Embed Size (px)
Citation preview
�������� ����� ��
Effect of a Reduction in glomerular filtration rate after nephrectomy on arterialstiffness and central hemodynamics: rationale and design of the EARNESTstudy
William E. Moody BMedSc(Hons), MRCP, Laurie A. Tomlinson MRCP,PhD, Charles J. Ferro MD, FRCP, Richard P. Steeds MA, MD, FRCP, PatrickB. Mark PhD, FRCP, Daniel Zehnder MD, PhD, Charles R. Tomson MA,DM, FRCP, John R. Cockcroft BSc(Hons), FRCP, Ian B. Wilkinson MA, DM,FRCP, Jonathan N. Townend MD, FRCP
PII: S0002-8703(13)00734-5DOI: doi: 10.1016/j.ahj.2013.10.024Reference: YMHJ 4495
To appear in: American Heart Journal
Received date: 20 May 2013Accepted date: 28 October 2013
Please cite this article as: Moody William E., Tomlinson Laurie A., Ferro Charles J.,Steeds Richard P., Mark Patrick B., Zehnder Daniel, Tomson Charles R., CockcroftJohn R., Wilkinson Ian B., Townend Jonathan N., Effect of a Reduction in glomeru-lar filtration rate after nephrectomy on arterial stiffness and central hemodynamics:rationale and design of the EARNEST study, American Heart Journal (2013), doi:10.1016/j.ahj.2013.10.024
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
1
Effect of A Reduction in glomerular filtration rate after NEphrectomy on
arterial STiffness and central hemodynamics: Rationale and design of the
EARNEST study
William E. Moody, BMedSc(Hons), MRCP,a Laurie A. Tomlinson, MRCP, PhD,b Charles J.
Ferro, MD, FRCP,a Richard P. Steeds, MA, MD, FRCP,a Patrick B. Mark, PhD, FRCP,c Daniel
Zehnder, MD, PhD,d Charles R. Tomson, MA, DM, FRCP,e John R. Cockcroft, BSc(Hons), FRCP,f
Ian B. Wilkinson, MA, DM, FRCP,b Jonathan N. Townend, MD, FRCP.a†
On behalf of the EARNEST study investigators
†Address for correspondence: Prof Jonathan N. Townend, Birmingham Cardio-Renal Group,
Centre for Clinical Cardiovascular Science, Nuffield House, Queen Elizabeth Hospital
Birmingham, Edgbaston, B15 2TH, United Kingdom.
Email: [email protected]
Tel: +44 (0)121 371 4623
Fax: +44 (0)121 371 4629
Web: www.birmingham.ac.uk/bcrg
NCT01769924
a Institution address for authors WEM, CJF, RPS and JNT: Birmingham Cardio-Renal Group,
Centre for Clinical Cardiovascular Science, Nuffield House, Queen Elizabeth Hospital
Birmingham, Edgbaston, B15 2TH, United Kingdom. b Institution address for authors LAT, IBW: Cambridge Clinical Trials unit, University of
Cambridge, Clinical School, Addenbrooke's Hospital, Hills Road, Cambridge, CB2 0QQ, UK. c Institution address for author PBM: BHF Cardiovascular Research Centre, Institute of
Cardiovascular and Medical Sciences, University of Glasgow, 126 University Place, Glasgow,
G12 8TA, UK. d Institution address for author DZ: Clinical Science Research Laboratory, University of
Warwick, Clifford Bridge Road, Coventry, CV2 2DX, UK. e Institution address for author CRT: Academic Renal Unit, Second Floor, Learning and
Research, Southmead Hospital, Westbury-on-Trym, Bristol, BS10 5NB, UK. f Institution address for author JRC: Department of Cardiology, Wales Heart Research
Institute, University Hospital, Cardiff, CF14 4XN, UK.
Keywords: Living kidney donor; Arterial stiffness; Blood pressure.
Total word count (excluding abstract, references, tables and legends): 4,011
Running head: Prospective assessment of arterial stiffness in living kidney donors
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
2
Abstract
Background: There is strong evidence of an association between chronic kidney disease
(CKD) and cardiovascular disease. To date, however, proof that a reduction in glomerular
filtration rate (GFR) is a causative factor in cardiovascular disease is lacking. Kidney donors
comprise a highly screened population without risk factors such as diabetes and
inflammation which invariably confound the association between CKD and cardiovascular
disease. There is strong evidence that increased arterial stiffness and left ventricular
hypertrophy and fibrosis rather than atherosclerotic disease mediate the adverse
cardiovascular effects of CKD. The expanding practice of live kidney donation provides a
unique opportunity to study the cardiovascular effects of an isolated reduction in GFR in a
prospective fashion. At the same time, the proposed study will address ongoing safety
concerns which persist because the majority of longitudinal outcome studies have been
undertaken at single centers and compared donor cohorts with an inappropriately selected
control group.
Hypotheses: The reduction in GFR accompanying uninephrectomy causes (1) a pressure-
independent increase in aortic stiffness (aortic pulse wave velocity) and (2) an increase in
peripheral and central blood pressure.
Methods: This is a prospective, multi-center, longitudinal, parallel group study of 440 living
kidney donors and 440 healthy controls. All controls will be eligible for living kidney
donation using current UK transplant criteria. Investigations will be performed at baseline
and repeated at 12 months in the first instance. These include measurement of arterial
stiffness using applanation tonometry to determine pulse wave velocity and pulse wave

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
3
analysis, office blood pressure, 24 hour ambulatory blood pressure monitoring and a series
of biomarkers for cardiovascular and bone-mineral disease.
Conclusions: These data will prove valuable by characterizing the direction of causality
between cardiovascular and renal disease. This should help inform whether targeting
reduced GFR alongside more traditional cardiovascular risk factors is warranted. In addition,
this study will contribute important safety data on living kidney donors by providing a
longitudinal assessment of well-validated surrogate markers of cardiovascular disease,
namely blood pressure and arterial stiffness. If any adverse effects are detected these may
be potentially reversed with the early introduction of targeted therapy. This should ensure
kidney donors do not come to long-term harm and thereby preserve the ongoing expansion
of the living donor transplant programme (NCT01769924).
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
4
Background and rationale
The robust epidemiological evidence that shows chronic kidney disease (CKD), as manifest
by reduced estimated glomerular filtration rate (eGFR), is associated with increased
cardiovascular morbidity and mortality, provides a strong rationale for a prospective study
to determine the cardiovascular effects of kidney donation. A graded inverse relationship
exists between cardiovascular risk and eGFR;1 deleterious cardiovascular effects are clearly
evident once eGFR falls to <60ml/min/1.73m2 although the exact threshold at which
cardiovascular risk becomes elevated remains contentious.2, 3 While most data indicate the
cut-off lies between 60-70 ml/min/1.73m2 it may be even higher; in a meta-analysis of
general population cohorts with a median follow-up of about 8 years, and more than 5
million person-years, mortality rose exponentially once eGFR fell below 75 mL/min/1.73m2.
Every year more than 6,000 US individuals undergo elective nephrectomy for the purposes
of live donation without apparent increased long-term mortality or cardiovascular risk.4, 5
Uninephrectomy may be qualified as an “acute kidney injury”, with an immediate 50%
reduction in GFR followed by an improvement related to hypertrophy in the remaining
kidney - but only to 60-70% of baseline.6 Up to two-thirds of donors following nephrectomy
fulfil criteria for CKD stage 3 (eGFR 30-59 ml/min/1.73m2) dependent upon baseline age and
renal function,7 which has an approximate odds ratio for cardiovascular disease of between
2 and 4 in the general population.8 To date however, all studies examining the long-term
consequences of kidney donation have been reassuring, often showing better health
outcomes in donors compared to the general population.4, 9, 10 Small adverse cardiovascular
effects of donation cannot be excluded, however, because of residual confounding from
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
5
selection and follow-up biases. Most donors are highly motivated individuals, often making
healthy lifestyle choices both before and after nephrectomy. This inherent altruistic nature,
in conjunction with the rigorous medical selection procedures for donors results in an
extreme low risk population, for whom it is near impossible to identify a control cohort of
equivalent health status from the general population. This makes well-controlled studies
difficult and thus far we are aware of only one published prospective, controlled
pathophysiological study of kidney donors.11
The mechanisms by which CKD exerts adverse effects on cardiovascular structure and
function are diverse and have been the subject of recent reviews.12, 13 Leading potential
mediators include increased arterial stiffness, hypertension, increased left ventricular (LV)
mass and abnormal bone mineral metabolism, which may lead to increased vascular
calcification.12 There is strong cross-sectional evidence that aortic pulse wave velocity
(aPWV, a validated measure of arterial stiffness) increases as GFR falls.14-16 In a community-
based study, among treated hypertensives, even minimally impaired baseline renal function
was associated with an increased rate of aortic stiffening.17 Aortic PWV is an independent
predictor of all-cause and cardiovascular mortality in many populations including patients
on dialysis18, 19 and failure to lower aPWV by ACE-inhibitors and blood pressure reduction
has been associated with reduced survival.20 To date, only one study examining arterial
stiffness in kidney donors post-nephrectomy has been published.21 This had a cross-
sectional observational design, comparing 101 kidney donors at a mean of 111±42 months
from donation with healthy controls matched only for age and gender, indicating that aPWV
was significantly higher in donors. In a recent uncontrolled study of 17 donors, although
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
6
aPWV was not examined, augmentation index and central arterial pressure were unchanged
at 6 months compared with baseline.22
With respect to the effects of kidney donation on peripheral blood pressure, the data are
inconclusive but the best available evidence from a meta-analysis suggests a moderate
increase of about 5 mmHg in systolic pressure at 10 years after donation.23 While high
quality prospective studies of donors are still required, in the general population, even a 2
mmHg increase in systolic blood pressure is associated with a long-term increase in
mortality of about 10% for stroke and 7% for ischaemic heart disease.24 Thus, it appears that
either the adverse effects of hypertension in kidney donors are small and as yet undetected
by clinical end point studies or, that regular medical supervision post-donation has allowed
early initiation of anti-hypertensive therapy and thereby prevented harmful sequelae.
Increased LV mass is an almost universal finding by late stage CKD25 and is recognised as an
important mediator of morbidity and mortality due to heart failure and lethal arrhythmia,
the commonest modes of death in CKD.26 Chronic Kidney Disease-Mineral and Bone
Disorder (CKD-MBD) is driven by impaired phosphate excretion resulting in both bone
disease and vascular calcification which in turn mediates increased arterial stiffness and
adverse LV remodelling.27, 28 Markers of CKD-MBD such as phosphate, FGF-23 and
parathyroid hormone predict mortality and adverse cardiovascular events in patients with
CKD.29 Furthermore, there is evidence from community-based studies of graded
associations between phosphate and LV mass, cardiovascular events and death.30 Further
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
7
detailed information is therefore required on the effect of kidney donation on both LV mass
and markers of CKD-MBD. A 23% increase in parathyroid hormone has already been
reported in kidney donors at 6 months post-nephrectomy compared with controls.11
Although reduced eGFR is strongly associated with increased cardiovascular risk this
relationship may not be causal: CKD has a powerful clustering effect for other cardiovascular
risk factors such as hypertension, diabetes, dyslipidemia and inflammation which may
confound the association. Kidney donors provide an ideal ‘human model’ that enables the
longitudinal study of the cardiovascular effects of a reduction in GFR in isolation without the
multiple confounding factors associated with renal disease. The proposed study will
prospectively examine the effects of unilateral nephrectomy on the potential
pathophysiological mechanisms that appear to mediate cardiovascular morbidity and
mortality in CKD, namely arterial stiffness and blood pressure as primary end points, and LV
mass and CKD-MBD parameters as nested sub-studies, in a cohort of kidney donors large
enough to allow the detection of small effect sizes.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
8
Hypotheses
In living kidney donors, the reduction in GFR which accompanies nephrectomy results in: (1)
a pressure-independent increase in aortic stiffness (aPWV); (2) an increase in blood
pressure; (3) an increase in LV mass and impairment in LV diastolic function; (4) adverse
effects on bone mineral metabolism.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
9
Methods
Study design
This is a prospective, multi-center, longitudinal, parallel group study of 440 living kidney
donors and 440 healthy controls to be recruited over two years with initial follow up of 12
months. All participants will undergo informed written consent in keeping with the
principles set out by the Declaration of Helsinki. The EARNEST study received research ethics
approval in February 2013. The study is funded by the British Heart Foundation and
registered with the U.S. National Institutes of Health database (NCT01769924). The authors
are solely responsible for the design and conduct of this study, all study analyses, the
drafting and editing of the paper and its final contents.
Study population
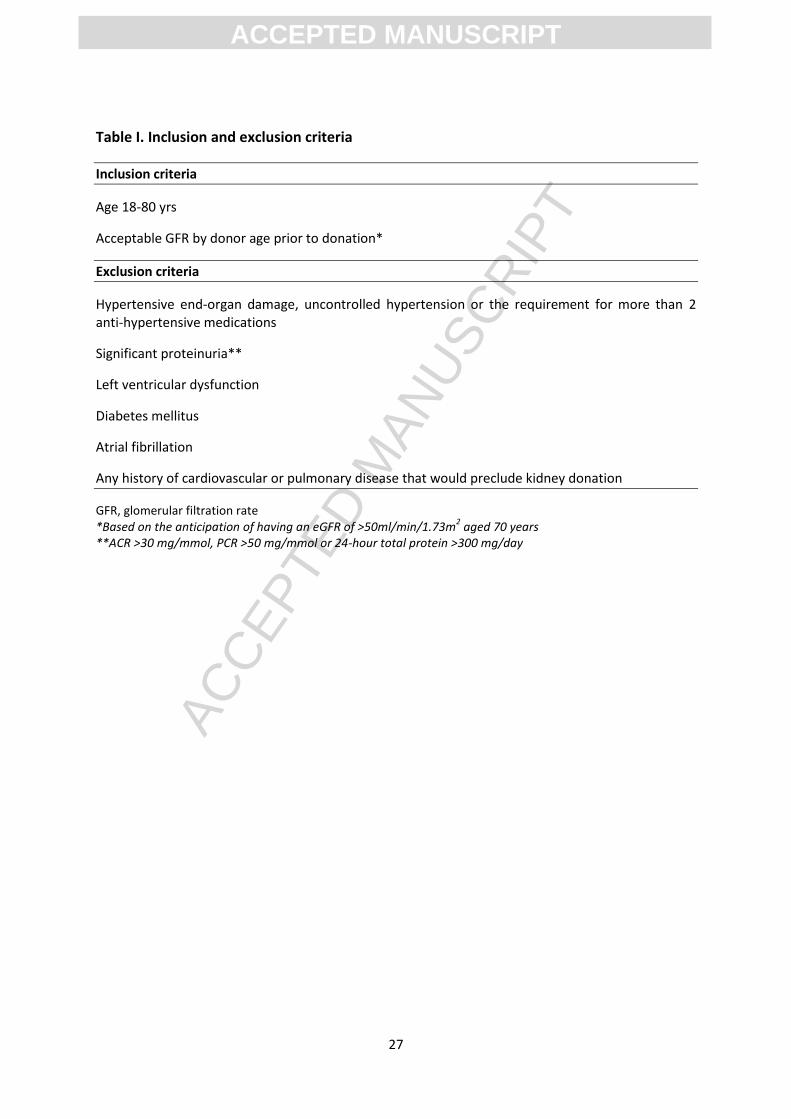
The inclusion and exclusion criteria for both donor subjects and controls are outlined in Table I
and are identical to those set by the UK living kidney donor guidelines compiled by the Joint
Working Party of The British Transplantation Society and The Renal Association.31 The only
inclusion criterion is that donor subjects will be scheduled for nephrectomy for the purpose of
kidney donation. A carefully matched series of control patients will be recruited from the same
living donor clinics at which subjects are identified, who after screening are found to be fit for
donation but do not proceed to surgery (e.g. because of arterial anatomy, immunological
mismatch). If appropriate, donor-related family members will also be invited to participate in the
study as healthy controls in order to provide a closely matched control population with
equivalent baseline health status to the donor cohort.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
10
Participants will be recruited from the following core centers, chosen because of their high
numbers of live donor transplants and strength in vascular research: (1) Queen Elizabeth
Hospital Birmingham, England (2) Addenbrooke’s Hospital, Cambridge, England (3) Western
Infirmary Glasgow, England (4) University Hospital Coventry and Warwick, England (5)
Southmead Hospital, Bristol, England (6) Northern General Hospital, Sheffield, England and (7)
Belfast City Hospital, Belfast, N. Ireland. This study remains open to the inclusion of additional
transplant centres from inside and outside the UK.
Study protocol
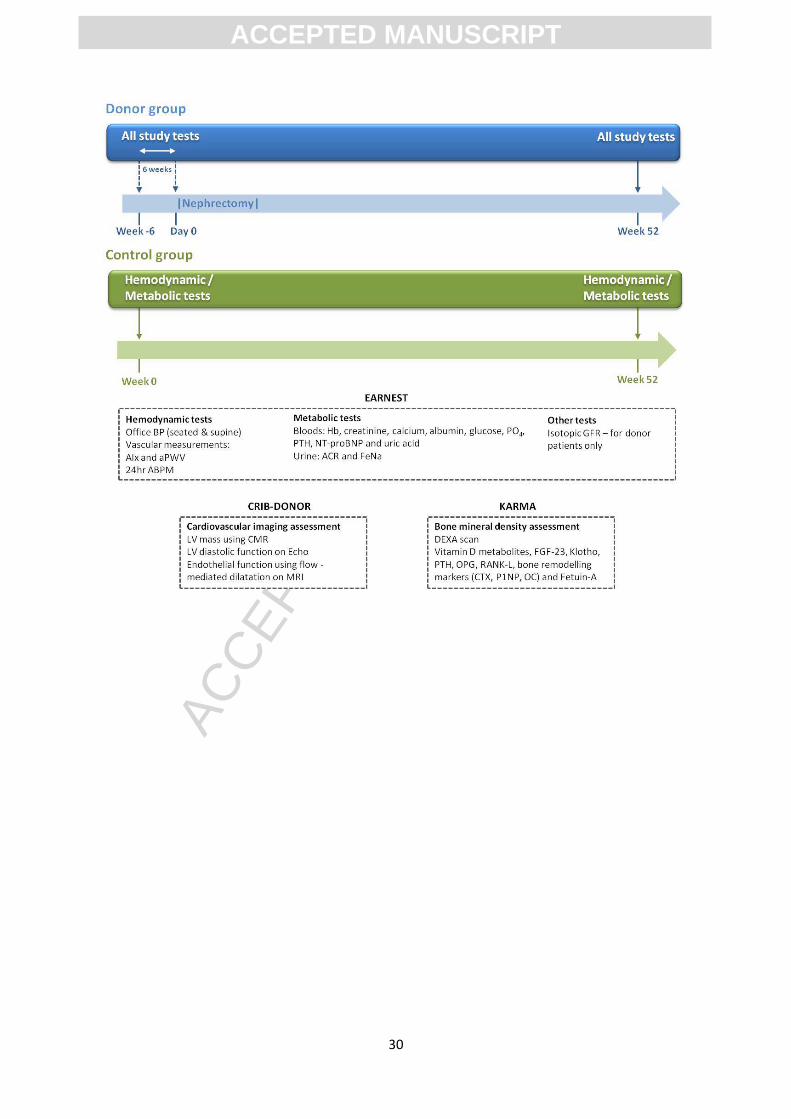
A flow chart of the study protocol is presented in Figure I. Investigations will be
performed in all participants at baseline in controls and within the 6 weeks prior to
nephrectomy in donors, with subsequent follow-up studies performed at 12 months.
Kidney donors will undergo routine follow up by their local medical and surgical team
with no alteration to normal care. No restrictions will be made to the introduction of
any treatment including anti-hypertensive drugs. At baseline and follow-up visits, body
mass index (BMI), blood pressure, heart rate and any clinical events will be recorded.
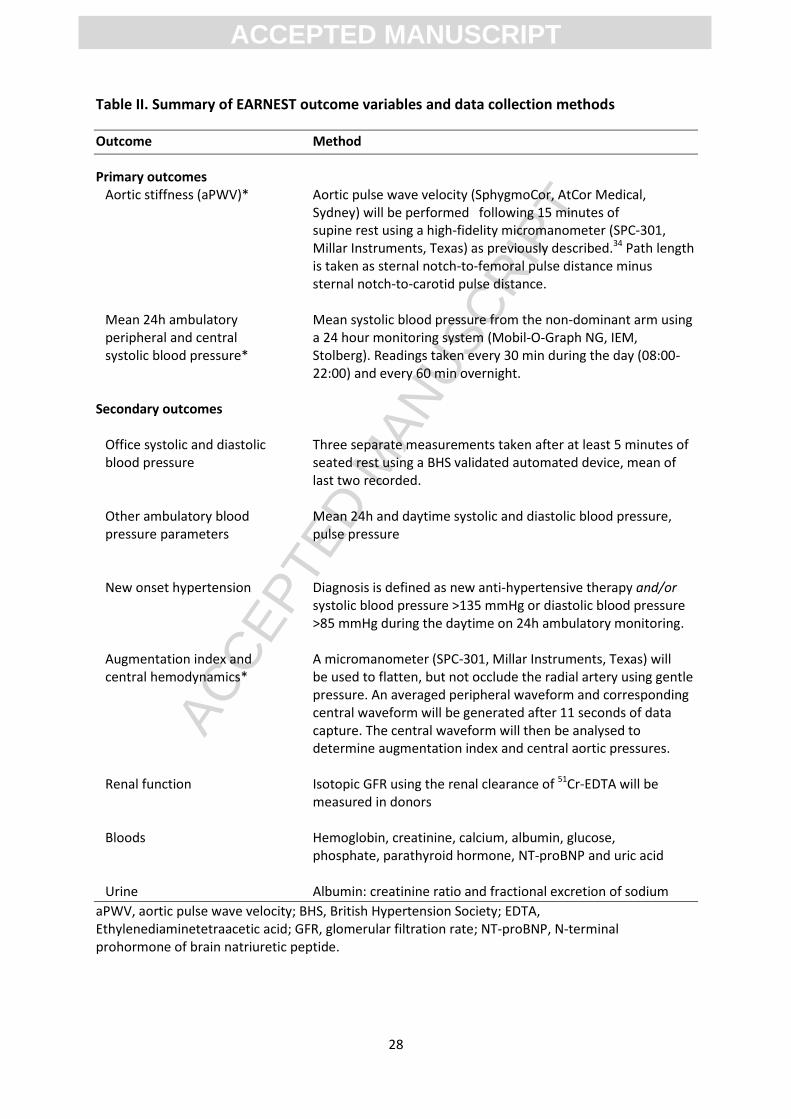
Table II summarises the main outcome variables of interest and the relevant data collection
methods. Office blood pressure will be measured on 3 occasions using a validated automated
device. The first measurement will be made following at least 5 minutes of seated rest. Two
further readings will be taken with at least one minute between readings. All measurements will
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
11
be made from the non-dominant arm using the same cuff size. Participants will also undergo 24h
ambulatory blood pressure monitoring using a British Hypertension Society validated oscillometric
recorder (Mobil-O-Graph NG, IEM, Stolberg, Germany) which will provide data on both peripheral
and central blood pressure.32, 33
Pulse wave velocity. Aortic PWV is the current gold-standard technique for measuring aortic
stiffness.34 Subjects will be studied in a quiet, temperature-controlled laboratory after 15 minutes
of lying supine. Pulse wave velocity (SphygmoCor, AtCor Medical, Sydney) will be determined by
sequential acquisition of pressure waveforms from the carotid and femoral arteries by use of a
high fidelity micromanometer (SPC-301, Millar Instruments, TX, USA) as previously described.35, 36
The path length will be calculated by subtracting the distance between the sternal notch and the
carotid recording site from the distance between the sternal notch and the femoral site.
Pulse wave analysis. Blood pressure measurement will be repeated supine before undertaking
applanation tonometry to record high fidelity arterial pressure waveforms from which indices
relating to large artery stiffness can be calculated. Central pressure waveforms will be derived and
analysed using the technique of pulse wave analysis as previously described.35, 37 A
micromanometer will be used to flatten, but not occlude the radial artery using gentle pressure.
An averaged peripheral waveform and corresponding central waveform will be generated after 11
seconds of data capture. The central waveform will then be analysed to determine the
augmentation index (AIx: the difference between the second and first peaks of the central
pressure waveform, expressed as a percentage of the pulse pressure) and central aortic pressures.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
12
The method has been shown to be reproducible in both healthy subjects and in patients with CKD.
Augmentation index and aPWV will also be recorded using ambulatory measurements taken from
the Mobilograph.38, 39
Training and reproducibility. Delegated study staff will receive formal training in
measurement techniques of arterial stiffness and undertake a reproducibility and
measurement quality study prior to study commencement. Measurements at each
center will only be performed by dedicated staff who have undergone this training.
Equipment will be calibrated at baseline and throughout the study at specific intervals.
Assessment of renal function. Isotopic GFR for kidney donors will also be measured
using the renal clearance of 51Cr-EDTA.40 Kidney function in controls will be estimated
from serum creatinine measurement.41, 42
Blood and urine. Routine hematological and biochemical parameters will be recorded
including hemoglobin, creatinine, calcium, albumin, glucose, phosphate and
parathyroid hormone. A series of biomarkers will also be measured including N-
terminal prohormone of brain natriuretic peptide, uric acid, urinary albumin:
creatinine ratio and fractional excretion of sodium.43-45
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
13
Long-term follow-up. Patients will also be asked to consent to longitudinal follow up
using the NHS Health & Social Care Information Centre’s (HSCIC) Data Linkage Service
(DLS) who provide the patient status and tracking service to examine long-term
outcomes after the study ends.
EARNEST sub-studies
The Chronic Renal Impairment in Birmingham - Kidney Donor (CRIB-DONOR) study: A
cardiac magnetic resonance and echocardiography study
Those participants enrolled into the study at Queen Elizabeth Hospital Birmingham and
some other centres will undergo cardiac magnetic resonance (CMR) imaging and
echocardiography at baseline and 12 months to determine the effects of an isolated
reduction in GFR on LV mass and function as well as aortic compliance and endothelial
function (Supplementary Table I). Arterial stiffness and office and ambulatory blood
pressure will also be measured at 6 months (in addition to the baseline and 12 month
measurement required for EARNEST). This study is registered separately with the U.S.
National Institutes of Health database (NCT01028703) and has a current recruitment target
of 140 participants.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
14
Cardiac magnetic resonance imaging. Cardiac magnetic resonance imaging will be
performed using a 1.5-T scanner (Magnetom Avanto, Siemens, Erlangen, Germany). Serial
contiguous short axis cines will be piloted from the vertical long axis and horizontal long axis
images of the left and right ventricles (ECG R-wave gated, steady-state free precession
imaging [True-FISP]; temporal resolution 40-50 ms, repetition time 3.2 ms, echo time 1.7
ms, flip angle 60°, slice thickness 7 mm with 3 mm gap) in accordance with previously
validated methodology.46 Analysis will be performed offline (Argus Software, Siemens,
Erlangen, Germany) by a single blinded observer for the assessment of ventricular volumes
(end-diastolic, end-systolic and stroke volumes), function (ejection fraction) and LV mass.46,
47 In the determination of ventricular mass, volumes and function, as compared with
transthoracic echocardiography, CMR has higher interstudy reproducibility thereby reducing
the number of participants required to adequately power such studies.48 Aortic distensibility
will be assessed at the ascending aorta and proximal descending aorta at the level of the
pulmonary artery and the distal descending aorta at the level of the diaphragm on held end-
expiration and calculated using previously validated formulae.49 Measurement of aortic
distensibility using CMR has low intra-observer variability and good reproducibility.50
Peripheral blood pressure will be performed synchronously, in triplicate, at the brachial
artery at the time of scanning for determination of pulse pressure.
Dynamic tissue-tagging MRI allows direct non-invasive assessment of regional systolic and diastolic
function and is a previously validated technique.51 Spatial modulation of magnetization will be
used to generate a uniform grid pattern with 8 mm tag separation on the LV myocardium at three
short axis sections (basal, mid and apex) and the horizontal long axis image using a fast filed echo
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
15
multi-shot sequence (temporal resolution 40-50 ms, repetition time 3.9 ms, echo time 4.4 ms,
voxel size 1.8/1.3/6.0 mm3, flip angel 14°, tag grid angle 45° with slice thickness 6 mm and a
minimum number of 15 phases per cardiac cycle) with prospective ECG gating as previously
described.52 Blinded analysis will be performed offline (CIMTag2D, University of Auckland, New
Zealand) for LV strain, strain rate and torsion calculation as previously described.52
Flow mediated dilatation of the brachial artery will also be measured using MR measurement of
brachial artery area before and after 5 minutes of arterial occlusion and also following 400mcg
GTN control.53 Brachial artery measurements will be performed off-line using semi-automated
contour tracking software (MATLAB R2008b, MathWorks Inc., Massachusetts, USA) calculating
flow-mediated dilatation as the proportional change in artery diameter in response to
hyperemia.54
Transthoracic echocardiography. A comprehensive transthoracic echocardiogram (iE33, Philips,
Eindhoven, Netherlands) will be performed at rest with the subject in the left lateral decubitus
position by a single experienced sonographer using second harmonic imaging and an S5-1 multi-
frequency transducer. All parameters will be measured in triplicate and averaged as per the
American Society of Echocardiography guidelines.55 Analysis will be performed offline by a single
blinded observer on an Xcelera workstation (Philips, Eindhoven, Netherlands). Ventricular
dimensions, wall thickness, chamber volumes and stroke volume will be determined using
standard methods.56 Left ventricular diastolic function will be determined using standard
techniques.57 Peak systolic (s’), early diastolic (e’) and late diastolic (a’) mitral annular velocities
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
16
will be measured at end expiration at the septal, lateral, inferior and anterior LV walls with real
time pulsed wave tissue Doppler (TDI).58
Grey-scale images for 2-dimensional LV strain, strain rate and torsion will be acquired in cineloop
format in triplicate from the apical 4-, 2- and 3-chamber views and parasternal short axis views at
basal, mid and apical levels at end expiration at frame rates >70Hz for offline analysis using
commercially available software (QLAB, Philips, Eindhoven, Netherlands). Myocardial contours will
be manually traced at end-systole and the software will then generate a region of interest over the
myocardium. This will enable frame-to-frame tracking of ultrasonic speckles that change position
according to surrounding tissue motion throughout the cardiac cycle. Peak systolic velocities,
strain, strain rate, rotation and twist will be measured for each myocardial segment in triplicate
and averaged.
In those subjects with appropriate image quality, transthoracic echocardiography will also be
performed during a progressive submaximal exercise test to derive stress related changes in LV
systolic and diastolic function using TDI and strain measures. Subjects will be installed on a
dedicated semisupine cycling ergometer (Schiller ERG 911 BP/L, Baar, Switzerland). After a 15-
minute rest period, each subject will undergo an exercise test that includes 3 workload stages of 4
minutes duration at 20%, 30% and 40% of their maximal aerobic power estimated via the
Wasserman equation [(body mass (50.72 – 0.372 X age))–350]/10.3 and corrected for semisupine
position (20% removed from normal values).59, 60
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
17
The KARMA Study: Effect of Kidney donAtion on bone-mineRal Metabolism and Arterial
stiffness
Participants enrolled into the study at Addenbrooke’s Hospital, Cambridge, will undergo a
more detailed biochemical assessment of the bone-mineral axis together with dual energy
X-ray absorptiometry (DEXA). It is planned to recruit 99 participants for the KARMA study, 2
controls for every living donor (Supplementary Table II).
DEXA scan. Dual energy X-ray absorptiometry is a means of measuring bone mineral density
(BMD) and soft tissue composition. A beam of X-ray, filtered into two energy bands, passes
through the patient's body. When soft tissue absorption is subtracted out, the BMD can be
determined from the absorption by bone at each energy. Dual energy X-ray absorptiometry
is the most widely used and most thoroughly studied bone density measurement
technology. For kidney donors, DEXA scans of the total body, hips and lumbar spine
scanning will be performed prior to surgery and one year later. The total body scan will
enable any changes in muscle mass to be estimated and their influence on bone density
factored out of the bone density analysis. The total effective dose of X-ray radiation for the
proposed scans will be approximately 4.5 micro Sieverts, comparable with a daily
background from atmospheric sources of 6 micro Sieverts. Pregnancy testing (urinary β-
HCG) will be performed in female participants of childbearing age in the donor group prior
to DEXA scanning.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
18
Blood Tests. These will be the same as for the main EARNEST study but for kidney donors
additional samples will be taken at days 1, 2 and 3 post-operatively and 6 weeks following
donation. Blood samples will be centrifuged within 30 minutes of venesection and serum
and plasma separated and frozen at -70◦C. Samples will later also be used for testing of
vitamin D metabolites (1, 25- and 25-vitamin D), FGF-23, Klotho, PTH, OPG, RANK-L, bone
remodelling markers (CTX, P1NP, OC) and Fetuin-A as well as renin and aldosterone.
Urine tests. Again, these will be the same as for the main EARNEST study but in addition for
kidney donors 100mL aliquots of urine will be taken at days 1, 2 and 3 post-operatively and
6 weeks following surgery and frozen at -70◦C for later measurement of Fetuin-A, calcium
and phosphate.
Statistical analysis
The formal comparison between arms of each of the co-primary endpoints will use a linear
regression model on the within-patient change from baseline, adjusting for baseline value,
sex, ethnicity, use of anti-hypertensives, age, eGFR at donation (and iGFR where available in
donors), and the other co-primary endpoint at baseline. To formally control the overall
significance level over both co-primary endpoints (aPWV and blood pressure) at 5%, a Holm-
Bonferroni method will be employed. Findings will be interpreted taking into consideration
that aPWV and blood pressure are correlated. A secondary analysis of the co-primary
endpoints will be performed according to age, ethnic group, baseline eGFR and change in
eGFR (and iGFR where available in donors), BMI and pre-donation hypertension.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
19
EARNEST Power calculations and sample size
Assuming that the SD of the within-patient change in aPWV is 1.0 m/s and in blood pressure
is 10 mmHg,35, 61 a sample size of 800 patients (control and donors, 400 subjects each,
assuming 9% dropout), will provide 80% power to detect a difference of 0.22 m/s or 2.2
mmHg for aPWV and blood pressure, respectively, under a two-sided t-test at the 2.5%
significance level. Power calculations for CRIB-DONOR and KARMA sub-studies are outlined
in Appendix I.
Discussion
There is strong evidence that patients with CKD have increased cardiovascular risk with a
graded relation with both eGFR and the level of albuminuria.62 However, previous studies
are limited by their cross-sectional and observational nature, and causation has not yet
been established. The true impact of CKD on the cardiovascular system remains hard to
define since the duration of the CKD is often unknown, the underlying causes are diverse
and there are numerous confounders, including associated diseases such as hypertension
and diabetes. Moreover, the level of GFR at which adverse structural and functional changes
occur within the heart and vasculature, and at which cardiovascular risk starts to rise, is not
clear. Kidney donors provide a unique healthy population who change at a known time
point from having normal to impaired renal function. This study should establish whether
reduced GFR leads directly to adverse cardiovascular effects such as increased arterial
stiffness, hypertension, LV mass and mineral bone disorder. Since the prevalence of CKD is
high and rising (14.0% in the US in 2005-10, as defined by eGFR<60ml/min/1.72m2 or
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
20
ACR≥30mg/g),26 it is important to establish if a causal relationship exists to determine
whether targeting CKD alongside more traditional risk factors could lead to reductions in
cardiovascular mortality and morbidity. The potential size of this effect is salutary. If
causative, it has been estimated that up to 10% of vascular events in middle age and 20% in
old age might be attributable to reduced eGFR.63
By careful prospective measurement of ambulatory blood pressure in living kidney donors
before and after nephrectomy, this study will also provide important practical information
needed for patient care. By clarifying whether there is an increased frequency of hypertension
and surrogate markers of CV disease post donation we will be able to better advise potential
donors in future and inform national guidance on the importance of long-term follow-up.
In an attempt to reduce the shortfall in the number of organs available for transplantation, the
opportunity to undergo donor nephrectomy is now being offered to people with pre-existing
medical conditions which include hypertension and raised BMI, as well as to subjects that are
older with lower baseline GFR. The potential renal and cardiovascular risks of kidney donation
may be most relevant to this group of donors, but those studies which have attempted to
address this issue are single-center, retrospective reports offering conflicting data.64-66 There
may also be increased risk in non-Caucasian donors although the data in this area remain
preliminary.9 The EARNEST study is large enough to prospectively examine the influences of age,
BMI, ethnicity and co-morbidity on changes in cardiovascular structure and function following
nephrectomy in kidney donors.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
21
We believe that the living kidney donation programme is a vital method of providing renal-
replacement therapy for individuals with end-stage kidney disease. The evidence to date
suggests that this practice is safe although there are data demonstrating an increased risk of
high blood pressure post-donation. Studying vascular parameters in detail both before and
after donation provides an excellent opportunity to examine prospectively the direction of
causality between loss of kidney function and cardiovascular disease. In addition, we may be
able to provide important information to guide the long-term management of kidney
donors. An open, critical approach is vital if we are to preserve public trust and the altruistic
goodwill of donors, with the aim of safeguarding the expansion of the living kidney
transplant programme.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
22
Acknowledgements
This manuscript has been prepared on behalf of the EARNEST study investigators. The study
is also heavily dependent upon the following collaborators: Professor Phil Kalra; Consultant
Nephrologist and Chair of the UKCRN Renal Specialty Group; Dr Katan Patel and Dr Mellone
Marchong, Study Coordinators and Mrs Jane Smith, Research Nurse, Cambridge Clinical
Trials unit; Ms Elizabeth Dwenger and Ms Lucia Sharpe, Cardiology Research Nurses,
University Hospital Birmingham NHS Foundation Trust; Dr Aisling Courtney, Consultant
Nephrologist and Ms Linda Trouton, Research Nurse, Belfast City Hospital; Mr Badri
Shrestha, Consultant Transplant Surgeon, Dr Martin Wilkie, Consultant Nephrologist and Ms
Louese Dunn, Renal Research Coordinator, Sheffield Kidney Institute; Ms Sue Dawson and
Ms Jo Vaz, Renal Research Nurses, Southmead Hospital, Bristol; Dr Neal Morgan, Southern
Health and Social Care Trust, Northern Ireland; Mr Marc Glancy, Director of Renal
Transplantation, Western Infirmary Glasgow.
The EARNEST study is funded by a British Heart Foundation Project Grant. WEM is
supported by a British Heart Clinical Research Fellowship. We are also grateful for the
resources provided by the BRC and CLRN, the Wellcome/NIHR Clinical Research Facilities in
Birmingham and Cambridge and The British Heart Foundation Research Centre in Glasgow.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
23
References
1. Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 2004;351(13):1296-305.
2. NKF. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 2002;39(2 Suppl 1):S1-266.
3. Eknoyan G, Lameire N, Barsoum R, Eckardt KU, Levin A, Levin N, et al. The burden of kidney disease: improving global outcomes. Kidney Int 2004;66(4):1310-4.
4. Segev DL, Muzaale AD, Caffo BS, Mehta SH, Singer AL, Taranto SE, et al. Perioperative mortality and long-term survival following live kidney donation. JAMA 2010;303(10):959-66.
5. Garg AX, Meirambayeva A, Huang A, Kim J, Prasad GV, Knoll G, et al. Cardiovascular disease in kidney donors: matched cohort study. Bmj 2012;344:e1203.
6. Krohn AG, Ogden DA, Holmes JH. Renal function in 29 healthy adults before and after nephrectomy. JAMA 1966;196(4):322-4.
7. Moody WE, Chue CD, Inston NG, Edwards NC, Steeds RP, Ferro CJ, et al. Understanding the effects of chronic kidney disease on cardiovascular risk: are there lessons to be learnt from healthy kidney donors? J Hum Hypertens 2011.
8. Schiffrin EL, Lipman ML, Mann JF. Chronic kidney disease: effects on the cardiovascular system. Circulation 2007;116(1):85-97.
9. Ibrahim HN, Foley R, Tan L, Rogers T, Bailey RF, Guo H, et al. Long-term consequences of kidney donation. N Engl J Med 2009;360(5):459-69.
10. Fehrman-Ekholm I, Elinder CG, Stenbeck M, Tyden G, Groth CG. Kidney donors live longer. Transplantation 1997;64(7):976-8.
11. Kasiske BL, Anderson-Haag T, Ibrahim HN, Pesavento TE, Weir MR, Nogueira JM, et al. A Prospective Controlled Study of Kidney Donors: Baseline and 6-Month Follow-up. Am J Kidney Dis 2013;62(3):577-86.
12. Moody WE, Edwards NC, Chue CD, Ferro CJ, Townend JN. Arterial disease in chronic kidney disease. Heart 2013;99(6):365-72.
13. Chue CD, Townend JN, Steeds RP, Ferro CJ. Arterial stiffness in chronic kidney disease: causes and consequences. Heart 2010;96(11):817-23.
14. Briet M, Bozec E, Laurent S, Fassot C, London GM, Jacquot C, et al. Arterial stiffness and enlargement in mild-to-moderate chronic kidney disease. Kidney Int 2006;69(2):350-7.
15. Wang MC, Tsai WC, Chen JY, Huang JJ. Stepwise increase in arterial stiffness corresponding with the stages of chronic kidney disease. Am J Kidney Dis 2005;45(3):494-501.
16. Townsend RR, Wimmer NJ, Chirinos JA, Parsa A, Weir M, Perumal K, et al. Aortic PWV in Chronic Kidney Disease: A CRIC Ancillary Study. Am J Hypertens 2009.
17. Benetos A, Adamopoulos C, Bureau JM, Temmar M, Labat C, Bean K, et al. Determinants of accelerated progression of arterial stiffness in normotensive subjects and in treated hypertensive subjects over a 6-year period. Circulation 2002;105(10):1202-7.
18. Blacher J, Guerin AP, Pannier B, Marchais SJ, Safar ME, London GM. Impact of aortic stiffness on survival in end-stage renal disease. Circulation 1999;99(18):2434-9.
19. Blacher J, Pannier B, Guerin AP, Marchais SJ, Safar ME, London GM. Carotid arterial stiffness as a predictor of cardiovascular and all-cause mortality in end-stage renal disease. Hypertension 1998;32(3):570-4.
20. Guerin AP, Blacher J, Pannier B, Marchais SJ, Safar ME, London GM. Impact of aortic stiffness attenuation on survival of patients in end-stage renal failure. Circulation 2001;103(7):987-92.
21. Bahous SA, Stephan A, Blacher J, Safar ME. Aortic stiffness, living donors, and renal transplantation. Hypertension 2006;47(2):216-21.
22. DeLoach SS, Meyers KE, Townsend RR. Living donor kidney donation: another form of white coat effect. Am J Nephrol 2012;35(1):75-9.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
24
23. Boudville N, Prasad GV, Knoll G, Muirhead N, Thiessen-Philbrook H, Yang RC, et al. Meta-analysis: risk for hypertension in living kidney donors. Ann Intern Med 2006;145(3):185-96.
24. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002;360(9349):1903-13.
25. Mark PB, Johnston N, Groenning BA, Foster JE, Blyth KG, Martin TN, et al. Redefinition of uremic cardiomyopathy by contrast-enhanced cardiac magnetic resonance imaging. Kidney Int 2006;69(10):1839-45.
26. USRDS. U S Renal Data System, Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2012. 2012.
27. Chue CD, Edwards NC, Moody WE, Steeds RP, Townend JN, Ferro CJ. Serum phosphate is associated with left ventricular mass in patients with chronic kidney disease: a cardiac magnetic resonance study. Heart 2012;98(3):219-24.
28. Faul C, Amaral AP, Oskouei B, Hu MC, Sloan A, Isakova T, et al. FGF23 induces left ventricular hypertrophy. J Clin Invest 2011;121(11):4393-408.
29. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl 2009(113):S1-130.
30. Foley RN. Phosphate levels and cardiovascular disease in the general population. Clin J Am Soc Nephrol 2009;4(6):1136-9.
31. British Transplantation Society / The Renal Association. United Kingdom Guidelines for Living Donor Kidney Transplantaton. 2005.
32. Wei W, Tolle M, Zidek W, van der Giet M. Validation of the mobil-O-Graph: 24 h-blood pressure measurement device. Blood Press Monit 2010;15(4):225-8.
33. Weiss W, Gohlisch C, Harsch-Gladisch C, Tolle M, Zidek W, van der Giet M. Oscillometric estimation of central blood pressure: validation of the Mobil-O-Graph in comparison with the SphygmoCor device. Blood Press Monit 2012;17(3):128-31.
34. Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, et al. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J 2006;27(21):2588-605.
35. Wilkinson IB, Fuchs SA, Jansen IM, Spratt JC, Murray GD, Cockcroft JR, et al. Reproducibility of pulse wave velocity and augmentation index measured by pulse wave analysis. J Hypertens 1998;16(12 Pt 2):2079-84.
36. Frimodt-Moller M, Nielsen AH, Kamper AL, Strandgaard S. Reproducibility of pulse-wave analysis and pulse-wave velocity determination in chronic kidney disease. Nephrol Dial Transplant 2008;23(2):594-600.
37. Savage MT, Ferro CJ, Pinder SJ, Tomson CR. Reproducibility of derived central arterial waveforms in patients with chronic renal failure. Clin Sci (Lond) 2002;103(1):59-65.
38. Hametner B, Wassertheurer S, Kropf J, Mayer C, Eber B, Weber T. Oscillometric estimation of aortic pulse wave velocity: comparison with intra-aortic catheter measurements. Blood Press Monit 2013;18(3):173-6.
39. Luzardo L, Lujambio I, Sottolano M, da Rosa A, Thijs L, Noboa O, et al. 24-h ambulatory recording of aortic pulse wave velocity and central systolic augmentation: a feasibility study. Hypertens Res 2012;35(10):980-7.
40. Martensson J, Groth S, Rehling M, Gref M. Chromium-51-EDTA clearance in adults with a single-plasma sample. J Nucl Med 1998;39(12):2131-7.
41. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, 3rd, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med 2009;150(9):604-12.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
25
42. Michels WM, Grootendorst DC, Verduijn M, Elliott EG, Dekker FW, Krediet RT. Performance of the Cockcroft-Gault, MDRD, and new CKD-EPI formulas in relation to GFR, age, and body size. Clin J Am Soc Nephrol 2010;5(6):1003-9.
43. Vickery S, Webb MC, Price CP, John RI, Abbas NA, Lamb EJ. Prognostic value of cardiac biomarkers for death in a non-dialysis chronic kidney disease population. Nephrol Dial Transplant 2008;23(11):3546-53.
44. Landray MJ, Emberson JR, Blackwell L, Dasgupta T, Zakeri R, Morgan MD, et al. Prediction of ESRD and death among people with CKD: the Chronic Renal Impairment in Birmingham (CRIB) prospective cohort study. Am J Kidney Dis 2010;56(6):1082-94.
45. Madero M, Sarnak MJ, Wang X, Greene T, Beck GJ, Kusek JW, et al. Uric acid and long-term outcomes in CKD. Am J Kidney Dis 2009;53(5):796-803.
46. Maceira AM, Prasad SK, Khan M, Pennell DJ. Normalized left ventricular systolic and diastolic function by steady state free precession cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2006;8(3):417-26.
47. Myerson SG, Bellenger NG, Pennell DJ. Assessment of left ventricular mass by cardiovascular magnetic resonance. Hypertension 2002;39(3):750-5.
48. Grothues F, Smith GC, Moon JC, Bellenger NG, Collins P, Klein HU, et al. Comparison of interstudy reproducibility of cardiovascular magnetic resonance with two-dimensional echocardiography in normal subjects and in patients with heart failure or left ventricular hypertrophy. Am J Cardiol 2002;90(1):29-34.
49. Groenink M, de Roos A, Mulder BJ, Spaan JA, van der Wall EE. Changes in aortic distensibility and pulse wave velocity assessed with magnetic resonance imaging following beta-blocker therapy in the Marfan syndrome. Am J Cardiol 1998;82(2):203-8.
50. Forbat SM, Mohiaddin RH, Yang GZ, Firmin DN, Underwood SR. Measurement of regional aortic compliance by MR imaging: a study of reproducibility. J Magn Reson Imaging 1995;5(6):635-9.
51. Yeon SB, Reichek N, Tallant BA, Lima JA, Calhoun LP, Clark NR, et al. Validation of in vivo myocardial strain measurement by magnetic resonance tagging with sonomicrometry. J Am Coll Cardiol 2001;38(2):555-61.
52. Young AA, Imai H, Chang CN, Axel L. Two-dimensional left ventricular deformation during systole using magnetic resonance imaging with spatial modulation of magnetization. Circulation 1994;89(2):740-52.
53. Wiesmann F, Petersen SE, Leeson PM, Francis JM, Robson MD, Wang Q, et al. Global impairment of brachial, carotid, and aortic vascular function in young smokers: direct quantification by high-resolution magnetic resonance imaging. J Am Coll Cardiol 2004;44(10):2056-64.
54. Jackson CE, Shirodaria CC, Lee JM, Francis JM, Choudhury RP, Channon KM, et al. Reproducibility and accuracy of automated measurement for dynamic arterial lumen area by cardiovascular magnetic resonance. Int J Cardiovasc Imaging 2009;25(8):797-808.
55. Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R, Feigenbaum H, et al. Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. J Am Soc Echocardiogr 1989;2(5):358-67.
56. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr 2005;18(12):1440-63.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
26
57. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr 2009;22(2):107-33.
58. Alam M, Wardell J, Andersson E, Samad BA, Nordlander R. Characteristics of mitral and tricuspid annular velocities determined by pulsed wave Doppler tissue imaging in healthy subjects. J Am Soc Echocardiogr 1999;12(8):618-28.
59. Arena R, Myers J, Abella J, Pinkstaff S, Brubaker P, Moore B, et al. Determining the preferred percent-predicted equation for peak oxygen consumption in patients with heart failure. Circ Heart Fail 2009;2(2):113-20.
60. Doucende G, Schuster I, Rupp T, Startun A, Dauzat M, Obert P, et al. Kinetics of left ventricular strains and torsion during incremental exercise in healthy subjects: the key role of torsional mechanics for systolic-diastolic coupling. Circ Cardiovasc Imaging 2010;3(5):586-94.
61. Rothwell PM, Howard SC, Dolan E, O'Brien E, Dobson JE, Dahlof B, et al. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet 2010;375(9718):895-905.
62. Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, et al. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet 2010;375(9731):2073-81.
63. Mafham M, Emberson J, Landray MJ, Wen CP, Baigent C. Estimated glomerular filtration rate and the risk of major vascular events and all-cause mortality: a meta-analysis. PLoS One 2011;6(10):e25920.
64. O'Brien B, Mastoridis S, Sabharwal A, Hakim N, Taube D, Papalois V. Expanding the donor pool: living donor nephrectomy in the elderly and the overweight. Transplantation 2012;93(11):1158-65.
65. Tavakol MM, Vincenti FG, Assadi H, Frederick MJ, Tomlanovich SJ, Roberts JP, et al. Long-term renal function and cardiovascular disease risk in obese kidney donors. Clin J Am Soc Nephrol 2009;4(7):1230-8.
66. Rook M, Bosma RJ, van Son WJ, Hofker HS, van der Heide JJ, ter Wee PM, et al. Nephrectomy elicits impact of age and BMI on renal hemodynamics: lower postdonation reserve capacity in older or overweight kidney donors. Am J Transplant 2008;8(10):2077-85.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
27
Table I. Inclusion and exclusion criteria
Inclusion criteria
Age 18-80 yrs
Acceptable GFR by donor age prior to donation*
Exclusion criteria
Hypertensive end-organ damage, uncontrolled hypertension or the requirement for more than 2 anti-hypertensive medications
Significant proteinuria**
Left ventricular dysfunction
Diabetes mellitus
Atrial fibrillation
Any history of cardiovascular or pulmonary disease that would preclude kidney donation
GFR, glomerular filtration rate *Based on the anticipation of having an eGFR of >50ml/min/1.73m
2 aged 70 years
**ACR >30 mg/mmol, PCR >50 mg/mmol or 24-hour total protein >300 mg/day
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
28
Table II. Summary of EARNEST outcome variables and data collection methods
Outcome Method
Primary outcomes Aortic stiffness (aPWV)* Aortic pulse wave velocity (SphygmoCor, AtCor Medical, Sydney) will be performed following 15 minutes of supine rest using a high-fidelity micromanometer (SPC-301, Millar Instruments, Texas) as previously described.34 Path length is taken as sternal notch-to-femoral pulse distance minus sternal notch-to-carotid pulse distance. Mean 24h ambulatory Mean systolic blood pressure from the non-dominant arm using peripheral and central a 24 hour monitoring system (Mobil-O-Graph NG, IEM, systolic blood pressure* Stolberg). Readings taken every 30 min during the day (08:00- 22:00) and every 60 min overnight. Secondary outcomes Office systolic and diastolic Three separate measurements taken after at least 5 minutes of blood pressure seated rest using a BHS validated automated device, mean of last two recorded. Other ambulatory blood Mean 24h and daytime systolic and diastolic blood pressure, pressure parameters pulse pressure New onset hypertension Diagnosis is defined as new anti-hypertensive therapy and/or systolic blood pressure >135 mmHg or diastolic blood pressure >85 mmHg during the daytime on 24h ambulatory monitoring. Augmentation index and A micromanometer (SPC-301, Millar Instruments, Texas) will central hemodynamics* be used to flatten, but not occlude the radial artery using gentle pressure. An averaged peripheral waveform and corresponding central waveform will be generated after 11 seconds of data capture. The central waveform will then be analysed to determine augmentation index and central aortic pressures. Renal function Isotopic GFR using the renal clearance of 51Cr-EDTA will be measured in donors Bloods Hemoglobin, creatinine, calcium, albumin, glucose, phosphate, parathyroid hormone, NT-proBNP and uric acid Urine Albumin: creatinine ratio and fractional excretion of sodium
aPWV, aortic pulse wave velocity; BHS, British Hypertension Society; EDTA, Ethylenediaminetetraacetic acid; GFR, glomerular filtration rate; NT-proBNP, N-terminal prohormone of brain natriuretic peptide.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
29
Figure I. EARNEST Study timeline
ABPM, ambulatory blood pressure monitoring; ACR, albumin: creatinine ratio; AIx, augmentation index; BP, blood pressure; CMR, cardiac magnetic resonance imaging; CTX, carboxy-terminal collagen crosslinks; DEXA, Dual energy X-ray absorptiometry; FeNa, fractional excretion of urinary sodium; FGF-23, fibroblast growth factor-23; GFR, glomerular filtration rate; Hb, haemoglobin; LV, left ventricular; MRI, magnetic resonance imaging; NT-proBNP, N-terminal prohormone of brain natriuretic peptide; OC, osteocalcin; OPG, osteoprotegerin; PO4, phosphate; PTH, parathyroid hormone; aPWV, aortic pulse wave velocity; P1NP, N-terminal
propeptides of type I procollagen; RANK-L, Receptor activator of nuclear factor kappa-B ligand.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
30




![[Miniinvasive laparoscopic or retroperitoneoscopic radical nephrectomy for the parenchymal tumor]](https://img.pdfslide.net/doc/110x75/63351f0e2670d310da0ef536/miniinvasive-laparoscopic-or-retroperitoneoscopic-radical-nephrectomy-for-the-parenchymal.jpg)
























