Embed Size (px)
Citation preview

1 3
DOI 10.1007/s12185-015-1799-8Int J Hematol
ORIGINAL ARTICLE
Curative haploidentical BMT in a murine model of X‑linked chronic granulomatous disease
Yasuo Takeuchi1,2 · Emiko Takeuchi2 · Takashi Ishida3,5 · Masafumi Onodera4 · Hiromitsu Nakauchi5 · Makoto Otsu5,6
Received: 4 November 2014 / Revised: 9 April 2015 / Accepted: 13 April 2015 © The Japanese Society of Hematology 2015
whole bone marrow cells achieved long-lasting mixed chi-merism in X-linked CGD mice in a haploidentical trans-plantation setting. Stable mixed chimerism was maintained for up to 1 year even at a low range (<20 % donor cells), indicating induction of donor-specific tolerance. The regi-men induced mild myelosuppression without severe acute complications. Stable chimerism was therapeutic, as it sup-pressed cutaneous granuloma formation in an in vivo test suited for evaluation of treatment efficacy in murine CGD models. These results warrant future development of a sim-plified allogeneic hematopoietic cell transplantation regi-men that would benefit CGD patients by allowing the use of haploidentical donor grafts without serious concerns of severe treatment-related toxicity.
Keywords Chronic granulomatous disease · Haploidentical hematopoietic cell transplantation · Non-myeloablative conditioning · Anti-CD40 ligand therapy · Tolerance
Introduction
Chronic granulomatous disease (CGD) is a form of con-genital immunodeficiency with an estimated prevalence between 1/200,000 and 1/250,000 live births [1]. The disease arises from a defect in one of the 4 components of the nicotinamide adenine dinucleotide phosphatase (NADPH) enzyme system, which results in failure of pro-duction of reactive oxygen species (ROS) in phagocytes. CGD patients are highly susceptible to infection with catalase-producing microorganisms, including Aspergil-lus sp. and Staphylococcus sp. [1–3]. Recurrent infections induce chronic inflammation through secretion of cytokines such as TNF-α, interleukin (IL)-6, IL-1, and IL-17, often
Abstract Chronic granulomatous disease (CGD) is a pri-mary immunodeficiency disorder characterized by defec-tive microbial killing in phagocytes. Long-term prognosis for CGD patients is generally poor, highlighting the need to develop minimally toxic, curative therapeutic approaches. We here describe the establishment of a mouse model in which X-linked CGD can be cured by allogeneic bone mar-row transplantation. Using a combination of non-myeloab-lative-dose total body irradiation and a single injection of anti-CD40 ligand monoclonal antibody, transplantation of
This work was performed in the Center for Stem Cell Biology and Regenerative Medicine, Institute of Medical Science, University of Tokyo.
Electronic supplementary material The online version of this article (doi:10.1007/s12185-015-1799-8) contains supplementary material, which is available to authorized users.
* Makoto Otsu [email protected]
1 Division of Nephrology, Department of Internal Medicine, Kitasato University School of Medicine, Sagamihara, Japan
2 Department of Immunology, Kitasato University School of Medicine, Sagamihara, Japan
3 Department of Hematology, Kitasato University School of Medicine, Sagamihara, Japan
4 Department of Human Genetics, National Center for Child Health and Development, Tokyo, Japan
5 Division of Stem Cell Therapy, Center for Stem Cell Biology and Regenerative Medicine, Institute of Medical Science, University of Tokyo, Tokyo, Japan
6 Stem Cell Bank and Division of Stem Cell Processing, Center for Stem Cell Biology and Regenerative Medicine, Institute of Medical Science, University of Tokyo, 4-6-1 Shirokanedai, Minato-ku, Tokyo 108-8639, Japan

Y. Takeuchi et al.
1 3
resulting in granuloma formation in vital organs [4–6]. Cur-rent management comprises the use of antibiotics, antimy-cotics, and/or IFN-γ for prophylaxis or treatment of infec-tion, and immunosuppressive drugs, when needed to target granulomata and autoimmune sequelae. Despite focused medical care, disease mortality is estimated at 3–5 % per year, and only 50 % of patients survive until age 30 years [1–3]. Therefore, establishment of a curative treatment is needed for CGD patients.
Allogeneic hematopoietic cell transplantation (allo-HCT) is one way to cure CGD. The outcome in X-linked CGD (X-CGD) patients receiving hematopoietic cell trans-plantation (HCT) with matched-related-donor or matched-unrelated-donor grafts is better than that in patients receiving conventional treatment alone [7, 8]. However, significant clinical problems associated with allo-HCT remain, including conditioning toxicity, graft failure, and graft-versus-host disease (GvHD) [9, 10]. In addition, in the absence of an HLA-matched sibling donor, although use of haploidentical grafts would improve the chance of finding a suitable donor, it also would likely increase the risk of transplant failure [8, 11]; accordingly, such donors usually are excluded from consideration. Therefore, to establish an HLA-haploidentical HCT (haplo-HCT) regi-men including bone marrow transplantation (haplo-BMT) with minimized toxicity would greatly benefit CGD patients [12–15].
We have described in mice a non-myeloablative regimen consisting of a low dose of total body irradiation (TBI) with a co-stimulatory blockade of CD40–CD40 ligand (CD40L) signaling followed by MHC-full mismatched allogeneic BMT (allo-BMT) [16]. The regimen reduced condition-ing toxicity and induced durable, long-lasting mixed bone marrow (BM) chimerism, along with donor-specific toler-ance without GvHD. We here tested if this regimen could be used in the mouse model of X-CGD [17], specifically by modeling a haplo-BMT setting. We expected that long-last-ing mixed chimerism would suffice to cure X-CGD recipi-ents without significant procedure-associated risk.
Materials and methods
Mice
X-CGD (B6: H-2b) mice [17] were kindly provided by Dr. Akihiro Kume (Jichi Medical University). Wild-type (WT) mice of strain origins C57BL/6 (B6: H-2b), DBA2 (H-2d), BDF1 (H-2b/d), and BCF1 (H-2b/k) were purchased from Japan SLC (Shizuoka, Japan). All mice were housed in a specific pathogen-free microisolator environment. All pro-tocols were approved by the Institutional Animal Use and
Care Committees of the Institute of Medical Science, Uni-versity of Tokyo, and of the Kitasato University School of Medicine.
Detection of specific reactive oxygen species in neutrophils
We employed 2-[6-(4′-amino) phenoxy-3H-xanthen-3-on-9-yl] benzoic acid (APF), a novel fluorescent probe, use-ful in detection of a limited spectrum of reactive oxygen species (sROS) that are strongly microbicidal [18]. The details of this probe are described in electronic supplemen-tary material. Peripheral blood (PB) samples were stained with allophycocyanin (APC)-conjugated anti-mouse Ly-6G monoclonal antibody (MoAb) (RB6-8C5; eBioscience, San Diego, CA) for 15 min at 4 °C to mark the neutrophil population. Erythrocytes were lysed and the remaining cells were loaded with an APF fluorescent probe (10 μΜ; Sekisui Chemical, Tokyo, Japan) for 20 min at room tem-perature. The cells taking up APF dye were stimulated with phorbol 12-myristate 13-acetate [(PMA); Sigma Aldrich Japan, Tokyo, Japan] at 2 ng/ml for 20 min at room temper-ature. After stimulation, fluorescence images were analyzed by flow cytometry. Polymorphonuclear leukocytes (PMNs) producing sROS were enumerated as APF+ cells within the Ly-6G+ cell population.
BMT procedures and evaluation of procedure‑related toxicity
Age-matched (8-week-old) recipient mice were treated with TBI 1 day before BMT (day −1), with varying doses (0, 1, 2, 3, 5, and 9.5 Gy). Twenty million unmodified BM cells (BMC) from donor mice were injected i.v. along with hamster anti-mouse CD40L MoAb (MR1; BioXCell, West Lebanon, NH) [16], 2 mg/mouse, administered i.p. In exper-iments to test hematologic recovery and severity of GvHD, mice in a control group received 9.5 Gy (two split doses ~4 h apart) on the day of transplantation (day 0). Where indi-cated, 1 × 106 CD3+ splenic T cells, obtained using APC-conjugated anti-CD3 MoAb and anti-APC microbeads (Miltenyi Biotech, Bergisch Gladbach, Germany), were co-infused into recipient mice in addition to whole BMC. Com-plete blood counts were monitored serially using a MEK-6450 Celltac-α automated hematology analyzer (Nihon Kohden, Tokyo, Japan). Body weight (BW) was monitored as an indicator of acute GvHD and conditioning toxic-ity. The reduction level of BW was calculated as follows: BW (g) after treatment
/
BW before treatment × 100 (%). Results were expressed as means ± SD. Histological anal-ysis for signs of GvHD was performed 7–10 days after transplantation.

Modeling haploidentical BMT for X-CGD
1 3
Analysis of multilineage donor chimerism in white blood cells
Flow-cytometry analysis was used to distinguish between donor and host cells of a particular lineage after BMT. The percentage of donor cells was calculated as described [19]. Donor- and recipient-derived cells were identified using fluorescein isothiocyanate (FITC)-conjugated anti-H-2Dk (KH95) and phycoerythrin (PE)-conjugated anti-H-2Dd MoAb (SF-1). Peripheral CD4+ and CD8+ T cells and B cells were identified, respectively using APC-conjugated anti-CD4- and CD8-MoAb and by PE-Cy7-conjugated anti-B220 MoAb (all PharMingen, San Diego, CA).
Subcutaneous inflammatory reactions to Aspergillus fumigatus in assays of in vivo therapeutic effects of mixed chimerism
An in vivo test developed for investigations into the hyper-inflammatory status of X-CGD mice was used to assess treatment efficacy in our BMT model [20]. Briefly, we tested if an intradermal injection of sterile Asper-gillus fumigatus (AF) debris induced neutrophil accu-mulations that resembled granulomata in human CGD patients. Detailed methods are described in supplementary information.
Statistical analysis
Data are expressed as means ± SD. Differences in the values between groups were analyzed by Mann–Whitney testing. Repeatedly measured BW values were assessed by a linear mixed model for detecting interaction between time and measurements. P values <0.05 were considered significant.
Results
Application of a pre‑established co‑stimulatory blockade‑based strategy to a haploidentical BMT model
We and others have shown that experimental BMT with an MHC-fully mismatched pair of donor and recipient mice (e.g., B6 and BALB/c) can, with costimulatory blockade-based conditioning, achieve mixed chimerism and immu-nological tolerance [16, 21, 22]. However, whether similar approaches could apply in a haplo-BMT setting remained uncertain; this was considered clinically relevant for mod-eling treatment of X-CGD patients. We therefore investi-gated whether the pre-established transplantation strategy could induce stable mixed chimerism in an MHC-haploi-dentical combination between BDF1 mice (H-2b/d) and
BCF1 mice (H-2b/k; Fig. 1a). We also tested the minimum dose of TBI in this conditioning regimen necessary to achieve therapeutically relevant levels of donor cell chimer-ism. As shown in Fig. 1b, most mice (5 of 6) given 5 Gy of TBI showed full chimerism, and all mice given 3 Gy showed mixed chimerism. In some mice, 2 Gy of TBI or less failed to induce donor chimerism and without TBI, no mouse showed donor chimerism. These results confirmed that the regimen could induce mixed chimerism even in a haplo-BMT setting. Based on titration results, we used 3 Gy as the optimal TBI dose for subsequent experiments.
Reduced‑intensity conditioning consisting of anti‑CD40L MoAb and 3 Gy TBI with haplo‑BMT allowed the induction of long‑lasting mixed chimerism in X‑CGD F1 mice
To mimic a haplo-BMT setting for X-CGD patients, X-CGD F1 male mice were generated as a recipient model (supplementary Fig. 1). We then treated X-CGD F1 mice (n = 18) and WT BDF1 littermates (n = 5) with 3 Gy TBI
Fig. 1 Determination of minimum dose of TBI for induction of robust mixed chimerism in an MHC-haploidentical BMT model. a Schematic representation of experimental transplantation. The conditioning for recipient mice consists of TBI on day −1 and sin-gle i.p. injection of anti-mouse CD40L MoAb (MR1; 2 mg/mouse) on day 0 (before BMT). On day 0, 2 × 107 unmodified, donor BM cells (BMC) were injected i.v. Varying doses of TBI were tested in the haploidentical combination of male BDF1 mice as recipients and male BCF1 mice as donors. b Percentages of peripheral donor B-cell chimerism in individual recipients were assessed by flow-cytometry analysis 12 weeks after BMT. Each symbol represents an individual recipient mouse in each group. The figures above the plots indicate number of mice with donor chimerism/number of mice treated

Y. Takeuchi et al.
1 3
(given on day −1) and MR1 MoAb (day 0), and trans-planted into them whole BMC obtained from donor BCF1 (H-2b/k) male mice. As shown in Fig. 2, stable and long-lasting mixed chimerism of peripheral blood lymphocytes (PBLs) was achieved in 16 of 18 X-CGD F1 mice. The per-centages of donor CD4+ T cells and B cells increased grad-ually up to 18 weeks after BMT in individual mice and then plateaued. Two of 16 chimeric X-CGD mice died at around 30–40 weeks after BMT (as indicated in each figure leg-end) without any appearances suggesting ongoing GvHD, such as emaciation or hair loss (not shown), and the cause of death remained uncertain. Ultimately, 14 of the chimeric X-CGD F1 mice were observed for 1 year after BMT. Stable donor chimerism was maintained throughout the observation period in all these mice regardless of chimer-ism level (Fig. 2). Results for percentages of donor CD8+ T
cells were similar (data not shown). Two of 18 mice eventu-ally showed no donor chimerism within the duration of the follow-up period. WT F1 littermate mice (5 of 5) treated with the same regimen showed a similar course in donor chimerism with respect to CD4+ T cells, CD8+ T cells and B cells (data not shown). Thus, this regimen achieved dura-ble and long-lasting mixed chimerism in X-CGD F1 mice subjected to BMT from MHC-haploidentical donors.
Safety features of reduced‑conditioning BMT strategy
GvHD and conditioning toxicity are serious obstacles to allo-BMT. We therefore evaluated the safety of the established costimulatory blockade-based regimen. Ini-tially, we examined hematologic recovery kinetics and the severity of GvHD using WT BDF1 recipients after transplantation. In a first experiment, recipient mice in the test group received exactly the same conditioning regimen as that described above (3 Gy TBI on day −1 and MR1 on day 0) followed by whole BMC of BCF1 origin, whereas mice in the control group were lethally irradiated (9.5 Gy), followed on the same day by receipt of haploidentical whole BMC. As shown in supple-mentary Fig. 2a, mild leukocytopenia was observed in the test group, suggesting that stable mixed chimerism induction might entail modest myelosuppresion. None of the mice in either group, however, manifested sub-stantial anemia and thrombocytopenia (supplementary Fig. 2a), and none exhibited any signs of GvHD (sup-plementary Fig. 2b, and data not shown). To test how robust the resistance to GvHD induction can be for the co-stimulatory blockade regimen, we then conducted a second experiment in which we infused haploidenti-cal splenic T cells in addition to whole BMC into the recipient mice to ensure induction of GvHD. As shown, myelosuppression was more evident than that seen in the first experiment, but outcomes in the recipient mice treated with 3 Gy TBI and MR1 MoAb were better than those in the control group, especially regarding sever-ity of anemia and thrombocytopenia (Fig. 3a). Remark-ably, signs of GvHD were obvious in this model for the mice that received haploidentical whole BM and splenic T cells with 9.5 Gy TBI, with marked reduction in BW (Fig. 3b) and decreased activity with hunched posture (supplementary video). In sharp contrast, the recipi-ent mice conditioned with the co-stimulatory blockade remained healthy with no decline in BW or activity (Fig. 3b and supplementary video). Overall, these results indicated that the established reduced-intensity regimen led to mild myelosuppression during mixed chimerism induction, but could confer robust GvHD resistance upon recipient mice. To address the safety issues spe-cifically in the context of transplantation with the CGD
Fig. 2 Achievement of stable and long-lasting mixed chimerism of PBLs in X-CGD recipients. Percentages of donor CD4+ T cells and B cells in peripheral blood of X-CGD F1 individuals were assessed by flow-cytometry analysis at each time point after BMT. Each line and symbol pair represents an individual X-CGD F1 recipient. Six-teen of 18 X-CGD F1 mice developed durable, long-lasting mixed chimerism of CD4+ T cells and B cells. Since two mice were found dead at 30 weeks (donor-cell contingent; 45.6 % for CD4+ cells and 70.0 % for B220+ cells) and 40 weeks (donor-cell contingent; 38.8 % for CD4+ cells and 76.2 % for B220+ cells) after BMT, only 14 of 16 chimeric X-CGD F1 mice were observed for one full year. Two of 18 X-CGD F1 mice showed no donor chimerism

Modeling haploidentical BMT for X-CGD
1 3
background, an experiment like the first was conducted with X-CGD F1 mice as recipients. X-CGD F1 recipient mice were divided into 2 groups; one cohort was con-ditioned with 3 Gy TBI and MR1 treatment, whereas another received 9.5 Gy TBI. Mice in both groups then received BCF1 whole BMC.
As shown in Fig. 4, BW decreased significantly in the X-CGD mice (n = 5) given 9.5 Gy with allo-BMT, with the maximum mean reduction level reaching 82.4 ± 3.6 % of baseline values at day 3 (P < 0.003 versus pre-treatment). In contrast, the X-CGD recipient mice (n = 5) given 3 Gy TBI and MR1 with allo-BMT did not show significant BW loss throughout the observation period. By day 32, BW eventually recovered to pre-treatment levels in all mice in the 9.5 Gy group. This result indicated that overt acute GvHD was not apparent in either group and that condition-ing toxicity was evident only in mice given 9.5 Gy of TBI. Conversely, within an observation period up to 30 days nei-ther complication manifested in X-CGD mice given 3 Gy of TBI with MR1 MoAb.
Stable maintenance of functional neutrophils derived from haploidentical transplants in PB of X‑CGD F1 recipient mice
We first confirmed that the APF dye assay was suitable for monitoring outcomes in transplantation experiments using X-CGD mouse models (supplementary Fig. 4). We then monitored emergence and maintenance of functional-neu-trophil populations in X-CGD F1 mice after haplo-BMT. As demonstrated, all the recipient mice that showed chi-merism in lymphocytes had both APF+ and APF− PMNs (Fig. 5a, chimeric X-CGD F1). As expected, two X-CGD F1 mice with no detectable donor lymphocytes showed no APF+ neutrophils (non-chimeric X-CGD F1), indicating failure in engraftment of transplanted hematopoietic stem cells (HSCs). The percentages of APF+ PMNs in 16 chi-meric X-CGD mice varied from 15.2 to 88.2 % 4 weeks after BMT. All the while, APF+ neutrophils in individu-als were both stable and long-lasting (Fig. 5b). The level of APF+ neutrophils in chimeric mice paralleled the level
Fig. 3 Favorable safety features of the CD40–CD40L blockade-based conditioning regimen. In this experiment (the second), mice in each of 2 groups received donor splenic CD3+ T cells (spT) in addi-tion to undergoing haploidentical BMT. a Complete blood count and b body weight (BW) were monitored over time. Seven recipient mice were treated in each group (n = 7), and one of them was killed for histological analysis on day 7 after transplantation (n = 6 thereafter).
WBC white blood cells, Hb hemoglobin, Plt platelet. Open square receiving 3 Gy of TBI and MR1 with donor BMT + spT; filled cir-cle receiving 9.5 Gy of TBI with donor BMT + spT. Results were expressed as means ± SD. With a linear mixed model, the overall difference in the kinetics of BW change was statistically significant between groups (P < 0.001). The differences between groups were also tested at each time point. *P < 0.05, **P < 0.01, ***P < 0.001

Y. Takeuchi et al.
1 3
of donor B cell chimerism shown in Fig. 2 and was main-tained for up to 1 year. Considering the short half-life of circulating neutrophils, a stable supply of functional neutrophils must indicate that robust engraftment was achieved for haploidentical donor HSCs in X-CGD F1 BM.
Chimeric X‑CGD F1 mice experienced remission of hyper‑inflammatory status via reconstitution of hematopoiesis with functional allogeneic neutrophils
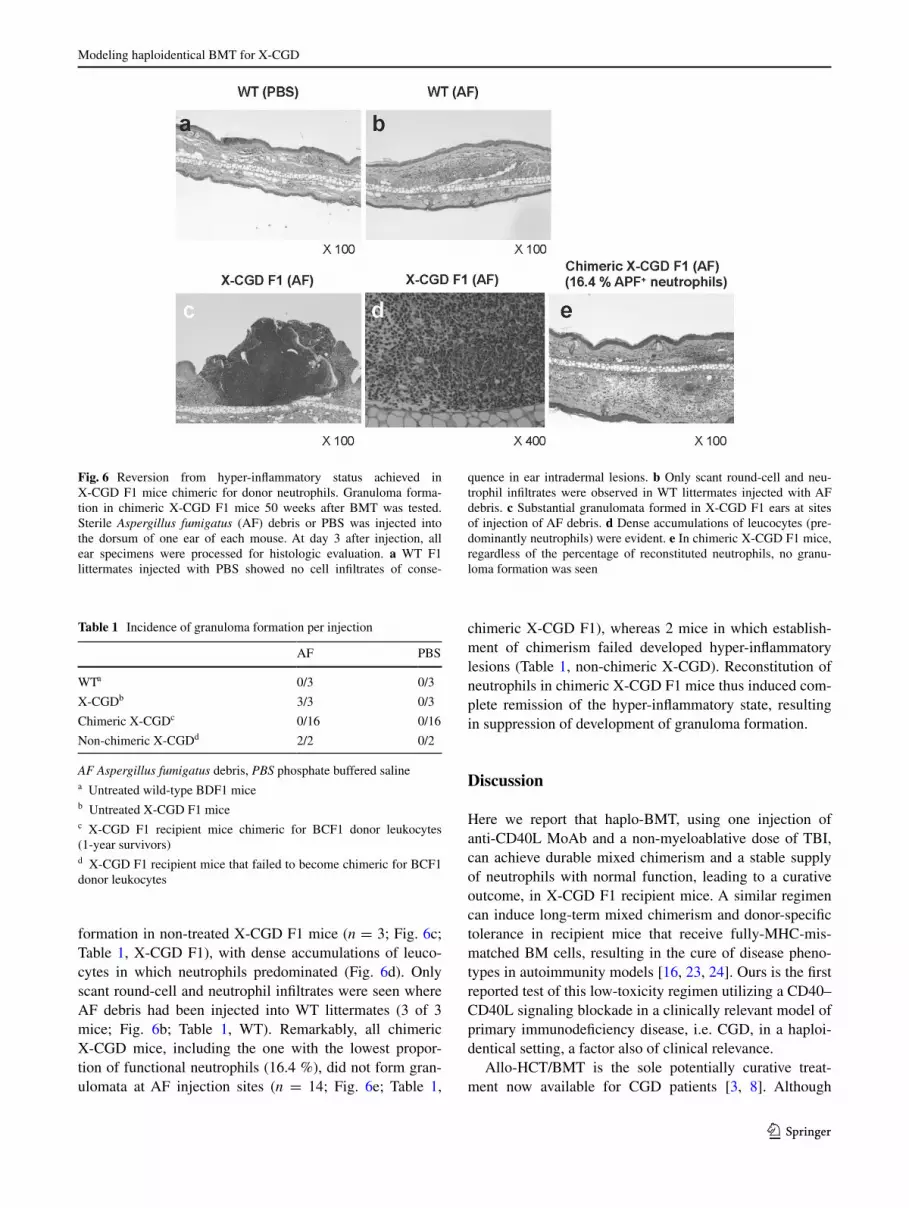
Finally, to assess whether reconstituted functional neutro-phils in chimeric X-CGD F1 mice conferred a therapeutic effect, we evaluated granuloma formation after intradermal injection of AF debris ~50 weeks after BMT, the endpoint for the observation of peripheral-donor chimerism. We took this approach (that of Petersen et al.) as an in vivo assay system [20] to evaluate the efficacy of experimental BMT in CGD mice. As expected, non-transplanted WT F1 lit-termates and X-CGD F1 mice (n = 3 each) injected with phosphate-buffered saline (PBS) showed no significant cell infiltrate in auricular intradermal lesions (Fig. 6a; and data not shown). Overall, PBS injection did not induce any inflammatory lesions in any mouse tested (Table 1). In con-trast, injection of AF debris induced significant granuloma
Fig. 4 Body weight loss not observed in X-CGD recipients treated with simplified haploidentical BMT. As an indicator of overt GvHD and conditioning toxicity, body weight (BW) was measured daily after treatment. The reduction level in BW reached 82.4 ± 3.6 % of baseline values at day 3 in X-CGD mice given 9.5 Gy with allogeneic BMT. In contrast, the mean level in BW did not alter significantly in X-CGD recipient mice given 3 Gy of TBI and MR1 with allo-BMT within the follow up period. Open square receiving 3 Gy of TBI and MR1 with donor BMT (n = 5); filled circle receiving 9.5 Gy of TBI with donor BMT (n = 5). Results were expressed as means ± SD. With a linear mixed model, the overall difference in the kinetics of BW change was statistically significant between groups (P < 0.001). The differences between groups were also tested at each time point. *P < 0.05, **P < 0.01, ***P < 0.001
Fig. 5 Achievement of stable and long-lasting supply of functional donor neutrophils in X-CGD recipients. Propor-tions of peripheral neutrophils showing sROS producing ability were evaluated at various times after BMT. a All neutrophils from donor BCF1 mice were APF+ (left). The neutrophils from chimeric X-CGD F1 mice included both APF+ and APF− populations, while all neutrophils from non-chimeric X-CGD mice were APF−. b The percentage of APF+ neutrophils in X-CGD F1 individuals was assessed by flow-cytometry analysis at each time point after BMT. Each line and symbol pair represents an individual X-CGD F1 recipient. Since two mice were found dead at 30 weeks (% APF+ 78.2 %) and 40 weeks (% APF+ 81.0 %) after BMT, only 14 of 16 chimeric X-CGD F1 mice were observed for one full year
Modeling haploidentical BMT for X-CGD
1 3
formation in non-treated X-CGD F1 mice (n = 3; Fig. 6c; Table 1, X-CGD F1), with dense accumulations of leuco-cytes in which neutrophils predominated (Fig. 6d). Only scant round-cell and neutrophil infiltrates were seen where AF debris had been injected into WT littermates (3 of 3 mice; Fig. 6b; Table 1, WT). Remarkably, all chimeric X-CGD mice, including the one with the lowest propor-tion of functional neutrophils (16.4 %), did not form gran-ulomata at AF injection sites (n = 14; Fig. 6e; Table 1,
chimeric X-CGD F1), whereas 2 mice in which establish-ment of chimerism failed developed hyper-inflammatory lesions (Table 1, non-chimeric X-CGD). Reconstitution of neutrophils in chimeric X-CGD F1 mice thus induced com-plete remission of the hyper-inflammatory state, resulting in suppression of development of granuloma formation.
Discussion
Here we report that haplo-BMT, using one injection of anti-CD40L MoAb and a non-myeloablative dose of TBI, can achieve durable mixed chimerism and a stable supply of neutrophils with normal function, leading to a curative outcome, in X-CGD F1 recipient mice. A similar regimen can induce long-term mixed chimerism and donor-specific tolerance in recipient mice that receive fully-MHC-mis-matched BM cells, resulting in the cure of disease pheno-types in autoimmunity models [16, 23, 24]. Ours is the first reported test of this low-toxicity regimen utilizing a CD40–CD40L signaling blockade in a clinically relevant model of primary immunodeficiency disease, i.e. CGD, in a haploi-dentical setting, a factor also of clinical relevance.
Allo-HCT/BMT is the sole potentially curative treat-ment now available for CGD patients [3, 8]. Although
Fig. 6 Reversion from hyper-inflammatory status achieved in X-CGD F1 mice chimeric for donor neutrophils. Granuloma forma-tion in chimeric X-CGD F1 mice 50 weeks after BMT was tested. Sterile Aspergillus fumigatus (AF) debris or PBS was injected into the dorsum of one ear of each mouse. At day 3 after injection, all ear specimens were processed for histologic evaluation. a WT F1 littermates injected with PBS showed no cell infiltrates of conse-
quence in ear intradermal lesions. b Only scant round-cell and neu-trophil infiltrates were observed in WT littermates injected with AF debris. c Substantial granulomata formed in X-CGD F1 ears at sites of injection of AF debris. d Dense accumulations of leucocytes (pre-dominantly neutrophils) were evident. e In chimeric X-CGD F1 mice, regardless of the percentage of reconstituted neutrophils, no granu-loma formation was seen
Table 1 Incidence of granuloma formation per injection
AF Aspergillus fumigatus debris, PBS phosphate buffered salinea Untreated wild-type BDF1 miceb Untreated X-CGD F1 micec X-CGD F1 recipient mice chimeric for BCF1 donor leukocytes (1-year survivors)d X-CGD F1 recipient mice that failed to become chimeric for BCF1 donor leukocytes
AF PBS
WTa 0/3 0/3
X-CGDb 3/3 0/3
Chimeric X-CGDc 0/16 0/16
Non-chimeric X-CGDd 2/2 0/2

Y. Takeuchi et al.
1 3
corrective gene transfer into HSCs has been attempted as a form of treatment for CGD patients, it has so far proven not to be curative, though surely beneficial [25]. Of note is that CGD treatment results with allo-HCT using HLA-matched unrelated donors have improved in recent years [15, 26, 27]. However, it remains uncertain what combi-nation of conditioning regimens and donor sources should be selected for each CGD patient. As a consequence of attempts to minimize conditioning toxicity, risk of graft failure, and incidence of GvHD, a wide variety of condi-tioning regimens has been reported [8, 14, 27–30], making it difficult to compare one regimen with another. Also to be noted is that only very limited numbers of CGD patients undergoing haplo-BMT have been reported [11, 26]. Our results thus propose a new strategy, one still at the stage of murine BMT modeling, which permits use of haploiden-tical donors in allo-BMT for CGD with a simplified regi-men. The dose of TBI proven effective in this experiment is the same as the one that Kang et al. [8] used for the patients who received unrelated donor grafts in their recent CGD allo-HCT trial. To use TBI with this dose may have advan-tages over other high intensity regimens that typically use treatment associated with significantly toxic effects on the recipients; such effects typically inhere in the use of busul-fan, a chemotherapeutic drug commonly used in condition-ing regimens for CGD allo-HCT [8]. In fact, an X-CGD patient who received a myeloablative dose of busulfan as a conditioning reagent in successful haplo-BMT experienced periods of myelosuppression that required frequent transfu-sions [26]. Although our regimen was found to induce mild myelosuppression, this effect was modest and “non-life-threatening”. We therefore think it reasonable to aim for the development of a low-toxicity regimen based on co-stimu-latory blockade, which is suitable in a haplo-BMT setting for CGD patients suffering from ongoing infections at the time of transplantation.
Also important is that long-lasting, stable mixed chi-merism was achieved in recipients of haploidentical donor grafts. Such stable mixed chimerism indeed has been reported in some CGD allo-HCT trials [14, 30]. Although our stance may excite controversy, we believe that mixed chimerism is to be favored for CGD patients receiving allo-HCT, because: (1) the regimen necessitates only con-ditioning milder than that aiming at full-donor chimerism; (2) even low level chimerism (~10 %) is expected to lead to disease cure [31]; (3) mixed chimerism may advanta-geously confer upon patients resistance to GvHD [32]. That no significant BW loss was observed indicates that the anti-CD40L MoAb-based regimen caused neither overt GvHD nor conditioning-related toxicity. This aspect of resistance to GvHD induction was further confirmed by the extreme experiment in which allogeneic T cells were added to maximize graft-versus-host effector forces. The induction
of stable mixed BM chimerism is thought to require dele-tional and non-deletional tolerance mechanisms, includ-ing T cell anergy or regulation for peripheral tolerance (effected by anti-CD40L MoAb in the early phase after BMT [33–35] ). Central tolerance will follow in the later phase (∼8–10 weeks after BMT) with negative selection of donor and recipient reactive T cells induced in the recipient thymus [33–35]. Accordingly, levels of donor cell chimer-ism remain strikingly stable up to as long as 50 weeks after BMT in our haploidentical model. Although all WT BDF1 recipients showed donor-cell chimerism in a TBI-dose titration experiment, 2 of 18 X-CGD F1 recipient mice (11.1 %) failed to establish detectable donor chimerism (Figs. 2, 5b). This may indicate that the minimum dose of TBI necessary to achieve donor chimerism in all recipients is higher for X-CGD mice than that for WT mice, due to the hyper-inflammatory status of the former [4, 20]. Lev-els of donor-cell chimerism varied greatly among 16 chi-meric X-CGD F1 mice, with the 2 lowest values 16.4 and 29.9 % (% APF+ neutrophils). Of importance is that all chimeric X-CGD F1 mice, including these 2 mice, showed resistance to cutaneous granuloma formation in response to sterile AF-debris injection. This in vivo assay is a demon-stratedly useful functional test in evaluation of the efficacy of curative treatment for X-CGD mice [20]. We therefore consider our strategy curative, as we have demonstrated that established long-term mixed chimerism with haploi-dentical hematopoietic cells suffices to return hyper-inflam-matory CGD status to normal in BMT recipients, thereby potentially sufficing to prevent the development of multiple granulomata in vital organs [4].
As selective blockade of CD40–CD40L signaling has emerged as an attractive target for modulation of immune reaction and inflammation, this was incorporated into the regimen in our study. Anti-CD40L therapy results in pro-tection from autoimmunity, inflammation, and transplant rejection in various preclinical models [36]. Based on the favorable features shown in these studies, several clinical trials of anti-CD40L therapy were initiated for certain types of autoimmune diseases [37, 38]. Although favorable clini-cal effects were achieved using anti-CD40L IgG1 MoAbs, serious concerns arose regarding safety after arterial and venous thromboembolic complications were reported in these clinical trials and in preclinical primate experiments [37, 39]. These events led to cessation of any clinical tri-als using anti-human CD40L MoAbs, but also prompted researchers to study mechanisms underlying the undesir-able complications. Recent data suggest that activation and aggregation of platelets are induced by binding of the anti-CD40L MoAb to the activating FcγRIIA (CD32a) receptor on platelets through its Fc domain [40]. Xie et al. [41] very recently reported a novel anti-human CD40L MoAb with a modified IgG1 tail that showed no binding to FcγRIIA,

Modeling haploidentical BMT for X-CGD
1 3
thus lacking the capacity to activate platelets. Remark-ably, this modified MoAb was thought to reduce the risk of thromboembolism, but still exhibited notably efficacious immunomodulatory activity in various preclinical models [41]. We thus believe that newly engineered anti-CD40L MoAb with enhanced safety features will be available for clinical applications. Although further preclinical studies are needed, as is re-assessment of anti-CD40L therapy in clinical settings, perhaps clinical application of our allo-HCT regimen will become realistic for CGD patients in future.
Acknowledgments We thank Dr. A. S. Knisely for critical read-ing of the manuscript, Dr. Michiko Abe for the Aspergillus fumigatus debris suspension, Dr. Yasuteru Urano for fluorescent probes and his technical advice, Dr. Yasunori Ota for histopathological analysis, and Dr. Masanori Nojima for statistical analysis. This work was supported in part of by a JSPS KAKENHI Grant-in-Aid for Yasuo Takeuchi and Makoto Otsu, and by grants from the Ministry of Health, Labor and Welfare and National Center for Child Health and Development (M. Onodera).
Conflict of interest The authors declare that they have no conflict of interest.
References
1. Winkelstein JA, Marino MC, Johnston RB Jr, Boyle J, Curnutte J, Gallin JI, et al. Chronic granulomatous disease. Report on a national registry of 368 patients. Medicine. 2000;79(3):155–69.
2. Holland SM. Chronic granulomatous disease. Clin Rev Allergy Immunol. 2010;38(1):3–10.
3. Seger RA. Advances in the diagnosis and treatment of chronic granulomatous disease. Curr Opin Hematol. 2011;18(1):36–41.
4. Kuijpers T, Lutter R. Inflammation and repeated infections in CGD: two sides of a coin. Cell Mol Life Sci. 2012;69(1):7–15.
5. Lindahl JA, Williams FH, Newman SL. Small bowel obstruction in chronic granulomatous disease. J Pediatr Gastroenterol Nutr. 1984;3(4):637–40.
6. Morgenstern DE, Gifford MA, Li LL, Doerschuk CM, Din-auer MC. Absence of respiratory burst in X-linked chronic granulomatous disease mice leads to abnormalities in both host defense and inflammatory response to Aspergillus fumigatus. J Exp Med. 1997;185(2):207–18.
7. Ahlin A, Fugelang J, de Boer M, Ringden O, Fasth A, Winiar-ski J. Chronic granulomatous disease-haematopoietic stem cell transplantation versus conventional treatment. Acta Paediatr. 2013;102(11):1087–94.
8. Kang EM, Marciano BE, DeRavin S, Zarember KA, Holland SM, Malech HL. Chronic granulomatous disease: overview and hematopoietic stem cell transplantation. J Allergy Clin Immunol. 2011;127(6):1319–26 (quiz 27–28).
9. Maeda Y. Pathogenesis of graft-versus-host disease: innate immunity amplifying acute alloimmune responses. Int J Hema-tol. 2013;98(3):293–9.
10. Paczesny S, Raiker N, Brooks S, Mumaw C. Graft-versus-host disease biomarkers: omics and personalized medicine. Int J Hematol. 2013;98(3):275–92.
11. Kikuta A, Ito M, Mochizuki K, Akaihata M, Nemoto K, Sano H, et al. Nonmyeloablative stem cell transplantation for
nonmalignant diseases in children with severe organ dysfunc-tion. Bone Marrow Transplant. 2006;38(10):665–9.
12. Gozdzik J, Pituch-Noworolska A, Skoczen S, Czogala W, Wedry-chowicz A, Baran J, et al. Allogeneic haematopoietic stem cell transplantation as therapy for chronic granulomatous disease—single centre experience. J Clin Immunol. 2011;31(3):332–7.
13. Gungor T, Halter J, Klink A, Junge S, Stumpe KD, Seger R, et al. Successful low toxicity hematopoietic stem cell transplan-tation for high-risk adult chronic granulomatous disease patients. Transplantation. 2005;79(11):1596–606.
14. Horwitz ME, Barrett AJ, Brown MR, Carter CS, Childs R, Gallin JI, et al. Treatment of chronic granulomatous disease with non-myeloablative conditioning and a T-cell-depleted hematopoietic allograft. N Engl J Med. 2001;344(12):881–8.
15. Hasegawa D, Fukushima M, Hosokawa Y, Takeda H, Kawasaki K, Mizukami T, et al. Successful treatment of chronic granu-lomatous disease with fludarabine-based reduced-intensity conditioning and unrelated bone marrow transplantation. Int J Hematol. 2008;87(1):88–90.
16. Takeuchi Y, Ito H, Kurtz J, Wekerle T, Ho L, Sykes M. Earlier low-dose TBI or DST overcomes CD8+ T-cell-mediated allore-sistance to allogeneic marrow in recipients of anti-CD40L. Am J Transplant. 2004;4(1):31–40.
17. Pollock JD, Williams DA, Gifford MA, Li LL, Du X, Fisher-man J, et al. Mouse model of X-linked chronic granulomatous disease, an inherited defect in phagocyte superoxide production. Nat Genet. 1995;9(2):202–9.
18. Setsukinai K, Urano Y, Kakinuma K, Majima HJ, Nagano T. Development of novel fluorescence probes that can reliably detect reactive oxygen species and distinguish specific species. J Biol Chem. 2003;278(5):3170–5.
19. Tomita Y, Sachs DH, Khan A, Sykes M. Additional monoclonal antibody (mAB) injections can replace thymic irradiation to allow induction of mixed chimerism and tolerance in mice receiving bone marrow transplantation after conditioning with anti-T cell mABs and 3-Gy whole body irradiation. Transplantation. 1996;61(3):469–77.
20. Petersen JE, Hiran TS, Goebel WS, Johnson C, Murphy RC, Azmi FH, et al. Enhanced cutaneous inflammatory reactions to Aspergillus fumigatus in a murine model of chronic granuloma-tous disease. J Invest Dermatol. 2002;118(3):424–9.
21. Durham MM, Bingaman AW, Adams AB, Ha J, Waitze SY, Pear-son TC, et al. Cutting edge: administration of anti-CD40 ligand and donor bone marrow leads to hemopoietic chimerism and donor-specific tolerance without cytoreductive conditioning. J Immunol. 2000;165(1):1–4.
22. Wekerle T, Kurtz J, Ito H, Ronquillo JV, Dong V, Zhao G, et al. Allogeneic bone marrow transplantation with co-stimulatory blockade induces macrochimerism and tolerance without cytore-ductive host treatment. Nat Med. 2000;6(4):464–9.
23. Nikolic B, Takeuchi Y, Leykin I, Fudaba Y, Smith RN, Sykes M. Mixed hematopoietic chimerism allows cure of autoimmune dia-betes through allogeneic tolerance and reversal of autoimmunity. Diabetes. 2004;53(2):376–83.
24. Takeuchi E, Shinohara N, Takeuchi Y. Cognate interaction plays a key role in the surveillance of autoreactive B cells in induced mixed bone marrow chimerism in BXSB lupus mice. Autoim-munity. 2011;44(5):363–72.
25. Grez M, Reichenbach J, Schwable J, Seger R, Dinauer MC, Thrasher AJ. Gene therapy of chronic granulomatous disease: the engraftment dilemma. Mol Ther. 2011;19(1):28–35.
26. Hoenig M, Niehues T, Siepermann K, Jacobsen EM, Schutz C, Furlan I, et al. Successful HLA haploidentical hematopoietic SCT in chronic granulomatous disease. Bone Marrow Trans-plant. 2014;49(10):1337–8.
27. Seger RA, Gungor T, Belohradsky BH, Blanche S, Bordigoni P, Di Bartolomeo P, et al. Treatment of chronic granulomatous

Y. Takeuchi et al.
1 3
disease with myeloablative conditioning and an unmodified hemopoietic allograft: a survey of the European experience, 1985–2000. Blood. 2002;100(13):4344–50.
28. Martinez CA, Shah S, Shearer WT, Rosenblatt HM, Paul ME, Chinen J, et al. Excellent survival after sibling or unrelated donor stem cell transplantation for chronic granulomatous disease. J Allergy Clin Immunol. 2012;129(1):176–83.
29. Soncini E, Slatter MA, Jones LB, Hughes S, Hodges S, Flood TJ, et al. Unrelated donor and HLA-identical sibling haemat-opoietic stem cell transplantation cure chronic granulomatous disease with good long-term outcome and growth. Br J Haema-tol. 2009;145(1):73–83.
30. Schuetz C, Hoenig M, Schulz A, Lee-Kirsch MA, Roesler J, Friedrich W, et al. Successful unrelated bone marrow transplan-tation in a child with chronic granulomatous disease complicated by pulmonary and cerebral granuloma formation. Eur J Pediatr. 2007;166(8):785–8.
31. Dinauer MC, Gifford MA, Pech N, Li LL, Emshwiller P. Vari-able correction of host defense following gene transfer and bone marrow transplantation in murine X-linked chronic granuloma-tous disease. Blood. 2001;97(12):3738–45.
32. Sykes M. Mixed chimerism and transplant tolerance. Immunity. 2001;14(4):417–24.
33. Fehr T, Takeuchi Y, Kurtz J, Wekerle T, Sykes M. Early regu-lation of CD8 T cell alloreactivity by CD4+ CD25- T cells in recipients of anti-CD154 antibody and allogeneic BMT is fol-lowed by rapid peripheral deletion of donor-reactive CD8+ T cells, precluding a role for sustained regulation. Eur J Immunol. 2005;35(9):2679–90.
34. Kurtz J, Shaffer J, Lie A, Anosova N, Benichou G, Sykes M. Mechanisms of early peripheral CD4 T-cell tolerance induction
by anti-CD154 monoclonal antibody and allogeneic bone mar-row transplantation: evidence for anergy and deletion but not regulatory cells. Blood. 2004;103(11):4336–43.
35. Wekerle T, Sayegh MH, Hill J, Zhao Y, Chandraker A, Swenson KG, et al. Extrathymic T cell deletion and allogeneic stem cell engraftment induced with costimulatory blockade is followed by central T cell tolerance. J Exp Med. 1998;187(12):2037–44.
36. Elgueta R, Benson MJ, de Vries VC, Wasiuk A, Guo Y, Noelle RJ. Molecular mechanism and function of CD40/CD40L engage-ment in the immune system. Immunol Rev. 2009;229(1):152–72.
37. Boumpas DT, Furie R, Manzi S, Illei GG, Wallace DJ, Balow JE, et al. A short course of BG9588 (anti-CD40 ligand antibody) improves serologic activity and decreases hematuria in patients with proliferative lupus glomerulonephritis. Arthritis Rheum. 2003;48(3):719–27.
38. Patel VL, Schwartz J, Bussel JB. The effect of anti-CD40 ligand in immune thrombocytopenic purpura. Br J Haematol. 2008;141(4):545–8.
39. Kawai T, Andrews D, Colvin RB, Sachs DH, Cosimi AB. Thromboembolic complications after treatment with monoclonal antibody against CD40 ligand. Nat Med. 2000;6(2):114.
40. Robles-Carrillo L, Meyer T, Hatfield M, Desai H, Davila M, Langer F, et al. Anti-CD40L immune complexes potently acti-vate platelets in vitro and cause thrombosis in FCGR2A trans-genic mice. J Immunol. 2010;185(3):1577–83.
41. Xie JH, Yamniuk AP, Borowski V, Kuhn R, Susulic V, Rex-Rabe S, et al. Engineering of a novel anti-CD40L domain antibody for treatment of autoimmune diseases. J Immunol. 2014;192(9):4083–92.





























