Embed Size (px)
Citation preview

ARTICLE IN PRESS
ORIGINAL ARTICLE
Abbr
plasm
CR-IM
geal
dysp
to tr
tion;
nar
Copy
0016
doi:1
www
Endoscopic ablation of Barrett’s esophagus: a multicenter studywith 2.5-year follow-up
eviatio
a coa
, com
cancer
lasia; I
eat; LG
PDT, p
junctio
right ª-5107/$
0.1016/
.giejou
David E. Fleischer, MD, Bergein F. Overholt, MD, Virender K. Sharma, MD, Alvaro Reymunde, MD,Michael B. Kimmey, MD, Ram Chuttani, MD, Kenneth J. Chang, MD, Charles J. Lightdale, MD,Nilda Santiago, MD, Douglas K. Pleskow, MD, Patrick J. Dean, MD, Kenneth K. Wang, MD
Scottsdale, Arizona, Knoxville, Memphis, Tennessee, Tacoma, Washington, Boston, Massachusetts, Irvine, California,New York, New York, Rochester, Minnesota, USA, Ponce, Puerto Rico
Background: For patients with Barrett’s esophagus (BE), life-long surveillance endoscopy is recommendedbecause of an elevated risk for developing dysplasia and esophageal adenocarcinoma. Various endoscopictherapies have been used to eradicate BE. Recently circumferential radiofrequency ablation has been usedwith encouraging short-term results.
Objective: To provide longer follow-up and to assess the long-term safety and efficacy of step-wise circumfer-ential ablation with the addition of focal ablation for BE.
Design: Prospective, multicenter clinical trial (NCT00489268).
Setting: Eight U.S. centers, between May 2004 and February 2007.
Patients: Seventy subjects with 2 to 6 cm of BE and histologic evidence of intestinal metaplasia (IM).
Interventions: Circumferential ablation was performed at baseline and repeated at 4 months if there was re-sidual IM. Follow-up biopsy specimens were obtained at 1, 3, 6, 12, and 30 months. Specimens were reviewed bya central pathology board. Focal ablation was performed after the 12-month follow-up for histological evidenceof IM at the 12-month biopsy (absolute indication) or endoscopic appearance suggestive of columnar-linedesophagus (relative indication). Subjects received esomeprazole for control of esophageal reflux.
Main outcome measurements: Complete absence of IM per patient from biopsy specimens obtained at 12and 30 months, defined as complete remission–IM (CR-IM).
Results: At 12 months, CR-IM was achieved in 48 of 69 available patients (70% per protocol [PP], 69% intentionto treat [ITT]). At 30 months after additional focal ablative therapy, CR-IM was achieved in 60 of 61 availablepatients (98% PP, 97% ITT). There were no strictures or buried glandular mucosa detected by the standardizedbiopsy protocol at 12 or 30 months, and there were no serious adverse events.
Limitations: This was an uncontrolled clinical trial with 2.5-year follow-up.
Conclusion: Stepwise circumferential and focal ablation resulted in complete eradication of IM in 98% ofpatients at 2.5-year follow-up. (Gastrointest Endosc 2008;-:---.)
ns: AIM, Ablation Intestinal Metaplasia trial; APC, argon
gulation; BE, Barrett’s esophagus; CR, complete remission;
plete remission of intestinal metaplasia; EAC, early esopha-
; GERD, gastroesophageal reflux disease; HGD, high-grade
D, inner diameter; IM, intestinal metaplasia; ITT, intention
D, low-grade dysplasia; MPEC, multipolar electrocoagula-
hotodynamic therapy; PP, per protocol; SCJ, squamocolum-
n; TGF, top of the gastric folds; VAS, visual analog scale.
2008 by the American Society for Gastrointestinal Endoscopy
32.00
j.gie.2008.03.008
rnal.org
A diagnosis of Barrett’s esophagus (BE) is suspectedupon the endoscopic finding of a salmon-colored colum-nar-lined distal esophagus and is confirmed by the histo-logic presence of intestinal metaplasia (IM) within thisarea.1-3 It is suspected that chronic injury from gastro-esophageal reflux induces the metaplastic change in theepithelium. The prevalence of BE in a general adultpopulation is estimated as 0.4% to 1.6%,4,5 whereas itsprevalence in more selected cohorts from gastroenterol-ogy practices is higher at 6.8% to 25.0%.6,7 The annual
Volume -, No. - : 2008 GASTROINTESTINAL ENDOSCOPY 1

ARTICLE IN PRESSEndoscopic ablation of Barrett’s esophagus Fleischer et al
incidence of BE, as reported in the ProGERD study,8 is0.65% per year for patients with GERD and 2.9% peryear for those with severe forms of esophagitis. In onereport, new cases of BE rose from 2.9 to 8.9 cases per1000 endoscopies over the last 10 years.9 In parallel withthese observations related to BE, the incidence of esoph-ageal adenocarcinoma (EAC) is also on the rise, marked bya 300% to 500% increase in annual new cases over the last4 decades.10 IM is a common precursor to EAC.8,11
Due to the elevated risk for progression from non-dysplastic IM to low-grade dysplasia (LGD), high-gradedysplasia (HGD), and EAC,8,12-19 these patients with BEundergo surveillance endoscopy with biopsy approxi-mately every 3 years to detect progression at the earliestpossible stage.20 Although nondysplastic IM has a risk ofprogression to EAC of 0.5% to 1.0% per patient-year offollow-up,12-19 Sharma et al13 reported that the aggre-gate risk of progression from nondysplastic IM to dyspla-sia or carcinoma over 4.2 years was 21.7% (5.2% perpatient-year of follow-up). Although the majority ofthese were LGD (16.2%), 3.6% were HGD, and 2.0%were EAC.
There are a number of resective and ablative tech-niques that have been studied for eliminating BE, includ-ing multipolar electrocoagulation (MPEC), argon plasmacoagulation (APC), laser ablation, cryotherapy, EMR, pho-todynamic therapy (PDT),21-30 and most recently, cir-cumferential and focal ablation with radiofrequencyenergy.31-34
Historically, there has been no rationale for ablatingIM (nondysplastic BE). Progression to carcinoma is infre-quent, and none of the ablative methods were establishedas safe, effective, and durable. In a recent multicenter trialusing circumferential ablation for nondysplastic IM, IMwas safely and completely eradicated in 70% of patients.31
We have extended this multicenter study with the objec-tive of determining whether selective ablation of persis-tent IM using a focal ablation device could furtherimprove the overall eradication rate while maintainingthe safety profile of this intervention.
PATIENTS AND METHODS
Study summaryThis is an extension of the Ablation of Intestinal Meta-
plasia (AIM) Trial,31 which was conducted in 2 serialphases, dosimetry and effectiveness, at 8 U.S. centers be-tween September 2003 and September 2005, and reportedwith 1-year patient follow-up after ablation in the February2007 issue of Gastrointestinal Endoscopy. An amendmentto the study protocol was approved by the institutional re-view board for each participating institution, allowing forsubsequent focal ablation in patients from the effective-ness phase of the study and longer-term follow-up (2.5years) of this cohort.
2 GASTROINTESTINAL ENDOSCOPY Volume -, No. - : 2008
Capsule Summary
What is already known on this topic
d Circumferential and focal ablation using radiofrequencyenergy has been recently introduced to eliminateBarrett’s esophagus (BE).
What this study adds to our knowledge
d In a prospective trial of 70 patients with BE, initialcircumferential radiofrequency ablation followed by focalablation resulted in eradication of all intestinalmetaplasia in 98% of patients at 2.5-year follow-up.
PatientsStudy patients were 18 to 75 years of age, had histologic
evidence of IM without dysplasia, and had reconfirmationof diagnosis with a new biopsy within 6 months of enroll-ment. Allowable endoscopic BE length (proximal marginof BE to the top of the gastric folds [TGF]) was 2 to 6 cm.Patients were not eligible if they had esophageal strictureor varices, active esophagitis, prior ablation, prior EMR,prior radiation therapy to the esophagus, history ofesophageal dysplasia or malignancy, or an implanted elec-trical device.
Study devicesCircumferential ablation was performed by using the
HALO360 system (BARRX Medical, Inc., Sunnyvale, Calif),consisting of a sizing balloon, a balloon-based ablationcatheter (Fig. 1A), and an energy generator. The ablationcatheter consists of a microelectrode array affixed to a bal-loon catheter. The array contains 60 tightly spaced bipolarelectrodes, which deliver ablative energy (radiofrequency)to the tissue.31
Focal ablation was performed by using the HALO90 ab-lation system (BARRX Medical, Inc., Sunnyvale, Calif); a de-vice that fits on the tip of a gastroscope (Fig. 1B) and iscoupled to an energy generator. The upper surface ofthe device is a 20-mm-long � 13-mm-wide articulated plat-form with an electrode array identical in pattern to the cir-cumferential device. Upward deflection of the endoscopebrings the electrode into contact with the BE tissue.
Both study device systems were evaluated in porcineand human treat-and-resect protocols, in which the devicedesign and treatment parameters were adjusted to achieveuniform ablation and avoid injury to the submucosa.32-34
Treatment parametersCircumferential ablation was performed by using an en-
ergy density setting of 10 J/cm2. Focal ablation was per-formed by using 12 J/cm2. All ablations were performedwith high-power density (40 W/cm2).31
www.giejournal.org
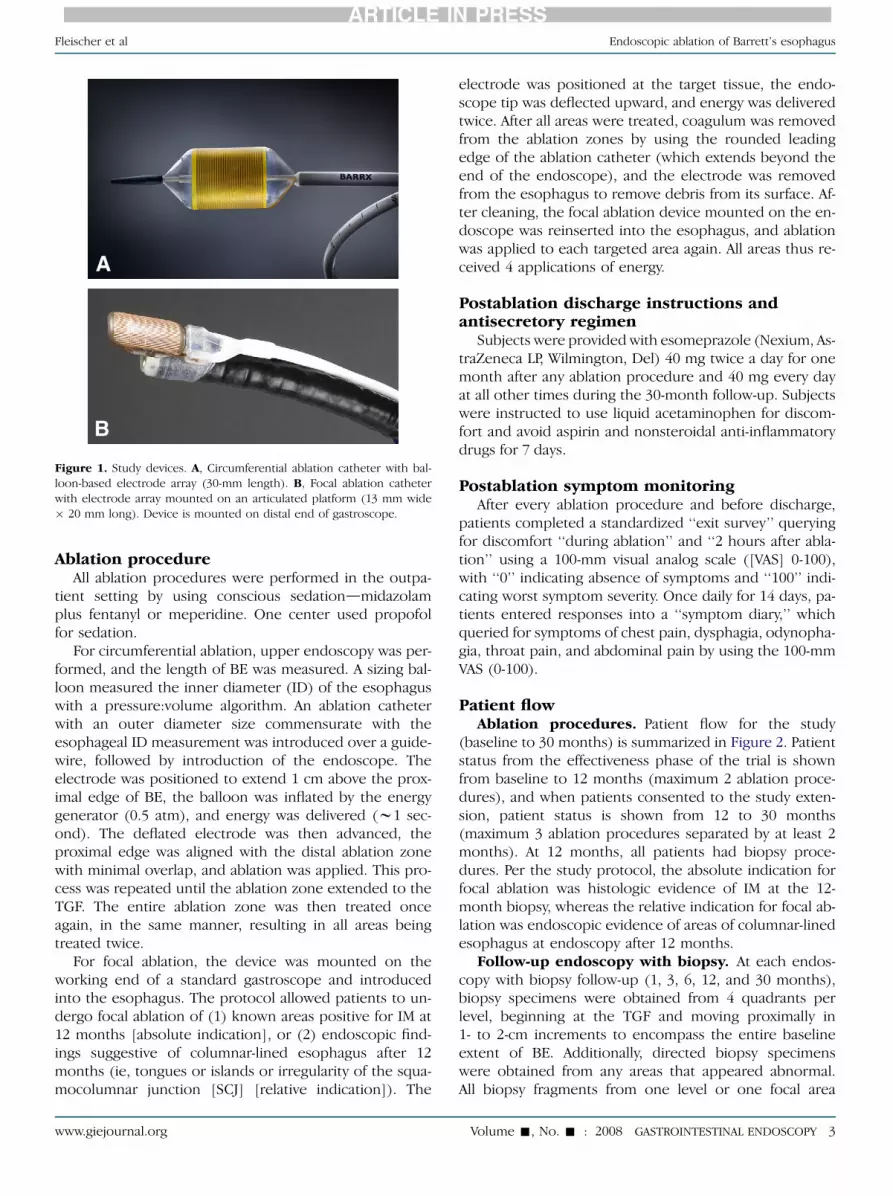
Figure 1. Study devices. A, Circumferential ablation catheter with bal-
loon-based electrode array (30-mm length). B, Focal ablation catheter
with electrode array mounted on an articulated platform (13 mm wide
� 20 mm long). Device is mounted on distal end of gastroscope.
ARTICLE IN PRESSFleischer et al Endoscopic ablation of Barrett’s esophagus
Ablation procedureAll ablation procedures were performed in the outpa-
tient setting by using conscious sedationdmidazolamplus fentanyl or meperidine. One center used propofolfor sedation.
For circumferential ablation, upper endoscopy was per-formed, and the length of BE was measured. A sizing bal-loon measured the inner diameter (ID) of the esophaguswith a pressure:volume algorithm. An ablation catheterwith an outer diameter size commensurate with theesophageal ID measurement was introduced over a guide-wire, followed by introduction of the endoscope. Theelectrode was positioned to extend 1 cm above the prox-imal edge of BE, the balloon was inflated by the energygenerator (0.5 atm), and energy was delivered (w1 sec-ond). The deflated electrode was then advanced, theproximal edge was aligned with the distal ablation zonewith minimal overlap, and ablation was applied. This pro-cess was repeated until the ablation zone extended to theTGF. The entire ablation zone was then treated onceagain, in the same manner, resulting in all areas beingtreated twice.
For focal ablation, the device was mounted on theworking end of a standard gastroscope and introducedinto the esophagus. The protocol allowed patients to un-dergo focal ablation of (1) known areas positive for IM at12 months [absolute indication], or (2) endoscopic find-ings suggestive of columnar-lined esophagus after 12months (ie, tongues or islands or irregularity of the squa-mocolumnar junction [SCJ] [relative indication]). The
www.giejournal.org
electrode was positioned at the target tissue, the endo-scope tip was deflected upward, and energy was deliveredtwice. After all areas were treated, coagulum was removedfrom the ablation zones by using the rounded leadingedge of the ablation catheter (which extends beyond theend of the endoscope), and the electrode was removedfrom the esophagus to remove debris from its surface. Af-ter cleaning, the focal ablation device mounted on the en-doscope was reinserted into the esophagus, and ablationwas applied to each targeted area again. All areas thus re-ceived 4 applications of energy.
Postablation discharge instructions andantisecretory regimen
Subjects were provided with esomeprazole (Nexium, As-traZeneca LP, Wilmington, Del) 40 mg twice a day for onemonth after any ablation procedure and 40 mg every dayat all other times during the 30-month follow-up. Subjectswere instructed to use liquid acetaminophen for discom-fort and avoid aspirin and nonsteroidal anti-inflammatorydrugs for 7 days.
Postablation symptom monitoringAfter every ablation procedure and before discharge,
patients completed a standardized ‘‘exit survey’’ queryingfor discomfort ‘‘during ablation’’ and ‘‘2 hours after abla-tion’’ using a 100-mm visual analog scale ([VAS] 0-100),with ‘‘0’’ indicating absence of symptoms and ‘‘100’’ indi-cating worst symptom severity. Once daily for 14 days, pa-tients entered responses into a ‘‘symptom diary,’’ whichqueried for symptoms of chest pain, dysphagia, odynopha-gia, throat pain, and abdominal pain by using the 100-mmVAS (0-100).
Patient flowAblation procedures. Patient flow for the study
(baseline to 30 months) is summarized in Figure 2. Patientstatus from the effectiveness phase of the trial is shownfrom baseline to 12 months (maximum 2 ablation proce-dures), and when patients consented to the study exten-sion, patient status is shown from 12 to 30 months(maximum 3 ablation procedures separated by at least 2months). At 12 months, all patients had biopsy proce-dures. Per the study protocol, the absolute indication forfocal ablation was histologic evidence of IM at the 12-month biopsy, whereas the relative indication for focal ab-lation was endoscopic evidence of areas of columnar-linedesophagus at endoscopy after 12 months.
Follow-up endoscopy with biopsy. At each endos-copy with biopsy follow-up (1, 3, 6, 12, and 30 months),biopsy specimens were obtained from 4 quadrants perlevel, beginning at the TGF and moving proximally in1- to 2-cm increments to encompass the entire baselineextent of BE. Additionally, directed biopsy specimenswere obtained from any areas that appeared abnormal.All biopsy fragments from one level or one focal area
Volume -, No. - : 2008 GASTROINTESTINAL ENDOSCOPY 3

Figure 2. Patient flow. Patients were enrolled and underwent circumfer-
ential ablation of BE at ‘‘0 months,’’ followed by endoscopy with biopsy
at 1, 3, 6, 12, and 30 months. A second circumferential ablation was
performed at 4 months if patient had IM at the 1- or 3-month biopsy.
Extension of the study provided for up to 3 focal ablation sessions after
the 12-month follow-up, with targeting of persistent endoscopically
evident BE and irregularity of the SCJ.
ARTICLE IN PRESSEndoscopic ablation of Barrett’s esophagus Fleischer et al
were submitted in one container and labeled with the lo-cation of the biopsy.
Central pathology processing andinterpretation
All tissue specimens were sent in a standardized kit toa pathology laboratory designated for the study (Gastroin-testinal Pathology, LLC, Memphis, Tenn). The formalin-fixedbiopsy fragments from each container were embedded inparaffin, affixed to a slide, and stained with hematoxylinand eosin. One slide represented each level or focal area.All slides were interpreted by a board-certified pathologistspecializing in GI pathology. Each fragment on each slidewas evaluated for the presence of IM. For each patient,a tally of fragments with and without IM was generated.These data were entered into a standardized pathologycase report form. A diagnosis of ‘‘buried glandular mucosa’’was made for any fragment that met the a priori definition
4 GASTROINTESTINAL ENDOSCOPY Volume -, No. - : 2008
of ‘‘any specialized columnar epithelium covered by a layerof squamous epithelium with no communication with thesurface.’’
Outcome measuresEffectiveness. The primary effectiveness outcome
was based on histologic assessment of esophageal biopsyspecimens obtained at 12 and 30 months (biopsy speci-mens from gastric cardia or corpus were excluded). Acomplete remission (CR) for a patient was defined as allbiopsy fragments (100%) negative for IM. Per protocol(PP) and intention to treat (ITT) analyses were performedseparately for the 12-month (effectiveness phase) and 30-month (extension) outcomes. In the PP analysis, patientswho consented for enrollment and underwent biopsyprocedure were included in the denominator. In the ITTanalysis, all patients who consented were considered inthe denominator, and those who did not undergo a biopsywere considered failures.
Patient safety and tolerability. Each site was re-sponsible for reporting all adverse events within 48 hoursby using a standardized form. The type, severity, and fre-quency of adverse events were tracked throughout thestudy. Patient tolerability was assessed by recording seda-tion medication during ablation, procedure time, exit sur-vey scores, 14-day symptom diary scores, and adverseevents.
Statistical analysisDescriptive statistics are provided for patient cohort de-
mographics and ablation procedure components. Patientresponses to the 14-day symptom diary, exit survey, andablation procedure components were segregated as to cir-cumferential versus focal ablation, and a 2-sample t testassuming unequal variances was applied to determinewhether there was a difference between the proceduretypes for continuous variables.
RESULTS
The effectiveness phase of the trial included 70 patientsenrolled at 8 centers, and 62 of the 70 (89%) were success-fully contacted and willing to participate in the study ex-tension. The demographics of both groups are shown inTable 1. Eight patients did not participate in the extensionfor the following reasons: could not be located (n Z 3),moved (n Z 1), had financial constraints (n Z 1), orknowledge of having no IM at 1 year prompted them toelect no further biopsy or ablation procedure (n Z 3).Of these 8 patients, 3 had CR-IM, and 4 had at least onefragment of IM. One patient had no pathology specimencollected. Fifty-nine of the 62 patients in the study exten-sion were treated with focal ablation.
Ablation procedure details are summarized in Table 2.Compared to circumferential ablation, focal ablation
www.giejournal.org

TABLE 1. Patient demographics
Effectiveness
phase Extension
No. patients 70 62
Sex (M/F) 52/18 45/17
Age (mean � SD), y 55.7 � 11.2 55.5 � 11.3
Age range, y 26-79 26-79
Body weight
(mean � SD), lbs
177.3 � 36.5 177.4� 38.2
Ethnicity, n (%)
White 47 (67) 42 (68)
Black 2 (3) 2 (3)
Hispanic/Latino 21 (30) 18 (29)
BE length
(mean � SD), cm
3.2 � 1.4 3.1 � 1.3
BE length (range), cm 2-6 2-6
Hiatal hernia (y/n) 60/10 52/10
Hiatal hernia length, when
present (mean � SD), cm
2.6 � 1.2 2.5 �1.1
BE, Barrett’s esophagus; PPI, proton pump inhibitor.
ARTICLE IN PRESSFleischer et al Endoscopic ablation of Barrett’s esophagus
required fewer minutes to perform (17 vs 28 minutes, P!.001) and less sedation (P ! .05). Exit survey symptomscores showed minimal symptoms for both procedures,with no difference between groups (P Z NS). Diary symp-tom scores were mildly elevated after circumferential andfocal ablation for some of the queried symptoms (Fig. 3Aand B), with no difference between the groups for anysymptom on any day (P Z NS).
There were 24 minor adverse events reported in 16 pa-tients after 106 circumferential ablation procedures(15.1%). All were transient, and all resolved completely.These included fever (2), chest/throat pain (9), superficiallinear mucosal injury (1), mild bleeding (1), mucosal scar-ring at 1-month endoscopy resolved by 3-month endoscopy(1), sedation-related airway obstruction (1), sedation-related hypotension (1), and nausea (8).
There were 4 minor adverse events reported in 3 patientsafter 115 focal ablation procedures (2.6%). These includedchest pain (1), nausea or vomiting (2), and sedation-relatedhypotension before ablation (1). All were transient, and allresolved completely.
As reported by us previously, 69 of the 70 enrolled pa-tients were available for 12-month follow-up after a meanof 1.5 circumferential ablation procedures (Table 2). Therewere 3007 biopsy fragments collected during the effective-ness phase. At 12 months, the percentage of patients withCR-IM was 70% (ITT, 69%).31 For the study extension, 61of the 62 enrolled patients were available for 30-month
www.giejournal.org
follow-up after a mean of 1.9 focal ablation procedures.There were 923 biopsy fragments collected at the 30-month follow-up (mean 15.1 per patient), and the per-centage of patients with CR-IM was 98% (ITT, 97%).
There were no strictures noted on any follow-up endos-copy. There was no buried glandular mucosa detected at 12or 30 months when using the standardized biopsy protocol.
Endoscopic images are shown in Figure 4A to D froma study patient who had 6 cm of BE at baseline, underwentcircumferential and focal ablation, and had no evidence ofIM at 30 months. Histologic specimens from this patientshow that the IM present at baseline was no longer pres-ent at 30 months (Fig. 5).
DISCUSSION
We know that BE is caused by chronic injury to theesophageal lining due to gastroesophageal reflux andthat, once present, BE does not regress despite controlof GERD symptoms. Due to the risk for developing dys-plasia and EAC, patients with nondysplastic IM undergoendoscopy with biopsy approximately every 3 years to de-tect progression at the earliest stage. The AIM Trial wasoriginally conducted in 2 serial phases to evaluate dose-response and effectiveness of circumferential ablationfor nondysplastic IM. After the initial dosimetry phase(n Z 32), the effectiveness phase of the trial (n Z 70)was conducted (10 J/cm2, 40 W/cm2). The CR-IM at 12months was 70%. There were no strictures and no buriedglandular mucosa detected when using a standardizedbiopsy protocol.31
In the dosimetry and effectiveness phases of the AIMTrial, we learned that accurate determination of the IDof the esophagus before ablation is challenging, and thatpresence of coagulum impedes the effect of a second ab-lation pass. This allowed us to incorporate specific refine-ments in the technique, such as adding an automatedsizing step and assiduously cleaning the electrode and ab-lation zone after the first pass. In addition, we learned thatthe circumferential treatment device is not ideally suitedfor certain anatomical areas, such as a widened gastro-esophageal junction due to hiatal hernia or dilated esoph-agus. We learned that a focal ablation device was effectivefor treating the flared SCJ. As per protocol, patients whohad negative biopsy results for IM at 12 months couldbe treated if the investigator felt it was appropriate. Be-cause ablation with either catheter may cause chest painin some patients, analgesics and sedatives used for the ab-lation procedure are given at higher doses than are usedwith standard endoscopy. The objectives of the subse-quent study extension were (1) to provide selective abla-tion to areas of visible BE and irregularity of the SCJ byusing a focal ablation device; (2) to improve the CR-IMby including focal ablation; and (3) to extend the follow-up from 12 to 30 months. Sixty-two of the original 70
Volume -, No. - : 2008 GASTROINTESTINAL ENDOSCOPY 5

TABLE 2. Ablation procedure details and histologic outcomes
Circumferential ablation Focal ablation
Patients 70 62
Total no. procedures 106 115
Mean no. procedures (range) 1.5 (1-2) 1.9 (0-3)
Procedure time Median (IQR), min 28 (24-34) 17 (11-22)*
Sedation
Median (IQR)
Midazolam, mg 8 (6-10) 7 (6-8)*
Fentanyl, mg 200 (150-212) 150 (100-200)*
Meperidine, mg 100 (75-132) 75 (50-100)y
Propofol, mg 650 (550-900) 425 (350-600)y
Exit survey results Circumferential ablation Focal ablation
Level of discomfort
Median (IQR) z
During procedure 2 (0-6) 0 (0-0)
2 hrs after procedure 9 (1-23) 0 (0-18)y
Histologic outcomes 12-month follow-up 30-month follow-up
Patients undergoing endoscopy with biopsy (n) 69 61
Analysis PP ITT PP ITT
CR-IM, n (%) 48 (70) 48 (69) 60 (98) 60 (97)
CR-IM, Complete remission, defined as all biopsies negative for IM at follow-up interval; PP, per protocol
analysis; ITT, intention-to-treat analysis; IQR, interquartile range.
*P ! .001; Student t test comparing circumferential and focal ablation parameter.
yP ! .05.
zExit survey scored with VAS (0-100); 0 Z no symptoms, 100 Z severe symptoms.
ARTICLE IN PRESSEndoscopic ablation of Barrett’s esophagus Fleischer et al
patients participated in the study extension, and therewere no serious adverse events. At the 30-month follow-up, 923 biopsy fragments were obtained from 61 of the62 patients, and CR-IM was achieved in 60 of these pa-tients (98% PP, 97% ITT). There was no evidence of buriedglandular mucosa detected when using the standardizedbiopsy protocol. There were no strictures. One patientelected not to undergo a final biopsy procedure.
One limitation of the study extension may be that 8 of70 eligible patients did not participate, creating a potentialfor bias. Demographic data for both patient cohorts areshown in Table 1. Nonparticipants in the study extensioninclude 3 with CR-IM at 12 months, 4 with focal IM at 12months, and 1 lost to follow-up at 1 month. When the 8nonparticipants are included in a post hoc ITT analysisand considered failures, CR-IM was achieved in 60 of 70patients (86%).
A strength of this study is that the primary outcome ishistology-based and, therefore, not subject to patientresponse bias. Although a control group (surveillance
6 GASTROINTESTINAL ENDOSCOPY Volume -, No. - : 2008
only) might have been helpful in establishing a rate ofspontaneous regression of IM, we believe that a controlgroup was not necessary for this study and that completespontaneous regression of IM is rare.
Another strength is that all pathologic specimens wereprepared and reviewed by a centralized service specializ-ing in GI pathology. Slides were reviewed in a blindedmanner. Although there may be discordance between pa-thologists related to the diagnosis of IM with dysplasia,this issue does not pertain to making a differentiation be-tween squamous mucosa and IM; therefore, we do not be-lieve there was significant bias related to the pathology orprimary outcome for this study. Finally, this study was per-formed in multiple centers to decrease the referral biasthat is present in many single centers.
One criticism is that achieving CR-IM in 98% of patientsrequired 1.5 circumferential and 1.9 focal ablation proce-dures, on average. We believe the number of ablations re-quired in future studies will be less, as the presentprotocol allowed for focal ablation for histologic evidence
www.giejournal.org
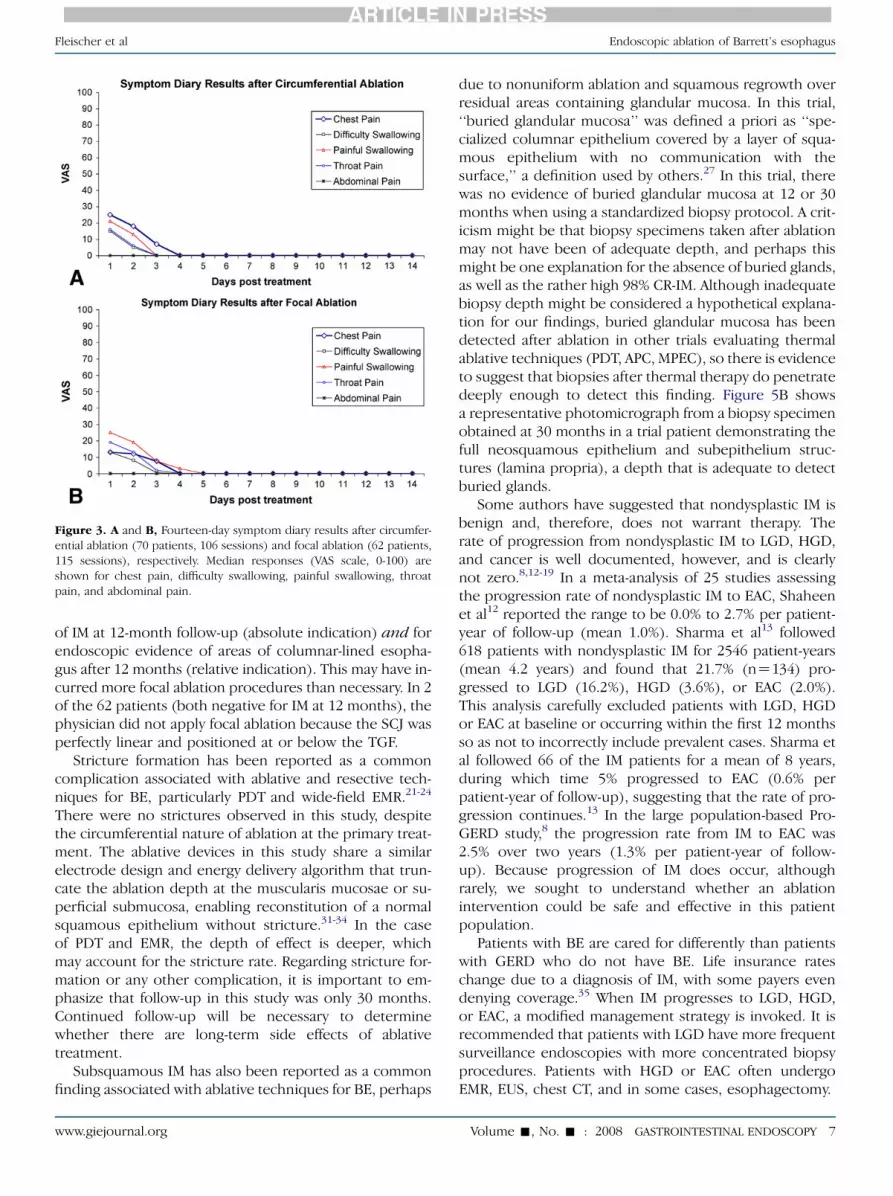
Figure 3. A and B, Fourteen-day symptom diary results after circumfer-
ential ablation (70 patients, 106 sessions) and focal ablation (62 patients,
115 sessions), respectively. Median responses (VAS scale, 0-100) are
shown for chest pain, difficulty swallowing, painful swallowing, throat
pain, and abdominal pain.
ARTICLE IN PRESSFleischer et al Endoscopic ablation of Barrett’s esophagus
of IM at 12-month follow-up (absolute indication) and forendoscopic evidence of areas of columnar-lined esopha-gus after 12 months (relative indication). This may have in-curred more focal ablation procedures than necessary. In 2of the 62 patients (both negative for IM at 12 months), thephysician did not apply focal ablation because the SCJ wasperfectly linear and positioned at or below the TGF.
Stricture formation has been reported as a commoncomplication associated with ablative and resective tech-niques for BE, particularly PDT and wide-field EMR.21-24
There were no strictures observed in this study, despitethe circumferential nature of ablation at the primary treat-ment. The ablative devices in this study share a similarelectrode design and energy delivery algorithm that trun-cate the ablation depth at the muscularis mucosae or su-perficial submucosa, enabling reconstitution of a normalsquamous epithelium without stricture.31-34 In the caseof PDT and EMR, the depth of effect is deeper, whichmay account for the stricture rate. Regarding stricture for-mation or any other complication, it is important to em-phasize that follow-up in this study was only 30 months.Continued follow-up will be necessary to determinewhether there are long-term side effects of ablativetreatment.
Subsquamous IM has also been reported as a commonfinding associated with ablative techniques for BE, perhaps
www.giejournal.org
due to nonuniform ablation and squamous regrowth overresidual areas containing glandular mucosa. In this trial,‘‘buried glandular mucosa’’ was defined a priori as ‘‘spe-cialized columnar epithelium covered by a layer of squa-mous epithelium with no communication with thesurface,’’ a definition used by others.27 In this trial, therewas no evidence of buried glandular mucosa at 12 or 30months when using a standardized biopsy protocol. A crit-icism might be that biopsy specimens taken after ablationmay not have been of adequate depth, and perhaps thismight be one explanation for the absence of buried glands,as well as the rather high 98% CR-IM. Although inadequatebiopsy depth might be considered a hypothetical explana-tion for our findings, buried glandular mucosa has beendetected after ablation in other trials evaluating thermalablative techniques (PDT, APC, MPEC), so there is evidenceto suggest that biopsies after thermal therapy do penetratedeeply enough to detect this finding. Figure 5B showsa representative photomicrograph from a biopsy specimenobtained at 30 months in a trial patient demonstrating thefull neosquamous epithelium and subepithelium struc-tures (lamina propria), a depth that is adequate to detectburied glands.
Some authors have suggested that nondysplastic IM isbenign and, therefore, does not warrant therapy. Therate of progression from nondysplastic IM to LGD, HGD,and cancer is well documented, however, and is clearlynot zero.8,12-19 In a meta-analysis of 25 studies assessingthe progression rate of nondysplastic IM to EAC, Shaheenet al12 reported the range to be 0.0% to 2.7% per patient-year of follow-up (mean 1.0%). Sharma et al13 followed618 patients with nondysplastic IM for 2546 patient-years(mean 4.2 years) and found that 21.7% (nZ134) pro-gressed to LGD (16.2%), HGD (3.6%), or EAC (2.0%).This analysis carefully excluded patients with LGD, HGDor EAC at baseline or occurring within the first 12 monthsso as not to incorrectly include prevalent cases. Sharma etal followed 66 of the IM patients for a mean of 8 years,during which time 5% progressed to EAC (0.6% perpatient-year of follow-up), suggesting that the rate of pro-gression continues.13 In the large population-based Pro-GERD study,8 the progression rate from IM to EAC was2.5% over two years (1.3% per patient-year of follow-up). Because progression of IM does occur, althoughrarely, we sought to understand whether an ablationintervention could be safe and effective in this patientpopulation.
Patients with BE are cared for differently than patientswith GERD who do not have BE. Life insurance rateschange due to a diagnosis of IM, with some payers evendenying coverage.35 When IM progresses to LGD, HGD,or EAC, a modified management strategy is invoked. It isrecommended that patients with LGD have more frequentsurveillance endoscopies with more concentrated biopsyprocedures. Patients with HGD or EAC often undergoEMR, EUS, chest CT, and in some cases, esophagectomy.
Volume -, No. - : 2008 GASTROINTESTINAL ENDOSCOPY 7
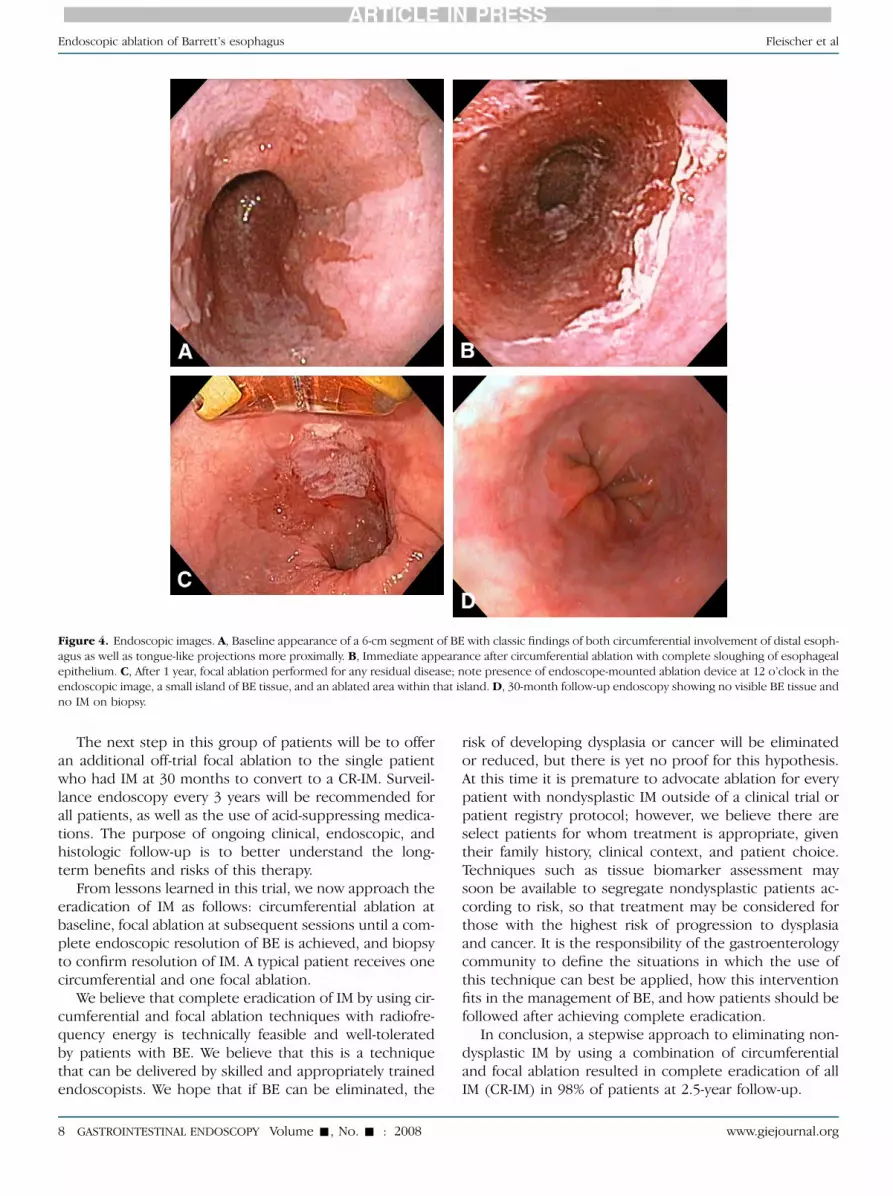
Figure 4. Endoscopic images. A, Baseline appearance of a 6-cm segment of BE with classic findings of both circumferential involvement of distal esoph-
agus as well as tongue-like projections more proximally. B, Immediate appearance after circumferential ablation with complete sloughing of esophageal
epithelium. C, After 1 year, focal ablation performed for any residual disease; note presence of endoscope-mounted ablation device at 12 o’clock in the
endoscopic image, a small island of BE tissue, and an ablated area within that island. D, 30-month follow-up endoscopy showing no visible BE tissue and
no IM on biopsy.
ARTICLE IN PRESSEndoscopic ablation of Barrett’s esophagus Fleischer et al
The next step in this group of patients will be to offeran additional off-trial focal ablation to the single patientwho had IM at 30 months to convert to a CR-IM. Surveil-lance endoscopy every 3 years will be recommended forall patients, as well as the use of acid-suppressing medica-tions. The purpose of ongoing clinical, endoscopic, andhistologic follow-up is to better understand the long-term benefits and risks of this therapy.
From lessons learned in this trial, we now approach theeradication of IM as follows: circumferential ablation atbaseline, focal ablation at subsequent sessions until a com-plete endoscopic resolution of BE is achieved, and biopsyto confirm resolution of IM. A typical patient receives onecircumferential and one focal ablation.
We believe that complete eradication of IM by using cir-cumferential and focal ablation techniques with radiofre-quency energy is technically feasible and well-toleratedby patients with BE. We believe that this is a techniquethat can be delivered by skilled and appropriately trainedendoscopists. We hope that if BE can be eliminated, the
8 GASTROINTESTINAL ENDOSCOPY Volume -, No. - : 2008
risk of developing dysplasia or cancer will be eliminatedor reduced, but there is yet no proof for this hypothesis.At this time it is premature to advocate ablation for everypatient with nondysplastic IM outside of a clinical trial orpatient registry protocol; however, we believe there areselect patients for whom treatment is appropriate, giventheir family history, clinical context, and patient choice.Techniques such as tissue biomarker assessment maysoon be available to segregate nondysplastic patients ac-cording to risk, so that treatment may be considered forthose with the highest risk of progression to dysplasiaand cancer. It is the responsibility of the gastroenterologycommunity to define the situations in which the use ofthis technique can best be applied, how this interventionfits in the management of BE, and how patients should befollowed after achieving complete eradication.
In conclusion, a stepwise approach to eliminating non-dysplastic IM by using a combination of circumferentialand focal ablation resulted in complete eradication of allIM (CR-IM) in 98% of patients at 2.5-year follow-up.
www.giejournal.org

Figure 5. A and B, Photomicrographs of esophageal biopsy specimens
obtained at baseline and at 30 months following ablation (H&E, orig.
mag. �200), respectively. Baseline biopsy specimen shows glandular mu-
cosa and goblet cells diagnostic of IM. Follow-up biopsy specimen shows
normal-appearing squamous epithelium, with a depth including subepi-
thelial structures (lamina propria) to confirm absence of buried glandular
mucosa.
ARTICLE IN PRESSFleischer et al Endoscopic ablation of Barrett’s esophagus
DISCLOSURE
The authors report that there are no disclosures rele-vant to this publication. This research was supported ateach research institution by a grant from BARRX Medi-cal, Inc., Sunnyvale, California. This research was sup-ported by the Investigator-Sponsored Study Program ofAstraZeneca (AstraZeneca LP, Wilmington, Delaware).
REFERENCES
1. Peters JH, Hagen JA, DeMeester SR. Barrett’s esophagus. J Gastrointest
Surg 2004;8:1-17.
2. Reid BJ. Barrett’s esophagus and adenocarcinoma. Gastroenterol Clin
North Am 1991;20:817-34.
3. Shaheen N, Ransohoff DR. Gastroesophageal reflux, Barrett’s esopha-
gus and esophageal cancer. JAMA 2002;287:1972-81.
www.giejournal.org
4. Cameron AJ, Zinsmeister AR, Ballard DJ, et al. Prevalence of columnar-
lined (Barrett’s) esophagus. Comparison of population-based clinical
and autopsy findings. Gastroenterology 1990;99:918-22.
5. Ronkainen J, Aro P, Storskrubb T, et al. Prevalence of Barrett’s esoph-
agus in the general population: an endoscopic study. Gastroenterol-
ogy 2005;129:1825-31.
6. Rex DK, Cummings OW, Shaw M, et al. Screening for Barrett’s esoph-
agus in colonoscopy patients with and without heartburn. Gastroen-
terology 2003;125:1670-7.
7. Gerson LB, Shetler K, Triadafilopoulos G. Prevalence of Barrett’s esoph-
agus in asymptomatic individuals. Gastroenterology 2002;123:636-9.
8. Labenz J, Nocon M, Lind T, et al. Prospective follow-up data from the
ProGERD Study suggest that GERD is not a categorical disease. Am
J Gastroenterol 2006;101:2457-62.
9. Kendall BJ, Whiteman DC. Temporal changes in the endoscopic fre-
quency of new cases of Barrett’s esophagus in an Australian health re-
gion. Am J Gastroenterol 2006;101:1178-82.
10. Shaheen NJ. Advances in Barrett’s esophagus and esophageal adeno-
carcinoma. Gastroenterology 2005;128:1554-66.
11. Chandrosoma P, Wickramasinghe K, Ma Y, et al. Is intestinal metaplasia
a necessary precursor lesion for adenocarcinoma of the distal esoph-
agus, gastroesophageal junction and gastric junction? Dis Esophagus
2007;20:36-41.
12. Shaheen NJ, Crosby MA, Bozymski EM, et al. Is there a publication bias
in reporting cancer risk in Barrett’s esophagus? Gastroenterology
2000;119:333-8.
13. Sharma P, Falk GW, Weston AP, et al. Dysplasia and cancer in a large
multicenter cohort of patients with Barrett’s esophagus. Clin Gastro-
enterol Hepatol 2006;4:566-72.
14. Drewitz DJ, Sampliner RE, Garewal HS. The incidence of adenocarci-
noma in Barrett’s esophagus: a prospective study of 170 patients fol-
lowed 4.8 years. Am J Gastroenterol 1997;92:212-5.
15. Rudolph RE, Vaughan TL, Storer BE, et al. Effect of segment length on
risk for neoplastic progression in patients with Barrett’s esophagus.
Ann Intern Med 2000;132:612-20.
16. O’Connor JB, Falk GW, Richter JE. The incidence of adenocarcinoma
and dysplasia in Barrett’s esophagus: report on the Cleveland Clinic
Barrett’s Esophagus Registry. Am J Gastroenterol 1999;94:2037-42.
17. Robertson CS, Mayberry JF, Nicholson DA, et al. Value of endoscopic
surveillance in the detection of neoplastic change in Barrett’s esoph-
agus. Br J Surg 1988;75:760-3.
18. Hameeteman, Tytgat GN, Houthoff HJ, et al. Barrett’s esophagus: de-
velopment of dysplasia and adenocarcinoma. Gastroenterology
1989;96:1249-56.
19. Vaughan TL, Dong LM, Blount PL, et al. Non-steroidal anti-inflamma-
tory drugs and risk of neoplastic progression in Barrett’s oesophagus:
a prospective study. Lancet Oncol 2005;6:945-52.
20. Sampliner RE. Updated guidelines for the diagnosis, surveillance, and
therapy of Barrett’s esophagus. Am J Gastroenterol 2002;97:1888-95.
21. Overholt BF, Lightdale CJ, Wang KK, et al. Photodynamic therapy with
porfimer sodium for ablation of high-grade dysplasia in Barrett’s
esophagus: international, partially blinded, randomized phase III trial.
Gastrointest Endosc 2005;62:488-98.
22. Webber J, Herman M, Kessel D, et al. Current concepts in gastrointes-
tinal photodynamic therapy. Ann Surg 1999;230:12-23.
23. Ell C, May A, Gossner L, et al. Endoscopic mucosal resection of early
cancer and high-grade dysplasia in Barrett’s esophagus. Gastroenter-
ology 2000;118:670-7.
24. Seewald S, Akaraviputh T, Seitz U, et al. Circumferential EMR and com-
plete removal of Barrett’s epithelium: a new approach to management
of Barrett’s esophagus containing high-grade intraepithelial neoplasia
and intramucosal carcinoma. Gastrointest Endosc 2003;57:854-9.
25. Gossner L, May A, Stolte M, et al. KTP laser destruction of dysplasia and
early cancer in columnar-lined Barrett’s esophagus. Gastrointest En-
dosc 1999;49:8-12.
26. Ginsberg GG, Barkun AN, Bosco JJ, et al. The argon plasma coagulator.
Gastrointest Endosc 2002;55:807-10.
Volume -, No. - : 2008 GASTROINTESTINAL ENDOSCOPY 9

ARTICLE IN PRESSEndoscopic ablation of Barrett’s esophagus Fleischer et al
27. Dulai GS, Jensen DM, Cortina G, et al. Randomized trial of argon
plasma coagulation vs. multipolar electrocoagulation for ablation of
Barrett’s esophagus. Gastrointest Endosc 2005;61:232-40.
28. Montes CG, Brandalise NA, Deliza R, et al. Antireflux surgery followed
by bipolar electrocoagulation in the treatment of Barrett’s esophagus.
Gastrointest Endosc 1999;50:173-7.
29. Sampliner RE, Faigel D, Fennerty MB, et al. Effective and safe endo-
scopic reversal of nondysplastic Barrett’s esophagus with thermal
electrocoagulation combined with high-dose acid inhibition: a multi-
center study. Gastrointest Endosc 2001;53:554-8.
30. Johnston MH, Eastone JA, Horwhat JD, et al. Cryoablation of Barrett’s
esophagus: a pilot study. Gastrointest Endosc 2005;62:842-8.
31. Sharma VK, Wang KK, Overholt BF, et al. Balloon-based, circumferen-
tial, endoscopic radiofrequency ablation of Barrett’s esophagus: 1-
year follow-up of 100 patients. Gastrointest Endosc 2007;65:185-95.
32. Ganz RA, Utley DS, Stern RA, et al. Complete ablation of esophageal
epithelium with a balloon-based bipolar electrode: a phased evalua-
tion in the porcine and in the human esophagus. Gastrointest Endosc
2004;60:1002-10.
33. Dunkin BJ, Martinez J, Bejarano PA, et al. Thin-layer ablation of human
esophageal epithelium using a bipolar radiofrequency balloon device
(BARRX). Surg Endosc 2006;20:125-30.
10 GASTROINTESTINAL ENDOSCOPY Volume -, No. - : 2008
34. Smith CD, Bejarano PA, Melvin WS, et al. Endoscopic ablation of intestinal
metaplasia containing high-grade dysplasia in esophagectomy patients
using a balloon-based ablation system. Surg Endosc 2007;21:560-9.
35. Shaheen NJ, Dulai GS, Ascher B, et al. Effect of a new diagnosis of Bar-
rett’s esophagus on insurance status. Am J Gastro 2005;100:577-80.
Received August 13, 2007. Accepted March 3, 2008.
Current affiliations: Mayo Clinic (D.E.F., V.K.S.), Scottsdale, Arizona,
Gastrointestinal Associates (B.F.O.), Knoxville, Tennessee, Ponce
Gastroenterology (A.R., N.S.), Ponce, Puerto Rico, Tacoma Digestive
Disease Center (M.B.K.) Tacoma, Washington, Beth Israel Deaconess
Medical Center (R.C., D.K.P.), Boston, Massachusetts, University of
California – Irvine (K.J.C.), Irvine, California, Columbia Presbyterian Medical
Center (C.J.L.), New York, NY, GI Pathology (P.J.D.), Memphis, Tennessee,
Mayo Clinic (K.K.W.) Rochester, Minnesota.
Presented at Digestive Disease Week, May 20-23, 2007, Washington, DC
(Gastrointest Endosc 2007;65:AB135).
Reprint requests: David E. Fleischer, MD, Mayo Clinic Arizona, 13400 East
Shea Blvd, Scottsdale, AZ 85259.
www.giejournal.org





























