Embed Size (px)
Citation preview

Clinical-Echocardiographic Correlation of Myocardial Infarction with Extension to Right Chambers JESUS VARGAS-BARRON, M.D., NILDA ESPINOLA-ZAVALETA, M.D., ANGEL ROMERO-ChDENAS, M.D., SILVINO SIMON-RUIZ, M.D., CANDACE KEIRNS, M.D., MARC0 PENA-DUQUE, M.D., MARIA RIJLAARSDAM, M.D., and EULO LUPI-HERRERA, M.D. Department of Echocardiography, Instituto Nacional de Cardiologia “Ignacio Chavez,” Tlalpan, Mexico
I n order to determine the transesophageal echocardiographic characteristics in patients with acute myocardial infarction of right ventricle and establish the relationship between these findings, the clinical condition, and their prognostic value, 38patients consecutively admitted to the Instituto Na- cional de Cardiologia with a diagnosis of acute left ventricular myocardial infarction with extension to right ventricle and lor atrium were retrospectively studied. Of the left ventricular infarctions, 37 were posteroinferior and one anterior. Significant elevations of CPK and DHL were found in 35. I n 30 patients (78%) electrocardiographic evidence of extension of infarction to the right ventricle was found, and in 3, evidence of right atrial infarction. Twenty-one patients presented clinical data com- patible with right ventricular infarction. I n 19, cardiac rhythm and atrioventricular conduction dis- turbances were documented. Coronary angiograms practiced on 34 patients demonstrated single- vessel (right coronary) disease in 12, affection of two vessels i n 14, and lesions in three or more in 6. Coronary arteries presented no significant lesions in two cases. With TEE, alterations of right ven- tricular segmental mobility were demonstrated in all patients, and in 6, alterations of right atrial mobility as well. As respects the ventricular wall movement index, 68.5% had total scores (RV + LV) of < 5. The other 31.5% had scores 2 5. I n 26%, the right ventricular wall movement index was 2 4. The RVDDILVDD ratio was 1 or less in 30 patients (78%) and > 1 in only 8 (22%). The conclu- sions from these findings are that: (1) TEE is an excellent diagnostic means of identifying right ven- tricular and lor atrial infarction; and (2) a relationship exists between the magnitude of right ven- tricular damage and a wall movement index of 5 or more or an RVILV diastolic diameter ratio > 1 postinfarction hemodynamic deterioration is significantly greater and the incidence of intrahospi- talary complications higher. (ECHOCARDIOGRAPHY, Volume 15, February 1998)
transesophageal echocardiography, myocardial infarction, enzymatic activity, functional class, right chambers
Over the last few years, interest in identify- ing right ventricular myocardial infarctions has grown, since these have been shown to be
frequently associated with left ventricular in- ferior infarction with an ample spectrum of clinical presentations. The repercussions of right ventricular damage may be minimal and masked by the manifestations of left ventricu- lar infarction. However, in some cases right ventricular necrosis may be associated with atrioventricular conduction disturbances; it is not unusual for thrombi to form in right cavi-
Address for correspondence and reprints: Jesus Vargas- Barrbn, M.D., Department of Echocardiography, Instituto Nacional de Cardiologia “Ignacio Chavez,” Juan Badiano N ~ . 1, c0l. seccibn m - y a l p a n , 14080 ~ b ~ i ~ ~ , D.F., M ~ ~ - ico. Fax: 573-09-94.
Vol. 15, No. 2, 1998 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 171

VARGAS-BARRON, ET AL.
172 ECHOCARDIOGRAPHY: A Jml. of CV Ultrasound & Allied Tech. Vol. 15, No. 2, 1998
ties, and right ventricular infarction can occa- sionally be responsible for cardiogenic shock.
From the point of view of noninvasive diag- nosis, the ECG may show ST segment eleva- tion of more than 1 mm in V4R. The sensitivity of this sign is 73% and the specificity
With radionuclide ventriculography, images of hemodynamically significant right ventricu- lar infarction have been identified by the pres- ence of abnormalities in wall movement with diminished ejection fraction. The sensitivity of these findings is 92% and the specificity 82%.2
When two-dimensional (2-D) echocardiogra- phy was limited to parasternal, apical, and subcostal images, the diagnostic criteria for right ventricular infarction were based on di- latation of the cavity and wall akinesis with abnormal movement of the interventricular septum because of the inversion of the pres- sure Doming of the interatrial sep- tum toward the left atrium was correlated with the appearance of arterial hypotension, atrio- ventricular block, and increased mortality. More recent studies have demonstrated that 2- D echocardiographic findings that aid in estab- lishing the hemodynamic significance of right ventricular infarction are the percentage of col- lapse of the inferior vena cava during inspira- tion as well as quantification of the descent of the base of the right ~en t r i c l e .~
Today, transesophageal echocardiography (TEE) has become a technique of great value for identifylng the extension of a left ventricular infarction into the right ventricle and atrium?’ It provides more information than is available from transthoracic echocardiography (TTE) and is particularly useful for locating intracav- itary thrombi and abnormalities of atrial and ventricular segmental wall movement.
The purpose of this article is to describe the findings obtained from TEE in patients with acute right ventricular myocardial infarction, define the relationship between these findings and the clinical state of the patient, and estab- lish their prognostic value.
Materials and Methods
The study included 38 patients who were ad- mitted to the Coronary Care Unit of the Insti-
tuto Nacional de Cardiologia “Ignacio Chavez” between January 1990 and May 1995. Their clinical follow-up after release from the hospi- tal varied from 6-60 months. A diagnosis of left ventricular myocardial infarction with ex- tension to right ventricle and/or atrium was es- tablished in all. In 37, the location of the in- farction was posteroinferior and in the other anterior.
The diagnosis of myocardial infarction was established on the basis of a history of chest pain, Q waves, and an ST elevation of at least one mm in different derivations of the ECG, in- cluding V4R and dorsal derivations. The diag- nosis of atrial infarction was based on the exis- tence of PR segment abnormalities or the ap- pearance of a negative deflection at the beginning of the P wave. Another finding used as a criterion for acute myocardial infarction was elevation of serum enzymes CPK and DHL. The group of patients included 35 men and 3 women with an average age of 56 years (range 38-75 years).
The variables evaluated in all patients in- cluded clinical data related to right atrial infarc- tion, rhythm and atrioventricular conduction disturbances, and location and degree of ob- struction of coronary arteries. Cardiac catheter- ization with coronary angiogram was performed in 34 patients between the second and thir- teenth day &r infarction. Coronary obstruc- tion of 75% or more was considered significant.
Echocardiographic Study
TEES were performed between the seventh and twelfth day after infarctions. Two ma- chines were used; in 31 cases, it was a Siemens Sonoline CF with color-coded Doppler and a 5- MHz biplanar transducer. The subsequent seven studies were practiced with a Hewlett- Packard machine with a multiplanar trans- ducer. Studies were carried out in the Coro- nary Care Unit with continuous monitoring of heart rate and blood pressure. A surface ECG was recorded during the echocardiographic study. Patients were lightly sedated with mi- dazolam for the procedure, which had an ap- proximate duration of 15 minutes.
Because of the limitations of biplanar TEE

CLINICAL-ECHOCARDIOGRAPHIC CORRELATION OF MYOCARDIAL INFARCTION
in visualizing the right ventricular apex and because this was a retrospective study, only transverse plane transgastric images at the level of papillary muscles (Fig. 1) and four- chamber transesophageal images were used for the general analysis of wall movement of both ventricles. With these recordings, left ventricular posteroinferior, anterior, and lat- eral walls and septum, and right ventricular inferior, lateral, and anterior walls were eval- uated. Only in the seven cases performed with the multiplanar transducer was it possible to evaluate basal, middle, and apical thirds of right ventricular inferior and anterior walls in the transgastric long-axis image. However, for scoring alterations in wall movement (Wall Movement Index = WMI) only transgastric im- ages at the level of papillary muscles and transesophageal four-chamber images were considered. Recordings were also obtained at the level of the atria in transverse and longitu- dinal planes; with simultaneous projection of 2-D images and pulsed wave Doppler spectra, the flow curves through the tricuspid and mi- tral valves were analyzed.
Alterations in wall movement supported right or left ventricular infarction. Depending on the amplitude of systolic movement, scores were given to the different walls. Normal wall movement was given a score of 0; hypokinesis
or diminished systolic wall thickening was scored as +l; akinesis or absence of systolic wall thickening as +2; dyskinesis or paradoxi- cal systolic movement as +3; and hyperkinesis or compensatory systolic movement of a wall without infarction as -1.
Another variable examined in both ventri- cles was end-diastolic diameter, which was measured using transverse plane recordings of four chambers at the level of the atrioventricu- lar annulus. The relationship between the dia- stolic diameters of the ventricles was calcu- lated (RVDDaVDD).
Echocardiographic findings supporting right atrial infarction included akinesis of the atrial wall, thrombosis at the site of akinesis, dilata- tion of the atrial cavity with spontaneous con- trast, and absence of atrial contribution to right ventricular filling in the presence of left atrial contraction.
The echocardiographic studies were ana- lyzed separately by two expert cardiologist- echocardiographers who were unaware of the clinical, electrocardiographic, and hemody- namic data of the patients. The conclusions were reached by consensus.
Statistical Analysis
Statistical analysis of the relationship of right ventricular wall movement index, total
L
Figure 1. Diagram of transgastric image at the level of the papillary muscles showing the right Ventricular wall. A = anterior; I = inferior; L = lateral.
Vol. 15, No. 2,1998 ECHOCARDIOGRAPHY: A Jml. of CV Ultrasound & Allied Tech. 173

VARGAS-BARRON, ET AL.
wall movement index, and the ratio of the dia- stolic diameters of the ventricles to NYHA functional class was performed using Student’s t- and Mann-Whitney U tests. The level of sig- nificance was P I 0.05.
Results
Clinical Findings
In 21 cases (55%) clinical data compatible with right ventricular infarction were present. These included arterial hypotension, right gal- lop rhythm, jugular plethora, and bradycar- dia. In all cases important enzymatic eleva- tion was documented, CPK had values from 300 mg% to 3785 mg% (mean 2042 mg%), and DHL was increased to 170 mg% to 1762 mg% (mean 966 mg%).
The enzymatic activity in the remaining pa- tients was the following: 14 had CPK between 55 mg% and 1687 mg% (mean 871 mg%) and DHL between 121 mg% and 1088 mg% (mean 604 mg%). Enzymatic activity was not deter- mined in three patients because they were hos- pitalized on the fifth and eighth day after in- farction (Table I).
Electrocardiographic Signs
All of the patients had ECG evidence of left ventricular infarction. In 37 cases, the location of the infarction was posteroinferior and was associated with Q waves with a duration of > 0.04 seconds and elevation of the ST segment of 1 mm or more in leads DII, DIII, and aW. In only one case, the location was anterior with Q waves and elevation of the ST segment in leads
Of the 38 patients, in 30 (78%) ECG evidence of extension of the infarction to right ventricle characterized by elevation of the ST segment of 1 mm or more in leads V,R and V,R was found. In 3 cases, right atrial infarction was diag- nosed; 1 showed a negative deflection at the beginning of the P wave and the other 2 eleva- tion of the PR segment (Table I).
In 19 of the 38 patients cardiac rhythm and atrioventricular conduction disturbances were documented. In 13 first- or second-degree atrioventricular blocks appeared; in 2 of these,
V,-V,.
right bundle branch blocks coexisted. In 3 pa- tients, atrioventricular junction rhythm was identified; in 2, atrial fibrillation; and in 1, right bundle branch block. It was necessary to use pacemakers in 11 of the 16 patients with atrioventricular conduction disturbances, 9 provisional and 2 definitive.
Coronary Angiogram
The findings of the coronary angiograms practiced on 34 patients (89%) appear in Table 11. In two cases, no significant coronary ob- structions were observed. In 12 patients, le- sions in a single vessel were identified, corre- sponding to the right coronary artery. In 14 pa- tients, lesions were found in two vessels; in 13 of them, obstructions existed in the right coro- nary and anterior descending branch, while in the other they were found in the right and cir- cumflex coronary arteries. Lesions of three or more vessels were observed in six patients.
Obstruction of the right coronary artery was demonstrated in the 34 coronary angiograms performed. The right coronary lesion was in the proximal third in 19 patients, in the middle third in 10, and in the distal third in 3. Right atrial circulation was evaluated and was con- sidered adequate because the atrial branches of the right coronary and/or circumflex artery were patent in 29 patients. In five cases, sig- nificant obstructions of atrial circulation were found. In two patients, atrial circulation had obstructions of 100%. Two patients only had one patent atrial branch from the circumflex artery and the other a very small branch from the right coronary artery.
Transesophageal Echocardiography
Alterations in left ventricular posteroinfe- rior wall movement were found in 37 cases and in the anterior wall in 1. All of the patients (38) had extension to right ventricle with alter- ations of inferior wall movement in 26 cases, inferior and lateral wall movement in 8, infe- rior wall and septal movement in 1, inferior and lateral wall and septal movement in 1, and alterations of movement of all right ventricular walls (anterior, inferior, lateral, and septal) in 2 (Figs. 2 and 3).
174 ECHOCARDIOGRAPHY: A Jml. of CV Ultrasound & Allied Tech. Vol. 15, No. 2, 1998

TABLE
I
Cha
ract
eris
tics
of P
atie
nts
~ ~
Ele
ctro
card
iogr
am
Enz
ymes
T
rans
esop
hage
al E
choc
ardi
ogra
phy
(mgO
/oo)
Func
tion
al
Loc
atio
n of
R
hyth
m a
nd A
V
RV
/LV
N
o.
Infa
rctio
n C
ondu
ctio
n D
istu
rban
ces
Cp
mH
L
rati
o T
WM
I R
V-W
MI
RA
Ext
C
ompl
icat
ions
C
lass
1
2 3 4 5 6 7 8
9 10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
LV
PI
LV
PI+R
V
LV
PI + R
V
LV
PI+R
V
LV
PI + R
V +
RA
LV
PI+R
V
LV
PI+R
V
LV
PI+R
V
LV
PI+R
V
LV
PI
LW
I L
VPI
+RV
L
VPI
+RV
L
VPI
L
VPI
+RV
L
VPI
L
VPI
+RV
L
VPI
+RV
L
VPI
+ RV
+ RA
L
VPI
+R
V
LV
PI+R
V
LV
PI+R
V
LV
PI+R
V
LV
PI+R
V+R
A
LV
PI + R
V
LV
PI
LV
PI+R
V
LV
PI+R
V
LV
PI
LV
PI+R
V
LV
PI+R
V
LV
PI
LV
PI +
RV
L
VPI
+RV
LV
PI+R
V
LV
PI+R
V
LV
Ant
+R
V
LV
PI+R
V
RB
BB
+ 1" &
2"
AV
Blo
ck
RB
BB
+2"
AV
Blo
ck
2" A
V B
lock
lo
& 2
" A
V B
lock
2"
AV
Blo
ck
AV
Jun
ctio
n R
hyth
m
-
-
1" A
V B
lock
AV
Jun
ctio
n R
hyth
m
1" A
V B
lock
R
BB
B
-
-
-
-
1" A
V B
lock
2"
AV
Blo
ck
AV
Jun
ctio
n R
hyth
m
1" &
2" A
V B
lock
-
-
-
1" &
2"
AV
Blo
ck
-
-
1" A
V B
lock
-
-
1" A
V B
lock
-
-
-
Atr
ial F
ibri
llat
ion
Atr
ial F
ibri
llat
ion
2650
/539
13
05/2
49
1817
/315
97
6/76
8 16
89/1
87
443/
524
2000
/479
20
00/3
90
1500
/899
37
85/1
265
662/
252
2636
/504
63
7/16
8 20
38/4
03
1080
/360
31
8/27
3 33
8717
35
2000
/529
60
0/28
9 17
56/2
53
3040
/944
25
38/1
762
-/- 55/1
70
7131
268
2311
205
544/
279
1687
/345
-/
- 20
4/12
1 11
52/3
44
1500
/321
30
0/28
2 -/
- 12
5813
87
1488
/108
8 11
61/3
96
330/
297
1.77
1.
10
1.13
1.
90
1.20
1.
21
0.66
0.
92
0.70
0.
88
1.0
1.0
0.69
0.
84
0.91
1.
0 0.
98
1.0
0.92
0.
93
1.0
1.0
1.0
1.0
1.77
0.
73
0.8
1.0
0.85
0.
92
0.8
0.93
1.
1 0.
74
0.92
1.
0 0.
73
0.76
13
8 5
4 5
4 5
4 14
8
5 5
1
1
3 2
3 2
3 2
2 1
3 2
1
1
1
1
3 2
4 1
2 2
5 4
3 3
2 1
3 1
4 3
6 4
10
4 6
4 2
1
3 1
3 1
5 2
1
1
3 2
1
1
2 1
4 2
2 1
2 1
4 2
5 2
Peri
card
ial e
ffus
ion
LV-P
B A
neur
ysm
V
entr
icul
ar s
epta
1 ru
ptur
e Pe
rica
rdia
l eff
usio
n
Rig
ht A
tria
l Thr
ombu
s -
-
-
-
-
Pat
ent F
oram
en O
vale
-
-
-
-
-
Peri
card
ial E
ffus
ion
Peri
card
ial E
ffus
ion
-
-
-
-
Peri
card
ial E
ffis
ion
+ Pa
pill
ary
Mus
cle
Rup
ture
-
-
Peri
card
ial E
ffus
ion
LW
B A
neur
ysm
-
-
-
-
-
-
Peri
card
ial E
ffus
ion
Papi
llar
y M
uscl
e R
uptu
re
-
-
-
IV (D
ied)
IV (D
ied)
IV (D
ied)
II
rn
111
IV (D
ied)
I I I1
I I I I I I I I I I I I I I I I I1
1-1
1
I I1
I I1
1 I1
I I -
-
-
AV
= A
trio
vent
ricu
lar;
LV
= L
eft v
entr
icul
e; P
B =
Pos
tero
basa
l; PI
= P
oste
roin
feri
or; R
A E
xt =
Rig
ht A
tria
l Ext
ensi
on; R
BB
B =
Rig
ht B
undl
e B
ranc
h B
lock
; RV
= R
ight
ven
tric
le; R
V-
WM
I =
Rig
ht V
entr
icul
ar W
all M
ovem
ent I
ndex
; SE
C =
Spo
ntan
eous
Ech
o C
ontr
ast;
TWMI =
Tot
al W
all M
ovem
ent I
ndex
.

VARGAS-BARRON, ET AL.
TABLE I1
Coronary Angiogram
Right Coronary Anterior Descending Circumflex Atrial Circulation
No. Segment ‘7c Obstruction L7C Obstruction 8 Obstruction % Obstruction
1 2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38
Proximal Proximal Vertical Proximal Proximal Proximal - -
-
Proximal Distal Vertical Vertical Vertical Vertical Distal Proximal Proximal Proximal Proximal Vertical Proximal Proximal
Proximal Vertical Proximal Proximal Proximal Proximal Proximal Vertical
-
- -
Vertical Vertical Distal Proximal
100 90 50
100 100 100
Not Performed 0
Not Performed 90 50 60 75 35
100 80 60 85
100 90
100 99
100 Not Performed
100 90
100 100 100 100 40 50 0
Not Performed 100 100 100 90
70 90 75
100 90
0 Not Performed
0 Not Performed
0 90 40
Diffuse 25 60 30 50
0 0 0
75 0 0
Not Performed 70 0
85 99 95
Diffuse 40 50 0
Not Performed 0 0 0 0
0 0 0 0 0 0
Not Performed 0
Not Performed 0
100 0
75 0 0 0 0
20 0 0 0 0 0
Not Performed 40 0
Diffuse 75 0
70 0 0 0
0 0 0 0
Not Performed
0 0 0
100 Small Circumflex Branch
100 Not Performed
0 Not Performed
0 0 0 0 0 0 0 0 0
0 0 0
Small Right Coronary Branch
Small Circumflex Branch Not Performed
0 0 0 0 0 0 0 0 0
0 0 0 0
Not Performed
As respects scoring of the severity of alter- ations in mobility of both ventricles (WMI), 26 patients (68.5%) were found to have total scores (RV + LV) of < 5 and the remaining 12 (31.5%) of 5 or more. The right ventricular WMI L 4 in 10 patients (26%). Included in these were the four patients who died in the hospital phase and two who are still alive in functional Class III/IV. Only four patients with
RV-WMI of 4 are in functional Class I. The re- maining 28 patients (74%) had right ventricu- lar WMI of < 4. The RVDDLVDD ratio ob- tained in the four-chamber transverse plane was 1 or less in 30 patients (78%) and > 1 in only 8 (22%).
In 6 patients, alterations in right atrial wall movement were documented, 2 with hypokine- sis (Fig. 4) and 2 with akinesis. In four of these
176 ECHOCARDIOGRAPHY. A Jml. of CV Ultrasound & Allied Tech. Vol. 15, No. 2,1998
CLINICAL-ECHOCARDIOGRAPHIC CORRELATION OF MYOCARDIAL INFARCTION
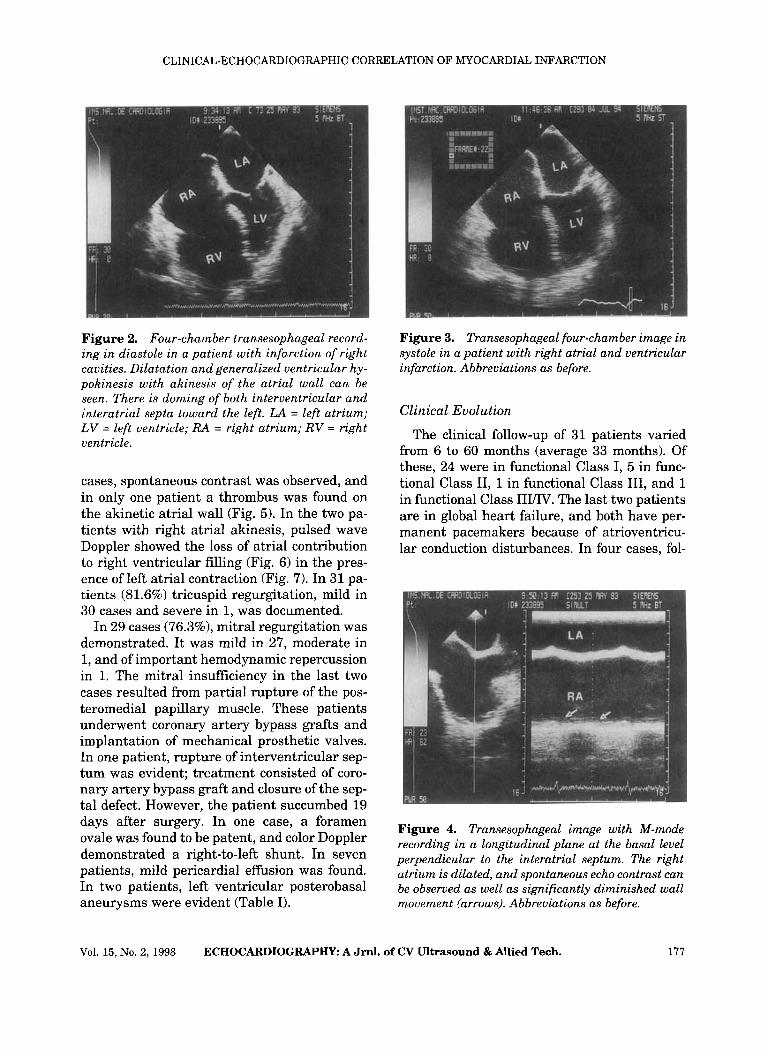
Figure 2. Four-chamber transesophageal record- ing in diastole in a patient with infarction of right cavities. Dilatation and generalized ventricular hy- pokinesis with akinesis of the atrial wall can be seen. There is doming of both interventricular and interatrial septa toward the left. LA = left atrium; LV = left ventricle; RA = right atrium; RV = right ventricle.
cases, spontaneous contrast was observed, and in only one patient a thrombus was found on the akinetic atrial wall (Fig. 5) . In the two pa- tients with right atrial akinesis, pulsed wave Doppler showed the loss of atrial contribution to right ventricular filling (Fig. 6) in the pres- ence of left atrial contraction (Fig. 7). In 31 pa- tients (81.6%) tricuspid regurgitation, mild in 30 cases and severe in 1, was documented.
In 29 cases (76.3%), mitral regurgitation was demonstrated. It was mild in 27, moderate in 1, and of important hemodynamic repercussion in 1. The mitral insufficiency in the last two cases resulted from partial rupture of the pos- teromedial papillary muscle. These patients underwent coronary artery bypass grafts and implantation of mechanical prosthetic valves. In one patient, rupture of interventricular sep- tum was evident; treatment consisted of coro- nary artery bypass graft and closure of the sep- tal defect. However, the patient succumbed 19 days after surgery. In one case, a foramen ovale was found to be patent, and color Doppler demonstrated a right-to-left shunt. In seven patients, mild pericardial effusion was found. In two patients, left ventricular posterobasal aneurysms were evident (Table I).
Figure 3. Transesophageal four-chamber image in systole in a patient with right atrial and ventricular infarction. Abbreviations as before.
Clinical Evolution
The clinical follow-up of 31 patients varied from 6 to 60 months (average 33 months). Of these, 24 were in functional Class I, 5 in func- tional Class 11, 1 in functional Class 111, and 1 in functional Class III/IV. The last two patients are in global heart failure, and both have per- manent pacemakers because of atrioventricu- lar conduction disturbances. In four cases, fol-
Figure 4. Transesophageal image with M-mode recording in a longitudinal plane at the basal level perpendicular to the interatrial septum. The right atrium is dilated, and spontaneous echo contrast can be observed as well as significantly diminished wall movement (arrows). Abbreviations as before.
Vol. 15, No. 2, 1998 ECHOCARDIOGRAPHY: A Jml. of CV Ultrasound & Allied Tech. 177

VARGAS-BARRON, ET AL.
Figure 5. Transesophageal echocardiographic im- age in a transverse plane at the level of the atria. A thrombus can be seen adhering to the akinetic right atrial wall (arrows). Abbreviations as before.
low-up was < 1 month. Two of these patients died in cardiogenic shock and two during surgery, one for removal of an aneurysm and the other for closure of a ventricular septa1 rup- ture. Three patients were lost to follow-up; in these, functional class could not be established.
Statistical Analysis
Statistical analysis was performed on the findings from 35 patients. A significant differ-
Figure 6. Transesophageal recording with pulsed Doppler spectrum of tricuspid diastolic flow. There is no atrial contribution to right ventricular filling (arrows). Abbreviations as before.
Figure 7. Transesophageal four-chamber image in a patient with infarction of right cavities. Doppler analysis shows left atrial contraction (arrows). Ab- breviations as before.
ence with P = 0.057 for Student’s t-test and P I 0.03 for Mann-Whitney U test was found for NYHA Functional Class I/II and a total WMI of > 5; and NYHA Class I I W and a total WMI of 5 or more.
The association of NYHA Functional Class I/II and an RV-WMI of c 4; and Functional Class I I W and an RV-WMI of 4 or more showed sig- nificance with P = 0.005 for Student’s t-test and P 5 0.01 for the Mann-Whitney U test.
Statistical significance also existed for the relationship of Functional Class 141 and an RVDDLVDD ratio of one or less; and Func- tional Class I I W and an RVDDLVDD > one with P = 0.022 for Student’s t-test and P I 0.001 for the Mann-Whitney U test.
Discussion
In this group of patients with left ventricular infarction, extension of the necrosis to right ventricle was suspected on the basis of clinical findings in only 21 (55%). As respects elevation of enzymes, we found that all patients with he- modynamic consequences of right ventricular infarction had significantly increased levels of CPK and DHL. However, similar enzymatic el- evations were observed in patients with small right ventricular infarctions.
The diagnosis of right ventricular infarction
178 ECHOCARDIOGRAPHY: A Jml. of CV Ultrasound & Allied Tech. Vol. 15, No. 2,1998

CLINICAL-ECHOCARDIOGRAPHIC CORRELATION OF MYOCARDIAL INFARCTION
by electrocardiography was achieved in only 30 cases (78%), a value in agreement with that re- ported in the literature. Those cases without electrocardiographic diagnosis could probably be explained by the transient nature of the ST elevation. In one series, 48% of the patients had resolution of electrocardiographic changes within 10 hours of the onset of symptoms.8 Moreover, the ECG showed evidence of right atrial infarction in only 3 of the 6 patients in which TEE demonstrated dyssynergy of the atrial wall. This indicates that correct diagno- sis requires a complete EGG with all of the right precordial leads as soon as possible.
It is noteworthy that half of the patients had rhythm or atrioventricular conduction distur- bances, particularly atrioventricular block. This supports the high incidence of the finding reported in the l i t e r a t~ re .~ In our series, con- duction disturbances occurred in 16 cases, or 42%. Of these, 13 were first- or second-degree atrioventricular blocks and in the other 3, com- plete blocks with junction rhythm. This high incidence of A-V block is not seen in patients with left ventricular posterior infarction with- out extension to right ventricle.
It was possible to evaluate the coronary an- giogram in only 34 of the 38 patients. In two cases, no significant atherosclerotic lesions could be found, while in the remaining 32, im- portant obstruction of the right coronary artery was seen. In 19 cases, there was coexistent ob- struction of the anterior descending artery, and in 7 patients of the circumflex artery.
When the right coronary artery lesion was proximal (19 cases), the patients had torpid evolution with arterial hypotension, right gal- lop rhythm, and atrioventricular conduction disturbances in 53% of the cases (10 patients).
When the total wall movement index was 5 or more, the RV-WMI 4 or more, and the RVDD/ LVDD ratio > 1, patients were in a worse func- tional Class (III/IV).
TEE was the diagnostic technique that best demonstrated the extension of the infarction to right chambers. In all 38 patients, it showed alterations of right inferior wall movement and in some cases dyssynergy that extended to lat- eral, septal, and even anterior walls. It also made it possible to demonstrate the extension
of the ischemic process to the right atrium. Atrial wall hypokinesis was evident in four cases and akinesis in two. In four of these cases, spontaneous contrast could be identified in the atrial cavity, and in one a thrombus ad- hering to the akinetic wall. In the two patients with right atrial akinesis, the tricuspid flow “a” wave could not be detected, confirming the lack of atrial contraction. The hemodynamic deteri- oration associated with extension of ischemia to the right atrium may be important; 3 of the 6 patients with atrial dyssynergy in TEE were in functional Class III/IV.
When alterations of right atrial wall move- ment were compared to findings from coronary angiograms, patients with right atrial akine- sis (2) proved to have total occlusion of the atrial circulation, while those with hypokine- sis received some blood supply from a small atrial branch of the circumflex (2) or right coronary artery (1). In one patient with right atrial hypokinesis, a coronary angiogram was not performed.
In one patient, TEE showed sudden right-to- left shunting through a previously unsus- pected patent foramen ovale; as right ventricu- lar function improved, the shunt diminished. This finding has been described in other re- p o r t ~ ~ ~ and may adversely affect the patient’s clinical course.
Color Doppler showed that regurgitation of atrioventricular valves is frequent. In 31 pa- tients (81.6%) tricuspid insufficiency, mild or moderate in all but one, was documented. In 29 cases (76.3%) mitral insufficiency was identified, which was mild to moderate in 27. In the two cases with severe mitral regurgitation, TEE demonstrated partial rupture of the posterome- dial papillary muscle. TEE also confirmed the rupture of the interventricular septum in an- other patient. In all three, the transesophageal echocardiographic findings provided the surgical indications.
Finally, as respects prognosis, the results of our series are in agreement with published re- ports. Mortality during hospitalization was 10%; in other series it has been as high as 31%.“ This contrasts dramatically with myocardial in- farction limited to the left ventricular pos- teroinferior wall, in which the mortality is e 6%.
Vol. 15, No. 2,1998 ECHOCARDIOGWHY: A Jrnl. of CV Ultrasound & Allied Tech. 179

VARGAS-BARRON, ET AL
Morbidity is also more important during hos- pitalization. In our series, rhythm and atrio- ventricular conduction disturbances were fre- quent, and in 11 of 16 patients with A-V con- duction disturbances, it was necessary to use pacemakers. Fortunately, in nine the require- ment was transitory. In only two were perma- nent pacemakers implanted.
On the basis of the results the following con- clusions were reached.
TEE is an excellent diagnostic technique for identifying myocardial infarction of the right ventricular inferior wall as well as its exten- sion to other walls. Likewise, TEE can docu- ment the extension of ischemia to the right atrium. A relationship exists between the mag- nitude of right ventricular damage and vari- ables available from transesophageal record- ings. A total WMI of 5 or more and a RV-WMI of 4 or more, or a ratio of RVLV diastolic di- ameters of > 1 are associated with greater he- modynamic deterioration after ventricular in- farction and a higher incidence of intrahospi- talary complications. I n these patients, short- or intermediate-term cardiac function will be more affected.
Extension of the ischemic process to right atrium is associated with greater intrahospital- ary morbidity.
References
1. Erhardt LR, Sjogren A, Wahlbers I: Single right- sided precordial lead in the diagnosis of right ventricular involvement in inferior myocardial infarction. Am Heart J 1976;91:571-576. Dell’Italia LJ, Starling MR, Crawford MH, et al: Right ventricular infarction: Identification by hemodynamic measurements before and af- ter volume loading and correlation with nonin-
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
vasive techniques. J Am Coll Cardiol 1984;4:
DArcy B, Nanda NC: Two-dimensional echo- cardiographic features of right ventricular in- farction. Circulation 1982;65:167-173. Lopez-Sendon J , Garcia-Fernandez MA, Coma- Canella I, et al: Segmental right ventricular function after acute myocardial infarction: Two-dimensional echocardiographic study in 63 patients. Am J Cardiol 1983;51:390-396. Goldberger JJ, Himelman RB, Wolfe ChL, et al: Right ventricular infarction: Recognition and assessment of its hemodynamic signifi- cance by two-dimensional echocardiography. J Am SOC Echocardiogr 1991;4:140-146. G6mez-Villalobos MJ, Vargas-Barron J, Romero- Cardenas A, et al: Right atrial and ventricular infarction: Evaluation with transesophageal echocardiography. Echocardiography 1995;12:
Vargas-Barron J, Romero-Cardenas A, Keirns C, et al: “ransesophageal echocardiography and right atrial infarction. J Am Soc Echocardiogr
Braat SH, Brugada P, de Zwaan C, et al: Value of electrocardiogram in diagnosing right ven- tricular involvement in patients with an acute inferior wall myocardial infarction. Br Heart J
Braat SH, de Zwaan C, Brugada P, et al: Right ventricular involvement with acute inferior wall myocardial infarction identifies high risk of developing atrioventricular nodal conduc- tion disturbances. Am Heart J 1984;107:1183- 1187. Laham RJ, Ho KKL, Douglas PS, et al: Right ventricular infarction complicated by acute right-to-left shunting. Am J Cardiol 1994;74:
Zehender M, Kasper W, Kauden E: Right ven- tricular infarction as an independent predictor of prognosis after acute inferior myocardial in- farction. N Engl J Med 1993;328:981-988.
93 1-939.
129-137.
1993 ;6:543-547.
1983;49:368-372.
824-826.
180 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 15, No. 2,1998





























