Embed Size (px)
Citation preview

K Okumura, B Olshansky, RW Henthorn, AE Epstein, VJ Plumb and AL Waldotachycardia in man: use of transient entrainment of the tachycardia
Demonstration of the presence of slow conduction during sustained ventricular
ISSN: 1524-4539 Copyright © 1987 American Heart Association. All rights reserved. Print ISSN: 0009-7322. Online
72514Circulation is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX
1987, 75:369-378Circulation
http://circ.ahajournals.org/content/75/2/369.citationlocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://www.lww.com/reprintsReprints: Information about reprints can be found online at [email protected]: 410-528-8550. E-mail: Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters http://circ.ahajournals.org//subscriptions/Subscriptions: Information about subscribing to Circulation is online at
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

PATHOPHYSIOLOGY AND NATURAL HISTORYVENTRICULAR TACHYCARDIA
Demonstration of the presence of slow conductionduring sustained ventricular tachycardia in man:use of transient entrainment of the tachycardiaKEN OKUMURA, M.D.,* BRIAN OLSHANSKY, M.D., RICHARD W. HENTHORN, M.D.,ANDREW E. EPSTEIN, M.D., VANCE J. PLUMB, M.D., AND ALBERT L. WALDO, M.D.
ABSTRACT To test the hypothesis that an area of slow conduction is present during reentrantventricular tachycardia in man, and that the earliest activation site during ventricular tachycardia iswithin or orthodromically just distal to the area of slow conduction in the reentry loop, we studied 12episodes of ventricular tachycardia (mean rate 185 + 32 beats/min) that were induced in nine patientswith ischemic heart disease. Rapid ventricular pacing was performed at selected sites during ventriculartachycardia while recording electrograms from an early activation site relative to the onset of the QRScomplex (site A) and from a site close to the pacing site (site B). Rapid pacing from the right ventricularapex during ventricular tachycardia with a right bundle branch block pattern and from selected leftventricular sites during ventricular tachycardia with a left bundle branch block pattern (mean pacingrate 202 ± 38 beats/min) resulted in constant ventricular fusion beats on the electrocardiogram exceptfor the last captured beat (i.e., the ventricular tachycardia was entrained) in 11 of 12 episodes. Duringentrainment: (1) sites A and B were activated at the pacing rate, (2) conduction time from the last pacingimpulse to the last captured ventricular electrogram at site A (St-A interval) was 359 ± 69 msec andspanned the diastolic interval, while that at site B (St-B interval) was only 28 + 13 msec, (3) site A hadthe same ventricular electrogram morphology as that during ventricular tachycardia, while site B had a
different electrogram morphology, indicating that site A was activated in the same direction duringentrainment as during ventricular tachycardia. Eight episodes of ventricular tachycardia were entrainedat two or more different pacing rates. The St-A interval increased during pacing at the faster rate(s) infour of eight episodes, while the St-B interval remained unchanged. Rapid ventricular pacing per-
formed from the same site during sinus rhythm (mean pacing rate 201 ± 37 beats/min) resulted in an
St-A interval of 103 + 37 msec (p < .001 vs the value during entrainment) and an St-B interval of 31+ 15 msec (p = NS vs the value during entrainment). It is concluded that an area of slow conductionnot demonstrable during sinus rhythm exists during ventricular tachycardia, and that the earliestactivation site during ventricular tachycardia is at or orthodromically distal to this area of slowconduction.Circulation 75, No. 2, 369-378, 1987.
REENTRY has been widely accepted as the majormechanism of ventricular tachycardia, especially thatassociated with ischemic heart disease.1"2 It is general-ly accepted that reentry usually requires a circuit with
From the Department of Medicine, Case Western Reserve Universi-ty/University Hospitals of Cleveland, Cleveland, Ohio, and The Uni-versity of Alabama at Birmingham, Birmingham.
Supported in part by grants 5P5OHL7667 and lRO1HL29381 fromthe National Institutes of Health, National Heart, Lung, and BloodInstitute, Bethesda.
Address for correspondence: Albert L. Waldo, M.D., Division ofCardiology, Case Western Reserve University, 2074 Abington Rd.,Cleveland, OH 44106.
Received April 18, 1986; revision accepted Oct. 2, 1986.*Present address: Division of Cardiology, Kumamoto University
Medical School, Kumamoto, Japan.
Vol. 75, No. 2, February 1987
unidirectional block for its initiation and an area ofslow conduction for both its initiation and its mainte-nance.3 Recent experimental studies of canine ventric-ular tachycardia after myocardial infarction not onlydemonstrated reentry as its mechanism, but also dem-onstrated slow conduction and unidirectional conduc-tion block (functional block) in the reentry circuit.` Inhuman ventricular tachycardia, the presence of an areaof slow conduction has generally been assumed,9 but ithas not been directly demonstrated.When a reentrant tachyarrhythmia is transiently en-
trained during rapid pacing, all the tissue related to thetachycardia, including the area of conduction in thereentry circuit, will be activated by the pacing impulse
369 by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

OKUMURA et al.
at the pacing rate. "" Thus, during transient entrain-ment it is possible to determine conduction time be-tween the pacing site and any selected site or in relationto the reentry loop simply by measuring the time inter-val between the pacing stimulus and the electrogramrecorded at the selected site(s) that results from thatpacing impulse.
In the present study, rapid ventricular pacing wasperformed from selected sites during sustained ventric-ular tachycardia induced in patients with ischemicheart disease. By analyzing data obtained during tran-sient entrainment of the tachycardia, we tested thehypothesis that an area of slow conduction is presentduring the tachycardia, and furthermore, that a siteactivated early relative to the onset of each QRS com-plex during the tachycardia is within or orthodromical-ly just distal to the area of slow conduction in thereentry loop.
MethodsNine patients with clinically sustained ventricular tachycardia
were studied in the cardiac catheterization laboratory after in-formed consent was obtained. All patients had a left ventricularaneurysm or akinetic region due to a previous myocardial in-farction (table 1). All antiarrhythmic drugs were discontinued atleast 24 hr before the study. Two patients had previously under-gone coronary artery bypass graft surgery and left ventricularaneurysmectomy. In one of these two patients, an electrophys-iologic study was performed both before and after the surgery.
Electrophysiologic study was performed by standard tech-niques." 2, 9. 11, 13-17 USCI Josephson quadripolar electrode
TABLE 1Clinical characteristics of the patients
Site of LVaneurysm
Patient Age Period after or akinetic OtherNo. (yr) Sex initial MI region relevant data
1 55 F 6 weeks AL,Ap2 69 M 4 years AL,Ap3 53 M 2 months D,PB4 46 M 4 years AL Post CABG
and aneu-rysmectomy
5 51 M 2years D6 60 M 11 years AL,Ap Study was
done bothbefore andafter CABGand aneu-rysmectomy
7 66 M 6 weeks D,PB8 66 M 4 months AL,Ap9 70 M <6 months D,PB
MI myocardial infarction; LV = left ventricular; AL = anterolat-eral portion; Ap = apical portion; D = diaphragmatic portion; PB =
posterobasal portion; CABG coronary artery bypass graft surgery.
catheters were placed in the right ventricular apex and in theright ventricular outflow tract of each patient. Also, a Josephsonor USCI octapolar electrode catheter was introduced in the leftventricular cavity to allow left ventricular endocardial mappingduring ventricular tachycardia. The interelectrode distances forthe Josephson electrode catheters were all 5 mm. The octapolarcatheter was of special design, consisting of four electrode pairs(pair Nos. 1, 2, 3, and 4, distal to proximal, respectively) inwhich the electrodes of each pair were separated by 2 mm. Pairs1 and 2 were separated by 1 cm, pairs 3 and 4 by 1 cm, and pairs2 and 3 by 5 cm, permitting electrograms to be recorded fromfour sites while the catheter sat in the left ventricle in a Uposition. The bend in the U was between pair 2 and pair 3.Bipolar electrograms filtered between a bandpass of 10 to 500Hz were recorded from all the electrode catheters on photo-graphic paper simultaneously with surface electrocardiographicleads I, II, III, and V, with use of an Electronics for MedicineVR-16 oscilloscopic recorder. All data were also recorded on aHoneywell 5600 FM tape recorder for subsequent playback andanalysis. A Medtronic 1349A battery-powered programmablepacemaker was used for the ventricular pacing. All the pacingwas done at a stimulus strength of twice the diastolic threshold.Study protocol. After ventricular tachycardia was induced
by standard pacing techniques, left ventricular endocardial cath-eter mapping was performed during the tachycardia to identifythe earliest activation site relative to the onset of the QRScomplex.'8 The position of the catheter in the left ventricle wasdetermined by the use of biplane fluoroscopy. An average of 26sites was mapped for each tachycardia (range eight to 40 sites).While bipolar electrograms were recorded from the electrodesplaced at this earliest activation site or at an early activation siteclose to the earliest site, transient entrainment of ventriculartachycardia by rapid ventricular pacing was attempted as fol-lows: Rapid pacing was initiated during ventricular tachycardiafrom the right ventricular apex and/or from a selected site in theleft ventricle at a rate 5 to 20 beats/min faster than the spontane-ous rate of the tachycardia. The ventricular pacing site wasusually in the ipsilateral chamber of the bundle branch blockpattern of the tachycardia, since rapid pacing from such a sitewas expected to demonstrate transient entrainment. 15, 19 Whenthe earliest activation site was located in the ventricular septumof the left ventricle and the ventricular tachycardia had a leftbundle branch block pattern, rapid pacing was performed fromthe posterobasal portion of the left ventricle with the use of themost distal pair of electrodes (pair No. 1) of the octapolarelectrode catheter while bipolar electrograms were recordedfrom the earliest or a relatively early activation site with one ofthe proximal two pairs (No. 3 or 4) of electrodes. Rapid pacingwas continued for up to 10 sec and then terminated abruptly. Ifthe tachycardia still continued, rapid ventricular pacing wasagain performed from the same site, but with an increment in thepacing rate of about 10 beats/min (range 9 to 17 beats/min). Thispacing procedure was repeated until either the ventricular tachy-cardia was interrupted or pacing had to be discontinued becauseof associated hemodynamic instability or concern that ventricu-lar pacing at too rapid a rate would precipitate ventricularfibrillation.
During subsequent sinus rhythm, rapid ventricular pacingfrom the same pacing site at about the same rate as used duringthe entrainment study was repeated while electrograms wererecorded from the same sites as before. During such pacing, therelative activation sequence of the ventricular electrograms andthe conduction times from the pacing stimulus to each recordingsite were compared with those obtained during the prior entrain-ment study.
All measurement data are the mean + SD. Statistical analysiswas performed with the Student t test.
CIRCULATION370 by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

PATHOPHYSIOLOGY AND NATURAL HISTORY-VENTRICULAR TACHYCARDIA
ResultsTwelve morphologically distinct episodes of sus-
tained ventricular tachycardia were induced in ninepatients. Eight episodes had a right bundle branchblock pattern (RB-VT) on the electrocardiogram andfour had a left bundle branch block pattern (LB-VT).The characteristics of each episode of ventriculartachycardia, including the rate of the tachycardia andthe earliest activation site during the tachycardia, areshown in table 2.
Transient entrainment of ventricular tachycardia. Rapidventricular pacing from the right ventricular apex dur-ing RB-VT and that from a selected site in the leftventricle (indicated in table 2) during LB-VT resultedin constant ventricular fusion beats on the electrocar-diogram, except for the last captured beat (the firstcriterion of entrainment),1' 12, 16 in seven of eight epi-sodes and four of four episodes, respectively. Themean pacing rate was 205 + 41 beats/min (14 ± 9beats/min higher than the rate of tachycardia) for RB-VT and 188 ± 37 beats/min (20 ± 14 beats/minhigher than the rate of tachycardia) for LB-VT. In theone remaining episode ofRB-VT (tachycardia rate 205beats/min), rapid pacing at 230 beats/min from multi-ple ventricular sites, including the right ventricularapex, right ventricular outflow tract, and left ventricu-lar apex, resulted in QRS complexes identical to those
TABLE 2
seen during rapid pacing from each of the respectivesites during sinus rhythm. Therefore, seven of eightepisodes of RB-VT and four of four episodes of LB-VT were found to be transiently entrained during rapidventricular pacing, permitting the conclusion that theywere due to reentry with an excitable gap.11 12, 16 Sinceone remaining episode of RB-VT was not shown to betransiently entrained during rapid pacing, its underly-ing mechanism could not be determined with certainty.Therefore, the latter episode was excluded from fur-ther analysis. The other 11 episodes of ventriculartachycardia were analyzed further. This analysis ispresented below.
Conduction times during transient entrainment. Ourprevious observations of transient entrainment oftachyarrhythmias indicate that when a tachycardia isentrained by rapid pacing, all the tissue responsible forsustaining the tachycardia is activated by the pacingimpulse at the pacing rate, either orthodromically (i.e.,just as during the spontaneous tachycardia) or anti-dromically (i.e., from a different direction than duringthe spontaneous tachycardia)."2' 1 As illustrated infigure 1, when rapid pacing is performed from a siterelatively proximal to the area of slow conduction inthe reentry loop, site A is activated by the orthodromicwave front of the pacing impulse from the same direc-tion as during spontaneous tachycardia. As a result, the
Characteristics of ventricular tachycardia and results of rapid ventricular pacing
Earliest Entrainment Study Pacing during sinus rhythmactivation
Patient VT rate site dur- Pacing Pacing Entrainment St-A St-B Pacing Pacing rate St-A St-BNo. (bpm) ing VT site rate criterion (msec) (msec) site (bpm) (msec) (msec)
RB-VT1 145 LV-AL RVA 156 + 467 20 RVA 130 75 262 182 LV-AL RVA 194 + 291 14 RVA 210 114 143 210 LV-D,L RVA 226 + 315 20 RVA 208 121 224 205 LV-AS RVA 2305 148 LV-L RVA 158 + 432 20 RVA 154 100 24
6 194 LV-BL RVA 200 + 360 18 RVA 250 200 18
7 237 LV-D RVA 269 + 290 28 RVA 225 109 28
8 224 LV-AL RVA 234 + 292 38 RVA 234 98 52
LB-VT1 153 LV-S LV-PB 163 + 430 52 LV-PB 167 95 48
RVA5 146 LV-S LV-PB 162 + 424 43 LV-PB 188 70 536 200 RVA LVA 240 + 289 17 LVA 214 65 17
9 176 LV-S LV-PB 190 + 360 38 LV-PB 231 81 43Mean 185 202 359 28 201 103 31
SD 32 38 69 13 37 37 15
VT = ventricular tachycardia; LV = left ventricle; AL = anterolateral portion; D = diaphragmmatic portion; L = lateral
portion; AS = apical septum; BL = basal lateral portion; S = septum; RVA = right ventricular apex; PB = posterobasalportion; LVA = left ventricular apex.
Vol. 75, No. 2, February 1987 371 by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

OKUMURA et al.
transient entrainment
FIGURE 1. Diagrams illustrating the activation sequence during spon-
taneous ventricular tachycardia (left) and during transient entrainmentof ventricular tachycardia by rapid pacing performed from a site rela-
tively proximal to an area of slow conduction (the central rectangularpart in each panel) (right). "A" indicates a ventricular electrogram(VEG) recording site orthodromically just distal to the area of slow
conduction, and "B" a VEG recording site close to the pacing site. Thepacing site is indicated by the large white arrow on the right. ORTHO= orthodromic wave front; ANTI = antidromic wave front; Xn = thewavefront from the pacing site; Xn- 1 = the previous orthodromic
pacing wavefront. See text for discussion.
electrogram recorded at that site shows the same mor-
phology during pacing as during the spontaneoustachycardia. However, during the same pacing epi-sode, site B is activated by the antidromic wave frontof the pacing impulse, i.e., from a different directionthan during the spontaneous tachycardia. As a result,the electrogram recorded from site B shows a differentmorphology during pacing than during the spontane-ous rhythm. Thus, the time interval between the pacingstimulus and the electrogram at each site that resultsfrom that pacing impulse represents conduction time ineither an orthodromic (stimulus-to-site A interval) or
an antidromic (stimulus-to-site B interval) direction atthe given pacing rate. In this study, we measured thetime interval between the stimulus artifact of the lastpacing impulse and the last electrogram at each sitethat resulted from that pacing impulse (i.e., the elec-trogram captured by the last pacing impulse) because itis then quite clear which pacing impulse is responsiblefor which electrogram.
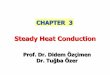
Figure 2 shows an example of transient entrainmentof RB-VT by rapid pacing from the right ventricularapex (patient No. 3). During the spontaneous tachycar-dia (the first half of panel A), the earliest identifiedactivation site was in the inferolateral portion of theleft ventricle, its activation time being -3 msec rela-tive to the onset of the QRS complex on the electrocar-diogram. When rapid ventricular pacing at 226 beats/min was initiated during the tachycardia (the second
372
half of panel A), ventricular fusion developed over
several beats until, as shown in panel B, constant ven-
tricular fusion beats developed. With the terminationof ventricular pacing (eighth beat in panel B), the lastcaptured beat was entrained but not fused and sponta-neous tachycardia resumed. Of note, for each pacedbeat, the two right ventricular recording sites (apex andoutflow tract) were activated by the pacing impulsewith a short conduction time, while the left ventricularsite (which was the earliest activation site identifiedduring the spontaneous tachycardia) was activated bythe previous pacing impulse with a long conductiontime. The time interval between the stimulus artifactand the electrogram recorded at the left ventricular site(St-A interval) was 315 msec, while that between thestimulus artifact and the electrogram recorded at a siteclose to the pacing site with use of the proximal pair ofelectrodes of a Josephson quadripolar electrode cath-eter (St-B interval) was only 20 msec.
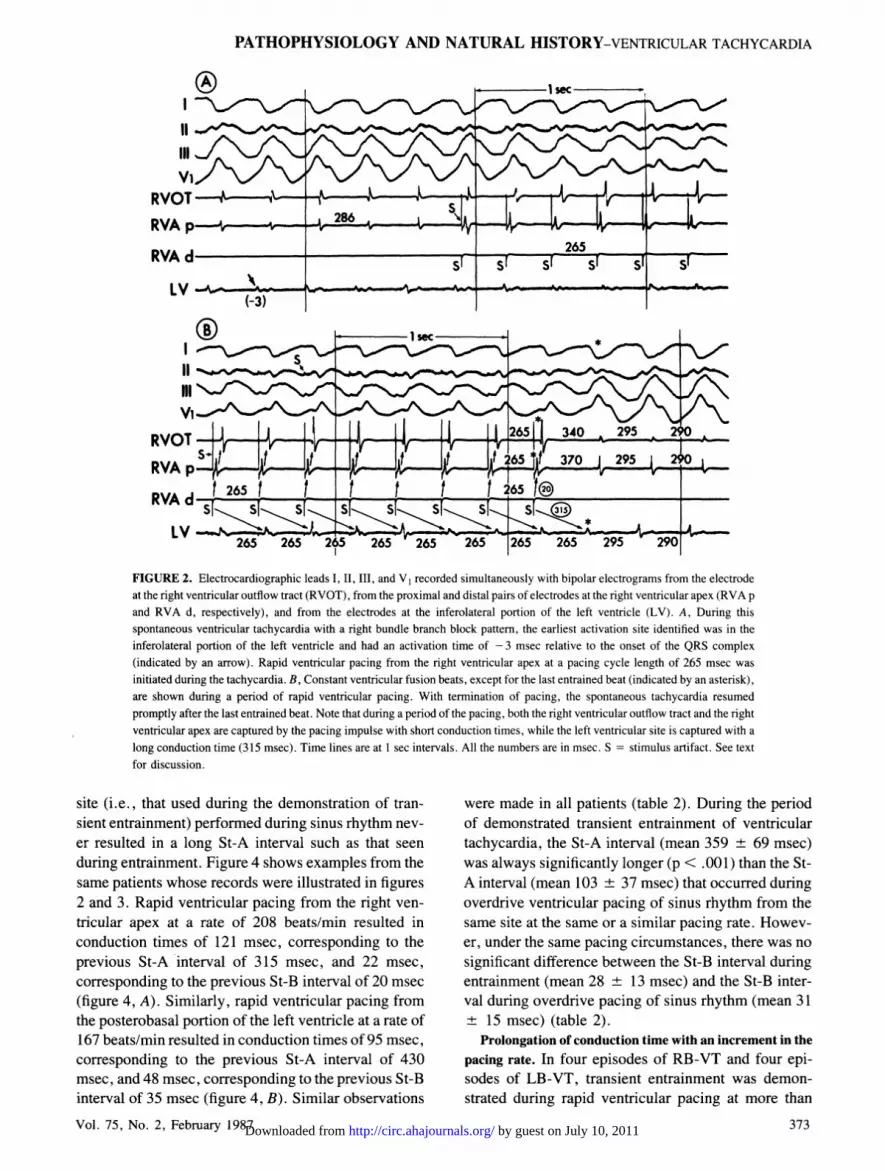
Figure 3 shows an example of transient entrainmentof LB-VT by rapid pacing from the posterobasal por-
tion in the left ventricle (patient No. 1). During thespontaneous tachycardia (panel A), the earliest activa-tion site identified was in the right ventricular apex, itsactivation time being -21 msec relative to the onset ofthe QRS complex on the electrocardiogram. Duringrapid ventricular pacing from the posterobasal portionof the left ventricle (panel B), constant ventricular fu-sion beats were demonstrated, except for the last cap-
tured beat, which was entrained but not fused. Thespontaneous tachycardia resumed after termination ofpacing. Again, for each paced beat, two left ventricu-lar sites (posterobasal portion and apex) and the rightventricular outflow tract were activated by the pacingimpulse with a short conduction time, while the rightventricular apex (the earliest activation site identifiedduring the spontaneous tachycardia) was activated bythe previous pacing impulse with a long conductiontime. The St-A interval was 430 msec, while the St-Binterval was only 52 msec.
Similar observations were made during transient en-
trainment in all the other episodes of RB-VT and LB-VT (table 2). The St-A interval for all studies was 359
69 msec (350 + 73 msec for RB-VT studies and376 ± 66 msec for LB-VT studies), while the St-Binterval was only 28 + 13 msec for all studies (23 + 8msec for RB-VT studies and 38 + 15 msec for LB-VTstudies). Thus, during periods of transient entrain-ment, the site that was activated earliest during thespontaneous tachycardia was activated by the pacingimpulse with a very long conduction time.
In contrast, rapid ventricular pacing from the same
CIRCULATION
spontaneousventricular tachycardia
, y111 ', 1
1/ \'v/*, \N '/ NIX
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from
PATHOPHYSIOLOGY AND NATURAL HISTORY-VENTRICULAR TACHYCARDIA
11.
111 !
Vi)RVOTRVA p.
RVA d
LV
(iIl
V,%T 1 ]_ _ 1 _
m 1 Xsec
11_ I 11 11i 26511_ 340 295 2
265 1 6-5ST FlFsX si si sl [ j\~~~~~~~~~~~~~~~~ A,265 ]265 265 295 29:0
FIGURE 2. Electrocardiographic leads I, II, III, and V1 recorded simultaneously with bipolar electrograms from the electrodeat the right ventricular outflow tract (RVOT), from the proximal and distal pairs of electrodes at the right ventricular apex (RVA p
and RVA d, respectively), and from the electrodes at the inferolateral portion of the left ventricle (LV). A, During thisspontaneous ventricular tachycardia with a right bundle branch block pattern, the earliest activation site identified was in theinferolateral portion of the left ventricle and had an activation time of - 3 msec relative to the onset of the QRS complex(indicated by an arrow). Rapid ventricular pacing from the right ventricular apex at a pacing cycle length of 265 msec was
initiated during the tachycardia. B, Constant ventricular fusion beats, except for the last entrained beat (indicated by an asterisk),are shown during a period of rapid ventricular pacing. With termination of pacing, the spontaneous tachycardia resumedpromptly after the last entrained beat. Note that during a period of the pacing, both the right ventricular outflow tract and the rightventricular apex are captured by the pacing impulse with short conduction times, while the left ventricular site is captured with a
long conduction time (315 msec). Time lines are at 1 sec intervals. All the numbers are in msec. S = stimulus artifact. See text
for discussion.
site (i.e., that used during the demonstration of tran-sient entrainment) performed during sinus rhythm nev-
er resulted in a long St-A interval such as that seen
during entrainment. Figure 4 shows examples from thesame patients whose records were illustrated in figures2 and 3. Rapid ventricular pacing from the right ven-
tricular apex at a rate of 208 beats/min resulted inconduction times of 121 msec, corresponding to theprevious St-A interval of 315 msec, and 22 msec,
corresponding to the previous St-B interval of 20 msec(figure 4, A). Similarly, rapid ventricular pacing fromthe posterobasal portion of the left ventricle at a rate of167 beats/min resulted in conduction times of 95 msec,
corresponding to the previous St-A interval of 430msec, and 48 msec, corresponding to the previous St-Binterval of 35 msec (figure 4, B). Similar observations
Vol. 75, No. 2, February 1987
were made in all patients (table 2). During the periodof demonstrated transient entrainment of ventriculartachycardia, the St-A interval (mean 359 ± 69 msec)was always significantly longer (p < .001) than the St-A interval (mean 103 + 37 msec) that occurred duringoverdrive ventricular pacing of sinus rhythm from thesame site at the same or a similar pacing rate. Howev-er, under the same pacing circumstances, there was no
significant difference between the St-B interval duringentrainment (mean 28 13 msec) and the St-B inter-val during overdrive pacing of sinus rhythm (mean 31+ 15 msec) (table 2).
Prolongation of conduction time with an increment in the
pacing rate. In four episodes of RB-VT and four epi-sodes of LB-VT, transient entrainment was demon-strated during rapid ventricular pacing at more than
373
nx a,RYU I
RVA p
RVAdI V
265 265 265 265 265
1__1 n --A 2 -A1-
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

OKUMURA et al.
fv_W~
1) 393
(-21)
* 4*ho .me &Nwt~
a 1 sec
360I
*
360 * 403 405
360 360. 360 * 405
60AA~ 360
4 d360 ~~467 405
*
-^ 1sec
FIGURE 3. Electrocardiographic leads I, I1, III, and V, recorded simultaneously with bipolar electrograms from the rightventricular outflow tract (RVOT), the right ventricular apex (RVA), the left ventricular apex (LVA), and from the proximal anddistal pairs of electrodes at the posterobasal portion of the left ventricle (LVPB p and LVPB d, respectively). A, During thespontaneous ventricular tachycardia with a left bundle branch block pattern, the earliest activation site identified was in the rightventricular apex (indicated by an arrow) and had an activation time of - 21 msec relative to the onset ofQRS complex. B, Duringrapid ventricular pacing from the posterobasal portion of the left ventricle at a pacing cycle length 360 msec, constant ventricularfusion beats are demonstrated except for the last entrained beat (indicated by an asterisk on the electrocardiogram). Thespontaneous tachycardia resumed promptly with the ternination of the pacing. Note that during the period of pacing, all therecording sites except for the right ventricular apex are captured by the pacing impulse with short conduction times, while theright ventricular apex is captured with a long conduction time (430 msec). The asterisk indicates the last captured beat by the lastpacing impulse. The time lines are at 1 sec intervals. All the numbers are in msec. S = stimulus artifact. See text for discussion.
one pacing rate. This permitted the demonstration ofprogressive fusion, the second criterion of entrainment(i.e., constant ventricular fusion beats at one constantpacing rate but a different degree of constant fusion atdifferent pacing rates)'" ", 16 ` in these eight episodes.
IVI,Vi
RVOT -rSXRVAP 4
RVA d-/ 288 2
LV
tr
v
0
Furthermore, in two episodes of RB-VT and in two ofLB-VT, the St-A interval was further prolonged witheach increment in the pacing rate, and the St-B intervalwas not. As illustrated in figure 5, during a spontane-ous RB-VT, the earliest activation site was recorded
FIGURE 4. A, Electrocardiographic leads I, II, III, and V, recorded simultaneously with the electrograms from the same sites inthe same patient as in figure 2. Results of rapid pacing from the right ventricular apex performed during sinus rhythm at a pacingcycle length of 288 msec are shown. B, Electrocardiographic leads I, II, III, and V, recorded simultaneously with electrogramsfrom the same sites in the same patient as in figure 3. Results of rapid pacing from the posterolateral portion of the left ventricleperformed during sinus rhythm at a pacing cycle length of 360 msec are shown. Note that for both panels, long conduction timessuch as demonstrated in figures 2 and 3 are no longer present during rapid ventricular pacing. Time lines are at 1 sec intervals. Allnumbers are in msec. S = stimulus artifact; other abbreviations are as in previous figures.
CIRCULATION
Il
RVOT-rRVA,V-
LVPB p-.~
LVPB d
-Vt\
374
r 1 r%
'......ALf- t
--v m n
1
LVA
A -Av
v
W
s-"-*-- - *-v.
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

PATHOPHYSIOLOGY AND NATURAL HISTORY-VENTRICULAR TACHYCARDIA
AJAJLEZ-5. - _ _
d
-1sec a
.1j A j- --- *m ----- --4
(-10)
FIGURE 5. Electrocardiographic leads 1, II, III,simultaneously with bipolar electrograms at the rigflow tract (RVOT) and the anterolateral portion ol(LV). During this ventricular tachycardia with a riblock pattern, the earliest activation site identifiedlateral portion of the left ventricle and had an activmsec relative to the onset of the QRS complex (indicRVA = right ventricular apex. The time lines are at
numbers are in msec.
.s c
IV
RVOT
RVA p
L v -___ _ __300 310
from the anterolateral portion of the left ventricle. Rap-id ventricular pacing from the right ventricular apex at200 beats/min (figure 6, A) showed constant fusion
V \A h beats, except for the last captured beat, which wasentrained but not fused. The St-A and St-B intervalswere 360 and 16 msec, respectively. When the pacingrate was increased to 214 beats/min (figure 6, B) andlater to 231 beats/min (figure 6, C), the tachycardia
HHIr C was entrained each time, but with different degrees ofconstant ventricular fusion beats. Note that the St-Ainterval was prolonged from 360 msec to 380 msec andthen to 390 msec at each pacing rate, respectively,while the St-B interval remained unchanged. When thepacing rate was further increased to 250 beats/min
and V1 recorded (figure 7, A), although the St-B interval remained con-;ht ventricular out- stant during the pacing, the St-A interval now gradual-f the left ventricle ly prolonged until localized conduction block betweenight bundle branch the pacing site and the left ventricular recording sitewas in the antero- occurred for 1 beat. This localized conduction blockation time of - 10 was associated with interiuption of the tachycardia.-ated by an arrow).1 sec intervals. All The following paced beats then activated the left ven-
tricular recording site from a different direction (note
280r *i 'Wt -a
SSS
280 316
me
26
1
1260S 'N
*t*
)18
0-A
260 326
FIGURE 6. Electrocardiographic leads 1, IL, III, and V,' recorded simultaneously with bipolar electrograms at the same sites in
the same patient as in figure 5. The proximal pair of electrodes at the right ventricular apex (RVA p) was used for recordingelectrograms and the distal pair (RVA d) was used for pacing. Rapid ventricular pacing from the right ventricular apex at a pacingcycle length of 300 msec (A), 280 msec (B), and 260 msec (C) was initiated during the tachycardia. Note that during each periodof pacing, constant fusion beats except for the last entrained beat are demonstrated and, moreover, progression fusion is
demonstrated with the shortening of the ventricular pacing cycle length. Also, note that the conduction time from the pacingimpulse to the earliest activation site (LV) progressively prolonged with the shortening of the pacing cycle length, althoughconduction time from the pacing impulse to the right ventricular outflow tract (RVOT) and right ventricular apex remainedunchanged. The asterisks indicate the last captured beats. The time lines are at 1 sec intervals. All numbers are in msec. S-stimulus artifact.
Vol. 75, No. 2, February 1987
I r\11Ill
RVOT
RVAA
LV.
j1
L
\1A-v-
1
_- -d 4
375 by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

OKUMURA et al.
1
*-0 -1 sec
F f t Fl F F~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~St St 2401 S/ SI St S[
Ai A A~0 , W, --0 _r -r --r -r
A-
240/0S1 S' S'\(>
Al-
FIGURE 7. Electrocardiographic leads I, II, III. and V1 recorded simultaneously with electrograms at the same sites in the samepatient as in figures 5 and 6. Rapid ventricular pacing from the right ventricular apex at a pacing cycle length of 240 msec wasinitiated during ventricular tachycardia (A). Note that localized conduction block occurred between the pacing site and the leftventricular recording site (indicated by a star) and was associated with interruption of the tachycardia. After this localized block,all the recording sites were now captured by the pacing impulse with the same activation sequence as when the pacing wasperformed during sinus rhythm (B). Also, note that after localized conduction block developed, the electrocardiographicmorphologies, especially in leads II and III, changed, as indicated by small notches at the end of QRS complex (curved arrow onthe electrocardiogram in A). Actually these electrocardiographic morphologies are identical to those seen during rapid pacingperformed during sinus rhythm (B). The time lines are at 1previous figures. See text for discussion.
the change in the ventricular electrogram morphology)and with a shorter conduction time (200 msec), fulfill-ing the third criterion of entrainment. 11 12 16 In fact,this site now was activated in the same way as duringrapid ventricular pacing at the same rate from the samesite during sinus rhythm (figure 7, B).The relationship between the pacing rate and St-A
and St-B intervals measured during each constant pac-ing rate is shown in figure 8 for all the episodes ofventricular tachycardia that were entrained by rapidpacing at two or more different rates. Although the St-B interval was always constant despite the incrementof the pacing rate, the St-A interval was prolonged bymore than 10 msec in four of eight episodes as thepacing rate increased. In two other episodes, prolonga-tion of less than 10 msec occurred, but pacing at onlytwo rates was performed. In the remaining two epi-sodes, no prolongation of conduction time occurreddespite pacing at three rates. Thus, while the St-A
376
sec intervals. All numbers are in msec. Abbreviations are as in
interval during transient entrainment of the tachycardiawas always long, the fact that it prolonged unpredict-ably suggests that the properties of this region varyfrom patient to patient.
DiscussionThe present study provides strong evidence for the
presence of an area of slow conduction in the reentrycircuit of ventricular tachycardia in man. First andforemost is the demonstration that during entrainmentof ventricular tachycardia, the site of earliest ventricu-lar activation is captured orthodromically with a long(mean 359 ms) conduction time (St-A interval). Sec-ond, this long conduction time is not present duringpacing from that same ventricular site at the same or asimilar rate performed during sinus rhythm. Third, thislong conduction time spans the diastolic interval at atime when there is no inscription of any portion of theQRS complex on the electrocardiogram. Fourth, after
CIRCULATION
11
V,
RVOT
RVA p
RVA d
LV W' -w- - v' - W' -W, - -
--Adb.-
by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

PATHOPHYSIOLOGY AND NATURAL HISTORY-VENTRICULAR TACHYCARDIA
(msec)500 r
450 -
400 -
350 -
300 -
250 -
50_
O L
St-A interval
St-B interval
150 200 250
Pacing rate (beats/min)FIGURE 8. The relationship between the pacing rate and St-A and St-B intervals measured during each constant pacing rate. These data wereobtained from eight episodes of ventricular tachycardia. Although theSt-B interval was always constant, the St-A interval was prolonged bymore than 10 msec in four of eight episodes as the pacing rate increased.See text for discussion.
termination of pacing that only transiently entrainedthe ventricular tachycardia, the spontaneous tachycar-dia resumed following activation of the earliest activa-tion site. Fifth, prolongation of conduction time to theearliest activation site (St-A interval) during transiententrainment at two or more different constant pacingrates was observed in half the episodes analyzed. Wesubmit that these observations can be best explained bythe presence of an area of slow conduction in a reentrycircuit, with the earliest activation site being locatedjust orthodromically distal to or perhaps within the area
of slow conduction.Other possible explanations of the long conduction
time (St-A interval) we observed include the possibil-ity of activation of the earliest activation site duringentrainment via a very long pathway. However, it
Vol. 75, No. 2, February 1987
seems unlikely that such a pathway without an area ofslow conduction exists during ventricular tachycardiabecause such a pathway would have to be longer thanis physically possible to accommodate the long con-duction time. Finally, the possibility of a long stimuluslatency period should be considered, but the short St-Binterval makes this alternative explanation also quiteunlikely.
Relationship of the area of slow conduction to the reentrycircuit. The demonstration of an area of slow conduc-tion does not necessarily mean it is a critical part of thereentry circuit. For example, ventriculoatrial conduc-tion time may increase with entrainment of a ventricu-lar tachycardia during ventricular pacing. This wouldbe an example of the demonstration of prolongation ofconduction time across an area of slow conduction notrelated to the reentry circuit of the tachycardia, sincethe ventricular tachycardia reentry circuit is inde-pendent of the area of slow conduction (the atrioven-tricular node) in this example.
That the area of slow conduction demonstrated inthe present study is indeed a critical part of the reentryloop is strongly supported by the following: (1) the siteof earliest activation during the spontaneous ventricu-lar tachycardia was activated during entrainment witha long conduction time, and after ternination of pac-ing, always preceded the first beat (i.e., the beat thatwas entrained but not fused) of the spontaneous tachy-cardia that resumed, and (2) localized conductionblock between the pacing site and the earliest activa-tion site was preceded by the demonstration of a longconduction time, and when it occurred, was alwaysassociated with interruption of the tachycardia. Thus,these observations indicate that the area of slow con-duction was not an innocent bystander,2' but rather wascentral to the reentry circuit.
References1. Wellens HJJ, Duren DR, Lie KI: Observations on mechanisms of
ventricular tachycardia in man. Circulation 54: 237, 19762. Josephson ME, Horowitz LN, Farshidi A, Kastor JA: Recurrent
sustained ventricular tachycardia. Circulation 57: 431, 19783. Cranefield PF: The conduction of the cardiac impulse. The slow
response and cardiac arrhythmias. Mt. Kisco, NY, 1975, FuturaPublishing Company, pp 153-198
4. El-Sherif N, Scherlag BJ, Lazzara R, Hope RR: Re-entrant ventric-ular arrhythmias in the late myocardial infarction period. 1. Con-duction characteristics in the infarction zone. Circulation 55: 686,1977
5. El-Sherif N, Hope RR, Scherlag BJ, Lazzara R: Re-entrant ventric-ular arrhythmias in the late myocardial infarction period. 2. Pat-terns of initiation and termination of re-entry. Circulation 55: 702,1977
6. El-Sherif N, Smith RA, Evans K: Canine ventricular arrhythmias inthe late myocardial infarction period. 8. Epicardial mapping ofreentrant circuits. Circ Res 49: 255, 1981
7. Wit AL, Allessie MA, Bonke FIM, Lammers W, Smeets J, Fenog-lio JJ Jr: Electrophysiologic mapping to determine the mechanism
377 by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from

OKUMURA et al.
of experimental ventricular tachycardia initiated by premature im-pulses. Experimental approach and initial results demonstratingreentrant excitation. Am J Cardiol 49: 166, 1982
8. Cardinal R, Savard P, Carson DL, Perry JB, Pagd P: Mapping ofventricular tachycardia induced by programmed stimulation in ca-nine preparations of myocardial infarction. Circulation 70: 136,1984
9. Josephson ME, Horowitz LN, Farshidi A: Continuous local electri-cal activity. A mechanism of recurrent ventricular tachycardia.Circulation 57: 659, 1978
10. Waldo AL, MacLean WAH, Karp RB, Kouchoukos NT, JamesTN: Entrainment and interruption of atrial flutter with atrial pacing.Studies in man following open heart surgery. Circulation 56: 737,1977
11. Waldo AL, Plumb VJ, Arciniegas JG, MacLean WAH, CooperTB, Priest MB, James TN: Transient entrainment and interruptionof the atrioventricular bypass pathway type of paroxysmal atrialtachycardia. A model for understanding and identifying reentrantarrhythmias. Circulation 67: 73, 1983
12. Waldo AL, Henthorn RW, Plumb VJ, MacLean WAH: Demon-stration of the mechanism of transient entrainment and interruptionof ventricular tachycardia with rapid atrial pacing. J Am Coll Car-diol 3: 422, 1984
13. Portillo B, Mejias J, Leon-Portillo N, Zaman L, Myerburg RJ,Castellanos A: Entrainment of atrioventricular nodal reentranttachycardias during overdrive pacing from high right atrium and
coronary sinus. With special reference to atrioventricular dissocia-tion and 2:1 retrograde block during tachycardias. Am J Cardiol 53:1570, 1984
14. Anderson KP, Swerdlow CD, Mason JW: Entrainment of ventricu-lar tachycardia. Am J Cardiol 53: 335, 1984
15. Mann DE, Lawrie GM, Luck JC, Griffin JC, Magro SA, Wynd-ham CRC: Importance of pacing site in entrainment of ventriculartachycardia. J Am Coll Cardiol 5: 781, 1985
16. Okumura K, Henthorn RW, Epstein AE, Plumb VJ, Waldo AL:Further observations on transient entrainment: importance of pac-ing site and properties of the components of the reentry circuit.Circulation 72: 1293, 1985
17. Almendral JM, Gottleib C, Marchlinski FE, Buxton AE, DohertyJU, Josephson ME: Entrainment of ventricular tachycardia by atrialdepolarizations. Am J Cardiol 56: 298, 1985
18. Josephson ME, Horowitz LN, Farshidi A, Spear JF, Kastor JA,Moore EN: Recurrent sustained ventricular tachycardia. 2. Endo-cardial mapping. Circulation 57: 440, 1978
19. Plumb VJ, Henthorn RW, Epstein AE, Waldo AL: Characteristicsof the transient entrainment of ventricular tachycardia by ventricu-lar pacing. PACE 7: 463, 1984 (abst)
20. MacLean WAH, Plumb VJ, Waldo AL: Transient entrainment andinterruption of ventricular tachycardia. PACE 4: 358, 1981
21. Spear JF, Horowitz LN, Hodess AB, McVaugh H III, Moore EN:Cellular electrophysiology of human myocardial infarction. I. Ab-normalities of cellular activation. Circulation 59: 247, 1979
CIRCULATION378 by guest on July 10, 2011http://circ.ahajournals.org/Downloaded from