Embed Size (px)
Citation preview

Effects of Ropivacaine on Pain After LaparoscopicCholecystectomy: A Prospective,Randomized Study
Murat Sozbilen, MDLevent Yeniay, MDOmerVedat Unalp, MDOzer Makay, MDDepartment of General Surgery
Alihan Pirim, MDSezgin Ulukaya, MDMeltem Uyar, MDDepartment of Anesthesiology
Sinan Ersin, MDDepartment of General SurgeryEge University School of MedicineIzmir, Turkey
ABSTRACT
Postoperative pain after laparoscopic cholecystectomy is an ongoing problem. To relieve this pain, practitioners have used many anesthetic and analgesic drugs.This study was undertaken to assess the effects of incisional and intraperitonealadministration of ropivacaine on postoperative pain and stress response inpatients undergoing laparoscopic cholecystectomy. In this prospective, single-blinded, randomized study, 45 patients with ASA (American Society of Anesthe-siologists) scores I and II who were about to undergo laparoscopic cholecystecto-my were divided into 3 groups. After cholecystectomy, a total of 40 mL of 3.75%ropivacaine was administered preincisionally and intraperitoneally to patients ingroup 1 (n=14); preincisionally and intraperitoneally to patients in group 2 (n=17);and intraperitoneally and locally at incision sites to patients in group 3 (n=14).Blood levels of epinephrine and norepinephrine were examined preoperatively,15 min after insufflation, and at the end of the operation. Visual analog pain scalescores and analgesic requirements were used for 24-h postoperative follow-up ofpain levels reported by patients. No statistically significant difference was foundamong the 3 groups with respect to visual analog pain scale scores, total analgesicrequirements, and accompanying pain, nausea, and vomiting. The earliest anal-gesic requirements were seen in group 2 (P<.005), and less shoulder pain was
247
Advancesin Therapy®
Volume 24 No. 2March/April 2007
Address correspondence toOmer V. Unalp, MDEge University School of MedicineDepartment of General SurgeryIzmir, 35100, TurkeyEmail: [email protected]
©2007 Health Communications IncTransmission and reproduction of this material in wholeor part without prior written approval are prohibited.
0953

noted in group 3 (P<.005). Norepinephrine and epinephrine levels showed no statistically sig-nificant differences between the 3 groups. Administration of ropivacaine preoperatively andpostoperatively for laparoscopic cholecystectomy has similar effects on postoperative painand the stress response of patients.
Keywords: laparoscopic cholecystectomy; postoperative pain; local anesthesia;ropivacaine
INTRODUCTION
Postoperative pain is a complex phenomenon that involves sensational, emotional,and behavioral factors. It remains a problem that impairs quality of life, especiallyduring the first postoperative 24 h.1,2 A total of 30% to 70% of patients who haveundergone an operation are known to experience severe postoperative pain.3Although laparoscopic cholecystectomy results in less pain than is produced by opencholecystectomy, it is not a painless procedure. No standard method of pain relief hasbeen devised for patients who experience post-laparoscopic cholecystectomy pain.Methods currently used for postoperative pain include systemic and local analgesicdrugs, local pain blockage, anti-inflammatory drugs, and heated gas.4 Several studieshave reported promising results1,2 with application of local anesthetics for reduction ofpostoperative pain after laparoscopic procedures. Modern analgesic medication regi-mens include preemptive analgesia, local techniques, neuraxial techniques, and com-bination treatment with opioid and nonopioid drugs. Recent studies have proved thatthis combination approach can shorten the length of hospital stay and reduce the post-operative recovery period.5
The study described here was undertaken to assess the effects of incisionally andintraperitoneally administered ropivacaine, a local anesthetic agent with long-last-ing efficacy, on postoperative pain and the stress response during the first 24 h afterelective laparoscopic cholecystectomy.
PATIENTS AND METHODS
This study consisted of a consecutive series of operations performed on 45 patientswho underwent elective laparoscopic cholecystectomy from April 2004 to November2004. The American Society of Anesthesiologists (ASA) score was I for 35 patients andII for the remaining 10. The study group included 19 male (42.2%) and 26 female(57.8%) patients with a mean age of 48.7±9.4 y.
General anesthesia included induction with 5 mg/kg thiopental sodium as a hyp-notic, 1 µg/kg remifentanyl as an analgesic, and 0.6 mg/kg rocuronium as a musclerelaxant, followed by intubation and maintenance with oxygen, 0.5% to 1.2% isoflu-rane, 0.25 to 0.5 µg/kg remifentanyl, and 0.15 mg/kg rocuronium. All operationswere performed by a consultant surgeon who specialized in laparoscopy and wasassisted by senior assistants. The standard 4-trocar technique was used for all opera-tions in which the target insufflation rate and intra-abdominal pressure were set at 1 L/min and 12 mm Hg, respectively. The deflation procedure was carried out care-fully for complete removal of residual carbon dioxide. Patients were randomlyassigned to group 1, 2, or 3.
248M. Sozbilen, et al
Effects of Ropivacaine on Pain After Laparoscopic Cholecystectomy

In group 1, 3.75% ropivacaine was administered to trocar sites preincisionally (intoskin, subcutaneous tissue, and fascia, 5 mL for each trocar site) and just after forma-tion of pneumoperitoneum. In addition, 40 mL of 3.75% ropivacaine was sprayed intothe intraperitoneum, the region of the gallbladder, and the subdiaphragmatic area; a lapse of 10 min was allowed before dissection was begun. In group 2, each trocar sitewas preincisionally infiltrated with 5 mL of 3.75% ropivacaine; at the end of the pro-cedure, just before desufflation, 40 mL of 3.75% ropivacaine was intraperitoneallysprayed onto the cholecystectomy site and the subdiaphragmatic space. In group 3, at the end of the procedure, just before desufflation, 40 mL of 3.75% ropivacaine wasintraperitoneally administered onto the cholecystectomy site and the subdiaphrag-matic space, and the periphery of each trocar site was infiltrated with 5 mL of 3.75%ropivacaine. Groups 1, 2, and 3 consisted of 14, 17, and 14 patients, respectively.
A visual analog pain scale (VAPS) and a patient satisfaction score (PSS) were usedto assess the postoperative pain level of patients at 0 min (at the end of the operation)and at 10 min, 20 min, 30 min, 1 h, 2 h, 4 h, 6 h, 12 h, 18 h, and 24 h after the operation.For VAPS measurements, patients were asked to mark a point on a grid that indicat-ed their current pain level and were advised that the bottom represented “no pain”and the top, “worst imaginable pain.” For PSS measurements, patients were askedhow much they appreciated the effects of the analgesic applied at that specific time.Additional parameters measured included shoulder tip pain, accompanying pain,nausea, vomiting, itchiness, urine retention, first urination time after operation, returntime of bowel sounds, first episode of flatulence after the operation, standing up forthe first time after the operation, and any adverse events due to drugs used. Patientswho needed additional analgesia or who had high VAPS scores received pethidine 1 mg/kg intramuscularly. No other oral or parenteral analgesic medication was used.In cases of nausea or vomiting, 10 mg metoclopropamide hydrochloride was givenintravenously.
Blood samples were taken for measurement of hormone levels before the operationand patency was maintained in veins 15 min after insufflation of the abdomen and atthe end of the surgical procedure; thus, 0.36 to 0.8 ng/dL and 0.14 to 0.3 ng/dL wereaccepted as normal ranges for norepinephrine and epinephrine levels, respectively.Results were expressed as median±standard deviation. Data obtained from the 3 groupswere analyzed via the χ2 test for cross-tables; by 1-way analysis of variance (ANOVA),repeated measure ANOVA, and the Friedman test for parametric data; and with theKruskall-Wallis and Mann-Whitney U tests for nonparametric data. A P value less than.05 was considered significant.
RESULTS
A comparison of demographic data among the 3 groups revealed a homogenousdistribution, yielding no significant difference (Table 1). The highest VAPS scoresduring the postoperative period were 6.7, 7.6, and 7.2 in groups 1, 2, and 3, respec-tively. The highest VAPS scores were attained at 10 min in groups 1 and 2, and at 0min (end of operation) in group 3. The highest VAPS score was reported in group 2.No significant difference was observed among VAPS scores of the 3 groups at anytime interval (P>.05) (Fig 1). Pain scores in each group decreased during the follow-up period, pointing to a statistically significant reduction (P<.05) (Fig 2).Comparison of PSSs among the 3 groups at any specific time interval revealed no
249Advances in Therapy®
Volume 24 No. 2, March/April 2007
statistically significant difference (P>.05) (Fig 3). The lowest PSSs were recorded at10 min in group 1 and at 0 min in groups 2 and 3; they were 1.5, 1.3, and 1.6, respec-tively. PSSs increased over the 24-h follow-up period, displaying a statistically sig-nificant elevation in each group (P<.05). The mean of the first additional analgesictime was 10.8±18.3 min in group 1, 8±15.6 min in group 2, and 12.3±32.9 min ingroup 3. No statistically significant difference was detected among the study groups(P>.05) (Fig 4). Approximately half of the patients (46.7%) needed the first dose ofanalgesic, whereas 24% needed the second dose and 17.8%, the third dose.Postoperative nausea and/or vomiting was recorded in a total of 25 patients, andthe difference among the groups was not statistically significant (P>.05). Percentagesof shoulder tip and back pain, which are defined as associated pain, in groups 1, 2,and 3 were 28%, 29%, and 7%, respectively (P>.05). Dizziness and headache werereported in only 2 patients (Table 2).
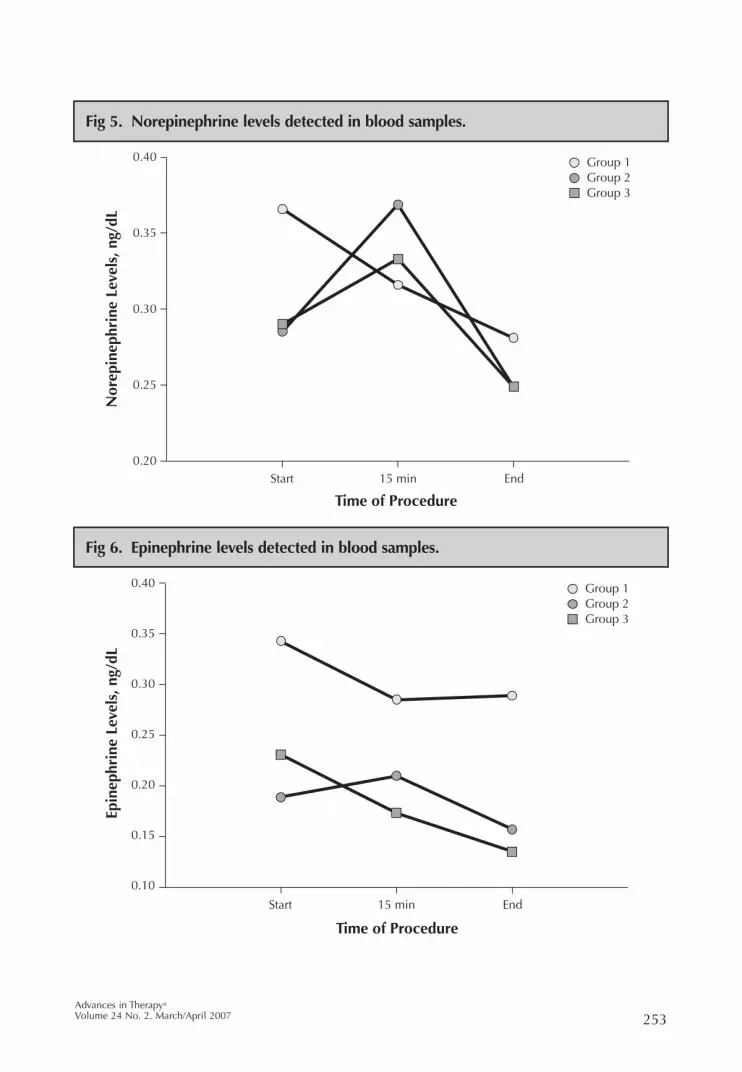
Norepinephrine levels in blood samples of patients were assessed at 3 differenttime periods (at the beginning of the procedure, at 15 min after insufflation, and at the end of the procedure). Respective levels in group 1 were 0.36±0.19 ng/dL,0.31±0.14 ng/dL, and 0.28±0.16 ng/dL; in group 2, 0.28±0.07 ng/dL, 0.36±0.09 ng/dL,and 0.24±0.15 ng/dL; and in group 3, 0.29±0.13 ng/dL, 0.33±0.09 ng/dL, and0.24±0.08 ng/dL. A marked decrease in norepinephrine levels was noted in eachgroup during the third period, but this change was not statistically significant withinany individual group or among the 3 groups (P>.05) (Fig 5).
Epinephrine levels were also detected at the same time periods, with corre-sponding results as follows: 0.34±0.25 ng/dL, 0.28±0.1 ng/dL, and 0.28±0.14 ng/dLin group 1; 0.18±0.05 ng/dL, 0.21±0.07 ng/dL, and 0.15±0.03 ng/dL in group 2; and0.23±0.18 ng/dL, 0.17±0.07 ng/dL, and 0.13±0.05 ng/dL in group 3. The third peri-od decrease in norepinephrine levels was not reflected in epinephrine levels. Despitethe insignificant difference within each individual group, the difference among the3 groups was statistically significant (P<.05) (Fig 6).
250M. Sozbilen, et al
Effects of Ropivacaine on Pain After Laparoscopic Cholecystectomy
Group 1 Group 2 Group 3 P Value
Age, y 46.31±10.66 50.35±7.48 48.93±10.54 >.05
Body weight, kg 71.69±11.59 71.41±8.78 76.21±4.64 >.05
BMI, kg/m2 26.315±3.636 26.53±3.416 27.584±2.695 >.05
Sex, M/F 4/10 7/10 8/6 >.05
ASA score, I/II 11/3 14/3 10/4 >.05
Operation time, min 68.33±21.25 71.47±32.97 62.50±22.77 >.05
Table 1. Demographic Data by Study Group

251Advances in Therapy®
Volume 24 No. 2, March/April 2007
10
8
6
4
2
0 T0 T1 T2 T3 T4 T5 T6
Group 1 Group 2 Group 3
Vis
ual A
nalo
g Pa
in S
cale
Sco
re
Time Interval
Fig 1. Postoperative visual analog pain scale scores of study groups.
10
9
8
7
6
5
4
3
2
1
0 2 0 4 6 8
Group 1 Group 2 Group 3
Vis
ual A
nalo
g Pa
in S
cale
Sco
re
Time Interval
Fig 2. Change in visual analog pain scale scores between time intervals.

252M. Sozbilen, et al
Effects of Ropivacaine on Pain After Laparoscopic Cholecystectomy
4
3
2
1
0 T0 T1 T2 T3 T4 T5 T6
Group 1Group 2Group 3
Pati
ent
Sati
sfac
tion
Sco
re
Time Interval
Fig 3. Postoperative PSS values by group.
15
10
5
0 Group 1 Group 2 Group 3
Tim
e, m
in
Fig 4. First analgesic requirements of study groups.
253Advances in Therapy®
Volume 24 No. 2, March/April 2007
0.40
0.35
0.30
0.25
0.20
Group 1 Group 2 Group 3
Start 15 min End
Nor
epin
ephr
ine
Leve
ls, n
g/dL
Time of Procedure
Fig 5. Norepinephrine levels detected in blood samples.
0.40
0.35
0.30
0.25
0.20
0.15
0.10
Group 1 Group 2 Group 3
Start 15 min End
Epin
ephr
ine
Leve
ls, n
g/dL
Time of Procedure
Fig 6. Epinephrine levels detected in blood samples.

DISCUSSION
Pain and vomiting are the most common complications after laparoscopic chole-cystectomy.6,7 Although postoperative pain is less frequent and more easily controlledafter minimally invasive procedures than after procedures performed by laparotomy,no general consensus has yet been reached on the effectiveness of control measures.1,8
Three types of pain occur after laparoscopy9: visceral pain, abdominal wall pain, andshoulder tip pain. Visceral pain occurs most often as a result of surgical manipulationand irritation of the parietal peritoneum and diaphragm by trapped and dissolvedcarbon dioxide gas within the abdomen. Placement of the patient in the Fowler posi-tion during the procedure also contributes to this. A somatic type of pain occurs at thesite where trocars enter the abdominal wall. Pain may also result from electrocauteryusage and irritation caused by peritoneal bile contamination. Previous studies haveshown that inflammation that occurs after cholecystectomy in the gallbladder bed,liver, diaphragm, and parietal peritoneum causes pain and nausea.10
Nonsteroidal anti-inflammatory drugs (NSAIDs) have been used to reduce painintensity after laparoscopic procedures through their anti-inflammatory and anal-gesic effects.11,12 Some studies have reported promising results with parenteral andintraperitoneal administration of NSAIDs.13
The effects of different types of local anesthetics on postoperative pain afterlaparoscopic cholecystectomy have been investigated in numerous studies; mostoften, these agents have been found to be effective in preventing postoperativepain.2,14,15 No consensus is evident in the literature as to (1) which local anestheticagent has the greatest superiority in laparoscopic procedures, and (2) where and atwhich stage of the operation local anesthetics should be applied. The most com-monly used and investigated local anesthetic drug is bupivacaine; studies done onropivacaine and L-bupivacaine are fewer in number but have been conducted morerecently.16-18 Ropivacaine is known for its less cardiotoxic and neurotoxic adverseeffects in comparison with bupivacaine.19 Investigators in this study therefore choseto use ropivacaine.
In the literature, local anesthetics were most frequently administered only to inci-sion sites or only intraperitoneally or as part of a combination regimen. Narchi et al20
reported that postoperative pain was reduced after intraperitoneal administration of local anesthetic at the end of the operation. In a study conducted by Inan et al,21
bupivacaine was administered to both trocar sites and the parietal peritoneum; theauthors concluded that administration at the end of the operation was most effective.Conversely, in a study by Pasquolucci et al,22 in which an intraperitoneal local anes-
254M. Sozbilen, et al
Effects of Ropivacaine on Pain After Laparoscopic Cholecystectomy
Group 1 Group 2 Group 3 P Value
Nausea/vomiting, % 57 52 64 >.05
Shoulder tip and back pain, % 28 29 7 >.05
Table 2. Postoperative Pain and Nausea and Vomiting Percentages

thetic drug (bupivacaine) was used similarly, a more potent analgesic effect wasreported for the group given this agent at the beginning of the operation. Studies byChundrigar et al23 and Mraovic et al24 could not, however, detect any statistically sig-nificant difference with respect to administration of bupivacaine at the beginning orthe end of the operation. In a study in which 0.25% intraperitoneal ropivacaine wasgiven to 37 patients who were about to undergo a laparoscopic cholecystectomy,Labaille et al25 reported a reduction in the severity of pain and in the need for analge-sia in a comparison with the placebo group. In the present study, no statistically sig-nificant difference was revealed with respect to postoperative pain and additionalanalgesic requirements between group 1, to which the drug was administered at thebeginning of the operation, and group 3, to which it was given at the end.
Some studies have reported that local anesthetic infiltration to incision sites wassomewhat potent in reducing pain but did not have a long-lasting effect.26 Once again,incisional administration before or after surgical trauma remains a matter of contro-versy. Pavlidis et al27 reported that preincisional, periportal ropivacaine infiltrationproduced better analgesic effects and reduced postoperative opioid requirementswhen compared with administration of placebo. With respect to incisional site infil-tration, Sarac et al28 found that preemptive application was not effective in relievingpostoperative pain. In the present study, investigators observed no effect with respectto postoperative pain in group 1, which may be viewed as the preemptive group.
Opioids are the recommended postoperative analgesics after laparoscopic proce-dures; therefore, investigators have used pethidine hydrochloride for relief of pain.29
Mouton et al30 reported in their study that up to 80% of patients needed opioids afterthey underwent laparoscopic cholecystectomy. In the present study, 89% of patientsrequired opioids during the postoperative period.
Postoperative nausea and vomiting are common complications after laparoscopy.6,7
In this study, nausea and vomiting occurred at a rate of up to 64% in all 3 groups,but nausea and vomiting are adverse effects of opioids, so it is difficult to establisha relationship among the groups in terms of this event.
This study was the first that has been undertaken to explore the effects of com-bined administration of incisional and intraperitoneal ropivacaine at different stagesof laparoscopic cholecystectomy.
Epinephrine levels were found to be significantly different among the 3 studygroups. The preemptive analgesia group had higher epinephrine levels than thegroup given intraperitoneal local anesthesia after cholecystectomy. Despite the factthat such a difference is significant, it is proposed here that additional studies shouldbe conducted with larger populations to support the significance of the differencesnoted in preoperative epinephrine levels. Although the differences in norepineph-rine levels were not statistically significant, these differences, along with differencesreported in epinephrine levels, highlight the need for additional studies.
Numerous studies have investigated the effectiveness of ropivacaine in reducingshoulder tip pain. In the present study, the severity of shoulder tip and back painwas markedly reduced in group 3, the group that received ropivacaine incisionallyand intraperitoneally after cholecystectomy, compared with the other 2 groups;however, these findings were statistically insignificant. Similar studies should beperformed with larger groups to find out whether ropivacaine is effective in reliev-ing shoulder tip pain.
255Advances in Therapy®
Volume 24 No. 2, March/April 2007

During the follow-up period, VAPS scores decreased and PSS scores increased ineach group, as expected. VAPS and PSS differences were not significantly differentbetween groups, but the change within each group was statistically significant.
The small number of patients studied precluded the possibility of conclusiveresults. The investigators believe that prospective, randomized studies with largerpopulations are needed so that more definite conclusions can be reached.
CONCLUSION
The investigators in the present study found that administration of 3.75% ropiva-caine at trocar sites and intraperitoneal spaces is a simple, quick, and safe approachfor use in laparoscopic cholecystectomy. Administration of ropivacaine at 3 differentstages of laparoscopic cholecystectomy revealed no significant difference in VAPS,PSS, and analgesic requirements during the postoperative period among the 3 groups.With respect to shoulder tip pain, administration of 3.75% ropivacaine intraperi-toneally and to trocar sites at the end of the operation seemed to produce effectiveresults, as was the case in group 3. Despite differences in stress hormone levelsbetween groups 1 and 3, studies with larger populations and a longer follow-up peri-od are needed to confirm the findings reported here.
NOTE
This study was presented at the 8th National Pain Congress of Turkey on May 18,2004, in Istanbul, Turkey.
REFERENCES
1. Lee IO, Kim SH, Kong MH, et al. Pain after laparoscopic cholecystectomy: the effect and timingof incisional and intraperitoneal bupivacaine. Can J Anaesth. 2001;48:545-550.
2. Alexander DJ, Ngoi SS, Lee L, et al. Randomized trial of periportal peritoneal bupivacaine forpain relief after laparoscopic cholecystectomy. Br J Surg. 1996;83:1223-1225.
3. Ure BM, Troidl H, Spanberger W, et al. Preincisional local anesthesia with bupivacaine and pain after laparoscopic cholecystectomy: a double-blind randomized clinical trial. Surg Endosc.1993;7:482-488.
4. Moote CA. The prevention of postoperative pain. Can J Anaesth. 1994;41:527-533.
5. Bardram L, Funch-Jensen P, Kehlet H. Rapid rehabilitation in elderly patients after laparoscopiccolonic resection. Br J Surg. 2000;87:1540-1545.
6. Nathanson LK, Shimi S, Cushieri A. Laparoscopic cholecystectomy: the Dundee technique. Br J Surg. 1991;78:155-159.
7. Salky BA, Bauer JJ, Kreel I, et al. Laparoscopic cholecystectomy: an initial report. GastrointestEndosc. 1991;37:1-4.
8. Soper NJ, Barteau JA, Clayman RV, Ashley SW, Dunnegan DL. Comparison of early postoperativeresults for laparoscopic versus standard open cholecystectomy. Surg Gynecol Obstet. 1992;174:114-118.
9. Joris J, Thiry E, Paris P, et al. Pain after laparoscopic cholecystectomy: characteristics and effectof intraperitoneal bupivacaine. Anesth Analg. 1995;81:379-384.
10. Schwenk W, Jacobi C, Mansmann U, et al. Inflammatory response after laparoscopic vs conven-tional colorectal resections—results of a prospective randomized trial. Langenbeck’s Arch Surg.2000;385:2-9.
256M. Sozbilen, et al
Effects of Ropivacaine on Pain After Laparoscopic Cholecystectomy
11. Gilberg LE, Harsten AS, Stahl LB. Preoperative diclofenac reduces post-laparoscopy pain. Can J Anaesth. 1993;40:406-408.
12. Rosenblum M, Weller RS, Conrad PL, Favley EA. Ibuprofen provides longer lasting analgesiathan fentanyl after laparoscopic surgery. Anesth Analg. 1991;73:255-259.
13. Elhakim M, Amine H, Kamel S, et al. Effects of intraperitoneal lidocaine combined with intravenous or intraperitoneal tenoxicam on pain relief and bowel recovery after laparoscopiccholecystectomy. Acta Anesthesiol Scand. 2000;44:929-933.
14. Bisgaard T, Klarskov B, Kristiansen VB, et al. Multi-regional local anesthetic infiltration during laparoscopic cholecystectomy in patients receiving prophylactic multi-modal analgesia:a randomized, double-blinded, placebo-controlled study. Anesth Analg. 1999;89:1017-1024.
15. Motamed C, Bouaziz H, Franco D, Benhamou D. Analgesic effect of low-dose intrathecal morphine and bupivacaine in laparoscopic cholecystectomy. Anaesthesia. 2000;55:118-124.
16. Goldstein A, Grimault P, Henique A, et al. Preventing postoperative pain by local anesthetic instillation after laparoscopic gynecologic surgery: placebo controlled comparison of bupivacaineand ropivacaine. Anesth Analg. 2000;91:403-407.
17. Horn EP, Schroeder F, Wilhelm S, et al. Wound infiltration and drain lavage with ropivacaineafter major shoulder surgery. Anesth Analg. 1999;89:1461-1466.
18. Mulroy MF, Burgess FW, Emanuelson BM. Ropivacaine 0.25% and 0.5% but not 0.125% provideeffective wound infiltration analgesia after outpatient hernia repair. Reg Anesth Pain Med. 1999;24:136-141.
19. Knudsen K, Beckmann Suurkula M, Blomberg S, Sjovall J, Edvardsson N. Central nervous andcardiovascular effects of i.v. infusions of ropivacaine, bupivacaine and placebo in volunteers. Br J Anaesth. 1997;78:507-514.
20. Narchi P, Benhamou D, Fernandez H. Intraperitoneal local anesthetic for shoulder pain afterday-case laparoscopy. Lancet. 1991;338:1569-1570.
21. Inan A, Sen M, Dener C. Local anesthesia use for laparoscopic cholecystectomy. World J Surg.2004;24:741-744.
22. Pasquolucci A, Contardo R, Donbrai U, et al. The effect of intraperitoneal local analgesics, analgesic requirement after laparoscopic cholecystectomy. Laparoendosc Surg. 1992;94:405-412.
23. Chundrigar T, Hedges AR, Morris R, Stamatakis JD. Intraperitoneal bupivacaine for effectivepain relief after laparoscopic cholecystectomy. Ann R Coll Surg Engl. 1993;75:437-439.
24. Mraovic B, Jurisic T, Kogler-Majeric V, Sustic A. Intraperitoneal bupivacaine for analgesia afterlaparoscopic cholecystectomy. Acta Anaesthesiol Scand. 1997;41:193-196.
25. Labaille T, Mazoit JX, Paqueron X, et al. The clinical efficacy and pharmacokinetics of intraperitonealropivacaine for laparoscopic cholecystectomy. Anesth Analg. 2002;94:100-105.
26. Wills VL, Hunt R. Pain after laparoscopic cholecystectomy. Br J Surg. 2000;87:273-284.
27. Pavlidis TE, Atmatzidis KS, Papaziogas BT, et al. The effect of preincisional periportal infiltrationwith ropivacaine in pain relief after laparoscopic procedures: a prospective randomized trial. JSLS. 2003;7:305-310.
28. Sarac AM, Aktan AO, Baykan N, et al. The effect and timing of local anesthesia in laparoscopiccholecystectomy. Surg Laparosc Endosc. 1996;6:362-366.
29. Alexander JI. Pain after laparoscopy. Br J Anaesth. 1997;79:369-378.
30. Mouton WG, Bessell JR, Otten KT, Maddern GJ. Pain after laparoscopy. Surg Endosc. 1999;13:445-448.
257Advances in Therapy®
Volume 24 No. 2, March/April 2007












![[Laparoscopic adrenalectomy]](https://img.pdfslide.net/doc/110x75/635b67f44028fc5adf01ad9d/laparoscopic-adrenalectomy.jpg)
















