Embed Size (px)
Citation preview
American Journal of Transplantation 2008; 8: 701–706Blackwell Munksgaard
C© 2008 The AuthorsJournal compilation C© 2008 The American Society of
Transplantation and the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2007.02120.xBrief Communication
Clinical Magnetic Resonance Imaging of PancreaticIslet Grafts After Iron Nanoparticle Labeling
C. Tosoa,b,∗, J.-P. Valleec, P. Morela, F. Risa,
S. Demuylder-Mischlera, M. Lepetit-Coiffec,
N. Marangond, F. Saudeke,
A. M. James Shapirob, D. Boscoa and T. Berneya
aCell Isolation and Transplantation Center, GenevaUniversity Hospitals, Geneva, SwitzerlandbClinical Islet Transplant Program, University of Alberta,Edmonton, CanadacDepartments of Radiology and dMedicine, GenevaUniversity Hospitals, Geneva, SwitzerlandeDiabetes Center, Institute for Clinical and ExperimentalMedicine, Prague, Czech Republic∗Corresponding author: Christian Toso,[email protected]
There is a crucial need for noninvasive assessmenttools after cell transplantation. This study investigateswhether a magnetic resonance imaging (MRI) strat-egy could be clinically applied to islet transplantation.The purest fractions of seven human islet preparationswere labeled with superparamagnetic iron oxide par-ticles (SPIO, 280 lg/mL) and transplanted into four pa-tients with type 1 diabetes. MRI studies (T2∗) wereperformed prior to and at various time points aftertransplantation. Viability and in vitro and in vivo func-tions of labeled islets were similar to those of con-trol islets. All patients could stop insulin after trans-plantation. The first patient had diffuse hypointenseimages on her baseline liver MRI, typical for sponta-neous high iron content, and transplant-related mod-ifications could not be observed. The other three pa-tients had normal intensity on pretransplant images,and iron-loaded islets could be identified after trans-plantation as hypointense spots within the liver. In oneof them, i.v. iron therapy prevented subsequent visu-alization of the spots because of diffuse hypointenseliver background. Altogether, this study demonstratesthe feasibility and safety of MRI-based islet graft mon-itoring in clinical practice. Iron overload (spontaneousor induced) represents the major obstacle to the tech-nique.
Key words: Islet assessment, islet transplantation,magnetic resonance imaging (MRI), monitoring
Received 21 September 2007, revised 15 November2007 and accepted for publication 04 December 2007
Introduction
Islets of Langerhans transplantation has come to the fore-front as a promising approach in the quest for a cure fortype 1 diabetes. Unfortunately, outcomes of 80% insulinindependence at 1 year have not been sustained (1–3),and the latest updates report insulin independence ratesof approximately 10–15% at 5 years, although graft func-tion (C-peptide positivity) was retained in a vast majority ofpatients (4).
Islet loss occurs in a two-step fashion. Early loss is linkedto the low rate of engraftment. It is thought to be the re-sult of damage during the isolation procedure or in the graftmicroenvironment within the liver, secondary to ischemia-reperfusion-like injury and to nonspecific inflammatory phe-nomena. Subsequent losses are usually more progres-sive, and are thought to involve allogeneic rejection, re-currence of autoimmunity, islet toxicity of the immunosup-pressive drugs or ‘exhaustion’ of the islet graft. Many ofthese events are likely to impact similarly on other types ofcell transplant, including bone marrow, hepatocytes, neu-ral cells and various types of stem cells, with wide areasof application.
There is undoubtedly a lot of room for improvement in theshort- and long-term survival rates of all types of cell trans-plants, but this will only be achieved when mechanisms ofdestruction have been fully understood and characterized.In this regard, there is a blatant lack of monitoring tools thatare able to detect graft damage or loss in a timely manner.
An ideal radiological monitoring modality should be nonin-vasive, should not be harmful to the graft, should enablea repeated and accurate assessment and should detectgraft damage early enough to allow treatment. In the situ-ation of islet transplantation, in order to be useful, a newtool should detect islet damage prior to a drop in serum C-peptide levels, an increase in fasting blood glucose levelsor the need to resume exogenous insulin intake.
Two strategies can be theoretically applied, namely, in situand ex vivo labeling. In situ labeling by posttransplant in-jection of a labeled tracer highly specific for islet cellswould be the preferred method, since it could be indefi-nitely repeated, and would not be confronted to half-lifeof the labeling agent issues. Unfortunately, this strategyhas been hampered by the lack of b-cell specificity of
701

Toso et al.
candidate molecules (5). For this reason, we have chosenan ex vivo labeling approach in which cells are labeled priorto transplantation.
The two main clinically relevant technologies for cell trans-plant monitoring include positron-emission tomography(PET) and MRI. The use of PET with pretransplant cell la-beling has thus far been limited by the short half-life of trac-ers, which prevents accurate monitoring beyond the firsthours posttransplant (6,7). In contrast, animal studies havedemonstrated that cell grafts labeled with superparamag-netic iron oxide (SPIO) particles could be monitored in vivoby MRI. The signal remained stable in syngeneic models,while it disappeared at the time of rejection in allogeneicmodels (8–13).
The aim of the present study is to investigate whether MRImonitoring of SPIO-labeled islets could be applied clinically,using the well-established islet transplantation procedureas a model.
Methods
This is a pilot study investigating the feasibility and safety of MRI monitor-ing of iron-labeled islet grafts. It was approved by the Ethical Committee forClinical Research at the University of Geneva Hospitals, and the off-labeluse of ferucarbotran (Resovist, Schering, Baar, Switzerland) was approvedby the Swiss Federal Office of Public Health. All patients on the waiting listfor islet transplantation at the University of Geneva Hospitals could poten-tially be included. Exclusion criteria included pregnancy, hypersensitivity tocomponents of Resovist and severe claustrophobia, and patients with pace-makers, implanted defibrillators, vascular clips (when implanted for less than2 weeks) or any other implant or device not allowed for MRI.
Islet culture, labeling and quality assessment
Islet labeling was performed by pooling approximately 20 000 isletequivalents (IEQ) per flask into 2–15 flasks (175 cm2, content: 650mL/flask, nonadherent; Sarstedt, Svelen, Switzerland) and culturing themin a serum-free Connaught’s Medical Research Labs (CMRL) 1066-basedmedium (30 ml/flask), supplemented with 10 lL/mL (280 lg iron/mL)
Table 1: Islet transplant characteristics
Labeled islets Total islets
Nb Purity Viability Duration of labeling∗ Nb Nb/kg PurityTransplant (IEQ) (%) (%) (h) (IEQ) (IEQ/kg) (%)
Patient 1 1 – – – 284 999 5439 782 50 000 80 90 48 294 500 5556 35
Patient 2 1 37 100 83 84 Overnight 288 615 6654 552 50 000 80 90 Overnight 354 333 6561 723 – – – 330 111 5948 33
Patient 3 1 374 916 87 85 Overnight 580 622 9841 442 100 000 87 90 Overnight 316 958 5372 60
Patient 4 1 287 166 85 90 Overnight 468 874 5860 662 306 250 80 90 Overnight 422 000 5103 43
Mean 172 205 83 88 371 224 6259 54SD ±144 690 ±3 ±3 ±100 640 ±1442 ±16∗Corresponding to the culture time from isolation to transplant
SPIO (ferucarbotran; Resovist, Schering, Baar, Switzerland). Other compo-nents of the medium included glutamax (2 mmol/L, final concentration),4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES) (25 mmol/L),sodium pyruvate (5 mmol/L), linoleic acid (5.35 mg/L), sodium hydroxide (2.5mmol/L), vitamin E (0.01 mmol/L), nicotinamide (10 mmol/L), penicillin (112kU/L), streptomycin (112 mg/L), zinc sulfate (4.8 mg/L), insulin (6.3 mg/L),transferrin (6.3 mg/L), selenium (6.3 lg/L) and human albumin (0.6%). Cul-ture temperature was 37◦C for the first 24 h, and 24◦C thereafter (whenapplicable). Culture (labeling) was performed at least overnight and up to 48h (Table 1). Only the purest islets were selected for labeling. Labeled andnonlabeled islets were pooled for transplant.
Viability was assessed by propidium iodide and fluorescein diacetate stain-ing. In vitro function of both labeled and nonlabeled islets was evaluatedby glucose-stimulated insulin release in static incubation assays run in trip-licate. Two hundred IEQ were preincubated at low glucose concentration(2.2 mmol/L) for 60 min. Basal and stimulated insulin concentrations weremeasured by enzyme-linked immunosorbent assay (ELISA) (Mercodia, Up-psala, Sweden) in the culture medium after further incubation at low andhigh glucose concentrations (2.2 and 22.2 mmol/L, for two periods of 90min each). At the end of static incubation, the insulin content was extractedby incubating the islets with acid-ethanol at 4◦C for 60 min. Results wereexpressed as absolute values and as ratios of basal or stimulated secretionover insulin content. Stimulation indexes (SI) were calculated by dividingeach stimulated response by each basal insulin secretion. The mean of theindexes was then reported. This in vitro test was performed with islets fromseven different isolations.
In vivo function of both labeled and nonlabeled human islets was also as-sessed by transplanting 2000 IEQ under the kidney capsule of athymic nu/nu(nude) mice (Janvier, Le Genest, France; 11 animals). This experiment wasperformed in accordance with a protocol approved by the Institutional An-imal Care and Use Committee. Animals were kept in the animal facility ofthe Faculty of Medicine at the University of Geneva. They had free accessto food and water at all times. Diabetes was induced by a single injection of220 mg/kg of streptozotocin (Sigma, St. Louis, MO). Only diabetic animalswith blood glucose levels higher than 20 mmol/L were used as recipients.Time to reverse diabetes (blood glucose <11 mmol/L) was recorded as theendpoint.
Magnetic Resonance Imaging (MRI)
MRI studies were performed prior to and at 5 days, 6 weeks and 6 monthsafter each transplant and whenever a significant metabolic event occurred.
702 American Journal of Transplantation 2008; 8: 701–706

MRI Monitoring After Islet Transplant
Images were acquired on a 1.5T Achieva MR system R1.5 (Philips MedicalSystems, Best, The Netherlands) using the standard abdominal flex coiland a sequence 2D T2∗-weighted breath hold gradient echo (fast field echo[FFE], repetition time [TR] = 220 ms, echo time [TE] = 18 ms, acquiredvoxel size: 1.8 × 2.7 × 5.0 mm, reconstructed voxel size: 1.31 × 1.31 ×5.00 mm, flip angle: 25◦, clear).
Analyses were performed blindly by four different investigators, studying allsections acquired over the liver. Iron-labeled islets appeared as dark signalspots on T2∗-weighted images. Images were analyzed in a dynamic fashion(on computer) in order to differentiate islet dark spots identified in oneimage, and vessels appearing tubular in several consecutive images. Theywere counted manually, and results were provided as an average of the fourcounts. The coefficients of variation (100∗mean/standard deviation [SD])among the four counts were also calculated for each time point, and themean of all coefficients was reported.
Liver (L) and paraspinous muscle (M) signal intensities were obtained inoperator-defined regions of interest on T2∗-weighted images. The L/M ratiowas calculated by dividing mean intensities (14).
Statistical analysis
Results were provided as mean ± SD. Continuous variables were comparedwith the Student’s t-test. Reversal of diabetes in nude mice was analyzedby the Kaplan-Meier method, and differences among groups were testedby the log-rank test. All tests were conducted using the standard alpha levelof 0.05. Analyses were done using the statistical software (StatSoft, Tulsa,OK).
Results
Patients, islets and transplants
Four patients were recruited (one female and three males,mean age of 52 ± 9 years). Types of transplant were: isletafter kidney (IAK) for patient 1, simultaneous islet kidney(SIK) for patient 2 and islet transplant alone (ITA) for pa-tients 3 and 4. They received a total of nine islet infusions(Table 1).
Figure 1: Clinical outcome. Clinicaloutcome after transplantation of iron-labeled (black bar) and nonlabeled(striped bar) islets. Grey histogramsshow periods of partial islet graftfunction (insulin dependence with de-tectable C-peptide), and white his-tograms show periods of full graftfunction (insulin independence). Allpatients underwent a baseline MRIprior to transplant; posttransplant MRIstudies are shown by black triangles.Numbers located over the trianglesrefer to the average of black spotsobserved within the liver by four dif-ferent investigators on each specificMRI; ‘-’refers to the fact that no spotcould be observed due to diffuse hy-pointense background.
Islets from seven isolations were labeled with SPIO (oneinfusion was performed before this study started, patient2 demonstrated high, spontaneous iron load and the lastinfusion was not labeled). Only the purest portions (83 ±3% purity) of the preparations were selected for labeling(39 ± 26% of total number of islets).
Posttransplant immunosuppression consisted of anti-CD25 antibody induction (daclizumab; Zenapax, Roche,Basel, Switzerland) for ITA and IAK recipients, and antithy-mocyte globulins (Thymoglobulin, Genzyme, Baar, Switzer-land) for the SIK recipient. Maintenance immunosup-pression consisted of sirolimus (Rapamune, Wyeth, Zug,Switzerland) and low-dose tacrolimus (Prograf, AstellasPharma, Villars-sur-Glane, Switzerland).
Labeled and nonlabeled islet assessment
After labeling, islet viability was 88 ± 4%. Islets demon-strated similar function as nonlabeled controls. In vitrobasal insulin secretions were 108 ± 106 and 282 ± 324mU/L (p = 0.2) for labeled and nonlabeled islets, respec-tively, stimulated secretions were 266 ± 224 and 395 ±454 mU/L (p = 0.5) and stimulation indexes 3.2 ± 2.2 and2 ± 1.3 (p = 0.2), respectively. When normalizing resultsfor the islet insulin content, basal ratios were 0.04 ± 0.03and 0.16 ± 0.20 (p = 0.2) for labeled and nonlabeled islets,respectively, and stimulated ratios were 0.13 ± 0.14 and0.2 ± 0.2 (p = 0.4), respectively. Two thousand human IEQreversed diabetes in 8 ± 4 and 6 ± 2 days in nude mice ofthe labeled and control groups (Log-rank test, p = 0.93).
Transplant outcome
All patients reached insulin independence (Figure 1), withnormalized hemoglobin A1c (HbA1c) under 6.5%. Patient 1had to restart insulin injections 15.5 months after thefirst transplant following a severe urinary sepsis. Somedegree of autoimmunity may also have occurred, as his
American Journal of Transplantation 2008; 8: 701–706 703
Toso et al.
anti-glutamic acid decarboxylase (GAD) antibody titre in-creased from 5000 U/L pretransplant to 29 000 U/L (normalrange <9.5 U/L). He was, at the time of writing, stable on9 U/day (32 U/day prior to transplant).
Two patients experienced significant anemia, which re-quired treatment with erythropoietin (patient 1, 2) and/ororal iron supplementation (patient 1). Patient 1 furtherrequired i.v. infusions of iron sucrose (Venofer, Vifor, StGallen, Switzerland) from 17 to 19 months, and from 24 to26 months after initial transplant (Figure 1).
Pretransplant ferritin levels were within normal ranges(from 36 lg/L to 195 lg/L), except in patient 2, who hada spontaneously high level (326 lg/L; normal ranges be-ing 11–137 lg/L in females and 26–417 lg/L in males).Subsequent ferritin levels remained overall stable, exceptin patient 1, who maintained high levels following i.v. ironsupplementation (400, 477, 333 and 368 lg/L at 11, 13, 16and 30 months after his first islet transplant).
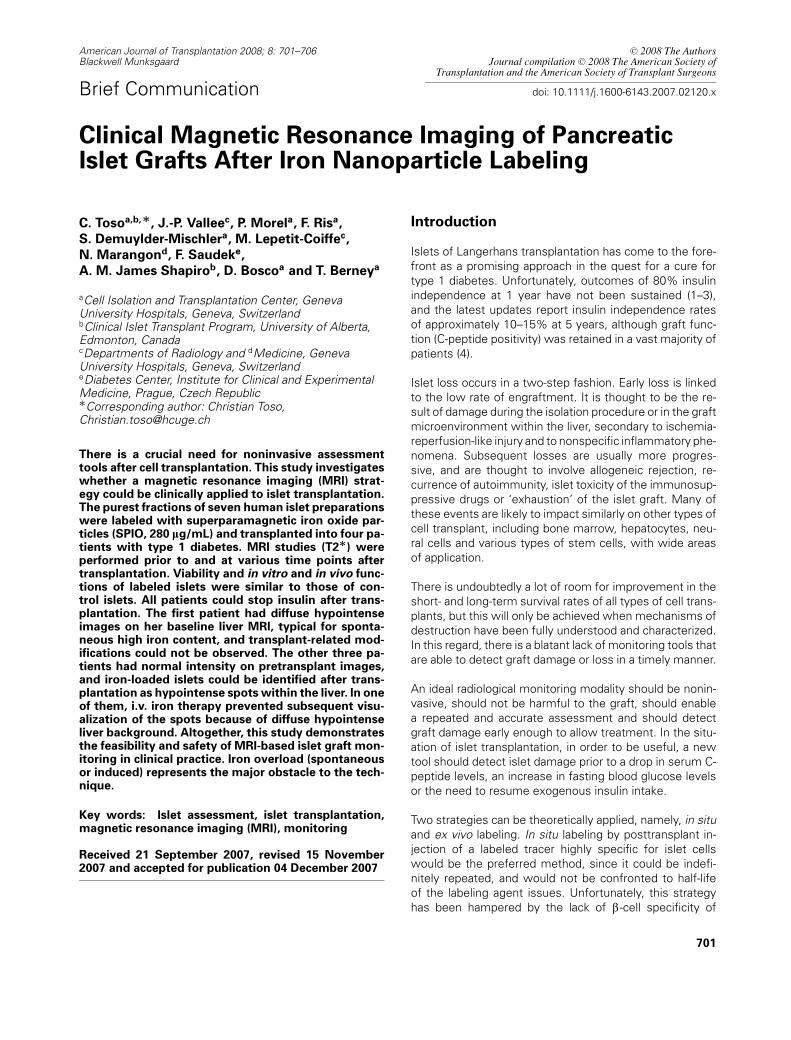
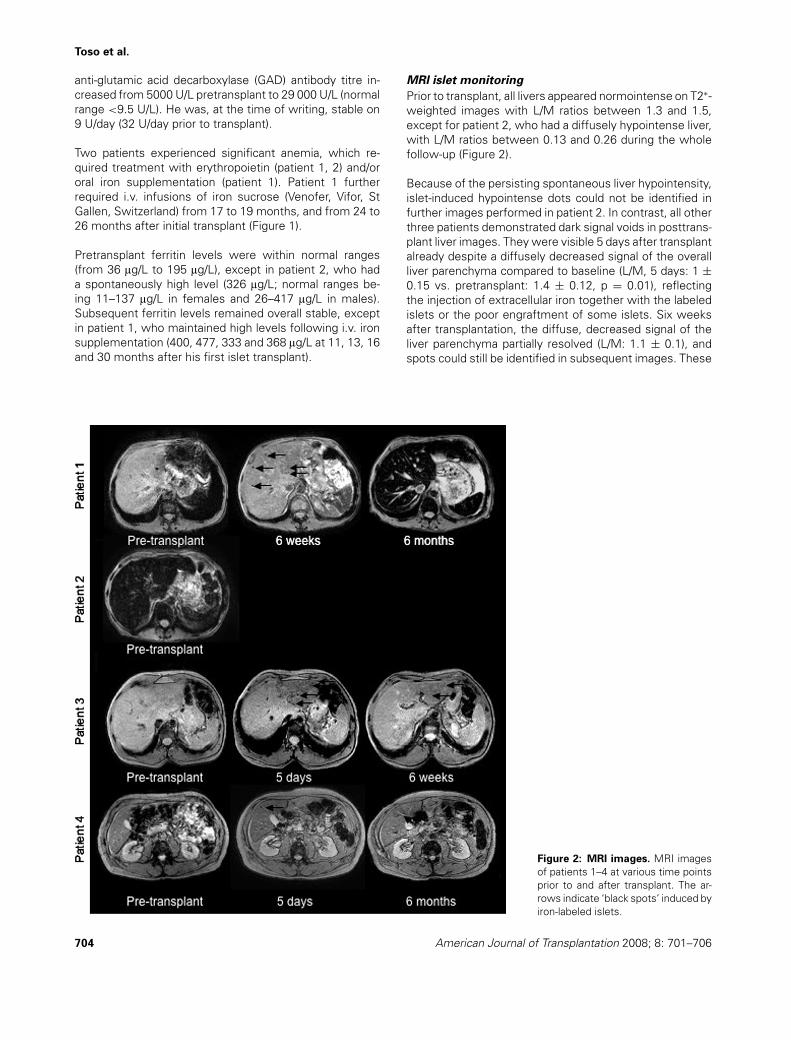
Figure 2: MRI images. MRI imagesof patients 1–4 at various time pointsprior to and after transplant. The ar-rows indicate ‘black spots’ induced byiron-labeled islets.
MRI islet monitoring
Prior to transplant, all livers appeared normointense on T2∗-weighted images with L/M ratios between 1.3 and 1.5,except for patient 2, who had a diffusely hypointense liver,with L/M ratios between 0.13 and 0.26 during the wholefollow-up (Figure 2).
Because of the persisting spontaneous liver hypointensity,islet-induced hypointense dots could not be identified infurther images performed in patient 2. In contrast, all otherthree patients demonstrated dark signal voids in posttrans-plant liver images. They were visible 5 days after transplantalready despite a diffusely decreased signal of the overallliver parenchyma compared to baseline (L/M, 5 days: 1 ±0.15 vs. pretransplant: 1.4 ± 0.12, p = 0.01), reflectingthe injection of extracellular iron together with the labeledislets or the poor engraftment of some islets. Six weeksafter transplantation, the diffuse, decreased signal of theliver parenchyma partially resolved (L/M: 1.1 ± 0.1), andspots could still be identified in subsequent images. These
704 American Journal of Transplantation 2008; 8: 701–706

MRI Monitoring After Islet Transplant
spots were located throughout the liver in two patients(patients 1 and 4), but only in the left lobe in patient 3(Figure 2).
The number of spots identified within the liver ranged from3 to 138 in the first imaging after transplant (Figure 1). Therewas no correlation between the number of injected isletsand the number of spots, but the only recipient (patient 1)of islets labeled during 48 h demonstrated higher counts.While the sharpness of the spots tended to decrease overtime, the number of dark signal voids remained stable inall patients. However, they could not be identified start-ing from the third posttransplant MRI of patient 1 becauseof the overall decreased intensity of the liver parenchyma(L/M between 0.09 and 0.51; Figure 2). This correlated tothe i.v. iron therapy and to an increased ferritin level, as de-scribed above. While the patient experienced a decreasein graft function, during the same time period, no clear cor-relation could be established between MRI signal and isletfunction.
Of note, counting results demonstrated a high interob-server variability, with a mean coefficient variation of 68± 34%.
Discussion
The present study demonstrates the feasibility and safetyof MRI-based monitoring after islet transplant. The tech-nique could be extended to all areas of cell transplantation,including hepatocyte, cardiac, neural and stem cell trans-plants.
Along with previous animal results (8–11), our results sug-gest that iron labeling is harmless to human islets in invitro static incubation and viability tests or in vivo testsafter transplantation in diabetic animals. As a further con-firmation, all transplanted patients did achieve insulin inde-pendence.
The labeling agent (ferucarbotran) is broadly used for clin-ical MR liver imaging. Labeling is the result of endocy-tosis. This process is not specific for b-cells, and SPIOcould be found in all islet cell types (11). As a conse-quence, we elected to label the purest transplanted isletsonly. All had 80% or over purity and represented about40% of islet grafts. This allowed a better specificity of thelabeling.
Importantly, the SPIO have been demonstrated to remainstable within cells, both in culture and after transplantation(10,15). This represents one of the main advantages of thedescribed MRI-based technique, and is in opposition to PETtracers, which have a low cell retention rate (5,6). In thepresent study, islet-induced spots could still be identified6 months after transplantation.
The main limitation of the described technique is linkedto the specific intraportal location of the islets, and is dueto the possible presence of iron overload and backgroundwithin the liver. This can be either spontaneous (patient 2)or following i.v. iron supplementation therapy (patient 1).Patients with pretransplant MRI L/M ratios of <1, suggest-ing high intrahepatic iron content (14), should be excluded.High ferritin levels are also suggestive of similar patterns.
While the described technique represents the first re-port of long-term clinical islet graft imaging, some ques-tions remain only partly answered. The monitoring modal-ity should ideally be able to correlate with the number oftransplanted cells. While this was demonstrated in animalmodels (11,12), in the present study, no correlation couldbe found between the number of transplanted islets andthe number of spots within the liver. Also, the number ofspots was low in regard to the number of transplantedislets. This likely reflects the fact that we only observedislets when several of them had engrafted at the samelocation, grouping iron particles together.
Counts were performed manually, and demonstrated ahigh variability from one investigator to the other (meancoefficient of variation: 68 ± 34%). This clearly empha-sizes the need for an accurate and automated countingtechnique.
A useful monitoring tool should also be able to detect dam-ages early enough to allow for appropriate intervention tosalvage the graft. In our series, only one patient experi-enced a loss of islet function (patient 1), and unfortunatelyrequired i.v. iron treatment around the same time period.Despite repeated images, the liver background remainedhigh up to 5 months after treatment. We were, therefore,unable to determine whether the subsequent absence ofspots within the liver was only linked to the backgroundor also to the loss of islets. Of note, animal studies havedemonstrated that the iron contained in rejected cells iscleared from the liver, and MRI can detect a decrease inthe number of spots at the time of rejection (9,11). In ad-dition, when injected i.v., Resovist is cleared from the liverwithin 10 days (earliest time point tested), with normalizedMRI imaging (16,17).
We believe that this study represents an important proof offeasibility of the MRI-based islet graft-imaging concept. Itopens the field to new studies aiming at optimizing MRIcontrast agents (18), increasing islet labeling efficiency,improving image resolution and quality and developingquantification methods to better correlate signal and isletmass.
Acknowledgments
The authors thank the fellows and the staff of the Cell Isolation and Trans-plantation Center (Dr. Mathieu Armanet, Dr. Reto Baertschiger, Solange
American Journal of Transplantation 2008; 8: 701–706 705

Toso et al.
Charvier, Raymond Mage, David Matthey, Florentina Naville, Nadine Pernin,Corinne Sinigalia and Dr. Anne Wojtusciszyn), the transplant coordinators,the radiology team, the immunology team, the diabetology team, thenephrology team and all Swiss and French pancreas-recovering teams. Thestudy was supported in part by grant 3200B0–113899 from the Swiss Na-tional Science Foundation (to TB, CT, JPV, DB), grant R01 AI 74225–01 fromNIH/NIDDK (to TB, DB, CT, JPV), a grant from the Research and Develop-ment Foundation at Geneva University Hospitals (to CT, TB, PM) and a grantfrom the ‘Fondation pour la lutte contre le cancer et pour des recherchesmedico-biologiques’ (to TB, CT, PM). CT is recipient of grant 118593/1 ofthe Swiss National Science Foundation and of a grant of the Alberta Her-itage Foundation for Medical Research; JPV is supported by the grant FNSPP00B-68778 and FS is recipient of grant no. MZO 00023001 from theMinistry of Health of the Czech Republic.
References
1. Benhamou PY, Oberholzer J, Toso C et al. Human islet transplan-tation network for the treatment of type I diabetes: First data fromthe Swiss-French GRAGIL consortium (1999–2000). Groupe deRecherche Rhin Rhjne Alpes Geneve pour la transplantation d’Ilotsde Langerhans. Diabetologia 2001; 44: 859–864.
2. Toso C, Baertschiger R, Morel P et al. Sequential kidney/islet trans-plantation: Efficacy and safety assessment of a steroid-free im-munosuppression protocol. Am J Transplant 2006; 6: 1049–1058.
3. Shapiro AM, Ricordi C, Hering BJ et al. International trial of theEdmonton protocol for islet transplantation. N Engl J Med 2006;355: 1318–1330.
4. Ryan EA, Paty BW, Senior PA et al. Five-year follow-up after clinicalislet transplantation. Diabetes 2005; 54: 2060–2069.
5. Sweet IR, Cook DL, Lernmark A et al. Systematic screening ofpotential beta-cell imaging agents. Biochem Biophys Res Commun2004; 314: 976–983.
6. Toso C, Zaidi H, Morel P et al. Positron-emission tomography imag-ing of early events after transplantation of islets of Langerhans.Transplantation 2005; 79: 353–355.
7. Eich T, Eriksson O, Lundgren T, and Nordic Network for ClinicalIslet Transplantation. Visualization of early engraftment in clinicalislet transplantation by positron-emission tomography. N Engl JMed 2007; 256: 2754–2755.
8. Jirak D, Kriz J, Herynek V et al. MRI of transplanted pancreaticislets. Magn Reson Med 2004; 52: 1228–1233.
9. Kriz J, Jirak D, Girman P et al. Magnetic resonance imaging ofpancreatic islets in tolerance and rejection. Transplantation 2005;80: 1596–1603.
10. Evgenov NV, Medarova Z, Dai G, Bonner-Weir S, Moore A. Invivo imaging of islet transplantation. Nat Med 2006; 12: 144–148.
11. Evgenov NV, Medrova Z, Pratt J et al. In vivo imaging of immune re-jection in transplanted pancreatic islets. Diabetes 2006; 55: 2419–2428.
12. Tai JH, Foster P, Rosales A et al. Imaging islets labeled withmagnetic nanoparticles at 1.5 tesla. Diabetes 2006; 55: 2931–2938.
13. Shapiro EM, Sharer K, Skrtic S, Koretsky AP. In vivo detection ofsingle cells by MRI. Magn Reson Med 2006; 55: 242–249.
14. Gandon Y, Olivie D, Guyader D et al. Non-invasive assessment ofhepatic iron stores by MRI. Lancet 2004; 363: 357–362.
15. Arbab AS, Bashaw LA, Miller BR et al. Characterisation of biophys-ical and metabolic properties of cells labeled with superparamag-netic iron oxide nanoparticles and transfection agent for cellularMR imaging. Radiology 2003; 229: 838–846.
16. Kalber TL, Smith CJ, Howe FA et al. A longitudinal study of R2∗ andR2 magnetic resonance imaging relaxation rate measurements inmurine liver after a single administration of 3 different iron oxide-based contrast agents. Invest Radiol 2005; 40: 784–791.
17. Briley-Saobo KC, Johansson LO, Hustvedt SO et al. Clearance ofiron oxide particles in rats liver: Effect of hydrated particle sizeand coating material on liver metabolism. Invest Radiol 2006; 41:560–571.
18. Biancone L, Crich GS, Cantaluppi V et al. Magnetic resonance imag-ing of gadolinium-labeled pancreatic islets for experimental trans-plantation. NMR Biomed 2007; 20: 40–48.
706 American Journal of Transplantation 2008; 8: 701–706





























