Embed Size (px)
Citation preview
Bashir Ali: 201316611 [email protected]
Ethiopia’s Demography Report: 1950-2012
Image: A picturesque image of a Sunday procession in one of Ethiopia’s oldest Orthodox Churches; the House of Saint George in
Lalibela, located in the Amhara region. Lalibela & Axum are both world, renowned for their ancient churches carved from living
rock and eleven of these churches are designated UNESCO World Heritage Sites (1978).
Ethiopia is one of the oldest nations in Africa and the entire world and it has the notable distinction of never being
colonised, despite a nine year Italian occupation from 1934-1942. The Federal Democratic Republic of Ethiopia is
located in East Africa and specifically the Horn of Africa. It is bordered by Eritrea to the Northeast, Djibouti and
Somalia to the east and Sudan and South Sudan to the West as well as Kenya to the south. Ethiopia is not only the
most populous landlocked country in the world, it is also comfortably Africa’s second most populous country after
Nigeria and its population has more than quadrupled from 18,434,000 in early 1950 to the current population of
91,728,849 as measured in 20131 (World Bank Data indicators, 1993). Ethiopia is a multi-ethnic Federal state and is
made up of over 80 ethnic groups with the Oromo group being the largest at approximately 40% of the population
along with the Amhara and Tigray groups which constitute approximately 32% of the population and have
traditionally been dominant politically. Other notable ethnic groups include; the Somalis and Afars. Ethiopia is
composed of 9 National Regional states: namely Tigray, Afar, Amhara, Oromia, Somali, Benishangul-Gumuz,
SNNPR, Gambella and Harari with Addis Ababa being its capital and largest city.2 In addition, Ethiopia is a
religiously diverse state and according to the 2007 Ethiopian Census; 62.8% are Christians with the majority followers
of the traditional, Orthodox Christianity. Also, 33.9% of the population are Muslims whereas a minority 2.6% are
followers of traditional religions (Ethiopian Central Statistical Agency).
Since Ethiopia’s new Constitution and designation as a Federal country in 1995, Ethiopia has achieved a great deal of
stability compared to the period 1974 to 1991 which was characterised by violent political conflict and severe famines.
Ethiopia has also achieved rapid economic growth in the last decade with growth averaging at 10.6% per year from
2004-2012 compared to the regional average of 4.9%. Yet, despite this Ethiopia has been characterised as one of the
world’s poorest countries, ranking 169 out of 179 on the UNDP Human Development Index as well as an average per
capita income of $410 which is substantially lower than the regional average.3 Ethiopia remains one of the least
urbanized countries in the world with the vast majority of the population based in rural areas, which was estimated at
83.7% in 2006 whereas around 16.3% lived in urban areas during the same period (World Development Indicators,
2008). In addition, the life expectancy of Ethiopia was estimated at 63 in 2012 which is relatively high for the region
(United Nations Population Division, World Population Prospects, 2012).
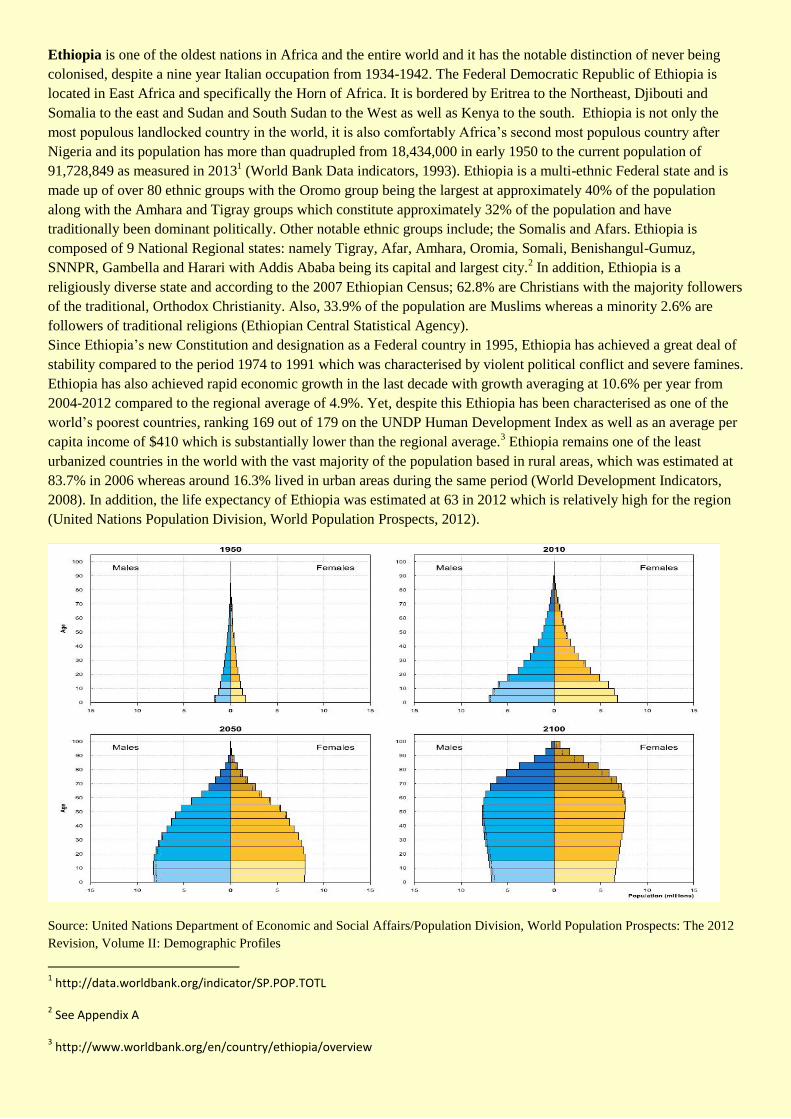
Source: United Nations Department of Economic and Social Affairs/Population Division, World Population Prospects: The 2012
Revision, Volume II: Demographic Profiles
1 http://data.worldbank.org/indicator/SP.POP.TOTL
2 See Appendix A
3 http://www.worldbank.org/en/country/ethiopia/overview
Population background:
Ethiopia was selected as a case study due to its intriguing demographic trends, whereby it has achieved
tangible successes in reducing mortality rates but slower progress in regards to stubbornly high fertility rates.
Ethiopia’s demographic challenge is not the substantial size of its population, but rather the rapid and
imbalanced distribution of population growth which it is experiencing. In fact the population trajectory of
Ethiopia as highlighted by its 2000 and 2005 Demography and Health Surveys (DHS) reveals a country in
the early stages of a demographic transition if it can replicate its mortality rate reductions to fertility rates.
Success in such interventions will enable Ethiopia to benefit from a potential “Demographic Dividend”
which refers to the accelerated economic growth that may result from reductions in fertility and mortality
rates which leads to a change in the age structure of the population. With fewer births each year, a country's
young dependent population grows smaller in relation to the working-age population. With the dependency
ratio being reduced; a country has a window of opportunity for rapid economic growth providing that sound
policies are adopted.
It is important to note that Ethiopia’s 1984 Census had hitherto been the first Census conducted in the
country. Based on this 1984 Census data, population growth was estimated at about 2.3 percent for the 1960-
70 period, 2.5 percent for the 1970-80 period, and 2.8 percent for the 1980-85 period (Ethiopian Central
Statistical Authority). In 2008 the population growth rate was 3.21%, which was the 11th
highest in the
world according to the CIA World Factbook. Throughout our demographic report of Ethiopia it is crucial to
note that for some indicators data is not available for the period prior to the 1980s and early 1990s due to a
combination of factors such as; political conflict, regime change etc. Yet, population projections compiled in
1988 by the Ethiopian Central Statistical Authority (CSA) projected a 2.83 percent growth rate for 1985-90
and a 2.96 percent growth rate for 1990-95. Estimated annual growth for 1995-2000 varied from 3.03
percent to 3.16 percent. Population estimates ranged from 67.4 million to 67.8 million by the year 2000. The
CSA projected that Ethiopia's population could range from 104 million to 115 million by the year 2015
which it is currently on track to meet. Ethiopia is only just now benefitting from the Demographic Dividend
whereby there will be a larger share of working age citizens amongst the population, thereby providing a
potential economic stimulus. For example; the average age of a citizen is 16.8 years and specifically 16.5
years for males and 17.1 years for females (CIA World Fact book 2011). Estimates have found that 45% of
the population in Ethiopia is under the age of 15.4 According to population projections, Ethiopia’s
population is expected to rise significantly to 125 million in 2025, 188 million in 2050 and a 244 million in
2100 (United Nations, Department of Economic and Social Affairs - Population Division, 2012).
4 http://www.healthpolicyinitiative.com/Publications/Documents/1332_1_Ethiopia_RAPID_Booklet_FINAL.pdf
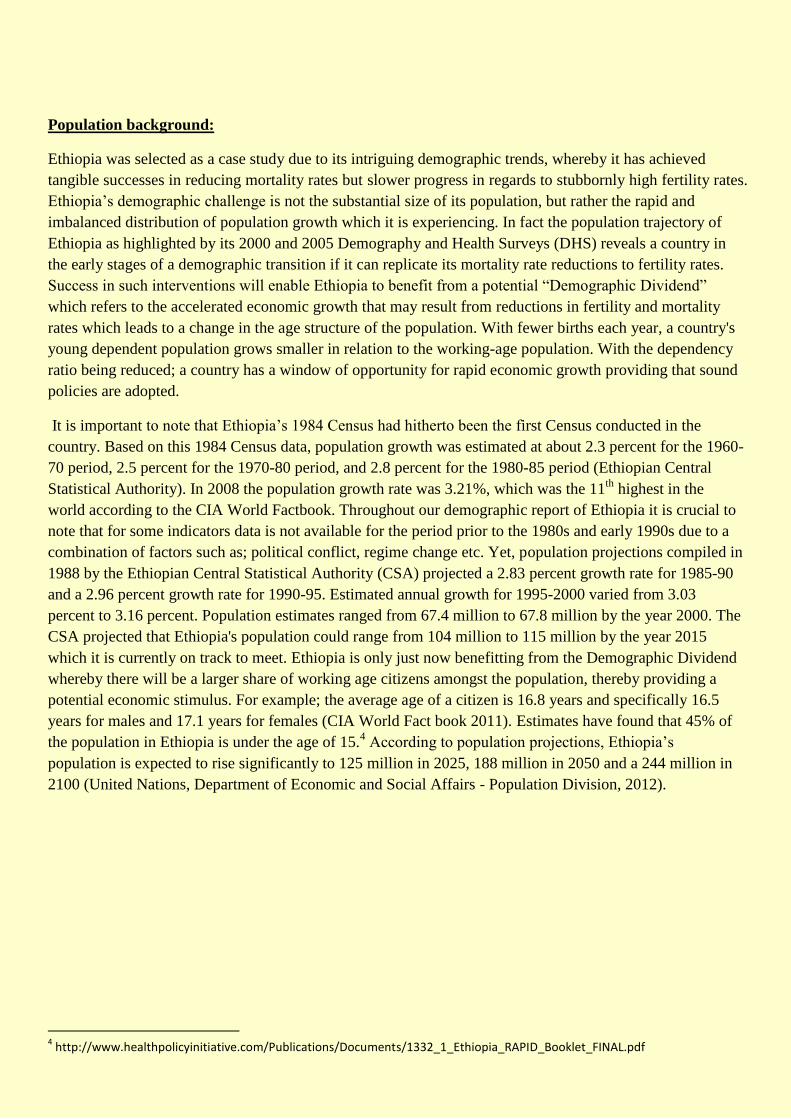
Source: World Development Indicators, July 2013 Source: World Development Indicators, July 2013
Fertility:
Interestingly, in the past couple of decades (particularly since the emergence of Ethiopia as a Federal state)
Fertility rates have declined gradually. In the period from 1950 – 1960 Ethiopia’s Total Fertility Rate was at
a very considerable 7.1 children per woman; this then dropped to 6.9 children per woman during the 1960s
and stood at 6.7 during the 1980s. Interestingly, the TFR then increased during the 1980s whereby it reached
7.0 again, yet this had again dropped by the 1990s to 6.4 (United Nations Population Division). The Total
Fertility Rate (TFR) in Ethiopia declined substantially to 5.7 children per woman in 2005 (DHS 2005, WB).
This interpretation of the TFR of Ethiopia was derived specifically from the 1984 and 1994 Censuses along
with the National Fertility Sample (NFS) Survey 1990 and Demographic and Health Survey (DHS) 2000 &
2005. However, according to current estimates of the TFR it stood at 4.6 in 2012 which is just below the
current 4.9 Sub Saharan African average (United Nations Population Division, World Population Prospects,
2012). It is important to note that it was only in the capital, Addis Ababa that the TFR had fallen below the
replacement level of 1.4 births per woman (Ethiopia, DHS, 2005). Therefore, it is important to make a
distinction between the TFR for urban areas as compared to the TFR for rural areas as there has always been
a gulf between the two from the 1950s to the present day. The urban TFR is 3.3 children per woman,
whereas the rural TFR is almost double at 6.4 children per woman (WB, p56). Indeed, there have been
various factors to explain this; namely; due to a lack of knowledge of family planning amongst rural levels
as well as the low educational levels of rural mothers, which economists have shown to impact on fertility
rates. This is especially important considering that over 80% of Ethiopia’s population live in rural areas and
thus explains the persistent population growth. In addition, studies have found that there are regional and
religious differences in terms of the TFR. For example, the TFR was higher amongst Muslims with no
education than among Christians with no education (7.7 compared with 6.1) in the largest region, Oromia 5
5 http://www.prb.org/Publications/Articles/2009/ethiopiamuslimdemographics.aspx
Furthermore, the current Crude Birth Rate (CBR) in Ethiopia is measured at 33.3 and has proved to be quite
significant when discussing Ethiopia’s demographic situation in the past 60 years. In the 1950s the CBR was
estimated to be 49.3 which then underwent a gradual decline to 48.3 during the 1980s and 45.4 during the
1990s as well as 41.3 between 2005 and 2010 (United Nations Department of Economics and Social Affairs
& Population Division, World Population Prospects: the 2012 Revision, Volume 2: Demographic Profiles).
The combined gradual declines in the TFR and CBR in Ethiopia have both coupled together to ensure that
Ethiopia is currently experiencing a gradual decline in fertility levels and is entering a potential
Demographic Dividend.
Marriage patterns/Education amongst women:
Marriage patterns in Ethiopia have changed significantly which has gradually led to a decrease in the
fertility levels. Statistics have markedly shown that women in Ethiopia are repeatedly delaying marriage
whereas in the past girls tended to marry at an extremely early age. This lower share of married women at
childbearing age can be felt in Ethiopia whereby the never married rate for women has increased to 27% in
the past two decades which is considerable for such a conservative nation. Also, the percentage of women
who were first married by age 15 has declined from 39% among women aged 45-49 to 8% amongst women
aged 15-19 (Ethiopia DHS, 2011, p61). This decline in early marriages is important for specific reasons,
namely, due to the fact that the most fertile age group are consistently delaying marriage which will push
down the TFR. Also, Ethiopia is a deeply conservative country with strong Christian communities as well as
Muslim communities and despite a decline in marriage; women are marginalised for having children out of
wedlock thus meaning the desire to postpone marriage has also coincided with women deciding not to have
children at the time. Indeed, it can be argued that this rapid decline in the proportion of women married has
been a crucial driver of such a fertility decline in Ethiopia and especially within its urban centres, principally,
Addis Ababa. In the capital a staggering 80% or more of the decline in fertility rates from 1990-2000 can be
attributed to the decline in the proportion of women married. Sibanda et al, (2003) found that the first two
factors driving this recent evolution – later age at first marriage and more women in their 20s and 30s
remaining single, while the dissolution of marriages had not fundamentally changed.
In Ethiopia, uneducated mothers tended to have twice as many children as women with at least a secondary
education. As a result when observing the changes in fertility patterns it is no surprise to see that during the
1950s to the 1980s more women tended to be uneducated and thus this provided upward pressures on the
fertility rates. For example, amongst the oldest age group (40 – 49) an overwhelming 95% of women have
no education. In particular, Ethiopia has significantly increased its female Labour force participation (ages
15-24) which was 74.40 as of 2011 and reached its peak of 76.20 in 2005.6 This is a considerable rise from
the 37% recorded in 1978. However, there is scope for improvement as there is still an imbalance between
education levels and labour participation rates in urban and rural areas with the latter lagging behind
significantly.
Contraception/family planning programmes:
Since the mid-1990s Ethiopia’s Federal government has attentively pursued family planning policies which
have made tangible gains. Ethiopia’s policies have in the past 11 years significantly increased access to
family planning and forms of contraception for its citizens. This is especially significant as Ethiopia has
historically had a very low level of contraceptive use. For example, according to the first ever national
6 http://www.indexmundi.com/facts/ethiopia/labor-participation-rate
survey on fertility and family planning in 1990; only 4% of women in their reproductive years were using
any family planning method at the time (Central Statistical Authority, 1993). Yet, in 2000 Ethiopia had a
modern Contraceptive Prevalence Rate (CPR) for women (of all ages) of less than 5%, however, in 11 years
that figure had increased significantly to around 20%. Moreover, according to the Minister of Health of the
Federal Democratic Republic of Ethiopia; Dr Keseteberhan Adamsu; “in 1991, just 3% of women in
Ethiopia were using modern contraception. By 2011, this has risen to 29% and recent surveys have shown
that this is expected to rise to 39%”.7 Ethiopia’s demographic situation is unique in that the rate of decline in
fertility rates is lower than might otherwise have been predicted given the substantial increase in the usage
of contraception.
However, Ethiopia’s fertility level declines have not been as significant as the mortality rate declines which
can be attributed to factors such as the substantial “unmet demand” for contraception in rural Ethiopia. This
unmet need refers to the difference between the total demand and the actual use of contraception. Statistics
show that while the CPR among married, urban women is 47%, it remains low and only 11% in rural areas.
There is also an income gulf whereby the DHS 2005 shows differentials between the rich and poor with 37%
of the former and only 4% of the latter using any method of contraception. Ethiopia’s Ministry of Health has
identified this inconsistency and is now focusing its family planning policies in rural areas with the aim to
tackle this unmet need which is highest amongst poor, rural women.
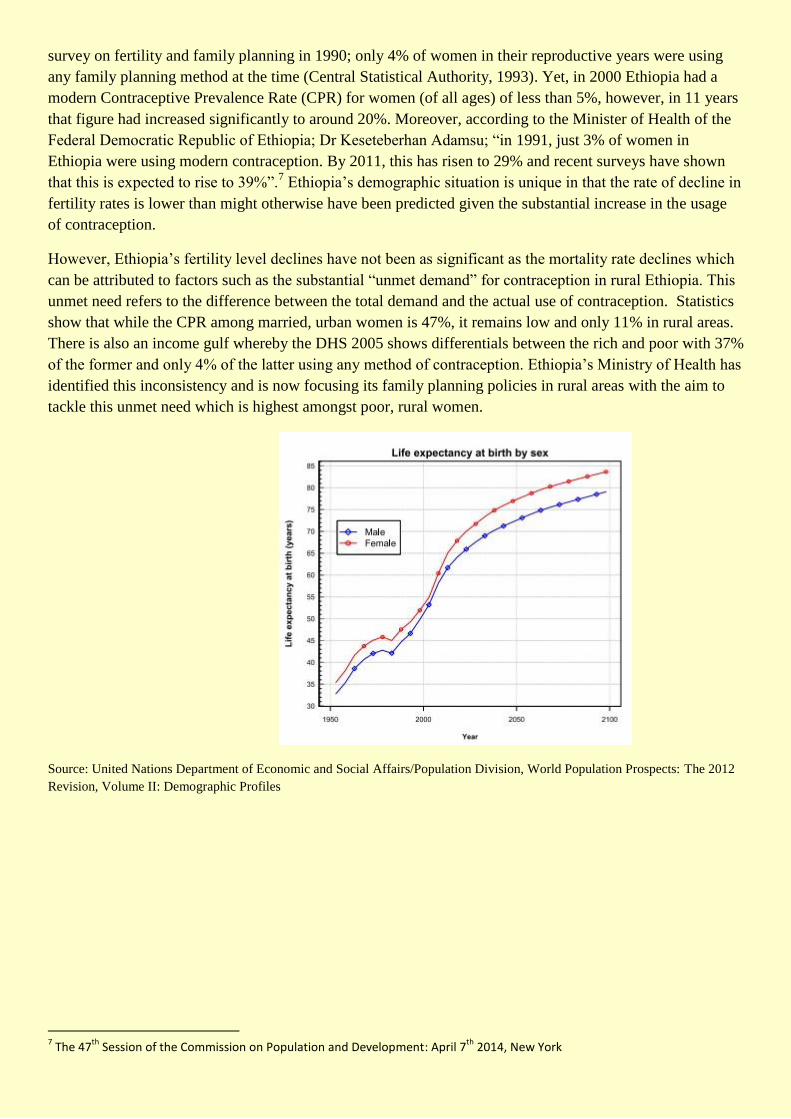
Source: United Nations Department of Economic and Social Affairs/Population Division, World Population Prospects: The 2012
Revision, Volume II: Demographic Profiles
7 The 47
th Session of the Commission on Population and Development: April 7
th 2014, New York
Mortality:
Ethiopia has experienced greater success in reducing mortality rates compared to fertility rates and at the
same time greatly improving life expectancy rates. Ethiopia’s improvement in combating previously high
mortality rates has resulted in life expectancy within Ethiopia rising to 63 in 2012 which is relatively high
for the region (United Nations Population Division, World Population Prospects, 2012). Historically,
Ethiopia’s life expectancy at birth was higher for females compared to males and this is the case today.
Interestingly, according to future projections the gap will only increase meaning that by 2050 the female life
expectancy rate will be a full 5 years higher than the male rate. This in turn will have considerable
demographic repercussions most notably for Ethiopia’s labour markets which will need to successfully
integrate women and increase their labour participation rates exponentially throughout.
According to the Ethiopian DHS (2000) 1 in 6 Ethiopians were under the age of 5 and this combined with
historically high infant and child mortality rates conveys how annual deaths are concentrated amongst
children under5. When one also takes into account the fact that 47% of Ethiopia’s current population is
under-15 it is clear to see that in the past 60 years, infant and child mortality rates contributed substantially
to the overall Crude Death Rate (CDR). Indeed, mortality rates in Ethiopia have been reduced over the past
50 years with the greatest gains in reduction made in regards to infant and child mortality rates. According
to Ethiopia’s DHS (2005) the infant mortality rate declined from 199 in 1950 to around 77 in 2005. Also,
crucially the under-five child mortality rates declined from 216 in 1984 (Ethiopia Central Statistical
Authority, 1984) to 123 (DHS, 2005). Recent data from the DHS (2011) has shown that Ethiopia’s
continued decline in mortality rates has been maintained with infant mortality being reduced by 42% from
the period 1995-2011 and likewise under-5 mortality has declined by 47% over the same period. As a result
the CDR of Ethiopia has also declined from about 30 per 1000 people in 1955 to an estimated 15 in 2005
(United Nations, 2006). As mentioned the major factor behind this rapid decline in the CDR is the
aforementioned decline in the infant and under-5 child mortality rates.
Government policies:
These relative advances made by Ethiopia in combating high infant & child mortality rates is due to the
robust Health Ministry decentralising its service delivery and enacting policies to overcome such high
mortality rates. Since the early 1990s Ethiopia has sought to aggressively pursue the Millennium
Development Goal (MDG 4) to reduce infant/child mortality. The Ethiopian Federal government has since
then put healthcare at the heart of its policies and namely combating the excessively high infant and child
mortality rates. Such has been its success that Ethiopia had by 2012 met its MDG 4 of reducing infant and
child mortality by two-thirds, which was three years ahead of schedule. Ethiopia was able to do this by
tackling the major communicable and preventable diseases which had caused the greatest infant and child
deaths such as; malaria, measles, polio and tuberculosis. Indeed, infant immunization rates for the major
vaccine-preventable diseases stood at a paltry 28% in the late 1990s and early 2000s according to UNICEF.
However, UNICEF had recorded an exponential rise to the current immunisation rates of around 80-90 per
cent in 2012. In addition, other government policies which have contributed to the reduced infant and child
mortality rates include improved early care treatment. In addition, the Health Ministry was able to do this
through hiring 38,000 health extension workers to provide direct care for children and women. Another
policy consisted of recruiting a “Health Development Army” of three million female volunteers, each
assigned to rural neighbourhood families, to encourage healthy behaviour, including infant immunization
(Dr Keseteberhan Adamsu, 2014).8
8 Minister of Health of the Federal Democratic Republic of Ethiopia; Dr Keseteberhan Adamsu - The 47th Session of the
Commission on Population and Development: April 7th 2014, New York
Changing marriage patterns and increased female education:
Another factor to explain mortality rate reductions can be linked to changing marriage patterns amongst
women as well as the improved status of women in Ethiopia. As we touched on earlier and the the EDHS
(2011) conveyed women are increasingly postponing marriage in recent decades. This is crucial as early
marriages are directly attributed to high infant and child mortality rates. For example, in 2000 infants born to
mothers aged 15-19 had a 32.3% higher mortality rate than those born to mothers aged 35 or over (EDHS,
2000). Furthermore, the contribution of higher levels of education was apparent amongst infants whose
mothers had secondary education or above who experienced the lowest mortality whereas infants who had
mothers with no primary education were 3 times more likely to die. (EDHS, 2000). Both factors, delayed
marriage age and increased female education contribute to child survival rates through women having fewer
children, utilizing prenatal care and as a result these women being more likely to immunize their children. A
final factor to explain the increased fall in the CDR can be linked to the robust economic growth levels that
Ethiopia has been experiencing for the past decade along with the proliferation of health related NGOs all
across Ethiopia since the 1990s. Such increased economic growth has led to greater female labour
participation rates.
Main causes of mortality:
As discussed, the main determinant of mortality rates throughout Ethiopia’s historical demographic situation
has been concentrated amongst the infant and child categories with the main cause being communicable
diseases such as malaria, pneumonia along with preventable deaths such as; acute malnutrition.
Socioeconomic factors contribute substantially to childhood mortality rates and as the table below conveys
there are mortality rate differences in terms of the educational level of the mother, regional differences as
well as household incomes. This is not a revelation considering that around 90% of mothers had not
completed primary education in the early 1990s (EDHS, 2000). The literature shows that even a modest
increase in female education, particularly within rural areas, had significant payoffs in improving child
health and survival rates. This in part explains why urban areas have succeeded in reducing their infant
mortality rates by a much greater amount. In addition, within rural areas in particular, infant and child
survival rates would benefit from the postponement of early motherhood. Another study found that infants
born to women under the age of 20 have a 40% higher chance of dying before their first birthday (Mekonnen
and Yimer, 2005). Access to clean water is another extremely important determinant of child mortality and
is sharply differentiated between rural and urban households. Rural households (around 38% in the EDHS,
2000) tend to rely on surface and rain water which is inherently more risky than piped water.
Rural and urban differentials in mortality rates:
Ethiopia’s mortality rate in terms of urban and rural differences is similar to its fertility levels. This can be
attributed to the fact that rural areas tend to have lower levels of educational attainment (amongst mothers)
and an early marriage age which are both contributors to higher levels of infant mortality. Indeed, with its
mosaic of different ethnic groups and religions there are distinctive differences in mortality rates. In the rural
sample group, ceteris paribus, being Muslim increased the probability of premature death by 5% relative to
being Protestant (EDHS, 2005). In addition, such mortality differences are also reflected in regional
variations amongst under-5 mortality rates. For example, children aged under-5 living in the rural Somali
region have an 8% higher probability of dying when compared to children in rural Gambella (EDHS, 2005).
Maternal Mortality Rates:
Ethiopia also has one of the highest rates of maternal mortality in Africa and the wider world as the rate
currently stands at 673 per 100,000 live births in 2005 (DHS, 2005). This can be attributed to the low levels
of antenatal care as well as birth attendance by healthcare professionals in Ethiopia, especially within rural,
poor areas. A major factor is the lack of qualified health professionals in the attendance of births which is
only 10% and also access to emergency obstetrical care is still limited. Also, in Ethiopia and particularly
rural areas; violence against women and harmful traditional practices (female genital mutilations, early
marriage, etc.) are prevalent, and are among the main factors that contribute to such a high maternal
mortality rate (World Health Organization, May 2013). According to the WHO it is estimated that more than
half of the population lives more than 10km away from the nearest health facility, usually in rural regions
with poor transportation infrastructure. Another key factor accounting for such unsustainably high levels of
maternal mortality rates is the early marriage patterns amongst girls as well as the young age of women
giving birth for the first time. Amongst women aged 20-35 maternal deaths at birth account for 30% of all
female adult deaths. Yet, it is important to note that “their expected declines following efforts to reach the
MDGs are unlikely to substantially affect the CDR or population growth given the limited contribution of
adult death to the current CDR” (World Bank 2007). When analysing Ethiopia’s historical mortality rates
one can see that the CDR spiked in the 1980s along with a fall in the life expectancy during the same period.
This can be attributed to the devastating 1984 famines that struck Ethiopia and gained worldwide notoriety
with around 1 million perishing.
Migration trends in Ethiopia:
Ethiopia is one of the world’s oldest states and has therefore experienced fluctuations in migration flows
throughout its history. However, according the pronounced movements of Ethiopians only became
significantly greater during the late 1960s and throughout the 1970s (Berhanu, Kassahun, Seid and Zekarias,
2004). Due to its strategic location in the Horn of Africa, one of the most volatile regions in the world,
Ethiopia has been prone to the various migratory patterns of the region.
Political conflict and migration:
The period between 1950 and 1974 can be marked as a relatively peaceful period of Ethiopia as the ruling
Emperor Haile Sellaise maintained power and the succession of emperors stretching back 2000 years.
However, it was only with his violent overthrow by the brutal Derg regime in 1974 that Ethiopia witnessed a
sustained period of political violence that would continue unabated until the early 1990s. It is no surprise
that this period of political violence coincided with a major increase in external emigration patterns with the
number of external refugees from Ethiopia increasing from 55,000 in 1972 to over 1 million in 1992
(Berhanu, Kassahun, Seid and Zekarias, 2004). During this period (1974-1992) most of the external
migrants who fled from Ethiopia were doing so as refugees escaping political conflict and repression as well
as devastating famines. There were various factors and often actions of the Ethiopian government that led to
increased external migration patterns. In particular, the Derg regime up until its fall in 1991 directly
increased refugee flows by persecuting specific ethnic groups and regions. Most notably, in the North an
ongoing war with Eritrea rebels led to the deaths of over 300,000 and a substantial rise in refugees fleeing to
neighbouring countries such as; Sudan. Another major conflict was the 1977-78 Ethiopian-Somali war over
the Somali region of Ethiopia. The fallout from the war was substantial as it led to massive external refugee
flows from 1978 to the early 1980s (Bariagaber, 1997). A UN survey estimated the number of Ethiopian
refugees who fled to Somalia as numbering around; 450,000 to 620,000. The United States Catholic Relief
Services (USCRS), however, estimated that by the 1990s about 410,000 refugees had returned to Ethiopia,
leaving about 430,000 in Somali refugee camps.
In addition, during the 1980s the Horn of Africa region became the largest refugee producing area in the
world, with Ethiopia being the largest contributor to refugee flows (Bariagaber, 1999). It is important to
remember that since the early 1990s the internal migration flows from neighbouring countries was more
substantial than Ethiopia’s own external flows. During the 1980s, according to the UN there was an
estimated 2.5 million refugees in East Africa and the majority of these refugees fled to Ethiopia thereby
impacting on the Net Migration Rate. Refugees came from a plethora of neighbouring countries and
included people fleeing conflicts in southern Sudan and northern Somalia, with the latter war leading to
hundreds of thousands of Somali fleeing to Ethiopia.
In addition, famine was a major factor in historical migration trends in Ethiopia and a major driver in
Ethiopia’s Net Migration Rate. Ethiopia’s economy is disproportionately dependent on agriculture with 80%
of the population employed in agriculture as well as it contributing to 46% of the country’s GDP. Also,
because only 1% of arable land is irrigated, therefore; droughts have a devastating effect on the economy as
witnessed during Ethiopia’s various famines (Financial Standards Forum, 2009). The earlier famines
includes; the 1964-65 famine and in 1973-74 a larger famine, also caused by low rainfall, affecting the
whole country negatively. According to Ezra and Kiros (2001) this led to people responding to these
ecological changes by moving from relatively dense population and low economic opportunity areas to areas
of less density and greater opportunity. The 1984-85 Famine proved to be especially fatal for Ethiopia’s
population and it mainly affected four Ethiopian provinces—Gojjam, Hararghe, Tigray, and Wollo as they
all received record low rainfalls in those years. Figures based on UN estimates have claimed that around 1
million people died during the famine making it easily one of the worst famines in recent memory. However,
scholars such as; De Waal (a known expert on famine) have contested these figures. Pertinent to our
demographic overview; the 1984-85 famine also contributed significantly to Ethiopia's refugee crises. The
1984-85 famine resulted in the death or displacement of hundreds of thousands of people within Ethiopia
and forced a further 100,000 to flee Somalia, 10,000 into Djibouti and more than 300,000 into Sudan.
Moreover, brutal “Resettlement” policies implemented by Ethiopia’s government served to exacerbate the
refugee crisis apparent in Ethiopia. In particular, according to De Waal (1991) the brutal “Villagization”
policy was a disaster and killed a minimum of around 50,000 and led to mass external and internal migration.
In addition, the famine caused increased rural-urban migration as “the rapid rate of urbanization was
primarily caused by poor, rural living conditions and persistent famine, forcing rural populations to migrate
to cities in search of alternative livelihoods” (Van Dijk and Fransen, 2008).
Current Migration Status
Finally when discussing Ethiopia’s migration patterns it is also important to take into account economic
factors which have played a major role in current migration patterns. Since the adoption of Ethiopia’s
Constitution in 1995 and the subsequent, relative peace, economic factors have played a major role in
driving external migration patterns. Despite its rapid economic growth in recent years; Ethiopia is still one
of poorest countries in the world, with a low per capita income and as a result since the 1990s many of its
inhabitants have consistently sought better economic opportunities abroad. According to the World Bank
Data Division; Ethiopia’s Net Migration Rate (as of 2012) was -60,001 meaning more of its citizens are still
leaving Ethiopia despite the absence of political violence or famines. It is for this reason that the Ethiopian
diaspora is one of the largest in Africa with significant communities in North America, the United Kingdom
and the Middle East. This has served to have a positive economic effect as these diaspora communities send
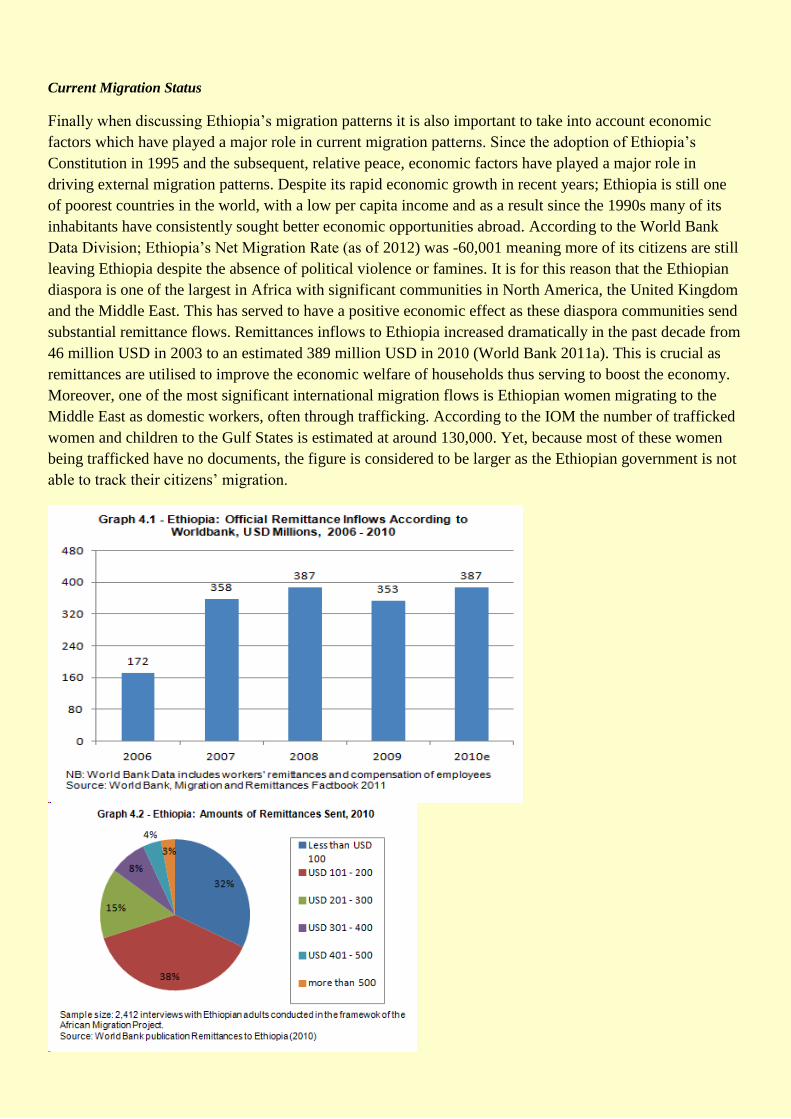
substantial remittance flows. Remittances inflows to Ethiopia increased dramatically in the past decade from
46 million USD in 2003 to an estimated 389 million USD in 2010 (World Bank 2011a). This is crucial as
remittances are utilised to improve the economic welfare of households thus serving to boost the economy.
Moreover, one of the most significant international migration flows is Ethiopian women migrating to the
Middle East as domestic workers, often through trafficking. According to the IOM the number of trafficked
women and children to the Gulf States is estimated at around 130,000. Yet, because most of these women
being trafficked have no documents, the figure is considered to be larger as the Ethiopian government is not
able to track their citizens’ migration.
In addition, when applying economic factors to Ethiopia’s internal migration patterns and specifically rural-
urban; one can observe that increasing numbers of citizens have moved to major urban centres such as;
Addis Ababa to improve their economic prospects. Berhanu and White (1998) reported an increase in the
rural-urban migration of women between 1960 and 1989.Indeed, statistics have shown that urbanisation in
Ethiopia has increased by a substantial 17% of the total population since the 1960s to 2011 (CIA Factbook,
2011). Also, according to the CIA Factbook (2011) the rate of urbanization in Ethiopia is undergoing a
3.57% annual rate of change. At the same time rural-to-rural migration is increasingly occurring in Ethiopia
as a response to poor agricultural conditions. The 1998 Migration, Gender and Health Survey had been
conducted in 5 regions of Ethiopia to gain an understanding of the impact of internal migration in Ethiopia.
These results conveyed that there were increasingly high levels of internal and rural-to-rural migration in
Ethiopia with inhabitants using this as survival strategy.
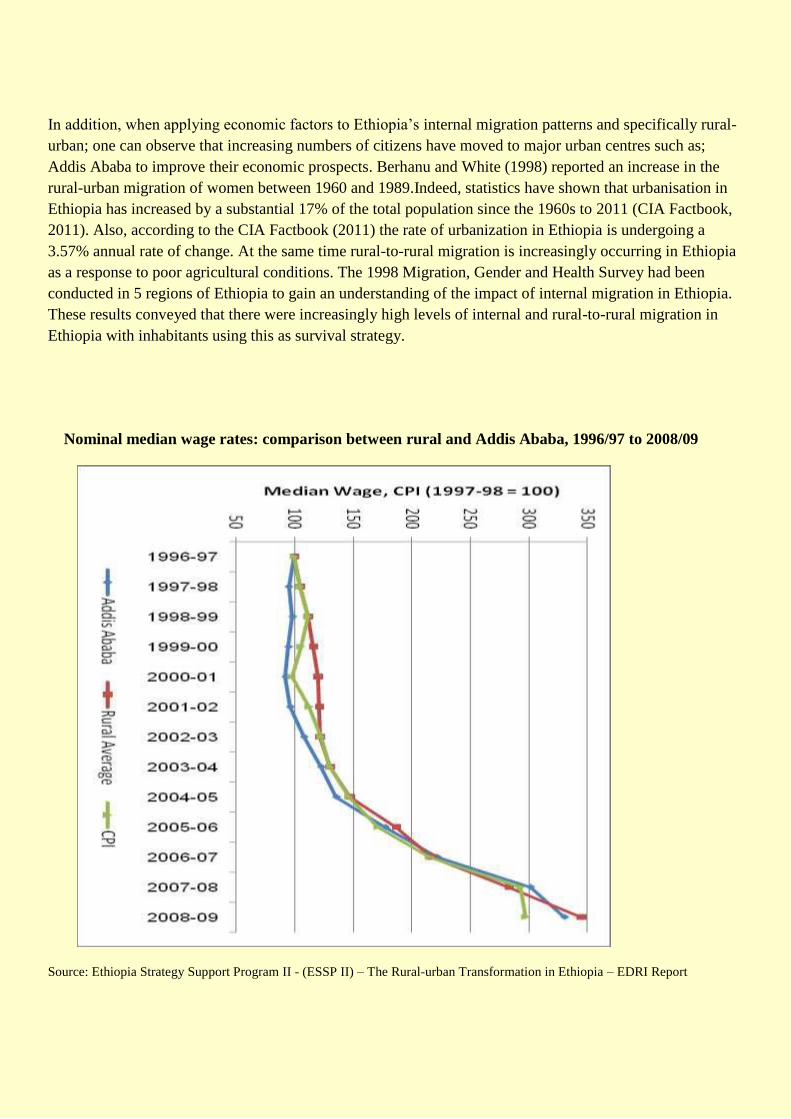
Nominal median wage rates: comparison between rural and Addis Ababa, 1996/97 to 2008/09
Source: Ethiopia Strategy Support Program II - (ESSP II) – The Rural-urban Transformation in Ethiopia – EDRI Report
Projected Fertility, Mortality and Migration trends with Policy recommendations:
With such a significant population and the Total Fertility Rate in Ethiopia still relatively high, it is estimated
that; Ethiopia’s population is expected to rise significantly to 188 million in 2050 and a 244 million in 2100.
Combined with the gains in reducing mortality rates and Crude Death Rates, Ethiopia will be experiencing a
“Youth Bulge” whereby a large proportion of the population will be made up of children and young adults.
Indeed, this presents the government with a double edged sword scenario whereby it could be the source of
economic prosperity or the source of instability in the coming decades. Therefore, it is paramount that the
Federal Government institute policies to benefit from this demographic window of opportunity. Their
policies should focus on decentralising economic opportunities to rural areas and providing increased
employment and education opportunities for these new generations of Ethiopians.
In addition, Ethiopia is suffering from a “Brain Dain” whereby many of the recent emigrants of the past two
decades are the most skilled including doctors and other professions. This has been exacerbated by the
failure of rapid economic growth to translate into genuine job creation. As a result it is crucial for the
government to utilise policies to overcome the high youth unemployment which is over 50% and
considerable as this represents 90 million people. By tackling these economic issues the government will be
able to stem the external migration of its most skilled whilst also limiting the substantial rural to urban
migration which is placing pressures on the state and economy.
Bibliography:
Ethiopia - Capturing the Demographic Bonus in Ethiopia: Gender, Development, and Demographic Actions
World Bank (2007) - Poverty Reduction and Economic Management 2, Country Department for Ethiopia
Ethiopia Demographic and Health Survey – 2011, Central Statistical Agency, Addis Ababa, Ethiopia -
http://dhsprogram.com/pubs/pdf/FR255/FR255.pdf
Ethiopia Demographic and Health Survey – 2005, Central Statistical Agency, Addis Ababa, Ethiopia
Ethiopia – World Bank Development Indicators - http://data.worldbank.org/country/ethiopia
Ethiopia Demographic and Health Survey – 2000, Central Statistical Agency, Addis Ababa, Ethiopia
Migration in Ethiopia: History, Current Trends and Future Prospects – Paper Series: Migration &
Development Country Profiles by Sonja Fransen and Katie Kuschminder, December 2009, Maastricht
Graduate School of Governance
Ethiopia Central Statistical Agency – 1984 CENSUS
DEMOGRAPHIC DATA FOR DEVELOPMENT ETHIOPIA - By: Yared Mekonnen & Population Council
CIA World Factbook for Ethiopia, 2011- http://cia-world-fact-book.findthedata.org/l/334/Ethiopia
Ethiopia Economic Outlook - http://www.afdb.org/countries/east-africa/ethiopia/ethiopia-economic-outlook/
IN-DEPTH STUDIES FROM THE 1994 POPULATION AND HOUSING CENSUS IN ETHIOPIA -
Central Statistical Authority (CSA) Addis Ababa, Ethiopia - Institute for Population Research – National
Research Council, Roma, Italy
Minister of Health of the Federal Democratic Republic of Ethiopia; Dr Keseteberhan Adamsu, Keynote
Address - The 47th Session of the Commission on Population and Development: April 7th 2014, New York
https://www.princeton.edu/~achaney/tmve/wiki100k/docs/Demographics_of_Ethiopia.html

APPENDICES
Figure 1: Regional Map of Ethiopia – Source: Wikipedia Commons





























