Embed Size (px)
Citation preview
Page 1 of 24 Document Development Template Guideline Reference number:
Digital Rectal Examination Guideline Version 4
The aim of this guideline is to ensure quality and consistency in the delivery of clinical care to people who require assessment, treatment and management of
rectum. The patient will receive a holistic assessment of their problem and will be offered appropriate treatment and management in a safe, timely and efficient manner
DOCUMENT NUMBER STHK0422
APPROVING COMMITTEE Patient Safety Council
DATE APPROVED 10/08/2016
DATE IMPLEMENTED 10/08/2016
NEXT REVIEW DATE 10/08/2019
ACCOUNTABLE DIRECTOR Medical Director and Director of Nursing, Midwifery and Governance
GUIDELINE AUTHOR Angela Sharman Continence Nurse Specialist, Siobainn Bathgate Pelvic Floor Nurse
TARGET AUDENCE All medical and nursing staff
KEY WORDS Digital Rectal Examination, Manual Removal of Faeces and Digital Rectal Stimulation
Important Note: The Intranet version of this document is the only version that is maintained. Any printed copies should therefore be viewed as “uncontrolled” and, as such, may not necessarily contain the latest updates and amendments.
Page 2 of 24 Document Development Template Guideline Reference number:
Contents
Item No.
Subject Page No.
1. Scope
3
2. Introduction
3
3. Statement of Intent
3
4. Definitions
4
5. Duties, Accountabilities and Responsibilities
4
6. 6. 1. 6. 2. 6. 3. 6. 4. 6. 5.
Guideline content Bowel examination Who can perform a Digital Rectal Examination Indication for performing a Digital Rectal Examination Consent, Exclusions and Caution Digital Rectal Examination/ Removal of faeces
5 5 5 5 6 6
7. Training
7
8. 8. 1. 8. 2.
Monitoring Compliance Key performance indicators Performance management guideline
8 8
9. Equality analysis 9
10. Procedure Appendix 1. Digital Rectal Examination Appendix 2. Manual Removal of Faeces Appendix 3. Digital Rectal Stimulation Appendix 4. Competency Framework Appendix 5. Digital rectal Examination
9 12 15 18 19
11. Autonomic Dysreflexia 21
12. References 24
3
1. SCOPE This guideline applies to the assessment, treatment and management of all adult patients requiring a digital rectal examination within St Helens and Knowsley Teaching Hospital NHS Trust, irrespective of their place of residence, i.e. hospital inpatient, care home or own home. It will apply to all hospital staff working within St Helens and Knowsley Teaching Hospital NHS Trust who undertakes a digital rectal examination after completing the relevant training. 2. INTRODUCTION The process of rectal emptying is usually initiated voluntarily. Movement of faeces into the rectum causing rectal distension evokes the desire to defecate, known as the “call to stool”. Under the appropriate circumstances, defecation is completed when a person adopts a sitting or squatting position. This allows abdominal pressure to rise by contraction of the diaphragm and abdominal muscles, followed by the relaxation of pubis rectalis muscle and external anal sphincter muscles, which results in the stool being expelled. Digital Rectal Examination (DRE) may be used a part of an assessment, providing
the health care professional is competent to carry out this procedure. DRE should be
used in conjunction with the assessment process, and not as a sole investigation for
evaluation and treatment of constipation. A failure to undertake a DRE during a
bowel assessment may result in a patient receiving inappropriate or ill-timed bowel
intervention (Nursing Times NT 2011).
Constipation is defecation that is unsatisfactory because of infrequent stools, difficult stool passage, or seemingly incomplete defecation. Stools are often dry and hard and may be abnormally large or abnormally small National Institute of Clinical Excellence NICE (2015). Rome II Criteria for Constipation The patient is said to be constipated when 2 or more of the following criteria are present for at least 12 weeks out of the preceding 12 months: • Straining at defecation on at least a quarter of occasions • Stools are lumpy or hard on at least a quarter of occasions • Sensation of incomplete evacuation on at least a quarter of the time • 3 or fewer bowel movements per week (Longstreth et al, 2006) This guideline is designed to ensure all staff working for and on behalf of St Helens
and Knowsley Teaching Hospitals NHS Trust provide an optimal level of service
delivery to this specific patient population. The advice and guidance contained within
this guideline is developed from the latest research based evidence.
3. STATEMENT OF INTENT
The aim of this guideline is to ensure quality and consistency in the delivery of
clinical care to people who require assessment, treatment and management of
4
rectum. The patient will receive a holistic assessment of their problem and will be
offered appropriate treatment and management in a safe, timely and efficient
manner.
4. DEFINITIONS DRE Digital Rectal Examination MRF Manual Removal of Faeces DRS Digital Rectal Stimulation NICE National Clinical Excellence NT Nursing Times RCN Royal College of Nursing NMC Nursing Midwifery Council SCI Spinal Cord Injury DOH Department of Health 5. DUTIES ACCOUNTABILITIES AND RESPONSIBILITIES Chief Executive Is responsible for ensuring Trust compliance with Governance arrangements Director of nursing, Midwifery and Quality Is responsible for ensuring systems are in place for all Nursing and Midwifery staff to enable compliance with this guideline
Medical Director Is responsible for ensuring systems are in place for all Medical Staff to enable compliance with this guideline
Assistant Director of Operations and assistant Medical Directors of Clinical Business Units Are responsible for ensuring all their staff are aware of this guideline, and that they are compliant with the guideline
All Medical and Nursing Staff It is the responsibility of the individual healthcare professional to maintain their knowledge and skills in line with professional, national, evidence and research based recommendations. All Trust staff are responsible for the development and implementation of St Helens and Knowsley Teaching Hospitals NHS Trust policies as part of their duties and responsibilities. All staff should have the knowledge to be able to access all policies via the Trust intranet and are responsible for arranging relevant training via the Training and Development department.
It is the responsibility of the individual healthcare professional to involve the patient/and or carer in the decision to catheterise. It is the responsibility of the individual health care professional to obtain and document in the medical notes verbal consent for the procedure and complete trust documentation.
5
Responsible for recommending this guideline Urology, Colorectal and Pelvic Floor Team. The above team have recommended the above guideline. 6. GUIDELINE CONTENT 6.1 Bowel Examination Prior to a bowel examination there should be a joint decision between the patient (where possible) and relevant health care professionals involved in the patient’s care to agree a bowel examination is needed and can be justified. Examination should take into account the possible sexual, physical, social, psychological and environmental impact on the examination.
6.2 Who can perform a DRE A trained healthcare professional can perform a DRE, DRF and MRF both male and female patients provided they have completed the DRE, DRF and MRF training session and completed the relevant competency. Registered practitioners are responsible for updating their practice to maintain competency (NMC 2008). 6.3 Indication for performing a DRE DRE is an invasive procedure and should only be performed when necessary, and after individual assessment (Kyle 2007).
To assess the presence of faecal matter in the rectum; the amount and consistency
To assess the anal tone and the ability to initiate a voluntary contraction and to what degree
To assess anal pathology
To assess anal and rectal sensation
To assess the need for and effects of rectal medication in certain circumstances
To assess the need for manual removal of faeces and evaluating bowel emptiness
To assess the outcome of faecal and colonic washout or irrigation if appropriate
To assess the need and outcome of using a digital stimulation to trigger defecation by stimulating the recto-anal reflex To assess the size, consistency and any abnormality with in the prostate 6.4 Consent, Exclusions and Caution
Health care professional must not undertake these procedures when: There is a lack of consent from the patient – written, verbal or implied as per Trust Policy Safeguarding Adults (2011)
6
The patient’s doctor has given specific instructions that these procedures are not to take place (Royal College of Nursing RCN guidance 2012) Caution should be exercised when performing these procedures with patients who have the following: Active inflammation of the bowel, including Crohn’s disease, ulcerative colitis and diverticulitis
Recent radiotherapy to the pelvic area
Rectal or anal pain
Rectal surgery or trauma to the anal or rectal area
Tissue fragility due to age, radiation, loss of muscle tone in neurological diseases or malnourishment
Obvious rectal bleeding
If the patient has a history of abuse
In certain spinal injured patients because of the risk of autonomic dysreflexia (Stephenson 2015)
The patient gains sexual satisfaction from these procedures (in these circumstances consultation with other members of the team is advised, involving the patient in that consultation).
6.5 Digital Rectal Examination/Removal of faeces DRE – the insertion of a non-latex gloved lubricated index finger into the patient’s rectum to ascertain the presence and consistency of faeces. . Digital Removal of Faeces DRF - the insertion of a non-latex lubricated index finger into the patient’s rectum to remove faeces. Digital Rectal Stimulation DRS – the insertion of a gloved lubricated finger in to the rectum followed by slow rotation of the finger in a circular movement against the rectal mucosa to promote peristalsis of the left colon. DRE is to be used as part of a nursing assessment, providing the nurse is able to demonstrate their professional skill and knowledge and competence to a level determined by their professional body (Nursing Midwifery Council NMC 2008) and Indications for DRE are to establish: • SCI (Spinal cord injury) patients as part of bowel management • The presence of faecal matter in the rectum, amount and consistency • Anal tone and the ability to initiate a voluntary contraction and to what degree • Anal/rectum sensation • Prior to giving any rectal medication to determine the state of the rectum • The need for the effects of rectal medication in certain circumstances • The need for manual removal of faeces and evaluating bowel emptiness • The outcome of rectal/colonic washout/irrigation if appropriate • The need and outcome of using digital stimulation to trigger defecation by stimulating the recto-anal reflex
7
IMPORTANT: it is vital to check for allergies, including allergies to latex, soap (lanolin), phosphate and peanut (present in arachis oil enemas) before proceeding with these procedures. Observation of the perineal and perianal area: Before these procedures can be performed, abnormalities of the perineal and perianal areas must be observed, documented and reported. You must observe for the following abnormalities: • Rectal prolapse –degree, ulceration • Haemorrhoids –number, position, grade, prolapse • Anal skin tags-number, position, condition • Wounds, dressings, discharge present • Anal lesions (malignancy) • Skin conditions, broken areas, pressure sores of all grades • Bleeding and colour of blood • Faecal matter • Infestation • Foreign bodies Presence of any abnormality would indicate that DRE or Manual removal of faeces must not be performed until advice has been sought from a specialist nurse or medical practitioner. Circumstances when extra care is required: You must exercise particular caution when performing these procedures with patients who have the following diseases and conditions: • Active inflammation of the bowel, including Crohns disease, ulcerative colitis and diverticulitis • Recent radiotherapy to the pelvic area • Rectal pain • Rectal surgery/trauma to the anal/rectal/area • Tissue fragility due to age, radiation, loss of muscle tone in neurological disease of malnourishment • Obvious rectal bleeding • If the patient has a known history of abuse • In spinal injury patients because of the risk of autonomic dysreflexia • If patients have a known history of allergies 7. TRAINING All registered nurses undertaking this procedure must have evidence of completed competency assessment and knowledge of the DRE. Undertake a one off practice assessment by appropriate assessor within the trust. Full day training will include both theory and practical. Please contact Angela Sharman 01744 646 264 or Siobainn Bathgate 0151 290 4407 for further information.
8
8 MONITORING OF COMPLIANCE with this document 8.1 Key performance Indicators of the guideline
Describe Key Performance Indicators (KPIs)
Frequency of Review Lead
DRE competency rates
Monthly Continence Nurse Specialist/ Pelvic Floor Nurse
8.2 Performance Management of guideline
Aspect of Compliance or effectiveness being monitored
Monitoring method
Job title of individual(s) responsible for monitoring and developing action plan
Frequency of the monitoring activity
Group/ committee which will receive the findings/monitoring report
Group/committee/individual responsible for ensuring that the actions are completed
Review of DRE competency rates
Review of staff ESR records
Continence Nurse Specialist / Pelvic Floor Nurse
Monthly Patient Safety Council
Angela Sharman Continence Nurse Specialist and Siobainn Bathgate Pelvic Floor
9. EQUALITY ANALYSIS Please refer to the overarching document which covers all chapters of the Digital Rectal Examination Guideline. http://nww.sthk.nhs.uk/MANAGE/library/documents/EqualityAnalysisforICM.pdf
9
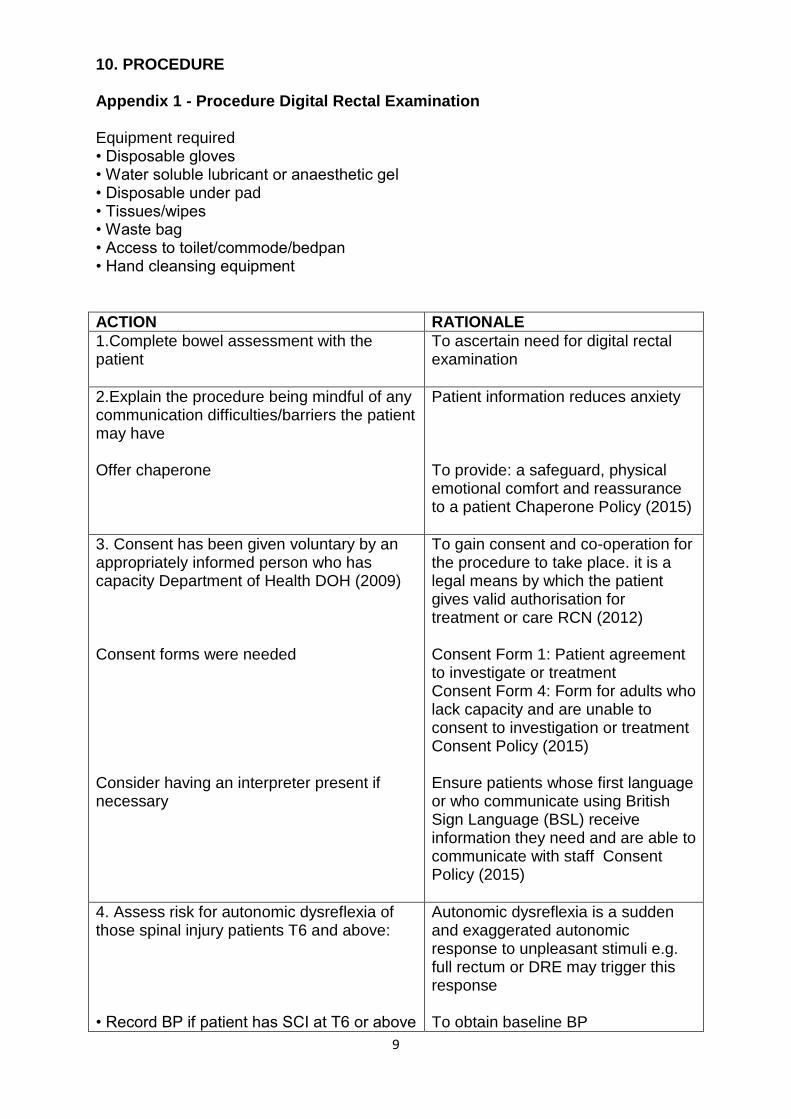
10. PROCEDURE Appendix 1 - Procedure Digital Rectal Examination Equipment required • Disposable gloves • Water soluble lubricant or anaesthetic gel • Disposable under pad • Tissues/wipes • Waste bag • Access to toilet/commode/bedpan • Hand cleansing equipment
ACTION RATIONALE
1.Complete bowel assessment with the patient
To ascertain need for digital rectal examination
2.Explain the procedure being mindful of any communication difficulties/barriers the patient may have Offer chaperone
Patient information reduces anxiety To provide: a safeguard, physical emotional comfort and reassurance to a patient Chaperone Policy (2015)
3. Consent has been given voluntary by an appropriately informed person who has capacity Department of Health DOH (2009) Consent forms were needed Consider having an interpreter present if necessary
To gain consent and co-operation for the procedure to take place. it is a legal means by which the patient gives valid authorisation for treatment or care RCN (2012) Consent Form 1: Patient agreement to investigate or treatment Consent Form 4: Form for adults who lack capacity and are unable to consent to investigation or treatment Consent Policy (2015) Ensure patients whose first language or who communicate using British Sign Language (BSL) receive information they need and are able to communicate with staff Consent Policy (2015)
4. Assess risk for autonomic dysreflexia of those spinal injury patients T6 and above: • Record BP if patient has SCI at T6 or above
Autonomic dysreflexia is a sudden and exaggerated autonomic response to unpleasant stimuli e.g. full rectum or DRE may trigger this response To obtain baseline BP
10
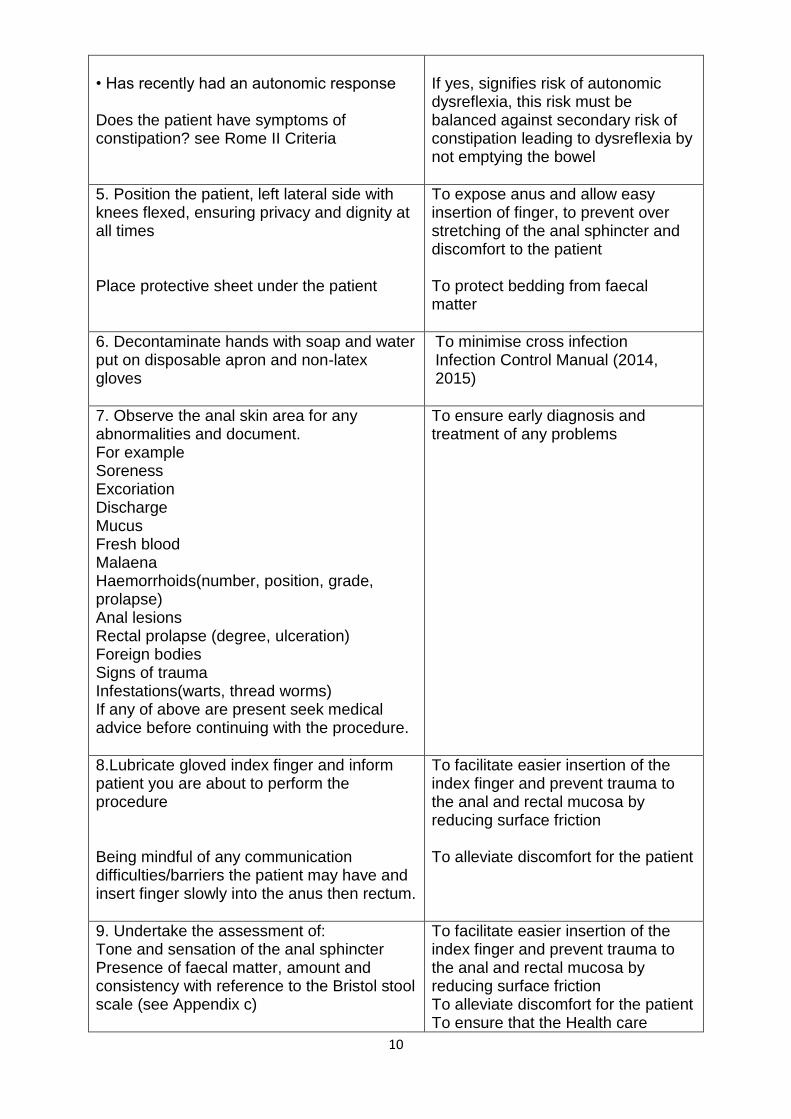
• Has recently had an autonomic response Does the patient have symptoms of constipation? see Rome II Criteria
If yes, signifies risk of autonomic dysreflexia, this risk must be balanced against secondary risk of constipation leading to dysreflexia by not emptying the bowel
5. Position the patient, left lateral side with knees flexed, ensuring privacy and dignity at all times Place protective sheet under the patient
To expose anus and allow easy insertion of finger, to prevent over stretching of the anal sphincter and discomfort to the patient To protect bedding from faecal matter
6. Decontaminate hands with soap and water put on disposable apron and non-latex gloves
To minimise cross infection Infection Control Manual (2014, 2015)
7. Observe the anal skin area for any abnormalities and document. For example Soreness Excoriation Discharge Mucus Fresh blood Malaena Haemorrhoids(number, position, grade, prolapse) Anal lesions Rectal prolapse (degree, ulceration) Foreign bodies Signs of trauma Infestations(warts, thread worms) If any of above are present seek medical advice before continuing with the procedure.
To ensure early diagnosis and treatment of any problems
8.Lubricate gloved index finger and inform patient you are about to perform the procedure Being mindful of any communication difficulties/barriers the patient may have and insert finger slowly into the anus then rectum.
To facilitate easier insertion of the index finger and prevent trauma to the anal and rectal mucosa by reducing surface friction To alleviate discomfort for the patient
9. Undertake the assessment of: Tone and sensation of the anal sphincter Presence of faecal matter, amount and consistency with reference to the Bristol stool scale (see Appendix c)
To facilitate easier insertion of the index finger and prevent trauma to the anal and rectal mucosa by reducing surface friction To alleviate discomfort for the patient To ensure that the Health care
11
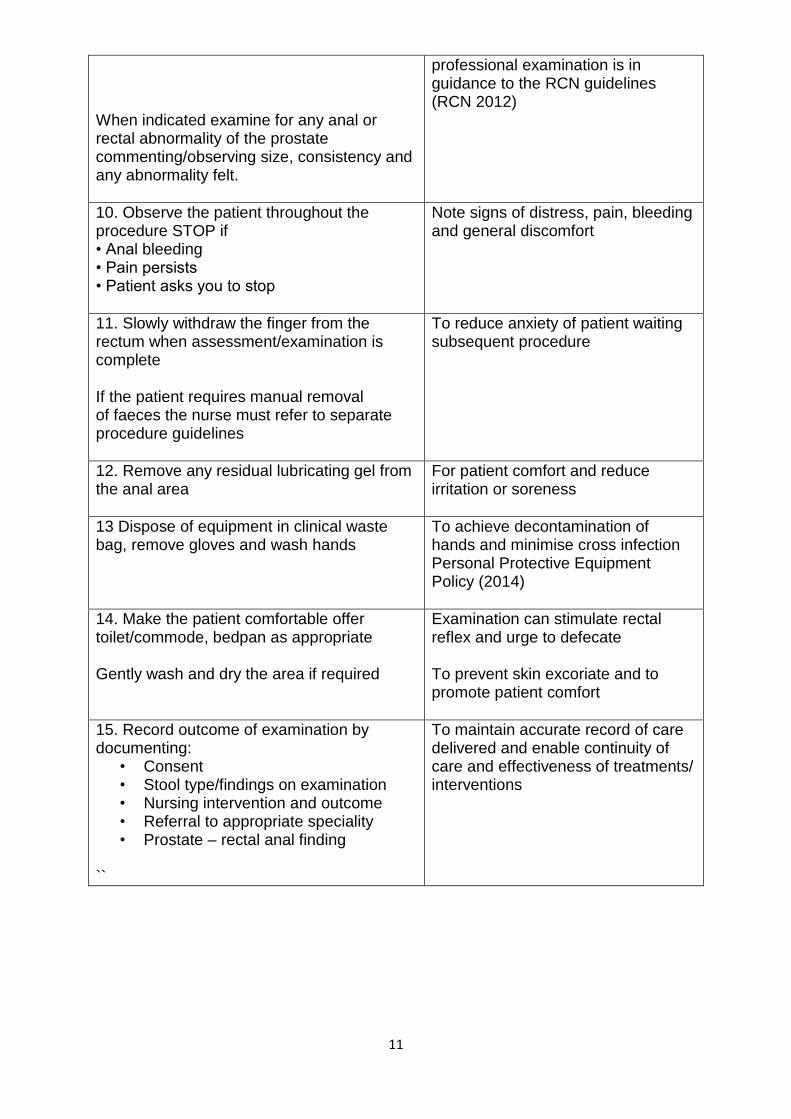
When indicated examine for any anal or rectal abnormality of the prostate commenting/observing size, consistency and any abnormality felt.
professional examination is in guidance to the RCN guidelines (RCN 2012)
10. Observe the patient throughout the procedure STOP if • Anal bleeding • Pain persists • Patient asks you to stop
Note signs of distress, pain, bleeding and general discomfort
11. Slowly withdraw the finger from the rectum when assessment/examination is complete
If the patient requires manual removal of faeces the nurse must refer to separate procedure guidelines
To reduce anxiety of patient waiting subsequent procedure
12. Remove any residual lubricating gel from the anal area
For patient comfort and reduce irritation or soreness
13 Dispose of equipment in clinical waste bag, remove gloves and wash hands
To achieve decontamination of hands and minimise cross infection Personal Protective Equipment Policy (2014)
14. Make the patient comfortable offer toilet/commode, bedpan as appropriate Gently wash and dry the area if required
Examination can stimulate rectal reflex and urge to defecate To prevent skin excoriate and to promote patient comfort
15. Record outcome of examination by documenting:
• Consent • Stool type/findings on examination • Nursing intervention and outcome • Referral to appropriate speciality • Prostate – rectal anal finding
``
To maintain accurate record of care delivered and enable continuity of care and effectiveness of treatments/ interventions
12
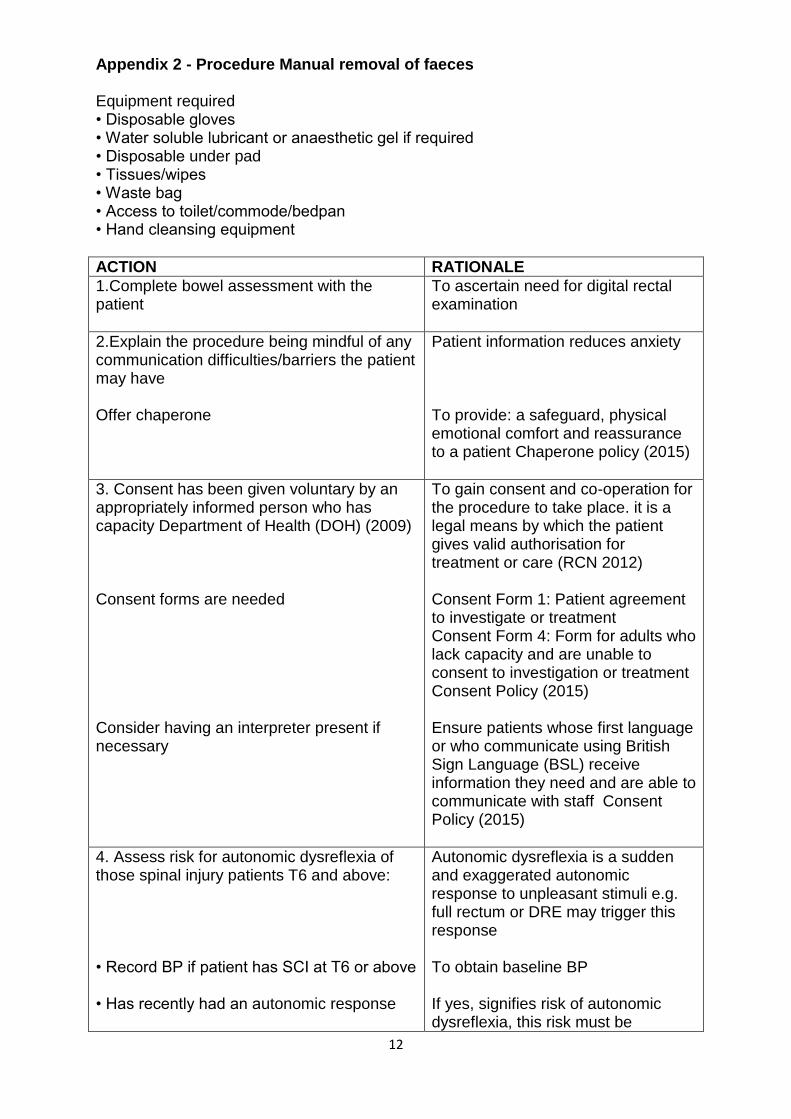
Appendix 2 - Procedure Manual removal of faeces Equipment required • Disposable gloves • Water soluble lubricant or anaesthetic gel if required • Disposable under pad • Tissues/wipes • Waste bag • Access to toilet/commode/bedpan • Hand cleansing equipment
ACTION RATIONALE
1.Complete bowel assessment with the patient
To ascertain need for digital rectal examination
2.Explain the procedure being mindful of any communication difficulties/barriers the patient may have Offer chaperone
Patient information reduces anxiety To provide: a safeguard, physical emotional comfort and reassurance to a patient Chaperone policy (2015)
3. Consent has been given voluntary by an appropriately informed person who has capacity Department of Health (DOH) (2009) Consent forms are needed Consider having an interpreter present if necessary
To gain consent and co-operation for the procedure to take place. it is a legal means by which the patient gives valid authorisation for treatment or care (RCN 2012) Consent Form 1: Patient agreement to investigate or treatment Consent Form 4: Form for adults who lack capacity and are unable to consent to investigation or treatment Consent Policy (2015) Ensure patients whose first language or who communicate using British Sign Language (BSL) receive information they need and are able to communicate with staff Consent Policy (2015)
4. Assess risk for autonomic dysreflexia of those spinal injury patients T6 and above: • Record BP if patient has SCI at T6 or above • Has recently had an autonomic response
Autonomic dysreflexia is a sudden and exaggerated autonomic response to unpleasant stimuli e.g. full rectum or DRE may trigger this response To obtain baseline BP If yes, signifies risk of autonomic dysreflexia, this risk must be
13
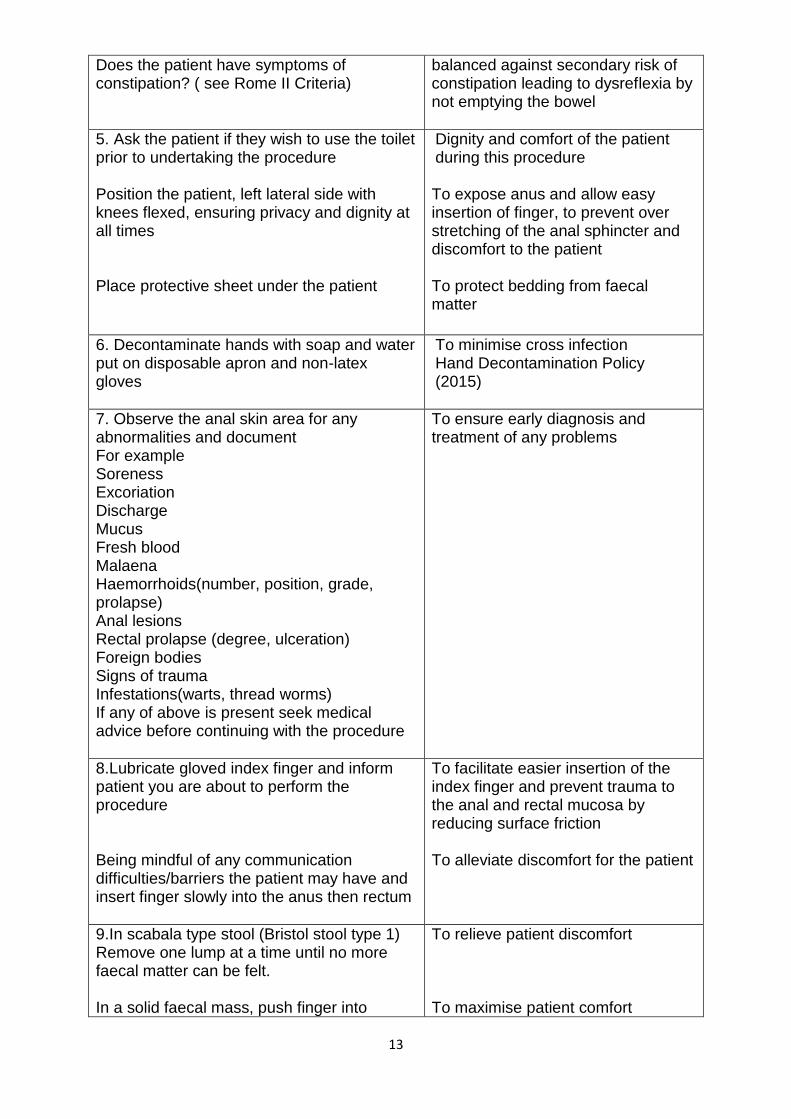
Does the patient have symptoms of constipation? ( see Rome II Criteria)
balanced against secondary risk of constipation leading to dysreflexia by not emptying the bowel
5. Ask the patient if they wish to use the toilet prior to undertaking the procedure Position the patient, left lateral side with knees flexed, ensuring privacy and dignity at all times Place protective sheet under the patient
Dignity and comfort of the patient during this procedure To expose anus and allow easy insertion of finger, to prevent over stretching of the anal sphincter and discomfort to the patient To protect bedding from faecal matter
6. Decontaminate hands with soap and water put on disposable apron and non-latex gloves
To minimise cross infection Hand Decontamination Policy (2015)
7. Observe the anal skin area for any abnormalities and document For example Soreness Excoriation Discharge Mucus Fresh blood Malaena Haemorrhoids(number, position, grade, prolapse) Anal lesions Rectal prolapse (degree, ulceration) Foreign bodies Signs of trauma Infestations(warts, thread worms) If any of above is present seek medical advice before continuing with the procedure
To ensure early diagnosis and treatment of any problems
8.Lubricate gloved index finger and inform patient you are about to perform the procedure Being mindful of any communication difficulties/barriers the patient may have and insert finger slowly into the anus then rectum
To facilitate easier insertion of the index finger and prevent trauma to the anal and rectal mucosa by reducing surface friction To alleviate discomfort for the patient
9.In scabala type stool (Bristol stool type 1) Remove one lump at a time until no more faecal matter can be felt. In a solid faecal mass, push finger into
To relieve patient discomfort To maximise patient comfort
14
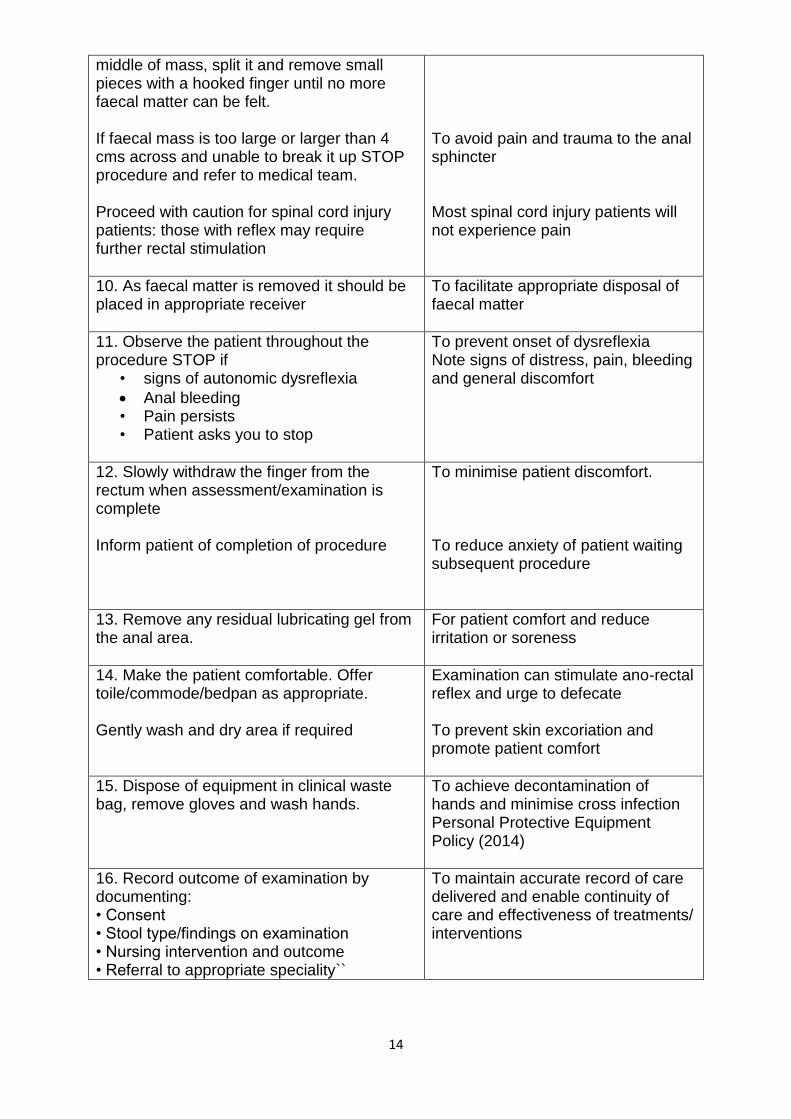
middle of mass, split it and remove small pieces with a hooked finger until no more faecal matter can be felt. If faecal mass is too large or larger than 4 cms across and unable to break it up STOP procedure and refer to medical team. Proceed with caution for spinal cord injury patients: those with reflex may require further rectal stimulation
To avoid pain and trauma to the anal sphincter Most spinal cord injury patients will not experience pain
10. As faecal matter is removed it should be placed in appropriate receiver
To facilitate appropriate disposal of faecal matter
11. Observe the patient throughout the procedure STOP if
• signs of autonomic dysreflexia
Anal bleeding • Pain persists • Patient asks you to stop
To prevent onset of dysreflexia Note signs of distress, pain, bleeding and general discomfort
12. Slowly withdraw the finger from the rectum when assessment/examination is complete
Inform patient of completion of procedure
To minimise patient discomfort. To reduce anxiety of patient waiting subsequent procedure
13. Remove any residual lubricating gel from the anal area.
For patient comfort and reduce irritation or soreness
14. Make the patient comfortable. Offer toile/commode/bedpan as appropriate. Gently wash and dry area if required
Examination can stimulate ano-rectal reflex and urge to defecate To prevent skin excoriation and promote patient comfort
15. Dispose of equipment in clinical waste bag, remove gloves and wash hands.
To achieve decontamination of hands and minimise cross infection Personal Protective Equipment Policy (2014)
16. Record outcome of examination by documenting: • Consent • Stool type/findings on examination • Nursing intervention and outcome • Referral to appropriate speciality``
To maintain accurate record of care delivered and enable continuity of care and effectiveness of treatments/ interventions
15
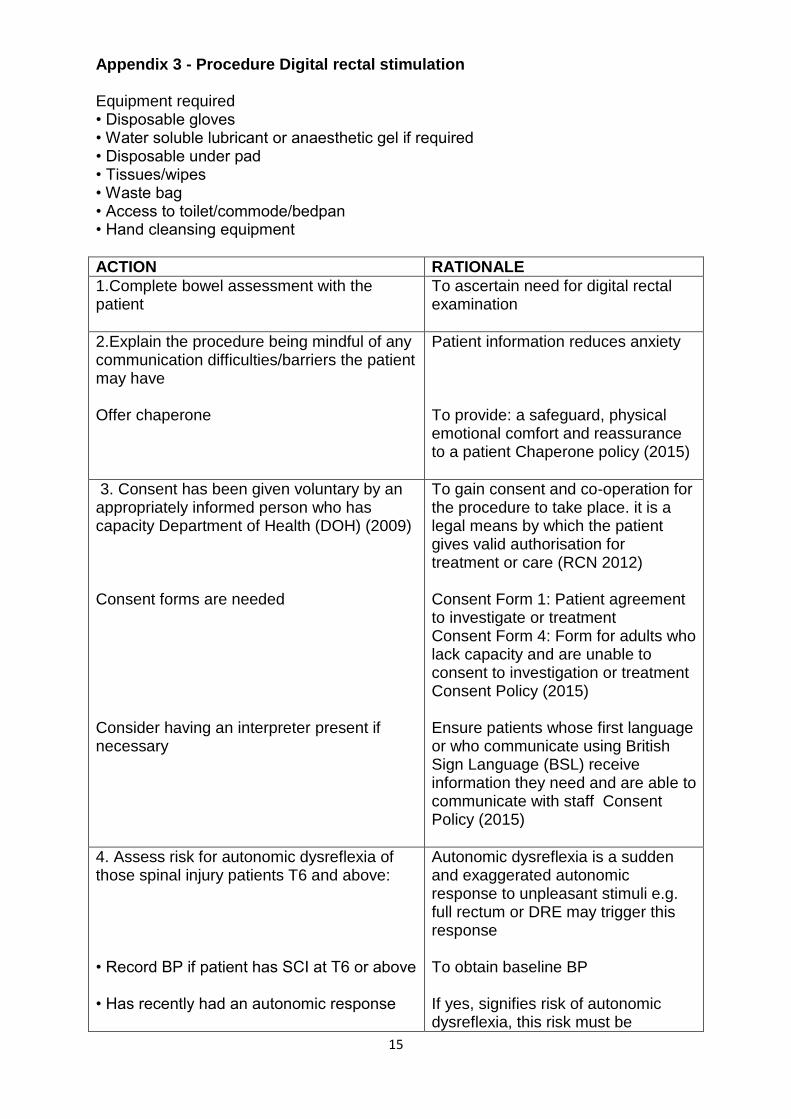
Appendix 3 - Procedure Digital rectal stimulation Equipment required • Disposable gloves • Water soluble lubricant or anaesthetic gel if required • Disposable under pad • Tissues/wipes • Waste bag • Access to toilet/commode/bedpan • Hand cleansing equipment
ACTION RATIONALE
1.Complete bowel assessment with the patient
To ascertain need for digital rectal examination
2.Explain the procedure being mindful of any communication difficulties/barriers the patient may have Offer chaperone
Patient information reduces anxiety To provide: a safeguard, physical emotional comfort and reassurance to a patient Chaperone policy (2015)
3. Consent has been given voluntary by an appropriately informed person who has capacity Department of Health (DOH) (2009) Consent forms are needed Consider having an interpreter present if necessary
To gain consent and co-operation for the procedure to take place. it is a legal means by which the patient gives valid authorisation for treatment or care (RCN 2012) Consent Form 1: Patient agreement to investigate or treatment Consent Form 4: Form for adults who lack capacity and are unable to consent to investigation or treatment Consent Policy (2015) Ensure patients whose first language or who communicate using British Sign Language (BSL) receive information they need and are able to communicate with staff Consent Policy (2015)
4. Assess risk for autonomic dysreflexia of those spinal injury patients T6 and above: • Record BP if patient has SCI at T6 or above • Has recently had an autonomic response
Autonomic dysreflexia is a sudden and exaggerated autonomic response to unpleasant stimuli e.g. full rectum or DRE may trigger this response To obtain baseline BP If yes, signifies risk of autonomic dysreflexia, this risk must be
16
Does the patient have symptoms of constipation? ( see Rome II Criteria)
balanced against secondary risk of constipation leading to dysreflexia by not emptying the bowel
5. Ask the patient if they wish to use the toilet prior to undertaking the procedure Position the patient, left lateral side with knees flexed, ensuring privacy and dignity at all times Place protective sheet under the patient
Dignity and comfort of the patient during this procedure To expose anus and allow easy insertion of finger, to prevent over stretching of the anal sphincter and discomfort to the patient To protect bedding from faecal matter
6. Decontaminate hands with soap and water put on disposable apron and non-latex gloves
To minimise cross infection Hand Decontamination Policy (2015)
7. Observe the anal skin area for any abnormalities and document. For example Soreness Excoriation Discharge Mucus Fresh blood Melena Haemorrhoids(number, position, grade, prolapse) Anal lesions Rectal prolapse (degree, ulceration) Foreign bodies Signs of trauma Infestations(warts, thread worms) If any of above is present seek medical advice before continuing with the procedure.
To ensure early diagnosis and treatment of any problems
8.Lubricate gloved index finger and inform patient you are about to perform the procedure Being mindful of any communication difficulties/barriers the patient may have and insert finger slowly into the anus then rectum
To facilitate easier insertion of the index finger and prevent trauma to the anal and rectal mucosa by reducing surface friction. To alleviate discomfort for the patient
9.Digital ano-rectal stimulation should last 20 seconds and stimulation no longer than 1 minute
To stimulate reflex emptying Stimulation can be repeated every 5 to 10 minutes until evacuation is completed, or no stool has been passed following 2 stimulations
17
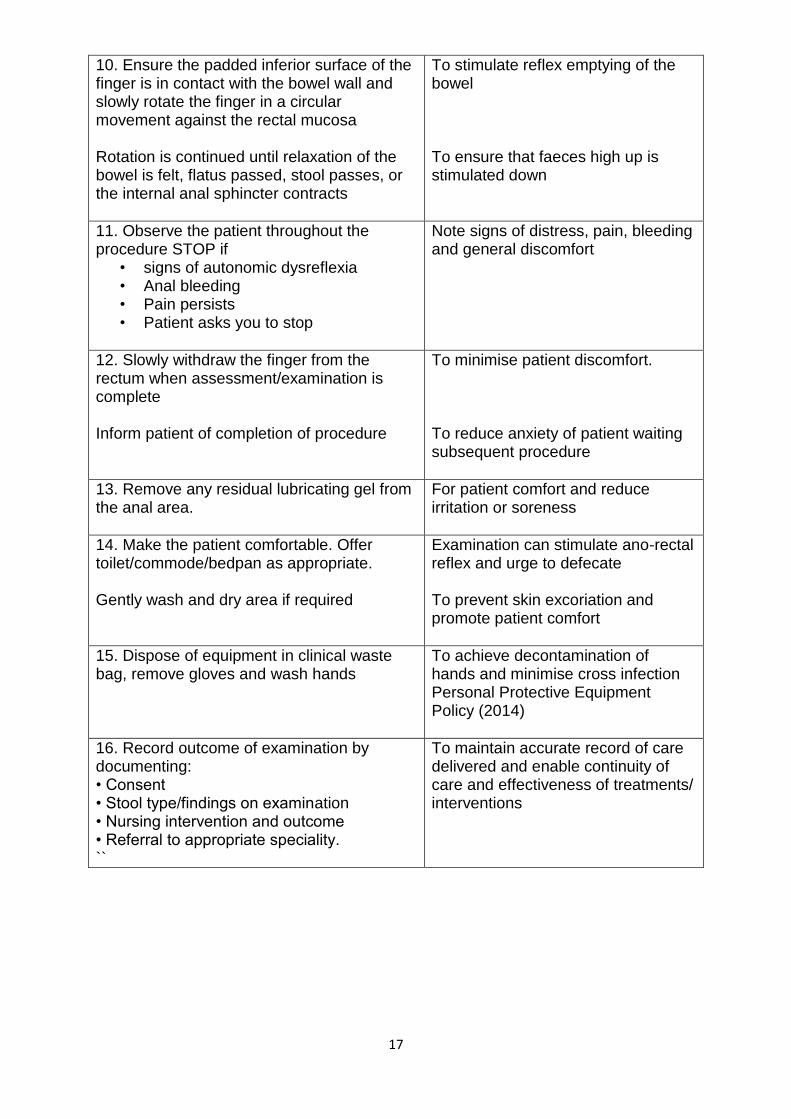
10. Ensure the padded inferior surface of the finger is in contact with the bowel wall and slowly rotate the finger in a circular movement against the rectal mucosa Rotation is continued until relaxation of the bowel is felt, flatus passed, stool passes, or the internal anal sphincter contracts
To stimulate reflex emptying of the bowel To ensure that faeces high up is stimulated down
11. Observe the patient throughout the procedure STOP if
• signs of autonomic dysreflexia • Anal bleeding • Pain persists • Patient asks you to stop
Note signs of distress, pain, bleeding and general discomfort
12. Slowly withdraw the finger from the rectum when assessment/examination is complete
Inform patient of completion of procedure
To minimise patient discomfort. To reduce anxiety of patient waiting subsequent procedure
13. Remove any residual lubricating gel from the anal area.
For patient comfort and reduce irritation or soreness
14. Make the patient comfortable. Offer toilet/commode/bedpan as appropriate. Gently wash and dry area if required
Examination can stimulate ano-rectal reflex and urge to defecate To prevent skin excoriation and promote patient comfort
15. Dispose of equipment in clinical waste bag, remove gloves and wash hands
To achieve decontamination of hands and minimise cross infection Personal Protective Equipment Policy (2014)
16. Record outcome of examination by documenting: • Consent • Stool type/findings on examination • Nursing intervention and outcome • Referral to appropriate speciality. ``
To maintain accurate record of care delivered and enable continuity of care and effectiveness of treatments/ interventions
18
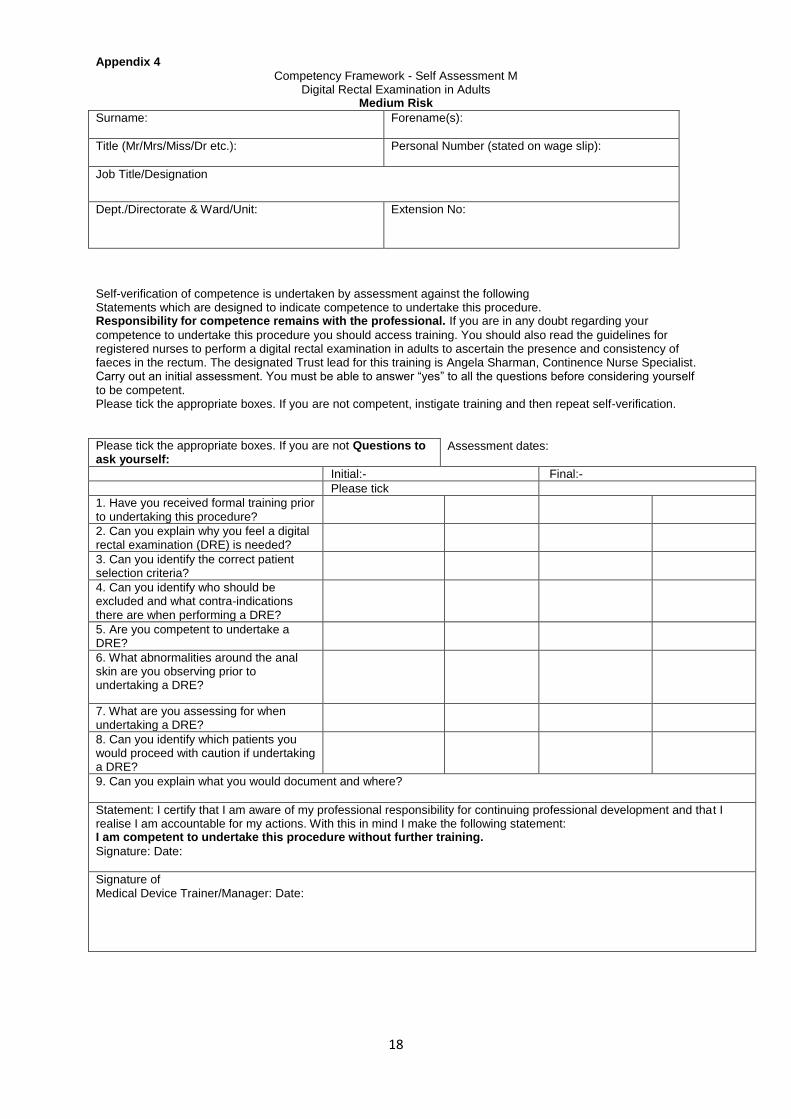
Appendix 4
Competency Framework - Self Assessment M Digital Rectal Examination in Adults
Medium Risk
Surname:
Forename(s):
Title (Mr/Mrs/Miss/Dr etc.):
Personal Number (stated on wage slip):
Job Title/Designation
Dept./Directorate & Ward/Unit: Extension No:
Self-verification of competence is undertaken by assessment against the following Statements which are designed to indicate competence to undertake this procedure. Responsibility for competence remains with the professional. If you are in any doubt regarding your
competence to undertake this procedure you should access training. You should also read the guidelines for registered nurses to perform a digital rectal examination in adults to ascertain the presence and consistency of faeces in the rectum. The designated Trust lead for this training is Angela Sharman, Continence Nurse Specialist. Carry out an initial assessment. You must be able to answer “yes” to all the questions before considering yourself to be competent. Please tick the appropriate boxes. If you are not competent, instigate training and then repeat self-verification.
Please tick the appropriate boxes. If you are not Questions to ask yourself:
Assessment dates:
Initial:- Final:-
Please tick
1. Have you received formal training prior to undertaking this procedure?
2. Can you explain why you feel a digital rectal examination (DRE) is needed?
3. Can you identify the correct patient selection criteria?
4. Can you identify who should be excluded and what contra-indications there are when performing a DRE?
5. Are you competent to undertake a DRE?
6. What abnormalities around the anal skin are you observing prior to undertaking a DRE?
7. What are you assessing for when undertaking a DRE?
8. Can you identify which patients you would proceed with caution if undertaking a DRE?
9. Can you explain what you would document and where?
Statement: I certify that I am aware of my professional responsibility for continuing professional development and that I realise I am accountable for my actions. With this in mind I make the following statement: I am competent to undertake this procedure without further training.
Signature: Date:
Signature of Medical Device Trainer/Manager: Date:
19
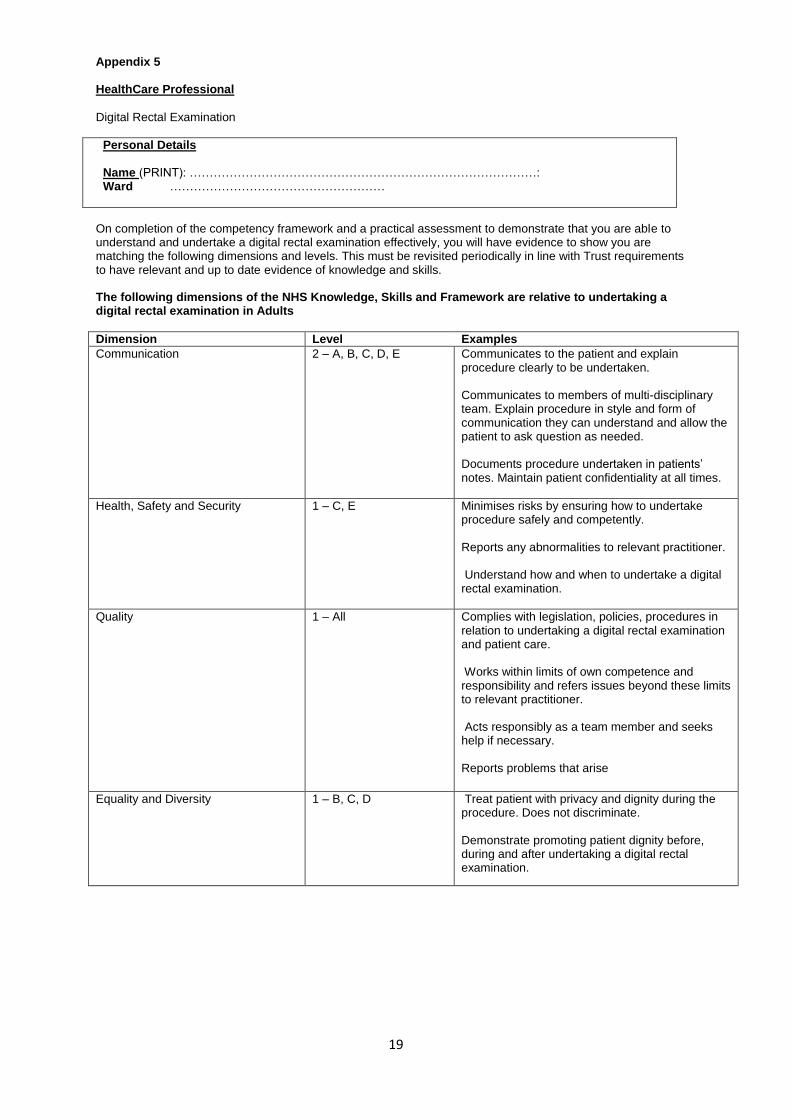
Appendix 5 HealthCare Professional
Digital Rectal Examination
Personal Details Name (PRINT): ……………………………………………………………………………: Ward ………………………………………………
On completion of the competency framework and a practical assessment to demonstrate that you are able to understand and undertake a digital rectal examination effectively, you will have evidence to show you are matching the following dimensions and levels. This must be revisited periodically in line with Trust requirements to have relevant and up to date evidence of knowledge and skills. The following dimensions of the NHS Knowledge, Skills and Framework are relative to undertaking a digital rectal examination in Adults
Dimension Level Examples
Communication 2 – A, B, C, D, E Communicates to the patient and explain procedure clearly to be undertaken. Communicates to members of multi-disciplinary team. Explain procedure in style and form of communication they can understand and allow the patient to ask question as needed. Documents procedure undertaken in patients’ notes. Maintain patient confidentiality at all times.
Health, Safety and Security 1 – C, E Minimises risks by ensuring how to undertake procedure safely and competently. Reports any abnormalities to relevant practitioner. Understand how and when to undertake a digital rectal examination.
Quality 1 – All Complies with legislation, policies, procedures in relation to undertaking a digital rectal examination and patient care. Works within limits of own competence and responsibility and refers issues beyond these limits to relevant practitioner. Acts responsibly as a team member and seeks help if necessary. Reports problems that arise
Equality and Diversity 1 – B, C, D Treat patient with privacy and dignity during the procedure. Does not discriminate. Demonstrate promoting patient dignity before, during and after undertaking a digital rectal examination.
20
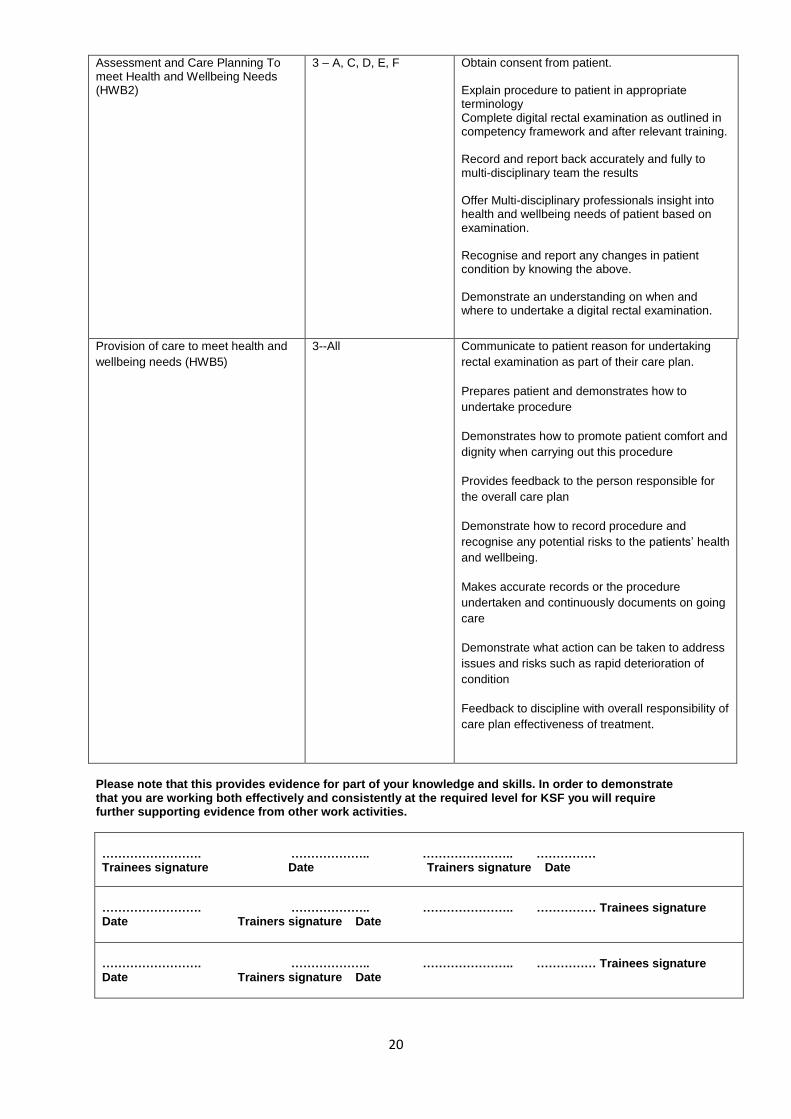
Assessment and Care Planning To meet Health and Wellbeing Needs (HWB2)
3 – A, C, D, E, F Obtain consent from patient. Explain procedure to patient in appropriate terminology Complete digital rectal examination as outlined in competency framework and after relevant training. Record and report back accurately and fully to multi-disciplinary team the results Offer Multi-disciplinary professionals insight into health and wellbeing needs of patient based on examination. Recognise and report any changes in patient condition by knowing the above. Demonstrate an understanding on when and where to undertake a digital rectal examination.
Provision of care to meet health and
wellbeing needs (HWB5)
3--All Communicate to patient reason for undertaking
rectal examination as part of their care plan.
Prepares patient and demonstrates how to
undertake procedure
Demonstrates how to promote patient comfort and
dignity when carrying out this procedure
Provides feedback to the person responsible for
the overall care plan
Demonstrate how to record procedure and
recognise any potential risks to the patients’ health
and wellbeing.
Makes accurate records or the procedure
undertaken and continuously documents on going
care
Demonstrate what action can be taken to address
issues and risks such as rapid deterioration of
condition
Feedback to discipline with overall responsibility of
care plan effectiveness of treatment.
Please note that this provides evidence for part of your knowledge and skills. In order to demonstrate that you are working both effectively and consistently at the required level for KSF you will require further supporting evidence from other work activities.
……………………. ……………….. ………………….. …………… Trainees signature Date Trainers signature Date
……………………. ……………….. ………………….. …………… Trainees signature Date Trainers signature Date
……………………. ……………….. ………………….. …………… Trainees signature Date Trainers signature Date
21
11. AUTONOMIC DYSREFLEXIA Autonomic Dysreflexia, also known as Hyperreflexia, is a condition where the blood pressure in a person with a spinal cord injury (SCI) above T5-6 becomes excessively high due to the over activity of the Autonomic Nervous System. Autonomic Dysreflexia is usually caused when a painful stimulus occurs below the level of spinal cord injury. The stimulus is then mediated through the Central Nervous System (CNS) and the Peripheral Nervous System (PNS). The CNS is made up of the spinal cord and brain, which control voluntary acts and end organs via their respective nerves. The PNS is made up from 12 pairs of cranial nerves, spinal nerves and peripheral nerves. The PNS also is divided into the somatic nervous system and the autonomic nervous system. The autonomic nervous system is responsible for the signs and symptoms of autonomic dysreflexia. The autonomic nervous system normally maintains body homeostasis via its two branches, the parasympathetic autonomic nervous system (PANS) and the sympathetic autonomic nervous system (SANS). These branches have complementary roles through a negative feedback system; that is, when one branch is stimulated, the other branch is suppressed. If continued painful stimuli are experienced below the level of the injury the messages of pain become ‘trapped’ at the level of the injury and the patient may develop autonomic dysreflexia. It can develop very suddenly and if not treated promptly it may lead to seizures, stroke and even death. Possible causes of Autonomic Dysreflexia Bladder (most common) - from overstretch or irritation of bladder wall
Urinary tract infection
Urinary retention
Blocked catheter
Overfilled collection bag
Non-compliance with intermittent catheterisation programme Bowel - over distension or irritation
Constipation / impaction
Distension during bowel programme (digital stimulation from manual evacuation of bowels)
Haemorrhoids or anal fissures
Infection or irritation (e.g. appendicitis) Skin-related Disorders
Any direct irritant below the level of injury (e.g. - prolonged pressure by object in shoe or chair, cut, bruise, abrasion)
Pressure sores (decubitus ulcer)
Ingrown toenails
Burns (e.g. - sunburn, burns from using hot water)
Tight or restrictive clothing or pressure to skin from sitting on wrinkled clothing Sexual Activity
Over stimulation during sexual activity (stimuli to the pelvic region which would ordinarily be painful if sensation were present)
Menstrual cramps
Labour and delivery
Other
22
Heterotopic ossification ("Myositis ossificans", "Heterotopic bone")
Acute abdominal conditions (gastric ulcer, colitis, peritonitis)
Skeletal fractures
The painful stimuli must be treated and removed for autonomic dysreflexia to be relieved.
Symptoms The patient will experience or display some or all of the following symptoms, most patients are aware of autonomic dysreflexia and know more about it than us, they will inform you they are experiencing autonomic dysreflexia symptoms.
Nasal congestion
Pounding headache
Anxiety, feeling of doom and apprehension
Sweating
Tightness in the chest
Blotching of the skin above level of cord lesion
Slow pulse
Hypertension (tetraplegic patients may have a low blood pressure of 90/60mmhg, therefore a rise to 120/80mmhg may represent a significant rise)
Pupillary dilation
Cardiac dysrhythmia Treatment 1. Immediate Action Reduce the blood pressure by placing the patient in the sitting position and/or raising the head. Take the blood pressure. Give sublingual Nifedipine 10mg. Pierced, bitten or chewed or GTN Spray (if possible monitor blood pressure every five minutes during the episode.) Treatment may be repeated up to four doses (40mg.) over one hour. (For all spinal injury patients please ensure they have 10mg. Sublingual Nifedipine, Lignocaine 2% gel and GTN Spray prescribed in the PRN section of the drug kardex on admission) 2. Remove cause Step one:
Check Bladder
Bladder distended
If catheters present check patency and if blocked/kinked correct the problem.
If not catheterised catheterise immediately and leave on free drainage (only if bladder distended)
IF IN ANY DOUBT RE-CATHETERISE (consider antibiotics for UTI) Step two:
Check bowel
Check rectum for faecal impaction using lubricating Gel or Lignocaine 2% gel. If impaction present gently carry out manual evacuation if trained to do so. (Ensure additional pain is not caused as this will aggravate the autonomic
23
dysreflexia symptoms). If rectum empty consider constipation as a cause and arrange appropriate treatment.
Step three:
Check Skin
Check skin for pressure ulcers, abscesses or tight uncomfortable clothing, relieve pressure from body weight or clothing, give analgesia and apply appropriate dressing.
Step four:
Check other causes
Check for other possibilities of stimuli such as in-growing toenails, fractures, deep vein thrombosis and treat accordingly.
Step five:
Continue to record observations,
Pulse, Blood pressure, Urine output, report and treat any abnormalities. Step six:
If condition has not resolved contact the spinal injuries unit for further advice. 3. Medical Management 1. Nifedipine, sublingual 10mg. Bitten or chewed. This may be repeated up to four doses (40mg.) over one hour. Or 2. GTN Spray 1-2 doses under tongue (as alternative to Nifedipine). 3. Diazepam (diazemules I.V) for treatment of associated spasms and for control of fits. 4. Ligoncaine 2% Gel per rectum (not licensed but considered best practice for autonomic dysreflexia management) or per urethra to relieve painful stimuli. 5. Pain – do not use Aspirin or NSAID for analgesia or for relief of headache. Use Paracetamol, Co-Proximal and/or consider morphine. CONTACT PHARMACY OR SPINAL INJURY UNIT FOR FURTHER ADVICE. Trust management of patients at risk of autonomic dysreflexia In the case of spinal cord injured (SCI) patients, then autonomic dysreflexia can occur in patients with faecal impaction and/or further stimulation brought on by digital removal. Southport Spinal unit treats SCI patients with regard to their pelvic floor issues and is fully aware of this potential problem. The majority of Trust patients requiring digital evacuation are managed at SpR level. These patients tend to be neurologically intact.
24
12. REFERENCES Chaperone Policy (2015) policy version 1.00 policy reference number STHK 0387 Consent Policy (2015) policy version 8.1 policy reference number: STHK 0058 Department of Health (2009) Reference guide to consent for examination or treatment http://www.gov.uk/.../reference-guide-to-consent-for-examination-or-treatment-second-edition Infection control manual (2015) – chapter 21 Hand Decontamination policy-version 10 (clinical) policy reference number: STHK 0079 Infection control manual (2014) – chapter 5 Personal Protective Equipment policy version 4 (clinical) policy reference number: STHK 0273 Kyle, G, (2007) Bowel care, part 5 – a practical guide to digital rectal examination. NursingTimes: 103, 45, 28-29. Longstreth, G. F., Thompson, W. G., Chey, W. D. et al (2006) Functional Bowel disorders. Gastroenterology 130 (5), 1480-1491 [Abstract(http://www.ncbi.nlm.nih.gov/pubmed/16678561)] Managing mental incapacity (2015) policy version 3 policy reference number: STHK 0169 National Institute for Clinical Excellence (NICE) (2015) Constipation http://cks.nice.org.uk/constipation Royal College of Nursing, (2012), Management of lower bowel dysfunction, including DRE and DRF: guidance for nurses. London: RCN. Publication code 000226 Nursing and Midwifery council (NMC) 2008 The code: Standards of conduct, performance and ethics for nurses and midwives, London: NMC. Stephenson R, (2015) automic dysreflexia in spinal cord injury http://emedicine.medscape.com/article/322809overview













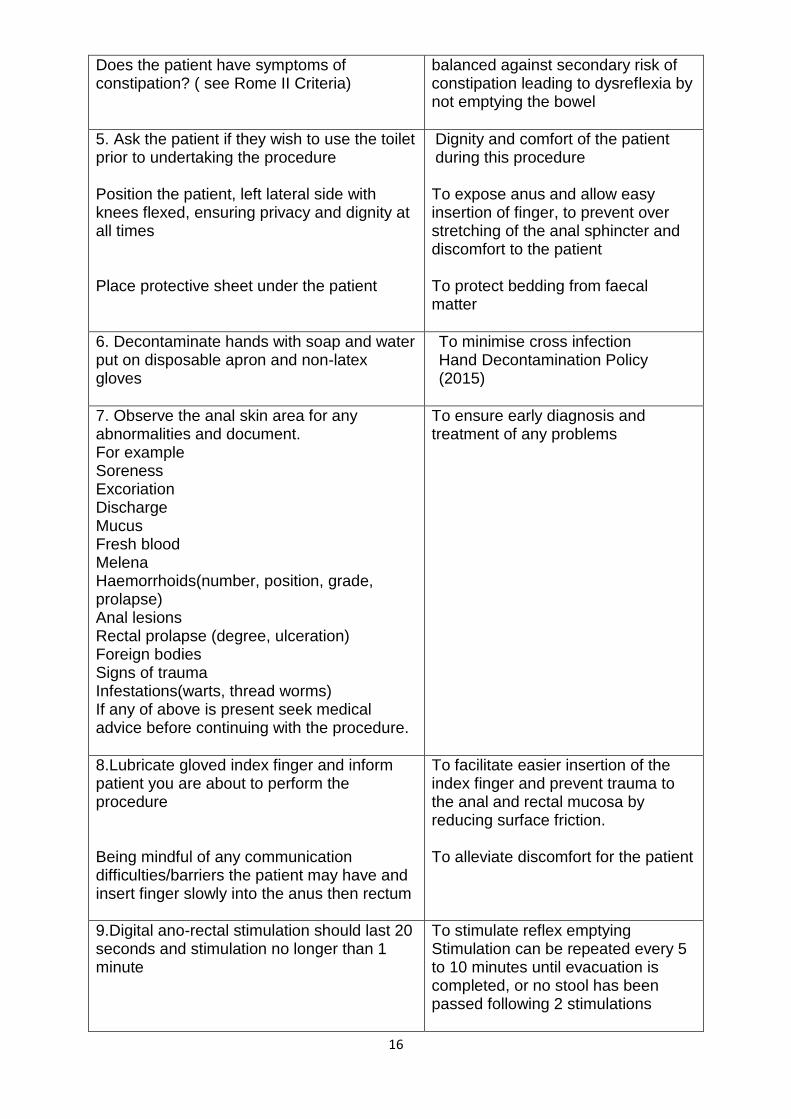
![[MRI of extraperitoneal rectal carcinoma]](https://img.pdfslide.net/doc/110x75/635a8910ef8fb73aab01ca90/mri-of-extraperitoneal-rectal-carcinoma.jpg)















