Embed Size (px)
Citation preview

Thorax 1996;51:841-845
Computed tomography-guided bronchoalveolarlavage in idiopathic pulmonary fibrosis
C Agusti, A Xaubet, P Luburich, MC Ayuso, J Roca, R Rodriguez-Roisin
AbstractBackground - High resolution computedtomography (HRCT) is now recognised asa sensitive tool for predicting the histo-logical characteristics of the lung paren-chymal abnormalities in patients with idi-opathic pulmonary fibrosis (IPF). Areticular pattern on HRCT scanning isindicative of fibrotic histology while aground glass pattern has been associatedwith inflammatory disease. The purposeof the present study was to investigatewhether the cell population in the bron-choalveolar lavage (BAL) fluid from dif-ferent lobes differs according to HRCTcharacteristics in patients with IPF.Methods - Twenty six patients with IPF (18men) of mean (SE) age 67 (2) years wereincluded in the study. A semiquantitativeanalysis of the extent of the abnormalitieson the HRCT scan was applied by summingthe proportion ofboth reticular and groundglass patterns in each lobe (expressed aspercentage of total area evaluated) and100 ml double BAL was then randomly per-formed in the lobe with the most extensiveinvolvement (lobe A) and that with the leastextensive involvement (lobe B).Results - Twenty three of the 26 patients(88%) had an abnormal cell count in theBAL fluid from lobe A compared with 18patients (69%) with abnormalities in theBAL fluid from lobe B. The median(range) percentage of 8.5% (0-34%) andthe absolute numbers ofneutrophils (1.3 x104iml, 0-14.6 x 104/ml) in lobe A were sig-nificantly higher than those in lobe B (5%(0-26%) and 1.2 x 104/ml (0-5 x 104/ml),respectively). The percentage (3%, 0-19%)and absolute numbers (0.65 x 104/ml, 0-4 x104/ml) of eosinophils were also higher inlobe A than in lobe B (1% (0-12%) and 0.1x 104/ml (0-4.8 x 104/ml), respectively). Forthe group as a whole a correlation wasfound between the percentage and abso-lute numbers of neutrophils in the BALfluid and the total score of abnormalitieson the HRCT scan in the most involvedlobe (lobe A). Multiple regression analysisindicated that both the percentage andabsolute numbers ofneutrophils were sig-nificantly and independently related to theextent of ground glass pattern.Conclusions - In patients with IPF thecell population in the BAL fluid is nothomogeneous and seems to be related tothe characteristics ofthe abnormalities onthe HRCT scan present in the lavagedlobe.(Thorax 1996;51:841-845)
Keywords: alveolitis, high resolutioninterstitial lung fibrosis.
CT scanning,
Idiopathic pulmonary fibrosis (IPF) is achronic progressive disorder of the lung paren-chyma manifested by both inflammation (al-veolitis) and fibrosis.' There is ample evidenceto suggest that alveolitis is the earliest manifes-tation of IPF since its cells are responsible forthe derangement of the connective tissuematrix and the subsequent development offibrosis.2" Bronchoalveolar lavage (BAL) pro-vides a safe, repeatable, and minimally invasivemethod of sampling inflammatory cells of thelungs.5 Several reports have suggested that theanalysis of the cellular constituents retrievedfrom BAL fluid could provide informationregarding the inflammatory activity of the dis-ease and therefore the prognosis.5"14 Broncho-alveolar lavage has usually been performed onthe middle lobe or lingula in patients with IPF,although some authors prefer the right lowerlobe as IPF predominantly affects the bases ofthe lung.9 10 A major concern related to the useof BAL in IPF is whether lavaging one lobe isrepresentative of the interstitial lung disorder,based on the assumption that the inflammatoryprocess is uniform throughout the lung paren-chyma. It is clear from ventilation-perfusionscanning, gallium-67 scans, and open lungbiopsies that inhomogeneity of lung involve-ment frequently occurs, some studies havingshown a lack of uniformity of cells in BAL fluidfrom different lung zones.15 Thus, the resultsobtained with BAL may misrepresent thedegree of underlying interstitial inflammationby sampling a relatively non-involved area oflung. 16
High resolution computed tomography(HRCT) is now recognised as a sensitivemeans of identifying disease in IPF.'7 Differentstudies have shown that the appearance of theHRCT scans can predict histological patternsmade evident in open lung biopsy specimens.Both reticular and honeycombing patternscorrelate with fibrosis, whereas a ground glasspattern identifies zones of alveolar and intersti-tial inflammation.'8-20The capacity of the HRCT scan to reflect
the histopathological substrate of the lungparenchyma in IPF may help to define the roleofBAL in this disease. It is our contention thatthe characteristics of the cell population in theBAL fluid may differ according to the extentand type of abnormalities of the lavaged lobe.To investigate this hypothesis we have applied asemiquantitative analysis of the extent of theabnormalities on the HRCT scan and per-formed a double BAL - one in the lobe with
Servei de Pneumologiai Al.lergia Respiratoriaand Servei deRadiodiagnostic,Departament deMedicina,Hospital Clinic,Universitat deBarcelona,Barcelona, SpainC AgustiA XaubetP LuburichMC AyusoJ RocaR Rodriguez-Roisin
Correspondence to:Dr A Xaubet, Servei dePneumologia, HospitalClinic, Villarroel 170,Barcelona 08036, Spain.
Received 30 August 1995Returned to authors5 December 1995Revised version received6 February 1996Accepted for publication14 February 1996
841
group.bmj.com on July 15, 2011 - Published by thorax.bmj.comDownloaded from

Agusti, Xaubet, Luburich, Ayuso, Roca, Rodriguez-Roisin
the most prominent pulmonary abnormalitiesand the other in the least extensively involvedlobe. The aims of the present study were toestablish whether cell populations retrievedfrom BAL fluid from these two lung zones were
comparable and to determine the relationshipsbetween the cell population in the BAL fluidand the characteristics of the HRCT scan.
MethodsPATIENTSThe population studied comprised 26 con-
secutive patients (18 men) ofmean (SE) age 67(2) years (range 49-88). Seven were smokers,two had ceased smoking at least five yearsbefore entry into study, and the remaining 17patients had never smoked. All patients had a
cough and 23 had some degree of dyspnoea,with a duration of symptoms of 11 (2) months(range 0-36). Bilateral widespread crackleswere heard in all patients and chest radiogra-phy showed bilateral interstitial infiltrates in allcases. The diagnosis of IPF was established byopen lung biopsy in eight cases (31%). Forthose 18 patients without histological confir-mation of the disease two conditions were
required for the diagnosis: (1) to fulfil the clini-cal criteria described by Turner-Warwick et al4which we have used previously2'l 22 and (2) todisplay findings compatible with IPF on theHRCT scan.23 24 At the time of the study noneof the patients had received glucocorticoids or
immunosuppressive therapy. The study was
performed as part of the current diagnosticassessment and outpatient monitoring forinterstitial lung diseases in our centre.2' Allpatients were informed of the nature of thestudy and gave full written informed consent.The study was approved by the ethicscommittee of the Hospital Clinic.
PULMONARY FUNCTION TESTSSpirometric tests (Stead-Wells spirometer, WECollins, Baintree, Massachusetts, USA), tho-racic gas volume and airway resistance (MedGraphics System 1085, St Paul, Minnesota,USA), single breath carbon monoxide transferfactor (TLCO) (Respirameter model A; PKMorgan, Chatham, Kent, UK), and arterialblood gases at rest while breathing room air (IL1302 Instrument Laboratories, Milan, Italy)were measured. The alveolar-arterial oxygentension difference (A-aPo2) was calculatedaccording to the standard formula assuming a
respiratory exchange ratio (R) of 0.80. The ref-erence values used were those from our own
laboratory.25 26 One patient was unable toperform pulmonary function tests due to seniledementia. TLCO was not performed in 12patients and total lung capacity (TLC) in ninebecause of severe reduction of lung volumesand/or lack of cooperation.
HIGH RESOLUTION CT SCANNINGComputed tomographic scans were performedin either a Somaton HiQ or a Somaton Plusscanner (Siemens, Erlanger, Germany). Allpatients underwent conventional computedtomographic scanning of the chest using a 10mm section thickness at 12 mm intervals.
HRCT scans were obtained at six predeter-mined levels: the great vessels, the aortic arch,the tracheal carina, the pulmonary hilae, thepulmonary venous confluence, and 1 cm abovethe right diaphragm. The scans were per-formed with a 1-2 mm section thickness and a1-2 second scanning time during breath hold-ing at the end of inspiration. These scans werereconstructed with a high spatial frequencyalgorithm and viewed at window levels appro-priate for pulmonary parenchyma (mean -500to -600 Hounsfield units; width 1400-1600Hounsfield units).Two radiologists (PL and MCA), without
knowledge of any of the clinical, functional andradiographic findings, examined the HRCTscans. The overall extent of lobar abnormalitieswas scored and a semiquantitative analysis ofthe relative proportion (to within 10%) of boththe ground glass and the reticular patterns wasperformed. By consensus, two pulmonarylobes were selected - the one with the mostextensive involvement (lobe A) and that withthe least extensive involvement (lobe B).
BRONCHOALVEOLAR LAVAGEBronchoalveolar lavage was performed byfibreoptic bronchoscopy as previously de-scribed.27 28 A 100 ml lavage of sterile salinesolution was performed at random in both thepulmonary lobe with the most extensiveinvolvement (lobe A) and the one less exten-sively involved on HRCT scanning (lobe B).The total cell count was obtained using aNeubauer s chamber and the cell viability wasassessed by trypan blue dye exclusion. Differ-ential cell counts were determined in cytocen-trifuge smears (Cytospin 3, Shandon) stainedwith May-Griinwald Giemsa. In our labora-tory, BAL differential cell counts are consid-ered abnormal if lymphocytes are > 12%,neutrophils > 3%, and eosinophils > 1%.Pulmonary function tests, HRCT scans, and
BAL were performed sequentially at the timeof clinical diagnosis and all three procedureswere carried out during an interval of less thanone week.
STATISTICAL ANALYSISWilcoxon's test was used for comparison ofpaired data and Mann-Whitney's test forunpaired data. Spearman's correlation coeffi-cients were used for correlation analyses. Amultivariate stepwise regression model wasused to identify independent determinants ofreticular and ground glass patterns on HRCTscans, taking the percentage and absolutenumbers of the different BAL cell typesseparately as a dependent variable. Whenappropriate, a logarithmic transformation(base 10) was used to normalise BAL cell dis-tribution. Statistical significance was estab-lished as p < 0.05.
ResultsLUNG FUNCTION STUDIESAll patients had a moderate to severe restrictiveventilatory impairment according to spiromet-ric tests and all but five had a TLC below 80%predicted (table 1). TLCO was below the lower
842
group.bmj.com on July 15, 2011 - Published by thorax.bmj.comDownloaded from
High resolution CT scanning in lungfibrosis
Table 1 Mean (SE) pulmonary function test results (with range of values) of thepopulation studied
Actual values % predicted
FVC (1) 2.2 (0.2) (0.9-4.3) 59 (3) (28-93)FEV1 (1) 1.8 (0.1) (0.9-3.4) 69 (3) (36-97)FEV,/FVC (%) 85 (4) (71-99)TLC (1) 4.4 (0.2) (3.3-7) 75 (4) (44-107)TLCO (ml/min/mm Hg) 13 (1) (6-9) 54 (4) (26-82)Kco (ml/min/mm Hg/mm) 3.9 (0.3) (2.4-6) 78 (6) (51-131)pH 7.41 (0)Pao2 (kPa) 9.3 (0.3) (4.1-11.9)Paco2 (kPa) 4.5 (0.5) (4.2-5.9)A-aPo0 (kPa) 4.9 (2.2) (1.9-9.9)
FVC = forced vital capacity; FEVy = forced expiratory volume in one second; TLC = total lungcapacity; TLCO = carbon monoxide transfer factor; Kco = carbon monoxide transfer coefficient;Pao2, Paco2 = arterial oxygen and carbon monoxide tensions; A-aPo2 = alveolar-arterial oxygentension difference.
limit of reference (80% predicted) in all butone patient, while the transfer coefficient(Kco) was below 80% predicted in seven.Arterial blood gases were performed in all butone patient. Arterial hypoxaemia (Pao2 < 10.7kPa) was present in 18 patients whilst theA-aPo2 was increased ( > 2.7 kPa) in 22.
BAL CELL ANALYSISTable 2 shows the lobes selected for perform-ing BAL, the individual differential cell countsin the BAL fluid, and their respective HRCTscoring analysis. As shown, BAL was per-formed on opposite lungs in 18 patients (69%)and in the same lung in eight cases (31%).The BAL differential cell count was normal
in three of the 26 patients (12%) in lobe A (nos20, 23 and 25, table 2) and in eight (31%) inlobe B (nos 6, 9, 13, 16, 17, 20, 24 and 25,table 2). Individually, the percentages oflymphocytes, neutrophils, and eosinophilswere above normal limits in three (12%), 20(77%), and 18 (69%) patients, respectively, inlobe A and in two (8%), 17 (61%), and nine(35%) patients, respectively, in lobe B.
40 r
a)
0
r=0-68p = 0-0001
30
0
0 0
* *
0
10
0
.-Qo.
_
* 0
0
0
0
0
0
0
*
*
0
0 20 40 60 80 100% of area of HRCT involvement
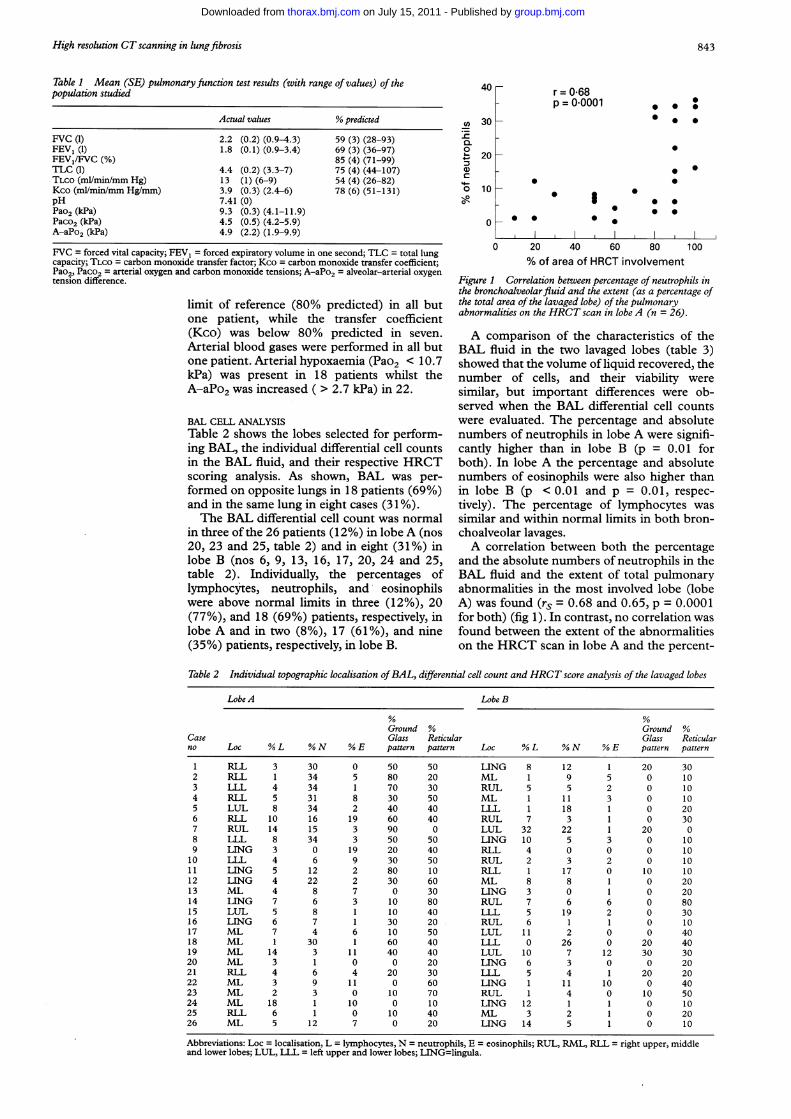
Figure 1 Correlation between percentage of neutrophils inthe bronchoalveolarfluid and the extent (as a percentage ofthe total area of the lavaged lobe) of the pulmonaryabnormalities on the HRCT scan in lobe A (n = 26).
A comparison of the characteristics of theBAL fluid in the two lavaged lobes (table 3)showed that the volume of liquid recovered, thenumber of cells, and their viability were
similar, but important differences were ob-served when the BAL differential cell countswere evaluated. The percentage and absolutenumbers of neutrophils in lobe A were signifi-cantly higher than in lobe B (p = 0.01 forboth). In lobe A the percentage and absolutenumbers of eosinophils were also higher thanin lobe B (p < 0.01 and p = 0.01, respec-tively). The percentage of lymphocytes wassimilar and within normal limits in both bron-choalveolar lavages.A correlation between both the percentage
and the absolute numbers of neutrophils in theBAL fluid and the extent of total pulmonaryabnormalities in the most involved lobe (lobeA) was found (rs = 0.68 and 0.65, p = 0.0001for both) (fig 1). In contrast, no correlation wasfound between the extent of the abnormalitieson the HRCT scan in lobe A and the percent-
Table 2 Individual topographic localisation ofBAL, differential cell count and HRCT score analysis of the lavaged lobes
Lobe A Lobe B
Ground % Ground %Case Glass Reticular Glass Reticularno Loc % L % N % E pattern pattern Loc % L % N % E pattern pattern
1 RLL 3 30 0 50 50 LING 8 12 1 20 302 RLL 1 34 5 80 20 ML 1 9 5 0 103 LLL 4 34 1 70 30 RUL 5 5 2 0 104 RLL 5 31 8 30 50 ML 1 11 3 0 105 LUL 8 34 2 40 40 LLL 1 18 1 0 206 RLL 10 16 19 60 40 RUL 7 3 1 0 307 RUL 14 15 3 90 0 LUL 32 22 1 20 08 LLL 8 34 3 50 50 LING 10 5 3 0 109 LING 3 0 19 20 40 RLL 4 0 0 0 1010 LLL 4 6 9 30 50 RUL 2 3 2 0 1011 LING 5 12 2 80 10 RLL 1 17 0 10 1012 LING 4 22 2 30 60 ML 8 8 1 0 2013 ML 4 8 7 0 30 LING 3 0 1 0 2014 LING 7 6 3 10 80 RUL 7 6 6 0 8015 LUL 5 8 1 10 40 LLL 5 19 2 0 3016 LING 6 7 1 30 20 RUL 6 1 1 0 1017 ML 7 4 6 10 50 LUL 11 2 0 0 4018 ML 1 30 1 60 40 LLL 0 26 0 20 4019 ML 14 3 11 40 40 LUL 10 7 12 30 3020 ML 3 1 0 0 20 LING 6 3 0 0 2021 RLL 4 6 4 20 30 LLL 5 4 1 20 2022 ML 3 9 11 0 60 LING 1 11 10 0 4023 ML 2 3 0 10 70 RUL 1 4 0 10 5024 ML 18 1 10 0 10 LING 12 1 1 0 1025 RLL 6 1 0 10 40 ML 3 2 1 0 2026 ML 5 12 7 0 20 LING 14 5 1 0 10
Abbreviations: Loc = localisation, L = lymphocytes, N = neutrophils, E = eosinophils; RUL, RML, RLL = right upper, middleand lower lobes; LUL, LLL = left upper and lower lobes; LING=lingula.
843
group.bmj.com on July 15, 2011 - Published by thorax.bmj.comDownloaded from
Agusti, Xaubet, Luburich, Ayuso, Roca, Rodriguez-Roisin
Table 3 Characteristics of the BAL performed on lobes A and B
Lobe A Lobe B p value
Volume recovered (ml) 30 (17-45) 32 (14-48) NSTotal cells (x 104/ml) 19.5 (5-51) 15 (5-77) NSCell viability (%) 75.5 (44-99) 73.5 (47-99) NSMacrophages (%) 77.5 (55-96) 84 (43-96) NSMacrophages (x 104/ml) 15.1 (4.3-38.7) 11.8 (3.6-73.1) NSLymphocytes (%) 5 (1-18) 5 (0-32) NSLymphocytes (x 104/ml) 0.77 (0.2-6.8) 0.70 (0-7.8) NSNeutrophils (%) 8.5 (0-34) 5 (0-26) 0.01Neutrophils (x 104/ml) 1.3 (0-14.6) 1.2 (0-5) 0.01Eosinophils (%) 3 (0-19) 1 (0-12) < 0.01Eosinophils (x 104/ml) 0.65 (0-4) 0.1 (0-4.8) 0.01
Values are medians (ranges).
Table 4 Correlations between bronchoalveolar cells andthe extent of the two HRCTpatterns in lobe A by multipleregression analysis (p values)
Reticular Ground-glasspattern pattern
Neutrophils (%) 0.11 0.0002Neutrophils (absolute) 0.66 0.001Eosinophils (%) 0.99 0.65Eosinophils (absolute) 0.84 0.91Lymphocytes (%) 0.11 0.77Lymphocytes (absolute) 0.20 0.12
age and absolute numbers of eosinophils (rs =-0. 1 1 and -0.01, respectively) or lymphocytes(rs = -0.11 and 0.06, respectively).To furtheridentify independent determinants of theextent ofground glass and reticular patterns onHRCT scans we performed a stepwise multipleregression analysis, taking as dependent variablesboth the percentage and absolute numbers ofneutrophils, eosinophils, and lymphocytes in theBAL fluid. A strong correlation was foundbetween the extent of the ground glass pattern inthe most involved lobe (lobe A) and both thepercentage and absolute numbers of neutrophilsin the BAL fluid (table 4), but no correlationswere found with eosinophils or lymphocytes.
DiscussionThe results of the present study support the viewthat, in patients with IPF, the cell population inthe BAL fluid may differ considerably betweendifferent pulmonary lobes, and HRCT scanningappears to be a useful method to identify pulmo-nary areas with different inflammatory activity.Bronchoalveolar lavage is considered the mostreliable procedure for the accurate assessment ofthe alveolitis in several interstitial lung disordersincluding IPF. In this disease BAL has been sys-tematically performed in several areas (middle,lingula, or right lower lobes) as it is consideredthat the cell population retrieved from thesezones is representative of the underlying intersti-tial process "-' However, few studies havecompared multiple lobe lavages in a systematicfashion.'5 29 30 Although the results of these stud-ies have shown a fairly close agreement betweenlobes, Garcia et al'5 showed a poor correlationbetween lobes in patients with IPF associatedwith collagen vascular disease, 35% of themhaving a greater than 10% discrepancy in thepercentage of neutrophils between the middlelobe and the lingula. It seems evident fromventilation-perfusion scanning, gallium-67scanning, and open lung biopsies that inhomo-geneity of lung involvement frequently occurs
in IPF' so that generalisations about the sever-ity of alveolitis based on the results obtainedfrom BAL systematically performed in onelobe may be incomplete. We have confirmedthat the cell population in the BAL fluid inpatients with IPF differs significantly betweenthe different pulmonary lobes evaluated. It isimportant to note, however, that, in contrast toGarcia et al'5 who systematically compared thecell population in BAL fluid obtained from themiddle lobe and the lingula, we preselected thepulmonary lobes to be explored bronchoscopi-cally from the HRCT findings.With the use of the HRCT scan it is possible
to obtain reliable information regarding theextent and histological characteristics of thepulmonary involvement in IPF. Different stud-ies have shown that areas of fine reticularabnormalities on the CT scan represent areasof fibrosis in the lung biopsy specimen, whileareas of ground glass opacification identify anincreased likelihood of an inflammatoryhistology.'8-20 Since pulmonary involvement inIPF is not homogeneous, HRCT scanningfacilitates differentiation of the specific areas ofthe lung parenchyma to be evaluated by BAL.Our results support this contention since (1)the percentage of both neutrophils and eosi-nophils in the BAL fluid from the mostinvolved areas of the lung parenchyma asdetermined by HRCT scanning was signifi-cantly higher, and (2) in contrast to areas ofmaximal involvement, the BAL cell populationin those areas minimally involved was fre-quently within normal limits. It is accepted thatboth neutrophils and eosinophils play animportant part in the pathogenesis of IPF byreleasing oxidants, potent proteinases, andvarious other potentially harmful agents,3' so itis reasonable to speculate that the presence ofthese cells can vary according to the activity ofthe disease, being more abundant in areas ofmore extensive involvement.32Our study also showed that BAL neu-
trophilia correlated with the total extent of pul-monary abnormalities on the HRCT scan andwith the extent of the ground glass pattern inthe lavaged lobe. These findings are supportedby the fact that the inflammatory process inIPF is characterised by a sustained accumula-tion of neutrophils in the alveolar spaces.2 In arecent study in which patients with pulmonaryfibrosis associated with systemic sclerosis wereevaluated, Wells et ar' also showed that thepercentage of neutrophils in the BAL fluid cor-related with the extent of the HRCT pulmo-nary abnormalities in the lavaged lobe. How-ever, in contrast with our results, they foundthat it was the extent of the reticular ratherthan the ground glass pattern that independ-ently correlated with neutrophilia in the BALfluid and, furthermore, they found that thepercentage counts of eosinophils correlatedwith the extension of the ground glass patternin the lavaged lobe. There are several explana-tions that could justify this apparent contradic-tion. Firstly, Wells et aP' studied a group ofpatients with pulmonary fibrosis associatedwith systemic sclerosis, possibly at an earlystage of evolution of the disease since almost
844
group.bmj.com on July 15, 2011 - Published by thorax.bmj.comDownloaded from
High resolution CT scanning in lungfibrosis
30% of the patients had no evidence of pulmo-nary involvement on the CT scan. It is of note,however, that both IPF and pulmonary fibrosisassociated with systemic sclerosis can have adifferent natural history so their BAL cell pro-files could be different.22 In the study by Wellset al an increase in the number of eosinophils,often without an associated neutrophilia, wasobserved in nine of 16 patients with limitedextensive disease (less than 50% pulmonaryabnormalities in the lavaged lobe) in theabsence of respiratory symptoms. To explaintheir results they postulated that eosinophilsmay play a pathogenetic role in early lung dis-ease in pulmonary fibrosis associated with sys-temic sclerosis. Secondly, although in thepresent study the use of 1 mm instead of 3 mmcollimation could have improved the distinc-tion between fibrosis and alveolitis, it seemslogical that, in some cases, it is not possible todistinguish clearly between thickening of alveo-lar walls due to inflammatory cell infiltrationand/or oedema from enhanced deposition ofconnective tissue; under these circumstances,areas with very fine fibrosis could not be differ-entiated from alveolitis.34 Thirdly, the fact that,in the present study, most of the involved lobesshared a "mixed" pattern of abnormalities(both with ground glass and reticular appear-ances) makes it difficult to separate the amountof each. Finally, it should be noted that aground glass pattern may be a consequence ofmovement artefact. However, our patients hadno difficulty in holding their breath for twoseconds during HRCT scanning.
In summary, the results of our study suggestthat, in patients with IPF, the cell population inthe BAL fluid from different pulmonary lobesis not uniform and appears to be related to theextent of the CT abnormalities present in thelavaged lobe. The relationship between theBAL cell population and the different CT pat-terns, and its usefulness in expanding theknowledge of the pathogenesis of this disease,merit further evaluation.
We thank Maite Carri6n and Teresa Sole for their technicalexpertise and Dr JM Montserrat and Dr E Ballester for theirunselfish cooperation.
This study was supported by grant 94/998 from the Fondo deInvestigaci6n Sanitaria de la Seguridad Social (FIS), theComissionat per Universitats i Recerca de la Generalitat deCatalunya (GRQ 94/9103) and the Fundaci6 Catalana dePneumologia.
1 Crystal RG, Fulmer JD, Roberts WC, Moss ML, Line BR,Reynolds HY. Idiopathic pulmonary fibrosis: clinical,histologic, radiographic, physiologic, scintigraphic, cyto-logic, and biochemical aspects. Ann Intern Med 1976;85:769-88.
2 Keogh BA, Crystal RG. Alveolitis: the key to the interstitiallung disorders. Thorax 1982;37: 1-10.
3 Carrington CB, Gaensler EA, Coutu RE, Fitzgerald MX,Gupta RG. Natural history and treated course of usual anddesquamative interstitial pneumonia. N EnglJ Med 1978;298:801-11.
4 Turner-Warwick M, Burrows B, Johnson A. Cryptogenicfibrosing alveolitis: clinical features and their influence onsurvival. Thorax 1980;35:171-80.
5 Hunninghake GW, Gadek JE, Kawanami 0, Ferrans VJ,Crystal RG. Inflammatory and immune processes in thehuman lung in health and disease: evaluation by broncho-alveolar lavage. Am J Pathol 1979;97:149-206.
6 Davis GS, Brody AR, Craighead JE. Analysis of airspace andinterstitial mononuclear cell populations in human diffuseinterstitial lung disease. Am Rev Respir Dis 1978;118:7-15.
7 Haslam PL. Bronchoalveolar lavage in interstitial lungdisease. Semin Respir Med 1984;6:55-70.
8 Haslam PL. Cryptogenic fibrosing alveolitis: pathogeneticmechanisms and therapeutic approaches. Eur Respir J1990;3:355-7.
9 Haslam PL, Turton CWG, Lukoszek A, Collins JV, SalsburyAJ, Turner-Warwick M. Bronchoalveolar lavage fluid cellcounts in cryptogenic fibrosing alveolitis and their relationto therapy. Thorax 1980;35:328-39.
10 Rudd RM, Haslam PL, Turner-Warwick M. Cryptogenicfibrosing alveolitis. Relationships of pulmonary physiologyand bronchoalveolar lavage to response to treatment andprognosis. Am Rev Respir Dis 1981; 124:1 -8.
11 Peterson MW, Monick M, Hunninghake GW. Prognosticrole of eosinophils in pulmonary fibrosis. Chest 1987;92:51-6.
12 Watters LC, Schwartz MI, Cherniack RM, Waldron JA,Dunn TL, Stanford RE, et al. Idiopathic pulmonary fibro-sis. Pretreatment bronchoalveolar lavage cellular constitu-ents and their relationships with lung histopathology andclinical response to therapy. Am Rev Respir Dis 1987;135:696-704.
13 Schwartz DA, Van Fossen DS, Davis CS, Helmers RA,Dayton CS, Burmeister LF, et al. Determinants ofprogression in idiopathic pulmonary fibrosis. Am J RespirCrit Care Med 1994;149:444-9.
14 Schwartz DA, Helmers RA, Dayton CS, Merchant RK,Hunninghake GW. Determinants of bronchoalveolarlavage cellularity in idiopathic pulmonary fibrosis. Jf ApplPhysiol 1991;71:1688-93.
15 Garcia JGN, Wolven RG, Garcia PL, Keogh BA. Assess-ment of interlobar variation of bronchoalveolar lavage cel-lular differentials in interstitial lung diseases. Am RevRespir Dis 1986;133:444-9.
16 Schwartz DA, Helmers RA, Galvin JR, Van Fossen DS,Frees KL, Dayton CS, et al. Determinants of survival inidiopathic pulmonary fibrosis. Am J Respir Crit Care Med1994;149:450-4.
17 Wells AU, Hansell DM, Rubens MB, Cullinan P, Black CM,du Bois RM. The predictive value of appearances on thin-section computed tomography in fibrosing alveolitis. AmRev Respir Dis 1993;148:1076-82.
18 Muller NL, Miller RR, Webb WR, Evans KG, Ostrow DN.Fibrosing alveolitis: CT-pathologic correlation. Radiology1986;160:585-8.
19 Muller NL, Stables CA, Miller RR, Vedal S, ThurbeckWM,Ostrow DN. Disease activity in idiopathic pulmonaryfibrosis: CT and pathologic correlation. Radiology 1987;165:731-4.
20 Nishimura K, Litaichi M, Izumi T, Nagai S, Kanaoka M,Itoh H. Usual interstitial pneumonia: histologic correla-tion with high resolution CT. Radiology 1992;182:337-42.
21 Agusti C, Xaubet A, Agusti AGN, Roca J, Ramirez J,Rodriguez-Roisin R. Clinical and functional assessment ofpatients with idiopathic pulmonary fibrosis: results of a 3year follow-up. Eur RespirJ 1994;7:643-50.
22 Agusti C, Xaubet A, Roca J, Agusti AGN, Rodriguez-RoisinR. Interstitial pulmonary fibrosis with and without associ-ated collagen vascular disease: results of a two year follow-up. Thorax 1992;47:1035-40.
23 Hansell DM, Kerr IH. The role of high resolutioncomputed tomography in the diagnosis of interstitial lungdisease. Thorax 1991;46:77-84.
24 Leung AN, Miller RR, Muller NL. Parenchymal opacifica-tion in chronic infiltrative lung diseases: CT-pathologiccorrelation. Radiology 1993;188:209-14.
25 Roca J, Sanchis J, Agusti-Vidal A, Segarra F, Navajas D,Rodriguez-Roisin R, et al. Spirometric reference valuesfrom a Mediterranean population. Bull Eur PhysiopatholRespir 1986;22:217-24.
26 Roca J, Rodriguez-Roisin R, Cobo E, Burgos F, Perez J,Clausen JL. Single-breath carbon monoxide diffusingcapacity (DLco) prediction equations from a Mediterra-nean population. Am Rev Respir Dis 1990;140: 1026-32.
27 Xaubet A, Rodriguez-Roisin R, Bombi JA, Marin A, Roca J,Agusti Vidal A. Correlation of bronchoalveolar lavage andclinical and functional findings in asbestosis. Am RevRespirDis 1986;133:848-54.
28 Xaubet A, Agusti C, Roca J, Picado C, Rodriguez-Roisin R.BAL lymphocyte activation antigens and diffusing capac-ity are related in mild to moderate pulmonary sarcoidosis.Eur RespirJ 1993;6:715-8.
29 Peterson MW, Nugent KM, Jolles H, Monick M, Hunning-hake GW. Uniformity ofbronchoalveolar lavage in patientswith pulmonary sarcoidosis. Am Rev Respir Dis 1988;137:79-84.
30 Scott Miller K, Smith EA, Kinsella M, Schabel SI, SilverRM. Lung disease associated with progressive systemicsclerosis. Am Rev Respir Dis 1990;141:301-6.
31 Daniele RP, Dantzker DR, Davis GS, Hunninghake GW,King TE Jr, Metzger WJ, et al. Clinical role of bronchoal-veolar lavage in adults with pulmonary disease. Am RevRespir Dis 1990;142:481-6.
32 Turner-Warwick M, Haslam PL. The value of serialbronchoalveolar lavages in assessing the clinical progressof patients with cryptogenic fibrosing alveolitis. Am RevRespir Dis 1987;135:26-34.
33 Wells AU, Hansell DM, Rubens MB, Cullinan P, HaslamPL, Black CM, et al. Fibrosing alveolitis in systemicsclerosis. Bronchoalveolar lavage findings in relation tocomputed tomographic appearance. Am J Respir Crit CareMed 1994;150:462-8.
34 Wells AU, Hansell DM, Corrin B, Harrison NK, GoldstrawP, du Bois RM. High resolution computed tomography asa predictor of lung histology in systemic sclerosis. Thorax1 992;47:508-1 2.
845
group.bmj.com on July 15, 2011 - Published by thorax.bmj.comDownloaded from
doi: 10.1136/thx.51.8.841 1996 51: 841-845Thorax
C. Agusti, A. Xaubet, P. Luburich, et al. pulmonary fibrosis.bronchoalveolar lavage in idiopathic Computed tomography-guided
http://thorax.bmj.com/content/51/8/841Updated information and services can be found at:
These include:
References http://thorax.bmj.com/content/51/8/841#related-urls
Article cited in:
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on July 15, 2011 - Published by thorax.bmj.comDownloaded from





























