Embed Size (px)
Citation preview
Max Stanley Chartrand, Ph.D.
(Behavioral Medicine)
CerumenManagement inthe Dispensing Practice
©2015 DigiCare® Behavioral Research

Attorney: Doctor, before you performed the autopsy, did you check for a
pulse?
Witness: No.
Attorney: Did you check for blood pressure? Breathing?
Witness: No, no.
Attorney: So, then it is possible the patient was alive when you began the
autopsy?
Witness: No.
Attorney: How can you be so sure, Doctor?
Witness: Because his brain was sitting on my desk in a jar.
Attorney: I see, but could the patient have still been alive, nevertheless?
Witness: Yes, I suppose he could have been alive…and practicing law.
Taken from an actual court transcription…

Cerumen Management in Dispensing: Expanded, Better Defined Scope of Practice in 2015
Section 101, 8c: Dispensing of hearing aids
includes…
Administering cerumen management in the course of
examining ears, taking ear impressions and/or fitting of
hearing aids,
Except…while engaged in routine cerumen removal [it is
discovered] trauma, continuous uncontrolled bleeding,
lacerations, or other traumatic injuries, [the dispenser] shall…
refer the patient to an otolaryngologist or a licensed
physician…”

Provisions re Cerumen Management in
New IHS Model Licensure Act: Section 113
(1) The licensee shall follow [state and] federal regulations, regarding Cerumen Management and referral of patients to a Medical Liaison.
(2) Training, Knowledge, and Skills.
(a) …[Obtain] training, knowledge, and skills necessary to perform [CM]
(b) Licensee shall obtain training that includes:
(i) Principles of [CM] including the anatomy of the ear canal and the ear
drum and classification of cerumen
(ii) Use of instruments [to remove/manage cerumen]
(iii) Techniques for cerumen removal
(iv) Recognition of complications
(v) Recognition of contraindications
(vi) Sanitation and safety procedures

Provisions re Cerumen Management in
New IHS Model Licensure Act: Section 113
(c) The licensee shall maintain documentation evidencing
…satisfactory completion of the training.
(3) Precautions:
(a) Licensee shall have established a Medical Liaison [within the
community] before performing cerumen removal
(b) Licensee may refer patients who exhibit contraindications [during]
cerumen removal requiring medical consultation or medical
intervention to a Medical Liaison
(c) Licensee shall carry appropriate Professional Liability insurance
before performing cerumen removal
(d) Licensee shall perform cerumen management using the customary
removal techniques commensurate with…training & experience

Practice Profile Scope of Practicere America’s Hearing Healthcare Team
0102030405060708090
100
Clin Assess Aud Assess
Dispenser
Audiologist
Physician
HA Related
Cerumen Management
Amp History
PT Audiometry
RE/SF/EA/CM
Amp Rec &/or
Referral
HA Related
Health History
Otoscopy
ME Assess
Flags/Referral
HA Related
Amplification
Servicing
Counseling
HA/Tinnitus/ALD/ADA
Clinical Assess
All Populations
Cochlear Impl
Pre/Post Op
Diagnose
Clin Tests
Clinical Assess
Cochlear Impl
Aud Function
Educational
Pre/post Op
Monitor Treat
Auditory Rehab
CI Prog/Rehab
Aud/Cognitive Treat
Balance Disorders
Post-Op Rehab
Peri-Post Treat Rehab
Tinnitus Management
Diagnose
Prescription/Treatment
Surgery

What are biomarkers? The National Institutes of Health (NIH) defines
biomarkers as:
“Characteristics that are objectively measured and evaluated as an indicator of normal biologic processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention”

The FDA Red Flags are the Biomarkers that brought the dispensing profession into the larger community of health professionals
Abbreviated list of Red Flags:
Pain in the ear
Significant cerumen
Rapidly progressive loss
Sudden unilateral loss
Deformity of the ear
Active drainage
Acute dizziness
Average air-bone gap at .5K, 1K, and 2KHz >15dB

This is important: The entire body
can be affected in some way by
what occurs in the EAC region.

For example:
Hyper-reactivity in
Arnold’s (Vagus)
Reflex Can Evoke:
-Watering eyes
-Cough
-Gag effect
-Effortful phonation
-Chest tightness
-Heart tension(Pseudopericarditis)
-Nausea

Normal EAC Behavior with amplification relies upon two main components of physiology
The corneum stratum of EAC (unlike other areas of the human body,
the ear canal’s “epidermis” is 100%
keratin, rather than 85% with live
epithelial cells)
EAC Nuerophysiology &
vasculature (the guardians of EAC
immunology)

A Physiological Review of Mechanoreceptors in Human Skin
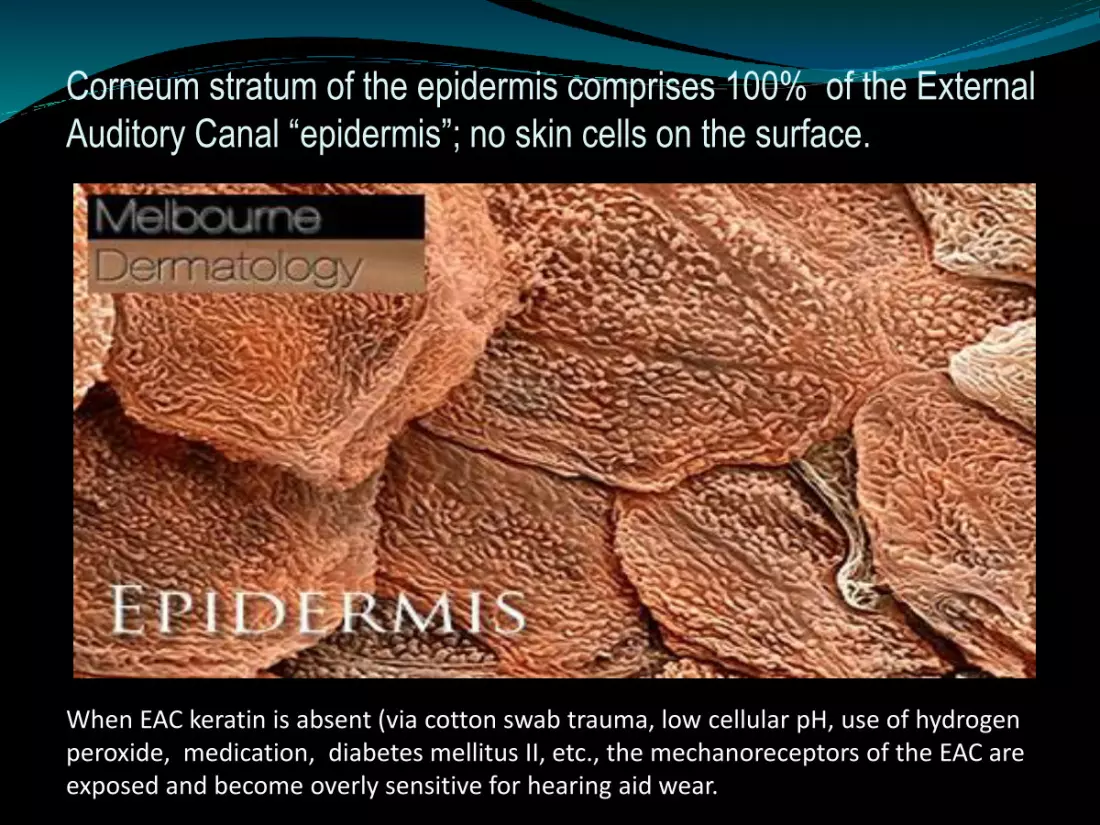
Corneum stratum of the epidermis comprises 100% of the External
Auditory Canal “epidermis”; no skin cells on the surface.
When EAC keratin is absent (via cotton swab trauma, low cellular pH, use of hydrogen peroxide, medication, diabetes mellitus II, etc., the mechanoreceptors of the EAC are exposed and become overly sensitive for hearing aid wear.

EAC Mechanoreceptors (You need to know them)
Hair follicles Senses slight air movement, incites vascular activity at TM
Meissner’s Corpuscles Senses light pressure near surface of epithelium, sends signal to tympanic plexus (Note: In complete reflex arc ceases
firing upon cessation of movement)
Pacinian Corpuscles Senses deep pressure in mid-level of tissue, sends signal to tympanic plexus region (Note: Excites cytokine and lymphocyte
production)
Vagal stimulation (via Arnold’s Branch)
Evokes various reflexes, including gag, cough, cardiac constriction, nausea in stomach
Trigeminal (Efferent neurons)
/Facial (Afferent neurons)
Controls vascularization & lymphatic activity (Note: Some aspects
have no parasympathetic response)

Evidence & Remediation of EAC
Neuroreflex Hyper-Reactivity
Trigeminal
(Red Reflex)
Hyper-vascularization re
Otoscope Speculum Placement
Requires increased gain/output after 15-30 minutes
Reduce/eliminate pressure in cartilaginous area of EAC or fit RIC
Vagus/Arnold’s Branch
(Cough Reflex)
Cough, gag reflex upon otoblock insertion
Complains of Non-acoustic occlusion, plugged sensation
Find most sensitive area & remove earmold material, or fit RIC
Lymphatic
(Tissue Swelling)
Painful sensitivity upon insertion of earmold in EAC—note missing keratin
HA becomes uncomfortable in short durations of wear, cannot acclimate
Improve keratin status before delivery, reduce pressure in EAC, or fit RIC
Reflex Label Observation Fitting Artifact Remedy

Use these one-of-a-kind tools to train staff, counsel patients, and sharpen your skills!

Since the introduction of video otoscopy in 1992, public health trends have changed dramatically
Chronic disease in every category has skyrocketed in the general population (Polypharmacy, DMII, Cancer, CVD & Neuropathies)
As cellular pH has dropped in the population in recent years, fungi, yeasts & pseudomonas, once rare , are now common
Incidence of absent EAC keratin has skyrocketed, making EAC mechanoreceptors overly sensitive to earmolds & hearings aids
Impacted cerumen has given way to keratosis obturans; untended cases progress to external ear cholesteatoma
Tympanosclerosis and other sclerotic plaques (due to acidosis) have proliferated approximately 5-fold in the general population

• Latent diabetes II case
Keratosis Obturans: Progression over 1-5
years into “the ingrown toenail of the ear”
• When cellular pH of the body falls below pH 7.1 (acidosis), external ear keratin can peel off at the rate of approx. 1mm per day. The example to the left is from a patient developing diabetes mellitus type 2 @ 6 months
• At year 4-5, several keratoses have formed, trapping dead skin cells, bacteria, amoeba, fungus, yeasts, etc., debris, and cerumen. Often mistaken for impacted cerumen
• Upon removal of just one of the keratoses, more are keratoses are revealed, each with their separate layers of keratin wrapped around the organisms listed above
• Upon removal of the final keratosis, a normal tympanic membrane is revealed

Potentially dangerous microorganisms
common to the external meatus
Acinetobacter Iwofii Long developing Impacted earwax
Sepsis; pneumonia; respiratory infections
Enterobacter Cloacae Untreated injury, infection (pseudomonas)
Sepsis, pneumonia, infection
Pseudomonas aeruginosa/anaerobic
Chronic EO, EM Irritation, pH<6.5
OE, Septicemia, pneumonia
S. areus Non-sterile earmolds, objects
Internal abscesses, carbuncles, boils
Aspergillus Favus -pH EM, hyper-natremia, DM II (dermatitis response)
Hypersensitive pneumonitis, other systemic disease
Candida Parapsilosis -pH EM, renal disease, thrush, DMII, gout
Candidiasis, skin Mucosal disease
Bacteria/Fungi Oto Culture Complications
DigiCare®

Introducing MiraCell’s ProEAR® Solution
16 years’ field observations:
Encourage keratin growth
Soothe ears re adaptation of earmolds
Help remove scar tissue, calcium plaque on eardrums, making amplification clearer
Soften hardened earwax for easier removal
Re-establish pH flora of ear canal (6.50-7.35)
Strengthen the ear’s immune system and dramatically reducing remakes & returns for credit

Standard Procedure for Using MiraCell’sProEAR® Botanical Solution in the Ear...
Tilt the head sideways & pour a generous amount of ProEAR solution into the ear (enough to cover the ear drum, evoking a shiver).
Place wad of tissue at the entrance of the canal and leave for at least 10-15 minutes
Do the same to opposite ear
Repeat procedure daily for 2 weeks & once weekly thereafter.
(Demonstration)DigiCare®

Patient: Doc, it’s been a month since my last visit with you and I still feel terrible.
Doctor: Did you follow the instructions on the medicine I gave you?
Patient: I sure did—the bottle said, “Keep Tightly Closed”

Video OtoscopyBiomarkers to Watch For

Peeled Keratin in EAC
Typical of many Pre-Diabetes and Diabetes Mellitus Type II cases, setting stage for a septic keratosis obturans, and ear canal overly sensitive. Other causes of this phenomena:
Hidden sepsis in jaw/teeth under crowns, root canals, periodontal disease
Prosthetic sepsis build-up (hips, knee, ankle, wrist, mesh screen, etc.)*
Other infections, eg recent upper respiratory infections (bronchitis, pneumonia, sinusitis
Intestinal infections, ulcerative colitis
In-grown toe nail, neuropathy of the legs/feet
*Note: Often accompanied by
persistent high blood sugar, A1C
scores.

Otitis Media/Acoustic & Barotrauma/
Tympanosclerosis/Scar Tissue
Mixed hearing loss
Flaccid Tympanometry
Bone loss
(otosclerosis/osteoporosis)
Programming challenges (resonance transfer abnormalities)
Medically intensive, refer for
cerumen management or risk
perforation

Epithelial/Congenital Abnormalities
Stenosis at Bony Isthmus
(Treacher-Collins)
Epidermis almost to the
bony isthmus
Yeasts growing from the TM
Absent keratin in EAC
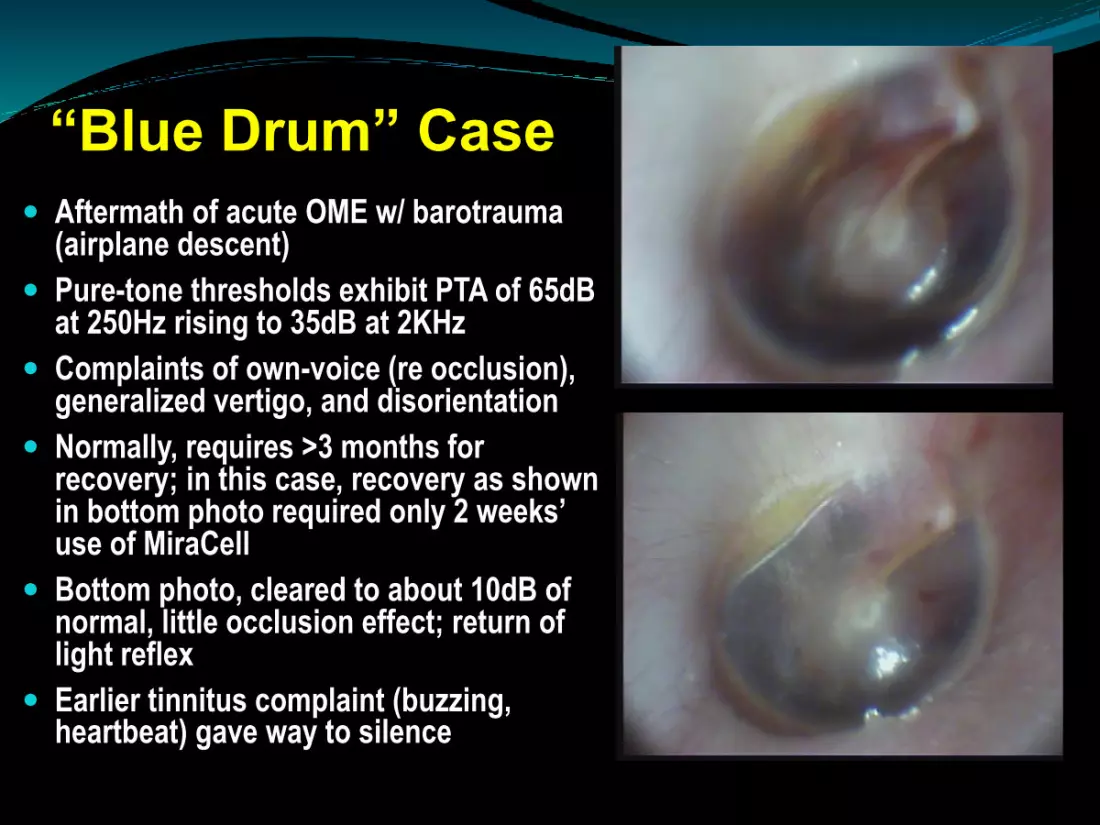
“Blue Drum” Case
Aftermath of acute OME w/ barotrauma(airplane descent)
Pure-tone thresholds exhibit PTA of 65dB at 250Hz rising to 35dB at 2KHz
Complaints of own-voice (re occlusion), generalized vertigo, and disorientation
Normally, requires >3 months for recovery; in this case, recovery as shown in bottom photo required only 2 weeks’ use of MiraCell
Bottom photo, cleared to about 10dB of normal, little occlusion effect; return of light reflex
Earlier tinnitus complaint (buzzing, heartbeat) gave way to silence

Informed Consent
Documentation
Disclaimers
Verbal notification
FDA/HIPAA/State
DigiCare®

Other Medico-Legal issues
Set up your Community Hearing Healthcare Team
Develop lines of communication
Standardize medical information re case history
Professional Liability Insurance (example: >$3 million
up to $1 million per incident)
Observe practice boundaries
DigiCare®

CM Rules of Hygiene
Separate servicing areas from test sites
where possible
Keep equipment, tools clean, sterile---
think bacteriologically!
Always wash hands thoroughly between
patients/tasks
Use disinfectant on speculae between
patients/ears (alcohol does not disinfect)
Never insert a hearing aid after handling
without cleaning it first
Teach patients proper earmold hygiene
DigiCare®

Good ear care rules to follow:
Never insert Q-tips more than 1/3 into the ear canal
Avoid boric acid, hydrogen peroxide, acetic acid solutions
Ask for a video otoscopy exam from your doctor or
healthcare professional periodically
To help removing water from the ear canal, simply pull back
and downward on the pinna
Use Miracell® solution to prepare for new hearing aids,
before/after cerumen removal; any time the ear itches
Maintain ears by using Miracell® once per week if you swim,
wear hearing aids, or undergo frequent altitude changes
(Consumer Counseling)

Types of Cerumen Management*
Secondary Management: Otoscopic inspection, Otoblock
insertion/removal, Impression-taking, Hearing insertion/removal
Minimally Invasive: V/O wax loop, tweezers@3/4” depth
Gentle, Moderately Invasive: Softening agent, syringing
method (warm water/antiseptic solution)
Maximally Invasive: Jet Irrigation, Manual Curette Removal,
High Pressure Suction (Vacuum Pump—Caution!)
DigiCare®*Caution: Always ascertain use
of anti-coagulants, aspirin

Observation & Preparation…

Warm, Antiseptic Water (98-102o F)

After softened, gently remove keratosis

Debris gone, keratin migrating outward

Use these one-of-a-kind tools to train staff, counsel patients, and sharpen your skills!





























