Embed Size (px)
Citation preview
Copyright © 2021 Contemporary Pediatric Dentistry
VOLUME 2 | ISSUE 1 | APRIL 2021 AIM and SCOPE Contemporary Pediatric Dentistry aims to serve as a forum for scientifically based information in pediatric dentistry, with the intention of continually expanding the knowledge base in this area. The journal aims to promote the highest standard of education, practice and research in paediatric dentistry world-wide. The Contemporary Pediatric Dentistry’s broad readership consists of pediatric dentists, dentists, and all academicians, researchers, specialists, and general practitioners interested in pediatric dentistry. This journal provides an open-access forum for the exchange of information about contemporary, new, and significant research in pediatric dentistry throughout the world. The scope is therefore broad, ranging from original research articles, case reports, reviews, editorial comments, and letters to the editor within all aspects of pediatric dentistry including education, practice and research. The journal covers the all aspects of pediatric dentistry. Author Guidelines is declared at its website; https://contemppediatrdent.org/author-guidelines/ COPYRIGHT and LICENSING Copyright on all articles published in Contemporary Pediatric Dentistry is retained by the Contemporary Pediatric Dentistry. When submitting an article to Contemporary Pediatric Dentistry, authors agree to transfer all copyright ownership, including the right to reproduce the article in all forms and media, to Contemporary Pediatric Dentistry. Contemporary Pediatric Dentistry publishes open access articles under a Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0). This license permits authors (users) to: Freely share (copy and redistribute material in any medium or format) under the following terms; Attribution: Authors (users) must give appropriate credit, provide a link to the license, and indicate if changes were made. Authors may do so in any reasonable manner, but not in any way that suggests the licensor endorses their use. NonCommercial: Authors (users) may NOT use the material for commercial purposes. NoDerivatives: If authors (users) remix, transform, or build upon the material, Authors (users) may NOT distribute the modified material. PUBLISHING RIGHTS When submitting an article to Contemporary Pediatric Dentistry, authors agree to transfer all copyright ownership, including the right to reproduce the article in all forms and media, to Contemporary Pediatric Dentistry by signing the copyright transfer agreement form. DISCLAIMER The Website: The Contemporary Pediatric Dentistry is provided by founding Editor-in-Chief, Dr. Burak Buldur, having its main place of at Department of Pediatric Dentistry, Cumhuriyet University, 58140, Sivas, Turkey, and/or its affiliates. By accessing or using the site, you accept and agree to the terms of this disclaimer and our online privacy policy, as outlined below. If you do not agree to the terms of this Disclaimer and/or online privacy policy, you may not access or otherwise use this Site or any of its content. The Contemporary Pediatric Dentistry is the copyright owner or licensee of the content and/or information on the Website, unless otherwise indicated. Individual documents in the Site may be subject to additional terms indicated in those documents. Contemporary Pediatric Dentistry has the disclaimer policy declared at its website: https://contemppediatrdent.org/privacy-policy/ OWNERSHIP AND PUBLISHER The journal is owned and published by Dr. Burak Buldur, the founding Editor-in-Chief, on behalf of Contemporary Pediatric Dentistry. The journal does not have any other sponsor or supporting body currently and self financed by Editor-in-Chief and Editorial Board.
Copyright © 2021 Contemporary Pediatric Dentistry
VOLUME 2 | ISSUE 1 | APRIL 2021
EDITOR-in-CHIEF Burak Buldur
Sivas Cumhuriyet University Turkey
ASSOCATE EDITORS EDITORIAL BOARD (2021) Vineet K. Dhar University of Maryland, USA
Zafer Cehreli Hacettepe University, Turkey
Anci Vukovic University of Belgrad, Serbia
Soraya Coelho Leal University of Brasilia, Brazil
Alessandro Leite Cavalcanti State University of Paraiba, Brazil
Meenakshi S. Kher Private Practice, India
Mohammed. H. Nekoofar Tehran University of Medical Sciences, Iran
Ola al-Batayneh Jordan University Science and Technologh, Jordan
Hasan Jamal University College London, United Kingdom
Juan Sebastian Lara Indiana University, USA
Esma J. Dogramaci University of Adelaide, Australia
Ines Guerra Pereira Porto University, Portugal
Ursula Albites Científica del Sur University, Peru
Marc Saadia Private practice, Mexico
Senchhema Limbu Kathmandu University, Nepal
Osama El Shahawy Future University, Egypt
Marina Belfer Peoples’ Friendship University, Russia
Mohamed Zayed Radwan Ain Shams University, Egypt
Gabriela Scagnet University of Buenos Aires, Argentina
Eveleyn Alvarez Vidigal Scientific University of south, Peru
Fatima Rosana Albertini Private clinic, Brazil
Sivakumar Nuvvula Narayana Dental College, India
Kaan Orhan Ku leuven University, Belgium
Virinder Goyal Guru Navak Dev Dental College, India
Alejandro Ramirez Universidad de Guadalajara, Mexico
Ece Eden Ege University, Turkey
Ikramul Ahmed Dhaka Dental College, Bangladesh
Ricardo Jorge Santos Polytechnic Institute of Porto, Portugal
Patricia Valerio The Federal University of Minas Gerais, Brazil
Om Prakash Kharbanda All India Institute of Medical Sciences, India
Riad Bacho Lebanese University, Lebanon
Figen Seymen Istanbul University, Turkey
Prasad K. Musale Private practice, India
Antonio Pedro Silva Private Practice, Belgium
Joana Monteiro Leeds Teaching Hospitals Nhs Trust, United Kingdom
STATISTICS EDITOR PRODUCTION EDITOR Ziynet Cinar Sivas Cumhuriyet University, Turkey
Kaan Sagtas

Copyright © 2021 Contemporary Pediatric Dentistry.
VOLUME 2 | ISSUE 1 | APRIL 2021
TABLE OF CONTENTS Review
Nanosilver fluoride as a caries arresting agent: A narrative review Mohammed Zameer, Sameen Badiujjama Birajdar, Syed Nahid Basheer, Syed Wali Peeran, Syed Ali Peeran, Arun Reddy
1-13
Original Research Assessment of communication words during dental treatment requiring with and without local anaesthesia between child and pediatric dentist Shital Kiran Davangere Padmanabh, Para Dave
14-20
Evaluation of the clinical efficiency of rotary and manual files for root canal instrumentation in primary teeth pulpectomies: A comparative randomized clinical trial KL Girish Babu, Guraj Hebbar Kavyashree
21-34
A survey on dental treatments provided under general anesthesia for pediatric patients: A hospital-based retrospective audit Sreekanth K Mallineni, Jayachandra Bhumireddy, Azher M Mohammed, Vinod Mukthineni
35-40
Retrospective evaluation of primary anterior teeth injuries and prevalence of sequelae in their successors Ozant Oncag, Candan Gurbuz Sarigol, Sevgi Arabulan
41-49
Case Report Composite odontoma with 23 denticles in a pediatric patient: A case report Paôla Caroline da Silva Mira, Jéssica Silva Peixoto Bem, Andresa Vieira da Silva, Marcio Santos de Carvalho, Marcelo Rodrigues Azenha, Christiano Oliveira-Santos, Maria Bernadete Sasso Stuani, Carolina Paes Torres
50-56
Management of internal root resorption in primary mandibular right first molar: A case report with four-year follow-up Prasad K Musale, Sneha S Kothare, Abhinav l Talekar
57-63
Correction of an anterior and posterior crossbite case with a modified McNamara appliance: A case report Wendes Dias Mendes, Luciane Macedo de Menezes, Fábio Romano, Mírian Aiko Nakame Matsumoto, Maria Bernadete Sasso Stuani
64-71
This journal is available online at: www.contemppediatrdent.org to search the articles and register.

Copyright © 2021 Contemporary Pediatric Dentistry. This work is licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International license. (CC BY-NC-ND 4.0)
Review
Nanosilver fluoride as a caries arresting agent: A narrative review
Mohammed Zameer 1✉, Sameen Badiujjama Birajdar 2, Syed Nahid Basheer 3, Syed Wali Peeran 4, Syed Ali Peeran 5, Arun Reddy 6
Abstract Dental caries is the most prevalent oral disease that continues to affect almost every country in the world. The contemporary management of dental caries focuses on non-restorative, non-invasive, and micro-invasive treatment approaches that arrest or reverse the caries process at a lesion level and reduce the loss of sound tooth structure. One of these approaches is the employment of caries arresting agents that possess antibacterial and remineralizing properties. Silver diamine fluoride (SDF) has drawn significant attention as an efficient caries arresting agent in children and adults. The major limitation with the use of SDF is the dark black staining of the carious tissue that compromises the esthetics. Silver ions are known for their antimicrobial effects, and silver nanoparticles (AgNPs) have the added advantage that it increases the surface area for exposure to the microbes. Literature reports that AgNPs have antimicrobial potential against predominant cariogenic flora. It has led to the development of nanosilver fluoride (NSF), a new colloid based on AgNPs, chitosan, and fluoride. It has shown to overcome the clinical limitations of SDF as it does not cause carious lesion staining. However, the current scientific literature lacks a comprehensive review of the benefits of using NSF for caries prevention and arrest. Thus, the purpose of this paper was to review the studies and clinical trials on NSF as a caries arresting agent, including antibacterial actions and modulation of the demineralization-remineralization balance. Keywords: Dental Caries; Fluoride; Tooth Demineralization
Highlights The current paper foregrounds the effectiveness of a non-invasive treatment approach for dental caries using caries arresting agents.
1 M.D.S (Pediatric Dentistry) Registrar Pedodontist, Armed Forces Hospital, Jazan, KSA
2 General Dentist, Sanjeevani Dental Clinic, Raichur, India 3 Assistant Professor, Department of Restorative Dental Sciences, Jazan University, Jazan, KSA 4 Senior Registrar periodontist, Armed Forces Hospital, Jazan, KSA 5 Registrar Prosthodontist, Armed Forces Hospital, Jazan, KSA 6 Associate Professor, Department of Oral & Maxillofacial Orthodontics, Navodaya Dental College, Raichur, India
Correspondence: Department of Pediatric Dentistry, Armed Forces Hospital, Jazan, KSA E-mail address: [email protected]
Received: 27 March 2021 Accepted: 05 May 2021 Online First: 05 May 2021
The silver nanoparticle-based preparations present to overcome the limitations of using silver ion-based solutions for caries arrest.
The newer nanotechnology-based caries arresting agent presents effective antibacterial properties against cariogenic bacteria and modulation of the demineralization-remineralization balance for teeth.
Contemporary Pediatric Dentistry Contemp Pediatr Dent 2021:2(1):1-13 DOI: 10.51463/cpd.2021.47

Zameer et al. 2 Contemp Pediatr Dent 2021:2(1):1-13
Copyright © 2021 Contemporary Pediatric Dentistry
INTRODUCTION Dental caries is the most prevalent oral disease
that continues to affect almost every country in the world.1 The contemporary dental practice focuses on non-restorative, non-invasive, and micro-invasive treatment approaches that arrest or reverse the caries process at a lesion level and reduce the loss of sound tooth structure. These treatment approaches include the employment of caries arresting agents, sealant, resin infiltration, fluoride varnish, fluoride toothpaste, and gel.2–4
Silver diamine fluoride (SDF), a metal ion-based topical fluoride solution, has drawn significant attention as an efficient caries arresting agent in children and adults.5–8 Studies9–13 have reported its effectiveness against cariogenic bacteria and fungi, and its remineralizing potential on enamel and dentin.13–16 Major limitation with the use of SDF is the dark black staining of the carious lesions due to the precipitation of silver particles on the carious tissue.17,18 Hence, its use in the aesthetic zone is not encouraging.19–21 The other limitations of SDF use include; metallic taste, short-term staining to the skin which resolves in 2 to 14days22 and mildly painful lesions on accidental contact of SDF solution with oral mucosa which generally heal within a couple of days.6,23 To counter the undesirable staining, it is suggested to follow a combination protocol; potassium iodide (KI) application immediately after the use of SDF17,24 or SDF mixed with glutathione(GSH) bio-molecule.25
The investigations on following the combination protocol revealed a positive effect in reducing the staining when compared to the use of SDF alone.25–27 However, the use of KI has been associated with poorer caries control28 and a certain degree of staining that can compromise the esthetics is observed in the carious arrested lesions.24,26,29,30 Furthermore, the use of KI is contraindicated in pregnant women and during
the first-six-months of breast-feeding because of the concern of overloading the developing thyroid with iodine.22
The advancement in nanotechnology led to the development of silver nanoparticles (AgNPs). The antibacterial properties of AgNPs have been well recognized in the medical field.31,32 These particles are assumed more efficient due to their greater surface area that would increase the contact with microbial cells.29 AgNPs have drawn attention from the dental researcher for their antibacterial potential that can be utilized in anti-caries approaches.33
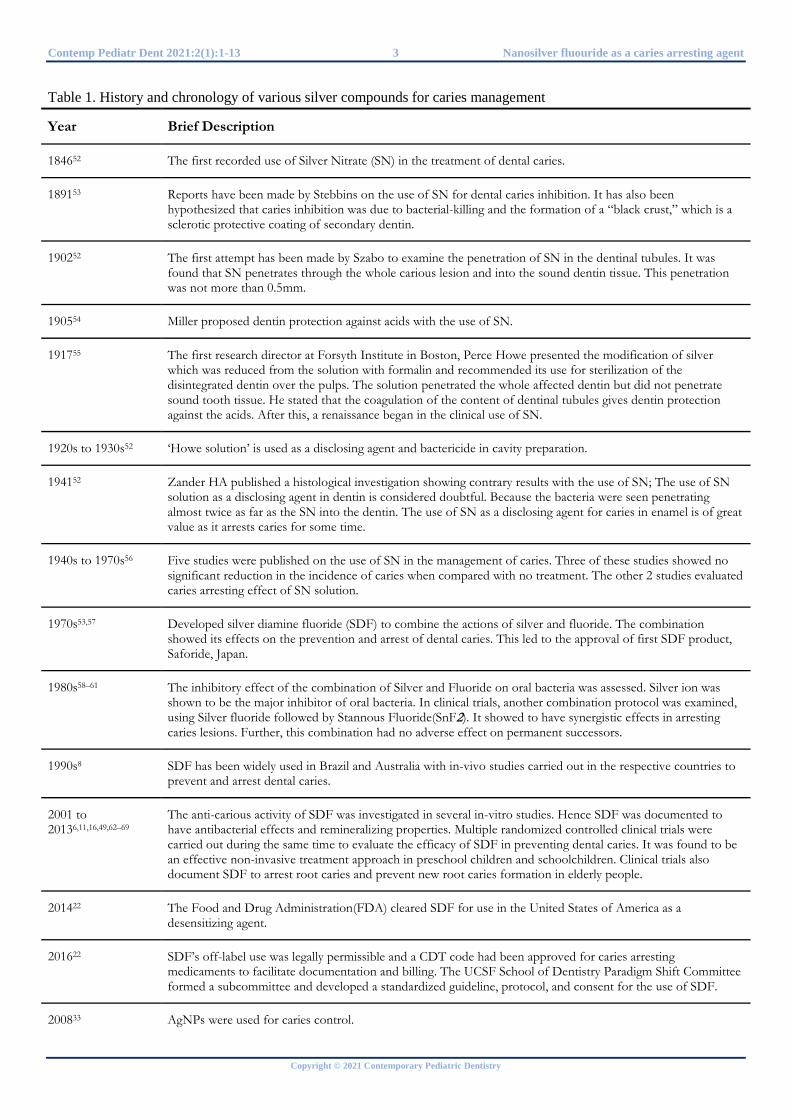
Table 1 summarizes history and chronology of various silver compounds for caries management. Literature12,34 reports that AgNPs have antimicrobial potential against predominant cariogenic flora. Furthermore, researchers have explored the combination of AgNPs and fluoride to include the advantages of each individual component.
Nano-silver fluoride (NSF), a new colloid based on AgNPs, chitosan, and fluoride was developed as a caries arresting agent that comprises both antibacterial and remineralizing properties.30 Hence, NSF is a promising agent as it overcomes the clinical limitations of SDF as it causes no carious lesion staining.29,30,35,36 This is due to the size of silver particles and also because the nanoparticles do not undergo oxidation.29 This new formulation is safe for use in humans, and controlled clinical trials have shown its anti-caries property.36–38 However, the current scientific literature lacks a comprehensive review of the benefits of using NSF in the treatment of dental caries. Thus, the purpose of this paper is to review NSF as a caries arresting agent, including antibacterial actions and modulation of demineralization-remineralization balance.
Contemp Pediatr Dent 2021:2(1):1-13 3 Nanosilver fluouride as a caries arresting agent
Copyright © 2021 Contemporary Pediatric Dentistry
Table 1. History and chronology of various silver compounds for caries management
Year Brief Description
184652 The first recorded use of Silver Nitrate (SN) in the treatment of dental caries.
189153 Reports have been made by Stebbins on the use of SN for dental caries inhibition. It has also been hypothesized that caries inhibition was due to bacterial-killing and the formation of a “black crust,” which is a sclerotic protective coating of secondary dentin.
190252 The first attempt has been made by Szabo to examine the penetration of SN in the dentinal tubules. It was found that SN penetrates through the whole carious lesion and into the sound dentin tissue. This penetration was not more than 0.5mm.
190554 Miller proposed dentin protection against acids with the use of SN.
191755 The first research director at Forsyth Institute in Boston, Perce Howe presented the modification of silver which was reduced from the solution with formalin and recommended its use for sterilization of the disintegrated dentin over the pulps. The solution penetrated the whole affected dentin but did not penetrate sound tooth tissue. He stated that the coagulation of the content of dentinal tubules gives dentin protection against the acids. After this, a renaissance began in the clinical use of SN.
1920s to 1930s52 ‘Howe solution’ is used as a disclosing agent and bactericide in cavity preparation.
194152 Zander HA published a histological investigation showing contrary results with the use of SN; The use of SN solution as a disclosing agent in dentin is considered doubtful. Because the bacteria were seen penetrating almost twice as far as the SN into the dentin. The use of SN as a disclosing agent for caries in enamel is of great value as it arrests caries for some time.
1940s to 1970s56 Five studies were published on the use of SN in the management of caries. Three of these studies showed no significant reduction in the incidence of caries when compared with no treatment. The other 2 studies evaluated caries arresting effect of SN solution.
1970s53,57 Developed silver diamine fluoride (SDF) to combine the actions of silver and fluoride. The combination showed its effects on the prevention and arrest of dental caries. This led to the approval of first SDF product, Saforide, Japan.
1980s58–61 The inhibitory effect of the combination of Silver and Fluoride on oral bacteria was assessed. Silver ion was shown to be the major inhibitor of oral bacteria. In clinical trials, another combination protocol was examined, using Silver fluoride followed by Stannous Fluoride(SnF2). It showed to have synergistic effects in arresting caries lesions. Further, this combination had no adverse effect on permanent successors.
1990s8 SDF has been widely used in Brazil and Australia with in-vivo studies carried out in the respective countries to prevent and arrest dental caries.
2001 to 20136,11,16,49,62–69
The anti-carious activity of SDF was investigated in several in-vitro studies. Hence SDF was documented to have antibacterial effects and remineralizing properties. Multiple randomized controlled clinical trials were carried out during the same time to evaluate the efficacy of SDF in preventing dental caries. It was found to be an effective non-invasive treatment approach in preschool children and schoolchildren. Clinical trials also document SDF to arrest root caries and prevent new root caries formation in elderly people.
201422 The Food and Drug Administration(FDA) cleared SDF for use in the United States of America as a desensitizing agent.
201622 SDF’s off-label use was legally permissible and a CDT code had been approved for caries arresting medicaments to facilitate documentation and billing. The UCSF School of Dentistry Paradigm Shift Committee formed a subcommittee and developed a standardized guideline, protocol, and consent for the use of SDF.
200833 AgNPs were used for caries control.

Zameer et al. 4 Contemp Pediatr Dent 2021:2(1):1-13
Copyright © 2021 Contemporary Pediatric Dentistry
Table 1. Continued
2009 to 201933,70 Researchers investigated AgNPs as an antimicrobial agent and confirmed it to inhibit the growth of cariogenic bacteria and biofilm adhesion. They were also found to preserve the collagen matrix and impede demineralization of enamel and dentin. AgNPs have been incorporated into dental materials for caries control. Sodium Fluoride(NaF) was combined with AgNPs to prevent and arrest caries. AgNPs were added to restorative materials such as restorative resin and adhesive systems with an intention to prevent secondary caries. Furthermore, AgNPs have been utilized in orthodontics accessories such as brackets, elastomeric ligatures, adhesives, and removable retainers.
2014 to 202029,30,35,48 Multiple studies have investigated the antibacterial properties of NSF. The AgNPs in the formulation have the added advantage that it increases the surface area for exposure to the microbes. It has shown to inhibit cariogenic bacterial growth and biofilm adhesion and cause bactericidal actions without harming human cells. Studies confirm effective remineralizing properties of NSF on both the primary and permanent tooth. NSF has shown to be a simple, inexpensive, non-toxic, non-invasive caries arresting agent, and it did not present carious lesion staining.
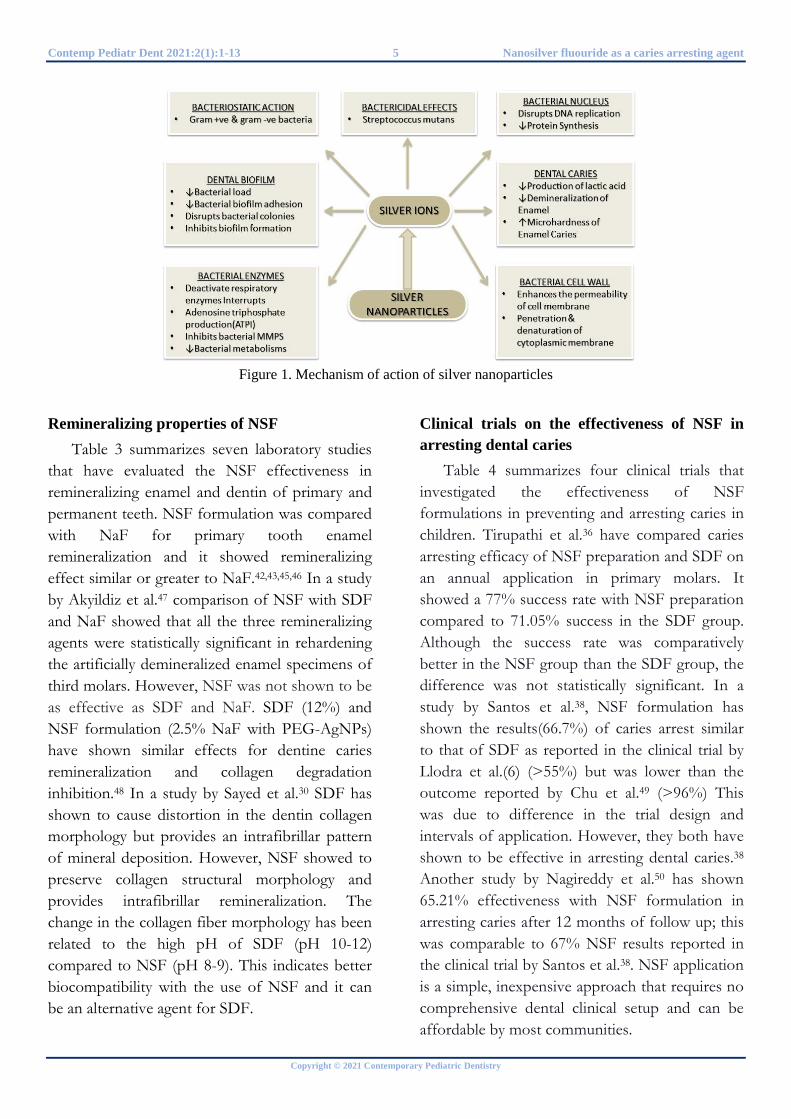
Mechanism of action of NSF
The antibacterial properties of nanomaterials have been investigated, and the antibacterial effect showed to come from AgNPs. Although the exact mechanism of antibacterial action of AgNPs has not been entirely understood, several antibacterial actions have been proposed and elaborated in Figure 1. Chitosan was added to the AgNPs as it acts as a carrier and stabilizes the compound. Further, to make this a more comprehensive agent, fluoride was added to the AgNPs-chitosan compound to fortify the antibacterial properties and prevent demineralization. This new formulation, called NSF, has been reported for caries prevention and arrest.33
Antibacterial properties of NSF Streptococcus mutans (SM) are the primary
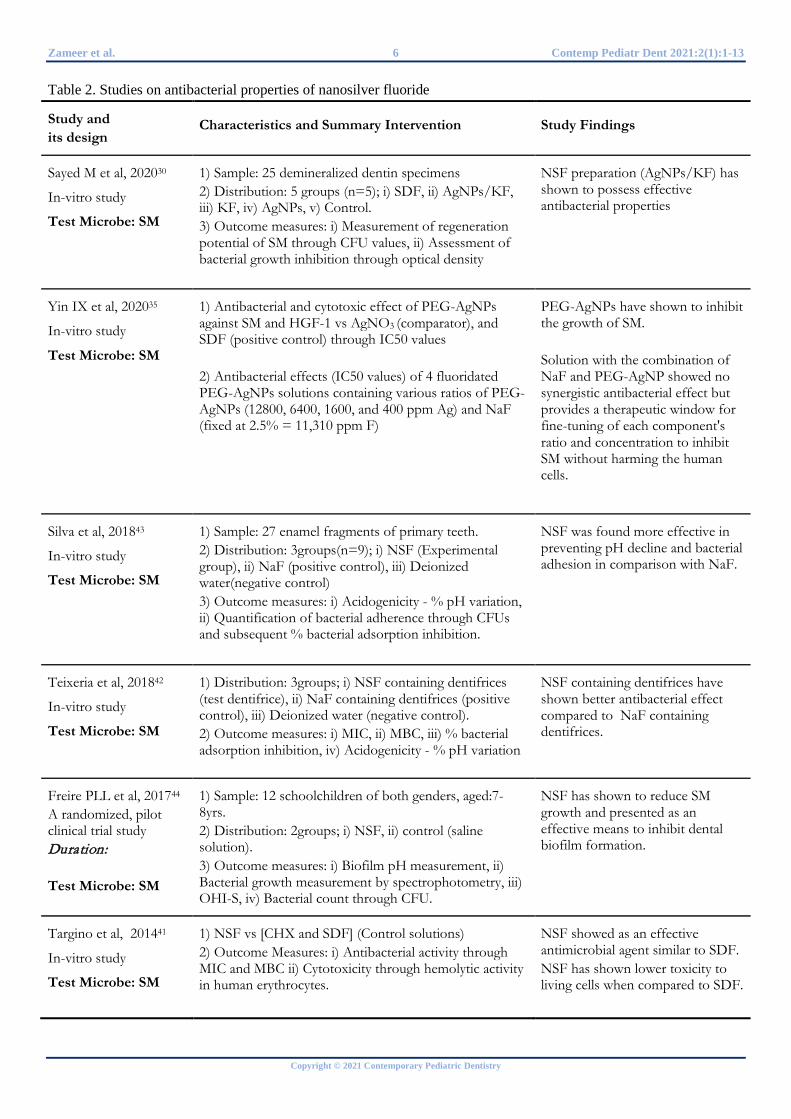
cariogenic bacteria, and they are associated with the initiation and progression of carious lesions. The oral bacteria exist collectively in the extracellular matrix to form a biofilm, which increases the resistance of microorganisms to antibacterial agents. Table 2 summarizes five in vitro studies and one clinical trial investigating the antibacterial effect of NSF on cariogenic bacteria.
Studies39,40 have shown that the antibacterial activity of AgNPs increases with a decrease in their particle size. Accordingly, few studies have shown AgNPs in the range of 2.56 + 0.43 nm, 3.2 + 1.2 nm and 5.9 + 3.8 nm in NSF formulations to favour the antibacterial activity against
SM.35,38,41 Sodium borohydride has been regularly used as a reducing agent in preparing NSF formulations.38,41,42 However, due to concerns over toxicity, some researchers have used thiolated polyethylene glycol (PEG) as both a reducing agent and a capping agent for its preparation. Several advantages have been reported for the use of PEG; it increases AgNPs stability to a level that they can be preserved at high ionic concentrations, PEG-coated AgNPs have shown to be less toxic than those with other capping agents and are less liable to oxidize.35 Comparison between NSF and SDF for minimum inhibitory concentration (MIC) and minimum bactericidal concentration (MBC) values showed better results with the NSF. Cytotoxicity assessment by hemolytic activity showed NSF to be less toxic to human erythrocytes than SDF. Another study by Yin et al.35 showed half-maximal inhibitory concentration (IC50) of PEG-AgNPs against SM to be half of IC50 against human gingival fibroblasts (HGF-1). This indicates the provision of bactericidal action without harming human cells. NSF showed greater anti-adherence and anti-acidogenicity effects against SM when compared to sodium fluoride (NaF).43 NSF has been suggested as an effective SM biofilm inhibitor because it has shown to reduce the CFU counts and dental biofilm inhibition values.30,42–44 Thus, NSF formulation can act as a more biocompatible antibacterial agent against SM.
Contemp Pediatr Dent 2021:2(1):1-13 5 Nanosilver fluouride as a caries arresting agent
Copyright © 2021 Contemporary Pediatric Dentistry
Figure 1. Mechanism of action of silver nanoparticles
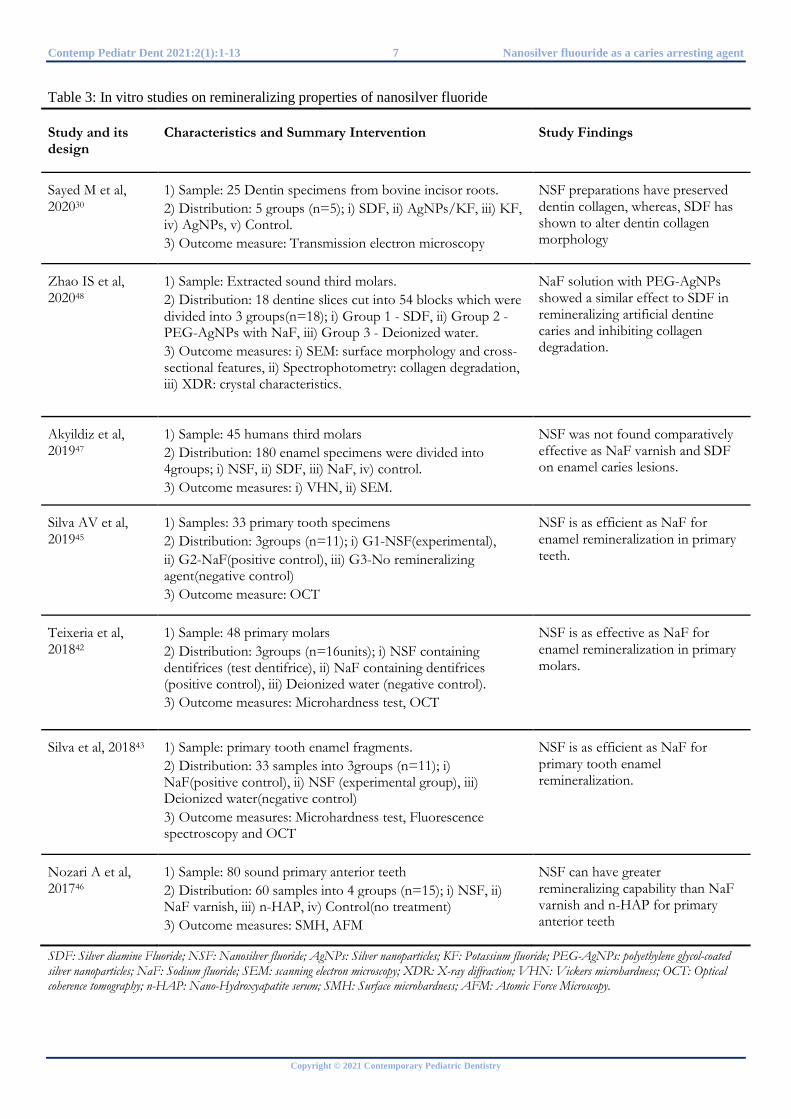
Remineralizing properties of NSF Table 3 summarizes seven laboratory studies
that have evaluated the NSF effectiveness in remineralizing enamel and dentin of primary and permanent teeth. NSF formulation was compared with NaF for primary tooth enamel remineralization and it showed remineralizing effect similar or greater to NaF.42,43,45,46 In a study by Akyildiz et al.47 comparison of NSF with SDF and NaF showed that all the three remineralizing agents were statistically significant in rehardening the artificially demineralized enamel specimens of third molars. However, NSF was not shown to be as effective as SDF and NaF. SDF (12%) and NSF formulation (2.5% NaF with PEG-AgNPs) have shown similar effects for dentine caries remineralization and collagen degradation inhibition.48 In a study by Sayed et al.30 SDF has shown to cause distortion in the dentin collagen morphology but provides an intrafibrillar pattern of mineral deposition. However, NSF showed to preserve collagen structural morphology and provides intrafibrillar remineralization. The change in the collagen fiber morphology has been related to the high pH of SDF (pH 10-12) compared to NSF (pH 8-9). This indicates better biocompatibility with the use of NSF and it can be an alternative agent for SDF.
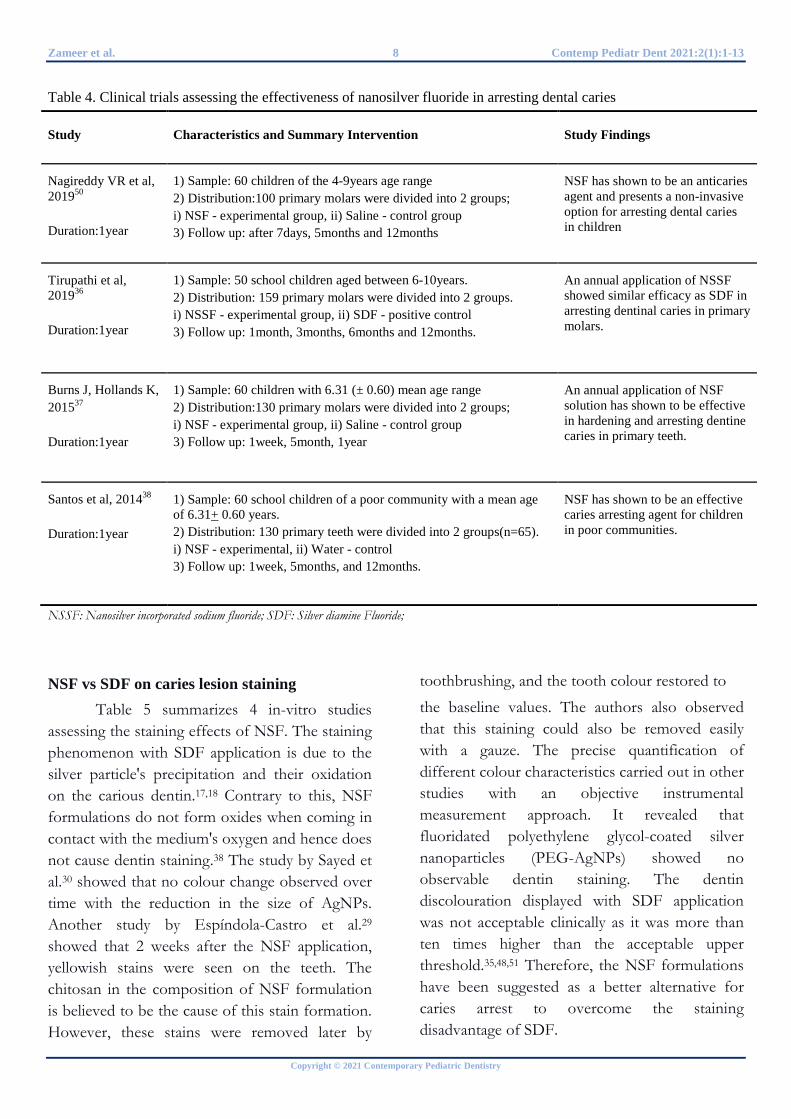
Clinical trials on the effectiveness of NSF in arresting dental caries
Table 4 summarizes four clinical trials that investigated the effectiveness of NSF formulations in preventing and arresting caries in children. Tirupathi et al.36 have compared caries arresting efficacy of NSF preparation and SDF on an annual application in primary molars. It showed a 77% success rate with NSF preparation compared to 71.05% success in the SDF group. Although the success rate was comparatively better in the NSF group than the SDF group, the difference was not statistically significant. In a study by Santos et al.38, NSF formulation has shown the results(66.7%) of caries arrest similar to that of SDF as reported in the clinical trial by Llodra et al.(6) (>55%) but was lower than the outcome reported by Chu et al.49 (>96%) This was due to difference in the trial design and intervals of application. However, they both have shown to be effective in arresting dental caries.38 Another study by Nagireddy et al.50 has shown 65.21% effectiveness with NSF formulation in arresting caries after 12 months of follow up; this was comparable to 67% NSF results reported in the clinical trial by Santos et al.38. NSF application is a simple, inexpensive approach that requires no comprehensive dental clinical setup and can be affordable by most communities.
Zameer et al. 6 Contemp Pediatr Dent 2021:2(1):1-13
Copyright © 2021 Contemporary Pediatric Dentistry
Table 2. Studies on antibacterial properties of nanosilver fluoride
Study and its design
Characteristics and Summary Intervention Study Findings
Sayed M et al, 202030
In-vitro study
Test Microbe: SM
1) Sample: 25 demineralized dentin specimens 2) Distribution: 5 groups (n=5); i) SDF, ii) AgNPs/KF, iii) KF, iv) AgNPs, v) Control. 3) Outcome measures: i) Measurement of regeneration potential of SM through CFU values, ii) Assessment of bacterial growth inhibition through optical density
NSF preparation (AgNPs/KF) has shown to possess effective antibacterial properties
Yin IX et al, 202035
In-vitro study
Test Microbe: SM
1) Antibacterial and cytotoxic effect of PEG-AgNPs against SM and HGF-1 vs AgNO3 (comparator), and SDF (positive control) through IC50 values 2) Antibacterial effects (IC50 values) of 4 fluoridated PEG-AgNPs solutions containing various ratios of PEG-AgNPs (12800, 6400, 1600, and 400 ppm Ag) and NaF (fixed at 2.5% = 11,310 ppm F)
PEG-AgNPs have shown to inhibit the growth of SM. Solution with the combination of NaF and PEG-AgNP showed no synergistic antibacterial effect but provides a therapeutic window for fine-tuning of each component's ratio and concentration to inhibit SM without harming the human cells.
Silva et al, 201843
In-vitro study
Test Microbe: SM
1) Sample: 27 enamel fragments of primary teeth. 2) Distribution: 3groups(n=9); i) NSF (Experimental group), ii) NaF (positive control), iii) Deionized water(negative control) 3) Outcome measures: i) Acidogenicity - % pH variation, ii) Quantification of bacterial adherence through CFUs and subsequent % bacterial adsorption inhibition.
NSF was found more effective in preventing pH decline and bacterial adhesion in comparison with NaF.
Teixeria et al, 201842
In-vitro study
Test Microbe: SM
1) Distribution: 3groups; i) NSF containing dentifrices (test dentifrice), ii) NaF containing dentifrices (positive control), iii) Deionized water (negative control). 2) Outcome measures: i) MIC, ii) MBC, iii) % bacterial adsorption inhibition, iv) Acidogenicity - % pH variation
NSF containing dentifrices have shown better antibacterial effect compared to NaF containing dentifrices.
Freire PLL et al, 201744
A randomized, pilot clinical trial study Duration: Test Microbe: SM
1) Sample: 12 schoolchildren of both genders, aged:7-8yrs. 2) Distribution: 2groups; i) NSF, ii) control (saline solution). 3) Outcome measures: i) Biofilm pH measurement, ii) Bacterial growth measurement by spectrophotometry, iii) OHI-S, iv) Bacterial count through CFU.
NSF has shown to reduce SM growth and presented as an effective means to inhibit dental biofilm formation.
Targino et al, 201441
In-vitro study
Test Microbe: SM
1) NSF vs [CHX and SDF] (Control solutions) 2) Outcome Measures: i) Antibacterial activity through MIC and MBC ii) Cytotoxicity through hemolytic activity in human erythrocytes.
NSF showed as an effective antimicrobial agent similar to SDF. NSF has shown lower toxicity to living cells when compared to SDF.
Contemp Pediatr Dent 2021:2(1):1-13 7 Nanosilver fluouride as a caries arresting agent
Copyright © 2021 Contemporary Pediatric Dentistry
Table 3: In vitro studies on remineralizing properties of nanosilver fluoride
Study and its design
Characteristics and Summary Intervention Study Findings
Sayed M et al, 202030
1) Sample: 25 Dentin specimens from bovine incisor roots. 2) Distribution: 5 groups (n=5); i) SDF, ii) AgNPs/KF, iii) KF, iv) AgNPs, v) Control. 3) Outcome measure: Transmission electron microscopy
NSF preparations have preserved dentin collagen, whereas, SDF has shown to alter dentin collagen morphology
Zhao IS et al, 202048
1) Sample: Extracted sound third molars. 2) Distribution: 18 dentine slices cut into 54 blocks which were divided into 3 groups(n=18); i) Group 1 - SDF, ii) Group 2 - PEG-AgNPs with NaF, iii) Group 3 - Deionized water. 3) Outcome measures: i) SEM: surface morphology and cross-sectional features, ii) Spectrophotometry: collagen degradation, iii) XDR: crystal characteristics.
NaF solution with PEG-AgNPs showed a similar effect to SDF in remineralizing artificial dentine caries and inhibiting collagen degradation.
Akyildiz et al, 201947
1) Sample: 45 humans third molars 2) Distribution: 180 enamel specimens were divided into 4groups; i) NSF, ii) SDF, iii) NaF, iv) control. 3) Outcome measures: i) VHN, ii) SEM.
NSF was not found comparatively effective as NaF varnish and SDF on enamel caries lesions.
Silva AV et al, 201945
1) Samples: 33 primary tooth specimens 2) Distribution: 3groups (n=11); i) G1-NSF(experimental), ii) G2-NaF(positive control), iii) G3-No remineralizing agent(negative control) 3) Outcome measure: OCT
NSF is as efficient as NaF for enamel remineralization in primary teeth.
Teixeria et al, 201842
1) Sample: 48 primary molars 2) Distribution: 3groups (n=16units); i) NSF containing dentifrices (test dentifrice), ii) NaF containing dentifrices (positive control), iii) Deionized water (negative control). 3) Outcome measures: Microhardness test, OCT
NSF is as effective as NaF for enamel remineralization in primary molars.
Silva et al, 201843
1) Sample: primary tooth enamel fragments. 2) Distribution: 33 samples into 3groups (n=11); i) NaF(positive control), ii) NSF (experimental group), iii) Deionized water(negative control) 3) Outcome measures: Microhardness test, Fluorescence spectroscopy and OCT
NSF is as efficient as NaF for primary tooth enamel remineralization.
Nozari A et al, 201746
1) Sample: 80 sound primary anterior teeth 2) Distribution: 60 samples into 4 groups (n=15); i) NSF, ii) NaF varnish, iii) n-HAP, iv) Control(no treatment) 3) Outcome measures: SMH, AFM
NSF can have greater remineralizing capability than NaF varnish and n-HAP for primary anterior teeth
SDF: Silver diamine Fluoride; NSF: Nanosilver fluoride; AgNPs: Silver nanoparticles; KF: Potassium fluoride; PEG-AgNPs: polyethylene glycol-coated silver nanoparticles; NaF: Sodium fluoride; SEM: scanning electron microscopy; XDR: X-ray diffraction; VHN: Vickers microhardness; OCT: Optical coherence tomography; n-HAP: Nano-Hydroxyapatite serum; SMH: Surface microhardness; AFM: Atomic Force Microscopy.
Zameer et al. 8 Contemp Pediatr Dent 2021:2(1):1-13
Copyright © 2021 Contemporary Pediatric Dentistry
Table 4. Clinical trials assessing the effectiveness of nanosilver fluoride in arresting dental caries
Study Characteristics and Summary Intervention Study Findings
Nagireddy VR et al, 201950
Duration:1year
1) Sample: 60 children of the 4-9years age range 2) Distribution:100 primary molars were divided into 2 groups; i) NSF - experimental group, ii) Saline - control group 3) Follow up: after 7days, 5months and 12months
NSF has shown to be an anticaries agent and presents a non-invasive option for arresting dental caries in children
Tirupathi et al, 201936
Duration:1year
1) Sample: 50 school children aged between 6-10years. 2) Distribution: 159 primary molars were divided into 2 groups. i) NSSF - experimental group, ii) SDF - positive control 3) Follow up: 1month, 3months, 6months and 12months.
An annual application of NSSF showed similar efficacy as SDF in arresting dentinal caries in primary molars.
Burns J, Hollands K, 201537
Duration:1year
1) Sample: 60 children with 6.31 (± 0.60) mean age range 2) Distribution:130 primary molars were divided into 2 groups; i) NSF - experimental group, ii) Saline - control group 3) Follow up: 1week, 5month, 1year
An annual application of NSF solution has shown to be effective in hardening and arresting dentine caries in primary teeth.
Santos et al, 201438
Duration:1year
1) Sample: 60 school children of a poor community with a mean age of 6.31+ 0.60 years. 2) Distribution: 130 primary teeth were divided into 2 groups(n=65). i) NSF - experimental, ii) Water - control 3) Follow up: 1week, 5months, and 12months.
NSF has shown to be an effective caries arresting agent for children in poor communities.
NSSF: Nanosilver incorporated sodium fluoride; SDF: Silver diamine Fluoride;
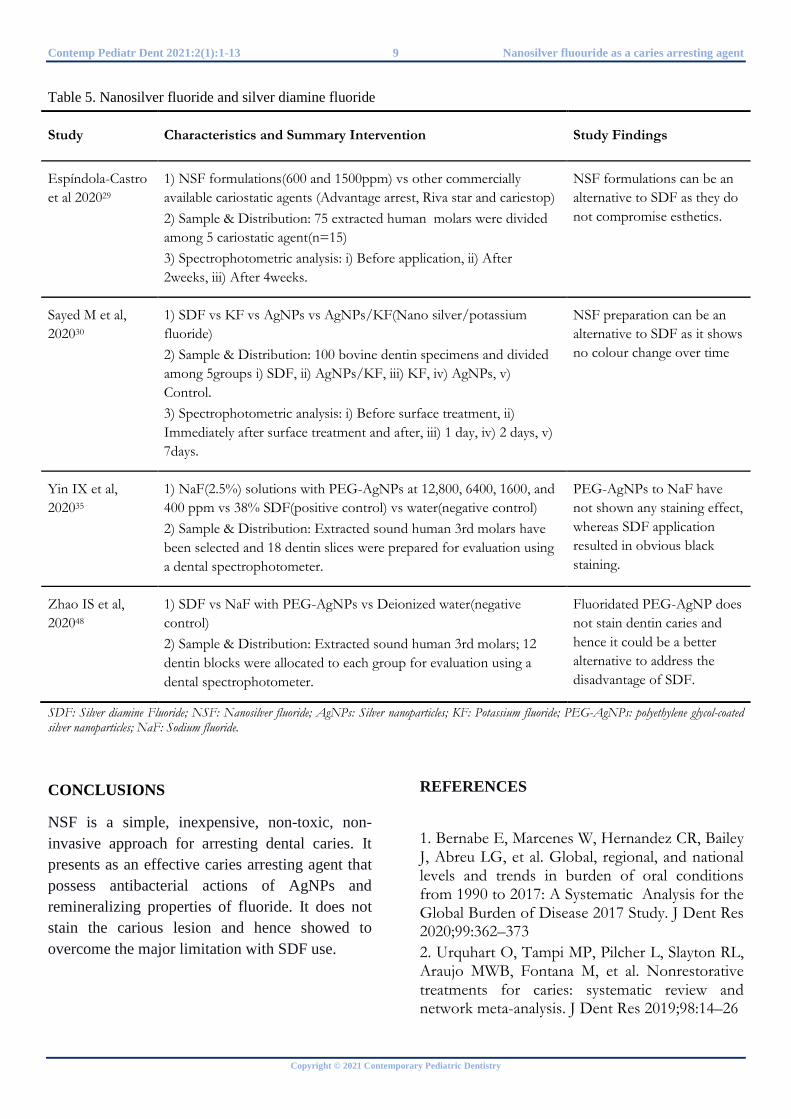
NSF vs SDF on caries lesion staining Table 5 summarizes 4 in-vitro studies
assessing the staining effects of NSF. The staining phenomenon with SDF application is due to the silver particle's precipitation and their oxidation on the carious dentin.17,18 Contrary to this, NSF formulations do not form oxides when coming in contact with the medium's oxygen and hence does not cause dentin staining.38 The study by Sayed et al.30 showed that no colour change observed over time with the reduction in the size of AgNPs. Another study by Espíndola-Castro et al.29 showed that 2 weeks after the NSF application, yellowish stains were seen on the teeth. The chitosan in the composition of NSF formulation is believed to be the cause of this stain formation. However, these stains were removed later by
toothbrushing, and the tooth colour restored to
the baseline values. The authors also observed that this staining could also be removed easily with a gauze. The precise quantification of different colour characteristics carried out in other studies with an objective instrumental measurement approach. It revealed that fluoridated polyethylene glycol-coated silver nanoparticles (PEG-AgNPs) showed no observable dentin staining. The dentin discolouration displayed with SDF application was not acceptable clinically as it was more than ten times higher than the acceptable upper threshold.35,48,51 Therefore, the NSF formulations have been suggested as a better alternative for caries arrest to overcome the staining disadvantage of SDF.
Contemp Pediatr Dent 2021:2(1):1-13 9 Nanosilver fluouride as a caries arresting agent
Copyright © 2021 Contemporary Pediatric Dentistry
Table 5. Nanosilver fluoride and silver diamine fluoride
Study Characteristics and Summary Intervention Study Findings
Espíndola-Castro et al 202029
1) NSF formulations(600 and 1500ppm) vs other commercially available cariostatic agents (Advantage arrest, Riva star and cariestop) 2) Sample & Distribution: 75 extracted human molars were divided among 5 cariostatic agent(n=15) 3) Spectrophotometric analysis: i) Before application, ii) After 2weeks, iii) After 4weeks.
NSF formulations can be an alternative to SDF as they do not compromise esthetics.
Sayed M et al, 202030
1) SDF vs KF vs AgNPs vs AgNPs/KF(Nano silver/potassium fluoride) 2) Sample & Distribution: 100 bovine dentin specimens and divided among 5groups i) SDF, ii) AgNPs/KF, iii) KF, iv) AgNPs, v) Control. 3) Spectrophotometric analysis: i) Before surface treatment, ii) Immediately after surface treatment and after, iii) 1 day, iv) 2 days, v) 7days.
NSF preparation can be an alternative to SDF as it shows no colour change over time
Yin IX et al, 202035
1) NaF(2.5%) solutions with PEG-AgNPs at 12,800, 6400, 1600, and 400 ppm vs 38% SDF(positive control) vs water(negative control) 2) Sample & Distribution: Extracted sound human 3rd molars have been selected and 18 dentin slices were prepared for evaluation using a dental spectrophotometer.
PEG-AgNPs to NaF have not shown any staining effect, whereas SDF application resulted in obvious black staining.
Zhao IS et al, 202048
1) SDF vs NaF with PEG-AgNPs vs Deionized water(negative control) 2) Sample & Distribution: Extracted sound human 3rd molars; 12 dentin blocks were allocated to each group for evaluation using a dental spectrophotometer.
Fluoridated PEG-AgNP does not stain dentin caries and hence it could be a better alternative to address the disadvantage of SDF.
SDF: Silver diamine Fluoride; NSF: Nanosilver fluoride; AgNPs: Silver nanoparticles; KF: Potassium fluoride; PEG-AgNPs: polyethylene glycol-coated silver nanoparticles; NaF: Sodium fluoride.
CONCLUSIONS
NSF is a simple, inexpensive, non-toxic, non-invasive approach for arresting dental caries. It presents as an effective caries arresting agent that possess antibacterial actions of AgNPs and remineralizing properties of fluoride. It does not stain the carious lesion and hence showed to overcome the major limitation with SDF use.
REFERENCES 1. Bernabe E, Marcenes W, Hernandez CR, Bailey J, Abreu LG, et al. Global, regional, and national levels and trends in burden of oral conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J Dent Res 2020;99:362–373 2. Urquhart O, Tampi MP, Pilcher L, Slayton RL, Araujo MWB, Fontana M, et al. Nonrestorative treatments for caries: systematic review and network meta-analysis. J Dent Res 2019;98:14–26
Zameer et al. 10 Contemp Pediatr Dent 2021:2(1):1-13
Copyright © 2021 Contemporary Pediatric Dentistry
3. Slayton RL, Urquhart O, Araujo MWB, Fontana M, Guzmán-Armstrong S, Nascimento MM, et al. Evidence-based clinical practice guideline on nonrestorative treatments for carious lesions: A report from the American Dental Association. J Am Dent Assoc 2018;149:837–849 4. Dorri M, Dunne SM, Walsh T, Schwendicke F. Micro-invasive interventions for managing proximal dental decay in primary and permanent teeth. Cochrane Database Syst Rev 2015;5:CD010431 5. Hendre AD, Taylor GW, Chávez EM, Hyde S. A systematic review of silver diamine fluoride: Effectiveness and application in older adults. Gerodontology 2017;34:411–419 6. Llodra JC, Rodriguez A, Ferrer B, Menardia V, Ramos T, Morato M. Efficacy of silver diamine fluoride for caries reduction in primary teeth and first permanent molars of schoolchildren: 36-month clinical trial. J Dent Res 2005;84:721–734 7. Oliveira BH, Rajendra A, Veitz-Keenan A, Niederman R. The Effect of Silver Diamine Fluoride in Preventing Caries in the Primary Dentition: A Systematic Review and Meta-Analysis. Caries Res 2019;53:24–32 8. Subbiah GK, Gopinathan NM. Is silver diamine fluoride effective in preventing and arresting caries in elderly adults? A systematic review. J Int Soc Prev Community Dent 2018;8:191–199 9. Fakhruddin KS, Egusa H, Ngo HC, Panduwawala C, Pesee S, Venkatachalam T, et al. Silver diamine fluoride (SDF) used in childhood caries management has potent antifungal activity against oral Candida species. BMC Microbiol 2020;20;95-105 10. Karched M, Ali D, Ngo H. In vivo antimicrobial activity of silver diammine fluoride on carious lesions in dentin. J Oral Sci 2019;61:19–24 11. Mei ML, Li Q-L, Chu C-H, Lo EC-M, Samaranayake LP. Antibacterial effects of silver diamine fluoride on multi-species cariogenic biofilm on caries. Ann Clin Microbiol Antimicrob 2013;26;12:4 12. Fakhruddin KS, Egusa H, Ngo HC, Panduwawala C, Pesee S, Samaranayake LP. Clinical efficacy and the antimicrobial potential of silver formulations in arresting dental caries: a systematic review. BMC Oral Health 2020;20:160-170
13. Zhao IS, Gao SS, Hiraishi N, Burrow MF, Duangthip D, Mei ML, et al. Mechanisms of silver diamine fluoride on arresting caries: a literature review. Int Dent J 2018;68:67–76 14. Punyanirun K, Yospiboonwong T, Kunapinun T, Thanyasrisung P, Trairatvorakul C. Silver diamine fluoride remineralized artificial incipient caries in permanent teeth after bacterial pH-cycling in-vitro. J Dent 2018;69:55–59 15. Yu OY, Zhao IS, Mei ML, Lo ECM, Chu CH. Caries-arresting effects of silver diamine fluoride and sodium fluoride on dentine caries lesions. J Dent 2018;78:65–71 16. Mei ML, Ito L, Cao Y, Li QL, Lo ECM, Chu CH. Inhibitory effect of silver diamine fluoride on dentine demineralisation and collagen degradation. J Dent 2013;41:809–817 17. Primus C. Potassium Iodide. The Solution to Silver Diamine Fluoride Discoloration? Adv Dent Oral Health 2017;5:555655 18. Patel J, Anthonappa RP, King NM. Evaluation of the staining potential of silver diamine fluoride: in vitro. Int J Paediatr Dent 2018;28;514-522 19. Crystal YO, Kreider B, Raveis VH. Parental expressed concerns about silver diamine fluoride (sdf) treatment. J Clin Pediatr Dent 2019 ;43:155–160 20. Crystal YO, Janal MN, Hamilton DS, Niederman R. Parental perceptions and acceptance of silver diamine fluoride staining. J Am Dent Assoc 2017;148:510–518 21. Alshammari AF, Almuqrin AA, Aldakhil AM, Alshammari BH, Lopez JNJ. Parental perceptions and acceptance of silver diamine fluoride treatment in Kingdom of Saudi Arabia. Int J Health Sci 2019;13:25–29 22. Horst JA, Ellenikiotis H, Milgrom PM. UCSF Protocol for caries arrest using silver diamine fluoride: rationale, ındications and consent. Pedia Dent 2017;84:16–26 23. Rosenblatt A, Stamford TCM, Niederman R. Silver diamine fluoride: a caries “silver-fluoride bullet.” J Dent Res 2009;88:116–125 24. Zhao IS, Mei ML, Burrow MF, Lo EC-M, Chu C-H. Effect of silver diamine fluoride and potassium ıodide treatment on secondary caries prevention and tooth discolouration in cervical glass ıonomer cement restoration. Int J Mol Sci 2017;18:340-345
Contemp Pediatr Dent 2021:2(1):1-13 11 Nanosilver fluouride as a caries arresting agent
Copyright © 2021 Contemporary Pediatric Dentistry
25. Sayed M, Matsui N, Hiraishi N, Nikaido T, Burrow MF, Tagami J. Effect of glutathione bio-molecule on tooth discoloration associated with silver diammine fluoride. Int J Mol Sci 2018;9:1322-1330 26. Roberts A, Bradley J, Merkley S, Pachal T, Gopal JV, Sharma D. Does potassium iodide application following silver diamine fluoride reduce staining of tooth? A systematic review. Aust Dent J 2020;65:109–117. 27. Turton B, Horn R, Durward C. Caries arrest and lesion appearance using two different silver fluoride therapies with and without potassium iodide: 6-month results. Heliyon. 2020;6:e04287 28. Turton B, Horn R, Durward C. Caries arrest and lesion appearance using two different silver fluoride therapies on primary teeth with and without potassium iodide: 12-month results. Clin Exp Dent Res 2020 Dec 02. Doi:10.1002/cre2.367 29. Espíndola-Castro LF, Rosenblatt A, Galembeck A, Monteiro G. Dentin staining caused by nano-silver fluoride: A comparative study. Oper Dent 2020;45:435–441 30. Sayed M, Hiraishi N, Matin K, Abdou A, Burrow MF, Tagami J. Effect of silver-containing agents on the ultra-structural morphology of dentinal collagen. Dent Mater 2020;36:936–944 31. Javan Bakht Dalir S, Djahaniani H, Nabati F, Hekmati M. Characterization and the evaluation of antimicrobial activities of silver nanoparticles biosynthesized from leaf extract. Heliyon 2020;6:e03624 32.Mikhailov OV, Mikhailova EO. Elemental silver nanoparticles: Biosynthesis and bio applications. Materials 2019;12:3177 33. Yin IX, Zhao IS, Mei ML, Li Q, Yu OY, Chu CH. Use of silver nanomaterials for caries prevention: A concise review. Int J Nanomedicine 2020;15:3181–3191 34.Yin IX, Yu OY, Zhao IS, Mei ML, Li Q-L, Tang J, et al. Developing biocompatible silver nanoparticles using epigallocatechin gallate for dental use. Arch Oral Biol 2019;102:106–112 35. Yin IX, Zhao IS, Mei ML, Lo ECM, Tang J, Li Q, et al. Synthesis and characterization of fluoridated silver nanoparticles and their potential as a non-staining anti-caries agent. Int J Nanomedicine 2020;15:3207–3215
36. Tirupathi S, Svsg N, Rajasekhar S, Nuvvula S. Comparative cariostatic efficacy of a novel Nano-silver fluoride varnish with 38% silver diamine fluoride varnish a double-blind randomized clinical trial. J Clin Exp Dent 2019;11:105–112 37. Burns J, Hollands K. Nano silver fluoride for preventing caries. Evid Based Dent 2015;16:8–9 38. Santos VE dos Jr, Vasconcelos Filho A, Targino AGR, Flores MAP, Galembeck A, Caldas AF Jr, et al. A new “silver-bullet” to treat caries in children--nano silver fluoride: a randomised clinical trial. J Dent 2014;42:945–951 39. Baker C, Pradhan A, Pakstis L, Pochan DJ, Shah SI. Synthesis and antibacterial properties of silver nanoparticles. J Nanosci Nanotechnol 2005;5:244–249 40. Morones JR, Elechiguerra JL, Camacho A, Holt K, Kouri JB, Ramírez JT, et al. The bactericidal effect of silver nanoparticles. Nanotechnology 2005;16:2346–2353 41. Targino AGR, Flores MAP, dos Santos Junior VE, de Godoy Bené Bezerra F, de Luna Freire H, Galembeck A, et al. An innovative approach to treating dental decay in children. A new anti-caries agent J Mater Sci Mater Med 2014;10: 2041–2047 42. Teixeira JA, Silva AVCE, Dos Santos Júnior VE, de Melo Júnior PC, Arnaud M, Lima MG, et al. Effects of a new nano-silver fluoride-containing dentifrice on demineralization of enamel and adhesion and acidogenicity. Int J Dent 2018;2018:1351925 43. Silva AVC, Amitis Vieira Costa, Teixeira JA, Cláudia C B, Emery Clayton Cabral, de Melo Júnior PC, et al. In Vitro morphological, optical and microbiological evaluation of nanosilver fluoride in the remineralization of deciduous teeth enamel Nanotechnol Rev 2018;7:509–520 44. Freire PLL, Albuquerque AJR, Sampaio FC, Galembeck A, Flores MAP, Stamford TCM, et al. AgNPs: The new allies against s. mutans biofilm - a pilot clinical trial and microbiological assay. Braz Dent J 2017;28:417–422 45. Silva AVC, Amitis Vieira Costa, de Araújo Teixeira J, de Melo Júnior PC, de Souza Lima MG, de Oliveira Mota CCB, et al. Remineralizing potential of nano-silver-fluoride for tooth enamel: An optical coherence tomography analysis. Pesqui Bras Odontopediatria Clin Integr 2019;19: 1–13 46. Nozari A, Ajami S, Rafiei A, Niazi E. Impact of nano hydroxyapatite, nano silver fluoride and
Zameer et al. 12 Contemp Pediatr Dent 2021:2(1):1-13
Copyright © 2021 Contemporary Pediatric Dentistry
sodium fluoride varnish on primary teeth enamel remineralization: An ın vitro study. J Clin Diagn Res 2017;11:97–100 47. Akyildiz M, Sönmez IS. Comparison of remineralising potential of nano silver fluoride, silver diamine fluoride and sodium fluoride varnish on artificial caries: an ın vitro study. Oral Health Prev Dent 2019;17:469–477 48. Zhao IS, Yin IX, Mei ML, Lo ECM, Tang J, Li Q, et al. Remineralising dentine caries using sodium fluoride with silver nanoparticles: An ın vitro study. Int J Nanomedicine 2020;15:2829–2839 49. Chu CH, Lo ECM, Lin HC. Effectiveness of silver diamine fluoride and sodium fluoride varnish in arresting dentin caries in Chinese pre-school children. J Dent Res 2002;81:767–770 50. Nagireddy VR, Reddy D, Kondamadugu S, Puppala N, Mareddy A, Chris A. Nanosilver fluoride-A paradigm shift for arrest in dental caries in primary teeth of schoolchildren: A randomized controlled clinical trial. Int J Clin Pediatr Dent 2019;12:484–490 51. Westland S, Luo W, Li Y, Pan Q, Joiner A. Investigation of the perceptual thresholds of tooth whiteness. J Dent 2017;67:11–14 52. Zander HA. use of silver nitrate in the treatment of caries. J Am Dent Assoc 1941;28:1260–1267 53. Crystal YO, Niederman R. Evidence-based dentistry update on silver diamine fluoride. Dent Clin North Am 2019;63:45–68 54. Köhler W. WD Miller. The micro-organisms of the human mouth 1974;14:84–84 55. Muntz JA, Dorfman A, Stephan RM. In vitro studies on sterilization of carious dentin. Evaluation of germicides. J Am Dent Assoc 1943;30:1893–900 56. Gao SS, Zhao IS, Duffin S, Duangthip D, Lo ECM, Chu CH. Revitalising silver nitrate for caries management. Int J Environ Res Public Health 2018;15:80-85 57. Yamaga R, Nishino M, Yoshida S, Yokomizo I. Diammine silver fluoride and its clinical application. J Osaka Univ Dent Sch 1972;12:1–20 58. Thibodeau EA, Handelman SL, Marquis RE. Inhibition and killing of oral bacteria by silver ıons generated with low ıntensity direct current. J Dent Res 1978;57:922–926
59. Craig GG, Powell KR, Cooper MH. Caries progression in primary molars: 24-month results from a minimal treatment programme. Community Dent Oral Epidemiol 1981;9:260–265 60. Craig GG, Powell KR, Cooper MH. Clinical appearance of permanent successors after nonextraction treatment of grossly carious primary molars in highly anxious children. ASDC J Dent Child 1987;54:170–175 61. Green E. A clinical evaluation of two methods of caries prevention in newly-erupted first permanent molars. Aust Dent J 1989;34: 407–419 62. Yee R, Holmgren C, Mulder J, Lama D, Walker D, van Palenstein Helderman W. Efficacy of silver diamine fluoride for arresting caries treatment. J Dent Res 2009;88:644–657 63. Zhi QH, Lo ECM, Lin HC. Randomized clinical trial on effectiveness of silver diamine fluoride and glass ionomer in arresting dentine caries in preschool children. J Dent 2012;40:962–967 64. Zhang W, McGrath C, Lo ECM, Li JY. Silver diamine fluoride and education to prevent and arrest root caries among community-dwelling elders. Caries Res. 2013;47:284–290 65. Dos Santos VE Jr, de Vasconcelos FMN, Ribeiro AG, Rosenblatt A. Paradigm shift in the effective treatment of caries in schoolchildren at risk. Int Dent J 2012;62:47–51 66. Jabin Z, Vishnupriya V, Agarwal N, Nasim I, Jain M, Sharma A. Effect of 38% silver diamine fluoride on control of dental caries in primary dentition: A systematic review. J Family Med Prim Care 2020;9:1302–1307 67. de Almeida L de FD, Cavalcanti YW, Valença AMG. In vitro antibacterial activity of silver diamine fluoride in different concentrations. Acta Odontol Latinoam 2011;24:127–131 68. Mei ML, Ito L, Cao Y, Lo ECM, Li QL, Chu CH. An ex vivo study of arrested primary teeth caries with silver diamine fluoride therapy. J Dent 2014;42:395–402 69. Chu C-H, Lee AH-C, Zheng L, Mei ML, Chan GC-F. Arresting rampant dental caries with silver diamine fluoride in a young teenager suffering from chronic oral graft versus host disease post-bone marrow transplantation: A case report. BMC Res Notes 2014:7:3-10

Contemp Pediatr Dent 2021:2(1):1-13 13 Nanosilver fluouride as a caries arresting agent
Copyright © 2021 Contemporary Pediatric Dentistry
70. Corrêa JM, Mori M, Sanches HL, da Cruz AD, Poiate E, Isis Andréa Venturini. Silver Nanoparticles in Dental Biomaterials. Int J Biomater 2015;1:1-9 How to cite this article: Mohammed Zameer, Sameen Badiujjama Birajdar, Syed Wali Peeran, Syed Nahid Basheer, Syed Ali Peeran, and Arun Reddy. Nanosilver fluoride as a caries arresting agent: A narrative review. Contemp Pediatr Dent 2021:2(1):1-13
Declarations
Acknowledgements: Not applicable. Conflict of Interest Statement: The authors disclose no potential conflicts of interest. Ethics Statement: This study does not require approval from the ethics committee. Informed Consent: Not required. Author contributions: Conception and design: MZ; Acquisition of data: MZ, SNB; Interpretation of data: MZ, SWP; Drafting article: MZ, SBB, AR; Revision artice: SBB, SNB, SAP, AR; Final approval: All Authors Funding: This work is not finantiated. Data Availability: The data used to support the findings of this study can be made available upon request to the corresponding author. Peer-review: Externally double-blinded peer-reviewed.
Copyright © 2021 Contemporary Pediatric Dentistry. This work is licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International license. (CC BY-NC-ND 4.0)
Original Research
Assessment of communication words during dental treatment requiring with and without local anaesthesia between child and pediatric dentist
Shital Kiran Davangere Padmanabh1✉, Para Dave2
Abstract Aim: To evaluate the widely used words by children and pediatric dentist during different dental procedures that involves treatment under local anaesthesia (LA) and without LA. Methods: 40 children aged between 6-12years were divided in to 2 groups, Group; I treated under local anaesthesia and Group II without anaesthesia. Each group comprising of 20 subjects (male- 10) (female -10) were recruited from the Department of Pediatric and Preventive Dentistry. The procedure was randomized only in one appointment by collecting the data conducted by recording the conversations between the child and dentist from the time the child walks in the dental operator until the session got over. The conversation was taped, transcribed and analyzed linguistically and statistically using chi-square test. Results: A total of 50 words were used with a minimum of 15 words in a session. There were no significant difference were found in words spoken by the child and the practitioner regarding gender, session, and duration of being acquainted with (p>0.05). Regarding age groups, (4–7-year-old) significantly used fewer words than the schoolers (6–12-year-old) (p<0.05). Conclusions: This study proved that the most commonly used words by the practitioner in treatment under LA and without LA were “syringe”, “pain” and “to identify” and “stop”, “open your mouth”, and “to identify” respectively. Keywords: Child; Dentist; Communication; Verbal Behavior
Highlights Regardless of local anaesthesia, communication played a vital role between pediatric dentist and child in the behaviour management during dental procedures.
1 Professor Dept. of Pedodontics and Preventive Dentistry, College of Dental Sciences At. Amargardh, Tal. Sihor, Dist Bhavnagar Gujarat -364210 2 Post Graduate student Dept. of Pedodontics and Preventive Dentistry, College of Dental Sciences At. Amargardh, Tal. Sihor, Dist Bhavnagar Gujarat -364210
Correspondence: Dept. of Pedodontics and Preventive Dentistry, College of Dental Sciences, At. Amargardh, Tal. Sihor, Dist Bhavnagar Gujarat -364210 E-mail address: [email protected]
Received: 06 February 2021 Accepted: 26 April 2021 Online First: 27 April 2021
Pediatric dentist needs to talk more often as possible in a directive to carry out successful behaviour managament regardless of the age of the child.
Treatment with local anaesthesia and no local anaesthesia, the words answered by the child were "na", "hmm", "hurt", and "ha", "aaa", "ok" respectively.
Contemporary Pediatric Dentistry Contemp Pediatr Dent 2021:2(1):14-20 DOI: 10.51463/cpd.2021.45

Padmanabh and Dave 15 Contemp Pediatr Dent 2021:2(1):14-20
Copyright © 2021 Contemporary Pediatric Dentistry
INTRODUCTION Noninvasive behaviour shaping in the form of
Communication places a vital role in the behaviour management of the children. Behaviour management is defined as that procedure which very slowly develops behaviour by reinforcing successive approximations of the desired conduct until it becomes to be.1 Behaviour shaping alters conduct according to the established principles based on a learning modem. Behaviour shaping requires positive behaviour throughout the procedure and it also retraces the steps in the form of positive reinforcement. It is a fact that establishing communication will lead to the successful management of the children. The children, when they meet the new people initially, they tend to be shy and reluctant to talk, However once children are comfortable in the familiar environment, they will gain confidence. In very young children, pediatric dentist has to use euphemisms which is like a second language for most pediatric dentist.1
Behaviour management is a part of pain-free local anaesthesia with the focus of controlling the child according to the concept of perceived control which regulates the pressure of an injection discomfort. Motor signaling such as lifting a hand2 or vocal signaling such as saying “Aaaa” may be used in the perceived controlled technique.3 Use of vocal signaling that is “Aaaa” is a natural reaction when the pain is perceived. The use of this natural signal can encourage children to overcome hesitation, thus cooperate with dental treatment. Communication (i.e., opinions, or information or interchange of thoughts or imparting) may ensue by various means but, however, in dental setup, it is proficient primarily via body language, tone of voice through dialogue and facial expression.4 Perceived control is the liberty fetched to children, which permits them to have control over the dental treatment. By utilizing stop signal by either saying “aaaaa or raising hand”, the pediatric dentist gives a pause in the
treatment procedure. Practicing perceived control brings down children's anxiety; thereby enhancing pain-free comfortable treatment session.5-7 A child's cognitive development will dictate the level and amount of information interchange that can take place.8
Communicative management of behaviour management is the essential component of Communication that requires no specific consent, whereas all other behaviour guidance techniques necessitate informed consent. Consistent with the American Association of Pediatric Dentistry (AAPD)'s guideline on informed consent, communicative supervision and proper use of commands are pragmatic unanimously in pediatric dentistry with both the uncooperative and cooperative child.9 AAPD guidelines words highlighted the importance of 'what is told' by the practitioner and 'what is understood' by the child. Language, verbal Communication, plays a significant role in the interface between the child patient and pediatric dentist. Dental procedures may provoke anxiety and fear. Very young age children are more disposed to dental fear due to lack of coping experience.10 Behaviour management technique along with appropriate communication between the child and the clinician, ensures reduction in the child's anxiety level.
The purpose of the study was to evaluate widely used words by children and pediatric dentist during different dental procedures, which involved treatment under local anaesthesia and without anaesthesia. The null hypothesis was to test whether the treatment requiring local anaesthesia or without anaesthesia required more communication between child and pediatric dentist.
METHODS Data source The study protocol was approved by the local institutional ethical committee board as per the
Contemp Pediatr Dent 2021:2(1):14-20 16 Communication words between child and pediaric dentist
Copyright © 2021 Contemporary Pediatric Dentistry
Helsinki declaration of human rights (Ref.No:CODS/IEC/128/2019 date 30.07.2019). Written consent was obtained from all the parents after explaining the objective of the study. This cross-sectional study adhered to Consolidated Standards of Reporting Trials (CONSORT) Guidelines and was conducted at department of pediatric and preventive dentistry, college of dental science, Amargadh, Gujarat, India, between December 2019 and January 2020. Sample size determination
The total sample sizes were determined with an error rate of 5% with 90% power. Therefore, the minimum required samples per group were found to be 20. Data collection
40 children who reported to pediatric dentistry department aged between 6-12 years old were recruited by the principle investigator randomly selected the subjects using coin toss method (one patient- one appointment- one procedural session) and were divided into 2 groups namely, Group I: children were treated under local anaesthesia (n=20); Group II: children without local anaesthesia dental procedures (n=20). Children aged between 6-12 years of age and their parents who gave informed consent for their child were included in the study. Specially- abled children and children with systemic conditions were excluded. Recruitment settings
A hidden audio recorder (Sony, Tokyo, Japan, ICD-PX240 MP3 digital voice recorder) was kept near the operator’s chair to record the conversation between the pediatric dentist and the child.Subjects who reported during the first session of the clinical hours (9 am to 12.00 pm) were allocated under Group I (local anaesthesia). Similarly, subjects who reported during the second session (1.00 pm to 4.00 pm) were
assigned under group II (without local anaesthesia).
The different treatment which was done under local anaesthesia lignocaine 2% (ICPA health products limited, Ankleshwar, Gujarat, India) were pulp therapies, tooth extractions, a restoration, which required local anaesthesia and stainless-steel crown placement. Similarly, the various treatments which were done without local anaesthesia were oral prophylaxis, topical fluoride application, a restoration which did not require local anaesthesia and fixed space maintainers. After completion of each procedure, the words which was spoken was played on the audio speaker (JBL Flip 3 by Harman, Los Angeles, California, United States), and all the conversed words were identified in their native language and converted to English language.
Data were subjected to statistical analysis by using the chi-square test for intergroup and intragroup. A p-value < 0.05 was considered statistically significant.
RESULTS The pediatric dentist used a total of 10,480 words throughout the study. Children who participated in the study were aged between 6-12 years with the mean age of Group I was 9.00 years, and group II were 9.20 years. A total of 2,895 different words were spoken by the pediatric dentist, whereas the child spoke 1,980 words as a response (Table1 and Table 2).
Comparison of various words used among males and females in Group I as well as in Group II was insignificant. Comparing of various words used between the Group I and II, the chi-square value was 40 and 17.1 for the word “tooth” and “syringe”, respectively. Similarly, for the “pain” the chi-square value was 29.5 and “dental cement” it was 13.9. It were observed that the word’s “tooth”, “pain”, “syringe”, and “dental cement”,were found highly significant (p=0.001) (Table3).
Padmanabh and Dave 17 Contemp Pediatr Dent 2021:2(1):14-20
Copyright © 2021 Contemporary Pediatric Dentistry
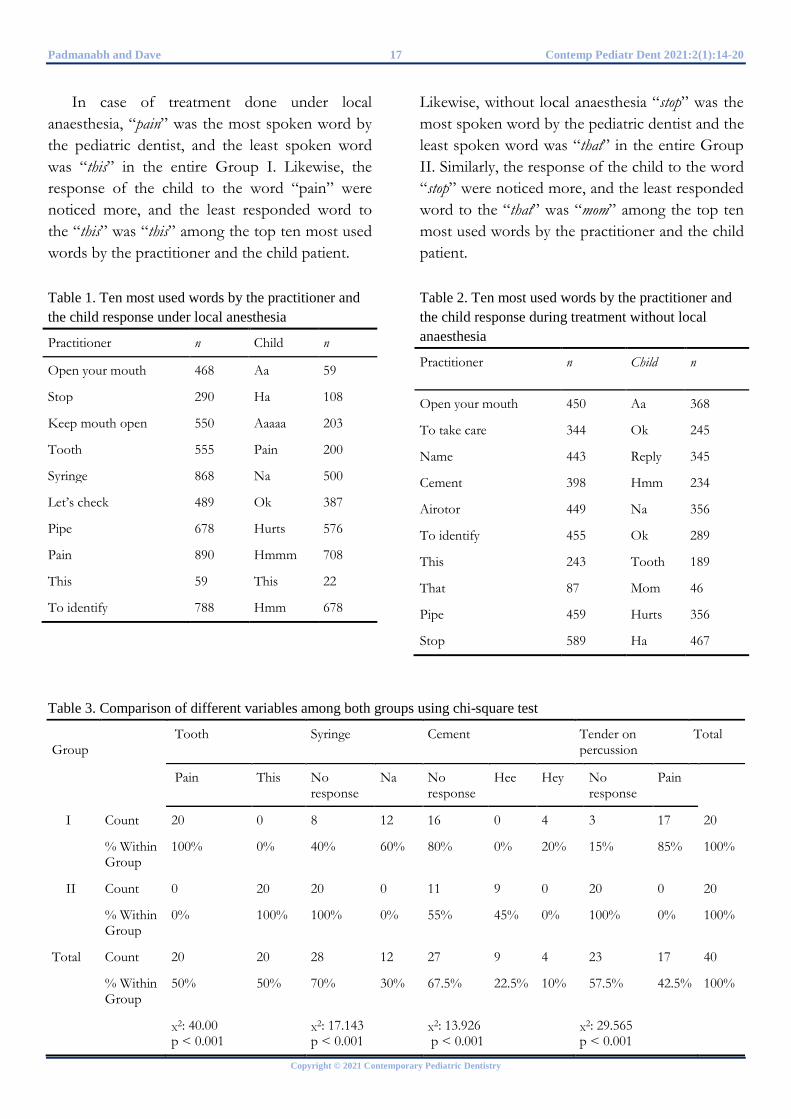
In case of treatment done under local anaesthesia, “pain” was the most spoken word by the pediatric dentist, and the least spoken word was “this” in the entire Group I. Likewise, the response of the child to the word “pain” were noticed more, and the least responded word to the “this” was “this” among the top ten most used words by the practitioner and the child patient. Table 1. Ten most used words by the practitioner and the child response under local anesthesia
Practitioner n Child n
Open your mouth 468 Aa 59
Stop 290 Ha 108
Keep mouth open 550 Aaaaa 203
Tooth 555 Pain 200
Syringe 868 Na 500
Let’s check 489 Ok 387
Pipe 678 Hurts 576
Pain 890 Hmmm 708
This 59 This 22
To identify 788 Hmm 678
Likewise, without local anaesthesia “stop” was the most spoken word by the pediatric dentist and the least spoken word was “that” in the entire Group II. Similarly, the response of the child to the word “stop” were noticed more, and the least responded word to the “that” was “mom” among the top ten most used words by the practitioner and the child patient. Table 2. Ten most used words by the practitioner and the child response during treatment without local anaesthesia
Practitioner n Child n
Open your mouth 450 Aa 368
To take care 344 Ok 245
Name 443 Reply 345
Cement 398 Hmm 234
Airotor 449 Na 356
To identify 455 Ok 289
This 243 Tooth 189
That 87 Mom 46
Pipe 459 Hurts 356
Stop 589 Ha 467
Table 3. Comparison of different variables among both groups using chi-square test
Group
Tooth Syringe Cement Tender on percussion
Total
Pain This No response
Na No response
Hee Hey No response
Pain
I Count 20 0 8 12 16 0 4 3 17 20
% Within Group
100% 0% 40% 60% 80% 0% 20% 15% 85% 100%
II Count 0 20 20 0 11 9 0 20 0 20
% Within Group
0% 100% 100% 0% 55% 45% 0% 100% 0% 100%
Total Count 20 20 28 12 27 9 4 23 17 40
% Within Group
50% 50% 70% 30% 67.5% 22.5% 10% 57.5% 42.5% 100%
X2: 40.00 p < 0.001
X2: 17.143 p < 0.001
X2: 13.926 p < 0.001
X2: 29.565 p < 0.001

Contemp Pediatr Dent 2021:2(1):14-20 18 Communication words between child and pediaric dentist
Copyright © 2021 Contemporary Pediatric Dentistry
DISCUSSION When pain was anticipated, local analgesia
supports behaviour management techniques (BMT)s in the dental treatment procedures.11 The regularity of linguistic techniques used throughout treatment procedure and its success in accomplishing patient cooperation have been studied. The majority of pediatric dentists agree on the importance of oral Communication to make the child's exposure to dentistry more pleasant and acceptable. Wurster et al.12 has demonstrated communication method used by the pediatric dentist depend upon behaviour of the child. Weinstein et al.13 demonstrated that inappropriate child behaviour results from ineffective approaches of the dentist, whereas the use of direction and reinforcement reduces the probability of unfavorable behaviour. They also showed the beneficial effects of empathic reactions compared to coercion and pleading.
Melamed et al. 14 tested the effect of reinforcement and concluded that it has a significant influence on the child's behaviour during dental treatment. The combination of negative and positive reinforcement consequences improved child cooperation. Dentists have used an assorted linguistic tactic during dental treatment, which has a precise outcome on the child's cooperation and behaviour. Collective strategies and different approaches would help the children overcome fear and therefore co-operating better. Verbal communication in the dental office is a part of what is termed as “institutional talk”15 which includes communication between patient and physician which is part of a wider sphere known as “conversational analysis”.16
The three models which define the features of talk between patient and physician are the activity-passivity, where the situation is controlled by the physician, especially in emergencies. Guidance-cooperation, in a condition wherein the patient, permits the physician to treat, with postulation considering physician knowledge and skill required to treat, thereby the patient complies
with instructions); Mutual participation, of both physician and patient make choices collectively.17 Decisions were presented, and the patient enthusiastically shares in the selecting treatment process.
Roter et al.18 advocated a supplementary model, consumerism, requests to the physician were made by the patient who is the consumer. Guidance cooperation which best designates the conversation between the child and dentist.19 Effective Communication is essential between the child and pediatric dentist to develop a trusting relationship and eventually gain the child’s cooperation.20 Communication is a reciprocal process where effective Communication occurs through a must sensory approach. The dentist acts as a transmitter, and the, child acts as a receiver and spoken words as a medium. Human being learns the rules according to the verbal descriptions whereas animal acquires by environmental contingencies. Therefore, behaviour in children should be contingency control and should show scheduled effects and also Communication between practitioner and child is bipolar in nature.21
Verbal communication effectiveness in the behaviour management of the children is tremendous, along with patient satisfaction. Even any instruction advised by the paediatric dentist depends upon how the parental attitude will be towards the dentistry. The relationship between parent and child is termed as one-tailed by Bell because of the influence on developing child. Here the children behave similar to the parental-maternal characteristic in various situation.22
By the age child reaches 5 to 6 years of age, the total vocabulary will be approximately 15,000 words with an increase of 10 words per day. According to Blinkhorn23, in 5 to 6 years old children, the total vocabulary wills 2,000 words per day. In the present study, the pediatric dentist used 2,895 different words to communicate with the child patient. In a similar study done by Caglar et al.24 in Turkish population, 626 different words

Padmanabh and Dave 19 Contemp Pediatr Dent 2021:2(1):14-20
Copyright © 2021 Contemporary Pediatric Dentistry
were used for communication, which indicates that in the Indian population, pediatric dentist speaks more words for the effective communication an behaviour management of the child. Blinkhorn23 stated that the importance of greeting the child by name instead of using generalized terms for them to feel special. In the present study, the most used word by the children in group I was “hmmm”, and by the pediatric dentist was “pain”. Likewise, in Group II the most used word by the children was “ha”, and by the pediatric dentist was “stop”. This study was conducted on normal healthy children, and it would be interesting to note whether the same number of words or any variations will be observed in the case of the specially-abled children.
CONCLUSIONS The present study proved that the most
commonly used words by the practitioner in treatment under LA were “syringe”, “pain”, and “to identify”. While the most common responded words by the child was “na”, “hmm”, and “hurts”. Similarly, the most commonly used words by the practitioner in treatment without LA were “stop”, “open your mouth”, and “to identify”. While the most common responded words by the child patient was “ha”,“ Aaa”, and “ok”.
REFERENCES 1. Schwartz S, Kupietzky A. Local Anesthesia. In: Wright GZ, Kupietzky A editors. Behavior Management in Dentistry for Children, Second Edition. New York: John Wiley & Sons, Inc; 2014. p.107-124 2. Chadwick BL, Honey MR. Behaviour management techniques in child training: How to Manage Children in Dental Practice. 2nd ed.London: Quintessence Publishing; 2003 3. Ram D, Kassirer J. Assessment of a palatal approach-anterior superior alveolar (P-ASA)
nerve block with the Wand in Pediatric dental patients. Int J Pediatric Dent 2006:16:348-351 4. Chambers DW. Communicating with the young dental patient. J Am Dent Assoc 1976;93:793-799 5. Corah NL. Effect of perceived control on stress reduction in pedodontic patients. J Dent Res 1973;52:1261-1264 6. Weinstein P, Milgrom P, Hoskuldsson O, Golletz D, Jeffcott E, Koday M. Situation-specific child control: a visit to the dentist. Behav Res Ther 1996;34:11-21 7. Weinstein P, Raadal M, Naidu S, Yoshida T, Kvale G, Milgrom P. A videotaped intervention to enhance child control and reduce anxiety of the pain of dental injections. Eur J Paediatr Dent 2003;4:181-185 8. Goleman J. Cultural factors affecting behavior guidance and family compliance. Pediatr Dent 2014;36:121-127 9. American Dental Association Division of Legal Affairs. Dental Records [Internet] 2021 [cited 2021 Apr 10]. Available from: https://success.ada.org/en/regulatory-legal/dental-records 10. Broberg AG, Klingberg G. Child and adolescent psychological development. In: Koch G, Poulsen S editors. Pediatric Dentistry - a clinical approach. West Sussex, UK: Wiley- Blackwell; 2009. p. 21-22 11. Kuscu OO, Çaglar E, Sandalli N. Local analgesia-a contemporary approach: What are the techniques that provide pain-free local analgesia for children? In: Spilieth CH editor. Revolutions in Pediatric Dentistry. Berlin: Quintessence Publishing; 2011. p. 135-150 12. Wurster GA, Weinstein P, Cohen AJ. Communication patterns in pedodontics. Percept Mot Skills 1979; 48:159-166 13. Weinstein P, Getz T, Ratener P, Domoto P. Dentists’ responses to fear and non-fear related behaviors in children. J Am Dent Assoc 1982;104:38-40 14. Melamed BG, Bennett CG, Jerrell G, Ross SL, Bush JP, Hill C, Courts F, Ronk S. Dentists’ behavior management as it affects compliance and fear in pediatric patients. J Am Dent Assoc 198;106:324-330 15. Schegloff EA. On talk and its institutional occasions. In: P Drew, J Heritage editors. Talk at
Contemp Pediatr Dent 2021:2(1):14-20 20 Communication words between child and pediaric dentist
Copyright © 2021 Contemporary Pediatric Dentistry
Work. Cambridge: Cambridge University Press, 1992. p. 101-134 16. Schiffrin D. Conversation analysis. Ann Rev Appl Linguistics 1990;11:13-16 17. Szasz TS, Hollender MH. A contribution to the philosophy of medicine: The basic models of doctor-patient relationships. Arch Int Med 1956; 97:585-592 18. Roter DL, Hall JA. Doctors Talking with Patients/Patients Talking to Doctors: Improving Communication in Medical Visits.1st ed. London: Auborn House; 1992 19. Haug MR, Lavin B. Practitioner or patient – Who’s in charge? J Health Soc Behav 1981; 22:212-229 20. Nash DA. Engaging children’s cooperation in the dental environment through effective communication. Pediatr Dent 2006; 28: 455-459 21. Broberg AG, Klingberg G. Child and adolescent psychological development. In: Koch G, Poulsen S, Pediatric Dentistry- a clinical approach. 2nd ed. West Sussex, UK: Wiley- Blackwell; 2009. p 21-22 22. Bell RQ. Stimulus control of parent or caretaker behavior by offspring. Dev Psychol 1971;4:63-72 23. Blinkhorn AS. Psychology of child development. In: Welbury RR. Paediatric Dentistry. 2nd ed. New York: Oxford University Press; 2001. p 23-28 24. Caglar E, Sandalli N, Kirant B, Kuscu O.O. Evaluation of words in child-paediatric dentist communication. Eur J Paediatr Dent 2015; 16: 236-238 How to cite this article: Shital Kiran Davangere Padmanabh, and Para Dave. Assessment of communication words during dental treatment requiring with and without local anesthesia between child and pediatric dentist. Contemp Pediatr Dent 2021:2(1):14-20
Declarations
Acknowledgements: Not applicable. Conflict of Interest Statement: The authors disclose no potential conflicts of interest. Ethics Statement: The study protocol was approved by the local institutional ethical committee board as per the Helsinki declaration of human rights (Ref. No:CODS/IEC/128/2019 date 30.07.2019). Informed Consent: Informed consent and assent were obtained from all participants. Author contributions: Conception and design: All Authors; Acquisition of data: All Authors; Interpretation of data: All Authors; Drafting article: All Author; Revision artice: SKDP; Final approval: All Authors Funding: This work is not finantiated. Data Availability: The data used to support the findings of this study can be made available upon request to the corresponding author. Peer-review: Externally double-blinded peer-reviewed.
Copyright © 2021 Contemporary Pediatric Dentistry. This work is licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International license. (CC BY-NC-ND 4.0)
Original Research
Evaluation of the clinical efficiency of rotary and manual files for root canal instrumentation in primary teeth pulpectomies: A comparative randomized clinical trial
KL Girish Babu1✉, Guraj Hebbar Kavyashree 2
Abstract Aim: To evaluate and compare the instrumentation time, obturation time, quality of obturation, and clinical and radiological success of pulpectomized teeth following root canal preparation of primary molars with rotary and manual file system. Methods: A total of 150 primary molars requiring pulpectomy were selected from children aged four to seven years. These teeth were divided into three groups of 50 teeth each. In Groups 1, 2, and 3, cleaning and shaping were carried out with Kedo-S pediatric rotary files, HERO Shaper rotary files, and manual NiTi K-files, respectively. Obturation was carried out with zinc oxide eugenol cement and an engine-driven Lentulo spiral. The instrumentation and obturation times were recorded. A radiographic assessment of the quality of the root filling was carried out immediately after obturation. Finally, the pulpectomized teeth were clinically and radiographically evaluated over a two-year period. Results: The mean instrumentation times for Groups 1, 2, and 3 were 14.56 ± 2.89 min, 17.93 ± 3.51 min, and 29.00 ± 2.08 min, respectively. The mean obturation times for Groups 1, 2, and 3 were 8.11 ± 1.7 min, 7.93 ± 1.3 min, and 9.64 ± 17.61 min, respectively. The mean difference in the quality of obturation was not statistically significant in primary molars instrumented with Kedo-S pediatric and HERO Shaper rotary file systems (p = 0.16). However, this mean difference was significant when compared between primary molar instrumented with rotary file systems and manual NiTi files (p = <0.001). At two years, the clinical success rate was 100% and the radiological success rates were 95.3%, 97.9%, and 89.5% in Groups 1, 2, and 3, respectively. Conclusions: The rotary file systems took significantly less instrumentation and obturation time than the manual NiTi files. There were no significant differences in obturation quality or success rates after two years. Keywords: Endodontic Obturation; Instrumentation; Pulpectomy; Root Canal Preparation
Highlights The application of rotary endodontics is still new in pediatric dentistry. Rotary files manufactured primarily for permanent teeth are routinely used in primary teeth.
1 Professor & Head, Department of Dentistry, Hassan Institute of Medical Sciences, Hassan-573201, India 2 Junior Resident, Department of Dentistry, Hassan Institute of Medical Sciences, Hassan-573201, India
Correspondence: Department of Dentistry, Hassan Institute of Medical Sciences, Hassan-573201, India E-mail address: [email protected]
Received: 20 February 2021 Accepted: 19 April 2021 Online First: 22 April 2021
The rotary file systems showed superior obturation quality, decreased instrumentation time, and decreased obturation time compared to manual files.
HERO Shaper rotary file system is manufactured for permanent teeth but its design makes it convenient to use in primary teeth. Recently, Kedo-S pediatric rotary file system was introduced for use in primary teeth.
Contemporary Pediatric Dentistry Contemp Pediatr Dent 2021:2(1):21-34 DOI: 10.51463/cpd.2021.42

Babu and Kavyashree 22 Contemp Pediatr Dent 2021:2(1):21-34
Copyright © 2021 Contemporary Pediatric Dentistry
INTRODUCTION
The use of rotary instruments in pediatric endodontics was introduced by Barr et al.,1,2 who found that the use of NiTi rotary files for root canal preparation in primary teeth is cost-effective, fast, and produces consistently uniform, predictable results. Since then, many rotary endodontic systems have been recommended for root canal cleaning and shaping in primary teeth.3–
7 However, NiTi file systems are primarily manufactured for use in permanent teeth. The use of these files in primary teeth may lead to lateral perforations, as primary teeth have shorter, thinner curved roots compared to permanent teeth and a ribbon-shaped morphology.8,9
One rotary file system that is manufactured for permanent teeth but convenient to use in primary teeth is the HERO Shaper rotary file system.10 The HERO Shaper rotary file system incorporates a conical design with high flexibility and a constant taper. The modified file design prevents a screw-like action and thus prevents the instrument from binding to the root canal.10 Additionally, HERO Shaper rotary files have short metallic shafts with non-cutting tips, making them more appropriate for use in primary teeth.11
The Endoflare is a separate #25 file, with a short blade length of 15 mm and a working length of 10 mm, that is suitable for the shorter root canal lengths of primary teeth. The 0.12 taper and positive cutting angle of the Endoflare allow for better cutting and excellent debridement, and its non-cutting tip makes it safer for use in primary teeth. The Endoflare is only used to flare the coronal third at the beginning of the shaping process.11,12 This is particularly suitable for primary molars where there is an abrupt cervical constriction and dentinal shelf covering the canal orifice.11,12
The Kedo-S pediatric file system is an exclusive, recently introduced pediatric rotary file system.13 This system consists of three NiTi files (D1, E1, and U1) with an altered working length
of 12 mm to expedite its use in primary teeth. The D1 and E1 files are designed for the instrumentation of molars, and the U1 files are designed for anterior teeth. Another added feature of this file system is the presence of a variably variable taper. 9,13
Independent studies10,11-18 have evaluated the immediate outcomes of the HERO Shaper rotary file system and Kedo-S pediatric rotary file systems and shown that they produce superior results. These trials are either in-vitro or cross-sectional in nature. No published scientific studies have evaluated the clinical efficiency of these two rotary file systems for the root canal instrumentation of primary teeth over a two-year period. Therefore, the objectives of the present study were to evaluate and compare (1) the instrumentation time, obturation time, and quality of obturation and (2) the clinical and radiological success of pulpectomized teeth following the root canal preparation of primary molars with Kedo-S pediatric rotary file system, HERO Shapers rotary file system, and manual NiTi K-files.
METHODS Prior to the beginning of this study, ethical
clearance was obtained from our institutional review board (IEC/HIMS/RR76). The study protocol followed the guidelines provided by the World Medical Association’s Declaration of Helsinki on Ethical Principles for Medical Research. The CONSORT guidelines for planning and reporting clinical trials in pediatric endodontics were followed throughout the different stages of the study (Figure 1). The study sample included normal, healthy, and cooperative children aged four to seven years visiting our department for pulpectomy of their primary molars.
The sample size was calculated based on previous studies.12,13,15,18 The prevalence of optimal fills in rotary file systems is 76.7%. Thus,

Contemp Pediatr Dent 2021:2(1):21-34 23 Clinical efficiency of rotary and manual files
Copyright © 2021 Contemporary Pediatric Dentistry
Z = 1.96 (constant for 95% CI)
P = 76.7% = 0.767
Q = 1 - P = 1 - 0.0767 = 0.233
d = Precision (5–20% of P) = 16% of 76.7% = 12.2% = 0.122
n = Z2PQ d2 = (1.96)2 X 0.767 X 0.233
(0.122)2
= 45
Thus, the estimated sample size was 45, which was rounded off to 50.
The nature and objectives of the study were explained to the parents of the participating children, who then provided their informed written consent. The participants’ confidentiality was ensured with the use of identification numbers, and their records were maintained by the principal investigator alone. Intraoral examinations were performed and standardized intraoral periapical radiographs were taken for the teeth to determine whether pulpectomy was indicated. The sample inclusion criteria covered teeth that exhibited one or more of the following features: 1) carious pulp exposure diagnosed with irreversible pulpits, 2) vital or non-vital primary molars without a sinus tract, 3) an absence of internal or external pathological root resorption, 4) radiographic signs of pulpal or inter-radicular involvement, or 5) the presence of two-thirds of root length.1,19,20 The exclusion criteria covered teeth with any of the following characteristics: 1) an abscess or sinus tract due to dental caries, 2) non-restorability, 3) pulpal floor perforation, 4) root resorption of more than one-third, or 5) an excessive pathologic loss of bone support with a loss of normal periodontal attachment. Additionally, children who had special care needs, had limited or lacking cooperative abilities, or required sedation/general anesthesia for behavior management were also not included.1,19,20
The study sample comprised 150 teeth from the selected children. Computer-generated randomization was used to sort these primary
molars into three groups (Group 1, Group 2, and Group 3), each consisting of 50 teeth, according to the type of instrumentation to be used for root canal preparation. The root canals in Group 1 were instrumented with the Kedo-S pediatric rotary file system (Reeganz Dental Care Pvt. Ltd., India), those in Group 2 were instrumented with the HERO Shaper rotary file system (Micromega, Geneva, Switzerland), and those in Group 3 were instrumented with manual NiTi K-files (Dentsply, Switzerland).
The pulpectomy procedure was carried out under stringent aseptic conditions by a single pediatric dentist with experience using both rotary and manual instrumentation techniques. Routine nonpharmacological behavior management techniques were used throughout the procedure. Following the administration of local anesthesia (2% lignocaine, Lignox, Bangalore, India), dental caries and overhanging enamel were removed with a #330 high-speed bur under a water spray. The coronal pulp was accessed using a #8 round bur, and the entire roof of the pulp chamber was removed. Necrotic tissue was removed from the pulp chamber with a sterile sharp spoon excavator (2 mm, EXC31W, #41 Round, 31W Endo Excavators, Hu-Friedy Mfg. Co., LLC). After straight-line access was obtained, pulp tissue was extirpated from the root canal using H-files (Mani, Inc., Tochigi, Japan). A #10 K-file (Mani, Inc., Tochigi, Japan) was then used to access the patency of the root canal. The working length was determined by superimposing an endodontic instrument over the preoperative radiograph and keeping it 1–2 mm short of the radiographic apex.12,13
The root canals in Group 1 were instrumented with the Kedo-S pediatric rotary file system (Reeganz Dental Care Pvt. Ltd., India) according to the manufacturer’s instructions. The D1 rotary files were used for preparation of the mesiobuccal and mesiolingual root canals of mandibular teeth and, mesiobuccal and distobuccal root canals of

Babu and Kavyashree 24 Contemp Pediatr Dent 2021:2(1):21-34
Copyright © 2021 Contemporary Pediatric Dentistry
maxillary teeth. E1 rotary file was used for preparation of the distal root canal of mandibular teeth and palatal canal of maxillary teeth with a lateral brushing motion.13 The root canals in Group 2 were instrumented with the HERO Shaper rotary file system (Micromega, Geneva, Switzerland) and a coronal-enlarging file (Endoflare-Micromega, Geneva, Switzerland) provided with the file system. The root canals were first instrumented up to the coronal one-third using an Endoflare file at 4-point torque. Then, the root canals were enlarged to working length according to the sequence recommended by the manufacturer.12 The rotary file systems used for Groups 1 and 2 were operated with an endodontic motor (X-Smart, Dentsply Maillefer, OK, USA) at 300 rpm and 2.2-Ncm torque.13 The root canals were not entered more than twice with each rotary file; this was ensured to prevent unexpected lateral perforation, especially in severely curved root canals.21 The root canals in Group 3 were instrumented with manual NiTi K-files (Dentsply, Maillefer, Ballaigues,Switzerland). A minimum-size file provided resistance for intracanal placement until the working length was determined as an initial file. The root canals were enlarged up to three times the size of the initial file. Then, the root canals were cleaned and shaped using a pullback motion.13
In all three groups, each file was used on up to five teeth to maintain uniformity during root canal preparation.13,21 If a point of resistance was encountered, no attempt was made to go beyond it; this was ensured to lower the risk of instrument fracture.21 All of the root canals were prepared with intermittent irrigation using a standard 5-ml volume of normal saline. During root canal preparation, 17% EDTA gel (RC Help, Prime Dental Products, Pvt. Ltd.) was used as a lubricating paste.13 Following complete root canal preparation, final irrigation was carried out with saline, and the root canals were dried with absorbent paper points. The root canals of the primary molars in all three groups were obturated
with zinc oxide eugenol cement (Zinc Oxide BP, Eugenol BP, Associated Dental Products Ltd.) using a Lentulo spiral mounted on a slow-speed handpiece. The selected Lentulo spiral was one size smaller than the last-used file size and was cut to half its length with a pair of sharp scissors to facilitate handling. A homogenous mixture of zinc oxide eugenol was mixed in a powder: liquid ratio of 1:1. The prepared paste was carried into the root canal using a slow-speed handpiece rotating in a clockwise direction, which was then gently withdrawn from the root canal while still rotating. A rubber stopper was used to keep the Lentulo spiral 1 mm short of the working length. This process was repeated five to seven times for each root canal until the canal orifice was filled with the paste.22,23 The pulp chamber was cleaned with a moist cotton pellet and then restored with type II glass ionomer cement (GC, India).13,20 Some of the younger children could not bear the long appointments required to maintain the standardized procedure. Hence, for these children, the final restoration with stainless steel crowns (3M ESPE, St. Paul, MN, USA) was carried out in a second appointment within one week of obturation. All the participants were instructed to report any symptoms following the procedure, such as pain or swelling.
The instrumentation and obturation times were calculated by a trained dental assistant using a stopwatch. Instrumentation time is the amount of time required to negotiate and shape all the root canals of a tooth to the desired size after root canal access opening and working length determination. Obturation time is the amount of time required to obturate all the root canals of a tooth after instrumentation.13,20 Immediate postoperative radiographs were taken with a dental X-ray unit operating at 60 kvp, 6 mA, 0.3 seconds, and 15 mm. These radiographs were evaluated for quality of obturation by two pediatric dentists who were blinded to the type of instrumentation used. A kappa test was performed for these examiners, producing scores
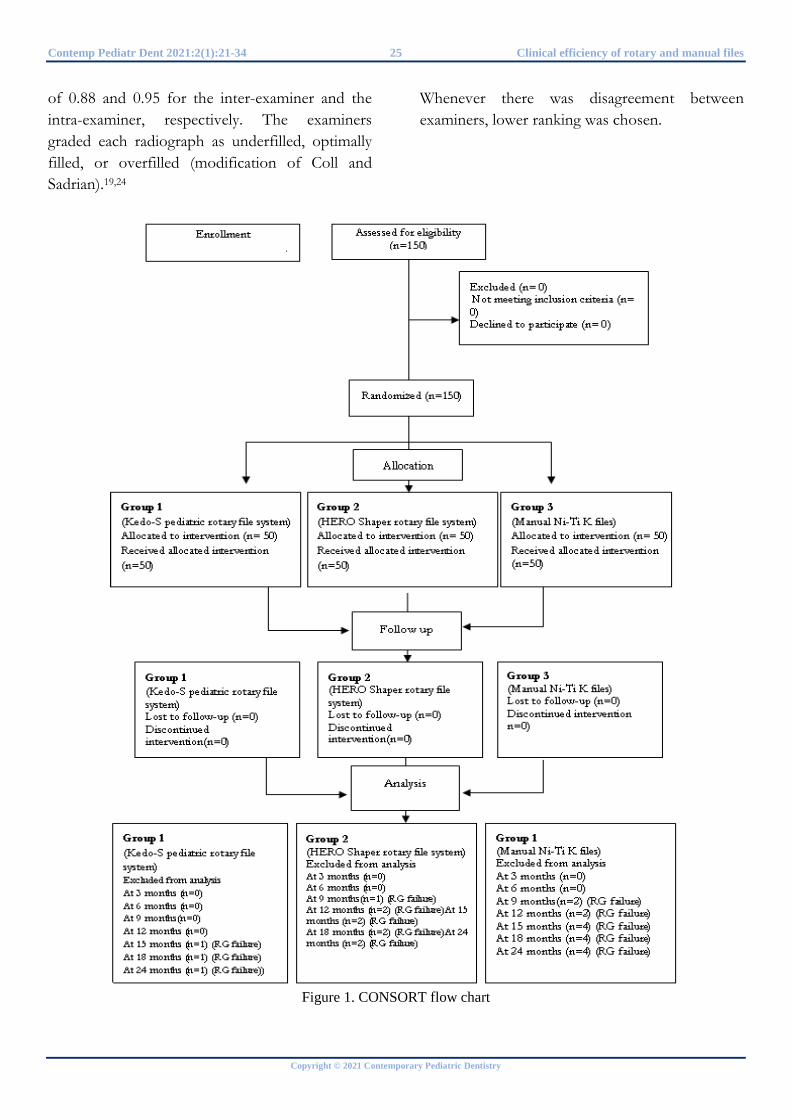
Contemp Pediatr Dent 2021:2(1):21-34 25 Clinical efficiency of rotary and manual files
Copyright © 2021 Contemporary Pediatric Dentistry
of 0.88 and 0.95 for the inter-examiner and the intra-examiner, respectively. The examiners graded each radiograph as underfilled, optimally filled, or overfilled (modification of Coll and Sadrian).19,24
Whenever there was disagreement between examiners, lower ranking was chosen.
Figure 1. CONSORT flow chart
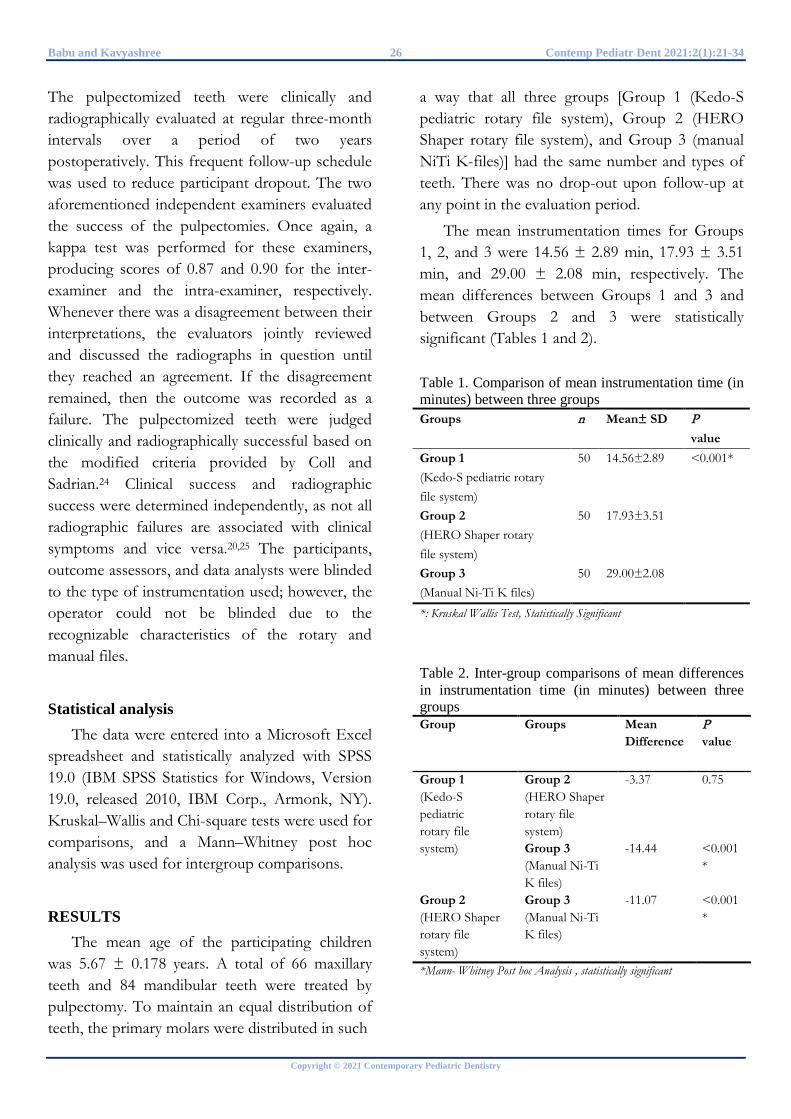
Babu and Kavyashree 26 Contemp Pediatr Dent 2021:2(1):21-34
Copyright © 2021 Contemporary Pediatric Dentistry
The pulpectomized teeth were clinically and radiographically evaluated at regular three-month intervals over a period of two years postoperatively. This frequent follow-up schedule was used to reduce participant dropout. The two aforementioned independent examiners evaluated the success of the pulpectomies. Once again, a kappa test was performed for these examiners, producing scores of 0.87 and 0.90 for the inter-examiner and the intra-examiner, respectively. Whenever there was a disagreement between their interpretations, the evaluators jointly reviewed and discussed the radiographs in question until they reached an agreement. If the disagreement remained, then the outcome was recorded as a failure. The pulpectomized teeth were judged clinically and radiographically successful based on the modified criteria provided by Coll and Sadrian.24 Clinical success and radiographic success were determined independently, as not all radiographic failures are associated with clinical symptoms and vice versa.20,25 The participants, outcome assessors, and data analysts were blinded to the type of instrumentation used; however, the operator could not be blinded due to the recognizable characteristics of the rotary and manual files.
Statistical analysis The data were entered into a Microsoft Excel
spreadsheet and statistically analyzed with SPSS 19.0 (IBM SPSS Statistics for Windows, Version 19.0, released 2010, IBM Corp., Armonk, NY). Kruskal–Wallis and Chi-square tests were used for comparisons, and a Mann–Whitney post hoc analysis was used for intergroup comparisons.
RESULTS The mean age of the participating children
was 5.67 ± 0.178 years. A total of 66 maxillary teeth and 84 mandibular teeth were treated by pulpectomy. To maintain an equal distribution of teeth, the primary molars were distributed in such
a way that all three groups [Group 1 (Kedo-S pediatric rotary file system), Group 2 (HERO Shaper rotary file system), and Group 3 (manual NiTi K-files)] had the same number and types of teeth. There was no drop-out upon follow-up at any point in the evaluation period.
The mean instrumentation times for Groups 1, 2, and 3 were 14.56 ± 2.89 min, 17.93 ± 3.51 min, and 29.00 ± 2.08 min, respectively. The mean differences between Groups 1 and 3 and between Groups 2 and 3 were statistically significant (Tables 1 and 2). Table 1. Comparison of mean instrumentation time (in minutes) between three groups Groups n Mean± SD P
value Group 1 (Kedo-S pediatric rotary file system)
50 14.56±2.89 <0.001*
Group 2 (HERO Shaper rotary file system)
50 17.93±3.51
Group 3 (Manual Ni-Ti K files)
50 29.00±2.08
*: Kruskal Wallis Test, Statistically Significant
Table 2. Inter-group comparisons of mean differences in instrumentation time (in minutes) between three groups Group Groups Mean
Difference P value
Group 1 (Kedo-S pediatric rotary file system)
Group 2 (HERO Shaper rotary file system)
-3.37 0.75
Group 3 (Manual Ni-Ti K files)
-14.44 <0.001*
Group 2 (HERO Shaper rotary file system)
Group 3 (Manual Ni-Ti K files)
-11.07 <0.001*
*Mann- Whitney Post hoc Analysis , statistically significant
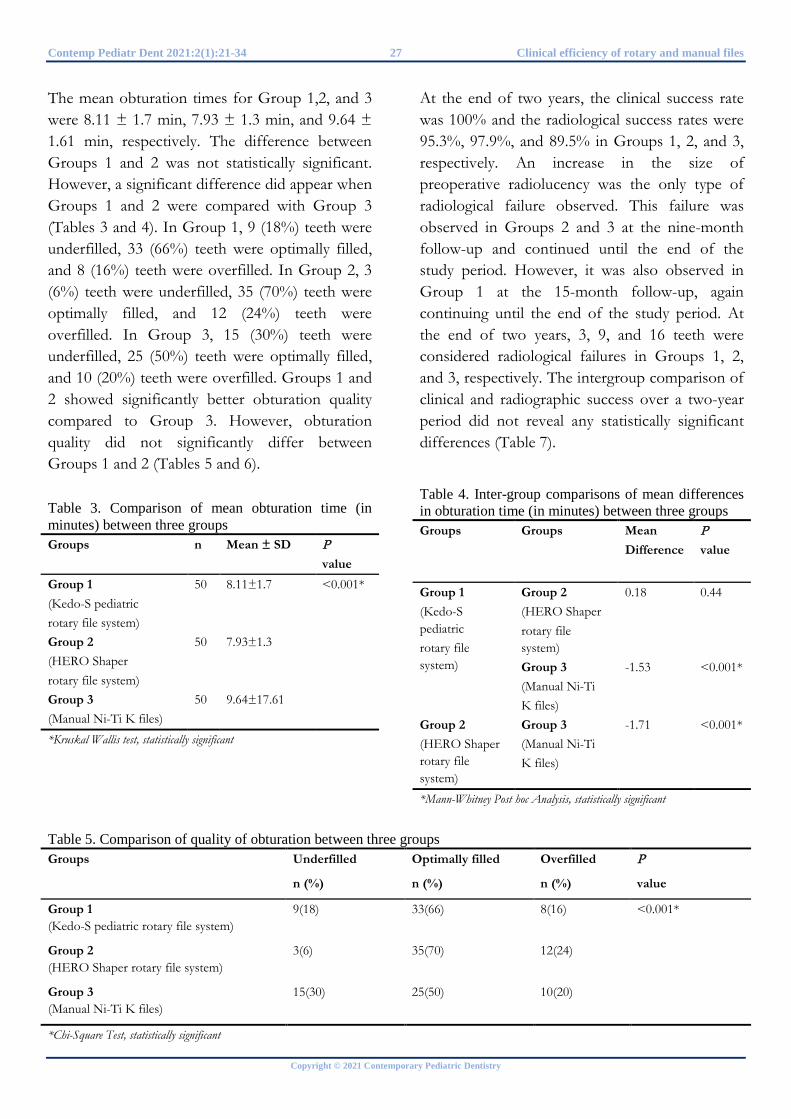
Contemp Pediatr Dent 2021:2(1):21-34 27 Clinical efficiency of rotary and manual files
Copyright © 2021 Contemporary Pediatric Dentistry
The mean obturation times for Group 1,2, and 3 were 8.11 ± 1.7 min, 7.93 ± 1.3 min, and 9.64 ± 1.61 min, respectively. The difference between Groups 1 and 2 was not statistically significant. However, a significant difference did appear when Groups 1 and 2 were compared with Group 3 (Tables 3 and 4). In Group 1, 9 (18%) teeth were underfilled, 33 (66%) teeth were optimally filled, and 8 (16%) teeth were overfilled. In Group 2, 3 (6%) teeth were underfilled, 35 (70%) teeth were optimally filled, and 12 (24%) teeth were overfilled. In Group 3, 15 (30%) teeth were underfilled, 25 (50%) teeth were optimally filled, and 10 (20%) teeth were overfilled. Groups 1 and 2 showed significantly better obturation quality compared to Group 3. However, obturation quality did not significantly differ between Groups 1 and 2 (Tables 5 and 6). Table 3. Comparison of mean obturation time (in minutes) between three groups Groups n Mean ± SD P
value Group 1 (Kedo-S pediatric rotary file system)
50 8.11±1.7 <0.001*
Group 2 (HERO Shaper rotary file system)
50 7.93±1.3
Group 3 (Manual Ni-Ti K files)
50 9.64±17.61
*Kruskal Wallis test, statistically significant
At the end of two years, the clinical success rate was 100% and the radiological success rates were 95.3%, 97.9%, and 89.5% in Groups 1, 2, and 3, respectively. An increase in the size of preoperative radiolucency was the only type of radiological failure observed. This failure was observed in Groups 2 and 3 at the nine-month follow-up and continued until the end of the study period. However, it was also observed in Group 1 at the 15-month follow-up, again continuing until the end of the study period. At the end of two years, 3, 9, and 16 teeth were considered radiological failures in Groups 1, 2, and 3, respectively. The intergroup comparison of clinical and radiographic success over a two-year period did not reveal any statistically significant differences (Table 7).
Table 4. Inter-group comparisons of mean differences in obturation time (in minutes) between three groups Groups Groups Mean
Difference P value
Group 1 (Kedo-S pediatric rotary file system)
Group 2 (HERO Shaper rotary file system)
0.18 0.44
Group 3 (Manual Ni-Ti K files)
-1.53 <0.001*
Group 2 (HERO Shaper rotary file system)
Group 3 (Manual Ni-Ti K files)
-1.71 <0.001*
*Mann-Whitney Post hoc Analysis, statistically significant
Table 5. Comparison of quality of obturation between three groups Groups
Underfilled
n (%)
Optimally filled
n (%)
Overfilled
n (%)
P
value
Group 1 (Kedo-S pediatric rotary file system)
9(18) 33(66) 8(16) <0.001*
Group 2 (HERO Shaper rotary file system)
3(6) 35(70) 12(24)
Group 3 (Manual Ni-Ti K files)
15(30) 25(50) 10(20)
*Chi-Square Test, statistically significant
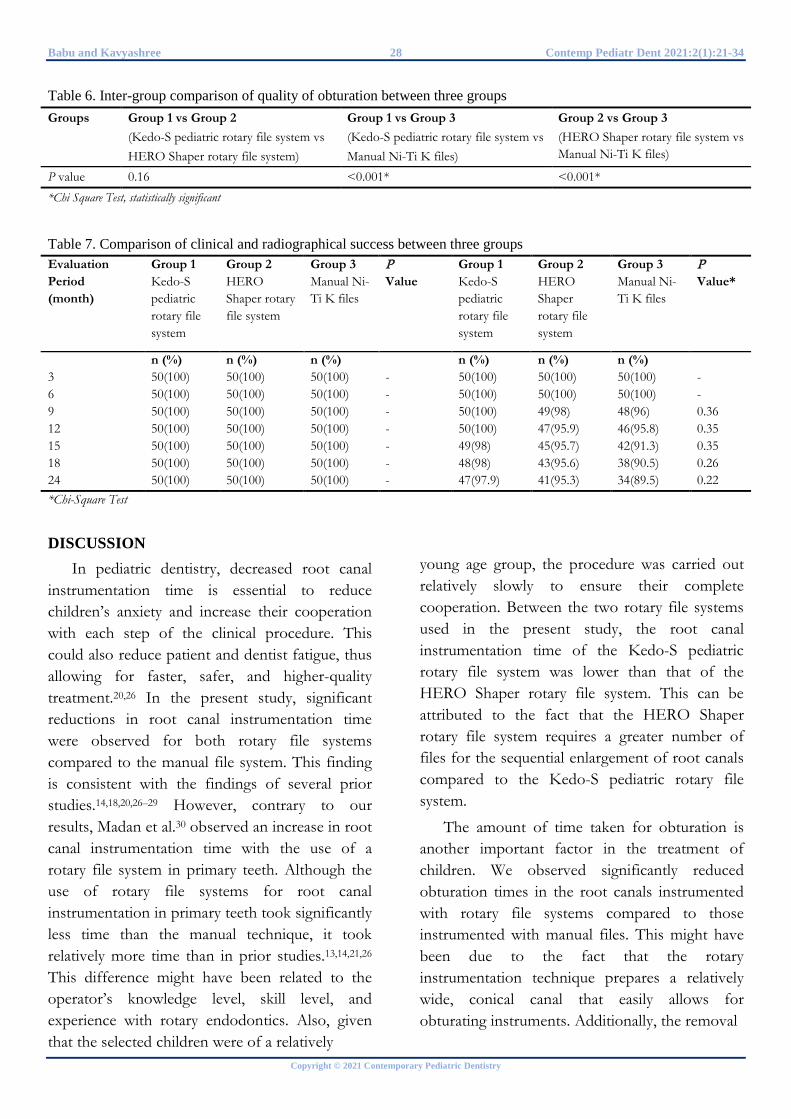
Babu and Kavyashree 28 Contemp Pediatr Dent 2021:2(1):21-34
Copyright © 2021 Contemporary Pediatric Dentistry
Table 6. Inter-group comparison of quality of obturation between three groups Groups Group 1 vs Group 2
(Kedo-S pediatric rotary file system vs HERO Shaper rotary file system)
Group 1 vs Group 3 (Kedo-S pediatric rotary file system vs Manual Ni-Ti K files)
Group 2 vs Group 3 (HERO Shaper rotary file system vs Manual Ni-Ti K files)
P value 0.16 <0.001* <0.001* *Chi Square Test, statistically significant
Table 7. Comparison of clinical and radiographical success between three groups Evaluation Period (month)
Group 1 Kedo-S pediatric rotary file system
Group 2 HERO Shaper rotary file system
Group 3 Manual Ni-Ti K files
P Value
Group 1 Kedo-S pediatric rotary file system
Group 2 HERO Shaper rotary file system
Group 3 Manual Ni-Ti K files
P Value*
n (%) n (%) n (%) n (%) n (%) n (%) 3 50(100) 50(100) 50(100) - 50(100) 50(100) 50(100) - 6 50(100) 50(100) 50(100) - 50(100) 50(100) 50(100) - 9 50(100) 50(100) 50(100) - 50(100) 49(98) 48(96) 0.36 12 50(100) 50(100) 50(100) - 50(100) 47(95.9) 46(95.8) 0.35 15 50(100) 50(100) 50(100) - 49(98) 45(95.7) 42(91.3) 0.35 18 50(100) 50(100) 50(100) - 48(98) 43(95.6) 38(90.5) 0.26 24 50(100) 50(100) 50(100) - 47(97.9) 41(95.3) 34(89.5) 0.22 *Chi-Square Test
DISCUSSION In pediatric dentistry, decreased root canal
instrumentation time is essential to reduce children’s anxiety and increase their cooperation with each step of the clinical procedure. This could also reduce patient and dentist fatigue, thus allowing for faster, safer, and higher-quality treatment.20,26 In the present study, significant reductions in root canal instrumentation time were observed for both rotary file systems compared to the manual file system. This finding is consistent with the findings of several prior studies.14,18,20,26–29 However, contrary to our results, Madan et al.30 observed an increase in root canal instrumentation time with the use of a rotary file system in primary teeth. Although the use of rotary file systems for root canal instrumentation in primary teeth took significantly less time than the manual technique, it took relatively more time than in prior studies.13,14,21,26 This difference might have been related to the operator’s knowledge level, skill level, and experience with rotary endodontics. Also, given that the selected children were of a relatively
young age group, the procedure was carried out relatively slowly to ensure their complete cooperation. Between the two rotary file systems used in the present study, the root canal instrumentation time of the Kedo-S pediatric rotary file system was lower than that of the HERO Shaper rotary file system. This can be attributed to the fact that the HERO Shaper rotary file system requires a greater number of files for the sequential enlargement of root canals compared to the Kedo-S pediatric rotary file system.
The amount of time taken for obturation is another important factor in the treatment of children. We observed significantly reduced obturation times in the root canals instrumented with rotary file systems compared to those instrumented with manual files. This might have been due to the fact that the rotary instrumentation technique prepares a relatively wide, conical canal that easily allows for obturating instruments. Additionally, the removal

Contemp Pediatr Dent 2021:2(1):21-34 29 Clinical efficiency of rotary and manual files
Copyright © 2021 Contemporary Pediatric Dentistry
of cervical obstructions in the root canals with rotary file systems could have decreased obturation times. However, the use of manual files results in irregularly shaped canals and thus takes more obturation time.20,26,28
The quality of root canal obturation is another key factor that determines the success of pulpectomized teeth. In the present study, rotary files produced a greater number of optimally filled root canals than manual files. This finding is similar to the findings of Romero et al.,26 Makarem et al.,27 and Jeevanadan et al.13 The root canals prepared by rotary files are conical in form, and this results in superior obturation quality.27,31 A rotary file has an elastic memory and a radial land that keeps the file in the center of the root canal via wall support and inactive tips, resulting in conical root canal shapes relative to those produced by manual files.31 Additionally, the greater taper of the rotary files could have contributed to the observed improvements in obturation quality. A higher number of underfilled root canals were observed with the use of manual NiTi files. The use of lesser tapered manual NiTi files could have resulted in narrow irregular root canals, which could have prevented the obturating material from flowing adequately.13,15 This observation is consistent with the findings of several prior studies.31,13,15–18,27 However, in contrast with our results, Morankar et al.20 reported that rotary and manual files performed equally in terms of obturation quality.
There was no statistically significant difference in obturation quality between the primary molars instrumented with the Kedo-S pediatric rotary file system and those instrumented with the HERO Shaper rotary file system. This result is consistent with the findings of prior studies that reported superior obturation quality with the use of a rotary file system in primary teeth, irrespective of the type of rotary file system used.17,21,32–34 Rotary files debride the uneven walls of primary root canals more effectively and provide dense obturation relative to manual files.1,2 The HERO
Shaper rotary file system produced a slightly higher percentage of optimally filled root canals relative to Kedo-S pediatric rotary file system. The use of an Endoflare to pre-enlarge the coronal third of the root canal could have contributed to the observed superior obturation quality. Coronal flaring removes any cervical interference from the root canal entrances, allowing endodontic instruments to freely access the apical portion of the root canal.11,12 Additionally, the increased taper of these rotary files could have shaped the canal into its final conical outline more easily than cylindrical instruments. With a greater taper, the prepared root canals should be wider and more conical, allowing the obturating material to flow up to the apical third more easily. These factors could produce a greater number of optimally filled canals.11,12 At the same time, the greatest number of overfilled root canals was noted in the primary teeth instrumented with this file system. This might have been due to the increased length and taper of the HERO Shaper file system, which could have resulted in over-instrumentation, as it is primarily designed for permanent teeth. Another probable explanation is that the correct root canal length might not have been maintained when the rubber stopper was fitted onto the Lentulo spiral. Consistent with the results of prior Indian studies,13,15–18 the Kedo-S pediatric rotary file system produced a greater number of optimally filled root canals. Furthermore, the pediatric rotary file system produced the fewest overfilled root canals. This might have occurred because the Kedo-S pediatric file system produces minimal apical enlargement, preventing the overpreparation and extrusion of the obturating material.18 Although the obturation materials and techniques varied between the cited studies13,15–18 and the present study, the quality of obturation did not vary significantly.
A pulpectomized tooth is considered to be a success when it remains in a functional state until it is replaced by its successor. At the end of two

Babu and Kavyashree 30 Contemp Pediatr Dent 2021:2(1):21-34
Copyright © 2021 Contemporary Pediatric Dentistry
years, we observed a clinical success rate of 100% in all groups. At the end of one year, Kuo et al.21 reported a clinical success rate of 95% using ProTaper® rotary files. At the end of two years, Morankar et al.20 reported a clinical success rate of 92.3% using HyFlex CM® rotary files. At the end of 18 months, Ozalp et al.25 reported a clinical success rate of 100% in primary teeth instrumented with manual files. Other researchers have reported clinical success rates ranging from 70–100% with varying follow-up periods.19,25,35–42 This variation in clinical success rates could be due to the influence of the individual body resistance and pathological condition of the tooth before treatment rather than the filling technique per se.24,37,41,42
At the end of two years, the radiographic success rates were 97.9%, 95.3%, and 89.5% in the primary teeth instrumented with the Kedo-S pediatric rotary file system, the HERO Shaper rotary file system, and the manual NiTi files, respectively. There was no statistically significant difference in radiographic success between these groups. This result is in consistent with the results obtained by Kuo et al.21 Root canals instrumented with manual files have yielded similar results24,25,35 to those of the present study. Ozalp et al.25 and Pandranki et al.38 both reported a success rate of 100% in primary teeth instrumented with manual file system at the end of a long-term follow-up period. However, in an Indian study,20 primary molars instrumented with manual and rotary files yielded very low rates of radiographic success (65.4% and 66.7%, respectively). The authors considered the radiographically failed teeth to have completely failed, even though they were clinically asymptomatic. Furthermore, the inclusion of pathological root resorption and radiological changes in furcal or periapical areas as radiographical failures could have influenced the success rate of this prior study relative to other studies.35,36 The high success rates of the pulpectomized teeth in the present study might have been due to the fact that clinical and
radiographic success were determined independently, as not all radiographic failures are associated with clinical symptoms and vice versa.25 Another probable reason for differences in the success rates reported in prior research and the present study is variation in the treatment selection criteria for primary molars.
A greater number of radiographic failures were observed in primary teeth instrumented with the HERO Shaper rotary file system than in those instrumented with the Kedo-S pediatric rotary file system. This might have been due to the greater number of overfilled root canals in the primary teeth instrumented with the HERO Shaper rotary file system. This is consistent with the results of Coll and Sadrian,24 Chawala et al.,35 and Pandranki et al.,38 who observed decreased success rates in overfilled teeth. On the other hand, Bawazir et al.19 and Yacobi et al.40 observed high success rates in overfilled root canals. Although care was taken not to apply excess pressure with each quarter-turn of the screw during the obturation process, extrusion of the obturating material was observed outside the root canals. Preexisting periradicular pathology and physiological root resorption are probable reasons for overfilling.19,36,38 The lack of apical constriction and relative difficulty of measuring the working length of primary teeth also contributed to the extrusion of the obturating material.38 The overfilling of root canals is unavoidable in some situations, as the dentinal wall of the root canal extending toward the succedaneous tooth are thin and weak and thus may give way during instrumentation.35 Furthermore, the zinc oxide cement carried by the Lentulo spiral had a low viscosity and flowed easily, taking the material apically further into the canal as the instrument rotated.41 The potential drawbacks of overfilling with zinc oxide-eugenol include foreign body reactions, necrosis of the bone and cementum, deflection of the unerupted permanent tooth, and development of a fibrous capsule that could prevent resorption.24 Hence, care should be taken

Contemp Pediatr Dent 2021:2(1):21-34 31 Clinical efficiency of rotary and manual files
Copyright © 2021 Contemporary Pediatric Dentistry
with the use of rotary files, especially with the use of a rotary file system designed for permanent teeth in primary teeth. Additionally, the correct root length should be maintained while fitting the rubber stopper onto the Lentulo spiral.
The low success rate of the primary teeth instrumented with manual files might have been due to a high number of underfilled root canals, which form a narrow channel for bacterial growth and can cause reinfection of the root canal.42 This explanation would be consistent with the results of Bawazir et al.19 and Yacobi et al.,40 who reported a higher failure rate in underfilled root canals than in overfilled or optimally filled root canals. However, contrary to our results, Coll and Sadrian24 reported a higher success rate in underfilled and optimally filled root canals than in overfilled root canals. At the end of the study period, there was no statistically significant difference between the success rates of the different groups of pulpectomized teeth. This might have occurred because the same pulpectomy procedure was used in all three groups, except for the type of root canal instrumentation. A similar result was reported by Pandranki et al.38 at the end of two years with the use of manual files.
The use of two-dimensional radiographic imaging is one potential limitation of the present study. The use of three-dimensional imaging, such as cone beam computed tomography (cone beam CT) or micro-CT, would allow researchers to assess every primary tooth. Limited clinical trials have been carried out to compare the success of pulpectomized teeth instrumented with rotary and manual files. Future longitudinal studies should be carried out to compare the use of different rotary file systems. Given that the success of pulpectomized teeth also depends on the type of obturating material, further investigations are in progress to evaluate the synergistic effect of the type of root canal instrumentation and the type of obturating material.
The results of the present study emphasize the use of rotary file systems for root canal instrumentation in primary teeth. Given that there were no differences in the studied parameters between the two studied rotary file systems, operators may choose to use either of these systems, as both are convenient to use with children. However, the added advantages of the Kedo-S pediatric rotary file system—such as a short file length, a short working length, and variable tapers with variable tip diameters—support its use in primary teeth.13,15–18 Additionally, the simple three-file system allows the operator to carry out the procedure more quickly and efficiently in children. However, given that rotary endodontics was only recently introduced to the field of pediatric dentistry, operators must improve their knowledge, skills, and experience with rotary file systems.
CONCLUSIONS Based on the results of the present study, it
can be concluded that rotary file systems require significantly less time for the instrumentation and obturation of root canals in primary molars compared to manual file systems. Although the HERO Shaper rotary file system took less time for obturation than the Kedo-S pediatric rotary file system, this difference was not statistically significant. The quality of obturation in primary molars instrumented with rotary file systems was found to be superior to that of primary molars instrumented with a manual NiTi file system. However, there was no significant difference in the quality of obturation between primary molars instrumented with a Kedo-S pediatric rotary file system and HERO Shaper rotary file system. At the end of two years, the clinical success rate was 100% and the radiographical success rates were 97.9%, 95.3%, and 89.5% in primary teeth instrumented with the Kedo-S pediatric rotary file system, the HERO Shaper rotary file system, and the manual NiTi file system, respectively.
Babu and Kavyashree 32 Contemp Pediatr Dent 2021:2(1):21-34
Copyright © 2021 Contemporary Pediatric Dentistry
However, there were no significant differences in success rates between these groups. REFERENCES 1. Barr ES, Kleier DJ, Barr NV. Use of nickel-titanium rotary files for root canal preparation in primary teeth. Pediatr Dent 1999;21:453-454 2. Barr ES, Kleier DJ, Barr NV. Use of nickel-titanium rotary files for root canal preparation in primary teeth. Pediatr Dent 2000;22:77-78 3. Moghaddam KN, Mehran M, Zadeh HF. Root canal cleaning efficacy of rotary and hand files instrumentation in primary molars. Iran Endod J 2009;4:53-71 4. Hidsmann, M., Gressmann, G., Schafers, F. A comparative study of root canal preparation using FlexMaster and HERO 642rotary NiTi instruments. Int Endod J 2003;36:358–366 5. Sonntag, D., Delschen, S., Stachniss, V. Root canal shaping with manual and rotary NiTi file performed by students. Int Endod J 2003;36:715–723 6. Bahrololoomi, Tabrizazadeh M, Salmani L. In vitro comparison of instrumentation time and cleaning capacity between rotary and manual preparation techniques in primary teeth. J Dent 2007;4:59-62 7. Katge F, Patil D, Poojari M, Pimpale J, Shitoot A, Rusawat B. Comparison of instrumentation time and cleaning efficacy of manual instrumentation, rotary systems and reciprocating systems in primary teeth: An in vitro study. J Ind Soc Pedod Prev Dent 2014;32:311–316 8. Finn SB. Morphology of primary teeth. In: Finn SB, editor. Clinical Pedodontics 4th ed. Philadelphia: Saunders Co;1973.p.59-70. 9. Jeevanandan G. Kedo-S Paediatric Rotary Files for Root Canal Preparation in PrimaryTeeth – Case Report. J Clin Diagn Res 2017;11:3-5 10. Kaptan F, Sert S, Kayahan B, HaznedarogluF,Tanalap J, Bayirli G. Comparative evaluation of the preparation efficacies of HERO shaper and Nitiflex root canal instruments in curved canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;100:636-64. 11. Subramaniam P, Girish Babu KL, Tabrez TA. Effectiveness of Rotary Endodontic Instruments on Smear Layer Removal in Root Canals of
Primary Teeth: A Scanning Electron Microscopy Study. J Clin Pediatr Dent 2016;40:141-146 12. Subramaniam P, Tabrez TA, Girish Babu KL. Microbiological assessment of root canals following use of rotary and manual instruments in primary molars. J Clin Pediatr Dent 2013;38:123-127 13. Jeevanandan G, Govindaraju L. Clinical comparison of Kedo-S paediatric rotary files vs manual instrumentation for root canal preparation in primary molars: a double blinded randomised clinical trial. Eur Arch Paediatr Dent 2018;19:273–278 14. Musale PK, Mujawar SAV. Evaluation of the efficacy of rotary vs. hand files in root canal preparation of primary teeth in vitro using CBCT. Eur Arch Paediatr Dent 2014;15:113-120 15. Panchal V, Jeevanandan G, Subramanian E. Comparison of instrumentation time and obturation quality between hand K-file, H-files, and rotary Kedo-S in root canal treatment of primary teeth: A randomized controlled trial. J Indian Soc Pedod Prev Dent 2019;37:75-79 16. Lakshmanan L, Mani G, Jeevanandan G, Ravindran V, Subramanian EMG. Assessing the quality of root canal filling and instrumentation time using Kedo-s files, reciprocating files and k-files. Braz Dent Sci 2020;23:1-7 17. Divya S, Jeevanandan G, Sujatha S, Subramanian EMG, Ravindran V. Comparison of quality of obturation and post-operative pain using manual vs rotary files in primary teeth - A randomised clinical trial. Indian J Dent Res 2019;30:904-908 18. Juliet S, Jeevanandan G, Govindaraju L, Ravindran V, Subramanian EMG. Comparison Between Three Rotary Files on Quality of Obturation and Instrumentation Time in Primary Teeth − A Double Blinded Randomized Controlled Trial. J Orofac Sci 2020;12:30-34. 19. Bawazir OA, Salama FS. Clinical evaluation of root canal obturation methods in primary teeth. Pediatr Dent 2006;28:39-47. 20. Morankar R, Goyal A, Gauba K, Kapur A, Bhatia SK. Manual versus rotary instrumentation for primary molar pulpectomies- A 24 months randomized clinical trial. Pedia Dent J 2020;28:96–102 21. Kuo C, Wang Y, Chang H, Huang G, Lin C, Li U, et al. Application of Ni-Ti rotary files for

Contemp Pediatr Dent 2021:2(1):21-34 33 Clinical efficiency of rotary and manual files
Copyright © 2021 Contemporary Pediatric Dentistry
pulpectomy in primary molars. J Dent Sci 2006;1:10-15 22. Dandashi MB, Nazif MM, Zullo T, Elliott MA, Schneider LG, Czonstkowsky M. An in vitro comparison of three endodontic techniques for primary incisors. Pediatr Dent. 1993;15:254-256 23. Memarpour M, Shahidi S, Meshki R. Comparison of different obturation techniques for primary molars by digital radiography. Pediatr Dent 2013;35:236-240 24. Coll JA, Sadrian R. Predicting pulpectomy success and its relationship to exfoliation and succedaneous dentition. Pediatr Dent 1996;18:57- 63 25. Ozalp N, Saroğlu I, Sönmez H. Evaluation of various root canal filling materials in primary molar pulpectomies: an in vivo study. Am J Dent 2005;18:347-350 26. Romero TO, Gonzalez VM. Comparison between rotary and manual techniques on duration of instrumentation and obturation times in primary teeth. J Clin Pediatr Dent 2011; 35:359-364 27. Makarem Abbas, Ravandeh Navid, Ebrahimi Masoumeh. Radiographic assessment and chair time of rotary instruments in the pulpectomy of primary second molar teeth: a randomized controlled clinical trial. J Dent Res Dent Clin Dent Prospects 2014; 8:84-89 28. Silva LA, Leonardo MR, Nelson-Filho P, Tanomaru JM. Comparison of rotary and manual instrumentation techniques on cleaning capacity and instrumentation time in deciduous molars. J Dent Child (Chic) 2004;71:45-47 29. Crespo S, Cortes O, Garcia C, Perez L. Comparison between rotary and manual instrumentation in primary teeth. J Clin Pediatr Dent 2008;32:295-298 30. Madan N, Rathnam A, Shigli AL, Indushekar KR. K-file vs ProFiles in cleaning capacity and instrumentation time in primary molar root canals: an in vitro study. J Indian Soc Pedod Prev Dent 2011;29:55-61 31. Moghaddam KN, Mehran M, Zadeh HF. Root canal cleaning efficacy of rotary and hand files instrumentation in primary molars. Iran Endod J 2009;4:53-71 32. Babji P, Mehta V, ManjooranT. Clinical Evaluation of rotary system over manual system
in deciduous molars: A clinical trial. Int J Pedod Rehabil 2019;4:13-16 33. Govindaraju L, Jeevanadan G, Subramaniam EM. Comparison of quality of obturation and instrumentation time using hand files and two rotary file system in primary molars: A single-blinded randomized controlled trial. Eur J Dent 2017:11:376-379 34. Govindaraju L, Jeevanadan G, Subramaniam EM. Clinical evaluation of quality of obturation and instrumentation time using two modified rotary file systems with manual instrumentation in primary teeth. J Clin Diagn Res 2017;77: 55-58 35. Chawla HS, Setia S, Gupta N, Gauba K, Goyal A. Evaluation of a mixture of zinc oxide, calcium hydroxide, and sodium fluoride as a new root canal filling material for primary teeth. J Indian Soc Pedod Prev Dent 2008;26:53-58 36. Fuks AB, Eidelman E, Pauker N. Rootfillings with endoflas in primary teeth: A retrospective study. J Clin Pediatr Dent 2002;27:41-45 37. Moskovitz M, Sammara E, Holan G. Success rate of root canal treatment in primary molars. J Dent 2005;33:41-47 38. Pandranki J, V Vanga NR, Chandrabhatla SK. Zinc oxide eugenol and Endoflas pulpectomy in primary molars: 24-month clinical and radiographic evaluation. J Indian Soc Pedod Prev Dent 2018;36:173-180 39. Ramar K, Mungara J. Clinical and radiographic evaluation of pulpectomies using three root canal filling materials: An in-vivo study. J Indian Soc Pedod Prev Dent 2010;28:25-29 40. Yacobi R, Kenny DJ, Judd PL, Johnston DH. Evolving primary pulp therapy techniques. J Am Dent Assoc 1991;122:83-85 41. Machida Y. Root canal obturation in primary teeth: a review. Jap Dent Assoc J 1983; 36:796-802. 42. Mortazavi M, Mesbahi M. Comparison of zinc oxide and eugenol, and Vitapex for root canal treatment of necrotic primary teeth. Int J Paediatr Dent 2004;14:417–424

Babu and Kavyashree 34 Contemp Pediatr Dent 2021:2(1):21-34
Copyright © 2021 Contemporary Pediatric Dentistry
How to cite this article: KL Girish Babu and Guraj Hebbar Kavyashree. Evaluation of the clinical efficiency of rotary and manual files for root canal instrumentation in primary teeth pulpectomies: A comparative randomized clinical trial. Contemp Pediatr Dent 2021:2(1):21-34 Declarations
Acknowledgements: Not applicable. Conflict of Interest Statement: The authors disclose no potential conflicts of interest. Ethics Statement: Ethical clearance to conduct this study was obtained from the Institutional Ethics Committee (IEC/HIMS/RR76). Informed Consent: Informed consent and assent were obtained from all participants. Author contributions: Conception and design: All Authors; Acquisition of data: All Authors; Interpretation of data: All Authors; Drafting article: All Authors; Revision artice: All Authors; Final approval: All Authors Funding: This work is not finantiated. Data Availability: The data used to support the findings of this study can be made available upon request to the corresponding author. Peer-review: Externally double-blinded peer-reviewed.
Copyright © 2021 Contemporary Pediatric Dentistry. This work is licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International license. (CC BY-NC-ND 4.0)
Original Research
A survey on dental treatments provided under general anesthesia for pediatric patients: A hospital-based retrospective audit
Sreekanth K Mallineni1✉, Jayachandra Bhumireddy2, Azher M Mohammed3, Vinod Mukthineni4
Abstract Aim: To evaluate the dental procedures carried out under general anesthesia (GA) on children with primary dentition in a pediatric hospital. Methods: The study comprised all children with primary dentition treated under GA at a private pediatric hospital from January 2014 to December 2017. The data was tabulated based on the dental records include reasons for dental treatment under general anesthesia (DGA), dental status, and treatment provided. Descriptive statistics were used for statistical analysis and chi-square test used for the comparison. Results: Forty-eight children with primary dentition were utilized the service of general anesthesia for dental treatment. Dental caries (78%) was the most common reason for DGA (p<0.05). More than 80% of children required treatment for more than ten teeth (p>0.05). Overall restorative procedures (60%), extractions (26%), and preventive procedures (14%) were performed under GA (p<0.05). Among, restorative procedures stainless steel crowns (54.2%) were given more priority than other restorative materials. Conclusions: Dental caries was found to be a common reason for DGA. Restorative procedures were given priority over surgical and preventive procedures. Stainless steel crowns were extensively used compared to other materials. Keywords: Children; Dental Care; General Anesthesia; Retrospective Study
Highlights General anesthesia is commonly used to facilitate dental treatment in children with anxiety or challenging behavior, many of whom are children.
1 Consultant, Vasan Dental Care, Hyderabad, Telangana, India Associate Professor, Pediatric Dentistry, Preventive Dental Science, College of Dentistry, Majmmah University, KSA 2 Consultant, Vasan Dental Care, Hyderabad, Telangana, India Assocaite professor, Pedodontics and Preventive Dentistry, Saraswati Dhanwantri Dental College and Hospital & Post Graduate Research Institute, Parbhani, Maharastra, India 3 Consultant, Vasan Dental Care, Hyderabad, Telangana, India Oral-maxillo-facial Surgery, Prince Sultan Military Medical City, Riyadh, KSA 4 Anesthesiologist, Udbhava Childrens’ Hospital, Hyderabad, Telanagana, India
Correspondence: Department of Preventive Dental Science, College of Dentistry, Majmaah University, Majmaah Saudi Arabia, 11952 E-mail address: [email protected]; [email protected]
Received: 04 February 2021 Accepted: 10 April 2021 Online First: 22 April 2021
Restorative procedures were given priority over the extractions in dental treatment under general anesthesia in the present study.
This study highlights a great need to develop the healthcare system regarding the appropriate management of caries among children with primary dentition.
Contemporary Pediatric Dentistry Contemp Pediatr Dent 2021:2(1):35-40 DOI: 10.51463/cpd.2021.40

Mallineni et al. 36 Contemp Pediatr Dent 2021:2(1):35-40
Copyright © 2021 Contemporary Pediatric Dentistry
INTRODUCTION General anesthesia (GA) is indicated in
patients with anxiety and fear associated with dental treatments.1 To facilitate dental treatment under GA for patients of motor dysfunction and/or cognitive impairment that precludes adequate treatment, provide treatment for these patients with a low age of reason, or extensive dental treatment procedures or traumatic injuries.1-3 Dental treatment under general anesthesia (DGA) is an effective way of treating pediatric dental patients who are uncooperative.1,2 It has the advantage of providing treatment under GA for children if they require multiple procedures at a time.4,5 Interest in delivering treatment under GA in children has increased over the recent years.6-8
The provision of dental treatment under GA for pediatric dental patients establishes and maintains the state of co-operation where the patient can receive assessment and treatment safely and successfully.8,9 The dental assessments involve attaining adequate evidence regarding dental problems to rationalize comprehensive oral rehabilitation under GA if the patient is not manageable for the treatment under local anesthesia (LA) in the clinical setting. The additional care beyond the LA may be necessary for pediatric patients to obtain dental treatment.7 Prior published studies reported that poor oral health might result in poor diet and nutrition, affecting systemic health. Nevertheless, the essential goal for DGA for children is providing comprehensive treatment for children.7,10 This type of management should be employed with a preventive program, behavioral remodeling, and a follow-up appointment to avoid further treatment and reduce multiple appointments. Even though many studies reported in the literature DGA for children, it is necessary to check the trends in dental treatment under GA in recent days in the Indian scenario. Therefore this study aimed to perform a retrospective audit on the
characteristics and treatment provided under GA for children with primary dentition.
METHODS This study followed the ethical standards
specified in the 1975 Declaration of Helsinki (revised in 2000) and its subsequent amendments. Written informed consent was obtained from participants.
Sample This retrospective audit of children with
primary dentition underwent dental treatment under general anesthesia at Udbhava Children Hospital, Hyderbad, Telangana, India. A single pediatric dentist referred all the patients from three different private clinics for DGA from January 2014 to December 2017. The healthy children with primary dentition, and with complete records were included in the study. The children without complete records, and children with mixed and permanent dentition were excluded from the study. The hospital authority approved the study, and the study details were collected retrospectively. All children received dental assessments and pre-anesthetic evaluation prior to DGA. The dental assessment included medical and dental history and clinical and radiographic examination. The complete data were collected based on the dental records (case sheet), dental status, management, and reasons for DGA were incorporated.
Procedure All the patients were admitted to the hospital
one day before the DGA. At the time of admission, a comprehensive treatment plan was discussed, and informed consent was obtained from parents. All the patients were discharged after complete recovery without any adverse conditions to the post-treatment. The anesthesia
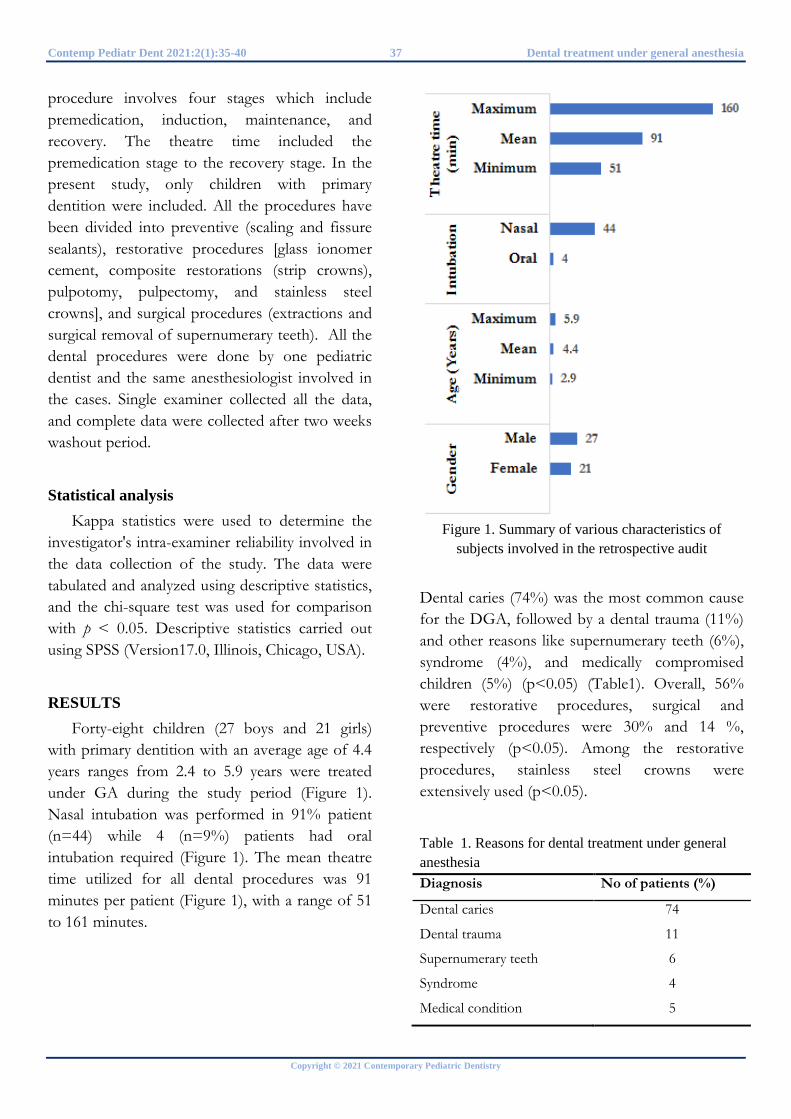
Contemp Pediatr Dent 2021:2(1):35-40 37 Dental treatment under general anesthesia
Copyright © 2021 Contemporary Pediatric Dentistry
procedure involves four stages which include premedication, induction, maintenance, and recovery. The theatre time included the premedication stage to the recovery stage. In the present study, only children with primary dentition were included. All the procedures have been divided into preventive (scaling and fissure sealants), restorative procedures [glass ionomer cement, composite restorations (strip crowns), pulpotomy, pulpectomy, and stainless steel crowns], and surgical procedures (extractions and surgical removal of supernumerary teeth). All the dental procedures were done by one pediatric dentist and the same anesthesiologist involved in the cases. Single examiner collected all the data, and complete data were collected after two weeks washout period.
Statistical analysis Kappa statistics were used to determine the
investigator's intra-examiner reliability involved in the data collection of the study. The data were tabulated and analyzed using descriptive statistics, and the chi-square test was used for comparison with p < 0.05. Descriptive statistics carried out using SPSS (Version17.0, Illinois, Chicago, USA).
RESULTS Forty-eight children (27 boys and 21 girls)
with primary dentition with an average age of 4.4 years ranges from 2.4 to 5.9 years were treated under GA during the study period (Figure 1). Nasal intubation was performed in 91% patient (n=44) while 4 (n=9%) patients had oral intubation required (Figure 1). The mean theatre time utilized for all dental procedures was 91 minutes per patient (Figure 1), with a range of 51 to 161 minutes.
Figure 1. Summary of various characteristics of subjects involved in the retrospective audit
Dental caries (74%) was the most common cause for the DGA, followed by a dental trauma (11%) and other reasons like supernumerary teeth (6%), syndrome (4%), and medically compromised children (5%) (p<0.05) (Table1). Overall, 56% were restorative procedures, surgical and preventive procedures were 30% and 14 %, respectively (p<0.05). Among the restorative procedures, stainless steel crowns were extensively used (p<0.05).
Table 1. Reasons for dental treatment under general anesthesia Diagnosis No of patients (%)
Dental caries 74
Dental trauma 11
Supernumerary teeth 6
Syndrome 4
Medical condition 5

Mallineni et al. 38 Contemp Pediatr Dent 2021:2(1):35-40
Copyright © 2021 Contemporary Pediatric Dentistry
The mean for stainless steel crowns, composites, glass ionomer cement, fissure sealants, preventive resin restorations, and strips crowns were 4.5, 1.5, 0.2, 1.1, 0.6, and 0.6, respectively (Table 2). Almost 80% of children required treatment for more than ten teeth (p>0.05), followed by 2% of 20 teeth, 10% of ≥15 teeth, and 8% of ≥5 teeth. Kappa statistics showed excellent (K=1.0) intra-examiner reliability.
Table 2. Details of restorative materials used for dental treatment under general anesthesia Procedure n % Mean
Fissure sealants 40 13.5 1.1
Composite 55 18.5 1.5
Glass ionomer cement 9 3.0 0.2
Preventive resin restoration 22 7.4 0.61
Stainless steel crowns 161 54.2 4.5
Strip crowns 10 3.4 0.3
DISCUSSION There are various types of dental
complications in pediatric patients that cannot be treated optimally in the clinical setting, and these are managed the better way in a pediatric hospital setting.11 The gender discrepancy was observed in the present study, and it was similar to prior studies.11,12 Inversely, few studies reported that females were predominantly treated under GA.13 In the present retrospective audit, dental caries (74%) is the most common reason for the DGA, followed by a dental trauma (11%) and other reasons (15%) like dental fear, supernumerary teeth, syndrome, and medically compromised children (p<0.05). These findings were in agreement with prior studies from Hong Kong13, Taiwan14, and Turkey15.
In the present study, 91 minutes utilized for DGA ranges between 54 and 160 minutes. Tsai and co-workers14 performed treatments under GA between 2.4 hours to 3.8 hours. In contrast to this study, Turkish study15 all the dental
procedures are finished at a mean of slightly more than 60 minutes. A recent Korean study16 reported that the mean duration of treatment was 101 min, almost in agreement with the present study findings. Shin and co-workers16 opined GA probably requires long treatment, is preferable to multiple sedation procedures in terms of both time and cost, and allows treatment to be completed in one visit without any psychological stress of treatment under restraint.
The mean number of teeth treats under GA was greater than 80% of children who required treatment for more than ten teeth. Nevertheless, a Taiwanese study14 reported that the mean no treated teeth under GA were slightly higher than the present study (15.2). A recent Turkish study15 reported that the mean value of teeth treated under GA was 10.4. These findings would explain that pediatric patients who required treatment for multiple teeth planned for DGA. This study opines that DGA recommended for pediatric patients who require treatment for ten or more teeth based on our findings.
Overall, in the present study, 56% were restorative procedures, 30% surgical procedures, and 14% were with preventive procedures were performed under DGA. It seems restorative procedures were given higher priority than surgical procedures. These findings are not in agreement with earlier studies reported by Kwok-Tung et al.6 and Shin et al.16. The present study findings are contrary to some other investigators6,12,17 where they have preferred surgical procedures more than restorative procedures under GA. Stainless steel crowns were given more precedence amongst all restorative procedures employed for multi-surface carious lesions. The provision of dental treatment under GA is a very efficient way of treating children with primary dentition because it allows the clinician to perform the entire treatment in one visit for highly uncooperative children and children with disabilities. Nonetheless, more

Contemp Pediatr Dent 2021:2(1):35-40 39 Dental treatment under general anesthesia
Copyright © 2021 Contemporary Pediatric Dentistry
parents and guardians would select DGA as an option based on the child’s psychological state, such as poor co-operation or dental anxiety.16
In the present study, only forty-eight children with primary dentition have utilized the service of the DGA. The sample involved in the study was significantly less compared with prior reported studies and considered a limitation. The possible reason was only children with primary dentition included in the present study. In the Indian subcontinent, dental treatment under general anesthesia was still confined to the urban areas. Hence, with this data, the study findings are not to be generalized. These findings could be used as a reference for further studies. Moreover, the study performed retrospectively from January 2014 to December 2017; this is another drawback. However, the early intervention of DGA for uncooperative children with more carious lesions improves their quality of life. Overall, the present study trend showed a conservative approach to a surgical approach, and these findings were in agreement with prior studies.6,8,16
CONCLUSIONS Dental caries was the most common reason
for DGA. Overall, restorative procedures were given priority over preventive and surgical procedures in DGA. Among restorative procedures, stainless steel crowns were extensively used. Nevertheless, DGA is also a viable option for pediatric patients if they require treatment for ten or more primary teeth. REFERENCES 1. Glassman P, Caputo A, Dougherty N, Lyons R, Messieha Z, Miller C, et al. Special Care Dentistry Association consensus statement on sedation, anesthesia, and alternative techniques for people with special needs. Spec Care Dentist 2009;29:2-8 2. Mallineni SK, Yiu CK. A retrospective review of outcomes of dental treatment performed for
special needs patients under general anaesthesia: 2-year follow-up. Scientific World J 2014;2014:748353 3. Jankauskiene B, Narbutaite J. Changes in oral health-related quality of life among children following dental treatment under general anaesthesia. A systematic review. Stomatologija 2010;12:60-64 4. Eaton J, McTigue D, Fields H, Beck F. Attitudes of contemporary parents toward behavior management techniques used in pediatric dentistry. Pediatr Dent 2005;27:107-113 5. White H, Lee J, Rozier G. The effects of general anesthesia legislation on operating room visits by preschool children undergoing dental treatment. Pediatr Dent 2008;30:70-75 6. Kwok-Tung L, King NM. Retrospective audit of caries management techniques for children under general anesthesia over an 18-year period. J Clin Pediatr Dent 2006;31:58-66 7. Mallineni SK, Yiu CK. Dental treatment under general anesthesia for special-needs patients: analysis of the literature. J Investig Clin Dent 2016;7:325-331 8. Lee PY, Chou MY, Chen YL, Chen LP, Wang CJ, Huang WH. Comprehensive dental treatment under general anesthesia in healthy and disabled children. Chang Gung Med J 2009;32:636-642 9. Mallineni SK, Priya V. Dental general anesthesia. Pediatric Dentistry for Special Child Edition: 1st ed. New Delhi:Jaypee Publishers; 2016 10. Khodadadi E, Mohammadpour M, Motamedian SR, Kouhestani F. Failure rate of pediatric dental treatment under general anesthesia. Dent J (Basel) 2018;6:25-30 11. Stanková M, Bucek A, Dostalova T, Ginzelova K, Pacakova Z, Seydlova M. Patients with special needs within treatment under general anesthesia - a meta-analysis. Prague Med Rep 2011;112:216-225 12. So-Youn An, Kwang-Suk Seo, Seungoh Kim, Jongbin Kim, Deok-Won Lee, Kyung-Gyun Hwang et al. Developmental procedures for the clinical practice guidelines for conscious sedation in dentistry for the Korean Academy of Dental Sciences. J Dent Anesth Pain Med 2016;16:253-261

Mallineni et al. 40 Contemp Pediatr Dent 2021:2(1):35-40
Copyright © 2021 Contemporary Pediatric Dentistry
13. Mallineni SK, Yiu CK. A retrospective audit of dental treatment provided to special needs patients under general anaesthesia during a ten-year period. J Clin Pediatr Dent 2018;42:155-160 14. Tsai CL, Tsai YL, Lin YT. A retrospective study of dental treatment under general anesthesia of children with or without a chronic illness and/or a disability. Chang Gung Med J 2006;29:412-418 15. Cantekin K, Dogan S, Avdinblege M, CanpolatDG, Yildirim MD, Avci S. Analysis of comprehensive dental rehabilitation under general anesthesia at a dental hospital in turkey. J Pediatr Dent 2014;2:49-55 16. Shin B, Yoo S, Kim J, Kim S, Kim J. A survey of dental treatment under general anesthesia in a Korean university hospital pediatric dental clinic. J Dent Anesth Pain Med 2016;16:203-208 How to cite this article: Sreekanth K Mallineni, Jayachandra Bhumireddy, Azher M Mohammed, Vinod Mukthineni. A survey on dental treatments provided under general anesthesia for pediatric patients: A hospital based retrospective audit. Contemp Pediatr Dent 2021:2(1):35-40
Declarations
Acknowledgements: Our sincere thanks to the management, Udbhava Children’s’ Hospital (MIG-196, Road no.1, K.P.H.B., Hyderabad, Telangana, India- 500072) for their support during this project. Conflict of Interest Statement: The authors disclose no potential conflicts of interest. Ethics Statement: This study followed the ethical standards specified in the 1975 Declaration of Helsinki (revised in 2000) and its subsequent amendments. Informed Consent: Informed consent and assent were obtained from all participants. Author contributions: Conception and design: All Authors; Acquisition of data: SKM, AMM,; Interpretation of data: All Authors; Drafting article: AMM; Revision artice: JB, AMM; Final approval: All Authors Funding: This work is not finantiated. Data Availability: The data used to support the findings of this study can be made available upon request to the corresponding author. Peer-review: Externally double-blinded peer-reviewed.
Copyright © 2021 Contemporary Pediatric Dentistry. This work is licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International license. (CC BY-NC-ND 4.0)
Original Research
Retrospective evaluation of primary anterior teeth injuries and prevalence of sequelae in their successors
Ozant Oncag1 ✉, Candan Gurbuz Sarigol2, Sevgi Arabulan3
Abstract Aim: Traumatic dental injuries occur frequently in children. Treatment and follow ups are important to avoid short and long term complications. The aim of this study was to investigate the prevalence of sequelae in the permanent anterior teeth following the trauma in their predecessors in the period of 2005 to 2011. Methods: This study was performed retrospectively according the data from the records of 79 children (53 boys, 26 girls), who were treated for anterior deciduous tooth trauma. Of the 79 affected children (186 teeth), 35 (91 teeth, 22 boys and13 girls) were available for the follow-up examination. Kappa coefficient was calculated for inter-examiner reliability. Descriptive statistics including percentage and mean values were also calculated. Results: Sequelae were detected on 45(49.5%) of 91 successors of the traumatized deciduous teeth and enamel hypoplasia and/or discoloration was observed in 14 (31.1%) teeth. Eruption was disturbed in 14 (31.1%). In 13 teeth (28.9%) crown and root malformation, in three teeth (6.7%) only crown and in one tooth (2.2%) only root malformation was detected. Most frequent sequela of successors were observed after the intrusive luxation of the deciduous teeth (33%). Crown-root malformations of the successor teeth were most frequently occurred after the trauma at the age of 0 to 2 (61.53%). Conclusions: Early diagnosis and treatment of primary dental injuries and routine clinical and radiological follow up would minimize the sequelae which were observed in permanent successors.
Keywords: Dental Trauma; Primary Teeth; Sequela; Tooth Injuries
Highlights Traumatic injuries of primary dentition are commonly seen in pediatric dental practice.
1 Professor, Department of Pediatric Dentistry, School of Dentistry, Ege University, Izmir, Turkey 2 Specialist, Alsancak Oral and Dental Health Center, Izmir, Turkey 3 Resident, Department of Pediatric Dentistry, School of Dentistry, Ege University, Izmir, Turkey
Correspondence: Department of Pediatric Dentistry, School of Dentistry, Ege University, Izmir, Turkey. E-mail address: [email protected]
Received: 10 January 2021 Accepted: 25 March 2021 Online First: 01 April 2021
Early detection of any sequelae and regular follow ups help better prognosis and provide more convenient treatment.
Trauma to primary dentition may cause sequelae in developing permanent dentition. It is important to know possible effects and detect as early as possible.
Contemporary Pediatric Dentistry Contemp Pediatr Dent 2021:2(1):41-49 DOI: 10.51463/cpd.2021.35

Oncag et al. 42 Contemp Pediatr Dent 2021:2(1):41-49
Copyright © 2021 Contemporary Pediatric Dentistry
INTRODUCTION Dental trauma in children and adolescents is a
common and serious problem. This injury has a high rate of incidence in deciduous teeth among children in the motor development phase.1-3 During this period, falls or tumbles are the most common reason4 and the most affected teeth are the upper deciduous central incisors.5-7 Different types of traumatic injuries affect the primary dentition. However, primary incisors are highly liable to luxation injuries, which constitute the 21% to 81% of traumatic injuries of these teeth.8-9 Due to the close relationship between the apices of the primary teeth and the germs of their permanent successors, developmental disturbances in the permanent dentition are common after trauma of the primary teeth, varying from 12% to 74%.10-12 The severity of the sequela depends on the age of the child at the time of injury, the grade of root resorption of the traumatized deciduous tooth, the type and extent of the injury, and the developmental stage of the successor at the time of injury.12-13 Traumatic avulsion and intrusive luxation are the most frequent types of trauma that affect the development of permanent successors.9 The sequelae in permanent teeth caused by traumatic injury in their predecessors are registered according to the following classifications: white or yellow-brown discoloration of enamel, enamel hypoplasia, crown dilaceration, root dilaceration, odontoma-like malformation, root duplication, partial or complete arrest of root formation, sequestration of the permanent tooth germ and eruption disturbances. The discoloration of enamel and the enamel hypoplasia are the most frequent sequelae.12-14 The treatment strategy after traumatic injuries of the primary dentition is determined by the concern for the safety of the permanent dentition.15-22
Management of traumatic dental injuries in children is challenging for both the child and the parents. It can also be challenging for the dental team. Correct treatment and follow-up are
important to give the child the best possible dental care. The risk of long-term complications may – if left affect the permanent teeth if left untreated. Thus, the aim of this study was to investigate the prevalence of sequelae in permanent anterior teeth following trauma in their predecessors.
METHODS This study was approved by the Ege
University Clinical Research Ethics Committee (20-3.1T/58).
This retrospective study was based on the clinical data of 79 patients (186 teeth). Of the 79 children (53 boys, 26 girls) who were treated for anterior primary tooth trauma in our university, a follow-up examination on 35 patients (91 teeth) were performed for the period of 2005 to 2011. Patients were recalled before for examination every 3-6 weeks, 3 months, 6 months and annually. The inclusion criteria were as follows; aged between 0-6 years at the time of injury; anterior primary tooth injuries; no systemic disease involvement; no medication taken; and attendance of regular follow up visits for 6 years. Clinical and radiological examinations data were evaluated for each patient retrospectively. The age, gender, etiology and time of trauma, presence or absence of soft tissue injury, number of injured teeth, type of trauma and type of tooth were investigated. The type of trauma was recorded according to the classification criteria of Andreassen and Andreassen.9 During the follow-up examination evaluations of 35 patients (91 teeth), clinical examinations and dental radiographs were investigated for each patient. The following information was determined: presence or absence of sequelae on permanent tooth, type of sequelae (hypoplasia, crown-root malformation, crown or root malformation), time of eruption of the permanent tooth (normal, delayed, premature), and the presence or absence of displacement. When the tooth presented more
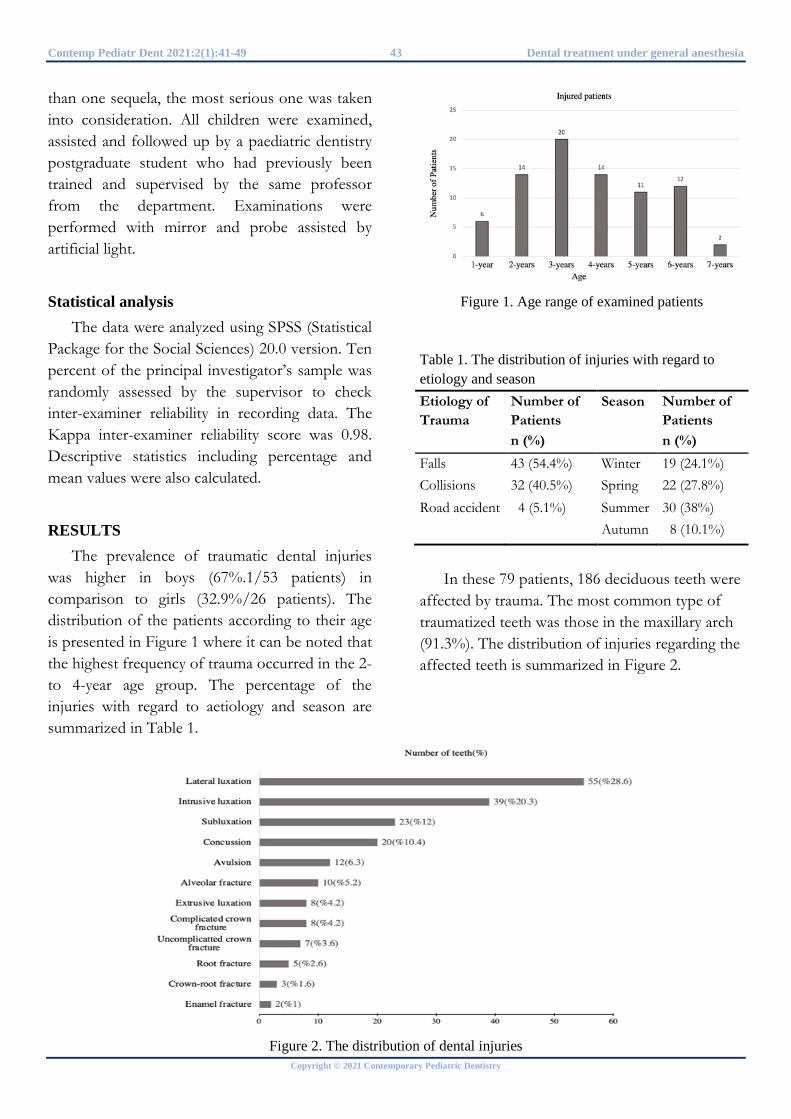
Contemp Pediatr Dent 2021:2(1):41-49 43 Dental treatment under general anesthesia
Copyright © 2021 Contemporary Pediatric Dentistry
than one sequela, the most serious one was taken into consideration. All children were examined, assisted and followed up by a paediatric dentistry postgraduate student who had previously been trained and supervised by the same professor from the department. Examinations were performed with mirror and probe assisted by artificial light.
Statistical analysis The data were analyzed using SPSS (Statistical
Package for the Social Sciences) 20.0 version. Ten percent of the principal investigator’s sample was randomly assessed by the supervisor to check inter-examiner reliability in recording data. The Kappa inter-examiner reliability score was 0.98. Descriptive statistics including percentage and mean values were also calculated.
RESULTS
The prevalence of traumatic dental injuries was higher in boys (67%.1/53 patients) in comparison to girls (32.9%/26 patients). The distribution of the patients according to their age is presented in Figure 1 where it can be noted that the highest frequency of trauma occurred in the 2-to 4-year age group. The percentage of the injuries with regard to aetiology and season are summarized in Table 1.
Figure 1. Age range of examined patients
Table 1. The distribution of injuries with regard to etiology and season Etiology of Trauma
Number of Patients n (%)
Season Number of Patients n (%)
Falls 43 (54.4%) Winter 19 (24.1%) Collisions 32 (40.5%) Spring 22 (27.8%) Road accident 4 (5.1%) Summer 30 (38%) Autumn 8 (10.1%)
In these 79 patients, 186 deciduous teeth were affected by trauma. The most common type of traumatized teeth was those in the maxillary arch (91.3%). The distribution of injuries regarding the affected teeth is summarized in Figure 2.
Figure 2. The distribution of dental injuries
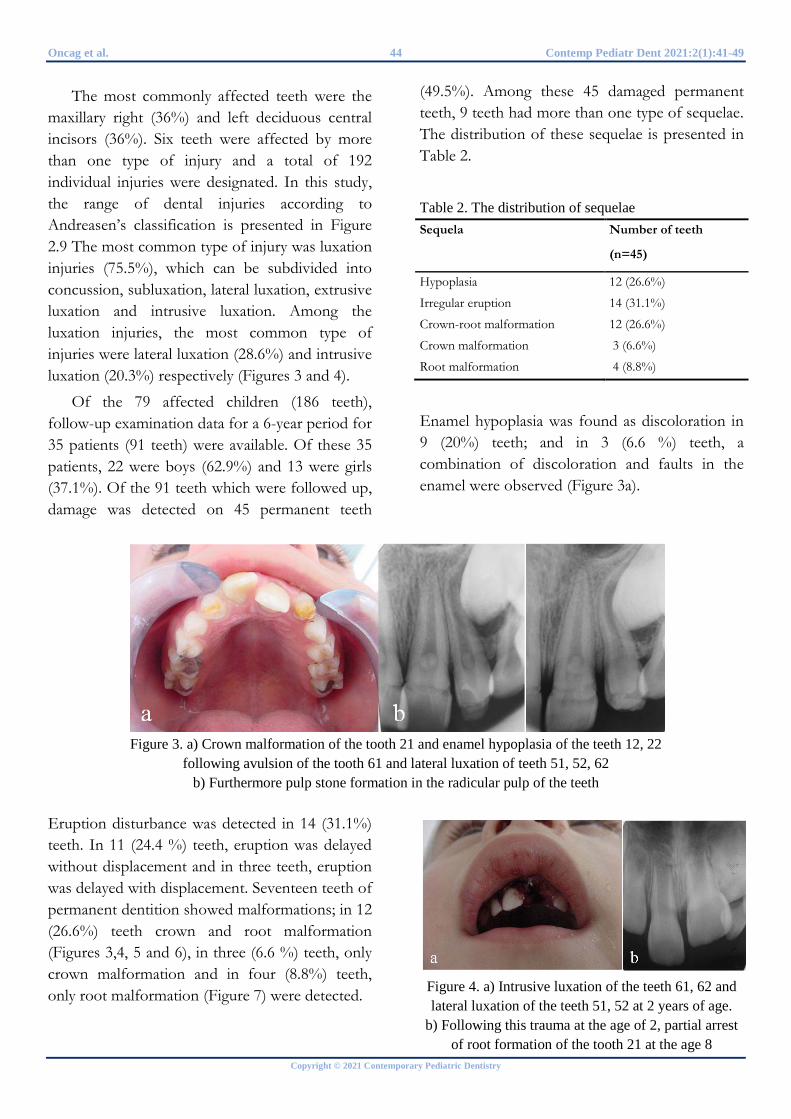
Oncag et al. 44 Contemp Pediatr Dent 2021:2(1):41-49
Copyright © 2021 Contemporary Pediatric Dentistry
The most commonly affected teeth were the maxillary right (36%) and left deciduous central incisors (36%). Six teeth were affected by more than one type of injury and a total of 192 individual injuries were designated. In this study, the range of dental injuries according to Andreasen’s classification is presented in Figure 2.9 The most common type of injury was luxation injuries (75.5%), which can be subdivided into concussion, subluxation, lateral luxation, extrusive luxation and intrusive luxation. Among the luxation injuries, the most common type of injuries were lateral luxation (28.6%) and intrusive luxation (20.3%) respectively (Figures 3 and 4).
Of the 79 affected children (186 teeth), follow-up examination data for a 6-year period for 35 patients (91 teeth) were available. Of these 35 patients, 22 were boys (62.9%) and 13 were girls (37.1%). Of the 91 teeth which were followed up, damage was detected on 45 permanent teeth
(49.5%). Among these 45 damaged permanent teeth, 9 teeth had more than one type of sequelae. The distribution of these sequelae is presented in Table 2.
Table 2. The distribution of sequelae Sequela Number of teeth
(n=45)
Hypoplasia 12 (26.6%)
Irregular eruption 14 (31.1%)
Crown-root malformation 12 (26.6%)
Crown malformation 3 (6.6%)
Root malformation 4 (8.8%)
Enamel hypoplasia was found as discoloration in 9 (20%) teeth; and in 3 (6.6 %) teeth, a combination of discoloration and faults in the enamel were observed (Figure 3a).
Figure 3. a) Crown malformation of the tooth 21 and enamel hypoplasia of the teeth 12, 22
following avulsion of the tooth 61 and lateral luxation of teeth 51, 52, 62 b) Furthermore pulp stone formation in the radicular pulp of the teeth
Eruption disturbance was detected in 14 (31.1%) teeth. In 11 (24.4 %) teeth, eruption was delayed without displacement and in three teeth, eruption was delayed with displacement. Seventeen teeth of permanent dentition showed malformations; in 12 (26.6%) teeth crown and root malformation (Figures 3,4, 5 and 6), in three (6.6 %) teeth, only crown malformation and in four (8.8%) teeth, only root malformation (Figure 7) were detected.
Figure 4. a) Intrusive luxation of the teeth 61, 62 and lateral luxation of the teeth 51, 52 at 2 years of age.
b) Following this trauma at the age of 2, partial arrest of root formation of the tooth 21 at the age 8
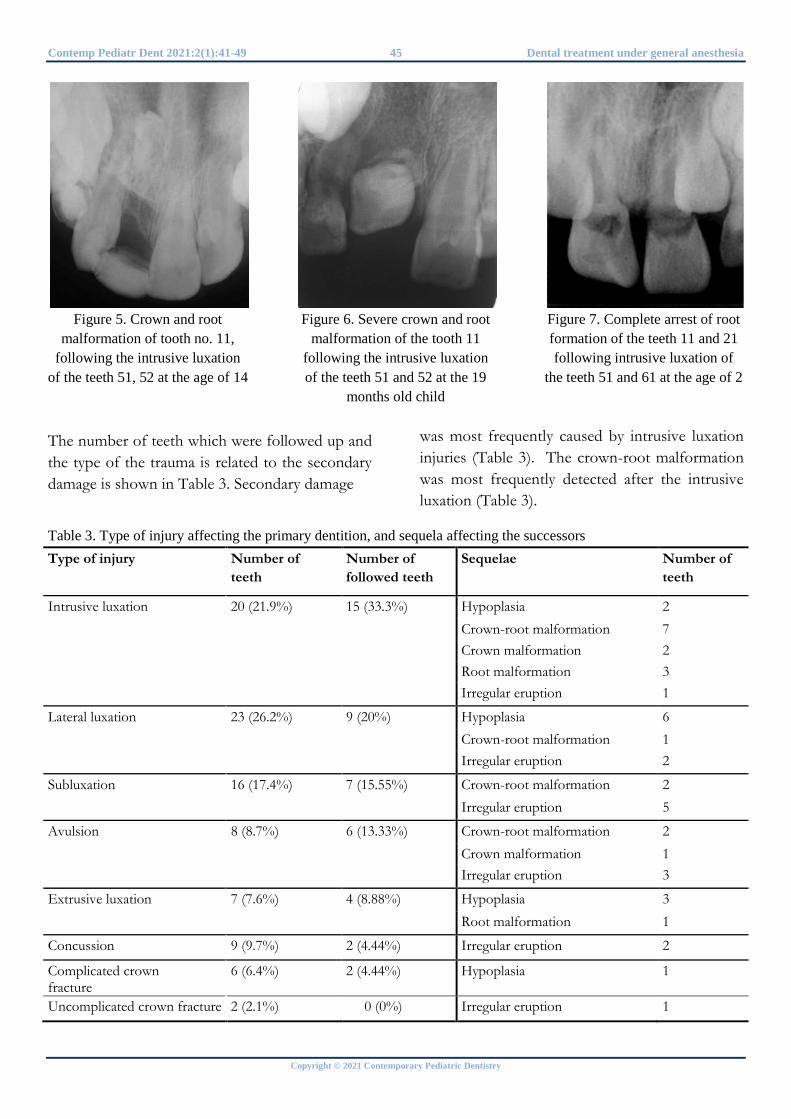
Contemp Pediatr Dent 2021:2(1):41-49 45 Dental treatment under general anesthesia
Copyright © 2021 Contemporary Pediatric Dentistry
Figure 5. Crown and root
malformation of tooth no. 11, following the intrusive luxation
of the teeth 51, 52 at the age of 14
Figure 6. Severe crown and root
malformation of the tooth 11 following the intrusive luxation of the teeth 51 and 52 at the 19
months old child
Figure 7. Complete arrest of root formation of the teeth 11 and 21 following intrusive luxation of
the teeth 51 and 61 at the age of 2
The number of teeth which were followed up and the type of the trauma is related to the secondary damage is shown in Table 3. Secondary damage
was most frequently caused by intrusive luxation injuries (Table 3). The crown-root malformation was most frequently detected after the intrusive luxation (Table 3).
Table 3. Type of injury affecting the primary dentition, and sequela affecting the successorsType of injury Number of
teeth Number of followed teeth
Sequelae Number of teeth
Intrusive luxation 20 (21.9%) 15 (33.3%) Hypoplasia 2 Crown-root malformation 7 Crown malformation 2 Root malformation 3 Irregular eruption 1
Lateral luxation 23 (26.2%) 9 (20%) Hypoplasia 6 Crown-root malformation 1 Irregular eruption 2
Subluxation 16 (17.4%) 7 (15.55%) Crown-root malformation 2 Irregular eruption 5
Avulsion 8 (8.7%) 6 (13.33%) Crown-root malformation 2 Crown malformation 1 Irregular eruption 3
Extrusive luxation 7 (7.6%) 4 (8.88%) Hypoplasia 3 Root malformation 1
Concussion 9 (9.7%) 2 (4.44%) Irregular eruption 2
Complicated crown fracture
6 (6.4%) 2 (4.44%) Hypoplasia 1
Uncomplicated crown fracture 2 (2.1%) 0 (0%) Irregular eruption 1
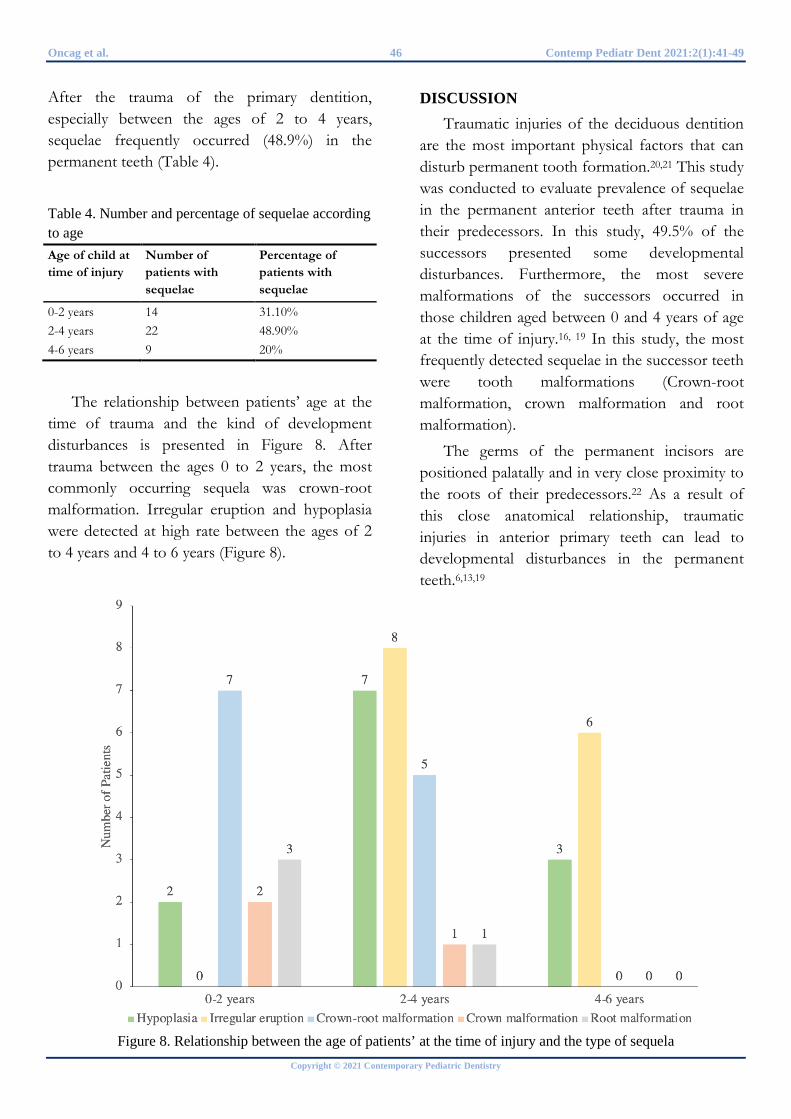
Oncag et al. 46 Contemp Pediatr Dent 2021:2(1):41-49
Copyright © 2021 Contemporary Pediatric Dentistry
After the trauma of the primary dentition, especially between the ages of 2 to 4 years, sequelae frequently occurred (48.9%) in the permanent teeth (Table 4).
Table 4. Number and percentage of sequelae according to age Age of child at time of injury
Number of patients with sequelae
Percentage of patients with sequelae
0-2 years 14 31.10% 2-4 years 22 48.90% 4-6 years 9 20%
The relationship between patients’ age at the time of trauma and the kind of development disturbances is presented in Figure 8. After trauma between the ages 0 to 2 years, the most commonly occurring sequela was crown-root malformation. Irregular eruption and hypoplasia were detected at high rate between the ages of 2 to 4 years and 4 to 6 years (Figure 8).
DISCUSSION
Traumatic injuries of the deciduous dentition are the most important physical factors that can disturb permanent tooth formation.20,21 This study was conducted to evaluate prevalence of sequelae in the permanent anterior teeth after trauma in their predecessors. In this study, 49.5% of the successors presented some developmental disturbances. Furthermore, the most severe malformations of the successors occurred in those children aged between 0 and 4 years of age at the time of injury.16, 19 In this study, the most frequently detected sequelae in the successor teeth were tooth malformations (Crown-root malformation, crown malformation and root malformation).
The germs of the permanent incisors are positioned palatally and in very close proximity to the roots of their predecessors.22 As a result of this close anatomical relationship, traumatic injuries in anterior primary teeth can lead to developmental disturbances in the permanent teeth.6,13,19
Figure 8. Relationship between the age of patients’ at the time of injury and the type of sequela

Contemp Pediatr Dent 2021:2(1):41-49 47 Dental treatment under general anesthesia
Copyright © 2021 Contemporary Pediatric Dentistry
The level of developmental disturbance in the permanent tooth depends on the stage of odontogenesis of the permanent tooth and the impact intensity and direction of the dental trauma.23
The number of trauma cases increases during the summer period. Results of this study match the results of previous studies conducted in Turkey.24, 25 This finding could be attributed to the fact that outdoor activities increase with warmer weather. In agreement with previous studies, we found a higher trauma percentage among boys than girls.26-28 This could be explained by the tendency of boys to take part in more dynamic outdoor activities compared to girls. As pointed out in another study24, Turkish society tends to raise girls in a more protective manner than boys. This could explain why boys have a higher percentage of traumatic injuries. Taking the age of the children at the time of accident into consideration, it becomes apparent that 80% of patients up to the age of 4 years suffered from sequelae in contrast to only 20% of patients older than 4 years. According to the previous studies, a possible cause could be the incomplete level of mineralization of bone and dental germ at that time.16,29-31 Moreover, in this research, irregular eruptions were considered as secondary sequela. 19,32 Although only the most serious sequelae were considered for classification, this type of secondary disturbance presented a high prevalence (31.1%). Crown malformation of the permanent teeth is more common following an intrusive luxation or avulsion of primary teeth, and the most vulnerable period is the early ages.9,14,19,22,32-34 The results of this study regarding the age of children at the time of injury and the type of traumatic injury are similar to those reported in the literature. 9,14,22,34 Within the scope of this research, it is noted that root malformation was observed in 4 of the 45 permanent successors. From these 4 teeth with root malformation, 3 were caused by intrusion in children aged between
2 and 4 years age. Crown-root malformation is the most common sequela (26.6%) in the tooth malformation. Predominantly, it is caused by intrusive luxations and avulsions in children between the ages of 0 to 2 years at the time of injury.11,19,35,36 In this study, similar to previous studies, it was found that intrusive luxation in primary teeth were the types of injury that most commonly caused sequela in their successors.8-12 Dental injuries are more common among preschool children.37 During this period, the permanent incisors are in continuous formation and any trauma can harm their constitution at different levels. The type of traumatic primary tooth injury connected with the age of the child at the time of accident can determine the possibility of subsequent secondary damages. Therefore, the importance of careful examination and documentation of the accident becomes significant. The purpose of the treatment of traumatic injuries in primary teeth can be regarded as an attempt to avoid major consequences in the involved tooth, and most importantly, to its developing successor.38 However, when the teeth and their surrounding tissues do not have any evident damage, parents only visit a dentist when a post traumatic sequela appears.19 In the aftermath of deciduous tooth trauma in children, the primary objective should be averting or minimizing the sequelae. Consequently, regular clinical follow-up examinations and periodic radiographs are necessary after the traumatic injuries of the deciduous teeth. However, one of the biggest difficulties in this study was to reach all previously traumatized patients. We determined that after the initial panic fades away, parents frequently do not come back for recall visits as other researchers have also pointed out.39,40 With regular follow-ups, early detection of any sequelae in the permanent anterior teeth can be established. Therefore, this approach can lead to a better prognosis which can minimize or avert the post traumatic sequelae in children and provide the possibility of a more effective treatment.
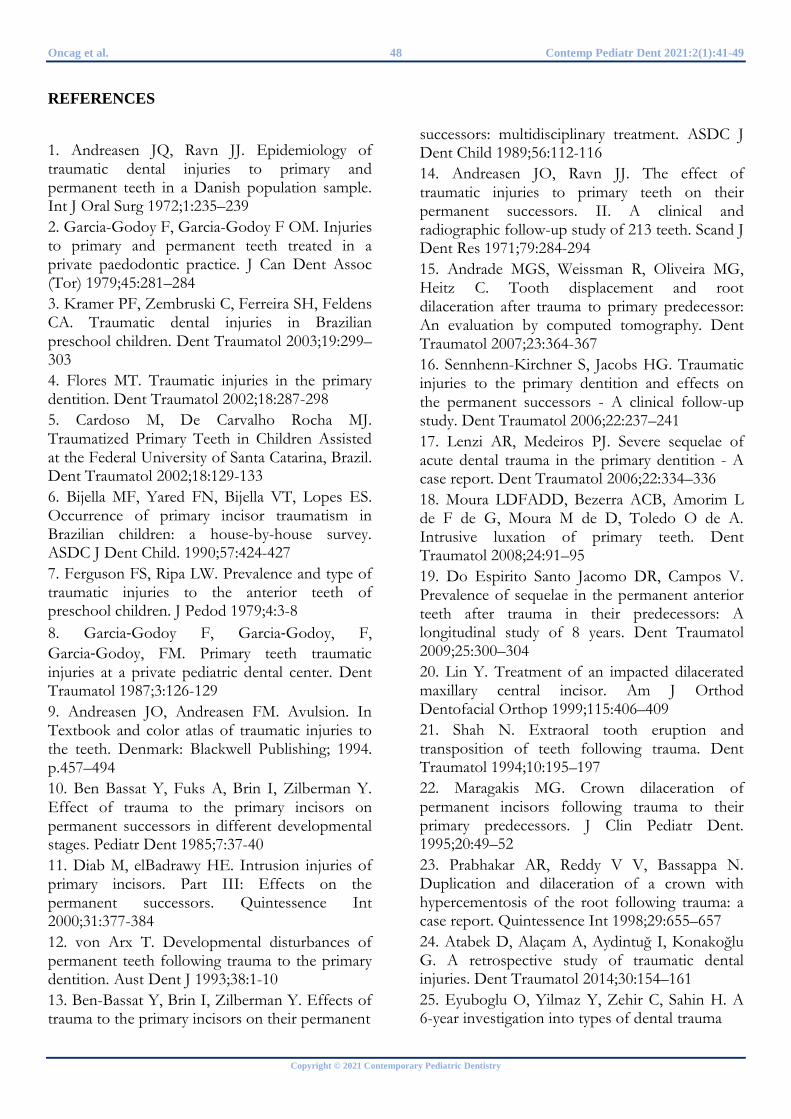
Oncag et al. 48 Contemp Pediatr Dent 2021:2(1):41-49
Copyright © 2021 Contemporary Pediatric Dentistry
REFERENCES 1. Andreasen JQ, Ravn JJ. Epidemiology of traumatic dental injuries to primary and permanent teeth in a Danish population sample. Int J Oral Surg 1972;1:235–239 2. Garcia-Godoy F, Garcia-Godoy F OM. Injuries to primary and permanent teeth treated in a private paedodontic practice. J Can Dent Assoc (Tor) 1979;45:281–284 3. Kramer PF, Zembruski C, Ferreira SH, Feldens CA. Traumatic dental injuries in Brazilian preschool children. Dent Traumatol 2003;19:299–303 4. Flores MT. Traumatic injuries in the primary dentition. Dent Traumatol 2002;18:287-298 5. Cardoso M, De Carvalho Rocha MJ. Traumatized Primary Teeth in Children Assisted at the Federal University of Santa Catarina, Brazil. Dent Traumatol 2002;18:129-133 6. Bijella MF, Yared FN, Bijella VT, Lopes ES. Occurrence of primary incisor traumatism in Brazilian children: a house-by-house survey. ASDC J Dent Child. 1990;57:424-427 7. Ferguson FS, Ripa LW. Prevalence and type of traumatic injuries to the anterior teeth of preschool children. J Pedod 1979;4:3-8 8. Garcia‐Godoy F, Garcia‐Godoy, F, Garcia‐Godoy, FM. Primary teeth traumatic injuries at a private pediatric dental center. Dent Traumatol 1987;3:126-129 9. Andreasen JO, Andreasen FM. Avulsion. In Textbook and color atlas of traumatic injuries to the teeth. Denmark: Blackwell Publishing; 1994. p.457–494 10. Ben Bassat Y, Fuks A, Brin I, Zilberman Y. Effect of trauma to the primary incisors on permanent successors in different developmental stages. Pediatr Dent 1985;7:37-40 11. Diab M, elBadrawy HE. Intrusion injuries of primary incisors. Part III: Effects on the permanent successors. Quintessence Int 2000;31:377-384 12. von Arx T. Developmental disturbances of permanent teeth following trauma to the primary dentition. Aust Dent J 1993;38:1-10 13. Ben-Bassat Y, Brin I, Zilberman Y. Effects of trauma to the primary incisors on their permanent
successors: multidisciplinary treatment. ASDC J Dent Child 1989;56:112-116 14. Andreasen JO, Ravn JJ. The effect of traumatic injuries to primary teeth on their permanent successors. II. A clinical and radiographic follow-up study of 213 teeth. Scand J Dent Res 1971;79:284-294 15. Andrade MGS, Weissman R, Oliveira MG, Heitz C. Tooth displacement and root dilaceration after trauma to primary predecessor: An evaluation by computed tomography. Dent Traumatol 2007;23:364-367 16. Sennhenn-Kirchner S, Jacobs HG. Traumatic injuries to the primary dentition and effects on the permanent successors - A clinical follow-up study. Dent Traumatol 2006;22:237–241 17. Lenzi AR, Medeiros PJ. Severe sequelae of acute dental trauma in the primary dentition - A case report. Dent Traumatol 2006;22:334–336 18. Moura LDFADD, Bezerra ACB, Amorim L de F de G, Moura M de D, Toledo O de A. Intrusive luxation of primary teeth. Dent Traumatol 2008;24:91–95 19. Do Espirito Santo Jacomo DR, Campos V. Prevalence of sequelae in the permanent anterior teeth after trauma in their predecessors: A longitudinal study of 8 years. Dent Traumatol 2009;25:300–304 20. Lin Y. Treatment of an impacted dilacerated maxillary central incisor. Am J Orthod Dentofacial Orthop 1999;115:406–409 21. Shah N. Extraoral tooth eruption and transposition of teeth following trauma. Dent Traumatol 1994;10:195–197 22. Maragakis MG. Crown dilaceration of permanent incisors following trauma to their primary predecessors. J Clin Pediatr Dent. 1995;20:49–52 23. Prabhakar AR, Reddy V V, Bassappa N. Duplication and dilaceration of a crown with hypercementosis of the root following trauma: a case report. Quintessence Int 1998;29:655–657 24. Atabek D, Alaçam A, Aydintuğ I, Konakoğlu G. A retrospective study of traumatic dental injuries. Dent Traumatol 2014;30:154–161 25. Eyuboglu O, Yilmaz Y, Zehir C, Sahin H. A 6-year investigation into types of dental trauma

Contemp Pediatr Dent 2021:2(1):41-49 49 Dental treatment under general anesthesia
Copyright © 2021 Contemporary Pediatric Dentistry
treated in a paediatric dentistry clinic in Eastern Anatolia Region, Turkey. Dent Traumatol 2009;25:110–114 26. Zuhal K, Semra ÖEM, Hüseyin K. Traumatic injuries of the permanent incisors in children in southern Turkey: A retrospective study. Dent Traumatol 2005;21:20–25 27. Cavalcanti AL, Bezerra PKM, De Alencar CRB, Moura C. Traumatic anterior dental injuries in 7- to 12-year-old Brazilian children. Dent Traumatol 2009;25:198–202 28. Güngör HC, Uysal S, Altay N. A retrospective evaluation of crown-fractured permanent teeth treated in a pediatric dentistry clinic. Dent Traumatol 2007;23:211–217 29. Ravn JJ. Sequelae of acute mechanical traumata in the primary dentition. A clinical study. ASDC J Dent Child 1968;35:281–289 30. Selliseth NE. The significance of traumatised primary incisors on the development and eruption of permenent teeth. Eur Orthod Soc 1970;443–459 31. Watzek G SJ. Milchzahntraumen und ihre Bedeutung für die bleibenden Zähne. Zahn Mund Kieferheilkd. 1976;64:126–133 32. Andreasen JO, Andreasen F. Injuries to primary teeth. In: Andreasen JO, Andreasen F. Essentials of Traumatic Injuries to the Teeth: A Step‐by‐Step Treatment Guide. Denmark: Munksgaard; 2001. p.141-154 33. Andreasen JO, J. RJ. Enamel changes in permanent teeth after trauma to their primary predecessors. Scand J Dent Res 1973;81:203–209 34. Ravn JJ. Developmental disturbances in permanent teeth after intrusion of their primary predecessors. Scand J Dent Res 1976;84:137–141 35. Zilberman Y, Fuks A, Ben Bassat Y, Brin I, Lustmann J. Effect of trauma to primary incisors on root development of their permanent successors. Pediatr Dent 1986;8:289–293 36. Nolla CM. The developmental of permanent teeth. J Dent Child 1960;27:254–266 37. Kilpatrick NM, Hardman PJ, Welbury RR. Dilaceration of a primary tooth. Int J Paediatr Dent 1991;1:151–153 38. Oliveira,BH; Moliterno,LF; Marcl, S; Balda A. Intrusão de incisive decíduos provocando distúrbio no desenvolvimento de dentes permanents: relato de caso. Rev Bras Odontol 1995;52:42–45
39. Da Silva Assuņão LR, Ferelle A, Iwakura MLH, Cunha RF. Effects on permanent teeth after luxation injuries to the primary predecessors: A study in children assisted at an emergency service. Dent Traumatol 2009;25:165–170 40. Brin I, Fuks A, Ben-Bassat Y, Zilberman Y. Trauma to the Primary Incisors and Its Effect on the Permanent Successors. Pediatr Dent 1984;6:78–82 How to cite this article: Ozant Oncag, Candan Gurbuz Sarigol, Sevgi Arabulan. Retrospective evaluation of primary anterior teeth injuries and prevalence of sequelae in their successors. Contemp Pediatr Dent 2021:2(1):41-49 Declarations
Acknowledgements: Not applicable. Conflict of Interest Statement: The authors disclose no potential conflicts of interest. Ethics Statement: This study was approved by the Ege University Clinical Research Ethics Committee (20-3.1T/58). Informed Consent: Informed consent and assent were obtained from all participants. Author contributions: Conception and design: All Authors; Acquisition of data: All Authors; Interpretation of data: All Authors; Drafting article: All Authors; Revision artice: All Authors; Final approval: All Authors Funding: This work is not finantiated. Data Availability: The data used to support the findings of this study can be made available upon request to the corresponding author. Peer-review: Externally double-blinded peer-reviewed.

Copyright © 2021 Contemporary Pediatric Dentistry. This work is licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International license. (CC BY-NC-ND 4.0)
Case Report
Composite odontoma with 23 denticles in a pediatric patient: A case report
Paôla Caroline da Silva Mira1 ✉, Jéssica Silva Peixoto Bem2, Andresa Vieira da Silva3, Marcio Santos de Carvalho4, Marcelo Rodrigues Azenha5, Christiano Oliveira-Santos6, Maria Bernadete Sasso Stuani7, Carolina Paes Torres8
Abstract Compound odontoma is an odontogenic tumor of ectomesenchymal origin containing tooth-like structures. Occasionally, this lesion may trigger occlusal, phonetic, and aesthetic disorders. The aim is to report a case of a compound odontoma containing 23 denticles in the anterior region of the maxilla of an infant patient. A 12-year-old male patient was referred for orthodontic treatment at Ribeirão Preto School of Dentistry, University of São Paulo (Ribeirão Preto, Brazil) complaining of a large diastema between the upper central incisors. Panoramic radiograph revealed the presence of a radiopaque lesion with tooth-like structures surrounded by a radiolucent rim in the anterior region of the maxilla, associated with distal displacement of the left central incisor. Surgical approach under general anesthesia revealed and extracted 23 denticles. Post-operative Cone beam computed tomography (CBCT) confirmed removal of all denticles, and further orthodontic treatment could be planned. Multidisciplinary involvement of pediatric dentist, oral and maxillofacial surgeon, and orthodontist was essential to achieve full functional, aesthetic, and psychosocial success. Keywords: Odontoma; Pediatric Dentistry; Surgery
Highlights Odontoma occurs more frequently during the permanent dentition phase in children, adolescents, and young adults.
1 Master, Department of Pediatric Clinics, University of São Paulo (USP), Brazil 2 Master student, Department of Pediatric Clinics, University of São Paulo (USP), Brazil 3 Specialization student, Department of Pediatric Clinics, University of São Paulo (USP), Brazil 4 Master student, Department of Pediatric Clinics, University of São Paulo (USP), Brazil 5 Professor, Department of Stomatology, Public Health, and Forensic Dentistry, University of São Paulo (USP), Brazil 6 Associate, Professor, Department of Stomatology, Public Health, and Forensic Dentistry, University of São Paulo (USP), Brazil 7 Associate, Professor, Department of Pediatric Clinics, University of São Paulo (USP), Brazil 8 Professor, Department of Pediatric Clinics, University of São Paulo (USP), Brazil
Correspondence: Department of Pediatric Clinics, School of Dentistry of Ribeirão Preto, University of São Paulo (USP) – Ribeirão Preto/SP, Brazil E-mail address: [email protected]
Received: 02 March 2021 Accepted: 15 April 2021 Online First: 21 April 2021
Treatment plan for odontomas should involve a more comprehensive approach considering not only its surgical removal, but also the potential consequences caused by presence of the lesion.
Even though odontomas are usually not associated with painful symptoms, their presence may trigger major occlusal, phonetic, and aesthetic disorders.
Contemporary Pediatric Dentistry Contemp Pediatr Dent 2021:2(1):50-56 DOI: 10.51463/cpd.2021.44

Mira et al. 51 Contemp Pediatr Dent 2021:2(1):50-56
Copyright © 2021 Contemporary Pediatric Dentistry
INTRODUCTION Odontoma is an odontogenic tumor of
ectomesenchymal origin containing anomalous tooth-like structures called denticles (i.e. compound odontoma), or characterized by a mass of irregular hard tissues (i.e. complex odontoma).1,2
Although idiopathic, the formation of an odontoma may be associated with a history of trauma and local infections. Odontoma occurs more frequently during the permanent dentition phase in children, adolescents, and young adults. The compound type tends to affect the anterior region of the maxilla, with a prevalence that varies between 9 to 37%, while the complex type is more common in the posterior region of the maxilla and mandible, with prevalence ranging from 5 to 30%.3
Even though odontomas are usually not associated with painful symptoms, their presence may trigger major occlusal, phonetic, and aesthetic disorders. The delay in the eruption of a permanent tooth in the anterior region of the maxilla is generally the chief complaint that leads to the radiographic investigation and subsequent diagnosis of the anomaly.4,5
Once diagnosed, the treatment plan for odontomas should involve a more comprehensive approach considering not only their surgical removal, but also the potential consequences caused by their presence. When a compound odontoma is associated with failure of the eruptive process of a permanent tooth, it is essential to establish a strategy including surgical approach and corrective orthodontic treatment to normalize occlusion, phonetics, and aesthetics, to minimize functional alterations, psychological effects, and to strengthen the patient's self-esteem. Therefore, the aim is to report a clinical case of a compound odontoma containing 23
denticles in the anterior region of the maxilla of an infant patient, emphasizing and discussing the surgical approach.
CASE REPORT A 12-year-old male patient was referred for
orthodontic treatment at Ribeirão Preto School of Dentistry, University of São Paulo (Ribeirão Preto, Brazil) complaining of a large diastema between the upper central incisors. Written informed consent was signed by his legal guardian during his first visit.
Upon clinical examination, the patient had overall good oral hygiene, and did not present active carious lesions or periodontal disease. However, in addition to the interincisal diastema, it was observed that the left lateral incisor was positioned palatally, behind the upper left central incisor (Figure 1). Medical history was unremarkable.
Panoramic radiograph revealed the presence of a heterogeneous radiopaque lesion surrounded by a radiolucent rim in the anterior region of the maxilla, close to the midline, associated with distal displacement of the left central incisor (Figure 1). The internal aspect of the lesion consisted of multiple tooth-like structures, with radiographic appearances of enamel, dentin and pulp, indicating the presence of multiple denticles. The typical radiographic presentation led to the diagnostic hypothesis of a compound odontoma.
The patient was referred to the Pediatric Dentistry clinic and the treatment plan was established in collaboration with an oral and maxillofacial surgeon. Considering the location of the lesion close to the nasal cavity, potential stress to the patient, and his history of anxiety and fear of dental treatment, a surgical approach under general anesthesia in a hospital environment was proposed.
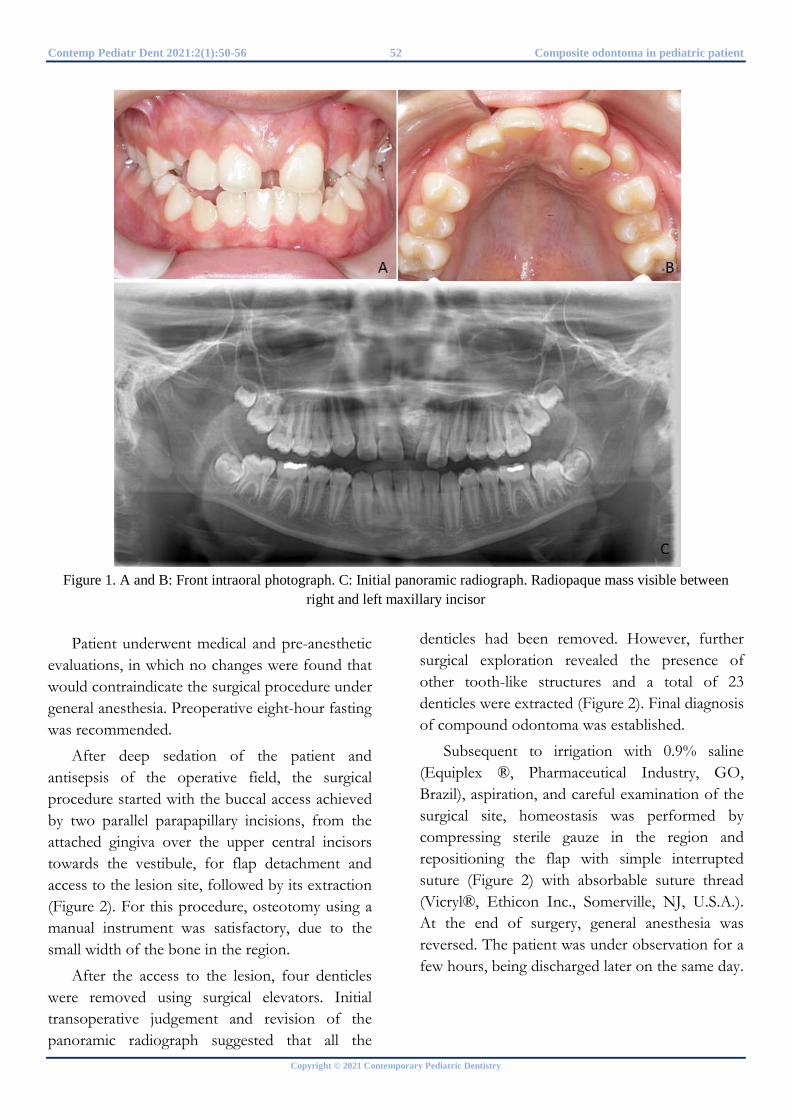
Contemp Pediatr Dent 2021:2(1):50-56 52 Composite odontoma in pediatric patient
Copyright © 2021 Contemporary Pediatric Dentistry
Figure 1. A and B: Front intraoral photograph. C: Initial panoramic radiograph. Radiopaque mass visible between
right and left maxillary incisor
Patient underwent medical and pre-anesthetic evaluations, in which no changes were found that would contraindicate the surgical procedure under general anesthesia. Preoperative eight-hour fasting was recommended.
After deep sedation of the patient and antisepsis of the operative field, the surgical procedure started with the buccal access achieved by two parallel parapapillary incisions, from the attached gingiva over the upper central incisors towards the vestibule, for flap detachment and access to the lesion site, followed by its extraction (Figure 2). For this procedure, osteotomy using a manual instrument was satisfactory, due to the small width of the bone in the region.
After the access to the lesion, four denticles were removed using surgical elevators. Initial transoperative judgement and revision of the panoramic radiograph suggested that all the
denticles had been removed. However, further surgical exploration revealed the presence of other tooth-like structures and a total of 23 denticles were extracted (Figure 2). Final diagnosis of compound odontoma was established.
Subsequent to irrigation with 0.9% saline (Equiplex ®, Pharmaceutical Industry, GO, Brazil), aspiration, and careful examination of the surgical site, homeostasis was performed by compressing sterile gauze in the region and repositioning the flap with simple interrupted suture (Figure 2) with absorbable suture thread (Vicryl®, Ethicon Inc., Somerville, NJ, U.S.A.). At the end of surgery, general anesthesia was reversed. The patient was under observation for a few hours, being discharged later on the same day.
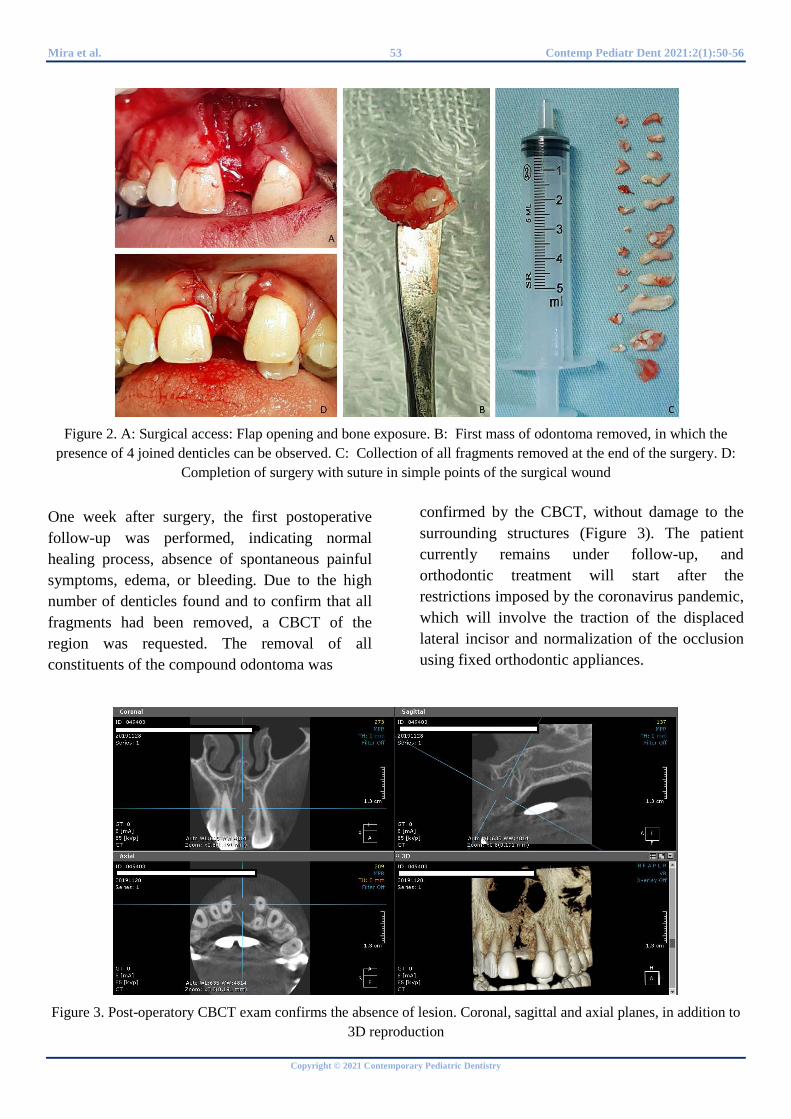
Mira et al. 53 Contemp Pediatr Dent 2021:2(1):50-56
Copyright © 2021 Contemporary Pediatric Dentistry
Figure 2. A: Surgical access: Flap opening and bone exposure. B: First mass of odontoma removed, in which the presence of 4 joined denticles can be observed. C: Collection of all fragments removed at the end of the surgery. D:
Completion of surgery with suture in simple points of the surgical wound
One week after surgery, the first postoperative follow-up was performed, indicating normal healing process, absence of spontaneous painful symptoms, edema, or bleeding. Due to the high number of denticles found and to confirm that all fragments had been removed, a CBCT of the region was requested. The removal of all constituents of the compound odontoma was
confirmed by the CBCT, without damage to the surrounding structures (Figure 3). The patient currently remains under follow-up, and orthodontic treatment will start after the restrictions imposed by the coronavirus pandemic, which will involve the traction of the displaced lateral incisor and normalization of the occlusion using fixed orthodontic appliances.
Figure 3. Post-operatory CBCT exam confirms the absence of lesion. Coronal, sagittal and axial planes, in addition to 3D reproduction

Contemp Pediatr Dent 2021:2(1):50-56 54 Composite odontoma in pediatric patient
Copyright © 2021 Contemporary Pediatric Dentistry
DISCUSSION
Imaging methods are relevant supplementary exams for diagnosis and treatment planning in Dentistry. Although radiographic examinations have been used for many years in Pediatric Dentistry, the use of three-dimensional imaging has gained more attention in more recent years with the use of CBCT in Dentistry, with its advantages related to elimination of problems related to image overlap in two-dimensional exams. However, its radiation dose is higher than conventional methods, therefore, its use should be performed according to well-established prescription criteria, particularly among pediatric patients.6,7 CBCT is indicated for diagnosis and treatment planning of supernumerary teeth, as well as for surgical-orthodontic approaches of impacted teeth.6-9
Invasive surgical interventions can be hindered by non-collaborative treatment during the clinical approach due to the dental anxiety presented by the patient according to his psychological maturity, social conditions, and emotional state.10 Furthermore, although several non-pharmacological techniques for adapting behavior are available11, the approach under general anesthesia was chosen. This option is justified because the diagnosis establish by the team allowed some predictability about the invasive nature of the intervention, and the need to minimize the risk of interference regarding patient's psycho-emotional reactions. Due to the location of the lesion, an appropriate hospital environment would be convenient in case of any complications. Moreover, conscious sedation through inhalation of nitrous oxide/oxygen would not be indicated since it could hinder access to the surgical site.
The 23 denticles removed during the complete excision of the compound odontoma represented, in fact, 19 fragments beyond the number anticipated at the beginning of the surgery. The initial imaging examination brought information from a perspective in two dimensions and did not
allow accurate measurement of the anomaly's extent in depth. Thus, adequate planning and diagnostic methods are crucial for an approach with greater predictability and security.8,12
The surgical plan was made using the panoramic radiography in order to reduce the patient's exposure to ionizing radiation. Despite that, a CBCT examination would have offered valuable information on the extent of the odontoma, and the choice for intervention under general anesthesia for this case would be even further validated.
General anesthesia promoted a smoother and overall faster procedure in addition to the monitorization of the patient's vital signs during the procedure. Also, as it consisted of a localized and short duration procedure, it provided quick recovery and absence of psychological trauma.
The multi-professional treatment planning was extremely important for the therapeutic success in this case. It could be verified by the lesion-free postoperative computed tomography associated with the uneventful healing process (Figure 3). The importance of multidisciplinary involvement is known to be relevant for success of complex treatments in Pediatric Dentistry.1,13
In this case, the involvement of the pediatric dentist and the oral and maxillofacial surgeon was essential. Subsequently, the orthodontist could carry out the following stage of the treatment, which would not be possible without the removal of the odontoma.
The presence of interincisal diastemas in children needs further investigation once it might represent a clinical sign of some alterations as dental agenesis, supernumerary teeth (mesiodens), or odontomas. Mesiodens are the most common dental anomaly related to number of teeth found in the anterior region. They are supernumerary teeth in the midline region, and their most common consequence is the delay or impaction of the permanent central incisor.13,14 However, compound odontomas should be investigated whenever there are clinical signs suggestive of this

Mira et al. 55 Contemp Pediatr Dent 2021:2(1):50-56
Copyright © 2021 Contemporary Pediatric Dentistry
alteration, such as bulging and delayed eruption of anterior teeth.1,15,16 Imaging is essential for establishing the diagnosis, and CBCT is the method of choice for adequate planning and, consequently, better prognosis.7-9
After surgery, corrective orthodontic intervention started to be studied and planned for the proper positioning of the upper incisors and satisfactory results of the occlusal and aesthetic conditions. The importance of adequate imaging exam is highlighted due to its contribution for better observation of diagnostic features of the lesion, treatment plan, and higher surgical predictability. Comprehensive planning involving professionals from different specialties is emphasized, as well as subsequent postoperative follow-up and orthodontic treatment, to maintain patient care until the global resolution of the lesion, aiming at full functional, aesthetic and psychosocial success.
REFERENCES 1. Altay MA, Ozgur B, Cehreli ZC. Management of a compound odontoma in the primary dentition. J Dent Child 2016;83:98-101 2. Philipsen HP, Reichart PA, Praetorius F. Mixed odontogenic tumours and odontomas. Considerations on interrelationship. Review of the literature and presentation of 134 new cases of odontomas. Oral Oncol 1997;33:86-99 3. de Oliveira BH, Campos V, Marçal S. Compound odontoma-diagnosis and treatment: three case reports. Pediatr Dent 2001;23:151-157 4. Sánchez OH, Berrocal MIL, González JMM. Metaanalysis of the epidemiology and clinical manifestations of odontomas. Med Oral Patol Oral Cir Bucal 2008;13:730-734 5. Janev EJ, Redzep E, Kanurkova L, Tosevska S. Compound odontoma in childhood population (Case Report). J. Morphol Sci 2020;3:73-78 6. Horner K, Islam M, Flygare L, Tsiklakis K, Whaites E. Basic principles for use of dental cone beam computed tomography: consensus guidelines of the European Academy of Dental and Maxillofacial Radiology. Dentomaxillofac Radiol 2020;38:187-195
7. Aps J. Radiography in pediatric dental practice. Clin Dent Rev 2020;4:5-6 8. Katheria BC, Kau CH, Tate R, Chen JW, English J, Bouquot J. Effectiveness of impacted and supernumerary tooth diagnosis from traditional radiography versus cone beam computed tomography. Pediatr Dent 2010;32:304-309 9. Mehta V, Ahmad N. Cone beamed computed tomography in pediatric dentistry: Concepts revisited. J Oral Biol Craniofac Res 2020;10:210-211 10. American Academy of Pediatric Dentistry. Management considerations for oral surgery and oral pathology. Pediatr Dent 2017;39:361-370 11. Townsend JA, Wells MH. Behavior guidance of the pediatric dental patient. Pediatr Dent 2019;41:352-370 12. Raupp S, Kramer PF, de Oliveira HW, da Rosa FM, Faraco Junior IM. Application of computed tomography for supernumerary teeth location in pediatric dentistry. Int J Clin Pediatr Dent 2008;32:273-276 13. Monteiro PM, Mira PCS, Arnez MFM, Silva FWGP, Stuani MBS. Mesiodens and maxillary central incisors impaction: multidisciplinary approach to reestablish esthetics and function. Rev Clín Ortod Dent Press 2019;18:120-129 14. Hong J, Lee DG, Park K. Retrospective analysis of the factors influencing mesiodentes eruption. Int J Paediatr Dent 2009;19:343-348 15. Shulman ER, Corio RL. Delayed eruption associated with an odontoma. ASDC J Dent Child 1987;54:205-207 16. Oliver RG, Hodges CG. Delayed eruption of a maxillary central incisor associated with an odontome: report of case. ASDC J Dent Child 1988;55:368-371

Contemp Pediatr Dent 2021:2(1):50-56 56 Composite odontoma in pediatric patient
Copyright © 2021 Contemporary Pediatric Dentistry
How to cite this article: Paôla Caroline da Silva Mira, Jéssica Silva Peixoto Bem, Andresa Vieira da Silva, Marcio Santos de Carvalho, Marcelo Rodrigues Azenha, Christiano Oliveira-Santos, Maria Bernadete Sasso Stuani, Carolina Paes Torres. Composite odontoma with 23 denticles in a pediatric patient: A case report. Contemp Pediatr Dent 2021:2(1):50-56 Declarations
Acknowledgements: Not applicable. Conflict of Interest Statement: The authors disclose no potential conflicts of interest. Ethics Statement: Procedure was explained to the legal guardian and written consent was obtained for the treatment and publication of the case report. Informed Consent: Written informed consent was signed by his legal guardian during his first visit. Author contributions: Conception and design: All Authors; Acquisition of data: COS, MBSS, CPT; Interpretation of data: PCSM, SSK; Drafting article: PCSM; Revision artice: JPB, AVS, MSC, MRA; Final approval: All Authors Funding: This work is not finantiated. Data Availability: The data used to support the findings of this study can be made available upon request to the corresponding author. Peer-review: Externally double-blinded peer-reviewed.
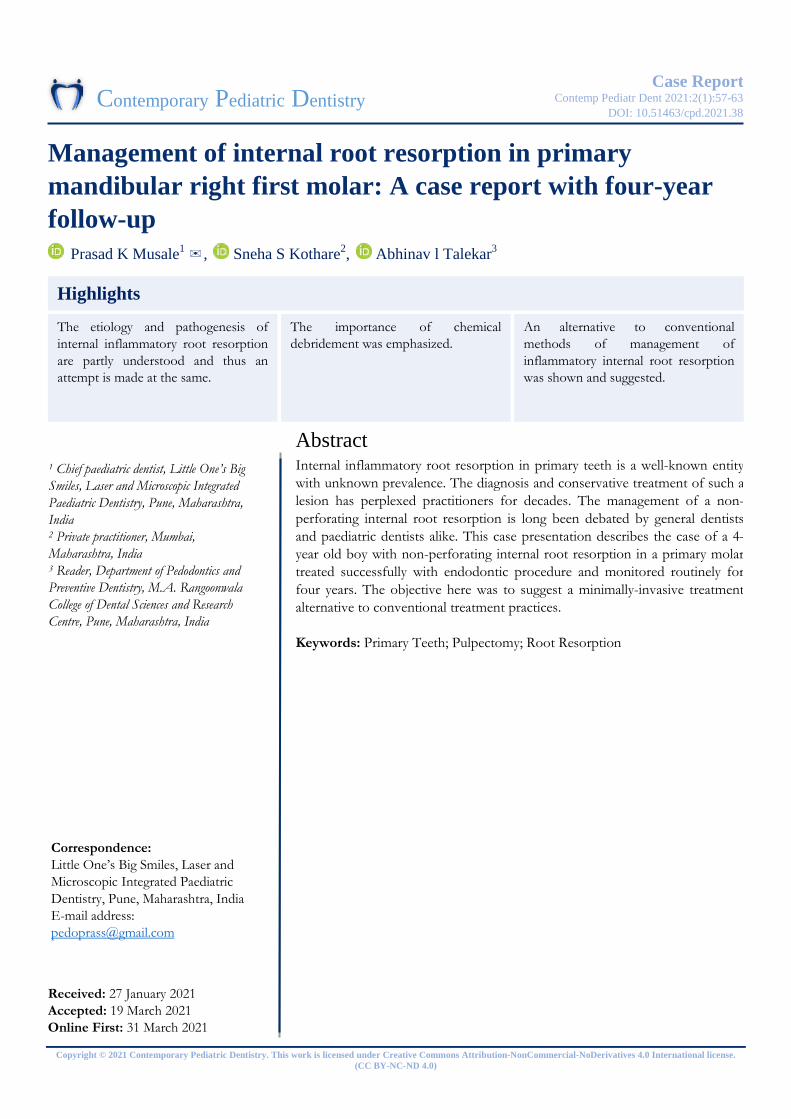
Copyright © 2021 Contemporary Pediatric Dentistry. This work is licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International license. (CC BY-NC-ND 4.0)
Case Report
Management of internal root resorption in primary mandibular right first molar: A case report with four-year follow-up
Prasad K Musale1 ✉, Sneha S Kothare2, Abhinav l Talekar3
Abstract Internal inflammatory root resorption in primary teeth is a well-known entity with unknown prevalence. The diagnosis and conservative treatment of such a lesion has perplexed practitioners for decades. The management of a non-perforating internal root resorption is long been debated by general dentists and paediatric dentists alike. This case presentation describes the case of a 4-year old boy with non-perforating internal root resorption in a primary molar treated successfully with endodontic procedure and monitored routinely for four years. The objective here was to suggest a minimally-invasive treatment alternative to conventional treatment practices. Keywords: Primary Teeth; Pulpectomy; Root Resorption
Highlights The etiology and pathogenesis of internal inflammatory root resorption are partly understood and thus an attempt is made at the same.
1 Chief paediatric dentist, Little One’s Big Smiles, Laser and Microscopic Integrated Paediatric Dentistry, Pune, Maharashtra, India 2 Private practitioner, Mumbai, Maharashtra, India 3 Reader, Department of Pedodontics and Preventive Dentistry, M.A. Rangoonwala College of Dental Sciences and Research Centre, Pune, Maharashtra, India
Correspondence: Little One’s Big Smiles, Laser and Microscopic Integrated Paediatric Dentistry, Pune, Maharashtra, India E-mail address: [email protected]
Received: 27 January 2021 Accepted: 19 March 2021 Online First: 31 March 2021
An alternative to conventional methods of management of inflammatory internal root resorption was shown and suggested.
The importance of chemical debridement was emphasized.
Contemporary Pediatric Dentistry Contemp Pediatr Dent 2021:2(1):57-63 DOI: 10.51463/cpd.2021.38

Musale et al. 58 Contemp Pediatr Dent 2021:2(1):57-63
Copyright © 2021 Contemporary Pediatric Dentistry
INTRODUCTION Tooth resorption in the primary and
permanent dentition has been studied extensively and the complex processes that lead to the loss of organic and inorganic components of tooth structure by clastic cells have been investigated. In recent times, Lindskog’s classification has subdivided tooth resorptions into three broad groups: trauma induced tooth resorption; infection induced tooth resorption; and hyperplastic invasive tooth.1
Inflammatory resorption is defined as an internal or external pathologic loss of tooth structure and possibly bone, resulting in a defect, occurs as a result of microbial infection; characterized radiographically by radiolucent areas of the root. More specifically, internal root resorption is defined as a process initiated within the pulp space with loss of dentin and possible invasion of cementum.2 Thus, internal inflammatory root resorption (IRR) is a relatively rare type of tooth resorption that begins in the root canal and destroys surrounding dental hard tissues. It is a well-known entity with most dentists able to diagnose the phenomenon accurately. Available literature has described its exact clinical as well as radiographic appearance. However, its etiology, pathogenesis is only partially understood and its subsequent management has perplexed practitioners. Further, the occurrence and management of internal inflammatory root resorption in primary teeth is poorly understood and scant literature is available in this regard.
Trauma is the most common cause of IRR followed by pulpitis. Pulpotomy, cracked tooth, tooth transplantation, restorative procedures, invagination, orthodontic treatment and Herpes zoster viral infection are the other predisposing factors to this type of resorption. Untreated carious teeth, carious pulp involvement, pulpotomy, pulpectomy lead to higher occurrence of IRR in primary teeth.3 It is postulated that
damage to the organic sheath, predentin and odontoblast cells covering mineralized dentine inside the root canal must occur to expose the mineralized tissue to pulpal cells with resorbing potential, thus resulting in loss of dentin and possible invasion of cementum. However, the exact initiating events leading to such denudation of root dentin are not fully understood.4
There is a general consensus that IRR is a rare phenomenon but its precise numbers are not known.5 Most of the available literature consists of case reports with emphasis on management of resorption. Haapsaalo and Endal4 theorized that the prevalence would be between 0.01 and 1%.4 Gabor et al.5 reported that 50% of teeth with pulpitis and 77% of teeth with pulpal necrosis showed IRR while it was absent in healthy teeth. In primary molars, the prevalence is found to be 16.2% with greater prevalence in 3-7 year old children (19.4%).3 Most of the lesions were in the middle third followed by apical third of the root while only one was in the coronal third.5
According to Wedenberg and Zetterqvist6, IRR in primary and permanent teeth is identical, both clinically and morphologically, except that the resorption is hastened in primary teeth. This difference could be attributed to the lesser number of clusters of epithelial cell rests of Mallassez in the periodontal ligament of primary teeth and lower expression of osteoprotegrin (OPG), factors usually associated with lower protection of primary teeth against root resorption.7
The development of root resorption requires two phases: injury to the protective tissues (mechanical or chemical) and then stimulation by infection or pressure.8
Bacteria-induced inflammation is typically accompanied by the production and release of potent stimulators of hard tissue resorption, such as osteoclast activating factor, prostaglandins, macrophage-chemotactic factor and bacterial

Contemp Pediatr Dent 2021:2(1):57-63 59 Internal root resorption in primary molar
Copyright © 2021 Contemporary Pediatric Dentistry
lipopolysaccharides. This stimulation may be necessary for the progression of internal resorption. Cessation of IRR usually occurs once either total pulp necrosis occurs or once a pulpectomy is carried out because the dentinoclasts require a viable blood supply for them to survive and be active.4
IRR is usually asymptomatic and is often first diagnosed as an inadvertent finding on radiographic examination. Alternatively, it is found when the patient develops symptoms as a result of the progression of the disease process to cause acute apical periodontitis at some stage after the entire root canal system has become infected or if it perforates through the root communicating with the periodontal ligament (PDL).9 The normal radiographic presentation is an area of enlargement of the root canal or the pulp chamber. This enlargement can be symmetrical or eccentric but has sharp, smooth and clearly defined margins. The root canal is indistinguishable within the resorptive lesion and the size and location of the resorptive defect is variable depending on the extent of damage.
Although digital intraoral radiography provides an acceptable level of accuracy, digital subtraction radiography shows superior results.10 However, in recent times, CBCT is found to be superior to any form of two-dimensional radiography and may result in a review of the radiographic techniques used for assessing the type of resorption lesion present. This superior diagnostic accuracy also results in an increased likelihood of correct management of resorption lesions.11
An internal resorption lacuna, when evident radiographically, is a definite indication for endodontic treatment. Since the resorbing cells in this type of resorption are pulpal in origin, a pulpectomy would eliminate the granulation tissue and cut off the blood supply of the resorptive cells.8 Debridement and filling of the canal and
the defect can be extremely challenging. Chemical debridement, which includes both irrigation and intracanal medication, has a major role to play in the elimination of the bacteria and the tissue present in the resorptive defect because this cannot be predictably achieved just with root canal instrumentation alone unless significant amounts of tooth structure are removed. However, such a mechanical approach will significantly weaken the tooth. Thus, the convention till date has been to extract the affected primary tooth and replace it with a suitable spacer maintainer.1 However, this case report discusses the management of a primary molar with non-perforating IRR and highlights the importance of chemical debridement with minimal mechanical preparation.
CASE REPORT
A 4-year old boy reported with a complain of severe pain and swelling associated with the primary mandibular right first molar since the previous night. His medical history was non-contributory. On clinical examination, a well-circumscribed swelling was seen in the region of #S on the buccal side. The gingiva overlying the region was reddish in color with reddish yellow color of the most prominent part. Clinically, the patient was diagnosed as a case acute dentoalveolar abscess of #84. Radiographic evaluation of the tooth revealed a large, ovoid radiolucency extending from the cervical-third of the distal root to the middle-third that was confined within the dentinal walls. Diffuse interfurcal radiolucency was seen extending up to the apical region of the distal root not involving the developing tooth bud (Figure 1). Thus, the radiographic diagnosis was non-perforating type of internal root resorption with pulpal etiology. A decision to perform multi-visit pulpectomy was made based on the clinical and radiographic evaluation and informed consent was obtained for the same from the parents.
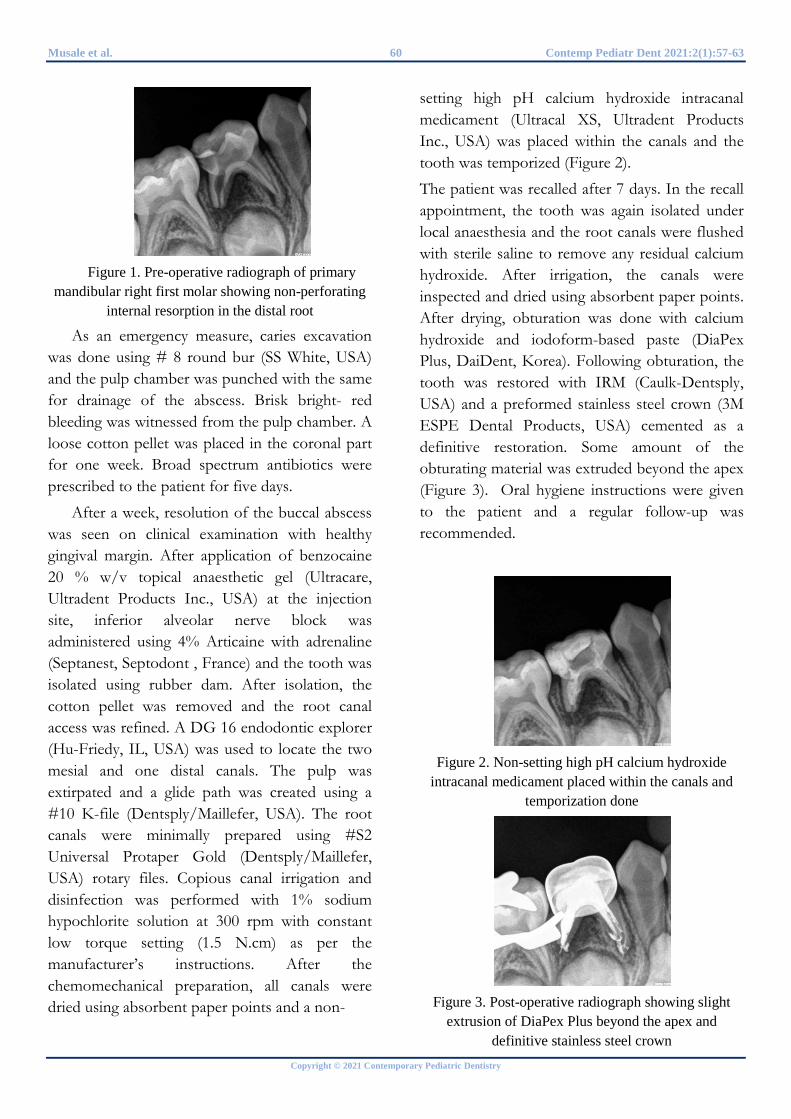
Musale et al. 60 Contemp Pediatr Dent 2021:2(1):57-63
Copyright © 2021 Contemporary Pediatric Dentistry
Figure 1. Pre-operative radiograph of primary
mandibular right first molar showing non-perforating internal resorption in the distal root
As an emergency measure, caries excavation was done using # 8 round bur (SS White, USA) and the pulp chamber was punched with the same for drainage of the abscess. Brisk bright- red bleeding was witnessed from the pulp chamber. A loose cotton pellet was placed in the coronal part for one week. Broad spectrum antibiotics were prescribed to the patient for five days.
After a week, resolution of the buccal abscess was seen on clinical examination with healthy gingival margin. After application of benzocaine 20 % w/v topical anaesthetic gel (Ultracare, Ultradent Products Inc., USA) at the injection site, inferior alveolar nerve block was administered using 4% Articaine with adrenaline (Septanest, Septodont , France) and the tooth was isolated using rubber dam. After isolation, the cotton pellet was removed and the root canal access was refined. A DG 16 endodontic explorer (Hu-Friedy, IL, USA) was used to locate the two mesial and one distal canals. The pulp was extirpated and a glide path was created using a #10 K-file (Dentsply/Maillefer, USA). The root canals were minimally prepared using #S2 Universal Protaper Gold (Dentsply/Maillefer, USA) rotary files. Copious canal irrigation and disinfection was performed with 1% sodium hypochlorite solution at 300 rpm with constant low torque setting (1.5 N.cm) as per the manufacturer’s instructions. After the chemomechanical preparation, all canals were dried using absorbent paper points and a non-
setting high pH calcium hydroxide intracanal medicament (Ultracal XS, Ultradent Products Inc., USA) was placed within the canals and the tooth was temporized (Figure 2).
The patient was recalled after 7 days. In the recall appointment, the tooth was again isolated under local anaesthesia and the root canals were flushed with sterile saline to remove any residual calcium hydroxide. After irrigation, the canals were inspected and dried using absorbent paper points. After drying, obturation was done with calcium hydroxide and iodoform-based paste (DiaPex Plus, DaiDent, Korea). Following obturation, the tooth was restored with IRM (Caulk-Dentsply, USA) and a preformed stainless steel crown (3M ESPE Dental Products, USA) cemented as a definitive restoration. Some amount of the obturating material was extruded beyond the apex (Figure 3). Oral hygiene instructions were given to the patient and a regular follow-up was recommended.
Figure 2. Non-setting high pH calcium hydroxide
intracanal medicament placed within the canals and temporization done
Figure 3. Post-operative radiograph showing slight
extrusion of DiaPex Plus beyond the apex and definitive stainless steel crown
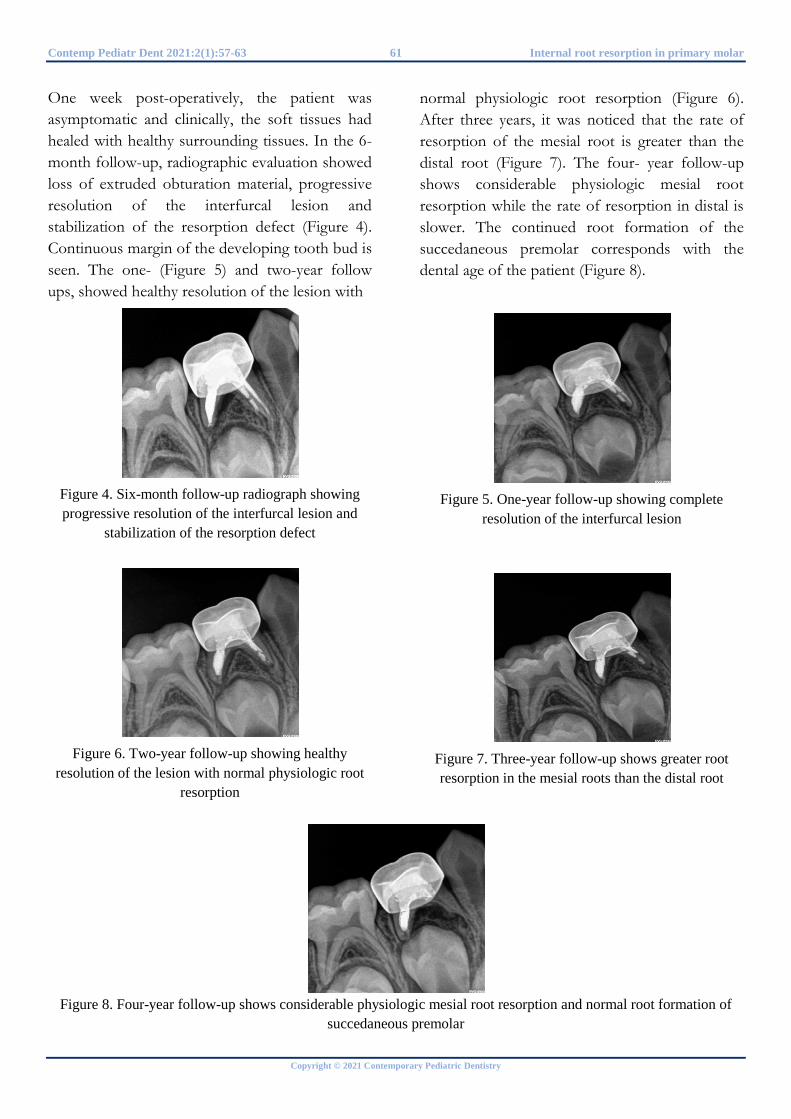
Contemp Pediatr Dent 2021:2(1):57-63 61 Internal root resorption in primary molar
Copyright © 2021 Contemporary Pediatric Dentistry
One week post-operatively, the patient was asymptomatic and clinically, the soft tissues had healed with healthy surrounding tissues. In the 6-month follow-up, radiographic evaluation showed loss of extruded obturation material, progressive resolution of the interfurcal lesion and stabilization of the resorption defect (Figure 4). Continuous margin of the developing tooth bud is seen. The one- (Figure 5) and two-year follow ups, showed healthy resolution of the lesion with
Figure 4. Six-month follow-up radiograph showing progressive resolution of the interfurcal lesion and
stabilization of the resorption defect
Figure 6. Two-year follow-up showing healthy
resolution of the lesion with normal physiologic root resorption
normal physiologic root resorption (Figure 6). After three years, it was noticed that the rate of resorption of the mesial root is greater than the distal root (Figure 7). The four- year follow-up shows considerable physiologic mesial root resorption while the rate of resorption in distal is slower. The continued root formation of the succedaneous premolar corresponds with the dental age of the patient (Figure 8).
Figure 5. One-year follow-up showing complete
resolution of the interfurcal lesion
Figure 7. Three-year follow-up shows greater root resorption in the mesial roots than the distal root
Figure 8. Four-year follow-up shows considerable physiologic mesial root resorption and normal root formation of succedaneous premolar

Musale et al. 62 Contemp Pediatr Dent 2021:2(1):57-63
Copyright © 2021 Contemporary Pediatric Dentistry
DISCUSSION
Inflammatory internal root resorption, once thought to have a poor prognosis and thus indicated for extraction, has a good prognosis after treatment if the lesion is small and not perforated.
Instrumentation in internal root resorption is kept minimal to prevent further weakening of the already thinned dentinal walls. Further, due to the ovoid shape of the resorption lesion, excessive instrumentation is of no consequence in debridement of the lesion and thus the emphasis has been on chemical debridement with minimal mechanical instrumentation.
In the present case, brisk bleeding, signifying active resorption process or vital nature of the pulp, was controlled with 1% sodium hypochlorite irrigation4 in the second appointment. This irrigation not only controlled the bleeding but also necrotized the vital tissue. In the following appointment, repeat sodium hypochlorite irrigation helped dissolve the residual necrotic tissue and disinfect the canals prior to obturation.
The inter-appointment calcium hydroxide medicament has two important functions as to control bleeding and necrotize residual pulp tissue to make it more soluble to sodium hypochlorite.3 In the present case, the high pH non-setting calcium hydroxide intracanal medicament was left in place for one week12 to facilitate removal of the residual tissue at the next appointment by irrigation and instrumentation.
The treatment of choice for IRR in primary teeth has been extraction followed by replacement with suitable space maintainer.13 However, several less invasive alternatives are now suggested. In this case report, the obturating material used was Diapex. Similar endodontic management was done in case of multiple idiopathic internal resorption lesions using Vitapex.14 Choi et al.15 reported stabilization of IRR following pulp therapy in a child with severe atopic dermatitis.
Mineral trioxide aggregate (MTA) has also been suggested as an alternative medicament for management of IRR in primary molars.16
CONCLUSIONS Inflammatory internal root resorption is a
treatable entity with a good prognosis. However, further research, in this regard, is necessary with longer follow-up periods and greater population under study.
REFERENCES 1. Wedenberg C, Lindskog S. Experimental internal resorption in monkey teeth. Dent Traumatol 1985;1:221-227 2. American Academy of Endodontists. Glossary of Endodontic Terms [Internet] 2016 [cited 2021 Feb 13]. Avaliable from: www.aae.org/glossary 3. Vieira-Andrade RG, Drumond CL, Alves LPA, Marques LS, Ramos-Jorge ML. Inflammatory root resorption in primary molars: prevalence and associated factors. Braz Oral Res 2012;26:335-340 4. Haapasalo M, Endal U. Internal inflammatory root resorption: the unknown resorption of the tooth. Endod Top 2006;14:60-79 5. Gabor C, Tam E, Shen Y, Haapasalo M. Prevalence of internal inflammatory root resorption. J Endod 2012;38:24-27 6. Wedenberg C, Zetterqvist L. Internal resorption in human teeth-a histological, scanning electron microscopic, and enzyme histochemical study. J Endod 1987;13:255-259 7. Cordeiro MMR, Santos BZ, Reyes-Carmona JF, Figueiredo CP. Primary teeth show less protecting factors against root resorption. Int J Paediatr Dent 2011;21:361-368 8. Fuss Z, Tsesis I, Lin S. Root resorption--diagnosis, classification and treatment choices based on stimulation factors. Dent Traumatol 2003;19:175-182 9. Tronstad L. Root resorption- etiology, terminology and clinical manifestations. Endod Dent Traumatol 1988;4:241-52 10 .Stephanopoulos G, Mikrogeorgis G, Lyroudia K. Assessment of simulated internal resorption

Contemp Pediatr Dent 2021:2(1):57-63 63 Internal root resorption in primary molar
Copyright © 2021 Contemporary Pediatric Dentistry
cavities using digital and digital subtraction radiography: A comparative study. Dent Traumatol 2011;27:344-349 11. Patel S, Dawood A, Wilson R, Horner K, Mannocci F. The detection and management of root resorption lesions using intraoral radiography and cone beam computed tomography- an in vivo investigation. Int Endod J 2009;42:831-838 12. Rodd HD, Waterhouse PJ, Fuks AB, Fayle SA, Moffat MA. UK National Clinical Guidelines in Paediatric Dentistry: stainless steel preformed crowns for primary molars. Int J Paediatr Dent 2008;18:20-28 13. Smith NL, Seale NS, Nunn ME. Ferric sulfate pulpotomy in primary molars: a retrospective study. Pediatr Dent 2000;22:192-199 14. Matsumoto-Nakano M, Kamakura N, Miyamoto E, Okawa R, Inagaki S, Fukuda Y, Ooshima T. Multiple sites of idiopathic internal resorption in primary dentition: A case report. Pediatr Dent J 2009;19:150-153 15. Choi EJ, Ahn BD, Lee JI , Kim JW. Multiple internal resorptions in deciduous teeth: a case report. J Oral Pathol Med 2007;36:250-251 16. Sari S, Sönmez D. Internal resorption treated with Mineral Trioxide Aggregate in a primary molar tooth: 18-month follow-up. J Endod 2006;32:69-71
How to cite this article: Prasad K Musale, Sneha S Kothare, Abhinav L Talekar. Management of internal root resorption in primary mandibular right first molar: A case report with four-year follow-up. Contemp Pediatr Dent 2021:2(1):57-63
Declarations
Acknowledgements: Not applicable. Conflict of Interest Statement: The authors disclose no potential conflicts of interest. Ethics Statement: Procedure was explained to the parents and written consent was obtained for the treatment and publication of the case report. Informed Consent: Written consent was taken for participation of parents and child in the study. Author contributions: Conception and design: All Authors; Acquisition of data: PKM; Interpretation of data: PKM, SSK; Drafting article: All Authors; Revision artice: All Authors; Final approval: All Authors Funding: This work is not finantiated. Data Availability: The data used to support the findings of this study can be made available upon request to the corresponding author. Peer-review: Externally double-blinded peer-reviewed.

Copyright © 2021 Contemporary Pediatric Dentistry. This work is licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International license. (CC BY-NC-ND 4.0)
Case Report
Correction of an anterior and posterior crossbite case with a modified McNamara appliance: A case report
Wendes Dias Mendes1 ✉, Luciane Macedo de Menezes2, Fábio Romano3, Mírian Aiko Nakame Matsumoto4, Maria Bernadete Sasso Stuani5
Abstract Anterior and posterior crossbites are malocclusions in the sagittal and transversal dimensions, respectively. As self-correction is rare in these alterations, early interception is recommended to allow normal occlusion and facial development. This case report aimed to discuss the treatment of an eight-year-old boy with an increased inferior facial third, who was submitted for rapid maxillary expansion with a modified bonded appliance to solve both transversal and anteroposterior deficiencies. The correction of both malocclusions was achieved within 21 days. The advantages of this procedure were to gain space in both arches, enlarge the maxillary arch, and improve nasal breathing. The interceptive therapy, as well as a well-planned appliance, proved to be effective and important for retrieving the patient´s normal condition and quality of life.
Keywords: Interceptive Orthodontics; Crossbites; Malocclusions; Treatment
Highlights Crossbites are frequent malocclusions in dental routine and their management by pediatric dentistry extends his/her field of work.
1 Master Student, Department of Basic and Oral Biology, School of Dentistry of Ribeirao Preto, University of São Paulo, Ribeirao Preto-SP, Brazil. 2 Full Professor, School of Health and Life Sciences, Pontifical Catholic University of Rio Grande do Sul, Porto Alegre- RS, Brazil. 3 Associate Professor, Department of Pediatric Dentistry, School of Dentistry of Ribeirao Preto, University of São Paulo, Ribeirao Preto-SP, Brazil. 4 Associate Professor, Department of Pediatric Dentistry, School of Dentistry of Ribeirao Preto, University of São Paulo, Ribeirao Preto-SP, Brazil. 5 Associate Professor, Department of Pediatric Dentistry, School of Dentistry of Ribeirao Preto, University of São Paulo, Ribeirao Preto-SP, Brazil.
Correspondence: Department of Basic and Oral Biology, School of Dentistry of Ribeirao Preto, University of Sao Paulo, Ribeirao Preto, SP, Brazil. E-mail address: [email protected]
Received: 31 January 2021 Accepted: 2 March 2021 Online First: 22 March 2021
This work allows the pediatric dentist to be familiarized with the smart treatment of combined posterior and anterior crossbite and encourages him/her to treat them.
Based on the correct diagnosis of crossbites, the clinician can manage more effective and less time-consuming treatments, leading to patient satisfaction and increasing their self-esteem.
Contemporary Pediatric Dentistry Contemp Pediatr Dent 2021:2(1):64-71 DOI: 10.51463/cpd.2021.39

Mendes et al. 65 Contemp Pediatr Dent 2021:2(1):64-71
Copyright © 2021 Contemporary Pediatric Dentistry
INTRODUCTION Early orthodontic treatment can be described
as the intervention in either primary or mixed dentition to allow normal occlusion and skeletal development before the establishment of the permanent dentition.1 Crossbites are malocclusions that frequently occur in children and whose prevalence are seen in the literature ranging from 8 - 22% relating to posterior crossbite and 2,2- 12% to anterior crossbite.2-3
Posterior crossbite is any atypical buccal-lingual relation between opposing arches in centric occlusion. Its occurrence can be attributed to impaired nasal breathing, muscular dysfunction, sucking habits, genetic factors, certain swallowing habits, chronic mouth breathing, traumas, and obstructive sleep apnea syndrome (OSAS).2,4,5 On the other hand, anterior crossbite is characterized as the reversed labiolingual relationship of the incisors, where the incisal edges of maxillary anterior teeth are located backwardly to those of the mandibular ones.3 Its etiological factors are described as skeletal dysplasia, where the mandible is positioned anteriorly to the maxilla, acquired muscular reflex pattern of mandibular closure, and a decrease in the axial inclination of one or more maxillary incisors. In some cases, this occlusal alteration is associated with Class III malocclusion.3-6
Spontaneous correction of crossbites is extremely unusual, therefore, early interceptive interventions are required.5 Consequences related to delay in the correction of the posterior crossbite for permanent dentition are reported as unpaired facial growth leading to asymmetry, altered muscle function, and temporomandibular joint dysfunction.2-5 Besides, the negative outcomes related to the anterior crossbite are gingival recession, loss of alveolar bone support, and mobility of the lower incisors, along with potential adverse growth influences on the anterior portion on the maxilla.7-8
Both abnormalities can be classified into three types regarding the etiological factor: skeletal, functional, and dental.2 One of the most common treatments to correct the normal transverse maxillary deficiency is the Rapid Maxillary Expansion (RME), which can be performed with different appliances.9 The correction of anterior crossbite depends on its specific type, and there is a range of treatment options.3 When the etiology is not skeletal, fixed or removable appliances can be used in the primary or late mixed dentition. However, if there is a skeletal bone implication, a reverse pull facemask is indicated.10
This case report aimed to present and offer to pediatric dentists a simple and time-saving clinical treatment option for the anterior and posterior crossbites simultaneously.
CASE REPORT An eight-year-old boy with no notable medical
history presented to the Preventive and Interceptive Clinic of our Dentistry Faculty with the chief complaint of "crooked" maxillary anterior teeth. He presented a symmetric pattern at the facial examination, competent lip sealing, obtuse nasolabial angle, good chin-neck line, convex profile, and an increased lower anterior facial third. The functional examination revealed mixed breathing with oral predominance. Written consent was taken for this case report.
The intraoral examination showed the patient was undergoing the inter-transitional period of mixed dentition with the presence of all primary teeth, Class I molars, canine relationships, and negative overjet (-2 mm), positive overbite, and no deviation of the midline (Figure 1). He presented a narrow maxilla with an ogival palate and the presence of bilateral posterior crossbite. According to Moyers mixed dentition space analysis method11 the maxillary arch presented a negative discrepancy of -4.9 mm and the mandibular arch of -1.0 mm.
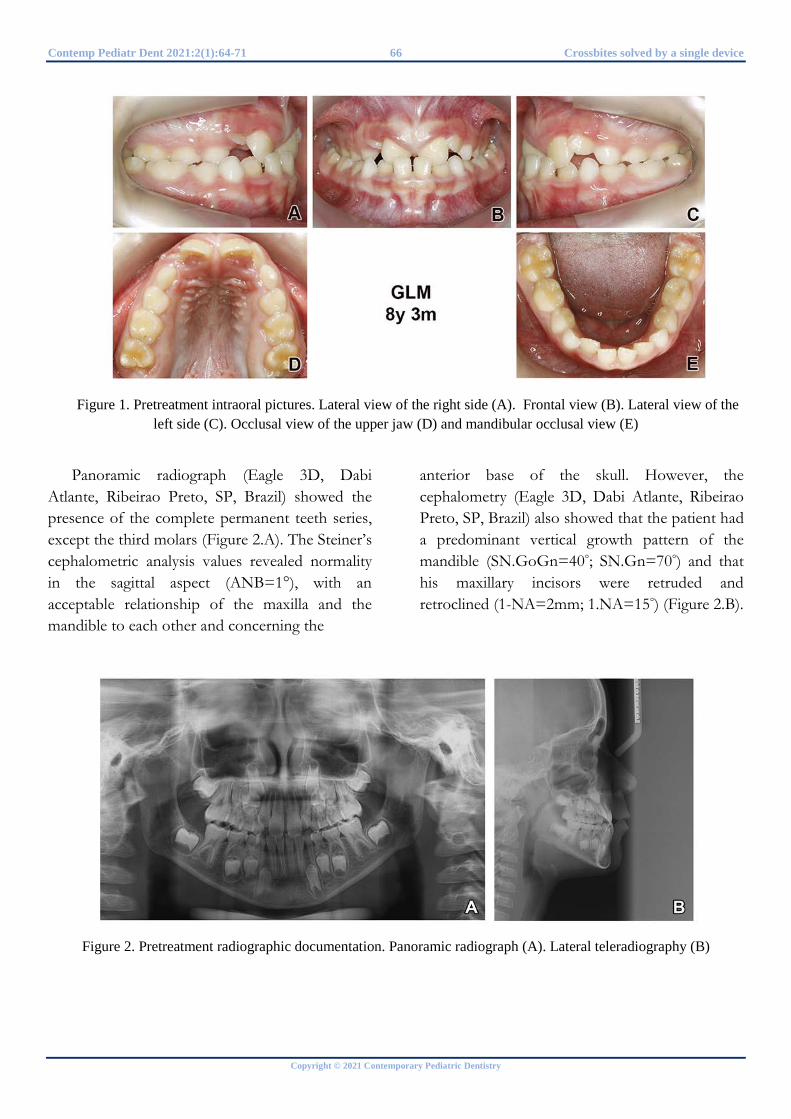
Contemp Pediatr Dent 2021:2(1):64-71 66 Crossbites solved by a single device
Copyright © 2021 Contemporary Pediatric Dentistry
Figure 1. Pretreatment intraoral pictures. Lateral view of the right side (A). Frontal view (B). Lateral view of the
left side (C). Occlusal view of the upper jaw (D) and mandibular occlusal view (E)
Panoramic radiograph (Eagle 3D, Dabi Atlante, Ribeirao Preto, SP, Brazil) showed the presence of the complete permanent teeth series, except the third molars (Figure 2.A). The Steiner’s cephalometric analysis values revealed normality in the sagittal aspect (ANB=1°), with an acceptable relationship of the maxilla and the mandible to each other and concerning the
anterior base of the skull. However, the cephalometry (Eagle 3D, Dabi Atlante, Ribeirao Preto, SP, Brazil) also showed that the patient had a predominant vertical growth pattern of the mandible (SN.GoGn=40°; SN.Gn=70°) and that his maxillary incisors were retruded and retroclined (1-NA=2mm; 1.NA=15°) (Figure 2.B).
Figure 2. Pretreatment radiographic documentation. Panoramic radiograph (A). Lateral teleradiography (B)
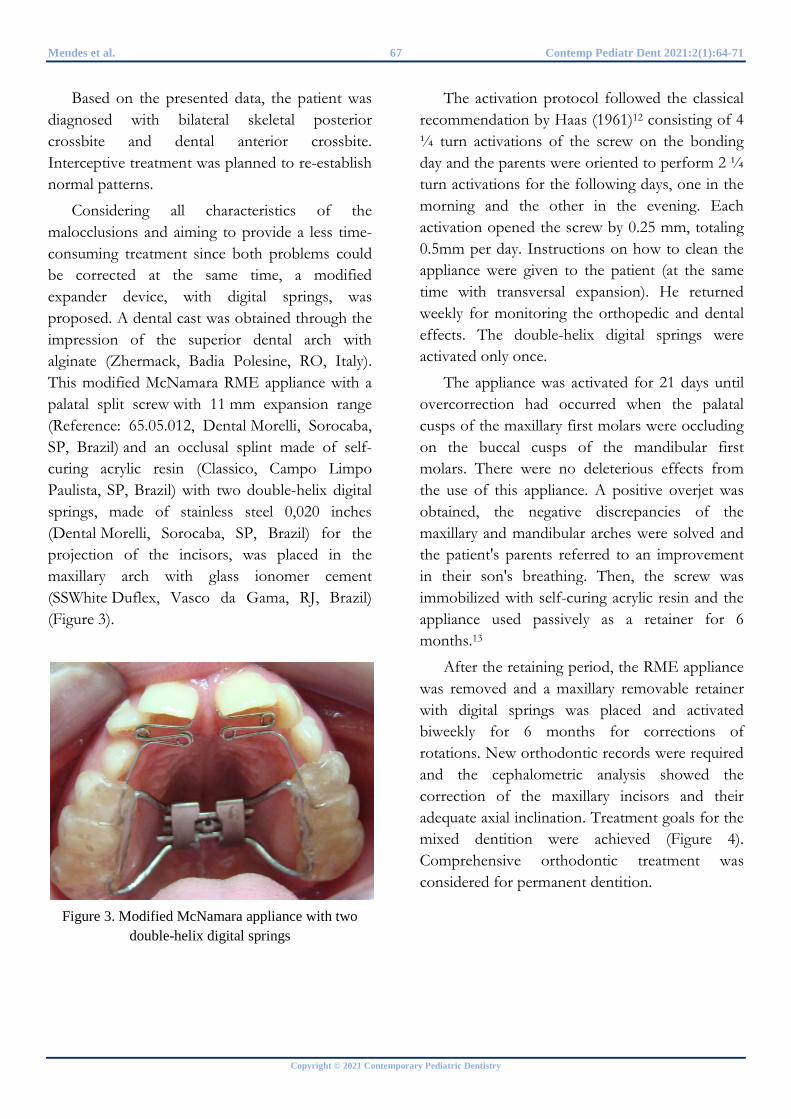
Mendes et al. 67 Contemp Pediatr Dent 2021:2(1):64-71
Copyright © 2021 Contemporary Pediatric Dentistry
Based on the presented data, the patient was diagnosed with bilateral skeletal posterior crossbite and dental anterior crossbite. Interceptive treatment was planned to re-establish normal patterns.
Considering all characteristics of the malocclusions and aiming to provide a less time-consuming treatment since both problems could be corrected at the same time, a modified expander device, with digital springs, was proposed. A dental cast was obtained through the impression of the superior dental arch with alginate (Zhermack, Badia Polesine, RO, Italy). This modified McNamara RME appliance with a palatal split screw with 11 mm expansion range (Reference: 65.05.012, Dental Morelli, Sorocaba, SP, Brazil) and an occlusal splint made of self-curing acrylic resin (Classico, Campo Limpo Paulista, SP, Brazil) with two double-helix digital springs, made of stainless steel 0,020 inches (Dental Morelli, Sorocaba, SP, Brazil) for the projection of the incisors, was placed in the maxillary arch with glass ionomer cement (SSWhite Duflex, Vasco da Gama, RJ, Brazil) (Figure 3).
Figure 3. Modified McNamara appliance with two
double-helix digital springs
The activation protocol followed the classical recommendation by Haas (1961)12 consisting of 4 ¼ turn activations of the screw on the bonding day and the parents were oriented to perform 2 ¼ turn activations for the following days, one in the morning and the other in the evening. Each activation opened the screw by 0.25 mm, totaling 0.5mm per day. Instructions on how to clean the appliance were given to the patient (at the same time with transversal expansion). He returned weekly for monitoring the orthopedic and dental effects. The double-helix digital springs were activated only once.
The appliance was activated for 21 days until overcorrection had occurred when the palatal cusps of the maxillary first molars were occluding on the buccal cusps of the mandibular first molars. There were no deleterious effects from the use of this appliance. A positive overjet was obtained, the negative discrepancies of the maxillary and mandibular arches were solved and the patient's parents referred to an improvement in their son's breathing. Then, the screw was immobilized with self-curing acrylic resin and the appliance used passively as a retainer for 6 months.13
After the retaining period, the RME appliance was removed and a maxillary removable retainer with digital springs was placed and activated biweekly for 6 months for corrections of rotations. New orthodontic records were required and the cephalometric analysis showed the correction of the maxillary incisors and their adequate axial inclination. Treatment goals for the mixed dentition were achieved (Figure 4). Comprehensive orthodontic treatment was considered for permanent dentition.
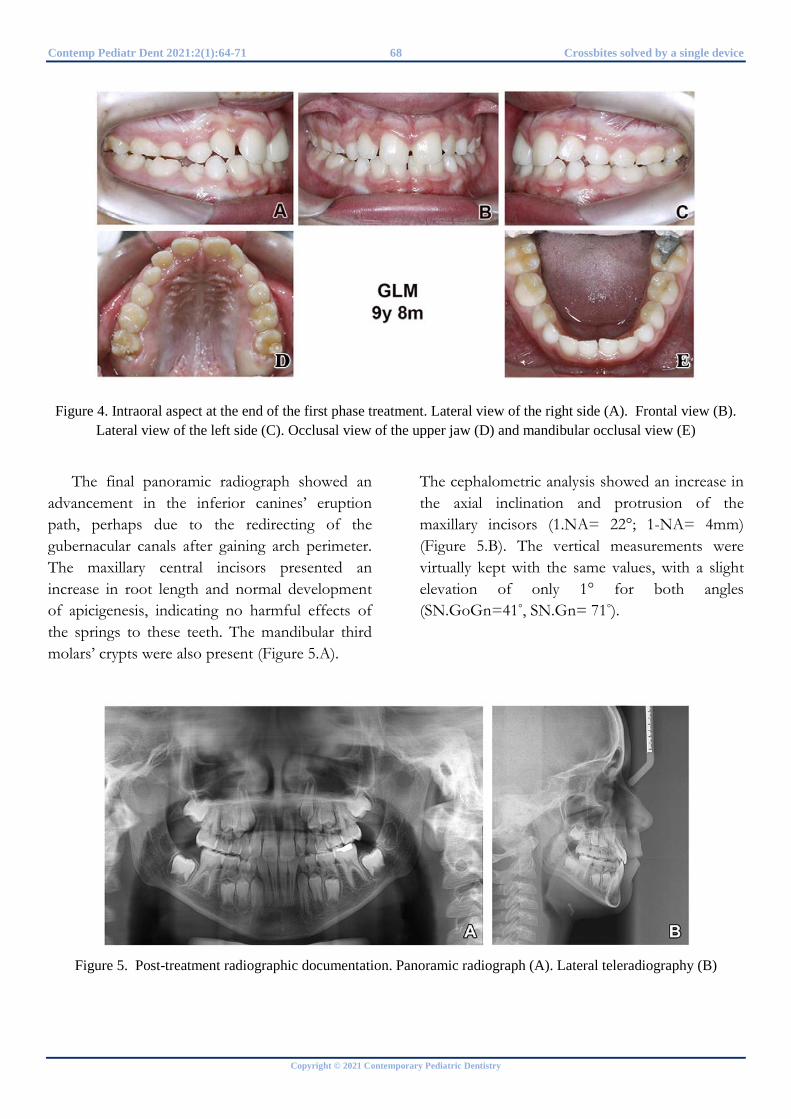
Contemp Pediatr Dent 2021:2(1):64-71 68 Crossbites solved by a single device
Copyright © 2021 Contemporary Pediatric Dentistry
Figure 4. Intraoral aspect at the end of the first phase treatment. Lateral view of the right side (A). Frontal view (B). Lateral view of the left side (C). Occlusal view of the upper jaw (D) and mandibular occlusal view (E)
The final panoramic radiograph showed an advancement in the inferior canines’ eruption path, perhaps due to the redirecting of the gubernacular canals after gaining arch perimeter. The maxillary central incisors presented an increase in root length and normal development of apicigenesis, indicating no harmful effects of the springs to these teeth. The mandibular third molars’ crypts were also present (Figure 5.A).
The cephalometric analysis showed an increase in the axial inclination and protrusion of the maxillary incisors (1.NA= 22°; 1-NA= 4mm) (Figure 5.B). The vertical measurements were virtually kept with the same values, with a slight elevation of only 1° for both angles (SN.GoGn=41°, SN.Gn= 71°).
Figure 5. Post-treatment radiographic documentation. Panoramic radiograph (A). Lateral teleradiography (B)
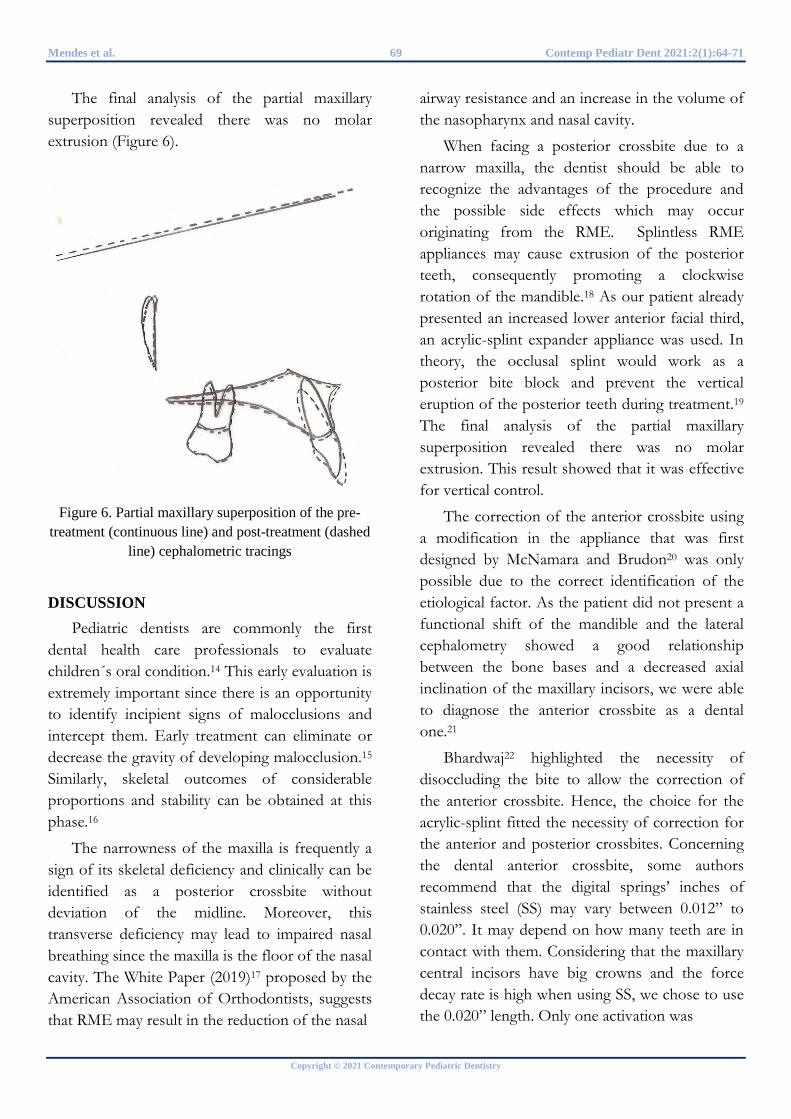
Mendes et al. 69 Contemp Pediatr Dent 2021:2(1):64-71
Copyright © 2021 Contemporary Pediatric Dentistry
The final analysis of the partial maxillary superposition revealed there was no molar extrusion (Figure 6).
Figure 6. Partial maxillary superposition of the pre-
treatment (continuous line) and post-treatment (dashed line) cephalometric tracings
DISCUSSION Pediatric dentists are commonly the first
dental health care professionals to evaluate children´s oral condition.14 This early evaluation is extremely important since there is an opportunity to identify incipient signs of malocclusions and intercept them. Early treatment can eliminate or decrease the gravity of developing malocclusion.15 Similarly, skeletal outcomes of considerable proportions and stability can be obtained at this phase.16
The narrowness of the maxilla is frequently a sign of its skeletal deficiency and clinically can be identified as a posterior crossbite without deviation of the midline. Moreover, this transverse deficiency may lead to impaired nasal breathing since the maxilla is the floor of the nasal cavity. The White Paper (2019)17 proposed by the American Association of Orthodontists, suggests that RME may result in the reduction of the nasal
airway resistance and an increase in the volume of the nasopharynx and nasal cavity.
When facing a posterior crossbite due to a narrow maxilla, the dentist should be able to recognize the advantages of the procedure and the possible side effects which may occur originating from the RME. Splintless RME appliances may cause extrusion of the posterior teeth, consequently promoting a clockwise rotation of the mandible.18 As our patient already presented an increased lower anterior facial third, an acrylic-splint expander appliance was used. In theory, the occlusal splint would work as a posterior bite block and prevent the vertical eruption of the posterior teeth during treatment.19 The final analysis of the partial maxillary superposition revealed there was no molar extrusion. This result showed that it was effective for vertical control.
The correction of the anterior crossbite using a modification in the appliance that was first designed by McNamara and Brudon20 was only possible due to the correct identification of the etiological factor. As the patient did not present a functional shift of the mandible and the lateral cephalometry showed a good relationship between the bone bases and a decreased axial inclination of the maxillary incisors, we were able to diagnose the anterior crossbite as a dental one.21
Bhardwaj22 highlighted the necessity of disoccluding the bite to allow the correction of the anterior crossbite. Hence, the choice for the acrylic-splint fitted the necessity of correction for the anterior and posterior crossbites. Concerning the dental anterior crossbite, some authors recommend that the digital springs’ inches of stainless steel (SS) may vary between 0.012” to 0.020”. It may depend on how many teeth are in contact with them. Considering that the maxillary central incisors have big crowns and the force decay rate is high when using SS, we chose to use the 0.020” length. Only one activation was

Contemp Pediatr Dent 2021:2(1):64-71 70 Crossbites solved by a single device
Copyright © 2021 Contemporary Pediatric Dentistry
required due to its effectiveness and, as the type of movement was as torque-like, the crowns went forward increasing the axial inclinations of those teeth.23-24
Reduction in the negative discrepancy of the maxillary arch after RME is well documented in the literature due to the increase in the perimeter of the arch.5,9,25,26,27 Furthermore, the expansion of mandibular arch widths can be explained by the presence of altered dental contacts, which could incline posterior mandibular teeth buccally.25 Our patient kept all his primary teeth during the whole treatment, not consuming the Leeway Space to solve the crowding.
When the professional keeps the benefits of early interception in mind and is concerned with mastering a good diagnosis and treatment plan for time and money-saving for his/her clinical practice, the pediatric dentist has much to gain overall.
CONCLUSIONS Early interception is a great strategy that
dentists should use to prevent many malocclusions in the future or even to avoid their worsening. The mechanics do not need expensive apparatus or complex mechanisms, nevertheless, a well-planned procedure based on the mastering of the diagnosis can present a great range of benefits not only to the patient but also to the dentist who may optimize his/her clinical work.
REFERENCES 1. Kerosuo H. The Role of Prevention and Simple Interceptive Measures in Reducing the Need for Orthodontic Treatment. Med Princ Pract 2002;11:16-21 2. Andrade AS, Gameiro GH, De Rossi M, Gavião MBD. Posterior Crossbite and Functional Changes: A Systematic Review. Angle Orthod 2008;79:380–386 3. Khalaf K and Mando M. Removable appliances to correct anterior crossbites in the mixed
dentition: a systematic review. Acta Odontol Scand 2020;78:118-125 4. Lippold C, Stamm T, Meyer U, Végh A, Moiseenko T, Danesh G. Early treatment of posterior crossbite - A randomized clinical trial. Trials 2013;14:1-10 5. Tanaka O, Fornazari I, Parra A, Castilhos B, Franco A. Complete Maxillary Crossbite Correction with a Rapid Palatal Expansion in Mixed Dentition Followed by a Corrective Orthodontic Treatment. Case Rep Dent 2016; 2016:1-6 6. Weinberg R. The anterior crossbite: report of cases. J Am Dent Assoc 1975;90:621-624 7. Miamoto C, Marques L, Abreu L, Paiva S. Comparison of two early treatment protocols for anterior dental crossbite in the mixed dentition: A randomized trial. Angle Orthod 2018;88:144-150 8. Borrie F, Bearn D. Early correction of anterior crossbites: A systematic review. J Orthod 2011; 38:175–184 9. McNamara J, Sigler L, Franchi L, Guest S, Baccetti T. Changes in occlusal relationships in mixed dentition patients treated with rapid maxillary expansion. Angle Orthod 2010;80:230-238 10. Jorge JO, Corradi-Dias L, Flores-Mir C, Pordeus IA, Paiva SM, Abreu LG. Comparison Between Removable and Fixed Devices for Nonskeletal Anterior Crossbite Correction in Children and Adolescents: A Systematic Review. J Evid Based Dent Pract 2020;20:1-10 11. Galvão M, Dominguez GC, Tormin ST, Akamine A, Tortamano A, de Fantini SM. Applicability of Moyers analysis in mixed dentition: A systematic review. Dental Press J Orthod 2013;18:100-105 12. Haas AJ. Rapid expansion of the maxillary dental arch and nasal cavity by opening the midpalatal suture. Angle Orthod 1961; 31:73–90 13. Lagravère MO, Carey J, Heo G, Toogood RW, Major PW. Transverse, vertical, and anteroposterior changes from bone-anchored maxillary expansion vs traditional rapid maxillary expansion: a randomized clinical trial. Am J Orthod Dentofacial Orthop 2010;137:304.e1-312e1 14. Aldrees A, Tashkandi N, AlWanis A, AlSanouni M, Al-Hamlan N. Orthodontic treatment and referral patterns: A survey of

Mendes et al. 71 Contemp Pediatr Dent 2021:2(1):64-71
Copyright © 2021 Contemporary Pediatric Dentistry
pediatric dentists, general practitioners, and orthodontists. Saudi Dent J 2015; 27:30-39 15. Burhan A, Nawaya F. Preventive and interceptive orthodontic needs among Syrian children. J Egyptian Public Health Assoc 2016; 91:90-94 16. Geran R, McNamara J, Baccetti T, Franchi L, Shapiro L. A prospective long-term study on the effects of rapid maxillary expansion in the early mixed dentition. Am J Orthod Dentofacial Orthop 2006;129:631-640 17. Behrents R, Shelgikar A, Conley R, Flores-Mir C, Hans M, Levine M, McNamara J, Palomo J, Pliska B, Stockstill J, Wise J, Murphy S, Nagel N, Hittner J. Obstructive sleep apnea and orthodontics: An American Association of Orthodontists White Paper. Am J Orthod Dentofacial Orthop 2019; 156:13-28 18. De Rossi M, De Rossi A, Abrão J. Skeletal Alterations Associated with the Use of Bonded Rapid Maxillary Expansion Appliance. Braz Dent J 2011;22: 334-339 19. Wendling L, Mcnamara J, Franchi L, Baccetti T. A Prospective Study of the Short-term Treatment Effects of the Acrylic-splint Rapid Maxillary Expander Combined with the Lower Schwarz Appliance. Angle Orthod 2005;75:7-14 20. McNamara Jr, Brudon WL. Orthodontic and orthopedic treatment in the mixed dentition. 5th ed. Ann Arbor: Needham Press; 1995 21. Wiedel A, Norlund A, Petrén S, Bondemark L. A cost minimization analysis of early correction of anterior crossbite - A randomized controlled trial. Eur J Orthod 2016;38:140-145 22. Bhardwaj P, Verma SK, Rastogi K, Bhushan R. An efficient method for correction of anterior crossbite without using bite plates. BMJ Case Rep 2013:1-3 23. White TC, Gardiner JH, Leighton BC. Orthodontics for Dental Students. 3rd ed. New Delhi: Macmillan India Ltd; 1976 24. Agarwal DK, Razdan A, Agarwal A, Bhattacharya P, Gupta A, Kapoor DN. A Comparative Study of Orthodontic Coil Springs. J Ind Orthod Soc. 2011; 45:160-168 25. Melgaço C, Neto J, Jurach E, da Nojima M, Sant’Anna E, Nojima L. Rapid maxillary expansion effects: An alternative assessment method by means of cone-beam tomography. Dental Press J Orthod 2014;19:88-96
26. Lagravere M, Major P, Flores-Mir C, Orth C. Long-Term Dental Arch Changes After Rapid Maxillary Expansion Treatment: A Systematic Review. Angle Orthod 2005;75:155–161 27. O'Grady P, McNamara J, Baccetti T, Franchi L. A long-term evaluation of the mandibular Schwarz appliance and the acrylic splint expander in early mixed dentition patients. Am J Orthod Dentofacial Orthop 2006;130:202-213
How to cite this article: Wendes Dias Mendes, Luciane Macedo de Menezes, Fábio Romano, Mírian Aiko Nakame Matsumoto, Maria Bernadete Sasso Stuani. Correction of an anterior and posterior crossbite case with a modified McNamara appliance: A case report. Contemp Pediatr Dent 2021:2(1):64-71
Declarations
Acknowledgements: Not applicable. Conflict of Interest Statement: The authors disclose no potential conflicts of interest. Ethics Statement: Procedure was explained to the parents and written consent was obtained for the treatment and publication of the case report. Informed Consent: Written consent was taken for participation of parents and child in the study. Author contributions: Conception and design: All Authors; Acquisition of data: MBSS; Interpretation of data: WDM; Drafting article: WDM; Revision artice: LMM, FLR, MANM; Final approval: All Authors Funding: This work is not finantiated. Data Availability: The data used to support the findings of this study can be made available upon request to the corresponding author. Peer-review: Externally double-blinded peer-reviewed.





























