Embed Size (px)
Citation preview

efcjta(Ugswovadcc1pahrwphsCp
ed
RA
The Journal of Emergency Medicine, Vol. xx, No. x, pp. xxx, 2009Copyright © 2009 Elsevier Inc.
Printed in the USA. All rights reserved0736-4679/09 $–see front matter
ARTICLE IN PRESS
doi:10.1016/j.jemermed.2009.09.028
Selected Topics:Toxicology
CYANIDE POISONING AND CARDIAC DISORDERS: 161 CASES
Jean-Luc Fortin, MD,* Thibault Desmettre, MD, PHD,* Cyril Manzon, MD,* Virginie Judic-Peureux, MD,*Caroline Peugeot-Mortier, MD,* Jean-Pascal Giocanti, MD,* Mohamed Hachelaf, MD,* Marie Grangeon, MD,*
Ulrike Hostalek, MD,† Julien Crouzet, MD,* and Gilles Capellier, MD, PHD*
*Department of Emergency and Critical Care Medicine, Jean Minjoz University Hospital, Besançon, France and †Merck KGaA,Darmstadt, Germany
Reprint Address: Ulrike Hostalek, Merck KGaA, Frankfurterstr. 250, Darmstadt D-64293, Germany
Acrkarcsmrap
aoah
AD1EMf
Abstract—Background: Inhalation of hydrogen cyaniderom smoke in structural fires is common, but cardiovas-ular function in these patients is poorly documented. Ob-ective: The objective was to study the cardiac complica-ions of cyanide poisoning in patients who received earlydministration of a cyanide antidote, hydroxocobalaminCyanokit®; Merck KGaA, Darmstadt, Germany [in thenited States, marketed by Meridian Medical Technolo-ies, Bristol, TN]). Methods: The medical records of 161 fireurvivors with suspected or confirmed cyanide poisoningere reviewed in an open, multicenter, retrospective reviewf cases from the Emergency Medical Assistance Unit (Ser-ice d’Aide Médical d’Urgence) in France. Results: Cardiacrrest (61/161, 58 asystole, 3 ventricular fibrillation), car-iac rhythm disorders (57/161, 56 supraventricular tachy-ardia), repolarization disorders (12/161), and intracardiaconduction disorders (5/161) were observed. Of the total61 patients studied, 26 displayed no cardiac disorder. Allatients were given an initial dose of 5 g of hydroxocobal-min. Non-responders received a second dose of 5 g ofydroxocobalamin. Of the patients initially in cardiac ar-est, 30 died at the scene, 24 died in hospital, and 5 survivedithout cardiovascular sequelae. Cardiac disorders im-roved with increasing doses of hydroxocobalamin, andigher doses of the antidote seem to be associated with auperior outcome in patients with initial cardiac arrest.onclusions: Cardiac complications are common in cyanideoisoning in fire survivors. © 2009 Elsevier Inc.
Keywords—cyanide poisoning; fire smoke; ECG; car-iac disorders; hydroxocobalamin
ECEIVED: 24 June 2009; FINAL SUBMISSION RECEIVED: 10
CCEPTED: 27 September 20091
INTRODUCTION
cute cyanide poisoning in humans is predominantlyaused by smoke inhalation in fires and, much morearely, by voluntary ingestion of cyanide salts. Little isnown about the pathophysiology, clinical expression,nd treatment perspectives. In addition to the classicespiratory and neurological clinical signs, there are alsoardiovascular manifestations that are indicative of poi-oning, the epidemiology of which is poorly docu-ented. Although cardiac arrest and hypotension are
apidly identified, other signs should be recognized, suchs rhythm, conduction, and repolarization disorders, es-ecially in patients poisoned with low doses.
The aim of this study was to evaluate the frequencynd type of electrocardiographic disorders in suspectedr confirmed acute hydrogen cyanide poisoning patients,nd also to assess the efficacy of early administration ofydroxocobalamin in correcting these disorders.
MATERIALS AND METHODS
n open, retrospective, multicenter (Paris, Besançon,ôle, Montbéliard) study was conducted from January995 to July 2008 through a systematic review of 161mergency Medical Assistance Unit (Service d’Aideédical d’Urgence; SAMU) medical records, and then
rom hospital admission records. As is common practice
ber 2009;
Septem
iSw(lbb
twpttctomwsawttotctpat
trs9obooWS
Opopifiwrt
pv3ehFcd3ows
dwssspb4v
E(icEdEmida
ab
T
C
R
C
R
T
2 J. L. Fortin et al.
ARTICLE IN PRESS
n France, the patients were first seen in the field by theAMU, and were then admitted to various locationsithin the hospital, including the Emergency Department
ED) or Intensive Care Unit (ICU). The selection of theocation did not depend on the patient’s condition alone,ut also on local habits or the availability of hospitaleds.
Patients with smoke inhalation or cyanide salts inges-ion were included in the study. All of them were treatedith hydroxocobalamin as early as possible within therehospital management. The analysis involved the elec-rocardiographic (ECG) tracings recorded on arrival ofhe medical team at the scene of the fire (n � 73) andontinuous cardiac monitoring data (n � 88). These ECGracings were recorded either before or at the beginningf antidotal administration. Blood cyanide levels wereeasured in 6 patients, 3 of whom were in cardiac arrest,hereas 2 had repolarization disorders, and 1 had
upraventricular tachycardia. The dose of epinephrinend the application of external direct current shocksere recorded, as well as the main clinical signs (ex-
ensive burns, alterations of consciousness) and the de-ermination of carboxyhemoglobin level. The patients’utcomes were assessed at the end of their hospitaliza-ion. This information was collected from the physician’slinical record, and by calling the doctor responsible forhe patient after hospitalization. In the majority of cases,atients were hospitalized in a medical ICU or the ICU ofburn center, with a few patients being admitted directly
o the ED.The statistical analysis of the response to antidotal
reatment was performed on the qualitative variables,epresented by the size (n) and percentage (%) of theample, and quantitative variables by their mean and5% confidence interval. Qualitative variables (numberf patients who survived, for example) were comparedy a chi-squared test or by Fisher’s exact test, dependingn the sample size. Quantitative variables, like the dosef antidote, were compared using Student’s and Kruskal-allis tests. Statistical analysis was performed using the
tata 9 program (StataCorp, College Station, TX).
RESULTS
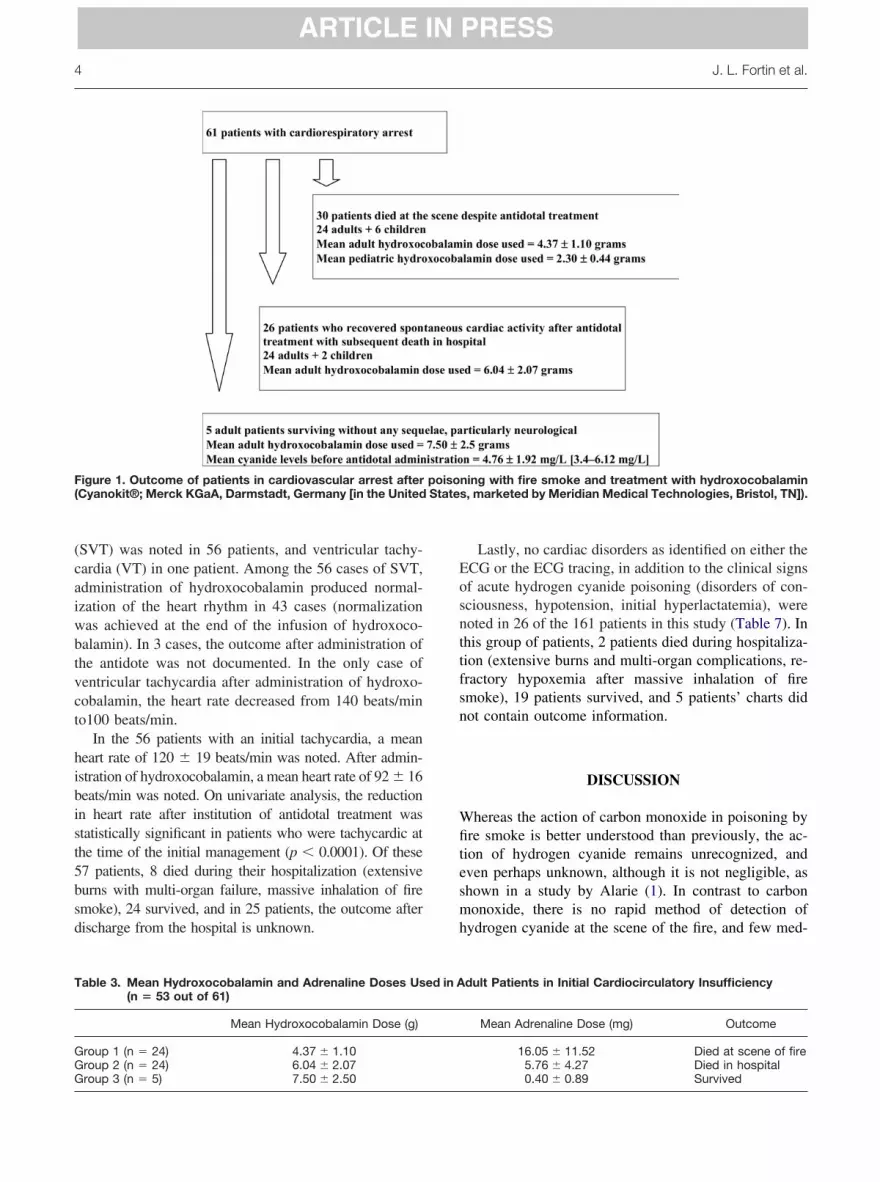
f the 161 patients with suspected acute hydrogen cyanideoisoning, 135 (84%) exhibited cardiac disorders confirmedn the initial ECG or monitor tracing (Table 1). Of the 61atients found in cardiac arrest (Table 2), 58 exhibited annitial asystole, and 3 patients initially had ventricularbrillation. Of the 31 patients (29 adults and 2 children)ho spontaneously recovered cardiac activity (sinus
hythm) after administration of hydroxocobalamin, 5 pa-
ients survived without any sequelae (Figure 1). (In the 24 adult patients who died in the prehospitalhase, the mean dose of hydroxocobalamin administeredia a peripheral venous route was 4.37 � 1.10 g (Table). In the 24 adult patients who had spontaneous recov-ry of cardiac activity after treatment, but who died in theospital, the mean dose of antidote was 6.04 � 2.07 g.inally, in the 5 patients who survived and were dis-harged from the hospital without sequelae, the meanosage used was 7.5 � 2.5 g. One of these patients (No.1) was 8 weeks pregnant (beta human chorionic gonad-tropin � 1838 IU/L on hospitalization) and recoveredithout any sequelae, but with an intrauterine fetal death
ubsequent to the poisoning.On univariate analysis, the differences in mean anti-
ote doses between the three groups—cardiac arrestithout recovery, cardiac arrest with early recovery but
ubsequent death, and cardiac arrest survivors—weretatistically significant (p � 0.01). In the 5 patients whourvived, cyanide levels in blood samples taken in therehospital phase before administration of hydroxoco-alamin showed a mean blood cyanide concentration of.76 � 1.92 mg/L (2.5 mg/L are considered lethal), withalues ranging from 3.4 to 6.12 mg/L.
Repolarization disorders were diagnosed after anCG at the time of initial management in 12 patients
Table 4), 5 in the form of myocardial ischemia (T-wavenversion on the ECG), and 7 in the form of a subendo-ardial injury current (ST-segment elevation on theCG). All of these patients received treatment with hy-roxocobalamin at a dose of 5 g, as well as a follow-upCG, performed either immediately after antidotal ad-inistration or on admission to the hospital after an
nterval of no more than 30 min. These traces showed theisappearance of the repolarization disorders after thedministration of treatment (Figures 2, 3).
Intracardiac conduction disorders were recorded in 5dult patients in the form of a left or right bundle branchlock, with a mean QRS complex duration of 0.35 s
able 1. Groupings of Cardiac Disorders Observed
Cardiac Disorder Number
ardiocirculatory arrestAsystole 58Ventricular fibrillation 3
epolarization disordersMyocardial ischemia 5Subendocardial lesion 7onduction disordersIntracardiac 5
hythm disordersSupraventricular tachycardia 56Ventricular tachycardia 1
otal 135
range 0.13–0.88 s, Table 5). These patients were not

kambm
4b
r
T
E heart
Cyanide Poisoning and Cardiac Disorders 3
ARTICLE IN PRESS
nown to have any history of conduction disorders. Thedministration of hydroxocobalamin produced rapid nor-alization of these disorders (left or right bundle branch
lock), which was substantiated by the second ECG. The
able 2. Doses of Hydroxocobalamin and Adrenaline Used
PatientAge
(Years) Sex
ECG or InitialElectrocardioscope
Trace
ECGElectroc
T
1 40 M Asystole Asysto2 37 F Asystole Asysto3 87 F Asystole Asysto4 4 M Asystole Asysto5 65 F Asystole Asysto6 47 F Asystole Asysto7 56 M Asystole Asysto8 5 M Asystole Asysto9 25 F Asystole Asysto
10 5 M Asystole Asysto11 40 M Asystole Asysto12 32 F Asystole Asysto13 36 M Asystole Asysto14 49 M Asystole Asysto15 4 M Asystole Asysto16 Adult F Asystole Asysto17 83 F Asystole Asysto18 75 M Asystole Asysto19 50 M Asystole Asysto20 48 F Asystole Asysto21 5 F Asystole Asysto22 53 F Asystole Asysto23 54 F Asystole Asysto24 40 M Asystole Asysto25 41 M Asystole Asysto26 20 M Asystole Asysto27 83 M Ventricular fibrillation Asysto28 60 M Asystole Asysto29 40 M Asystole Asysto30 5 M Asystole Sinus31 43 F Asystole Sinus,32 30 F Asystole Sinus,33 31 F Asystole Sinus,34 42 F Asystole Sinus,35 86 F Asystole Sinus,36 55 F Asystole Sinus,37 5 F Asystole Sinus,38 79 F Asystole Sinus,39 67 M Asystole Sinus,40 69 M Asystole Sinus,41 52 F Asystole Sinus,42 65 M Asystole Sinus,43 47 M Asystole Sinus,44 Adult Asystole Sinus,45 52 F Ventricular fibrillation Sinus,46 2 F Asystole Sinus,47 46 F Asystole Sinus,48 30 M Ventricular fibrillation Sinus,49 74 F Asystole Sinus50 64 M Asystole Sinus,51 47 F Asystole Sinus,52 49 F Asystole Sinus,53 56 M Asystole Sinus,54 50 M Asystole Sinus55 60 M Asystole Sinus56 58 F Asystole Atrial fi57 82 M Asystole Sinus58 60 F Asystole Sinus59 42 M Asystole Sinus,60 27 F Asystole Sinus61 23 M Asystole Sinus
CG � electrocardiogram; EC � electrical cardioversion; HR �
ean hydroxocobalamin dose used in these patients was b
.50 � 1.11 g. All of the patients with a bundle branchlock survived (Table 5).
Rhythm disorders in the form of tachycardia wereecorded for 57 patients (Table 6). No cases of sinus
ents with Cardiorespiratory Insufficiency (n � 61)
pe HydroxocobalaminDose (g)
Adrenaline Dose(mg)/Electric
Shocks Outcome
5 45 Died5 40 Died5 15 Died1.5 1.45 (Pediatric) Died5 8 Died5 10 Died2.5 10 Died2.5 1.1 (Pediatric) Died2.5 10 Died2.5 3 (Pediatric) Died5 Not documented Died5 Not documented Died5 14 Died5 15 Died2.5 1.4 (Pediatric) Died5 15 Died5 15 Died5 16 Died5 10 Died5 10 Died2.5 1.4 (Pediatric) Died5 35 Died5 10 Died5 13 Died5 Not documented Died5 5 Died5 Not documented Died5 8 Died5 15 Died5 1.1 (Pediatric) Died
8 5 0 Survived5 5 Died in hospital
0 5 5 Died in hospital0 5 6 Died in hospital
5 0 Died in hospital3 5 Not documented Died in hospital7 2.5 5 (Pediatric) Died in hospital
5 1 Died in hospital5 6 Died in hospital
1 5 0 Survived5 5 Died in hospital
0 10 15 Died in hospital5 2 Died in hospital
1 7.5 2 Survived10 15/3 EC Died in hospital
6 1 1 (Pediatric) Died in hospital5 6 Died in hospital
0 5 3/2 EC Died in hospital5 Not documented Died in hospital
10 7 Died in hospital10 3 Died in hospital5 1.5 Died in hospital
7 5 12 Died in hospital5 Not documented Died in hospital5 6 Died in hospital5 8 Died in hospital5 Not documented Died in hospital
10 0 Survived5 5 3 Died in hospital
10 Not documented Died in hospital10 0 Survived
rate (in beats/min).
in Pati
or Finalardioscorace
lelelelelelelelelelelelelelelelelelelelelelelelelelelelele
HR � 12HR � 75HR � 10HR � 11HR � 97HR � 10HR � 11HR � 85HR � 80HR � 10HR � 77HR � 10HR � 89HR � 10HR � 85HR � 11HR � 77HR � 10
HR � 95HR � 74HR � 77HR � 10
brillation
HR � 12
radycardia were noted. Supraventricular tachycardia
(caiwbtvct
hibist5bsd
Eosnttfsn
Wfitesmh
F poiso( State
T
GGG
4 J. L. Fortin et al.
ARTICLE IN PRESS
SVT) was noted in 56 patients, and ventricular tachy-ardia (VT) in one patient. Among the 56 cases of SVT,dministration of hydroxocobalamin produced normal-zation of the heart rhythm in 43 cases (normalizationas achieved at the end of the infusion of hydroxoco-alamin). In 3 cases, the outcome after administration ofhe antidote was not documented. In the only case ofentricular tachycardia after administration of hydroxo-obalamin, the heart rate decreased from 140 beats/mino100 beats/min.
In the 56 patients with an initial tachycardia, a meaneart rate of 120 � 19 beats/min was noted. After admin-stration of hydroxocobalamin, a mean heart rate of 92 � 16eats/min was noted. On univariate analysis, the reductionn heart rate after institution of antidotal treatment wastatistically significant in patients who were tachycardic athe time of the initial management (p � 0.0001). Of these7 patients, 8 died during their hospitalization (extensiveurns with multi-organ failure, massive inhalation of firemoke), 24 survived, and in 25 patients, the outcome afterischarge from the hospital is unknown.
igure 1. Outcome of patients in cardiovascular arrest afterCyanokit®; Merck KGaA, Darmstadt, Germany [in the United
able 3. Mean Hydroxocobalamin and Adrenaline Doses Us(n � 53 out of 61)
Mean Hydroxocobalamin Dose (g)
roup 1 (n � 24) 4.37 � 1.10roup 2 (n � 24) 6.04 � 2.07
roup 3 (n � 5) 7.50 � 2.50Lastly, no cardiac disorders as identified on either theCG or the ECG tracing, in addition to the clinical signsf acute hydrogen cyanide poisoning (disorders of con-ciousness, hypotension, initial hyperlactatemia), wereoted in 26 of the 161 patients in this study (Table 7). Inhis group of patients, 2 patients died during hospitaliza-ion (extensive burns and multi-organ complications, re-ractory hypoxemia after massive inhalation of firemoke), 19 patients survived, and 5 patients’ charts didot contain outcome information.
DISCUSSION
hereas the action of carbon monoxide in poisoning byre smoke is better understood than previously, the ac-
ion of hydrogen cyanide remains unrecognized, andven perhaps unknown, although it is not negligible, ashown in a study by Alarie (1). In contrast to carbononoxide, there is no rapid method of detection of
ydrogen cyanide at the scene of the fire, and few med-
ning with fire smoke and treatment with hydroxocobalamins, marketed by Meridian Medical Technologies, Bristol, TN]).
dult Patients in Initial Cardiocirculatory Insufficiency
Mean Adrenaline Dose (mg) Outcome
16.05 � 11.52 Died at scene of fire5.76 � 4.27 Died in hospital
ed in A
0.40 � 0.89 Survived

ifi
i
dTtp
T
*E
Fcma
Cyanide Poisoning and Cardiac Disorders 5
ARTICLE IN PRESS
cal laboratories perform a blood cyanide assay to con-rm the diagnosis retrospectively.
These two gases impair tissue oxygenation, each hav-ng a distinct inhibitory mechanism that is exerted at two
able 4. Outcome of Electrocardiographic Abnormalities, DPatients Presenting with Repolarization Disorders
Patient No. Age Sex Initial ECG Trace Fina
62 66 F Myocardial ischemia Norm63 55 F Myocardial ischemia Norm64 81 F Myocardial ischemia Norm65 27 F Myocardial ischemia Norm66 45 M Myocardial ischemia Norm67 30 F Myocardial lesion Norm68 80 M Myocardial lesion Norm69 58 M Myocardial lesion Norm70 67 M Myocardial lesion Norm71 47 F Myocardial lesion Norm72 48 M Myocardial lesion Norm73 23 M Myocardial lesion Norm
Threshold for positivity � 0.15 ng/L.CG � electrocardiogram.
igure 2. Patient No. 73: discovered with disorders of conscioyanide serum level 6.12 mg/L. (A) Initial electrocardiogram
in); (B) Normalized electrocardiographic trace with disappearandministration of hydroxocobalamin.
ifferent levels of the respiratory chain (Figure 4) (2).hus, by binding to hemoglobin, carbon monoxide in-
erferes with arterial oxygen transport. This effect isotentiated by that of hydrogen cyanide that binds at the
Hydroxocobalamin and Troponin Levels and Outcome ofeated with Hydroxocobalamin (HC; n � 12)
Outcome HC Dose (g) Initial Troponin Assay (ng/L)*
Survival 5 0Survival 5 0Survival 5 0Survival 5 0.15Survival 5 Not documentedUnknown 5 Not documentedSurvival 7.5 Not documentedSurvival 5 0Survival 5 Not documentedSurvival 10 0.04Survival 10 0.27Survival 10 0.17
s, Glasgow Coma Scale score 11, pulse 151 beats/min, initialbefore administration of hydroxocobalamin) lead II (10 h, 37
ose ofand Tr
l ECG
alizedalizedalizedalizedalizedalizedalizedalizedalizedalizedalizedalized
usnestrace (
ce of initial repolarization disorders at 13 h, 06 min after

cdosEp
pecot
dstatt
smr(t
Fic amin);h
T
E
6 J. L. Fortin et al.
ARTICLE IN PRESS
ellular level, inhibiting mitochondrial cytochrome oxi-ase. Inhibition of this enzyme causes the cessation ofxygen consumption at the cellular level, involving ahift in its metabolism toward an anaerobic process.nergy depletion with a reduction in adenosine triphos-hate, intracellular acidosis, and cell death then ensues.
The energy blockade of cardiac cytochrome oxidaseroduced by hydrogen cyanide poisoning exerts an earlyffect on calcium homeostasis, particularly in cardiacells (3). Malis and Bonventre showed that calcium andxygen free radicals reduce adenosinetriphosphatase ac-ivity by 55% and adenine nucleotide transferase by 66%
igure 3. Patient No. 127: discovered with disorders of consnhalation of fire smoke, soot, burns, and repolarization dardiogram trace (before administration of hydroxocobalydroxocobalamin.
able 5. Outcome of Patients Presenting with Conduction D
Patient No. Age Sex Initial ECG
74 67 M Conduction disorder,75 51 M Conduction disorder,76 42 M Conduction disorder,77 55 M Conduction disorder,78 68 M Conduction disorder,
CG � electrocardiogram.
uring an ischemic event or after poisoning (4). Animaltudies suggest a dose-effect relationship, which explainshe increase in calcium in the intracellular environmentfter exposure to cyanide. There is a correlation betweenhe elevation of intracellular calcium and the intensity ofhe clinical manifestations, particularly cardiac (5–7).
The presence or absence of hydrogen cyanide in firemoke will depend on the composition of the burningaterials (8,9). The release of hydrogen cyanide may
esult from the combustion both of natural materialswool, cotton, silk) and of synthetic materials (polyure-hane, polyacrylonitrile, polyamide). The more nitrogen
ness, Glasgow Coma Scale score 14, pulse 120 beats/min,rs. Initial blood lactate level 8 mmol/L. (A) Initial electro-(B) Electrocardiogram trace after administration of 5 g
rs and Treated with Hydroxocobalamin (HC; n � 5)
Final ECG Outcome HC Dose (g)
0.13 s Normalized Survived 50.12 s Normalized Survived 50.13 s Normalized Survived 50.88 s Normalized Survived 50.14 s Normalized Survived 2.5
ciousisorde
isorde
QRS �QRS �QRS �QRS �QRS �

cr
d
pad
T
E ; HR �c rn surf
Cyanide Poisoning and Cardiac Disorders 7
ARTICLE IN PRESS
ompounds a substance contains, the greater the potentialelease of hydrogen cyanide during combustion (10).
The clinical signs of hydrogen cyanide poisoning are
able 6. Outcome of Patients Exhibiting Rhythm Disorders
PatientNo.
Age(Years) Sex Initial ECG Final ECG Ou
79 83 F SVT, HR � 120 Normalized, HR � 65 Unkn80 88 F SVT, HR � 120 Normalized, HR � 90 Surv81 40 M SVT, HR � 100 Normalized, HR � 75 Surv82 33 M SVT, HR � 125 Normalized, HR � 95 Surv83 50 M SVT, HR � 100 Normalized, HR � 85 Unkn84 58 M SVT, HR � 130 Normalized, HR � 72 Surv85 55 M SVT, HR � 140 SVT, HR � 120 Died86 56 F SVT, HR � 115 SVT, HR � 100 Surv87 32 M SVT, HR � 120 SVT, HR � 100 Died88 Adult M SVT, HR � 100 SVT, HR � 100 Unkn89 51 M SVT, HR � 100 Normalized, HR � 96 Surv90 35 F SVT, HR � 100 Normalized, HR � 79 Surv91 61 F SVT, HR � 110 SVT, HR � 110 Died92 65 M SVT, HR � 120 SVT, HR � 100 Unkn93 40 M SVT, HR � 120 Normalized, HR � 90 Unkn94 42 M SVT, HR � 140 Normalized, HR � 70 Surv95 40 M SVT, HR � 105 SVT, HR � 120 Unkn96 21 M SVT, HR � 110 Normalized, HR � 95 Surv97 50 F SVT, HR � 120 Normalized, HR � 94 Surv98 28 F SVT, HR � 130 SVT, HR � 100 Died99 50 F SVT, HR � 125 SVT, HR � 100 Died
100 27 F SVT, HR � 114 Normalized, HR � 87 Surv101 26 M SVT, HR � 100 Normalized, HR � 96 Unkn102 14 M SVT, HR � 120 SVT, HR � 101 Unkn103 24 M SVT, HR � 110 Normalized, HR � 95 Died104 64 F SVT, HR � 109 Normalized, HR � 60 Unkn105 55 M SVT, HR � 100 SVT, HR � 100 Surv106 23 M SVT, HR � 135 SVT, HR � 120 Surv107 60 F SVT, HR � 107 Not documented Unkn108 90 F SVT, HR � 135 SVT, HR � 131 Surv
109 52 F SVT, HR � 105 Normalized, HR � 96 Unkn110 34 M SVT, HR � 121 Normalized, HR � 90 Surv111 35 M SVT, HR � 110 Normalized, HR � 80 Surv
112 47 M SVT, HR � 105 SVT, HR � 101 Unkn113 26 M SVT, HR � 156 Normalized, HR � 78 Unkn
114 1 F SVT, HR � 200 SVT, HR � 128 Unkn115 56 F SVT, HR � 108 Normalized, HR � 80 Unkn116 30 M SVT, HR � 120 SVT, HR � 101 Unkn117 53 F SVT, HR � 100 SVT, HR � 100 Unkn118 34 M SVT, HR � 120 Not documented Died119 52 F SVT, HR � 105 Normalized, HR � 88 Unkn120 55 M SVT, HR � 126 SVT, HR � 110 Unkn121 48 M SVT, HR � 100 Normalized, HR � 75 Unkn122 61 M SVT, HR � 140 SVT, HR � 100 Died123 47 F SVT, HR � 140 Normalized, HR � 80 Unkn124 31 M SVT, HR � 120 Normalized, HR � 72 Surv
125 30 M SVT, HR � 180 Normalized, HR � 75 Unkn126 37 M SVT, HR � 112 Normalized, HR � 98 Surv127 25 F SVT, HR � 120 Normalized, HR � 81 Unkn
128 26 M SVT, HR � 114 Normalized, HR � 63 Surv129 40 M SVT, HR � 160 SVT � 110 Surv130 74 M SVT, HR � 120 Normalized, HR � 70 Unkn131 45 F SVT, HR � 102 Normalized, HR � 74 Surv132 42 F SVT, HR � 110 SVT � 100 Unkn133 58 F VT, HR � 140 SVT � 100 Died134 73 M SVT, HR � 120 Normalized, HR � 80 Surv135 56 M SVT, HR � 139 Normalized, HR � 79 Surv
CG � electrocardiogram; SVT � supraventricular tachycardiaonsciousness; GCS � Glasgow Coma Scale score; BSA � bu
ifficult to distinguish from those of carbon monoxide p
oisoning. Whereas both asphyxiating gases cause vari-ble neurological impairment, hydrogen cyanide pro-uces an effect on respiratory rate with bradypnea, hy-
eated with Hydroxocobalamin (HC; n � 56)
HCDose (g) Main Initial Accompanying Signs
5 Dis. consciousness (GCS � 13), burns, hyperpnea5 Dis. consciousness, burns5 Dis. consciousness (GCS � 9), burns5 Dis. consciousness (GCS � 13), burns5 Dis. consciousness (GCS � 12), HbCO � 15%5 Dis. consciousness (GCS � 7)5 Dis. consciousness (GCS � 3), burns (BSA � 40%)5 Dis. consciousness, burns2.5 Dis. consciousness, burns5 Dis. consciousness, burns5 HbCO � 20%5 Dis. consciousness (GCS � 3), HbCO � 24.5%5 Dis. consciousness (GCS � 6), burns, HbCO � 25%2.5 Dis. consciousness (GCS � 7), burns (BSA � 35%)5 Dis. consciousness (GCS � 6)5 Dis. consciousness, burns5 Dis. consciousness (GCS � 11)5 Dis. consciousness (GCS � 10), Hyperpnea (VR � 40)5 Dis. consciousness (GCS � 14), HbCO � 14%5 Dis. consciousness (GCS � 11), HbCO � 5%5 Transient dis. consciousness, burns (BSA � 25%)5 Dis. consciousness (GCS � 14), HBCO � 17%, hyperpnea5 Soot5 Dis. consciousness (GCS � 9)5 Dis. consciousness, burns5 Dis. consciousness, burns5 Dis. consciousness, burns5 Burns (BSA � 90%)5 Dis. consciousness (GCS � 7), burns (BSA � 17%)5 Dis. consciousness (GCS � 10), burns (BSA � 5%),
HbCO � 5.2%5 Dis. consciousness (GCS � 12), burns (BSA � 25%)2.5 HbCO � 5.5%5 Dis. consciousness (GCS � 5), burns (BSA � 63%),
HbCO � 13%5 Burns (BSA � 5%)5 Dis. consciousness (GCS � 5), hyperpnea (VR � 34),
SpO2 � 70%2.5 Dis. consciousness (GCS � 8), SpO2 � 92%5 Dis. consciousness (GCS � 12), burns (BSA � 12%)5 Dis. consciousness (GCS � 4)5 Dis. consciousness (GCS � 10), burns (BSA � 10%)5 Dis. consciousness (GCS � 3), burns (BSA � 45%)2.5 Burns (BSA � 10%)5 Dis. consciousness (GCS � 6), ventilatory pauses5 Dis. consciousness (GCS � 11), burns (BSA � 27%)5 Burns (BSA � 70%)5 Dis. consciousness (GCS � 3), SpO2 � 76%
10 Dis. consciousness (GCS � 3 ), SpO2 � 90%,bradypnea(VR � 10), HbCO � 7.8%
5 Dis. consciousness (GCS � 6), burns (BSA � 2%)5 Dis. consciousness GCS � 3), HbCO � 27%, SpO2 � 81%5 Dis. consciousness (GCS � 4), burns (BSA � 4%) lactate �
8 mmol/L55
10 Dis. consciousness5 Dyspnea (VR � 24)5 Dis. consciousness
8 5 Dis. consciousness (GCS � 3), burns (BSA � 3%)5 Burns (BSA � 36%), HbCO � 6%
10 Dis. consciousness (GCS � 14), burns, SpCO � 40%,lactate � 12.9 mmol/L, CN � 3.04 mg/L
heart rate (in beats/min); Dis. Consciousness � disorders oface area; VR � ventilatory rate.
and Tr
tcome
ownivedivedivedown
ived
ived
ownivedived
ownown
ivedown
ivedived
ivedownown
ownivedivedown
ived
ownivedived
ownown
ownownownown
ownownown
ownived
ownivedown
ivedivedown
ivedownat H�4
ivedived
otension and shock, and a marked increase in blood

lsaIlwwc
tslcTdEcb
snadsmao
dnt
uaii1fa4impaptToocimau
T
E conscS breath
8 J. L. Fortin et al.
ARTICLE IN PRESS
actate. With carbon monoxide poisoning, clinical signsuch as loss of consciousness, polypnea, or tachycardiappear at carboxyhemoglobin values of about 40–50%.n our study, 15 patients had their carboxyhemoglobinevels determined in the prehospital phase before theyere placed on oxygen therapy (in the context of a fireith medical facilities already on site), with the resulting
arboxyhemoglobin values ranging from 5% to 33.9%.In our study, we found cardiac disorders in 135 pa-
ients. Whereas the majority of cardiac disorders ob-erved were cardiac arrests (asystole or ventricular fibril-ation) in 61 (38%) patients, 74 patients exhibited eitheronduction disorders, rhythm or repolarization disorders.his shows the benefit of systematically testing for theseisorders after smoke inhalation by recording a 12-leadCG or single-lead ECG tracing. These manifestationsan be easily corrected by administration of hydroxoco-alamin, a rapidly effective antidote.
Among the 61 patients in cardiocirculatory arrest, 5urvived without sequelae and, in particular, withouteurological sequelae. Four of the 5 patients were notdministered epinephrine (Table 2); these patients wereiscovered in cardiac arrest by the fire brigade, andpontaneous cardiac activity was obtained after cardiacassage and oxygen therapy. Although hydroxocobal-
min was not responsible for the recovery of spontane-
able 7. Outcome of Patients with No Electrocardiographic
PatientNo.
Age(Years) Sex ECG Initial Outcome H
136 53 M Normal, HR � 88 Survived137 Adult M Normal, HR � 99 Survived138 55 M Normal, HR � 86 Survived139 45 M Normal, HR � 82 Survived140 37 F Normal, HR � 90 Unknown141 36 M Normal, HR � 80 Died142 60 M Normal, HR � 80 Unknown143 32 F Normal, HR � 90 Survived144 40 M Normal, HR � 96 Survived145 79 F Normal, HR � 95 Survived146 47 F Normal, HR � 90 Survived
147 39 F Normal, HR � 60 Survived148 77 M Normal, HR � 90 Survived149 38 F Normal, HR � 95 Unknown150 64 F Normal, HR � 70 Survived151 29 M Normal, HR � 80 Survived152 28 M Normal, HR � 90 Survived153 60 M Normal, HR � 67 Survived154 25 F Normal, HR � 80 Unknown155 52 M Normal, HR � 75 Survived156 11 M Normal, HR � 99 Survived 2.5157 80 F Normal, HR � 80 Died158 38 F Normal, HR � 81 Survived
159 45 M Normal, HR � 76 Unknown160 76 F Normal, HR � 85 Survived161 36 M Normal, HR � 84 Survived
CG � electrocardiogram; HR � heart rate (in beats/min); Dis. ofcale score; BSA � burn surface area; VR � ventilatory rate (in
us cardiac activity in these patients, this antidote very s
efinitely enabled a satisfactory hemodynamic state andormal cardiac rhythm to be maintained subsequently inhese 4 patients.
Although there are alternative antidotes that can besed in this situation, they are not all equally effective,nd some cause significant adverse side effects. Histor-cally, the protective effect of methemoglobin related tots affinity for the cyanide ion has been known since930, resulting in the development of methemoglobin-orming substances for the treatment of hydrogen cy-nide poisoning (amyl nitrile, sodium nitrite, and-dimethylaminophenol). The use of these substancess falling out of favor in view of the resultant methe-oglobinemia with reduced oxygen transport and the
ossibility of severe side effects (sudden hypotensionnd severe shock). Methemoglobinemia may also com-romise, if not dramatically reduce, arterial oxygenransport that is already impaired by carboxyhemoglobin.he use of sodium thiosulphate for its ability to metab-lize cyanide to an atoxic substance, thiocyanate, may bef theoretical interest in the treatment of acute hydrogenyanide poisoning, but its delayed onset of action makest more of an adjuvant treatment. Dicobalt ethylene dia-ine tetra-acetic acid acts by binding the cyanide ion,
nd forms an atoxic complex that is eliminated in therine. However, it causes considerable cardiovascular
ers Treated with Hydroxocobalamin (HC; n � 26)
(g) Main Accompanying Signs
Dis. of consciousness (GCS � 14), HbCO � 33.9%, burns, sootDis. of consciousness (GCS � 9), burns, sootDis. of consciousness (GCS � 9), burns (BSA � 60%), hyperpneaSoot, HbCO � 10%, burns (BSA � 5%)Dis. of consciousness (GCS � 8), burns (BSA � 15%), sootDis. of consciousness (GCS � 13), burns (BSA � 30%), sootDis. of consciousness (GCS � 3)Dis. of consciousness (GCS � 6), HbCO � 11.1%Dis. of consciousness (GCS � 3), sootDis. of consciousness (GCS � 11), hyperpnea, sootHistory of 3 episodes of loss of consciousness, burns (BSA � 5%),
sootBurns (BSA � 16%), hyperpnea (VR � 30/min)Initial loss of consciousness, expired CO � 27%Dis. of consciousness (GCS � 6), hyperpnea (VR � 28), sootDis. of consciousness (GCS � 8), burns (BSA � 10%)Dis. of consciousness (GCS � 14), hypotension, burnsDis. of consciousness, burns, sootDis. of consciousness, burns, sootBurns, sootDis. of consciousness (GCS � 12), burns (BSA � 30%) hyperpnea
ric) Dis. of consciousness (GCS � 3), status epilepticusRespiratory distress, sootDis. of consciousness (GCS � 14), burns (BSA � 11%),
hyperpnea, sootDis. of consciousness (GCS � 6), hypotension (SBP � 80 mm Hg)Dis. of consciousness (GCS � 14), HbCO � 13,4%, sootHbCO � 32%, burns (BSA � 35%), blood alcohol � 2.5 g/l
iousness � disorders of consciousness; GCS � Glasgow Comas/min).
Disord
C Dose
55555555555
555555555
(Pediat55
555
ide effects (sudden hypotension or hypertension, tachy-

cna
rSkTcfbai(tlheooafoCpss
aoaaspiang
L
Tcseusas
Ifosttieosot
bsesde(ttfic
FsL
Cyanide Poisoning and Cardiac Disorders 9
ARTICLE IN PRESS
ardia, extrasystoles) and is sometimes associated withausea, vomiting, diarrhea, profuse sweating, and annaphylactoid reaction.
The antidote currently used in France, and which hasecently received marketing authorization in the Unitedtates, Japan, and Europe, is hydroxocobalamin, mar-eted under the name Cyanokit® (Meridian Medicalechnologies, Bristol, TN). It acts in acute hydrogenyanide poisoning by substituting a cyano (CN�) groupor a hydroxyl (OH�) group, thus producing cyanoco-alamin, which is entirely eliminated in the urine. Thisntidote is supplied in the form of a lyophilisate forntravenous use after reconstitution. This lyophilisate2.5 g) is contained in a glass vial, with each kit con-aining two vials of 2.5 g of hydroxocobalamin, equiva-ent to a dose of 70 mg/kg in adults. The efficacy ofydroxocobalamin has been demonstrated in differentxperimental and clinical conditions (11–13). Its speedf action and its good tolerability, apart from a red colorf the mucosa and urine, make it the drug of choice forcute hydrogen cyanide poisoning, and it should be in-used without delay at the scene of the fire in the eventf suspected severe hydrogen cyanide poisoning (14).yanokit® should be given to patients presenting with arolonged exposure to smoke inhalation in a closedpace, with soots, altered neurological status, hypoten-
igure 4. Metabolism of glucose and cell respiration andite of action of the cyanide ion according to Dehon andhermitte (2).
ion, cardiac disorders (dysrhythmia, repolarization, r
nd conduction disorders), or cardiac arrest. In casesf cardiac arrest or persistent hypotension after thedministration of 5 g of hydroxocobalamin, a seconddministration of 5 g may be indicated. Cardiac arresteems to be evidence of severe hydrogen cyanideoisoning (15). In the case of a cardiac arrest ornsufficiency, a dose of 10 g of hydroxocobalamindministered at the outset seems to improve the prog-osis for recovery without sequelae. Further investi-ation is needed to confirm this.
imitations
his was a retrospective chart review. There was noontrol group. Hydroxocobalamin has been demon-trated to be an effective antidote to cyanide poisoning inxperimental studies (see above), and has been in routinese in the emergency medicine setting in France forome years. Thus, ethics dictated that no patients withoutdministration of hydroxocobalamin were available toerve as controls.
CONCLUSIONS
n conclusion, in these 161 cases, the cardiac disordersound were principally cardiac arrests, repolarization dis-rders, and rhythm disorders. These must be screened forystematically at the outset, and monitored continuouslyhroughout the patient’s management. Early administra-ion of the antidote seems to be an essential factor tomprove outcome in the case of cardiac arrest. In thevent of pure hydrogen cyanide poisoning (on ingestionf cyanide salts) or of hydrogen cyanide poisoning as-ociated with carbon monoxide poisoning (on inhalationf fire smoke), hydroxocobalamin should be adminis-ered without delay.
In the absence of the possibility of a rapid assay oflood cyanides, treatment must be administered pre-umptively on the basis of the patient’s history (enclosednvironment, fire, or ingestion), the clinical signs ob-erved (disorders of consciousness, hypotension, or car-iac arrest) and laboratory findings (disorders on thelectrocardiogram, raised lactate levels � 8 mmol/L)16,17). An ECG should be recorded routinely wheneverhere is a possibility of hydrogen cyanide poisoning. Inhe event of manifest cardiac arrest or circulatory insuf-ciency, the dose of hydroxocobalamin must be in-reased, or even repeated in the absence of a rapid
esponse.
1
1
1
1
1
1
1
1
10 J. L. Fortin et al.
ARTICLE IN PRESS
REFERENCES
1. Alarie Y. Toxicity of fire smoke. Crit Rev Toxicol 2002;32:259 – 89.
2. Dehon B, Lhermitte M. Cyanides and anions. In: Kintz P, ed.Toxicologie and Pharmacologie Médico-Légales. Paris: Elsevier;1998:147–55.
3. O’Flaherty EJ, Thomas WC. The cardiotoxicity of hydrogen cya-nide as a component of polymer pyrolysis smokes. Toxicol ApplPharmacol 1982;63:373–81.
4. Malis CD, Bonventre JV. Mechanism of calcium potentiation ofoxygen free radical injury to renal mitochondria. A model forpost-ischemic and toxic mitochondrial damage. J Biol Chem 1986;261:4201–8.
5. Franchini KG, Krieger EM. Cardiovascular responses of consciousrats to carotid body chemoreceptor stimulation by intravenousKCN. J Auton Nerv Syst 1993;42:63–9.
6. Allen DG, Eisner DA, Pirolo JS, Smith GL. The relationshipbetween intracellular calcium and contraction-overloaded ferretpapillary muscles. J Physiol 1985;364:169–82.
7. US Department of Health and Human Services. Toxicologicalprofile for cyanide. July 2006. Available at: http://www.atsdr.cdc.gov/toxprofiles/tp8.html#bookmark09. Accessed December2008.
8. Tuovinen H, Blomquist P. Modelling of hydrogen cyanide forma-tion in room fires. Borås, Sweden: Swedish National Testing and
Research Institute; 2003.9. Hertzberg T, Blomquist P, Dalene M, Skarping G. Particles andisocyanate from fire. Borås, Sweden: Swedish National Testingand Research Institute; 2003.
0. Ballantyne B. Toxicology of cyanides. In: Ballantyne B, Marrs TC,eds. Clinical and experimental toxicology of cyanides. Bristol, UK:Wright Publishers; 1987:41–6.
1. Megarbane B, Delahaye A, Goldgran-Toledano D, Baud FJ. An-tidotal treatment of cyanide poisoning. J Chin Med Assoc 2003;66:193–203.
2. Fortin JL, Ruttimann M, Domanski L, et al. Use of hydroxocobal-amin. Fire Rescue International Med Congress, Las Vegas, April15–18, 2004.
3. Fortin JL, Giocanti JP, Ruttimann M, Kowalski JJ. Prehospitaladministration of hydroxocobalamin for smoke inhalation associ-ated cyanide poisoning: 8 years of experience in the Paris FireBrigade. Clin Toxicol (Phila) 2006;44(Suppl 1):37–44.
4. Fortin JL, Ruttimann M, Domanski L, Kowalski JJ. Hydroxocobalamintreatment for smoke inhalation associated cyanide poisoning. Meeting theneeds of fire victims. JEMS 2004;29(Suppl):18–21.
5. Baud F, Barriot P, Toffis V, et al. Elevated blood cyanide concentrationsin victims of smoke inhalation. N Engl J Med 1991;325:1761–6.
6. Renard C, Fortin JL, Baud F. Terrorisme chimique et cyanides. In:de Revel MC, Gourmelon MCS, Vidal PC, Renaudeau PCS, eds.Menace terroriste: Approche Médicale [French]. Montrouge,France: John Libbey Eurotext; 2005: 353–9.
7. Grangeon M. Les intoxications aux cyanures, prise en charge ettraitement [French]. Besançon, France: Université de Franche-Comté, Faculté de médecine et de pharmacie de Besançon. Thèse,
Année 2008 – n°08–22.ARTICLE SUMMARY1. Why is this topic important?
Cardiac sequelae are an important facet of cyanidepoisoning, but have not been well studied.2. What does this study attempt to show?
We set out to measure cardiac electrocardiographicfunction in a systematic manner among patients withsuspected cyanide poisoning who were attended to by theemergency services in France.3. What are the key findings?
Most survivors of cyanide poisoning demonstrated car-diac rhythm disorders (mostly cardiac arrest or dysrhyth-mias). Early administration of hydroxocobalamin (an anti-dote to cyanide) was significantly associated with improvedelectrocardiographic outcome.4. How is patient care impacted?
Our data support the routine administration of hydr-oxocobalamin to patients with suspected cyanide poison-ing, for example, in the setting of structural fires.





























