Embed Size (px)
Citation preview

Chronic exposure to sour gasemissions: meeting a community concernwith epidemiologic evidence
Walter 0. Spitzer, MD, MPH, FRCPRobert E. Dales, MD, MSc, FRCPCMartin T. Schechter, MD, MSc, PhDSamy Suissa, PhDPierre Tousignant, MD, MSc, FRCPCNicolas Steinmetz, MD, MPH, FRCPCMarian E. Hutcheon, MD, MHSc, FRCPC
For 25 years residents of a rural area in south-western Alberta have complained of healthproblems attributed to sour gas emissions fromnearby natural gas refineries. We undertook alarge epidemiologic study of the current healthstatus and the selected morbidity rates among2152 people in the exposed area. We establishedtwo comparison groups: one was a demographi-cally similar unexposed population and theother a demographically different group alsoexposed to sour gas emissions in another region.The methods included a cross-sectional surveyof current residents and separate historical co-hort studies involving registry linkage to inves-tigate cancer incidence and all-cause mortality.The cross-sectional survey involved a compre-hensive health questionnaire, standardized clin-ical examinations by physicians blinded to thesubjects' symptoms and concerns, and severallaboratory tests. We were able to contact justunder 60% of the people who we knew hadmoved from each area since 1958 and found noevidence of selective migration for health rea-sons. Although the residents of the exposed areareported an excess number of symptoms andhealth problems there were no significant dif-ferences in the mortality rate, incidence of can-cer, reproductive problems, major ailments, hairlevels of arsenic and certain metals or respirato-ry function between the groups.
From the Department of Epidemiology and Biostatistics, McGillUniversity, Montreal, and the Department of Health Care andEpidemiology, University of British Columbia, Vancouver
Reprint requests to: Dr. Walter 0. Spitzer, Department ofEpidemiology and Biostatistics, McGill University, 1020 PineAve. W, Montreal, PQ H3A 1A2
Depuis 25 ans les habitants d'une region ruraledu sud-ouest de l'Alberta se plaignent detroubles de la sante qu'ils attribuent aux ema-nations fetides de raffineries de gaz natureldans le voisinage. Aussi avons-nous entreprisun vaste travail epidemiologique aupres de2152 personnes dans la region en question,portant sur l'tat de sante actuel et des tauxchoisis de morbidite. Pour fins de comparaisonnous prenons deux groupes: l'un a les memescaracteres demographiques mais n'est pasexpose aux gaz; le second, dans une autreregion ou il y a egalement des gaz fetides, ades caracteres demographiques differents. Nosmethodes comprennent d'une part une enquetetransversale aupres des habitants actuels,d'autre part l'etude rdtrospective de cohortesportant sur les taux consignds de cancer etde mortalite globale. L'enquete transversalecomprend un interrogatoire medical complet,un examen clinique normalise par des mede-cins non informes des symptomes et des sou-cis accuses par les sujets, et plusieurs exa-mens de laboratoire. Nous pouvons retracerpres de 60% des personnes qui ont quittechacune des regions depuis 1958 et netrouvons aucune preuve d'une migrationselective pour raisons de sante. Bien queles habitants de la region k l'etude fassentetat d'un plus grand nombre de sympt6meset de troubles de la sante que les sujets desgroupes de comparaison, nous ne trouvons au-cune difference significative entre les diversgroupes quant a la mortalitE, aux taux de can-cer, d'anomalies de la reproduction et de mala-dies graves, d la fonction respiratoire et auxconcentrations de l'arsenic et de certainsmetaux.
CMAJ, VOL. 141, OCTOBER 1, 1989 685- For prescribing information see page 730

O ne of the most difficult challenges incommunity epidemiology is the investiga-
lqt,rltion of an "epidemic" based not on databut on anecdotal observations that generate com-munity concern about an unusually high preva-lence of adverse health effects. In some instancesthe challenge is posed by a purported cluster ofcases without any suspected environmental cause,'but more frequently the alleged outbreak is linkedwith a noxious or potentially toxic substance suchas polycyclic aromatic hydrocarbons2 or forestrypesticide emulsifiers.3 This sort of open epidemio-logic study should be distinguished from a clusterinvestigation,4 in which a group of reported andvalidated cases of a disease appears to exceed theexpected frequency for the area.
Since 1957 several refineries in southwesternAlberta have been converting natural "sour" gasinto marketable "sweet" gas by removing contami-nants. Shortly after operation began at one plantresidents downwind began to complain of a dis-agreeable odour and of various adverse healtheffects. Town council members, journalists andpolitical leaders sounded alarms about ocular,respiratory, skin and neurologic symptoms, excessrates of cancer and birth defects, adverse pregnan-cy outcomes, abnormal childhood development,trace metal poisoning and even excess mortalityrates.
During the ensuing 25 years the complaintswere examined in isolated studies by governmentand university groups. Three studies of air pollu-tants were carried out; in 1964 the chief pollutantswere identified as hydrogen sulfide and sulfurdioxide, but environmental experts of the provin-cial government felt the levels were well belowthose that could produce adverse health effects. In1971 an investigation revealed that air quality inthe area met the standards of the Clean Air Act; in1980 and 1981 additional studies showed that themaximum peak levels of hydrogen sulfide occa-sionally exceeded recommended long-term expo-sure levels but were felt to be far below levelsassociated with adverse health effects.5
Despite these reassurances community con-cerns increased. In 1984 the Alberta Acid Depo-sition Research Program, a joint government-industry agency founded to study the effects ofacid-forming emissions produced by refining sul-fur-containing natural resources, convened a scien-tific advisory board comprising specialists in toxi-cology, environmental health, respirology and car-cinogenesis. The board recommended that urgentand concerted action be taken to determine theimpact of airborne industrial pollution on thehealth of Albertans. The McGill EpidemiologyRapid Response Unit was asked to design andcarry out a study, the field work to be completed in3 months and the final report to be submittedwithin 1 year.
The investigators decided at the outset thatexisting health status data derived from the medi-cal care system would not be adequate, since
health records were not uniformly or universallyavailable, were not sufficiently comprehensive forthe purposes of the study, were subject to bias dueto self-selection and were of uneven quality.
The general objective was to assess the overallhealth of the affected population and to discernany measurable excess of adverse health events incomparison with the most demographically similar"unexposed" population available. Since there wasno evidence for unsafe levels of the sour gasemissions and since other possible factors - pesti-cides, herbicides and traces of heavy metals in thesoil - were also blamed for adverse health effectsthe investigation was not intended to be an etio-logic study of an exposure-outcome relation. Be-cause the community concern about adverse healtheffects was spread over a geographic area expo-sures in individuals or subgroups were not mea-sured. The principal challenges were to selectsuitable comparison groups, to ensure a high levelof participation in the study and to perform medi-cal examinations that would be acceptable toscientists, clinicians and the community underinvestigation.
By June 1, 1985, 118 staff members wereassembled; these included 23 university-basedphysicians from Canada and the United States, 20professional interviewers, 11 laboratory techni-cians and 15 data coders as well as support staff forhousing, transportation, child care and routineclerical duties. Eleven mobile homes housed theexamination and laboratory rooms; communityfacilities were also used.
A detailed description of the administration,methods and analyses of this investigation wasprepared for the Alberta government.6'7 In thisarticle we will describe the three methodologicfeatures necessary to understand and assess thestudy: the selection of the reference populations,the use and integration of existing databases, andthe comprehensive medical examinations. Otheressential features will be summarized.
Methods
Study populations
Index area (IA) referred to the region contain-ing the contiguous communities of Twin Butte,Glenwood, Mountain View, Hill Spring, WillowCreek and a portion of Pincher Creek that wasexposed, as determined by the Alberta govern-ment's assessment of airborne emissions down-wind of the two sour gas processing plants. Usinga combination of house-to-house enumeration andchecks of municipal tax records we conducted acomplete census of the region and found 2328eligible people, about half of whom were Mormon(Table I).
The population in the control or primaryreference area (PRA) comprised people in anunexposed area who had demographic character-
686 CMAJ, VOL. 141, OCTOBER 1, 1989
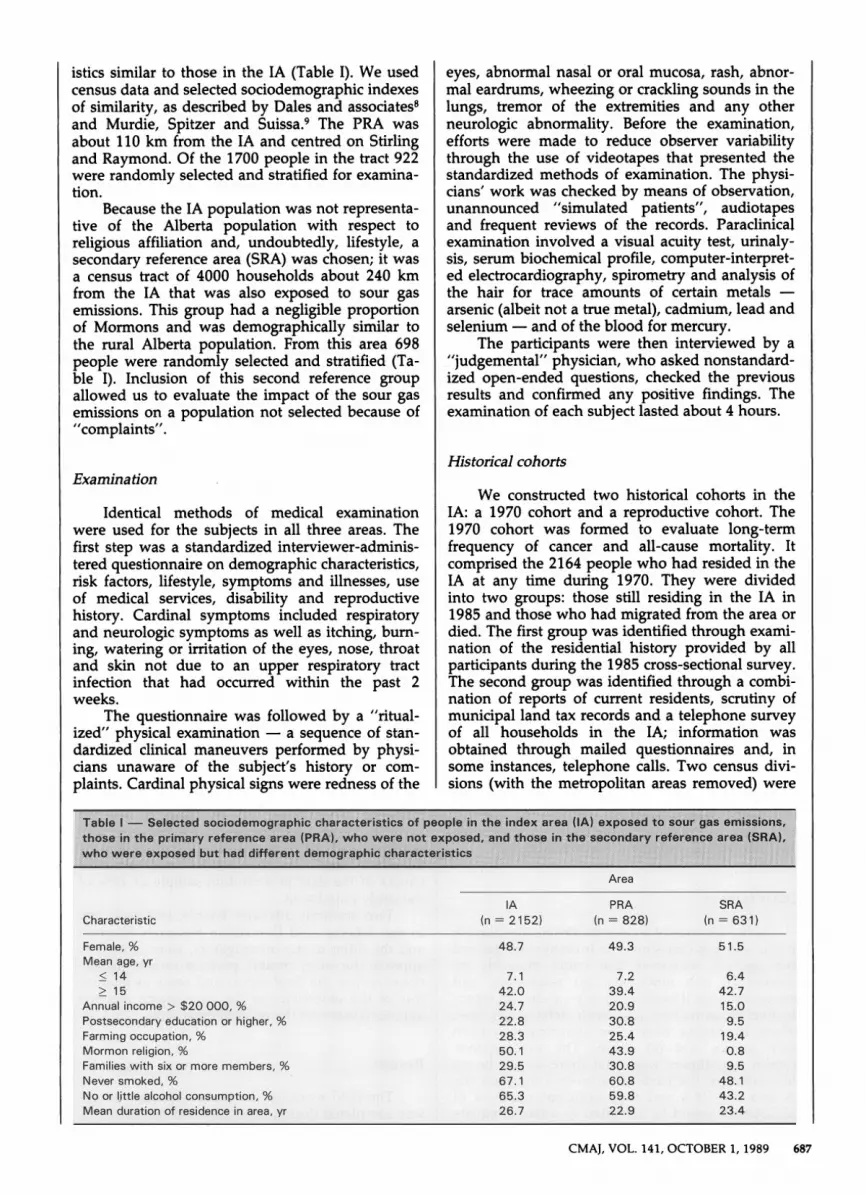
istics similar to those in the IA (Table I). We usedcensus data and selected sociodemographic indexesof similarity, as described by Dales and associates8and Murdie, Spitzer and Suissa.9 The PRA wasabout 110 km from the IA and centred on Stirlingand Raymond. Of the 1700 people in the tract 922were randomly selected and stratified for examina-tion.
Because the IA population was not representa-tive of the Alberta population with respect toreligious affiliation and, undoubtedly, lifestyle, asecondary reference area (SRA) was chosen; it wasa census tract of 4000 households about 240 kmfrom the IA that was also exposed to sour gasemissions. This group had a negligible proportionof Mormons and was demographically similar tothe rural Alberta population. From this area 698people were randomly selected and stratified (Ta-ble I). Inclusion of this second reference groupallowed us to evaluate the impact of the sour gasemissions on a population not selected because of"complaints".
Examination
Identical methods of medical examinationwere used for the subjects in all three areas. Thefirst step was a standardized interviewer-adminis-tered questionnaire on demographic characteristics,risk factors, lifestyle, symptoms and illnesses, useof medical services, disability and reproductivehistory. Cardinal symptoms included respiratoryand neurologic symptoms as well as itching, bum-ing, watering or irritation of the eyes, nose, throatand skin not due to an upper respiratory tractinfection that had occurred within the past 2weeks.
The questionnaire was followed by a "ritual-ized" physical examination - a sequence of stan-dardized clinical maneuvers performed by physi-cians unaware of the subject's history or com-plaints. Cardinal physical signs were redness of the
eyes, abnormal nasal or oral mucosa, rash, abnor-mal eardrums, wheezing or crackling sounds in thelungs, tremor of the extremities and any otherneurologic abnormality. Before the examination,efforts were made to reduce observer variabilitythrough the use of videotapes that presented thestandardized methods of examination. The physi-cians' work was checked by means of observation,unannounced "simulated patients", audiotapesand frequent reviews of the records. Paraclinicalexamination involved a visual acuity test, urinaly-sis, serum biochemical profile, computer-interpret-ed electrocardiography, spirometry and analysis ofthe hair for trace amounts of certain metals -arsenic (albeit not a true metal), cadmium, lead andselenium - and of the blood for mercury.
The participants were then interviewed by a"judgemental" physician, who asked nonstandard-ized open-ended questions, checked the previousresults and confirmed any positive findings. Theexamination of each subject lasted about 4 hours.
Historical cohorts
We constructed two historical cohorts in theIA: a 1970 cohort and a reproductive cohort. The1970 cohort was formed to evaluate long-termfrequency of cancer and all-cause mortality. Itcomprised the 2164 people who had resided in theIA at any time during 1970. They were dividedinto two groups: those still residing in the IA in1985 and those who had migrated from the area ordied. The first group was identified through exami-nation of the residential history provided by allparticipants during the 1985 cross-sectional survey.The second group was identified through a combi-nation of reports of current residents, scrutiny ofmunicipal land tax records and a telephone surveyof all households in the IA; information wasobtained through mailed questionnaires and, insome instances, telephone calls. Two census divi-sions (with the metropolitan areas removed) were
Table I - Selected sociodemographic characteristics of people in the index area (IA) exposed to sour gas emissions.those in the primary reference area (PRA), who were not exposed, and those in the secondary reference area (SRA),who were exposed but had different demographic characteristics
Area
IA(n = 2152)Characteristic
PRA(n = 828)
SRA(n = 631)
Female, % 48.7 49.3 51.5Mean age, yr
* 14 7.1 7.2 6.4* 15 42.0 39.4 42.7
Annual income > $20 000, % 24.7 20.9 15.0Postsecondary education or higher, % 22.8 30.8 9.5Farming occupation, % 28.3 25.4 19.4Mormon religion, % 50.1 43.9 0.8Families with six or more members, % 29.5 30.8 9.5Never smoked, % 67.1 60.8 48.1No or little alcohol consumption, % 65.3 59.8 43.2Mean duration of residence in area, yr 26.7 22.9 23.4
CMAJ, VOL. 141, OCTOBER 1, 1989 687

used to approximate the PRA and the SRA. Thecancer and mortality rates in the 1970 cohort, asdetermined through the Alberta Cancer Registryand the Alberta Bureau of Vital Statistics respec-tively, were compared with the rates of the tworeference populations by means of indirect stan-dardization.
The reproductive cohort was constructed totrack fertility rates, prematurity and low birthweight, congenital defects and childhood develop-ment. According to the outcome being studied thecohort comprised either women of childbearingage who had resided at least 1 year in the surveyareas between 1958 and 1985, women who hadhad at least one pregnancy during the same periodor children who were under 15 years of age whenexamined during the 1985 cross-sectional survey.Information on current residents was obtainedthrough a questionnaire that was supplemented bythe physical examination.
Community involvement
Community involvement was required tojudge the relevance of the investigation to the IApopulation, to approve the basic research plan andto encourage participation of the residents infinding former residents and interpreting the find-ings to other members of the community. Theresidents of each study area were invited to formcommunity advisory boards.
The required participation rate of 90% wasrelatively easy to achieve in the IA and the SRAbecause of exposure to sour gas; however, thesubjects in the PRA had little motivation to under-go 4-hour medical examinations, particularly dur-ing the harvest season. Attempts to enhance par-ticipation included frequent radio and televisionappearances by the investigators, support by min-isters and priests, and lotteries in which the win-ning numbers matched study registration numbers.A mobile unit allowed a nearly complete examina-tion to be performed in the participant's home.This tactic was particularly helpful for farmers,who could be examined in the early morning whiletheir harvesting equipment was warming up.
Other features
In the absence of a clear syndrome attributableto the sour gas emissions the investigators definedfive cardinal outcomes that could plausibly beaffected by the emissions: (a) respiratory andmucocutaneous illnesses, (b) any cancer, (c) repro-ductive abnormalities and birth defects, (d) toxiceffects (including neurologic abnormalities) fromtrace metals and (e) death. The investigators'a priori hypotheses were that there would be nodifferences in the cardinal outcomes between theIA and the PRA and that sufficient numbers ofparticipants would be recruited to attain adequate
statistical power to support a negative finding. Thesample size yielded 90% power to detect differ-ences of 10% in the prevalence data for infrequentoutcomes and differences of 20% for frequentoutcomes at an alpha level of 0.05. The investiga-tors insisted that the participation rates had to begreater than 90% for the study to be valid.
Restricting the number of primary compari-sons to the five cardinal outcomes, as well as thecommitment to the a priori hypotheses, reducedthe chance of false-positive results without theneed for lowering the alpha level, which mighthave reduced the power of the study to detectmeaningful differences. Statistical testing wasbased on paired comparisons of the IA with thetwo reference areas independently, chi-squared orgroup t-tests being used as needed.
Despite the size and complexity of the studyextensive precautions were taken to guard againstbias. These included the uniform interviews andritualized examination. In addition, those whocollected and coded the data were kept unaware ofthe specific hypotheses of the study, and theinvestigators were kept blind to the areas fromwhich the data came until a late phase of theanalysis.
A substudy of hair analysis for trace metalsinvolved 94 people from each of two colonies ofHutterites - one in the IA and the other in acontrol area near Lethbridge. Hutterites were cho-sen because most of the food they eat is locallygrown, and any changes in the metal compositionof the soil in the areas near the refineries could bereflected in the food.
Numerous quality checks were carried out atvarious phases of the study; these included (a) a"dress rehearsal" of the field techniques in Quebecbefore the main study began, (b) assessment of therole of seasonal variation by means of interviewinga sample of the study population and performingan abbreviated examination with an emphasis onrespiratory conditions 6 months after the mainstudy, in the coldest time of winter, (c) periodicanalysis of 10% of the hair specimens by tworeference laboratories, (d) checking of selectedvariables in the questionnaire by a supervisor, whoreinterviewed 10% of the study population bytelephone and (e) double-entry and accuracychecks of the data in a random sample of 10% ofthe study population.
Two scientific advisory boards, one reportingto the Alberta Acid Deposition Research Programand the other to the investigators, were formed toapprove the study design, perform on-site inspec-tions, review the final report and serve as guaran-tors of the objectivity of the conclusions and theappropriateness of the recommendations.
Results
The field work for the cross-sectional surveyswas completed during June, July and August 1985.
688 CMAJ, VOL. 141, OCTOBER 1, 1989

The participation rates for the three areas were93% for the IA (2157 people), 91% for the PRA(839) and 91% for the SRA (632). Information fromthe questionnaire was available for 2152, 828 and631 of the subjects respectively. As expected theSRA group differed from the other two withrespect to the proportion of farming families, sizeof family, religion, and abstinence from smokingand drinking (Table I).
We were able to contact just under 60% of thepeople who had been living in the three areasbetween 1958 and 1985 and who had subsequent-ly moved away; the rates were 63% (1969/3140)in the IA, 53% (330/625) in the PRA and 61%(332/546) in the SRA. Among those who respond-ed to the mailed questionnaires 1.3% in the IA,0.4% in the PRA and 1.1% in the SRA reportedthat they moved because of health reasons.
The prevalence of subjectively reported healthproblems, physical impairment and use of healthcare facilities among children and adults wasconsistently higher in the IA group than in the tworeference groups, although the differences werenot significant (Table II). However, the prevalenceof cardinal signs was not uniformly higher in theIA group than in the two reference groups (Table
III); in fact, the PRA had a much higher incidenceof red eyes and red nasal or oral mucosa, althoughthe difference was not significant. The proportionof people with clinical diagnoses was generallylow, but the rate of hay fever and allergic rhinitisin the IA was double that in the SRA (Table IV).
The prevalence rates of any abnormal serumbiochemical test result or electrocardiographic find-ing did not differ by more than 1% between thethree groups. For urinalysis the prevalence rates ofabnormal findings differed by no more than 3.1%.Spirometric measurements (obtained for 2863 sub-jects at least 7 years of age) did not differ betweenthe three groups.
In the IA and the PRA the respective propor-tions of women with reported fertility problemswere 11.8% and 8.6%, of miscarriages 14.9% and8.6%, of low-birth-weight infants 5% and 5%, andof birth defects 6.3% and 4.6%. Parents' satisfac-tion with the development of their children andthe reported developmental characteristics werethe same across the areas. In contrast, on the basisof clinical examination the incidence was lower inthe IA than in the PRA for congenital anomalies(1.9% and 3.3% respectively) and for observed:ex-pected ratios of major birth defects (0.96% and
Table 11 - Prevalence of subjectively reported health problems, physical impairment and use of health care facilitiesamong children and adults
Area; % of people
Indicator IA PRA SRA
Medication used on physician's advice in past 2 daysOne or more cardinal symptoms reported in past 2 weeksAny health problem reported in past 2 weeks
(n = 762)
19.050.713.2
(n= 1390)
Any activity loss in past 2 weeksBedridden in past 2 weeksOvernight admission to a health care facility in past 12 monthsEncounter with a health professional in past 2 weeksMedication used on physician's advice in past 2 daysAny health problem reported in past 2 weeksOne or more cardinal symptoms reported in past 2 weeks
21.67.5
19.714.337.830.179.4
Children, < 14 yr of age(n = 343)
1 7.246.31 1.4
Adults, > 15 yr of age(n = 485)
17.77.4
17.413.237.526.274.2
Table Ill - Prevalence of cardinal signs
Area; % of people
IA PRA SRASign (n = 2151) (n = 816) (n = 616)
Red eyes 10.7 17.5 8.8Impaired visual acuity 9.4 8.5 8.7Red nasal or oral mucosa 12.8 24.5 10.4Rash 3.8 2.3 2.1Ear drum abnormalities 9.3 7.5 8.0Wheezing or crackling sounds in lungs 2.8 2.6 1 .8Tremor 0.6 0 0.7Abnormal neurologic findings 11.9 7.1 7.6At least one of the above signs 36.5 45.2 30.4
CMAJ, VOL. 141, OCTOBER 1, 1989 689
(n -265)
17.749.17.7
(n = 366)
18.85.2
15.610.735.322.674.3

1.00%Y). The measurements of height and weight,the degree of sexual maturity and the results of theDenver Developmental Screening Test for childrenaged 4 years did not differ between the three areas.
Trace metal levels in the hair and bloodsamples were close to the lower limits of normaland were similar in all the areas. When the levelsin all of the participants were combined more than94% of them were within normal limits or un-detectable. In comparison with the PRA the IA hadan equal or lower proportion of people with levelsclose to the upper limit of normal for each of thetrace metals. Among the Hutterites the serummercury levels and the arsenic and cadmiumvalues in the hair samples were all within normallimits. People with abnormal results were testedagain and followed up; however, the findings didnot change.
In the 1970 cohort 123 cases of cancer werereported in 109 people from 1970 to 1984; thisincluded 45 cases of nonmelanotic skin cancer. Theobserved numbers of cancer reports in the IA werecompared with those expected on the basis ofincidence rates in the PRA, the SRA and in ruralsouthern Alberta derived from census data. Thestandardized incidence ratios (and the 95% confi-
Table >V Proportion of people with clinical diagnoses
dence limits) were 1.03 (0.80 and 1.33), 1.09 (0.84and 1.41) and 1.05 (0.81 and 1.36) respectively.
A total of 163 people (112 men) in the 1970cohort died from 1970 to 1984. To these wereadded 21 reported but unconfirmed deaths derivedfrom census and registry data. Relative to the tworeference areas the standardized mortality ratios(and 95% confidence limits) were 0.88 (0.73 and1.08) and 0.84 (0.69 and 1.03). None of thestandardized ratios in the cancer or mortalityanalyses differed significantly between the IA andthe two reference areas.
Discussion
The increase in the number of reports ofsymptoms in the absence of any excess in confir-matory clinical findings was not unexpected. Spe-cifically, the excess of symptoms in the IA wasexpected because the residents' complaints hadinitiated the study. Of relevance is the fact that thisdissonance was consistently greater in the IA thanin the other two areas. Table V shows this relationfor a few selected variables.
In designing the study we carefully considered
Table V -- Discordance between subjective reports and objective findings
690 CMAJ, VOL. 141, OCTOBER 1, 1989

any factors that could have biased the findings.The high participation rate and low rate of migra-tion from the IA, strong demographic similaritiesbetween the IA and the PRA, and the reliance onobjective data collected in the field and fromregistries support our impression that we haveobtained a non-biased estimate of health status inthe IA population.
As in previous reports of investigations ofcommunity health emergencies, our work wasdesigned to meet the expressed needs of thecommunity as well as the scientific and medicalrequirements of the research question. Bender andassociates2 described an inexpensive "feasibilitystudy" approach to public concems about theimpact of contaminated water supplies on the ratesof breast cancer in a suburb of Minneapolis.However, they also attempted to produce a judge-ment that would diminish community concem. Inour situation such an approach would have beenneither feasible nor acceptable. First, existing medi-cal records were not sufficiently complete, accurateor uniform to provide a usable database. Second,previous pilot studies and informal surveys in thearea had failed to alleviate community concemsand, because of inadequate methods and biasedresults in some cases, had indeed resulted inadditional anxiety. It was our feeling and that ofthe extemal advisory panel that only a definitivestudy of all putative adverse outcomes with the useof objective data collection, well-chosen compari-son populations and confirmatory clinical assess-ment could address the long-standing controversy.
We acknowledge that the size and expense ofour study, the budget having approached $4 mil-lion, preclude the use of all our methods as toolsfor dealing with community concems. Neverthe-less, we believe that similar empirical investiga-tions, even if conducted on a far smaller scale, mayprovide evidence to reassure and inform othercommunities convinced of an environmentalthreat.
Given our initial goal, to gather informationthat could help the residents make decisions abouttheir health and justify appropriate communityaction, a follow-up survey was necessary. This wasdone 3 years after the end of the study. At therequest of the Alberta Acid Deposition ResearchProgram, Decima Research of Toronto polled aprobability sample of 700 of the residents in March1988. Of the respondents 94% were aware of thestudy, and 69% knew that the study had shown nodifference between the health status of unexposedrural Albertans and those living downwind of therefining plants; most important, 73% of thosesurveyed found the results of the study reassuring(jean Andryiszyn, Acid Deposition Research Pro-gram, Calgary: personal communication, 1988).
In March 1989 the principal investigator(W.O.S.) visited the area and interviewed thecommunity advisory board members. They report-ed that the original concerns were no longer anissue among the residents except for a very small
number of people. Informal discussions with otherpeople confirmed this assessment.
It is important to remember that this researchwas done not to study any etiologic relationbetween sour gas emissions and health problemsbut simply to investigate empirically whether theresidents had experienced higher than expectedadverse health outcomes. Although the negativefindings of this study did not implicate the sour gasprocess as a health hazard, none of the findingscan or should be interpreted as justification forrelaxing efforts to control the potentially hazardousconstituents of sour gas emissions and other envi-ronmental contaminants. We have recommended asustained short-term and socially responsible long-term plan for environmental protection in Alberta.In addition, we recommend that Alberta upgradeits registry of birth defects through mandatoryreporting and more active surveillance of theenvironment.
Any further investigations of health outcomesin the IA will be hampered by the unavoidably lowstatistical power for detecting small differences oflarge proportional differences in uncommon find-ings and by selective recall of symptoms andhealth events. We believe that further clinical,epidemiologic or demographic research into thequestion we pursued is no longer necessary in theIA.
This study was supported by the Government of Albertaand the Alberta Acid Deposition Research Program.
References
1. Spitzer WO, Shenker SC, Hill GB: Cancer in a Montrealsuburb: the investigation of a nonepidemic. Can AMed AssocJ1982; 127: 971-974
2. Bender AP, Williams AN, Sprafka M et al: Usefulness ofcomprehensive feasibility studies in environmental epidemi-ology investigations: a case study in Minnesota. Am I PublicHealth 1987; 78: 287-290
3. Spitzer WO: Report of the New Brunswick Task Force on theEnvironment and Reye's syndrome. Clin Invest Med 1982; 5:203-214
4. Schulte PA, Ehrenberg RL, Singal M: Investigation of cancerclusters: theory and practice. Am J Public Health 1987; 77:52-56
5. O'Laney JM: History of the Twin Butte EnvironmentalHealth Concerns, Alberta Ministry of Social Services andCommunity Health, Edmonton, 1985
6. Acid Deposition Research Program: Methods, vol 1 of TheSouthwestern Alberta Medical Diagnostic Review, Govt ofAlberta, June 1986
7. Idem: Results, vol 2. Ibid8. Dales RE, Spitzer WO, Suissa S et al: Respiratory health of a
population living downwind from natural gas refineries. AmRev Respir Dis 1989; 138: 595-600
9. Murdie RA, Spitzer WO, Suissa S: Application of a euclidiandistance measure to the selection of reference areas inepidemiologic research concerning environmental issues.ScandiJ Work Health 1988; 14: 168-174
CMAJ, VOL. 141, OCTOBER 1, 1989 691





























