Embed Size (px)
Citation preview

Contrast-Enhanced Ultrasound of Histologically ProvenLiver Hemangiomas
Christoph F. Dietrich,1 Joachim C. Mertens,1 Barbara Braden,2 Gudrun Schuessler,1 Michaela Ott,1 and Andre Ignee1
Differentiation of small and atypical hemangiomas from other hepatic masses using imagingmethods can be difficult, especially in patients with underlying malignant disease. There-fore, contrast-enhanced ultrasound was assessed in patients with histologically confirmedhemangiomas with respect to contrast-enhancing kinetics and tumor characteristics. In 58patients with indeterminate hepatic lesions demonstrated with at least 2 imaging methods(ultrasound/computed tomography/magnetic resonance imaging), ultrasound-guided liverbiopsy revealed hemangioma. In all patients a hepatic neoplasm had been suspected becauseof underlying malignant disease (n � 41), liver cirrhosis (n � 15), or growth of the lesion(n � 2). All patients underwent nonlinear, low mechanical index real-time contrast-en-hanced ultrasound scanning with bolus injections of SonoVue. Peripheral nodular arterialenhancement was detected in 43 patients (74%), whereas the typical metastatic peripheralrim-like enhancement was not observed at all. Strong homogenous arterial enhancement wasfound in 9 of 58 (16%) patients. In 6 patients (10%), the arterial contrast enhancementpattern could not be determined because of the very small size of the lesions or fibroticnodules. Forty-five (78%) of the hemangiomas showed homogenous centripetal fillingwithin 180 seconds. Conclusion: Contrast-enhanced ultrasound demonstrates typical hem-angioma imaging characteristics, that is, peripheral nodular contrast enhancement andiris-diaphragm sign in a high percentage of patients with undetermined lesions. This tech-nique may therefore improve noninvasive functional characterization and differentiation ofhemangiomas. (HEPATOLOGY 2007;45:1139-1145.)
Hepatic hemangiomas are known to be the mostcommon benign liver tumors, with an inci-dence in autopsy and imaging studies of up to
7%.1-10 As incidentally discovered hepatic tumors aremore frequently detected with the increasing use of mod-ern abdominal imaging techniques, reliable noninvasivecharacterization and differentiation of such liver tumors ishighly important in the clinical routine.
Although ultrasound (US) has long been consideredinferior to computed tomography (CT) and magnetic res-onance imaging (MRI),10,11 new US imaging techniques,especially contrast-enhanced techniques, have changed
this view.12-15 Contrast-enhanced US (CEUS) has beendemonstrated to significantly improve the detection ofliver metastases in comparison with B-mode US, includ-ing a multicenter trial study.16 The results are within thesame range as for CT. CEUS also can differentiate be-tween most benign and malignant liver lesions by analyz-ing the portal venous phase in patients with normal liverparenchyma.17,18 In addition, CEUS could differentiatebetween typical focal nodular hyperplasia and hepatocel-lular adenoma. This differentiation is essential because ofdifferent therapeutic approaches.19 In contrast, the role ofreal-time CEUS in characterizing hemangiomas has notyet been determined.
We examined the contrast-enhancing imaging featuresof atypical liver hemangiomas with inconclusive comple-mentary imaging results to assess the accuracy of CEUS.
Patients and MethodsBetween 2000 and 2006, 58 patients [29 female, 29
male; 56 � 13 (24-77) years] with histologically con-firmed hemangiomas were included in this prospectivestudy. Indications for liver biopsy were indeterminate le-
Abbreviations: CEUS, contrast-enhanced ultrasound; CT, computed tomogra-phy; MRI, magnetic resonance imaging; US, ultrasound.
From the 1Second Department of Internal Medicine, Caritas Hospital Bad Mer-gentheim, Bad Mergentheim, Germany; and 2John Radcliffe Hospital, Oxford, UK.
Received September 19, 2006; accepted December 12, 2006Address reprint requests to: Christoph F. Dietrich, M.D., 2nd Department of
Internal Medicine, Caritas Hospital Bad Mergentheim, Uhlandstr. 7, D-97980Bad Mergentheim, Germany. E-mail: [email protected]; fax: (49)7931–58–2290.
Copyright © 2007 by the American Association for the Study of Liver Diseases.Published online in Wiley InterScience (www.interscience.wiley.com).DOI 10.1002/hep.21615Potential conflict of interest: Nothing to report.
1139

sions shown in at least 2 imaging methods (US/CT/MRI).
Examination Techniques. All patients underwentB-mode ultrasound and color or power Doppler exami-nation with a 3.5-MHz and 7-MHz multifrequencytransducer as described.18,20 Siemens Elegra Advanced orAcuson Sequoia (Sonoline Elegra, Siemens, Erlangen,Germany, or Acuson Sequoia, Siemens, Erlangen, Ger-many) were used with a low mechanical index � 0.2 to0.3 setting (no split screen imaging was used). All exami-nations were carried out by the same examiner (C.F.D.);however, image analysis was performed by at least 2 addi-tional examiners. All examinations were digitally storedand documented by a commercially available system orvideotapes. The images of a particular patient were alwaysshown to the additional readers in the same sequence:baseline followed by CEUS.
The patients received up to 3 bolus injections (1 bolusinjection in 50 patients) of 2.4 (Acuson Sequoia) or 4.8ml (Siemens Elegra) of the contrast agent SonoVue(Bracco, Milan, Italy). The criteria reported for this set-ting were peripheral nodular enhancement during the ar-terial phase, iris-diaphragm sign using time-analysis ofcontrast enhancement within 0-180 seconds to analyzethe arterial phase in comparison with the hepatic arteryand portal venous phase in comparison with the sur-rounding portal vein (branches) as described.13,19
Reference Imaging Examinations and Liver Biopsy.Reference imaging examinations (e.g., CT, MRI, andscintigraphy) were performed as part of the clinicalworkup of the patients—in several cases outside of ourinstitution—and not for the purpose of this study. Thestandard practice used in our department includes 2 dif-ferent imaging procedures (US: n � 59/CT: n � 55/MRI: n � 33) (re)evaluated by at least 2 experts.
All hemangiomas were histologically confirmed be-cause of inconclusive findings in the imaging methodsand suspected malignancy. In 41 cases (41 of 58, 71%),an underlying malignant disease was found. In all cases,the diagnosis of a liver metastasis would have changed thetherapeutic approach. Fifteen patients (15 of 58, 26%)had a liver lesion in a (suspected) liver cirrhosis attribut-able to HCV infection (10 of 15, 67%), primary biliarycirrhosis (4 of 15, 27%), or cystic fibrosis (1 of 15, 7%). Inthose cases, a HCC could not be excluded. In 2 cases(2/58, 3%), significant growth within a year was observedin patients with history of ovarian tumors under hormonetherapy, and the former diagnosis of a hemangioma was indoubt.
Liver biopsy was performed closely to and always afterthe US examination. The size of the lesion was stableduring the interval between liver biopsy and the study in
all patients. Clotting indices were considered adequate forbiopsy in all patients, following the general rules. Biopsyunder US guidance using a device and avoiding directpuncture of superficial lesions was performed with aTemno 1.2-mm cutting needle to allow accurate histolog-ical evaluation (with a minimum required sample size of15 mm and in most cases 20 mm). Liver biopsy specimenswere fixed in formalin and embedded in paraffin for rou-tine staining and immunohistochemistry. In 3 of 58 pa-tients (3 of 58, 5%) more than one biopsy was necessaryto determine the correct histological nature of the lesion.No complications were recorded.
Statistics. Clinical characteristics of patients were ex-pressed as mean � standard deviation (SD) and as medianvalues with limits of 50% interquartile ranges when ap-propriate.
Institutional Board Approval. Institutional Boardapproval and informed consent according to the ethicalguidelines from Helsinki was obtained from all patientsafter informing the patient about the purpose and aim ofthe study before the ultrasound examination was started.Patient characteristics are summarized in Table 1.
ResultsIn contrast to other reports with female preponder-
ance, the sex ratio (male/female ratio) was equal in thisstudy. In all patients, adequate visualization of the respec-tive contrast phases was possible. No adverse events werereported. In 10 patients, the histologically confirmedhemangiomas were not visualized by CT (n � 6) or MRI(n � 4). These patients had lesions below 15 mm.
Coincidence of Hemangiomas with Malignant Tu-mors. A single tumor was seen in 21 patients, whereas inthe remaining 38 patients two (n � 15) or more tumorswere observed. Coincidence of metastases (lymphoma)and hemangiomas occurred in 8 of 58 (14%), and coin-cidence of hepatocellular carcinoma and hemangiomasoccurred in 2 of 58 (4%) patients, which means a coinci-
Table 1. Demographic Characteristics and Indications forBiopsy
Characteristics Percentage
DemographyNo. (M/F) 58 (29/29)Mean age (years) 56 � 13 (24-77)
Indication for biopsyUnderlying malignant disease 41/58 (81%)Growing tumor* 2/58 (3%)(Suspected) liver cirrhosis (HCV/PBC/CF) 15/58 (19%) (10/4/1)
Abbreviations: M, male; F, female; HCV, hepatitis C virus infection; PBC, primarybiliary cirrhosis; CF, cystic fibrosis.
*An impressive growth pattern from less than 20 mm to more than 50 mmwithin 2 years was seen in a patient with a malignant ovarian tumor.
1140 DIETRICH ET AL. HEPATOLOGY, May 2007

dence of 10 of 58 (17%) hemangiomas with malignantlesions also proven by histology.
Ultrasound Findings. On conventional B-mode, wefound a single lesion in 21 patients (21 of 58, 36%) andmore than one lesion in 37 patients (37 of 58, 64%).
Using color Doppler imaging in 25 patients (25 of 58,43%), at least one feeding or draining vessel was found.This sign is thought to be the corresponding Doppler signto the peripheral nodular enhancement pattern of con-trast-enhanced methods. A homogenous hypervascularitywas found in 4 patients (4 of 58, 7%). In all other patients(29 of 58, 50%) no vascularization inside the lesion couldbe demonstrated at all (Table 2).
In 43 patients (43 of 58, 74%), a peripheral nodulararterial enhancement could be demonstrated. In no pa-tients could the peripheral rim-like enhancement be visu-alized (0 of 58, 0%), which is typically seen in metastasis.In 6 patients (6 of 58, 10%), the pattern could not bedetermined because of very small size of the lesion orfibrotic nodules. A strong homogenous arterial enhance-ment could be seen in 9 patients (9 of 58, 16%).
Complete homogenous fill-in could be seen in 45 pa-tients (45 of 58, 78%). In most patients (27 of 45, 60%),the time to complete fill-in was between 61 and 180 sec-onds. In 12 patients (12 of 45, 27%), the time was equalto or faster than 30 seconds. In 6 patients (6/45, 13%),the time to complete fill-in was between 31 and 60 sec-onds. An incomplete (inhomogenous, incomplete iris-di-aphragm sign, including 1 with complete sparing that wasinterpreted as a solitary necrotic nodule) was seen in 13patients (13 of 58, 22%).
Peripheral nodular arterial enhancement as well ascomplete portal venous fill-in was seen in 31 of 58 (54%)patients. In 12 of 58 (21%) patients, peripheral nodulararterial enhancement but no complete fill-in was seen. In
14 of 58 (24%) patients, a complete fill-in but no periph-eral nodular enhancement was seen. In 1 of 58 (2%) pa-tients, neither peripheral nodular enhancement norcomplete fill-in was seen. The sensitivity for peripheralnodular arterial enhancement was 74% (95% confidenceinterval, 61%-85%); for complete portal venous fill-inwas 78% (65%-88%); and for the combination of both,98% (91%-100%). The results are summarized in Table 3.
DiscussionUp to now only a few imaging studies have investigated
hepatic hemangiomas, and most of them did not confirmthe diagnosis by histology.18,21-24 To our knowledge, lowmechanical index real-time CEUS has never been used tocharacterize atypical hemangiomas. We demonstrate thatCEUS can reliably compile typical signs of hemangiomasin most patients with undetermined findings using non-enhanced US, CT, and MRI, which might be useful inavoiding biopsy.
Hemangiomas show peripheral nodular enhancementwith gradual centripetal filling and are regarded as havinga large, slowly enhancing blood volume. Atypical featuresinclude small (�15 mm) or huge hemangiomas [�4-7cm (depending on the literature published)], so-called“shunt hemangiomas”25 with abundant arterio(porto-)venous shunts (functionally described as high-flow hem-angiomas), sclerosing hemangiomas, and hemangiomaswith regressive changes such as calcifications, thrombosis,and phlebolith. Hemangiomas below 10 mm, in particu-lar, tend to lack the typical hemangioma contrast en-hancement and are a particular challenge.
The best, though most expensive, imaging method forhemangiomas is MRI with a sensitivity and specificity
Table 3. Contrast-Enhancing Pattern of 58 HistologicallyProven Lesions
Characteristics Percentage
Contrast enhancement, arterialPeripheral nodular arterial enhancement 43/58 (74%)Peripheral rimlike enhancement 0/58 (0%)Not determinable (e.g., due to size of the lesion, solitaryfibrotic nodule) 6/58 (10%)
Strong homogenous arterial enhancement* 9/58 (16%)Centripetal filling
Complete (homogenous) fill-in �180 seconds 45/58 (78%)�30 seconds 12 (21%)�30 seconds and �60 seconds 6 (10%)�60 seconds and �180 seconds 27 (47%)Incomplete (inhomogenous, incomplete iris diaphragm sign,including one with non-enhancing solitary necrotic nodule) 13/58 (22%)
SensitivityPeripheral nodular arterial enhancement 43/58 (74%)Complete portal venous fill-in 45/58 (78%)Combination of both 57/58 (98%)
*In 2 patients with liver cirrhosis, shunt-hemangiomas were found.
Table 2. B-Mode and Color Doppler Imaging Characteristicsof 58 Histologically Proven Lesions
Number of Lesions Percentage
One lesion 21/58 (36%)Multiple lesions 37/58 (64%)Size [mm]� 35 � 28 (6-130)Echogenicity
Hyperechoic 45/58 (78%)Isoechoic 4/58 (7%)Hypoechoic 9/58 (15%)Halo 0/58 (0%)
Color Doppler imagingFeeding and draining vessels* 25/58 (43%)Homogenous hypervascularity 4/58 (7%)
*Representing the color Doppler imaging (CDI) sign of peripheral nodularcontrast enhancement. In patients with liver cirrhosis, the tumors were hyperechoicin 14 and isoechoic in 1. CDI was not helpful in identifying shunts in any of thepatients because vascularity cannot be displayed.
HEPATOLOGY, Vol. 45, No. 5, 2007 DIETRICH ET AL. 1141
between 85% and 95%. Bright signal intensity on T2-weighted images, and similar enhancement pattern to en-hanced CT are very specific and effective for accuratediagnosis.26 However, atypical findings of hemangiomassuch as cystic hemangiomas or small hemangiomas withimmediate homogeneous enhancement are also seen.27,28
In these cases, histological confirmation via needle biopsyis required.26
Atypical hemangioma behavior includes the differen-tial diagnosis of hemangiomas versus hypervascular ma-lignancy, hemangiomas with arterioportal shunts,hemangiomas in liver cirrhosis, hemangiomas in fattyliver, small hypoattenuating hemangiomas, atypical sig-nal on T2-weighted MR imaging, and attenuation rela-tive to vascular pool.28
Differentiation of hemangiomas from other benignand from malignant hypervascular tumors can be a chal-lenge because some can mimic peripheral nodular (glob-ular) enhancement (which is especially true in very smalltumors), and not all hemangiomas show this characteris-tic pattern.27,29 Neuroendocrine tumors or metastasesfrom gastrointestinal cancer and other organs also mayshow strong T2 hyperintensity,29 and a prolonged con-trast enhancement may be seen in certain hypervascularmalignancies.27 It is helpful to know that hemangiomascan remain unenhanced (e.g., due to thrombosis). There-
fore, image interpretation based on the combination of allimaging phases is required.
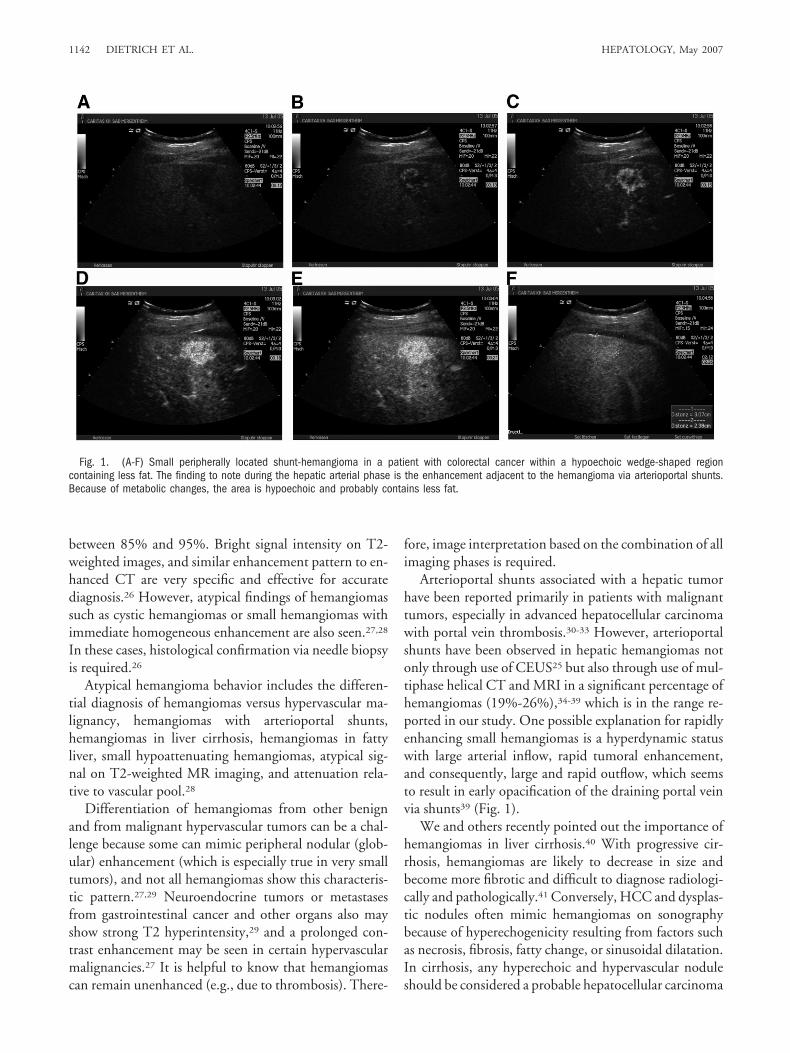
Arterioportal shunts associated with a hepatic tumorhave been reported primarily in patients with malignanttumors, especially in advanced hepatocellular carcinomawith portal vein thrombosis.30-33 However, arterioportalshunts have been observed in hepatic hemangiomas notonly through use of CEUS25 but also through use of mul-tiphase helical CT and MRI in a significant percentage ofhemangiomas (19%-26%),34-39 which is in the range re-ported in our study. One possible explanation for rapidlyenhancing small hemangiomas is a hyperdynamic statuswith large arterial inflow, rapid tumoral enhancement,and consequently, large and rapid outflow, which seemsto result in early opacification of the draining portal veinvia shunts39 (Fig. 1).
We and others recently pointed out the importance ofhemangiomas in liver cirrhosis.40 With progressive cir-rhosis, hemangiomas are likely to decrease in size andbecome more fibrotic and difficult to diagnose radiologi-cally and pathologically.41 Conversely, HCC and dysplas-tic nodules often mimic hemangiomas on sonographybecause of hyperechogenicity resulting from factors suchas necrosis, fibrosis, fatty change, or sinusoidal dilatation.In cirrhosis, any hyperechoic and hypervascular noduleshould be considered a probable hepatocellular carcinoma
Fig. 1. (A-F) Small peripherally located shunt-hemangioma in a patient with colorectal cancer within a hypoechoic wedge-shaped regioncontaining less fat. The finding to note during the hepatic arterial phase is the enhancement adjacent to the hemangioma via arterioportal shunts.Because of metabolic changes, the area is hypoechoic and probably contains less fat.
1142 DIETRICH ET AL. HEPATOLOGY, May 2007
until proven otherwise, and therefore operation or biopsyand histological evaluation are mandatory.
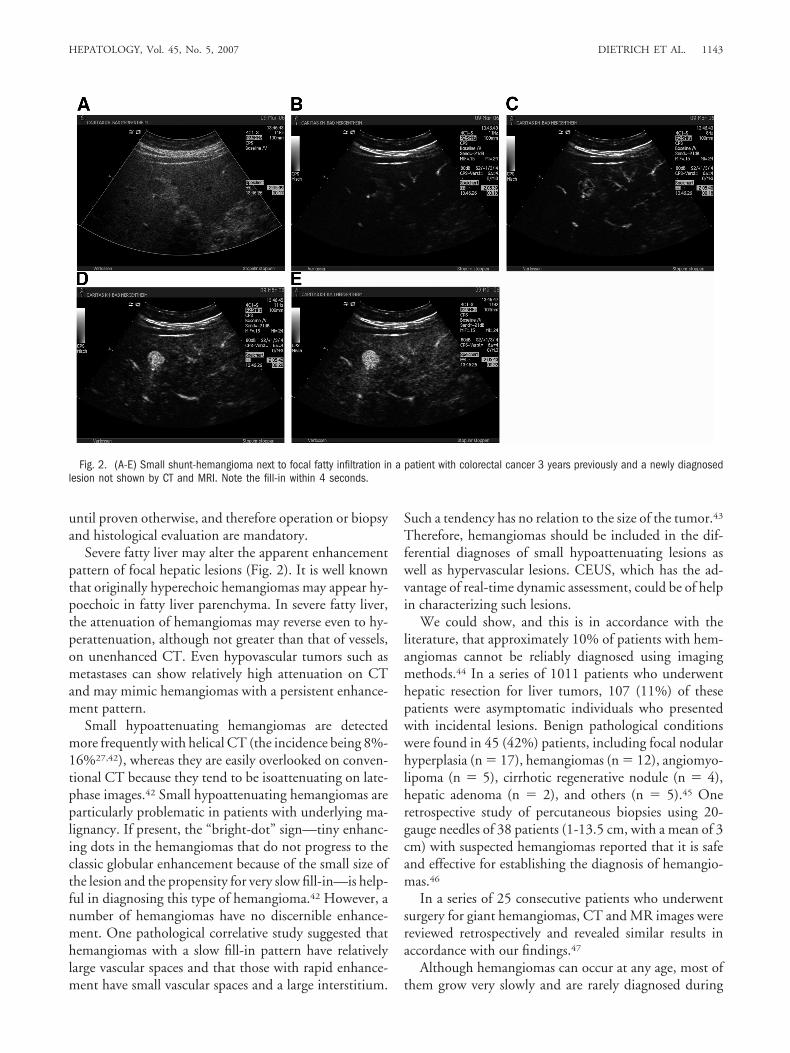
Severe fatty liver may alter the apparent enhancementpattern of focal hepatic lesions (Fig. 2). It is well knownthat originally hyperechoic hemangiomas may appear hy-poechoic in fatty liver parenchyma. In severe fatty liver,the attenuation of hemangiomas may reverse even to hy-perattenuation, although not greater than that of vessels,on unenhanced CT. Even hypovascular tumors such asmetastases can show relatively high attenuation on CTand may mimic hemangiomas with a persistent enhance-ment pattern.
Small hypoattenuating hemangiomas are detectedmore frequently with helical CT (the incidence being 8%-16%27,42), whereas they are easily overlooked on conven-tional CT because they tend to be isoattenuating on late-phase images.42 Small hypoattenuating hemangiomas areparticularly problematic in patients with underlying ma-lignancy. If present, the “bright-dot” sign—tiny enhanc-ing dots in the hemangiomas that do not progress to theclassic globular enhancement because of the small size ofthe lesion and the propensity for very slow fill-in—is help-ful in diagnosing this type of hemangioma.42 However, anumber of hemangiomas have no discernible enhance-ment. One pathological correlative study suggested thathemangiomas with a slow fill-in pattern have relativelylarge vascular spaces and that those with rapid enhance-ment have small vascular spaces and a large interstitium.
Such a tendency has no relation to the size of the tumor.43
Therefore, hemangiomas should be included in the dif-ferential diagnoses of small hypoattenuating lesions aswell as hypervascular lesions. CEUS, which has the ad-vantage of real-time dynamic assessment, could be of helpin characterizing such lesions.
We could show, and this is in accordance with theliterature, that approximately 10% of patients with hem-angiomas cannot be reliably diagnosed using imagingmethods.44 In a series of 1011 patients who underwenthepatic resection for liver tumors, 107 (11%) of thesepatients were asymptomatic individuals who presentedwith incidental lesions. Benign pathological conditionswere found in 45 (42%) patients, including focal nodularhyperplasia (n � 17), hemangiomas (n � 12), angiomyo-lipoma (n � 5), cirrhotic regenerative nodule (n � 4),hepatic adenoma (n � 2), and others (n � 5).45 Oneretrospective study of percutaneous biopsies using 20-gauge needles of 38 patients (1-13.5 cm, with a mean of 3cm) with suspected hemangiomas reported that it is safeand effective for establishing the diagnosis of hemangio-mas.46
In a series of 25 consecutive patients who underwentsurgery for giant hemangiomas, CT and MR images werereviewed retrospectively and revealed similar results inaccordance with our findings.47
Although hemangiomas can occur at any age, most ofthem grow very slowly and are rarely diagnosed during
Fig. 2. (A-E) Small shunt-hemangioma next to focal fatty infiltration in a patient with colorectal cancer 3 years previously and a newly diagnosedlesion not shown by CT and MRI. Note the fill-in within 4 seconds.
HEPATOLOGY, Vol. 45, No. 5, 2007 DIETRICH ET AL. 1143
childhood. We observed 2 patients with more than 50%growth in 1 year. The pathogenesis of hemangiomas andespecially the growth pattern is not well understood.Growth of hemangiomas is thought to be due to ectasiarather than hypertrophy or hyperplasia. Some of thesehemangiomas have estrogen receptors, and acceleratedgrowth has been observed during estrogen influence dur-ing puberty, pregnancy, oral contraceptive use, and withandrogen treatment.26,46,48,49 Growing tumors are mainlyseen in women.49,50
In summary, for typical hemangiomas in an asymp-tomatic patient without risk factors for malignancy, con-ventional B-mode ultrasound is sufficient and no furtherimaging method is recommended.
For atypical hemangiomas in an asymptomatic patientwithout risk factors for malignancy, contrast-enhancedimaging techniques (US, CT, MRI) should be addition-ally used. This is especially true in larger lesions, thosewith uncertain imaging features, or those at risk for anytype of malignancy. Hemangiomas demonstrate a repro-ducible and apparently specific pattern of enhancementeven in small lesions, echogenicity rapidly becomingequal to or greater than that of the liver through the portalvenous phase and beyond because of the real-time natureof CEUS, which is an essential for confident diagnosis.Complete enhancement does not always occur, especially
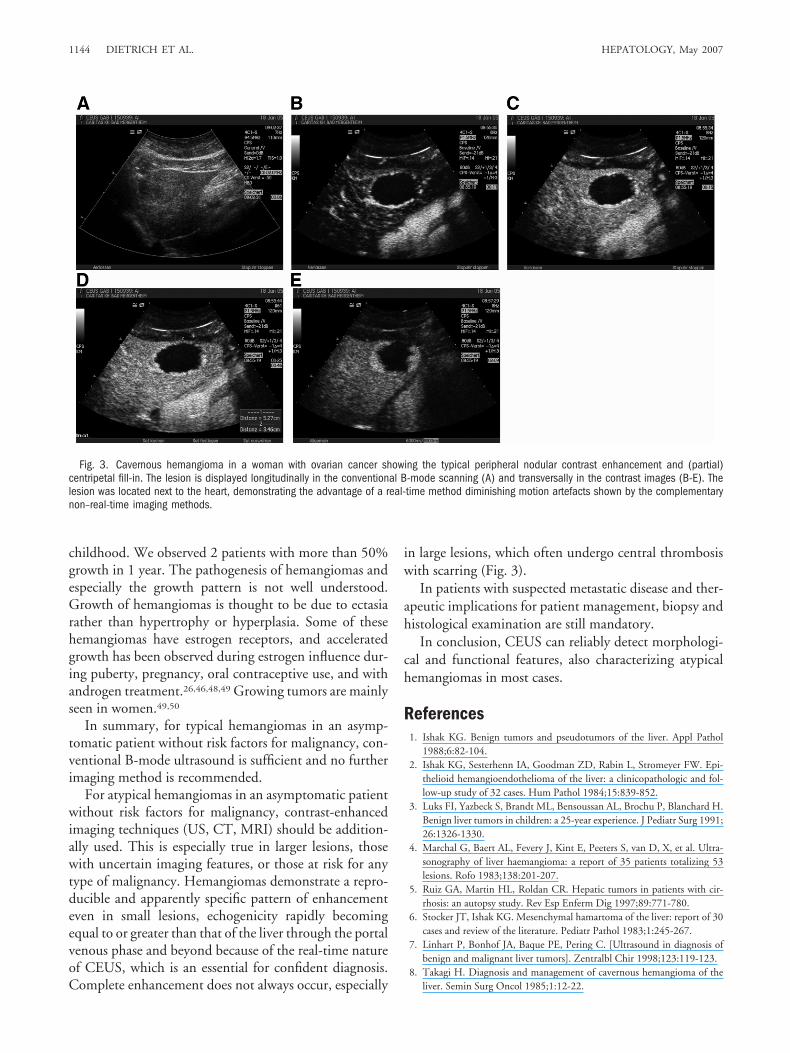
in large lesions, which often undergo central thrombosiswith scarring (Fig. 3).
In patients with suspected metastatic disease and ther-apeutic implications for patient management, biopsy andhistological examination are still mandatory.
In conclusion, CEUS can reliably detect morphologi-cal and functional features, also characterizing atypicalhemangiomas in most cases.
References1. Ishak KG. Benign tumors and pseudotumors of the liver. Appl Pathol
1988;6:82-104.2. Ishak KG, Sesterhenn IA, Goodman ZD, Rabin L, Stromeyer FW. Epi-
thelioid hemangioendothelioma of the liver: a clinicopathologic and fol-low-up study of 32 cases. Hum Pathol 1984;15:839-852.
3. Luks FI, Yazbeck S, Brandt ML, Bensoussan AL, Brochu P, Blanchard H.Benign liver tumors in children: a 25-year experience. J Pediatr Surg 1991;26:1326-1330.
4. Marchal G, Baert AL, Fevery J, Kint E, Peeters S, van D, X, et al. Ultra-sonography of liver haemangioma: a report of 35 patients totalizing 53lesions. Rofo 1983;138:201-207.
5. Ruiz GA, Martin HL, Roldan CR. Hepatic tumors in patients with cir-rhosis: an autopsy study. Rev Esp Enferm Dig 1997;89:771-780.
6. Stocker JT, Ishak KG. Mesenchymal hamartoma of the liver: report of 30cases and review of the literature. Pediatr Pathol 1983;1:245-267.
7. Linhart P, Bonhof JA, Baque PE, Pering C. [Ultrasound in diagnosis ofbenign and malignant liver tumors]. Zentralbl Chir 1998;123:119-123.
8. Takagi H. Diagnosis and management of cavernous hemangioma of theliver. Semin Surg Oncol 1985;1:12-22.
Fig. 3. Cavernous hemangioma in a woman with ovarian cancer showing the typical peripheral nodular contrast enhancement and (partial)centripetal fill-in. The lesion is displayed longitudinally in the conventional B-mode scanning (A) and transversally in the contrast images (B-E). Thelesion was located next to the heart, demonstrating the advantage of a real-time method diminishing motion artefacts shown by the complementarynon–real-time imaging methods.
1144 DIETRICH ET AL. HEPATOLOGY, May 2007
9. Takagi H, Kido C, Morimoto T, Yasue M, Kato H. Surgical treatment ofcavernous hemangioma of the liver. J Surg Oncol 1984;26:91-99.
10. Karhunen PJ. Benign hepatic tumours and tumour like conditions in men.J Clin Pathol 1986;39:183-188.
11. Wernecke K, Rummeny E, Bongartz G, Vassallo P, Kivelitz D, WiesmannW, et al. Detection of hepatic masses in patients with carcinoma: compar-ative sensitivities of sonography, CT, and MR imaging. AJR Am J Roent-genol 1991;157:731-739.
12. Albrecht T, Blomley MJ, Burns PN, Wilson S, Harvey CJ, Leen E, et al.Improved detection of hepatic metastases with pulse-inversion US duringthe liver-specific phase of SHU 508A: multicenter study. Radiology 2003;227:361-370.
13. Albrecht T, Blomley M, Bolondi L, Claudon M, Correas JM, Cosgrove D,et al. Guidelines for the use of contrast agents in ultrasound. January 2004.Ultraschall Med 2004;25:249-256.
14. Bryant TH, Blomley MJ, Albrecht T, Sidhu PS, Leen EL, Basilico R, et al.Improved characterization of liver lesions with liver-phase uptake of liver-specific microbubbles: prospective multicenter study. Radiology2004;232:799-809.
15. Oldenburg A, Hohmann J, Foert E, Skrok J, Hoffmann CW, Frericks B, etal. Detection of hepatic metastases with low MI real time contrast en-hanced sonography and SonoVue. Ultraschall Med 2005;26:277-284.
16. Dietrich CF, Kratzer W, Strobe D, Danse E, Fessl R, Bunk A, et al.Assessment of metastatic liver disease in patients with primary extrahepatictumors by contrast-enhanced sonography versus CT and MRI. World JGastroenterol 2006;12:1699-1705.
17. von Herbay A, Vogt C, Haussinger D. Late-phase pulse-inversion sonog-raphy using the contrast agent levovist: differentiation between benign andmalignant focal lesions of the liver. AJR Am J Roentgenol 2002;179:1273-1279.
18. Dietrich CF, Ignee A, Trojan J, Fellbaum C, Schuessler G. Improvedcharacterisation of histologically proven liver tumours by contrast en-hanced ultrasonography during the portal venous and specific late phase ofSHU 508A. Gut 2004;53:401-405.
19. Dietrich CF, Schuessler G, Trojan J, Fellbaum C, Ignee A. Differentiationof focal nodular hyperplasia and hepatocellular adenoma by contrast-en-hanced ultrasound. Br J Radiol 2005;78:704-707.
20. Dietrich CF, Chichakli M, Hirche TO, Bargon J, Leitzmann P, WagnerTO. Sonographic findings of the hepatobiliary-pancreatic system in adultpatients with cystic fibrosis. J Ultrasound Med 2002;21:409-416.
21. Mathieu D, Zafrani ES, Anglade MC, Dhumeaux D. Association of focalnodular hyperplasia and hepatic hemangioma. Gastroenterology 1989;97:154-157.
22. Quaia E, Bartolotta TV, Midiri M, Cernic S, Belgrano M, Cova M. Anal-ysis of different contrast enhancement patterns after microbubble-basedcontrast agent injection in liver hemangiomas with atypical appearance onbaseline scan. Abdom Imaging 2006;31:59-64.
23. Quaia E, Bertolotto M, Dalla PL. Characterization of liver hemangiomaswith pulse inversion harmonic imaging. Eur Radiol 2002;12:537-544.
24. Vilgrain V, Boulos L, Vullierme MP, Denys A, Terris B, Menu Y. Imagingof atypical hemangiomas of the liver with pathologic correlation. Radio-graphics 2000;20:379-397.
25. Schuessler G, Ignee A, Hirche T, Dietrich CF. [Improved detection andcharacterisation of liver tumors with echo-enhanced ultrasound]. Z Gas-troenterol 2003;41:1167-1176.
26. Choi BY, Nguyen MH. The diagnosis and management of benign hepatictumors. J Clin Gastroenterol 2005;39:401-412.
27. Kim T, Federle MP, Baron RL, Peterson MS, Kawamori Y. Discrimina-tion of small hepatic hemangiomas from hypervascular malignant tumorssmaller than 3 cm with three-phase helical CT. Radiology 2001;219:699-706.
28. Jang HJ, Kim TK, Lim HK, Park SJ, Sim JS, Kim HY, et al. Hepatichemangioma: atypical appearances on CT, MR imaging, and sonography.AJR Am J Roentgenol 2003;180:135-141.
29. Bennett GL, Petersein A, Mayo-Smith WW, Hahn PF, Schima W, Saini S.Addition of gadolinium chelates to heavily T2-weighted MR imaging:limited role in differentiating hepatic hemangiomas from metastases. AJRAm J Roentgenol 2000;174:477-485.
30. Shimada M, Matsumata T, Ikeda Y, Urata K, Hayashi H, Shimizu M, et al.Multiple hepatic hemangiomas with significant arterioportal venousshunting. Cancer 1994;73:304-307.
31. Oliver JH III, Baron RL, Federle MP, Jones BC, Sheng R. Hypervascularliver metastases: do unenhanced and hepatic arterial phase CT imagesaffect tumor detection? Radiology 1997;205:709-715.
32. Oliver JH III, Baron RL. Helical biphasic contrast-enhanced CT of theliver: technique, indications, interpretation, and pitfalls. Radiology 1996;201:1-14.
33. Taylor KJ, Ramos I, Morse SS, Fortune KL, Hammers L, Taylor CR. Focalliver masses: differential diagnosis with pulsed Doppler US. Radiology1987;164:643-647.
34. Byun JH, Kim TK, Lee CW, Lee JK, Kim AY, Kim PN, et al. Arterioportalshunt: prevalence in small hemangiomas versus that in hepatocellular car-cinomas 3 cm or smaller at two-phase helical CT. Radiology 2004;232:354-360.
35. Kim KW, Kim TK, Han JK, Kim AY, Lee HJ, Choi BI. Hepatic heman-giomas with arterioportal shunt: findings at two-phase CT. Radiology2001;219:707-711.
36. Hanafusa K, Ohashi I, Himeno Y, Suzuki S, Shibuya H. Hepatic heman-gioma: findings with two-phase CT. Radiology 1995;196:465-469.
37. Tanaka A, Morimoto T, Yamamori T, Moriyasu F, Yamaoka Y. Atypicalliver hemangioma with shunt: long-term follow-up. J Hepatobiliary Pan-creat Surg 2002;9:750-754.
38. Itai Y, Ohtomo K, Kokubo T, Yamauchi T, Tanioka H, Yoshikawa K, etal. Atypical cavernous hemangioma of the liver. Radiat Med 1988;6:135-140.
39. Jeong MG, Yu JS, Kim KW. Hepatic cavernous hemangioma: temporalperitumoral enhancement during multiphase dynamic MR imaging. Ra-diology 2000;216:692-697.
40. Ignee A, Weiper D, Schuessler G, Teuber G, Faust D, Dietrich CF. Sono-graphic characterisation of hepatocellular carcinoma at time of diagnosis. ZGastroenterol 2005;43:289-294.
41. Brancatelli G, Federle MP, Blachar A, Grazioli L. Hemangioma in thecirrhotic liver: diagnosis and natural history. Radiology 2001;219:69-74.
42. Jang HJ, Choi BI, Kim TK, Yun EJ, Kim KW, Han JK, et al. Atypical smallhemangiomas of the liver: “bright dot” sign at two-phase spiral CT. Radi-ology 1998;208:543-548.
43. Yamashita Y, Ogata I, Urata J, Takahashi M. Cavernous hemangioma ofthe liver: pathologic correlation with dynamic CT findings. Radiology1997;203:121-125.
44. Descottes B, Glineur D, Lachachi F, Valleix D, Paineau J, Hamy A, et al.Laparoscopic liver resection of benign liver tumors. Surg Endosc 2003;17:23-30.
45. Liu CL, Fan ST, Lo CM, Chan SC, Tso WK, Ng IO, et al. Hepaticresection for incidentaloma. J Gastrointest Surg 2004;8:785-793.
46. Biecker E, Fischer HP, Strunk H, Sauerbruch T. Benign hepatic tumours.Z Gastroenterol 2003;41:191-200.
47. Coumbaras M, Wendum D, Monnier-Cholley L, Dahan H, Tubiana JM,Arrive L. CT and MR imaging features of pathologically proven atypicalgiant hemangiomas of the liver. AJR Am J Roentgenol 2002;179:1457-1463.
48. Cobey FC, Salem RR. A review of liver masses in pregnancy and a proposedalgorithm for their diagnosis and management. Am J Surg 2004;187:181-191.
49. Trotter JF, Everson GT. Benign focal lesions of the liver. Clin Liver Dis2001;5:17-42, v.
50. Mergo PJ, Ros PR. Benign lesions of the liver. Radiol Clin North Am1998;36:319-331.
HEPATOLOGY, Vol. 45, No. 5, 2007 DIETRICH ET AL. 1145





























