Embed Size (px)
Citation preview

J Neurosurg Spine 21:867–876, 2014
J Neurosurg: Spine / Volume 21 / December 2014 867
©AANS, 2014
Anterior lumbar interbody fusion (ALIF) is per-formed in patients suffering pain and/or neuro-logical symptoms associated with degenerative
disorders of the lumbar spine or posttraumatic instability. The earliest reports of ALIF include those by Capener for the surgical management of spondylolisthesis in 1932,
Mercer for the treatment of disc pathology, and perfor-mance by Burns in 1933.12,13,34 The objectives of an ALIF procedure are to achieve solid arthrodesis of the degen-erative segment, which is critically influenced by bone graft selection.36 Currently, iliac crest bone graft (ICBG) remains the gold standard to achieve lumbar fusion, al-though patient dissatisfaction stemming from donor site morbidity, lengthier operating times, and finite supply of ICBG support the pursuit for comparable alternatives.35
Graft incorporation and healing for bony fusion in-
Clinical outcomes and fusion rates following anterior lumbar interbody fusion with bone graft substitute i-FACTOR, an anorganic bone matrix/P-15 composite
Clinical article
Ralph J. Mobbs, b.sc., M.b.b.s., M.s., F.R.a.c.s.,1,2 Monish MahaRaJ, M.D.,2 anD pRashanth J. Rao, M.D.1,2
1NeuroSpineClinic, Prince of Wales Private Hospital; and 2Faculty of Medicine, University of New South Wales, Sydney, Australia
Object. Despite limited availability and the morbidity associated with autologous iliac crest bone graft (ICBG), its use in anterior lumbar interbody fusion (ALIF) procedures remains the gold standard to achieve arthrodesis. The search for alternative grafts yielding comparable or superior fusion outcomes with fewer complications continues. In particular, i-FACTOR, a novel bone graft substitute composed of anorganic bone matrix (ABM) with P-15 small pep-tide, is one example currently used widely in the dental community. Although preclinical studies have documented its usefulness, the role of i-FACTOR in ALIF procedures remains unknown.
The authors’ goal was to determine the safety and efficacy of i-FACTOR bone graft composite used in patients who underwent ALIF by evaluating fusion rates and clinical outcomes.
Methods. A nonblinded cohort of patients who were all referred to a single surgeon’s practice was prospectively studied. One hundred ten patients with degenerative spinal disease underwent single or multilevel ALIF using the ABM/P-15 bone graft composite with a mean of 24 months (minimum 15 months) of follow-up were enrolled in the study. Patient’s clinical outcomes were assessed using the Oswestry Disability Index for low-back pain, the 12-Item Short Form Health Survey, Odom’s criteria, and a visual analog scale for pain. Fine-cut CT scans were used to evalu-ate the progression to fusion.
Results. All patients who received i-FACTOR demonstrated radiographic evidence of bony induction and early incorporation of bone graft. At a mean of 24 months of follow-up (range 15–43 months), 97.5%, 81%, and 100% of patients, respectively, who had undergone single-, double-, and triple-level surgery exhibited fusion at all treated levels. The clinical outcomes demonstrated a statistically significant (p < 0.05) difference between preoperative and postoperative Oswestry Disability Index, 12-Item Short Form Health Survey, and visual analog scores.
Conclusions. The use of i-FACTOR bone graft substitute demonstrates promising results for facilitating success-ful fusion and improving clinical outcomes in patients who undergo ALIF surgery for degenerative spinal patholo-gies.(http://thejns.org/doi/abs/10.3171/2014.9.SPINE131151)
Key WoRDs • anterior lumbar interbody fusion • i-FACTOR • ABM/P-15 • degenerative disc disease • bone graft substitute
This article contains some figures that are displayed in color on line but in black-and-white in the print edition.
Abbreviations used in this paper: ABM = anorganic bone matrix; ALIF = anterior lumbar interbody fusion; BMP = bone morphoge-netic protein; DDD = degenerative disc disease; ICBG = iliac crest bone graft; ODI = Oswestry Disability Index; rhBMP = recombinant human BMP; SF-12 = 12-Item Short Form Health Survey; VAS = visual analog scale.

R. J. Mobbs, M. Maharaj, and P. J. Rao
868 J Neurosurg: Spine / Volume 21 / December 2014
volves the processes of hematoma formation, inflamma-tion, vascularization, and the formation and remodeling of bone, all factors that affect overall graft response. The ideal graft should possess the following properties: os-teogenicity, osteoinductivity, and osteoconductivity.17,36,50
Only autograft encompasses all 3 properties, and re-cent ALIF studies with autograft demonstrate arthrodesis rates for single-level noninstrumented fusions ranging between 78.8% and 100%.16,23,37,39 Other interbody fusion studies using autograft supplemented with posterior fixa-tion exhibited fusion rates of 71%–98.6% in either single- or double-level fusions.40,41,48 However, its disadvantages have led to the development and use of graft alternatives including allograft, bone morphogenetic proteins (BMPs), and ceramics (Table 1).14
Allograft is obtained mostly from cadaveric femur or iliac crest, and its use in ALIF procedures has demonstrat-ed fusion rates varying between 60% and 100%.1,6,25,26,30,43 Limitations to its use stem from the possible risk of host rejection and disease transmission from donor to host. Fusion rates for ceramics as a grafting option for spinal procedures have been reported to be greater than 90%; however, very few reports have described their use in ALIF procedures.31,47 Recombinant BMP-2 (rhBMP-2; INFUSE, Medtronic) is widely used in many countries. INFUSE is currently considered the most effective alter-native to autograft as it possesses potent osteoinductive properties. INFUSE studies with significant sample sizes have described a high rate of early postsurgical fusion success ranging from 94.5% to 100%.7–9,11,27,44,51 Although they have good osteoinductive properties, BMPs are very expensive. In addition, the literature has demonstrated a high risk of complications, notably ectopic bone formation and bony osteolysis, leading to graft subsidence, and pro-nounced inflammatory and edematous reactions.4,15,24,32,49
Recently, a novel bone graft substitute, i-FACTOR, an anorganic bone matrix (ABM) with P-15 small peptide (ABM/P-15 composite, Cerapedics Inc.), has been used within the orthopedic community. The ABM provides osteoconductive properties in the form of the calcium phosphate matrix necessary for cellular invasion and migration. The bioactive P-15 peptide represents the bio-logically active component of the graft. It is a synthetic 15–amino acid residue, which acts as a biomimetic to the cell binding domain of Type I human collagen for osteo-genic cells.49 When combined with ABM, it provides the necessary scaffold to initiate cell invasion, binding, and osteogenesis. Attachment of P-15 to osteogenic cells initi-ates a cascade of intracellular signaling that triggers the synthesis of extracellular matrix and growth factors. This induces cell proliferation and differentiation and subse-quent osteogenesis.5,21,28 Although i-FACTOR possesses many of the desired criteria of an ideal bone graft, the lack of published data on its use in spinal fusion in hu-mans makes it a uncommon bone graft choice. Currently, i-FACTOR is still considered an investigational device and has not been approved for use in the US, and clinical use has been permitted in Europe only since 2008, which explains the scarcity of clinical data.
Consequently, the literature does not yet include a prospective study demonstrating the clinical efficacy of i- TA
BLE
1: Su
mm
ary o
f bon
e gra
ft al
tern
ative
s in
ALIF
pro
cedu
res*
Graf
t Opti
on
Fusio
n Rate
(%
)Ty
pe of
Gra
ftPr
oper
ties
Adva
ntag
es
Disa
dvan
tage
sCo
mplic
ation
s w/ G
raft
Cost†
OGOC
OISt
reng
th
auto
graf
t51
.9–1
00ca
ncell
ous b
one
+++
+++
++–
host
tissu
e; na
tural
biolog
ical
pr
oper
ties
finite
supp
ly, in
crea
sed s
urgi-
cal ti
me, b
lood l
oss,
pain
DSM
nilco
rtica
l bon
e+
++
–all
ogra
ft 42
.8–1
00no
DSM
; abu
ndan
t sup
ply; v
er-
sa
tility
as ex
tende
r &/or
graf
t
risk o
f bac
terial
cont
amina
-
tion,
viral
trans
miss
ion,
ho
st re
jectio
n
graf
t coll
apse
++
canc
ellou
s fre
sh-fr
ozen
–++
+–
freez
e-dr
ied–
+++
–DB
M90
‡–
+++
–no
DSM
; use
ful a
s bon
e
exten
ders
lacks
stre
ngth,
only
1 ALIF
clinic
al tri
algr
aft c
ollap
se++
cera
mics
79.3
–100
–++
+–
+no
DSM
not e
ffecti
ve as
stan
d-alo
ne;
lac
k of A
LIF cl
inica
l trial
sca
ge su
bside
nce
+
rhBM
P-2
44–1
00–
++++
+++
no D
SM, v
ery p
otent
oste
oin-
du
ctive
prop
ertie
s, hig
h
fusio
n rate
s
rare
, cos
tly, u
ncer
taint
y sur
-
roun
ding a
ppro
priat
e clin
i-
cal d
osag
e
heter
otopic
bone
form
ation
,
early
osteo
lysis,
graf
t
subs
idenc
e, infl
amma
tion
+++
* DB
M =
demi
nera
lized
bon
e ma
trix;
DSM
= do
nor s
ite m
orbid
ity; O
C =
oste
ocon
ducti
on; O
G =
oste
ogen
esis;
OI =
oste
oindu
ction
; + =
pre
senc
e of
the
prop
erty;
++
= str
onge
r pre
senc
e; ++
+ =
stron
gest
pres
ence
; – =
abse
nce o
f pro
perty
.†
Cost
of gr
afts
are a
ppro
ximate
and r
elativ
e only
.‡
Only
one c
linica
l stu
dy on
the a
pplic
ation
of de
mine
raliz
ed bo
ne m
atrix
to AL
IF w
as co
nduc
ted.

Clinical outcomes and fusion rates following ALIF with i-FACTOR
869J Neurosurg: Spine / Volume 21 / December 2014
FACTOR in human ALIF procedures. Thus, the purpose of this study is to prospectively evaluate the radiological and clinical success of ABM/P-15 composite in its use in anterior spondylodesis.
MethodsEthics Approval
Approval was obtained from the South Eastern Syd-ney Local Health District, New South Wales, Australia.
Patient RecruitmentThe study was a consecutive, single-surgeon prospec-
tive series, supported through a grant from Cerapedics, Inc. Patients were enrolled between July 2009 and Janu-ary 2012 by the senior author (R.J.M.), who performed all ALIF procedures. Exclusion criteria were infection, osteoporosis, and cancer. Indications for surgical inter-vention were as outlined in Radiographic Assessment.
Surgical TechniqueAll patients underwent an open ALIF using an anteri-
or approach to the lumbosacral spine. A vascular surgeon assisted with the approach to the spine in all procedures. A retroperitoneal exposure of the affected anterior ver-tebral disc and retraction with a Synframe (Synthes) was performed. Major anterior vessels were mobilized and retracted. The level of pathology was confirmed using ra-diography prior to disc removal. After initial disc prepa-ration and removal of the cartilaginous endplate with a Cobb elevator, a range of spine curettes and a high-speed drill with a 3-mm round bur were used to even out the endplates to facilitate an even, press-fit of the interbody cage upon insertion. A Synfix intergral fixation (Synthes) stand-alone polyetheretherketone cage was packed with i-FACTOR, inserted, and fixed with 4 divergent screws. Radiography was used to confirm correct placement, and antibiotic irrigation was used prior to closure.
Postoperative CareIn the postoperative period, patients were encouraged
to ambulate within 24 hours of surgery. Determinations regarding rehabilitation and the level of physical exercise were based on the recommendation of the treating surgeon.
Data Collection and Analysis
Radiographic Assessment. Neurological examina-tions, standing radiography, bone mineral density, bone scan/SPECT CT, and MRI were performed in all patients in the preoperative phase to determine the type and level of pathology. The following 6 indications for ALIF sur-gery were included in this study: 1) degenerative disc disease (DDD) with back pain and no radiculopathy; 2) DDD with back pain and radiculopathy; 3) spondylolis-thesis (degenerative or isthmic); 4) adjacent-segment de-generation; 5) scoliosis; and 6) failed union of a posterior fusion.
While ALIF is indicated for a variety of degenerative spinal pathologies, there is no consensus on which specif-
ic technique is most favorable to treat these pathologies. In the present study, the surgeon’s training and experi-ence was the fundamental basis for the choice of the ante-rior approach and implants used. Unrelieved pain and dis-ability despite prolonged conservative management and a multidisciplinary clinic evaluation were prerequisites to having surgery.
Fine-cut, high-resolution CT scans were obtained to evaluate fusion after surgery. All patients consented to undergo postoperative standing radiography on Day 1 and CT scanning at 3, 6, and 9–12 months, with addition-al scans obtained based on individual patient recovery. Scans were used to monitor progression of the incorpora-tion of the graft (Fig. 1).
A solid fusion was defined as bridging bone forma-tion between adjacent vertebral bodies as evidenced by bony continuity between the upper and lower endplates, and the absence of radiolucent lines covering greater than 50% of the implant (Fig. 2). All patients had a minimum radiological follow-up period of 15 months. The mean follow-up was 24 months (range 15–43 months). Radio-logical evaluation of coronal, sagittal, and axial CT scans for fusion was performed by 2 radiologists with experi-ence in evaluation of spinal and musculoskeletal radiol-ogy. All radiological data were statistically analyzed us-ing a paired sample t-test.
Clinical Outcome Assessment. Patient clinical out-comes were measured using well-established instruments for spinal procedures: the Oswestry Disability Index (ODI), 12-Item Short Form Health Survey (SF-12), and the 10-point visual analog scale (VAS).18,52 Outcomes were measured pre- and postoperatively at each visit. Patients who had incomplete outcome assessment forms were excluded from statistical analysis; however, more than 95% of patients (105 of 110) completed all follow-up clinical outcome assessments. The pre- and postoperative scores were compared using a 2-tailed, paired sample t-test, and the mean difference between the scores was also determined. A p value < 0.05 was considered signifi-cant. All statistical analyses were performed using SPSS software (version 22.0, IBM). At follow-up, patients were also assessed using Odom’s criteria to obtain insight into their quality of life and satisfaction of outcome postsur-gery.52 Patients rated their postoperative pain from excel-lent to poor based on resolution, reduction, or persistence of preoperative symptoms (Table 2). Adverse events were collected by a practice nurse who met with patients sepa-rately from the operative surgeon, and were prospectively entered into a custom database.
Results
Patient Characteristics
A total of 110 patients were included in the study. All patients satisfied the minimum 15-month radiological and clinical follow-up period. Demographic findings are il-lustrated in Table 3 with the ALIF indication distribution shown in Fig. 3. The most common indication was DDD with radiculopathy representing almost half of the cohort, followed by those with DDD without radiculopathy.

R. J. Mobbs, M. Maharaj, and P. J. Rao
870 J Neurosurg: Spine / Volume 21 / December 2014
Radiological OutcomesThe rate of solid arthrodesis was dependent on the
specific level operated on and the number of surgically treated levels per patient. In total, surgery was performed at 142 levels in 110 patients. The total observed fusion rate in the cohort was 93.6%. Patients who underwent sur-gery at 2 levels reported a lower fusion rate of 82% than patients who underwent surgery at 1 level (98%) at the time of radiological follow-up (Table 4). All 3 patients who underwent 3-level surgery reported solid fusion. A high fusion rate of 98% was reported for the L5–S1 level, which was also the most common level operated on, com-paratively higher than the other levels (Table 5). It was in-teresting to note that patients who smoked, had diabetes, or claimed workers’ compensation demonstrated compa-rably lower fusion rates than those who did not have those factors (Table 6), although only diabetes proved statisti-cally significant (p = 0.004).
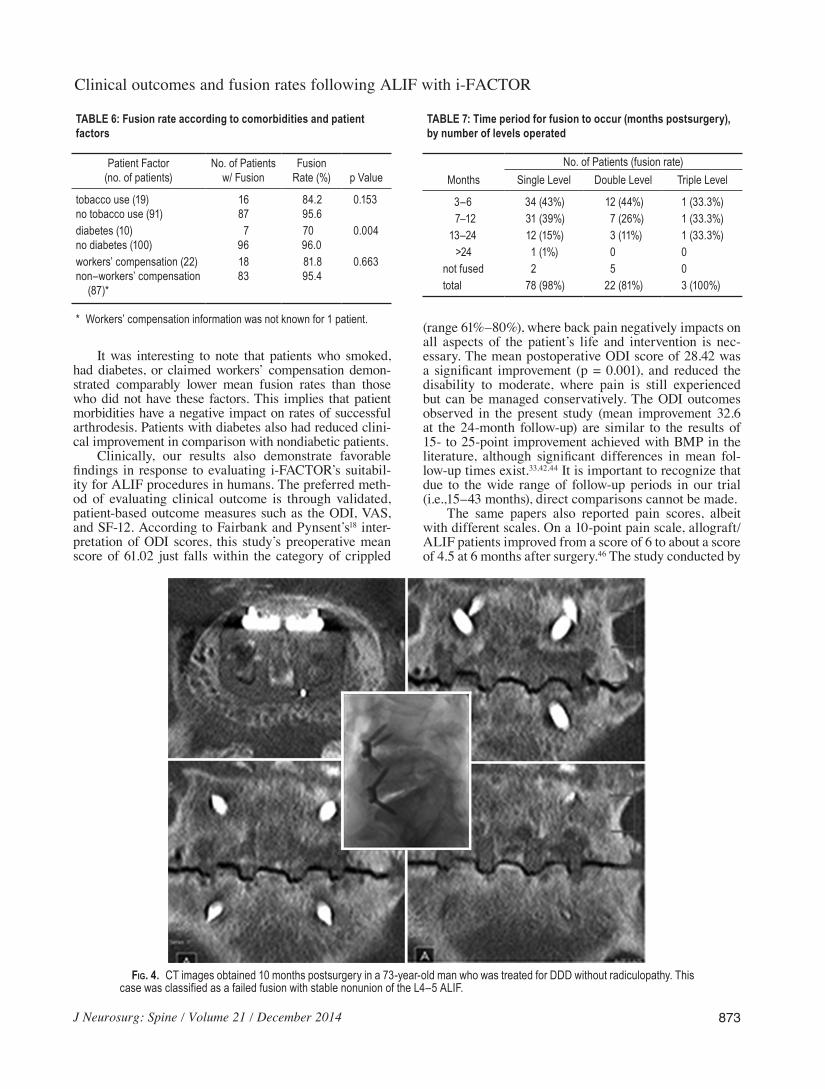
The mean follow-up time for collection of radiologi-cal data was 24 months (range 15–43 months), although evidence of fusion was demonstrated as early as 3 months postsurgery in some patients (Fig. 2). One patient who had undergone a 2-level ALIF had solid fusion at the L5–S1 level at 10 months with a stable nonunion (no movement on flexion/extension radiographs) of the L4–5 ALIF. This case was classified as “not fused” as there was no indi-cation of bone bridging (Fig. 4). All patients undergoing
surgery at 3 levels demonstrated evidence of fusion in all 3 levels postsurgery.
Of the patient population, 82% of patients undergo-ing single-level surgery exhibited fusion by 12 months and 98% by 24 months (Table 7). Lower fusion rates were reported in patients who underwent surgery at 2 levels within the same time period, whereas 70% and 81% of patients showed evidence of fusion at 12 and 24 months, respectively. Overall, 86 patients (78.2%) exhibited fusion by 12 months and 102 patients (92.7%) exhibited fusion by 24 months (Fig. 5). Seven of the 104 patients who had radiological follow-up had not exhibited fusion at the time of this study. These patients were observed at a minimum of 15 months after surgery and therefore the fusion rate may increase further as time passes.
For patients who did not exhibit fusion at the 12-month mark or who had complications, further clinical follow-up was offered at either 18, 24, or 36 months postoperatively. Patients were offered further CT assessment, as the senior author (R.J.M.) prefers CT analysis over radiography as the primary assessment of arthrodesis.
Clinical OutcomesPostoperative ODI, SF-12, and VAS scores were as-
sessed at a mean of 24 months postsurgery. The clinical results collected demonstrated a statistically significant (p < 0.05) difference between preoperative and postop-
Fig. 1. Images demonstrating progression of interbody fusion in a 45-year-old woman treated for DDD without radiculopa-thy. A: Radiograph of the L5–S1 level 1 day postsurgery. B: Coronal CT images obtained 1 month postoperatively. C: CT images obtained 5 months postoperatively. D: CT images obtained 12 months postoperatively demonstrating solid fusion.

Clinical outcomes and fusion rates following ALIF with i-FACTOR
871J Neurosurg: Spine / Volume 21 / December 2014
erative scores (Table 8). Patients with incomplete pre- and postoperative clinical outcome data were excluded from the statistical analysis, leaving a total of 105 patients. Im-provements were noted across all 3 measures, with statis-tical significance attained in all. Across patient comor-bidities and factors (diabetes, tobacco use, and worker’s compensation), although improvements were observed across cohorts, statistical significance was not attained.
Based on Odom’s criteria, 85.3% of 109 patients available for follow-up had excellent to good outcomes (Table 9). Patients with fair to poor outcomes experienced no or minimal symptom relief of their preoperative pain despite adequate decompression and fusion.
Adverse Events and ComplicationsThe overall complications rate (all postoperative com-
plications) was 10%, with 11 complications in total (6 major and 5 minor). Major complications included 4 cases of ret-rograde ejaculation, a postoperative hematoma, and an in-cisional hernia that required further surgery. Two patients with retrograde ejaculation recovered within 4 months postsurgery. Minor complications included postoperative deep vein thrombosis and prolonged (> 7 days) postop-erative ileus. Notably, there were no reports of wound infection or hardware failure. All complications were as-sociated with the surgical exposure and approach involved with the ALIF procedure. Graft migration was evident on postoperative CT scanning due to the radiodense nature of the i-FACTOR graft material. Despite a minor volume of graft migration in the majority of cases, we did not ob-serve an increased rate of abdominal issues, infection, or retrograde ejaculation in this series as compared with re-sults of similar studies. In the later stages of the study, the anterior hole in the ALIF implant was blocked to stop any graft migration as the material was wholly contained within the implant. One minor complication, unlikely re-lated to i-FACTOR, was vague abdominal pain in a patient in whom a volume of graft had migrated.
Fig. 2. CT images obtained 4 months postoperatively in a 62-year-old patient who was treated for degenerative spondylolis-thesis with radiculopathy at L4–5.
TABLE 2: Adapted definitions of Odom’s criteria
Outcome Criteria Definitionexcellent all preop symptoms relieved; pain reducedgood minimal persistence of preoperative symptoms;
abnormal findings unchanged or improvedfair definite relief of some preoperative symptoms; other
symptoms unchanged or slightly improvedpoor symptoms & signs worsened, or unchanged

R. J. Mobbs, M. Maharaj, and P. J. Rao
872 J Neurosurg: Spine / Volume 21 / December 2014
Cost Comparator DataAs i-FACTOR is not currently an FDA-approved
product in the US, no cost comparison data are available to assess its potential benefits versus existing FDA ap-proved products for similar indications. In the Australian health care system, the Prostheses List provides a fee structure for payment for the use of various medical de-
vices including biological materials and bone graft sub-stitutes. i-FACTOR, compared with rh-BMP2 (INFUSE) and rhBMP-7 (OP-1), is significantly less expensive with the added benefit of fewer complications and acceptable/similar fusion results.
DiscussionDespite being the current gold standard, harvested
autologous ICBG has many disadvantages both peri- and postoperatively, with donor site pain being the most fre-quent complication reported with an incidence of 25%–31%.2,3,29,45,51 Despite the extensive list of associated compli-cations with autograft, including graft collapse, neurologi-cal injury, and sacroiliac joint–related complications, the primary reason deterring patients and surgeons from using ICBG harvest is the subjective perception that the harvest is the most painful part of the fusion procedure.16,19,20,22,23,38 The presence of these factors justifies the necessity and use of bone graft substitutes as illustrated in Table 1.
While promising results have been observed in both animal and human studies evaluating ABM/P-15 use as a bone graft, our study is the first to investigate its use composite in human ALIF procedures. Overall our data, following a mean 24-month (minimum 15 months) fol-low-up, demonstrated a fusion rate of 92.7% in the cohort. This is consistent with the prospective trial by Sherman et al.42 in which they used ABM/P-15 in an ovine mod-el (n = 6, fusion rate = 100%) and Lauweryns’ unpub-lished prospective trial33 utilizing ABM/P-15 in posterior lumbar interbody fusion in humans (autograft 82.2% vs ABM/p-15 97.8%, 12-month follow-up). Lauweryns’ find-ings, as presented at the 2011 Global Spine Congress in Barcelona, also concluded that in addition to being “sta-tistically superior,” ABM/P-15 achieved solid fusion faster than autologous bone graft with data at 6 months showing a 38.6% difference in fusion. There were no un-expected complications and the complication rate (10%) in our prospective study is comparable to the complica-tion rate of 9.5% in the large retrospective study of BMP in ALIF by Williams et al.53
TABLE 3: Patient demographics and characteristics
Patient Demographics Value*
no. of patients 110no. of levels 142age in yrs mean 57.6 range 25–86M/F 48/62BMI underweight (<18.5) normal range (18.5–25) overweight (25–30) obese (>30)
570314
tobacco use 19 (17)diabetes 10 (9)workers’ compensation 22 (20)follow-up period in mos mean 24 range 15–43length of stay in days mean 4.6 range 1–19intraop blood loss in ml mean 102 range 80–700total operation time in mins mean 97 range 40–195
* Values are the number of patients (%) unless noted otherwise.
Fig. 3. Surgical indications for which ALIF was performed. ASD = adjacent-segment disease; R = radiculopathy.
TABLE 4: Fusion rates of 1-, 2-, and 3-level ALIF proceedures
No. of Levels No of Patients w/ Fusion (%)
1 78/80 (98)2 22/27 (82)3 3/3 (100)
total 103/110 (94)
TABLE 5: Fusion rate per surgically treated level
Level No. of Levels Fused (%)
L2–3 3/3 (100)L3–4 14/17 (82)L4–5 50/59 (85)L5–S1 62/63 (98)total 130/142 (92)
Clinical outcomes and fusion rates following ALIF with i-FACTOR
873J Neurosurg: Spine / Volume 21 / December 2014
It was interesting to note that patients who smoked, had diabetes, or claimed workers’ compensation demon-strated comparably lower mean fusion rates than those who did not have these factors. This implies that patient morbidities have a negative impact on rates of successful arthrodesis. Patients with diabetes also had reduced clini-cal improvement in comparison with nondiabetic patients.
Clinically, our results also demonstrate favorable findings in response to evaluating i-FACTOR’s suitabil-ity for ALIF procedures in humans. The preferred meth-od of evaluating clinical outcome is through validated, patient-based outcome measures such as the ODI, VAS, and SF-12. According to Fairbank and Pynsent’s18 inter-pretation of ODI scores, this study’s preoperative mean score of 61.02 just falls within the category of crippled
(range 61%–80%), where back pain negatively impacts on all aspects of the patient’s life and intervention is nec-essary. The mean postoperative ODI score of 28.42 was a significant improvement (p = 0.001), and reduced the disability to moderate, where pain is still experienced but can be managed conservatively. The ODI outcomes observed in the present study (mean improvement 32.6 at the 24-month follow-up) are similar to the results of 15- to 25-point improvement achieved with BMP in the literature, although significant differences in mean fol-low-up times exist.33,42,44 It is important to recognize that due to the wide range of follow-up periods in our trial (i.e.,15–43 months), direct comparisons cannot be made.
The same papers also reported pain scores, albeit with different scales. On a 10-point pain scale, allograft/ALIF patients improved from a score of 6 to about a score of 4.5 at 6 months after surgery.46 The study conducted by
TABLE 6: Fusion rate according to comorbidities and patient factors
Patient Factor (no. of patients)
No. of Patients w/ Fusion
Fusion Rate (%) p Value
tobacco use (19)no tobacco use (91)
1687
84.295.6
0.153
diabetes (10)no diabetes (100)
796
7096.0
0.004
workers’ compensation (22)non–workers’ compensation (87)*
1883
81.895.4
0.663
* Workers’ compensation information was not known for 1 patient.
Fig. 4. CT images obtained 10 months postsurgery in a 73-year-old man who was treated for DDD without radiculopathy. This case was classified as a failed fusion with stable nonunion of the L4–5 ALIF.
TABLE 7: Time period for fusion to occur (months postsurgery), by number of levels operated
No. of Patients (fusion rate)Months Single Level Double Level Triple Level
3–6 34 (43%) 12 (44%) 1 (33.3%)7–12 31 (39%) 7 (26%) 1 (33.3%)
13–24 12 (15%) 3 (11%) 1 (33.3%)>24 1 (1%) 0 0
not fused 2 5 0total 78 (98%) 22 (81%) 3 (100%)

R. J. Mobbs, M. Maharaj, and P. J. Rao
874 J Neurosurg: Spine / Volume 21 / December 2014
Burkus et al. was analyzed using a 20-point pain scale, and hence, the outcomes cannot be directly compared with the outcomes of our current study, although positive outcomes were maintained at the 6-year follow-up.10 The mean differences were 7.3 and 7.1 for BMP and autograft, respectively, at 6 months postsurgery,9 while a larger im-provement from 7.40 preoperatively to 2.65 postopera-tively (p = 0.013) was seen in our study. This demonstrates that i-FACTOR is a promising graft substitute to achieve fusion and to assist with the ALIF procedure to reduce pain caused by certain spinal pathologies, without the po-tential adverse events and complications associated with autograft and BMPs. Although migration of i-FACTOR was seen in patients when not contained, there were no confirmed adverse effects from the graft material located outside the interbody space.
Our study used the SF-12 survey to assess clinical outcomes on the basis of increased patient convenience and compliance, demonstrating a mean increase in the score from 68.27 to 92.99 (mean difference 24.72; p = 0.043). The results suggest i-FACTOR use as an adjunct to spinal arthrodesis, significantly improving the qual-ity of life and mental state of patients. Comparisons with other recent studies were not possible due to their imple-mentation of the SF-36.
Odom outcomes demonstrated that 85.3% of patients in the current study for whom follow-up was available had excellent to good outcomes. These patients experienced a significant improvement in their quality of life and noted that ALIF using i-FACTOR was an appropriate choice.
It is of paramount importance that evaluation of the suc-cess of a graft is made on the basis of both radiological and clinical patient outcome measures, as successful fu-sion does not always correlate with satisfactory patient outcome.
Limitations of our study are the lack of direct con-trol and the potential for respondent bias. Patients who participate in research are more likely to comply with postoperative medications and physiotherapy, thus result-ing in better health outcomes. For instance, a few patients declined completing the postoperative outcome data be-cause they were discontent with their outcome. These pa-tients were subsequently excluded from statistical analy-sis, which may have positively skewed results.
ConclusionsAnterior lumbar interbody fusion using i-FACTOR
(ABM/P-15) synthetic bone graft substitute is a useful treatment option for degenerative pathologies of the lum-bar spine. The present study demonstrates a high fusion rate and clinical improvements comparable to the pub-lished results for ALIF using autograft or BMP. At the same time the use of ABM/P-15 as a graft material avoids the complications specific to those 2 materials. Further studies comparing rate of arthrodesis, clinical outcome, and cost between ABM/P-15 and other graft alternatives are warranted.
Disclosure
Dr. Mobbs reports receiving clinical or research support for the study described from Cerapedics.
Author contributions to the study and manuscript preparation include the following. Conception and design: Mobbs. Acquisition of data: all authors. Analysis and interpretation of data: all authors. Drafting the article: Mobbs. Critically revising the article: all au -thors. Reviewed submitted version of manuscript: Mobbs, Rao. Approved the final version of the manuscript on behalf of all authors: Mobbs. Statistical analysis: Mobbs, Maharaj. Administrative/techni-cal/material support: Rao. Study supervision: Mobbs.
References
1. Anderson DG, Sayadipour A, Shelby K, Albert TJ, Vaccaro AR, Weinstein MS: Anterior interbody arthrodesis with per-cutaneous posterior pedicle fixation for degenerative condi-tions of the lumbar spine. Eur Spine J 20:1323–1330, 2011
2. Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity. A statistical evaluation. Spine (Phila Pa 1976) 20:1055–1060, 1995
3. Bednar DA, Al-Tunaib W: Failure of reconstitution of open-section, posterior iliac-wing bone graft donor sites after lum-bar spinal fusion. Observations with implications for the etiol-ogy of donor site pain. Eur Spine J 14:95–98, 2005
TABLE 8: Summary of clinical outcome score data within the entire patient cohort
Variable SF-12 ODI VAS
preop score 68.57 ± 14.06 61.02 ± 21.38 7.38 ± 1.53postop score 92.99 ± 15.72 28.42 ± 19.53 2.65 ± 2.13p value 0.043* 0.001* 0.013*
* Statistically significant.
TABLE 9: Odom outcomes
Variable Excellent Good Fair Poor
1-level 36 33 12 22-level 13 8 2 03-level 1 2 0 0total 50 43 14 2
Fig. 5. Pie chart showing the overall fusion for patients undergoing 1-, 2-, and 3-level surgery. The values indicate time points in months.

Clinical outcomes and fusion rates following ALIF with i-FACTOR
875J Neurosurg: Spine / Volume 21 / December 2014
4. Benglis D, Wang MY, Levi AD: A comprehensive review of the safety profile of bone morphogenetic protein in spine sur-gery. Neurosurgery 62 (5 Suppl 2):ONS423–ONS431, 2008
5. Bhatnagar RS, Qian JJ, Gough CA: The role in cell binding of a beta-bend within the triple helical region in collagen alpha 1 (I) chain: structural and biological evidence for conforma-tional tautomerism on fiber surface. J Biomol Struct Dyn 14: 547–560, 1997
6. Blumenthal SL, Baker J, Dossett A, Selby DK: The role of an-terior lumbar fusion for internal disc disruption. Spine (Phila Pa 1976) 13:566–569, 1988
7. Boden SD, Zdeblick TA, Sandhu HS, Heim SE: The use of rhBMP-2 in interbody fusion cages. Definitive evidence of os-teoinduction in humans: a preliminary report. Spine (Phila Pa 1976) 25:376–381, 2000
8. Burkus JK, Dorchak JD, Sanders DL: Radiographic assess-ment of interbody fusion using recombinant human bone mor-phogenetic protein type 2. Spine (Phila Pa 1976) 28:372–377, 2003
9. Burkus JK, Gornet MF, Dickman CA, Zdeblick TA: Anterior lumbar interbody fusion using rhBMP-2 with tapered inter-body cages. J Spinal Disord Tech 15:337–349, 2002
10. Burkus JK, Gornet MF, Schuler TC, Kleeman TJ, Zdeblick TA: Six-year outcomes of anterior lumbar interbody arthrod-esis with use of interbody fusion cages and recombinant hu-man bone morphogenetic protein-2. J Bone Joint Surg Am 91:1181–1189, 2009
11. Burkus JK, Transfeldt EE, Kitchel SH, Watkins RG, Balder-ston RA: Clinical and radiographic outcomes of anterior lumbar interbody fusion using recombinant human bone mor-phogenetic protein-2. Spine (Phila Pa 1976) 27:2396–2408, 2002
12. Burns BH: An operation for spondylolisthesis. Lancet 221: 1233–1239, 1933
13. Capener N: Spondylolisthesis. Br J Surg 19:374–386, 193214. Chau AM, Xu LL, Wong JH, Mobbs RJ: Current status of
bone graft options for anterior interbody fusion of the cervical and lumbar spine. Neurosurg Rev 37:23–37, 2014
15. Chen Z, Ba G, Shen T, Fu Q: Recombinant human bone mor-phogenetic protein-2 versus autogenous iliac crest bone graft for lumbar fusion: a meta-analysis of ten randomized controlled trials. Arch Orthop Trauma Surg 132:1725–1740, 2012
16. Cheung KM, Zhang YG, Lu DS, Luk KD, Leong JC: Reduc-tion of disc space distraction after anterior lumbar interbody fusion with autologous iliac crest graft. Spine (Phila Pa 1976) 28:1385–1389, 2003
17. Ehrler DM, Vaccaro AR: The use of allograft bone in lumbar spine surgery. Clin Orthop Relat Res (371):38–45, 2000
18. Fairbank JC, Pynsent PB: The Oswestry Disability Index. Spine (Phila Pa 1976) 25:2940–2952, 2000
19. Fowler BL, Dall BE, Rowe DE: Complications associated with harvesting autogenous iliac bone graft. Am J Orthop 24: 895–903, 1995
20. Greenough CG, Taylor LJ, Fraser RD: Anterior lumbar fusion: results, assessment techniques and prognostic factors. Eur Spine J 3:225–230, 1994
21. Gomar F, Orozco R, Villar JL, Arrizabalaga F: P-15 small peptide bone graft substitute in the treatment of non-unions and delayed union. A pilot clinical trial. Int Orthop 31:93–99, 2007
22. Heary RF, Schlenk RP, Sacchieri TA, Barone D, Brotea C: Persistent iliac crest donor site pain: independent outcome as-sessment. Neurosurgery 50:510–517, 2002
23. Ishihara H, Osada R, Kanamori M, Kawaguchi Y, Ohmori K, Kimura T, et al: Minimum 10-year follow-up study of anterior lumbar interbody fusion for isthmic spondylolisthesis. J Spi-nal Disord 14:91–99, 2001
24. Kanatani M, Sugimoto T, Kaji H, Kobayashi T, Nishiyama K, Fukase M, et al: Stimulatory effect of bone morphogenetic
protein-2 on osteoclast-like cell formation and bone-resorbing activity. J Bone Miner Res 10:1681–1690, 1995
25. Kim JS, Choi WG, Lee SH: Minimally invasive anterior lum-bar interbody fusion followed by percutaneous pedicle screw fixation for isthmic spondylolisthesis: minimum 5-year fol-low-up. Spine J 10:404–409, 2010
26. Kim JS, Kim DH, Lee SH, Park CK, Hwang JH, Cheh G, et al: Comparison study of the instrumented circumferential fusion with instrumented anterior lumbar interbody fusion as a sur-gical procedure for adult low-grade isthmic spondylolisthesis. World Neurosurg 73:565–571, 2010
27. Kleeman TJ, Ahn UM, Talbot-Kleeman A: Laparoscopic an-terior lumbar interbody fusion with rhBMP-2: a prospective study of clinical and radiographic outcomes. Spine (Phila Pa 1976) 26:2751–2756, 2001
28. Kübler A, Neugebauer J, Oh JH, Scheer M, Zöller JE: Growth and proliferation of human osteoblasts on different bone graft substitutes: an in vitro study. Implant Dent 13:171–179, 2004
29. Kurz LT, Garfin SR, Booth RE Jr: Harvesting autogenous iliac bone grafts. A review of complications and techniques. Spine (Phila Pa 1976) 14:1324–1331, 1989
30. Lee DY, Lee SH, Maeng DH: Two-level anterior lumbar in-terbody fusion with percutaneous pedicle screw fixation: a minimum 3-year follow-up study. Neurol Med Chir (Tokyo) 50:645–650, 2010
31. Linovitz RJ, Peppers TA: Use of an advanced formulation of beta-tricalcium phosphate as a bone extender in interbody lumbar fusion. Orthopedics 25 (5 Suppl):s585–s589, 2002
32. Mannion RJ, Nowitzke AM, Wood MJ: Promoting fusion in minimally invasive lumbar interbody stabilization with low-dose bone morphogenic protein-2—but what is the cost? Spine J 11:527–533, 2011
33. McAdoo S: Prospective, randomized, controlled trial demon-strates 98% fusion rate at 6-months and 12-months with i-FAC-TOR™ biologic bone graft and superiority versus autograft in single- and multi-level PLIF spine surgery. Cerapedics. (http://www.cerapedics.com/intl/news/story6/) [Accessed September 3, 2014]
34. Mercer W: Spondylolisthesis: with a description of a new meth-od of operative treatment and notes of ten cases. Edinburgh Med J 43:545–572, 1936
35. Mobbs RJ, Chung M, Rao PJ: Bone graft substitutes for an-terior lumbar interbody fusion. Orthop Surg 5:77–85, 2013
36. Mobbs RJ, Loganathan A, Yeung V, Rao PJ: Indications for anterior lumbar interbody fusion. Orthop Surg 5:153–163, 2013
37. Motosuneya T, Asazuma T, Nobuta M, Masuoka K, Ichimura S, Fujikawa K: Anterior lumbar interbody fusion: changes in area of the dural tube, disc height, and prevalence of cauda equina adhesion in magnetic resonance images. J Spinal Dis-ord Tech 18:18–22, 2005
38. Newman MH, Grinstead GL: Anterior lumbar interbody fu-sion for internal disc disruption. Spine (Phila Pa 1976) 17: 831–833, 1992
39. Ohtori S, Koshi T, Yamashita M, Takaso M, Yamauchi K, In-oue G, et al: Single-level instrumented posterolateral fusion versus non-instrumented anterior interbody fusion for lumbar spondylolisthesis: a prospective study with a 2-year follow-up. J Orthop Sci 16:352–358, 2011
40. Pavlov PW, Meijers H, van Limbeek J, Jacobs WC, Lemmens JA, Obradov-Rajic M, et al: Good outcome and restoration of lordosis after anterior lumbar interbody fusion with additional posterior fixation. Spine (Phila Pa 1976) 29:1893–1900, 2004
41. Saraph V, Lerch C, Walochnik N, Bach CM, Krismer M, Wimmer C: Comparison of conventional versus minimally in-vasive extraperitoneal approach for anterior lumbar interbody fusion. Eur Spine J 13:425–431, 2004
42. Sherman BP, Lindley EM, Turner AS, Seim HB III, Benedict J, Burger EL, et al: Evaluation of ABM/P-15 versus autog-

R. J. Mobbs, M. Maharaj, and P. J. Rao
876 J Neurosurg: Spine / Volume 21 / December 2014
enous bone in an ovine lumbar interbody fusion model. Eur Spine J 19:2156–2163, 2010
43. Shim CS, Lee SH, Jung B, Sivasabaapathi P, Park SH, Shin SW: Fluoroscopically assisted percutaneous translaminar fac-et screw fixation following anterior lumbar interbody fusion: technical report. Spine (Phila Pa 1976) 30:838–843, 2005
44. Slosar PJ, Josey R, Reynolds J: Accelerating lumbar fusions by combining rhBMP-2 with allograft bone: a prospective analy-sis of interbody fusion rates and clinical outcomes. Spine J 7:301–307, 2007
45. Summers BN, Eisenstein SM: Donor site pain from the ilium. A complication of lumbar spine fusion. J Bone Joint Surg Br 71:677–680, 1989
46. Thalgott JS, Fogarty ME, Giuffre JM, Christenson SD, Ep-stein AK, Aprill C: A prospective, randomized, blinded, single-site study to evaluate the clinical and radiographic dif-ferences between frozen and freeze-dried allograft when used as part of a circumferential anterior lumbar interbody fusion procedure. Spine (Phila Pa 1976) 34:1251–1256, 2009
47. Thalgott JS, Klezl Z, Timlin M, Giuffre JM: Anterior lumbar interbody fusion with processed sea coral (coralline hydroxy-apatite) as part of a circumferential fusion. Spine (Phila Pa 1976) 27:E518—E527, 2002
48. Tiusanen H, Seitsalo S, Osterman K, Soini J: Anterior interbody lumbar fusion in severe low back pain. Clin Orthop Relat Res (324):153–163, 1996
49. US Food and Drug Administration: Summary of Safety and Effectiveness Data. InFUSE™ Bone Graft/LT-CAGE™ Lumbar Tapered Fusion Device. (http://www.accessdata.
fda.gov/cdrh_docs/pdf/P000058b.pdf) [Accessed September 3, 2014]
50. Vaccaro AR, Chiba K, Heller JG, Patel TC, Thalgott JS, Tru-umees E, et al: Bone grafting alternatives in spinal surgery. Spine J 2:206–215, 2002
51. Vaidya R, Weir R, Sethi A, Meisterling S, Hakeos W, Wybo CD: Interbody fusion with allograft and rhBMP-2 leads to consistent fusion but early subsidence. J Bone Joint Surg Br 89:342–345, 2007
52. Ware J Jr, Kosinski M, Keller SD: A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care 34:220–233, 1996
53. Williams BJ, Smith JS, Fu KM, Hamilton DK, Polly DW Jr, Ames CP, et al: Does bone morphogenetic protein increase the incidence of perioperative complications in spinal fu-sion? A comparison of 55,862 cases of spinal fusion with and without bone morphogenetic protein. Spine (Phila Pa 1976) 36:1685–1691, 2011
Manuscript submitted December 18, 2013.Accepted September 2, 2014.Please include this information when citing this paper: published
online October 17, 2014; DOI: 10.3171/2014.9.SPINE131151.Address correspondence to: Ralph J. Mobbs, B.Sc., M.B.B.S.,
M.S., F.R.A.C.S., NeuroSpineClinic, Suite 7a, Level 7, Prince of Wales Private Hospital, Randwick, NSW 2031, Australia. email: [email protected].





























