Embed Size (px)
Citation preview
Accepted Manuscript
Low flows after Tubularized Incised Plate (TIP) urethroplasty: increased fibrogenesis, elastin fibers loss or none of the above?
L.E. Jesus, A. Schanaider, T. Kirwan, K.J. Aitken, M.L.R. Caldas, E. Fonseca, A. Marchenko, D.J. Bagli, J.L. Pippi-Salle
PII: S0022-5347(13)06070-9 DOI: 10.1016/j.juro.2013.11.098
Reference: JURO 10941
To appear in: The Journal of Urology Accepted date: 25 November 2013 Please cite this article as: Jesus, L.E., Schanaider, A., Kirwan, T., Aitken, K.J., Caldas, M.L.R., Fonseca, E., Marchenko, A., Bagli, D.J., Pippi-Salle, J.L., Low flows after Tubularized Incised Plate (TIP) urethroplasty: increased fibrogenesis, elastin fibers loss or none of the above?, The Journal of Urology® (2013), doi: 10.1016/j.juro.2013.11.098. DISCLAIMER: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our subscribers we are providing this early version of the article. The paper will be copy edited and typeset, and proof will be reviewed before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to The Journal pertain. All press releases and the articles they feature are under strict embargo until uncorrected proof of the article becomes available online. We will provide journalists and editors with full-text copies of the articles in question prior to the embargo date so that stories can be adequately researched and written. The standard embargo time is 12:01 AM ET on that date.
Low flows after Tubularized Incised Plate (TIP) urethroplasty: increased fibrogenesis, elastin fibers loss or none of the
above?
Jesus, LE1,2; Schanaider, A 1; Kirwan, T4; Aitken, KJ4; Caldas, MLR 5; Fonseca, E 5; Marchenko, A3; Bagli, DJ 3,4, Pippi-Salle, JL 3.
1. Center for Experimental Surgery. Post-Graduation in Surgical Sciences, Federal University of Rio de Janeiro, Rio de Janeiro, CAPES, CNPq, Brazil.
2. Department of Surgery, Division of Pediatric Surgery and Pediatric Urology, Federal Fluminense University and Servidores do Estado Hospital, Rio de Janeiro, Brazil.
3. Division of Pediatric Urology, The Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada.
4. Division of Developmental & Stem Cell Biology, The Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada
5. Department of Pathology, Federal Fluminense University, Rio de Janeiro, Brazil.
Original Scientific article, Pediatric Section
Descriptive runninghead: Elastic fibers and collagen profile after TIP and dorsal inlay urethroplasty. Acknowledgements: Paula Pflugfelder and Marvin Estrada, Experimental Surgery Department, The Hospital for Sick Children, Toronto University, Toronto, Canada, Greg Patterson, Engineering Technician, The Hospital for Sick Children, Toronto University, Toronto, Canada, Alexandre Santos Aguiar, independent consultant in biostatistics.
Word countings: abstracts: 249; manuscript: 2500; Figures: 6; Tables: 0.
Author for correspondence:
Lisieux Eyer de Jesus, MD, MsC, PhD – Fellow of the Brazilian College of Surgeons. Hospital Universitário Antônio Pedro, Universidade Federal Fluminense, Rio de Janeiro, Brazil. 52 Presidente Domiciano St, apt 801. Niterói, Rio de Janeiro, Brazil. CEP 24210-270. e-mail [email protected]
ABSTRACT:
INTRODUCTION: Low flows rates are common after TIP urethroplasty but their etiology remains unclear and may related to low urethral compliance, maybe due to abnormal collagen concentrations and/or less elastic fibers in the healed urethral plate. We also hypothesized that inserting a preputial mucosal graft over the dorsal raw area after the midline incision (TIPG) may avoid scarring and improve urethral compliance.
METHODS: Adult rabbits were submitted to TIP and TIPG operations according to a previously described protocol. Tissular concentrations of collagens I/III/IV/VI/VIII/XIII were measured. Histomorphometry was used to quantify elastic fibers in the urethra. TIP, TIPG and normal rabbits’ urethras (controls) were compared.
RESULTS: The mRNA concentrations for collagens I, II and XIII were similar between controls and operated rabbits. The proportions between collagen I and III were, respectively, 1.05, 1.21 and 0.87, in controls, TIP and TIPG animals. mRNA concentrations for collagen IV and for collagens VI/VIII tended to be higher and lower, respectively, in the operated urethras, despite showing statistical significance only for collagen VIII in TIPG animals versus controls (p=0.02). The operated animals did not show a lower number of elastic fibers in the urethral tissues, as compared to controls.
CONCLUSION: Elastic fiber number and distribution was similar between TIP and controls, suggesting that lower concentrations of elastic fibers are not the explanation for low urethral compliances after TIP. The raw area determined by the dorsal urethral incision regenerated after TIP, while cicatrization with fibrosis occurred in correspondence to the grafted areas after TIPG surgery.
KEY-WORDS: hypospadias; collagen profile; elastin fibers; urethral compliance, TIP, Tubularized incised plate, Snodgrass procedure, onlay preputial graft.
INTRODUCTION:
TIP urethroplasty 1 is widely used for hypospadias repairs. Abnormal post-
operative flow rates are common, despite the absence of anatomical urethral
obstruction in most cases 2. Previous experimental results indicate that TIP does not
induce extensive urethral fibrosis 3-5, but modifications of the collagen distribution or
loss of elastic fibers in the operated area are still possible.
We decided to study these aspects further in a previously described animal
model 2, departing from the hypothesis of a loss of urethral compliance in TIP models,
maybe due either to fibrosis, differential collagen distribution or paucity of elastic fibers
after cicatrization of the median incision. We also studied how the addition of a free
graft over the raw dorsal area after the midline incision modified urethral cicatrization.
Our objectives are to evaluate tissular concentration of different collagens, to
quantify and to describe the distribution of elastic fibers in normal urethras, TIP and
TIPG models.
METHODS:
The experimental protocol was approved by our institution’s Animal Care
Committee (REB 1000007883). All handling and procedures were performed following
the Canadian Council on Animal Care guidelines.
Twenty-five adult male 3-3.5 kg New Zealand rabbits were kept in individual
cages receiving standard rabbit’s diet, water ad libitum and routine care and pre-
anesthetized with Ketamine and Azepromazine. Anesthesia was accomplished by a
mixture of halothane, nitrous oxide and oxygen through a mask and penile block with
2% lidocaine.
The animals were distributed into 3 groups:
1. Control (G1): n=9: non-operated normal male adult rabbits.
2. TIP (figure 1) (G2): n=8: animals underwent a segmental TIP urethroplasty
after resection of the ventro-lateral portion of the urethral wall (not adherent
to the CC), leaving approximately ½ of the urethral circumference, followed
by a midline dorsal incision (limited to the adventicia of the CC) and ventral
tubularization (single layered continuous polydioxanone 6.0 suture over a 10
F catheter that was removed immediately after finishing the procedure). The
operated segment was 2.5 cm long, beginning 1 cm proximal to the glans.
3. TIPG model (figure 1) (G3): n=8: same procedure done in G2 animals,
except for placing a mucosal preputial graft over the incised area, sutured to
the edges of the incision and quilted to the corporal albuginea with
interrupted 7.0 polyglactin stitches.
The animals received routine care after recovering from anesthesia. Analgesics
were not necessary in the post-operative period. All animals were observed for 6
weeks and then sacrificed using anesthetic overdose.
Penile dissection and degloving was done immediately after death. Urethral
compliance was evaluated by measuring tension in an isolated urethral segment, after injections of specific volumes of air, as previously reported 6. A 3 cm urethra
plus CC segment distal to the penopubic junction was isolated and sectioned in 3 equal
parts, each of them containing a segment of operated urethra in G2 and G3 animals.
One segment was selected for histological studies, preserved in phosphate
buffered formalin and sectioned (4 μm thick sections). Four sections for each animal
were stained using hematoxilyn-eosin (routine histological evaluation), Movat
pentachrome (specific for elastic fibers), Masson and Picrosirius Red. The last two staining methods are specific to evaluate collagen deposition. A stained section
for each rabbit was then photographed (software Mirax Viewer®, Carl Zeiss
MicroImaging GmbH). Using 20x augment 4 sections were selected for elastin fibers
counting and tissue description, starting from the mucosa inwards: area 1: median
dorsal, areas 2 and 4, lateral; area 3: median ventral (Figure 2). The selected areas
were uploaded for manual counting of elastic fibers using grid mask tool, spaced 40 x
40 (software Image-Pro Plus® Version 4.5.0.29 for Windows 98/NT/2000, Media
Cybernetics Inc.).
Another urethral segment was used for PCR. The tissue was washed with
saline, immediately frozen in dry ice and kept in -8oC freezer. Measurement of collagen
mRNA was done for collagens I, III, IV, VI, VIII and XIII. RNA corresponding to each
collagen was obtained by using oligoDT primers and reverse transcriptase
(Invitrogen®). The primers were custom-designed and tested before usage. DNA was
induced with TRIzol® solution. Normalization of the results used the reference genes b
actin and HPRT. Amplification was counted with fluorescence (SYBRgreen), with 90-
110% efficiency.
The third segment of the specimen was preserved for future evaluations with
other methods, if pertinent.
Correlation analyses were done with Spearman test. Non-parametrical variance
analyses were also used (Wilcoxon between groups and Kruskall-Wallis inside
groups)(Software R, The R Foundation for Statistical Computing, Vienna, Austria,
version 2.15.1). p values < 0.05 were considered significant.
RESULTS:
All animals were operated uneventfully, without perioperative deaths. One
animal (G3) died in 19th post-operative day and was excluded. Its necropsy did not
reveal any problems related to the urethral surgery. There were no urethral fistulae or
stenoses in G2 and G3 animals. Three animals from G1 and 2 from G3 were excluded
because of problems with identification and preservation of the specimens. One animal
from G1 and another from G3 were also excluded because appropriate slides for
elastic fibers counting could not be obtained (Figure 3). As reported on reference 6,
there were no significant differences in segmental urethral compliance between groups 6.
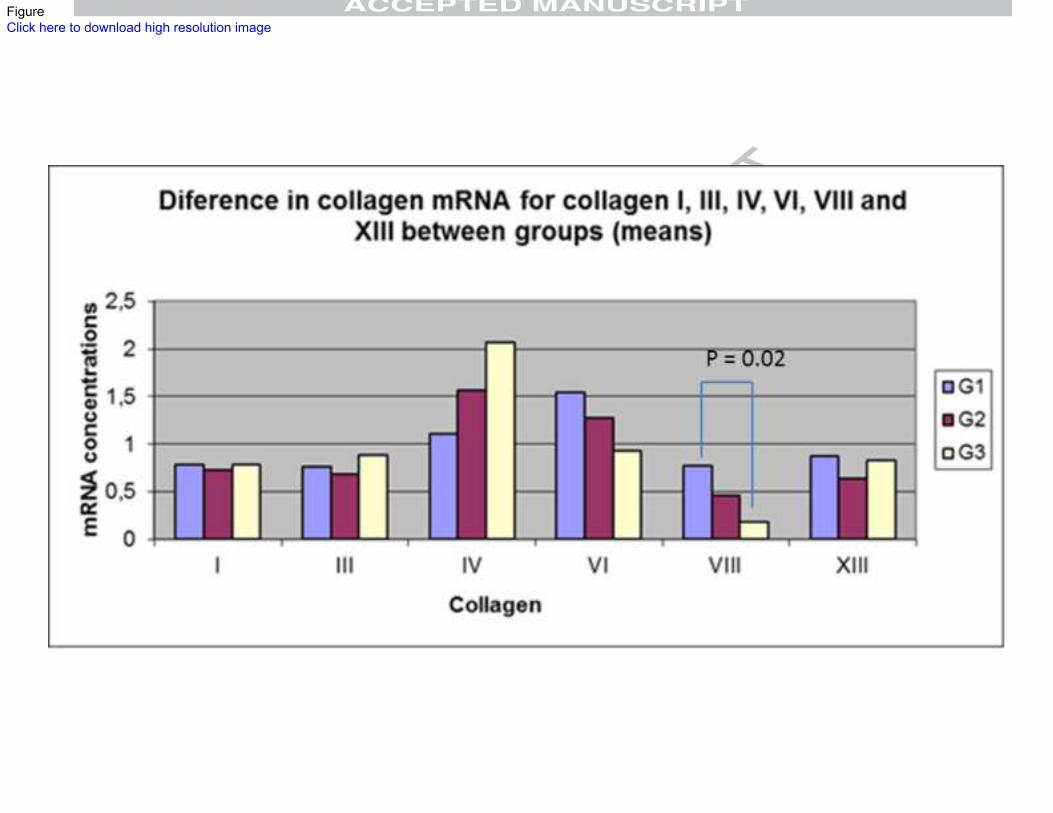
One animal was excluded for Collagen XIII analysis by technical criteria
(outlier). mRNA expressions for collagens I, III and XIII were similar between groups.
Expressions for collagen VI and VIII were lower in the operated animals (G1>G2>G3).
Collagen IV mRNA was higher in the operated animals (G1<G2<G3) (figure 4). The
difference for collagen VIII between G1 and G3 was significant (p=0.02), but
differences were not significant between G1 and G2 (p=0.33) or G2 and G3 (p=0.48).
The proportions between collagens I/III differed between groups (1.05, 1.21 and 0.87
for G1, G2 and G3, respectively).
G2 and G3 urethras showed ventral fibrosis, disorganization and dispersion of
muscle fibers, corresponding to the tubularization sutures. All grafts were taken in G3 rabbits. Those animals showed fibrosis corresponding to the area of the graft. G2
animals did not show signs of cicatrization/fibrosis in the dorsal area, suggesting that
regeneration occurs in the area of the dorsal incision in our TIP model (figure 5).
G1 animals showed more elastic fibers in the ventral than in the dorsal part of
the urethra (normal pattern for the species). Histomorphometry showed that the
number of elastic fibers were comparable between groups (p> 0.05 for all
comparisons)(figure 6).
DISCUSSION:
Urethral healing after TIP seems to occur by centripetal progressive
epithelialization and is not related to higher total concentrations of collagen or
discernible fibrosis in various hypospadias models, by histological, histomorphometrical
and/or biochemical methods 3-5. Our group has also demonstrated the absence of
significant fibrosis after TIP in the same model used in this research 2. Our findings
demonstrated that acute post-operative tissue responses had subsided after 6 weeks,
which bases our choice of this interval for urethral harvest 2.
The absence of fibrosis in TIP models suggests similar concentrations of
structural collagens (I/III) as compared to normal controls, but different concentrations
of other collagens, which have diverse functions and present in much lower tissular
concentrations, may present. Different concentrations of non-structural collagens could
explain different tissular biophysical characteristics by modulating ECM components.
Alternatively, varying proportions between collagens I and III may modify elastic
properties and justify divergent biophysical tissular responses.
Specific collagens have distinct biological functions related to modulation of
tissue metabolism, reconstruction, angiogenesis, healing and remodeling processes,
programmed by complex interactions with cell receptors and ECM components,
including biophysical signaling. Besides the concentration of the protein per se, the
three-dimensional collagen architecture contributes to mechanical tissue properties.
We chose to study collagens related to tissue structure (fibril forming – I and III,
microfibrilar - VI and short chain - VIII), basal membrane (collagen IV) and a
transmembrane regulator (XIII). Collagens I and III directly relate to tissue biophysical
properties, collagens VI and VIII are thought to be fibrogenic through fibroblasts
recruiting, collagen IV is the most important structural component of basal membranes
and collagen XIII regulates growth and regenerative tissular processes 7-9.
Collagen I:III proportion increases in the initial phases of urethral healing 4.
Collagen III is abundant in elastic tissues and visceral reticular fibers, possibly relating
to elasticity and organization of elastic fibers 7, 10. Baskin et al suggest that the normal
human urethra is composed by 75% collagen I and 25% collagen III, while in strictured
urethras the proportion was 83% collagen I vs 16% collagen III 11. In our model,
involving animals without stenoses in a late phase of healing, the mean proportions of
mRNA for collagen I:III were 1.05 (controls), 1.21 (TIP) and 0,87 (TIPG), suggesting
that maybe TIP increases and TIPG decreases collagen I:III proportion. Contrastingly,
Hayashi et al assert that collagen III is absent in urethral plates. Interpreting these
opposite results is difficult, as their paper evaluate real human urethral plates in
prepubertal children and use immunohistochemistry to map collagen distributions,
while our study deals with normal urethras in rabbits and estimates collagen
concentrations with PCR, without dealing with tissular architectural distribution of the
protein 12.
Collagen IV RNA was higher in the experimental groups, predominating in TIPG
animals. In their paper Hayashi et al 12 studied collagen IV distribution in biopsies taken
from the tissue between the urethral plate and the adventitia of the corpora in human
children and suggest that collagen IV is restricted to basal membranes of the
capillaries. However, collagen IV has been described in the basement membrane of
the urothelium and detrusor muscle by other authors 13, that related focal losses of
collagen IV reactivity to inflammation, dysplasia and non-invasive bladder cancer 14. It
is possible that the restricted distribution of collagen IV described by Hayashi et al 12 is
due to the restricted biopsies taken, which did not include urethral epithelium.
In our research collagen VI mRNA expression tended to be lower in the
experimental groups. This collagen is ubiquitous and forms networks linking either cells
and basement membranes to the matrix or collagen I and III fibrils to the basement
membranes, suggesting an important role in regulation of tissular architecture. In
humans it stimulates fibroblast proliferation and is upregulated in skin from 3 days after
tissue trauma, persisting during the late healing phase, possibly with an active role in
fibrogenesis 15.
Collagen VIII may be related to ECM stabilization,16 active remodelling, myocyte
migration and dedifferentiation into fibroblasts17-18. Data suggest that it is actively
secreted by myocytes in the remodelling processes of biological tubes (vessels and
bronchi) exposed to intermittent continued mechanical stresses and in tissue trauma 18-
19. We did not expect this collagen to be lower in the experimental groups, especially in
TIPG models, considering its role in remodelling and fibroblasts recruiting. Lower
synthesis of type VIII collagen may be due to a lower number of myocytes in our
model, which could modify tissue remodelling after trauma. Assessing the differential
cell populations in the wounds may help to find an explanation for the lower levels of
collagen VIII in the operated animals in the near future.
Concerning elastic fibers, our intention was to estimate the number and
distribution of mature fibers, reflecting the effective elasticity of the tissue and excluding
non-functional elastin (elastosis). This is the reason for us to choose direct counting of
the fibers instead of measurement of elastin. We opted for manual grid counting in
order to eliminate errors that could happen because of wrong automatic counting of
other deep dark structures (such as cell nuclei) by software automatic systems after
Movat’s dyeing method.
Tissular compliance combines resilience, deformability and morphological stability
and involves interactions between elastin and collagen, as well as their tridimensional
distribution. The system is dynamic and interactions between ECM, cells and
mechanical stimuli modulate tissue conformation. Elastic fibers are essential in organs
that suffer periodic changes in shape, such as the male urethra, periodically distended
and elongated for micturition and erections.
Urethral connective tissue contains abundant elastin fibers distributed in the ECM
and forming a net. The urethral submucosa shows the highest volumetric proportion
between elastic fibers/tissue among all human tissues 20. Elastic fibers are long,
numerous and tortuous, distributing mainly in the spongiosum and immediately
beneath the basement membrane 21-22. Human fetuses show progressive accumulation
of elastin fibers from the second trimester to term: the number, size and thickness of
elastic fibers increase almost 4 times from the fetal 2nd trimester to the adult.
Interestingly, the concentration of elastic fibers in the adult is 1,3x higher than in term
fetuses, implying that some effective elastogenesis occurs after birth 21.
Studies about elastic fibers distribution in the urethra are rare. Most of the
information available concerns the cavernosum and spongiosum bodies and deal with
erection mechanisms. To the best of our knowledge, there are no published papers
concerning the relationship between elastin fibers and micturition.
Our results confirm a lower concentration of elastin fibers in the dorsal urethra of
the normal rabbits. Elastin fibers countings were comparable between the groups,
implying that elastic fibers loss may not be the explanation for the post-operative
biomechanical problems.
The absence of spongiosum influences the determination of the biomechanical
properties of neourethras constructed to treat hypospadias, but we were unable to find
data comparing urethral function with or without spongioplasty. Our model does not
consider that specific aspect, as it departs from normal urethras that are not devoid of
spongiosum.
Our paper has several limitations:
1. Our experimental model, in spite of being well accepted for
hypospadias surgery, is carried out in adult rabbits, which urethras
are anatomically different from human counterparts and were
exposed to androgenic stimuli. Besides, the reconstructions are done
in urethral remnants, which are not real hypospadiac urethral plates.
These limitations are also present in other experimental research
papers dealing with hypospadias, as there is still no easily available
and predictable animal model of congenital hypospadias.
2. Assessment of elastin fibers in a unidimensional frame and
measurement of collagen concentrations do not show the tissular
tridimensional structure, which may be important in biomechanical
functions.
3. Although there are no published data specifically concerning the
urethra, the collagen structure of the penis changes with maturation
and age 23. It is possible that some of our findings would be different
in immature animals, especially concerning collagen XIII, which
overexpresses in immature and growing tissues 9.
4. Our study looked at quantitative mRNA expression for collagen,
which may differ from final protein expression, despite a direct
relationship between mRNA and final protein concentrations being
expected.
Future research regarding specific collagens tissular distribution by
immunohistochemistry would be a further step to explain the relationship between
tissular proteins, collagen and biophysical properties of the virgin and post-operated
urethra, by showing the architectural pattern of distribution of different types of
collagen. Also, studying the cell populations in each model, especially myofibroblasts
and myocytes, could help to understand different circumstantial patterns of collagen
secretion.
CONCLUSIONS:
Lower concentrations of elastic fibers does not explain lower urethral compliances
after TIP surgery in this model. The dorsal urethral segment regenerated after TIP
incision, but healing with fibrosis occurred in the ventral sutured areas in the operated
animals and grafted areas after TIPG surgery.
REFERENCES:
1. Snodgrass, W. Tubularized incised plate for distal hypospadias. J Urol 1994, 151(2):464-5.
2. Leslie, B; Jesus, LE; ElHout, Y et al. Comparative histological and functional analysis of tabularized incised plate urethroplasty with and without dorsal inlay graft: a preliminary experimental study in rabbits. J Urol 2011, 186(4 suppl):1631-7.
3. Bleustein, CB; Esposito, MP; Soslow, RA et al. Mechanism of healing following the Snodgrass repair. J Urol 2001, 165:277-9.
4. Taneli, F; Ulman, C; Genc, A et al. Biochemical analysis of urethral collagen after tubularized incised plate urethroplasty: an experimental study in rabbits. Urol Res 2004, 32:219-22.
5. Somuncu, S; Caglayan, O; Cakmak, M et al. The effect of indwelling catheter on OH-proline in the urethral wound: an experimental study. J Pediatr Urol 2006, 2:182-4.
6. Jesus, LE; Schanaider, A; Patterson, G et al. Urethral compliance in hypospadias operated by tubularized incised urethral plate (TIP) with and without a dorsal inlay graft: an experimental controlled study. World J Urol 2013, 31:971-5.
7. Gelse, K; Poschl, E; Aigner, T. Collagens: structure, function and biosynthesis. Adv Drug Delivery Ver 2003, 55:1531-46.
8. Gordon, MK; Hahn, RA. Collagens. Cell Tissue Res 2010, 339:247-57.
9. Hiekkinen, A; Tu, H; Pihlajaniemi, T. Collagen XIII: a type II transmembrane protein with relevance to musculoskeletal tissues, microvessels and inflammation. Int J Biochem Cell Biol 2012, 44:714-7.
10. von der Mark, K. Localization of collagen types in tissues. Tissue Res 1981; 9:265-34.
11. Baskin, LS; Constantinescu, SC; Howard, OS et al. Biochemical characterization and quantitation of the collagenous components of urethral stricture tissue. J Urol 1993, 150:642-7.
12. Hayashi, Y; Mizuno, K; Kojuma, Y et al. Characterization of the urethral plate and the underlying tissue defined by expression of collagen subtypes and microarchitecture in hypospadias. Int J Urol 2011, 18(4):217-22.
13. Borza, DB; Bondar, O; Ninomiya, Y et al. The NC1 domain of collagen IV encodes a novel network composed of the alpha 1, alpha 2, alpha 5 and alpha 6 chains in smooth muscle basement membranes. J Biol Chem 2001, 276(30):28532-40.
14. Deen, S; Ball, RY. Basement membrane and extracellular interstitial matrix components in bladder neoplasia – evidence of angiogenesis. Histopathology 1994, 25(5):475-81.
15. Oono, T; Specks, U; Eckes, B et al. Expression of type VI collagen mRNA during wounk healing. J Investig Dermatol 1993, 100(3):329-34.
16. MacBeath, JR; Kielty, CM; Shuttleworth, CA. Type VIII collagen is a product of vascular smooth-muscle cells in development and disease. Biochem J 1996, 319(pt3):993-8.
17. Cherepanova, OA; Pidkovka, NA; Sarmento, OF et al. Oxidized phospholipids induce type VIII collagen expression and vascular smooth cell migration. Circ Res 2009, 104(5):609-18.
18. Hou, G; Mulholland, D; Gronska, MA et al. Type VIII collagen stimulates smooth muscle cell migration and matrix metalloproteinase synthesis after arterial injury. Am J Pathol 2000, 156(2):467-76.
19. Hasaneen, NA; Zucker, S; Lin, RZ et al. Angiogenesis is induced by airway smooth muscle strain. Am J Physiol Lung Cell Mol Physiol 2007, 293(4):L1059-68.
20. Testut, L. Traité d’anatomie humaine. Octave Doin et Fils, Paris, 1912, 16 ed, v4. p 507-534; 627-30.
21. Bastos, AL; Silva, EA; Costa, WS et al. Concentration of elastic fibers in the male urethra during human fetal development. Br J Urol 2004, 94:620-3.
22. Hsu, GL; Brock, A; Von Heyden, B et al. The distribution of elastic fibrous elements within the human penis. Br J Urol 1994, 73:566-71.
23. Goldstein, AM; Meehan, JP; Morrow, JW et al. Ultrastructural changes in impotent penile tissue; comparison of 65 patients. J Urol 1991, 145:749-58.

Figure 1: A: Markings for the urethral reduction (degloved penis); B: TIP model, pre‐tubularization; C: TIPG model, pre‐tubularization.
Figure 2: Areas selected for histological description and elastic fibers histomorphometry.
Figure 3: Description of the cohort and exclusions.
Figure 4: PCR results for collagen mRNAs (means). The only statistically significant difference found (collagen VIII, comparing G1 and G3) is marked in the graph.
Figure 5: Panoramic views of the urethras. The arrows show fibrotic areas on the dorsal urethra, corresponding to the areas where the grafts were inserted. CB = cavernosum body; VU = ventral urethra.
Figure 6: Elastic fibers countings.
ABBREVIATIONS:
TIP: tubularized incised plate urethroplasty
CC: corpus cavernosum
TIPG: tubularized incised plate urethroplasty with inlay preputial graft
ECM: extracellular matrix
*Key of Definitions for Abbreviations (only include abbreviations used 3 times or more in manuscript)

Figure 1Click here to download high resolution image
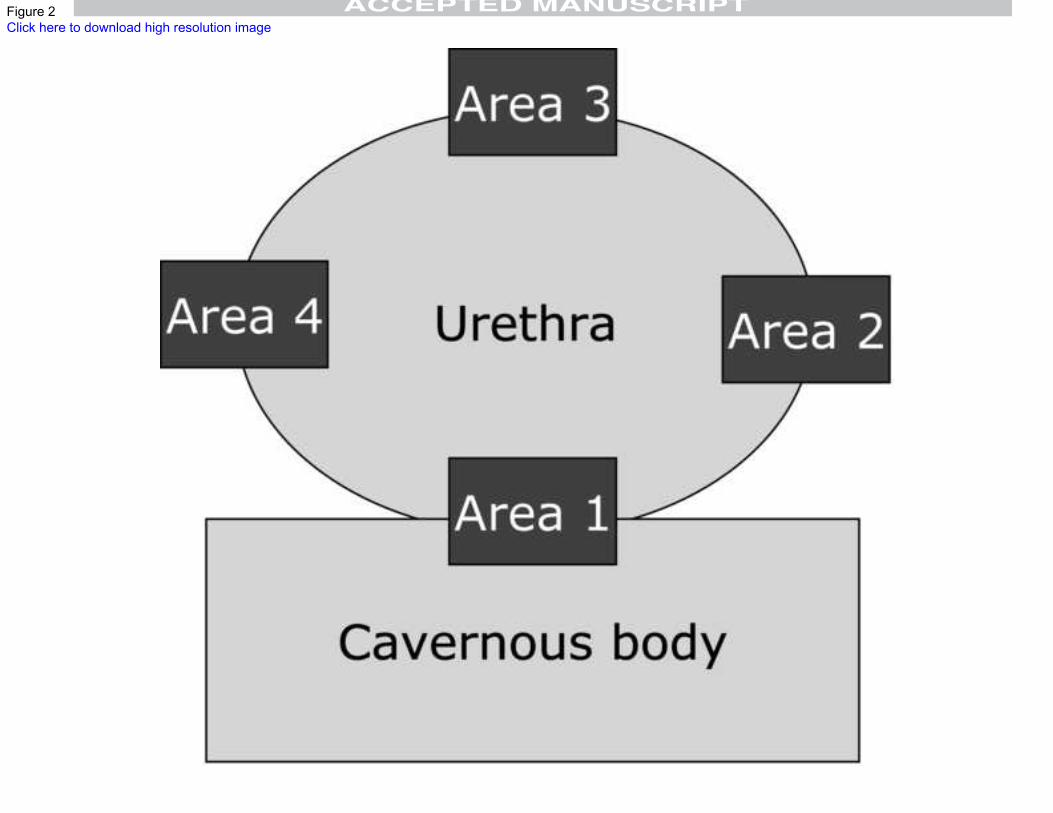
Figure 2Click here to download high resolution image
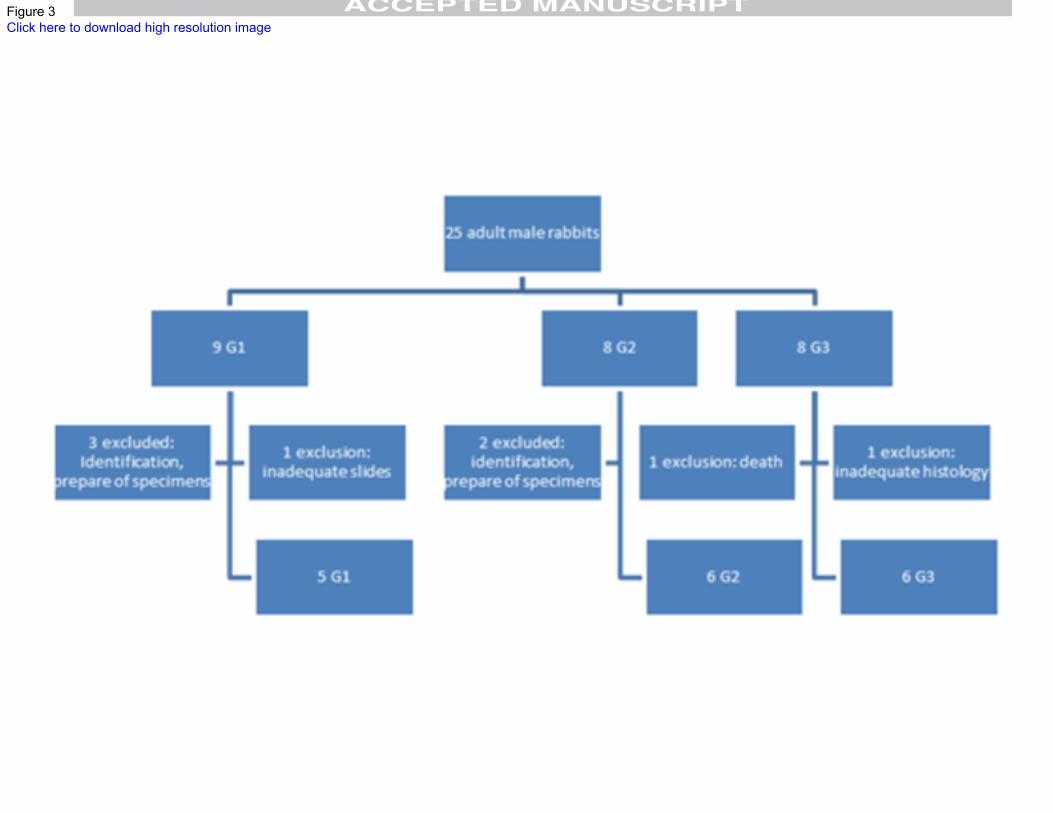
Figure 3Click here to download high resolution image
FigureClick here to download high resolution image
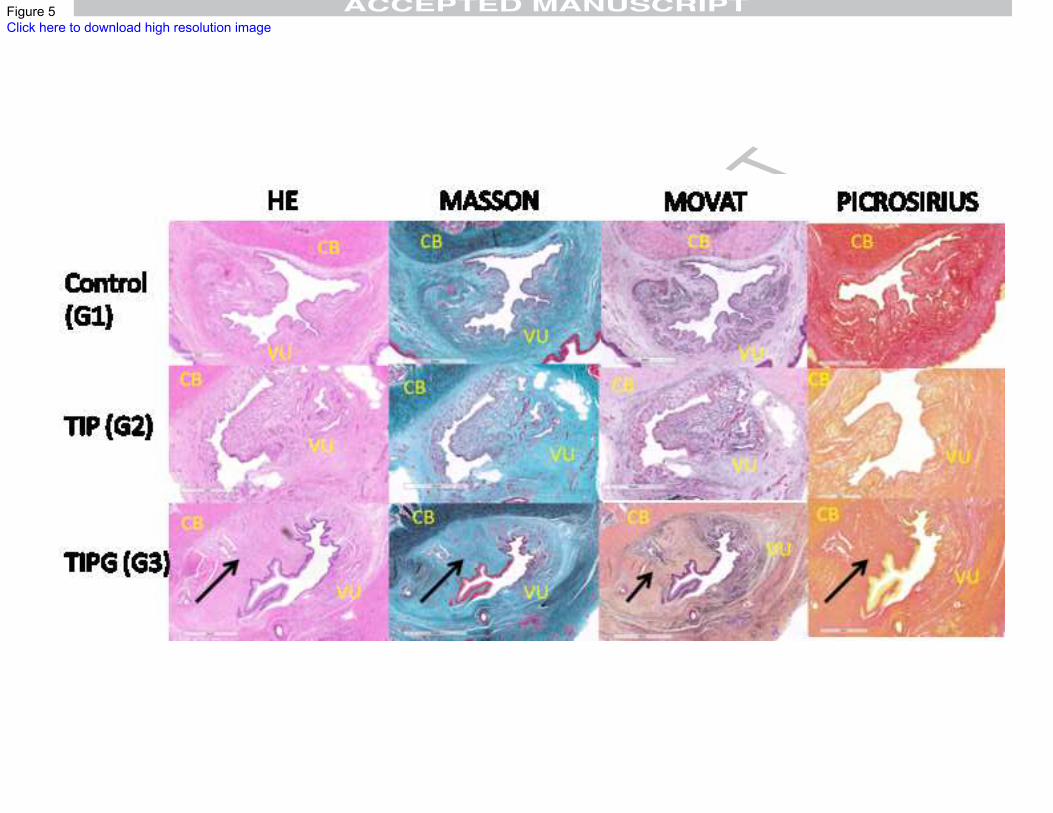
Figure 5Click here to download high resolution image
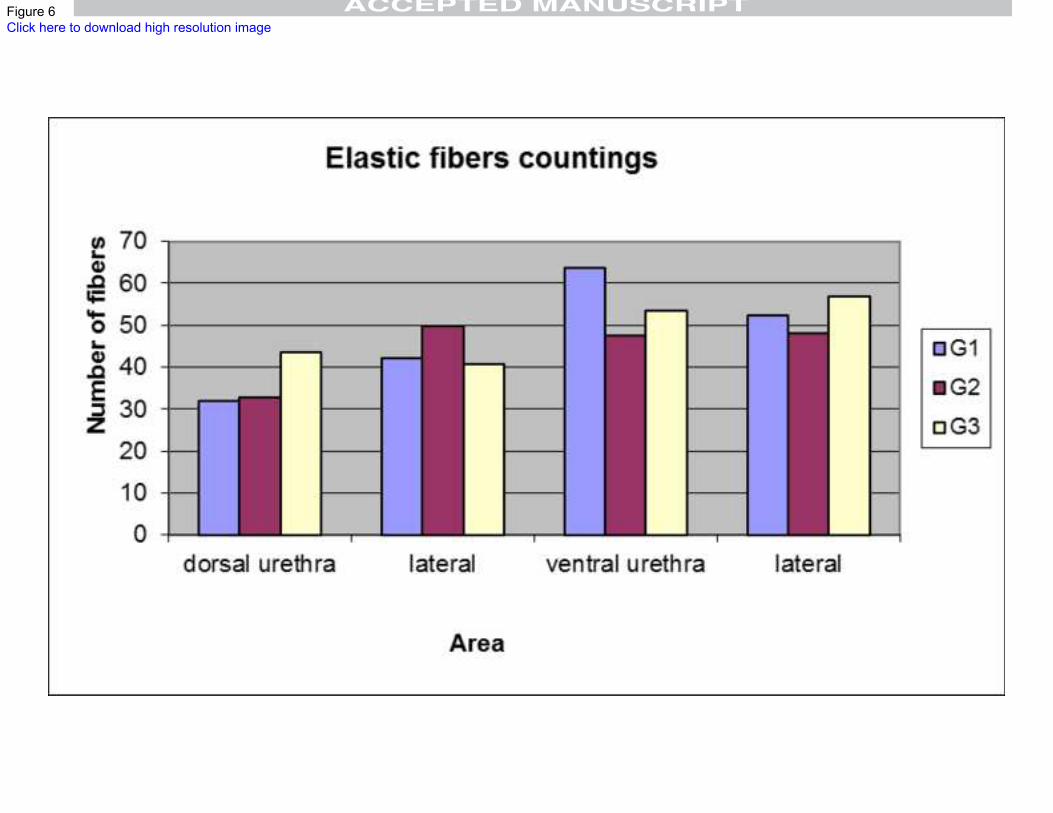
Figure 6Click here to download high resolution image





























