Embed Size (px)
Citation preview

This article was downloaded by: [University of South Florida]On: 16 May 2014, At: 10:56Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Children's Health CarePublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/hchc20
Correlates and Mediators of Life Satisfaction amongYouth with Attention-Deficit/Hyperactivity DisorderJoshua M. Nadeau Ph.D a , Marni L. Jacob Ph.D a , Amanda C. Keene B.A. a , Shawn M.Alderman B. A. a , Leah E. Hacker B.A. a , Mark A. Cavitt M.D. b , Jeffrey L. Alvaro M.D. b &Eric A. Storch Ph.D. aa Department of Pediatrics , University of South Floridab Pediatric Psychiatry Services , All Children's Hospital/John Hopkins MedicineAccepted author version posted online: 16 May 2014.Published online: 16 May 2014.
To cite this article: Joshua M. Nadeau Ph.D , Marni L. Jacob Ph.D , Amanda C. Keene B.A. , Shawn M. Alderman B. A. , LeahE. Hacker B.A. , Mark A. Cavitt M.D. , Jeffrey L. Alvaro M.D. & Eric A. Storch Ph.D. (2014): Correlates and Mediators of LifeSatisfaction among Youth with Attention-Deficit/Hyperactivity Disorder, Children's Health Care
To link to this article: http://dx.doi.org/10.1080/02739615.2014.896215
Disclaimer: This is a version of an unedited manuscript that has been accepted for publication. As a serviceto authors and researchers we are providing this version of the accepted manuscript (AM). Copyediting,typesetting, and review of the resulting proof will be undertaken on this manuscript before final publication ofthe Version of Record (VoR). During production and pre-press, errors may be discovered which could affect thecontent, and all legal disclaimers that apply to the journal relate to this version also.
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 1
Running head: LIFE SATISFACTION AMONG YOUTH WITH ADHD
Correlates and Mediators of Life Satisfaction among Youth with Attention-Deficit/Hyperactivity Disorder Joshua M. Nadeau, Ph.D.1, Marni L. Jacob, Ph.D.1, Amanda C. Keene, B.A.1, Shawn M. Alderman, B. A.1, Leah E. Hacker, B.A.1, Mark A. Cavitt, M.D.2, Jeffrey L. Alvaro, M.D.2,
and Eric A. Storch, Ph.D.1
1Department of Pediatrics, University of South Florida
2Pediatric Psychiatry Services, All Children’s Hospital/John Hopkins Medicine
Author Note
Correspondence concerning this article should be addressed to Dr. Joshua Nadeau, Department of Pediatrics, Rothman Center for Neuropsychiatry, University of South Florida, Box 7523, 880 6th Street South, St. Petersburg, FL 33701; email: [email protected].
Abstract
The current study examined factors associated with life satisfaction among 111 youth, ages 8-17
years, presenting for outpatient treatment of attention-deficit/hyperactivity disorder (ADHD).
Youth completed the Students’ Life Satisfaction Scale, Vanderbilt ADHD Diagnostic Rating
Scale – Child, and the Generalized Anxiety Disorder (GAD) and Major Depressive Disorder
(MDD) modules of the Revised Child’s Anxiety and Depression Scale. A primary caregiver
completed a standard demographic form, and the Vanderbilt ADHD Diagnostic Rating Scale –
Parent. Results indicated that child-rated ADHD symptoms, depressive symptoms, and
generalized anxiety symptoms were negatively related to life satisfaction. Parent-rated ADHD
symptoms in the child were related to child-rated ADHD symptoms, but not to depressive
symptoms, generalized anxiety symptoms, or life satisfaction. Depressive symptoms predicted
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4
ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 2
life satisfaction above and beyond parent-rated ADHD symptom severity; however, neither
depressive nor generalized anxiety symptoms were found to uniquely predict life satisfaction
above and beyond child-rated ADHD symptom severity. Depressive symptoms mediated the
relationship between child-rated ADHD symptom severity and life satisfaction. Assessment and
treatment implications are discussed; specifically, we highlight how the variables of interest may
impact clinical presentation and treatment course.
Research on subjective well being has provided insight into individual resilience and positive
outcomes, offering a different perspective from the traditional focus on symptoms and
impairment and encouraging investigation of comprehensive treatment strategies (Frisch, 1999;
Gilman & Huebner, 2003). It is generally understood that subjective well being is a binary
construct, consisting of an emotional (e.g., positive and negative affect) and a cognitive
component (e.g., life satisfaction; Diener, 1984). Life satisfaction is defined as “a global
assessment of a person’s quality of life according to his/her chosen criteria” (Dew & Huebner,
1994). Life satisfaction is considered more stable than positive and negative affect across time
(Diener, Suh, Lucas, & Smith, 1999), being relatively unaffected by changes in life experiences
(Fujita & Diener, 2005; Huebner, Funk, & Gilman, 2000). Among youth, life satisfaction has
demonstrated weak correlations with demographics (Gilman & Huebner, 2003), suggesting that
life satisfaction ratings are not significantly associated with race, gender, or school grade
(Huebner et al., 2000).
Despite weak associations between demographic variables and life satisfaction, emerging data
suggest that life satisfaction is strongly associated with personal characteristics and perceptions.
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 3
For example, adolescents endorsing high life satisfaction also report higher GPA, self-esteem,
levels of hope, and quality of relationships with their parents, as well as being less likely to
experience anxiety or depression (Gilman & Huebner, 2006) as compared to peers endorsing
lower levels of life satisfaction. Conversely, research has identified direct associations between
low life satisfaction and internalizing and externalizing behaviors (Lewinsohn, Redner, &
Seeley, 1991; McKnight, Huebner, & Suldo, 2002). For example, Lewinsohn et al. (1991)
demonstrated that low life satisfaction was associated with depressive symptoms.
Among clinical populations, a number of positive indicators have been linked to high life
satisfaction, with data suggesting that life satisfaction may mitigate functional impairment
among youth with chronic conditions (e.g., Huebner, Funk, & Gilman, 2000; Nadeau et al.,
2013). Similarly, low life satisfaction among youth with psychopathology has been associated
with increased internalizing symptoms and externalizing behaviors, as youth with low life
satisfaction were more likely to endorse engagement in risk-taking behavior (e.g., drug and
alcohol use; Zullig, Valois, Huebner, Oeltmann, & Drane, 2001). Despite the associations
between maladaptive behavior and low life satisfaction, it is unclear to what extent specific
symptoms of psychopathology are associated with life satisfaction levels. In particular, given the
presence of significant impairment that is often associated with attention-deficit/hyperactivity
disorder (ADHD) in youth (DuPaul et al., 2004; Hoza et al., 2005; Mikami & Hinshaw, 2006),
children diagnosed with ADHD may be at an elevated risk for experiencing low life satisfaction,
potentially leading to greater negative outcomes and symptomology (Gilman & Huebner, 2003;
Gudjonsson et al., 2009, Mick, Faraone, Spencer, Zhang, & Biederman, 2008).
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 4
An externalizing disorder characterized by inattention and/or hyperactivity and impulsivity
(American Psychiatric Association [APA], 2013), ADHD affects 5-8% of school-aged children
(Froehlich, Lanphear, Epstein, Barbaresi, Katusic, & Kahn, 2007; Polanczyk, de Lima, Horta,
Biederman, & Rohde, 2007). A diagnosis of ADHD is often comorbid with both externalizing
and internalizing behaviors (Biederman, 2005), as approximately 25% of children with ADHD
are also diagnosed with a comorbid anxiety disorder – commonly Generalized Anxiety Disorder
(GAD; Angold, Costello, & Erkanli, 1999; Jarrett & Ollendick, 2008). As such, in addition to the
significant impairment in social (Mikami & Hinshaw, 2006) and academic (DuPaul et al., 2004)
domains of functioning associated with ADHD, symptoms of comorbid generalized anxiety
and/or depression may compound the degree of impairment experienced (Biederman et al., 1996;
Safren et al., 2001). Further, symptoms associated with GAD may overlap with or mimic
symptoms consistent with ADHD; specifically, worry or intrusive thoughts may appear as
inattention, while restlessness or nervousness may be difficult to distinguish from hyperactivity
or impulsivity (Jarrett & Ollendick, 2008). Within the social domain, children with ADHD
experience frequent peer rejection and fewer dyadic friendships (Hoza et al., 2005). In the
academic domain, children with ADHD are often placed in special education classes and are
likely to have comorbid learning disorders, lower performance on standardized testing, failing
grades, grade retention, and lower graduation rates (DeShazo-Barry, Lyman & Klinger, 2002;
DuPaul, 2004). Familial relationships are also affected by the presence of ADHD, with studies
demonstrating greater levels of parent-child conflict (Whalen et al., 2006), higher levels of
divorce (Wymbs et al., 2008), and lower levels of family functioning (Counts et al., 2005;
Deault, 2010) in families among youth with ADHD.
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 5
Given the significant level of impairment associated with the presence of ADHD, it is reasonable
to hypothesize that ADHD symptom severity would be negatively associated with life
satisfaction; however, the available research on life satisfaction among children with ADHD is
sparse. Currently, only one study has examined the relationship between life satisfaction and
ADHD symptoms in a sample of university students (Gudjonsson et al., 2009). Although the
researchers found that life satisfaction was negatively associated with inattentive symptoms of
ADHD, life satisfaction levels were more strongly associated (directly) with social functioning
and symptoms of anxiety and depression than with ADHD symptoms (Gudjonsson et al., 2009).
However, as this study sampled a community population of college-age students, it is unclear to
what extent these relationships are representative of those found within a clinical pediatric
population. Nevertheless, these findings align with the general associations between life
satisfaction and internalizing symptoms that have been observed among non-clinical populations
(Mahmoud, Staten, Hall, & Lennie, 2012; Ollendick, Raishevich, Davis, Sirbu, & Ost, 2010;
Proctor, Linley, & Maltby, 2009).
Understanding the relationship between ADHD symptoms and life satisfaction among children
may inform more effective intervention, leading to the increased likelihood of long-term positive
outcomes as children mature. Accordingly, this study sought to identify relationships among
child-reported life satisfaction, child- and parent-rated symptoms of ADHD, and child-reported
generalized anxiety and depressive symptoms. More specifically, this study examined three
research questions. First, what are the relationships among life satisfaction, ADHD symptoms,
and depressive and generalized anxiety symptoms in youth? Second, do depressive and
generalized anxiety symptoms predict life satisfaction over and above ADHD symptom severity?
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 6
Finally, does life satisfaction mediate the relationship between child-rated ADHD symptom
severity and depressive symptoms? Based on previous research, it was expected that ADHD
symptoms and depressive symptoms would show significant inverse associations with self-
reported life satisfaction levels.
Method
Participants
Participants included 111 children and adolescents (39 female) and their parent(s) who presented
at a hospital-based outpatient pediatric psychiatric clinic specializing in the treatment of ADHD.
The youth ranged in age from 8 to 17 years (M=11.59 + 2.55 years). The vast majority of
participants were Caucasian (90.1%), with the remaining youth identified by parents as African-
American (4.5%), Hispanic (3.6%), Asian (0.9%), or other (0.9%). Approximately 27% of
families had an income of $40,000 or less, 37% of families had an income between $41,000 and
$82,000, and 36% of families had an income above $82,000.
All participants had a primary or co-primary diagnosis of ADHD according to the Diagnostic and
Statistical Manual (Fourth Edition, Text Revision; American Psychiatric Association [APA],
2000). Diagnoses were determined via best estimate procedures (Leckman, Sholomaskas,
Thompson, Belanger, & Weissman, 1982) in which consensus between two board certified child
and adolescent psychiatrists (one the treating clinician) regarding the primary diagnosis and the
presence of comorbid diagnoses was required for inclusion. In this procedure, the two
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4
ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 7
psychiatrists discussed clinical information provided by the child and his/her family, together
with reviewing the participants’ completed measures and past clinical records to provide an
accurate diagnostic profile. Participants were excluded in the absence of 100% agreement for the
primary or comorbid diagnoses, or if they received co-occurring diagnoses of psychosis, autism
spectrum disorder, or mental retardation. Of note, no youth were excluded based upon diagnostic
disagreement.
Measures
Demographic Form. Parents/caregivers provided information about their child’s age, gender,
grade level, medication, how long the child has been on their current medication regimen, and
other current treatments (e.g., therapy, etc.).
Students’ Life Satisfaction Scale. The SLSS (Huebner, 1991) consists of seven 4-point Likert-
type items assessing youth perceptions of satisfaction with life, with higher scores indicating
higher levels of life satisfaction. The SLSS exhibits strong psychometric properties (Marques,
Pais-Ribeiro, & Lopez, 2011). Internal consistency for the SLSS in this sample was strong (α =
.86).
Vanderbilt ADHD Diagnostic Rating Scale - Parent/Child (VADRS - P/C; Wolraich et al.,
2003). The VADRS is a 47-item rating scale utilized to assess the presence of ADHD,
oppositional-defiant disorder (ODD), and conduct disorder (CD) symptoms in clinical youth
populations. Given the nature of the current study, only items relevant to ADHD symptoms in
youth (e.g., inattention, hyperactivity/impulsivity) were utilized. The VADRS has shown
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 8
excellent reliability (α = .90) and adequate concurrent validity (r = .79) for inattention and
hyperactivity/impulsivity subscales (Wolraich et al., 2003). Internal consistency ratings for the
VADRS-P/C in this sample were strong for child (α = .88 overall, .79 for inattention and .86 for
hyperactivity/impulsivity) and parent (α = .91 overall, .87 for inattention and .92 for
hyperactivity/impulsivity) versions.
Revised Child’s Anxiety and Depression Scale (RCADS; Chorpita et al., 2000). The RCADS
is a 47-item youth self-report inventory that assesses anxiety and depressive symptoms within six
separate subscales. For this study, only the major depressive disorder (MDD; 10 items) and
generalized anxiety disorder (GAD; 6 items) subscales were completed. The RCADS has
demonstrated excellent psychometric properties (Chorpita, Moffit, & Gray, 2005). Internal
consistency ratings for the RCADS in this sample were strong (α = .82 overall, .84 for GAD and
.70 for MDD).
Procedures
Study procedures were approved by the local Institutional Review Board. During their regularly
scheduled appointments, patients were screened by their clinician and provided with a general
description of the study. Patients meeting inclusion criteria and expressing interest in
participating were provided the full details of study participation by study staff, who then
obtained written consent from the parent and written assent from the youth. Participating parents
and youth were separated into private rooms to complete study measures. A member of the
research staff remained available to answer any questions and/or assist the child in completing
the assessment packet.
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 9
Data Analysis
Descriptive statistics were generated for all measures, with zero-order correlations used to assess
univariate relationships. Two hierarchical regression analysis models were used to determine the
independent predictors of life satisfaction, with the first model utilizing parent-rated ADHD
symptom severity and the second model incorporating child-rated ADHD symptom severity. In
both models, ADHD symptom severity was included in the first step, and depressive and
generalized anxiety symptoms incorporated within the second step. To evaluate the possibility of
the association between child-rated ADHD symptom severity and depressive symptoms being
mediated by life satisfaction, bootstrapping methods of indirect effect (Preacher & Hayes, 2004)
were performed using the PROCESS macro in SPSS 21 (SPSS Inc., Chicago, IL) with 5,000
resamples and bias-corrected 95% confidence intervals (an indirect effect was considered
significant if the confidence interval did not include zero). This model set child-rated ADHD
symptom severity as the predictor, life satisfaction ratings as the mediator, and RCADS MDD
subscale score as the outcome.
Results
Sample characteristics
Of the 111 participating youth, 33 (29.7%) met criteria for at least one comorbid disorder, with
13 (11.7%) having an anxiety disorder, 12 (10.8%) a disruptive behavior disorder, 10 (9%) a
depressive disorder, 5 (4.5%) an unspecified mood disorder, and 5 (4.5%) a tic disorder. In
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 10
addition, of the 111 participants, 108 (97.3%) were taking at least one prescribed medication,
with 26 (23.4%) taking three or more medications. Eighty-six (77.5%) were taking stimulant
medication, 30 (27%) a serotonin reuptake inhibitor (SRI), 23 (20.7%) an antihypertensive, 14
(12.6%) an atypical antipsychotic, and 13 (11.7%) a non-SRI antidepressant.
Associations between clinical characteristics
Zero-order univariate correlations between child-rated life satisfaction, child-rated depressive
and generalized anxiety symptoms, and measures of parent- and child-rated ADHD symptoms
are presented in Table 1. As can be seen, child-rated ADHD symptoms, symptoms of generalized
anxiety, and depressive symptoms displayed moderate negative correlations with life
satisfaction, while parent-rated ADHD symptoms were associated with child-rated ADHD
symptoms but not with depressive symptoms, symptoms of generalized anxiety, or child-rated
life satisfaction. Further, generalized anxiety and depressive symptoms were strongly correlated,
and both showed a strong positive relationship with child-rated ADHD symptoms.
Regression analysis for overall depressive and anxiety symptoms
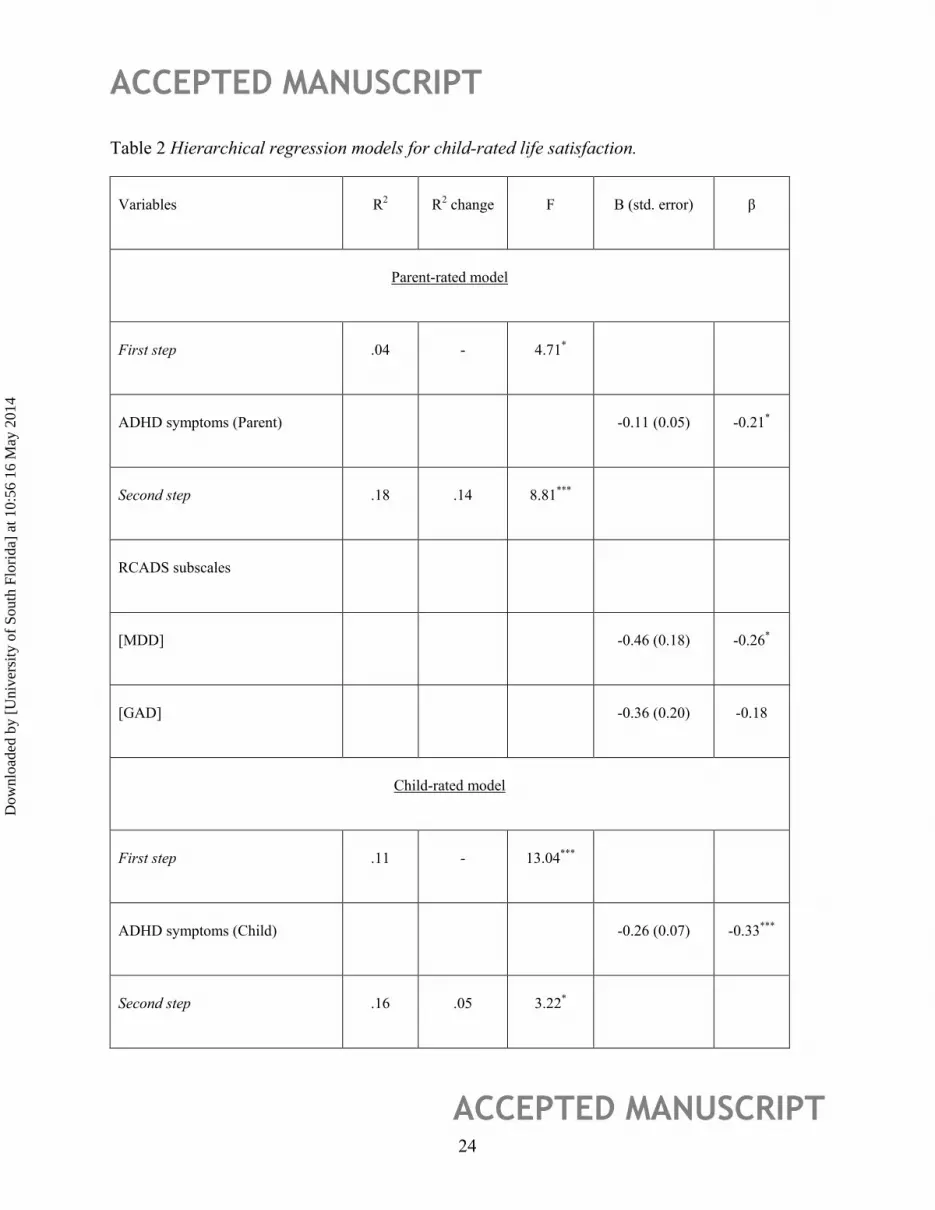
Findings of the parent- and child-rated hierarchical regression models with life satisfaction as the
dependent variable are summarized in Table 2. Severity of parent-rated ADHD symptoms was a
significant predictor of life satisfaction, explaining 4% of the variance observed. Addition of
depressive and anxiety symptoms improved the overall model, explaining an additional 14% of
the variance in life satisfaction. Individual coefficients suggest that depressive symptoms
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 11
predicted additional variance in life satisfaction beyond parent-rated ADHD symptom severity,
while generalized anxiety symptoms did not.
In the child-rated model, ADHD symptom severity was a significant predictor of life satisfaction,
explaining 11% of the variance observed. Addition of depressive and anxiety symptoms
improved the overall model, explaining an additional 5% of the variance in life satisfaction.
However, individual coefficients suggest that generalized anxiety and depressive symptoms did
not individually predict additional variance in life satisfaction beyond child-rated ADHD
symptom severity.
Mediational analysis
Regarding the potential for perceived life satisfaction to explain increased depressive symptoms
(as measured by the RCADS depressive subtotals) among youth with ADHD, an indirect effect
was observed wherein life satisfaction mediated the effect between ADHD symptom severity and
depressive symptoms (point estimate = –2.27, 95% confidence interval [CI] = .003 to .070).
Discussion
The purpose of this study was to examine the nature of life satisfaction among youth with ADHD
by examining the contributions of child- and parent-rated ADHD symptom severity, child-rated
generalized anxiety symptoms, and child-rated depressive symptoms. We also sought to
determine whether life satisfaction could account for the impact of child-rated ADHD symptoms
upon child-rated depressive symptoms. Of note, although the rate of anxiety disorder
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 12
comorbidity was relatively low (11.7%) in the current sample, 27% of the sample were being
treated with SRI medications. While ADHD symptoms (and the associated academic and social
impairment) often drive treatment-seeking behavior, comorbidity rates found in this study
collectively suggest that mood disturbances were witnessed with relative frequency which may
necessitate pharmacotherapy with SRIs.
As expected, and consistent with previous findings (Gudjonsson et al., 2009; McKnight et al.,
2002), child-rated ADHD symptoms, and generalized anxiety and depressive symptoms were
inversely and moderately associated with life satisfaction. This can be understood by considering
the potential impact that such symptoms might have upon life satisfaction. In terms of ADHD
symptoms, youth who exhibit difficulty maintaining attention and focus will likely find it harder
to follow-through with tasks and goals, perhaps providing fewer opportunities for them to build
self-efficacy and confidence; hence, they might experience lower life satisfaction. Youth who
exhibit hyperactivity and/or impulsivity might be perceived negatively in their interpersonal
relationships due to the exhibition of disruptive behavior, which might also negatively impact
life satisfaction. Thus, the presence of significant ADHD symptoms might make it more difficult
for youth to successfully manage the varied experiences that impact life satisfaction. The finding
that youth who exhibited greater generalized anxiety symptoms also reported less life satisfaction
is consistent with research linking anxiety and life satisfaction in young adults (Mahmoud,
Staten, Hall, & Lennie, 2012). Youth who experience generalized anxiety symptoms may worry
over the potential consequences of trying new situations or interacting with new people, and may
be in general less confident in their abilities to meet their goals – all of which may negatively
impact their life satisfaction. We also found significant links between depressive symptoms and
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 13
life satisfaction, which is also consistent with previous work (Lewinsohn et al., 1991). Youth
who experience depressive symptoms, particularly in the presence of an ADHD diagnosis, are
more likely to experience problems with sleep (Mayes et al., 2009), and are more likely to have
encountered adverse life events (e.g., arguments with parents, parent in prison, parent divorce,
death of relative, financial hardship among family; Daviss & Diler, 2012). Both of these
phenomena interfere with daily functioning across settings, and therefore seem likely to have a
negative impact upon perceived satisfaction with life.
Although not the primary focus of this paper, the weak association between child- and parent-
rated ADHD symptoms warrants comment and is consistent with previous research examining
the phenomenon of positive illusory bias, namely an overestimation of self-competence among
youth with ADHD, particularly as compared to parent- and/or clinician-rated competence
(Owens et al., 2007). Further, it is not uncommon for youth and parent reports to be discrepant,
as each informant may have a different perspective in terms of the youth’s coping and emotion
regulation abilities (Hourigan, Goodman, & Southam-Gerow, 2011). However, it is surprising
that parent-rated ADHD symptoms showed no significant association with clinical variables
aside from child-rated ADHD symptoms. If positive illusory bias was culpable in the differences
between child- and parent-rated ADHD symptoms – that is to say, if a child’s underestimation of
his or her ADHD symptoms accounted for discrepancies between ratings of youth and their
parents – then it would be expected that the relationships between child-rated ADHD symptoms
and other clinical variables (e.g., life satisfaction, depressive symptoms) would be attenuated, as
there is little in the literature to suggest a similar underestimation bias with respect to these
variables among youth with ADHD (Mick et al., 2008; Owens et al., 2007). These patterns of
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 14
association may reflect shared method variance in which reports by the same individual may be
inter-related partially independent of construct assessed.
Although the combination of child-rated depressive and generalized anxiety symptoms predicted
life satisfaction over and above ADHD symptoms independent of rater in the current sample,
depressive symptoms were the only significant independent predictor, and only in the parent-
rated model. This is surprising, given previous findings suggesting that life satisfaction is more
strongly associated with anxiety and depression symptoms than with ADHD symptoms
(Gudjonsson et al., 2009). However, this finding was consistent with the observation that
depressive and generalized anxiety symptoms were more strongly correlated with ADHD
symptoms than was life satisfaction, and that depressive and generalized anxiety symptoms were
of generally equivalent correlative strength. These findings, although difficult to interpret
meaningfully, indicate the need for further research to clearly articulate the nature of these
relationships.
The finding that life satisfaction mediated the relationship between child-rated ADHD symptoms
and depressive symptoms is consistent with prior research in this area (e.g., McKnight, Huebner,
& Suldo, 2002). Youth with ADHD are likely to find academic tasks and social interactions
more challenging than their peers (DuPaul et al., 2004), and their subjective experience of daily
life – particularly within the school-age portions of the developmental arc – may become more
negative as a result (Gudjonsson et al., 2009). The lowered perception of life satisfaction could
contribute to concomitant manifestation of negative emotion as anxious and depressive
symptoms, discouragement, and low confidence among youth with ADHD. Clinically, this
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 15
suggests that youth with ADHD may benefit from activities that foster a sense of self-worth and
enhance life satisfaction. For instance, incorporation of commonly used treatment strategies such
as behavioral activation, problem-solving skills, use of positive reinforcement, and social skills
training may have a positive impact on youth life satisfaction and may therefore foster better
adjustment (Davidson & Memaray, 2007; Demaray & Malecki, 2003; McKnight et al., 2002).
This study has several limitations. First, the design was cross-sectional, thereby preventing
inference of causal effects. Second, the sample was treatment-seeking and relatively
homogeneous demographically, limiting the potential for generalization of findings to the larger
population of youth with ADHD. Third, the majority of data were collected via self-report, so
same-reporter bias may have impacted the results. Similarly, the lack of parent-reported GAD
and depressive symptoms, and of teacher-reported ADHD symptoms, decreases the
interpretability of the study’s results due to increased need for inference. Future research should
stress triangulation of data by incorporating multiple rater perspectives, and examine more
closely the direction of observed relationships among youth with ADHD.
Implications for Practice
The findings of this study have important implications for clinical practice. First, treatment
efforts for ADHD in youth should explicitly address life satisfaction in addition to targeting
ADHD symptoms. Utilizing comprehensive treatment may engender a more positive outcome, in
that heightened life satisfaction predicts decreased risk for depressive and generalized anxiety
symptoms in this population. Significant progress in the area of interventions addressing life
satisfaction has been made, with interventions typically targeting character strengths assessed by
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 16
the Values in Action Inventory of Strengths (VIA-IS; Peterson et al., 2005); however, further
research is necessary to determine the appropriateness and effectiveness of such interventions
among youth with ADHD. Second, as an extension to the first point, youth presenting with
ADHD symptoms should also be assessed utilizing a measure of life satisfaction. Deficits in this
area, particularly within the context of ADHD, should alert the clinician to the risk of depressive
and/or generalized anxiety symptoms, as well as possible additional academic and social
impairment.
References
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental
Disorders (5th Ed.). Washington D.C.: Author.
American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental
Disorders (Revised 4th Ed.). Washington D.C.: Author.
Angold, A., Costello, J. E., Erkanli, A. (1999). Comorbidity. Journal of Child Psychology and
Psychiatry, 40, 57-87.
Biederman, J., (2005). Attention-deficit/hyperactivity disorder: A selective overview. Biological
Psychiatry, 57, 1215-1220.
Biederman, J., Faraone, S., Milberger, S., Curtis, S., Chen, L., Marrs, A., Ouellette, C., Moore,
P., & Spencer, T. (1996). Predictors of persistence and remission of ADHD into adolescence:
results from a four-year prospective follow-up study. Journal of the American Academy of Child
and Adolescent Psychiatry, 35, 343-351.
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4
ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 17
Chorpita, B. F., Yim, L. M., Moffitt, C. E., Umemoto L. A., & Francis, S. E. (2000). Assessment
of symptoms of DSM-IV anxiety and depression in children: A Revised Child Anxiety and
Depression Scale. Behaviour Research and Therapy, 38, 835-855.
Chorpita, B. F., Moffitt, C. E., & Gray, J. (2005). Psychometric properties of the revised child
anxiety depression scale in a clinical sample. Behaviour Research and Therapy, 43, 309-322.
Counts, C., Nigg, J., Stawicki, J., Rappley, M., and Von Eye, A. (2005). Family adversity in
DSM-IV ADHD combined and inattentive subtypes and associated disruptive behavior problems.
Journal of American Academy of Child and Adolescent Psychiatry, 44, 690-698.
Davidson, L. M., & Demaray, M. K. (2007). Social support as a moderator between
victimization and internalizing-externalizing distress from bullying. School Psychology Review,
36, 383-405.
Daviss, W. B., & Diler, R. (2012). Does comorbid depression predict subsequent adverse life
events in youth with attention-deficit/hyperactivity disorders? Journal of Child and Adolescent
Psychopharmacology, 22, 65-71.
Deault, L. C. (2010). A systematic review of parenting in relation to the development of
comorbidities and functional impairments in children with attention-deficit/hyperactivity
disorder (ADHD). Child Psychiatry & Human Development, 41, 168-192.
Demaray, M. K., & Malecki, C. K. (2003). Perceptions of the frequency and importance of social
support by students classified as victims, bullies, and bully/victims in an urban middle school.
School Psychology Review, 32, 471-489.
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 18
DeShazo-Barry, T., Lyman, R. D., & Klinger, L. G. (2002). Academic underachievement and
attention-deficit/hyperactivity disorder: the negative impact of symptom severity on school
performance. Journal of School Psychology, 40, 259-283.
Dew, T., & Huebner, S. E. (1994). Adolescents' perceived quality of life: An exploratory
investigation. Journal of School Psychology, 32, 185-199.
Diener, E. (1984). Subjective well-being. Psychological Bulletin, 95, 542-575.
Diener, E., Suh, E. M., Lucas, R. E., & Smith, H. L. (1999). Subjective well-being: Three
decades of progress. Psychological Bulletin, 125, 276-302.
DuPaul, G., Volpe, R., Asha, J., Lutz, G., Lorah, K. & Gruber, R., (2004). Elementary school
students with AD/HD: Predictors of academic achievement. Journal of School Psychology, 42,
285-301.
Fujita, F., & Diener, E. (2005). Life satisfaction set point: stability and change. Journal of
Personality and Social Psychology, 88, 158-164.
Frisch, M. B. (1999). Quality of life assessment/intervention and the Quality of Life Inventory
(QOLI). In M. R. Maruish (Ed.), The use of psychological testing for treatment planning and
outcome assessment (2nd ed., pp.1227-1331). Hillsdale, NJ: Lawrence Erlbaum.
Froehlich, T. E., Lanphear, B. P., Epstein, J. N., Barbaresi, W. J., Katusic, S. K., & Kahn, R. S.
(2007). Prevalence, recognition, and treatment of attention-deficit/hyperactivity disorder in a
national sample of US children. Archives of Pediatrics and Adolescent Medicine, 161, 857.
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 19
Gilman, R., & Huebner, S. (2003). A review of life satisfaction research with children and
adolescents. School Psychology Quarterly, 18, 192-205.
Gudjonsson, G. H., Sigurdsson, J. F., Eyjolfsdottir, G. A., Smari, J., & Young, S. (2009). The
relationship between satisfaction with life, ADHD symptoms, and associated problems among
university students. Journal of Attention Disorders, 12, 507-515.
Hourigan, S. E., Goodman, K. L., Southam-Gerow, M. A. (2011). Discrepancies in parents’ and
children’s reports of child emotion regulation. Journal of Experimental Child Psychology, 110,
198-212.
Hoza, B., Mrug, S., Gerdes, A., Bukowski, W., Kraemer, H., Wigal, T., Hinshaw, S., Gold, J.,
Pelham, W., & Arnold, L. (2005). What aspects of peer relationships are impaired in children
with attention-deficit/hyperactivity disorder? Journal of Consulting and Clinical Psychology, 73,
411-423.
Huebner, S. E. (1991). Initial development of the Students’ Life Satisfaction Scale. School
Psychology International, 12, 231-243.
Huebner, S. E., Funk, B. A., & Gilman, R. (2000). Cross-sectional and longitudinal
psychosocial correlates of adolescent life satisfaction reports. Canadian Journal of School
Psychology, 16, 53-64.
Jarrett, M. A., & Ollendick, T. H. (2008). A conceptual review of the comorbidity of attention-
deficit/hyperactivity disorder and anxiety: implications for future research and practice. Clinical
Psychology Review, 28, 1266-1280.
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 20
Leckman, J. F., Sholomaskas, D., Thompson, W. E., Belanger, A., & Weissman, M. M. (1982).
Best estimate of lifetime psychiatric diagnosis: a methodological study. Archives of General
Psychiatry, 39, 879-883.
Lewinsohn, P. M., Redner, J., & Seeley, J. (1991). The relationship between life satisfaction and
psychosocial variables: New perspectives. In F. Strack, M. Argyle, and N. Schwarz (Eds.),
Subjective well-being: An interdisciplinary perspective, pp.141-169. New York: Pergamon Press.
Mahmoud, J. S. R., Staten, R. T., Hall, L. A., & Lennie, T. A. (2012). The relationship among
young adult college students’ depression, anxiety, stress, demographics, life satisfaction, and
coping styles. Issues in Mental Health Nursing, 33, 149-156.
Marques, S. C., Pais-Ribeiro, J. L., & Lopez, S. J. (2011). The role of positive psychology
constructs in predicting mental health and academic achievement in children and adolescents: A
two-year longitudinal study. Journal of Happiness Studies, 12, 1049-1062.
Mayes, S. D., Calhoun, S. L., Bixler, E. O., Vgontzas, A. N., Mahr, F., Hillwig-Garcia, j.,
Elamir, B., Edhere-Ekezie, L., & Parvin, M. (2009). ADHD subtypes and comorbid anxiety,
depression, and oppositional-defiant disorder: Differences in sleep problems. Journal of
Pediatric Psychology, 34, 328-337.
McKnight, C. G., Huebner, E. S., & Suldo, S. (2002). Relationships among stressful life events,
temperament, problem behavior, and global life satisfaction in adolescents. Psychology in the
Schools, 39, 677-687.
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4
ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 21
Mick, E., Faraone, S. V., Spencer, T., Zhang, H. F., & Biederman, J. (2008). Assessing the
validity of the Quality of Life Enjoyment and Satisfaction Questionnaire – Short Form in adults
with ADHD. Journal of Attention Disorders, 11, 504-509.
Mikami, A. & Hinshaw, S. (2006). Resilient adolescent adjustment among girls: Buffers of
childhood peer rejection and attention-deficit/hyperactivity disorder. Journal of Abnormal Child
Psychology, 34, 825-839.
Nadeau, J. M., Lewin, A. B., Arnold, E. B., Crawford, E. A., Murphy, T. K., & Storch, E. A.
(2013). Clinical correlates of functional impairment in children and adolescents with obsessive–
compulsive disorder. Journal of Obsessive-Compulsive and Related Disorders, 2, 432-436.
Ollendick, T. H., Raishevich, N., Davis III, T. E., Sirbu, C., & Ost, L. G. (2010). Specific phobia
in youth: phenomenology and psychological characteristics. Behavior Therapy, 41, 133-141.
Owens, J. S., Goldfine, M. E., Evangelista, N. M., Hoza, B., & Kaiser, N. M. (2007). A critical
review of self-perceptions and the positive illusory bias in children with ADHD. Clinical Child
and Family Psychology Review, 10, 335-351.
Peterson, C., Park, N., & Seligman, M. E. P. (2005). Assessment of character strengths. In G. P.
Koocher, J. C. Norcross, & S. S. Hill III (Eds.), Psychologists’ Desk Reference (2nd ed., pp. 93–
98). New York: Oxford University Press.
Polanczyk, G., de Lima, M., Horta, B., Biederman, J., & Rohde, L. (2007). The worldwide
prevalence of ADHD: a systematic review and meta-regression analysis. American Journal of
Psychiatry, 164, 942-948.
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 22
Preacher, K. J., & Hayes, A. F. (2004). SPSS and SAS procedures for estimating indirect effects
in simple mediation models. Behavior Research Methods, Instruments, & Computers, 36, 717-
731.
Proctor, C. L., Linley, P. A., & Maltby, J. (2009). Youth life satisfaction: A review of the
literature. Journal of Happiness Studies, 10, 583-630.
Safren, S. A., Lanka, G. D., Otto, M. W., & Pollack, M. H. (2001). Prevalence of childhood
ADHD among patients with generalized anxiety disorder and a comparison condition, social
phobia. Depression and Anxiety, 13, 190-191.
Whalen, C., Henker, B., Jamner, L., Ishikawa, S., Floro, J., Swindle, R., Perwien, A., &
Johnston, J. (2006). Toward mapping daily challenges of living with ADHD: Maternal and child
perspectives using electronic diaries. Journal of Abnormal Child Psychology, 34, 115-130.
Wolraich, M. L., Lambert, W., Doffing, M. A., Bickman, L., Simmons, T., & Worley, R. (2003).
Psychometric properties of the Vanderbilt ADHD Diagnostic Parent Rating Scale in a referred
population. Journal of Pediatric Psychology, 28, 559-567.
Wymbs, B., Pelham, W., Gnagy, E., Molina, B., Wilson, T., and Greenhouse, J. (2008). Rate and
predictors of divorce among parents of youths with ADHD. Journal of Consulting and Clinical
Psychology, 76, 735-744.
Zullig, K. J., Valois R. F., Huebner, S. E., Oeltmann, J. E., & Drane, J. W. (2001). Relationship
between perceived life satisfaction and adolescents' substance abuse. Journal of Adolescent
Health, 29, 279-288.
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 23
Table 1 Correlations and Descriptive Statistics for Clinical Variables
Variable LS ADHD (Child) ADHD (Parent) RCADS Reliability Mean (SD)
Life Satisfaction - -.327** -.165 -.367** .86 30.39 (7.97)
ADHD (Child) -.327** - .231* .553** .88 20.41 (9.92)
Inattention -.381** .849** .129 .573** .79 11.76 (5.22)
Hyperactivity/Impulsivity -.204* .894** .263** .406** .86 8.66 (6.15)
ADHD (Parent) -.165 .231* - .069 .91 31.68 (10.77)
Inattention -.144 .226* .226* .228 .87 18.57 (5.38)
Hyperactivity/Impulsivity -.138 .175 .894** .068 .92 13.11 (7.24)
RCADS -.367** .553** .069 - .82 15.90 (7.05)
Anxiety -.288** .462** .124 .831** .84 6.42 (3.88)
Depression -.333** .479** .000 .870** .70 9.48 (4.39)
Note: LS=Life Satisfaction, refers to Student Life Satisfaction Scale scores; ADHD scores refer to Inattentive,
Hyperactive/Impulsive, and Combined subscale scores from the Vanderbilt ADHD Rating Scale – Child or Parent version;
RCADS=Revised Child Anxiety and Depressive Scales. *ρ<.05; **ρ<.01
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4
ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 24
Table 2 Hierarchical regression models for child-rated life satisfaction.
Variables R2 R2 change F B (std. error) β
Parent-rated model
First step .04 - 4.71*
ADHD symptoms (Parent) -0.11 (0.05) -0.21*
Second step .18 .14 8.81***
RCADS subscales
[MDD] -0.46 (0.18) -0.26*
[GAD] -0.36 (0.20) -0.18
Child-rated model
First step .11 - 13.04***
ADHD symptoms (Child) -0.26 (0.07) -0.33***
Second step .16 .05 3.22*
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4

ACCEPTED MANUSCRIPT
ACCEPTED MANUSCRIPT 25
RCADS subscales
[MDD] -0.35 (0.19) -1.84
[GAD] -0.24 (0.21) -0.12
Note: ADHD symptoms) = Combined subscale scores from the Vanderbilt ADHD Rating Scale – Parent or Child
version; RCADS = Revised Child Anxiety and Depressive Scales; MDD = Major Depressive Disorder subscale;
GAD = Generalized Anxiety Disorder subscale. *ρ<.05; **ρ<.01; ***ρ<.001
Dow
nloa
ded
by [
Uni
vers
ity o
f So
uth
Flor
ida]
at 1
0:56
16
May
201
4





























