Embed Size (px)
Citation preview
This article was downloaded by: [University of Bristol]On: 13 October 2014, At: 00:55Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH,UK
Psychology, Health & MedicinePublication details, including instructions for authorsand subscription information:http://www.tandfonline.com/loi/cphm20
Determinants of socialengagement in older menR. H. Harwood , P. Pound & S. EbrahimPublished online: 19 Aug 2010.
To cite this article: R. H. Harwood , P. Pound & S. Ebrahim (2000) Determinants ofsocial engagement in older men, Psychology, Health & Medicine, 5:1, 75-85, DOI:10.1080/135485000106025
To link to this article: http://dx.doi.org/10.1080/135485000106025
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all theinformation (the “Content”) contained in the publications on our platform.However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, orsuitability for any purpose of the Content. Any opinions and views expressedin this publication are the opinions and views of the authors, and are not theviews of or endorsed by Taylor & Francis. The accuracy of the Content shouldnot be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions,claims, proceedings, demands, costs, expenses, damages, and other liabilitieswhatsoever or howsoever caused arising directly or indirectly in connectionwith, in relation to or arising out of the use of the Content.
This article may be used for research, teaching, and private study purposes.Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly
forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Uni
vers
ity o
f B
rist
ol]
at 0
0:55
13
Oct
ober
201
4

PSYCHOLOGY, HEALTH & M EDICINE, VOL. 5, NO. 1, 2000
Determinants of social engagement in older
men
R. H. HARWOOD, P. POUND & S. EBRAHIM
University Department of Primary Care and Population Sciences, Royal Free Hospital School of
Medicine, London, UK
Abstract The objective of this study was to investigate associations between social engagement and
health and social variables. Cross-sectional analysis of questionnaire data from a national cohort
study was carried one. Participants were 5,905 men aged 51± 70 years, from 24 general practices
from 24 British towns. A nine-item social engagement scale was used as the outcome measurement.
Greater social engagement was associated with younger age, higher social class, house and car
ownership, being married, having fewer medical diagnoses, no disability and better self-perceived
health. Men who had suffered a stroke or heart attack had less engagement than men who had not.
Confound ing by age and socio-economic factors explained the relationship between social engagement
and heart attack. Confounding did not explain the poorer social engagement experienced by men who
had had a stroke, which appeared to be mediated by poorer self-perceived health. We have found age,
social class, marital status, home and car ownership and physical health to be associated with social
engagement. A diagnosis of stroke was associated with poorer social engagement, independently of
social and economic factors.
Introduction
The importance of considering quality of life in health research is now well established.
Global quality of life is hard to de® ne (Ebrahim, 1995), and is therefore hard to measure.
Another approach is to concentrate on more limited but measurable elements of quality of life
(Lawton et al., 1999). The World Health Organization have recently rede® ned the conse-
quences of disease in terms of body function, activity and participation, replacing the
concepts of impairment, disability and handicap from the International classi ® cation of impair-
ments, disabilities and handicaps (World Health Organization, 1980). These positive concepts
of activity Ð the nature and extent of activities associated with everyday life Ð and partici-
pation Ð the nature and extent of a person’ s involvement in life situations Ð are of particular
relevance in de® ning successful aging.
Study of `social engagement’ has its roots in social gerontology. It is de® ned as `the
degree of participation in the social milieu’ (Morgan et al., 1987), almost identical to the new
W HO de® nition of `participation’ . Social disengagement was originally hypothesized as a
normal, adaptive reaction to old age (Cumming & Henry, 1961). This view is generally
Address for correspondence: Dr Rowan Harwood, Consultant Geriatrician, Department of Health Care of the
Elderly, A Floor East Block, Queen’ s Medical Centre, Nottingham NG7 2UH, UK. Tel: 1 44 0115 924 9924 ext 42809;
Fax: 1 44 0115 970 9947; E-mail: [email protected]
ISSN 1354-8506 print /ISSN 1465-3966 online/00/010075-11 Ó Taylor & Francis Ltd
Dow
nloa
ded
by [
Uni
vers
ity o
f B
rist
ol]
at 0
0:55
13
Oct
ober
201
4

76 R. H . HARW OOD ET AL.
rejected now (Gordon, 1975), but it is likely that some people `disengage’ from the life of
their community for alternative reasons (Lahniers, 1975; Spence, 1975), such as ill health.
Chronic illness is known to diminish roles, activities, social networks and relationships
(Anderson & Bury, 1988; Locker, 1983; Williams & Bury, 1989). The extent to which this
depends upon the type of condition or associated confounding factors is not known.
A social engagement scale was developed for the Nottingham Activity and Ageing Study
(Dallosso et al., 1986; 1988). The scale asks about nine activities that involve contact with
people outside the immediate household (telephoning, letter writing, attending religious
services, going on holiday this year or next, and membership of a club or society), or
indicating interest in the wider community (taking a magazine or journal, voting in elections,
using a public library). Previous validation work showed that the scale was capable of
discriminating between active elderly people attending a swimming group, elderly people
drawn from a general practice register, and frail elderly people attending a day hospital
(Morgan et al., 1985). In a population survey of older people (Morgan et al., 1987), the social
engagement scale was strongly correlated with Neugarten’ s Life Satisfaction Index (Neu-
garten et al., 1961), but not with a scale measuring aspects of personality (Bedford et al.,
1976), and gave higher scores in younger people and in those who were more physically
active.
In this study we measured associations between social engagement in men and a variety
of social, economic and health factors. In particular we considered the effects of heart attack
and stroke, both of which are acute in onset, life threatening and may recur. They have
profound consequences for patients and their families (Anderson, 1992; Schott & Badura,
1988; Speedling, 1982) in terms of disruption of lifestyle, roles and social relationships. For
people who survive a stroke the consequences are likely to be more diverse, visible and
long-lasting than for those who survive a heart attack. We have previously demonstrated high
levels of handicap in stroke survivors (Harwood et al., 1994). Among the possible conse-
quences of stroke are speech impairment, cognitive impairment, abnormal gait, incontinence,
hemiparesis, depression and emotionalism, while after heart attack, there may be disability
from angina or heart failure, apprehension towards strenuous activities or fear of recurrence.
W e hypothesized that stroke survivors would be disproportionately likely to withdraw from
social activities, even after their levels of disability are taken into account.
Methods
The British Regional Heart Study
The British Regional Heart Study is a national prospective investigation into the fundamental
causes of cardiovascular disease (Shaper et al., 1981). In 1978± 80, 7,735 men aged 40± 59
were drawn at random from one general practice in each of 24 towns in England, Wales and
Scotland and had a detailed examination including a questionnaire on personal and family
factors, an electrocardiogram, lung function tests and a blood sample for 24 biochemical and
haematological measurements. Men have been followed for all-cause mortality and for fatal
and non-fatal cardiovascular events, with contact being maintained with 99% of surviving
men.
In 1992, the men were sent a questionnaire by post which included questions on
self-rated health, medical diagnoses, occupation, marital status, housing tenure, car owner-
ship, physical disability and social engagement. Self-rated health was classi® ed as excellent,
good, fair or poor (Wannamethee & Shaper, 1991). Subjects were asked if they had ever been
told by a doctor that they had any of the following medical diagnoses: heart attack, stroke,
Dow
nloa
ded
by [
Uni
vers
ity o
f B
rist
ol]
at 0
0:55
13
Oct
ober
201
4

SOCIAL ENGAG EMENT IN OLDER M EN 77
angina, other heart trouble, high blood pressure, aortic aneurysm, diabetes, peptic ulcer,
gout, gall bladder disease, thyroid disease, arthritis, bronchitis, asthma or cancer. Disability
items comprised bending and straightening, keeping balance, climbing stairs, getting out of
the house and walking 400 yards (365 metres).
Statistical analyses
W e examined the effect of heart attack and stroke on social engagement, and conducted
analyses to investigate the origins of any differences seen. Mean social engagement scores
(SES) were calculated for people who had and had not reported heart attack and stroke, and
for possible confounding and explanatory factors. Men were categorized according to
® ve-year age bands, social class (Registrar General’ s classi® cation), whether or not any of the
six disability items could not be performed, and whether none, one, two or three or more
co-morbid conditions were reported. Disability was dichotomized as the distribution was
heavily skewed, with the majority of subjects recording no disability. The signi® cance of
differences were tested using t-tests, chi-square tests or tests of linear trend in means as
appropriate.
Multiple regression analysis (SAS procedure GLM) was used to investigate the relation-
ship between social engagement score (the dependent variable) and diagnosis (heart attack,
stroke, both or neither), once the effects of other variables had been taken into account. The
® rst model included only the diagnosis. The second model added age and socio-economic
variables. Thirdly, the co-morbidity variable was included. Finally, all the measured variables
were entered, including current health status measured according to self-rated health and
disability status. It is possible that these last two variables lie on the causal pathway between
diagnosis and social engagement score, and so are not true confounders. They were included
to investigate whether the diagnosis of stroke or heart attack per se led to social disengagement
or whether this was mediated via poor physical health.
For each model the statistical signi® cance of including the diagnosis variable was tested,
the R-squared statistic examined for the ® t of the model and least squares adjusted mean
estimates for social engagement score calculated for the different diagnostic groups. These
adjusted means are comparable within models but not between different models. Con ® dence
intervals were calculated for differences in adjusted SES according to diagnosis.
Results
Of the original 7,735 men, 6,528 were known to be alive in 1992. Of these, 5,905 responded
(90.4% of survivors); 5,681 (96%) had complete data for the social engagement questions,
and 4,772 men had data complete for all variables, these forming the subjects for the
multivariate analyses. Internal consistency for the scale was reasonable (Cronbach’ s al-
pha 5 0.61).
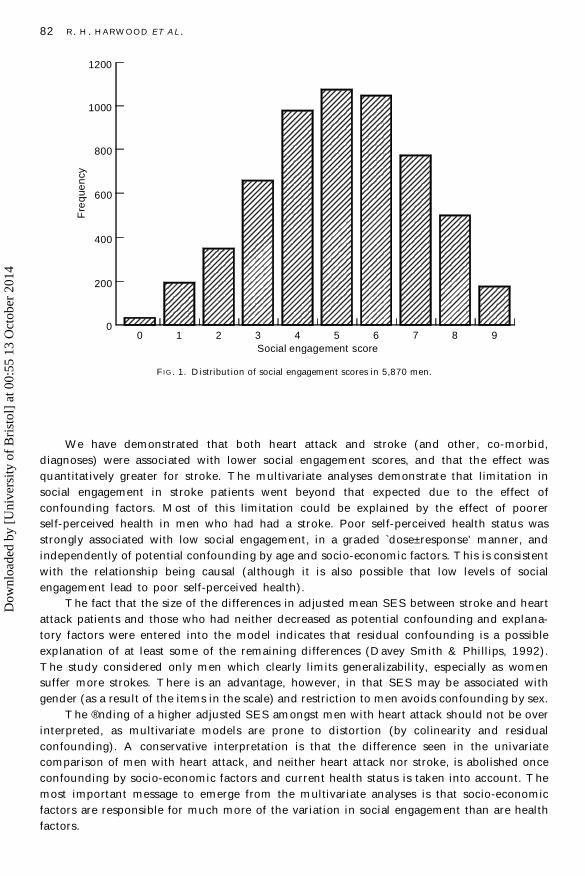
Distribution of scores
The distribution of social engagement scores (SES) in this population is shown in Figure 1.
Mean SES was 5.1 out of nine, standard deviation was 2.0. Social engagement scores were
lower in men who had had a heart attack (M 5 4.9, SD 5 1.9) or stroke (M 5 4.3, SD 5 2.1)
compared with those who had neither (M 5 5.2, SD 5 1.9). The difference in SES between
heart attack and stroke was statistically signi® cant (p 5 0.0001).
Dow
nloa
ded
by [
Uni
vers
ity o
f B
rist
ol]
at 0
0:55
13
Oct
ober
201
4
78 R. H . HARW OOD ET AL.
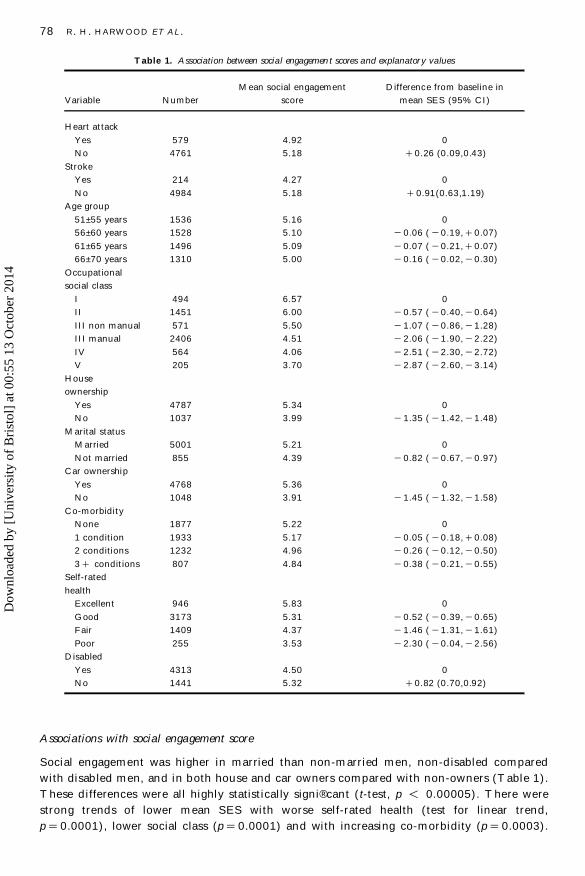
Table 1. Association between social engagemen t scores and explanator y values
Mean social engagement Difference from baseline in
Variable Number score mean SES (95% CI)
Heart attack
Yes 579 4.92 0
No 4761 5.18 1 0.26 (0.09,0.43)
Stroke
Yes 214 4.27 0
No 4984 5.18 1 0.91(0.63,1.19)
Age group
51± 55 years 1536 5.16 0
56± 60 years 1528 5.10 2 0.06 ( 2 0.19, 1 0.07)
61± 65 years 1496 5.09 2 0.07 ( 2 0.21, 1 0.07)
66± 70 years 1310 5.00 2 0.16 ( 2 0.02, 2 0.30)
Occupational
social class
I 494 6.57 0
II 1451 6.00 2 0.57 ( 2 0.40, 2 0.64)
III non manual 571 5.50 2 1.07 ( 2 0.86, 2 1.28)
III manual 2406 4.51 2 2.06 ( 2 1.90, 2 2.22)
IV 564 4.06 2 2.51 ( 2 2.30, 2 2.72)
V 205 3.70 2 2.87 ( 2 2.60, 2 3.14)
House
ownership
Yes 4787 5.34 0
No 1037 3.99 2 1.35 ( 2 1.42, 2 1.48)
Marital status
Married 5001 5.21 0
Not married 855 4.39 2 0.82 ( 2 0.67, 2 0.97)
Car ownership
Yes 4768 5.36 0
No 1048 3.91 2 1.45 ( 2 1.32, 2 1.58)
Co-morbidity
None 1877 5.22 0
1 condition 1933 5.17 2 0.05 ( 2 0.18, 1 0.08)
2 conditions 1232 4.96 2 0.26 ( 2 0.12, 2 0.50)
3 1 conditions 807 4.84 2 0.38 ( 2 0.21, 2 0.55)
Self-rated
health
Excellent 946 5.83 0
Good 3173 5.31 2 0.52 ( 2 0.39, 2 0.65)
Fair 1409 4.37 2 1.46 ( 2 1.31, 2 1.61)
Poor 255 3.53 2 2.30 ( 2 0.04, 2 2.56)
Disabled
Yes 4313 4.50 0
No 1441 5.32 1 0.82 (0.70,0.92)
Associations with social engagement score
Social engagement was higher in married than non-m arried men, non-disabled compared
with disabled men, and in both house and car owners compared with non-owners (Table 1).
These differences were all highly statistically signi® cant (t-test, p , 0.00005). There were
strong trends of lower mean SES with worse self-rated health (test for linear trend,
p 5 0.0001), lower social class (p 5 0.0001) and with increasing co-morbidity (p 5 0.0003).
Dow
nloa
ded
by [
Uni
vers
ity o
f B
rist
ol]
at 0
0:55
13
Oct
ober
201
4
SOCIAL ENGAG EMENT IN OLDER M EN 79
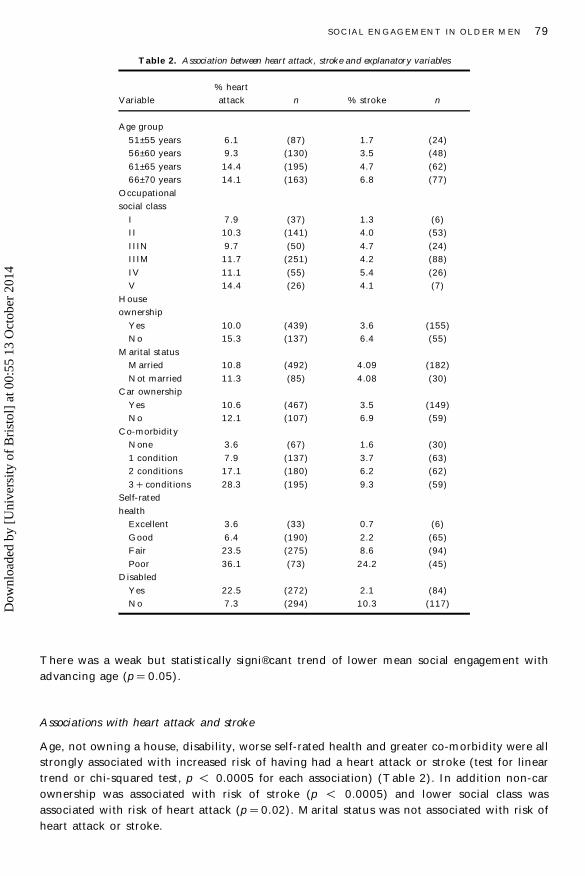
Table 2. Association between heart attack, stroke and explanator y variable s
% heart
Variable attack n % stroke n
Age group
51± 55 years 6.1 (87) 1.7 (24)
56± 60 years 9.3 (130) 3.5 (48)
61± 65 years 14.4 (195) 4.7 (62)
66± 70 years 14.1 (163) 6.8 (77)
Occupational
social class
I 7.9 (37) 1.3 (6)
II 10.3 (141) 4.0 (53)
IIIN 9.7 (50) 4.7 (24)
IIIM 11.7 (251) 4.2 (88)
IV 11.1 (55) 5.4 (26)
V 14.4 (26) 4.1 (7)
House
ownership
Yes 10.0 (439) 3.6 (155)
No 15.3 (137) 6.4 (55)
Marital status
Married 10.8 (492) 4.09 (182)
Not married 11.3 (85) 4.08 (30)
Car ownership
Yes 10.6 (467) 3.5 (149)
No 12.1 (107) 6.9 (59)
Co-morbidity
None 3.6 (67) 1.6 (30)
1 condition 7.9 (137) 3.7 (63)
2 conditions 17.1 (180) 6.2 (62)
3 1 conditions 28.3 (195) 9.3 (59)
Self-rated
health
Excellent 3.6 (33) 0.7 (6)
Good 6.4 (190) 2.2 (65)
Fair 23.5 (275) 8.6 (94)
Poor 36.1 (73) 24.2 (45)
Disabled
Yes 22.5 (272) 2.1 (84)
No 7.3 (294) 10.3 (117)
There was a weak but statistically signi® cant trend of lower mean social engagement with
advancing age (p 5 0.05).
Associations with heart attack and stroke
Age, not owning a house, disability, worse self-rated health and greater co-morbidity were all
strongly associated with increased risk of having had a heart attack or stroke (test for linear
trend or chi-squared test, p , 0.0005 for each association) (Table 2). In addition non-car
ownership was associated with risk of stroke (p , 0.0005) and lower social class was
associated with risk of heart attack (p 5 0.02). Marital status was not associated with risk of
heart attack or stroke.
Dow
nloa
ded
by [
Uni
vers
ity o
f B
rist
ol]
at 0
0:55
13
Oct
ober
201
4
80 R. H . HARW OOD ET AL.
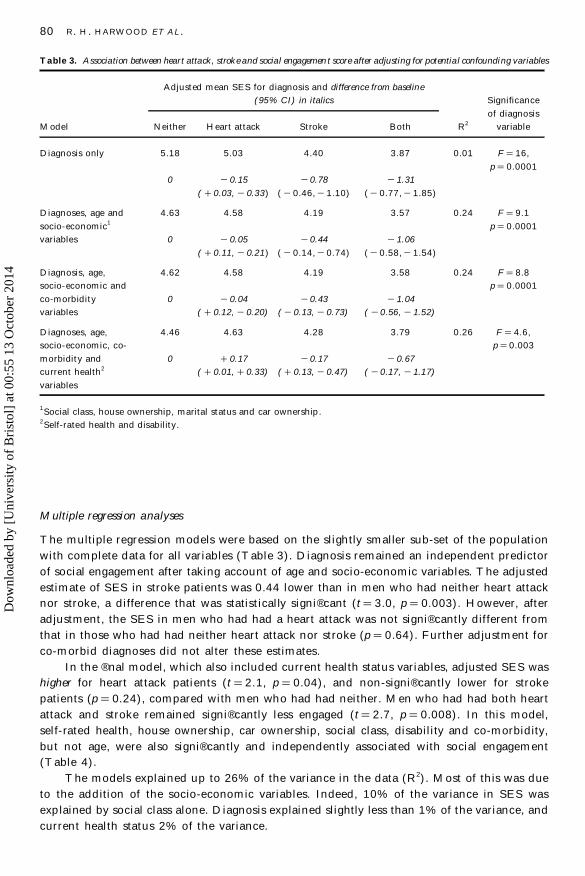
Table 3. Association between heart attack, stroke and social engagemen t score after adjusting for potential confounding variable s
Adjusted mean SES for diagnosis and difference from baseline
(95% CI) in italics Significance
of diagnosis
Model Neither Heart attack Stroke Both R2 variable
Diagnosis only 5.18 5.03 4.40 3.87 0.01 F 5 16,
p 5 0.0001
0 2 0.15 2 0.78 2 1.31
( 1 0.03, 2 0.33) ( 2 0.46, 2 1.10) ( 2 0.77, 2 1.85)
Diagnoses, age and 4.63 4.58 4.19 3.57 0.24 F 5 9.1
socio-economic1
p 5 0.0001
variables 0 2 0.05 2 0.44 2 1.06
( 1 0.11, 2 0.21) ( 2 0.14, 2 0.74) ( 2 0.58, 2 1.54)
Diagnosis, age, 4.62 4.58 4.19 3.58 0.24 F 5 8.8
socio-economic and p 5 0.0001
co-morbidity 0 2 0.04 2 0.43 2 1.04
variables ( 1 0.12, 2 0.20) ( 2 0.13, 2 0.73) ( 2 0.56, 2 1.52)
Diagnoses, age, 4.46 4.63 4.28 3.79 0.26 F 5 4.6,
socio-economic, co- p 5 0.003
morbidity and 0 1 0.17 2 0.17 2 0.67
current health2( 1 0.01, 1 0.33) ( 1 0.13, 2 0.47) ( 2 0.17, 2 1.17)
variables
1Social class, house ownership, marital status and car ownership .
2Self-rated health and disability.
Multiple regression analyses
The multiple regression models were based on the slightly smaller sub-set of the population
with complete data for all variables (Table 3). Diagnosis remained an independent predictor
of social engagement after taking account of age and socio-economic variables. The adjusted
estimate of SES in stroke patients was 0.44 lower than in men who had neither heart attack
nor stroke, a difference that was statistically signi® cant (t 5 3.0, p 5 0.003). However, after
adjustment, the SES in men who had had a heart attack was not signi® cantly different from
that in those who had had neither heart attack nor stroke (p 5 0.64). Further adjustment for
co-morbid diagnoses did not alter these estimates.
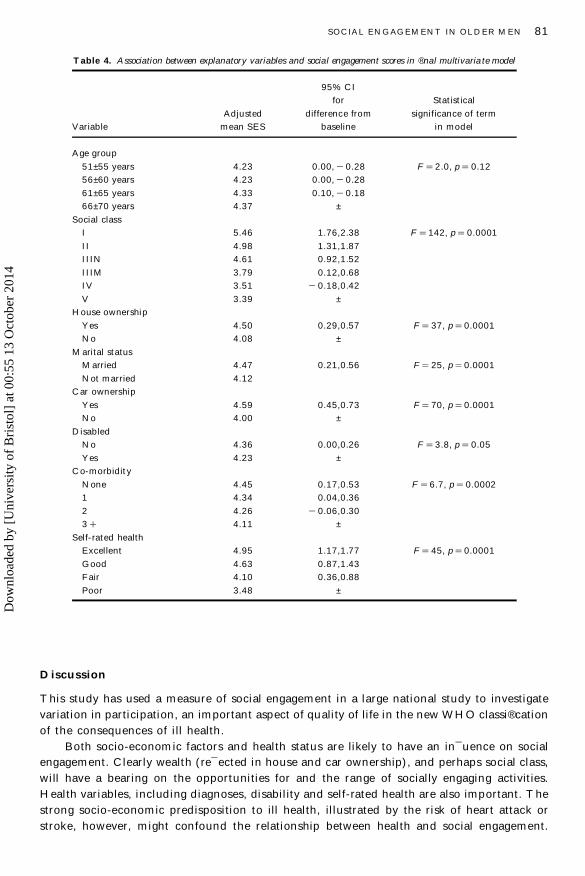
In the ® nal model, which also included current health status variables, adjusted SES was
higher for heart attack patients (t 5 2.1, p 5 0.04), and non-signi® cantly lower for stroke
patients (p 5 0.24), compared with men who had had neither. Men who had had both heart
attack and stroke remained signi® cantly less engaged (t 5 2.7, p 5 0.008). In this model,
self-rated health, house ownership, car ownership, social class, disability and co-morbidity,
but not age, were also signi® cantly and independently associated with social engagement
(Table 4).
The models explained up to 26% of the variance in the data (R2). Most of this was due
to the addition of the socio-economic variables. Indeed, 10% of the variance in SES was
explained by social class alone. Diagnosis explained slightly less than 1% of the variance, and
current health status 2% of the variance.
Dow
nloa
ded
by [
Uni
vers
ity o
f B
rist
ol]
at 0
0:55
13
Oct
ober
201
4
SOCIAL ENGAG EMENT IN OLDER M EN 81
Table 4. Association between explanatory variable s and social engagement scores in ® nal multivaria te model
95% CI
for Statistical
Adjusted difference from significance of term
Variable mean SES baseline in model
Age group
51± 55 years 4.23 0.00, 2 0.28 F 5 2.0, p 5 0.12
56± 60 years 4.23 0.00, 2 0.28
61± 65 years 4.33 0.10, 2 0.18
66± 70 years 4.37 ±
Social class
I 5.46 1.76,2.38 F 5 142, p 5 0.0001
II 4.98 1.31,1.87
IIIN 4.61 0.92,1.52
IIIM 3.79 0.12,0.68
IV 3.51 2 0.18,0.42
V 3.39 ±
House ownership
Yes 4.50 0.29,0.57 F 5 37, p 5 0.0001
No 4.08 ±
Marital status
Married 4.47 0.21,0.56 F 5 25, p 5 0.0001
Not married 4.12
Car ownership
Yes 4.59 0.45,0.73 F 5 70, p 5 0.0001
No 4.00 ±
Disabled
No 4.36 0.00,0.26 F 5 3.8, p 5 0.05
Yes 4.23 ±
Co-morbidity
None 4.45 0.17,0.53 F 5 6.7, p 5 0.0002
1 4.34 0.04,0.36
2 4.26 2 0.06,0.30
3 1 4.11 ±
Self-rated health
Excellent 4.95 1.17,1.77 F 5 45, p 5 0.0001
Good 4.63 0.87,1.43
Fair 4.10 0.36,0.88
Poor 3.48 ±
Discussion
This study has used a measure of social engagement in a large national study to investigate
variation in participation, an important aspect of quality of life in the new W HO classi® cation
of the consequences of ill health.
Both socio-economic factors and health status are likely to have an in¯ uence on social
engagement. Clearly wealth (re¯ ected in house and car ownership), and perhaps social class,
will have a bearing on the opportunities for and the range of socially engaging activities.
Health variables, including diagnoses, disability and self-rated health are also important. The
strong socio-economic predisposition to ill health, illustrated by the risk of heart attack or
stroke, however, might confound the relationship between health and social engagement.
Dow
nloa
ded
by [
Uni
vers
ity o
f B
rist
ol]
at 0
0:55
13
Oct
ober
201
4
00
Fre
que
ncy
Social engagement score1 2 3 4 5 6 7 8 9
200
400
600
800
1000
1200
82 R. H . HARW OOD ET AL.
FIG . 1. Distribution of social engagement scores in 5,870 men.
We have demonstrated that both heart attack and stroke (and other, co-morbid,
diagnoses) were associated with lower social engagement scores, and that the effect was
quantitatively greater for stroke. The multivariate analyses demonstrate that limitation in
social engagement in stroke patients went beyond that expected due to the effect of
confounding factors. Most of this limitation could be explained by the effect of poorer
self-perceived health in men who had had a stroke. Poor self-perceived health status was
strongly associated with low social engagement, in a graded `dose± response’ manner, and
independently of potential confounding by age and socio-economic factors. This is consistent
with the relationship being causal (although it is also possible that low levels of social
engagement lead to poor self-perceived health).
The fact that the size of the differences in adjusted mean SES between stroke and heart
attack patients and those who had neither decreased as potential confounding and explana-
tory factors were entered into the model indicates that residual confounding is a possible
explanation of at least some of the remaining differences (Davey Smith & Phillips, 1992).
The study considered only men which clearly limits generalizability, especially as women
suffer more strokes. There is an advantage, however, in that SES may be associated with
gender (as a result of the items in the scale) and restriction to men avoids confounding by sex.
The ® nding of a higher adjusted SES am ongst men with heart attack should not be over
interpreted, as multivariate models are prone to distortion (by colinearity and residual
confounding). A conservative interpretation is that the difference seen in the univariate
comparison of men with heart attack, and neither heart attack nor stroke, is abolished once
confounding by socio-economic factors and current health status is taken into account. The
most important message to emerge from the multivariate analyses is that socio-economic
factors are responsible for much more of the variation in social engagement than are health
factors.
Dow
nloa
ded
by [
Uni
vers
ity o
f B
rist
ol]
at 0
0:55
13
Oct
ober
201
4
SOCIAL ENGAG EMENT IN OLDER M EN 83
Implications of lower social engagement
Poor social engagement is important in its own right, re¯ ecting disadvantage, exclusion and
missed opportunities, making it important that health services address its causes if possible.
Rehabilitation aims at re-ablement, re-integration and the maximizing of potential (Ebrahim,
1992). Fortunately, poor levels of social engagement are potentially reversible, by tackling
medical, psychological, environmental and social barriers to participation, even in very
disabled subjects (Schroll et al., 1997). Lawton et al. (1999) describe social engagement as
being `close to the core of overall quality of life’ , and demonstrated direct and indirect
associations between social engagement and measures of psychological wellbeing in elderly
subjects.
Diminished social engagement may also have wider implications for health. For example,
low levels of social engagement have been associated with the onset of cognitive decline
(Basuk et al., 1999). The items in the social engagement scale relate to elements of social
networks and social support. Studies investigating the impact of social networks, or network
size, on people with stroke point to the bene® ts associated with them in terms of recovery
(Vogt et al., 1992) and reduction in physical limitation (Colantonio et al., 1993). After a heart
attack social isolation has been associated with a two- to three-fold increase in mortality over
nine years compared with those most socially engaged (Kaplan, 1988). Additionally, in-
creased levels of social support have been associated with functional recovery after stroke
(Glass et al., 1993) and community social support has been found to produce a strong
protective effect on psychosocial outcomes after stroke (Friesland & McColl, 1987). The
perception am ongst stroke patients and their carers that support is lacking has been associ-
ated with depression after stroke (Morris et al., 1991).
It is possible that the lower social engagement in the stroke group might be explained
by depression, which is common and often undiagnosed after stroke (Ebrahim & Harwood,
1999; House, 1987), or by the stigmatizing consequences of stroke which are arguably
greater than those of heart attack or other conditions (by virtue of the range, nature and
visibility of the resulting problems). Either might lead men to perceive their health as worse
and to engage in fewer social activities. The experience or anticipation of stigma by subjects
might lead them to withdraw from social activities in order to avoid discrediting situations.
Support for this theory comes from the ® ndings that people with rectal cancer who felt
stigmatized were more likely to withdraw from social activities (MacDonald & Anderson,
1984).
Educating the public about disability and its causes might go some way towards
lessening any associated stigma. Rehabilitation staff have a role to play in helping to promote
self-con ® dence and self-esteem. Stroke, for example, has been described as an assault on
the `taken for granted’ self (Kaufman, 1991); people’ s sense of identity and, sometimes, their
personality may be affected (Charmaz, 1983). In this context it is easy to understand
how important it is for rehabilitation staff to help patients maintain a sense of identity
and continuity with the life they had before the onset of health problems (Bury, 1982), and
to recognize depression. This means that people should be encouraged and enabled to
continue in their customary roles, so that participation in their community and their social
networks might be maintained. However, it also goes beyond this. It has been argued that
rehabilitation staff need biographical knowledge of the people they are working with (Kauf-
man, 1988). This would facilitate understanding of the meaning of the illness to the
individual and an appreciation of its impact on them, given their lifestyle, previous roles and
interests.
Dow
nloa
ded
by [
Uni
vers
ity o
f B
rist
ol]
at 0
0:55
13
Oct
ober
201
4
84 R. H . HARW OOD ET AL.
Acknowledgements
The BRHS was funded by the Department of Health and the British Heart Foundation. RH
was an MRC Health Services Research Training Fellow and PP was funded by the Stroke
Association. Richard Morris advised on statistical methods, and Andy Thompson ran the
computer analyses.
References
ANDERSON, A. (1992). The aftermath of stroke: the experienc e of patient s and their familie s. Cambridge: Cambridge
University Press.
ANDERSON, R. & BURY, M. (1988). Living with chronic illness. London: Unwin Hyman.
BASSUK, S. S., GLASS, T. A. & BERKMAN, L. F. (1999). Social disengagement and incident cognitive decline in
community-dwelling elderly persons. Annals of Internal Medicin e, 131, 165± 173.
BEDFORD , A., FOULDS, G. A. & SHEFFIELD, B. F. (1976). A new personality disturbance scale. British Journa l of Social
and Clinica l Psychology, 15 , 387± 394.
BURY, M. (1982). Chronic illness as biographical disruption. Sociolog y of Health and Illnes s, 4, 167± 182.
CHARMAZ, K. (1983). Loss of self: a fundamental form of suffering in the chronically ill. Sociolog y of Health and Illness,
5, 168± 195.
COLANTONIO, A., KASL, S. V., OSTFIELD, A. M. & BERKMAN, L. F. (1993). Psychosocial predictors of stroke outcomes
in an elderly population. Journa l of Gerontolog y, 48, S261± S268.
CUMMING , E. & HENRY, W. E. (1961). Growing old: the process of disengagement. New York: Basic Books.
DALLOSSO, H., M ORGAN, K., BASSEY, J., EBRAHIM , S., FENTEM, P. & ARIE, T. (1988). Levels of customary physical
activity among the old and the very old living at home. Journa l of Epidemiology and Communi ty Health, 42, 121± 127.
DALLASSO, J., MORGAN, K., EBRAHIM , S., SMITH, C., BASSEY, J., FENTEM , P. & ARIE, T. (1986). Health and contact
with medical service among the elderly in Greater Nottingham. East Midlands Geographe r, 9, 37± 44.
DAVEY SMITH, G. & PHILLIPS, A. (1992). Confounding in epidemiological studies: why `independent’ effects may not
be all they seem. British Medical Journal, 305 , 757± 759.
EBRAHIM, S. (1992). Rehabilitation. In: J. C. BROCKELHURST, R. C. TALLIS & H. M. FILLET (Eds), Textbook of geriatric s
and gerontology, 4th edition (pp. 1038± 1054). Edinburgh: Churchill Livingstone.
EBRAHIM, S. (1995). Clinical and public health perspectives and applications of health related quality of life. Social
Science and Medicine, 41, 1383± 1394.
EBRAHIM, S. & HARWOOD, R. H. (1999). Stroke: epidemiolog y, evidence and clinica l practice (pp. 237± 244). Oxford:
Oxford University Press.
FRIESLAND, J. & MCCOLL, M. (1987). Social support and psychosocial dysfunction after stroke: buffering effects in a
community sample. Archives of Physical Medicin e and Rehabilitat ion, 68, 475± 480.
GLASS, T. A., MATCHAR, D. B., BELYEA, M. & FEUSSNER, J. R. F. (1993). Impact of social support on outcome in ® rst
stroke. Stroke , 24, 64± 70.
GORDON, J. B. (1975). A disengaged look at disengagement theory. International Journal of Aging and Human
Developmen t, 6, 215± 227.
HARWOOD, R. H., GOMPERTZ, P. & EBRAHIM, S. (1994). Handicap one year after a stroke: validity of a new scale.
Journal of Neurology , Neurosurgery and Psychiatry, 57, 825± 829.
HOUSE, A. (1987). Mood disorders after stroke: a review of the evidence. International Journal of Geriatric Psychiatry,
2, 211± 221.
KAPLAN, G. A. (1988). Social contacts and ischaemic heart disease. Annals of Clinica l Research, 20, 131± 136.
KAUFMAN, S. R. (1988). Stroke rehabilitation and the negotiation of identity. In: S. REINHARZ & G. D. ROWLES (Eds),
Qualitativ e gerontology. New York: Springer .
KAUFMAN, S. R. (1991). Content and boundaries of medicine in long-term care: physicians talk about stroke. The
Gerontologis t, 31, 238± 245.
LAHNIERS, C. E. (1975). Perceptions of aging parents in the context of disengagement theory. Genetic Psychology
Monographs , 92, 299± 320.
LAWTON, M. P., W INTER, L., KLEBAN, M. H. & RUCKDESCHEL, K. (1999). Affect and quality of life Ð objective and
subjective. Journal of Aging and Health, 11 , 169± 198.
LOCKER, D. (1983). Disability and disadvantage: the consequen ces of chronic illness. London: Tavistock Publications.
M ACDONALD , L. D. & ANDERSON, H. R. (1984). Stigma in patients with rectal cancer: a community study. Journal of
Epidemiolog y and Community Health, 38, 284± 290.
Dow
nloa
ded
by [
Uni
vers
ity o
f B
rist
ol]
at 0
0:55
13
Oct
ober
201
4

SOCIAL ENGAG EMENT IN OLDER M EN 85
M ORGAN, K., DALLOSSO, H. & ARIE, T. (1987). Mental health and psychological well-being among the old and very
old living at home. British Journal of Psychiatry, 150, 801± 807.
M ORGAN, K., DALLOSSO, H. & EBRAHIM , S. (1985). A brief self-report scale for assessing personal engagement in the
elderly: reliabilit y and validity. In: A. BUTLER (Ed.), Ageing: recent advances and creative responses (pp. 298 ± 304).
Beckenham: Croom Helm.
M ORRIS, P. I., ROBINSON, R. G., RAPHAEL, B. & BISHOP, D. (1991). The relationship between the perception of social
support and post-stroke depression in hospitalised patients. Psychiatry, 54, 306± 316.
NEUGARTEN, B. L., HAVINGHURST, R. J. & TOBIN, S. S. (1961). The measurement of life satisfaction. Journal of
Gerontolog y, 16, 134± 143.
SCHOTT, T. & BADURA, B. (1988). Wives of heart attack patients: the stress of caring. In: R. ANDERSON & M. BURY
(Eds), Living with chronic illness. London: Unwin Hyman.
SCHROLL, M., JONSSON, P. V., M OR, V., BERG, K. & SHERWOOD, S. (1997). An international study of social engage-
ment among nursing home residents. Age and Ageing, 26 (Suppl. 2), 55± 59.
SHAPER, A. G., POCOCK, S. J., WALKER, M., COHEN, N. M., WALE, C. J. & THOMPSON, A. G. (1981). British Regional
Heart Study: cardiovascular risk factors in middle-aged men in 24 towns. British Medical Journa l, 283, 179± 186.
SPEEDLING, E. J. (1982). Heart attack: the family response at home and in the hospital. London: Tavistock Publications.
SPENCE, D. L. (1975). The meaning of engagement. International Journa l of Aging and Human Development, 6,
193± 198.
VOGT, T. M., MULLOOLY, J. P., ERNST, D., POPE, C. R. & HOLLIS, J. F. (1992). Social networks as predictors of
ischemic heart disease, cancer, stroke and hypertension: incidence, survival and mortality. Journa l of Clinica l
Epidemiolog y, 45, 659± 666.
WANNAM ETHEE, G. & SHAPER, A. G. (1991). Self-assessment of health status and mortality in middle-aged British
men. International Journa l of Epidemiology, 20 , 239± 245.
W ILLIAMS, S. J. & BURY, M. (1989). `Breathtaking’ : the consequences of chronic respiratory disorder. International
Disability Studies, 11 , 114± 120.
WORLD HEALTH ORGANIZATION (1980). International classi ® cation of impairments, disabilitie s and handicap s. Geneva:
WHO. Revised taxonomy (ICIDH-2) is at http://www.who.int/msa/mnh/ems/icidh/index.htm
Dow
nloa
ded
by [
Uni
vers
ity o
f B
rist
ol]
at 0
0:55
13
Oct
ober
201
4





























