Embed Size (px)
Citation preview
Creating partnerships between researchers, health care
providers and Indigenous Australians to improve
Indigenous health: a demonstration model
Bianca Calabria
BPsych(Hons)
A thesis in fulfilment of the requirements for the degree of
Doctor of Philosophy
National Drug and Alcohol Research Centre
School of Public Health and Community Medicine
Faculty of Medicine
University of New South Wales
August 2013
i
Originality Statement
I hereby declare that this submission is my own work and to the best of my knowledge it
contains no materials previously published or written by another person, or substantial
proportions of material which have been accepted for the award of any other degree or
diploma at UNSW or any other educational institution, except where due acknowledgement is
made in the thesis. Any contribution made to the research by others, with whom I have
worked at UNSW or elsewhere, is explicitly acknowledged in the thesis. I also declare that the
intellectual content of this thesis is the product of my own work, except to the extent that
assistance from others in the project's design and conception or in style, presentation and
linguistic expression is acknowledged.
Bianca Calabria August 2013
ii
Copyright Statement
I hereby grant the University of New South Wales or its agents the right to archive and to
make available my thesis or dissertation in whole or part in the University libraries in all forms
of media, now or here after known, subject to the provisions of the Copyright Act 1968. I
retain all proprietary rights, such as patent rights. I also retain the right to use in future works
(such as articles or books) all or part of this thesis or dissertation. I also authorise University
Microfilms to use the 350 word abstract of my thesis in Dissertation Abstract International
(this is applicable to doctoral theses only). I have either used no substantial portions of
copyright material in my thesis or I have obtained permission to use copyright material; where
permission has not been granted I have applied/will apply for a partial restriction of the digital
copy of my thesis or dissertation.
Bianca Calabria March 2014
iii
Authenticity Statement
I certify that the Library deposit digital copy is a direct equivalent of the final officially
approved version of my thesis. No emendation of content has occurred and if there are any
minor variations in formatting, they are the result of the conversion to digital format.
Bianca Calabria March 2014

iv
Supervisor Statement
I hereby certify that all co-authors of the published or submitted papers agree to Bianca
Calabria submitting those papers as part of her doctoral thesis.
Anthony Shakeshaft August 2013
Thesis by Publication Statement
Six papers are included in this thesis by publication. Four papers have been published in peer-
reviewed journals and two papers have been submitted for editorial review to peer-reviewed
journals. I attest to the publishable quality of the two papers currently under editorial review.
Anthony Shakeshaft August 2013
v
Acknowledgements
Firstly, I would like to thank my supervisors Anthony Shakeshaft and Anton Clifford for their
dedicated supervision. Through working with Anthony and Anton over the duration of my
candidature I have learnt about the kind of researcher I aspire to be. I would like to thank
Anthony for his enthusiasm for research which motivated me to get through the next stage of
thesis writing. Anthony’s flexibility, compassion, and dedication to teaching have helped me to
develop my research skills on many levels. I am grateful for the ongoing discussions Anton and
I had about the day by day project challenges. Anton’s drive, open mindedness and
commitment have taught me to look for the benefit in the unexpected hurdles of research. I
would also like to thank my co-supervisor Christopher Doran for helping to develop my
research skills and professional networks, which will be a part of my career in academia in the
years to come.
I would like to thank the co-authors on the six published papers that constitute my thesis:
Julaine Allan, Donna Bliss, Anton Clifford, Kate Conigrave, Christopher Doran, Wayne Hall, Alys
Havard, Miranda Rose, Anthony Shakeshaft, Lynette Simpson, and Theo Vos. The contributions
made by each have improved the content of the co-authored papers, and therefore my thesis.
I would also like to thank Mark Deady, Joanne Gilsenan, Melissa Haswell-Elkins, Sonja
Memedovic, Tim Slade, Chiara Stone, and Komla Tsey who provided input into this research.
Thank you to the Aboriginal people involved in this research. As this thesis demonstrates, input
from Aboriginal people is imperative for Aboriginal-specific research. I value the time they
volunteered and the conversations we had, in addition to the comments and suggestions they
provided about the research project.
vi
I am grateful to the staff of Yoorana Gunya Family Healing Centre and the Lyndon Community
who were involved in this research. This research would be nothing without their commitment
and dedication to achieving the project’s goals. I would like to especially thank the counsellors
who worked so hard to be trained and certified in the interventions.
I am grateful to the National Drug and Alcohol Research Centre (NDRAC) for providing a
supportive environment during my candidature and the opportunity for me to work closely
with many talented researchers. Thank you to NDARC, the National Health and Medical
Research Council, the Australian Research Council, the Australian Government Department of
Health and Ageing, and the Alcohol Education and Rehabilitation Foundation for providing
funding that supported this research.
To my loving family and friends, thank you for everything you have done to help me get
through my candidature; the listening ear, the needed distraction, and the child minding all
helped me to complete my thesis. I’d especially like to thank my husband and my son for their
understanding when I was absorbed by my research, and for their constant love and support.
vii
Abstract
Alcohol misuse imposes a disproportionately high burden of harm on Indigenous Australians.
Alcohol-related harms affect the physical, psychological, and spiritual wellbeing of Indigenous
Australians. Harms extend beyond the problem drinker to their families and communities.
The primary aim of this thesis was to develop and implement a process of researchers, health
care providers and Indigenous Australians working in partnership to more effectively respond
to the deleterious impact of alcohol misuse on Indigenous families and communities. The
process was highly interactive in that it sought to combine the methodological skills of
researchers, the clinical knowledge and skills of health care providers, and the community
knowledge and experience of Indigenous Australians. Specifically, research was used to
identify interventions with potential to address alcohol-related harms that could be tailored to
be consistent with Indigenous Australians’ concepts of health and wellbeing (Papers 1 and 6),
to ensure the reliability and validity of potential measures of impact (Paper 2), and to identify
more precisely the nature of alcohol-related harm experienced by Indigenous Australians
(Paper 5). Indigenous Australians’ perceptions of the acceptability of potential interventions
were obtained (Paper 4). Health care providers’ views on how the potential interventions
might best be tailored for routine delivery (Paper 3), and on undertaking a certification process
to improve and standardise their skills in delivering the potential interventions (Paper 3), were
also obtained.
This thesis is presented for examination as a series of publications, which means it presents a
series of papers that were published in, or submitted for editorial review to, a peer-reviewed
journal during the student’s candidature, rather than the traditional model of presenting thesis
chapters. Consistent with the University of New South Wales’ thesis requirements, preambles

viii
have been added to the papers to facilitate a coherent logical flow across the thesis, and
appendices are included to complement the published content, but otherwise the papers are
unaltered from the published or submitted versions. Papers 1, 4, 5 and 6 are published and
Papers 2 and 3 are currently under editorial review. The introduction, and the implications and
future directions chapter, provide a broader context for this thesis.
1
Table of Contents
Originality Statement i
Copyright Statement ii
Authenticity Statement iii
Supervisors Statement iv
Thesis by Publication Statement iv
Acknowledgements v
Abstract vii
List of Tables 5
List of Figures 7
List of Abbreviations 8
List of Presentations 10
Introduction 13
Paper 1: A systematic review of family-based interventions targeting alcohol misuse
and their potential to reduce alcohol-related harm in Indigenous communities
28
Copyright statement 29
Preamble 30
Abstract 31
Introduction 32
Method 34
Results 39
Discussion 53
Paper 2: Identifying Aboriginal-specific AUDIT-C and AUDIT-3 cut-off scores for at-risk,
high-risk and likely dependent drinkers using measures of agreement with the 10-item
2
Alcohol Use Disorders Identification Test 58
Copyright statement 59
Preamble 60
Abstract 62
Background 63
Methods 64
Results 69
Discussion 75
Paper 3: Tailoring a family-based alcohol intervention for Aboriginal Australians, and
the experiences and perceptions of the health care providers trained in its delivery
80
Copyright statement 81
Preamble 82
Abstract 84
Introduction 85
Methods 86
Results 94
Discussion 102
Paper 4: The acceptability to Aboriginal Australians of a family-based intervention to
reduce alcohol-related harms
107
Copyright statement 108
Preamble 109
Abstract 110
Introduction 111
Methods 112
Results 114

3
Discussion 117
Paper 5: Epidemiology of alcohol-related burden of disease among Indigenous
Australians
121
Copyright statement 122
Preamble 123
Abstract 124
Introduction 125
Method 126
Results 129
Discussion 133
Paper 6: A systematic and methodological review of interventions for young people
experiencing alcohol-related harm
137
Copyright statement 138
Preamble 139
Abstract 140
Introduction 141
Method 143
Results 148
Discussion 160
Implications and future directions 167
References 181
Appendix A: Search strings for systematic search for family-based alcohol
interventions
216
Appendix B: Formulae for analysis 218
Appendix C: Health care provider consent form 219
4
Appendix D: Qualitative data analysis 223
Appendix E: CRA and CRAFT intervention resources 242
Appendix F: Advertising poster for recruitment for the acceptability study 264
Appendix G: Acceptability survey information for participants 265
Appendix H: Intervention information and acceptability survey 268
Appendix I: Slides used to present the acceptability survey in a standardised manner 289
Appendix J: Group record sheet for acceptability survey 351
Appendix K: Additional methods and results not included in the published paper
(Calabria et al. 2013)
352
Appendix L: Search strings for systematic search for interventions addressing
problematic alcohol use among young people
360
5
List of Tables
Paper 1: A systematic review of family-based interventions targeting alcohol misuse and their
potential to reduce alcohol-related harm in Indigenous communities
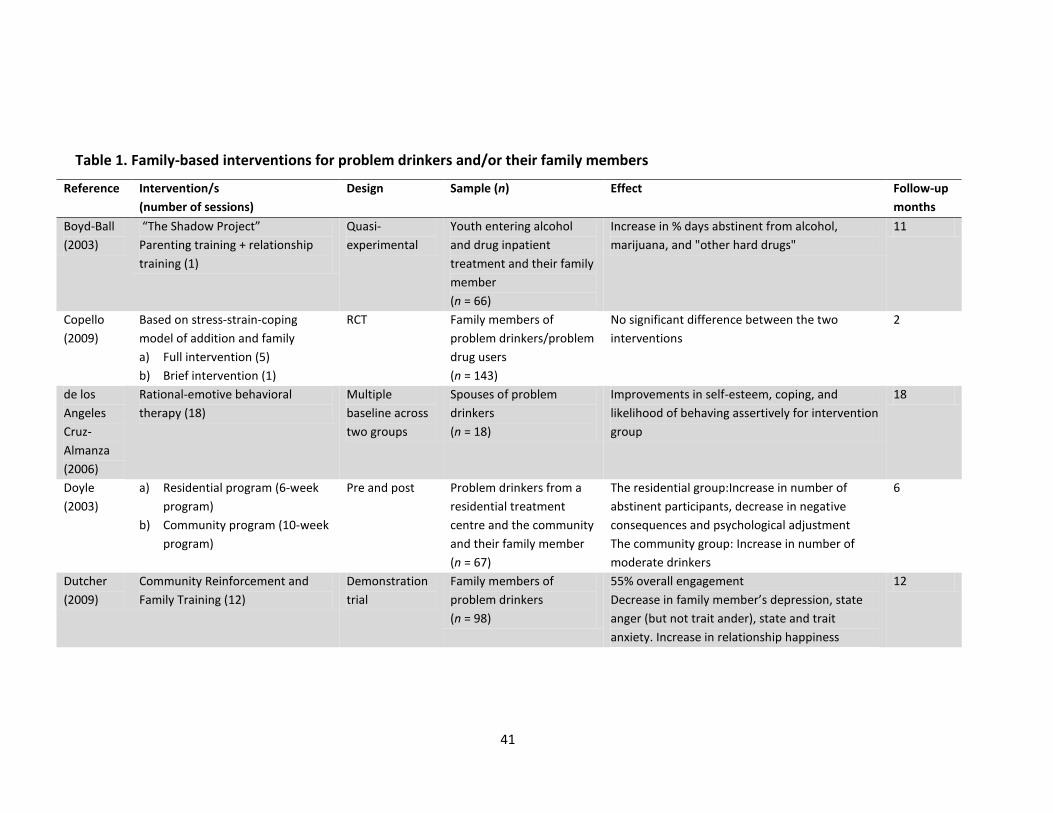
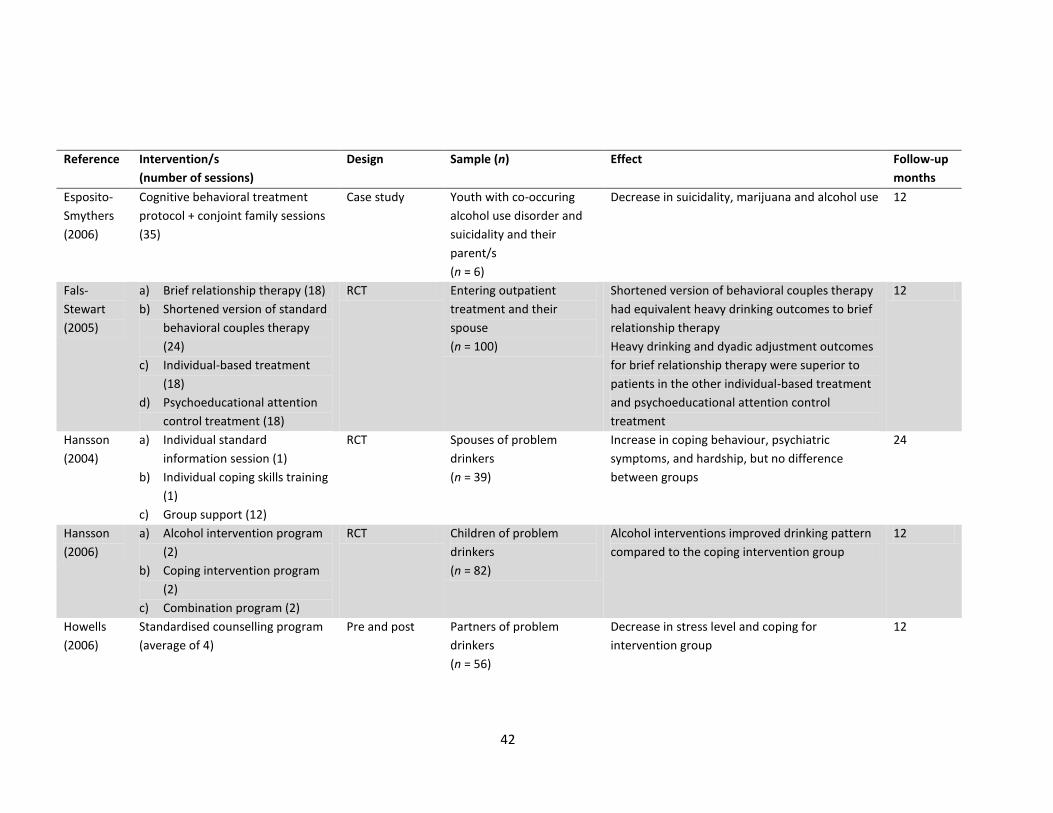
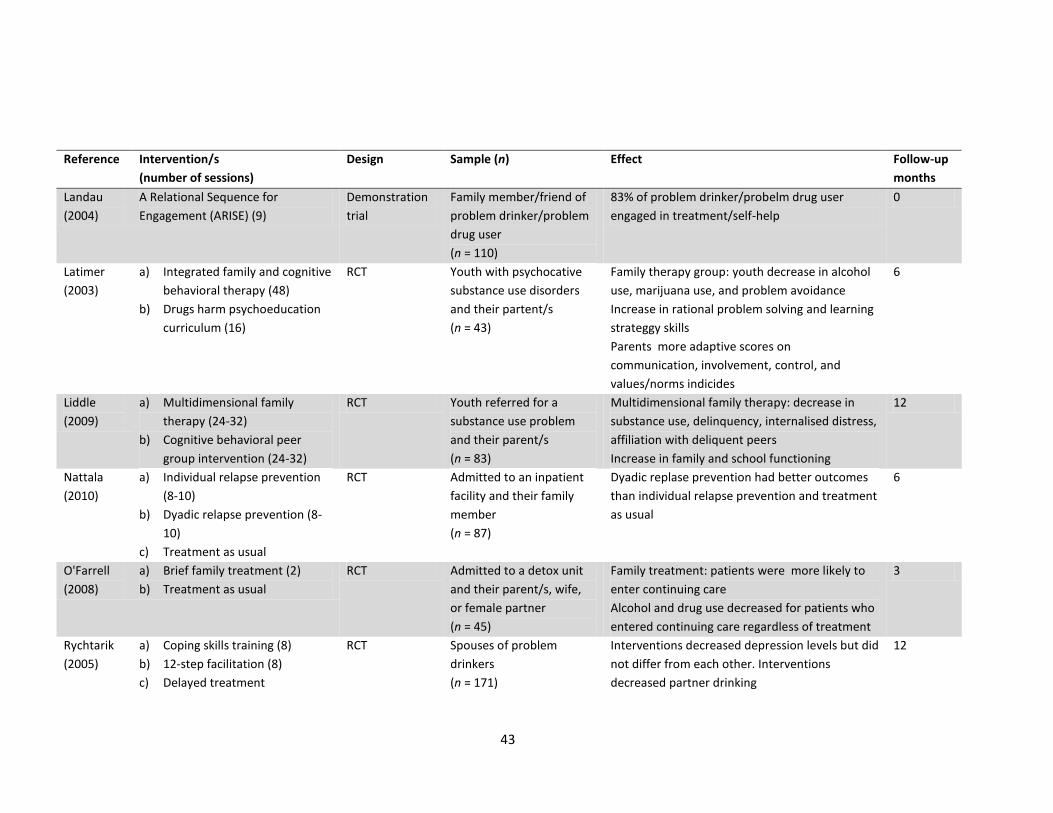
Table 1: Family-based interventions for problem drinkers and/or their family
members
41
Table 2: Methodological adequacy 50
Paper 2: Identifying Aboriginal-specific AUDIT-C and AUDIT-3 cut-off scores for at-risk, high-risk
and likely dependent drinkers using measures of agreement with the 10-item Alcohol Use
Disorders Identification Test
Table 1: Alcohol Use Disorders Identification Test (AUDIT) adapted wording for
Aboriginal Australians
66
Table 2: Measures of agreement for AUDIT-C and AUDIT-3 cut-off scores 71
Paper 3: Tailoring a family-based alcohol intervention for Aboriginal Australians, and the
experiences and perceptions of the health care providers trained in its delivery
Table 1: Health care providers’ role and qualifications 91
Table 2: Focus of working group meetings 92
Paper 4: The acceptability to Aboriginal Australians of a family-based intervention to reduce
alcohol-related harms
Table 1: Demographic characteristics of the sample (n = 116) 115
Table 2: Preference for intervention delivery 116
Paper 5: Epidemiology of alcohol-related burden of disease among Indigenous Australians
Table 1: Rates (DALYs per 1,000) of alcohol-related disease and injury, Australia 131
Paper 6: A systematic and methodological review of interventions for young people
experiencing alcohol-related harm
Table 1: Interventions for young people experiencing alcohol-related harm 150

6
Table 2: Methodological adequacy of reviewed studies 156
7
List of Figures
Paper 1: A systematic review of family-based interventions targeting alcohol misuse and their
potential to reduce alcohol-related harm in Indigenous communities
Figure 1: Flowchart indicating search strategy and classification of articles 35
Paper 2: Identifying Aboriginal-specific AUDIT-C and AUDIT-3 cut-off scores for at-risk, high-risk
and likely dependent drinkers using measures of agreement with the 10-item Alcohol Use
Disorders Identification Test
Figure 1: ROC curve for at-risk drinker (AUDIT score ≥ 8) 72
Figure 2: ROC curve for high-risk drinker (AUDIT score ≥ 13) 73
Figure 3: ROC curve for likely dependent drinker (AUDIT score ≥ 20) 74
Paper 3: Tailoring a family-based alcohol intervention for Aboriginal Australians, and the
experiences and perceptions of the health care providers trained in its delivery
Figure 1: Process of tailoring the CRA and CRAFT interventions 88
Paper 5: Epidemiology of alcohol-related burden of disease among Indigenous Australians
Figure 1: Alcohol-related disease and injury by sex: males 132
Figure 2: Alcohol-related disease and injury by sex: females 132
Paper 6: A systematic and methodological review of interventions for young people
experiencing alcohol-related harm
Figure 1: Flowchart indicating search strategy and classification of articles 145
8
List of Abbreviations
In each chapter/paper, abbreviations are used after the phrase has been written in full.
A-CRA Adolescent Community Reinforcement Approach
ACCHS Aboriginal Community Controlled Health Service
AH&MRC Aboriginal Health and Medical Research Council
AQoL-6D Assessment of Quality of Life – 6D
ARISE A Relational Sequence for Engagement
AUROC Areas under the receiver operating characteristic
AUDIT Alcohol Use Disorders Identification Test
AUDIT-C First three items of AUDIT
AUDIT-3 Third item of AUDIT
BMI Brief motivational interviewing
CBT Cognitive behavioural therapy
CI Confidence interval
CRA Community Reinforcement Approach
CRAFT Community Reinforcement and Family Training
CRAFFT Car Relax Alone Forget Friends Trouble
CVD Cardiovascular disease
DALY Disability adjusted life year
DAST Drug Abuse Screening Test
DSM-IV Diagnostic and Statistical Manual of Mental Disorders, Volume 4
DUI Driving under the influence
etc. Et cetera
e.g. For example
Fig. Figure
9
g Grams
GEM Growth Empowerment Measure
HIV Human immunodeficiency virus
HREC Human Research Ethics Committee
i.e. That is
MBD Multiple baseline design
MI Motivational interviewing
N/A Not applicable
NATSIHS National Aboriginal and Torres Strait Islander Health Survey
NDARC National Drug and Alcohol Research Centre
NHMRC National Health and Medical Research Council
NHS National health survey
NSW New South Wales
PAF Population attributable fraction
RCT Randomised control trial
ROC Receiver operating characteristic
SD Standard deviation
UNSW University of New South Wales
U.S. United States
YLD Year of life lived with disability
YLL Years of life lost
10
List of Presentations
1. Bianca Calabria, Anthony Shakeshaft, Anton Clifford, Komla Tsey, Julaine Allan, Christopher
Doran, Miranda Rose, Rod MacQueen. Family-based intervention for Indigenous people
who have alcohol use problems, National Drug and Alcohol Research Centre Seminar
Series, May 2010: Sydney, Australia [oral presentation].
2. Bianca Calabria, Anton Clifford, Anthony Shakeshaft, Christopher Doran. Reducing alcohol-
related harms among Indigenous Australians: A systematic review of family-based
approaches, National Drug and Alcohol Research Centre Annual Symposium, August 2010:
Sydney, Australia [poster presentation].
3. Bianca Calabria, Anton Clifford, Anthony Shakeshaft, Christopher Doran, Julaine Allan,
Miranda Rose, Komla Tsey. Family-based approaches to reduce alcohol-related harms
among Indigenous Australians, Australian Professional Society on Alcohol and Other Drugs
(APSAD) Conference, November 2010: Canberra, Australia [oral presentation].
4. Bianca Calabria, Anthony Shakeshaft, Anton Clifford, Komla Tsey, Julaine Allan, Christopher
Doran, Miranda Rose, Rod MacQueen. Development and evaluation of a family-based
intervention to reduce alcohol-related harms among Indigenous Australians: Acceptability
and study design, National Drug and Alcohol Research Centre Seminar Series, April 2011:
Sydney, Australia [oral presentation].
5. Bianca Calabria, Anton Clifford, Anthony Shakeshaft, Christopher Doran, Julaine Allan,
Miranda Rose, Rod MacQueen. The acceptability of a family-based alcohol intervention to
Indigenous clients of a rural Aboriginal Community Controlled Health Service and drug and
alcohol treatment agency, 3rd Aboriginal Health Research Conference, Coalition for
11
Research to Improve Aboriginal Health (CRIAH), May 2011: Sydney, Australia [oral
presentation].
6. Bianca Calabria, Anton Clifford, Anthony Shakeshaft, Christopher Doran, Julaine Allan,
Miranda Rose, Komla Tsey, Rod MacQueen. The acceptability of a family-based alcohol
intervention to Indigenous clients of a rural Aboriginal Community Controlled Health
Service and drug and alcohol treatment agency, University of New South Wales, School of
Public Health and Community Medicine Research Symposium, August 2011: Sydney,
Australia [oral presentation].
7. Bianca Calabria, Anton Clifford, Anthony Shakeshaft, Christopher Doran, Julaine Allan,
Miranda Rose, Komla Tsey, Rod MacQueen. A family-based approach to reducing alcohol-
related harms among Aboriginal Australians in rural New South Wales, National Drug and
Alcohol Research Centre Annual Symposium, August 2011: Sydney, Australia [oral
presentation].
8. Bianca Calabria, Anton Clifford, Anthony Shakeshaft, Christopher Doran, Julaine Allan,
Miranda Rose, Komla Tsey, Rod MacQueen. The acceptability of a family-based alcohol
intervention to Indigenous clients of a rural Aboriginal Community Controlled Health
Service and drug and alcohol treatment agency, National Drug and Alcohol Research
Centre Annual Symposium, August 2011: Sydney, Australia [poster presentation].
9. Bianca Calabria, Anton Clifford, Anthony Shakeshaft, Katherine Conigrave, Lynette
Simpson, Julaine Allan. Identifying risky and dependent Aboriginal drinkers using AUDIT-C
and AUDIT-3, National Drug and Alcohol Research Centre Annual Symposium, August
2012: Sydney, Australia [poster presentation].

12
10. Bianca Calabria, Anton Clifford, Anthony Shakeshaft, Katherine Conigrave, Lynette
Simpson, Donna Bliss and Julaine Allan. AUDIT-C and AUDIT-3 cut-off scores for Aboriginal
Australians, National Drug and Alcohol Research Centre Seminar Series, November 2012:
Sydney, Australia [oral presentation].
11. Bianca Calabria, Anton Clifford, Miranda Rose, Anthony Shakeshaft. Tailoring two
evidence-based interventions for delivery to Aboriginal Australians: Perception of, and
suggestions by, health care providers, National Drug and Alcohol Research Centre Annual
Symposium, September 2013: Sydney, Australia [poster presentation].
12. Bianca Calabria, Anthony Shakeshaft, Anton Clifford. Improving Indigenous intervention
research by establishing partnerships between researchers, Indigenous Australians and
health care providers, University of New South Wales, School of Public Health and
Community Medicine Research Symposium, October 2013: Sydney, Australia [oral
presentation].
13
Introduction
14
A brief overview of Indigenous Australian history and alcohol
Indigenous Australians1 have one of the oldest continuing cultures in the world (Rasmussen et
al. 2011). They share a strong connection to their past and to their traditional lands which is
communicated through varied cultural practices (Coates 2004), both traditional and
contemporary. The colonisation of Australia and government policies and practices had, and
continues to have, a negative and significant impact on Indigenous Australians’ physical, social,
emotional and mental health and wellbeing (Gracey & King 2009). The health status of
Indigenous Australians is, therefore, worse than any other identifiable group in Australia
(Australian Institute of Health and Welfare 2011d). The socio-economic determinants of poor
health for Indigenous and non-Indigenous people include income, education, employment,
living conditions, social support and access to health care services (King, Smith & Gracey 2009).
Indigenous Australians have worse outcomes on each of these determinants compared to non-
Indigenous Australians (Altman 2003; Australian Medical Association 2011). Additionally,
Indigenous Australians’ health is negatively affected by factors inextricably linked to the
process of colonisation, such as racism, loss of language and connection to the land,
environmental deprivation, and spiritual, emotional and mental disconnectedness from culture
and community (King, Smith & Gracey 2009). The presence of these socio-economic
determinants of poor health has, in turn, been shown to be significantly associated with an
increased incidence of a number of health risk behaviours, including alcohol misuse, which has
1 Australia’s first peoples have two distinct cultural identities: Aboriginal and Torres Strait Islander
groups. The first inhabitants of Australia are referred to in this thesis as Indigenous Australians,
Aboriginal people, Aboriginal Australians, and Aboriginal and Torres Strait Islander people. Referential
terms for Australia’s first peoples vary across the chapters/papers of this thesis to represent the
preference of Aboriginal and/or Torres Strait Islander people involved in each chapter.
15
been shown to further worsen Indigenous Australians’ health status (Australian Institute of
Health and Welfare 2011d; King, Smith & Gracey 2009; Vos et al. 2007).
The colonisation of Australia had a particularly detrimental effect on alcohol consumption
patterns among Indigenous Australians. Prior to colonisation, Indigenous Australians
participated in controlled consumption of mild fermented beverages made from local plants
(Brady 1991) for ceremonial and trade purposes (Brady 2008). Alcohol was also introduced to
Indigenous Australians by Makassans, the Dutch, the French and the Russians, before the
British arrived in 1788 (Brady 2008). When the British settled in Australia, patterns of
consuming large quantities of alcohol on a single occasion were introduced (Lewis 1992) and
Indigenous Australians learned these patterns of drinking (Brady 2008). State Prohibition Laws
denying Indigenous Australians legal access to alcohol were introduced in New South Wales in
1838, Western Australia in 1843, Victoria in 1864, South Australia and the Northern Territory
in 1869, Queensland in 1885, Tasmania in 1908, and the Australian Capital Territory in 1929
(Brady 1991; Brady 2008). These laws had the effect of segregating Indigenous and non-
Indigenous drinking, effectively increasing the temptation of alcohol to Indigenous Australians,
and encouraging Indigenous Australians to get drunk very quickly in an uncontrolled
environment (Brady 2008). When prohibition eased in the 1900s, conditional citizenship, and
the legal right to drink, were restored in the legislation, but only for Indigenous Australians
who had abandoned their tribal associations, served in the armed forces, or were deemed to
have acquired the ‘habits of civilised life’ (Lewis 1992). Indigenous Australians classified as
‘mixed decent’ (that is those who were part Indigenous and part European) were also allowed
to drink alcohol (Brady 1991). The right to drink alcohol, therefore, was equated to citizenship
and assimilation with the prevailing European values and lifestyle (Lewis 1992).
16
Alcohol use in Australia’s Indigenous and general populations
The National Drug Strategy Household Survey collects alcohol consumption data for
Australians aged 14 years or older. The most comprehensive and methodologically sound data
(Chikritzhs & Brady 2006) on Indigenous Australian alcohol use was collected in 1994 and is
reported in the Urban Aboriginal and Torres Strait Islander Peoples Supplement (Australian
Department of Human Services and Health 1995). This supplement compares 1994 Indigenous-
specific data to 1993 general population data. Thirty-seven percent of Indigenous Australians
reported that they did not currently drink alcohol (28% of males and 44% of females),
compared to 22% of general population Australians (16% of males and 26% of females).
Among the current drinkers, hazardous (two to four standard drinks per occasion for females
and four to six for males) and harmful (more than four standard drinks per occasion for
females and more than six for males) drinking was reported by 14% and 68% of Indigenous
respondents respectively, and 17% and 11% of general population respondents respectively.
Although limited, more recent data show a similar trend. A greater proportion of Indigenous
Australians abstain from drinking alcohol, compared to general population Australians: 21.3%
compared to 16.4% in 2004; 23.4% compared to 17.1% in 2007; and 24.5% compared to 19.5%
in 2010 (Australian Institute of Health and Welfare 2005; Australian Institute of Health and
Welfare 2008a; Australian Institute of Health and Welfare 2011a). A higher proportion of
Indigenous Australians, however, drink at levels that increase their risk of alcohol-related
harm. The proportion of those who report short-term risky alcohol consumption for
Indigenous Australians, relative to general population Australians, in 2004 (defined as the
consumption of at least seven (males) or five (females) standard drinks per occasion) was
38.7% and 20.7% respectively. In 2007 the comparable proportions were 27.4% and 20.4%
respectively. Results from 2010 showed a substantial reduction for both Indigenous and
general population Australians (24.6% and 15.9%, respectively) (defined as the consumption of
17
more than four standard drinks per occasion for both males and females). The proportion of
those who report long-term risky alcohol consumption for Indigenous Australians, relative to
general population Australians, in 2004 (defined as the consumption of at least 29 (males) or
15 (females) standard drinks in a week) was 22.7% and 9.9% respectively. In 2007 the
comparable proportions were 12.5% and 10.3% respectively. Results from 2010 showed a
large increase for both Indigenous and general population Australians (31.0% and 20.1%
respectively), although this most likely reflects the introduction of a more conservative
definition of long-term risky drinking (the consumption of at least two standard drinks on any
day for males and females) (Australian Institute of Health and Welfare 2005; Australian
Institute of Health and Welfare 2008a; Australian Institute of Health and Welfare 2011a). As a
consequence of these relatively higher proportions of both short-term and long-term risky
drinkers, Indigenous Australians experience a disproportionately high burden of alcohol-
related harm, relative to general population Australians (Begg et al. 2007; Vos et al. 2003).
Contribution of alcohol use to the burden of disease and health care costs imposed
on Indigenous Australians
The health related burden of disease is commonly measured using the Disability Adjusted Life
Year (DALY) which is equivalent to one lost year of ‘healthy’ life due to death or disability
(Murray et al. 2012). Mortality and morbidity health data are incorporated into the DALYs from
hospital records, vital registration, surveys and other sources (Vos et al. 2007). In the
Indigenous Australian population, alcohol is estimated to contribute 5.4% to the total burden
of disease (6.2% of harmful effects and -0.8% of beneficial effects) (Vos et al. 2007), compared
to 2.3% of the total burden of disease (3.3% of the harmful effects and -1.0% of the beneficial
effects) in the general Australian population (Begg et al. 2007). The greatest contributors to
the estimated alcohol-related harm among Indigenous Australians are alcohol abuse and
harmful use (40%), homicide and violence (14%), suicide (14%) and road traffic accidents (14%)
18
(Vos et al. 2003). Relative to other risk factors, alcohol is estimated as being responsible for the
greatest proportion of the burden of disease imposed on Indigenous males aged 15-34 years
and the second greatest proportion of the burden of disease imposed on Indigenous females
of the same age (eclipsed only by intimate partner violence) (Vos et al. 2003). Alcohol is also
the leading risk factor for injury among Indigenous Australians (Vos et al. 2007). In addition,
mental health disorders is estimated as being responsible for 15.5% of the total disease burden
among Indigenous Australians, 19% of which is directly associated with alcohol dependence
and harmful use (Vos et al. 2003).
As well as attempting to estimate the relative contribution of different diseases and injuries to
mortality and morbidity, the burden of disease data are used to quantify the health gap
between Indigenous and general population Australians. The health gap is defined as the
difference between the number of ‘healthy’ years of life lost through disability or death and
the number of healthy years that would have been lost if a difference between Indigenous
Australian and general Australian population disease and injury rates did not exist (Vos et al.
2009). The Indigenous health gap accounts for 59% of the total burden of disease among
Indigenous Australians. Alcohol is in the top five main risk factors and contributes 4% to the
Indigenous health gap. The other four main risk factors are tobacco (17%), high body mass
(16%), physical inactivity (12%), and high blood cholesterol (7%) (Vos et al. 2009).
The health gap is reflected in the difference in health costs for Indigenous, compared to
general population, Australians. The estimated per person expenditure on health care costs for
2008-09, for services where cost has been estimated, was $3,887.20 for Indigenous Australians
and $2,509.20 for non-Indigenous Australians (Australian Institute of Health and Welfare
2011c). Hospital separations refer to an episode of admitted patient care that is completed by
discharge, dying, being transferred to another hospital, or by change of type of care (Australian

19
Institute of Health and Welfare 2011b). Hospital separation rates (public and private) for
alcohol dependence and other harmful use during 2008-09 were 3.7 times higher for
Indigenous compared to non-Indigenous Australians (7.3 for Indigenous and 2.0 for non-
Indigenous). These hospital separations cost an estimated $17.6 million for Indigenous and
$135.9 million for non-Indigenous, translating to $32.30 for each Indigenous individual and
$6.40 for each non-Indigenous individual (Australian Institute of Health and Welfare 2011c).
Governments provided 69.7% of the total health care funding for 2008-09 with the remaining
30.3% paid by individuals, private health insurance and other non-government sources
(Australian Institute of Health and Welfare 2010). An effective government response to reduce
these harms and costs is, therefore, essential.
Closing the Gap Framework
In March 2008, the Council of Australian Governments (including the Prime Minister, State
Premiers, Territory Chief Ministers and the President of the Australian Local Government
Association) formally committed to the Closing the Gap Framework, aimed at achieving
Indigenous health equality within 25 years (Council of Australian Governments 2012). Six
specific targets were agreed: 1) closing the life expectancy gap within a generation; 2) halving
the gap in mortality rates for Indigenous children under five within a decade; 3) ensuring all
Indigenous four year olds in remote communities have access to early childhood education
within five years; 4) halving the gap for Indigenous students in reading, writing and numeracy
within a decade; 5) halving the gap for Indigenous young people attaining Year 12
qualifications or equivalent by 2020; and 6) halving the gap in employment outcomes between
Indigenous and non-Indigenous Australians within a decade (Council of Australian
Governments 2012; Australian Institute of Health and Welfare 2011d). Seven building blocks
were also defined in the Closing the Gap Framework as underpinning the achievement of the
targets: 1) early childhood; 2) schooling; 3) health; 4) healthy homes; 5) economic
20
participation; 6) safe communities; and 7) governance and leadership. Among other things, the
‘health’ and ‘safe communities’ building blocks are aimed at reducing alcohol-related harms
among Indigenous Australians by expanding health care services for alcohol dependence and
abuse, increasing the number of alcohol and drug workers, reducing Foetal Alcohol Spectrum
Disorders, reducing alcohol-related road traffic accidents, reducing community violence and
dysfunction, and supporting community chosen Alcohol Management Plans (Australian
Government 2013). Improved efforts to identify best evidence interventions for reducing
alcohol misuse among Indigenous Australians, and effective methods for tailoring them to the
specific circumstances of Indigenous communities would help to achieve the alcohol-related
aims of the Closing the Gap building blocks.
Improving intervention research
Systematic reviews of the published Indigenous health literature have identified a
predominance of descriptive research in the Indigenous health research field, and a need for
more Indigenous-specific intervention research (Sanson-Fisher et al. 2006; Gray et al. 2000).
Specifically, with respect to alcohol research there is a lack of intervention and measures
research, and the limited number of intervention evaluations that have been published tend to
focus on primary interventions (e.g. health promotion, alcohol restrictions) with little attention
to secondary interventions (e.g. brief interventions, cognitive-behavioural interventions) (Gray
et al. 2000; Clifford et al. 2010; Shakeshaft, Clifford & Shakeshaft 2010). The main
consequence of continuing the current trend in Indigenous alcohol research would be an
ongoing lack of reliable evidence for the types of interventions that are likely to be most cost-
effective for difference types of alcohol-related problems, and an increased likelihood that
interventions of unknown effectiveness and cost will continue to be implemented.
21
To adequately determine their cost-effectiveness, Indigenous-specific interventions require
careful consideration and development, comprising both meaningful consultation and
collaboration with Indigenous communities and rigorous evaluation using practical and
rigorous evaluation designs, and valid, reliable and acceptable measurement instruments
(Gray et al. 2000; Clifford et al. 2010). Rigorous evaluations that use valid and reliable
instruments to measure outcomes are required to determine the true effect of an intervention
(Sanson-Fisher & Campbell 1994). Indigenous-specific measures with published validity and
reliability are rare (Clifford et al. 2010; Shakeshaft, Clifford & Shakeshaft 2010) and, as such,
their development should be a priority for researchers.
Tailoring evidence-based interventions with potential to reduce alcohol-related harms to the
needs and preferences of Indigenous communities and health care services increases both the
likelihood that they will prove to be cost-effective and that those shown to be cost-effective
will be able to be integrated into routine care (Shakeshaft, Clifford & Shakeshaft 2010). Family-
based approaches have been shown to be effective for reducing alcohol-related harms in non-
Indigenous populations (Miller & Wilbourne 2002; Smit et al. 2008; Templeton, Velleman &
Russell 2010), and they are likely to be acceptable to Indigenous Australians for four main
reasons: 1) family members in close contact with problem drinkers are at risk of alcohol-
related violence, conflict, sexual assault, psychological abuse and/or neglect (Kelly &
Kowalyszyn 2003; Laslett et al. 2010); 2) positive family relationships are the foundation for
community cohesion in Indigenous communities (McLennan & Khavarpour 2004) and can
promote behavioural change (Nagel & Thompson 2010); 3) family-based approaches align with
the Indigenous Australian cultural practice of including family members in health care
communications (McGrath et al. 2006); and 4) family-based approaches are consistent with
the Indigenous Australian concept of health that incorporates physical, social, emotional, and
cultural wellbeing (Brady 2004).
22
Evidence-based interventions tailored for Indigenous Australians and delivered through
Indigenous-specific health care services improves the likelihood that they will be accessed by
Indigenous Australians, because they are more likely to seek culturally appropriate care
(Henry, Houston & Mooney 2004). Aboriginal Community Controlled Health Services (ACCHSs)
are primary care services aimed at providing high quality holistic and culturally appropriate
care through local Indigenous community planning and management. ACCHSs often provide
primary and secondary interventions aimed at addressing low and risky alcohol consumption
(Hunter et al. 2005). Tertiary interventions, addressing high-risk alcohol use and high levels of
alcohol dependence, are usually delivered to Indigenous Australians through drug and alcohol
treatment agencies (Brady, Dawe & Richmond 1998). Although drug and alcohol treatment
agencies are not always governed by Indigenous Australians, they can provide specialist care
through health care providers who have experience working with Indigenous Australians.
Irrespective of the specific nature of the health care service, the extent to which it is utilised by
Indigenous people, and their willingness to engage in research, is fundamentally determined
by the level of trust that exists between the health care service and the local Indigenous
community (Allan & Campbell 2011).
Working in partnership with Indigenous Australians and health care providers
The development of Indigenous-specific interventions for delivery through routine health care
services requires ongoing consultation with Indigenous people (Gray et al. 1995). This includes,
but is not limited to, a steering committee that comprises Indigenous Australian
representatives (Henderson et al. 2002). The process of consultation addresses Indigenous
people’s right to self-determination (United Nations 2008) and provides acknowledgment of,
and respect for, differences in cultural beliefs and systems between Indigenous and non-
Indigenous Australians, and the diversity of Indigenous peoples (Australian Institute of

23
Aboriginal and Torres Strait Islander Studies 2010; National Health and Medical Research
Council 2003). To optimise the feasibility and likely cost-effectiveness of Indigenous-specific
interventions, they must be acceptable to the needs and circumstances of Indigenous people
and to the health care providers who will deliver them to Indigenous people. The support of
health care providers for a proposed intervention is integral to the success with which it is
likely to be delivered in the context of routine care.
Historically evidence-based research has been developed in an academic setting without
consultation with health care providers or community members and presented to health care
providers for implementation into routine practice (Green 2008). This method has not been
successful in ensuring that evidence-based research is used in clinical practice settings,
because what works in a controlled environment under strict conditions, as is the case for
rigorously designed trials, is not always effective or appropriate in a real world setting
(Westfall, Mold & Fagnan 2007). The participation of health care providers and community
members in the development of locally targeted evidence-based interventions is more likely to
result in implementation into routine practice, than if research evidence is developed and
disseminated to health care services without consultation (Green 2008). The process of
consultation provides an opportunity for the perceived needs of health care providers and of
community members to be incorporated into research.
Translational research aims to achieve the balance between research informing practice and
practice and perceived needs informing research (Marincola 2003; Havard Catalyst 2013), and
has been categorised into five different types: T1) basic research into clinical effect; T2) clinical
effect into clinical intervention; T3) clinical intervention into clinical practice; T4) specific public
health intervention at a population level; and T5) clinical, public health and determinants-
related interventions applied to the population or specific sub-population (Thompson 2012).
24
Since T5 research is most relevant to intervention research that is integrated into the routine
delivery of health care services, its applicability to Indigenous Australians is most likely to be in
the context of health care services provided by ACCHSs, or provided by health care providers
who are employed by mainstream treatment agencies but have experience working with
Indigenous Australians (Brady, Dawe & Richmond 1998; Hunter et al. 2005). Researchers
working in consultation with health care providers who routinely interact with Indigenous
Australians, and with Indigenous Australians themselves, creates the opportunity for
Indigenous-specific research to inform practice and, conversely, for the requirements of
clinical practice and the perceived needs of Indigenous clients and communities, to inform
research. Factors that may limit the practical application of this dynamic model of integrated
clinical practice and evaluation include: limited clinician access to existing research findings
and evaluation expertise; no encouragement from the health care organisation for staff to
continue learning; the lack of incentive for researchers to engage with health care providers;
and a range of individual-level factors (e.g. personal beliefs, lack of motivation) (Barratt 2003).
One potential way to address these barriers is to develop formal partnerships between
researchers, health care providers and Indigenous Australians, that allow each of them to
contribute their own skills to identify best evidence interventions, tailor them to meet the
needs and fit the circumstances of relevant Indigenous communities, families and health care
providers, implement them in the context of routine service delivery and, ultimately, evaluate
their impact and costs. Given the historical nature of the relationship between Indigenous and
non-Indigenous Australians, these partnerships are most likely to be effective if they explicitly
foster Indigenous control of, or at a minimum meaningful Indigenous participation in, all
phases of their own health research.
25
This thesis aimed to demonstrate one such process of researchers working in partnership with
health care providers and Indigenous Australians in the context of routine provision of health
care services. The partnership identified and tailored promising interventions to reduce rates
of alcohol-related harm experienced by Indigenous Australians, and devised Indigenous-
specific reliable and valid measures of alcohol misuse and harm to identify at-risk individuals
and provide a psychometrically tested outcome measure. It also sought to respond to concerns
specifically raised by Indigenous participants about the particular negative impact of alcohol on
Indigenous young people. Following from this doctoral research, participants are being
recruited to take part in the tailored interventions and baseline and follow-up data is being
collected to assess their cost-effectiveness. The evaluation of the tailored interventions will
occur as part of the ongoing partnership that has been established by this doctoral research.
Overview of chapters
Paper 1 presents the results of a systematic review of family-based interventions aimed at
reducing alcohol-related harms. The review was limited to family-based interventions because
they are most consistent with the intervention approach that both the Indigenous community
and the health care providers involved in the partnership thought would be most acceptable in
their communities. The review identified 1,369 studies, of which 142 were classified as
intervention studies. Nineteen intervention studies were family-based alcohol interventions:
eleven included the family member in the treatment of the problem drinker; and eight
specifically targeted family members of problem drinkers. Community Reinforcement and
Family Training (CRAFT) was identified as an intervention approach that had at least some
evidence for its effectiveness and had potential to be successfully tailored for delivery to
Indigenous people. CRAFT is an intervention that targets family members of problem drinkers
and teaches them skills to support their problem drinking relative to reduce their alcohol
consumption by removing positive reinforcement for drinking behaviour. CRAFT also teaches

26
family members of problem drinkers how to increase their own social and emotional
wellbeing.
Paper 2 identifies Indigenous-specific cut-off scores for two short versions of the Alcohol Use
Disorders Identification Test (AUDIT), a measure of problematic alcohol use: AUDIT-C and
AUDIT-3. Indigenous-specific AUDIT-C and AUDIT-3 cut-off scores could be used to screen
Indigenous people for enrolment into interventions and to measure intervention outcomes.
Paper 3 presents health care providers’ suggestions for tailoring CRAFT and the Community
Reinforcement Approach (CRA) (an intervention that targets problem drinkers from which
CRAFT was modelled) for Indigenous Australians, and their perceptions of the CRA and CRAFT
certification process. Changes to technical language, fewer sessions and the availability of
group sessions were suggested. The certification process was viewed positively.
Paper 4 presents Indigenous Australians’ perceptions of, and suggestions for, tailoring CRA and
CRAFT for delivery in their local community. The interventions were viewed favourably. In
addition to reaffirming the communities’ commitment to trialling a family-based approach, a
perception that young Indigenous people were at particular risk of alcohol-related harm was
highlighted; an issue explored in papers 5 and 6.
Paper 5 investigates differences in experienced alcohol-related harm for Indigenous
Australians, compared to the general Australian population, by age and sex. The findings are
consistent with the perceptions of the participants in Paper 4 that young Indigenous people
generally experience a disproportionately high burden of alcohol-related harm, relative to the
general Australian population.

27
Paper 6 presents the results of a systematic review of the peer-reviewed literature on
intervention evaluations for young people at high risk of alcohol-related harm. The review
identified 1,697 studies, of which 148 were classified as intervention studies. Nine studies
evaluating interventions targeting young people at high risk of alcohol-related harm were
identified. This review identified that the interventions with the most potential to help reduce
alcohol-related harms among high risk young people were cognitive-behavioural therapy,
family therapy and CRA.
The final section of this thesis discusses the implications of the findings of Papers 1 to 6 and
presents avenues for future research, including proposed guiding principles for researchers
developing partnerships with health care providers and Indigenous Australians to help improve
the quality of Indigenous intervention research and, ultimately, the health of Indigenous
Australians.

28
Paper 1
A systematic review of family-based interventions targeting alcohol misuse
and their potential to reduce alcohol-related harm in Indigenous
communities
Bianca Calabria1, Anton Clifford2, Anthony P. Shakeshaft1, Christopher M. Doran3,4,5
1. National Drug and Alcohol Research Centre, University of New South Wales, Sydney, New South Wales,
Australia
2. Queensland Alcohol and Drug Research and Education Centre, School of Population Health, University
of Queensland, Brisbane, Queensland, Australia
3. Hunter Medical Research Centre, Newcastle, New South Wales, Australia
4. University of Newcastle, Newcastle, New South Wales, Australia
5. Hunter Valley Research Foundation, Newcastle, New South Wales, Australia
Paper 1 has been published in the Journal of Studies on Alcohol and Drugs (Calabria et al. 2012).
29
Copyright Statement
I certify that this publication was a direct result of my research towards this PhD, and that
reproduction in this thesis does not breach copyright regulations.
Calabria, B, Clifford, A, Shakeshaft, A & Doran, C 2012, 'Systematic review of family-based
interventions targeting alcohol misuse and their potential to reduce alcohol-related harm in
Indigenous communities', Journal of Studies on Alcohol and Drugs, vol. 73, no. 3, pp. 477-488.
Bianca Calabria August 2013

30
Preamble
Paper 1 systematically reviews the peer-review literature to identify the family-based approaches
for reducing alcohol-related harm that have the most potential to be tailored for delivery to
Indigenous people. An initial systematic search of the peer-reviewed literature, using the same
methodology described in this paper, was undertaken to identify published evaluations of family-
based alcohol interventions specifically targeting Indigenous Australians; however, this search
identified no relevant studies. When evidence about intervention effectiveness that has been
established specifically in Indigenous health care settings is not available, it may be possible to
tailor interventions that have been evaluated in non-Indigenous health care settings to Indigenous
settings, provided there is little likelihood of harmful outcomes for participants (Shakeshaft,
Clifford & Shakeshaft 2010). A broader systematic search of the peer-review literature was
therefore undertaken to identify published evaluations of family-based alcohol interventions
targeting any population group. The acceptability and feasibility to health care providers and
Indigenous Australians of the most promising interventions would subsequently be explored.
Although the findings of this systematic review are applicable to both Indigenous and non-
Indigenous populations, the main purpose of the review is to identify which family-based
interventions appear most promising to reduce alcohol-related harm in Indigenous communities.
31
Abstract
Objective: Alcohol misuse is a major risk factor for harm in Indigenous communities. The
Indigenous family unit is often the setting for, and is most adversely affected by, alcohol-related
harm. Therefore, family-based alcohol interventions offer great potential to reduce alcohol-related
harm in Indigenous communities. This systematic review aims to identify peer-reviewed
publications of evaluations of family-based alcohol interventions, critique the methodological
quality of those studies and describe their intervention characteristics, and identify which
interventions appear most promising to reduce alcohol-related harm in Indigenous communities.
Method: Eleven electronic databases were searched. The reference lists of reviews of family-based
approaches focused on alcohol interventions were hand-searched for additional relevant studies
not identified by the electronic database search.
Results: Initially, 1,369 studies were identified, of which 21% (n = 142) were classified as
intervention studies. Nineteen intervention studies were family-based alcohol interventions.
Eleven of these studies included family members in the treatment of problem drinkers, and eight
studies specifically targeted family members of problem drinkers. Methodological quality of
studies varied, particularly in relation to study design, including confounding variables in the
analyses, and follow-up rates.
Conclusions: The evidence for the effectiveness of family-based alcohol interventions is less than
optimal, although the reviewed studies did show improved outcomes. Given the important role of
family in Indigenous communities, there is merit in exploring family-based approaches to reduce
alcohol-related harms. Tailored family-based approaches should be developed with direct
consultation with targeted Indigenous communities.

32
Introduction
Indigenous peoples have a historical continuity with pre-colonial traditional societies. They derive
a sense of identify from, and have a strong connection to, their traditional lands. Indigenous
peoples communicate their strong understanding of and connection with their past through varied
and distinct lifestyle and cultural practices. Adaptations away from traditional land, lifestyle and
culture do not negate Indigenous identity (Coates 2004).
In countries where alcohol use is culturally acceptable, a greater proportion of Indigenous people
abstain from alcohol use compared to the general population; however, among those that do
drink, Indigenous people consume alcohol at riskier levels (Australian Department of Human
Services and Health 1995; First Nations/First Nationals Information Governance Committee 2007;
Bramley et al. 2003). In other countries, where alcohol is only consumed by a minority of the
population, Indigenous people are more likely to consume alcohol than those in the general
population (Subramanian, Smith & Subramanyam 2006). As a result, Indigenous people experience
a disproportionately high burden of alcohol-related harm compared with the general population
(Centre for Disease Control 2008; Calabria et al. 2010). Alcohol-related mortality rates are
between two (Centre for Disease Control 2008; Connor et al. 2004) and eight (Vos et al. 2003;
Begg et al. 2007) times higher among Indigenous populations compared to the general population.
The main contributors to alcohol-related mortality among Indigenous people are homicide and
violence, injury, suicide (including self-inflicted injury), and road traffic accidents (Centre for
Disease Control 2008; Vos et al. 2003; Connor et al. 2004; Calabria et al. 2010; Begg et al. 2007).
Despite these extraordinarily high rates of alcohol-related harm, Indigenous peoples’ access to
health services and programs to reduce these harms is disproportionately low (Berry & Crowe
33
2009; KnowledgeAssets 2009). Mainstream services and programs are generally unacceptable
and/or inappropriate for Indigenous peoples (Dodgson & Struthers 2005; Hayman, White &
Spurling 2009), and Indigenous-specific alcohol services are often lacking and/or inadequately
resourced (Gray et al. 2010; Allison, Rivers & Fottler 2004). As a consequence, Indigenous peoples
require improved access to acceptable and appropriate alcohol intervention services and
programs.
The harms resulting from alcohol misuse extend beyond drinkers to their families and
communities. Family members and friends who have regular contact with a problem drinker are at
increased risk of alcohol-related violence, conflict, sexual assault, psychological abuse, and/or
neglect (Laslett et al. 2010; Kelly & Kowalyszyn 2003; Seale et al. 2002). These negative personal
relationships can result in psychological distress (Laslett et al. 2010; Seale et al. 2002). Conversely,
positive family relationships are the foundation for community cohesion among Indigenous groups
(McLennan & Khavarpour 2004) and can promote behavioural change (Nagel & Thompson 2010).
Given the increased risk of alcohol-related harm among relatives of problem drinkers and the
central role that family relationships play in Indigenous communities, family member participation
in interventions to help problem drinkers reduce their alcohol consumption is likely to result in
better outcomes than interventions that target problem drinkers only.
Family-based interventions have proven to be effective in non-Indigenous populations
(Templeton, Velleman & Russell 2010; Smit et al. 2008; Miller & Wilbourne 2002). Cultural
adaptation of evidence-based interventions to increase their likelihood of proving acceptable and
effective for Indigenous people is, however, necessary and appropriate because of differences in
their cultural values, knowledge bases and levels of exposure to risk factors (Bernal, Jime´nez-
34
Chafey & Rodreguez 2009; Lau 2006). Despite calls for increased family support services for
Indigenous communities (Gray et al. 2010; Seale et al. 2006), the effectiveness and
appropriateness of family-based interventions for reducing alcohol-related harm in Indigenous
communities is yet to be rigorously examined.
The aims of this paper are threefold: first, to identify peer-reviewed publications of evaluations of
family-based alcohol interventions; second, to critique the methodological quality of those studies
and describe their intervention characteristics; and third, to identify which interventions appear
most promising to reduce alcohol-related harm in Indigenous communities.
Method
Sample
The search was limited to publications dated 2003-2010 (inclusive) to complement, rather than
replicate, a previous review of family-based interventions, published in 2005 (Copello, Velleman &
Templeton 2005).
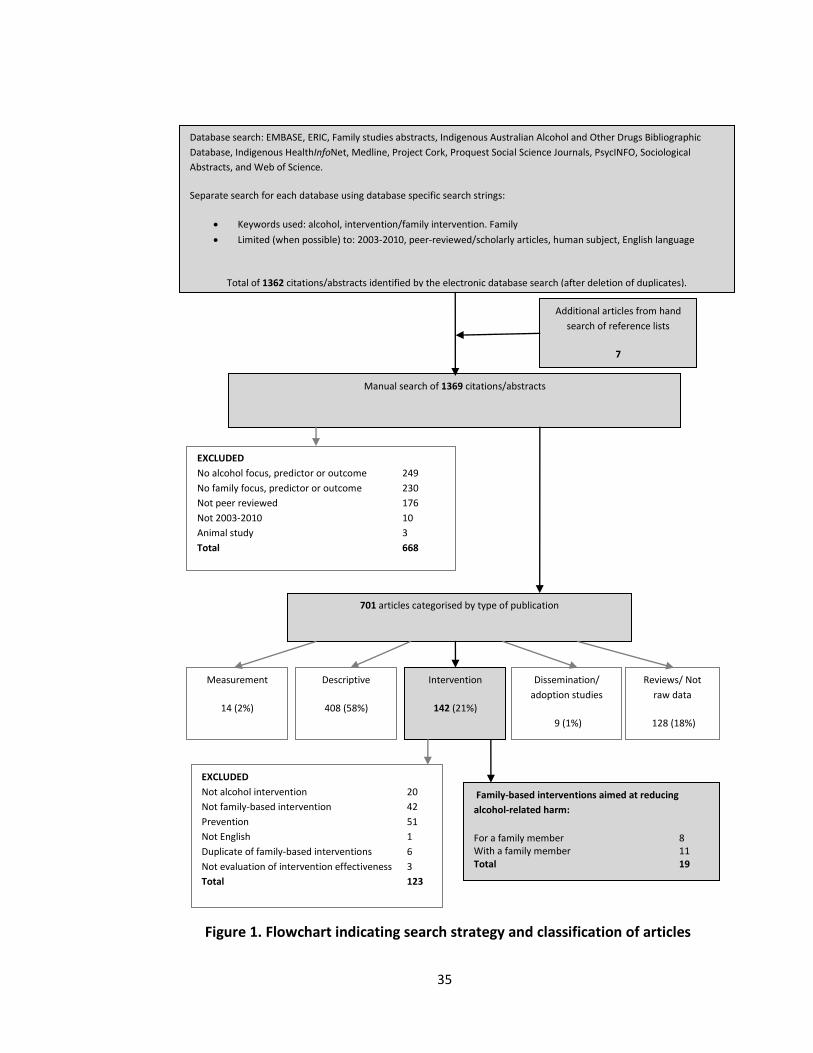
Search strategy
Figure 1 summarises the databases searched, the search terms used, the exclusion criteria, and
classification of included studies (see Appendix A for search strings).
35
Database search: EMBASE, ERIC, Family studies abstracts, Indigenous Australian Alcohol and Other Drugs Bibliographic
Database, Indigenous HealthInfoNet, Medline, Project Cork, Proquest Social Science Journals, PsycINFO, Sociological
Abstracts, and Web of Science.
Separate search for each database using database specific search strings:
Keywords used: alcohol, intervention/family intervention. Family
Limited (when possible) to: 2003-2010, peer-reviewed/scholarly articles, human subject, English language
Total of 1362 citations/abstracts identified by the electronic database search (after deletion of duplicates).
Manual search of 1369 citations/abstracts
701 articles categorised by type of publication
Measurement
14 (2%)
Descriptive
408 (58%)
Intervention
142 (21%)
Dissemination/
adoption studies
9 (1%)
Reviews/ Not
raw data
128 (18%)
EXCLUDED
No alcohol focus, predictor or outcome 249
No family focus, predictor or outcome 230
Not peer reviewed 176
Not 2003-2010 10
Animal study 3
Total 668
EXCLUDED
Not alcohol intervention 20
Not family-based intervention 42
Prevention 51
Not English 1
Duplicate of family-based interventions 6
Not evaluation of intervention effectiveness 3
Total 123
Family-based interventions aimed at reducing
alcohol-related harm:
For a family member 8 With a family member 11 Total 19
Additional articles from hand
search of reference lists
7
Figure 1. Flowchart indicating search strategy and classification of articles
36
Consistent with methods detailed in the Cochrane Collaboration’s Handbook on Systematic
Reviews of Health Promotion and Public Health Interventions (Jackson 2007) and with previous
reviews (Havard, Shakeshaft & Sanson-Fisher 2008; Webb et al. 2009; Wood et al. 2006; Calabria,
Shakeshaft & Havard 2011; Shakeshaft, Bowman & Sanson-Fisher 1997), the search strategy
comprised two steps. First, consultation with a qualified archivist identified nine relevant
electronic databases to search: Project Cork, EMBASE, ERIC, Family Studies Abstract, MEDLINE,
Proquest Social Science Journals, PsycINFO, Sociological Abstracts, and Web of Science. Electronic
databases were searched individually with specific search strings as this search method is more
effective at identifying relevant articles than a simultaneous search using generic search terms
(Jackson 2007). The search terms (modelled from a previous review (Calabria, Shakeshaft &
Havard 2011)) “alcohol”, “family” and “intervention” were integrated into database specific search
strings. The combined searches of the nine databases located 3,032 references that were
imported into Endnote. An Endnote search for “intervention” was conducted to identify a
manageable number of citations for review. The Endnote search identified 1,250 articles for
classification. To maximise coverage of Indigenous-specific studies, the Indigenous Australian
Alcohol and Other Drugs Bibliographic Database (National Drug Research Institute) and the
Indigenous HealthInfoNet (Australian Government Department of Health and Ageing) were
searched using the same search terms. A total of 112 studies were identified for classification.
These were reviewed by hardcopy printouts because the databases lack the capacity to export
references to Endnote.
Second, reference lists of reviews of family-based approaches targeting alcohol (n = 44), identified
by Step 1, were hand-searched for relevant studies not yet identified. This process identified seven
37
relevant studies (Dutcher et al. 2009; Howells & Orford 2006; Latimer et al. 2003; Rychtarik &
McGillicuddy 2005; Walitzer & Dermen 2004; Doyle et al. 2003; Fals-Stewart et al. 2005).
Classification of studies
The abstracts of the 1,369 identified references were classified in a three-step process.
Step 1: Identification of studies for exclusion. Articles were excluded if: (a) they did not focus on
alcohol or if the outcome or predictor variables did not include alcohol (n = 249); (b) the subject of
the research was not defined as a family member (e.g. parent, spouse, sibling, or child) or the
outcome or predictor variables did not include family (e.g. family functioning or heritability)
(n = 230); (c) they were not peer-reviewed (n = 176); (d) they were not conducted in 2003-2010
(n = 10); or (e) they were animal studies (n = 3). Step 1 excluded 668 articles.
Step 2: Classification of studies. The remaining studies (n = 701) were classified as either
intervention studies or one of four other criteria derived and adapted from previous similar
reviews (Havard, Shakeshaft & Sanson-Fisher 2008; Webb et al. 2009; Wood et al. 2006; Calabria,
Shakeshaft & Havard 2011): (a) interventions, defined as evaluations or trials of family-based
intervention approaches designed to reduce alcohol-related harm, or evaluations or trials of
intervention approaches that include alcohol or family as an outcome or predictor variable
(n = 142); (b) measurement, defined as articles concerned primarily with developing measurement
instruments and/or testing the psychometric properties of measurement instruments (n = 14); (c)
descriptive, defined as data-based descriptive, analytical research on alcohol-related harm and
families (n = 408); (d) dissemination/adoption and acceptability/feasibility, defined as studies
evaluating approaches for improving the uptake and delivery of alcohol interventions by health
38
care practitioners, and/or the acceptability and/or feasibility of alcohol intervention delivery
(n = 9); and (e) reviews, defined as literature reviews, non-data-based articles and comments
(n = 128). Step 2 excluded 559 articles. Ten percent (n = 71) of classified articles were re-classified
by a blinded co-author (A.C.) to crosscheck classifications performed by the first author (B.C.). The
articles excluded in Step 1 were not cross-checked because they were not relevant for the review.
Agreement between co-authors was approaching substantial ( = 0.58). Discrepancies were
discussed and resolved. Sufficient agreement between co-authors deemed crosschecking more
than 10% of article classifications unnecessary.
Step 3: Identification of family-based alcohol intervention studies. Of the 142 intervention papers
identified, 123 were excluded for the following reasons: (a) they were not an alcohol intervention
(n = 20), (b) they were not a family-based alcohol intervention (n = 42), (c) they were preventive
interventions (n = 51), (d) they were not published in English (n = 1), (e) they were duplicate
articles based on intervention studies already included (n = 6), or (f) they did not report on the
effectiveness of an intervention (e.g. compared outcomes of ethnic groups participating in the
intervention) (n = 3). Step 3 excluded 123 articles and identified 19 family-based intervention
studies for critical review.
Data extraction from studies
Criteria for data extraction from studies were adapted from the Cochrane Collaboration’s
Handbook for Systematic Reviews of Health Promotion and Public Health Interventions (Jackson
2007). The criteria relate to the intervention/s sample (including eligibility, size, age range, and
percent male), outcomes measured, and cost calculations performed.
39
Methodological critique of intervention studies
Methodological quality was assessed using the Dictionary for the Effective Public Health Practice
Project Quality Assessment Tool for Quantitative Studies (Jackson 2007). Sections A to F (A =
selection bias; B = allocation bias; C = confounders; D = blinding; E = data collection methods; and
F = withdrawal and drop-outs) were coded weak, moderate, or strong, consistent with the
component rating scale of the Dictionary (Jackson 2007). For Sections G (analysis) and H
(intervention integrity) descriptive information was recorded, using dictionary recommendations
as a guide.
Results
Intervention type and setting
All family-based interventions identified were counselling-based interventions: 11 targeted
problem drinkers and their family members, and 8 targeted family members of problem drinkers
only (Table 1). The delivery mode for interventions targeting problem drinkers and their family
members included individual sessions (Boyd-Ball 2003; Liddle et al. 2009; Nattala et al. 2010;
O'Farrell et al. 2008; Slesnick & Prestopnik 2009; Vedel, Emmelkamp & Schippers 2008), individual
sessions with concurrent group and/or family/couples sessions (Doyle et al. 2003; Esposito-
Smythers et al. 2006; Fals-Stewart et al. 2005; Slesnick & Prestopnik 2009), group sessions with
concurrent family/couples sessions (Doyle et al. 2003; Latimer et al. 2003), family/couples sessions
(Fals-Stewart et al. 2005; Nattala et al. 2010; Slesnick & Prestopnik 2009; Vedel, Emmelkamp &
Schippers 2008), or group sessions (Walitzer & Dermen 2004; Fals-Stewart et al. 2005; Latimer et
al. 2003; Liddle et al. 2009). Interventions targeting problem drinkers and their family members
were delivered in tertiary health care settings (Boyd-Ball 2003; Doyle et al. 2003; Esposito-
40
Smythers et al. 2006; Fals-Stewart et al. 2005; Latimer et al. 2003; Liddle et al. 2009; Nattala et al.
2010; O'Farrell et al. 2008; Vedel, Emmelkamp & Schippers 2008); a research centre (Walitzer &
Dermen 2004); and within a home, an office or runaway shelter (Slesnick & Prestopnik 2009). The
delivery mode for interventions targeting family members of problem drinkers included individual
sessions (Copello et al. 2009; Dutcher et al. 2009; Hansson et al. 2006; Hansson et al. 2004;
Howells & Orford 2006; Landau et al. 2004), group sessions (de los Angeles Cruz-Almanza, Gaona-
Marquez & Sanchez-Sosa 2006; Hansson et al. 2004; Rychtarik & McGillicuddy 2005), or a
combination of both (Rychtarik & McGillicuddy 2005). Interventions targeting family members of
problem drinkers were delivered in primary health care settings (de los Angeles Cruz-Almanza,
Gaona-Marquez & Sanchez-Sosa 2006; Copello et al. 2009), tertiary health care settings (Dutcher
et al. 2009; Howells & Orford 2006; Landau et al. 2004), and a university (Hansson et al. 2006).
41
Table 1. Family-based interventions for problem drinkers and/or their family members
Reference Intervention/s
(number of sessions)
Design Sample (n) Effect Follow-up
months
Boyd-Ball
(2003)
“The Shadow Project”
Parenting training + relationship
training (1)
Quasi-
experimental
Youth entering alcohol
and drug inpatient
treatment and their family
member
(n = 66)
Increase in % days abstinent from alcohol,
marijuana, and "other hard drugs"
11
Copello
(2009)
Based on stress-strain-coping
model of addition and family
a) Full intervention (5)
b) Brief intervention (1)
RCT Family members of
problem drinkers/problem
drug users
(n = 143)
No significant difference between the two
interventions
2
de los
Angeles
Cruz-
Almanza
(2006)
Rational-emotive behavioral
therapy (18)
Multiple
baseline across
two groups
Spouses of problem
drinkers
(n = 18)
Improvements in self-esteem, coping, and
likelihood of behaving assertively for intervention
group
18
Doyle
(2003)
a) Residential program (6-week
program)
b) Community program (10-week
program)
Pre and post Problem drinkers from a
residential treatment
centre and the community
and their family member
(n = 67)
The residential group:Increase in number of
abstinent participants, decrease in negative
consequences and psychological adjustment
The community group: Increase in number of
moderate drinkers
6
Dutcher
(2009)
Community Reinforcement and
Family Training (12)
Demonstration
trial
Family members of
problem drinkers
(n = 98)
55% overall engagement
Decrease in family member’s depression, state
anger (but not trait ander), state and trait
anxiety. Increase in relationship happiness
12
42
Reference Intervention/s
(number of sessions)
Design Sample (n) Effect Follow-up
months
Esposito-
Smythers
(2006)
Cognitive behavioral treatment
protocol + conjoint family sessions
(35)
Case study Youth with co-occuring
alcohol use disorder and
suicidality and their
parent/s
(n = 6)
Decrease in suicidality, marijuana and alcohol use 12
Fals-
Stewart
(2005)
a) Brief relationship therapy (18)
b) Shortened version of standard
behavioral couples therapy
(24)
c) Individual-based treatment
(18)
d) Psychoeducational attention
control treatment (18)
RCT Entering outpatient
treatment and their
spouse
(n = 100)
Shortened version of behavioral couples therapy
had equivalent heavy drinking outcomes to brief
relationship therapy
Heavy drinking and dyadic adjustment outcomes
for brief relationship therapy were superior to
patients in the other individual-based treatment
and psychoeducational attention control
treatment
12
Hansson
(2004)
a) Individual standard
information session (1)
b) Individual coping skills training
(1)
c) Group support (12)
RCT Spouses of problem
drinkers
(n = 39)
Increase in coping behaviour, psychiatric
symptoms, and hardship, but no difference
between groups
24
Hansson
(2006)
a) Alcohol intervention program
(2)
b) Coping intervention program
(2)
c) Combination program (2)
RCT Children of problem
drinkers
(n = 82)
Alcohol interventions improved drinking pattern
compared to the coping intervention group
12
Howells
(2006)
Standardised counselling program
(average of 4)
Pre and post Partners of problem
drinkers
(n = 56)
Decrease in stress level and coping for
intervention group
12
43
Reference Intervention/s
(number of sessions)
Design Sample (n) Effect Follow-up
months
Landau
(2004)
A Relational Sequence for
Engagement (ARISE) (9)
Demonstration
trial
Family member/friend of
problem drinker/problem
drug user
(n = 110)
83% of problem drinker/probelm drug user
engaged in treatment/self-help
0
Latimer
(2003)
a) Integrated family and cognitive
behavioral therapy (48)
b) Drugs harm psychoeducation
curriculum (16)
RCT Youth with psychocative
substance use disorders
and their partent/s
(n = 43)
Family therapy group: youth decrease in alcohol
use, marijuana use, and problem avoidance
Increase in rational problem solving and learning
strateggy skills
Parents more adaptive scores on
communication, involvement, control, and
values/norms indicides
6
Liddle
(2009)
a) Multidimensional family
therapy (24-32)
b) Cognitive behavioral peer
group intervention (24-32)
RCT Youth referred for a
substance use problem
and their parent/s
(n = 83)
Multidimensional family therapy: decrease in
substance use, delinquency, internalised distress,
affiliation with deliquent peers
Increase in family and school functioning
12
Nattala
(2010)
a) Individual relapse prevention
(8-10)
b) Dyadic relapse prevention (8-
10)
c) Treatment as usual
RCT Admitted to an inpatient
facility and their family
member
(n = 87)
Dyadic replase prevention had better outcomes
than individual relapse prevention and treatment
as usual
6
O'Farrell
(2008)
a) Brief family treatment (2)
b) Treatment as usual
RCT Admitted to a detox unit
and their parent/s, wife,
or female partner
(n = 45)
Family treatment: patients were more likely to
enter continuing care
Alcohol and drug use decreased for patients who
entered continuing care regardless of treatment
3
Rychtarik
(2005)
a) Coping skills training (8)
b) 12-step facilitation (8)
c) Delayed treatment
RCT Spouses of problem
drinkers
(n = 171)
Interventions decreased depression levels but did
not differ from each other. Interventions
decreased partner drinking
12

44
Reference Intervention/s
(number of sessions)
Design Sample (n) Effect Follow-up
months
Slesnick
(2009)
a) Home-based ecological family
therapy (16)
b) Office-based functional family
therapy (16)
c) Treatment as usual
RCT Primary alcohol problem
runaway youth and their
primary caretaker/s
(n = 119)
Home-based family therapy: decreased alcohol
use for adolescents
Office-based family therapy: decreased alcohol
use for adolescents
15
Vedel
(2008)
a) Behavioral couples therapy
(10)
b) Cognitive behavioral therapy
(10)
RCT Patients and their spouse
(n = 64)
Couples therapy and cognitive-behavioral
therapy were both effective in changing drinking
behavior
Marital satisfaction of the spouse increased in
the couples therapy
Self-efficacy to withstand alcohol-related high-
risk situations increased more in cognitive
behavioral therapy than in couples therapy
6
Walitzer
(2004)
a) Treatment for problem
drinkers only (10)
b) Couples alcohol treatment (10)
c) Couples alcohol treatment and
behavioral couples therapy
(10)
RCT Drinkers (≥10 drinks per
week) and their female
spouse
(n = 64)
Couples treatmemt: decrease in alcohol
consumption
The additional of behavioral couples therapy to
couples alcohol treatment did not significantly
improve outcomes
12
Note. RCT = Randomised control/clinical trial.
45
Sample population targeted by interventions
One intervention specifically targeted an Indigenous population: Native Americans (Boyd-Ball
2003). Across interventions for problem drinkers and their family members, problem drinking
youth (Boyd-Ball 2003; Esposito-Smythers et al. 2006; Latimer et al. 2003; Liddle et al. 2009;
Slesnick & Prestopnik 2009) or adults (Doyle et al. 2003; Fals-Stewart et al. 2005; Nattala et al.
2010; O'Farrell et al. 2008; Vedel, Emmelkamp & Schippers 2008; Walitzer & Dermen 2004) were
targeted. Types of family members targeted in the treatment of problem drinkers included parents
(Esposito-Smythers et al. 2006; Latimer et al. 2003; Liddle et al. 2009) or other family members
(Boyd-Ball 2003; Slesnick & Prestopnik 2009) for adolescent problem drinkers, and spouse (Fals-
Stewart et al. 2005; Vedel, Emmelkamp & Schippers 2008; Walitzer & Dermen 2004) or other
family members (Doyle et al. 2003; Nattala et al. 2010; O'Farrell et al. 2008) for adult problem
drinkers. Interventions for family members only targeted a spouse (de los Angeles Cruz-Almanza,
Gaona-Marquez & Sanchez-Sosa 2006; Hansson et al. 2004; Howells & Orford 2006; Rychtarik &
McGillicuddy 2005) or other family members (Dutcher et al. 2009; Landau et al. 2004; Copello et
al. 2009; Hansson et al. 2006) of a problem drinker. Samples ranged in age from 12 to 78 years.
The percentage range of male participants was 17% (Esposito-Smythers et al. 2006) to 100% (Fals-
Stewart et al. 2005; Nattala et al. 2010; Walitzer & Dermen 2004) for interventions targeting
problem drinkers and 0% (de los Angeles Cruz-Almanza, Gaona-Marquez & Sanchez-Sosa 2006) to
31% (Landau et al. 2004) for interventions targeting family members.
Eligibility criteria
Alcohol use/dependence eligibility criteria for problem drinkers whose family members were
involved in their treatment varied across studies and were treatment samples (Boyd-Ball 2003;
Doyle et al. 2003; Liddle et al. 2009), alcohol dependence/abuse diagnosis (Fals-Stewart et al.
46
2005; Latimer et al. 2003; Vedel, Emmelkamp & Schippers 2008; Nattala et al. 2010; Esposito-
Smythers et al. 2006; O'Farrell et al. 2008), or problem alcohol use (Slesnick & Prestopnik 2009;
Walitzer & Dermen 2004).
Eligibility criteria for family members of problem drinkers were the family member’s perception
that their relative had a drinking problem defined by the family member’s reports of problematic
patterns of alcohol consumption (Dutcher et al. 2009; Hansson et al. 2004; Hansson et al. 2006;
Howells & Orford 2006; Landau et al. 2004; Rychtarik & McGillicuddy 2005) or the family
member’s perceptions of the impact of the problem drinker’s negative behaviour on their
wellbeing (Copello et al. 2009; de los Angeles Cruz-Almanza, Gaona-Marquez & Sanchez-Sosa
2006).
Data collection methods
Self-report and non-self-report measures. All 19 studies used self-report measures. Eight studies
conducted interviews (Hansson et al. 2006; Hansson et al. 2004; Rychtarik & McGillicuddy 2005;
Doyle et al. 2003; Fals-Stewart et al. 2005; Latimer et al. 2003; Walitzer & Dermen 2004; Vedel,
Emmelkamp & Schippers 2008), and five used corroborated reports (Rychtarik & McGillicuddy
2005; Fals-Stewart et al. 2005; Latimer et al. 2003; Nattala et al. 2010; Walitzer & Dermen 2004).
In six studies, non-self-report measures were also used: Two used urine tests (Latimer et al. 2003;
Slesnick & Prestopnik 2009), two used observational methods (Liddle et al. 2009; Boyd-Ball 2003),
and two checked medical records (Landau et al. 2004; O'Farrell et al. 2008).
Measurement instruments for alcohol use and/or dependence. Ten of the eleven studies targeting
problem drinkers and their family members measured alcohol use and/or dependence with a

47
validated instrument. Instruments were Timeline Follow-back Interview (O'Farrell et al. 2008;
Liddle et al. 2009; Doyle et al. 2003; Esposito-Smythers et al. 2006; Fals-Stewart et al. 2005), the
Alcohol Dependence Scale (Doyle et al. 2003; Walitzer & Dermen 2004), Structured Clinical
Interview for DSM-IV (Vedel, Emmelkamp & Schippers 2008; Fals-Stewart et al. 2005), Diagnostic
Interview of Children and Adolescents (Latimer et al. 2003), the Adolescent Diagnostic Interview-
Revised (Latimer et al. 2003), the Personal Experience Inventory (Latimer et al. 2003), the Problem
Oriented Screening Instrument for Teenagers (Liddle et al. 2009), Form 90 (Nattala et al. 2010;
Slesnick & Prestopnik 2009), and the Alcohol Use Disorders Identification Test (AUDIT) (Vedel,
Emmelkamp & Schippers 2008). Two studies also used quantity and frequency questions (Vedel,
Emmelkamp & Schippers 2008; Walitzer & Dermen 2004).
Two of the eight studies targeting only family members of problem drinkers measured their
alcohol consumption using the following validated instruments: the AUDIT (Hansson et al. 2004;
Hansson et al. 2006) and the Estimated Blood Alcohol Concentration Method (Hansson et al.
2006).
Outcome measures. The most frequently measured outcome for problem drinkers was alcohol
consumption (Boyd-Ball 2003; Doyle et al. 2003; Esposito-Smythers et al. 2006; Fals-Stewart et al.
2005; Latimer et al. 2003; Liddle et al. 2009; Nattala et al. 2010; O'Farrell et al. 2008; Slesnick &
Prestopnik 2009; Vedel, Emmelkamp & Schippers 2008; Walitzer & Dermen 2004), followed by
illicit drug use (Boyd-Ball 2003; Esposito-Smythers et al. 2006; Fals-Stewart et al. 2005; Latimer et
al. 2003; Liddle et al. 2009; O'Farrell et al. 2008; Slesnick & Prestopnik 2009). Primary outcomes
recurrently measured for family members of problems drinkers were coping (Howells & Orford
2006; Hansson et al. 2006; Hansson et al. 2004; de los Angeles Cruz-Almanza, Gaona-Marquez &
48
Sanchez-Sosa 2006; Copello et al. 2009), self-esteem (Howells & Orford 2006; Copello et al. 2009;
de los Angeles Cruz-Almanza, Gaona-Marquez & Sanchez-Sosa 2006), and engagement in
treatment service and/or help seeking (Howells & Orford 2006; Dutcher et al. 2009; Landau et al.
2004; Rychtarik & McGillicuddy 2005).
Family/marital functioning/satisfaction/cohesion was measured by eight studies (Doyle et al.
2003; Latimer et al. 2003; Liddle et al. 2009; Nattala et al. 2010; Slesnick & Prestopnik 2009; Vedel,
Emmelkamp & Schippers 2008; Walitzer & Dermen 2004; Rychtarik & McGillicuddy 2005). Eleven
studies were conducted in the United States (Dutcher et al. 2009; Landau et al. 2004; Rychtarik &
McGillicuddy 2005; Boyd-Ball 2003; Esposito-Smythers et al. 2006; Fals-Stewart et al. 2005;
Latimer et al. 2003; Liddle et al. 2009; O'Farrell et al. 2008; Slesnick & Prestopnik 2009; Walitzer &
Dermen 2004), three in the United Kingdom (Copello et al. 2009; Howells & Orford 2006; Doyle et
al. 2003), one in Mexico (de los Angeles Cruz-Almanza, Gaona-Marquez & Sanchez-Sosa 2006),
three in Europe (Sweden and Holland) (Hansson et al. 2006; Hansson et al. 2004; Vedel,
Emmelkamp & Schippers 2008), and one in India (Nattala et al. 2010).
Methodological Adequacy
Table 2 summarizes the methodological adequacy of the 19 studies. Two studies minimized
selection bias by identifying a representative sample and obtaining a high consent rate (Dutcher et
al. 2009; Liddle et al. 2009). Sixty-three percent of studies utilised a randomized control/clinical
trial, thereby reducing the risk of allocation bias (Copello et al. 2009; Hansson et al. 2006; Hansson
et al. 2004; Rychtarik & McGillicuddy 2005; Fals-Stewart et al. 2005; Latimer et al. 2003; Liddle et
al. 2009; Nattala et al. 2010; O'Farrell et al. 2008; Slesnick & Prestopnik 2009; Vedel, Emmelkamp
& Schippers 2008; Walitzer & Dermen 2004). Three quarters of the studies that reported
49
differences between groups did not control for these baseline variations, making it difficult to
ascertain whether post-test differences were attributed to the intervention (Hansson et al. 2006;
Hansson et al. 2004; Esposito-Smythers et al. 2006; Fals-Stewart et al. 2005; Nattala et al. 2010;
Slesnick & Prestopnik 2009).
Twelve studies allocated participants evenly across groups (de los Angeles Cruz-Almanza, Gaona-
Marquez & Sanchez-Sosa 2006; Hansson et al. 2006; Hansson et al. 2004; Rychtarik & McGillicuddy
2005; Fals-Stewart et al. 2005; Latimer et al. 2003; Liddle et al. 2009; Nattala et al. 2010; O'Farrell
et al. 2008; Slesnick & Prestopnik 2009; Vedel, Emmelkamp & Schippers 2008; Walitzer & Dermen
2004). Outcome assessors were blinded in one third of the applicable studies (Copello et al. 2009;
Hansson et al. 2006; Hansson et al. 2004; Rychtarik & McGillicuddy 2005; Vedel, Emmelkamp &
Schippers 2008). Measures with established psychometric properties were used by 84% of studies
(Copello et al. 2009; de los Angeles Cruz-Almanza, Gaona-Marquez & Sanchez-Sosa 2006; Dutcher
et al. 2009; Hansson et al. 2006; Hansson et al. 2004; Howells & Orford 2006; Rychtarik &
McGillicuddy 2005; Doyle et al. 2003; Fals-Stewart et al. 2005; Latimer et al. 2003; Liddle et al.
2009; Nattala et al. 2010; O'Farrell et al. 2008; Slesnick & Prestopnik 2009; Vedel, Emmelkamp &
Schippers 2008; Walitzer & Dermen 2004). Eight studies reported follow-up rates between 80%
and 100% (Copello et al. 2009; Hansson et al. 2006; Hansson et al. 2004; Boyd-Ball 2003; Esposito-
Smythers et al. 2006; Latimer et al. 2003; Nattala et al. 2010; O'Farrell et al. 2008).
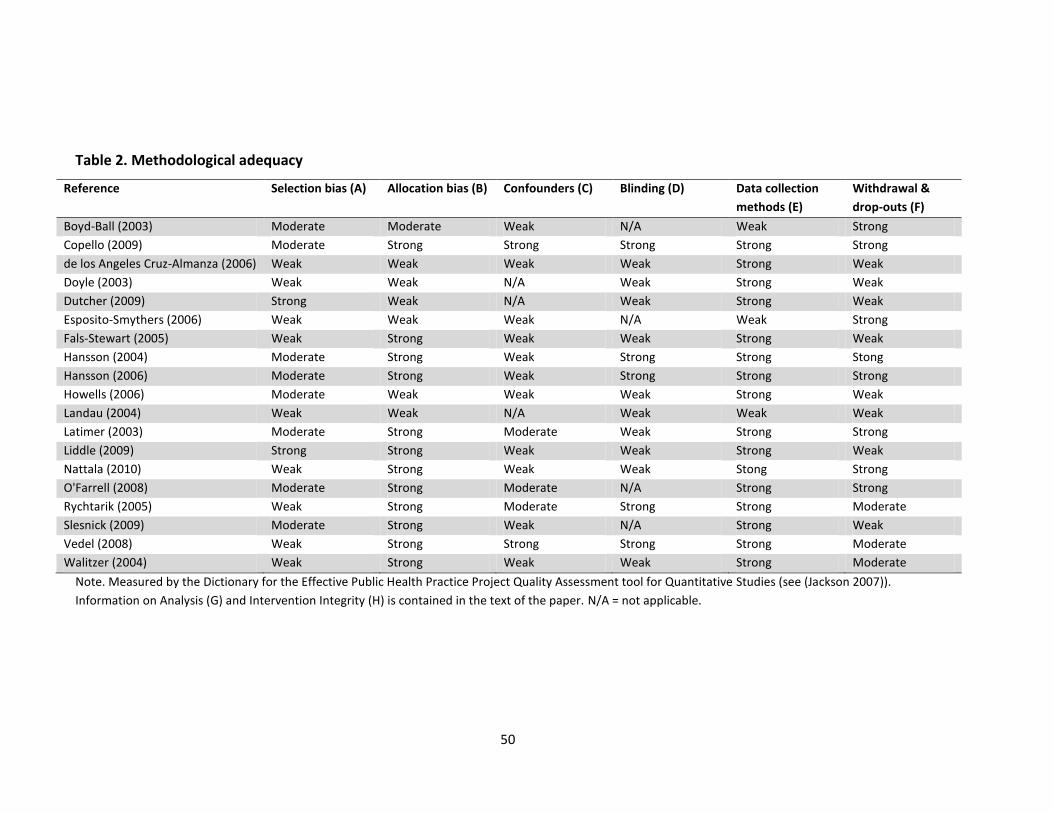
50
Table 2. Methodological adequacy
Reference Selection bias (A) Allocation bias (B) Confounders (C) Blinding (D) Data collection
methods (E)
Withdrawal &
drop-outs (F)
Boyd-Ball (2003) Moderate Moderate Weak N/A Weak Strong
Copello (2009) Moderate Strong Strong Strong Strong Strong
de los Angeles Cruz-Almanza (2006) Weak Weak Weak Weak Strong Weak
Doyle (2003) Weak Weak N/A Weak Strong Weak
Dutcher (2009) Strong Weak N/A Weak Strong Weak
Esposito-Smythers (2006) Weak Weak Weak N/A Weak Strong
Fals-Stewart (2005) Weak Strong Weak Weak Strong Weak
Hansson (2004) Moderate Strong Weak Strong Strong Stong
Hansson (2006) Moderate Strong Weak Strong Strong Strong
Howells (2006) Moderate Weak Weak Weak Strong Weak
Landau (2004) Weak Weak N/A Weak Weak Weak
Latimer (2003) Moderate Strong Moderate Weak Strong Strong
Liddle (2009) Strong Strong Weak Weak Strong Weak
Nattala (2010) Weak Strong Weak Weak Stong Strong
O'Farrell (2008) Moderate Strong Moderate N/A Strong Strong
Rychtarik (2005) Weak Strong Moderate Strong Strong Moderate
Slesnick (2009) Moderate Strong Weak N/A Strong Weak
Vedel (2008) Weak Strong Strong Strong Strong Moderate
Walitzer (2004) Weak Strong Weak Weak Strong Moderate
Note. Measured by the Dictionary for the Effective Public Health Practice Project Quality Assessment tool for Quantitative Studies (see (Jackson 2007)).
Information on Analysis (G) and Intervention Integrity (H) is contained in the text of the paper. N/A = not applicable.
51
Three studies justified the appropriateness of their analyses by referencing a source for their
statistical approach (Copello et al. 2009; de los Angeles Cruz-Almanza, Gaona-Marquez &
Sanchez-Sosa 2006; Liddle et al. 2009). Follow-up rates varied from 9% (Vedel, Emmelkamp &
Schippers 2008) to 98% (Latimer et al. 2003; O'Farrell et al. 2008; Slesnick & Prestopnik 2009),
and intent-to-treat analyses were reported by one third of studies (Copello et al. 2009;
Rychtarik & McGillicuddy 2005; Latimer et al. 2003; Liddle et al. 2009; O'Farrell et al. 2008;
Slesnick & Prestopnik 2009; Walitzer & Dermen 2004).
Methods to optimise intervention fidelity were not reported by two studies (Hansson et al.
2004; Boyd-Ball 2003). When reported, most commonly reported methods to optimise
intervention fidelity were therapist training (Walitzer & Dermen 2004; Vedel, Emmelkamp &
Schippers 2008; Slesnick & Prestopnik 2009; Nattala et al. 2010; Latimer et al. 2003; Doyle et
al. 2003; Rychtarik & McGillicuddy 2005; Landau et al. 2004; Howells & Orford 2006; de los
Angeles Cruz-Almanza, Gaona-Marquez & Sanchez-Sosa 2006; Copello et al. 2009; Dutcher et
al. 2009; Hansson et al. 2006), therapist supervision (Walitzer & Dermen 2004; Vedel,
Emmelkamp & Schippers 2008; Slesnick & Prestopnik 2009; O'Farrell et al. 2008; Nattala et al.
2010; Latimer et al. 2003; Rychtarik & McGillicuddy 2005; Landau et al. 2004; Howells & Orford
2006; Copello et al. 2009), and intervention manuals/protocol (Walitzer & Dermen 2004;
Vedel, Emmelkamp & Schippers 2008; O'Farrell et al. 2008; Fals-Stewart et al. 2005; Esposito-
Smythers et al. 2006; Rychtarik & McGillicuddy 2005; Landau et al. 2004; Hansson et al. 2006;
Copello et al. 2009). Of the 14 studies with more than one group, participants were evenly
recruited into groups for 12 studies (de los Angeles Cruz-Almanza, Gaona-Marquez & Sanchez-
Sosa 2006; Fals-Stewart et al. 2005; Hansson et al. 2006; Hansson et al. 2004; Latimer et al.
2003; Liddle et al. 2009; Nattala et al. 2010; O'Farrell et al. 2008; Rychtarik & McGillicuddy
2005; Slesnick & Prestopnik 2009; Vedel, Emmelkamp & Schippers 2008; Walitzer & Dermen

52
2004). Contamination was likely for six studies (Vedel, Emmelkamp & Schippers 2008;
Rychtarik & McGillicuddy 2005; Walitzer & Dermen 2004; Esposito-Smythers et al. 2006; de los
Angeles Cruz-Almanza, Gaona-Marquez & Sanchez-Sosa 2006; Howells & Orford 2006).
Effects
A meta-analysis using the most commonly reported outcomes (which were alcohol use among
problem drinkers and coping among their family members) was explored but judged
inappropriate, given the variability between studies in the outcomes reported. The most
commonly reported effect for problem drinkers was decreased alcohol consumption (Walitzer
& Dermen 2004; Slesnick & Prestopnik 2009; O'Farrell et al. 2008; Nattala et al. 2010; Latimer
et al. 2003; Boyd-Ball 2003; Doyle et al. 2003; Esposito-Smythers et al. 2006; Liddle et al. 2009;
Fals-Stewart et al. 2005). The most commonly reported effect for family members of problem
drinkers was improved coping (Howells & Orford 2006; Hansson et al. 2004; de los Angeles
Cruz-Almanza, Gaona-Marquez & Sanchez-Sosa 2006). Of the eight studies measuring family
functioning, four reported improvements in family functioning (Nattala et al. 2010; Vedel,
Emmelkamp & Schippers 2008; Slesnick & Prestopnik 2009; Liddle et al. 2009). In addition to
measures of effect, three studies measured level of participant engagement in treatment to be
55% (Dutcher et al. 2009), 83% (Landau et al. 2004), and 92% (O'Farrell et al. 2008). Two
interventions investigated the cost of the evaluated interventions: one based solely on the
length of sessions (Vedel, Emmelkamp & Schippers 2008) and the other calculated cost-
effectiveness ratios for participants using the change in percentage of days of heavy drinking
from baseline to follow-up (Fals-Stewart et al. 2005).
53
Discussion
Although an encouraging 18 of the 19 family-based interventions yielded a positive effect,
methodological deficiencies in evaluation designs across all studies resulted in less-than-
optimal evidence.
Methodological adequacy
The rating of studies across methodological review criteria was variable. For example, although
84% of studies were rated as strong for data collection methods, selection bias was rated as
weak for 47% of studies. Most studies did not control for confounders, even when identified.
Follow-up rates varied from 9% to 98%, and one third of studies performed an intent-to-treat
analysis. Methodological quality was similar for reviewed interventions targeting problem
drinkers and their family members, compared to interventions for family members of problem
drinkers only, although allocation bias was rated more strongly for the former and blinding
was rated more strongly for the latter. Variable reporting of an intervention evaluation makes
it difficult for the intervention to be replicated or adapted for other populations and settings
or for wider implementation.
Limitations of the available literature
Large variation in eligibility criteria for different studies limits their comparability.
Measurement of the primary criteria of an alcohol use disorder or problem was diverse for
studies that targeted problem drinkers and their family members. Comparability between
studies would be improved by using a standard measure of alcohol misuse, such as the AUDIT
(Saunders et al. 1993) or the Diagnostic and Statistical Manual of Mental Disorders, Fourth
Edition (DSM-IV) criteria (American Psychiatric Association 1994).
54
All studies (n = 19) used self-report measures. Non-self-report measures were used by six
studies. Reliance on self-report to measure health outcomes is problematic as the method is
prone to biases, even when bias is minimised by using psychometrically validated tools (Hogan
2003). A combination of objective non-self-report and self-report measures would increase
confidence in the validity of outcome findings. For example, information from medical records
has been shown to be both suitable and efficient for evaluating interventions targeting a range
of health and social outcomes (Samet et al. 2003; Landau et al. 2004; O'Farrell et al. 2008),
particularly if common challenges to its collection and use, such as limitations in data access
and poor data quality (Safran 1991), can be overcome.
Intervention costs were measured by two studies, but neither completed a full economic
evaluation. An economic evaluation is increasingly recognised as an integral component of any
evaluation because it provides relevant information on the potential efficiency of allocating
health care resources (Drummond & McGuire 2001). An integral component of any economic
evaluation is a rigorous assessment of both intervention costs and consequences compared to
current practice. Comparability of results between economic evaluation studies is further
made possible by the adoption of a commonly used validated health outcome measure such as
the quality adjusted life year or disability adjusted life year.
Interventions with potential to be tailored to Indigenous communities
This review only identified one intervention study targeting an Indigenous population (Native
Americans) (Boyd-Ball and Boyd-Ball, 2003), a study that was not methodologically strong. The
lack of evaluations of family-based interventions targeting Indigenous people is somewhat
surprising given that Indigenous family members are typically present at health services and
participate in communication about familial health problems with health practitioners
(McGrath et al. 2006; McCubbin 2006; King & Turia 2002). Therefore, their involvement in
55
programs to reduce alcohol-related harm fits with usual care practices. This review identified
family and cognitive-behavioral therapy (Latimer et al. 2003) and multidimensional family
therapy (Liddle et al. 2009) as effective and robustly evaluated problem drinker targeted
interventions that include a family member. Family members of problem drinkers experience
negative consequences of their relative’s drinking (Laslett et al. 2010; Kelly & Kowalyszyn 2003;
Seale et al. 2002), and therefore programs targeting family members in their own right that
also address problem drinker outcomes are likely to be acceptable and appropriate for delivery
in Indigenous communities to reduce alcohol-related harms. Effective programs identified by
this review, targeting family members and focusing on outcomes of the problem drinker and
those of their family member are Community Reinforcement and Family Training (CRAFT)
(Dutcher et al. 2009), coping skills training, and 12-step facilitation (Rychtarik & McGillicuddy
2005).
To ensure that these best evidence family-based approaches are appropriate and acceptable
for delivery to Indigenous people, they should be adapted for integration into Indigenous-
specific health care in collaboration with locally targeted Indigenous communities.
Potential limitations of the review
Although a rigorous and thorough search strategy was used, there is a possibility that the
review did not locate all relevant studies. Relevant intervention evaluations may have been
misclassified; however, a sufficient agreement between blinded coders ( = 0.58) suggests
otherwise. Last, because evaluations with statistically significant findings are more likely to be
published it is possible that the published evaluations reviewed overestimate the
interventions’ true effectiveness (Dickersin et al. 1987; Easterbrook et al. 1991).
56
Conclusions
Although family-based approaches appear effective in engaging problem drinkers into
treatment and reducing their risk of alcohol-related harms, the evidence-base for their cost-
effectiveness would be strengthened by evaluation studies that recruit more representative
samples, include confounding variables in analyses, improve consent and follow-up rates, and
conduct high quality economic evaluations. Given the central role that family relationships play
in reinforcing behaviour and maintaining social cohesion in Indigenous communities, family-
based approaches offer considerable promise for reducing alcohol-related harms among
Indigenous peoples. Family-based interventions are more likely to be acceptable, appropriate
and effective for Indigenous peoples if (a) adapted with the input of Indigenous community
members (Masotti et al. 2006); (b) the involvement of family members who are themselves
problem drinkers is not automatically excluded, because their exclusion is not practical in the
context of routine delivery of health care services due to clustering of alcohol problems within
racial minority family groups (Seale et al. 2010); (c) therapists delivering the intervention are
trained and supervised to optimise intervention fidelity (Miller et al. 2006); and (d) the
intervention is manualized for integration into health service protocols and procedures but has
sufficient flexibility to meet the needs of individual clients (Liddle 2004).
57
Points of clarification for Paper 1
The Journal of Studies on Alcohol and Drugs owns the copyright of this published paper. The
points of clarification have been added to provide additional information about the research
for this thesis without modifying the content of the published paper.
Resolution of classification discrepancies
Coders met to discuss classification discrepancies. Consensus was reached through re-
examining the identified studies and agreeing on the appropriate classification.
58
Paper 2
Identifying Aboriginal-specific AUDIT-C and AUDIT-3 cut-off scores for at-
risk, high-risk and likely dependent drinkers using measures of
agreement with the 10-item Alcohol Use Disorders Identification Test
Bianca Calabria1, Anton Clifford2,3, Anthony P. Shakeshaft1, Katherine M. Conigrave1,4,5,
Lynette Simpson6, Donna Bliss7, Julaine Allan8
1. National Drug and Alcohol Research Centre, University of New South Wales, Sydney, New South
Wales, Australia
2. Institute for Urban Indigenous Health, University of Queensland, Bowen Hills, Queensland, Australia
3. Queensland Alcohol and Drug Research and Education Centre, University of Queensland, Brisbane,
Australia
4. Drug Health Services, Royal Prince Alfred Hospital, Missenden Road, Camperdown, New South
Wales, Australia
5. Sydney Medical School, University of Sydney, Sydney, New South Wales, Australia
6. Drug Health Services, South Western Sydney Local Health District, Croydon Health Centre, Croydon,
New South Wales, Australia.
7. Yoorana Gunya Family Healing Centre Aboriginal Corporation, Forbes, New South Wales, Australia
8. The Lyndon Community, Orange, New South Wales, Australia
Paper 2 has been submitted to Addiction Science & Clinical Practice (Calabria et al. submitted-
b).

59
Copyright Statement
I certify that this publication was a direct result of my research towards this PhD, and that
reproduction in this thesis does not breach copyright regulations.
Calabria, B, Clifford, A, Shakeshaft, A, Conigrave, K, Simpson, L, Bliss, D & Allan, J submitted,
'Identifying Aboriginal-specific AUDIT-C and AUDIT-3 cut-off scores for at-risk, high-risk and
likely dependent drinkers using measures of agreement with the 10-item AUDIT', Addiction
Science & Clinical Practice.
Bianca Calabria August 2013
60
Preamble
Paper 1 identified Community Reinforcement and Family Training (CRAFT) as a family-based
intervention that has considerable potential to reduce alcohol-related harms among
Indigenous Australians and that has some evidence for its effectiveness (Calabria et al. 2012).
Although the study evaluating CRAFT identified in Paper 1 (Dutcher et al. 2009) was
methodologically weak, primarily due to its non-randomised design, failure to blind outcome
assessors and its low follow-up rates, CRAFT offers considerable promise for implementation in
Indigenous communities for at least three main reasons. Firstly, controlled research published
outside of the Paper 1 review timeframe has shown CRAFT to be superior to
Alcoholics/Narcotics Anonymous and the Johnson Institute Intervention for engaging
treatment resistant individuals into treatment (Miller, Meyers & Tonigan 1999; Roozen, de
Waart & van der Kroft 2010; Meyers et al. 2002), and the CRAFT approach has demonstrated
ability to be tailored for delivery across different drug types, family member types, and cultural
groups (Meyers, Villanueva & Smith 2005; Lopez Viets 2008; Villarreal 2008). Second, CRAFT
offers a flexible mode of delivery: trained therapists choose from a selection of manualised
evidence-based therapeutic approaches and can apply them to individual clients (Smith &
Meyers 2007) who are likely to have complex comorbidities (Kelly 2006). Third, multiple family
members can be included in the program, allowing for Indigenous peoples’ extended family
groups and their holistic concept of health, in which the health of individuals is linked to the
health of families and communities (Brady 2004).
To increase the likelihood that individuals with a particular health risk behaviour will be
identified and offered an appropriate intervention, and that the effect of the intervention can
be accurately assessed, reliable and valid measures should be identified and used. The Alcohol
Use Disorders Identification Test (AUDIT) was designed as a cross-cultural screening
instrument and has been recommended for use in Indigenous health care settings (Babor et al.

61
2001; Saunders et al. 1993); however the time it takes to complete all 10-items has proven to
be a barrier to delivery. Although appropriate cut-off scores have been identified for other
cultural groups (Cherpitel 1998; Cherpitel & Clark 1995), Indigenous-specific cut-off scores
have not been published in the peer-reviewed literature. Paper 2 identifies Indigenous-specific
cut-off scores for two shorter versions of AUDIT, AUDIT-C and AUDIT-3, relative to cut-off
scores for the full 10-item AUDIT (Calabria et al. submitted-b). Indigenous-specific cut-off
scores for AUDIT-C and AUDIT-3 could be used to more accurately and efficiently identify
problem drinkers for enrolment into Aboriginal-specific family-based intervention programs
aimed at reducing alcohol-related harms, and to more accurately assess changes in their levels
of alcohol consumption and risk of harm before and after intervention delivery.
62
Abstract
Background: The Alcohol Use Disorders Identification Test (AUDIT) is a 10-item alcohol
screener that has been recommended for use in Aboriginal health care settings. The time it
takes respondents to complete AUDIT, however, has proven to be a barrier to its routine
delivery. Two shorter versions, AUDIT-C and AUDIT-3, have been used as screening
instruments in health care settings. This paper aims to identify the AUDIT-C and AUDIT-3 cut-
off scores that most closely identify individuals classified as being at-risk drinkers, high-risk
drinkers or likely alcohol dependent by the 10-item AUDIT.
Methods: Two cross-sectional surveys were conducted in June 2009 to May 2010 and July 2010
to June 2011. Aboriginal Australian participants (n = 136) were recruited through an Aboriginal
Community Controlled Health Service and a community-based drug and alcohol treatment
agency in rural New South Wales (NSW), and through community-based Aboriginal groups in
Sydney (NSW). Sensitivity, specificity, and positive and negative predictive values of each score
on the AUDIT-C and AUDIT-3 were calculated, relative to standard cut-off scores on the 10-
item AUDIT for at-risk, high-risk and likely dependent drinkers. Receiver operating
characteristic curve analysis was conducted to measure the detection characteristics of AUDIT-
C and AUDIT-3 for at-risk, high-risk and likely dependent drinkers, as classified by the 10-item
AUDIT.
Results: Recommended cut-off scores for Aboriginal Australians are: at-risk drinkers AUDIT-C ≥
5, AUDIT-3 ≥ 1; high-risk drinkers AUDIT-C ≥ 6, AUDIT-3 ≥ 2; and likely dependent drinkers
AUDIT-C ≥ 9, AUDIT-3 ≥ 3. Adequate sensitivity and specificity were achieved for
recommended cut-off scores for AUDIT-C and AUDIT-3, relative to the 10-item AUDIT. All areas
under the receiver operating characteristic curves were above 0.90.
Conclusions: Identified cut-off scores for AUDIT-C and AUDIT-3 have potential to detect
Aboriginal Australians as being problem drinkers in Aboriginal-specific health care settings.

63
Background
Problem drinkers are at high risk of causing physical and psychological harm to themselves,
their family and their community (Laslett et al. 2010). Although Aboriginal Australians are
more likely to abstain from drinking alcohol than other Australians, a greater proportion of
Aboriginal Australians who drink alcohol do so to levels that increase their risk of alcohol-
related harm (Australian Department of Human Services and Health 1995; Calabria et al.
2010). Screening Aboriginal people to assess their level of alcohol consumption is recognised
as an important initial step for determining their risk of alcohol-related harm and need for
alcohol intervention (Australian Government Department of Health and Ageing 2004;
Australian Government Department of Health and Ageing 2007; NACCHO and the Chronic
Disease Alliance of NGOs 2008). Alcohol screening can also be effective for engaging Aboriginal
patients in discussions about their drinking (Clifford & Shakeshaft 2011) and can result in
reduced alcohol consumption independent of intervention (Conigliaro, Lofgren & Hanusa
1998; Jenkins, McAlaney & McCambridge 2009).
The Alcohol Use Disorders Identification Test (AUDIT) was developed by the World Health
Organization as a cross cultural screening instrument for problematic alcohol use (Saunders et
al. 1993; Babor et al. 2001). AUDIT has ten items comprising three domains: recent alcohol
use; alcohol dependence symptoms; and alcohol-related problems (Babor et al. 2001). Cut-off
scores aim to identify non-drinkers, low-risk drinkers, at-risk drinkers, high-risk drinkers and
likely dependent drinkers (Babor et al. 2001; Conigrave, Hall & Saunders 1995; Tsai et al. 2005).
AUDIT has high internal consistency across diverse samples and settings (median alpha = 0.83)
and demonstrated validity for the English language version (Reinert & Allen 2007).
The Alcohol Treatment Guidelines for Indigenous Australians recommend using AUDIT to
screen for alcohol use problems among Aboriginal Australians (Australian Government
64
Department of Health and Ageing 2007). The Guideline’s recommended classification scores
are 0-7 for non-drinkers or low-risk drinkers, 8-12 for at-risk drinkers, and 13+ for high-risk
drinkers. A key limitation of AUDIT for routine screening in Aboriginal-specific (Brady et al.
2002; Clifford & Shakeshaft 2011) and mainstream (Hearne, Connolly & Sheehan 2002) health
care settings has been the time it takes respondents to complete all 10 items. Two shorter
versions of AUDIT, AUDIT-C (comprising the first three questions of AUDIT) and AUDIT-3 (the
third question of AUDIT), have been shown to perform well to identify risky drinking when
compared with a ‘gold standard’ measure of problematic alcohol consumption, for example
Diagnostic and Statistical Manual of Mental Disorders alcohol dependence criteria (American
Psychiatric Association 1994), in non-Indigenous-specific health care settings (Reinert & Allen
2007),.
Despite evidence from qualitative studies that shorter versions of AUDIT are more feasible to
deliver in Aboriginal-specific primary health care settings (Brady et al. 2002; Clifford &
Shakeshaft 2011; Brit et al. 2009), and the shorter versions of AUDIT being used to measure
Aboriginal Australians’ drinking in general practice settings (Brit et al. 2009), no published
studies have identified cut-off scores specifically for Aboriginal Australians. This paper aims to
identify AUDIT-C and AUDIT-3 cut-off scores for detecting problematic alcohol use, as defined
by the 10-item AUDIT, among Aboriginal clients in health care settings.
Methods
Ethics
Ethics approval for the study was granted by: the Human Research Ethics Committee (HREC),
University of New South Wales (NSW), Sydney; South West Area Health Service HRECs, Sydney;
and the Aboriginal Health and Medical Research Council (AH&MRC) Ethics Committee, NSW.
65
The study was also either formally approved by the board of the participating Aboriginal
Community Controlled Health Services (ACCHSs) or had a representative of the ACCHS on its
steering committee. All participants were provided with study and consent information.
Setting and participants
A convenience sample of Australian Aboriginal participants was recruited through a NSW rural
ACCHS and a rural community-based drug and alcohol treatment agency from July 2010 to
June 2011, as part of a study investigating the acceptability of an evidence-based cognitive
behavioural alcohol intervention to Aboriginal people (Calabria et al. 2013). Participants were
also recruited through existing Aboriginal community-based groups in metropolitan Sydney
from June 2009 to May 2010, as part of a pilot study of community education and brief
intervention (Conigrave et al. 2012). Participants recruited in rural NSW were reimbursed $A40
to cover their out-of-pocket expenses for involvement in the study. Reimbursement was not
available for participants in the Sydney based sample.
Questionnaires
A version of the 10-item AUDIT which has been modified for, and is acceptable to, Aboriginal
Australians (Table 1) (Conigrave et al. 2012), was self-completed by participants, with literacy
support available. Total scores range from zero to forty, with higher scores indicating more
problematic alcohol use. Cut-off scores recommended by the Alcohol Treatment Guidelines for
Indigenous Australians (Australian Government Department of Health and Ageing 2007) were
used to classify drinker status. Given Indigenous Australians who drink alcohol are more likely
to do so at levels that places them at increased risk of alcohol-related harm than the general
Australian population (Australian Department of Human Services and Health 1995), the
Guideline’s high-risk drinker classification was divided into high-risk drinkers and likely
dependent drinkers (Babor et al. 2001) to more clearly investigate this group. Therefore
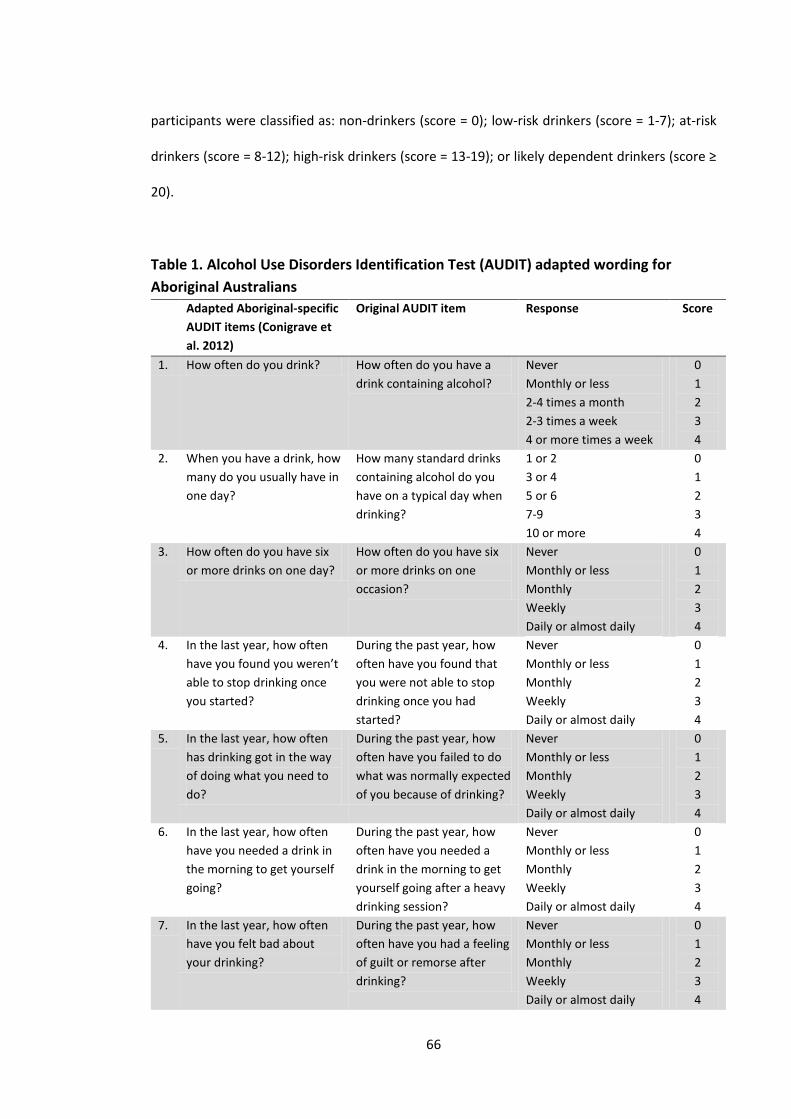
66
participants were classified as: non-drinkers (score = 0); low-risk drinkers (score = 1-7); at-risk
drinkers (score = 8-12); high-risk drinkers (score = 13-19); or likely dependent drinkers (score ≥
20).
Table 1. Alcohol Use Disorders Identification Test (AUDIT) adapted wording for
Aboriginal Australians
Adapted Aboriginal-specific
AUDIT items (Conigrave et
al. 2012)
Original AUDIT item Response Score
1. How often do you drink? How often do you have a
drink containing alcohol?
Never
Monthly or less
2-4 times a month
2-3 times a week
4 or more times a week
0
1
2
3
4
2. When you have a drink, how
many do you usually have in
one day?
How many standard drinks
containing alcohol do you
have on a typical day when
drinking?
1 or 2
3 or 4
5 or 6
7-9
10 or more
0
1
2
3
4
3. How often do you have six
or more drinks on one day?
How often do you have six
or more drinks on one
occasion?
Never
Monthly or less
Monthly
Weekly
Daily or almost daily
0
1
2
3
4
4. In the last year, how often
have you found you weren’t
able to stop drinking once
you started?
During the past year, how
often have you found that
you were not able to stop
drinking once you had
started?
Never
Monthly or less
Monthly
Weekly
Daily or almost daily
0
1
2
3
4
5. In the last year, how often
has drinking got in the way
of doing what you need to
do?
During the past year, how
often have you failed to do
what was normally expected
of you because of drinking?
Never
Monthly or less
Monthly
Weekly
Daily or almost daily
0
1
2
3
4
6. In the last year, how often
have you needed a drink in
the morning to get yourself
going?
During the past year, how
often have you needed a
drink in the morning to get
yourself going after a heavy
drinking session?
Never
Monthly or less
Monthly
Weekly
Daily or almost daily
0
1
2
3
4
7. In the last year, how often
have you felt bad about
your drinking?
During the past year, how
often have you had a feeling
of guilt or remorse after
drinking?
Never
Monthly or less
Monthly
Weekly
Daily or almost daily
0
1
2
3
4

67
Adapted Aboriginal-specific
AUDIT items (Conigrave et
al. 2012)
Original AUDIT item Response Score
8. In the last year, how often
have you had a memory
lapse or blackout because of
your drinking?
During the past year, have
you been unable to
remember what happened
the night before because
you had been drinking?
Never
Monthly or less
Monthly
Weekly
Daily or almost daily
0
1
2
3
4
9. Have you injured yourself or
anyone else because of your
drinking?
Have you or someone else
been injured as a result of
your drinking?
No
Yes, but not in the past
year
Yes, during the past year
0
2
4
10. Has anyone (family, friend,
doctor) been worried about
your drinking or asked you
to cut down?
Has a relative or friend,
doctor or other health
worker been concerned
about your drinking or
suggested you cut down?
No
Yes, but not in the past
year
Yes, during the past year
0
2
4
AUDIT-C assesses frequency and quantity of alcohol use, and frequency of heavy drinking (six
or more drinks on one day) (Table 1, items 1-3). Total scores range from zero to twelve. As
with the 10-item AUDIT, higher scores indicate more problematic alcohol use. AUDIT-3 (the
third item of the 10-item AUDIT) measures frequency of heavy drinking (Table 1, item 3). Total
scores range from zero to four: greater consumption of alcohol is reflected in a higher score.
Exclusion criterion
Participants who did not complete all 10 AUDIT items were excluded, except for those who
appropriately did not answer item two because they indicated being a non-drinker on item
one. In that circumstance, item two was scored zero, reflecting the participant’s status as a
non-drinker.
Data analysis
Sensitivity, specificity, and positive and negative predictive values (Lemeshow et al. 1990) of
each score on the AUDIT-C and AUDIT-3 were calculated, relative to cut-off scores on the 10-
68
item AUDIT: at-risk drinkers (score ≥ 8); high-risk drinkers (score ≥ 13); and likely dependent
drinkers (score ≥ 20) (Australian Government Department of Health and Ageing 2007; Babor et
al. 2001; Conigliaro, Lofgren & Hanusa 1998) (see Appendix B for formulae used in analysis).
For this study, sensitivity is the proportion of respondents identified as risky drinkers on the
10-item AUDIT who are also identified as risky drinkers on AUDIT-C and/or AUDIT-3. Specificity
is the proportion of respondents identified as non-risky drinkers on the 10-item AUDIT who are
also identified as non-risky drinkers on AUDIT-C and/or AUDIT-3. The positive predictive value
is the proportion of respondents identified as risky drinkers on AUDIT-C and/or AUDIT-3 who
are also identified as risky drinkers on the 10-item AUDIT. The negative predictive value is the
proportion of respondents identified as non-risky drinkers on AUDIT-C and/or AUDIT-3 who are
also identified as non-risky drinkers on the 10-item AUDIT (Lemeshow et al. 1990).
Factors specific to Aboriginal health care settings were used to guide decisions about optimal
cut-off scores. Since Aboriginal drinkers are more likely to drink at risky levels than non-
Aboriginal drinkers (Australian Department of Human Services and Health 1995) there is a
higher probability that Aboriginal drinkers will require an alcohol-specific intervention
(Australian Government Department of Health and Ageing 2007). Consequently, higher
sensitivity (to detect true positive cases) took preference over higher specificity (to detect true
negative cases). For dependent drinkers, minimising the number of people who receive
referral unnecessarily is important given their treatment is relatively expensive and typically
involves multiple health care providers and inpatient care (Australian Government Department
of Health and Ageing 2007). Consequently, higher specificity (to detect true negative cases)
was favoured over higher sensitivity (to detect true positive cases) for optimal cut-off scores in
relation to likely alcohol dependence.
69
Receiver operating characteristic (ROC) curve analysis was conducted to measure the
detection characteristics of AUDIT-C and AUDIT-3 for at-risk, high-risk and likely dependent
drinkers identified by the 10-item AUDIT (Metz 1978). A value of one for the area under the
ROC (AUROC) curve represents a test with 100% accuracy. Ninety five percent confidence
intervals were calculated.
Data analysis used IBM® SPSS® Statistics 19 (IBM 2010), and Microsoft® Excel 2007 (Microsoft
2007).
Results
Sample characteristics
One hundred and fifty seven Aboriginal Australian participants took part in the surveys, 21 of
whom did not answer all 10 items of AUDIT. Of the 136 participants in the final sample (71%
from rural NSW and 29% from Sydney), 11% were aged 18 to 24 years, 24% were aged 25 to 34
years, 27% were aged 35 to 44 years, 25% were aged 45 to 55 years, 10% were 55 years or
older (3% did not indicate their age), 49% were male.
Alcohol use
AUDIT scores of participants ranged from zero to forty (median = 8.0; standard deviation =
11.0). Applying standard cut-off scores for the 10-item version of AUDIT resulted in the
following distribution of participants across risk categories: 15% were non-drinkers (score = 0);
31% were low-risk drinkers (score = 1-7); 15% were at-risk drinkers (score = 8-12); 16% were
high-risk drinkers (score = 13-19); and 22% were likely dependent drinkers (score ≥ 20). There
were more at-risk drinkers in Sydney (30%) than rural NSW (9%), and more likely dependent
drinkers in rural NSW (30%), compared to Sydney (3%). Of the total sample, 73 (54%) were
70
classified as being at least at-risk drinkers (AUDIT score ≥ 8) and 38% (n = 52) were classified as
being at least high-risk drinkers (AUDIT score ≥ 13).
The distribution of participants across risk categories varied for males (and females): 10%
(21%) were non-drinkers; 18% (44%) were low-risk drinkers; 21% (10%) were at-risk drinkers;
16% (15%) were high-risk drinkers; and 34% (10%) were likely dependent drinkers.
At-risk drinkers
The AUROC for AUDIT-C was high for drinkers classified as being at increased risk by the 10-
item AUDIT (0.93, 95%CI = 0.89 – 0.97) (Figure 1). The optimal combination of sensitivity and
specificity for at-risk drinkers was reached using a cut-off score of ≥ 5 for AUDIT-C. This cut-off
score identified 85% of at-risk drinkers, as classified by the 10-item AUDIT, and 81% of those
identified as not being at increased risk. The positive and negative predictive values were both
greater than 0.80 (Table 2).
The AUROC for AUDIT-3 was also high for drinkers classified as being at increased risk by the
10-item AUDIT (0.91, 95%CI = 0.85 – 0.96) (Figure 1). The optimal combination of sensitivity
and specificity for at-risk drinkers was reached using a cut-off score of ≥ 1 for AUDIT-3. This
cut-off score identified 95% of at-risk drinkers, as classified by the 10-item AUDIT, and 65% of
those identified as not being at increased risk drinkers. A lower positive predictive value (0.76)
than for AUDIT-C, however, indicated a number of false positive cases would be identified
relative to the 10-item AUDIT. A cut-off score of ≥ 2 reduces the number of false positive cases
(positive predictive value = 0.91), but decreases the number of true positive cases (sensitivity =
0.81) (Table 2).
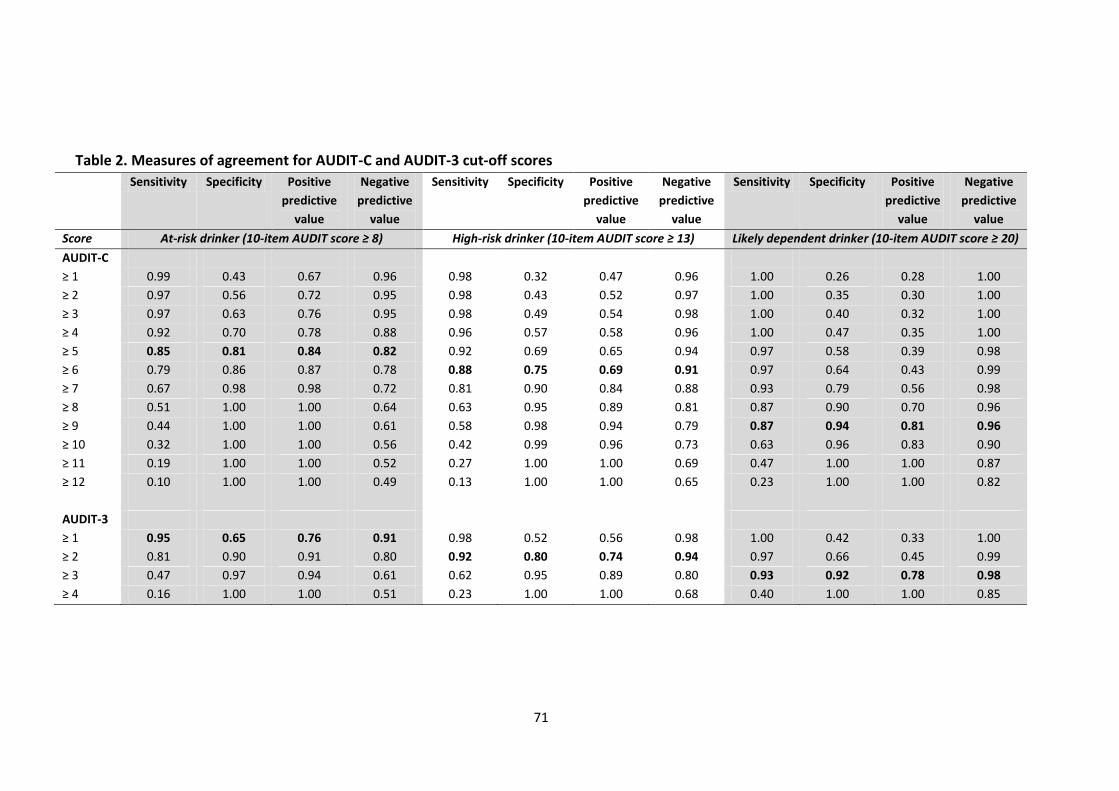
71
Table 2. Measures of agreement for AUDIT-C and AUDIT-3 cut-off scores
Sensitivity Specificity Positive
predictive
value
Negative
predictive
value
Sensitivity Specificity Positive
predictive
value
Negative
predictive
value
Sensitivity Specificity Positive
predictive
value
Negative
predictive
value
Score At-risk drinker (10-item AUDIT score ≥ 8) High-risk drinker (10-item AUDIT score ≥ 13) Likely dependent drinker (10-item AUDIT score ≥ 20)
AUDIT-C
≥ 1 0.99 0.43 0.67 0.96 0.98 0.32 0.47 0.96 1.00 0.26 0.28 1.00
≥ 2 0.97 0.56 0.72 0.95 0.98 0.43 0.52 0.97 1.00 0.35 0.30 1.00
≥ 3 0.97 0.63 0.76 0.95 0.98 0.49 0.54 0.98 1.00 0.40 0.32 1.00
≥ 4 0.92 0.70 0.78 0.88 0.96 0.57 0.58 0.96 1.00 0.47 0.35 1.00
≥ 5 0.85 0.81 0.84 0.82 0.92 0.69 0.65 0.94 0.97 0.58 0.39 0.98
≥ 6 0.79 0.86 0.87 0.78 0.88 0.75 0.69 0.91 0.97 0.64 0.43 0.99
≥ 7 0.67 0.98 0.98 0.72 0.81 0.90 0.84 0.88 0.93 0.79 0.56 0.98
≥ 8 0.51 1.00 1.00 0.64 0.63 0.95 0.89 0.81 0.87 0.90 0.70 0.96
≥ 9 0.44 1.00 1.00 0.61 0.58 0.98 0.94 0.79 0.87 0.94 0.81 0.96
≥ 10 0.32 1.00 1.00 0.56 0.42 0.99 0.96 0.73 0.63 0.96 0.83 0.90
≥ 11 0.19 1.00 1.00 0.52 0.27 1.00 1.00 0.69 0.47 1.00 1.00 0.87
≥ 12 0.10 1.00 1.00 0.49 0.13 1.00 1.00 0.65 0.23 1.00 1.00 0.82
AUDIT-3
≥ 1 0.95 0.65 0.76 0.91 0.98 0.52 0.56 0.98 1.00 0.42 0.33 1.00
≥ 2 0.81 0.90 0.91 0.80 0.92 0.80 0.74 0.94 0.97 0.66 0.45 0.99
≥ 3 0.47 0.97 0.94 0.61 0.62 0.95 0.89 0.80 0.93 0.92 0.78 0.98
≥ 4 0.16 1.00 1.00 0.51 0.23 1.00 1.00 0.68 0.40 1.00 1.00 0.85
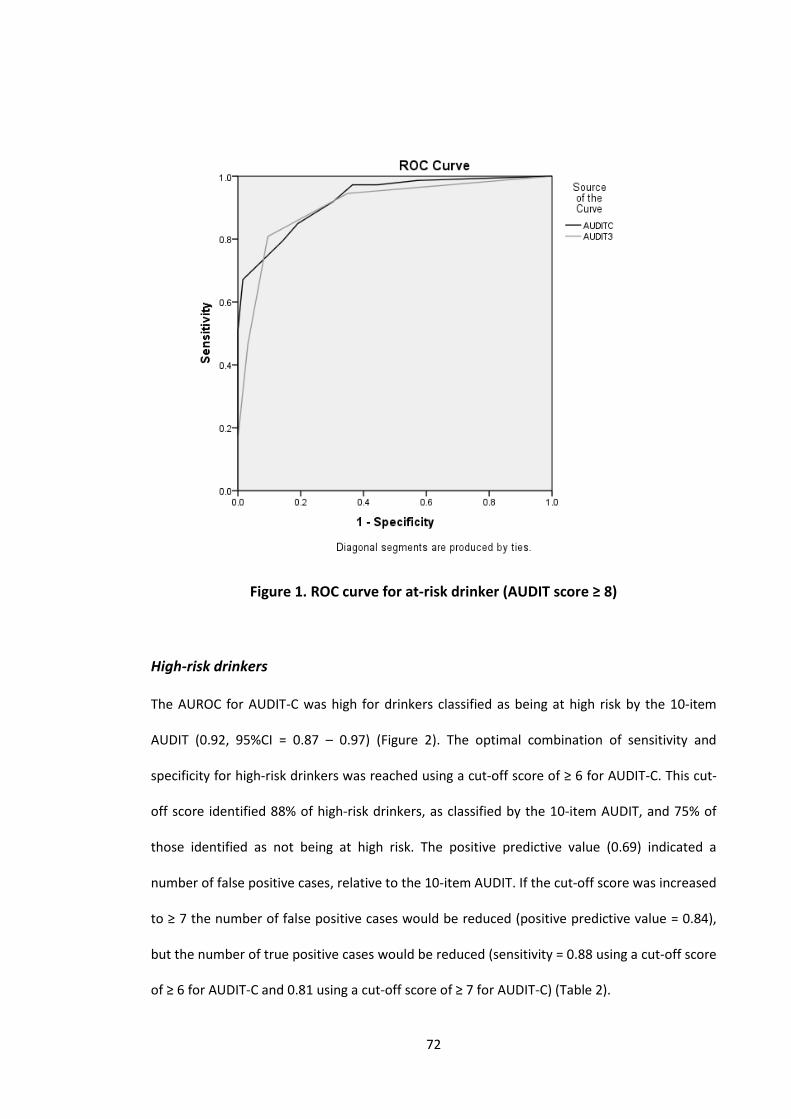
72
Figure 1. ROC curve for at-risk drinker (AUDIT score ≥ 8)
High-risk drinkers
The AUROC for AUDIT-C was high for drinkers classified as being at high risk by the 10-item
AUDIT (0.92, 95%CI = 0.87 – 0.97) (Figure 2). The optimal combination of sensitivity and
specificity for high-risk drinkers was reached using a cut-off score of ≥ 6 for AUDIT-C. This cut-
off score identified 88% of high-risk drinkers, as classified by the 10-item AUDIT, and 75% of
those identified as not being at high risk. The positive predictive value (0.69) indicated a
number of false positive cases, relative to the 10-item AUDIT. If the cut-off score was increased
to ≥ 7 the number of false positive cases would be reduced (positive predictive value = 0.84),
but the number of true positive cases would be reduced (sensitivity = 0.88 using a cut-off score
of ≥ 6 for AUDIT-C and 0.81 using a cut-off score of ≥ 7 for AUDIT-C) (Table 2).
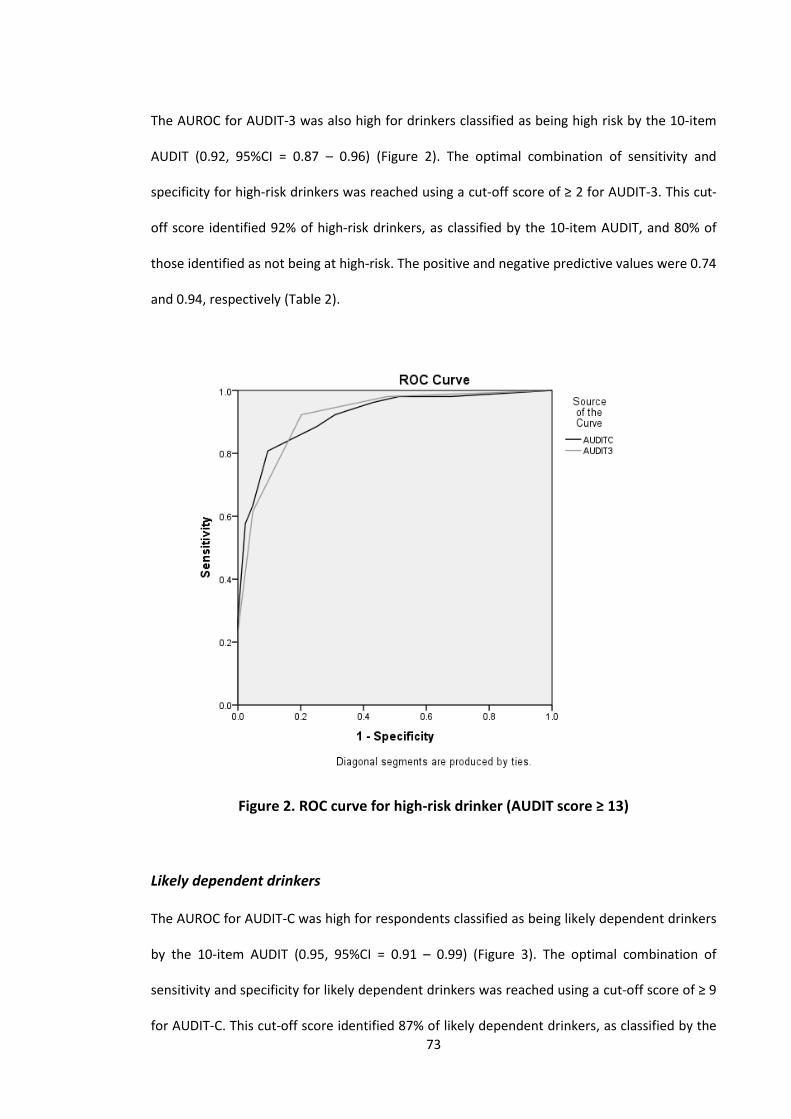
73
The AUROC for AUDIT-3 was also high for drinkers classified as being high risk by the 10-item
AUDIT (0.92, 95%CI = 0.87 – 0.96) (Figure 2). The optimal combination of sensitivity and
specificity for high-risk drinkers was reached using a cut-off score of ≥ 2 for AUDIT-3. This cut-
off score identified 92% of high-risk drinkers, as classified by the 10-item AUDIT, and 80% of
those identified as not being at high-risk. The positive and negative predictive values were 0.74
and 0.94, respectively (Table 2).
Figure 2. ROC curve for high-risk drinker (AUDIT score ≥ 13)
Likely dependent drinkers
The AUROC for AUDIT-C was high for respondents classified as being likely dependent drinkers
by the 10-item AUDIT (0.95, 95%CI = 0.91 – 0.99) (Figure 3). The optimal combination of
sensitivity and specificity for likely dependent drinkers was reached using a cut-off score of ≥ 9
for AUDIT-C. This cut-off score identified 87% of likely dependent drinkers, as classified by the

74
10-item AUDIT, and 94% of those identified as unlikely to be dependent drinkers. Positive and
negative predictive values were both above 0.80 (Table 2).
The AUROC for AUDIT-3 was also high for respondents classified as being likely dependent
drinkers by the 10-item AUDIT (0.96, 95%CI = 0.92 – 0.99) (Figure 3). The optimal combination
of sensitivity and specificity for likely dependent drinkers was reached using a cut-off score of
≥ 3 for AUDIT-3. This cut-off score identified 93% of likely dependent drinkers, as classified by
the 10-item AUDIT, and 92% of those identified as unlikely to be dependent drinkers. Positive
and negative predictive values were 0.78 and 0.98, respectively (Table 2).
Figure 3. ROC curve for likely dependent drinker (AUDIT score ≥ 20)
75
Discussion
Summary of results
This is the first study to identify the sensitivity and specificity, and positive and negative
predictive values, of shorter forms of the 10-item AUDIT questionnaire for urban and rural
Aboriginal Australians. When using AUDIT-C to identify at-risk, high-risk and likely dependent
drinkers, as classified by the 10-item AUDIT, recommended cut-off scores are ≥ 5, ≥ 6 and ≥ 9,
respectively. When using AUDIT-3 to identify at-risk, high-risk and likely dependent drinkers, as
classified by the 10-item AUDIT, recommended cut-off scores are≥ 1, ≥ 2 and ≥ 3, respectively.
All AUROC were above 0.90 indicating good performance of both AUDIT-C and AUDIT-3 in
identifying the at-risk, high-risk and likely dependent drinkers that were classified as such by
the 10-item AUDIT.
Implications
These recommended AUDIT-C and AUDIT-3 cut-off scores for detecting at-risk, high-risk or
likely dependent Aboriginal Australian drinkers are generally higher than those identified for
non-Aboriginal Australian populations (Reinert & Allen 2007), although one study found
comparable cut-off scores for at-risk drinkers in a primary care sample (Seale et al. 2006).
These differences in cut-off scores potentially reveal a unique response pattern by Aboriginal
Australians which may reflect the fact that participants in this study were asked questions
about drinks. Participants in this study were asked questions about drinks, rather than
standard drinks, to cut down the need for mental arithmetic in a population that has often
been educationally disadvantaged. The Australian standard drink is 10 g of ethanol whereas a
can of beer, for example, is approximately 1.3 standard drinks, and most people drink wine in
at least 1.8 standard drink serves (National Health and Medical Research Council 2009). It is
76
unclear how the participants’ calculation of the number of drinks they consume compares to
these standard drink definitions (Lee, Dawson & Conigrave in press).
The two results for which recommended cut-off scores are most difficult to determine are
AUDIT-3 cut-off scores for at-risk drinkers and AUDIT-C cut-off scores for high-risk drinkers.
The recommended cut-off scores prioritise higher sensitivity over higher specificity; however,
this creates an issue of false positives which may result in additional work following up cases to
distinguish false positives from true positives. If brief intervention is done appropriately and
respectfully, however, then this checking process can be done as part of a reminder of current
recommended drinking guidelines. A larger study may be able to more definitively determine
appropriate cut-off scores in these cases.
From a clinical services perspective, a decision about which screening instrument is most
appropriate for Aboriginal clients would be required in consultation with Aboriginal health
professionals and/or Aboriginal communities. For at-risk drinkers, AUDIT-C has a greater
specificity, albeit a slightly lower sensitivity than AUDIT-3 (sensitivity: 0.85 and 0.95,
respectively; specificity: 0.81 and 0.65, respectively) indicating a slight preference for using
AUDIT-C to identify at-risk Aboriginal drinkers. For high-risk and likely dependent Aboriginal
drinkers using either AUDIT-C or AUDIT-3 would be appropriate, based on similar sensitivities
and specificities for the two measures. The decision may be made on practical grounds:
whether saving time during the screening process or in following-up on positive results is more
important. If screening is automated, with touch-screen computers for example, then the
three item AUDIT-C (or indeed the 10-item AUDIT) may be desirable given its greater
specificity. If screening is manual, however, or screening is also required for a number of other
health risk factors (e.g. smoking, nutrition and obesity), asking only a single alcohol question
(AUDIT-3) may be preferred, with a later discussion about drinking and other health risk
77
factors during the clinical interview. Community consultation could help to determine which of
AUDIT-C or AUDIT-3 is more acceptable to Aboriginal people in different circumstances.
Limitations
A convenience sample was used. This method of recruitment which resulted in a sample of
Aboriginal Australians likely to access the participating health services or community groups,
probably resulted in low recruitment of treatment resistant individuals with alcohol problems.
Self-report data are prone to bias, even when this is minimised by using psychometrically
validated tools (Hogan 2003). Self-reports of alcohol consumption are more likely to be
accurate under optimal conditions: when participants are alcohol free; when assured
confidentiality; when questions are clear; and in situations not likely to promote under-
reporting (e.g., clinical compared to legal) (National Institute on Alcohol Abuse and Alcoholism
1995). These conditions were likely to be met by our study.
Although it has been recommended that measures to detect alcohol misuse be tested
separately for men and women (Reinert & Allen 2007), this study did not attempt to do so due
to the small number of men and women in each group. Given lower cut-off scores have been
recommended for women, compared to men, in other populations (Reinert & Allen 2007),
these analyses would be worthwhile undertaking for studies with larger sample sizes.
The method used in this study of comparing results on AUDIT-C and AUDIT-3 to the 10-item
AUDIT differs from other validation studies that compare the short versions of AUDIT with a
‘gold standard’ measure (Reinert & Allen 2007). The method for this study, however, was
required because a ‘gold standard’ measure for Aboriginal Australians is not available. The 10-
item AUDIT questionnaire was used because it has been recommended for use in Aboriginal
health care settings (Australian Government Department of Health and Ageing 2007), despite
78
not having been formally validated itself with Aboriginal Australian populations. Although
comparison with other validation studies should be made with caution, because different
results may have been found if AUDIT-C and AUDIT-3 were evaluated against some other ‘gold
standard measure’, any such differences are likely to be minor.
The AUDIT scoring was developed at a time when international and Australian drinking
guidelines were more liberal. Further study is required to see if the current recommended
AUDIT cut-off scores (and hence AUDIT-C and AUDIT-3 cut-off scores) should be revised
downward, to allow detection of anyone drinking over current recommended limits (e.g. 20 g
daily or 40 g on any one occasion in Australia) (National Health and Medical Research Council
2009), and whether the use of open ended responses to questions one and two result in more
accurate drink risk identification.
Finally, the diagnostic error of the 10-item AUDIT questionnaire is expected to be highly
correlated with the error of AUDIT-C and AUDIT-3 and, therefore, the AUROC analyses are
likely to be biased upwards. AUROCs in this study ranged from 0.91 to 0.96, and therefore if
the results were revised downwards to account for bias they are likely to still be comparable to
other validation studies (Reinert & Allen 2007).
Conclusions
The optimal performance of AUDIT-C and AUDIT-3 in detecting at-risk, high-risk and likely
dependent Aboriginal Australian drinkers, as classified by the 10-item AUDIT, was achieved
using cut-off scores of AUDIT-C ≥ 5 and AUDIT-3 ≥ 1, AUDIT-C ≥ 6 and AUDIT-3 ≥ 2, and AUDIT-
C ≥ 9 and AUDIT-3 ≥ 3, respectively. These findings provide an empirical basis for defining cut-
off scores, which complements existing evidence that both short form versions of AUDIT are
79
suitable for routinely screening Aboriginal Australian clients for alcohol problems in Aboriginal
specific health care settings.
Acknowledgements
We would like to thank the many colleagues and community members who helped with this
research. We are also grateful for the statistical advice provided by Dr Tim Slade. This work
was supported by the Australian Government Department of Health and Ageing, a linkage
grant from the Australian Research Council and by a grant from the National Drug Research
Institute, Curtin University. This research was conducted without input from the funders.

80
Paper 3
Tailoring a family-based alcohol intervention for Aboriginal Australians,
and the experiences and perceptions of health care providers trained in
its delivery
Bianca Calabria1, Anton Clifford2,3, Miranda Rose4, Anthony Shakeshaft1
1. National Drug and Alcohol Research Centre, University of New South Wales, Sydney, New South
Wales, Australia
2. Institute for Urban Indigenous Health, University of Queensland, Bowen Hills, Queensland, Australia
3. Queensland Alcohol and Drug Research and Education Centre, University of Queensland, Brisbane,
Australia
3. University of Technology, Sydney, New South Wales, Australia
Paper 3 has been submitted to Health Service Research (Calabria et al. submitted-a) .
81
Copyright Statement
I certify that this publication was a direct result of my research towards this PhD, and that
reproduction in this thesis does not breach copyright regulations.
Calabria, B, Clifford, A, Rose, M & Shakeshaft, A submitted, 'Tailoring a family-based alcohol
intervention for Aboriginal Australians, and the experiences and perceptions of healthcare
practitioners trained in its delivery', Health Services Research.
Bianca Calabria August 2013
82
Preamble
The identification of Indigenous-specific AUDIT-C and AUDIT-3 cut-off scores in Paper 2 gives
some certainly that alcohol consumption risk levels can be accurately assigned to Indigenous
clients who present at health care services which, in turn, increases the likelihood that their
health care needs can be more precisely met. Providing Indigenous-specific interventions
aimed at reducing alcohol-related harms to Indigenous Australians, who are screened using
Indigenous-specific cut-off scores for AUDIT-C and AUDIT-3, will help address Indigenous-
specific needs more cost-effectively.
Paper 1 identified CRAFT as a family-based alcohol intervention with potential to be tailored
for Indigenous people, when modified in consultation with targeted community members
(Calabria et al. 2012). CRAFT targets family members of problem drinkers and teaches them
how to support their problem drinking relative to reduce their alcohol consumption, increase
participation in rewarding non-drinking behaviours, and to engage in appropriate treatment.
CRAFT also has a focus on the family member’s personal safety and increasing their own
wellbeing (Smith & Meyers 2007). Although CRAFT has been successfully adapted for use
among Native Americans (Miller, Meyers & Hiller-Sturmhofel 1999), it has not been evaluated
with Indigenous people in other countries. The modified CRAFT program used with Native
Americans was consistent with Indigenous holistic concepts of health and wellbeing by
emphasising the connectedness with family, community and spirituality in the treatment
approach. The suitability of this approach for Native Americans reflects that it is highly likely to
be acceptable and feasible if adapted for Indigenous communities elsewhere.
CRAFT uses cognitive-behavioural principles and procedures modelled from the Community
Reinforcement Approach (CRA). CRA is an evidence-based cognitive-behavioural intervention
aimed at working with problem drinkers to reduce their alcohol consumption and has a focus
83
on changing behavioural patterns to spend more time in enjoyable non-drinking situations
(Meyers & Smith 1995; Miller & Wilbourne 2002). Given the parallels between CRAFT and CRA,
CRA would be a highly relevant treatment for relatives of individuals participating in CRAFT.
For CRA and CRAFT to be feasible for delivery to Indigenous Australians, both interventions
need to be acceptable to the Indigenous people who are likely to access the interventions and
to the health care providers who will deliver the programs.
Paper 3 presents health care providers perceptions of the applicability of CRA and CRAFT for
Indigenous Australians and suggestions for suitable modifications to the interventions to
increase their appropriateness. Paper 3 also presents the experiences of health care providers
participating in an internationally recognised counsellor certification program for CRA and
CRAFT (Calabria et al. submitted-a).
84
Abstract
Objective. To describe the process of tailoring the Community Reinforcement Approach (CRA)
and Community Reinforcement and Family Training (CRAFT) for delivery to Aboriginal
Australians, explore the perceptions of health care providers participating in the tailoring
process, and their experiences of participating in CRA and CRAFT counselor certification.
Data Sources/Study Setting. Notes recorded from eight working group meetings with 22 health
care providers of a drug and alcohol treatment agency and Aboriginal Community Controlled
Health Service (November 2009-February 2013), and transcripts of semi-structured interviews
with seven health care providers participating in CRA and CRAFT counselor certification (May
2012).
Study Design. Qualitative content analysis was used.
Data Collection/Extraction Methods. Data from working group meeting notes and interview
transcripts were categorized into key themes.
Principle Findings. Health care providers perceived counselor certification it to be beneficial for
developing their skills and confidence in delivering CRA and CRAFT, but reported the
challenges of time constraints and competing tasks. Modification to the technical language, a
reduction in the number of sessions, and inclusion of group delivery, were suggested to make
to interventions more applicable for Aboriginal Australians.
Conclusions. Tailoring CRA and CRAFT was an iterative process involving ongoing consultations
and feedback from health care providers.
85
Introduction
Aboriginal Australians experience a disproportionately high burden of alcohol-related harm,
compared to the general Australian population (Calabria et al. 2010; Vos et al. 2003).
Approaches that simultaneously target individuals and families at risk of alcohol-related harm
are likely to be acceptable to, and feasible for, delivery to Aboriginal Australians (Calabria et al.
2012), given that positive interaction with family members influences behavioral change in
Aboriginal Australians (Nagel & Thompson 2010), and family relationships are fundamental to
the cohesion and wellbeing of Indigenous communities (McLennan & Khavarpour 2004; Nagel
& Thompson 2010).
The Community Reinforcement Approach (CRA) (Meyers & Smith 1995) is an evidence-based
cognitive-behavioral intervention for problem drinkers (Miller & Wilbourne 2002). CRA aims to
reduce alcohol consumption by using social, recreational, family and vocational reinforcers to
motivate people towards making their non-drinking lifestyle more rewarding than drinking
alcohol. Community Reinforcement and Family Training (CRAFT) (Smith & Meyers 2007) is a
family-based intervention modelled on CRA and has been identified as an effective cognitive-
behavioral intervention with potential to be tailored, in collaboration with locally targeted
Aboriginal communities, for delivery in Aboriginal-specific health care settings (Calabria et al.
2012). CRAFT provides structured, personalised training and support to a family member of a
problem drinker. The aims of CRAFT are to teach family members how to effectively and safely
remove positive reinforcement for the problem drinker’s drinking behavior, increase positive
reinforcement for non-drinking behavior, and help to engage the problem drinker into
treatment. In addition, CRAFT aims to improve family members’ own social and emotional
wellbeing. CRA and CRAFT were both developed in the United States and include a structured
certification program for counselors. CRA and CRAFT have been found to be acceptable to
Aboriginal Australians in rural New South Wales (NSW) for delivery in their local community,
86
when tailored to optimise their cultural appropriateness (Calabria et al. 2013). Although both
interventions have been successfully modified for other minority groups (Lopez Viets 2008;
Villarreal 2008; Meyers, Villanueva & Smith 2005; Miller, Meyers & Hiller-Sturmhofel 1999),
they have not been tailored for Aboriginal Australians.
This paper reports on a project that involved researchers working with health care services and
Aboriginal community members to tailor CRA and CRAFT for Aboriginal Australians in rural
NSW, Australia. The paper has three aims. Firstly, to describe the process of tailoring CRA and
CRAFT for delivery to Aboriginal Australians in rural New South Wales (NSW). Second, to
explore the perceptions of health care providers participating in the tailoring process. Third, to
explore the experiences of health care providers participating in CRA and CRAFT counselor
certification.
Methods
Ethics
Ethical approval for this study was provided by the Human Research Ethics Committee,
University of NSW, and the Aboriginal Health and Medical Research Council, Ethics Committee
of NSW. All interview participants provided informed consent (see Appendix C for consent
form).
Tailoring CRA and CRAFT
The process of tailoring CRA and CRAFT for Aboriginal Australians was an iterative process
comprising four key phases, as summarised in Figure 1. Each phase yielded data that informed
the tailoring process.
87
1. Working group meetings with health care providers to adapt CRA and CRAFT for
routine delivery to Aboriginal Australians at risk of alcohol-related harm;
2. Survey of Aboriginal clients from participating health care services to examine their
perceptions of the acceptability of, and suggestions for tailoring, CRA and CRAFT for
delivery in their community (Calabria et al. 2013);
3. Certification of health care providers in CRA and CRAFT to develop their knowledge
and skills to deliver CRA and CRAFT in practice; and
4. Interviews with health care providers participating in CRA and CRAFT counselor
certification to explore their experiences of undertaking the counselor certification
programs and perceptions of the feasibility of CRA and CRAFT procedures for delivery
to Aboriginal Australians.
This paper presents results from Steps 1, 3 and 4. Results from Step 2 are reported elsewhere
(Calabria et al. 2013). This method of working in consultation with Aboriginal Australians and
health care providers to tailor CRA and CRAFT to be more acceptable to Aboriginal Australians
has been previously demonstrated to be feasible in other family-based research with different
Aboriginal Australians groups (Turner & Sanders 2007).
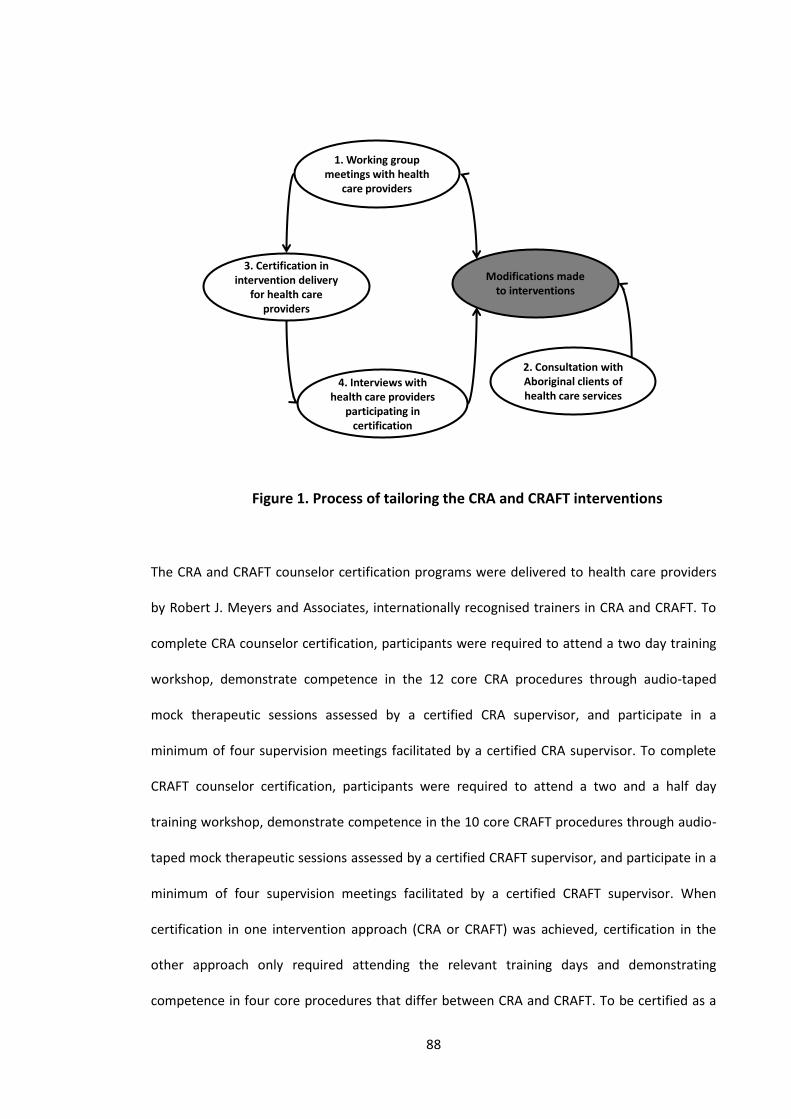
88
1. Working group meetings with health
care providers
3. Certification in intervention delivery
for health care providers
4. Interviews with health care providers
participating in certification
Modifications made to interventions
2. Consultation with Aboriginal clients of health care services
Figure 1. Process of tailoring the CRA and CRAFT interventions
The CRA and CRAFT counselor certification programs were delivered to health care providers
by Robert J. Meyers and Associates, internationally recognised trainers in CRA and CRAFT. To
complete CRA counselor certification, participants were required to attend a two day training
workshop, demonstrate competence in the 12 core CRA procedures through audio-taped
mock therapeutic sessions assessed by a certified CRA supervisor, and participate in a
minimum of four supervision meetings facilitated by a certified CRA supervisor. To complete
CRAFT counselor certification, participants were required to attend a two and a half day
training workshop, demonstrate competence in the 10 core CRAFT procedures through audio-
taped mock therapeutic sessions assessed by a certified CRAFT supervisor, and participate in a
minimum of four supervision meetings facilitated by a certified CRAFT supervisor. When
certification in one intervention approach (CRA or CRAFT) was achieved, certification in the
other approach only required attending the relevant training days and demonstrating
competence in four core procedures that differ between CRA and CRAFT. To be certified as a
89
CRA or CRAFT supervisor participants were required to complete the relevant counselor
certification, facilitate five relevant supervision sessions, and assess five relevant audio-taped
therapeutic sessions.
The tailoring process involved input and feedback from health care providers on: CRA and
CRAFT core procedures; printed resource materials used to work through core procedures with
clients (including worksheets for goals of counselling, Happiness Scale, Relationship Happiness
Scale, perfect relationship, problem solving, session checklist, and functional analysis); their
delivery of CRA and CRAFT; and Aboriginal-specific CRA and CRAFT manuals. Aboriginal-specific
CRA and CRAFT manuals were developed from CRA and CRAFT clinical practice manuals
(Meyers & Smith 1995; Smith & Meyers 2007). The tailored manuals summarized and
simplified the content of the original manuals and included scenarios relevant to Aboriginal
Australians, in order to better contextualize each intervention’s content and procedures. The
manuals were designed to be used for training health care providers in CRA and CRAFT and as
a resource to support them to deliver both interventions. Both manuals were written by a
researcher with more than 20 years of experience working in Aboriginal primary health care.
Input and feedback was also sought from health care providers regarding the most appropriate
and feasible research methods for examining the implementation of CRA and CRAFT in their
setting and evaluating its effectiveness among their client population using valid outcome
measures.
Setting and participants
Study participants were 19 health care providers from a drug and alcohol treatment agency
and three health care providers from an Aboriginal Community Controlled Health Service
(ACCHS) in rural NSW, Australia (n = 22). All participants attended at least one working group
90
meeting and interviews were conducted with working group meeting participants who had
completed CRAFT counselor certification and CRA training days at the time of the interviews.
Table 1 summarises the professional role of participants, their level of participation in working
group meetings, and the current level of CRA and CRAFT qualifications they had attained.
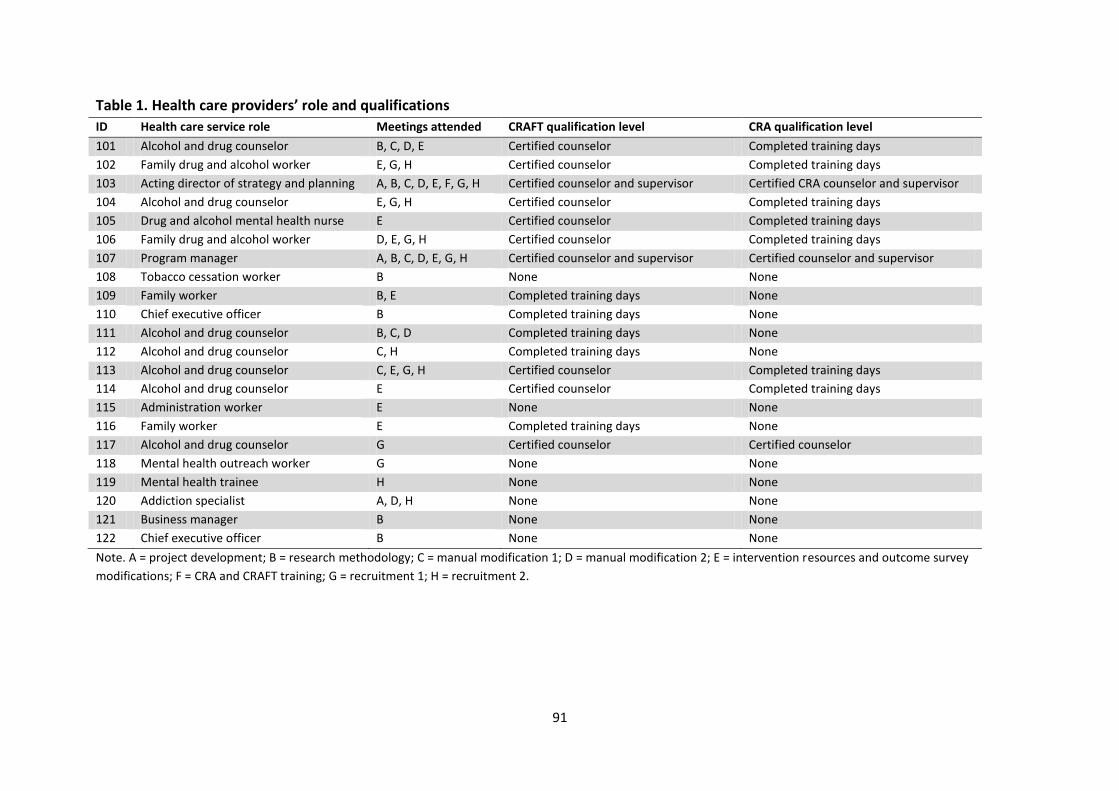
91
Table 1. Health care providers’ role and qualifications
ID Health care service role Meetings attended CRAFT qualification level CRA qualification level
101 Alcohol and drug counselor B, C, D, E Certified counselor Completed training days
102 Family drug and alcohol worker E, G, H Certified counselor Completed training days
103 Acting director of strategy and planning A, B, C, D, E, F, G, H Certified counselor and supervisor Certified CRA counselor and supervisor
104 Alcohol and drug counselor E, G, H Certified counselor Completed training days
105 Drug and alcohol mental health nurse E Certified counselor Completed training days
106 Family drug and alcohol worker D, E, G, H Certified counselor Completed training days
107 Program manager A, B, C, D, E, G, H Certified counselor and supervisor Certified counselor and supervisor
108 Tobacco cessation worker B None None
109 Family worker B, E Completed training days None
110 Chief executive officer B Completed training days None
111 Alcohol and drug counselor B, C, D Completed training days None
112 Alcohol and drug counselor C, H Completed training days None
113 Alcohol and drug counselor C, E, G, H Certified counselor Completed training days
114 Alcohol and drug counselor E Certified counselor Completed training days
115 Administration worker E None None
116 Family worker E Completed training days None
117 Alcohol and drug counselor G Certified counselor Certified counselor
118 Mental health outreach worker G None None
119 Mental health trainee H None None
120 Addiction specialist A, D, H None None
121 Business manager B None None
122 Chief executive officer B None None
Note. A = project development; B = research methodology; C = manual modification 1; D = manual modification 2; E = intervention resources and outcome survey
modifications; F = CRA and CRAFT training; G = recruitment 1; H = recruitment 2.
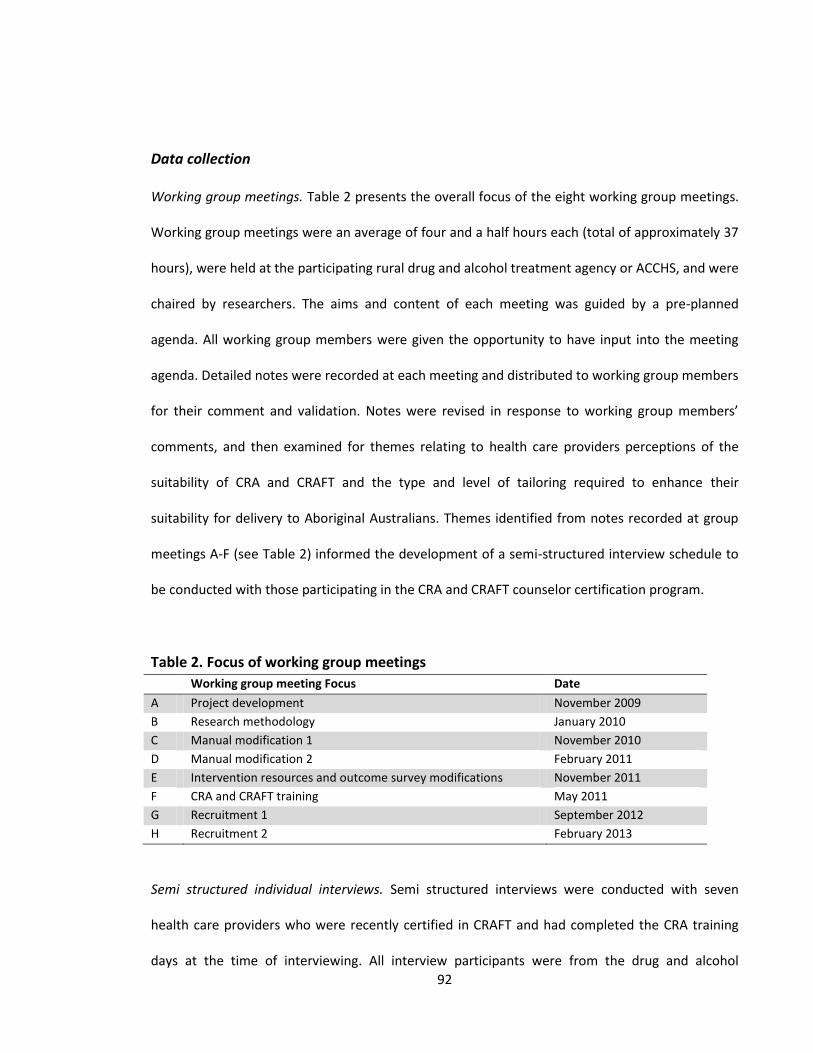
92
Data collection
Working group meetings. Table 2 presents the overall focus of the eight working group meetings.
Working group meetings were an average of four and a half hours each (total of approximately 37
hours), were held at the participating rural drug and alcohol treatment agency or ACCHS, and were
chaired by researchers. The aims and content of each meeting was guided by a pre-planned
agenda. All working group members were given the opportunity to have input into the meeting
agenda. Detailed notes were recorded at each meeting and distributed to working group members
for their comment and validation. Notes were revised in response to working group members’
comments, and then examined for themes relating to health care providers perceptions of the
suitability of CRA and CRAFT and the type and level of tailoring required to enhance their
suitability for delivery to Aboriginal Australians. Themes identified from notes recorded at group
meetings A-F (see Table 2) informed the development of a semi-structured interview schedule to
be conducted with those participating in the CRA and CRAFT counselor certification program.
Table 2. Focus of working group meetings
Working group meeting Focus Date
A Project development November 2009
B Research methodology January 2010
C Manual modification 1 November 2010
D Manual modification 2 February 2011
E Intervention resources and outcome survey modifications November 2011
F CRA and CRAFT training May 2011
G Recruitment 1 September 2012
H Recruitment 2 February 2013
Semi structured individual interviews. Semi structured interviews were conducted with seven
health care providers who were recently certified in CRAFT and had completed the CRA training
days at the time of interviewing. All interview participants were from the drug and alcohol
93
treatment agency. Interviews were conducted over two days in May 2012 in a private room at the
drug and alcohol treatment agency. The interview schedule included questions relating to health
care providers’ experiences of participating in CRA counselor training days and CRAFT counselor
certification, perceptions of the certification process, and perceptions of the suitability of CRA and
CRAFT for the treatment and management of Aboriginal people at risk of alcohol-related harm.
Interviews were conducted by a qualitative researcher with more than 20 years experience
working in Aboriginal primary health care and were an average of 39 minutes duration (range = 29
– 50 minutes). Interviews were audio-taped and recordings were transcribed verbatim for analysis.
Data analysis
Qualitative content analysis was used to systematically categorize text data into categories derived
inductively, and to summarize the data qualitatively (Forman & Damschroder 2008). Inductively
deriving the coding categories was appropriate given interviews were conducted with health care
providers about CRA and CRAFT used in an Aboriginal Australians health care setting for the first
time. The unit of analysis for the group meetings was the group and the unit of analysis for semi-
structured interview data was the individual. The qualitative content analysis followed three steps:
1) immersion resulted in listing memos (nine for working group meeting data and 23 for interview
data); 2) reduction summarized the memos into codes (five for working group meeting data:
CRAFT counselor certification, therapeutic issues, adaptability of CRA and CRAFT for Aboriginal
Australians, modifications to outcome measures, and possible referral pathways; and six for the
interview data: CRAFT counselor certification, CRA training, therapeutic issues, organisational
support, qualifications of therapists, and adaptability of CRA and CRAFT for Aboriginal Australians);
and 3) interpretation identified examples from specific working group meeting notes or from
individual health care provider interview transcripts relating to each code (Forman & Damschroder
94
2008). Data pertaining to common codes across working group meeting notes and interview
transcripts were combined for interpretation (see Appendix D for qualitative data analysis).
Results
CRAFT counsellor certification
Health care providers initially perceived the CRAFT counselor certification process as daunting, but
having commenced the process perceived training days, audio-taped sessions for review and
feedback, and supervision sessions, as valuable for developing their skills and confidence in
delivering CRAFT.
(I) enjoyed the CRAFT training, I thought it was really good...(the CRAFT counselor
certification process has) been really, really valuable (health care provider 103).
As a component of CRAFT counselor certification, fortnightly supervision sessions were delivered
to health care providers via videoconferencing using Skype (Microsoft 2013) or ooVoo (LLC 2013).
These sessions were delivered regularly to enable the United States based CRA and CRAFT
certified supervisors to meet with health care providers undertaking CRAFT counselor certification
in Australia. The purpose of these meetings was for supervisors to redemonstrate CRAFT
procedures to health care providers and provide them with group level feedback on their
performance to date. Health care providers reported that supervision sessions were important for
developing their confidence and skills to deliver CRAFT procedures to the standard required to
complete the certification process, and for addressing their questions or concerns relating to
delivering CRAFT in practice.
95
I think the Skype concept was definitely a recommendation that I would put in (health
care provider 102).
I thought that (supervision on Skype) was a very useful tool, rather than reading. I
think it was good because you could then ask questions directly (health care provider
103).
Although feedback about the supervision sessions was positive, health care providers reported
experiencing some technical difficulties when using the Internet-based programs for video
conferencing. Two health care providers are now certified CRAFT supervisors so ongoing CRAFT
supervision can be delivered face-to-face and will resolve these technical issues.
CRA training days
The two day CRA training was delivered after the two and a half day CRAFT training. Given that
some core CRA and CRAFT procedures are identical, there was some repetition. Nonetheless, the
CRA training days were well received by health care providers.
For those of us who had done CRAFT, we found the first day (of CRA training) a little
boring...but the second day, we did quite a few more exercises and...some group stuff
(health care provider 103).
...the CRA training...was fantastic... (health care provider 104).
96
Therapeutic issues
There were three main challenges to health care providers completing CRAFT counselor
certification. First, staying motivated to complete all the audio-taped sessions in addition to their
usual workload was difficult for health care providers, all of whom identified this as a challenge.
...the negatives was the time and the pressure that (counselor certification) put on
you (health care provider 104).
...(the CRAFT counselor certification process) was challenging...fitting it in with work
(health care provider 105).
This challenge was resolved by nominating an individual to co-ordinate the CRA and CRAFT
counselor certification process and by scheduling specific days for health care providers to
complete the required audio-taped sessions, without the distraction of competing work tasks.
The worst part was trying to get everyone motivated to do (the audio-taped sessions),
and actually co-ordinating them all to actually do them. So we set aside days...and
that worked well because everybody could just concentrate on that (health care
provider 107).
The second challenge of the CRAFT counselor certification process was initial reluctance by health
care providers to role play therapeutic procedures; however, the benefits of role plays for
consolidating and applying knowledge acquired from training days became apparent to health
care providers once they participated in role plays, and their reluctance appeared to diminish.
97
...it was kind of hard to do (role plays) and feel natural about it...the more we did it,
the more you got used to that (health care provider 104).
...I am a lot more confident with using (CRAFT) now than I would have been if we
hadn’t have done the role plays before and just getting the feedback was good to
know this bit you did really well, this bit you probably need to work on (health care
provider 106).
The third challenge was the incongruence of some core procedures with health care providers’
previous counseling training. Concern was raised, in interviews and working group meetings,
about a process included in CRAFT that asks the family member of the drinker how they think their
relative feels about his/her own drinking and what they believe their relative is thinking when
he/she drinks. Health care providers generally perceived this question to be inappropriate.
I’d always learnt in counseling that you don’t get people to theorise or hypothesise
about how someone else feels (health care provider 103).
...trying to get an understanding of what does your loved one think right before he
drinks?, or what does he feel right before he drinks? I think that’s going to be pretty
hard for people and I guess how accurate that’s going to be is a bit of a concern I think
(health care provider 106).
The role of organizational support
98
Health care providers felt well supported by their organization and identified this support as
important. Support and encouragement from managers and other team members increased their
motivation to continue with CRA and CRAFT counselor certification.
It was really good to sort of work in a team that was doing it together... we sort of
kept pushing each other along and we needed to keep going with it, because we were
all doing it together (health care provider 104).
Qualifications of counselors
Although CRA and CRAFT have previously been delivered, in different settings, by individuals who
hold a university degree and have completed CRA and CRAFT counselor certification, health care
providers generally held the view that individuals with different levels of qualifications could
effectively deliver the interventions once certified in the approaches.
...so long as you had those people skills and sort of the willingness to sort of learn
something different, and then to apply it. Sometimes I think there’s some resistance
to apply it, maybe from some lack of confidence. But that’s - I think that’s more down
to an individual, rather than their level of knowledge and experience...sometimes
probably experience is a more useful thing than having the university education
(health care provider 104).
One health care provider suggested that the manner in which certified counselors will deliver
intervention procedures is likely to be dependent upon their existing skills.
99
I think that there’s quite a lot of high level practice required to implement CRAFT in
the way that it’s intended...I think people will vary in the way they implement the
procedures (health care provider 103).
Adaptability of CRA and CRAFT for Aboriginal Australians
Health care providers were generally of the view that CRA and CRAFT could successfully be
delivered to Aboriginal Australians if it tailored to their needs, preferences and literacy levels.
So I find using this kind of model, an American model, for an Indigenous population, it
doesn’t quite fit with me at the moment...there’s components within this training...I
think will work for indigenous people (health care provider 103).
In particular, changing the language used to suit the Aboriginal Australian population was
mentioned in both the interviews and the working group meetings. History, low literacy and
Aboriginal-specific use of the English language were commonly identified as reasons for changing
the language to make it more appropriate to Aboriginal people.
We’re going to have to modify (CRA and CRAFT) a bit for...Australia, for the
clients...just the wording and that sort of stuff...maybe use some pictures (health care
provider 107).
...you’re working with people who live in these worlds of chaos, you’ve really got to
look at the language so that everyday people in that country can relate to it. So I think
it really needs to be - an Australian version of it really needs to be looked at. The
100
concepts are still the same but again, you need to look at it in a different way (health
care provider 102).
...(with Aboriginal people) you really need to look at what’s happened to them in the
past, how would you present this...I think it’s all doable with the Aboriginal
community, it’s just that the language might just need to be adapted a little bit to suit
them a bit better (health care provider 101).
Working group meetings and interviews were used to assess health care providers’ perceptions of
the CRA and CRAFT resources used to deliver the core procedures to clients. Overall the recourses
were believed to be useful, in particular, the Happiness Scale, that asks clients to rate health,
social, emotional and economic aspects of their life on a ten-point scale (1= completely unhappy,
10 = completely happy).
To maximize the likelihood of Aboriginal clients attending and completing the CRA and CRAFT
interventions it was suggested at working group meetings that less than eight sessions comprise
the Aboriginal-specific CRA and CRAFT interventions (the original United States based CRA and
CRAFT interventions are twelve sessions each), and that the interventions be available in a group
setting as well as to individuals, consistent with the usual model of care used by the health care
services.
Working group meetings with health care providers were used to gain feedback on early drafts of
the CRA and CRAFT manuals. Health care providers said that they wanted “...something to take
and something to refer to...not too detailed...more of a guideline” (working group meeting C).
101
When the final versions of the manuals were made available to health care providers for comment
and review their feedback was generally positive.
...(the manual) made it a lot easier to understand what each component was (health care
provider 106).
...the scenarios out of the manual...were good (health care provider 107).
Outcome measures
In tailoring CRA and CRAFT for delivery to Aboriginal Australians, the research team proposed
reliable and valid clinical alcohol measures that could be used to identify Aboriginal people likely
to benefit from CRA and CRAFT and assess the effectiveness of CRA and CRAFT for reducing
alcohol-related harms among those identified to be at risk. These outcome measures not only had
to be valid and reliable for the identification and assessment of Aboriginal people at risk, but also
acceptable to those health care providers who were responsible for administering them to
Aboriginal people, and feasible for them to do so in the context of routine practice. Health care
providers deemed the package of outcome measures originally proposed by researchers as too
lengthy and time consuming to complete. The package of outcome measures originally proposed
aimed to measure drug and alcohol consumption, and social, emotional and physical wellbeing.
The package of outcome measures comprised demographic questions, the Emotional
Empowerment Scale (EES14) (Haswell et al. 2010), K-5 (Cunningham & Paradies 2012), Growth
Empowerment Measure (GEM) scenarios (Haswell et al. 2010), Alcohol Use Disorders
Identification Test (AUDIT) (Saunders et al. 1993), frequency of illicit drug use, Assessment of
Quality of Life - 6D (AQoL-6D) (Allen et al. 2013), time spent caring for a problem drinking relative
102
(in CRAFT outcomes only), and health care service use questions. In response to health care
providers’ feedback, the package of outcome measures was revised to include demographics
questions, the Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST) (Humeniuk,
Ali & WHO ASSIST Phase II Study Group 2006), K-5 (Cunningham & Paradies 2012), GEM scenarios
(Haswell et al. 2010), and health care service use questions. The aims of the intervention
evaluation were not compromised by changes to the main outcome measures.
Recruitment options
Working group meetings G and H were used to identify and discuss recruitment options that
would have the potential to develop into ongoing referral pathways into CRA and CRAFT once
implemented into routine practice. Health care providers suggested a number of options including
through probation and parole, and other local health care services that do not currently provide
alcohol treatment services for Aboriginal Australians.
Discussion
CRA and CRAFT counselor certification involved a lengthy process that was positively reviewed by
health care providers at participating health care services. Initial challenges of time constraints
and reluctance to perform role plays were resolved by organising specific days to complete
certification measures and by ongoing organizational and peer support. Underfunding of
Aboriginal health care services (Allison, Rivers & Fottler 2004; Gray et al. 2010) often means that
employed health care providers have a large workload, and reiterates the importance of
organizations assigning a co-ordinator to ensure health care providers are motivated and given
time to participate in activities designed to improve their knowledge and skills to undertake their
103
professional role. Underfunding also affects continuity of staff employment (Adams et al. 2005). In
this study, high staff turnover prompted the establishment of a locally based training and
certification program run by the two certified CRA and CRAFT supervisors. In addition to training
days and reviewing audio-taped sessions, these supervisors have developed a system whereby a
certified CRAFT counselor delivering CRA or CRAFT group sessions is assisted by a counselor in
training, rather than another certified counselor. This process ensures new staff have exposure to
the delivery of CRA and CRAFT in practice while they are undertaking the certification process, and
increases the number of staff available to deliver the interventions.
CRA and CRAFT counselor certification were completed in the original United States versions of
CRA and CRAFT. The CRA and CRAFT concepts and resources were thought to be applicable to
Aboriginal Australians, when tailored specifically for this population group. In particular, technical
language needed to be changed to words more regularly used by Aboriginal Australians. In
response, CRA and CRAFT resources have been modified to include more appropriate language,
and clear formatting in large font. For example, “Who is your loved one usually with when
drinking?” was changed to “Who is your relative usually with when drinking?” (see Appendix E for
tailored CRA and CRAFT intervention resources). Aboriginal-specific CRA and CRAFT manuals were
developed in consultation with group meeting attendees and identified as important resources for
health care providers to refer to. The modified examples of how to deliver the interventions,
included in the manuals, presented CRA and CRAFT in the Australian context which helped health
care providers to translate the United States CRA and CRAFT interventions into an Aboriginal
Australian based model of care. Changing the contextual focus has been the aim of other research
projects tailoring CRA or CRAFT for minority groups (Villarreal 2008; Miller, Meyers & Hiller-
Sturmhofel 1999). For example, alcohol dependent Native Americans were reconnected with their

104
cultural spirituality through cultural practices, such as the talking circle, while participating in CRA
(Miller, Meyers & Hiller-Sturmhofel 1999). Other Aboriginal-specific interventions have also
focused on changing the context of an intervention, such as using story telling with parents and
children to improve behavioral problems and decrease parental psychological distress (Robinson
et al. 2012; Stock, Mares & Robinson 2012).
To ensure that CRA and CRAFT can be delivered in routine practice, Aboriginal-specific group
programs for CRA and CRAFT have been developed by CRAFT certified health care providers. These
group programs include the same content as the individual programs; however, the individual
programs are designed to use the core procedures in an order that is appropriate for each client
and the group programs presents the core procedures in a standardized order using a PowerPoint
presentation. Client workbook exercises are also included in the group programs. Clients attend six
group sessions and are given the opportunity to attend additional individual sessions if required.
Group delivery of intervention programs is appropriate for Aboriginal Australians and has been
successfully demonstrated by an Aboriginal-specific family-based intervention targeting parents
and children aimed at reducing Aboriginal disadvantage (Robinson et al. 2012; Stock, Mares &
Robinson 2012), and a healthy behaviours program promoted through an Aboriginal men’s group
(Bindon et al. 2009).
The variation in qualifications held by health care providers involved in CRA and CRAFT counselor
certification was not perceived to be a barrier for delivery but was believed to impact on how the
interventions would be delivered. This finding is consistent with studies exploring the optimum
mix of qualifications, experience and commitment required to effectively deliver CRAFT (Smith &

105
Meyers 2007). Two individuals have completed CRAFT supervisor certification, providing the
opportunity for ongoing local supervision of certified counselors to assist in intervention fidelity.
Limitations
The purpose of the interviews with health care providers was to explore their experiences of
participating in the process of tailoring CRA and CRAFT for Aboriginal Australians and undertaking
CRA and CRAFT counselor certification. Interviews were conducted with a small number of health
care providers from one drug and alcohol agency in NSW; however the sample represents 77%
(7/9) of all health care providers who had completed CRAFT certification and CRA training days at
the time of interviewing. Aboriginal Australian individuals were involved in the working group
meetings but none participated in the interviews, predominantly because they were no longer
working at the health care service, they were unable to participate in the certification process due
to competing priorities, or they appeared unwilling to participate due to fears and concerns they
would not be able to successfully complete to certification process. When health care services
who work with Aboriginal Australians become involved in research, changes are often required
within that service to accommodate the research process. Researchers must also make changes to
accommodate the delivery of interventions in a real world setting, as long as the changes do not
compromise the integrity and aims of the research.
The self-report nature of the data mean they are prone to bias, in particular social desirable
responding is likely. Social desirable responding is likely to have been minimized by anonymity
being assured to all participants, and interviews conducted in a private room (Hogan 2003).
Responses in working group meetings may have been biased by group think, but such data are
important for the modification of the CRA and CRAFT interventions.

106
Conclusion
CRA and CRAFT were tailored through an iterative process of which consultation between health
researchers and health care providers was a main component. The CRA and CRAFT counselor
certification process was perceived to be useful and informative to learn skills and build
confidence to deliver the interventions. The content of CRA and CRAFT were believed to be
appropriate for Aboriginal Australians; however core intervention procedures and methods for
their delivery required tailoring.
Acknowledgements
We would like to thank the health care providers for their participation in this project. Their
ongoing contributions have benefited this research greatly. This work was supported by a project
grant from the National Health and Medical Research Council and by the Australian Government
Department of Health and Ageing.
107
Paper 4
The acceptability to Aboriginal Australians of a family-based intervention to
reduce alcohol-related harms
Bianca Calabria1, Anton Clifford2,3, Anthony Shakeshaft1, Julaine Allan4,5, Donna Bliss6,
Christopher Dorn7,8
1. National Drug and Alcohol Research Centre, University of New South Wales, Sydney, New South Wales,
Australia
2. Institute of Urban Indigenous Health, Brisbane, Queensland, Australia
3. University of Queensland, Brisbane, Queensland, Australia
4. Lyndon Community, Orange, New South Wales, Australia
5. Centre for Inland Health, Charles Sturt University, Orange, New South Wales, Australia
6. Yoorana Gunya Family Violence Healing Centre Aboriginal Corporation, Forbes, New South Wales,
Australia
7. Hunter Medical Research Centre, University of Newcastle, Newcastle, New South Wales, Australia
8. Hunter Valley Research Foundation, Newcastle, New South Wales, Australia
Paper 4 has been published in Drug and Alcohol Review (Calabria et al. 2013).
108
Copyright Statement
I certify that this publication was a direct result of my research towards this PhD, and that
reproduction in this thesis does not breach copyright regulations.
Calabria, B, Clifford, A, Shakeshaft, A, Allan, J, Bliss, D & Doran, C 2013, 'The acceptability to
Aboriginal Australians of a family-based intervention to reduce alcohol-related harms', Drug and
Alcohol Review, vol. 32, no. 3, pp. 328-332.
Bianca Calabria August 2013

109
Preamble
Paper 3 presented the experiences of health care providers participating in CRA and CRAFT
counsellor certification, and their suggestions for tailoring the interventions to be more applicable
for Indigenous Australians (Calabria et al. submitted-a). This consultation process resulted in
modifications made to intervention resources and method of delivery. Health care providers were
self-declared advocates for the delivery of CRA and CRAFT to Indigenous Australians after
completing CRAFT counsellor certification and, although all had experience working with
Indigenous Australians, none were of Indigenous origin. Consequently, their perceptions of the
appropriateness of CRA and CRAFT for Indigenous Australians needed to be complemented with
the views and preferences of Indigenous Australian people themselves. Paper 4 presents the
perceptions of the Indigenous clients of participating health care services of the acceptability of
CRA and CRAFT for delivery in their local community, and their suggestions for tailoring both
interventions (Calabria et al. 2013).
110
Abstract
Introduction: Cognitive-behavioural interventions that utilise familial and community reinforcers in
an individual’s environment are effective for reducing alcohol-related harms. Such interventions
have considerable potential to reduce the disproportionately high burden of alcohol-related harm
among Aboriginal Australians if they can be successfully tailored to their specific needs and
circumstances.
Aim: The overall aim of this paper is to describe the perceived acceptability of two cognitive-
behavioural interventions, the Community Reinforcement Approach (CRA) and Community
Reinforcement and Family Training (CRAFT), to a sample of Aboriginal people.
Design and Methods: Descriptive survey administered to 116 Aboriginal people recruited through
an Aboriginal Community Controlled Health Service and a community-based drug and alcohol
treatment agency in rural New South Wales, Australia.
Results: Participants perceived CRA and CRAFT to be highly acceptable for delivery in their local
Aboriginal community. Women were more likely than men to perceive CRAFT as highly acceptable.
Participants expressed a preference for counsellors to be someone they knew and trusted, and
who has experience working in their local community. CRA was deemed most acceptable for
delivery to individuals after alcohol withdrawal and CRAFT for people who want to help a
relative/friend start alcohol treatment. There was a preference for five or more detailed sessions.
Discussion and Conclusions: Findings of this study suggest that CRA and CRAFT are likely to be
acceptable for delivery to some rural Aboriginal Australians, and that there is potential to tailor
these interventions to specific communities.

111
Introduction
Aboriginal Australians experience a disproportionately high burden of alcohol-related harm
relative to the general Australian population (Calabria et al. 2010). Cognitive-behavioural
interventions that utilise positive familial and community reinforcers for low-risk drinking have
proven to be effective for reducing alcohol-related harms and improving the social and emotional
wellbeing of at-risk drinkers (Calabria et al. 2012; Miller & Wilbourne 2002). The influential role of
family and community factors in modifying health risk behaviours among Aboriginal people is
widely acknowledged (Australian Government Department of Health and Ageing 2007; Nagel &
Thompson 2010), and suggests that integrating these factors into cognitive-behavioural
interventions is likely to be effective for reducing alcohol-related harms among Aboriginal
Australians.
The Community Reinforcement Approach (CRA) uses social, familial and recreational positive
reinforcers to modify the behaviour of problem drinkers and is ranked among the most effective
cognitive-behavioural interventions (Meyers & Smith 1995; Miller & Wilbourne 2002). A family-
focused version of CRA, Community Reinforcement and Family Training (CRAFT) (Smith & Meyers
2007), is likely to be highly relevant to Aboriginal communities because it teaches practical skills to
family members of treatment resistant problem drinkers. Specifically, it aims to improve their own
health and well-being and assist them to encourage their problem drinking relative into treatment.
This study identifies the extent to which CRA and CRAFT are acceptable to Aboriginal Australians,
their preferences for how CRA and CRAFT ought to be delivered and a process of tailoring these
interventions for Aboriginal people.
112
Methods
Ethics
Ethics approval for the study was granted by the Human Research Ethics Committee, University of
New South Wales (NSW), the Ethics Committee of the Aboriginal Health and Medical Research
Council, NSW, and the board of the participating Aboriginal Community Controlled Health Service
(ACCHS). A steering committee, including Aboriginal health workers and researchers who live in
the participating communities, oversaw the over-arching project of which this study is a part.
Setting and participants
Aboriginal participants who were over 18 years of age were recruited through existing groups
organised by one ACCHS and new clients of a community-based drug and alcohol treatment
agency in rural NSW, from July 2010 to June 2011, by researchers or Aboriginal health workers.
Participants were reimbursed $A40 to cover out-of-pocket travel expenses.
The survey
Survey development. The survey was adapted from the Treatment Acceptability Questionnaire
(Hunsley 1992) in consultation with health service staff, non-Aboriginal and Aboriginal researchers,
and Aboriginal clients of the participating drug and alcohol agency. The survey was initially
administered to four Aboriginal people, who were either receiving treatment or who had recently
completed treatment for alcohol use problems, to assess its appropriateness and
comprehensibility.
113
Overall acceptability of CRA and CRAFT was assessed using a 5-point Likert scale (1 = very bad, 5 =
very good) by asking ‘what do you think about CRA/CRAFT being delivered in your community?’
The acceptability of intervention delivery in rural settings was assessed as ‘okay’ or ‘not okay’.
Participants’ drinking risk status was measured, using the Alcohol Use Disorders Identification Test
(AUDIT) (Conigrave et al. 2012; Saunders et al. 1993; Saunders & Aasland 1987), to determine the
extent to which their drinking status was associated with their preferences for CRA and CRAFT
delivery.
Survey administration. Key information on CRA and CRAFT interventions was initially presented to
participants by a researcher or Aboriginal health worker, including the target client population, the
overall purpose, the therapeutic approach and the mode of delivery. Participants then self-
completed the survey (with literacy support available). Space was provided for participants to
write down additional comments. Survey completion was voluntary and responses confidential
(see Appendix F for survey advertising poster, Appendix G for participant study information sheet,
Appendix H for the survey, Appendix I for slides used by researchers or Aboriginal Health Workers
to standardise the presentation of intervention and survey information, and Appendix J for group
attendance record sheet).
Data analysis
Given few participants rated the acceptability of CRA and CRAFT as 1, 2 or 3, multinomial logistic
regression analyses were not appropriate. Consequently, ratings of the acceptability of CRA and
CRAFT were dichotomously coded as ‘bad’ (1 to 3) or ‘good’ (4 and 5). Predictors of ‘good’
[gender, drinking status (not/at risk or high risk drinker), family member drinking problem
(no/family member with a drinking problem), and health service (ACCHS/drug and alcohol

114
treatment agency)] were identified for CRA and for CRAFT, using separate binary logistic
regressions (Hosmer & Lemeshow 2000). Additional comments were examined for themes.
Results
The sample consisted of 116 Aboriginal Australians (n = 110) or non-Aboriginal Australians who
have an Aboriginal spouse and/or child (n = 6). Eleven individuals who completed the survey were
excluded because they were non-Aboriginal without an Aboriginal spouse or child. The response
rate was 94% (116/124). Table 1 shows the demographic characteristics of participants, 95% of
whom rated CRA as acceptable and 90% of whom rated CRAFT as acceptable. Women were more
likely than men to rate CRAFT as ‘good’ (odds ratio = 0.07, 95%CI = 0.01 – 0.56). Table 2 shows
that CRA was more acceptable as a post-withdrawal, rehabilitation or incarceration option and
CRAFT was more acceptable for people who want to help a problem-drinking relative/friend start
alcohol treatment. Preference was for a counsellor who was known and trusted, with experience
working in the local community.
Increased access to follow-up support (listed six times) and more interventions for young people
(listed seven times) were the most common additional comment by participants (see Appendix K
for additional methods and results not included in the published paper).
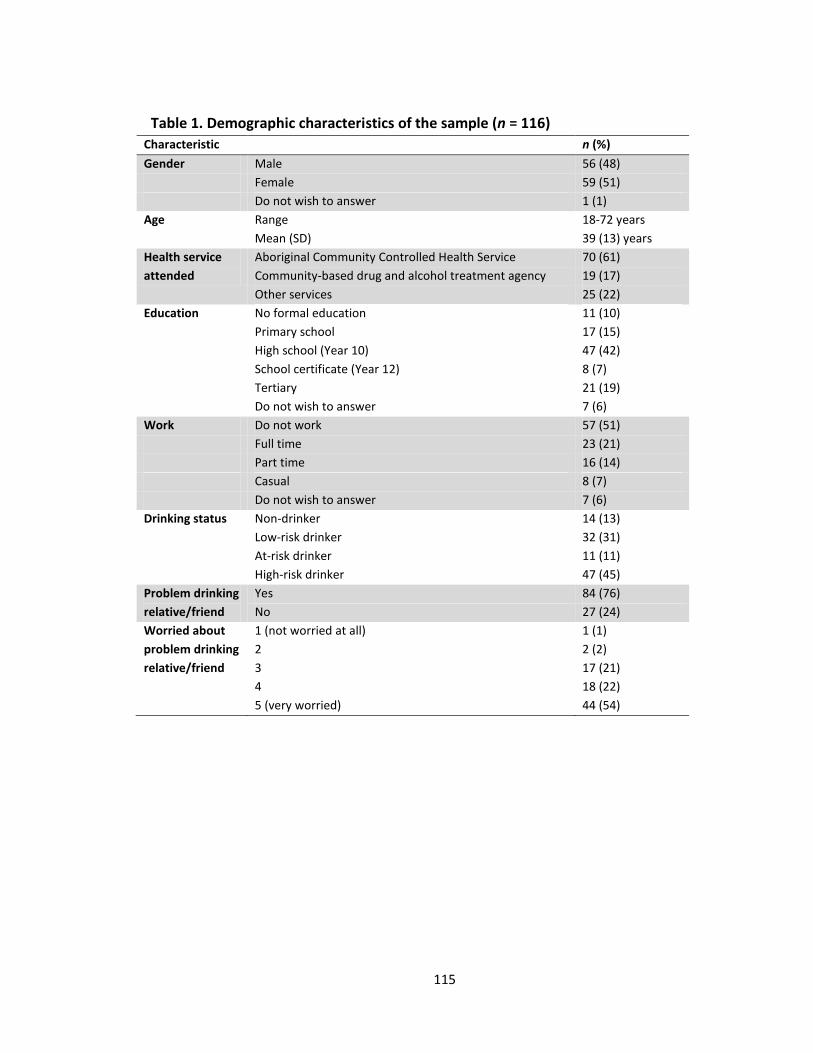
115
Table 1. Demographic characteristics of the sample (n = 116)
Characteristic n (%)
Gender Male 56 (48)
Female 59 (51)
Do not wish to answer 1 (1)
Age Range 18-72 years
Mean (SD) 39 (13) years
Health service
attended
Aboriginal Community Controlled Health Service 70 (61)
Community-based drug and alcohol treatment agency 19 (17)
Other services 25 (22)
Education No formal education 11 (10)
Primary school 17 (15)
High school (Year 10) 47 (42)
School certificate (Year 12) 8 (7)
Tertiary 21 (19)
Do not wish to answer 7 (6)
Work Do not work 57 (51)
Full time 23 (21)
Part time 16 (14)
Casual 8 (7)
Do not wish to answer 7 (6)
Drinking status Non-drinker 14 (13)
Low-risk drinker 32 (31)
At-risk drinker 11 (11)
High-risk drinker 47 (45)
Problem drinking
relative/friend
Yes 84 (76)
No 27 (24)
Worried about
problem drinking
relative/friend
1 (not worried at all) 1 (1)
2 2 (2)
3 17 (21)
4 18 (22)
5 (very worried) 44 (54)
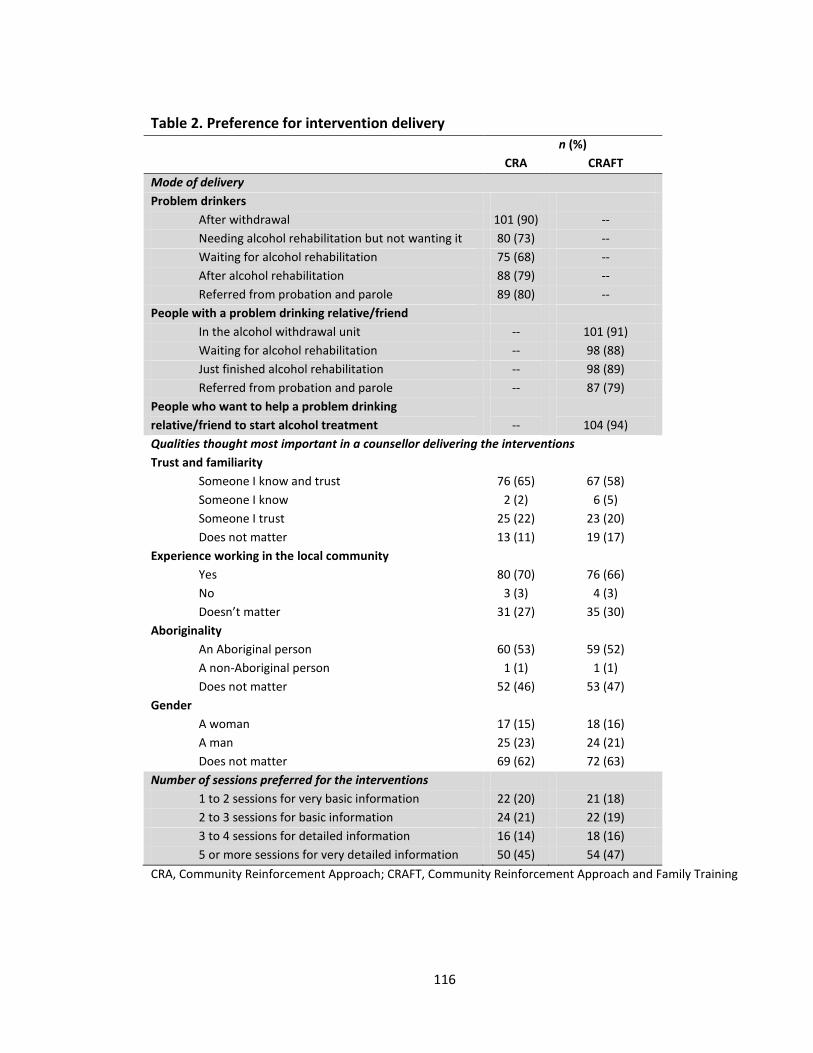
116
Table 2. Preference for intervention delivery
n (%)
CRA CRAFT
Mode of delivery
Problem drinkers
After withdrawal 101 (90) --
Needing alcohol rehabilitation but not wanting it 80 (73) --
Waiting for alcohol rehabilitation 75 (68) --
After alcohol rehabilitation 88 (79) --
Referred from probation and parole 89 (80) --
People with a problem drinking relative/friend
In the alcohol withdrawal unit -- 101 (91)
Waiting for alcohol rehabilitation -- 98 (88)
Just finished alcohol rehabilitation -- 98 (89)
Referred from probation and parole -- 87 (79)
People who want to help a problem drinking
relative/friend to start alcohol treatment
--
104 (94)
Qualities thought most important in a counsellor delivering the interventions
Trust and familiarity
Someone I know and trust 76 (65) 67 (58)
Someone I know 2 (2) 6 (5)
Someone I trust 25 (22) 23 (20)
Does not matter 13 (11) 19 (17)
Experience working in the local community
Yes 80 (70) 76 (66)
No 3 (3) 4 (3)
Doesn’t matter 31 (27) 35 (30)
Aboriginality
An Aboriginal person 60 (53) 59 (52)
A non-Aboriginal person 1 (1) 1 (1)
Does not matter 52 (46) 53 (47)
Gender
A woman 17 (15) 18 (16)
A man 25 (23) 24 (21)
Does not matter 69 (62) 72 (63)
Number of sessions preferred for the interventions
1 to 2 sessions for very basic information 22 (20) 21 (18)
2 to 3 sessions for basic information 24 (21) 22 (19)
3 to 4 sessions for detailed information 16 (14) 18 (16)
5 or more sessions for very detailed information 50 (45) 54 (47)
CRA, Community Reinforcement Approach; CRAFT, Community Reinforcement Approach and Family Training

117
Discussion
Both CRA and CRAFT were highly acceptable to Aboriginal people. Counsellors who were known
and trusted, and delivery of five or more sessions, were preferred. CRA was deemed most
acceptable for individuals post alcohol withdrawal, and CRAFT for those wanting to help a
relative/friend start alcohol treatment. Improved follow-up support and more interventions for
young people were identified most frequently as important.
Recommended tailoring of each intervention
First, health workers who are known and trusted by the community should be available to deliver
CRA and CRAFT interventions. Health workers building trusting relationships with Aboriginal
community members has been shown to increase access to drug and alcohol services (Allan &
Campbell 2011) and, as a minimum, provides an alternative for those Aboriginal Australians whose
preference for a known counsellor outweighs their confidentiality concerns (Vicary & Westerman
2004). Second, five or more detailed sessions should be offered, which is consistent with findings
that the median number of CRAFT sessions attended is 4.7 (Miller, Meyers & Tonigan 1999). Third,
the tailored interventions should include follow-up support for participants, a need that has been
recognised through government consultations with Indigenous communities (Kurti et al. 2009).
Fourth, there is a need for the interventions to be available for young people, which reflects the
findings of a recent review that found no methodologically rigorous evaluations of interventions
targeting young people at high risk of alcohol-related harm that have a broader focus than the
individual (Calabria, Shakeshaft & Havard 2011). Given a CRA intervention designed specifically for
adolescents has been found to improve outcomes in non-Aboriginal groups (Dennis et al. 2004;
Slesnick et al. 2007), its acceptability to Aboriginal adolescents should be examined.

118
Limitations
A convenience sample was recruited, resulting in a sample of Aboriginal people likely to access
interventions through the participating health services and a high response rate (94%), as well as
under-representation of high-risk individuals resistant to treatment. Although 5% of the sample
perceived CRA as unacceptable and 10% perceived CRAFT as unacceptable, these relatively small
proportions suggest alternative interventions ought to be made available for them, rather than
further adaptation of CRA or CRAFT. Self-report data are prone to biases, even when bias is
minimised by using psychometrically validated tools (Hogan 2003). Repeating the survey after
trialling the intervention would provide further evidence about the acceptability of CRA and CRAFT
in practice.
Conclusion
The CRA and CRAFT interventions were acceptable to the majority of Aboriginal people recruited
through a rural ACCHS and a community-based drug and alcohol treatment agency, which has
both reinforced that a trial of their cost-effectiveness is warranted and helped tailor the specific
versions of the interventions to local Aboriginal communities.
Acknowledgements
We would like to thank the participating services (Lyndon Community and Yoorana Gunya Family
Violence Healing Centre Aboriginal Corporation), communities and their members for their
support and input, without which this research would not be possible. The CEOs of the
participating services have approved publication of these results in this format. We gratefully
acknowledge Barbara Toson for providing statistical advice. This work was supported by the

119
Australian Government Department of Health and Ageing and by a linkage grant from the
Australian Research Council.
120
Points of clarification for Paper 4
Drug and Alcohol Review owns the copyright of this published paper. The points of clarification
have been added to provide additional information about the research for this thesis without
modifying the content of the published paper.
Table 1
The number of responses in Table 1 varies depending on missing data, with the exception of the
‘worried about problem drinking relative/friend’ which was only applicable to participants who
indicated that they had a problem drinking relative/friend.
Predictors of acceptability
Predictors of the acceptability of CRA and CRAFT were investigated using separate binary logistic
regressions (gender, drinking status, family member drinking problem, health service). The
analysis using gender had the only significant result. Non-significant results were not reported in
the paper.
121
Paper 5
Epidemiology of alcohol-related burden of disease among Indigenous
Australians
Bianca Calabria1, Christopher M Doran1, Theo Vos2, Anthony P Shakeshaft1,3 Wayne Hall4
1. National Drug and Alcohol Research Centre, University of New South Wales, Sydney, Australia
2. School of Population Health, University of Queensland, Brisbane, Queensland, Australia
3. Sax Institute, University of Technology, Sydney, New South Wales, Australia
4. University of Queensland Centre for Clinical Research, Brisbane, Queensland, Australia
Paper 5 has been published in the Australian and New Zealand Journal of Public Health (Calabria et
al. 2010).
122
Copyright Statement
I certify that this publication was a direct result of my research towards this PhD, and that
reproduction in this thesis does not breach copyright regulations.
Calabria, B, Doran, CM, Vos, T, Shakeshaft, AP & Hall, W 2010, 'Epidemiology of alcohol-related
burden of disease among Indigenous Australians', Australian and New Zealand Journal of Public
Health, vol. 34, no. S1, pp. S47-S51.
Bianca Calabria August 2013

123
Preamble
Paper 4 demonstrated the high level of perceived acceptability of CRA and CRAFT by Indigenous
clients of an Aboriginal Community Controlled Health Service and a rural drug and alcohol
treatment agency in New South Wales, for delivery in their community (Calabria et al. 2013).
Additionally, Paper 4 identified a perceived need among a sample of rural Indigenous Australians
for interventions to reduce alcohol-related harms among Indigenous young people. As a result,
Paper 5 examines alcohol-related harms experienced by Indigenous people by age and sex,
compared to the general population of Australia, in order to determine differences in the
magnitude and type of alcohol-related harms experienced by young Indigenous people versus
other age groups (Calabria et al. 2010).

124
Abstract
Objective: To compare the burden of alcohol-related harm and underlying factors of this harm, by
age and sex, for Indigenous and general population Australians.
Methods: Population attributable fractions are used to estimate the disability adjusted life years
(DALYs) for alcohol-related disease and injury. The DALYs were converted to rates per 1,000 by age
and sex for the Indigenous and general populations.
Results: Homicide and violence rates were much higher for Indigenous males: greatest population
difference was for 30-44 years, Indigenous rate 8.9 times higher. Rates of suicide were also
greater: the largest population difference was for 15-29 years, Indigenous rate 3.9 times higher.
Similarly for Indigenous females, homicide and violence rates were much higher: greatest
population difference was for 30-44 years, Indigenous rate 18.1 times higher. Rates of suicide
were also greater: the largest population difference was for 15-29 years, Indigenous rate 5.0 times
higher.
Conclusions: Alcohol consumption and associated harms are of great concern for Indigenous
Australians across all ages. Violent alcohol-related harms have been highlighted as a major
concern.
Implications: To reduce the disproportionate burden of alcohol-related harm experienced by
Indigenous Australians, targeted interventions should include the impact on families and
communities and not just the individual.
125
Introduction
Although the deleterious impact of alcohol on Indigenous Australians and their communities has
been extensively documented (Australian Bureau of Statistics & Australian Institute of Health and
Welfare 2005; Australian Bureau of Statistics & Australian Institute of Health and Welfare 2008;
Australian Department of Human Services and Health 1995; Australian Government Department
of Health and Ageing 2007; Chikritzhs, Fillmore & Stockwell 2009; Gray et al. 1997), obtaining
accurate estimates of the extent of harm across a range of health indicators (including death,
hospitalisations, quality of life and social costs) has been challenging. One approach to this task
has been to use Disability Adjusted Life Years (DALYs), a summary measure of health that
combines years of life lost (YLL) and years lived with disability (YLD) as a consequence of a disease
or injury.
Two reports using DALYs to describe the drug and alcohol-related burden of disease and injury in
Australia have recently been published: one for Australia generally (Begg et al. 2007); and one
specific to Indigenous Australians (Vos et al. 2003). In the general Australian population, alcohol is
responsible for 3.3%, and prevents 1% of the total disease burden, a net effect of 2.3%, equivalent
to 61,091 DALYs and 0.8% (1,084) of all deaths (Begg et al. 2007). For Indigenous Australians,
alcohol harm causes 6.2%, and prevents 0.8% of the total burden, a net effect of 5.4% (5,171) of
DALYs and 6.7% (192) of all deaths (Vos et al. 2003). The disproportionate burden of alcohol-
related harm experienced by Indigenous people results in an estimated life expectancy of 15 years
less, on average, than in the general population (Vos et al. 2003).
Using DALY estimates as the basis for developing, implementing and evaluating policies and
interventions will be critical given the clear lack of Indigenous alcohol intervention research to
126
date (Sanson-Fisher et al. 2006). Such policies and interventions, however, are likely to be more
effective if they are tailored to specific sub-populations and disease types (Sackett et al. 1996;
Ockene et al. 2007), rather than remaining restricted to broad-based, population-level
comparisons between general population and Indigenous Australians. This paper aims to compare
alcohol consumption DALYs for Indigenous and general population Australians by age and sex and
by disease or injury related to use.
Method
The methodology has been described in detail elsewhere (Begg et al. 2007; Vos et al. 2003; 2008);
a summary follows. The population attributable fraction (PAF), representing the expected
proportional reduction in mortality if alcohol exposure were reduced to an alternative
(counterfactual) distribution, was calculated before determining the number of attributed deaths.
The PAF uses the exposure level, actual population distribution of the exposure; counterfactual
(alternative) population distribution of the exposure, relative risk of mortality at exposure level
and maximum exposure level (see equations 1A for continuous exposures and 1B for categorical
exposures).
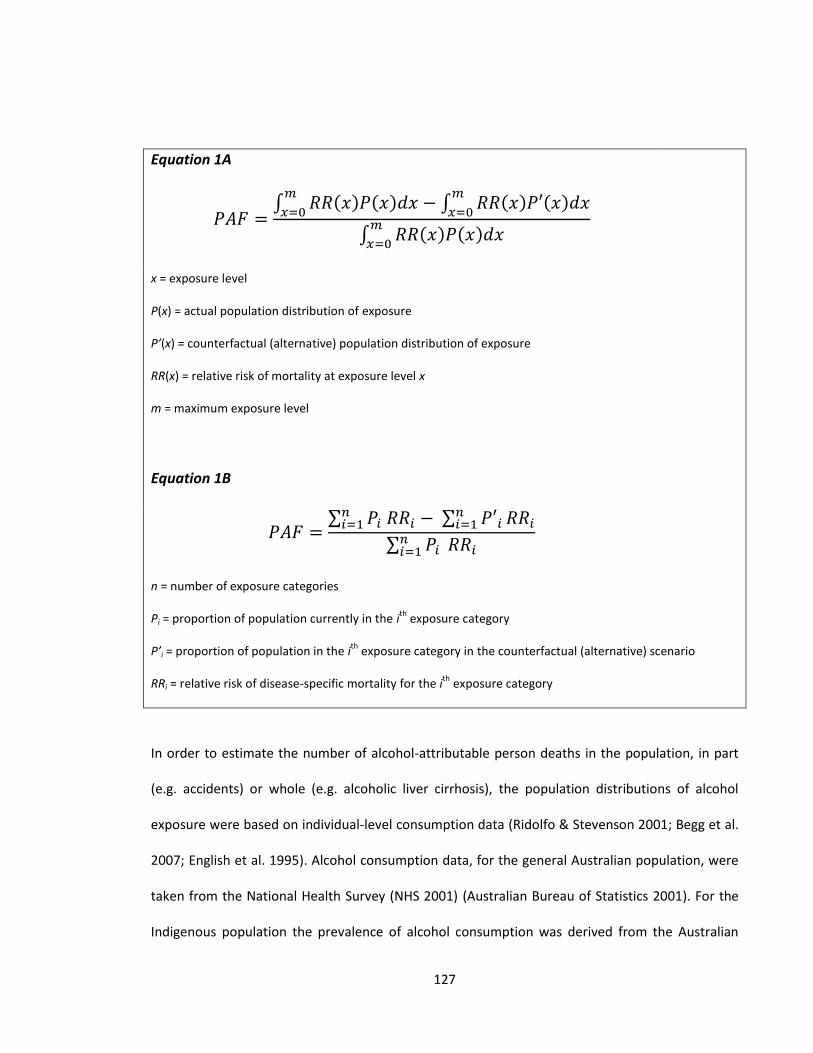
127
Equation 1A
∫ ( ) ( )
∫ ( ) ( )
∫ ( ) ( )
x = exposure level
P(x) = actual population distribution of exposure
P’(x) = counterfactual (alternative) population distribution of exposure
RR(x) = relative risk of mortality at exposure level x
m = maximum exposure level
Equation 1B
∑ ∑
∑
n = number of exposure categories
Pi = proportion of population currently in the ith
exposure category
P’i = proportion of population in the ith
exposure category in the counterfactual (alternative) scenario
RRi = relative risk of disease-specific mortality for the ith
exposure category
In order to estimate the number of alcohol-attributable person deaths in the population, in part
(e.g. accidents) or whole (e.g. alcoholic liver cirrhosis), the population distributions of alcohol
exposure were based on individual-level consumption data (Ridolfo & Stevenson 2001; Begg et al.
2007; English et al. 1995). Alcohol consumption data, for the general Australian population, were
taken from the National Health Survey (NHS 2001) (Australian Bureau of Statistics 2001). For the
Indigenous population the prevalence of alcohol consumption was derived from the Australian
128
Bureau of Statistics National Aboriginal and Torres Strait Islander Health Survey (NATSIHS) 2004-05
(Australian Bureau of Statistics 2006). Prevalence of alcohol consumption was categorised into the
four levels used in English and colleagues’ analysis of the risks of alcohol consumption (English et
al. 1995), in accordance with the NHMRC’s recommendations on alcohol consumption (National
Health and Medical Research Council 1992). The population distributions of alcohol exposure for
each level of alcohol intake were estimated by age and sex for both Indigenous and general
population Australians.
Relative risks and PAFs from Ridolfo and Stevenson (Ridolfo & Stevenson 2001) were used for
conditions for which there is evidence of causation by alcohol consumption. Included in these
estimates are harms, i.e., injury or diseases, that are causally related and completely attributed to
alcohol exposure as well as related harms that are causally but not solely attributed to alcohol
exposure (contributing factors) (Rehm et al. 2004).
The following diseases and injuries were included: ischemic heart disease; other cardiovascular
disease (CVD) (including stroke, hypertensive heart disease and inflammatory heart disease);
cancer; road traffic accidents; homicide and violence; suicide (including self-inflicted injuries);
alcohol use disorders (including dependence, harmful use, alcoholic cirrhosis); and other (including
fire, burns and scalds, gallbladder and bile duct disease, surgical and medical misadventure,
striking and crushing accidents, poisoning, cutting and piercing accidents, sports injuries, other
transport accidents, natural and environmental factors, machinery accidents, suffocation and
foreign bodies, drowning, pancreatitis, and falls).
129
Age standardisation was applied to DALYs to account for the variation in age structure between
Indigenous and the general population, resulting in comparable age specific estimates. The DALYs
for alcohol-related harm and contributing factors were converted to rates per 1,000 by age and
sex for the Indigenous and general populations.
Results
Alcohol-related burden of harm
Rates of alcohol-related harm among Indigenous males are three times higher than in the general
Australian population: rates were more than twice as high for Indigenous males aged 0-29 years
and more than three times higher thereafter. Rates for Indigenous females were seven times
higher than general population females, consistently more than five times higher from age 15-59
years (see Table 1).
Contributing factors to alcohol injury and disease
Males. In terms of underlying alcohol-related disease and injury, rates of DALYs for Indigenous
males were higher than general population males across all age groups (see Figure 1, Table 1).
Road traffic accidents were the main contributing factor for alcohol-related harm in Indigenous
males aged 0-14 years (2.3 times higher). Homicide and violence rates were much higher for
Indigenous males: 6.1 times higher for 15-29 year olds; 8.9 times higher for 30-44 year olds; 7.5
times higher for 45-59 year olds; and 5.0 times higher for 60 years or more. Rates of suicide were
also greater for Indigenous males: the largest difference between populations was for 15-29 year
olds with the Indigenous rate 3.9 times higher. Alcohol use disorders made a larger contribution in
later years of life with rates 5.8 times higher for 45-59 year olds and 4.8 times higher for
130
Indigenous males aged 60 years or more. On the positive side, the protective effects of ischemic
heart disease were higher in Indigenous males compared to the general population: 6.6 times
higher for 15-29 year olds; 8.3 times higher for 30-44 year olds; 4.0 times higher for 45-59 year
olds; and 2.0 times higher for 60 years or more (see Table 1).
Females. Among Indigenous females, rates of DALYs were higher than general population females
(with the exception of similar rates for both groups for cancer) across all age groups (see Figure 2,
Table 1). Similarly to Indigenous males, road traffic accidents were the main contributor to
alcohol-related harm for Indigenous females aged 0-14 years (2.4 times higher). Homicide and
violence rates were much higher for Indigenous females: 13.9 times higher for 15-29 year olds;
18.1 times higher for 30-44 year olds; 6.0 times higher for 45-59 year olds; and 20.7 times higher
for 60 years of more. Rates of suicide were also greater for Indigenous females: the largest
difference between populations was for 15-29 year olds with the Indigenous rate 5.0 times higher.
Alcohol use disorders made a larger contribution later in life with rates 10.9 times higher for 45-59
year olds and 9.9 times higher for Indigenous females aged 60 years or more.
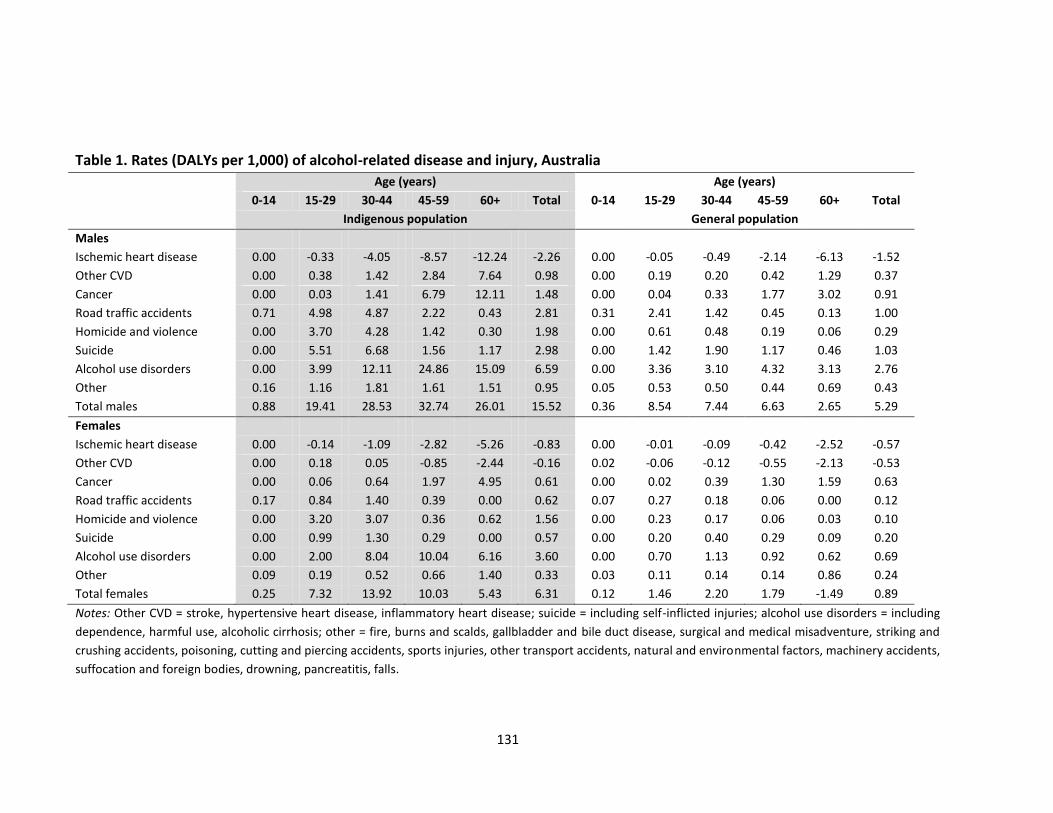
131
Table 1. Rates (DALYs per 1,000) of alcohol-related disease and injury, Australia
Age (years) Age (years)
0-14 15-29 30-44 45-59 60+ Total 0-14 15-29 30-44 45-59 60+ Total
Indigenous population General population
Males
Ischemic heart disease 0.00 -0.33 -4.05 -8.57 -12.24 -2.26 0.00 -0.05 -0.49 -2.14 -6.13 -1.52
Other CVD 0.00 0.38 1.42 2.84 7.64 0.98 0.00 0.19 0.20 0.42 1.29 0.37
Cancer 0.00 0.03 1.41 6.79 12.11 1.48 0.00 0.04 0.33 1.77 3.02 0.91
Road traffic accidents 0.71 4.98 4.87 2.22 0.43 2.81 0.31 2.41 1.42 0.45 0.13 1.00
Homicide and violence 0.00 3.70 4.28 1.42 0.30 1.98 0.00 0.61 0.48 0.19 0.06 0.29
Suicide 0.00 5.51 6.68 1.56 1.17 2.98 0.00 1.42 1.90 1.17 0.46 1.03
Alcohol use disorders 0.00 3.99 12.11 24.86 15.09 6.59 0.00 3.36 3.10 4.32 3.13 2.76
Other 0.16 1.16 1.81 1.61 1.51 0.95 0.05 0.53 0.50 0.44 0.69 0.43
Total males 0.88 19.41 28.53 32.74 26.01 15.52 0.36 8.54 7.44 6.63 2.65 5.29
Females
Ischemic heart disease 0.00 -0.14 -1.09 -2.82 -5.26 -0.83 0.00 -0.01 -0.09 -0.42 -2.52 -0.57
Other CVD 0.00 0.18 0.05 -0.85 -2.44 -0.16 0.02 -0.06 -0.12 -0.55 -2.13 -0.53
Cancer 0.00 0.06 0.64 1.97 4.95 0.61 0.00 0.02 0.39 1.30 1.59 0.63
Road traffic accidents 0.17 0.84 1.40 0.39 0.00 0.62 0.07 0.27 0.18 0.06 0.00 0.12
Homicide and violence 0.00 3.20 3.07 0.36 0.62 1.56 0.00 0.23 0.17 0.06 0.03 0.10
Suicide 0.00 0.99 1.30 0.29 0.00 0.57 0.00 0.20 0.40 0.29 0.09 0.20
Alcohol use disorders 0.00 2.00 8.04 10.04 6.16 3.60 0.00 0.70 1.13 0.92 0.62 0.69
Other 0.09 0.19 0.52 0.66 1.40 0.33 0.03 0.11 0.14 0.14 0.86 0.24
Total females 0.25 7.32 13.92 10.03 5.43 6.31 0.12 1.46 2.20 1.79 -1.49 0.89
Notes: Other CVD = stroke, hypertensive heart disease, inflammatory heart disease; suicide = including self-inflicted injuries; alcohol use disorders = including
dependence, harmful use, alcoholic cirrhosis; other = fire, burns and scalds, gallbladder and bile duct disease, surgical and medical misadventure, striking and
crushing accidents, poisoning, cutting and piercing accidents, sports injuries, other transport accidents, natural and environmental factors, machinery accidents,
suffocation and foreign bodies, drowning, pancreatitis, falls.
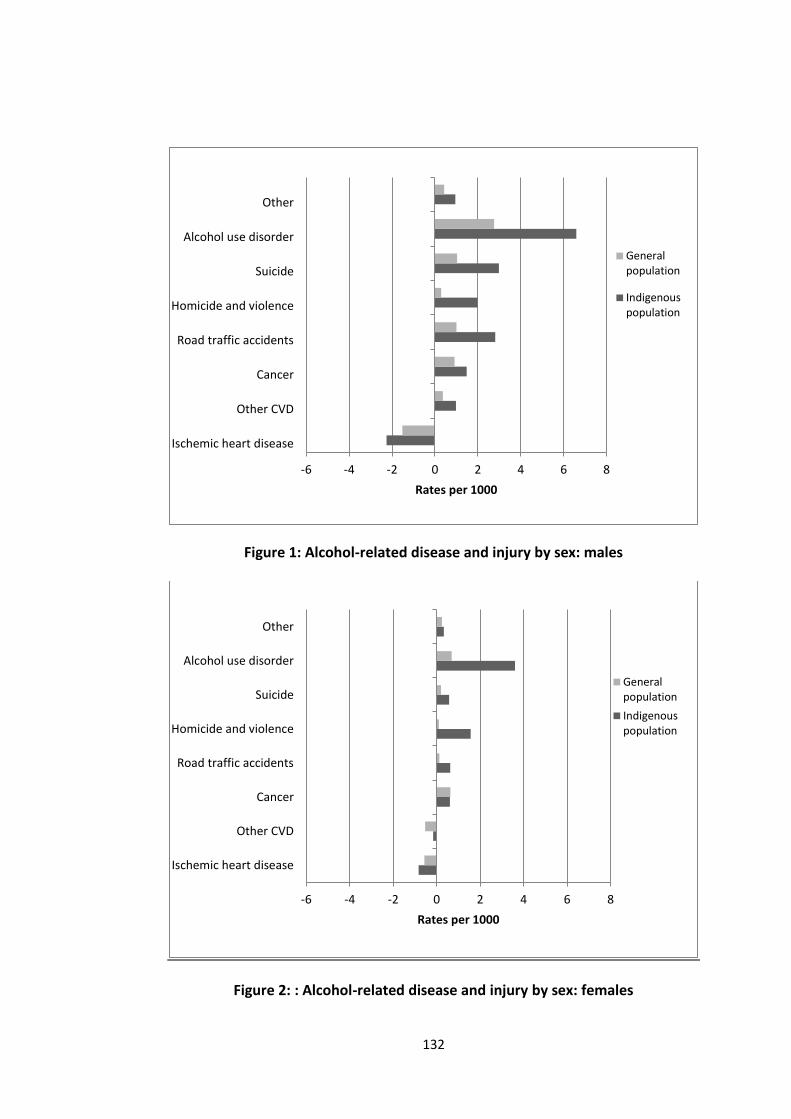
132
Figure 1: Alcohol-related disease and injury by sex: males
Figure 2: : Alcohol-related disease and injury by sex: females
-6 -4 -2 0 2 4 6 8
Ischemic heart disease
Other CVD
Cancer
Road traffic accidents
Homicide and violence
Suicide
Alcohol use disorder
Other
Rates per 1000
Generalpopulation
Indigenouspopulation
-6 -4 -2 0 2 4 6 8
Ischemic heart disease
Other CVD
Cancer
Road traffic accidents
Homicide and violence
Suicide
Alcohol use disorder
Other
Rates per 1000
Generalpopulation
Indigenouspopulation
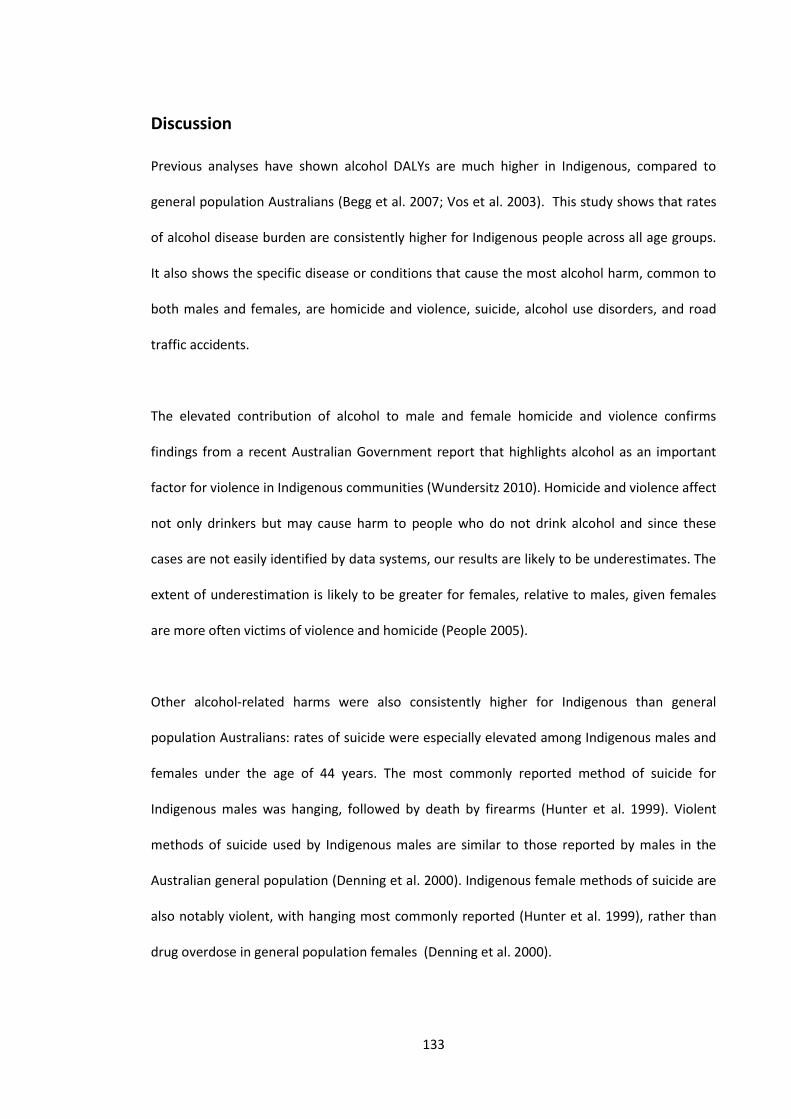
133
Discussion
Previous analyses have shown alcohol DALYs are much higher in Indigenous, compared to
general population Australians (Begg et al. 2007; Vos et al. 2003). This study shows that rates
of alcohol disease burden are consistently higher for Indigenous people across all age groups.
It also shows the specific disease or conditions that cause the most alcohol harm, common to
both males and females, are homicide and violence, suicide, alcohol use disorders, and road
traffic accidents.
The elevated contribution of alcohol to male and female homicide and violence confirms
findings from a recent Australian Government report that highlights alcohol as an important
factor for violence in Indigenous communities (Wundersitz 2010). Homicide and violence affect
not only drinkers but may cause harm to people who do not drink alcohol and since these
cases are not easily identified by data systems, our results are likely to be underestimates. The
extent of underestimation is likely to be greater for females, relative to males, given females
are more often victims of violence and homicide (People 2005).
Other alcohol-related harms were also consistently higher for Indigenous than general
population Australians: rates of suicide were especially elevated among Indigenous males and
females under the age of 44 years. The most commonly reported method of suicide for
Indigenous males was hanging, followed by death by firearms (Hunter et al. 1999). Violent
methods of suicide used by Indigenous males are similar to those reported by males in the
Australian general population (Denning et al. 2000). Indigenous female methods of suicide are
also notably violent, with hanging most commonly reported (Hunter et al. 1999), rather than
drug overdose in general population females (Denning et al. 2000).

134
Limitations
There is an urgent need to improve the evidence base for alcohol policy in Australia
(Shakeshaft, Doran & Byrnes 2009). Although this research is based on epidemiological studies
that apply an accepted methodology, the underlying data used to calculate alcohol-related
harm are drawn from a range of sources from varying quality including: specific Indigenous and
general population alcohol prevalence data; relative risks from international literature for
chronic diseases; Australian general population data on alcohol-related injuries; and variety of
other sources that were predominantly Australian. Self-reported consumption data used are
prone to biases (Hogan 2003): however, this method of estimating alcohol-attributed deaths
has been commonly used (Ridolfo & Stevenson 2001; English et al. 1995). Although estimates
of alcohol disease and injury include a wide range of conditions, they are likely to be an
underestimate of the true proportion of alcohol-related harm because: 1) they exclude
alcohol-related injuries experienced by individuals who have not consumed alcohol, primarily
because there are no valid and reliable estimates of the extent of alcohol harm experienced by
non-drinking victims; and 2) it is likely that not all perpetrators who have consumed alcohol
are identified. Few direct data sources for Indigenous estimates were found so relativities
found in proxy measurements were largely used (Begg et al. 2007; Vos et al. 2003). Further,
the data from the Australia Burden of Disease and Injury study (Begg et al. 2007) did not
explicitly separate Indigenous from non-Indigenous populations. The substantial alcohol-
related harm reported in these studies reinforces the need for improved data collection.
Policy implications
Information is available on potential strategies to reduce alcohol harm, although most of the
recent studies tend to focus on strategies to curb alcohol-misuse in the general population,
such as changes to the taxation of alcoholic beverages (Cobiac et al. 2009; Byrnes et al. 2010).
The cost-effective population-wide approaches to reducing alcohol harm would be improved
135
by implementing complementary interventions tailored specifically to high-risk sub-
populations or diseases and conditions (Doran et al. 2010). The analyses in this paper suggest
interventions that focus on reducing homicide and violence in Indigenous males and females,
and with specific attention to lowering rates of suicide for Indigenous males and decreasing
the number of Indigenous females who have an alcohol use disorder, are most likely to have
the biggest impact in reducing alcohol-related harm for Indigenous Australians and their
communities (Wundersitz 2010).
Indigenous Australians have a unique pattern of alcohol-related disease and harm that justifies
implementation of specific interventions for this population. Implementing more than one
intervention strategy would increase the likelihood of significantly reducing alcohol-related
problems (Cobiac et al. 2009; Doran & Shakeshaft 2008). Given the disproportionately high
rates of alcohol use disorders, homicide and violence, and suicide, it may be that interventions
specific to factors critical to the functioning of Indigenous communities and individuals would
be highly cost-effective. Positive interaction with family, for example, has been identified by
Indigenous Australians as the most important characteristic to facilitate behaviour change
generally (Nagel & Thompson 2010) and the major reason for reducing or ceasing alcohol use
specifically (Hunter, Hall & Spargo 1991; Nagel & Thompson 2010). This highlights the potential
importance of developing intervention strategies that include families, as well as communities
and individuals. It is critical, however, that any intervention is developed and implemented in
consultation with Indigenous community members, families and individuals, to ensure they are
culturally acceptable, reflecting the knowledge base and world view of Indigenous Australians
(Dixon et al. 2007; Vos et al. 2003).
In addition to social harms, there is clearly a need for more effective interventions to reduce
deaths and injuries associated with traffic accidents, especially among young people. Despite
136
the effectiveness of random breath testing (Cobiac et al. 2009) road traffic accidents are a
substantial problem for Indigenous and general population Australians, except females 60
years or more. A recent analysis relevant to the Australian population generally, indicated that
the most cost-effective strategies for reducing alcohol-related road deaths among young
Australians are likely to be a zero-tolerance policy for alcohol and driving until the age of 22
years (Hall et al. 2010).
Conclusions
Indigenous males had a higher alcohol-related burden of disease than general population
males attributable to all contributing factors. Indigenous males also had a higher protective
effect of ischemic heart disease. Key problem areas for alcohol-related harm among
Indigenous Australian males were: homicide and violence, suicide and road traffic accidents.
Indigenous females had a higher alcohol-related burden of disease than general population
females with the exception of similar rates for cancer across groups. Although Indigenous
females had a higher protective effect of ischemic heart disease, general population females
had a higher protective effect for other CVD. Key problem areas for alcohol-related harm
among Indigenous females were: homicide and violence, alcohol use disorders and road traffic
accidents.
An informed policy response first requires a detailed characterisation of the contributions that
alcohol use makes to disease burden by age, sex and Indigenous status as we present in this
paper. It also requires methodologically rigorous evaluation of culturally sensitive
interventions to reduce Indigenous alcohol-related harm and should, in the Indigenous
context, include the impact on families and communities and not just the individual.

137
Paper 6
A systematic and methodological review of interventions for young
people experiencing alcohol-related harm
Bianca Calabria1, Anthony P. Shakeshaft1, Alys Havard1
1. National Drug and Alcohol Research Centre, University of New South Wales, Sydney, Australia
Paper 6 has been published in Addiction (Calabria, Shakeshaft & Havard 2011).
138
Copyright Statement
I certify that this publication was a direct result of my research towards this PhD, and that
reproduction in this thesis does not breach copyright regulations.
Calabria, B, Shakeshaft, AP & Havard, A 2011, 'A systematic and methodological review of
interventions for young people experiencing alcohol-related harm', Addiction, vol. 106, no. 8,
pp. 1406-1418.
Bianca Calabria August 2013
139
Preamble
Paper 5 demonstrated that Indigenous people have a unique pattern of alcohol-related disease
and harm and young Indigenous people experience alcohol-related harms differently to older
Indigenous people. Most notably, road traffic accidents and violent alcohol-related harms
were of concern for young Indigenous Australians, compared to alcohol use disorders and
violent alcohol-related harms among older Indigenous Australians. Paper 6 investigates which
interventions are available for, and offer the greatest potential to reduce harms among, young
people at high risk of alcohol-related harm. The systematic and methodological review focuses
on interventions delivered outside of educational settings because school-based interventions
are usually prevention focused and are, therefore, unlikely to impact on high-risk young
people, predominately because they attend school infrequently (Best et al. 2006). As with
Paper 1 (Calabria et al. 2012), Paper 6 (Calabria, Shakeshaft & Havard 2011) does not focus
specifically on Indigenous people, because of the lack of published evaluations of interventions
specifically targeting Indigenous young people at high risk of alcohol-related harm (Gray et al.
2010). The identified mainstream interventions could be tailored for young Indigenous
Australians, if they are found to be acceptable to this group.
140
Abstract
Aims: This review identified published studies evaluating interventions delivered outside of
educational settings, designed for young people with existing alcohol use problems, or who
participate in behaviour that places them at high risk of alcohol-related harm, critiqued their
methodology and identified future opportunities for new interventions.
Methods: A systematic search of the peer-reviewed literature interrogated ten electronic
databases using specific search strings, limited to 2005-09. No additional studies were found
by a librarian searching other collections and clearing-houses, or by hand-searching review
paper reference lists. The 1697 articles identified were reviewed against criteria from the
Dictionary for the Effective Public Health Practice Project Quality Assessment Tool for
Quantitative Studies.
Results: The methodological quality of existing studies is variable, and needs to be both more
rigorous and more consistent. Particular problems include the lack of blinding outcome
assessors, a reliance solely on self-report measures, highly variable consent and follow-up
rates, infrequent use of intention-to-treat analyses and the absence of any economic or cost
analyses. The range of interventions evaluated is currently limited to individually focused
approaches, almost exclusively implemented in the United States.
Conclusions: There is a great need for more intervention trials for young people at high risk of
experiencing alcohol-related harm that are both methodologically rigorous and have a broader
community focus, to complement the psychological interventions that currently dominate the
relevant literature. Such trials would improve outcomes for high-risk young people themselves
and would improve the evidence base, both in their own right and by facilitating future meta-
analyses.
141
Introduction
Alcohol consumption guidelines recommend that healthy females and males limit their alcohol
consumption to minimise their risk of alcohol-related harm (National Health and Medical
Research Council 2009; U.S. Department of Health and Human Services & U.S. Department of
Agriculture 2005). Current Australian guidelines, for example, recommend that both males and
females drink no more than two standard drinks per day (a standard drink is defined as 10 g of
alcohol) to minimise the likelihood of experiencing harms associated with risky drinking over
the longer term, including dependence, depression and cancer (Fergusson, Boden & Horwood
2009; Seitz & Cho 2009; Calabria et al. 2010; National Health and Medical Research Council
2009), and limiting consumption on one occasion to no more than four standard drinks (both
males and females), to minimize the risk of short-term alcohol-related harms (National Health
and Medical Research Council 2009), such as driving under the influence of alcohol (DUI),
accidents, injuries, violence and crime (Begg & Gulliver 2008; Cherpitel & Ye 2008; Calabria et
al. 2010). These deleterious outcomes (both short- and long-term) impose substantial costs on
both the individuals experiencing the harm (Collins & Lapsley 2008; Petrie et al. 2008) and
their communities (Rehm et al. 2009; Petrie et al. 2008; Czech et al. 2010; Breen et al. 2011b).
A greater proportion of young people, relative to other age groups, consume alcohol at a level
that places them at increased risk of harm in the short and long term (Australian Institute of
Health and Welfare 2008b). In the United States, for example, consuming five or more
standard alcoholic drinks (a standard drink is defined as 14 g of alcohol) on the same occasion
is reported by over 40% of young people aged 21-29 years (21 is the minimum legal drinking
age in the United States), compared to fewer than 30% for older age groups, a proportion that
decreases with increasing age. A substantial proportion of young people under the United
States’ minimum legal drinking age also report alcohol use at this level: over 30% of 18-20-
142
year-olds; almost 20% of 16-17-year-olds; approximately 5% of 14-15-year-olds; and about 1%
of 12-13-year-olds (Substance Abuse and Mental Health Services Administration 2009).
Attempts to reduce alcohol harm experienced by young people have largely focused on school-
based education and prevention interventions for students and/or parents (Wood et al. 2006;
Foxcroft et al. 2002). It is likely school-based interventions are routinely implemented because
schools provide access to a large number of young people across a broad geographic area and
interventions can be easily incorporated into diverse curricula. The evidence for their
effectiveness in modifying drinking behaviour (as opposed to increasing awareness or
knowledge) is limited (Vogl et al. 2009; McBride et al. 2004; Wood et al. 2006). Harm
minimization approaches have been found to be effective in increasing knowledge and
attitudes related to safe drinking choices (Vogl et al. 2009; McBride et al. 2004) and decreasing
alcohol-related harms experienced by the drinking individual, but not harms from other
peoples’ alcohol use (McBride et al. 2004). Despite this, broad-based educational strategies
may be justified on the basis that they are relatively inexpensive to implement and could
achieve small benefits for individuals across large population groups (Newton et al. 2010).
These broad-based educational interventions, however, generally aim to prevent alcohol use
or misuse among the general student population and are unlikely to impact significantly on the
minority of young people who currently experience substantial alcohol-related harm, primarily
because they do not regularly attend school (Best et al. 2006).
Interventions delivered outside of educational settings that are designed for young people
who are experiencing alcohol-related harm or are participating in high-risk drinking behaviour,
are likely to be highly cost-beneficial even if they are expensive to implement, if they can
achieve relatively modest improvements in personal and employment trajectories over a life-
time (Cohen 1998; Pacileo & Fattore 2009; McGorry et al. 2007) Despite reviews of alcohol
143
interventions for young people being previously published (Tripodi et al. 2010; Fletcher, Bonell
& Hargreaves 2008; Gates et al. 2006; Smit et al. 2008; Spoth, Greenberg & Turrisi 2008;
Toumbourou et al. 2007; Velleman, Templeton & Copello 2005; Coombes et al. 2008; Williams
& Chang 2000), none have recently focused on youth who are experiencing alcohol-related
harm or participating in behaviour that increases their risk of harm.
This systematic review aims to: (1) identify published studies evaluating interventions
delivered outside formal educational settings, designed for young people with existing alcohol
use problems or who participate in behaviour that places them at high risk of alcohol-related
harm; (2) describe and critique their methodology; and (3) identify future opportunities for
methodologically adequate intervention studies.
Methods
Sample
Rather than specify an arbitrary age range a priori, which may have resulted in good-quality
intervention studies failing to be detected, the search strategy used the more general search
term ‘youth’. Studies were included for review if the young people met any of four alcohol-
related criteria. First, a diagnosis of alcohol dependence or abuse according to the Diagnostic
and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) (American Psychiatric
Association 1994); secondly, at-risk alcohol use as assessed by a formal screening instrument,
such as the Alcohol Use Disorders Identification Test (AUDIT) (Saunders et al. 1993); thirdly,
referral for treatment for an alcohol use problem; fourthly, engagement in high-risk alcohol-
related behaviour, such as drinking above recommended guidelines or DUI.
144
Search strategy
Figure 1 summarizes the databases searched, the search terms used, the exclusion criteria and
classification of included studies (see Appendix L for search strings).
Consistent with methods detailed in the Cochrane Collaboration Handbook on Systematic
Reviews of Health Promotion and Public Health Interventions (Jackson 2007), and with previous
reviews (Shakeshaft, Bowman & Sanson-Fisher 1997; Havard, Shakeshaft & Sanson-Fisher
2008; Webb et al. 2009; Wood et al. 2006), the search strategy comprised three steps. First, 10
electronic databases were searched: ACP Journal Club; CCTR; CDSR; Project Cork; DARE;
EMBASE; ERIC; MEDLINE; PsycINFO; and Web of Science. Electronic databases were searched
individually so that database-specific search strings could be used to identify relevant articles
more effectively, compared to using generic search terms for searching all databases
simultaneously. CDSR, ACP Journal Club and DARE were the exception; they were searched
simultaneously so that CDSR could be accessed via the OvidSP platform. The search terms
‘youth’ (‘basic’ and ‘advanced terms’), ‘alcohol’, ‘alcohol abuse/dependence’, ‘intervention’
(‘basic’ and ‘advanced terms’), ‘risk’ and ‘disruptive’ were integrated into database-specific
search strings (including subheadings, MESH terms, EMTREE terms and explode terms).
Combinations of these search strings were tested and resultant data coverage was reviewed.
The most parsimonious combination used the search terms ‘youth’ (‘basic terms’), ‘alcohol’,
‘intervention’ (‘basic terms’) and ‘risk’. To be as inclusive as possible, no specific age range was
defined by the search terms. The combined searches of all databases (CDSR, ACP Journal Club,
DARE, CCTR, EMBASE, Medline, PSYCInfo, ERIC, Project Cork and Web of Science) located 2243
references. Duplicates were electronically deleted leaving 1697 references for classification.
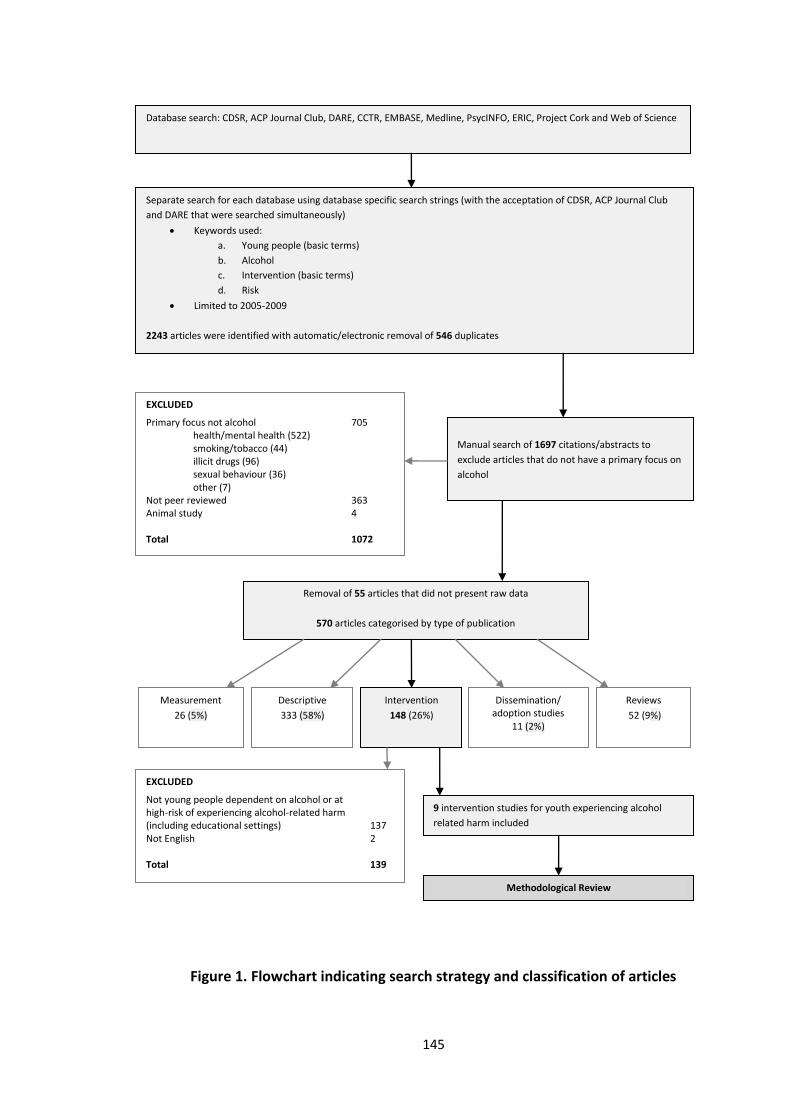
145
Figure 1. Flowchart indicating search strategy and classification of articles
Database search: CDSR, ACP Journal Club, DARE, CCTR, EMBASE, Medline, PsycINFO, ERIC, Project Cork and Web of Science
Separate search for each database using database specific search strings (with the acceptation of CDSR, ACP Journal Club
and DARE that were searched simultaneously)
Keywords used:
a. Young people (basic terms)
b. Alcohol
c. Intervention (basic terms)
d. Risk
Limited to 2005-2009
2243 articles were identified with automatic/electronic removal of 546 duplicates
Manual search of 1697 citations/abstracts to
exclude articles that do not have a primary focus on
alcohol
Removal of 55 articles that did not present raw data
570 articles categorised by type of publication
Measurement
26 (5%)
Descriptive
333 (58%)
Intervention
148 (26%)
Dissemination/ adoption studies
11 (2%)
Reviews
52 (9%)
EXCLUDED
Primary focus not alcohol 705 health/mental health (522) smoking/tobacco (44) illicit drugs (96) sexual behaviour (36) other (7) Not peer reviewed 363 Animal study 4
Total 1072
EXCLUDED
Not young people dependent on alcohol or at high-risk of experiencing alcohol-related harm (including educational settings)
137
Not English 2
Total 139
9 intervention studies for youth experiencing alcohol
related harm included
Methodological Review
146
Secondly, an experienced librarian conducted searches to identify additional studies that the
original search may have missed. DRUG, APAIS, Health, DrugInfo Clearinghouse, SafetyLit and
the National Drug and Alcohol Research Centre library collection were searched using search
terms ‘young people’ or ‘youth’, ‘alcohol’ and ‘intervention’. This additional search did not
locate any relevant articles that had not already been identified.
Finally, the reference lists of all review articles, identified by the electronic database search
and focused on alcohol interventions for youth, were hand-searched for any relevant studies
that had not been identified. No relevant studies were identified during this process.
All searches were limited to 2005-09 for two reasons. First, since broad search terms were
used to maximize the range of intervention types identified, the number of years searched was
limited to 5 to ensure a realistic number of studies could be categorized and to ensure that a
realistic number of intervention studies could be critiqued; and secondly, to optimize the
likelihood that the most recent intervention studies would be included, on the assumption that
the interventions being evaluated would represent current best-evidence practice.
Classification of studies
The titles and abstracts (if the title did not contain enough descriptive information to classify
the article) of the 1697 identified references were classified in a three-step process.
Step 1: applying exclusion criteria. Papers were excluded if: (i) they did not focus on alcohol
use, alcohol abuse, alcohol dependence or alcohol problems (n = 705); (ii) they were not peer-
reviewed (n = 363), including a number of books identified by Project Cork; or (iii) they were an
animal study (n = 4). A total of 1072 papers were excluded.
147
Step 2: study type. Fifty-five papers were removed because they did not present raw data
(non-data based papers and comments). The 570 remaining papers were classified using
categories derived and adapted from previous, similar reviews (Havard, Shakeshaft & Sanson-
Fisher 2008; Webb et al. 2009; Wood et al. 2006): (i) measurement, defined as papers
concerned primarily with developing measurement instruments and/or the psychometric
properties of measurement instruments (n = 26); (ii) descriptive, defined as data-based
descriptive, analytical research on alcohol-related harm (n = 333); (iii) interventions, defined as
evaluation or intervention trials aimed at reducing alcohol-related harm (n = 148); (iv)
dissemination/adoption, defined as studies evaluating methods of ensuring effective
interventions to reduce alcohol-related harm are adopted into routine practice (n = 11); and
(v) reviews, defined as literature reviews (n = 52).
Step 3: exclusion criteria for interventions. Of the 148 intervention papers, 139 were excluded
because: (i) they did not meet the alcohol-related criteria, they did not specifically target
young people or they were delivered in an educational setting (i.e. school, college, or
university) (n = 137); or (ii) they were not published in English (n = 2). The nine remaining
intervention studies were included in the review.
Twenty percent of the articles focused on alcohol (not excluded in Step 1, n = 625) were
classified a second time by a blinded co-author (A.H.) to cross-check the classifications
conducted originally by the first author (B.C.). The articles excluded in Step 1 were not cross-
checked because they were not relevant for the review. Agreement between co-authors was
86%. Discrepancies were discussed and resolved. Due to high agreement between co-authors
and the failure of the hand-searched reference lists to identify additional intervention studies
that met the inclusion criteria, cross-checking more than 20% of article classifications was
deemed unnecessary.
148
Information extraction and summary
Review criteria for data extraction were adapted from the Cochrane Collaboration Handbook
for Systematic Reviews of Health Promotion and Public Health Interventions (Jackson 2007).
The criteria, shown in Table 1, summarize the intervention/s, the sample (including eligibility,
size, age range and percent male), the outcomes measured and the cost calculations
performed.
Methodological critique of intervention studies
Methodological quality was assessed using the Dictionary for the Effective Public Health
Practice Project Quality Assessment Tool for Quantitative Studies (see (Jackson 2007)). Sections
A-F (A, selection bias; B, allocation bias; C, confounders; D, blinding; E, data collection
methods; and F, withdrawal and drop-outs) were coded weak, moderate or strong as advised
by the component rating scale of the Dictionary. For example, a strong rating for section B
(allocation bias) indicates a randomized control trial; a moderate rating for section B indicates
a two-group quasi-experimental design; and a weak rating indicates a case control,
before/after study or no control group (Jackson 2007). Sections G (analysis) and H
(intervention integrity) included descriptive information guided by the Dictionary.
Results
Interventions
Nine intervention studies were included: eight counselling-based interventions and one
medically-based intervention. Of the counselling interventions, seven had individual session/s
for the young person (D'Amico et al. 2008; Esposito-Smythers et al. 2006; Peterson et al. 2006;
149
Slesnick et al. 2007; Stein et al. 2006; Kemp et al. 2007), three included family-based therapy
(Esposito-Smythers et al. 2006; Liddle et al. 2009; Slesnick et al. 2006) and one included group-
based therapy (Liddle et al. 2009). Counselling interventions were based on motivational
interviewing (MI) (D'Amico et al. 2008; Peterson et al. 2006; Stein et al. 2006; Kemp et al.
2007), cognitive-behavioural therapy (CBT) (Esposito-Smythers et al. 2006; Liddle et al. 2009;
Kemp et al. 2007), family therapy (Esposito-Smythers et al. 2006; Liddle et al. 2009; Slesnick et
al. 2006) and/or an operant perspective community-reinforcement approach (Slesnick et al.
2007; Slesnick et al. 2006). The number of reported counselling sessions ranged from one
(D'Amico et al. 2008; Peterson et al. 2006; Stein et al. 2006) to 32 (Liddle et al. 2009). The
medically-based intervention investigated the efficacy of medicating alcohol-dependent
adolescents with a serotonin-3 antagonsit (ondansetron) (Dawes et al. 2005).
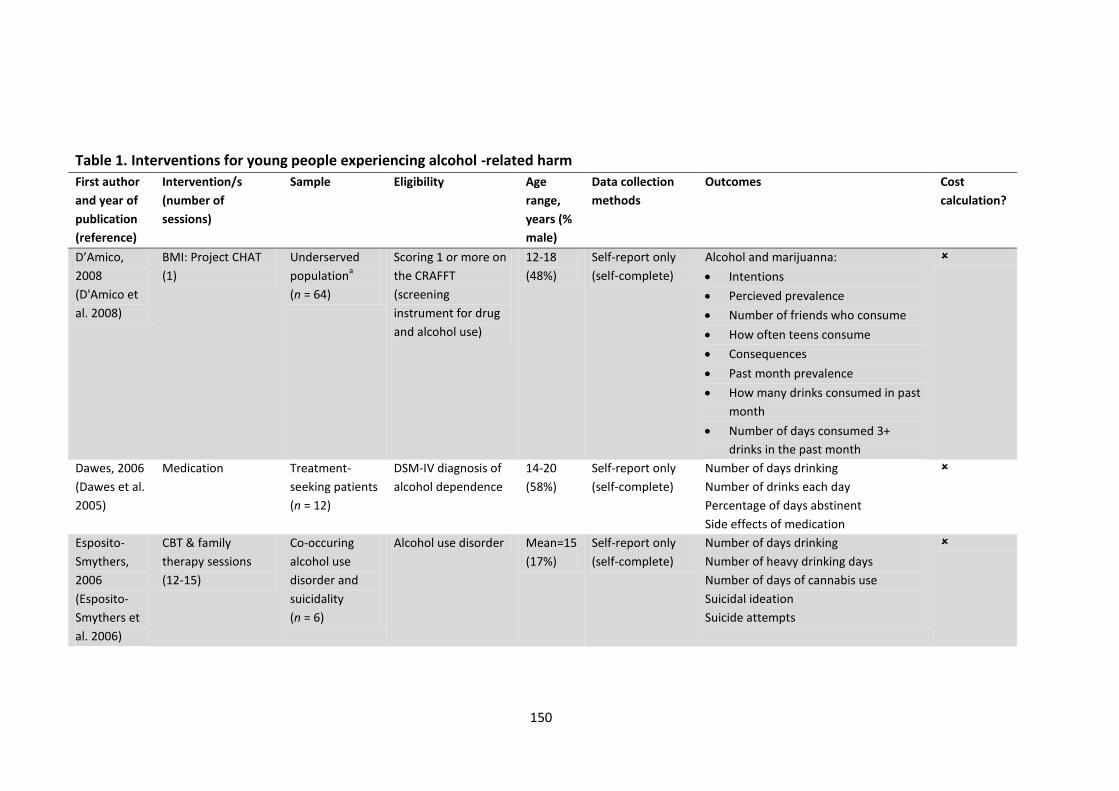
150
Table 1. Interventions for young people experiencing alcohol -related harm
First author
and year of
publication
(reference)
Intervention/s
(number of
sessions)
Sample Eligibility Age
range,
years (%
male)
Data collection
methods
Outcomes Cost
calculation?
D’Amico,
2008
(D'Amico et
al. 2008)
BMI: Project CHAT
(1)
Underserved
populationa
(n = 64)
Scoring 1 or more on
the CRAFFT
(screening
instrument for drug
and alcohol use)
12-18
(48%)
Self-report only
(self-complete)
Alcohol and marijuanna:
Intentions
Percieved prevalence
Number of friends who consume
How often teens consume
Consequences
Past month prevalence
How many drinks consumed in past
month
Number of days consumed 3+
drinks in the past month
Dawes, 2006
(Dawes et al.
2005)
Medication Treatment-
seeking patients
(n = 12)
DSM-IV diagnosis of
alcohol dependence
14-20
(58%)
Self-report only
(self-complete)
Number of days drinking
Number of drinks each day
Percentage of days abstinent
Side effects of medication
Esposito-
Smythers,
2006
(Esposito-
Smythers et
al. 2006)
CBT & family
therapy sessions
(12-15)
Co-occuring
alcohol use
disorder and
suicidality
(n = 6)
Alcohol use disorder Mean=15
(17%)
Self-report only
(self-complete)
Number of days drinking
Number of heavy drinking days
Number of days of cannabis use
Suicidal ideation
Suicide attempts
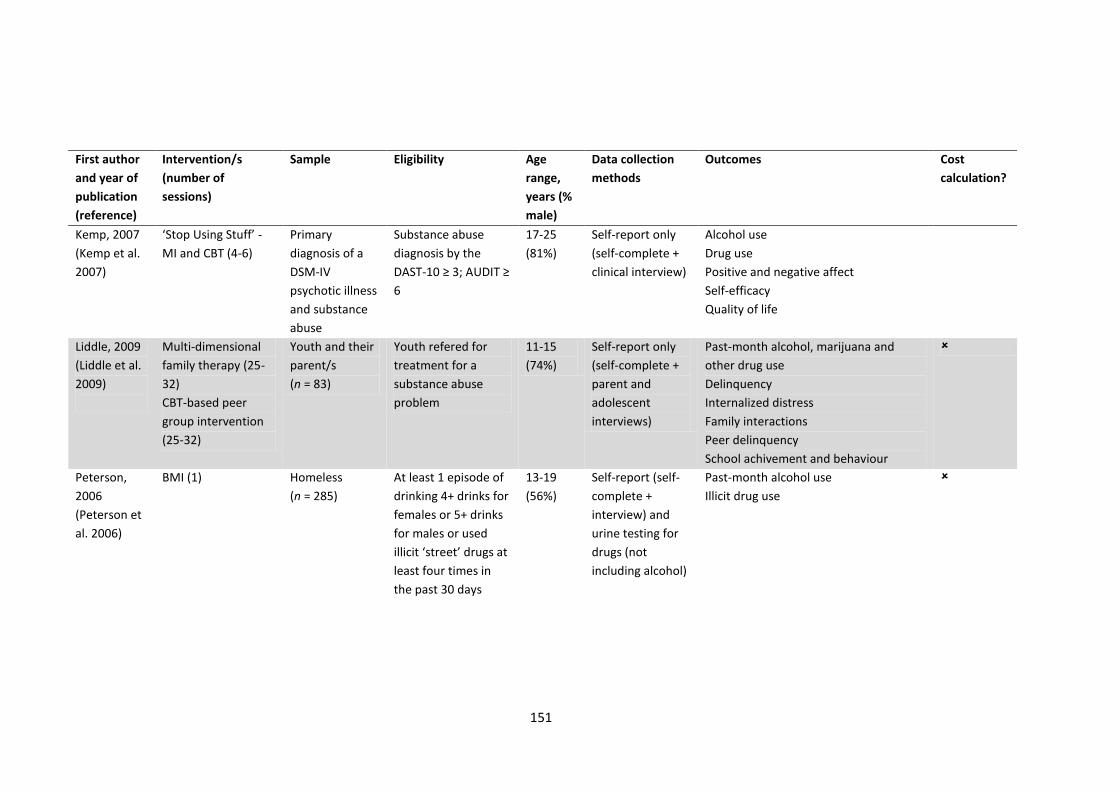
151
First author
and year of
publication
(reference)
Intervention/s
(number of
sessions)
Sample Eligibility Age
range,
years (%
male)
Data collection
methods
Outcomes Cost
calculation?
Kemp, 2007
(Kemp et al.
2007)
‘Stop Using Stuff’ -
MI and CBT (4-6)
Primary
diagnosis of a
DSM-IV
psychotic illness
and substance
abuse
Substance abuse
diagnosis by the
DAST-10 ≥ 3; AUDIT ≥
6
17-25
(81%)
Self-report only
(self-complete +
clinical interview)
Alcohol use
Drug use
Positive and negative affect
Self-efficacy
Quality of life
Liddle, 2009
(Liddle et al.
2009)
Multi-dimensional
family therapy (25-
32)
CBT-based peer
group intervention
(25-32)
Youth and their
parent/s
(n = 83)
Youth refered for
treatment for a
substance abuse
problem
11-15
(74%)
Self-report only
(self-complete +
parent and
adolescent
interviews)
Past-month alcohol, marijuana and
other drug use
Delinquency
Internalized distress
Family interactions
Peer delinquency
School achivement and behaviour
Peterson,
2006
(Peterson et
al. 2006)
BMI (1) Homeless
(n = 285)
At least 1 episode of
drinking 4+ drinks for
females or 5+ drinks
for males or used
illicit ‘street’ drugs at
least four times in
the past 30 days
13-19
(56%)
Self-report (self-
complete +
interview) and
urine testing for
drugs (not
including alcohol)
Past-month alcohol use
Illicit drug use
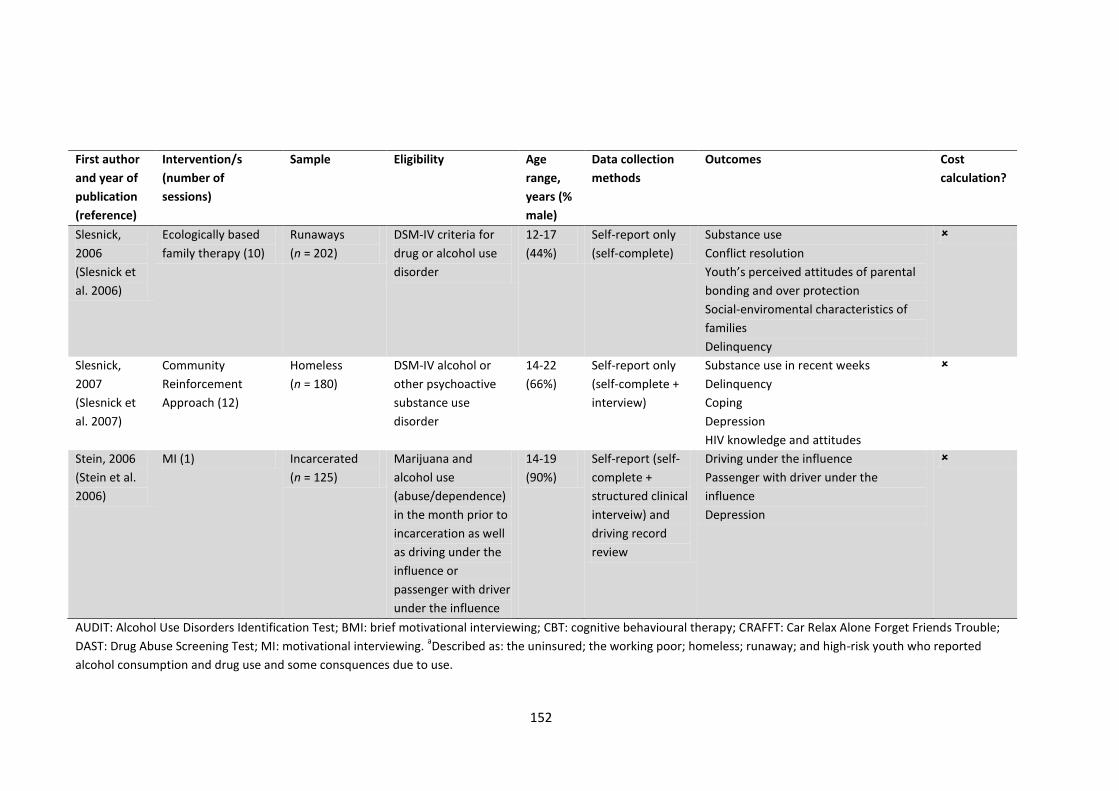
152
First author
and year of
publication
(reference)
Intervention/s
(number of
sessions)
Sample Eligibility Age
range,
years (%
male)
Data collection
methods
Outcomes Cost
calculation?
Slesnick,
2006
(Slesnick et
al. 2006)
Ecologically based
family therapy (10)
Runaways
(n = 202)
DSM-IV criteria for
drug or alcohol use
disorder
12-17
(44%)
Self-report only
(self-complete)
Substance use
Conflict resolution
Youth’s perceived attitudes of parental
bonding and over protection
Social-enviromental characteristics of
families
Delinquency
Slesnick,
2007
(Slesnick et
al. 2007)
Community
Reinforcement
Approach (12)
Homeless
(n = 180)
DSM-IV alcohol or
other psychoactive
substance use
disorder
14-22
(66%)
Self-report only
(self-complete +
interview)
Substance use in recent weeks
Delinquency
Coping
Depression
HIV knowledge and attitudes
Stein, 2006
(Stein et al.
2006)
MI (1) Incarcerated
(n = 125)
Marijuana and
alcohol use
(abuse/dependence)
in the month prior to
incarceration as well
as driving under the
influence or
passenger with driver
under the influence
14-19
(90%)
Self-report (self-
complete +
structured clinical
interveiw) and
driving record
review
Driving under the influence
Passenger with driver under the
influence
Depression
AUDIT: Alcohol Use Disorders Identification Test; BMI: brief motivational interviewing; CBT: cognitive behavioural therapy; CRAFFT: Car Relax Alone Forget Friends Trouble;
DAST: Drug Abuse Screening Test; MI: motivational interviewing. aDescribed as: the uninsured; the working poor; homeless; runaway; and high-risk youth who reported
alcohol consumption and drug use and some consquences due to use.
153
Samples and eligibility
The sampled youth population varied across studies, including: the underserved, described as
the uninsured, working poor, homeless, runaway and high-risk youth (D'Amico et al. 2008);
treatment seeking individuals (Dawes et al. 2005); those with comorbid suicidality (Esposito-
Smythers et al. 2006); those with a primary diagnosis of a psychotic illness and substance
abuse (Kemp et al. 2007); young people and their parents (Liddle et al. 2009); runaways
(Slesnick et al. 2006); the homeless (Peterson et al. 2006; Slesnick et al. 2007); and
incarcerated youth (Stein et al. 2006). The young people ranged in age from 11 to 25 years and
the percent of male participants from 17% to 90%. Although participants were screened
appropriately for an alcohol/substance use disorder (Esposito-Smythers et al. 2006; Liddle et
al. 2009; Slesnick et al. 2007; Dawes et al. 2005; Slesnick et al. 2006; Kemp et al. 2007) or
problematic alcohol use (D'Amico et al. 2008; Peterson et al. 2006; Stein et al. 2006), two
studies gave no clear definition of the cut-off score for eligibility for inclusion (Esposito-
Smythers et al. 2006; Liddle et al. 2009) and all except one (Stein et al. 2006) used self-report
eligibility criteria.
Data collection methods and outcomes
All studies used self-report measures. Table 1 shows seven studies used self-report measures
only; three of these used both self-complete and interview techniques (Liddle et al. 2009;
Slesnick et al. 2007; Kemp et al. 2007) and four used self-complete only (D'Amico et al. 2008;
Dawes et al. 2005; Esposito-Smythers et al. 2006; Slesnick et al. 2006). Of the two studies that
used non-self-report measures, one used urine tests for drugs (not including alcohol) (Peterson
et al. 2006) and one used driving record checks for reports of driving under the influence of
alcohol (only amongst participants who where old enough to obtain a driving permit) (Stein et
al. 2006).
154
Alcohol use outcomes were measured across all studies but varied: recent alcohol use
(D'Amico et al. 2008; Liddle et al. 2009; Peterson et al. 2006; Slesnick et al. 2007; Kemp et al.
2007); frequency/quantity of alcohol use (D'Amico et al. 2008; Esposito-Smythers et al. 2006;
Dawes et al. 2005; Slesnick et al. 2006; Kemp et al. 2007); heavy alcohol use or alcohol use
disorders (D'Amico et al. 2008; Esposito-Smythers et al. 2006); and driving under the influence
of alcohol (Stein et al. 2006). Other outcome measures included: other drug use/abuse
(D'Amico et al. 2008; Peterson et al. 2006; Slesnick et al. 2007; Slesnick et al. 2006; Kemp et al.
2007; Esposito-Smythers et al. 2006); alcohol and/or drug perceptions and intentions to use
(D'Amico et al. 2008); suicide ideation and attempts (Esposito-Smythers et al. 2006); family
interactions (Liddle et al. 2009); conflict resolution (Slesnick et al. 2006); social-environmental
characteristics of families (Slesnick et al. 2006); youth’s perceived attitudes of parental
bonding and overprotection (Slesnick et al. 2006); delinquency (Liddle et al. 2009; Slesnick et
al. 2007; Slesnick et al. 2006); school achievement and behaviour (Liddle et al. 2009);
experienced affect or affective disorders (Stein et al. 2006; Liddle et al. 2009; Slesnick et al.
2007; Kemp et al. 2007); coping (Slesnick et al. 2007); human immunodeficiecy virus (HIV)
knowledge and attitudes (Slesnick et al. 2007); self-efficacy (Kemp et al. 2007); quality of life
(Kemp et al. 2007); and medication side effects (Dawes et al. 2005).
Eight studies were conducted in the United States (D'Amico et al. 2008; Esposito-Smythers et
al. 2006; Liddle et al. 2009; Peterson et al. 2006; Slesnick et al. 2007; Stein et al. 2006; Dawes
et al. 2005; Slesnick et al. 2006) and one study was from Australia (Kemp et al. 2007).
Methodological adequacy
Table 2 summarises the methodological adequacy of the nine studies. Two studies obtained a
100% consent rate, obviating the possibility of selection bias (Liddle et al. 2009; Stein et al.
2006). A randomized control trial was employed by seven of the nine studies (D'Amico et al.

155
2008; Liddle et al. 2009; Peterson et al. 2006; Slesnick et al. 2007; Stein et al. 2006; Kemp et al.
2007; Slesnick et al. 2006), minimizing the risk of allocation bias. Baseline differences in
comparison groups were not controlled in the analyses, so it is difficult to know the extent to
which reported post-test differences are attributable to the intervention. More than half the
studies used outcome assessors that were not blinded (Liddle et al. 2009; Peterson et al. 2006;
Slesnick et al. 2007; Stein et al. 2006; Kemp et al. 2007). Six studies used measures with
demonstrated validity and reliability (Liddle et al. 2009; Peterson et al. 2006; Slesnick et al.
2007; Stein et al. 2006; Slesnick et al. 2006; Kemp et al. 2007), one used measures of known
validity but unknown reliability (D'Amico et al. 2008) and two studies used measures that were
not tested psychometrically (Esposito-Smythers et al. 2006; Dawes et al. 2005). Five studies
had follow-up rates between 80% and 100% (Esposito-Smythers et al. 2006; Slesnick et al.
2007; Stein et al. 2006; Slesnick et al. 2006; Kemp et al. 2007), one study had a follow-up rate
between 60% and 79% (Peterson et al. 2006), and three studies had follow-up rates less than
60%: 50% (Dawes et al. 2005; Liddle et al. 2009) and 34% (D'Amico et al. 2008).
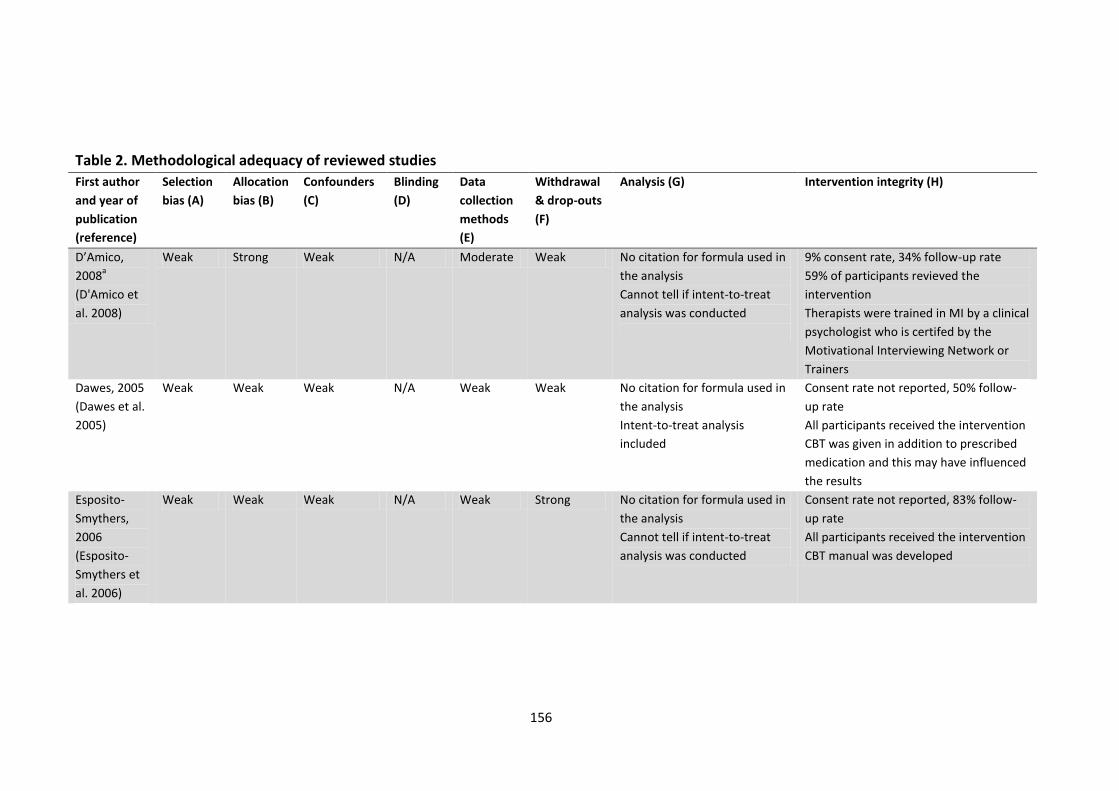
156
Table 2. Methodological adequacy of reviewed studies
First author
and year of
publication
(reference)
Selection
bias (A)
Allocation
bias (B)
Confounders
(C)
Blinding
(D)
Data
collection
methods
(E)
Withdrawal
& drop-outs
(F)
Analysis (G) Intervention integrity (H)
D’Amico,
2008a
(D'Amico et
al. 2008)
Weak Strong Weak N/A Moderate Weak No citation for formula used in
the analysis
Cannot tell if intent-to-treat
analysis was conducted
9% consent rate, 34% follow-up rate
59% of participants revieved the
intervention
Therapists were trained in MI by a clinical
psychologist who is certifed by the
Motivational Interviewing Network or
Trainers
Dawes, 2005
(Dawes et al.
2005)
Weak Weak Weak N/A Weak Weak No citation for formula used in
the analysis
Intent-to-treat analysis
included
Consent rate not reported, 50% follow-
up rate
All participants received the intervention
CBT was given in addition to prescribed
medication and this may have influenced
the results
Esposito-
Smythers,
2006
(Esposito-
Smythers et
al. 2006)
Weak Weak Weak N/A Weak Strong No citation for formula used in
the analysis
Cannot tell if intent-to-treat
analysis was conducted
Consent rate not reported, 83% follow-
up rate
All participants received the intervention
CBT manual was developed
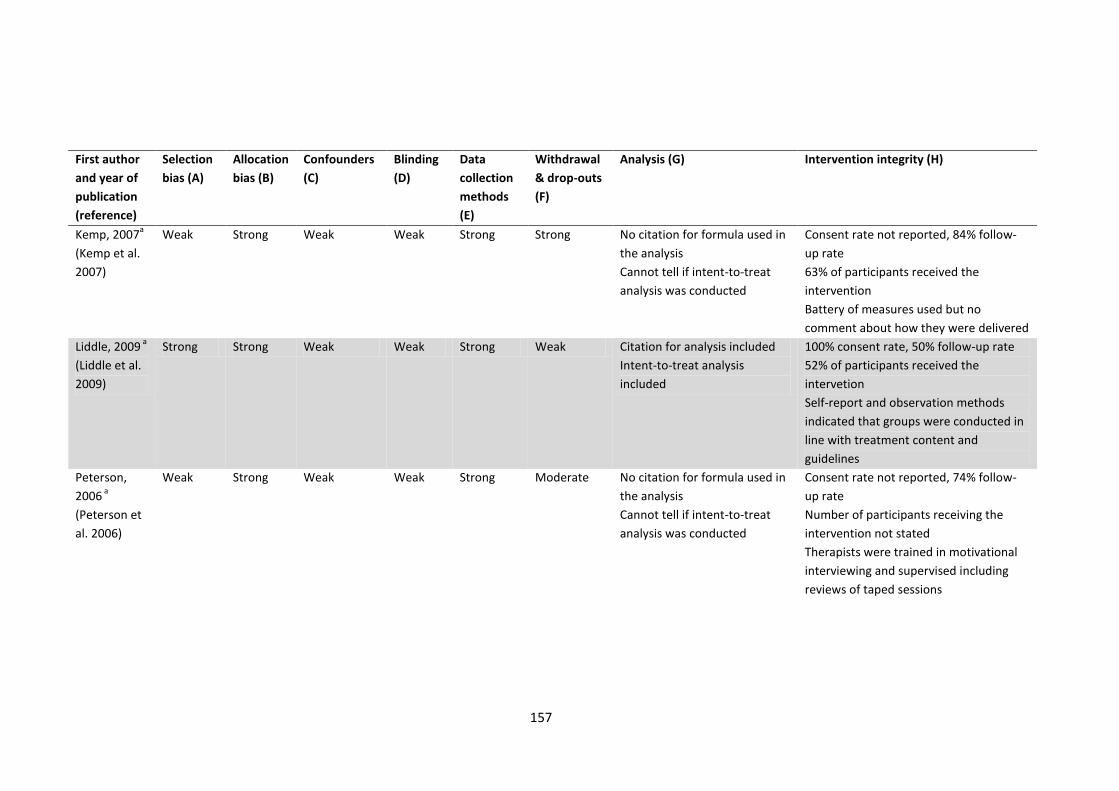
157
First author
and year of
publication
(reference)
Selection
bias (A)
Allocation
bias (B)
Confounders
(C)
Blinding
(D)
Data
collection
methods
(E)
Withdrawal
& drop-outs
(F)
Analysis (G) Intervention integrity (H)
Kemp, 2007a
(Kemp et al.
2007)
Weak Strong Weak Weak Strong Strong No citation for formula used in
the analysis
Cannot tell if intent-to-treat
analysis was conducted
Consent rate not reported, 84% follow-
up rate
63% of participants received the
intervention
Battery of measures used but no
comment about how they were delivered
Liddle, 2009 a
(Liddle et al.
2009)
Strong Strong Weak Weak Strong Weak Citation for analysis included
Intent-to-treat analysis
included
100% consent rate, 50% follow-up rate
52% of participants received the
intervetion
Self-report and observation methods
indicated that groups were conducted in
line with treatment content and
guidelines
Peterson,
2006 a
(Peterson et
al. 2006)
Weak Strong Weak Weak Strong Moderate No citation for formula used in
the analysis
Cannot tell if intent-to-treat
analysis was conducted
Consent rate not reported, 74% follow-
up rate
Number of participants receiving the
intervention not stated
Therapists were trained in motivational
interviewing and supervised including
reviews of taped sessions
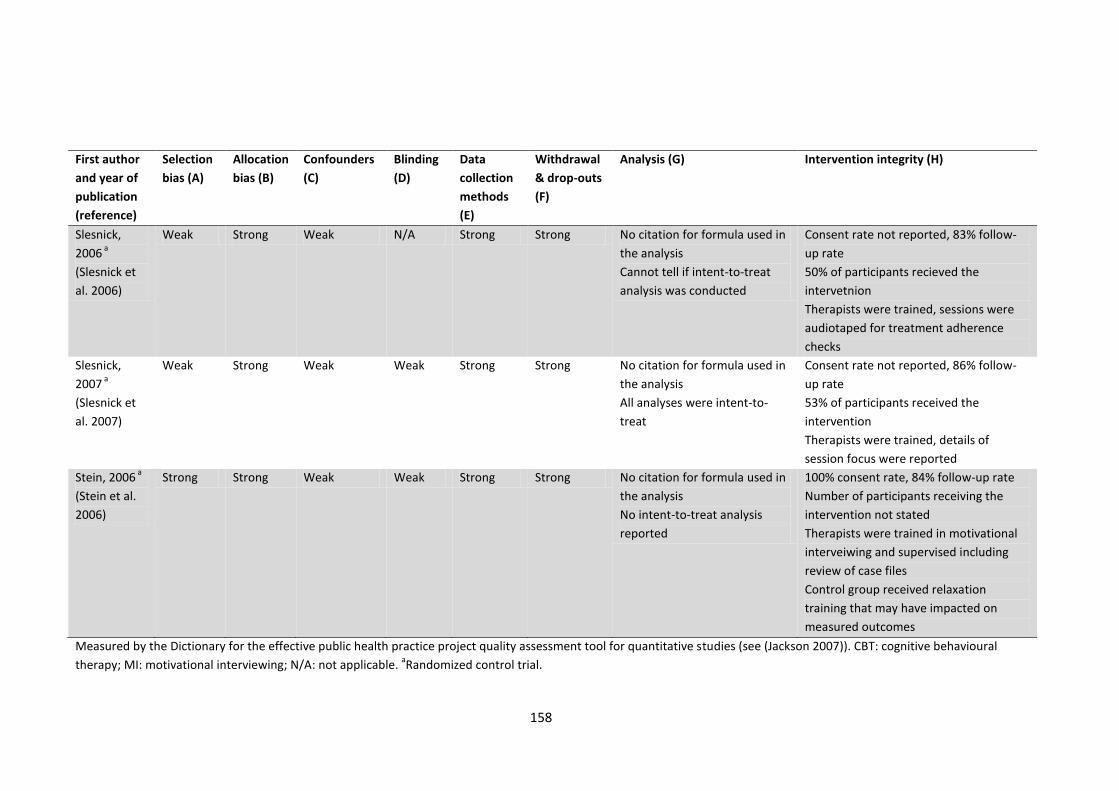
158
First author
and year of
publication
(reference)
Selection
bias (A)
Allocation
bias (B)
Confounders
(C)
Blinding
(D)
Data
collection
methods
(E)
Withdrawal
& drop-outs
(F)
Analysis (G) Intervention integrity (H)
Slesnick,
2006 a
(Slesnick et
al. 2006)
Weak Strong Weak N/A Strong Strong No citation for formula used in
the analysis
Cannot tell if intent-to-treat
analysis was conducted
Consent rate not reported, 83% follow-
up rate
50% of participants recieved the
intervetnion
Therapists were trained, sessions were
audiotaped for treatment adherence
checks
Slesnick,
2007 a
(Slesnick et
al. 2007)
Weak Strong Weak Weak Strong Strong No citation for formula used in
the analysis
All analyses were intent-to-
treat
Consent rate not reported, 86% follow-
up rate
53% of participants received the
intervention
Therapists were trained, details of
session focus were reported
Stein, 2006 a
(Stein et al.
2006)
Strong Strong Weak Weak Strong Strong No citation for formula used in
the analysis
No intent-to-treat analysis
reported
100% consent rate, 84% follow-up rate
Number of participants receiving the
intervention not stated
Therapists were trained in motivational
interveiwing and supervised including
review of case files
Control group received relaxation
training that may have impacted on
measured outcomes
Measured by the Dictionary for the effective public health practice project quality assessment tool for quantitative studies (see (Jackson 2007)). CBT: cognitive behavioural
therapy; MI: motivational interviewing; N/A: not applicable. aRandomized control trial.
159
One study provided support for the appropriateness of its analysis by referencing a book about
their general statistical approach (Liddle et al. 2009). Participation consent rates varied from
9% (D'Amico et al. 2008) to 100% (Liddle et al. 2009; Stein et al. 2006) and intent-to-treat
analyses were reported by three studies (Slesnick et al. 2007; Dawes et al. 2005; Liddle et al.
2009). In two studies, all participants received the intervention (Dawes et al. 2005; Esposito-
Smythers et al. 2006). Of the seven studies with a control group, five reported that more than
half the participants were in the intervention group (Slesnick et al. 2007; D'Amico et al. 2008;
Liddle et al. 2009; Slesnick et al. 2006; Kemp et al. 2007). Methods to optimize consistency in
the delivery of interventions were not described in two studies (Dawes et al. 2005; Kemp et al.
2007). When they were described, methods included training therapists (D'Amico et al. 2008;
Peterson et al. 2006; Slesnick et al. 2007; Stein et al. 2006; Slesnick et al. 2006), developing
manuals (Esposito-Smythers et al. 2006), audio-taping for adherence to treatment protocols
(Peterson et al. 2006; Slesnick et al. 2006) and self-report or observation (Liddle et al. 2009).
Contamination was likely for Dawes et al. because CBT was provided in addition to the medical
intervention that was the focus of the study (Dawes et al. 2005).
Effects
Due to the generally weak methodological quality of the included studies, especially their
susceptability to intervention confounding and lack of blinding, the effect sizes are likely to be
biased and, therefore, were not summarized. A meta-analysis using the most commonly
reported outcomes was explored but judged inappropriate, given the variability between
studies in the outcomes reported. No interventions included a cost or economic analysis.
160
Discussion
This systematic review of available peer-reviewed studies evaluating interventions delivered
outside educational settings, designed for young people with existing alcohol use problems or
who participate in behaviour that places them at high-risk of alcohol-related harm, identified
eight counselling-based interventions (Kemp et al. 2007; D'Amico et al. 2008; Esposito-
Smythers et al. 2006; Liddle et al. 2009; Peterson et al. 2006; Slesnick et al. 2007; Stein et al.
2006; Slesnick et al. 2006) and one medically-based intervention (Dawes et al. 2005). Six
counselling studies had an individual focus (D'Amico et al. 2008; Esposito-Smythers et al. 2006;
Peterson et al. 2006; Slesnick et al. 2007; Stein et al. 2006; Kemp et al. 2007) and three
included family and peers (Liddle et al. 2009; Esposito-Smythers et al. 2006; Slesnick et al.
2006). Counselling types varied across the eight studies: family-based, MI, CBT and community
reinforcement. Length of the interventions were also diverse: three used brief interventions
(one session) (D'Amico et al. 2008; Peterson et al. 2006; Stein et al. 2006), four had between
two and fifteen sessions (Esposito-Smythers et al. 2006; Kemp et al. 2007; Slesnick et al. 2006;
Slesnick et al. 2007), and one had 25-32 sessions (Liddle et al. 2009).
Methodological adequacy
None of the included intervention studies had consistently strong methodology. Weak ratings
were commonly recorded for selection bias and confounding, while allocation bias was mainly
rated strongly across studies. Blinding was rated weakly when applicable. Data collection
methods were generally appropriate, with seven studies using measures with some published
evidence of their reliability and validity. Withdrawal and dropout ratings also varied across
studies, ranging from 22% to 86%. Statistical analyses used were rarely supported by a citation
of source and intent-to-treat analyses were conducted for only a third of studies. Consent
rates varied from 9% to 100% and follow-up rates ranged from 34% to 86%, when reported.
Therapists were trained and supervised.
161
Limitations of the available literature
In addition to methodological adequacy, the substantial variation in the eligibility criteria
across studies limits the validity of comparisons between them. Although a primary eligibility
criterion was either an alcohol use disorder or problem, no studies screened participants in the
same way. Screening using standardized measures of alcohol dependence or misuse, such as
the AUDIT (Saunders et al. 1993) or DSM-IV criteria (American Psychiatric Association 1994),
would improve comparability between studies.
Another limitation of the available literature relates to measurement. First, one study grouped
alcohol and drug use outcomes together, increasing the difficulty of determining the impact of
their intervention specifically on alcohol-related harm (Slesnick et al. 2007). Secondly, since
self-report data are prone to bias, even when bias is minimized by using psychometrically
validated tools (Hogan 2003), complementary objective measures would increase the rigour of
intervention outcome measures. Despite this, seven studies in this review only used self-report
measures (D'Amico et al. 2008; Esposito-Smythers et al. 2006; Liddle et al. 2009; Slesnick et al.
2007; Dawes et al. 2005; Slesnick et al. 2006; Kemp et al. 2007). Of the two that used objective
measures, one used urine tests for drug use but did not test for alcohol use (Peterson et al.
2006), and the other reviewed driving records (Stein et al. 2006). A number of more objective
measures suitable for evaluating alcohol harm interventions are emerging, including measures
of alcohol-related crime, traffic accidents and emergency department presentations (Breen et
al. 2011a; Czech et al. 2010; Shakeshaft, Doran & Byrnes 2009).
Eight of the nine identified studies were conducted in the United States which limits
generalizability to other countries. Although outcomes of interventions evaluated in the
United States may be applicable to other high-income countries in so far as they share similar
162
socio-economic factors and infrastructure for young people, between-country differences in
drinking prevalence and patterns (World Health Organization 2004), as well as different legal
drinking ages, might lead to different intervention effects in different countries. Rigorous
evaluation trials, conducted in countries other than the United States, would be valuable
additions to the evidence base.
Finally, there was no consideration of costs in any of the included studies. Economic analysis
provides an important contribution by costing and valuing reductions in alcohol-related harm,
as well as providing a benchmark to evaluate potential savings associated with interventions.
Although the economic cost of alcohol misuse among young people has not been measured
(Doyle, Delaney & Tobin 1994), the associated rates of alcohol-related health service utilization
and crime are high. Accumulated over a life-time, these harms are likely to result in a
substantial cost to society with minimal off-set of those costs through tax contributions
(McGorry et al. 2007; Pacileo & Fattore 2009; Cohen 1998).
Intervention effects
Despite their methodological limitations, the studies identified by this systematic review
represent best evidence for the effectiveness of interventions for young people with existing
alcohol use problems or who participate in behaviour that places them at high risk of harm.
The most promising approaches to reduce such harms are CBT (Esposito-Smythers et al. 2006;
Kemp et al. 2007), family therapy (Liddle et al. 2009; Slesnick et al. 2006) and community
reinforcement (Slesnick et al. 2007). Evaluations using more rigorous methodologies are
required before clear conclusions can be reached about the most effective interventions to
reduce alcohol-related harms among youth who have existing alcohol use problems, or who
participate in behaviour that places them at high risk of harm.
163
Limitations of the review
The possibility that this systematic review did not locate all relevant studies is unlikely: 10
electronic databases were searched by researchers, seven collections checked by a senior
librarian and reference lists of review articles examined. Relevant identified studies may have
been excluded or misclassified, but this is also unlikely given high agreement between blinded
coders (86%).
Because this review is limited to intervention studies published in 2005-09, effective
interventions published prior to 2005 are excluded. A comprehensive review of relevant
interventions published prior to 2000, however, identified only family therapy and community
reinforcement as interventions with evidence for their effectiveness (Williams & Chang 2000).
For the period 2000-04, the 52 reviews identified in this review (Fig. 1) were examined and 14
reviews of intervention studies were identified. Hand-searching their reference lists located
four individual treatment outcome studies (Kaminer, Burleson & Goldberger 2002; Liddle et al.
2001; Wells-Parker & Williams 2002; Kypri et al. 2004), only two of which showed significant
effects: one for CBT (Kaminer, Burleson & Goldberger 2002) and the other for family therapy
(Liddle et al. 2001). In total, therefore, prior to 2005 three intervention types have been
identified with evidence for their effectiveness, all of which were included in this review. This
suggests effective interventions are unlikely to have been omitted. As might be expected, it
also indicates that the number of intervention studies is increasing over time: four between
2000 and 2004 and nine between 2005 and 2009. It is likely, however, that these published
evaluations overestimate the true intervention effectiveness, as evaluations with statistically
significant findings are more likely to be published (Dickersin et al. 1987; Easterbrook et al.
1991).
164
Although this review focused on interventions to reduce alcohol-related harm, multi-modal
interventions that address alcohol and other common comorbid issues are likely to increase
benefits for young people and their communities (Bauman & Phongsavan 1999), because
alcohol misuse is associated commonly with other harms, particularly illicit drug use (Regier et
al. 1990; Teesson et al. 2010). All but one study in this review included illicit drug use in the
sample characteristics and/or as an outcome (D'Amico et al. 2008; Esposito-Smythers et al.
2006; Kemp et al. 2007; Liddle et al. 2009; Peterson et al. 2006; Slesnick et al. 2006; Slesnick et
al. 2007; Stein et al. 2006).
Future opportunities for methodologically adequate intervention studies
The published intervention studies delivered outside of educational settings, designed for
young people with existing alcohol use problems or who participate in behaviour that places
them at high risk of alcohol-related harm, have substantial methodological limitations that
make it difficult to interpret their results. Future intervention trials need to be more rigorous,
particularly in terms of their study designs, sample recruitment and follow-up and statistical
analyses. It is also clear that individualistic approaches have been the focus of interventions
evaluated to date. Given the complex, multi-dimensional nature of problems experienced by
highly disadvantaged young people, it is likely that programs that engage with the broader
social context and community resources, as well as individual factors, will be more cost-
effective (Mortimer & Segal 2005). As a minimum, replication of these interventions in studies
outside the United States would increase the generalizability of their results.
Conclusions
Given the extent of costs and harms associated with risky alcohol use by young people, there is
a clear need for a greater number of methodologically rigorous evaluations of interventions

165
targeting high-risk young people and those experiencing alcohol-related harm, particularly
with a focus broader than the individual.
Acknowledgements
We would like to thank Associate Professor Christopher Doran for providing advice on the
paper’s content. Funding was provided by the Alcohol Education and Rehabilitation
Foundation as part of the Alcohol Action in Rural Communities project.
166
Points of clarification for Paper 6
Addiction owns the copyright of this published paper. The points of clarification have been
added to provide additional information about the research for this thesis without modifying
the content of the published paper.
Resolution of classification discrepancies
Coders met to discuss classification discrepancies. Consensus was reached through re-
examining the identified studies and agreeing on the appropriate classification.

167
Implications and future directions

168
The feasibility and benefits of creating partnerships between researchers, health care
providers and Indigenous Australians
The work contained in this thesis demonstrates a process of researchers working in
partnership with health care providers and Indigenous Australians to improve the
development of Indigenous-specific interventions for implementation into routine health care.
The systematic review of the peer-reviewed literature completed in Paper 1 (Calabria et al.
2012) identified family-based interventions as having some evidence for their effectiveness
and having the most potential to be tailored to Indigenous people to reduce their experience
of alcohol-related harm, specifically Community Reinforcement and Family Training (CRAFT).
CRAFT and the Community Reinforcement Approach (CRA) (an evidence-based intervention for
problem drinkers on which the development of CRAFT was based) were then tailored to the
requirements of the health care providers who would be likely to deliver them (Paper 3
(Calabria et al. submitted-a)) and their level of acceptability to potential Indigenous clients of
health care services was examined (Paper 4 (Calabria et al. 2013)).
This consultation process determined that CRA and CRAFT could be modified to optimise their
acceptability to Indigenous people in the local community and local health care providers. The
major modifications to CRA and CRAFT were to convert the technical language in the
intervention resources and CRA and CRAFT manuals to a more local dialect, and to introduce
the possibility of group sessions to complement individual counselling sessions. Health care
providers at a rural drug and alcohol treatment agency have now been trained and certified in
the delivery of both interventions, and a local supervision and training program has been
established to provide ongoing support for certified health care providers delivering CRA and
CRAFT. Furthermore, sufficient capacity has now been built to enable the training and
certification of new health care providers in other local communities. Ongoing referral
pathways into CRA and CRAFT have been newly established, or existing pathways improved,
169
through a range of different agencies including, for example, probation and parole, and local
Aboriginal Medical Services. Finally, a package of outcome measures has been developed that
is acceptable for use by health care providers, and could be used by researchers or health care
providers to assess the outcomes of clients participating in the tailored CRA and CRAFT
interventions.
The consultation process also identified a perceived need for interventions targeting young
Indigenous people at high risk of alcohol-related harm. Research evidence was found to
support this perceived need in two separate ways: an epidemiological analysis which
confirmed the disproportionately high negative impact on young Indigenous people (Paper 5
(Calabria et al. 2010); and a systematic review of the literature that identified the potential
effectiveness of CRA with adolescents (Paper 6 (Calabria, Shakeshaft & Havard 2011)). An
adolescent version of CRA (A-CRA) has been recently developed, that includes parents in the
therapeutic approach (Garner, Barnes & Godley 2009; Garner et al. 2009; Godley et al. 2007;
Godley, Hedges & Hunter 2011; Godley et al. 2001; Godley et al. 2009; Smith et al. 2011).
Although A-CRA is also a United States based intervention, it derives from the same principles
as CRA and CRAFT and the evidence presented in this thesis strongly suggests that it could also
be tailored to optimise its acceptability to both health care providers (Paper 3 (Calabria et al.
submitted-a)) and Indigenous adolescents (Paper 4 (Calabria et al. 2013)).
This demonstrated process of tailoring interventions, through evidence informing practice and
practice and perceived needs informing research, is highly consistent with the definition of
translational research (Marincola 2003; Havard Catalyst 2013). This process is not linear; what
matters is the maintenance of the complementary relationship between research and practice.
This optimises the likelihood that current best evidence will be used to inform the
development of Indigenous-specific interventions aimed to meet the identified and perceived
170
needs of Indigenous Australians in an acceptable and feasible manner. Evidence-based
medicine is defined as integrating clinical experience with clinical research evidence (Sackett et
al. 1996), which is clearly consistent with the principle of translation research. The next step
after an intervention has been identified and tailored for health care providers and Indigenous
Australians is to evaluate both its effectiveness and costs. Intervention evaluation that
demonstrates cost-effectiveness has the potential to contribute to improvements in
Indigenous health (Paul et al. 2010). The evaluation itself will require effective and consultative
partnerships (Gray et al. 2000), primarily to provide ongoing feedback to health care providers
and Indigenous communities on outcomes and to facilitate ongoing modification of
intervention programs to improve their effectiveness, or the economic efficiency with which
they can be delivered. Although cost-effectiveness analyses are important in determining the
relative efficiency with which different interventions are provided, they are limited by the
assumptions that underpin the models used and the quality of the data available to populate
them (Drummond et al. 2005). Furthermore, interventions that are not cost-effective, but do
have evidence for their effectiveness, can still provide health benefits.
Developing guiding principles for researchers working in partnership with Indigenous
Australians and health care providers to improve intervention research
Through the process of working in partnership with health care providers and Indigenous
Australians to improve intervention research, three guiding principles began to emerge that
could be useful for other groups aiming to tailor, implement and evaluate Indigenous-specific
interventions: 1) consultation between researchers, health care providers and Indigenous
Australians is required from intervention identification and modification, through to
implementation and evaluation; 2) finding a balance between methodologically rigorous
research and intervention implementation in a real world setting; 3) building capacity to
171
ensure the delivery of effective interventions is sustained beyond the timeframe of any
research project.
Guiding principles have been previously published for implementing community interventions
among Indigenous people in Canada (Potvin et al. 2003). The authors of those guiding
principles state that similar principles date back to the 1950s, but highlight the importance of
demonstrating the principles in their current research context. Therefore, although the
Canadian guiding principles are similar to those proposed by this thesis, there is merit in
attempting to demonstrate the applicability of these types of principles to the Australian
Indigenous context.
Principle 1: consultation between researchers, health care providers and Indigenous
Australians is required from intervention identification and modification, through to
implementation and evaluation
Consultation between researchers and Indigenous Australians about Indigenous-specific
research acknowledges and respects Indigenous people’s right to self-determination, their
differences in cultural beliefs and systems, and the diversity of Indigenous people (United
Nations 2008; Australian Institute of Aboriginal and Torres Strait Islander Studies 2010;
National Health and Medical Research Council 2003). For these reasons consultation is an
ethical requirement for Indigenous research (National Health and Medical Research Council
2003). Consultation with health care providers that are likely to deliver Indigenous-specific
interventions increases the likelihood of the interventions being feasible to implement and
being sustained beyond the life of a defined research project. Indigenous Australians and
health care providers who work with Indigenous people should be actively involved in
Indigenous-specific research from conception to evaluation. This thesis has demonstrated that
172
it is feasible to establish a process whereby evidence informs practice, and practice and
perceived needs informs research. Although this is a lengthy process, it has the potential to
improve the quality of Indigenous-specific research, which to date has been shown to be less
than adequate (Sanson-Fisher et al. 2006; Clifford et al. 2010; Shakeshaft, Clifford &
Shakeshaft 2010). Researcher consultation with health care providers and Indigenous
Australians should continue after the specific intervention has been developed, to improve
both the implementation and evaluation phase.
Ensuring the acceptability of rigorous research design and measures to health care providers
who delivered the interventions, and to Indigenous Australians, was a key requirement
identified in this thesis. This did not mean that the methodological quality of the research had
to be diluted to ensure its acceptability to health care providers and Indigenous Australians.
Rather, it meant that the type of, and need for, various research methods needed to be clearly
communicated to health care providers involved in the evaluation, specifically highlighting the
stages of intervention development through to evaluation: 1) tailor the intervention; 2)
implement tailored intervention; 3) measure its effectiveness (ensuring that the agreed
intervention is delivered consistently); and 4) analyse the outcome data. For this doctoral
project the needs and suggestions of health care providers and Indigenous Australians were
incorporated into the research, even when they led to modification to the original research
plan, providing the modifications did not excessively dilute the reliability and validity of the
outcomes. Finding this balance was difficult and required ongoing communication and
negotiations between all those engaged in the partnership.
Principle 2: finding a balance between methodologically rigorous research and
intervention implementation in a real world setting

173
A balance between rigorous research design and methods, and real world service delivery
must be reached. Research methods need to be sufficiently flexible to fit into the routine care
of clients and health care providers need to be open to incorporate some evaluation
components into their usual work. Establishing a trusting and co-operative relationship
between researchers and health care providers aimed at benefiting the local Indigenous
community is essential to finding the research-real-world-balance (Clapham 2011; Potvin et al.
2003).
Rigorous evaluation gives the best chance of determining the true effects of an intervention.
The absence of a controlled design can limit the findings of an evaluation because any
observed differences between pre- and post-intervention outcomes cannot confidently be
attributed to the intervention being evaluated, independently of other co-occurring factors
that may have influenced the outcome over time (Jackson 2007; Chambless & Hollon 1998).
Despite being the ‘gold standard’ for efficacy research (Sibbald & Roland 1998), randomised
controlled trials (RCTs) are not always appropriate when interventions are delivered in
naturalistic settings (Seligman 1995).
Randomised controlled trials randomly allocate recruited participants or groups into the
intervention or control condition (Sibbald & Roland 1998). When individuals are the unit of
analysis, eligible individuals are randomised to receive either the intervention or the control
condition, which could be treatment as usual or no treatment. Individual outcome measures
are used to evaluate the effectiveness of the intervention and can include self-reported survey
data or routinely collected individual data (e.g. Medicare data). Group randomisation is
appropriate for evaluating interventions that are implemented across whole communities, or
within schools, or health care services, such as Indigenous primary care practices. The two
most rigorous evaluation designs appropriate to group randomisation have been identified as:
174
1) a cluster RCT where the groups are randomly assigned to the intervention or control
condition (Campbell et al. 2000); and 2) a stepped wedge or multiple baseline design (MBD)
where groups are randomised to start intervention delivery at staggered intervals (e.g. 6
months, 12 months and 18 months) (Hawkins et al. 2007). Both these design options allow
active engagement of a range of health and other community services. Self-reported and
routinely collected community-level, or service-level, data (e.g. community surveys, police
counts of alcohol-related assaults, or audits of client medical records) are outcome measures
that are highly appropriate to cluster RCT or MBD evaluation designs.
Randomised controlled trials that randomise individuals are not feasible to implement in
Indigenous communities and Indigenous-specific health care services where there are many
familial connections and strong community cohesion (Stewart et al. 2010). Randomising whole
communities or services would minimise the potential for contamination between intervention
and control groups, but cluster RCTs are an expensive and time consuming evaluation design
(Biglan, Ary & Wagenaar 2000). For example, a recent community-level cluster RCT conducted
with rural communities in New South Wales (NSW) to reduce alcohol harm cost approximately
$A2.3 million and took six years to complete (Shakeshaft et al. 2012). These practical reasons
could help explain the lack of rigorous evaluation research focused on Indigenous health (Paul
et al. 2010; Sanson-Fisher et al. 2006; Clapham 2011). The MBD, as an alternative to a cluster
RCT, is less expensive to implement because each community effectively acts as its own
control, meaning this evaluation could be done with as few as two communities or health care
services. Although the level of evidence it generates is less rigorous than in a cluster RCT, it is
sufficiently rigorous to be used as the basis for policy and health service delivery decisions
(Hawkins et al. 2007). Nevertheless, MBD evaluations are still expensive compared to simpler
designs, such as a pre- and post-evaluation design with one group, because they typically
evaluate complex interventions that involve multiple key stakeholders and are logistically
175
difficult, time consuming and require high level research skills to implement (Hawkins et al.
2007).
The relatively high cost and complexity of both cluster RCTs and MBDs potentially highlights
the particular value of a more staged approach to real world intervention research. These
stages could involve a process of defining and tailoring an intervention and outcome measures,
as has been the focus of this thesis. The next stage could be a relatively simple evaluation of
the agreed intervention using a pre- and post-evaluation design. Although a pre- and post-
evaluation design does not provide the strength of evidence of an RCT or MBD, it does provide
sufficient evidence to justify the expense and time commitment required for a large-scale trial,
the conduct of which could be the final stage in this stepped approach to real world
Indigenous intervention research. It is probable that a key criticism of this approach would be
the time that is required to go through these stages in order to produce rigorous evidence, but
existing reviews have clearly shown that very little high quality Indigenous evaluation research
has been published over the last 20 years in Australia or internationally (Sanson-Fisher et al.
2006; Clifford et al. 2010; Shakeshaft, Clifford & Shakeshaft 2010), which suggests
implementing this staged approach over a period of approximately 5-6 years would produce
more high quality outcomes than has been achieved to date.
Reliable and valid measures are necessary to accurately assess the outcomes of an
intervention, regardless of the evaluation design (Streiner & Norman 2008). Specifically,
measures designed, or validated, for Indigenous people should be used when conducting
research with this group. Paper 2 (Calabria et al. submitted-b) identified Indigenous-specific
cut-off scores on two shorter versions of the Alcohol Use Disorders Identification Test (AUDIT):
AUDIT-C and AUDIT-3. These measures can be used to classify the drinking risk status of new
clients, to determine the most appropriate intervention for them, or to measure participant
176
outcomes before and after intervention delivery. AUDIT was designed as a cross cultural
screening instrument (Babor et al. 1989; Saunders et al. 1993) but Indigenous-specific cut-off
scores for two shorter versions (AUDIT-C and AUDIT-3) have not previously been published. As
well as identifying Indigenous drinking risk status using AUDIT-C and AUDIT-3, the Indigenous-
specific cut-off scores on these shorter versions of the AUDIT can be used to reduce the time it
takes to complete the AUDIT, an issue that has previously been identified as a barrier to its
routine use (Brady et al. 2002; Clifford & Shakeshaft 2011).
Another measure, that was designed for Indigenous Australians and has been validated among
this population, is the Growth Empowerment Measure (GEM) (Haswell et al. 2010). The GEM
measures Indigenous people’s social and emotional wellbeing. The measure consists of the
Emotion Empowerment Scale (EES14) and twelve scenarios (12S). This Indigenous-specific
measure shows great potential to be used in intervention evaluations.
An issue identified in this research was the problem of researchers imposing an additional data
collection burden on both health care providers and clients, as a consequence of requiring
evaluation-specific outcomes to be assessed pre- and post- intervention. A solution that was
identified in this project was to ensure that, as far as possible, the outcome measures were
brief (e.g. testing shorter forms of AUDIT) and aligned with the routine reporting requirements
of health care providers and the health care services. Anecdotally, this project showed
acceptable compromises about which questions needed to be asked, and the required data
collection time points were able to be successfully negotiated. Indeed, the counsellors valued
the additional information the measures provided (e.g. a specific indicator of each individual
client’s level of risk regarding their alcohol use, smoking status and other drug use), as
evidenced by their updating their intake assessment forms to allow them to easily continue to
collect these additional data routinely.
177
In addition to the use of valid and reliable measures, the method of delivery of measures is
also important to consider for an evaluation. Computerised survey delivery has potential to
improve the efficiency of data collection and processing, for example by tailoring questions for
participants based on previous responses, providing instant feedback, and automatically
extracting data into computerised statistical computer programs for analysis (Bonevski et al.
1997). Further, computer programs can include verbal versions of survey questions to assist
participants with low literacy (Newell et al. 1997), which is applicable for Indigenous
Australians who have lower literacy levels than non-Indigenous Australians (Australian
Government 2013). The use of computerised surveys minimises missing data and achieves at
least comparable reliability and validity to pen and paper surveys or interviews (Bonevski et al.
1997; Newell et al. 1997). The use of computers to present surveys has also been shown to be
acceptable to clients in health care settings (Shakeshaft, Bowman & Sanson-Fisher 1998;
Bonevski et al. 1997; Newell et al. 1997). With new Tablet technology (e.g. Apple iPads), using
computers to present surveys is easy because of the convenient travel size and the novelty of
Tablet use with participants. Tablet use to deliver surveys could provide benefits to
researchers and participants, and when appropriate, could be considered for evaluating
interventions, although the acceptability of their use to health care providers and Indigenous
Australians should be assessed prior to their routine use.
Principle 3: building capacity to ensure the delivery of effective interventions is
sustained beyond the timeframe of the research project
Building capacity in health care services involved in the development, implementation and
evaluation of Indigenous-specific interventions can help ensure that the delivery of effective
interventions to Indigenous Australians is sustained beyond the timeframe of the research
project. This doctoral project, for example, demonstrated that it is feasible in the context of
178
routine health care service delivery, to provide benefit beyond the life of the research project
(Paper 3 (Calabria et al. submitted-a)). Key factors to facilitate this were that: 1) a local training
program was established to build the intervention skills of health care providers; 2)
intervention components and standardised delivery was documented (e.g. an intervention
manual written for the intervention context in consultation with health care providers); 3)
regular local supervisory meetings were organised to provide support for health care
providers; and 4) referral pathways into the intervention were established and transparent.
Nevertheless, a key challenge to sustaining interventions in routine health care service delivery
is that Indigenous health care has historically been under-funded (Allison, Rivers & Fottler
2004; Gray et al. 2010), resulting in low numbers of health care providers and a high turnover
of staff. Under staffing creates additional challenges when health care providers are asked to
incorporate research methods into their usual practice. Health care providers, who are already
busy, have previously identified that they perceive that they do not have the time to add to
their workload, nor the skills to address additional health issues that might be identified
(Shakeshaft & Frankish 2003; Solberg, Maciosek & Edwards 2008).
One way to address these challenges could be for supervisors and managers to discuss with
health care providers how they can best deliver health care services and incorporate research
methods into their routine workload. High staff turnover means that training health care
providers to deliver the tailored interventions needs to be ongoing to ensure that new staff
have the opportunity to deliver the intervention. It is therefore important to establish local
training programs that are sustainable over time: organising specific training days can provide
time free from competing tasks that is dedicated to intervention training. To facilitate this
process, this doctoral research found that the appointment of a nominated individual based at
the health care service who was specifically responsible for managing the intervention within
179
that service was instrumental to its successful implementation (see Paper 3 (Calabria et al.
submitted-a)). This finding reflects earlier health care service research which shows that
advantages of engaging a respected and influential study champion to promote new
interventions and problem solve issues as they arise (Fiore, Keller & Curry 2007; Ziedonis et al.
2007). The nominated individual can motivate health care providers to co-ordinate additional
intervention procedures into their routine practice. The nominated individual can also discuss
with health care providers their client outcomes, in a simple, comprehensible format at regular
intervals, which has been shown to improve the frequency and quality of their delivery of
clinical care (Barker 2000).
Another potential solution to the problem of integrating research into routine delivery of
health care services that has emerged from this research is to apply the same intervention to
multiple issues, where appropriate, to avoid health care providers having to learn multiple
intervention approaches. The CRA and CRAFT interventions, for example, have been used with
other population groups to address problem drug use (Roozen, de Waart & van der Kroft 2010)
and so, if the need is identified, it is likely that these programs could also be used to address
Indigenous drug use.
Conclusions
This thesis demonstrates a process of researchers working in partnership with health care
providers and with Indigenous Australians to tailor interventions for delivery to Indigenous
Australians through routine health care. It shows how the specific skills and expertise of
different groups can be combined: research skills in reviewing evidence and designing
evaluations and outcome measures; health care provider experience of working with
Indigenous Australians and skills in implementing interventions; and the knowledge and
expertise of Indigenous Australians in determining the type and format of interventions, as
180
well as highlighting new areas of concern. Three guiding principles are proposed for tailoring,
implementing and evaluating Indigenous-specific interventions: 1) consultation between
researchers, health care providers and Indigenous Australians is required from intervention
identification and modification, through to implementation and evaluation; 2) finding a
balance between methodologically rigorous research and intervention implementation in a
real world setting; 3) building capacity to ensure the delivery of effective interventions is
sustained beyond the timeframe of the research project. Specifically, health care providers and
Indigenous Australians should be actively involved in research projects aimed at tailoring,
implementing and evaluating Indigenous-specific interventions, and should work with
researchers to incorporate Indigenous Australian values and needs into routine service
delivery, using rigorous research methodology. This process requires compromise and
negotiation among researchers, health care providers and Indigenous Australians, as well as
confidence and trust that all those involved have improving the health and wellbeing of
Indigenous Australians at the forefront of decisions made. Local training and supervisory
programs should be overseen by a nominated individual, with the goal of maintaining
motivation among health care providers for training in intervention delivery, implementing the
intervention, collecting outcome data, and driving the intervention. Although these guiding
principles are the result of research into family-based intervention aimed at reducing alcohol-
related harm among Indigenous Australians, they are likely to be applicable to the evaluation
of a wide-range of Indigenous-specific interventions.
181
References
182
Adams, M, Aylward, P, Heyne, N, Hull, C, Misan, G, Taylor, J & Walker-Jeffreys, M 2005,
'Integrated support for Aboriginal tertiary students in health-related courses: The Pika
Wiya Learning Centre', Australian Health Review, vol. 29, no. 4, pp. 482-488.
Allan, J & Campbell, M 2011, 'Improving access to hard-to-reach services: A soft entry
approach to drug and alcohol services for rural Australian Aboriginal communities',
Social Work in Health Care, vol. 50, no. 6, pp. 443-465.
Allen, J, Inder, KJ, Lewin, TJ, Attia, JR & Kelly, BJ 2013, 'Construct validity of the Assessment of
Quality of Life - 6D (AQoL-6D) in community samples', Health and Quality of Life
Outcomes, vol. 11, no. 61, p. 2.
Allison, M, Rivers, PA & Fottler, MD 2004, 'Can community health center funding enhance
health services for Native American tribes and organizations?', Journal of Health Care
for the Poor and Underserved, vol. 15, no. 2, pp. 193-205.
Altman, J 2003, 'The economic and social context of Indigenous health', in The Health of
Indigenous Australians, ed. N Thompson, Oxford University Press, South Melbourne,
pp. 25-43.
American Psychiatric Association 1994, Diagnostic and statistical manual of mental health
disorders (4th edition), 4th edn, Author, Washington DC.
Australian Bureau of Statistics 2001, National Health Survey 2001, Expanded CURF, RADL, ABS
data available on request
Australian Bureau of Statistics 2006, National Aboriginal and Torres Strait Islander Health
Survey 2004-05, Expanded CURF, RADL, Findings based on use of ABS CURF data
Australian Bureau of Statistics & Australian Institute of Health and Welfare 2005, The health
and welfare of Australia's Aboriginal and Torres Strait Islander peoples Australian
Bureau of Statistics and Australian Institute of Health and Welfare, Canberra
183
Australian Bureau of Statistics & Australian Institute of Health and Welfare 2008, The health
and welfare of Australia's Aboriginal and Torres Strait Islander peoples, Australian
Bureau of Statistics and Australian Institute of Health and Welfare, Canberra
Australian Department of Human Services and Health 1995, National Drug Strategy Household
Survey: Urban Aboriginal and Torres Strait Islander peoples supplement 1994,
Australian Government Publishing Service, Canberra.
Australian Government 2013, Closing the Gap Prime Minister's Report 2013, Canberra.
Australian Government Department of Health and Ageing, Australian Indigenous
HealthInfoNet. Available from: <http://www.healthinfonet.ecu.edu.au/>.
Australian Government Department of Health and Ageing 2004, Helping you to stay healthy:
Information on the Aboriginal and Torres Strait Islander adult health check, Australian
Government Publishing Service, Canberra.
Australian Government Department of Health and Ageing 2007, Alcohol Treatment Guidelines
for Indigenous Australians, Commonwealth of Australia, Canberra.
Australian Institute of Aboriginal and Torres Strait Islander Studies 2010, Guidelines for ethical
research in Australian Indigenous studies, Australian Institute of Aboriginal and Torres
Strait Islander Studies, Canberra.
Australian Institute of Health and Welfare 2005, 2004 National Drug Strategy Household
Survey: Detailed findings, Australian Institute of Health and Welfare, Canberra.
Australian Institute of Health and Welfare 2008a, 2007 National Drug Strategy Household
Survey: Detailed findings, Australian Institute of Health and Welfare, Canberra.
Australian Institute of Health and Welfare 2008b, 2007 National Drug Strategy Household
Survey: First results, Australian Institute of Health and Welfare, Canberra.
Australian Institute of Health and Welfare 2010, Health expenditure Australia, 2008-09,
Australian Institute of Health and Welfare, Canberra.
184
Australian Institute of Health and Welfare 2011a, 2010 National Drug Strategy Household
Survey report, Australian Institute of Health and Welfare, Canberra.
Australian Institute of Health and Welfare 2011b, Australian hospital statistics 2009-10,
Australian Institute of Health and Welfare, Canberra.
Australian Institute of Health and Welfare 2011c, Expenditure on health for Aboriginal and
Torres Strait Islander people, 2008-09: An analysis by remoteness and disease,
Australian Institute of Health and Welfare, Canberra.
Australian Institute of Health and Welfare 2011d, The health and welfare of Australia's
Aboriginal and Torres Strait Islander people, an overview 2011, Australian Institute of
Health and Welfare, Canberra.
Australian Medical Association 2011, Aboriginal and Torres Strait Islander health report card:
Best practice in primary health care for Aboriginal peoples and Torres Strait Islanders,
2010-2011, Australian Medical Association, Canberra.
Babor, TF, de la Fuente, JR, Saunders, JB & Grant, M 1989, AUDIT the Alcohol Use Disorders
Identification Test: Guidelines for use in primary health care, World Health
Organization, Division of Mental Health, Geneva.
Babor, TF, Higgins-Biddle, JC, Saunders, JB & Monteiro, M 2001, The Alcohol Use Disorders
Identification Test: Guidelines for use in primary care, World Health Organization,
Geneva.
Barker, R 2000, 'Managing quality in primary health care: The need for valid information about
performance ', Quality in Health Care, vol. 9, no. 2, p. 83.
Barratt, M 2003, 'Organizational support for evidence-based practice within child and family
social work: A collaborative study', Child & Family Social Work, vol. 8, no. 2, pp. 143-
150.
185
Bauman, A & Phongsavan, P 1999, 'Epidemiology of substance use in adolescence: Prevalence,
trends and policy implications', Drug and Alcohol Dependence, vol. 55, no. 3, pp. 187-
207.
Begg, DJ & Gulliver, P 2008, 'A longitudinal examination of the relationship between
adolescent problem behaviors and traffic crash involvement during young adulthood',
Traffic Injury Prevention, vol. 9, no. 6, pp. 508-514.
Begg, S, Vos, T, Barker, B, Stevenson, C, Stanley, L & Lopez, A 2007, The burden of disease and
injury in Australia 2003, AIHW cat. no. PHE 82, The Australian Institute of Health and
Welfare, Canberra.
Bernal, G, Jime´nez-Chafey, MI & Rodreguez, MMD 2009, 'Cultural adaptation of treatments: A
resource for considering culture in evidence-based practice', Professional Psychology-
Research and Practice, vol. 40, no. 4, pp. 361-368.
Berry, SL & Crowe, TP 2009, 'A review of engagement of Indigenous Australians within mental
health and substance abuse services', Advances in Mental Health, vol. 8, no. 1, pp. 16-
27.
Best, D, Manning, V, Gossop, M, Gross, S & Strang, J 2006, 'Excessive drinking and other
problem behaviours among 14-16 year old school children', Addictive Behaviors, vol.
31, no. 8, pp. 1424-1435.
Biglan, A, Ary, D & Wagenaar, A 2000, 'The value of interupted time-series experiements for
community intervention research', Prevention Science, vol. 1, no. 1, pp. 31-49.
Bindon, J, Headley, EJ, Rissel, C & Wade, V 2009, 'Improving the health and wellbeing of an
urban Aboriginal men's group through a cycling program', Aboriginal and Islander
Health Worker Journal, vol. 33, no. 4, pp. 3-5.
Bonevski, B, Sanson-Fisher, RW, Campbell, EM & Ireland, MC 1997, 'Do general practice
patients find computer health risk surveys acceptable? A comparison with pen-and-
paper method', Health Promotion Journal of Australia, vol. 7, no. 2, pp. 100-106.
186
Boyd-Ball, AJ 2003, 'A culturally responsive, family-enhanced intervention model', Alcoholism,
Clinical and Experimental Research, vol. 27, no. 8, pp. 1356-1360.
Brady, M 1991, 'Drug and alcohol use among Aboriginal people', in The health of Aboriginal
Australia, eds J Reid & P Trompf, Harcourt Brace Jovanovich Publishers, Sydney, pp.
173-217.
Brady, M 2004, Indigenous Australia and alcohol policy: Meeting difference with indifference,
University Of New South Wales Press, Sydney.
Brady, M 2008, First taste: How Indigenous Australians learned about grog, The Alcohol
Education & Rehabilitation Foundation Ltd, Canberra.
Brady, M, Dawe, S & Richmond, R 1998, 'Expanding knowledge among Aboriginal service
providers on treatment options for excessive alcohol use', Drug and Alcohol Review,
vol. 17, no. 1, pp. 69-76.
Brady, M, Sibthorpe, B, Bailie, R, Ball, S & Sumnerdodd, P 2002, 'The feasibility and
acceptability of introducing brief intervention for alcohol misuse in an urban Aboriginal
medical service', Drug and Alcohol Review, vol. 21, no. 4, pp. 375-380.
Bramley, D, Broad, J, Harris, R, Reid, P, Jackson, R & for the Alcohol Burden of Disease and
Disability Group 2003, 'Differences in patterns of alcohol consumption between Maori
and non-Maori in Aotearoa (New Zealand)', New Zealand Medical Journal, vol. 116, no.
1184, pp. 1-17.
Breen, C, Shakeshaft, A, Slade, T, D'Este, C & Mattick, RP 2011a, 'Assessing reliability of
measures using routinely collected data', Alcohol and Alcoholism, vol. 46, no. 4, pp.
501-502.
Breen, C, Shakeshaft, A, Slade, T, Love, S, D'Este, C & Mattick, RP 2011b, 'Do community
characteristics predict alcohol-related crime?', Alcohol & Alcoholism, vol. 46, no. 4, pp.
464-470.
187
Brit, H, Miller, GC, Charles, J, Henderson, J, Bayram, C, Pan, Y, Valenti, L, Harrison, C, Fahridin, S
& O'Halloran, J 2009, General practice activity in Australia 2008-09: BEACH bettering
the evaluation and care of health, Australian Institute of Health and Welfare, Canberra.
Byrnes, JM, Cobiac, LJ, Doran, CM, Vos, T & Shakeshaft, AP 2010, 'Cost-effectiveness of
volumetric taxation in Australia', Medical Journal of Australia, vol. 192, no. 8, pp. 439-
43.
Calabria, B, Clifford, A, Rose, M & Shakeshaft, A submitted-a, 'Tailoring a family-based alcohol
intervention for Aboriginal Australians, and the experiences and perceptions of health
care providers trained in its delivery', BMC Public Health.
Calabria, B, Clifford, A, Shakeshaft, A, Allan, J, Bliss, D & Doran, C 2013, 'The acceptability to
Aboriginal Australians of a family-based intervention to reduce alcohol-related harms',
Drug and Alcohol Review, vol. 32, no. 3, pp. 328-332.
Calabria, B, Clifford, A, Shakeshaft, A, Conigrave, K, Simpson, L, Bliss, D & Allan, J submitted-b,
'Identifying Aboriginal-specific AUDIT-C and AUDIT-3 cut-off scores for at-risk, high-risk
and likely dependent drinkers using measures of agreement with the 10-item Alcohol
Use Disorders Identification Test', Addiction Science & Clinical Practice.
Calabria, B, Clifford, A, Shakeshaft, A & Doran, C 2012, 'Systematic review of family-based
interventions targeting alcohol misuse and their potential to reduce alcohol-related
harm in Indigenous communities', Journal of Studies on Alcohol and Drugs, vol. 73, no.
3, pp. 477-488.
Calabria, B, Doran, CM, Vos, T, Shakeshaft, AP & Hall, W 2010, 'Epidemiology of alcohol-related
burden of disease among Indigenous Australians', Australian and New Zealand Journal
of Public Health, vol. 34, no. S1, pp. S47-S51.
Calabria, B, Shakeshaft, AP & Havard, A 2011, 'A systematic and methodological review of
interventions for young people experiencing alcohol-related harm', Addiction, vol. 106,
no. 8, pp. 1406-1418.
188
Campbell, MK, Mollison, J, Steen, N, Grimshaw, JM & Eccles, M 2000, 'Analysis of cluster
randomized trials in primary care: A practical approach', Family Practice, vol. 17, no. 2,
pp. 192-196.
Centre for Disease Control 2008, 'Alcohol-attributable deaths and years of potential life lost
among American Indians and Alaska Natives, United States, 2001-2005', MMWR
Weekly, vol. 57, no. 34, pp. 938-941.
Chambless, DL & Hollon, SD 1998, 'Defining empirically supported therapies', Journal of
Consulting and Clinical Psychology, vol. 66, no. 1, pp. 7-18.
Cherpitel, C 1998, 'Differences in performance of screening instruments for problem drinking
among blacks, whites and Hispanics in an emergency room', Journal of Studies on
Alcohol, vol. 59, no. 4, pp. 420-426.
Cherpitel, C & Clark, W 1995, 'Ethnic differences in performance of screening instruments for
identifying harmful drinking and alcohol dependence in the emergency room',
Alcoholism, Clinical and Experimental Research, vol. 19, no. 3, pp. 628-634.
Cherpitel, CJ & Ye, Y 2008, 'Trends in alcohol- and drug-related ED and primary care visits: Data
from three US national surveys (1995-2005)', American Journal of Drug and Alcohol
Abuse, vol. 34, no. 5, pp. 576-583.
Chikritzhs, T & Brady, M 2006, 'Fact or fiction? A critique of the national Aboriginal and Torres
Strait Islander social survey 2002', Drug and Alcohol Review, vol. 25, no. 3, pp. 277-
287.
Chikritzhs, T, Fillmore, K & Stockwell, T 2009, 'A healthy dose of scepticism: four good reasons
to think again about protective effects of alcohol on coronary heart disease', Drug and
Alcohol Review, vol. 28, no. 4, pp. 441-444.
Clapham, K 2011, 'Indigenous-led intervention research: The benefits, challenges and
opportunities', International Journal of Critical Indigenous Studies, vol. 4, no. 2, pp. 40-
48.
189
Clifford, A, Pulver, LJ, Richmond, R, Shakeshaft, A & Ivers, R 2010, 'Smoking, nutrition, alcohol
and physical activity interventions targeting Indigenous Australians: Rigorous
evaluations and new directions', Australian and New Zealand Journal of Public Health,
vol. 34, pp. 640-645.
Clifford, A & Shakeshaft, A 2011, 'Evidence-based alcohol screening and brief intervention in
Aboriginal Community Controlled Health Services: Experiences of healthcare
providers', Drug and Alcohol Review, vol. 30, no. 1, pp. 55-62.
Coates, KS 2004, A global history of Indigenous peoples: Struggle and survival, Palgrave
MacMillan, New York.
Cobiac, L, Vos, T, Doran, C & Wallance, A 2009, 'Cost-effectiveness of interventions to prevent
alcohol-related disease and injury in Australia', Addiction, vol. 104, no. 10, pp. 1646-
1655.
Cohen, MA 1998, 'The monetary value of saving a high-risk youth', Journal of Quantitative
Criminology, vol. 14, no. 1, pp. 5-33.
Collins, DJ & Lapsley, HM 2008, The costs of tobacco, alcohol and illicit drug abuse to Australian
society in 2004/2005, Commonwealth of Australia, Canberra.
Conigliaro, J, Lofgren, RP & Hanusa, BH 1998, 'Screening for problem drinking: Impact on
physician behavior and patient drinking habits', Journal of General Internal Medicine,
vol. 13, no. 4, pp. 251-256.
Conigrave, K, Freeman, B, Caroll, T, Simpson, L, Lee, K, Wade, V, Kiel, K, Ella, S, Becker, K &
Freeburn, B 2012, 'The Alcohol Awareness project: Community education and brief
intervention in an urban Aboriginal setting', Health Promotion Journal of Australia, vol.
23, no. 3, pp. 219-225.
Conigrave, KM, Hall, WD & Saunders, JB 1995, 'The AUDIT questionnaire: Choosing a cut-off
score', Addiction, vol. 90, no. 10, pp. 1349-1356.
190
Connor, J, Broad, J, Jackson, R, Vander Hoorn, S & Rehm, J 2004, The burden of death, disease
and disability due to alcohol in New Zealand: Research summary, University of
Auckland, Auckland.
Coombes, L, Allen, D, Foxcroft, D & Guydish, J 2008, 'Motivational interviewing for the
prevention of alcohol misuse in young people (protocol)', Cochrane Database of
Systematic Reviews, vol. Issue 2.
Copello, A, Templeton, L, Orford, J, Velleman, R, Patel, A, Moore, L, MacLeod, J & Godfrey, C
2009, 'The relative efficacy of two levels of a primary care intervention for family
members affected by the addiction problem of a close relative: A randomized trial',
Addiction, vol. 104, no. 1, pp. 49-58.
Copello, AG, Velleman, RDB & Templeton, LJ 2005, 'Family interventions in the treatment of
alcohol and drug problems', Drug and Alcohol Review, vol. 24, no. 4, pp. 369-385.
Council of Australian Governments 2012, National Indigenous reform agreement (Closing the
Gap).
Cunningham, J & Paradies, YC 2012, 'Socio-demographic factors and psychological distress in
Indigenous and non-Indigenous Australian adults aged 18-64 years: Analysis of
national survey data', BMC Public Health, vol. 12, p. 95.
Czech, S, Shakeshaft, AP, Byrnes, JM & Doran, CM 2010, 'Comparing the cost of alcohol-related
traffic crashes in rural and urban environments', Accident Analysis & Prevention, vol.
42, pp. 1195-98.
D'Amico, EJ, Miles, JNV, Stern, SA & Meredith, LS 2008, 'Brief motivational interviewing for
teens at risk of substance use consequences: A randomized pilot study in a primary
care clinic', Journal of Substance Abuse Treatment, vol. 35, no. 1, pp. 53-61.
Dawes, MA, Johnson, BA, Ait-Daoud, N, Ma, JZ & Cornelius, JR 2005, 'A prospective, open-label
trial of ondansetron in adolescents with alcohol dependence', Addictive Behaviors, vol.
30, no. 6, pp. 1077-1085.
191
de los Angeles Cruz-Almanza, M, Gaona-Marquez, L & Sanchez-Sosa, JJ 2006, 'Empowering
women abused by their problem drinker spouses: Effects of a cognitive-behavioral
intervention', Salud Mental, vol. 29, no. 5, pp. 25-31.
Denning, DG, Conwell, Y, King, D & Cox, C 2000, 'Method, choice, intent, and gender in
completed suicide', Suicide and Life-Threatening Behavior, vol. 30, no. 3, pp. 282-288.
Dennis, M, Godley, SH, Diamond, G, Tims, FM, Babor, T, Donaldson, J, Liddle, H, Titus, JC,
Kaminer, Y, Webb, C, Hamilton, N & Funk, R 2004, 'The Cannabis Youth Treatment
(CYT) study: Main findings from two randomized trials', Journal of Substance Abuse
Treatment, vol. 27, no. 3, pp. 197-213.
Dickersin, K, Chan, S, Chalmersx, TC, Sacks, HS & Smith Jr, JH 1987, 'Publication bias and clinical
trials', Controlled Clinical Trials, vol. 8, no. 4, pp. 343-353.
Dixon, AL, Yabiku, ST, Okamoto, SK, Tann, SS, Marsiglia, FF, Kulis, S & Burke, AM 2007, 'The
efficacy of a multicultural prevention intervention among urban American Indian youth
in the southwest U.S.', Journal of Primary Prevention, vol. 28, no. 6, pp. 547-568.
Dodgson, JE & Struthers, R 2005, 'Indigenous women's voices: Marginalization and health',
Journal of Transcultural Nursing, vol. 16, no. 4, pp. 339-346.
Doran, CM, Hall, WD, Shakeshaft, AP, Vos, T & Cobiac, LJ 2010, 'Alcohol policy reform in
Australia: What can we learn from the evidence?', Medical Journal of Australia, vol.
192, no. 8, pp. 468-470.
Doran, CM & Shakeshaft, AP 2008, 'Using taxes to curb drinking in Australia', Lancet vol. 372,
no. 9640, pp. 701-702.
Doyle, H, Delaney, W & Tobin, J 1994, 'Follow-up study of young attenders at an alcohol unit',
Addiction, vol. 89, no. 2, pp. 183-189.
Doyle, M, Carr, A, Rowan, S, Galvin, P, Lyons, S & Cooney, G 2003, 'Family-oriented treatment
for people with alcohol problems in Ireland: A comparison of the effectiveness of
192
residential and community-based programmes', Journal of Family Therapy, vol. 25, no.
1, pp. 15-40.
Drummond, M & McGuire, A 2001, Economic evaluation in health care, Oxford University
Press, Oxford.
Drummond, MF, Sculpher, MJ, Torrance, GW, O'Brien, BJ & Stoddart, GL 2005, Methods for the
economic evaluation of health care programmes, third edition, Oxford University Press,
New York.
Dutcher, LW, Anderson, R, Moore, M, Luna-Anderson, C, Meyers, RJ, Delaney, HD & Smith, JE
2009, 'Community Reinforcement and Family Training (CRAFT): An effectiveness
study', Journal of Behavior Analysis in Health, Sports, Fitness and Medicine, vol. 2, no.
1, pp. 80-90.
Easterbrook, PJ, Gopalan, R, Berlin, JA & Matthews, DR 1991, 'Publication bias in clinical
research', Lancet, vol. 337, no. 8746, pp. 867-872.
English, DR, Holman, CDJ, Milne, E, Winter, MG, Hulse, GK, Coddle, JP, Bower, CJ, Corti, B, De
Klerk, N, Knuiman, MW, Kurinczuk, JJ, Lewin, GF & Ryan, GA 1995, The quantification
of drug caused morbidity and mortality in Australia 1995, Part 2, Canberra
Esposito-Smythers, C, Spirito, A, Uth, R & Lachance, H 2006, 'Cognitive behavioral treatment
for suicidal alcohol abusing adolescents: Development and pilot testing', American
Journal on Addictions, vol. 15, no. S1, pp. 126-130.
Fals-Stewart, W, Klostermann, K, Yates, BT, O'Farrell, TJ & Birchler, GR 2005, 'Brief relationship
therapy for alcoholism: A randomized clinical trial examining clinical efficacy and cost-
effectiveness', Psychology of Addictive Behaviors, vol. 19, no. 4, pp. 363-371.
Fergusson, DM, Boden, JM & Horwood, LJ 2009, 'Tests of causal links between alcohol abuse or
dependence and major depression', Archives of General Psychiatry, vol. 66, no. 3, pp.
260-266.
193
Fiore, MC, Keller, PA & Curry, SJ 2007, 'Health system changes to facilitate the delivery of
tobacco-dependence treatment', American Journal of Preventative Medicine, vol. 33,
no. S6, pp. S349-S356.
First Nations/First Nationals Information Governance Committee 2007, First Nations Regional
Longitudinal Health Survey (RHS) 2002/03: Results for adults, youth and children living
in First Nation communities, Assembly of First Nations/First Nations Information
Governance Committee, Ottawa.
Fletcher, A, Bonell, C & Hargreaves, J 2008, 'School effects on young people's drug use: A
systematic review of intervention and observational studies', Journal of Adolescent
Health, vol. 42, no. 3, pp. 209-220.
Forman, J & Damschroder, L 2008, 'Qualitative content analysis', in Empirical Methods For
Bioethics: A Primer, vol. 11, eds L Jacoby & LA Siminoff, Elsevier, Amsterdam, pp. 39-
62.
Foxcroft, DR, Ireland, D, Lister-Sharf, DJ, Lowe, G & Breen, R 2002, Primary prevention for
alcohol misuse in young people (Cochrane Review), Oxford.
Garner, BR, Barnes, B & Godley, SH 2009, 'Monitoring Fidelity in the Adolescent Community
Reinforcement Approach (A-CRA): The training process for A-CRA raters', Journal of
Behavior Analysis in Health, Sports, Fitness and Medicine, vol. 2, no. 1, pp. 43-54.
Garner, BR, Godley, SH, Funk, RR, Dennis, ML, Smith, JE & Godley, MD 2009, 'Exposure to
Adolescent Community Reinforcement Approach (A-CRA) treatment procedures as a
mediator of the relationship between adolescent substance abuse treatment retention
and outcome', Journal of Substance Abuse Treatment, vol. 36, no. 3, pp. 252-264.
Gates, S, McCambridge, J, Smith, LA & Foxcroft, D 2006, 'Interventions for prevention of drug
use by young people delivered in non-school settings', Cochrane Database of
Systematic Reviews, vol. 25, no. 1.
194
Global Burden of Disease study group 2008, The global burden of diseases, injuries, and risk
factors study: Operations manual final draft, January 31, 2008, Harvard Initiative for
Global Health, Institute for Health Metrics and Evaluation at the University of
Washington, John Hopkins University, University of Queensland, World Health
Organization
Godley, MD, Godley, SH, Dennis, ML, Funk, R & Passetti, LL 2007, 'The effect of assertive
continuing care on continuing care linkage, adherence, and abstinence following
residential treatment for substance use disorders in adolescents', Addiction, vol. 102,
no. 1, pp. 81-93.
Godley, SH, Hedges, K & Hunter, B 2011, 'Gender and racial differences in treatment process
and outcome among participants in the Adolescent Community Reinforcement
Approach', Psychology of Addictive Behaviors, vol. 25, no. 1, pp. 143-154.
Godley, SH, Meyers, RJ, Smith, JE, Karvinen, T, Titus, JC, Godley, MD, Dent, G, Passetti, L &
Kelberg, P 2001, The Adolescent Community Reinforcement Approach for adolescent
cannabis users, Center for Substance Abuse Treatment, Substance Abuse and Mental
Health Services Administration, Rockville.
Godley, SH, Smit, JE, Meyers, RJ & Godley, MD 2009, 'Adolescent community reinforcement
approach (A-CRA)', in Substance abuse treatment for youth and adults, eds DW
Springer & A Rubin, John Wiley & Sons Inc., Hoboken New Jersey, pp. 109-201.
Gracey, M & King, M 2009, 'Indigenous health part 1: Determinants and disease patterns',
Lancet, vol. 374, no. 9683, pp. 65-75.
Gray, D, Morfitt, B, Ryan, K & Williams, S 1997, 'The use of tobacco, alcohol and other drugs by
young Aboriginal people in Albany, Western Australia', Australian and New Zealand
Journal of Public Health, vol. 21, no. 1, pp. 71-76.
195
Gray, D, Saggers, S, Drandich, M, Wallam, D & Plowright, P 1995, 'Evaluating government
health and substance abuse programs for Indigenous peoples: A comparative review',
Australian Journal of Public Health, vol. 19, no. 6, pp. 567-572.
Gray, D, Saggers, S, Sputore, B & Bourbon, D 2000, 'What works? A review of evaluated alcohol
misuse interventions among Aboriginal Australians', Addiction, vol. 95, no. 1, pp. 11-
22.
Gray, D, Stearne, A, Wilson, M & Doyle, M 2010, Indigenous-specific alcohol and other drug
interventions: Continuities, changes and areas of greatest need, ANCD research paper
20, National Indigenous Drug and Alcohol Committee and Australian National Council
on Drugs, Canberra.
Green, A 2008, 'Making research relevant: If it is an evidence-based practice, where's the
practice-based evidence?', Family Practice, vol. 25, no. S1, pp. i20-i24.
Hall, WD, Wallance, AL, Cobiac, LJ, Doran, CM & Vos, T 2010, 'How can we reduce alcohol-
related road crash deaths among young Australians?', Medical Journal of Australia, vol.
192, no. 8, pp. 464-466.
Hansson, H, Rundberg, J, Zetterlind, U, Johnsson, KO & Berglund, M 2006, 'An intervention
program for university students who have parents with alcohol problems: A
randomized controlled trial', Alcohol and Alcoholism, vol. 41, no. 6, pp. 655-663.
Hansson, H, Zetterlind, U, Aberg-Orbeck, K & Berglund, M 2004, 'Two-year outcome of coping
skills training, group support and information for spouses of alcoholics: A randomized
controlled trial', Alcohol and Alcoholism, vol. 39, no. 2, pp. 135-140.
Haswell, MR, Kavanagh, D, Tsey, K, Reilly, L, Cadet-James, Y, Laliberte, A, Wilson, A & Doran, C
2010, 'Psychometric validation of the Growth and Empowerment Measure (GEM)
applied with Indigenous Australians', Australian and New Zealand Journal of
Psychiatry, vol. 44, no. 9, pp. 791-799.
196
Havard, A, Shakeshaft, A & Sanson-Fisher, R 2008, 'Systematic review and meta-analyses of
strategies targeting alcohol problems in emergency departments: Interventions reduce
alcohol-related injuries', Addiction, vol. 103, no. 3, pp. 368-376.
Havard Catalyst, Pathfinder: Training and tools for researchers like you, The Harvard Clinical
and Translational Science Centre. Available from: <http://catalyst.harvard.edu/>.
Hawkins, NG, Sanson-Fisher, RW, Shakeshaft, A, D'Este, C & Green, LW 2007, 'The multiple
baseline design for evaluating population-based research', American Journal of
Preventative Medicine, vol. 33, no. 2, pp. 162-168.
Hayman, NE, White, NE & Spurling, GK 2009, 'Improving Indigneous patients' access to
mainstream health services: The Inala experience', Medical Journal of Australia, vol.
190, no. 10, pp. 604-606.
Hearne, R, Connolly, A & Sheehan, J 2002, 'Alcohol abuse: Prevalence and detection in a
general hospital', Journal of the Royal Society of Medicine, vol. 95, no. 2, pp. 84-87.
Henderson, R, Simmons, DS, Bourke, L & Muir, J 2002, 'Development of guidelines for non-
Indigenous people undertaking research among the Indigenous population of north-
east Victoria', Medical Journal of Australia, vol. 176, no. 10, pp. 482-485.
Henry, BR, Houston, S & Mooney, GH 2004, 'Institutional racism in Australian healthcare: A
plea for decency', Medical Journal of Australia, vol. 180, no. 10, pp. 517-520.
Hogan, T 2003, Psychological testing: A practical introduction, John Wiley & Sons Inc., United
States.
Hosmer, DW & Lemeshow, S 2000, Applied Logistic Regression, John Wiley & Sons Inc., New
York.
Howells, E & Orford, J 2006, 'Coping with a problem drinker: A therapeutic intervention for the
partners of problem drinkers, in their own right', Journal of Substance Use, vol. 11, no.
1, pp. 53-71.
197
Humeniuk, R, Ali, R & WHO ASSIST Phase II Study Group 2006, Validation of the Alcohol,
Smoking and Substance Involvement Screening Test (ASSIST) and pilot brief
intervention: A technical report of Phase II findings of the WHO ASSIST Project,
Management of Substance Abuse, Department of Mental Health and Substance Abuse,
Geneva.
Hunsley, J 1992, 'Development of the Treatment Acceptability Questionnaire', Journal of
Psychopathology and Behavioral Assessment, vol. 14, no. 1, pp. 55-64.
Hunter, E, Hall, W & Spargo, R 1991, The distribution and correlates of alcohol consumption in
a remote Aboriginal population, National Drug and Alcohol Research Centre Sydney.
Hunter, E, Reser, J, Baird, M & Reser, P 1999, An analysis of suicide in Indigenous Communities
of North Queensland: The historical, cultural and symbolic landscape, University of
Queensland, Gurriny Yealamucka, James Cook University Canberra.
Hunter, P, Mayers, P, Couzos, S, Daniels, J, Murray, R, Bell, K, Kehoe, H, Brice, G & Tynan, M
2005, 'Aboriginal Community Controlled Health Services', in General Practice in
Australia, Commonwealth Department of Health and Ageing, Canberra, pp. 337-356.
IBM 2010, SPSS Statistics 19.
Jackson, N 2007, Handbook: Systematic Reviews of Health Promotion and Public Health
Interventions, Cochrane Health Promotion and Public Health Field, Victorian Health
Promotion Foundation.
Jenkins, R, McAlaney, J & McCambridge, J 2009, 'Change over time in alcohol consumption in
control groups in brief intervention studies: Systematic review and meta-regression
study', Drug and Alcohol Dependence, vol. 100, no. 1-2, pp. 107-114.
Kaminer, Y, Burleson, JA & Goldberger, R 2002, 'Cognitive-behavioural coping skills and
psychoeducation therapies for adolescent substance use', The Journal of Nervous and
Mental Disease, vol. 190, no. 11, pp. 737-745.
198
Kelly, AB 2006, 'Alcohol problems and psychological health in a remote Indigenous Australian
community: A preliminary quantitative study', Australian Journal of Rural Health, vol.
14, no. 2, pp. 86-87.
Kelly, AB & Kowalyszyn, M 2003, 'The association of alcohol and family problems in a remote
Indigenous Australian community', Addictive Behaviors, vol. 28, no. 4, pp. 761-767.
Kemp, R, Harris, A, Vurel, E & Sitharthan, T 2007, 'Stop using stuff: Trial of a drug and alcohol
intervention for young people with comorbid mental illness and drug and alcohol
problems', Australasian Psychiatry, vol. 15, no. 6, pp. 490-93.
King, A & Turia, T 2002, He Korowai Oranga: Maori health strategy, Wellington.
King, M, Smith, A & Gracey, M 2009, 'Indigenous health part 2: The underlying causes of the
health gap', Lancet, vol. 374, no. 9683, pp. 76-85.
KnowledgeAssets, Racial and ethnic disparities in substance abuse treatment, Knol. Available
from: <http://saprp.org/knowledgeassets/knowledge_detail.cfm?KAID=11>.
Kurti, L, Piggott, R, Keevy, N & Jones, L 2009, Evaluation of the National Drug Strategy
Aboriginal and Torres Strait Islander Peoples Complementary Action Plan 2003-2009
(CAP): Final report, Canberra.
Kypri, K, Saunders, JB, Williams, SM, McGee, RO, Langley, JD, Cashell-Smith, ML & Gallagher, SJ
2004, 'Web-based screening and breif intervention for hazardous drinking: A double-
blind randomized controlled trial', Addiction, vol. 99, no. 11, pp. 1410-1417.
Landau, J, Stanton, MD, Brinkman-Sull, D, Ikle, D, McCormick, D, Garrett, J, Baciewicz, G, Shea,
RR, Browning, A & Wamboldt, F 2004, 'Outcomes with the ARISE approach to engaging
reluctant drug- and alcohol-dependent individuals in treatment', American Journal of
Drug and Alcohol Abuse, vol. 30, no. 4, pp. 711-748.
Laslett, A-M, Catalano, P, Chikritzhs, T, Dale, C, Doran, C, Ferris, J, Jainullabudeen, T, Livingston,
M, Matthews, S, Mugavin, J, Room, R, Schlotterlein, M & Wilkinson, C 2010, The range
199
and magnitude of alcohol's harm to others, AER Centre for Alcohol Policy Research,
Turning Point Alcohol and Drug Centre, Eastern Health, Canberra.
Latimer, WW, Winters, KC, D'Zurilla, T & Nichols, M 2003, 'Integrated family and cognitive-
behavioral therapy for adolescent substance abusers: A Stage I efficacy study', Drug
and Alcohol Dependence, vol. 71, no. 3, pp. 303-317.
Lau, AS 2006, 'Making the case for selective and directed cultural adaptations of evidence-
based treatments: Examples from parent training', Clinical Psychology: Science and
Practice, vol. 13, no. 4, pp. 295-310.
Lee, K, Dawson, A & Conigrave, K in press, 'The role of an Aboriginal women’s group in meeting
the high needs of clients attending outpatient alcohol and other drug treatment', Drug
and Alcohol Review.
Lemeshow, S, Hosmer, DW, Klar, J & Lwanga, SK 1990, Adequacy of sample size in health
studies, John Wiley & Sons Inc., Chichester.
Lewis, M 1992, A rum state: Alcohol and state policy in Australia 1788-1988, Australian
Government Publishing Service, Canberra.
Liddle, HA 2004, 'Family-based therapies for adolescent alcohol and drug use: Research
contributions and future research needs', Addiction, vol. 99, no. S2, pp. 76-92.
Liddle, HA, Dakof, GA, Parker, K, Diamond, GS, Barret, K & Tejeda, K 2001, 'Multidimensional
family therapy for adolecents substance abuse: Results of a randomized clinical trial',
American Journal of Drug and Alcohol Abuse, vol. 27, no. 4, pp. 651-688.
Liddle, HA, Rowe, CL, Dakof, GA, Henderson, CE & Greenbaum, PE 2009, 'Multidimensional
Family Therapy for young adolescent substance abuse: Twelve-month outcomes of a
randomized controlled trial', Journal of Consulting and Clinical Psychology, vol. 77, no.
1, pp. 12-25.
LLC, o 2013, ooVoo.

200
Lopez Viets, V 2008, 'CRAFT: Helping Latino families concerned about a loved one', Alcoholism
Treatment Quarterly, vol. 25, no. 4, pp. 111-123.
Marincola, FM 2003, 'Translational medicine: A two-way road', Journal of Translational
Medicine, vol. 1, no. 1, pp. 1-2.
Masotti, P, George, MA, Szala-Meneok, K, Morton, AM, Loock, C, Van Bibber, M, Ranford, J,
Fleming, M & MacLeod, S 2006, 'Preventing fetal alcohol spectrum disorder in
Aboriginal communities: A methods development project', PLoS Medicine, vol. 3, no. 1,
pp. 24-29.
McBride, N, Farringdon, F, Miford, R, Meuleners, L & Phillips, M 2004, 'Harm minimisation in
school drug education. Final results of the School Health and Alcohol Harm Reduction
Project (SHAHRP)', Addiction, vol. 99, no. 3, pp. 278-91.
McCubbin, LD 2006, 'Indigenous values, cultural safety and improving health care: The case of
Native Hawaiians', Contemporary Nurse, vol. 22, no. 2, pp. 214-217.
McGorry, PD, Purcell, R, Hickie, IB & Jorm, AF 2007, 'Investing in youth mental health is a best
buy: The logic and plan for achieving early intervention in youth mental health in
Australia', Medical Journal of Australia, vol. 187, no. 7, pp. S5-S7.
McGrath, P, Patton, MA, Holewa, H & Rayner, R 2006, 'The importance of the 'family meeting'
in health care communication with Indigenous people: Findings from an Australian
study', Australian Journal of Primary Health, vol. 12, no. 1, pp. 56-64.
McLennan, V & Khavarpour, F 2004, 'Culturally appropriate health promotion: Its meaning and
application in Aboriginal communities', Health Promotion Journal of Australia, vol. 15,
no. 3, pp. 237-239.
Metz, CE 1978, 'Basic principles of ROC analysis', Seminars in Nuclear Medicine, vol. 8, no. 4,
pp. 283-298.
201
Meyers, RJ, Miller, WR, Smith, JE & Tonigan, JS 2002, 'A randomized trial of two methods for
engaging treatment-refusing drug users through concerned significant others', Journal
of Consulting and Clinical Psychology, vol. 70, no. 5, pp. 1182-1185.
Meyers, RJ & Smith, JE 1995, Clinical guide to alcohol treatment: The Community
Reinforcement Approach, The Guilford Press, New York.
Meyers, RJ, Villanueva, M & Smith, JE 2005, 'The Community Reinforcement Approach: History
and new directions', Journal of Cognitive Psychotherapy, vol. 19, no. 3, pp. 247-260.
Microsoft 2007, Excel.
Microsoft 2013, Skype, ed.^eds 6.11.0.102.
Miller, WR, Meyers, RJ & Hiller-Sturmhofel, S 1999, 'CRA and special populations', Alcohol
Research & Health, vol. 23, no. 2, p. 121.
Miller, WR, Meyers, RJ & Tonigan, JS 1999, 'Engaging the unmotivated in treatment for alcohol
problems: A comparison of three strategies for intervention through family members',
Journal of Consulting and Clinical Psychology, vol. 67, no. 5, pp. 688-697.
Miller, WR, Sorensen, JL, Selzer, JA & Brigham, GS 2006, 'Disseminating evidence-based
practices in substance abuse treatment: A review with suggestions', Journal of
Substance Abuse Treatment, vol. 31, no. 1, pp. 25-39.
Miller, WR & Wilbourne, PL 2002, 'Mesa grande: A methodological analysis of clinical trials of
treatments for alcohol use disorders', Addiction, vol. 97, no. 3, pp. 265-277.
Mortimer, D & Segal, L 2005, 'Economic evaluation of interventions for problem drinking and
alcohol dependence: Cost per QALY estimates', Alcohol and Alcoholism, vol. 40, no. 6,
pp. 549-555.
Murray, CJL, Vos, T, Lozano, R, Naghavi, M, Flaxman, AD, Michaud, C, Ezzati, M, Shibuya, K,
Salomon, JA, Abdalla, S, Aboyans, V, Abraham, J, Ackerman, I, Aggarwa, R, Ahn, SY, Ali,
MK, AlMazroa, MA, Alvarado, M, Anderson, HR, Anderson, LM, Andrews, KG, Atkinson,
C, Baddour, LM, Bahalim, AN, Barker-Collo, S, Barrero, LH, Bartels, DH, Basáñez, M-G,
202
Baxter, A, Bell, ML, Benjamin, EJ, Bennett, D, Bernabé, E, Bhalla, K, Bhandari, B, Bikbov,
B, Abdulhak, AB, Birbeck, G, Black, JA, Blencowe, H, Blore, JD, Blyth, F, Bolliger, I,
Bonaventure, A, Boufous, Sa, Bourne, R, Boussinesq, M, Braithwaite, T, Brayne, C,
Bridgett, L, Brooker, S, Brooks, P, Brugha, TS, Bryan-Hancock, C, Bucello, C, Buchbinder,
R, Buckle, Gr, Budke, CM, Burch, M, Burney, P, Burstein, R, Calabria, B, Campbell, B,
Canter, CE, Carabin, H, Carapetis, J, Carmona, L, Cella, C, Charlson, F, Chen, H, Cheng,
AT-A, Chou, D, Chugh, SS, eng, LEC, Cola, SD, Colquhoun, S, Colson, KE, Condon, J,
Connor, MD, Cooper, LT, Corriere, M, Cortinovis, M, Vaccaro, KCd, Couser, W, Cowie,
BC, Criqui, MH, Cross, M, Dabhadkar, KC, Dahiya, M, Dahodwala, N, Damsere-Derry, J,
Danaei, G, Davis, A, Leo, DD, Degenhardt, L, Dellavalle, R, Delossantos, A, Denenberg, J,
Derrett, S, Jarlais, DCD, Dharmaratne, SD, Dherani, M, Diaz-Torne, C, Dolk, H, Dorsey,
ER, Driscoll, T, Duber, H, Ebel, B, Edmond, K, Elbaz, A, Ali, SE, Erskine, H, Erwin, PJ,
Espindola, P, Ewoigbokhan, SE, Farzadfar, F, Feigin, V, Felson, DT, Ferrari, A, Ferri, CP,
Fèvre, EM, Finucane, MM, Flaxman, S, Flood, L, Foreman, K, Forouzanfar, MH, Fowkes,
FGR, Fransen, M, Freeman, MK, Gabbe, BJ, Gabriel, SE, Gakidou, E, Ganatra, HA,
Garcia, B, Gaspari, F, Gillum, RF, Gmel, G, Gonzalez-Medina, D, Gosselin, R, Grainger, R,
Grant, B, Groeger, J, Guillemin, F, Gunnell, D, Gupta, R, Haagsma, J, Hagan, H, Halasa,
YA, Hall, W, Haring, D, Haro, JM, Harrison, JE, Havmoeller, R, Hay, RJ, Higashi, H, Hill, C,
Hoen, B, man, HH, Hotez, PJ, Hoy, D, Huang, JJ, Ibeanusi, SE, Jacobsen, KH, James, SL,
Jarvis, D, Jasrasaria, R, Jayaraman, S, Johns, N, Jonas, JB, Karthikeyan, G, Kassebaum, N,
Kawakami, N, Keren, A, Khoo, J-P, King, CH, Knowlton, LM, Kobusingye, O, Koranteng,
A, Krishnamurthi, R, Laden, F, Lalloo, R, Laslett, LL, Lathlean, T, Leasher, JL, Lee, YY,
Leigh, J, Levinson, D, Lim, SS, Limb, E, Lin, JK, Lipnick, M, Lipshultz, SE, Liu, W, Loane, M,
Ohno, SL, Lyons, R, Mabweijano, J, MacIntyre, MF, Malekzadeh, R, Mallinger, L,
Manivannan, S, Marcenes, W, March, L, Margolis, DJ, Marks, GB, Marks, R, Matsumori,
A, Matzopoulos, R, Mayosi, BM, McAnulty, JH, McDermott, MM, McGill, N, McGrath, J,
203
Medina-Mora, ME, Meltzer, M, Memish, ZA, Mensah, GA, Merriman, TR, Meyer, A-C,
Miglioli, V, Miller, M, Miller, TR, Mitchell, PB, Mock, C, Mocumbi, AO, tt, TEM, Mokdad,
AA, Monasta, L, Montico, M, Moradi-Lakeh, M, Moran, A, Morawska, L, Mori, R,
Murdoch, ME, Mwaniki, MK, Naidoo, K, Nair, MN, Naldi, L, Narayan, KMV, Nelson, PK,
Nelson, RG, Nevitt, MC, Newton, CR, Nolte, S, Norman, P, Norman, R, O’Donnell, M,
O’Hanlon, S, Olives, C, Omer, SB, Ortblad, K, Osborne, R, Ozgediz, D, Page, A, Pahari, B,
Pandian, JD, Rivero, AP, Patten, SB, Pearce, N, Padilla, RP, Perez-Ruiz, F, Perico, N,
Pesudovs, K, Phillips, D, Phillips, MR, Pierce, K, Pion, S, Polanczyk, GV, Polinder, S, III,
CAP, Popova, S, Porrini, E, Pourmalek, F, Prince, M, Pullan, RL, Ramaih, KD,
Ranganathan, D, Razavi, H, Regan, M, Rehm, JT, Rein, DB, Remuzzi, G, Richardson, K,
Rivara, FP, Roberts, T, Robinson, C, Leòn, FRD, Ronfani, L, Room, R, Rosenfeld, LC,
Rushton, L, Sacco, RL, Saha, S, Sampson, U, Sanchez-Riera, L, Sanman, E, Schwebel, DC,
Scott, JG, Segui-Gomez, M, Shahraz, S, Shepard, DS, Shin, H, Shivakoti, R, Singh, D,
Singh, GM, Singh, JA, Singleton, J, Sleet, DA, Sliwa, K, Smith, E, Smith, JL, Stapelberg,
NJC, Steer, A, Steiner, T, Stolk, WA, Stovner, LJ, Sudfeld, C, Syed, S, Tamburlini, G,
Tavakkoli, M, Taylor, HR, Taylor, JA, Taylor, WJ, Thomas, B, Thomson, WM, Thurston,
GD, Tleyjeh, IM, Tonelli, M, Towbin, JrA, Truelsen, T, Tsilimbaris, MK, Ubeda, C,
Undurraga, EA, Werf, MJvd, Os, Jv, Vavilala, MS, Venketasubramanian, N, Wang, M,
Wang, W, Watt, K, Weatherall, DJ, Weinstock, MA, Weintraub, R, Weisskopf, MG,
Weissman, MM, White, RA, Whiteford, H, Wiebe, N, Wiersma, ST, Wilkinson, JD,
Williams, HC, Williams, SRM, Witt, E, Wolfe, F, Woolf, AD, Wulf, S, Yeh, P-H, Zaidi,
AKM, Zheng, Z-J, Zonies, D & Lopez, AD 2012, 'Disability-adjusted life years (DALYs) for
291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the
Global Burden of Disease Study 2010', Lancet, vol. 380, no. 9859, pp. 2197-2223.
204
NACCHO and the Chronic Disease Alliance of NGOs 2008, 'The well person's health check', in
Aboriginal primary health care: An evidence based approach, eds S Couzos & R Murray,
Oxford University Press, South Melbourne, pp. 131-194.
Nagel, TM & Thompson, C 2010, 'The central role of Aboriginal families in motivational
counselling: Family support and family 'humbug'', Australian Indigenous
HealthBulletin, vol. 10, no. 1, pp. 1-17.
National Drug Research Institute, Indigenous Australian Acohol and Other Drugs Bibliographic
Database Available from: <http://www.db.ndri.curtin.deu.au/>.
National Health and Medical Research Council 1992, Is there a safe level of daily consumption
of alcohol for men and women: Recommendations regarding responsible drinking
behaviour, National Health and Medical Research Council, Canberra
National Health and Medical Research Council 2003, Values and ethics: Guidelines for ethical
conduct in Aboriginal and Torres Strait Islander health research, Commonwealth of
Australia, Canberra.
National Health and Medical Research Council 2009, Australian guidelines to reduce health
risks from drinking alcohol, Commonwealth of Australia, Canberra.
National Institute on Alcohol Abuse and Alcoholism 1995, Assessing alcohol problems: A guide
for clinicians and researchers, National Institutes of Health, Bethesda.
Nattala, P, Leung, KS, Nagarajaiah & Murthy, P 2010, 'Family member involvement in relapse
prevention improves alcohol dependence outcomes: A prospective study at an
addiction treatment facility in India', Journal of Studies on Alcohol and Drugs, vol. 71,
no. 4, pp. 581-587.
Newell, S, Girgis, A, Sanson-Fisher, RW & Stewart, J 1997, 'Are touchscreen computer surveys
acceptable to medical oncology patients?', Journal of Psychosocial Oncology, vol. 15,
no. 2, pp. 37-46.
205
Newton, NC, Teesson, M, Vogl, LE & Anderson, G 2010, 'Internet-based prevention for alcohol
and cannabis use: Final results of the Climate Schools course', Addiction, vol. 105, no.
4, pp. 749-759.
O'Farrell, TJ, Murphy, M, Alter, J & Fals-Stewart, W 2008, 'Brief family treatment intervention
to promote continuing care among alcohol-dependent patients in inpatient
detoxification: A randomized pilot study', Journal of Substance Abuse Treatment, vol.
34, no. 3, pp. 363-369.
Ockene, JK, Edgerton, EA, Teutsch, SM, Marion, LN, Miller, T, Genevro, JL, Loveland-Cherry, CJ,
Fielding, JE & Briss, PA 2007, 'Integrating evidence-based clinical and community
strategies to improve health', American Journal of Preventative Medicine, vol. 32, no.
3, pp. 244-52.
Pacileo, G & Fattore, G 2009, 'Alcohol abuse prevention in young people: An economic
simulation', Journal of Substance Use, vol. 14, no. 6, pp. 385-392.
Paul, CL, Sanson-Fisher, R, Stewart, J & Anderson, AE 2010, 'Being sorry is not enough: The
sorry state of the evidence base for improving the health of Indigenous populations',
American Journal of Preventative Medicine, vol. 38, no. 5, pp. 566-568.
People, J 2005, Trends and patterns in domestic violence assaults, NSW Bureau of Crime
Statistics and Research
Peterson, PL, Baer, JS, Wells, EA, Ginzler, JA & Garrett, SB 2006, 'Short-term effects of a brief
motivational intervention to reduce alcohol and drug risk among homeless
adolescents', Psychology of Addictive Behaviors, vol. 20, no. 3, pp. 254-264.
Petrie, D, Doran, C, Shakeshaft, A & Sanson-Fisher, R 2008, 'The relationship between alcohol
consumption and self reported health status using the EQ5D: Evidence from rural
Australia', Social Science and Medicine, vol. 67, no. 11, pp. 1717-1726.
Potvin, L, Cargo, M, McComber, AM, Delormier, T & Macaulay, AC 2003, 'Implementing
participatory intervention and research in communities: Lessons from the Kahnawake
206
Schools Diabetes Prevention Project in Canada', Social Science and Medicine, vol. 56,
no. 6, pp. 1295-1305.
Rasmussen, M, Guo, X, Wang, Y, Lohmueller, KE, Rasmussen, S, Albrechtsen, A, Skotte, L,
Lindgreen, S, Metspalu, M, Jombart, T, Kivisild, T, Tridico, S, Metspalu, E, Nielsen, K,
Avila-Arcos, MC, Moreno-Mayar, JV, Muller, C, Dortch, J, Gilbert, MTP, Lund, O,
Wesolowska, A, Karmin, M, Weinert, LA, Wang, B, Li, J, Tai, S, Xiao, F, Hanihara, T, van
Driem, G, Jha, AR, Ricaut, F-X, de Knijff, P, Migliano, AB, Romero, IG, Kristiansen, K,
Lambert, DM, Brunak, S, Forster, P, Brinkmann, B, Nehlich, O, Bunce, M, Richards, M,
Gupta, R, Bustamante, CD, Krogh, A, Foley, RA, Lahr, MM, Balloux, F, Sicheritz-Ponten,
T, Villems, R, Nielsen, R, Wang, J & Willerslev, E 2011, 'An Aboriginal Australian
genome reveals separate human dispersals into Asia', Science, vol. 334, no. 6052, pp.
94-98.
Regier, DA, Farmer, ME, Rae, DS, Locke, BZ, Keith, SJ, Judd, LL & Goodwin, FK 1990,
'Comorbidity of mental disorders with alcohol and other drug abuse: Results from the
Epidemiologic Catchment Area (ECA) study', Journal of the American Medical
Association, vol. 264, no. 19, pp. 2511-2518.
Rehm, J, Mathers, C, Popova, S, Thavorncharoensap, M, Teerawattananon, Y & Patra, J 2009,
'Global burden of disease and injury and economic cost attributable to alcohol use and
alcohol-use disorders', Lancet, vol. 373, no. 9682, pp. 2223-2233.
Rehm, J, Room, R, Monteiro, M, Gmel, G, Graham, K, Rehm, N, Sempos, CT, Frick, U & Jernigan,
D 2004, 'Alcohol use', in Comparative quantification of health risks: Global and regional
burden of disease attributable to selected major risk factors, vol. 1, eds M Ezzati, AD
Lopez, A Rodgers & CLJ Murray, World Health Organization, Geneva.
Reinert, DF & Allen, JP 2007, 'The Alcohol Use Disorders Identification Test: An update of
research findings', Alcoholism Clinical and Experimental Research, vol. 31, no. 2, pp.
185-199.

207
Ridolfo, B & Stevenson, C 2001, The quantification of drug-caused mortality and morbidity in
Australia, 1998, Australian Institute of Health and Welfare, Canberra
Robinson, G, Tyler, W, Jones, Y, Silburn, S & Zubrick, SR 2012, 'Context, diversity and
engagement: Early intervention with Australian Aboriginal families in urban and
remote contexts', Children & Society, vol. 26, no. 5, pp. 343-355.
Roozen, HG, de Waart, R & van der Kroft, P 2010, 'Community Reinforcement and Family
Training: An effective option to engage treatment-resistant substance-abusing
individuals in treatment', Addiction, vol. 105, no. 10, pp. 1729-1738.
Rychtarik, RG & McGillicuddy, NB 2005, 'Coping skills training and 12-step facilitation for
women whose partner has alcohooism: Effects on depression, the partner's drinking,
and partner physical violence', Journal of Consulting and Clinical Psychology, vol. 73,
no. 2, pp. 249-261.
Sackett, DL, Rosenberg, WM, Gray, JA, Haynes, RB & Richardson, WS 1996, 'Evidence based
medicine: What it is and what it isn't', British Medical Journal, vol. 312, no. 7023, pp.
71-72.
Safran, C 1991, 'Using routinely collected data for clinical research', Statistics in Medicine, vol.
10, no. 4, pp. 559-564.
Samet, JH, Larson, MJ, Horton, NJ, Doyle, K, Winter, M & Saitz, R 2003, 'Linking alcohol- and
drug-dependent adults to primary medical care: A randomized controlled trial of a
multi-disiplinary health intervention in a detoxification unit', Addiction, vol. 98, no. 4,
pp. 509-516.
Sanson-Fisher, R & Campbell, E 1994, 'Health research in Australia: It's role in achieving the
goals and targets', Health Promotion Journal of Australia, vol. 4, no. 3, pp. 28-33.
Sanson-Fisher, RW, Campbell, EM, Perkins, JJ, Blunden, SV & Davis, BB 2006, 'Indigenous
health research: A critical review of outputs over time', Medical Journal of Australia,
vol. 184, no. 10, pp. 502-505.
208
Saunders, JB & Aasland, OG 1987, WHO Collaborative Project on Identification and Treatment
of Persons with Harmful Alcohol Consumption. Report on phase I: Development of a
screening instrument, World Health Organization, Division of Mental Health, Geneva.
Saunders, JB, Aasland, OG, Babor, TF, de la Fuente, JR & Grant, M 1993, 'Development of the
Alcohol Use Disorders Idenfication Test (AUDIT): WHO collaborative project on early
detection of persons with harmful alcohol consumption-II', Addiction, vol. 88, no. 6,
pp. 791-804.
Seale, JP, Boltri, JM, Shellenberger, S, Velasquez, MM, Cornelius, M, Guyinn, M, Okosun, I &
Sumner, H 2006, 'Primary care validation of a single screening question for drinkers',
Journal of Studies on Alcohol, vol. 67, no. 5, pp. 778-784.
Seale, JP, Shellenberger, S, Rodriguez, C, Seale, JD & Alvarado, M 2002, 'Alcohol use and
cultural change in an Indigenous population: A case study from Venezuela', Alcohol
and Alcoholism, vol. 37, no. 6, pp. 603-608.
Seale, JP, Shellenberger, S, Sanchez, N, Vogel, RL, Villalobos, E, Girton, FS, Seale, DM & Okosun,
IS 2010, 'Characteristics of problem drinking in an urban South American Indigenous
population', Substance Use and Misuse, vol. 45, no. 13, pp. 2185-2202.
Seitz, HK & Cho, CH 2009, 'Contribution of alcohol and tobacco use in gastrointestinal cancer
development', Methods in Molecular Biology, vol. 472, pp. 217-241.
Seligman, MEP 1995, 'The effectiveness of psychotherapy: The consumer reports study',
American Psychologist, vol. 50, no. 12, pp. 965-974.
Shakeshaft, A, Doran, C, Petrie, D, Breen, C, Havard, A, Abudeen, A, Harwood, E, Clifford, A,
D'Este, C, Gilmour, S, Byrnes, J, Navarro, H & Sanson-Fisher, R 2012, The Alcohol Action
in Rural Communities (AARC) Project: Working with communities to select, implement
and measure the impact of strategies to reduce alcohol-related harm, Foundation for
Alcohol Research and Education, Canberra.
209
Shakeshaft, A, Doran, CM & Byrnes, J 2009, 'The role of research in the failure of the alcopops
excise in Australia: What have we learned?', Medical Journal of Australia, vol. 191, no.
4, pp. 223-225.
Shakeshaft, AP, Bowman, JA & Sanson-Fisher, RW 1997, 'Behavioural alcohol research: New
directions or more of the same?', Addiction, vol. 92, no. 11, pp. 1411-1422.
Shakeshaft, AP, Bowman, JA & Sanson-Fisher, RW 1998, 'Computers in community-based drug
and alcohol clinical settings: Are they acceptable to respondents?', Drug and Alcohol
Dependence, vol. 50, no. 2, pp. 177-180.
Shakeshaft, AP, Clifford, A & Shakeshaft, M 2010, 'Reducing alcohol-related harm experienced
by Indigenous Australians: Identifying opportunities for Indigenous primary health care
services', Australian and New Zealand Journal of Public Health, vol. 34, no. S1, pp. S41-
S45.
Shakeshaft, AP & Frankish, CJ 2003, 'Using patient-driven computers to provide cost-effective
prevention in primary care: A conceptual framework', Health Promotion International,
vol. 18, no. 1, pp. 67-77.
Sibbald, B & Roland, M 1998, 'Understanding controlled trials: Why are randomised controlled
trials important?', British Medical Journal, vol. 316, no. 7126, p. 201.
Slesnick, N, Bartle-Haring, S, Glebova, T & Glade, A 2006, 'Primary alcohol versus primary drug
use among adolescents: An examination of differences', Addictive Behaviors, vol. 31,
no. 11, pp. 2080-2093.
Slesnick, N & Prestopnik, JL 2009, 'Comparison of family therapy outcome with alcohol-
abusing, runaway adolescents', Journal of Marital and Family Therapy, vol. 35, no. 3,
pp. 255-277.
Slesnick, N, Prestopnik, JL, Meyers, RJ & Glassman, M 2007, 'Treatment outcome for street-
living, homeless youth', Addictive Behaviors, vol. 32, no. 6, pp. 1237-51.
210
Smit, E, Verdurmen, J, Monshouwer, K & Smit, F 2008, 'Family interventions and their effect on
adolescent alcohol use in general populations: A meta-analysis of randomized
controlled trials', Drug and Alcohol Dependence, vol. 97, no. 3, pp. 195-206.
Smith, DC, Godley, SH, Godley, MD & Dennis, ML 2011, 'Adolescent Community Reinforcement
Approach outcomes differ among emerging adults and adolescents', Journal of
Substance Abuse Treatment, vol. 41, no. 4, pp. 422-430.
Smith, JE & Meyers, RJ 2004, Motivating substance abusers to enter treatment: Working with
family members, The Guildford Press, New York.
Smith, JE & Meyers, RJ 2007, Motivating substance abusers to enter treatment: Working with
family members, The Guilford Press, New York.
Solberg, LI, Maciosek, MV & Edwards, NM 2008, 'Primary care intervention to reduce alcohol
misuse ranking its health impact and cost effectiveness', American Journal of
Preventative Medicine, vol. 34, no. 2, pp. 143-152.
Spoth, R, Greenberg, M & Turrisi, R 2008, 'Preventive interventions addressing underage
drinking: State of the evidence and steps toward public health impact', Paediatrics, vol.
121, no. S4, pp. S311-S336.
Stein, LAR, Colby, SM, Barnett, NP, Monti, PM, Golembeske, C & Lebeau-Craven, R 2006,
'Effects of motivational interviewing for incarcerated adolescents on driving under the
influence after release', American Journal on Addictions, vol. 15, no. S1, pp. 50-57.
Stewart, JM, Sanson-Fisher, RW, Eades, SJ & Mealing, NM 2010, 'Strategies for increasing high-
quality intervention research in Aboriginal and Torres Strait Islander health: Views of
leading researchers', Medical Journal of Australia, vol. 192, no. 10, pp. 612-615.
Stock, C, Mares, S & Robinson, G 2012, 'Telling and re-telling stories: The use of drawing in a
group intervention with parents and children in a remote Aboriginal community',
Australian and New Zealand Journal of Family Therapy, vol. 33, no. 2, pp. 157-170.
211
Streiner, DL & Norman, GR 2008, Health measurement scales: A practical guide to their
development and use, Oxford University Press, New York.
Subramanian, SV, Smith, GD & Subramanyam, M 2006, 'Indigenous health and socioeconomic
status in India', PLoS Medicine, vol. 3, no. 10, pp. 1794-1804.
Substance Abuse and Mental Health Services Administration 2009, Results from the 2008
National Survey on Drug Use and Health: National findings, Office of Applied Studies,
U.S. Department of Health and Human Services, Rockville, MD.
Teesson, M, Hall, W, Slade, T, Mills, K, Grove, R, Mewton, L, Baillie, A & Harber, P 2010,
'Prevalence and correlates of DSM-IV alcohol abuse and dependence in Australia:
Findings of the 2007 National Survey of Mental Health and Wellbeing', Addiction, vol.
105, no. 12, pp. 2085-2094.
Templeton, L, Velleman, R & Russell, C 2010, 'Psychological interventions with families of
alcohol misusers: A systematic review', Addiction Research & Theory, vol. 18, no. 6, pp.
616-648.
Thompson, N 2012, Translational research and the Australian Indigenous HealthInfoNet,
Australian Indigenous HealthInfoNet,
[http://www.healthinfonet.ecu.edu.au/about/translational_research].
Toumbourou, J, Stockwell, T, Neighbors, C, Marlatt, GA, Sturge, J & Rehm, J 2007,
'Interventions to reduce harm associated with adolescent substance use', Lancet, vol.
369, no. 9570, pp. 1391-1401.
Tripodi, SJ, Bender, K, Litschge, C & Vaughn, MG 2010, 'Interventions for reducing adolescent
alcohol abuse: A meta-analytic review', Archives of Pediatrics & Adolescent Medicine,
vol. 164, no. 1, pp. 85-91.
Tsai, M-C, Tsai, T-F, Chen, C-Y & Liu, C-Y 2005, 'Alcohol Use Disorders Identification Test
(AUDIT): Establishment of cut-off scores in a hospitalized Chinese population',
Alcoholism, Clinical and Experimental Research, vol. 29, no. 1, pp. 53-57.
212
Turner, K & Sanders, M 2007, 'Family intervention in Indigenous communities: Emergent issues
in conducting outcome research', Australasian Psychiatry: Bulletin of Royal Australian
and New Zealand College of Psychiatrists, vol. 15, no. S1, pp. S39-S43.
U.S. Department of Health and Human Services & U.S. Department of Agriculture 2005, Dietary
guidelines for Americans, 2005, Washington DC.
United Nations 2008, United Nations declaration on the rights of Indigenous peoples,
[http://www.un.org/esa/socdev/unpfii/documents/DRIPS_en.pdf].
Vedel, E, Emmelkamp, PMG & Schippers, GM 2008, 'Individual cognitive-behavioral therapy
and behavioral couples therapy in alcohol use disorder: A comparative evaluation in
community-based addiction treatment centers', Psychotherapy & Psychosomatics, vol.
77, no. 5, pp. 280-288.
Velleman, RDB, Templeton, LJ & Copello, AG 2005, 'The role of the family in preventing and
intervening with substance use and misuse: A comprehensive review of family
interventions, with a focus on young people', Drug and Alcohol Review, vol. 24, no. 2,
pp. 93-109.
Vicary, D & Westerman, T 2004, ''That's just the way he is': Some implications of Aboriginal
mental health beliefs', Australian e-Journal for the Advancement of Mental Health, vol.
3, no. 3, pp. 1-10.
Villarreal, MI 2008, 'Women and health disparities: Implications for treating Hispanic women in
rural and urban communities', Alcoholism Treatment Quarterly, vol. 25, no. 4, pp. 91-
110.
Vogl, L, Teeson, M, Andrews, G, Bird, K, Steadman, B & Dillon, P 2009, 'A computerized harm
minimzation prevention program for alcohol misuse and related harms: Randomized
controlled trial', Addiction, vol. 104, no. 4, pp. 564-75.
213
Vos, T, Barker, B, Begg, S, Stanley, L & Lopez, AD 2009, 'Burden of disease and injury in
Aboriginal and Torres Strait Islander peoples: The Indigenous health gap', International
Journal of Epidemiology, vol. 38, no. 2, pp. 470-477.
Vos, T, Barker, B, Stanley, L & Lopez, A 2003, The burden of disease and injury in Aboriginal and
Torres Strait Islander peoples 2003, Centre for the Burden of Disease and Cost-
effectiveness, School of Population Health, University of Queensland, Brisbane.
Vos, T, Barker, B, Stanley, L & Lopez, A 2007, The burden of disease and injury in Aboriginal and
Torres Strait Islander peoples: Summary report, Centre for Burden of Disease and Cost-
effectiveness, School of Population Health, University of Queensland, Brisbane.
Walitzer, KS & Dermen, KH 2004, 'Alcohol-focused spouse involvement and behavioral couples
therapy: Evaluation of enhancements to drinking reduction treatment for male
problem drinkers', Journal of Consulting and Clinical Psychology, vol. 72, no. 6, pp. 944-
955.
Webb, G, Shakeshaft, A, Sanson-Fisher, R & Havard, A 2009, 'A systematic review of work-place
interventions for alcohol-related problems', Addiction, vol. 104, no. 3, pp. 365-377.
Wells-Parker, E & Williams, M 2002, 'Enhancing the effectiveness of traditional interventions
with drinking drivers by adding brief individual intervention components', Journal of
Studies on Alcohol, vol. 63, no. 6, pp. 655-664.
Westfall, JM, Mold, J & Fagnan, L 2007, 'Practice-based research - "blue highways" on the NIH
roadmap', Journal of the American Medical Association, vol. 297, no. 4, pp. 403-406.
Williams, RJ & Chang, SY 2000, 'A comprehensive and comparative review of adolescent
substance abuse treatment outcome', Clinical Psychology: Science and Practice, vol. 7,
no. 2, pp. 138-166.
Wood, E, Shakeshaft, A, Gilmour, S & Sanson-Fisher, R 2006, 'A systematic review of school-
based studies involving alcohol and the community', Australian and New Zealand
Journal of Public Health, vol. 30, no. 6, pp. 541-549.
214
World Health Organization 2004, Global status report on alcohol 2004, World Health
Organization. Department of Mental Health and Substance Abuse, Geneva.
Wundersitz, J 2010, Indigenous perpetrators of violence: Prevalence and risk factors for
offending, Canberra.
Ziedonis, DM, Zammarelli, L, Seward, G, Oliver, K, Guydish, J, Hobart, M & Meltzer, B 2007,
'Addressing tobacco use through organizational change: A case study of an addiction
treatment organization', Journal of Psychoactive Drugs, vol. 39, no. 4, pp. 451-459.

215
Appendices
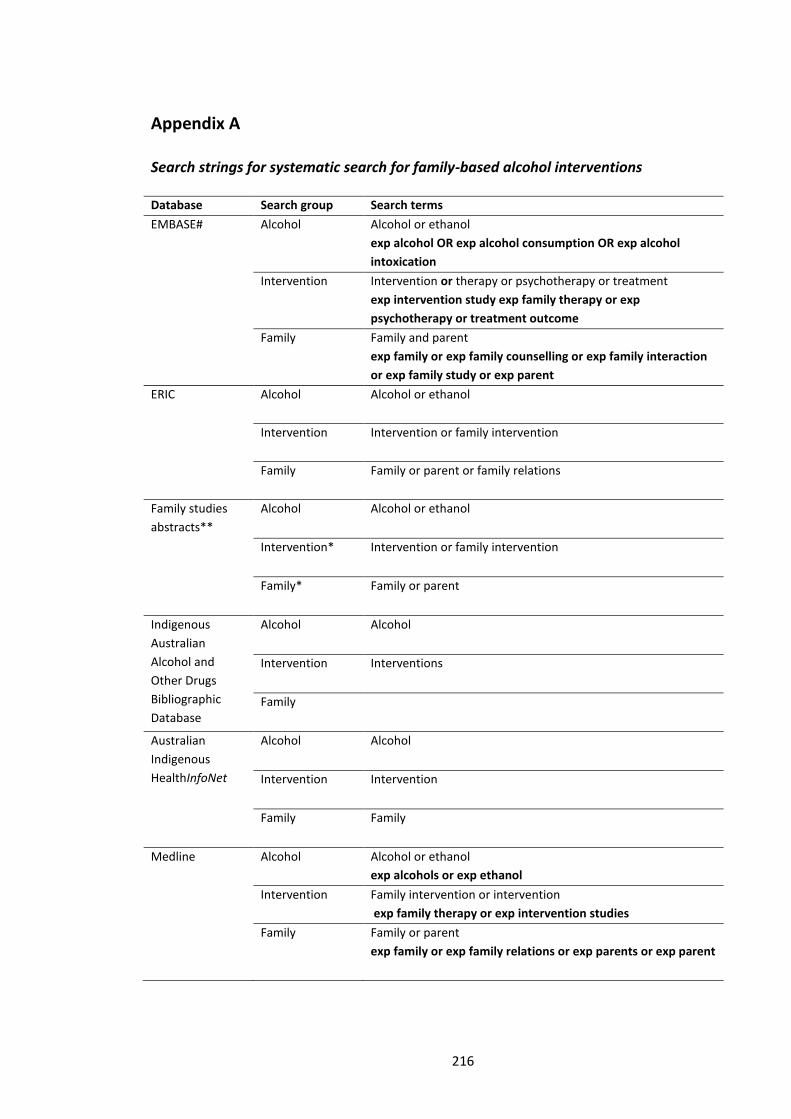
216
Appendix A
Search strings for systematic search for family-based alcohol interventions
Database Search group Search terms
EMBASE# Alcohol Alcohol or ethanol
exp alcohol OR exp alcohol consumption OR exp alcohol
intoxication
Intervention Intervention or therapy or psychotherapy or treatment
exp intervention study exp family therapy or exp
psychotherapy or treatment outcome
Family Family and parent
exp family or exp family counselling or exp family interaction
or exp family study or exp parent
ERIC Alcohol Alcohol or ethanol
Intervention Intervention or family intervention
Family Family or parent or family relations
Family studies
abstracts**
Alcohol Alcohol or ethanol
Intervention* Intervention or family intervention
Family* Family or parent
Indigenous
Australian
Alcohol and
Other Drugs
Bibliographic
Database
Alcohol Alcohol
Intervention Interventions
Family
Australian
Indigenous
HealthInfoNet
Alcohol Alcohol
Intervention Intervention
Family Family
Medline Alcohol Alcohol or ethanol
exp alcohols or exp ethanol
Intervention Family intervention or intervention
exp family therapy or exp intervention studies
Family Family or parent
exp family or exp family relations or exp parents or exp parent
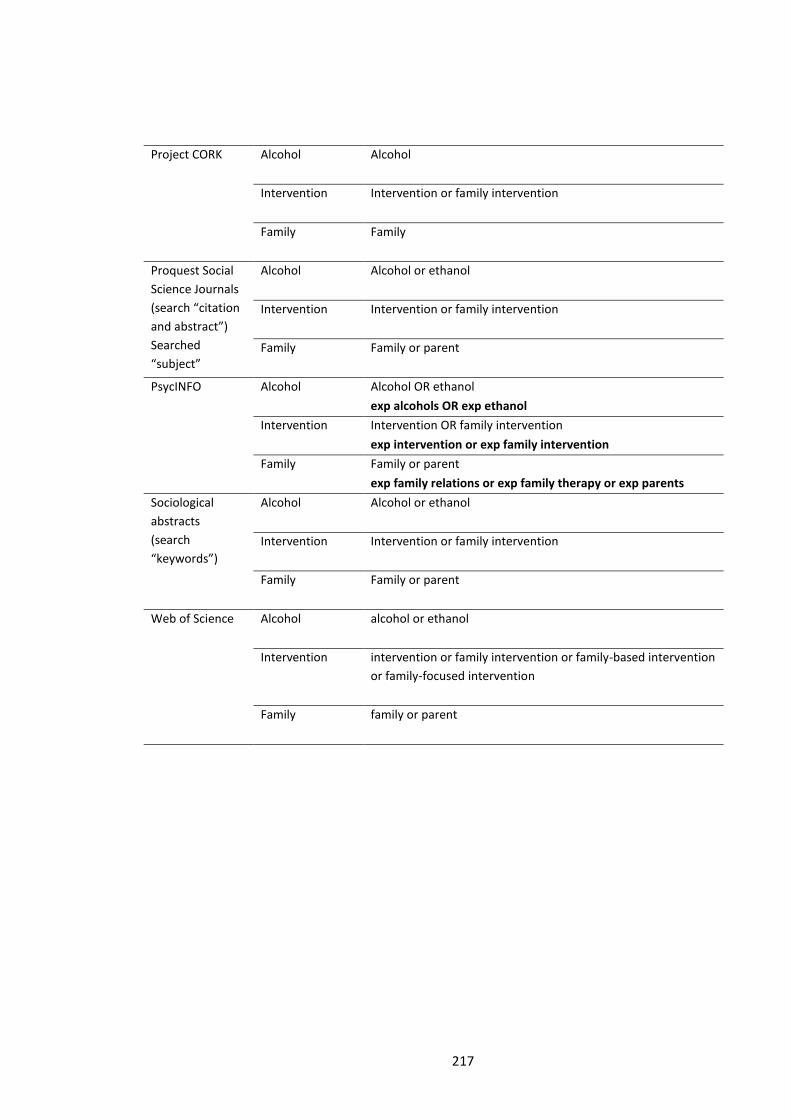
217
Project CORK
Alcohol Alcohol
Intervention Intervention or family intervention
Family Family
Proquest Social
Science Journals
(search “citation
and abstract”)
Searched
“subject”
Alcohol Alcohol or ethanol
Intervention Intervention or family intervention
Family Family or parent
PsycINFO
Alcohol Alcohol OR ethanol
exp alcohols OR exp ethanol
Intervention Intervention OR family intervention
exp intervention or exp family intervention
Family Family or parent
exp family relations or exp family therapy or exp parents
Sociological
abstracts
(search
“keywords”)
Alcohol Alcohol or ethanol
Intervention Intervention or family intervention
Family Family or parent
Web of Science
Alcohol alcohol or ethanol
Intervention intervention or family intervention or family-based intervention
or family-focused intervention
Family family or parent
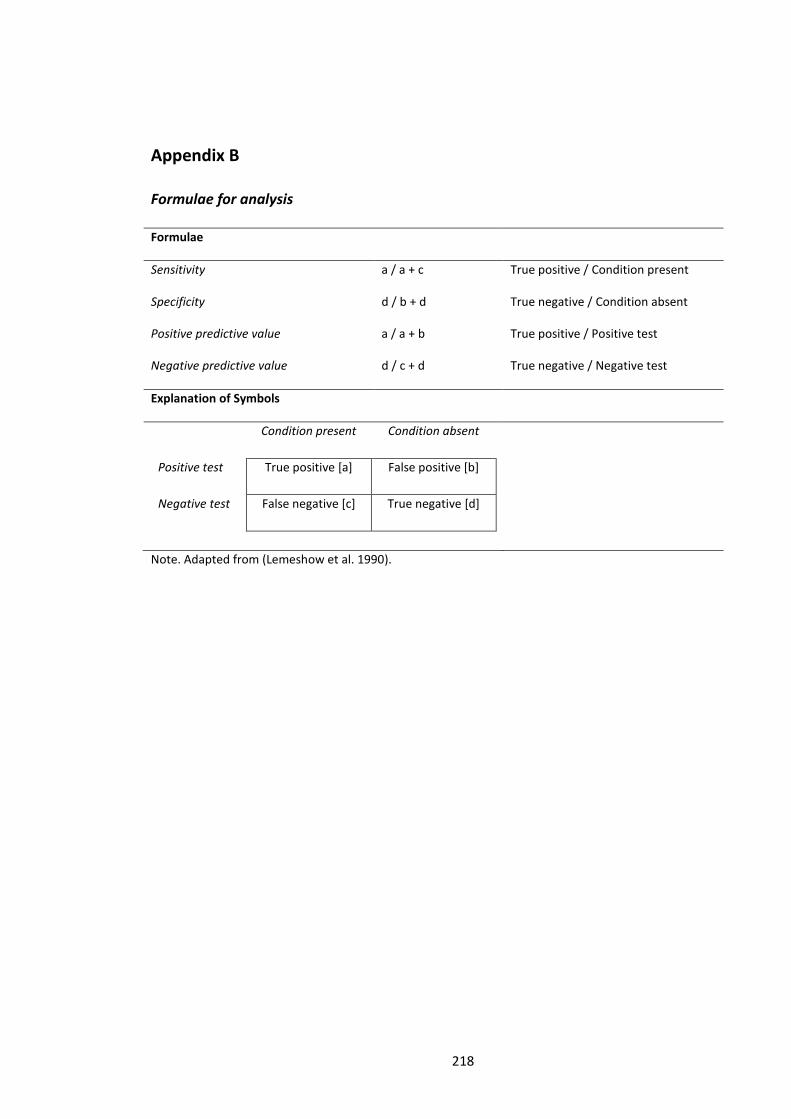
218
Appendix B
Formulae for analysis
Formulae
Sensitivity a / a + c True positive / Condition present
Specificity d / b + d True negative / Condition absent
Positive predictive value a / a + b True positive / Positive test
Negative predictive value d / c + d True negative / Negative test
Explanation of Symbols
Condition present Condition absent
Positive test True positive [a] False positive [b]
Negative test False negative [c] True negative [d]
Note. Adapted from (Lemeshow et al. 1990).

219
Appendix C
Health care provider consent form
Yoorana Gunya Family Violence
Healing Centre Aboriginal
Corporation
Condobolin Aboriginal Health
Service
Information for Participants: Health Worker
Name of research project
The cost benefit of a Community Reinforcement and Family Training (CRAFT) alcohol
intervention for Indigenous Australians.
What is the project?
We are trialling two alcohol programs for Aboriginal people. Program One, The Community
Reinforcement Approach (CRA), is a program of counselling and support to help Aboriginal
people who drink too much alcohol to cut down or stop drinking. Program Two, Community
Reinforcement and Family Training (CRAFT), is a program of training and support for family
members and/or friends of Aboriginal people who drink too much alcohol. Both programs will
be delivered by workers from Yoorana Gunya Family Violence Healing Centre Aboriginal
Corporation (Forbes) and the Lyndon Community (Orange). The National Drug and Alcohol
Research Centre (NDARC) at the University of New South Wales (UNSW) will work with
Yoorana Gunya and Lyndon Community to assess how well both programs work.
What it means to be a part of the Community Reinforcement and Family Training (CRAFT)
alcohol intervention project?
If you agree to be part of the project you will be asked to participate in professional
development training to provide you with the knowledge and skills you need to deliver the
Community Reinforcement Approach (CRA) or Community Reinforcement and Family Training
(CRAFT). If you are trained and/or certified in CRA you will be asked to deliver the program to
clients who have alcohol problems and have agreed to participate in the project. If you are
trained and/or certified in CRAFT you will be asked to deliver the program to clients who have
220
a relative/s with alcohol problems and have agreed to participate in the project. You will also
be asked to participate in interviews after you have completed training and/or certification.
Interviews will be held at Yoorana Gunya Family Violence Healing Centre Aboriginal
Corporation and/or at the Lyndon Community, and will take up to one hour. The interviews
will be conducted by a researcher involved in the project. The researcher will ask you
questions about your experiences completing the training and certification programs. All
interviews will be audio taped. You may also be asked by researchers to provide access to your
outreach diary so researchers can gain information about how much time is required to
provide outreach services. Brief access to your diary will only be required at a time that is
mutually suitable for the researcher and the worker.
Name, address and telephone number of principal researcher, for the purposes of this
document, unless otherwise stated, also called the Data Custodian
A/Prof Anthony Shakeshaft
National Drug and Alcohol Research Centre
University of New South Wales
Sydney NSW 2052 Australia
Phone: 02 9385 0285, or Email: [email protected]
Name, address and telephone number of institution, for the purposes of this document,
unless otherwise stated, also called the Data Repository.
National Drug and Alcohol Research Centre
Faculty of Medicine
University of New South Wales
Sydney NSW 2052 Australia
Phone: 02 9385 0333, Fax: 02 9385 0222
Right to withdrawal
Participation is voluntary. At any time you can choose not to be a part project and may ask for
the information that you have given not to be used. Withdrawing from the project will not
result in any personal or financial penalty to you. Taking part in the CRAFT Project is not a
condition of your employment.
Confidentiality and privacy
Any information you give will be private and confidential and will not be used in any way that
will identify you. All data will be stored in secure facilities, and accessed only by authorised
personnel for up to seven years, after which it will be destroyed. Specific information about
you will not be published in a manner that could identify you as an individual, during or after
221
the conclusion of this project. Published information may identify Yoorana Gunya Family
Violence Healing Centre Aboriginal Corporation and the Lyndon Community.
Potential risks and discomforts
As part of the CRA and CRAFT programs you will need to ask sensitive questions that may
result in psychological distress experienced by your client or by yourself. You will be provided
with training on how to ask sensitive questions and respond accordingly. If you experience
psychological distress specialist counsellors, mental health workers and medical addiction
specialists will be available to provide additional advice and support.
Community consultation
The Aboriginal community, through the representative members of the board of Yoorana
Gunya Family Violence Healing Centre Aboriginal Corporation, Orange Aboriginal Medical
Service and Lyndon Community has been consulted and agreed to be a part of the CRAFT
project.
Ethical provision
The CRAFT project abides by ethical conduct relating to health research in Aboriginal
communities as stated in National Aboriginal Community Controlled Health Organisation
(NACCHO), Aboriginal Health & Medical Research Council (AH&MRC), National Health &
Medical Research Council (NHMRC), UNSW ethics publications, and the Human Research Ethics
Committee (HREC) of the Greater Western Area Health Service and that, where required,
ethics approval has been granted by these organisations.
Questions and concerns
If you have any questions about the CRAFT project you can contact the principal researcher
listed on page 2. If you have any complaints you should contact the three ethics committees
listed below:
The Chairperson
AHMRC Ethics Committee
PO Box 1565
Strawberry Hills NSW 2012
Phone: 02 9212 4777
Fax: 02 9212 7211
Email: [email protected]
UNSW Ethics Secretariat
University of New South Wales
Sydney 2052 AUSTRALIA
Phone: 02 9385 4234
Fax: 02 9385 6648
Email: [email protected]
The Executive Officer
Greater Western AHS
HREC
PO Box 143
Bathurst NSW 2795
Phone: 02 6339 5601
222
Health Worker Consent for the CRAFT project
I, ................................................................................................................ [print full name], have
read and understood the Information for Participants: Health Worker.
I have been made aware of the procedures involved in the study, including any known or
expected inconvenience, risk, discomfort or potential side effect and of their implications as
far as they are currently known by the researchers. I understand that I can withdraw my
participation from the study at any time.
I hereby agree to participate in this research study.
Signature of participant: Date:
Witnessed by [print name]:
Signature of Witness: Date:

223
Appendix D
Qualitative data analysis
Memos: Working group meeting notes data
1. Literacy issues working with Aboriginal clients so keep language simple.
2. 4-6 sessions max
3. Certification helpful, in addition to training day (good supervision, designated days for
CRAFT have been good)
4. Problems with asking family member why a drinker is behaving in a certain way
5. Problem with fit of US training (where their language must be used) and real world
delivery to Aboriginal clients (language needs to be changed).
6. Resources good but language needs to be simplified
7. Delivery of CRAFT and CRA in groups (rather than individual)
8. Shorter package of outcome measures
9. Recruitment options: probation and parole and other health care services

224
Code Book: Working group meeting notes data
Code Description
CRAFT certification
(CERT)
Usefulness of the CRAFT certification process
Therapeutic issues
(THERA)
Problems with aspects of the therapeutic approach
Adapt CRA and CRAFT
(ADAPT)
Information about adapting CRA and CRAFT to be` appropriate for
Aboriginal Australians
Measures (MES) Information about modification to outcome measure
Recruitment (RECRUIT) Information about possible referral pathways
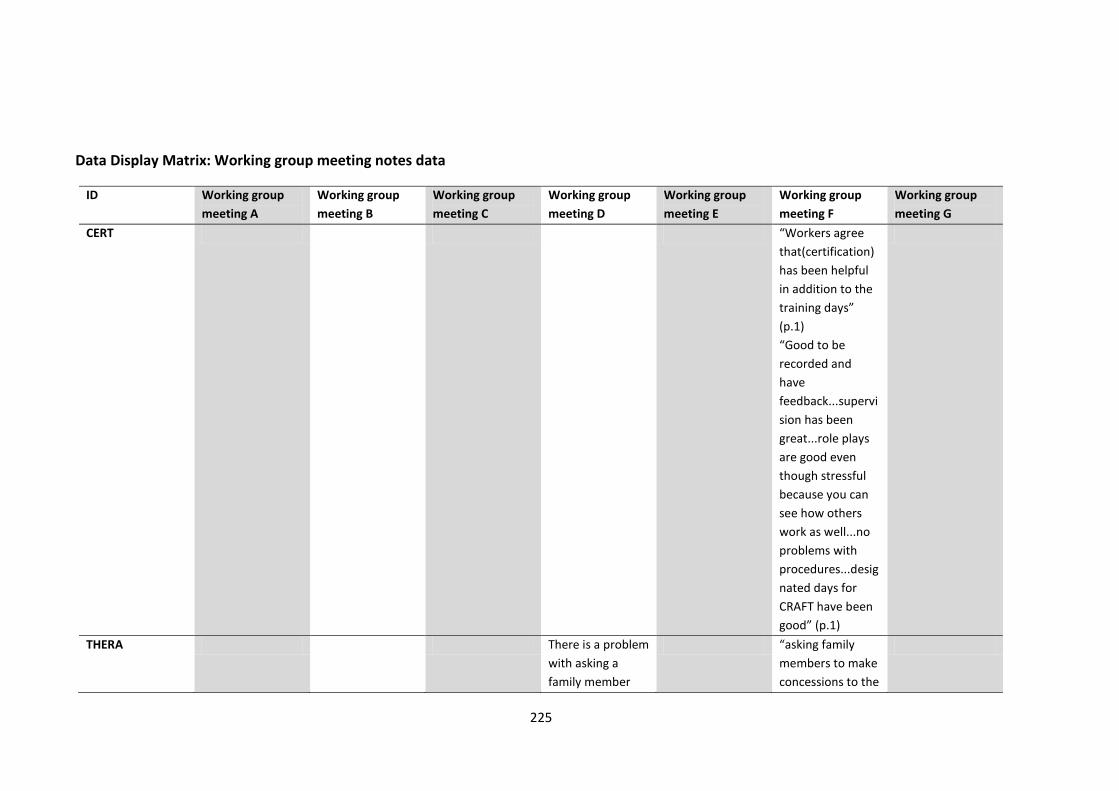
225
Data Display Matrix: Working group meeting notes data
ID Working group
meeting A
Working group
meeting B
Working group
meeting C
Working group
meeting D
Working group
meeting E
Working group
meeting F
Working group
meeting G
CERT “Workers agree
that(certification)
has been helpful
in addition to the
training days”
(p.1)
“Good to be
recorded and
have
feedback...supervi
sion has been
great...role plays
are good even
though stressful
because you can
see how others
work as well...no
problems with
procedures...desig
nated days for
CRAFT have been
good” (p.1)
THERA There is a problem
with asking a
family member
“asking family
members to make
concessions to the
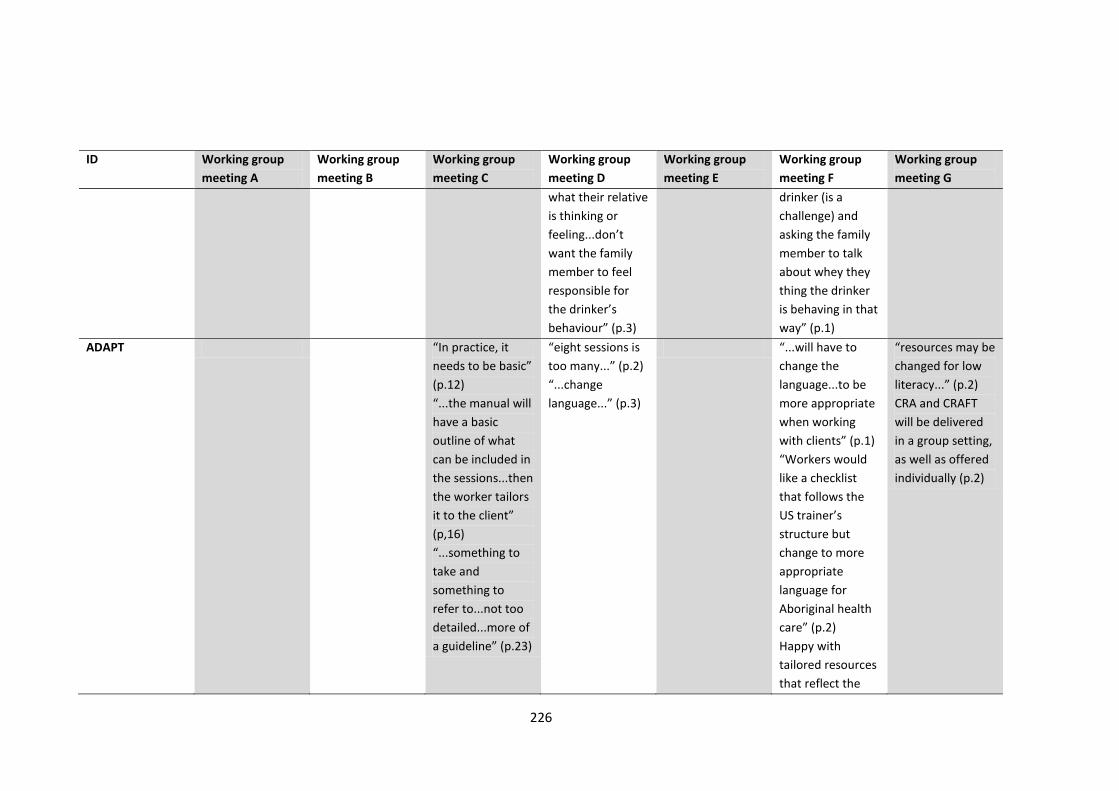
226
ID Working group
meeting A
Working group
meeting B
Working group
meeting C
Working group
meeting D
Working group
meeting E
Working group
meeting F
Working group
meeting G
what their relative
is thinking or
feeling...don’t
want the family
member to feel
responsible for
the drinker’s
behaviour” (p.3)
drinker (is a
challenge) and
asking the family
member to talk
about whey they
thing the drinker
is behaving in that
way” (p.1)
ADAPT “In practice, it
needs to be basic”
(p.12)
“...the manual will
have a basic
outline of what
can be included in
the sessions...then
the worker tailors
it to the client”
(p,16)
“...something to
take and
something to
refer to...not too
detailed...more of
a guideline” (p.23)
“eight sessions is
too many...” (p.2)
“...change
language...” (p.3)
“...will have to
change the
language...to be
more appropriate
when working
with clients” (p.1)
“Workers would
like a checklist
that follows the
US trainer’s
structure but
change to more
appropriate
language for
Aboriginal health
care” (p.2)
Happy with
tailored resources
that reflect the
“resources may be
changed for low
literacy...” (p.2)
CRA and CRAFT
will be delivered
in a group setting,
as well as offered
individually (p.2)
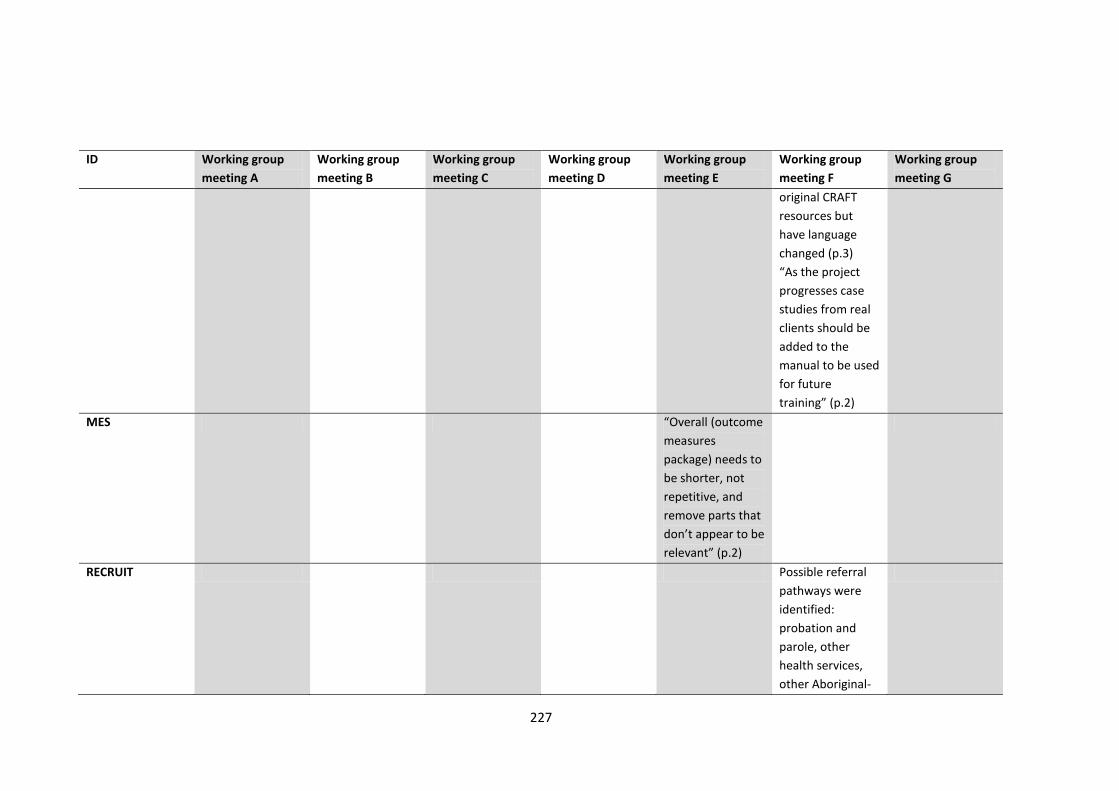
227
ID Working group
meeting A
Working group
meeting B
Working group
meeting C
Working group
meeting D
Working group
meeting E
Working group
meeting F
Working group
meeting G
original CRAFT
resources but
have language
changed (p.3)
“As the project
progresses case
studies from real
clients should be
added to the
manual to be used
for future
training” (p.2)
MES “Overall (outcome
measures
package) needs to
be shorter, not
repetitive, and
remove parts that
don’t appear to be
relevant” (p.2)
RECRUIT Possible referral
pathways were
identified:
probation and
parole, other
health services,
other Aboriginal-
228
ID Working group
meeting A
Working group
meeting B
Working group
meeting C
Working group
meeting D
Working group
meeting E
Working group
meeting F
Working group
meeting G
specific services
229
Memos: Interview data
1. Language changes required
2. Good structured program but prescribed sessions not practical
3. Role plays critical/useful to cement training even though uncomfortable at first
4. Ease of Skype and ooVoo use
5. Resources good
6. Manual - Not used - Use – scenarios were good
7. Training intense but useful
8. Time constraints and other commitments for audio taping sessions, no time constraints for
supervision
9. Supervision positive and needed for motivation
10. Team member support important
11. CRAFT is adaptable to Aboriginal Australians
12. Function analysis – not right to ask someone what they think someone else is feeling
13. Training in Indigenous specific
14. Need experience working with Aboriginal Australians to give comment on changes to
CRAFT
15. Don’t need a degree to be a therapist but do need experience
16. Complex clients don’t fit with original CRAFT
17. Training fostered personal growth
18. Happiness scale and positive communication skills both useful
19. Positive reinforcement for drinker hard for family member to do
20. Similar to what done/doing before/now
21. Role plays for certification – didn’t always work with the same partner
22. Obstacle – role plays and recordings but people got use to it
23. Training pitched fine but need a level of counselling experience
230
Code Book: Interview data
Code Description
CRAFT Certification
(CERT)
Usefulness of CRAFT training days and CRAFT certification INCLUDE
information about experiences during role plays
CRA Training (TRAIN) Usefulness of CRA training day
Therapeutic issues
(ISSUES)
Issues raised with the training and delivery of CRA and CRAFT
Organisational support
(SUPPORT)
Therapist supervision, team member support, supervision sessions
with the U.S. supervisor
Qualifications of
therapists (QUALS)
Information on the pitch of training and what qualifications would
be appropriate for health workers interested in doing CRAFT
certification
Adaptability of CRA
and CRAFT for
Aboriginal Australians
(ADAPT)
Adaptability of CRAFT for Aboriginal Australians INCLUDE
information about changes required to language to be appropriate
for Aboriginal Australians INCLUDE statements about the manual
and intervention resources (e.g. Functional Analysis, Happiness
Scale, Positive Communication, etc.)

231
Data Display Matrix: Interview data
ID Health care provider
101
Health care
provider 102
Health care
provider 103
Health care
provider 104
Health care provider
105
Health care
provider 106
Health care provider
107
CERT “I’m actually quite an
advocate for it now
and particularly with
the tools like with the
happiness scales and
with things like that,
that’s something that
really people can look
at and they can see
where they’ve
changed and made
progress and things
that they really want
to look at and things
like that.” (p.17)
“I think it was all
really good, I wouldn’t
change anything, I
don’t think.(p.19)
“Doing the role-plays
and talking to (the
supervisor) there a
couple of weeks ago
was really good”
(p.17)
“I tried not to do the
role plays...but it was
“...at first it was a
bit overwhelming”
(p. 8)
“...I liked the fact
that it had...some
group work...gave
the opportunity
to...getting the
concept of
(CRAFT)” (p. 9).
“...having an open
discussion with
the other people
who were in
training for the
supervision (was
useful)” (p.10)
“...doing some role
playing during the
workshops, I think,
was valuable for
people to
understand the
concept rather
than being talked
at” (p. 8)
“...we had a few
“...enjoyed the
CRAFT training, I
thought it was
really good”
(p.3)
“(the workshop
format) was a
little bit dated”
(p. 4)
“...(the
accreditation
process has)
been really,
really valuable
for the people
who have gone
through it to get
feedback about
their skills in
counselling,
regardless of
doing the
procedures
which are part
of the program”
(p.11)
“I thought that
“It was really
good to have -
see the role play
and do a reverse
role play and
that sort of
thing...” (during
Skype
supervision
sessions) (p.7)
I think (the
audio-taped
sessions) was a
kind of a tough
process to start
with... I was not
quite sure if I
was doing things
right... I
found...it really
good to get back
the feedback”
(p.11)
“To start with, it
was tricky ‘cause
... co-ordinating
time and getting
Oh, (the workshop
with the US trainer)
was good...I really
enjoyed it” (p4)
“...(Skyping with the
US supervisor) was
excellent...really,
really good...” (p.5)
“...I just found it
really, really good,
and just the support
that the US
supervisor’s given
us, fantastic.
Difficult in getting
my old head to think
in a different way
with some of the
procedures, so I did
send off a few tapes
where I just didn’t
get it, but then I’ve
got it, if you know
what I mean? “ (p.4)
“I’ve learnt more
from talking to the
US supervisor
“I thought the
workshop was
good... that
made it sort of
sink in a little bit
better than if we
had of just gone
through the
information but
yeah, I thought
it was good
training” (p.4)
“We just found
it really draining
to be – because
it was so
structured” (p.7)
“I actually found
(Skyping) pretty
useful” (p.4)
“Like I guess
ideally it would
probably be
better to be able
to do
(supervision) in
person but there
“...the actual content
was good (of the
workshop)...nothing
really that I hadn’t
done before, but it
was just packaged
differently” (p.4)
“the whole process
has been good for
everybody, I think”
(p.17)
“I can’t really think of
anything negative
about the training.
It’s good for people to
get that feedback on
the counselling, too”
(p.24)
“...(Skyping) was very
good, I thought... he
gave us a lot of good
feedback... he’d
demonstrate...the
difference ways of
asking people and
that sort of stuff”
(p.5)
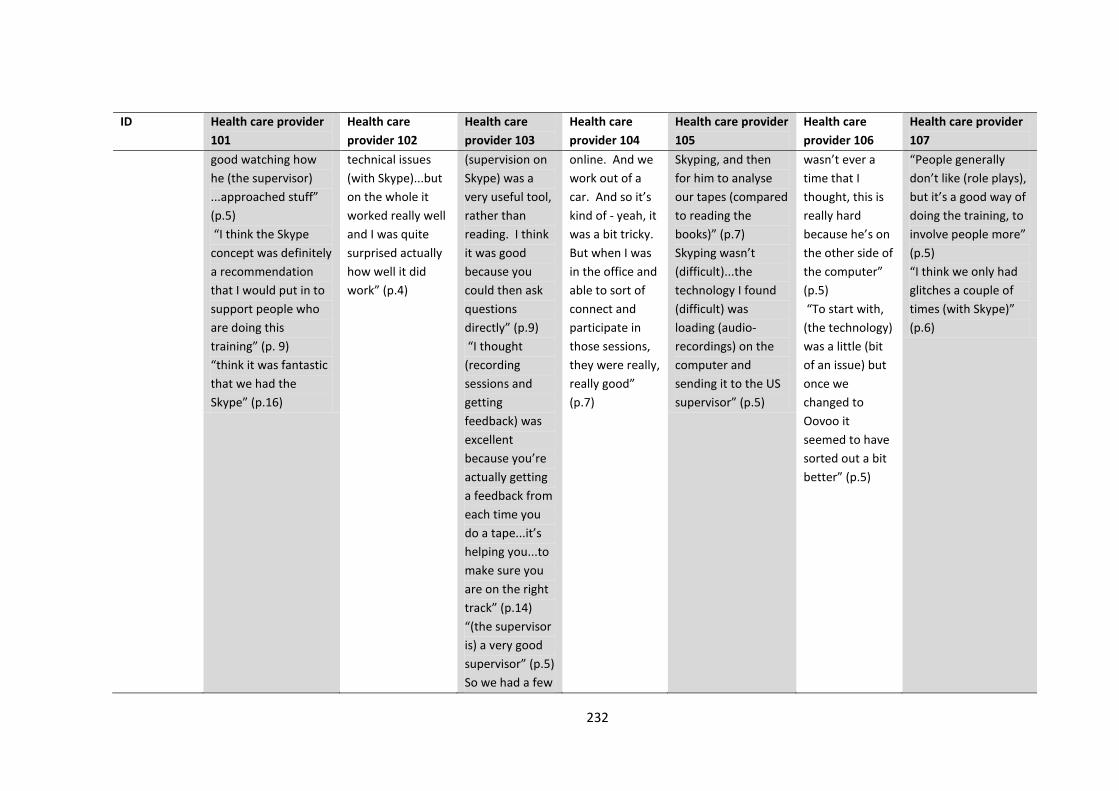
232
ID Health care provider
101
Health care
provider 102
Health care
provider 103
Health care
provider 104
Health care provider
105
Health care
provider 106
Health care provider
107
good watching how
he (the supervisor)
...approached stuff”
(p.5)
“I think the Skype
concept was definitely
a recommendation
that I would put in to
support people who
are doing this
training” (p. 9)
“think it was fantastic
that we had the
Skype” (p.16)
technical issues
(with Skype)...but
on the whole it
worked really well
and I was quite
surprised actually
how well it did
work” (p.4)
(supervision on
Skype) was a
very useful tool,
rather than
reading. I think
it was good
because you
could then ask
questions
directly” (p.9)
“I thought
(recording
sessions and
getting
feedback) was
excellent
because you’re
actually getting
a feedback from
each time you
do a tape...it’s
helping you...to
make sure you
are on the right
track” (p.14)
“(the supervisor
is) a very good
supervisor” (p.5)
So we had a few
online. And we
work out of a
car. And so it’s
kind of - yeah, it
was a bit tricky.
But when I was
in the office and
able to sort of
connect and
participate in
those sessions,
they were really,
really good”
(p.7)
Skyping, and then
for him to analyse
our tapes (compared
to reading the
books)” (p.7)
Skyping wasn’t
(difficult)...the
technology I found
(difficult) was
loading (audio-
recordings) on the
computer and
sending it to the US
supervisor” (p.5)
wasn’t ever a
time that I
thought, this is
really hard
because he’s on
the other side of
the computer”
(p.5)
“To start with,
(the technology)
was a little (bit
of an issue) but
once we
changed to
Oovoo it
seemed to have
sorted out a bit
better” (p.5)
“People generally
don’t like (role plays),
but it’s a good way of
doing the training, to
involve people more”
(p.5)
“I think we only had
glitches a couple of
times (with Skype)”
(p.6)
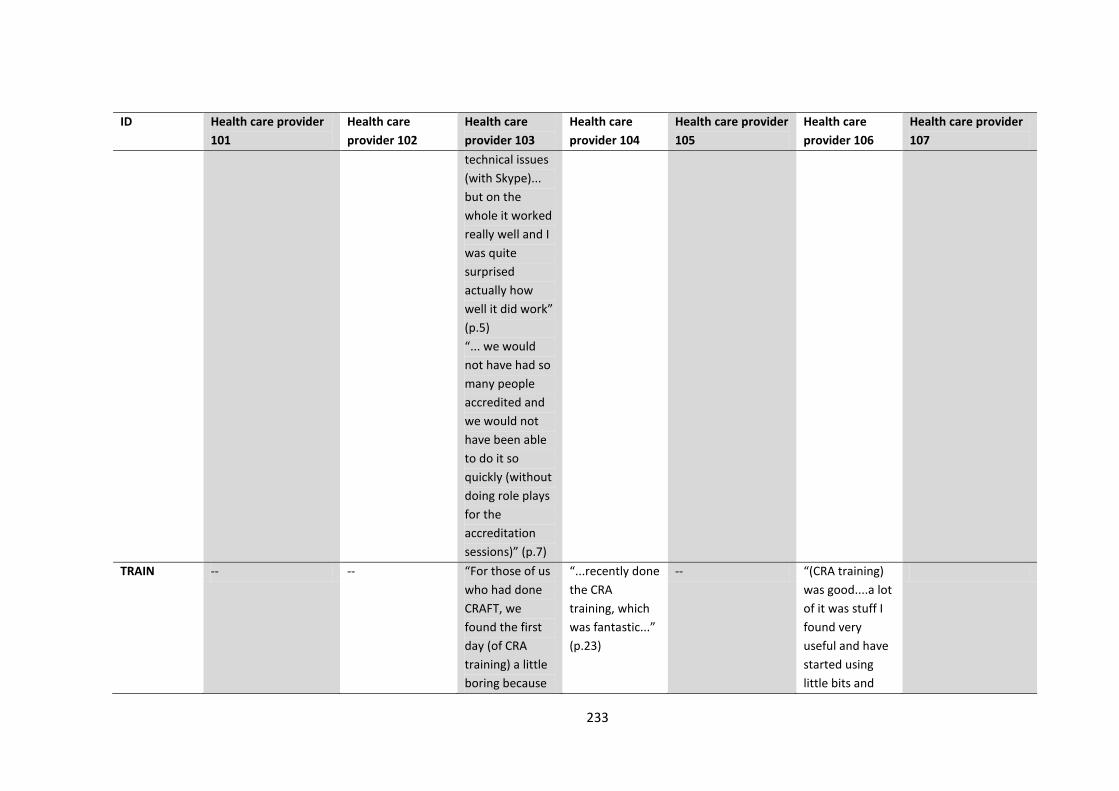
233
ID Health care provider
101
Health care
provider 102
Health care
provider 103
Health care
provider 104
Health care provider
105
Health care
provider 106
Health care provider
107
technical issues
(with Skype)...
but on the
whole it worked
really well and I
was quite
surprised
actually how
well it did work”
(p.5)
“... we would
not have had so
many people
accredited and
we would not
have been able
to do it so
quickly (without
doing role plays
for the
accreditation
sessions)” (p.7)
TRAIN -- -- “For those of us
who had done
CRAFT, we
found the first
day (of CRA
training) a little
boring because
“...recently done
the CRA
training, which
was fantastic...”
(p.23)
-- “(CRA training)
was good....a lot
of it was stuff I
found very
useful and have
started using
little bits and

234
ID Health care provider
101
Health care
provider 102
Health care
provider 103
Health care
provider 104
Health care provider
105
Health care
provider 106
Health care provider
107
it was talking
about functional
analysis and
that sort of
stuff...but the
second day, we
did quite a few
more exercises
and ...some
group stuff
(p.15)
pieces with
clients already
when I’ve been
talking to them,
so that’s good”
(p.17)
ISSUES “I only did a few
(supervision sessions)
because they were on
Thursday...” (p.5)
“what was good for”
me personally, is
when we had
identified CRAFT days
because sometimes
fitting it in was
difficult...and that
really motivated all of
us, I think, to just get
stuck in” p.8)
“...(role playing) was
excruciating but it was
really good. It was
good putting it in
Didn’t look at
manual “mainly
due to time
restraints” (p.10)
“sometimes you
didn’t want to do
the sessions,
mainly because of
overload from
other areas of
your work” (p.15)
“Some sessions I
missed because I
was committed to
other things”
(p.19)
“...it really was a
significant time
and effort
commitment for
the last 10
months” (p.5)
“I’d always
learnt in
counselling that
you don’t get
people to
theorise or
hypothesise
about how
someone else
feels...it was a
different spin
when...you ask a
“I mean the
negatives was
the time and the
pressure that it
put on you”
(p.15)
“...it was kind of
hard to do (role
plays) and feel
natural about
it...the more we
did it, the more
you got used to
that (p.11)
“(the certification
process) was
challenging...fitting
it in with work” (p.8)
“....(role plays with
other therapists
was) a bit
confrontational in
that you’re seeing
another therapist
see your style and
then you wonder if
that’s okay, if you’ve
done okay, am I
doing it okay” (p.8)
“The hardest
part of it was
finding the time
to get (the role
plays) done”
(p.7)
“I am a lot more
confident with
using it now
than I would
have been if we
hadn’t have
done the role
plays before and
just getting the
feedback was
good to know
this bit you did
“The worst part was
trying to get everyone
motivated to do (the
audio-taped
sessions), and actually
co-ordinating them all
to actually do them.
So we set aside days –
specific days – to get
a couple done each of
those days. And that
worked well because
everybody could just
concentrate on that.
So I thought it was
good, especially
because I was
listening to other
235
ID Health care provider
101
Health care
provider 102
Health care
provider 103
Health care
provider 104
Health care provider
105
Health care
provider 106
Health care provider
107
practice.” (p.8)
woman ...when
you are doing a
functional
analysis...how
do you think he
feels?” (p.11)
really well, this
bit you probably
need to work
on” (p.8)
“...so I think
trying to get
people to really
look at their
family member’s
behaviours and
trying to reward
them and things
like that, might
be a bit tough...
And I think the
difference
between trying
to get people to
understand
between
positive
reinforcement
and enabling
that is going to
be pretty tricky
as well... (time
out for positive
reinforcement)
has the potential
people, so I could see
where their skill level
was at, and that sort
of thing. So it was a
good learning curve
for, yeah, everybody.”
(p.8)
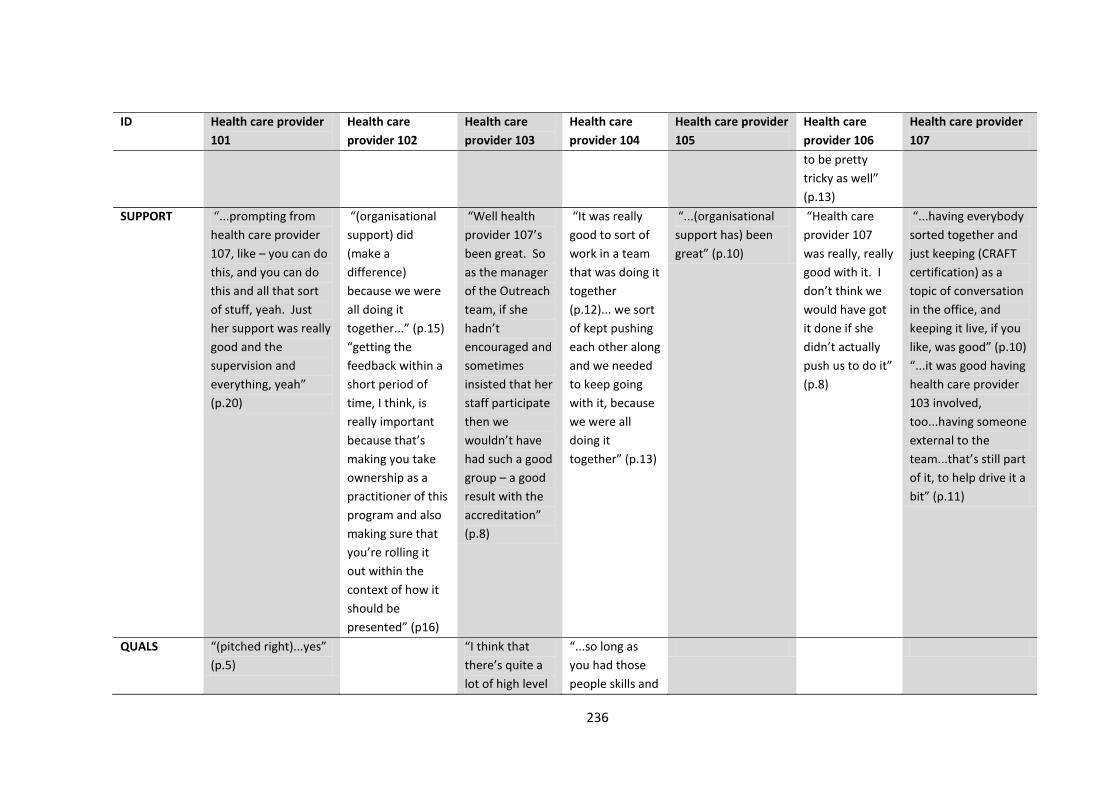
236
ID Health care provider
101
Health care
provider 102
Health care
provider 103
Health care
provider 104
Health care provider
105
Health care
provider 106
Health care provider
107
to be pretty
tricky as well”
(p.13)
SUPPORT “...prompting from
health care provider
107, like – you can do
this, and you can do
this and all that sort
of stuff, yeah. Just
her support was really
good and the
supervision and
everything, yeah”
(p.20)
“(organisational
support) did
(make a
difference)
because we were
all doing it
together...” (p.15)
“getting the
feedback within a
short period of
time, I think, is
really important
because that’s
making you take
ownership as a
practitioner of this
program and also
making sure that
you’re rolling it
out within the
context of how it
should be
presented” (p16)
“Well health
provider 107’s
been great. So
as the manager
of the Outreach
team, if she
hadn’t
encouraged and
sometimes
insisted that her
staff participate
then we
wouldn’t have
had such a good
group – a good
result with the
accreditation”
(p.8)
“It was really
good to sort of
work in a team
that was doing it
together
(p.12)... we sort
of kept pushing
each other along
and we needed
to keep going
with it, because
we were all
doing it
together” (p.13)
“...(organisational
support has) been
great” (p.10)
“Health care
provider 107
was really, really
good with it. I
don’t think we
would have got
it done if she
didn’t actually
push us to do it”
(p.8)
“...having everybody
sorted together and
just keeping (CRAFT
certification) as a
topic of conversation
in the office, and
keeping it live, if you
like, was good” (p.10)
“...it was good having
health care provider
103 involved,
too...having someone
external to the
team...that’s still part
of it, to help drive it a
bit” (p.11)
QUALS “(pitched right)...yes”
(p.5)
“I think that
there’s quite a
lot of high level
“...so long as
you had those
people skills and
237
ID Health care provider
101
Health care
provider 102
Health care
provider 103
Health care
provider 104
Health care provider
105
Health care
provider 106
Health care provider
107
practice
required to
implement
CRAFT in the
way that it’s
intended...I
think people will
vary in the way
they implement
the procedures”
(p.12)
sort of the
willingness to
sort of learn
something
different, and
then to apply it.
Sometimes I
think there’s
some resistance
to apply it,
maybe from
some lack of
confidence. But
that’s - I think
that’s more
down to an
individual,
rather than their
level of
knowledge and
experience...
sometimes
probably
experience is a
more useful
thing than
having the
university
education”
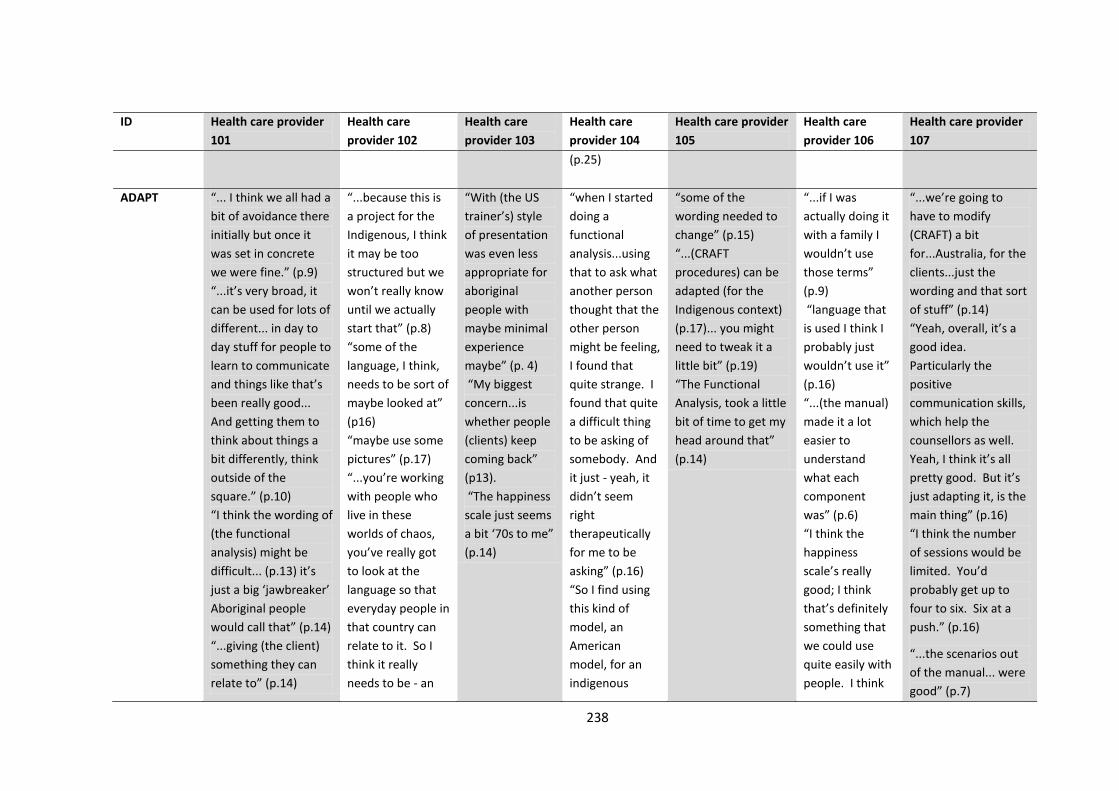
238
ID Health care provider
101
Health care
provider 102
Health care
provider 103
Health care
provider 104
Health care provider
105
Health care
provider 106
Health care provider
107
(p.25)
ADAPT “... I think we all had a
bit of avoidance there
initially but once it
was set in concrete
we were fine.” (p.9)
“...it’s very broad, it
can be used for lots of
different... in day to
day stuff for people to
learn to communicate
and things like that’s
been really good...
And getting them to
think about things a
bit differently, think
outside of the
square.” (p.10)
“I think the wording of
(the functional
analysis) might be
difficult... (p.13) it’s
just a big ‘jawbreaker’
Aboriginal people
would call that” (p.14)
“...giving (the client)
something they can
relate to” (p.14)
“...because this is
a project for the
Indigenous, I think
it may be too
structured but we
won’t really know
until we actually
start that” (p.8)
“some of the
language, I think,
needs to be sort of
maybe looked at”
(p16)
“maybe use some
pictures” (p.17)
“...you’re working
with people who
live in these
worlds of chaos,
you’ve really got
to look at the
language so that
everyday people in
that country can
relate to it. So I
think it really
needs to be - an
“With (the US
trainer’s) style
of presentation
was even less
appropriate for
aboriginal
people with
maybe minimal
experience
maybe” (p. 4)
“My biggest
concern...is
whether people
(clients) keep
coming back”
(p13).
“The happiness
scale just seems
a bit ‘70s to me”
(p.14)
“when I started
doing a
functional
analysis...using
that to ask what
another person
thought that the
other person
might be feeling,
I found that
quite strange. I
found that quite
a difficult thing
to be asking of
somebody. And
it just - yeah, it
didn’t seem
right
therapeutically
for me to be
asking” (p.16)
“So I find using
this kind of
model, an
American
model, for an
indigenous
“some of the
wording needed to
change” (p.15)
“...(CRAFT
procedures) can be
adapted (for the
Indigenous context)
(p.17)... you might
need to tweak it a
little bit” (p.19)
“The Functional
Analysis, took a little
bit of time to get my
head around that”
(p.14)
“...if I was
actually doing it
with a family I
wouldn’t use
those terms”
(p.9)
“language that
is used I think I
probably just
wouldn’t use it”
(p.16)
“...(the manual)
made it a lot
easier to
understand
what each
component
was” (p.6)
“I think the
happiness
scale’s really
good; I think
that’s definitely
something that
we could use
quite easily with
people. I think
“...we’re going to
have to modify
(CRAFT) a bit
for...Australia, for the
clients...just the
wording and that sort
of stuff” (p.14)
“Yeah, overall, it’s a
good idea.
Particularly the
positive
communication skills,
which help the
counsellors as well.
Yeah, I think it’s all
pretty good. But it’s
just adapting it, is the
main thing” (p.16)
“I think the number
of sessions would be
limited. You’d
probably get up to
four to six. Six at a
push.” (p.16)
“...the scenarios out
of the manual... were
good” (p.7)
239
ID Health care provider
101
Health care
provider 102
Health care
provider 103
Health care
provider 104
Health care provider
105
Health care
provider 106
Health care provider
107
“The language...as it is
written, might need to
be broken...maybe
just simplified” (p.15)
“I think it’s all doable
with the Aboriginal
community, it’s just
that the language
might just need to be
adapted a little bit to
suit them a bit better”
(p.15)...tweak then
here and there for the
individuals” (p.17)
“The language used
definitely needs to be
different and just a
little bit simplified or
it needs to be put in
Aboriginal language
and I don’t mean a
dialect I mean in the
way Aboriginal people
speak English” (p.17)
“I’m sure it can be
adapted. In its
present probably
form, it might be a bit
daunting for
Australian version
of it really needs
to be looked at.
The concepts are
still the same but
again, you need to
look at it in a
different way”
(p.23)
“(with Indigenous
people)... you
really need to look
at what’s
happened to them
in the past, how
would you present
this, because if
anything looks
government-like,
word-like, they
shut down, which
you can
understand” (p.
23)
“So you’ve really
got to do what we
call a soft entry
approach” (p. 24)
“...it was good to
population, it
doesn’t quite fit
with me at the
moment” (p.17)
“...so yes,
there’s
components
within this
training, and
certainly that I
think will work
for Indigenous
people” (p.21)
“We’re going to
get the
opportunity to
now go out and
look at what will
and won’t work
about that. And
I think that’s a
great thing.
Yeah” (p.24)
“if we could sort
of take away
some of the sort
of more
American based
language” (p.26)
some of the
things like with
the functional
analysis, trying
to get an
understanding
of: what does
your loved one
think right
before he
drinks, or what
does he feel
right before he
drinks? I think
that’s going to
be pretty hard
for people and I
guess how
accurate that’s
going to be is a
bit of a concern I
think.” (p.11)
“I think they’re all
(resources)pretty
good” (p.14)
240
ID Health care provider
101
Health care
provider 102
Health care
provider 103
Health care
provider 104
Health care provider
105
Health care
provider 106
Health care provider
107
Aboriginal people but
if it can be adapted
and a bit more user
friendly for their
community I think it
will be a really good
program” (p.19)
“That was all really
good...the copies of
the happiness
scale...the
worksheets...all that
stuff...” (p.6)
“Yeah, they were
good, they were very
good because they
were concise and they
told you exactly what
you needed to do and
that was how I
identified my little
gaps, things that I
might have missed.”
(p.7)
“I like those pieces of
paper, they were
good. When we were
doing recordings I’d
have them near me –
read (the
PowerPoint
presentation
handouts)...to get
your head around
it” (p. 10)
“I really liked the
Happiness Scale, I
liked ...functional
analysis” (p.13)
“Happiness
Scale...maybe
have it sort of
different (terms)...
(p. 18)
“The Domestic
Violence
Precautions, I
thought that was a
good warning sign
because the whole
idea is not to make
the situation
worse for the
family.” (p. 20)
“that to me is
how I feel
comfortable
using CRAFT is
having an
Aboriginal
worker. Yeah,
yeah, yeah,
come along and
walk alongside.”
(p.27)
“...(the manual)
was great” (p.9)
“The manual’s
great” (p.10)
“I think the
functional
analysis is a
fantastic tool to
use say in the
CRA which I’ve
just done the
training on. And
I think that’s a
fantastic tool to
use directly with
somebody who
is using. But I
just - and I still

241
ID Health care provider
101
Health care
provider 102
Health care
provider 103
Health care
provider 104
Health care provider
105
Health care
provider 106
Health care provider
107
okay, I need to do this
now” (p.12)
“...it was hard doing
the rewarding the
positive
behaviour...and then
practicing the
withdrawing of
rewards...that was
tricky. The
communications stuff
was really...good. But
the consequences was
a bit tricky to get
them to understand”
(p.12)
have my doubts
about that with
CRAFT” (p.17)
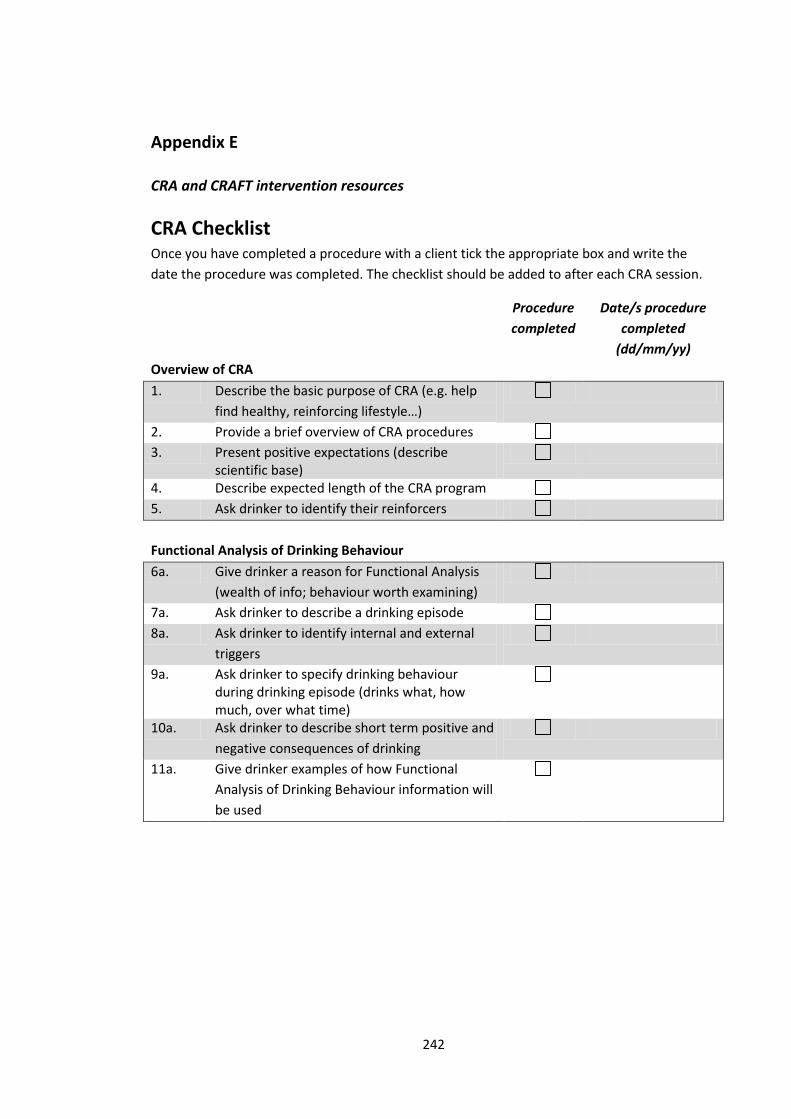
242
Appendix E
CRA and CRAFT intervention resources
CRA Checklist Once you have completed a procedure with a client tick the appropriate box and write the
date the procedure was completed. The checklist should be added to after each CRA session.
Procedure
completed
Date/s procedure
completed
(dd/mm/yy)
Overview of CRA
1. Describe the basic purpose of CRA (e.g. help
find healthy, reinforcing lifestyle…)
2. Provide a brief overview of CRA procedures
3. Present positive expectations (describe scientific base)
4. Describe expected length of the CRA program
5. Ask drinker to identify their reinforcers
Functional Analysis of Drinking Behaviour
6a. Give drinker a reason for Functional Analysis
(wealth of info; behaviour worth examining)
7a. Ask drinker to describe a drinking episode
8a. Ask drinker to identify internal and external
triggers
9a. Ask drinker to specify drinking behaviour during drinking episode (drinks what, how much, over what time)
10a. Ask drinker to describe short term positive and
negative consequences of drinking
11a. Give drinker examples of how Functional
Analysis of Drinking Behaviour information will
be used
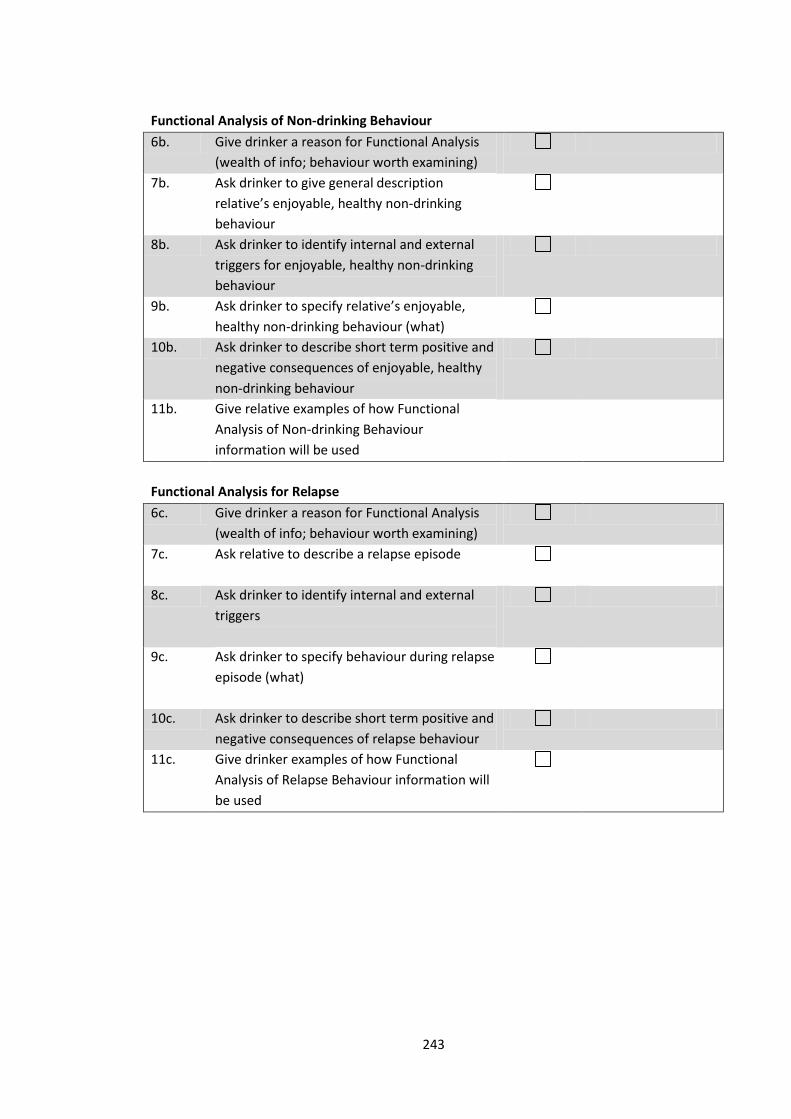
243
Functional Analysis of Non-drinking Behaviour
6b. Give drinker a reason for Functional Analysis
(wealth of info; behaviour worth examining)
7b. Ask drinker to give general description
relative’s enjoyable, healthy non-drinking
behaviour
8b. Ask drinker to identify internal and external
triggers for enjoyable, healthy non-drinking
behaviour
9b. Ask drinker to specify relative’s enjoyable,
healthy non-drinking behaviour (what)
10b. Ask drinker to describe short term positive and
negative consequences of enjoyable, healthy
non-drinking behaviour
11b. Give relative examples of how Functional
Analysis of Non-drinking Behaviour
information will be used
Functional Analysis for Relapse
6c. Give drinker a reason for Functional Analysis
(wealth of info; behaviour worth examining)
7c. Ask relative to describe a relapse episode
8c. Ask drinker to identify internal and external
triggers
9c. Ask drinker to specify behaviour during relapse
episode (what)
10c. Ask drinker to describe short term positive and
negative consequences of relapse behaviour
11c. Give drinker examples of how Functional
Analysis of Relapse Behaviour information will
be used
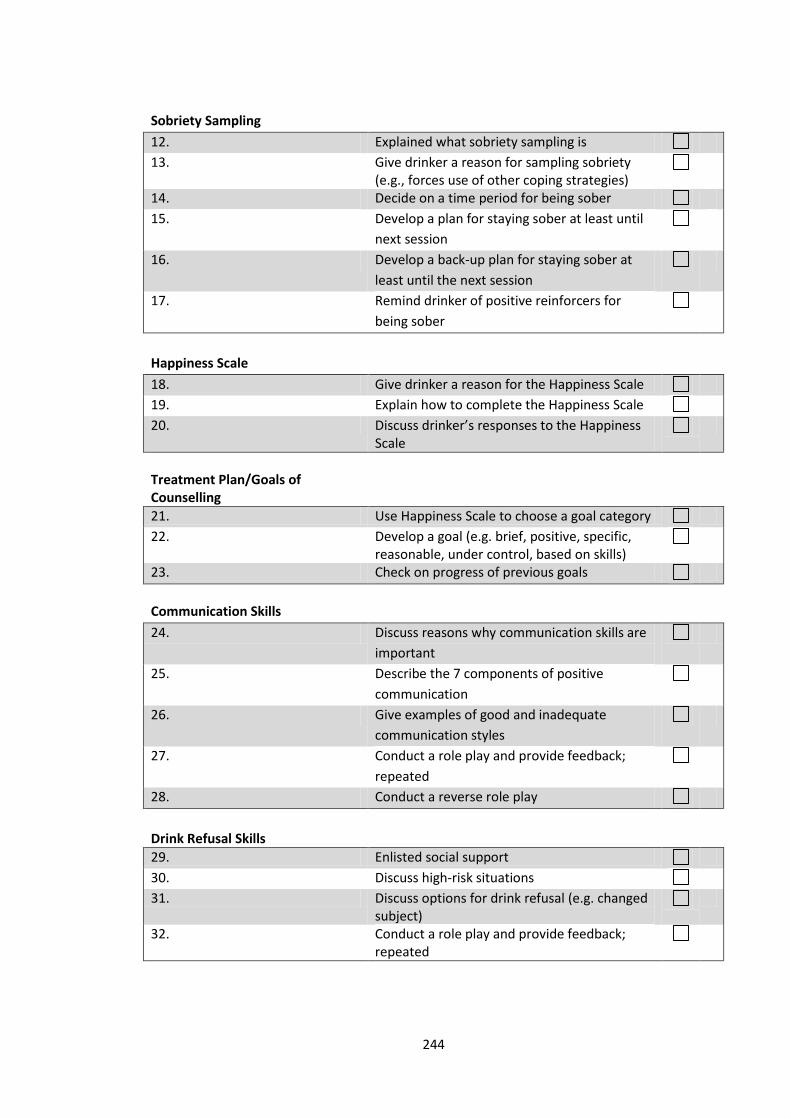
244
Sobriety Sampling
12. Explained what sobriety sampling is
13. Give drinker a reason for sampling sobriety (e.g., forces use of other coping strategies)
14. Decide on a time period for being sober
15. Develop a plan for staying sober at least until
next session
16. Develop a back-up plan for staying sober at
least until the next session
17. Remind drinker of positive reinforcers for
being sober
Happiness Scale
18. Give drinker a reason for the Happiness Scale
19. Explain how to complete the Happiness Scale
20. Discuss drinker’s responses to the Happiness Scale
Treatment Plan/Goals of Counselling
21. Use Happiness Scale to choose a goal category
22. Develop a goal (e.g. brief, positive, specific, reasonable, under control, based on skills)
23. Check on progress of previous goals
Communication Skills
24. Discuss reasons why communication skills are
important
25. Describe the 7 components of positive
communication
26. Give examples of good and inadequate
communication styles
27. Conduct a role play and provide feedback;
repeated
28. Conduct a reverse role play
Drink Refusal Skills
29. Enlisted social support
30. Discuss high-risk situations
31. Discuss options for drink refusal (e.g. changed subject)
32. Conduct a role play and provide feedback; repeated
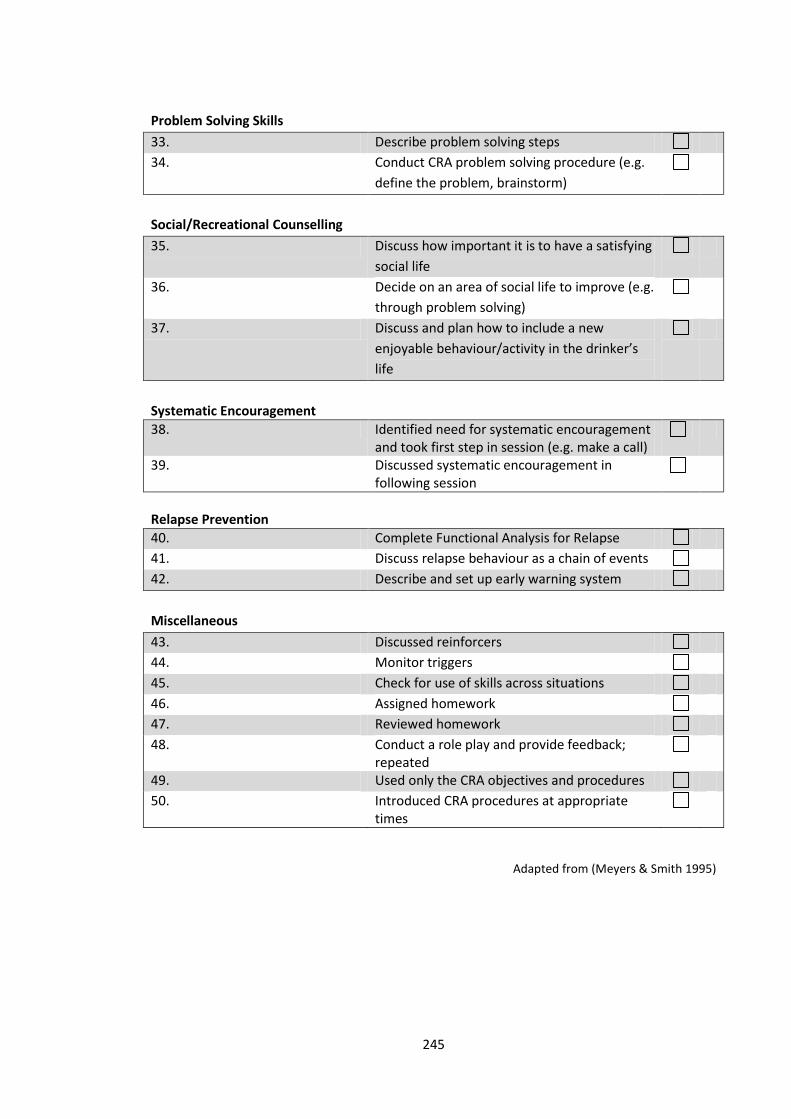
245
Problem Solving Skills
33. Describe problem solving steps
34. Conduct CRA problem solving procedure (e.g.
define the problem, brainstorm)
Social/Recreational Counselling
35. Discuss how important it is to have a satisfying
social life
36. Decide on an area of social life to improve (e.g.
through problem solving)
37. Discuss and plan how to include a new
enjoyable behaviour/activity in the drinker’s
life
Systematic Encouragement
38. Identified need for systematic encouragement and took first step in session (e.g. make a call)
39. Discussed systematic encouragement in following session
Relapse Prevention
40. Complete Functional Analysis for Relapse
41. Discuss relapse behaviour as a chain of events
42. Describe and set up early warning system
Miscellaneous
43. Discussed reinforcers
44. Monitor triggers
45. Check for use of skills across situations
46. Assigned homework
47. Reviewed homework
48. Conduct a role play and provide feedback; repeated
49. Used only the CRA objectives and procedures
50. Introduced CRA procedures at appropriate times
Adapted from (Meyers & Smith 1995)
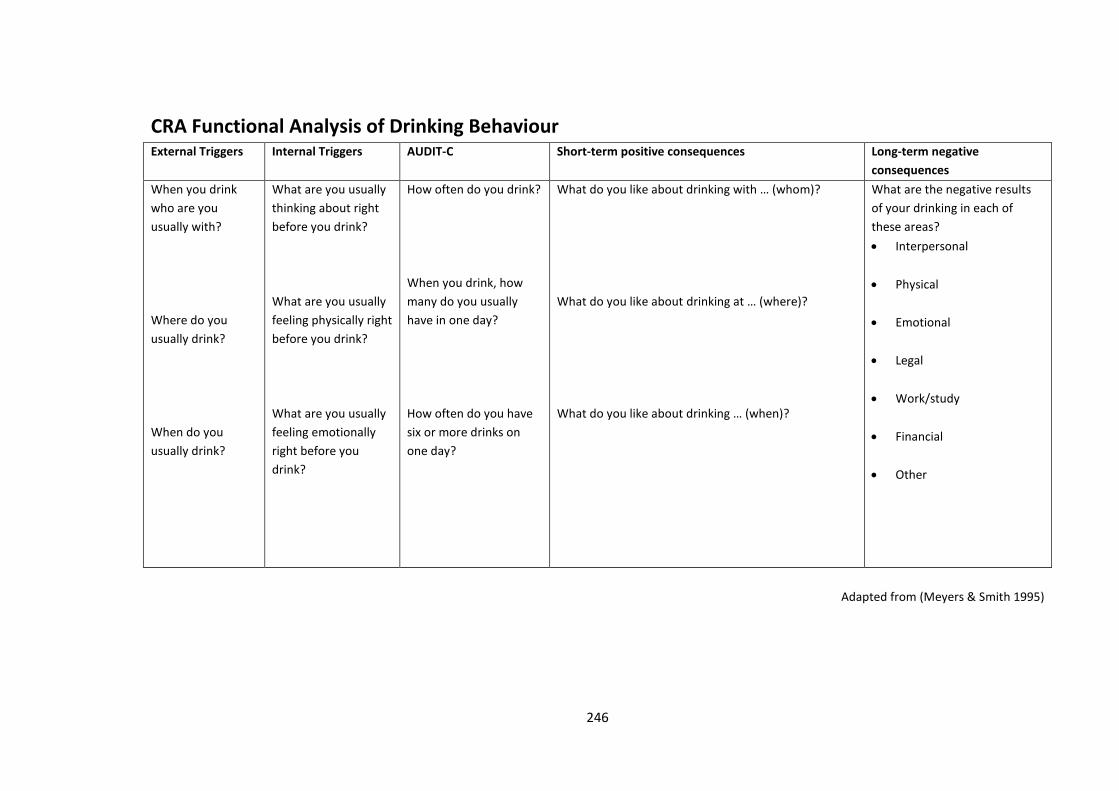
246
CRA Functional Analysis of Drinking Behaviour External Triggers Internal Triggers AUDIT-C Short-term positive consequences Long-term negative
consequences
When you drink
who are you
usually with?
Where do you
usually drink?
When do you
usually drink?
What are you usually
thinking about right
before you drink?
What are you usually
feeling physically right
before you drink?
What are you usually
feeling emotionally
right before you
drink?
How often do you drink?
When you drink, how
many do you usually
have in one day?
How often do you have
six or more drinks on
one day?
What do you like about drinking with … (whom)?
What do you like about drinking at … (where)?
What do you like about drinking … (when)?
What are the negative results
of your drinking in each of
these areas?
Interpersonal
Physical
Emotional
Legal
Work/study
Financial
Other
Adapted from (Meyers & Smith 1995)
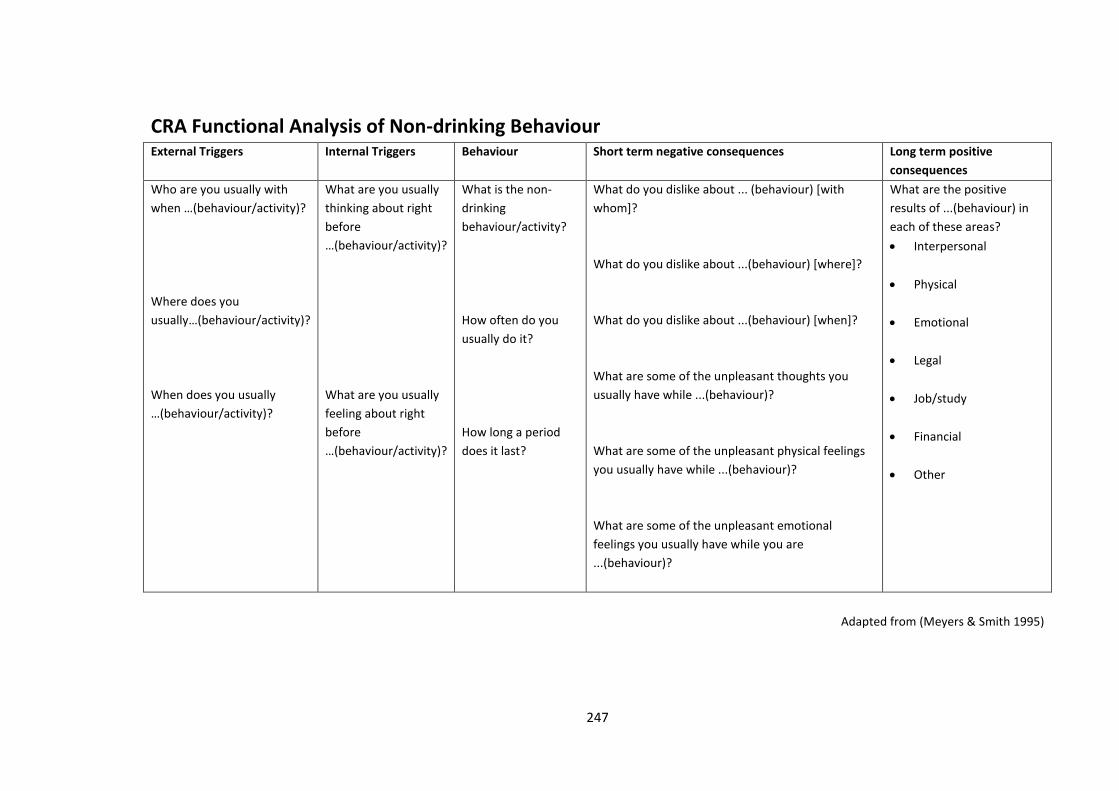
247
CRA Functional Analysis of Non-drinking Behaviour External Triggers Internal Triggers Behaviour Short term negative consequences Long term positive
consequences
Who are you usually with
when …(behaviour/activity)?
Where does you
usually…(behaviour/activity)?
When does you usually
…(behaviour/activity)?
What are you usually
thinking about right
before
…(behaviour/activity)?
What are you usually
feeling about right
before
…(behaviour/activity)?
What is the non-
drinking
behaviour/activity?
How often do you
usually do it?
How long a period
does it last?
What do you dislike about ... (behaviour) [with
whom]?
What do you dislike about ...(behaviour) [where]?
What do you dislike about ...(behaviour) [when]?
What are some of the unpleasant thoughts you
usually have while ...(behaviour)?
What are some of the unpleasant physical feelings
you usually have while ...(behaviour)?
What are some of the unpleasant emotional
feelings you usually have while you are
...(behaviour)?
What are the positive
results of ...(behaviour) in
each of these areas?
Interpersonal
Physical
Emotional
Legal
Job/study
Financial
Other
Adapted from (Meyers & Smith 1995)
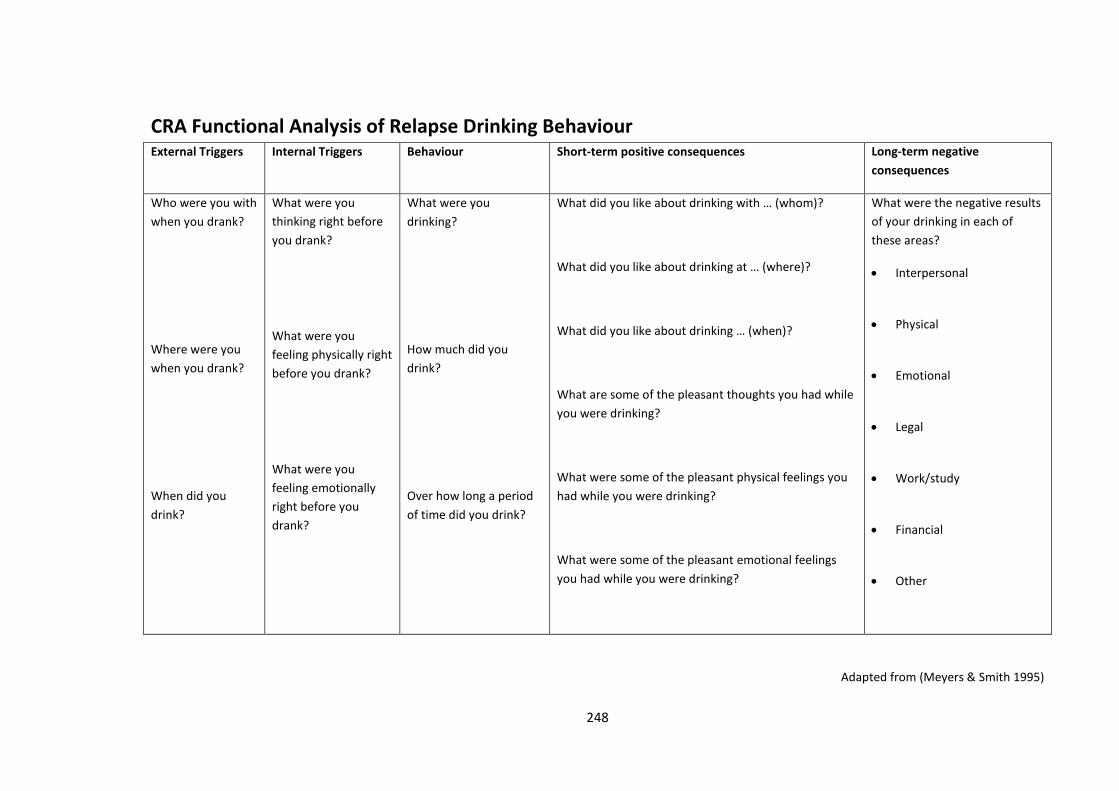
248
CRA Functional Analysis of Relapse Drinking Behaviour External Triggers Internal Triggers Behaviour Short-term positive consequences Long-term negative
consequences
Who were you with
when you drank?
Where were you
when you drank?
When did you
drink?
What were you
thinking right before
you drank?
What were you
feeling physically right
before you drank?
What were you
feeling emotionally
right before you
drank?
What were you
drinking?
How much did you
drink?
Over how long a period
of time did you drink?
What did you like about drinking with … (whom)?
What did you like about drinking at … (where)?
What did you like about drinking … (when)?
What are some of the pleasant thoughts you had while
you were drinking?
What were some of the pleasant physical feelings you
had while you were drinking?
What were some of the pleasant emotional feelings
you had while you were drinking?
What were the negative results
of your drinking in each of
these areas?
Interpersonal
Physical
Emotional
Legal
Work/study
Financial
Other
Adapted from (Meyers & Smith 1995)
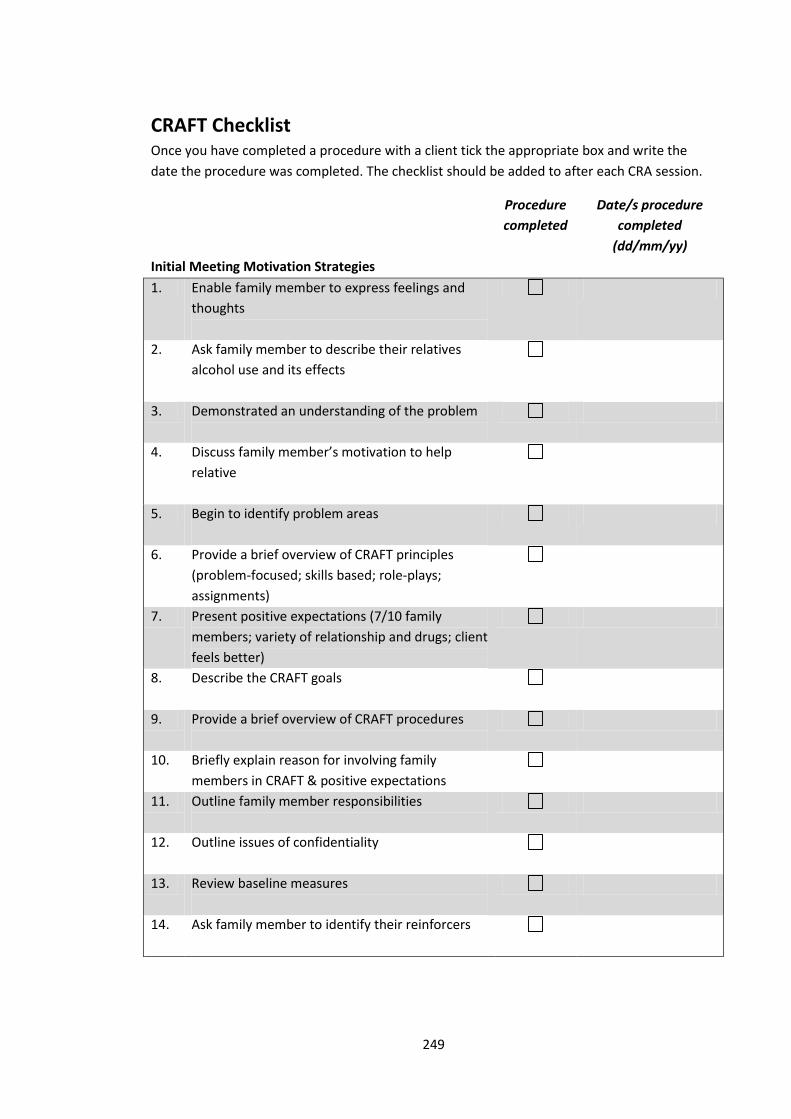
249
CRAFT Checklist Once you have completed a procedure with a client tick the appropriate box and write the
date the procedure was completed. The checklist should be added to after each CRA session.
Procedure
completed
Date/s procedure
completed
(dd/mm/yy)
Initial Meeting Motivation Strategies
1. Enable family member to express feelings and
thoughts
2. Ask family member to describe their relatives
alcohol use and its effects
3. Demonstrated an understanding of the problem
4. Discuss family member’s motivation to help
relative
5. Begin to identify problem areas
6. Provide a brief overview of CRAFT principles
(problem-focused; skills based; role-plays;
assignments)
7. Present positive expectations (7/10 family
members; variety of relationship and drugs; client
feels better)
8. Describe the CRAFT goals
9. Provide a brief overview of CRAFT procedures
10. Briefly explain reason for involving family
members in CRAFT & positive expectations
11. Outline family member responsibilities
12. Outline issues of confidentiality
13. Review baseline measures
14. Ask family member to identify their reinforcers
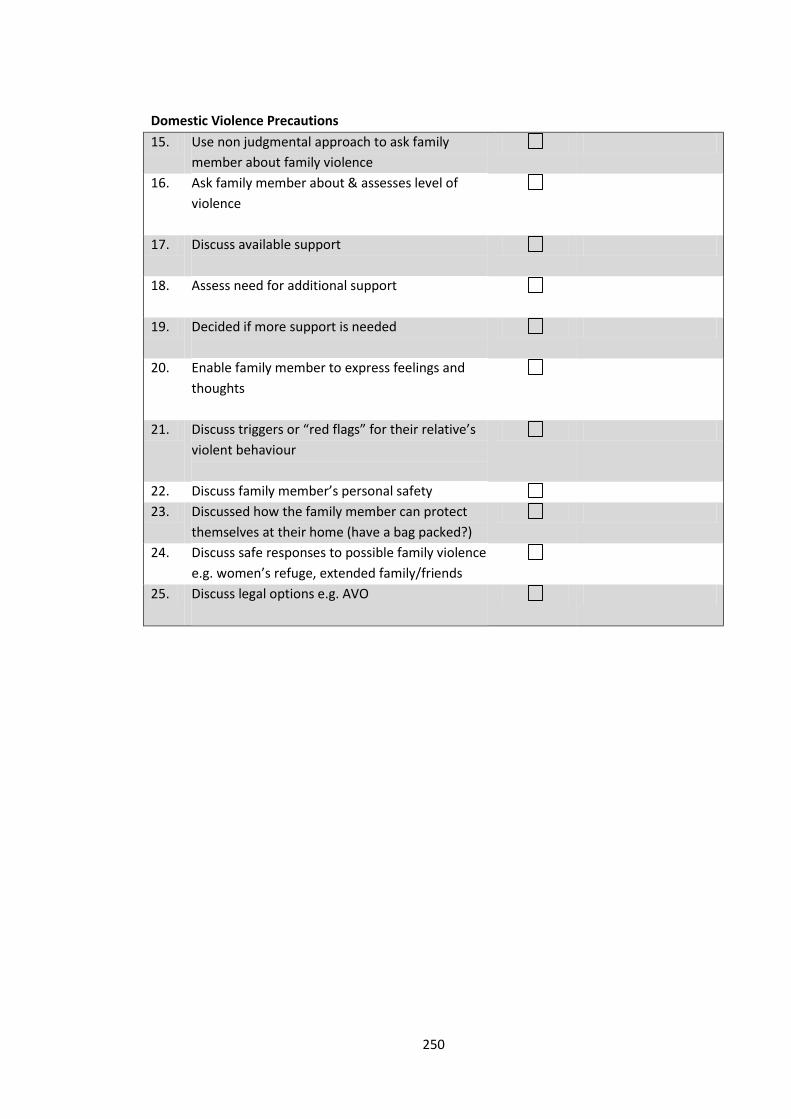
250
Domestic Violence Precautions
15. Use non judgmental approach to ask family
member about family violence
16. Ask family member about & assesses level of
violence
17. Discuss available support
18. Assess need for additional support
19. Decided if more support is needed
20. Enable family member to express feelings and
thoughts
21. Discuss triggers or “red flags” for their relative’s
violent behaviour
22. Discuss family member’s personal safety
23. Discussed how the family member can protect
themselves at their home (have a bag packed?)
24. Discuss safe responses to possible family violence
e.g. women’s refuge, extended family/friends
25. Discuss legal options e.g. AVO

251
Functional Analysis of Drinking Behaviour
26a. Give family member reason for Functional
Analysis (wealth of info; family member
behaviour worth examining)
27a. Ask family member to describe a drinking
episode
28a. Ask family member to identify internal and
external triggers
29a. Ask family member to specify drinking behaviour
during drinking episode (drinks what, how much,
over what time)
30a. Ask family member to describe short term
positive and negative consequences of relative’s
drinking
31a. Give family member examples of how Functional
Analysis of Drinking Behaviour information will
be used
Functional Analysis of Non-drinking Behaviour
26b. Give family member reason for Functional
Analysis (wealth of info; family member
behaviour worth examining)
27b. Ask family member to give general description
relative’s enjoyable, healthy non-drinking
behaviour
28b. Ask family member to identify internal and
external triggers for enjoyable, healthy non-
drinking behaviour
29b. Ask family member to specify relative’s
enjoyable, healthy non-drinking behaviour (what)
30b. Ask family member to describe short term
positive and negative consequences of relative’s
enjoyable, healthy non-drinking behaviour
31b. Give family member examples of how Functional
Analysis of Non-drinking Behaviour information
will be used

252
Functional Analysis of Violent Behaviour
26c. Give family member reason for Functional
Analysis (wealth of info; family member
behaviour worth examining)
27c. Ask family member to describe a violent episode
28c. Ask family member to identify internal and
external triggers
29c. Ask family member to specify behaviour during
violent episode (what)
30c. Ask family member to describe short term
positive and negative consequences of relative’s
violent behaviour
31c. Give family member examples of how Functional
Analysis of Violent Behaviour information will be
used
Positive Communication Skills
32. Discuss reasons why communication skills are
important
33. Describe the 7 components of positive
communication
34. Give examples of good and inadequate
communication styles
35. Conduct a role play and provides feedback;
repeated
36. Conduct a reverse role play
37. Discuss positive communication skills at an
appropriate time
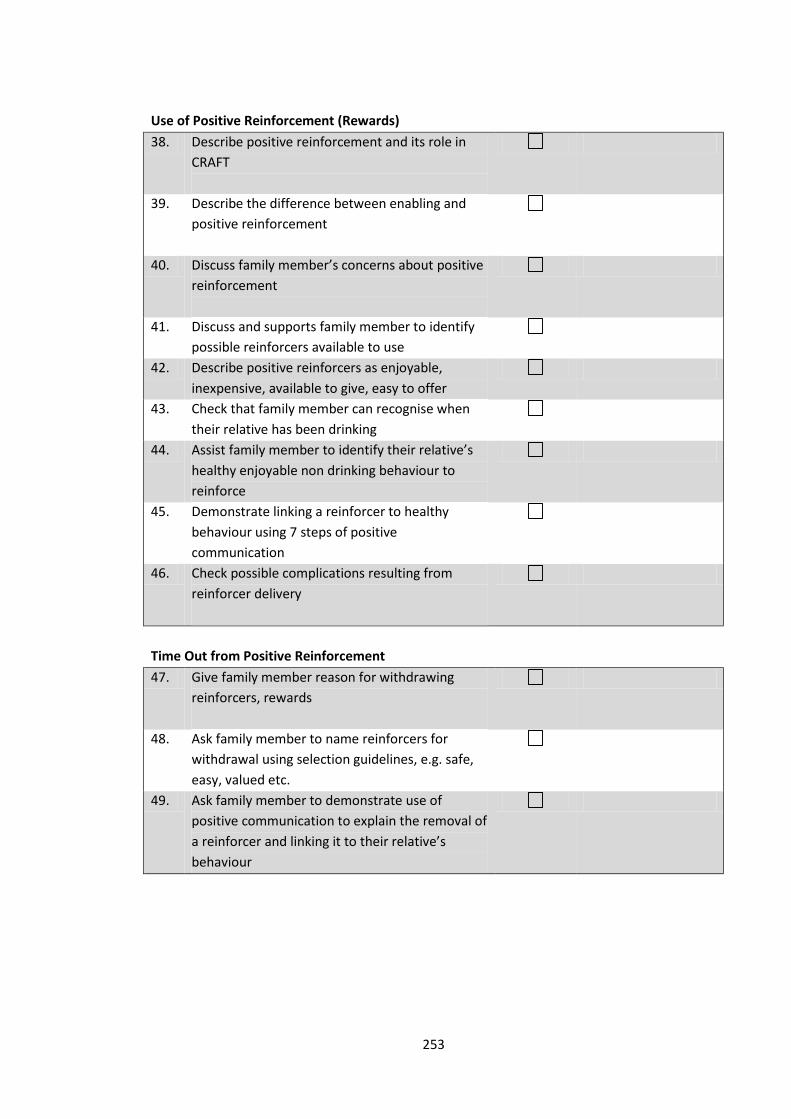
253
Use of Positive Reinforcement (Rewards)
38. Describe positive reinforcement and its role in
CRAFT
39. Describe the difference between enabling and
positive reinforcement
40. Discuss family member’s concerns about positive
reinforcement
41. Discuss and supports family member to identify
possible reinforcers available to use
42. Describe positive reinforcers as enjoyable,
inexpensive, available to give, easy to offer
43. Check that family member can recognise when
their relative has been drinking
44. Assist family member to identify their relative’s
healthy enjoyable non drinking behaviour to
reinforce
45. Demonstrate linking a reinforcer to healthy
behaviour using 7 steps of positive
communication
46. Check possible complications resulting from
reinforcer delivery
Time Out from Positive Reinforcement
47. Give family member reason for withdrawing
reinforcers, rewards
48. Ask family member to name reinforcers for
withdrawal using selection guidelines, e.g. safe,
easy, valued etc.
49. Ask family member to demonstrate use of
positive communication to explain the removal of
a reinforcer and linking it to their relative’s
behaviour
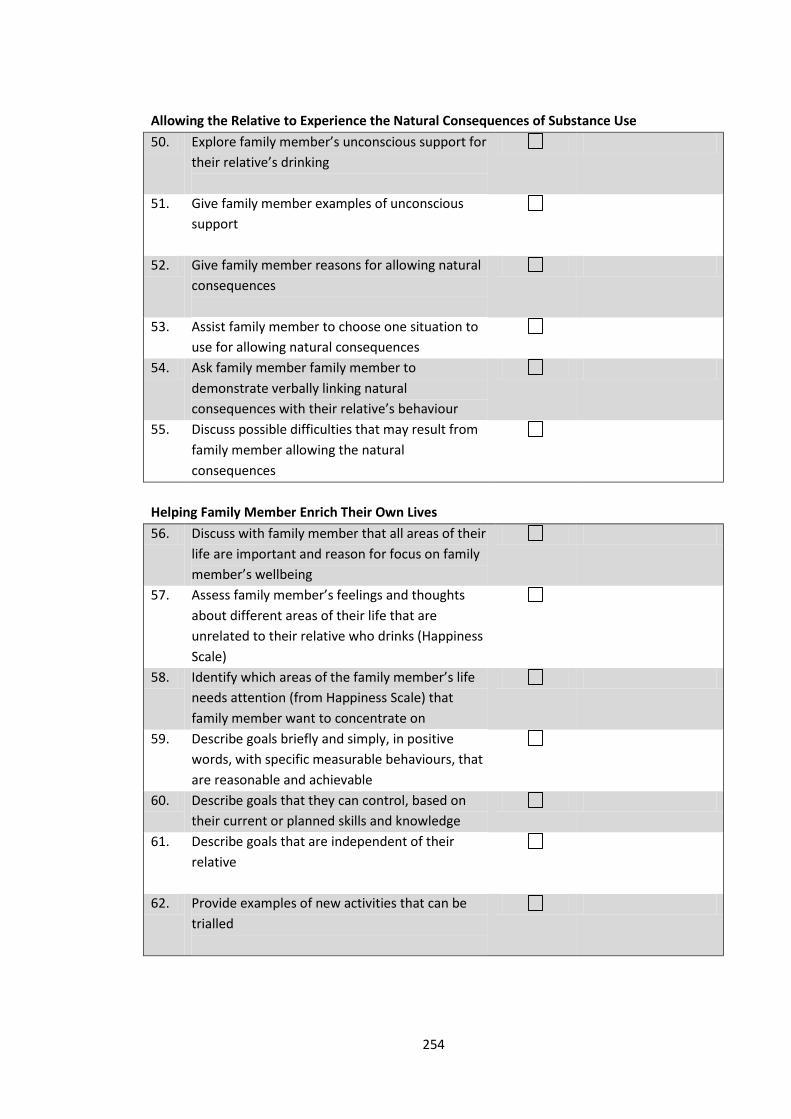
254
Allowing the Relative to Experience the Natural Consequences of Substance Use
50. Explore family member’s unconscious support for
their relative’s drinking
51. Give family member examples of unconscious
support
52. Give family member reasons for allowing natural
consequences
53. Assist family member to choose one situation to
use for allowing natural consequences
54. Ask family member family member to
demonstrate verbally linking natural
consequences with their relative’s behaviour
55. Discuss possible difficulties that may result from
family member allowing the natural
consequences
Helping Family Member Enrich Their Own Lives
56. Discuss with family member that all areas of their
life are important and reason for focus on family
member’s wellbeing
57. Assess family member’s feelings and thoughts
about different areas of their life that are
unrelated to their relative who drinks (Happiness
Scale)
58. Identify which areas of the family member’s life
needs attention (from Happiness Scale) that
family member want to concentrate on
59. Describe goals briefly and simply, in positive
words, with specific measurable behaviours, that
are reasonable and achievable
60. Describe goals that they can control, based on
their current or planned skills and knowledge
61. Describe goals that are independent of their
relative
62. Provide examples of new activities that can be
trialled
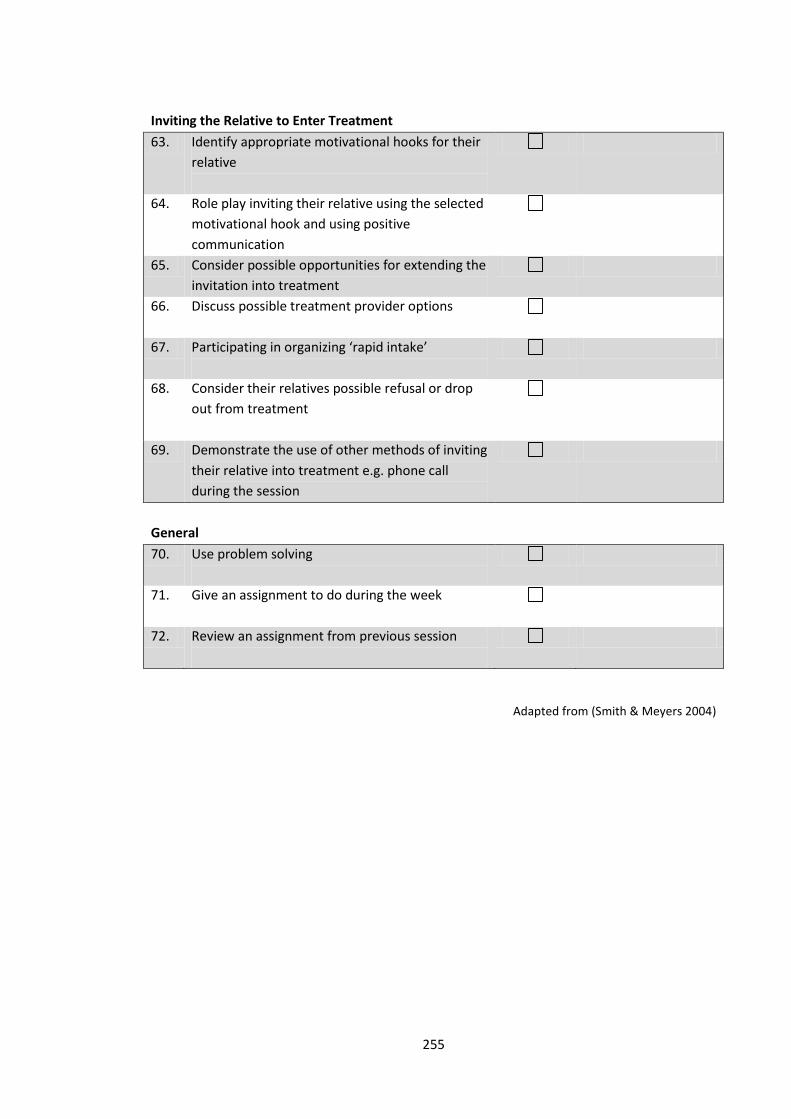
255
Inviting the Relative to Enter Treatment
63. Identify appropriate motivational hooks for their
relative
64. Role play inviting their relative using the selected
motivational hook and using positive
communication
65. Consider possible opportunities for extending the
invitation into treatment
66. Discuss possible treatment provider options
67. Participating in organizing ‘rapid intake’
68. Consider their relatives possible refusal or drop
out from treatment
69. Demonstrate the use of other methods of inviting
their relative into treatment e.g. phone call
during the session
General
70. Use problem solving
71. Give an assignment to do during the week
72. Review an assignment from previous session
Adapted from (Smith & Meyers 2004)

256
CRAFT Functional Analysis of a Relative’s (or Friend’s) Drinking Behaviour External Triggers Internal Triggers Behaviour Short-term positive consequences Long-term negative
consequences
Who is your
relative usually
with when
drinking?
Where does he/she
usually drink?
When does he/she
usually drink?
What do you think
your relative might be
thinking about right
before drinking?
What do you think
he/she might be
feeling right before
drinking?
What does your relative
usually drink?
How much does he/she
usually drink?
Over how long a period
of time does he/she
usually drink?
What do you think your relative likes about drinking
with … (whom)?
What do you think your relative likes about drinking at
… (where)?
What do you think your relative likes about drinking …
(when)?
What pleasant thoughts do you think he/she might
have while drinking?
What pleasant feelings do you think he/she might have
while drinking?
What do you think are the
negative results of your
relative’s drinking in each of
these areas (* the ones he/she
would agree with)?
Interpersonal
Physical
Emotional
Legal
Work/study
Financial
Other
Adapted from (Smith & Meyers 2004)
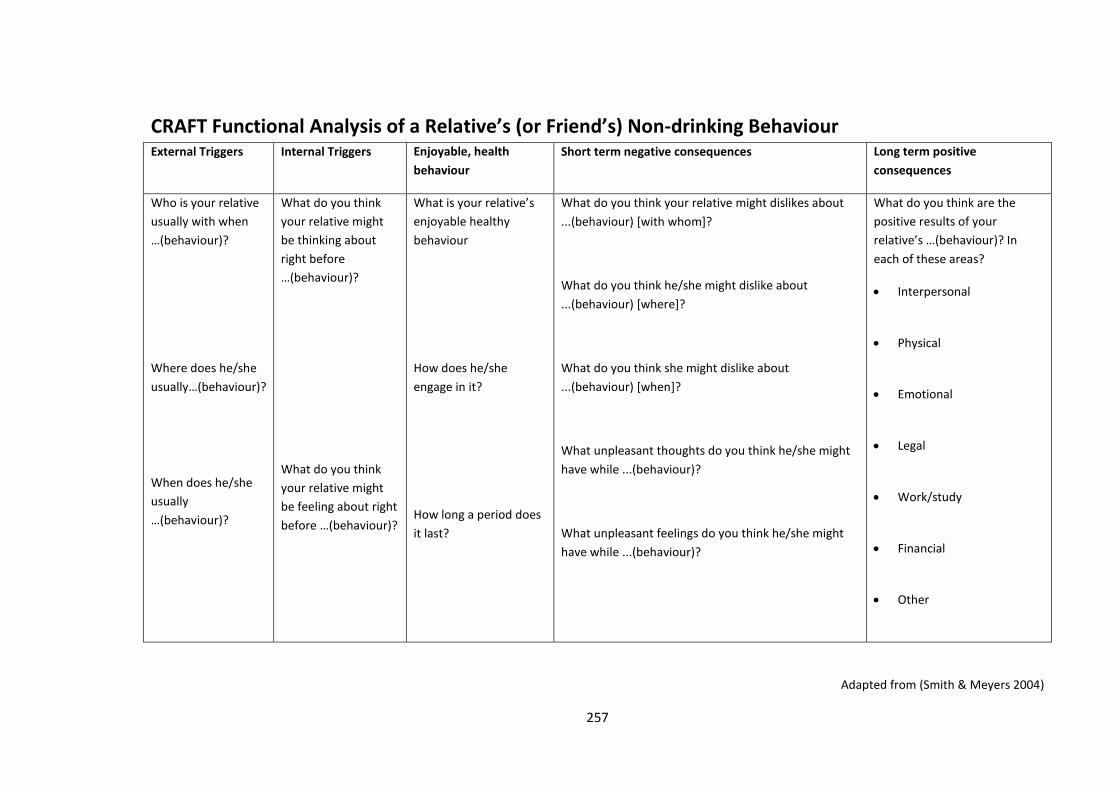
257
CRAFT Functional Analysis of a Relative’s (or Friend’s) Non-drinking Behaviour External Triggers Internal Triggers Enjoyable, health
behaviour
Short term negative consequences Long term positive
consequences
Who is your relative
usually with when
…(behaviour)?
Where does he/she
usually…(behaviour)?
When does he/she
usually
…(behaviour)?
What do you think
your relative might
be thinking about
right before
…(behaviour)?
What do you think
your relative might
be feeling about right
before …(behaviour)?
What is your relative’s
enjoyable healthy
behaviour
How does he/she
engage in it?
How long a period does
it last?
What do you think your relative might dislikes about
...(behaviour) [with whom]?
What do you think he/she might dislike about
...(behaviour) [where]?
What do you think she might dislike about
...(behaviour) [when]?
What unpleasant thoughts do you think he/she might
have while ...(behaviour)?
What unpleasant feelings do you think he/she might
have while ...(behaviour)?
What do you think are the
positive results of your
relative’s …(behaviour)? In
each of these areas?
Interpersonal
Physical
Emotional
Legal
Work/study
Financial
Other
Adapted from (Smith & Meyers 2004)
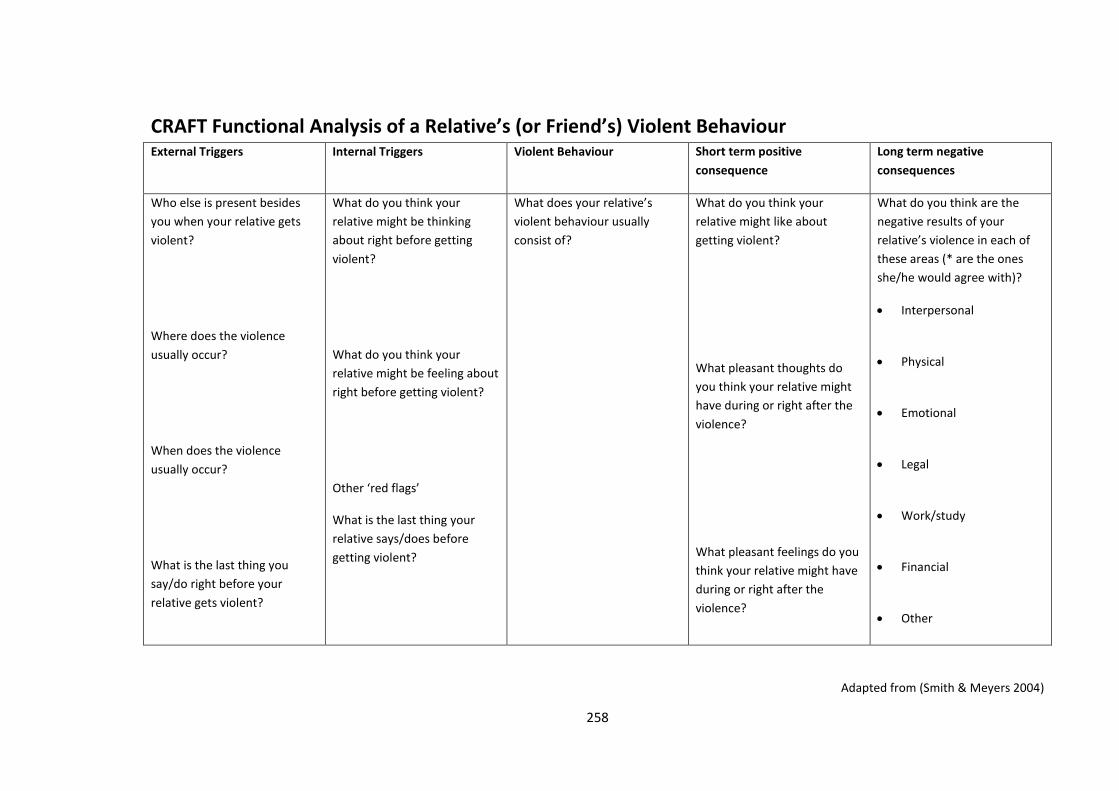
258
CRAFT Functional Analysis of a Relative’s (or Friend’s) Violent Behaviour External Triggers Internal Triggers Violent Behaviour Short term positive
consequence
Long term negative
consequences
Who else is present besides
you when your relative gets
violent?
Where does the violence
usually occur?
When does the violence
usually occur?
What is the last thing you
say/do right before your
relative gets violent?
What do you think your
relative might be thinking
about right before getting
violent?
What do you think your
relative might be feeling about
right before getting violent?
Other ‘red flags’
What is the last thing your
relative says/does before
getting violent?
What does your relative’s
violent behaviour usually
consist of?
What do you think your
relative might like about
getting violent?
What pleasant thoughts do
you think your relative might
have during or right after the
violence?
What pleasant feelings do you
think your relative might have
during or right after the
violence?
What do you think are the
negative results of your
relative’s violence in each of
these areas (* are the ones
she/he would agree with)?
Interpersonal
Physical
Emotional
Legal
Work/study
Financial
Other
Adapted from (Smith & Meyers 2004)
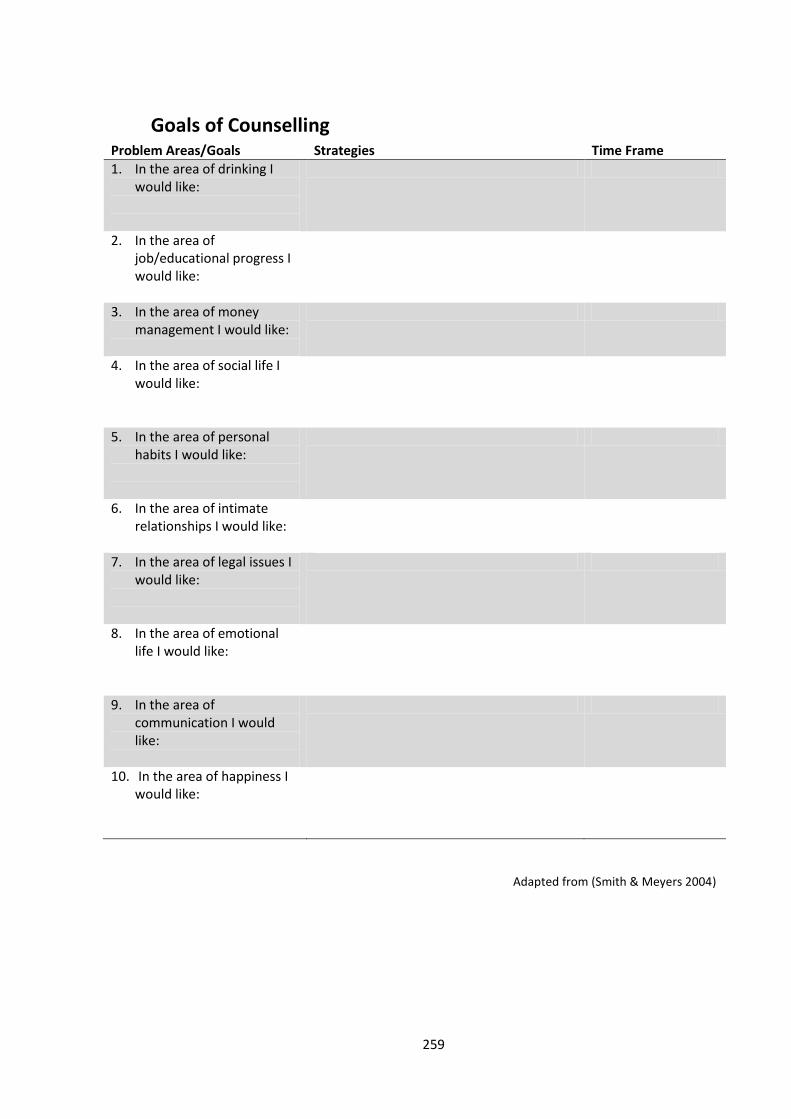
259
Goals of Counselling Problem Areas/Goals Strategies Time Frame
1. In the area of drinking I would like:
2. In the area of job/educational progress I would like:
3. In the area of money management I would like:
4. In the area of social life I would like:
5. In the area of personal habits I would like:
6. In the area of intimate relationships I would like:
7. In the area of legal issues I would like:
8. In the area of emotional life I would like:
9. In the area of communication I would like:
10. In the area of happiness I would like:
Adapted from (Smith & Meyers 2004)

260
Happiness Scale The scale is intended to estimate your current happiness with your life in each of the ten areas
listed below. Ask yourself the following question as you rate each area:
How happy am I with this area of my life?
Then circle one of the numbers (1-10) beside each area.
Numbers toward the left (lower numbers) indicate different levels of unhappiness, and
numbers toward the right (higher numbers) reflect different levels of happiness.
In other words, mark on the scale (1-10) exactly how you feel today. Also, try not to allow one
area to influence the results of the other areas.
Completely unhappy Completely happy
Drinking 1 2 3 4 5 6 7 8 9 10
job/education 1 2 3 4 5 6 7 8 9 10
Money 1 2 3 4 5 6 7 8 9 10
social life 1 2 3 4 5 6 7 8 9 10
personal habits 1 2 3 4 5 6 7 8 9 10
marriage/relations
hips
1 2 3 4 5 6 7 8 9 10
legal issues 1 2 3 4 5 6 7 8 9 10
emotional life 1 2 3 4 5 6 7 8 9 10
communication 1 2 3 4 5 6 7 8 9 10
general happiness 1 2 3 4 5 6 7 8 9 10
Adapted from (Smith & Meyers 2004)
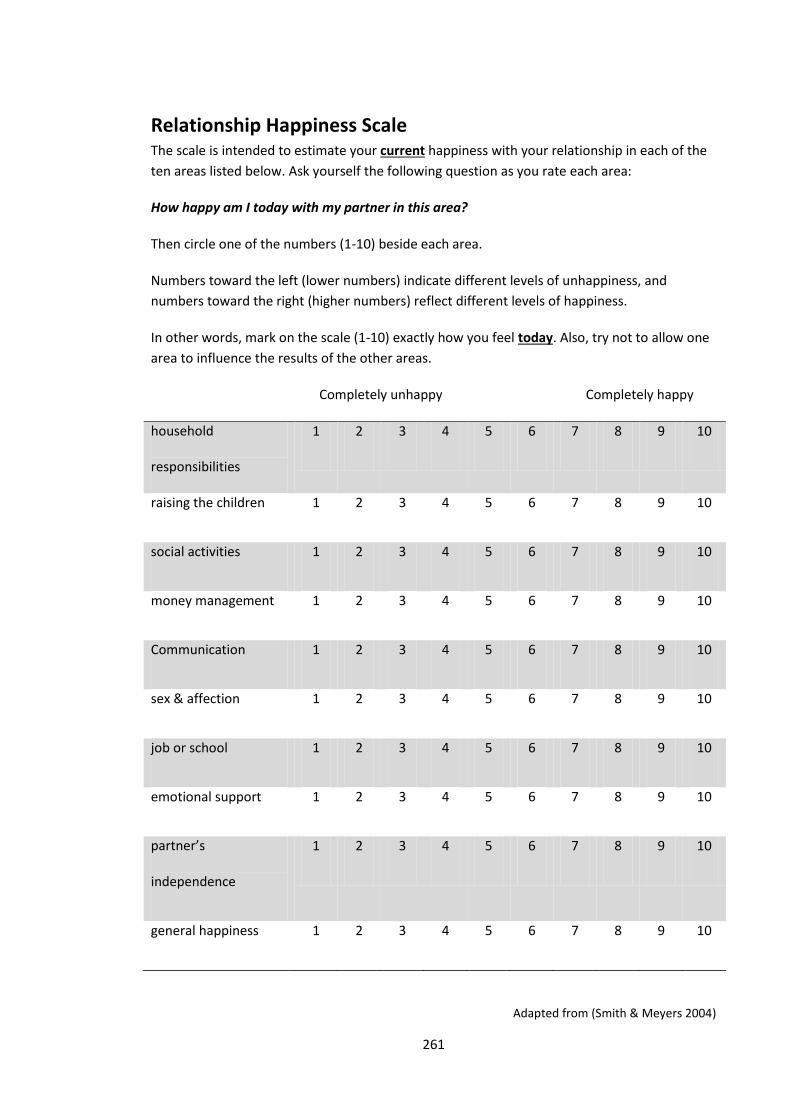
261
Relationship Happiness Scale The scale is intended to estimate your current happiness with your relationship in each of the
ten areas listed below. Ask yourself the following question as you rate each area:
How happy am I today with my partner in this area?
Then circle one of the numbers (1-10) beside each area.
Numbers toward the left (lower numbers) indicate different levels of unhappiness, and
numbers toward the right (higher numbers) reflect different levels of happiness.
In other words, mark on the scale (1-10) exactly how you feel today. Also, try not to allow one
area to influence the results of the other areas.
Completely unhappy Completely happy
household
responsibilities
1 2 3 4 5 6 7 8 9 10
raising the children 1 2 3 4 5 6 7 8 9 10
social activities 1 2 3 4 5 6 7 8 9 10
money management 1 2 3 4 5 6 7 8 9 10
Communication 1 2 3 4 5 6 7 8 9 10
sex & affection 1 2 3 4 5 6 7 8 9 10
job or school 1 2 3 4 5 6 7 8 9 10
emotional support 1 2 3 4 5 6 7 8 9 10
partner’s
independence
1 2 3 4 5 6 7 8 9 10
general happiness 1 2 3 4 5 6 7 8 9 10
Adapted from (Smith & Meyers 2004)

262
Positive Communication
1. Be brief
2. Be positive
3. Refer to specific behaviours
4. Label your feelings
5. Offer an understanding statement
6. Accept partial responsibility
7. Offer to help
Adapted from (Smith & Meyers 2004)
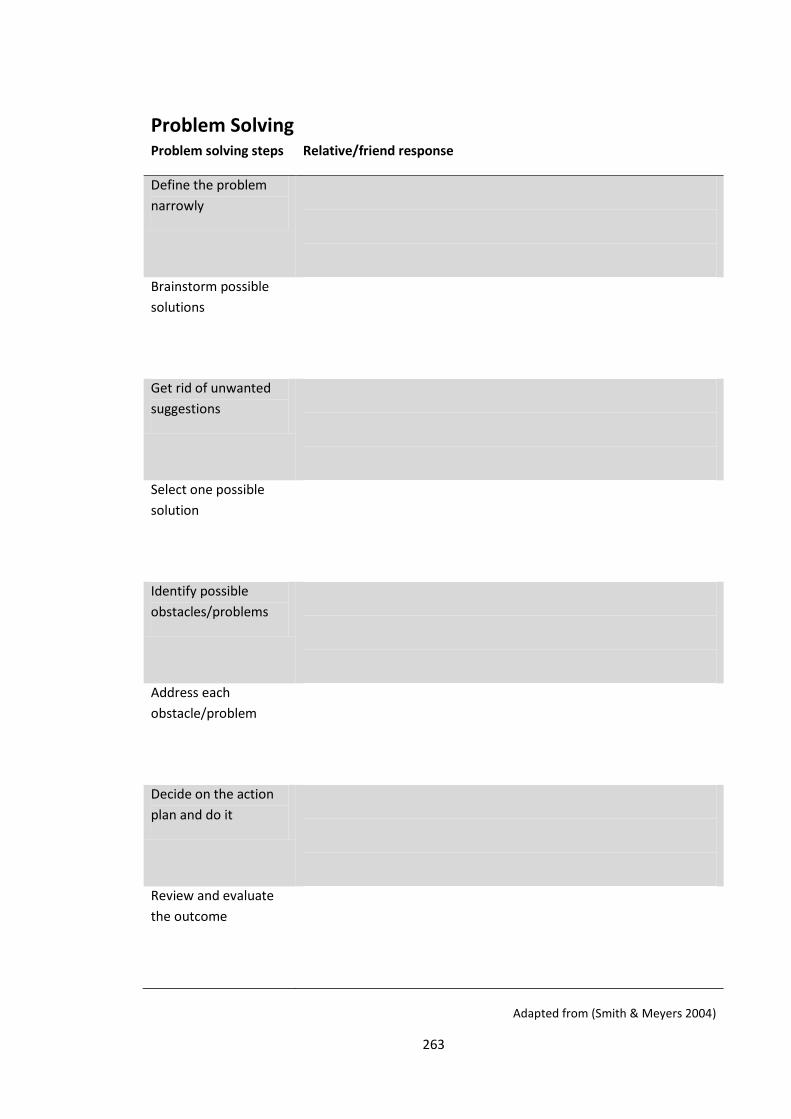
263
Problem Solving Problem solving steps Relative/friend response
Define the problem
narrowly
Brainstorm possible
solutions
Get rid of unwanted
suggestions
Select one possible
solution
Identify possible
obstacles/problems
Address each
obstacle/problem
Decide on the action
plan and do it
Review and evaluate
the outcome
Adapted from (Smith & Meyers 2004)
264
Appendix F
Advertising poster for recruitment for the acceptability study
What do you think?
We are developing two programs to support Aboriginal and Torres Strait
Islander people who drink too much alcohol to cut down or stop drinking:
Individual Counselling & Family Training.
We want to know what Aboriginal and Torres Strait Islander community
members of Orange, Forbes, Condobolin and surrounding areas think about
the two programs.
[DATE]
[TIME]
[ADDRESS]
You will be given $40 for your time
For more information call [PARTICIPATING SERVICE DETAILS].

265
Appendix G
Acceptability survey information for particiapnts
Please note that the the names of the programs were changed from the Community
Reinforcement Approach (CRA) to the Personalised Alcohol Treatment (PAT) program, and from
Community Reinforcement and Family Training (CRAFT) to Family Training (FT), to avoid
confusion about the local community playing a role in each individually focused treatment
program. All other aspects of the CRA and CRAFT programs were maintained.
Drinking too much alcohol causes physical and mental health problems as well as social
problems, not just for people who drink, but also for their families and community.
Health workers can help people who need to cut down or stop drinking alcohol to
improve their physical and mental wellbeing. Health workers can also help families and
communities by teaching them how to better support family members and friends,
who need to cut down or stop drinking alcohol.
What we would like to do
We would like to deliver two programs to see if they work to help Aboriginal (including
Torres Strait Islander) people who need to cut down or stop drinking alcohol.
Personalised Alcohol Treatment
(PAT) program for Aboriginal people
who need to cut down or stop
drinking alcohol.
Family Training (FT) program for
family members/friends of Aboriginal
people who need to cut down or stop
drinking alcohol.
Who will be delivering these programs?
The programs will be delivered through Yoorana Gunya Family Violence Healing Centre
Aboriginal Corporation and the Lyndon Community to Aboriginal people in Forbes,
Orange and surrounding areas.
Program One Program Two
266
Who else will be involved?
The National Drug and Alcohol Research Centre at the University of New South Wales
will work closely with the services delivering the programs to see if they work to help
Aboriginal people who need to cut down or stop drinking alcohol.
Why are we inviting you to answer these questions?
You are being invited to answer the questions in this survey because you are a new or
existing client of Yoorana Gunya Family Violence Healing Centre Aboriginal Corporation
or the Lyndon Community.
What we would like to know from you
Before we start delivering the two programs, we would like to find out what Aboriginal
clients of Yoorana Gunya and the Lyndon Community think of each one. We are also
interested in any suggestions you have to improve each program (there is a section in
the survey where you can write down your suggestions).
How confidential are you answers?
All your answers are confidential. Researchers from the University of New South Wales
and the Lyndon Community will be able to look at your answers. The answers to the
survey will be stored on a computer file at the University of New South Wales. If you
provide us with your name and address, these details will not be linked to your survey
answers.
If you are not sure about any of these questions, or would like more information about
the study, please call Anton Clifford on (02) 9385 0386 at the Faculty of Medicine,
University of New South Wales.
If you have any concerns as a result of completing this survey please contact the
closest health service:
Lyndon Community Julaine Allan (02) 6361 1521
Yoorana Gunya Donna Bliss (02) 6851 5111
If you have any complaints you should contact the AHMRC Ethics Committee and the
UNSW Ethics Committee as follows:
The Chairperson, AHMRC Ethics
Committee
PO Box 1565, Strawberry Hills NSW 2012
Ph (02) 9212 4777, Fax (02) 9212 7211
Email [email protected]
UNSW Ethics Secretariat, The University of
New South Wales, SYDNEY 2052
AUSTRALIA
Ph (02) 9385 4234, Fax (02) 9385 6648
Email [email protected]

267
How to answer the questions
The questions require you to choose an answer that best describes what you think.
Please ask a group leader if you do not understand a question. Please be as honest and
accurate as you can be. Remember all your answers are confidential and we will not
give your name and address to anyone who is not a health practitioner in this service.
Be aware that you may withdraw your participation at any time without needing a
reason.
THANK YOU.
268
Appendix H
Intervention information and acceptability survey
Please note that the the names of the programs were changed from the Community
Reinforcement Approach (CRA) to the Personalised Alcohol Treatment (PAT) program, and from
Community Reinforcement and Family Training (CRAFT) to Family Training (FT), to avoid
confusion about the local community playing a role in each individually focused treatment
program. All other aspects of the CRA and CRAFT programs were maintained.
Personalised Alcohol Treatment (PAT)
Who is PAT for?
o Aboriginal and Torres Strait Islander people from Orange, Forbes
and surrounding areas who need help to cut down or stop
drinking alcohol.
What is PAT?
o One-on-one counselling with a drug and alcohol counsellor who
has been trained to deliver the program.
o To reduce alcohol-related harms experienced by the drinker,
their family and their community.
o Assessment of risk of harms from alcohol.
o Personalised treatment plan.
o Support to cut down or stop drinking alcohol.
When can PAT be delivered?
o After withdrawal.
o If needing rehab but not wanting to go.
o Waiting for rehab.
o After rehab.
269
PART A: Personalised Alcohol Treatment (PAT)
Please circle ONE number for question 1.
1. What do you think about PAT being delivered in your community?
1 2 3 4 5
very bad very good
Please tick () ONE box for each part of question 2.
2. Do you think it is okay for PAT to be available for Aboriginal people:
2a. After withdrawal?
not okay
okay
2b. Needing rehab but not wanting to go?
not okay
okay
2c. Waiting for rehab?
not okay
okay
2d. After rehab?
not okay
okay
2e. Referred from probation and parole?
not okay
okay
ID:
270
Imagine you drink too much alcohol and want help to cut down or stop.
Please tick () ONE box for each part of questions 3 to 8.
3. What are the qualities that you think are most important in a counsellor:
3a. Trust and familiarity?
someone I know and trust
someone I know
someone I trust
doesn’t matter
3b. Experience working in your local community?
no
yes
doesn’t matter
3c. Aboriginality?
a non-Aboriginal person
an Aboriginal person
doesn’t matter
3d. Gender?
a woman
a man
doesn’t matter
4. Would you feel okay to talk one-on-one with a counsellor, who has the qualities
you have described above, about:
4a. How much alcohol you usually drink?
okay
not okay
4b. How you feel about your drinking?
okay
not okay
4c. What you do when you are drinking?
okay
not okay
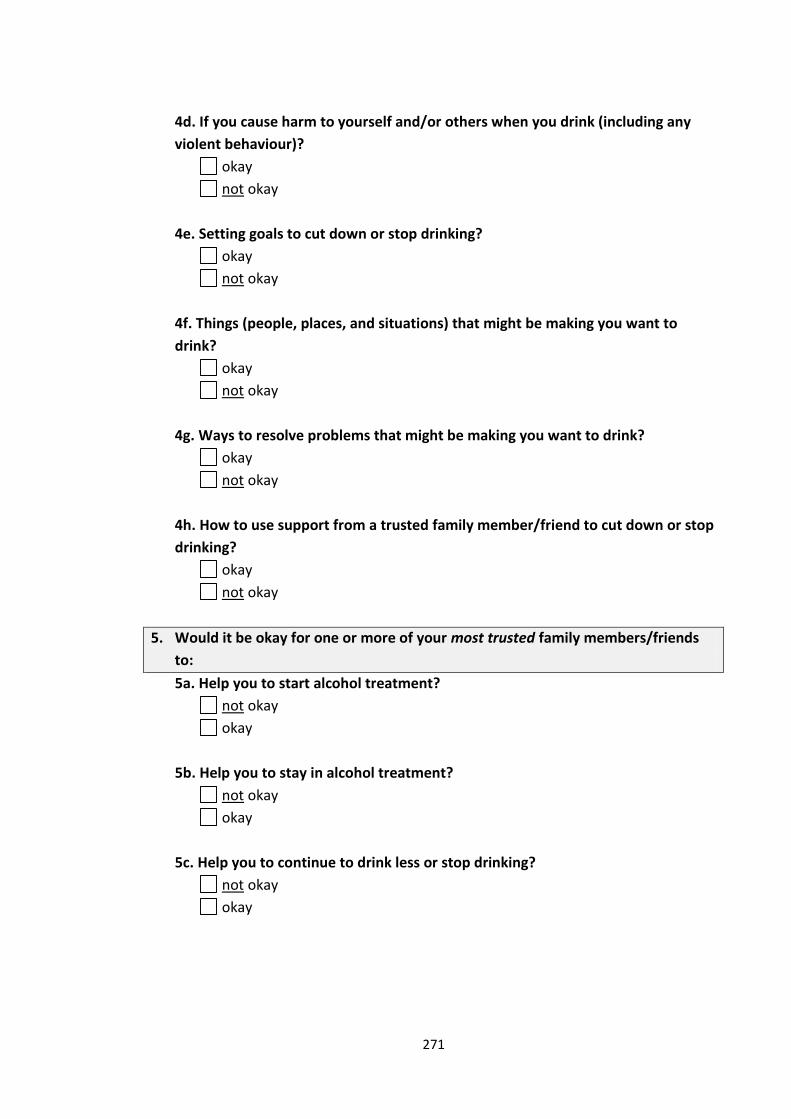
271
4d. If you cause harm to yourself and/or others when you drink (including any
violent behaviour)?
okay
not okay
4e. Setting goals to cut down or stop drinking?
okay
not okay
4f. Things (people, places, and situations) that might be making you want to
drink?
okay
not okay
4g. Ways to resolve problems that might be making you want to drink?
okay
not okay
4h. How to use support from a trusted family member/friend to cut down or stop
drinking?
okay
not okay
5. Would it be okay for one or more of your most trusted family members/friends
to:
5a. Help you to start alcohol treatment?
not okay
okay
5b. Help you to stay in alcohol treatment?
not okay
okay
5c. Help you to continue to drink less or stop drinking?
not okay
okay
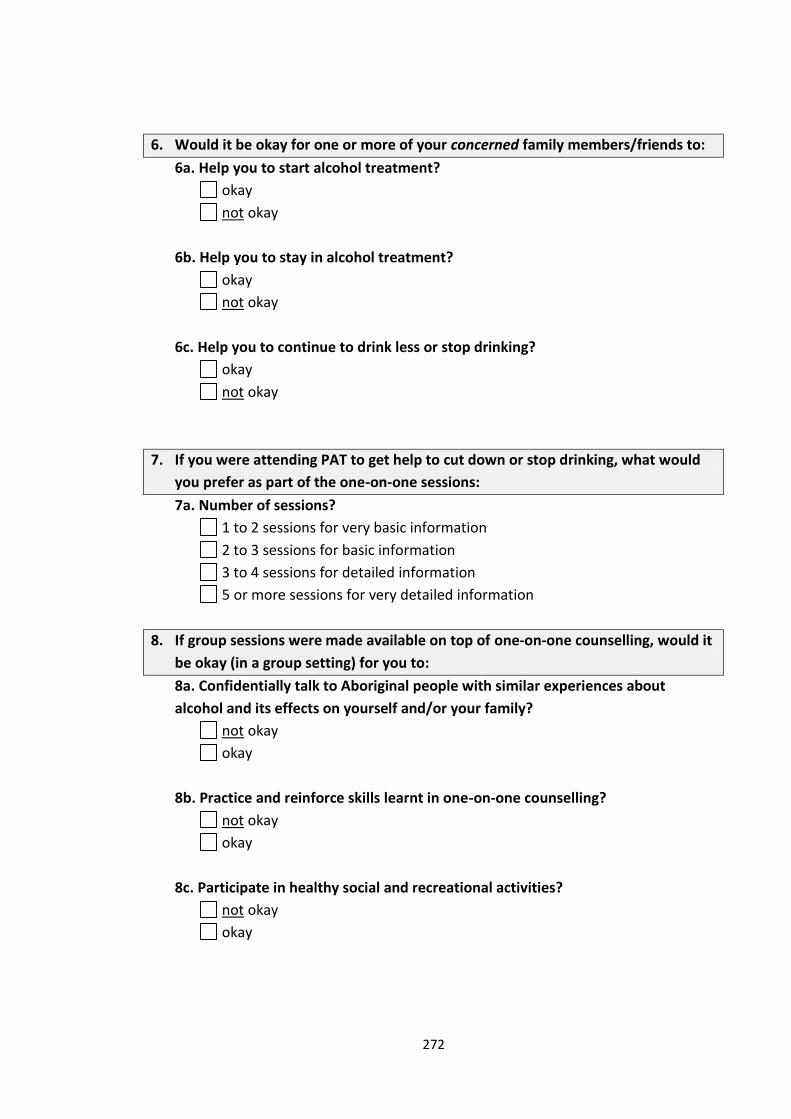
272
6. Would it be okay for one or more of your concerned family members/friends to:
6a. Help you to start alcohol treatment?
okay
not okay
6b. Help you to stay in alcohol treatment?
okay
not okay
6c. Help you to continue to drink less or stop drinking?
okay
not okay
7. If you were attending PAT to get help to cut down or stop drinking, what would
you prefer as part of the one-on-one sessions:
7a. Number of sessions?
1 to 2 sessions for very basic information
2 to 3 sessions for basic information
3 to 4 sessions for detailed information
5 or more sessions for very detailed information
8. If group sessions were made available on top of one-on-one counselling, would it
be okay (in a group setting) for you to:
8a. Confidentially talk to Aboriginal people with similar experiences about
alcohol and its effects on yourself and/or your family?
not okay
okay
8b. Practice and reinforce skills learnt in one-on-one counselling?
not okay
okay
8c. Participate in healthy social and recreational activities?
not okay
okay
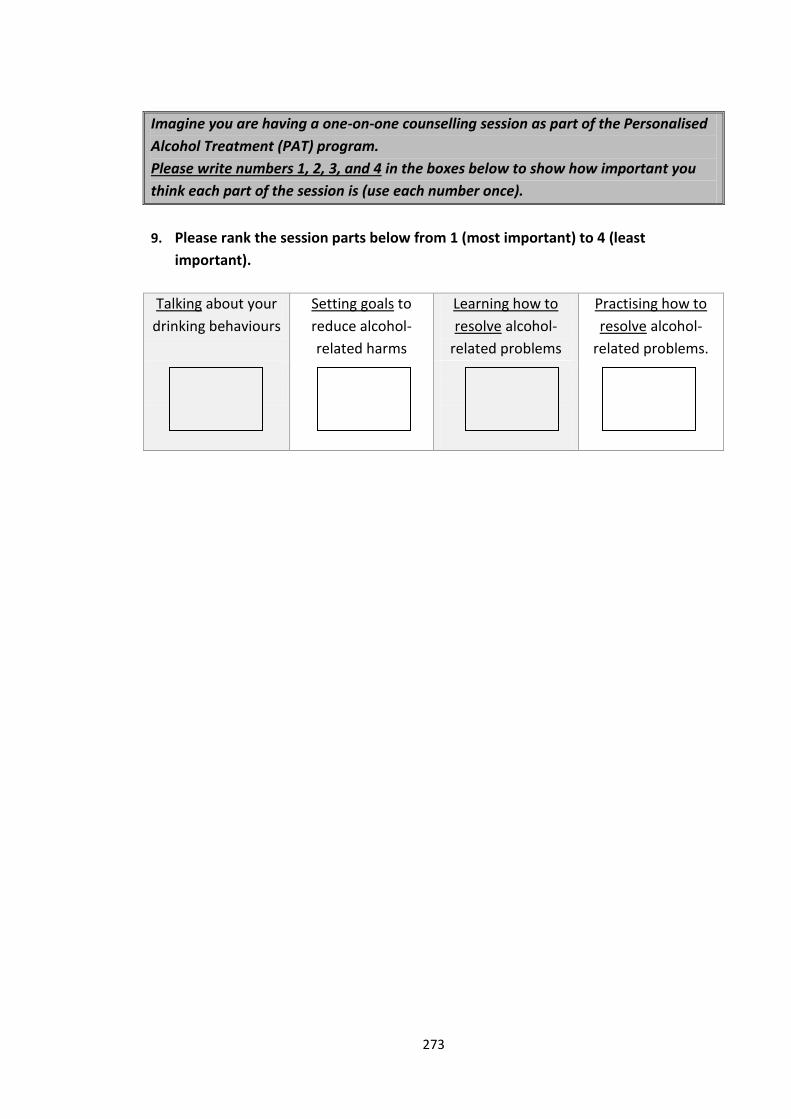
273
Imagine you are having a one-on-one counselling session as part of the Personalised
Alcohol Treatment (PAT) program.
Please write numbers 1, 2, 3, and 4 in the boxes below to show how important you
think each part of the session is (use each number once).
9. Please rank the session parts below from 1 (most important) to 4 (least
important).
Talking about your
drinking behaviours
Setting goals to
reduce alcohol-
related harms
Learning how to
resolve alcohol-
related problems
Practising how to
resolve alcohol-
related problems.
274
Please write your suggestions for the PAT program in the box below.
10. Is there anything we haven’t asked you about that you think we should include in
the Personalised Alcohol Treatment (PAT) program?
END OF PART A
275
Family Training (FT)
Who is FT for?
o Aboriginal and Torres Strait Islander people from Orange,
Forbes and surrounding areas who have a family
member/friend who drinks too much alcohol.
What is FT?
o One-on-one counselling with a drug and alcohol worker who
has been trained to deliver the program.
o To talk about affects of family member’s/friend’s drinking.
o Training and support for people who want to help a family
member/friend who needs to cut down or stop drinking
alcohol.
o To increase the wellbeing of people with a family
member/friend who drinks too much alcohol.
When can FT be delivered?
o For people who have a family member/friend in the
withdrawal unit.
o For people who want to help a family member/friend to start
alcohol treatment.
o For people who have a family member/friend who is waiting
for rehab.
o For people who have a family member/friend who has
finished rehab.
276
PART B: Family Training (FT)
Please circle ONE number for question 1.
1. What do you think about FT being delivered in your community?
1 2 3 4 5
very bad very good
Please tick () ONE box for each part of question 2.
2. Do you think it is okay for FT to be available for Aboriginal people:
2a. With a family member/friend in the withdrawal unit?
okay
not okay
2b. Who want to help a family member/friend who drinks too much alcohol to
start treatment?
okay
not okay
2c. With a family member/friend who is waiting for rehab?
okay
not okay
2d. With a family member/friend who has just finished rehab?
okay
not okay
2e. With a family member/friend who has been referred from probation and
parole?
okay
not okay
ID:
277
Imagine you want to help a family member/friend who drinks too much alcohol.
3. Would you be comfortable asking your family member/friend who drinks too
much alcohol:
3a. How much alcohol he/she drinks?
not comfortable
comfortable
3b. How he/she feels about his/her own drinking?
not comfortable
comfortable
3c. What he/she does when drinking alcohol?
not comfortable
comfortable
Please tick () ONE box for each part of questions 3 to 7.
4. What are the qualities you think are most important in a drug and alcohol
worker:
4a. Trust and familiarity?
someone I know and trust
someone I know
someone I trust
doesn’t matter
4b. Experience working in your local community?
yes
no
doesn’t matter
4c. Aboriginality?
an Aboriginal person
a non-Aboriginal person
doesn’t matter
4d. Gender?
a man
a woman
doesn’t matter
278
5. Would you feel okay to talk one-on-one with a drug and alcohol worker, who has
the qualities you have described, about:
5a. How much alcohol your family member/friend drinks?
okay
not okay
5b. What your family member/friend does when he/she drinks alcohol?
okay
not okay
5c. If your family member/friend harms themselves or others when he/she drinks
alcohol (including any violent behaviour)?
okay
not okay
6. Would you feel okay about using FT to work on:
6a. How to talk to your family member/friend about his/her drinking?
not okay
okay
6b. Ways to talk to your family member/friend about how alcohol is causing
difficulty in your community?
not okay
okay
6c. Ways you can support your family member/friend to start treatment?
not okay
okay
6d. Ways you can support your family member/friend to stay in treatment?
not okay
okay
6e. Ways to support your family member/friend to continue to drink less?
not okay
okay
6f. Ways to set boundaries when alcohol causes difficulty in your community?
not okay
okay
279
6g. Ways you can stay strong living in a community where alcohol causes
difficulty?
not okay
okay
6h. Ways to you can help your community stay strong when alcohol causes
difficulty?
not okay
okay
7. If you were attending FT so that you could help a family member/friend who
drinks too much alcohol, what would you prefer as part of the one-on-one
sessions:
7a. Number of sessions?
1 to 2 sessions for very basic information
2 to 3 sessions for basic information
3 to 4 sessions for detailed information
5 or more sessions for very detailed information
8. If group sessions were made available on top of one-on-one counselling, would it
be okay (in a group setting) for you to:
8a. Confidentially talk to Aboriginal people with similar experiences about
alcohol and its effects on yourself and/or your family?
okay
not okay
8b. Practise and reinforce skills learnt in one-on-one counselling?
okay
not okay
8c. Participate in healthy social and recreational activities?
okay
not okay
280
Imagine you are having one-on-one sessions as part FT.
Please write numbers 1, 2, 3, & 4 in the boxes below to show how important you
think each part of the session is (use each number once).
9. Please rank the session parts below from 1 (most important) to 4 (least
important).
Talking about your family
member’s/friend’s drinking behaviour
Learning how to communicate with
your family member/friend about his/her
drinking
Learning how to support your family member/friend to cut down or stop
drinking
Practicing how to support your family member/friend to cut down or stop
drinking

281
Please WRITE your suggestions for the FT program in the box.
10. Is there anything we haven’t asked you about that you think we should include in
the Family Training (FT) program?
END OF PART B
282
PART C: Information about you
The questions in this section provide us with some information about you. Remember that this information is confidential and so will only be used for the research project and will not forwarded on to any authorities or other organisations.
Please tick () ONE box for each part of questions 1 to 12 and WRITE answers where shown.
1. Health service attended
Lyndon Community
Yoorana Gunya
other (please write)
2. Gender
female
male
3. Date of birth
(day) (month) (year) (please write)
4. Did you guess any part of your birth date?
no
yes, I estimated (please write)
ID:
283
5. Are you of Aboriginal or Torres Strait Islander origin?
no (if no, go to question 7)
yes, Aboriginal
yes, Torres Strait Islander
yes, Aboriginal and Torres Strait Islander
6. What clan, tribal or language group do you identify with?
I identify with (please write)
7. Do you have a spouse (husband/wife) or child who is of Aboriginal or Torres Strait Islander origin?
no
yes, spouse and child
yes, spouse only
yes, child only
8. Were you born in Australia?
yes
no, I was born in (please write)
9. What language do you prefer to speak at home?
English
other, I prefer to speak (please write)
10. Have you completed any formal education?
no formal education
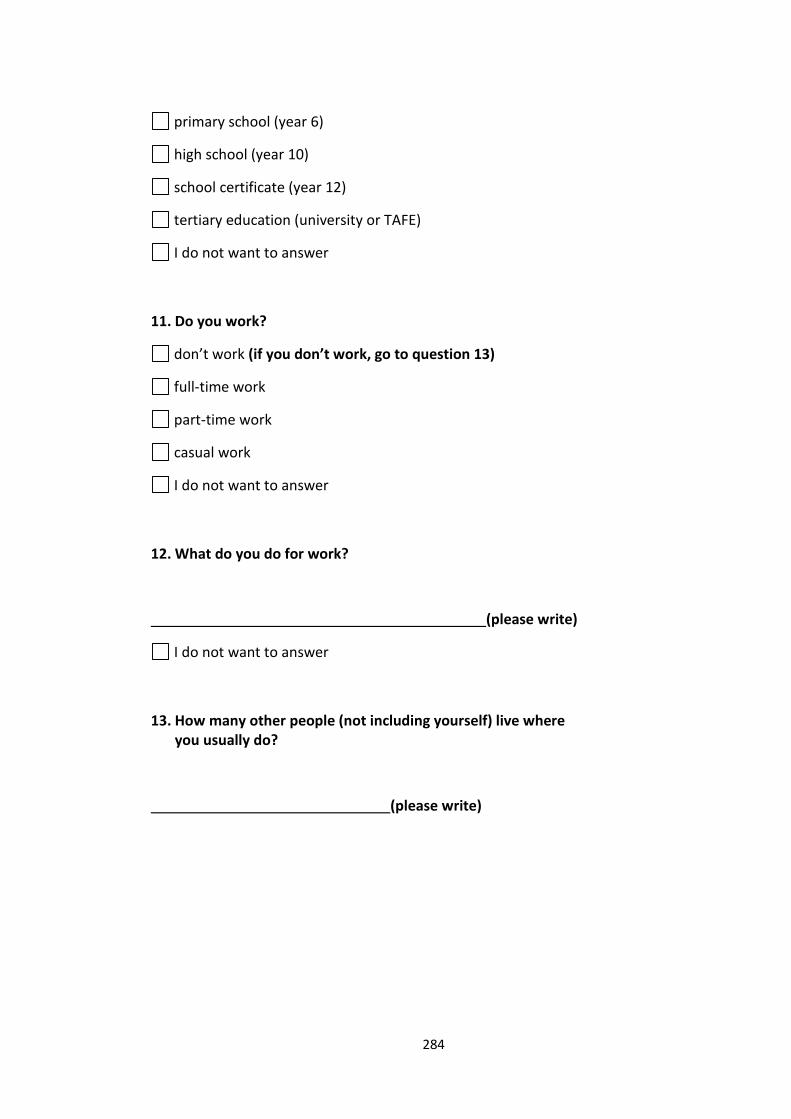
284
primary school (year 6)
high school (year 10)
school certificate (year 12)
tertiary education (university or TAFE)
I do not want to answer
11. Do you work?
don’t work (if you don’t work, go to question 13)
full-time work
part-time work
casual work
I do not want to answer
12. What do you do for work?
(please write)
I do not want to answer
13. How many other people (not including yourself) live where you usually do?
(please write)
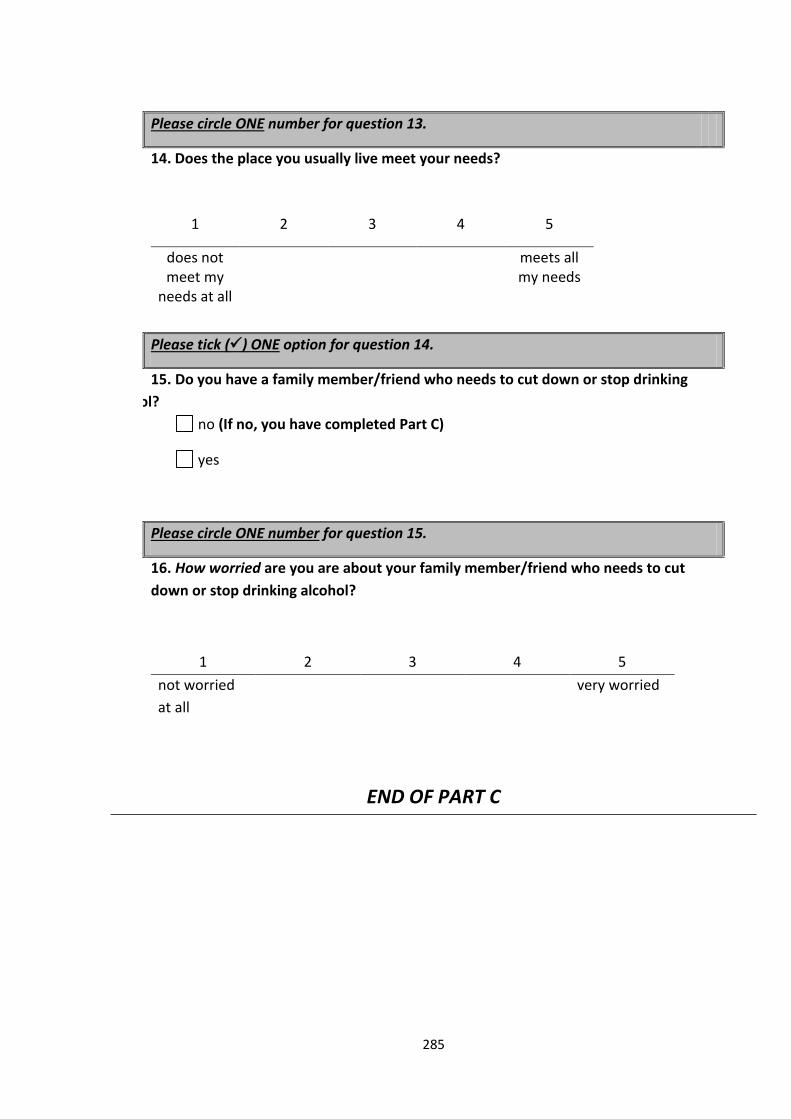
285
Please circle ONE number for question 13.
14. Does the place you usually live meet your needs?
1 2 3 4 5
does not meet my
needs at all
meets all my needs
Please tick () ONE option for question 14.
39. 15. Do you have a family member/friend who needs to cut down or stop drinking
alcohol?
no (If no, you have completed Part C)
yes
Please circle ONE number for question 15.
40. 16. How worried are you are about your family member/friend who needs to cut
down or stop drinking alcohol?
41.
1 2 3 4 5
not worried
at all
very worried
END OF PART C
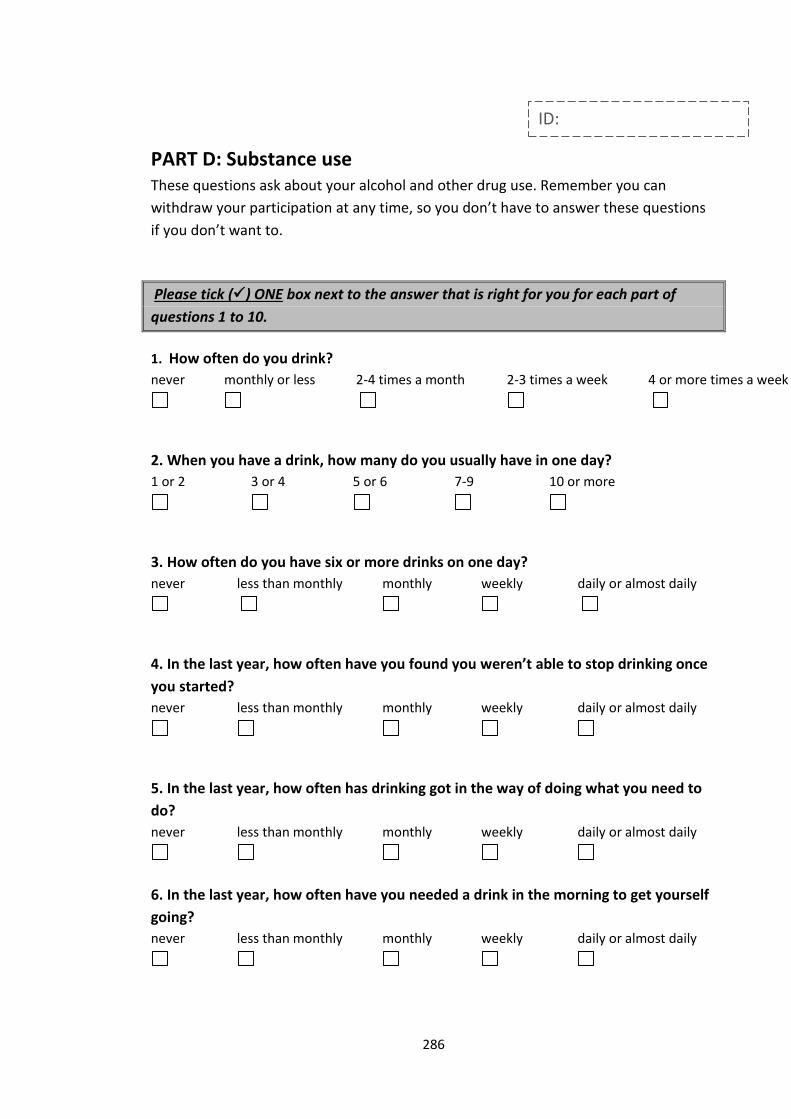
286
PART D: Substance use These questions ask about your alcohol and other drug use. Remember you can
withdraw your participation at any time, so you don’t have to answer these questions
if you don’t want to.
Please tick () ONE box next to the answer that is right for you for each part of
questions 1 to 10.
1. How often do you drink?
never
monthly or less
2-4 times a month
2-3 times a week
4 or more times a week
2. When you have a drink, how many do you usually have in one day?
1 or 2
3 or 4
5 or 6
7-9
10 or more
3. How often do you have six or more drinks on one day?
never
less than monthly
monthly
weekly
daily or almost daily
4. In the last year, how often have you found you weren’t able to stop drinking once
you started?
never
less than monthly
monthly
weekly
daily or almost daily
5. In the last year, how often has drinking got in the way of doing what you need to
do?
never
less than monthly
monthly
weekly
daily or almost daily
6. In the last year, how often have you needed a drink in the morning to get yourself
going?
never
less than monthly
monthly
weekly
daily or almost daily
ID:
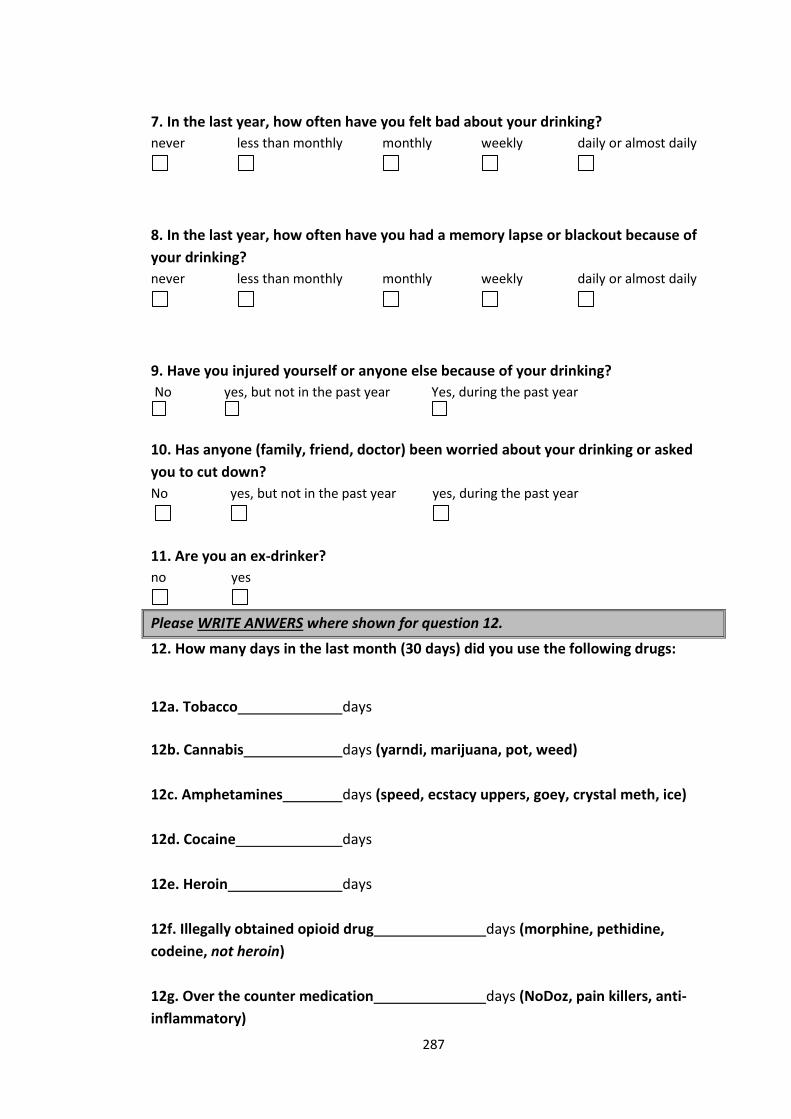
287
7. In the last year, how often have you felt bad about your drinking?
never
less than monthly
monthly
weekly
daily or almost daily
8. In the last year, how often have you had a memory lapse or blackout because of
your drinking?
never
less than monthly
monthly
weekly
daily or almost daily
9. Have you injured yourself or anyone else because of your drinking?
No
yes, but not in the past year
Yes, during the past year
10. Has anyone (family, friend, doctor) been worried about your drinking or asked
you to cut down?
No
yes, but not in the past year
yes, during the past year
11. Are you an ex-drinker?
no
yes
Please WRITE ANWERS where shown for question 12.
12. How many days in the last month (30 days) did you use the following drugs:
12a. Tobacco days
12b. Cannabis days (yarndi, marijuana, pot, weed)
12c. Amphetamines days (speed, ecstacy uppers, goey, crystal meth, ice)
12d. Cocaine days
12e. Heroin days
12f. Illegally obtained opioid drug days (morphine, pethidine,
codeine, not heroin)
12g. Over the counter medication days (NoDoz, pain killers, anti-
inflammatory)
288
12h. Tranquilisers days (benzos, valium, rohypnol)
12i. Other drug not listed above days
Please specify which drug
END OF PART D
Thank you for completing the survey!
289
Appendix I
Slides used to present the acceptability survey in a standardised manner
What do you think?
Programs to help Aboriginal and Torres Strait Islander people who drink too much alcohol and their family members/friends
1
2
Information sheets are handed out
by the group leader
290
Overview
3
Drinking too much alcohol causes:
Health problems (physical & mental)
Social problems
Problems are experienced by the people who drink as
well as their families & community
Health workers can help
Teaching families & communities how to better support people
who need to cut down or stop drinking
What we would like to do
4
Program 1 Program 2
Personalised Alcohol Treatment
(PAT) program
For Aboriginal and Torres Strait Islander
people who need to cut down or stop
drinking alcohol
Family Training
(FT) program
For family members/friends of Aboriginal
and Torres Strait Islander people who
need to cut down or stop drinking alcohol

291
Who will be delivering these programs?
5
Yoorana Gunya Family Violence Healing Centre Aboriginal Corporation
Who else will be involved?
6

292
Why are we inviting you to answer these
questions?
7
New or existing clients of to health services:
Lyndon Community
Yoorana Guyna
What we would like to know from you
8
What you think of the two programs
Personalised Alcohol Treatment (PAT) program
Family Training (FT) program
Suggestions you have to improve the programs
293
How confidential are your answers?
9
All answers are confidential.
Researchers from UNSW and the Lyndon Community
will have access to your survey answers.
If you provide us with your name and address, these
details will not be linked to your survey answers.
Questions & Concerns
10
Questions
Anton Clifford, UNSW, (02) 93850386
Concerns
Julaine Allan, Lyndon Community, (02) 63611521
Donna Bliss, Yoorana Guyna, (02) 68515111

294
Complaints
11
The Chairperson
AHMRC Ethics Committee
PO Box 1565, Strawberry Hills NSW 2012
Ph: (02) 9212 4777, Fax: (02) 9212 7211
Email: [email protected]
UNSW Ethics Secretariat
UNSW, SYDNEY 2052 AUSTRALIA
Ph: (02) 9385 4234, Fax: (02) 9385 6648
Email: [email protected]
How to answer the questions?
12
Follow instructions carefully. We cannot use your answers if you do not follow the instructions.
Choose an answer that best describes what you think.
Ask if you do not understand.
Be honest & accurate.
You may withdraw your participation at any time without needing a reason.
295
13
Any questions?
Your ID code
14
Survey will be given out in parts.
Your ID code will only be used to link different parts of your
survey together.
296
Create your ID code
15
Create your ID code (e.g. 16DIA)
The date you were born (e.g. 16)
AND
First three letters of your mother’s name (e.g. DIA)
Please write your ID CODE on the top of your information sheet
16
PAT information sheets are handed out
by the group leader
297
Personalised Alcohol Treatment (PAT)
17
Who is PAT for? Aboriginal and Torres Strait Islander people from Orange, Forbes and
surrounding areas who need help to cut down or stop drinking alcohol.
What is PAT?
One-on-one counselling with a drug and alcohol counsellor who has been trained to deliver the program.
To reduce alcohol-related harms experienced by the drinker, their family and their community.
Assessment of risk of harms from alcohol.
Personalised treatment plan.
Support to cut down or stop drinking alcohol.
When can PAT be delivered? After withdrawal.
If needing rehab but not wanting to go.
Waiting for rehab.
After rehab.
Part A: PAT program
18
Part A is handed out by the group leader
Please write your ID CODE at the top of Part A

298
Part A: PAT program
19
1. What do you think about PAT being delivered in your
community? [page 1]
Please circle one number
1 2 3 4 5
very bad very good
Part A: PAT program
20
2. Do you think it is okay for PAT to be available for Aboriginal
people: [page 1]
2a. After withdrawal?
not okay
okay
Please tick () one box
299
Part A: PAT program
21
2. Do you think it is okay for PAT to be available for Aboriginal
people: [page 1]
2b. Needing rehab but not wanting to go?
not okay
okay
Please tick () one box
Part A: PAT program
22
2. Do you think it is okay for PAT to be available for Aboriginal
people: [page 1]
2c. Waiting for rehab?
not okay
okay
Please tick () one box

300
Part A: PAT program
23
2. Do you think it is okay for PAT to be available for Aboriginal
people: [page 1]
2d. After rehab?
not okay
okay
Please tick () one box
Part A: PAT program
24
2. Do you think it is okay for PAT to be available for Aboriginal
people: [page 1]
2e. Referred from probation and parole?
not okay
okay
Please tick () one box

301
25
Imagine you drink too much alcohol
and want help to cut down or stop
Part A
26
3. What are the qualities that you think are most important in a
counsellor? [page 2]
3a. Trust & familiarity:
someone I know and trust
someone I know
someone I trust
doesn’t matter
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
302
Part A
27
3. What are the qualities that you think are most important in a
counsellor? [page 2]
3b. Experience working in your local community:
no
yes
doesn’t matter
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
Part A
28
3. What are the qualities that you think are most important in a
counsellor? [page 2]
3c. Aboriginality:
a non-aboriginal person
an Aboriginal person
doesn’t matter
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
303
Part A
29
3. What are the qualities that you think are most important in a
counsellor? [page 2]
3d. Gender:
a woman
a man
doesn’t matter
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
Part A
30
4. Would you feel okay to talk one-on-one with a counsellor, who
has the qualities you have described above, about: [page 2]
4a. How much alcohol you usually drink?
okay
not okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
304
Part A
31
4. Would you feel okay to talk one-on-one with a counsellor, who
has the qualities you have described above, about: [page 2]
4b. How you feel about your drinking?
okay
not okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
Part A
32
4. Would you feel okay to talk one-on-one with a counsellor, who
has the qualities you have described above, about: [page 2]
4c. What you do when you are drinking?
okay
not okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
305
Part A
33
4. Would you feel okay to talk one-on-one with a counsellor, who
has the qualities you have described above, about: [page 3]
4d. If you cause harm to yourself and/or others when you drink
(including any violent behaviour)?
okay
not okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
Part A
34
4. Would you feel okay to talk one-on-one with a counsellor, who
has the qualities you have described above, about: [page 3]
4e. Setting goals to cut down or stop drinking?
okay
not okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
306
Part A
35
4. Would you feel okay to talk one-on-one with a counsellor, who
has the qualities you have described above, about: [page 3]
4f. Things (people, places, and situations) that might be making you
want to drink?
okay
not okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
Part A
36
4. Would you feel okay to talk one-on-one with a counsellor, who
has the qualities you have described above, about: [page 3]
4g. Ways to resolve problems that might be making you want to
drink?
okay
not okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop

307
Part A
37
4. Would you feel okay to talk one-on-one with a counsellor, who
has the qualities you have described above, about: [page 3]
4h. How to use support from a trusted family member/friend to cut
down or stop drinking?
okay
not okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
Part A
38
5. Would it be okay for one of your most trusted family
members/friends to: [page 3]
5a. Help you to start alcohol treatment?
not okay
okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop

308
Part A
39
5. Would it be okay for one of your most trusted family
members/friends to: [page 3]
5b. Help you to stay in treatment?
not okay
okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
Part A
40
5. Would it be okay for one of your most trusted family
members/friends to: [page 3]
5c. Help you to continue to drink less or stop drinking?
not okay
okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
309
Part A
41
6. Would it be okay for one of your concerned family
members/friends to: [page 4]
6a. Help you to start alcohol treatment?
okay
not okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
Part A
42
6. Would it be okay for one of your concerned family
members/friends to: [page 4]
6b. Help you to stay in treatment?
okay
not okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
310
Part A
43
6. Would it be okay for one of your concerned family
members/friends to: [page 4]
6c. Help you to continue to drink less or stop drinking?
okay
not okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
Part A
44
7. If you were attending PAT to get help to cut down or stop
drinking, what would you prefer as part of the one-on-one
sessions? [page 7]
7a. Number of sessions?
1 to 2 sessions for very basic information
2 to 3 sessions for basic information
2 to 4 sessions for detailed information
5 or more sessions for very detailed information
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
311
Part A
45
8. If group session were made available on top of one-on-one
counselling, would it be okay (in a group setting) for you to: [page 4]
8a. Confidentially talk to Aboriginal people with similar experiences
about alcohol and its effects on yourself and/or your family?
not okay
okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
Part A
46
8. If group session were made available on top of one-on-one counselling, would it be okay (in a group setting) for you to: [page 4]
8b. Practice and reinforce skills learnt in one-on-one counselling?
not okay
okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
312
Part A
47
8. If group session were made available on top of one-on-one counselling, would it be okay (in a group setting) for you to: [page 4]
8c. Participate in healthy social and recreational activities?
not okay
okay
Please tick () one box
Imagine you drink too much alcohol
and want help to cut down or stop
Part A
48
Remember you can withdraw your
participation at any time without
needing a reason
313
49
Imagine you are having a
one-on-one counselling session as
part of PAT
Part A
50
9. Please rank the session parts below from 1 (most important)
to 4 (least important) [page 5]
Please write numbers 1, 2, 3 or 4 in the boxes (use each number once)
Imagine you are having a one-on-one
counselling session as part of
PAT
Talking about your
drinking behaviours
Setting goals to
reduce alcohol-
related harms
Learning how to
resolve alcohol-
related problems
Practicing how to
resolve alcohol-
related problems
314
Part A
51
10. Is there anything we haven’t asked you about that you think we should include in the Personalised Alcohol Treatment (PAT) program? [page 6]
Please write your suggestions in the box
I think that
Part A
52
END OF PART A
The group leader will collect Part A
when you have finished

315
53
FT information sheets are handed out
by the group leader
Family Training (FT)
54
Who is FT for?
Aboriginal and Torres Strait Islander people from Orange, Forbes and surrounding areas who have a family member/friend who drinks too much alcohol.
What is FT?
One-on-one counselling with a drug and alcohol worker who has been trained tpdeliver the program.
To talk about affects of family member’s/friend’s drinking.
Training and support for people who want to help a family member/friend who needs to cut down or stop drinking alcohol.
To increase the wellbeing of people with a family member/friend who drinks too much alcohol.
When can FT be delivered?
For people who have a family member/friend in the withdrawal unit.
For people who want to help a family member/friend to start alcohol treatment.
For people who have a family member/friend who is waiting for rehab.
For people who have a family member/friend who has finished rehab.
316
Part B: FT program
55
Part B is handed out by the group leader
Please write your ID CODE at the top of Part B
Part B: FT program
56
1. What do you think about FT being delivered in your
community? [page 1]
Please circle one number
1 2 3 4 5
very bad very good
317
Part B: FT program
57
2. Do you think it is okay for FT to be available for Aboriginal
people: [page 1]
2a. With a family member/friend in the withdrawal unit?
okay
not okay
Please tick () one box
Part B: FT program
58
2. Do you think it is okay for FT to be available for Aboriginal
people: [page 1]
2b. Who want to help a family member/friend who drinks too much
alcohol to start treatment?
okay
not okay
Please tick () one box
318
Part B: FT program
59
2. Do you think it is okay for FT to be available for Aboriginal
people: [page 1]
2c. With a family member/friend who is waiting for rehab?
okay
not okay
Please tick () one box
Part B: FT program
60
2. Do you think it is okay for FT to be available for Aboriginal
people: [page 1]
2d. With a family member/friend who has just finished rehab?
okay
not okay
Please tick () one box
319
Part B: FT program
61
2. Do you think it is okay for FT to be available for Aboriginal people: [page 1]
2e. With a family member/friend who has been referred from probation and parole?
okay
not okay
Please tick () one box
62
Imagine you want to help
a family member/friend
who drinks too much alcohol
320
Part B
63
3. Would you be comfortable asking your family member/friend
who drinks too much alcohol: [page 2]
3a. How much alcohol he/she drinks?
not comfortable
comfortable
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
Part B
64
3. Would you be comfortable asking your family member/friend
who drinks too much alcohol: [page 2]
3b. How he/she feels about his/her own drinking?
not comfortable
comfortable
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
321
Part B
65
3. Would you be comfortable asking your family member/friend
who drinks too much alcohol: [page 2]
3c. What he/she does when drinking alcohol?
not comfortable
comfortable
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
Part B
66
4. What are the qualities that you think are most important in a drug and alcohol worker: [page 2]
4a. Trust & familiarity?
someone I know and trust
someone I know
someone I trust
doesn’t matter
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
322
Part B
67
4. What are the qualities that you think are most important in a
drug and alcohol worker? [page 2]
4b. Experience working in your local community:
yes
no
doesn’t matter
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
Part B
68
4. What are the qualities that you think are most important in a
drug and alcohol worker? [page 2]
4c. Aboriginality:
an Aboriginal person
a non-Aboriginal person
doesn’t matter
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
323
Part B
69
4. What are the qualities that you think are most important in a
drug and alcohol worker? [page 3]
4d. Gender:
a man
a woman
doesn’t matter
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
Part B
70
5. Would you feel okay to talk one-on-one with a drug and
alcohol worker, who has the qualities you have described
above, about: [page 3]
5a. How much alcohol your family member/friend drinks?
okay
not okay
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
324
Part B
71
5. Would you feel okay to talk one-on-one with a drug and
alcohol worker, who has the qualities you have described
above, about: [page 3]
5b. What your family member/friend does when he/she drinks
alcohol?
okay
not okay
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
Part B
72
5. Would you feel okay to talk one-on-one with a drug and
alcohol worker, who has the qualities you have described
above, about: [page 3]
5c. If your family member/friend harm themselves or others when
he/she drinks alcohol (including any violent behaviour)?
okay
not okay
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
325
Part B
73
6. Would you feel okay about using FT to work on: [page 3]
6a. How to talk to your family member/friend about his/her drinking?
not okay
okay
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
Part B
74
6. Would you feel okay about using FT to work on: [page 3]
6b. Ways to talk to your family member/friend about how alcohol is
causing difficulty in your community?
not okay
okay
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
326
Part B
75
6. Would you feel okay about using FT to work on: [page 3]
6c. Ways you can support your family member/friend to start
treatment?
not okay
okay
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
Part B
76
6. Would you feel okay about using FT to work on: [page 3]
6d. Ways you can support your family member/friend to stay in
treatment?
not okay
okay
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
327
Part B
77
6. Would you feel okay about using FT to work on: [page 4]
6e. Ways to support your family member/friend to continue to drink?
not okay
okay
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
Part B
78
6. Would you feel okay about using FT to work on: [page 4]
6f. Ways to set boundaries when alcohol causes difficulty in your
community?
not okay
okay
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol

328
Part B
79
6. Would you feel okay about using FT to work on: [page 4]
6g. Ways you can stay strong living in a community where alcohol
causes difficulty?
not okay
okay
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
Part B
80
6. Would you feel okay about using FT to work on: [page 4]
6h. Ways to you can help your community stay strong when alcohol
causes difficulty?
not okay
okay
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
329
Part B
81
7. If you were attending FT so that you could help a family member/friend who drinks too much alcohol, what would you prefer as part of the one-on-one sessions: [page 4]
7a. Number of sessions?
1 to 2 sessions for very basic information
2 to 3 sessions for basic information
2 to 4 sessions for detailed information
5 or more sessions for very detailed information
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
Part B
82
8. If group session were made available on top of one-on-one
counselling, would it be okay (in a group setting) for you to: [page 4]
8a. Confidentially talk to Aboriginal people with similar experiences
about alcohol and its effects on yourself and/or your family?
okay
not okay
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
330
Part B
83
8. If group session were made available on top of one-on-one counselling, would it be okay (in a group setting) for you to: [page 4]
8b. Practice and reinforce skills learnt in one-on-one counselling?
okay
not okay
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
Part B
84
8. If group session were made available on top of one-on-one counselling, would it be okay (in a group setting) for you to: [page 4]
8c. Participate in healthy social and recreational activities?
okay
not okay
Please tick () one box
Imagine you want to help a family
member/friend who drinks too much
alcohol
331
85
Imagine you are having a
one-on-one counselling session as
part of FT
Part B
86
9. Please rank the session parts below from 1 (most important) to 4 (least important) [page 5]
Please write numbers 1, 2, 3, & 4 in the boxes (use each number once)
Imagine you are having one-on-one
sessions as part of
FT
Talking about your
family
member’s/friend’s
drinking behaviour
Learning how to
communicate with
your family
member/friend
about his/her
drinking
Learning how to
support your family
member/friend to
cut down or stop
drinking
Practicing how to
support your family
member/friend to
cut down or stop
drinking
332
Part B: FT program
87
10. Is there anything we haven’t asked you about that you think we should include in the Family Training (FT) program? [page 6]
Please write your suggestions in the box
The FT program would be better if
Part B: FT program
88
END OF PART B
The group leader will collect Part B
when you have finished

333
Part C: Information about you
89
Part C is handed out by the group leader
Please write your ID CODE at the top of Part C
Part C: Information about you
90
Remember that this information will be
used for the research project and not
forwarded on to any authorities

334
Part C: Information about you
91
1. Health service attended [page 1]
Lyndon Community
Yoorana Gunya
other (please write)
Please tick () one box and write answer where shown
Part C: Information about you
92
2. Gender [page 1]
female
male
I do not want to answer
Please tick () one box

335
Part C: Information about you
93
3. Date of birth [page 1]
(day) (month) (year)
Please write answer where shown
Part C: Information about you
94
4. Did you guess any part of your birth date? [page 1]
no
yes, I estimated (please write)
Please tick () one box and write answer where shown

336
Part C: Information about you
95
5. Are you of Aboriginal or Torres Strait Islander origin? [page 2]
no (if no, go to question 22)
yes, Aboriginal
yes, Torres Strait Islander
yes, Aboriginal and Torres Strait Islander
Please tick () one box
Part C: Information about you
96
6. What clan, tribal or language group do you identify with? [page 2]
I identify with (please write)
Please write answer where shown

337
Part C: Information about you
97
7. Were you born in Australia? [page 2]
yes
no, I was born in (please write)
Please tick () one box and write answer where shown
Part C: Information about you
98
8. What language do you prefer to speak at home? [page 2]
English
other, I prefer to speak (please write)
Please tick () one box and write answer where shown
338
Part C: Information about you
99
9. Have you completed any formal education? [page 2]
no formal education
primary school (year 6)
high school (year 10)
school certification (year 12)
tertiary education (university or TAFE)
I do not want to answer
Please tick () one box
Part C: Information about you
100
10. Do you work? [page 3]
don’t work (if you don’t work, go to question 12)
full-time work
part-time work
casual work
other
I do not want to answer
Please tick () one box
339
Part C: Information about you
101
11. What do you do for work? [page 3]
(please write)
I do not want to answer
Please tick () one box or write answer where shown
Part C: Information about you
102
12. How many other people (not including yourself) live where you usually do? [page 3]
(please write)
Please write answer where shown
340
Part C: Information about you
103
13. Does the place where you usually live meet your
needs? [page 3]
Please circle one number
1 2 3 4 5
does not
meet my
needs at all
meets all my
needs
Part C: Information about you
104
14. Do you have a family member who needs to cut down or stop drinking? [page 4]
no (if no, you have completed Part C)
yes
Please tick () one box
341
Part C: Information about you
105
15. How worried are you about your family member/friend
who needs to cut down or stop drinking alcohol? [page 4]
Please circle one number
1 2 3 4 5
not worried
at all
very worried
Part C: Information about you
106
END OF PART C
The group leader will collect Part C
when you have finished
342
107
Expression of interest sheet is handed out
by the group leader
Interested in being involved?
108
If you are interested in being involved in the PAT or FT programs
please fill in your contact details.
These details will be used by Yoorana Gunya and Lyndon
Community staff to contact you about your participation in the
program/s.
Providing your contact details is voluntary.
Your contact details will not be linked to your survey answers.
343
Interested in being involved?
109
Name: (please write)
Address: (please write)
Home phone: (please write)
Mobile phone: (please write)
I am a person who needs to cut down or stop drinking alcohol
AND/OR
I have a family member/friend who needs to cut down or stop
drinking alcohol
Please tick () one or both boxes that apply to you
110
The group leader will collect
your expression of interest sheet
when you are finished
344
Part D: Alcohol use
111
Part D
• Questions in Part D ask about your drinking.
• Examples of questions that could be used in the programs.
• Remember you can withdraw your participation at any time, so you do not have to answer these questions
• if you do not want to.
• You will be able to get feedback on your answers if you complete Part D.
Part D: Alcohol use
112
Part D is handed out by the group leader
Please write your ID CODE at the top of Part D
345
Part D: Alcohol use
113
1. How often do you drink? [page 1]
never
monthly or less
2-4 times a month
2-3 times a week
4 or more times a week
Please tick () one box
Part D: Alcohol use
114
2. When you drink, how many do you usually have in one day? [page 1]
1 or 2
3 or 4
5 or 6
7-9
10 or more
Please tick () one box
346
Part D: Alcohol use
115
3. How often do you have six or more drinks on one day? [page 1]
never
less than monthly
monthly
weekly
daily or almost daily
Please tick () one box
Part D: Alcohol use
116
4. In the last year, how often have you found you weren’t able to stop drinking once you started? [page 1]
never
less than monthly
monthly
weekly
daily or almost daily
Please tick () one box
347
Part D: Alcohol use
117
5. In the last year, how often has drinking got in the way of doing what you need to do? [page 1]
never
less than monthly
monthly
weekly
daily or almost daily
Please tick () one box
Part D: Alcohol use
118
6. In the last year, how often have you needed a drink in the morning to get yourself going? [page 2]
never
less than monthly
monthly
weekly
daily or almost daily
Please tick () one box
348
Part D: Alcohol use
119
7. In the last year how often have you felt bad about your drinking? [page 2]
never
less than monthly
monthly
weekly
daily or almost daily
Please tick () one box
Part D: Alcohol use
120
8. In the last year, how often have you has a memory lapse or blackout because of your drinking? [page 2]
never
less than monthly
monthly
weekly
daily or almost daily
Please tick () one box
349
Part D: Alcohol use
121
9. Have you injured yourself or anyone else because of
your drinking? [page 2]
no
yes, but not in the last year
yes, during the last year
Please tick () one box
Part D: Alcohol use
122
10. Has anyone (family, friend, doctor) been worried about
your drinking or asked you to cut down? [page 2]
no
yes, but not in the last year
yes, during the last year
Please tick () one box
350
Part D: Alcohol Use
123
END OF PART D
351
Appendix J
Group record sheet for acceptability survey
Acceptability study: group record sheet
Please fill in this form for each group that is involved in the acceptability study.
Date:
Service:
Start time:
End time:
Group leaders name:
Number of clients invited to
participate:
Number of clients consented to
participate:
Number of clients completed the
survey:
Comments:
352
Appendix K
Additional methods and results not included in the published paper (Calabria et al.
2013)
Additional acceptability survey content
In addition to asking about the overall acceptability of the program, parts A and B of the survey
asked whether particular content and delivery options were acceptable. The Community
Reinforcement Approach (CRA) program survey (part A) asked about the acceptability of
program setting and delivery, counsellor characteristics, session discussion topics, and family
member’s involvement in treatment. The Community Reinforcement and Family Training
(CRAFT) program survey (part B) asked about the acceptability of setting and delivery,
communication with the drinker, counsellor characteristics, and session discussion topics.
Participants were also asked to rank in order of importance four session components. The CRA
program components to be ranked were: talking about your drinking behaviour, setting goals
to reduce alcohol-related harms, learning how to resolve alcohol-related problems, and
practicing how to resolve alcohol-related problems. The CRAFT program components to be
ranked were: talking about your family member’s/friend’s drinking behaviour, learning how to
communicate with your family member/friend about his/her drinking, learning how to support
your family member/friend to cut down or stop drinking, and practicing how to support your
family member/friend to cut down or stop drinking.
In addition to demographic information (part C) presented in the published paper participants
were asked which health service he/she attended, clan/tribal/language group, country of birth,
preferred language, how many people usually lived with, whether residence meets needs
(rated on a five-point scale, 1=does not meet my needs at all, 5=meets all my needs).
353
Alcohol use (part D) was measured using the Alcohol Use Disorders Identification Test (AUDIT)
(Saunders et al. 1993; Saunders & Aasland 1987). The AUDIT measures hazardous and harmful
alcohol consumption in the past 12 months and covers the domains of alcohol consumption,
drinking behaviour, and alcohol-related problems. The AUDIT is a ten item scale: items one to
eight are scored on a 5-point Likert scale and items nine and ten are scored on a 3-point Likert
scale. Total scores range from zero to forty and a high score indicates problematic alcohol
misuse. Universally used cut-off scores determine participants’ drinking behaviour: non-
drinker (score of 0); drinks within recommended limits (score of 1-7); at-risk drinking (score of
8-12); or high-risk drinking (score of 13 or more) (Conigrave, Hall & Saunders 1995; Tsai et al.
2005; Babor et al. 2001). Although the measure has not been validated for Aboriginal
Australians, it has been designed as a cross-cultural instrument (Saunders et al. 1993) and is
recommended by the Alcohol Treatment Guidelines for Indigenous Australians (Australian
Government Department of Health and Ageing 2007). The AUDIT has high internal consistency
across diverse samples and settings (median alpha = 0.83) and the English language version has
demonstrated validity (Reinert & Allen 2007). The wording used for the AUDIT in the current
study was taken from an Aboriginal-specific adaptation developed by researchers at the
University of Sydney and Sydney South West Area Health Service: the content is the same but
phasing slightly altered to be more appropriate for Aboriginal Australians. For example, instead
of “how many standard drinks do you have on a typical day?” the Aboriginal-specific version
asks “when you drink, how many do you usually have?”. Participants were also asked if they
had a family member/friend who needed to cut down or stop drinking and how worried they
were about that family member/friend (rated on a 5-point Likert scale, 1=not worried at all,
5=very worried). Tobacco and illicit drug consumption was measured using frequency
questions. Formal and slang names of drugs were listed to maximise comprehension.
354
Additional procedure information
Participants were lead through the survey process and sections of the survey were handed out
separately. The process was guided by a researcher or Aboriginal Health Worker who followed
steps outlined in a PowerPoint presentation designed to standardise the process of survey
delivery (see Appendix I for PowerPoint slides). First, the study aims were explained and an
information sheet was given to participants including information on consent. Consenting
participants were asked to generate an identification number for themselves, which they
wrote on the information sheet for future reference, and were then asked to write on each
section of their survey, later used to link their sections of the survey. The identification number
consisted of the date the participant was born and the first three letters of their mother’s
name (e.g. 16DIA). Second, general information was presented on the CRA program, including
who the program was for, what the program involved (e.g. individual one-on-one counselling
with a trained counsellor to reduce alcohol-related harms experienced by the drinker, their
family and their community), and when the program could be delivered. After program
information was presented participants were given part A of the survey and asked to imagine
that they had a drinking problem and needed help to cut down or stop, before recording their
opinions on the content of the CRA program. Third, general information was presented on the
CRAFT program including who the program was for, what the program involved (e.g. individual
one-on-one counselling with a trained counsellor to talk about the affects of their relative’s
drinking, learn how to support non-drinking behaviour, and increase their own social and
emotional wellbeing), and when the program could be delivered. Participants were then given
part B of the survey and asked to imagine that they had a relative/friend who drank too much
who they wanted to help, before recording their opinions on the content of the CRAFT
program. Fourth, the demographic section of the survey (part C) was handed out to
participants for completion. Finally, the alcohol and drug use section of the survey (part D) was
given to participants for completion.
355
Researchers and/or Aboriginal Health Workers were present throughout the process and were
available to answer any questions from participants. The surveys were self completed;
however, assistance was provided for participants who were illiterate or had difficulty with
reading. Participation was voluntary and responses were confidential.
When the survey was administered in a group setting discussion time, facilitated by a
researcher, was given after each program survey (parts A and B). A section was provided on
the survey for participants to write down any comments they wanted to make about the
programs, serving the purpose of gaining the opinions of those who participated individually
and those who did not wish to speak in a group discussion.
Additional analysis
The proportion of participants who endorsed each response option for the survey items were
calculated. Predictors of overall acceptability of CRA and CRAFT were investigated using logistic
regression (Hosmer & Lemeshow 2000). Multinomial logistic regression (Hosmer & Lemeshow
2000) was performed to investigate predictors of the ranked session components. Predictors
included: gender; drinking status (not/at risk or high risk drinker); family member drinking
problem (no/family member with a drinking problem); and health service (Aboriginal
Community Controlled Health Service/drug and alcohol treatment agency). A difference was
statistically significant at 0.05.
Additional Results
Eight percent of participants lived alone and the others lived with up to eight other people.
When rating whether their place of usual residence met their needs, 69% endorsed a four or
five on a 5-point Likert scale (1=does not meet my needs at all, 5=meets all my needs).
356
Alcohol use. AUDIT scores ranged the capacity of the measure from zero to forty. Thirteen
percent were non-drinkers, 31% drank within recommended limits, 11% were at-risk drinkers,
and 45% were high-risk drinkers (44% not risky drinkers and 56% risky drinkers). Seventy six
percent had a family member or friend that they believed needed to cut down or stop drinking
alcohol and of those, 74% endorsed a four or five on a 5-point Likert scale to indicate that they
were worried about their family member or friend (1=not worried at all, 5=very worried).
Among at-risk and high-risk drinkers 81% could identify a family member or friend who drank
too much, this proportion was reduced to 70% for non-drinkers and those who drank within
recommended limits. Seventy percent had used tobacco in the past month. Illicit drug use was
less prevalent in the last 30 days: cannabis (29%); amphetamines (5%); cocaine (1%); heroin
(2%); and illegally obtained opioid drug (2%). The use of over the counter medications in the
past month was reported by 20% and tranquilizer use by 5%.
Community Reinforcement Approach. All presented topics of discussion for a CRA session were
endorsed as acceptable by a proportion of the sample, which varied: how much alcohol you
usually drink (86%); how you feel about your drinking (73%); what you do when you are
drinking (72%); if you cause harm to yourself and/or others when you drink (61%); setting
goals to cut down or stop drinking (93%); things (people, places, and situations) that might be
making you want to drink (64%); ways to resolve problems that might be making you want to
drink (83%); and how to use support from a trusted family member/friend to cut down or stop
drinking (88%). The role of a trusted family member/friend in a problem drinker’s treatment
was more acceptable (help you start alcohol treatment (82%), stay in alcohol treatment (89%),
and continue to drink less or stop drinking (85%)) than the role of a concerned family
member/friend (help you start alcohol treatment (80%), stay in alcohol treatment (87%), and
continue to drink less or stop drinking (84%)).
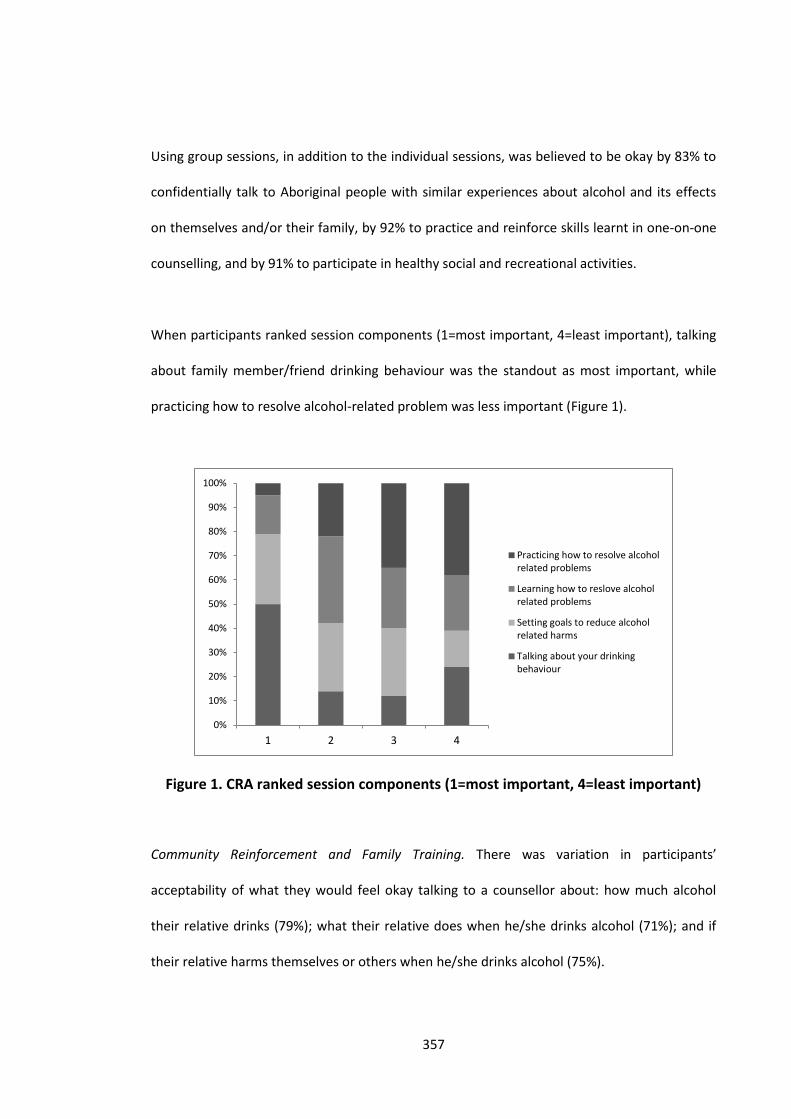
357
Using group sessions, in addition to the individual sessions, was believed to be okay by 83% to
confidentially talk to Aboriginal people with similar experiences about alcohol and its effects
on themselves and/or their family, by 92% to practice and reinforce skills learnt in one-on-one
counselling, and by 91% to participate in healthy social and recreational activities.
When participants ranked session components (1=most important, 4=least important), talking
about family member/friend drinking behaviour was the standout as most important, while
practicing how to resolve alcohol-related problem was less important (Figure 1).
Figure 1. CRA ranked session components (1=most important, 4=least important)
Community Reinforcement and Family Training. There was variation in participants’
acceptability of what they would feel okay talking to a counsellor about: how much alcohol
their relative drinks (79%); what their relative does when he/she drinks alcohol (71%); and if
their relative harms themselves or others when he/she drinks alcohol (75%).
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1 2 3 4
Practicing how to resolve alcoholrelated problems
Learning how to reslove alcoholrelated problems
Setting goals to reduce alcoholrelated harms
Talking about your drinkingbehaviour
358
All presented topics areas for a CRAFT session were endorsed as acceptable by a proportion of
the sample, which varied: how to talk to their relative about his/her drinking (88%); ways to
talk to their relative about how alcohol is causing difficulty in their community (84%); ways to
support their relative to start treatment (89%); ways to support their relative to stay in
treatment (90%); ways to support their relative to continue to drink less (93%); ways to set
boundaries when alcohol causes difficulty in your community (91%); ways to stay strong living
in a community where alcohol causes difficulty (89%); and ways to help their community stay
strong when alcohol causes difficulty (91%).
Group sessions, in addition to one-on-one counselling, were acceptable to a proportion of the
sample in varied situations: to confidentially talk to Aboriginal people with similar experiences
about alcohol and its effects on themselves and/or their family by 85%; to practice and
reinforce skills learnt in one-on-one counselling by 89%; and to participate in health social and
recreational activities by 89%.
When participants ranked session components (1=most important, 4=least important),
practicing how to a support family member/friend to cut down or stop drinking was less
important than other session components (Figure 2).
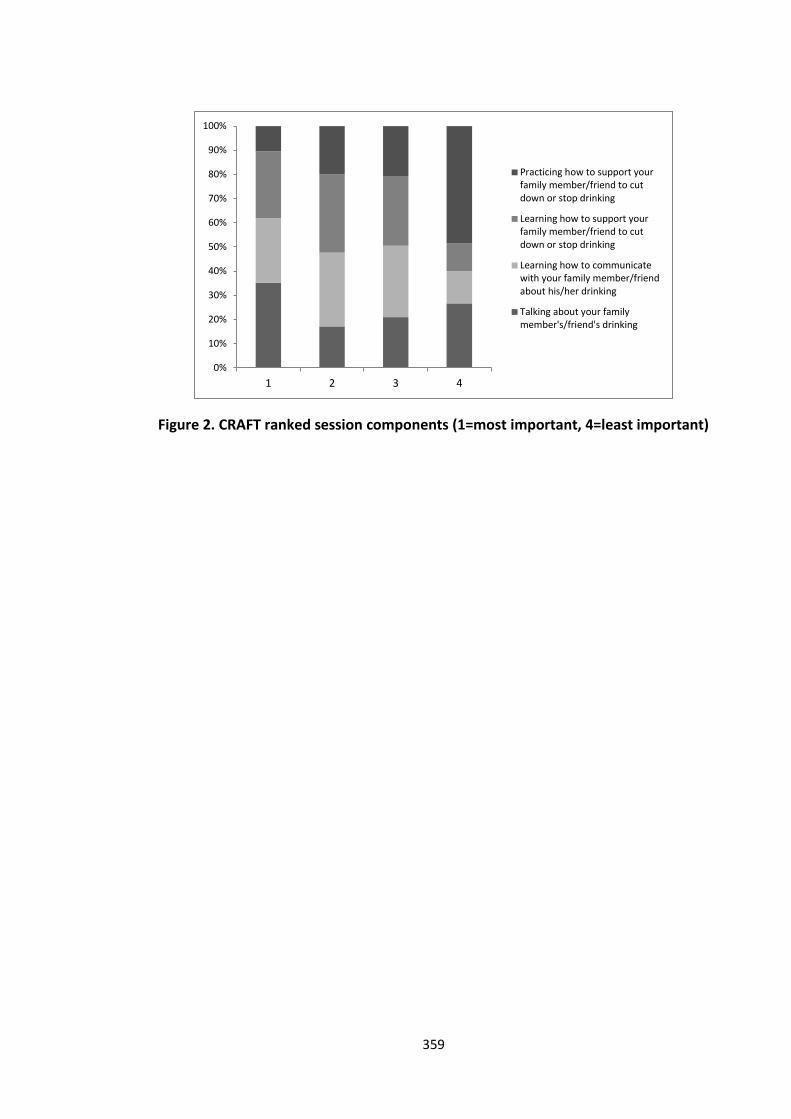
359
Figure 2. CRAFT ranked session components (1=most important, 4=least important)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1 2 3 4
Practicing how to support yourfamily member/friend to cutdown or stop drinking
Learning how to support yourfamily member/friend to cutdown or stop drinking
Learning how to communicatewith your family member/friendabout his/her drinking
Talking about your familymember's/friend's drinking
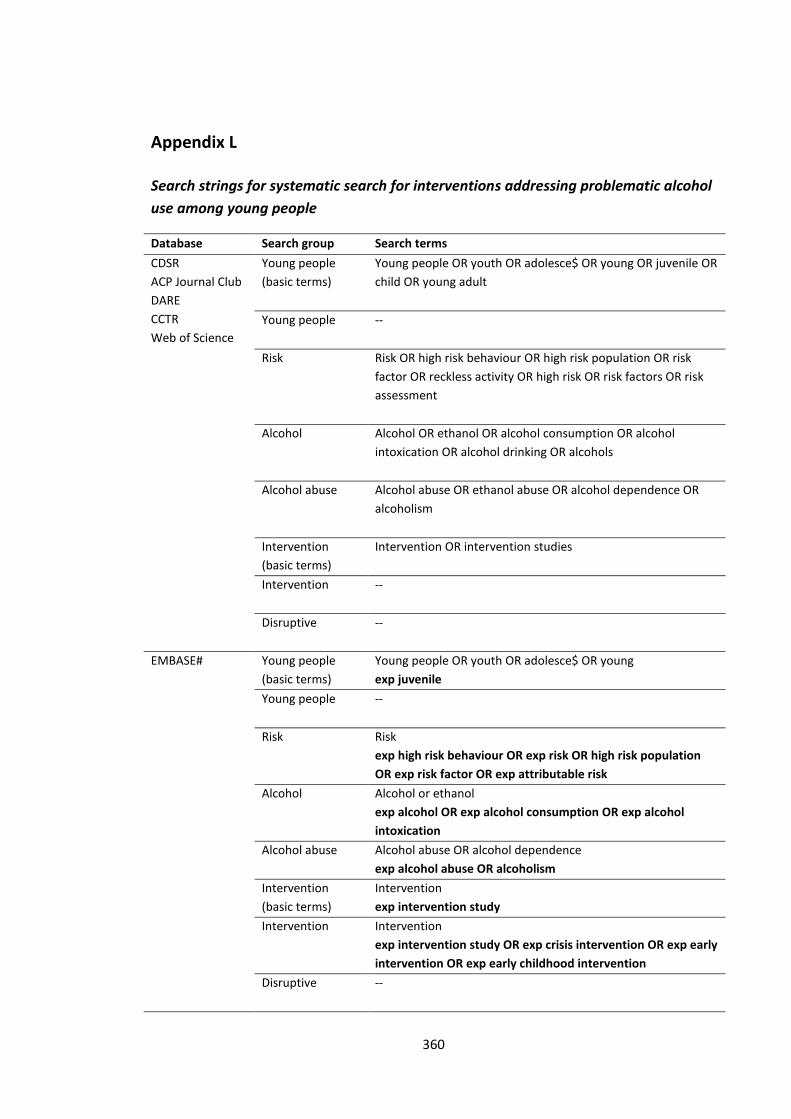
360
Appendix L
Search strings for systematic search for interventions addressing problematic alcohol
use among young people
Database Search group Search terms
CDSR
ACP Journal Club
DARE
CCTR
Web of Science
Young people
(basic terms)
Young people OR youth OR adolesce$ OR young OR juvenile OR
child OR young adult
Young people --
Risk Risk OR high risk behaviour OR high risk population OR risk
factor OR reckless activity OR high risk OR risk factors OR risk
assessment
Alcohol Alcohol OR ethanol OR alcohol consumption OR alcohol
intoxication OR alcohol drinking OR alcohols
Alcohol abuse Alcohol abuse OR ethanol abuse OR alcohol dependence OR
alcoholism
Intervention
(basic terms)
Intervention OR intervention studies
Intervention --
Disruptive --
EMBASE# Young people
(basic terms)
Young people OR youth OR adolesce$ OR young
exp juvenile
Young people --
Risk Risk
exp high risk behaviour OR exp risk OR high risk population
OR exp risk factor OR exp attributable risk
Alcohol Alcohol or ethanol
exp alcohol OR exp alcohol consumption OR exp alcohol
intoxication
Alcohol abuse Alcohol abuse OR alcohol dependence
exp alcohol abuse OR alcoholism
Intervention
(basic terms)
Intervention
exp intervention study
Intervention Intervention
exp intervention study OR exp crisis intervention OR exp early
intervention OR exp early childhood intervention
Disruptive --
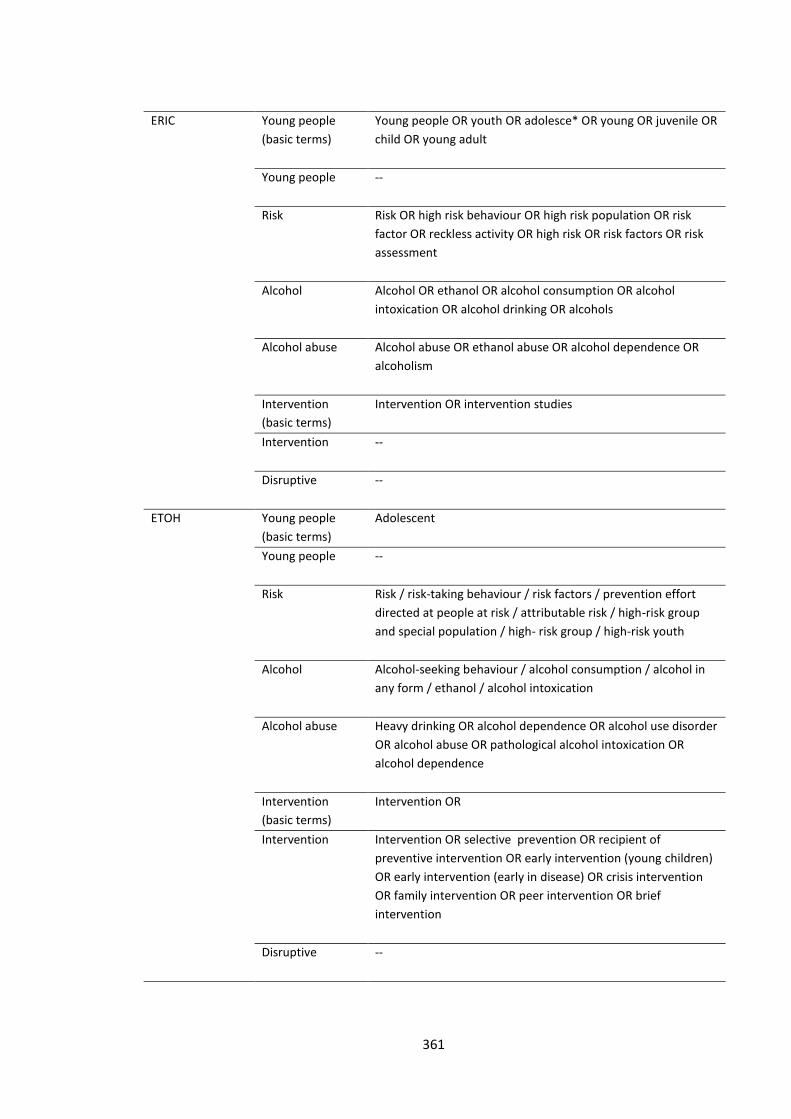
361
ERIC Young people
(basic terms)
Young people OR youth OR adolesce* OR young OR juvenile OR
child OR young adult
Young people --
Risk Risk OR high risk behaviour OR high risk population OR risk
factor OR reckless activity OR high risk OR risk factors OR risk
assessment
Alcohol Alcohol OR ethanol OR alcohol consumption OR alcohol
intoxication OR alcohol drinking OR alcohols
Alcohol abuse Alcohol abuse OR ethanol abuse OR alcohol dependence OR
alcoholism
Intervention
(basic terms)
Intervention OR intervention studies
Intervention --
Disruptive --
ETOH Young people
(basic terms)
Adolescent
Young people --
Risk Risk / risk-taking behaviour / risk factors / prevention effort
directed at people at risk / attributable risk / high-risk group
and special population / high- risk group / high-risk youth
Alcohol Alcohol-seeking behaviour / alcohol consumption / alcohol in
any form / ethanol / alcohol intoxication
Alcohol abuse Heavy drinking OR alcohol dependence OR alcohol use disorder
OR alcohol abuse OR pathological alcohol intoxication OR
alcohol dependence
Intervention
(basic terms)
Intervention OR
Intervention Intervention OR selective prevention OR recipient of
preventive intervention OR early intervention (young children)
OR early intervention (early in disease) OR crisis intervention
OR family intervention OR peer intervention OR brief
intervention
Disruptive --
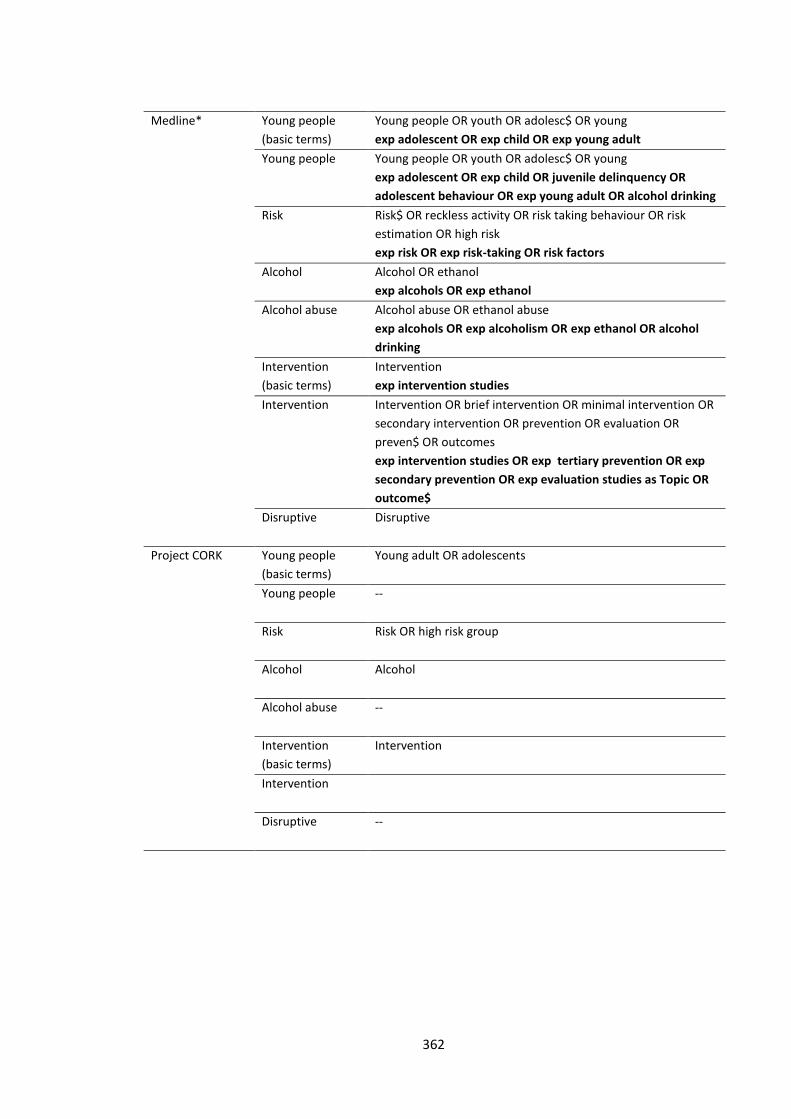
362
Medline* Young people
(basic terms)
Young people OR youth OR adolesc$ OR young
exp adolescent OR exp child OR exp young adult
Young people Young people OR youth OR adolesc$ OR young
exp adolescent OR exp child OR juvenile delinquency OR
adolescent behaviour OR exp young adult OR alcohol drinking
Risk Risk$ OR reckless activity OR risk taking behaviour OR risk
estimation OR high risk
exp risk OR exp risk-taking OR risk factors
Alcohol Alcohol OR ethanol
exp alcohols OR exp ethanol
Alcohol abuse Alcohol abuse OR ethanol abuse
exp alcohols OR exp alcoholism OR exp ethanol OR alcohol
drinking
Intervention
(basic terms)
Intervention
exp intervention studies
Intervention Intervention OR brief intervention OR minimal intervention OR
secondary intervention OR prevention OR evaluation OR
preven$ OR outcomes
exp intervention studies OR exp tertiary prevention OR exp
secondary prevention OR exp evaluation studies as Topic OR
outcome$
Disruptive Disruptive
Project CORK Young people
(basic terms)
Young adult OR adolescents
Young people --
Risk Risk OR high risk group
Alcohol Alcohol
Alcohol abuse --
Intervention
(basic terms)
Intervention
Intervention
Disruptive --
363
PsycINFO^ Young people
(basic terms)
Young people OR youth OR adolesc$ OR young
exp adolescent development OR exp juvenile delinquency
Young people --
Risk Risk
exp at risk populations OR exp risk factors OR exp risk taking
OR exp risk assessment
Alcohol Alcohol OR ethanol
exp alcohols OR exp ethanol
Alcohol abuse Alcohol abuse OR ethanol abuse OR alcohol dependence OR
alcohol drinking
exp alcohols OR exp alcoholism OR exp ethanol OR drug
abuse OR alcohol abuse
Intervention
(basic terms)
Intervention OR intervention studies
exp intervention
Intervention Intervention OR intervention studies
exp intervention OR exp crisis intervention OR exp crisis
intervention services OR exp family intervention OR exp
group intervention OR exp early intervention
Disruptive --
* ‘key-words’ in lowercase, ‘MeSH’ terms in bold
^ ‘key words’ in lowercase, explode terms in bold
# ‘key-words’ in lowercase, ‘EMTREE’ terms in bold





























