Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Elevated thrombopoietin in plasma of burned patientswithout and with sepsis enhances platelet activation
E . LUP IA ,* 1 O . B OS C O, * 1 F . MAR IANO,� A. E . DONDI ,* A . GOFF I , * T . SPATOLA ,*
A . CUCCURULLO,* P . T IZZANI , * G . BRONDINO,§ M. STELLA� and G . M O NT R UC C H IO **Department of Clinical Pathophysiology, University of Turin, Turin; �Department of Medicine Area, Nephrology and Dialysis Unit, and
�Department of Plastic Surgery and Burns Unit, CTO Hospital, Turin; and §Department of Housing and City, Polytechnic University of Turin,
Turin, Italy
To cite this article: Lupia E, Bosco O, Mariano F, Dondi AE, Goffi A, Spatola T, Cuccurullo A, Tizzani P, Brondino G, Stella M, Montrucchio G.
Elevated thrombopoietin in plasma of burned patients without and with sepsis enhances platelet activation. J Thromb Haemost 2009; 7:
1000–8.
Summary. Background: Thrombopoietin (TPO) is a humoral
growth factor that does not induce platelet aggregation per se,
but enhances platelet activation in response to several agonists.
Circulating levels of TPO are increased in patients with sepsis
and are mainly related to sepsis severity. Objectives: To
investigate the potential contribution of elevated TPO levels
in platelet activation during burn injury complicated or not by
sepsis.Methods: Westudied 22 burned patients, 10without and
12 with sepsis, and 10 healthy subjects. We measured plasma
levels of TPO, as well as leukocyte-platelet binding and P-
selectin expression. The priming activity of plasma fromburned
patients or healthy subjects on platelet aggregation and
leukocyte-platelet binding, and the role of TPO in these effects
were also studied in vitro.Results: Burned patients without and
with sepsis showed higher circulating TPO levels and increased
monocyte-platelet binding compared with healthy subjects.
Moreover, TPO levels, monocyte-platelet binding and P-
selectin expression were significantly higher in burned patients
with sepsis than in burned patients without sepsis. In vitro,
plasma from burned patients without and with sepsis, but not
from healthy subjects, primed platelet aggregation, monocyte-
platelet binding and platelet P-selectin expression. The effect of
plasma fromburnedpatientswith sepsiswas significantly higher
than that of plasma from burned patients without sepsis. An
inhibitor of TPO prevented the priming effect of plasma from
burned patients. Conclusions: Increased TPO levels may
enhance platelet activation during burn injury and sepsis,
potentially participating in the pathogenesis of multi-organ
failure in these diseases.
Keywords: burn, leukocyte-platelet adhesion, platelet activation
markers, platelet aggregation, sepsis, thrombopoietin.
Introduction
Thrombopoietin (TPO) is a humoral growth factor originally
identified for its ability to stimulate the proliferation and
differentiation of megakaryocytes [1,2]. TPO is constitutively
produced by the liver and kidneys, and is then cleared from
circulation upon binding with its receptor, c-Mpl, expressed
mainly on platelets and megakaryocytes [1,2]. We and others
have shown that, in addition to its action on megakaryocytes
and bone marrow progenitor cells [1,2], TPO also directly
modulates the response of mature platelets to several stimuli
and thereby their homeostatic potential [3,4]. In particular
TPO, which does not induce platelet aggregation per se,
enhances platelet activation in response to different agonists
[3,4], and the subsequent leukocyte-platelet adhesion via P-
selectin [5].
Elevated TPO levels have been reported in different clinical
conditions, from acute coronary syndromes [6] to hematolog-
ical diseases, where increased circulating TPO may be a
response to altered bone marrow hematopoiesis [7–9]. Several
investigations show that dysregulation of the TPO/Mpl
receptor system is also present in sepsis. In particular, elevated
TPO levels have been reported in healthy volunteers after
endotoxin infusion [10], as well as in septic children and
neonates [11–15] and septic adult patients [16,17]. In particular,
Zakynthinos et al. showed that TPO levels were greatly
increased in patients with sepsis compared with control
subjects, and that sepsis severity is the major determinant of
elevated TPO levels in these patients [17].
The aim of the present study was to investigate the potential
role of TPO in sustaining platelet aggregation and leukocyte-
Correspondence: Giuseppe Montrucchio, Dipartimento di Fisiopatologia
Clinica, Universita degli Studi di Torino, Via Genova 3, 10126 Torino,
Italy.
Tel.: +39 011 6705386; Fax: +39 011 6705367.
E-mail: [email protected]
1These authors contributed equally.
Received 22 December 2008, accepted 12 March 2009
Journal of Thrombosis and Haemostasis, 7: 1000–1008 DOI: 10.1111/j.1538-7836.2009.03348.x
� 2009 International Society on Thrombosis and Haemostasis

platelet interaction in patients with burn injury complicated or
not by the occurrence of sepsis.
Materials and methods
Patients
We studied 12 burned patients with sepsis, 10 patients with
burns and no evidence of infection, and 10 healthy subjects
(Table 1). All patients had burns covering 15–40% of their
total body surface area.
The diagnosis of sepsis was confirmed before blood collec-
tion by an experienced intensivist, blinded to the goals of the
study, according to the modified criteria for the diagnosis of
sepsis proposed in burned patients [18]. During the first 24 h
after the diagnosis of sepsis, burned patients with sepsis were
enrolled in the study.
Patients with burns and no evidence of infection were
monitored after enrollment for the appearance of signs of
infection, and kept in the study only if they did not match the
criteria for sepsis in burned patients within the following 72 h.
Exclusion criteria included the following: (i) age <16 years;
(ii) presence of overt disseminated intravascular coagulation
(DIC) [19] or platelet count <100 · 109 L)1; (iii) presence of
chronic hepatic failure, chronic renal failure, or hematological
disease affecting coagulation, platelet, or TPO production
[1,7,8,16]; (iv) the presence of malignancies under chemother-
apy or malignancies related to coagulation or platelets; and (v)
assumption of medications affecting platelet behaviour.
Severity of organ dysfunction was estimated using the
sequential organ failure assessment (SOFA) score [20].
The control group consisted of healthy volunteers, receiving
nomedications. None had shown any evidence of febrile illness
during the previous 2 weeks. Their hematological indices, and
liver and kidney function tests were within normal ranges.
The study was conducted according to the Helsinki Decla-
ration and it was approved by the Institutional Ethical
Committee �A.O.U. San Giovanni Battista di Torino - A.O.
C.T.O./Maria Adelaide di Torino�, dossier n. CEI/221.
Informed consent was obtained from the patients or their
caring relatives.
Blood collection protocol
Blood collection was performed using a central venous catheter
or, for healthy subjects, by clean venipuncture using a 19-gauge
butterfly infusion set, without venous stasis. After discarding
the first 4 mL, blood entered Vacutainers containing EDTA or
3.8% trisodium citrate, as appropriate.
To obtain plasma samples, EDTA-anticoagulated tubes
were centrifuged at 1600 ·g for 10 min at 4 �C. Plasma was
then centrifuged again at 12 500 ·g for 10 min at 4 �C, andimmediately frozen and stored at )70 �C.
Platelet-rich plasma (PRP) was prepared by centrifugation
of 3.8% trisodium citrate-anticoagulated blood for 15 min at
180 ·g [3].
Thrombopoietin measurement
TPO levels in EDTA-anticoagulated plasma were measured
using an ELISA assay (R&D Systems Inc., Minneapolis, MN,
USA) according to the manufacturer�s instructions.
Flow cytometry
All experiments were conducted using 3.8% trisodium citrate-
anticoagulated blood. Leukocyte-platelet aggregates in vivo
were analyzed using three-colour staining of whole blood
samples, as previously described [6]. Briefly, blood was diluted
1:1 with Tyrodes�s HEPES buffered saline (pH 7.4), and added
to a mixture of FITC-conjugated anti-CD45 (Beckman Coul-
ter, Miami, FL, USA), ECD-conjugated anti-CD14 (Beckman
Coulter), and PE-conjugated anti-CD41 (Dako Cytomation,
Glostrup,Denmark)monoclonal antibodies, and incubated for
15 min at room temperature. Cells were then fixed with 1%
paraformaldehyde and resuspended in 0.5 mL of phosphate-
buffered saline (PBS), after removal of erythrocytes by
hypotonic lysis.
Table 1 Clinical characteristics
Characteristics
Healthy subjects
(n = 10)
Burned patients
(n = 10)
Septic burned
patients (n = 12) P-value
Age (years) 50.0 ± 4.0 54.4 ± 6.0 57.8 ± 6.4 0.631
Gender (Male/female) 5/5 6/4 10/2
Outcome (Dead/alive) NA 2/8 8/4�
SOFA score* NA 4.80 ± 0.29 9.50 ± 0.75� <0.0001
Platelets (109 L)1)* 216.9 ± 16.7 177.1 ± 26.2 218.1 ± 25.7 0.856
Leukocytes (106 L)1)* 6153 ± 589 9070 ± 1408 13058 ± 1566§,� 0.004
Monocytes (106 L)1)* 474 ± 49 870 ± 204 965 ± 173 0.122
Thrombopoietin (pg mL)1)* 68.90 ± 17.16 153.79 ± 33.07§ 374.93 ± 62.41**,– <0.0001
Data represent means ± standard error. The last right column reports the P-value obtained by comparing the three experimental groups using
one-way ANOVA.
NA, non applicable; SOFA, sequential organ failure assessment. *Data at enrollment. �P < 0.05 vs. burned patients. �P < 0.0001 vs. burned
patients. §P < 0.01 vs. healthy subjects. –P < 0.01 vs. burned patients. **P < 0.001 vs. healthy subjects.
TPO enhances platelet activation in burn injury 1001
� 2009 International Society on Thrombosis and Haemostasis

Samples were analyzed on an EPICS–XL flow cytometer
(Coulter Corp, Hialeah, FL, USA) using adequate compensa-
tion for different fluorochromes. Total leukocytes were iden-
tified by their positive staining with anti-CD45, and
lymphocyte, polymorphonuclear and monocyte populations
were discriminated on the ground of CD45 vs. forward scatter.
The percentage of leukocyte subgroups co-expressing CD45-
CD41 (polymorphonuclear leukocytes-platelets) or CD14-
CD41 (monocytes-platelets) over the total population of
leukocytes expressing CD45 or CD14 was used as an index
of leukocyte-platelet adhesion [6].
P-selectin expression was evaluated in whole blood using a
mixture of FITC-conjugated anti-CD62P/P-selectin (Ancell
corporation, Bayport, MN, USA) or the appropriate isotypic
control, and PE-conjugated anti-CD41monoclonal antibodies.
Platelets were identified by their characteristic light scatter and
the positive signal provided by the platelet marker PE-anti-
CD41 monoclonal antibody.
For in vitro experiments, 100 lL of diluted blood from
healthy adult donors was pre-incubated at 37 �Cwith 25 lL of
plasma of patients or normal subjects for 5 min and then
stimulated with adenosine 5¢-diphosphate (ADP, 0.8 lM;Helena Laboratories, Beaumont, TX, USA) or epinephrine
(EPI, 3 lM; Helena Laboratories). Samples were then pro-
cessed and analyzed as described above.
In separate experiments, plasma was incubated with a
humanTPO receptor (TPOR)-Fc chimera (2.5 lg mL)1; R&D
Systems Inc.) for 5 min at 37 �C; the mixture of sample and
TPOR-Fc chimera was added to whole blood, further
incubated for 5 min at 37 �C and stimulated with ADP or
EPI. We have previously reported that the TPOR-Fc chimera
inhibited the priming effect exerted by recombinant human
TPO in PRP and whole blood, but did not affect the
aggregation induced by ADP or EPI [6].
Platelet aggregation
Platelet aggregation was evaluated in 3.8% trisodium citrate-
anticoagulated PRP and whole blood as previously described
[3,6]. PRPorwholebloodwasobtained fromhealthy subjects as
described above and incubated with 25 or 100 lL of plasma,
respectively, at 37 �C. In selected experiments, the effect of
tumor necrosis factor-a (TNF-a), interleukin (IL)-1, IL-6, IL-3,granulocyte colony stimulating factor (GCSF), or granulocyte
macrophage-colony stimulating factor (GMCSF) was evalu-
ated.When evaluating priming activity, ADPorEPIwas added
as secondary agonist. For each experiment, the ADP (0.8–
2 lmol L)1) or EPI (0.1–3 lmol L)1) concentration that
induced theminimummeasurable aggregationwas determined.
The priming index (PI)was calculated as the response to plasma
and agonist together, divided by the sum of the individual
responses elicited by plasma and the agonist separately [3,6].
Using this calculation, a PI > 1 indicated synergism, a PI = 1
indicated additive response, and PI < 1 indicated inhibition.
In separate experiments, plasma was incubated with the
human TPOR-Fc chimera (2.5 lg mL)1) for 5 min at 37 �C;
the mixture of sample and TPOR-Fc chimera was added to
PRP or whole blood, further incubated for 5 min at 37 �C and
stimulated with ADP or EPI.
Statistical analysis
Values are represented by means ± standard error (SE).
Comparisons between groups were carried out using ANOVA
followed by Newman–Keuls multicomparison test or Student�st-test where appropriate; categorical variables were compared
using two-way cross-tabulation with the chi-square test.
Normality was assessed using the Shapiro–Wilk analysis,
whereas the Bartlett test was used to test variance hetero-
geneity. When ANOVA assumptions were violated, data
were transformed using the Box–Cox power transformation
method.
The relationship between variables was investigated using
Pearson�s correlation test.
A P value <0.05 was considered significant.
All statistics were done using GRAPHPAD PRISM 4.00
(GraphPad Software, La Jolla, CA, USA) and R 2.7.1.
Results
Patient clinical characteristics and TPO levels
Table 1 gives demographic and clinical data for patients and
healthy subjects. Burned patients with sepsis did not differ
regarding demographic characteristics either from burned
patients without sepsis or from healthy subjects. All septic
patients required vasopressors, and the intra-hospital mortality
in this group of patients was about 66% (eight out of 12).
Platelet counts were not different between the groups. Leuko-
cyte counts were significantly higher in burned patients with
sepsis (13058 ± 1566 · 106 L)1) than in burned patients
without sepsis (9070 ± 1408 · 106 L)1) and healthy subjects
(6153 ± 589 · 106 L)1); in contrast, absolute monocyte
counts were not different between the groups (healthy subjects
474 ± 49, burned patients 870 ± 204, septic burned patients
965 ± 173 · 106 L)1) (Table 1). Plasma TPO concentrations
were significantly higher in burned patients, both without
(153.79 ± 33.07 pg mL)1) and with sepsis (374.93 ± 62.41
pg mL)1), than in healthy subjects (68.90 ± 17.16 pg mL)1);
moreover, burned patients who developed sepsis had higher
circulating levels of TPO than burned patients without sepsis
(Table 1). No significant correlation was found between
circulating TPO levels and platelet count (not shown).
In vivo platelet activation
A significantly higher percentage of monocyte-platelet binding
was found in burned patients, both without (36.25 ± 2.58%)
and with sepsis (57.61 ± 7.87%), compared with healthy
subjects (23.21 ± 2.72%); burned patients with sepsis had a
significantly higher percentage of monocyte-platelet binding
than burned patients without sepsis (Fig. 1A, B). On the
1002 E. Lupia et al
� 2009 International Society on Thrombosis and Haemostasis

contrary, polymorphonuclear-platelet aggregates were not
significantly different between the three groups, although a
tendency towards an increase in polymorphonuclear-platelet
adhesionwas observed in burned patients who developed sepsis
(not shown).
The percentage of platelets expressing P-selectin was signif-
icantly higher in burned patients with sepsis (14.16 ± 2.63%)
than in burned patients without sepsis (2.78 ± 0.26%) or
healthy subjects (2.38 ± 0.18%) (Fig. 1C, D).
TPO levels in plasma significantly correlated withmonocyte-
platelet aggregation (r = 0.52; P < 0.005), and with platelet
P-selectin expression (r = 0.67; P < 0.0001).
Effect of plasma from burned patients on platelet activation
in vitro
The effect of plasma fromburnedpatients or normal subjects on
platelet aggregation was tested in vitro on PRP from healthy
donors. Plasma from burned patients, both without and with
sepsis, did not induce platelet aggregation per se, but it
significantly enhanced the aggregation induced by ADP
(PI = 1.57 ± 0.10 for burned patients without sepsis;
PI = 2.04 ± 0.20 for burned patients with sepsis) (Fig. 2A)
or EPI (PI = 1.84 ± 0.16 for burned patients without sepsis;
PI = 2.83 ± 0.25 for burned patients with sepsis) (Fig. 2B).
When EPI was used as a secondary agonist to trigger platelet
aggregation in PRP, the priming effect induced by plasma from
burned patients with sepsis was significantly higher than that
observed with plasma from burned patients without sepsis
(Fig. 2B), whereas no difference was seen when ADP was used
as a secondary agonist (Fig 2A). This priming effect on platelet
aggregation inPRPwas seenwith all plasma samples examined.
Also in whole blood, pre-incubation of samples with plasma
obtained from burned patients primed aggregation induced by
ADP(Fig. 3A)orEPI (Fig. 3B). In this experimental condition,
the priming effect induced in whole blood by plasma from
burned patients with sepsis was significantly higher
(PI = 2.23 ± 0.15 for ADP; PI = 2.49 ± 0.34 for EPI) than
that induced by plasma from burned patients without sepsis
(PI = 1.75 ± 0.08 forADP;PI = 1.81 ± 0.09 forEPI)when
both ADP and EPI were used as secondary agonists (Fig. 3).
Plasma from healthy subjects did neither prime platelet
aggregation in PRP nor in whole blood (Figs 2 and 3).
In parallel experiments, we tested the activity of several
cytokines known to be released during sepsis [21] to assess their
potential contribution to the priming effect exerted by plasma
samples of burned patients with sepsis. We did not detect any
priming activity on ADP- or EPI-induced platelet aggregation
using TNF-a, IL-1, IL-6, IL-3, GCSF or GMCSF (data not
shown).
Healthy subject Burned patient
Burned patient
Septic burned patient
aggr
egat
es (
%)
Healthy subject Septic burned patient
CD41 PE
CD41 PE
CD41 PE
CD41 PE
E1
E3 E4
E2
E1
E3 E4
E2
E1
E3 E4
E2
E1
E3 E4
E2
103
103
102
102
101
101
100
103
102
101
100
103
102
101
100
103
102
101
100
100
103102101100
103102101100
103102101100
CD
14 E
CD
CD
62P
FIT
C
CD
62P
FIT
C
CD
62P
FIT
C
CD
14 E
CD
CD41 PE
E1
E3 E4
E2
80P < 0.001
P < 0.001
P < 0.05
P < 0.001
P < 0.01
Health
y
Burne
d
burn
edSep
tic
Health
y
Burne
d
burn
edSep
tic
60
40
20
20
15
10
5
0
0
103
102
101
100
103
102
101
100
103102101100
CD41 PE
E1
E3 E4
E2
103102101100
CD
14 E
CD
Mon
ocyt
e-pl
atel
etP
late
let P
-sel
ectin
(%
)
A B
C D
Fig. 1. Representative flow cytometry analysis (Panels A, C) and data quantification (Panels B, D) of the percentage of monocyte (CD14-positive)-platelet
(CD41-positive) aggregates and platelet CD62P/P-selectin expression detected in vivo in healthy subjects and in burned patients without and with sepsis.
Data represent means ± SE. One-way ANOVA with Newman–Keuls multicomparison test was performed.
TPO enhances platelet activation in burn injury 1003
� 2009 International Society on Thrombosis and Haemostasis

Neither plasma from burned patients, both without andwith
sepsis, nor from healthy subjects increased monocyte-platelet
binding and platelet P-selectin expression in whole blood per se.
On the contrary, plasma from burned patients without and
with sepsis, but not from healthy subjects, significantly
enhanced monocyte-platelet binding and platelet P-selectin
expression induced byADP (Fig. 4A, B) or EPI (Fig. 4C,D) in
whole blood, as determined using flow-cytometric analysis. The
effect induced by plasma from burned patients with sepsis was
significantly higher than that induced by plasma from burned
patients without sepsis when EPI was used as secondary
agonist to trigger platelet activation, as evaluated in terms of
both monocyte-platelet binding (52.20 ± 3.06% vs. 36.63
± 2.10%) and platelet P-selectin expression (19.39 ± 1.81%
vs. 14.83 ± 0.84%) in whole blood (Fig. 4C, D). However,
whenADPwas used as a secondary agonist, only the difference
in monocyte-platelet binding was statistically significant
(41.67 ± 2.48% vs. 33.13 ± 2.52%) (Fig. 4A), whereas no
difference was seen in terms of P-selectin expression
(16.28 ± 1.52% vs. 13.28 ± 1.02%) (Fig. 4B).
Role of TPO in the priming activity of plasma from burned
patients
Circulating TPO levels measured in vivo correlated with the
in vitro priming activity exerted by plasma samples on platelet
aggregation both in PRP and in whole blood. In particular,
plasma TPO levels significantly correlated with the ADP-
induced priming index in PRP (r = 0.39;P < 0.05) andwhole
blood (r = 0.58; P < 0.02), as well as with the EPI-induced
priming index in PRP (r = 0.42; P < 0.02) and whole blood
(r = 0.52; P < 0.05).
Moreover, pre-incubation of plasma from burned patients
without and with sepsis with an inhibitor of TPO biological
activity, a human TPOR-Fc chimera, significantly reduced the
priming effect exerted on platelet aggregation in PRP by ADP
(from PI = 1.57 ± 0.10 to 1.29 ± 0.07 for burned patients
without sepsis; from PI = 2.04 ± 0.20 to 1.35 ± 0.06 for
burned patients with sepsis) (Fig. 5A, B) or EPI (from
PI = 1.84 ± 0.16 to 1.38 ± 0.09 for burned patients without
sepsis; from PI = 2.83 ± 0.25 to 1.44 ± 0.03 for burned
patients with sepsis) (Fig. 5C, D). A similar reduction in the
priming effect on platelet aggregation induced by ADP (from
PI = 1.75 ± 0.08 to 1.31 ± 0.08 for burned patients without
sepsis; from PI = 2.23 ± 0.15 to 1.40 ± 0.11 for burned
patients with sepsis) (Fig. 6A, B) or EPI (from
PI = 1.81 ± 0.09 to 1.20 ± 0.07 for burned patients without
sepsis; from PI = 2.49 ± 0.34 to 1.46 ± 0.16 for burned
patients with sepsis) (Fig. 6C, D) was also observed in whole
blood. Pre-treatment of plasma from burned patients without
and with sepsis with the TPOR-Fc chimera also significantly
decreased monocyte-platelet binding induced in whole blood
using ADP (from 33.13 ± 2.52% to 24.67 ± 2.46% for
Prim
ing
inde
x
Ligh
t tra
nsm
issi
on (
%)
Ligh
t tra
nsm
issi
on (
%)
5%5%
Septic burned
Burned
Healthy
patient
Septic burnedpatient
4
P < 0.001
P < 0.001
P < 0.01
P < 0.01
P < 0.01
Health
y
Burne
d
burn
edSep
tic
Health
y
Burne
d
burn
edSep
tic
3
2
0
1
Prim
ing
inde
x4
3
2
0
1
patient
Burnedpatient
subject
Healthysubject
1 min
1 min
Plasma
Plasma
ADP
EPI
A
B
Fig. 2. Representative aggregation traces and quantification of the in vitro
priming activity induced by plasma from healthy subjects and burned
patients without and with sepsis on ADP- (Panel A) or EPI- (Panel B)
induced platelet aggregation in platelet-rich plasma. Data represent
means ± SE. One-way ANOVA with Newman–Keuls multicomparison
test was performed. ADP, adenosine 5¢-diphosphate; EPI, epinephrine.
Impe
danc
e (Ω
)Im
peda
nce
(Ω)
Septic burned
Burned
Healthy
patient
patient
subject1 min
ADP
EPI
Plasma
2Ω
Septic burned
Burned
Healthy
patient
patient
subject1 min
Plasma
2Ω
P < 0.001
P < 0.05
P < 0.01
3
2
0
1
Prim
ing
inde
x
Health
y
Burne
d
burn
edSep
tic
P < 0.001
P < 0.05
P < 0.001
Health
y
Burne
d
burn
edSep
tic
Prim
ing
inde
x
3
2
0
1
A
B
Fig. 3. Representative aggregation traces and quantification of the in vitro
priming activity induced by plasma from healthy subjects and burned
patients without and with sepsis on ADP- (Panel A) or EPI- (Panel B)
induced platelet aggregation in whole blood. Data represent means ± SE.
One-way ANOVA with Newman–Keuls multicomparison test was per-
formed. ADP, adenosine 5¢-diphosphate; EPI, epinephrine.
1004 E. Lupia et al
� 2009 International Society on Thrombosis and Haemostasis

burned patients without sepsis; from 41.67 ± 2.48% to
26.87 ± 1.99 for burned patients with sepsis) (Fig. 7A) or
EPI (from 36.63 ± 2.10% to 26.53 ± 1.18% for burned
patients without sepsis; from 52.20 ± 3.06 to 36.19 ± 2.79 for
burned patients with sepsis) (Fig. 7C), as evaluated by flow-
cytometric analysis. An analogous inhibitory effect of TPOR-
Fc chimera was seen on platelet P-selectin expression (ADP:
from 13.28 ± 1.02% to 10.23 ± 1.26% for burned patients
without sepsis; from 16.28 ± 1.52% to 10.62 ± 1.25% for
burned patients with sepsis; EPI: from 14.83 ± 0.44% to
12.18 ± 0.49% for burned patients without sepsis; from
19.39 ± 1.81% to 12.80 ± 1.54% for burned patients with
sepsis) (Fig. 7B, D). On the contrary, pre-incubation of plasma
from healthy subjects with the TPOR-Fc chimera had no
significant effect (data not shown).
Discussion
The first result of our study is that patients with a burn injury
have increased monocyte-platelet aggregates and platelet P-
selectin expression comparedwith healthy subjects. In addition,
monocyte-platelet aggregates were significantly higher in
burned patients with sepsis than burned patients without
sepsis. It is known that monocyte-platelet aggregation is not
only a sensitive measure of platelet activation, but also has
significant pro-inflammatory and pro-thrombotic conse-
quences, in particular in acute coronary syndrome [22]. Our
present findings show that increased platelet activation (i.e. P-
selectin expression) and eterotypic aggregation (i.e. monocyte-
platelet adhesion) also occur in burn injury, especially after
sepsis development, suggesting that activated platelets amplify
the inflammatory reactions and favor the insurgence of organ
damage in these pathological conditions.
Moreover, we found that burn injury is associated with a
significant increase in the circulating levels of TPO, about 2-
fold the levels measured in healthy subjects. TPO levels further
increase upon development of sepsis, suggesting that the
development of sepsis, in addition to burn injury, may
contribute to increase circulating TPO levels in these patients.
These results are substantially in agreement with those already
reported by Zakynthinos et al. [17] in a larger population of
patients with sepsis. However, our data are the first to evaluate
TPO levels in burned patients without and with sepsis.
Thrombocytopenia has been correlated with poor outcome
in extensive burns and may be considered a sensitive marker of
sepsis [18,23]. However, septic patients in our study had a
platelet count within the normal range. As thrombocytopenia
and DIC are common complications of sepsis, and TPO levels
are elevated during DIC [16], we excluded from the study those
patients whomatched the diagnostic criteria for overt DIC [19],
and in particular had a platelet count <100 · 109 L)1. The
application of this exclusion criterionmay explain our failure to
detect thrombocytopenia in burned and septic burned patients,
which may also be related to the small number of patients
studied and to the relatively early enrollment of septic patients.
The precise origin of the rise in TPO levels observed in
burned patients without and with sepsis remains unclear. TPO
levels are well known to be primarily regulated by platelet mass
[1,2], and yet we did not detect thrombocytopenia in septic
patients in our study. Burned patients without and with sepsis
also showed increased indices of in vivo platelet activation
compared with healthy subjects.Moreover, we found a positive
correlation between (i) TPO levels and monocyte-platelet
binding in vivo, and (ii) TPO levels and platelet P-selectin
expression in vivo. Therefore, platelets themselves may repre-
sent a major contributor to increased TPO levels, as they are
known to release full-length biological active TPO upon
stimulation [16]. Finally, as IL-6, themain acute-phase reactant
produced in the liver, enhances TPO synthesis [24], high TPO
levels in burned and septic patients may also depend on
increased hepatic synthesis.
The presence of TPO in the circulation precludes the
evaluation of its role on platelet aggregation directly on blood
samples obtained from patients. Therefore, we studied the
contribution of TPO to platelet aggregation by adding patient
plasma samples to platelets of healthy subjects in vitro and
inhibiting TPO biological activity using the TPOR-Fc chimera.
In these experimental conditions, plasma from burned patients
without and with sepsis, but not from healthy subjects,
Mon
ocyt
e-pl
atel
etag
greg
ates
(%
)M
onoc
yte-
plat
elet
aggr
egat
es (
%)
60
Health
y
Burne
d
Septic
burn
ed
Health
y
Burne
d
Septic
burn
ed
Health
y
Burne
d
Septic
burn
ed
P < 0.001
P < 0.001
P < 0.001
P < 0.05
P < 0.001
P < 0.001
P < 0.05
P < 0.05
P < 0.05
P < 0.001P < 0.05
0
20
20
25
15
10
5
0
25
40
20
0
40
Pla
tele
t P-s
elec
tin (
%)
Health
y
Burne
d
Septic
burn
ed
20
25
15
10
5
0
Pla
tele
t P-s
elec
tin (
%)
A B
C D
Fig. 4. In vitro effect of plasma from healthy subjects and burned patients
without and with sepsis on ADP- (Panels A, B) or EPI- (Panels C, D)
induced monocyte-platelet aggregation and platelet P-selectin expression,
analyzed by flow cytometry in whole blood. Data represent means ± SE.
One-way ANOVA with Newman–Keuls multicomparison test was
performed. ADP, adenosine 5¢-diphosphate; EPI, epinephrine.
TPO enhances platelet activation in burn injury 1005
� 2009 International Society on Thrombosis and Haemostasis

enhances platelet aggregation as well as monocyte-platelet
binding and platelet P-selectin expression in blood samples
from healthy donors. The priming effect induced by plasma
from burned patients with sepsis was significantly higher than
that induced by plasma from burned patients without sepsis in
all the experimental conditions tested. However, when ADP
was used as a secondary agonist in PRP for platelet aggregation
studies or in whole blood for the evaluation of P-selectin
Plasma
Burned patient
Burned patient
Septic burned
Septic
burn
ed
4
3
2
1
0
Burne
d
Septic burned
patient
Septic burnedpatient
patientBurned patient+ TPORFc
Burned patient+ TPORFc
+ TPORFc
Burne
d
+ TPORFc
Septic
burn
ed
+ TPORFc
Septic
burn
ed
Burne
d
Burne
d
+ TPORFc
Septic
burn
ed
+ TPORFc
Septic burnedpatient
+ TPORFc
1 min
1 min
1 min
1 min
ADP
Plasma EPI
Plasma ADP
Plasma EPI
Ligh
t tra
nsm
issi
on (
%)
Ligh
t tra
nsm
issi
on (
%)
5%5%
5%
Prim
ing
inde
xP
rimin
g in
dex
5%
P < 0.001
P < 0.0001
P < 0.005
P < 0.005
4
3
2
1
0
A B
DC
Fig. 5. Representative aggregation traces and quantification of the effect of plasma from burned patients without andwith sepsis pre-incubated or not with
the TPOR-Fc chimera on ADP- (Panels A, B) or EPI- (Panels C, D) induced platelet aggregation in platelet-rich plasma. Data represent means ± SE.
Student�s t-test was performed. ADP, adenosine 5¢-diphosphate; EPI, epinephrine.
Impe
danc
e (Ω
)Im
peda
nce
(Ω)
Burned patient
Septic burned
Septic
burn
ed
3
2
1
0
Prim
ing
inde
x
2
1
0
Prim
ing
inde
x
Burne
d
patient
Septic burnedpatient
Burned patient+ TPORFc
+ TPORFc
Septic burnedpatient
Septic burnedpatient
+ TPORFc
Burne
d
+ TPORFc
Septic
burn
ed
+ TPORFc
Septic
burn
ed
Burne
d
Burne
d
+ TPORFc
Septic
burn
ed
+ TPORFc
Burned patient
Burned patient+ TPORFc
Plasma ADP Plasma ADP
Plasma EPI Plasma EPI
2Ω
1 min 1 min
1 min 1 min
2Ω
2Ω2Ω
2Ω
P < 0.005
P < 0.01
P < 0.013
P < 0.001BA
C D
Fig. 6. Representative aggregation traces and quantification of the effect of plasma from burned patients without andwith sepsis pre-incubated or not with
the TPOR-Fc chimera onADP- (Panels A, B) or EPI- (Panels C, D) induced platelet aggregation in whole blood. Data represent means ± SE. Student�s t-test was performed. ADP, adenosine 5¢-diphosphate; EPI, epinephrine.
1006 E. Lupia et al
� 2009 International Society on Thrombosis and Haemostasis
expression by flow cytometry, the priming effect was not
different between burned patients without and with sepsis.
These results may be related to the higher variability of the
experimental data in these settings. The contribution of TPO to
the priming effect exerted by plasma samples from burned
patients without and with sepsis is suggested by: (i) the
correlation analysis showing that TPO levels and ADP- and
EPI-induced priming index in PRP and whole blood consen-
sually increased in the three groups; and (ii) the inhibitory effect
of the TPOR-Fc chimera. Taken together, our in vivo and in
vitro data support the hypothesis that TPO present in the
circulation of burned patients, especially those developing
sepsis, may facilitate platelet activation by sensitizing circulat-
ing platelets to the action of other agonists, thus precipitating
the occurrence of microvascular thrombosis and the clinical
onset of multi-organ failure. This model is in agreement with
the priming effect observed in vivo on platelet activation after
TPO infusion in non-human primates; platelets isolated from
TPO-treated animals showed indeed a heightened sensitivity to
substances that stimulate platelet aggregation during the first
few days of treatment [25].
Other humoral mediators may also be evoked as potential
candidates for the initiation of leukocyte-platelet activation and
microvascular damage during burn injury and/or sepsis
[21,22,26]. In our experimental model, no priming effect on
platelet aggregation in both PRP and whole blood was seen
using TNF-a, IL-1, IL-6, IL-3, GCSF, or GMCSF, as also
previously shown by others [27]. However, platelets express
Toll-like receptors, which, upon binding with bacterial lipo-
polysaccharides, are responsible for sepsis-induced thrombo-
cytopenia and microvascular injury [28–30]. Therefore,
endotoxins may also cooperate with TPO in sustaining
enhanced platelet activation in burned patients who develop
sepsis.
We studied burned patients, who may be considered a good
model to evaluate the pathogenesis of organ failure in sepsis.
They are a homogeneous population in which the initial insult
can be quantified, and sepsis often develops in severe burns [31].
However, cautionmust be taken when generalizing conclusions
drawn by studies in selected populations, as that considered in
our study, to all patients affected by sepsis, or to patients with
sepsis originated from other infectious sites.
In conclusion, increased TPO levels may enhance platelet
activation during burn injury and sepsis and have a role in the
pathogenesis of multi-organ failure in these pathological
conditions.
Mon
ocyt
e-pl
atel
etag
greg
ates
(%
)
Burne
d
Septic
burn
ed
Septic
burn
ed
+ TPORFc
Burne
d
+ TPORFc
Burne
d
Septic
burn
ed
Septic
burn
ed
+ TPORFc
Burne
d
+ TPORFc
Burne
d
Septic
burn
ed
Septic
burn
ed
+ TPORFc
Burne
d
+ TPORFc
60
40
20
0
P < 0.05
P < 0.0001 P < 0.001
P < 0.01
P < 0.005
P < 0.005
20
25
15
10
5
0
Pla
tele
t P-s
elec
tin (
%)
Burne
d
Septic
burn
ed
Septic
burn
ed
+ TPORFc
Burne
d
+ TPORFc
20
25
15
10
5
0
Pla
tele
t P-s
elec
tin (
%)
Mon
ocyt
e-pl
atel
etag
greg
ates
(%
)
60
P < 0.005
P < 0.0001
0
20
40
A
C D
B
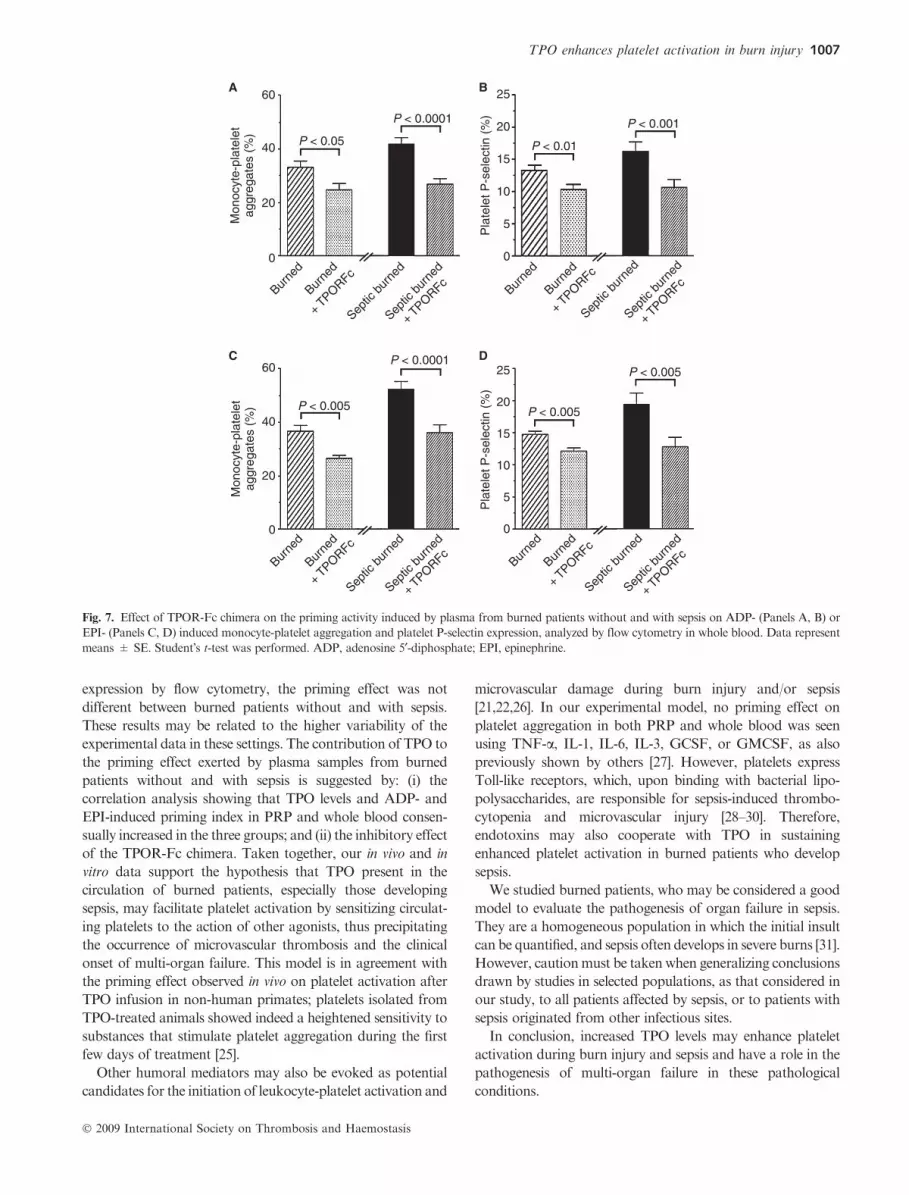
Fig. 7. Effect of TPOR-Fc chimera on the priming activity induced by plasma from burned patients without and with sepsis on ADP- (Panels A, B) or
EPI- (Panels C, D) induced monocyte-platelet aggregation and platelet P-selectin expression, analyzed by flow cytometry in whole blood. Data represent
means ± SE. Student�s t-test was performed. ADP, adenosine 5¢-diphosphate; EPI, epinephrine.
TPO enhances platelet activation in burn injury 1007
� 2009 International Society on Thrombosis and Haemostasis

Addendum
Conception and design: E. Lupia, G. Montrucchio, F.
Mariano. Patient recruitment: M. Stella, F. Mariano. Analysis
and interpretation of data: E. Lupia, O. Bosco, A. Cuccurullo,
T. Spatola, A.E. Dondi, A. Goffi, P. Tizzani, G. Montrucchio.
Statistical Analysis: G. Brondino. Drafting, critical revision
and final approval of the manuscript: E. Lupia, O. Bosco, G.
Montrucchio.
Acknowledgement
This work was supported by MURST ex-60% to GM, and
Progetto di Ricerca Sanitaria Finalizzata – Regione Piemonte
2006 to EL and GM.
Disclosure of Conflict of Interests
The authors state that they have no conflict of interest.
References
1 Kaushansky K. Thrombopoietin: a tool for understanding thrombo-
poiesis. J Thromb Haemost 2003; 1: 1587–92.
2 Kuter DJ, Begley CG. Recombinant human thrombopoietin:
basic biology and evaluation of clinical studies. Blood 2002; 100: 3457–
69.
3 Montrucchio G, Brizzi MF, Calosso G, Marengo S, Pegoraro L,
Camussi G. Effects of recombinant humanmegakaryocyte growth and
development factor on platelet activation. Blood 1996; 87: 2762–8.
4 Oda A,Miyakawa Y, Druker BJ, Ozaki K, Yabusaki K, Shirasawa Y,
Handa M, Kato T, Miyazaki H, Shimosaka A, Ikeda Y. Thrombo-
poietin primes human platelet aggregation induced by shear stress and
by multiple agonists. Blood 1996; 87: 4664–70.
5 Tibbles HE, Navara CS, Hupke MA, Vassilev AO, Uckun FM.
Thrombopoietin induces P-selectin expression on platelets and sub-
sequent platelet/leukocyte interactions. Biochem Biophys Res Commun
2002; 292: 987–91.
6 Lupia E, Bosco O, Bergerone S, Dondi AE, Goffi A, Oliaro E,
Cordero M, Del Sorbo L, Trevi G, Montrucchio G. Thrombopoietin
contributes to enhanced platelet activation in patients with unstable
angina. J Am Coll Cardiol 2006; 48: 2195–203.
7 Emmons RV, Reid DM, Cohen RL, Meng G, Young NS, Dunbar
CE, Shulman NR. Human thrombopoietin levels are high when
thrombocytopenia is due to megakaryocyte deficiency and low when
due to increased platelet destruction. Blood 1996; 87: 4068–71.
8 Kosugi S, Kurata Y, Tomiyama Y, Tahara T, Kato T, Tadokoro S,
Shiraga M, Honda S, Kanakura Y, Matsuzawa Y. Circulating
thrombopoietin level in chronic immune thrombocytopenic purpura.
Br J Haematol 1996; 93: 704–6.
9 Cerutti A, Custodi P, Duranti M, Noris P, Balduini CL. Thrombo-
poietin levels in patients with primary and reactive thrombocytosis.
Br J Haematol 1997; 99: 281–4.
10 Stohlawetz P, Folman CC, von dem Borne AE, Pernerstorfer T,
Eichler HG, Panzer S, Jilma B. Effects of endotoxemia on thrombo-
poiesis in men. Thromb Haemost 1999; 81: 613–7.
11 Ishiguro A, Suzuki Y, Mito M, Shimbo T, Matsubara K, Kato T,
Miyazaki H. Elevation of serum thrombopoietin precedes thrombo-
cytosis in acute infections. Br J Haematol 2002; 116: 612–8.
12 Colarizi P, Fiorucci P, Caradonna A, Ficuccilli F, MancusoM, Papoff
P. Circulating thrombopoietin levels in neonates with infection. Acta
Paediatr 1999; 88: 332–7.
13 Bjerre A, OvsteboR, Kierulf P, Halvorsen S, Brandtzaeg P. Fulminant
meningococcal septicemia: dissociation between plasma thrombo-
poietin levels and platelet counts. Clin Infect Dis 2000; 30: 643–7.
14 Reinhold A, Zhang J, Gessner R, Felderhoff-Mueser U, Obladen M,
Dame C. High thrombopoietin concentrations in the cerebrospinal
fluid of neonates with sepsis and intraventricular hemorrhage may
contribute to brain damage. J Interferon Cytokine Res 2007; 27: 137–
45.
15 Oygur N, Tunga M, Mumcu Y, Yesilipek A, Gura A, Coskun M,
Yegin O. Thrombopoietin levels of thrombocytopenic term and pre-
term newborns with infection. Am J Perinatol 2001; 18: 279–86.
16 Folman CC, Linthorst GE, vanMourik J, vanWilligen G, de Jonge E,
Levi M, de Haas M, von dem Borne AE. Platelets release thrombo-
poietin (Tpo) upon activation: another regulatory loop in thrombo-
cytopoiesis? Thromb Haemost 2000; 83: 923–30.
17 Zakynthinos SG, Papanikolaou S, Theodoridis T, Zakynthinos EG,
Christopoulou-Kokkinou V, Katsaris G, Mavrommatis AC. Sepsis
severity is the major determinant of circulating thrombopoietin levels
in septic patients. Crit Care Med 2004; 32: 1004–10.
18 Jeschke MG, Chinkes DL, Finnerty CC, Przkora R, Pereira CT,
HerndonDN. Blood transfusions are associated with increased risk for
development of sepsis in severely burned pediatric patients. Crit Care
Med 2007; 35: 579–83.
19 Taylor FB, Jr, Toh CH, Hoots WK, Wada H, Levi M. Towards
definition, clinical and laboratory criteria, and a scoring system for
disseminated intravascular coagulation. Thromb Haemost 2001; 86:
1327–30.
20 Vincent JL, Moreno R, Takala J, Willatts S, De Mendonca A,
Bruining H, Reinhart CK, Suter PM, Thijs LG. The SOFA (sepsis-
related organ failure assessment) score to describe organ dysfunction/
failure. On behalf of the Working Group on Sepsis-Related Problems
of the European Society of Intensive Care Medicine. Intensive Care
Med 1996; 22: 707–10.
21 Bone RC. The pathogenesis of sepsis. Ann Intern Med 1991; 115: 457–
69.
22 Freedman JE, Loscalzo J. Platelet-monocyte aggregates: bridging
thrombosis and inflammation. Circulation 2002; 105: 2130–2.
23 Housinger TA, Brinkerhoff C, Warden GD. The relationship between
platelet count, sepsis, and survival in pediatric burn patients.Arch Surg
1993; 128: 65–6.
24 Wolber EM, Jelkmann W. Interleukin-6 increases thrombopoietin
production in human hepatoma cells HepG2 and Hep3B. J Interferon
Cytokine Res 2000; 20: 499–506.
25 Harker LA, Marzec UM, Hunt P, Kelly AB, Tomer A, Cheung E,
Hanson SR, Stead RB. Dose-response effects of pegylated human
megakaryocyte growth and development factor on platelet production
and function in nonhuman primates. Blood 1996; 88: 511–21.
26 Vincent JL, Yagushi A, Pradier O. Platelet function in sepsis.Crit Care
Med 2002; 30: S313–7.
27 Leytin V, Shakoor S, Mody M, Allen D, Garvey B, Freedman J.
Sepsis- and endotoxemia-generated cytokines do not trigger activation
of human platelets. Crit Care Med 2002; 30: 2771–3.
28 Semple JW, AslamR, KimM, Speck ER, Freedman J. Platelet-bound
lipopolysaccharide enhances Fc receptor-mediated phagocytosis of
IgG-opsonized platelets. Blood 2007; 109: 4803–5.
29 Clark SR, Ma AC, Tavener SA, McDonald B, Goodarzi Z, Kelly
MM, Patel KD, Chakrabarti S, McAvoy E, Sinclair GD, Keys EM,
Allen-Vercoe E, Devinney R, Doig CJ, Green FH, Kubes P. Platelet
TLR4 activates neutrophil extracellular traps to ensnare bacteria in
septic blood. Nat Med 2007; 13: 463–9.
30 Andonegui G, Kerfoot SM, McNagny K, Ebbert KV, Patel KD,
Kubes P. Platelets express functional toll-like receptor-4. Blood 2005;
106: 2417–23.
31 Lingnau WW, Nguyen TT, Woodsen LC, Herndon DN, Prough DS
Critical care of burn complications. In:Total Burn Care. HerndonDN.
New York: Saunders; 1996: 319–45.
1008 E. Lupia et al
� 2009 International Society on Thrombosis and Haemostasis




























