Embed Size (px)
Citation preview

Current Issues in the Staging of Esophageal Cancer Michael T.Jaklitsch, David H. Harpole, Jr, Elizabeth A. Healey, and DavidJ. Sugarbaker Staging technology and the 1983 international staging system for esophageal cancer have changed. The 1988 system is based on depth of wall penetration and regional lymph node involvement; it abandons the previ- ous criteria of tumor length and degree of obstruction. The clinical reasoning behind this change is reviewed. New staging technology includes chest computed to- mography (CT), magnetic resonance imaging (MRI), transesophageal ultrasound (EUS), and invasive surgical staging. Overall accuracy of CT to predict depth of penetration is 80% to 85%. CT accuracy of regional lymph node status is less than 69%, but it is 90% accurate in the detection of distant metastases. MRI is comparable. EUS is 71% to 98% accurate in predicting depth of tumor invasion. Although highly sensitive (85%
to 95%), the accuracy of EUS in predicting the status of lymph nodes is adversely affected by low specificity (50% to 60%), reducing its overall accuracy of node prediction to 70% to 88%. EUS may fail to assess intra-abdominal disease in 21% to 36% of patients secondary to esophageal obstruction. Regional nodes on both sides of the diaphragm can be assessed by laparoscopy combined with thoracoscopy. Thoracos. copy and laparoscopy have a greater than 92% accuracy in staging regional nodes. Such information is indispens- able for the design of treatment fields. Combinations of these new technologies may provide improved preresec- tional staging. Copyright �9 1994 by W.B. Saunders Company
C arcinoma of the esophagus continues to be a major health problem. Currently, it accounts
for 4% of all cancers in the United States, and the American Cancer Society estimates 13,000 new cases will be diagnosed in this country in 1993. L Although basic science knowledge of the disease has increased, overall survival has remained disappointingly low, with most reports in the range of 15%. This is probably because of the aggressive biological behav- ior of the disease and to the late presentation of patients with esophageal cancer. Most presenting lesions are full thickness of the esophagus (T3, T4) or involve lymph nodes (N1).
There has been great interest in the possible role of induction chemotherapy and radiotherapy for esophageal cancer to increase the number of curative resections and ultimate survivals. Treatment strate- gies based on careful surgical-pathological staging facilitate the critical assessment of treatment effi- cacy. If it were possible to achieve exact preoperative staging information in esophageal cancer, patients could be stratified into those felt to be at "high risk" and, thus, likely to benefit from preoperative chemo- therapy and radiation therapy, and those felt to be at "low risk" who might be better treated with immedi-
From the Division of Thoracic Surgery, Brigham and Women's Hospital, and The Joint Center for Radiation Therapy, Boston, MA.
Address reprint requests to David Sugarbaker, MD, Division of Thoracic Surgery, Brigham and Women's Hospital, 75 Francis St, Boston, MA 02115.
Copyright �9 1994 by W.B. Saunders Company 1053-4296/94/0403-0002505.00/0
ate resection. This strategy might enable the physi- cian to tailor treatment options to appropriate pa- tient populations and thereby spare certain subgroups the morbidity associated with one or more treatment modalities. Unfortunately, the staging tools for esophageal cancer have not been precise.
Over the past decade, staging technology and the international staging system for esophageal cancer have changed. There is a growing body of knowledge of the disease and an increasingly sophisticated methodology to assess the degree of spread before resection. Esophageal cancer staging has evolved from the diagnostic tools of a physical examination, chest radiograph, barium swallow, and esophagos- copy, to chest computed tomography (CT) scanning, and consideration of transesophageal ultrasound and various invasive staging procedures. Admittedly, this has led to more costly workups involving multiple specialists, but it is driven by the belief that accurate staging information will provide a foundation upon which to tailor therapy to specific patient subgroups.
Several controversies have developed regarding the best methods to adequately evaluate the esopha- geal cancer patient and what variables should be emphasized to stratify patients for treatment. The goal of this article is to accurately review assessment and staging in esophageal cancer.
Esophageal Staging Systems Accurate staging is important to assess new treat- ments, and advise individual patients of prognosis. The TNM classification, based on independent mea-
Seminars in Radiation Oncology, Vol 4, No 3 (July), 1994.'pp 135-145 1 3 5

136 Jaklitsch et al
sures of primary Tumor size, regional lymph Node involvement, and distant Metastases, forms the basis of stratifying esophageal cancer patients into prognos- tic stage groups.
International consensus for esophageal cancer staging was reached in 1988 with worldwide approval from all national TNM committees for the fourth edition of the Union Internationale Contre le Cancer (UICC) classification 2 and the third edition of the American Joint Committee on Cancer (AJCC) Manual for Staging of Cancer. 3 The new system is based on depth of wall penetration and lymph node involvement, these two variables being most predic- tive of long-term survival. However, controversy ex- ists about whether this new system is practical for most patients, and whether it properly stratifies groups by prognosis.
An historical perspective helps in understanding the controversies associated with the current staging system. The first widely used international staging system for esophageal cancer was developed by the AJCC, published by the UICC in 1968, and revised in 1974 and 1978. 4 There have been four editions of the AJCC classification: 1978, 5 1983, 6 1988, 3 and 1992. 7 The only major changes occurred between the 1983 and the current 1988 editions (Table 1).
Current controversies in preresectional staging of esophageal cancer stem from the changes in the 1988 AJCC edition. At that time, the 1983 clinical classification based on palpable supraclavicular nodes, length of tumor, and degree of esophageal obstruc- tion by tumor was abandoned for the new pathological classification based on regional nodes and depth of wall penetration in the resection specimen. In the 1983 clinical classification, regional nodes were not assessed for the intrathoracic esophagus because these were "not ordinarily accessible for clinical evaluation. ''6 In 1988, tumor classification was changed so that it was based solely on depth of invasion. Invasion of adjacent structures was classi- fied as T4. Nodal stage was simplified to NO disease for no regional node metastases and N1 for any regional node metastases. The perigastric lymph nodes were classified as regional nodes for the intra- thoracic esophagus, instead of M1 disease. Further- more, stage II disease was further subdivided into stage IIA and IIB, depending on whether regional nodes were involved.
T (Primary Tumor) Classification
Japan has organized a large retrospective cohort of patients treated with surgical resection for analysis of
Table 1. Comparison Between the 1983 and 1987 AJCC TNM Classification and Stage Grouping For Esophageal Cancer
1983 Classification 1988 Classification
Primary tumor (T) clinical classification T1 Tumor involves 5 cm or less of esophageal length,
T2
T3 T4
Nodal involvement (N) NO N1 N2 N3
Distant metastasis (M) M0 M1
Staging grouping Stage I Stage II Stage IIA Stage IIB Stage III Stage IV
produces no obstruction, and no circumferen- tial involvement
Tumor involves more than 5 cm of esophageal length or causes obstruction or involves the circumference of the esophagus
Extraesophageal spread
pathological classification No regional node metastasis Unilateral regional nodes involved Bilateral regional nodes involved Multiple regional nodes involved clinical classification No distant metastasis Distant metastasis
T1, NO, M0 T1, N1-N2, M0 or T2, N0-N2, M0
T3, any N, M0 or any T, N3, M0 AnyT, any N, M1
Tumor invades lamina propria or submucosa
Tumor invades muscularis propria
Tumor invades adventitia Tumor invades adjacent structures
No regional node metastasis Regional node metastasis
No distant metastasis Distant metastasis
TI, NO, M0
T2-T3, NO, M0 T1-T2, N1, M0 T3, N1, M0 or T4, any N, M0 Any T, any N, M1
Data from 19836 and 19883 editions of the AJCC Manual for Cancer Staging.
Staging of Esophageal Cancer 13 7
prognostic variables. The Japanese Society for Esopha- geal Disease published guidelines for clinical and pathological studies on carcinoma of the esophagus in 1969. 8 These guidelines have standardized report- ing of data for esophageal carcinoma in that country and have enabled the study of a large cohort of Japanese patients from 1969 to the present. In 1975, the Japanese Committee for Registration of Esopha- geal Carcinoma Cases began a 234-institute registra- tion of patients with esophageal cancer treated with resection after 1969. By the end of the 1980s, 10,113 patients had been registered?
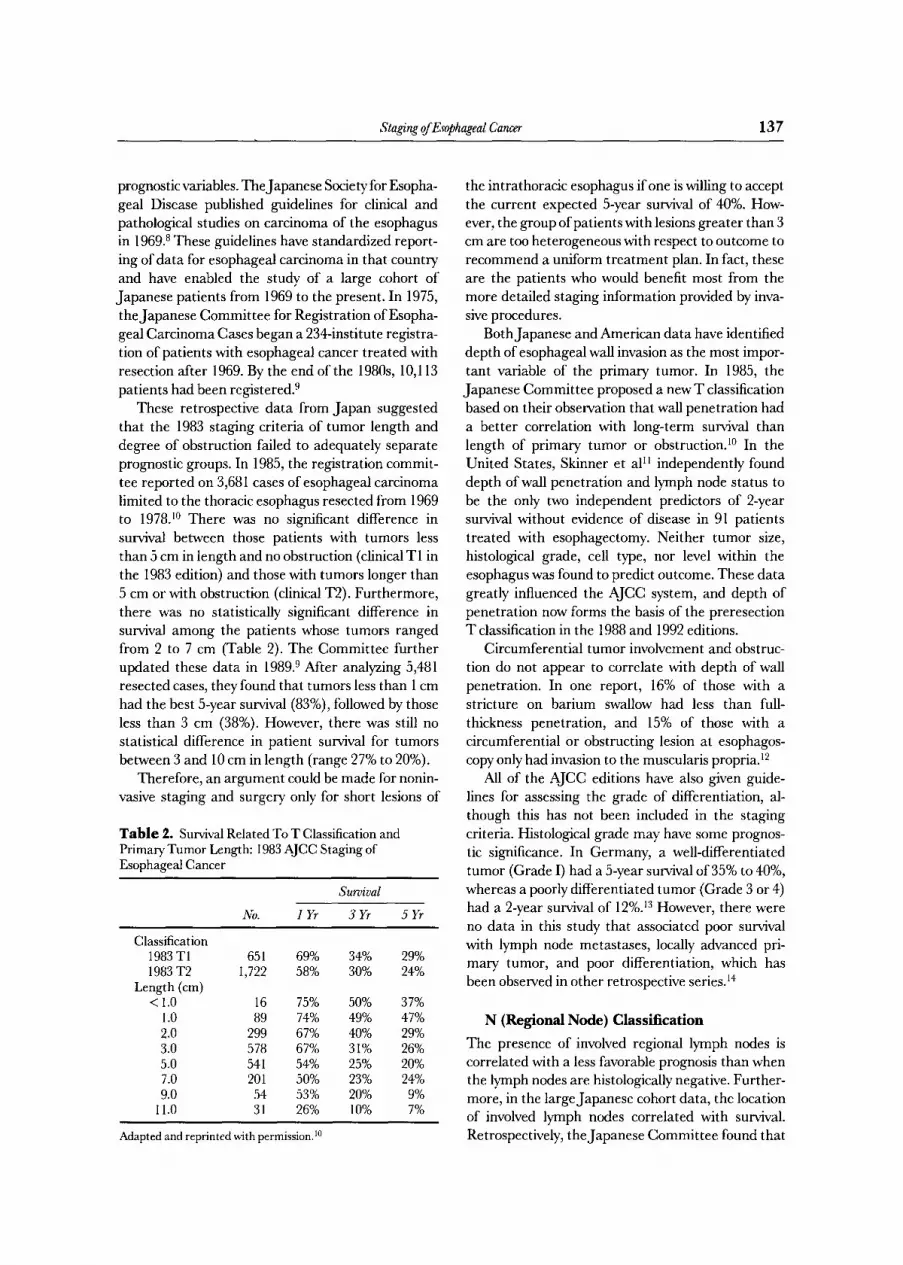
These retrospective data from Japan suggested that the 1983 staging criteria of tumor length and degree of obstruction failed to adequately separate prognostic groups. In 1985, the registration commit- tee reported on 3,681 cases of esophageal carcinoma limited to the thoracic esophagus resected from 1969 to 1978. l~ There was no significant difference in survival between those patients with tumors less than 5 cm in length and no obstruction (clinical T1 in the 1983 edition) and those with tumors longer than 5 cm or with obstruction (clinical T2). Furthermore, there was no statistically significant difference in survival among the patients whose tumors ranged from 2 to 7 cm (Table 2). The Committee further updated these data in 1989. 9 After analyzing 5,481 resected cases, they found that tumors less than 1 cm had the best 5-year survival (83%), followed by those less than 3 cm (38%). However, there was still no statistical difference in patient survival for tumors between 3 and 10 cm in length (range 27% to 20%).
Therefore, an argument could be made for nonin- vasive staging and surgery only for short lesions of
Table 2. Survival Related To T Classification and Primary Tumor Length: 1983 AJCC Staging of Esophageal Cancer
Survival
No. 1 D 3 D 5 D
Classification 1983 T1 651 69% 34% 29% 1983 T2 1,722 58% 30% 24%
Length (cm) < 1.0 16 75% 50% 37%
1.0 89 74% 49% 47% 2.0 299 67% 40% 29% 3.0 578 67% 31% 26% 5.0 541 54% 25% 20% 7.0 201 50% 23% 24% 9.0 54 53% 20% 9%
11.0 31 26% 10% 7%
Adapted and reprinted with permission. 1~
the intrathoracic esophagus if one is willing to accept the current expected 5-year survival of 40%. How- ever, the group of patients with lesions greater than 3 cm are too heterogeneous with respect to outcome to recommend a uniform treatment plan. In fact, these are the patients who would benefit most from the more detailed staging information provided by inva- sive procedures.
Both Japanese and American data have identified depth of esophageal wall invasion as the most impor- tant variable of the primary tumor. In 1985, the Japanese Committee proposed a new T classification based on their observation that wall penetration had a better correlation with long-term survival than length of primary tumor or obstruction, l~ In the United States, Skinner et al I1 independently found depth of wall penetration and lymph node status to be the only two independent predictors of 2-year survival without evidence of disease in 91 patients treated with esophagectomy. Neither tumor size, histological grade, cell type, nor level within the esophagus was found to predict outcome. These data greatly influenced the AJCC system, and depth of penetration now forms the basis of the preresection T classification in the 1988 and 1992 editions.
Circumferential tumor involvement and obstruc- tion do not appear to correlate with depth of wall penetration. In one report, 16% of those with a stricture on barium swallow had less than full- thickness penetration, and 15% of those with a circumferential or obstructing lesion at esophagos- copy only had invasion to the muscularis propria. 12
All of the AJCC editions have also given guide- lines for assessing the grade of differentiation, al- though this has not been included in the staging criteria. Histological grade may have some prognos- tic significance. In Germany, a well-differentiated tumor (Grade I) had a 5-year survival of 35% to 40%, whereas a poorly differentiated tumor (Grade 3 or 4) had a 2-year survival of 12%. 13 However, there were no data in this study that associated poor survival with lymph node metastases, locally advanced pri- mary tumor, and poor differentiation, which has been observed in other retrospective series. 14
N (Regional Node) Classification
The presence of involved regional lymph nodes is correlated with a less favorable prognosis than when the lymph nodes are histologically negative. Further- more, in the large Japanese cohort data, the location of involved lymph nodes correlated with survival. Retrospectively, the Japanese Committee found that

13 8 Jaklitsch eta I
patients with involved paraesophageal, mediastinal, and perigastric metastases had similar long-term survivals, whereas patients with other involved ab- dominal nodes and further distant nodes had a much worse prognosis.l~
Although there is no published analysis of the Japanese cohort data with respect to the prognostic value of the number of histologically involved lymph nodes, other investigators have reported varying thresholds relating the number of involved nodes to different prognostic categories. Abe et al, 14 reporting on 4l Japanese patients, found that no patient with two or more regional nodal metastases lived for 4 years after surgery, whereas the 5-year survival for patients with no or only one metastatic node was 50.9%. These authors do not state what percentage of the latter group had zero nodes involved, although they do observe that there were 3 long-term survivors (45 to 89 months) in the group with a single positive node. When three or more nodes were involved, no patient survived more than 3 years.
As previously mentioned, Skinner's group identi- fied lymph node status and wall penetration as the only independent predictors of 2-year survival for their patients treated with esophagectomy.H Further- more, this group observed that some patients with one to four positive nodes were without evidence of disease at 2 years follow-up, whereas all patients with five or more nodes had died or had recurrent disease at the same time point.
In the German experience, five positive mediasti- nal nodes was an important bench mark) 5 Siewart's analysis of 107 patients treated with en bloc esophage- ctomy showed that none of the 29 patients with five or more positive mediastinal lymph nodes survived greater than 25 months compared with approxi- mately 35% 5-year survival for the 78 patients with fewer than five lymph nodes involved. Furthermore, he reports the survival of patients with fewer than five positive nodes was equal to that of patients without lymph node metastases.
This analysis, which minimizes the clinical signifi- cance of a small number of positive regional nodes, must be viewed with skepticism in view of data from other organ systems. Regional node disease in adeno- carcinoma of other organs is viewed as a harbinger of systemic spread and is often an indication for adju- vant systemic therapy to improve survival. In addi- tion, the overall 35% survival remains unacceptably low for patients with limited nodal disease.
The demographics of esophageal cancer are differ- ent in the United States and Europe compared with Japan. The Japanese series generally involve large
patient numbers with predominantly squamous cell carcinoma. The American series tend to be much smaller, and have a larger percentage of adenocarci- noma, usually involving the gastro-esophageal (GE) junction. Adenocarcinoma of the esophagus may have a different biological behavior than squamous cell carcinoma of the esophagus. Therefore, compari- sons of series including both histologies between the two countries is problematic. The better prognosis of one to four positive nodes identified in the American and German literature may be attributable to the subgroup of patients with adenocarcinoma of the GE junction. This may be a group that benefits from en bloc resection that contains a limited number of involved regional nodes. The United States series that have reported survival advantages associated with radical lymphadenectomy have included large numbers of patients with adenocarcinoma. For in- stance, in the report by DeMeester et al, 16 seven of eight long-term survivors among the curative resec- tion group were diagnosed with adenocarcinoma.
M (Distant Metastases) Classification All reports recognize the dismal prognosis of distant metastatic disease with an average 2-year survival rate of 4%. 1~ However, the definition of distant metastasis has changed. Based on data from the Japanese Committee for Registration of Esophageal Carcinoma, metastases to perigastric lymph nodes from the intrathoracic esophagus is now considered N1 disease, whereas celiac lymph node involvement for tumor at any level of the esophagus is considered M1 disease. The legitimacy of this M1 designation is in doubt given the regional nature of the celiac nodes for tumors on the gastric side of the GEjunction.
The Prognostic Accuracy of the Current Staging System
The ability of the current AJCC classification to accurately predict prognosis in Japanese patients with squamous cell carcinoma of the intrathoracic esophagus was analyzed by an additional report by Iizuka et al in 1989. 9 The 10-year survival rates of 5,071 survivors of resection were analyzed according to the 1988 TNM stage of disease (Fig 1). There was a clear difference between each of the five groups, supporting the use of esophageal wall penetration and regional node status as important prognostic factors.
Application of the AJCC 1988 TNM system to patients in the United States has not been as success- ful as in Japan. Ellis et a117 analyzed 265 patients surviving esophageal resection from 1970 to 1988 but

Staging of Esophageal Cancer 139
F igure 1. Survival of Japa- nese patients according to stage of disease using the new- est (1988 and 1992) AJCC TNM classification of esopha- geal cancer. (Data from Ii- zuka et al. 9)
1 0 0
(.9 8 0 z > > it" 6 0
03
I - z 4 0 LLI O r r LLI 13. 2 0
\ -. ,, " - , .
'.,, ........... "\
*~'~
I I I I
1 2 3 4 5
YEARS
S T A G E I
. . . . . S T A G E I IA
. . . . . S T A G E l iB
.......... S T A G E II I
. . . . S T A G E IV
found no difference in survival between stages I and HA, nor between stages IIB and llI (Fig 2). Interest- ingly, they also found one to four positive lymph nodes to have intermediate survival compared with zero or more than four positive nodes.
The greatest on-going controversy concerns the number of positive regional lymph nodes required to be clinically significant. According to the current international staging system, a single positive node relegates a patient to an advanced stage (IIB) and thus to potential candidacy for more aggressive therapy. However, a number of small phase II Ameri- can and German studies suggest that patients with one to four regional node metastases still have limited disease and could be considered candidates for immediate esophagectomy with curative intent, if one is willing to accept the overall survival rate currently reported. At present, there is not sufficient data to resolve this debate.
New Esophageal Cancer Staging Techniques
CT and Magnetic Resonance Imaging (MRI)
CT of the chest and upper abdomen with oral and intravenous contrast has been used over the past decade to evaluate the primary esophageal tumor, supraclavicular nodes, mediastinal nodes, lungs, liver, adrenals, and abdominal nodes. Although initially endorsed enthusiastically for its ability to accurately stage esophageal cancer before resection, recent reports have been more skeptical. 18-22 In general, the
overall accuracy of CT images is 80% to 85% when compared with resection specimens. 23
Evaluation of the primary tumor by CT is not without limitations. The wall thickness of the normal esophagus varies because of the distensibility of the lumen, but 5 mm on a CT image is generally considered the upper limit of normal. Because indi- vidual wall layers cannot be discerned with certainty by CT, T1 tumors cannot be definitively differenti- ated from T2 tumors. 18
CT accuracy of regional lymph node status is less than 69%. 24,25 A recent report found the sensitivity of CT in predicting celiac nodal metastases to be only 48%, but the specificity was 93%? l The current radiologic criterion for an abnormal mediastinal or celiac lymph node is a transverse axis of 10 mm or greater. Thus, nodes less than 10 mm that are infiltrated by tumor will be falsely interpreted as negative and swollen inflammatory nodes may be falsely interpreted as positive. Furthermore, en- larged nodes adjacent to a tumor may be overlooked on a CT scan if such structures are radiographically inseparable.
The CT scan is a very accurate tool for the detection of distant metastases in the chest (lungs) or abdomen (adrenals, nonperigastric nodes, liver). Abdominal metastases in the liver or nodal stations other than the celiac nodes can be detected with 80% sensitivity and 98% specificity by CT scan or with 80% sensitivity and 99% specificity by extracorporeal ultra- sound (US)? I
Siewart et a113 found little difference between the

140 Jaklitsch et al
Percent Survival
100 I I I t I
80
60
40
20
0
~
l _ I l i i
, I !
I I I I I
"., Stage 0 I
" ~ I
"1
.... i. S tage I
0 1
I I I I
I I
. . . . i I
"_.~
.., .......... :,.., Stage I la
~ " i . . . . Stage lib
: . . . . Sta,(]e IV Stage III
2 3 4 5 6 7 8 Years
Figure 2. Survival of Ameri- can patients according to stage of disease using the newest (1988 and 1992) AJCC TNM classification of esophageal cancer. (Copyright �9 1993. Re- printed by permission of John Wiley & Sons, Inc) 7)
predictive values of CT and MRI when compared prospectively with histology in 60 patients. The diag- nostic accuracy for CT was only 60% (sensitivity 31%, specificity 86%). The accuracy of MRI was virtually identical. Assessment of mediastinal nodes was accu- rate in 56% for both modalities (sensitivity 47% to 50%, specificity 59%). Accuracy in assessing abdomi- nal nodes was even less, with only 45% accuracy for CT (sensitivity 12%, specificity 47%) and 46% for MRI (sensitivity 50%, specificity 46%).
Thus, CT scans are very accurate for the assess- ment of distant metastases, yet less accurate in the determination of tumor or node classification. To further improve the accuracy of staging patients with esophageal cancer, CT would need to be combined with other techniques that are better at determining the T and N classification.
Endoesophageal US (EUS) EUS is a relatively new tool used for staging. It consists of a probe at the end of an endoscope and an inflatable balloon to distend the esophagus and provide an ultrasonic interface between the probe
and the mucosa. Transducer heads between 7.5 and 12 MHz (million cycles per second) are available for EUS. In general, the lower the frequency the greater the depth of penetration but the poorer the resolu- tion) 8
The esophageal wall is composed of five layers of alternating hyperechoic and hypoechoic signals in vivo (Fig 3). The first two layers correspond to the mucosa, the third layer to the submucosa, the fourth to the muscularis propria, and the fifth layer to the adventitia. These five layers are seen consistently throughout the entire gastrointestinal tract, al- though overdistension of the examining balloon may make the first three layers appear as one. 26 Unlike CT, the normal wall thickness of the undiseased esophagus as shown by EUS is 3 mm.
EUS is a good tool for the detection of the depth of tumor invasion. A broad range of accuracy is reported, ranging from 71% overall to 98% of those without obstruction. 13,tSa6,27 EUS understages the primary tumor in about 5% of cases. 13,27 It overstages the primary tumor in approximately I I%, especially in tumors that do not extend through the muscutaris

Staging of Esophageal Cancer 141
Figure 3. Diagram and EUS scan of a normal esophagus. Concentric rings of alternating echo density represent: 1, mucosa (hyperechoic); 2, mucosa-submucosa interface (hypoechoic); 3, submucosa (hyperechoic); 4, muscularis propria (hypoechoic); 5, adventitial interface (hyperechoic); and 6, EUS transducer. (Reprinted with permission.18)
propria. Overcompression of the balloon or fibrosis and inflammation in the esophageal wall can blur the five distinct layers. 26 Thus, EUS may prove to have limited ability to "re-stage" patients after a period of induction chemotherapy or radiotherapy.
Unlike CT and MRI, EUS can assess the shape, margin, and internal structure, as well as the size of mediastinal and celiac nodes. However, it has been difficult to distinguish inflammatory lymph nodes from metastatic disease by EUS. Quantification of EUS accuracy for node status has generally ranged between 70% and 88%. 13,18,26,27 Although highly sensi- tive (85% to 95%), the accuracy of predicting the status of lymph nodes is adversely affected by the low specificity (50% to 60%). 13,27 Although EUS is more accurate at assessing regional nodes than CT or MRI, it still tends to overestimate histological involve- ment. This is important to keep in mind for those patients declared "unresectable" based on EUS.
EUS is not very useful in identifying distant metastatic disease. The left lobe of the liver can be seen by EUS overlying the stomach, but the right hepatic lobe and evidence of pulmonary metastases cannot be reliably evaluated with this method. EUS has been reported to have a 69% accuracy in detect- ing metastatic disease, compared with 90% for CT scan.18
At present, EUS fails in a significant number of patients (21% to 36%) secondary to obstruction of the esophagus such that the endoscope cannot be
passed through the lesion and consequently visualiza- tion is greatly limited. 26-28 This, in turn, decreases the sensitivity of EUS to determine abdominal disease into the 45% to 60% range. Smaller echo probes are becoming commercially available, and this may in- crease the utility of EUS. EUS alone is a poor predictor of stage grouping (58% accuracy) because of its inability to pass through stenoses and its lack of specificity in evaluating regional nodes. 27
Accuracy is expected to improve with combina- tions of staging procedures. Botet et a118 compared EUS and CT prospectively in 42 patients. EUS only had a 60% accuracy in predicting clinical stage of disease (primarily because of poor prediction of distant metastases) whereas CT only had a 64% accuracy (primarily because of poor prediction of tumor and nodal classification). Combining these two modalities produced an 86% accuracy in predict- ing disease stage.
Although EUS has certain limitations concerning the N classification, it can provide reliable informa- tion about the degree of wall penetration. If com- bined with a highly accurate means of assessing the regional nodes and distant metastases, such a combi- nation may provide very accurate preresectional staging.
Minimally Invasive Surgical Staging Complete surgical staging requires systematic sam- pling of nodes and identification of distant spread
142 Jaklitsch et al
both above and below the diaphragm. Up to 33% of upper and midthoracic esophageal cancers and 66% of lower thoracic esophageal cancers can be expected to have metastases to the perigastric nodesfl 9 These can be assessed by laparoscopy combined with thora- coscopy in a single two-part procedure.
Preresectional surgical staging was advocated by Murray et al in the 1970s. 3~ They prospectively studied 30 patients with mediastinoscopy and mini- laparotomy before esophageal resection. Seven (23%) had positive mediastinal nodes and 16 (53%) were found to have metastases to the celiac nodes. None of these patients survived more than 1 year after resection. Thus, surgical staging identified a signifi- cant subgroup of patients who might have benefitted from an alternative treatment strategy such as induc- tion chemoradiation. Recent advances in thoracos- copy have opened new vistas for surgical staging of esophageal cancer. Unlike mediastinoscopy, nodes accessible through the thoracoscope are not confined to the anterior mediastinal nodes. Thoracoscopy allows evaluation of the entire thoracic esophagus and periesophageal nodes in the right chest, and the aorto-pulmonary window nodes as well as the mid to lower thoracic esophagus and periesophageal nodes in the left chest. Pleural and pulmonary metastases missed by EUS can be readily identified at thoracos- copy. Furthermore, thoracoscopy can be particularly useful in evaluating the significant number of tumors through which an EUS probe could not be passed. Generally, the right chest is used to gain access to the mediastinum, unless a previous staging procedure has suggested the pathological process is concen- trated in the left hemithorax.
This minimally invasive surgical staging proce- dure allows direct visualization of the adventitia of the esophagus and can accurately judge deep wall invasion and involvement of adjacent organs. The location and nature of contiguous spread to impor- tant mediastinal adjacent structures can be directly assessed. Palpating instruments can be used to judge depth of wall penetration and mobility of the esopha- gus. Regional lymph nodes can be visualized and directly sampled for histological analysis, providing the most specific system for evaluation of mediasti- nal node status.
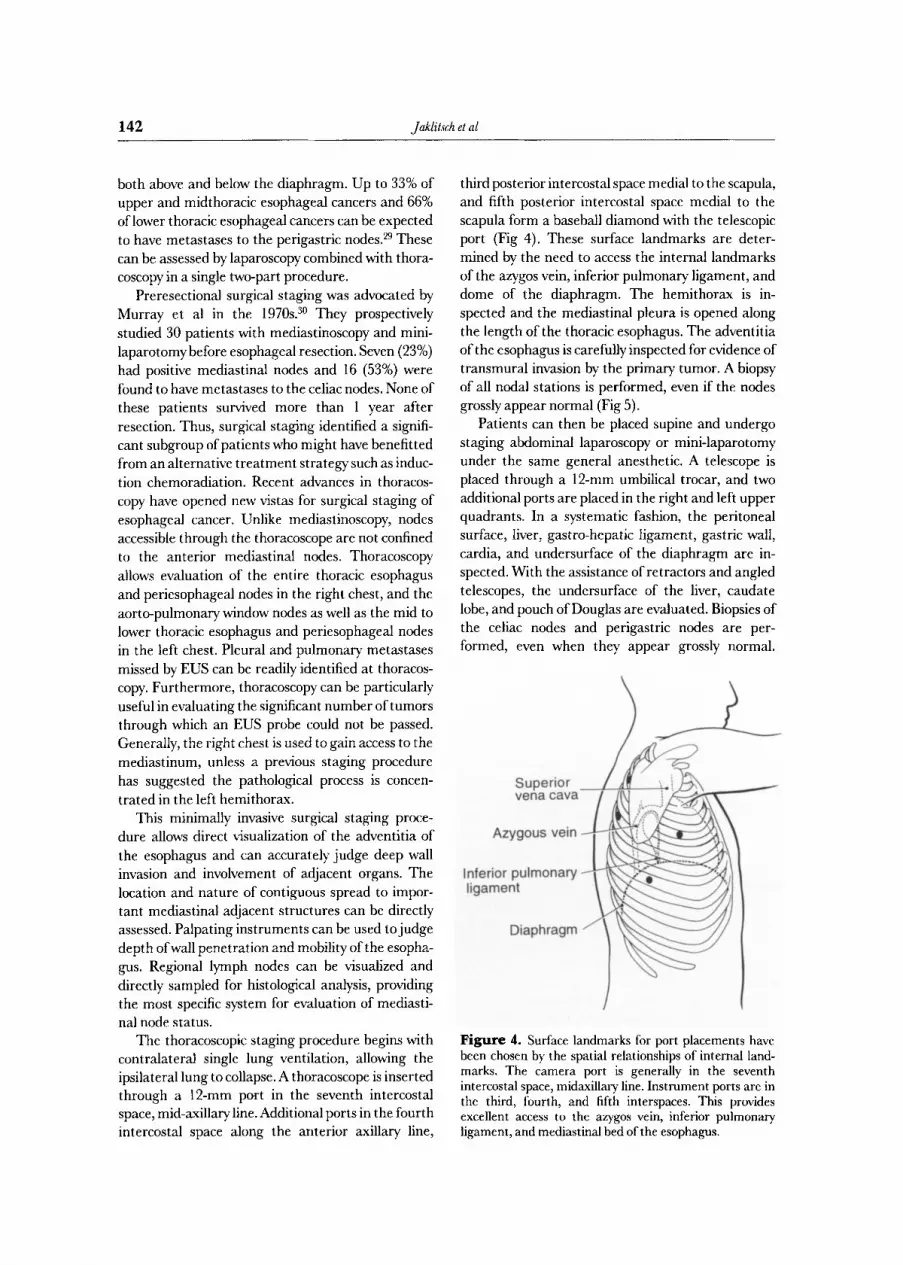
The thoracoscopic staging procedure begins with contralateral single lung ventilation, allowing the ipsilateral lung to collapse. A thoracoscope is inserted through a 12-mm port in the seventh intercostal space, mid-axillary line. Additional ports in the fourth intercostal space along the anterior axillary line,
third posterior intercostal space medial to the scapula, and fifth posterior intercostal space medial to the scapula form a baseball diamond with the telescopic port (Fig 4). These surface landmarks are deter- mined by the need to access the internal landmarks of the azygos vein, inferior pulmonary ligament, and dome of the diaphragm. The hemithorax is in- spected and the mediastinal pleura is opened along the length of the thoracic esophagus. The adventitia of the esophagus is carefully inspected for evidence of transmural invasion by the primary tumor. A biopsy of all nodal stations is performed, even if the nodes grossly appear normal (Fig 5).
Patients can then be placed supine and undergo staging abdominal laparoscopy or mini-laparotomy under the same general anesthetic. A telescope is placed through a 12-rnm umbilical trocar, and two additional ports are placed in the right and left upper quadrants. In a systematic fashion, the peritoneal surface, liver, gastro-hepatic ligament, gastric wall, cardia, and undersurface of the diaphragm are in- spected. With the assistance of retractors and angled telescopes, the undersurface of the liver, caudate lobe, and pouch of Douglas are evaluated. Biopsies of the celiac nodes and perigastric nodes are per- formed, even when they appear grossly normal.
Az
Inferior ligamel
Figure 4. Surface landmarks for port placements have been chosen by the spatial relationships of internal land- marks. The camera port is generally in the seventh intercostal space, midaxillary line. Instrument ports are in the third, fourth, and fifth interspaces. This provides excellent access to the azygos vein, inferior pulmonary ligament, and mediastinal bed of the esophagus.

Staging of Esophageal Cancer 143
F igure 5. View through the camera of the sampling of the azygos node. The mediastinal pleura overlying the esopha- gus has been opened, and the deflated lung retracted anteri- orly. The entire node is re- moved by gentle traction with an endoscopic forceps while a hemostatic clip is placed at the pedicle.
Patients deemed to be candidates for multimodality protocols can then have a mediport and feeding jejunostomy placed at the end of the staging proce- dures.
The Brigham and Women's Hospital, the Univer- sity of Maryland, and the Medical University of South Carolina, have undertaken a prospective trial of thoracoscopic staging for patients with biopsy- proven esophageal cancer. Of the first 49 patients evaluated, 95% had correct staging of the mediasti- nal nodes. Three patients (6%) were correctly down- staged to T3 by direct visualization and assessment of mobility, when other preoperative staging tests had suggested T4 lesions. Thoracoscopic staging was associated with minimal morbidity.
The addition oflaparoscopy to thoracoscopy offers multiple advantages. The diagnostic accuracy of laparoscopy is reported to be 92%. 31 It is superior to CT or US in detecting liver metastases, peritoneal metastases, and celiac node metastases. It can effec- tively diagnose occult cirrhosis of the liver. It also allows histological confirmation of suspected meta- static disease by allowing biopsy under direct vision. The combination of these two minimally invasive staging procedures also enables the clinician to assess the efficacy of drug and radiotherapy by clearly documenting the extent of disease before therapy.
In the series of patients with cancers of the lower third of the esophagus reported by Dagnini et al, 32 metastases to intra-abdominal nodes was detected by
laparoscopy in 3%, and metastases to the stomach wall, peritoneum, or omentum were found in 17%. The false-negative rate was only 4% (1 l of 250) when compared with resection pathology. Watt et a133 reported a 51% sensitivity and 93% specificity for laparoscopic evaluation of abdominal nodes, a 96% accuracy in detecting hepatic metastases, and an 89% accuracy in detecting peritoneal implants. Addi- tionally, there was no morbidity or mortality associ- ated with laparoscopy in any of these reports.
Laparoscopy has little added benefit to offer the subgroup of patients identified to have hepatic metas- tases by CT or US. CT and US have equally high specificity in evaluating hepatic metastases (97%). However, in Watt's series, 8 of 74 patients (11%) with a negative CT and US scan proved to have hepatic metastases and 8 patients had peritoneal implants at laparoscopy. Therefore, laparoscopy offers signifi- cant advantages to those patients with negative CT or ultrasound scans, as well as for those patients with adenopathy identified by CT or US.
The main advantage of the combined thoraco- scopic/laparoscopic staging procedure described above is that it provides greater accuracy in evalua- tion of regional and celiac lymph nodes. Such informa- tion is indispensable in patient stratification and selection of therapy, especially in the setting of new treatment protocols. Furthermore, for patients who will be receiving radiotherapy, the histological status of thoracic and abdominal lymph nodes is critical for

144 Jaklitsch et al
the design of t rea tment fields. For example, for patients with tumors of the lower esophagus, the supraclavicular lymph nodes may be omit ted from the t reatment field in the absence of involved nodes. However, if thoracic nodes are involved, t rea tment fields may be increased to cover the supraclavicular regions because they would represent a higher risk site in this setting. Moreover, the t rea tment of celiac nodes with radiotherapy is controversial because of the M1 status of these nodes and the potential morbidity of upper abdominal radiotherapy. There- fore, some radiation oncologists may choose only to treat perigastric and celiac lymph nodes in the setting of documented involvement. For all these reasons, we believe histological confirmation of the mediastinal and upper abdominal lymph nodes is an important complement to CT and EUS staging information.
We believe these minimally invasive surgical stag- ing techniques could provide preresectional pathologi- cal information regarding the status of the mediasti- nal and celiac nodes. For selected patients we would add a chest CT scan and consideration of EUS, thoracoscopic, and laparoscopic staging to the stan- dard esophageal cancer staging workup of a physical exam, chest radiograph, barium swallow, and esopha- goscopy of a decade ago. This added staging informa- tion is particularly important for patient stratifica- tion and assessment of t reatment efficacy in clinical trials. In an era where alternative induction therapy protocols are available for esophageal cancer, mini- mally invasive surgical staging may provide a new
standard of staging accuracy and protocol assess- ment. Randomized, prospective, multi-institutional trials are needed to validate these techniques. Such trials are currently being developed.
Conclusion
The new staging system requires assessment of depth of wall penetrat ion and lymph node status before resection. To do this with a high degree of accuracy generally requires some combination of CT, MR/, EUS, or surgical staging. This may not be practical at the community hospital level. Yet the stratification of patients obtained with just a physical exam, bar ium swallow, and CT scan is not of suffi- cient quality to judge the results of multi-modality protocols. Surgical pathological staging of patients with esophageal cancer, we believe, should form the basis of protocol development, design, and evalua- tion. It is hoped that refinement of such protocols will
ult imately affect the dismal survival rates reported in this disease over the past 30 years.
Acknowledgment The authors thank Mary, Sullivan Visciano for editorial assistance.
References 1. Boring CC, Squires TS, Tong T: Cancer statistics. CA Cancer
J Clin 43:7-26, 1993 2. Union Internationale Contre le Cancer: TNM classification of
malignant tumors (ed 4). Berlin, Germany, Springer-Verlag, 1987
3. American Joint Committee on Cancer: Manual for Staging of Cancer (ed 3). Philadelphia, PA, Lippincott, 1988
4. Union Internationale Contre le Cancer: TNM classification of malignant tumors (ed 3). Geneva, Switzerland, International Union Against Cancer, 1982
5. American Joint Committee on Cancer Staging and End Results Reporting: Manual for Staging of Cancer, 1978. Chicago, IL, American Joint Committee for Cancer Staging and End Results Reporting, 1978
6. American Joint Committee on Cancer: Manual for Staging of Cancer (ed 2). Philadelphia, PA, Lippincott, 1983
7. American Joint Committee on Cancer: Manual for Staging of Cancer (ed 4). Philadelphia, PA, Lippincon, 1992
8. Japanese Society for Esophageal Disease: Guidelines for clini- cal and pathologic studies on carcinoma of the esophagus.Jpn J Surg 6:69-86, 1976
9. Iizuka T, Isono K, Kakegawa T, et al for the Japanese Committee for Registration of Esophageal Carcinoma Cases: Parameters linked to ten-year survival in Japan of resected esophageal carcinoma. C best 96:1005-1011, 1989
10. Iizuka T, Akiyama H, Isono K, et al for the Japanese Committee for Registration of Esophageal Carcinoma Cases: A proposal for a new TNM classification for carcinoma of the esophagus.JpnJ Clin Oneo114:625-636, 1985
11. Skinner DB, Dowlatshahi KD, DeMeester TR: Potentially curable cancer of the esophagus. Cancer 50:2571-2575, 1982
12. Skinner DB, Little AG, Ferguson MK, et al: Selection of operation for esophageal cancer based on staging. Ann Surg 204:391-401, 1986
13. Siewart JR, Holscher AH, Dittler HJ: Preoperative staging and risk analysis in esophageal carcinoma. Hepatogastroenter- ology 37:382-387, 1990
14. Abe S, Tachibana M, Shiraishi M, et al: Lymph node metasta- sis in resectable esophageal cancer. J Thorac Cardiovasc Surg 100:287-291, 1990
15. Siewart JR: Esophageal cancer from the German point of view.JpnJ Surg 19:11-20, 1989
16. DeMeester TR, Zaninono G, Johansson KE: Selective thera- peutic approach to cancer of the lower esophagus and cardia.J Thorac Cardiovasc Surg 95:42-54, 1988
17. Ellis FH Jr, Watkins E Jr, Krasna MJ, et al: Staging of carcinoma of the esophagus and cardia: A comparison of different staging criteria.J Surg Onco152:231-235, 1993
18. BotetJF, Lightdale CJ, Zauber AG, et al: Preoperative staging of esophageal cancer: Comparison of endoscopic US and dynamic CT. Radiology 181:419-425, 1991
19. Takashima S, Takeuchi N, Shiozaki H, et al: Carcinoma of the

Staging of Esophageal Cancer 145
esophagus: CT vs MR imaging in determining resectability. AJR 156:297-302, 1991
20. Tio TL, Cohen P, Coene PP, et al: Endosonography and computed tomography of esophageal carcinoma: Preoperative classification compared to the now (1987) TNM system. Gastroenterology 96:1478-1486, 1989
21. Van Overhagen H, Lameris JS, Berger MY, et al: Improved assessment of supraclavicular and abdominal metastases in oesophageal and gastro-oesophageal junction carcinoma with the combination of ultrasound and computed tomography. Br J Radio166:203-208, 1993
22. Vilgrain V, Mompoint D, Palazzo L, et al: Staging of esopha- geal carcinoma: Comparison of results with endoscopic sonog- raphy and CT. AJR 155:277-281, 1990
23. Inculet RI, Keller SM, Dwyer A, et al: Evaluation of noninva- sive tests for the preoperative staging of carcinoma of the esophagus. Ann Thorac Surg 40:561, 1985
24. Thompson WM, Halvorsen RA, Foster WK, et al: Computed tomography for staging esophageal cancer: reevaluation. AJR 141:951, 1983
25. LeaJWV, Prager RL, Bender HWJr: The questionable role of computed tomography in preoperative staging of esophageal carcinoma. Ann Thorac Surg 38:479-481, 1984
26. Rice TW, Boyce GA, Sivak MV, et al: Esophageal ultrasound
and the preoperative staging of carcinoma of the esophagus.J Thorac Cardiovasc Surg 101:536-544, 1991
27. Tio TL, Coene PPLO, den HartogJager FCA, et al: Preopera- tive TNM Classification of esophageal carcinoma by endo- sonography. Hepatogastroenterology 37:376-381, 1990
28. Fok M, Cheng SWK, Wong J: Endosonography in patient selection for surgical treatment of esophageal carcinoma. WorldJ Surg 16:1098-1103, 1992
29. Akiyama H, Tsurumaru M, Kawamura T, et al: Principles of surgical treatment for carcinoma of the esophagus: Analysis of lymph node involvement. Ann Surg 194:438-446, 1981
30. Murray GF, Wilcox BR, Starek PJK: The assessment of operability of esophageal carcinoma. Ann Thorac Surg 23:393- 399, 1977
31. Kriplani AK, Kapur BML: Laparoscopy for pre-operative staging and assessment of operability in gastric carcinoma. Gastrointest Endosc 37:441-443, 1991
32. Dagnini G, Caldironi MW, Marin G, et al: Laparoscopy in abdominal staging of esophageal carcinoma: Report of 369 cases. Gastrointest Endosc 32:400-402, 1986
33. Watt I, Stewart I, Anderson D, et al: Laparoscopy, ultrasound and computed tomography in cancer of the oesophagus and gastric cardia: A prospective comparison for detecting intra- abdominal metastases. BrJ Surg 76:1036-1039, 1989





























