Embed Size (px)
Citation preview

European Journal of Cancer (2013) 49, 3806–3812
A v a i l a b l e a t w w w . s c i e nc e d i r e c t . c o m
ScienceDirect
jour na l homepage : www.e jcancer . com
Cetuximab, gemcitabine and capecitabine in patientswith inoperable biliary tract cancer: A phase 2 study
G. Rubovszky a,⇑, I. Lang a, E. Ganofszky a, Z. Horvath a, E. Juhos a, T. Nagy a,E. Szabo a, Z. Szentirmay b, B. Budai c, E. Hitre a
a Department of Medical Oncology and Clinical Pharmacology “B”, National Institute of Oncology, Budapest, Hungaryb Surgical and Molecular Tumour Pathology Centre, National Institute of Oncology, Budapest, Hungaryc Department of Molecular Immunology and Toxicology, National Institute of Oncology, Budapest, Hungary
Available online 2 September 2013
09
ht
⇑R
KEYWORDS
Biliary tract cancerGemcitabineCapecitabineCetuximab
59-8049/$ - see front matter
tp://dx.doi.org/10.1016/j.ejca.
Corresponding author: Addrath Gy. u. 7-9, 1122 Budapes
E-mail address: garub@onc
� 2013 E
2013.07.1
ess: Depat, Hungaol.hu (G
Abstract Purpose: Biliary tract cancer is rare and has dismal prognosis. Chemotherapy hasits role in inoperable disease but the role of targeted agents like cetuximab remains to bedefined. On the basis of high epidermal growth factor receptor expression of biliary tract can-cers this study aims to investigate the efficacy of cetuximab, gemcitabine and capecitabine inan exploratory phase 2 trial.Patients and methods: Inoperable biliary tract cancer patients were treated with the combina-tion of gemcitabine (1000 mg/m2 on day 1 and 8), capecitabine (1300 mg/m2/d on day 1–14)and weekly cetuximab (400 mg/m2 loading and 250 mg/m2 maintenance dose) in 21-d cyclesuntil progression or the appearance of intolerable side-effects.Results: Out of 34 patients (mean age 59.7 years) accrued in this study 16 had intrahepatic,eight extrahepatic cholangiocarcinoma and 10 gall bladder cancer. The best overall responserate was 17.6% (two complete responses and four partial responses) and the clinical benefitrate was 76.5%. After a median of 15.4 months follow-up the median progression free survivalwas 34.3 weeks and the median overall survival was 62.8 weeks. The performance status andchemotherapy efficacy were independent and significant markers of survival. Only moderateside-effects were registered in this study. KRAS mutation was evaluable in 24 tumours, allof these were of wild type.Conclusion: The efficacy of cetuximab, gemcitabine and capecitabine combination is encour-aging and a well tolerated treatment of inoperable biliary tract cancers.� 2013 Elsevier Ltd. All rights reserved.
lsevier Ltd. All rights reserved.
43
rtment of Oncological Internal Medicine and Clinical Pharmacology “B”, National Institute of Oncology,ry. Tel.: +36 1 2248600; fax: +36 1 2248744.
. Rubovszky).
G. Rubovszky et al. / European Journal of Cancer 49 (2013) 3806–3812 3807
1. Introduction
Biliary tract cancer is a rare disease with poor prog-nosis. Its incidence is increasing, accounting for 3% ofall gastrointestinal tumours [1], but regional differencesare well described [2,3]. The incidence of the disease inHungary is 13 cases per 100,000 inhabitants. The diag-nosis of biliary tract cancer is usually made between ages50 and 70. The only curative treatment is surgery,although even after complete resection or transplanta-tion the cancer often recurs with the probability of a5 year survival of about 15% [4,5]. Locoregionalapproaches, like chemoembolization, show promisingresults, although in metastatic disease this modality isnot feasible [6–8]. In cases where systemic chemotherapyis the only therapeutic choice the expected survival isshort (rarely exceeds 12 months) [1,9,10]. The basic com-pound of palliative chemotherapy is gemcitabine with aresponse rate of 5–30% when used alone [11]. Its combi-nation with other agents may have a superior effect. Onthe grounds of the results of two randomised trials com-paring gemcitabine versus gemcitabine plus cisplatin thegemcitabine and cisplatin combination is the currentstandard chemotherapeutic treatment [12,13]. However,the fluoropyrimidines, like capecitebine also have clini-cal activity, both as monotherapy or combined withgemcitabine [9,14,15], without such severe side-effectssuch as neuropathy.
Cetuximab is a monoclonal antibody targeting epi-dermal growth factor receptor (EGFR) with provenclinical efficacy in head and neck and colorectal cancers.Biliary tract cancers are predominantly EGFR positiveby immunohistochemistry and dysfunction in theEGFR-RAS-RAF-MEK signal transduction pathwayhas an important role in carcinogenesis [11]. This makesbiliary tract cancer a potential target to cetuximab. Inthree clinical trials (one of them a randomised phase2) cetuximab combined with gemcitabine and oxalipla-tin proved to have clinical activity in the biliary tractcancer [1,16,17].
On the basis of high EGFR expression in biliary tractcancers we launched an exploratory phase 2 trial in 2009with cetuximab, gemcitabine and capecitabine. As far aswe know there is no published trial with thiscombination.
2. Patients and methods
In this explorative single centre study 34 patients withhistologically confirmed unresectable biliary tract cancerhave been recruited from July 2009 to March 2012. Theprotocol has been approved by the Medical ResearchCouncil of the Ethics Committee for Clinical Pharma-cology, the National Institute of Pharmacy and theLocal Ethics Committee and registered at the EuropeanMedicines Agency (EMEA) (EudraCT No. 2006-
001694-23). Patients were informed in detail before theygave consent. Patients were eligible if the tumour wasinoperable and the loco-regional therapy was not achoice. Previous surgery and chemotherapy other thangemcitabine and capecitabine were allowed, previouscetuximab therapy was an exclusion criterion. All partic-ipants had to have measurable disease by ResponseEvaluation Criteria in Solid Tumours (RECIST) 1.0,preserved performance status (Eastern Clinical Oncol-ogy Group (ECOG) 0-2), sufficient cardiac (New YorkHeart Association (NYHA) Functional Classification0-1), hepatic (aspartate aminotransferase (AST)/alanineaminotransferase (ALT) 6 5� upper limit of normal(ULN)) and renal function (creatinin 6 2� ULN), abil-ity to swallow and absorb oral medication. Patientsmust have had adequate bone marrow reserve (Absoluteneutrophil count (ANC) P 1.5 G/l, platelets P 100 G/l). Stent implantation was allowed before recruitment,but during the treatment phase it was considered as pro-gression. The EGFR positive status was confirmed byimmunohistochemistry (Ventana confirm 3C6) beforeentering the study. KRAS mutation status (exon 2,codons 12 and 13) was analysed prospectively only fromMay 2010 and retrospectively only if suitable paraffinembedded blocks were available. After whole genomeamplification and real-time polynerase chain reaction(PCR), melting-point analysis was performed with posi-tive and negative controls. The KRAS status of allpatients was evaluated with the same method in thesame accredited laboratory.
2.1. Study design
This was a phase 2a, open-label, investigator initi-ated, single-centre trial. We planned first interim analy-sis after enroling at least 30 patients on the basis of aprevious calculation [1].
Patients received gemcitabine 1000 mg/m2 i.v. on day1 and 8 over 60–90 min, followed by a 1 week rest. Cape-citabine was administered at a dose of 1300 mg/m2 everyday on days 1–14. Capecitabine daily dose had beenrounded down to a dose maintained with 500 mg tablets.The capecitabine daily dose was divided into two dosesand given in 12-h intervals. Cycle duration was 21 d.Cetuximab was administered every week with a dose of250 mg/m2 daily after a loading dose of 400 mg/m2.Patients were monitored for toxicity weekly by the treat-ing physician and laboratory tests were performed beforeevery chemotherapy administration. In the case of grade3 or 4 side-effects either dose modification or temporaryor permanent discontinuation of drugs was at the treat-ing physician’s discretion taking into account relatedguidelines. It was recommended for physicians that aftergrade 3 or 4 haematological or grade 3 non-haematolog-ical side-effects the dose should be reduced by 25% as thefirst step and by 50% as the second step. After grade 4

Table 1Main characteristics of patients.
Characteristics N (%)
Age (years)Mean 59.7Range 34.5–76
SexMale 11 (32)Female 23 (68)
Site of primary tumourIntrahepatic 16 (47)Extrahepatic 8 (23.5)Gall bladder 10 (29.5)
StageLocoregional 7 (20.6)Metastatic 27 (79.4)
Site of metastasis
3808 G. Rubovszky et al. / European Journal of Cancer 49 (2013) 3806–3812
non-haematological side-effects the study treatment musthave been permanently discontinued. If the administra-tion of one compound of therapy had to be modified(dose reduction or discontinuation), the other compoundcould be continued at the treating physician’s discretion.The treatment was planned to be continued until radio-logical progression according to RECIST 1.0 criteria orunacceptable toxicity. Radiological assessment with heli-cal CT was carried out within 28 d before the first cycle oftherapy and then every 8–12 weeks. No confirmatoryevaluation was planned. Before every new cycle thepatient’s medical history was checked and an evaluationof side-effects, physical examination and laboratory eval-uation (blood count, hepatic and renal function) wasperformed.
Liver 21 (61.8)Lymph node 18 (53)Lung 2 (5.9)Bone 5 (14.7)Peritoneum 6 (17.6)Local (infiltrating) 3 (8.8)Other 2 (5.9)
ECOG PS0 6 (17.6)1 11 (32.4)2 17 (50)
BMI<25 17 (50)P25 17 (50)
EGFR (rate of positive tumour cells)630% 6 (17.6)>30% 22 (64.7)NA 6 (17.6)
Prior surgery 14 (41.2)Prior chemotherapy (for stage IV disease) 5 (14.7)
Abbreviations: ECOG PS, Eastern Cooperative Oncology Groupperformance status; BMI, body mass index; EGFR, epidermal growthfactor receptor; NA, not available
2.2. Statistical analysis
The primary objective of the study was to assessresponse rate, secondary objectives were progressionfree survival, overall survival and adverse events. Bestoverall response rate, measured according to RECIST1.0 criteria, was evaluated by computed tomography.Progression free survival was considered from the begin-ning of therapy to radiological or clinical progression,whichever occurred first. Overall survival was calculatedfrom the beginning of therapy until the date of death.Factors involved in analysis were age, sex, the site of ori-gin (intrahepatic, extrahepatic or gall bladder), stage(locoregional or metastatic), performance status (ECOG0 versus 1 versus 2), body mass index (BMI, <25 kg/m2
versus P25 kg/m2), best response and EGFR expressionlevel (rate of positive tumour cells 630% versus >30%).Best response was analysed with two groupings for sur-vival analysis: objective response (complete response(CR) + partial response (PR)) versus stable disease(SD) versus progressive disease (PD) or clinical benefitrate (CR + PR + SD) versus PD. Progression freesurvival and overall survival were analysed withKaplan–Meier curves and the log-rank test. Multivari-ate regression was performed with stepwise method.Estimates were considered statistically significant fortwo tailed values of p < 0.05. The toxic effects wereevaluated according to Common Terminology Criteriafor Adverse Events v3.0 (CTC AE). Statistical analysiswas performed using SAS 9 (SAS Institute Inc., 2011).
3. Results
Patient recruitment lasted from February 2009 toMarch 2012. Data collection was closed on 13th July2012. A total of 34 patients were accrued in the study.The main characteristics of recruited patients are shownin table 1. Five of them received chemotherapy beforethe study entry. Fluorouracil, epiadriamycin andmitomycin combination was intravenously applied in
three cases and in two cases as transarterial intrahepaticchemoembolisation. The best clinical response evalua-tion was possible for all patients. There were twopatients with CR (5.9%), four patients with PR(11.8%), 20 patients with SD (58.8%) and eight patientswith PD (23.5%). The objective response rate was 17.6%and the clinical benefit rate was 76.5%. Eight patientswere still in the study without evidence of progressionat the closure of data collection. In one patient withKlatskin’s tumour the therapy was interrupted forapplying additional radiotherapy for not-progressingdisease after which the patient’s condition did not per-mit chemotherapy continuation. During the analysedperiod with a median follow-up of 15.4 months (95%confidence interval (CI) 9.1–27.7 months) 26 patientsprogressed and 19 patients died. The median progres-sion free and overall survivals were 34.3 weeks (95%CI 24.4–38.3 weeks) and 62.8 weeks (95% CI 43.7–67.4 weeks), respectively.
In this trial a confirmatory computed tomography(CT) was not compulsory after PR or CR. To
G. Rubovszky et al. / European Journal of Cancer 49 (2013) 3806–3812 3809
demonstrate confirmed regression we have chosenpatients whose therapy lasted at least until the thirdCT (two consecutive CT scans showed at least SD).These criteria were fulfilled by 15 patients (44.1%),who mostly had SD (73%), but one CR and three PRwere also confirmed. Despite objective responses noneof the patients became candidates for curativeoperation.
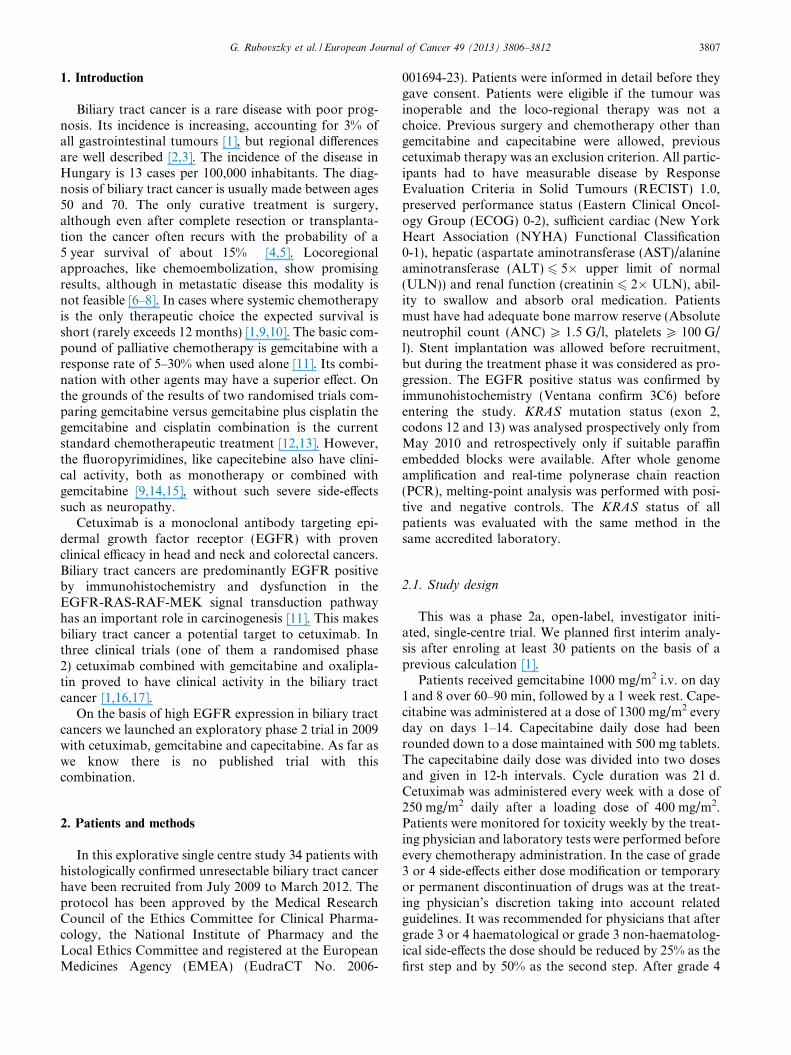
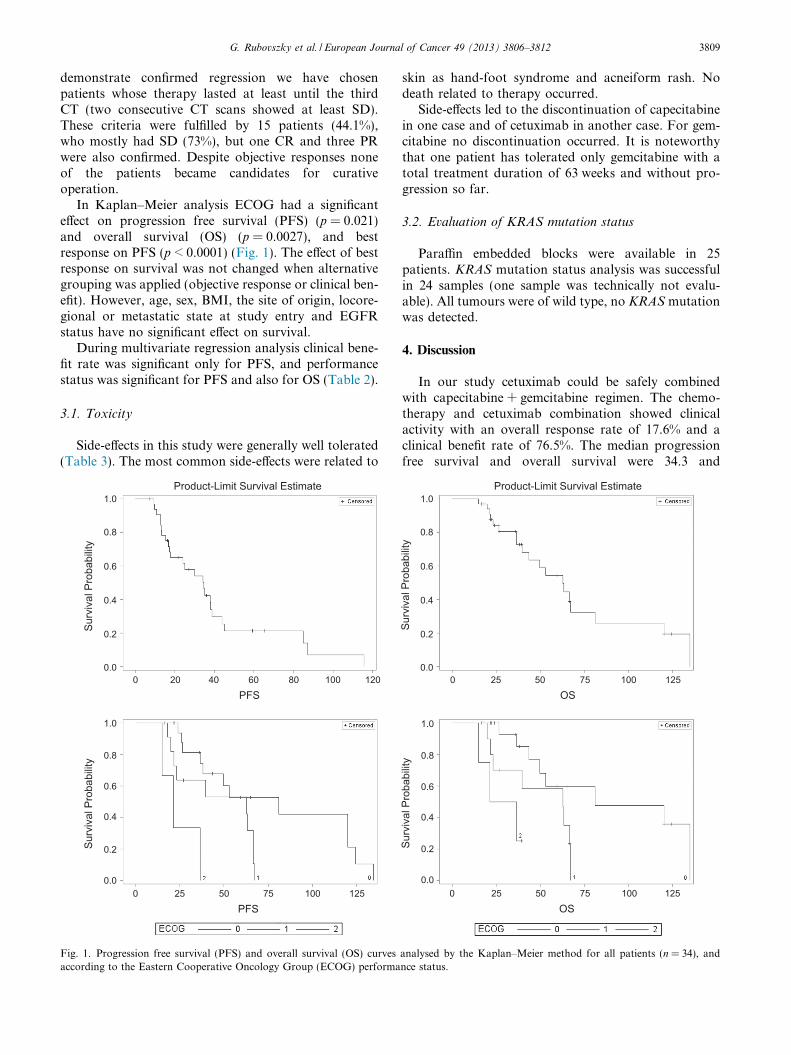
In Kaplan–Meier analysis ECOG had a significanteffect on progression free survival (PFS) (p = 0.021)and overall survival (OS) (p = 0.0027), and bestresponse on PFS (p < 0.0001) (Fig. 1). The effect of bestresponse on survival was not changed when alternativegrouping was applied (objective response or clinical ben-efit). However, age, sex, BMI, the site of origin, locore-gional or metastatic state at study entry and EGFRstatus have no significant effect on survival.
During multivariate regression analysis clinical bene-fit rate was significant only for PFS, and performancestatus was significant for PFS and also for OS (Table 2).
3.1. Toxicity
Side-effects in this study were generally well tolerated(Table 3). The most common side-effects were related to
1.0
0.8
0.6
0.4
0.2
0.00 20 40 60 80 100 120
Surv
ival
Pro
babi
lity
1.0
0.8
0.6
0.4
0.2
0.0
Surv
ival
Pro
babi
lity
Product-Limit Survival Estimate
PFS
0 25 50 75 100 125PFS
Fig. 1. Progression free survival (PFS) and overall survival (OS) curvesaccording to the Eastern Cooperative Oncology Group (ECOG) performa
skin as hand-foot syndrome and acneiform rash. Nodeath related to therapy occurred.
Side-effects led to the discontinuation of capecitabinein one case and of cetuximab in another case. For gem-citabine no discontinuation occurred. It is noteworthythat one patient has tolerated only gemcitabine with atotal treatment duration of 63 weeks and without pro-gression so far.
3.2. Evaluation of KRAS mutation status
Paraffin embedded blocks were available in 25patients. KRAS mutation status analysis was successfulin 24 samples (one sample was technically not evalu-able). All tumours were of wild type, no KRAS mutationwas detected.
4. Discussion
In our study cetuximab could be safely combinedwith capecitabine + gemcitabine regimen. The chemo-therapy and cetuximab combination showed clinicalactivity with an overall response rate of 17.6% and aclinical benefit rate of 76.5%. The median progressionfree survival and overall survival were 34.3 and
1.0
0.8
0.6
0.4
0.2
0.00 25 50 75 100 125
1.0
0.8
0.6
0.4
0.2
0.0
Surv
ival
Pro
babi
lity
Surv
ival
Pro
babi
lity
Product-Limit Survival Estimate
0 25 50 75 100 125OS
OS
analysed by the Kaplan–Meier method for all patients (n = 34), andnce status.

Table 2Results of multivariate regression analysis.
Variables HR 95% CI p
PFS ECOG PS0 11 2.7 1.05–7.04 0.042 9.0 2.25–35.8 0.0018
Best responseCBR 1 13.5–127.7 <0.0001PD 131
OS ECOG PS0 11 3.2 0.92–10.9 0.072 13.8 2.24–84.9 0.005
Abbreviations: HR, hazard ratio; CI, confidence interval; PFS, progression free survival; OS, overallsurvival, ECOG PS, Eastern Cooperative Oncology Group performance status; CBR, clinical benefitrate; PD, progressive disease.
Table 3Adverse events, all grades (occurred at least in 10% of patients) andgrade 3 or 4.
All grades Grades 3–4
N (%) N (%)
Hand-foot syndrome (HFS) 16 47.1 2 5.9Acneiform rash 27 79.4 4 11.8Fatigue 13 38.2 5 14.7Constipation 6 17.6 –Diarrhoea 5 14.7 –Nausea/vomiting 12 35.3 –Anorexia 4 11.8 1 2.9Anaemia 20 58.8 –Leukopaenia/neutropenia 14 41.2 6 17.6Febric neutropenia 2 5.9Thrombocytopenia 9 26.5 1 2.9Fever/infection 19 55.9 1 2.9Pain 13 38.2 1 2.9Allergic reaction 3 8.8Hypercalcaemia 7 20.6 4 11.8Dyspnoea 1 2.9Hyperbilirubinemia 12 35.3 8 23.5Hyperglycaemia 2 5.9Liver enzyme elevation 20 59 1 2.9
3810 G. Rubovszky et al. / European Journal of Cancer 49 (2013) 3806–3812
62.8 weeks, respectively. These results fit in well withpreviously published data by Eckel et al. Although theresponse rate was lower than reported in a pooled anal-ysis, tumour control rate, progression free and overallsurvival are more favourable. In the pooled analysisresponse rate, tumour control rate, time to progressionand overall survival were 22.6%, 57.3%, 4.1 and8.2 months, respectively [18]. In two randomised trials(one phase 3 and one phase 2) gemcitabine monotherapywas compared to its combination with cisplatin resultingin a significant benefit of 3.5 months for the combina-tion arm [12,13]. The combination of gemcitabine withoxaliplatin also had promising clinical activity [3]. Flu-oropyrimidines were also evaluated as counterpart togemcitabine. In a non-randomised trial leucovorin, fluo-rouracil and gemcitabine combination produced signifi-cantly higher response rate and survival data than
gemcitabine monotherapy (11 versus 8 months, respec-tively) [19]. The S-1/gemcitabine combination is alsoan active regimen [20]. Reichelmann et al. investigatedthe gemcitabine/capecitabine combination recruiting 75patients in a phase 2 trial. There was a high responserate (29%) with three CR and 6.2 months median PFS[21]. Iqbal et al. published similar results [14]. Koeberleet al. found in a series of 44 patients that this combina-tion can alleviate symptoms and ameliorate the qualityof life [9]. There are no published data on cetuximabco-administered with gemcitabine/capecitabine so far.
Malka et al. investigated gemcitabine/oxaliplatinwith or without cetuximab in the phase 2 BINGO trial.It was reported that the progression free survival rate in36 patients after 4 months of therapy was 61% on gem-citabine/oxaliplatin plus cetuximab and 44% on gemcit-abine/oxaliplatin [17]. In the updated analysis of thistrial PFS and OS were similar in both arms [22]. Inthe other recently presented phase 2 trial with similartreatment arms only the disease control rate and PFSand not the response rate and OS proved to be signifi-cantly favourable in the cetuximab combination arm[23]. It is worth noting that erlotinib added to gemcita-bin/oxaliplatin in a phase 3 trial has also not alteredthe survival significantly [24].
In some diseases the success of an anti-EGFR ther-apy can be predicted by the presence of biomarkers. Inour study the EGFR expression level had no significanteffect on the efficacy of therapy or survival and none ofthe 24 evaluable tissue samples harboured the KRAS
gene mutation. In 1996 Malats et al. reported an overallmutation prevalence of 40.4% (59/146) on codon 12 inthe bile duct and gall bladder cancer and shorter sur-vival for mutated tumours [25]. In other trials the muta-tion rate fell between 10% and 35% [1,22,23]. TheK-RAS and also B-RAF mutation status, and EGFRoverexpression had no statistically significant prognosticor predictive effect. The higher rate of mutationoccurred most commonly in Eastern studies and the

G. Rubovszky et al. / European Journal of Cancer 49 (2013) 3806–3812 3811
lower rate reported in Western studies suggest that thereare geographical differences in aetiology and the geneticsof this tumour type [11]. Our findings of high percentageof wild type tumours may be explained by the low num-ber of tumours analysed. In line with early trials withother targeted agents like bevacizumab, erlotinib or sun-itinib [24,26,27] results with cetuximab make the use ofthis agent debatable in this patient population untilthe exploration of a predictive biomarker.
In some studies investigating the effect of gemcita-bine-based combination chemotherapy survival datawere reported to be more favourable than in our study.This can be explained by several causes. In these phase 2and 3 studies the previous chemotherapy was an exclu-sion criterion, but in our trial five patients had been trea-ted earlier with chemotherapy. In other trials it wasquite strictly determined how the dose modificationshould be performed. In our study the dose modifica-tions were left to the discretion of the physician keepingin mind the quality of life issues, and this could lead to alower total dose given during a certain time period.
In previous studies detrimental effect on bone mar-row, gastrointestinal tract (nausea, vomiting and diar-rhoea) and skin, pain and fatigue were also reported[9,17,20,28]. In our trial side-effects were generally mild,only three grade 3 allergic reactions and one grade 4infection and four serious (grade 3/4) hypercalcaemiaoccurred.
It can be concluded that chemotherapy has its role inthe treatment of bile duct and gall bladder cancers. It isclear that surgery is the only curative intervention and inselected cases transplantation might be considered, too.Chemotherapy may add to the cure rate in the neoadju-vant and adjuvant setting, and clearly has a role in pal-liation. The standard first line therapy is nowgemcitabine combined with cisplatin or oxaliplatin,however in certain cases gemcitabine with a fluoropyr-imidine may be a reasonable and active alternative.Until the exploration of a biomarker for cetuximab effi-cacy, cetuximab remains investigational.
Conflict of interest statement
None declared.
Acknowledgements
The authors thank Monika Nagy for her help in datamanagement and Tibor Deak for his help in statisticalwork-up.
References
[1] Gruenberger B, Schueller J, Heubrandtner U, et al. Cetuximab,gemcitabine, and oxaliplatin in patients with unresectableadvanced or metastatic biliary tract cancer: a phase 2 study.Lancet Oncol 2010;11:1142–8.
[2] von Hahn T, Ciesek S, Wegener G, et al. Epidemiological trendsin incidence and mortality of hepatobiliary cancers in Germany.Scand J Gastroenterol 2011;46:1092–8.
[3] Sharma A, Dwary AD, Mohanti BK, et al. Best supportive carecompared with chemotherapy for unresectable gall bladdercancer: a randomized controlled study. J Clin Oncol2010;28:4581–6.
[4] Uchiyama K, Yamamoto M, Yamaue H, et al. Impact of nodalinvolvement on surgical outcomes of intrahepatic cholangiocar-cinoma: a multicenter analysis by the Study Group for HepaticSurgery of the Japanese Society of Hepato-Biliary-PancreaticSurgery. J Hepatobiliary Pancreat Sci 2011;18:443–52.
[5] Hong JC, Jones CM, Duffy JP, et al. Comparative analysis ofresection and liver transplantation for intrahepatic and hilarcholangiocarcinoma: a 24-year experience in a single center. ArchSurg 2011;146:683–9.
[6] Kiefer MV, Albert M, McNally M, et al. Chemoembolization ofintrahepatic cholangiocarcinoma with cisplatinum, doxorubicin,mitomycin C, ethiodol, and polyvinyl alcohol: a 2-center study.Cancer 2011;117:1498–505.
[7] Wijlemans JW, Van Erpecum KJ, Lam MG, et al. Trans-arterial(90)yttrium radioembolization for patients with unresectabletumors originating from the biliary tree. Ann Hepatol2011;10:349–54.
[8] Park SY, Kim JH, Yoon HJ, Lee IS, Yoon HK, Kim KP.Transarterial chemoembolization versus supportive therapy in thepalliative treatment of unresectable intrahepatic cholangiocarci-noma. Clin Radiol 2011;66:322–8.
[9] Koeberle D, Saletti P, Borner M, et al. Swiss Group for ClinicalCancer Research. Patient-reported outcomes of patients withadvanced biliary tract cancers receiving gemcitabine plus capecit-abine: a multicenter, phase II trial of the Swiss Group for ClinicalCancer Research. J Clin Oncol 2008;26:3702–8.
[10] Sharma A, Dwary AD, Mohanti BK, et al. Best supportive carecompared with chemotherapy for unresectable gall bladdercancer: a randomized controlled study. J Clin Oncol2010;28:4581–6.
[11] Marino D, Leone F, Cavalloni G, Cagnazzo C, Aglietta M.Biliary tract carcinomas: from chemotherapy to targeted therapy.Crit Rev Oncol Hematol 2013;85:136–48.
[12] Valle J, Wasan H, Palmer DH, et al. ABC-02 trial investigators.Cisplatin plus gemcitabine versus gemcitabine for biliary tractcancer. N Engl J Med 2010;362:1273–81.
[13] Okusaka T, Nakachi K, Fukutomi A, et al. Gemcitabine alone orin combination with cisplatin in patients with biliary tract cancer:a comparative multicentre study in Japan. Br J Cancer2010;103:469–74.
[14] Iqbal S, Rankin C, Lenz HJ, et al. A phase II trial of gemcitabineand capecitabine in patients with unresectable or metastaticgallbladder cancer or cholangiocarcinoma: Southwest OncologyGroup study S0202. Cancer Chemother Pharmacol2011;68:1595–602.
[15] Lassen U, Jensen LH, Sorensen M, Rohrberg KS, Ujmajuridze Z,Jakobsen A. A phase I–II dose escalation study of fixed-dose rategemcitabine, oxaliplatin and capecitabine every two weeks inadvanced cholangiocarcinomas. Acta Oncol 2011;50:448–54.
[16] Paule B, Herelle MO, Rage E, et al. Cetuximab plus gemcitabine–oxaliplatin (GEMOX) in patients with refractory advancedintrahepatic cholangiocarcinomas. Oncology 2007;72:105–10.
[17] Malka D, Trarbach T, Fartoux L. Et al A multicenter, random-ized phase II trial of gemcitabine and oxaliplatin (GEMOX) aloneor in combination with biweekly cetuximab in the first-linetreatment of advanced biliary cancer: Interim analysis of theBINGO trial. J Clin Oncol 2009;27:15s [Suppl. abstr 4520].
[18] Eckel F, Schmid RM. Chemotherapy in advanced biliary tractcarcinoma: a pooled analysis of clinical trials. Br J Cancer2007;96:896–902.

3812 G. Rubovszky et al. / European Journal of Cancer 49 (2013) 3806–3812
[19] Gebbia V, Giuliani F, Maiello E, et al. Treatment of inoperableand/or metastatic biliary tree carcinomas with single-agentgemcitabine or in combination with levofolinic acid and infu-sional fluorouracil: results of a multicenter phase II study. J ClinOncol 2001;19:4089–91.
[20] Kanai M, Yoshimura K, Tsumura T, et al. A multi-institutionphase II study of gemcitabine/S-1 combination chemotherapy forpatients with advanced biliary tract cancer. Cancer ChemotherPharmacol 2011;67:1429–34.
[21] Riechelmann RP, Townsley CA, Chin SN, et al. Expanded phaseII trial of gemcitabine and capecitabine for advanced biliarycancer. Cancer 2007;110:1307–12.
[22] Malka D, Cervera P, Heurteau-Foulon S, et al. Gemcitabine andoxaliplatin (GEMOX) alone or with cetuximab in first-linetreatment of advanced biliary cancers (ABC): exploratory anal-yses according to tumor KRAS/BRAF mutations and EGFRexpression in a randomized phase II trial (BINGO). J Clin Oncol2013;31 [Suppl. abstr 4127].
[23] Chen LT, Chen JS, Chao Y, et al. KRAS mutation status-stratified randomized phase II trial of GEMOX with and withoutcetuximab in advanced biliary tract cancer (ABTC): the TCOGT1210 trial. J Clin Oncol 2013;31 [Suppl. abstr 4018].
[24] Lee J, Park SH, Chang HM, et al. Gemcitabine and oxaliplatinwith or without erlotinib in advanced biliary-tract cancer: amulticentre, open-label, randomised, phase 3 study. Lancet Oncol2012;13:181–8.
[25] Malats N, Porta M, Pinol JL, Corominas JM, Rifa J, Real FX.Ki-ras mutations as a prognostic factor in extrahepatic bile systemcancer. PANK-ras I Project Investigators. J Clin Oncol1995;13:1679–86.
[26] Kemeny NE, Schwartz L, Gonen M, et al. Treating primary livercancer with hepatic arterial infusion of floxuridine and dexa-methasone: does the addition of systemic bevacizumab improveresults? Oncology 2011;80:153–9.
[27] Yi JH, Thongprasert S, Lee J, et al. A phase II study of sunitinibas a second-line treatment in advanced biliary tract carcinoma: amulticentre, multinational study. Eur J Cancer 2012;48:196–201.
[28] Maughan TS, Adams RA, Smith CG, et al. MRC COIN trialinvestigators. Addition of cetuximab to oxaliplatin-based first-linecombination chemotherapy for treatment of advanced colorectalcancer: results of the randomised phase 3 MRC COIN trial.Lancet 2011;377:2103–14.





























