Embed Size (px)
Citation preview
La Revue de Santé de la Méditerranée orientale
Eastern Mediterranean Health Journal
Volume 27 No. 11November/Novembre
المجلد السابع والعشرون عدد 112021 نوفمبر/تشرين الثاني
The COVID-19 pandemic is the first in human history in which innovative digital technologies are being used on an unprecedented scale to keep people connected, safe and productive while being physically and socially apart. During the World Health Assembly in 2019, Member States endorsed the Global Strategy for Digital Health. This has proven timely for implementation of digital technologies in response to different national priorities, including more efficient health care delivery and pandemic response
Eastern Mediterranean Health Journal
IS the official health journal published by the Eastern Mediterranean Regional Office of the World Health Organization. It is a forum for the presentation and promotion of new policies and initiatives in public health and health services; and for the exchange of ideas, concepts, epidemiological data, research findings and other information, with special reference to the Eastern Mediterranean Region. It addresses all members of the health profession, medical and other health educational institutes, interested NGOs, WHO Collaborating Centres and individuals within and outside the Region.
املجلة الصحية لرشق املتوسط هى املجلة الرسمية التى تصدر عن املكتب اإلقليمى لرشق املتوسط بمنظمة الصحة العاملية. وهى منرب لتقديم السياسات واملبادرات اجلديدة يف الصحة العامة بإقليم رشق يتعلق منها املعلومات، وخاصة ما الوبائية ونتائج األبحاث وغري ذلك من واخلدمات الصحية والرتويج هلا، ولتبادل اآلراء واملفاهيم واملعطيات املتوسط. وهى موجهة إىل كل أعضاء املهن الصحية، والكليات الطبية وسائر املعاهد التعليمية، وكذا املنظامت غري احلكومية املعنية، واملراكز املتعاونة مع منظمة
الصحة العاملية واألفراد املهتمني بالصحة ىف اإلقليم وخارجه.
La Revue de Santé de la Méditerranée Orientale
EST une revue de santé officielle publiée par le Bureau régional de l’Organisation mondiale de la Santé pour la Méditerranée orientale. Elle offre une tribune pour la présentation et la promotion de nouvelles politiques et initiatives dans le domaine de la santé publique et des services de santé ainsi qu’à l’échange d’idées, de concepts, de données épidémiologiques, de résultats de recherches et d’autres informa-tions, se rapportant plus particulièrement à la Région de la Méditerranée orientale. Elle s’adresse à tous les professionnels de la santé, aux membres des instituts médicaux et autres instituts de formation médico-sanitaire, aux ONG, Centres collaborateurs de l’OMS et personnes concernés au sein et hors de la Région.
Correspondence
Editor-in-chief
Eastern Mediterranean Health JournalWHO Regional Office for the Eastern MediterraneanP.O. Box 7608 Nasr City, Cairo 11371 Egypt Tel: (+202) 2276 5000 Fax: (+202) 2670 2492/(+202) 2670 2494 Email: [email protected]
Members of the WHO Regional Committee for the Eastern Mediterranean Afghanistan . Bahrain . Djibouti . Egypt . Islamic Republic of Iran . Iraq . Jordan . Kuwait . Lebanon Libya . Morocco . Oman . Pakistan . Palestine . Qatar . Saudi Arabia . Somalia . Sudan . Syrian Arab RepublicTunisia . United Arab Emirates . Yemen
البلدان أعضاء اللجنة اإلقليمية ملنظمة الصحة العاملية لرشق املتوسط األردن . أفغانستان . اإلمارات العربية املتحدة . باكستان . البحرين . تونس . ليبيا . مجهورية إيران اإلسالمية
اجلمهورية العربية السورية . جيبويت . السودان . الصومال . العراق . عامن . فلسطني . قطر . الكويت . لبنان . مرص . املغرباململكة العربية السعودية . اليمن
Membres du Comité régional de l’OMS pour la Méditerranée orientale Afghanistan . Arabie saoudite . Bahreïn . Djibouti . Égypte . Émirats arabes unis . République islamique d’Iran Iraq . Libye . Jordanie . Koweït . Liban . Maroc . Oman . Pakistan . Palestine . Qatar . République arabe syrienne Somalie . Soudan . Tunisie . Yémen
Subscriptions and Permissions
Publications of the World Health Organization can be obtained from Knowledge Sharing and Production, World Health Organization, Regional Office for the Eastern Mediterranean, PO Box 7608, Nasr City, Cairo 11371, Egypt (tel: +202 2670 2535, fax: +202 2670 2492; email: [email protected]). Requests for permission to reproduce, in part or in whole, or to translate publications of WHO Regional Office for the Eastern Mediterranean – whether for sale or for noncommercial distribution – should be addressed to WHO Regional Office for the Eastern Mediterranean, at the above address; email: [email protected].
EMHJ is a trilingual, peer reviewed, open access journal and the full contents are freely available at its website: http://www/emro.who.int/emhj.htm
EMHJ information for authors is available at its website: http://www.emro.who.int/emh-journal/authors/
EMHJ is abstracted/indexed in the Index Medicus and MEDLINE (Medical Literature Analysis and Retrieval Systems on Line), ISI Web of knowledge, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Embase, Lexis Nexis, Scopus and the Index Medicus for the WHO Eastern Mediterranean Region (IMEMR).
© World Health Organization (WHO) 2021. Some rights reserved.This work is available under the CC BY-NC-SA 3.0 IGO licence (https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Disclaimer The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.
The authors alone are responsible for the views expressed in this publication and they do not necessarily represent the views, decisions or policies of the institutions with which they are affiliated.
If authors are staff members of the World Health Organization, the authors alone are responsible for the views expressed in this publication and do not necessarily represent the decisions, policy or views of the World Health Organization.
ISSN 1020-3397
Cover image © WHO
Cover 27-11.indd 4,6Cover 27-11.indd 4,6 06/12/2021 12:38 PM06/12/2021 12:38 PM
Vol. 27 . 11 – 2021
La Revue de Santé de la Méditerranée orientale
Eastern Mediterranean Health Journal
Editorial
Enhancing capacity and use of digital health in the Eastern Mediterranean Region: an urgent priority for actionAhmed Mandil, Arash Rashidian, Mohamed Nour, Heba Fouad and Rana Hajjeh..............................................................................................1031
Commentary
Waste management of used personal protective equipment during the COVID-19 pandemic in the Eastern Mediterranean RegionRola Al-Emam and Basel Al-Yousfi .......................................................................................................................................................................................1034
Research articlesNoncommunicable disease, clinical course and COVID-19 prognosis: results based on I-CORE RegistryShaghayegh Javanmard, Noushin Mohammadifard, Maryam Nasirian, Golnaz Vaseghi, Kamal Heidari, Behrouz Kelidari, Tahereh Changiz and Nizal Sarrafzadegan ................................................................................................................................... 1036
Adapting the ethical review process for COVID-19 research: reviewers’ perspectives from PakistanSualeha Shekhani, Saima Iqbal and Aamir Jafarey .........................................................................................................................................................1045
Prevalence of and risk factors for Enterobius vermicularis infestation in preschool children, West Bank, PalestineRasha Khayyat, Souad Belkebir, Sameh Abuseir, Majd Barahmeh, Lujain Alsadder and Walid Basha ........................................................ 1052
Association between type of physical activity and risk factors for cardiovascular disease, Islamic Republic of IranOmid Aminian, Maryam Saraei, Saeed Najieb Pour and Sahar Eftekhari ...............................................................................................................1061
Determinants of the Early Childhood Development Index among children aged < 5 years in Bangladesh, Costa Rica and Ghana: a comparative studyIqramul Haq, Md. Ismail Hossain, Maliha Afroj Zinnia, Md Rifat Hasan and Imru-Al-Quais Chowdhury ..............................................1069
Association of clinical features of typhoid fever with socioeconomic status in PakistanMuhammad Samsoor Zarak, Hamaiyal Sana, Muzhgan Shah, Shabir Lehri, Mahekan Saghir, Qandeel Gul, Muhammad Saood, Aqeel Nasim and Noman ul haq. ........................................................................................................................1078
Incidence of and factors associated with metabolic syndrome, south-east Islamic Republic of IranKhadijeh Farmanfarma, Alireza Ansari-Moghaddam, Mahmoud Kaykhaei, Mehdi Mohammadi, Hosein Adineh and Hasan Aliabd .........................................................................................................................................................................................1084
Health effects of desert dust storm events in the south-eastern Mediterranean: perceptions and practices of local stakeholdersParaskevi Kinni, Panayiotis Kouis, Helen Dimitriou, Shaked Yarza, Stefania I. Papatheodorou, Eirini Kampriani, Melanie Charalambous, Nicos Middleton, Victor Novack, Emmanouil Galanakis and Panayiotis K. Yiallouros...................................1092
Short research communication
The brain drain: why medical students and young physicians want to leave EgyptIbrahim Kabbash, Rania El-Sallamy, Hanaa Zayed, Ibrahim Alkhyate, Ahmed Omar and Sanaa Abdo .........................................................1102
ReportMERS-CoV in the COVID-19 era: update from Saudi Arabia, 2019–2020Anas Khan, Sharafaldeen Bin Nafisah, Bandr Mzahim, Bakhitah Aleid, Daliah Almatrafi,Abdullah Assiri and Hani Jokhdar .........................................................................................................................................................................................1109
ReviewCOVID-19 in Saudi Arabia: the national health response
Anas Khan, Yousef Alsofayan, Ahmed Alahmari, Jalal Alowais, Abdullah Algwizani, Haleema Alserehi,Abdullah Assiri and Hani Jokhdar ......................................................................................................................................................................................... 1114
WHO events addressing public health prioritiesNational workshop for health research prioritization in Jordan ...................................................................................................... 1125
Book 27-11.indb 1029Book 27-11.indb 1029 06/12/2021 12:39 PM06/12/2021 12:39 PM
Ahmed Al-Mandhari Editor-in-ChiefArash Rashidian Executive EditorAhmed Mandil Deputy Executive Editor
Editorial BoardMahmoud Fahmy Fathalla Akbar Fotouhi Rita Giacaman Rana Hajjeh Ahmed Mandil Ziad Memish Arash Rashidian Abla Mehio Sibai Sameen Siddiqi Huda Zurayk
International Advisory Panel Mansour M. Al-Nozha Fereidoun Azizi Rafik Boukhris Zulfiqar Bhutta Majid Ezzati Hans V. Hogerzeil Mohamed A. Ghoneim Alan Lopez Hossein Malekafzali El-Sheikh Mahgoub Hooman Momen Sania Nishtar Hikmat Shaarbaf Salman Rawaf
Editorial assistantsNadia Abu-Saleh, Suhaib Al Asbahi (graphics), Diana Tawadros (graphics)
Editorial supportGuy Penet (French editor)Eva Abdin, Fiona Curlet, Cathel Kerr, Marie-France Roux (Technical editors)Ahmed Bahnassy, Abbas Rahimiforoushani, Manar El Sheikh Abdelrahman (Statistics editors)
Administration Iman Fawzy, Marwa Madi
Web publishingNahed El Shazly, Ihab Fouad, Hazem Sakr
Library and printing supportHatem Nour El Din, Gehane Al Garraya, Mariam Zaki, Fouad Abdelghaffar Ahmed Magdy, Amin El Sayed
Cover and internal layout designed by Diana Tawadros and Suhaib Al AsbahiPrinted by WHO Regional Office for the Eastern Mediterranean, Cairo, Egypt
Book 27-11.indb 1030Book 27-11.indb 1030 06/12/2021 12:39 PM06/12/2021 12:39 PM

1031
EMHJ – Vol. 27 No. 11 – 2021Editorial
Enhancing capacity and use of digital health in the Eastern Mediterranean Region: an urgent priority for action
Ahmed Mandil,1 Arash Rashidian,2 Mohamed Nour,3 Heba Fouad4 and Rana Hajjeh5
1Coordinator, Research and Innovation; 2Director, Science, Information & Dissemination; 3Technical Officer, Digital Health & Innovation; 4Regional Surveillance Officer; 5Director, Programme Management, World Health Organization Regional Office for the Eastern Mediterranean, Cairo, Egypt (Correspondence to: Arash Rashidian: [email protected]).
Citation: Mandil A; Rashidian A; Nour M; Fouad H; Hajjeh R. Enhancing capacity and use of digital health in the Eastern Mediterranean Region: an urgent priority for action. East Mediterr Health J. 2021;27(11):1031−1033. https://doi.org/10.26719/2021.27.11.1031
Copyright © World Health Organization (WHO) 2021. Open Access. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license (https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
The Eastern Mediterranean Region (EMR) faces massive challenges that threaten people’s livelihood and health due to multiple factors, including socioeconomic disparities, conflicts and emergencies in many countries of the Region (1). The COVID-19 pandemic has further exacerbated these challenges and significantly disrupted access to essential health services. As highlighted in recent flagship reports, the region is unlikely to achieve health-related Sustainable Development Goals (2,3), unless crucial changes are made in the way the goals are pursued (4,5). Effective implementation of digital health technologies could provide opportunities to enhance the response to the pandemic, as well as improve the access to health services and develop stronger and more resilient health systems (6,7). Such technologies are widely used to provide more efficient connectivity and access to health information; better access and quality of health care services; cost-effective systems and services; reaching out to remote, rural and migrant settings; monitoring health outcomes; supporting health decision-making as well as facilitating emergency response (7). However, the adoption of digital health solutions without a strategy that identifies country priorities and community context could lead to fragmented short-living implementations that have limited impact on individuals’ well-being (7).Countries need to develop a vision and a strategy to guide selection of appropriate digital health technologies, that are relevant to their health priorities. This would lead to an implementation plan that better suits their context, and more sustainable commitment and impact (6,8,9,10).
WHO is expanding its efforts to support countries in engaging stakeholders and coordinating the the core components of digital health (including leadership and governance, capital investment, services and applications, standards and interoperability, infrastructure, legislations and compliance, workforce) required for sustainable implementation to enhance health systems’ capabilities in provision of equitable and efficient health services (6,9,10,11). Using digital health in support of healthcare delivery and health systems has been discussed in several WHO/EMR ministerial meetings (12−15), most recently
during a pre-Regional Committee (RC) 68th session titled: “Is the Eastern Mediterranean Region ready for digitalizing health? Implications from Global Strategy on Digital health (2020–2025)” (16). The focus was on adaptation of the global strategy (adopted globally in the 71st World Health Assembly in 2018) to the regional needs and context (6,16). The Be He@lthy, Be Mobile (BHBM) is a global mobile health (mHealth) initiative, led by the World Health Organization (WHO) and International Telecommunication Union (ITU), to assist governments in using mobile technology to address priority health topics and reinforce existing national health activities to prevent, manage and treat health conditions and diseases (11). The BHBM platform has been used to deliver reliable information to tens of millions of people through SMS messages and mobile applications, for health promotion, disease prevention, management, and preventing complications.
The COVID-19 pandemic is probably the first in human history in which innovative digital technologies and social media are being used on an unprecedented scale to keep people connected, safe and productive, while being physically and socially apart (17). This has been witnessed in using digital technologies in all phases of pandemic response, including surveillance, prevention & promotion, screening, diagnostics, therapeutics, follow up, communication and community engagement (11). Such applications were observed in the fields of telemedicine including online consultations, referrals to diagnostics and inpatient care, and management; mobile applications: used for diagnosing and managing patients (e-MCH; e-NCDs); telehealth applications: used for teaching, diagnosis, management, follow-up; e-Census; digital contact tracing; home delivery of medicines especially for NCDs, just to name a few examples from most if not all countries of the EMR, regardless of their economic or logistic resources. In fact. digital health and telemedicine modalities were adopted during the COVID-19 pandemic to ensure the continuity of services to People Living with NCDs (PLWNDs) and minimize their exposure to the infection while visiting health
Book 27-11.indb 1031Book 27-11.indb 1031 06/12/2021 12:39 PM06/12/2021 12:39 PM
EMHJ – Vol. 27 No. 11 – 2021Editorial
1032
facilities. Remote care for hypertensive and diabetic patients during the COVID-19 pandemic, via telemedicine services, was shown to be very successful in several EMR countries including IR of Iran, Jordan, Oman, Qatar, Saudi Arabia, Sudan, UAE among others (17).
Nevertheless, the region is a good example of what is referred to as the “digital divide”, which could be described as the “gap which exists between people who have access to modern information and communication technology and those who lack such access”; including gender gap, geographical gaps, and gaps related to other determinants such as education, income, residence (urban / rural / remote / settlements) and digital literacy (18). Such divide is also reflected by great discrepancies between national resources available to other different countries of the region. Several countries are affected by scarcity or fragmentation of digital health and
innovation infrastructures or suffer from challenges in interoperability and connectivity, and inadequacy of trained and capable human resources to enable digital health infrastructure, and health care workers that are adequately trained to use them. However, the pandemic presented many opportunities to accelerate use of digital technologies in countries. WHO can support countries in their efforts to strengthen digital platforms, and strengthen collaboration with other key players such as the International Telecommunication Union (ITU) and other stakeholders. Moreover, digital solutions should ensure ethically sound policies that will protect populations from the potential adverse impact of the inappropriate use of technologies, and enhance governance capacities so that countries ensure that expansion of digital health will contribute to the enhancement of population health in an efficient and equitable manner (6).
References1. Brennan R, Hajjeh R, Al-Mandhari A. Responding to health emergencies in the Eastern Mediterranean region in times of con-
flict. Lancet. 2020 Mar 2:S0140-6736(20)30069-6. doi: 10.1016/S0140-6736(20)30069-6
2. WHO/EMRO. Progress on the health-related Sustainable Development Goals and targets in the Eastern Mediterranean Region, 2020. Cairo: WHO Regional Office for the Eastern Mediterranean; 2020.
3. WHO/EMRO. Health and well-being profile of the Eastern Mediterranean Region: an overview of the health situation in the Region and its countries in 2019. Cairo: WHO Regional Office for the Eastern Mediterranean; 2020. 9789290223399-eng.pdf (who.int)
4. Doctor HV; Mabry R; Kabudula CW; Rashidian A; Hajjeh R; Hussain SJ; et al. Progress on the health-related Sustainable Develop-ment Goals in Eastern Mediterranean Region countries: getting back on track in the time of COVID-19. East Mediterr Health J. 2021;27(6):530–534. https://doi. org/10.26719/2021.27.6.530
5. Al-Mandhari A; Marmot M; Ghaffar A; Hajjeh R; Allen J; Khan W; et al. COVID-19 pandemic: a unique opportunity to ‘build back fairer’ and reduce health inequities in the Eastern Mediterranean Region. East Mediterr Health J. 2021;27(3):217-219 https://doi.org/10.26719/2021.27.3.217
6. WHO. Global Digital Health Strategy 2020-2025. Geneva: WHO, 2019. https://apps.who.int/iris/bitstream/handle/10665/344249/9789240020924-eng.pdf
7. WHO guideline: recommendations on digital interventions for health system strengthening. Geneva: World Health Organiza-tion; 2019. 9789241550505-eng.pdf (who.int)
8. WHO. Global diffusion of eHealth: making universal health coverage achievable. Report of the third global survey on eHealth. Geneva: World Health Organization, 2016. https://apps.who.int/iris/bitstream/handle/10665/252529/9789241511780-eng.pdf
9. WHO/EMRO. Vision 2023: Eastern Mediterranean region, 2018 http://www.emro.who.int/about-who/vision2023/vision-2023.html
10. Narasimhan, M., Lucido, B., Say, L. et al. Changing national health policies for introduction, uptake and scale-up of self-care interventions for sexual and reproductive health and rights in the Eastern Mediterranean Region. Health Res Policy Sys 19, 60 (2021). https://doi.org/10.1186/s12961-021-00705-1
11. WHO/EMRO. Advancing Be He@lthy, Be Mobile in the Eastern Mediterranean Region: Combating noncommunicable diseases through mobile technology. Cairo: WHO Regional Office for the Eastern Mediterranean; 2021. 9789290225225-eng.pdf (who.int)
12. WHO/EMRO. WHO Regional Committee for the Eastern Mediterranean. Health informatics and telematics (EM/RC44/R.4) 1997 https://www.who.int/medical_devices/policies/resolution_emro_rc44r3.pdf?ua=1
Book 27-11.indb 1032Book 27-11.indb 1032 06/12/2021 12:39 PM06/12/2021 12:39 PM
1033
EMHJ – Vol. 27 No. 11 – 2021Editorial
13. WHO/EMRO. WHO Regional Committee for the Eastern Mediterranean. Regional strategy for knowledge management to sup-port public health (EM/RC48/R.6) 2006 https://applications.emro.who.int/docs/em_rc53_r10_en.pdf
14. WHO/EMRO. WHO Regional Committee for the Eastern Mediterranean. Use and potential of geographic information sys-tems for health mapping in the Eastern Mediterranean Region (EM/RC54/R.6) 2007 https://apps.who.int/iris/bitstream/han-dle/10665/122590/em_rc54_r6_en.pdf?sequence=1&isAllowed=y
15. WHO/EMRO. WHO Regional Committee for the Eastern Mediterranean technical paper EM/RC66/11 on Summary of the draft global strategy on digital health. Cairo: WHO Regional Office for the Eastern Mediterranean; 2019 https://applications.emro.who.int/docs/RC_Technical_Papers_2019_11_en.pdf?ua=1
16. WHO/EMRO. Is the Eastern Mediterranean Region ready for digitalizing health? Implications from Global Strategy on Digital health (2020–2025)”. WHO 68th Regional Committee, 11-14 Oct 2021. Cairo: WHO/EMRO. http://www.emro.who.int/about-who/rc68/live-streaming.html
17. WHO/EMRO. Digital innovation stories during COVID-19. (http://www.emro.who.int/noncommunicable-diseases/publications/success-stories.html?format=html).
18. Digital Divide Council. What is digital divide? http://www.digitaldividecouncil.com/what-is-the-digital-divide/
Book 27-11.indb 1033Book 27-11.indb 1033 06/12/2021 12:39 PM06/12/2021 12:39 PM

1034
Commentary EMHJ – Vol. 27 No. 11 – 2021
Waste management of used personal protective equipment during the COVID-19 pandemic in the Eastern Mediterranean RegionRola Al-Emam1 and Basel Al-Yousfi1
1World Health Organization Regional Office for the Eastern Mediterranean, Regional Centre for Environmental Health Action, Amman, Jordan. (Correspondence to: Basel Al-Yousfi: [email protected])
Citation: Al-Emam R; Al-Yousfi B. Waste management of used personal protective equipment during the COVID-19 pandemic in the Eastern Mediterranean Region. East Mediterr Health J. 2021;27(11):1034–1035. https://doi.org/10.26719/2021.27.11.1034 Received: 23/02/21; accepted: 06/10/21Copyright © World Health Organization (WHO) 2021. Open Access. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license (https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
The COVID-19 pandemic continues to take a heavy toll on various sectors globally, including in the Eastern Medi-terranean Region. While the world witnessed positive (but perhaps short-lived) environmental impacts from lockdowns and curtailed human activities, such as im-proved air and water quality and reduced greenhouse gas emissions, the impact of COVID-19 waste management has been less positive (1,2), in particular the improper disposal of personal protective equipment (PPE) such as used face masks, coveralls, gowns and gloves. Waste management is an essential infection prevention and control activity and public health service that cannot be disregarded during these difficult times. Concerted ef-forts are needed to protect human health and the envi-ronment during and after the pandemic.
Wearing face masks is recommended by the World Health Organization (WHO) and other national disease control centres as part of the nonpharmaceutical interventions to control the spread of COVID-19. The continued use of masks by health workers and the public, indoors (such as in supermarkets or shopping malls), in public transport facilities and outdoors in crowded places, results in millions of items of PPE being manufactured and used daily. In Jordan, an estimated 1.1 million masks and 2.2 million gloves are used and disposed of on average every day (3). In the Islamic Republic of Iran, a study found that 5.6 million masks and more than 11 million gloves were discarded daily on average over a 3-month period (4).
Poverty, negligence, limited supply and high demand for masks may increase the likelihood of people collecting used face masks and reselling them (5). The improper disposal of used masks and gloves poses a major health threat and undermines national efforts to control the spread of infection in communities. Moreover, masks and other items of PPE may clog sewers and waterways, resulting in negative human health effects and broader environmental impacts (9). WHO has warned against disadvantages that may result from the increased use and improper handling and disposal of masks by the public such as random mask disposal leading to increased litter in public places, risk of contamination for street cleaners and environmental hazards (6). Several media articles in
the Region have raised the issue of abandoned used face masks and gloves outside shopping malls, supermarkets and mosques, and along beaches (7,8). Recognizing that so far there is limited evidence on transmission through fomites, such improperly discarded masks and gloves, which may be contaminated not only with the COVID-19 virus (SARS-CoV-2) but with other pathogens, can be blown around by the wind and lead to the dispersion of pathogens. Waste handlers and street sweepers are at especially high occupational health risk since they are in direct contact with such waste, but all outdoor workers (construction workers, policemen, etc.) and pedestrians are at risk of exposure to infection from improperly discarded masks and gloves.
The increased numbers of discarded PPE items exceed the capacity of the already limited and compromised waste management services observed in many developing countries, including those in the Eastern Mediterranean Region. In such countries, solid waste may be dumped in poorly designed and managed landfills or openly burned (with the latter leading to the release of harmful pollutants as dioxins and furans). A World Bank report states that 53% of solid waste in the Middle East and North Africa is disposed of in open dumps (9), putting waste handlers and pickers scavenging for recyclable items and neighbouring communities at major health risk in addition to nuisance. Waste collection, which is curtailed during lockdowns, is a critical step in managing waste. However, waste collection rates significantly vary by country income levels, with upper middle- and high-income countries providing nearly universal waste collection.
WHO has published several interim guidance notes on the safe management of COVID-19 waste. Waste generated from caring for COVID-19 patients at home as well as used PPE in the community should be disposed of in strong bags which are closed completely before collection by municipal waste services. Additionally, general noninfectious waste in health care facilities should be properly segregated from infectious waste such as sharps, bandages, pathological waste, and treated appropriately prior to safe disposal.
Book 27-11.indb 1034Book 27-11.indb 1034 06/12/2021 12:39 PM06/12/2021 12:39 PM

1035
Commentary EMHJ – Vol. 27 No. 11 – 2021
WHO interim guidance lists preferred environmentally friendly treatment options as high temperature, dual-chamber incineration or autoclaving. If such services are unavailable, safe burying or controlled burning are interim measures until more sustainable and environmentally friendly procedures can be arranged. To prevent scavenging and reselling of used masks, efforts are needed to ensure safe waste disposal in fenced and regulated waste areas (9). The WHO Regional Centre for Environmental Health Action in the Eastern Mediterranean Region has been providing capacity-building and technical support to Member States for the safe integrated management of waste, including COVID-19 waste, and the occupational safety and health of waste handlers.
Safe management of COVID-19 waste requires proper classification and urgent action at all levels of society. Enforcement of regulations, provision of adequate safe waste management services and individual responsibility are all needed to control the improper disposal of used PPE. Unless waste (including PPE and infectious waste) is handled with due care, we risk the creation of new
epicentres of diseases within our health care facilities and across society at large.
Health care waste management related to COVID-19 vaccination campaigns requires even closer attention. Large volumes of immunization waste including syringes, vials and PPE will be generated. To minimize waste from vaccination, use of PPE must be rational based on risk assessment as part of standard precautions. PPE additional to masks, for example gloves, is not indicated if skin is intact.
Countries should ensure that a safe and effective waste management plan, including training of health workers and provision of bins and treatment technologies, is in place prior to vaccine deployment (10). Unless safe waste management protocols and practices are established and monitored, such waste will pose a risk to health workers, the public and the environment. Perhaps the current pandemic will focus the attention of policy- and decision-makers on the dire need to invest in safe waste management practices, ensure green recovery and build back better towards achieving the United Nations Sustainable Development Goals.
References1. Saadat, S., Rawtani, D., Hussain, C.M. Environmental perspective of COVID-19. Sci. Total Environ. 2020;728(8), 138870. https://
doi.org/10.1016/j.scitotenv.2020.138870.
2. Zambrano-Monserrate, M.A., Ruano, M.A., Sanchez-Alcalde, L. Indirect effects of COVID-19 on the environment. Sci. Total Envi-ron. 2020;728, 138813. https://doi.org/10.1016/j.scitotenv.2020.138813.
3. Royal Scientific Society (2020). Technical Opinion on Masks and Gloves Disposal Management during COVID-19. Retrieved from: https://www.rss.jo/news/technical-opinion-on-masks-and-gloves-disposal-management-during-covid-19/
4. Zand A.D., Heir A.V. Emerging challenges in urban waste management in Tehran, Iran during the COVID-19 pandemic. ResourcD-es, Conservation and Recycling. 2020; 162(11). https://doi.org/10.1016/j.resconrec.2020.105051
5. WHO. Water, sanitation, hygiene, and waste management for SARS-CoV-2, the virus that causes COVID-19: Interim guidance. https://www.who.int/publications/i/item/water-sanitation-hygiene-and-waste-management-for-the-covid-19-virus-inter-im-guidance
6. WHO. Advice on the use of masks in the context of COVID-19: Interim guidance. https://www.who.int/publications/i/item/advice-on-the-use-of-masks-in-the-community-during-home-care-and-in-healthcare-settings-in-the-context-of-the-novel-coro-navirus-(2019-ncov)-outbreak
7. Ayyasrah, R (2020, August 26). Throwing masks and gloves on the streets is a health and environmental threat to citizens. Addus-tour. Retrieved from https://www.addustour.com/articles/1168434
8. Abed, A and Bayoumi, A (2020, May 19). Throwing masks and gloves in the streets is a source of spreading “Corona” ... and calls for tougher punishment for violators. Emaratalyoum. Retrieved from https://www.emaratalyoum.com/local-section/otha-er/2020-05-19-1.1351311
9. Kaza, Silpa; Yao, Lisa C.; Bhada-Tata, Perinaz; Van Woerden, Frank (2018). What a Waste 2.0 : A Global Snapshot of Solid Waste Management to 2050. Urban Development;. Washington, DC: World Bank. © World Bank. https://openknowledge.worldbank.org/handle/10986/30317
10. WHO. COVID-19 vaccination: supply and logistics guidance: Interim guidance. https://www.who.int/publications/i/item/who-2019-ncov-vaccine-deployment-logistics-2021-1
Book 27-11.indb 1035Book 27-11.indb 1035 06/12/2021 12:39 PM06/12/2021 12:39 PM

1036
Research article EMHJ – Vol. 27 No. 11 – 2021
Noncommunicable disease, clinical course and COVID-19 prognosis: results based on I-CORE Registry Shaghayegh Javanmard,1 Noushin Mohammadifard,2 Maryam Nasirian,3 Golnaz Vaseghi,4 Kamal Heidari,5 Behrouz Kelidari,6 Tahereh Changiz7 and Nizal Sarrafzadegan4,8
1Applied Physiology Research Center, Isfahan Cardiovascular Research Institute, Isfahan University of Medical Sciences, Isfahan, Islamic Republic of Iran. 2Hypertension Research Center, Cardiovascular Research Institute, Isfahan University of Medical Sciences, Isfahan, Islamic Republic of Iran. 3Infectious Diseases and Tropical Medicine Research Center; and Department of Epidemiology and Biostatistics, Health School, Isfahan University of Medical Sciences, Isfahan, Islamic Republic of Iran. 4Isfahan Cardiovascular Research Center, Cardiovascular Research Institute, Isfahan University of Medical Sciences, Isfahan, Islamic Republic of Iran (Correspondence to: N. Sarrafzadegan: [email protected]). 5Social Determinants of Health Research Center, Isfahan University of Medical Sciences, Isfahan, Islamic Republic of Iran. 6Department of Surgery, Isfahan Minimally Invasive Surgery and Obesity Research Center, Alzahra Hospital, Isfahan University of Medical Sciences, Isfahan, Islamic Republic of Iran. 7Department of Medical Education, Medical Educational Research Center, Isfahan University of Medical Science, Isfahan, Islamic Republic of Iran. 8School of Population and Public Health, Faculty of Medicine, University of British Columbia, Vancouver, Canada.
Abstract Background: There are no data on the association between clinical course and comorbidity in Iranian patients with COVID-19. Aims: To determine noncommunicable disease (NCD), clinical characteristics and prognosis of patients hospitalized with COVID-19 in Isfahan, Islamic Republic of Iran.Methods: This multicentric retrospective observational study was performed on all patients hospitalized with COVID-19 in Isfahan from 17 February to 6 April 2020. We recruited 5055 patients. Data on clinical course and comorbid NCDs such as hypertension, coronary heart disease (CHD), diabetes mellitus (DM), cancer, chronic kidney disease (CKD) and chronic respiratory disease (CRD) were collected. Statistical analyses were done by Mann–Whitney U, χ2 and logistic regression tests using Stata version 14. Results: DM and hypertension were the most prevalent comorbidities in patients with positive and negative reverse tran-scription polymerase chain reaction (RT-PCR). Odds ratio (95% confidence interval) of mortality-associated factors was significant for DM [1.35 (1.07–1.70)], CHD [1.58 (1.26–1.96)], CRD [2.18 (1.58–3.0)], and cancer [3.55 (2.42–5.21)]. These results remained significant for cancer after adjustment for age, sex and clinical factors. Among patients with positive RT-PCR, death was significantly associated with CRD and cancer, while this association disappeared after adjustment for all po-tential confounders. There was a significant association between NCDs and higher occurrence of low oxygen saturation, mechanical ventilation requirement and intensive care unit admission after adjustment for age and sex. Conclusion: The presence of NCDs alone did not increase mortality in patients with COVID-19, after adjustment for all potential confounders including clinical factors. Keywords : COVID-19, noncommunicable disease, mortality, cardiovascular disease, kidney diseaseCitation: Javanmard S; Mohammadifard N; Nasirian M; Vaseghi G; Heidari K; Kelidari B et al. Noncommunicable disease, clinical course and COVID-19 prognosis: results based on I-CORE Registry. East Mediterr Health J. 2021;27(11):1036-1044. https://doi.org/10.26719/emhj.21.052 Received: 19/11/20; accepted: 06/04/21 Copyright © World Health Organization (WHO) 2021. Open Access. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license (https://creativecommons.org/licenses/by-nc-sa/3.0/igo)
IntroductionIn November 2019, the first cases of an epidemic of COV-ID-19 were detected in Wuhan, China, and it spread rap-idly around the world (1). It has been acknowledged as a major international public health crisis, leading to a ma-jor global economic burden (2). According to the World Health Organization (WHO) announcement, the COV-ID-19 outbreak became a pandemic on 11 March 2020 (3). Up to 29 April 2020, this novel virus involved 210 coun-tries and its territories with > 3 100 000 confirmed cases and 218 000 deaths worldwide (4). On 19 February 2020, the Islamic Republic of Iran reported its first cases of COVID-19 (5) and until 29 April 2020, it ranked eighth in the world for number of cases (n = 92 584) and had the seventh highest death toll (n =5877) (4).
Over 50% of the global burden of disease (6) and 70% of deaths have been attributed to the epidemic of noncommunicable diseases (NCDs) worldwide (7). In the Islamic Republic of Iran, NCDs account for 79% of all deaths and 74% of the disease burden (8). The COVID-19 pandemic has affected all aspects of life and health services worldwide. Initial case series have shown that people with NCDs are more likely to have critical disease when infected with the novel coronavirus (9,10). Some measures for reducing the spread of COVID-19, including lockdowns, quarantine, social distancing, and travel limitations, could lead to restriction of physical activity, unavailability of healthy food, limited access to health services and postponement of routine medical examinations; all of which could interrupt NCD care.
Book 27-11.indb 1036Book 27-11.indb 1036 06/12/2021 12:39 PM06/12/2021 12:39 PM

1037
Research article EMHJ – Vol. 27 No. 11 – 2021
Additionally, the economic crisis due to the pandemic can increase stressful conditions and worsen NCD status (11).
In February 2020, Isfahan COVID-19 Registry (I-CORE) was established to register all patients hospitalized with COVID-19 in Isfahan (12). The catchment area included Isfahan Province except Kashan. According to WHO interim guidance for global surveillance (1), all confirmed and probable cases of COVID-19 that were hospitalized in Isfahan University of Medical Sciences (IUMS) affiliated hospitals were recruited in this registry.
This paper presents the clinical course and comorbidities such as hypertension, coronary heart disease (CHD), diabetes mellitus (DM), cancer, chronic kidney disease (CKD) and chronic respiratory disease (CRD), in patients hospitalized with COVID-19, and the impact of NCDs on outcomes of COVID-19.
Methods Design and participantsThis multicentre retrospective observational study was performed on all registered patients in I-CORE who were hospitalized in IUMS affiliated hospitals from 17 Febru-ary to 6 April 2020. Isfahan is the second largest prov-ince in the Islamic Republic of Iran, with a population of850 120 5 based on the national census in 2016. All pa-tients who were hospitalized because of possible diagno-sis of COVID-19 based on WHO criteria were recruited to this study, irrespective of their prognosis or real-time re-verse transcription polymerase chain reaction (RT-PCR) results. COVID-19 was diagnosed according to WHO classification and consisted of having severe or moderate symptoms such as respiratory rate > 30 breaths/minute, oxygen saturation < 94% in room air at sea level, ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) < 300 mmHg, or lung infiltrates > 50% (13). Written consent was obtained from all patients or close relatives upon admission. We analysed the data of 6831 patients who were admitted or transferred from oth-er hospitals and health centres to the referral hospitals. All hospitalized COVID-19 cases were either confirmed by positive RT-PCR, unconfirmed by negative RT-PCR, or were untested. Detailed analysis was limited to 5055 patients who were tested with RT-PCR. The study was approved by the Ethics Committee of IUMS.
Data collection Data gathering forms were completed first by nurses upon patient admission. Our data comprised demograph-ics, medical history of underlying comorbidities, oxygen saturation on admission, transfer to intensive care unit (ICU), mechanical ventilation, as well as clinical out-comes that consisted of death or recovery and discharge. Questions on comorbid NCDs were completed based on patients’ self-report or their close relatives’ answers if they were in a critical medical condition. We defined co-morbidities as coexisting NCDs, including hypertension, CHD, DM, cancer, CKD and CRD. Regarding the history of these NCDs, we asked “Have you ever been diagnosed
for any of these diseases by a physician?” If the answer was yes, then all medical records of the patients were re-viewed by the physicians. To determine history of DM or hypertension, we added other questions such as “Do you take any hypoglycaemic or antihypertensive med-ication?”. Attending specialized physicians completed clinical examination on admission and throughout hos-pitalization. Their daily notes on the clinical situation of patients were accompanied by those of registered nurses. All were reported in the medical records that were linked to the electronic health information system of the hos-pitals. Our clinical outcomes were death or recovery and discharge after COVID-19. Death due to COVID-19 was defined according to WHO guidelines and through med-ical certification in hospital (14). The data were extracted on an Excel sheet from that system to I-CORE (12). RT-PCR was used to detect SARS-CoV-2 RNA according to the WHO protocol from samples of throat swabs (15). Sam-ples were sent to 2 designated laboratories related to the provincial health centre. All routine and other necessary laboratory tests were done for patients. I-CORE Web-based software was developed to retrieve, save, manage and integrate collected patients’ data from admission and the health information system of referral hospitals. If there were missing data, nurses went back to patients’ medical records to fill the gaps.
Statistical analysisContinuous variables including age were presented as means and standard deviation and were compared by Mann–Whitney U test. Categorical variables, frequency and percentage of patients with oxygen saturation < 93%, mechanical ventilation needed, ICU transfer, and clinical outcome based on sex and different RT-PCR results were compared by χ2 test. A logistic regression model was used to determine the association of comorbidity with death as well as clinical characteristics including oxygen satu-ration, need for mechanical ventilation and ICU admis-sion. Odds ratio (OR) and 95% confidence interval (CI) were reported. Age as continuous variable, sex, oxygen saturation, mechanical ventilation, ICU, and NCDs were adjusted in the logistic regression model. P < 0.05 was considered statistically significant. Statistical analyses were done using Stata version 14.
ResultsDemographics and clinical characteristicsFrom 17 February to 6 April 2020, 6831 patients with a WHO definition of COVID- 19 were admitted to referral hospitals in Isfahan Province; among whom, 5055 had RT-PCR results, with a higher frequency of male com-pared to female patients (54.9% vs 45.1%). Table 1 presents the demographic and clinical characteristics of these patients. Mean age was 56.1 (20.5) years for RT-PCR-pos-itive patients compared to 59.3 (17.3) years for negative patients. Older age distribution was significantly higher in positive patients. Although low oxygen saturation and ICU admission were significantly higher in the positive
Book 27-11.indb 1037Book 27-11.indb 1037 06/12/2021 12:39 PM06/12/2021 12:39 PM
1038
Research article EMHJ – Vol. 27 No. 11 – 2021
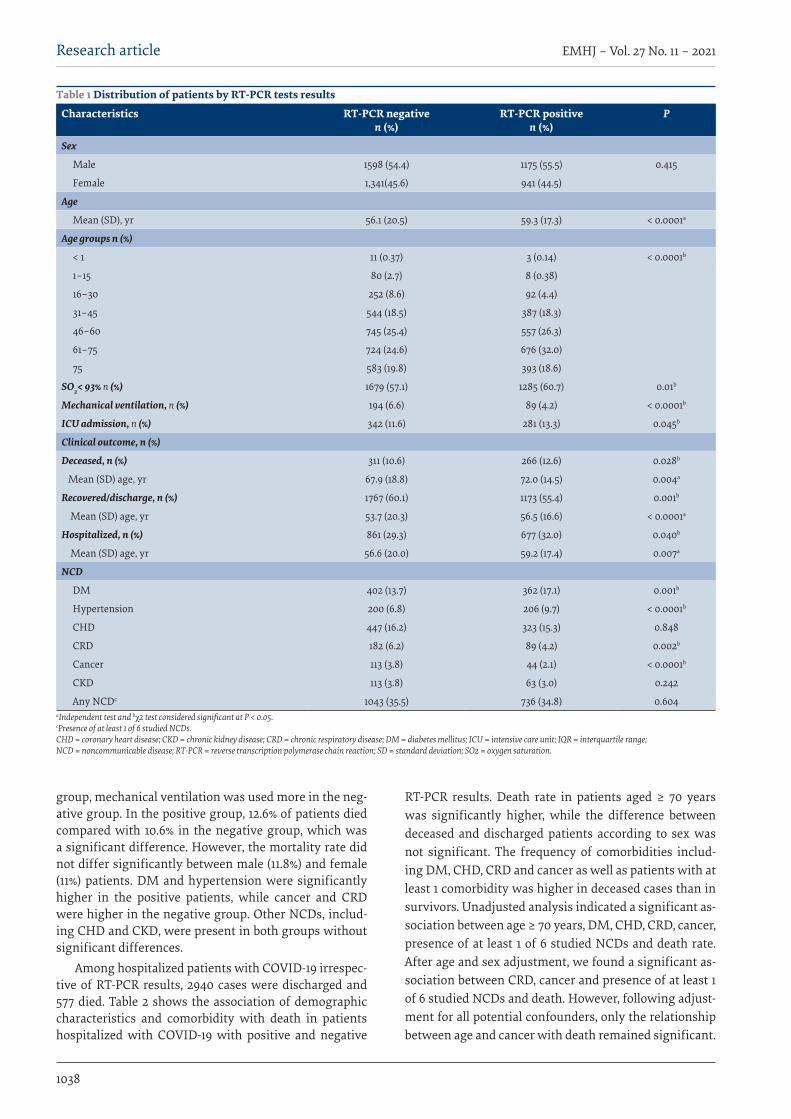
group, mechanical ventilation was used more in the neg-ative group. In the positive group, 12.6% of patients died compared with 10.6% in the negative group, which was a significant difference. However, the mortality rate did not differ significantly between male (11.8%) and female (11%) patients. DM and hypertension were significantly higher in the positive patients, while cancer and CRD were higher in the negative group. Other NCDs, includ-ing CHD and CKD, were present in both groups without significant differences.
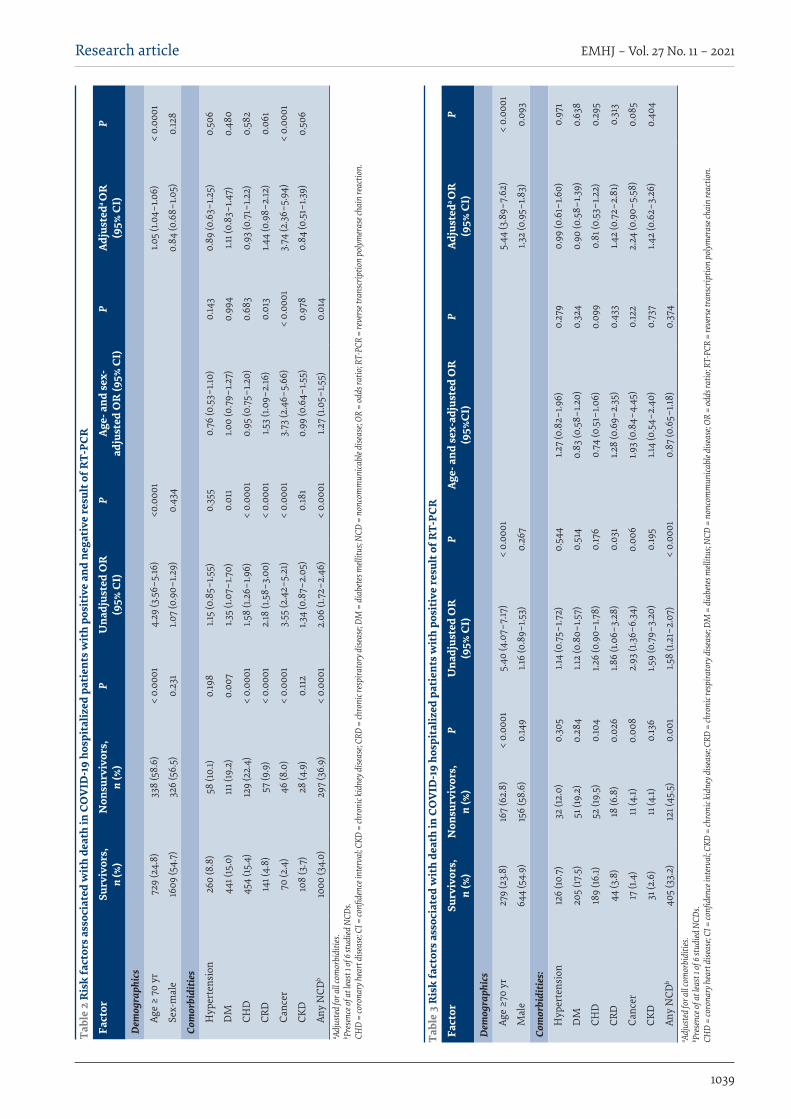
Among hospitalized patients with COVID-19 irrespec-tive of RT-PCR results, 2940 cases were discharged and 577 died. Table 2 shows the association of demographic characteristics and comorbidity with death in patients hospitalized with COVID-19 with positive and negative
RT-PCR results. Death rate in patients aged ≥ 70 years was significantly higher, while the difference between deceased and discharged patients according to sex was not significant. The frequency of comorbidities includ-ing DM, CHD, CRD and cancer as well as patients with at least 1 comorbidity was higher in deceased cases than in survivors. Unadjusted analysis indicated a significant as-sociation between age ≥ 70 years, DM, CHD, CRD, cancer, presence of at least 1 of 6 studied NCDs and death rate. After age and sex adjustment, we found a significant as-sociation between CRD, cancer and presence of at least 1 of 6 studied NCDs and death. However, following adjust-ment for all potential confounders, only the relationship between age and cancer with death remained significant.
Table 1 Distribution of patients by RT-PCR tests results
Characteristics RT-PCR negative n (%)
RT-PCR positive n (%)
P
Sex
Male 1598 (54.4) 1175 (55.5) 0.415
Female 1,341(45.6) 941 (44.5)
Age
Mean (SD), yr 56.1 (20.5) 59.3 (17.3) < 0.0001a
Age groups n (%)
< 1 11 (0.37) 3 (0.14) < 0.0001b
1–15 80 (2.7) 8 (0.38)
16–30 252 (8.6) 92 (4.4)
31–45 544 (18.5) 387 (18.3)
46–60 745 (25.4) 557 (26.3)
61–75 724 (24.6) 676 (32.0)
75 583 (19.8) 393 (18.6)
SO2< 93% n (%) 1679 (57.1) 1285 (60.7) 0.01b
Mechanical ventilation, n (%) 194 (6.6) 89 (4.2) < 0.0001b
ICU admission, n (%) 342 (11.6) 281 (13.3) 0.045b
Clinical outcome, n (%)
Deceased, n (%) 311 (10.6) 266 (12.6) 0.028b
Mean (SD) age, yr 67.9 (18.8) 72.0 (14.5) 0.004a
Recovered/discharge, n (%) 1767 (60.1) 1173 (55.4) 0.001b
Mean (SD) age, yr 53.7 (20.3) 56.5 (16.6) < 0.0001a
Hospitalized, n (%) 861 (29.3) 677 (32.0) 0.040b
Mean (SD) age, yr 56.6 (20.0) 59.2 (17.4) 0.007a
NCD
DM 402 (13.7) 362 (17.1) 0.001b
Hypertension 200 (6.8) 206 (9.7) < 0.0001b
CHD 447 (16.2) 323 (15.3) 0.848
CRD 182 (6.2) 89 (4.2) 0.002b
Cancer 113 (3.8) 44 (2.1) < 0.0001b
CKD 113 (3.8) 63 (3.0) 0.242
Any NCDc 1043 (35.5) 736 (34.8) 0.604aIndependent test and bχ2 test considered significant at P < 0.05. cPresence of at least 1 of 6 studied NCDs. CHD = coronary heart disease; CKD = chronic kidney disease; CRD = chronic respiratory disease; DM = diabetes mellitus; ICU = intensive care unit; IQR = interquartile range; NCD = noncommunicable disease; RT-PCR = reverse transcription polymerase chain reaction; SD = standard deviation; SO2 = oxygen saturation.
Book 27-11.indb 1038Book 27-11.indb 1038 06/12/2021 12:39 PM06/12/2021 12:39 PM
1039
Research article EMHJ – Vol. 27 No. 11 – 2021
Tabl
e 2
Ris
k fa
ctor
s ass
ocia
ted
wit
h de
ath
in C
OV
ID-1
9 ho
spit
aliz
ed p
atie
nts w
ith
posi
tive
and
neg
ativ
e re
sult
of R
T-PC
R
Fact
or
Surv
ivor
s,n
(%)
Non
surv
ivor
s,n
(%)
P U
nadj
uste
d O
R
(95%
CI)
P Ag
e- a
nd se
x-ad
just
ed O
R (9
5% C
I)P
Adju
sted
a O
R
(95%
CI)
P
Dem
ogra
phic
s
Age
≥ 70
yr
729
(24.
8)33
8 (5
8.6)
< 0.
0001
4.29
(3.5
6–5.
16)
<0.0
001
1.05
(1.04
–1.0
6)<
0.00
01
Sex-
mal
e16
09 (5
4.7)
326
(56.
5)0.
231
1.07
(0.9
0–1.2
9)0.
434
0.84
(0.6
8–1.0
5)0.
128
Com
orbi
ditie
s
Hyp
erte
nsio
n26
0 (8
.8)
58 (1
0.1)
0.19
81.1
5 (0
.85–
1.55)
0.35
50.
76 (0
.53–
1.10)
0.14
30.
89 (0
.63–
1.25)
0.50
6
DM
441 (
15.0
)11
1 (19
.2)
0.00
71.3
5 (1.
07–1
.70)
0.01
11.0
0 (0
.79–
1.27)
0.99
41.1
1 (0.
83–1
.47)
0.48
0
CHD
454
(15.4
)12
9 (2
2.4)
< 0.
0001
1.58
(1.26
–1.9
6)<
0.00
010.
95 (0
.75–
1.20)
0.68
30.
93 (0
.71–
1.22)
0.58
2
CRD
141 (
4.8)
57 (9
.9)
< 0.
0001
2.18
(1.5
8–3.
00)
< 0.
0001
1.53
(1.09
–2.16
)0.
013
1.44
(0.9
8–2.
12)
0.06
1
Canc
er70
(2.4
)46
(8.0
)<
0.00
013.
55 (2
.42–
5.21
)<
0.00
013.
73 (2
.46–
5.66
)<
0.00
013.
74 (2
.36–
5.94
)<
0.00
01
CKD
108
(3.7
)28
(4.9
)0.
112
1.34
(0.8
7–2.
05)
0.18
10.
99 (0
.64–
1.55)
0.97
80.
84 (0
.51–
1.39)
0.50
6
Any
NCD
b10
00 (3
4.0)
297
(36.
9)<
0.00
012.
06 (1
.72–
2.46
) <
0.00
011.2
7 (1.
05–1
.55)
0.01
4a Ad
just
ed fo
r all c
omor
bidi
ties.
b Pres
ence
of at
leas
t 1 of
6 st
udied
NCD
s. CH
D =
coro
nary
hea
rt d
iseas
e; CI
= co
nfide
nce i
nter
val; C
KD =
chro
nic k
idne
y dise
ase;
CRD
= ch
roni
c res
pira
tory
dise
ase;
DM =
dia
bete
s mell
itus;
NCD
= n
onco
mm
unica
ble d
iseas
e; OR
= od
ds ra
tio; R
T-PC
R =
reve
rse t
rans
crip
tion
poly
mer
ase c
hain
reac
tion.
Tabl
e 3
Ris
k fa
ctor
s ass
ocia
ted
wit
h de
ath
in C
OV
ID-1
9 ho
spit
aliz
ed p
atie
nts w
ith
posi
tive
resu
lt o
f RT-
PCR
Fact
or
Surv
ivor
s,n
(%)
Non
surv
ivor
s,n
(%)
P U
nadj
uste
d O
R
(95%
CI)
P Ag
e- a
nd se
x-ad
just
ed O
R
(95%
CI)
PAd
just
eda O
R
(95%
CI)
P
Dem
ogra
phic
s
Age
≥70
yr
279
(23.
8)16
7 (6
2.8)
< 0.
0001
5.40
(4.0
7–7.
17)
< 0.
0001
5.44
(3.8
9–7.
62)
< 0.
0001
Mal
e64
4 (5
4.9)
156
(58.
6)0.
149
1.16
(0.8
9–1.5
3)0.
267
1.32
(0.9
5–1.8
3)0.
093
Com
orbi
ditie
s:
Hyp
erte
nsio
n12
6 (10
.7)
32 (1
2.0)
0.30
51.1
4 (0
.75–
1.72)
0.54
41.2
7 (0
.82–
1.96)
0.27
90.
99 (0
.61–
1.60)
0.97
1
DM
205
(17.5
)51
(19.
2)0.
284
1.12
(0.8
0–1.5
7)0.
514
0.83
(0.5
8–1.2
0)0.
324
0.90
(0.5
8–1.3
9)0.
638
CHD
189
(16.1)
52 (1
9.5)
0.10
41.2
6 (0
.90–
1.78)
0.17
60.
74 (0
.51–
1.06)
0.09
90.
81 (0
.53–
1.22)
0.29
5
CRD
44 (3
.8)
18 (6
.8)
0.02
61.8
6 (1.
06–3
.28)
0.03
11.2
8 (0
.69–
2.35
)0.
433
1.42
(0.7
2–2.
81)
0.31
3
Canc
er17
(1.4
)11
(4.1)
0.00
82.
93 (1
.36–
6.34
)0.
006
1.93
(0.8
4–4.
45)
0.12
22.
24 (0
.90–
5.58
)0.
085
CKD
31 (2
.6)
11 (4
.1)0.
136
1.59
(0.7
9–3.
20)
0.19
51.1
4 (0
.54–
2.40
)0.
737
1.42
(0.6
2–3.
26)
0.40
4
Any
NCD
b40
5 (3
3.2)
121 (
45.5
)0.
001
1.58
(1.21
–2.0
7)<
0.00
010.
87 (0
.65–
1.18)
0.37
4a Ad
just
ed fo
r all c
omor
bidi
ties.
b Pres
ence
of at
leas
t 1 of
6 st
udied
NCD
s. CH
D =
coro
nary
hea
rt d
iseas
e; CI
= co
nfide
nce i
nter
val; C
KD =
chro
nic k
idne
y dise
ase;
CRD
= ch
roni
c res
pira
tory
dise
ase;
DM =
dia
bete
s mell
itus;
NCD
= n
onco
mm
unica
ble d
iseas
e; OR
= od
ds ra
tio; R
T-PC
R =
reve
rse t
rans
crip
tion
poly
mer
ase c
hain
reac
tion.
Book 27-11.indb 1039Book 27-11.indb 1039 06/12/2021 12:39 PM06/12/2021 12:39 PM
1040
Research article EMHJ – Vol. 27 No. 11 – 2021
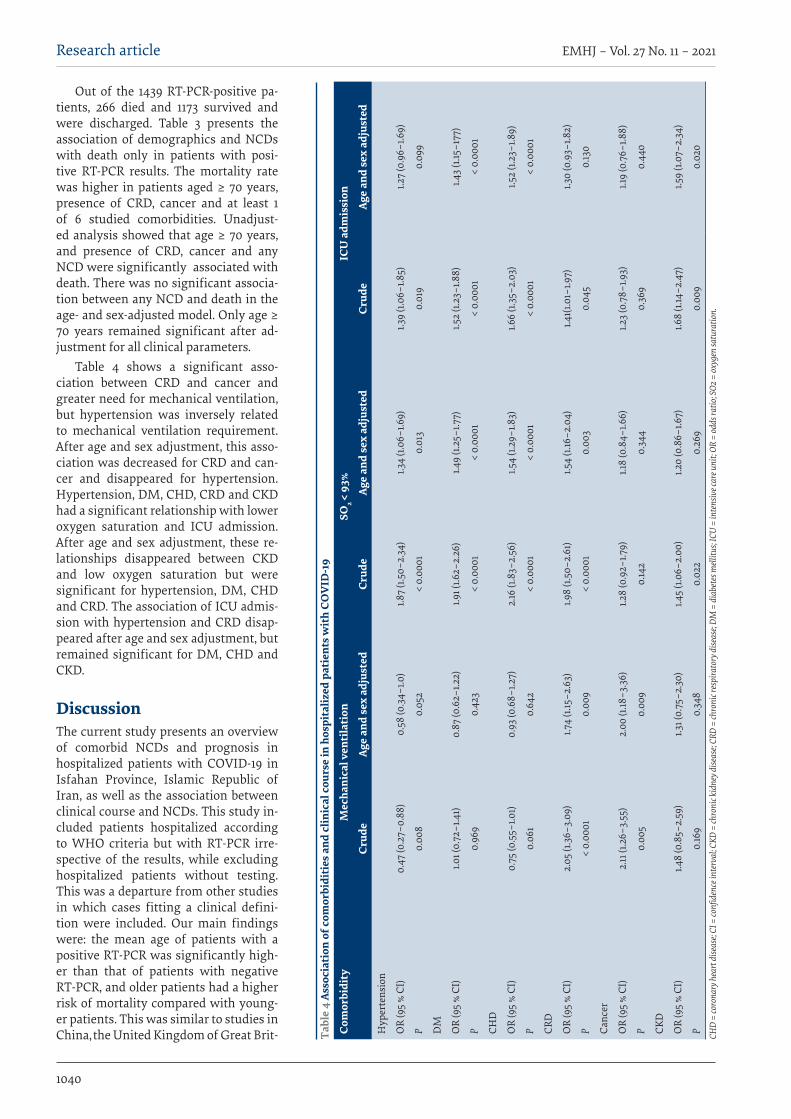
Out of the 1439 RT-PCR-positive pa-tients, 266 died and 1173 survived and were discharged. Table 3 presents the association of demographics and NCDs with death only in patients with posi-tive RT-PCR results. The mortality rate was higher in patients aged ≥ 70 years, presence of CRD, cancer and at least 1 of 6 studied comorbidities. Unadjust-ed analysis showed that age ≥ 70 years, and presence of CRD, cancer and any NCD were significantly associated with death. There was no significant associa-tion between any NCD and death in the age- and sex-adjusted model. Only age ≥ 70 years remained significant after ad-justment for all clinical parameters.
Table 4 shows a significant asso-ciation between CRD and cancer and greater need for mechanical ventilation, but hypertension was inversely related to mechanical ventilation requirement. After age and sex adjustment, this asso-ciation was decreased for CRD and can-cer and disappeared for hypertension. Hypertension, DM, CHD, CRD and CKD had a significant relationship with lower oxygen saturation and ICU admission. After age and sex adjustment, these re-lationships disappeared between CKD and low oxygen saturation but were significant for hypertension, DM, CHD and CRD. The association of ICU admis-sion with hypertension and CRD disap-peared after age and sex adjustment, but remained significant for DM, CHD and CKD.
DiscussionThe current study presents an overview of comorbid NCDs and prognosis in hospitalized patients with COVID-19 in Isfahan Province, Islamic Republic of Iran, as well as the association between clinical course and NCDs. This study in-cluded patients hospitalized according to WHO criteria but with RT-PCR irre-spective of the results, while excluding hospitalized patients without testing. This was a departure from other studies in which cases fitting a clinical defini-tion were included. Our main findings were: the mean age of patients with a positive RT-PCR was significantly high-er than that of patients with negative RT-PCR, and older patients had a higher risk of mortality compared with young-er patients. This was similar to studies in China, the United Kingdom of Great Brit- Ta
ble
4 As
soci
atio
n of
com
orbi
diti
es a
nd c
linic
al c
ours
e in
hos
pita
lized
pat
ient
s wit
h CO
VID
-19
Com
orbi
dity
Mec
hani
cal v
enti
lati
on
SO2
< 93
%IC
U a
dmis
sion
Crud
e Ag
e an
d se
x ad
just
ed
Crud
e Ag
e an
d se
x ad
just
ed
Crud
e Ag
e an
d se
x ad
just
ed
Hyp
erte
nsio
n
OR
(95
% CI
)0.
47 (0
.27–
0.88
)0.
58 (0
.34–
1.0)
1.87
(1.50
–2.3
4)1.3
4 (1.
06–1
.69)
1.39
(1.06
–1.8
5)1.2
7 (0
.96–
1.69)
P 0.
008
0.05
2<
0.00
010.
013
0.01
90.
099
DM
OR
(95
% CI
)1.0
1 (0.
72–1
.41)
0.87
(0.6
2–1.2
2)1.9
1 (1.6
2–2.
26)
1.49
(1.25
–1.7
7)
1.52
(1.23
–1.8
8)1.4
3 (1.
15–1
77)
P 0.
969
0.42
3<
0.00
01<
0.00
01<
0.00
01<
0.00
01
CHD
OR
(95
% CI
)0.
75 (0
.55–
1.01)
0.93
(0.6
8–1.2
7)2.
16 (1
.83–
2.56
)1.5
4 (1.
29–1
.83)
1.66
(1.35
–2.0
3)1.5
2 (1.
23–1
.89)
P 0.
061
0.64
2<
0.00
01<
0.00
01<
0.00
01<
0.00
01
CRD
OR
(95
% CI
)2.
05 (1
.36–
3.09
)1.7
4 (1.
15–2
.63)
1.98
(1.50
–2.6
1)1.5
4 (1.
16–2
.04)
1.41(1
.01–
1.97)
1.30
(0.9
3–1.8
2)
P <
0.00
010.
009
< 0.
0001
0.00
30.
045
0.13
0
Canc
er
OR
(95
% CI
)2.
11 (1
.26–
3.55
)2.
00 (1
.18–3
.36)
1.28
(0.9
2–1.7
9)1.1
8 (0
.84–
1.66)
1.23
(0.7
8–1.9
3)1.1
9 (0
.76–
1.88)
P 0.
005
0.00
90.
142
0.34
40.
369
0.44
0
CKD
OR
(95
% CI
)1.4
8 (0
.85–
2.59
)1.3
1 (0.
75–2
.30)
1.45
(1.06
–2.0
0)1.2
0 (0
.86–
1.67)
1.68
(1.14
–2.4
7)1.5
9 (1.
07–2
.34)
P 0.
169
0.34
80.
022
0.26
90.
009
0.02
0CH
D =
coro
nary
hea
rt d
iseas
e; CI
= co
nfide
nce i
nter
val; C
KD =
chro
nic k
idne
y dise
ase;
CRD
= ch
roni
c res
pira
tory
dise
ase;
DM =
dia
bete
s mell
itus;
ICU
= in
tens
ive c
are u
nit;
OR =
odds
ratio
; SO2
= ox
ygen
satu
ratio
n.
Book 27-11.indb 1040Book 27-11.indb 1040 06/12/2021 12:39 PM06/12/2021 12:39 PM

1041
Research article EMHJ – Vol. 27 No. 11 – 2021
ain and Northern Ireland, United States of America (USA)
and Republic of Korea (9,15–17). Male predominance ob-served in this study was similar to that in other published studies on COVID-19 (9,15–17). Patients aged ≥ 70 years had a higher mortality risk and this was similar to that reported in the USA (16). In contrast to global findings, mortality rate showed no significant difference between men and women (4), although hospitalization was higher in men.
While low oxygen saturation and ICU admission rates were significantly more frequent in patients with positive RT-PCR tests, mechanical ventilation was significantly higher in patients with negative results. These results may be explained by limited validity of our RT-PCR tests. Similar results were reported in other countries, such as 30–50% false-negative rate in China and > 5% in the USA (18,19). Multiple factors can play a role in such results, like the method of obtaining samples, method of transfer, technical issues and nonvalid kits.
One of our main findings was that CHD and DM were the most common NCDs in our patients with positive or negative RT-PCR tests. This is similar to other studies (5,9,15–17,20,21). Similarly, studies in China and Italy showed that the most prevalent underlying condition was hypertension (9,21,22). Other comorbidities reported in our study were cancer, CKD and CRD, which were similar to other studies (5,9,10,15–17,20–23). Differences between our and other studies may be due to methodology as our data on the presence of NCDs were self-reported which may have resulted in underestimation.
The presence of any of the 6 studied NCDs increased mortality by more than twice in patients with positive or negative RT-PCR results and by 58% only in patients with positive RT-PCR results. Unadjusted analysis showed that DM, CHD, CRD and cancer were significant risk factors for death in all COVID-19 patients with negative and positive RT-PCR results; however, in our full adjustment analysis, only cancer showed a significant association with death. Among patients with positive RT-PCR results, CRD and cancer were significantly associated with death, which vanished after adjustment for confounders including clinical course. A strong association between NCDs and some clinical characteristics may affect COVID-19 prognosis and cause disappearance of the association of NCDs and COVID-19 death after adjustment for clinical factors. CRD and cancer were associated with increased
frequency of mechanical ventilation by 1.74 and 2 times, respectively. Hypertension, DM, CHD and CRD had 34–54% greater occurrence of oxygen saturation < 93%. DM, CHD and CKD were associated with increased frequency of ICU transfer by 43%, 52% and 59%, respectively . Similarly, previous studies have shown the predictive effects of underlying NCDs in increasing the number of patients with clinical features such as ICU transfer, oxygen saturation and mechanical ventilation (24,25).
A meta-analysis of 40 studies on 18 012 COVID-19 patients showed that DM, hypertension and CVD were important risk factors for COVID-19 mortality (26). However, most studies did not adjust all the confounders that we did in our study. A study in Italy showed that hypertension was not an independent predictor of COVID-19 outcomes (27). Consistent with the current study, cancer comorbidity was associated with more adverse COVID-19 outcomes (28). In patients with DM, immune dysfunction, proinflammatory and prothrombotic hypercoagulable state are related to COVID-19 mortality (29).
To the best of our knowledge, this is the first report from the Islamic Republic of Iran on the association of some clinical characteristics of COVID-19 with comorbid NCDs that worsen the prognosis of hospitalized patients. The study had some limitations. Firstly, comorbidities were self-reported by patients or their close relatives which may have led to under-reporting the frequency due to lack of awareness. Secondly, the limited validity of RT-PCR testing may have underestimated the number of confirmed cases of COVID-19.
Conclusion We conclude that COVID-19 infection and death were as-sociated with age and male sex in patients hospitalized with COVID-19 in the Islamic Republic of Iran. DM, CHD and hypertension were the most prevalent underlying comorbidities. The presence of at least 1 of the studied NCDs increased mortality in patients with positive or negative RT-PCR results. However, none of the NCDs was associated significantly with death after adjustment of all confounders in patients with positive RT-PCR re-sults. This analysis and other reports from I-CORE can be helpful for policy-makers to make proper decisions on referring patients, facilities, management and treatment of high-risk patients.
Acknowledgment We express our special thanks to all physicians, nurses and other staff who were frontline healthcare providers in our COVID-19 referral hospitals. We also thank all the patients and their families who provided consent to use their data in our analysis. The efforts of all staff of health centres and laboratories who test COVID-19 in Isfahan Province is appreciated.
Funding: None.
Competing interests: None declared.
Book 27-11.indb 1041Book 27-11.indb 1041 06/12/2021 12:39 PM06/12/2021 12:39 PM
1042
Research article EMHJ – Vol. 27 No. 11 – 2021
األمراض غي السارية، واملسار الرسيري، والتنبؤ بسي كوفيد-19: نتائج مستندة لسجل كوفيد-19 شقايق جافانامرد، نوشني حممدي-فرد، مريم نارصيان، جولناز واسيغي، كامل حيدري، هبروز كليداري، طاهرة تشانجيز، نزال رصافزاجيان
اخلالصة اخللفية: ال تتوافر بيانات عن االرتباط بني املسار الرسيري واألمراض املصاحبة يف املرىض اإليرانيني املصابني بكوفيد-19.
إصابتهم جراء املستشفى إىل أدخلوا الذين للمرىض الرسيرية واخلصائص السارية غري األمراض حتديد اىل الدراسة هذه هدفت األهداف: بكوفيد-19 يف أصفهان، بجمهورية إيران اإلسالمية، والتنبؤ بسري املرض لدهيم.
طرق البحث: أجريت هذه الدراسة الرصدية االسرتجاعية املتعددة املراكز عىل مجيع املرىض الذين أدخلوا إىل املستشفى جراء إصابتهم بكوفيد-19 يف أصفهان يف الفرتة من 17 فرباير / شباط وحتى 6 أبريل / نيسان 2020. واشرتك فيها 5055 مريضا. ومجعت بيانات عن املسار الرسيري واألمراض غري السارية املصاحبة مثل ارتفاع ضغط الدم، وأمراض القلب التاجية، والسكري، والرسطان، وأمراض الكىل املزمنة، وأمراض اجلهاز التنفيس املزمنة. وأجريت حتليالت إحصائية بواسطة اختبار مان-ويتني، واختبار مربع كاي )χ2(، واختبار االنحدار اللوجستي باستخدام اإلصدار
14 من برنامج Stata احلاسويب. ري وارتفاع ضغط الدم أكثر األمراض املصاحبة انتشارا يف صفوف املرىض الذين كانت نتائج اختبار "التنسخ العكيس لتفاعل ك النتائج: كان السالبوليمرياز املتسلسل" RT PCR-لدهيم اجيابية أو سلبية. وكانت نسبة األرجحية )فاصل ثقة 95%( للعوامل املرتبطة بالوفيات ملحوظة يف السكري ،])3.00-1.58( 2.18[ املزمنة التنفيس اجلهاز وأمراض ،])1.96-1.26( 1.58[ التاجية القلب وأمراض ،])1.70-1.07( 1.35[والرسطان ]3.55 )2.42-5.21([. وبقيت تلك النتائج مهمة بالنسبة للرسطان بعد التصحيح بالعمر، واجلنس والعوامل الرسيرية. ومن بني املرىض الذين كان نتائج اختبار "التنسخ العكيس لتفاعل البوليمرياز املتسلسل" لدهيم إجيابية، كانت الوفاة مرتبطة بشكل ملحوظ بأمراض اجلهاز التنفيس املزمنة والرسطان، يف حني اختفى هذا االرتباط بعد التصحيح للسيطرة عىل مجيع عوامل اإلرباك املحتملة. وكان هناك ارتباط كبري بني ع األكسجيني، واالحتياج إىل التهوية امليكانيكية، واإلدخال إىل وحدة الرعاية املركزة األمراض غري السارية وارتفاع معدل حدوث انخفاض التشب
بعد التصحيح وفقا للعمر واجلنس. االستنتاجات: مل يؤد وجود األمراض غري السارية وحدها إىل زيادة الوفيات يف صفوف املرىض املصابني بكوفيد-19، وذلك بعد التصحيح للسيطرة
عىل مجيع عوامل اإلرباك املحتملة، ومن بينها العوامل الرسيرية.
Maladies non transmissibles, évolution clinique et pronostic de COVID-19 : résultats basés sur le registre I-CORE Résumé Contexte : Il n'existe pas de données sur le lien entre comorbidités et évolution clinique chez les patients iraniens atteints de COVID-19. Objectifs : Déterminer les maladies non transmissibles (MNT), les caractéristiques cliniques et le pronostic des patients hospitalisés pour COVID-19 à Ispahan (République islamique d'Iran).Méthodes : La présente étude observationnelle rétrospective multicentrique a été réalisée sur tous les patients hospitalisés pour COVID-19 à Ispahan entre le 17 février et le 6 avril 2020. Nous avons recruté 5055 patients. Des données sur l’évolution clinique et les comorbidités avec des maladies non transmissibles telles que l'hypertension, les coronaropathies, le diabète sucré, le cancer, la maladie rénale chronique et les maladies respiratoires chroniques ont été recueillies. Des analyses statistiques ont été effectuées à l'aide de tests de Mann-Whitney (U), χ2 et de régression logistique avec le logiciel Stata version 14. Résultats : Le diabète sucré et l'hypertension constituaient les comorbidités les plus prévalentes chez les patients présentant une réaction en chaîne par polymérase après transcription inverse (RT-PCR) positive et négative. L'odds ratio (intervalle de confiance à 95 %) des facteurs associés à la mortalité était significatif pour le diabète sucré [1,35 (1,07-1,70)], les coronaropathies [1,58 (1,26-1,96)], les maladies respiratoires chroniques [2,18 (1,58-3,0)] et le cancer [3,55 (2,42-5,21)]. Ces résultats restaient significatifs pour le cancer après ajustement en fonction de l’âge, du sexe et des facteurs cliniques. Chez les patients dont les tests RT-PCR étaient positifs, la mortalité était significativement associée aux maladies respiratoires chroniques et au cancer, tandis que cette association disparaissait après ajustement en fonction de tous les facteurs de confusion possibles. Il existait un lien important entre les maladies non transmissibles et la survenue plus fréquente d'une faible saturation en oxygène, d'un besoin en ventilation mécanique et d'une admission en unité de soins intensifs après ajustement en fonction de l'âge et du sexe. Conclusion : La présence de maladies non transmissibles à elle seule n'a pas augmenté la mortalité chez les patients atteints de COVID-19, après ajustement en fonction de tous les facteurs de confusion possibles, y compris les facteurs cliniques.
Book 27-11.indb 1042Book 27-11.indb 1042 06/12/2021 12:39 PM06/12/2021 12:39 PM
1043
Research article EMHJ – Vol. 27 No. 11 – 2021
References 1. Report of the WHO-China joint mission on coronavirus disease 2019 (COVID-19). Geneva: World Health Organization; 2020
(https://www.who.int/publications/i/item/report-of-the-who-china-joint-mission-on-coronavirus-disease-2019-(covid-19), acp-cessed 6 July 2021).
2. Zheng J. SARS-CoV-2: an emerging coronavirus that causes a global threat. Int J Biol Sci. 2020 Mar 15;16(10):1678–85. https://doi.org/10.7150/ijbs.45053 PMID:32226285
3. WHO Director-General’s opening remarks at the media briefing on COVID-19. 11 March 2020 [website]. Geneva: World Health Organization; 2020 (https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-me-dia-briefing-on-covid-19---11-march-2020).
4. COVID-19 coronavirus pandemic [website] (https://www.worldometers.info/coronavirus/, accessed 6 July 2021).
5. Xu X-W, Wu X-X, Jiang X-G, Xu K-J, Ying L-J, Ma C-L, et al. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: retrospective case series. BMJ. 2020 Feb 19;368:m606. https://doi.org/10.1136/bmj.m606 PMID:32075786
6. Benziger CP, Roth GA, Moran AE. The Global Burden of Disease Study and the preventable burden of NCD. Glob Heart. 2016 Dec;11(4):393–7. https://doi.org/10.1016/j.gheart.2016.10.024 PMID:27938824
7. NCD Countdown 2030 collaborators: worldwide trends in non-communicable disease mortality and progress towards Sus-tainable Development Goal target 3.4. Lancet. 2018 Sep 22;392(10152):1072–88. https://doi.org/10.1016/S0140-6736(18)31992-5 PMID:30264707
8. Khosravi Shadmani F, Farzadfar F, Larijani B, Mirzaei M, Haghdoost AA. Trend and projection of mortality rate due to non-com-municable diseases in Iran: a modeling study. PLoS One. 2019 Feb 14;14(2):e0211622. https://doi.org/10.1371/journal.pone.0211622 PMID:30763320
9. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coro-navirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020 Feb 15;395(10223):P507–13. https://doi.org/10.1016/S0140-6736(20)30211-7
10. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coro-navirus-infected pneumonia in Wuhan, China. JAMA. 2020 Mar 17; 323(11):1061–9. https://doi.org/10.1001/jama.2020.1585 PMID:32031570
11. Kluge HHP, Wickramasinghe K, Rippin HL, Mendes R, Peters DH, Kontsevaya A, et al. Prevention and control of non-commu-nicable diseases in the COVID-19 response. Lancet. 2020 May 30;395(10238):1678–80. https://doi.org/10.1016/S0140-6736(20)31067 PMID:32401713
12. Javanmard S, Nasirian M, Ataei B, Vaseghi G, Vaezi A, Changiz T. Isfahan COvid-19 REgistry (I-CORE): Design and methodology. J Res Med Sci. 2020 Mar 30;25:32. https://doi.org/10.4103/jrms.JRMS_271_20 PMID:32582338
13. Clinical management of severe acute respiratory infection when novel coronavirus (2019-nCoV) infection is suspected: interim guidance, 28 January 2020. Geneva: World Health Organization; 2020 (https://apps.who.int/iris/handle/10665/330893, accessed 6 July 2021).
14. International guidelines for certification and classification (coding) of covid-19 as cause of death based on ICD international statistical classification of diseases. Geneva: World Health Organization (https://www.who.int/classifications/icd/Guidelines_Cause_of_Death_COVID-19.pdf?ua=1, accessed 1 April 2021).
15. Docherty AB, Harrison EM, Green CA, Hardwick HE, Pius R, Norman L, et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO clinical characterisation protocol: prospective observational cohort study. BMJ. 2020 May 22;369:m1985. https://doi.org/10.1136/bmj.m1985 PMID:32444460
16. Petrilli CM, Jones SA, Yang J, Rajagopalan H, Luke O’Donnell, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ. 2020;369:m1966. https://doi.org/10.1136/bmj.m1966
17. Report on the Epidemiological Features of Coronavirus Disease 2019 (COVID-19) Outbreak in the Republic of Korea from Janu-ary 19 to March 2, 2020. J Korean Med Sci. 2020 Mar 16;35(10):e112. https://doi.org/10.3346/jkms.2020.35.e112 PMID:32174069
18. Pan Y, Long L, Zhang D, Yan T, Cui S, Yang P, et al. Potential false-negative nucleic acid testing results for severe acute respira-tory syndrome coronavirus 2 from thermal inactivation of samples with low viral loads. Clin Chem. 2020 Jun 1;66(6):794–801. https://doi.org/10.1093/clinchem/hvaa091 PMID:32246822
19. West CP, Montori VM, Sampathkuma P. COVID-19 testing: the threat of false-negative results. Mayo Clin Proc. 2020 Jun;95(6):1127–9. https://doi.org/10.1016/j.mayocp.2020.04.004 PMID:32376102
20. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020 Feb 15;395(10223):497–506. https://doi.org/10.1016/S0140-6736(20)30183-5
21. Guan WJ, Liang WH, Zhao Y, Liang HR, Chen ZS, Li YM, et al. Comorbidity and its impact on 1590 patients with COV-ID-19 in China: a nationwide analysis. Eur Respir J. 2020 May 14;55(5):2000547. https://doi.org/10.1183/13993003.00547-2020 PMID:32217650
22. Liu K, Fang YY, Deng Y, Liu W, Wang MF, Ma JP, et al. Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei Province. Chin Med J (Engl). 2020 May 5;133(9):1025–31. https://doi.org/10.1097/CM9.0000000000000744 PMID:32044814
Book 27-11.indb 1043Book 27-11.indb 1043 06/12/2021 12:39 PM06/12/2021 12:39 PM
1044
Research article EMHJ – Vol. 27 No. 11 – 2021
23. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COV-ID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020 Mar 28;395(10229):1054–62. https://doi.org/10.1016/S0140-6736(20)30566-3 PMID:32171076
24. Ioannou GN, Locke E, Green P, Berry K, O’Hare AM, Shah JA, et al. Risk factors for hospitalization, mechanical ventilation, or death among 10 131 US veterans with SARS-CoV-2 infection. JAMA Netw Open. 2020 Sep 1;3(9):e2022310. https://doi.org/10.1001/jamanetworkopen.2020.22310 PMID:32965502
25. Ahlström B, Frithiof R, Hultström M, Larsson IM, Strandberg G, Lipcsey M. The swedish covid-19 intensive care cohort: risk factors of ICU admission and ICU mortality. Acta Anaesthesiol Scand. 2021 Jan 12. https://doi.org/10.1111/aas.13781 PMID:33438198
26. de Almeida-Pititto B, Dualib PM, Zajdenverg L, Dantas JR, de Souza FD, Rodacki M, et al. Severity and mortality of COVID 19 in patients with diabetes, hypertension and cardiovascular disease: a meta-analysis. Diabetol Metab Syndr. 2020 Aug 31;12:75. https://doi.org/10.1186/s13098-020-00586-4 PMID:32874207
27. Iccarino G, Grassi G, Borghi C, Ferri C, Salvetti M, Vole M, et al. Age and multimorbidity predict death among COVID-19 pa-tients. Results of the SARS-RAS Study of the Italian Society of Hypertension. Hypertension. 2020 Aug;76(2):366–72. https://doi.org/10.1161/HYPERTENSIONAHA.120.15324 PMID:32564693
28. Jee J, Foote MB, Lumish M, Stonestrom AJ, Wills B, Narendra V, et al. Chemotherapy and COVID-19 outcomes in patients with cancer. J Clin Oncol. 2020 Oct 20;38(30):3538–46. https://doi.org/10.1200/JCO.20.01307 PMID:32795225
29. Morra ME, Van Thanh L, Kamel MG, Ghazy AA, Altibi AMA, Dat LM. Clinical outcomes of current medical approaches for Middle East respiratory syndrome: a systematic review and meta-analysis. Rev Med Virol. 2018 May;28(3):e1977. https://doi.org/10.1002/rmv.1977 PMID:29664167
Book 27-11.indb 1044Book 27-11.indb 1044 06/12/2021 12:39 PM06/12/2021 12:39 PM

1045
Research article EMHJ – Vol. 27 No. 11 – 2021
Adapting the ethical review process for COVID-19 research: reviewers’ perspectives from PakistanSualeha Shekhani,1 Saima Iqbal2 and Aamir Jafarey1
1Centre of Biomedical Ethics and Culture, Sindh Institute of Urology and Transplantation (SIUT), Karachi, Pakistan (Correspondence to: A.M. Jafarey: [email protected]). 2Department of Family Medicine, Shifa College of Medicine, Shifa Tameer-e-Millat University, Islamabad, Pakistan.
AbstractBackground: Research ethics committees (RECs) globally have adapted their responses to provide timely reviews of re-search proposals in the wake of the COVID-19 pandemic. The REC of the National Bioethics Committee (NBC) of Pakistan has followed suit.Aims: To explore perceptions of NBC-REC reviewers who reviewed COVID-19 research proposals while describing the newly instituted Rapid Turnaround Review (RTR) system.Methods: This cross-sectional study used 3 methods of data collection: a demographic questionnaire filled in by perma-nent members and co-opted reviewers; qualitative in-depth interviews conducted with both groups; and document review related to COVID-19 research proposals.Results: Eight permanent members and 3 co-opted members participated. Under the RTR system, the time for review was established as 72 hours after receipt of the proposal. The Committee reviewed 55 projects over 10 months. Participants de-scribed numerous strengths of the new system, including introduction of online discussions via Zoom as well as presence of co-opted members leading to learning opportunities, particularly for junior members. The RTR system also allowed NBC-REC to gain recognition it had not enjoyed previously. Challenges identified by respondents included initial diffi-culty in initiating the system and tighter deadlines that may have compromised review quality. Poor scientific quality of proposals, compounded by external pressures to provide rapid approval, added to reviewers’ frustrations. While fruitful, the RTR system was considered unsustainable beyond a public health emergency. Conclusion: Adaptation of ethical review processes is essential in emergencies, however, existing guidelines have to be modified to suit contextual needs.Citation: Shekhani S; Iqbal S; Jafarey A. Adapting the ethical review process for COVID-19 research: reviewers’ perspectives from Pakistan. East Mediterr Health J. 2021;27(11):1045−1051. https://doi.org/10.26719/emhj.21.053 Received: 05/01/21; accepted: 13/04/21Copyright © World Health Organization (WHO) 2021. Open Access. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license (https://creativecommons.org/licenses/by-nc-sa/3.0/igo)
IntroductionEthical review is a core aspect of human research. In the wake of the COVID-19 pandemic, there has been an expo-nential increase globally in the number of research pro-jects investigating its various aspects. For instance, 4094 clinical trials in various phases were listed for COVID-19 on clinicaltrials.gov as of December 2020 (1). While it is an ethical imperative to conduct research during public health emergencies, cutting corners in scientific or eth-ical aspects is never acceptable. Instead, research ethics committees (RECs), tasked with the responsibility of eth-ical review, have to adapt their processes to facilitate re-search in such times, while reducing obstacles (2). Ethical preparedness is therefore essential during humanitarian emergencies to ensure unhindered research (3).
According to a 2009 mapping exercise conducted in the World Health Organization Eastern Mediterranean Region, Pakistan was among the 15 countries that reported having a national REC (4). The Pakistani REC is a subcommittee of the National Bioethics Committee (NBC). Since 2004, the NBC-REC has been reviewing all human research that has foreign or Pakistani
Government funding, or research proposed to be conducted in multiple provinces of Pakistan. Additionally, all clinical trials, irrespective of location, or funding come to the NBC-REC. Prior to the COVID-19 pandemic, all NBC-REC reviews were conducted asynchronously, with proposal packages being sent electronically to members with a 6-week turnaround time. The Committee had no mechanism for rapid review prior to the pandemic and all proposals were reviewed according to the regular schedule. However, the anticipated increase in research reviews in the wake of the COVID-19 pandemic led to the introduction of a national rapid turnaround review (RTR) system, catering specifically to the public health emergency situation. While devising this system within the Pakistani context, it was important to ensure that it was not open to misuse for rapid reviews for routine research merely because the researchers were in a hurry, or could use their influence to pass through the system quickly. Cognizant of the challenges, the NBC-REC modified its terms of reference (TORs) to adapt to an RTR system, with a 72-hour response time for research proposals studying situations related to public health emergencies, such as COVID-19. To ensure immediate
Book 27-11.indb 1045Book 27-11.indb 1045 06/12/2021 12:39 PM06/12/2021 12:39 PM

1046
Research article EMHJ – Vol. 27 No. 11 – 2021
deliberation by the Committee, videoconferencing for each review was also instituted. This meant that such virtual meetings were happening up to 3 times a week at the peak of the first wave of the COVID-19 pandemic. The NBC-REC also made a provision in the TORs to co-opt relevant reviewers, as needed. The TORs were adapted from a guidance document by WHO (5).
The present study investigated the procedural aspects of the RTR system through a document review, and explored the perspectives of the reviewers with respect to the strengths and challenges encountered with the system. Some descriptive reports have recently summarized the experience of RECs during the COVID-19 pandemic (6,7); however, to the best of our knowledge, this is the first study to utilize qualitative methods to explore the perspectives of national REC members. This study will contribute a useful low and middle income country perspective in an area with, as yet, little empirical analysis.
MethodsThis cross-sectional study used 3 methods of data collec-tion, including: a document review of projects reviewed under the RTR system; a demographic questionnaire to collect basic information about NBC-REC members; and a semistructured interview guideline, prepared specifi-cally for the purpose of this study, to explore perceptions of members regarding the RTR system.
After obtaining informed consent from all participants, which included both permanent and co-opted members, demographic information was collected by email and in-depth interviews were conducted online via the Zoom platform. Ethical clearance was obtained from the Institutional Review Board of Shifa Tameer-e-Millat University, Islamabad.
Interviews, conducted in a mixture of English and Urdu, lasted 25 minutes to 1 hour. Interviews were audiorecorded to aid recordkeeping and later transcribed verbatim. Two authors of this paper, serving on the NBC-REC, provided narratives regarding their experiences that contributed towards triangulation of data.
All transcriptions (and the 2 narrative experiences) were deidentified and assigned unique identification codes. Data from all sources were collated for analysis. For the qualitative part, themes and subthemes were developed inductively from the collated data using a modified version of the grounded theory known as constant comparison method (8). This method involved a series of steps that included: 1) reading transcripts multiple items by all 3 authors individually, and assigning codes in the process, known as open coding; 2) comparing codes from collated data, and identifying common patterns using axial coding; and 3) the eventual emergence of themes and subthemes. All 3 authors agreed upon the thematic framework presented in the Results.
ResultsThere were 11 participants included in the demograph-ic and qualitative arms of this study, which included 8 permanent NBC-REC members and 3 co-opted reviewers. In-depth interviews were conducted with 9 participants and 2 members shared their experiences in a written narrative form. Data from demographic questionnaire, document review and the thematic framework from the qualitative arm (Table 1) are presented below.
Demographic characteristics of participantsParticipants’ demographic characteristics are summa-rized in Table 2.
Characteristics of proposals reviewed under RTR systemA review of NBC-REC records revealed that from April to the first week of December 2020, when these data were compiled, the Committee reviewed 55 COVID-19-related research proposals. Forty-seven proposals were given ap-proval to proceed; 3 on first review, 42 after more than 1review, and 2 were granted exemption. Each review oc-curred within the mandated 72 hours. However, on aver-age, the back and forth between the Committee and the applicant took 3–4 weeks before approval. Out of the 5 cases for which approval was not granted, the prime rea-son was inadequate response to concerns raised by the reviewers. One of these projects was the only instance in which the NBC-REC took > 72 hours to review, since external scientific input was required. Concerns of the reviewers and the scientific experts were conveyed to the research team, in writing and during a special video-conference with the applicants. However, the Committee had not heard back from the researchers at the time of this study. One proposal was withdrawn by the research-er and 2 proposals were rejected.
Overall, 135 proposals were reviewed by the Committee when 77 non-COVID-19 proposals were included. Ten of these were pending final approval at the time of finalizing this dataset. Many of the non-COVID-
Table 1 Thematic framework for qualitative arm
Sr. no. Themes Subthemes1 Strengths of the
RTR systemAddition of video meetings
Logistic advantages of RTR system
Presence of co-opted members
Increased recognition of NBC-REC
2 Challenges of the RTR system
Roadblocks in initiating the system
Difficulties in time management
Poor quality of proposals
Lack of preparedness
External pressures
3 Sustainability of the RTR system
N/A
N/A = not available; NBC-REC = National Bioethics Committee Research Ethics Committee; RTR = rapid turnaround review.
Book 27-11.indb 1046Book 27-11.indb 1046 06/12/2021 12:39 PM06/12/2021 12:39 PM
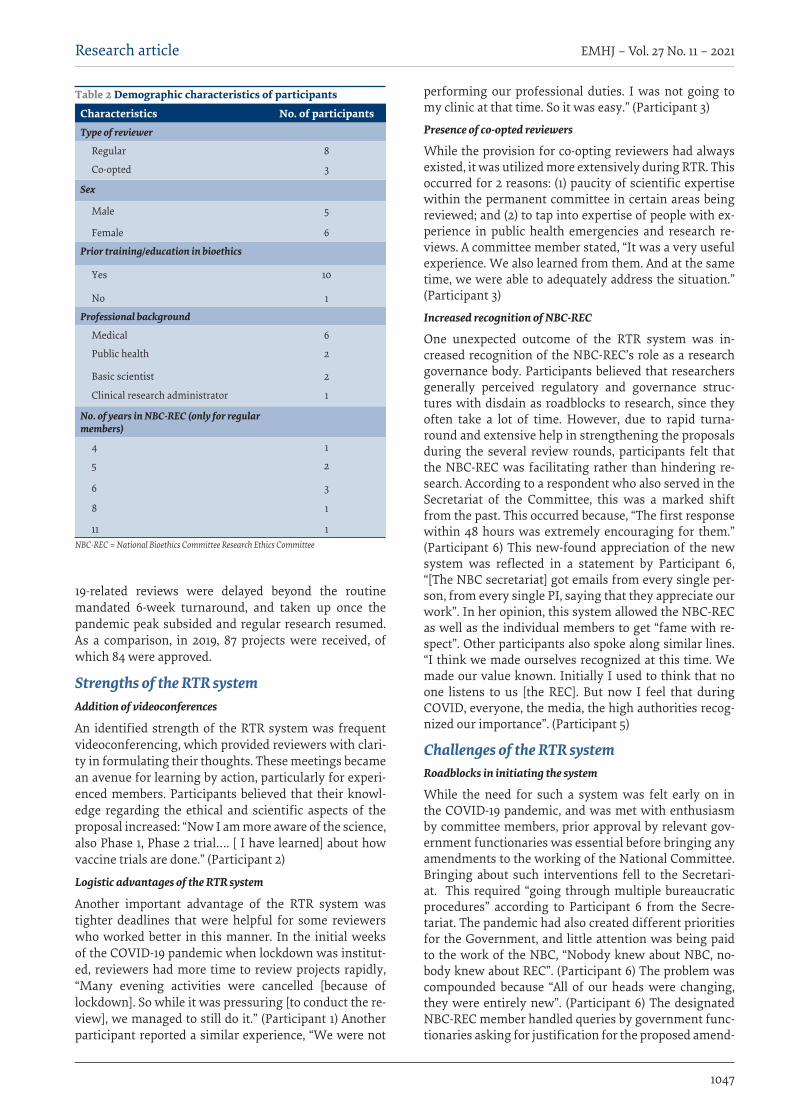
1047
Research article EMHJ – Vol. 27 No. 11 – 2021
19-related reviews were delayed beyond the routine mandated 6-week turnaround, and taken up once the pandemic peak subsided and regular research resumed. As a comparison, in 2019, 87 projects were received, of which 84 were approved.
Strengths of the RTR systemAddition of videoconferences
An identified strength of the RTR system was frequent videoconferencing, which provided reviewers with clari-ty in formulating their thoughts. These meetings became an avenue for learning by action, particularly for experi-enced members. Participants believed that their knowl-edge regarding the ethical and scientific aspects of the proposal increased: “Now I am more aware of the science, also Phase 1, Phase 2 trial…. [ I have learned] about how vaccine trials are done.” (Participant 2)
Logistic advantages of the RTR system
Another important advantage of the RTR system was tighter deadlines that were helpful for some reviewers who worked better in this manner. In the initial weeks of the COVID-19 pandemic when lockdown was institut-ed, reviewers had more time to review projects rapidly, “Many evening activities were cancelled [because of lockdown]. So while it was pressuring [to conduct the re-view], we managed to still do it.” (Participant 1) Another participant reported a similar experience, “We were not
performing our professional duties. I was not going to my clinic at that time. So it was easy.” (Participant 3)
Presence of co-opted reviewers
While the provision for co-opting reviewers had always existed, it was utilized more extensively during RTR. This occurred for 2 reasons: (1) paucity of scientific expertise within the permanent committee in certain areas being reviewed; and (2) to tap into expertise of people with ex-perience in public health emergencies and research re-views. A committee member stated, “It was a very useful experience. We also learned from them. And at the same time, we were able to adequately address the situation.” (Participant 3)
Increased recognition of NBC-REC
One unexpected outcome of the RTR system was in-creased recognition of the NBC-REC’s role as a research governance body. Participants believed that researchers generally perceived regulatory and governance struc-tures with disdain as roadblocks to research, since they often take a lot of time. However, due to rapid turna-round and extensive help in strengthening the proposals during the several review rounds, participants felt that the NBC-REC was facilitating rather than hindering re-search. According to a respondent who also served in the Secretariat of the Committee, this was a marked shift from the past. This occurred because, “The first response within 48 hours was extremely encouraging for them.” (Participant 6) This new-found appreciation of the new system was reflected in a statement by Participant 6, “[The NBC secretariat] got emails from every single per-son, from every single PI, saying that they appreciate our work”. In her opinion, this system allowed the NBC-REC as well as the individual members to get “fame with re-spect”. Other participants also spoke along similar lines. “I think we made ourselves recognized at this time. We made our value known. Initially I used to think that no one listens to us [the REC]. But now I feel that during COVID, everyone, the media, the high authorities recog-nized our importance”. (Participant 5)
Challenges of the RTR systemRoadblocks in initiating the system
While the need for such a system was felt early on in the COVID-19 pandemic, and was met with enthusiasm by committee members, prior approval by relevant gov-ernment functionaries was essential before bringing any amendments to the working of the National Committee. Bringing about such interventions fell to the Secretari-at. This required “going through multiple bureaucratic procedures” according to Participant 6 from the Secre-tariat. The pandemic had also created different priorities for the Government, and little attention was being paid to the work of the NBC, “Nobody knew about NBC, no-body knew about REC”. (Participant 6) The problem was compounded because “All of our heads were changing, they were entirely new”. (Participant 6) The designated NBC-REC member handled queries by government func-tionaries asking for justification for the proposed amend-
Table 2 Demographic characteristics of participants
Characteristics No. of participants Type of reviewer
Regular 8
Co-opted 3
Sex
Male 5
Female 6
Prior training/education in bioethics
Yes 10
No 1
Professional background
Medical 6
Public health 2
Basic scientist 2
Clinical research administrator 1
No. of years in NBC-REC (only for regular members)
4 1
5 2
6 3
8 1
11 1NBC-REC = National Bioethics Committee Research Ethics Committee
Book 27-11.indb 1047Book 27-11.indb 1047 06/12/2021 12:39 PM06/12/2021 12:39 PM

1048
Research article EMHJ – Vol. 27 No. 11 – 2021
ments in the TORs: “I answered that a lot of research is going to happen. I told them that this will be a situation [a large number of proposals] which will happen. I believe we must put in this system”. (Participant 6)
Difficulties in time management
Once the system was in place, most members believed that strict timelines for reviewing the projects and re-sponding to the investigators took a toll. This was height-ened with the lifting of lockdown and people resuming their professional obligations. According to one, “When my official duties started, I could not fit in the review process”. (Participant 5) For the Chair of the Committee, her professional obligations suffered due to extra time required for the RTR system. According to some respond-ents, because of multiple competing responsibilities, they were concerned about the quality of their review. One stated, “I did not review them as thoroughly as I would have liked to”. (Participant 2) The number of proposals proved to be challenging as well, because according to Participant 5, “Before COVID-19, we did not have that many proposals that required review at so much speed”.
Poor quality of proposals
Another challenge for all participants was the poor qual-ity of proposals. This was attributed to overeager re-searchers wishing to join the fray, and hence submitting hastily put together proposals. Another challenge associ-ated with poor quality was the bad science presented in the proposals: “Much of our time was spent fixing the sci-ence, rather than the ethics of it”. (Participant 10) While this proved to be frustrating for many members, Partic-ipant 11 believed that it was their responsibility to do so in order to promote good research, “even if it meant the project going back and forth several times”.
Lack of preparedness
Adding to the poor quality of proposals was the review-ers own discomfort and concern in reviewing technically challenging projects. For instance, studies involving mo-lecular biology, stem cell approaches, vaccine trials, and testing of indigenously prepared ventilators led to sig-nificant discomfort among reviewers. This was circum-vented by co-opting relevant members. Another problem while reviewing was a lack of preparedness or training for research reviews based on public health emergencies.
External pressures
Poor quality of proposals combined with political pres-sures to approve quickly, particularly for high-profile projects, also increased the burden of REC members, according to Participant 10. The Chair of the Committee and the Secretariat primarily absorbed these pressures. However, a senior member reported getting calls from the highest government quarters to proceed with quickly with the review process. Sometimes, external pressures on the Committee came via the NBC Secretariat, who would receive requests for rapid approvals (Participant 10). This happened when back and forth communication was going on between the Committee and the research-ers asked to amend their proposals to conform to ethical
and scientific requirements. However, members believed that the Secretariat should not have been used to put pressure on the Committee. As Participant 5 stated, “We should be free to work with our peace of mind”.
Sustainability of RTR systemWhile the REC members took the RTR system in their stride, they believed that the process required a lot of commitment that would not be sustainable indefinitely (Participant 3). Increased risk of burnout for the review-ers was cited as one reason. In addition, in retrospect, the reviewers believed that the 72-hour commitment was ambitious (Participant 9). Given the gradual change in research proposals from clinical to sociological research, the deadline “could have been relaxed a bit”. All respond-ents believed that while this system was excellent as a short-term emergency response, it could not exist under normal circumstances because “it really exhausts your energies” (Participant 6).
DiscussionThe response of national health research organizations and ethical review committees after the onset of the COVID-19 pandemic was noteworthy in many parts of the world, with authorities developing and implement-ing processes to ensure timely review of research relat-ed to COVID-19 (9–11). The Pakistan NBC-REC developed its own response that, as this study demonstrated, was appreciated by reviewers and researchers. Furthermore, analysis of this RTR system has useful learning points for RECs within the developing world.
The new system necessitated online, real-time discussions through videoconferencing. This system was acknowledged as an advantage by all respondents. While videoconferencing is not a novel idea, this was never considered as an option by the NBC-REC prior to the COVID-19 pandemic (12). This system proved successful and provided guidance for the future since members of the REC are spread across the country, and allows real-time exchange of opinions and consensus building. The videoconferencing experience from the pandemic has provided guidance for the conduct of future committee meetings as well. If necessary, the Committee now meets online weekly to review COVID-19-related projects. Regular meetings are now scheduled fortnightly to clear the backlog of non-COVID-related projects delayed due to the pandemic.
Several guidelines have recommended that, to prepare for emergency public health research reviews, RECs should include relevant members (2). Since the TORs had this provision, a list of potential co-opted reviewers was developed and their inclusion in the review process started early. The presence of co-opted reviewers provided learning opportunities and enhanced review quality. However, it was easy to co-opt reviews since several senior members in the Committee personally knew people with relevant expertise who could provide high-quality input for the review process. It was useful
Book 27-11.indb 1048Book 27-11.indb 1048 06/12/2021 12:39 PM06/12/2021 12:39 PM

1049
Research article EMHJ – Vol. 27 No. 11 – 2021
to harness external expertise from overseas as well as national reviewers.
A welcome and unexpected outcome of the new rapid review system was that this Committee acquired a recognition and respect it previously did not enjoy. This is intriguing since ethical review processes are often considered impediments to research (12–14). This recognition of the positive role of the NBC was a direct result of its rapid response to researchers, in addition to extensive feedback to enhance the quality of proposals. Since it is mandatory for all clinical trials to be approved by the NBC-REC before commencing, a poorly functioning national review system would have derailed important research and earned a bad name for the Committee. As it transpired, the newly installed RTR system worked and was well received, with the NBC-REC earning a good name and being propelled into the national limelight; something that members considered their personal accomplishment. The new system also helped to build trust in the system of research ethics governance (12).
The RTR system naturally faced challenges and constraints. The regular workload on the Committee is reflected by its caseload in 2019, which was 87 proposals, with a 6-week response time. From April to December 2020, the Committee handled 55 COVID-19-related projects; all but 1 being responded to within 72 hours. Respondents therefore found their review responsibilities overwhelming due to the short turnaround time and frequent virtual meetings, at times happening thrice weekly. This increase in workload and changes in modus operandi of committees has emerged from other countries including Italy (15), the Philippines (16), China (16) and Islamic Republic of Iran (18). For example, in China, a committee that met only once a month prior to the pandemic met 4 times within 34 days (18).
In retrospect however, the 72-hour deadline could have been applied selectively to pertinent COVID-19 proposals, and in particular, social sciences projects could have been given longer turnaround periods. After the first peak of the COVID-19 pandemic, the REC saw a decrease in the number of proposals received, which led to increasing the turnaround time to 1 week for COVID-19-related proposals.
Another serious challenge that study respondents recounted was the poor quality of proposals received. This was not considered surprising as disaster-related protocols are often developed in a hurry, without proper planning (15,16). While improving science and methodology is not considered the domain of RECs, there was a strong feeling among committee members that bad science leads to bad ethics (17). The time involved in the back and forth communication between the Committee and researchers reflected the commitment by the members to their voluntary task. To bring about improvement in proposals, it is important to develop an adequate research culture within developing countries.
This study also highlights the importance of ethical review in going beyond just ethics and into the science of the proposal itself, to strengthen the structure of research ethics governance.
Apart from the challenge of poor-quality research proposals, another area of concern was external pressures from influential quarters, primarily to further expedite reviews stuck in a re-review process. The majority of proposals were reviewed and a decision conveyed to the researchers within the stipulated 72 hours, with only 1 exception. While it is important to facilitate the research process during a pandemic, no compromises on review quality should be made since the primary responsibility of RECs is to provide quality reviews. Such pressures were brought on by the Committee particularly for those proposals that were regarded as projects of national importance. However, members believed that these pressures were unfair since their job and responsibility was to ensure review quality rather than cater to the demands of powerful offices. However, such external pressures are not uncommon from this part of the world (3,19).
An important finding of this study was that, while quick turnaround is essential for emergencies, it ought not be prolonged beyond a certain point, since it taxes the energies of the entire committee. The changes that COVID-19 has brought offers a unique window of opportunity for national and institutional RECs to develop innovative systems of oversight. We believe that the RTR system of the NBC-REC presents a workable model that other RECs can emulate.
This study had some limitations. Inclusion of 2 members from the NBC-REC in the research team may be perceived as a limitation because it may have induced bias, but the presence of a third researcher, unrelated to the REC, ensured that any bias was neutralized. The findings of this study reflect the experience of 1 national REC, and the small number of participants in the study may be regarded as a limitation. However, a qualitative analysis that included perspectives of all reviewers involved in the review process ensured richness of data.
We make the following recommendations in light of our study. The WHO guidance document for public health emergency research reviews is a good template, and can be contextualized for the needs of particular countries. Provisions must be made by national and institutional RECs to avail relevant outside expertise to maintain review quality and credibility. Face to face meetings enhance review quality, and videoconferencing is an excellent tool to enable such meetings when physical meetings are not possible. Additional training, even for seasoned members, particularly within the field of disaster ethics, should be provided. As epidemics and health disasters and emergencies continue to emerge, it is essential that RECs are equipped in ethics preparedness.
Book 27-11.indb 1049Book 27-11.indb 1049 06/12/2021 12:39 PM06/12/2021 12:39 PM
1050
Research article EMHJ – Vol. 27 No. 11 – 2021
AcknowledgementThe authors wish to acknowledge Mr. Hamza Jafarey who transcribed all the interviews.Funding: Supported by a grant from WHO/EMRO Division of Science, Information and Dissemination: 2020/1068517-0.
Competing interests: None declared.
تكييف املراجعة األخالقية لبحوث كوفيد-19: وجهات نظر املراجعني من باكستانصواحلة شيخاين، سايام إقبال، عامر جعفري
اخلالصةم مراجعات مناسبة التوقيت للمشاريع البحثية يف أعقاب انتشار اخللفية: واءمت جلان مراجعة أخالقيات البحوث حول العامل استجاباهتا كي تقد
جائحة كوفيد-19. وسارت جلنة مراجعة أخالقيات البحوث املنبثقة عن اللجنة الوطنية لألخالقيات احليوية يف باكستان عىل نفس املنوال.األهداف: هدفت هذه الدراسة اىل استكشاف تصورات مراجعي جلنة مراجعة أخالقيات البحوث املنبثقة عن اللجنة الوطنية لألخالقيات احليوية
الذين استعرضوا املرشوعات البحثية املتعلقة بكوفيد-19 مع وصف نظام االستعراض رسيع الدوران الذي أنشئ حديثا.طرق البحث: استخدمت هذه الدراسة املقطعية ثالث طرق جلمع البيانات، وهي: استبيان سكاين يملؤه األعضاء الدائمون واملراجعون املنضمون
باالختيار؛ ومقابالت نوعية متعمقة أجريت مع كال املجموعتني؛ واستعراض الوثائق املتعلقة باملشاريع البحثية التي تتناول كوفيد-19.النتائج: شارك يف الدراسة ثامنية أعضاء دائمني وثالثة أعضاء منضمني باالختيار. ويف إطار نظام االستعراض رسيع الدوران، حدد وقت املراجعة ا عىل مدى 10 أشهر. ووصف املشاركون العديد من مواطن عىل أنه 72 ساعة بعد تلقي املرشوع البحثي. واستعرضت اللجنة 55 مرشوعا بحثيالقوة يف النظام اجلديد، ومن ذلك استحداث املناقشات عرب اإلنرتنت عن طريق تطبيق »زووم«، فضال عن وجود أعضاء منضمني باالختيار، األمر يتحقق هلا من قبل. باعرتاف مل للجنة أن حتظى أيضا الدوران املراجعة رسيع نظام املبتدئني. وسمح للتعلم، ال سيام لألعضاء فرصا يتيح الذي وشملت التحديات التي حددها املستجيبون الصعوبة األولية التي اتسم هبا بدء العمل بالنظام، واملواعيد النهائية األكثر رصامة مما مىض التي قد تؤثر عىل جودة املراجعة. وما زاد من إحباط املراجعني تدين النوعية العلمية للمرشوعات، إضافة إىل الضغوط اخلارجية إلبداء املوافقة برسعة. وعىل
الرغم من الفائدة التي عاد هبا النظام، فقد اعترب غري قابل لالستمرار يف حال حدوث حالة طوارئ صحية عامة. االستنتاجات: يعد تكييف عمليات مراجعة األخالقيات البحثية أمرا أساسيا يف حاالت الطوارئ، غري أنه ينبغي تعديل املبادئ التوجيهية القائمة
لتتناسب مع االحتياجات التي يتطلبها السياق.
Adaptation du processus d'examen éthique de la recherche sur la COVID-19 : points de vue des examinateurs au PakistanRésuméContexte : Partout dans le monde, les comités d'éthique de la recherche (CER) ont adapté leurs réponses afin d'examiner en temps utile les propositions de recherche formulées dans le sillage de la pandémie de COVID-19. Le CER du Comité national de bioéthique (CNB) du Pakistan s'est lui aussi adapté.Objectifs : Explorer les points de vue des examinateurs du CER-CNB qui ont étudié les propositions de recherche sur la COVID-19 et décrire en parallèle le nouveau système d'examen accéléré mis en place.Méthodes : La présente étude transversale a utilisé trois méthodes de collecte de données : un questionnaire démographique rempli par les membres permanents et les examinateurs cooptés ; des entretiens qualitatifs approfondis menés avec les deux groupes ; et un examen documentaire relatif aux propositions de recherche sur la COVID-19.Résultats : Huit membres permanents et trois membres cooptés ont participé à l'étude. Dans le cadre du système d'examen accéléré, le délai d'examen a été fixé à 72 heures après réception de la proposition. Le comité a examiné 55 projets sur 10 mois. Les participants ont décrit les nombreux points forts du nouveau système, notamment l'introduction de discussions en ligne via Zoom, ainsi que la présence de membres cooptés, ces deux nouveautés offrant des possibilités d'apprentissage, en particulier pour les examinateurs juniors. Le système d'examen accéléré a également permis au CER-CNB d'obtenir un degré de reconnaissance sans précédent. Les défis identifiés par les répondants comprenaient la difficulté initiale à mettre en place le système, et des délais plus serrés qui auraient pu compromettre la qualité de l'examen. La piètre qualité scientifique des propositions, aggravée par des pressions externes en faveur d'une approbation rapide, a accentué la frustration des examinateurs. Bien que concluant, le système d'examen accéléré a été jugé comme non viable en dehors d'une situation d'urgence de santé publique.Conclusion : L'adaptation des processus d'examen éthique est indispensable en situation d'urgence. Cependant, les lignes directives existantes doivent être modifiées en fonction des besoins du contexte.
Book 27-11.indb 1050Book 27-11.indb 1050 06/12/2021 12:39 PM06/12/2021 12:39 PM
1051
Research article EMHJ – Vol. 27 No. 11 – 2021
References 1. Covid-19 information [website]. ClinicalTrials.gov.; 2021 (https://clinicaltrials.gov/ct2/results?cond=Covid-19&term=&cnt-
try=&state=&city=&dist, accessed 13 July 2021.
2. Guidance and strategies to streamline ethics review and oversight of COVID-19-related research. Washington DC: Pan American Health Organization; 2020 (https://www.paho.org/en/documents/guidance-and-strategies-streamline-ethics-review-and-over-sight-covid-19-related-research, accessed 13 July 2021).
3. Kumar NK, Muthuswamy V. Fostering ethical biomedical and health research in India during the COVID-19 pandemic. Research Ethics. 2020 Jul;16(3–4). https://doi.org/10.1177/1747016120941632
4. Abou-Zeid A, Afzal M, Silverman HJ. Capacity mapping of national ethics committees in the Eastern Mediterranean Region. BMC Med Ethics. 2009 Jul 4;10:8. https://doi.org/10.1186/1472-6939-10-8 PMID:19575813
5. Guidance for research ethics committees for rapid review of research during public health emergencies. Geneva: World Health Organization; 2020 (https://www.who.int/publications/i/item/9789240006218, accessed 13 July 2021.
6. Agrawal V, Nath C, Mishra SK. Ethics committee meeting by video-conferencing during Covid-19. Indian J Med Ethics. 2020 May 27. https://doi.org/10.20529/IJME.2020.062 PMID:32546456
7. Sheehy A, James JR, Horgan M. Implementing a national approach to research ethics review during a pandemic – the Irish expe-rience. HRB Open Research. 2020 Nov 16;3:63. https://doi.org/10.12688/hrbopenres.13146.2 PMID:33490861
8. Boeije H. A purposeful approach to the constant comparative method in the analysis of qualitative interviews. Qual Quant. 2002 Nov 1; 36(4):391–409. https://doi.org/10.1023/A:1020909529486
9. Position of the European Network of Research Ethics Committees (EUREC) on the Responsibility of Research Ethics Committees during the COVID-19 pandemic. EUREC; 2020 (https://ancei.es/wp-content/uploads/2020/05/EUREC-Positionpaper_COVID_19.pdf, accessed 13 July 2021).
10. Fast track review guidance for COVID-19 studies [website]. London: NHS Health Research Authority; 2020 (https://www.hra.nhs.uk/covid-19-research/fast-track-review-guidance-covid-19-studies/, accessed 13 July 2021).
11. ICMR, WHO India and ISCR jointly organized a webinar on ethics review for bio-medical projects during the pandemic [web-site]. World Health Organization South-East Asia Region; 2020 (https://www.who.int/india/news/detail/27-06-2020-icmr-who-in0-dia-and-iscr-jointly-organized-a-webinar-on-ethics-review-for-bio-medical-projects-during-the-pandemic, accessed 13 July 2021).
12. Ghooi RB. Ethics committee meetings – online or face to face?. Perspect Clin Res. 2020 Jul–Sep;11(3):121–3. https://doi.org/10.4103/picr.picr_97_20 PMID:33033701
13. Brown C, Spiro J, Quinton S. The role of research ethics committees: friend or foe in educational research? An exploratory study. Br Educ Res J. 2020 Aug; 46(4):747–69. https://doi.org/10.1002/berj.3654
14. Jafarey AM, Iqbal SP, Hassan M. Ethical review in Pakistan: the credibility gap. J Pak Med Assoc. 2012 Dec;62(12):1354–7. PMID:23866494
15. Alirol E, Kuesel AC, Guraiib MM, de la Fuente-Núñez V, Saxena A, Gomes MF. Ethics review of studies during public health emergencies – the experience of the WHO ethics review committee during the Ebola virus disease epidemic. BMC Med Ethics. 2017 Dec 1;18(1):43. https://doi.org/10.1186/s12910-017-0201-1 PMID:28651650
16. Zhang H, Shao F, Gu J, Li L, Wang Y. Ethics committee reviews of applications for research studies at 1 hospital in China during the 2019 novel coronavirus epidemic. JAMA. 2020 May 12;323(18):1844–6. https://doi.org/10.1001/jama.2020.4362 PMID:32202608
17. Gelling L. Role of the research ethics committee. Nurse Educ Today. 1999 Oct 1;19(7):564–9. https://doi.org/10.1054/nedt.1999.0349
18. Hashemi A, Bahmani F, Saeedi Tehrani S, Forouzandeh M, Koohpayehzadeh J, Ashrafi M, et al. Ethical considerations and interdisciplinary approach to research on COVID-19 pandemic: the response of Iran University of Medical Sciences. Med J Islam Repub Iran. 2020 Jul 29;34:87. https://doi.org/10.34171/mjiri.34.87 PMID:33306052
19. Bompart F. Ethical rationale for better coordination of clinical research on COVID-19. Res Ethics. 2020 Jul;16(3–4):1–10. https://doi.org/10.1177/1747016120931998
Book 27-11.indb 1051Book 27-11.indb 1051 06/12/2021 12:39 PM06/12/2021 12:39 PM

1052
Research article EMHJ – Vol. 27 No. 11 – 2021
Prevalence of and risk factors for Enterobius vermicularis infestation in preschool children, West Bank, Palestine, 2015Rasha Khayyat,1 Souad Belkebir,1 Sameh Abuseir,2 Majd Barahmeh,1 Lujain Alsadder1 and Walid Basha1
1Faculty of Medicine and Health Sciences, An-Najah National University, Nablus, West Bank, Palestine. 2Department of Veterinary Medicine, Faculty of Agriculture and Veterinary Medicine, An-Najah National University, Nablus, West Bank, Palestine (Correspondence to: Walid Basha: [email protected]).
AbstractBackground: Enterobius vermicularis (pinworm) infestation is a common condition that primarily affects children. Aims: The aim of this study was to assess the prevalence of and the risk factors for E. vermicularis infestation in preschool children in north West Bank.Methods: A cross-sectional study that included the six main governorates in north West Bank was carried out on a sample of 384 preschool children from 86 day-care centres. The perianal cellophane tape method was used to detect E. vermicularis infestation. Parents/guardians of participating children completed a questionnaire to collect information about: demo-graphic characteristics; hygiene behaviour; socioeconomic status; history of previous infestation; and presence of symp-toms. Risk factors for infestation were assessed using logistic regression analysis.Results: Of the 384 children, 85 (22.1%) had E. vermicularis infestation. Age (P = 0.04), governorate (P = 0.01), residency (P = 0.03), number of household members (P < 0.001) and washing hands after toilet use (P = 0.01) were significantly asso-ciated with E. vermicularis infestation. In the logistic regression analysis, factors that increased the probability of infection were: living in villages (odds ratio (OR) 2.25; 95% confidence interval (CI): 1.01–5.00), living in a household with ≥ nine family members (OR 3.63; 95% CI: 1.42–9.26) and not washing hands after using the toilet (OR 2.4; 95% CI: 1.30–4.40). Conclusions: E. vermicularis is an important helminthic infestation among preschool children in Palestine. Efforts are needed to ensure the availability of treatment for infected children at primary care centres and to reinforce hygiene be-haviour.Keywords: Enterobius vermicularis, prevalence, risk factors; preschool children, Palestine.Citation: Khayyat R; Belkebir S; Abuseir S; Barahmeh M; Alsadder L; Basha W. Prevalence of and risk factors for Enterobius vermicularis infestation in preschool children, West Bank, Palestine, 2015. East Mediterr Health J. 2021;27(11):1052–1060. https://doi.org/10.26719/emhj.21.022Received: 23/12/20; accepted: 23/03/21Copyright © World Health Organization (WHO) 2021. Open Access. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license (https://creativecommons.org/licenses/by-nc-sa/3.0/igo)
IntroductionParasitic infestations are prevalent throughout the world and are a public health burden, especially in developing countries where they cause more morbidity and mortali-ty than other infectious diseases (1,2). Enterobius vermicula-ris (pinworms) is the least harmful of the gastrointestinal nematode helminths; it is considered more of a nuisance than a serious disease. It has the widest distribution of any parasitic helminths and humans are its only natu-ral host (3,4). Enterobius vermicularis also appears to be the oldest parasitic helminth to infect ancient populations (5). Studies in several countries around the world have shown a high prevalence of E. vermicularis in different age groups: for example, 30–80% in North America, 18% in China and 17% in Tanzania (6,7). Other studies indicate that a prevalence of more than 20% is common in many parts of the world (8).
Most infestations with gastrointestinal nematodes are asymptomatic. This may be why gastrointestinal nematode infestations including E. vermicularis infestation have been neglected in terms of public health recognition and research funding (1).
Enterobius vermicularis is most common in crowded residences among all ages, but is particularly common in children and affects between 4% and 28% of children worldwide (9,10). This parasite is mostly found in children in kindergartens, institutions or in families with a large number of children. It spreads easily between all family members, with frequent reinfestation (11–13). Mother’s employment and household income have also been shown to be risk factors for E. vermicularis infestation (14).
E. vermicularis can cause itching around the anus which can lead to difficulty sleeping and restlessness. This pruritus may also produce secondary lesions as mechanical dermatitis of the perianal or vulvar tissues (15). The presence of large numbers of adult worms in the bowel can cause abdominal pain, constipation, tenesmus and vaginitis (4,15,16). Some evidence exists that E. vermicularis infestation may be a cause of secondary enuresis (17,18). There have also been reported cases of appendicitis complicated by E. vermicularis infestation (19,20). E. vermicularis was found responsible for 7% of acute cases of appendicitis (21).
Furthermore, this infestation has been reported to have the potential to cause inflammation that can
Book 27-11.indb 1052Book 27-11.indb 1052 06/12/2021 12:39 PM06/12/2021 12:39 PM

1053
Research article EMHJ – Vol. 27 No. 11 – 2021
affect children’s growth, including salpingitis, ileocolitis, mesenteric abscess and urinary tract infection (22). It has been further reported to cause rectal malignancy (23) and create granuloma in the cecum, sigmoid colon, anal canal and extraintestinal tissues such as liver and ovary (24–26).
The main objective of this study was to determine the prevalence and risk factors of E. vermicularis infestation in preschool children in north West Bank, Palestine.
MethodsStudy design and setting We conducted a descriptive analytic cross-sectional study in north West Bank, Palestine. Samples were col-lected over a period of 7 months (May–November 2015) from six governorates in north West Bank, Palestine: Nablus, Jenin, Qalqilia, Salfeet, Tubas and Tulkarm. The population of these governorates was estimated to be more than1.1 million people, about 38% of the Palestinian population in the West Bank (27).
We used Raosoft sample size calculator (Raosoft, Inc., USA) to calculate the sample size, with a 95% confidence interval (CI) and a 0.05 margin of error. As there were no previous studies in Palestine on the prevalence of E. vermicularis infestation, we assumed the expected population proportion to be 0.5. The resulting sample size needed was 377 and the final sample size was 384.
We obtained information from bureau of statistics on the number of children aged 3–5 years in each governorate. We approached day-care centres and we included those that were willing to collaborate. From these centres, we selected a convenience sample of children aged 3–5 years proportionate to the number in each governorate.
A total of 86 day-care centres agreed to collaborate and 1300 sample kits, each containing a questionnaire and two scotch tapes, were distributed to children aged 3–5 years old who attended these centres over a period of 7 months from May to November 2015. We included children whose parents/guardians completed the questionnaire and provided the cellophane samples for testing.
E. vermicularis detectionTwo cellophane tapes were given to each child’s parent or guardian to use over two consecutive nights. Parents were given written and visual instructions on how to use the cellophane tapes and were asked to return them to the day-care centre. The tapes were sent to the microbiol-ogy laboratories of An-Najah National University where they were attached to glass slides and examined under light microscope. E. vermicularis infestation was consid-ered positive if E. vermicularis eggs were found on at least one cellophane tape.
QuestionnaireA questionnaire (completed by parents/guardians) was used to collect data on demographic characteristics of the child and his/her parents, family socioeconomic status, personal hygiene, medical history of previous infesta-
tion and clinical symptoms. The demographic section asked about the age and sex of the child, residency (city, village or refugee camp), number of children under the age of 9 years in the family, occupation of the mother and monthly income of the household. The personal hygiene section asked about certain behaviours, including wash-ing hands after using the toilet and before meals, playing outdoors, biting nails, daily change of underwear, and the type and location of the toilet. Finally, the question-naire asked about history of previous infestation with E. vermicularis, history of previous use of antihelminthic treatment for pinworms and the type of treatment used (herbal or pharmaceutical), and complaints of five clini-cal symptoms associated with E. vermicularis infestation: abdominal pain and discomfort, perianal itching, sleep disturbance, enuresis and change in appetite.
The questionnaire was based on an extensive literature review about risk factors of the development of E. vermicularis infestation (6,7,12,14,28). We independently reviewed the items included for content and face validity to determine the extent to which the questions reflected the scope of the study objectives and covered all essential factors presumed to be related to E. vermicularis. We gave the final version to volunteer mothers to evaluate the face validity, language adequacy and time required to fill it; no further changes to its content were made.
Statistical analysisWe only included completed questionnaires for analysis. We used SPSS, version 21 for data processing and analysis. We report data as means and standard deviations (SD) and frequencies as appropriate. We used the chi-squared test for statistical analysis with P < 0.05 set as the level of significance. We also used multivariable logistic regres-sions analysis to assess the association between the prev-alence of E. vermicularis and potential risks factors.
Ethical considerationsThe institutional review board committee at An-Najah National University approved the study protocol (archive number 20/March/2015).
The proposed procedure (use of cellophane tape for diagnosis) and the possible risks and benefits were explained to day-care centre principals and teachers. Communication with the parents/guardians of the participating children was mainly through teachers and principals of day-care centres. A written consent form was obtained from the parent/guardian of each participating child and they were informed if their child was found to be infected. Treatment for enterobiasis is available for free in primary health care centres and medical insurance for all children up to 5 years of age is provided by the Palestinian government without fees.
ResultsThe parents/guardians of 384 children complied with the instructions to use the tape over 2 consecutive nights, completed the questionnaire and returned both to the
Book 27-11.indb 1053Book 27-11.indb 1053 06/12/2021 12:39 PM06/12/2021 12:39 PM
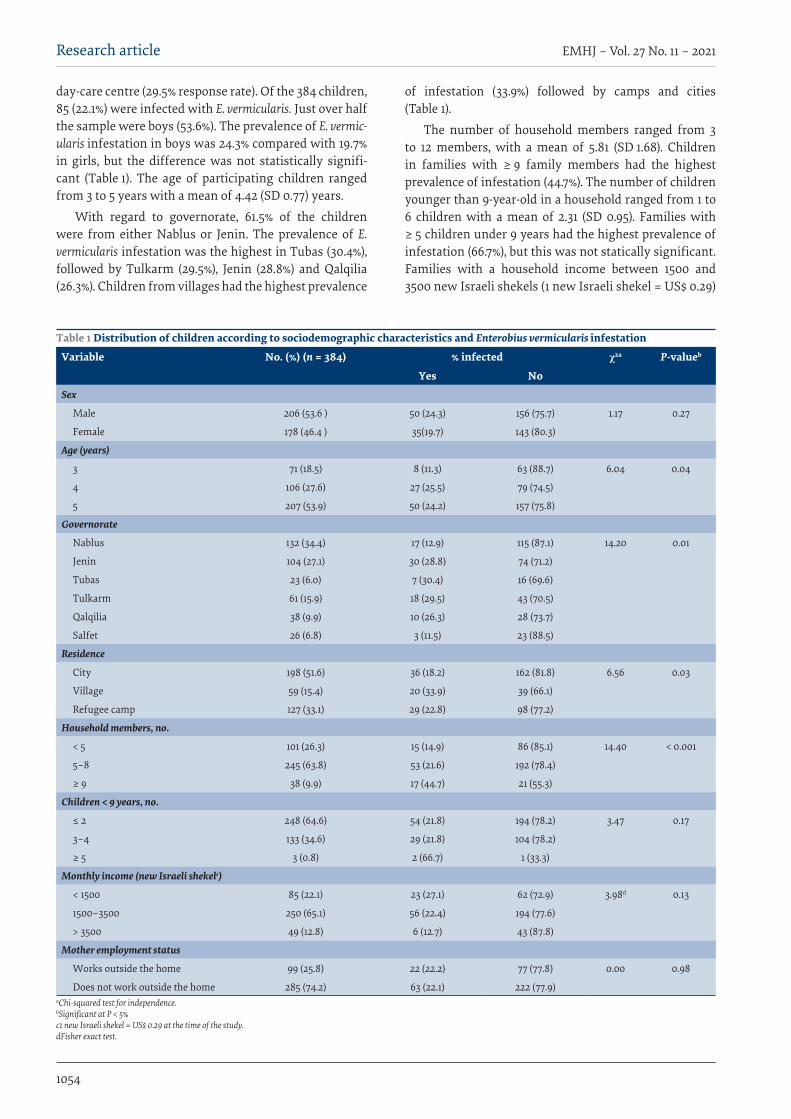
1054
Research article EMHJ – Vol. 27 No. 11 – 2021
day-care centre (29.5% response rate). Of the 384 children, 85 (22.1%) were infected with E. vermicularis. Just over half the sample were boys (53.6%). The prevalence of E. vermic-ularis infestation in boys was 24.3% compared with 19.7% in girls, but the difference was not statistically signifi-cant (Table 1). The age of participating children ranged from 3 to 5 years with a mean of 4.42 (SD 0.77) years.
With regard to governorate, 61.5% of the children were from either Nablus or Jenin. The prevalence of E. vermicularis infestation was the highest in Tubas (30.4%), followed by Tulkarm (29.5%), Jenin (28.8%) and Qalqilia (26.3%). Children from villages had the highest prevalence
of infestation (33.9%) followed by camps and cities (Table 1).
The number of household members ranged from 3 to 12 members, with a mean of 5.81 (SD 1.68). Children in families with ≥ 9 family members had the highest prevalence of infestation (44.7%). The number of children younger than 9-year-old in a household ranged from 1 to 6 children with a mean of 2.31 (SD 0.95). Families with ≥ 5 children under 9 years had the highest prevalence of infestation (66.7%), but this was not statically significant. Families with a household income between 1500 and 3500 new Israeli shekels (1 new Israeli shekel = US$ 0.29)
Table 1 Distribution of children according to sociodemographic characteristics and Enterobius vermicularis infestation
Variable No. (%) (n = 384) % infected χ2a P-valueb
Yes NoSex
Male 206 (53.6 ) 50 (24.3) 156 (75.7) 1.17 0.27
Female 178 (46.4 ) 35(19.7) 143 (80.3)
Age (years)
3 71 (18.5) 8 (11.3) 63 (88.7) 6.04 0.04
4 106 (27.6) 27 (25.5) 79 (74.5)
5 207 (53.9) 50 (24.2) 157 (75.8)
Governorate
Nablus 132 (34.4) 17 (12.9) 115 (87.1) 14.20 0.01
Jenin 104 (27.1) 30 (28.8) 74 (71.2)
Tubas 23 (6.0) 7 (30.4) 16 (69.6)
Tulkarm 61 (15.9) 18 (29.5) 43 (70.5)
Qalqilia 38 (9.9) 10 (26.3) 28 (73.7)
Salfet 26 (6.8) 3 (11.5) 23 (88.5)
Residence
City 198 (51.6) 36 (18.2) 162 (81.8) 6.56 0.03
Village 59 (15.4) 20 (33.9) 39 (66.1)
Refugee camp 127 (33.1) 29 (22.8) 98 (77.2)
Household members, no.
< 5 101 (26.3) 15 (14.9) 86 (85.1) 14.40 < 0.001
5–8 245 (63.8) 53 (21.6) 192 (78.4)
≥ 9 38 (9.9) 17 (44.7) 21 (55.3)
Children < 9 years, no.
≤ 2 248 (64.6) 54 (21.8) 194 (78.2) 3.47 0.17
3–4 133 (34.6) 29 (21.8) 104 (78.2)
≥ 5 3 (0.8) 2 (66.7) 1 (33.3)
Monthly income (new Israeli shekelc)
< 1500 85 (22.1) 23 (27.1) 62 (72.9) 3.98d 0.13
1500–3500 250 (65.1) 56 (22.4) 194 (77.6)
> 3500 49 (12.8) 6 (12.7) 43 (87.8)
Mother employment status
Works outside the home 99 (25.8) 22 (22.2) 77 (77.8) 0.00 0.98
Does not work outside the home 285 (74.2) 63 (22.1) 222 (77.9)aChi-squared test for independence. bSignificant at P < 5% c1 new Israeli shekel = US$ 0.29 at the time of the study. dFisher exact test.
Book 27-11.indb 1054Book 27-11.indb 1054 06/12/2021 12:39 PM06/12/2021 12:39 PM
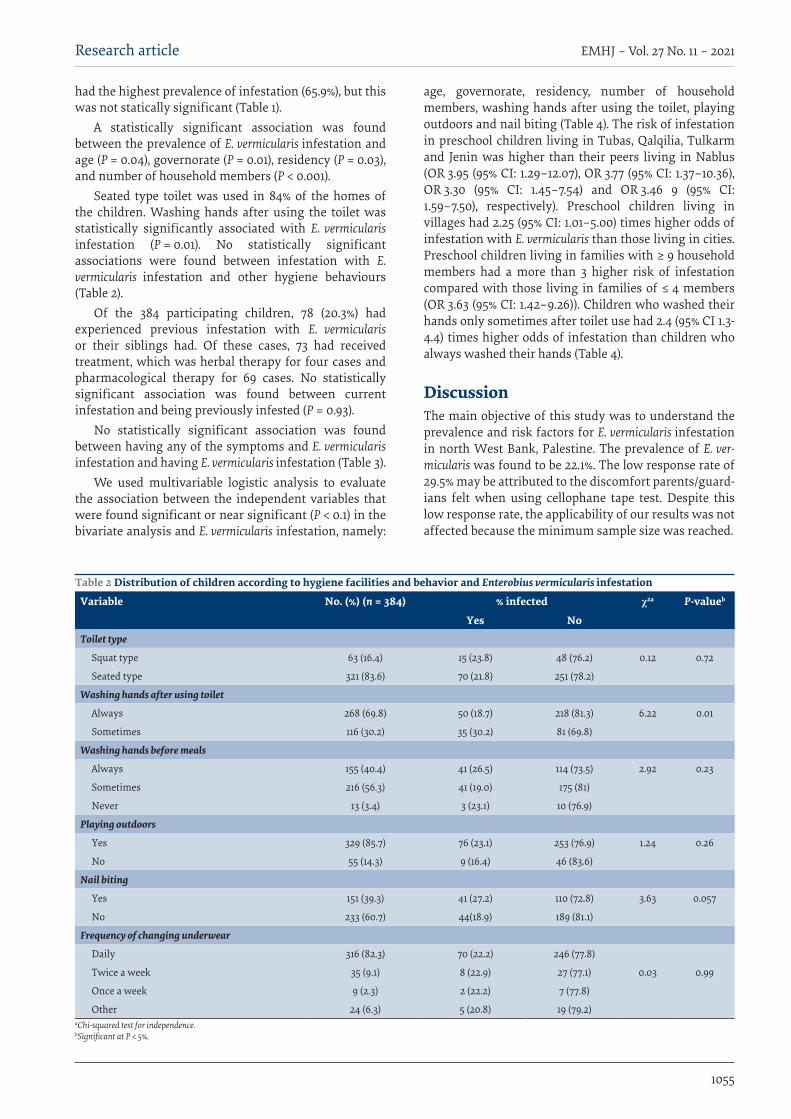
1055
Research article EMHJ – Vol. 27 No. 11 – 2021
had the highest prevalence of infestation (65.9%), but this was not statically significant (Table 1).
A statistically significant association was found between the prevalence of E. vermicularis infestation and age (P = 0.04), governorate (P = 0.01), residency (P = 0.03), and number of household members (P < 0.001).
Seated type toilet was used in 84% of the homes of the children. Washing hands after using the toilet was statistically significantly associated with E. vermicularis infestation (P = 0.01). No statistically significant associations were found between infestation with E. vermicularis infestation and other hygiene behaviours (Table 2).
Of the 384 participating children, 78 (20.3%) had experienced previous infestation with E. vermicularis or their siblings had. Of these cases, 73 had received treatment, which was herbal therapy for four cases and pharmacological therapy for 69 cases. No statistically significant association was found between current infestation and being previously infested (P = 0.93).
No statistically significant association was found between having any of the symptoms and E. vermicularis infestation and having E. vermicularis infestation (Table 3).
We used multivariable logistic analysis to evaluate the association between the independent variables that were found significant or near significant (P < 0.1) in the bivariate analysis and E. vermicularis infestation, namely:
age, governorate, residency, number of household members, washing hands after using the toilet, playing outdoors and nail biting (Table 4). The risk of infestation in preschool children living in Tubas, Qalqilia, Tulkarm and Jenin was higher than their peers living in Nablus (OR 3.95 (95% CI: 1.29–12.07), OR 3.77 (95% CI: 1.37–10.36), OR 3.30 (95% CI: 1.45–7.54) and OR 3.46 9 (95% CI: 1.59–7.50), respectively). Preschool children living in villages had 2.25 (95% CI: 1.01–5.00) times higher odds of infestation with E. vermicularis than those living in cities. Preschool children living in families with ≥ 9 household members had a more than 3 higher risk of infestation compared with those living in families of ≤ 4 members (OR 3.63 (95% CI: 1.42–9.26)). Children who washed their hands only sometimes after toilet use had 2.4 (95% CI 1.3-4.4) times higher odds of infestation than children who always washed their hands (Table 4).
DiscussionThe main objective of this study was to understand the prevalence and risk factors for E. vermicularis infestation in north West Bank, Palestine. The prevalence of E. ver-micularis was found to be 22.1%. The low response rate of 29.5% may be attributed to the discomfort parents/guard-ians felt when using cellophane tape test. Despite this low response rate, the applicability of our results was not affected because the minimum sample size was reached.
Table 2 Distribution of children according to hygiene facilities and behavior and Enterobius vermicularis infestation
Variable No. (%) (n = 384) % infected χ2a P-valueb
Yes NoToilet type
Squat type 63 (16.4) 15 (23.8) 48 (76.2) 0.12 0.72
Seated type 321 (83.6) 70 (21.8) 251 (78.2)
Washing hands after using toilet
Always 268 (69.8) 50 (18.7) 218 (81.3) 6.22 0.01
Sometimes 116 (30.2) 35 (30.2) 81 (69.8)
Washing hands before meals
Always 155 (40.4) 41 (26.5) 114 (73.5) 2.92 0.23
Sometimes 216 (56.3) 41 (19.0) 175 (81)
Never 13 (3.4) 3 (23.1) 10 (76.9)
Playing outdoors
Yes 329 (85.7) 76 (23.1) 253 (76.9) 1.24 0.26
No 55 (14.3) 9 (16.4) 46 (83.6)
Nail biting
Yes 151 (39.3) 41 (27.2) 110 (72.8) 3.63 0.057
No 233 (60.7) 44(18.9) 189 (81.1)
Frequency of changing underwear
Daily 316 (82.3) 70 (22.2) 246 (77.8)
Twice a week 35 (9.1) 8 (22.9) 27 (77.1) 0.03 0.99
Once a week 9 (2.3) 2 (22.2) 7 (77.8)
Other 24 (6.3) 5 (20.8) 19 (79.2)aChi-squared test for independence. bSignificant at P < 5%.
Book 27-11.indb 1055Book 27-11.indb 1055 06/12/2021 12:39 PM06/12/2021 12:39 PM
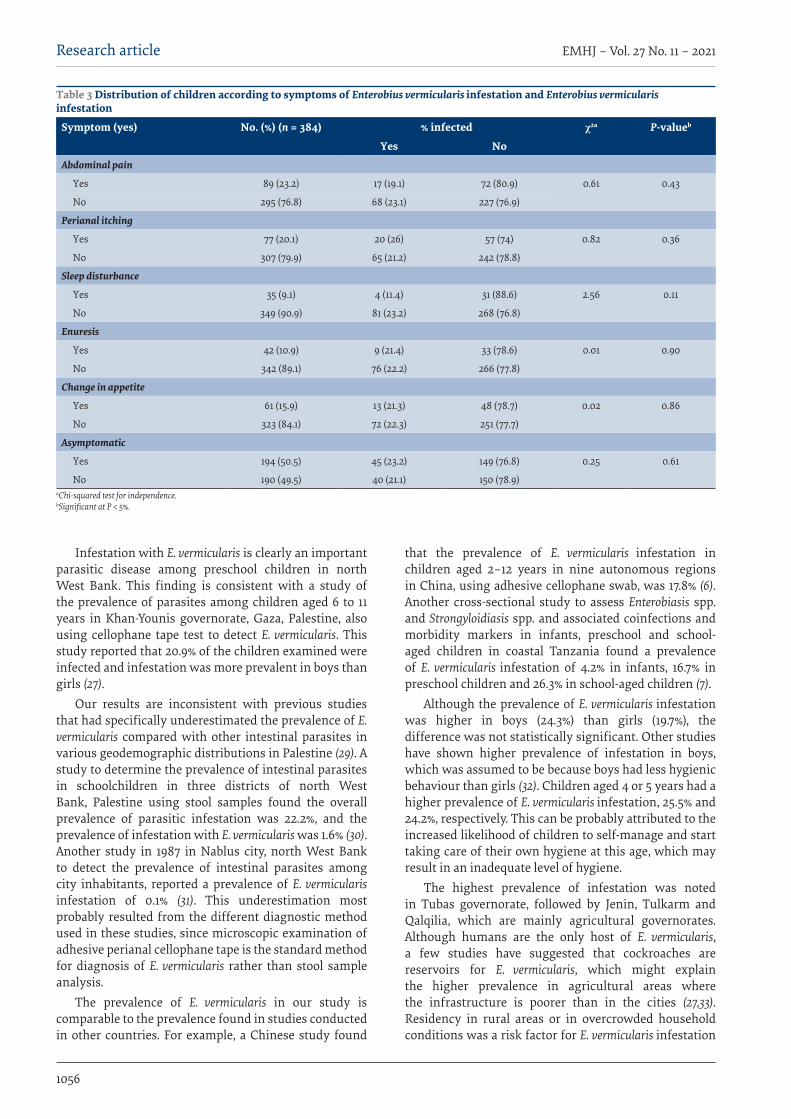
1056
Research article EMHJ – Vol. 27 No. 11 – 2021
Infestation with E. vermicularis is clearly an important parasitic disease among preschool children in north West Bank. This finding is consistent with a study of the prevalence of parasites among children aged 6 to 11 years in Khan-Younis governorate, Gaza, Palestine, also using cellophane tape test to detect E. vermicularis. This study reported that 20.9% of the children examined were infected and infestation was more prevalent in boys than girls (27).
Our results are inconsistent with previous studies that had specifically underestimated the prevalence of E. vermicularis compared with other intestinal parasites in various geodemographic distributions in Palestine (29). A study to determine the prevalence of intestinal parasites in schoolchildren in three districts of north West Bank, Palestine using stool samples found the overall prevalence of parasitic infestation was 22.2%, and the prevalence of infestation with E. vermicularis was 1.6% (30). Another study in 1987 in Nablus city, north West Bank to detect the prevalence of intestinal parasites among city inhabitants, reported a prevalence of E. vermicularis infestation of 0.1% (31). This underestimation most probably resulted from the different diagnostic method used in these studies, since microscopic examination of adhesive perianal cellophane tape is the standard method for diagnosis of E. vermicularis rather than stool sample analysis.
The prevalence of E. vermicularis in our study is comparable to the prevalence found in studies conducted in other countries. For example, a Chinese study found
that the prevalence of E. vermicularis infestation in children aged 2–12 years in nine autonomous regions in China, using adhesive cellophane swab, was 17.8% (6). Another cross-sectional study to assess Enterobiasis spp. and Strongyloidiasis spp. and associated coinfections and morbidity markers in infants, preschool and school-aged children in coastal Tanzania found a prevalence of E. vermicularis infestation of 4.2% in infants, 16.7% in preschool children and 26.3% in school-aged children (7).
Although the prevalence of E. vermicularis infestation was higher in boys (24.3%) than girls (19.7%), the difference was not statistically significant. Other studies have shown higher prevalence of infestation in boys, which was assumed to be because boys had less hygienic behaviour than girls (32). Children aged 4 or 5 years had a higher prevalence of E. vermicularis infestation, 25.5% and 24.2%, respectively. This can be probably attributed to the increased likelihood of children to self-manage and start taking care of their own hygiene at this age, which may result in an inadequate level of hygiene.
The highest prevalence of infestation was noted in Tubas governorate, followed by Jenin, Tulkarm and Qalqilia, which are mainly agricultural governorates. Although humans are the only host of E. vermicularis, a few studies have suggested that cockroaches are reservoirs for E. vermicularis, which might explain the higher prevalence in agricultural areas where the infrastructure is poorer than in the cities (27,33). Residency in rural areas or in overcrowded household conditions was a risk factor for E. vermicularis infestation
Table 3 Distribution of children according to symptoms of Enterobius vermicularis infestation and Enterobius vermicularis infestation
Symptom (yes) No. (%) (n = 384) % infected χ2a P-valueb
Yes NoAbdominal pain
Yes 89 (23.2) 17 (19.1) 72 (80.9) 0.61 0.43
No 295 (76.8) 68 (23.1) 227 (76.9)
Perianal itching
Yes 77 (20.1) 20 (26) 57 (74) 0.82 0.36
No 307 (79.9) 65 (21.2) 242 (78.8)
Sleep disturbance
Yes 35 (9.1) 4 (11.4) 31 (88.6) 2.56 0.11
No 349 (90.9) 81 (23.2) 268 (76.8)
Enuresis
Yes 42 (10.9) 9 (21.4) 33 (78.6) 0.01 0.90
No 342 (89.1) 76 (22.2) 266 (77.8)
Change in appetite
Yes 61 (15.9) 13 (21.3) 48 (78.7) 0.02 0.86
No 323 (84.1) 72 (22.3) 251 (77.7)
Asymptomatic
Yes 194 (50.5) 45 (23.2) 149 (76.8) 0.25 0.61
No 190 (49.5) 40 (21.1) 150 (78.9)aChi-squared test for independence. bSignificant at P < 5%.
Book 27-11.indb 1056Book 27-11.indb 1056 06/12/2021 12:39 PM06/12/2021 12:39 PM
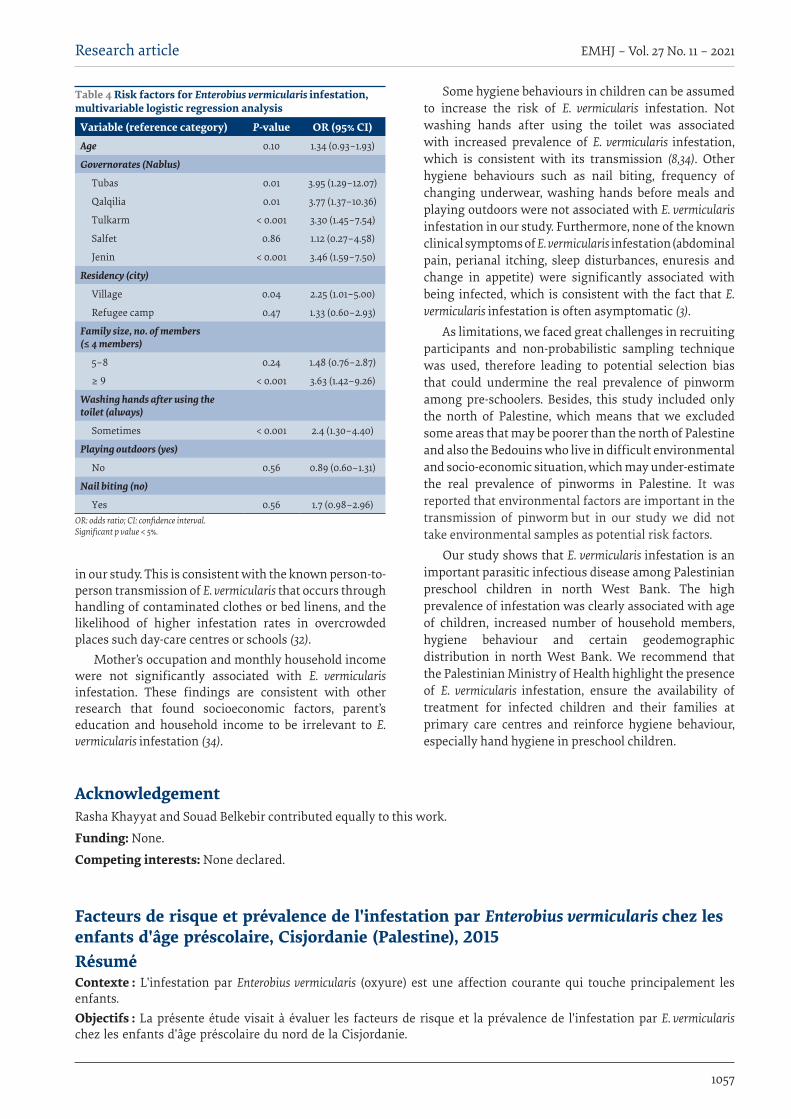
1057
Research article EMHJ – Vol. 27 No. 11 – 2021
in our study. This is consistent with the known person-to-person transmission of E. vermicularis that occurs through handling of contaminated clothes or bed linens, and the likelihood of higher infestation rates in overcrowded places such day-care centres or schools (32).
Mother’s occupation and monthly household income were not significantly associated with E. vermicularis infestation. These findings are consistent with other research that found socioeconomic factors, parent’s education and household income to be irrelevant to E. vermicularis infestation (34).
Some hygiene behaviours in children can be assumed to increase the risk of E. vermicularis infestation. Not washing hands after using the toilet was associated with increased prevalence of E. vermicularis infestation, which is consistent with its transmission (8,34). Other hygiene behaviours such as nail biting, frequency of changing underwear, washing hands before meals and playing outdoors were not associated with E. vermicularis infestation in our study. Furthermore, none of the known clinical symptoms of E. vermicularis infestation (abdominal pain, perianal itching, sleep disturbances, enuresis and change in appetite) were significantly associated with being infected, which is consistent with the fact that E. vermicularis infestation is often asymptomatic (3).
As limitations, we faced great challenges in recruiting participants and non-probabilistic sampling technique was used, therefore leading to potential selection bias that could undermine the real prevalence of pinworm among pre-schoolers. Besides, this study included only the north of Palestine, which means that we excluded some areas that may be poorer than the north of Palestine and also the Bedouins who live in difficult environmental and socio-economic situation, which may under-estimate the real prevalence of pinworms in Palestine. It was reported that environmental factors are important in the transmission of pinworm but in our study we did not take environmental samples as potential risk factors.
Our study shows that E. vermicularis infestation is an important parasitic infectious disease among Palestinian preschool children in north West Bank. The high prevalence of infestation was clearly associated with age of children, increased number of household members, hygiene behaviour and certain geodemographic distribution in north West Bank. We recommend that the Palestinian Ministry of Health highlight the presence of E. vermicularis infestation, ensure the availability of treatment for infected children and their families at primary care centres and reinforce hygiene behaviour, especially hand hygiene in preschool children.
Table 4 Risk factors for Enterobius vermicularis infestation, multivariable logistic regression analysis
Variable (reference category) P-value OR (95% CI)Age 0.10 1.34 (0.93–1.93)
Governorates (Nablus)
Tubas 0.01 3.95 (1.29–12.07)
Qalqilia 0.01 3.77 (1.37–10.36)
Tulkarm < 0.001 3.30 (1.45–7.54)
Salfet 0.86 1.12 (0.27–4.58)
Jenin < 0.001 3.46 (1.59–7.50)
Residency (city)
Village 0.04 2.25 (1.01–5.00)
Refugee camp 0.47 1.33 (0.60–2.93)
Family size, no. of members (≤ 4 members)
5–8 0.24 1.48 (0.76–2.87)
≥ 9 < 0.001 3.63 (1.42–9.26)
Washing hands after using the toilet (always)
Sometimes < 0.001 2.4 (1.30–4.40)
Playing outdoors (yes)
No 0.56 0.89 (0.60–1.31)
Nail biting (no)
Yes 0.56 1.7 (0.98–2.96)OR: odds ratio; CI: confidence interval. Significant p value < 5%.
AcknowledgementRasha Khayyat and Souad Belkebir contributed equally to this work.
Funding: None.
Competing interests: None declared.
Facteurs de risque et prévalence de l'infestation par Enterobius vermicularis chez les enfants d'âge préscolaire, Cisjordanie (Palestine), 2015RésuméContexte : L'infestation par Enterobius vermicularis (oxyure) est une affection courante qui touche principalement les enfants. Objectifs : La présente étude visait à évaluer les facteurs de risque et la prévalence de l'infestation par E. vermicularis chez les enfants d'âge préscolaire du nord de la Cisjordanie.
Book 27-11.indb 1057Book 27-11.indb 1057 06/12/2021 12:39 PM06/12/2021 12:39 PM
1058
Research article EMHJ – Vol. 27 No. 11 – 2021
References1. Stepek G, Buttle DJ, Duce IR, Behnke JM. Human gastrointestinal nematode infections: are new control methods required? Int J
Exp Pathol. 2006;87:325–41. https://doi.org/10.1111/j.1365-2613.2006.00495.x
2. Medkour HH, Amona I, Laidoudi Y, Davoust B, Bitam I, Levasseur A, et al. Parasitic infections in African humans and non-hu-man primates. Pathogens. 2020;9(7):561. https://doi.org/10.3390/pathogens9070561
3. Parasites [Internet]. Atlanta: Centers for Disease Control and Prevention; (https://www.cdc.gov/parasites/index.html, accessed 17 June 2021).
4. Chitnis A, Azimi DY, Sabri S, Dhebri A. Enterobius vermicularis: a parasitic cause of appendicular colic. Cureus. 2020;12(6):e8524. https://doi.org/10.7759/cureus.8524
مية الدودية وعوامل اخلطر املسببة هلا يف صفوف األطفال دون سن املدرسة، الضفة معدل انتشار اإلصابة بالرسالغربية، فلسطني
رشا خياط، سعاد بلكبري، سامح أبوصري، ماجد برامهة، جلني الصدر، وليد باشا
اخلالصةمية الدودية )الدودة الدبوسية( تعد حالة شائعة تصيب األطفال يف املقام األول. اخللفية: اإلصابة بالرس
قبل ما املرتبطة هبا يف صفوف األطفال يف سن الدودية وعوامل اخلطر مية بالرس انتشار اإلصابة تقييم معدل اىل الدراسة هدفت هذه األهداف: املدرسة يف شامل الضفة الغربية.
قبل ما الغربية عىل عينة ضمت 384 طفال يف مرحلة الضفة الست يف شامل الرئيسية املحافظات البحث: أجريت دراسة مقطعية شملت طرق آباء/ مأل الدودية. مية بالرس اإلصابة عن للكشف الرشج حول السيلوفان رشيط طريقة واستخدمت النهارية. للرعاية مركزا 86 من املدرسة أوصياء األطفال املشاركني استبيانا جلمع معلومات عن: اخلصائص السكانية؛ والسلوك من حيث النظافة العامة؛ والوضع االجتامعي واالقتصادي؛
وسوابق اإلصابة؛ ووجود األعراض. وقيمت عوامل خطر اإلصابة باستخدام حتليل االنحدار اللوجستي.مية الدودية. وارتبط العمر )قيمة احتاملية = 0.04(، واملحافظة النتائج: من بني األطفال البالغ عددهم 384 طفال، أصيب 85 )22.1%( بالرسبعد استخدام اليدين > 0.001( وغسل احتاملية أفراد األرسة )قيمة احتاملية = 0.03(، وعدد اإلقامة )قيمة احتاملية = 0.01(، ومكان )قيمة مية الدودية. ويف حتليل االنحدار اللوجستي، متثلت العوامل التي زادت من املرحاض )قيمة احتاملية = 0.01( ارتباطا ملحوظا باإلصابة بالرساحتامل اإلصابة بالعدوى يف: العيش يف القرى )نسبة أرجحية 2.25؛ فاصل ثقة 95%: 1.01 - 5.00(، والعيش يف منزل به تسعة أفراد من األرسة أو أكثر )نسبة أرجحية 3.63؛ فاصل ثقة 95%: 1.42–9.26( وعدم غسل اليدين بعد استخدام املرحاض )نسبة أرجحية 2.4؛ فاصل ثقة %95:
.)4.40 - 1.30مية الدودية هي إصابة دودية خطرية حتدث يف صفوف األطفال يف سن ما قبل املدرسة يف فلسطني. ويلزم بذل جهود لضامن االستنتاجات: الرس
توافر عالج األطفال املصابني يف مراكز الرعاية األولية وتعزيز سلوك النظافة العامة.
Méthodes : Une étude transversale qui incluait les six principaux gouvernorats du nord de la Cisjordanie a été menée dans un échantillon de 384 enfants d'âge préscolaire fréquentant 86 garderies. La méthode de l’application d’un ruban adhésif autour de l’anus a été utilisée pour détecter l'infestation par E. vermicularis. Les parents/tuteurs des enfants participants ont rempli un questionnaire servant à recueillir diverses informations : caractéristiques démographiques ; comportement en matière d'hygiène ; statut socioéconomique ; antécédents d'infestation ; et présence de symptômes. Les facteurs de risque d'infestation ont été évalués à l'aide d'une analyse de régression logistique.Résultats : Sur les 384 enfants, 85 (22,1 %) présentaient une infestation par E. vermicularis. L'âge (p = 0,04), le gouvernorat (p = 0,01), le lieu de résidence (p = 0,03), le nombre de membres du foyer (p < 0,001) et le non-lavage des mains après utilisation des toilettes (p = 0,01) étaient associés de manière significative à l'infestation par E. vermicularis. À l'analyse de régression logistique, les facteurs augmentant la probabilité d'infection étaient les suivants : le fait de vivre dans un village (odds ratio [OR] 2,25 ; intervalle de confiance (IC) à 95 % : 1,01-5,00), de vivre dans un foyer comptant au moins neuf membres d'une même famille (OR 3,63 ; IC à 95 % : 1,42-9,26) et de ne pas se laver les mains après un passage aux toilettes (OR 2,4 ; IC à 95 % : 1,30-4,40). Conclusions : E. vermicularis cause une helminthiase importante chez les enfants d'âge préscolaire en Palestine. Des efforts doivent être déployés afin de garantir la disponibilité du traitement dans les centres de soins de santé primaires pour les enfants infestés et de renforcer les comportements en matière d'hygiène.
Book 27-11.indb 1058Book 27-11.indb 1058 06/12/2021 12:39 PM06/12/2021 12:39 PM
1059
Research article EMHJ – Vol. 27 No. 11 – 2021
5. Paknazhad N, Mowlavi G, Dupouy Camet J, Jelodar ME, Mobedi I, Makki M, et al. Paleoparasitological evidence of pinworm (Enterobius vermicularis) infection in a female adolescent residing in ancient Tehran (Iran) 7000 years ago. Parasit Vectors. 2016;22:9:33. https://doi.org/10.1186/s13071-016-1322-y
6. Chen YD, Wang JJ, Zhu HH, Zhu TJ, Zang W, Qian M-B, et al. [Enterobius vermicularis infection status among children in 9 provinces/autonomous regions/municipalities of China.] [Chinese J Parasitol Parasit Dis]. 2013;31(4):251–55. [in Chinese]
7. Salim N, Schindler T, Abdul U, Rothen J, Genton B, Lweno O, et al. Enterobiasis and strongyloidiasis and associated co-infections and morbidity markers in infants, preschool- and school-aged children from rural coastal Tanzania: a cross-sectional study. BMC Infect Dis. 2014;14:644. https://doi.org/10.1186/s12879-014-0644-7
8. Chen KY, Yen CM, Hwang KP, Wang LC. Enterobius vermicularis infection and its risk factors among pre-school children in Taipei, Taiwan. J Microbiol Immunol Infect. 2018;51(4):559–64. https://doi.org/10.1016/j.jmii.2016.12.013
9. Altun E, Avci V, Azatcam M. Parasitic infestation in appendicitis. A retrospective analysis of 660 patients and brief literature review. Saudi Med J. 2017;38(3):314–8. https://doi.org/10.15537/smj.2017.3.18061
10. Zouari M, Louati H, Abid I, Trabelsi F, Ben Dhaou M, Jallouli M, et al. Enterobius vermicularis: a cause of abdominal pain mim-icking acute appendicitis in children. A retrospective cohort study. Arch Iran Med. 2018;21(2):67–72.
11. Gonzalez S, De la Cabada FJ. Parasitic infections of the colon and rectum. Baillieres Clin Gastroenterol. 1987;1(2):447–67. https://doi.org/10.1016/0950-3528(87)90013-3
12. Cook GC. Enterobius vermicularis infections. Gut. 1994;35(9):1159–62. https://doi.org/10.1136/gut.35.9.1159
13. Kucik CJ, Martin GL, Sortor BV. Common intestinal parasites. Am Fam Physician. 2004;69(5):1161–9.
14. Muge OA, Baykan Z, Artan C. Enterobiasis among preschool children: a study from Kayseri, Turkey. Jpn J Infect Dis. 2008;61(6):482–3.
15. Kacker PP. Vulvo-vaginitis in an adult with thread-worms in the vagina. Br J Vener Dis. 1973;49(3):314–5. https://doi.org/10.1136/sti.49.3.314
16. Mentessidou A, Theocharides C, Patoulias I, Panteli C. Enterobius vermicularis-associated pelvic inflammatory disease in a child. J Pediat Adolescent Gynecol. 2016;29(2):e25–e7. https://doi.org/10.1016/j.jpag.2015.10.010
17. Mayers CP, Purvis RJ. Manifestations of pinworms. Can Med Assoc J. 1970;103(12):489–93.
18. Al-Qadhi BN, Al-Warid HSJ, Al-Qadhi MN. Enterobiasis and its relationship with enuresis among one of orphanage care children in Baghdad-Iraq. Iraqi J Sci. 2011;52(3):394–9.
19. Maki AC, Combs B, McClure B, Slack P, Matheson P, Wiesenauer C. Enterobius vermicularis: a cause of acute appendicitis in children. Am Surg. 2012;78(12):E523–4.
20. Martinez-Criado Y, Millan-Lopez A, Galan N, De-Agustin-Asensio JC. Acute appendicitis by Enterobius vermicularis: an unusual etiology in children. Rev Esp Enferm Dig. 2012;104(7):393–4. https://doi.org/10.4321/s1130-01082012000700016
21. Fleming CA, Kearney DE, Moriarty P, Redmond HP, Andrews EJ. An evaluation of the relationship between Enterobius vermicu-laris infestation and acute appendicitis in a paediatric population: a retrospective cohort study. Int J Surg. 2015;18:154–8. https://doi.org/10.1016/j.ijsu.2015.02.012
22. Sodergren MH, Jethwa P, Wilkinson S, Kerwat R. Presenting features of Enterobius vermicularis in the vermiform appendix. Scand J Gastroenterol. 2009;44:457–61. https://doi.org/10.1080/00365520802624227
23. Akıncı A, Kepil N, Erzin YZ, Zengin AK. Enterobius vermicularis infestation mimicking rectal malignancy. Turkiye Parazitol Derg. 2020;44(1):58–60. https://doi.org/10.4274/tpd.galenos.2019.6617
24. Bharathi K, Anuradha S, Chandrasekar VA, Thirunarayanan R. Enterobius vermicularis worm granuloma mimicking like a pseudo tumor in the anal canal: an unusual clinical presentation. Trop Parasitol. 2012;2(2):124–6. https://doi.org/10.4103/2229-5070.105178
25. Arkoulis N, Zerbinis H, Simatos G, Nisiotis A. Enterobius vermicularis (pinworm) infection of the liver mimicking malig-nancy: presentation of a new case and review of current literature. Int J Surg Case Rep. 2012;3(1):6–9. https://doi.org/10.1016/j.ijscr.2011.10.003
26. Elsaid N, Mahmood H, Tekkis P, Tan E. Enterobiasis-related inflammatory caecal polyp masquerading as a malignancy. BMJ Case Rep. 2014;2014:bcr2013201599. https://doi.org/10.1136/bcr-2013-201599.
27. Estimated population in Palestine mid-year by governorate, 1997–2021. Ramallah: Palestinian Central Bureau of Statistics; 2021 (http://www.pcbs.gov.ps/Portals/_Rainbow/Documents/%D8%A7%D9%84%D9%85%D8%AD%D8%A7%D9%81%D8%B8%D8%A7%D8%AA%20%D8%A7%D9%86%D8%AC%D9%84%D9%8A%D8%B2%D9%8A%2097-2017.html, accessed 17 June 2021).
28. Astal Z. Epidemiological survey of the prevalence of parasites among children in Khan Younis governorate, Palestine. Parasitol Res. 2004;94(6):449–51. https://doi.org/10.1007/s00436-004-1234-1
29. Mezeid N, Shaldoum F, Al-Hindi AI, Mohamed FSA, Darwish ZEA. Prevalence of intestinal parasites among the population of the Gaza Strip, Palestine. Ann Parasitol. 2014;60(4):281–9.
30. Hussein AS. Prevalence of intestinal parasites among children in northern districts of West Bank, Palestine. Trop Med Int Health. 2011;16(2):240–4. https://doi.org/10.1111/j.1365-3156.2010.02674.x
Book 27-11.indb 1059Book 27-11.indb 1059 06/12/2021 12:39 PM06/12/2021 12:39 PM
1060
Research article EMHJ – Vol. 27 No. 11 – 2021
31. Ali-Shtayeh MS, Hamdan AH, Shaheen SF, Abu-Zeid I, Faidy YR. Prevalence and seasonal fluctuations of intestinal parasitic infections in the Nablus area, West Bank of Jordan. Ann Trop Med Parasitol. 1989;83(1):67–72. https://doi.org/10.1080/00034983.1989.11812312
32. Gunawardena NK, Chandrasena TN, de Silva NR. Prevalence of enterobiasis among primary school children in Ragama, Sri Lanka. Ceylon Med J. 2013;58(3):106–10. https://doi.org/10.4038/cmj.v58i3.5039
33. Chan OT, Lee EK, Hardman JM, Navin JJ. The cockroach as a host for Trichinella and Enterobius vermicularis: implications for public health. Hawaii Med J. 2004;63(3):74–7.
34. Li HM, Zhou CH, Li ZS, Deng ZH, Ruan CW, Zhang QM, et al. Risk factors for Enterobius vermicularis infection in children in Gaozhou, Guangdong, China. Infect Dis Poverty. 2015;4:28. https://doi.org/10.1186/s40249-015-0058-9
Book 27-11.indb 1060Book 27-11.indb 1060 06/12/2021 12:39 PM06/12/2021 12:39 PM

1061
Research article EMHJ – Vol. 27 No. 11 – 2021
Association between type of physical activity and risk factors for cardiovascular disease, Islamic Republic of IranOmid Aminian,1 Maryam Saraei,1 Saeed Najieb Pour1 and Sahar Eftekhari1
1Center for Research on Occupational Diseases, Tehran University of Medical Sciences, Tehran, Islamic Republic of Iran (Correspondence to: Sahar Eftekhari: [email protected]).
AbstractBackground: Little is known about the role of occupational-related physical activity and risk factors for cardiovascular disease.Aims: This study aimed to assess the association between different types of physical activity (work-related, transport-re-lated, home-time and leisure-time) and risk factors for cardiovascular disease in a sample of Iranian workers.Methods: This cross-sectional study was conducted from February to November 2018 among 415 workers of a rubber factory in Tehran province. Physical activity levels of the participants were measured using the International Physical Activity Questionnaire. Blood sample were analysed for cardiovascular disease risk factors (fasting blood sugar ≥ 100 mg/dL, triglycerides ≥ 150 mg/dL, total cholesterol ≥ 200 mg/dL, systolic blood pressure ≥ 130 mmHg, diastolic blood pres-sure ≥ 85 mmHg and waist circumference ≥ 102 cm). Alanine aminotransferase and aspartate aminotransferase were also measured, as was body mass index (BMI). Results: Risk factors for cardiovascular disease differed significantly according to type of physical activity. Fasting blood sugar ≥ 100 mg/dL and BMI ≥ 25 kg/m2 had a significant negative association with overall physical activity level (P < 0.001). In a logistic regression analysis, leisure-time physical activity had a significant negative correlation with all risk factors for cardiovascular disease after adjusting for age and smoking.Conclusion: Leisure-time physical activity has a more important role in reducing cardiovascular disease risk factors than other types of activity, including work-related physical activity.Key words: cardiovascular disease, risk factors, exercise, leisure activities, IranCitation: Aminian O; Saraei M; Najieb Pour S; Eftekhari S. Association between type of physical activity and risk factors for cardiovascular disease, Islamic Republic of Iran. East Mediterr Health J. 2021;27(11):1061–1068. https://doi.org/10.26719/emhj.21.060Received: 30/09/20; accepted: 23/03/21Copyright © World Health Organization (WHO) 2021. Open Access. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license (https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
IntroductionCardiovascular disease (CVD) is one of the most impor-tant causes of mortality and morbidity in the general population worldwide (1–3). CVD has increased in de-veloping countries (4–6). Many risk factors for CVD are modifiable with specific prevention measures. A global study in 52 countries, found that nine modifiable risk fac-tors – smoking, dyslipidaemia, hypertension, diabetes, abdominal obesity, psychosocial factors, fruit and vege-table consumption, alcohol use, and daily physical activi-ty accounted for over 90% of the population-attributable risk of a first myocardial infarction (7,8). Many studies have estimated that more than half of mortality due to CVD is associated with five leading modifiable risk fac-tors – hypercholesterolaemia, diabetes, hypertension, obesity and smoking (9). Moreover, the absence of these major risk factors predicts much lower CVD risk factors (10). According to the American Heart Association, seven ideal cardiovascular health metrics have been included in its CVD screening programme to improve risk factors in the general population (11), namely: not smoking, being physically active, having normal blood pressure, having normal blood glucose, having normal total cholesterol
level, being normal weight, and eating a healthy diet. Even moderate physical activity gives some protection against coronary heart disease, one of the four main CVD categories (7,12–16). Some studies maintain that individ-uals with mild to moderate physical activity levels, even as a part of their occupation, appear to have a lower risk of myocardial infarction compared with sedentary work-ers (17,18). Some studies mentioned that patients with NAFLD have an increased risk of CVD that is independ-ent of traditional CVD risk factors and components of metabolic syndrome (19,20). Also, we have much evidence of the association between physical inactivity and fatty liver disease (21).
Globalization and computerization of workplace, technological changes, highly automated work processes have resulted in an increasing prevalence of sedentary work. Studies on the association between physical work activities and cardiovascular risks give inconsistent results. A systematic review found limited evidence to support a positive relationship between sedentary work and poor health (22). A prospective cohort study among 4819 male industrial workers concluded that moderately hard occupational physical activity may adversely affect
Book 27-11.indb 1061Book 27-11.indb 1061 06/12/2021 12:39 PM06/12/2021 12:39 PM
1062
Research article EMHJ – Vol. 27 No. 11 – 2021
health and should not be a substitute for leisure-time physical activity which is known to protect against coronary heart disease mortality (23). On the other hand, a study showed a significant risk reduction in CVD mortality with moderate work and household physical activity, moderate to vigorous leisure time and total physical activity compared to light physical activity (24). Similarly, a meta-analysis of 21 prospective cohort studies found a strong protective effect of moderate levels of occupational physical activity in both men and women (25).
While the relationship between physical inactivity and CVD is established, clear evidence is lacking that occupational physical activity decreases the prevalence of CVD risk factors. Therefore, we need to research physical activity categories separately to determine which ones have a significant effect on CVD risk factors.
MethodsThe survey was conducted from February to November 2018 in a rubber factory in Tehran province which had 583 workers. We collected data on demographic variables, physical activity and cardiovascular disease risk factors. We excluded from the analysis, men who did not partici-pate in measurement of physical activity or in blood test-ing or who submitted incomplete questionnaires. Thus, 415 male workers aged 21–57 years were included in the study (response rate: 71%): 326 blue collar and 89 white collar workers. Blue collar workers worked in different stations of rubber processing, including mastication, when the elastomer is sheared, and the molecules are broken down to give easier flow, mixing with a Banbury mixer when additives are incorporated, shaping of the viscous mass by extrusion, calendaring and vulcanizing (curing) when the polymer molecules become interlinked and the shape is fixed. White collar workers had clerical, administrative, marketing or managerial duties.
Height was assessed using a digital scale (InBody stadiometer, USA), and for weight, we used an electronic scale (Fitbit Aria 2, USA). Waist circumference was measured with measuring tape from the midpoint of the subcostal region and the upper iliac crest on both sides to the nearest 0.1 cm in the standing position. Blood pressure was measured after sitting for 10 minutes using an electronic haematomanometer (Rossmax X9 blood pressure monitor, Taiwan). Blood was collected after the participant had fasted for more than 10 hours and fasting blood glucose, total cholesterol, triglycerides, alanine aminotransferase (ALT) and aspartate aminotransferase (AST) were measured.
Physical activity of rubber industry workers was measured using an interviewer-administered version of the International Physical Activity Questionnaire (IPAQ) modified and validated for use with the Iranian population (26). The grade of physical activity was based on the IPAQ score conversion system.
IPAQ assesses physical activity undertaken across a comprehensive set of areas, including work-related
activity (physical activity as part of paid or unpaid work), transport-related activity (physical activity for travelling from place to place including to work, shops and the cinema). Home-time activity included housework, gardening, yard work, general maintenance work and caring for family and leisure time activity included physical activity solely for recreation, sport, exercise or leisure. The questionnaire asks the time spent being physically active in the past 7 days. Frequency (measured in days per week) and duration (length of time per day) of physical activity are collected separately for each specific type of activity. To calculate the total physical activity score duration (in minutes) and frequency (days) of physical activity are summed.
Physical activity status was divided into three groups according to the IPAQ scoring system as follows (27–29):
1. Low physical activity: not enough activity reported to meet categories 2 or 3.
2. Moderate physical activity: any of the following three criteria:
i. 3 or more days of vigorous-intensity activity of at least 20 minutes a day.
ii. 5 or more days of moderate-intensity activity and/or walking for at least 30 minutes a day.
iii. 5 or more days of any combination of walking, moderate-intensity or vigorous-intensity activi-ties, achieving a minimum of at least 600 metabol-ic equivalent task (MET) minutes/week.
3. High physical activity. Either of the following two criteria:
i. Vigorous-intensity activity of at least 3 days a week achieving at least 1500 MET minutes/week.
ii. 7 or more days of any combination of walking or moderate- or vigorous-intensity activity achieving at least 3000 MET minutes/week.
Statistical analysisWe used SPSS, version 24 for statistical analyses. We as-sessed differences in CVD risk factors among individuals with varying physical activity levels (low, moderate and high) using the Kruskal–Wallis test (one-way ANOVA). To confirm the association of cardiovascular risk factors and type of physical activity, we calculated the Pearson correlation coefficient using bivariate correlation analy-sis. P-value of ≤ 0.05 was considered statistically signifi-cant. We also used logistic regression analysis to examine the association between type of physical activity (contin-uous variables) and CVD risk factors (fasting blood sugar ≥ 100 mg/dl, triglycerides ≥ 150 mg/dl, total cholesterol ≥ 200 mg/dl, systolic blood pressure ≥ 130 mmHg, diastolic blood pressure ≥ 85 mmHg, and waist circumference ≥ 102 cm) adjusting for age and smoking.
Ethical considerationsThe study was approved by the ethics and research com-mittee of Tehran University of Medical Sciences (regis-
Book 27-11.indb 1062Book 27-11.indb 1062 06/12/2021 12:39 PM06/12/2021 12:39 PM
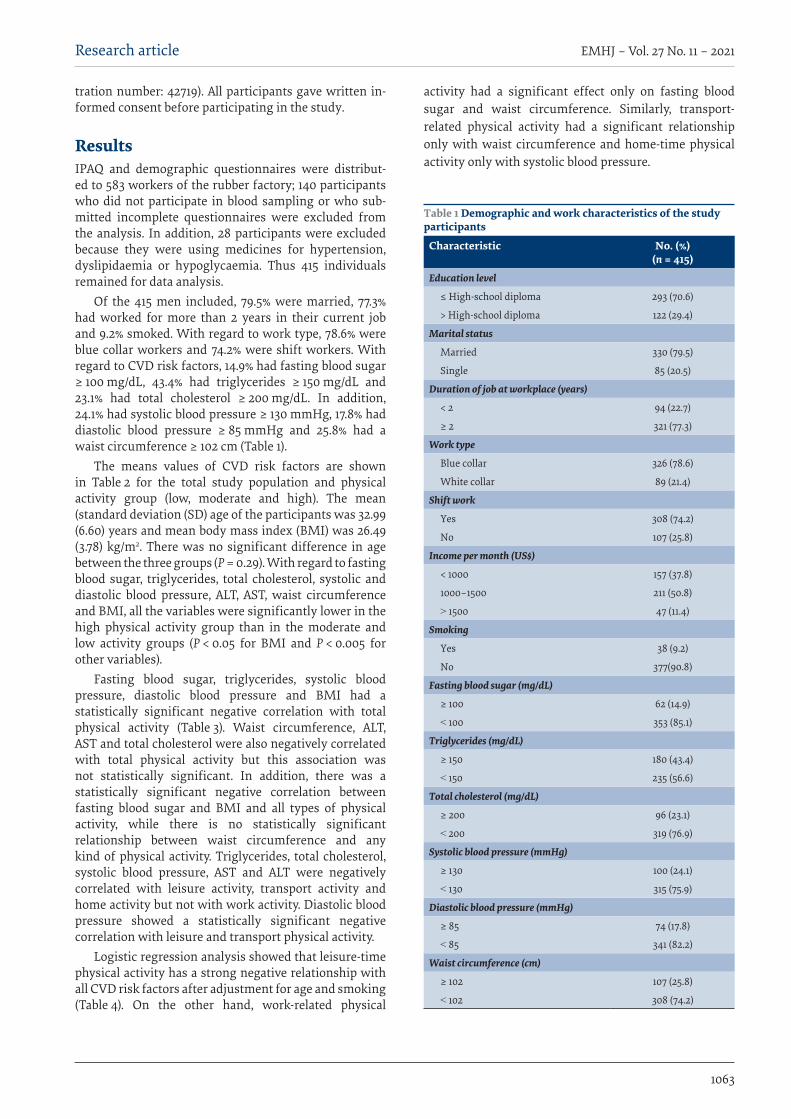
1063
Research article EMHJ – Vol. 27 No. 11 – 2021
tration number: 42719). All participants gave written in-formed consent before participating in the study.
ResultsIPAQ and demographic questionnaires were distribut-ed to 583 workers of the rubber factory; 140 participants who did not participate in blood sampling or who sub-mitted incomplete questionnaires were excluded from the analysis. In addition, 28 participants were excluded because they were using medicines for hypertension, dyslipidaemia or hypoglycaemia. Thus 415 individuals remained for data analysis.
Of the 415 men included, 79.5% were married, 77.3% had worked for more than 2 years in their current job and 9.2% smoked. With regard to work type, 78.6% were blue collar workers and 74.2% were shift workers. With regard to CVD risk factors, 14.9% had fasting blood sugar ≥ 100 mg/dL, 43.4% had triglycerides ≥ 150 mg/dL and 23.1% had total cholesterol ≥ 200 mg/dL. In addition, 24.1% had systolic blood pressure ≥ 130 mmHg, 17.8% had diastolic blood pressure ≥ 85 mmHg and 25.8% had a waist circumference ≥ 102 cm (Table 1).
The means values of CVD risk factors are shown in Table 2 for the total study population and physical activity group (low, moderate and high). The mean (standard deviation (SD) age of the participants was 32.99 (6.60) years and mean body mass index (BMI) was 26.49 (3.78) kg/m2. There was no significant difference in age between the three groups (P = 0.29). With regard to fasting blood sugar, triglycerides, total cholesterol, systolic and diastolic blood pressure, ALT, AST, waist circumference and BMI, all the variables were significantly lower in the high physical activity group than in the moderate and low activity groups (P < 0.05 for BMI and P < 0.005 for other variables).
Fasting blood sugar, triglycerides, systolic blood pressure, diastolic blood pressure and BMI had a statistically significant negative correlation with total physical activity (Table 3). Waist circumference, ALT, AST and total cholesterol were also negatively correlated with total physical activity but this association was not statistically significant. In addition, there was a statistically significant negative correlation between fasting blood sugar and BMI and all types of physical activity, while there is no statistically significant relationship between waist circumference and any kind of physical activity. Triglycerides, total cholesterol, systolic blood pressure, AST and ALT were negatively correlated with leisure activity, transport activity and home activity but not with work activity. Diastolic blood pressure showed a statistically significant negative correlation with leisure and transport physical activity.
Logistic regression analysis showed that leisure-time physical activity has a strong negative relationship with all CVD risk factors after adjustment for age and smoking (Table 4). On the other hand, work-related physical
activity had a significant effect only on fasting blood sugar and waist circumference. Similarly, transport-related physical activity had a significant relationship only with waist circumference and home-time physical activity only with systolic blood pressure.
Table 1 Demographic and work characteristics of the study participants
Characteristic No. (%)(n = 415)
Education level
≤ High-school diploma 293 (70.6)
> High-school diploma 122 (29.4)
Marital status
Married 330 (79.5)
Single 85 (20.5)
Duration of job at workplace (years)
< 2 94 (22.7)
≥ 2 321 (77.3)
Work type
Blue collar 326 (78.6)
White collar 89 (21.4)
Shift work
Yes 308 (74.2)
No 107 (25.8)
Income per month (US$)
< 1000 157 (37.8)
1000–1500 211 (50.8)
˃ 1500 47 (11.4)
Smoking
Yes 38 (9.2)
No 377(90.8)
Fasting blood sugar (mg/dL)
≥ 100 62 (14.9)
˂ 100 353 (85.1)
Triglycerides (mg/dL)
≥ 150 180 (43.4)
˂ 150 235 (56.6)
Total cholesterol (mg/dL)
≥ 200 96 (23.1)
˂ 200 319 (76.9)
Systolic blood pressure (mmHg)
≥ 130 100 (24.1)
˂ 130 315 (75.9)
Diastolic blood pressure (mmHg)
≥ 85 74 (17.8)
˂ 85 341 (82.2)
Waist circumference (cm)
≥ 102 107 (25.8)
˂ 102 308 (74.2)
Book 27-11.indb 1063Book 27-11.indb 1063 06/12/2021 12:39 PM06/12/2021 12:39 PM
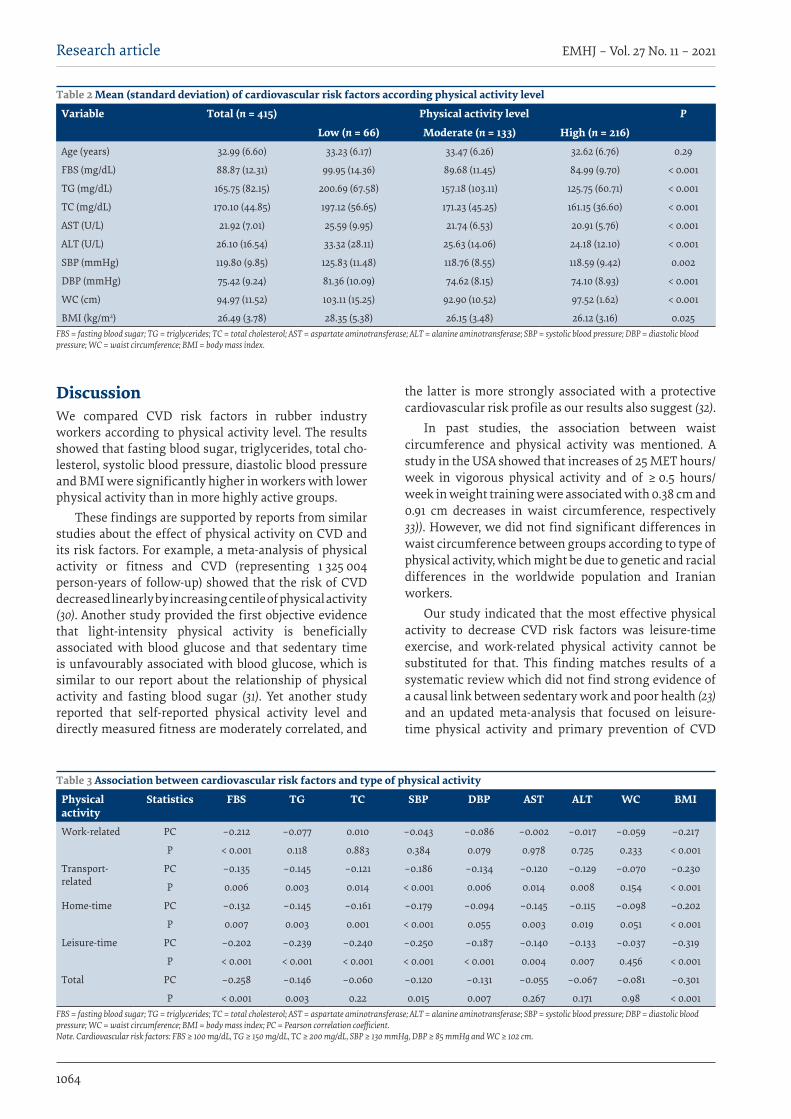
1064
Research article EMHJ – Vol. 27 No. 11 – 2021
DiscussionWe compared CVD risk factors in rubber industry workers according to physical activity level. The results showed that fasting blood sugar, triglycerides, total cho-lesterol, systolic blood pressure, diastolic blood pressure and BMI were significantly higher in workers with lower physical activity than in more highly active groups.
These findings are supported by reports from similar studies about the effect of physical activity on CVD and its risk factors. For example, a meta-analysis of physical activity or fitness and CVD (representing 1 325 004 person-years of follow-up) showed that the risk of CVD decreased linearly by increasing centile of physical activity (30). Another study provided the first objective evidence that light-intensity physical activity is beneficially associated with blood glucose and that sedentary time is unfavourably associated with blood glucose, which is similar to our report about the relationship of physical activity and fasting blood sugar (31). Yet another study reported that self-reported physical activity level and directly measured fitness are moderately correlated, and
the latter is more strongly associated with a protective cardiovascular risk profile as our results also suggest (32).
In past studies, the association between waist circumference and physical activity was mentioned. A study in the USA showed that increases of 25 MET hours/week in vigorous physical activity and of ≥ 0.5 hours/week in weight training were associated with 0.38 cm and 0.91 cm decreases in waist circumference, respectively 33)). However, we did not find significant differences in waist circumference between groups according to type of physical activity, which might be due to genetic and racial differences in the worldwide population and Iranian workers.
Our study indicated that the most effective physical activity to decrease CVD risk factors was leisure-time exercise, and work-related physical activity cannot be substituted for that. This finding matches results of a systematic review which did not find strong evidence of a causal link between sedentary work and poor health (23) and an updated meta-analysis that focused on leisure-time physical activity and primary prevention of CVD
Table 2 Mean (standard deviation) of cardiovascular risk factors according physical activity level
Variable Total (n = 415) Physical activity level P
Low (n = 66) Moderate (n = 133) High (n = 216)Age (years) 32.99 (6.60) 33.23 (6.17) 33.47 (6.26) 32.62 (6.76) 0.29
FBS (mg/dL) 88.87 (12.31) 99.95 (14.36) 89.68 (11.45) 84.99 (9.70) < 0.001
TG (mg/dL) 165.75 (82.15) 200.69 (67.58) 157.18 (103.11) 125.75 (60.71) < 0.001
TC (mg/dL) 170.10 (44.85) 197.12 (56.65) 171.23 (45.25) 161.15 (36.60) < 0.001
AST (U/L) 21.92 (7.01) 25.59 (9.95) 21.74 (6.53) 20.91 (5.76) < 0.001
ALT (U/L) 26.10 (16.54) 33.32 (28.11) 25.63 (14.06) 24.18 (12.10) < 0.001
SBP (mmHg) 119.80 (9.85) 125.83 (11.48) 118.76 (8.55) 118.59 (9.42) 0.002
DBP (mmHg) 75.42 (9.24) 81.36 (10.09) 74.62 (8.15) 74.10 (8.93) < 0.001
WC (cm) 94.97 (11.52) 103.11 (15.25) 92.90 (10.52) 97.52 (1.62) < 0.001
BMI (kg/m2) 26.49 (3.78) 28.35 (5.38) 26.15 (3.48) 26.12 (3.16) 0.025FBS = fasting blood sugar; TG = triglycerides; TC = total cholesterol; AST = aspartate aminotransferase; ALT = alanine aminotransferase; SBP = systolic blood pressure; DBP = diastolic blood pressure; WC = waist circumference; BMI = body mass index.
Table 3 Association between cardiovascular risk factors and type of physical activity
Physical activity
Statistics FBS TG TC SBP DBP AST ALT WC BMI
Work-related PC –0.212 –0.077 0.010 –0.043 –0.086 –0.002 –0.017 –0.059 –0.217
P < 0.001 0.118 0.883 0.384 0.079 0.978 0.725 0.233 < 0.001
Transport-related
PC –0.135 –0.145 –0.121 –0.186 –0.134 –0.120 –0.129 –0.070 –0.230
P 0.006 0.003 0.014 < 0.001 0.006 0.014 0.008 0.154 < 0.001
Home-time PC –0.132 –0.145 –0.161 –0.179 –0.094 –0.145 –0.115 –0.098 –0.202
P 0.007 0.003 0.001 < 0.001 0.055 0.003 0.019 0.051 < 0.001
Leisure-time PC –0.202 –0.239 –0.240 –0.250 –0.187 –0.140 –0.133 –0.037 –0.319
P < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 0.004 0.007 0.456 < 0.001
Total PC –0.258 –0.146 –0.060 –0.120 –0.131 –0.055 –0.067 –0.081 –0.301
P < 0.001 0.003 0.22 0.015 0.007 0.267 0.171 0.98 < 0.001FBS = fasting blood sugar; TG = triglycerides; TC = total cholesterol; AST = aspartate aminotransferase; ALT = alanine aminotransferase; SBP = systolic blood pressure; DBP = diastolic blood pressure; WC = waist circumference; BMI = body mass index; PC = Pearson correlation coefficient. Note. Cardiovascular risk factors: FBS ≥ 100 mg/dL, TG ≥ 150 mg/dL, TC ≥ 200 mg/dL, SBP ≥ 130 mmHg, DBP ≥ 85 mmHg and WC ≥ 102 cm.
Book 27-11.indb 1064Book 27-11.indb 1064 06/12/2021 12:39 PM06/12/2021 12:39 PM
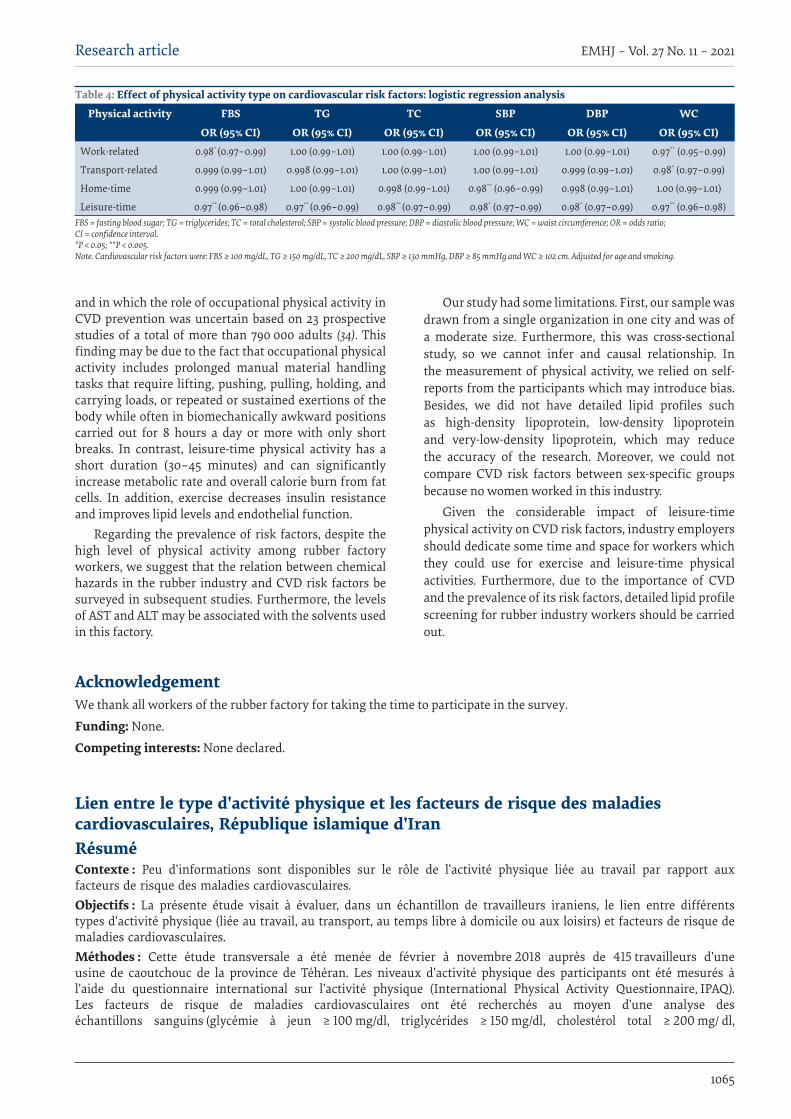
1065
Research article EMHJ – Vol. 27 No. 11 – 2021
and in which the role of occupational physical activity in CVD prevention was uncertain based on 23 prospective studies of a total of more than 790 000 adults (34). This finding may be due to the fact that occupational physical activity includes prolonged manual material handling tasks that require lifting, pushing, pulling, holding, and carrying loads, or repeated or sustained exertions of the body while often in biomechanically awkward positions carried out for 8 hours a day or more with only short breaks. In contrast, leisure-time physical activity has a short duration (30–45 minutes) and can significantly increase metabolic rate and overall calorie burn from fat cells. In addition, exercise decreases insulin resistance and improves lipid levels and endothelial function.
Regarding the prevalence of risk factors, despite the high level of physical activity among rubber factory workers, we suggest that the relation between chemical hazards in the rubber industry and CVD risk factors be surveyed in subsequent studies. Furthermore, the levels of AST and ALT may be associated with the solvents used in this factory.
Our study had some limitations. First, our sample was drawn from a single organization in one city and was of a moderate size. Furthermore, this was cross-sectional study, so we cannot infer and causal relationship. In the measurement of physical activity, we relied on self-reports from the participants which may introduce bias. Besides, we did not have detailed lipid profiles such as high-density lipoprotein, low-density lipoprotein and very-low-density lipoprotein, which may reduce the accuracy of the research. Moreover, we could not compare CVD risk factors between sex-specific groups because no women worked in this industry.
Given the considerable impact of leisure-time physical activity on CVD risk factors, industry employers should dedicate some time and space for workers which they could use for exercise and leisure-time physical activities. Furthermore, due to the importance of CVD and the prevalence of its risk factors, detailed lipid profile screening for rubber industry workers should be carried out.
Table 4: Effect of physical activity type on cardiovascular risk factors: logistic regression analysis
Physical activity FBS TG TC SBP DBP WC
OR (95% CI) OR (95% CI) OR (95% CI) OR (95% CI) OR (95% CI) OR (95% CI)Work-related 0.98* (0.97–0.99) 1.00 (0.99–1.01) 1.00 (0.99–1.01) 1.00 (0.99–1.01) 1.00 (0.99–1.01) 0.97** (0.95–0.99)
Transport-related 0.999 (0.99–1.01) 0.998 (0.99–1.01) 1.00 (0.99–1.01) 1.00 (0.99–1.01) 0.999 (0.99–1.01) 0.98* (0.97–0.99)
Home-time 0.999 (0.99–1.01) 1.00 (0.99–1.01) 0.998 (0.99–1.01) 0.98** (0.96–0.99) 0.998 (0.99–1.01) 1.00 (0.99–1.01)
Leisure-time 0.97** (0.96–0.98) 0.97** (0.96–0.99) 0.98** (0.97–0.99) 0.98* (0.97–0.99) 0.98* (0.97–0.99) 0.97** (0.96–0.98)FBS = fasting blood sugar; TG = triglycerides; TC = total cholesterol; SBP = systolic blood pressure; DBP = diastolic blood pressure; WC = waist circumference; OR = odds ratio; CI = confidence interval. *P < 0.05; **P < 0.005. Note. Cardiovascular risk factors were: FBS ≥ 100 mg/dL, TG ≥ 150 mg/dL, TC ≥ 200 mg/dL, SBP ≥ 130 mmHg, DBP ≥ 85 mmHg and WC ≥ 102 cm. Adjusted for age and smoking.
AcknowledgementWe thank all workers of the rubber factory for taking the time to participate in the survey.
Funding: None.
Competing interests: None declared.
Lien entre le type d'activité physique et les facteurs de risque des maladies cardiovasculaires, République islamique d'IranRésuméContexte : Peu d'informations sont disponibles sur le rôle de l'activité physique liée au travail par rapport aux facteurs de risque des maladies cardiovasculaires.Objectifs : La présente étude visait à évaluer, dans un échantillon de travailleurs iraniens, le lien entre différents types d'activité physique (liée au travail, au transport, au temps libre à domicile ou aux loisirs) et facteurs de risque de maladies cardiovasculaires.Méthodes : Cette étude transversale a été menée de février à novembre 2018 auprès de 415 travailleurs d'une usine de caoutchouc de la province de Téhéran. Les niveaux d'activité physique des participants ont été mesurés à l'aide du questionnaire international sur l'activité physique (International Physical Activity Questionnaire, IPAQ). Les facteurs de risque de maladies cardiovasculaires ont été recherchés au moyen d’une analyse des échantillons sanguins (glycémie à jeun ≥ 100 mg/dl, triglycérides ≥ 150 mg/dl, cholestérol total ≥ 200 mg/ dl,
Book 27-11.indb 1065Book 27-11.indb 1065 06/12/2021 12:39 PM06/12/2021 12:39 PM
1066
Research article EMHJ – Vol. 27 No. 11 – 2021
References4. Laslett LJ, Alagona P, Clark BA, Drozda JP, Saldivar F, Wilson SR, et al. The worldwide environment of cardiovascular disease:
prevalence, diagnosis, therapy, and policy issues: a report from the American College of Cardiology. Am Coll Cardiol. 2012;60(25 Suppl):S1–49. https://doi.org/10.1016/j.jacc.2012.11.002
5. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-spe-cific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385(9963):117–71. https://doi.org/10.1016/S0140-6736(14)61682-2
6. Roth GA, Huffman MD, Moran AE, Feigin V, Mensah GA, Naghavi M, et al. Global and regional patterns in cardiovascular mor-tality from 1990 to 2013. Circulation. 2015;132(17):1667–78. https://doi.org/10.1161/CIRCULATIONAHA.114.008720
7. Hajat C, Harrison O. The Abu Dhabi cardiovascular program: the continuation of Framingham. Prog Cardiovasc Dis. 2010;53(1):28–38. https://doi.org/10.1016/j.pcad.2010.05.002
8. Reddy KS, Satija AJ. The Framingham Heart Study: impact on the prevention and control of cardiovascular diseases in India. Prog Cardiovasc Dis. 2010;53(1):21–7. https://doi.org/10.1016/j.pcad.2010.02.011
9. Vartiainen E, Laatikainen T, Peltonen M, Juolevi A, Männistö S, Sundvall J, et al. Thirty-five-year trends in cardiovascular risk factors in Finland. Int J Epidemiol. 2010;39(2):504–18. https://doi.org/10.1093/ije/dyp330
10. Yusuf S, Hawken S, Ôunpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937–52. https://doi.org/10.1016/S0140-6736(04)17018-9
االرتباط بني نوع النشاط البدين وعوامل خطر أمراض القلب واألوعية الدموية، مجهورية إيران اإلسالميةأوميد أمينيان، مريم ساراي، سعيد نجيب بور، سحر افتخاري
اخلالصةاخللفية: ال يعرف سوى القليل عن دور النشاط البدين املرتبط بمامرسة املهنة وعوامل خطر اإلصابة بأمراض القلب واألوعية الدموية.
األهداف: هدفت هذه الدراسة إىل تقييم االرتباط بني خمتلف أنواع النشاط البدين )املتصل بالعمل، واملتصل بالنقل، ويف املنزل، ويف وقت الفراغ( وبني عوامل خطر اإلصابة بأمراض القلب واألوعية الدموية لدى عينة من العاملني اإليرانيني.
طرق البحث: أجريت هذه الدراسة املقطعية يف الفرتة من فرباير / شباط وحتى نوفمرب / ترشين الثاين 2018 عىل 415 عامال يف مصنع للمطاط يف حمافظة طهران. وقيست مستويات النشاط البدين للمشاركني باستخدام االستبيان الدويل للنشاط البدين. وحللت عينة من الدم ملعرفة عوامل خطر اإلصابة بأمراض القلب واألوعية الدموية )سكر الدم أثناء الصيام يساوي أو يزيد عن 100 جمم/ دل )ميليجرام بالدييس لرت(، والدهون الثالثية تساوي أو تزيد عن 150 جمم/ دل، والكولسرتول اإلمجايل يساوي أو يزيد عن 200 جمم/ دل، وضغط الدم االنقبايض يساوي أو يزيد عن 130 مليمرت زئبق، وضغط الدم االنبساطي يساوي أو يزيد عن 85 مليمرت زئبق، وحميط اخلرص يساوي أو يزيد عن 102 سم. كام قيس إنزيم ناقلة أمينو
أالنني وإنزيم ناقلة أمينو أسبارتيت، وكذلك منسب كتلة اجلسم. النتائج: تتفاوت عوامل خطر اإلصابة بأمراض القلب واألوعية الدموية بشكل كبري حسب نوع النشاط البدين. وتبني وجود ارتباط سلبي ملحوظ بني سكر الدم أثناء الصيام الذي يساوي أو يزيد عن 100 جمم/ دل ومنسب كتلة اجلسم الذي يساوي أو يزيد عن 25 كجم/م2 ومستوى النشاط ا ملحوظا بجميع > 0.001(. ويف حتليل االنحدار اللوجستي، ارتبط النشاط البدين أثناء وقت الفراغ ارتباطا سلبي البدين اإلمجايل )قيمة احتاملية
عوامل خطر أمراض القلب واألوعية الدموية بعد التصحيح مع العمر والتدخني.االستنتاجات: يؤدي النشاط البدين يف وقت الفراغ دورا أكثر أمهية يف احلد من عوامل خطر اإلصابة بأمراض القلب واألوعية الدموية من سائر
أنواع النشاط األخرى، ال سيام النشاط البدين املتصل بالعمل.
tension artérielle systolique ≥ 130 mm Hg, tension artérielle diastolique ≥ 85 mm Hg et tour de taille ≥ 102 cm). L'alanine aminotransférase et l'aspartate aminotransférase ont également été mesurées, ainsi que l'indice de masse corporelle (IMC). Résultats : Les facteurs de risque des maladies cardiovasculaires différaient considérablement selon le type d'activité physique. Une glycémie à jeun supérieure ou égale à 100 mg/dl et un IMC supérieur ou égal à 25 kg/m2 étaient liés de façon négative et significative au niveau global d'activité physique (p < 0,001). Dans une analyse de régression logistique, l'activité physique de loisir était corrélée de façon négative et significative avec tous les facteurs de risque des maladies cardiovasculaires après ajustement en fonction de l'âge et du tabagisme.Conclusion : L'activité physique de loisir joue un rôle plus important dans la réduction des facteurs de risque des maladies cardiovasculaires que les autres types d'activité, y compris l'activité physique liée au travail.
Book 27-11.indb 1066Book 27-11.indb 1066 06/12/2021 12:39 PM06/12/2021 12:39 PM

1067
Research article EMHJ – Vol. 27 No. 11 – 2021
11. Orkaby AR, Forman DE. Physical activity and CVD in older adults: an expert’s perspective. Expert Rev Cardiovasc Ther. 2018;16(1):1–10. https://doi.org/10.1080/14779072.2018.1419062
12. Patel SA, Winkel M, Ali MK, Narayan KV, Mehta NK. Cardiovascular mortality associated with 5 leading risk factors: national and state preventable fractions estimated from survey data. Ann Intern Med. 2015;163(4):245–53. https://doi.org/10.7326/M14-1753
13. Stamler J, Stamler R, Neaton JD, Wentworth D, Daviglus ML, Garside D, et al. Low risk-factor profile and long-term cardiovascu-lar and noncardiovascular mortality and life expectancy: findings for 5 large cohorts of young adult and middle-aged men and women. JAMA. 1999;282(21):2012–8. https://doi.org/10.1001/jama.282.21.2012
14. Lloyd-Jones DM, Hong Y, Labarthe D, Mozaffarian D, Appel LJ, Van Horn L, et al. Defining and setting national goals for car-diovascular health promotion and disease reduction: the American Heart Association’s strategic impact goal through 2020 and beyond. Circulation. 2010;121(4):586–613. https://doi.org/10.1161/CIRCULATIONAHA.109.192703
15. Powell KE, Thompson PD, Caspersen CJ, Kendrick JS. Physical activity and the incidence of coronary heart disease. Annu Rev Public Health. 1987;8(1):253–87. https://doi.org/10.1146/annurev.pu.08.050187.001345
16. Paffenbarger Jr RS, Hyde RT, Wing AL, Lee I-M, Jung DL, Kampert JB. The association of changes in physical-activity level and other lifestyle characteristics with mortality among men. New Engl J Med. 1993;328(8):538–45. https://doi.org/10.1056/nejm199302253280804
17. Leon AS, Connett J, Jacobs D, Rauramaa R. Leisure-time physical activity levels and risk of coronary heart disease and death. JAMA. 1987;258(17):2388–95. https://doi:10.1001/jama.1987.03400170074026
18. Lee D-C, Sui X, Artero EG, Lee I-M, Church TS, McAuley PA, et al. Long-term effects of changes in cardiorespiratory fitness and body mass index on all-cause and cardiovascular disease mortality in men: the Aerobics Center Longitudinal Study. Circulation. 2011;124(23):2483–90. https://doi.org/10.1161/CIRCULATIONAHA.111.038422
19. Kubota Y, Evenson KR, MacLehose RF, Roetker NS, Joshu CE, Folsom AR, et al. Physical activity and lifetime risk of cardiovascu-lar disease and cancer. Med Sci Sports Exerc. 2017;49(8):1599.https://doi.org/10.1249/mss.0000000000001274
20. Held C, Iqbal R, Lear SA, Rosengren A, Islam S, Mathew J, et al. Physical activity levels, ownership of goods promoting seden-tary behaviour and risk of myocardial infarction: results of the INTERHEART study. Eur Heart J. 2012;33(4):452–66. https://doi.org/10.1093/eurheartj/ehr432
21. Roberts LM, Jaeger BC, Baptista LC, Harper SA, Gardner AK, Jackson EA, et al. Wearable technology to reduce sedentary behavior and CVD risk in older adults: a pilot randomized clinical trial. Clin Interv Aging. 2019;14:1817. https://dx.doi.org/10.2147%2FCIA.S222655
22. Targher G, Day CP, Bonora EJ. Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. New Engl J Med 2010;363(14):1341–50. https://doi.org/10.1056/nejmra0912063
23. Wong VW-S, Wong GL-H, Yip GW-K, Lo AO-S, Limquiaco J, Chu WC-W, et al. Coronary artery disease and cardiovascular out-comes in patients with non-alcoholic fatty liver disease. Gut. 2011.242016. https://doi.org/10.1136/gut.2011.242016
24. Qiu S, Cai X, Sun Z, Li L, Zügel M, Steinacker JM, et al. Association between physical activity and risk of nonalcoholic fatty liver disease: a meta-analysis. Therap Adv Gastroenterol. 2017;10(9):701–13. https://doi.org/10.1177/1756283x17725977
25. Van Uffelen JG, Wong J, Chau JY, Van Der Ploeg HP, Riphagen I, Gilson ND, et al. Occupational sitting and health risks: a sys-tematic review. Am J Prev Med. 2010;39(4):379–88. https://doi.org/10.1016/j.amepre.2010.05.024
26. Harari G, Green MS, Zelber-Sagi S. Combined association of occupational and leisure-time physical activity with all-cause and coronary heart disease mortality among a cohort of men followed-up for 22 years. Occup Environ Med. 2015;72(9):617–24. https://doi.org/10.1136/oemed-2014-102613
27. Autenrieth CS, Baumert J, Baumeister SE, Fischer B, Peters A, Döring A, et al. Association between domains of physical activity and all-cause, cardiovascular and cancer mortality. Eur J Epidemiol. 2011;26(2):91–9. https://doi.org/10.1007/s10654-010-9517-6
28. Li J, Siegrist J. Physical activity and risk of cardiovascular disease—a meta-analysis of prospective cohort studies. Int J Environ Res Public Health. 2012;9(2):391–407. https://doi.org/10.3390/ijerph9020391
29. Vasheghani-Farahani A, Tahmasbi M, Asheri H, Ashraf H, Nedjat S, Kordi R. The Persian, last 7-day, long form of the Interna-tional Physical Activity Questionnaire: translation and validation study. Asian J Sports Med. 2011;2(2):106. https://doi.org/10.5812/asjsm.34781
30. Sjöström M, Ainsworth B, Bauman A, Bull F, Hamilton-Craig C, Sallis J. Guidelines for data processing analysis of the In-ternational Physical Activity Questionnaire (IPAQ) – short and long forms. 2005 (https://www.scienceopen.com/docu-ment?vid=b223350f-d159-4043-9b48-e2031f210a3c, accessed 24 June 2021).
31. Hagströmer M, Oja P, Sjöström M. The International Physical Activity Questionnaire (IPAQ): a study of concurrent and con-struct validity. Public Health Nutr. 2006;9(6):755–62. https://doi.org/10.1079/phn2005898
32. Ko K-J, Kim E-H, Baek U-H, Gang Z, Kang S-J. The relationship between physical activity levels and metabolic syndrome in male white-collar workers. J Phys Ther Sci. 2016;28(11):3041–6. https://doi.org/10.1589/jpts.28.3041
33. Williams PTJM, sports si, exercise. Physical fitness and activity as separate heart disease risk factors: a meta-analysis. Med Sci Sports Exerc. 2001;33(5):754. https://doi.org/10.1097/00005768-200105000-00012
Book 27-11.indb 1067Book 27-11.indb 1067 06/12/2021 12:39 PM06/12/2021 12:39 PM
1068
Research article EMHJ – Vol. 27 No. 11 – 2021
34. Healy GN, Dunstan DW, Salmon J, Cerin E, Shaw JE, Zimmet PZ, et al. Objectively measured light-intensity physical activity is independently associated with 2-hr plasma glucose. Diabetes Care. 2007;30(6):1384–9. https://doi.org/10.2337/dc07-0114
35. Minder CM, Shaya GE, Michos ED, Keenan TE, Blumenthal RS, Nasir K, et al. Relation between self-reported physical activity level, fitness, and cardiometabolic risk. Am J Cardiol. 2014;113(4):637–43. https://doi.org/10.1016/j.amjcard.2013.11.010.
36. Koh-Banerjee P, Chu N-F, Spiegelman D, Rosner B, Colditz G, Willett W, et al. Prospective study of the association of changes in dietary intake, physical activity, alcohol consumption, and smoking with 9-y gain in waist circumference among 16 587 US men. Am J Clin Nutr. 2003;78(4):719–27. https://doi.org/10.1093/ajcn/78.4.719
37. Li J, Loerbroks A, Angerer P. Physical activity and risk of cardiovascular disease: what does the new epidemiological evidence show? Curr Opin Cardiol. 2013;28(5):575–83. https://doi.org/10.1097/hco.0b013e328364289c
Book 27-11.indb 1068Book 27-11.indb 1068 06/12/2021 12:39 PM06/12/2021 12:39 PM

1069
Research article EMHJ – Vol. 27 No. 11 – 2021
Determinants of the Early Childhood Development Index among children aged < 5 years in Bangladesh, Costa Rica and Ghana: a comparative studyIqramul Haq,1 Md. Ismail Hossain,2 Maliha Afroj Zinnia,3 Md Rifat Hasan2 and Imru-Al-Quais Chowdhury4
1Department of Agricultural Statistics, Sher-e-Bangla Agricultural University, Dhaka, Bangladesh. (Correspondence to: Iqramul Haq , [email protected]). 2Department of Statistics, Jagannath University, Dhaka, Bangladesh. 3Department of Pharmacy, East West University, Dhaka, Bangladesh. 4Armed Forces Medical Institute, Dhaka Cantonment, Bangladesh.
AbstractBackground: Early child development is a crucial factor for children that controls health and well-being in later life. Aims: To determine the influence of sociodemographic factors on the Early Child Development Index (ECDI) among children aged < 5 years.Methods: The analysis was performed using cross-sectional survey data from 2019, 2017–2018 and 2018 Multiple Indica-tor Cluster Surveys from Bangladesh, Ghana and Costa Rica, respectively. We used the χ2 test for bivariate analysis and binary logistic regression model for multivariate analysis for all 3 countries. All the statistical analyses were performed with IBM SPSS version 25 and R version 4.0.0.Results: Child age and sex, followed by maternal education level, economic status, child nutritional status, reading chil-dren’s books, and maternal functional difficulties had the greatest effect on ECDI. Children aged 36–47 months had lower odds of development than those aged 48–59 months, and boys had lower odds of development than girls in Bangladesh, Costa Rica and Ghana. Urban children had lower odds of development than rural children in Costa Rica but higher odds in Ghana. Conclusion: We recommend that governments should take the necessary steps to enhance children’s early development and well-being in all 3 countries by raising education, improving economic conditions and providing balanced nutrition.Keywords: child development, child nutrition, child mortality, cognitive, early childhood developmentCitation: Haq I; Hossain MI; Zinnia MA; Hasan MR; Chowdhury I. Determinants of the Early Childhood Development Index among children aged < 5 years in Bangladesh, Costa Rica and Ghana: a comparative study. East Mediterr Health J. 2021;27(11):1069-1077. https://doi.org/10.26719/emhj.21.055 Received: 18/11/20; accepted: 25/04/21Copyright © World Health Organization (WHO) 2021. Open Access. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license (https://creativecommons.org/licenses/by-nc-sa/3.0/igo)
IntroductionEarly childhood development (ECD) comprises the phys-ical, cognitive, motor and socioemotional growth of children up to 8 years of age (1,2). Approximately 20% of children aged < 5 years develop slowly, 5% show signs of wasting, and 11% are underweight. Child development starts during conception and the initial years are signifi-cant because the brain advances most rapidly during this time and builds capacity for improvements, as this foun-dation is involved in health and quality of life (3). A child’s brain improves by 90% within the first 5 years, thus these years are critical (4). The Sustainable Development Goals (SDGs) Agreement indicates that ECD will be a priority for the 21st century (5). The new sustainable development agenda includes 1 target (4.2) relevant for ECD. Target 4.2 states that, by 2030, countries should ensure that all girls and boys have access to quality early childhood de-velopment, care and preprimary education so that they are ready for primary education (5). However, the contri-butions of the SDGs to ECD are wider than this educa-tion-oriented goal. The key to achieving at least 7 of the SDGs is to strengthen ECD by tackling poverty, hunger,
health (including child mortality), education, gender, wa-ter and sanitation, and inequality.
Children must be provided with responsive care, balanced nutrition, nurturing, and a safe environment to live, learn, grow and develop to full potential (6). Several studies conducted in 2007 concluded that > 200 million children under the age of 5 years did not achieve their developmental potential in low- and middle-income countries (LMICs) as a result of nutritional deficiencies and insufficient learning opportunities (7–9). Economic depression and climate diversity have also raised the number of children affected (10,11). Biological and psychosocial risk factors accompanied by poverty lead to an imbalance in ECD that threaten educational attainment and adult productivity (7,12).
High-quality preschool education has a significant influence on cognitive and socioemotional development (13,14). Costa Rica has become a global leader in ECD by making it mandatory for all young children to enrol in preprimary education (4). In Costa Rica, preschool allowances are increased, particularly in kindergarten, and to be admitted to the first-grade school, 3- and 4-year-old children must attend first-grade preprimary
Book 27-11.indb 1069Book 27-11.indb 1069 06/12/2021 12:39 PM06/12/2021 12:39 PM
1070
Research article EMHJ – Vol. 27 No. 11 – 2021
education (15,16). One in 5 children in Ghana experiences stunted growth due to insufficient nutrition, recurrent illness and an unhealthy environment, resulting in disrupted physical, social and cognitive development that successively affects their early learning, school performance, and ultimately, their socioeconomic development (17). In 2007, Ghana launched a 2-year preprimary education for children between 3 and 4 years of age. In recent years, preprimary school attendance has increased and education in Ghana has improved (18,19).
In Bangladesh, understanding of ECD is still emerging as a result of severe constraints, such as poverty, lack of qualified educators and health professionals, as well as funding (20). Most parents have little knowledge of childcare and rearing, and the Bangladeshi Ministry of Women’s and Children’s Affairs and the Ministry of Health and Family Welfare have formed the Centre of Early Childhood Care and Development. The Centre aims to provide essential elements of child growth, such as early nutrition, stimulation, security and learning (21). While most of the activities of the Centre are targeted at preschool children, a few are aimed at parents or children under 3 years of age (21).
Several studies have shown that the development of many children aged < 5 years has not progressed in the right way in LMICs due to many factors such as poverty and education. The present study aimed to measure the effects of various sociodemographic and economic factors on ECD, and to determine which risk factors are associated with Early Childhood Development Index
(ECDI) in 3 LMICs, Bangladesh, Costa Rica and Ghana. This should provide researchers and policy-makers with updated insights on early childhood development and help them develop appropriate guidance and programmes.
MethodsStudy design and data sourcesThe analysis was performed on cross-sectional survey data obtained from the 2019 Multiple Indicator Clus-ter Survey (MICS) for Bangladesh, 2018 MICS for Costa Rica, and 2017–2018 MICS for Ghana. For survey sample selection, we used a 2-stage stratified cluster sampling approach and the same sampling frame was adopted for the Bangladesh Census of Population and Housing, 2011 (22), the Housing Sample Frame (Marco Muestral de Viviendas), 2011 (for Costa Rica) (23), and Population and Housing Census, 2010 (for Ghana) (19). Household and independent (mothers) questionnaires were utilized to collect information about children aged < 5 years. Follow-ing weighting of the samples, 23 099 children aged < 5 in Bangladesh, 37 0096 in Costa Rica, and 8879 in Ghana were included in this study. The geographical locations of the children in the 3 countries are shown in Figure 1.
Dependent variableThe dependent variable was ECD among children aged 36–59 months and was calculated by using 4 domains (19,22,23): literacy–numeracy, physical, social–emotional,
Figure 1 Map showing the geographical locations of samples in 3 countries. ECDI = Early Child Development Index
<caption>Figure 1. Map showing the geographical locations of samples in 3 countries. ECDI = Early Child Development Index.
Book 27-11.indb 1070Book 27-11.indb 1070 06/12/2021 12:39 PM06/12/2021 12:39 PM
1071
Research article EMHJ – Vol. 27 No. 11 – 2021
and learning. To distinguish domain compliance for each child i aged 36–59 months in country j (Bangladesh, Costa Rica or Ghana), for domain r (literacy–numeracy, physi-cal, social–emotional, or learning),
ECD compliance was defined as child i, in country , that satisfied at least 3 of 4 domains r. That is,
For the aim of the study, children whose development was on track in at least 3 domains were categorized as 1 and the remainder as 0.
The created binary variable was considered as the dependent variable for our study.
Independent variableBesides the dependent variable, we also considered child age, childsex, residence, maternal education, economic status, child nutritional status, reading children’s books, and maternal functional difficulties as potential factors for early development among children aged < 5 years in Bangladesh, Costa Rica and Ghana. Descriptions and classifications of the study explanatory variables are list-ed in Table 1.
Data analysisThe IBM SPSS version 25 and R version 4.0.0 were used for data management, analysis and geographical map-ping. Appropriate statistical methods for data analysis were used to obtain different objectives of this study. To examine the association between dependent variables and selected covariates, we applied the χ2 test for bivar-
iate analysis. The binary logistic regression model in a multivariable setup was applied to identify factors that contributed to ECDI among children aged < 5 years.
ResultsECDI characteristics of children aged < 5 yearsThe overall ECDI was 69.1% in Ghana, 74.9% in Bangla-desh, and 86.0% in Costa Rica during this study period.
Effect of sociodemographic factors on ECDChildren’s age and sex, residence, maternal education, economic status, child nutritional status, reading chil-dren’s books, and maternal functional difficulties were significantly correlated with ECD in Bangladesh, Costa Rica and Ghana (Table 2).
Collinearity for independent variableMulticollinearity statistics for all explanatory variables are shown in Table 3. In a regression model, multicol-linearity is observed as high levels of interdependence among predictors, which can be particularly burdensome for studies. Multicollinearity is indicated by a threshold of 5 or 10 for variance inflation factor (VIF) and 0.1 or 0.2 for tolerance. Table 3 shows that there was no multicol-linearity in the present study. The range of VIF values was 1.003–1.342 for Bangladesh, 1.007–1.290 for Costa Rica and 1.006–1.629 for Ghana.
Multivariate analysis for identifying factorsTable 4 illustrated the odds of child development status among children aged 3–5 years in Bangladesh, Costa Rica and Ghana. For all countries in the model, significant (P < 0.001, P < 0.01 and P < 0.05) odds ratios for child age, child sex, maternal education, economic status, reading children books, and maternal functional difficulties were distinguished. Several risk factors were not significant for different countries; in particular, residence for Bang-ladesh, severe child nutritional status and moderate nu-tritional status for Ghana and Bangladesh, respectively.
Table 1 Summary of explanatory variables
Variable CategorizationChild age, months 36–47, 48–59
Child sex Male or female
Residence Urban or rural
Maternal education None education, primary education, secondary and above education
Economic status Poor, middle or rich
Child nutritional status In 2019, MICS Bangladesh used weight and height calculations to explore the nutritional status of children aged < 5 years and used common measures of height for age Z score, weight for age Z score, and weight for height Z score to determine the nutritional health of children. We used weight for age Z score as child nutritional status variable and categories as:severely malnourished: WAZ < -3.0 moderately malnourished: -3.0 < WAZ < -2.01 nourished: WAZ > -2.01
Reading children books < 3 or ≥ 3
Maternal functional difficulties Yes or no
ECDI
Book 27-11.indb 1071Book 27-11.indb 1071 06/12/2021 12:39 PM06/12/2021 12:39 PM
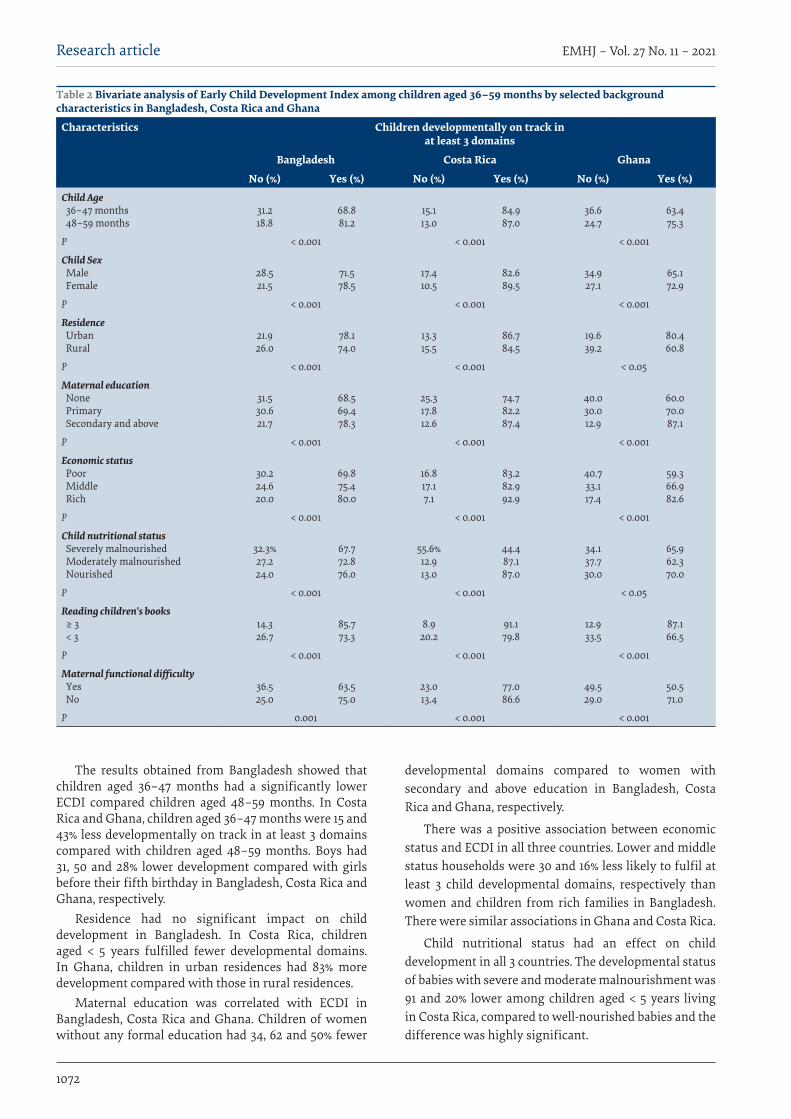
1072
Research article EMHJ – Vol. 27 No. 11 – 2021
The results obtained from Bangladesh showed that children aged 36–47 months had a significantly lower ECDI compared children aged 48–59 months. In Costa Rica and Ghana, children aged 36–47 months were 15 and 43% less developmentally on track in at least 3 domains compared with children aged 48–59 months. Boys had 31, 50 and 28% lower development compared with girls before their fifth birthday in Bangladesh, Costa Rica and Ghana, respectively.
Residence had no significant impact on child development in Bangladesh. In Costa Rica, children aged < 5 years fulfilled fewer developmental domains. In Ghana, children in urban residences had 83% more development compared with those in rural residences.
Maternal education was correlated with ECDI in Bangladesh, Costa Rica and Ghana. Children of women without any formal education had 34, 62 and 50% fewer
developmental domains compared to women with secondary and above education in Bangladesh, Costa Rica and Ghana, respectively.
There was a positive association between economic status and ECDI in all three countries. Lower and middle status households were 30 and 16% less likely to fulfil at least 3 child developmental domains, respectively than women and children from rich families in Bangladesh. There were similar associations in Ghana and Costa Rica.
Child nutritional status had an effect on child development in all 3 countries. The developmental status of babies with severe and moderate malnourishment was 91 and 20% lower among children aged < 5 years living in Costa Rica, compared to well-nourished babies and the difference was highly significant.
Table 2 Bivariate analysis of Early Child Development Index among children aged 36–59 months by selected background characteristics in Bangladesh, Costa Rica and Ghana
Characteristics Children developmentally on track in at least 3 domains
Bangladesh Costa Rica Ghana
No (%) Yes (%) No (%) Yes (%) No (%) Yes (%)Child Age 36–47 months 48–59 months
31.218.8
68.881.2
15.113.0
84.987.0
36.624.7
63.475.3
P < 0.001 < 0.001 < 0.001
Child Sex Male Female
28.521.5
71.578.5
17.410.5
82.689.5
34.927.1
65.172.9
P < 0.001 < 0.001 < 0.001
Residence Urban Rural
21.926.0
78.174.0
13.315.5
86.784.5
19.639.2
80.460.8
P < 0.001 < 0.001 < 0.05
Maternal education None Primary Secondary and above
31.530.621.7
68.569.478.3
25.317.812.6
74.782.287.4
40.030.012.9
60.070.087.1
P < 0.001 < 0.001 < 0.001
Economic status Poor Middle Rich
30.224.620.0
69.875.480.0
16.817.17.1
83.282.992.9
40.733.117.4
59.366.982.6
P < 0.001 < 0.001 < 0.001
Child nutritional status Severely malnourished Moderately malnourished Nourished
32.3%27.224.0
67.772.876.0
55.6%12.913.0
44.487.187.0
34.137.730.0
65.962.370.0
P < 0.001 < 0.001 < 0.05
Reading children’s books ≥ 3 < 3
14.326.7
85.773.3
8.920.2
91.179.8
12.933.5
87.166.5
P < 0.001 < 0.001 < 0.001
Maternal functional difficulty Yes No
36.525.0
63.575.0
23.013.4
77.086.6
49.529.0
50.571.0
P 0.001 < 0.001 < 0.001
Book 27-11.indb 1072Book 27-11.indb 1072 06/12/2021 12:39 PM06/12/2021 12:39 PM
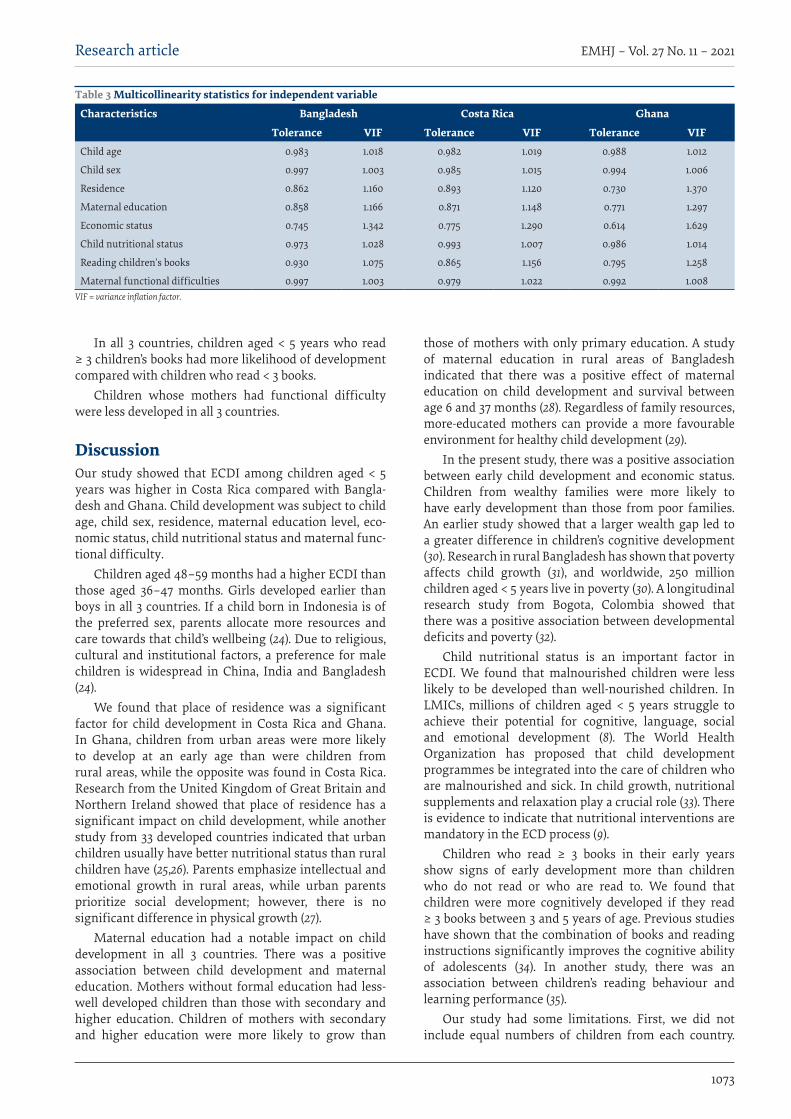
1073
Research article EMHJ – Vol. 27 No. 11 – 2021
In all 3 countries, children aged < 5 years who read ≥ 3 children’s books had more likelihood of development compared with children who read < 3 books.
Children whose mothers had functional difficulty were less developed in all 3 countries.
DiscussionOur study showed that ECDI among children aged < 5 years was higher in Costa Rica compared with Bangla-desh and Ghana. Child development was subject to child age, child sex, residence, maternal education level, eco-nomic status, child nutritional status and maternal func-tional difficulty.
Children aged 48–59 months had a higher ECDI than those aged 36–47 months. Girls developed earlier than boys in all 3 countries. If a child born in Indonesia is of the preferred sex, parents allocate more resources and care towards that child’s wellbeing (24). Due to religious, cultural and institutional factors, a preference for male children is widespread in China, India and Bangladesh (24).
We found that place of residence was a significant factor for child development in Costa Rica and Ghana. In Ghana, children from urban areas were more likely to develop at an early age than were children from rural areas, while the opposite was found in Costa Rica. Research from the United Kingdom of Great Britain and Northern Ireland showed that place of residence has a significant impact on child development, while another study from 33 developed countries indicated that urban children usually have better nutritional status than rural children have (25,26). Parents emphasize intellectual and emotional growth in rural areas, while urban parents prioritize social development; however, there is no significant difference in physical growth (27).
Maternal education had a notable impact on child development in all 3 countries. There was a positive association between child development and maternal education. Mothers without formal education had less-well developed children than those with secondary and higher education. Children of mothers with secondary and higher education were more likely to grow than
those of mothers with only primary education. A study of maternal education in rural areas of Bangladesh indicated that there was a positive effect of maternal education on child development and survival between age 6 and 37 months (28). Regardless of family resources, more-educated mothers can provide a more favourable environment for healthy child development (29).
In the present study, there was a positive association between early child development and economic status. Children from wealthy families were more likely to have early development than those from poor families. An earlier study showed that a larger wealth gap led to a greater difference in children’s cognitive development (30). Research in rural Bangladesh has shown that poverty affects child growth (31), and worldwide, 250 million children aged < 5 years live in poverty (30). A longitudinal research study from Bogota, Colombia showed that there was a positive association between developmental deficits and poverty (32).
Child nutritional status is an important factor in ECDI. We found that malnourished children were less likely to be developed than well-nourished children. In LMICs, millions of children aged < 5 years struggle to achieve their potential for cognitive, language, social and emotional development (8). The World Health Organization has proposed that child development programmes be integrated into the care of children who are malnourished and sick. In child growth, nutritional supplements and relaxation play a crucial role (33). There is evidence to indicate that nutritional interventions are mandatory in the ECD process (9).
Children who read ≥ 3 books in their early years show signs of early development more than children who do not read or who are read to. We found that children were more cognitively developed if they read ≥ 3 books between 3 and 5 years of age. Previous studies have shown that the combination of books and reading instructions significantly improves the cognitive ability of adolescents (34). In another study, there was an association between children’s reading behaviour and learning performance (35).
Our study had some limitations. First, we did not include equal numbers of children from each country.
Table 3 Multicollinearity statistics for independent variable
Characteristics Bangladesh Costa Rica Ghana
Tolerance VIF Tolerance VIF Tolerance VIFChild age 0.983 1.018 0.982 1.019 0.988 1.012
Child sex 0.997 1.003 0.985 1.015 0.994 1.006
Residence 0.862 1.160 0.893 1.120 0.730 1.370
Maternal education 0.858 1.166 0.871 1.148 0.771 1.297
Economic status 0.745 1.342 0.775 1.290 0.614 1.629
Child nutritional status 0.973 1.028 0.993 1.007 0.986 1.014
Reading children’s books 0.930 1.075 0.865 1.156 0.795 1.258
Maternal functional difficulties 0.997 1.003 0.979 1.022 0.992 1.008VIF = variance inflation factor.
Book 27-11.indb 1073Book 27-11.indb 1073 06/12/2021 12:39 PM06/12/2021 12:39 PM
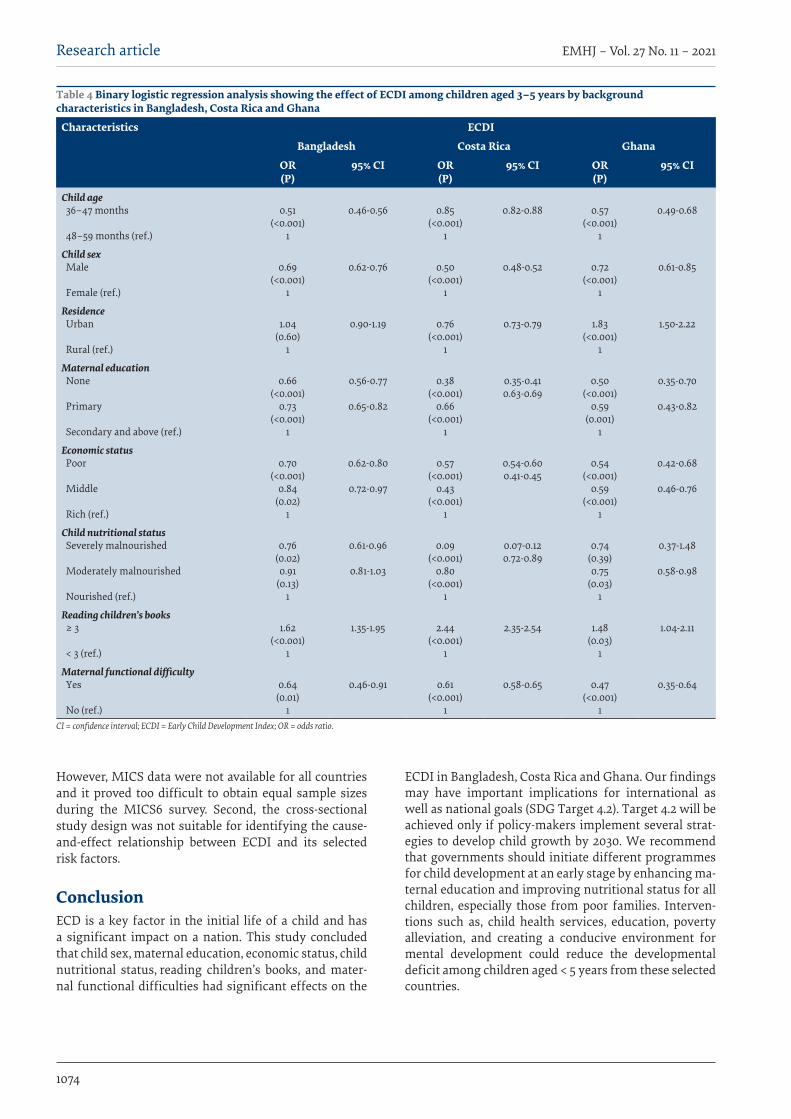
1074
Research article EMHJ – Vol. 27 No. 11 – 2021
However, MICS data were not available for all countries and it proved too difficult to obtain equal sample sizes during the MICS6 survey. Second, the cross-sectional study design was not suitable for identifying the cause-and-effect relationship between ECDI and its selected risk factors.
ConclusionECD is a key factor in the initial life of a child and has a significant impact on a nation. This study concluded that child sex, maternal education, economic status, child nutritional status, reading children’s books, and mater-nal functional difficulties had significant effects on the
ECDI in Bangladesh, Costa Rica and Ghana. Our findings may have important implications for international as well as national goals (SDG Target 4.2). Target 4.2 will be achieved only if policy-makers implement several strat-egies to develop child growth by 2030. We recommend that governments should initiate different programmes for child development at an early stage by enhancing ma-ternal education and improving nutritional status for all children, especially those from poor families. Interven-tions such as, child health services, education, poverty alleviation, and creating a conducive environment for mental development could reduce the developmental deficit among children aged < 5 years from these selected countries.
Table 4 Binary logistic regression analysis showing the effect of ECDI among children aged 3–5 years by background characteristics in Bangladesh, Costa Rica and Ghana
Characteristics ECDI
Bangladesh Costa Rica Ghana
OR (P)
95% CI OR(P)
95% CI OR(P)
95% CI
Child age 36–47 months
48–59 months (ref.)
0.51(<0.001)
1
0.46-0.56 0.85(<0.001)
1
0.82-0.88 0.57(<0.001)
1
0.49-0.68
Child sex Male
Female (ref.)
0.69(<0.001)
1
0.62-0.76 0.50(<0.001)
1
0.48-0.52 0.72(<0.001)
1
0.61-0.85
Residence Urban
Rural (ref.)
1.04(0.60)
1
0.90-1.19 0.76(<0.001)
1
0.73-0.79 1.83(<0.001)
1
1.50-2.22
Maternal education None
Primary
Secondary and above (ref.)
0.66(<0.001)
0.73(<0.001)
1
0.56-0.77
0.65-0.82
0.38(<0.001)
0.66(<0.001)
1
0.35-0.410.63-0.69
0.50(<0.001)
0.59(0.001)
1
0.35-0.70
0.43-0.82
Economic status Poor
Middle
Rich (ref.)
0.70(<0.001)
0.84(0.02)
1
0.62-0.80
0.72-0.97
0.57(<0.001)
0.43(<0.001)
1
0.54-0.600.41-0.45
0.54(<0.001)
0.59(<0.001)
1
0.42-0.68
0.46-0.76
Child nutritional status Severely malnourished
Moderately malnourished
Nourished (ref.)
0.76(0.02)0.91
(0.13)1
0.61-0.96
0.81-1.03
0.09(<0.001)
0.80(<0.001)
1
0.07-0.120.72-0.89
0.74(0.39)0.75
(0.03)1
0.37-1.48
0.58-0.98
Reading children’s books ≥ 3
< 3 (ref.)
1.62(<0.001)
1
1.35-1.95 2.44(<0.001)
1
2.35-2.54 1.48(0.03)
1
1.04-2.11
Maternal functional difficulty Yes
No (ref.)
0.64(0.01)
1
0.46-0.91 0.61(<0.001)
1
0.58-0.65 0.47(<0.001)
1
0.35-0.64
CI = confidence interval; ECDI = Early Child Development Index; OR = odds ratio.
Book 27-11.indb 1074Book 27-11.indb 1074 06/12/2021 12:39 PM06/12/2021 12:39 PM
1075
Research article EMHJ – Vol. 27 No. 11 – 2021
AcknowledgementSpecial thank goes to the United Nations Children’s Fund (UNICEF) for enabling us to use Multiple Indicator Cluster Survey data from Bangladesh, Costa Rica and Ghana for our study (http://mics.unicef.org/).
Funding: None.
Competing interests: None declared.
حمددات مؤرش النامء يف مرحلة الطفولة املبكرة يف صفوف األطفال الذين تقل أعامرهم عن 5 سنوات يف بنجالديش، وكوستاريكا، وغانا: دراسة مقارنة
إكرام احلق، إسامعيل حسني، مليحة عفروج زينيا، رفعت حسن، إمرؤ القيس شودري
اخلالصةاخللفية: يمثل النامء يف مرحلة الطفولة املبكرة عامال حاسام يتحكم يف صحة األطفال ورفاههم يف مراحل عمرهم الالحقة.
األهداف: هدفت هذه الدراسة اىل حتديد تأثري العوامل االجتامعية السكانية عىل مؤرش النامء يف مرحلة الطفولة املبكرة يف صفوف األطفال الذين تقل أعامرهم عن 5 سنوات.
طرق البحث: أجري التحليل باستخدام بيانات مسح مقطعي مستمدة من مسوح عنقودية متعددة املؤرشات جرت يف األعوام 2018-2017، ونموذج املتغريات ثنائي حتليل إلجراء )χ2( كاي مربع اختبار واستخدمنا التوايل. عىل وكوستاريكا وغانا، بنجالديش، عىل 2019 ،2018االنحدار اللوجستي الثنائي إلجراء التحليل املتعدد املتغريات للبلدان الثالثة. وأجريت مجيع التحليالت اإلحصائية باستخدام اإلصدار 25 من
برنامج IBM SPSS احلاسويب واإلصدار 4.0.0 من برنامج R احلاسويب.األطفال، كتب وقراءة لألطفال، التغذوية واحلالة االقتصادي، والوضع األمهات، تعليم مستوى يليهام وجنسه، الطفل لعمر كان النتائج: والصعوبات التي تواجهها األمهات يف أداء الوظائف أكرب أثر عىل مؤرش النامء يف مرحلة الطفولة املبكرة. وأظهر األطفال الذين ترتاوح أعامرهم بني 36 و47 شهرا مؤرش نامء يف مرحلة الطفولة املبكرة أقل من األطفال الذين ترتاوح أعامرهم بني 48 و59 شهرا، وأظهر الفتيان مؤرش نامء يف مرحلة الطفولة املبكرة أقل من الفتيات يف بنجالديش، وكوستاريكا، وغانا. وأظهر األطفال يف املناطق احلرضية مؤرش نامء يف مرحلة الطفولة املبكرة أقل
من نظريه يف صفوف األطفال يف املناطق الريفية يف كوستاريكا، ولكنه كان أعىل يف غانا. التعليم، البلدان الثالثة من خالل رفع مستوى االستنتاجات: نويص احلكومات باختاذ اخلطوات الالزمة لتعزيز نامء األطفال املبكر ورفاههم يف
وحتسني الظروف االقتصادية، وتوفري التغذية املتوازنة.
Déterminants de l'indice de développement dans la petite enfance chez les enfants de moins de cinq ans au Bangladesh, au Costa Rica et au Ghana : étude comparativeRésuméContexte : Le développement du jeune enfant est un facteur crucial qui influence la santé et le bien-être à l'âge adulte. Objectifs : Déterminer l'influence des facteurs sociodémographiques sur l'indice de développement dans la petite enfance chez les enfants de moins de cinq ans.Méthodes : L'analyse a été réalisée à partir de données d'études transversales menées dans le cadre des enquêtes en grappes à indicateurs multiples effectuées respectivement en 2019, 2017-2018 et 2018 au Bangladesh, au Ghana et au Costa Rica. Pour les trois pays, nous avons utilisé le test χ2 pour l'analyse bivariée et le modèle de régression logistique binaire pour l'analyse multivariée. Toutes les analyses statistiques ont été réalisées à l'aide des logiciels SPSS version 25 et R version 4.0.0 d'IBM.Résultats : L'âge et le sexe de l'enfant, suivis par le niveau d'éducation de la mère, la situation économique, l'état nutritionnel de l'enfant, la lecture de livres pour enfants et les difficultés fonctionnelles de la mère, correspondaient aux facteurs influençant le plus l'indice de développement du jeune enfant. Les enfants âgés de 36 à 47 mois affichaient de plus faibles chances de développement que ceux âgés de 48 à 59 mois, de même que les garçons par rapport aux filles au Bangladesh, au Costa Rica et au Ghana. Les enfants vivant en zone urbaine présentaient des chances de développement inférieures à celles des enfants des zones rurales au Costa Rica, tandis que la situation était inverse au Ghana. Conclusion : Nous recommandons aux gouvernements de prendre les mesures nécessaires afin d'améliorer le développement et le bien-être des jeunes enfants dans les trois pays. Cela passe par le renforcement de l'accès à l’éducation et à une nutrition équilibrée, et par l'amélioration des conditions économiques.
Book 27-11.indb 1075Book 27-11.indb 1075 06/12/2021 12:39 PM06/12/2021 12:39 PM
1076
Research article EMHJ – Vol. 27 No. 11 – 2021
References1. Lerner RM. Concepts and theories of human development. Taylor & Francis; 2015.
2. Sk R, Banerjee A, Mishra R, Barua S. Quality of care and early childhood developmental status in Nepal: a multilevel analysis. Early Child Dev Care. 2019;190(14):2264–77. https://doi.org/10.1080/03004430.2019.1570503
3. Britto PR, Lye SJ, Proulx K, Yousafzai AK, Matthews SG, Vaivada T, et al. Nurturing care: promoting early childhood develop-ment. Lancet. 2017 Jan 7;389(10064):91–102. https://doi.org/10.1016/S0140-6736(16)31390-3 PMID:27717615
4. Hunter E. Costa Rica shows the way by providing pre-primary education for all children [website]. Their World; 2018 (https://theirworld.org/news/costa-rica-shows-the-way-provides-pre-primary-education-for-every-child#:~:text=Costa%20Rica%20has%20become%20a, accessed 2 August 2021).
5. Transforming our world: the 2030 Agenda for Sustainable Development. United Nations, Department of Economic and Social Affairs; 2015 (https://sustainabledevelopment.un.org/post2015/transformingourworld, accessed 2 August 2021).
6. Nurturing care for early childhood development a global framework for action and results. Geneva: World Health Organization; 2018 (https://www.who.int/maternal_child_adolescent/child/nurturing-care-framework-first-draft.pdf, accessed 18 November 2020).
7. Walker SP, Wachs TD, Grantham-McGregor S, Black MM, Nelson CA, Huffman SL, et al. Inequality in early childhood: risk and protective factors for early child development. Lancet. 2011 Oct 8;378(9799):1325–38. https://doi.org/10.1016/S0140-6736(11)60555-2 PMID:21944375
8. Walker SP, Wachs TD, Meeks Gardner J, Lozoff B, Wasserman GA, Pollitt E, et al. Child development: risk factors for ad-verse outcomes in developing countries. Lancet. 2007 Jan 13;369(9556):145–57. https://doi.org/10.1016/S0140-6736(07)60076-2 PMID:17223478
9. Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L, Strupp B. Developmental potential in the first 5 years for chil-dren in developing countries. Lancet. 2007 Jan 6;369(9555):60–70. https://doi.org/10.1016/S0140-6736(07)60032-4 PMID:17208643
10. Friedman J, Sturdy J. The influence of economic crisis on early childhood development: a review of pathways and measured im-pact. In: Alderman H, editor. No small matter: the impact of poverty, shocks, and human capital investments in early childhood development. World Bank; 2011:51–83.
11. Sheffield PE, Landrigan PJ. Global Climate change and children’s health: threats and strategies for prevention. Environ Health Perspect. 2011 Mar;119(3):291–8. https://doi.org/10.1289/ehp.1002233 PMID:20947468
12. Engle PL, Black MM, Behrman JR, Cabral de Mello M, Gertler PJ, Kapiriri L, et al. Strategies to Avoid the Loss of Developmen-tal Potential in More than 200 Million Children in the Developing World. Lancet. 2007 Jan 20;369(9557):229–42. https://doi.org/10.1016/S0140-6736(07)60112-3 PMID:17240290
13. Bowman BT, Donovan S, Burns MS, National Research Council (US). Committee on Early Childhood Pedagogy. Eager to learn: educating our preschoolers. Washington, Dc: National Academy Press; 2001.
14. Sylva K, Melhuish E, Sammons P, Siraj-Blatchford I, Taggart B. The Effective Provision of Pre-School Education (EPPE) Project: findings from pre-school to end of key stage 1. 2004 (https://dera.ioe.ac.uk/8543/7/SSU-SF-2004-01.pdf, accessed 3 August 2021).
15. San Francisco AR, Arias M, Villers R. Quality early childhood education in Costa Rica? Policy, practice, outcomes and challenges. Early Years. 2005;25(2):113–27. https://doi.org/10.1080/09575140500127956
16. Apolitical. Should preschool be mandatory? Costa Rica thinks so [website]. 2018 (https://apolitical.co/en/solution_article/should-preschool-be-mandatory-costa-rica-thinks-so, accessed 3 August 2021).
17. Early childhood development [website]. UNICEF; 2012 (https://www.unicef.org/early-childhood-development, accessed 3 August 2021).
18. Bago J-L, Ouédraogo M, Akakpo K, Lompo ML, Souratié W dite M, Ouédraogo E. Early childhood education and child develop-ment: new evidence from Ghana. Child Youth Services Rev. 2020; 108:104620. https://doi.org/10.1016/j.childyouth.2019.104620
19. Multiple Indicator Cluster Survey (MICS 2017/18), survey findings report. Accra: Ghana Statistical Service; 2018.
20. Sikder S, Banu LFA. Early childhood care and education in Bangladesh: a review of policies, practices and research. In: Fleer M, van Oers B, editors. International Handbook of Early Childhood Education. Springer; 2018;569–87.
21. Hamadani JD, Nahar B, Huda SN, Tofail F. Integrating early child development programs into health and nutrition services in Bangladesh: benefits and challenges. Ann N Y Acad Sci. 2014 Jan;1308(1):192–203. https://doi.org/10.1111/nyas.12366 PMID:24571219
22. Bangladesh Bureau of Statistics (BBS) and UNICEF Bangladesh. Progotir pathey, Bangladesh Multiple Indicator Cluster Survey 2019, survey findings report. Dhaka: BBS; 2019 (https://www.unicef.org/bangladesh/media/3281/file/Bangladesh%202019%20MICS%20Report_English.pdf, accessed 3 August 2021).
23. Ministerio de Salud (MS), Instituto Nacional de Estadistica y Censos (INEC) y Fondo de las Naciones Unidas para la Infancia (UNICEF). Encuesta de Mujeres, Niñez y Adolescencia (EMNA), Informe de resultados de la encuesta. San José, Costa Rica; 2018 (https://www.unicef.org/costarica/media/436/file/Encuesta-de-mujeres-ninez-y-adolescencia-2018.pdf, accessed 3 August 2021).
24. Palloni G. Childhood health and the wantedness of male and female children. J Dev Econ. 2017;126:19–32. https://doi.org/10.1016/j.jdeveco.2016.11.005
Book 27-11.indb 1076Book 27-11.indb 1076 06/12/2021 12:39 PM06/12/2021 12:39 PM
1077
Research article EMHJ – Vol. 27 No. 11 – 2021
25. Little M, Kohm A, Thompson R. The impact of residential placement on child development: research and policy implications. Int J Soc Welf. 2005 Jul;14(3):200–9. https://doi.org/10.1111/j.1468-2397.2005.00360.x
26. Smith LC, Ruel MT, Ndiaye A. Why is child malnutrition lower in urban than in rural areas? Evidence from 36 developing coun-tries. World Dev. 2005 Aug;33(8):1285–305. https://doi.org/10.1016/j.worlddev.2005.03.002
27. Coleman M, Ganong LH, Clark JM, Madsen R. Parenting perceptions in rural and urban families: is there a difference? J Mar-riage Fam. 1989 May;51(2):329–35. https://doi.org/10.2307/352496
28. Bhuiya A, Streatfield K. Mothers’ education and survival of female children in a rural area of Bangladesh. Popul Stud. 1991 Jul;45(2):253–64. https://www.jstor.org/stable/2174782
29. Cui Y, Liu H, Zhao L. Mother’s education and child development: evidence from the compulsory school reform in China. J Comp Econ. 2019 Sep;47(3):669–92. https://doi.org/10.1016/j.jce.2019.04.001
30. Black MM, Walker SP, Fernald LCH, Andersen CT, DiGirolamo AM, Lu C, et al. Early childhood development coming of age: science through the life course. Lancet. 2017 Jan 7;389(10064):77–90. https://doi.org/10.1016/S0140-6736(16)31389-7 PMID:27717614
31. Hamadani JD, Mehrin SF, Tofail F, Hasan MI, Huda SN, Baker-Henningham H, et al. Integrating an early childhood develop-ment programme into Bangladeshi primary health-care services: an open-label, cluster-randomised controlled trial. Lancet Glob Health. 2019 Mar 1;7(3):e366–75. https://doi.org/10.1016/S2214-109X(18)30535-7
32. Rubio‐Codina M, Grantham‐McGregor S. Evolution of the wealth gap in child development and mediating pathways: evidence from a longitudinal study in Bogota, Colombia. Dev Sci. 2019 Sep;22(5):e12810. https://doi.org/10.1111/desc.12810
33. Aboud FE, Akhter S. A cluster-randomized evaluation of a responsive stimulation and feeding intervention in Bangladesh. Pedi-atrics. 2011 May;127(5):e1191–7. https://doi.org/10.1542/peds.2010-2160 PMID:21502222
34. Dickinson DK, Griffith JA, Golinkoff RM, Hirsh-Pasek K. How reading books fosters language development around the world. Child Dev Res. 2012;Article ID 602807. https://doi.org/10.1155/2012/602807
35. Dünser A, Hornecker E. An observational study of children interacting with an augmented story book. In: Pan Z, Zhang X, El Rhalibi A, Woo W, Li Y, editors. Technologies for e-learning and digital entertainment. Springer Nature; 2007:305–15.
Book 27-11.indb 1077Book 27-11.indb 1077 06/12/2021 12:39 PM06/12/2021 12:39 PM

1078
Research article EMHJ – Vol. 27 No. 11 – 2021
Association of clinical features of typhoid fever with socioeconomic status in PakistanMuhammad Samsoor Zarak,1 Hamaiyal Sana,2 Muzhgan Shah,2 Shabir Lehri,2 Mahekan Saghir,2 Qandeel Gul,2 Muhammad Saood,3 Aqeel Nasim3 and Noman ul haq3.
1West Virginia University Health Sciences Centre, Morgantown, West Virginia, United States of America (Correspondence to: M Samsoor Zarak: [email protected]). 2Bolan Medical College, Brewery Road, Quetta, Pakistan. 3Department of Pharmacy Practice, University of Balochistan, Quetta, Pakistan.
AbstractBackground: Typhoid fever is spread by ingestion of contaminated food or water, which is linked to infrastructure; spe-cifically, sewage and sanitation. In developing countries, infrastructure varies according to socioeconomic status (SES). Balochistan is the least developed province of Pakistan. Aims: To analyse the association between the clinical features of typhoid fever and socioeconomic status.Methods: A quantitative, cross-sectional study was conducted in Quetta, Balochistan, Pakistan. Between May and Oc-tober 2017, 143 patients presented to tertiary care hospitals and private clinics with a complaint of fever lasting ~3 days, along with a clinical history of headache, malaise, diarrhoea or constipation, abdominal pain, dry cough, and anorexia. All patients had a positive blood culture for Salmonella enterica serotype Typhi. Eighteen patients dropped out of the study, leaving 125.Results: Seventy (56%) participants had low socioeconomic status (SES), 40 (32%) middle SES and 15( 12%) high SES. The strongest predictors of presenting with typhoid fever were patients’ clinical condition when presenting to health facilities, followed by SES. Most respondents had a treatment duration of 1–2 weeks. SES had a high impact on source of drinking water supply.Conclusion: The strongest predictor of reporting typhoid fever was the current clinical condition of the patients, followed closely by SES. The incidence of typhoid fever in the low SES patients was almost the same as in the middle and high SES patients. Patients with low SES were more susceptible to contracting typhoid fever due to poor health status and facilities.Keywords: Balochistan, socioeconomic status, typhoid fever, enteric fever, Pakistan.Citation: Samsoor Zarak M; Sana H; Shah M; Lehri S; Saghir M; Gul Q. et al. Association of clinical features of typhoid fever with socioeconomic status in Pakistan. East Mediterr Health J. 2021;27(11):1078−1083. https://doi.org/10.26719/emhj.21.054Received: 25/09/19; accepted: 19/04/21 Copyright © World Health Organization (WHO) 2021. Open Access. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license (https://creativecommons.org/licenses/by-nc-sa/3.0/igo)
IntroductionTyphoid fever is a severe illness caused primarily by Gram-negative Salmonella enterica serotype Typhi (1). It is indicated by nonspecific symptoms such as continuous fever, headache, nausea, poor appetite, lethargy, diar-rhoea and sometimes constipation (2). Other clinical fea-tures include splenomegaly, hepatomegaly, rose spots, and lethal intestinal perforation (1). It is contracted via the faecal–oral route by ingestion of food or water contami-nated with Salmonella species. Poor hygiene and sewage are considered to be contributing factors. The global bur-den of typhoid fever over the past few decades shows that there are 21.6 million cases globally and ~216 500 deaths annually (3). The annual incidence of typhoid fever in Asia is > 100/100 000 cases (4). More than 90% of typhoid fever cases arise from South and Southeast Asia (3), main-ly Pakistan, India, China, Indonesia and Viet Nam, where the disease is still considered to be endemic (4).
Pakistan is a developing country with a rapidly growing population and less than satisfactory water, food and hygiene measures that result in a flourishing habitat for infectious diseases. According to a study in
2013 in Quetta, 18.6% of paediatric patients had positive serological tests for typhoid fever (5). In Karachi, the incidence of typhoid fever was 710/100 000 when diagnosed by serological tests, and almost 170/100 000 when diagnosed by blood culture (6).
Health issues are frequently related to socioeconomic status (SES), which serves as a reliable indicator of population mortality and morbidity (7). Most studies have shed light on health-related issues associated with low SES; mainly because individuals with low SES are more susceptible to illness and death compared with middle and high SES. Typhoid fever remains a poorly characterized disease, with uncertain and often inaccessible methods of diagnosis and lack of data about the total global burden (8). It is hard to understand the incidence and prevalence patterns of typhoid fever among the population due to its often random occurrence without much distinction for SES or age.
The present study is believed to be the first to analyse the association of typhoid fever and its clinical features, such as signs and symptoms, duration and treatment, with SES.
Book 27-11.indb 1078Book 27-11.indb 1078 06/12/2021 12:39 PM06/12/2021 12:39 PM
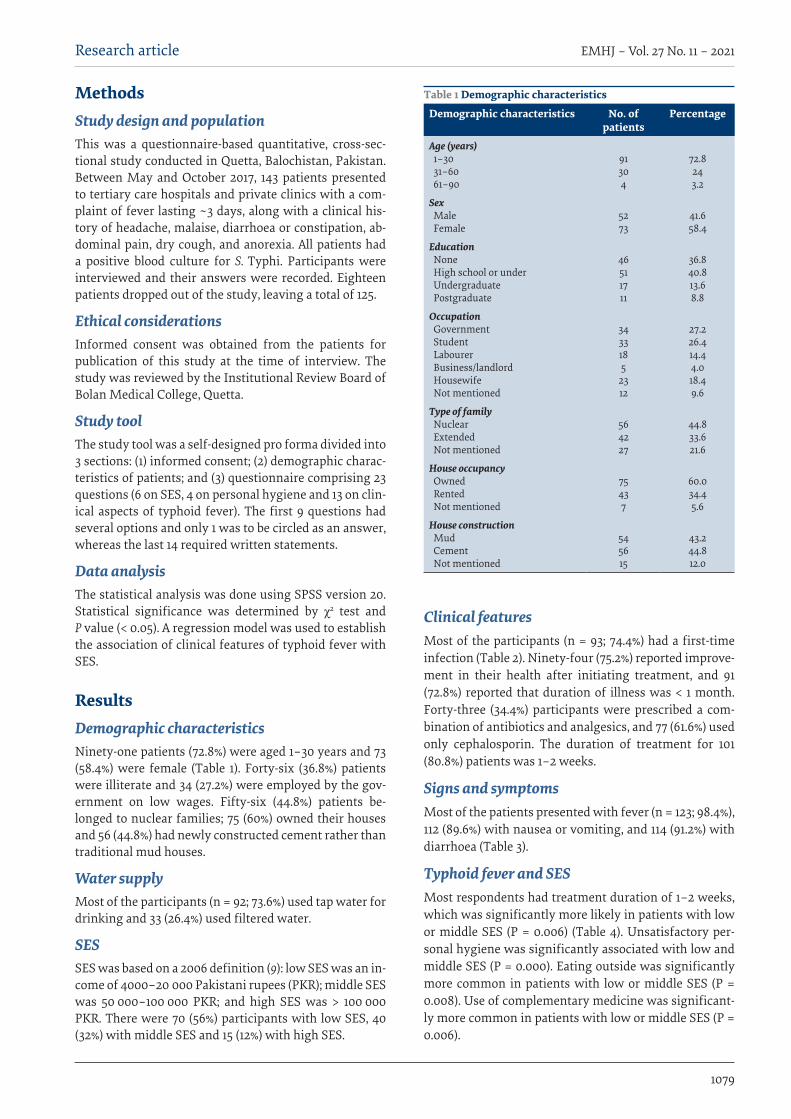
1079
Research article EMHJ – Vol. 27 No. 11 – 2021
Methods Study design and populationThis was a questionnaire-based quantitative, cross-sec-tional study conducted in Quetta, Balochistan, Pakistan. Between May and October 2017, 143 patients presented to tertiary care hospitals and private clinics with a com-plaint of fever lasting ~3 days, along with a clinical his-tory of headache, malaise, diarrhoea or constipation, ab-dominal pain, dry cough, and anorexia. All patients had a positive blood culture for S. Typhi. Participants were interviewed and their answers were recorded. Eighteen patients dropped out of the study, leaving a total of 125.
Ethical considerationsInformed consent was obtained from the patients for publication of this study at the time of interview. The study was reviewed by the Institutional Review Board of Bolan Medical College, Quetta.
Study toolThe study tool was a self-designed pro forma divided into 3 sections: (1) informed consent; (2) demographic charac-teristics of patients; and (3) questionnaire comprising 23 questions (6 on SES, 4 on personal hygiene and 13 on clin-ical aspects of typhoid fever). The first 9 questions had several options and only 1 was to be circled as an answer, whereas the last 14 required written statements.
Data analysisThe statistical analysis was done using SPSS version 20. Statistical significance was determined by χ2 test and P value (< 0.05). A regression model was used to establish the association of clinical features of typhoid fever with SES.
ResultsDemographic characteristicsNinety-one patients (72.8%) were aged 1–30 years and 73 (58.4%) were female (Table 1). Forty-six (36.8%) patients were illiterate and 34 (27.2%) were employed by the gov-ernment on low wages. Fifty-six (44.8%) patients be-longed to nuclear families; 75 (60%) owned their houses and 56 (44.8%) had newly constructed cement rather than traditional mud houses.
Water supplyMost of the participants (n = 92; 73.6%) used tap water for drinking and 33 (26.4%) used filtered water.
SESSES was based on a 2006 definition (9): low SES was an in-come of 4000–20 000 Pakistani rupees (PKR); middle SES was 50 000–100 000 PKR; and high SES was > 100 000 PKR. There were 70 (56%) participants with low SES, 40 (32%) with middle SES and 15 (12%) with high SES.
Clinical featuresMost of the participants (n = 93; 74.4%) had a first-time infection (Table 2). Ninety-four (75.2%) reported improve-ment in their health after initiating treatment, and 91 (72.8%) reported that duration of illness was < 1 month. Forty-three (34.4%) participants were prescribed a com-bination of antibiotics and analgesics, and 77 (61.6%) used only cephalosporin. The duration of treatment for 101 (80.8%) patients was 1–2 weeks.
Signs and symptoms Most of the patients presented with fever (n = 123; 98.4%), 112 (89.6%) with nausea or vomiting, and 114 (91.2%) with diarrhoea (Table 3).
Typhoid fever and SES Most respondents had treatment duration of 1–2 weeks, which was significantly more likely in patients with low or middle SES (P = 0.006) (Table 4). Unsatisfactory per-sonal hygiene was significantly associated with low and middle SES (P = 0.000). Eating outside was significantly more common in patients with low or middle SES (P = 0.008). Use of complementary medicine was significant-ly more common in patients with low or middle SES (P = 0.006).
Table 1 Demographic characteristics
Demographic characteristics No. of patients
Percentage
Age (years) 1–30 31–60 61–90
91304
72.8243.2
Sex Male Female
5273
41.658.4
Education None High school or under Undergraduate Postgraduate
46511711
36.840.813.68.8
Occupation Government Student Labourer Business/landlord Housewife Not mentioned
3433185
2312
27.226.414.44.018.49.6
Type of family Nuclear Extended Not mentioned
564227
44.833.621.6
House occupancy Owned Rented Not mentioned
75437
60.034.45.6
House construction Mud Cement Not mentioned
545615
43.244.812.0
Book 27-11.indb 1079Book 27-11.indb 1079 06/12/2021 12:39 PM06/12/2021 12:39 PM
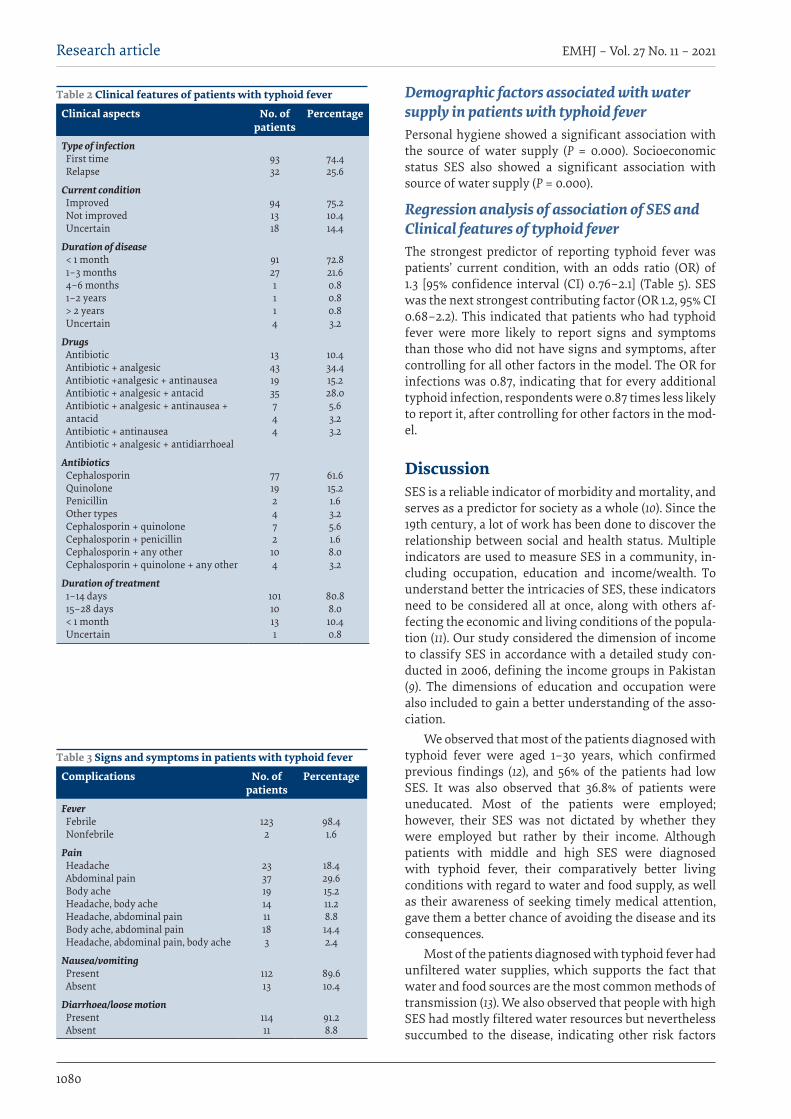
1080
Research article EMHJ – Vol. 27 No. 11 – 2021
Demographic factors associated with water supply in patients with typhoid fever Personal hygiene showed a significant association with the source of water supply (P = 0.000). Socioeconomic status SES also showed a significant association with source of water supply (P = 0.000).
Regression analysis of association of SES and Clinical features of typhoid feverThe strongest predictor of reporting typhoid fever was patients’ current condition, with an odds ratio (OR) of 1.3 [95% confidence interval (CI) 0.76–2.1] (Table 5). SES was the next strongest contributing factor (OR 1.2, 95% CI 0.68–2.2). This indicated that patients who had typhoid fever were more likely to report signs and symptoms than those who did not have signs and symptoms, after controlling for all other factors in the model. The OR for infections was 0.87, indicating that for every additional typhoid infection, respondents were 0.87 times less likely to report it, after controlling for other factors in the mod-el.
DiscussionSES is a reliable indicator of morbidity and mortality, and serves as a predictor for society as a whole (10). Since the 19th century, a lot of work has been done to discover the relationship between social and health status. Multiple indicators are used to measure SES in a community, in-cluding occupation, education and income/wealth. To understand better the intricacies of SES, these indicators need to be considered all at once, along with others af-fecting the economic and living conditions of the popula-tion (11). Our study considered the dimension of income to classify SES in accordance with a detailed study con-ducted in 2006, defining the income groups in Pakistan (9). The dimensions of education and occupation were also included to gain a better understanding of the asso-ciation.
We observed that most of the patients diagnosed with typhoid fever were aged 1–30 years, which confirmed previous findings (12), and 56% of the patients had low SES. It was also observed that 36.8% of patients were uneducated. Most of the patients were employed; however, their SES was not dictated by whether they were employed but rather by their income. Although patients with middle and high SES were diagnosed with typhoid fever, their comparatively better living conditions with regard to water and food supply, as well as their awareness of seeking timely medical attention, gave them a better chance of avoiding the disease and its consequences.
Most of the patients diagnosed with typhoid fever had unfiltered water supplies, which supports the fact that water and food sources are the most common methods of transmission (13). We also observed that people with high SES had mostly filtered water resources but nevertheless succumbed to the disease, indicating other risk factors
Table 2 Clinical features of patients with typhoid fever
Clinical aspects No. of patients
Percentage
Type of infection First time Relapse
9332
74.425.6
Current condition Improved Not improved Uncertain
941318
75.210.414.4
Duration of disease < 1 month 1–3 months 4–6 months 1–2 years > 2 years Uncertain
91271114
72.821.60.80.80.83.2
Drugs Antibiotic Antibiotic + analgesic Antibiotic +analgesic + antinausea Antibiotic + analgesic + antacid Antibiotic + analgesic + antinausea + antacid Antibiotic + antinausea Antibiotic + analgesic + antidiarrhoeal
13431935744
10.434.415.228.05.63.23.2
Antibiotics Cephalosporin Quinolone Penicillin Other types Cephalosporin + quinolone Cephalosporin + penicillin Cephalosporin + any other Cephalosporin + quinolone + any other
77192472104
61.615.21.63.25.61.68.03.2
Duration of treatment 1–14 days 15–28 days < 1 month Uncertain
10110131
80.88.010.40.8
Table 3 Signs and symptoms in patients with typhoid fever
Complications No. of patients
Percentage
Fever Febrile Nonfebrile
1232
98.41.6
Pain Headache Abdominal pain Body ache Headache, body ache Headache, abdominal pain Body ache, abdominal pain Headache, abdominal pain, body ache
2337191411183
18.429.615.211.28.814.42.4
Nausea/vomiting Present Absent
11213
89.610.4
Diarrhoea/loose motion Present Absent
11411
91.28.8
Book 27-11.indb 1080Book 27-11.indb 1080 06/12/2021 12:39 PM06/12/2021 12:39 PM
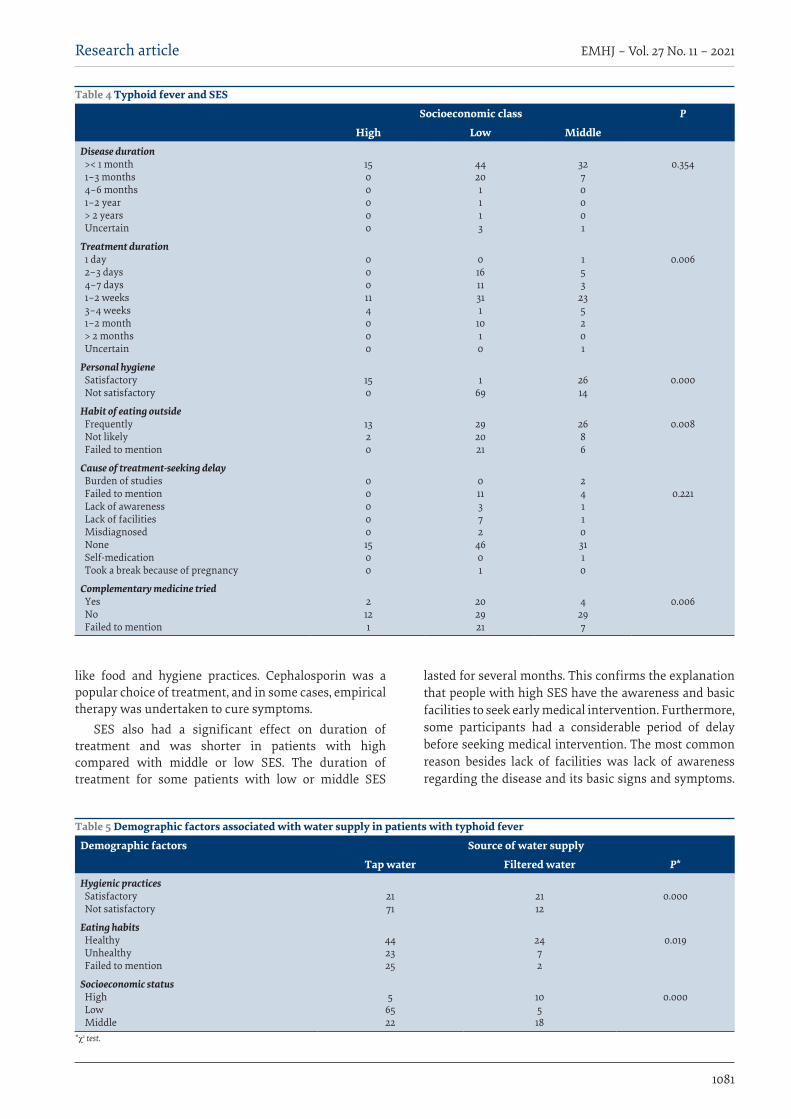
1081
Research article EMHJ – Vol. 27 No. 11 – 2021
like food and hygiene practices. Cephalosporin was a popular choice of treatment, and in some cases, empirical therapy was undertaken to cure symptoms.
SES also had a significant effect on duration of treatment and was shorter in patients with high compared with middle or low SES. The duration of treatment for some patients with low or middle SES
lasted for several months. This confirms the explanation that people with high SES have the awareness and basic facilities to seek early medical intervention. Furthermore, some participants had a considerable period of delay before seeking medical intervention. The most common reason besides lack of facilities was lack of awareness regarding the disease and its basic signs and symptoms.
Table 4 Typhoid fever and SES
Socioeconomic class P
High Low MiddleDisease duration >< 1 month 1–3 months 4–6 months 1–2 year > 2 years Uncertain
1500000
44201113
3270001
0.354
Treatment duration 1 day 2–3 days 4–7 days 1–2 weeks 3–4 weeks 1–2 month > 2 months Uncertain
000114000
01611311
1010
153
235201
0.006
Personal hygiene Satisfactory Not satisfactory
150
1
69
2614
0.000
Habit of eating outside Frequently Not likely Failed to mention
1320
292021
2686
0.008
Cause of treatment-seeking delay Burden of studies Failed to mention Lack of awareness Lack of facilities Misdiagnosed None Self-medication Took a break because of pregnancy
000001500
011372
4601
241103110
0.221
Complementary medicine tried Yes No Failed to mention
2121
202921
4297
0.006
Table 5 Demographic factors associated with water supply in patients with typhoid fever
Demographic factors Source of water supply
Tap water Filtered water P* Hygienic practices Satisfactory Not satisfactory
2171
2112
0.000
Eating habits Healthy Unhealthy Failed to mention
442325
2472
0.019
Socioeconomic status High Low Middle
5
6522
10518
0.000
*χ2 test.
Book 27-11.indb 1081Book 27-11.indb 1081 06/12/2021 12:39 PM06/12/2021 12:39 PM

1082
Research article EMHJ – Vol. 27 No. 11 – 2021
Patients, especially those with low SES, were in the habit of seeking treatment with complementary medicine.
SES played a significant role in patients’ hygiene, indicating poor hygienic practice in those with low SES. Typhoid fever was most commonly observed in patients with low SES but it was also seen in those with high SES, which suggests that SES does not necessarily dictate the causative pattern of typhoid fever. Its occurrence in less-privileged people is understandable due to lack of education regarding the disease and collective poor living conditions and health facilities. The fact that typhoid fever affects the middle and high SES groups in roughly the same measure gives it a unique and confounding causative pattern.
The largest contributor to reporting a case of typhoid fever was the current condition of the patients, followed closely by SES. We also observed that patients who had typhoid fever were more likely to report signs and symptoms of the disease than were those who did not have signs and symptoms, after controlling for other factors in the model.
One limitation of the present study was that it was based on a small sample. Further research in a larger population-based study may give better and more consistent results.
ConclusionTyphoid fever remains one of the most poorly character-ized diseases even today. This is mainly due to the lack of data on the global burden of the disease and controversies regarding the accuracy of the diagnostic tests, and lack of awareness in the general population. Our study con-cluded that the largest contributor to reporting typhoid fever was the current condition of the patients followed closely by SES. We showed that the incidence pattern of typhoid fever had no distinction for SES and the disease affected people with low SES in almost the same meas-ure as those with middle and high SES. However, patients with low SES are more susceptible to contracting typhoid fever with more distressing signs, symptoms and disease duration due to meagre health education and facilities. There is a need for health professionals and the general population to address typhoid fever, prioritizing low and middle SES and poor health facilities, which pose a threat as great as multidrug-resistant bacteria.
Funding: None.
Competing interests: None declared.
Lien entre le tableau clinique de la fièvre typhoïde et le statut socio-économique au PakistanRésuméContexte : La fièvre typhoïde se propage par ingestion d'eau ou d'aliments contaminés, elle-même liée aux infrastructures, et plus particulièrement aux systèmes d'égout et d'assainissement de l'eau. Dans les pays en développement, les infrastructures varient en fonction du statut socio-économique. Le Baloutchistan est la province la moins développée du Pakistan. Objectifs : Analyser le lien entre le tableau clinique de la fièvre typhoïde et le statut socio-économique des patients.Méthodes : Une étude transversale quantitative a été menée à Quetta, au Baloutchistan (Pakistan). Entre mai et octobre 2017, 143 patients ont consulté dans des hôpitaux de soins tertiaires et des cliniques privées pour une fièvre qui persistait depuis environ trois jours, accompagnée d’antécédents cliniques de céphalées, de malaise, de diarrhée ou de constipation, de douleurs abdominales, de toux sèche et d'anorexie. Tous les patients présentaient une hémoculture positive pour la Salmonella enterica sérotype Typhi. Dix-huit patients ont quitté l'étude, qui s'est poursuivie avec les 125 restants.Résultats : Soixante-dix participants (56 %) avaient un statut socio-économique faible, 40 (32 %) avaient un statut moyen et 15 (12 %) avaient un statut élevé. L'état clinique des patients lors de leur arrivée dans les établissements de santé, suivis par le statut socio-économique étaient les principaux facteurs prédictifs de consultation pour symptômes de fièvre typhoïde. La plupart des participants ont reçu un traitement dont la durée était d’une à deux semaines. Le statut socio-économique avait un impact important sur la source d'approvisionnement en eau potable.Conclusion : Le principal facteur prédictif de déclaration de symptômes de fièvre typhoïde était l'état clinique des patients au moment de leur arrivée dans l’établissement de santé, suivi de près par le statut socio-économique. L'incidence de la fièvre typhoïde chez les patients de faible statut socio-économique était presque la même que chez les patients de statut moyen ou élevé. Les patients ayant un statut socio-économique faible étaient plus susceptibles de contracter la fièvre typhoïde en raison de leur mauvais état de santé et d'installations sanitaires médiocres.
Book 27-11.indb 1082Book 27-11.indb 1082 06/12/2021 12:39 PM06/12/2021 12:39 PM
1083
Research article EMHJ – Vol. 27 No. 11 – 2021
References1. Hosoglu S, Aldemir M, Akalin S, Geyik MF, Tacyildiz IH, Loeb M. Risk factors for enteric perforation in patients with typhoid
fever. Am J Epidemiol. 2004 Jul 1;160(1):46–50. https://doi.org/10.1093/aje/kwh172 PMID:15229116
2. Klotz SA, Jorgensen JH, Buckwold FJ, Craven PC. Typhoid fever: an epidemic with remarkably few clinical signs and symptoms. Arch Intern Med. 1984 Mar;144(3):533–7. https://doi.org/10.1001/archinte.144.3.533 PMID:6703825
3. Crump JA, Luby SP, Mintz ED. The global burden of typhoid fever. Bull World Health Organ. 2004 May;82(5):346–53. PMID:15298225
4. Ochiai RL, Acosta CJ, Danovaro-Holliday M, Baiqing D, Bhattacharya SK, Agtini MD, et al. A study of typhoid fever in five Asian countries: disease burden and implications for controls. Bull World Health Organ. 2008 Apr;86(4):260–8. https://doi.org/10.2471/blt.06.039818 PMID:18438514
5. Khan MN, Shafee M, Hussain K, Samad A, Awan MA, Manan A, et al. Typhoid fever in paediatric patients in Quetta, Balochistan, Pakistan. Pak J Med Sci. 2013 Jul;29(4):929–32. https://doi.org/10.12669/pjms.294.3251 PMID:24353661
6. Siddiqui FJ, Rabbani F, Hasan R, Nizami SQ, Bhutta ZA. Typhoid fever in children: some epidemiological considerations from Karachi, Pakistan. Int J Infect Dis. 2006 May;10(3):215–22. https://doi.org/10.1016/j.ijid.2005.03.010 PMID:16431148
7. Feinstein JS. The relationship between socioeconomic status and health: a review of the literature. Milbank Q. 1993;71(2):279–322. PMID:8510603
8. Crump J, Ram P, Gupta S, Miller M, Mintz E. Part I. Analysis of data gaps pertaining to Salmonella enterica serotype Typhi infec-tions in low and medium human development index countries, 1984–2005. Epidemiol Infect. 2008 Apr;136(4):436–48. https://doi.org/10.1017/S0950268807009338 PMID:17686194
9. Subohi A. Defining income groups. Dawn. 20 November 2006 (https://www.dawn.com/news/219652/defining-income-groups, accessed 22 July 2021).
10. Winkleby MA, Jatulis DE, Frank E, Fortmann SP. Socioeconomic status and health: how education, income, and occupation con-tribute to risk factors for cardiovascular disease. Am J Public Health. 1992 Jun;82(6):816–20. https://doi.org/10.2105/ajph.82.6.816 PMID:1585961
11. Durkin MS, Islam S, Hasan Z, Zaman S. Measures of socioeconomic status for child health research: comparative results from Bangladesh and Pakistan. Soc Sci Med. 1994 May;38(9):1289–97. https://doi.org/10.1016/0277-9536(94)90192-9 PMID:8016692
12. Parry CM. Epidemiological and clinical aspects of human typhoid fever. Cambridge: Cambridge University Press; 2006.
13. Crump JA, Mintz ED. Global trends in typhoid and paratyphoid fever. Clin Infect Dis. 2010 Jan 15;50(2):241–6. https://doi.org/10.1086/649541 PMID:20014951
االرتباط بني السامت الرسيرية حلمى التيفود والوضع االجتامعي واالقتصادي يف باكستانحممد سمسور زراك، محايال ثناء، مژگان شاہ، شبري هلري، ، ماهيكان صغري، قنديل جل، حممد سعود، عقيل نسيم، نعامن احلق
اخلالصةاخللفية: تنترش محى التيفود عن طريق تناول أغذية أو مياه ملوثة، وهو ما يرتبط بالبنية التحتية؛ وعىل وجه التحديد، مياه املجاري والرصف الصحي.
ويف البلدان النامية، تتفاوت البنى التحتية حسب الوضع االجتامعي واالقتصادي. وتعد بلوشستان املقاطعة األقل تنمية يف باكستان.األهداف: هدفت هذه الدراسة اىل حتليل االرتباط بني السامت الرسيرية حلمى التيفود والوضع االجتامعي واالقتصادي.
طرق البحث: أجريت دراسة كمية مقطعية يف كويتا، ببلوشستان، باكستان. ويف الفرتة ما بني مايو / أيار و أكتوبر/ ترشين األول 2017، قدم 143 مريضا إىل مستشفيات الرعاية التخصصية والعيادات اخلاصة بشكوى من محى استمرت 3 أيام تقريبا، إىل جانب وجود سوابق رسيرية متثلت يف ك، واإلسهال أو اإلمساك، وآالم البطن، والسعال اجلاف، وفقدان الشهية. وكانت نتيجة مزرعة الدم التي أجريت جلميع املرىض الصداع، والتوع
للكشف عن السلمونيال املعوية من النمط املصيل التيفي إجيابية. وخرج ثامنية عرش مريضا من الدراسة تاركني 125 آخرين.بينام كان متوسطا لدى 40 مشاركا )32%(، ومرتفعا لدى كان الوضع االجتامعي واالقتصادي منخفضا لدى سبعني مشاركا )%56(، النتائج: يتبعها الصحية، املرافق إىل قدومهم عند للمرىض الرسيرية احلالة التيفود بحمى التبليغ يف املنبئة العوامل أقوى وكانت .)%12( مشاركا 15وضعهم االجتامعي واالقتصادي. واستمرت مدة العالج لدى معظم املستجيبني مدة ترتاوح بني أسبوع واحد وأسبوعني. وكان للوضع االجتامعي
واالقتصادي تأثري كبري عىل مصدر إمدادات مياه الرشب.االستنتاجات: كان العامل املنبئ األقوى يف التبليغ بحمى التيفود هو احلالة الرسيرية احلالية للمرىض، يليها مبارشة الوضع االجتامعي واالقتصادي. وكان معدل اإلصابة بحمى التيفويد يف صفوف املرىض من ذوي الوضع االجتامعي واالقتصادي املنخفض مماثال تقريبا لنظريه يف صفوف املرىض من ذوي الوضع االجتامعي واالقتصادي املتوسط واملرتفع. وكان املرىض من ذوي الوضع االجتامعي واالقتصادي املنخفض أكثر عرضة لإلصابة
بحمى التيفود بسبب تدين الوضع الصحي واملرافق.
Book 27-11.indb 1083Book 27-11.indb 1083 06/12/2021 12:39 PM06/12/2021 12:39 PM

1084
Research article EMHJ – Vol. 27 No. 11 – 2021
Incidence of and factors associated with metabolic syndrome, south-east Islamic Republic of IranKhadijeh Farmanfarma,1 Alireza Ansari-Moghaddam,1 Mahmoud Kaykhaei,1 Mehdi Mohammadi,1 Hosein Adineh2 and Hasan Aliabd1
1Department of Epidemiology & Biostatistics, Health Promotion Research Center, Zahedan University of Medical Sciences, Zahedan, Islamic Republic of Iran. 2Department of Epidemiology & Biostatistics, School of Health, Iranshahr University of Medical Sciences, Iranshahr, Islamic Republic of Iran. (Correspondene to: Hasan O. Aliab: [email protected]).
AbstractBackground: Metabolic syndrome is an important cause of cardiovascular disease. Mortality from cardiovascular disease is 12.82 deaths/100 000 population in Zahedan, south-east Islamic Republic of Iran.Aims: This study aimed to determine the incidence of metabolic syndrome and its predicting factors in Zahedan city.Methods: All participants without metabolic syndrome in a 2009 study in Zahedan, available in 2017, were included in this study. Metabolic syndrome was diagnosed based on the criteria of several organizations. Anthropometric indices and blood pressure were measured and blood tests were done. Age-standardized incidence of metabolic syndrome was calcu-lated and its predictors were evaluated in a logistic regression analysis.Results: Mean age (standard deviation) of the participants was 45.46 (12.63) years in 2017. The incidence of metabolic syndrome varied from 17.21% to 27.18% depending on the criteria used and it was higher in women. High age-standardized incidence was associated with large waist circumference (55.81%) and high blood pressure (25.32%). The highest adjust-ed odds ratios (OR) for metabolic syndrome were for high triglycerides (OR = 23.75; 95% confidence interval (CI): 9.92–56.84%), large waist circumference (OR = 22.42; 95% CI: 9.03–55.70%), high blood pressure (OR = 16.91; 95% CI: 8.54–33.50%) and high fasting blood sugar (OR = 13.22; 95% CI: 6.74–25.94%). Waterpipe smoking, sex, low-density lipoprotein and wrist circumference were also associated with metabolic syndrome. Conclusions: The incidence of metabolic syndrome has increased in Zahedan. Effective, interventions, including to pro-mote healthy diet, physical activity and avoidance of waterpipe smoking, are needed to control this condition.Keywords: metabolic syndrome, incidence, risk factors, IranCitation: Farmanfarma K; Ansari-Moghaddam A; Kaykhaei M; Mohammad M; Adineh H; Aliab H. Incidence of and factors associated with metabolic syndrome, south-east Islamic Republic of Iran. East Mediterr Health J. 2021;27(11):1084–1091. https://doi.org/10.26719/emhj.21.051Received: 10/06/20; accepted: 04/04/21Copyright © World Health Organization (WHO) 2021. Open Access. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license (https://creativecommons.org/licenses/by-nc-sa/3.0/igo)
IntroductionMetabolic syndrome is an asymptomatic pathophysio-logical condition characterized by high blood pressure, central obesity, insulin resistance, dyslipidaemia and hyperglycaemia (1). The prevalence of this disorder has been increasing in recent years and stands at about 25% globally; it is therefore among the main health problems in the world (2,3). The incidence of metabolic syndrome has been reported to range from 28 persons per 1000 persons-year to more than 70 per 1000 persons-year in different regions of the world (4,5). As a result of rapid economic changes, the increased popularity of the west-ern lifestyle and lack of physical activity, the world faces the threat of obesity and type 2 diabetes epidemics. If the current trend in obesity and type 2 diabetes continues unchanged, the incidence of metabolic syndrome will be expected to increase, especially in developing countries (2,6). According to epidemiological studies, the incidence of metabolic syndrome is higher in women than men (5,7). Factors, such as socioeconomic status, lack of phys-ical activity, smoking, family history of diabetes, obesity and the western lifestyle, increase the risk of metabolic syndrome (8). Most studies on the incidence and risk fac-
tors of metabolic syndrome have been conducted in de-veloped countries or regions where the populations have a relatively high socioeconomic status. Few studies have been done in more deprived regions and regions with low income (9). Therefore, we aimed to determine the inci-dence and predictors of metabolic syndrome in Zahedan city (Sistan and Baluchestan province), south-eastern Is-lamic Republic of Iran. This city is among the most de-prived regions of the country and is situated in vicinity of Pakistan and Afghanistan.
MethodsStudy design and sampleA cohort study was conducted on the urban population of Zahedan city, south-eastern Islamic Republic of Iran.
A cross-sectional study was conducted on 1802 participants from September 2008 to March 2009 (10). The participants were Iranians aged more than 20 years with no intellectual disability or haemorrhagic diseases. According to random cluster sampling method, Zahedan was divided into 20 regions and number of participants were selected from each area proportional to size.
Book 27-11.indb 1084Book 27-11.indb 1084 06/12/2021 12:39 PM06/12/2021 12:39 PM
1085
Research article EMHJ – Vol. 27 No. 11 – 2021
In 2017, all participants without metabolic syndrome in 2009 were followed and invited to participate in the current study. In the 2009 study, 1351 people were found not to have metabolic syndrome based on International Diabetes Federation (IDF) criteria (11), 1424 based on National Cholesterol Education Program-Adult Treatment Panel, (NCEP-ATP) III criteria (11), and 1333 based on American Heart Association and National Heart, Lung and Blood Institute (AHA/NHLBI) criteria (11). In 2017, samples were selected based on IDF criteria (n = 585), NCEP-ATP III criteria (n = 622), and AHA/NHLBI criteria (n = 578).
Although, it was impossible to reach all eligible individuals from the study conducted in 2009, the number of missing participants was similar in all the clusters and the people surveyed were a reasonably good representation of the city. In 2017, the research team contacted the study participants through their profile recorded in 2009. An appointment was made with the participants and a trained team, including interviewers and a laboratory expert, visited them at their homes.
Data collectionThe objectives of the study were explained to individuals and those who signed the written informed consent form were enrolled in the study. Data were collected using standard questionnaires. Blood samples were collected after an 8–12 hours fasting period. Anthropometric indi-ces were measured.
Blood samples of the participants were centrifuged to separate serum and maintained for 24 hours at –20 °C and for 6 months at –80 °C. Serum glucose, triglycerides and cholesterol were measured based on calorimetric methods by standard kits (Bioteck) using an ELAN 2000 autoanalyser. High-density lipoprotein (HDL) and low-density lipoprotein (LDL) were measured by direct methods. Anthropometric indices (height, weight and waist circumference) were measured. Weight was measured using a Seca scale (precision: 100 g) while in light clothing and no shoes. Height was measured using a Seca stadiometer in a standing position without shoes and shoulders in a natural position (precision: 1 cm). Waist circumference was measured at the narrowest point at the end of natural exhalation, using a stretch-resistant cloth tape without any pressure on body (precision: 0.1 cm). Blood pressure (systolic and diastolic) was measured twice with 10 minutes between measurements using a standard sphygmomanometer with an appropriate arm cuff placed on the right arm after sitting for 15 minutes. The average of the two measurements was calculated and considered the final blood pressure.
Each participant had a face-to-face interview to complete a semistructured questionnaire to evaluate nutritional information, physical activity and waterpipe smoking.
Statistical analysisData were entered in SPSS, version 16. Mean and standard deviation (SD) were used to describe quantitative vari-
ables. Numbers and percentages were used to describe qualitative variables. Data were analysed the chi-squared test and logistic regression analysis with data presented as odds ratios (OR) and 95% confidence intervals (95% CI). For calculating age-standardized incidence rates of met-abolic syndrome and its components, participants were first classified into age groups based on their age in 2013, which was midpoint of study duration (2009–2017). The adjusted incidence rate in 2017 was the weighted mean of incidence rates in age groups weighted by the proportion of the population in 2015 census.
Ethical concernsThe review board of Zahden University of Medical Sciences appproved the study (number: 8140).
ResultsParticipants were selected based on IDF criteria (n = 585), NCEP-ATP III criteria (n = 622) and AHA/NHLBI criteria (n = 578). AHA/NHLBI criteria were used to describe the participants’ information because there were no statis-tically significant differences between different defini-tions. Thus, based on AHA/NHLBI criteria, 578 partici-pants (47.4% women and 52.6% men) were included in the 2017 study. Mean age of participants was 45.46 (SD 12.63) years at the end of follow-up period. About half of the par-ticipants (48.4%) had up to a high-school diploma, 34.6% had a university degree and 17.0% were illiterate in 2017.
Metabolic syndromeThe direct age-standardized incidence rate of metabolic syndrome was 27.18% (95% CI: 23.50–31.09%) based on AHA/NHLBI criteria, 24.48% (95% CI: 21.03–28.34%) based on IDF criteria, 19.73% (95% CI: 16.57–23.12%) based on NCEP-ATP III criteria and 17.21% (95% CI: 14.29–20.47%) based on ATP III criteria (Table 2). Crude and age-stand-ardized incidence rates of metabolic syndrome were higher in women than men based on all the criteria (Table 2). Incidence rate varied in men from 9.22% (95% CI: 6.33–12.95%) to 20.74% (95% CI: 16.25–25.83%), and in women from 26.86% (95% CI: 21.69–32.37%) to 35.27% (95% CI: 29.44–41.43%).
Components of metabolic syndromeBased on all the criteria used for measuring metabolic syndrome, the highest crude and age-standardized inci-dence rates of metabolic syndrome were associated with waist circumference and blood pressure and the lowest rates were associated with HDL cholesterol level (Table 4)
Based on the different diagnostic criteria, the age-standardized incidence rate for abnormal fasting blood sugar varied from 14.04% (11.39–17.10%) to 23.35% (95% CI: 19.89–27.12%). In all the calculations, the incidence rate was higher in women than men. The age-standardized incidence rate for abnormal triglycerides varied from 12.22% (95% CI: 9.53–15.15%) to 13.40% (95% CI: 10.79–16.39%). In all the calculations, the incidence rate was lower in women than men. The age-standardized
Book 27-11.indb 1085Book 27-11.indb 1085 06/12/2021 12:39 PM06/12/2021 12:39 PM
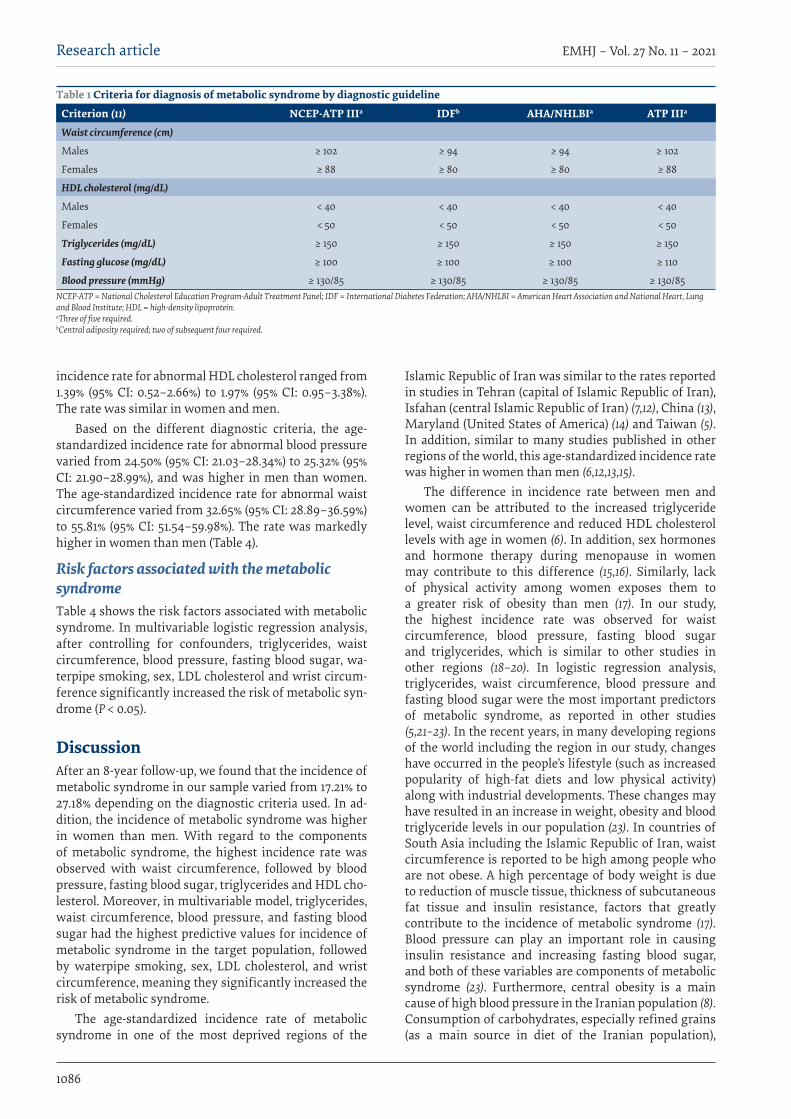
1086
Research article EMHJ – Vol. 27 No. 11 – 2021
incidence rate for abnormal HDL cholesterol ranged from 1.39% (95% CI: 0.52–2.66%) to 1.97% (95% CI: 0.95–3.38%). The rate was similar in women and men.
Based on the different diagnostic criteria, the age-standardized incidence rate for abnormal blood pressure varied from 24.50% (95% CI: 21.03–28.34%) to 25.32% (95% CI: 21.90–28.99%), and was higher in men than women. The age-standardized incidence rate for abnormal waist circumference varied from 32.65% (95% CI: 28.89–36.59%) to 55.81% (95% CI: 51.54–59.98%). The rate was markedly higher in women than men (Table 4).
Risk factors associated with the metabolic syndromeTable 4 shows the risk factors associated with metabolic syndrome. In multivariable logistic regression analysis, after controlling for confounders, triglycerides, waist circumference, blood pressure, fasting blood sugar, wa-terpipe smoking, sex, LDL cholesterol and wrist circum-ference significantly increased the risk of metabolic syn-drome (P < 0.05).
DiscussionAfter an 8-year follow-up, we found that the incidence of metabolic syndrome in our sample varied from 17.21% to 27.18% depending on the diagnostic criteria used. In ad-dition, the incidence of metabolic syndrome was higher in women than men. With regard to the components of metabolic syndrome, the highest incidence rate was observed with waist circumference, followed by blood pressure, fasting blood sugar, triglycerides and HDL cho-lesterol. Moreover, in multivariable model, triglycerides, waist circumference, blood pressure, and fasting blood sugar had the highest predictive values for incidence of metabolic syndrome in the target population, followed by waterpipe smoking, sex, LDL cholesterol, and wrist circumference, meaning they significantly increased the risk of metabolic syndrome.
The age-standardized incidence rate of metabolic syndrome in one of the most deprived regions of the
Islamic Republic of Iran was similar to the rates reported in studies in Tehran (capital of Islamic Republic of Iran), Isfahan (central Islamic Republic of Iran) (7,12), China (13), Maryland (United States of America) (14) and Taiwan (5). In addition, similar to many studies published in other regions of the world, this age-standardized incidence rate was higher in women than men (6,12,13,15).
The difference in incidence rate between men and women can be attributed to the increased triglyceride level, waist circumference and reduced HDL cholesterol levels with age in women (6). In addition, sex hormones and hormone therapy during menopause in women may contribute to this difference (15,16). Similarly, lack of physical activity among women exposes them to a greater risk of obesity than men (17). In our study, the highest incidence rate was observed for waist circumference, blood pressure, fasting blood sugar and triglycerides, which is similar to other studies in other regions (18–20). In logistic regression analysis, triglycerides, waist circumference, blood pressure and fasting blood sugar were the most important predictors of metabolic syndrome, as reported in other studies (5,21–23). In the recent years, in many developing regions of the world including the region in our study, changes have occurred in the people’s lifestyle (such as increased popularity of high-fat diets and low physical activity) along with industrial developments. These changes may have resulted in an increase in weight, obesity and blood triglyceride levels in our population (23). In countries of South Asia including the Islamic Republic of Iran, waist circumference is reported to be high among people who are not obese. A high percentage of body weight is due to reduction of muscle tissue, thickness of subcutaneous fat tissue and insulin resistance, factors that greatly contribute to the incidence of metabolic syndrome (17). Blood pressure can play an important role in causing insulin resistance and increasing fasting blood sugar, and both of these variables are components of metabolic syndrome (23). Furthermore, central obesity is a main cause of high blood pressure in the Iranian population (8). Consumption of carbohydrates, especially refined grains (as a main source in diet of the Iranian population),
Table 1 Criteria for diagnosis of metabolic syndrome by diagnostic guideline
Criterion (11) NCEP-ATP IIIa IDFb AHA/NHLBIa ATP IIIa
Waist circumference (cm)
Males ≥ 102 ≥ 94 ≥ 94 ≥ 102
Females ≥ 88 ≥ 80 ≥ 80 ≥ 88
HDL cholesterol (mg/dL)
Males < 40 < 40 < 40 < 40
Females < 50 < 50 < 50 < 50
Triglycerides (mg/dL) ≥ 150 ≥ 150 ≥ 150 ≥ 150
Fasting glucose (mg/dL) ≥ 100 ≥ 100 ≥ 100 ≥ 110
Blood pressure (mmHg) ≥ 130/85 ≥ 130/85 ≥ 130/85 ≥ 130/85NCEP-ATP = National Cholesterol Education Program-Adult Treatment Panel; IDF = International Diabetes Federation; AHA/NHLBI = American Heart Association and National Heart, Lung and Blood Institute; HDL = high-density lipoprotein. aThree of five required. bCentral adiposity required; two of subsequent four required.
Book 27-11.indb 1086Book 27-11.indb 1086 06/12/2021 12:39 PM06/12/2021 12:39 PM
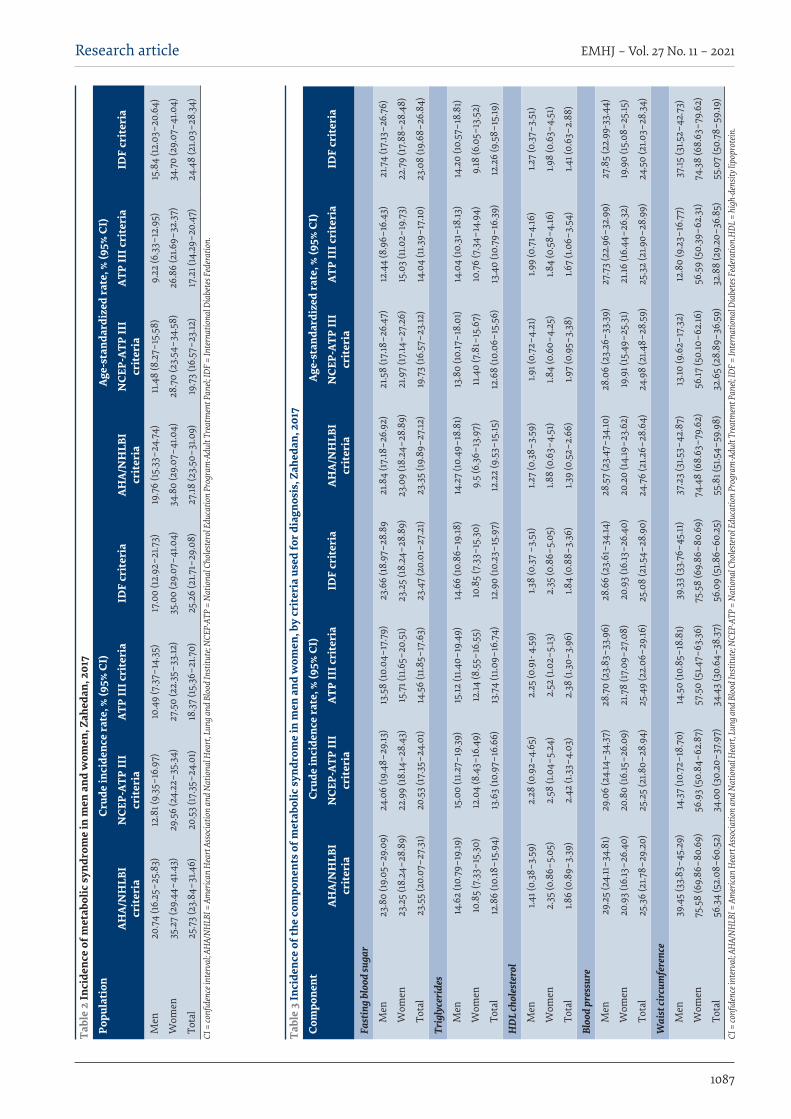
1087
Research article EMHJ – Vol. 27 No. 11 – 2021
Tabl
e 2
Inci
denc
e of
met
abol
ic sy
ndro
me
in m
en a
nd w
omen
, Zah
edan
, 201
7
Popu
lati
onCr
ude
inci
denc
e ra
te, %
(95%
CI)
Age-
stan
dard
ized
rate
, % (9
5% C
I)
AHA/
NH
LBI
crit
eria
NCE
P-AT
P II
I cr
iter
iaAT
P II
I cri
teri
aID
F cr
iter
iaAH
A/N
HLB
I cr
iter
iaN
CEP-
ATP
III
crit
eria
ATP
III c
rite
ria
IDF
crit
eria
Men
20.7
4 (16
.25–
25.8
3)12
.81 (
9.35
–16.
97)
10.4
9 (7
.37–
14.3
5)17
.00
(12.9
2–21
.73)
19.7
6 (15
.33–
24.7
4)11
.48
(8.2
7–15
.58)
9.22
(6.3
3–12
.95)
15.8
4 (12
.03–
20.6
4)
Wom
en35
.27
(29.
44–4
1.43)
29.5
6 (2
4.22
–35.
34)
27.5
0 (2
2.35
–33.
12)
35.0
0 (2
9.07
–41.0
4)34
.80
(29.
07–4
1.04)
28.7
0 (2
3.54
–34.
58)
26.8
6 (2
1.69–
32.3
7)34
.70
(29.
07–4
1.04)
Tota
l25
.73
(23.
84–3
1.46)
20.5
3 (17
.35–
24.0
1)18
.37
(15.3
6–21
.70)
25.2
6 (2
1.71–
29.0
8)27
.18 (2
3.50
–31.0
9)19
.73
(16.5
7–23
.12)
17.2
1 (14
.29–
20.4
7)24
.48
(21.0
3–28
.34)
CI =
confi
denc
e int
erva
l; AH
A/N
HLB
I = A
mer
ican
Hea
rt A
ssoc
iatio
n an
d N
atio
nal H
eart
, Lun
g and
Blo
od In
stitu
te; N
CEP-
ATP
= N
atio
nal C
holes
tero
l Edu
catio
n Pr
ogra
m-A
dult
Trea
tmen
t Pan
el; ID
F = In
tern
atio
nal D
iabe
tes F
eder
atio
n.
Tabl
e 3
Inci
denc
e of
the
com
pone
nts o
f met
abol
ic sy
ndro
me
in m
en a
nd w
omen
, by
crit
eria
use
d fo
r dia
gnos
is, Z
ahed
an, 2
017
Com
pone
ntCr
ude
inci
denc
e ra
te, %
(95%
CI)
Age-
stan
dard
ized
rate
, % (9
5% C
I)
AHA/
NH
LBI
crit
eria
NCE
P-AT
P II
I cr
iter
iaAT
P II
I cri
teri
aID
F cr
iter
iaAH
A/N
HLB
I cr
iter
iaN
CEP-
ATP
III
crit
eria
ATP
III c
rite
ria
IDF
crit
eria
Fast
ing
bloo
d su
gar
Men
23.8
0 (19
.05–
29.0
9)24
.06
(19.4
8–29
.13)
13.5
8 (10
.04–
17.7
9)23
.66
(18.9
7–28
.89
21.8
4 (17
.18–2
6.92
)21
.58
(17.18
–26.
47)
12.4
4 (8
.96–
16.4
3)21
.74
(17.13
–26.
76)
Wom
en23
.25
(18.2
4–28
.89)
22.9
9 (18
.14–2
8.43
)15
.71 (
11.6
5–20
.51)
23.2
5 (18
.24–
28.8
9)23
.09
(18.2
4–28
.89)
21.9
7 (17
.14–2
7.26
)15
.03
(11.0
2–19
.73)
22.7
9 (17
.88–
28.4
8)
Tota
l23
.55
(20.
07–2
7.31
)20
.53
(17.3
5–24
.01)
14.5
6 (11
.85–
17.6
3)23
.47
(20.
01–2
7.21
)23
.35
(19.8
9–27
.12)
19.7
3 (16
.57–
23.12
)14
.04
(11.3
9–17
.10)
23.0
8 (19
.68–
26.8
4)
Trig
lyce
ride
s
Men
14.6
2 (10
.79–
19.19
)15
.00
(11.2
7–19
.39)
15.12
(11.4
0–19
.49)
14.6
6 (10
.86–
19.18
)14
.27
(10.4
9–18
.81)
13.8
0 (10
.17–1
8.01
)14
.04
(10.3
1–18
.13)
14.2
0 (10
.57–
18.8
1)
Wom
en10
.85
(7.3
3–15
.30)
12.0
4 (8
.43–
16.4
9)12
.14 (8
.55–
16.5
5)10
.85
(7.3
3–15
.30)
9.5
(6.3
6–13
.97)
11.4
0 (7
.81–
15.6
7)10
.76
(7.3
4–14
.94)
9.18
(6.0
5–13
.52)
Tota
l12
.86
(10.18
–15.
94)
13.6
3 (10
.97–
16.6
6)13
.74
(11.0
9–16
.74)
12.9
0 (10
.23–
15.9
7)12
.22
(9.5
3–15
.15)
12.6
8 (10
.06–
15.5
6)13
.40
(10.7
9–16
.39)
12.2
6 (9
.58–
15.19
)
HD
L ch
oles
tero
l
Men
1.41 (
0.38
–3.5
9)2.
28 (0
.92–
4.65
)2.
25 (0
.91-
4.59
)1.3
8 (0
.37
–3.5
1)1.2
7 (0
.38–
3.59
)1.9
1 (0.
72–4
.21)
1.99
(0.7
1–4.
16)
1.27
(0.3
7–3.
51)
Wom
en2.
35 (0
.86–
5.05
)2.
58 (1
.04–
5.24
)2.
52 (1
.02–
5.13
)2.
35 (0
.86–
5.05
)1.8
8 (0
.63–
4.51
)1.8
4 (0
.60–
4.25
)
1.8
4 (0
.58–
4.16
)1.9
8 (0
.63–
4.51
)
Tota
l1.8
6 (0
.89–
3.39
)2.
42 (1
.33–
4.03
)2.
38 (1
.30–
3.96
)1.8
4 (0
.88–
3.36
)1.3
9 (0
.52–
2.66
)
1.97
(0.9
5–3.
38)
1.67
(1.06
–3.5
4)
1.4
1 (0.
63–2
.88)
Bloo
d pr
essu
re
Men
29.2
5 (2
4.11
–34.
81)
29.0
6 (2
4.14
–34.
37)
28.7
0 (2
3.83
–33.
96)
28.6
6 (2
3.61
–34.
14)
28.5
7 (2
3.47
–34.
10)
28.0
6 (2
3.26
–33.
39)
27.7
3 (2
2.96
–32.
99)
27.8
5 (2
2.99
-33.
44)
Wom
en20
.93
(16.13
–26.
40)
20.8
0 (16
.15–2
6.09
)21
.78
(17.0
9–27
.08)
20.
93 (1
6.13
–26.
40)
20.2
0 (14
.19–2
3.62
)19
.91 (
15.4
9–25
.31)
21.16
(16.
44–2
6.32
)19
.90
(15.0
8–25
.15)
Tota
l25
.36
(21.7
8–29
.20)
25.2
5 (2
1.80–
28.9
4)25
.49
(22.
06–2
9.16
)25
.08
(21.5
4–28
.90)
24.7
6 (2
1.26–
28.6
4)24
.98
(21.4
8–28
.59)
25.3
2 (2
1.90–
28.9
9)24
.50
(21.0
3–28
.34)
Wai
st ci
rcum
fere
nce
Men
39.4
5 (3
3.83
–45.
29)
14.3
7 (10
.72–
18.7
0)14
.50
(10.8
5–18
.81)
39.3
3 (3
3.76
–45.
11)
37.2
3 (3
1.53–
42.8
7)13
.10 (9
.62–
17.3
2)12
.80
(9.2
3–16
.77)
37.15
(31.5
2–42
.73)
Wom
en75
.58
(69.
86–8
0.69
)56
.93
(50.
84–6
2.87
)57
.50
(51.4
7–63
.36)
75.5
8 (6
9.86
–80.
69)
74.4
8 (6
8.63
–79.
62)
56.17
(50.
10–6
2.16
)56
.59
(50.
39–6
2.31
)74
.38
(68.
63–7
9.62
)
Tota
l56
.34
(52.
08–6
0.52
)34
.00
(30.
20–3
7.97
)34
.43
(30.
64–3
8.37
)56
.09
(51.8
6–60
.25)
55.8
1 (51
.54–
59.9
8)32
.65
(28.
89–3
6.59
)32
.88
(29.
20–3
6.85
)55
.07
(50.
78–5
9.19
)CI
= co
nfide
nce i
nter
val; A
HA/
NH
LBI =
Am
erica
n H
eart
Ass
ocia
tion
and
Nat
iona
l Hea
rt, L
ung a
nd B
lood
Inst
itute
; NCE
P-AT
P =
Nat
iona
l Cho
leste
rol E
duca
tion
Prog
ram
-Adu
lt Tr
eatm
ent P
anel;
IDF =
Inte
rnat
iona
l Dia
bete
s Fed
erat
ion.
HDL
= h
igh-
dens
ity li
popr
otein
.
Book 27-11.indb 1087Book 27-11.indb 1087 06/12/2021 12:39 PM06/12/2021 12:39 PM
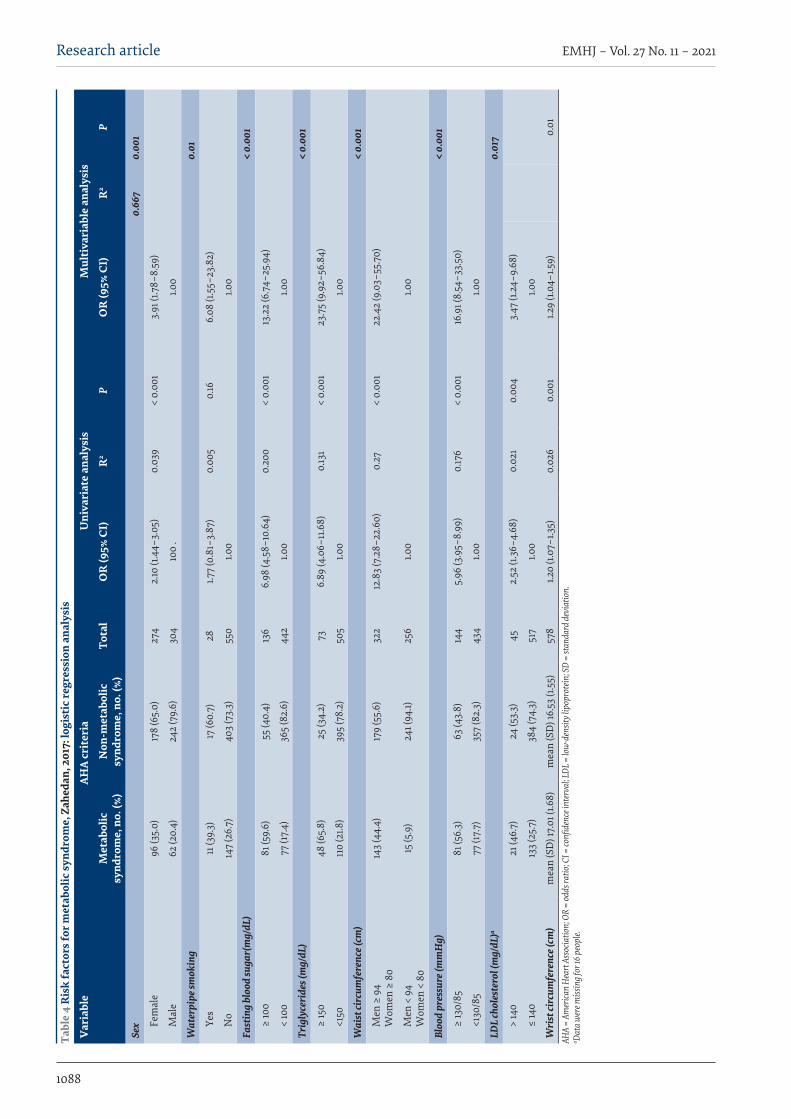
1088
Research article EMHJ – Vol. 27 No. 11 – 2021Ta
ble
4 R
isk
fact
ors f
or m
etab
olic
synd
rom
e, Z
ahed
an, 2
017:
logi
stic
regr
essi
on a
naly
sis
Var
iabl
eAH
A cr
iter
iaU
niva
riat
e an
alys
isM
ulti
vari
able
ana
lysi
s
Met
abol
ic
synd
rom
e, n
o. (%
)N
on-m
etab
olic
sy
ndro
me,
no.
(%)
Tota
lO
R (9
5% C
I)R
2P
OR
(95%
CI)
R2
P
Sex
0.66
70.
001
Fem
ale
96 (3
5.0)
178
(65.
0)27
42.
10 (1
.44–
3.05
)0.
039
< 0.
001
3.91
(1.7
8–8.
59)
Mal
e62
(20.
4)24
2 (7
9.6)
304
100
.1.0
0
Wat
erpi
pe sm
okin
g0.
01
Yes
11 (3
9.3)
17 (6
0.7)
281.7
7 (0
.81–
3.87
)0.
005
0.16
6.08
(1.5
5–23
.82)
No
147
(26.
7)
403
(73.
3)55
01.0
01.0
0
Fast
ing
bloo
d su
gar(
mg/
dL)
< 0.
001
≥ 10
081
(59.
6)55
(40.
4)13
66.
98 (4
.58–
10.6
4)0.
200
< 0.
001
13.2
2 (6
.74–
25.9
4)
< 10
077
(17.
4)36
5 (8
2.6)
442
1.00
1.00
Trig
lyce
ride
s (m
g/dL
)<
0.00
1
≥ 15
048
(65.
8)25
(34.
2)73
6.89
(4.0
6–11
.68)
0.13
1<
0.00
123
.75
(9.9
2–56
.84)
<150
110
(21.8
)39
5 (7
8.2)
505
1.00
1.00
Wai
st ci
rcum
fere
nce (
cm)
< 0.
001
Men
≥ 9
4 W
omen
≥ 8
014
3 (4
4.4)
179
(55.
6)32
212
.83
(7.2
8–22
.60)
0.27
< 0.
001
22.4
2 (9
.03–
55.7
0)
Men
< 9
4 W
omen
< 8
015
(5.9
)24
1 (94
.1)25
61.0
01.0
0
Bloo
d pr
essu
re (m
mH
g)<
0.00
1
≥ 13
0/85
81 (5
6.3)
63 (4
3.8)
144
5.96
(3.9
5–8.
99)
0.17
6<
0.00
116
.91 (
8.54
–33.
50)
<130
/85
77 (1
7.7)
357
(82.
3)43
41.0
01.0
0
LDL
chol
este
rol (
mg/
dL)a
0.01
7
> 14
021
(46.
7)24
(53.
3)45
2.52
(1.3
6–4.
68)
0.02
10.
004
3.47
(1.2
4–9.
68)
≤ 14
013
3 (2
5.7)
384
(74.
3)51
71.0
01.0
0
Wri
st ci
rcum
fere
nce (
cm)
mea
n (S
D) 1
7.01
(1.6
8)m
ean
(SD
) 16.
53 (1
.55)
578
1.20
(1.07
–1.3
5)0.
026
0.00
11.2
9 (1.
04–1
.59)
0.01
AHA
= Am
erica
n H
eart
Ass
ocia
tion;
OR
= od
ds ra
tio; C
I = co
nfide
nce i
nter
val; L
DL =
low
-den
sity l
ipop
rote
in; S
D =
stan
dard
dev
iatio
n.
a Data
wer
e miss
ing f
or 16
peo
ple.
Book 27-11.indb 1088Book 27-11.indb 1088 06/12/2021 12:39 PM06/12/2021 12:39 PM

1089
Research article EMHJ – Vol. 27 No. 11 – 2021
contributes to the incidence of metabolic syndrome due to their high glycaemic load (8,24).
Our results also showed that sex, waterpipe smoking, LDL cholesterol level and wrist circumference increased the risk of metabolic syndrome. As previously reported, sex hormones, such as androgen and estrogen play a determining role in the incidence of metabolic syndrome (25) because metabolic changes in women are associated with sex hormones both before and after menopause (26). In addition, waterpipe smoking reduces blood HDL cholesterol and increases triglycerides, which contributes to the incidence of metabolic syndrome (27). Moreover, LDL cholesterol causes insulin resistance and thus contributes to the incidence of metabolic syndrome (28). The predictive role of wrist circumference in the incidence of metabolic syndrome can also be attributed to the relationship between this component and weight, body mass index, waist circumference, insulin resistance and LDL cholesterol level (29). Other studies on the Iranian
population have also reported a relationship between wrist circumference and metabolic syndrome (29,30).
Our study has some limitations. First, the sample size was small and there was no annual follow-up of the target population. Despite these limitations, to the best of our knowledge, this study is the first of its kind conducted in this geographical region to measure the incidence of metabolic syndrome. Thus, our results can provide Iranian health policy-makers with useful information on the trend in metabolic syndrome.
ConclusionWaist circumference, blood pressure, fasting blood sug-ar and triglycerides had the highest incidence rate of the components of metabolic syndrome, indicating inappro-priate health-related behaviours, high-fat diets or low physical activity. Our results highlight the need for effec-tive interventions to encourage people to adopt a healthy and safe diet, have more physical activity and modify their unhealthy behaviour (e.g. waterpipe smoking).
AcknowledgmentWe thank the Health Promotion Research Center and Zahedan University of Medical Sciences for their support.
Funding: This manuscript is part of the PhD thesis of Khadijeh K. Farmanfarma who was funded by a scholarship from Zahedan University of Medical Sciences (Grant no. 8140).
Competing interests: None declared.
Incidence du syndrome métabolique et facteurs associés dans le sud-est de la République islamique d'IranRésuméContexte : Le syndrome métabolique est une cause importante de maladies cardiovasculaires. La mortalité imputable aux maladies cardiovasculaires est de 12,82 décès pour 100 000 habitants à Zahedan, dans le sud-est de la République islamique d'Iran.Objectifs : La présente étude visait à déterminer l'incidence du syndrome métabolique ainsi que ses facteurs prédictifs dans la ville de Zahedan.Méthodes : Toutes les personnes qui n’étaient pas atteintes de syndrome métabolique, ayant participé à une étude en 2009 à Zahedan et disponibles en 2017, ont été incluses dans la présente étude. Le syndrome métabolique a été diagnostiqué selon les critères de plusieurs organisations. Les indices anthropométriques et la tension artérielle ont été mesurés et des tests sanguins ont été effectués. L'incidence standardisée selon l'âge a été calculée pour le syndrome métabolique, et ses facteurs prédictifs ont été évalués dans une analyse de régression logistique.Résultats : L'âge moyen (écart type) des participants était de 45,46 (12,63) ans en 2017. L'incidence du syndrome métabolique était comprise entre 17 , 21 % et 27 , 18 % selon les critères utilisés ; elle était plus élevée chez les femmes. Une incidence standardisée selon l'âge élevée était associée à un grand tour de taille (55,81 %) et à une hypertension artérielle (25,32 %). Les odds ratios (OR) ajustés les plus élevés pour le syndrome métabolique concernaient les participants qui avaient un taux de triglycérides élevé (OR = 23,75 ; intervalle de confiance [IC] à 95 % : 9,92-56,84 %), un grand tour de taille (OR = 22,42 ; IC à 95 % : 9,03-55 , 70 %), une hypertension artérielle (OR = 16,91 ; IC à 95 % : 8,54-33,50 %) et un taux de glycémie élevé à jeun (OR = 13,22 ; IC à 95 % : 6,74-25,94 %). Le tabagisme par pipe à eau, le sexe, les lipoprotéines de basse densité et la circonférence du poignet étaient également associés au syndrome métabolique. Conclusions : L'incidence du syndrome métabolique a augmenté à Zahedan. Des interventions efficaces, notamment pour promouvoir une alimentation saine et l'activité physique et pour décourager l'usage de la pipe à eau, sont nécessaires afin de lutter contre cette affection.
Book 27-11.indb 1089Book 27-11.indb 1089 06/12/2021 12:39 PM06/12/2021 12:39 PM
1090
Research article EMHJ – Vol. 27 No. 11 – 2021
References1. Nolan PB, Carrick-Ranson G, Stinear JW, Reading SA, Dalleck LC. Prevalence of metabolic syndrome and metabolic syndrome
components in young adults: a pooled analysis. Prev Med Rep. 2017;7:211–5. https://doi.org/10.1016/j.pmedr.2017.07.004
2. Herath H, Weerasinghe N, Weerarathna T, Amarathunga A. A comparison of the prevalence of the metabolic syndrome among Sri Lankan patients with type 2 diabetes mellitus using WHO, NCEP-ATP III, and IDF definitions. Int J Chronic Dis. 2018;2018:7813537. https://doi.org/10.1155/2018/7813537
3. Garralda-Del-Villar M, Carlos-Chillerón S, Diaz-Gutierrez J, Ruiz-Canela M, Gea A, Martinez-González MA, et al. Healthy life-style and incidence of metabolic syndrome in the SUN cohort. Nutrients. 2019;11(1):65. https://doi.org/10.3390/nu11010065
4. Sarebanhassanabadi M, Mirhosseini SJ, Mirzaei M, Namayandeh SM, Soltani MH, Pedarzadeh A, et al. The incidence of meta-bolic syndrome and the most powerful components as predictors of metabolic syndrome in central Iran: a 10-year follow-up in a cohort study. Iran Red Crescent Med J. 2017;19(7):e14934.
5. Sheu WH-H, Chuang S-Y, Lee W-J, Tsai S-T, Chou P, Chen C-H. Predictors of incident diabetes, metabolic syndrome in middle-aged adults: a 10-year follow-up study from Kinmen, Taiwan. Diabetes Res Clin Pract. 2006;74(2):162–8. https://doi.org/10.1016/j.diabres.2006.03.011
6. Hwang JH, Kam S, Shin J-Y, Kim J-Y, Lee K-E, Kwon G-H, et al. Incidence of metabolic syndrome and relative importance of five components as a predictor of metabolic syndrome: 5-year follow-up study in Korea. J Korean Med Sci. 2013;28(12):1768–73. https://doi.org/10.3346/jkms.2013.28.12.1768
7. Zabetian A, Hadaegh F, Sarbakhsh P, Azizi F. Weight change and incident metabolic syndrome in Iranian men and women: a 3 year follow-up study. BMC Public Health. 2009;9(1):138. https://doi.org/10.1186/1471-2458-9-138
8. Hadaegh F, Hasheminia M, Lotfaliany M, Mohebi R, Azizi F, Tohidi M. Incidence of metabolic syndrome over 9 years follow-up; the importance of sex differences in the role of insulin resistance and other risk factors. PLoS One. 2013;8(9):e76304. https://doi.org/10.1371/journal.pone.0076304
9. Pietroiusti A, Neri A, Somma G, Coppeta L, Iavicoli I, Bergamaschi A, et al. Incidence of metabolic syndrome among night-shift healthcare workers. Occup Environ Med. 2010;67(1):54–7. https://doi.org/10.1136/oem.2009.046797
10. Kaykhaei MA, Hashemi M, Narouie B, Shikhzadeh A, Jahantigh M, Shirzaei E, et al. Prevalence of metabolic syndrome in adult population from zahedan, southeast iran. Iran J Public Health. 2012;41(2):70–6.
11. Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint inter-im statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International aAtherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640–45. https://doi.org/10.1161/circulationaha.109.192644
معدل حدوث املتالزمة االستقالبية والعوامل املرتبطة هبا، جنوب رشق مجهورية إيران اإلسالميةخدجية فرمانفارما، عيل-رضا أنصاري-مقدم، حممود كيخاي، مهدي حممدي، حسني عدينة، حسن عيل- عبد
اخلالصةاخللفية: تعترب املتالزمة االستقالبية سببا مهام ألمراض القلب واألوعية الدموية. ويبلغ معدل الوفيات النامجة عن أمراض القلب واألوعية الدموية
12.82 وفاة لكل 100000 نسمة يف زاهدان، جنوب رشق مجهورية إيران اإلسالمية.األهداف: هدفت هذه الدراسة إىل حتديد معدل حدوث املتالزمة االستقالبية والعوامل التي تنبئ هبا يف مدينة زاهدان.
من يعانون ال ممن 2017 عام يف وأتيحت زاهدان يف 2009 عام أجريت دراسة يف شاركوا الذين مجيع الدراسة هذه يف أدرج البحث: طرق صت املتالزمة االستقالبية بناء عىل معايري تطبقها عدة منظامت. وقيست مؤرشات القياسات األنثروبومرتية وضغط املتالزمة االستقالبية. وشخالدم وأجريت اختبارات الدم. وحسب معدل احلدوث املعياري حسب العمر للمتالزمة االستقالبية وقيمت عوامل التنبؤ هبا يف حتليل االنحدار
اللوجستي.النتائج: بلغ متوسط عمر املشاركني )االنحراف املعياري( 45.46 عاما )12.63( يف عام 2017. وتراوحت نسبة اإلصابة باملتالزمة االستقالبية بني 17.21% و27.18% حسب املعايري املستخدمة، وكانت أعىل يف صفوف النساء. وارتبط ارتفاع معدل احلدوث املعياري حسب العمر بضخامة الثالثية الدهون يف االستقالبية للمتالزمة حة املصح األرجحية نسب أعىل ومتثلت .)%25.32( الدم ضغط وارتفاع )%55.81( اخلرص حميط املرتفعة )نسبة أرجحية = 23.75؛ فاصل ثقة 95%: 9.92 - 56.84(، وحميط اخلرص الكبري )نسبة أرجحية = 22.42؛ فاصل ثقة %95: 9.03 - 55.70(، وارتفاع ضغط الدم )نسبة أرجحية = 16.91؛ فاصل ثقة 95%: 8.54 - 33.50( وارتفاع نسبة السكر يف الدم أثناء الصيام )نسبة الكثافة، وحميط اخلرص املنخفض والليبوبروتني الشيشة، واجلنس، ارتبط تدخني ثقة 95%: 6.74 - 25.94(. كام أرجحية = 13.22؛ فاصل
باملتالزمة االستقالبية. االستنتاجات: ارتفعت نسبة اإلصابة باملتالزمة االستقالبية يف زاهدان. ومتس احلاجة إىل إجراء تدخالت فعالة ملكافحة تلك احلالة، بحيث تشمل
تعزيز النظام الغذائي الصحي، والنشاط البدين، وجتنب تدخني الشيشة.
Book 27-11.indb 1090Book 27-11.indb 1090 06/12/2021 12:39 PM06/12/2021 12:39 PM
1091
Research article EMHJ – Vol. 27 No. 11 – 2021
12. Janghorbani M, Amini M. Incidence of metabolic syndrome and its risk factors among type 2 diabetes clinic attenders in Isfa-han, Iran. ISRN Endocrinol. 2012;2012:167318. https://doi.org/10.5402/2012/167318
13. Jiang B, Li B, Wang Y, Han B, Wang N, Li Q, et al. The nine-year changes of the incidence and characteristics of metabolic syn-drome in China: longitudinal comparisons of the two cross-sectional surveys in a newly formed urban community. Cardiovas Diabetol. 2016;15(1):84. https://doi.org/10.1186/s12933-016-0402-9
14. Scuteri A, Morrell CH, Najjar SS, Muller D, Andres R, Ferrucci L, et al. Longitudinal paths to the metabolic syndrome: can the incidence of the metabolic syndrome be predicted? The Baltimore Longitudinal Study of Aging. J Gerontol A Biol Sci Med Sci. 2009;64(5):590–8. https://doi.org/10.1093/gerona/glp004
15. Chen S-P, Chang H-C, Hsiao T-M, Yeh C-J, Yang H-J. Gender differences in the effects of the frequency of physical activity on the incidence of metabolic syndrome: results from a middle-aged community cohort in Taiwan. Metab Syndr Relat Disord. 2018;16(5):224–31. https://doi.org/10.1089/met.2017.0154
16. Bhalavi V, Deshmukh PR, Goswami K, Garg N. Prevalence and correlates of metabolic syndrome in the adolescents of rural Wardha. Indian J Community Med. 2015;40(1):43-48. https://doi.org/10.4103/0970-0218.149270
17. Kumar SV, Nagesh A, Leena M, Shravani G, Chandrasekar V. Incidence of metabolic syndrome and its characteristics of patients attending a diabetic outpatient clinic in a tertiary care hospital. J Nat Sci Biol Med. 2013;4(1):57–62. https://doi.org/10.4103/0976-9668.107261
18. Santos AC, Severo M, Barros H. Incidence and risk factors for the metabolic syndrome in an urban south European population. Prev Med. 2010;50(3):99–105. https://doi.org/10.1016/j.ypmed.2009.11.011
19. Zanchetti A, Hennig M, Baurecht H, Tang R, Cuspidi C, Carugo S, et al. Prevalence and incidence of the metabolic syndrome in the European Lacidipine Study on Atherosclerosis (ELSA) and its relation with carotid intima–media thickness. J Hypertens. 2007;25(12):2463–70. https://doi.org/10.1097/HJH.0b013e3282f063d5
20. Carroll MD, Lacher DA, Sorlie PD, Cleeman JI, Gordon DJ, Wolz M, et al. Trends in serum lipids and lipoproteins of adults, 1960–2002. JAMA. 2005;294(14):1773–81. https://doi.org/10.1001/jama.294.14.1773
21. Palaniappan L, Carnethon MR, Wang Y, Hanley AJ, Fortmann SP, Haffner SM, et al. Predictors of the incident metabolic syndrome in adults: the Insulin Resistance Atherosclerosis Study. Diabetes Care. 2004;27(3):788–93. https://doi.org/10.2337/dia-care.27.3.788
22. Hosseinpanah F, Nazeri P, Ghareh S, Tohidi M, Azizi F. Predictors of the incident metabolic syndrome in healthy obese sub-jects: a decade of follow-up from the Tehran Lipid and Glucose Study. Eur J Clin Nutr. 2014;68(3):295–9. https://doi.org/10.1038/ejcn.2013.142
23. Heidari Z, Hosseinpanah F, Mehrabi Y, Safarkhani M, Azizi F. Predictive power of the components of metabolic syndrome in its development: a 6.5-year follow-up in the Tehran Lipid and Glucose Study (TLGS). Eur J Clin Nutr. 2010;64(10):1207–14. https://doi.org/10.1038/ejcn.2010.111
24. Hadaegh F Ghasemi A, Padyab M, Tohidi M, Azizi F. The metabolic syndrome and incident diabetes: assessment of alternative definitions of the metabolic syndrome in an Iranian urban population. Diabetes Res Clin Pract. 2008;80(2):328–34. https://doi.org/10.1016/j.diabres.2008.01.003
25. Agirbasli M, Agaoglu NB, Orak N, Caglioz H, Ocek T, Poci N, et al. Sex hormones and metabolic syndrome in children and adoles-cents. Metabolism. 2009;58(9):1256–62. https://doi.org/10.1016/j.metabol.2009.03.024
26. Jiang B, Zheng Y, Chen Y, Chen Y, Li Q, Zhu C, et al. Age and gender-specific distribution of metabolic syndrome components in East China: role of hypertriglyceridemia in the SPECT-China study. Lipids Health Dis. 2018;17(1):92. https://doi.org/10.1186/s12944-018-0747-z
27. Soflaei SS, Darroudi S, Tayefi M, Tirkani AN, Moohebati M, Ebrahimi M, et al. Hookah smoking is strongly associated with diabetes mellitus, metabolic syndrome and obesity: a population-based study. Diabetol Metab Syndr. 2018;10(1):33. https://doi.org/10.1186/s13098-018-0335-4
28. Hajian-Tilaki K, Heidari B, Hajian-Tilaki A, Firouzjahi A, Bakhtiari A. Does the low-density lipoprotein cholesterol play a key role in predicting metabolic syndrome in the Iranian adult population? Caspian J Intern Med. 2017;8(4):289–95.
29. Hajsadeghi S, Firouzi A, Bahadoran P, Hassanzadeh M. The value of wrist circumference for predicting the presence of coronary artery disease and metabolic syndrome. Indian Heart J. 2016;68(Suppl 3):S5–9. https://doi.org/10.1016/j.ihj.2016.10.011
30. Jahangiri Noudeh Y, Hadaegh F, Vatankhah N, Momenan AA, Saadat N, Khalili D, et al. Wrist circumference as a novel predictor of diabetes and prediabetes: results of cross-sectional and 8.8-year follow-up studies. J Clin Endocrinol Metab. 2013;98(2):777–84. https://doi.org/10.1210/jc.2012-2416
Book 27-11.indb 1091Book 27-11.indb 1091 06/12/2021 12:39 PM06/12/2021 12:39 PM

1092
Research article EMHJ – Vol. 27 No. 11 – 2021
Health effects of desert dust storm events in the south-eastern Mediterranean: perceptions and practices of local stakeholders Paraskevi Kinni,1 Panayiotis Kouis,1 Helen Dimitriou,2 Shaked Yarza,3,4 Stefania I. Papatheodorou,5,6 Eirini Kampriani,7 Melanie Charalambous,8 Nicos Middleton,9 Victor Novack,3.4 Emmanouil Galanakis2 and Panayiotis K. Yiallouros1
1Respiratory Physiology Laboratory, Medical School, University of Cyprus, Nicosia, Cyprus. (Correspondence to: Paraskevi Kinni: [email protected]). 2Medical School, University of Crete, Heraklion, Crete, Greece. 3Clinical Research Center, Soroka University Medical Center, Beer-Sheva, Israel. 4Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel. 5Department of Epidemiology, Harvard T.H. Chan School of Public Health, Harvard University, Boston, United States of America. 6Cyprus International Institute for Environmental & Public Health; 7Department of Social and Political Sciences, University of Cyprus, Nicosia, Cyprus. 8Educational Sector, Nursing Services, Ministry of Health, Nicosia, Cyprus. 9Department of Nursing, School of Health Sciences, Cyprus University of Technology, Limassol, Cyprus.
AbstractBackground: The south-eastern Mediterranean experiences frequent desert dust storm events (DDS) that have been shown to be associated with adverse health effects.Aims: This study assessed the perceptions and practices towards DDS of local authorities and stakeholders from 3 coun-tries in the region, Cyprus, Greece and Israel. Methods: Between October 2017 and April 2018, we administered a semi-structured questionnaire to regulatory authori-ties involved in public protection from DDS as well as social stakeholders in the 3 countries. The questionnaire addressed their knowledge regarding DDS, perceptions on the relationship between DDS and health effects and relevant actions taken towards public protection.Results: Out of 58 stakeholders contacted, 49 participated in the study (84.5% response rate). Fourteen (28.6%) were reg-ulatory authorities and 35 (71.4%) were social stakeholders. All responders were familiar with DDS but several underesti-mated the frequency of events while the majority (73%) instinctively reported that elders, children and respiratory patients are susceptible subpopulations. Nevertheless, 71% were unaware of a national policy on DDS, or considered that this was lacking in their country. Although several stakeholders reportedly receive questions from the public regarding DDS ef-fects, only few reply according to a pre-determined action plan. Conclusions: Regulatory authorities and social stakeholders in Cyprus, Greece and Israel are characterized by good knowledge of DDS and associated health effects, although implementation of pre-determined action plans for public pro-tection is limited. Future efforts should concentrate on increasing awareness among stakeholders and the public and developing national policies, including effective measures to minimize DDS exposure. Keywords: desert dust storm, public health, perceptions, questionnaire, stakeholders Citation: Kinni P; Kouis P; Dimitriou H; Yarza S; Papatheodorou S; Kampriani E; et al. Health effects of desert dust storm events in the south eastern Mediterranean: perceptions and practices of local stakeholders. East Mediterr Health J. 2021;27(11):1092–1101. https://doi.org/10.26719/emhj.21.037Received: 04/06/20; accepted: 03/01/21Copyright © World Health Organization (WHO) 2021. Open Access. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license (https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
IntroductionThe south-eastern Mediterranean region is affected by frequent and often severe desert dust storms (DDS) last-ing several days. These are characterized by extremely high levels of coarse particles with aerodynamic diam-eter between 2.5 μm and 10 μm (PM10) as well as by in-creases in fine particles with aerodynamic diameter < 2.5 μm (PM2.5) (1,2). Cyprus, Crete (Greece) and Israel are in the centre of this region experiencing DDS events that originate from both the Sahara and the Arabian Penin-sula deserts (3). With reducing precipitation and advanc-ing desertification in the region due to ongoing climat-ic change, these countries are expected to experience further increases in the frequency and severity of DDS events in the future (4,5).
Consistent evidence from toxicological and epidemiological studies has demonstrated the negative impact of desert dust on cardiorespiratory health. More specifically, data generated from rodent and cell-line assays have highlighted the potential of naturally generated particles to inhibit immunoglobulin-mediated suppression of inflammation (6), amplify pro-inflammatory cytokines and oxidative stress in respiratory epithelial cells (7) and exacerbate pulmonary eosinophilia (8) and tissue injury (9). Through systemic circulation, smaller particles and toxic substances in desert dust may be transported to all tissues and previous studies have reported increased endothelial dysfunction (10), increased heart rate and mean blood pressure and decreased cardiac contractility (11). These findings are in line with epidemiological studies from around the world, which reported significant associations with both
Book 27-11.indb 1092Book 27-11.indb 1092 06/12/2021 12:39 PM06/12/2021 12:39 PM
1093
Research article EMHJ – Vol. 27 No. 11 – 2021
respiratory (asthma, pneumonia, chronic obstructive pulmonary disease, allergic rhinitis, coccidiomycosis) and cardiovascular (stroke, arrhythmia, ischaemic heart disease, cerebrovascular disease) outcomes (12). Preliminary evidence, also supports the association of desert dust with reproductive (13), neurological (14) and dermatological (15) health effects, as well as with a higher incidence of meningococcal meningitis (16) and conjunctivitis (17).
In previous years, studies from the region have reported associations of PM10 during DDS outbreaks with increased hospital admissions for asthma, chronic obstructive pulmonary disease and cardiovascular disease as well as increased mortality (18–21). However, evidence on the societal concerns and risk perception in relation to DDS events and the associated health problems in these countries is limited (22). Furthermore, there are no data on either the current knowledge and relevant practices of the regulatory authorities or the knowledge and perceptions of involved social stakeholders in the region regarding the health effects of DDS events. As shown before, research in stakeholder perceptions and knowledge has been useful in identifying and prioritizing problems that could and should be resolved, especially in situations where there is no single organization or individual totally in charge, but many are partially involved or affected (23). Thus, in order to introduce effective, easy to implement and sustainable policy interventions towards the mitigation of DDS health effects, it is important to interrelate evidence on the concerns of stakeholders and the capabilities of the regulatory authorities in science-based stakeholder dialogues (24).
The aim of this study was to capture the current state of knowledge and consensus about DDS events and their impact on human health among relevant regulatory authorities (governmental) and societal stakeholders (patients, parents, municipalities, academics, nongovernmental organizations) in Cyprus, Crete (Greece) and Israel.
MethodsStudy participants In order to include a wide range of considerations on DDS events, we adopted an inclusive definition of stake-holders (25). As described elsewhere (25–27), we defined stakeholders as “every person or organization who/which can influence discussions about the development of policy measures for mitigating the health effects of DDS events”. The International Risk Governance Coun-cil classifies stakeholders in 4 types: regulatory author-ities, affected stakeholders, external scientists and civil society organizations (28). However, we adopted some changes to this classification to address the needs of the study. Thus, we considered 2 types of stakeholders: reg-ulatory authorities and social stakeholders. Regulatory authorities were defined as governmental institutions involved in public protection in relation to DDS events. A subcategorization for regulatory authorities was created
depending on whether these were educational, health or environmental bodies. Social stakeholders were subdi-vided into patients’ support groups, medical associations, parents’ associations, trade unions, municipalities and academic/research institutions.
For the purposes of the study we adopted a judgmental sampling method where participants were identified based on their professional backgrounds, affiliations and experience with DDS events and this allowed us to collect and examine the perceptions and views from different perspectives. In the category of regulatory authorities, representatives holding key positions in organizations that influence the development and management of public health, environmental and education policies were contacted (e.g. ministries of environment, health, labour, education). In the case of municipalities and trade unions, occupational health safety professionals who are involved in the management of occupational health safety risks were identified. Patients’ support groups, medical associations and parents’ associations were chosen because they act as liaisons with the respective patient groups and the relevant health care and education professionals. In the category of academic/research institutions, we selected experts from various fields who are involved in environmental, air pollution and public health studies.
The survey was conducted between October 2017 and April 2018 and 6 researchers were involved in data collection, 2 from each country.
Data acquisition and survey procedureThis study employed a cross-sectional survey study de-sign and used semi-structured questionnaires for data collection, which is considered a suitable approach that can yield a significant amount of information related to the phenomenon under study and also be able to focus on the specific study objectives (29).
The semi-structured questionnaires examined the knowledge of participants on DDS events, their perception on the relationship between DDS events and health effects and the relevant actions taken by their organization towards protecting public health from DDS events. The questionnaires were developed through critical comparative analysis and adaptation of existing international questionnaires that were originally used to assess the awareness of professionals in regard to environmental health issues and early warning systems (30,31). The questionnaire was initially developed in English and forward translated in Greek. Two independent bilingual speakers, then back translated the agreed Greek version. The agreed back translation was sent to the authors for their comments and their suggestions were included into the final Greek version. Prior to implementation of the main study, the questionnaires were administered to a restricted sample in order to assess efficacy and applicability and ensure that the questionnaire was culturally acceptable, comprehensible and readable in Cyprus, Crete and Israel.
Book 27-11.indb 1093Book 27-11.indb 1093 06/12/2021 12:39 PM06/12/2021 12:39 PM
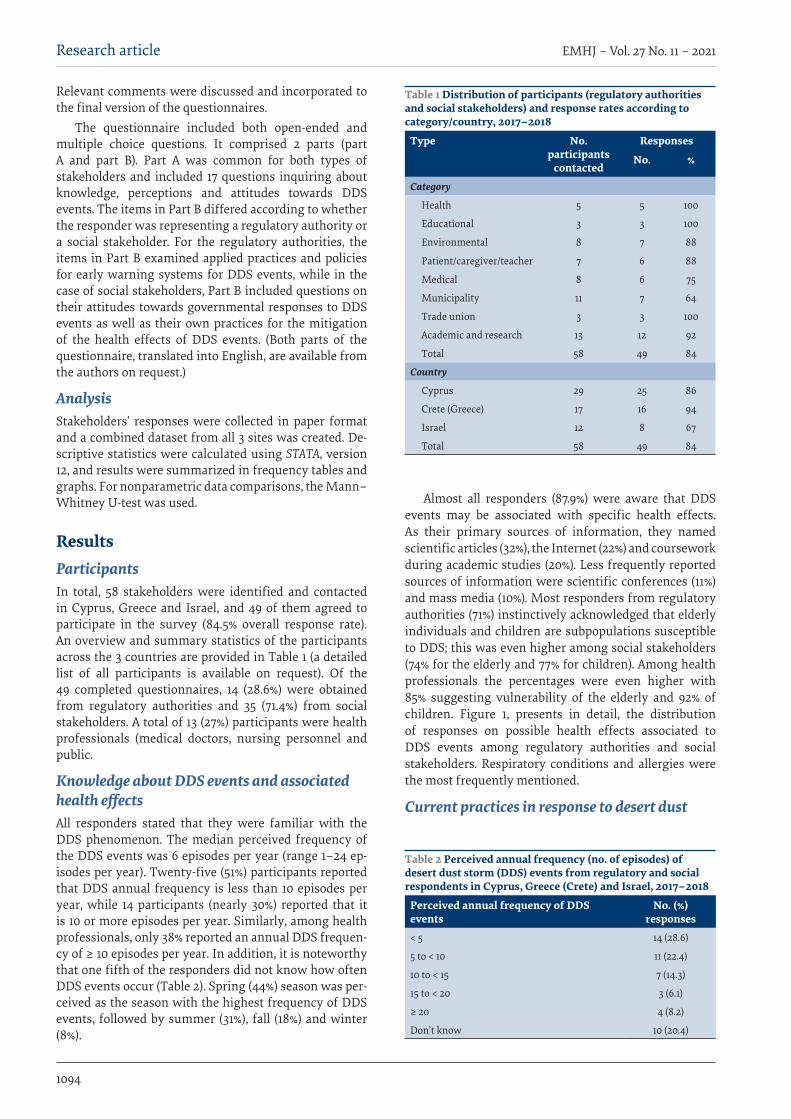
1094
Research article EMHJ – Vol. 27 No. 11 – 2021
Relevant comments were discussed and incorporated to the final version of the questionnaires.
The questionnaire included both open-ended and multiple choice questions. It comprised 2 parts (part A and part B). Part A was common for both types of stakeholders and included 17 questions inquiring about knowledge, perceptions and attitudes towards DDS events. The items in Part B differed according to whether the responder was representing a regulatory authority or a social stakeholder. For the regulatory authorities, the items in Part B examined applied practices and policies for early warning systems for DDS events, while in the case of social stakeholders, Part B included questions on their attitudes towards governmental responses to DDS events as well as their own practices for the mitigation of the health effects of DDS events. (Both parts of the questionnaire, translated into English, are available from the authors on request.)
AnalysisStakeholders’ responses were collected in paper format and a combined dataset from all 3 sites was created. De-scriptive statistics were calculated using STATA, version 12, and results were summarized in frequency tables and graphs. For nonparametric data comparisons, the Mann–Whitney U-test was used.
ResultsParticipantsIn total, 58 stakeholders were identified and contacted in Cyprus, Greece and Israel, and 49 of them agreed to participate in the survey (84.5% overall response rate). An overview and summary statistics of the participants across the 3 countries are provided in Table 1 (a detailed list of all participants is available on request). Of the 49 completed questionnaires, 14 (28.6%) were obtained from regulatory authorities and 35 (71.4%) from social stakeholders. A total of 13 (27%) participants were health professionals (medical doctors, nursing personnel and public.
Knowledge about DDS events and associated health effectsAll responders stated that they were familiar with the DDS phenomenon. The median perceived frequency of the DDS events was 6 episodes per year (range 1–24 ep-isodes per year). Twenty-five (51%) participants reported that DDS annual frequency is less than 10 episodes per year, while 14 participants (nearly 30%) reported that it is 10 or more episodes per year. Similarly, among health professionals, only 38% reported an annual DDS frequen-cy of ≥ 10 episodes per year. In addition, it is noteworthy that one fifth of the responders did not know how often DDS events occur (Table 2). Spring (44%) season was per-ceived as the season with the highest frequency of DDS events, followed by summer (31%), fall (18%) and winter (8%).
Almost all responders (87.9%) were aware that DDS events may be associated with specific health effects. As their primary sources of information, they named scientific articles (32%), the Internet (22%) and coursework during academic studies (20%). Less frequently reported sources of information were scientific conferences (11%) and mass media (10%). Most responders from regulatory authorities (71%) instinctively acknowledged that elderly individuals and children are subpopulations susceptible to DDS; this was even higher among social stakeholders (74% for the elderly and 77% for children). Among health professionals the percentages were even higher with 85% suggesting vulnerability of the elderly and 92% of children. Figure 1, presents in detail, the distribution of responses on possible health effects associated to DDS events among regulatory authorities and social stakeholders. Respiratory conditions and allergies were the most frequently mentioned.
Current practices in response to desert dust
Table 1 Distribution of participants (regulatory authorities and social stakeholders) and response rates according to category/country, 2017–2018
Type No. participants
contacted
Responses
No. %
Category
Health 5 5 100
Educational 3 3 100
Environmental 8 7 88
Patient/caregiver/teacher 7 6 88
Medical 8 6 75
Municipality 11 7 64
Trade union 3 3 100
Academic and research 13 12 92
Total 58 49 84
Country
Cyprus 29 25 86
Crete (Greece) 17 16 94
Israel 12 8 67
Total 58 49 84
Table 2 Perceived annual frequency (no. of episodes) of desert dust storm (DDS) events from regulatory and social respondents in Cyprus, Greece (Crete) and Israel, 2017–2018
Perceived annual frequency of DDS events
No. (%) responses
< 5 14 (28.6)
5 to < 10 11 (22.4)
10 to < 15 7 (14.3)
15 to < 20 3 (6.1)
≥ 20 4 (8.2)
Don’t know 10 (20.4)
Book 27-11.indb 1094Book 27-11.indb 1094 06/12/2021 12:39 PM06/12/2021 12:39 PM
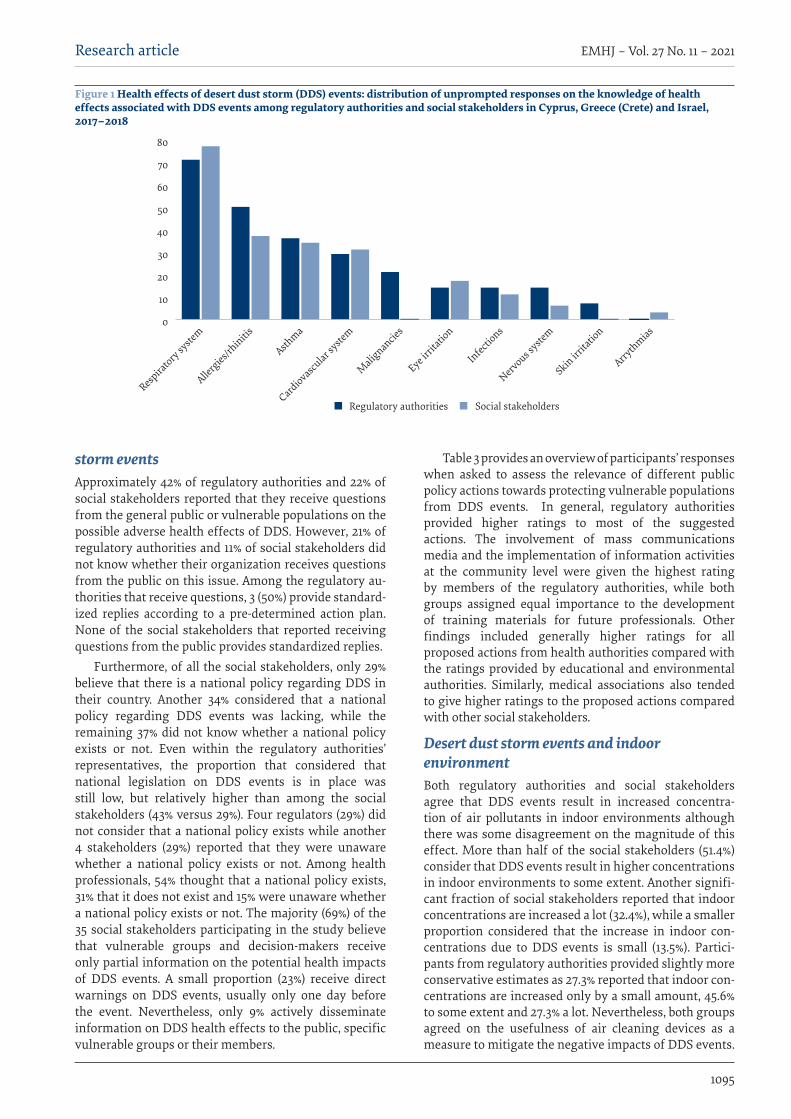
1095
Research article EMHJ – Vol. 27 No. 11 – 2021
storm eventsApproximately 42% of regulatory authorities and 22% of social stakeholders reported that they receive questions from the general public or vulnerable populations on the possible adverse health effects of DDS. However, 21% of regulatory authorities and 11% of social stakeholders did not know whether their organization receives questions from the public on this issue. Among the regulatory au-thorities that receive questions, 3 (50%) provide standard-ized replies according to a pre-determined action plan. None of the social stakeholders that reported receiving questions from the public provides standardized replies.
Furthermore, of all the social stakeholders, only 29% believe that there is a national policy regarding DDS in their country. Another 34% considered that a national policy regarding DDS events was lacking, while the remaining 37% did not know whether a national policy exists or not. Even within the regulatory authorities’ representatives, the proportion that considered that national legislation on DDS events is in place was still low, but relatively higher than among the social stakeholders (43% versus 29%). Four regulators (29%) did not consider that a national policy exists while another 4 stakeholders (29%) reported that they were unaware whether a national policy exists or not. Among health professionals, 54% thought that a national policy exists, 31% that it does not exist and 15% were unaware whether a national policy exists or not. The majority (69%) of the 35 social stakeholders participating in the study believe that vulnerable groups and decision-makers receive only partial information on the potential health impacts of DDS events. A small proportion (23%) receive direct warnings on DDS events, usually only one day before the event. Nevertheless, only 9% actively disseminate information on DDS health effects to the public, specific vulnerable groups or their members.
Table 3 provides an overview of participants’ responses when asked to assess the relevance of different public policy actions towards protecting vulnerable populations from DDS events. In general, regulatory authorities provided higher ratings to most of the suggested actions. The involvement of mass communications media and the implementation of information activities at the community level were given the highest rating by members of the regulatory authorities, while both groups assigned equal importance to the development of training materials for future professionals. Other findings included generally higher ratings for all proposed actions from health authorities compared with the ratings provided by educational and environmental authorities. Similarly, medical associations also tended to give higher ratings to the proposed actions compared with other social stakeholders.
Desert dust storm events and indoor environmentBoth regulatory authorities and social stakeholders agree that DDS events result in increased concentra-tion of air pollutants in indoor environments although there was some disagreement on the magnitude of this effect. More than half of the social stakeholders (51.4%) consider that DDS events result in higher concentrations in indoor environments to some extent. Another signifi-cant fraction of social stakeholders reported that indoor concentrations are increased a lot (32.4%), while a smaller proportion considered that the increase in indoor con-centrations due to DDS events is small (13.5%). Partici-pants from regulatory authorities provided slightly more conservative estimates as 27.3% reported that indoor con-centrations are increased only by a small amount, 45.6% to some extent and 27.3% a lot. Nevertheless, both groups agreed on the usefulness of air cleaning devices as a measure to mitigate the negative impacts of DDS events.
Figure 1 Health effects of desert dust storm (DDS) events: distribution of unprompted responses on the knowledge of health effects associated with DDS events among regulatory authorities and social stakeholders in Cyprus, Greece (Crete) and Israel, 2017–2018
0
10
20
30
40
50
60
70
80
Social stakeholdersRegulatory authorities
Arrythmias
Skin irrita
tion
Nervous syste
m
Infections
Eye irrita
tion
Malig
nancies
Cardiovascular s
ystem
Asthma
Allergies/r
hinitis
Respira
tory syste
m
Book 27-11.indb 1095Book 27-11.indb 1095 06/12/2021 12:39 PM06/12/2021 12:39 PM
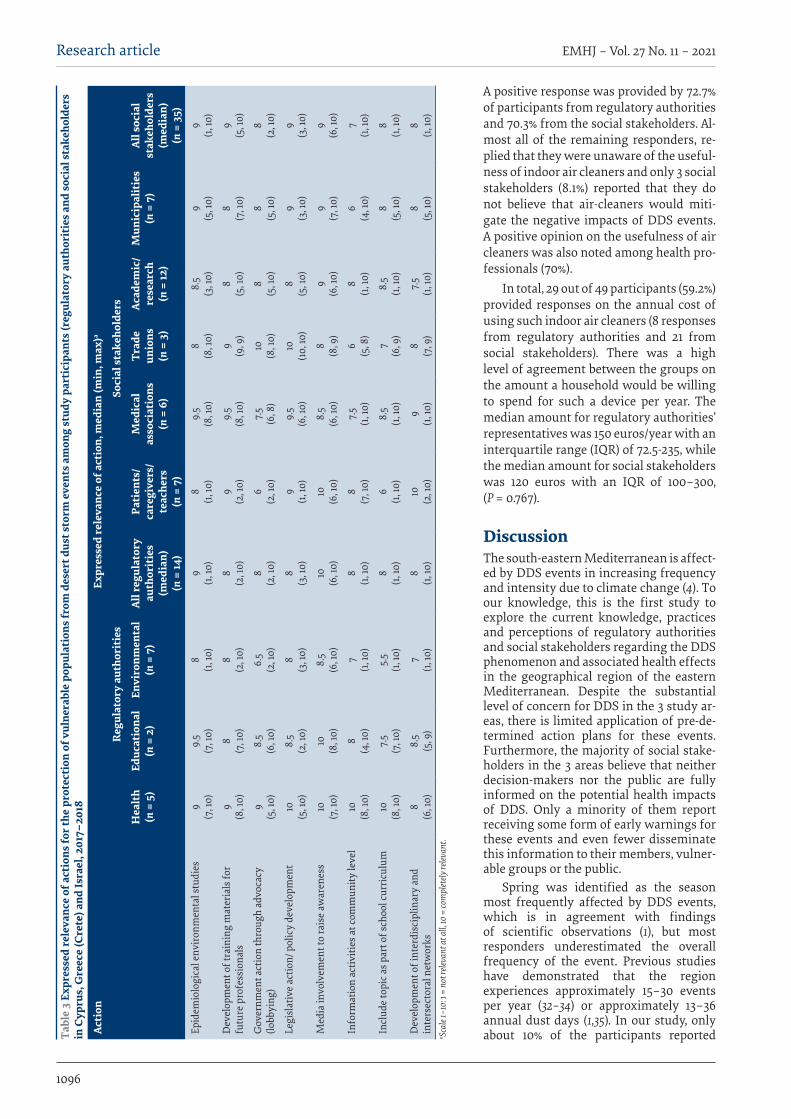
1096
Research article EMHJ – Vol. 27 No. 11 – 2021
A positive response was provided by 72.7% of participants from regulatory authorities and 70.3% from the social stakeholders. Al-most all of the remaining responders, re-plied that they were unaware of the useful-ness of indoor air cleaners and only 3 social stakeholders (8.1%) reported that they do not believe that air-cleaners would miti-gate the negative impacts of DDS events. A positive opinion on the usefulness of air cleaners was also noted among health pro-fessionals (70%).
In total, 29 out of 49 participants (59.2%) provided responses on the annual cost of using such indoor air cleaners (8 responses from regulatory authorities and 21 from social stakeholders). There was a high level of agreement between the groups on the amount a household would be willing to spend for such a device per year. The median amount for regulatory authorities’ representatives was 150 euros/year with an interquartile range (IQR) of 72.5-235, while the median amount for social stakeholders was 120 euros with an IQR of 100–300, (P = 0.767).
DiscussionThe south-eastern Mediterranean is affect-ed by DDS events in increasing frequency and intensity due to climate change (4). To our knowledge, this is the first study to explore the current knowledge, practices and perceptions of regulatory authorities and social stakeholders regarding the DDS phenomenon and associated health effects in the geographical region of the eastern Mediterranean. Despite the substantial level of concern for DDS in the 3 study ar-eas, there is limited application of pre-de-termined action plans for these events. Furthermore, the majority of social stake-holders in the 3 areas believe that neither decision-makers nor the public are fully informed on the potential health impacts of DDS. Only a minority of them report receiving some form of early warnings for these events and even fewer disseminate this information to their members, vulner-able groups or the public.
Spring was identified as the season most frequently affected by DDS events, which is in agreement with findings of scientific observations (1), but most responders underestimated the overall frequency of the event. Previous studies have demonstrated that the region experiences approximately 15–30 events per year (32–34) or approximately 13–36 annual dust days (1,35). In our study, only about 10% of the participants reported Ta
ble
3 Ex
pres
sed
rele
vanc
e of
act
ions
for t
he p
rote
ctio
n of
vul
nera
ble
popu
lati
ons f
rom
des
ert d
ust s
torm
eve
nts a
mon
g st
udy
part
icip
ants
(reg
ulat
ory
auth
orit
ies a
nd so
cial
stak
ehol
ders
in
Cyp
rus,
Gre
ece
(Cre
te) a
nd Is
rael
, 201
7–20
18
Acti
onEx
pres
sed
rele
vanc
e of
act
ion,
med
ian
(min
, max
)a
Reg
ulat
ory
auth
orit
ies
Soci
al st
akeh
olde
rs
Hea
lth
(n =
5)
Educ
atio
nal
(n =
2)
Envi
ronm
enta
l(n
= 7
)Al
l reg
ulat
ory
auth
orit
ies
(med
ian)
(n =
14)
Pati
ents
/ ca
regi
vers
/ te
ache
rs(n
= 7
)
Med
ical
as
soci
atio
ns(n
= 6
)
Trad
e un
ions
(n =
3)
Acad
emic
/ re
sear
ch(n
= 12
)
Mun
icip
alit
ies
(n =
7)
All s
ocia
l st
akeh
olde
rs(m
edia
n)(n
= 3
5)Ep
idem
iolo
gica
l env
iron
men
tal s
tudi
es9
(7
, 10)
9.5
(7
, 10)
8
(1, 10
)9
(1,
10)
8
(1, 10
)9.
5
(8, 1
0)8
(8
, 10)
8.5
(3
, 10)
9
(5, 1
0)9
(1,
10)
Dev
elop
men
t of t
rain
ing
mat
eria
ls fo
r fu
ture
pro
fess
iona
ls9
(8
, 10)
8
(7, 1
0)8
(2
, 10)
8
(2, 1
0)9
(2
, 10)
9.5
(8
, 10)
9
(9, 9
)8
(5
, 10)
8
(7, 1
0)9
(5
, 10)
Gov
ernm
ent a
ctio
n th
roug
h ad
voca
cy
(lobb
ying
)9
(5
, 10)
8.5
(6, 1
0)6.
5
(2, 1
0)8
(2
, 10)
6
(2, 1
0)7.
5
(6, 8
)10
(8
, 10)
8
(5, 1
0)8
(5
, 10)
8
(2, 1
0)
Legi
slat
ive
actio
n/ p
olic
y de
velo
pmen
t10
(5
, 10)
8.5
(2
, 10)
8
(3, 1
0)8
(3
, 10)
9
(1, 10
)9.
5
(6, 1
0)10
(10
, 10)
8
(5, 1
0)9
(3
, 10)
9
(3, 1
0)
Med
ia in
volv
emen
t to
rais
e aw
aren
ess
10
(7, 1
0)10
(8
, 10)
8.5
(6
, 10)
10
(6, 1
0)10
(6
, 10)
8.5
(6
, 10)
8
(8, 9
)9
(6
, 10)
9
(7, 1
0)9
(6
, 10)
Info
rmat
ion
activ
ities
at c
omm
unity
leve
l10
(8
, 10)
8
(4, 1
0)7
(1,
10)
8
(1, 10
)8
(7
, 10)
7.5
(1,
10)
6
(5, 8
)8
(1,
10)
6
(4, 1
0)7
(1,
10)
Incl
ude
topi
c as p
art o
f sch
ool c
urri
culu
m10
(8
, 10)
7.5
(7
, 10)
5.5
(1,
10)
8
(1, 10
)6
(1,
10)
8.5
(1,
10)
7
(6, 9
)8.
5
(1, 10
)8
(5
, 10)
8
(1, 10
)
Dev
elop
men
t of i
nter
disc
iplin
ary
and
inte
rsec
tora
l net
wor
ks8
(6
, 10)
8.5
(5
, 9)
7
(1, 10
)8
(1,
10)
10
(2, 1
0)9
(1,
10)
8
(7, 9
)7.
5
(1, 10
)8
(5
, 10)
8
(1, 10
)a Sc
ale 1
–10:
1 =
not r
eleva
nt at
all, 1
0 =
com
plet
ely re
levan
t.
Book 27-11.indb 1096Book 27-11.indb 1096 06/12/2021 12:39 PM06/12/2021 12:39 PM

1097
Research article EMHJ – Vol. 27 No. 11 – 2021
a similar or higher frequency. Almost all responders instinctively identified respiratory complications as the main health effect of DDS events, while other effects, particularly from the cardiovascular system, were greatly underestimated and were reported by fewer responders. In fact, numerous studies have already demonstrated a strong and consistent link between DDS events and cardiovascular mortality and morbidity both in Asia and Europe (20,36,37). This discrepancy underlines the lack of knowledge of the wide body of evidence on the main health effects of DDS events (12) and poor dissemination of existing evidence to regional stakeholders.
Although both social stakeholders and regulatory authorities acknowledge that DDS may affect indoor air quality, their opinion on the magnitude of this effect was variable. Few studies have examined this aspect and shown that there is high infiltration of outdoor PM to the indoor environment during DDS events (38,39). More specifically, in Israel the infiltration factor reached 0.82 for PM2.5 and 0.72 for PM10 during DDS events (39), while a study in Japan has shown that just leaving the window open for 10 minutes during a dust event resulted in a rapid increase in indoor particulate matter counts up to 70% of the outside particulate matter (38). However, it should be noted that infiltration factors also vary depending on the ventilation system, household floor level and presence of pets (38–40), and fine particles are able to infiltrate more efficiently into the indoor environment compared with larger particles even when windows are closed (39). In this respect, the majority of the responders not surprisingly considered as beneficial the use of an indoor air cleaner as a measure to mitigate the negative impacts of DDS events. This view is in agreement with the findings of recent studies demonstrating the effectiveness of air cleaners to remove particulates from indoor air in households (41–43) and schools (44). Also of interest is that most of the responders were willing to spend 70 to 300 euros per year for such a device (including electricity consumption). This amount is realistic, taking into consideration that the retail cost of quality HEPA air cleaners ranges between US$ 200 and US$ 400 and electricity consumption of the most recent models is low (< 120 Watts) (45).
The main strength of our study is that it captures for the first time the current perspectives and practices in regard to DDS events of regulatory authorities and a wide range of social stakeholders across 3 countries in the south-eastern Mediterranean. The only other study that focused on public health policy for DDS events was recently carried out in the Islamic Republic of Iran and focused on the preparedness challenges of the local health system in response to DDS. It demonstrated that senior policy-makers and executives were not fully familiar with DDS and the related health effects, the severity of the phenomenon, and the identification of high-risk areas. It also highlighted the lack of DDS-specific action plans and the need for integrated training programmes and increasing population awareness (46). Collectively these findings may assist the intercalation of scientists and stakeholders, which is an integral part of any participatory decision making process for the development of national and international policies (27). Failure to attend carefully to stakeholder interests, state of knowledge and perceptions in the past has been repeatedly shown to result in negative outcomes (47).
The findings of this study are expected to enhance cooperation among various actors and provide the foundation for stakeholders and regulatory authorities to define their responsibilities towards a range of intervention measures aiming to minimize DDS exposure and associated health problems. Furthermore, as DDS events constitute a common environmental health risk that is usually transboundary, originating from multiple dust sources and affecting multiple countries at once (48–50), our study contributes towards the dissemination of knowledge and sharing of public health policies between the countries of the region. Although not all countries of the region experience the same intensity and frequency of DDS, international collaboration between regulatory authorities (meteorological forecasters, air pollution monitoring stations and health authorities) may facilitate the development of a regional, or even global, desert dust health warning system and transfer of best practices between countries, as suggested previously (51). In line with this approach, the ongoing European Union-funded InDust COST action aims to facilitate the development of an international network of scientists working on linking dust forecasting models and ground measurements with early warning systems (52).
It is suggested that DDS warnings be disseminated through multiple, pre-defined and well maintained notification channels and must be clear, consistent and accurate, targeting distinct audiences such as health care professionals, educators and outdoor workers as well as the general public (53). Warning messages should also be accompanied by specific evidence-based guidelines aimed at reducing the health impact of DDS, especially among vulnerable population groups. These guidelines can include behavioural adaptations to reduce exposure to PM10 by limiting time spend outdoors and reducing outdoor physical activities during DDS, while indoor concentrations of PM10 can be controlled using a HEPA air cleaner. The feasibility and effectiveness of these guidelines will be assessed in 2 large field studies focusing on children with asthma and elderly patients with atrial fibrillation as part of the demonstration project MEDEA (Mitigating the Health Effects of Desert Dust Storms Using Exposure-Reduction Approaches), which is funded by the European Union LIFE Programme (54).
Our study is also characterized by some limitations. We acknowledge that some of the organizations contacted, did not participate in the study and the possibility that our results may have been influenced by non-responder bias cannot be ruled out. Furthermore, the response rate was higher in Greece and Cyprus than in Israel, which may reflect cultural differences (mentality, unwillingness to share information), unfamiliarity with European collaborative projects as well as possible security concerns. Secondly, the participation in some categories, such as the medical and municipalities groups, was lower than in other categories. This could be largely attributed to their possible different attitudes toward DDS events (perceived less relevant to them) and their possible hesitation to share information due to lack of specific knowledge on the subject. Nevertheless, although the sample of surveyed participants was not homogeneous (particularly in terms of ethnicity and background), its diversity is representative of the study area and the researchers tried to saturate concepts by many well experienced participants.
Book 27-11.indb 1097Book 27-11.indb 1097 06/12/2021 12:39 PM06/12/2021 12:39 PM
1098
Research article EMHJ – Vol. 27 No. 11 – 2021
Conclusion This study analysed the perceptions and practices of regulatory authorities and social stakeholders regarding DDS events in 3 countries in the south-eastern Mediter-ranean region. Our results demonstrate high awareness for this phenomenon and a good understanding of some
of the related health effects among stakeholders in the 3 countries but also limited existence and hence appli-cation of pre-determined action plans for DDS events. Our findings are expected to inform and further support an ongoing public dialogue in the region for the devel-opment of intervention measures aimed at minimizing DDS exposure and associated health effects.
AcknowledgementThe authors would like to thank the representatives from the different stakeholders for their participation in the study.
Funding: This study was supported by the European Union LIFE project MEDEA (LIFE16 CCA/CY/000041).
Competing interests: None declared.
Effets sanitaires des tempêtes de poussières désertiques dans le sud-est de la Méditerranée : perceptions et pratiques des parties prenantes locales RésuméContexte : Le sud-est de la Méditerranée subit fréquemment des tempêtes de poussières désertiques qui se sont révélées être associées à des effets néfastes sur la santé. Objectifs : La présente étude a évalué les perceptions et les pratiques des autorités locales et des parties prenantes concernant les tempêtes de poussières, dans trois pays de la région : Chypre, la Grèce et Israël.Méthodes : Entre octobre 2017 et avril 2018, nous avons demandé aux autorités de réglementation impliquées dans la protection du public contre les tempêtes de poussières ainsi qu'aux parties prenantes sociales des trois pays de remplir un questionnaire semi-structuré. Ce questionnaire portait sur leurs connaissances au sujet des tempêtes de poussières, leur perception de la relation entre ces dernières et les effets sur la santé et les mesures pertinentes adoptées pour protéger le public.Résultats : Sur les 58 parties prenantes contactées, 49 ont participé à l'étude (taux de réponse de 84,5 %). Quatorze (28,6 %) étaient des autorités de réglementation et 35 (71,4 %) des parties prenantes sociales. Tous les répondants avaient des connaissances sur les tempêtes de poussières désertiques, mais plusieurs d'entre eux sous-estimaient la fréquence des événements, tandis que la majorité (73 %) avait instinctivement indiqué que les personnes âgées, les enfants et les patients souffrant de troubles respiratoires étaient des sous-populations qui y sont sensibles. Néanmoins, 71 % d'entre eux n'avaient pas connaissance de l'existence d'une politique nationale en matière de protection contre les tempêtes de poussières, ou considéraient qu'elle faisait défaut dans leur pays. Même si plusieurs parties prenantes ont indiqué avoir reçu des questions du grand public concernant les effets des tempêtes de poussières désertiques, seules quelques-unes y ont répondu selon un plan d'action prédéterminé. Conclusions : À Chypre, en Grèce et en Israël, les autorités de réglementation et les parties prenantes sociales font preuve d’une bonne connaissance des tempêtes de poussières et de leurs effets sur la santé, bien que la mise en œuvre de plans d’action prédéterminés pour la protection du grand public soit limitée. À l'avenir, il sera nécessaire d’augmenter la sensibilisation à ce sujet parmi les parties prenantes et le grand public et d'élaborer des politiques nationales, notamment des mesures efficaces pour minimiser l'exposition aux tempêtes de poussières désertiques.
اآلثار الصحية ألحداث العواصف الرتابية الصحراوية يف جنوب رشق البحر املتوسط: تصورات وممارسات اجلهات صاحبة املصلحة املحلية
باراسكيفي كيني، بانايوتيس كويس، هيلني ديميرتيو، شاكد يرزا، ستيفانيا باباثيودورو، إيريني كامربياين،، ميالين شاراالمبوس، نيكوس ميدلتون، فيكتور نوفاك، إمانويل جاالناكيس، بانايوتيس يالوروس
اخلالصةاخللفية: تشهد منطقة جنوب رشق املتوسط العديد من أحداث العواصف الرتابية الصحراوية التي ثبت ارتباطها بآثار صحية ضارة.
األهداف: هدفت هذه الدراسة اىل تقييم تصورات وممارسات السلطات املحلية واجلهات صاحبة املصلحة إزاء العواصف الرتابية الصحراوية يف ثالثة بلدان يف املنطقة، وهي قربص واليونان وإرسائيل.
Book 27-11.indb 1098Book 27-11.indb 1098 06/12/2021 12:39 PM06/12/2021 12:39 PM
1099
Research article EMHJ – Vol. 27 No. 11 – 2021
References 1. Achilleos S, Evans JS, Yiallouros PK, Kleanthous S, Schwartz J, Koutrakis P. PM10 Concentration levels at an urban and back-
ground site in Cyprus: The impact of urban sources and dust storms. J Air Waste Manag Assoc. 2014;64(12):1352–60. doi:10.1080/10962247.2014.923061
2. Querol X, Pey J, Pandolfi M, Alastuey A, Cusack M, Pérez N, et al. African dust contributions to mean ambient PM10 mass-levels across the Mediterranean Basin. Atmos Environ. 2009;43(28):4266–77. doi:10.1016/j.atmosenv.2009.06.013
3. Pey J, Querol X, Alastuey A, Forastiere F, Stafoggia M. African dust outbreaks over the Mediterranean Basin during 2001–2011: PM10 concentrations, phenomenology and trends, and its relation with synoptic and mesoscale meteorology. Atmos Chem Phys. 2013;13(3):1395–410.
4. Ganor E, Osetinsky I, Stupp A, Alpert P. Increasing trend of African dust, over 49 years, in the eastern Mediterranean. J Geophys Res Atmos. 2010;115(7).
5. Goudie AS, Middleton NJ. The changing frequency of dust storms through time. Climatic Change. 1992;(20):197–225. doi:10.1007/BF00139839
6. Keil DE, Buck B, Goossens D, McLaurin B, Murphy L, Leetham-Spencer M, et al. Nevada desert dust with heavy metals suppress-es IgM antibody production. Toxicol reports. 2018 Feb 9;5:258–69. doi:10.1016/j.toxrep.2018.01.006
7. Ghio AJ, Kummarapurugu ST, Tong H, Soukup JM, Dailey LA, Boykin E, et al. Biological effects of desert dust in respiratory epithelial cells and a murine model. Inhal Toxicol. 2014;26(5):299–309. doi:10.3109/08958378.2014.888109
8. He M, Ichinose T, Song Y, Yoshida Y, Bekki K, Arashidani K, et al. Desert dust induces TLR signaling to trigger Th2-domi-nant lung allergic inflammation via a MyD88-dependent signaling pathway. Toxicol Appl Pharmacol. 2016 Apr;296:61–72. doi:10.1016/j.taap.2016.02.011
9. Wang B, Li N, Deng F, Buglak N, Park G, Su S, et al. Human bronchial epithelial cell injuries induced by fine particulate mat-ter from sandstorm and non-sandstorm periods: association with particle constituents. J Environ Sci (China). 2016;47:201–10. doi:10.1016/j.jes.2015.12.015
10. Münzel T, Gori T, Al-Kindi S, Deanfield J, Lelieveld J, Daiber A, et al. Effects of gaseous and solid constituents of air pollution on endothelial function. Eur Heart J. 2018 Oct 7;39(38):3543–50. doi:10.1093/eurheartj/ehy481
11. Chang C-C, Hwang J-S, Chan C-C, Wang P-Y, Cheng T-J. Effects of concentrated ambient particles on heart rate, blood pressure, and cardiac contractility in spontaneously hypertensive rats during a dust storm event. Inhal Toxicol. 2007 Jan 1;19(11):973–8. doi:10.1080/08958370701515399
12. Zhang X, Zhao L, Tong DQ, Wu G, Dan M, Teng B. A systematic review of global desert dust and associated human health ef-fects. Atmosphere (Basel). 2016;7(12):158. https://doi.org/10.3390/atmos7120158
13. Moreira I, Linares C, Follos F, Sánchez-Martinez G, Vellón JM, Diaz J. Short-term effects of Saharan dust intrusions and biomass combustion on birth outcomes in Spain. Sci Total Environ. 2020;701:134755. doi:10.1016/j.scitotenv.2019.134755
14. Cox PA, Richer R, Metcalf JS, Banack SA, Codd GA, Bradley WG. Cyanobacteria and BMAA exposure from desert dust: a possible link to sporadic ALS among Gulf War veterans. Amyotroph Lateral Scler . 2009 Jan 1;10(Suppl. 2):109–17. doi:10.3109/17482960903286066
م إىل كل من السلطات التنظيمية املعنية طرق البحث: يف الفرتة بني أكتوبر / ترشين األول2017 و أبريل / نيسان 2018، أرسلنا استبيانا شبه منظباحلامية العامة من العواصف الرتابية الصحراوية واجلهات صاحبة املصلحة يف املجال االجتامعي يف البلدان الثالثة. وتناول االستبيان معرفة هذه السلطات واجلهات بالعواصف الرتابية الصحراوية وتصوراهتا إزاء العالقة بني العواصف الرتابية الصحراوية واآلثار الصحية، واإلجراءات ذات
الصلة املتخذة من أجل محاية اجلمهور.النتائج: شاركت يف الدراسة 49 جهة من اجلهات صاحبة املصلحة من أصل 58 جهة جرى االتصال هبا )بمعدل استجابة بلغ 84.5%(. وبلغ عدد املستجيبني من السلطات التنظيمية 14 )28.6%(، و35 جهة من اجلهات صاحبة املصلحة يف املجال االجتامعي )71.4%(. وكان مجيع املستجيبني املسنني أن بعفوية إىل تواتر األحداث، يف حني أشار غالبيتهم )%73( نوا من الصحراوية، ولكن كثريين منهم هو الرتابية بالعواصف عىل دراية واألطفال ومرىض اجلهاز التنفيس هم الفئات الفرعية من السكان التي تتأثر هبذه العواصف. ومع ذلك، مل يكن 71% منهم عىل علم بوجود سياسة وطنية معنية بالعواصف الرتابية الصحراوية، أو رأوا أن بلدهم يفتقر إىل مثل هذه السياسة. وعىل الرغم من ورود تقارير تفيد بأن العديد من اجلهات صاحبة املصلحة تتلقى أسئلة من اجلمهور تتعلق بآثار العواصف الرتابية الصحراوية، مل جيب سوى عدد قليل من هذه اجلهات وفقا خلطة عمل
حمددة سلفا. االستنتاجات: تتميز السلطات التنظيمية واجلهات صاحبة املصلحة يف املجال االجتامعي يف قربص واليونان وإرسائيل بمعرفتها اجليدة بالعواصف ينبغي أن تركز اجلهود العامة حمدود. لذلك، املحددة سلفا للحامية العمل تنفيذ خطط أن املرتبطة هبا، رغم الرتابية الصحراوية واآلثار الصحية يف املستقبل عىل زيادة الوعي بني اجلهات صاحبة املصلحة واجلمهور ووضع سياسات وطنية، بام يف ذلك اختاذ تدابري فعالة للتقليل من التعرض
للعواصف الرتابية الصحراوية إىل أدنى حد.
Book 27-11.indb 1099Book 27-11.indb 1099 06/12/2021 12:39 PM06/12/2021 12:39 PM
1100
Research article EMHJ – Vol. 27 No. 11 – 2021
15. Otani S, Onishi K, Mu H, Yokoyama Y, Hosoda T, Okamoto M, et al. The relationship between skin symptoms and allergic reac-tions to Asian dust. Int J Environ Res Public Health. 2012 Dec 10;9(12):4606–14. doi:10.3390/ijerph9124606
16. Tobias A, Caylà JA, Pey J, Alastuey A, Querol X. Are Saharan dust intrusions increasing the risk of meningococcal meningitis? Int J Infect Dis. 2011;15(7):e503. doi:10.1016/j.ijid.2011.03.008
17. Yang C-Y. Effects of Asian dust storm events on daily clinical visits for conjunctivitis in Taipei, Taiwan. J Toxicol Environ Health A. 2006 Oct 1;69(18):1673–80. doi:10.1080/15287390600630096
18. Mallone S, Stafoggia M, Faustini A, Paolo Gobbi G, Marconi A, Forastiere F. Saharan dust and associations between particulate matter and daily mortality in Rome, Italy. Environ Health Perspect. 2011;119(10):1409–14. https://doi.org/10.1289/ehp.1003026
19. Vodonos A, Friger M, Katra I, Avnon L, Krasnov H, Koutrakis P, et al. The impact of desert dust exposures on hospitalizations due to exacerbation of chronic obstructive pulmonary disease. Air Qual Atmos Heal. 2014;7:433–9. doi 10.1007/s11869-014-0253-z
20. Middleton N, Yiallouros P, Kleanthous S, Kolokotroni O, Schwartz J, Dockery DW, et al. A 10-year time-series analysis of respira-tory and cardiovascular morbidity in Nicosia, Cyprus: The effect of short-term changes in air pollution and dust storms. Environ Health. 2008;7:1–16. doi:10.1186/1476-069X-7-39
21. Neophytou AM, Yiallouros P, Coull BA, Kleanthous S, Pavlou P, Pashiardis S, et al. Particulate matter concentrations during desert dust outbreaks and daily mortality in Nicosia, Cyprus. J Expo Sci Environ Epidemiol. 2013;23(3):275–80. doi:10.1038/jes.2013.10
22. Im H-J, Kwon H-J, Ha M, Lee SG, Hwang S-S, Ha EH, et al. [Public perceptions of the risk of Asian dust storms in Seoul and its metropolitan area.] J Prev Med Public Health]. 2006 May;39(3):205–12 (in Korean). PMID:16764494
23. Crosby BC, Bryson JM. Leadership for the common good: tackling public problems in a shared-power world, 2nd ed. San Francis-co: John Wiley & Sons; 2005.
24. Welp M, de la Vega-Leinert A, Stoll-Kleemann S, Jaeger CC. Science-based stakeholder dialogues: theories and tools. Glob Envi-ron Chang. 2006;16(2):170–81. doi:10.1016/j.gloenvcha.2005.12.002
25. Bryson JM. What to do when stakeholders matter: Stakeholder identification and analysis techniques. Public Manag Rev. 2004;6(1):21–53. doi:10.1080/14719030410001675722
26. Brugha R, Varvasovszky Z. Stakeholder analysis: a review. Health Policy Plan. 2000;15(3):239–46. doi:10.1093/heapol/15.3.239
27. Reed MS. Stakeholder participation for environmental management: a literature review. Biol Conserv. 2008;141(10):2417–31. https://doi.org/10.1016/j.biocon.2008.07.014
28. Renn O. White paper on risk governance: toward an integrative framework. In: Renn O, Walker KD, eds. Global risk governance. International Risk Governance Council Bookseries, vol 1. Dordrecht: Springer; 2005. doi:10.1007/978-1-4020-6799-0_1
29. Gill P, Stewart K, Treasure E, Chadwick B. Methods of data collection in qualitative research: interviews and focus groups. Bdj. 2008 Mar 22;204:291.
30. Callaghan S, Corra L, Hanvey L, Leoni M, Monti V. Profile of children’s environmental health in Argentina. Buenos Aires: Min-isterio de Salud de la Argentina, la Sociedad Argentina de Pediatria, la Asociación Argentina de Médicos por el Medio Ambient, Canadian Institute of Child Health; 2007.
31. Golnaraghi M. Global assessment report on disaster reduction: thematic progress review sub-component on early warning systems. Geneva: World Meteorological Organization; 2009:1–32.
32. Kopanakis I, Mammi-Galani ‐, Pentari D, Glytsos T, Lazaridi M. Ambient particulate matter concentration levels and their ori-gin during dust event episodes in the Eastern Mediterranean. Aerosol Sci Engineer 2. 2018:61–73. doi:10.1007/s41810-018-0023-7
33. Ganor E. The frequency of Saharan dust episodes over Tel Aviv, Israel. Atmos Environ. 1994;28(17):2867–71. doi:10.1016/1352-2310(94)90087-6
34. Kaskaoutis DG, Kosmopoulos PG, Nastos PT, Kambezidis DH, Sharma M, Mehdi W. Transport pathways of Sahara dust over Athens, Greece as detected by MODIS and TOMS. Geomatics, Nat Hazards Risk. 2012 Feb 1;3(1):35–54.
35. Trianti SM, Samoli E, Rodopoulou S, Katsouyanni K, Papiris SA, Karakatsani A. Desert dust outbreaks and respiratory morbidity in Athens, Greece. Environ Heal A Glob Access Sci Source. 2017;16(1):1–9. doi:10.1186/s12940-017-0281-x
36. Renzi M, Forastiere F, Calzolari R, Cernigliaro A, Madonia G, Michelozzi P, et al. Short-term effects of desert and non-desert PM10on mortality in Sicily, Italy. Environ Int. 2018;120(April):472–9. doi:10.1016/j.envint.2018.08.016
37. Alessandrini ER, Stafoggia M, Faustini A, Gobbi GP, Forastiere F. Saharan dust and the association between particulate matter and daily hospitalisations in Rome, Italy. Occup Environ Med. 2013;70(6):432–4. doi:10.1136/oemed-2012-101182
38. Kanatani KT, Okumura M, Tohno S, Adachi Y, Sato K, Nakayama T. Indoor particle counts during Asian dust events under every-day conditions at an apartment in Japan. Environ Health Prev Med. 2014;19(1):81–8. doi:10.1007/s12199-013-0356-4
39. Krasnov H, Katra I, Novack V, Vodonos A, Friger MD. Increased indoor PM concentrations controlled by atmospheric dust events and urban factors. Build Environ. 2015;87:169–76. doi:10.1016/j.buildenv.2015.01.035
40. Kuo HW, Shen HY. Indoor and outdoor PM2.5 and PM10 concentrations in the air during a dust storm. Build Environ. 2010;45(3):610–4. doi:10.1016/j.buildenv.2009.07.017
41. Ciuzas D, Prasauskas T, Krugly E, Jurelionis A, Seduikyte L, Martuzevicius D. Indoor air quality management by combined venti-lation and air cleaning: an experimental study. Aerosol Air Qual Res. 2016;16(10):2550–9. doi:10.4209/aaqr.2015.10.0577
Book 27-11.indb 1100Book 27-11.indb 1100 06/12/2021 12:39 PM06/12/2021 12:39 PM
1101
Research article EMHJ – Vol. 27 No. 11 – 2021
42. Lanphear BP, Hornung RW, Khoury J, Yolton K, Lierl M, Kalkbrenner A. Effects of HEPA air cleaners on unscheduled asthma visits and asthma symptoms for children exposed to secondhand tobacco smoke. Pediatrics. 2011;127(1):93–101. doi:10.1542/peds.2009-2312
43. Butz AM, Matsui EC, Breysse P, Curtin-Brosnan J, Eggleston P, Diette G, et al. A randomized trial of air cleaners and a health coach to improve indoor air quality for inner-city children with asthma and secondhand smoke exposure. Arch Pediatr Adolesc Med. 2011;165(8):741–8. doi:10.1001/archpediatrics.2011.111
44. Jhun I, Gaffin JM, Coull BA, Huffaker MF, Petty CR, Sheehan WJ, et al. School environmental intervention to reduce particulate pollutant exposures for children with asthma. J Allergy Clin Immunol Pr. 2017;5(1):154–9. doi:10.1016/j.jaip.2016.07.018
45. Liu G, Xiao M, Zhang X, Gal C, Chen X, Liu L, et al. A review of air filtration technologies for sustainable and healthy building ventilation. Sustain Cities Soc. 2017;32(April):375–96.
46. Allahbakhshi K, Ghomian Z, Jazani RK, Khorasani-Zavareh D. Preparedness challenges of the Iranian health system for dust and sand storms: a qualitative study. J Educ Health Promot. 2019 Jun 27;8:114. doi:10.4103/jehp.jehp_470_18
47. Nutt PC. Why decisions fail: avoiding the blunders and traps that lead to debacles. San Francisco: Berrett-Koehler Publishers; 2002.
48. Achilleos S, Mouzourides P, Kalivitis N, Katra I, Kloog I, Kouis P, et al. Spatio-temporal variability of desert dust storms in Eastern Mediterranean (Crete, Cyprus, Israel) between 2006 and 2017 using a uniform methodology. Sci Total Environ. 2020 Apr;714:136693. doi:10.1016/j.scitotenv.2020.136693
49. Soleimani Z, Teymouri P, Darvishi Boloorani A, Mesdaghinia A, Middleton N, Griffin DW. An overview of bioaerosol load and health impacts associated with dust storms: A focus on the Middle East. Atmos Environ. 2020;223:117187.
50. Gherboudj I, Naseema Beegum S, Ghedira H. Identifying natural dust source regions over the Middle-East and North-Africa: estimation of dust emission potential. Earth-Science Rev. 2017;165:342–55.
51. Sprigg WA. Dust storms, human health and a global early warning system. In: Steinberg SL, Sprigg WA, eds. Extreme weather, health, and communities: interdisciplinary engagement strategies. Cham: Springer International Publishing; 2016:59–87.
52. Nemuc A, Mona L, Waldhauserova P, Tobias A, Monteiro A, Kazadzis S, et al. COST Lecture 2019 AE GM Barcelona: International Network to Encourage the Use of Monitoring and Forecasting Dust Products (InDust) How does Cambridge Core Share work? European Review: 2020;1-15
53. Kuligowski E, Dootson P. Emergency notification: warnings and alerts. Encyclopedia of wildfires and wildland-urban interface (WUI) fires. Cham: Springer International Publishing; 2018:1–9. https://doi.org/10.1007/978-3-319-51727-8_48-1
54. Mitigating the health effects of desert dust storms using exposure-reduction approaches (MEDEA). ClinicalTrials.gov identifier: NCT03503812. Bethesda, Maryland: US National Library of Medicine; 2018 (https://clinicaltrials.gov/ct2/show/NCT03503812, accessed 25 April 2021).
Book 27-11.indb 1101Book 27-11.indb 1101 06/12/2021 12:39 PM06/12/2021 12:39 PM

1102
Short research communication EMHJ – Vol. 27 No. 11 – 2021Short research communication
The brain drain: why medical students and young physicians want to leave EgyptIbrahim Kabbash,1 Rania El-Sallamy,2 Hanaa Zayed,2 Ibrahim Alkhyate,3 Ahmed Omar3 and Sanaa Abdo1
1Department of Public Health and Community Medicine, Faculty of Medicine, Tanta University, Tanta, Egypt. 2Occupational Medicine, Department of Public Health and Community Medicine, Faculty of Medicine, Tanta University, Tanta, Egypt. 3Faculty of Medicine, Tanta University, Tanta, Egypt (Correspondence to: Ibrahim A. Kabbash: [email protected], [email protected]).
AbstractBackground: Egypt has a shortage of physicians despite thousands of medical students graduating annually. Aims: This study aimed to explore the reasons for Egyptian medical students and young physicians wanting to emigrate.Methods: This cross-sectional study, conducted from February to April 2019, included 711 fifth- and sixth-year medical students and 174 residents from two medical faculties in Egypt, Tanta and Kafrelshiekh. A questionnaire was used to collect data on sociodemographic factors, desire to emigrate and motives for wanting to emigrate.Results: Most participant (89.4%) wanted to emigrate, and thought their salary was not compatible with their working hours or risks. About half the participants (52.8%) worked part-time in private hospitals. Only 4.9% of participants felt appreciated by the country. Most participants (75.9%) were not satisfied with their relationship with patients and 40.2% were not satisfied with their relationship with colleagues. Verbal abuse was reported by 55.5% of participants and physical assaults by 35.4%. Most participants who wanted to emigrate (85.1%) said they would change their minds if improvements were made in the health sector. Residents generally had less negative attitudes to workplace and professional factors than students.Conclusion: Physicians emigrate to seek better work and financial incentives. A retention policy needs to be developed to prevent Egyptian physicians from emigrating.Keywords: emigration, physicians, workplace, motivation, EgyptCitation: Kabbash I; El-Sallamy R; Zayed H; Alkhyate I; Omar A; Abdo S. The brain drain: why medical students and young physicians want to leave Egypt. East Mediterr Health J. 2021;27(11):1102–1108. https://doi.org/10.26719/emhj.21.050 Received: 18/01/21; accepted: 04/04/21Copyright © World Health Organization (WHO) 2021. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license https://creativecommons.org/licenses/by-nc-sa/3.0/igo
IntroductionUniversal health coverage is a priority goal for the World Health Organization (WHO) that needs an adequate, skilled and motivated health workforce to be achieved (1). Migration of physicians from low- and middle-income countries (LMICs) to high-income countries (HICs), the so-called brain drain, is an area of concern that threatens the sustainability of health systems in LMICs (2). Health workers are under pressure for a number of reasons: high cost of training, attrition, migration and increasing de-mands of ageing populations (3).
In 2013, WHO estimated a global shortage of 7.2 million health care providers (1). This shortage is predicted to reach 15 million by 2030 (4). This shortage is worsened in LMICs by migration of educated health workers to HICs (5–7). The brain drain is especially affecting Africa, which has 25% of the global disease burden and only 3% of the health workforce (8). Losses in health workforce in some African countries may reach up to 70% due to migration, with one fifth of African-born physicians estimated to be working in HICs (9). Losses of trained health personnel from already stressed health systems leave the remaining professionals overwhelmed and demoralized. This exacerbates the problem of low doctor-to-population ratios in many developing countries, leading to a critical
lack of services and a reduction in the quality of care provided (10–12).
Egypt suffers from a shortage of physicians despite thousands of medical students graduating annually. In 2016, the density of physicians was estimated to be 1 physician per 12 285 inhabitants (13). Emigration of physicians intensifies physician shortages in Egypt and the loss cannot be replaced by recruitment (14). Despite being a major supplier of immigrant medical graduates, little is known about the pattern of physician migration and its associated factors. Therefore, we explored factors associated with migration among medical students, who are the future physicians, and junior resident physicians in two university hospitals in Egypt.
MethodsStudy design, setting and participantsWe carried out a cross-sectional study in the Nile Del-ta region university hospitals during the period from February to April 2019. The Nile Delta Region has eight faculties of medicine, from which two medical faculties were chosen randomly, Tanta and Kafrelshiekh. The tar-get population of this study were undergraduate medical students in the final clinical grades (5th and 6th years)
Book 27-11.indb 1102Book 27-11.indb 1102 06/12/2021 12:39 PM06/12/2021 12:39 PM
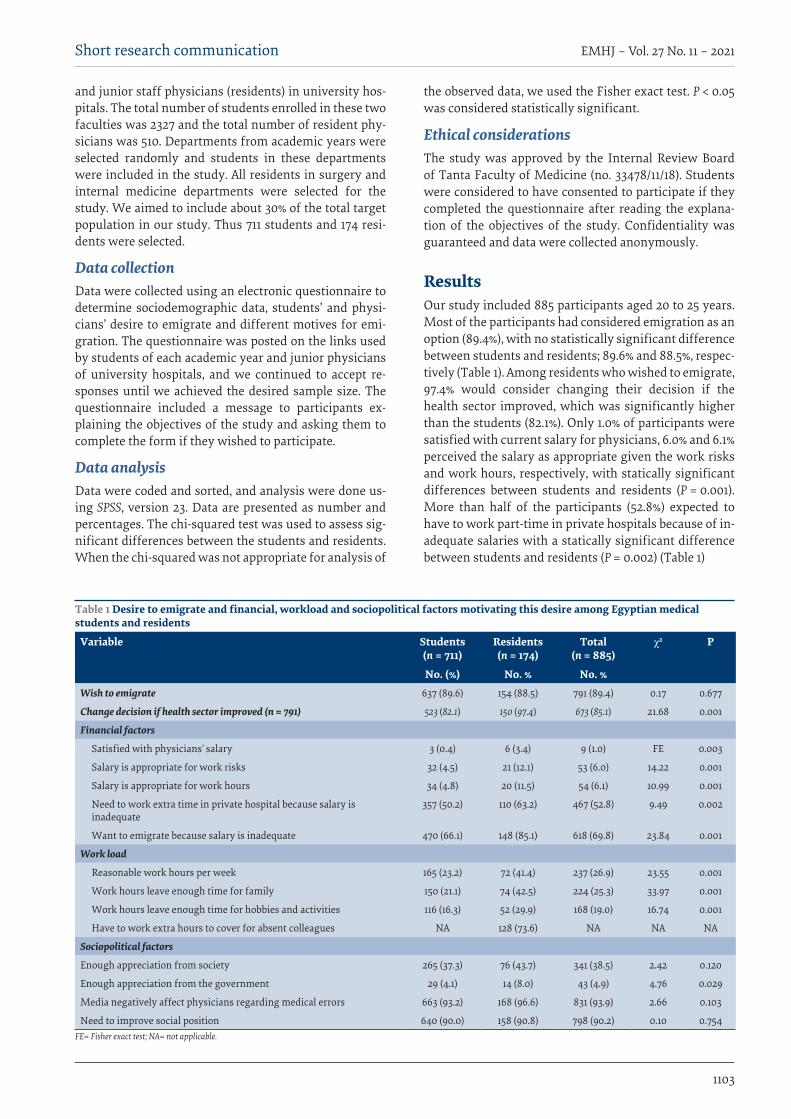
1103
Short research communication EMHJ – Vol. 27 No. 11 – 2021
and junior staff physicians (residents) in university hos-pitals. The total number of students enrolled in these two faculties was 2327 and the total number of resident phy-sicians was 510. Departments from academic years were selected randomly and students in these departments were included in the study. All residents in surgery and internal medicine departments were selected for the study. We aimed to include about 30% of the total target population in our study. Thus 711 students and 174 resi-dents were selected.
Data collectionData were collected using an electronic questionnaire to determine sociodemographic data, students’ and physi-cians’ desire to emigrate and different motives for emi-gration. The questionnaire was posted on the links used by students of each academic year and junior physicians of university hospitals, and we continued to accept re-sponses until we achieved the desired sample size. The questionnaire included a message to participants ex-plaining the objectives of the study and asking them to complete the form if they wished to participate.
Data analysis Data were coded and sorted, and analysis were done us-ing SPSS, version 23. Data are presented as number and percentages. The chi-squared test was used to assess sig-nificant differences between the students and residents. When the chi-squared was not appropriate for analysis of
the observed data, we used the Fisher exact test. P < 0.05 was considered statistically significant.
Ethical considerationsThe study was approved by the Internal Review Board of Tanta Faculty of Medicine (no. 33478/11/18). Students were considered to have consented to participate if they completed the questionnaire after reading the explana-tion of the objectives of the study. Confidentiality was guaranteed and data were collected anonymously.
ResultsOur study included 885 participants aged 20 to 25 years. Most of the participants had considered emigration as an option (89.4%), with no statistically significant difference between students and residents; 89.6% and 88.5%, respec-tively (Table 1). Among residents who wished to emigrate, 97.4% would consider changing their decision if the health sector improved, which was significantly higher than the students (82.1%). Only 1.0% of participants were satisfied with current salary for physicians, 6.0% and 6.1% perceived the salary as appropriate given the work risks and work hours, respectively, with statically significant differences between students and residents (P = 0.001). More than half of the participants (52.8%) expected to have to work part-time in private hospitals because of in-adequate salaries with a statically significant difference between students and residents (P = 0.002) (Table 1)
Table 1 Desire to emigrate and financial, workload and sociopolitical factors motivating this desire among Egyptian medical students and residents
Variable Students (n = 711)
Residents (n = 174)
Total (n = 885)
χ2 P
No. (%) No. % No. %Wish to emigrate 637 (89.6) 154 (88.5) 791 (89.4) 0.17 0.677
Change decision if health sector improved (n = 791) 523 (82.1) 150 (97.4) 673 (85.1) 21.68 0.001
Financial factors
Satisfied with physicians’ salary 3 (0.4) 6 (3.4) 9 (1.0) FE 0.003
Salary is appropriate for work risks 32 (4.5) 21 (12.1) 53 (6.0) 14.22 0.001
Salary is appropriate for work hours 34 (4.8) 20 (11.5) 54 (6.1) 10.99 0.001
Need to work extra time in private hospital because salary is inadequate
357 (50.2) 110 (63.2) 467 (52.8) 9.49 0.002
Want to emigrate because salary is inadequate 470 (66.1) 148 (85.1) 618 (69.8) 23.84 0.001
Work load
Reasonable work hours per week 165 (23.2) 72 (41.4) 237 (26.9) 23.55 0.001
Work hours leave enough time for family 150 (21.1) 74 (42.5) 224 (25.3) 33.97 0.001
Work hours leave enough time for hobbies and activities 116 (16.3) 52 (29.9) 168 (19.0) 16.74 0.001
Have to work extra hours to cover for absent colleagues NA 128 (73.6) NA NA NA
Sociopolitical factors
Enough appreciation from society 265 (37.3) 76 (43.7) 341 (38.5) 2.42 0.120
Enough appreciation from the government 29 (4.1) 14 (8.0) 43 (4.9) 4.76 0.029
Media negatively affect physicians regarding medical errors 663 (93.2) 168 (96.6) 831 (93.9) 2.66 0.103
Need to improve social position 640 (90.0) 158 (90.8) 798 (90.2) 0.10 0.754FE= Fisher exact test; NA= not applicable.
Book 27-11.indb 1103Book 27-11.indb 1103 06/12/2021 12:39 PM06/12/2021 12:39 PM
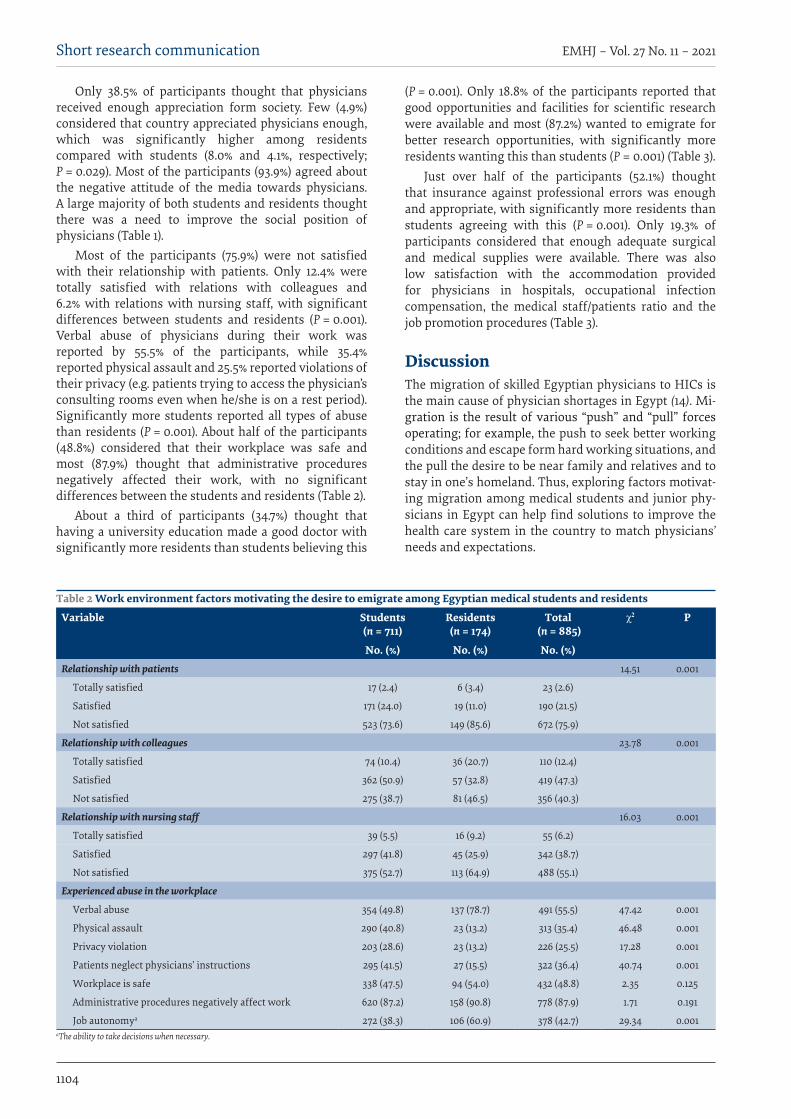
1104
Short research communication EMHJ – Vol. 27 No. 11 – 2021
Only 38.5% of participants thought that physicians received enough appreciation form society. Few (4.9%) considered that country appreciated physicians enough, which was significantly higher among residents compared with students (8.0% and 4.1%, respectively; P = 0.029). Most of the participants (93.9%) agreed about the negative attitude of the media towards physicians. A large majority of both students and residents thought there was a need to improve the social position of physicians (Table 1).
Most of the participants (75.9%) were not satisfied with their relationship with patients. Only 12.4% were totally satisfied with relations with colleagues and 6.2% with relations with nursing staff, with significant differences between students and residents (P = 0.001). Verbal abuse of physicians during their work was reported by 55.5% of the participants, while 35.4% reported physical assault and 25.5% reported violations of their privacy (e.g. patients trying to access the physician’s consulting rooms even when he/she is on a rest period). Significantly more students reported all types of abuse than residents (P = 0.001). About half of the participants (48.8%) considered that their workplace was safe and most (87.9%) thought that administrative procedures negatively affected their work, with no significant differences between the students and residents (Table 2).
About a third of participants (34.7%) thought that having a university education made a good doctor with significantly more residents than students believing this
(P = 0.001). Only 18.8% of the participants reported that good opportunities and facilities for scientific research were available and most (87.2%) wanted to emigrate for better research opportunities, with significantly more residents wanting this than students (P = 0.001) (Table 3).
Just over half of the participants (52.1%) thought that insurance against professional errors was enough and appropriate, with significantly more residents than students agreeing with this (P = 0.001). Only 19.3% of participants considered that enough adequate surgical and medical supplies were available. There was also low satisfaction with the accommodation provided for physicians in hospitals, occupational infection compensation, the medical staff/patients ratio and the job promotion procedures (Table 3).
DiscussionThe migration of skilled Egyptian physicians to HICs is the main cause of physician shortages in Egypt (14). Mi-gration is the result of various “push” and “pull” forces operating; for example, the push to seek better working conditions and escape form hard working situations, and the pull the desire to be near family and relatives and to stay in one’s homeland. Thus, exploring factors motivat-ing migration among medical students and junior phy-sicians in Egypt can help find solutions to improve the health care system in the country to match physicians’ needs and expectations.
Table 2 Work environment factors motivating the desire to emigrate among Egyptian medical students and residents
Variable Students (n = 711)
Residents (n = 174)
Total (n = 885)
χ2 P
No. (%) No. (%) No. (%)Relationship with patients 14.51 0.001
Totally satisfied 17 (2.4) 6 (3.4) 23 (2.6)
Satisfied 171 (24.0) 19 (11.0) 190 (21.5)
Not satisfied 523 (73.6) 149 (85.6) 672 (75.9)
Relationship with colleagues 23.78 0.001
Totally satisfied 74 (10.4) 36 (20.7) 110 (12.4)
Satisfied 362 (50.9) 57 (32.8) 419 (47.3)
Not satisfied 275 (38.7) 81 (46.5) 356 (40.3)
Relationship with nursing staff 16.03 0.001
Totally satisfied 39 (5.5) 16 (9.2) 55 (6.2)
Satisfied 297 (41.8) 45 (25.9) 342 (38.7)
Not satisfied 375 (52.7) 113 (64.9) 488 (55.1)
Experienced abuse in the workplace
Verbal abuse 354 (49.8) 137 (78.7) 491 (55.5) 47.42 0.001
Physical assault 290 (40.8) 23 (13.2) 313 (35.4) 46.48 0.001
Privacy violation 203 (28.6) 23 (13.2) 226 (25.5) 17.28 0.001
Patients neglect physicians’ instructions 295 (41.5) 27 (15.5) 322 (36.4) 40.74 0.001
Workplace is safe 338 (47.5) 94 (54.0) 432 (48.8) 2.35 0.125
Administrative procedures negatively affect work 620 (87.2) 158 (90.8) 778 (87.9) 1.71 0.191
Job autonomya 272 (38.3) 106 (60.9) 378 (42.7) 29.34 0.001 aThe ability to take decisions when necessary.
Book 27-11.indb 1104Book 27-11.indb 1104 06/12/2021 12:39 PM06/12/2021 12:39 PM
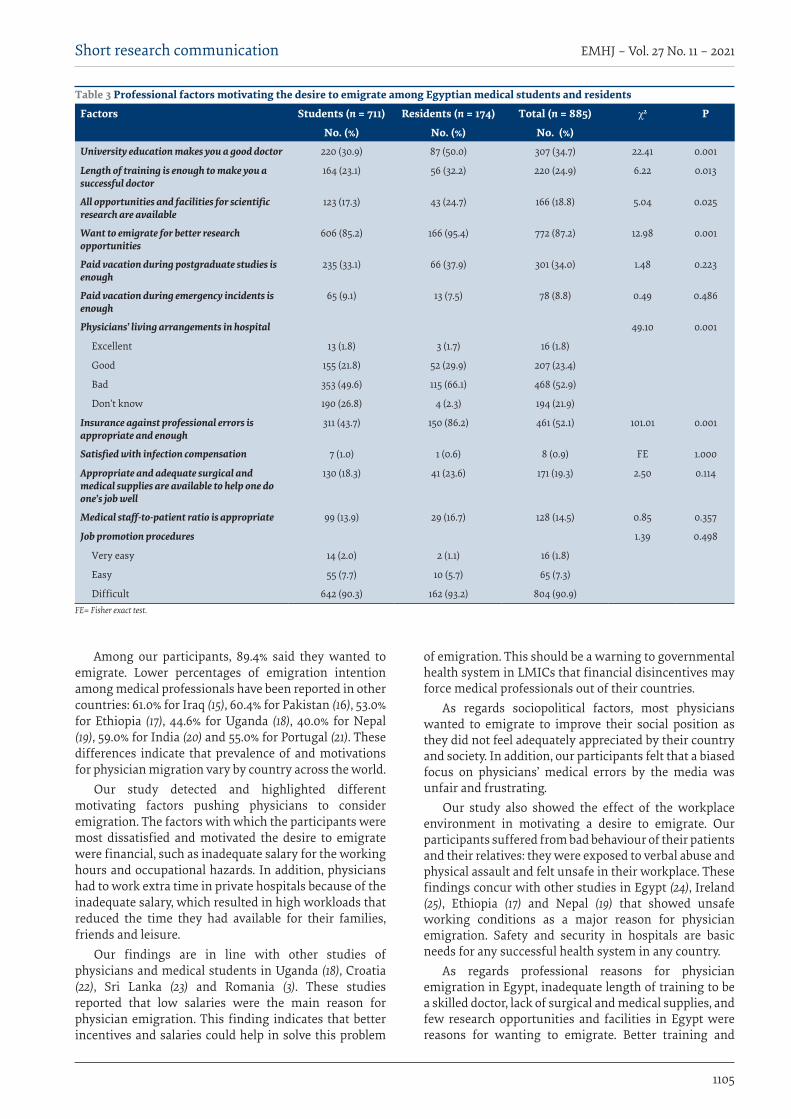
1105
Short research communication EMHJ – Vol. 27 No. 11 – 2021
Among our participants, 89.4% said they wanted to emigrate. Lower percentages of emigration intention among medical professionals have been reported in other countries: 61.0% for Iraq (15), 60.4% for Pakistan (16), 53.0% for Ethiopia (17), 44.6% for Uganda (18), 40.0% for Nepal (19), 59.0% for India (20) and 55.0% for Portugal (21). These differences indicate that prevalence of and motivations for physician migration vary by country across the world.
Our study detected and highlighted different motivating factors pushing physicians to consider emigration. The factors with which the participants were most dissatisfied and motivated the desire to emigrate were financial, such as inadequate salary for the working hours and occupational hazards. In addition, physicians had to work extra time in private hospitals because of the inadequate salary, which resulted in high workloads that reduced the time they had available for their families, friends and leisure.
Our findings are in line with other studies of physicians and medical students in Uganda (18), Croatia (22), Sri Lanka (23) and Romania (3). These studies reported that low salaries were the main reason for physician emigration. This finding indicates that better incentives and salaries could help in solve this problem
of emigration. This should be a warning to governmental health system in LMICs that financial disincentives may force medical professionals out of their countries.
As regards sociopolitical factors, most physicians wanted to emigrate to improve their social position as they did not feel adequately appreciated by their country and society. In addition, our participants felt that a biased focus on physicians’ medical errors by the media was unfair and frustrating.
Our study also showed the effect of the workplace environment in motivating a desire to emigrate. Our participants suffered from bad behaviour of their patients and their relatives: they were exposed to verbal abuse and physical assault and felt unsafe in their workplace. These findings concur with other studies in Egypt (24), Ireland (25), Ethiopia (17) and Nepal (19) that showed unsafe working conditions as a major reason for physician emigration. Safety and security in hospitals are basic needs for any successful health system in any country.
As regards professional reasons for physician emigration in Egypt, inadequate length of training to be a skilled doctor, lack of surgical and medical supplies, and few research opportunities and facilities in Egypt were reasons for wanting to emigrate. Better training and
Table 3 Professional factors motivating the desire to emigrate among Egyptian medical students and residents
Factors Students (n = 711) Residents (n = 174) Total (n = 885) χ2 P
No. (%) No. (%) No. (%)University education makes you a good doctor 220 (30.9) 87 (50.0) 307 (34.7) 22.41 0.001
Length of training is enough to make you a successful doctor
164 (23.1) 56 (32.2) 220 (24.9) 6.22 0.013
All opportunities and facilities for scientific research are available
123 (17.3) 43 (24.7) 166 (18.8) 5.04 0.025
Want to emigrate for better research opportunities
606 (85.2) 166 (95.4) 772 (87.2) 12.98 0.001
Paid vacation during postgraduate studies is enough
235 (33.1) 66 (37.9) 301 (34.0) 1.48 0.223
Paid vacation during emergency incidents is enough
65 (9.1) 13 (7.5) 78 (8.8) 0.49 0.486
Physicians’ living arrangements in hospital 49.10 0.001
Excellent 13 (1.8) 3 (1.7) 16 (1.8)
Good 155 (21.8) 52 (29.9) 207 (23.4)
Bad 353 (49.6) 115 (66.1) 468 (52.9)
Don’t know 190 (26.8) 4 (2.3) 194 (21.9)
Insurance against professional errors is appropriate and enough
311 (43.7) 150 (86.2) 461 (52.1) 101.01 0.001
Satisfied with infection compensation 7 (1.0) 1 (0.6) 8 (0.9) FE 1.000
Appropriate and adequate surgical and medical supplies are available to help one do one’s job well
130 (18.3) 41 (23.6) 171 (19.3) 2.50 0.114
Medical staff-to-patient ratio is appropriate 99 (13.9) 29 (16.7) 128 (14.5) 0.85 0.357
Job promotion procedures 1.39 0.498
Very easy 14 (2.0) 2 (1.1) 16 (1.8)
Easy 55 (7.7) 10 (5.7) 65 (7.3)
Difficult 642 (90.3) 162 (93.2) 804 (90.9)FE= Fisher exact test.
Book 27-11.indb 1105Book 27-11.indb 1105 06/12/2021 12:39 PM06/12/2021 12:39 PM
1106
Short research communication EMHJ – Vol. 27 No. 11 – 2021
research opportunities were important reasons in other studies among physicians in Pakistan (16), Lebanon (26), India (20) and Mongolia (27).
An encouraging result of this study was that responders said that their desire to emigrate could change if the health sector in Egypt improved. Another study of Egyptian medical students found that 81.8% of the participants planned to return to Egypt after training to serve their home country (24). Another promising point in our results is that residents generally had less of a negative attitude to workplace and professional factors than students. The perceptions of students is more based on observation and experiences of others, while those of
residents reflect their own experience after starting work as a doctor.
Our study reflects the experience of medical students and junior physicians in Lower Egypt, which could be different from students and residents in Upper Egypt and the main cities of Cairo and Alexandria. Our large sample size can ensure representativeness of the results to the target population.
To conclude, Egyptian medical students and young physicians have a strong desire to emigrate abroad to seek better working conditions, lifestyle, financial incentives and research opportunities. A retention policy needs to be developed with strategic actions to prevent Egyptian physicians from emigrating to other countries.
AcknowledgementWe thank the students of the fourth academic year who shared in data collection.
Funding: None
Competing interests: None declared.
هجرة األدمغة: ملاذا يريد طالب الطب وشباب األطباء مغادرة مرص؟إبراهيم كباش، رانيا السالمي، هناء زايد، إبراهيم اخلياط، أمحد عمر، سناء عبده
اخلالصةا. ج اآلالف من طالب الطب سنوي اخللفية: تعاين مرص من نقص يف عدد األطباء، برغم ختر
األهداف: هدفت هذه الدراسة إىل استكشاف أسباب رغبة طالب الطب وشباب األطباء املرصيني يف اهلجرة.
Fuite des cerveaux : pourquoi les étudiants en médecine et les jeunes médecins veulent quitter l’ÉgypteRésuméContexte : L’Égypte fait face à une pénurie de médecins malgré les milliers d’étudiants en médecine qui obtiennent leur diplôme chaque année. Objectifs : La présente étude visait à explorer les raisons pour lesquelles les étudiants en médecine et les jeunes médecins égyptiens souhaitent émigrer.Méthodes : Cette étude transversale, menée de février à avril 2019, incluait 711 étudiants de cinquième et sixième année et 174 médecins résidents de deux facultés de médecine en Égypte, à savoir celle de Tanta et de Kafr el-Cheikh. Un questionnaire a été utilisé pour recueillir des données sur les facteurs sociodémographiques, la volonté d’émigrer et les motifs sous-jacents.Résultats : La plupart des participants (89,4 %) souhaitaient émigrer, et pensaient que leur salaire n’était pas compatible avec leur temps de travail ou les risques du métier. Près de la moitié des participants (52,8 %) travaillaient à temps partiel dans des hôpitaux privés. Seuls 4,9 % des participants se sentaient valorisés par le pays. La plupart des participants (75,9 %) n’étaient pas satisfaits de leurs relations avec les patients et 40,2 % n’étaient pas satisfaits de leurs relations avec leurs collègues. Des agressions verbales ont été rapportées par 55,5 % des participants et des agressions physiques par 35,4 %. La plupart des participants qui souhaitaient émigrer (85,1 %) ont déclaré qu’ils changeraient d’avis si des améliorations étaient apportées dans le secteur de la santé. Les médecins résidents avaient généralement une attitude moins négative que les étudiants à l’égard de l’environnement de travail et des facteurs professionnels.Conclusion : Les médecins émigrent en quête de meilleures conditions de travail et d’un meilleur salaire. Une politique de fidélisation doit être mise en place pour empêcher les médecins égyptiens d’émigrer.
Book 27-11.indb 1106Book 27-11.indb 1106 06/12/2021 12:39 PM06/12/2021 12:39 PM
1107
Short research communication EMHJ – Vol. 27 No. 11 – 2021
References1. Global Health Workforce Alliance and World Health Organization. A universal truth: no health without a workforce. Geneva:
World Health Organization; 2013. (http://www.who.int/workforcealliance/knowledge/resources/GHWA_AUniversalTruthRee-port.pdf, accessed 13 October 2020).
2. OECD data. Doctors [Internet]. Paris: Organisation for Economic Co-operation and Development; 2016 (https://data.oecd.org/healthres/doctors.htm, accessed 13 October 2020.
3. Suciu SM, Popescu CA, Ciumageanu MD, Buzoianu AD. Physician migration at its roots: a study on the emigration preferences and plans among medical students in Romania. Hum Resour Health. 2017;15(1):6. https://doi.org/10.1186/s12960-017-0181-8
4. Liu JX, Goryakin Y, Maeda A, Bruckner T, Scheffler R. Global health workforce labor market projections for 2030. Hum Resour Health. 2017;15(1):11. https://doi.org/10.1186/s12960-017-0187-2
5. Crisp N, Chen L. Global supply of health professionals. N Engl J Med. 2014;370(10):950–7. https://doi.org/10.1056/NEJMra1111610
6. Moszynski P. One billion people are affected by global shortage of healthcare workers. BMJ. 2011;342:d696. https://doi.org/10.1136/bmj.d696
7. Aluttis C, Bishaw T, Frank MW. The workforce for health in a globalized context: global shortages and international migration. Glob Health Action. 2014;7:23611. https://doi.org/10.3402/gha.v7.2361
8. The World Health Report, 2006. Working together for health. Geneva: World Health Organization; 2006 (https://apps.who.int/iris/handle/10665/43432, accessed 13, August 2021).
9. Duvivier RJ, Burch VC, Boulet JR. A comparison of physician emigration from Africa to the United States of America between 2005 and 2015. Hum Resour Health. 2017;15(1):41. https://doi.org/10.1186/s12960-017-0217-0
10. Asongu S. The impact of health worker migration on development dynamics: evidence of wealth effects from Africa. Yaoundé, African Governance and Development Institute; 2012 (http://www.afridev.org/RePEc/agd/agd-wpaper/The-imu-pact-of-health-worker-migration-on-development-dynamics.-Evidence-of wealth-effects-from-Africa.pdf, accessed 6 August 2021).
11. Bhargava A, Docquier F, Moullan Y. Modeling the effects of physician emigration on human development. Econ Hum Biol. 2011;9(2):172–83. https://doi.org/10.1016/j.ehb.2010.12.004
12. Okeke EN. Do higher salaries lower physician migration? Health Policy Plann. 2014;29(5):603–14 https://doi.org/10.1093/heapol/czt046
13. Global Health Observatory data repository [Internet]. Geneva: World Health Organization (http://apps.who.int/gho/data/node.main.A1444, accessed 6 August 2021).
14. Abdelaziz A, Kassab SE, Abdelnasser A, Hosny S. Medical education in Egypt: historical background, current status, and challeng-es. Health Prof Educ. 2018;4(4):236–44. https://doi.org/10.1016/j.hpe.2017.12.007
15. Burnham G, Malik S, Al-Shibli ASD, Mahjoub AR, Baqer AQ, Baqer ZQ et al. Understanding the impact of conflict on health services in Iraq: information from 401 Iraqi refugee doctors in Jordan. Int J Health Plann Manage. 2012;27(1):e51–e64. https://doi.org/10.1002/hpm.1091
16. Sheikh A, Naqvi SH, Sheikh K, Naqvi SH, Bandukda MY. Physician migration at its roots: a study on the factors contribut-ing towards a career choice abroad among students at a medical school in Pakistan. Global Health. 2012;8:43. https://doi.org/10.1186/1744-8603-8-43
17. Deressa W, Azazh A. Attitudes of undergraduate medical students of Addis Ababa University towards medical practice and mi-gration, Ethiopia. BMC Med. Educ. 2012;12(68). https://doi.org/10.1186/1472-6920-12-68
18. Kizito S, Mukunya D, Nakitende J, Nambasa S, Nampogo A, Kalyesubula R, et al. Career intentions of final year medical students in Uganda after graduating: the burden of brain drain. BMC Med. Educ. 2015;15:122. https://doi.org/10.1186/s12909-015-0396-0
19. Lakhey M, Lakhey S, Niraula SR. Comparative attitude and plans of the medical students and young Nepalese doctors. Kathman-du Univ Med J (KUMJ). 2009;7(26):177–82. https://doi.org/10.1097/00001888-200602000-00015
طرق البحث: اشتملت هذه الدراسة املقطعية، التي أجريت يف الفرتة من فرباير/ شباط إىل أبريل/ نيسان 2019، عىل 711 طالبا و174 طبيبا من كليتني للطب يف مرص، مها طنطا وكفر الشيخ. واستخدم استبيان جلمع البيانات عن العوامل االجتامعية السكانية والرغبة يف اهلجرة والدوافع هلذه
الرغبة.النتائج: أراد معظم املشاركني اهلجرة )89.4%( واعتقدوا أن رواتبهم ال تتوافق وساعات عملهم، أو املخاطر التي يتعرضون هلا. وذكر أكثر من يرض معظم بالتقدير. ومل املشاركني يشعر سوى 4.9% من اخلاصة. ومل املستشفيات بدوام جزئي يف يعملون أهنم املشاركني )%52.8( نصف ضهم إلساءات تعر املشاركني عن وأبلغ 55.5% من بزمالئهم. يرض 40.2% عن عالقتهم مل باملرىض، كام املشاركني )75.9%( عن عالقتهم لفظية، و35.4% العتداءات جسدية. وقال معظم املشاركني الذين رغبوا يف اهلجرة )85.1%( إهنم سيغريون رأهيم إذا أدخلت حتسينات عىل القطاع
الصحي. وكان لدى األطباء املقيمني عموما مواقف سلبية أقل جتاه أماكن العمل والعوامل املهنية مقارنة بالطالب.االستنتاجات: هياجر األطباء بحثا عن عمل وحوافز مالية أفضل. وهكذا جيب وضع سياسة استبقاء ملنع األطباء املرصيني من اهلجرة.
Book 27-11.indb 1107Book 27-11.indb 1107 06/12/2021 12:39 PM06/12/2021 12:39 PM

1108
Short research communication EMHJ – Vol. 27 No. 11 – 2021
20. Rao NR, Rao UK and Cooper RA. Indian medical students’ views on immigration for training and practice. Acad Med. 2006;81(2):185–8. https://doi.org/10.1097/00001888-200602000-00015
21. Ramos P, Alves H. Migration intentions among Portuguese junior doctors: results from a survey. Health Policy. 2017; 121(12):1208–14. https://doi.org/10.1016/j.healthpol.2017.09.016
22. Bojanic A, Bojanic K and Likic R. Brain drain: final year medical students’ intentions of training abroad. Postgrad Med J. 2015;91(1076):315–21. https://doi.org/10.1136/postgradmedj-2014-132908
23. de Silva NL, Samarasekara K, Rodrigo C, Samarakoon L, Fernando SD, Rajapakse S. Why do doctors emigrate from Sri Lanka? A survey of medical undergraduates and new graduates. BMC Res Notes. 2014;7:918. https://doi.org/10.1186/1756-0500-7-918
24. Fouad YA, Fahmy YM, Abdel Hady SM, Elsabagh AE. Egyptian future physicians are packing to leave but may be willing to return. Int Health. 2015;7(3):190–4. https://doi.org/10.1093/inthealth/ihu072
25. Gouda P, Kitt K, Evans DS, Goggin D, McGrath D, Last J, Hennessy M, et al. Ireland’s medical brain drain: migration intentions of Irish medical students. Hum. Resour Health. 2015;13:11. https://doi.org/10.1186/s12960-015-0003-9
26. Akl EA, Maroun N, Major S, Afif C, Abdo A, Choucair J, et al., Post-graduation migration intentions of students of Lebanese medi-cal schools: a survey study. BMC Public Health. 2008;8:191. https://doi.org/10.1186/1471-2458-8-191
27. Wells KM, Shalabi H, Sergelen O, Wiessner P, Zhang C, deVries C, et al. Patient and Physician perceptions of changes in surgical care in Mongolia 9 years after roll-out of a national training program for laparoscopy. World J Surg. 2016;40(8):1859–64. https://doi.org/10.1007/s00268-016-3498-x
Book 27-11.indb 1108Book 27-11.indb 1108 06/12/2021 12:39 PM06/12/2021 12:39 PM

1109
Report EMHJ – Vol. 27 No. 11 – 2021
MERS-CoV in the COVID-19 era: update from Saudi Arabia, 2019–2020Anas Khan,1 Sharafaldeen Bin Nafisah,2 Bandr Mzahim,2 Bakhitah Aleid,3 Daliah Almatrafi,2 Abdullah Assiri4 and Hani Jokhdar4
1Emergency Department, College of Medicine, King Saud University, Riyadh, Saudi Arabia. 2Emergency Department, King Fahd Medical City, Riyadh, Saudi Arabia. 3Internal Medicine Department, King Fahd Medical City, Riyadh, Saudi Arabia. 4Ministry of Health, Riyadh, Saudi Arabia (Correspondence to: Sharafaldeen Bin Nafisah: [email protected]).
AbstractBackground: The prevalence of Middle East respiratory syndrome coronavirus (MERS-CoV) infection during the period of coronavirus disease 2019 (COVID-19) remains uncertain. Aims: This study aimed to provide an update on the epidemiology of MERS-CoV in Saudi Arabia from January 2019 to October 2020.Methods: Data on all laboratory-confirmed cases of MERS-CoV infection in Saudi Arabia from January 2019 to 20 October 2020 were retrieved from the Health Electronic Surveillance Network of the Ministry of Health of Saudi Arabia. Data col-lected were: demographic characteristics of cases, clinical course of the infection, related mortality and association with exposure to confirmed cases or camels. Results: In total, 299 cases of MERS-CoV infection were reported in the study period. The mean age of cases was 52.4 years. Most of the cases were males (78.9%) and had comorbidities (72.7%), and 11.9% of cases were health care providers. Of the 299 cases, 83 (27.7%) died. Older age and having comorbidities were associated with higher mortality. Exposure to camels was associated with lower mortality. Health care providers also had a lower mortality rate than non-health care providers. Compared with COVID-19, MERS-CoV infection still has a higher mortality rate but with a more predictable pattern and an anticipated deterioration.Conclusion: MERS-CoV infection remains a public health concern. The percentage of cases that were health care provid-ers (11.9%) is lower than previously reported (19.1–25.0%), possibly due to the various preventive measures put in place to control COVID-19.Keywords: Middle East respiratory syndrome coronavirus, COVID-19, health personnel, public health, Saudi ArabiaCitation: Khan A; Bin Nafisah S; Mzahim B; Aleid B; Almatrafi D; Assiri A; Jokhdar H. MERS-CoV in COVID-19 era: an update from Saudi Arabia, 2019–2020. East Mediterr Health J. 2021;27(11): 1109−1113. https://doi.org/10.26719/emhj.21.049 Received: 25/10/20; accepted: 04/04/21Copyright © World Health Organization (WHO) 2021. Open Access. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license (https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
IntroductionMiddle East respiratory syndrome coronavirus (MERS-CoV) was first reported in Saudi Arabia in 2012 (1). The outbreak of this infection progressed to an epidemic with more than 2494 cases reported worldwide by No-vember 2019, of which 2102 cases were from Saudi Ara-bia (2). Several attempts have been made to understand the behaviour of this coronavirus strain (3,4). It tends to affect elderly people and those with comorbidities, and several outbreaks have occurred in health care settings (3,5). Nonetheless, the emergence of a new coronavirus in 2019 (acute respiratory syndrome coronavirus 2 (SARS-CoV-2)) uncovered the need for repeated in-depth so-ciodemographic analysis of patients who are infected to uncover any change in the behaviour of the strain. The ongoing COVID-19 pandemic prompts another look at how MERS-CoV survived and whether such outbreaks should be foreseen.
Epidemiological data on MERS-CoV have been reported until 2019. In this study, we aimed to provide an update on the epidemiology of MERS-CoV in Saudi
Arabia, from January 2019 to October 2020. We also aimed to investigate the behaviour of MERS-CoV during the COVID-19 pandemic, to understand the difference between MERS-CoV and COVID-19.
MethodsWe retrieved data on all laboratory-confirmed cases of MERS-CoV in Saudi Arabia from January 2019 to 20 October 2020 from the Health Electronic Surveillance Network of the Ministry of Health of Saudi Arabia. We collected data on: demographic characteristics of cases, clinical course of the infection, related mortality and as-sociation with exposure to confirmed cases or camels. We followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for reporting observational studies (6).
This study was reviewed by the King Fahd Medical City research committee and because it did not involve direct patient contact and data were anonymised, the committee decided it did not require institutional review board approval.
Book 27-11.indb 1109Book 27-11.indb 1109 06/12/2021 12:39 PM06/12/2021 12:39 PM
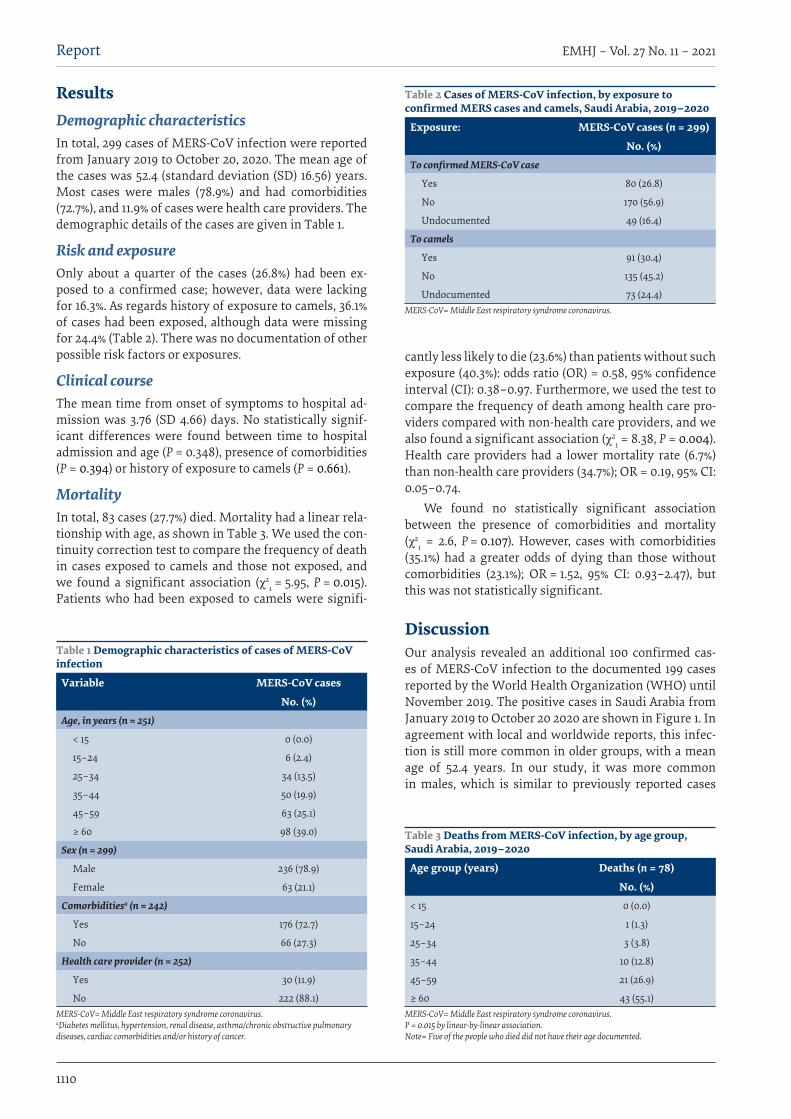
1110
Report EMHJ – Vol. 27 No. 11 – 2021
ResultsDemographic characteristicsIn total, 299 cases of MERS-CoV infection were reported from January 2019 to October 20, 2020. The mean age of the cases was 52.4 (standard deviation (SD) 16.56) years. Most cases were males (78.9%) and had comorbidities (72.7%), and 11.9% of cases were health care providers. The demographic details of the cases are given in Table 1.
Risk and exposureOnly about a quarter of the cases (26.8%) had been ex-posed to a confirmed case; however, data were lacking for 16.3%. As regards history of exposure to camels, 36.1% of cases had been exposed, although data were missing for 24.4% (Table 2). There was no documentation of other possible risk factors or exposures.
Clinical courseThe mean time from onset of symptoms to hospital ad-mission was 3.76 (SD 4.66) days. No statistically signif-icant differences were found between time to hospital admission and age (P = 0.348), presence of comorbidities (P = 0.394) or history of exposure to camels (P = 0.661).
MortalityIn total, 83 cases (27.7%) died. Mortality had a linear rela-tionship with age, as shown in Table 3. We used the con-tinuity correction test to compare the frequency of death in cases exposed to camels and those not exposed, and we found a significant association (χ2
1 = 5.95, P = 0.015). Patients who had been exposed to camels were signifi-
cantly less likely to die (23.6%) than patients without such exposure (40.3%): odds ratio (OR) = 0.58, 95% confidence interval (CI): 0.38–0.97. Furthermore, we used the test to compare the frequency of death among health care pro-viders compared with non-health care providers, and we also found a significant association (χ2
1 = 8.38, P = 0.004). Health care providers had a lower mortality rate (6.7%) than non-health care providers (34.7%); OR = 0.19, 95% CI: 0.05–0.74.
We found no statistically significant association between the presence of comorbidities and mortality (χ2
1 = 2.6, P = 0.107). However, cases with comorbidities (35.1%) had a greater odds of dying than those without comorbidities (23.1%); OR = 1.52, 95% CI: 0.93–2.47), but this was not statistically significant.
DiscussionOur analysis revealed an additional 100 confirmed cas-es of MERS-CoV infection to the documented 199 cases reported by the World Health Organization (WHO) until November 2019. The positive cases in Saudi Arabia from January 2019 to October 20 2020 are shown in Figure 1. In agreement with local and worldwide reports, this infec-tion is still more common in older groups, with a mean age of 52.4 years. In our study, it was more common in males, which is similar to previously reported cases
Table 1 Demographic characteristics of cases of MERS-CoV infection
Variable MERS-CoV cases
No. (%)Age, in years (n = 251)
< 15 0 (0.0)
15–24 6 (2.4)
25–34 34 (13.5)
35–44 50 (19.9)
45–59 63 (25.1)
≥ 60 98 (39.0)
Sex (n = 299)
Male 236 (78.9)
Female 63 (21.1)
Comorbiditiesa (n = 242)
Yes 176 (72.7)
No 66 (27.3)
Health care provider (n = 252)
Yes 30 (11.9)
No 222 (88.1)MERS-CoV= Middle East respiratory syndrome coronavirus. aDiabetes mellitus, hypertension, renal disease, asthma/chronic obstructive pulmonary diseases, cardiac comorbidities and/or history of cancer.
Table 2 Cases of MERS-CoV infection, by exposure to confirmed MERS cases and camels, Saudi Arabia, 2019–2020
Exposure: MERS-CoV cases (n = 299)
No. (%)To confirmed MERS-CoV case
Yes 80 (26.8)
No 170 (56.9)
Undocumented 49 (16.4)
To camels
Yes 91 (30.4)
No 135 (45.2)
Undocumented 73 (24.4)MERS-CoV= Middle East respiratory syndrome coronavirus.
Table 3 Deaths from MERS-CoV infection, by age group, Saudi Arabia, 2019–2020
Age group (years) Deaths (n = 78)
No. (%)< 15 0 (0.0)
15–24 1 (1.3)
25–34 3 (3.8)
35–44 10 (12.8)
45–59 21 (26.9)
≥ 60 43 (55.1)MERS-CoV= Middle East respiratory syndrome coronavirus. P = 0.015 by linear-by-linear association. Note= Five of the people who died did not have their age documented.
Book 27-11.indb 1110Book 27-11.indb 1110 06/12/2021 12:39 PM06/12/2021 12:39 PM
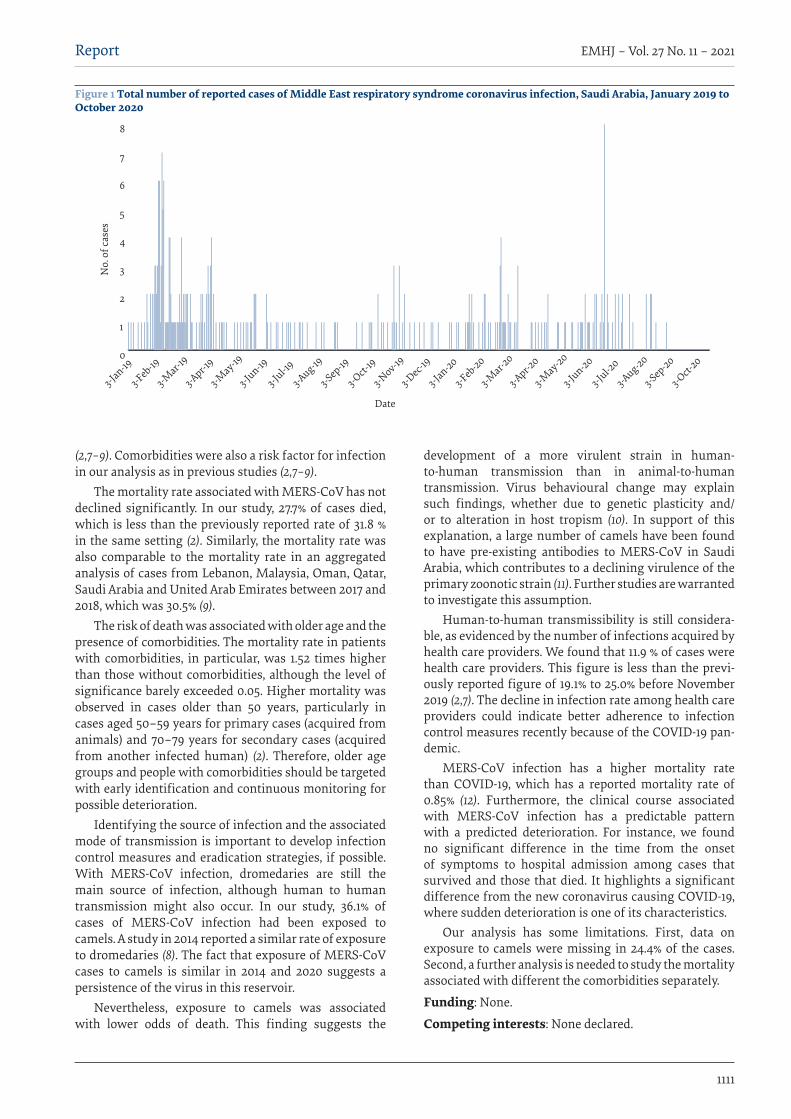
1111
Report EMHJ – Vol. 27 No. 11 – 2021
(2,7–9). Comorbidities were also a risk factor for infection in our analysis as in previous studies (2,7–9).
The mortality rate associated with MERS-CoV has not declined significantly. In our study, 27.7% of cases died, which is less than the previously reported rate of 31.8 % in the same setting (2). Similarly, the mortality rate was also comparable to the mortality rate in an aggregated analysis of cases from Lebanon, Malaysia, Oman, Qatar, Saudi Arabia and United Arab Emirates between 2017 and 2018, which was 30.5% (9).
The risk of death was associated with older age and the presence of comorbidities. The mortality rate in patients with comorbidities, in particular, was 1.52 times higher than those without comorbidities, although the level of significance barely exceeded 0.05. Higher mortality was observed in cases older than 50 years, particularly in cases aged 50–59 years for primary cases (acquired from animals) and 70–79 years for secondary cases (acquired from another infected human) (2). Therefore, older age groups and people with comorbidities should be targeted with early identification and continuous monitoring for possible deterioration.
Identifying the source of infection and the associated mode of transmission is important to develop infection control measures and eradication strategies, if possible. With MERS-CoV infection, dromedaries are still the main source of infection, although human to human transmission might also occur. In our study, 36.1% of cases of MERS-CoV infection had been exposed to camels. A study in 2014 reported a similar rate of exposure to dromedaries (8). The fact that exposure of MERS-CoV cases to camels is similar in 2014 and 2020 suggests a persistence of the virus in this reservoir.
Nevertheless, exposure to camels was associated with lower odds of death. This finding suggests the
development of a more virulent strain in human-to-human transmission than in animal-to-human transmission. Virus behavioural change may explain such findings, whether due to genetic plasticity and/or to alteration in host tropism (10). In support of this explanation, a large number of camels have been found to have pre-existing antibodies to MERS-CoV in Saudi Arabia, which contributes to a declining virulence of the primary zoonotic strain (11). Further studies are warranted to investigate this assumption.
Human-to-human transmissibility is still considera-ble, as evidenced by the number of infections acquired by health care providers. We found that 11.9 % of cases were health care providers. This figure is less than the previ-ously reported figure of 19.1% to 25.0% before November 2019 (2,7). The decline in infection rate among health care providers could indicate better adherence to infection control measures recently because of the COVID-19 pan-demic.
MERS-CoV infection has a higher mortality rate than COVID-19, which has a reported mortality rate of 0.85% (12). Furthermore, the clinical course associated with MERS-CoV infection has a predictable pattern with a predicted deterioration. For instance, we found no significant difference in the time from the onset of symptoms to hospital admission among cases that survived and those that died. It highlights a significant difference from the new coronavirus causing COVID-19, where sudden deterioration is one of its characteristics.
Our analysis has some limitations. First, data on exposure to camels were missing in 24.4% of the cases. Second, a further analysis is needed to study the mortality associated with different the comorbidities separately.
Funding: None.
Competing interests: None declared.
Figure 1 Total number of reported cases of Middle East respiratory syndrome coronavirus infection, Saudi Arabia, January 2019 to October 2020
0
1
2
3
4
5
6
7
8
Date
No.
of c
ases
3-Jan-19
3-Feb-19
3-Mar-1
9
3-Apr-19
3-May-19
3-Jun-19
3-Jul-19
3-Aug-19
3-Sep-19
3-Oct-
19
3-Jan-20
3-Feb-20
3-Mar-2
0
3-Apr-20
3-May-20
3-Jun-20
3-Jul-2
0
3-Aug-20
3-Sep-20
3-Oct-
20
3-Nov-19
3-Dec-1
9
Book 27-11.indb 1111Book 27-11.indb 1111 06/12/2021 12:39 PM06/12/2021 12:39 PM
1112
Report EMHJ – Vol. 27 No. 11 – 2021
فيوس كورونا املسبب ملتالزمة الرشق األوسط التنفسية يف حقبة كوفيد-19: حتديث من اململكة العربية السعودية، 2020-2019
أنس خان، رشف الدين بن نفيسه، بندر مزاحم، بخيتة العيد، دالية املطريف، عبد اهلل عسريي، هاين جوخدار
اخلالصة 2019 كورونا فريوس مرض حقبة خالل التنفسية األوسط الرشق ملتالزمة املسبب كورونا بفريوس العدوى انتشار معدل زال ما اخللفية:
)كوفيد-19( غري مؤكد. األهداف: هدفت هذه الدراسة إىل تقديم أحدث املعلومات عن اخلصائص الوبائية لفريوس كورونا املسبب ملتالزمة الرشق األوسط التنفسية يف
اململكة العربية السعودية يف الفرتة من يناير / كانون الثاين 2019 وحتى أكتوبر/ ترشين األول 2020.العربية اململكة يف التنفسية األوسط الرشق ملتالزمة املسبب كورونا فريوس لعدوى خمتربيا املؤكدة احلاالت مجيع بيانات مجعت البحث: طرق السعودية من يناير / كانون الثاين 2019 وحتى أكتوبر/ ترشين األول 2020 من نظام "حصن" اإللكرتوين التابع لوزارة الصحة يف اململكة العربية السعودية. ومتثلت البيانات التي مجعت يف: اخلصائص السكانية للحاالت، واملسار الرسيري للعدوى، والوفيات ذات الصلة وارتباطها بالتعرض
للحاالت املؤكدة أو اإلبل. النتائج: إمجاال، أبلغ بوجود 299 حالة عدوى بفريوس كورونا املسبب ملتالزمة الرشق األوسط التنفسية أثناء فرتة الدراسة. وكان متوسط عمر احلاالت 52.4 عاما. وكانت معظم احلاالت من الذكور )78.9%(، وكانت لدهيم اعتالالت مصاحبة )72.7%(، فيام كان 11.9% من احلاالت من يت 83 )27.7%(. وارتبط التقدم يف العمر ووجود اعتالالت مصاحبة بارتفاع معدل الوفيات. مقدمي الرعاية الصحية. ومن بني 299 حالة توفمقدمي منه يف صفوف غري أقل الصحية الرعاية مقدمي الوفيات يف صفوف معدل كان كام الوفيات. معدل بانخفاض لإلبل التعرض وارتبط الرعاية الصحية. وباملقارنة مع كوفيد-19، ال يزال معدل الوفيات النامجة عن عدوى فريوس كورونا املسبب ملتالزمة الرشق األوسط التنفسية أكثر
ارتفاعا، ولكنه يسري بنمط أكثر قابلية للتنبؤ به وبتدهور أكثر توقعا.االستنتاجات: ال تزال عدوى فريوس كورونا املسبب ملتالزمة الرشق األوسط التنفسية تسبب قلقا صحيا عاما. وتقل نسبة احلاالت التي كانت يف ذت صفوف مقدمي خدمات الرعاية الصحية )11.9%( عام سبق التبليغ به )19.1-25.0%(، وربام يعود ذلك إىل خمتلف التدابري الوقائية التي اخت
ملكافحة كوفيد-19.
Le coronavirus du syndrome respiratoire du Moyen-Orient à l'ère de la COVID-19 : le point sur la situation en Arabie saoudite en 2019-2020RésuméContexte : La prévalence de l'infection par le coronavirus du syndrome respiratoire du Moyen-Orient (MERS-CoV) pendant la pandémie de maladie à coronavirus 2019 (COVID-19) reste incertaine. Objectifs : La présente étude visait à faire le point sur l'épidémiologie du MERS-CoV en Arabie saoudite entre janvier 2019 et octobre 2020.Méthodes : Les données sur tous les cas d'infection par le MERS-CoV en Arabie saoudite, confirmés en laboratoire, entre janvier 2019 et le 20 octobre 2020 ont été extraites du réseau de surveillance électronique sanitaire du ministère saoudien de la Santé. Les données recueillies étaient les suivantes : caractéristiques démographiques des cas, évolution clinique de l'infection, mortalité associée et lien avec une exposition à des cas confirmés ou à des chameaux. Résultats : Au total, 299 cas d'infection par le MERS-CoV ont été rapportés pendant la période de l'étude. L'âge moyen des personnes concernées était de 52,4 ans. La plupart des cas étaient de sexe masculin (78,9 %) et présentaient des comorbidités (72,7 %) ; 11,9 % des cas étaient des prestataires de soins de santé. Sur les 299 cas, 83 (27 , 7 %) sont décédés. Un âge avancé et la présence de comorbidités étaient des facteurs associés à une mortalité plus élevée. En revanche, l'exposition à des chameaux était corrélée à une moindre mortalité. Le taux de mortalité des prestataires de soins de santé était également inférieur à celui du reste des sujets. Par rapport à la COVID-19, l'infection par le MERS-CoV présente toujours un taux de mortalité plus élevé, mais affiche un schéma plus prévisible et un processus de détérioration de l'état anticipé.Conclusion : L'infection par le MERS-CoV demeure un problème de santé publique. Le pourcentage des cas correspondant à des prestataires de soins de santé (11,9 %) est inférieur aux valeurs rapportées précédemment (19,1-25,0 %), peut-être grâce aux différentes mesures de prévention mises en place pour lutter contre la COVID-19.
Book 27-11.indb 1112Book 27-11.indb 1112 06/12/2021 12:39 PM06/12/2021 12:39 PM
1113
Report EMHJ – Vol. 27 No. 11 – 2021
References1. Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneu-
monia in Saudi Arabia. N Engl J Med. 2012;367:1814–20. https://doi.org/10.1056/NEJMoa1211721
2. MERS situation update, November 2019. Cairo: World Health Organization Regional Office for the Eastern Mediterranean; 2019 (http://www.emro.who.int/pandemic-epidemic-diseases/mers-cov/mers-situation-update-november-2019.html, accessed 30 June 2020).
3. Mubarak A, Alturaiki W, Hemida MG. Middle East respiratory syndrome coronavirus (MERS-CoV): infection, immunological response, and vaccine development. J Immunol Res. 2019 6491738. https://doi.org/10.1155/2019/6491738
4. Zhao J, Li K, Wohlford-Lenane C, Agnihothram SS, Fett C, Zhao J, et al. Rapid generation of a mouse model for Middle East res-piratory syndrome. Proc Natl Acad Sci USA. 2014;111(13):4970–5. https://doi.org/10.1073/pnas.1323279111
5. Updated information on the epidemiology of Middle East respiratory syndrome coronavirus (MERS-CoV) infection and guid-ance for the public, clinicians, and public health authorities, 2012-2013. MMWR Morb Mortal Wkly Rep. 2013;62(38):793–6.
6. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The strengthening the report-ing of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemi-ol. 2008 Apr;61(4):344–9. https://doi.org/10.1016/j.jclinepi.2007.11.008
7. Altamimi A, Abu-Saris R, El-Metwally A, Alaifan T, Alamri A. Demographic variations of MERS-CoV infection among suspected and confirmed cases: an epidemiological analysis of laboratory-based data from Riyadh regional laboratory. BioMed Res Int. 2020. 2020:9629747. https://doi.org/10.1155/2020/9629747
8. Alraddadi BM, Watson JT, Almarashi A, Abedi GR, Turkistani A, Sadran M, et al. Risk factors for primary Middle East respira-tory syndrome coronavirus illness in humans, Saudi Arabia, 2014. Emerg Infect Dis. 2016;22(1):49–55. https://doi.org/10.3201/eid2201.151340
9. Mobaraki K, Ahmadzadeh J. Current epidemiological status of Middle East respiratory syndrome coronavirus in the world from 1.1.2017 to 17.1.2018: a cross-sectional study. BMC Infect Dis. 2019;19(1):351. https://doi.org/10.1186/s12879-019-3987-2
10. Widagdo W, Sooksawasdi Na Ayudhya S, Hundie GB, Haagmans BL. Host determinants of MERS-CoV transmission and patho-genesis. Viruses. 2019;11(3):280. https://doi.org/10.3390/v11030280
11. Alharbi NK, Ibrahim OH, Alhafufi A, Kasem S, Aldowerij A, Albrahim R, et al. Challenge infection model for MERS-CoV based on naturally infected camels. Virol J. 2020; 17(1):77. https://doi.org/10.1186/s12985-020-01347-5
12. Ritchie H, Ortiz-Ospina E, Beltekian D, Mathieu E, Hasell J, Mcdonals B, et al. Coronavirus pandemic (COVID-19) [online]. Our-WorldInData.org. 2020 (https://ourworldindata.org/coronavirus, accessed 13 May 2021).
Book 27-11.indb 1113Book 27-11.indb 1113 06/12/2021 12:39 PM06/12/2021 12:39 PM

1114
Review EMHJ – Vol. 27 No. 11 – 2021
COVID-19 in Saudi Arabia: the national health responseAnas Khan,1 Yousef Alsofayan,2 Ahmed Alahmari,2 Jalal Alowais,3 Abdullah Algwizani,4 Haleema Alserehi,5 Abdullah Assiri6 and Hani Jokhdar7
1Department of Emergency Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia. 2Global Center for Mass Gatherings Medicine, Ministry of Health, Riyadh, Saudi Arabia. 3Department of Surgery, College of Medicine, Imam Mohammed ibn Saud Islamic University, Riyadh, Saudi Arabia. 4Saudi Center for Disease Prevention and Control, Riyadh, Saudi Arabia. 5Executive Department for Global Health, Saudi Center for Disease Prevention and Control, Riyadh, Saudi Arabia. 6Ministry of Health, Riyadh, Saudi Arabia. 7Deputyship of Public Health, Ministry of Health, Riyadh, Saudi Arabia. (Correspondence to: Yousef M. Alsofayan: [email protected]).
AbstractBackground: With the spread of coronavirus disease 2019 (COVID-19), most countries rushed to take early measures to control this disease. Aims: This paper describes and evaluates the Saudi Arabian strategic preparedness and response plan on COVID-19 up to 31 December 2020.Methods: Saudi Arabia adopted the World Health Organization’s guidelines on response to COVID-19, which are based on nine pillars of public health preparedness and response. The measures Saudi Arabia took are assessed against these pillars.Results: In response to COVID-19, Saudi Arabia prepared public and private institutions to deal with the pandemic. Saudi authorities established a governance system comprised of responsible committees to continuously monitor national and international updates, trace contacts, screen the population, raise awareness and take proper actions to contain the spread of this disease. After the announcement of the first case in Saudi Arabia, all schools, social events, sports activities, do-mestic travel and international flights were suspended. Restrictions on social movement, social and religious gatherings, travel and businesses were imposed ahead of the first 100 confirmed COVID-19 cases. The Hajj pilgrimage for 2020 was scaled down to limit participants and no cases of COVID-19 were detected among pilgrims. The country maintained all basic health services and immunization programmes and supported all proposals for COVID-19 drugs and vaccines. The country is working to develop its capacity to produce these products and achieve self-sufficiency.Conclusion: Saudi Arabia took extreme measures to respond to COVID-19 which contributed to limiting the spread and effect of the disease.Keywords: COVID-19, pandemics, public health, Saudi ArabiaCitation: Khan A; Alsofayan Y; Alahmari A; Alowais J; Algwizani A; Alserehi H; et al. COVID-19 in Saudi Arabia: the national health response. East Mediterr Health J. 2021;27(11):1114–1124. https://doi.org/10.26719/emhj.21.048Received: 05/01/21; accepted: 04/04/21Copyright © World Health Organization (WHO) 2021. Open Access. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license (https://creativecommons.org/licenses/by-nc-sa/3.0/igo)
IntroductionThe World Health Organization (WHO) advised all coun-tries to contain the spread of the coronavirus disease 2019 (COVID-19) pandemic (1,2). A well structured response should include: (i) active surveillance measures; (ii) con-tinuous prevention and control of infection; (iii) effective plans for health care facilities; (iv) postponement of mass gathering events; and (v) raising public awareness and understanding of the disease (3).
According to WHO, each government is the natural leader in national risk management for overall coordination and communication. However, due to the increased burden on health systems, the strategic response to COVID-19 varied worldwide, in terms of prevention, response and operational readiness (4).
Saudi Arabia is the largest county in the Arabian Peninsula. It has a well established health care system that is offered for free to all residents. The health care system has 494 hospitals and 22.5 beds per 10 000 people (5). In 2019, the country had 113 000 physicians (6).
In the WHO Eastern Mediterranean Region, trends in the COVID-19 pandemic differed substantially across the region in virus transmission, number of COVID-19 cases, deaths and hospitalizations. These differences could be due to the preparedness of the public health sector, early precautionary measures, restrictions on mass gathering events, restricted international arrivals and the proportion of the population with risk factors (older people and people with comorbidities) (7). We aim to describe the Saudi Arabian strategic preparedness and response plan on COVID-19 in line with the WHO operational planning guidelines to support country preparedness and response during December 2019 to December 2020 (8). These guidelines were based on nine pillars of public health preparedness and response – pillar 1: country-level coordination, planning, and monitoring; pillar 2: risk communication and community engagement; pillar 3: surveillance, rapid response teams, and case investigation; pillar 4: points of entry, international travel, and transport; pillar 5: national laboratories;
Book 27-11.indb 1114Book 27-11.indb 1114 06/12/2021 12:39 PM06/12/2021 12:39 PM
1115
Review EMHJ – Vol. 27 No. 11 – 2021
pillar 6: infection prevention and control; pillar 7: case management; pillar 8: operational support and logistics; and pillar 9: maintaining essential health services and systems. We also describe Saudi Arabia vaccine response and contribution to research on COVID-19.
Country-level coordination, planning and monitoring National emergency response committeeTo facilitate an effective response to COVID-19, a nation-al emergency response committee was established to develop measures across all sectors. This committee was chaired by the Minister of Health (8). The National Com-mand and Control Center within the health ministry was activated to continuously monitor international, national and regional updates and take operational action (9).
Early measures were taken by the committee to limit the spread of COVID-19, including managing confirmed cases, repatriating Saudi citizens abroad, upgrading port procedures, facilitating and supplying the health sector with essential resources and requirements, and assessing the risks of mass gathering events (9,10). Based on the risk assessment tool of the Saudi Center for Disease Control, Saudi Arabia, at an early stage of the pandemic, issued warnings against travelling to risky countries with high incidence of COVID-19. Then, when the global spread of COVID-19 was rising, all international and domestic flights were suspended on 15 and 21 March, 2020, respectively (11).
Risk assessment tools for mass gathering eventsSaudi Arabia has unique experience in using scientif-ic tools for planning and conducting mass gathering events (12). In 2010, the Saudi health ministry estab-lished the Global Center for Mass Gatherings Medi-cine and developed a set of risk assessment tools for mass gathering events, including the Jeddah tool for religious mass gathering events and the Salem tool for small to medium mass gathering events. With COV-ID-19, the Salem tool was modified to the Salem COV-ID tool, which was used to assess the health risks of COVID-19 in mass gathering events (13,14). The Jeddah tool was used to conduct a strategic assessment of the health risks due to the pandemic of Umrah and Hajj (13). All decisions on holding mass gathering events were based on these tools, including suspension of Umrah and its phased limited return, and performing “Safe Hajj 2020”. All factors related to these decisions were taken into account, including the impact on national health resources and global health security (5,15–19).
Risk communication and community engagementRisk communication and community engagement is a vital public health intervention that helps detect and respond to concerns, rumours and misinformation (20). The Saudi Arabian Ministry of Health organized a daily press conference to ensure a reliable source of information for the community on the ongoing situation, procedures and efforts (21,22). Further-more, in collaboration with other sectors, the Minis-try of Health produced professional media materials that provided effective and reliable information for both the general population and health care workers. Through various media platforms (e.g. video and text messages), the Ministry of Health conveyed scientific information in non-technical language – in Arabic, as well as in the languages of the many expatriates living in Saudi Arabia – to reach the maximum number of people nationwide with reliable, official information. Of note, the Ministry of Health implemented several community empowerment strategies, such as moni-toring citizens’ response to precautionary measures in social media so measures could be adjusted and modified accordingly (5).
Furthermore, the health hotline centre (no. 937) was scaled up to over 2000 employees to: (i) provide immediate support to the public and address their concerns; (ii) provide medical advice for the general population and at-risk people; and (iii) provide psychological support to the citizens to prevent anxiety and panic. This service is provided around the clock. It was supplemented by other communication channels such as Sehaty (Ministry of Health application (App)), WhatsApp and chatbots services. The needs of special populations were not overlooked; for example, the Sign Language app was developed to ensure effective messages to people with hearing disabilities (5,23).
The Ministry of Health also developed Tetamman and Mawid applications to assess suspected cases and monitor confirmed ones by providing protection and guidance to the public (24,25). The applications ensured the safety of cases and promoted recovery measures through educational information, test results, updates of contact details, daily follow-up of patients’ health status, contact with the health hotline centre (no. 937) and a countdown indicator for self-isolation (24,25).
In its national response document, the Ministry of Health presented data on the utilization of its different risk communication and community engagement messages. Over six and half billion messages were sent up to the end of August 2020, while the educational videos had over 150 million views. Furthermore, over nine million people benefited from public awareness campaigns (5). As of the 24 November 2020, the health hotline centre (no. 937) had received nearly 22 million calls.
Book 27-11.indb 1115Book 27-11.indb 1115 06/12/2021 12:39 PM06/12/2021 12:39 PM

1116
Review EMHJ – Vol. 27 No. 11 – 2021
Surveillance, rapid response teams and case investigation The Ministry of Health activated rapid response teams of specialists in infectious diseases and infection pre-vention and control, including physicians, nurses, epidemiologists and public health professionals. The main functions of these teams were to evaluate and monitor confirmed cases, analyse daily data on the global burden of COVID-19, prepare daily reports, pre-pare periodic instructions and guidelines, update the COVID-19 manual and prepare information and train-ing courses for the public (26).
Health electronic surveillance networkThe health electronic surveillance network provided a robust online solution in response to the pandemic. The system was an integrated public health information sys-tem that created an extensive and easily accessible data-base on one platform to overcome the challenges of link-ing all health care sectors in the country. This network contributed to disease detection, response, prevention, control and community health monitoring, and ena-bled decision-makers to implement necessary measures based on timely and high-quality data (27).
Mass screening programmesSaudi Arabia launched a mass screening programme for early detection and immediate control of the spread of COVID-19. The first stage focused on screen-ing individuals in highly populated districts through field tests; this was implemented in 807 locations (5). The second stage was facilitated through the Mawid app self-assessment tool, which classifies users as low or high risk. The low-risk group was the targeted pop-ulation and was screened in designated primary care centres (25,28,29). The third stage was screening sus-pected COVID-19 cases with no symptoms at special-ized drive-through testing centres, so-called takkad centres (30) – 1 847 573 tests had been administered up to mid-August 2020 (5).
The implementation of Tetamman clinics (specialized fever clinics) was another initiative devoted to screening people suspected of having COVID-19 without prior appointments. This service was free of charge, and provided diagnostic tests and therapeutic options for people with suspected COVID-19 symptoms, such as fever, shortness of breath, cough and other common clinical characteristics of COVID-19. These clinics had an immediate effect on relieving the pressure on emergency departments (31,32). More than 239 Tetamman clinics were opened and had received more than 1.5 million visitors by the end of November 2020 (5,33).
Points of entry, international travel and transportMany efforts and resources focused on surveillance ac-tivities at land, sea and air points of entry to control the
spread of COVID-19 (34). This included screening travel-lers after filling the health declaration forms, intensify-ing epidemiological surveillance, applying precautionary measures, developing a mechanism to detect travellers from high-risk countries, and direct them as needed. Na-tional COVID-19 guidelines were issued and personnel at ports were trained on precautionary measures. Saudi airports enhanced COVID-19 awareness through posters and educational videos. Airport authorities continuously monitored and evaluated all activities in terms of pre-paredness and effectiveness of measures (28,35). Of note, Saudi Arabia was ranked as the safest place in the region and the sixth safest place to travel worldwide according to the standards of the European Union for coordination of travel restrictions (36).
National laboratories Saudi Arabia increased its laboratory readiness and abili-ty to manage and analyse COVID-19 samples, and collab-orated with international reference laboratories. The Na-tional Public Health Laboratory of the Saudi Center for Disease Control, as well as many regional laboratories, actively received and analysed the increasing number of COVID-19 samples. The national laboratory adopted and monitored all standard operating procedures for sam-ples to achieve the highest validity and reliability and rapid turnaround time (28). The results of the samples were linked immediately to the database of the Health Electronic Surveillance Network. The laboratory of the Center for Disease Control also developed readiness plans for urgent surge capacity through the activation of all regional laboratories and laboratories of other sectors in Saudi Arabia (37). At the same time, analysis of samples of other viruses continued so as to prevent the spread of other epidemics in conjunction with COVID-19 (28).
Infection prevention and controlThe Ministry of Health prepared guidelines for case treatment, epidemiological surveillance, health facili-ties and all segments of society. Furthermore, the Sau-di Center for Disease Control published the infection prevention and control manual to guide all sectors during the COVID-19 pandemic (28). Details of these guidelines are given in the national response document issued online by the Ministry of Health (5).
Health care awareness guidance The Ministry of Health developed procedures and guide-lines for infection prevention and control and health facility preparations, which included updated criteria for respiratory screening, isolation rooms, hand hy-giene stations and staff training on the basic principles of infection prevention and control, such as the use of personal protective equipment and methods of hand hy-giene (26). In collaboration with infection prevention and control teams, supply teams and stock control teams, the Ministry of Health continuously identified the required
Book 27-11.indb 1116Book 27-11.indb 1116 06/12/2021 12:39 PM06/12/2021 12:39 PM
1117
Review EMHJ – Vol. 27 No. 11 – 2021
quantities of personal protective equipment and hand disinfection products, and their estimated use in health facilities. The Ministry of Health also established a mech-anism to monitor, record and investigate COVID-19 cases in health workers and confirmed COVID-19 cases. Daily indicators were created and monitored by the Command and Control Center for appropriate action (9).
Public awareness guidanceIn collaboration with the Saudi Center for Disease Con-trol, the Ministry of Health issued and distributed public guidelines targeting high-risk locations (38). Moreover, these guidance materials were issued in various languag-es to ensure maximum accessibility to all citizens and residents in the country (21).
Case management Readiness of health care facilities in Saudi Arabia All Saudi primary health care centres, hospitals and quar-antine facilities were prepared to receive large numbers of suspected and confirmed cases of COVID-19. This high level of preparedness put the health care system under constant pressure. Personnel at these facilities were aware of the definition of COVID-19 and gave priority and appropriate care to patients at risk of infection. In the early phases of the pandemic, the General Directorate of Hospitals designated reference hospitals to receive COV-ID-19 cases and continuously assessed their readiness. Reference hospitals reported their estimated isolation capacity, intensive care beds and their occupancy rates.
Moreover, the General Directorate of Hospitals monitored respirators and respiratory consumables, calculated the workforce required for escalation of cases and planned all necessary measures (28). Dedicated ambulance teams were allocated to transport confirmed and suspected cases to and from health facilities in cooperation with the Ministry of Health referral programme (28). Ensuring that field hospitals were prepared and ready to support the health system was a priority at the early phases of the pandemic, as these facilities were used to provide COVID-19 vaccination in large numbers. Four field hospitals with a capacity of 1100 beds were put into operation in order to increase capacity during the pandemic (5). Psychological counselling and support were provided to patients, health workers and the community in the early stages of the pandemic in cooperation with mental health teams (39). In addition, private health care facilities, home medical care and telemedicine centres were activated to relieve the strain on Ministry of Health facilities.
Digital health services were used extensively to reduce the number of visits to health care facilities, and hence reduce the possibility of infection (40). The Ministry of Health also implemented mobile apps to help affected patients and their contacts. For example, the Tawakkalna app offered a secure way to report confirmed and/or suspected cases, thus breaking the chain of infection. The
app had almost seven million user at the end of August 2020 (41). Likewise, the Tabaud app provided users with a notification if they came in close contact with a COVID-19 case, or somebody later found positive for COVID-19; this app started with 15 000 participants (42). Telemedicine services served more than five million users during the pandemic; besides, the Tetamman app was used by more than one and half million users from April to August 2020 (5,43).
Quarantine processQuarantines played an essential role in preventing the spread of COVID-19 by separating confirmed and sus-pected cases (44). Before reaching the designated quar-antine locations, each traveller returning from abroad is provided with information on the pandemic and quaran-tine. On arrival, educational materials, masks and hand sanitizers are offered. The medical team then completes screening procedures and triages cases to either hospi-tal or quarantine according to their condition (45). By the end of the quarantine period, any additional polymerase chain reaction testing for cases is coordinated by the medical teams (28). With the availability of electronic bracelets and apps, the choice for home quarantine is pro-vided if housing conditions are appropriate, and many choose this option (46).
Free health care servicesThe health care services in Saudi Arabia are free-of-charge for all citizens, and residents are required to have medical insurance from their employers (47). As of the 30 March, 2020, the Saudi health authority announced that COVID-19 treatment is free for all citizens and residents. This includes residency violators without any legal con-sequences (5).
National treatment protocolThe Ministry of Health issued a national treatment protocol for suspected and confirmed cases of COV-ID-19, which is updated regularly according to scientific studies and international protocols. This protocol aims to provide treating physicians with the best evidence-based approach for the management of COVID-19 cases, with-out replacing their clinical judgement. The protocol covers supportive care and pharmacotherapy for man-agement of asymptomatic, mild-to-moderate, and severe cases. It also highlights recent evidence on the manage-ment of special populations, such as pregnant women and patients on thromboprophylaxis (48). The Ministry of Health set up several monitoring teams who were trained to evaluate compliance with the protocol to en-sure effective implementation of the treatment protocol in intensive care units. Furthermore, the Ministry of Health followed up on COVID-19 management in hospi-tals and issued recommendations for the use of the pro-tocol and minimization of side-effects (5).
Book 27-11.indb 1117Book 27-11.indb 1117 06/12/2021 12:39 PM06/12/2021 12:39 PM

1118
Review EMHJ – Vol. 27 No. 11 – 2021
Operational support and logistics Inventory controlInventory control includes monitoring the exchange and consumption rates of medical stocks to ensure the need-ed supply. Several national factories joined initiatives to produce sterilizers, masks and ventilators locally to en-sure the sustainability of medical equipment during the COVID-19 pandemic (49,50).
Electronic health supportElectronic health support (E-health) had a significant role in responding to COVID-19; it provided several key indicators for health care facility preparedness and epidemiological surveillance. These indicators included: isolation hospital health staff dashboard; blood sample reports; sample carrier shipments; sup-ply dashboard; COVID-19 mortality reports; work-force; blood bank dashboard; and many others (51). E-health was also supported by the launch of electron-ic apps to educate, assess and monitor confirmed and suspected cases (24,25). Moreover, COVID-19 scientific materials were summarized and translated into differ-ent languages and uploaded onto a unified electronic platform to help communication with the public (21). E-health also supported the role of virtual clinics, tele-medicine, teleconsultations, teleradiology and use of robotics to prevent the spread of COVID-19 (5).
Community volunteeringCommunity participation and health volunteering have a role in responding to pandemics (52). Volunteer teams underwent general and specialized training to deal with the pandemic in public places and health care facilities. The Ministry of Health estimated that these volunteering activities involved about 32 000 volunteers and 1.1 million volunteer hours as of end of August 2020 (5).
Maintaining essential health services and systemsAlthough all efforts of the Ministry of Health were direct-ed towards tackling the COVID-19 pandemic as a top pri-ority, this did not replace their primary role in maintain-ing essential health services for all people as required. Hospitals and health care centres ensured the provision of their services through virtual clinics and/or hospital clinics, and provided special teams to follow and monitor patients (8). Examples included diabetes, rehabilitation and specialized oncology services (53).
In various regions within Saudi Arabia, health centres provided medication and vaccination delivery services to people’s homes. To prevent further spread of communicable diseases in the community, the scheduling and monitoring of routine vaccinations for children were enhanced in the early stages of the COVID-19 pandemic, in accordance with WHO recommendations (54). The number of available appointments for routine vaccinations (seasonal influenza and paediatric immunizations) reached
more than 10 million appointments as of the end of August 2020, and the efficiency of vaccination in primary care centres was monitored closely (54,55).
COVID-19 vaccinationOn the 10 December 2020, Saudi Arabia approved the Pfizer/BioNTech COVID-19 vaccine through the Saudi Food and Drug Authority and prioritized targeted popu-lations – elderly people and frontline health care work-ers in the first phase (56). The vaccine programme was launched in mid-December 2020 and, as of 7 February 2021, 431 608 doses have been administered through four sites. The programme aims to cover 17.4 million adults (70% of the adult population of Saudi Arabia) by the third quarter of 2021. Saudi Arabia also approved the Astra-Zeneca/Oxford vaccine and an expected ten million doses were planned for delivery in February 2021.
Research Studies have shown the importance of exploring the etiologies, clinical characteristics and therapeutic options in many previous pandemics. Saudi Arabia paid great attention to supporting urgent medical research programmes and publishing data on COV-ID-19. In this context, the National Committee for Pandemic Research was formed. Its main objectives were to support and encourage scientific research, es-tablish and publish priorities for COVID-19 research, and announce the opening of proposals for scientific research support programmes (57,58). From the start of the pandemic until May 2020, 100 proposals were granted ethical approval. Moreover, Saudi Arabia as-sured the use of the best protocols for new treatments and vaccines from international and national research institutions. Saudi Arabia had an important role in the research efforts for the development of COVID-19 vac-cines: the contribution of the country to international trials on MERS-CoV, including trials for the develop-ment of the new ChAdOX1 vaccine and the MIRACLE tri-al, provided a solid basis of the country’s participation in the international efforts against COVID-19 (59–61). The Ministry of Health has supported a national clin-ical study of blood plasma transfusion as a treatment in more than 21 sites (62). Furthermore, Saudi Arabia has drawn up a plan to restudy the infrastructure needed to develop new drugs and vaccines to achieve local sufficiency (63). Overall, Saudi Arabia was the leading country in the Arab world, and the 18th global-ly, in COVID-19 research (64).
Summary of Saudi Arabia’s responseFigure 1 and Box 1 summarize the measures taken by Sau-di Arabia in preparing and responding to COVID-19. In its national response document, the Ministry of Health evaluated whether each of the above-mentioned strate-gies achieved its aim with regard to each preparedness and response pillar and presented the relevant statistics (Table 1).
Book 27-11.indb 1118Book 27-11.indb 1118 06/12/2021 12:39 PM06/12/2021 12:39 PM
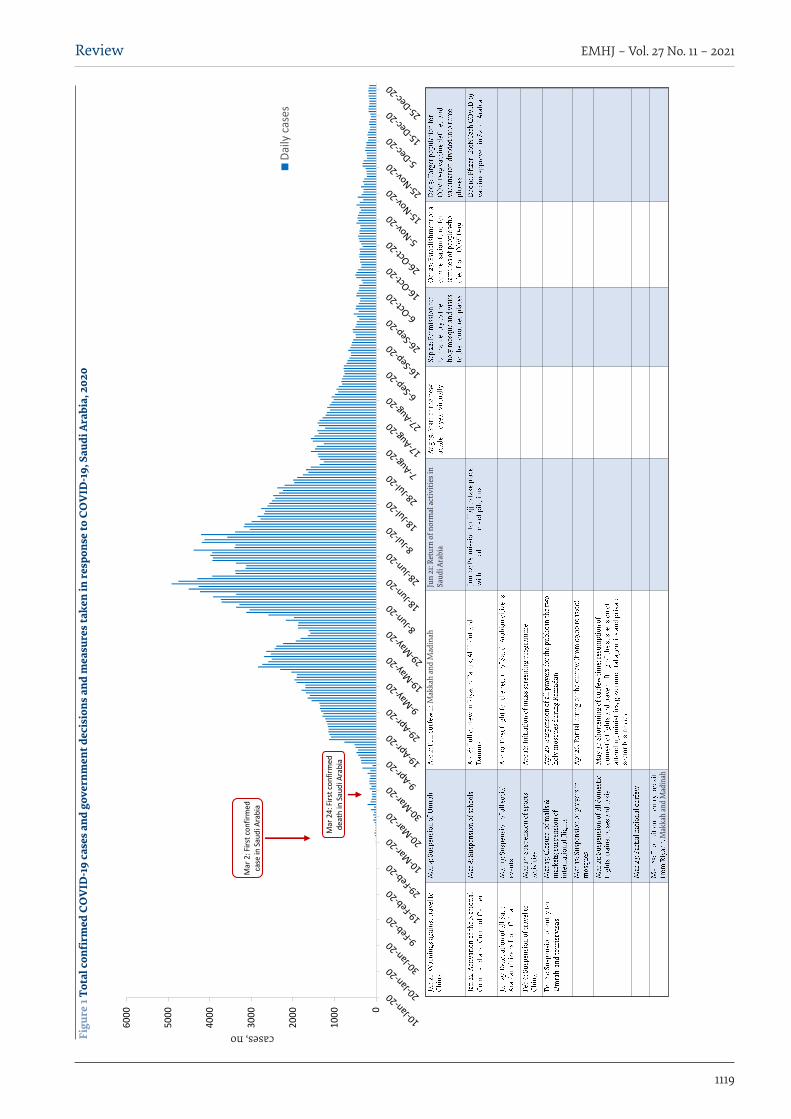
1119
Review EMHJ – Vol. 27 No. 11 – 2021
Figu
re 1
Tota
l con
firm
ed C
OV
ID-1
9 ca
ses a
nd g
over
nmen
t dec
isio
ns a
nd m
easu
res t
aken
in re
spon
se to
CO
VID
-19,
Sau
di A
rabi
a, 2
020
0
1000
2000
3000
4000
5000
6000
Cases, no.
Daily
case
s
Mar
24:
Firs
t con
firm
ed
deat
h in
Sau
di A
rabi
a
Mar
2: F
irst c
onfir
med
ca
se in
Sau
di A
rabi
a
cases, no
Jun
21: R
etur
n of
nor
mal
act
iviti
es in
Sa
udi A
rabi
aM
akka
h an
d M
adin
ah
Mak
kah
and
Mad
inah
Book 27-11.indb 1119Book 27-11.indb 1119 06/12/2021 12:39 PM06/12/2021 12:39 PM
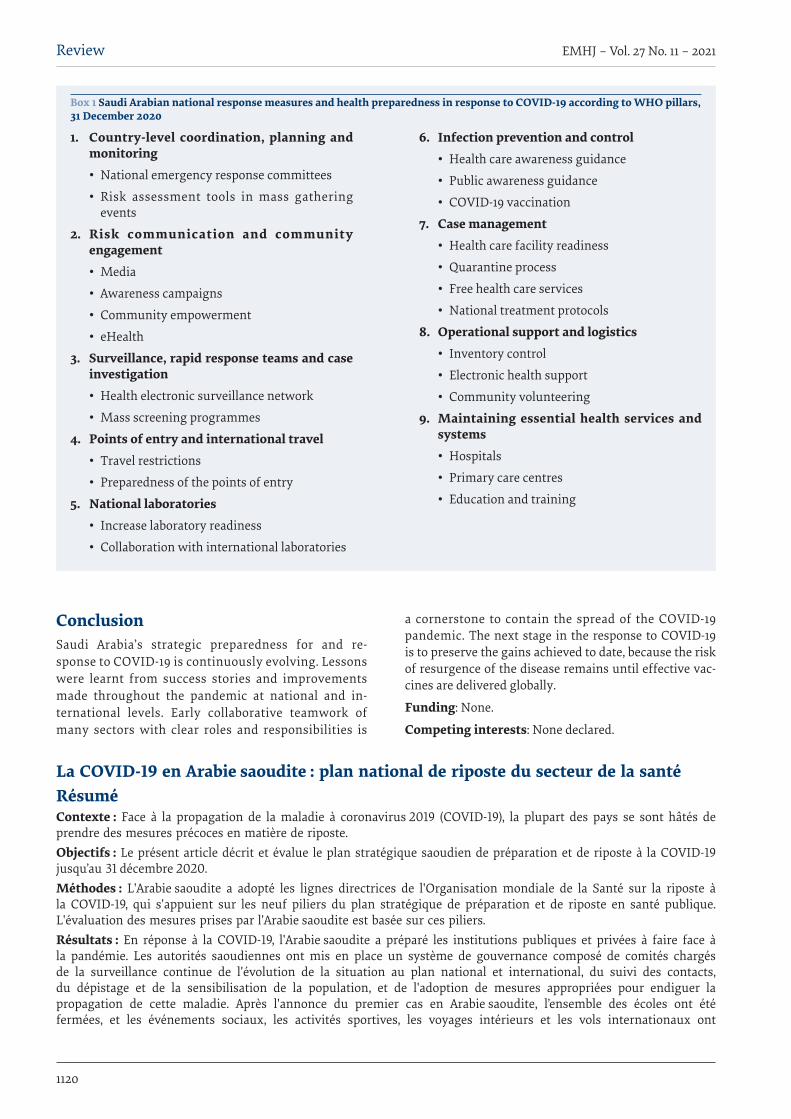
1120
Review EMHJ – Vol. 27 No. 11 – 2021
Box 1 Saudi Arabian national response measures and health preparedness in response to COVID-19 according to WHO pillars, 31 December 2020
1. Country-level coordination, planning and monitoring• National emergency response committees
• Risk assessment tools in mass gathering events
2. Risk communication and community engagement• Media
• Awareness campaigns
• Community empowerment
• eHealth
3. Surveillance, rapid response teams and case investigation• Health electronic surveillance network
• Mass screening programmes
4. Points of entry and international travel• Travel restrictions
• Preparedness of the points of entry
5. National laboratories• Increase laboratory readiness
• Collaboration with international laboratories
6. Infection prevention and control• Health care awareness guidance
• Public awareness guidance
• COVID-19 vaccination
7. Case management• Health care facility readiness
• Quarantine process
• Free health care services
• National treatment protocols
8. Operational support and logistics• Inventory control
• Electronic health support
• Community volunteering
9. Maintaining essential health services and systems• Hospitals
• Primary care centres
• Education and training
ConclusionSaudi Arabia’s strategic preparedness for and re-sponse to COVID-19 is continuously evolving. Lessons were learnt from success stories and improvements made throughout the pandemic at national and in-ternational levels. Early collaborative teamwork of many sectors with clear roles and responsibilities is
a cornerstone to contain the spread of the COVID-19 pandemic. The next stage in the response to COVID-19 is to preserve the gains achieved to date, because the risk of resurgence of the disease remains until effective vac-cines are delivered globally.
Funding: None.
Competing interests: None declared.
La COVID-19 en Arabie saoudite : plan national de riposte du secteur de la santéRésuméContexte : Face à la propagation de la maladie à coronavirus 2019 (COVID-19), la plupart des pays se sont hâtés de prendre des mesures précoces en matière de riposte. Objectifs : Le présent article décrit et évalue le plan stratégique saoudien de préparation et de riposte à la COVID-19 jusqu’au 31 décembre 2020.Méthodes : L'Arabie saoudite a adopté les lignes directrices de l'Organisation mondiale de la Santé sur la riposte à la COVID-19, qui s'appuient sur les neuf piliers du plan stratégique de préparation et de riposte en santé publique. L'évaluation des mesures prises par l'Arabie saoudite est basée sur ces piliers.Résultats : En réponse à la COVID-19, l'Arabie saoudite a préparé les institutions publiques et privées à faire face à la pandémie. Les autorités saoudiennes ont mis en place un système de gouvernance composé de comités chargés de la surveillance continue de l'évolution de la situation au plan national et international, du suivi des contacts, du dépistage et de la sensibilisation de la population, et de l'adoption de mesures appropriées pour endiguer la propagation de cette maladie. Après l'annonce du premier cas en Arabie saoudite, l’ensemble des écoles ont été fermées, et les événements sociaux, les activités sportives, les voyages intérieurs et les vols internationaux ont
Book 27-11.indb 1120Book 27-11.indb 1120 06/12/2021 12:39 PM06/12/2021 12:39 PM
1121
Review EMHJ – Vol. 27 No. 11 – 2021
كوفيد-19 يف اململكة العربية السعودية: االستجابة الصحية الوطنيةأنس خان، يوسف السفيان ، أمحد األمحري، جالل العويس، عبد اهلل القويزاين، حليمة الرسحيي، عبد اهلل عسريي، هاين جوخدار
اخلالصةاخللفية: مع انتشار مرض فريوس كورونا 2019 )كوفيد-19(، سارع معظم البلدان إىل اختاذ تدابري مبكرة ملكافحة هذا املرض.
األهداف: هدفت هذه الدراسة اىل وصف وتقييم خطة التأهب واالستجابة االسرتاتيجية للمملكة العربية السعودية بشأن كوفيد-19 حتى 31 ديسمرب / كانون األول 2020.
طرق البحث: اعتمدت اململكة العربية السعودية املبادئ التوجيهية الصادرة عن منظمة الصحة العاملية بشأن االستجابة لكوفيد-19، والتي تستند إىل تسع ركائز للتأهب واالستجابة يف جمال الصحة العامة. وجيري تقييم التدابري التي اختذهتا اململكة العربية السعودية يف ضوء تلك الركائز.
النتائج: استجابة لكوفيد-19، جهزت اململكة العربية السعودية مؤسسات عامة وخاصة للتعامل مع اجلائحة. حيث أنشأت السلطات السعودية مستوى ورفع السكان، وفحص املخالطني، ع وتتب والدولية، الوطنية للتحديثات املستمر الرصد عن مسؤولة جلان من يتألف للحوكمة نظاما الوعي، واختاذ اإلجراءات املناسبة الحتواء انتشار هذا املرض. وبعد اإلعالن عن احلالة األوىل يف السعودية، أوقفت مجيع املدارس، واملناسبات ل االجتامعي، والتجمعات االجتامعية والدينية، والسفر االجتامعية، واألنشطة الرياضية، والسفر الداخيل، والطريان الدويل. وفرضت قيود عىل التنقض عدد حجاج بيت اهلل احلرام لعام 2020 من أجل احلد من واألعامل التجارية قبل ظهور أول 100 حالة مؤكدة من حاالت كوفيد-19. وخفاملشاركني فيه، ومل يكشف عن وجود أية حاالت إصابة بكوفيد-19 يف صفوف احلجاج. وواصل البلد تقديم مجيع اخلدمات الصحية األساسية وبرامج التحصني ووفر الدعم جلميع املقرتحات املتعلقة بعقاقري كوفيد-19 ولقاحاته. كام يعمل البلد عىل تطوير قدرته عىل إنتاج تلك املنتجات
وحتقيق االكتفاء الذايت منها.دة للتصدي ملرض كوفيد-19 ما ساهم يف احلد من انتشار املرض وتأثريه. االستنتاجات: اختذت اململكة العربية السعودية تدابري مشد
tous été suspendus. Des restrictions sur les mouvements sociaux, les rassemblements publics et religieux, les déplacements et les entreprises ont été imposées avant la survenue des 100 premiers cas confirmés de COVID-19. La participation au pèlerinage du Hadj de 2020 a aussi été soumise à des restrictions, si bien qu'aucun cas de COVID-19 n'a été détecté parmi les pèlerins. Le pays a maintenu tous les services de santé et les programmes de vaccination de base et a soutenu toutes les propositions de médicaments et de vaccins contre la COVID-19. L'Arabie saoudite travaille au renforcement de sa capacité à fabriquer ces produits et à son objectif d'autosuffisance.Conclusion : L'Arabie saoudite a pris des mesures extrêmes pour lutter contre la COVID-19, ce qui a contribué à y limiter la propagation et les effets de la maladie.
References1. Preparedness, prevention and control of coronavirus disease (COVID-19) for refugees and migrants in non-camp settings. Gene-
va: World Health Orgnaization; 2020 (https://apps.who.int/iris/handle/10665/331777, accessed 2 November 2020).
2. Health Cluster. COVID-19 response [Internet]. Geneva: World Health Organization; 2020(https://www.who.int/health-cluster/news-and-events/news/COVID19/en/, accessed 5 November 2020).
3. Bedford J, Enria D, Giesecke J, Heymann DL, Ihekweazu C, Kobinger G, et al. COVID-19: towards controlling of a pandemic. Lan-cet. 2020;395(10229):1015–8. https://doi.org/10.1016/S0140-6736(20)30673-5
4. Strengthening preparedness for COVID-19 in cities and urban settings. Geneva: World Health Organization; 2020 (https://www.who.int/publications-detail/strengthening-preparedness-for-covid-19-in-cities-and-urban-settings, accessed 10 November 2020).
5. The Kingdom of Saudi Arabia’s experience in health preparedness and response to COVID-19 pandemic. Riyadh: Government of Saudi Arabia; 2020 (https://www.moh.gov.sa/en/Ministry/MediaCenter/Publications/Documents/COVID-19-NATIONAL.pdf, accessed 6 December 2020).
6. Saudi Arabia physicians total number 2010–2019 [Internet]. Hamburg: Statista; 2021 (https://www.statista.com/statistics/608539/total-number-of-physicians-in-saudi-arabia/, accessed 1 March 2021).
7. Al-Mandhari AS, Brennan RJ, Abubakar A, Hajjeh R. Tackling COVID-19 in the Eastern Mediterranean Region. Lancet. 2020;396(10265):1786–1788. https://doi.org/10.1016/S0140-6736(20)32349-7
8. Operational planning guidelines to support country preparedness and response. Geneva: World Health Organization; 2020 (https://www.who.int/publications-detail-redirect/draft-operational-planning-guidance-for-un-country-teams, accessed 1 Noo-vember 2020).
Book 27-11.indb 1121Book 27-11.indb 1121 06/12/2021 12:39 PM06/12/2021 12:39 PM
1122
Review EMHJ – Vol. 27 No. 11 – 2021
9. About command and control center [Internet]. Riyadh: Saudi Arabia Ministry of Health; 2020 (https://www.moh.gov.sa/en/ccc/about/Pages/default.aspx, accessed 25 December 2020).
10. Ventilators are readily available at all MOH’s facilities, COVID-19 Monitoring Committee stresses. Riyadh: Saudi Arabia Minis-try of Health; 2020 (https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-04-07-004.aspx, accessed 10 December 2020).
11. Official Source at Ministry of Interior: Kingdom’s government decides to suspend international flights for two weeks starting tomorrow, Sunday [Internet]. Saudi Press Agency. 14 March 2020 (https://www.spa.gov.sa/viewfullstory.php?lang=en&newsid=2047488, accessed 1 October 2020).
12. McCloskey B, Zumla A, Lim PL, Endericks T, Arbon P, Cicero A, et al. A risk-based approach is best for decision making on hold-ing mass gathering events. Lancet. 2020;395(10232):1256–7. https://doi.org/10.1016/S0140-6736(20)30794-7
13. Yezli S, Khan AA. The Jeddah tool. A health risk assessment framework for mass gatherings. Saudi Med J. 2020;41(2):121–2. https://doi.org/10.15537/smj.2020.2.24875
14. COVID-19 – Salem tool [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://www.moh.gov.sa/en/HealthAware.-ness/EducationalContent/PublicHealth/Pages/016.aspx, accessed 1 December 2020).
15. COVID-19 health risk assessment (HRA) related to infection transmission in events and gatherings. Novel coronavirus (COV-ID-19) [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://www.moh.gov.sa/en/HealthAwareness/EducationalA-Content/Corona/Documents/COVID-19Health_Risk_Assessment-Salem_Tool.pdf, accessed 6 Dece,ebr 2020).
16. Khan A, Lezor Bieh K, El-Ganainy A, Ghallab S, Assiri A, Jokhdar H, et al. Estimating the COVID-19 risk during the Hajj pilgrim-age. J Travel Med. 2020;27(8):taaa157. https://doi.org/10.1093/jtm/taaa157
17. Ministry of Hajj and Umrah: Hajj 1441H is decided to take place this year with limited number of pilgrims from all na-tionalities residing in Saudi Arabia [Internet]. Saudi Press Agency. 22 June 2020 (https://www.spa.gov.sa/viewfullstory.php?lang=en&newsid=2100951, accessed 1 October 2020).
18. Jokhdar H, Khan A, Asiri S, Motair W, Assiri A, Alabdulaali M. COVID-19 mitigation plans during Hajj 2020: a success story of zero cases. Health Secur. 2021;19(2):133–9. https://doi.org/10.1089/hs.2020.0144
19. Interior Ministry official source: suspension of Umrah temporarily for citizens, residents in the Kingdom [Internet]. Saudi Press Agency. 4 March 2020 (https://www.spa.gov.sa/viewfullstory.php?lang=en&newsid=2042815, accessed 1 October 2020).
20. Costantino C, Fiacchini D. Rationale of the WHO document on risk communication and community engagement (RCCE) readiness and response to the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and of the Italian decalogue for prevention departments. J Prev Med Hyg. 2020;61(1):E1–E2. https://doi.org/10.15167/2421-4248/jpmh2020.61.1.1502
21. Protect against COVID-19 [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://covid19awareness.sa/en/home-page, accessed 1 October 2020).
22. MOH news – coronavirus follow-up committee holds its 20th meeting [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-03-10-008.aspx, accessed 1 October 2020).
23. MOH news – MOH: Call (937) service center for inquires about novel coronavirus [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-02-29-002.aspx, accessed 1 October 2020).
24. E-services. Tetamma app [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://www.moh.gov.sa/en/eServices/Pag.-es/Rest-assured.aspx, accessed 31 December 2020).
25. E-services. Mawid service [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://www.moh.gov.sa/en/eServices/Pagt-es/cassystem.aspx, accessed 31 December 2020).
26. Professionals & health workers [Internet]. Riyadh: Saudi Center for Diseases Pevention and Control; 2020 (https://covid19.cdc.gov.sa/professionals-health-workers/, accessed 10 December 2020).
27. Health Electronic Surveillance Network. What Is HESN? [Internet]. 2020. (https://hesn.moh.gov.sa/webportal/what-is-hesn-, accessed 31 December 2020).
28. Coronavirus disease 19 guidelines. Riyadh: Ministry of Health, Saudi Arabia; 2020. (https://www.moh.gov.sa/en/Ministry/Mes-diaCenter/Publications/Pages/covid19.aspx, accessed 31 December 2020).
29. MOH news. Over 600,000 self-assessment exams through “Mawid” App, COVID-19 monitoring committee says [Internet]. Ri-yadh: Ministry of Health, Saudi Arabia; 2020. Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-04-25-001.aspx, accessed 13 November 2020).
30. MOH news. Third stage of (Takkad) initiative centers launched [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-06-17-004.aspx, accessed 24 November 2020).
31. Alsofayan YM, Althunayyan SM, Khan AA, Hakawi AM, Assiri AM. Clinical characteristics of COVID-19 in Saudi Arabia: a nation-al retrospective study. J Infect Public Health. 2020;13(7):920–5. https://doi.org/10.1016/j.jiph.2020.05.026
32. Tetamman clinics at healthcare centers and hospitals [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://www.moh.gov.sa/en/HealthAwareness/Tataman-Clinics/Pages/default.aspx, accessed 11 October 2020).
Book 27-11.indb 1122Book 27-11.indb 1122 06/12/2021 12:39 PM06/12/2021 12:39 PM
1123
Review EMHJ – Vol. 27 No. 11 – 2021
33. MOH news. Jeddah: 1.5M+ beneficiaries served by “Tetamman” clinics to date [Internet]. Riyadh: Ministry of Health, Saudi Ara-bia; 2020Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-11-26-009.aspx accessed 24 December 2020).
34. Global surveillance for human infection with coronavirus disease (COVID-19). Interim guidance. Geneva: World Health Organi-zation; 2020 (https://apps.who.int/iris/handle/10665/331231, accessed 12 November 2020).
35. Domestic and International Aviation Protocols [Internet]. Riyadh: Saudi Center for Disease Prevention and Control; 2020 (https://covid19.cdc.gov.sa/professionals-health-workers/preventive-protocols-from-29-10-1441/domestic-and-international-aviaa-tion-protocols-en/, accessed 22 November 2020).
36. Safe places to travel during COVID pandemic - which countries are safe for travel now? [Internet]. Wego Travel Blog; 2020 (https://blog.wego.com/safe-travel-destinations-after-the-coronavirus-pandemic/, accessed 7 Decemebr 2020).
37. Covid-19 laboratory testing [Internet]. Riyadh: Saudi Center for Disease Prevention and Control; 2020 (https://covid19.cdc.gov.sa/covid-19-laboratory-testing/, accessed 31 December 2020).
38. Community & public [Internet]. Riyadh: Saudi Center for Disease Prevention and Control; 2020 (https://covid19.cdc.gov.sa/comn-munity-public/, accessed 10 December 2020).
39. Operational considerations for case management of COVID-19 in health facility and community. Intermim guidance. Geneva: World Health Organization; 2020 (https://apps.who.int/iris/handle/10665/331492, accessed 24 November 2020).
40. Jalabneh R, Zehra Syed H, Pillai S, Hoque Apu E, Hussein MR, Kabir R, et al. Use of mobile phone apps for contact tracing to control the COVID-19 Pandemic: a literature review [preprint]. SSRN 1 July 2020. http://dx.doi.org/10.2139/ssrn.3641961
41. Tawakkalna application [Internet]. Riyadh: Ministry of Health, Saudi Arabia (https://ta.sdaia.gov.sa/, accessed 9 March 2021).
42. Tabaud application [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://tabaud.sdaia.gov.sa/, accessed 9 March 2021).
43. Alghamdi S, Alqahtani J, Aldhahir A. Current status of telehealth in Saudi Arabia during COVID-19. J Family Community Med. 2020;27(3):208–11. https://doi.org/10.4103/jfcm.JFCM_295_20
44. Considerations for quarantine of contacts of COVID-19 cases. Interim guidance. Geneva: World Health Orgnaization; 2020 (https://www.who.int/publications/i/item/considerations-for-quarantine-of-individuals-in-the-context-of-containment-for-coroo-navirus-disease-(covid-19), accessed 1 October 2020).
45. MOH news. MOH shows period of home isolation or quarantine for COVID-19 patients [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-07-07-002.aspx, accessed 1 October 2020).
46. MOH news.Tetamman smart bracelet a must for citizens returning from abroad [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020. (https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-05-22-002.aspx, accessed 16 Novems-ber 2020).
47. Alshammari TM, Altebainawi AF, Alenzi KA. Importance of early precautionary actions in avoiding the spread of COVID-19: Saudi Arabia as an example. Saudi Pharm J. 2020;28(7):898–902. https://doi.org/10.1016/j.jsps.2020.05.005
48. Saudi MoH protocol for patients suspected of/confirmed with COVID-19. Supportive care and antiviral treatment of suspected or confirmed COVID-19 infection [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://covid19.cdc.gov.sa/, accessed 7 December 2020).
49. Ranney ML, Griffeth V, Jha AK. Critical supply shortages – the need for ventilators and personal protective equipment during the Covid-19 pandemic. N Engl J Med. 2020;382(18):e41. https://doi.org/10.1056/NEJMp2006141
50. SCE invites industrial companies to manufacture ventilators [Internet]. Saudi Press Agency. 9 April 2020 (https://www.spa.gov.sa/viewfullstory.php?lang=en&newsid=2072078, accessed 12 November 2020).
51. COVID 19 dashboard: Saudi Arabia [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://covid19.moh.gov.sa/, ac -cessed 31 December 2020).
52. MOH news. 3 million individuals benefit from health volunteer center’s services across the Kingdom, [Internet]. Riyadh: Minis-try of Health, Saudi Arabia; 2020 (https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-05-13-004.aspx, accessed 14 November 2020).
53. Jazieh A-R, Al Hadab A, Al Olayan A, AlHejazi A, Al Safi F, Al Qarni A, et al. Managing oncology services during a major coronavi-rus outbreak: lessons from the Saudi Arabia experience. JCO Glob Oncol. 2020;6:518–24. https://doi.org/10.1200/GO.20.00063
54. At least 80 million children under one at risk of diseases such as diphtheria, measles and polio as COVID-19 disrupts routine vaccination efforts, warn Gavi, WHO and UNICEF [Internet]. Geneva: World Health Organization; 2020 (https://www.who.int/news-room/detail/22-05-2020-at-least-80-million-children-under-one-at-risk-of-diseases-such-as-diphtheria-measles-and-polio-as-covid-19-disrupts-routine-vaccination-efforts-warn-gavi-who-and-unicef, accessed 14 November 2020).
55. MOH news. COVID-19 monitoring committee confirms number of recoveries has risen to 7798 [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-05-07-004.aspx, accessed 16 November 2020).
56. MOH news. MOH: COVID-19 vaccine to be received in phases [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-12-13-007.aspx, accessed 24 December 2020).
Book 27-11.indb 1123Book 27-11.indb 1123 06/12/2021 12:39 PM06/12/2021 12:39 PM
1124
Review EMHJ – Vol. 27 No. 11 – 2021
57. MOH news. COVID-19 monitoring committee reviews positive outcomes of the precautionary measures [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-04-04-005.aspx, accessed 21 November 2020).
58. KSA Ministry of Health leads advance clinical studies, on 4 innovative techniques for coronavirus treatment [Internet]. Saudi Arabia Press Agency. 2 May 2020 (https://www.spa.gov.sa/viewfullstory.php?lang=en&newsid=2081616, accessed 26 November 2020).
59. MOH news. MOH: our research continues, new COVID-19 vaccine trials to be conducted [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020 (https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-08-08-003.aspx, accessed 1 October 2020).
60. Modjarrad K, Roberts CC, Mills KT, Castellano AR, Paolino K, Muthumani K, et al. Safety and immunogenicity of an anti-Middle East respiratory syndrome coronavirus DNA vaccine: a phase 1, open-label, single-arm, dose-escalation trial. Lancet Infect Dis. 2019;19(9):1013–22. https://doi.org/10.1016/S1473-3099(19)30266-X
61. Arabi YM, Asiri AY, Assiri AM, Balkhy HH, Al Bshabshe A, Al Jeraisy M, et al. Interferon beta-1b and lopinavir–ritonavir for Mid-dle East respiratory syndrome. N Engl J Med. 2020;383(17):1645–56. https://doi.org/10.1056/NEJMoa2015294
62. MOH news. Over 100 COVID-19 patients benefited from blood plasma treatment [Internet]. Riyadh: Ministry of Health, Saudi Arabia; 2020. (https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-07-03-001.aspx, accessed 11 Novems-ber 2020).
63. COVID-19 research efforts draw on Saudi Arabia’s MERS experience [Internet]. Riyadh: King Abdullah International Medical Research Center (KAIMRC); 2020 (https://innovations.kaimrc.med.sa/en/feature/416/covid-19-research-efforts-draw-on-saudi-arabia’s-mers-experience, accessed 6 November 2020).
64. Saudi Arabia advances in global COVID-19 research ranking [Internet]. Arab News. 25 January 2021 (https://www.arabnews.com/node/1797876/saudi-arabia, accessed 1 March 2021).
Book 27-11.indb 1124Book 27-11.indb 1124 06/12/2021 12:39 PM06/12/2021 12:39 PM

1125
WHO events addressing public health priorities EMHJ – Vol. 27 No. 11 – 2021
Introduction The Eastern Mediterranean Region (EMR) is confronting unprecedented challenges, exacerbated by demographic and epidemiologic changes, large burden of noncommu-nicable and communicable diseases, increasing health care expenditure, as well as the effects of chronic emer-gencies, social conflicts and population movements (1–3). Research for health is essential for generating evidence that can contribute to health improvement, economic growth and equity. Health research priority-setting is one the four pillars of WHO’s strategy on research for health (4). Research prioritization is crucial, as it assists in best utilization of available resources in areas that maximize the research impact on population health. To achieve this goal, in September 2020, WHO published guidance on adopting a systematic approach to undertaking research priority setting (5). The systemic approach outlined in the guidance suggests four phases for health research prior-itization: Plan, Implement, Publish and Evaluate (PIPE). Jordan was the first country in the Region to conduct a national health research priority-setting exercise using the WHO guidance. A workshop was held virtually using the interactive Zoom platform on 15 February 2021. It was attended by more than 50 participants from Jordan’s pub-lic sector and from different national and international organizations. The main aim of the workshop was to en-hance research for health through research mapping ac-tivities and prioritizing a list of research areas for Jordan. Objectives of the workshop were to: review the national health research priority-setting exercise in Jordan; develop a short list of research statements for each of the three research areas from pre-developed long lists, through voting on two criteria: public health importance and feasibility.
Summary of discussions A nominal group technique (NGT) methodology was used for the priority-setting exercise. NGT uses small group discussion to generate a list of research options, then the facilitator asks the participants to independent-
ly prioritize the ideas by voting, rating or ranking. The facilitator summarizes the scores to determine the prior-ities. In an agreement between WHO and the Ministry of Health, three main research areas were chosen accord-ing to national strategies, plans and prioritized action plans. These were: health systems, including universal health coverage and resource management; health ser-vices, including digital health and health migration, and COVID-19 response, including public health surveillance. Ministry of Health experts, with the support of WHO, provided a long list of research statements covering these three identified main research areas. During the workshop, participants worked in three groups to review the long list of research statements. Each participant pri-vately voted on each research statement on a scale of 0–9, based on the two criteria: 1) public health importance; and 2) feasibility (a composite criterion covering tech-nical, financial and logistic feasibility). An average score was calculated by the facilitators, ranking the research statements. All scores were recorded by facilitators on a dedicated spreadsheet for each group. An average score for each research statement was calculated which was ranked by sorting from the largest to smallest of aver-age scores. The three parallel groups successfully prior-itized the long list of research statements and provided short lists of 10–15 research statements. The short lists of health research priorities were subsequently shared with participants for further comments/ suggestions, be-fore endorsement and dissemination to stakeholders in Jordan. This would concludes the first two steps in the WHO guide for national health research prioritization exercises (the planning and implementation phases).
RecommendationsThe Jordan Ministry of Health and WHO country office will collaborate to formalize a national technical working group, which will be tasked to oversee the implementa-tion of the outcomes of the national workshop. Other ac-tions will include developing a timeline and a monitoring and evaluation plan, which will also be spearheaded by the Ministry of Health.
1 This summary is extracted from the report on the National workshop on health research in Jordan, 15 Feb 2021 (https://applications.emro.who.int/docs/WHOEMRPC049E-eng.pdf?ua=1)
National workshop for health research prioritization in Jordan1 Citation: National workshop for health research prioritization in Jordan. East Mediterr Health J. 2021;27(11):1125–1126. https://doi.org/10.26719/2021.27.11.1125Copyright © World Health Organization (WHO) 2021. Open Access. Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO license (https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Book 27-11.indb 1125Book 27-11.indb 1125 06/12/2021 12:39 PM06/12/2021 12:39 PM

WHO events addressing public health priorities
1126
EMHJ – Vol. 27 No. 11 – 2021
References1. World Health Organization Regional Office for the Eastern Mediterranean (WHO/EMRO). EMR Vision 2023 Eastern Mediterra-
nean Region. Cairo: WHO/EMRO; 2019 (http://www.emro.who.int/about-who/vision2023/vision-2023.html).
2. Al-Mandhari A. Public health in the Eastern Mediterranean Region: profound challenges, huge opportunities. Lancet. 2019 Sep 21;394(10203):992-993. DOI: 10.1016/S0140-6736(19)32138-5.
3. Al-Mandhari A. Achieving “Health for All by All” in the Eastern Mediterranean Region. East Mediterr Health J. 2019 Oct 13;25(9):595-596. DOI: 10.26719/2019.25.9.595
4. World Health Organization. WHO strategy on research for health. Geneva: World Health Organization; 2012 https://apps.who.int/iris/bitstream/handle/10665/77935/9789241503259_eng.pdf;jsessionid=D92838E04CE129646D43DE0F267168C5?sequence=1
5. World Health Organization. A systematic approach for undertaking a research priority-setting exercise. Guidance for WHO staff. Geneva: World Health Organization; 2020 https://apps.who.int/iris/bitstream/handle/10665/334408/9789240009622-eng.pdf?sequence=1&isAllowed=y
Book 27-11.indb 1126Book 27-11.indb 1126 06/12/2021 12:39 PM06/12/2021 12:39 PM
Eastern Mediterranean Health Journal
IS the official health journal published by the Eastern Mediterranean Regional Office of the World Health Organization. It is a forum for the presentation and promotion of new policies and initiatives in public health and health services; and for the exchange of ideas, concepts, epidemiological data, research findings and other information, with special reference to the Eastern Mediterranean Region. It addresses all members of the health profession, medical and other health educational institutes, interested NGOs, WHO Collaborating Centres and individuals within and outside the Region.
املجلة الصحية لرشق املتوسط هى املجلة الرسمية التى تصدر عن املكتب اإلقليمى لرشق املتوسط بمنظمة الصحة العاملية. وهى منرب لتقديم السياسات واملبادرات اجلديدة يف الصحة العامة بإقليم رشق يتعلق منها املعلومات، وخاصة ما الوبائية ونتائج األبحاث وغري ذلك من واخلدمات الصحية والرتويج هلا، ولتبادل اآلراء واملفاهيم واملعطيات املتوسط. وهى موجهة إىل كل أعضاء املهن الصحية، والكليات الطبية وسائر املعاهد التعليمية، وكذا املنظامت غري احلكومية املعنية، واملراكز املتعاونة مع منظمة
الصحة العاملية واألفراد املهتمني بالصحة ىف اإلقليم وخارجه.
La Revue de Santé de la Méditerranée Orientale
EST une revue de santé officielle publiée par le Bureau régional de l’Organisation mondiale de la Santé pour la Méditerranée orientale. Elle offre une tribune pour la présentation et la promotion de nouvelles politiques et initiatives dans le domaine de la santé publique et des services de santé ainsi qu’à l’échange d’idées, de concepts, de données épidémiologiques, de résultats de recherches et d’autres informa-tions, se rapportant plus particulièrement à la Région de la Méditerranée orientale. Elle s’adresse à tous les professionnels de la santé, aux membres des instituts médicaux et autres instituts de formation médico-sanitaire, aux ONG, Centres collaborateurs de l’OMS et personnes concernés au sein et hors de la Région.
Correspondence
Editor-in-chief
Eastern Mediterranean Health JournalWHO Regional Office for the Eastern MediterraneanP.O. Box 7608 Nasr City, Cairo 11371 Egypt Tel: (+202) 2276 5000 Fax: (+202) 2670 2492/(+202) 2670 2494 Email: [email protected]
Members of the WHO Regional Committee for the Eastern Mediterranean Afghanistan . Bahrain . Djibouti . Egypt . Islamic Republic of Iran . Iraq . Jordan . Kuwait . Lebanon Libya . Morocco . Oman . Pakistan . Palestine . Qatar . Saudi Arabia . Somalia . Sudan . Syrian Arab RepublicTunisia . United Arab Emirates . Yemen
البلدان أعضاء اللجنة اإلقليمية ملنظمة الصحة العاملية لرشق املتوسط األردن . أفغانستان . اإلمارات العربية املتحدة . باكستان . البحرين . تونس . ليبيا . مجهورية إيران اإلسالمية
اجلمهورية العربية السورية . جيبويت . السودان . الصومال . العراق . عامن . فلسطني . قطر . الكويت . لبنان . مرص . املغرباململكة العربية السعودية . اليمن
Membres du Comité régional de l’OMS pour la Méditerranée orientale Afghanistan . Arabie saoudite . Bahreïn . Djibouti . Égypte . Émirats arabes unis . République islamique d’Iran Iraq . Libye . Jordanie . Koweït . Liban . Maroc . Oman . Pakistan . Palestine . Qatar . République arabe syrienne Somalie . Soudan . Tunisie . Yémen
Subscriptions and Permissions
Publications of the World Health Organization can be obtained from Knowledge Sharing and Production, World Health Organization, Regional Office for the Eastern Mediterranean, PO Box 7608, Nasr City, Cairo 11371, Egypt (tel: +202 2670 2535, fax: +202 2670 2492; email: [email protected]). Requests for permission to reproduce, in part or in whole, or to translate publications of WHO Regional Office for the Eastern Mediterranean – whether for sale or for noncommercial distribution – should be addressed to WHO Regional Office for the Eastern Mediterranean, at the above address; email: [email protected].
EMHJ is a trilingual, peer reviewed, open access journal and the full contents are freely available at its website: http://www/emro.who.int/emhj.htm
EMHJ information for authors is available at its website: http://www.emro.who.int/emh-journal/authors/
EMHJ is abstracted/indexed in the Index Medicus and MEDLINE (Medical Literature Analysis and Retrieval Systems on Line), ISI Web of knowledge, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Embase, Lexis Nexis, Scopus and the Index Medicus for the WHO Eastern Mediterranean Region (IMEMR).
© World Health Organization (WHO) 2021. Some rights reserved.This work is available under the CC BY-NC-SA 3.0 IGO licence (https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Disclaimer The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.
The authors alone are responsible for the views expressed in this publication and they do not necessarily represent the views, decisions or policies of the institutions with which they are affiliated.
If authors are staff members of the World Health Organization, the authors alone are responsible for the views expressed in this publication and do not necessarily represent the decisions, policy or views of the World Health Organization.
ISSN 1020-3397
Cover image © WHO
Cover 27-11.indd 4,6Cover 27-11.indd 4,6 06/12/2021 12:38 PM06/12/2021 12:38 PM
La Revue de Santé de la Méditerranée orientale
Eastern Mediterranean Health Journal
EMHJ – Vol. 27 No. 11 – 2021
Volume 27 No. 11November/Novembre
المجلد السابع والعشرون عدد 112021 نوفمبر/تشرين الثاني
Eastern Mediterranean H
ealth Journal Vol. 27 No. 11 – 2021
The COVID-19 pandemic is the first in human history in which innovative digital technologies are being used on an unprecedented scale to keep people connected, safe and productive while being physically and socially apart. During the World Health Assembly in 2019, Member States endorsed the Global Strategy for Digital Health. This has proven timely for implementation of digital technologies in response to different national priorities, including more efficient health care delivery and pandemic response
Editorial
Enhancing capacity and use of digital health in the Eastern Mediterranean Region: an urgent priority for actionAhmed Mandil, Arash Rashidian, Mohamed Nour, Heba Fouad and Rana Hajjeh .......................................................................................................................... 1031
Commentary
Waste management of used personal protective equipment during the COVID-19 pandemic in the Eastern Mediterranean RegionRola Al-Emam and Basel Al-Yousfi .................................................................................................................................................................................................................... 1034
Research articlesNoncommunicable disease, clinical course and COVID-19 prognosis: results based on I-CORE RegistryShaghayegh Javanmard, Noushin Mohammadifard, Maryam Nasirian, Golnaz Vaseghi, Kamal Heidari, Behrouz Kelidari, Tahereh Changiz and Nizal Sarrafzadegan ................................................................................................................................................................ 1036
Adapting the ethical review process for COVID-19 research: reviewers’ perspectives from PakistanSualeha Shekhani, Saima Iqbal and Aamir Jafarey ..................................................................................................................................................................................... 1045
Prevalence of and risk factors for Enterobius vermicularis infestation in preschool children, West Bank, PalestineRasha Khayyat, Souad Belkebir, Sameh Abuseir, Majd Barahmeh, Lujain Alsadder and Walid Basha ..................................................................................... 1052
Association between type of physical activity and risk factors for cardiovascular disease, Islamic Republic of IranOmid Aminian, Maryam Saraei, Saeed Najieb Pour and Sahar Eftekhari ........................................................................................................................................... 1061
Determinants of the Early Childhood Development Index among children aged < 5 years in Bangladesh, Costa Rica and Ghana: a comparative studyIqramul Haq, Md. Ismail Hossain, Maliha Afroj Zinnia, Md Rifat Hasan and Imru-Al-Quais Chowdhury ........................................................................... 1069
Association of clinical features of typhoid fever with socioeconomic status in PakistanMuhammad Samsoor Zarak, Hamaiyal Sana, Muzhgan Shah, Shabir Lehri, Mahekan Saghir, Qandeel Gul, Muhammad Saood, Aqeel Nasim and Noman ul haq. .................................................................................................................................................... 1078
Incidence of and factors associated with metabolic syndrome, south-east Islamic Republic of IranKhadijeh Farmanfarma, Alireza Ansari-Moghaddam, Mahmoud Kaykhaei, Mehdi Mohammadi, Hosein Adineh and Hasan Aliabd ..................................................................................................................................................................................................................... 1084
Health effects of desert dust storm events in the south-eastern Mediterranean: perceptions and practices of local stakeholdersParaskevi Kinni, Panayiotis Kouis, Helen Dimitriou, Shaked Yarza, Stefania I. Papatheodorou, Eirini Kampriani, Melanie Charalambous, Nicos Middleton, Victor Novack, Emmanouil Galanakis and Panayiotis K. Yiallouros ............................................................... 1092
Short research communication
The brain drain: why medical students and young physicians want to leave EgyptIbrahim Kabbash, Rania El-Sallamy, Hanaa Zayed, Ibrahim Alkhyate, Ahmed Omar and Sanaa Abdo ..................................................................................... 1102
ReportMERS-CoV in the COVID-19 era: update from Saudi Arabia, 2019–2020Anas Khan, Sharafaldeen Bin Nafisah, Bandr Mzahim, Bakhitah Aleid, Daliah Almatrafi,Abdullah Assiri and Hani Jokhdar ......................................................................................................................................................................................................................1109
ReviewCOVID-19 in Saudi Arabia: the national health response
Anas Khan, Yousef Alsofayan, Ahmed Alahmari, Jalal Alowais, Abdullah Algwizani, Haleema Alserehi,Abdullah Assiri and Hani Jokhdar .......................................................................................................................................................................................................................1114
WHO events addressing public health prioritiesNational workshop for health research prioritization in Jordan ................................................................................................... 1125
Cover 27-11.indd 1,3Cover 27-11.indd 1,3 06/12/2021 12:38 PM06/12/2021 12:38 PM





























