Embed Size (px)
Citation preview
28
Electroencephalography and Over-‐diagnosis of Epilepsy; A Cross-‐sectional Study in Sulaimaniya City, Iraq” Osama S. Amin, MRCPI, MRCPS (Glasg), FCCP, FACP (1), Haw S. Namiq MBChB MSc (2) Hero M. Zangan MBChB (3), Nawa A. Ameen MBChB (4) 1. Neurologist, Department of Neurology, Sulaimaniya General Teaching Hospital, Sulaimaniya City, Iraq 2. Assistant lecturer, Neurophysiology, College of Pharmacy, Sulaimaniya University, Iraq 3. Senior House Officer in Neurology, Department of Neurology, Sulaimaniya General Teaching Hospital, Sulaimaniya City, Iraq. 4. Junior house officer, Department of Neurology, Sulaimaniya General Teaching Hospital, Sulaimaniya City, Iraq. Corresponding author: Osama Shukir Muhammed Amin Sulaimaniya Post-‐Office, PO BOX 196 Sulaimaniya City, Iraq E-‐mail: [email protected]
Abstract The aim of this study was to investigate the extent of misdiagnosing epilepsy in Sulaimaniya city in Iraq. This cross-‐sectional study involved 65 epileptic patients who were receiving antiepileptic drugs for a variable duration. Most of the diagnoses were made solely on an abnormal EEG. The study was conducted in Sulaimaniya general teaching hospital and its neurology/neurophysiology departments, outpatients clinic and private neurology/neurophysiology clinics from November 1st, 2009 to January 30th, 2010. All patients had their EEG done prior to the initiation of the study. We interviewed the patients, re-‐examined them, and re-‐interpreted their EEGs. Results showed that twelve out of the 65 “epileptic” patients (18%) were found to have a genuine seizure disorder after a careful review of their clinical presentation and EEG findings. The rest (n=53, 82%) had no epilepsy and their diagnosis ranged from syncope and pre-‐syncope (n=9) to malingering (n=1). The first routine EEG was
29
reported as normal in 12 (out of 65) patients and a further of three EEGs were inconclusive; the other 50 EEGs were labelled as demonstrating epileptiform activities. In Conclusion the lack of Iraqi national guidelines for EEG referrals, the absence of audit of these EEG referrals, the common misbelieves that EEG can solve many cases of abnormal movements, and the poor expertise in the interpretation of EEG have resulted in misuse/abuse of EEG with secondary over-‐diagnosis of epilepsy among Sulaimaniya city patients. Key words: Electroencephalogram, epilepsy, movements, wrong diagnosis, and EEG Misinterpretation.
Introduction In 1929, the German neuropsychiatrist, Hans Berger, discovered the human electroencephalogram, but at that time, its clinical applications were still unclear. Several years later, Gibbs and co-‐workers in Boston found the 3-‐Hz spike-‐and-‐wave discharge of what was then named absence seizures [1]. In spite of the usefulness of EEG as an investigating tool in seizure disorders, there are many drawbacks and the potential for misuse and abuse may secondarily arise; when EEG is being ordered to diagnose/exclude seizure as an explanation behind “funny turns”, over-‐diagnosis of epilepsy would occur by the inexperienced physician. [2]
Patients and Methods In conducting this study, we tried to investigate why the number of epileptic disorders has increased dramatically in Sulaimaniya city in Iraq. We reviewed the registry of the Ali Kamal Primary Public Health Centre in Sulaimaniya city; this centre dispenses a variety of medications of chronic illnesses (including anti-‐epileptics) to the public at a very low cost. We noticed that the number of epileptic patients attending that Centre has increased from an average of two patients per day in October 2006 to six patients per day in October 2009 (i.e., 300% increment). This study was conducted in Sulaimaniya general teaching hospital and its neurology/neurophysiology outpatients’ clinic from November 1st 2009 to January 30th, 2010. The aforementioned medical centre is the largest medical care provider in Sulaimaniya city and contains the only tertiary neurology facility. Table 1 summarizes various patients’ characteristics.
30
Inclusion criteria and initial work-‐up To be enrolled in this cross-‐sectional study, the individual should have been given a diagnosis of epilepsy by a doctor practicing in Sulaimaniya city after having an electroencephalographic examination in one of the EEG centres in this city, regardless of the duration of epilepsy and anti-‐epileptic medications ingested. Individuals who underwent more than one EEG examination at two or more different EEG centres were excluded; the latter criterion would lessen inter-‐observer variation in the initial EEG interpretation. Patients (or their parents, in paediatric cases) attending Ali Kamal Primary Public Health Centre were asked to be enrolled in this study; sixty-‐five patients participated within three months. Patients (or their parents) who agreed signed a consent form and they brought their very first EEG trace. For history re-‐taking, a questionnaire was formulated in the English language, which was then translated into Kurdish language by an independent translation office. After we interviewed the patients (or their parents), back-‐translation of the findings from Kurdish to English was done by the same office. Another independent office validated the translation. All patients (n=65) underwent routine blood tests (complete blood counts, ESR, fasting blood sugar, urea and electrolytes, liver function tests, and urine examination), thyroid function, brain imaging (CT scan and/or MRI), and EEG. Other investigations were ordered according to the clinical picture of the patient; ECG (n=43), trans-‐thoracic echocardiography (n=29), chest X-‐ray (n=28), CSF examination (n=12), EMG/nerve conduction studies (n=7), cervical spine X-‐ray (n=4). The EEG examination was done with the use of Micromed Brain Quick EEG machine and SystemPlus Evolution software. The duration of EEG examination in all patients was 20 minutes. Sixty-‐five patients (100%) underwent a single EEG that included manoeuvres such as eye opening, eye closure, and activation procedures (such as photic stimulation and hyperventilation). Sleep EEG was done in four patients (all were children). A second EEG recording was obtained in five patients only because the initial trace was disorganized with many artefacts. None of the patients has had his/her EEG done after sleep deprivation or during a suspected seizure. Video EEG monitoring is not available in our hospital. The EEG examination was done in the neurophysiology division of our outpatients’ clinic (n=28) and various private clinics (n=37). Technicians carried out the outpatients’ clinic EEG recording, and neurologists attending the same outpatient clinic interpreted these EEGs. Twenty-‐one EEGs were performed in private neurophysiology clinics by
31
neurophysiologists, who also interpreted the trace and wrote the report of the EEG. The remaining (n=16) EEGs were obtained in private neurology clinics; medical personnel who have had no training in neurophysiology did the EEG while the neurologist of that clinic interpreted the results. All EEGs were re-‐examined thoroughly by an expert neurophysiologist in Sulaimaniya city who did not know the diagnosis beforehand. We labelled the EEG trace as abnormal (and epileptogenic) if it demonstrated abnormal spike (duration < 70 ms), sharp wave (duration 70-‐200 ms), polyspike, or spike-‐and-‐wave discharges.
Results This study involved 65 patients with a presumed epileptic disorder and who were prescribed a medical therapy for these seizures. The age of the patients ranged from one week to 69 years with a mean of 25.3 years. Twenty-‐one patients (32%) were below the age of 18 years. Thirty-‐seven patients were males (56%) while the rest (n=28, 44%) were females. All (n=65) patients were residents of Sulaimaniya city. The presenting complaints of these patients (for which the EEG was arranged) are summarized in figure 1. We reviewed 65 EEGs with their given report (figure 2), and the results are shown in figure 3 (the results were quoted from the patients’ EEG reports). Who interpreted the EEG and wrote the report in the first place? 1. Neurophysiologists: neurophysiologists read twenty-‐one EEGs. Neurophysiologists reported fifteen EEGs as normal, normal with normal wave variants, or inconclusive. Neurophysiologists reported only six abnormal EEGs. 2. Neurologists: this physician’s category interpreted and wrote the reports of 37 EEGs; they reported these EEGs as abnormal. 3. Various: psychiatrists (n=3), neurosurgeons (n=2), and internists (n=2). All of these EEGs were reported as abnormal. After we interviewed the patients thoroughly and carefully examined their initial EEG (figure 3), we came-‐up with the following diagnoses: 1. Generalized tonic-‐clonic seizures (n=5). 2. Complex partial epilepsy (n=4). 3. Absence seizures (n=2). 4. Benign Rolandic epilepsy (n=1). 5. The rest of the patients (n=53) were found to have an alternative diagnosis; see table 2
32
The misdiagnosis of epilepsy was statistically significantly and higher in the study group (Chi square = 25.86 and P value < 0.0005).
Discussion The diagnosis of epilepsy is not always a straightforward mission, and misdiagnosis (both under-‐ and over-‐diagnosis) is not rare. In a study conducted in the UK to assess the quality of epilepsy care, Sheepers and colleague found that 49 of their 214 patients with a primary diagnosis of epilepsy were subsequently found to have been misdiagnosed following a specialist review and investigations, and another group of 26 patients had their diagnoses disputed [3]. A detailed and reliable history of the possible epileptic event by an eyewitness is a very important part of the diagnosis; however, this may not be available in all cases [4]. Electroencephalography (EEG) is a useful adjunctive tool to support the preliminary diagnosis of epilepsy and it may help classify the epilepsy type. It, at times, may direct the physician start/stop the antiepileptic therapy. However, this investigation has many drawbacks and it should not be used solely to make or refute the diagnosis of epilepsy for the following reasons [5, 6]: 1-‐ Some brain diseases are not associated with any particular EEG abnormality, especially if the underlying pathology is small and/or deep-‐seated. 2-‐ The EEG trace can be abnormal in otherwise healthy individuals. 3-‐ Many brain diseases may impart more than one abnormality because the underlying pathology could result in multiple seizure types. 4-‐ The intermittent epileptiform discharges may not be picked-‐up during a single brief EEG recording. All patients (n=65) in this study underwent a single brief EEG recording of approximately 20 minutes. Many studies suggested a sensitivity of 20-‐55% for the “first routine” EEG to detect an epileptiform abnormality [7, 8]. Therefore, it is unlikely that the patient's usual spell will be recorded during a routine EEG [9]. It should be kept in mind that the presence of interictal abnormal spikes is not pathognomonic for epilepsy, as 1-‐3% of the general population display such a finding, and the vast majority of these individuals never develop epilepsy [10-‐12]. Electroencephalograms may display a multitude of normal wave variants, such as benign epileptiform transients of sleep, wicket spikes, rhythmical mid-‐temporal theta of drowsiness, 6-‐Hz spike-‐and-‐wave burst, subclinical rhythmic EEG discharge of adult,
33
positive occipital transient sharp waves of sleep, hyperventilation-‐induced high voltage paroxysmal slow waves, “artefacts”, repetitive vertex waves (especially in children), and breach rhythm [13]. Many clinicians without a specific training in epilepsy misinterpret these normal waveforms as being epileptiform in nature because of their “sharp acute margins” [14-‐16]: see figure 4-‐6. Several patients in this study presented with non-‐specific complaints, such as dizziness, poor sleep, malaise, muscle cramps, memory problems, etc. In our opinion, neither the history nor the clinical examination warranted referral for EEG testing in most patients. Many of these EEGs were interpreted as abnormal and epileptic in nature. We found that 12 out of 65 patients (18%) had genuine epilepsy. Of this subgroup, five patients had a typical picture of idiopathic grand mal epilepsy. A careful assessment of another four patients pointed towards complex partial epilepsy. Two children had absence seizures. One child presented with abnormal hand movements (focal motor seizures) and he displayed the characteristic EEG findings of benign Rolandic epilepsy. The city of Sulaimaniya is about 400 Km northeast of Baghdad, the capital of Iraq. This city is populated by 1 500 000 individuals, including its suburbs (2009). Until the end of 2007, Sulaimaniya city (hospitals and clinics) were not equipped with any EEG machine. The first MSc post-‐graduate study in neurophysiology was conducted around that time and EEG was brought into action then.
Limitations of the study 1. This is a single institutional study and does not reflect the epileptology practice in the whole of Iraq. 2. The number of the patients was small as the duration of the study was short (three months only). For the same reason, paediatric patients were taken with adults. 3. The lack of well-‐trained EEG technicians affected the performance of the EEG examination.
Conclusions 1-‐ Many of the EEG referrals were not justified in the first place and did not follow any of the international guidelines (as Iraq has no national guidelines) [17-‐20]. This is because many physicians believe that EEG can confirm or exclude epilepsy as a cause of involuntary movements or any intermittent “strange” complaints.
34
2-‐ The bulk of the EEGs were interpreted by clinical neurologists, who have had no specialized/advanced training in EEG. In fact, many of the abnormal waves reported by neurologists were normal variants [14]. 3-‐ The EEG requests and referrals, whether to the neurophysiology outpatients’ clinic or to the private sector, were not audited, as there is no Iraqi law governs this subject. The potential for misuse and abuse therefore exists [22, 23]. The cost of doing EEG is $51 in Sulaimaniya city private clinics. The government charges $22 for doing this investigation if the latter is performed in the neurophysiology outpatients’ clinic evening shift; this figure falls abruptly to less than $1 if the EEG test is performed during the morning working hours of the day. The lack of national Iraqi guidelines for EEG referral, the absence of audit of these EEG referrals, the common misbelieves that EEG can solve many cases of ‘funny turns’, and the poor expertise in the interpretation of EEG have resulted in misuse/abuse of EEG with secondary over-‐diagnosis of epilepsy among Sulaimaniya city patients. The majority of these patients (81.5%) presented with a variety of complaints that turned out to be non-‐epileptic in nature. Defeating the shortage of experienced neurophysiologist and well-‐trained technicians, setting standards for EEG referrals with well-‐designed guidelines, and creating an audit of these referrals will prevent the misuse/abuse of EEG and lessen the misdiagnosis of epilepsy.
Acknowledgments A special gratitude goes to our patients and their families; without their kind help, this study would have not been accomplished.
References 1. Niedermeyer E. Historical aspects. In: Niedermeyer E, Lopez de Silva FH. Electroencephalography: basic principles, clinical applications, and related fields, 5th edition. Philadephia: Lippincott Williams & Wilkins; 2005: p 7-‐9. 2. Ferrie CD. Preventing misdiagnosis of epilepsy. Arch Dis Child 2006 March; 91(3):206-‐9. 3. Scheepers B, Clough P, Pickles C. The misdiagnosis of epilepsy: findings of a population study. Seizure 1998b; 7:403. 4. van Donselaar CA, Stroink H, Arts WF, Dutch Study Group of Epilepsy in Childhood. How confident are we of the diagnosis of epilepsy? Epilepsia 2006; 47 Suppl 1:9.
35
5. Buzsaki G, Traub RD, Pedley TA. The Cellular Basis of EEG Activity. In: Ebersole JS, Pedley TA (eds).Current Practice of Clinical Electroencephalography. Philadelphia: Lippincott Williams & Wilkins, 2003: p 1. 6. Walczak T, Scheuer M, Resor S, Pedley T. Prevalence and features of epilepsy without interictal epileptiform discharges. Neurology 1993; 43:287. 7. King MA, Newton MR, and Jackson GD, et al. Epileptology of the first-‐seizure presentation: a clinical, electroencephalographic, and magnetic resonance imaging study of 300 consecutive patients. Lancet 1998; 352:1007. 8. Van Donselaar CA, Schimsheimer RJ, Geerts AT, Declerck AC. Value of the electroencephalogram in adult patients with untreated idiopathic first seizures. Arch Neurol 1992; 49:231. 9. Mendez OE, Brenner RP. Increasing the yield of EEG. J Clin Neurophysiol 2006; 23:282. 10. George RP, Oates T, Merry RT. Electroencephalogram epileptiform abnormalities in candidates for aircrew training. Electroencephalogram Clin Neurophysiol 1993; 86:75-‐77. 11. Trojaborg W. EEG abnormalities in 5893 jet pilot applicants registered in a 20-‐year period. Clin Electroencephalogr 1992; 23:72-‐78. 12. Everett WD, Akhavi MS. Follow-‐up of 14 abnormal electroencephalograms in asymptomatic US Air Force Academy cadets. Aviat Space Environ Med 1982; 53:277-‐80. 13. Mushtaq R, Van Cott AC. Benign EEG variants. Am J Electroneurodiagnostic Technol 2005; 45:88. 14. Benbadis SR, Tatum WO. Overintepretation of EEGs and misdiagnosis of epilepsy. J Clin Neurophysiol 2003; 20:42. 15. Fowle AJ, Binnie CD. Uses and abuses of the EEG in epilepsy. Epilepsia 2000; 41 Suppl 3:S10. 16. Krauss GL. Clinical and EEG features of patients with EEG wicket rhythms misdiagnosed with epilepsy. Neurology 2005; 64:1879.
36
17. NICE. The epilepsies: the diagnosis and management of the epilepsies in adults and children in primary and secondary care, Clinical guideline. London: National Institute for Clinical Excellence; 2004:201-‐73. 18. Scottish Intercollegiate Guidelines Network. Diagnosis and management of epilepsy in adults. A national clinical guideline, Edinburgh: Scottish Intercollegiate Guidelines Network; 2003:70. 19. Flink R, Pedersen B, Guekht AB, et al., Guidelines for the use of EEG methodology in the diagnosis of epilepsy-‐International League against Epilepsy: Commission Report Commission on European Affairs: Subcommission on European Guidelines. Acta Neurol Scand 2002; 106 Suppl 1:1-‐7. 20. Krumhols A, Wiebe S, and Gronseth G, et al. Practice parameter: evaluating an apparent unprovoked first seizure in adults (an evidence-‐based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology 2007; 69:1996-‐2007. 21. Pillai J, Sperling MR. Interictal EEG and the diagnosis of epilepsy. Epilepsia 2006; 47 Suppl 1:14. 22. Pearce KM, Cock HR. An audit of electroencephalography requests: use and misuse. Seizures 2006; 15:184-‐89. 23. Smith D, Bartolo R, Pickles RM, Tedman BM. Requests for electroencephalography in a district general hospital: retrospective and prospective audit. Br Med J 2001; 322:954-‐57.
37
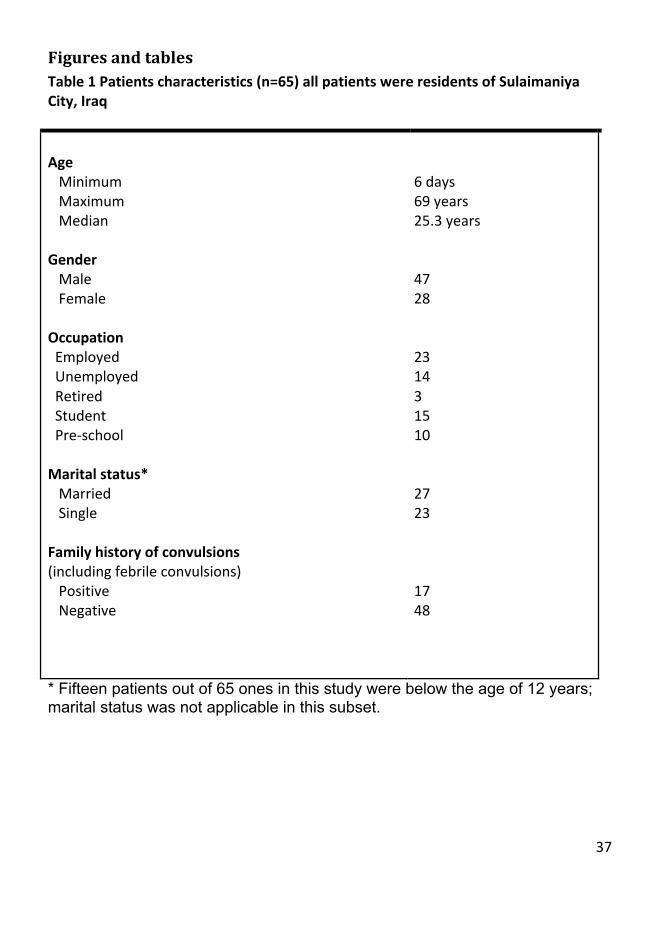
Figures and tables Table 1 Patients characteristics (n=65) all patients were residents of Sulaimaniya City, Iraq Age Minimum Maximum Median Gender Male Female Occupation Employed Unemployed Retired Student Pre-‐school Marital status* Married Single Family history of convulsions (including febrile convulsions) Positive Negative
6 days 69 years 25.3 years 47 28 23 14 3 15 10 27 23 17 48
* Fifteen patients out of 65 ones in this study were below the age of 12 years; marital status was not applicable in this subset.
38
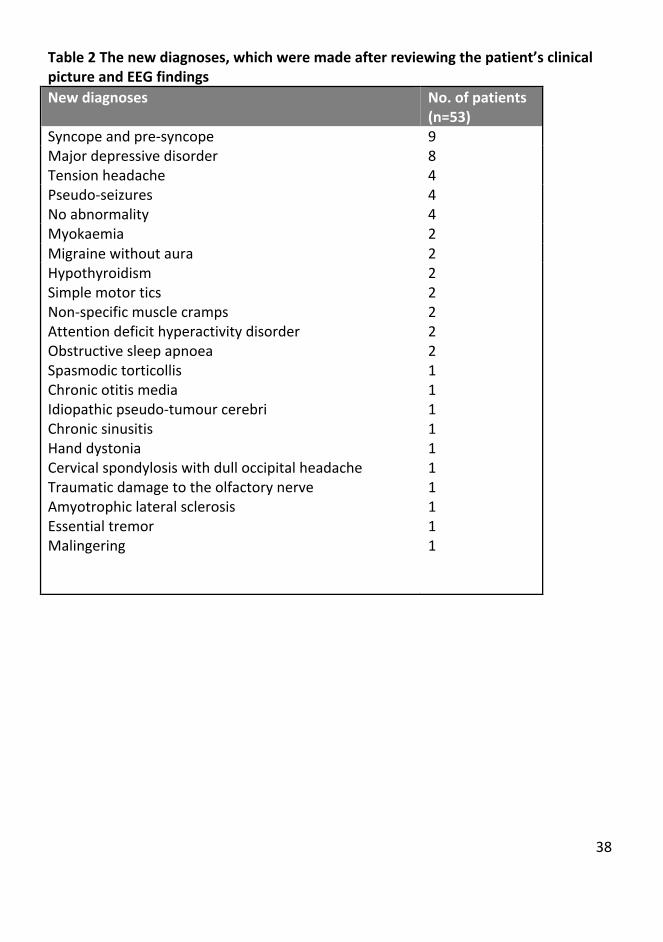
Table 2 The new diagnoses, which were made after reviewing the patient’s clinical picture and EEG findings New diagnoses No. of patients
(n=53) Syncope and pre-‐syncope 9 Major depressive disorder 8 Tension headache 4 Pseudo-‐seizures 4 No abnormality 4 Myokaemia 2 Migraine without aura 2 Hypothyroidism Simple motor tics Non-‐specific muscle cramps Attention deficit hyperactivity disorder Obstructive sleep apnoea Spasmodic torticollis Chronic otitis media Idiopathic pseudo-‐tumour cerebri Chronic sinusitis Hand dystonia Cervical spondylosis with dull occipital headache Traumatic damage to the olfactory nerve Amyotrophic lateral sclerosis Essential tremor Malingering
2 2 2 2 2 1 1 1 1 1 1 1 1 1 1
39
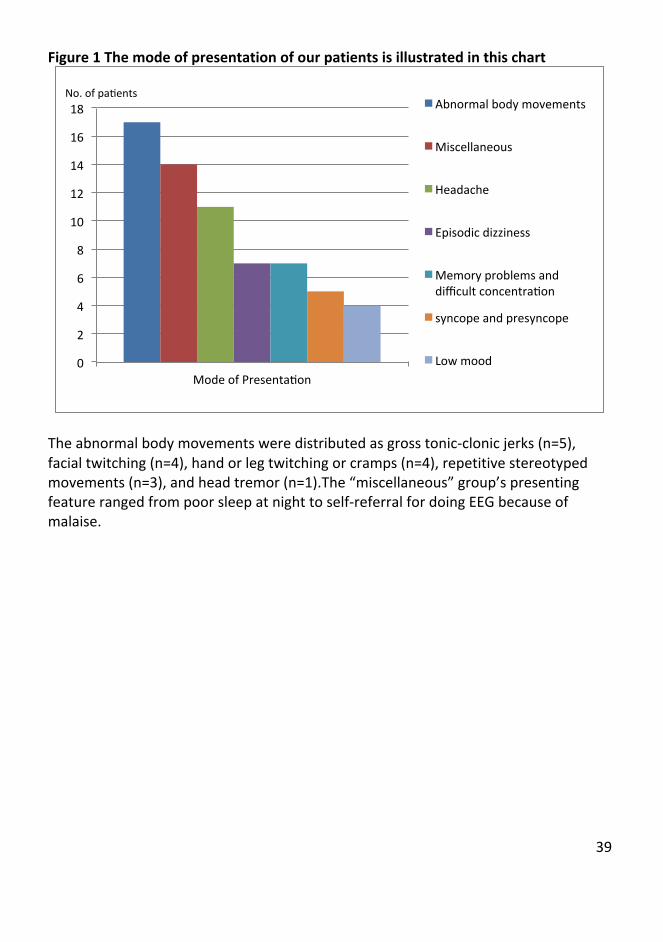
Figure 1 The mode of presentation of our patients is illustrated in this chart
The abnormal body movements were distributed as gross tonic-‐clonic jerks (n=5), facial twitching (n=4), hand or leg twitching or cramps (n=4), repetitive stereotyped movements (n=3), and head tremor (n=1).The “miscellaneous” group’s presenting feature ranged from poor sleep at night to self-‐referral for doing EEG because of malaise.
0
2
4
6
8
10
12
14
16
18
Mode of Presentazon
Abnormal body movements
Miscellaneous
Headache
Episodic dizziness
Memory problems and difficult concentrazon
syncope and presyncope
Low mood
No. of pazents
40
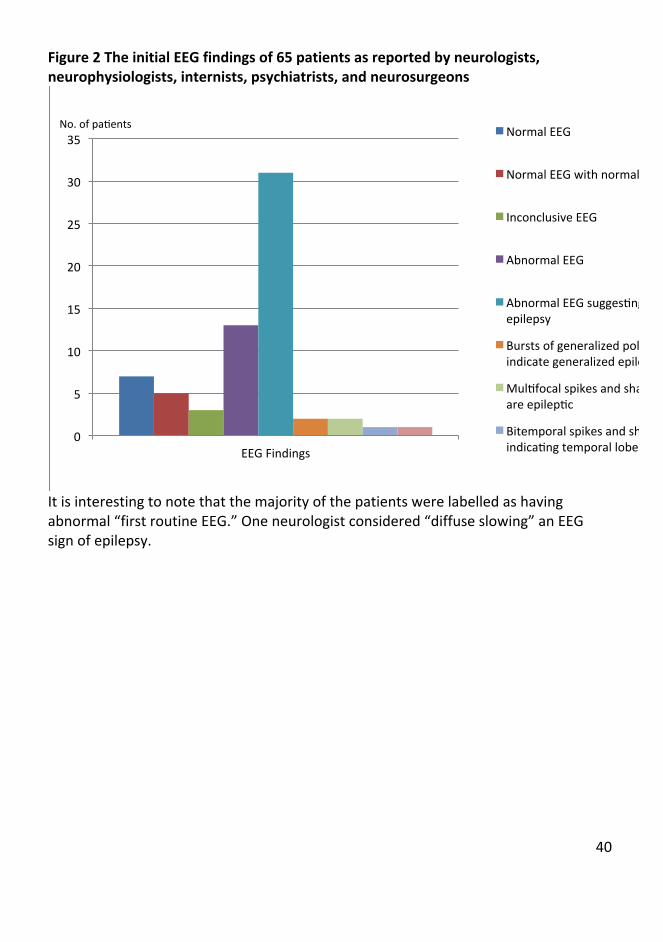
Figure 2 The initial EEG findings of 65 patients as reported by neurologists, neurophysiologists, internists, psychiatrists, and neurosurgeons
It is interesting to note that the majority of the patients were labelled as having abnormal “first routine EEG.” One neurologist considered “diffuse slowing” an EEG sign of epilepsy.
0
5
10
15
20
25
30
35
EEG Findings
Normal EEG
Normal EEG with normal variants
Inconclusive EEG
Abnormal EEG
Abnormal EEG suggeszng generalized epilepsy
Bursts of generalized poly-‐spikes that indicate generalized epilepsy
Mulzfocal spikes and sharp waves that are epilepzc
Bitemporal spikes and sharp waves indicazng temporal lobe epilepsy
No. of pazents
41
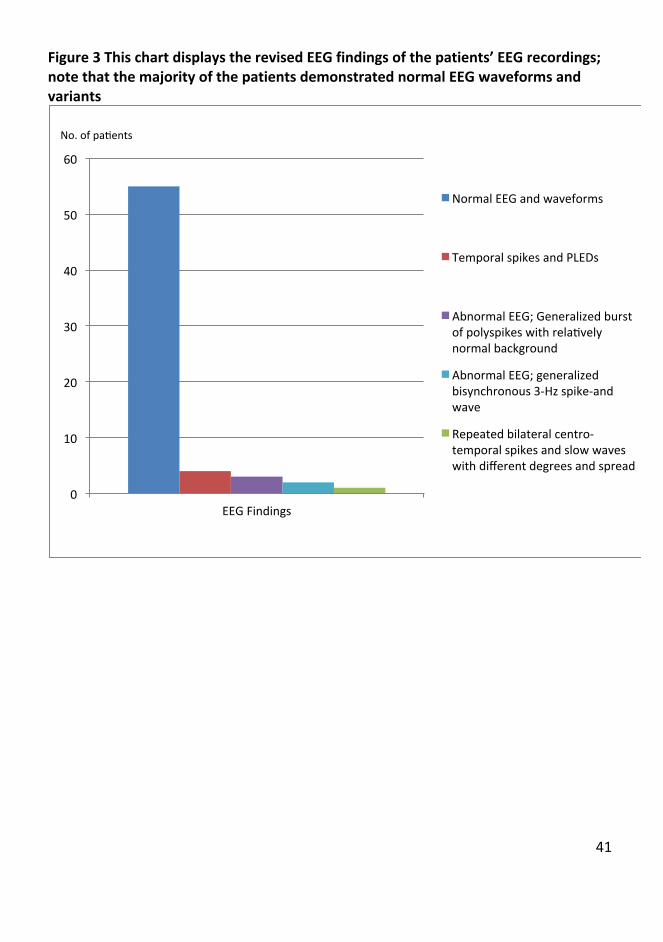
Figure 3 This chart displays the revised EEG findings of the patients’ EEG recordings; note that the majority of the patients demonstrated normal EEG waveforms and variants
0
10
20
30
40
50
60
EEG Findings
Normal EEG and waveforms
Temporal spikes and PLEDs
Abnormal EEG; Generalized burst of polyspikes with relazvely normal background
Abnormal EEG; generalized bisynchronous 3-‐Hz spike-‐and wave
Repeated bilateral centro-‐temporal spikes and slow waves with different degrees and spread
No. of pazents
42
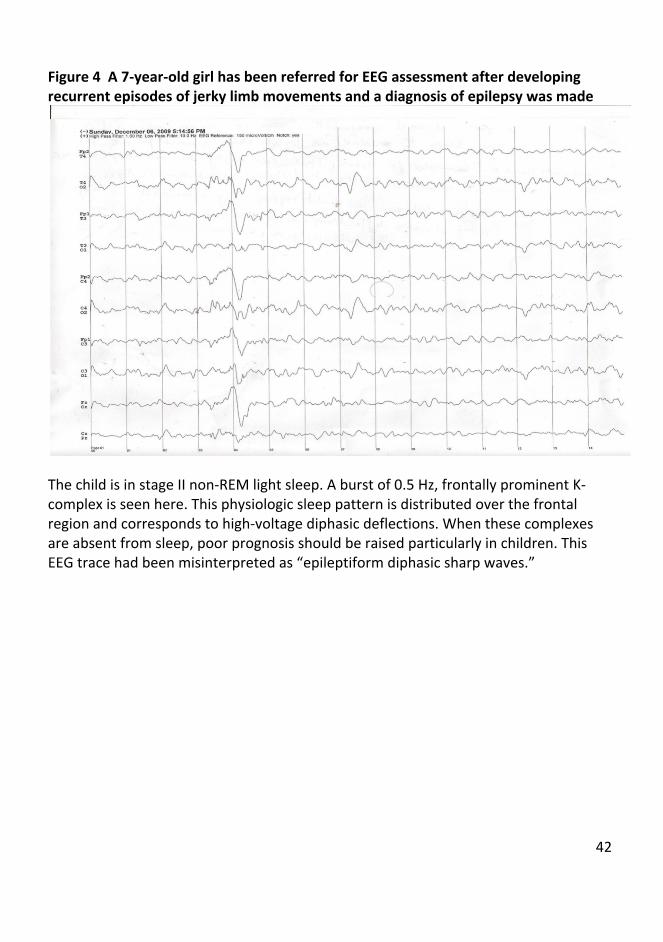
Figure 4 A 7-‐year-‐old girl has been referred for EEG assessment after developing recurrent episodes of jerky limb movements and a diagnosis of epilepsy was made
The child is in stage II non-‐REM light sleep. A burst of 0.5 Hz, frontally prominent K-‐complex is seen here. This physiologic sleep pattern is distributed over the frontal region and corresponds to high-‐voltage diphasic deflections. When these complexes are absent from sleep, poor prognosis should be raised particularly in children. This EEG trace had been misinterpreted as “epileptiform diphasic sharp waves.”
43
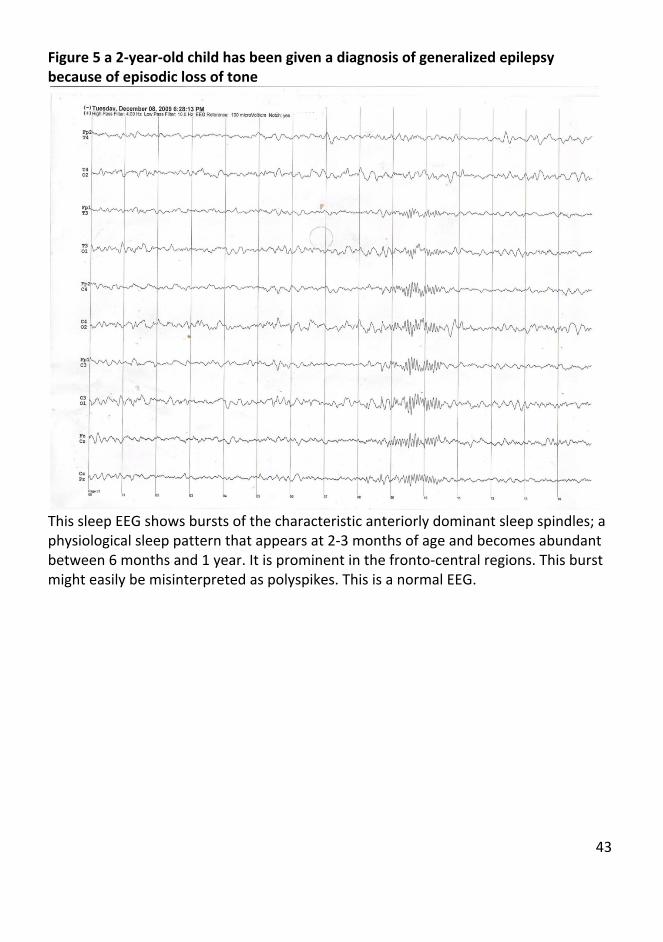
Figure 5 a 2-‐year-‐old child has been given a diagnosis of generalized epilepsy because of episodic loss of tone
This sleep EEG shows bursts of the characteristic anteriorly dominant sleep spindles; a physiological sleep pattern that appears at 2-‐3 months of age and becomes abundant between 6 months and 1 year. It is prominent in the fronto-‐central regions. This burst might easily be misinterpreted as polyspikes. This is a normal EEG.
44
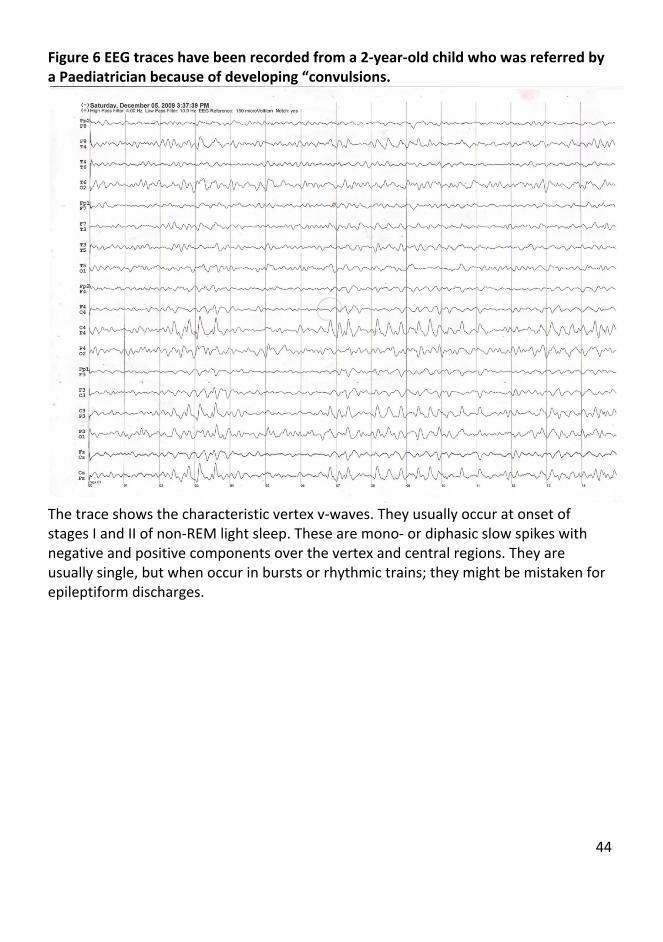
Figure 6 EEG traces have been recorded from a 2-‐year-‐old child who was referred by a Paediatrician because of developing “convulsions.
The trace shows the characteristic vertex v-‐waves. They usually occur at onset of stages I and II of non-‐REM light sleep. These are mono-‐ or diphasic slow spikes with negative and positive components over the vertex and central regions. They are usually single, but when occur in bursts or rhythmic trains; they might be mistaken for epileptiform discharges.





























