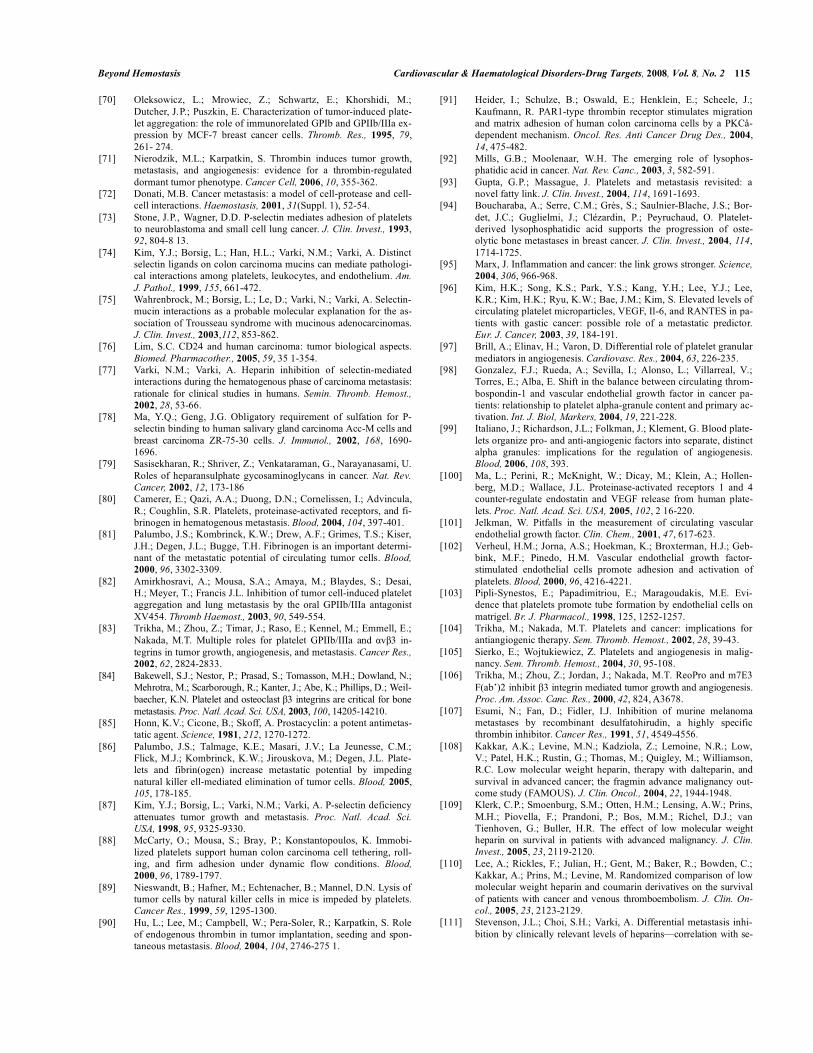
Beyond Hemostasis Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 115
[70] Oleksowicz, L.; Mrowiec, Z.; Schwartz, E.; Khorshidi, M.; Dutcher, J.P.; Puszkin, E. Characterization of tumor-induced plate-let aggregation: the role of immunorelated GPIb and GPIIb/IIIa ex-pression by MCF-7 breast cancer cells. Thromb. Res., 1995, 79,261- 274.
[71] Nierodzik, M.L.; Karpatkin, S. Thrombin induces tumor growth, metastasis, and angiogenesis: evidence for a thrombin-regulated dormant tumor phenotype. Cancer Cell, 2006, 10, 355-362.
[72] Donati, M.B. Cancer metastasis: a model of cell-protease and cell-cell interactions. Haemostasis, 2001, 31(Suppl. 1), 52-54.
[73] Stone, J.P., Wagner, D.D. P-selectin mediates adhesion of platelets to neuroblastoma and small cell lung cancer. J. Clin. Invest., 1993,92, 804-8 13.
[74] Kim, Y.J.; Borsig, L.; Han, H.L.; Varki, N.M.; Varki, A. Distinct selectin ligands on colon carcinoma mucins can mediate pathologi-cal interactions among platelets, leukocytes, and endothelium. Am. J. Pathol., 1999, 155, 661-472.
[75] Wahrenbrock, M.; Borsig, L.; Le, D.; Varki, N.; Varki, A. Selectin-mucin interactions as a probable molecular explanation for the as-sociation of Trousseau syndrome with mucinous adenocarcinomas. J. Clin. Invest., 2003,112, 853-862.
[76] Lim, S.C. CD24 and human carcinoma: tumor biological aspects. Biomed. Pharmacother., 2005, 59, 35 1-354.
[77] Varki, N.M.; Varki, A. Heparin inhibition of selectin-mediated interactions during the hematogenous phase of carcinoma metastasis: rationale for clinical studies in humans. Semin. Thromb. Hemost., 2002, 28, 53-66.
[78] Ma, Y.Q.; Geng, J.G. Obligatory requirement of sulfation for P-selectin binding to human salivary gland carcinoma Acc-M cells and breast carcinoma ZR-75-30 cells. J. Immunol., 2002, 168, 1690-1696.
[79] Sasisekharan, R.; Shriver, Z.; Venkataraman, G., Narayanasami, U. Roles of heparansulphate gycosaminoglycans in cancer. Nat. Rev. Cancer, 2002, 12, 173-186
[80] Camerer, E.; Qazi, A.A.; Duong, D.N.; Cornelissen, I.; Advincula, R.; Coughlin, S.R. Platelets, proteinase-activated receptors, and fi-brinogen in hematogenous metastasis. Blood, 2004, 104, 397-401.
[81] Palumbo, J.S.; Kombrinck, K.W.; Drew, A.F.; Grimes, T.S.; Kiser, J.H.; Degen, J.L.; Bugge, T.H. Fibrinogen is an important determi-nant of the metastatic potential of circulating tumor cells. Blood, 2000, 96, 3302-3309.
[82] Amirkhosravi, A.; Mousa, S.A.; Amaya, M.; Blaydes, S.; Desai, H.; Meyer, T.; Francis J.L. Inhibition of tumor cell-induced platelet aggregation and lung metastasis by the oral GPIIb/IIIa antagonist XV454. Thromb Haemost., 2003, 90, 549-554.
[83] Trikha, M.; Zhou, Z.; Timar, J.; Raso, E.; Kennel, M.; Emmell, E.; Nakada, M.T. Multiple roles for platelet GPIIb/IIIa and v 3 in-tegrins in tumor growth, angiogenesis, and metastasis. Cancer Res., 2002, 62, 2824-2833.
[84] Bakewell, S.J.; Nestor, P.; Prasad, S.; Tomasson, M.H.; Dowland, N.; Mehrotra, M.; Scarborough, R.; Kanter, J.; Abe, K.; Phillips, D.; Weil-baecher, K.N. Platelet and osteoclast 3 integrins are critical for bone metastasis. Proc. Natl. Acad. Sci. USA, 2003, 100, 14205-14210.
[85] Honn, K.V.; Cicone, B.; Skoff, A. Prostacyclin: a potent antimetas-tatic agent. Science, 1981, 212, 1270-1272.
[86] Palumbo, J.S.; Talmage, K.E.; Masari, J.V.; La Jeunesse, C.M.; Flick, M.J.; Kombrinck, K.W.; Jirouskova, M.; Degen, J.L. Plate-lets and fibrin(ogen) increase metastatic potential by impeding natural killer ell-mediated elimination of tumor cells. Blood, 2005,105, 178-185.
[87] Kim, Y.J.; Borsig, L.; Varki, N.M.; Varki, A. P-selectin deficiency attenuates tumor growth and metastasis. Proc. Natl. Acad. Sci. USA, 1998, 95, 9325-9330.
[88] McCarty, O.; Mousa, S.; Bray, P.; Konstantopoulos, K. Immobi-lized platelets support human colon carcinoma cell tethering, roll-ing, and firm adhesion under dynamic flow conditions. Blood, 2000, 96, 1789-1797.
[89] Nieswandt, B.; Hafner, M.; Echtenacher, B.; Mannel, D.N. Lysis of tumor cells by natural killer cells in mice is impeded by platelets. Cancer Res., 1999, 59, 1295-1300.
[90] Hu, L.; Lee, M.; Campbell, W.; Pera-Soler, R.; Karpatkin, S. Role of endogenous thrombin in tumor implantation, seeding and spon-taneous metastasis. Blood, 2004, 104, 2746-275 1.
[91] Heider, I.; Schulze, B.; Oswald, E.; Henklein, E.; Scheele, J.; Kaufmann, R. PAR1-type thrombin receptor stimulates migration and matrix adhesion of human colon carcinoma cells by a PKCå-dependent mechanism. Oncol. Res. Anti Cancer Drug Des., 2004,14, 475-482.
[92] Mills, G.B.; Moolenaar, W.H. The emerging role of lysophos-phatidic acid in cancer. Nat. Rev. Canc., 2003, 3, 582-591.
[93] Gupta, G.P.; Massague, J. Platelets and metastasis revisited: a novel fatty link. J. Clin. Invest., 2004, 114, 1691-1693.
[94] Boucharaba, A.; Serre, C.M.; Grès, S.; Saulnier-Blache, J.S.; Bor-det, J.C.; Guglielmi, J.; Clézardin, P.; Peyruchaud, O. Platelet-derived lysophosphatidic acid supports the progression of oste-olytic bone metastases in breast cancer. J. Clin. Invest., 2004, 114,1714-1725.
[95] Marx, J. Inflammation and cancer: the link grows stronger. Science, 2004, 306, 966-968.
[96] Kim, H.K.; Song, K.S.; Park, Y.S.; Kang, Y.H.; Lee, Y.J.; Lee, K.R.; Kim, H.K.; Ryu, K.W.; Bae, J.M.; Kim, S. Elevated levels of circulating platelet microparticles, VEGF, Il-6, and RANTES in pa-tients with gastic cancer: possible role of a metastatic predictor. Eur. J. Cancer, 2003, 39, 184-191.
[97] Brill, A.; Elinav, H.; Varon, D. Differential role of platelet granular mediators in angiogenesis. Cardiovasc. Res., 2004, 63, 226-235.
[98] Gonzalez, F.J.; Rueda, A.; Sevilla, I.; Alonso, L.; Villarreal, V.; Torres, E.; Alba, E. Shift in the balance between circulating throm-bospondin-1 and vascular endothelial growth factor in cancer pa-tients: relationship to platelet alpha-granule content and primary ac-tivation. Int. J. Biol, Markers, 2004, 19, 221-228.
[99] Italiano, J.; Richardson, J.L.; Folkman, J.; Klement, G. Blood plate-lets organize pro- and anti-angiogenic factors into separate, distinct alpha granules: implications for the regulation of angiogenesis. Blood, 2006, 108, 393.
[100] Ma, L.; Perini, R.; McKnight, W.; Dicay, M.; Klein, A.; Hollen-berg, M.D.; Wallace, J.L. Proteinase-activated receptors 1 and 4 counter-regulate endostatin and VEGF release from human plate-lets. Proc. Natl. Acad. Sci. USA, 2005, 102, 2 16-220.
[101] Jelkman, W. Pitfalls in the measurement of circulating vascular endothelial growth factor. Clin. Chem., 2001, 47, 617-623.
[102] Verheul, H.M.; Jorna, A.S.; Hoekman, K.; Broxterman, H.J.; Geb-bink, M.F.; Pinedo, H.M. Vascular endothelial growth factor-stimulated endothelial cells promote adhesion and activation of platelets. Blood, 2000, 96, 4216-4221.
[103] Pipli-Synestos, E.; Papadimitriou, E.; Maragoudakis, M.E. Evi-dence that platelets promote tube formation by endothelial cells on matrigel. Br. J. Pharmacol., 1998, 125, 1252-1257.
[104] Trikha, M.; Nakada, M.T. Platelets and cancer: implications for antiangiogenic therapy. Sem. Thromb. Hemost., 2002, 28, 39-43.
[105] Sierko, E.; Wojtukiewicz, Z. Platelets and angiogenesis in malig-nancy. Sem. Thromb. Hemost., 2004, 30, 95-108.
[106] Trikha, M.; Zhou, Z.; Jordan, J.; Nakada, M.T. ReoPro and m7E3 F(ab’)2 inhibit 3 integrin mediated tumor growth and angiogenesis. Proc. Am. Assoc. Canc. Res., 2000, 42, 824, A3678.
[107] Esumi, N.; Fan, D.; Fidler, I.J. Inhibition of murine melanoma metastases by recombinant desulfatohirudin, a highly specific thrombin inhibitor. Cancer Res., 1991, 51, 4549-4556.
[108] Kakkar, A.K.; Levine, M.N.; Kadziola, Z.; Lemoine, N.R.; Low, V.; Patel, H.K.; Rustin, G.; Thomas, M.; Quigley, M.; Williamson, R.C. Low molecular weight heparin, therapy with dalteparin, and survival in advanced cancer; the fragmin advance malignancy out-come study (FAMOUS). J. Clin. Oncol., 2004, 22, 1944-1948.
[109] Klerk, C.P.; Smoenburg, S.M.; Otten, H.M.; Lensing, A.W.; Prins, M.H.; Piovella, F.; Prandoni, P.; Bos, M.M.; Richel, D.J.; van Tienhoven, G.; Buller, H.R. The effect of low molecular weight heparin on survival in patients with advanced malignancy. J. Clin. Invest., 2005, 23, 2119-2120.
[110] Lee, A.; Rickles, F.; Julian, H.; Gent, M.; Baker, R.; Bowden, C.; Kakkar, A.; Prins, M.; Levine, M. Randomized comparison of low molecular weight heparin and coumarin derivatives on the survival of patients with cancer and venous thromboembolism. J. Clin. On-col., 2005, 23, 2123-2129.
[111] Stevenson, J.L.; Choi, S.H.; Varki, A. Differential metastasis inhi-bition by clinically relevant levels of heparins—correlation with se-
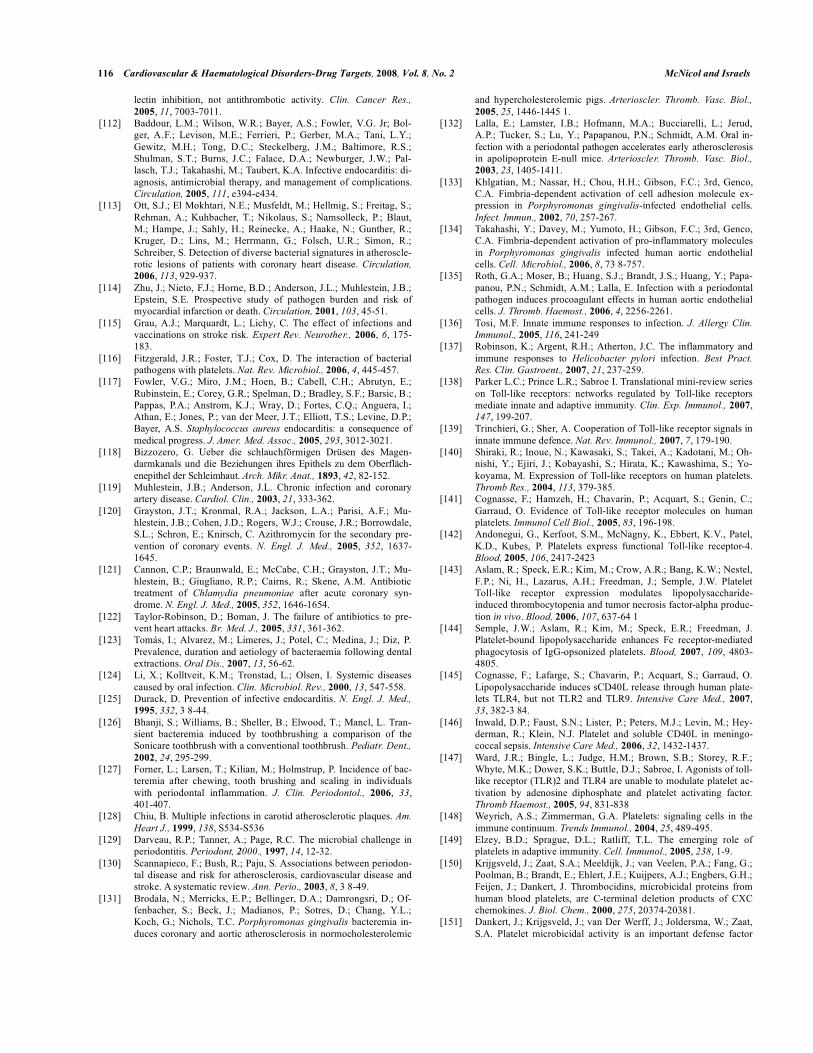
116 Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 McNicol and Israels
lectin inhibition, not antithrombotic activity. Clin. Cancer Res., 2005, 11, 7003-7011.
[112] Baddour, L.M.; Wilson, W.R.; Bayer, A.S.; Fowler, V.G. Jr; Bol-ger, A.F.; Levison, M.E.; Ferrieri, P.; Gerber, M.A.; Tani, L.Y.; Gewitz, M.H.; Tong, D.C.; Steckelberg, J.M.; Baltimore, R.S.; Shulman, S.T.; Burns, J.C.; Falace, D.A.; Newburger, J.W.; Pal-lasch, T.J.; Takahashi, M.; Taubert, K.A. Infective endocarditis: di-agnosis, antimicrobial therapy, and management of complications. Circulation, 2005, 111, e394-e434.
[113] Ott, S.J.; El Mokhtari, N.E.; Musfeldt, M.; Hellmig, S.; Freitag, S.; Rehman, A.; Kuhbacher, T.; Nikolaus, S.; Namsolleck, P.; Blaut, M.; Hampe, J.; Sahly, H.; Reinecke, A.; Haake, N.; Gunther, R.; Kruger, D.; Lins, M.; Herrmann, G.; Folsch, U.R.; Simon, R.; Schreiber, S. Detection of diverse bacterial signatures in atheroscle-rotic lesions of patients with coronary heart disease. Circulation, 2006, 113, 929-937.
[114] Zhu, J.; Nieto, F.J.; Horne, B.D.; Anderson, J.L.; Muhlestein, J.B.; Epstein, S.E. Prospective study of pathogen burden and risk of myocardial infarction or death. Circulation, 2001, 103, 45-51.
[115] Grau, A.J.; Marquardt, L.; Lichy, C. The effect of infections and vaccinations on stroke risk. Expert Rev. Neurother., 2006, 6, 175-183.
[116] Fitzgerald, J.R.; Foster, T.J.; Cox, D. The interaction of bacterial pathogens with platelets. Nat. Rev. Microbiol., 2006, 4, 445-457.
[117] Fowler, V.G.; Miro, J.M.; Hoen, B.; Cabell, C.H.; Abrutyn, E.; Rubinstein, E.; Corey, G.R.; Spelman, D.; Bradley, S.F.; Barsic, B.; Pappas, P.A.; Anstrom, K.J.; Wray, D.; Fortes, C.Q.; Anguera, I.; Athan, E.; Jones, P.; van der Meer, J.T.; Elliott, T.S.; Levine, D.P.; Bayer, A.S. Staphylococcus aureus endocarditis: a consequence of medical progress. J. Amer. Med. Assoc., 2005, 293, 3012-3021.
[118] Bizzozero, G. Ueber die schlauchförmigen Drüsen des Magen-darmkanals und die Beziehungen ihres Epithels zu dem Oberfläch-enepithel der Schleimhaut. Arch. Mikr. Anat., 1893, 42, 82-152.
[119] Muhlestein, J.B.; Anderson, J.L. Chronic infection and coronary artery disease. Cardiol. Clin., 2003, 21, 333-362.
[120] Grayston, J.T.; Kronmal, R.A.; Jackson, L.A.; Parisi, A.F.; Mu-hlestein, J.B.; Cohen, J.D.; Rogers, W.J.; Crouse, J.R.; Borrowdale, S.L.; Schron, E.; Knirsch, C. Azithromycin for the secondary pre-vention of coronary events. N. Engl. J. Med., 2005, 352, 1637-1645.
[121] Cannon, C.P.; Braunwald, E.; McCabe, C.H.; Grayston, J.T.; Mu-hlestein, B.; Giugliano, R.P.; Cairns, R.; Skene, A.M. Antibiotic treatment of Chlamydia pneumoniae after acute coronary syn-drome. N. Engl. J. Med., 2005, 352, 1646-1654.
[122] Taylor-Robinson, D.; Boman, J. The failure of antibiotics to pre-vent heart attacks. Br. Med. J., 2005, 331, 361-362.
[123] Tomás, I.; Alvarez, M.; Limeres, J.; Potel, C.; Medina, J.; Diz, P. Prevalence, duration and aetiology of bacteraemia following dental extractions. Oral Dis., 2007, 13, 56-62.
[124] Li, X.; Kolltveit, K.M.; Tronstad, L.; Olsen, I. Systemic diseases caused by oral infection. Clin. Microbiol. Rev., 2000, 13, 547-558.
[125] Durack, D. Prevention of infective endocarditis. N. Engl. J. Med., 1995, 332, 3 8-44.
[126] Bhanji, S.; Williams, B.; Sheller, B.; Elwood, T.; Mancl, L. Tran-sient bacteremia induced by toothbrushing a comparison of the Sonicare toothbrush with a conventional toothbrush. Pediatr. Dent., 2002, 24, 295-299.
[127] Forner, L.; Larsen, T.; Kilian, M.; Holmstrup, P. Incidence of bac-teremia after chewing, tooth brushing and scaling in individuals with periodontal inflammation. J. Clin. Periodontol., 2006, 33,401-407.
[128] Chiu, B. Multiple infections in carotid atherosclerotic plaques. Am. Heart J., 1999, 138, S534-S536
[129] Darveau, R.P.; Tanner, A.; Page, R.C. The microbial challenge in periodontitis. Periodont, 2000., 1997, 14, 12-32.
[130] Scannapieco, F.; Bush, R.; Paju, S. Associations between periodon-tal disease and risk for atherosclerosis, cardiovascular disease and stroke. A systematic review. Ann. Perio., 2003, 8, 3 8-49.
[131] Brodala, N.; Merricks, E.P.; Bellinger, D.A.; Damrongsri, D.; Of-fenbacher, S.; Beck, J.; Madianos, P.; Sotres, D.; Chang, Y.L.; Koch, G.; Nichols, T.C. Porphyromonas gingivalis bacteremia in-duces coronary and aortic atherosclerosis in normocholesterolemic
and hypercholesterolemic pigs. Arterioscler. Thromb. Vasc. Biol., 2005, 25, 1446-1445 1.
[132] Lalla, E.; Lamster, I.B.; Hofmann, M.A.; Bucciarelli, L.; Jerud, A.P.; Tucker, S.; Lu, Y.; Papapanou, P.N.; Schmidt, A.M. Oral in-fection with a periodontal pathogen accelerates early atherosclerosis in apolipoprotein E-null mice. Arterioscler. Thromb. Vasc. Biol., 2003, 23, 1405-1411.
[133] Khlgatian, M.; Nassar, H.; Chou, H.H.; Gibson, F.C.; 3rd, Genco, C.A. Fimbria-dependent activation of cell adhesion molecule ex-pression in Porphyromonas gingivalis-infected endothelial cells. Infect. Immun., 2002, 70, 257-267.
[134] Takahashi, Y.; Davey, M.; Yumoto, H.; Gibson, F.C.; 3rd, Genco, C.A. Fimbria-dependent activation of pro-inflammatory molecules in Porphyromonas gingivalis infected human aortic endothelial cells. Cell. Microbiol., 2006, 8, 73 8-757.
[135] Roth, G.A.; Moser, B.; Huang, S.J.; Brandt, J.S.; Huang, Y.; Papa-panou, P.N.; Schmidt, A.M.; Lalla, E. Infection with a periodontal pathogen induces procoagulant effects in human aortic endothelial cells. J. Thromb. Haemost., 2006, 4, 2256-2261.
[136] Tosi, M.F. Innate immune responses to infection. J. Allergy Clin. Immunol., 2005, 116, 241-249
[137] Robinson, K.; Argent, R.H.; Atherton, J.C. The inflammatory and immune responses to Helicobacter pylori infection. Best Pract. Res. Clin. Gastroent., 2007, 21, 237-259.
[138] Parker L.C.; Prince L.R.; Sabroe I. Translational mini-review series on Toll-like receptors: networks regulated by Toll-like receptors mediate innate and adaptive immunity. Clin. Exp. Immunol., 2007,147, 199-207.
[139] Trinchieri, G.; Sher, A. Cooperation of Toll-like receptor signals in innate immune defence. Nat. Rev. Immunol., 2007, 7, 179-190.
[140] Shiraki, R.; Inoue, N.; Kawasaki, S.; Takei, A.; Kadotani, M.; Oh-nishi, Y.; Ejiri, J.; Kobayashi, S.; Hirata, K.; Kawashima, S.; Yo-koyama, M. Expression of Toll-like receptors on human platelets. Thromb Res., 2004, 113, 379-385.
[141] Cognasse, F.; Hamzeh, H.; Chavarin, P.; Acquart, S.; Genin, C.; Garraud, O. Evidence of Toll-like receptor molecules on human platelets. Immunol Cell Biol., 2005, 83, 196-198.
[142] Andonegui, G., Kerfoot, S.M., McNagny, K., Ebbert, K.V., Patel, K.D., Kubes, P. Platelets express functional Toll-like receptor-4. Blood, 2005, 106, 2417-2423
[143] Aslam, R.; Speck, E.R.; Kim, M.; Crow, A.R.; Bang, K.W.; Nestel, F.P.; Ni, H., Lazarus, A.H.; Freedman, J.; Semple, J.W. Platelet Toll-like receptor expression modulates lipopolysaccharide-induced thrombocytopenia and tumor necrosis factor-alpha produc-tion in vivo. Blood, 2006, 107, 637-64 1
[144] Semple, J.W.; Aslam, R.; Kim, M.; Speck, E.R.; Freedman, J. Platelet-bound lipopolysaccharide enhances Fc receptor-mediated phagocytosis of IgG-opsonized platelets. Blood, 2007, 109, 4803-4805.
[145] Cognasse, F.; Lafarge, S.; Chavarin, P.; Acquart, S.; Garraud, O. Lipopolysaccharide induces sCD40L release through human plate-lets TLR4, but not TLR2 and TLR9. Intensive Care Med., 2007,33, 382-3 84.
[146] Inwald, D.P.; Faust, S.N.; Lister, P.; Peters, M.J.; Levin, M.; Hey-derman, R.; Klein, N.J. Platelet and soluble CD40L in meningo-coccal sepsis. Intensive Care Med., 2006, 32, 1432-1437.
[147] Ward, J.R.; Bingle, L.; Judge, H.M.; Brown, S.B.; Storey, R.F.; Whyte, M.K.; Dower, S.K.; Buttle, D.J.; Sabroe, I. Agonists of toll-like receptor (TLR)2 and TLR4 are unable to modulate platelet ac-tivation by adenosine diphosphate and platelet activating factor. Thromb Haemost., 2005, 94, 831-838
[148] Weyrich, A.S.; Zimmerman, G.A. Platelets: signaling cells in the immune continuum. Trends Immunol., 2004, 25, 489-495.
[149] Elzey, B.D.; Sprague, D.L.; Ratliff, T.L. The emerging role of platelets in adaptive immunity. Cell. Immunol., 2005, 238, 1-9.
[150] Krijgsveld, J.; Zaat, S.A.; Meeldijk, J.; van Veelen, P.A.; Fang, G.; Poolman, B.; Brandt, E.; Ehlert, J.E.; Kuijpers, A.J.; Engbers, G.H.; Feijen, J.; Dankert, J. Thrombocidins, microbicidal proteins from human blood platelets, are C-terminal deletion products of CXC chemokines. J. Biol. Chem., 2000, 275, 20374-20381.
[151] Dankert, J.; Krijgsveld, J.; van Der Werff, J.; Joldersma, W.; Zaat, S.A. Platelet microbicidal activity is an important defense factor

Beyond Hemostasis Cardiovascular & Haematological Disorders-Drug Targets, 2008, Vol. 8, No. 2 117
against viridans streptococcal endocarditis. J. Infect. Dis., 2001,184, 597-605.
[152] Tang, Y.Q.; Yeaman, M.R.; Selsted, M.E. Antimicrobial peptides from human platelets. Infect. Immun., 2002, 70, 6524-6533.
[153] Zahn, A.; Jennings, N.; Ouwehand, W.H.; Allain, J.P. Hepatitis C virus interacts with human platelet glycoprotein VI. J. Gen. Virol., 2006, 87, 2243-225 1.
[154] Iannacone, M.; Sitia, G.; Ruggeri, Z.M.; Guidotti, L.G. HBV pathogenesis in animal models: recent advances on the role of platelets. J. Hepatol., 2007, 46, 7 19-726.
[155] Lee, T.H.; Stromberg, R.R.; Heitman, J.W.; Sawyer, L.; Hanson, C.V.; Busch, M.P. Distribution of HIV type 1 (HIV-1) in blood components: detection and significance of high levels of HIV- 1 as-sociated with platelets. Transfusion, 1998, 38, 580-588.
[156] Chaipan, C.; Soilleux, E.J.; Simpson, P.; Hofmann, H.; Gramberg, T.; Marzi, A.; Geier, M.; Stewart, E.A.; Eisemann, J.; Ste-inkasserer, A.; Suzuki-Inoue, K.; Fuller, G.L.; Pearce, A.C.; Wat-son, S.P.; Hoxie, J.A.; Baribaud, F.; Pohlmann, S. DC-SIGN and
CLEC-2 mediate human immuno-deficiency virus type 1 capture by platelets. J. Virol., 2006, 80, 8951-8960.
[157] Boukour, S.; Masse, J.M.; Benit, L.; Dubart-Kupperschmitt, A.; Cramer, E.M. Lentivirus degradation and DC-SIGN expression by human platelets and megakaryocytes. J. Thromb. Haemost., 2006,4, 426-435.
[158] Collins, S.J.; Lawson, V.A.; Masters, C.L. Transmissible spongi-form encephalopathies. Lancet, 2004, 363, 51-61.
[159] Starke, R.; Harrison, P.; Mackie, I.; Wang, G.; Erusalimsky, J.D.; Gale, R.; Masse, J.M.; Cramer, E.; Pizzey, A.; Biggerstaff, J.; Ma-chin, S. The expression of prion protein (PrP(C)) in the megakar-yocyte lineage. J. Thromb. Haemost., 2005, 3, 1266-1273.
[160] Robertson, C.; Booth, S.A.; Beniac, D.R.; Coulthart, M.B.; Booth, T.F.; McNicol, A. Cellular prion protein is released on exosomes from activated platelets. Blood, 2006, 107, 3907-3911.
[161] Holada, K.; Glierova, H.; Simak, J.; Vostal, J.G. Expression of cellu-lar prion protein on platelets from patients with gray platelet or Hermansky-Pudlak syndrome and the protein's association with al-pha-granules. Haematologica, 2006, 91, 1126-1129.
Received: 14 July, 2007 Revised: 07 November, 2007 Accepted: 12 November, 2007





























