Embed Size (px)
Citation preview

©2011 Landes Bioscience.Do not distribute.
Virulence 2:6, 528-537; November/December 2011; © 2011 Landes Bioscience
ReseaRch papeR
528 Virulence Volume 2 Issue 6
*Correspondence to: Karen Ejrnæs; Email: [email protected]: 05/20/11; Revised: 09/21/11; Accepted: 09/22/11http://dx.doi.org/10.4161/viru.2.6.18189
Introduction
Urinary tract infections (UTIs) are among the most common bacterial infectious diseases encountered in clinical practice and account for significant morbidity and high medical costs.1 Escherichia coli is the most predominant pathogen causing 80 to 90% of community-acquired UTIs and more than 30% of nosocomially acquired UTIs.2-4 Recurrent UTIs (RUTIs) are reported in 16–25% of women within six months and in 40–50% of women within one year of an UTI episode, and thus pose a major clinical problem.5-9 We previously showed that up to 77% of RUTIs are caused by E. coli identical to the primary infecting E. coli, but characteristics of E. coli
Recurrent urinary tract infections (RUTIs) pose a major problem but little is known about characteristics of Escherichia coli associated with RUTI. This study includes E. coli from 155 women with community-acquired lower urinary tract infections (UTIs) randomized to one of three dosing regiments of pivmecillinam and aimed to identify associations between the presence of 29 virulence factor genes (VFGs), phylogenetic groups and biofilm formation and the course of infection during follow-up visits at 8–10 and 35–49 d post-inclusion, respectively.
E. coli causing persistence or relapse were more often of phylogenetic group B2 and had a significantly higher aggre-gate VFG score than E. coli that were not detectable at follow-up. specifically, these E. coli causing persistence or relapse were characterized by a higher prevalence of hemolysis and 12 VFGs (sfa/focDE, papAH, agn43, chuA, fyuA, iroN, kpsM II, kpsM II K2, cnf1, hlyD, malX and usp). KpsM II K2 and agn43aCFT073 were independently associated with persistence or relapse. No specific combination of presence/absence of VFGs could serve as a marker to predict RUTI. stratifying for VFGs, seven days of pivmecillinam treatment reduced the prevalence of persistence or relapse of UTI compared with three days.
In vitro biofilm formation was not higher among E. coli causing persistence or relapse. The presence of agn43aCFT073 or agn43bCFT073 was associated with biofilm forming capacity.
In conclusion, our results show potential targets for prevention and treatment of persistence/relapse of UTI and po-tential markers for selecting treatment lengths and warrant studies of these and new VFGs.
Characteristics of Escherichia coli causing persistence or relapse of urinary tract infections
Phylogenetic groups, virulence factors and biofilm formation
Karen ejrnæs,1,2,* Marc stegger,1 andreas Reisner,3,4 sven Ferry,5,6 Tor Monsen,5 stig e. holm,5,7 Bettina Lundgren8,9 and Niels Frimodt-Møller1
1Department of Microbiological surveillance and Research; statens serum Institut; copenhagen, Denmark; 2Department of pathology; herlev hospital; herlev, Denmark; 3Molecular Microbial ecology Group; center for Biomedical Microbiology; Technical University of Denmark; Lyngby, Denmark; 4Biomedical science;
University of applied sciences; Graz, austria; 5Department of clinical Microbiology; Umea, sweden, 6Teg primary health care centre; Vännäs, sweden; 7Department of Medical Microbiology and Immunology; University of Gothenburg; Gothenburg, sweden; 8Department of clinical Microbiology; hvidovre hospital;
hvidovre, Denmark; 9centre of Diagnostic Investigations; Rigshospitalet; copenhagen, Denmark
Key words: E. coli, biofilm, recurrence, virulence factor, urinary tract infection, phylogenetic group
Abbreviations: UTI, urinary tract infection; RUTI, recurrent urinary tract infection; VF, virulence factor; VFG, virulence factor gene; PIV, pivmecillinam; IBC, intracellular bacterial communities
associated with persistence or relapse of UTI remain poorly defined.10,11
E. coli can be separated in four phylogenetic groups (A, B1, B2 and D) that appear to have different ecological niches and pro-pensity to cause disease.12-17 It is so far unknown whether there is an association between phylogenetic groups and E. coli causing RUTIs.
Epidemiological and in vivo studies suggest a large number of virulence factor genes (VFGs) to be associated with uro-pathogenic E. coli (UPEC).18,19 However, only a few studies have addressed the relation between virulence factors (VFs) and relapse of UTI in women and none of these had a combination of a large study population and a broad spectrum of VFGs.7,20,21

©2011 Landes Bioscience.Do not distribute.
www.landesbioscience.com Virulence 529
ReseaRch papeR ReseaRch papeR
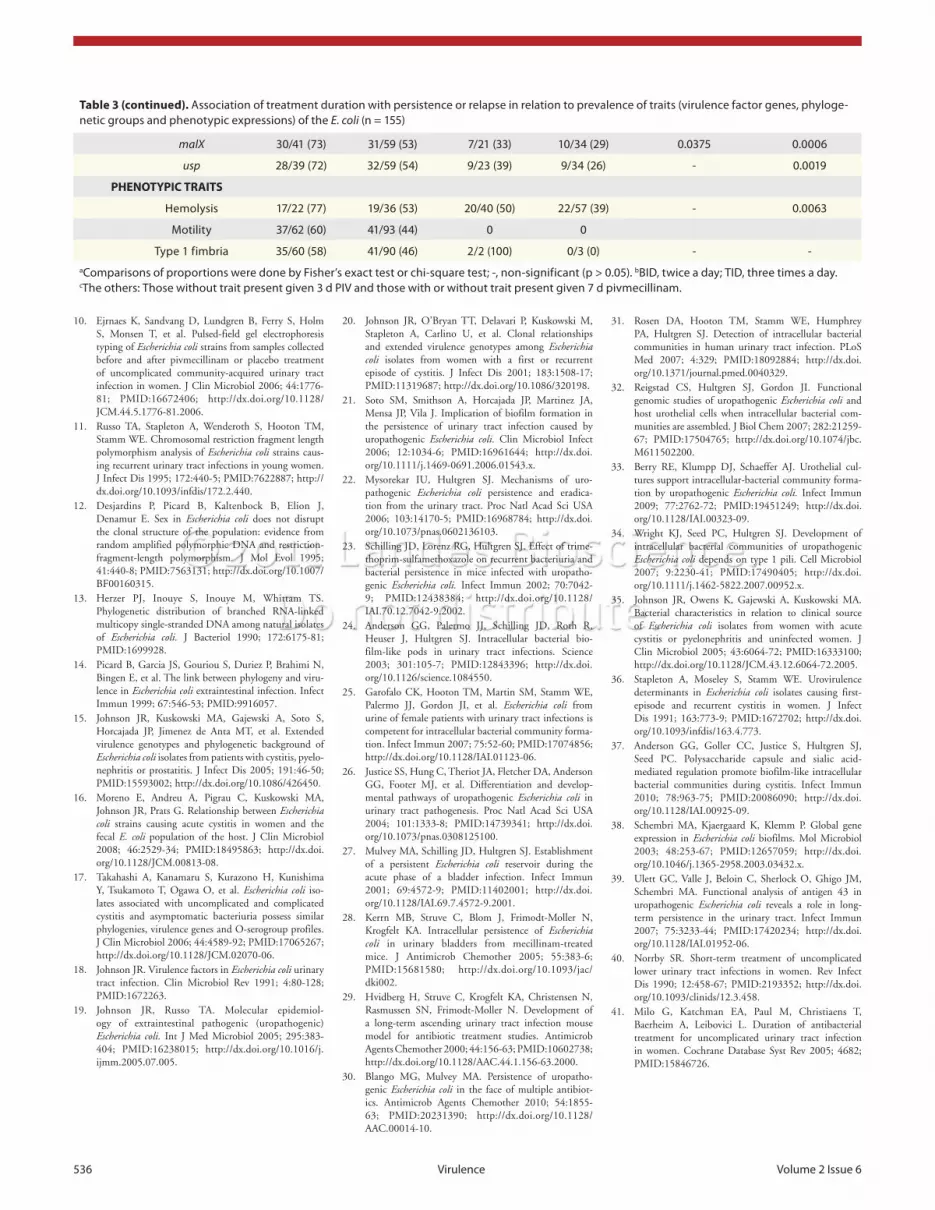
Duration of treatment. E. coli being positive for a least one of five traits (phylogenetic group B2, ireA, iroN, ibeA and malX ) was associated with significantly higher prevalence of persistence or relapse when given 3 d PIV therapy compared with those given 7 d. However, E. coli not being positive for these traits did not show any difference in prevalence of persistence/relapse between 3 d and 7 d PIV treatment (Table 3).
E. coli being positive for at least one of 16 traits (phylogenetic group B2, papAH, sfa/focDE, agn43, chuA, fyuA, iroN, kpsM II, kpsM II K2, traT, cnf1, hlyD, ibeA, malX, usp and phenotypic hemolysis) was associated with significantly higher prevalence of persistence or relapse when given 3 d compared with those with-out these traits given 3 d PIV therapy or those with/or without these traits given 7 d PIV therapy (Table 3).
Cluster analysis did not show E. coli causing persistence/relapse and those followed by cure/reinfection to segregate in separate clusters characterized by a specific combination of pres-ence or absence of traits and treatment regimen.
VFGs and phylogenetic groups. Strains of phylogenetic group B2 had a significantly higher aggregate VFG score than strains from non-B2 groups (B2 VFG score
Median (range) = 15 (3–21) vs.
non-B2 VFG scoreMedian (range)
= 5 (1–14), p < 0.0001).Biofilm formation of E. coli in different growth media. The
capacity of the E. coli to form biofilms in vitro was assessed in three different growth media, which promoted biofilm forma-tion differently (p < 0.001) in the following order: ABTCAA (A
595, Median, ABTCAA = 1.07) > ABTG (A
595, Median, ABTG = 0.46) > LB
(A595, Median, LB
= 0.15).There was no significant difference in biofilm formation
capacity between E. coli causing persistence or relapse compared with E. coli followed by cure or reinfection in any of the three media. The biofilm formation capacity did not differ among the phylogenetic groups in any of the three media.
Biofilm formation in vitro and antigen 43. The biofilm for-mation capacity in vitro of the E. coli strains was analyzed in relation to the presence or absence of the four allelic variants of the gene agn43 encoding Antigen 43 (Ag43). We found no significant associations for agn43 and agn43
K12 alleles. However,
E. coli positive for agn43bCFT073
exhibited stronger biofilm forma-tion than those negative for this gene when tested in the ABTG medium (A
595 Median, pos = 0.5200 vs. A
595 Median,
neg = 0.3800; p =
0.0005) and in the ABTCAA medium (A595 Median, pos
= 1.235 vs. A
595 Median,
neg = 1.010; p = 0.0016). Also E. coli positive for
agn43aCFT073
had a higher biofilm score in the ABTG medium compared with those negative for this gene (A
595 Median, pos = 0.4450
vs. A595 Median, neg
= 0.3600; p = 0.0327).Antimicrobial resistance. The prevalence of antimicrobial
resistance to the nine tested antimicrobials among the primary infecting E. coli was generally low: ampicillin (10%), cefpodox-ime (1%), chloramphenicol (1%), ciprofloxacin (0%), gentami-cin (0%), streptomycin (7%), sulfamethizole (8%), tetracycline (8%) and trimethoprim (3%). Antibiotic resistance profiles of the E. coli strains were not associated with a specific course of infection such as cure, persistence, reinfection or relapse (data not shown).
E. coli can invade and replicate within the murine bladder forming biofilm-like intracellular bacterial communities (IBCs) and establish quiescent intracellular reservoirs that may repre-sent stable reservoirs for RUTI.22-28 No antibiotics have proven efficient in eradicating the UPEC reservoirs in the bladder in mice.23,28-30 Exfoliated IBCs and filamentous E. coli have been detected in urine from women with acute uncomplicated cystitis indicating that this pathogenic pathway may occur in women with UTIs.31 The mechanisms behind the IBC pathogenic path-way are only partially established. Some VFs have been suggested to have a potential role in the formation of IBCs.24,32-34 Despite the potential role of these VFs in the pathogenesis of relapse of UTI in women it is unknown whether these VFGs are associated with E. coli causing relapse in women.
The aim of the present study was to identify and analyze pos-sible associations between characteristics of E. coli (VFGs, phy-logenetic groups and biofilm formation) and the course of UTI with focus on E. coli causing persistence or relapse.
Results
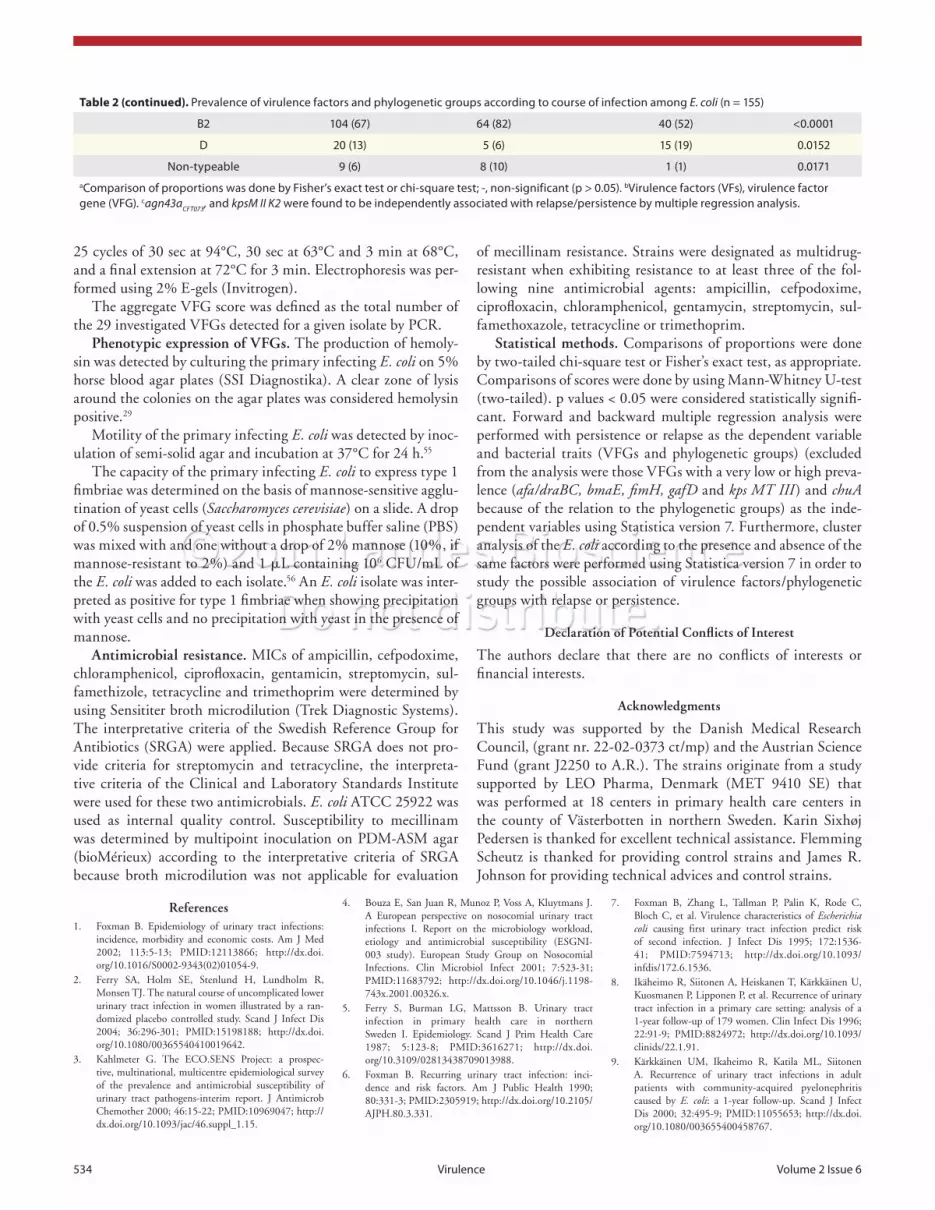
Association between phylogenetic groups and course of infection. A total of nine (6%) E. coli strains were classified as non-typeable. Phylogenetic group B2 was dominating (67%), followed by group D (13%), A (11%) and B1 (3%) (Table 2). Phylogenetic group B2 dominated among E. coli that caused persistence or relapse at fol-low-up (82% vs. 52%; p < 0.0001) whereas phylogenetic group D dominated among E. coli that were followed by cure or reinfection at follow-up (6% vs. 19%; p = 0.0152) (Table 2). Groups A and B1 showed no significant association with the course of infection.
Distribution of VFGs. The prevalence of 29 VFGs among the E. coli strains varied significantly also within the six functional groups (Table 2). The median of aggregate VFG scores was 13 (range 0–21). Only one isolate was negative for all tested VFGs.
Phenotypic expression of selected VFs. All (155, 100%) of the E. coli were found to be motile. A total of 99% (150/152) of the E. coli positive for fimH also expressed type 1 fimbriae and 87% (58/67) of the E. coli positive for hlyD also exhibited pheno-typic hemolysis (Table 2).
Association between VFGs and course of infection. The median of the aggregate VFG score was significantly higher for E. coli causing persistence or relapse at follow-up than for those followed by cure or reinfection (14 vs. 10; p = 0.0038, Table 2). The E. coli causing persistence or relapse exhibited a significantly higher prevalence of hemolysis and 12 VFGs distributed among all six functional groups (papAH, sfa/focDE, agn43, chuA, fyuA, iroN, kpsM II, kpsM II K2, cnf1, hlyD, malX and usp) compared with those followed by cure or reinfection (Table 2). Multiple regression analysis showed that kpsM II K2 and agn43a
CFT073
were independently and significantly associated with persistence or relapse (p < 0.05). Cluster analysis did not show E. coli causing persistence/relapse and those followed by cure/reinfection to seg-regate in separate clusters characterized by a specific combination of VFGs. No clear distinction based on the presence and absence of VFGs could thus be made between the two groups.

©2011 Landes Bioscience.Do not distribute.
530 Virulence Volume 2 Issue 6
showed that the polysialic acid K1 capsule is significant in the maintenance of IBC morphology.37 Our study concerning genes encoding for parts of the heme receptor (chuA), salmochelin siderophore receptor (iroN ), α hemolysin (hlyD), cytotoxic nec-rotizing factor 1 (cnf1), and group II capsular polysaccharides (kpsMII, kpsMII K2) that have been speculated to be related to the formation of IBC is to our knowledge the first study to show correlation between E. coli strains causing persistence or relapse in the patients and these VFGs. Interestingly it should be noticed here that we also found kpsM II K2 to be independently associ-ated with persistence or relapse in multiple regression analysis. Our results may further support the theory of IBC formation in the bladder and warrants further studies of these VFs.
We found that E. coli causing persistence/relapse had a higher median aggregate VFG score than those followed by cure or rein-fection. This is an interesting result; however, a higher aggregate VFG score per se is not sufficient to serve as a marker for detect-ing E. coli that might cause RUTI. Unfortunately cluster analysis did not reveal a specific combination of presence/absence of the tested VFGs that clustered together among the group causing persistence/relapse or cure/reinfection. The bacterial characteris-tics that were investigated in this study could not serve to predict the potential for E. coli to cause RUTI and further genetic char-acterization of these strains is undertaken.
The apparent cell-cell interactions during IBC formation in the bladder suggest that E. coli causing RUTI might have a selec-tive advantage based on their ability to form biofilms. Only one former study of 43 women has addressed the question of biofilm in relation to RUTI and found that biofilm formation in vitro to be more frequent among E. coli causing relapse as opposed to E. coli associated with reinfection.21 Our study of 155 women did not confirm the finding of a correlation between biofilm forma-tion in vitro and strains causing persistence or relapse. However, it would be interesting to further study biofilm formation of the E. coli strains in model systems closer mimicking the natural sys-tem and the role in IBC formation.
Genes encoding the autotransporter Ag43 has been reported to be associated with cell aggregation and biofilm formation in laboratory strain E. coli K12.38 Our study is to our knowledge the first to reveal that the presence of Ag43 alleles (agn43a
CFT073 and
agn43bCFT073
) known from UPEC CFT073 is associated with bio-film formation in vitro of uropathogenic E. coli. Ag43 has been found to be expressed on the surface of UPEC cells located in IBCs in the bladder epithelium.24 Recently, it was shown that the variant Ag43a from the UPEC CFT073 promotes long-term persistence in the urinary bladder in a mouse model.39 Our study showed a correlation between relapse or persistence and E. coli strains being positive for agn43 and multiple regression analysis showed agn43a
CFT073 to be related to relapse or persistence. This
correlation between agn43 and allele with E. coli strains causing relapse or persistence of UTI in women has not been reported before and further supports a possible role of Ag43 in IBCs and RUTI and further studies of these VFs.
Analysis of bacterial traits of the primary infecting E. coli at time of clinical presentation in relation to treatment regi-men and outcome showed that E. coli being positive for certain
Discussion
A better understanding of the characteristics that predispose pathogens to cause RUTI would facilitate the development of new therapeutic strategies. We present a study of 155 primary infecting E. coli isolated from 155 women with community-acquired symptomatic lower UTI experiencing cure, persistence, reinfection or relapse during the follow-up period. The study compared the presence of 29 VFGs, phylogenetic groups, biofilm formation and antimicrobial resistance with the course of UTI during follow-up and is to our knowledge the largest study pub-lished of this kind.
The finding of group B2 being the predominant phylogenetic group followed by group D, A and B1 agrees with other studies concerning phylogenetic groups in UPEC.15-17 We found phylo-genetic groups B2 to be associated with persistence or relapse. To our knowledge no former studies have evaluated phylogenetic groups in relation to RUTI in women. Our interesting finding might be explained by the fact, that E. coli strains belonging to phylogenetic group B2 contained a greater number of VFGs than E. coli belonging to a non-B2 phylogenetic group as also reported by other studies of UPEC.15,35 It argues for exploring VFs or other bacterial characteristics associated with phylogenetic B2 in unveiling the pathogenesis behind RUTI.
In general, the prevalence of the tested VFGs among the E. coli strains was found to correlate well with other studies of cystitis in women.15,20,35 This indicates that the selected strains constitute a representative sample of E. coli strains causing UTI.
Interestingly, we found that E. coli causing persistence or relapse during follow-up had a higher prevalence of 12 VFGs indicating that these VFs may play a role in the pathogenesis of RUTI. These 12 VFGs are equally distributed among all six functional VFG groups encoding adhesins, a biofilm related fac-tor, iron uptake systems but also protectins and toxins and thus do not indicate a specific pathogenic strategy that predisposes E. coli strains to cause persistence or relapse of UTI.
Only four previous studies have analyzed the presence of VFGs in relation to RUTI in women.7,20,21,36 These studies were based on study population sizes ranging from 43 to 174 patients and a spectrum of 13 to 27 VFGs but none of these studies had a combination of a large study population and a broad spectrum of VFGs comparable to ours. One study did not find a correla-tion between VFGs and RUTI.36 The others found VFGs such as papA, papG, iha, iutA, fyuA and drb to be associated with RUTI. However, these studies differ in many aspects from each other and from our present study, e.g., definition and criteria for RUTI, selection of VFGs, methods used etc. making compari-sons difficult.7,20,21
Recently, three studies aimed to explore the mechanisms behind the observed formation of biofilm-like IBCs by E. coli in the murine bladder.32,33,37 One study showed that chuA, iroN and hlyA were expressed at significantly higher levels among E. coli (UTI89) in IBCs compared with those in the intestine.32 Another study reported in an in vitro model that mimics IBC formation, that iroN, hlyA, cnf1, fliC and kpsD were upregulated under intra-cellular conditions.33 Finally, the recent study by Anderson et al.

©2011 Landes Bioscience.Do not distribute.
www.landesbioscience.com Virulence 531
to be asymptomatic. Their risk for misclassification may thus be fairly limited.
In summary, our results did not find a specific marker based on bacterial traits for RUTI that could be a useful diagnostic tool. However we showed interesting potential targets for preven-tion and treatment of persistence and relapse of UTI and inter-esting potential markers for selecting treatment lengths. Future studies must explore the function of these VFGs and other puta-tive or new VFGs of UPEC in relation to persistence and relapse and their possible role in establishment of IBCs and quiescent intracellular reservoirs. Defining the repertoire and mechanism of VFGs could facilitate the development of new diagnostic tools, regimens and drugs for prevention and treatment of RUTI.
Materials and Methods
Strain collection. This present study focused on a subgroup of 155 E. coli strains selected from a large prospective, multicenter, randomized, double-blind, placebo-controlled comparative study of community-acquired lower UTI in women.42 The women were randomized to one of three dosing regimens of pivmecil-linam (pivoxil amdinocillin, PIV) or placebo and evaluated clini-cally and bacteriologically at inclusion and at two follow-up visits after 8–10 d and 35–49 d post-inclusion, respectively. The Ethics Committee of Umea University, Sweden, approved the study (Um Dnr 93–178), and informed written consent to participate was obtained from the included patients.2 Urine sample collec-tion, quantification and identification were done as previously described by Ferry et al.42 Symptoms suggestive of lower UTI (urgency, dysuria, suprapubic pain or low lumbar/flank pain) were graded and a total score of zero classified the patients as being asymptomatic and ≥1 as being symptomatic. Significant bacteriuria was defined according to current European guide-lines.43 For E. coli this was defined as a bacterial count of E. coli of ≥103 CFU/ml for symptomatic women and a bacterial count of E. coli of ≥105 CFU/ml for asymptomatic women.
The E. coli strains for the present study were isolated at inclu-sion prior to therapy from 155 women with symptoms of lower UTI treated with PIV in the large parent study. E. coli from women receiving placebo were not included in the present study since we aimed at studying persistence/relapse following antimi-crobial treatment. The strains selected for the present study con-sisted of all primary infecting E. coli susceptible to mecillinam from women having significant E. coli bacteriuria at one or both of the follow-up visits (two strains that could not be assigned to an infection profile, two strains resistant to mecillinam, and one strain with at mixed infection were excluded),10 and a ran-domly selected group of 20 (if possible) primary infecting E. coli from patients who had a negative urine culture at both follow-up visits from each of the three dosing regimens of PIV (Table 1). Thus, we were able to study in detail a collection of E. coli strains isolated from patients with UTI before treatment who experi-enced relapse/persistence or cure/reinfection after treatment, i.e., we could compare virulence and other bacterial factors among E. coli strains disappearing from or able to remain in the urinary tract.
bacterial traits was associated with a higher prevalence of persis-tence or relapse of UTI when given 3 d PIV as compared with those given 7 d PIV therapy. We have not seen any other stud-ies, which have found such significant links between presence of virulence factors in UPEC, duration of treatment and the risk of RUTI. Unfortunately cluster analysis did not reveal a specific combination of bacterial traits (presence/absence of traits) that could serve as a marker for choosing treatment regimen. Given the commonality of some of these traits, the predictive value of some of the traits might be limited and our interesting results should therefore be pursued in future studies including other bacterial characteristics and prospective studies, where rapid molecular methods could be used to detect genetic factors that predict higher risk of RUTI and to choose treatment duration to reduce this risk.
A meta-analysis of duration of therapy for lower UTI rec-ommended 5–7 d also for other β-lactam antimicrobials.40 Additionally, a Cochrane review concluded that 3 d therapy was less effective than a 5–10 d therapy of uncomplicated UTI with respect to bacteriological failure.41 Of course, increased con-sumption of antimicrobials may increase the risk of emergence of antibiotic-resistant strains. Furthermore, therapy above 3 d may increase the prevalence of adverse effects.41 Treatment above 3 d could thus be speculated to be reserved for a selected group of women, and similar studies like ours also with other antimicrobi-als than PIV could help identifying potential markers in UPEC that could be used in selecting a more differentiated and optimal treatment duration for uncomplicated UTI.
The E. coli strains were collected in Sweden, an area charac-terized by a low level of resistance, and the level of antimicrobial resistance among our E. coli collection was also found to be low. Antibiotic resistance profiles were not found to be related to per-sistence or relapse.
The strengths of the present study include a large study popu-lation, which is well-characterized with respect to clinical and epidemiological data, availability of outcome data, differentiation between same-strain vs. different-strain recurrence, the exten-sive number of bacterial traits analyzed, a rather long follow-up period of 5–7 weeks and information of treatment regimen given. The limitations of the study include the lack of vaginal and rectal cultures limiting the discussion regarding a possible vaginal, rec-tal or bladder (IBCs) reservoir for E. coli causing RUTI. Another limitation of the study is the use of multiple comparisons, which may increase the risk of type I errors. However, the present study was designed to analyze for possible associations that could be pursued in future studies. Interdependence or closely linkage of VFGs may also confound the observations. Finally the first fol-low-up visit was placed on day 8–10 implying a risk for the two treatment cohorts of 7 d PIV that the first follow-up was placed within the washout period for mecillinam. There is a risk that a negative urine culture at first follow-up, in some of the cases with 7 d PIV treatment, does not represent the infectious state of the urine. However in 49% of these cases it was found that the first follow-up was placed on day 9 or later where residual antibiotic is not a problem. Among the group with 7 d PIV and a negative urine culture and a first follow-up placed at day 8, 65% showed

©2011 Landes Bioscience.Do not distribute.
532 Virulence Volume 2 Issue 6
negative for yjaA were additionally screened for the gene ibeA. In the presence of ibeA the E. coli strain was classified as B2.
Genotypic detection of VFGs. The primary infecting E. coli was screened for the presence of the following 29 VFGs repre-senting six functional groups (Table 2): (1) Adhesins: afa/draBC (Dr. binding adhesin), bmaE (blood group M fimbriae), fimH (type 1 fimbriae), focG (F1C fimbriae), gafD (G fimbriae), iha (Iron-regulated gene A homolog adhesin, siderophore recep-tor), papAH (P fimbriae), sfa/focDE (S fimbriae, FIC fimbriae); (2) Biofilm related: agn43 (Antigen 43, common), agn43a
CFT073
(Antigen 43, allele a CFT073), agn43bCFT073
(Antigen 43, allele b CFT073), agn43
K12 (Antigen 43, allele K12); (3) Iron uptake:
chuA (heme receptor), fyuA (yersiniabactin siderophore receptor), iroN (salmochelin siderophore receptor), ireA (iron-regulated element, siderophore receptor), iutA (aerobactin siderophore receptor); (4) Protectins: iss (increased serum survival), kpsM II (group II capsule), kpsM II K2 (group II capsule, K2), kpsMT III (group III capsule), traT (serum resistance); (5) Toxins: cdtB (cytolethal distending toxin), cnf1 (cytotoxic necrotizing fac-tor 1), hlyD (α hemolysin), sat (secreted autotransporter toxin); (6) Miscellaneous: ibeA (invasion of brain endothelium), malX (pathogenicity-associated island marker of CFT073), usp (uro-pathogenic specific protein).
The gene chuA was detected by the PCR for phylogenetic groups (see paragraph for phylogenetic analysis). The rest of the genes were detected by using a modified multiplex PCR protocol described by Johnson and Steel.49 There were six primer pools: Pool 1: malX, papAH, fimH, focG, traT, ibeA; Pool 2: gafD, fyuA, iroN, sfa/focDE, kpsM II; Pool 3: hlyD, iha, afa/draBC, iss, ireA; Pool 4: cnf, usp, bmaE, agn43b
CFT073, kpsMT III; Pool 5: sat, kpsM
II K2, cdtB, agn43K12
, iutA; and Pool 6: agn43, agn43aCFT073
.17,49-54 PCR was performed in a final volume of 25 μL containing 2 μL of template DNA (boiled lysate), 0.6 μM of each primer, 1x PCR Buffer (Invitrogen, 10966034), 4 mM MgCl
2 (Invitrogen,
10966034), 40 μM dNTPs (Invitrogen, 10966034), and 0.5 U Platinum Taq DNA polymerase (Invitrogen, 10966034). Amplification conditions were denaturation for 12 min at 95°C;
The primary infecting E. coli isolates were categorized into four infection profiles as previously described: cure, persis-tence, reinfection or relapse (Table 1).10 This classification did not include clinical parameters as symptom score or paraclini-cal parameters as inflammatory biomarkers but was based on only urine culture results and pulsed-field gel electrophoresis (PFGE). Cure was defined by a negative urine culture at both follow-up visits. Persistence was defined as significant bacteri-uria with the same E. coli as the primary infecting E. coli at the first follow-up. Relapse was defined as a negative culture at first follow-up followed by significant bacteriuria with the same E. coli as the primary infecting E. coli at the second follow-up. Reinfection was defined as significant bacteriuria with E. coli different from the primary infecting E. coli at first follow-up or a negative culture at first follow-up followed by significant bacte-riuria with a new E. coli at second follow-up. Among the group with persistence at first follow-up 81% were symptomatic and among the group with persistence or relapse at second follow-up 71% were symptomatic. For comparisons, two groups of courses of infection were defined and compared: persistence or relapse against cure or reinfection.
Biofilm assay. Cultivation and quantification of biofilms were performed as previously described except that 96-well u-bottom plates (Sterilin) were used for biofilm cultivation.44 Briefly, test strains were grown in micro-titer plates containing LB medium or minimal medium AB containing thiamine and supplemented with glucose (ABTG) or casaminoacids (ABTCAA) for 48 h before quantification of biofilm formation by staining with crys-tal violet.45,46 Biofilm score was defined as the A
595 nm measured at
a VICTOR2 multilabel counter (PerkinElmer) after extraction of surface-bound crystal violet with 180 μL of ethanol (96%).
Phylogenetic analysis. Phylogenetic grouping into the phy-logenetic group A, B1, B2 and D was determined by a triplex PCR assay.47 Assigning E. coli to the four phylogenetic groups A, B1, B2 and D was done according to modified interpretive crite-ria.48 Strains failing to yield any PCR product were classified as non-typeable, while strains positive for chuA and TSPE4.C2 and
Table 1. Distribution according to course of infection and treatment group of the E. coli (n = 155)
Culture Results Course of Infectiona Pivmecillinam Groups (n = 155)
Initial Visit 1st follow-upb 2nd follow-upc n 400 mg BIDd for 3 d 200 mg BIDd for 7 d 200 mg TIDd for 7 d
E. coli Negative Negative cure 57 17 20 20
E. coli same E. colie same E. coli persistence 15 7 4 4
E. coli same E. coli Negative persistence 5 3 1 1
E. coli same E. coli Missing persistence 12 10 0 2
E. coli Negative same E. coli Relapse 46 17 16 13
E. coli Negative New E. coli f Reinfection 14 4 5 5
E. coli New E. coli New E. coli Reinfection 2 1 0 1
E. coli New E. coli Negative Reinfection 2 1 0 1
E. coli New E. coli Missing Reinfection 2 2 0 0
Total 155 62 46 47acourse of infection according to pFGe results by ejrnaes et al.10 b8–10 d post-inclusion. c35–49 d post-inclusion. dBID, twice a day; TID, three times a day. esame E. coli as the primary infecting E. coli at inclusion according to pFGe.10 fE. coli different from the primary infecting E. coli at inclusion according to pFGe.10

©2011 Landes Bioscience.Do not distribute.
www.landesbioscience.com Virulence 533
Prevalence of Bacterial Traits (Column %)
Total n = 155 Relapse or Persistence n = 78 Cure or Reinfection n = 77 p-valuesa
aggregate VFG score median (range)b 13 (1–21) 14 (1–21) 10 (1–20) 0.0038
VIRULENCE FACTOR GENES
Adhesins
afa/draBC 6 (4) 3 (4) 3 (4) -
bmaE 0 0 0 -
fimH 152 (98) 76 (97) 76 (99) -
focG 32 (21) 16 (21) 16 (21) -
gafD 0 0 0 -
iha 35 (23) 17 (22) 18 (28) -
papAH 72 (47) 43 (55) 29 (38) 0.0293
sfa/focDE 71 (46) 47 (60) 24 (31) 0.0003
Biofilm-related
agn43 123 (79) 67 (86) 56 (73) 0.0428
agn43aCFT073 c 35 (23) 17 (22) 18 (23) -
agn43bCFT073 44 (28) 25 (32) 19 (25) -
agn43K12 40 (26) 18 (23) 22 (29) -
Iron uptake
chuA 124 (80) 69 (88) 55 (71) 0.0080
fyuA 121 (78) 69 (88) 52 (66) 0.0016
iroN 87 (56) 55 (71) 32 (42) 0.0003
ireA 27 (17) 14 (18) 13 (17) -
iutA 55 (36) 30 (38) 25 (32) -
Protectins
iss 20 (13) 10 (13) 10 (13) -
kpsM II 103 (67) 61 (78) 42 (55) 0.0018
kpsM II K2 c 109 (70) 61 (78) 48 (62) 0.0306
kpsMT III 3 (2) 2 (3) 1 (1) -
traT 55 (36) 31 (40) 24 (31) -
Toxins
cdtB 27 (17) 16 (21) 11 (14) -
cnf1 60 (39) 40 (51) 20 (26) 0.0012
hlyD 67 (43) 43 (55) 24 (31) 0.0026
sat 34 (23) 17 (22) 17 (22) -
Miscellaneous
ibeA 34 (23) 21 (17) 13 (17) -
malX 100 (65) 61 (78) 39 (51) 0.0003
usp 98 (63) 60 (77) 38 (49) 0.0004
PHENOTYPIC EXPRESSION OF VFsb
hemolysis 58 (37) 36 (46) 22 (29) 0.0237
Motility 155 (100) 78 (100) 77 (100) -
Type 1 fimbriae 150 (97) 76 (97) 74 (96) -
PHYLOGENETIC GROUPS
a 17 (11) 6 (7) 11 (14) -
B1 5 (3) 2 (3) 3 (4) -acomparison of proportions was done by Fisher’s exact test or chi-square test; -, non-significant (p > 0.05). bVirulence factors (VFs), virulence factor gene (VFG). cagn43aCFT073, and kpsM II K2 were found to be independently associated with relapse/persistence by multiple regression analysis.
Table 2. prevalence of virulence factors and phylogenetic groups according to course of infection among E. coli (n = 155)
©2011 Landes Bioscience.Do not distribute.
534 Virulence Volume 2 Issue 6
of mecillinam resistance. Strains were designated as multidrug-resistant when exhibiting resistance to at least three of the fol-lowing nine antimicrobial agents: ampicillin, cefpodoxime, ciprofloxacin, chloramphenicol, gentamycin, streptomycin, sul-famethoxazole, tetracycline or trimethoprim.
Statistical methods. Comparisons of proportions were done by two-tailed chi-square test or Fisher’s exact test, as appropriate. Comparisons of scores were done by using Mann-Whitney U-test (two-tailed). p values < 0.05 were considered statistically signifi-cant. Forward and backward multiple regression analysis were performed with persistence or relapse as the dependent variable and bacterial traits (VFGs and phylogenetic groups) (excluded from the analysis were those VFGs with a very low or high preva-lence (afa/draBC, bmaE, fimH, gafD and kps MT III) and chuA because of the relation to the phylogenetic groups) as the inde-pendent variables using Statistica version 7. Furthermore, cluster analysis of the E. coli according to the presence and absence of the same factors were performed using Statistica version 7 in order to study the possible association of virulence factors/phylogenetic groups with relapse or persistence.
Declaration of Potential Conflicts of Interest
The authors declare that there are no conflicts of interests or financial interests.
Acknowledgments
This study was supported by the Danish Medical Research Council, (grant nr. 22-02-0373 ct/mp) and the Austrian Science Fund (grant J2250 to A.R.). The strains originate from a study supported by LEO Pharma, Denmark (MET 9410 SE) that was performed at 18 centers in primary health care centers in the county of Västerbotten in northern Sweden. Karin Sixhøj Pedersen is thanked for excellent technical assistance. Flemming Scheutz is thanked for providing control strains and James R. Johnson for providing technical advices and control strains.
25 cycles of 30 sec at 94°C, 30 sec at 63°C and 3 min at 68°C, and a final extension at 72°C for 3 min. Electrophoresis was per-formed using 2% E-gels (Invitrogen).
The aggregate VFG score was defined as the total number of the 29 investigated VFGs detected for a given isolate by PCR.
Phenotypic expression of VFGs. The production of hemoly-sin was detected by culturing the primary infecting E. coli on 5% horse blood agar plates (SSI Diagnostika). A clear zone of lysis around the colonies on the agar plates was considered hemolysin positive.29
Motility of the primary infecting E. coli was detected by inoc-ulation of semi-solid agar and incubation at 37°C for 24 h.55
The capacity of the primary infecting E. coli to express type 1 fimbriae was determined on the basis of mannose-sensitive agglu-tination of yeast cells (Saccharomyces cerevisiae) on a slide. A drop of 0.5% suspension of yeast cells in phosphate buffer saline (PBS) was mixed with and one without a drop of 2% mannose (10%, if mannose-resistant to 2%) and 1 μL containing 106 CFU/mL of the E. coli was added to each isolate.56 An E. coli isolate was inter-preted as positive for type 1 fimbriae when showing precipitation with yeast cells and no precipitation with yeast in the presence of mannose.
Antimicrobial resistance. MICs of ampicillin, cefpodoxime, chloramphenicol, ciprofloxacin, gentamicin, streptomycin, sul-famethizole, tetracycline and trimethoprim were determined by using Sensititer broth microdilution (Trek Diagnostic Systems). The interpretative criteria of the Swedish Reference Group for Antibiotics (SRGA) were applied. Because SRGA does not pro-vide criteria for streptomycin and tetracycline, the interpreta-tive criteria of the Clinical and Laboratory Standards Institute were used for these two antimicrobials. E. coli ATCC 25922 was used as internal quality control. Susceptibility to mecillinam was determined by multipoint inoculation on PDM-ASM agar (bioMérieux) according to the interpretative criteria of SRGA because broth microdilution was not applicable for evaluation
Table 2 (continued). prevalence of virulence factors and phylogenetic groups according to course of infection among E. coli (n = 155)
B2 104 (67) 64 (82) 40 (52) <0.0001
D 20 (13) 5 (6) 15 (19) 0.0152
Non-typeable 9 (6) 8 (10) 1 (1) 0.0171acomparison of proportions was done by Fisher’s exact test or chi-square test; -, non-significant (p > 0.05). bVirulence factors (VFs), virulence factor gene (VFG). cagn43aCFT073, and kpsM II K2 were found to be independently associated with relapse/persistence by multiple regression analysis.
References1. Foxman B. Epidemiology of urinary tract infections:
incidence, morbidity and economic costs. Am J Med 2002; 113:5-13; PMID:12113866; http://dx.doi.org/10.1016/S0002-9343(02)01054-9.
2. Ferry SA, Holm SE, Stenlund H, Lundholm R, Monsen TJ. The natural course of uncomplicated lower urinary tract infection in women illustrated by a ran-domized placebo controlled study. Scand J Infect Dis 2004; 36:296-301; PMID:15198188; http://dx.doi.org/10.1080/00365540410019642.
3. Kahlmeter G. The ECO.SENS Project: a prospec-tive, multinational, multicentre epidemiological survey of the prevalence and antimicrobial susceptibility of urinary tract pathogens-interim report. J Antimicrob Chemother 2000; 46:15-22; PMID:10969047; http://dx.doi.org/10.1093/jac/46.suppl_1.15.
4. Bouza E, San Juan R, Munoz P, Voss A, Kluytmans J. A European perspective on nosocomial urinary tract infections I. Report on the microbiology workload, etiology and antimicrobial susceptibility (ESGNI-003 study). European Study Group on Nosocomial Infections. Clin Microbiol Infect 2001; 7:523-31; PMID:11683792; http://dx.doi.org/10.1046/j.1198-743x.2001.00326.x.
5. Ferry S, Burman LG, Mattsson B. Urinary tract infection in primary health care in northern Sweden I. Epidemiology. Scand J Prim Health Care 1987; 5:123-8; PMID:3616271; http://dx.doi.org/10.3109/02813438709013988.
6. Foxman B. Recurring urinary tract infection: inci-dence and risk factors. Am J Public Health 1990; 80:331-3; PMID:2305919; http://dx.doi.org/10.2105/AJPH.80.3.331.
7. Foxman B, Zhang L, Tallman P, Palin K, Rode C, Bloch C, et al. Virulence characteristics of Escherichia coli causing first urinary tract infection predict risk of second infection. J Infect Dis 1995; 172:1536-41; PMID:7594713; http://dx.doi.org/10.1093/infdis/172.6.1536.
8. Ikäheimo R, Siitonen A, Heiskanen T, Kärkkäinen U, Kuosmanen P, Lipponen P, et al. Recurrence of urinary tract infection in a primary care setting: analysis of a 1-year follow-up of 179 women. Clin Infect Dis 1996; 22:91-9; PMID:8824972; http://dx.doi.org/10.1093/clinids/22.1.91.
9. Kärkkäinen UM, Ikaheimo R, Katila ML, Siitonen A. Recurrence of urinary tract infections in adult patients with community-acquired pyelonephritis caused by E. coli: a 1-year follow-up. Scand J Infect Dis 2000; 32:495-9; PMID:11055653; http://dx.doi.org/10.1080/003655400458767.

©2011 Landes Bioscience.Do not distribute.
www.landesbioscience.com Virulence 535
Proportions with Persistence or Relapse vs. Trait status (row %)
Trait Present Trait Absent p-valuesa
Pivmecillinam Group Pivmecillinam Group
Traits400 mg BIDb
for 3 d200 mg BIDb or
TIDb for 7 d400 mg BIDb
for 3 d200 mg BIDb or
TIDb for 7 dTrait present-3 d vs.
Trait present-7 dTrait present-3 d
vs. the othersc
PHYLOGENETIC GROUPS
Group a 2/8 (25) 4/9 (44) 35/54 (65) 37/84 (44) - -
Group B1 2/3 (67) 0/2 (0) 35/59 (59) 41/91 (45) - -
Group B2 31/42 (74) 33/62 (53) 6/20 (30) 7/31 (23) 0.0343 0.0004
Group D 2/8 (25) 3/12 (25) 35/54 (65) 38/81 (47) - -
Non-typeable 0 1/9 (11) 37/61 (61) 40/85 (47) - -
VIRULENCE FACTOR GENES
Adhesins
afa/draBC 1/1 (100) 2/5 (40) 36/61 (59) 39/88 (44) - -
bmaE 0 0 0 0 - -
fimH 36/61 (59) 40/91 (44) 1/1 (100) 1/2 (50) - -
focG 8/13 (62) 8/19 (42) 29/49 (59) 33/74 (45)
gafD 0 0 0 0
iha 7/14 (50) 10/21 (48) 30/48 (63) 31/72 (43)
papAH 23/33 (70) 20/39 (51) 14/29 (48) 21/54 (39) - 0.0121
sfa/focDE 23/29 (79) 24/42 (57) 14/33 (42) 17/51 (33) - 0.0005
Biofilm-related
agn43 32/51 (63) 35/72 (49) 5/11 (45) 6/21 (29) - 0.0303
agn43aCFT073 8/14 (57) 9/21 (43) 29/48 (60) 32/72 (44)
agn43bCFT073 11/17 (65) 14/27 (52) 26/45 (58) 27/66 (41) - -
agn43K12 11/20 (55) 7/20 (35) 26/42 (59) 24/73 (47) - -
Iron uptake
chuA 33/50 (66) 36/74 (49) 4/12 (33) 5/19 (26) 0.0071
fyuA 32/47 (68) 37/74 (50) 5/15 (33) 4/19 (21) - 0.0035
iroN 28/35 (80) 27/52 (52) 9/27 (33) 14/41 (34) 0.0077 <0.0001
ireA 9/12 (75) 5/15 (33) 28/50 (56) 36/78 (46) 0.0313 -
iutA 13/22 (59) 17/33 (52) 24/40 (60) 24/60 (40) - -
Protectins
iss
kpsM II 29/42 (69) 32/61 (52) 8/20 (40) 9/23 (39) - 0.0162
kpsM II K2 29/44 (66) 32/65 (49) 8/18 (44) 9/28 (32) - 0.0145
kpsMT III 1/1 (100) 1/2 (50) 36/61 (59) 40/91 (44)
traT 18/26 (69) 13/29 (45) 19/36 (53) 28/64 (44) - 0.0345
Toxins
cdtB 10/14 (71) 6/13 (46) 27/48 (56) 35/80 (44) - -
cnf1 19/24 (79) 21/36 (58) 18/37 (49) 20/57 (35) - 0.0024
hlyD 19/25 (76) 24/42 (57) 18/38 (47) 17/51 (33) - 0.0046
sat 7/14 (54) 10/20 (50) 30/48 (64) 31/73 (42) - -
Miscellaneous
ibeA 13/16 (81) 8/18 (44) 24/46 (52) 33/75 (44) 0.0275 0.0090acomparisons of proportions were done by Fisher’s exact test or chi-square test; -, non-significant (p > 0.05). bBID, twice a day; TID, three times a day. cThe others: Those without trait present given 3 d pIV and those with or without trait present given 7 d pivmecillinam.
Table 3. association of treatment duration with persistence or relapse in relation to prevalence of traits (virulence factor genes, phylogenetic groups and phenotypic expressions) of the E. coli (n = 155)
©2011 Landes Bioscience.Do not distribute.
536 Virulence Volume 2 Issue 6
31. Rosen DA, Hooton TM, Stamm WE, Humphrey PA, Hultgren SJ. Detection of intracellular bacterial communities in human urinary tract infection. PLoS Med 2007; 4:329; PMID:18092884; http://dx.doi.org/10.1371/journal.pmed.0040329.
32. Reigstad CS, Hultgren SJ, Gordon JI. Functional genomic studies of uropathogenic Escherichia coli and host urothelial cells when intracellular bacterial com-munities are assembled. J Biol Chem 2007; 282:21259-67; PMID:17504765; http://dx.doi.org/10.1074/jbc.M611502200.
33. Berry RE, Klumpp DJ, Schaeffer AJ. Urothelial cul-tures support intracellular-bacterial community forma-tion by uropathogenic Escherichia coli. Infect Immun 2009; 77:2762-72; PMID:19451249; http://dx.doi.org/10.1128/IAI.00323-09.
34. Wright KJ, Seed PC, Hultgren SJ. Development of intracellular bacterial communities of uropathogenic Escherichia coli depends on type 1 pili. Cell Microbiol 2007; 9:2230-41; PMID:17490405; http://dx.doi.org/10.1111/j.1462-5822.2007.00952.x.
35. Johnson JR, Owens K, Gajewski A, Kuskowski MA. Bacterial characteristics in relation to clinical source of Escherichia coli isolates from women with acute cystitis or pyelonephritis and uninfected women. J Clin Microbiol 2005; 43:6064-72; PMID:16333100; http://dx.doi.org/10.1128/JCM.43.12.6064-72.2005.
36. Stapleton A, Moseley S, Stamm WE. Urovirulence determinants in Escherichia coli isolates causing first-episode and recurrent cystitis in women. J Infect Dis 1991; 163:773-9; PMID:1672702; http://dx.doi.org/10.1093/infdis/163.4.773.
37. Anderson GG, Goller CC, Justice S, Hultgren SJ, Seed PC. Polysaccharide capsule and sialic acid-mediated regulation promote biofilm-like intracellular bacterial communities during cystitis. Infect Immun 2010; 78:963-75; PMID:20086090; http://dx.doi.org/10.1128/IAI.00925-09.
38. Schembri MA, Kjaergaard K, Klemm P. Global gene expression in Escherichia coli biofilms. Mol Microbiol 2003; 48:253-67; PMID:12657059; http://dx.doi.org/10.1046/j.1365-2958.2003.03432.x.
39. Ulett GC, Valle J, Beloin C, Sherlock O, Ghigo JM, Schembri MA. Functional analysis of antigen 43 in uropathogenic Escherichia coli reveals a role in long-term persistence in the urinary tract. Infect Immun 2007; 75:3233-44; PMID:17420234; http://dx.doi.org/10.1128/IAI.01952-06.
40. Norrby SR. Short-term treatment of uncomplicated lower urinary tract infections in women. Rev Infect Dis 1990; 12:458-67; PMID:2193352; http://dx.doi.org/10.1093/clinids/12.3.458.
41. Milo G, Katchman EA, Paul M, Christiaens T, Baerheim A, Leibovici L. Duration of antibacterial treatment for uncomplicated urinary tract infection in women. Cochrane Database Syst Rev 2005; 4682; PMID:15846726.
20. Johnson JR, O’Bryan TT, Delavari P, Kuskowski M, Stapleton A, Carlino U, et al. Clonal relationships and extended virulence genotypes among Escherichia coli isolates from women with a first or recurrent episode of cystitis. J Infect Dis 2001; 183:1508-17; PMID:11319687; http://dx.doi.org/10.1086/320198.
21. Soto SM, Smithson A, Horcajada JP, Martinez JA, Mensa JP, Vila J. Implication of biofilm formation in the persistence of urinary tract infection caused by uropathogenic Escherichia coli. Clin Microbiol Infect 2006; 12:1034-6; PMID:16961644; http://dx.doi.org/10.1111/j.1469-0691.2006.01543.x.
22. Mysorekar IU, Hultgren SJ. Mechanisms of uro-pathogenic Escherichia coli persistence and eradica-tion from the urinary tract. Proc Natl Acad Sci USA 2006; 103:14170-5; PMID:16968784; http://dx.doi.org/10.1073/pnas.0602136103.
23. Schilling JD, Lorenz RG, Hultgren SJ. Effect of trime-thoprim-sulfamethoxazole on recurrent bacteriuria and bacterial persistence in mice infected with uropatho-genic Escherichia coli. Infect Immun 2002; 70:7042-9; PMID:12438384; http://dx.doi.org/10.1128/IAI.70.12.7042-9.2002.
24. Anderson GG, Palermo JJ, Schilling JD, Roth R, Heuser J, Hultgren SJ. Intracellular bacterial bio-film-like pods in urinary tract infections. Science 2003; 301:105-7; PMID:12843396; http://dx.doi.org/10.1126/science.1084550.
25. Garofalo CK, Hooton TM, Martin SM, Stamm WE, Palermo JJ, Gordon JI, et al. Escherichia coli from urine of female patients with urinary tract infections is competent for intracellular bacterial community forma-tion. Infect Immun 2007; 75:52-60; PMID:17074856; http://dx.doi.org/10.1128/IAI.01123-06.
26. Justice SS, Hung C, Theriot JA, Fletcher DA, Anderson GG, Footer MJ, et al. Differentiation and develop-mental pathways of uropathogenic Escherichia coli in urinary tract pathogenesis. Proc Natl Acad Sci USA 2004; 101:1333-8; PMID:14739341; http://dx.doi.org/10.1073/pnas.0308125100.
27. Mulvey MA, Schilling JD, Hultgren SJ. Establishment of a persistent Escherichia coli reservoir during the acute phase of a bladder infection. Infect Immun 2001; 69:4572-9; PMID:11402001; http://dx.doi.org/10.1128/IAI.69.7.4572-9.2001.
28. Kerrn MB, Struve C, Blom J, Frimodt-Moller N, Krogfelt KA. Intracellular persistence of Escherichia coli in urinary bladders from mecillinam-treated mice. J Antimicrob Chemother 2005; 55:383-6; PMID:15681580; http://dx.doi.org/10.1093/jac/dki002.
29. Hvidberg H, Struve C, Krogfelt KA, Christensen N, Rasmussen SN, Frimodt-Moller N. Development of a long-term ascending urinary tract infection mouse model for antibiotic treatment studies. Antimicrob Agents Chemother 2000; 44:156-63; PMID:10602738; http://dx.doi.org/10.1128/AAC.44.1.156-63.2000.
30. Blango MG, Mulvey MA. Persistence of uropatho-genic Escherichia coli in the face of multiple antibiot-ics. Antimicrob Agents Chemother 2010; 54:1855-63; PMID:20231390; http://dx.doi.org/10.1128/AAC.00014-10.
Table 3 (continued). association of treatment duration with persistence or relapse in relation to prevalence of traits (virulence factor genes, phyloge-netic groups and phenotypic expressions) of the E. coli (n = 155)
malX 30/41 (73) 31/59 (53) 7/21 (33) 10/34 (29) 0.0375 0.0006
usp 28/39 (72) 32/59 (54) 9/23 (39) 9/34 (26) - 0.0019
PHENOTYPIC TRAITS
hemolysis 17/22 (77) 19/36 (53) 20/40 (50) 22/57 (39) - 0.0063
Motility 37/62 (60) 41/93 (44) 0 0
Type 1 fimbria 35/60 (58) 41/90 (46) 2/2 (100) 0/3 (0) - -acomparisons of proportions were done by Fisher’s exact test or chi-square test; -, non-significant (p > 0.05). bBID, twice a day; TID, three times a day. cThe others: Those without trait present given 3 d pIV and those with or without trait present given 7 d pivmecillinam.
10. Ejrnaes K, Sandvang D, Lundgren B, Ferry S, Holm S, Monsen T, et al. Pulsed-field gel electrophoresis typing of Escherichia coli strains from samples collected before and after pivmecillinam or placebo treatment of uncomplicated community-acquired urinary tract infection in women. J Clin Microbiol 2006; 44:1776-81; PMID:16672406; http://dx.doi.org/10.1128/JCM.44.5.1776-81.2006.
11. Russo TA, Stapleton A, Wenderoth S, Hooton TM, Stamm WE. Chromosomal restriction fragment length polymorphism analysis of Escherichia coli strains caus-ing recurrent urinary tract infections in young women. J Infect Dis 1995; 172:440-5; PMID:7622887; http://dx.doi.org/10.1093/infdis/172.2.440.
12. Desjardins P, Picard B, Kaltenbock B, Elion J, Denamur E. Sex in Escherichia coli does not disrupt the clonal structure of the population: evidence from random amplified polymorphic DNA and restriction-fragment-length polymorphism. J Mol Evol 1995; 41:440-8; PMID:7563131; http://dx.doi.org/10.1007/BF00160315.
13. Herzer PJ, Inouye S, Inouye M, Whittam TS. Phylogenetic distribution of branched RNA-linked multicopy single-stranded DNA among natural isolates of Escherichia coli. J Bacteriol 1990; 172:6175-81; PMID:1699928.
14. Picard B, Garcia JS, Gouriou S, Duriez P, Brahimi N, Bingen E, et al. The link between phylogeny and viru-lence in Escherichia coli extraintestinal infection. Infect Immun 1999; 67:546-53; PMID:9916057.
15. Johnson JR, Kuskowski MA, Gajewski A, Soto S, Horcajada JP, Jimenez de Anta MT, et al. Extended virulence genotypes and phylogenetic background of Escherichia coli isolates from patients with cystitis, pyelo-nephritis or prostatitis. J Infect Dis 2005; 191:46-50; PMID:15593002; http://dx.doi.org/10.1086/426450.
16. Moreno E, Andreu A, Pigrau C, Kuskowski MA, Johnson JR, Prats G. Relationship between Escherichia coli strains causing acute cystitis in women and the fecal E. coli population of the host. J Clin Microbiol 2008; 46:2529-34; PMID:18495863; http://dx.doi.org/10.1128/JCM.00813-08.
17. Takahashi A, Kanamaru S, Kurazono H, Kunishima Y, Tsukamoto T, Ogawa O, et al. Escherichia coli iso-lates associated with uncomplicated and complicated cystitis and asymptomatic bacteriuria possess similar phylogenies, virulence genes and O-serogroup profiles. J Clin Microbiol 2006; 44:4589-92; PMID:17065267; http://dx.doi.org/10.1128/JCM.02070-06.
18. Johnson JR. Virulence factors in Escherichia coli urinary tract infection. Clin Microbiol Rev 1991; 4:80-128; PMID:1672263.
19. Johnson JR, Russo TA. Molecular epidemiol-ogy of extraintestinal pathogenic (uropathogenic) Escherichia coli. Int J Med Microbiol 2005; 295:383-404; PMID:16238015; http://dx.doi.org/10.1016/j.ijmm.2005.07.005.

©2011 Landes Bioscience.Do not distribute.
www.landesbioscience.com Virulence 537
52. Russo TA, Carlino UB, Johnson JR. Identification of a new iron-regulated virulence gene, ireA, in an extrain-testinal pathogenic isolate of Escherichia coli. Infect Immun 2001; 69:6209-16; PMID:11553562; http://dx.doi.org/10.1128/IAI.69.10.6209-16.2001.
53. Restieri C, Garriss G, Locas MC, Dozois CM. Autotransporter-encoding sequences are phylogeneti-cally distributed among Escherichia coli clinical iso-lates and reference strains. Appl Environ Microbiol 2007; 73:1553-62; PMID:17220264; http://dx.doi.org/10.1128/AEM.01542-06.
54. Johnson JR, O’Bryan TT. Detection of the Escherichia coli group 2 polysaccharide capsule synthesis Gene kpsM by a rapid and specific PCR-based assay. J Clin Microbiol 2004; 42:1773-6; PMID:15071046; http://dx.doi.org/10.1128/JCM.42.4.1773-6.2004.
55. Tittsler RP, Sandholzer LA. The use of semi-solid agar for the detection of bacterial motility. J Bacteriol 1936; 31:575-80; PMID:16559914.
56. Hagberg L, Jodal U, Korhonen TK, Lidin-Janson G, Lindberg U, Svanborg EC. Adhesion, hemagglutina-tion and virulence of Escherichia coli causing uri-nary tract infections. Infect Immun 1981; 31:564-70; PMID:7012012.
48. Gordon DM, Clermont O, Tolley H, Denamur E. Assigning Escherichia coli strains to phylogenetic groups: multi-locus sequence typing versus the PCR triplex method. Environ Microbiol 2008; 10:2484-96; PMID:18518895; http://dx.doi.org/10.1111/j.1462-2920.2008.01669.x.
49. Johnson JR, Stell AL. Extended virulence genotypes of Escherichia coli strains from patients with urosepsis in relation to phylogeny and host compromise. J Infect Dis 2000; 181:261-72; PMID:10608775; http://dx.doi.org/10.1086/315217.
50. Johnson JR, Russo TA, Tarr PI, Carlino U, Bilge SS, Vary JC Jr, et al. Molecular epidemiological and phy-logenetic associations of two novel putative virulence genes, iha and iroN (E. coli), among Escherichia coli isolates from patients with urosepsis. Infect Immun 2000; 68:3040-7; PMID:10769012; http://dx.doi.org/10.1128/IAI.68.5.3040-7.2000.
51. Guyer DM, Henderson IR, Nataro JP, Mobley HL. Identification of sat, an autotransporter toxin pro-duced by uropathogenic Escherichia coli. Mol Microbiol 2000; 38:53-66; PMID:11029690; http://dx.doi.org/10.1046/j.1365-2958.2000.02110.x.
42. Ferry SA, Holm SE, Stenlund H, Lundholm R, Monsen TJ. Clinical and bacteriological outcome of different doses and duration of pivmecillinam compared with placebo therapy of uncomplicated lower urinary tract infection in women: the LUTIW project. Scand J Prim Health Care 2007; 25:49-57; PMID:17354160; http://dx.doi.org/10.1080/02813430601183074.
43. European Confederation of Laboratory Medicine. European urinalysis guidelines. Scand J Clin Lab Invest 2000; 231:1-86; PMID:12647764.
44. Reisner A, Krogfelt KA, Klein BM, Zechner EL, Molin S. In vitro biofilm formation of commen-sal and pathogenic Escherichia coli strains: impact of environmental and genetic factors. J Bacteriol 2006; 188:3572-81; PMID:16672611; http://dx.doi.org/10.1128/JB.188.10.3572-81.2006.
45. Bertani G. Studies on lysogenesis. I. The mode of phage liberation by lysogenic Escherichia coli. J Bacteriol 1951; 62:293-300; PMID:14888646.
46. Clark DJ, Maaløe O. DNA replication and the division cycle in Escherichia coli. J Mol Biol 1967; 23:99-112; http://dx.doi.org/10.1016/S0022-2836(67)80070-6.
47. Clermont O, Bonacorsi S, Bingen E. Rapid and simple determination of the Escherichia coli phyloge-netic group. Appl Environ Microbiol 2000; 66:4555-8; PMID:11010916; http://dx.doi.org/10.1128/AEM.66.10.4555-8.2000.





























