Embed Size (px)
Citation preview

INT’L. J. AGING AND HUMAN DEVELOPMENT, Vol. 69(3) 221-244, 2009
CAREGIVERS—WHO COPES HOW?*
NEENA L. CHAPPELL
CARREN DUJELA
University of Victoria, British Columbia
ABSTRACT
Within gerontological caregiving research, there is a major emphasis on
stresses and burdens of this role. Yet there has been little attention directed
toward the coping strategies that caregivers engage in to cope with this role
and the factors that influence their adoption of different coping strategies.
This article examines coping strategies and change in coping strategy over a
1-year period. In particular the differential importance of caregiver capacity
(such as social support, health, and personality) compared with careload
(such as hours of caregiving and need of the care recipient) is examined
within a path model. Data came from a purposive sample of caregivers
experiencing heavy demands. Overall, problem-focused coping is used
more often than emotion-focused coping (either positive or negative) or
seeking social support, but caregivers use all types simultaneously. Caregiver
capacity, specifically neuroticism, is the strongest predictor of problem-
focused coping with those high in neuroticism less likely to use this strategy.
High neuroticism also predicts less use overall and negative emotion-
focused coping strategies. Few significant predictors emerge of change; those
that did were caregiver capacity, not careload variables. The use of all coping
strategies, except seeking social support which remained stable, decreased
over a 1-year period.
*The research reported here was funded by the Social Sciences & Humanities Research Council
of Canada in a grant to Chappell.
221
� 2009, Baywood Publishing Co., Inc.
doi: 10.2190/AG.69.3.d
http://baywood.com

INTRODUCTION
Much emphasis in gerontological research on caregiving has focused on the
stress and burden experienced by these individuals (George, 1987, 1990;
Vitaliano, Young, & Russo, 1991). Despite this focus, data reveal that, at any one
time, the majority of caregivers are not overly burdened (Chappell & Litkenhaus,
1995; Vitaliano & Zhang, 2004). Rather, while experiencing burden, most
caregivers are able to simultaneously meet their demands without becoming
dysfunctional (Schulz & Williamson, 1991) and are able to name satisfactions
derived from this role (Chappell, Reid, & Dow, 2001). Compared with the
overwhelming interest in the stress and burden of caregiving, there is less research
on how most caregivers cope with this role despite the demands placed on them.
The long tradition of research on coping (Folkman & Moskowitz, 2004) tends
to not focus on caregivers. In fact, in the late 1990s Gignac and Gottlieb (1997)
noted that research on coping in the area of chronic stress was almost non-existent.
While the research that examines coping among caregivers has been growing
over the last half dozen years, it is almost entirely on the relationship between
coping and caregiver outcomes such as well-being and is especially targeted to
caregivers of those living with Alzheimer’s disease (Garity, 1997; Kneebone &
Martin, 2003). In contrast, this article examines coping per se, that is, not as a
mediator between the demands of caregiving and caregiver well-being. Rather,
it examines the types of coping strategies caregivers use, the co-existence of
different types of coping, and change in the use of coping strategies over a 1-year
period. It also examines who uses what type of coping, that is, the caregiver
capacities (such as caregiver social support, health, and personality) versus
careload (referring to the demands of caregiving) as predictors of coping strategy.
The data are from a sample of caregivers to care recipients living in the com-
munity (not restricted to only those with dementia).
LITERATURE REVIEW
Coping, the thoughts and behaviors used to manage the internal and external
demands of situations that are appraised as stressful (Folkman & Moskowitz,
2004), has received widespread attention outside of gerontology since the 1970s
and 80s. The most frequently cited types of coping strategies are problem-
focused and emotion-focused (Shaw et al., 1997). While problem-focused coping
has been related to better outcomes and emotional-focused coping to more
distress, results are mixed (Folkman & Moskowitz, 2004). Hooker, Frazier, and
Monahan (1994) name social support as the third commonly identified coping
strategy and conclude after their review of the literature that mixed results
are also evident when relating it to outcomes. Also popular for classifying
coping strategies are distinctions based on topological features rather than
functions. The most popular classification is approach versus avoidance with
the distinction between whether the activity is oriented toward or away from
222 / CHAPPELL AND DUJELA

the stressor (Skinner, Edge, Altman, & Sherwood, 2003). In this instance
approach and avoidance can each include cognitive and emotional activity.
However, problem solving and support seeking are typically considered approach
strategies whereas emotional and escape actions are typically considered
avoidance strategies.
Others such as Stanton, Kirk, Cameron, and Donoff-Burg (2000) note that
emotional coping may be adaptive in the short term. Garity (1997) argues that
problem-focused forms of coping are often used in encounters appraised as
changeable and emotion-focused coping in encounters considered unchangeable.
Furthermore, while initially problem-focused and emotion-focused strategies
were viewed as exclusive of one another, subsequent research has established that
different coping strategies often co-occur although one type may predominate
(O’Rourke & Cappeliez, 2002).
Like the research on coping generally, that focused on caregivers is also replete
with different conceptualizations and operationalizations of the different types
of coping (O’Rourke & Cappeliez, 2002; Skinner et al., 2003) and often reports
inconsistent findings. After their review of research on coping by family care-
givers of persons with dementia, Gottlieb and Wolfe (2002) conclude that the
cross-sectional designs, different coping and outcome measures, lack of
specificity and incomparability of target stressors, and the reliance on retro-
spective reports mean that the interpretability of the cumulative body of empirical
findings is questionable. Kneebone and Martin (2003), however, conclude other-
wise. After their review of coping among those caring for persons with dementia
in the community, they conclude that there is a general tendency toward problem
solving and acceptance strategies of coping to be advantageous (for a more
recent study, see Wells, Dywan, & Dumas, 2005).
Irrespective of whether a particular type of coping strategy is ultimately
judged to be positive or negative, it is also important to understand which
caregivers adopt particular types of coping strategies, a topic about which there
is little known. This article seeks to address this gap in knowledge concerning
who uses what coping techniques, that is, the predictors of different coping
strategies by caregivers.
Both the general gerontological caregiving literature and that specifically on
coping strategies suggest the potential importance of caregiver capacities and
careload for differentially distinguishing the type of coping strategy caregivers are
most likely to adopt. Like the conceptualizations of coping style, the predictors
chosen for study tend to vary considerably and findings are mixed. The extent
to which the relative absence of an examination of indirect, as well as direct,
effects of potential influences might account for differential findings is unknown.
Borrowing from the popular stress process model (originally proposed by Pearlin,
Mullan, Semple, & Skaff, 1990) designed to examine caregiver outcomes such
as well-being, background characteristics can be added as another potential
factor preceding primary stressors and current caregiver capacity. If coping
CAREGIVERS—WHO COPES HOW? / 223

strategy is specified as the caregiver outcome, then careload and demands can be
viewed as primary stressors, predicting coping strategy that could have direct
and/or indirect effects on coping style. If indirect, they could act through caregiver
capacity (including personality and social support) to affect coping strategy.
This model is specified in Figure 1.
Demands of the caregiving situation can affect the coping strategy adopted by
the caregiver. For example, Dell’Aquila (2003) find among caregivers to persons
suffering from Parkinson’s disease, that the more time spent as a caregiver the
less the caregiver uses seeking social support coping strategy. While much
research has reported that behavioral problems of care recipients are particularly
difficult for caregivers (see, for example, Chappell & Penning, 1996), the effects
of problem behaviors on the adoption of different coping strategies are unknown.
The illness suffered by the care recipient and/or the stage of that disease could
also affect caregiving coping strategies.
Caregiver capacities include social support caregivers draw on. While there is
much research on social support in old age (Lawrence, Tennestedt, & Assmann,
1998; Vachon, 1999), little examines social support as a predictor of coping.
Dell’Aquila (2003) reports the larger the social network the more likely caregivers
seek social support as a coping strategy but no relationship with emotion-focused
coping. However, some have found that it is the quality and not the quantity of
social support that has the most influence on well-being (Deal, Dunst, & Trivette,
1989), so it could be that those with “better” social relationships are more likely
to seek social support from others. One might speculate that availability of others
and in particular availability of others who are assisting with caregiving might
lead to a greater use of seeking social support. There is also some suggestion
that, depending on the relationship one has with the care recipient, different types
of coping may or may not be effective. Quayhagen and Quayhagen (1988) report
that, among spouses, but not daughters, problem solving, help seeking, and
low self-blame are effective in relation to well-being. Conversely, Knight (1992)
224 / CHAPPELL AND DUJELA
Direct and Indirect Paths to Coping Styles
Context/BackgroundCharacteristics
Primary Stressor/Careload
Mediators/CaregiverCapacity
Outcome Coping/Strategy
– Age– Gender
– Care receiverphysical relatedhealth problems
– Social support– Personality– Caregiver health
– Problem focused– Emotion focused– Negative emotion– Positive emotion– Seeking social
support
Figure 1. Predicting caregiver coping strategy, a modified stressprocess model (Pearlin et al., 1990).

reports no significant differences between spouse caregivers and other types of
caregivers, in terms of help seeking.
Caregiver personality is another potential caregiver resource. Little of the per-
sonality literature examines its importance for determining coping strategies and
even less applies to informal caregivers to seniors. Hooker and colleagues (1994)
though find that neuroticism is significantly related to both problem-focused and
emotion-focused coping but not social support coping among a sample of spouse
caregivers to persons with dementia. Among the non-caregiver research, high
hardy individuals (consisting of a sense of personal control, commitment to people
and activities which one is involved, and perceiving change as a challenge) have
been found to use more approach or problem-focused types of coping strategies
and low hardy individuals to use more avoidance or emotion-focused coping
(Florian, Mikulincer, & Taubman, 1995; Maddi, 1999; Soderstrom, Dolbier,
Leiferman, & Steinhardt, 2000). Among family caregivers of disabled older
adults, Clark (1998) finds those with higher hardiness use more overall transfor-
mational coping (including help-seeking). Sussman (2003) finds caregiver hardi-
ness positively related to problem-focused and support seeking coping strategies
and negatively associated with wishful thinking and avoidant coping strategies
among caregivers to persons with Alzheimer’s disease living in institutions.
Hardiness is sometimes viewed as an aspect of resilience (the ability to
withstand and rebound from crisis and adversity or the ability to transform disaster
into a growth experience and move forward) (Bergeman & Wallace, 1999; Polk,
1997; Walsh, 1996). Resilience is believed to consist of high levels of self-esteem,
personal control, and optimism. Optimism has been associated with use of problem-
focused coping and seeking social support (Scheier, Weintraub, & Carver, 1986).
Braithwaite (1996) reported that caregivers with low personal resiliency had
higher burden, more psychiatric symptoms, and poorer affect but did not examine
the effect of resiliency on the differing use of coping strategies among caregivers.
Different ways of approaching situations and putting forth one’s experience
influence how situations are viewed (McCrae, 1996). The ability to tolerate
change and a willingness to make adjustments to new or different situations
characterizes Openness to Experience. Those individuals who are high in
Openness tend to be more imaginative and creative (McCrae, 1987); they demon-
strate an interest in considering other options and are less fearful of taking risks
(Flynn, 2005). Openness differentiates those who are original, liking variety,
and interested in academic and artistic endeavors from those who are more
conventional, down-to-earth, and preferring routine.
In terms of caregiver health, Dell’Aquila (2003) finds that the more stress
caregivers report, the more likely they are to use seeking social support as a coping
strategy but that global stress or time spent in caregiving is related to neither
problem-solving or emotion-focused coping. Whether caregivers experiencing
worse health seek additional social support is not known but one could speculate
that their own health could affect the coping strategies they use.
CAREGIVERS—WHO COPES HOW? / 225

Contextual background factors include age and gender. Empirical studies on
the effect of age are extremely limited; those which exist are contradictory.
Stephens and colleagues (1988) find that younger caregivers are more likely
to use escape/avoidance coping. On the other hand, Folkman, Lazarus, Pimley,
and Novacek (1987) report that older people are more likely to use passive
interpersonal emotion-focused forms of coping partially because they appraise
their encounters as less changeable than do younger people. Gender has received
attention in the coping literature with the argument that men are more task-
oriented and therefore more likely to use problem solving whereas women are
more likely to use emotion-focused coping. However, research tends to find
that women are more likely to use emotion-focused coping strategies but no
gender difference in the use of problem solving (Folkman et al., 1987; Kvam &
Lyons, 1991; Soderstrom et al., 2000) although some studies show men use more
approach or problem-focused coping (Holahan, Moos, Holahan, & Brennan,
1995; Ptacek, Smith, & Dodge, 1994).1*
In sum, this article examines different coping strategies used by informal
caregivers to older adults to gain understanding about who among caregivers is
more likely to adopt which type of coping strategy, more specifically, to assess
the differential contributions of caregiver capacities and careload in the choice
of coping strategy. Analyses begin by examining the predominance of different
coping strategies and their co-existence. Multi-variate analyses assess the pre-
dictors of different coping strategies at t1 using path models to assess both
direct and indirect effects. In particular, the article assesses the role of personality
factors (specifically resilience, hardiness, neuroticism, and openness to experi-
ence), social support, and demands on caregivers as potential predictors of coping
styles. Sex and age are introduced as background variables. Change in coping
styles between t1 and 1 year later are then examined.
METHODS
Data were collected in face-to-face interviews, lasting on average 2 hours
4 minutes, with caregivers to persons age 65 or over living in the community
from April 2003 to January 2004, in greater Victoria, British Columbia, Canada
and communities “up island” from greater Victoria to 1½ hours drive. The
sample was purposive, obtained through referrals from a variety of health service
agencies, such as the Family Caregivers’ Network, the Alzheimer’s Society, and
the Geriatric Outreach program within the local area. Agencies were asked to
refer those who, in their opinion, were providing heavy caregiving. Once referred,
individuals were screened to assess whether they were providing care for a
minimum of 4 hours/3 days/week. This criterion was created by an expert steering
committee that included caregivers and health care service providers who worked
226 / CHAPPELL AND DUJELA
1*See “Endnotes” and end of chapter for all footnotes.

with seniors, to target those providing heavy caregiving. It exceeds the cutoff
of over 3 hours/week that Keefe and Rosenthal (2000) found differentiated
employed caregivers to elderly relatives from those providing no help, on both
cultural and structural dimensions. In total, 92 caregivers were included; 52
(56.5%) were interviewed in greater Victoria and 40 (43.5%) “up island.”
Caregivers were re-interviewed 1 year later. At t2 N = 80 or 87% of the
original sample. Over the year, caregivers increased the numbers of hours per
week of care on average by 2, bringing the sample 0 to 88; those living with
the care recipient decreased, down from 63% to 48.8%. At t2 21% of care
receivers were in an institution and 14% were deceased; 65% were living in
the community, of whom 75% were living with the caregiver. Data were collected
from informal caregivers, irrespective of the illness of the care recipient because
our interest was in the use of coping strategies in the general population of
informal caregivers to counter the general focus in the literature on caregivers
only to those with dementia.
The primary variable of interest was coping. The brief Ways of Coping Scale
(WOC) which correlates highly with the long version (Folkman et al., 1987)
was used. First, respondents were asked to describe a time when they found it
difficult to cope with supporting the care recipient and the circumstances. Then
they were asked to respond to 31 items using a 4-point Likert scale for each item
ranging from 0 (not used) to 3 (used a great deal). The three most commonly
referenced strategies of coping were computed. Problem-solving coping consisted
of summing the items for the confrontive coping and planful coping (alpha = .69).
An emotion-focused scale combined distancing coping, control, accepting respon-
sibility, escape, and reappraisal (alpha = .72). Because emotion-focused coping
includes both negative-focused and positive-focused emotions, separate scales
measured each: negative emotion-focused coping included distancing coping,
control, and escape (alpha = .64). Positive emotion-focused coping included
accepting responsibility and reappraisal (alpha = .64). Seeking social support
consisted of the original five items comprising this scale in the WOC scale
(alpha = .75).
Change in coping strategy was computed using the Reliability Change Index
(RCI) consisting of t2-t1/SE meas. This classical approach is suitable when there
is no known intervening variable between t1 and t2, does not require uniform
distribution of the data and rules out high probability of measurement error. It
provides a means of assessing true change (Maassen, 2004; Wu & Hart, 2002).
Social support was measured with several items. A single item asked whether
they received unpaid assistance from anyone and was coded as 0, 1, 2, or 3+.
They were asked whether they received emotional support from family (0 = no;
1 = yes), their living arrangement (number of people in household) and their
marital status (married or not). They were asked about whether their relationship
with their care recipient had changed since they had begun caregiving and if
so, how (primarily negative – 1, no change – 2, primarily positive – 3). No one said
CAREGIVERS—WHO COPES HOW? / 227

it had not changed. The relationship of the caregiver to the care receiver was
also recorded (husband, wife, daughter, son, other).
The personality factors of resilience, hardiness, neuroticism, and openness to
experience were measured using five separate scales (alphas = .92; .85; .84, and
.60 respectively). The Resilience Scale (Wagnild & Young, 1990, 1993) is a
25-item measure of the positive emotional stamina people use to manage diffi-
cult life events. It uses a 7-point scale, from 1 (disagree) to 7 (agree) with a
higher score indicating more resilience. The Family Hardiness Index (McCubbin,
McCubbin, & Thompson, 1986) is a 20-item scale with four subscales (commit-
ment, confidence, challenge, and control) but the overall score has been shown
to be the best indicator of hardiness. It uses a 4-point scale from 0 (false) to
3 (totally true). The Big Five Test (Costa & McCrae, 1987) measured personality
traits. The BFT is a 25-item scale that uses 5 points from 1 (not at all true of
me) to 5 (very true of me); the neuroticism and openness to experience scales
were used here. Neuroticism is calculated by summing the reverse scored items
of tense, anxious, nervous, worrying, and self-pitying. Openness to experience
is calculated by summing the scores of imaginative, original, warm, outgoing,
and clever.
Measurement of the health of the caregiver included the number of chronic
conditions: “For each problem that I read, please tell me if this health issue is
something that you are currently managing or facing in your life”; conditions
included: high blood pressure or hypertension (with or without medication);
coronary heart disease, stroke, or effects of stroke; paralyses or paraplegia;
Parkinson’s disease; other neurological problems; eye trouble not relieved by
glasses; ear trouble including hearing loss, etc. The number of chronic conditions
was summed. Perceived health was measured: “For your age, would you say,
in general, your health is excellent, good for your age, fair for your age, poor for
your age, or bad for your age.” Because poor and bad response categories had
so few responses, they were combined.
Demands of caregiving were measured in terms of the health of the care receiver
and other characteristics of the caregiving role. Functional disability was asked
in terms of the level of assistance required with daily activities, coded as requires
no assistance or requires assistance for each of a list of 14 areas such as: bathing;
toileting; using the telephone; transportation; and financial responsibilities
(alpha = .78). Chronic conditions of the care receiver were asked using the same
question as above in relation to the caregiver but in reference to the care recipient.
Behavioral problems of the care receiver were also asked: “Do you have to
deal with behavioral problems?” Categories were: verbal agitation, physically
non-aggressive, and physically aggressive behavior. The mental health of the
care receiver was solicited: “Are there any mental health issues facing the care
receiver?” In addition, caregivers were asked how many years they had been
providing care (coded in years) and hours/week of caregiving (coded in hours).
Sex (male, female) and age (left continuous) were used as control variables.
228 / CHAPPELL AND DUJELA

Analyses began with an examination of the existence of the different coping
strategies (raw score means divided by number of items to allow comparison
between the different types of coping), and their co-existence using Pearson’s r.
Multiple regression analyses were performed in a path model with each of the
variables in the categories in Figure 1 as a dependent variable (DV), with each
of the five different coping strategies as final DVs. Because of the small sample
size relative to the number of IV and control variables, each group was entered
in a separate regression (a separate regression for each: personality factors,
social support factors, caregiver health, demands of caregiving, and control
variables). Only those variables that revealed a statistical significance of p < .10
were entered into a final regression for that coping strategy. In the final regres-
sions, only variables with a p < .05 were considered significant. The final
regressions are shown here. Data were examined for colinearity, linearity,
homescedasticity, and normality.
RESULTS
Sample characteristics are shown in Table 1. Females, not surprisingly, con-
stitute the majority of the sample (68.5%) with male caregivers under a third.
Caregivers are primarily married (83.3%); half are caring for a spouse (50%).
These caregivers are relatively highly educated with 28.3% having a bachelor
degree or more and 23.9% having a college diploma or associate degree. The
average age of the caregivers is 60.7; the average age of the care recipient is
80.1 years. Caregivers have been providing care on average for 8 years and on
average provide 86 hours of care per week. Almost two-thirds (63.0%) live
with the person they are providing care to. The sample, while not representative,
successfully included caregivers who are under heavy demands, as intended.
The occurrences of the different strategies of coping appear in Table 2. Overall,
problem-focused coping is used more than any other type of coping with seeking
social support a close second (1.53 and 1.50 respectively). Negative emotion is
used less than the other types. That is, caregivers engage in problem-focused
coping and seeking social support more than emotion-focused coping. Turning
to the correlations of the coping strategies with one another, Table 3 shows that
they are related to one another. Problem-focused coping is significantly and
positively related to all other forms of coping, with the highest correlations with
positive emotion coping (r = .45; p < .001) and the overall emotion coping scale
(r = .41; p < .001). In other words, those engaged in problem solving are likely
to also be engaged in emotion-focused coping and for that emotion-focused
coping to be positively oriented. Seeking social support is also correlated with
problem-focused coping (r = .40; p < .001). Not surprisingly, the highest cor-
relations are between the overall emotion-focused scale and the two sub-scales
of which it consists, namely, negative-emotion coping (r = .89; p < .001) and
positive-emotion coping (r = .76; p < .001). Seeking social support is least likely
CAREGIVERS—WHO COPES HOW? / 229
to co-occur with overall or negative emotion-focused coping. While these
different strategies co-exist, by no means are they synonymous, at most there
is a 20% overlap.
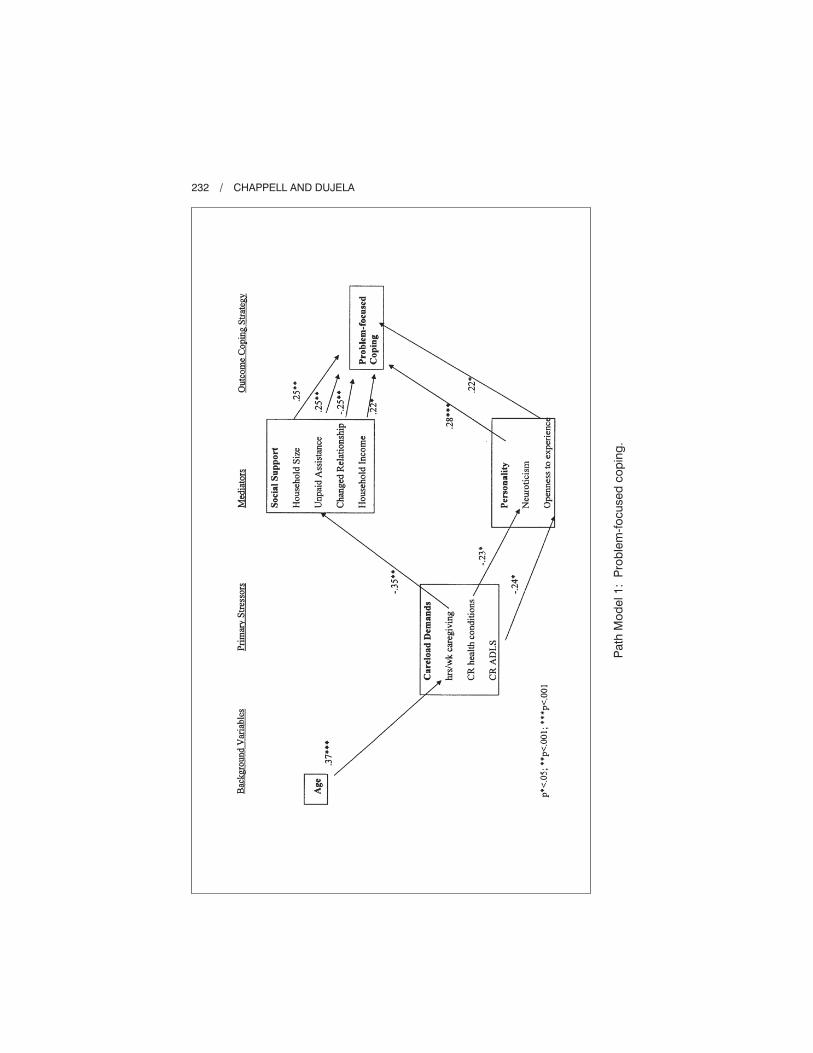
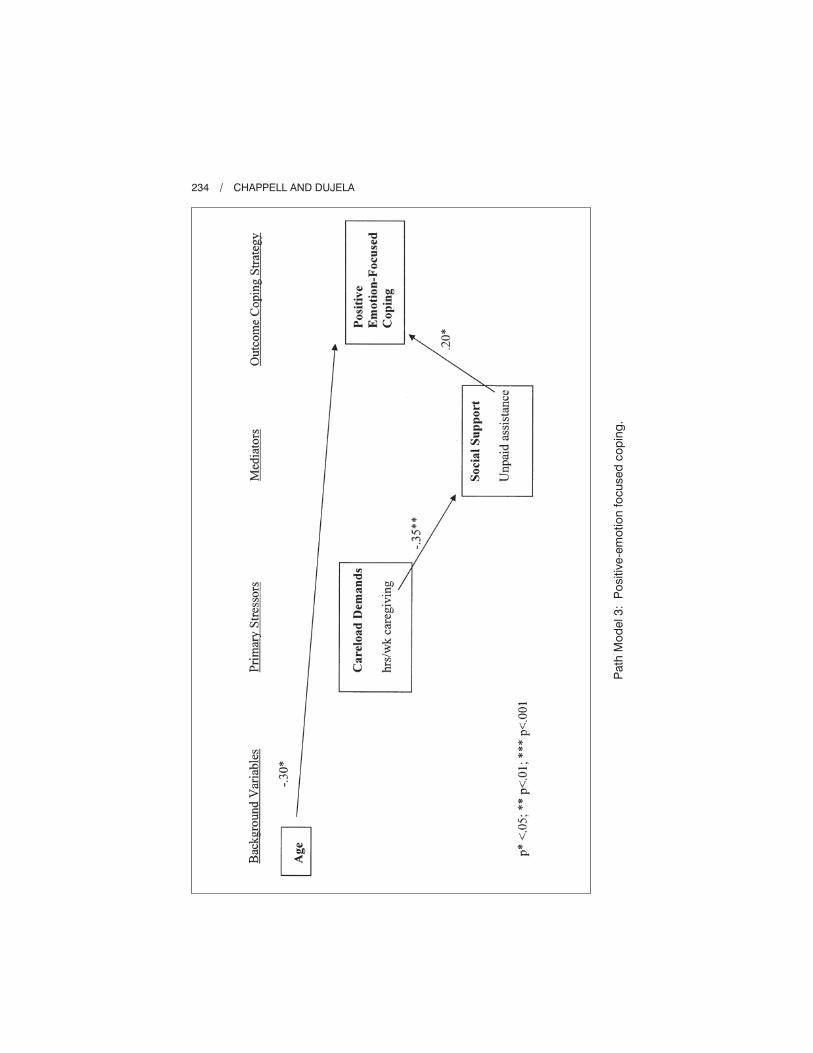
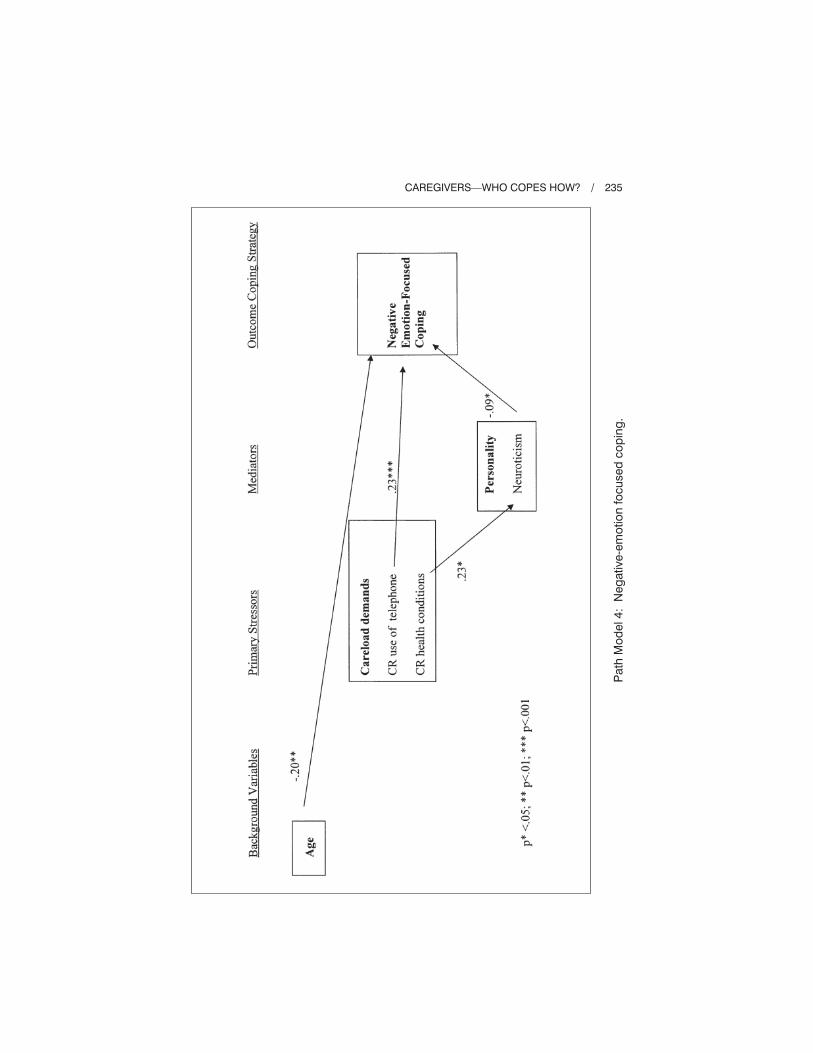
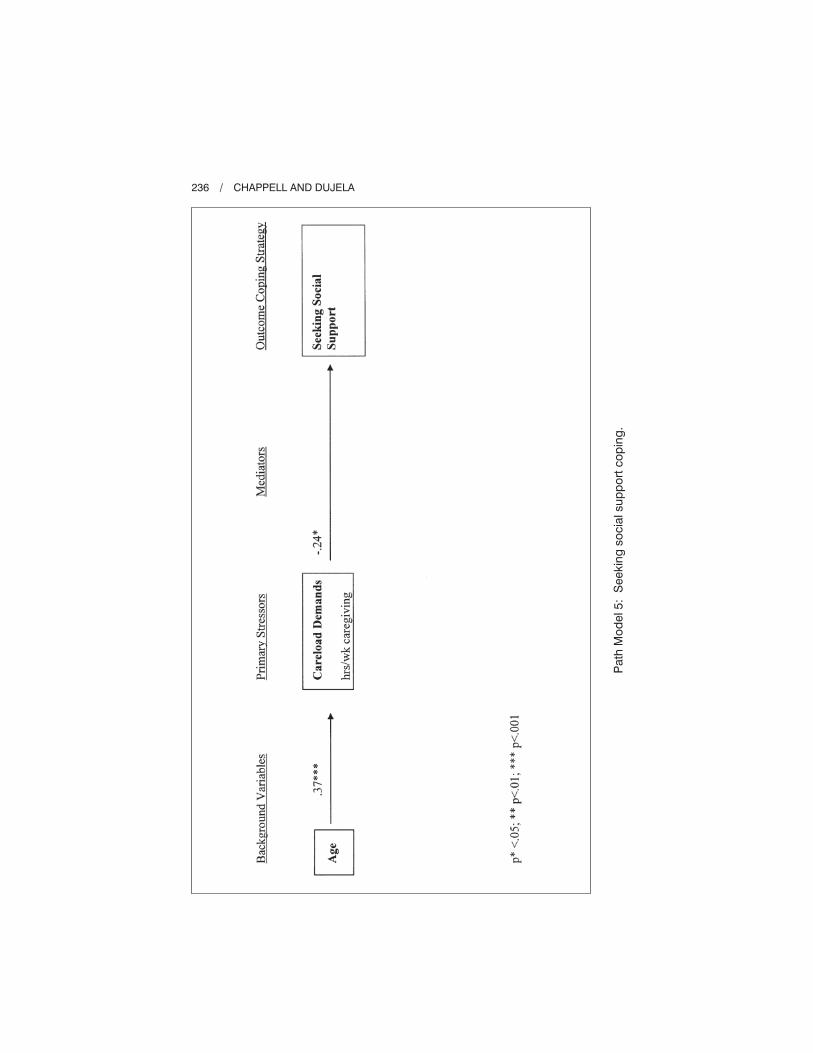
The predictors of different strategies of coping appear in Path Models 1-5.
Table 4 summarizes the significant direct predictors and the DVs for which
they were significant. The model was most successful in explaining variance in
problem-focused coping (44%). While significant predictors emerged for the
other strategies of coping, they explain less of the variance (17% for negative
emotion-focused coping; 21% for positive-emotion focused coping; 19% for
230 / CHAPPELL AND DUJELA
Table 1. Selected Sample Characteristics t1 (N = 92)
A) Sex %
Male
Female
31.5
68.5
B) Marital Status %
Married
Divorced/Separated
Other
83.3
6.7
9.8
C) Relation to Care Recipient (Caregiver is _______) %
Wife
Husband
Daughter
Son
Other
38.0
12.0
35.9
10.9
3.0
D) Education %
� High School
Trade diploma/some university
College diploma/assoc. degree
� Bachelor degree
26.1
18.5
23.9
28.3
E) Caregiver Lives with Care Recipient %
Yes
No
63.0
37.0
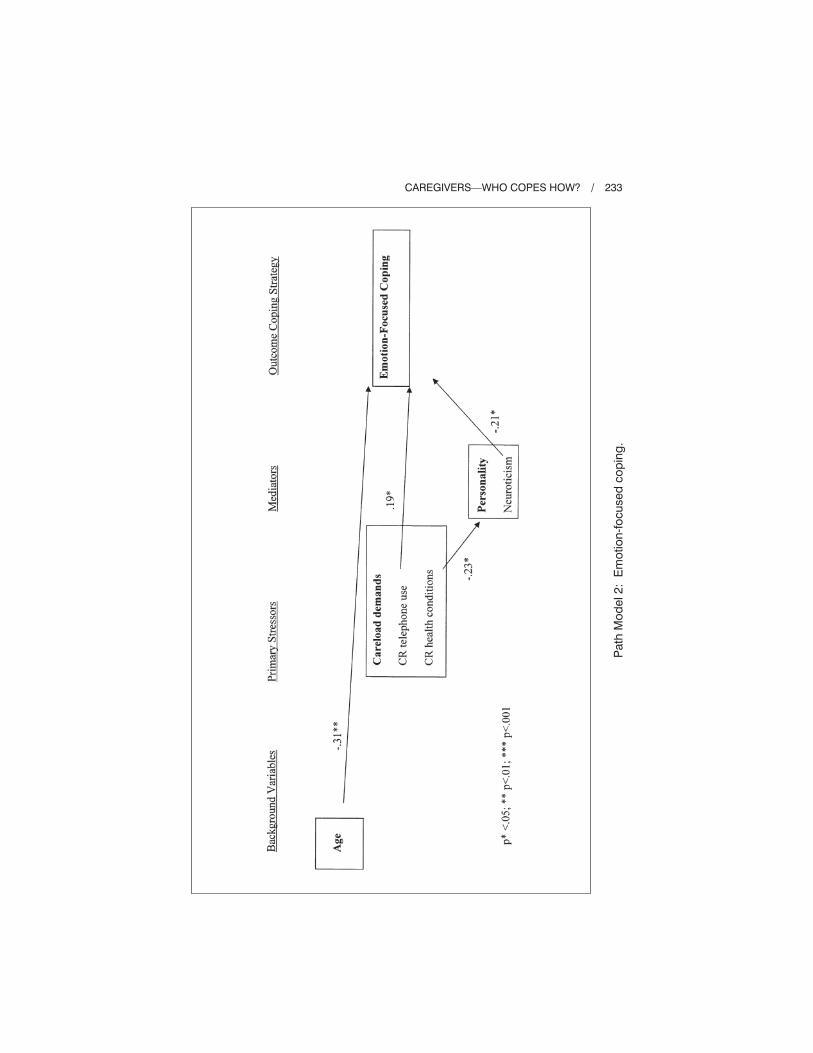
overall emotion-focused coping; 19% for seeking social support). Gender is
unrelated to type of coping strategy used. Men and women are equally likely to
engage in problem-focused, emotion-focused coping, and seeking social support.
Age, however, is significantly and directly related to all types of emotion-focused
coping, overall, positive and negative. Specifically, those who are younger tend
to engage in each of these types of emotion-focused coping compared with
those who are older. While age is not directly related to the use of problem-
focused coping or seeking social support it is related indirectly through careload
demands, specifically hours/week caregiving which in turn is negatively related
to social support (specifically those providing more hours/week of care tend to
have less unpaid assistance) which is related to problem-focused coping. Age
is similarly indirectly related to seeking social support, through hours/week
of caregiving.
Demands of caregiving are related to coping style. Care receiver functional
disability, specifically with using the telephone, is related to overall and negative
CAREGIVERS—WHO COPES HOW? / 231
Table 2. Ways of Coping, Raw Scores/
Number of Items
Problem-focused
Emotion-focused
Negative emotion
Positive emotion
Seek social support
1.53
1.37
1.18
1.23
1.50
Table 3. Coping Strategies—Correlation Matrix
Problem-
focused
Emotion-
focused
Emotion-
negative
Emotion-
positive
Seeking
social
support
Problem-focused
Emotion-focused
Emotion-negative
Emotion-positive
Seeking social support
1
.41***
.26**
.45***
.40***
1
.89***
.76***
ns
1
.39***
ns
1
.23* 1
*p < .05; **p < .01; ***p < .001.
232 / CHAPPELL AND DUJELA
Path
Mo
del1:
Pro
ble
m-f
ocu
sed
co
pin
g.
CAREGIVERS—WHO COPES HOW? / 233
Path
Mo
del2:
Em
otio
n-f
ocu
sed
co
pin
g.
234 / CHAPPELL AND DUJELA
Path
Mo
del3:
Po
sitiv
e-e
mo
tio
nfo
cu
sed
co
pin
g.
CAREGIVERS—WHO COPES HOW? / 235
Path
Mo
del4:
Neg
ative
-em
otio
nfo
cu
sed
co
pin
g.
236 / CHAPPELL AND DUJELA
Path
Mo
del5:
Seekin
gso
cia
lsu
pp
ort
co
pin
g.

emotion-focused coping. Those caring for individuals with greater disability
are more likely to use overall and negative emotion-focused coping. It is the
strongest predictor of negative emotion-focused coping, explaining 5% of
the variance. The sum of functional disability has an indirect effect on
problem-focused coping, through openness to experience (those caring for
persons with more disability tend lower on openness to experience). Another
careload demand, sum of care receiver’s chronic conditions, has an indirect
effect through neuroticism (those caring for persons with greater disability
are more likely to be high on neuroticism) also directly effecting the use
of negative emotion-focused coping. A similar indirect effect is found for
emotion-focused coping, and negative-emotion focused coping, and problem-
focused coping. Hours of care provided per week is the only significant predictor
of seeking social support, where those providing fewer hours of care are more
likely to seek social support, perhaps because they have the time to do so.
However, it is indirectly related to both problem-focused coping and positive
emotion-focused coping through unpaid assistance (in both instances the more
hours of care is related to less unpaid assistance) which is directly related to
both styles of coping.
In terms of social support, caregivers who have more unpaid assistance from
others are more likely to use problem-focused and positive emotion-focused
coping strategies. Those for whom their relationship with the care recipient has
changed for the worse, those in smaller households, and those with more income
are also more likely to problem solve, irrespective of age.
CAREGIVERS—WHO COPES HOW? / 237
Table 4. Summary of Direct Predictors of Coping
Problem-
focused
Emotion-
focused
Negative
emotion
Positive
emotion
Seeking
social
support
Age
Relation changed
IADL – telephone
Unpaid assistance
Household size
Household income
Openness to Experience
Neuroticism
Hours of caregiving
–
+
–
+
+
–
–
+
–
–
+
–
–
+
– –

In terms of personality factors, neuroticism is related to three of the four
strategies, specifically those who are high on neuroticism are less likely to use
problem-focused coping, overall or negative emotion-focused coping strategies.
Personality factors are unrelated to the use of positive emotion-focused coping.
Neuroticism, furthermore, is the strongest predictor of problem-focused coping,
explaining 8% of the variance. Openness to experience is also a significant
predictor of problem-focused coping with those more open to experience more
likely to problem solve.
Of the five coping strategies, all showed significant change over the 1-year
period except seeking social support. Change for all other strategies of coping is
negative; in all instances caregivers decrease their use of the coping strategy (other
than seeking social support which remains stable) over the course of 1 year.
CONCLUSIONS
Despite the preoccupations within gerontological research with stressors and
burdens of caregiving, there is surprisingly little on coping strategies caregivers
use in order to deal with the demands made on them. If one asks the question,
who are the caregivers who adopt different coping strategies, the literature cannot
provide an answer. The intent of this article was to begin filling this gap by
examining the types of coping strategies used by caregivers under heavy demands
to a senior living in the community. It was a deliberate decision to seek a sample
of caregivers that was not restricted to one disease group. However, the relatively
small sample size precludes an analysis of differences by disease type. It is
important to pursue further research, asking whether the predictors of coping
strategy are similar or different across disease and disability groups and if so,
how. In order to recruit a sample of caregivers who were under heavy demands
from this role, a purposive sample was drawn so the results cannot be generalized.
Nevertheless, among this group of caregivers, these data support the co-existence
of different coping strategies. Caregivers do not choose either emotion-focused or
problem-focused but tend to engage in different types of coping simultaneously.
These findings add to previous work that has noted the co-existence of coping
strategies (O’Rourke & Cappeliez, 2002).
Furthermore, these data reveal problem- and emotion-focused coping strategies
change over time; their use decreases, lending support to Folkman and Lazarus’
(1985) contention that they are fluid. Seeking social support though remains
stable. A gender difference is not supported; men are no more likely to adopt
problem-focused coping than are women and women are no more likely to adopt
emotion-focused coping than are men. Age, though, emerges as an important
factor effecting all styles of coping either directly or indirectly through care
demands, specifically hours/week of care provided. Those who are younger are
more likely to engage in emotion-focused coping contrary to the finding reported
by Folkman et al. (1987). The reasons for this are unknown although it might be
238 / CHAPPELL AND DUJELA

speculated that younger caregivers have yet to come to terms with the aging
process and its declines in health, finding the experience more emotionally
charged. Kramer (1993) suggests that those with a shorter duration of caregiving
use more emotional strategies because they have not adjusted to the onset and
progression of disease.
Given that these caregivers are providing, on average, more hours per week
than a full-time job, the effects of the actual demands of that job warrant comment.
The number of years providing care is unrelated to coping strategy as are health
of the caregiver, supporting notions that caregivers tend to their loved ones and
not to themselves. Increased functional disability of the care recipient results
in more negative emotion-focused coping. More hours of caregiving per week is
related to seeking social support. Both factors reveal additional indirect effects:
functioning is indirectly related to problem-focused and negative emotion-focused
coping through personality. Hours per week caregiving is indirectly related to
problem-focused and positive emotion-focused coping through unpaid assistance
and to negative emotion-focused coping through personality. Interestingly, func-
tioning is more related to emotional coping, and directly so; chronic conditions
are more related to problem-focused as well as emotion-focused coping but tends
to operate indirectly through personality.
Social support, particularly unpaid assistance, emerges as related to both
problem-focused and emotion-focused coping with other measures of social
support, such as household size and change in relationship, also related to problem-
focused coping. That is, social support appears to be particularly important for
individuals who engage in problem-focused coping. More specifically, those
who are in a relationship with a care recipient whom they perceive to have
worsened, who are in a smaller household, with unpaid assistance and with
more income engage in problem-focused coping. This suggests that although
their situation is perceived as having deteriorated, with the help of others and
with some economic resources, they turn to problem solving perhaps because
they feel they have the means to do so both in terms of drawing on others and
in terms of income.
A comment is also warranted on the fact that the amount of unpaid assistance
and therefore in some senses the availability of others from which one might
seek social support does not correlate with seeking social support as a coping
strategy. Whether they receive emotional support from their family, the number
of people living in the household, their marital status, whether their relationship
with the care recipient has changed, their relationship with the care recipient
that is, spouse or child, none of these are correlated with seeking social support.
If the social networks within which one is embedded do not affect whether
one seeks social support, it might be speculated that it is personality factors, but
at least among this group of caregivers, none of the personality factors correlate
with seeking social support. Whether this particular group is providing so much
care and is under such heavy demands that they do not have the time to seek out
CAREGIVERS—WHO COPES HOW? / 239

others is not known and would require comparative data to answer. It is however,
an important question to address in future research.
The personality factor of neuroticism is the strongest correlate of problem-
focused coping and emerges as a correlate of both problem-focused and emotion-
focused coping with less neuroticism related to a greater likelihood of using
each coping style. This supports earlier research for example by Hooker and
colleagues (1994). The findings reported here are also consistent with earlier
research in that neuroticism is unrelated to seeking social support. Interestingly,
neither hardiness nor resilience are related to any of the strategies of coping
examined. Perhaps this is because the constructs of hardiness and resilience
suggest “better” coping whereas the coping strategies examined here could be
either advantageous or disadvantageous to the caregivers. This research did
not examine whether the coping strategies were beneficial to the caregivers
involved. The fact that neuroticism is related to coping strategies indicates that
high neuroticism interferes with coping whether that coping strategy is ultimately
beneficial or not.
Caregiver capacity emerges as a more important predictor of coping strategy
than does workload, except for negative emotion-focused coping where functional
disability is the most significant predictor. Otherwise, caregiver resources and
especially the personality characteristic of neuroticism are particularly important.
The decomposition of overall emotion-focused coping into negative emotion-
focused coping and positive emotion-focused coping suggests that each has
somewhat different correlates. This may be a fruitful avenue for future research.
Finally, there are, in addition, many areas to be probed in future research
that were not incorporated here. We asked about coping during a difficult time.
It is equally important to ask about coping during daily hassles and compare how
this differs from coping with major events. Our primary interest centred on the
caregiver but it is also important to know more about the care recipient, such as
the number of children they have and other aspects of their support network.
Data on both caregiver and care receiver perceptions of the caregiving experience
is equally interesting.
ENDNOTE
1We know almost nothing about predictors of change in coping strategies used
by caregivers over time even though coping is viewed as situation specific, that is,
as a dynamic process (Folkman & Lazarus, 1985). Powers, Gallagher-Thompson, and
Kraemer (2002) report stability in cognitive, behavioral, and avoidant coping over 2
years, measured at 6 month intervals, among non-depressed caregivers to those with
dementia. They did not examine predictors of change but speculate that changes in
coping may occur only when major events such as institutionalization of the loved one.
Regression analyses were conducted to assess the predictors of change. The same strategy
as noted in the text was followed except t2 was the DV and t1 of that variable was forced
in first. Variance explained after the effect of t1 is removed refers to the predictors of
240 / CHAPPELL AND DUJELA

change. Then t2 IVs were added as a block after those significant at t1 were entered. The t2IVs included: care receiver status at t2 (remains in the community, now institutionalized,
or deceased) and change in: care receiver’s behavioral problems, care receiver’s ADLs,
and chronic conditions, caregivers’ chronic conditions, resilience, neuroticism, and hardi-
ness. All other variables showed no significant change.
Few significant predictors emerge and they are most often dissimilar from the predictors
of engaging in that coping strategy at t1. The predictors are t1 variables. For example,
it is not change in the health of the care recipient or the caregiver that predicts coping
strategy at t2 but rather it is their health at t1. Similarly with other predictors. Less of the
variance is explained in change than at t1 for all coping strategies except negative-focused
coping (the large amounts of variance are explained by the DV at t1, not by the explanatory
factors entered into the model).
Gender is significant, for problem-focused coping with caregivers to female recipients
less likely to use this coping strategy at t2 and those caring for male recipients more likely
to use it at t2, explaining 4% of the t2 variance. Age is a predictor of emotion-focused
coping; those who are younger use this type of coping more than those who are older,
explaining 7% of the t2 variance. Self-rated health is also a significant predictor, explaining
4% of the t2 variance. Those who rate their health as better, tend to use this strategy less at
t2. Self-rated health also predicts the use of negative emotion-focused coping at t2, in the
same direction and explaining 6% of the t2 variance. Perceived change in the relationship
at t1 (when asked about change since beginning caregiving) also predicts the use of negative
emotion-focused coping; those who perceive the relationship to have changed for the
better were more likely to use this strategy at t2 (explaining 4% of the variance). No
significant predictors emerged for positive emotion-focused coping. It is to be noted that
all of the significant variables refer to caregiver capacity, none to careload. It is also
noteworthy that care recipient status, whether they are still in the community, in a facility,
or deceased at t2 is unrelated to change in coping strategy. This suggests that Powers,
Gallagher-Thompson, and Kraemer’s (2002) speculation that changes in coping occur
only when major events such as institutionalization occur is, at least at times, inaccurate.
While few predictors of change emerge, those that do, all refer to caregiver capacity.
None refer to careload. This suggests that there are ways for caregivers to cope, despite
heavy care demands. It is also notable that the predictors of change are not the same as
the predictors of coping strategy at a given point in time. The forces that lead us to change
our coping strategies differ from those that influence us to adopt a particular strategy
at one point in time. This is important for those who examine how to influence coping
strategies. Typically, we examine the correlates of coping strategies rather than the factors
that lead us to change the particular techniques that we have been engaged in.
REFERENCES
Bergeman, C. S., & Wallace, K. A. (1999). Resiliency and aging. In T. Whitman, T.
Merluzzi, & R. White (Eds.), Psychology and medicine (pp. 207-225). Hillsdale, NJ:
Erlbaum.
Braithwaite, V. (1996). Understanding stress in informal caregiving: Is burden a problem
of the individual or of society? Research on Aging 18(2), 139-174.
Chappell, N. L., & Litkenhaus, R. (1995). Informal caregivers to adults in British
Columbia. The Caregivers Association of British Columbia, 54. Canada: University
of Victoria: Centre on Aging.
CAREGIVERS—WHO COPES HOW? / 241

Chappell, N. L., & Penning, M. P. (1996). Behavioural problems and distress among
caregivers of people with dementia. Ageing and Society, 16, 57-73.
Chappell, N. L., Reid, R. C., & Dow, E. (2001). Respite reconsidered: A typology of
meanings based on the caregiver’s point of view. Journal of Aging Studies, 15(2),
201-216.
Clark, P. C. (1998). Effect of individual and family hardiness on the stress of caregivers
of older adults. Dissertation Abstracts International, 59B(3), 1045.
Costa, P. T., & McCrae, R. R. (1987). Neuroticism, somatic complaints, and disease: Is
the bark worse than the bite? Journal of Personality, 55, 299-316.
Deal, A. G., Dunst, C. J., & Trivette, C. M. (1989). A flexible and functional approach
to developing individualized family support plans. Infants and Young Children, 1(4),
32-43.
Dell’Aquila, R. D. (2003). Parkinson’s disease: Factors related to coping. Dissertation
Abstracts International, 63A(8), 2975.
Florian, V., Mikulincer, M., & Taubman, O. (1995). Does hardiness contribute to mental
health during a stressful real life situation? The roles of appraisal and coping. Journal
of Personality and Social Psychology, 68(4), 687-695.
Flynn, F. (2005). Having an open mind: The impact of openness to experience on interracial
attitudes and impression formation. Journal of Personality and Social Psychology,
88(5), 816-826.
Folkman, S., & Lazarus, R. S. (1985). If it changes it must be a process: A study of emotion
and coping during three stages of a college examination. Journal of Health and Social
Behavior, 21, 219-239.
Folkman, S., Lazarus, R. S., Pimley, S., & Novacek, J. (1987). Age differences in stress
and coping processes. Psychology and Aging, 2(2), 171-184.
Folkman, S., &. Moskowitz, J. (2004). Coping: Pitfalls and promise. Annual Review of
Psychology, 55, 745-774.
Garity, J. (1997). Stress, learning style, resilience factors, and ways of coping in Alzheimer
family caregivers. American Journal of Alzheimer’s Disease, 12(4), 171-178.
George, L. K. (1987). Easing caregiver burden: The role of informal and formal supports.
In R. W. Ward & S. S. Tobin (Eds.), Health in aging: Sociological issues and policy
directions (pp. 133-158). New York: Springer.
George, L. K. (1990). Caregiver stress studies—There really is more to learn (editorial).
The Gerontologist, 30(5), 580-581.
Gignac, M. A. M., & Gottlieb, B. H. (1997). Changes in coping with chronic stress: The
role of caregivers’ appraisals of coping efficacy. In B. H. Gottlieb (Ed.), Coping with
chronic stress (pp. 245-267). New York: Plenum.
Gottlieb, B. H., & Wolfe, J. (2002). Coping with family caregiving to persons with
dementia: A critical review. Aging and Mental Health, 6(4), 325-342.
Holahan, C. J., Moos, R. H., Holahan, C. K., & Brennan, P. L. (1995). Social support,
coping, and depressive symptoms in a late-middle-aged sample of patients reporting
cardiac illness. Health Psychology, 14, 152-163.
Hooker, K., Frazier, L. D., & Monahan, D. J. (1994). Personality and coping among
caregivers of spouses with dementia. The Gerontologist, 34(3), 386-392.
Keefe, J., & Rosenthal, C. J. (2000). The impact of ethnicity on helping older relatives:
Findings from a sample of employed Canadians. Canadian Journal of Aging, 19(3),
317-342.
242 / CHAPPELL AND DUJELA

Kneebone, I., & Martin, P. (2003). Coping and caregivers of people with dementia.
British Journal of Health Psychology, 8(1), 1-17.
Knight, B. G. (1992). Emotional distress and diagnosis among helpseekers: A comparison
of dementia caregivers and older adults. Journal of Applied Gerontology, 11(3),
361-373.
Kramer, B. J. (1993). Expanding the conceptualization of caregiver coping: The impor-
tance of relationship-focused coping strategies. Family Relations, 42, 383-391.
Kvam, S. H., & Lyons, J. S. (1991). Assessment of coping strategies, social support, and
general health status in individuals with diabetes mellitus. Psychological Reports,
68(2), 286-293.
Lawrence, R. H., Tennstedt, S., & Assmann, S. F. (1998). Quality of the caregiver—
Care recipient relationship: Does it offset negative consequences of caregiving for
family caregivers? Psychology and Aging, 13(1), 150-158.
Maassen, G. H. (2004). The standard error in the Jacobson and Truax Reliable Change
Index: The classical approach to the assessment of reliable change. Journal of the
International Neuropsychological Society, 10, 888-893.
Maddi, S. R. (1999). The personality construct of hardiness: I. Effects on experiencing,
coping and strain. Consulting Psychology Journal: Practice and Research, 51(2),
83-94.
McCrae, R. (1987). Creativity, divergent thinking, and openness to experience. Journal
of Personality and Social Psychology, 52(6), 1258-1265.
McCrae, R. (1996). Social consequences of experiential openness. Psychological Bulletin,
120(3), 323-337.
McCubbin, M. A., McCubbin, H. I., & Thompson, A. I. (1986). FHI: Family Hardiness
Index. In H. I. McCubbin & A. I. Thompson (Eds.), Family assessment inventories for
research and practice (2nd ed., pp. 124-130). Madison, WI: University of Wisconsin.
O’Rourke, N., & Cappeliez, P. (2002). Perceived control, coping, and expressed burden
among spouses of suspected dementia patients: Analysis of the goodness-of-fit
hypothesis. Canadian Journal on Aging, 21(3), 385-392.
Pearlin, L. I., Mullan, J. T., Semple, S. J., & Skaff, M. M. (1990). Caregiving and
the stress process: An overview of concepts and their measures. The Gerontologist, 30,
583-594.
Polk, L. V. (1997). Toward a middle-range theory of resilience. Advances in Nursing
Science, 19(3), 1-13.
Powers, D. V., Gallagher-Thompson, D., & Kraemer, H. C. (2002). Coping and depression
in Alzheimer’s caregivers. The Journals of Gerontology Series B: Psychological
Sciences and Social Sciences, 57, 205-211.
Ptacek, J. T., Smith, R. E., & Dodge, K. L. (1994). Gender differences in coping with
stress: When stressor and appraisals do not differ. Personality and Social Psychology
Bulletin, 20, 421-430.
Quayhagen, M. P., & Quayhagen, M. (1988). Alzheimer’s stress: Coping with the
caregiving role. The Gerontologist, 28(3), 391-396.
Scheier, M. F., Weintraub, J. K., & Carver, C. S. (1986). Coping with stress: Divergent
strategies of optimists and pessimists. Journal of Personality and Social Psychology,
57, 1024-1040.
Schulz, R., & Williamson, G. M. (1991). Two year longitudinal study of depression
among Alzheimer’s caregivers. Psychology and Aging, 6(4), 569-578.
CAREGIVERS—WHO COPES HOW? / 243

Shaw, W. S., Patterson, T. L., Semple, S. J., Grant, I., Yu, E. S. H., Zhang, M. Y., et al.
(1997). A cross-cultural validation of coping strategies and their associations with
caregiver distress. The Gerontologist, 37(4), 490-504.
Skinner, E. A., Edge, K., Altman, J., & Sherwood, H. (2003). Searching for the structure
of coping: A review and critique of category systems for classifying ways of coping.
Psychological Bulletin, 129(2), 216-269.
Soderstrom, M., Dolbier, C., Leiferman, J., & Steinhardt, M. (2000). The relationship of
hardiness, coping strategies, and perceived stress to symptoms of illness. Journal
of Behavioral Medicine, 23(3), 311-328.
Stanton, A. L., Kirk, S. B., Cameron, C. L., & Danoff-Burg, S. (2000). Coping through
emotional approach: Scale construction and validation. Journal of Personal Social
Psychology, 78, 1150-1169.
Stephens, P. M., Norris, V. K., Kinney, J. M., Ritchie, S. W., & Grotz, R. C. (1988).
Stressful situations in caregiving: Relations between caregiver coping and well-being.
Psychology and Aging, 3(2), 208-209.
Sussman, G. M. (2003). Hardiness, coping, and distress among caregivers of institu-
tionalized Alzheimer’s patients. Dissertation Abstracts International, 63B(8), 3942.
Vachon, D. O. (1999). The health effects of caregiving for adults in later life. In T. L.
Whitman, T. Merluzzi, & R. D. White (Eds.), Life span perspectives on health and
illness (pp. 227-248). Mahwah, NJ: Lawrence Erlbaum.
Vitaliano, P., & Zhang, J. (2004). Is caregiving hazardous to one’s physical health? A
meta-analysis. Psychological Bulletin, 129(6), 946-972.
Vitaliano, P. P, Young, H. M., & Russo, J. (1991). Burden: A review of measures used
among caregivers of individuals with dementia. The Gerontologist, 31, 65-75.
Wagnild, G. M., & Young, H. M. (1990). Resilience among older women. Journal of
Nursing Scholarship, 22(4), 252-255.
Wagnild, G. M., & Young, H. M. (1993). Development and psychometric evaluation of
the Resilience Scale. Journal of Nursing Measurement 1(2), 165-178.
Walsh, F. (1996). The concept of family resilience: Crisis and challenge. Family Processes,
35(3), 261-281.
Wells, R., Dywan, J., & Dumas, J. (2005). Life satisfaction and distress in family
caregivers as related to specific behavioural changes after traumatic brain injury.
Brain Injury, 19(13), 1105-1115.
Wu, Z., & Hart, R. (2002). The effects of marital and nonmarital union transition on
health. Journal of Marriage and Family, 64, 420-432.
Direct reprint requests to:
Neena L. Chappell
Canada Research Chair in Social Gerontology
Professor, Centre on Aging and Department of Sociology
University of Victoria
Sedgewick Building, Rm A136
P.O. Box 1700 STN CSC
Victoria, BC V8W 2Y2
e-mail: [email protected]
244 / CHAPPELL AND DUJELA





























