Embed Size (px)
Citation preview

C A C a n c e r J C l i n 1 9 9 6 ; 4 6 : 7 0 - 9 2
70 Ca—A cancer Journal for Clinicians
IntroductionAlthough occupationally related cancersmake up only a small fraction of all can-cers, many environmental carcinogenshave first been discovered in occupation-al settings. The estimate typically foundin the scientific literature is that abouttwo to eight percent of all human cancersare of occupational origin.1 However, byaveraging the unexposed population inwith the exposed, such estimates tend toobscure the heavy toll that occupationalcancer can take on specific populations ofexposed workers. Among persons actual-ly exposed to carcinogens at work, risk es-timates are much higher. For instance,Morabia et al2 have put the attributablerisk for lung cancer at 9.2 percent for menemployed in occupations characterizedby exposure to established carcinogens.For bladder cancer, the population attrib-utable risk from occupational exposuresmay exceed one case in five for men3 andone in ten for women.4
Indeed, despite the relatively small“contribution” that occupational cancer
makes to the total cancer burden, recog-nition and concern for cancers related toworkplace exposures have been centralthemes in control of environmental car-cinogens. There are several good reasonsfor this. One is the unique nature of theworkplace, which serves as a focal pointin which large numbers of people maybe exposed to high concentrations ofchemicals or other hazardous situations.Another is that the very nature of workcreates a cohort for the kinds of epidemi-ologic studies described below that canhelp establish a cause-effect relationshipbetween an environmental exposure andcancer. It is because of the exposures tolarge doses and the opportunities to im-plement effective procedures for risk as-sessment and control in the workplacethat the study of occupational cancerplays so important a role in the control ofcancer in general.
Finally, perhaps the most importantreason to identify occupational carcino-gens and to elucidate their role in cancercausation is that occupational cancersare, for the most part, entirely pre-ventable through appropriate engineer-ing, personnel practices, and strict gov-ernmental protective legislation.
The ultimate goal of collecting, eval-uating, and disseminating data on car-cinogenicity of occupational exposures isto develop strategies for prevention ofdisease. The most efficient strategy relieson primary prevention, that is, identifica-tion and elimination of sources of expo-
Cancer and the Workplace
Jeanne Mager Stellman, PhDSteven D. Stellman, PhD, MPH
Dr. Jeanne Stellman is an Associate Professor ofClinical Public Health in the Division of HealthPolicy and Management in the School of PublicHealth at Columbia University in New York, NewYork.
Dr. Steven Stellman is Chief of the Division ofEpidemiology at the American Health Foundationin New York, New York.
This work was supported in part by National CancerInstitute grants CA-17613, CA-63021, CA-68384,and CA-32617.
sure. Secondary prevention throughscreening of asymptomatic illness plays alesser role, but may still be valuable inspecific workplaces. Recent advances inmolecular biology have led to identifica-tion of tests that can identify workers ex-posed to various carcinogens. Such tests,however, are at present extremely expen-sive, and their predictive value is nogreater than that of traditional industrialhygiene workplace evaluations. Occupa-tional screening may have its greatestusefulness as a tool for educating workersto potential hazards in the workplace.
Identifying Human CarcinogensDespite the fact that more than six mil-lion chemicals have already been identi-fied and registered with the ChemicalAbstracts Service and more than 50,000are estimated to be regularly used in com-merce, probably fewer than 1,000 chemi-cals or exposure situations have beenscrutinized as to their potential for cancercausation.5 Even so, the literature onevaluation of cancer risks for even thissmall fraction of known exposures is mas-sive and not altogether consistent formany specific substances. Estimation ofactual cancer risks to humans requirescareful sifting and evaluation of largequantities of data from many differentstudies. Since the early 1970s, an exten-sive effort has been made to systematizethe available data on cancer risks. A com-prehensive methodology for assessmentof human cancer risks has been devel-oped by the International Agency for Re-search on Cancer (IARC) that draws ondata from a variety of disciplines.
The IARC methods, which arewidely regarded as definitive, rely on thejudgment of internationally recognizedexperts. Groups of scientists with exper-tise in various disciplines are convened todiscuss and summarize the literature onindividual carcinogens, groups of relatedcarcinogens, or in some cases entire in-dustries. These critical evaluations are ul-
timately presented as monographs, eachof which contains a critical evaluation ofthe carcinogenicity of one or more targetexposures. The evaluations take into ac-count many different types of informa-tion, including data from epidemiology,experimental studies on rodents and oth-er laboratory animals, in vitro studieswhere appropriate, and other relevantdata including toxicity, metabolism,genotoxicity, and metabolic studies.
According to the IARC, “Eachmonograph consists of a brief descriptionof the chemical and physical propertiesof the agent; methods for its analysis; adescription of the methods and volumesof production and use; data on occur-rence and human exposure; summariesof case reports and epidemiologic studiesof cancer in humans; summaries of ex-perimental carcinogenicity tests; a briefdescription of other relevant biologicdata, such as toxicity and genetic effects,that may indicate its possible mechanismof action; and an evaluation of its car-cinogenicity.”6 Because the IARC peri-odically revises its evaluations to reflectaccumulation of new data and evolutionof methods of assessment, the informa-tion in these monographs is generallycurrent and forms the basis of the sum-mary tables in this paper.
Categories of Carcinogenicity toHumansThe IARC classifies the evidence for car-cinogenicity of specific exposures intofour categories: sufficient, limited, or in-adequate evidence of carcinogenicity orevidence suggesting lack of carcinogenici-ty. Sufficient evidence of carcinogenicityimplies that a causal relationship hasbeen established between exposure to theagent, mixture, or exposure circumstanceand human cancer and that chance, bias,and confounding have been ruled outwith reasonable confidence.
Limited evidence of carcinogenicityimplies that a positive association has
C A C a n c e r J C l i n 1 9 9 6 ; 4 6 : 7 0 - 9 2
Vol. 46 No. 2 March/April 1996 71

been observed between exposure to theagent, mixture, or exposure circumstanceand cancer for which a causal interpreta-tion is considered to be credible, butchance, bias, or confounding cannot beruled out with reasonable confidence.
Inadequate evidence of carcino-genicity means that the available studiesare of insufficient quality, consistency, orstatistical power to permit a conclusionregarding the presence or absence of acausal association or that no data on can-cer in humans are available.
Evidence suggesting lack of carcino-genicity means that there are several ade-quate studies covering the full range ofexposure levels that human beings areknown to encounter that are mutuallyconsistent in not showing a positive asso-ciation between exposure to the agentand the studied cancer at any observedlevel of exposure.
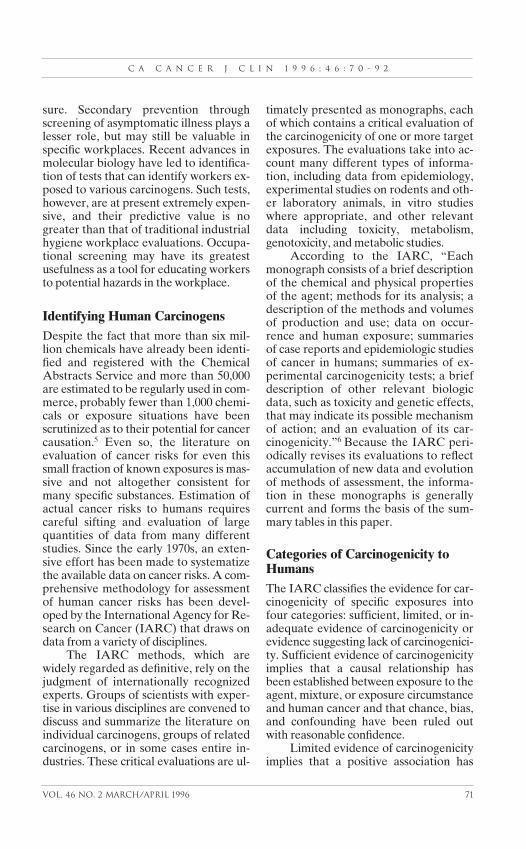
Criteria for EvaluatingCarcinogenicity Based on TotalEvidenceA set of criteria analogous to those for as-sessing risk in human studies is used toclassify cancer risk even when definitivehuman data are not available. Thisprocess takes into account informationfrom carcinogenesis bioassays and otherexperimental studies of animals alongwith toxicity and other biologic data. Theexpert committee deliberations take intoaccount epidemiologic, animal, and othertypes of data, including in vitro and meta-bolic studies where appropriate, fromwhich an overall assessment of carcino-genicity to humans is synthesized within ascheme that consists of four broadgroups. To date, 61 volumes of IARCMonographs have been published, and782 agents or exposure circumstanceshave been classified.
The distribution of these 782 agentsor exposure circumstances within the car-cinogenicity groupings is shown in Table1. Group 2, likely carcinogens, is subdi-
vided into Group 2A, probably carcino-genic to humans, and Group 2B, possiblycarcinogenic to humans. These catego-rizations take explicit note of the rele-vance of animal studies to human cancerrisk and are most often used to classifysubstances for which human data may belimited or inadequate but where animaldata are deemed sufficient and mechanis-tically relevant to humans (Group 2A) orless than sufficient but strongly support-ive of existing human data (Group 2B).
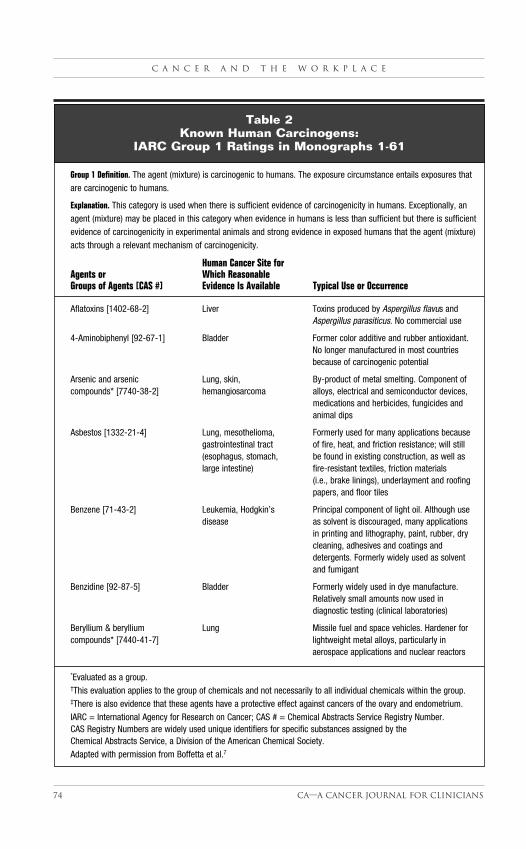
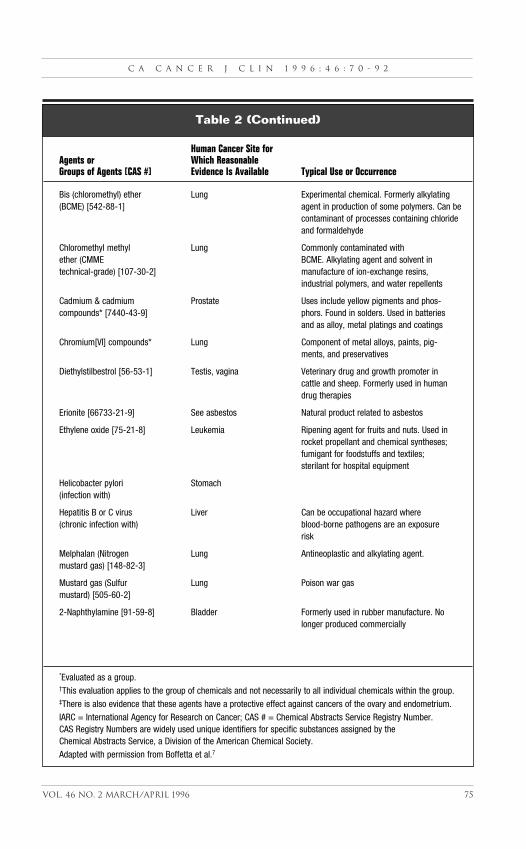
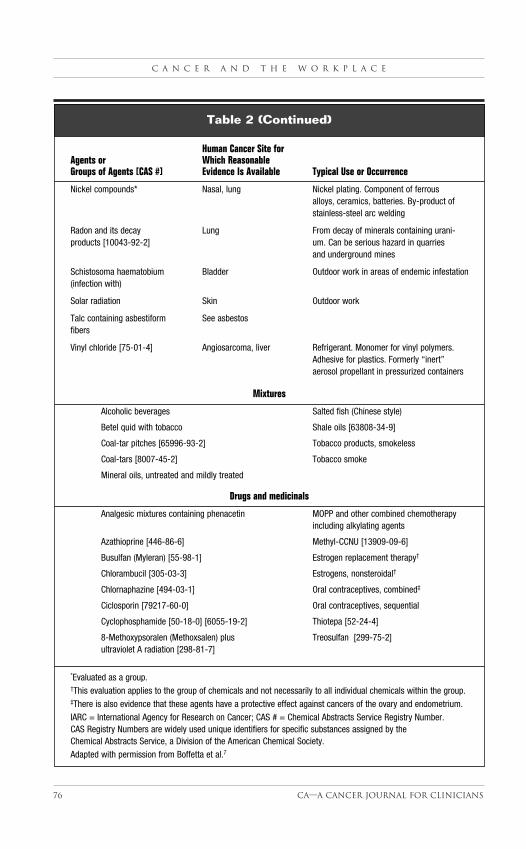
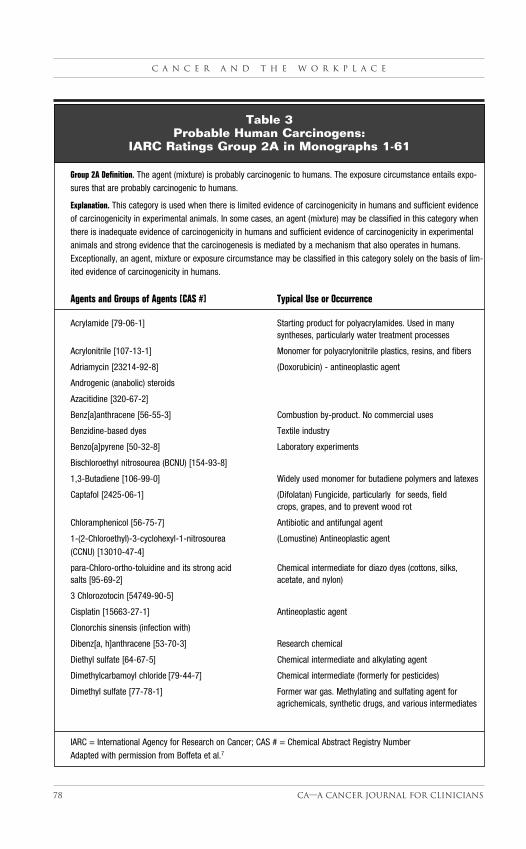
The seemingly large number ofagents denoted as carcinogenic or proba-bly carcinogenic (Groups 1 and 2A,N=117) is a reflection of the selectionprocess for inclusion in the monographs.Agents are generally evaluated only whensubstantial data bases already exist. Thesedata bases, in turn, have usually evolvedover a period of years in response to con-cerns of industry, workers, or the public.Tables 2 and 3 present the IARC Mono-graph groupings of known and probablehuman carcinogens (Groups 1 and 2A)and typical uses or occurrences.7 Table 4summarizes occupational exposure situa-tions that have been classified as fallinginto Groups 1, 2A, and 2B.
Some Examples of Exposures andControls in Health CareThe history of occupational cancer identi-fication and control has been recountedby many authors.8 The potential forwork-related cancers has been recog-nized at least since the work of Ramazziniin the sixteenth century, and in fact ourmodern understanding of the influence ofenvironmental factors on human canceris due in large measure to occupationalstudies, ironically many of them drawnfrom the exposures of people in thehealth care professions. Examination ofthe known and probable occupationalcarcinogens and exposure situations, giv-en in Tables 2 to 4, reveals a number thatare found in health care situations and forwhich work practices are still inadequate
C a n c e r a n d t h e w o r k p l a c e
72 Ca—A cancer Journal for Clinicians
to protect health care personnel with po-tential exposures.
X-rays provide a good case study.Much of the knowledge about the dan-gers of the industrial use of x-rays is basedon the “lamentable history” of the pio-neers in the medical field, according tooccupational medicine pioneer DonaldHunter.9 The first death recognized to bethe result of the action of x-rays occurredin 1914 to the Italian radiologist, EmilioTiraboschi. By 1922 at least one hundredradiologists had died from malignant dis-eases arising from their occupation. Muchof the natural course of radiation poison-ing was elucidated by following the pro-gression of disease among these early vic-tims. It is estimated that many hundredsof people have died as a result of occupa-tional exposures to medical x-rays.
The recognition of the potentialdeadliness of exposure to x-rays led tothe relatively early establishment of na-tional and international regulatory bod-ies, such as the International Commis-sion on Radiological Protection, whichwas formed in 1928. Important safety
concepts, such as maximum permissibledose, appropriate design and control ofx-ray equipment, and basic principlesfor the elimination of unnecessary expo-sures, were developed over the years,along with systems of administrative con-trol for registration and surveillance ofpeople occupationally exposed to radia-tion.
In many ways the control of expo-sure to x-rays is a paradigm for the basicprinciples for prevention of occupationalcancer. The primary means of preventionis to reduce exposure to x-rays. This is fa-cilitated by providing equipment de-signed to be as safe as possible and bytesting and maintaining the equipment ona specified schedule. Exposure is alsominimized through the use of appropriateshielding. Other preventive measures in-clude administrative procedures to con-trol potential exposures and rigorous pro-grams of registration and surveillance(medical record keeping and exposuremonitoring by radiation badges). All per-sonnel who work with x-rays must receivetraining, and some job categories require
C A C a n c e r J C l i n 1 9 9 6 ; 4 6 : 7 0 - 9 2
Vol. 46 No. 2 March/April 1996 73
Number of Agentsor ExposureSituations
Category Carcinogenicity (1972-1995)
Group 1: Carcinogenic to humans 66
Group 2A: Probably carcinogenic to humans 51
Group 2B: Possibly carcinogenic to humans 210
Group 3: Data insufficient to decide carcinogenicity 454
Group 4: Probably not carcinogenic to humans 1
Total Evaluated 782
Table 1International Agency for Research on Cancer
Assessments of Chemical Carcinogenicity
C a n c e r a n d t h e w o r k p l a c e
74 Ca—A cancer Journal for Clinicians
Group 1 Definition. The agent (mixture) is carcinogenic to humans. The exposure circumstance entails exposures thatare carcinogenic to humans.
Explanation. This category is used when there is sufficient evidence of carcinogenicity in humans. Exceptionally, anagent (mixture) may be placed in this category when evidence in humans is less than sufficient but there is sufficientevidence of carcinogenicity in experimental animals and strong evidence in exposed humans that the agent (mixture)acts through a relevant mechanism of carcinogenicity.
Human Cancer Site for Agents or Which ReasonableGroups of Agents [CAS #] Evidence Is Available Typical Use or Occurrence
Aflatoxins [1402-68-2] Liver Toxins produced by Aspergillus flavus andAspergillus parasiticus. No commercial use
4-Aminobiphenyl [92-67-1] Bladder Former color additive and rubber antioxidant.No longer manufactured in most countries because of carcinogenic potential
Arsenic and arsenic Lung, skin, By-product of metal smelting. Component ofcompounds* [7740-38-2] hemangiosarcoma alloys, electrical and semiconductor devices,
medications and herbicides, fungicides and animal dips
Asbestos [1332-21-4] Lung, mesothelioma, Formerly used for many applications because gastrointestinal tract of fire, heat, and friction resistance; will still(esophagus, stomach, be found in existing construction, as well as large intestine) fire-resistant textiles, friction materials
(i.e., brake linings), underlayment and roofing papers, and floor tiles
Benzene [71-43-2] Leukemia, Hodgkin’s Principal component of light oil. Although usedisease as solvent is discouraged, many applications
in printing and lithography, paint, rubber, dry cleaning, adhesives and coatings and detergents. Formerly widely used as solvent and fumigant
Benzidine [92-87-5] Bladder Formerly widely used in dye manufacture. Relatively small amounts now used in diagnostic testing (clinical laboratories)
Beryllium & beryllium Lung Missile fuel and space vehicles. Hardener forcompounds* [7440-41-7] lightweight metal alloys, particularly in
aerospace applications and nuclear reactors
*Evaluated as a group.†This evaluation applies to the group of chemicals and not necessarily to all individual chemicals within the group.‡There is also evidence that these agents have a protective effect against cancers of the ovary and endometrium.IARC = International Agency for Research on Cancer; CAS # = Chemical Abstracts Service Registry Number. CAS Registry Numbers are widely used unique identifiers for specific substances assigned by the Chemical Abstracts Service, a Division of the American Chemical Society.Adapted with permission from Boffetta et al.7
Table 2Known Human Carcinogens:
IARC Group 1 Ratings in Monographs 1-61
C A C a n c e r J C l i n 1 9 9 6 ; 4 6 : 7 0 - 9 2
Vol. 46 No. 2 March/April 1996 75
Human Cancer Site for Agents or Which ReasonableGroups of Agents [CAS #] Evidence Is Available Typical Use or Occurrence
Bis (chloromethyl) ether Lung Experimental chemical. Formerly alkylating(BCME) [542-88-1] agent in production of some polymers. Can be
contaminant of processes containing chloride and formaldehyde
Chloromethyl methyl Lung Commonly contaminated with ether (CMME BCME. Alkylating agent and solvent intechnical-grade) [107-30-2] manufacture of ion-exchange resins,
industrial polymers, and water repellents
Cadmium & cadmium Prostate Uses include yellow pigments and phos-compounds* [7440-43-9] phors. Found in solders. Used in batteries
and as alloy, metal platings and coatings
Chromium[VI] compounds* Lung Component of metal alloys, paints, pig-ments, and preservatives
Diethylstilbestrol [56-53-1] Testis, vagina Veterinary drug and growth promoter in cattle and sheep. Formerly used in human drug therapies
Erionite [66733-21-9] See asbestos Natural product related to asbestos
Ethylene oxide [75-21-8] Leukemia Ripening agent for fruits and nuts. Used in rocket propellant and chemical syntheses;fumigant for foodstuffs and textiles; sterilant for hospital equipment
Helicobacter pylori Stomach(infection with)
Hepatitis B or C virus Liver Can be occupational hazard where (chronic infection with) blood-borne pathogens are an exposure
risk
Melphalan (Nitrogen Lung Antineoplastic and alkylating agent.mustard gas) [148-82-3]
Mustard gas (Sulfur Lung Poison war gasmustard) [505-60-2]
2-Naphthylamine [91-59-8] Bladder Formerly used in rubber manufacture. No longer produced commercially
*Evaluated as a group.†This evaluation applies to the group of chemicals and not necessarily to all individual chemicals within the group.‡There is also evidence that these agents have a protective effect against cancers of the ovary and endometrium.IARC = International Agency for Research on Cancer; CAS # = Chemical Abstracts Service Registry Number. CAS Registry Numbers are widely used unique identifiers for specific substances assigned by the Chemical Abstracts Service, a Division of the American Chemical Society.Adapted with permission from Boffetta et al.7
Table 2 (Continued)
C a n c e r a n d t h e w o r k p l a c e
76 Ca—A cancer Journal for Clinicians
Human Cancer Site forAgents or Which ReasonableGroups of Agents [CAS #] Evidence Is Available Typical Use or Occurrence
Nickel compounds* Nasal, lung Nickel plating. Component of ferrous alloys, ceramics, batteries. By-product of stainless-steel arc welding
Radon and its decay Lung From decay of minerals containing urani-products [10043-92-2] um. Can be serious hazard in quarries
and underground mines
Schistosoma haematobium Bladder Outdoor work in areas of endemic infestation(infection with)
Solar radiation Skin Outdoor work
Talc containing asbestiform See asbestosfibers
Vinyl chloride [75-01-4] Angiosarcoma, liver Refrigerant. Monomer for vinyl polymers. Adhesive for plastics. Formerly “inert” aerosol propellant in pressurized containers
Mixtures
Alcoholic beverages Salted fish (Chinese style)
Betel quid with tobacco Shale oils [63808-34-9]
Coal-tar pitches [65996-93-2] Tobacco products, smokeless
Coal-tars [8007-45-2] Tobacco smoke
Mineral oils, untreated and mildly treated
Drugs and medicinals
Analgesic mixtures containing phenacetin MOPP and other combined chemotherapy including alkylating agents
Azathioprine [446-86-6] Methyl-CCNU [13909-09-6]
Busulfan (Myleran) [55-98-1] Estrogen replacement therapy†
Chlorambucil [305-03-3] Estrogens, nonsteroidal†
Chlornaphazine [494-03-1] Oral contraceptives, combined‡
Ciclosporin [79217-60-0] Oral contraceptives, sequential
Cyclophosphamide [50-18-0] [6055-19-2] Thiotepa [52-24-4]
8-Methoxypsoralen (Methoxsalen) plus Treosulfan [299-75-2]ultraviolet A radiation [298-81-7]
*Evaluated as a group.†This evaluation applies to the group of chemicals and not necessarily to all individual chemicals within the group.‡There is also evidence that these agents have a protective effect against cancers of the ovary and endometrium.IARC = International Agency for Research on Cancer; CAS # = Chemical Abstracts Service Registry Number. CAS Registry Numbers are widely used unique identifiers for specific substances assigned by the Chemical Abstracts Service, a Division of the American Chemical Society.Adapted with permission from Boffetta et al.7
Table 2 (Continued)

specific licensure. A regulatory structureprovides guidance and specifies the mini-mum legal requirements.
Cancer Chemotherapeutic Agents:An Apposite ExampleUnlike the medical use of x-rays, whichrepresents a paradigm for proper engi-neering and administrative controls inthe use of dangerous substances, the mix-ing and administration of cancer chemo-therapeutic agents provide an exampleof working conditions that have in manycases remained poorly conceived andcontrolled. The toxicity of drugs used asantineoplastics is well documented, yetuntil 1979, when a serendipitous experi-ment revealed elevated levels of muta-gens in the urine of nurses who adminis-ter the drugs,10 no routine precautionswere taken to prevent potential expo-sure, particularly to pharmacy and nurs-ing staff.
The major route for possible expo-sure arises from the aerosolization ofdrugs during mixing and administration.The presence of a vacuum in the syringein which drugs are dissolved and fromwhich they are administered leads to animperceptible spraying of droplets un-less a special “blow-back” device is used.Other preventive methods for avoidingcontamination include the use of chemi-cal hoods to provide exhaust ventilationduring mixing and the use of personalprotective equipment—such as dispos-able gloves, masks, and clothing—duringdrug administration. Such precautionsare straightforward, yet they are notroutinely followed in all health caresettings. Indeed, as the number of pa-tients requiring treatment with cancerchemotherapeutic agents grows and asthe availability of in-hospital facilitiesdecreases, one can envision that the pos-sibilities of occupational exposures willincrease rather than decrease.
Despite the extreme biologic poten-cy of antineoplastic drugs, including car-
cinogenicity, and the large number ofantineoplastic agents that appear on theIARC lists of known and probablehuman carcinogens, no regulations re-quiring safe handling procedures havebeen promulgated, although the Occupa-tional Safety and Health Administration(OSHA) published guidelines a few yearsafter the exposure became widely recog-nized.11 This is in sharp contrast to therapid growth of information, training,and regulation to control unnecessary ex-posure to medical x-rays. Thus, the ex-tent of current exposure among healthcare personnel to these drugs is notknown. While most major academicmedical centers have, in fact, incorporat-ed the recommended OSHA guidelinesinto their routine practices, many situa-tions still exist in physician offices andamong professionals who provide treat-ment at patient homes, for example, inwhich staff may be unnecessarily ex-posed to these drugs.
Epidemiology and OccupationalCancer Hazard IdentificationIdentification of human carcinogens in anoccupational setting is a laborious andtime-consuming process. Accumulationof enough evidence to classify a chemicalor exposure as Group 1 can take years ordecades. The process is an ongoing one,and lists such as those in Tables 2 to 4 arealways incomplete because (1) estab-lished exposures are periodically reevalu-ated as more data become available andas industrial practices and hence expo-sure situations shift and (2) new chemi-cals and exposures are constantly beingintroduced into the workplace.
Thus, health professionals, and clini-cians in particular, must be alert to thechanging spectrum of workplace expo-sures and the possibility that new expo-sure situations will lead to shifts in exist-ing patterns of disease and perhaps tonew occupational cancer hazards. Theprocess of identifying or confirming sus-
C A C a n c e r J C l i n 1 9 9 6 ; 4 6 : 7 0 - 9 2
Vol. 46 No. 2 March/April 1996 77
C a n c e r a n d t h e w o r k p l a c e
78 Ca—A cancer Journal for Clinicians
Group 2A Definition. The agent (mixture) is probably carcinogenic to humans. The exposure circumstance entails expo-sures that are probably carcinogenic to humans.
Explanation. This category is used when there is limited evidence of carcinogenicity in humans and sufficient evidenceof carcinogenicity in experimental animals. In some cases, an agent (mixture) may be classified in this category whenthere is inadequate evidence of carcinogenicity in humans and sufficient evidence of carcinogenicity in experimentalanimals and strong evidence that the carcinogenesis is mediated by a mechanism that also operates in humans.Exceptionally, an agent, mixture or exposure circumstance may be classified in this category solely on the basis of lim-ited evidence of carcinogenicity in humans.
Agents and Groups of Agents [CAS #] Typical Use or Occurrence
Acrylamide [79-06-1] Starting product for polyacrylamides. Used in many syntheses, particularly water treatment processes
Acrylonitrile [107-13-1] Monomer for polyacrylonitrile plastics, resins, and fibers
Adriamycin [23214-92-8] (Doxorubicin) - antineoplastic agent
Androgenic (anabolic) steroids
Azacitidine [320-67-2]
Benz[a]anthracene [56-55-3] Combustion by-product. No commercial uses
Benzidine-based dyes Textile industry
Benzo[a]pyrene [50-32-8] Laboratory experiments
Bischloroethyl nitrosourea (BCNU) [154-93-8]
1,3-Butadiene [106-99-0] Widely used monomer for butadiene polymers and latexes
Captafol [2425-06-1] (Difolatan) Fungicide, particularly for seeds, field crops, grapes, and to prevent wood rot
Chloramphenicol [56-75-7] Antibiotic and antifungal agent
1-(2-Chloroethyl)-3-cyclohexyl-1-nitrosourea (Lomustine) Antineoplastic agent(CCNU) [13010-47-4]
para-Chloro-ortho-toluidine and its strong acid Chemical intermediate for diazo dyes (cottons, silks, salts [95-69-2] acetate, and nylon)
3 Chlorozotocin [54749-90-5]
Cisplatin [15663-27-1] Antineoplastic agent
Clonorchis sinensis (infection with)
Dibenz[a, h]anthracene [53-70-3] Research chemical
Diethyl sulfate [64-67-5] Chemical intermediate and alkylating agent
Dimethylcarbamoyl chloride [79-44-7] Chemical intermediate (formerly for pesticides)
Dimethyl sulfate [77-78-1] Former war gas. Methylating and sulfating agent for agrichemicals, synthetic drugs, and various intermediates
IARC = International Agency for Research on Cancer; CAS # = Chemical Abstract Registry NumberAdapted with permission from Boffeta et al.7
Table 3Probable Human Carcinogens:
IARC Ratings Group 2A in Monographs 1-61
C A C a n c e r J C l i n 1 9 9 6 ; 4 6 : 7 0 - 9 2
Vol. 46 No. 2 March/April 1996 79
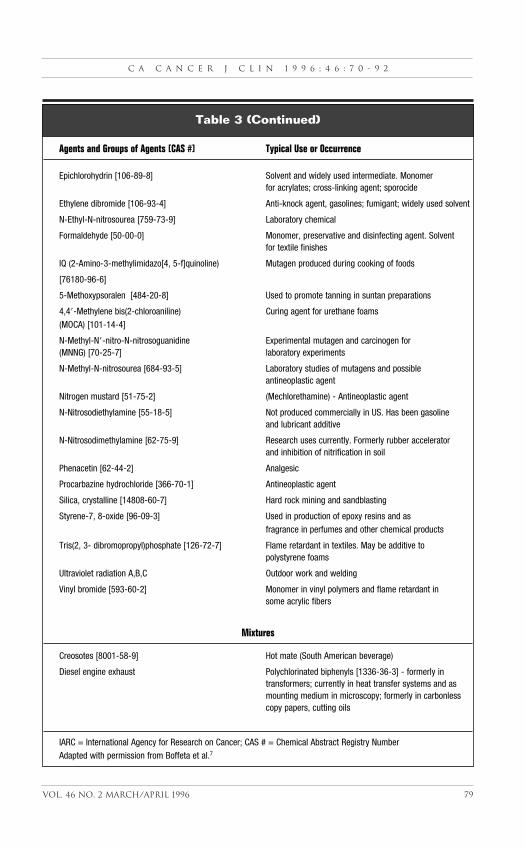
Agents and Groups of Agents [CAS #] Typical Use or Occurrence
Epichlorohydrin [106-89-8] Solvent and widely used intermediate. Monomerfor acrylates; cross-linking agent; sporocide
Ethylene dibromide [106-93-4] Anti-knock agent, gasolines; fumigant; widely used solvent
N-Ethyl-N-nitrosourea [759-73-9] Laboratory chemical
Formaldehyde [50-00-0] Monomer, preservative and disinfecting agent. Solvent for textile finishes
IQ (2-Amino-3-methylimidazo[4, 5-f]quinoline) Mutagen produced during cooking of foods
[76180-96-6]
5-Methoxypsoralen [484-20-8] Used to promote tanning in suntan preparations
4,4�-Methylene bis(2-chloroaniline) Curing agent for urethane foams(MOCA) [101-14-4]
N-Methyl-N�-nitro-N-nitrosoguanidine Experimental mutagen and carcinogen for(MNNG) [70-25-7] laboratory experiments
N-Methyl-N-nitrosourea [684-93-5] Laboratory studies of mutagens and possible antineoplastic agent
Nitrogen mustard [51-75-2] (Mechlorethamine) - Antineoplastic agent
N-Nitrosodiethylamine [55-18-5] Not produced commercially in US. Has been gasoline and lubricant additive
N-Nitrosodimethylamine [62-75-9] Research uses currently. Formerly rubber acceleratorand inhibition of nitrification in soil
Phenacetin [62-44-2] Analgesic
Procarbazine hydrochloride [366-70-1] Antineoplastic agent
Silica, crystalline [14808-60-7] Hard rock mining and sandblasting
Styrene-7, 8-oxide [96-09-3] Used in production of epoxy resins and as fragrance in perfumes and other chemical products
Tris(2, 3- dibromopropyl)phosphate [126-72-7] Flame retardant in textiles. May be additive to polystyrene foams
Ultraviolet radiation A,B,C Outdoor work and welding
Vinyl bromide [593-60-2] Monomer in vinyl polymers and flame retardant in some acrylic fibers
Mixtures
Creosotes [8001-58-9] Hot mate (South American beverage)
Diesel engine exhaust Polychlorinated biphenyls [1336-36-3] - formerly in transformers; currently in heat transfer systems and as mounting medium in microscopy; formerly in carbonless copy papers, cutting oils
IARC = International Agency for Research on Cancer; CAS # = Chemical Abstract Registry NumberAdapted with permission from Boffeta et al.7
Table 3 (Continued)
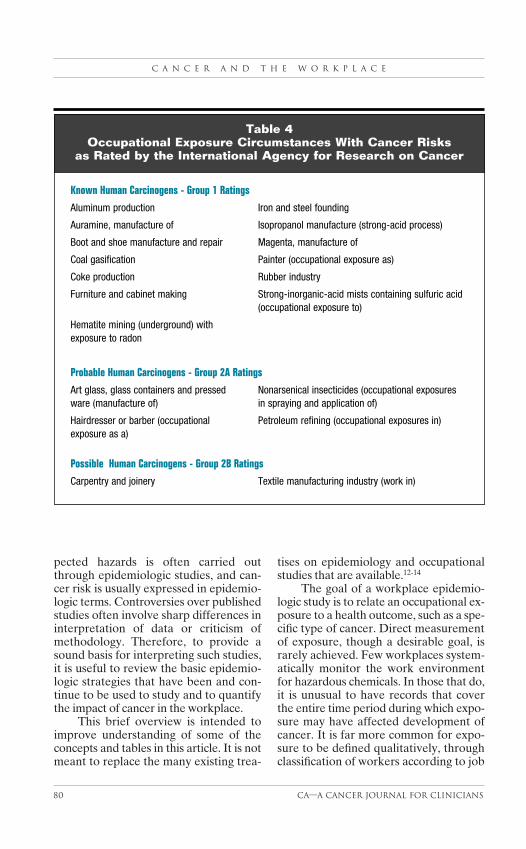
pected hazards is often carried outthrough epidemiologic studies, and can-cer risk is usually expressed in epidemio-logic terms. Controversies over publishedstudies often involve sharp differences ininterpretation of data or criticism ofmethodology. Therefore, to provide asound basis for interpreting such studies,it is useful to review the basic epidemio-logic strategies that have been and con-tinue to be used to study and to quantifythe impact of cancer in the workplace.
This brief overview is intended toimprove understanding of some of theconcepts and tables in this article. It is notmeant to replace the many existing trea-
tises on epidemiology and occupationalstudies that are available.12-14
The goal of a workplace epidemio-logic study is to relate an occupational ex-posure to a health outcome, such as a spe-cific type of cancer. Direct measurementof exposure, though a desirable goal, israrely achieved. Few workplaces system-atically monitor the work environmentfor hazardous chemicals. In those that do,it is unusual to have records that coverthe entire time period during which expo-sure may have affected development ofcancer. It is far more common for expo-sure to be defined qualitatively, throughclassification of workers according to job
C a n c e r a n d t h e w o r k p l a c e
80 Ca—A cancer Journal for Clinicians
Known Human Carcinogens - Group 1 Ratings
Aluminum production Iron and steel founding
Auramine, manufacture of Isopropanol manufacture (strong-acid process)
Boot and shoe manufacture and repair Magenta, manufacture of
Coal gasification Painter (occupational exposure as)
Coke production Rubber industry
Furniture and cabinet making Strong-inorganic-acid mists containing sulfuric acid (occupational exposure to)
Hematite mining (underground) with exposure to radon
Probable Human Carcinogens - Group 2A Ratings
Art glass, glass containers and pressed Nonarsenical insecticides (occupational exposuresware (manufacture of) in spraying and application of)
Hairdresser or barber (occupational Petroleum refining (occupational exposures in)exposure as a)
Possible Human Carcinogens - Group 2B Ratings
Carpentry and joinery Textile manufacturing industry (work in)
Table 4Occupational Exposure Circumstances With Cancer Risks
as Rated by the International Agency for Research on Cancer
title, work location, or industry of em-ployment. For studies based solely ondeath certificates, the recorded occupa-tion and/or industry serves as an exposuresurrogate.
In recent years occupational studieshave frequently used industrial hygieniststo help reconstruct likely exposure sce-narios. In addition, a technique that usesa “job exposure matrix” has been devel-oped to assign probable exposures to var-ious combinations of occupations andindustries of employment.15 Finally, ex-posure to toxic chemicals is sometimes es-timated from human-derived measure-ment of the chemicals themselves, theirmetabolites, or other effects of their in-teraction with biologic materials, such asadducts with DNA. These methods arecollectively known as biomarker meth-ods.16 While biomarker methods are be-coming increasingly popular, their relia-bility still remains to be fully established,chiefly because they usually require ex-trapolation from current or relatively re-cent measurements to exposures thatmay have taken place in the distant pastwhen carcinogenic effects may have, infact, been more relevant.
Types of Epidemiologic StudiesCASE REPORTS AND SENTINEL EVENTS
The appearance of a highly unusual can-cer, such as angiosarcoma of the liver inchemical workers or scrotal cancer inchimneysweeps,17 or the appearance ofan otherwise common cancer among agroup ordinarily at low risk, such as lungcancer in very young workers exposed tobis (chloromethyl) ether, is termed a sig-nal cancer. The first identified chemicalcarcinogen, �-naphthylamine, was dis-covered in 1895 after an astute clinicianreported a large excess of bladder cancerin chemical dye industry workers.18,19
Vinyl chloride was first identified asa human carcinogen following reports ofangiosarcoma of the liver in chemical
workers. Animal studies showing car-cinogenicity of vinyl chloride appeared atabout the same time as the case reports.20
Angiosarcoma of the liver is so rare thatfew physicians ever see such a patient in alifetime of practice, yet three workerswere diagnosed in a brief period in a tireplant in Kentucky in 1974.21
Bis (chloromethyl) ether, an un-wanted by-product in the production ofpolymeric resins, was initially reported in1971 as a lung carcinogen by a pulmonaryphysician at a local hospital serving thearea of residence of many Rohm & Haasworkers in Philadelphia,22 but only afterthe workers themselves identified a num-ber of their colleagues who had contract-ed the disease.23
A signal cancer is a special case of asentinel health event, which was definedby Rutstein et al24 as a preventable dis-ease, disability, or untimely death whoseoccurrence serves as a warning signal of apotentially hazardous situation that mayrequire investigation and correction. Thediscovery of a signal or sentinel cancer, ifpromptly and properly followed up, canresult in identification and elimination ofan unsuspected hazard. However, sen-tinel health events rarely occur, andworkplace cancer hazards are more oftendiscovered through clinical observationsand traditional epidemiologic methods. Itshould be noted that unlike many currentepidemiologic investigations, which focuson “weak associations” (i.e., those char-acterized by a risk increase smaller thantwofold), many of the occupational car-cinogens in Tables 2 and 3 were originallyrecognized because their effects were suf-ficiently large to be noticeable at the clini-cal level.
ECOLOGIC STUDIES
All modern countries systematically col-lect data on cause of death in their popu-lation. Ecologic studies are built on thehypothesis that workers in specific indus-tries may have higher rates of cancer than
C A C a n c e r J C l i n 1 9 9 6 ; 4 6 : 7 0 - 9 2
Vol. 46 No. 2 March/April 1996 81

the general population. By comparingcancer death rates in those industries withpopulation rates of the same cancers,conclusions as to whether workers are atincreased risk can be drawn. The advan-tage of this type of analysis is that itmakes use of existing death records and,therefore, requires no new data acquisi-tion—provided occupational informationis available. The drawback is that suchdata normally do not contain any infor-mation about exposures of individuals tospecific substances. The primary contri-bution of this descriptive epidemiology isto uncover new associations between par-ticular occupations or industries and dis-ease. The drawback of ecologic methodsis that they are very weak tools that areinadequate to establish cause-effect rela-tionships.25 Stronger methods requirecomparison of cancer risks betweengroups of people with and without estab-lished exposures. These are often provid-ed by analytic methods such as cohortand case-control studies.
In Great Britain, the Registrar-Gen-eral (equivalent to the National Centerfor Health Statistics in the United States)has published “Decennial Supplements”to the vital statistics reports that specifi-cally compare age-adjusted death rates ofworkers in various occupations and in-dustries with each other and with the gen-eral population.26 These valuable reportshave identified, for instance, the high rateof lung cancer in woodworkers, which hasbeen confirmed in other studies.27
In the Nordic countries, where citi-zens are assigned identification numbersthat are used in a variety of governmen-tal data systems, census data can belinked electronically with occupationaldata and with cancer registration data topermit direct calculation of cancer ratesin workers in specific industries. A num-ber of studies of occupational cancerhave been published on workers in Den-mark,28 Norway,29 and Sweden.30 Bylinking census data with national cancerregistries, a collaborative group found
increased risks for bladder and lung can-cer in hairdressers in Denmark, Norway,and Sweden.31
ANALYTIC EPIDEMIOLOGY
The most common types of epidemiolog-ic studies are those in which exposuresand health outcomes are determined forindividuals. Many treatises now exist thatexplain the application of analytic epi-demiology to occupational cancer.32-36
The two study methodologies most com-monly encountered are cohort studiesand case-control studies. In ideal circum-stances, they ought to yield equivalent re-sults, but in practice the availability ofworkers and the quality of work-relatedrecords and/or measurements usually dic-tate choice of study design.
In a typical cohort or follow-upstudy, a group of workers with some com-mon characteristic, such as employmentin a target industry or well-characterizedexposure to a known hazardous sub-stance, is identified as of a specific timeand their vital status (in a mortality study)or cancer occurrence (in an incidencestudy) is ascertained as of a later time.Subjects may be identified throughrecords and followed into the present orfuture (a design sometimes called retro-spective), or they may be identified cur-rently and followed up prospectively. Theclassic studies of Selikoff et al37 on as-bestos insulation workers that linked as-bestos exposure to cancer of the lung andother sites were of this design. Occupa-tional cohorts have been used to investi-gate the etiology of cancer in workers ex-posed to sulfuric acid mists,38 in rubberworkers,39 and in workers occupationallyexposed to formaldehyde.40
Cancer risk as determined by a co-hort study is commonly expressed as astandard incidence ratio (SIR) or stan-dard mortality ratio (SMR), depending onwhether the outcome is a newly diagnosedcancer or cancer death. The simplest SIR(or SMR) is calculated as the number of
C a n c e r a n d t h e w o r k p l a c e
82 Ca—A cancer Journal for Clinicians
observed cases (or deaths) in a populationexposed to a suspected carcinogen dividedby the number expected based on rates inan unexposed population (the referenceor control group). SIRs and SMRs areusually adjusted statistically for possibleconfounding factors, most commonly age.
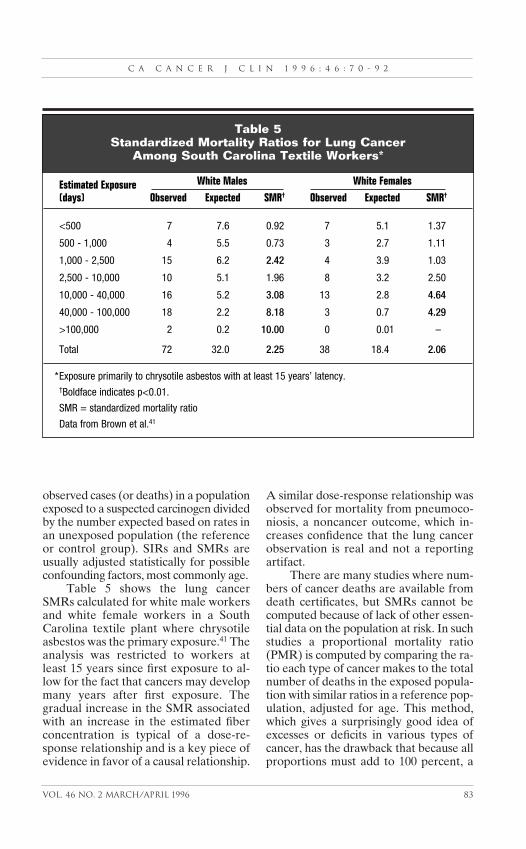
Table 5 shows the lung cancerSMRs calculated for white male workersand white female workers in a SouthCarolina textile plant where chrysotileasbestos was the primary exposure.41 Theanalysis was restricted to workers atleast 15 years since first exposure to al-low for the fact that cancers may developmany years after first exposure. Thegradual increase in the SMR associatedwith an increase in the estimated fiberconcentration is typical of a dose-re-sponse relationship and is a key piece ofevidence in favor of a causal relationship.
A similar dose-response relationship wasobserved for mortality from pneumoco-niosis, a noncancer outcome, which in-creases confidence that the lung cancerobservation is real and not a reportingartifact.
There are many studies where num-bers of cancer deaths are available fromdeath certificates, but SMRs cannot becomputed because of lack of other essen-tial data on the population at risk. In suchstudies a proportional mortality ratio(PMR) is computed by comparing the ra-tio each type of cancer makes to the totalnumber of deaths in the exposed popula-tion with similar ratios in a reference pop-ulation, adjusted for age. This method,which gives a surprisingly good idea ofexcesses or deficits in various types ofcancer, has the drawback that because allproportions must add to 100 percent, a
C A C a n c e r J C l i n 1 9 9 6 ; 4 6 : 7 0 - 9 2
Vol. 46 No. 2 March/April 1996 83
Estimated Exposure White Males White Females
(days) Observed Expected SMR† Observed Expected SMR†
<500 7 7.6 0.92 7 5.1 1.37
500 - 1,000 4 5.5 0.73 3 2.7 1.11
1,000 - 2,500 15 6.2 2.42 4 3.9 1.03
2,500 - 10,000 10 5.1 1.96 8 3.2 2.50
10,000 - 40,000 16 5.2 3.08 13 2.8 4.64
40,000 - 100,000 18 2.2 8.18 3 0.7 4.29
>100,000 2 0.2 10.00 0 0.01 –
Total 72 32.0 2.25 38 18.4 2.06
*Exposure primarily to chrysotile asbestos with at least 15 years’ latency.†Boldface indicates p<0.01.
SMR = standardized mortality ratio
Data from Brown et al.41
Table 5Standardized Mortality Ratios for Lung Cancer
Among South Carolina Textile Workers*
PMR for one particular cause may artifi-cially appear to be very high or very low ifsome other common cause of death, suchas heart disease, is unusually high or lowin the study population. Nevertheless, thePMR method is well accepted as an inex-pensive and valid way to obtain a firstlook at a possible cancer problem.
In the United States, the ready avail-ability of death certificates, many ofwhich list the industry and occupation ofthe decedent, makes PMR analysis a use-ful screen for unexpected cancer risks.The US National Institute for Occupa-tional Safety and Health supports an oc-cupationally coded data base of deathcertificates containing nearly five millionentries. This data base has been used toevaluate age-adjusted and race-specificPMRs for women in eleven broad occu-pational groupings and over 400 specific
occupations.42,43 For both white and blackwomen, significantly elevated lung cancerPMRs were noted for the categories ofexecutive-managerial, technician, sales,administrative support (clerical), preci-sion production, and operator-laborer.
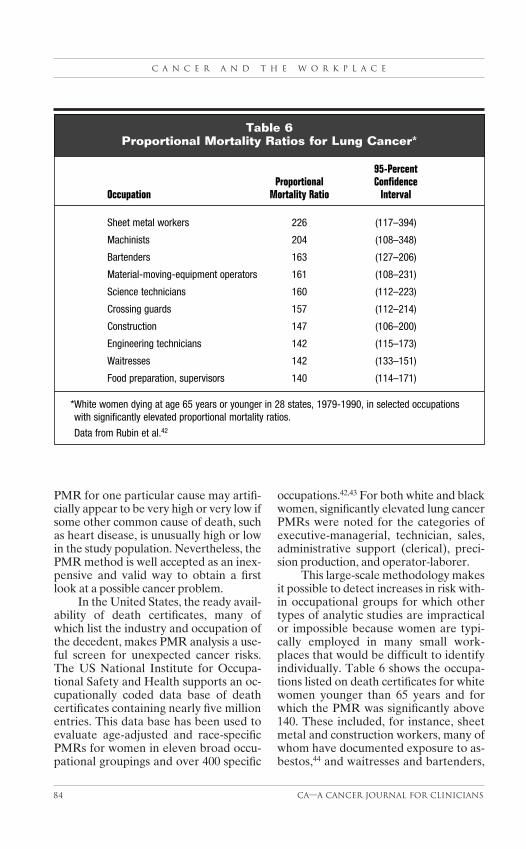
This large-scale methodology makesit possible to detect increases in risk with-in occupational groups for which othertypes of analytic studies are impracticalor impossible because women are typi-cally employed in many small work-places that would be difficult to identifyindividually. Table 6 shows the occupa-tions listed on death certificates for whitewomen younger than 65 years and forwhich the PMR was significantly above140. These included, for instance, sheetmetal and construction workers, many ofwhom have documented exposure to as-bestos,44 and waitresses and bartenders,
C a n c e r a n d t h e w o r k p l a c e
84 Ca—A cancer Journal for Clinicians
95-PercentProportional Confidence
Occupation Mortality Ratio Interval
Sheet metal workers 226 (117–394)
Machinists 204 (108–348)
Bartenders 163 (127–206)
Material-moving-equipment operators 161 (108–231)
Science technicians 160 (112–223)
Crossing guards 157 (112–214)
Construction 147 (106–200)
Engineering technicians 142 (115–173)
Waitresses 142 (133–151)
Food preparation, supervisors 140 (114–171)
*White women dying at age 65 years or younger in 28 states, 1979-1990, in selected occupationswith significantly elevated proportional mortality ratios.
Data from Rubin et al.42
Table 6Proportional Mortality Ratios for Lung Cancer*

among whom the prevalence of cigarettesmoking is higher than for many otheroccupations.45
A case-control study is conducted byidentifying subjects who already havecontracted or died of a specific diseaseand comparing their exposures with ex-posures of subjects diagnosed with someother disease or with no disease at all. Acase-control study has the advantage ofbeing highly efficient for study of rare dis-eases such as cancer. It has two majorweaknesses. First, by definition it can beused to investigate only one disease out-come, whereas cohort studies provideinformation about practically all observ-able health outcomes. Second, case-con-trols studies are limited by the frequencywith which subjects with specific occupa-tions present at hospitals or die within thegeographic area where the study is car-ried out. The people who make up thecases may be identified through hospitalcanvass or by examining local or regionaltumor registries and subsequently inter-viewed. Cases may also be constructed byselecting decedents from death certificateregistries, in which case exposure infor-mation is ordinarily restricted to informa-tion recorded on the death certificate, al-though interviews with family membersare sometimes conducted.
The case-control design has beenused to study bladder cancer, for whichoccupational risks arise in chemical andother industries,46-48 and lung cancer inshipyard workers, many of whom havebeen exposed to high levels of asbestos.49
Cancer risks ascertained in case-con-trol studies are commonly expressed bymeans of an odds ratio, which is a statisti-cal estimate of the relative risk. Blot andFraumeni50 combined data from fourcase-control studies of lung cancer in re-lation to cigarette smoking and shipyardwork and reported a relative risk of 21.7for men employed as shipyard workerswho smoked at least two packs of ciga-rettes per day and a relative risk of 10.3for men who were not shipyard workers
but smoked two packs a day. The refer-ence group (relative risk, 1.0) was non-smoking, nonshipyard workers.
Case-control studies are less fre-quently used to screen occupations andindustries for increased risk, but the avail-ability of large data files has improved thefeasibility of this approach. Cantor et al51
examined death certificates covering over59,000 female breast cancer deaths in 24states from 1984 through 1989 that werecoded for occupation and industry. Theyused noncancer deaths from the samedata base as a comparison group. Afteradjusting for age and socioeconomic sta-tus, they reported suggestive associationsfor probability and level of exposure forstyrene, several organic solvents (methyl-ene chloride, carbon tetrachloride, andformaldehyde), several metals/metal ox-ides, and acid mists. Such associationswould have to be investigated in specificworkplaces before causal inferencescould be made.
Methodological Issues inEpidemiology StudiesBecause epidemiologic studies are obser-vational and thus are rarely subject to thetypes of controls that operate in experi-mental laboratory science, to be crediblethey must deal rigorously with method-ological issues. Some of the more impor-tant ones are described in this section.
Exposure assessment is obviously anessential element of any occupationalstudy. Exposures may be ascertainedthrough company records, which underfavorable circumstances might includeactual industrial hygiene measurementsof ambient levels of hazardous materials,or exposures may be inferred indirectlythrough job titles or even more crudely asemployment in a specific plant or indus-try. Obviously, the more informationavailable regarding exposures incurredby individuals, the more precisely cancerrisks can be related to such exposures.However, reconstruction of historical ex-
C A C a n c e r J C l i n 1 9 9 6 ; 4 6 : 7 0 - 9 2
Vol. 46 No. 2 March/April 1996 85
C a n c e r a n d t h e w o r k p l a c e
86 Ca—A cancer Journal for Clinicians
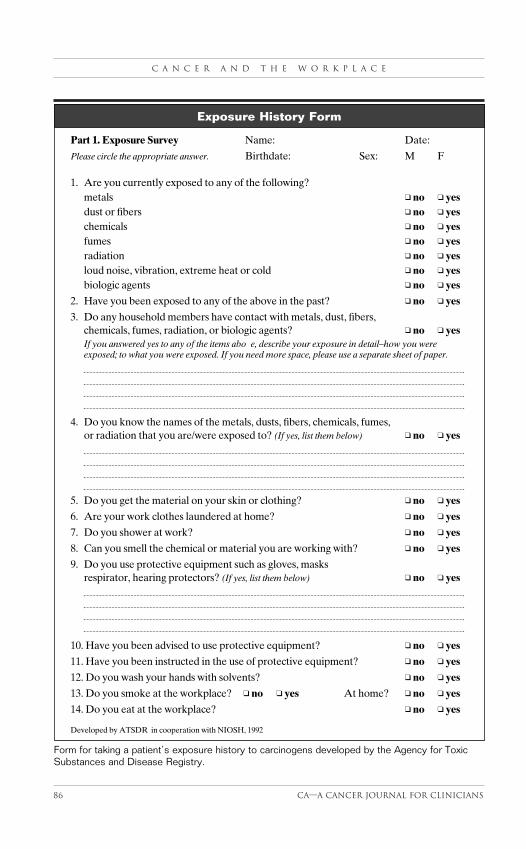
Part 1. Exposure Survey Name: Date:
Please circle the appropriate answer. Birthdate: Sex: M F
1. Are you currently exposed to any of the following?metals ❑ no ❑ yesdust or fibers ❑ no ❑ yeschemicals ❑ no ❑ yesfumes ❑ no ❑ yesradiation ❑ no ❑ yesloud noise, vibration, extreme heat or cold ❑ no ❑ yesbiologic agents ❑ no ❑ yes
2. Have you been exposed to any of the above in the past? ❑ no ❑ yes
3. Do any household members have contact with metals, dust, fibers, chemicals, fumes, radiation, or biologic agents? ❑ no ❑ yesIf you answered yes to any of the items above, describe your exposure in detail–how you were exposed; to what you were exposed. If you need more space, please use a separate sheet of paper.
4. Do you know the names of the metals, dusts, fibers, chemicals, fumes, or radiation that you are/were exposed to? (If yes, list them below) ❑ no ❑ yes
5. Do you get the material on your skin or clothing? ❑ no ❑ yes
6. Are your work clothes laundered at home? ❑ no ❑ yes
7. Do you shower at work? ❑ no ❑ yes
8. Can you smell the chemical or material you are working with? ❑ no ❑ yes
9. Do you use protective equipment such as gloves, masks respirator, hearing protectors? (If yes, list them below) ❑ no ❑ yes
10. Have you been advised to use protective equipment? ❑ no ❑ yes
11. Have you been instructed in the use of protective equipment? ❑ no ❑ yes
12. Do you wash your hands with solvents? ❑ no ❑ yes
13. Do you smoke at the workplace? ❑ no ❑ yes At home? ❑ no ❑ yes
14. Do you eat at the workplace? ❑ no ❑ yes
Developed by ATSDR in cooperation with NIOSH, 1992
Exposure History Form
Form for taking a patient’s exposure history to carcinogens developed by the Agency for ToxicSubstances and Disease Registry.
posures over a long period of time is chal-lenging and has been done accuratelyonly in a few industries.
In recent years exposure recordshave been supplemented by “biologicdosages,” exemplified by levels of certainchemicals in serum or other body fluids.52
As these biomarker methods becomemore refined, they will increasingly be in-corporated into future studies.
Outcome assessment is also impor-tant, particularly for cohort studies wherefailure to obtain complete follow-up dataon a proportion of the cohort might leadto biased results. Some occupational mor-tality studies rely solely on death certifi-
cates as a source of outcome data. Thissource may be less accurate for sometypes of cancer than for others.53
A basic concept of carcinogenesis islatency, the time from an initial exposureto a carcinogen to the clinical appearanceof disease. Latency of occupational can-cers is generally measured in decades.This greatly complicates the epidemio-logic study of these illnesses because ofthe difficulty of reconstructing past levelsof exposure. The latency for occupationalskin cancer can be as brief as one year. Incontrast, the latency for lung cancer at-tributed to exposure to bis (chloromethyl)ether was reported to range from eight to
C A C a n c e r J C l i n 1 9 9 6 ; 4 6 : 7 0 - 9 2
Vol. 46 No. 2 March/April 1996 87
The American College of Occupational and Environmental Medicine: 55West Seegers Road, Arlington Heights, IL 60005. Tel: 847-228-6850. Officialpublication: Journal of Occupational and Environmental Medicine.
The Association of Occupational and Environmental Clinics: 1010 VermontAvenue, NW Suite 513, Washington, DC 20005. Tel: 202-347-4976.
The National Institute for Occupational Safety and Health can provide a listof the Education Resource Centers established throughout the United States.Contact the NIOSH Division of Training and Manpower Development. Tel:1-800-536-4674.
The American Association of Poison Control Centers is a clearinghouse forRegional Poison Control Centers. Regional centers can be found in the bluepages of the telephone directory. Most operate under the aegis of the localdepartment of health.
The Agency for Toxic Substances and Disease Registries, a branch of theCenters for Disease Control and Prevention: 1600 Clifton Road, NE, Room3726 - Mail Stop E28, Atlanta, GA 30333. Tel: 404-639-0700.
The National Library of Medicine is connected to a vast network of on-linedata resources, including Medline, PDQ, and Toxnet. The library can be con-tacted directly by telephone at 301-496-6095. Many physicians andresearchers may already have access to these resources through their institu-tional libraries, which should be consulted first.
Appendix For Further Information

26 years,54 while the latency for bladdercancer can be more than 40 years.55
A second fundamental idea is thatexposure to certain combinations of car-cinogens can result in cancer risk that notonly exceeds the risk from exposure to ei-ther alone, but exceeds the risk from bothexposures combined. This phenomenonis known as synergism. The best knownsynergistic risk is that of lung cancer in as-bestos workers who also smoke ciga-rettes, which is at least fifty times the riskin nonsmoking asbestos workers.56
BIAS
Because epidemiologic studies are largelyobservational, their interpretation reliesstrongly on comparison of risks betweenpersons with and without disease or withand without exposure (depending on thestudy design). In either case, the informa-tion from the comparison group is as im-portant as that from the study group, andinformation from both groups is potential-ly subject to bias.57 Problems may arise ifcontrols are selected in a manner that isnot comparable to the way in which casesare selected. For instance, if cases are se-lected from a regional tumor registry andcontrols are selected through a popula-tion sampling method, such as random-digit telephone dialing, a low responserate among those called may result in abiased risk estimate based on those whoare actually contacted and interviewed.
Confounding is the introduction ofartifacts into risk estimates when criticalvariables, such as age, are distributed dif-ferently in a study group relative to con-trols. Confounding can be controlledthrough statistical methods, but onlywhen it is initially identified and relevantinformation on confounding variablescollected.58
Choice of an appropriate compari-son group is sometimes complicated bylack of acceptable alternatives. Compar-ison of death rates between a specificoccupational group and the general pop-
ulation is likely to be biased against re-porting an association due to the well-known healthy worker effect. This arisesbecause workers are recruited, possiblyvia medical screening, from a pool of peo-ple healthy enough to work in industrywhere continuation of employment isconditional on continued good health. Bycontrast, the general population, whichfurnishes the comparison rates, containspeople who are very sick. Therefore,death rates in an employed group are ex-pected to be lower than those of the gen-eral population even before consideringpossible work-related hazards.59
SAMPLE SIZE AND STATISTICAL POWER
A fundamental requirement of an epi-demiologic study is that there be enoughexposed workers or cases of the diseaseof interest to permit meaningful statisticaltesting. Where the relative risk is veryhigh, as with asbestos and lung cancer,this is less of a concern, but for cancersthat are very rare or where few peopleare exposed, even a well-designed studymight not uncover a provable effect dueto small numbers. A study by the Centersfor Disease Control that was originallydesigned to look for a possible relation-ship between exposure to phenoxy herbi-cides in Vietnam and nasal cancer inVietnam veterans had to be given up asinconclusive after only two of 48 veteransinterviewed were found to have actuallyseen Vietnam service.60
OTHER EXPOSURES
While studies of occupational cancers fo-cus by definition on potential carcino-genic exposures in the workplace, work-ers can be exposed to cancer-causing orcancer-preventing substances or condi-tions outside of the workplace. Cigarettesmoking is the most-recognized nonoccu-pational carcinogenic exposure, and it iswell recognized that information onsmoking habits should be collected when
C a n c e r a n d t h e w o r k p l a c e
88 Ca—A cancer Journal for Clinicians

feasible. Unfortunately, this is sometimesimpossible, especially in studies whereexposure data are reconstructed frompast employment and medical records orfrom death certificates.
Less well understood is the possibleinfluence of diet and nutrition on occupa-tional cancer. Fruits and vegetables havebeen associated with reduced lung cancerrisk in many studies, even after adjust-ment for smoking. In a large-scale,prospective study in Japan, Hirayama61
found independent (additive) effects foremployment as a “material metal work-er” and cigarette smoking on the risk ofdeath from lung cancer. The study alsofound an independent protective effectfor regular consumption of green-yellowvegetables. Nevertheless, few occupa-tional studies have actually taken nutri-tion into account as a possible etiologicfactor, and the negative association be-tween consumption of fruits and vegeta-bles with cigarette smoking62 makes it dif-ficult to generalize such findings tooccupational settings.
REPLICABILITY
The foregoing discussion has highlight-ed most of the methodological factorsthat must be considered in interpretingepidemiologic studies of occupationalcancer. However, even the most meticu-lous studies have limitations, often be-cause of imperfect estimation of expo-sure to specific substances over the longtime period during which cancer devel-ops. Acceptance by the scientific com-munity that a specific occupational ex-posure causes cancer nearly alwaysrequires replication by different investi-gators in a variety of populations or oc-cupational settings.
Evaluating Occupational Exposuresin a Clinical SettingIn this era of increased public awarenessand concern about occupational and en-
vironmental health hazards, cliniciansshould be alert to the possibility thatcancers may have occupational origins.This concern is appropriate if only be-cause it may lead to reduction of theharmful exposure for the patient and hisor her coworkers. As we have noted pre-viously, it is especially important to keepthe patient fully informed of any findingsrelating his or her illness to the work-place, as there may be many other work-ers who can benefit from this knowl-edge.63 Also, while physicians shouldtake every opportunity to counsel theirpatients who smoke to give up the habit,the possibility that smoking may exacer-bate cancer risk simply increases the im-portance of this step.
While there has been dramaticgrowth in the number of professionalswith formal training in occupational andenvironmental health and parallel growthin the resources available to clinicians fordiagnosing occupational diseases, mostclinicians require assistance when facedwith determining whether a particularcancer can be linked to an occupationalor environmental origin.
A work or exposure history is an es-sential component for diagnosis of an oc-cupational cancer. The Agency for ToxicSubstances and Disease Registry has de-veloped a form for taking a patient’s ex-posure history.64 The form (Figure) is de-signed for quick scanning of importantdetails. The form comprises three com-ponents: a survey of possible exposuresto physical and chemical agents, a workhistory of every job held over the work-ing lifetime, and an environmental histo-ry of hobbies and conditions in the homeenvironment that could be associatedwith the cancer.
In general, it is not necessary to un-derstand the jargon of a particular tradeto take an adequate exposure history. Ac-cording to the Agency for Toxic Sub-stances and Disease Registry, persistentquestioning by the clinician can clarifythe tasks involved in most jobs and can
C A C a n c e r J C l i n 1 9 9 6 ; 4 6 : 7 0 - 9 2
Vol. 46 No. 2 March/April 1996 89

reveal possible exposures. It may be, however, that further
technical information is required. Thiscan usually be obtained from the employ-er or a local government or university re-source. The American College of Occu-pational and Environmental Medicinecan provide a list of board-certified occu-pational physicians, and the Associationof Occupational and EnvironmentalClinics is a network of clinics affiliatedwith medical schools throughout theUnited States. The National Institute forOccupational Safety and Health has es-tablished Education Resource Centersthat can also provide information as wellas formal training opportunities. Oftenthe local Poison Control Center can pro-
vide specific information about the toxici-ty and health effects of hazardous expo-sures involved in poisonings. This may beof use in attempting to evaluate the morechronic effects generally associated withlong-term environmental exposures. Fi-nally, systematic and extensive informa-tion is now available in electronic formaton the toxicology of thousands of chemi-cals used in the occupational environ-ment. Many are available on CD-ROM.The National Library of Medicine inBethesda, MD, and the Agency for ToxicSubstances and Disease Registry in At-lanta, Ga, are two important resourcesfor obtaining such information. The Ap-pendix lists addresses and telephonenumbers for these resources.
C a n c e r a n d t h e w o r k p l a c e
90 Ca—A cancer Journal for Clinicians
References1. Doll R, Peto R: The Causes of Cancer:Quantitative Estimates of Avoidable Risks ofCancer in the United States Today. New York,Oxford University Press, 1981.2. Morabia A, Markowitz S, Garibaldi K, WynderEL: Lung cancer and occupation: Results of a mul-ticentre case-control study. Br J Ind Med 1992;49:721-727.3. Goldstein MD, Brandt-Rauf PW: Bladder car-cinogens and surveillance, in Rom WN (ed):Environmental and Occupational Medicine.Boston, Little, Brown, 1992, pp. 881-886.4. Silverman DT: Occupational risks of bladder can-cer among white women in the United States. Am JEpidemiol 1990;132:453-461.5. Agency for Toxic Substances and DiseaseRegistry: Annual Report. Atlanta, United StatesPublic Health Service, 1993.6. Vainio H, Wilbourn J: Approaches to hazardidentification, in Stellman JM (ed): Encyclopedia ofOccupational Health and Safety, ed 4. Geneva,ILO, in press.7. Boffetta P, Saracci R, Kogevinas M, et al:Occupational carcinogens, in Stellman JM (ed):Encyclopedia of Occupational Health and Safety,ed 4. Geneva, ILO, in press.8. Schottenfeld D, Haas JF: Carcinogens in theworkplace. CA Cancer J Clin 1979;29:144-168.9. Hunter D: The Diseases of Occupations, ed 4.Boston, Little, Brown, 1969.10. Falck K, Grohn P, Sorsa M, et al: Mutagenicityin urine of nurses handling cytostatic drugs. Lancet1979;1:1250-1251. Letter.11. Occupational Safety and Health Adminis-
tration: Guidelines for Handling of CancerChemotherapeutic Drugs. Washington, DC, USDepartment of Labor, 1986.12. Breslow N, Day N: Statistical Methods inCancer Research. Vol. 1: The Analysis of Case-Control Studies. Lyon, International Agency forResearch on Cancer, 1980.13. Breslow N, Day N: Statistical Methods inCancer Research. Vol. 2: The Design and Analysisof Cohort Studies. Lyon, International Agency forResearch on Cancer, 1987.14. Checkoway H, Pearce N, Crawford-Brown DJ:Research Methods in Occupational Epidemiology.New York, Oxford University Press, 1989. 15. Siemiatycki J, Dewar R, Richardson L: Costsand statistical power associated with five methodsof collecting occupation exposure information forpopulation-based case-control studies. Am JEpidemiol 1989;130:1236-1246.16. Hemminki K: Use of chemical, biochemical, andgenetic markers in cancer epidemiology and riskassessment. Am J Ind Med 1992;21:65-76.17. Pott P: Chirurgical observations relative to thecataract, the polypus of the nose, the cancer of thescrotum, the different kinds of ruptures, and themortification of the toes and feet. London, Hawes,Clarke, & Collins, 1775, in Natl Cancer Inst Monogr1962;10:7-13.18. Rehn L: Blasengeschwülste bei fuchsin-arbeit-ern. Arch Klin Chir 1895;50:588-600.19. Case RA, Pearson JT: Tumors of the urinarybladder in workmen engaged in the manufactureand use of certain dyestuff intermediates in theBritish chemical industry. Part II. Further consider-ation of the role of aniline (fuchsine) as possible
CA
causative agents. Br J Indust Med 1954;11:213-216.20. Viola PL, Bigotti A, Caputo A: Oncogenicresponse of rat skin, lungs, and bones to vinyl chlo-ride. Cancer Res 1971;31:516-519.21. Falk H, Creech JL Jr, Heath CW Jr, et al:Hepatic disease among workers at a vinyl chloridepolymerization plant. JAMA 1973;230:59-63.22. Figueroa WG, Raszkowski R, Weiss W: Lungcancer in chloromethyl methyl ether workers. NEngl J Med 1973;288:1096-1097.23. Randall WS, Solomon SD: Building 6: TheTragedy at Bridesburg. Boston, Little, Brown, 1977.24. Rutstein DD, Mullan RJ, Frazier TM, et al:Sentinel health events (occupational): A basis forphysician recognition and public health surveil-lance. Am J Public Health 1983;73:1054-1062.25. Marsh G: Epidemiology of occupational dis-eases, in Rom WN (ed): Environmental andOccupational Medicine, ed 2. Boston, Little,Brown, 1992, pp. 35-50.26. Logan WP: Cancer mortality by occupation andsocial class: 1851-1971. IARC Sci Publ 1982;36:1-253.27. Stellman SD, Garfinkel L: Cancer mortalityamong woodworkers. Am J Ind Med 1984;5:343-357.28. Lynge E: A follow-up study of cancer incidenceamong workers in manufacture of phenoxy herbi-cides in Denmark. Br J Cancer 1985;52:259-270.29. Hilt B, Andersen A, Rosenberg J, Langard S:Cancer incidence among asbestos-exposed chemi-cal industry workers: An extended observationperiod. Am J Ind Med 1991;20:261-264.30. Jakobsson R, Ahlbom A, Bellander T,Lundberg I: Acute myeloid leukemia among petrolstation attendants. Arch Environ Health 1993;48:255-259.31. Skov T, Andersen A, Malker H, et al: Risk forcancer of the urinary bladder among hairdressers inthe Nordic countries. Am J Ind Med 1990;17:217-223.32. Monson RR: Occupational Epidemiology, ed 2.Boca Raton, Fla, CRC Press, 1990.33. Checkoway H, Pearce N, Dement JM: Designand conduct of occupational epidemiology studies:I. Design aspects of cohort studies. Am J Ind Med1989;15:363-373.34. Checkoway H, Pearce N, Dement JM: Designand conduct of occupational epidemiology studies:II. Analysis of cohort data. Am J Ind Med 1989;15:375-394.35. Pearce N, Checkoway H, Dement JM: Designand conduct of occupational epidemiology studies:III. Design aspects of case-control studies. Am JIndust Med 1989;15:395-402.36. Pearce N, Checkoway H, Dement JM: Designand conduct of occupational epidemiology studies:IV. The analysis of case-control data. Am J IndMed 1989;15:403-416.37. Selikoff IJ, Hammond EC, Seidman H:Mortality experience of insulation workers in theUnited States and Canada: 1943-1976. Ann NYAcad Sci 1979;330:91-116.
38. Steenland K, Beaumont J: Further follow-upand adjustment for smoking in a study of lung can-cer and acid mists. Am J Ind Med 1989;16:347-354.39. Monson RR, Nakano KK: Mortality among rub-ber workers. I. White male union employees inAkron, Ohio. Am J Epidmiol 1976;103:284-296.40. Blair A, Stewart PA, O’Berg M, et al: Mortalityamong industrial workers exposed to formalde-hyde. J Natl Cancer Inst 1986;76:1071-1084.41. Brown DP, Dement JM, Okun A: Mortality pat-terns among female and male chrysotile asbestostextile workers. J Occup Med 1994;36:882-888.42. Rubin CH, Burnett CA, Halperin WE,Seligman PJ: Occupation and lung cancer mortalityamong women: Using occupation to target smokingcessation programs for women. J Occup Med1994;36:1234-1238.43. Rubin CH, Burnett CA, Halperin WE,Seligman PJ: Occupation as a risk identifier forbreast cancer. Am J Public Health 1993;83:1311-1315.44. Muscat JE, Stellman SD, Wynder EL:Insulation, asbestos, smoking habits, and lung can-cer cell types. Am J Ind Med 1995;27:257-269.45. Stellman SD, Boffetta P, Garfinkel L: Smokinghabits of 800,000 American men and women inrelation to their occupations. Am J Ind Med1988;13:43-58.46. Cole P, Hoover R, Friedell GH: Occupation andcancer of the lower urinary tract. Cancer 1972;29:1250-1260.47. Wynder EL, Goldsmith R: The epidemiology ofbladder cancer: A second look. Cancer 1977;40:1246-1268.48. Siemiatycki J, Dewar R, Nadon L, Gerin M:Occupational risk factors for bladder cancer:Results from a case-control study in Montreal,Quebec, Canada. Am J Epidemiol 1994;140:1061-1080.49. Blot WJ, Harrington JM, Toledo A, et al: Lungcancer after employment in shipyards during WorldWar II. N Engl J Med 1978;229:620-624.50. Blot WJ, Fraumeni JF Jr: Cancer among ship-yard workers, in Peto R, Schneiderman M (eds):Banbury Report 9: Quantification of OccupationalCancer. Cold Spring Harbor, NY, Cold SpringHarbor Laboratory, 1981.51. Cantor KP, Stewart PA, Brinton LA, DosemeciM: Occupational exposures and female breast can-cer mortality in the United States. J Occup EnvironMed 1995;37:336-348.52. Fingerhut MA, Halperin WE, Marlow DA, etal: Cancer mortality in workers exposed to 2,3,7,8-tetrachlorodibenzo-p-dioxin. N Engl J Med 1991;324:212-218.53. Percy C, Stanek E, Gloeckler L: Accuracy ofcancer death certificates and its effect on cancermortality statistics. Am J Public Health 1981;71:242-250.54. Lemen RA, Johnson WM, Wagoner JK, et al:Cytologic observations and cancer incidence fol-lowing exposure to BCME. Ann NY Acad Sci1976;271:71-80.
C A C a n c e r J C l i n 1 9 9 6 ; 4 6 : 7 0 - 9 2
Vol. 46 No. 2 March/April 1996 91
55. Goldwater LJ, Rosso AJ, Kleinfeld M: Bladdertumors in a coal tar dye plant. Arch Environ Health1965;11:814-817.56. Stellman SD: Interactions between smoking andother exposures: Occupation and Diet, inHoffmann D, Harris C (eds): Banbury Report No.23, Mechanisms in Tobacco Carcinogenesis. ColdSpring Harbor, NY, Cold Spring HarborLaboratory, 1986, pp. 377-393.57. Wynder EL, Stellman SD: The “over-exposed”control group. Am J Epidemiol 1992;135:459-461.58. Stellman SD: Workshop on guidelines to theepidemiology of weak associations: Confounding.Prev Med 1987;16:165-182.59. Fox AJ, Collier PF: Low mortality rates inindustrial cohort studies due to selection for workand survival in the industry. Br J Prev Soc Med1976;30:225-230.60. The Selected Cancers Cooperative Study
Group: The association of selected cancers with ser-vice in the US military in Vietnam. III. Hodgkin’sdisease, nasal cancer, nasopharyngeal cancer, andprimary liver cancer. Arch Intern Med 1990;150:2495-2505.61. Hirayama T: Diet and cancer. Nutr Cancer1979;1:67-81.62. Stellman SD: Chairman’s Remarks, in GarfinkelL, Ochs O, Mushinski M (eds): Selection, Follow-up, and Analysis in Prospective Studies: AWorkshop. Natl Cancer Inst Monogr 1985;67:145-147.63. Stellman SD, Stellman JM: Women’s occupa-tions, smoking, and cancer and other diseases. CACancer J Clin 1981;31:29-43.64. Agency for Toxic Substances and DiseaseRegistry: Taking an Exposure History, Case Studiesin Environmental Medicine #26. Atlanta, US PublicHealth Service, 1992.
C a n c e r a n d t h e w o r k p l a c e
92 Ca—A cancer Journal for Clinicians
American Cancer Society and International Union Against Cancer On-Line Information Resources
The American Cancer Society and the International Union Against Cancerboth have sites on the World Wide Web offering information resources for pa-tients and health care professionals.
The American Cancer Society’s site provides general information about programs and events, meetings, publications, and grants and awards and alsoincludes educational information about cancer, including fact sheets and data on various topics. The site also features information on breast cancer through the Society’s Breast Cancer Network. The Internet address is http://www.cancer.org. For further information, call Derrick Wheeler at 404-329-7931.
The International Union Against Cancer’s site includes information aboutprograms and publications, a calendar of events, and a membership directory.The site also allows membership access to GLOBALink, an electronic net-work designed to serve those active in tobacco control, cancer control, andpublic health. Sponsored by the Europe Against Cancer Programme and theAmerican Cancer Society, GLOBALink provides members of the networkwith electronic services including news bulletins, electronic conferences, inter-active forums, electronic mail, and full text data bases. The Internet address ishttp://www.uicc.ch/. For further information, contact International UnionAgainst Cancer GLOBALink Department, 3, rue du Conseil-General, 1205Geneva-Switzerland, telephone +41 22 809 18 50; fax +41 22 809 18 10; e-mail:[email protected].





























