Embed Size (px)
Citation preview
Clinical Governance: An International JournalEmerald Article: Clinical governance: a review of key concepts in the literatureJoanne F. Travaglia, Deborah Debono, Allan D. Spigelman, Jeffrey Braithwaite
Article information:
To cite this document: Joanne F. Travaglia, Deborah Debono, Allan D. Spigelman, Jeffrey Braithwaite, (2011),"Clinical governance: a review of key concepts in the literature", Clinical Governance: An International Journal, Vol. 16 Iss: 1 pp. 62 - 77
Permanent link to this document: http://dx.doi.org/10.1108/14777271111104592
Downloaded on: 04-02-2013
References: This document contains references to 32 other documents
Citations: This document has been cited by 1 other documents
To copy this document: [email protected]
This document has been downloaded 1780 times since 2011. *
Users who downloaded this Article also downloaded: *
Joanne F. Travaglia, Deborah Debono, Allan D. Spigelman, Jeffrey Braithwaite, (2011),"Clinical governance: a review of key concepts in the literature", Clinical Governance: An International Journal, Vol. 16 Iss: 1 pp. 62 - 77http://dx.doi.org/10.1108/14777271111104592
Joanne F. Travaglia, Deborah Debono, Allan D. Spigelman, Jeffrey Braithwaite, (2011),"Clinical governance: a review of key concepts in the literature", Clinical Governance: An International Journal, Vol. 16 Iss: 1 pp. 62 - 77http://dx.doi.org/10.1108/14777271111104592
Joanne F. Travaglia, Deborah Debono, Allan D. Spigelman, Jeffrey Braithwaite, (2011),"Clinical governance: a review of key concepts in the literature", Clinical Governance: An International Journal, Vol. 16 Iss: 1 pp. 62 - 77http://dx.doi.org/10.1108/14777271111104592
Access to this document was granted through an Emerald subscription provided by University of New South Wales For Authors: If you would like to write for this, or any other Emerald publication, then please use our Emerald for Authors service. Information about how to choose which publication to write for and submission guidelines are available for all. Please visit www.emeraldinsight.com/authors for more information.
About Emerald www.emeraldinsight.comWith over forty years' experience, Emerald Group Publishing is a leading independent publisher of global research with impact in business, society, public policy and education. In total, Emerald publishes over 275 journals and more than 130 book series, as well as an extensive range of online products and services. Emerald is both COUNTER 3 and TRANSFER compliant. The organization is a partner of the Committee on Publication Ethics (COPE) and also works with Portico and the LOCKSS initiative for digital archive preservation.
*Related content and download information correct at time of download.
AUSTRALIAN PERSPECTIVE
Clinical governance: a review ofkey concepts in the literature
Joanne F. Travaglia and Deborah DebonoCentre for Clinical Governance Research, Faculty of Medicine,
University of New South Wales, Sydney, Australia
Allan D. SpigelmanSt Vincent’s Clinical School, Faculty of Medicine,
University of New South Wales, Sydney, Australia, and
Jeffrey BraithwaiteCentre for Clinical Governance Research and
Australian Institute of Health Innovation, Faculty of Medicine,University of New South Wales, Sydney, Australia
Abstract
Purpose – This paper aims to explore the development of the concept of clinical governance as aninternational approach to addressing quality and safety issues in healthcare.
Design/methodology/approach – The authors reviewed and analysed published clinicalgovernance abstracts from 1966 to 2009. Citations were identified through a systematic search ofMedline, Embase and CINAHL databases. A time series analysis was undertaken on the citations. Thecontents of the abstracts were then examined using an automated data-mining software package inorder to identify underlying concepts.
Findings – A total of 2,000 publications which made direct mention of clinical governance wereidentified across the 43-year search period. All were produced after 1998. This was when the conceptwas first seriously mobilised. Of the 2,000 citations, 2.3 per cent were published in 1998 and 6.3 percent in 2008 (the last complete year available). The peak was reached in 2003, when 12.7 per cent of allclinical governance citations were published. The years 1998 to 2003 accounted for 59.2 per cent of allcitations (to September 2009). There has been a steady decrease in the number of citations makingdirect reference to clinical governance since 2003.
Originality/value – This paper maps the development and peak of clinical governance as amobilising concept in healthcare in the late twentieth and early twenty-first centuries and shows howits conceptual underpinnings have been taken up by wider quality and safety agendas. Fads andfashions rise and fall in healthcare, as in other areas of life.
Keywords Clinical governance, Literature, Medical care
Paper type Literature review
IntroductionClinical governance has been one of the driving forces behind the healthcareimprovement agenda over the last decade. Emerging as a response to the Bristol RoyalInfirmary Inquiry (Department of Health, 2001) in the UK, the purpose of clinicalgovernance, that is, the “systematic joining up of initiatives to improve quality”(Halligan and Donaldson, 2001, p. 1413) transcends healthy systems and service types(Eeckloo et al., 2007; Spigelman, 2008). Clinical governance is said to provide the
The current issue and full text archive of this journal is available at
www.emeraldinsight.com/1477-7274.htm
CGIJ16,1
62
Clinical Governance: An InternationalJournalVol. 16 No. 1, 2011pp. 62-77q Emerald Group Publishing Limited1477-7274DOI 10.1108/14777271111104592
overarching structure within which health systems, clinicians and staff work towards,and are held accountable for, the safety and continuous quality improvement of theirservice (Allen, 2000).
In an earlier paper (Braithwaite and Travaglia, 2008) we undertook a review of theliterature on clinical governance and its associated concepts, in an effort to understandthe types of clinical governance initiatives and practices that have emerged over the lastdecade. That model identified four components of clinical governance, that is the: use ofclinical governance to promote quality and safety; creation of clinical governancestructures to improve safety and quality; effective use of data and evidence; sponsoringof a patient-centred approach. Clinical governance is also utilised, fifthly, to strengthenlinks between the health services clinical and corporate governance arenas.
In this paper we seek to provide a more detailed discussion, through an analysis ofrelevant literature, of the way in which the concept of clinical governance has emerged,and how that concept is manifest. We provide an appraisal of the ideas that underpinthe literature (objective one) and map the major concepts, strategies, approaches andprocesses encouraged by clinical governance against our original model (objectivetwo). We aim to reflect on the way in which the clinical governance literature hasevolved, and to examine the underlying “sense-making” (Weick, 1995) process whichhas occurred within the public narrative on clinical governance.
MethodAs our typology shows (Braithwaite and Travaglia, 2008), clinical governance is arelatively new term for a number of long-standing, inter-related activities aimed atimproving the quality and safety of health care. Although originally flagged by theWorld Health Organisation in 1983 (Penny, 2000) the concept’s substantive roots are inthe “modernisation” of the UK’s National Health Service (NHS) in the late 1990s. Weinterrogated in depth the published literature that has directly addressed clinicalgovernance as an approach, rather than each component of clinical governance (forexample, incident reporting, patient centred care etc). To do so we reviewed theliterature on clinical governance in four separate databases from their inception untilSeptember 2009. The databases included were: Medline and Medline in process(medicine, from 1950); Embase (medicine, from 1947); and CINAHL (nursing and alliedhealth, including in press, from 1981).
The search term used was clinical governance. The initial search utilised thestandardised Medical Subject Heading (MeSH) term. As the results from this searchwere limited, we then searched using clinical governance as a keyword. Keywordsearches identify the sequence of words in publications, and may therefore identifyarticles which contain references to clinical governance, but which have not beencategorised as such. The results are presented in Table I.
Term MedlineaMedline in
process CINAHLb Embase TotalTotal minusduplicates
Clinicalgovernance 777 44 1,174 874 2,869 2,000
Notes: aMeSH results yielded 33; bMeSH results yielded 321
Table I.Search findings for the
term clinical governance
Clinicalgovernance
63
The results were downloaded into Endnote X3, a reference management softwarepackage. We analysed the resulting data using Leximancer, a data-mining package.We took four samples of the data in order to compare the changes in the conceptsunderlying the clinical governance approach: all citations and abstracts, those from1998, 2003 and 2008 (the last full year of data available). The identified citations andabstracts were analysed by one author to identify type and frequency, and thecategorisation validated by a second author. An analysis of the database search resultswas then conducted using the automated software. Leximancer is able to produce botha ranked list of concepts emerging from a body of data, and a map showing therelationships between these concepts (Travaglia et al., 2009; Stockwell et al., 2009;Smith and Humphreys, 2006; Watson et al., 2005). This enabled us to explore thepeer-reviewed literature available on clinical governance to date, and to compare thisliterature to our own typology as a way of assessing the concepts that underpin thisapproach.
FindingsThe first published literature on clinical governance appeared in 1998. In all, 46citations were identified for that year. The most number of citations relating to clinicalgovernance were produced in 2003, when 253 articles, books or conference papersrelating to the term appeared in the databases searched. Since that peak the overallnumber of citations on clinical governance has decreased steadily, although not evenly.
Of the 2,000 citations, 2.3 per cent were published in 1998 and 6.3 per cent in 2008(the last complete year available). The peak was reached in 2003, when 12.7 per cent ofall clinical governance citations were published. The years 1998 to 2003 accounted for59.2 per cent of all citations (to September 2009). There has been a steady decrease inthe number of citations making direct reference to clinical governance since that time.Figure 1 presents the results of number of citations identified by year to September2009.
Table II presents the 25 journals with the highest number of citations relating toclinical governance. The list locates the clinical governance research primarily withinBritish journals, with nursing dominant amongst professional journals. Articles onclinical governance and published within the British Journal of Clinical Governance(BJCG), Clinical Performance and Quality Healthcare (which was incorporated into theBJCG) or its successor Clinical Governance: An International Journal make up 8.5 percent of clinical governance citations. These are not all articles in the journal, but thosethat address the issue directly.
We subjected the literature to a data-mining process in order to examine changes inthe concepts underpinning clinical governance. The analysis of the data from 1998 ispresented in Figure 2. The analysis shows that literature from that year was focused onten broad themes: clinical, audit, care, practice, quality, evidence, future, drugs,responsibilities, and article. The dots within each circle are the individual concepts.Their location is significant, in that the closer the physical proximity between conceptsthe stronger the conceptual association. The absence of a concept from either theconcept map or ranked list does not mean that it is absent from the literature, butrather that its impact on the literature is not as great as that of other concepts.
Figure 2 shows that the literature in 1998 was concerned with the quality of care, theuse of audit and evidence as governance tools, and the impact of these tools and policy
CGIJ16,1
64
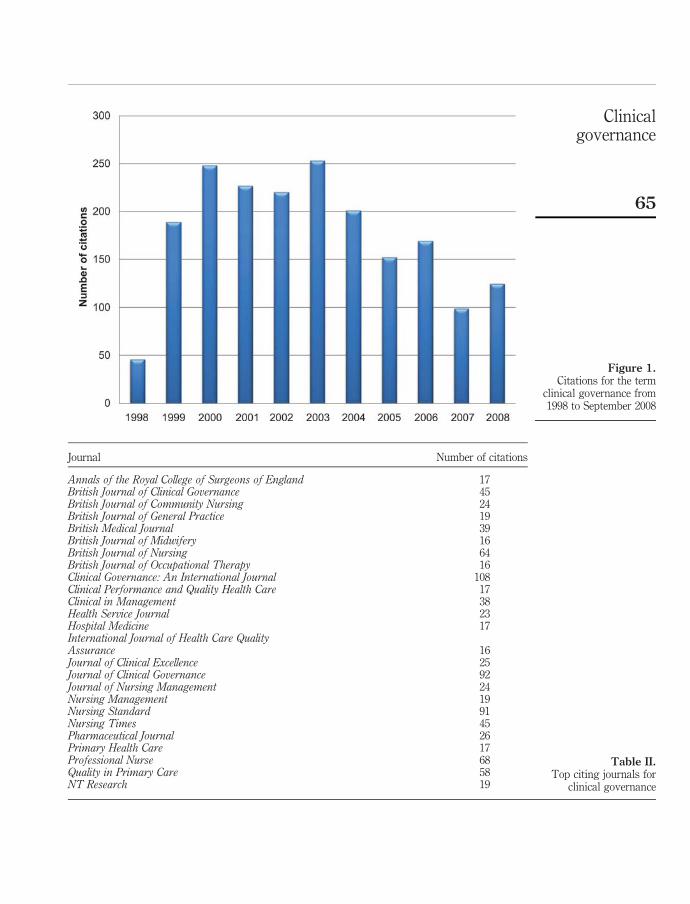
Figure 1.Citations for the term
clinical governance from1998 to September 2008
Journal Number of citations
Annals of the Royal College of Surgeons of England 17British Journal of Clinical Governance 45British Journal of Community Nursing 24British Journal of General Practice 19British Medical Journal 39British Journal of Midwifery 16British Journal of Nursing 64British Journal of Occupational Therapy 16Clinical Governance: An International Journal 108Clinical Performance and Quality Health Care 17Clinical in Management 38Health Service Journal 23Hospital Medicine 17International Journal of Health Care QualityAssurance 16Journal of Clinical Excellence 25Journal of Clinical Governance 92Journal of Nursing Management 24Nursing Management 19Nursing Standard 91Nursing Times 45Pharmaceutical Journal 26Primary Health Care 17Professional Nurse 68Quality in Primary Care 58NT Research 19
Table II.Top citing journals for
clinical governance
Clinicalgovernance
65
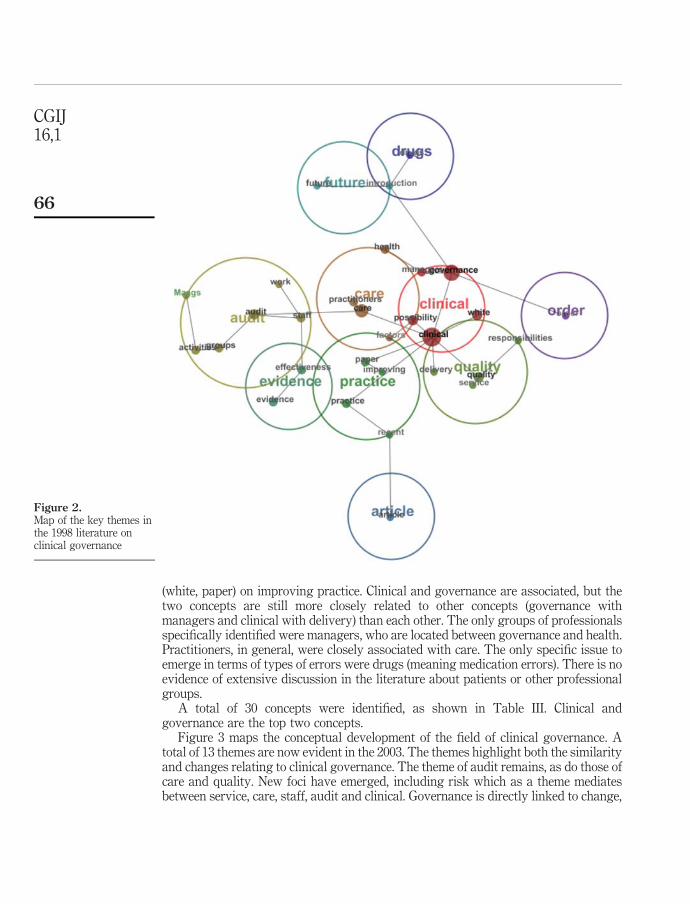
(white, paper) on improving practice. Clinical and governance are associated, but thetwo concepts are still more closely related to other concepts (governance withmanagers and clinical with delivery) than each other. The only groups of professionalsspecifically identified were managers, who are located between governance and health.Practitioners, in general, were closely associated with care. The only specific issue toemerge in terms of types of errors were drugs (meaning medication errors). There is noevidence of extensive discussion in the literature about patients or other professionalgroups.
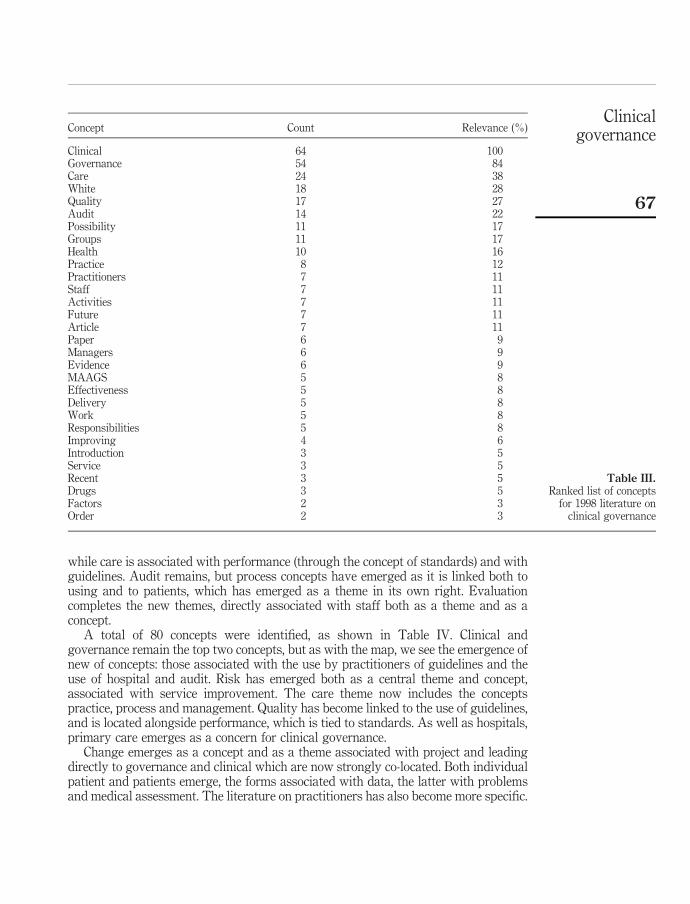
A total of 30 concepts were identified, as shown in Table III. Clinical andgovernance are the top two concepts.
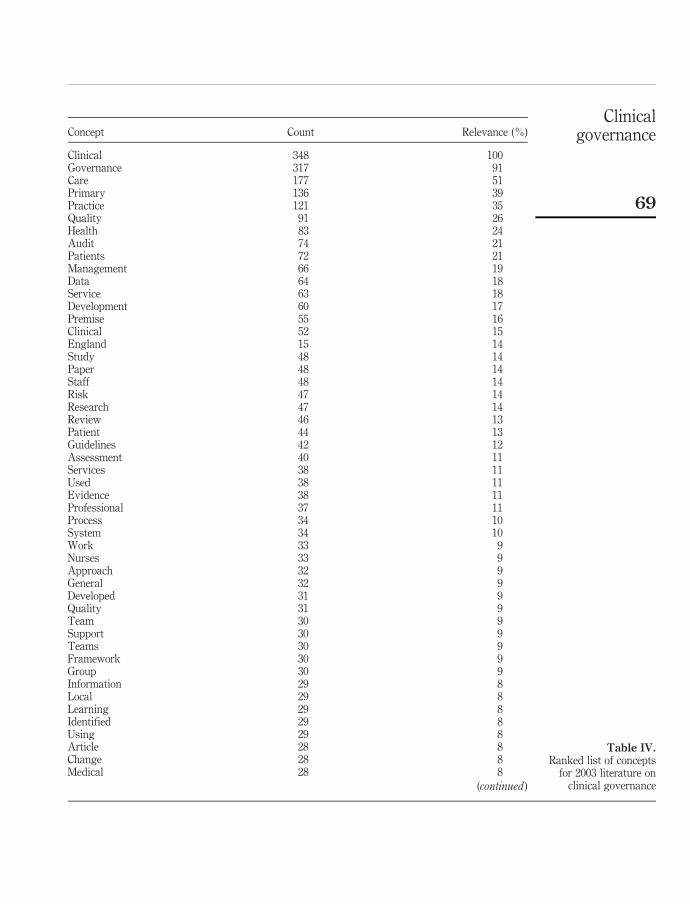
Figure 3 maps the conceptual development of the field of clinical governance. Atotal of 13 themes are now evident in the 2003. The themes highlight both the similarityand changes relating to clinical governance. The theme of audit remains, as do those ofcare and quality. New foci have emerged, including risk which as a theme mediatesbetween service, care, staff, audit and clinical. Governance is directly linked to change,
Figure 2.Map of the key themes inthe 1998 literature onclinical governance
CGIJ16,1
66
while care is associated with performance (through the concept of standards) and withguidelines. Audit remains, but process concepts have emerged as it is linked both tousing and to patients, which has emerged as a theme in its own right. Evaluationcompletes the new themes, directly associated with staff both as a theme and as aconcept.
A total of 80 concepts were identified, as shown in Table IV. Clinical andgovernance remain the top two concepts, but as with the map, we see the emergence ofnew of concepts: those associated with the use by practitioners of guidelines and theuse of hospital and audit. Risk has emerged both as a central theme and concept,associated with service improvement. The care theme now includes the conceptspractice, process and management. Quality has become linked to the use of guidelines,and is located alongside performance, which is tied to standards. As well as hospitals,primary care emerges as a concern for clinical governance.
Change emerges as a concept and as a theme associated with project and leadingdirectly to governance and clinical which are now strongly co-located. Both individualpatient and patients emerge, the forms associated with data, the latter with problemsand medical assessment. The literature on practitioners has also become more specific.
Concept Count Relevance (%)
Clinical 64 100Governance 54 84Care 24 38White 18 28Quality 17 27Audit 14 22Possibility 11 17Groups 11 17Health 10 16Practice 8 12Practitioners 7 11Staff 7 11Activities 7 11Future 7 11Article 7 11Paper 6 9Managers 6 9Evidence 6 9MAAGS 5 8Effectiveness 5 8Delivery 5 8Work 5 8Responsibilities 5 8Improving 4 6Introduction 3 5Service 3 5Recent 3 5Drugs 3 5Factors 2 3Order 2 3
Table III.Ranked list of concepts
for 1998 literature onclinical governance
Clinicalgovernance
67
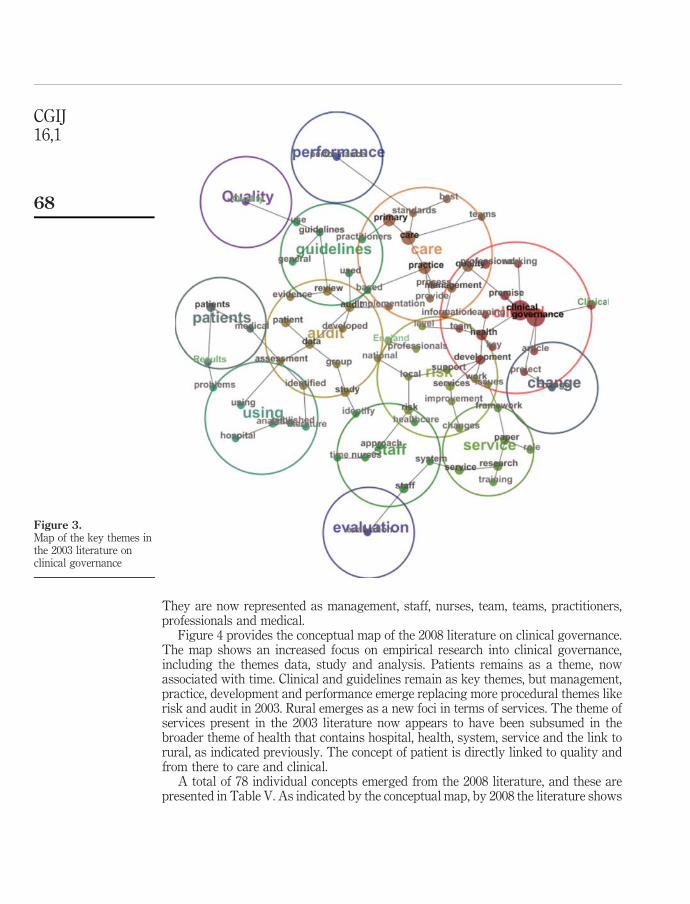
They are now represented as management, staff, nurses, team, teams, practitioners,professionals and medical.
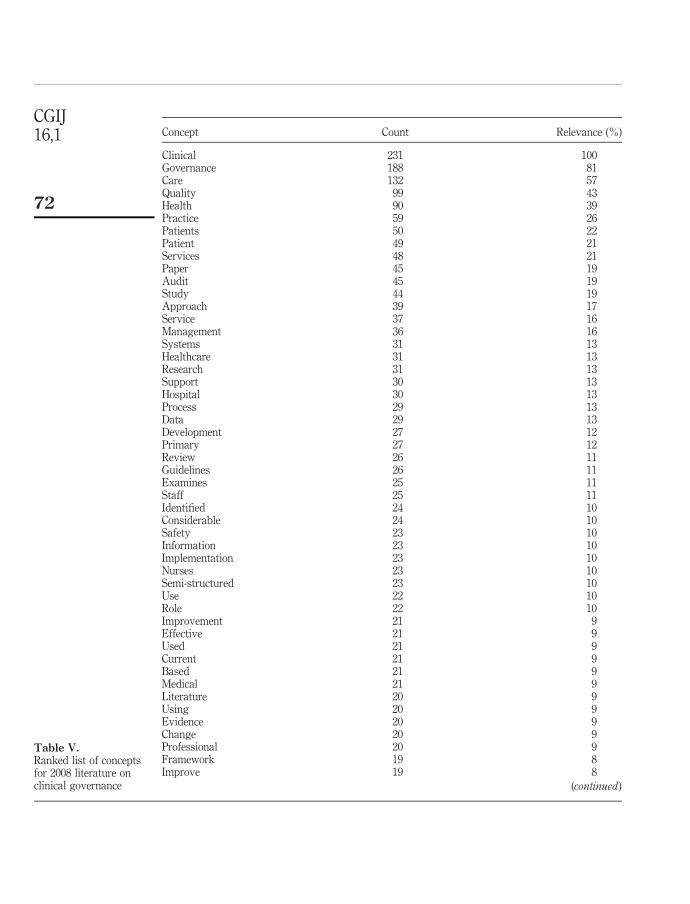
Figure 4 provides the conceptual map of the 2008 literature on clinical governance.The map shows an increased focus on empirical research into clinical governance,including the themes data, study and analysis. Patients remains as a theme, nowassociated with time. Clinical and guidelines remain as key themes, but management,practice, development and performance emerge replacing more procedural themes likerisk and audit in 2003. Rural emerges as a new foci in terms of services. The theme ofservices present in the 2003 literature now appears to have been subsumed in thebroader theme of health that contains hospital, health, system, service and the link torural, as indicated previously. The concept of patient is directly linked to quality andfrom there to care and clinical.
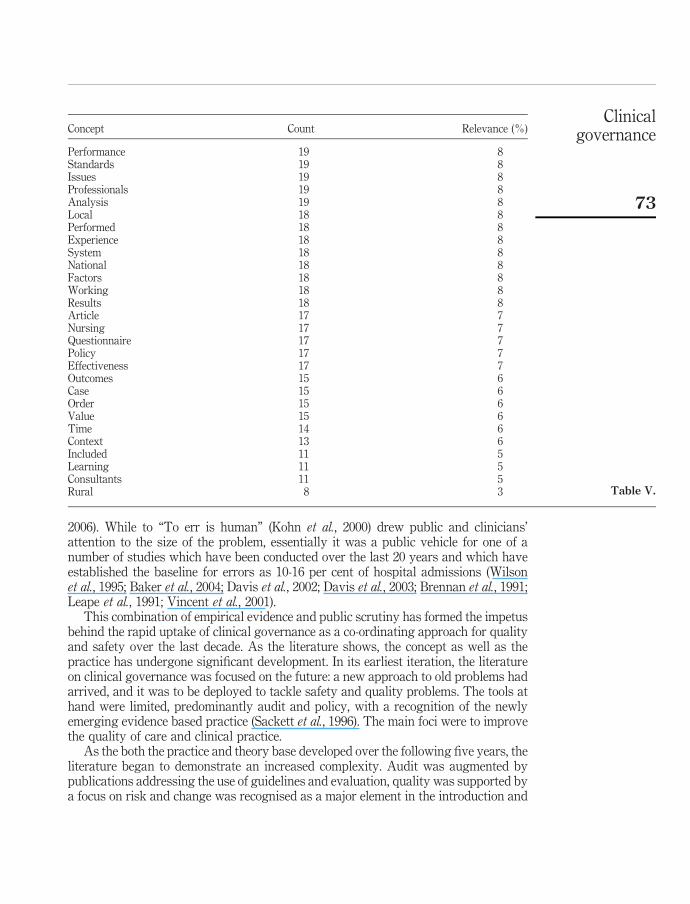
A total of 78 individual concepts emerged from the 2008 literature, and these arepresented in Table V. As indicated by the conceptual map, by 2008 the literature shows
Figure 3.Map of the key themes inthe 2003 literature onclinical governance
CGIJ16,1
68
Concept Count Relevance (%)
Clinical 348 100Governance 317 91Care 177 51Primary 136 39Practice 121 35Quality 91 26Health 83 24Audit 74 21Patients 72 21Management 66 19Data 64 18Service 63 18Development 60 17Premise 55 16Clinical 52 15England 15 14Study 48 14Paper 48 14Staff 48 14Risk 47 14Research 47 14Review 46 13Patient 44 13Guidelines 42 12Assessment 40 11Services 38 11Used 38 11Evidence 38 11Professional 37 11Process 34 10System 34 10Work 33 9Nurses 33 9Approach 32 9General 32 9Developed 31 9Quality 31 9Team 30 9Support 30 9Teams 30 9Framework 30 9Group 30 9Information 29 8Local 29 8Learning 29 8Identified 29 8Using 29 8Article 28 8Change 28 8Medical 28 8
(continued )
Table IV.Ranked list of concepts
for 2003 literature onclinical governance
Clinicalgovernance
69
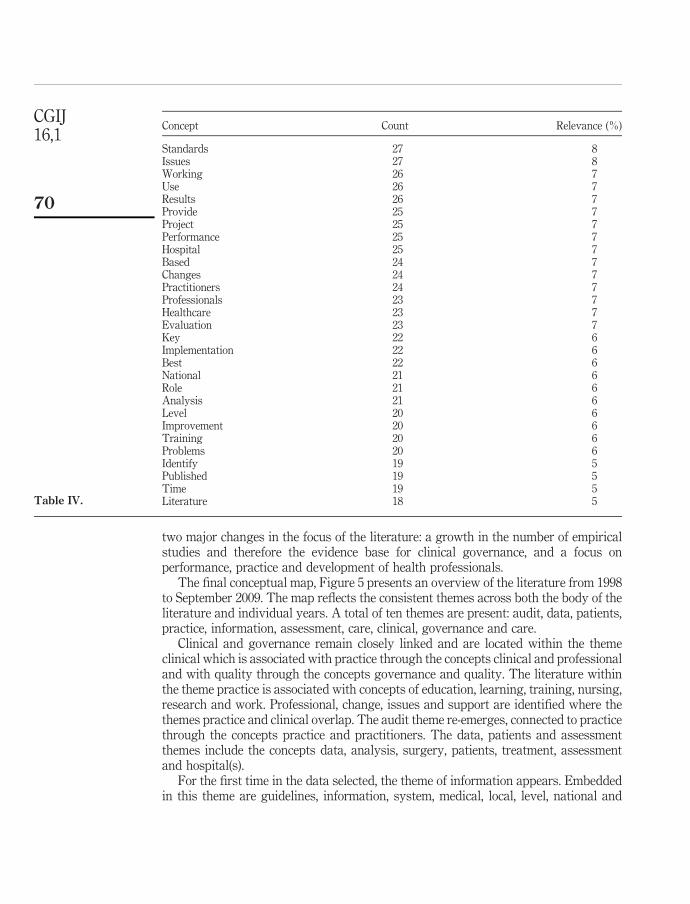
two major changes in the focus of the literature: a growth in the number of empiricalstudies and therefore the evidence base for clinical governance, and a focus onperformance, practice and development of health professionals.
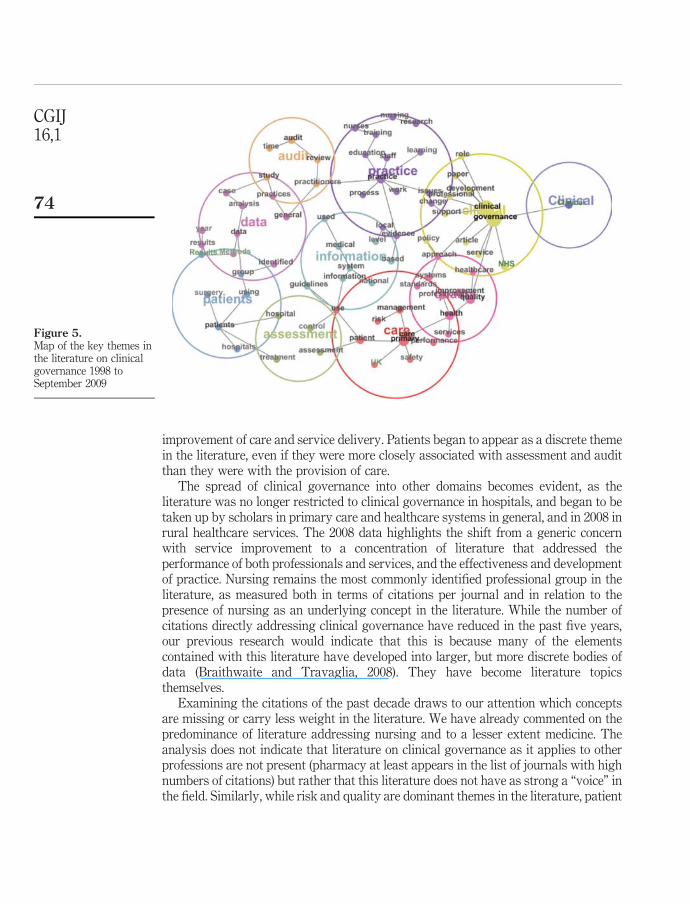
The final conceptual map, Figure 5 presents an overview of the literature from 1998to September 2009. The map reflects the consistent themes across both the body of theliterature and individual years. A total of ten themes are present: audit, data, patients,practice, information, assessment, care, clinical, governance and care.
Clinical and governance remain closely linked and are located within the themeclinical which is associated with practice through the concepts clinical and professionaland with quality through the concepts governance and quality. The literature withinthe theme practice is associated with concepts of education, learning, training, nursing,research and work. Professional, change, issues and support are identified where thethemes practice and clinical overlap. The audit theme re-emerges, connected to practicethrough the concepts practice and practitioners. The data, patients and assessmentthemes include the concepts data, analysis, surgery, patients, treatment, assessmentand hospital(s).
For the first time in the data selected, the theme of information appears. Embeddedin this theme are guidelines, information, system, medical, local, level, national and
Concept Count Relevance (%)
Standards 27 8Issues 27 8Working 26 7Use 26 7Results 26 7Provide 25 7Project 25 7Performance 25 7Hospital 25 7Based 24 7Changes 24 7Practitioners 24 7Professionals 23 7Healthcare 23 7Evaluation 23 7Key 22 6Implementation 22 6Best 22 6National 21 6Role 21 6Analysis 21 6Level 20 6Improvement 20 6Training 20 6Problems 20 6Identify 19 5Published 19 5Time 19 5Literature 18 5Table IV.
CGIJ16,1
70
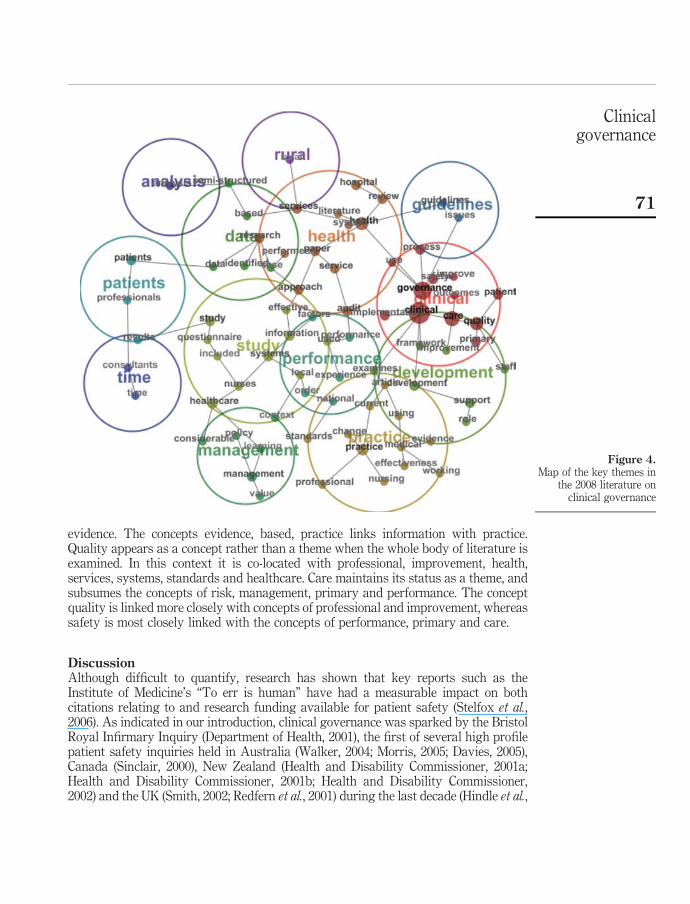
evidence. The concepts evidence, based, practice links information with practice.Quality appears as a concept rather than a theme when the whole body of literature isexamined. In this context it is co-located with professional, improvement, health,services, systems, standards and healthcare. Care maintains its status as a theme, andsubsumes the concepts of risk, management, primary and performance. The conceptquality is linked more closely with concepts of professional and improvement, whereassafety is most closely linked with the concepts of performance, primary and care.
DiscussionAlthough difficult to quantify, research has shown that key reports such as theInstitute of Medicine’s “To err is human” have had a measurable impact on bothcitations relating to and research funding available for patient safety (Stelfox et al.,2006). As indicated in our introduction, clinical governance was sparked by the BristolRoyal Infirmary Inquiry (Department of Health, 2001), the first of several high profilepatient safety inquiries held in Australia (Walker, 2004; Morris, 2005; Davies, 2005),Canada (Sinclair, 2000), New Zealand (Health and Disability Commissioner, 2001a;Health and Disability Commissioner, 2001b; Health and Disability Commissioner,2002) and the UK (Smith, 2002; Redfern et al., 2001) during the last decade (Hindle et al.,
Figure 4.Map of the key themes in
the 2008 literature onclinical governance
Clinicalgovernance
71
Concept Count Relevance (%)
Clinical 231 100Governance 188 81Care 132 57Quality 99 43Health 90 39Practice 59 26Patients 50 22Patient 49 21Services 48 21Paper 45 19Audit 45 19Study 44 19Approach 39 17Service 37 16Management 36 16Systems 31 13Healthcare 31 13Research 31 13Support 30 13Hospital 30 13Process 29 13Data 29 13Development 27 12Primary 27 12Review 26 11Guidelines 26 11Examines 25 11Staff 25 11Identified 24 10Considerable 24 10Safety 23 10Information 23 10Implementation 23 10Nurses 23 10Semi-structured 23 10Use 22 10Role 22 10Improvement 21 9Effective 21 9Used 21 9Current 21 9Based 21 9Medical 21 9Literature 20 9Using 20 9Evidence 20 9Change 20 9Professional 20 9Framework 19 8Improve 19 8
(continued )
Table V.Ranked list of conceptsfor 2008 literature onclinical governance
CGIJ16,1
72
2006). While to “To err is human” (Kohn et al., 2000) drew public and clinicians’attention to the size of the problem, essentially it was a public vehicle for one of anumber of studies which have been conducted over the last 20 years and which haveestablished the baseline for errors as 10-16 per cent of hospital admissions (Wilsonet al., 1995; Baker et al., 2004; Davis et al., 2002; Davis et al., 2003; Brennan et al., 1991;Leape et al., 1991; Vincent et al., 2001).
This combination of empirical evidence and public scrutiny has formed the impetusbehind the rapid uptake of clinical governance as a co-ordinating approach for qualityand safety over the last decade. As the literature shows, the concept as well as thepractice has undergone significant development. In its earliest iteration, the literatureon clinical governance was focused on the future: a new approach to old problems hadarrived, and it was to be deployed to tackle safety and quality problems. The tools athand were limited, predominantly audit and policy, with a recognition of the newlyemerging evidence based practice (Sackett et al., 1996). The main foci were to improvethe quality of care and clinical practice.
As the both the practice and theory base developed over the following five years, theliterature began to demonstrate an increased complexity. Audit was augmented bypublications addressing the use of guidelines and evaluation, quality was supported bya focus on risk and change was recognised as a major element in the introduction and
Concept Count Relevance (%)
Performance 19 8Standards 19 8Issues 19 8Professionals 19 8Analysis 19 8Local 18 8Performed 18 8Experience 18 8System 18 8National 18 8Factors 18 8Working 18 8Results 18 8Article 17 7Nursing 17 7Questionnaire 17 7Policy 17 7Effectiveness 17 7Outcomes 15 6Case 15 6Order 15 6Value 15 6Time 14 6Context 13 6Included 11 5Learning 11 5Consultants 11 5Rural 8 3 Table V.
Clinicalgovernance
73
improvement of care and service delivery. Patients began to appear as a discrete themein the literature, even if they were more closely associated with assessment and auditthan they were with the provision of care.
The spread of clinical governance into other domains becomes evident, as theliterature was no longer restricted to clinical governance in hospitals, and began to betaken up by scholars in primary care and healthcare systems in general, and in 2008 inrural healthcare services. The 2008 data highlights the shift from a generic concernwith service improvement to a concentration of literature that addressed theperformance of both professionals and services, and the effectiveness and developmentof practice. Nursing remains the most commonly identified professional group in theliterature, as measured both in terms of citations per journal and in relation to thepresence of nursing as an underlying concept in the literature. While the number ofcitations directly addressing clinical governance have reduced in the past five years,our previous research would indicate that this is because many of the elementscontained with this literature have developed into larger, but more discrete bodies ofdata (Braithwaite and Travaglia, 2008). They have become literature topicsthemselves.
Examining the citations of the past decade draws to our attention which conceptsare missing or carry less weight in the literature. We have already commented on thepredominance of literature addressing nursing and to a lesser extent medicine. Theanalysis does not indicate that literature on clinical governance as it applies to otherprofessions are not present (pharmacy at least appears in the list of journals with highnumbers of citations) but rather that this literature does not have as strong a “voice” inthe field. Similarly, while risk and quality are dominant themes in the literature, patient
Figure 5.Map of the key themes inthe literature on clinicalgovernance 1998 toSeptember 2009
CGIJ16,1
74
safety remains relatively weakly represented, as do concepts about patient centredcare.
ConclusionWe have demonstrated in this paper how clinical governance has developed over thelast decade, and how while the overall number of citations has peaked and is declining,the complexity of the concepts underlying this approach continues to grow.Understanding how this important concept has developed provides us with insightsinto which areas may require further development, and provide suggestions as tofuture strategies to increase the safety and wellbeing of staff and patients. It tells usthat scholarly literature, like fads and fashions in other areas of life, goes throughphases, and waves of popularity.
References
Allen, P. (2000), “Clinical governance in primary care. Accountability for clinical governance:developing collective responsibility for quality in primary care”, British Medical Journal,Vol. 321, pp. 608-11.
Baker, G.R., Norton, P.G., Flintoft, V., Blais, R., Brown, A., Cox, J., Etchells, E., Ghali, W.A.,Hebert, P., Majumdar, S.R., O’Beirne, M., Palacios-Derflingher, L., Reid, R.J., Sheps, S. andTamblyn, R. (2004), “The Canadian adverse events study: the incidence of adverse eventsamong hospital patients in Canada”, Canadian Medical Association Journal, Vol. 170,pp. 1678-86.
Braithwaite, J. and Travaglia, J.F. (2008), “An overview of clinical governance policies, practicesand initiatives”, Australian Health Review, Vol. 32, pp. 10-22.
Brennan, T.A., Leape, L.L., Laird, N., Herbert, L., Localio, A.R., Lawthers, A.G., Newhouse, J.P.,Weiler, P.C. and Hiatt, H. (1991), “The nature of adverse events in hospitalized patients:results of the Harvard Medical Practice Study I”, New England Journal of Medicine,Vol. 324, pp. 370-6.
Davies, G. (2005), Queensland Public Hospitals Commission of Inquiry, Queensland Government,Brisbane.
Davis, P., Lay-Yee, R., Briant, R., Ali, W., Scott, A. and Schug, S. (2002), “Adverse events in NewZealand public hospitals I: occurrence and impact”, New Zealand Medical Journal, Vol. 115,p. 271.
Davis, P., Lay-Yee, R., Briant, R., Ali, W., Scott, A. and Schug, S. (2003), “Adverse events in NewZealand public hospitals II: preventability and clinical context”, New Zealand MedicalJournal, Vol. 116, p. U624.
Department of Health (2001), The Report of the Public Inquiry into Children’s Heart Surgery at theBristol Royal Infirmary 1984-1995: Learning From Bristol, Stationery Office, London,available at: www.bristol-inquiry.org.uk/final_report/index.htm (accessed 10 June 2009).
Eeckloo, K., Delesie, L. and Vleugels, A. (2007), “Where is the pilot? The changing shapes ofgovernance in the European hospital sector”, Journal of the Royal Society for the Promotionof Health, Vol. 127, pp. 78-86.
Halligan, A. and Donaldson, L. (2001), “Implementing clinical governance: turning vision intoreality”, British Medical Journal, Vol. 322, pp. 1413-7.
Health and Disability Commissioner (2001a), Gisbourne Hospital 1999-2000, Health andDisability Commissioner, Auckland, available at: www.hdc.org.nz/files/hdc/publications/172522_health_&_disability.pdf (accessed 10 November 2009).
Clinicalgovernance
75

Health and Disability Commissioner (2001b), Mental Health Services of a Public Hospital, Healthand Disability Commission, Auckland, (accessed 10 November 2009).
Health and Disability Commissioner (2002), Southland District Health Board Mental HealthServices: February-March 2001, Health and Disability Commissioner, Auckland, availableat: www.hdc.org.nz/files/hdc/publications/other-southlandreport.pdf (accessed 10 November2009).
Hindle, D., Braithwaite, J., Iedema, R. and Travaglia, J. (2006), Patient Safety: A ComparativeAnalysis of Eight Inquiries in Six Countries, Centre for Clinical Governance Research inHealth, University of NSW and Clinical Excellence Commission, Sydney.
Kohn, L.T., Corrigan, J.M. and Donaldson, M.S. (Eds) (2000), To Err Is Human: Building A SaferHealth System, Institute of Medicine and The National Academies Press, Washington, DC.
Leape, L.L., Brennan, T.A., Laird, N., Lawthers, A.G., Localio, A.R., Barnes, B.A., Herbert, L.,Newhouse, J.P., Weiler, P.C. and Hiatt, H. (1991), “The nature of adverse events inhospitalized patients, Results of the Harvard Medical Practice Study II”, New EnglandJournal of Medicine, Vol. 324, pp. 377-84.
Morris, A. (2005), Bundaberg Base Hospital Commission of Inquiry, Bundaberg Base HospitalCommission of Inquiry, Brisbane.
Penny, A. (2000), “Clinical governance in Britain defined”, Healthcare Review Online, Vol. 4.
Redfern, M., Keeling, J. and Powell, E. (2001), The Royal Liverpool Children’s Inquiry, The Houseof Commons, London, available at: www.rlcinquiry.org.uk/ (accessed 8 November 2008).
Sackett, D.L., Rosenberg, W.M.C., Gray, J.A.M., Haynes, R.B. and Richardson, W.S. (1996),“Evidence based medicine: what it is and what it isn’t”, BMJ, Vol. 312, pp. 71-2.
Sinclair, C.M. (2000), The Report of the Manitoba Pediatric Cardiac Surgery Inquest: An Inquiryinto Twelve Deaths at the Winnipeg Health Sciences Centre in 1994, Provincial Court ofManitoba, Winnipeg, available at: www.pediatriccardiacinquest.mb.ca/pdf/pcir_intro.pdf(accessed 10 November 2009).
Smith, A.E. and Humphreys, M.S. (2006), “Evaluation of unsupervised semantic mapping ofnatural language with Leximancer concept mapping”, Behavior Research Methods, Vol. 38,pp. 262-79.
Smith, J. (2002), Shipman Inquiry: First Report, Crown Copyright, Norwich, available at: www.the-shipman-inquiry.org.uk/reports.asp (accessed 9 October 2008).
Spigelman, A.D. (2008), “Australian perspectives”, Clinical Governance: An International Journal,Vol. 13, pp. 225-6.
Stelfox, H.T., Palmisani, S., Scurlock, C., Orav, E.J. and Bates, D.W. (2006), “The “to err is human”report and the patient safety literature”, Quality and Safety in Health Care, Vol. 15,pp. 174-8.
Stockwell, P., Colomb, R.M., Smith, A.E. and Wiles, J. (2009), “Use of an automatic contentanalysis tool: a technique for seeing both local and global scope”, International Journal ofHuman Computer Studies, Vol. 67, pp. 424-36.
Travaglia, J.F., Westbrook, M.T. and Braithwaite, J. (2009), “Implementation of a patient safetyincident management system as viewed by doctors, nurses and allied healthprofessionals”, Health, Vol. 13, pp. 277-96.
Vincent, C., Neale, G. and Woloshynowych, M. (2001), “Adverse events in British hospitals:preliminary retrospective record review”, British Medical Journal, Vol. 322, pp. 517-9.
Walker, B. (2004), Final Report of the Special Commission of Inquiry into Campbelltown andCamden Hospitals, New South Wales Attorney General’s Department, Sydney.
CGIJ16,1
76

Watson, M., Smith, A. and Watter, S. (2005), “Leximancer concept mapping of patient casestudies”, Lecture Notes in Computer Science, Vol. 3683, pp. 1232-8.
Weick, K.E. (1995), Sensemaking in Organizations, Sage, Thousand Oaks, CA.
Wilson, R., Runciman, W., Gibberd, R.W., Harrison, B.T., Newby, L. and Hamilton, J.D. (1995),“The quality in Australian health care study”, Medical Journal of Australia, Vol. 163,pp. 458-71.
About the authorsJoanne F. Travaglia is a Sociologist with a particular interest in the health and safety ofvulnerable groups, both patients and staff. She is currently a research fellow with the Centre forClinical Governance, Australian Institute of Health Innovation, Faculty of Medicine, Universityof New South Wales. Her research explores the creation and construction of patient safetyknowledge and practice through mechanisms such as patient safety inquires; the implementationand impact of incident reporting and safety improvement, clinical governance, and accreditationprogrammes; the risks faced by vulnerable groups within the health system; and the impact ofclinician and patient diversity on the quality and safety of care. Joanne F. Travaglia is thecorresponding author and can be contacted at: [email protected]
Deborah Debono is a Research Assistant with the Centre for Clinical Governance, AustralianInstitute of Health Innovation, Faculty of Medicine, University of New South Wales. She iscurrently undertaking a PhD empirically examining workarounds and the use of electronicmedication systems. Electronic medication systems aim to improve patient safety. However,these systems are not perfect and limitations, including the potential to create new types ofadverse events, pose challenges for patient safety improvement. Ms Debono’s PhD aims toexamine factors that contribute to the development and proliferation of workarounds in relationto electronic medication systems.
Allan D. Spigelman is the Clinical Associate Dean in the Department of Surgery at StVincent’s Clinical School of the University of New South Wales, Director of Cancer Services at StVincent’s and Mater Health Sydney and Professor of Surgery at the University of New SouthWales. He has published four books and over 130 peer reviewed papers and books chapters. Hispublications cover both his scientific research in areas such as familial adenomatous polyposisand upper gastrointestinal tract cancers, and broader health services management issues, suchas the development and implementation of clinical governance.
Jeffrey Braithwaite is Professor and Foundation Director, Australian Institute of HealthInnovation and Director, Centre for Clinical Governance Research, Faculty of Medicine,University of New South Wales, Australia. His research examines the changing nature of healthsystems, particularly patient safety, leadership and management, the structure and culture oforganisations and their network characteristics, attracting funding of more than $34 million,chiefly from National Health and Medical Research Council and Australian Research Councilgrants. He has presented over 400 times and contributed to over 400 publications includingmultiple times in the British Medical Journal, The Lancet, Social Science and Medicine, Qualityand Safety in Health Care and many other prestigious journals. Jeffrey Braithwaite has receivednumerous national and international awards including a Vice-Chancellor’s award for teachingfrom UNSW and six separate awards for research papers in 2007 and 2008, and safety in healthcare and international health policy development and implementation.
Clinicalgovernance
77
To purchase reprints of this article please e-mail: [email protected] visit our web site for further details: www.emeraldinsight.com/reprints





























