Embed Size (px)
Citation preview

An international publication dealing with medicolegal issues. Articles, court decisions, and legislation on:Medical law, forensic medicine, sexology and law, psychiatry and law, psychology and law, dentistry and law, nursing law, pharmaceutical law, medical ethics, clinical criminology, drugs, alcohol, child abuse, medical experimentation, genetic engineering, organ transplantation, abortion, contraception, sterilization, euthanasia, religion, AIDS, etc.
© PROBOOK 2013
Manuscripts should be submitted to the Editorial Office:The International Center for Health, Law and Ethics, University of Haifa, Haifa 31905, IsraelE-Mail: [email protected]
Founder and Editor-in-Chief (1980-2010): Prof. Amnon CarmiEditor-in-Chief: Dr. Mohammed S. WattadEditor’s Executive Assistant: Ava Van DamEnglish Editor: Dorothy Fajans, Yehuda Levy, LL.B.Layout: Ayala GordonIndexing: Natali Goldring
Editorial BoardAbu Ramadan, Dr. MoussaAdlan, Dr. Abdallah Aguiar-Guevara, Prof. RafaelBeran, Dr. RoyBerger, Dr. KenBeyleveld, Prof. DeryckBlum, Prof. JohnCook, Prof. RebeccaCotler, Prof. MiriamDantas, Prof. Eduardoden Exter, Dr. AndreDickens, Prof. BernardDoron, Dr. IsraelDubinsky, Dr. Isser
Subscription Information:Volume 32: 4 issues will appear in 2013Worldwide annual subscription rate: US$ 180.00Single Copies: US$ 50.00Index 1982-1991 available: US$ 45.00Rates are inclusive of delivery by Surface Airmail Lifted (SAL) service.Full airmail delivery supplementary cost available on request.Place subscriptions with a recognized bookseller or directly with:PROBOOK Ltd., P.O.Box 56055, Tel Aviv 61560, ISRAELTEL: 972-3-5257999 FAX: 972-3-5285397 E-MAIL: [email protected]
Change of address: Send mailing label from a recent issue with full new address, including Zip/Postal Code. Allow six weeks for changes to become effective.Back numbers are still available. Prices available on request.Advertisment inquiries: PROBOOK Ltd., P.O.Box 56055, Tel Aviv 61560, Israel [email protected]
DuMont, Prof. JaniceDute, Prof. JosephEfron, Adv. YaelFerris, Prof. LorraineFimate, Prof. LallukhumFrenkel, Prof. DavidGevers, Prof. SjefHrevtsova, Dr. RadmilaKassim, Dr. Puteri N. J.Kegley, Prof. JacquelynKhalaila, Dr. RabeiLe Blang, Prof. TheodoreLevy, Ms. SharonLupton, Prof. Michael
Martens, Dr. WillemMester, Prof. RobertoNissim, Dr. Sara Noguchi, Prof. ThomasPiga, Prof. AntonioRudnick Dr. AbrahamShalata, Dr. AbedSlovenko, Prof. RalphStrous, Prof. RaelTabak, Prof. NiliTalib, Prof. NorchayaVan Wyk, Prof. ChristaWolfman, Dr. SamuelZaremski, Mr. Miles
WORLD ASSOCIATION FOR MEDICAL LAWBoard of Governors
President
Prof. Thomas T. Noguchi (United States)
Vice PresidentsBerna Arda (Turkey) Kenneth Berger (Canada) Eduardo Dantas (Brazil) Muh Nasser (Indonesia)Chongqi Wu (China)
Executive CommitteeOren Asman (Israel) Roy G. Beran (Australia)Thomas T. Noguchi (United States)Andre G. Dias Pereira (Portugal)
Executive Vice PresidentOren Asman (Israel)
Secretary GeneralRoy G. Beran (Australia)
TreasurerAndre G. Dias Pereira (Portugal)
Board of GovernorsBerna Arda (Turkey) Oren Asman (Israel) Roy G. Beran (Australia)Kenneth Berger (Canada)David Collins (New Zealand)Eduardo Dantas (Brazil)Sanjin Dekovic (Bosnia and Herzegovina)Anne-Marie Duguet (France)Terhi Hermanson (Finland)Radmyla Hrevtsova (Ukraine)
Mitsuyasu Kurosu (Japan)Natalia Lojko (Poland)Vugar Mammadov (Azerbaijan)Muh Nasser (Indonesia)Thomas T. Noguchi (United States)Herman Nys (Belgium)Andre G. Dias Pereira (Portugal)Yuriy Sergeyev (Russian Federation)Chongqi Wu (China)
R. Dierkens WAML Medalion (2002)Hon Secretary General and Founder (2004)
Koichi BaiWAML Medalion (2006)
Arthur LewisHonorary Governor (2004)
Sonderland Honorary Governor (2004)
Members of HonorAntonio PigaHonorary Governor (2006)
Jose Pinto De CostaHonorary Governor (2006)
Amnon Carmi Honorary President (2010)
Bernard DickensHonorary Vice President (2010)

Ethics: Submission of a manuscript for publication in this Journal confirms that all standard ethics procedures were conducted; such as but not restricted to, voluntary informed consent of research participants when applicable and approval of the responsible Research Ethics Board(s).
I
List of Contents
VOLUME 32 NUMBER 4
IIIEduardo DantasEditorialBrief Words from the Guest Editor
429Helena PeterkováPreviously Expressed Wishes in the Czech Republic - A Missed Chance of the Czech Legislator
441Nicole Marie Saitta and Samuel D. Hodge, Jr.What Are the Consequences of Disregarding a “Do Not Resuscitate Directive” in the United States?
459Eduardo DantasAdvanced Directives and Living Wills - The Role of Patient’s Autonomy in the Brazilian Experience
481Carla A. Arena Ventura et alRethinking Ethical and Legal Issues at the End of Life in the UK and Brazil: A Role for Solidarity?
497André Dias PereiraLiving Will and Health Care Proxy - The Portuguese Legal Situation
503Shane CampbellTitle to Life: Time for Reform?
II
List of Contents (Continued)
515Marianna ChavesAdvance Directives: The Consecration of Autonomy and Dignity of the Human Being
525Sara Leitão Moreira Brief Notes on the Portuguese Criminal Regimeof Homicide upon Request of the Victim and Physician Assisted Suicide
541Luciana DadaltoCompetence X Cognition: Who can make a Living Will?
549Nuket Ornek Buken and Aysun Balseven-OdabasiPhysicians’ Attitudes at the End-of-Life: A Cross-Cultural Evaluation
567Maria do Céu Rueff “Leges Artis, End(ing) of Life, and Compassion”
577Denard Veshi Ethical and Legal Issues in Cases of Withdrawing Treatment From an Incompetent Patient in Italy
587Ernest Owusu-DapaaEuthanasia, Assisted Dying and the Right to Die in Ghana: A Socio-Legal Analysis
601María Luisa ArcosNotes on Patients with Disabilities Autonomyin Spanish Law
613Index
II III
THEME ISSUE
END OF LIFE ISSUES AND ADVANCE DIRECTIVES
BRIEF WORDS FROM THE GUEST EDITOR
When I received - and promptly accepted - the invitation to serve as guest editor to this theme issue of Medicine & Law, I knew we were going to deal with a subject that is, at the same time, controversial, exciting and challenging.
Controversial, because it involves not only legal concepts, but also personal beliefs, religious dogmas, and an endless number of ethical and philosophical questions that have been haunting mankind for centuries.
Exciting, because we are living in a time where science is developing faster than in any other period of history, bringing advanced technologies to medical devices, and creating the possibility to artificially postponing death but, at the same time, bringing along the questions: should we (?); and who gets to decide.
Challenging, because by discussing it over and over again, we have the opportunity to observe the issues under new parameters, discovering that sometimes we don´t need to focus on the answer, but on reformulating the questions.
As a result, we deliver to you a theme issue with no less than fourteen papers, from all over the world. Fourteen different views, proposals and experiences that - combined - will provide an excellent source for research and discussion, hopefully breeding new ideas, provoking new debates, and delivering alternatives and ways to balance ethics, human dignity, science and law.
And without any further delay, I hope that your reading experience will be fruitful and positive.
With my warmest regards,
Eduardo DantasWarsaw, May 2013

©PROBOOK 2013and Law
Medicine Med Law (2013) 32:429-440
429
PREVIOUSLY EXPRESSED WISHES IN THE CZECH REPUBLIC - A MISSED CHANCE OF THE CZECH LEGISLATORHelena Peterková*
Abstract: By ratification of the Convention on Human rights and Biomedicine, previously expressed wishes as a completely new institute have been, via Article 9, implemented in the Czech legal system. With no history of practical experience with previously expressed wishes, and after more than 6 years of legislative work on the new Act on Healthcare Service, a unique provision was enacted which is actually not meant to serve as an instrument enabling withdrawal of the mechanical support of vital functions. In this paper, the great paradox of the Czech legal provision on previously expressed wishes is to be discussed and critically analyzed in order to explain the seriousness of the consequences of initial misunderstanding of the purposes and context of previously expressed wishes.
Keywords: Previously Expressed Wishes; Withdrawal of Mechanical Support of Vital Functions; Autonomy.
1. INTRODUCTION
Previously expressed wishes are an institute relatively new in the Czech law, arousing a very large number of doubts and uncertainties due to the not quite clear legal status of the patient, persons close to him/her and the attending physician and healthcare provider when it has to be decided whether to follow the previously expressed wish, especially in cases whenthe previously expressed wish is regarding withdrawal of a life-saving or life-prolonging treatment.
Previously expressed wishes were adopted into the legal system of the Czech Republic through the ratification of the Convention on Human Rights
* Centre for Medical Law, Law Faculty, Charles University in Prague Email: [email protected] This paper could be written thanks to the financial support received from the Grant
Agency of Charles Universityin Prague, Project No. GAUK6506/2012.
Medicine and Law 430
and Biomedicine,1 which for the Czech concept of the doctor and patient relationship meant a next major shift from paternalism to the patient‘s autonomy recognition. In connection with the adoption of the Convention on Biomedicine there was an amendment of Section 23 of the former Act on National Healthcare2, setting the informed consent to treatment to better reflect the general rule for the area of healthcare provision, i.e. that the intervention in the area of healthcare can be performed only if the person concerned has given a free informed consent.3 The new Act on Healthcare Services then in Section 34 et seq. takes over the general rule and elaborates it in detail.
We can succinctly summarize that the previously expressed wish according to Article 9 of the Convention on Biomedicine is de facto an informed consent with an extended time effect, when the patient eligible for legal acts in case of their possible future incompetence in advance formulates his/her position in regard to the treatment, the provision of which could possibly be considered for the patient in the future.
In this context, we ask the question to what extent is the structure of the previously expressed wish adopted by Article 9 of the Convention on Biomedicine and taken over by Section 36 (1) of the Act on Healthcare Services - i.e. the previously expressed wish understoodboth as assent/consent anda dissent/refusal - appropriate. Looking across the borders we may actually find only one quite specific previously expressed assent, namely the assent of the future donor of organs with tasks related to the preparation of the body for transplantation.
All other cases of the previously expressed wish could be supposed to be actually the previously expressed dissent with treatment, and it can be assumed, even with validity for the Czech legal system, that such narrowed content4 of previously expressed wish would suffice: In the event that in the future a treatment for an incompetent patient would be considered as medically indicated, the treatment can be provided based on a substitute consent,
1 Convention for the Protection of Human Rights and Dignity of the Human Being with regard to the Application of Biology and Medicine, published under No. 96/2001 Coll. of International Treaties.
2 Act on National Healthcare, Act No. 20/1966 Coll.3 Article 5 of the Convention on Biomedicine.4 With regard to the primary purpose of the so called Advanced Directives, it is probably
not the case of tampering the previously expressed wish, but merely giving the concept its original content. Comp. to this footnote No. 25.
Medicine and Law 431
whether granted by a judicially appointed guardian, healthcare proxy by the patient concerned or quasi - representative according to Section 38 of Act on Healthcare Services. The patient, therefore, does not have to express his/her assent. Conversely, if the treatment is not indicated, the previously expressed assent shall never be a reason for the treatment to be granted.
That previously expressed assent can move the meaning and the purpose of the previously expressed wish in the direction at least debatable, can be illustrated in the attempt of the psychiatric hospital to use the previously expressed consent even for restrictive measures of psychiatrically ill patients, thus avoiding the mandatory reporting (and judicial inspection) of the use of these measures.
Article 9 of the Convention on Biomedicine states that the previously expressed wishes relating to a medical intervention by a patient who is not, at the time of the intervention, in a state to express his or her wishes shall be taken into account. Due to the system of the Convention on Biomedicine it is clear that the previously expressed wishes should especially serve as an exception to the procedure predicted by Article 8 (emergency situation), i.e. through the previously expressed wishes it should be possible to prevent situations in emergencies, in which the appropriate consent could not be obtained, and procedures necessary for the benefit of health and saving the life of the person concerned were immediately implemented5. In addition to eliminating the emergency mode, the previously expressed wishes should serve as an expression of the will if the patient anticipated future decline in his cognitive abilities (e.g. due to progressive dementia6), a coma or a permanent vegetative state.
There are legitimate disputes about the extent of the binding effect of the previously expressed wish; neither the Convention on Biomedicine itself, nor its Explanatory Report are helpful enough as to the explanation. The Explanatory Report to the Convention on Biomedicine states that when persons have previously expressed their wishes, these shall be taken into account.78
5 Article 8 of the Convention on Biomedicine and conversely6 Not quite exact Czech translation of the Explanatory Report to the Convention on
Biomedicine7 Paragraph 62 of Explanatory Report to the Convention on Biomedicine8 Amazingly, in the Czech version of the Explanatory Report the wording taken into
consideration instead of taken intoaccount is aplied. Furthermore, the Czech Explanatory report states that by taken into consideration it is actually meant the obligation to respect the previously expressed wish.

Medicine and Law 432
However, almost immediately, this obligation to respect the previously expressed wish that according to the linguistic interpretation does not arise from the wording of Article 9, is more or less relativized (or denied) when it adds that nevertheless, taking previously expressed wishes into account does not mean that they should necessarily be followed. For example, when the wishes were expressed a long time before the intervention and science has since progressed, there may be grounds for not heeding the patient's opinion. The practitioner should thus, as far as possible, be satisfied that the wishes of the patient apply to the present situation and are still valid, taking in account particular or technical progress in medicine.
The above clearly illustrates a fundamental problem associated with the institute of the previously expressed wish and its legislation, because no matter how precisely defined by the law, in no national legal system the previously expressed wishes have an absolute binding effect. On the contrary, they essentially serve always as anevidence (albeit very important), on the basis of which the presumed current patient’s will at the decisive moment is inferred as a mosaic.
However, the autonomists claim that if the meaning of the previously expressed wish is to be a primary protection of the individual's right to self-determination and autonomy, then it is the duty of the legislator not to allow, at any cost, for a fully informed patient who validly formulated the previously expressed wish, to be treated, or kept alive in a way that he/she had demonstratively refused in advance, and previously expressed wishes should be at all times absolutely binding. Another possible approach is to protect the current will of the patient because the patient's wish could have changed since the previously expressed wish had been written. Finally, we cannot ignore the views that completely rejectthe institute of the previously expressed wish and accentuate the, so called, best current interest of the patient (the, so called, new person argument9).10
9 LAMB, D.: Autonomy and the refusal of life-prolonging therapy, (1995) Vol. I. Res Publica no. 2, on pages 153-159.
10 GETH, C., MONA, M.: Widersprüche bei der Regelung der Patientenverfügung im neuen Erwachsenenschutzgerecht: Verbindlichkeit, mutmasslicher Wille oder objektive Interessen? ZSR 2009 I, onpages 155-178, on page 156

Medicine and Law 433
2. THE ACT ON HEALTHCARE SERVICES
From April 1, 2012, Section 36 of Act on Healthcare Services sets that the patient may, in case where he/she got into such a state of health, in which he/she will not be able to assent or dissent with the provision of healthcare services and the way they are provided, give the assent or dissent in advance.11 The provider of healthcare services has an obligation to take into consideration the previously expressed wish of the patient, if it is available, and provided that at the time of delivery of healthcare services a predictable situation occurred, to which the previously expressed wish applies, and the patient is in such a state of health, in which he/she is unable to express a new assent or dissent. Only such a previously expressed wish will be respected, if it was made based on the written instructions of the physician to the patient about the consequences of this decision.12
The law essentially requires a written form of the previously expressed wish, including the officially authenticated signature of the patient, and it restricted the validity of the previously expressed wish to fiveyears in the original version.13 However, it admits the possibility that the patient will make the previously expressed wish when received to the care of the provider or anytime during hospitalization, for the provision of healthcare services provided by this provider. Such an expressed wish is recorded in the kept medical records of the patient; the record is signed by the patient, a healthcare worker and a witnesses.14
Apart from the conditions, under which the previously expressed wish of the patient will be respected, the law then introduced the circumstances under which the previously expressed wish does not need to be respected (from the time it was expressed there has been such development in the provision of healthcare services, to which this wish relates, that it can be reasonably assumed that the patient would have agreed to their provision15), and under which the previously expressed wish must not be respected (it encourages
11 Provision of Section 36 (1) of Act on Healthcare Services.12 Provision of Section 36 (2) of Act on Healthcare Services.13 Provision of Section 36 (3) of Act on Healthcare Services. The time restriction of the
previously expressed wishes was in November 2012 annulled by the Czech Constitutional Court.
14 Provision of Section 36 (4) of Act on Healthcare Services.15 Provision of Section 36 (5)(a) of Act on Healthcare Services.
Medicine and Law 434
such practices which result in the active cause of death;16 its fulfilment could endanger other persons17; at the time when the provider did not have the previously expressed wish such medical procedures had already been started and their interruption would lead to an active cause of death18).
2.1 Validity of the previously expressed wish
Still in the vacatiolegis period the provision of Section 36 was subjected to relatively considerable criticism - primarily because according to the Explanatory Report with respect to the rapid progress in medicine, the Act limited the validity of the previously expressed wish to fiveyears.However, the Act does not, allow in situations where the patient is no longer competent due to objective reasons, to restore the previously expressed wish after five years, and in particular, the Explanatory Report, to the detriment of the matter, did not imply that in such a case the previously expressed wish does not lose its validity.
The claim that the restriction of validity contradicts the wording of Article 9 of the Convention on Biomedicine was also inquired by the Constitutional Court of the Czech Republic, which by the finding from November 27, 2012, annulled the five years validity period. It also pronounced that it is not compatible with the patient's right under Article 9 of the Convention on Human Rights and Biomedicine, for his/her previously expressed wish not to be taken into consideration only as a result of the expiry of the statutory period of its validity, if this patient does not have at the same time a real possibility to restore this wish through his/her expression of will. Given that the contested provision allows such a possibility, it is necessary to consider it a restriction of the concerned right devoid of any constitutionally qualified reason (comp. Articles 26 and 27 of the stated Convention), as a result of which it is contrary to Article 9 of the stated Convention.19 For this reason, the last sentence of Section 36 (3), according to which the validity of the previously expressed wish is five years, was annulled by the Constitutional Court of the Czech Republic.
As already outlined above, neither the wording of Article 9 of the Convention on Biomedicine, nor of the Explanatory Report to it imply the binding nature
16 Provision of Section 36 (5)(b) of Act on Healthcare Services.17 Provision of Section 36 (5)(c) of Act on Healthcare Services.18 Provision of Section 36 (5)(d) of Act on Healthcare Services.19 Finding of the Constitutional Court of the Czech Republic PI.ÚS 1/12

Medicine and Law 435
of the previously expressed wish itself; it only determines the obligation to take the previously expressed wish into account, into consideration respectively.
The time limit on the validity of the previously expressed wish established originally by Section 36 of Act on Healthcare Services was undoubtedly based on the Austrian model of binding advanced directives (verbindliche Patientenverfügung20) but without the Czech legislation consistently taking over also the, so called, considerable advanced directives (beachtliche Patientenverfügung21). Yet this dichotomy is apparent also in Section 36 (2) of Act on Healthcare Services, when the previously expressed wish will be under certain circumstances taken into consideration and under other circumstances be respected.
Therefore, I believe that the legal determination of the limited validity itself was not in breach of Article 9 of the Convention on Biomedicine, because the wishes written before the period of more than five years would still have to be taken into consideration. However, the weakness of the original wording of Section 36 (3) of Act on Healthcare Services can be clearly identified in the fact that the Act did not provide for the conditions, under which the running of the time limit is stopped - as is typical in case of the loss of legal capacity.
2.2 Previously expressed wish requiring termination of life on request
The Act do not recognise the binding nature of such previously expressed wish that would require active cause of death, just as is the case in the vast majority of countries that adopted the institute of the previously expressed wish. In the present context, when termination of life on request is not regulated by the Criminal Code in the Czech Republic even as an expressively privileged crime, the concept of Section 36 is fully in place; moreover, the Dutch, Belgian and Luxembourg legislations that allow under certain conditions taking the life of another at the latter’s expressed advanced request22 can be considered in this respect as rather extreme exceptions, which is probably even more problematic than the decriminalized actualtermination of life on request itself in the real time context to the patient's request for termination of life.
20 Provision of Section 4 et. seq. of the Australian Act on Advanced Directives (Patientenverfügungsgesetz)
21 Provision of Section 8 et. seq. of the Australian Act on Advanced Directives.22 It should be noted that this kind previously expressed wish is not very successful (i.e.
frequent and followed) in practice.
Medicine and Law 436
The current Czech legal regulation regarding the previously expressed wish, however, arouses an urgent question whether active cause of death defined by the Explanatory Report of the Act on Healthcare Services and involving also disconnecting from the device, which is by the Report even equated to the administration of a lethal dose of drugs, is not too dogmatic. Disconnecting from life support devices is actually by its very nature undoubtedly a withdrawal of a specific professional procedure (treatment - instrumental life support), in which the doctor no longer continues, i.e. a procedure fundamentally diametrically distinguish to the administration of a lethal dose of drugs.
In December 2011, the Parliament of the CR approved the Act on Healthcare Services with effect from April 1, 2012, which in Section 36 (5) explicitly states that the previously expressed wish:
a) does not need to be followed if, from the time it was expressed there has been such development in the provision of healthcare services, to which this wish relates, that it can be reasonably assumed that the patient would have agreed to their provision; ...
b) cannot be followed if it encourages such practices, which result in active cause of death,
c) cannot be followed if its fulfilment could endanger other persons,
d) cannot be followed if at the time when the provider did not have the previously expressed wish available such medical procedures were started the interruption of which would lead to an active cause of death.
The Act on Healthcare Services thus refuses to sanction the binding nature of such previously expressed wish that would require active cause of death, just as is the case in the vast majority of countries that adopted the institute of the previously expressed wish. As has already been stated in the text above, the very ban of the previously expressed wish requiring active cause of death is undoubtedly understandable in the context of the Czech healthcare and criminal law, similarly, one can also in some context understand the fact that the legislator, with regard to the reality perceived by senses, declared the disconnecting from life support devices (movement consisting in switching off a machine) as active causing of death. However, one cannot leniently ignore fact that these two thought structures are connected in Section 36 (5) in such an unfortunate way that they make it impossible to terminate the
Medicine and Law 437
already initiated instrumental support of vital functions through the previously expressed wish of the patient.
The structure of Section 36 (5) of Act on Healthcare Services, including the Explanatory Report to it is all the more incomprehensible since the Act in the light of the Explanatory Report indicates that the patient is not allowed through previously expressed wish to require to be disconnected from the life support device, although on the other hand, he/she may require not be connected to the device at all.23 This concept is, nevertheless, completely inconsistent with the whole legal framework of refusing healthcare, because, as already explained in the text above, the patient, which has legal capacity at the relevant time, may require an immediate withdrawal of a treatment, including a mechanical support of vital functions (e.g. dialysis)24, without inferring that the medic will thus actively cause damage to health or death.
It can therefore be concluded that the Czech legislation on the previously expressed wish according to Section 36 of Act on Healthcare Services not only disregards the general (and constitutional) law on autonomy and providing healthcare, but by not permitting switching off a life supporting device based on a previously expressed wish, without exaggeration, denies the main and original meaning of the previously expressed wish.25
3. LEGAL CONSEqUENCES OF THE PREVIOUSLY EXPRESSED WISH IN CZECH LAW
If the previously expressed wish refuses life-saving or life-prolonging treatment, one can speak, in terms of the traditional classification, with some
23 Although one can certainly argue that in the first case (not to be connected from the beginning) it is a pure omission, while in the second case (to disconnect the already connected patient) it is a rather a sort of metonymic quasi-omission (omission to the effect that no further treatment will be provided).
24 Provision of Section 34 (5) of Act on Healthcare Services (The retraction of the consent is not effective if the implementation of health care procedures has already started and its disruption can cause severe damage to health or death to the patient) is inconsistent with Article 5 et seq. Convention on Biomedicine, as well as the opinion of the Constitutional Court.
25 The term advanced directive was first used in the U.S. in the 60s of the last century by lawyer L. Kutner, specifically in connection with the previously expressed wish, by which the patient refuses to be, even with the help of instruments, kept alive against his/her will. In.: EMANUEL, L. How living wills can help doctors and patients talk about dying. BMJ 2000, 320: 1618-1619.

Medicine and Law 438
reservations, in case of following such previously expressed wish, of passive euthanasia.
The right of a patient with full legal capacity to refuse treatment was for decades confirmed in Section 23 (2) of Act on National Healthcare, and is currently enacted especially in the provisions of Section 28 (1) and Section 34 (6) of Act on Healthcare Services and is explicitly recognized also by the judicature. The patient's consent to the doctor’s actions, the aim and the result of which will be the patient's death, does not constitute according to Section 30 (3) of the Criminal Code any legal defence for a crime against life. Conversely, an informed dissent of the same patient, as a result of which life-saving treatment will not be initiated or it will be discontinued, thus causing the death of the patient is a reason for impunity.
In other words, the refusal of a life-saving treatment, which will lead to no treatment (doctor’s failure to treat) that will result in the patient's death, is a circumstance excluding illegality, unlike the informed consent to termination of life that would have happened through the doctor’s active action, although both of these actions will be in causal connection with the death of the patient.
Whoever respects a valid refusal of the treatment is not acting illegally and is not responsible for the death. According to the pure medical-legal science then, as in the case of omission on the basis of informed dissent, also the omission on the basis of the previously expressed dissent will be in accordance with the law. The will not to undergo treatment formulated through the previously expressed wish must be free, serious, expressed clearly and definitely.
In practice, however, the physician may always face the risk that the validity of the previously expressed wish will be questioned, for instance, because when the patient wrote the previously expressed wish, he/she could not be legally capable to such an (irrational) legal action as a result of mental disorder, or because it can be inferred that if the patient had known about his/her situation what the doctor knows now, he/she would never have spoken the previously expressed wish and would never have refused the treatment.26
26 In this respect, it is very interesting how the existence of the previously expressed wish is accepted - without the necessity of a greater formalism - by Swiss authorities active in criminal proceedings (which express much confidence in the submitted written evidence in the implementation of feedback controls in cases of assistance in suicide - e.g. they do not at all require certified signatures on the declarations of the will to commit suicide, etc.). Similarly, in the matter of the previously expressed wish requesting disconnecting

Medicine and Law 439
The judicature on this issue is missing in the Czech Republic. However, it can be deduced from the Czech legal system as well as from foreign experience that if the objected invalidity of the previously expressed wish is recognized as legitimate, the doctor who with regard to the alleged existence of the previously expressed wish did not treat the patient, thus causing his/her death, considering the physician's guarantor status and the special duties of a doctor to act resulting from it pursuant to Section 112 of the Criminal Code, will be found criminally responsible for some criminal offence against life, most likely for manslaughter under Section 141, 143 respectively of the Criminal Code. If, on the contrary, the doctor does not observe the previously expressed wish, he/she may be found liable for infringement of the right of privacy under Section 11 et seq. Civil Code.
In this context, it is interesting how the treatment against the explicitly expressed will of a legally competent patient was evaluated by the British courts in the case of Mrs. B. who demanded switching off the ventilator, on which she was dependent. The court in her case stated that after Mrs. B’s legal competence had been proven, and yet after a few months she was not disconnected from the ventilator, an unauthorized interference with her autonomy occurred. The court, however, tended to assess this unlawful interference rather as, in its effect, the underrated and actually respectable doctors’ care of the patient. The patient was awarded damages of £100 compensation for interference with the right to self-determination and autonomy, stating that the doctors did not commit a mistake and the amount will be paid to her from the public healthcare system resources.27
4. SUMMARY
The issues of previously expressed wishes, whether relating to patients with poor prognosis in terms of maintaining their cognitive functions, patients with little or no chance of recovery, or patients in a coma or in a permanent irreversible vegetative state, is a topic undoubtedly complex, complicated, moreover arousing emotions not only in theory, but also in everyday medical practice.
from a probe, also the German court was satisfied with the statement of the patient‘s daughter that her mother had once expressed such wish.
27 Ms. B in An NHS Hospital Trust (2002) EWHC 429. Similarly, the case of Edwards in the USA.

Medicine and Law 440
The informed consent, which was introduced by the Convention on Biomedicine as a general rule, has become one of the principal axes of the medical law, and from which is further derived the previously expressed wish, which, hypothetically, may have in its effect also a completely unlimited time effect. The provisions regulating the previously expressed wishes, Article 9 of the Convention on Biomedicine, together with Section 36 of Act on Healthcare Services, however, represent an imperfect legislation that in places, to the detriment of the cause, disregards the teleological understanding of the institute of the previously spoken wish.
I consider the legislation in the Benelux countries, which allows the patient to even require the termination of life on request through the previously expressed wish, as potentially very problematic because it further shifts the role of the doctor in ending the patient's life - in the name of the patient’s autonomy it will in fact be the doctor who will not only end the patient's life, but will also at some point decide about the right moment (based on the interpretation of the previously expressed wish).
However, I perceive the Czech legislation on the previously expressed wish as a similar extreme, but in the opposite direction because the previously expressed wish, through which it is not possible to require the withdrawal of the mechanical life support, is a completely facade institute of the Czech medical law.

©PROBOOK 2013and Law
Medicine Med Law (2013) 32:441-458
441
WHAT ARE THE CONSEqUENCES OF DISREGARDING A “DO NOT RESUSCITATE DIRECTIVE” IN THE UNITED STATES?Nicole Marie Saitta* and Samuel D. Hodge, Jr.**
Abstract: Does a valid cause of action exist against a health care provider who intentionally disregards a “do-not resuscitate order,” prolonging a patient’s life? Wrongful prolongation of life has not gained traction in the United States. Although the issue has garnered media attention and has raised awareness of advanced directives, physicians still may disregard a patient’s last wishes for fear of legal reprisal or due to lack of communication. This article examines key cases and explains the differences between living wills, advanced directives and proxies. Claims have been advanced under theories of battery, Constitutional violations, breach of contract, infliction of emotional distress, and negligence, but no cause of action has allowed monetary damages. Courts maintain that it is not their place to judge an impaired life as being less valuable than no life.A state-by-state analysis of legislation concerning advanced directives follows along with a discussion of the Patient Self-Determination Act.
Keywords: Wrongful Life; Wrongful Birth; Wrongful Prolongation of Life; Advanced Directives; Patient Self-Determination Act; Do Not Resuscitate Order; The Right to Die; Damages; Constitutionally Protected Right to Die
* Temple University Beasley School of Law, J.D. expected 2015. Villanova University, M.A.
** Temple University Beasley School of Law, J.D., 1974 Temple University, Legal Studies Department, Chair and Professor
Medicine and Law 442
"The right to a good death is a basic human freedom. The Supreme Court's decision to uphold aid in dying allows us to view and act on death as a dignified moral and godly choice for those suffering with terminal illnesses."
- John Shelby Spong
The courts in the United States have considered at least three theories of liability concerning the inception and expiration of life: “wrongful life,” “wrongful birth” and “wrongful living.”1 A claim for “wrongful life” is initiated by a child seeking damages against a health care provider for negligently failing to properly sterilize the parent.2“Wrongful birth” deals with the parents of an impaired child who are requesting damages for the birth of that child.3 These individuals maintain that, as the result of malpractice, the parents were prevented from exercising their right to terminate the pregnancy or avoid conception.4 However, in a “wrongful living” or “wrongful prolongation of life” case, the claimant asserts a right to enforce an informed, competent decision to reject life-saving treatment.5
A wrongful prolongation of life claim is inextricably linked to the constitutionally protected right to die.6 Thus, the claimant is maintaining a liberty interest in refusing undesired medical treatment. It is the denial of this liberty interest, caused by a health care provider who either negligently or intentionally disregards the wishes of a patient that gives rise to this cause of action.7 Nevertheless, the reported decisions for wrongful prolongation of life reflect a general reluctance by the courts to grant monetary recovery, especially for pain and suffering damages, claiming it is not their place to judge an impaired life as being inherently less valuable than non-life.8
1 Anderson v. St. Francis-St. George Hosp., Inc., 671 N.E. 2d 225, 227 (Ohio 1996).2 Id.3 Id.4 Id.5 Id.6 The right to die was recognized by the United States Supreme Court in Cruzan v. Dir.,
Mo. Dep’t of Health,497 U.S. 261(1990).7 Anderson, 671 N.E. 2d at 227.8 See generally Burks v. St. Joseph’s Hosp., 596 N.W.2d 391 (Wis. 1999) (discussing a
doctor’s responsibility to make medically based decisions whether to treat patients).

Medicine and Law 443
ADVANCE DIRECTIVES: THE LESSONS OF KAREN ANN qUINLAN AND TERRY SCHIAVO
Advance directives and prolongation of life questions are not foreign to the courts. This topic became a public issue in 1976 with the tragic case of Karen Ann Quinlan.9 A father sought guardianship of his 21-year-old daughter who was in a persistent vegetative state.10 Mr. Quinlan wanted to discontinue all extraordinary procedures necessary to sustain his daughter’s life.11 The New Jersey Supreme Court, reliant on the physician’s statement that there was no reasonable possibility of Karen ever emerging from her comatose state, agreed that life-support systems could be withdrawn on the basis of her right to privacy without criminal or civil liability.12 In this case, the court began to address questions concerning “prolongation of life” and noted the paucity of legislation in this area, a recurrent theme cited by the courts in subsequent years.13 Ultimately, this litigation paved the way for future courts to issue declaratory or injunctive relief against health care providers who refuse to carry out advance directives, and it has led to the enactment of state statutes that aim to protect a patient’s right to die while upholding a physician’s obligation to prolong life.14
These issues were again prominently brought to the public’s attention in 2005 with the case of Terry Schiavo, which addressed the issue of a woman being kept alive on artificial life support.15 The patient’s husband disagreed with Terry’s parents over the removal of their daughter’s food, fluids, and medical treatment.16 The parents alleged that the husband was violating their daughter’s rights, and they sought a temporary restraining order to reverse his decision to withhold the patient’s medical treatment.17 Throughout the
9 See Time Specials, Top 10 Comas, http://www.time.com/time/specials/packages/article/0,28804,1864940_18649 39_1864909,00.html (last visited Nov. 4, 2011) (stating that the Quinlan case became the first “right to die” case in U.S. legal history).
10 In re Quinlan, 355 A.2d 647, 651 (N.J. 1976).11 Id.12 Id at 669. According to Mack v. Mack, 618 A.2d 744, 755 (Md. 1993), a number of
courts have found that a person's right to refuse treatment is premised on a federal or state constitutional right of privacy.
13 In re Quinlan, 355 A.2d at 652, 664.14 Diane E. Hoffman & Jack Schwartz, Who Decides Whether a Patient Lives or Dies?,
Trial, Oct. 2006, at 30-31.15 Schiavo ex relv. Schiavo, 403 F.3d 1223 (11th Cir. 2005).16 Id. at 1231.17 Id. at 1225. Florida's legislation contemplates a process for designation of a proxy in the
Medicine and Law 444
proceedings, both parties argued over what they believed were the patient’s intentions concerning artificial life support, though no concrete document regarding her wishes existed.18 The fierce debate that ensued reawakened the public’s interest in advance directives. For instance, the National Hospice and Palliative Care Organization (NHPCO) received over 900 calls and 2,000 emails during the pending of the litigation from individuals interested in state-specific advance directives so they could avoid the controversy that was taking place in the Schiavo matter.19
THE PROLIFERATION OF ADVANCE DIRECTIVES AND THE DESIRE TO ENFORCE THEM
States have attempted to regulate this area by enacting living will legislation.20 California passed the first living will statute in 1976,21 and every state,22 and certain U.S. territories such as Guam, Puerto Rico,23 and the Virgin Islands,24 have statutes that address this topic. Although no two laws are identical, all address the formality with which a living will must be executed.25 Many state laws specifically mention the duties and obligations of health care providers with regards to honoring advance directives while also acting in the best interest of the patient.26 For instance, New Jersey’s law upholds the right of
absence of an executed advance directive and allows for judicial resolution of disputes concerning decisions made by the proxy. Where a decision by the proxy is challenged by the patient's other family members, it is ripe for the parties to seek “expedited judicial intervention.” Id. at 1233.
18 Id. at 1235.19 Holly Fernandez Lynch et al., Compliance with Advance Directives: Wrongful Living
and Tort Incentives, 29 J. Legal Med. 133, 138 (2008). 20 Linda Shields Stiefel, A Time to Live, A Time to Die, 24 Akron L. Rev. 699 (1991).21 Id. at 700.22 Frequently Asked Questions (FAQ) about the U.S. Living Will Registry, U.S. Living Will
Registry, http://www.uslwr. com/faq.shtm (last visited Oct. 24, 2011).23 Arthur S. Berger, When Life Ends, 34 (Greenwood Publg, 1995),http://books.google.
com/books?id =n3j40KnvR8YC&pg=PA34&lpg=PA34&dq=US+territories+with+living+will+statutes&source=bl&ots=ZX0TRESJZt&sig=noUYqes8CXoXXFdgMnBGSavGAYM&hl=en&ei=IgCmTt6YOOre0QGcq834DQ&sa=X&oi=book_result&ct=result&resnum=6&ved=0CGIQ6AEwBQ#v=onepage&q=US%20territories%20with%20living%20will%20statutes&f=false.
24 Daniel J. Gravel, The Importance of Estate Planning, Virgin Islands Law Blog (June 25, 2010), http://lawblog.vilaw.com/2010/06/articles/tax-estate-planning/the-importance-of-estate-planning/.
25 Stiefel, supra note 43, at 703.26 Martha S. Swartz, “Conscience Clauses” or “Unconscionable Clauses”: Personal Beliefs
Versus Professional Responsibilities, 6 Yale J. Health Pol’y L. & Ethics 269, 282 (2006).

Medicine and Law 445
health care providers to refuse to participate in withholding or withdrawing life sustaining measures while also requiring physicians to document patients’ advance directives.27 South Dakota, while recognizing a patient’s right to execute a living will, allows health care professionals to provide treatment to alleviate pain or discomfort.28 Oklahoma protects the patient’s wishes by overriding the obligations of a physician or health care provider who may desire to render care to preserve life.29
Even more prevalent than legislative pronouncements concerning the rights of a patient30 and the duties of physicians to honor advance directives31 are statutes that provide for immunity so long as the physician uses his or her best judgment in treating the patient.32 Sixteen states, along with the U.S. Virgin Islands, mention “immunity” when discussing advance directives.33At least seventeen states, along with Puerto Rico, specifically mention the word “liability” with regards to treating patients with advance directives, either by the administering of treatment or the following of a DNR order.34 Most of these statutes do not hold the health care provider criminally or civilly liable for removing life support in the presence of an advance directive.35 Some states, however, expand on this law by stating, as in Oklahoma, “the physician shall use his or her best judgment” when delivering a standard of care.36 Texas mandates that the standard of care provided by a physician in the presence of an advance directive shall be equal to the “prudence and skill...exercised under the same or similar circumstances in the same or similar community.”37 Statutes appear to contain this general language so that, if a doctor ignores an advance directive under the pretense of following a certain standard of care, the physician will not be held liable for the disregard of it.
27 N.J. Stat. Ann. § 26:2H-62 (West 1992).28 S.D. Codified Laws § 34-12D-9 (West 2007).29 Okla. Stat. Ann. tit.63, § 3101.2 (West 2006).30 Id.31 S.D. Codified Laws § 34-12D-9.32 E.g., Matthew S. Ferguson, Ethical Postures of Futility and California’s Uniform Health
Care Decisions Act, 75 S. Cal. L. Rev. 1217, 1236-37 (2002).33 See OHIO, Rhode Island, Virginia, Vermont, Wisconsin, Virgin Islands, ARIZONA,
Colorado, Florida. Illinois, Iowa, Louisiana, Maine,Mississippi, Nebraska, Nevada and New York.
34 See Oklahoma, Tennessee,Texas, Virginia,Washington, Puerto Rico, Arizona, Connecticut, Florida, Georgia, Kentucky, Louisiana, Massachusetts, Michigan., Missouri, Nevada and New York..
35 E.g., Mass. Gen. Laws Ann. ch. 201D § 8 (West 2011).36 Okla. Stat. Ann. tit.63, § 3101.10 (West 2011).37 Tex. Health & Safety Code Ann. §166.160 (West 2011).
Medicine and Law 446
State statutes that mention civil and/or criminal liability with regards to advance directives and/or using professional discretion include Arizona, Colorado, Connecticut, Florida, Georgia, Iowa, Kentucky, Louisiana, Massachusetts, Mississippi, Nebraska, Nevada, New York, Ohio, Oklahoma, Rhode Island, Tennessee, Texas, Virginia, Washington, Wisconsin, and the Virgin Islands.38 The language contained in these laws seems intentionally vague, allowing for physicians to comply with advance directives without liability while also protecting them if they do not act in accordance with a patient’s directive but within “reasonable medical standards.”39 The bottom line is that these statutes recognize the existence of advance directives, but there is a disconnection between what the law requires and a physician’s actual practice.40
A natural question arises as to why physicians would resuscitate individuals with DNR orders.41 One reason may be the lack of communication between patient/care providers and the subsequent hospital/doctor,42 and this problem is only compounded when individuals are transported between facilities, nursing homes, and hospitals, often without the accompanying paperwork.43 As one physician noted:
Lack of communication about the wishes of the patient in a time of medical crisis is the main cause for unintentionally bypassing “do not resuscitate”/ “do not intubate” orders. In these cases, the patient suddenly collapses from a heart attack or stroke. Often, a cardiac or respiratory arrest occurs at night when neither the family nor the patient’s physician is on site. In these cases, the person is witnessed to collapse or is found unresponsive and a “code” is instantly called. At that moment, everyone comes running - nurses, any available physicians, respiratory therapists - to start resuscitation efforts. The intent is to save the life. In the haste to come to the aid of the patient, the DNR/
38 See Oklahoma, Tennessee, Texas, Virginia, Washington, ARIZONA, Connecticut, Florida, Georgia., Kentucky, Louisiana, MASSACHUSETTS, Michigan, Nevada, New York, Iowa, Colorado, Virgin Islands, Wisconsin, Rhode Island, Ohio , and Nebraska.
39 E.g., V.I. Code Ann. tit. 19, § 194 (West 2011).40 See M. Rose Gasner, Financial Penalties for Failing to Honor Patient Wishes to Refuse
Treatment, 11 St. Louis U. Pub. L. Rev. 499, 502 (1992).41 See Jo-Anne Herina Jeffreys, Advance Directives: Are They Worth the Paper They’re
Written On?, 190 N.J. Lawyer 17, Apr. 1998 (stating “Despite the enactment of state and federal statutes which provide for advance directives, studies indicate that at least 25 percent of these validly executed documents are not honored.”).
42 Id. at 18.43 See Rodriguez, supra note 16 (stating in cases where a doctor is unfamiliar with a patient
they do not have the time or incentive to learn the details of treatment refusal).

Medicine and Law 447
DNI status may not be appreciated, especially if the medical event occurs at the start of a shift before the nursing staff has become familiar with all of their patients.44
Some states provide the option of wearing a “Do-Not-Resuscitate” bracelet to inform doctors of a patient’s resuscitative choice.45 For example, Pennsylvania defines an “Out-of-hospital do-not-resuscitate bracelet” as one “supplied by the [Department of Health of the Commonwealth] and issued by the attending physician, which may be worn at the patient’s option to notify emergency medical services providers of the presence of an order.”46 Wisconsin allows doctors to “provide a DNR order in the form of a bracelet for adults with terminal illnesses who choose not to receive cardiopulmonary resuscitation (CPR), including cardiac compression, endotracheal intubation, artificial ventilation and defibrillation should they have a medical emergency while not hospitalized.”47 Montana and the District of Columbia use a “Comfort One”48 and “comfort care”49 bracelet to alert EMS of an advance directive. Virginia and several other states use bracelets and/or necklaces that have DNR instructions printed on them to notify emergency personnel when a person is not a patient in a hospital, nursing home, or licensed hospice.50 Interestingly, Wisconsin51 and a few other jurisdictions provide that the defacing or removing of a DNR bracelet by the patient is considered a revocation of the order.52 While bracelets may help to communicate a patient’s final wishes, most of these measures are aimed at alerting EMS first-responders. Therefore, if the bracelet is inadvertently marred or removed in the chaotic activity of an emergency situation, physicians may not be properly informed when patients are transferred from one location to another.53
44 E-mail from Jack E. Hubbard, Ph.D., M.D., Dr. of Adult Neurology, Minneapolis Clinic of Neurology (June 24, 2011) (on file with the author).
45 Wis. Stat Ann. § 154.19(2)(a)(1) (West 2011).46 20 Pa. Stat. Ann. § 5483 (West 2011).47 Jane Barclay Mandel, Wisconsin’s Do Not Resuscitate Bracelet Law Raises Legal and
Medical Issues, 70 Wis. Law. 14, 14 (1997).48 Mont. Admin. R. 37.10.105 (2011).49 D.C. Code § 70651.04 (West 2011).50 National Association of Emergency Medical Services Directors & National Association
of Emergency Medical Services Physicians, National Guidelines for Statewide Implementation of EMS “Do Not Resuscitate” (DNR) Programs (1994); Ga. Code Ann.§ 31-39-6.1.
51 Wis. Stat. Ann. § 154.21.52 N.H. Rev. Stat. Ann. § 137-J:29 (West 2011).53 Id.

Medicine and Law 448
WHY ARE ADVANCE DIRECTIVES IGNORED?
Communication errors may be one reason why doctors fail to adhere to a patient’s advance directives. However, the fear of reprisal from family members when following such instructions weighs heavily on doctors’ minds.54 While statutes exist to protect physicians in these situations,55 this does not always insulate them from lawsuits. Some doctors, therefore, err on the side of human life when making decisions about resuscitation and other life saving measures, thereby ignoring a living will and adhering to the belief that they might be subject to a damages lawsuit.56 This is what happened in Allore v. Flower Hospital57 where the patient’s living will was ignored by his health care providers despite their awareness of its existence.58 Under the terms of the living will, the patient wanted “no life-sustaining treatment” in the event of a terminal condition or “permanently unconscious state.”59 After being repeatedly admitted to the hospital for pulmonary problems associated with asbestosis, Allore was intubated and mechanically ventilated because his advance directive was unknown to the treating physicians.60 In fact, the patient’s chart read, “In the event of cardiac standstill, ventricular fibrillation or respiratory arrest, resuscitation measures are to be initiated immediately using ACLS protocols,” measures which directly contradicted the patient’s wishes.61 Unfortunately, Mr. Allore’s repeated hospitalizations caused his end-of-life directions to be miscommunicated in the shuffle of paperwork and changing of physicians. In a subsequent lawsuit, the estate was barred from recovering damages for the wrongful prolongation of life.62 The court noted that, since the “harm” was the benefit of life, it would not provide compensation.63 The only damages allowed were those related to the alleged battery for the resuscitation efforts against the patient’s wishes.64 Thus, the recovery of medical costs and pain and suffering could not be awarded since
54 Renee Martin, Liability for Failing to Follow Advance Directives, Physician’s News Digest (1999), available at www.physiciansnews.com/law/999martindv.html.
55 Ohio Rev. Code Ann. § 2133.22.56 Martin, supra note 77.57 699 N.E.2d 560, 561 - 62 (Ohio Ct. App. 1997).58 Id.59 Id. at 561.60 Id. at 561-62.61 Id. at 561.62 Allore,699 N.E.2d at 565. 63 Id. at 563.64 Id.

Medicine and Law 449
they related to the wrongful prolongation of the decedent’s life and not a direct result of a battery or negligence.65
Allore was decided under the doctrine of implied consent, a policy which protects physicians when providing treatment in emergencies “without the specter of liability for lack of consent.”66 This policy is not applicable when an advance directive exists since an individual has already made a choice regarding life-sustaining measures. However, a physician can still act within means of a standard of care, especially when an advance directive is not clearly known.67 In this regard, the court recognized that there was no evidence that the attending physician was aware of Allore’s refusal of treatment, and since he signed a consent form for treatment when admitted to the hospital, “no issue of material fact existed as to implied consent on the part of Frank Allore to the patient’s intubation and ventilation.”68
Allore might seem like an isolated incident of ignoring a patient’s wishes, but it is not. One survey found that only 36% of individuals with advance directives had mention of this fact in their medical records and less than 1% actually had the document filed with their chart.69 The study concluded that advance directives fail to have a significant effect on orders regarding resuscitation.70 Other studies have revealed that the medical profession’s ambivalence toward advance directives often leads to their failure to comply with these orders for several reasons: (1) the fear of liability; (2) the perception that directives interpose an unnecessary additional control over, and interfere with, the physician’s professional actions; and (3) the perception that directives implicitly question the physician’s judgment of the patient’s best interests.71
65 Id.66 Lawcore.com, What is Implied Consent?, http://www.lawcore.com/dui-dwi/what-is-
implied-consent.html.67 Rodriguez, supra note 16.68 Allore, 699 N.E.2d 560. In a variation of a wrongful prolongation of life claim, a number
of courts have considered wrongful life claims in the context of the birth of child with a physical impairment. As noted in Lininger v. Eisenbaum, 764 P.2d 1202 (Colo. 1988), courts have disallowed wrongful life claims on the theory that the baby sustained no injury or on the grounds that if the child did suffer an injury, damages would be impossible to determine. For other examples, see: Elliott v. Brown, 361 So. 2d 546 (Ala. 1978); Moores v. Lucas, 405 So.2d 1022 (Fla. App. 1981); Blake v. Cruz, 698 P.2d 315 (1984); and Siemieniec v. Lutheran General Hosp., 512 N.E.2d 691 (1987).
69 Lynch et al., supra note 40, at 137.70 Id. at 137.71 Jeffreys, supra note 64, at 18.
Medicine and Law 450
This last factor lends itself to the moral extremism that some physicians may feel. As noted: “In rare instances, a health care provider may have a powerful personal moral bias that all life is worth saving and that everything possible should be done for every patient.”72
Despite possible feelings of moral obligations, physicians are ultimately required to assess the degree of severity of the patient and treat the person accordingly. This, in and of itself, may affect a physician’s prescribed course of treatment.
While a patient may have a DNI [do not intubate] order on the chart, they may develop a treatable pneumonia or other respiratory difficulty responsive to antibiotics or other medications. In these cases of a reversible respiratory problem, intubation and ventilatory support may be necessary to buy time until the medications have time to work. Thus, while the intubation is contrary to the DNI request, it is temporary and does not represent a long term commitment. This decision and its reasoning must be discussed with the patient and/or the family.73
Doctors often walk a fine line between a patient’s wishes and medical necessity. Another factor that might influence the disregarding of a DNR order includes the financial motivation to prolong treatment.74 Even when an advance directive exists, the patient’s decisions are not always clear since living wills often contain general language that does not refer to specific life-sustaining treatment.75This situation may frustrate a conflicted family that might be in disagreement about an individual’s end-of-life care. “While a DNR/DNI status may be indicated in the chart, the division within the family creates a hostile environment for the medical staff. As such, should a cardiac or respiratory arrest occur, the nurses and physicians prefer to resuscitate the patient until the family reaches a consensus.”76 Thus, it is important to be quite specific with end-of-life directives and to apprise one’s family of these decisions.
While overly cautious resuscitation might have been the practice in the past, a recent study found “do-not-resuscitate” orders to be an independent risk
72 Hubbard, supra note 67.73 Id.74 Jeffreys, supra note 64, at 18.75 Rodriguez, supra note 16.76 Hubbard, supra note 67.
Medicine and Law 451
factor for poor surgical outcome.77 The researchers concluded that surgical patients with DNR orders sustain more postoperative complications, with 1 in 4 dying within 30 days of surgery.78 In fact, people with DNR orders may be twice as likely to die soon after surgery regardless of the procedure or health status of the individual before the operation.79 Some attribute this statistic to the overall poorer health of this population, but the Director of Clinical Ethics at Stanford’s Center for Biomedical Ethics claims that these directives “subconsciously affect how doctors and nurses treat patients. For example, they order fewer tests and don’t enter the patient’s room as often.”80
THE PATIENT SELF-DETERMINATION ACT
The Patient Self-Determination Act (PSDA) was found by the United States Supreme Court in Cruzan v Missouri Department of Health81 to recognize the constitutional right of an individual to make medical decisions.82 As noted, “A competent person has a liberty interest under the Due Process Clause in refusing unwanted medical treatment.”83 By way of background, PSDA requires health care providers receiving Medicare and Medicaid funds to inform patients of their right to make a living will and have a health care proxy.84Hospitals, nursing facilities, home health agencies, hospice programs, and certain health maintenance organizations are included in this legislation, and they are required to ask patients about their advance directives and to document those instructions in the medical records.85 This federal law is important because it reinforces the patient’s ability to make his final wishes for medical care known, and it offers an added layer of protection to the various state statutes
77 Hadiza Kazaure, Sanziana Roman & Julia A. Sosa, High Mortality in Surgical Patients with Do-Not-Resuscitate Orders, 146 Archives of Surgery 8 (2011) available at
http://archsurg.amaassn.org/cgi/content/abstract/146/8/922 (last visited Dec. 27, 2011). 78 Id.79 Jennifer Warner, DNR Orders May Affect Surgical Outcomes, WebMD, April 18, 2011,
http://www.webmd.com/palliative-care/news/20110418/dnr-orders-may-affect-surgical-outcomes.
80 Id.81 497 U.S. 261 (1990).82 Id.; Pub. L. No. 101-508 codified at 42 U.S.C. 1395cc.83 Cruzan, 497 U.S. at 278. By way of contrast, the New York Court of Appeals in In re
Storar, 420 N.E. 2d 64, cert. denied, 454 U.S. 858(1981), refused to base a right to refuse medical treatment by the constitutional right of privacy. Rather, it found such a right “adequately supported” by the informed consent doctrine. Id. at 377.
84 Lynch et al., supra note 40 at 135.85 Martin, supra note 77.
Medicine and Law 452
on living wills.86 Equally as important, the term “wrongful prolongation of life” has made its way into legal vernacular based on the increasing number of claims in recent years using this term to recover damages.87 In these cases, the “wrongful prolongation of life” has required a close look at state and federal laws with regards to death, living wills, and advance directives.88 While state laws might be used as the basis for a cause of action against a health care provider who ignores a living will or advance directive, a violation of these statutes alone has not been utilized as the foundation for a wrongful prolongation of life lawsuit; rather, theories of liability for battery, negligence, violation of constitutional rights, and infliction of emotional distress have been the basis for these lawsuits.89
Cruzan has been used as a precedent for a number of wrongful prolongation of life cases that have made their way to the courts since the inception of the PSDA.90 For instance, in Rosebush v. Oakland County Prosecutor,91 a Michigan court cited Cruzan to reinforce the principle that a competent adult has the right to decline medical treatment or lifesaving methods.92 The facts
86 Id.87 See Maxwell J. Mehlman, Wrongful Prolongation of Life?, The Doctor Will See You
Now, Feb. 1, 2001, http://www.thedoctorwillseeyounow.com/content/bioethics/art1973.html?getPage=1.
88 Wright v. Johns Hopkins Health Sys. Corp., 728 A.2d 166, 169 (Md. 1999) (citing Maryland’s Health Care Decisions Act, which overlies an individual’s right to refuse life-sustaining medical treatment); Rosebush v. Oakland Cnty. Prosecutor, 491 N.W.2d 633, 638 (Mich. Ct. App. 1992) (mentioning M.C.L. § 700.496 which addresses the appointment of “a patient advocate to make medical-treatment decisions”); Anderson v. St. Francis-St. George Hosp.,No. C-930819, 1995 WL 109128 (Ohio Ct. App. 1995); Scheible v. Joseph L. Morse Geriatric Ctr., Inc.,988 So.2d 1130, 1132 (Fla. Dist. Ct. App. 2008).
89 Rodriguez, supra note 16, at 7-8.90 See Wright, 728 A.2d at 172 (Md. 1999) (involving an AIDS patient whose life had been
prolonged through heart resuscitation); Schiavo v. Schiavo, 403 F.3d 1223, 1223 (11th Cir. 2005) (involving the death of a girl who was removed from life support pursuant to a court order); Rosebush, 491 N.W.2d at 635 (involving parents of a minor wishing to remove their vegetative daughter from life support); Grace Plaza of Great Neck v. Elbaum, 623 N.E.2d 513, 513 (N.Y. 1993) (involving the spouse of a vegetative patient who refused to pay for the services of a nursing home after the spouse requested that a feeding tube be removed); Montalvo v. Borkovec, 647 N.W.2d 413, 413 (Wis. Ct. App. 2002) (involving a patient suing doctors for performing life-saving resuscitation on a premature baby without consent); HCA, 36 S.W.3d 187 (involving lawsuit against hospital for performing resuscitation on premature infant despite the parents giving specific instructions not to do so).
91 Rosebush, 491 N.W.2d 633.92 Id. at 635-36.

Medicine and Law 453
show that Joelle Rosebush was left in a vegetative state after a car accident, but her injuries did not leave her “brain dead.”93 The patient’s family sought to have her life-sustaining treatments stopped, and the court recognized theories of battery and informed consent of the patient when a doctor refused to adhere to such requests.94 While the court ordered the removal of life support, a dissenting judge noted:
Courts in foreign jurisdictions have recognized the unique policy and societal implications of removing the life-support system of a person in a persistent vegetative state. Because of the complex and sensitive nature of issues that are related to the removal of life-support systems, these courts urged that judicial policy gives way to the legislative process in order to insure that the interests of the constituency are served. Similarly, this Court has recognized that where moral and public policy matters are at issue, intermediate appellate judges should forgo their desire to create new law in favor of the legislative process.95
This comment aptly pinpoints the reason for the hesitancy of the courts to prescribe rules for cases concerning these sensitive issues. The courts do not want to legislate and would rather leave the matter to the legislature to create a new cause of action for wrongful prolongation of life. Nevertheless, the majority in Rosebush acknowledged that a state’s interests may outweigh the right to refuse life-sustaining treatment when the issue involves the preservation of life, protection of innocent third parties, prevention of suicide, and maintenance of ethical standards in the medical profession.96 Thus, while acknowledging advance directives, the court cited caveats that require at least two physicians’ diagnoses that a patient is terminally ill and the prognosis that there is no reasonable possibility of future recovery.97
Wright v. Johns Hopkins Health Systems98 is another case that draws attention to a state’s law regarding advance directives.99 This Maryland case involved
93 Id. at 635.94 Id. 95 Id. at 641.96 Rosebush, 491 N.W.2d at 637-38 (suggesting that the state can intervene in these
decisions when it is absolutely necessary, but only when it is absolutely necessary).97 Id. at 637-38.98 728 A.2d 166 (Md. 1999).99 Id.
Medicine and Law 454
an individual with Acquired Immune Deficiency Syndrome (AIDS) who was resuscitated after a cardiac arrest.100 The person’s estate sued the health care providers, claiming they “wrongfully prolonged the patient’s life” when he had a living will that stated his desire for no resuscitation.101 Ultimately, the court noted that the patient’s statements in the emergency room about a DNR order were insufficient.102 The court skirted the issue of wrongful prolongation of life by denying the claim for damages on other grounds and concluded that it is up to the legislature to decide whether wrongful prolongation of life is a proper tort.103 This case is yet another example of how the courts have found ways to not recognize causes of action for wrongful prolongation of life.104
The Indiana court in Taylor v. Muncie Medical Investors105 also refused to recognize this cause of action.106 The facts demonstrate that Taylor executed a living will before entering a nursing home, and a DNR order while in the nursing home, both of which were ignored after she suffered a stroke that left her comatose.107 An action was brought against the nursing home for the wrongful prolongation of life, but the court denied the claim, noting that its state’s Health Care Consent Act108 provides a remedy that already exists under the Indiana Code.109
New York considered the issue of wrongful prolongation of life in Cronin v. Jamaica Hospital Medical Center110 and ruled that such a case could not be maintained since being alive does not constitute an injury.111 In Grace Plaza of Great Neck, Inc. v. Elbaum,112 another New York court issued a similar ruling113
100 Id. at 171.101 Id. at 173.102 Id. at 177.103 Id. at 179 (citing previous instances where the court deferred to comprehensive legislation
related to a patient's right to refuse medical treatment).104 See Slawek v. Stroh, 215 N.W. 2d 9, 22 (Wis. 1974) (stating that recognition of such
cause of action “would have vast social ramifications and the creation of such a cause of action is the type of public policy decision that should be made by the people of this state or elected legal representatives”).
105 727 N.E.2d 466 (Ind. Ct. App. 2000).106 Id. at 472.107 Id. at 467-68.108 Ind.Code §§ 16-36-1-1 to 16-36-1-14.109 Id. at 471.110 60 A.D.3d 803 (N.Y. App. Div. 2009).111 Id.112 623 N.E.2d 513 (N.Y. 1993).113 Id.

Medicine and Law 455
and even found that the nursing home did not forfeit its right to payment for treatment provided to the patient after the nursing home refused to follow the spouse’s instruction to remove the patient’s feeding tube.114
Illinois discussed the issue in Gragg v. Calandra,115 a case in which a patient underwent open-heart surgery without consent and was placed on life-support despite a living will that contained instructions to the contrary.116
The defendant’s medical staff director stated that he would not honor the living will.117 The facts show that the patient never regained consciousness and died.118 A lawsuit was filed premised upon violations of the Illinois Family Expense Act and Consumer Fraud and Deceptive Business Practices Act.119 In this regard, the plaintiff claimed that the defendants “represented to the public that patients for cardiology services would promptly receive care for cardiac patients who would be in surgery within an hour.”120 The decedent’s family also stated that the medical center claimed it had a complete cardiovascular unit with a catheterization lab and that staff would help patients choose the right doctor.121 The court denied the claim under the Family Expense Act, asserting that the legislation only allowed a spouse to recover expenses incurred due to an injury.122 The court also stated that the plaintiff failed to establish how the medical center’s advertisements were false and that there was no causal connection between the alleged false advertising and the particular heart surgery that led to the plaintiff’s injuries.123 In addition, the family sought damages for intentional infliction of emotional distress caused by the doctor’s public accusations that they were trying to kill their family member by withholding life-sustaining treatment.124 Surprisingly, the appellate court found that the trial judge erred
114 Id. at 516 (“[u]nder these circumstances, plaintiff did not breach its contract, and defendant was not excused from paying for his wife's care”).
115 696 N.E.2d 1282 (Ill. App. Ct. 1998).116 Id. at 1285.117 Id.118 Id.119 Id.120 Gragg, 696 N.E.2d at 1288.121 Id. 122 Id. at 1286.123 Id. at 1288-89.124 Id. at 1289-90.
Medicine and Law 456
in dismissing the count for intentional infliction of emotional distress.125
Some attorneys have crafted lawsuits for wrongful prolongation of life under a breach of contract theory126 such as in Scheible v. Joseph L. Morse Geriatric Center, Inc.127 In this Florida litigation, it was alleged that a nursing home disregarded the patient’s advance directives under the Patient Self-Determination and Nursing Home Resident’s Rights Acts.128 The latter legislation provides that a patient has “[t]he right to refuse medication or treatment and to be informed of the consequences of such decisions, unless determined unable to provide informed consent under state law.”129 The breach of contract claim was premised upon the theory that the living will/advance directive was incorporated into the contract for the patient’s care.130 A jury was favorably impressed with the contract claim and awarded $150,000.131 On appeal, the court had to decide whether the resuscitative measures taken contrary to the decedent’s wishes resulted in “a manner of death other than that which would have occurred absent those measures.”132 The court ultimately
125 Gragg, 696 N.E.2d at 1290.Despite a favorable outcome in Gragg, appellants are not always successful in their claims of emotional distress as was the case with Bartling v. Glendale Adventist Medical Center, 184 Cal. App. 3d 961 (1986). In this case, much like in Gragg, the plaintiffs sought damages from emotional distress arising out of the hospital’s efforts to preserve the patient’s life; however, the California Court of Appeals upheld the trial courts verdict in favor of the defendants. Bartling, 184 Cal. App. 3d at 970-72. The difference between these cases is the public nature with which the defendant, in Gragg, accused the decedent’s family of ultimately trying to kill him by withholding life-sustaining measures , 696 N.E.2d at 1290, versus the private emotional distress endured when caring for a persistently vegetative family member in Bartling, 184 Cal. App. 3d at 971.
126 Filing a suit under violations of state and federal laws has proven to be a better avenue than filing under a violation of Constitutional Law. Pennsylvania considered the issue in a case based upon an alleged violation of the Pennsylvania Advance Directive for Health Care Act, 20 Pa.C.S. § 5401 et seq..in Klavan v. Crozer-Chester Medical Center, 60 F. Supp. 2d 436 (E.D. Pa. 1999), where the plaintiff attempted suicide but was resuscitated despite an advance directive to the contrary. Suit was subsequently filed for a violation of the patient’s due process and constitutional rights, a claim that was not upheld by the court. Id. at 444-45.
127 988 So. 2d 1130 (Fla. Dist. Ct. App. 2008).128 Id. at 1132.See also Fla. Stat. Ann. § 400.022(1) (West 1995) (nursing home residents’
rights);Kush v. Lloyd, 616 So. 2d 415, 417 (Fla. 1992) (court rejected the tort of wrongful life).
129 Fla. Stat. Ann. § 400.022(1)(k)(West 2011).130 Scheible, 988 So. 2d at 1132 n.1.131 Id.132 Id. at 1133.
Medicine and Law 457
concluded that the estate had no cause of action for violating the patient’s bill of rights.133
Prior to the 1997 Allore case,134 Ohio had other wrongful prolongation of life claims which were influenced by legislation in this area. In 1991, the state adopted a version of the Uniform Right of the Terminally Ill Act135 and also expanded the powers under a durable power of attorney for health care.136 This Act details the right to refuse life-sustaining treatment,137 the right to die, and acknowledges living wills.138 In Anderson v. St. Francis-St. George Hospital,139 just two years before Allore, damages were sought for the wrongful prolongation of life of an 82 year-old man who wanted no extraordinary measures utilized to prolong his life, but was resuscitated despite a “no code blue” order in his chart.140 In the first appeal, the court held that “wrongful living is not a compensable loss in Ohio.”141 The patient’s estate could not recover damages just for the patient being alive after resuscitation.142 However, the violation of an adult patient’s right to refuse treatment was addressed, a right affirmed by the Ohio statutes and federal law which included the Uniform Right of the Terminally Ill Act.143 The second appeal defined a claim of wrongful living as a damages concept, and thus looked at the facts under claims of negligence and battery.144 Ultimately, the Ohio Supreme Court held that (1) there is no cause of action for “wrongful living,’’ and (2) the patient suffered no legally compensable damages as a result of the defibrillation of his heart.145 Thus, while the first appeal established that one has the right to decline life-saving treatment and health-care providers can be forced to comply with these directives, the second review established that
133 Id.134 Allore v. Flower Hospital, 699 N.E.2d 560 (Ohio Ct. App. 1997).135 Ohio Rev. Code Ann. § 2133.01-.16 (West 2011).136 Ohio Rev. Code Ann. §§ 1337.11-.17 (West 2011); see also Anderson v. St. Francis-St.
George Hospital, 671 N.E.2d 225 (Ohio1996)(stating Ohio adopted both a version of the Uniform Right of the Terminally Ill Act and expanded the powers of a durable power of attorney for health care).
137 See 22A Am. Jur. 2d Death§ 552 (2011) (defining “life-sustaining treatment” as “any medical procedure or intervention that, when administered to a qualified patient, will serve only to prolong the process of dying”).
138 Ohio Rev. Code Ann. § 2133.01-.16 (West 2011).139 No. C-930819, 1995 WL 109128 (Ohio App. 1 Dist., 1995).140 Id. at *1.141 Id. at *3.142 Id.143 Id. at *4.144 Anderson v. St. Francis-St. George Hospital, Inc., 671 N.E.2d 225, 226 (Ohio 1996).145 Id. at 228-29.
Medicine and Law 458
tort law is not a means of redress when life-sustaining measures have already been taken.146
CONCLUSION
Wrongful prolongation of life cases have been advanced under theories of negligence, battery, violations of the Constitution, breach of contract, and infliction of emotional distress, but no recognized cause of action has really emerged allowing for the awarding of monetary damages.147 Various legislative enactments and high-profile cases have made the public more aware of the importance of advance directives,148 but the recognition of these documents by health care professionals does not remain consistent.149 Until legislation creates a cause of action for the wrongful prolongation of life, living wills and advanced directives merely remain a way of making one’s end of life wishes known, which wishes may or may not be honored.150
146 Hoffman & Schwartz, supra note 35, at 31. 147 See, e.g., Scheible v. Joseph L. Morse Geriatric Ctr., Inc., 988 So. 2d 1130, 1132 (Fla.
Dist. Ct. App. 2008)(using a breach of contract claim); Klavan v. Crozer-Chester Med. Ctr., 60 F. Supp. 2d 436, 440 (E.D. Pa. 1999)(claiming a violation of the patient’s constitutional due process rights); Gragg v. Calandra, 696 N.E.2d 1282, 1289-90 (Ind. Ct. App. 1998) (advancing a claim of intentional infliction of emotional distress).
148 See discussion supra pp. 6-8.149 See discussion supra pp. 13-18. 150 Seeid. (suggesting that DNR agreements are ignored sometimes because physicians are
worried about future litigation for not resuscitating a patient; this suggests that possible litigation is a motivating force that physicians respond to. Thus, allowing a claim of wrongful life would act as a deterrent for violation of DNR agreements).
©PROBOOK 2013and Law
Medicine Med Law (2013) 32:459-481
459
ADVANCE DIRECTIVES AND LIVING WILLS:THE ROLE OF PATIENT´S AUTONOMY IN THE BRAZILIAN EXPERIENCEEduardo Dantas*
Vice-President World Association for Medical LawPresident Brazilian Association for Health Law
To violate a person´s autonomy is to treat that person merely as a means, that is, in accordance with others´ goals without regard to that person´s own goals. Such treatment is a fundamental moral violation because autonomous persons are ends in themselves capable of
determining their destinies.1
Abstract: This paper aims to discuss the development of the notion that the patient has the right to refuse treatment, and how the Brazilian legal system is dealing with bioethical dilemmas, such as the possibility of exercising autonomy through advance directives. The paper discusses the lack of legislation to regulate important issues in the end of life healthcare, and what ethical guidelines exist, providing physicians with ethical and legal parameters to deal with the patient´s will.
Keywords: Autonomy; Living Will; Advance Directives; End of Life; Informed Consent; Brazilian Law
* Lawyer, registered in both Brazilian and Portuguese BAR associations. Specialist in Consummer Law by the University of Castilla-La Mancha, Spain. LL.M. in Medical Law by the University of Glasgow, Scotland. PhD student at the University of Coimbra, Portugal. Vice-President of the World Association for Medical Law. Vice-President of the Asociación Latinoamericana de Derecho Médico.President of the Brazilian Association for Health Law.Member of the European Association of Health Law. Author of several articles published in Brazil, Portugal, USA, Israel, Czech Republic and France. Author of the booksDireito Médico (Editora GZ, 2009),Comentários ao Código de Ética Médica (Editora GZ, 2010) and Droit Médical au Brésil: essais et reflexionssous la perspective du droit comparé (Editora GZ, 2013).
E-mail: [email protected] Beauchamp and Childress, Principles of Biomedical Ethics, 1994, 4th ed., p. 125.
Medicine and Law 460
1. INTRODUCTION
All over the world, one of the more controversial ethical issues is how to deal with the patient´s wishes in a scenario surrounded by the approximation of death. Physicians are trained to postpone death at all costs, but sometimes the patient´s will is to avoid senseless pain when staying alive is not viable anymore (or when life cannot be lived with dignity).
So many questions arise from this conflict: Until when a patient is competent to decide? What are the limits of the patient´s autonomy? What are the limits of medicine, and at what point the thin line of saving a patient´s life and making him suffer for no reason other than keeping him alive is crossed?
And more: in a society where medical issues are brought to the courts in a speed that challenges even common sense, and where the law and statutes can´t keep up to the pace of medical development, what are the limits to what is legal, what is acceptable, what is moral, what is ethical and what is right?
Medicine has evolved in such a speed in the last six decades, that now it is possible to keep a patient artificially alive for years, even against what could be called “the laws of Nature”. There are huge debates over the purposes of postponing death at all costs, even if it means leaving the patient alive and suffering in a vegetative state, just to satisfy the family´s wishes. For some, this is a natural response (and obligation) of medicine. To others, it is just playing God beyond the limits of science.
There is no easy answer to these issues, but a consistent solution is under construction in different parts of the world, leading towards the respect of the patient´s will, and recognizing the importance of obtaining the patient´s consent, whenever it is possible, respecting autonomy and choice.
2. DEFINING CONCEPTS, OR UNDERSTANDING AUTONOMY IN END OF LIFE SITUATIONS
Informed consent is the authorization given by the patient to undergo treatment, based on the knowledge of the nature of a medical procedure, and be submitted to risks, side effects, possible complications, benefits and alternatives to the proposed treatment. In other words, it is the acceptance of the services to be delivered by a healthcare professional, after understanding what is being consented to.
Medicine and Law 461
A long time has passed from the days when physicians told patients what they needed and patients agreed without question. Although some patients still have an “I will do whatever you say, doctor” attitude, they’re in the minority. In today’s world, different people react to proposed treatments or tests differently, often as a result of their varied backgrounds, financial status, values, attitudes and perspectives.
The paradox of contemporary medicine is that a constant expansion of therapeutic options makes decoding these options increasingly difficult. In legal terms, this new situation has been transposed into a growing demand for patient participation in decision-making which seems to express the notion that anxiety caused by being subjected to some kind of medical dictatorship creates the need to even out a relationship which is by essence asymmetrical. To this recent culture is added a growing trend to judiciarisation2 which challenges medicine to respond to two contradictory imperatives: to give the best possible care, but within mandatory limits and constraints, or to be confronted with hostility.
When it comes to end of life situation, another piece of human drama is added: the patient - as a corollary of the principle of respect for human dignitiy, has the right to be informed about his situation, the prognosis and the possible or expected outcome, and then be an active player in the decision-making process.
In other words: in a terminal situation, the patient has the right to refuse treatment, if there is no possibility of staying alive without suffering or a minimum standard of quality, and opt to receive just palliative care, leaving life to follow its natural course, without artificially postponing death.
One of the biggest problems in accepting this decision is that some segments of society still thinks that refusing treatment is the same as authorizing euthanasia.
Euthanasia is the act of provoking, or facilitating the death of another person who is suffering from a serious and, for the most part, painful illness. It depends on a clear act, such as the application of high doses of sedating, or lethal substances toa terminal patient, which differs from the assisted suicide,
2 On this topic, DEMICHEL’s “Au nom de quoi? Libre propos d’une juriste sur la médicalisation de la vie”.
Medicine and Law 462
because in the latter, the help to die is explicitly requested by a patient who is no longer able to move, or to act on hisown in this regard.
The orthotanasia, is the suspension, reduction or withdrawal of medication, equipment, or procedures that serve to artificially prolong the life of a patient, abbreviating his suffering, and allowing life follow its natural path to extinction. Not resuscitating one patient who is suffering a cardiorespiratory arrest seems to be a good example of it.
In a diverse path follows the dysthanasia, which is prolonging life of a patient without any viable prospect of cure or improvement by artificial means.
The treatment of terminally ill patients, and the postponing of end of life issues, has always been one of the greatest dilemmas faced by doctors, who were trained and taught to face death as a defeat, and the prolongation of life as the only acceptable procedure.
Just recently, the issue has become subject of legislation in different countries, strenghtening the idea that the patients needed to play a major role, regulating thus how autonomy could be exercised, in order to bring legal safety to the decisions, pushing liability and criminal responsibility away from the doctor-patient relationship.
3. THE DEVELOPMENT OF THE PATIENT´S CHOICE - ETHICAL AND LEGAL ASPECTS
Refusing treatment is always an event situated at the centre of a profusion of concerns. The need for recognition is probably one of the most significant of them. This need for recognition that Paul Ricoeur3 analyzed with great precision exists in both patient and doctor.
Patients want doctors to recognize their individuality and their complexity. Refusal can be an expression of this need and a request for euthanasia is frequently a call for help rather than evidence of any real desire to end life.
But doctors also need recognition from patients, not so much in the form of gratitude, but in terms of recognition for their competence, their sense of responsibility and the legitimacy and specificity of the values which the medical profession upholds.
3 P. Ricoeur, Parcours de la reconnaissance, Paris, Stock, 2004

Medicine and Law 463
To these two components could probably be added the expression of a need for social recognition, recognition of a need expressed by a public call for help from both protagonists in the act of caring. One specific characteristic of caring is the statement of an act of solidarity so that the “private” dialogue between patient and physician is frequently part of a quest for social harmony. When these demands are claimed by both parties, it is easy to understand that the two (or three) recognitions may not coincide. This may be the case when a sick person entertains iron-bound convictions that do not allow him to take account of the concern for professional - not to mention legal - responsibilities that inhabit the doctor,or a doctor who is excessively infatuated with some therapeutic project and resents criticism from the patient.
Or it could also be a recognition in the medicine as a culture that finds it unacceptable for traditional beliefs it considers as irrational to be allowed to challenge their modern practices backed by scientific evidence. As can be seen from all these examples, solving the issues on a pragmatic case by case basis is not the way to developing guidelines.
One answer lies in the fact that the way many of us can expect to live, age and die has changed dramatically over the past quarter of a century. In many countries, advances in basic living conditions, healthcare and medical technology mean that most of us are living to a good age, and that many of us are living to a very good age in spite of the illnesses or fragility which ordinarily beset us. When in the past we had good reasons to fear an early death, today many of us fear living too long, and we fear that medical interventions will unreasonably prolong our dying as well. When in the past we had good reasons to fear a painful and uncomfortable aging and dying, today with advances in the management of chronic illnesses and palliative medicine, we are more likely to be fearful of living not with pain and discomfort, but instead with the perceived degradation of physical dependence or mental incompetence.
Boundaries of this subject are yet to be discovered. In Old Law, New Medicine4, Sheila McLeanpoints out:
“The fundamental taboos which surround the very subject of death permit the perpetuation of an approach to it which may have a number of consequences. First, those who actively choose death may be regarded as irrational or lacking legal competence.
4 (1999), London, Pandora, p. 140-141.
Medicine and Law 464
This is particularly so when medicine can offer hope of a cure or palliation of symptoms.…Second, some individuals may be so afraid of a life without prolonged quality that they choose suicide as an option. Angell, for example, has noted that: ‘The very high suicide rate in older Americans is due partly to their being concerned that they will not be ableto stop treatment if hospitalized… Some people now fear living more than dying, because they dread becoming prisoners of technology.’…Finally, medical advances require resolution of the question of what is to be done in respect of the person who is incompetent, with no hope of recovery and with no clear advance expression of wishes. Strict adherence to the principle of the sanctity of life results in such individuals being maintained in an insentient form for what, in some cases, may be a very long time. Without clear justifications for the termination of treatment, life which has no quality for the person living will be prolonged merely because the technology to do so exists.”
The discussion about patient´s autonomy is neither new nor original5. But it is interesting to see that all movements made, both in the legal and ethical fields, lead towards the same conclusion. Different jurisdictions, with completely unrelated legal backgrounds, eventually end in finding the same solutions.
Historically, the ability to force treatment on unwilling patients derives from a need-for-treatment justification. This approach started to change in the 1960's, mostly in the United States, when there was a gradual move toward the "dangerous patient" justification-unwanted treatment could be imposed only if, or when, the patient presented a significant risk of harming himself or others. Under this new system, patients' advocates began to press for the patient's right to determine what is to bedone to his own body, creating instances in which the committed patient could decline treatment with medication. As these matters began to make countrywide legal appearances
5 Regarding the historical background on this issue, I refer to my paper entitled “When consent is not enough: the construction and development of the modern concept of autonomy”, published by Lex Medicinae (Portugal, vol. 15, 2011, p. 101-112).
Medicine and Law 465
in the U.S., virtually every involved court recognized some substantial patient interest in a right to refuse treatment6.
In 1989, deciding a case in the British courts7, Lord Donaldson MR stated in his ruling that:
“The ability of the ordinary adult to exercise a free choice in deciding whether to accept or refuse medical treatment and to choose between treatments is not to be dismissed as desirable but inessential. It is a crucial factor in relation to all medical treatment”.
In 1997, Article 5 of the Oviedo Convention (European Convention of Human Rights and Biomedicine), clearly stated:
“An intervention in the health field may only be carried out after the person concerned has given free and informed consent. This person shall beforehand be given appropriate information as to the purpose and nature of the intervention as well as on its consequence and risks. The person concerned may freely withdraw at any time.”
Very similar to that, and just a few years later, UNESCO´s Universal Declaration on Biomedicine and Human Rights (2005) recognized the same principle of respect for autonomy, also in its article 5:
“The autonomy of persons to make decisions, while taking responsibility for those decisions and respecting the autonomy of others, is to be respected”.
In 1994, the United States Congress acknowledged patients' overall rights to refuse medical treatment in certain circumstances, even if such refusal would result in death, enacting the Patient Self Determination Act8 (the "Act") in an effort to encourage patients to exercise their common law rights to refuse treatment. The Act applies to licensed health care facilities which receive Medicare or Medicaid program funds. The Act requires hospitals, nursing homes and hospices to furnish certain information to the patient/resident at the
6 In the same sense, see Vacco v. Quill, 117 S.Ct. 2293 (1997) or Washington v. Glucksberg, 117 S.Ct. 2258 (1997).
7 In Re F (Mental Patient: Sterilisation) (1990) 2 AC 1.8 (a.k.a. the "Danforth Act") See 42 U.S.C. §1395cc (1994).
Medicine and Law 466
time of admission. This written information concerns the patient's rights under State law and the written policies of the provider regarding implementation of the patient's advance directives. The facility must also document in the patient's medical record whether he holds an advance medical directive. The provision of the patient's care may not be conditioned upon execution of an advance directive.
In France,the patient´s right to advance directive and to appoint a person to act as proxy (not necessarily a relative, but someone who will be entrusted on enforcing the patient´s will in case of unconsciousness, or inability to speak for itself) is regulated by the law of March 4th, 2004 (commonly known as Loi Kouchner).
Recently, Portugal enacted the Law 25/2012, which regulates advance directives, living wills and healthcare proxy and creates a National Registry of Advance Directives.
All of this combined represents a quick but comprehensive view on the complexity of the situation, and how seriously the debate over autonomy and the patient´s right to decide his own fate when facing a terminal disease is.
In the precise words of Kristinsson9,
“Personal deliberation might be valued for its ability to bring out, express, and create the distinct point of view of the individual in question, and for making it possible for the individual to steer the course of her life according to that distinct point of view. An individual´s “point of view” is a complex, dynamic outcome of emotions, judgments, beliefs, desires, habits, and character, and all of these are in turn affected by upbringing and other contingent circumstances”.
From all this comparative background, it seems that there is no doubt that we are heading towards the recognition of the patient´s right to exercise autonomy, not only during treatment, but also deciding when it should finish.
9 KRISTINSSON, Sigurdur. Autonomy and informed consent: A mistaken Association? Medicine, Health Care and Philosophy. DOI 10.1007/s11019-007-9048-4, Springer, 2007.
Medicine and Law 467
4. THE BRAZILIAN SCENARIO - THE ACTIVE ROLE OF THE FEDERAL COUNCIL OF MEDICINE
The Brazilian situation regarding advance directives is very peculiar. While other countries have long been discussing the subject, either in court or through legislation, the issue has been solemnly ignored by politicians, leaving a void in legislation, and thus creating insecurity for the health care professionals.
There is no provision in Brazilian law, regulation or establishing guidelines for the use (and even validity) of advance directives in a terminal situation. Physicians have to rely on the interpretation of various codes and legal norms in an exercise of legal interpretation they are not used (or trained) to.
According to the Federal Constitution, based on Article 5, section II, which states that nobody can be forced to do, or be compelled not to do something against his or her will, unless determined by law, a patient has the right to refuse medical treatment,.
In the same sense, according to sections VI and VIII of the same article, which guarantees such freedom, medical treatment can be refused in respect for the patients' philosophical convictions and religious beliefs. In other words, it’s a constitutional right that the patient’s will prevails over the therapeutic options chosen by the doctor, even if technical and professional arguments are ignored. Being a conscious decision, taken by a competent patient, after proper information, the patient’s will must be respected.
References to the patient’s right to refuse treatment are scattered all over Brazilian legislation, without a specific legal act. The Civil Code states, in Article 15, that “no one can be constrained to submit, with risk to life, to a medical treatment or surgical intervention”.
The terms of the article are imprecise, because the expression “with risk to life” may lead to the false conclusion that, if there’s no risk of dying, the patient could be constrained, or forced, to accept treatment or surgical intervention, which is not the spirit of the law.
The new Civil Code, enacted in 2002, presents a twist in medical responsibility, changing what was considered the main physician’s obligation - saving human lives by all means - and giving powers (and, as a consequence, responsibilities) to patients and legal surrogates, letting them interfere and decide their own
Medicine and Law 468
fate, according to the bioethical principles of autonomy.
In the same spirit of law, Article 17 of the Elder’s Statute (Estatuto do Idoso) guarantees to people of more than 65 years of age, which are sound mind and sane, the right to choose what they consider to be the most favorable health treatment.
The aforementioned Statute does not make any reference to risk of death as a condition to carry out the right to choose a therapeutic option. Regardless of his clinical condition, the only possibility of restraint for the patient is to be insane and lacking mental integrity. In this situation, the doctor can only proceed his own personal option of treatment if: a) the patient cannot express his will; b) the relatives or legal surrogates cannot be found; and; c) there is immediate and real risk of death.
Another expression of the patient’s autonomy in the Brazilian legal system is contained in Article 10 of the Statute of Organ Donations and Transplants. This Article favours, the patient’s consent in any situation, in spite of the doctor’s decision, demanding the express consent of the receiver, after counseling about the risks of the transplant procedure. That means that, even in real and immediate risk of death, the patient can decide to submit or not to the risks of transplantation.
The same reasoning, though, can be applied to radical surgical procedures, administration of medicine, chemotherapy and blood transfusion, considered bymany as a form of “transplantation”
It is perhaps worth mentioning, at this point, a law enforced by the State of São Paulo10, which guarantees to the State’s health service users the right to receive clear and adequate information on therapies and therapeutic procedures, in respect for ethical and cultural values.
Two other States - Paraná and Minas Gerais - also passed laws for public health services users’ protection11, stressing patient’s autonomy as a principle to be observed and enforced.
It is clear then, that these modern pieces of legislation take into consideration the patient’s will, in spite of his clinical state and condition, presenting legal
10 State Law n. 10.241/1999 - São Paulo11 State Law n. 14.254/2003 - Paraná and State Law n. 16.279/2006 - Minas Gerais
Medicine and Law 469
mechanisms to enforce his right of choice, rejecting medical or judicial impositions and respecting the principles of dignity of the human being.
Another conclusion that can be reached is that the bioethical principle of Beneficence must be interpreted under the patient’s view, since he is the addressee of medical intervention, and even if the Medical Ethics Code guarantees the physician (Article 22) discretionary action in a life and death situation, this discretion cannot oppose constitutional rights.
There are, though, winds of change, provided not by legislators, but by physicians themselves. By August 2012, the Federal Council of Medicine approved a new resolution (CFM n. 1995/2012) allowing doctors to withhold procedures or withdraw treatments designed to keep a terminal patient alive, provided the patient or his legal surrogate expresses the wish to do so.
RESOLUTION CFM 1.995/2012 (August 31st, 2012)
Article 1 - Defining advanced directives as a set of wishes, previously and expressely manifested by the patient, about the health care or treatments he/she wants - or not - to receive in the moment he/she loses the ability freely and autonomously express, his/her will.
Article 2 - When deciding about health care or treatment of patients who are incapable of communicating, or to freely and independently express their will, the physician shall take into consideration their advanced directives.
Section 1 - If the patient has designated a proxy for that purpose, the proxy´s informations should be taken into consideration by the physician.
Section 2 - The physician shall disregard the patient´s advanced directives or proxy´s informations when they are, after his analysis, conflicting with the principles established by the Medical Ethics Code.
Section 3 - The advance directives shall prevail against any medical opinion and against the patient´s family wishes.
Section 4 - The physician will register, on the patient´s chart, the advanced directives that are directly communicated to him by the patient.
Medicine and Law 470
Section 5 - If no advanced directives are established, nor a proxy has been designated, and if there is no family members available to decide, or if they have conflicting requests, the physician - when found necessary and convenient - shall submit the case to the hospital´s Ethics Committee. If thereis no such committee, the case must be submitted to the Regional and Federal Council of Medicine, to provide solid grounds in order to solve ethical conflicts.
Article 3 - This Resolution shall enter into force on the date of its publication.
Such a Resolution is not an statute, but rather than just being an ethical guideline, and facing the lack of regulation on the matter, it assumes capital importance and (at least temporarily) fulfills the legal gap, since the Federal Council of Medicine was created by a Federal Law, and among the competencies that were given to it, there is the power to enact guidelines that will oblige physicians during the exercise of the medical profession.
Itis an important step towards giving the patient the possibility of regaining control over his own life, thus allowing him to die with dignity. The main result of this Resolution is to recognize that dying with dignity is the culmination of a greater scenario, which is living with dignity.
Although it may seem justifiable to state that patients may wish to be and remain at all times in complete control over matters regarding their personal health, this simple statement of principle bears little relationship to reality. People who are confronted with pain, disease or approaching death, are bound to feel diminished by the awareness of their own weakness and therefore lose some of their autonomy to the extent that they no longer know what it is they realy want or can accept and are not even able to express themselves.
By their side, more often than not, facing them, are physicians or carers whose strength, despite some doubts and hesitation at times, is, reinforced by their own science and who wish to accomplish their mission, which is to apply in full a treatment they consider to be the most appropriate, under the circumstances, to alleviate, cure, or delay the advent of death.
But can what is left of patient autonomy, of the notion of consent that the patient is requested to give and of the need to create conditions in which freedom of
Medicine and Law 471
consent - which everyone agrees must be “informed” - be exercised? Can there be consent if, as we have seen, there is no possibility of refusal?
This was the question that the Brazilian Code of Medical Ethics (another Resolution from the Federal Council of Medicine) dated 2009 attempted to answer, so as to provide patients with more autonomy of decision as regards medical care and ensure more equality in the relationship between doctors and patients.
The Code enshrines the notion that patient consent must prevail and in other words states that, in the light of information and advice supplied by healthcare providers and in consultation with them, patients are entitled to take decisions regarding their own health. Doctors must respect wishes expressed by patients after informing them of the consequences of their decisions.
When refusing to undergo or continue treatment represents a threat to life, physicians must do their utmost to convince patients that they should accept essential treatment. No medical act or treatment may be applied without securing free and informed consent from the person concerned. There is, though, a legal gap in here, since consent may be withdrawn at any time, but the criminal code forbids physicians to interrupt life-saving treatments. This inconsistency has yet to be faced by Court, since no claim has posed this issue up to now.
These are, therefore, the ethical foundations of patient autonomy and right to refuse treatment, as inserted in Brazilian Code of Medical Ethics:
Art. 41-[The doctor shall not] Shorten the patient's life, albeit at his request or at his legal representative.
Sole paragraph - In cases of incurable and terminal disease, the doctor must provide all palliative care available without undertaking unnecessary diagnostic, therapeutic or obstinate actions, always taking into consideration the wishes expressed by the patient or, in his impossibility, of his legal representative ".
Amongst the Fundamental Principles of Medicine, elected by the Medical Ethics Code, the one described in section XXII says verbatim that "in terminal and irreversible clinical situations, physicians avoid carrying out unnecessary diagnostic and therapeutic procedures and allow the patients under his care all appropriate palliative care. "

Medicine and Law 472
The aforementioned resolution is grounded in the claim of the defense of constitutional principles such as human dignity, and the prohibition of inhuman or degrading treatment, clearly stated in Articles 1°, III and 5º, III - of the Federal Constitution. While these effectively important principles add up to the bioethical principle of autonomy, they do conflict with the protection of life (the sanctity of life, as found in the foreign doctrine).
When dealing with the existence and recognition of a patient's right to die with dignity and autonomy, Leticia Ludwig Möller shows well the conflict faced between the ethically desirable and legally permissible:12
“The excessive and inappropriate use of technologies applied to the medical treatment of patients in the terminal stage, leading to the prolongation of a painful end of life (often beyond what would be desired by the patient himself, disregarding his right to exercise autonomy, conforming the idea and the need to affirm the existence of a right to die with dignity. The expression "right to die" or "right to a dignified death" can now be found in studies about end of life seeking the dialogue between different areas of knowledge, such as medicine, ethics and law. The advocates of the right to die with dignity, in general, are glimpsing the patient's terminal condition that is exposed to treatments that merely extend the time of his death, bringing him no benefits, but only pain and suffering - not often wishing these authors extend this defense to the practice of euthanasia (active). Dying with dignity so often relates to the idea of dying in peace, with physical and spiritual integrity, or even, to die at the right time, with comfort and relief from suffering.(...)We share the understanding of Ronald Dworkin, that the way we die has importance, and in general, the right of the individual to his death is a reflex of how he lived and must be respected, that this time keeps a consistency with the values and beliefs expressed in life - especially if this is the manifest desire of the ailing, and within the limits (as stated above).”
12 In Right to die with dignity and autonomy. Ed (Publisher). Juruá, Curitiba, 2007. pages 95-98.

Medicine and Law 473
Another important aspect to be considered is the fact that the practice of palliative medicine is now a reality in the vast majority of hospitals in Brazil, being positive in order not to deprive the conviviality of terminally ill patient from their families. This stance, according to its advocates, meets one of the pillars of bioethics, which is the principle of autonomy, the patient's right to decide the course of their own treatment. It would still be consistent with respect for human dignity, the principle developed in the first article of our Federal Constitution.
Examining the Medical Ethics Code, Leo Pessini adds:13
“(...) we noticed significant change of emphasis. The goal of medicine is not only maximizing the lifetime of a person. The aim of medical attention is the health of the human being and the criterion to evaluate their procedures is whether they will benefit the patientor not (cf. art. 2nd). The commitment to health, especially if understood as global welfare of the person and not just the absence of disease, opens up the possibility for other issues in the treatment of the terminally ill, and the healing issues. Even so, it remains a steadfast conviction, also found in earlier codes, that "The doctor must keep absolute respect for human life (...)" (art. 6). This tension between benefiting the patient with palliative treatments, which may shorten his life but promote his physical and mental well-being, and the absolutism of the value of human life in its biological sense, produces a dilemma that some doctors prefer to settle in favour of prolonging life.”
From a strictly rational point of view, death is just one of many aspects of life. Nothing more natural. However, talking about death, this companion that is increasingly present from the moment we are born, causes us such discomfort, that we turned it into a real taboo. We associate it with fear, frustration, pain, suffering and despair. Trying to ignore the undeniable reality of its existence, we avoid talking about it: we deny children the understanding of the phenomenon of death and the right to bid farewell to the beloved ones; we deny ourselves share the grief with loved ones; we deny health professions students a deep discussion on the topic that would help them to better deal with the matter within their professional practice. We created an illusion of
13 In his article "Dysthanasia: some reflections from the bioethical Brazilian reality", published in the journal Bioethics 2004, Vol. 12, No. 01.

Medicine and Law 474
immortality, thus wasting the opportunity that the acceptance of our finitude gives us: the opportunity to reflect on life and the perception that the time we have is limited, and therefore precious. Live it with quality is the true translation of what it is a life well lived.
It is within this perspective of emphasis to a life of dignity and quality that the healthcare professionals who are dedicated to palliative care work. Such care seek to relieve the suffering of patients whose medical diagnostics indicate that they have no chance of healing, through symptom control (not only physical, but in different orders) and the promotion of a lifetime with the best possible quality until the last moment. It is the quest for "good death".
Inherent to palliative care is the attempt to rescue an experience more human in the relationship between the patient and the professional staff that takes care of him. Special attention is also given to the humanization of the processes of death and mourning in prolonged illnesses that are usually intense and characterized by long periods of emotional burnout and stress.
In palliative care, the person is treated, not the disease. This seemingly simple change makes a big difference. It opens space for a perception of singularities of the individual, thus leading to a more accurate understanding of their real needs. Treating the patient with respect and preserving his dignity is only possible when it is considered in its context and its nuances. This is a sine qua non condition, so that we can see him in his condition of human being, rather than sick and we are open to listen to their concerns, fears, desires and feelings, whether they manifest in verbal or unsaid.
Kübler-Ross points out five stages of dying, each with its own characteristics. At the denial stage, the patient uses this defense mechanism in an attempt to cope with the anxiety facing his own the death. At the stage of anger, arises a revolt against the diagnosis, the prognosis, and often against God and against those who are around him. The patient may show up aggressive toward his family members and the professionals who take care of him. At the bargaining stage, there is an attempt to negotiate his healing, doing good deeds to be rewarded for them. The fourth stage described by the author is depression, in which the patient comes into contact with a profound sense of loss and may prove to be silent and isolated from others. Finally, there is the stage of acceptance, in which the despair gives place to a feeling of peace. It is important to stress that, although these stages serve as parameters for the
Medicine and Law 475
understanding of the process by which the patient passes, they do not present themselves in a rigid order and the way they are experienced, as well as the duration of each, is variable for each individual. It is important to respect each of these phases allowing the patient to experience them.14
While in traditional medicine the health professional seem encouraged to turn to attempt to extend the duration of life avoiding death, medicine that resorts to palliative care is seeking to prolong what makes us human, preserving the maximum freedom of making conscious choices. Life is not only considered in its biological sense, but also includes social, psychological and relational aspects. While there is life, there is also the potential for intra and interpersonal emotional growth..
Implied to a discussion about palliative care is the issue of how human beings are perceived, because the vision of man that the healthcare professional has, directly affects his attitude and his work - whether he is aware of his ideas or not.
If the ideas of the professionals are inserted within a paradigm that assigns to the man an essence of identity, he will not be seen as amenable to changes and growth, but as someone always equal to himself, thus not affected by the other. From this perspective there is an appreciation of stability: the human conflicts are viewed negatively, taken as imbalances that must be banned for threatening stability. This man is thought of as a passive being, and therefore being incumbent to the health professional's keeping of knowledge and total responsibility for the course of his treatment.
There is, however, another paradigm that has been strengthening and which provides the basis for the changes requested by the palliative medicine: the man seen as a procedural being, i.e. a man that builds himself, actively, as he lives. This means that he never remains static or reaches the end of constructing himself. On the contrary, it lies in a continuous becoming, overtaking what is from what is about to become . The processuality of man takes place through the meeting with the other, in a dialectical relationship which affects and is also affected, being the mutual affectation the requirement for growth. The conflicts, far from being seen as negative, are the promoters of growth and they stimulate and develop the potential of adaptation.
14 KÜBLER-ROSS, E. On death and dying: what patients have to teach doctors, nurses, religious and their own relatives. Ed (Publisher). Martins Fontes Sao Paulo, 1996.
Medicine and Law 476
The emphasis, in this paradigmatic vision, is in the potential of human beings to make changes, to reframe their experiences and establish life projects for themselves. His ability to make conscious choices gives the possibility to seek self-fulfilment creatively and responsibly. Within this perspective, the patient is not passive towards health professionals and diagnoses received.
The paradigm that sees the patient as a whole human being has autonomy over his lifetime. So there is no space for a health professional who presents himself authoritatively: possible interventions and the implications of each of them must necessarily be discussed with clarity and directness between doctor, team, patient and family, whence the dignity of the patient is mantained and he is allowed to make choices that, in his concern, are the most appropriate, i.e. meeting his best interests. When talking about choices, we do not mean only those that involve the balancing of risks and benefits of possible treatments and medical interventions, but rather we include the resolutions of life and farewells.
To deny the patient the clarification on his actual conditions is not a way to protect him. Rather, it means leaving him alone without the chance to share his woes and feeling himself betrayed by realizing that he cannot fully rely on those whose care he is submitted to. When the family decides to keep secrets or lie to the patient about his diagnosis and prognosis, it will create an emotional barrier that will hamper the free expression of affections in relationships.
Being able to go through the end of life consciously and feeling himself valued and respected enriches the life of the patient in order to promote a greater sense of emotional strengthening. This is an important prerequisite for the establishment of clearer priorities and for a deeper connection with the loved ones.
Palliative care also fulfills the role of helping the relatives of the patient to face the process of coming across the pain of the situation impending loss of a beloved (family) member.
The familiar universe is systemic, and therefore the impact of the existence of a member in need of palliative care is impacting to each of the other members and to the family unit as a whole. The family faces a long and anticipatory mourning, since the feeling of loss is settled from the diagnosis, and the emotional issues that arise during this period of stress need to be recognized and addressed.

Medicine and Law 477
Being able to express the pain and share feelings promotes the individuals and his family's strengthening. Depart from the patient does not relieve pain from anyone and causes to the patient the extra pain of abandonment in life.
To be empowered to act appropriately in palliative care, a health care professional needs some training which goes beyond the technical field. As important as the safety in knowledge acquired is personal preparation which allows coming across his own limitations and with the confrontation of doubts and anguish that the theme of death rises, and yet what we call interpersonal preparation, is indispensable when the proposal is truly monitoring the patient, taking him and his family in his afflictions and acting as facilitator of the relationship between both of them, in favor of a dignified life.
The great virtue of this resolution was to bring onto the stage the debate which hitherto remained confined to the corridors of hospitals. Science has evolved to the point of allowing to artificially prolong a terminal life indefinitely, under suffering, mechanically, without purpose and at any cost, whereby medicine is avoiding its primary objective.
5. CONCLUSIONS
It is important to recognize, however, that some people who express support for a ‘right to die,’ only do so in a highly qualified way. Many people who think that medicine often sustains or prolongs life unreasonably, and who feel helpless to oppose its momentum, often assert a ‘right to die’ when what they are really claiming is the ‘right to refuse burdensome or futile treatment’. They are not interested in asserting complete control over death, but seek instead, to reclaim some control over the manner of their dying.
There is, of course, a clear and established ethical tradition describing the legitimate scope and limit of choice with respect to the circumstances and timing of death. Mindful of the dignity and consequent inviolability of human life, the Catholic ethical tradition stands with traditional Western medical ethics, in recognizing that the direct and voluntary killing of an innocent human person, at every stage and in every state of life, is always gravely wrong.15 When life-saving or life-sustaining treatment is withdrawn or withheld with the intention of ending a person’s life, this is an unethical action or omission, irrespective of
15 John Paul II. Evangelium Vitae: Encyclical Letter on the Value and Inviolability of Human Life. Homebush: St Pauls, 1995, n. 57.

Medicine and Law 478
any good motive, and morally equivalent to euthanasia or suicide.16
Yet this tradition also recognizes that, sometimes, respecting human dignity and caring for patients can require the avoidance of over-treatment as well as under-treatment. Within the life of every human person there are limits to the extent to which life and health should or can be actively pursued. While there will often be good reasons to do things which protect or prolong life, there may concurrently be good reasons not to do so, such as great risks or burdens of various kinds for the person whose life would be prolonged or for those who would be engaged in her care.
Therefore, Catholic medical ethics describes treatments which have become, or are likely to be, futile or overly-burdensome as ‘extraordinary’, ‘heroic’ or ‘disproportionate’. To forego such treatments is not the equivalent of euthanasia or suicide, but an acceptance of the human condition in the face of death.17 This is not a choice for death, but a choice about how to live while dying.
Provided that the ‘right to refuse treatment’ does not embrace any right to refuse treatment precisely so that death will occur sooner, this right is substantially different from any alleged right to become or to be made dead, by whatever means. What we are to make of this latter right - whether or not there is a specific ‘natural’ or ‘basic human’ right to have one’s life intentionally shortened through suicide, assisted suicide or voluntary euthanasia - is asking ‘is there a right to die?’
It is the central thesis of the common law doctrine of trespass to the person that the voluntary choices and decisions of an adult person of sound mind concerning what is or is not done to his or her body must be respected and accepted, irrespective of what others, including doctors, may think is in the interests of that particular person. To this general thesis there is an exception: a person cannot consent to the infliction of grievous bodily harm without ‘good reason’. But save in this exceptional case, the common law respects and preserves the autonomy of adult persons of sound mind with respect to their bodies. By doing so, the common law accepts that a person has rights of control and self-determination in respect of her or his body that other persons must respect. Those rights can only be altered with the consent of the person
16 EV n. 6517 ibid

Medicine and Law 479
concerned. Thus the legal requirement of consent to bodily interference protects the autonomy and dignity of the individual and limits the power of others to interfere with that person’s body.
Although the law’s respect for the unique dignity of every person is the same, the protection of the physical integrity which is required to preserve the dignity of one person may change from time to time and it may differ from the protection of physical integrity required to preserve the dignity of another. Differing measures of protection are required according to the physical and mental capabilities of individuals at particular times; the baby whose dignity is respected by being carried and cared for by his or her parents grows into a man or woman whose dignity would be offended by such treatment; a donation of blood by a person of full age and understanding may enhance dignity, while the extraction of blood from a person who is incapable of consenting is an invasion of that person’s physical integrity. Human dignity requires the whole personality to be respected: the right to physical integrity is a condition of human dignity but the gravity of any invasion of physical integrity depends on its effect not only on the body but also on the mind and on the self-perception.
Refusal of treatment is never simply a confrontation, be it rebellion against what is perceived as the medical “order”, or a claim for absolute freedom of choice or a misapprehension of the true situation. In the wings, there is always a misunderstanding, something left unsaid, on the part of the doctor, the family, or a person who may, or may not, be ailing. But perhaps it is in just such situations that the medical profession must show the true colours of its ethics.
6. REFERENCES
BEAUCHAMP, Tom L., CHILDRESS, J. Principles of biomedical ethics. New York, Oxford University Press, 1979.
DANTAS, Eduardo. Direito Médico. Rio de Janeiro, Editora GZ, 2009.
DANTAS, Eduardo. When consent is not enough: the construction and development of the modern concept of autonomy. In Lex Medicinae - Revista Portuguesa de Direito da Saúde. Year 8, n. 15, Coimbra, Coimbra Editora, 2011, p. 101-112.
Medicine and Law 480
DANTAS, Eduardo. How informed should consent be? A brief analysis on consent and autonomy under the European Convention on Human Rights and Biomedicine. In Lex Medicinae - Revista Portuguesa de Direito da Saúde. Year 9, n. 17, Coimbra, Coimbra Editora, 2012, p. 51-64.
DEMICHEL, F.. Au nom de quoi? Libre propos d’une juriste sur la médicalisation de la vie. Bordeaux, Les Études Hospitalières, 2006.
Federal Council of Medicine - Brazil. Resolution 1.931 (2009) [Medical Ethics Code]
Federal Council of Medicine - Brazil. Resolution 1.995 (2012)
HOWARTH, L., Autonomy, A Study in Philosophical Psychology and Ethics. New Haven, Yale University Press, 1986.
John Paul II.Evangelium Vitae: Encyclical Letter on The Value and Inviolability of Human Life. Homebush: St Pauls, 1995.
KRISTINSSON, Sigurdur. Autonomy and informed consent: A mistaken Association?Medicine, Health Care and Philosophy. DOI 10.1007/s11019-007-9048-4, Springer, 2007.
KÜBLER-ROSS, E. Sobre a morte e o morrer: o que os doentes têm para ensinar a médicos, enfermeiras, religiosos e aos seus próprios parentes. Martins Fontes, São Paulo, 1996.
McLEAN, Sheila. Old Law, New Medicine. London, Pandora, 1999.
MöLLER , Leticia Ludwig.Direito à morte com dignidade e autonomia. Juruá, Curitiba, 2007.
PESSINI, Leo. "Distanásia: algumas reflexões bioéticas a partir da realidade brasileira ", in Revista Bioética,CFM, Brasília, 2004, Vol. 12, n. 01.
RICOEUR, Paul. Parcours de la reconnaissance. Paris, Stock, 2004.
©PROBOOK 2013and Law
Medicine Med Law (2013) 32:481-496
481
RETHINKING ETHICAL AND LEGAL ISSUES AT THE END OF LIFE IN THE UK AND BRAZIL: A ROLE FOR SOLIDARITY?Carla A. Arena Ventura, LLM, PhD,* Ann Gallagher RN, PhD,** Robert Jago, BA (Hons), MPhil. (Cantab)*** and Isabel Amélia Costa Mendes, RN, PhD****
Abstract: There are currently high profile debates about legal and ethical aspects of end of life care and treatment in the UK and Brazil. Unlike some other jurisdictions, neither country has legalised assisted dying or euthanasia. We argue that it is timely to consider the issues from the perspectives of an evolving concept in bioethics, that of solidarity.
Keywords: End-of-Life Care; Assisted Dying; Euthanasia; Solidarity; Ethics; Law.
INTRODUCTION
At the time of writing, a legal challenge was being pursued by a 58 year old British man, for the right to die. Paul Lamb was paralysed in a car accident in 1990 and was quoted as saying: ‘I am in pain every single hour of every single day for a lot of years and have given it my best shot. Now I feel worn out and I am genuinely fed up with my life. I feel I cannot and do not want to keep living. I feel trapped by the situation and have no way out1.’ The case of * Associate Professor, University of São Paulo at Ribeirão Preto College of Nursing, WHO
Collaborating Centre for Nursing Research Development, Brazil Correspondence Address: Av. Bandeirantes, 3900 - Campus Universitário Ribeirão Preto, São Paulo, Brazil, CEP 14040-902 Email: [email protected]** Reader in Nursing Ethics, Chair, University Ethics Committee, Director, International
Centre for Nursing Ethics, Editor, Nursing Ethics, School of Health and Social Care Faculty of Health and Medical Sciences, University of Surrey, Guildford, Surrey GU2
7TE. Email: [email protected]*** Senior Lecturer, Deputy Head of School, Director of Undergraduate Studies School of Law, University of Surrey, Guildford, Surrey GU2 7TE Email: [email protected]**** Full Professor, University of São Paulo at Ribeirão Preto College of Nursing WHO Collaborating Centre for Nursing Research Development, Brazil Correspondence Address: Av. Bandeirantes, 3900 - Campus Universitário Ribeirão Preto, São Paulo, Brazil. CEP 14040-902 Email:[email protected] See: http://www.bbc.co.uk/news/uk-22191059

Medicine and Law 482
Mr. Lamb will join the case of Tony Nicklinson, whose family are challenging the rejection of his case in the British High Court. Mr Nicklinson had locked in syndrome as a result of a stroke and died from pneumonia in 2012. He said ‘I am saddened that the law wants to condemn me to a life of increasing indignity and misery’2. As neither Mr Lamb nor Mr. Nicklinson could self-administer a fatal dose, the assistance requested would amount to euthanasia3. Some other UK citizens are opting for assisted dying and travelling to Dignitas, a clinic in Switzerland that provides this service. It has also been condemned as promoting ‘death tourism’ and the Swiss government had considered imposing restrictions on this activity4. Whereas suicide has been decriminalised in the UK, assisted suicide and euthanasia remain against the law.
In Brazil, the debate about euthanasia and assisted suicide is still superficial among the different members of society, including health professionals and legislators. However, there are two main cases showing legal and ethical attempts to propose limits to the use of technology to prolong life without the consent of the patient. The first one was in the State of São Paulo, with the so-called Covas Act, sanctioned in 1999 by Governor Mario Covas, himself a victim of cancer. This emphasized the right of patients to refuse painful treatment strategies to prolong life. The other document is the Federal Council of Medicine (CFM) Resolution No. 1,805/06, which allowed physicians to restrict or suspend medical procedures and treatment to prolong the patients’ life, in accordance with patients or their legal representatives’ wishes. In 2007, this resolution was brought to the courts and was suspended as judges considered orthotanasia a homicide behaviour5.
The challenges for patients and families seem obvious as they seek release from seemingly relentless suffering and frustration. For lawyers and ethicists, the arguments have focused on autonomy, dignity, beneficence and the potential adverse consequences of changes in the law, for example, slippery
2 http://www.bbc.co.uk/news/uk-england-wiltshire-193415713 Paterson C. Assisted Suicide and Euthanasia: A Natural Law Approach: Aldershot,
Ashgate Publishing Limited, 2008.4 http://www.guardian.co.uk/society/2009/oct/28/swiss-consider-ban-assisted-suicide5 Santos OM. Suffering and pain in palliative care: ethical reflections. Rev. Bioet 2011;
19(3): 683-95.
Medicine and Law 483
slope arguments6,7,8. It is, in our view, time to take a fresh look at the issues relating to assisted suicide and euthanasia and consider the helpfulness of another value: solidarity. This value is well-developed in Brazilian political and bioethical discourse and is just beginning to be recognised in the UK.
This paper discusses some of the legal issues focussing on the cases of UK and Brazil, considering that the national laws of both countries are shaped by their history, community values, economics, culture, religious orientation, and current predominant legal philosophy. We will consider solidarity in the light of the framework of legal principles established in UK and Brazil regarding end-of-life care.
BACKGROUND - A GOOD DEATH?
A substantial share of the literature in bioethics and related law is devoted to questions surrounding the beginning of life and its end. With respect to the end of life, studies show that in spite of recent advances in palliative care and treatment, intolerable physical incapacity, pain and suffering remain a daily reality for thousands of terminally ill patients9. In the UK General Medical Council’s (2010) document,10 ‘Treatment and care at the end of life: good practice in decision-making’ it is emphasised that doctors should adhere to five principles: equalities and human rights; presumption in favour of prolonging life; presumption of capacity; maximising capacity to make decisions; and overall benefit. In response to UK nurses’ concerns about patients and family requests for guidance regarding assisted dying, the Royal College of Nursing (RCN) published ‘When someone asks for your assistance to die’ (RCN 2011)11. This document clarifies the UK legal position for nurses.
6 Tulloch G. Euthanasia-Choice and Death. Edinburgh University Press, 2005. 7 Dworking G, Frey RG, Bok S. Euthanasia and Physician-Assisted Suicide: For and
Against. Cambridge University Press, 1998.8 Dworkin R. Life´s Dominion: An argument about Abortion and Euthanasia. Haper
Collins Publishers, London: 1993.9 Florencio PS, Keller RH. End-of-life decision making: rethinking the principles of
fundamental justice in the context of emerging empirical data. Health Law Journal 1999; 7: 233-258.
10 http://www.gmc-uk.org/static/documents/content/Treatment_and_care_towards_the_end _of_life-_English_1011.pdf
11 http://www.rcn.org.uk/__data/assets/pdf_file/0004/410638/004167.pdf
Medicine and Law 484
In Brazil, the Code of Ethics for Medical Professionals12 sets forth in Article 41, a single paragraph: in cases of incurable and terminal disease, the physician should offer available all palliative care without useless therapeutic or diagnostic obstinacy actions, always taking into consideration the patient’s expressed wish or, when he/she is unable to do so, his/her legal representative’s. For instance, the Code of Ethics for Nursing Professionals13 does not explicitly mention the situation of care for the terminally ill but, in general terms, the Code reaffirms nursing as a profession committed to health and the quality of life, based on the respect for ethical and legal principles, such as the respect for life, dignity and the human rights of patients.
On a governmental level, the Brazilian Health Ministry has stated its concern regarding the growing need for palliative care and pain management in the country and, in 2002, created the National Program for Pain Management and Palliative Care. After this, there have been many national initiatives, and studies were developed about the need to implement palliative care at all health care levels. However, in spite of these initiatives, there is a lot to be accomplished in order to implement this therapeutic approach. We must deal with the difficult access to health care services, the flaws of health policy guidelines, the deficient education of health professionals and, mainly, the lack of information to patients along with the need to manage these patients’ pain, relieve their symptoms, and promote a better quality of life for them14.
The development of the palliative care movement in the UK has contributed significantly to the improvement in symptom control at the end of life. Cecily Saunders, a pioneer of the UK palliative care and hospice movements, expressed her hope that assisted dying would not be necessary:
‘All who work with dying people are anxious that what is known already should be developed and extended so that terminal care everywhere should become so good that no one need ever ask for voluntary euthanasia.’ 15
12 Federal Medicine Council (CFM). Resolution CFM 1931/09. Code of Ethical Medicine. Brasília: CFM; 2010 .
13 Federal Nursing Council (COFEN). Resolution COFEN-311/2007. Code of Ethics for Nursing Professionals. Diário Oficial da República Federativa do Brasil, Brasília (DF); 2007 Fev 8; Seção I.
14 Boemer M. About palliative care. Revista da Escola de Enfermagem da USP 2009; 43(3):502-3.
15 Glover J. Causing Death and Saving Lives. Penguim Books, London: 1997, p. 182.
Medicine and Law 485
In Brazil, however, this is at an earlier stage of development16. The palliative care movement has done much to improve pain management and symptom control, recognizing that dying and suffering patients have a right to adequate symptom and management. Nevertheless, many patients, including those seriously ill and dying, are routinely undertreated for pain. Medical research has established that perhaps 10% of dying patients have conditions in which the alleviation of pain is truly difficult or impossible. The fact that one out of two dying patients endures pain unnecessarily is a little noticed human rights tragedy17.
On the other hand, even when patients are provided with excellent pain and symptom management, a fraction of dying patients wants the option of a humane hastened death if their pain and suffering becomes intolerable17. Several studies show a substantial majority of citizens and health professionals alike to believe that competent terminally ill patients should have this option18. A British survey19, for example, found that 75% of the population favour a change in the law to permit ‘some degree of assisted suicide’. A UK Royal College of Nursing (RCN) consultation20 suggested that 49% of the nurses who responded were in favour of assisted suicide and 40% against.
In Brazil, this discussion focuses on religious beliefs including the sanctity of life. Thus, in Brazil and the UK, as in many other countries, laws prohibit assisted suicide or euthanasia. Some patients then experience suffering they consider intolerable and surveys suggests that a majority of the public and professionals consider that the law should be changed. This seems to support a new engagement with the issues and a reconsideration of legal position, however, these need to be defended by drawing on pertinent principles.
16 Sousa A.França J.Nóbrega M.Fernandes M.Costa S. Palliative care: a conceptual analysis Online Brazilian Journal of Nursing 2010 August 30 [Cited 2013 Apr 21] 9(2): Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/2947.
doi: http://dx.doi.org/10.5935/1676-4285.20102947.17 Trucker K. End of Life Care: a human rights issue. Human Rights, 2003; 30: 11-13.18 Johnson S. End-of-life decision making: what we don’t know, we make up; what we do
know, we ignore. Indiana Law Review 1998; 31(1): 13-47. 19 http://yougov.co.uk/news/2010/03/05/majority-would-support-more-compassionate-
euthana/20 http://news.bbc.co.uk/1/hi/health/8167454.stm

Medicine and Law 486
ETHICAL ISSUES
Much of the philosophical discussion relating to assisted dying is couched in terms of autonomy, dignity, beneficence and weighing up benefits and harms for the individuals and groups drawing on, for example, slippery slope arguments6,7,8. Rights discourse has also been very prominent in supporting arguments for assisted dying. Decisions to withhold or withdraw treatment are both profoundly important and challenging. There may be conflict between the perspectives of patients and professionals, and between professionals and family members. In relation to the latter, this is particularly so when patients lack capacity. As such, it is helpful if there is a carefully defined process that everyone involved understands in a particular instance, and one that the majority of society agrees with in the wider social and philosophical setting21. About this, Boff wrote on the right to die, affirming that health professionals must make all efforts to cure a patient. However, this does not mean to use treatments to prolong life. The author affirms that “let the person die” is not the same than “making the person die”. One of the main ethical aspects is the patients´ right to decide and the health professional’s obligation to respect this decision22. Therefore, humane care must not be treated as an intervention on the patient: it is not a subject-object relationship, but a subject-subject interaction.
This discussion is essential because when health providers are taking clinical decisions of such magnitude, they have to be sure that they understand the ethical, legal, professional and personal invectives that apply17.
In spite of the importance of these issues, early research illustrated how health professionals in a hospital environment avoided direct communication about dying with the hope that the patient would discover this by himself23.
Health professionals are all subject to a code of professional conduct produced by their regulatory body. The UK Nursing and Midwifery Code (2008), for example, emphasises prioritising the interests of patients and respecting their individuality and dignity. The Code also emphasises the importance of collaboration, openness, honesty and advocacy and of acting with integrity. The Code of Ethics for Nursing Professionals in Brazil is based on these same principles.
21 Fullbrook, S. End-of-life issues: common law and the Mental Capacity Act 2005. British Journal of Nursing; 2007, 16(13): 816-818.
22 Boff, L. Saber cuidar. Petrópolis: Vozes, 1999. 23 Glaser BG, Strauss AL. Awareness of dying. Chicago: Aldine, 1965.

Medicine and Law 487
Therefore, there is much potential for value conflict in end of life care and health professionals need to be cautious not to substitute their beliefs for those of their patients. As such, health professionals have to be aware that some patients that they care for will hold opposing views to them.
It is also crucial that health professionals understand that terminally ill patients face several problems simultaneously: the fight against the disease and its treatments, emotional reactions (such as anger, depression, lack of hope and guilt); and the change of life plans as they leave behind long term plans to focus on a short term plan. Therefore, the care provided should include: compassion, humility and honesty in a multidisciplinary context and vision24,25.
Health providers’ perceptions of constraints on their professional authority, regarding decisions about seriously ill patients, is an area in which significant differences might be expected among practitioners between countries in which different legal systems apply and in which traditions of health ethics vary26. On the other hand, health professionals cannot be forced to undertake a procedure that they do not deem to be in the patient’s best clinical interests.
One of the most commonly referred to ethical frameworks in both the UK and Brazil is the four principles approach27, health professionals should respect patient´s autonomy, balance benefits (principle of beneficence) and risks (principle of non-maleficence) of treatment and treat people justly (principle of justice). This approach, we suggest, would be enhanced by drawing an ethics of care needs that emphasizes, essentially, the vulnerable nature of human beings and concepts such as relationality, dignity and care28.Therefore, ethics does not only involve the process of deciding, but also the quality of the relationships, such as openness and trust. In this sense, one must face death not as an isolated event, but as a process. Health professionals must be prepared to share this experience with their patients. Therefore, countries must
24 Pessini L, Bertachini L. New perspectives in palliative care: ethics, geriatrics, gerontology, communication and spirituality. O Mundo da Saúde, 2005; 29(4): 491-509.
25 Marengo MO, Flavio DA, Alves da Silva RH. Completion of life: bioethics and humanization in health. Medicina (RP) 2009; 42(3): 350-357.
26 McCrary S; Swanson J. Physicians’ legal defensiveness and knowledge of medical law: comparing Denmark and the USA. Scandinavian Journal of Public Health, 1999; 27(1): 18-21.
27 Beauchmp T, Childress J. Princípios de Ética Biomédica, São Paulo: Loyola, 2002.28 Gastman C. Dignity-enhancing care: A foundational ethical framework. Nursing Ethics
2013; 20(2): 142-149.

Medicine and Law 488
design and implement specific policies that do not happen on a moral vacuum and are only based on technical hegemony29.
A value that has been well established in Brazilian political and bioethical discourse is solidarity. Recent UK work by the Nuffield Council on Bioethics has described solidarity as ‘an emerging concept in bioethics’30. The Nuffield report examines the wide-ranging literature relating to this concept and arrives at ‘its most bare-bone form, solidarity signifies shared practices reflecting a collective commitment to carry ‘costs’ (financial, social, emotional, or otherwise) to assist others’ (30). The authors outline ‘three tiers of solidarity’ as follows:
Tier 1 - interpersonal level - this applies to the individual level whereby ‘solidarity comprises manifestations of the willingness to carry costs to assist others with whom a person recognises sameness or similarity in at least one relevant respect’ (30, p.47). This kind of solidarity needs to be enacted by responding to and helping people.
Tier 2 - group practices - this occurs when solidarity at the inter-personal level becomes institutionalised and when ‘solidarity can be described as manifestations of a collective commitment to carry costs to assist others (who are all linked by means of a shared situation or cause)’ (30, p. 48). This is enacted by groups where ‘people negotiate ways of conduct’ in a situation and they agree how best to support each other or organise resulting in the emergence of shared values.
Tier 3 - contractual and legal manifestations - this is evident when ‘values or principles solidify not only into social norms but manifest themselves in contractual or other legal norms’ (30, p. 49). It is described as the ‘hardest’ and ‘most fixed form of solidarity’. The example is given of a welfare state. It is pointed out that while the lower levels of solidarity (1 and 2) can exist without higher levels, the higher levels need to follow from the lower levels’ (30, p. 49).
29 Rego S, Palácios M. Human finitude and public health. Cad. Saúde Pública, Rio de Janeiro 2006; 22(8): 1755-1760.
30 Praisack B, Buyx A. Solidarity: reflections on an emerging concept in bioethics; Nuffield Council on Bioethics 2011. p.46
Medicine and Law 489
Whereas the ‘bare bones’ description of solidarity do not prescribe an approach to assisted dying, the work does suggest a deliberative process for ethical and legal discourse that necessarily involves collaboration with patients and families, professionals and takes into account the health care system and legal contexts. This will include a consideration of adequate provision of palliative care services. We turn next to legal issues relating to assisted dying.
LEGAL ISSUES
Health professionals often assist patients, patients’ family members and significant others in facing end-of-life situations. Most of these situations are resolved among themselves without the need for legal intervention as patients often decide, where possible, to refuse life prolonging treatment and this is sometimes with the patient’s family. However, in the absence of consensus, or perhaps as a consequence of advances in medical technology, some of the difficult end-of-life questions have been brought to the national courts for resolution and the International courts for state influencing judgment31.
The legal analysis of end-of-life and pain treatment is complex. It can involve issues of criminal law and the law of battery as well as issues concerning human rights and the right to non-discrimination within any constitutional framework. The legal analysis of these problems is shaped by the juridical system and philosophy of each country, as well as being influenced by international conventions that have been incorporated into the law of the respective countries32.
As difficult decisions concerning people’s lives follow on from the legal concerns of each system, the courts have found that competent adults do have the right to refuse or discontinue medical interventions. In this sense, the termination or withdrawal of life-prolonging treatment is legal in most western democracies. However active euthanasia, regardless of the circumstances, is still generally illegal (Belgium, the Netherlands and the US State of Oregon being the exceptions rather than the rule).
The legal acceptance of the patient’s right to refuse life prolonging treatment and the medical professions willingness to withdraw life prolonging treatment
31 McGowan C. Legal aspects of end-of-life care. Critical Care Nurse 2011; 31(5): 64-69.32 Mendelson D, Jost TSA. Comparative Study of the Law of Palliative Care and End-of-
Life Treatment. Journal of Law, Medicine & Ethics 2003; 31(1): 130-143.
Medicine and Law 490
in cases of medical futility is now so widespread among both opponents and proponents of euthanasia that it is easy to forget that these issues were bitterly contested but a short time ago9.
It is only over the last decades that a majority of health professionals have become more comfortable with the idea of respecting their patient’s requests for the withdrawal of life-sustaining treatments 9. In this sense, there exists no right to die per se, even where international and national instruments guarantee a right to life, but there are clear limitations on the ability of healthcare providers or the state to impose undesired life prolonging interventions against the wishes of the patient or the patient’s authorized surrogate decision maker’s.
Thus, a competent patient has the right to refuse or discontinue life-sustaining treatments, even if that desire conflicts with the desires of the patient’s family33.
When these decisions are made, health professionals are not only performing a clinical role, but are also acting in a significant legal role. For example, they may decide whether an adult lacks capacity, or guardianship legislation may grant them power to be a decision-maker or to supervise the decisions made by others. Undertaking these roles can be challenging because of insufficient training and because of complexity and ambiguity in the law34,35.
To reinforce these decisions, individuals may attempt to use rights based discourse as a way of framing any argument to support the end of life decision chosen by the patient. A number of rights can be asserted in this way36. Firstly the focus is often on the legal right to liberty where freedom provides the choice for all individuals to manage their own death. If they require support to assist them with their choice then this too is seen as causing no harm and therefore supporting liberty. Linked to this argument is the focus on the legal right to autonomy which is inherent in any rights based discussion on end of life decision making. It has been argued that anyone wishing to end their life
33 Emanuel EJ. A review of the ethical and legal aspects of terminating medical care. Am. J. Med. 1988; 84(2):291-301.
34 Pawl R.J. Patient care decision making at end of life: law lags behind medical advances. ED Legal Letter, 2007; 17(5): 49-60.
35 White, B; Willmott, L; Parker, M; Cartwright, C; Williams, G. Should law have a role in end-of-life care? Internal Medicine Journal. Editorial, 2012: 966-967.
36 Lewis, P. Assisted Dying and Legal Change. Oxford: Oxford University Press, 2007.

Medicine and Law 491
is a sign of mental illness37, but this is not universally supported and the desire for self-determination, for autonomy, especially in cases where individuals are terminally ill is well supported in the literature38.
It has been argued that the right to life (as enshrined in Article 2 of the European Convention on Human Rights) should include a right to die. This has not been successfully argued as the European Court has made it clear that the two are not synonymous (Pretty v UK 2002). Similarly, when it has been argued that the right not to be tortured or suffer inhuman or degrading treatment (Article 3 of the European Convention on Human Rights), the courts have been quick to note that it is the individual’s medical condition which may be causing it, but it is not the state and so this right cannot be mobilised.
The legal right to privacy (as enshrined in Article 8 of the European Convention on Human Rights) has been mobilised where it has been argued that suicide, in this context, is the ‘ultimate exercise of one’s right to privacy’ (Bouvia v Superior Court (Glenchur) (1986)). It has been argued that just as individuals should be able to die naturally, so those who need assistance when choosing a painless death should be permitted the opportunity. The reason for asserting this right is often linked with the right to dignity. Dworkin (1993)39 champions this right as preferable to indignity, although it is appreciated that if an end of life decision was not undertaken in dignified circumstances and by dignified means then this right would be overridden.
In most developed societies discrimination is outlawed. Consequently those patients, who wish to manage their end of life decisions in a particular way, especially if they require assistance, can argue that if they are unable to effect these decisions and require assistance, the system discriminates against them if it does not permit them to use that assistance. An example of this was in Pretty v UK (2002) where Mrs Pretty argued that the prohibition on assisted suicide discriminated against her because she was unable, due to her physical disabilities, to carry out the act of suicide. This prohibition on assistance was, she argued, discriminating against her, when compared with able bodied
37 Rosenblum V, Clarke G. The Right to Assisted Suicide: Protection of Autonomy or an Open Door to Social Killing. Issues in Law and Medicine, 1990; 6(1): 3-31.
38 Quill, T., Cassel, CK., Meier, DE. Care of the Hopelessly Ill: Proposed Clinical Criteria for Physician Assisted Suicide, New England Journal of Medicine, 1992; 327(19); 1380-1384
39 Dworkin R. Life’s Dominion: An Argument about Abortion, Euthanasia and Individual Freedom. New York: A.A. Knopf, 1993.

Medicine and Law 492
people. Mrs Pretty was therefore arguing in favour of a right to equality. Able bodied people could end their life as they wanted to but those who were in some way disabled could not.
Another less regularly articulated right here is the legal right to freedom of conscience and religion. It is noted that this tends to be articulated in cases of abortion rather than end of life decision making but the tenet of this claim is that for the state to interfere in the end of life choices of the individual is a violation of the individual’s right to freedom of conscience32. A similarly limited right in this context is the individuals’ right to their property, which in this context, is their body. The assertion of these rights focusses on the individuals’ moral and physical being and although subject to certain limitations they do compliment the range of rights that can be asserted in these cases. In discussing the third ‘wave’ or phase of rights, Klug (2000)40 identifies a less individualistic phase, that is, one that emphasises solidarity, fraternité, mutuality and participation. She states:
While there is still the same recognition of the values of liberty and community as in the second wave, there is now a growing emphasis on participation and mutuality [...] because of this participation - and because rights are increasingly presented as more than claims against governments but also as a set of obligations that individuals owe to each other - a new value of mutuality can be said to characterise an emerging third wave of rights’ (40, p. 196).
This development of rights discourse suggests that it is timely to consider a different approach to end of life of life decision-making.
UK
There has been a historical societal reluctance to regulate how people die. Believing that people’s lives come to an end when their Creator deemed it appropriate was the overriding principle that guided the legal position in England and Wales until 1961. If an individual unsuccessfully attempted to end his life, he was guilty of a crime, as were those who might have assisted him in his endeavour. The Suicide Act 1961 abrogated the rule of law that suicide is a crime, although it was never a criminal offence in Scotland to commit suicide. Up until that time, end of life decisions were not routinely
40 Klug F. Values for a godless age - The story of the United Kingdom´s new bill of rights; London, Penguin Books: 2000.
Medicine and Law 493
discussed and the law was clear, but it did retain the offence of assisted suicide under section 2(1) of the 1961 Act. This provides that: ‘a person who aids, abets, counsels or procures the suicide of another, or attempt by another to commit suicide shall be liable, on conviction, on indictment to imprisonment for a term not exceeding fourteen years’.
It is worth noting, at this stage, that the consent of the Director of Public Prosecutions (DPP) is required before an individual may be prosecuted41.
Having decriminalized suicide the courts have, in recent years, found themselves considering a range of issues relating to end of life decision-making. Where clinicians have decided to end patients’ lives for their own gain, this has been dealt with under the law of homicide (see R v Shipman [2000]). Similarly, if there have been concerns about the nature of a clinician’s treatment, then the issue has been brought before the courts even if a conviction has not followed (see R v Adams [1957], R v Cox [1992] and R v Moor [1999]). These later cases have focused on the concerns surrounding the doctrine of double effect where clinicians understand that they are administering pain relief medication but at the same time are also conscious that this may hasten the end of a patient’s life42.
Some patients take control of their lives, often upon diagnosis of a chronic or terminal illness, by making an advance treatment refusal, which is made for the time of potential future incompetence43. These ‘advance directives’ are legally binding (see Re C (Adult: Refusal of Medical Treatment) (1994) but will only be so if the patient was, at the time, competent, informed, free from controlling influences and intended the refusal to apply to future circumstances. Maclean (2008)44 has argued that these criteria can ensure that where the Court believes a ‘worthwhile’ life is worth protecting and refusal of life saving treatment is ‘unreasonable’, then regardless of the patient’s original wishes the courts will ensure that treatment continues. In fact it is recommended at the present time that rather than rely on an ‘advance directive’ and the decisions of the medical profession, the individual is better placed to appoint a trusted proxy who has lasting power of attorney under section 10 of the Mental Capacity Act 2005.
41 www.cps.gov.uk42 Jackson E. Death, Euthanasia and the Medical Profession in Brooks Gordon, B et al
Death Rites and Rights. Oxford: Hart, 2007.43 Michalowski S. Advance Refusal of Life-Sustaining Medical Treatment: The Relativity
of an Absolute Right. Modern Law Review, 2005; 68(6): 958-982.44 Maclean A. Advance Directives and the Rocky Waters of Anticipatory Decision Making.
Medical Law Review, 2008; 16(1): 1-22.

Medicine and Law 494
Where a patient refuses medical treatment in the knowledge that this will result in their death, the UK courts have taken the view that as long as the individual has full capacity and is not being coerced by anyone, then they can refuse medical treatment (see Re B (Adult: Refusal of Medical Treatment) (2002). Just as the courts have respected autonomy, some individuals have explored the possibility of securing treatment in the future, when they have been concerned that it might be withdrawn once the patient has lost capacity (see Re (Burke) v GMC 2005). Since 2000 the UK courts have been obliged to consider the European Convention on Human Rights in their decision making as a result of the Human Rights Act 1998. This has led to a number of cases where the courts have been required to navigate their way through the relevant rights within the convention (see R(Purdy) v DPP (2009)). Some individuals have chosen to travel abroad to Switzerland where they are able to secure the requisite medication to end their lives (Re Z (An Adult: Capacity) (2004)).
Whilst capacity is the key issue for the courts when it comes to end of life decisions, those who lack capacity are dealt with in accordance with the principle of best interests. Where individuals find themselves in a persistent vegetative state (PVS), then the courts will permit withdrawal of life prolonging treatment (Airedale NHS Trust v Bland (1993)). The final area of concern in the UK in these cases of end of life decision-making is the role and responsibility of carers. It has been argued that there is a long tradition of non-professional caring which is actively encouraged in UK society. Biggs and Mackenzie (2006)45 note: ‘care of the elderly, the infirm and children, has always taken place within the home, relying on the good will and fortitude of genetically related emotional carers.’ (45, p. 118). In end of life decision making, carers may actively assist in the suicide of the patient by providing the means for the suicide to take place. These instances have left carers being dubbed as ‘assisted dying outlaws’46 and without changes to existing legislation the risk of prosecution remains.
45 Biggs H, Mackenzie R. End of life decision making, policy and the criminal justice system: Untrained carers assuming responsibility and their uncertain legal liabilities. Genomics, Society and Policy 2006; 2: 118-128.
46 Biggs H. Criminalising Carers in Brooks Gordon, B et al Death Rites and Rights. Oxford: Hart, 2007.

Medicine and Law 495
BRAZIL
Brazil is a predominantly Catholic country, with a civil law tradition, and religious values have generally influenced the debate and legislation regarding end-of-life issues.
Suicide was never considered a crime in the country and the actual Brazilian Constitution47recognizes the right to life and to body integrity, based on the fundamental principle of human dignity. In addition, the Brazilian Constitution also recognizes rights to free development of personality, inviolable freedom, and inviolable dignity. Therefore, Brazil takes a strong pro-life position in several medico-legal controversies.
In this perspective, the 1940 Criminal Code (still in force) considers euthanasia and orthotanasia as evidences of homicide. According to Article 19, assisted suicide is also a crime. In this perspective, even with patients’ consent, physicians can be prosecuted. This legislation presents several gaps and deficiencies, if one takes into account Article 5 of the 1988 Constitution. In order to respond to that a state Law was, in 1999, approved in São Paulo, assuring the patient’s rights to choose treatment and decide about the use of life prolonging procedures. In the same direction, the Federal Council of Medicine adopted resolutions to support the patient’s rights to withdraw treatment, without mentioning about euthanasia and assisted suicide, which are still considered illegal and unethical practices.
As a consequence of this movement the rights to self-determination and to autonomous medical decision making, in Brazil, underlie the right of patients to demand that treatment, including life prolonging treatment. Competent adults have the legal prerogative to decide how to respond to medical conditions that threaten their well-being and even their lives. A competent adult has a privacy right to be free from unwanted interventions. Generally, incompetent adults and minors require some sort of surrogate medical decision making. In case of minors, the surrogate decision makers are typically that minor’s parents.
Failure to disclose to patients the nature of a proposed medical intervention, its gravity, and any material risk attendant upon its performance gives rise to a tort of negligence. However, the rights to self-determination and to autonomous decision making end where euthanasia begins. Both physician
47 Brazil. Constitution of the Federal Republic of Brazil,1988.
Medicine and Law 496
assisted suicide and mercy-killing are illegal in Brazil, being punishable as the crime of murder. No exception exists, including the case of competent terminally ill patients seeking assistance in dying, regardless of their state of physical incapacity or degree of pain and suffering.
In sum, the paternalistic foundation of Brazilian criminal law, at the same time as the ethical value of autonomy, mainly recognized by health professionals and their Ethical Codes in the country, are based on the principle of human dignity, pointing, however, to opposite directions when facing death and end-of-life decisions. In this context, the 1988 Brazilian Constitution is a landmark as, for the first time in the country, individual and social rights were fully and universally recognized, giving elements to sustain decisions taken in accordance to patients’ wishes, valuing their self-determination.
FINAL CONSIDERATIONS
Human Dignity, as autonomy, translates demands for keeping and expanding human freedom, since third-parties rights are respected and there are material, psychological and physical conditions for the exercise of the self-determination capacity. In the context of ethical and legal debates regarding end-of-life decisions, solidarity was highlighted as offering a new perspective. We also need a sea change in our attitude to death and dying as, despite their inevitability, in both countries there is considerable stigma and reluctance to engage in open discussion. There is an opportunity here for lawyers, ethicists, professionals and patient groups to consider these complex issues together and ask if, for example, the mandatory institutionalisation of advance directives would reduce dilemmas and enhance autonomy at the end of life.

©PROBOOK 2013and Law
Medicine Med Law (2013) 32:497-502
497
LIVING WILL AND HEALTH CARE PROXY - THE PORTUGUESE LEGAL SITUATIONAndré Dias Pereira*
Abstract: The article describes the recent Portuguese Act of 16 July 2012 on Living wills and Health care proxy, in a comparative perspective. After six years of parliamentary debate, the law was approved by unanimity and provides binding advance declaration of will, as long as it respects strict procedural control (Notary control, non-compulsory medical information and a (declarative) National Registry of Advance Declarations). The Author considers the Law a step forward in the right direction for the promotion of health care planning and ageing, especially for people suffering from dementia, and the autonomy of the patient in the end-of-life.
Keywords: Living Will; Health Care Proxy; End-of-Life, Dementia; Alzheimer; Portugal
INTRODUCTION
People, increasingly educated and aware of their rights, wish to declare in advance their desire with regard to health care. Others, for religious or conscience grounds, refuse a particular type of medical intervention, including a blood transfusion or transplantation of tissues or organs. These people want to ensure that this right is respected even if they become incompetent. Other situations include the decision to refuse resuscitation following a car accident or a stroke, due to the deep desire of not wanting to risk a life of lower quality, in terms of the communication capacity of mobility or life of relationship:think of do-not-resuscitate orders or even the refusal of hydration or nutrition in case of persistent vegetative state. These and other cases brought to the emergence of the prospective autonomy. In a word, the anticipated informed consent1 that has been consolidated by the Portuguese Law no. 25/2012, of July 16th, 2012.
* Centre for Biomedical Law - University of Coimbra. Email: [email protected] See DWORKIN R, Life’s Dominion: an argument about abortion and euthanasia,
London, Harpen Collins Publishers, 1993, 226
Medicine and Law 498
DEBATE BEFORE THE LAW
After a debate in the legal and medical community that lasted for more than twenty years2, the Portuguese legislator enacted an Act on living will.
We could synthetize that there were two main trends: for some, the living will should have a binding effect, for others, the living will should have merely an indicatory effect.3
In its 2010 opinion, the National Council of Ethics for Life Sciences also made some statements concerning the issue and finally reached a progressive model, in favor of the autonomy of the patient.
The Parliament was confronted with the topic in 2006 with a proposal from the civil society, more exactly for the Portuguese Bioethics Association; in 2009 the Socialist Party presented another proposal and finally in 2011 and 2012 a large political debate came to an end with the approval, by unanimity of the Law.
THE LAW 25/2012, OF JULY 16TH, 2012
After years of debate in the legal, bioethical and political community, the Parliament enacted the Law 25/2012; it regulates Advance directives, namely Living will, Health-care proxy and creates a National Registry of Advance directives.4
Although the right to refuse a life saving treatment is the dominant doctrine in Portugal, there were some doubts in accepting the advanced refusal. Notwithstanding the option for a strict procedural control through the Notary was the key to solve the bioethical conflict.
2 SeeLOUREIRO J, “Metáfora do Vegetal ou Metáfora do Pessoal? - Considerações Jurídicas em torno do Estado Vegetativo Crónico”, Cadernos de Bioética, 8, 1994, p. 41
3 See PEREIRA A, “Advance Directives: Binding or Merely Indicative? Incoherence of the Portuguese National Council of Ethics for the Life Sciences and Insufficiencies of Newly Proposed Regulation”, European Journal of Health Law 16 (2009) 165-171.
4 The National Registry of Advance Directives has not yet been created by the Government, however, as it is merely declarative, living wills are already binding. It is up to the patients to give publicity to their advance directives: inserting a copy in the medical file, offering a copy to close relatives and so on.
Medicine and Law 499
According to the National Council of Ethics and some Authors5, a medical consultation before the drafting of the living will should not only be advised but compulsory.6
The Doctor would inform the patient about her concrete doubts; however, the fact that many citizens don’t have a very easy access to family doctors and the fear of some that such solution would be paternalistic,7 led to a different solution. According to Art. 3., No. 2: In the event the grantee call on the assistance of a doctor for the preparation of advance directives will, the identification and signature of the doctor may be contained in the document.
On the other hand, the law states that in order to be binding, the document must be signed before a Notary, who guarantees the capacity, information and freedom of the patient.
THE LIVING WILL: DEFINITION, CONTENT, FORMAND EFFICACY
A living will is defined by law as anunilateral document, freely revocable, written, whereby an adult and competent person declares in advance his/ her will, in a conscious and free manner, in what concerns healthcare treatment she/he wants or not to receive in case she/he becomes, by any reason, incompetent to consent.
The Law gives some examples of what a person can accept or refuse in advance. Thus, a person can declare in advance, that he/she: a) does not accept to be submitted to artificial support of vital functions; b) does not accept to be submitted to futile or useless or disproportional treatment according to good clinical practice, namely in what concerns the basic measures of life support and hydration and nutrition measures that only aim to delay the
5 PEREIRA A, “Advance Directives: Binding or Merely Indicative? Incoherence of the Portuguese National Council of Ethics for the Life Sciences and Insufficiencies of Newly Proposed Regulation”, EJHL, 16, 2009, p. 1-7.
6 That is the solution in Austria: § 5 of Patientenverfügungsgesetz, of 8 May 2006.7 That is the opinion of the GERMAN NATIONAL ETHICS COUNCIL, The advance
directive: an instrument of self-determination, June 2005: “11.The majority view of the National Ethics Council is that the validity of an advance directive should not be made conditional on its maker’s having obtained prior expert advice. However, all members of the National Ethics Council recommend that expert advice be taken before an advance directive is drawn up.”
Medicine and Law 500
natural process of death; c) accepts receiving palliative care; d) accepts to be submitted to treatment that is in an experimental phase; e) authorizes or refuses to participate in clinical trials or research.
In order to overcome some ethical dilemmas presented by the acceptance of a living will, the law opted for a bureaucratic model, in which a written document, signed by the person at the Notary or at the National Registry of Advance Directives is required. This way, one is sure of the will of the persons and his/her capacity and freedom to sign the document. Following this procedure, the living will must be respected. If there is a simple written living will, without notarial intervention, I understand it should, nevertheless, be taken into account, as stated by Art. 9 of the Oviedo Convention.
The law further states that, in case there was a collaboration of a doctor, the identification and signature of the doctor may be part of the document. This norm represents a compromise between two distinct views: the one that supports the engagement of a doctor in the drafting of the living will, and the opposite view that argues for the freedom of the citizen to refuse treatments, without any medical counseling or influence. I would defend the first thesis, and I have been instructing the Notaries that they shall explain the persons that they should have an interview with a doctor before writing and signing some more radical advance directives.
The competence to draft a living will and to designate a health care proxy is exclusively for adult persons, that is, over 18 years old, and that are not under guardianship for mental incapacity and that are able to give a free and informed consent.
The law states some limits of the living will. The advance directives are not valid ifthey are contrary to law, public order or that determine an action against good clinical practice, if the respect for the living will deliberately cause non-natural and avoidable consequences, as foreseen in articles 134 and 135 Penal Code (involuntary and voluntary euthanasia) and c) if the patient did not explain clearly his/ her will.
As a rule, the living will is binding: “the medical team shall respect the content of the living will”.
However, the advance directive may be not respected if: a) one proves that the patient would not want to keep the advance decision; b) if the will is evidently
Medicine and Law 501
out of time, because of the progresses of the technologies. The decision not to respect must be written in the clinical file.
The living will is valid only for five years after its signature. However, if the patient becomes incompetent during these five years, the time limit does not apply. Moreover, and this must be stressed, even after five years, the living will shall be taken into consideration (Art. 9 Convention on Human Rights and Biomedicine).
The law provides some special rules, namely the right to conscientious objection and non-discrimination.
HEALTH CARE PROXY: A STEP TOWARDS BETTER COMMUNICATION BETWEEN THE MEDICAL TEAM AND THE FAMILY AND CLOSE PERSONS
Of capital importance for ageing and health-care planning is the nomination of a health care proxy. This designation can be done simultaneously with the drafting of advance directives and follows the same substantial and formal requirements as explained above. The proxy can take binding decisions in the moment the patient becomes incompetent. The designation of the durable power of attorney will help the communication between the medical team and the family and close persons and will increase the respect for the patient’s values and expressed wishes.
CONCLUSION
Modern western societies face the challenge of health care planning in ageing societies. The demography of Portugal shows that a rising number of aged and lonely persons, dementia and mental illness, bring to the forefront the need to regulate this period of life with respect for the fundamental principles of human dignity, autonomy and solidarity.
This law is a very positive step in the direction of ageing planning. The bureaucratic model that has been followed, as the intervention of the Notary is compulsory, can have virtues, if the notaries - together with health care providers - contribute for the planning of the moments of incompetence.

Medicine and Law 502
However, patrimonial issues still need to be regulated as this law does not deal with it. A judicial action of interdiction is the adequate legal tool for the purpose of giving legal powers of representation to another person, including patrimonial matters (guardianship).

©PROBOOK 2013and Law
Medicine Med Law (2013) 32:503-513
503
TITLE TO LIFE: TIME FOR REFORM?Shane Campbell*
Abstract: This article seeks to outline the law relating to euthanasia and assisted-suicide in New Zealand, and to critically examine whether there are any practical justifications for retaining the current prohibition. The paper initially discusses terminology, then what is and what is not permissible in New Zealand under the present legal regime. The paper then very briefly reviews the other jurisdictions which have euthanasia or assisted-suicide laws. Finally, the paper looks at the practical arguments for and against reform.
Keywords: Euthanasia; Assisted-suicide; Law; Legal; Regime; New Zealand; Reform; End-of-life; End of Life Choice Bill.
INTRODUCTION
Arthur Schopenhauer once wrote:1
“They tell us that suicide is the greatest piece of cowardice; that only a madman could be guilty of it; and other insipidities of the same kind; or else they make the nonsensical remark that suicide is wrong; when it is quite obvious that there is nothing in the world to which every man has a more unassailable title than to his own life and person.”
Euthanasia and assisted suicide are immensely polarising topics which have a remarkable ability to evoke emotive responses. One result of this polarisation is that the concepts are incredibly topical, resulting in the existence of a sizeable body of literature in which scholars have rigorously debated the morality of euthanasia and assisted suicide. Perhaps because of this intense focus on the moral and ethical arguments, there exists, what is arguably, a disproportionately smaller body of literature considering the practical arguments for and against the two concepts. The aim of this paper is to make some inroads into rectifying that situation.
* Studying towards a Bachelor of Laws (LL.B. (Hons.) at the University of Canterbury, New Zealand. This paper, in a slightly altered form, was submitted in partial completion for a paper in Medical Law.
1 Arthur Schopenhauer, Volume Four: Studies in Pessimism, translated by T Bailey Saunders (Penn State, Electronic, 2005) at 22.
Medicine and Law 504
The paper will first discuss relevant terminology. It will then set out what end of life assistance from third parties is presently permissible under New Zealand law, and what is not. Then, very briefly, the paper will consider the position in other jurisdictions. Finally, the paper will contemplate whether the law in New Zealand ought to be amended, taking sole account of the practical justifications for and against reform.
TERMINOLOGY
It is prudent to first outline relevant concepts and associated terminology. This paper will be focusing on the role of third parties, predominantly physicians, in end of life decisions. In particular, this paper will be reviewing voluntary active euthanasia, and assisted suicide.2
Voluntary active euthanasia describes the situation in which a person has resolved that they no longer wish to live but, for some reason, they require another person to commit the final overt act which causes death. An example of this would be a physician, injecting a terminally ill person with sufficient lethal drugs to induce death.
Assisted suicide describes the situation in which a person wants to die, and obtains assistance from a third party to do so, though the final overt act causing death is taken by the individual, not the third party. An example of assisted suicide would be where a physician prescribes an individual with sufficient pills to induce death, but where the individual themselves takes and swallows the pills, thus inducing death.
WHAT IS PERMISIBLE IN NEW ZEALAND?
It is uncontroversial that in New Zealand, as with most common law countries, a competent adult has the right to refuse treatment, even where the consequences of that refusal, or non-treatment, would result in their death.3
2 See, Lorana Bartels and Margaret Otlowski, “A Right to Die? Euthanasia and the Law in Australia” (2010) 17 JLM 532, at 532 - 533, for further terminology.
3 See, Ben White, Lindy Willmott and John Allen, “Withholding and Withdrawing Life Sustaining medical Treatment: Criminal Responsibility for Established Medical Practice?” (2010) 17 JLM 849. See also: Auckland Area Health Board v Attorney-General [1993] 1 NZLR 235; Re G [1997] 2 NZLR 201; s 11, New Zealand Bill of Rights Act 1990; Brightwater Care Group (Inc) v Rossiter [2009] WASC 229; Re B [2002] 2 All

Medicine and Law 505
Related to the above category is the parens patriae jurisdiction of the Court, in which a declaration may be granted by the court that life supporting treatment can be withdrawn, where the patient is unable to consent or communicate, despite the fact that such action will result in death.4
The doctrine of double effect has recently been held to be extant in New Zealand law.5 This doctrine holds that a doctor, and in New Zealand it must be a doctor, is entitled to administer pain relief to any patient so long as in so doing the doctor does not intend to cause death, despite knowing that death will occur as a result.6
Finally, it is very important to note that in New Zealand, suicide is not a crime. The result of this in practice is that no person will be held liable for any attempt on their own life, or for succeeding in terminating their own life.7
WHAT IS NOT PERMISIBLE IN NEW ZEALAND?
In New Zealand, no form of voluntary active euthanasia or assisted suicide is permitted by law, unless the act could be considered to fall within the purview of one of the permissible acts identified above.
Assisted suicide is prohibited by virtue of s 179(b) of the Crimes Act 1961. This provides a punishment of “a term not exceeding 14 years” for any person who “…aids or abets any person in the commission of suicide.” Were it not for the existence of s 179, assisted suicide would not be a crime as the ordinary sections relating to party liability8 would not be operative as there is no principal crime of suicide from which party liability could be derived. It ought to be noted that the crime established by s 179 is anomalous as it makes it a crime to assist that which is not a crime.9
ER 449; Cruzan v Director, Missouri Department of Health 497 US 261 (1990); Nancy B v Hotel-Dieu de Quebec (1992) 86 DLR (4th) 385. See also Hutt District Health Board v B [2011] NZFLR 873 (HC); Airedale NHS Trust v Bland [1993] AC 789 (HL).
4 Re G [1997] 2 NZLR 201.5 R v Martin (No 3) [2004] 3 NZLR 69. See also R v Adams [1957] Crim LR 365.6 See also, Airedale NHS Trust v Bland [1993] AC 789 (HL); Auckland Health Board v
ttorney-General [1993] NZLR 235; R v Cox (1992) 12 BMLR 38.7 See below for details.8 Crimes Act 1961, s 66(1)(b)-(d).9 Shaun Pattinson, Medical Law and Ethics (3rd ed, Sweet and Maxwell, London, 2011), at
541.
Medicine and Law 506
Voluntary active euthanasia is prohibited by virtue of the ordinary murder provisions of the Crimes Act 1961.10 If a doctor, or any person, intentionally kills another, that constitutes murder, even if done for altruistic reasons.
Despite the absolute prohibition, an analysis of the cases concerning assisted death which have been decided in New Zealand,11 serve to exemplify the fact that even where a case is brought to trial, the courts are willing to impose lenient sentences upon the defendants. The sentences are varied, but include short terms of imprisonment, community work, community detention, supervision and even discharge without conviction.
WHAT IS PERMISIBLE IN OTHER JURISDICTIONS?
Voluntary active euthanasia is only permissible in a handful of jurisdictions around the world. The jurisdictions of which the author is aware at the time of writing are Albania,12 Belgium,13 Luxembourg,14
10 Crimes Act 1961, ss 158, 160, 167.11 See: R v Mott [2012] NZHC 2366; R v Davison24/11/2011, HC Dunedin, French J CRI-
2010-012-4876; R v Crutchley 9/07/2008, HC Hamilton, Keane J CRI-2007-069-83; R v KJK 18 February 2010, HC Christchurch, Chisholm J CRI-2009-009-14397; R v W (No 1) (2004) 21 CRNZ 926; R v Martin 31/03/2004, HC Wanganui, Wild J CRI-2003-083-432E; R v Bell 8/03/2002, HC Wanganui, Hammond J S011886; R v Law (2002) 19 CRNZ 500; R v Karnon 29/4/1999, HC Auckland, Paterson J S-14-99; R v Albury-Thompson (1998) 16 CRNZ 79; R v Ruscoe (1992) 8 CRNZ 68; R v Stead (1991) 7 CRNZ 291; R v M 11 December 2007, HC Dunedin, John Hansen J CRI-2007-012-211, subsequently varied in R v M 24 September 2008, HC Dunedin, French J CRI-2007-012-211; R v Faithfull 14 March 2008, HC Auckland, Venning J CRI-2007-044-007451; R v Novis 5 February 1988, HC Hamilton, Anderson J T42-87.
12 The precise Albanian position is not entirely clear. For more detail refer, Abdul Haseeb Ansari, A O Sambo and A B Abdulkadir, “The Right to Die via Euthanasia: An Expository Study of Shari’ah and Laws in Selected Jurisdictions” (2012) 6(5) Advances in Natural and Applied Sciences 673, at 678.
13 The Act Concerning Euthanasia of 2002 (Bel.). An unofficial translation of the Belgian Act was carried out by Dale Kidd, and can be found at: http://www.ethical-perspectives.be/viewpic.php?LAN =E&TABLE =EP &ID=59>, retrieved on 26 February 2013. See also, Maurice Adams and Herman Nys, “Comparative Reflections on the Belgian Euthanasia Act 2002” (2003) 11 Medical Law Review 353.
14 The Law of 16 March 2009 relating to Euthanasia and Assisted Suicide (Lux.). See also, Rory Watson, “Luxembourg is to Become Third Country to Allow Euthanasia” (2009) 338 BMJ 738.
Medicine and Law 507
The Netherlands,15 Colombia,16 and Japan.17
Assisted suicide is also only permissible in a few jurisdictions around the world. These are, in addition to those that permit voluntary active euthanasia, Switzerland,18 the state of Montana,19 the state of Oregon20 and the state of Washington.21
The Northern Territory of Australia deserves mention in this section. It passed legislation in 1995 rendering both physician assisted suicide and voluntary active euthanasia permissible, subject to conditions.22 However, in 1997 the Federal Parliament brought about the death of that legislation.23
It should be observed that in all of the above states which legalise some form of assisted death, various safeguards exist over the practice of such. However, the details of each jurisdiction’s precise legal control, including strengths and weaknesses, cannot be traversed in a paper of this length.
WHAT OUGHT TO BE PERMISSIBLE IN NEW ZEALAND?
Because the moral arguments for and against euthanasia have previously been traversed in great depth,24 this paper will focus only on the practical arguments.
15 Termination of Life on Request and Assistance with Suicide (Review Procedures) Act 2001 (Neths.). See also Kelisiana Thynne, “Implications of Legalising Euthanasia in the Netherlands: Greater Regulatory Control?” (2002) 10 JLM 232.
16 For an excellent overview of the Colombian legal position refer, Sabine Michlowski, “Legalising Euthanasia through the Courts: Some Lessons from Colombia” [2009] 17 MLR 183.
17 Refer, Stanley Yeo, “Right to Die” (2003) 28(2) Alternative Law Journal 89.18 Swiss Penal Code, Art. 115. See also, Olivier Guillod and Aline Schmidt, “Assisted
Suicide under Swiss law” (2005) 12 EJHL 25.19 Baxter v Montana (2009) MT 449.20 Death with Dignity Act 1995 (Oregon). See also, SP Calandrillo, “Legislative Activity:
Physician Assisted Suicide under Managed Care” (1998) 26(1) The Journal of Law Medicine and Ethics 72.
21 Death with Dignity Act 2008 (Washington). See also, Karen Feldt (et al), “Washington State Death with Dignity Act: Implications for Long-Term Care” (2011) 37(10) Journal of Gerontological Nursing 32.
22 Rights of the Terminally Ill Act 1995 (NT).23 Euthanasia Laws Act 1997 (Cth.).24 See for example: Julia Werren, Necef Yuksel and Saxon Smith, “Avoiding a Fate Worse
than Death: An Argument for Legalising Voluntary Physician Based Euthanasia” (2012) 20 JLM 184; H. Kuhse, “From Merely ‘Letting Die’ to ‘Helping Die’: The Case for Voluntary Euthanasia” (2001) 58-59 Australian Rationalist 33; Cynthia Cohen, “Christian
Medicine and Law 508
In this paper practical is used to refer to arguments which are not moral or ethical. They are both legal and otherwise. Once the practical arguments have been outlined, the paper will then consider whether, on the strength of these arguments, the legal framework in New Zealand should be reformed.
Prior to traversing the substantive arguments in this section it is worth noting that in June 2012 Maryan Street, a Member of Parliament for Labour, a New Zealand political party, introduced into the ballot a private member’s Bill which is called the End of Life Choice Bill 2012. An in depth analysis of this Bill would be out of place in a paper of this length,25 however, it is important to note that New Zealand may be on the cusp of reform. If this does prove to be the case then the arguments contained herein will hopefully prove thought provoking when the issues are being debated.
The Arguments in Favour
An excellent starting point for contemplating reform of the laws relating to lethal treatment and assisted suicide is the stage of public opinion. Various studies have consistently indicated that a majority of people in New Zealand consider that some form of lethal treatment or assisted suicide should be made legal.26 In addition, New Zealand is the fifth most democratic country on earth,27 with the most transparent government on earth.28 If it is accepted that “[t]he law is in effect the codification of the will of the people”,29 then one could be forgiven for wondering why such a politically admirable country and Government continues to maintain the general prohibition outlined above.
Perspectives on Assisted Suicide and Euthanasia: The Anglican Tradition” (1996) 24 J. L. Med. & Ethics 369; Andrew McGee, “Defending the Sanctity of Life Principle: A Reply to John Keown” (2011) 18 JLM 820; JM Finnis, “Bland: Crossing the Rubicon?” (1993) 109 LQR 329; Rachael Patterson and Katrina George, “Euthanasia and Assisted Suicide: A Liberal Approach versus the Traditional Moral View” (2005) 12 JLM 494.
25 For a discussion of this Bill refer A D Macleod, “Euthanasia and Physician-assisted Death” (2012) 125 The New Zealand Medical Journal 127. See also Jack Havill, “Medically Assisted Dying” (2013) 126 The New Zealand Medical Journal (letters).
26 The website <www.policyprojects.ac.nz> provides an excellent overview of the general public sentiment on this issue, with surveys dating back to 1982. Anon, “Legalisation of Euthanasia in New Zealand” retrieved from http://policyprojects.ac.nz/jasonrenwick/surveys-in-new-zealand/#_edn1, 20 February 2013.
27 Economist Intelligence Unit, “Democracy Index”, retrieved from <http://www.eiu.com/index.asp?layout=info&info_name=infographic_democracy>, 20 February 2013.
28 Transparency International, “Accountability: Corruption by Country”, retrieved from http://www.transparency.org/country#NZL, 20 February 2013.
29 R Smith, “Euthanasia: Time For a Royal Commission” (1992) 305(6856) BMJ 728, at 728.
Medicine and Law 509
This paper submits that this alone represents a very compelling argument in favour of reform.
As was noted above, suicide is not a crime in New Zealand, and has not been since 1893 when the Criminal Code Act 1893 defined homicide as:30
the killing of a human being by another directly or indirectly, by any means whatsoever.
This definition required a human to be killed by another human, which removed the possibility of self-murder. Prior to this, suicide was considered a crime. This fact was observed by Bracton, who said:31
Just as a man may commit a felony by slaying another, so he may do so by slaying himself, the felony is said to be done to himself.
Coke also observed this when he stated:32
Felo de se is a man, or woman, which being compos mentia, of second memory, and of the age of discretion, killeth himself, which being lawfully found by the oath of twelve men, all the goods and chattels of the party so offending are forfeited.
The fact that suicide is no longer a crime does require consideration as to the justification for making it a crime to assist, irrespective of whether that assistance comes in the form of helping the person wanting to die commit the final overt act themselves, or by committing that final overt act for them. If the law does not condemn suicide, it can be difficult to understand why the law does condemn those who seek to assist a person to commit suicide. It is acknowledged that there is potential for abuse, but as will be identified below, that is able to be ameliorated. Thus, legal consistency would be an argument in favour of reform.
Another issue which arises with respect to suicide is the position of those who are not capable of terminating their own life due to physical or mental issues.
30 Criminal Code Act 1893, s 154.31 G Neeley, The Constitutional Right to Suicide: A Legal & Philosophical Examination
(1996, Peter Lang Publishing, New York) at 46, citing G. Woodbine, Bracton on the Laws and Customs of England, translated S. Thompson (1968).
32 G Neeley, The Constitutional Right to Suicide: A Legal & Philosophical Examination (1996, Peter Lang Publishing, New York), at 49, citing Coke, Third Institute, at 54.
Medicine and Law 510
The harsh reality of the matter is that many people are physically incapable of committing suicide.33 The rendering of assistance in such cases is still illegal despite the fact that often the individual would take their own life if they had the ability to do so. This seems, prima facie, to constitute discrimination based on disability - there seems to be little principled reason for denying these people a right to death which other able bodied or able minded people could enjoy, and certainly no reason which cannot be overcome. Reform could go some way to removing this apparent discrimination.
Medical reality indicates that medical practitioners, and likely ordinary people, are already helping people to die, in spite of the current legal regime prohibiting such behaviour. Papers have been published in New Zealand,34 Australia,35 the United States,36 the United Kingdom,37 and other countries,38 which all testify to the fact that at least some proportion of medical practitioners participate in euthanasia or assisted suicide, despite the prohibitive legal regime. This flagrant contravention of the strict legal position shows that the current legal regime is not efficacious, and identifies very real issues with the detection of the offences. This paper submits that these reasons represent compelling practical justifications for reviewing the present legal position and considering reform.
Finally, legal reality is another indicator that the present legal regime is ineffective. Despite voluntary lethal treatment and assisted suicide being criminal acts in New Zealand, and irrespective of the fact that the laws are not followed, the judiciary looks upon those who contravene the strict legal position with great sympathy. The sentence imposed on those people
33 Jean Davies, “The Case for Legalising Voluntary Euthanasia”, in John Keown (ed), Euthanasia Examined: Ethical, Clinical and Legal Perspectives (Cambridge University Press, Cambridge, 1997), at 89.
34 Kay Mitchell and R Glynn Owens, “National Survey of Medical Decisions at End of Life Made by New Zealand General Practitioners” (2003) 327 BMJ 202.
35 H Kuhse, P Singer, P Baume, M Clark, and M Richard, “End of Life Decisions in Australian Medical Practice” (1997) 166 Med. J. Australia 191; CD Douglas, IH Kerridge, KJ Rainbird et. al., “The Intention to Hasten Death: A Survey of Attitudes and Practices of Surgeons in Australia” (2001) 175 Medical Journal of Australia 511.
36 See Roger Magnusson, “’Underground Euthanasia’ and the Harm Minimization Debate” (2004) 32 Journal of Law Medicine and Ethics 486, which traverses, inter alia, the pertinent US studies.
37 Clive Seale, “National Survey of End-of-life Decisions Made by UK Medical Practitioners” (2006) 20 Palliative Medicine 3.
38 See for example A van der Heide, L Deliens, K Faisse et al., “End-of-life Decision-making in Six European Countries: Descriptive Study” (2003) 362 Lancet 345.

Medicine and Law 511
is typically exceedingly lenient.39 It is submitted that the degree of leniency which is found in these sentences effectively amounts to judicial circumvention of the law under the guise of the Sentencing Act.40 It is suggested that there is little utility in a law which the judiciary appears to strive to circumvent, to a greater or lesser extent, by the imposition of either the least harsh punishment possible in the circumstances, or certainly punishments at the lower end of the sentencing scale.
The Arguments Against
The question may arise as to whether physicians would even participate in such procedures if they were legal. This could be a potential practical reason for retaining the status quo. However, studies have consistently indicated that sufficient numbers of medical practitioners would be willing to participate in end of life activities should it be legalised, and, as identified above, there are those who would do so despite the fact it is not presently legal. One Waikato University study indicated that 54 out of 102 doctors surveyed would engage in such practices if it were permitted by law.41
It has been suggested that one consequence of allowing physicians to assist in the death of their patients is that it may be “harmful to the standards and role of the medical profession.”42 However, this argument seems to be particularly weak, especially since it is ordinarily relied on with no reference to any substantiating evidence. It is rarely, if not never, acknowledged that underground euthanasia already occurs, including non-voluntary euthanasia, when this argument is proffered. In the absence of evidence to the contrary, this argument should not be considered compelling.
An argument against assisted death which appears with alarming regularity is that of the slippery slope. The argument posits that if one form of assisted death was permitted, it would effectively place humanity on a slippery slope to permitting non-voluntary, and even involuntary, euthanasia. However, there is no evidential basis for such an assertion. One study by Lewis concluded that
39 See above.40 Sentencing Act 2002.41 Parliamentary Library, Background Note, Voluntary Euthanasia and New Zealand (22
November 2003), at 19.42 Martin Gunderson, “A Right to Suicide Does Not Entail a Right to Assisted Death”
(1997) 23 Journal of Medical Ethics 51, at 52; Karl Lorenz and Joanne Lynn, “Moral and Practical Challenges of Physician Assisted Suicide” (2003) 289(17) JAMA 2282, at 2282.

Medicine and Law 512
“the current evidence does not support the drawing of inferences either that legalisation causes an increase in the rate of non-voluntary euthanasia or that such rates are higher under a prohibitive approach.”43
There is a wider question which subsumes the slippery slope argument, which is whether such a regime would result in abuse of any sort. This paper submits that while any framework is open to abuse, New Zealand is in a position whereby it can analyse the legal position of the jurisdictions which do permit assisted death, and the safeguards therein, and construct a robust legal framework which would diminish to less than negligible, the risks for abuse.
Reform?
A review of the practical justifications identified above, considered in aggregate, but in isolation from ethical consideration, tends towards the conclusion that the law as it presently stands is unsatisfactory, ineffective, and ought to be reformed. The practical justifications against reform do not, it is suggested, proffer any compelling argument in favour of retention of the status quo, and certainly not any that cannot be overcome.
A majority of individuals, in what is apparently a deeply democratic nation, would prefer that some form of assisted death was rendered permissible. Suicide has not been a crime in this country for 120 years, yet it remains a crime to assist a person to commit suicide. Moreover, medical and legal reality indicate that the law is ineffective - it is contravened, often without detection, and when it is detected the offender escapes with exceedingly lenient sentences.
It is respectfully submitted that none of the practical justifications which may be used to oppose reform are compelling. There would be sufficient numbers of physicians willing to participate if such procedures were legal. There is no substantiated evidence positively indicating that any harm to the medical profession would result from such practices being legalised. Finally, the slippery slope argument has no evidential basis, and any potential for abuse can be mitigated, and rendered negligible by a robust legal framework.
43 Penney Lewis, “The Empirical Slippery Slope from Voluntary to Non-Voluntary Euthanasia” (2007) 35 Journal of Law, Medicine and Ethics 197, at 205. See also Stephen Smith, “Fallacies of the Logical Slippery Slope in the Debate on Physician-Assisted Suicide and Euthanasia” (2005) 13 Medical Law Review 224.

Medicine and Law 513
This paper supports the legalisation of physician assisted suicide and voluntary active euthanasia, but only where the physician is the person who undertakes the ultimate overt act causing the death of the person so requesting, and provided that the activities were subject to a rigorous medical and legal procedure which would render less than negligible any potential for abuse. Such a framework could be developed by a thorough and considered analysis of the jurisdictions which permit assisted death. This would allow New Zealand to benefit from all of the strengths and obviate all of the weaknesses extant in the legal regimes of various jurisdictions, while obviating all of the weaknesses. Finally, and perhaps more importantly, an analysis of such regimes would also provide evidence as to whether the regimes were being abused, or whether incidences of abuse had increased under the regulated, as opposed to prohibitive, regimes.
CONCLUSION
This paper has sought to deal with the practical justifications for and against reform of the law relating to voluntary active euthanasia and assisted suicide. It has been seen that a multiplicity of exemptions exist in which it is possible for a person to acquire assistance in inducing their death, yet the general prohibition on assisted suicide and voluntary active euthanasia remains.
It is suggested that the practical justifications in favour of reforming the law are compelling, while the practical justifications for retention of the status quo are comparatively weak, all of which can be overcome with reasonable ease. A review of the jurisdictions which presently permit some form of assisted death would provide a solid foundation on which New Zealand could base its new regime.
This paper would favour a regime in which assisted suicide and voluntary active euthanasia were rendered permissible, though only when carried out by a physician. Such a solution, it is suggested, would remove a significant burden from the shoulders of friends and family, and place it squarely on the medical profession, which is in the best position to address it.

©PROBOOK 2013and Law
Medicine Med Law (2013) 32:515-523
515
ADVANCE DIRECTIVES: THE CONSECRATION OF AUTONOMY AND DIGNITY OF THE HUMAN BEINGMarianna Chaves*
Abstract: Advance directives emerge in the doctor-patient relationship as a way to ensure that the autonomy of the patient is observed, prior to a potential state of incapacity. Thus, autonomy can be exercised ensuring patient´s dignity and self-determination. Advance directives yet have the power to drive the medical practitioner and his staff so that it is given the treatment and care previously chosen by the patient. The main purpose of this paper is to show the lack of legislation on the matter in Brazil versus the recognition of Advance Directives by the Brazilian Federal Council of Medicine. Can a mere resolution of the Council transform directives into enforceable wishes? This is an answer we intend to offer throughout the text.
Keywords: Advance Directives; Autonomy; Human Dignity; Brazil
Summary: Introduction. 1. The Advance Directives in the Brazilian system. 2. Founding principles of the Advance Directives; 2.1 Human dignity; 2.2 Autonomy. 3.The conclusion of a right to a dignified death. References.
INTRODUCTION
We intend to analyze the right that every individual has to decide in advance about the end of his life, choosing what seems best and most convenient, before being affected by incurable disease, in end-stage, or irreversible incapacity and being unable to express his will regarding how he wants to spend his last moments of life and which treatments he wishes or do not wish to receive.
* PhD Candidate in Civil Law at Coimbra University- Portugal, Masters Degree in Legal Sciences from Lisbon University - Portugal, Member of the World Association for Medical Law, Legal Consultant, Rua Infanta D. Maria, 426/ 3ºD, 3030-330, Coimbra - Portugal. Email: [email protected]
Medicine and Law 516
In Brazil, the doctrine had already been understanding to the possibility for a person to express himself by way of a declaration of will - in a document that holds resemblance with the will - about procedures or decisions regarding their own body or their life and future decisions, to be taken when suffering from serious illness or unconsciousness, the so called living will.
André Pereira conceptualized the living will as a document written by a person of legal age and capable, generally in the presence of witnesses, that contains directives regarding the treatment in the last moments of life, having in sight eventual situations of incapacity to make decisions for and about himself.1
Much has been criticized the nomenclature used, considering that in the Brazilian legal system, the will is a typical institute mortis causa.2 Considering that the document in question has efficacy in life, the terminology “Advance Directives” (AD) proves to be more suitable. The uproar over the terminological issue seems - apparently - to have come to an end after the emergence of Resolution nº 1.995/2012 of the Brazilian Federal Council of Medicine, which expressly provides for Advance Directives of willingness of the patients.
1. THE ADVANCE DIRECTIVES IN THE BRAZILIAN SYSTEM
Recognizing the need for regulation and the lack of legislation on advance directives from the patient's will in the context of Brazilian medical ethics; Considering the need to regulate the conduct of the physician in front of advance directives; Pondering the relevance of the matter of patient´s autonomy in the context of the doctor-patient relationship, as well as its interface with the advance directives; Emphasizing that in professional practice physicians may be faced with this ethical situation yet not covered by current national ethics provisions; Recalling that new technological resources enable the adoption of measures that disproportionate prolong the suffering of the terminally ill patient without benefits and that these measures may have been rejected in advance by the patient, the Federal
1 EREIRA, André Gonçalo Dias. O consentimento informado na relação médico-paciente: um estudo de direito civil. Coimbra: Coimbra Editora: 2004, p. 240.
2 For a deeper critique of the terminology, see TARTUCE, Flávio. “A questão do testamento vital ou biológico - primeiras reflexões”, In: Novos Direitos Após Seis Anos de Vigência do Código Civil de 2002/Inácio de Carvalho Neto (org.). Curitiba, Juruá, pp. 433-458, 2009, p. 433.
Medicine and Law 517
Council of Medicine adopted, in 2012,the aforementioned resolution on advance directives.
The resolution is quite simple and its content is restricted to two articles. The key issue is to know if the content of the document may or not be enforceable under Brazilian law. We will try to provide this response later.
The first article of Federal Council of Medicine (CFM) Resolution (1955/2012) defines what are AD for the Council. The AD´s are defined as the set of wishes, previously and expressly, manifested by the patient about care and treatment he wants or does not want to receive at the time he is incapable to freely and autonomously express his will.
The second article of the resolution is a bit more complex than the first, since it deals with different issues relating to the same matter. The head of this article indicates that in decisions regarding care and treatment of patients who are unable to communicate or to freely express their will, the physician will consider their AD.
The resolution uses the term "consider" since a physician may fail to take into consideration the patient's or his representative´s advance directives that, in his understanding, are in variance with the precepts dictated by the Brazilian Code of Medical Ethics (article 2, § 1 and 2).
If AD's are in accordance with the Code of Medical Ethics, the patient's wishes shall take precedence over any other non-medical opinion, including family members (article 2, § 3).
The CFM Resolution establishes a mandatory way to formalize AD's. These desires are not required to be a notarized document such as a will, for example. They may be spoken orally to the physician that will register, in the patient's medical records, the wishes reported to him directly by the patient (article 2, § 4). This paragraph clearly emphasizes the importance of the doctor-patient relationship. But, obviously, in absence of a declaration before the physician it is necessary to have a written document.
In absence of AD's from the patient or his designated representative, family members, or if there is a lack of consensus among them , the physician will resort to the Bioethics Committee of the institution, if any. In its absence, and when he understands that this measure is necessary and convenient (article
Medicine and Law 518
2, § 5), he will resort to the Medical Ethics Committee of the hospital or the Regional/Federal Council of Medicine in order to base his decision about ethical conflicts..
Within the Code of Medical Ethics, two articles have particular relevance in this matter and harmonize with possibility of AD's. Article 24 states that it is prohibited for the physician to fail to ensure the patients' right to freely decide about their person or their well-being as well as exercise his authority to limit it.
Article 41 states that it is prohibited for the physician to abbreviate the patient´s life even if it is at his own request or his legal representative's. But the same disposition clarifies that in cases of incurable and terminal disease, the physician must provide all palliative care available without taking futile or obstinate diagnostic or therapeutic actions, always taking into consideration the wishes of the patient or, in its absence, his legal representative´s. In summary, we can state that there is an express prohibition to euthanasia, but an opening for orthothanasia in Brazilian legal system.
2. FOUNDING PRINCIPLES OF THE ADVANCE DIRECTIVES
As previously stated, it can be said that there is space in the Brazilian legal system - within certain limits -for people to have their wishes of life and death, respected. In other words, to have their dignity honored in all stages of life, including the very end of it. But which are the principles that lead to the understanding that there is a right to a dignified death?
2.1 Human dignity
Human dignity is not a constitutional creation. It is, prior to any speculative attempt, a fact, just as the human person. The Brazilian Constitution, recognizing its existence and eminence, made it an exalted value of the legal order and one of the grounds of the Republic.3 To clarify the meaning of human dignity as the foundation of the Republic, the Portuguese doctrine asserts that it is the recognition of the individual as the limit and foundation of political dominance of the Republic.
3 With the same understanding, see SILVA, José Afonso da. Comentário Contextual à Constituição. 5. ed. São Paulo: Malheiros Editores, 2008, p. 39.

Medicine and Law 519
This statement results from historical reoccurrences of attempted extermination of human beings, such as: ethnic genocide, slavery, the Inquisition, Nazism, among others.4
It can be stated that the principle of human dignity is currently one of the supporting bases of modern legal systems. It is impractical to disconnect thinking about rights from the concept and idea of dignity.
Dignity is a term under which emerge a collection of other ethical principles and essential values such as freedom, autonomy, citizenship, equality and solidarity. These inscriptions are the result and consequence of political struggles and achievements associated with the evolution of thinking, development of the sciences and new technologies. The notion of dignity and indignity is what made thinking, organizing and developing the human rights possible.5
Ingo Sarlet's classifies the dignity of the human being as a distinctive and inherent quality of every human being, making him worthy of the same respect and consideration by the State and the community, implying, in this sense, a complex of fundamental rights and duties to ensure his protection against any degrading act and inhumane treatment. In addition to providing and promoting their active participation and co-responsibility in the destinations of their own existence, it must also ensure minimal existential conditions for a healthy life.6
Dieter Grimm asserts that the dignity as the condition of intrinsic value of the human being creates for individuals the right to decide autonomously about their existential projects, happiness, life and even when this autonomy is absent or can not be updated, the person should still be regarded and respected for his human condition.7
4 See CANOTILHO, J. J. Gomes. Direito constitucional e teoria da constituição. 7. ed. 5ª reimp. Coimbra: Almedina, 2003, p. 225.
5 PEREIRA, Rodrigo da Cunha. Direito de Família: uma abordagem psicanalítica 2. ed. rev. atual. ampl. Belo Horizonte: Del Rey, 2003, p. 94.
6 SARLET, Ingo Wolfgang. Dignidade da pessoahumana e direitosfundamentaisna Constituição Federal de 1988. Porto Alegre: Livraria do Advogado Editora, 2001, p. 60.
7 GRIMM, Dieter apud SARLET, Ingo Wolfgang. “As dimensões da dignidade da pessoahumana: construindou ma compreensão jurídico-constitucional necessária e possível”. In: SARLET, Ingo Wolfgang (Org.). Dimensões de dignidade: ensaios de filosofia do direito e direitoconstitucional. Porto Alegre: Livraria do Advogado, pp. 13-44, 2005, p. 34.
Medicine and Law 520
Much we talk about dignity in the early stages of life but it is important to emphasize that the final moment of life is just as deserving of care as its beginning. Each individual should have the right to freely express their will about their end of life and it is the role of the legal system give effect to fulfillment of these provisions. In attention to the dignity, these wishes should take effect prior to the time of death of the holder of the legal interests life and willingness.8
2.2 Autonomy
To Luis Roberto Barroso, autonomy is the ethical element of human dignity. It is the foundation of the people´s free will, allowing them to get - on their own way - their ideals of good living and good life. Here, the central notion is self-determination: an autonomous person defines the rules that will govern his life.9
Merely to differentiate autonomy and freedom, the same author recalls that freedom has a broader scope, which may be limited by external lawful forces. But autonomy is the part of freedom that cannot be suppressed by interference from the state or society as it covers basic personal decisions. Therefore, autonomy is the ability of someone to make decisions and personal choices throughout life, based on their own conception of good, without undue external influences.10
The biotechnological and medical advances now allow a prolongation of life (and death delay) that can transform the process of end of life in an extremely long and painful journey. Undignified. That's where the autonomy of will has more relevance in this matter. Everyone should have the right to die with dignity and not be forced to suffer for a futilely prolonged period of time, deprived of the domain over his body.11
8 See CABRAL, Vivian Boechat. “O Testamento Vital e a Efetividade da Vontade do Titular do Bem Jurídico Vida”, In: Revista Brasileira de Direito das Famílias e Sucessões. Vol. 28, Jun./Jul. Porto Alegre: Magister, pp. 22-47, 2012, p. 24.
9 BARROSO, Luís Roberto. A dignidade da pessoa humana no direito constitucional contemporâneo: a construção de um conceito jurídico à luz da jurisprudência mundial. Belo Horizonte: Fórum, 2013, p. 81.
10 BARROSO, Luís Roberto. A dignidade da pessoa humana no direito constitucional contemporâneo: a construção de um conceito jurídico à luz da jurisprudência mundial. Belo Horizonte: Fórum, 2013, p. 82.
11 In the same sense, see BARROSO, Luís Roberto. A dignidade da pessoa humana no direito constitucional contemporâneo: a construção de um conceito jurídico à luz da

Medicine and Law 521
3. THE CONCLUSION OF A RIGHT TO A DIGNIFIED DEATH
As previously mentioned, in Brazil there is still no legislation regulating the matter. But are we thus in a total legal vacuum? A document containing advance directives would be legally null and void? It does not seem.
The suspension of futile therapeutic efforts have support in the Constitution (Art. 1, III and Art. 5, III), which recognizes the dignity of the human person as the foundation of the democratic state and specifically states that no one will be subjected to torture or to degrading treatment; in the Civil Code (Art. 15), which allows the patient to refuse certain medical procedures; in the Organic Health Law (law nº 8.080/90, Art. 7, III), which recognizes the right to autonomy of the patient, and in the Code of Medical Ethics, which prohibits the physician to perform therapeutic procedures against the patient's will, outside a framework of medical emergency of salvation, which is not the case of a patient with irreversible disease, which gives no response to any type of treatment.12
More than that, we can state that this "legislative vacuity" is at least temporarily supplied by the Federal Council of Medicine´s Resolution on Advance Directives that according to doctrine13 is hierarchically equal to the law as it complements the legal system, filling gap where the legislature was silent.
Finally, there is nothing in the Brazilian Civil Code that rejects the legal force of advance directives. Pursuant to Art. 14 of the Civil Code, the validity of the legal transaction has three requirements: capable agent; lawful, possible, determined or determinable object; species prescribed or not prohibited by law.
So while the document that contains the advance directives comply with such formal requirements, it should be considered fully valid under penalty to affront several constitutional principles such as the dignity of the human being and freedom, embodied in the autonomy to determine what will be done with his body, within his notion of health.
jurisprudência mundial. Belo Horizonte: Fórum, 2013, p. 109. 12 RIBEIRO, Diaulas Costa. Um novo testamento: testamentos vitais e diretivas antecipadas.
In: PEREIRA, Rodrigo da Cunha (Coord.). Família e dignidade humana: Anais do V Congresso de Direito de Família. Belo Horizonte: IBDFAM, 2005, pp. 281-282
13 DANTAS, Eduardo; COLTRI, Marcos. Comentáriosao Código de Ética Médica. Rio de Janeiro: GZ, 2010, p. 99.
Medicine and Law 522
In summary: the Brazilian legal system currently allows a person to dispose of his body and his life, within the limits of orthothanasia, which represents a significant advance in terms of autonomy and self-determination.
REFERENCES
BARROSO, Luís Roberto. A dignidade da pessoa humana no direito constitucional contemporâneo: a construção de um conceito jurídico à luz da jurisprudência mundial. Belo Horizonte: Fórum, 2013.
CABRAL, Vivian Boechat. “O Testamento Vital e a Efetividade da Vontade do Titular do Bem Jurídico Vida”, In: Revista Brasileira de Direito das Famílias e Sucessões. Vol. 28, Jun./Jul. Porto Alegre: Magister, pp. 22-47, 2012.
CANOTILHO, J. J. Gomes. Direito constitucional e teoria da constituição. 7. ed. 5ª reimp. Coimbra: Almedina, 2003.
DANTAS, Eduardo; COLTRI, Marcos. Comentáriosao Código de Ética Médica. Rio de Janeiro: GZ, 2010.
PEREIRA, André Gonçalo Dias. O consentimento informado na relação médico-paciente: um estudo de direito civil. Coimbra: Coimbra Editora: 2004.
PEREIRA, Rodrigo da Cunha. Direito de Família: uma abordagem psicanalítica. 2. ed. rev. atual. ampl. Belo Horizonte: Del Rey, 2003.
RIBEIRO, Diaulas Costa. Um novo testamento: testamentos vitais e diretivas antecipadas. In: PEREIRA, Rodrigo da Cunha (Coord.). Família e dignidade humana: Anais do V Congresso de Direito de Família. Belo Horizonte: IBDFAM, 2005.
SARLET, Ingo Wolfgang. Dignidade da pessoa humana e direitos fundamentais na Constituição Federal de 1988. Porto Alegre: Livraria do Advogado Editora, 2001.
“As dimensões da dignidade da pessoa humana: construindo uma compreensão jurídico - constitucional necessária e possível”. In: SARLET, Ingo Wolfgang (Org.). Dimensões de dignidade: ensaios de filosofia do direito e direito constitucional. Porto Alegre: Livraria do Advogado, pp. 13-44, 2005.
Medicine and Law 523
SILVA, José Afonso da. Comentário Contextual à Constituição. 5. ed. São Paulo: Malheiros Editores, 2008.
TARTUCE, Flávio. “A questão do testamento vital ou biológico - primeiras reflexões”, In: Novos Direitos Após Seis Anos de Vigência do Código Civil de 2002/Inácio de Carvalho Neto (org.). Curitiba, Juruá, pp. 433-458, 2009

©PROBOOK 2013and Law
Medicine Med Law (2013) 32:527-541
525
BRIEF NOTES ON THE PORTUGUESE CRIMINAL REGIME OF HOMICIDE UPON REqUEST OF THE VICTIM AND PHYSICIAN ASSISTED SUICIDE Sara Leitão Moreira*
Abstract: Society is changing at an unprecedented rate. Several areas of knowledge are evolving on a daily basis, namely medicine and connected sciences. Hence it is needed that the legislator walks at least right behind this evolution, in order not to be considered retrograde.
One of the areas that need the constant attention of the legislator is medicine, as far as prolonging life is considered. We have witnessed several cases along the decades of people who are not living a long and healthy life, but rather just a long life, with little quality in it. Therefore, it is also known that issues such as euthanasia have been discussed at several levels. Criminal law, in most countries, namely in Portugal, does not admit any type of euthanasia. We will briefly analyse the two Articles in the Portuguese Penal Code concerning this matter, in order to come to the conclusion of its pertinence and adequacy to today’s society.
Keywords: Euthanasia; Homicide Upon Request; Physician Assisted Auicide; Medicine; Criminal Law; Portugal.
INTRODUCTION
The Portuguese society has come a long way when it comes to adapting its legislation to current times. The legislator has tried to keep up with the constant evolution of science, although sometimes it is not always possible to assimilate everything and change the values that are inherent to our society in due time.
Considering that asymmetry, many issues are raised and the evolution of certain areas, like medicine and other sciences, are not being accompanied by, for instance, law. We are not affirming that the Portuguese law is regressive, it evolves at the rate that is permitted and adequate to its society, but truth is
* Assistant Professor at the Higher Institute Bissaya Barreto. Email: [email protected]

Medicine and Law 526
that some matters are kept in the dark and in need of a different approach, or at least to be thought about according to different perspectives, and be scrutinized by the ones who are affected by it, the people1.
The thought of a referendum is considered to be convenient in these types of issues, yet there has been a certain refrain to use it in the case of euthanasia, but we will have the opportunity to talk about this matter in another instance.
Man, in abstract terms, is an unsatisfied being who, in the same way that he moves towards socialisation, also tends to move away from it. Meaning that, he tends to make ways to prolong his life in order to stay longer in this society, just to make ways to move away from it once again. Let’s just say that an intrinsic unsocial sociability is natural to us as human beings, just as Bronze tells us (2010, p. 201)2 and Immanuel Kant once wrote (2003, p.8).3 We understand that this is one of the most important lengths of our human nature and of irrefutable relevance to the evolution of the society in which we live in. Society depends on the history of the non-finite character of Man, his lack of satisfaction, and the reality in which he settles.
The shift in values, the shift in the way that we consider certain issues and reality itself4, has a tremendous influence in law, especially criminal law, and we witness this permeability through decriminalisation and de-penalisation, or on the contrary, through criminalisation or penalisation, of certain behaviours. That is, what was once considered as criminally relevant behaviour may become irrelevant (or precisely the inverse situation) due to the powerlessness of the legislator to foresee everything.
1 In this sense see NUNES, R., 2009.Referendo Nacional sobre a Prática da Eutanásia. In: R. Nunes, G. Rego, I. Duarte, ed. 2009.Eutanásia e outras questões éticas no fim da vida. Coimbra: Gráfica de Coimbra, pp.263-273.
2 Bronze, F. J., 2010.Lições de Introdução ao Direito. 2nd ed. Coimbra: Coimbra Editora, p. 201.
3 Kant, I., 1785.Ideia de uma história universal com um propósito cosmopolita. Translated by R. Naves and R. Terra., 2003. São Paulo: Martins Fontes, p. 8.
4 For a different perspective on the Hippocratic Oath, and the effects it has on various practices of today’s medicine, namely euthanasia and abortion (“I will neither give a deadly drug to anybody if asked for it, nor will I make a suggestion to this effect. Similarly I will not give to a woman an abortive remedy. In purity and holiness I will guard my life and my art”), due precisely to shifts in mentality and society, see Pellegrino, E.D., 1998. Rethinking the Hippocratic Oath. In M. Uhlmann, ed. 1998. Last Rights? Assisted Suicide and Euthanasia Debated. Washington D. C.: William B. Eerdmans Publishing Company, pp. 257-261.
Medicine and Law 527
Considering the constant changes that man witnesses on a daily basis he questions the “who”, the “what”, the “where”, the “why” and the “how” of his existence, and comes to the conclusion that he is not satisfied with what is presented to him in his present tense (or past tense, for that matter). We have witnessed several changes in medicine that have driven us to rethinking the way we consider life and the values that subdue us.
Nowadays medicine has ways to make us live longer, almost indefinitely, just as Costa points out (2005, pp. 116-120), and that has serious consequences in legal terms, for it does not always mean that this is the same as quality of life. The same author, very eloquently says that (Costa, 2005, pp.110-113) death is the only phenomenon in life that is truly opaque, or just as Edward Ward in his 1724 'Dancing Devils' 'Death and Taxes, they are certain’, yet we are witnessing some changes in that certainty. The life expectancy has been increasing due to advances in medicine and has made our hour of “natural death” quite uncertain. Well, what if, even having that possibility of having a few more years (maybe even decades), does not really interest us and we need help to end our life, either through someone else, or with help us do it ourselves?
The aim of this paper is thus to analyse the way the Portuguese legislator faces the euthanasia phenomenon, be it through the homicide upon request or assistance to suicide. These are two completely different scenarios, yet they reflect the way society portrays death, when it does not come about in a “natural way”, and is carried out by, or somehow has the participation of, a third part. Criminal law in Portugal does not accept any type of third party “life disposal” actions, homicide, murder, manslaughter, always foreseeing prison as a necessary penalty for that type of crime. Nor does it permit the violation of a non-available good, such as Life, except in precluding wrongfulness circumstances, such as self-defence, or exculpatory circumstances, and even then it is dubious, due to the fact that life is never available to be pondered upon.
We therefore propose to look at the Portuguese criminal legislation in the face and see what standards it meets towards the euthanasia issue nowadays.

Medicine and Law 528
EUTHANASIA - AN ATTEMPT TO SIMPLIFY A COMPLICATED REALITY
Article 245 of the Portuguese Constitution of 19766, which is presently in force7, stipulates that the human life is said to be inviolable. Well, what is euthanasia? Many of us have questioned ourselves about this, somewhere along our journey, be it due to personal issues, or by cases that have come to our knowledge.
All words are polysemous and therefore their meaning can be expressed by various forms, however, we found a particular definition by Pattinson8 (2006, p. 476) which translates the general view of euthanasia, “Euthanasia is a word of Greek origin. To some it conjures up images of a gentle passing chosen by a person at peace with himself; to others it conjures up Nazi-inspired fear of the brutal slaughter of unwilling innocents. It originally referred to a gentle death.” Besides this brief reference to what euthanasia is, in general terms, we must not forget that the doctrine has presented us with different types of this alleged “mercy killing”.
The mentioned existence of different types of euthanasia, and other end of life choices submitted to the scrutiny of criminal law, affects especially the way it is put into practice, namely voluntary, non-voluntary and involuntary
5 Article 24, n. 1 of the Portuguese Constitution states ‘human life in inviolable’.6 This Article is considered to contain a subjective right, which means that the one that holds
that right to a certain conduct from anyone else, on the other hand have the duty to put into practice that conduct. In this sense see Canotilho, J. J. G., 2003, Direito Constitucional e Teoria da Constituição.5th ed. Coimbra: Almedina, p.1238, who concludes the following about the Article 24 of the Portuguese Constitution“1. The individual has the right, before the State, to not being killed by it (“prohibition of a legal death penalty”); the State has an obligation to refrain itself from attempt against the life of an individual; 2. The individual has the right to life before other individuals; these must refrain from practicing acts (active or omissive) that attempt against someone’s life.” We may also conclude that fundamental rights are subjective rights and therefore of utmost importance in any Rule of Law. See the same author, p. 1240-1245.
7 For further developments see: Costa, J. F., 2005. O fim da vida e o direito penal. In. Costa, J. F., ed. 2005. Linhas de direito penal e de filosofia: alguns cruzamentos reflexivos.Coimbra: Coimbra Editora, p. 136-138.
8 Pattinson, S. D., 2006. Medical Law & Ethics. London: Sweet and Maxwell, p. 476. This author also states that there are different definitions of euthanasia such as the ones mentioned in footnote number 2 of the referenced page “Keown 1995b, 1 (“Euthanasia - the intentional killing of a patient by act or omission, as part of his or her medical care”) with Lord Goff in Airedale NHS Trust v Bland (1993) A.C. 789, 865 (“euthanasia - actively causing his death to avoid or to end his suffering”)”.
Medicine and Law 529
euthanasia and active and passive euthanasia. Simplifying the discussion, voluntary euthanasia implies that the patient requests that his life comes to an end9, while involuntary euthanasia comes about when the patient does not ask the physician or anyone else to “put an end to his misery”, which means that it is done without his informed consent, when he could actually give it; whereas non-voluntary euthanasia comes about as a symbiosis of certain aspects of the previous two, due to the fact that the consent to euthanize is not given because the patient is incapable of giving it10.
As far as active and passive euthanasia are concerned, either of them might be related both to voluntary, involuntary or non-voluntary euthanasia, because it means that the termination of the patient’s life is at the hands of a third party, be it with or without his consent11.
The difference here lies in the fact that passive euthanasia comes about as a way for the doctor to simply omit the advised treatment for the patient, from which the patient will die, and in active euthanasia the doctor actually has to do something, be it administering a pharmaceutical cocktail or turning off the life support machines.
Still in the range of end of life decisions, we have the assisted suicide. The major difference between this situation and the one above stated for euthanasia, is the fact that the doctor helps the patient to commit suicide, therefore the doctor does not “kill” the patient himself, meaning he does not subjectively, by his own hand, through an action or omission, contribute to the termination of the patient’s life. It is basically a suicide, yet with the help of someone else, therefore the dominion of the act and the moment that brings about the death of the ‘victim’ is in the victim’s hands12. Suicide itself has been a controversial issue in the criminal law doctrine, yet, gladly, nowadays there’s an overall tradition of not criminalizing that action, especially considering, namely in the Portuguese legislation, that one can only be held liable for his or her actions13.
9 Keown, J,, 2009.Evaluating Euthanasia., In: R. Nunes, G. Rego, I. Duarte, ed. 2009. Eutanásia e outras questões éticas no fim da vida. Coimbra: Gráfica de Coimbra, pp. 184-186,
10 See Campbell, A., Gillet, G., Jones, G., 2001.Medical Ethics. Oxford: Oxford Press, pp. 208-210.
11 Idem pp. 208-210.12 Andrade, M. C., 1999. Incitamento ou Ajuda ao Suicídio.In J. F. Dias, ed. 1999.
Comentário Conimbricense ao Código Penal, Parte Especial, Tomo I. Coimbra: Coimbra Editora, p. 134.
13 As stated in Article 30. N. 3 of the Portuguese Constitution ‘Criminal liability is not transmissible’.
Medicine and Law 530
Considering what has been stated above, the Portuguese legislation has not been insensitive to the euthanasia matter and until today has faced it as a homicide phenomenon. Thus, in addition to the Constitutional commandment that human life is inviolable14, the Portuguese Penal Code states in its Articles 131 through 137,that homicide is punishable by imprisonment, therefore considering any form of life withholding as homicide. Although it is faced as a criminally sanctionable behaviour, euthanasia and assisted suicide have been debated over the years, especially considering the latest developments from some of our European neighbours, namely Belgium15, the Netherlands16, Luxembourg and France17. It is precisely in that scenario that we will develop the theme in this brief presentation.
HOMICIDE UPON REqUEST OF THE VICTIM - ARTICLE 134 OF THE PORTUGUESE PENAL CODE - AN OUTDATED PROVISION?
Article 134 of The Portugal Penal Code states as follows:
14 Although we do not contest the fact that this constitutional determination is to be treated as if irrefutable, due to the importance of the good called life, there is not always a correspondence between what is stated in the Constitution and what is determined by the Penal Code. The Constitution gives us the general principles of criminal law, for sure, yet there is some dissimilarity between the two and the protection that is ought to be done by both of the juridical areas. See Costa, J. F., 2007. Direito Penal Especial, Contributo de uma sistematização dos problemas “especiais” da Parte Especial. Coimbra: Coimbra Editora, pp. 28-34, and also Dias, J. F., Direito Penal, Parte Geral, Tomo I, Questões Fundamentais da Doutrina Geral do Crime, 2nd Edition, Coimbra: Coimbra Editora, pp. 129-130, who states that “there are no juridical-constitutional criminalization impositions”.
15 See Herring, J., 2011. Medical Law and Ethics, 4th Edition. Oxford: Oxford University Press, p. 531.
16 For more developments see Pattinson (2006, pp. 492-494), Costa (2005, pp.138-140), Louro, M. A., 2004, Diante da Vida- Eutanásia, Aborto, Pena de Morte, Toxixodependência. Paulinas: Prior Velho, pp. 37-40.
17 As far as France is concerned, the French President François Holland considered the possibility of legalizing this assisted death, for the French Medical Ethics Council has pondered the effected that unlawful euthanasia has had on society. According to what was stated in the news, legal euthanasia would be allowed when sick patients were persistent and conscious about their requests to end their lives.
Samuel, H., 2013. France moves one step closer to legalising euthanasia. Telegraph Online. April 14th 2013. http://www.telegraph.co.uk/news/worldnews/europe/france/9870407/France-moves-one-step-closer-to-legalising-euthanasia.html. (Accessed 20 April 2013).
Medicine and Law 531
1. Whoever kills another person determined by a serious, instant and expressed request that has been made by her is punished with imprisonment until three years.
2. Attempt is punishable.
Well, considering what was above stated, the Portuguese criminal law considers that any type of euthanasia is against the law for it is considered murder. Just like Dias (1999, p. 14)18 so eloquently states: “an intentional or necessary active shortening of the life period is what is called direct active euthanasia. It fulfils the objective elements of the homicidal offense, even when the lethal effect is pursued with the intention of putting an end to the pain or suffering of the dying person; and even when consent has been verified in that same sense or even due to several requests from the patient”19.
Therefore, considering the way the Portuguese legal system is founded, without a serious and flexible revision of its legal standards, namely the possibility of trespassing the material limits of constitutional revision, it will always consider any hetero form of life ending as murder20.
The way this offense was set in the Penal Code indicates that it was already the result of a well thought manner to enter some sort of compromise between two constitutional values and indisputable rights, self-determination and life. Both of them must be considered in any life ending circumstances, due to the fact that both are in the personal sphere of the one who wants to enact upon them. Anyone can put into practice acts that compromise his or her life, be it to enhance it or to shorten it, making suicide a legal way to dispose of our life, as long as we do not request someone else’s aid or participation.
In homicide upon request, the pondering of life and self-determination is of a conflicting nature, because life should never be in conflict with other juridical goods, due to the fact that it is constitutionally considered to be inviolable. Yet there seems to be a renunciation of the good called life and an enhancement of
18 Dias, J. F., 1999, Homicídio. In J. F. Dias, ed. 1999. Comentário Conimbricense ao Código Penal, Parte Especial, Tomo I. Coimbra: Coimbra Editora, p. 14.
19 Translation by the present author and not revised by the original author.20 We will not dedicate any attention to the decision made by the doctor as far as futile
treatment is concerned, meaning that the doctor can decide to withdraw or withhold treatment when it will no longer do any good to the ailing patient. We will leave that issue, and its pertinence to criminal law, for another instance. For an interesting view on this issue see Peterkova, H. 2011, Rationing: a marginal argument in the end-of-life debate?Lex Medicinae, Revista Portuguesa de Direito da Saúde, Year 8 (16), pp. 67-78.
Medicine and Law 532
self-determination21, and a choice22 made by the author of the “crime”, letting the victim decide what good she would prefer to keep, almost as if we were facing a precluding wrongfulness circumstance, such as a state of necessity23. It is a farfetched scenario24, but it somehow reflects the legislator’s choice in penalties.
Even though he did not exclude the offensiveness of the conduct, the legislator somehow reduced the level of culpability in these cases25, which is clearly reflected upon the choice of penalties. For instance, homicide26 is punishable with imprisonment from 8 to 16 years and homicide upon request of the victim is punishable with imprisonment up to three years, and that is a significant difference, which is precisely explainable through the reduction of guilt. However, there has to be the intent of satisfying the victim’s wish of death, not a secret selfish intention of the author, because then we would be either in the range of homicide or aggravated homicide.
As far as the conduct is concerned, the victim has to be serious about her request, and it cannot be a simple consent to the ending of her life, but a true request, supported by a personal and factual will to die. This request must be done to a specific person, which means that if the person with whom the victim talked to, or directed her request to, cannot kill her and if another person, who heard the conversation, for instance, decided to end the victim’s life, this person’s conduct would not have been the result of a true request from the victim27, and hence the crime in question would not be homicide upon request,
21 For an inside look on the principle of autonomy and self-determination, see Dantas, E., 2009.Direito Médico.Rio de Janeiro: GZ Editora, pp. 79-82, and also Herring, J., 2011.Medical Law and Ethics, pp. 512-516.
22 Still concerning patient autonomy and the nebulous conflict between certain interests and goods, such as life and self-determination, see Huxtable, R., 2013.Law, Ethics and Compromise at the Limits of Life - To treat or not to treat? London and New York: Routledge, pp. 90-95 and for different types of autonomy see pp. 116-119.
23 Andrade, M. C., 1999, ‘Homicídio a pedido da vítima’, p. 56.24 That is defended by some authors, namely Merkel, who states that “the active and wanted
production of death upon request is justified by the necessity right, in cases where the communicated interest of someone who clearly puts the interest of ending her life upon the interest in life itself”, cited by Andrade, M. C., 1999.Idem, p. 72.
25 We do not refute the fact human life should be inviolable, but undoubtedly the legislator considered that it should not be considered as an irrefutable dogma. In this sense see Costa, J. F., 2007, pp. 140-141.
26 Article 131of the Portuguese Penal Code.27 Nonetheless we could find ourselves before an error issue, which may be relevant in
terms of guilt or mens rea - intent.
Medicine and Law 533
but eventually, homicide28 or privileged homicide.
The request done by the victim has to be serious, therefore not influenced by a third party, through coercion or instigation. It also has to result from some insistence of the victim29, and the request also has to be explicit, meaning not ambiguous, in order to exclude any doubts of the victim’s intention to end her life.
The legal regime is very clear with the Article that is now under our scope and the constitutional irrefutable provision of life, yet we believe that some adjustments may be able to be done. We consider, if we are allowed at this stage, that self-determination must be seen as a fundamental right equivalent to life, in the extent that both of them are subjective rights, and that an individual must be free to do as he pleases with his life as long as that does not interfere with the freedom of others and it is put into practice in restricted circumstances30. Thus we are of the opinion that a regime like the one present either in the Netherlands31 or Belgium would have positive effects on the
28 Just as Pattinson, S. D., 2006, wrote “intentionally taking another person’s life is murder”, p. 486. This author also claims that there are differences between an intentional murder and the foresight of death by administering a certain substance into the ailing patient, called a double effect, among other perspectives. He hence states that this distinction without certain fixed boundaries could be claimed as being somewhat of an arbitrary nature “if the distinction between intention and foresight is a morally relevant distinction, then it should not matter whether the context is one of medical treatment. If the distinction is not morally relevant, then to rely on it at all is problematic. Proper medical treatment could be held no to constitute that actus reus of murder (an unlawful or omission causing death) without invoking the doctrine of double effect with regard to the mens rea of murder.” p. 288. The author refers as well a necessity doctrine, in the same sense that we have stated above. He sums it up by stating in the same page that “the lethal administration of treatment that has no palliative effects is illegal”, yet there is still some uncertainty concerning the boundaries of this question, whether it can be seen as legal or illegal in similar circumstances. See also Herring, J., 2011, p. 510.
29 At least insisting enough to make the perpetrator want to obtain the victim’s death, meaning enough to inflict upon that person the mens rea needed to commit this type of crime. As Moos said, the victim “has to convince the agent of the definite subjective need of the death request”, cited by Andrade, M. C., 1999. Homicídio a pedido da vítima, p.65.
30 Just like it was foreseen in the Project for a Law on Euthanasia in Germany, in which, besides the referred premises of an insisting, serious and explicit request, and eventual exemption of criminal liability would be possible if it were a case of “putting an end to a state of suffering, the most painful and unbearable to the patient, and that could not be avoided or mitigated by any other means”, in Andrade, M. C., 1999, ‘Homicídio a pedido da vítima’, p.59.
31 For a different approach, with empirical data that reflect the phenomenon a few years after it was put into practice, see Osswald, W., 2004.Um fio de ética.Coimbra: Gráfica de Coimbra, pp. 151-154, and also Keown, J., Evaluating Euthanasia. In: R. Nunes, G. Rego, I. Duarte, ed. 2009. Eutanásia e outras questões éticas no fim da vida. Coimbra: Gráfica de Coimbra, pp. 199-204.
Medicine and Law 534
Portuguese society. Let’s consider, for instance the Dutch regime on this issue, namely the doctor’s reporting procedure and requirements that must be shown to the committee that:
1. The patient has made a “voluntary and well considered” request;
2. The patient’s suffering is “lasting and unbearable”;3. He has consulted with another, independent doctor; and4. Has terminated the patient’s life or assisted in his suicide with
due medical care32.”
We are not proclaiming that euthanasia should be put into practice in any given circumstances, because we own our lives and we should be able to determine whether we want to live or die, by our hands or by the hands of another individual. Au contraire, we think that life is precious and it shouldn’t be portrayed as a good or a right that is disposable of whenever we feel like it, but only when there is absolutely no way out of the pain and condition that we are suffering from. And if certain limits or boundaries are not set from the very beginning, then we might slip into areas of abuse, such as decisions without a true intent behind it, and/or determined by a transitory and not permanent state of mind and infirmity, which, just like Dr. Timothy Quill once said “it puts the doctor in a very powerful position33”.
Thus we can conclude that homicide upon request of the victim, the way that it is set in the Portuguese Penal Code does not leave any margin for the alleged victim to ask someone to end his or her life as a form of expression of self-determination34, due to the fact that it might lead to imprisonment of the person
32 Pattinson, S. D., 2006, p. 494.33 Kamisar, Y., 1998.Are Laws Against Assisted Suicide Unconstitutional? In M. Uhlmann,
ed. 1998. Last Rights? Assisted Suicide and Euthanasia Debated. Washington D. C.: William B. Eerdmans Publishing Company, p. 453.
34 For a very elucidative view on self-determination and the individual as the center of the juridical system as far as rights as concerned, see Costa, J. F., 2005, pp. 127-129. This author states, for instance, that “the vertical line of apprehension of self-determination - and it is not randomly that we say vertical line - settles on the idea that it is the individual that, in auto-reflection, must find the way he settles in society and the way he lives with himself and, most of all, that he is the only center of decision of his behaviour with other individuals” (our translation). Further on the author says that “The individual that decides, that decides with full autonomy, cannot be understood as an individual that decides in a solipsistic manner. The obscuration, the effective and real disappearance of the individual happens, paradoxically, when he, due to autistic corruption phenomena, believes that world is centered and revolves around that ideal and discarnate “self” that
Medicine and Law 535
that carries out the insistent, explicit and serious request. Hence, considering the example of some of our neighbouring countries, the Portuguese legislator should seriously consider an alteration of that Article in order to come to some sort of consensus, as far as the leverage between the good of life and self-determination is concerned.
ASSISTED SUICIDE - AN OVERALL PERSPECTIVE
Before we start the analysis of assisted suicide, we consider pertinent the understanding of what is considered to be suicide and how it is relevant to criminal law.
As we understand nowadays, suicide or attempted suicide are not considered to be crimes in the Portuguese jurisdiction, and that is truly understandable because if suicide35 is the act of a “person intentionally killing themselves”36, then who would be object to a criminal procedure? A third party? Well, that makes absolutely no sense, especially considering what we have already said about criminal liability not being transmissible.
Yet, is there a right to commit suicide? We may say that we are free to do it, yet, is there an actual right to do it? It is permitted, but we cannot say with full property that it is a right, even though life itself is a fundamental and subjective constitutional right. In similar terms, then we have a right to death, and that is not exact. We can demand from other people that they refrain from doing anything that could compromise our life, because we have a right to, but we cannot demand that every other person refrains from stopping us from killing ourselves37. Due to our way of thought, we find interesting the words
he believes to be fully representing. Nothing could be more false. So, this is one of the bigger dangers - if not the biggest - of an erroneous comprehension of what self-determination is” (again our translation).
35 Durkheim gave us a more extensive definition of suicide “The term suicide is applied to any death which is a direct or indirect result of a positive or negative act accomplished by the victim himself, which he knows should produce this result (death)”, cited by Herring, J., 2011,p. 542
36 Ob cit. idem p. 486.37 We follow the in part the opinion of Campbell, A. et al., 2001, when the authors state that
“There is clearly a point beyond which we regard it as immoral and unjust to interfere with the lives of autonomous beings because of our own moral convictions; and it is debatable where this point is reached in dealing with the diverse reality of suicide. Suicide has already been considered in the context of psychiatric ethics, but in general we seem to have good reasons to intervene in suicide even when this may seem to be against

Medicine and Law 536
of Baroness Hale in a case that took place in the UK, R (Purdy) v DPP, “It is not for society to tell people what to value about their own lives. But it may be justifiable for society to insist that we value their lives even if they do not”38. Cory J, a Canadian Judge, concerning the matter of life and death as rights to which every single one of us in entitled to, stated in the case Rodriguez v A-G of British Columbia: “Dying is an integral part of living…It follows that the right to die with dignity should be as well protected as is any other aspect of the right to life. State prohibitions that would force a dreadful death on a rational but incapacitated terminally ill patient are an affront to human dignity”39. We can agree with this position, once it meets the one we have above stated about the rethinking of euthanasia and the way it should/could be portrayed in the Portuguese society.
Yet there are still a couple of conceptual problems that need to be attended to, namely the difference between the refusal of treatment by the patient and assisted suicide. Where and how can we set the boundaries? In practical terms it reveals to be much easier, than theoretically, due to the fact that both situations come out as a form of self-determination and self-inflicted offense, but one might go as far as the refusal of treatment40as an impediment for the doctor to do what he considers to be more adequate to the situation, and the assisted suicide is actually giving him a green light to do something to end our life. It may seem odd to make a distinction at all, but as Andrade says “The doctor who, respecting the will of the patient, does not intervene and does not save him, does not commit the crime. It will be considered differently if the patient decides to end his life by his own hands: whoever helps him commits the crime of incited or assisted suicide.”41
the wishes of the victim.”, p. 208, yet we consider that there have to be boundaries to the stalling of someone’s wish to end his or her life, namely in the same sense that we mentioned above concerning homicide upon request of the victim.
38 Herring, J., 2011, p. 491.39 Example taken from Mason, J.K., Smith, R. A., Laurie, G.T., 2012.Law and Medical
Ethics, London: Butterworths, p. 423.40 For further reading see Herring, J., 2011, p. 491, where the author gives the example of
the Jehovah’s Witnesses, who cannot receive blood transfusions, therefore if they require them the doctor cannot administer it, because then he could be charged with the criminal offense of battery, pp. 552-553.
41 Andrade, M. C., 1999. Incitamento e Ajuda ao Suicídio, In: J. F. Dias, ed. 1999. Comentário Conimbricense ao Código Penal, Parte Especial, Tomo I. Coimbra: Coimbra Editora, p.81.
Medicine and Law 537
Article 135 of The Portuguese Penal Code says:1. Whoever urges someone else to commit suicide, or assists them
for that end, is punishable with imprisonment up to three years, whether the suicide is actually tempted or consummated.
2. If the urged person or the one who helps her is under the age of 16 or has, by any reason, a significantly decreased evaluation or determination capacity, the agent is punished with imprisonment from one to five years.
Just a fore note, we will not discuss number two of the above transcribed Article and we will restrict our investigation to the assistance in the medical area and not to the incitement. Therefore the mentioned assisted suicide shall be considered as physician assisted suicide, leaving out the assistance by someone other than a professional of the health industry.
Due to the irrelevancy of suicide in the criminal system, some authors question the fact that assisted suicide42is considered a crime. As we have already mentioned, suicide is a form of taking our own life, deliberately, and without the help of anyone else. Assisted suicide, on the other hand, already implicates an interaction with someone else, a certain someone that will aid in the materialization of the death. Nonetheless, the victim is the one who dominates the fact; therefore there is only a mediate authorship in this type of crime and not an immediate one43.
As far as the boundaries between suicide and homicide are concerned, Andrade tells us44, according to Roxin, that there are two lines that separate these actions, an external border and an internal border. The first one differentiates assisted suicide from homicide upon request “from the definition and value of the contributions of the victim and the third party, seen from their exterior profile. On the other hand, the internal border looks to determine itself in which way, regardless of the exterior lineout, things apart themselves from the psychic and spiritual situation of the victim”45. Basically, as already above said, it is a matter of dominion of the fact and what is completely decisive for
42 See also Herring, J., 2011, p. 487.43 See also Kamisar, Y., 1998. Are Laws Against Assisted Suicide Unconstitutional? In M.
Uhlmann, ed. 1998. Last Rights? Assisted Suicide and Euthanasia Debated. Washington D. C.: William B. Eerdmans Publishing Company, p. 452.
44 Andrade, M. C., 1999, Incitamento e Ajuda ao Suicídio, p.81.45 Idem., pp. 81-82.
Medicine and Law 538
the distinction and the pertinence of the incrimination of assisted suicide is the ability of the alleged victim to be able to represent that her behaviour is in fact self-destructive and irreparable, due to the fact that there is no way to amend death46.
The assistance itself has to abide to a couple of characteristics, namely the fact that it is not an incitement, but rather a consequence of the victim’s previous determination to kill herself. It can be any type of aid, be it moral or material, physical or psychological, and it must be in the exact measure that the victim conveyed with the “assistant”, because if there is excessiveness it might implicate that we will be before a homicide, in plain terms, and not an assisted suicide.
We can conclude that this type of help is in fact harmful to the victim and legislators must not look at it lightly, in order to prevent any type of excessive abuses. We mention this because we consider that the patient’s autonomy should be taken into account, and that self-determination, materialized in the act of suicide, might be considered to be the only way out of an irreparable situation (or terminal illness47, for instance), for a couple of people. It should be considered as a last resort, yet some ruling is definitely needed in order for it to become less difficult upon the patients (and consequently, the “possible assistants”) to take a stand on what they really want for their “final hour”.
To conclude, we can say that assisted suicide has a mixture of mediate and immediate authorship, but the Portuguese legislator should take into consideration the fact that the alleged victim wants to die, but does not have to means to put it into practice. There should be some restrictions if the legislator in fact enables this type of behaviour, through decriminalization, namely that it could only be done by a doctor and if in fact there is absolutely no way for the victim to go back on her decision, which should be scrutinized by professionals. We cannot face this reality lightly because it implicates the overrunning of numerous values which are sunk into our society, on the other hand, our society is constantly changing, and one must be able to evolve with
46 We have to understand that Life is considered to be inviolable, especially by someone else rather than ourselves, therefore Kamisar concludes that “moreover, in principle, it would seem that the interest in the sanctity of life that are represented by the criminal homicide laws are threatened by one who expresses a willingness to participate in taking the life of another, even though the act may be accomplished with the consent, or at the request, of the suicide victim”, Kamisar, Y., 1998, p. 448.
47 About the question whether ‘legal’ assisted suicide should only be limited to the terminally ill, see Kamisar, 1998, idem. pp. 454-457.

Medicine and Law 539
it, and must be able to take under his wing the utmost consequences of his choice, as long as it does not undermine our neighbours autonomy as well.
5. SOME FINAL THOUGHTS
The issue that we have taken up in this brief exposure of ideas is not of a peaceful nature. The idea of death and all other connected scenarios are not attended to with carelessness, and sometimes are even considered to be taboo, unspoken of, and without a full disclosure. With the critical advances in medicine, and the constant racing in any type of science, everything is speeding up, meaning the way we live our life, the way we want to fulfil our dreams and aspirations, but also our vulnerabilities, and the way we actually feel and think about death.
Most of us do not think about, or dwell upon our time of death, or dream about our “final hour”, but it so happens that people with little left to live for, who are terminally ill, do consider that possibility. As many authors have already said, death is one of our only certainties in this thing called life, but we can choose when we die. This ability to choose is something that is exclusively ours as human beings, due to the fact that we can represent what our actions mean and what consequences might come from them.
Hence we conclude this brief investigation with minor reflections concerning euthanasia, homicide upon request, and assisted suicide. We agree that life is a major good and that it is considered to be our utmost fundamental right, yet it is our right to live the way we want to live, as long as it does not interfere with the life of our neighbour. Well, what if we do not want to live anymore, should we not be able to end this life, since it is our own and nobody else has a prerogative to it? We believe that self-determination and autonomy should have a saying in all of this. Life is ours to decide upon however we like it, then why can we not ask someone to put an end to it, or help us terminate it? We do not agree with a full arbitrariness of this possibility, but the legislator should work in the sense of a permission with well-set boundaries, just like in Belgium and the Netherlands.
Making a long story short, we believe that the Portuguese community is on the right track to overcome some issues that were, until not so long ago, unable to be discussed, take the next step, and really ponder the value the of the goods that are at stake, at the present time, in a sense of flexibility, directed by a principle of autonomy, without trespassing the admissible boundaries of self-determination.

©PROBOOK 2013and Law
Medicine Med Law (2013) 32:541-548
541
COMPETENCE X COGNITION: WHO CAN MAKE A LIVING WILL?Luciana Dadalto*
Abstract: This article discusses who can write a valid Advanced Directive by analyzing the classical theory of disabilities and the introduction of the criterion of judgment in civil law. In the search for the answer of the proposed problem, this article examines how countries that have legislated on the AD deals with it and, such as Brazil, which still has no legislation on policies can advance the issue, equalizing the age criterion with the personality rights of considered incapable.
Keywords: Advance Directives; Capacity, Discernment
1. INTRODUCTION
A review of the classic Theory of incapability has been widely discussed in Brazil. The reason for this is that Brazil like most countries of Civil Law adopts an objective age criteria to attribute legal competence, depriving the incapable person of ample personal rights. Thus, the criterion of discretion begins to be defended, in detriment of capacity, for the exercise of personal rights.
Making a living will is a way to exercise the exclusive personal right of bodily autonomy; the present article will discuss which criteria should be used regarding the legitimacy of the individual to manifest his wishes through a living will.
2. UNDERSTANDING THE CLASSIC THEORY OF COMPETENCE
Competence, has been historically understood as agenre in which are two species the legal competence and the “de facto” competence. While the first refers to the acquiring of rights and obligations, the second is the exercise
* Attorney. Master in Private Law by PUCMinas. Doctorate in Health Sciences - Medical School UFMG. Administrator of the site: www.testamentovital.com.br.
Medicine and Law 542
of these rights and obligations, meaning that legal competence is inherent to human beings, while “de facto” competence is related to cognition.
Rodrigues states that the disability scheme has as an assumption the protection of people or principles that do not possess enough cognition - considering cognition as comprehension and understanding- to form and express their wishes. In this system we use an objective age criteria, that is to say, an age limit is established, starting at which the individual acquires the “de facto” competence.
Countries like Brazil, France, Spain and Portugal use this criteria in their civil legislation, meaning that the individual who has not yet reached the age foreseen by law, which is in general 18, possesses only legal competence, having to be assisted or represented by a legal representative or a third party in civil acts such as marriage, judicial estate affairs and even medical decisions. These individuals acquire “de facto“ competency when they reach the determined age. That means, in Brazil for example, an individual who on the fortnight of his 18th birthday needs to undergo surgery must, as a rule, obtain the consent of his parents, to undergo such a procedure. If the same procedure had to take place the next day, he would not need parental consent.
3. CRITIC TO THE CLASSIC THEORY OF INCAPACITY
The classic theory of incapacity creates a subjective problem for the Law: the existence of individuals considered incompetent by civil law but are completely capable of giving consent. This situation is too reckless and should be avoided in a contemporary democratic state of law, where the coexistence of individual life projects is attempted. Moreover, going deeper into the issue of consent with regards to issues concerning health, this situation can spawn the outrageous case of a minor who is seventeen and wishes to undergo a medical procedure and whose parents, for a moral or legal reason, refuse to give their consent.
The contrary is also possible, that is, it is possible for a patient to be considered legally competent, but the doctor realizes that he is using medication that affects his mental faculties or that an illness is affecting his capability to make autonomous choices.
Therefore, Beauchamp and Childress state that a patient or individual is capable of making a decision if he is capable of understanding the material

Medicine and Law 543
information, makes judgment of that information in light of his own values, has in mind a certain result and freely communicates his wishes to those who treat him or who want to know what his wishes are.1
It should be noted that Portuguese doctrinist André Pereira2 understands that cognition, which he calls the competence to consent, is a new kind of competence, that will figure beside the “de facto” competence and the legal competence. This, according to the author, would be established by the doctor and would be subject to judicial control, through the filing of a lawsuit questioning the capacity of the patient.
Having said that, there is a strong movement in these countries which, through the relativization of these objective criterion that define competence, strives to make it possible for the incompetent to make decisions which affect his personal rights understood as the rights inherent to the human being and that cannot be disposed of by themselves or by others3.
4. WHO CAN FORMULATE A LIVING WILL?
Taking into account the rereading of the classic theory of incapacity it is necessary to establish who are the individuals who have legitimacy to formulate a Living Will. Noticeably the guiding criteria of this legitimacy should be cognition and not legal competence, the statement of incapacity cannot, as a matter of fact, jeopardize, completely private autonomy given by law to the human being, even when they are taken by physical or mental inabilities or illnesses which affect their cognition. [...]Flexibilizing the institutes of incompetence and custodianship is a new hermeneutical mechanism capable of ensuring the wishes of the incapable individual, always when it is possible to make his psychological wishes compatible with legal determination, cloaking it thus with jurisdiction4.
1 BEAUCHAMP, Tom L; CHILDRESS, James F. Princípios de ética biomédica. Trad. Luciana Pudenzi. São Paulo: Loyola, 2002, p.154.
2 PEREIRA, André Gonçalo Dias. O consentimento informado na relação médico-paciente. Coimbra: Coimbra Editora, 2004.
3 For the best understanding of the subject: TEIXEIRA, Ana Carolina Brochado. Saúde, corpo e autonomia privada. Rio de Janeiro: Renovar, 2010, is recommended.
4 RODRIGUES, Renata de Lima. Incapacidade, curatela e autonomia rivada:estudos no marco do Estado Democrático de Direito. 2005. 200f. Dissertação (Mestrado) Pontifícia Universidade Católica de Minas Gerais, Faculdade Mineira de Direito, Belo Horizonte, p.169-170.
Medicine and Law 544
We must keep in mind that objective age criterion predetermined by norm, make it impossible, in many cases, to exercise the rights of personality of the incapable individual in this way hindering him from living out in a complete sense of dignity.
Despite this, cognition is not easily measured, once it cannot be done in abstrato. Thus, it is necessary to verify, in a concrete case, if the individual who is legally incompetent possesses specific cognition which allows him to consent or refuse the undergoing of a medical procedure through a living will.
Here we have a complex situation, for this verification must happen in the environment of the Legal Power, that is to say, a legal procedure must take place to verify, in concreto, the existence or absence of this cognition. This procedure must be analogous to the procedure for the interdiction of individuals, that is to say, a serious psychological study of the individual must be done with the ends of verifying if he possesses the cognition to consent.
From a practical point of view, this procedures, noticeably of voluntary jurisdiction, can be proposed by the person, by his doctor or by his legal representatives and can only be denied by a magistrate if it is proven, in the records, that the person does not possess cognition to refuse or consent to treatment in a living will. Especially, the disagreement of the doctors or legal representatives will not be taken into account in the judicial decision, which should be taken, strictly, based on the psychological report of the person.
4.1 Who may write up a living will in countries which have already legislated on the issue?
As it is known there is still no legislation about living wills in Brazil. What exists up to that moment, is Resolution 1995 of the Federal Medical Council, which acknowledges the patient’s right to refuse futile treatments, also known as extraordinary, understood as “treatments that do not offer real benefits to the patient be cause death is inevitable”5, by means of a living will.
Resulting from a class action, this resolution, is effective only among the medical class, for which reason for we cannot state that living wills are legal in the country.
5 Beauchamp, TL; Childress, JF. Princípios de ética biomédica. Trad. Luciana Pudenzi. São Paulo: Loyola, 2002, p-197
Medicine and Law 545
It is exactly because the CFM does not have legitimacy to legislate that the resolution mentions that only the civilly capable can write their directives. Even if the CFM understood that the cognition criteria should prevail it could not mention this in the resolution because it would be seizing competency that belongs to the Brazilian Legislative Power.
That means that only a Law will have power to institute that any person with cognition can make a living will. This is understood to be of absolute importance to protect the individuals’ right to self - determination in an egalitarian manner.
In countries that have already legislated on this subject we notice, in general, the permanence of the classic theory of incompetence, that is, the use of the objective age criteria to determine who can refuse or accept treatment by means of a living will.
In Spain, despite the Federal Law, 41/2002, that textually states about the need of the principal being of age, the autonomous communities of Aragon, Cataluña, Navarra and La Rioja adopt the criteria of cognition, allowing the minor, who is capable of consent to write a living will. When making a statement on the living wills in these provinces, Cristina Sanchez states that a minor with enough intellectual and cognitive capacity can write a document with those characteristics, being that no one better than he knows what his wishes are, and especially because, once they are written they do not become irrevocable, being subject to modification and periodic review6.
In Portugal there Law 25/2012, establishes in its fourth 4o article, three accumulative criteria about the capacity of the principals: to be legally of age, to be not declared incapable, to possess full capacity to consent.
Verifiably Portuguese legislation holds within it a real mix up between the competence to consent and the “de facto” competence, accumulating both. Despite this, it is forgotten that it is possible to have the competence to consent without the existence of “de facto” competence, better would be if the criteria
6 Defendemos que el menor de edad con suficiente capacidad intelectiva y volitiva podría redactar un documento de estas características, puesto que nadie mejor que él sabrá cuáles son sus deseos que, además, una vez plasmados por escrito no se convierten en irrevocables, sino que no sólo podrán ser modificados sino que, además, resulta sumamente conveniente su revisión periódica. SÁNCHEZ, Cristina López. Testamento vital y voluntad del paciente: conforme a la Ley 41/2002, de 14 de noviembre. Madrid: Dykinson, 2003.
Medicine and Law 546
foreseen in this article were excluding and not accumulative.
The United States of America, a country which despite having its normative system based on Common Law, is a reference in the study of living wills for being the first country in the world to have legislation on this issue, also adopts the objective age criterion with regards to the principal of this documents.
5. CONCLUSION
It is noticeable, by what has been exposed, that the issue of the principal´s cognition for living wills is not a unanimous issue, much on the contrary. The replacement of the “de facto” competence criterion for the competence to consent criteria or, in other words, from the objective age criterion to the subjective discretionary criterion is a measure that will bring a number of reflexes to legal ordinances based on the classic theory of incompetence.
But, despite the complexity of the issue herein proposed, it is necessary to have in mind that it is an imperious issue, aimed at adjusting the archaic incompetence theory to the changes brought about by contemporary society and by the recognition of the individual´s right to self determination. To deny this fact is to deny the effectiveness of this right, an important achievement of the second half of the XXth century.
So, what is here proposed is that when legislating on living wills, it should be established that all individuals with cognition can draw up a living will for medical treatment. However, those who are legally incompetent will need an express legal authorization for this purpose, to be obtained through a procedure of voluntary jurisdiction, where the only evidence will be a psychological report which states the principal’s capacity to consent.
With regard to the countries that have already legislated on this issue, a legislative reform is proposed in the above stated model of the autonomous Spanish communities. This model stipulates that people who are legally incompetent but have proven cognition may make a Living Will.
In fact, here we defend the assumption that cognition is not linked to age and that the freedom of the individual´s self-determination cannot be verified in a prior manner. It is necessary that the legal systems that adopt Civil Law take unto themselves, in this aspect of the teachings brought by Common Law regarding the importance of verifying, in concreto, the specificities of each
Medicine and Law 547
case, treating the law only as an instrument that should guide the decision do judge.
In summary, the right to self determination regarding medical care for the end of life should be preserved for all individuals who present capacity to self-determine in this sphere. This is what is expected from a Lawful Democratic state, which guarantees the coexistence of different life projects of autonomous individuals.
REFERENCES
BEAUCHAMP, Tom L; CHILDRESS, James F. Princípios de ética biomédica. Trad. Luciana Pudenzi. São Paulo: Loyola, 2002.
CONSELHO FEDERAL DE MEDICINA. Resolução 1995/2012. Disponível: http://www.portalmedico.org.br/resolucoes/CFM/2012/1995_2012.pdf. Acesso 13 mar. 2013.
DADALTO, Luciana. Testamento Vital. Rio de Janeiro: Lumen Juris, 2010.
JUSTIÇA FEDERAL DO ESTADO DE GOIÁS. DecisãoliminarAção Civil Pública n. 0001039-86.2013.4.01.3500.Disponívelem: http://processual.trf1.jus.br/consultaProcessual/processo.php?trf1_captcha_id=776c1b3b3122047f40e7eb4a116dc9b4&trf1_captcha=hbm6&enviar=Pesquisar&secao=GO&proc=10398620134013500>. Acesso em 17 mar. 2013.
MINISTÉRIO PÚBLICO FEDERAL. Ação Civil Pública n. 0001039-86.2013.4.01.3500. Disponível em: http://www.prgo.mpf.gov.br/images/stories/ascom/ACP-CFM-ortotanasia.pdf . Acesso em 13 mar. 2013.
PEREIRA, André Gonçalo Dias. O consentimento informado na relação médico- paciente. Coimbra: Coimbra Editora, 2004.
RODRIGUES, Renata de Lima. Incapacidade, curatela e autonomia privada:estudos no marco do Estado Democrático de Direito. 2005. 200f. Dissertação (Mestrado) Pontifícia Universidade Católica de Minas Gerais, Faculdade Mineira de Direito, Belo Horizonte.
SÁNCHEZ, Cristina López. Testamento vital y voluntad del paciente: conforme a la Ley 41/2002, de 14 de noviembre. Madrid: Dykinson, 2003.

Medicine and Law 548
TEIXEIRA, Ana Carolina Brochado.Saúde, corpo e autonomia privada. Rio de Janeiro: Renovar, 2010.

©PROBOOK 2013and Law
Medicine Med Law (2013) 32:549-565
549
PHYSICIANS’ ATTITUDES AT THE END-OF-LIFE: A CROSS-CULTURAL EVALUATIONNuket Ornek Buken* and Aysun Balseven-Odabasi**
Abstract: Physician’s attitudes towards patients with incurable cancer or at the end-of-life process - treatment of patients, withholding ventilation support, physician-assisted suicide - have changed rapidly in recent years.
In cases such as incurable cancer, illnesses in the terminal phase, some neurologic diseases and AIDS, physicians and other health care workers experience dilemmas, arguments and problems on the subjects of whether or not to tell the truth or how to do it,who should inform the patient or his/her guardian, and then, how to give treatment to patients with incurable cancer or withhold ventilation support. All of these issues are affected by the country’s' sociocultural and economic structures, the physician’s attitudes at the end of life,the medical practice and the form of health structures.
In this study our objectives are to assess physicians’ views in Turkey regarding the process of the end of life and decision-making, to compare them with views from the USA, Japan and Saudi Arabia and to cristalize a cross-cultural assessment.
Our study contains three clinical situations covering the following areas: (1) a patient’s right to be informed of incurable cancer, (2) doctor-assisted suicide (3) the conflicting rights of patients, doctors and the family in issues such as refusing ventilatory support or witholding treatment. The four-point Likert Scale was used to mark the responses to the statements.
The significant cultural, social and economic differences that exist in health care services between regions in our country affect physician-patient communication and end of life decision-making, as reflected in the process of obtaining informed consent.
* (MD, PhD), Professor of Medical Ethics at the University of Hacettepe School of Medicine, Dept. of Medical Ethics, Sihhiye, Ankara, 06100, Turkey.
[email protected] [email protected]** (MD, PhD), Associate Professor of Forensic Medicine at the University of Hacettepe
School of Medicine, Ankara, Turkey.

Medicine and Law 550
Keywords: Terminal Patients; End of life; Withholding Treatment; Comparative Law; Right to Information.
INTRODUCTION
Any medical intervention directed only towards curing and avoiding harm to patients while disregarding the patient’s autonomy causes a paternalistic relationship in which physicians are the only decision makers. At present, in many countries, including Turkey, an emphatic communication that requires both physicians and patients to participate in decision-making processes is not realized and traditional paternalistic attitudes are transmitted from generation to generation through a master-apprenticeship relationship. As in other countries, where the social structure is determined by paternalistic attitudes, the Turkish physicians have the authority in patient-physician relationships.
There is a heated debate over end of life decisions in medical practice. Physicians’ attitudes towards patients with cancer, terminal illnesses, and fatal diseases in intensive care units and several geriatric diseases and ethical dilemmas experienced during end-of-life care are debated and are the different subjects of research in many countries. Coping with these dilemmas, the clinical and ethical decisions made by all parties concerned, including physicians, patients, patients’ families, hospital administrations and ethical committees of hospitals, are affected by moral, religious, social, cultural and legal characteristics of societies, health policies of countries and physicians’ traditional attitudes. It is also of importance that all parties play a role in end-of-life decisions.1
There have been many quantitative and qualitative studies about who the primary end-of-life decision maker is and how clinical and ethical decisions are made and these studies have attempted to reveal cross-cultural differences.
Clinician-patient communication in end of life issues does not operate outside ofthe context of culture. Culture can be defined as the socially transmitted body of values, beliefs, behaviors, social and political institutions, arts, crafts and science that are shared by a given group of people. This concept of culture can also be applied to groups who share characteristics other than geography or ethnicity.
Medicine and Law 551
AIM
Physicians who are aware of cross-cultural differences in end-of-life decisions can better understand that patients with end-of-life illnesses create appropriate problem solving methods and start decision making mechanisms. The aim of this study is to reveal mechanisms of end-of-life decisions in Turkey and differences in these mechanisms between our country and other countries, to discuss the reasons for these differences and to reach pragmatic conclusions. To this aim, using three different scenarios, we investigated Turkish physicians’ attitudes towards end-of-life decisions and made a cross cultural comparison between Turkey, the United States, Japan and Saudi Arabia.
METHODS
Data were collected with a questionnaire used by Ruhnke et al. in a comparative study including American and Japanese physicians.2 The questionnaire was also used in a study by Mobeireeket al.3 This allowed us to compare between the countries. The questionnaire was translated into Turkish and back into English. It was first piloted on a group of physiciansin order to determine whether it was understandable.
The questionnaire contains three clinical situations covering the following areas: (1) the patient’s right to be informed of incurable cancer, (2) doctor-assisted suicide (3) the conflicting rights of patients, doctors, and the family in refusing ventilatory support and witholding treatment. It was a four-point Likert Scale (strongly agree, agree, disagree, and strongly disagree).
The questionnaire was sent, between November 2007 and January 2008, to 30.000 physicians via e-mail through the website of the Turkish Medical Association. The web-based data collection allowed contact between physicians in various disciplines in various parts of the country and members of Turkish Medical Association. Out of 30.000 questionnaires, 4,084 were completed and sent back.
Approval was obtained from the Ethical Committee of Hacettepe University and the study was funded by the Scientific Research Unit of Hacettepe University.
SPSS11.5 was used to analyse the data. The Chi-square test and an extension of Fisher’s exact test to mxn table were used for statistical analyses. p<0.05 was considered significant.

Medicine and Law 552
RESULTS
The averageage of the participants was 40,3±8,7 years. Out of 4,084 participants, 68,1% were male and 31,9% female.
31.6% of the participants were general practitioners, 6,2% were pediatricians, 5,6% general surgeons, 5,5% internists, 4,9% anesthetists, 4,4% gynecologists, 3,7% psychiatrists, 3,4% radiologists, 2,3% urologists, 2,4% orthopedists and 2,3% otolaryngologists. The rest of the participants were from other medical disciplines.
Eighty percent of the American physicians agreed that first patients should be informed about the diagnosis of cancer and that the decision whether patients’ families should be informed about, should be left to the patients’ discretion. 67% of the Saudi Arabian physicians, 61% of the Turkish physicians and 17% of the Japanese physicians were in agreement with the American physicians. The above mentioned distribution shows that the highest rate of physicians who agreed to inform patients rather than their relatives about their diseases were American, followed by Turkish, Saudi Arabian and Japanese with a significant difference (P<0,05). The difference in scenario 1.1 was significant between the American and Turkish physicians, between Turkish and Japanese physicians and between Saudi Arabian and Turkish physicians (P<0,05) (Table I).
80% of the Japanese physicians, 48% of the Turkish and Saudi Arabian physicians and only 6% of the American physicians agreed that physicians should inform patients’ relatives about patients’ diagnoses and leave the decision to inform the patients to their relatives.As in scenario 1, both Turkish and Saudi Arabian physicians were in favour of the idea that the decision maker was the family, but the rate of the American physicians favouring this approach was very low. The difference between physicians from different nations was significant (P<0,05). The difference between the American and Turkish physicians and between the Japanese and Turkish physicians was significant (P<0,05), though there was no significant difference between the Saudi Arabian and Turkish physicians (P>0,05) (Table 1).
79% of the American physicians, 59% of the Turkish physicians and 56% of the Saudi Arabian physicians held the opinion that physicians have to inform patients about their diagnosis of cancer although their families did not agree.
Medicine and Law 553
Only 8% of the Japanese physicians had the same opinion, which suggested that the Japanese physicians were sticking to their traditional attitudes.The difference in scenario 1.3 between physicians from different nations was significant (P<0,05). In fact, there was a significant difference in scenario 1.3 between the American and Turkish physicians and between the Japanese and Turkish physicians (P<0,05), though the difference between the Saudi Arabian and Turkish physicians was not significant (P>0,05) (Table 1).
As for physician assisted suicides (scenario 2), 12% of the Turkish physicians, 7% of the Saudi Arabian physicians, 8% of the Japanese physicians and 5% of the American physicians approved physician provision of large doses of drug for patients they encountered once (In Clinical scenario 2,Table 2). There was a significant difference in scenario 2.1.1 and 2.1.2 between the American and Turkish physicians, between the Japanese and Turkish physicians and between the Saudi Arabian and Turkish physicians (P<0,05). However, there was no significant difference between the physicians in scenario 2.1.3 (p=0.090) (In Clinical scenario 2, Table 2).
In a similar scenario, in which a physician has known the patient for 20 years, 39% of the American physicians, 29% of the Turkish physicians, 25% of the Japanese physicians and 7% of the Saudi Arabian physicians accepted supplying large doses of drugs to patients. Although the rate of the Saudi Arabian physicians in favor of assisted suicide in patients they had known for 20 years did not change, the rate of the American physicians increased.The rates of Turkish and Japanese physicians were similar (P>0,05) (In Clinical scenario 2, Table 2).
In Clinical scenario 3 the patient needs ventilation support in order to avoid immediate death. Table 3 shows the results regarding ventilation support in case of incurable illness with short life expectancy. The patient is first described as mentally competent and, subsequently, as being mentally incapacitated. When the patient was described as mentally competent, 50% of the Japanese, 43% of the Saudi Arabian physicians and 61% of Turkish physicians agreed that such a patient should be ventilated in accordance with the wishes of the patient’s family, despite the opposition of the physician. Relatively to the Saudi Arabian, American and Japanese physicians,a higher rate of Turkish physicians (61%) advocated the use of a ventilator, although the family refused it. Whereas the Turkish doctors were significantly influenced by the family and the wishes of the patient, the family or the treating physician had minor effects on the

Medicine and Law 554
responses of the American, Japanese and Saudi Arabian physicians. Only very small proportions of the American physicians (1%) agreed (3.1.1.).
In contrast, when the patient’s wish to be allowed to die conflicts with that of both doctor and family, 86% of the American physicians agreed that the patient should be allowed to die and should not be ventilated. 44% of the Japanese physicians, 56% of the Saudi Arabian physicians and 36% of the Turkish physicians agreed (3.1.2).
Significantly more Turkish (46%) than Saudi Arabian (35%), Japanese (22%) and American physicians (1%) agreed that such a patient should be ventilated despite the opposition of all parties (3.1.3)
There was a significant difference in scenarios 3.1.1, 3.1.2 and 3.1.3 between the physicians from different nations (P<0,05). In fact, the difference was between the American and Turkish physicians, between the Japanese and Turkish physicians and between the Saudi Arabian and Turkish physicians (P<0,05) (Table 3).
In a scenario in which the doctor wants to connect the patient to the ventilator, but both the patient and his family want him to be allowed to die immediately, 95% of the American physicians and 69% of the Japanese physicians agreed that the patient should not be connected, but 48% of the Saudi Arabian physicians and 46% of the Turkish physicians agreed that the patient should be connected (3.1.4). There was a significant difference between the physicians from different nations in their responses to this scenario (P<0,05). In fact, while the difference between the American and Turkish physicians and between the Japanese and Turkish physicians was significant (P<0,05), the difference between the Saudi Arabian and Turkish physicians was not (P>0,05) (Table 3).
In a scenario in which the patient is mentally incapacitated, 18% of the American physicians, 35% of the Japanese physicians, 53% of the Saudi Arabian physicians, and 74% of the Turkish physicians agreed that such a patient should be ventilated in accordance with the doctor’s wishes and despite family opposition. Significantly fewer American physicians agreed with it (3.2.1).
In a scenario in which the patient had an advance directive and stated his desire to be allowed to die, 92% of the American physicians, 55% of the Japanese

Medicine and Law 555
physicians, 57% of the physicians and 43% of the Turkish physicians said that the patient should not be connected to the ventilator (3.2.2).There was a significant difference between the physicians from different nations in their responses to scenarios 3.2.1 and 3.2.2 (P<0,05) (Table 3).
DISCUSSION
Telling the patient the truth ensures that the correct information is given and the correct choice for the patient is made. Explaining the truth to the patient is a more complicated process than simply giving information. In this process the physician's attitude is important. A physician who has developed communication skills and suitable approaches for informing can give the desired messages,including the amount of information that the patient wants to know and the timing, when the patient is ready. The attitude to truth-telling may vary from country to country and culture to culture. The reason is reflected in different ethnic roots, religious beliefs, cultural differences and legal regulations. At present, physicians in both developing and developed countries are more concerned to tell the truth about the diagnosis to the patients themselves. However, most of them prefer to inform the patients’ relatives first. In other words, patients’ relatives rather than patients themselves are informed.4-7
One of the most important problems concerning the relationship between physicians and patients is that decisions about the treatment of patients are mostly made by patients’ relatives and/or physicians. This is especially true in end-of-life decisions. The reasons why patients’ relatives think they have the right to decide on behalf of patients arethe intensive care unit patients’ inability to make decisions their suffer and pain, financial difficulties, ineffective treatment and the idea that efforts to improve their health quality merely lengthen the time to death.5-8
Interventions in intensive care units should be considered in terms of the principles of gaining benefits, avoiding harm to patients and a fair distribution of already limited resources. Risks of a given treatment which outweigh its benefits make its administration difficult to justify. However, it is difficult to answer the questions of what the benefits of the treatment are and who will determine its benefits. In Turkey, although health staff may find treatment useless in some cases, they cannot decide to end treatment for reasons such as administrative, social and legal considerations. This causes problems with a
Medicine and Law 556
fair use of already limited medical resources. When an end-of-life decision is to be made and should the treatment be considered futile, issues like so-called prolonged life- time to death- assessment of quality of life and its costs, and who will provide the necessary financial support are not yet clear.7
As in some other countries, paternalistic attitudes shape sociological structure in our country as well. A relationship in which one person controls the other is considered more valid than a physician-patient relationship. Since the society is often faced with different types of such a relationship, which in time develop into a norm, it is impossible for the society to find this relationship odd and to force the existing system to change.9,10
The importance of individual autonomy, however, is challenged in many Eastern cultures such as Turkey. In the Turkish context, there are several other factors to consider in crucial decision-making situations. In some cases, the patient opts to exclude himself from receiving information and participating in discussions regarding his management, delegating family members to make the decisions. Alternatively he may invite his physician to use his best judgment and choose the best option for him. In other situations, the family members may insist on excluding the patient from the decision-making loop.
Turkish society offers challenges to the decision making process because crucial decision making is often done by family members or is left entirely up to the attending physician. There seems to be a general acceptance of this shifting of focus from the individual to other players. This also raises certain ethical dilemmas for physicians who may feel uncomfortable with communication which excludes the patient or in accepting a paternalistic primary decision making role. The objective of this informal qualitative study is to ascertain physicians’ perceptions regarding the process of information delivery to the patient in the Turkish context and the various influences acting upon it.
The significant cultural, social and economic differences that exist in health care services between regions in our country affect physician-patient communication and end-of-life decision-making and is reflected in the process of obtaining informed consent. In this context there are differences not just between western and eastern countries but also between regions within our country and these differences have gained importance in the context of our subjects. 9,10
Medicine and Law 557
In the present study, 61% of the physicians in Turkey thought the patient should be told about a diagnosis of incurable illness instead of telling the family and 52% of the physicians thought it was inappropriate for the family to deny the patients full disclosure. A comparison of these findings with those of Ruhnkeet al. shows that the Turkish physicians’ attitudes concerning scenario 1 are similar to the Saudi Arabian’s and that the American physicians prioritize patient autonomy. The Japanese physicians tend to inform patients’ relatives rather than the patients themselves11.
Physician assisted suicide is one of the most important and controversial issues in end-of-life. Nowadays physician-assistaned suicide is known to be provided in several countries in varying frequencies.12,13 In the present study we found that the highest and the lowest rates of the physicians in favour of physician assisted suicide for the patients they encountered once were Turkish and American respectively. When patients’ families approved physician-assisted suicide, the rates of American, Japanese and Turkish physicians in favour of physician assisted suicide increased, but the rates of the Saudi Arabian physicians who agreed decreased. Mobeireek in his study of SaudiArabian physicians attributed it to religious beliefs and the sanctity of human life;3 however, the rate of physicians who agreed with physician assisted suicide in Turkey, where the majority of the population is Muslim, was higher. Considering that human life is important in all monotheist belief systems, the Saudi Arabian physicians’ attitudes can be ascribed to traditions, culture and behaviour typical of eastern societies rather than religious beliefs.
Withholding of life-prolonging treatment in the context of a terminal illness remains a topic of considerable controversy, even within the same culture. Not surprisingly, remarkable differences were again observed between the Turkish, Saudi Arabian, American and Japanese physicians. The great majority of Americans were against the use of such therapy despite the family or treating physician’s consent, whereas the Japanese and the Turkish physicians, who would honour the family’s wishes, were in favor. In the present study, many participants supported the use of mechanical ventilation against the wishes of the patient, family or treating doctor.
The ventilation support scenarioalso suggests that Americans wish to preserve patient autonomy at the end of life while Turkish, Japanese and Saudi Arabian respondents exhibit a greater deference to family and physician authority.

Medicine and Law 558
While most Turkish respondents disagreed with a patient’s right to die, given unified family-physician opposition, most respondents agreed with this right to die whenever expressed through an advance directive. It is also very possible that the patient’s incompetence itself influenced the responses in favour of withholding mechanical ventilation.
CONCLUSION
It may not be possible to know all cultures and their approaches to decision-making. Culture shapes individuals’ attitudes towards diseases, suffering and death. At present one can encounter patients and physicians of different races, nationalities, religions and cultures in the global world. This may increase the risk of misunderstandings concerning patient care at the end of life between patients and physicians from different cultures. Using appropriate intercultural communication approaches and techniques will increase satisfaction with the process and outcomes of patient care for all parties. When health staff integrates the principles of telling the truth and receiving informed consent with cultural appropriateness, they encourage patients to make sound end-of-life decisions and help patients to receive appropriate health care. Besides, patients will have the chance to make decisions about their treatment based on scientific knowledge.14,15
However, physicians’ cultural values may affect their attitudes towards various ethical dilemmas. Modern medicine requires that the primary decision maker should be the patient, he should be provided with all the information needed before making a decision about his illness and he should base his given consent on this information. It has been observed that this is not the case in Turkey. Therefore, it is of importance that research is required to describe the present situation and that obtained data should be discussed to achieve desirable outcomes. This will allow patients and their relatives to get involved in clinical and ethical decision making processes, help to reveal that end-of-life decisions are not only medical decisions and to create awareness among physicians. These issues should be included into medical curricula, and appropriate pre-service and in-service education should be provided. In fact, there have already been attempts to incorporate these subjects into undergraduate, graduate and in-service medical education curricula. Besides, it is important that education programs directed towards patients and their relatives, do improve the sense of responsibility for their problems and help them understand the concept of patient authonomy.1
Medicine and Law 559
Physicians should make decisions and perform interventions in accordance with ethical principles and values. It is essential that physicians should make every effort to put ethical principles into practice whatever approaches and methods they use. Physicians should not depend on their conscience and should not shoulder the responsibility for their decisions alone when they have to solve ethical dilemmas. The responsibilities for those decisions should be shared by all members of the staff. Patient autonomy and the patients’ right to be informed about their health and to make their own decisions should be of central importance. Hospital Ethics Committees should be formed in hospitals so that decisions can be made in the best interest of the patients.
Guidelines are required to help both the members of the committees and health staff working in intensive care units to make decisions. The Turkish Medical Association has prepared a guide for end-of-life decisions.16 Associations of all medical disciplines, doctors’ chambers and other relevant institutions should play a role in putting this guide into practice. All discussions about ethics and the guidelines will help to draft necessary regulations.
Acknowledgement: We would like to thank the Central Council of Turkish Medical Association and Dr. Orhan Odabaşı & Uğur Okmanfor Informatics Group of Turkish Medical Association and Dr. Erdem Karabulut for statistical evaluation of the data.
REFERENCES
1. Balseven Odabasi A, Ornek Buken N. “Informed Consent and Ethical Decision Making in the End of Life: Hacettepe Example” Turkiye Klinikleri J Med Sci 2009; 29: 1041-54.
2. Ruhnke GW, Wilson SR, Akamatsu T, et al. Ethical decision making and patient autonomy: a comparison of physicians and patients in Japan and the United States. Chest 2000; 118: 1172-82.
3. Mobeireek AF, Al-Kassimi F, Al-Zahrani K,et al. Information disclosure and decision-making: the Middle East versus the Far East and the West. J Med Ethics 2008; 34; 225-29.
4. Mystakidou K, Parpa E, Tsilika E, et al. Cancer information disclosure in different cultural contexts. Support Care Cancer 2004; 12: 147-54.
5. Oguz NY,Tepe H, Buken NO, Kucur D. “Tedavininreddi”, “Tedaviyisonlandırma”, Biyoetik Terimleri Sözlügü, 1. Baski, Turk
Medicine and Law 560
Felsefe Kurumu Yayini; 2005; 231-32. Bioethics Terminology Dictionary; (Dictionary Study), Supported by the Bioethics Section of the Turkish Philosophy Institute, to be published by the Turkish Philosophy Institute. Ankara.
6. Erer S, Atici E, Erdemir AD. The views of cancer patients on patient rights in the context of information and autonomy. J Med Ethics 2008; 34: 384-88.
7. Buken NO. "Truth-telling information and communication with cancer patients in Turkey". JISHIM 2003; 2: 31-37.
8. Oguz NY, Miles SH, Buken N.O,et al."End of life care in Turkey", The Cambridge Quarterly of Health Care Ethics 2003; 12:279-84.
9. Buken NO “The Health System, Health Policies and Health Transformation Program in Turkey”, Medicine and Law 2009; 28: 23-47.
10. Buken NO. Arapgirlioğlu K. “Bioethics Committees and Examining Consent within the Patient-Doctor Relationship in Turkey”, The International Conference on Bioethics Committees in Hospitals, Book of Abstracts, pg: 8-9, Zefat, Israil, May 17-20, 2009.
11. Csaba L Dégi Non-disclosure of cancer diagnosis: an examination of personal, medical, and psychosocial factors. Support Care Cancer, 2009; 17( 8 ): 1101-107.
12. Seale C. Characteristics of end-of-life decisions: survey of UK medical practitioners.Palliat Med 2006; 20: 653-59.
13. Van der Heide A, Deliens L, Faisst K, et al. End-of-life decision-making in six European countries: descriptive study.Lancet 2003; 362: 345-50.
14. Singer MK, Blackhall LJ. Negotiating cross-cultural issues at the end of life: “You got to Where the lives”. JAMA 2001; 286: 2993-3001.
15. Gastin Lawrence O. Informed consent, cultural sensitivity, and respect for person. JAMA 1995; 274: 844-45.
16. Turk Tabipleri Birligi Etik Bildirgeler Calıştayı Sonuç Raporu (Turkish Medical Association Ethical Guidelines), 1. Baski, 1. Press, Ankara: TTB Yayınlari, to be published by TMA, Haziran, June, 2008: 27-34.
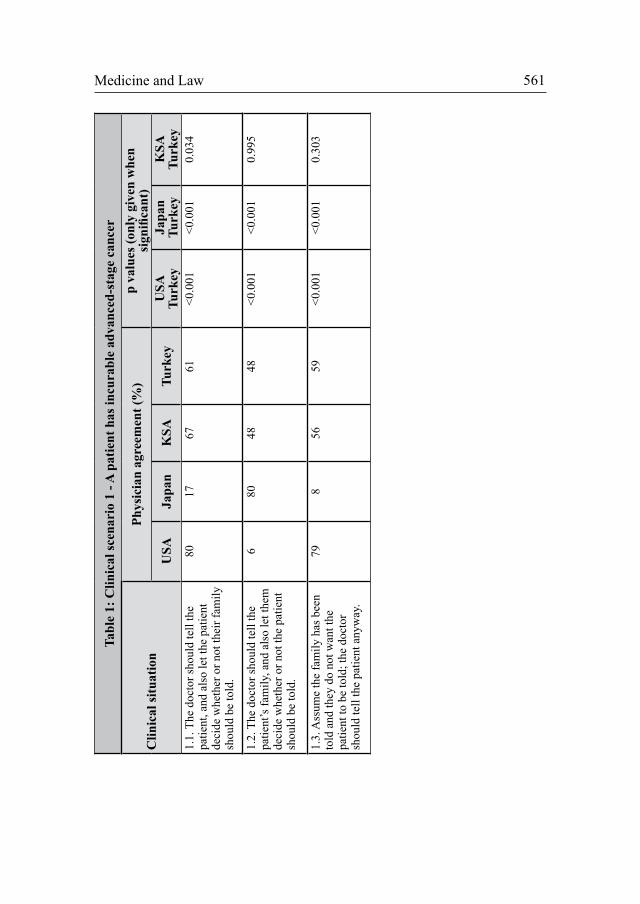
Medicine and Law 561
Tabl
e 1:
Clin
ical
scen
ario
1 -
A p
atie
nt h
as in
cura
ble
adva
nced
-sta
ge c
ance
r
Clin
ical
situ
atio
nPh
ysic
ian
agre
emen
t (%
)
p
valu
es (o
nly
give
n w
hen
sign
ifica
nt)
USA
Japa
nK
SATu
rkey
USA
Tu
rkey
Japa
n Tu
rkey
KSA
Turk
ey1.
1. T
he d
octo
r sho
uld
tell
the
patie
nt, a
nd a
lso
let t
he p
atie
nt
deci
de w
heth
er o
r not
thei
r fam
ily
shou
ld b
e to
ld.
8017
6761
<0.0
01<0
.001
0.03
4
1.2.
The
doc
tor s
houl
d te
ll th
e pa
tient
’s fa
mily
, and
als
o le
t the
m
deci
de w
heth
er o
r not
the
patie
nt
shou
ld b
e to
ld.
680
4848
<0.0
01<0
.001
0.99
5
1.3.
Ass
ume
the
fam
ily h
as b
een
told
and
they
do
not w
ant t
he
patie
nt to
be
told
; the
doc
tor
shou
ld te
ll th
e pa
tient
any
way
.
798
5659
<0.0
01<0
.001
0.30
3
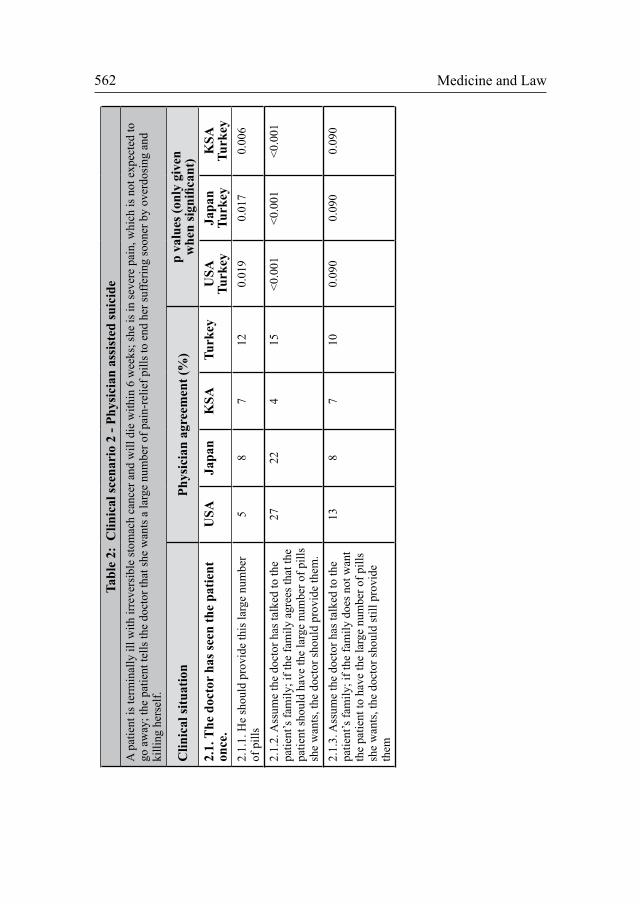
Medicine and Law 562
Tabl
e 2:
Clin
ical
scen
ario
2 -
Phys
icia
n as
sist
ed su
icid
eA
pat
ient
is te
rmin
ally
ill w
ith ir
reve
rsib
le st
omac
h ca
ncer
and
will
die
with
in 6
wee
ks; s
he is
in se
vere
pai
n, w
hich
is n
ot e
xpec
ted
to
go a
way
; the
pat
ient
tells
the
doct
or th
at sh
e w
ants
a la
rge
num
ber o
f pai
n-re
lief p
ills t
o en
d he
r suf
ferin
g so
oner
by
over
dosi
ng a
nd
killi
ng h
erse
lf.
Clin
ical
situ
atio
nPh
ysic
ian
agre
emen
t (%
)
p va
lues
(onl
y gi
ven
whe
n si
gnifi
cant
)2.
1. T
he d
octo
r ha
s see
n th
e pa
tient
on
ce.
USA
Japa
nK
SATu
rkey
USA
Tu
rkey
Japa
n Tu
rkey
KSA
Turk
ey2.
1.1.
He
shou
ld p
rovi
de th
is la
rge
num
ber
of p
ills
58
712
0.01
90.
017
0.00
6
2.1.
2. A
ssum
e th
e do
ctor
has
talk
ed to
the
patie
nt’s
fam
ily; i
f the
fam
ily a
gree
s tha
t the
pa
tient
shou
ld h
ave
the
larg
e nu
mbe
r of p
ills
she
wan
ts, t
he d
octo
r sho
uld
prov
ide
them
.
2722
415
<0.0
01<0
.001
<0.0
01
2.1.
3. A
ssum
e th
e do
ctor
has
talk
ed to
the
patie
nt’s
fam
ily; i
f the
fam
ily d
oes n
ot w
ant
the
patie
nt to
hav
e th
e la
rge
num
ber o
f pill
s sh
e w
ants
, the
doc
tor s
houl
d st
ill p
rovi
de
them
138
710
0.09
00.
090
0.09
0
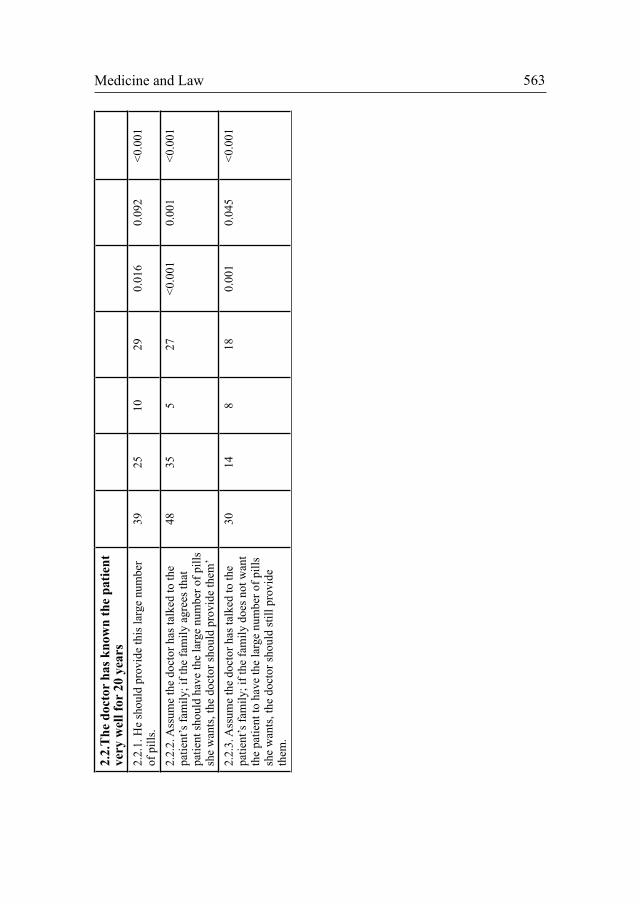
Medicine and Law 563 2.
2.T
he d
octo
r ha
s kno
wn
the
patie
nt
very
wel
l for
20
year
s2.
2.1.
He
shou
ld p
rovi
de th
is la
rge
num
ber
of p
ills.
3925
1029
0.01
60.
092
<0.0
01
2.2.
2. A
ssum
e th
e do
ctor
has
talk
ed to
the
patie
nt’s
fam
ily; i
f the
fam
ily a
gree
s tha
t pa
tient
shou
ld h
ave
the
larg
e nu
mbe
r of p
ills
she
wan
ts, t
he d
octo
r sho
uld
prov
ide
them
’
4835
527
<0.0
010.
001
<0.0
01
2.2.
3. A
ssum
e th
e do
ctor
has
talk
ed to
the
patie
nt’s
fam
ily; i
f the
fam
ily d
oes n
ot w
ant
the
patie
nt to
hav
e th
e la
rge
num
ber o
f pill
s sh
e w
ants
, the
doc
tor s
houl
d st
ill p
rovi
de
them
.
3014
818
0.00
10.
045
<0.0
01
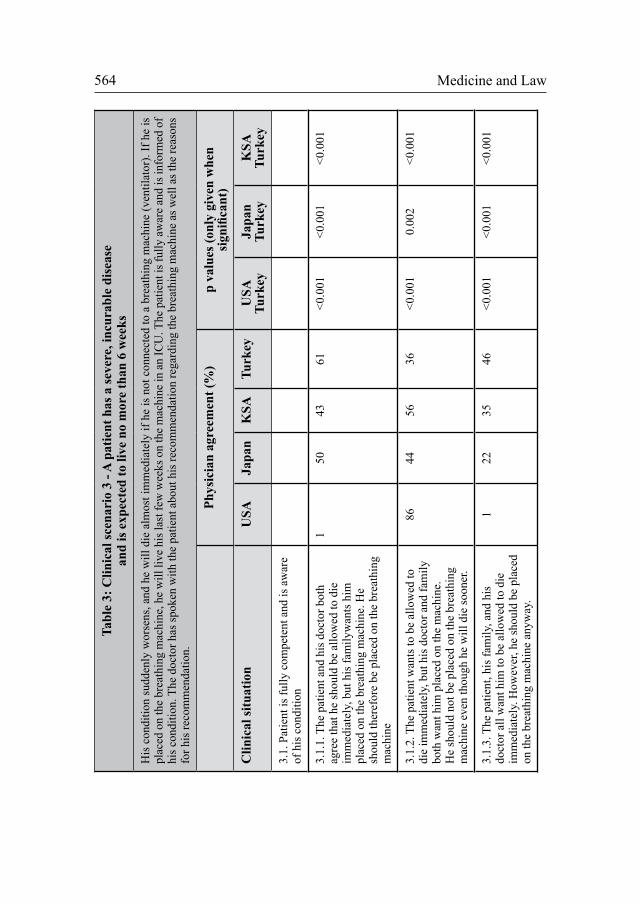
Medicine and Law 564
Tabl
e 3:
Clin
ical
scen
ario
3 -
A p
atie
nt h
as a
seve
re, i
ncur
able
dis
ease
an
d is
exp
ecte
d to
live
no
mor
e th
an 6
wee
ks
His
con
ditio
n su
dden
ly w
orse
ns, a
nd h
e w
ill d
ie a
lmos
t im
med
iate
ly if
he
is n
ot c
onne
cted
to a
bre
athi
ng m
achi
ne (v
entil
ator
). If
he
is
plac
ed o
n th
e br
eath
ing
mac
hine
, he
will
live
his
last
few
wee
ks o
n th
e m
achi
ne in
an
ICU
. The
pat
ient
is fu
lly a
war
e an
d is
info
rmed
of
his c
ondi
tion.
The
doc
tor h
as sp
oken
with
the
patie
nt a
bout
his
reco
mm
enda
tion
rega
rdin
g th
e br
eath
ing
mac
hine
as w
ell a
s the
reas
ons
for h
is re
com
men
datio
n.
Phys
icia
n ag
reem
ent (
%)
p
valu
es (o
nly
give
n w
hen
sign
ifica
nt)
Clin
ical
situ
atio
nU
SAJa
pan
KSA
Turk
eyU
SA
Turk
eyJa
pan
Turk
eyK
SATu
rkey
3.1.
Pat
ient
is fu
lly c
ompe
tent
and
is a
war
e of
his
con
ditio
n
3.1.
1. T
he p
atie
nt a
nd h
is d
octo
r bot
h ag
ree
that
he
shou
ld b
e al
low
ed to
die
im
med
iate
ly, b
ut h
is fa
mily
wan
ts h
im
plac
ed o
n th
e br
eath
ing
mac
hine
. He
shou
ld th
eref
ore
be p
lace
d on
the
brea
thin
g m
achi
ne
1 50
4361
<0.0
01<0
.001
<0.0
01
3.1.
2. T
he p
atie
nt w
ants
to b
e al
low
ed to
di
e im
med
iate
ly, b
ut h
is d
octo
r and
fam
ily
both
wan
t him
pla
ced
on th
e m
achi
ne.
He
shou
ld n
ot b
e pl
aced
on
the
brea
thin
g m
achi
ne e
ven
thou
gh h
e w
ill d
ie so
oner
.
8644
5636
<0.0
010.
002
<0.0
01
3.1.
3. T
he p
atie
nt, h
is fa
mily
, and
his
do
ctor
all
wan
t him
to b
e al
low
ed to
die
im
med
iate
ly. H
owev
er, h
e sh
ould
be
plac
ed
on th
e br
eath
ing
mac
hine
any
way
.
122
3546
<0.0
01<0
.001
<0.0
01
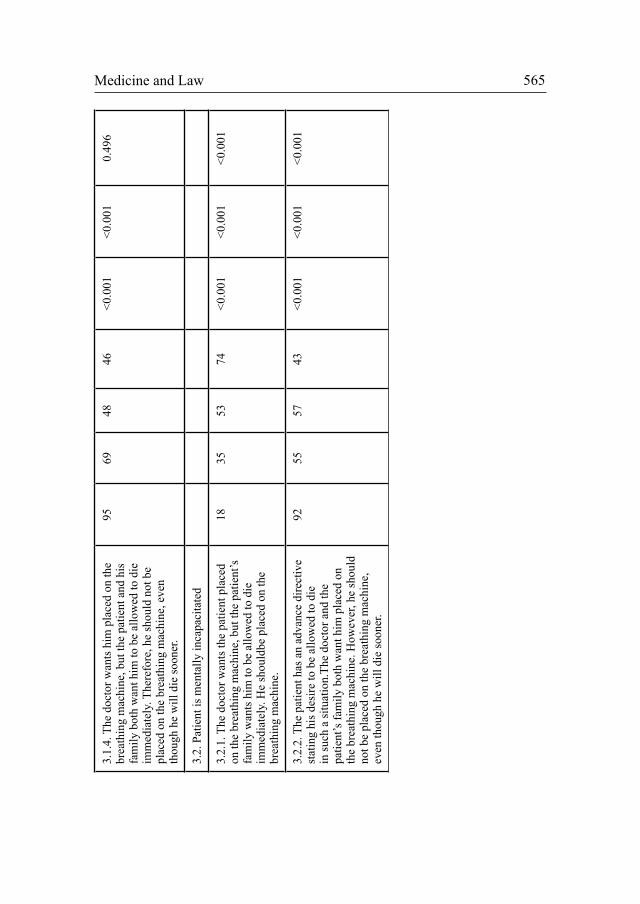
Medicine and Law 565 3.
1.4.
The
doc
tor w
ants
him
pla
ced
on th
e br
eath
ing
mac
hine
, but
the
patie
nt a
nd h
is
fam
ily b
oth
wan
t him
to b
e al
low
ed to
die
im
med
iate
ly. T
here
fore
, he
shou
ld n
ot b
e pl
aced
on
the
brea
thin
g m
achi
ne, e
ven
thou
gh h
e w
ill d
ie so
oner
.
9569
4846
<0.0
01<0
.001
0.49
6
3.2.
Pat
ient
is m
enta
lly in
capa
cita
ted
3.2.
1. T
he d
octo
r wan
ts th
e pa
tient
pla
ced
on th
e br
eath
ing
mac
hine
, but
the
patie
nt’s
fa
mily
wan
ts h
im to
be
allo
wed
to d
ie
imm
edia
tely
. He
shou
ldbe
pla
ced
on th
e br
eath
ing
mac
hine
.
1835
53
74<0
.001
<0.0
01<0
.001
3.2.
2. T
he p
atie
nt h
as a
n ad
vanc
e di
rect
ive
stat
ing
his d
esire
to b
e al
low
ed to
die
in
such
a si
tuat
ion.
The
doct
or a
nd th
e pa
tient
’s fa
mily
bot
h w
ant h
im p
lace
d on
th
e br
eath
ing
mac
hine
. How
ever
, he
shou
ld
not b
e pl
aced
on
the
brea
thin
g m
achi
ne,
even
thou
gh h
e w
ill d
ie so
oner
.
9255
5743
<0.0
01<0
.001
<0.0
01


©PROBOOK 2013and Law
Medicine Med Law (2013) 32:567-576
567
“LEGES ARTIS, END(ING) OF LIFE, AND COMPASSION”Maria do Céu Rueff*
Abstract: I will problematize medical performances at the end of life, confronting them with the responses of Portuguese Criminal Law. By starting from a review of literature, both in Portugal and abroad, I will cross the criminal doctrine with a broader, interdisciplinary approach, including the reconsideration of medicine ethical tradition (notably the Hippocratic Writings) and the present developments in neurosciences.
The frame of homeostasis (neurobiology of emotions) by Damásio, with compassion in the top, helps to clarify to which extent medical act according to legesart is becomes the centre of the problem. Indeed, it is within the medical act, understood as the meeting of two autonomies - patient’s and doctor’s autonomies - that the compassion takes place as a result of the agreement/compromise between the patient’s will of ceasing her/his life in a situation of unbearable suffering and the doctor’s duty to relieve that suffering. Compassion arises here as a “homeostasis instrument”, that is, an emotion which is important in the regulation of life, even when we are speaking about end(ing) of life.
This new perspective allows us to guess a shift of paradigm on the ethical and social levels.
On the other hand, in so far as we have passed from the compassionate response in medical setting to its discussion, successively, in medical ethics, in the courts, and as a normative instrument, I claim that we are before the “transition from an automatic homeostasis to a deliberate homeostasis” (Damásio). Therefore, I seek for a balance between the spontaneous and the planned, concerning the issue of praxis. Indeed, what increasingly happens in medical praxis should be brought together with theory, whereby medical law has a word to say.
* Universidade Lusíada, CEJEA/FCT, Centro de Direito Biomédico da Faculdade de Direito da Universidade de Coimbra. [email protected] [email protected]
Medicine and Law 568
Keywords: Medical Ethics; Medical Law; Leges Artis; Euthanasia; Homeostasis; Social Change
1. THE LEGAL-CRIMINAL SETTING OF AID TO DEATH AND DYING
I will approach the legal-medical issue of direct aid to death. As “aid to dying”, in the legal criminal field, Dias understands the aid provided in accordance with the patient’s real or perceived request, when the patient is severely and hopelessly ill, often in unbearable suffering. This request is in the sense that the patient may reach his/her death in a way that he believes, or may have reasons to believe, will preserve his/her human dignity.1
Nowadays we tend to highlight three forms of aid to death and dying: Direct active aid to death: when an active form of behavior causes death or hastens its occurrence (e.g. by administration of lethal injection); Indirect active aid to death: when we cannot exclude or it is not safe to conclude that the medication given with the sole purpose of alleviating the pain or induce unconsciousness may result in unintentionally hastening the moment of death (e.g. administration of increased doses of morphine); Passive aid to death, for the cases in which the failure and interruption of treatment are likely the cause of a shorter life span. This is understood as objectively attributed to those situations (e. g. denial of surgical intervention or intensive care that is likely to prolong the patient’s life span).
Here we have various principles at stake and we begin with the protection of the human life. The Portuguese Penal Code (Art. 134) incriminates the homicide by request consisting in the act of providing death to another person according to the serious and clear request that he/she has made to the agent. The incitement or aid to suicide builds a type of illicit (Art. 135), but even though we tolerate suicide, because it is not punishable in our Penal Code. We should note that the Penal Code maintains criminal accountability and the type of homicide (privileged - Art. 133) for the person who practiced this for “compassion”, although with significant reduction of the guilt.
In these normative predictions several factors are not taken into account, namely: the situation of the disease; the situation of the terminal illness;
1 Dias, J. F. (2008), “A ‘Ajuda à Morte’: uma consideração jurídico-penal”, Revista de Legislação e Jurisprudência, Ano 137, No 3949, 2008 (pp. 202-215), p. 203.

Medicine and Law 569
the unbearable suffering; the possible proximity for the ending of life; the occurrence or necessity of medical care; the doctor-patient relationship at the end of life and the possibility to alleviate suffering, according to the means available to the medical science today; the exercise of compassion due to the suffering that we can witness in the moment of transition - but yet belonging to life - which we call death.
The Portuguese legislator took into consideration the medical activity in the special part of the Penal Code (Art. 150), where the procedures carried out by the physicians according to the Leges Artis (considered as professional, technical norms) are just considered as atypical. Among other aims implicit in this norm, the expression “to suppress or minimize suffering” is also found.
This justifies the question that already arises as self-assertion on the title of this paper: what (kind of) Leges Artis at the end(ing) of life? How to articulate Leges Artis, end(ing) of life, compassion and criminal law?
2. LEGES ARTIS AND END(ING) OF LIFE
The relevance of the principle of autonomy, resulting from the eminent dignity of the human being and the consequent right of self-determination of the individual, is not negotiable. It is interesting how Dias stresses its validity in this matter. He says that the principle of autonomy conforms “a true fundamental ethical rule that should govern the medical activity”. He further clarifies that the physician’s respect for the patient’s will corresponds to a healthy understanding of the physician’s function, and advances the following about the role of this function: It may not consist in keeping alive at any price the patients who are entrusted to the physician, nor is it allowed keeping them alive contrary to their true will; It shall consist in providing patients “the best conditions to die naturally with peace and dignity”, by giving up “the paraphernalia of technical instruments which are today available to artificially maintain the vital functions”; having in view the progress of the medical technology, what determines the limits of the duty of medical care is not the efficiency of the machines, but the decision, case by case, addressed to human life and dignity.2
2 Dias, op.cit., p. 206.

Medicine and Law 570
These are some of the Leges Artis in end(ing) of life. The question that still remains is how to deal with the cases of direct active aid to death. It is here that the author admits, in principle, the incrimination by Art. 133 to 135.3 He puts, however, the question whether we shouldn’t go further and produce a very strong reduction of the ambit of protection of the incriminating norm. This by taking into account the motives ruling the act, and since there is a reasonable and objectively founded request towards death by patient. He foresees that the courts may, in some cases, deliberate the exemption of punishment (de lege ferenda or future law).
Costa has a similar point of view but goes further. The author underlines the aspect of self-determination of whomever consents and requests, and arrives at the medical act, in which the issue is in fact centered, then placing here the argumentative locus. In his words: “Throughout this reflection it has become clear that active euthanasia, sustained by serious, firm and expressed request, may not be carried out by anyone. It is common ground that such an act must have the dignity that it can be carried out by a physician only”.4
On the other hand, taking into consideration the medical advances, above all medical support, Costa states that the end of life was thrown into “unthinkable chronological ages” making the perception of the end(ing) of life for the person who goes through this experience not so much a perception of death, but rather a perception of “ceasing to live”. Therefore, the ethical-juridical sense of who claims for him/herself the power of “ceasing to live” is a value that the juridical order cannot fail to consider.5
The acceptance of impunity of an active euthanasia carried out by a physician presupposes a very rigorous procedural system which should be based on the following six requirements: active euthanasia, based on a serious, firm and expressed request, cannot be but a clearly exceptional and justified practice; it is justified only in the terminal phase of an incurable and severe illness; the provision of palliative care is absolutely an indispensable procedure; it cannot, in any case, be practiced on minors of age, even if emancipated, nor on mentally ill patients, even though they have expressed their wish, when in
3 Dias, op. cit., pp. 214-215.4 Costa, J. F., “O Fim da Vida e o Direito Penal”, in: Liber Discipulorum Para Jorge de
Figueiredo Dias, ed. by Andrade, M. C. / Costa, J. F. / Rodrigues, A. M., / Antunes, M. J., Coimbra, Coimbra Editora, 2003 (pp. 759-807), p. 791.
5 Costa, J. F., op. cit., pp. 791-795.

Medicine and Law 571
a perfect state of mind; only a physician can practice euthanasia; the physician can always enforce the right of conscientious objection.6
Concerning the legal frame, within Criminal Law, of the act of “ceasing to live”, Costa comes to prefer a solution that he defines as “not even filling the legal type of crime”. He justifies this position saying that Art. 150 of Penal Code expresses unambiguously a medical privilege.7 As long as medical procedures are carried out under the intentions previously mentioned, they do not even fill the type of legal crime of offences against physical integrity. Within this normative architecture, it would not make sense or have little sense to split the unity of the medical act. What would imply that the active euthanasia, practiced by the physician, while executor of the medical act, should not even qualify the legal type of homicide. This only makes sense and legal-criminal sense, if it is accepted, within the actual medical thinking, that such acts, those of “ceasing to live”, are still and will always be medical acts.8
I could not agree more with this position, except when the author put all the emphasis - in my point of view excessively - in the patient’s self-determination. Instead, the focus should be directed to the encounter of two autonomies - that of the physician and of the patient - that the medical act should always presuppose. For it is at that moment of unbearable suffering that the patient mostly needs the help from another human being. It is also then that the physician as a human being is able to be self-determined in his/her performance by the experience of condoling/compassion (meaning to suffer together with another).
3. HIPPOCRATIC AUTHORS, COMPASSION, LETHAL DRUG
The word “compassion” does not exist in the Hippocratic Oath, but its observation and the necessity to act in conformity with the Greek medical practice results from the so called “Hippocratic Corpus”.9 The reading of nowadays called “clinical” cases, in one of those treaties, denominated
6 Costa, J. F., op. cit., p. 796.7 Costa, J. F., op. cit., p. 801.8 Costa, J. F., op. cit., p. 802.9 See further development in Rueff, M. C., O Segredo Médico Como Garantia de Não-
Discriminação - Estudo de Caso: HIV/SIDA, Coimbra, Coimbra Editora and Centro de Direito Biomédico da Faculdade de Direito da Universidade de Coimbra, 2009, pp. 37-80.

Medicine and Law 572
Epidemics, clearly transmits the idea of the compassionate physician at the patient’s bedside. Also in the treaty The Art or Science of Medicine is written that medical care may be given until the end, but that the death is something natural.10
As pointed out in other cases that I will briefly leave aside for now, the aid to death is not unfamiliar to the physicians of the Hippocratic tradition. What is difficult to articulate is this reality with the passage of the Hippocratic Oath condemning the administration of any lethal substance to the patient. So it is necessary to clarify interpretations already made on this part of the oath, notably by João Lobo Antunes when he says - and I agree with him - that: “Making the Hippocratic Oath normative and not understanding its symbolic meaning is one of the unfortunate and double-faced confusions of our [medical] profession.”11
Miles means that the expression “I will not give a fatal drug to anyone if I am asked, nor will I suggest any such thing” has nothing to do with nowadays concepts of medically assisted suicide, voluntary/involuntary euthanasia or withdrawal of life support measures. Accordingly, he explains that the term suicide in the Greek language did not arise until long after the Oath was written. Afterwards, because even when it arises, it appears associated with concepts such as acceptance of heroic death by another, or giving yourself the death for shame, which has nothing to do with an intentional termination of life as a way of ending the suffering caused by disease. Miles also puts in evidence that the Greek word euthanasia, which literally means good death, was not coined until 280 (B.C.), that is, about a century after the Oath was written and that this new term did not refer to aiding death (or assisting death), but to the natural death without agony, and therefore it does not coincide with the meaning it has today.12
10 Thus: “Our practice is limited by the instruments made available by nature or art. When a man is attacked by a disease which is more powerful than the medical instruments, there should be no expectation that medicine is victorious. (…) When the physician fails it is the power of the disease which is responsible and not the deficiencies of the medical science.” See Hippocratic Writings, Edited with an introduction by G.E.R. Lloyd, London, etc., Penguin Classics,1983, p. 143.
11 Antunes, J. L., Inquietação Interminável - Ensaio sobre ética das ciências da vida, Lisbon, Gradiva, 2010, p. 166.
12 Miles, S. H., The Hippocratic Oath and the Ethics of Medicine, Auckland/Bangkok, etc., Oxford University Press, 2004, pp. 67-68.
Medicine and Law 573
So - and by taking also into account the positions of Diego Gracia13, Albert Jonsen14,Littré and Geoffrey Lloyd (both apud Miles)15 - I have no doubt to conclude that none of the conceptions about this passage of the Oath has any similarity with aiding in situations of unbearable pain or compassion during all the care moments, even at the end of life. Rather, such part of the Oath is related to the maximum of prudence that should regulate the medical action and also to the preservation of the physician’s exemption by providing medical care. Its aim is to guarantee that the confident relationship between doctor and patient is always established to help the patient and never to cause damage (harm or injury) to him. Any other limitation or moral value is not the most important at stake here.
4. AID IN DEATH, AS A MEDICAL ACT
Today some countries in the world allow either active direct euthanasia or assisted suicide.16 I will not go into the analysis of the measures taken by those legal systems leading to the legalization of such practices. Studies by Penny Lewis17 and Laura Santos18 follow this path. I retain from both the role they ascribe to the Dutch case, to accentuate how the normative change was processed.
The legal framework of the issue in Netherlands was based on the Art. 293 of the Penal Code that provides for homicide by express and serious request. What took place before this legislation19 was that some cases went to trial, having been judged by the Supreme Court, based on Art. 40 of the Penal Code that allows the justification by necessity. It was then declared that a physician before the conflict of duties - life preservation and pain relief of the patient
13 Gracia, D., Fundamentos de Bioética, 2nd Edition, Coimbra, Gráfica de Coimbra, Lda, 2007, pp. 69-93.
14 Jonsen, A. R., A Short History of Medical Ethics, Oxford, New York, etc., Oxford University Press, 2008, p. 5.
15 Miles, op. cit., pp. 73-74.16 This is the case of Holland, Belgium, Switzerland, Luxemburg, or the state of Oregon in
the USA.17 Lewis, P., Assisted Dying and Legal Change, Oxford and New York, Oxford University
Press, 2007.18 Santos, L. F., Ajudas-me amorrer? - A morte assistida na culturaocidental do século XXI,
Lisbon, Sextante Editora, 2009.19 Carried out by the legal instrument titled “Termination of Life on Request and Assisted
Suicide (Review Procedures) act 2001”. See Lewis, op. cit., p. 77; Santos, op. cit., p. 42.
Medicine and Law 574
- may defend him/herself by justifying necessity, if he/she chooses the latter for being most important under an objective point of view, even if this implies something which is in itself forbidden.
The Supreme Court recognized that the physician’s duty to relieve a “hopeless and unbearable suffering” could justify the application of defense by clause of necessity, which became the basis of the decriminalization of euthanasia and the opening for the assisted suicide. This means that the recognized defense basis resides in the patient’s experience of unbearable suffering, but also means that this basis is sustained by the verification that only a physician may find him/herself faced with such conflict of duties: that is, concomitantly, preservation of life and relief of suffering.20
In the motives which led to this, we find the prominent role of the physicians and of the Royal Medical Association of Holland, the first, and apparently only, medical association in the world to support from the beginning the explicit voluntary termination in the absolute respect for autonomy, and demands the repeated expression of that will. Therefore, in Holland euthanasia is a medical act.21
5. MEDICAL COMPASSION IN DYING: FROM AN AUTOMATIC HOMEOSTASIS TO A DELIBERATE HOMEOSTASIS
António Damásio questions the origins of the ethical behavior, notably whether it is molded by the genome or through culture transmitted by learning and socialization processes. The author states that emotions are the key to the mystery. To explain this, he summarizes the neurobiology of emotions (fundamental to life-regulation or homeostasis) facing them in a complex picture that has to do with life regulation, which he calls the homeostasis frame.22 At the top of the list he places the so-called social emotions and among them, the compassion, in which “the competent emotional stimulus is the suffering of the other individual. The feeling that follows it has as a
20 Lewis, P., op. cit., pp. 78, 80,125.21 Antunes, J. L., op. cit.,p. 165.22 Damásio, A., “A Neurobiologia da ética: sob o Signo de Espinosa”, Ordem dos
Advogados, 29 Especial (Conferências de S. Domingos: O Cérebro entre o Bem e o Mal, O Corpo / A Alma), 2003, pp. 31- 39.

Medicine and Law 575
consequence the comfort and re-balancing of the other or the group”.23
Damásio emphasizes the difference between genetic behavior and ethical principles and states that ethics consists in the construction of the principles that took place through the human civilizations and not only by something brought by a genome. The ethical behavior results from double influence: one that has to do with biological evolution, through the genome, and another that results from the construction of a social, cultural space, which can only occur in the humans, who are endowed with conscience and emotion.24
Damásio puts the question why emotions have so much importance in the construction of Ethics and Law, and the answer comes from a fact that he says being curious: notably, that emotions, in their basic aspect, have to do with the regulation of life. They are instruments of homeostasis. Without emotions and the mechanisms that are underlying them, it is not possible to survive in well-being. Accordingly, the ethical principles, the laws and socio-political organizations are also homeostasis mechanisms, even though they are not seen in this manner.
In conclusion, Damásio states: “I consider Ethics, in general, and everything else that belongs to it, as an extended homeostasis, a homeostasis that does not come directly from genome, a homeostasis that we have been building. And, it is curious to think that that is a recent construction. Contrary to what happens with the emotions, which have millions of biological evolution, we have a few thousand years behind us in the construction of these new homeostasis techniques. This is a gradual process (...), a process that is also a work in progress. (...) The beauty of this idea has to do with the transition of an automatic homeostasis to a deliberate homeostasis.”25
I do not hesitate in seeing in discussion of the dilemma I am dealing with a “transition of an automatic homeostasis to a deliberate homeostasis”. To the extent that we passed, successively, from the response of automatic compassion in medical care, to its discussion in medical ethics, afterwards in the courts, and now as a normative instrument.
23 Damásio, op. cit., pp. 32-34.24 Damásio, op. cit., p. 76.25 Damásio, op. cit., p. 38.
Medicine and Law 576
In fact, it is within the medical act that the question of the aid to death is to be ‘focused medical act’ determined by the will of the patient, but also, concomitantly, in a balanced way, by the other pole of the relationship: the physician. Thus, it is in the encounter between both that an agreement will take place, where we see the will to cease life and the duty to alleviate suffering, that is, the moment of compassion.
An integrated perspective of the medical law - where the medical and legal methods are crossed -,26 will integrate certainly all situations of medical compassion at the end of life (a development that we are observing), in order to embrace the widest spectrum of situations.
Not listening in a situation of incurable disease to the insistent request of the patient to the physician to alleviate suffering means not humanely responding to such request. If it is difficult to see in this situation the accomplishment of the principle of beneficence - because beneficence without life and body is something that cannot be objectified - at least we may consider the case as an accomplishment of the principle of non-maleficence. In fact, the omission of the physician’s intervention would mean, during the entire period of the inaction, an evil - that is, the unbearable suffering -, that the patient precisely implored to be ceased.
Here the physician has the domain of the fact, in the double sense of the term: the exclusivity of means, and the opportunity of putting an end to suffering, or rather, not causing further harm. The Criminal Law cannot be indifferent to this reality, be it called compassion, or not.
26 See Rueff, op. cit., and Eser, A., “Von sektoralem zu integrativem Medizinrecht”, in: Perspektiven des Medizinrechts, ed. by Eser, A. / Just, H. / Koch, H.-G., Baden-Baden, Nomos Verlagsgesellschaft, 2004, pp. 247-256.
©PROBOOK 2013and Law
Medicine Med Law (2013) 32:577-585
577
ETHICAL AND LEGAL ISSUES IN CASES OF WITHDRAWING TREATMENT FROM AN INCOMPETENT PATIENT IN ITALYDenard Veshi*, **
Abstract: The traditional approach towards end-of-life decision-making in Italy has changed. Whilst article 32 of the Italian Constitution recognizes the ‘right to health’ that grants patients to withhold or withdraw medical treatment, the Italian Medical Ethics Code neglects any kind of assistance during death or euthanasia.
Although norms seem clear, ethicists and lawyers continue to discuss if withdrawing treatment from an incompetent patient should be classified as immoral and/or illegal. This is the result of acceptance of concepts such as patient’s autonomy and the “right to die”. On one hand, ethicist and lawyers, valuing the patient’s autonomy, believe that letting die cannot be punished. On the other hand, however, some conservative ethicists and lawyers argue that the right to life is absolute and imperative and therefore a physician must do everything possible to protect one's life.
Keywords: Withdrawing Treatment; Incompetent Patient; Advance Directives; Physician; Homicide; Kidnapping; Duress.
1. INTRODUCTION
In Italy, bioethical debates about end-of-life decision making has increased in the last decades. This is the result of new medical discoveries. The establishment of the Italian National Bioethics Committee, decreased the influence of the Roman Catholic Church within Italian society, the new interpretation of article 32 of the Italian Constitution and the importance given by the media to cases connected with refusal of medical treatment.
* Ph.D. fellow in Joint International Doctoral (Ph.D.) Degree in “Law, Science and Technology”, 2012-2015 University of Bologna. Via San Donato, 9, Bologna (BO) 40126, Italy. Email: [email protected]
** All the translation from Italian into English has been done by the author and all on-line documents were consultable during April 2013.
Medicine and Law 578
The advances of medicine have brought about the existence of a grey zone between life and death within which the promulgation of life or the anticipation of death depends on the individual’s or the doctor’s decision to inject or reject life-sustaining treatment. New medical discoveries can prolong the life of a patient with incurable disease for an unlimited time. The best examples are those of patients in a persistent vegetative state (PVS) wherein the person is not dead but has lost mental activity and consciousness1.
In 1990, a Prime Minister’s Decree led to the establishment of the Italian National Bioethics Committee, an advisory body to the Government, composed of experts in the medical, ethical and legal field. The debate about end-of-life decision-making started only in the last decade of the last century. Before this debate, the Roman Catholic Church, condemning such decisions, has had a big influence on the Italian society2.
Meanwhile, Article 32 of the Italian Constitution recognizes the “right to health” that grants patients the right to consent or even withhold medical treatment. “Right to health” is safeguarded as “a fundamental right of the individual and as a collective interest” and can be limited only “under the provisions of the law”.
It is also important to highlight the role of the media’s attention on the case of Eluana Englaro who was in a PVS for more than fifteen years and the controversy following the final decision of the Court of Cassation.
In the last decades, due to changing cultural tendances within Italian society, there has been an incredible increase in public debate about end-of-life decision-making.
1 The brain is divided into two main parts: the “higher brain”, in particular the cerebral cortex where mental and consciousness activity are realized, and the “lower brain” which consists of the brainstem responsible for the somatic functions of the organism even when the brain has lost the capacity to support mental activity. In case of damage to the cerebral cortex, the patient is in a permanent vegetative state and in case of damage to the brainstem the patient is described as “locked in”. More information in Singer, M., 1995, Rethinking Life and Death: The Collapse of Our Traditional Ethics, New York: St. Martin’s Press and Dworking, R., 1993, Life’s Dominion, New York: Alfred A. Knopf.
2 Griffith, J., Weyers, H. and Adam M., 2008, Euthanasia and the law in Europe, Oxford; Portland, Or.: Hart Publishing, p. 396.

Medicine and Law 579
2. REJECTING MEDICAL TREATMENT: BIOETHICS ISSUES
The right to decide the exact moment of death has been discussed for many centuries. Under the Greek and Roman empires' rules, suicide and euthanasia were considered immoral, however, the Renaissance and Enlightenment eras brought about an increase in their social acceptance.
The debate about the ownership of life and the right to die grew in the 20th century following discoveries in the medical field. This entailed a division between “natural” and “artificial” life or between “biological life” and “life with dignity”3. Therefore, death was no longer considered a natural event but a long process of steps involving medical treatment where the relationship between duty of care and quality of life became ever more ambiguous, contentious and controversial. Article 32 of the Italian Constitution recognizes the “right to health” that grants patients the right to withhold or withdraw medical treatment. As was confirmed by the Italian Constitutional Court (decision 282/2002)4, medical treatment has to protect not only the patient’s health but also his dignity. Furthermore, according to decision 307/90 of the Italian Constitution Court5, this right can only be limited when medical treatment protects not only the health of the single patient but also that of all the society. These are the cases of vaccination of a population or the cases of caregiving in the context of HIV. This limitation must be predicted and specified by the Italian national law.
However, the Italian Medical Ethics Code neglects any kind of assistance during death or euthanasia (Article 17). In case of assistance, the assisting physicians will be liable for homicide of the consenting person (Article 579 Penal Code; PC) or, in case of incompetent patient, for intentional homicide Article 575 PC). However, it recognizes the patient’s autonomy by rejecting all kinds of futile treatment (Article 16) and by ruling the patient’s consent (Articles 33-38). The decision is made difficult in practical terms, because the Italian scientific community is divided with respect to the classification of artificial nutrition and hydration as being considered "basic care" or "medical
3 Zullo, S., 2010, Interruzione delle cure e morte cerebrale. Profili bioetici e filosofici In Faralli, C., 2010, Biodiritto. Problemi, casi e materiali, Torino: Giappichelli Editore, pp. 122-131.
4 Italian Constitutional Court, decision n. 282/02 of 19 June 2002, in Official Journal, July 3, 2002.
5 Italian Constitutional Court, decision n. 307/90 of 14 June 1990, in Official Journal, June 27, 1990.
Medicine and Law 580
treatment". The “Oleari Commission” formed by the Minister of Health in 2000, states that artificial nutrition and hydration constitute medical treatment6. Meanwhile, the National Bioethics Committee in its document of September 2005 argues that artificial nutrition and hydration are basic care7, implying that cases, as the withdrawal of artificial ventilation, may be punishable as active euthanasia.
It is necessary to review the classification of artificial nutrition and hydration as being basic care or medical treatment. If qualified as medical treatment, and unless there is an emergency or a necessity, the patient’s consent is mandatory to start it. Furthermore, if considered as medical treatment and the patient requests to stop artificial nutrition and hydration, withdrawing treatment by the doctor will not be considered as homicide of the consenting person (article 579 PC).
Since the reality of new medical discoveries of the last decades puts forward novel ethical and legal issues that were previously dictated by natural law8, end-of-life decision-making has become, nowadays, an integral part of the public philosophical discourse. The existence of new technologies pushes us to re-examine and re-consider the physician’s duty of care and the patient’s rights.
3. WITHDRAWING TREATMENT FROM AN INCOMPETENT PATIENT AND THE IMPORTANCE OF ADVANCE DIRECTIVES
The complexity of legal and ethical issues concerning withdrawing treatment from an incompetent patient arises from the need to reconstruct the patient’s will. Lawyers claim that withdrawing treatment from an incompetent patient fulfils all the objective and subjective criteria for the act to be classified as a crime. This is a direct result of the acceptance of the idea of self-determination
6 Casini, M., Di Pietro, M. L. and Casini, C., 2007, Profili storici del dibattito italiano sul testamento biologico ed esame comparato dei disegni di legge all’esame della XII Commissione (igiene e sanità) del Senato. Medicina Morale, 1, pp. 19-60.
7 Presidenza del Consiglio dei Ministri, Comitato Nazionale per la Bioetica, 2005, L’alimentazione e l’idratazione nei pazienti in stato vegetativo permanente. [online] Available at: http://www.palazzochigi.it/bioetica/testi/PEG.pdf. (accessed on DATA!) This document received many critics and thirteen members (out of thirty-five in total) redact a dissenting statement in which artificial alimentation and hydration were considered as medical treatment.
8 Rodotà, S., 2006, La vita e le regole, tra diritto e non diritto, Bologna: Feltrinelli.

Medicine and Law 581
and of the ethical decision to choose the exact time to die. The majority of them believe that “letting die” cannot be punished because despite the facts being similar to those of homicide of the consenting person (article 579 PC), there is the exculpation act of fulfilment of duty (article 51 PC)9. However, conservative lawyers argue that humans do not have the moral right to die and therefore in case of incompetent patient, even if the patient has, during some point of his life given consent, there is the necessity to save the patient’s life (article 54 PC). In these cases the doctor is neither liable for kidnapping nor duress (articles 605, 610 and 613 of PC)10.
In Italy, the most famous case of withdrawing treatment from an incompetent patient is that of Eluana Englaro (25th November 1970 - 9th February 2009) from Lecco, who, following a car accident, entered into a PVS on the 18thof January 1992. The case of Englaro is also similar to that of Quilan (29th March 1954 - 11thJune 11, 1985) in the USA. Mr. Beppino Englaro asked, for the first time in 1999, the Tribunal of Lecco to discontinue Eluana's hydration and nutrition supply. The Tribunal of Lecco11 and the Court of Appeal of Milan12 dismissed the case because of the absence of any legislation regarding withdrawing treatment from an incompetent patient. According to the judges, Article 2 of the Italian Constitution gives absolute and imperative protection of the right to life. Even the Court of Cassation13, based on the absence of a special guardian or guardian in litem (administratore di sostegno) to confirm withdrawing treatment as the patient’s own decision, dismissed the case in 2005.
Even after Franca Alessio was appointed as a special guardian, the Tribunal of Lecce, based on the fact that an incompetent patient lacks the right to reject medical treatment, declined Mr. Englaro’s second request to stop life-sustaining treatment. Moreover, according to this decree, supplied hydration and nutrition is not a medical treatment but basic care14. The Court of Appeal
9 Canestrari, S., 2003, Le diverse tipologie di eutanasia. Riv. It. Med. Leg. XXV, pp. 751-775.
10 Iadecola, G., 2003, Note critiche in tema di “testamento biologico”, Riv. It. Med. Leg. XXV, p. 477.
11 Tribunal of Lecco, Persons, minors and family sector, decree n. 59/99 of 1 March 1999.12 Court of Appeal of Milan, Persons, minors and family sector, decree n. 99/99 of 31
December 1999.13 Court of Cassation, section I civil, ordinance n. 8291 of 10 April 2005. 14 Tribunal of Lecco, section 1 civil, decree n. 1094/05 of 20 December 2005.
Medicine and Law 582
of Milan15 reversed the Tribunal’s decision by declaring that everyone has the right to reject medical treatment, but, in this concrete case, the evidence was insufficient to clearly indicate that Ms. Eluana Englaro would have wanted to terminate her medically supplied nutrition and hydration. Mr. Beppino Englaro continued his legal battle, and on the 16th of October 2007 the Court of Cassation16 decided that judges could authorise removal of life-sustaining treatment for patients who have been declared incompetent when two conditions are met: (1) it is clear that the patient is in a PVS; and (2) it can be determined by clear and convincing evidence, provided by the patient’s representative and based on knowledge of the patient’s lifestyle, personality and conviction that the patient would not wish to be kept alive through artificial means. In the case of Eluana Engluaro the second condition was hardest to satisfy. As it can be understood, based on the difficulty of the issue, the Court did not conclude whether artificial nutrition and hydration are medical treatment or basic care.
Thus, “advance directives” assume a big importance, because this might be the only way of increasing the patient’s autonomy, or, as in Englaro's case, to understand the patient’s desire. Furthermore, advance directives play down the distinction between basic and medical treatment, or between proportional and excessive medical invasion17. It should further be noted, that the concept of ‘actual wish’ should not be chronologically limited to the nearest future, but should be considered as the last wish of the patient18.
Additionally, advance directives can’t be considered as part of the concepts of ‘right to die’ or euthanasia. This is confirmed by empirical evidence from the Netherlands. Here, euthanasia is legal and there exist two different types of advance directives: one for the medical treatment that the person would like or would not like to have in case of incompetence which can be considered as part of informed consent, and the other concerning euthanasia19. Further, Balestra20 concludes that the introduction of living will or advance directives
15 Court of Appeal of Milan, section I civil, decree of 16 December 2006. 16 Court of Cassation, decree n. 21748 of 16 October 2006.17 Lecaldano E., 2005, Bioetica. Le scelte morali, Bari-Roma: Laterza, p. 59.18 This is based on the advice of the Italian National Bioethics Committee of December
2003 and on Giunta, F., 1997, Diritto di morire e diritto penale. I termini di una relazione problematica. Rivista Italiana del diritto e della procedura penale, p. 108.
19 Vezzoni, C., 2005, The legal status and social practice of treatment directives in the Netherlands, Groningen: RUG (Rijksuniversiteit Groningen).
20 Balestra, L., Efficacia del testamento biologico e ruolo del medico, In VV: AA. (edited by Fondazione Veronesi), 2006, Il testamento biologico: riflessioni di dieci giuristi, Milano, pp. 89-106.

Medicine and Law 583
in the Italian legal system has no connection to the legalization of euthanasia.
The role of advance directives has been recognized within the Charter of Self-Determination approved by the Italian National Bioethics Committee on February 1992, and included in the Italian Medical Ethics Code in 2006. The advance directive has to be precise, authentic and spontaneous, and should be reviewed by a group of medical experts. There is no space for a doctor’s discretional opinion21. A small group of lawyers, such as Rodotà22, believe that advance directives should have blinding legal force. According to Rodotà, advance directives are an expression of the patient’s autonomy and, when provided, the doctor's position remains a discreet one. Moreover, in case a doctor acts against the patient’s advance directives, a judge’s decision shall be based on the validity of these advance directives. In addition, according to Amato23, advance directives should have blinding force to avoid loopholes within the legal system. The recognition of blinding force solely for withholding or withdrawing treatment from a competent patient means that an unconscious person may not be considered a human being and all his wishes may lose their validity.
Other lawyers, such as Balestra24, argue against the blinding force of advance directives as this may interfere in the doctor’s duty of care. Based on this argument, although Article 38 of the Italian Medical Ethics Code considers the importance of advance directives it does not give them a blinding force.
Meanwhile, Article 9 of the Convention of Oviedo states that the wishes of the incompetent patient should be taken into account. However, it should be noted that the “European Convention on Human Rights and Biomedicine” has been approved but not ratified in Italy. Therefore, this convention can be used as an interpretative resource and not as “source of law”25. Finally, Article 38
21 Canestrari, S., 2003, Le diverse tipologie di eutanasia. Riv. It. Med. Leg. XXV, pp. 751-775.
22 Rodotà, S., 2006, La vita e le regole, tra diritto e non diritto, Bologna: Feltrinelli. 23 Vincenti Amato, D., Il silenzio della legge e il testamento di vita, In VV: AA. (edited by
Fondazione Veronesi), 2006, Il testamento biologico: riflessioni di dieci giuristi, Milano, pp. 177-188.
24 Balestra, L., Efficacia del testamento biologico e ruolo del medico, In VV: AA. (edited by Fondazione Veronesi), 2006, Il testamento biologico: riflessioni di dieci giuristi, Milano, pp. 89-106.
25 Faenza, F., 2010, Il rifiuto informato di cure salvavita: il caso del paziente in stato d’incoscienza in Faralli, C., 2010, Biodiritto. Problemi, casi e materiali, Torino: Giappichelli Editore, pp. 148-151.

Medicine and Law 584
of the Italian Medical Ethics Code highlights the importance of the advance wishes too.
In case of advance directives, the weight of a doctor’s word is limited. By recognizing the importance of advance directives and by limiting weight given to a doctor’s decision a balance between duty of care and patient’s self-determination is created. With respect to advance directives, Patti26 highlights the limitation of the patients’ lack of knowledge regarding medical treatment they might need in the future.
According the Italian National Bioethics Committee’s27 advice, even in cases of planning the medical treatment of a patient who is suffering from a chronic illness, advance directives are not reliable. According to this advice, advance directives cannot be considered as a blinding force. The doctor has to take into account the patient’s wishes, but he is not obliged to follow them.
What is sure is that advance directives cannot be considered with blinding force until there is no specific law specifying their form, content, temporal validity and the degree of right that the person would have. The idea of a doctor having to follow a patient's wish; based on an advance directive; written by a competent person and on informed consent, is here put forward, as a competent person who has expressed his wish must be trusted to have taken responsibility toward himself in case of a future state of unconsciousness and to have chosen his own best and revokable interest Advance directive has to be specific and clear unless the patient’s best interest is to be decided by a group of doctors. Advance directives should exist in writing and avoid any space for interpretation. Further, they should avoid bureaucratic and expensive procedures by being signed with no need for notary verification. Moreover, the decision has to be based on informed consent as the only way to ensure patient’s autonomy, avoid paternal influence approaches and exclude advance directives of general or abstract nature.
26 Patti, S., 2006, L’autonomia decisionale della persona alla fine della vita, In VV: AA. (edited by Fondazione Veronesi), 2006, Il testamento biologico: riflessioni di dieci giuristi, Milano, pp. 1-14.
27 The advice of the Italian National Bioethics Committee about Advance Directives is available in: http://www.sitiarcheologici.palazzochigi.it/www.governo.it/maggio%202006/www.governo.it/bioetica/testi/Dichiarazioni_anticipate_trattamento.pdf

Medicine and Law 585
4. CONCLUSION
There has been, in the last decades, a remarkable increase in public debate about end-of-life decision making in Italy. Although Article 32 of the Italian Constitution of 1948 recognizes the “right to health”, which grants patients the right to consent to or refuse medical treatment; ethicist and lawyers continue to discuss the morality and legality of withdrawing treatment from an incompetent patient.
Advance directives are here presented as the only instruments able to emphasize a patient’s autonomy and right to his wish. Although the Italian Medical Ethics Code does not grant blinding force, it is here argued that in cases of case-specific advance directives, written by a competent person and based on informed consent, the doctor must follow the patient’s wish. Finally, an individual, through the official expression of his own wishes, takes responsibility of himself even in possible future states of unconsciousness.
Whilst western society is undergoing tremendous change it must be counteracted by a new interpretation of the current norms. Although there is no Italian law directly supporting end-of-life decision making, judges' interpretation of existing laws should be facilitated though the formalization of patients' autonomy with advance directives.

©PROBOOK 2013and Law
Medicine Med Law (2013) 32:587-599
587
EUTHANASIA, ASSISTED DYING AND THE RIGHT TO DIE IN GHANA: A SOCIO-LEGAL ANALYSISErnest Owusu-Dapaa*
Abstract: There is unanimity among states to protect the continuation of life of the individual as a safeguard against their collective extinction. The right to life is accordingly guaranteed but its antithesis, the right to die is the subject of an unending debate. The controversy over the right to die is deepened by rapid advances in medicine, creating the capability for prolongation of life beyond the span which one’s natural strength can endure. Ghana’s supreme law explicitly guarantees the right to life but remains ambiguous on right to die, particularly euthanasia and assisted dying. Thus, some of the other rights, such as the right to dignity and not to be tortured, can creatively be exploited to justify some instances of euthanasia. Ghana’s criminal code largely proscribes euthanasia. Notwithstanding, proscription of euthanasia and assisted dying by the law, in Ghana’s empirical work undertaken in some of the communities in Ghana, suggests that euthanasia is quietly practisedin health facilities and private homes, especially in the rural areas. Contrary to the popular reasons assigned in the literature of the Western world, with respect to the practice or quest for legalization of euthanasia as being a necessity for providing relief from pain or hopeless quality of life, empirical data from social and anthropological studies conducted in Ghana reveal that poverty is the motivation for informal euthanasia practice in Ghana rather than genuine desire on part of patients to die or their relatives to see to their accelerated death. Apart from poverty, traditional cultural values of African societies consider non-natural death as a taboo and ignominy to the victim and his family. Thus, any move by the government to legalize euthanasia will need to be informed by widely held consultations and a possible referendum; otherwise the law may be
* Barrister at Law, Lecturer, Faculty of Law, Kwame Nkrumah University of Science and Technology, Ghana and PhD Candidate, Lancaster University School of Law, UK.
Email: [email protected]. I wish to express my appreciation to Rodrigo Cespedes of Lancaster University School of
Law, for his helpful comments and criticism. I remain solely responsible for all limitations.

Medicine and Law 588
just a mere transplant of Western models of legislation on euthanasia without reflecting the ethos of the African people.
Keywords: Euthanasia; Right to Die; Assisted Dying; Ghana; Sanctity of Life; Criminal Law; Bad Death.
INTRODUCTION
‘Euthanasia is a hotly debated issue in almost every country, even those states with reasonably well settled constitutions find them tested by medico-legal decision at the end of life.'1 The desire for life, to remain alive and keep living is deeply seated in the ethos of human society regardless of geography, race, gender, religion or class. Indeed, life has been mentioned as the first irreducible condition for human flourishing. Indeed, John Finn is has noted that ‘a first basic value, corresponding to the drive for self-preservation, is the value of life.’2 The consensus of the international community after the devastating and grueling World War II culminated in the legal protection of the right to life.3The sanctity of life principle in international human rights law has been one of the prominent bases for advocating the abolition of death penalty.4
Medical advances have unleashed both relief and challenges to human beings everywhere. Geography is no immunity to the radical and sweeping revolution in medical intervention technology. Thus, patients in Ghana can experience the life prolonging capacity of medical advances accomplished in the developed world. In recent times respirators and artificial hydration among others are available to sustain life even beyond what the natural capacity a human body can endure. Advances are so cumulative that the standard definition of biological death is being revised constantly within the medical research world, especially in the light of the medical technology of organ transplantation’s achievements. The concept of death is no longer cast in stone because it shifts
1 M. Davies, Textbook on Medical Law, 2nd ed. (Oxford: Oxford University Press, 1998), p.342.
2 J. Finnis, Natural Law and Natural Rights, 2nd ed., (Oxford: Oxford University Press, 2011), p.86.
3 See Article 3 of the UN Universal Declaration on Human Rights http://www.un.org/en/documents/udhr/index.shtml (last visited: 3/4/2013); Article 6 of the International Covenant on Civil and Political Rights http://www.unhcr.org/refworld/docid/3ae6b3aa0.html (last visited: 3/4/2013).
4 http://www.amnesty.org/en/death-penalty (last visited: 3/4/2013).
Medicine and Law 589
with progress in medical capabilities to sustain life beyond a person’s natural ability to remain alive. For a long time it was thought that the vital functions of a human body were breathing, heartbeat and the capacity for consciousness or sentience; thus, death was understood as the absence of these vital functions.5
However, the introduction of respirator and life support machines meant that the generally accepted medical definition of death in the late 1950s has become obsolete. In 1976 the Royal Colleges of Medicine in England and Wales adopted brain-stem death as the new definition of death.6 The question of the definition of death has several ethical and legal implications. To begin with, the determination of when the dying process begins and ends has significant implications on euthanasia. In this paper, I explore the extent to which euthanasia assisted dying and the right to die exist under Ghanaian law; and the social and anthropological attitudes and ethos of Ghanaians towards the end of life issues. The segment after this general introduction is an exploration of the nature of euthanasia and assisted dying.
UNPACKING EUTHANASIA, ASSISTED DYING AND THE RIGHT TO DIE
It is incontestable that euthanasia remains a phenomenon of universal concern. But what exactly constitutes euthanasia. The term ‘euthanasia’ is succinctly defined in Black’s Law Dictionary as ‘the act or practice of painlessly putting to death persons suffering from incurable and distressing disease as an act of mercy.’7 This definition is consistent with the etymology of the term. Etymologically, 'euthanasia' originates from the Greek words, eu (good) and thantos (death).8Physician assisted dying is the practice of a doctor or healthcare professional providing the means for a patient to end his own life. Subject to the relationship between the roles of the doctor and the patient, we may have voluntary active euthanasia, passive euthanasia and involuntary euthanasia.9
5 I. Kennedy, The Unmasking of Medicine (England: St Albans, 1983), pp.162-1646 Ibid.7 H. C. Black, Black’s Law Dictionary, 16th edn, (St Paul Minn-West Publishing Co,
(1991)), p. 554.8 S. Ost, An Analytical Study of the Legal, Moral, and Ethical Aspects of the Living
Phenomenon of Euthanasia, (Lampter: Edwin Mellen Press, 2003), p.15.9 J.K. Mason, G.T. Laurie, Mason and McCall Smith’s Law and Medical Ethics, 6th ed.
(Oxford: Oxford University Press, 2006), p.566.
Medicine and Law 590
Voluntary active euthanasia refers to ‘hastening one’s own death by use of drugs or other means, with a doctor’s direct assistance.’10 On the other hand passive euthanasia connotes’ hastening death by withdrawing life sustaining treatment and letting nature take its course.’ Involuntary euthanasia involves causing or accelerating the death of someone who has not asked for assistance with dying, such as a persistent vegetative patient. The right to die is the very antithesis of the right to life. It is clear that all the various forms of euthanasia including assisted dying fall within the ambit of the right to die but it is possible for some other forms of death to be subsumed under the right to die. It is submitted that the right to die should be narrowly understood to encapsulate only those instances of death meant to alleviate pain and suffering in a situation where there is no hope whatsoever of being restored to meaningful life. To that extent, right to life, euthanasia and assisted dying are not mutually exclusive strictosensu.
There is no consensus as to the rightness or wrongness11 of helping someone to die.12A positive act leading to death as euthanasia was unequivocally denounced by Bingham, MR, in the English case of Airedale NHS Trust v Bland, which deals with the issue of removal of life support from a patient in a persistent or permanent vegetative state. His Lordship considered that such practice is not about euthanasia, if by that is meant the taking of positive action to cause death. It is not about putting down the old and infirm, the mentally defective or the physically imperfect. It has nothing to do with the eugenic practices associated with fascist Germany.13
IS EUTHANASIA LEGALISED IN GHANA?
There is no direct legal framework for lawful euthanasia in Ghana. The default provision of the law as reflected in disparate statutory and customary law
10 S. C. Chima, A Primer on Medical Law, Bioethics & Human Rights for African Scholars (Durban- SA: Chimason Educational Books, 2011), 324.
11 Pretty v. the United Kingdom (Application no. 2346/02) (2002)35 EHRR 1; , Sue Rodriguez v A-G of British Columbia 107 DLR (4th ), 342 ; Also see Dr Jack Kevorkian who assisted over 100 euthanasia cases http://www.pbs.org/wgbh/pages/frontline/kevorkian/chronology.html (last visited: 1/4/2013)
12 A. Norrie, ‘Legal Form and Moral Judgment: The Problem of Euthanasia’ March 23, 2010). Warwick School of Law Research Paper No. 2010-05. Available at SSRN: http://ssrn.com/abstract=1577163 or http://dx.doi.org/10.2139/ssrn.157716 (last visited 1/4/2013).
13 [1993] 1 All ER 821.

Medicine and Law 591
provisions is proscription of euthanasia. It is important to survey the laws of Ghana which are relevant to the subject in order to bolster this observation that Ghanaian law, by default, outlaws euthanasia.
The search for the legal position on euthanasia in Ghana must begin from the 1992’s Constitution (hereinafter‘ the Constitution’), which is the fundamental and supreme law of the land.14 The right to life is guaranteed by the Constitution. Article 13 of the Constitution stipulates:
1. No person shall be deprived of his life intentionally except in the exercise of the execution of a sentence of a court in respect of a criminal offence under the laws of Ghana of which he has been convicted.’
2. A person shall not be held to have deprived another person of his life in contravention of clause (1) of this article if that other person dies as the result of a lawful act of war or if that other person dies as the result of the use of force to such an extent as is reasonably justifiable in the particular circumstances.- (a) for the defence of any person from violence or for the defence of property; or (b) in order to effect a lawful arrest or to prevent the escape of a person lawfully detained; or (c) for the purposes of suppressing a riot, insurrection or mutiny; or (d) in order to prevent the commission of a crime by that person.15
The wording of the provision suggests that it is deprivation or termination of a person’s life by another which is generally outlawed by the Constitution. Thus a doctor or any person who seeks to assist a suffering patient even in a persistent vegetative state in Ghana could be guilty of depriving another person’s life contrary to the provision in Article 13 of the Constitution. In one leading English case16, a health authority responsible for the treatment of a persistent vegetative state patient brought an application to the court for a declaration that it and the responsible physicians could lawfully discontinue all life-sustaining treatment and medical support measures designed to keep the patient alive in his existing PVS, including ventilation, nutrition and hydration by artificial means.17 The House of Lords granted the declaration but reiterated the need for doctors to seek the guidance of the courts before
14 1992 Constitution of the Republic of Ghana (Accra, Assembly Press, 1992), Art.2.15 1992 Constitution.16 By virtue of colonial connection, Ghana’s legal system is based upon the common law
tradition. English decisions are of persuasive authority.17 Airedale NHS Trust v Bland [1993] 1 All ER 821.
Medicine and Law 592
withholding treatment in such cases.18 The trial judge in Bland, Sir Stephen Brown P, noted that the term persistent vegetative state (PVS) was first coined in 1972 by some medical professors to ‘describe a syndrome that was being increasingly encountered as the life-saving and life-sustaining technologies of intensive care were securing the survival of some patients with brain damage of a severity that would previously have proved fatal.’19
Commenting on article 3 of the European Convention on Human Rights (ECHR) which is substantially in pari material with Article 13 of the Constitution, Suzanne Ost rightly contended that although euthanasia does not fall within the permitted derogations of the provision on right to life, the fact that ‘there are circumstances in which the deprivation of life does not amount to a breach of this Article provides indication that the right to life is not an absolute right.’20 Indeed, if the right to life is not so sacrosanct or absolute, then it is apposite to explore other provisions of the Constitution for support or rejection of euthanasia, assisted dying or right to die.
The right to personal dignity under the constitution is worth exploring to ascertain if it lends some support to the right to die or euthanasia in Ghana. Article 13 states that:
No person shall, whether or not he is arrested, restricted or retained, be subjected to -(a) torture or other cruel, inhuman or degrading treatment or punishment; (b) any other condition that detracts or is likely to detract from his dignity and worth as a human being.21
This provision raises interesting possible interpretations which may provide some support for the antithesis of the right to life, that is, right to die or euthanasia and assisted dying. It may be contended that a refusal to terminate the life of a suffering patient in irretrievably excruciating terminal condition may constitute violation of the right not to be subjected to torture or un-dignifying treatment. Reflecting on a similar provision in Article 3 of ECHR, Ost noted that it may be theoretically possible to construe omission
18 Airedale NHS Trust v Bland [1993] 1 All ER 821 at 874 per Lord Goff of Chieveley; at 880 per Lord Brown-Wilkinson.
19 Airedale NHS Trust v Bland [1993] 1 All ER 821 at 82720 S. Ost, ‘Conceptions of the Euthanasia Phenomenon: A Comparative Discussion of the
Law, Individual Rights and Morality within Three Jurisdictions,’ (2000) 5 Journal of Civil Liberties 155, 158; Also see generally, B. Brody, ‘Life and Death Decision Making,' (Oxford: Oxford University Press, 1988).
21 1992 Constitution.
Medicine and Law 593
by doctors to end a suffering patient’s life as cruel treatment.22She opines that such possibility may exist where a suffering patient who feels humiliated by his condition voluntarily requests for assistance to die from the doctor. Notwithstanding, the persuasiveness of Ost’s argument, the derivative right to die based upon right to personal dignity, has not yet been tested in health care related litigation in Ghana.
Apart from the constitutional provisions, it is apposite to explore the extent to which the practice of euthanasia is prohibited or permitted by other statutes of Ghana. The Criminal Code of Ghana, 1960 (Act 29) is the most relevant piece of legislation which needs to be analysed here. Sections 42,23 47, 52 and 57 are the material provisions of Act 29 with respect to exploration of euthanasia and assisted suicide. The infliction of harm may be justified by consent under Act 29, but section 42 expressly excludes consent as a justification for killing another person. Thus, euthanasia and assisted dying may not be justified by merely pleading consent. Also, a patient who does not succeed in terminating his life shall be guilty of attempted suicide, punishable as misdemeanour under section 47(2) of Act 29.
However, any person who abets the commission of attempted suicide, that is assisted dying in medical law taxonomy, is guilty of first degree felony punishable by life imprisonment.24According to section 20 of Act 29, ‘every person who, directly or indirectly, instigates, commands, counsels, procures, solicits, or in any manner purposely aids, facilitates, encourages, or promotes, whether by his act or presence or otherwise, and every person who does any act for the purpose of aiding, facilitating, encouraging or promoting the
22 Ost, n.24 above, p. 159.23 Section 42 - ‘The use of force against a person may be justified on the ground of his
consent, but - (a) the killing of a person cannot be justified on the ground of consent;
(b) a wound or grievous harm cannot be justified on the ground of consent, unless the consent is given, and the wound or harm is caused, in good faith, for the purposes or in the course of medical or surgical treatment. (c) consent to the use of force for the purposes of medical or surgical treatment does not extend to any improper or negligent treatment. (e) if a person is intoxicated or insensible, or is from any cause unable to give or withhold consent, any force is justifiable which is used, in good faith and without negligence, for the purposes of medical or surgical treatment or otherwise for his benefit, unless some person authorised by him or by law to give or refuse consent on his behalf dissents from the use of that force;’
24 Criminal Code, 1960 (Act 29), s. 47 (1).
Medicine and Law 594
commission of a crime by any other person, whether known or unknown, certain or uncertain, is guilty of abetting that crime, and of abetting the other person in respect of that crime.’
The import of this provision in the context of end of life discourse is that it is not only the doctor or health care professional that may be liable for the offence of attempted suicide but relatives of the patients who aided or facilitated or anyway encouraged the provision of assistance towards the termination of the patient’s life are equally culpable as accessories.
What remains unclear from statutory law in Ghana is the extent to which the use of force (such as painless in relation to insensate patients) can be used to bring an end to suffering.
There appears to be an ambiguity in the law which can be exploited to justify a limited version of euthanasia in Ghana. Section 42 of Act 30 stipulates:
The use of force against a person may be justified on the ground of his consent, but -
(e) if a person is intoxicated or insensible, or is from any cause unable to give or withhold consent, any force is justifiable which is used, in good faith and without negligence, for the purposes of medical or surgical treatment or otherwise for his benefit, unless some person authorised by him or by law to give or refuse consent on his behalf dissents from the use of that force.
A close analysis of the above provision reveals a certain degree of ambiguity which can be interpreted liberally to encapsulate some forms of euthanasia in Ghana particularly in relation to persistent or permanent vegetative state patients as was noted above in relation to Bland. It is striking that the law does not limit application of force to only medical or surgical treatment but also ‘otherwise for his benefit’. It is submitted that the provisions tacitly recognises that it is not all the time that medical or surgical therapy may achieve the traditional purpose for restoration of health.
Indeed, in the case of medical futility where therapeutic intervention does not in any way prolongs life or relief pain it may be beneficial to the patient in some situations to exit. Thus, the phrase ‘otherwise for his benefit’ is quite elastic as it stands until a court of law has competently interpreted it. A number

Medicine and Law 595
of questions arise from the potential import of that phrase. Can termination of life in a severe and excruciating pain with no hope of recovery be considered as benefiting that patient? Can a patient who does not have means to afford palliative care be assisted to die for his benefit? The answers to these questions cannot be known until the provisions have been tested in a court of law. A search conducted in all the law reports in Ghana as at January, 2013 did not reveal any decided case in relation to this provision. An equally important test for operationalization of the justification in section 42 of Act 29 is whether the doctor or healthcare professional acted in good faith.
The determination of good faith in this context may impinge on issues of medical ethics and in particular the Hippocratic Oath which doctors in Ghana subscribe before being enrolled. I submit that the doctrine of double effect established in 1957 by the English case, R v Bokin Adams25 may properly be invoked under Section 42(e) of Act 29 to exculpate liability for physician assisted death in appropriate situations.26 The doctrine is basically that a doctor is not culpable where in discharging his primary obligation in treating terminally ill patient; he administers a form of treatment for his patient’s benefit with the awareness that it has secondary effect of accelerating or likely to accelerate the patient’s death.27 In 1957, Dr. John Bodkin Adams was tried for the murder of an eighty-four year old woman in his care, who had named him as beneficiary in her will. The patient was terminally ill and succumbed following the administration of large doses of narcotics prescribed by Dr. Adams. Other similar cases were also suspected in his practice. Devlin J advised the jury that, regardless of the health of the victim and the motive of the accused, the law would treat as murder any action which intended to kill and did in fact kill. Despite this he also ruled that if the first purpose of medicine, the restoration of health, can no longer be achieved there is still much for a doctor to do, and he is entitled to do all that is proper and necessary to relieve pain and suffering, even if the measures he takes may incidentally shorten human life.28
25 [1957] Crim. L R. 365.26 This decision can be a persuasive authority in Ghanaian court since Ghana’s Criminal
Code was passed in 1960 barely three years after the Bodkin Adams case.27 I. Kennedy, ‘The Law Relating to the Treatment of the Terminally ill’ in I. Kennedy, Treat
Me Right - Essays in Medical Law and Ethics (Oxford: Oxford University Press, 1988), ch.16, p.325.
28 [1957] Crim. L R. 365.
Medicine and Law 596
Regardless of the interpretive window of opportunity lending support for a certain degree of euthanasia and assisted dying in Ghana, it remains a mere conjecture or phantom of legal speculation until a court of competent jurisdiction has pronounced upon the matter. Consequently, the current position is that Ghanaian law, by default, proscribes euthanasia and assisted dying in all its forms.
The rational of the default position of the law in Ghana in preventing euthanasia is not clearly discernible. However, we can situate the legal position in the moral context. Two competing moral arguments may be explored. The sanctity of life theory holds that life must be protected and sustained under all conditions possible.29 It trumps even the right of the individual to self-determination or autonomy. The sanctity of life argument postulates further that human being is a relational being such that there is an important sense in which a person’s life is not just her own but also belongs to the group of which she is part of.30 The countervailing argument to sanctity of life is the libertarian notions of autonomy. It has been argued that the autonomy of a person should find expression in the exercise of his or her self-determination to life or die especially having regard to irretrievably diminished quality of life.31 Thus, a person can exercise his or her autonomy and choose one’s own death in terms of time and place. In this way, a person is able to have a good death which underscores the etymology of euthanasia, that is eu (good) and thantos (death).
THE VIEWS OF GHANAIANS ON EUTHANASIA AND ASSISTED DYING FROM SOCIO-ANTHROPOLOGICAL STUDIES
Euthanasia occurs in Ghana in various forms. Geest has noted that certain family members continue to request physicians to withhold care from their relatives because of lack of funds to sustain such treatment.32 Whereas in the developed countries euthanasia is undertaken predominantly to end suffering
29 A. O. Nwafor, ‘Comparative Perspective on Euthanasia in Nigeria and Ethiopia,’ (2010) 18 Africa Journal of Comparative and International Law, 170, 173.
30 A. Norrie, n.15 above, p.3.31 Mason, Laurie, n.9 above, ch.18.32 S. Van der Geest ‘I want to go: How elderly people in Ghana look forward to death’
(2002) 22(1) Ageing and Society, 7-28.
Medicine and Law 597
of a patient in irretrievably difficult medical condition,33 the motivation for instances of euthanasia in Africa, and in particular Ghana, is probably more of poverty, inability to meet medical bills and inadequacy of health care facilities than the need to release patient from suffering.34
According to empirical research undertaken by other scholars, there is a divided sociological and anthropological opinion on the phenomenon of euthanasia in Ghana. A properly contextualised understanding of the debate on euthanasia in Ghana ought to begin from understanding the perceptions of Ghanaians on death and dying due to the inextricable linkage between the two stages of the same phenomena.35 The inevitability of death is beyond realm of disputation due to the ultimate immortality of humankind.36 In his empirical studies conducted in 2002 Van der Geestidentified two kinds of deaths in the Kwahu-Tafo region of Ghana, namely ‘good death’ and ‘bad death.’37 An individuals who lived a descent life and died naturally is said to have had a good death.38 On the contrary, an individual is considered to have had a bad death if he or she died through an unnatural cause such as accidents, suicide or a woman who dies during childbirth.39 It is a widely held view in Ghana that euthanasia is a form of suicide and is therefore considered a ‘bad death.’40
Euthanasia which is generally categorised by people in Ghana as bad death has unpleasant consequences for the deceased and his or her relatives. Agyemang has noted that it attracts incalculable shame and social stigma upon the existing family.41 Due to weak law enforcement coupled with the predominantly rural areas where euthanasia often takes place in Ghana, it is the adverse social consequences rather than the deterrence potential of law which discourage rampant resort to euthanasia even in the face of poverty and lack of adequate
33 Ost, n. 8 above.34 K. Agyemang, ‘The Impact of new medical technology upon attitudes towards euthanasia
among Akans, Cultural Heritage and Contemporary Change, http://www.crvp.org/book/Series02/II-5/chapter_ix.htm (last visited: 6/4/2013)
35 M. Luguterah, The Experiences and Perceptions of Ghanaian Medical Professionals towards the Practice of Passive Euthanasia in Ghana (Cappella University, PhD Dissertation: 2012), p.32-33.
36 F. Brennan, ‘Palliative Care as an International Human Right’ (2007) 33(5) Journal of Pain and Symptom Management, 494-499.
37 Van der Geest, n.31 above, p.20.38 Ibid.39 Ibid.40 Agyemang, n.33 above.41 Ibid.
Medicine and Law 598
health care facilities. Moreover, the heavily religious and traditional nature of Ghanaian society even in modern times suggest that practice of euthanasia is against what the people consider to be the wishes of the Almighty God. Indeed, an empirical survey in the rural town of Kwahu-Tafo in Southern Ghana confirmed that euthanasia was not accepted as a possible means of death because both the young and old held the view that life and death are and should remain in God’s hands.42 This finding is further corroborated by the philosophical reflection on the impact of new medical technology by Kwasi Agyeman:
The absolute sanctity and dignity of life, as well as reverence for life, and the analytic claim that every event has a cause, are among the everyday truisms which go unquestioned even when state-of-the-art medical wonders appear to challenge the given realities of the natural world. Such convictions concerning nkrabea or destiny run contrary to approving of euthanasia.43
CONCLUSION
It is undoubted that society is readily jealous to protect the continuation of human life as a safeguard against its collective extinction. The right to life is accordingly guaranteed but its antithesis, the right to die is the subject of unending debate. The controversy over the right to die is deepened by rapid advances in medicine creating the capability for prolongation of life beyond the span one’s natural strength can endure. Ghana’s supreme law, the constitution, explicitly guarantees the right to life but remains ambiguous on the right to die, particularly euthanasia and assisted dying.
Thus, some of the other rights, such as the right to dignity and not to be tortured, can creatively be exploited to justify some instances of euthanasia. But no court has yet taken that stance. The statute law, particularly Ghana’s criminal code, largely proscribes euthanasia. Notwithstanding, proscription of euthanasia and assisted dying by the law in Ghana’s empirical work undertaken in some of the communities in Ghana, suggests that euthanasia is quietlypractisedin health facilities and private homes, especially in the rural areas. Due to generally weak law enforcement in Ghana, there is no decided case on euthanasia or assisted dying in Ghana. Contrary, to the popular
42 Van der Geest, n.31.43 Agyemang, n.33 above.

Medicine and Law 599
reasons assigned in the literature of the Western world for the practice or quest for euthanasia being a relief from pain or hopeless quality of life, empirical data from social and anthropological studies conducted in Ghana reveal that poverty is the motivation for informal euthanasia practice in Ghana rather than genuine desire on part of patients to die or their relatives to see to their accelerated death.
Apart from poverty, traditional cultural values of African societies consider non-natural death as a taboo and ignominy to the victim and his family. Thus, any move by the government to legalize euthanasia will need to be informed by widely held consultations and a possible referendum; otherwise the law may be just a mere transplant of Western models of legislation on euthanasia without reflecting the ethos of the people.

©PROBOOK 2013and Law
Medicine Med Law (2013) 32:601-614
601
NOTES ON PATIENTS WITH DISABILITIES AUTONOMY IN SPANISH LAWMaría Luisa Arcos*
Abstract: The UN Convention on the Rights of Persons with Disabilities recognizes as the first of its general principles the “Respect for inherent dignity, individual autonomy including the freedom to make one’s own choice, and independence of persons” (Art.3.a). With regard to health, States Parties recognize that persons with disabilities have the right to the enjoyment of the highest attainable standard of health without being discriminated on the basis of disability (Article 25), which includes requiring health professionals to provide care of the same quality to persons with disabilities as to others, including on the basis of free and informed consent (subsection d).These guidelines must enlighten the interpretation of the Spanish legal system as for the scope of autonomy of people with disabilities. Nevertheless, they still bear some handicaps in order to preserve their autonomy from third-party interferences.
Keywords: Persons with Disabilities; Autonomy; Informed Consent; Advanced Directives, Third-Party Intervention, End-of-Life Decisions.
1. DIGNITY, AUTONOMY AND DISABILITY
According to the international instruments on human rights approved since the Universal Declaration of Human Rights of 1948, Art. 10.1 of the Spanish Constitution (1978) states the principle of human dignity1, on which the fundamental rights and the principle of patient’s autonomy are based2. The
* Tenured Professor of Civil Law, Public University of Navarra (Spain). Email: [email protected] This article is framed within the research project entitled “Rethinking the principle of
autonomy in Health Law and its limits; specially, freedom to choose and conscientious objection” (DER2012-32735), funded by the Spanish Ministry of Economy and Competitiveness (2013-2015).
1 Art. 10.1: “The dignity of the person, the inviolable rights which are inherent, the free development of the personality, the respect for the law and for the rights of others are the foundation of political order and social peace”
2 Art. 1 Council of Europe Convention for the Protection of Human Rights and Dignity of the Human Being with regard to the Application of Biology and Medicine.
Medicine and Law 602
regulation of the right to clinical information, informed consent and advanced directives is, consequently, lying in the intrinsic worth of human being that implies equality and respect for the individuals’ integrity and for their capacity to take their own decisions3.
Regarding disability, the Spanish Constitution received the prevailing model at that time, which considered persons with disabilities as people who were basically perceived as ill and in need of help because of their impairments4. This model aimed to “rehabilitate” these persons and so reintegrate them into the “normal-people” society, which adopted a paternalistic attitude in relation to “their” problem and tried to sort it out5. The model, frequently described as “medical model”, also corresponded with the hierarchical relationship between the doctor and the handicapped person, thus the latter has scarcely any control about the decisions concerning his/her life.
Since the last quarter of the past century this “medical model” of disability has, at an international level, been losing relevance in front of the “social model”.
This new perspective emphasizes that the society consists of persons with functional diversity, and every one must be accepted as he/she is. People with disabilities should receive the assistance they need while always respecting, as much as possible, their autonomy, understood as the ability to guide one’s life, as this is one of the components of human dignity. Nobody should take anyone’s place in charge of his/her life unless it is imperative.
On May 3, 2008 entered into force the UN Convention on the Rights of Persons with Disabilities (CRPD) which is going to spread a wide range of consequences in every State Party, both at a legal and a social level. This binding international instrument reflects that new approach to disability6,recognizing that it is an evolving concept which shall be now considered from the perspective of the human rights.
3 Art. 2.1 Law 41/2002, of 14th November, on patient’s autonomy and on rights and obligations with regard to clinical information and documentation.
4 Art. 49: “The public authorities shall carry out a policy of preventive care, treatment, rehabilitation and integration of the physically, sensorially and mentally handicapped by giving them the specialized care they require, and affording them special protection for the enjoyment of the rights granted by this Part to all citizens”.
5 Palacios, A.: El modelo social de discapacidad: orígenes, caracterización y plasmación en la Convención Internacional sobre los Derechos de las Personas con Discapacidad, Colección CERMI, nº 6, 2008, p. 66 ss.
6 Palacios, A: op.cit., p. 313 ss.
Medicine and Law 603
The Convention affirms that disability is the result of the interaction between the individual with some impairment and the barriers existing in the society to which the former belongs. Obviously, the result of this interaction will vary as a consequence of modifying either the physical, mental or sensory personal conditions or the circumstances in which people must develop their lives. So, the more and harder physical and attitudinal barriers and obstaclesst and in a given society, the more people will not be able to overcome them7.
On the contrary, reducing these barriers will decrease the impact of disability, which hinders persons with impairments from reaching the highest level of autonomy in every sphere of their lives. The CRPD aims to redress what is seen as a “profound social disadvantage to persons with disabilities” and to enforce these people’s rights in a number of fields such as education, employment, privacy and access to justice, among others. The Convention also states their right “to the enjoyment of the highest attainable standard of health without being discriminated on the basis of disability” (Art. 25), which includes requiring health professionals to provide care of the same quality to persons with disabilities as to others, including on the basis of free and informed consent (subsection d).
The core regulation on patient’s autonomy in Spanish Law is set out in the Law 14/1986, of 25th April, on Health (LGS), and in the Law 41/2002, of 14thNovember, on Patient’s Autonomy and on Rights and Obligations with regard to Clinical Information and Documentation (LBAP)8. Based on the binding effect of the CRPD and on the obligations that it imposes to the State Parties9, the Spanish Parliament has passed the Law 26/2011, of 1st August, the purpose of which is adapting Spanish Law to the requirements laid down by the Convention10.
Both Law 14/1986 and Law 41/2002 are among the nineteen Acts that have been modified, although in these two cases the reforms have not been
7 See “Inequalities and multiple discrimination in access to and quality of healthcare”, European Union Agency for Fundamental Rights, 2013.
8 Both are national laws, implemented by regional regulation.9 Art. 4 CRPD: among others, to adopt all appropriate legislative, administrative and other
measures for the implementation of the rights recognized in the Convention; and to take all appropriate measures, including legislation, to modify or abolish existing laws, regulations, customs and practices that constitute discrimination against persons with disabilities.
10 Each region shall adapt its pre-existing regulation to the CPRD within their constitutional competences (D.Ad. 1st of Law 26/2011).
Medicine and Law 604
substantial. Basically, they deal about: (1) explicitly including disability among the personal circumstances that don’t justify any kind of unfair discrimination-reform that was not strictly needed11, and; (2) adding to several articles12 that the information shall be given in accessible formats according to the principles of the Design for All or Universal Design13.
Recently, three regions have passed laws on rights and guarantees of the dying person’s dignity, all of them later than the entry into force of the CRPD: Andalucía (Law 2/2010, of 8th March -LAndDGDPM-), Aragón (Law 10/2011, of 24th March -LArDGDPM-) and Navarra (Law 8/2011, of 24th
March -LFDGDPM-).
Analyzing the legal frame of end-of-life decisions of patients with disabilities imposes distinguishing, as for the rest of patients, the right to clinical information, the right to consent or to refuse the treatment, and the right to explain their will by giving advanced directives. The respect to personality, human dignity and privacy, and the proscription of discrimination of persons with disabilities are guidelines to take account of in any case.
2. THE RIGHT TO CLINICAL INFORMATION.
Every patient, with or without disabilities, has the right to be informed of everything that is related to his/her health unless he/she prefers to refuse receipt of the information14 or where doctors, based on objective reasons, notice that this would seriously worsen their health conditions15.
The LBAP states also that the information shall be given in a comprehensible way according to every patient’s needs16 which, in my opinion, is one of the guidelines of the legal system, reflecting the special interest with regard to persons with disabilities. This Law lays down such obligation expressly as
11 Art. 10.1 LGS12 Art. 10.2 LGS, Art. 9.5 LBAP, several articles of Law 14/2006, of 26th May (Human
assisted reproduction techniques), and Art. 4 Law 30/1979, of 27th October (Organs Donation and Transplantation).
13 As explained by CRPD, "Universal design" means the design of products, environments, programmes and services to be usable by all people, to the greatest extent possible, without the need for adaptation or specialized design.
14 Art. 4.1 LBAP.15 Art. 5.4 LBAP.16 Art. 4.2 LBAP.
Medicine and Law 605
regards incompetence: also in this case the patient shall be informed as far as possible depending on his/her capacity to understand the information and to take decisions17.This principle does not change at all for dying patients, so that they shall receive the information about their process according to their ability to understand it18.
Consequently, the obligation to inform that concerns the healthcare professional entails making an effort to adapt the information to the patient’s circumstances, that is, looking for the way to communicate with him/her.
Contrary to Art. 25.d CRPD, avoiding to do that effort under the pretext of the patient’s disability means, on one hand, not to provide care “of the same quality to persons with disabilities as to others, including on the basis of free and informed consent”. On the other hand, in a certain number of cases, it also means to interpose a third-party to whom personal information is going to be disclosed regardless of the patient’s opinion: it must be taken into account that, in general, a third-party (even closest relatives) could be informed only to the degree that the patient allows it explicitly or tacitly19. So before making such a decision, the healthcare professional must be able to justify the impossibility of establishing an effective communication with his/her patient.
As stated in Art. 12.3 CRPD “States Parties shall take appropriate measures to provide access by persons with disabilities to the support they may require in exercising their legal capacity”, what is of special interest for persons with physical or sensory disabilities but intellectually able to make a decision. For instance, sign-languages interpreter services should be, where possible, offered to a deaf patient as an option in front of requesting anyone else’s intervention20; more efforts could be probably done to translate into Braille information useful to blind patients, so they could have documents at their disposal21; and so on.
17 Art. 5.2 LBAP.18 Art. 6 LFDGDPM, Art. 6 LAndDGDPM, and Art. 6 LArDGDPM.19 Art. 5.1 LBAP.20 The Law 27/2007, of 23rd October, regulates Spanish sign-languages and the oral
communication support facilities for deaf and blind-and-deaf people, and people with hearing disabilities.
21 The number of initiatives is increasing in the last years. For instance, in 2008 instructions of care needed after discharge were translated into Braille in Valencia; in 2009 the Punta de Europa Hospital (Cádiz) has translated into Braille information of Clinical and Biochemical Laboratory.

Medicine and Law 606
A case considered in the judgment of the Spanish Supreme Court of July 14th, 2004, dealt with a man affected by a complete tetraplegia who was unable to speak or write. His cognitive and volitional abilities were undamaged and he was able to read and to understand what he read or heard. His only way to communicate with others was by moving his eyes: someone stood in front of him with a paper in which the alphabet is written, and slowly pointed at each of the letters until the patient moved the eyes up and down, and selected the letter he wanted. This process had to be repeated as many times as letters were needed to express the patient’s thought. The man was declared totally incompetent, albeit the possibility to communicate existed and it would have been more effective with the appropriate instruments and measures. Even without them, however, in my opinion every medical treatment should require the patient’s previous informed consent.
When a patient is not able to properly understand the information, it will be given to a third-party. That condition - incompetence - must be established with enough certainty: either because the patient is a minor under the age of making his/her own decisions, or because he/she has been legally declared incompetent, or because that is the professional opinion. In the second case (people legally declared incompetent) the judgment shall state the kind of acts that the person cannot carry out by his/herself and, then, whether he/she needs to be replaced by a legal representative or merely assisted by a curator.
The national Law does not state any criteria to guide de doctor’s decision on the patient’s incompetence, but regional Laws on end-of-life process do22. Among other factors, it will be taken into account if the patient has difficulty understanding the information, retains it or not, use it logically or not, realize it or not what would be the consequences of every option and, finally, if he/she can make a decision and communicate it.
In assessing the patient’s competence, the doctor can take into consideration another professionals’ opinion (necessarily, in LFDGDPM), and consult the family (it is an obligation in LArDGDPM) or even the loved ones (LFDGDPM). Either way, some guidelines, deriving from the principle of human dignity, must be taken into account. Firstly, reaching the conclusion of the lack of someone’s capacity must be based on certainty: if in doubt, the patient’s incompetence must not be presumed. Secondly, every judgment or rule dealing with restrictions to legal capacity must be interpreted restrictively.
22 Art. 20 LArDGDPM, Art. 19LFDGDPM, Art. 20 LAndDGDPM.

Medicine and Law 607
And over all, every decision on behalf of a person with disabilities who is unable to consent must always be adopted in his/her best interest.
When the patient has a legal representative (parents, tutor), or a curator, this person will receive the information. If not, relatives or unmarried partners will be informed23. Since the national Law does not specify any order or legal preference at this point, the doctor’s criteria should inevitably be adopted in consideration to the patient’s personal environment and the doctor’s professional experience. It seems obvious that the person designated by the patient as his/her representative in the advanced directives should logically be the only person, except for the patient, to be informed. In any other cases, the preferences stated in regional Laws regarding information to dying patients can be useful: representative appointed in advanced directives, legal representative, married or unmarried partner, and closest relatives. Two of the Laws lay down that the older person will be preferred among the same-degree relatives but, in a more reasonable way, the LArDGDPM gives preference to the relative in charge of the patient24. Finally, the judicial authority can appoint the person25 it deem the fittest.
The patient can also refuse to be informed26 but in absence of such a decision the information must be given to him/her according to the previous rules, even to persons with disabilities or in process of dying27.
3. THE RIGHT TO INFORMED CONSENT
The right to informed consent, as the patient’s right to allow any kind of healthcare after being informed28,requires the capacity of making one’s own free will, which could be not sufficient in persons with disabilities. This capacity will vary, depending on both the seriousness of the patient’s conditions and the complexity and potential risks of the medical intervention29.
23 Art. 5.3 LBAP.24 Art. 10.1.25 Art. 10 LArDGDPM, Art. 11 LFDGDPM.26 Art. 4.1 LBAP.27 Art. 10.3 LAndDGDPM, Art. 7 LFDGDPM, Art. 10.3 LArDGDPM.28 The basic information to be given will include the nature and purpose of the medical
intervention, its certain relevant consequences, risks involved (those specific for each patient -in view of his/her personal or professional circumstances-, and the likely ones under normal conditions) and contraindications (Arts. 4 and 10.1 LBAP).
29 This is why minors can consent by themselves if they are mentally and emotionally capable of understanding the importance of the planned intervention: Art. 9.3.c LBAP, a contrario.
Medicine and Law 608
In relation to persons with disabilities the same principle must be applied as required by Art. 12.2 CRPD, which lays down that “States Parties shall recognize that persons with disabilities enjoy legal capacity on an equal basis with others in all aspects of life”. The only reform introduced in the LBAP as a result of CRPD is just on informed consent. Based on the new Art. 9.5, if the patient is a person with disability, supporting measures shall be offered to him/her, including information in appropriate formats according to the principles of the Universal Design and in such a way that the information becomes accessible and understandable, so that the patient can give the informed consent by himself/herself.
If the patient with disability has been legally declared incompetent, it will be necessary to carefully analyze the judgment in order to know if the ability of giving informed consent is or not included among the acts or decisions out of the patient’s competence, or if he/she needs to be assisted -but not replaced -for that purpose by a third-party30. In case of patients with disabilities not legally declared incompetent, the doctor’s opinion31, as said for clinical information, is decisive for determining whether they are or not naturally incompetent to make the required decisions or to realize their actual situation.
One of the following representatives is to be appointed if the patient is not able to consent: the one appointed in advanced directives, the legal representative (parents, tutor) or, finally, relatives or unmarried partners. Just like the right to information, any legal order that can guide the doctor’s choice regarding the right to consent, lacks in the national Law; however, unlike that right, relatives or unmarried partners are not merely receiving information but making a decision on the patient’s healthcare. As seen in relation to the right to be informed, the order laid down by regional Laws on end-of-life decisions could be helpful to the doctor.
The respect for patient’s dignity gains special relevance when the decision to make is part of the dying process. People who are in this situation have also the right to make their own decisions32, and the incompetence on the basis of a disability must be reduced to the minimum. The scope of the patient’s autonomy includes the right to refuse a treatment or to revoke a previous
30 The Art. 9.3.a LBAP must be interpreted as stating that a third-party is going to give informed consent if the patient has been legally declared incompetent just for giving it for his/her own.
31 This is referred to the doctor in charge of the patient.32 Art. 7.2 LArDGDPM, Art. 7.1 LAndDGDPM.
Medicine and Law 609
consent, even if it endangers his/her life33, but adopting such a decision requires being aware of its consequences.
When the patient is not able to consent, the refusal or withdrawal could be decided by a third-party, adducing to act according to the patient’s will. If the doctors think that this decision is against the patient’s interests or rights, then they should inform the judicial authority34, which is not going to happen if both family or representatives and doctors are in agreement35. The problems related to the patient’s consent or refusal to treatment are, at an international level, of special importance in case of persons with mental problems36.
4. THE RIGHT TO THE RESPECT FORPATIENT’S ADVANCED DIRECTIVES
Based on Art. 9 of the Convention on Human Rights and Biomedicine,37 the LBAP admitted the patient’s right to the respect of his/her will in regard to healthcare preferences, even in case of current incompetence, provided this will had previously been expressed, in writing.
The advanced directives on living wills are especially useful in foreseeing one’s end-of-life scene, taking advantage of the current autonomy for organizing that moment. Moreover, they can avoid burdening closest relatives and family environment with the responsibility of taking very difficult decisions. They also contribute some helpful guidelines to the third-party who has to take that decisions, and can be used to settle the issue of who is entitled to decide instead of the patient. Finally, by giving an advanced directives document a patient that becomes unable to consent or refuse any healthcare remains in charge of his/her life to the end, getting any kind of treatment (for instance, life sustaining treatment) he/she may want or, on the contrary, not being forced
33 Art. 8 LAndDGDPM, Art. 8 LArDGDPM, Art. 8LFDGDPM.34 Beltrán, J.L.: “La relación médico-paciente en situaciones de riesgo grave, de enfermedad
invalidante e irreversible, y en el proceso del final de la vida: supuestos y respuestas bioéticas y jurídicas”, Revista Aranzadi Civil, 6/2011.
35 About the scope of the problem -in United States- of third-parties decisions regarding disabled patients’ healthcare, see Carson, D.; Smith, C., Wilker, N.: “Devaluing People with Disabilities. Medical procedures that violate civil rights”, National Disability Rights Network, may 2012.
36 “Involuntary placement and involuntary treatment of persons with mental health problems”, Eurpean Union Agency for Fundamental Rights (FRA), 2012.
37 Convention (Council of Europe) for the Protection of Human Rights and Dignity of the Human Being with regard to the Application of Biology and Medicine.
Medicine and Law 610
to undergo unwanted medical procedures..
As it represents a decision about the healthcare one person wants - or not - to receive, the effectiveness of such a document requires also the capacity of making one’s own free will. In fact, at a national level, an advanced directives document could be binding upon health professionals only if given by people over the age of eighteen38, capable and free: that is, it requires the full capacity to act.
On one hand, the advanced directives document is an interesting precautionary measure against the risk of lacking in the future the capacity to take decisions or when the patient knows that he/she is suffering from a progressive and disabling disease. Unfortunately, however, it has not had as much an impact as it would be expected39.
On the other hand, this possibility can be precluded for a number of people with disabilities, as Spanish statements are limited to written advanced directives and these ones require full capacity to act. Nevertheless, neither professionals, nor the family should ignore the disabled patient’s preferences, if they know them.
Several reasons base this duty. Art. 9 of the Convention on Human Rights and Biomedicine stated the need of taking into account the patients’ previously expressed wishes, without limiting it to written wishes. This formal requirement is essential from the perspective of the burden of proof in case of conflict, and, when necessary, for imposing its content in front of third-parties’ opinions, but it must not justify acting against the patient’s known will.
The LBAP states that every patient, even in case of being replaced by a legal representative, shall participate as far as possible in the healthcare decision-making process40. There is no reason to restrict this principle to current
38 Art. 11.1 LBAP. It does not seem coherent with allowing sixteen year-old minors to give informed consent by their own. However, certain minors are able to give this document regarding to regional laws. For instance, in Navarre that is possible for sixteen year-old people.
39 Recently, “The previously expressed wishes relating to health care. Common principles and differing rules in national legal systems”, Steering Committee on Bioethics (CDBI), Report 2008. In Navarra less than 1900 documents have been registered in the last ten years. Although it must be taken into account that it is not necessary to register such documents, the population in this region is about 650.000. In Andalucía the registered documents are around 23.400 for a population of more than 8.400.000.
40 Art. 9.5.

Medicine and Law 611
processes. Given that in these cases patients with disabilities must be informed and at least heard, their expressed wishes will, should they become absolutely unable to express them by themselves, continue to echo. This is the way in which a third-party can respect the replaced patient’s dignity, a respect always due. Regarding people with disabilities, the CRPD demands the respect for their inherent dignity, individual autonomy including the freedom to make one's own choices, and independence (Art. 3.a CRPD). Regarding people in process of death, regional Spanish legislation states that should a third-party make a decision on behalf of the patient, the former shall decide on the basis of both the advanced directives and the will that the patient would express in case of being able to do it41.
In addition, regarding Spanish laws, the advanced directives document could be given with the sole assistance of witnesses. Even being required that these persons are of age, fully competent and not very close relatives42, the effectiveness of the document - given the general requirements, such as the patient’s age - relies on them. While they are supposed to confirm the patient’s competence for deciding about healthcare preferences, a medical opinion is needed in this case. The lack of professional control could be in favor of or against the disabled patient’s interests, although it can be assumed that it is more likely that witnesses will be well-disposed to the patient’s preferences.
5. CONCLUSIONS
Once the dignity of every person is recognized at a constitutional level, the entire legal system should be consistent with this fundamental principle and the society should act accordingly. This means that negative impact of the impairments on people’s life should be reduced to a minimum, respecting as much as possible the scope of their legal capacity and their personal autonomy. Yet, even in industrialized countries, some important tasks remain undone. A healthcare of the same quality provided to the rest of the society concerning the patient’s autonomy is one of them.
Regarding to healthcare, it is time to remember all those demands that some decades ago put an end to the misunderstood medical paternalism. Even being ill, week and ignorant, people asserted their rights, their autonomy
41 Art. 11.4 LFDGDPM, Art. 10.4 LArDGDPM, Art. 9.5 LAndDGDPM.42 In Navarra, Art. 55 Law 17/2010, of 8th November: three people, at least two of them not
having any economic relation with the patient, nor being even a second-degree relative.
Medicine and Law 612
and their dignity against the imposition of others’ decision on what was the best for them. Now it is the turn of people with disabilities, their rights, their autonomy and their dignity, and the CRPD is an important step forward in this process.
©PROBOOK 2013and Law
Medicine Med Law (2013) 32:613-634
613
Index Volume 32 No 4
Vol 32 No PageAAdvance Directives 2 175
3 373, 376-8, 389, 393, 401, 414, 416-21
4 443-6, 448-9, 451-3, 456, 458-9, 466-7, 469, 493, 496, 498-501, 515-7, 521, 541, 577, 580, 582-5
Altruism 1 115, 119-21, 123-7, 129Alzheimer 2 209
3 389, 391-2, 401, 404-5, 415-64 497
Attitudes 1 11, 60, 81, 106, 115, 118-21, 123-7, 129
2 163, 169, 202 3 281, 283-4, 287, 303 4 461, 549-51, 553, 556-8, 589
Assessment 1 36, 39-40, 46, 48, 50, 52, 119 2 141, 143-4, 146, 148-50, 152,
1813 262, 273, 280, 327, 341, 403 4 549, 556
Assisted Dying 4 481-4, 486, 489, 494, 587-90, 592-3, 596, 598
Assisted-Suicide 4 503Asylum 3 327, 329-30, 335-9, 341Auschwitz 2 140, 191-3, 196-200, 203Authenticity 2 153, 156-9, 161
Medicine and Law 614
Index Volume 32 No 4 (Continued)
Vol 32 No PageAutonomy 2 153-162, 170, 173, 180, 199
3 242, 244, 247, 251-4, 281, 289, 305, 313, 315, 376, 400, 404-5, 414-5, 417
4 429-30, 432, 437, 439-40, 459-60, 462, 464-6, 468, 470-3, 476, 478-9, 482, 486-7, 490-1, 494, 496-8, 501, 515-6, 519-22, 538-9, 541, 543, 550, 556-7, 559, 569, 574, 577,579, 582-5, 596, 601-3, 608-9, 611-2
Avastin 1 65-74
BBad Death 4 588, 597Bioethics 1 1, 6, 10
2 139, 141, 151, 153-5, 158, 162-6, 168-70, 172-3, 175-6, 200, 205-6, 208-10
3 235, 248, 252, 254, 305, 3914 473, 481, 483, 488, 498, 517,
577-80, 583-4Brazil 4 473, 481-7, 495, 515, 521, 541-2,
544Brazilian Law 4 459, 467, 517Brüstle v Greenpeace 3 347-8, 354, 365, 372
615Medicine and Law
Index Volume 32 No 4 (Continued)
Vol 32 No PageCCapacity 1 11, 36-9, 45, 47, 51-2, 57
2 155-8, 160-1, 166, 179 3 325, 335, 338, 386, 400-4, 414,
416-84 435, 437-8, 483, 486, 490, 493-4,
496-7, 499-500, 537, 541, 543, 545-7, 588-9, 602, 605-8, 610-1
Choice 1 68, 96, 112 2 158, 162, 191, 193-4, 201, 203,
211 3 272, 312-3, 330, 401, 413 4 442, 447, 449, 460, 462, 465,
469, 477-9, 490, 503, 532, 539, 555, 601, 608
Clinical Bias 2 205Clinical Case
Consultations2 205
Clinical Ethics 2 141-2, 152, 159, 161-2, 175, 207, 212
4 451Communism 2 191, 195Comparative Law 4 550Computerized Medical
Records Systems 1 14
(Human) Connections 3 327, 330, 334-6, 339, 342, 344Constitutionally
Protected Right to Die
4 441-2
Medicine and Law 616
Index Volume 32 No 4 (Continued)
Vol 32 No PageConsultation 1 23, 106
2 141-4, 146-52, 205, 208-103 272, 282, 4124 471, 485, 499
Control 1 25, 39, 42, 49, 54, 60, 80, 1112 141, 148, 152, 160, 179, 2013 252-3, 263, 270, 321-2, 344, 353,
366, 377, 416 4 449, 470, 474, 477-8, 484-5, 493,
497-8, 507, 543, 602, 611Cost 1 65, 68-71, 74
2 141, 144-50, 1543 2514 432, 477
Criminal Law 1 33, 35-6, 45, 512 217, 2214 436, 489, 496, 525-9, 531, 535,
567, 569, 571, 588Criminal Responsibility 1 33, 37-8, 40, 44, 49, 52
4 462Critical Reasoning 3 305Cryobank 3 252, 267Culture 1 88-9, 106
2 146, 156, 169, 193, 206-73 248, 291, 303, 327, 333-5, 337,
343-4, 352, 3814 461, 463, 483, 550, 555, 557-8,
574
617Medicine and Law
Index Volume 32 No 4 (Continued)
Vol 32 No PageDDamages 3 239
4 439, 441-2, 448, 452, 454-5, 457-8
Death 1 5, 8, 10-1, 45, 86, 88, 117-8, 120, 122
2 163, 168, 180, 182, 185-6, 191-3,198-202, 215-8, 220-2, 224-9
3 258-9, 265-8, 294, 300, 335, 340, 387, 397
4 434-9, 442, 452, 456, 460-3, 465, 468-70, 472-5, 477-8, 482-3, 485, 487, 490-1, 494, 496, 500, 504-7, 510-3, 515, 518, 520-1, 527-9, 532, 535-9, 544, 553, 555-6, 558, 568-70, 572-3, 576-9, 587-90, 595-9, 611
Dementia 1 603 389, 391-3, 397, 399, 401, 404,
407, 414-5, 4214 431, 497, 501
Diffusion of Innovation 1 14Discernment 2 175
4 541Dissociative Identity
Disorder1 33, 35, 37, 39-42, 49-52
Do Not Resuscitate Order
3 378
4 441
Medicine and Law 618
Index Volume 32 No 4 (Continued)
Vol 32 No PageDonor Anonymity 1 95-6, 98-101, 105, 107, 109,
112-3Donor Relations 1 95, 107-9, 111DSR 1 95, 103, 109, 111-3Duress 2 156
3 3394 577, 581
Dutch NICU-Practice 2 215
EEducation 1 8, 11, 91, 112, 121
2 146, 1933 241, 248, 288, 292, 305, 379-80,
4214 484, 558, 603
Elders 3 389, 398-400, 403, 414, 416, 420Empirical Research 1 14
2 143 4 597
End-of-Life 1 1172 145, 222 4 458-62, 472, 476, 481, 483-4,
487, 490-4, 496, 503-4, 508, 511, 520, 528-9, 547, 549, 550, 557-8, 567, 569-70, 573, 576, 588-9, 594
End-of-Life Care 2 2213 373, 377, 381 4 450, 481, 483, 550
619Medicine and Law
Index Volume 32 No 4 (Continued)
Vol 32 No PageEnd-of-Life Choice Bill 4 503, 508End-of-Life Decisions 2 215-6, 218-9, 221-2
4 496, 550-1, 555, 558-9, 601, 604, 608
Ethical Decisions 2 143, 2053 283, 306 4 550
Ethical Principles 2 1643 236-7, 249, 252-4, 273-4, 3154 519, 559, 575
Ethics 1 1, 8-10, 53, 1082 142-4, 146-50, 159, 161-3, 165-
6, 168, 171-3, 175-6, 184-5, 191, 193, 196, 199-201, 203, 206-8, 212
3 235-46, 248-55, 259-61, 263, 266, 268, 271, 273-4, 277, 282, 284-5, 305-6, 312, 314-5, 322, 330, 337, 342, 367, 377, 389-91, 395, 399, 407
4 451, 472, 479, 481, 487, 498-9, 516, 559, 575
ECatPB = Ethics Committee at the Patient’s Bedside
3 277-85
Ethics Discourses 3 277Euthanasia 1 3-4
2 251, 289
Medicine and Law 620
Vol 32 No PageEuthanasia (continued) 4 437, 461-2, 472, 478, 481-90,
495, 500, 503-7, 510-3, 518, 525-31, 534, 536, 539, 568, 570-4, 577, 579-80, 582-3, 587-94, 596-9
Evaluation 1 21, 74, 952 141, 143, 145, 2273 250, 330, 337, 341-2, 3474 537, 549, 559
Experience 1 14, 27-8, 30, 43, 68, 70, 722 163-6, 168, 174, 191-2, 201, 207,
209 3 247, 250, 253, 266, 279, 285,
288, 302, 306, 311, 316, 332, 337-8, 341, 343, 380, 383-4, 415
4 429, 439, 459, 474-5, 485, 487, 549, 570-1, 574, 588, 607
FFamilies 1 53, 79, 95-7, 104, 107, 109, 112-
3, 1162 150, 211-23 284, 330, 373-6, 378, 381-3, 385,
3874 473, 482, 489, 550, 552, 557
France 1 142 1983 319-20, 322, 324, 357, 3614 466, 530, 542
Index Volume 32 No 4 (Continued)
621Medicine and Law
Vol 32 No PageGGamete Donation 1 95, 99-101, 106, 109Ghana 4 587-8, 590-9Guardians 1 7
3 277, 281, 284
HHealth 1 1-4, 7, 10, 13-30, 40, 43, 46, 48,
50, 57, 59, 61, 65, 71-2, 74, 91, 98, 100-2, 104, 106, 110, 121-3, 126, 128-9
2 144-5, 151, 170, 172, 177, 180, 184-7, 189, 195, 210-1, 216, 227
3 236, 248, 254, 265, 269, 271, 279, 287-8, 290, 294, 296, 300-1, 305-6, 310, 313-6, 319-21, 324-6, 330, 332, 349, 353, 367, 373-7, 379-81, 383-4, 387-8, 393-4, 396-9, 406-7, 410, 412-3, 418
4 431, 433, 437, 441-5, 447-8, 450-4, 457-8, 465, 467-71, 473, 475-8, 482, 484-7, 489-90, 496-7, 500-1, 521, 537, 547, 549-50, 555-6, 558-9, 577-80, 585, 587, 591, 593, 595, 597-8, 601, 603-4, 610
Health Authorities 1 65, 71, 74, 106Health Care Ethics 3 288
Index Volume 32 No 4 (Continued)
Medicine and Law 622
Vol 32 No PageHealth Care Providers 1 13-7, 19-30
2 180, 1853 373-7, 379-814 443-5, 448, 451, 454, 501
Health Care Proxy 4 451, 497, 500-1Health Legislation 1 14, 46Hermeneutics 2 164-5, 169Heuristic 2 150, 211
3 327, 336, 344History of Medicine 3 288-9Holocaust 1 1-2, 8-10
2 191, 202Homicide 2 217, 227
4 482, 493, 495, 509, 527, 530, 532-3, 537-8, 568, 571, 573, 577, 579-81
Homicide upon Request 4 525, 527, 530-2, 534, 537, 539Homeostasis 4 567-8, 574-5Human Dignity 1 47, 107
2 191, 193, 198, 203 3 320, 356-7, 368, 3724 472-3, 478-9, 495-6, 501, 515,
518-20, 536, 568, 601-2, 604, 606
Human Embryonic Stem Cells
3 347-9, 351-3, 355, 360, 363
Index Volume 32 No 4 (Continued)
623Medicine and Law
Vol 32 No PageHusband 1 96
2 196, 2103 252-3, 255-60, 263-6, 3004 443
IIncompetent Patient 4 430, 577, 579-81, 583, 585Influenza 2 177-9, 183-5, 187-9
3 299Informed Consent 1 73-4, 119
2 1703 277, 281, 284, 289, 389, 393-4,
400-1, 408, 411, 420 4 430, 438, 440, 453, 456, 459-60,
465, 471, 497, 500, 529, 549, 556, 558, 582, 584-5, 601-3, 605-8
Informed Consent and Informed Refusal (decision-making)
3 277
(Specific) Intent 3 264, 267-8, 327, 330, 335-6, 343Israel 1 10, 55-7, 59, 61, 95, 97, 101-5,
107, 109, 115-7, 119, 122, 127 3 237, 239, 244, 245, 247-8
JJewish Pre-Modern
Society 3 288
Judaism 1 116-72 191-3, 199-201
Index Volume 32 No 4 (Continued)
Medicine and Law 624
Vol 32 No PageJustice 1 1, 10, 49, 53, 95, 102
2 170, 184, 2013 252, 279, 327, 336, 338, 347, 396,
403, 4164 487, 603
KKidnapping 1 46, 48
4 577, 581Knowledge Level 1 115, 129
LLaw 1 1, 3-5, 10, 33, 35-7, 40, 45, 48-9,
51-3, 61, 68, 72-4, 87, 101-3, 107, 116-7, 121
2 172, 202, 217, 221, 228 3 235-40, 242-4, 246-7, 250-1, 253-
4, 256, 258, 260, 263, 265, 267, 281, 284, 298, 300, 310, 319-20, 322, 324, 327, 330, 336, 339, 344, 347- 51, 354, 356-7, 363, 366-8, 371-3, 375-83, 388-9 , 393-6, 398, 401, 405-8, 410-1, 414, 416-8, 422
4 429, 432-3, 436-8, 440, 444-6, 451, 453, 456-8, 459-60, 463, 465-8, 470, 472, 478, 481-3, 485, 489-90, 492-3, 495-505, 508-9, 511-3, 517, 521, 525-9, 531, 535, 541-3, 545-7, 550, 567-71, 575-6, 578-80, 583-5, 587-91, 593-601, 603-4, 606-8
Index Volume 32 No 4 (Continued)
625Medicine and Law
Vol 32 No PageLegal 1 13-7, 19-21, 23-30, 33, 36-7, 39-
40, 48-53, 55, 57-8, 60, 65-6, 73, 84, 95, 102, 105, 111, 113, 117
2 141, 149, 172, 202, 209, 215-8, 221-5, 227-9
3 235-9, 242-3, 247, 250-2, 255-6, 267-8, 273, 281, 298, 300, 305, 309, 319, 322-4, 326, 329, 335, 337, 342-3, 348-9, 353, 358, 364-5, 372-3, 375, 377-8, 380-3, 389-90, 394, 398-402, 406, 408, 417-22
4 429-30, 432, 435-9, 441, 452, 459-64, 467-71, 479, 481-92, 495-8, 502-3, 507-13, 516, 518-22, 527, 531, 533, 541-4, 546, 550, 555, 568, 571, 573, 576-7, 578, 580, 582-3, 587-91, 596, 601-2, 604-8, 610-1
Legal Aspects 1 532 215-6, 2214 462
Leges Artis 4 567-70Legislation 1 19, 24, 26, 28, 30, 46, 57, 59, 67,
72, 101, 1052 1423 241, 252-5, 257-61, 266-7, 273,
349, 356-7, 373-5, 377-9, 382, 387, 393-5, 406, 408-10, 418, 420
Index Volume 32 No 4 (Continued)
Medicine and Law 626
Vol 32 No PageLegislation (continued) 4 432, 435, 437, 440-1, 443-4, 451,
455-9, 462, 467-8, 490, 494-5, 507, 515-6, 521, 525, 527, 529-30, 541-2, 544-6, 573, 581, 588, 593, 599, 611
Living Will 3 3844 444-5, 448, 451-2, 454-6, 459,
464, 497-501, 516, 541, 543-6, 582
Lucentis 1 65-6, 68-72, 74
MMaltreatment of Older
Persons1 53, 61
Meaning 1 2, 40, 1202 147, 153-9, 161-6, 168-76,
193,199, 2223 282, 330, 335-6, 338, 341-2, 347-
8, 356, 3714 431-2, 437, 518, 526, 528-9, 533,
539, 542, 571-2Medical Education 1 1
4 558Medical Ethics 1 9
2 184, 2083 238, 240-1, 246, 253, 274, 306,
3214 469, 471, 473, 477-8, 516-8, 521,
567-8, 575, 577, 579, 583-5, 595
Index Volume 32 No 4 (Continued)
627Medicine and Law
Vol 32 No PageMedical Law 3 253
4 567-8, 576, 593Medical Staff (health
workers) 3 277-81, 283, 295
Medication Regimes 2 215-6, 229Medicine 1 2, 4-5, 8-10, 35, 37, 40, 48-9,
67-9, 72, 101, 1082 163-9, 176, 180, 211, 2283 237, 239-40, 252-4, 263, 287-93,
301-2, 325, 331, 337, 382 4 432, 434, 460-1, 463-4, 467-73,
475, 477, 482, 495, 515-8, 525, 527, 539, 558, 567, 572, 578, 587, 589, 595, 598
Moral Distress 3 277-9, 282, 285Morality Clause 3 347-9, 352-6, 359, 366, 368-72
NNeonates 2 215, 218Neutrality 3 305-17Neuroethics 3 389-91, 410, 421Neuroscience 3 389-91, 395-7, 399-402, 404,
408, 412, 414-6, 419-22New Zealand 4 503-10, 512-3
OOff-Label 1 65-9, 71-4Older Persons 1 53-60
3 389-91, 393, 396-402, 405, 407-9, 419-21
Index Volume 32 No 4 (Continued)
Medicine and Law 628
Vol 32 No PageOrgan Donation 1 115-27, 129
3 259Outcome 1 46, 54, 70, 123-5
2 141, 143-52, 1833 261, 274, 3824 451, 461, 466
PPandemic 2 177-9, 183-9Participatory Approach 3 277, 279, 285Patents 3 347-50, 353-4, 356-8, 360-4,
366-7, 369-70, 372 Patient Self-
Determination Act4 441, 451
Pathological Criminal Incapacity
1 33, 35-41, 44, 48-50, 52
Patient Decisions 2 153-4, 159, 1623 386
Pedagogy 3 305, 312Persons with
Disabilities 4 601-5, 607-8
Physician 1 10, 34, 72, 96, 1002 150, 160-1, 183, 207-10, 212,
217, 2253 239, 246, 249, 267, 288-9, 291-8,
300-2, 320, 322-4, 331, 337, 373-4, 376, 384, 387, 410
Index Volume 32 No 4 (Continued)
629Medicine and Law
Vol 32 No PagePhysician (continued) 4 429, 433, 438, 445-7, 449, 463,
469-70, 484, 495, 504, 507, 513, 516-8, 521, 525, 529, 537, 549-50, 553, 555-8, 561-2, 564, 569-74, 576-7, 589, 595
Physician Assisted Suicide
4 507, 525, 537, 553, 557, 562
Policy 1 4, 53, 65-6, 71, 74, 95, 97-9, 101, 104, 106-7
2 144, 170-1, 208, 219, 221, 2233 235-6, 250, 256, 319, 348-51, 353,
358, 360-2, 364, 366-7, 372, 375- 6, 378, 381, 387-9, 393-400, 407- 8, 410, 412-3, 416-7, 419-20, 422
4 449, 453, 484POLST 3 373-88Portugal 3 294
4 466, 497-8, 501, 525, 527, 530, 542, 545, 567
Posthumous 3 251-3, 255, 257-61, 264-8Previously Expressed
Wishes 4 429, 431-2, 439-40
Process 1 1, 10, 19, 66-7, 71, 107, 127 2 141, 143-4, 146, 148, 150-2,158,
164, 167, 175, 180-1, 212, 218-9, 222-6, 229
3 235-7, 246, 250, 256, 280, 284, 290, 299, 316, 329, 335-6, 342, 350, 357, 371, 377, 380, 383, 386, 391, 397, 400-1, 403, 405, 414, 417, 420
Index Volume 32 No 4 (Continued)
Medicine and Law 630
Vol 32 No PageProcess (continued) 4 451, 453, 461, 475-6, 486-7, 489,
500, 520, 549, 555-6, 558, 575, 579, 589, 605-8, 610-2
Procreation 1 1003 251-2, 255, 259-61, 263-6, 268
Professional 1 1, 6-9, 21, 23, 39, 43, 55, 59-602 216-7, 222, 225-6, 228-93 235-6, 238-45, 247-50, 282-5,
290, 298, 305-7, 311, 315, 345, 377, 379-81, 383, 394, 413
4 436, 446, 449, 460, 469, 467, 473-7, 486-7, 494, 516, 537, 569, 589, 594-5, 605-7, 611
Professional Ethics 1 1, 8, 533 235-6, 238-41, 243-4, 246, 250,
288Psychiatry 1 33, 35-6, 40, 52
3 300, 327, 329-30, 336, 339, 344-5
PTSD 3 327, 329, 335-7, 339, 341Public Policy 1 107
2 144, 170-13 256, 348-9, 366, 373-4, 383, 3874 453
qQuality 1 13-4, 17, 21-6, 28-9, 45, 56, 60-1
2 141, 143, 146-52, 194, 201, 210 3 272, 319, 321, 338, 413
Index Volume 32 No 4 (Continued)
631Medicine and Law
Vol 32 No PageRRashomon 2 205, 207-8, 211Recruitment Strategies 1 95, 112Reduction 2 145, 163, 168-9, 174, 186
3 252, 269-71, 3864 462, 532, 568, 570
Regime 1 1, 92 216-7, 221-93 3624 503, 510, 512-3, 525, 533-4
Regulatory 1 65, 67-8, 71, 73-4, 1092 142-3, 165, 171-23 319, 322, 374-6, 378-81, 387-8,
394-54 486
Reform 3 383, 4084 503-4, 508-10, 512-3, 546, 604,
608Relativism 3 305, 313-4Religiosity 1 115, 118-9, 121, 123-4, 128-9Research 1 2-3, 5-6, 14, 19, 25, 27, 29, 37,
42, 53, 55, 66, 89, 95, 101, 104, 110, 112, 125-6
2 141, 143-4, 152, 165, 179, 215-6 3 245, 250, 252, 255, 288, 295,
320, 347-9, 352-3, 357-60, 363-6, 368-72, 374-6, 383, 387, 389-422
4 485-6, 500, 550-1, 558, 588, 597
Index Volume 32 No 4 (Continued)
Medicine and Law 632
Vol 32 No PageResearch Ethics 2 206
3 389-91, 393-7, 402, 412-3, 419Residential Institutions 1 53, 59Right 1 6, 11, 15, 23, 47, 53-4, 74, 79-80,
89, 97, 100, 102-3, 106, 112, 116 2 158, 184, 193, 196-7, 199, 202-3,
207-83 237, 240, 249, 251, 253, 258-60,
264, 267, 270-1, 274, 293, 307-8, 313-4, 316, 319-20, 324, 327, 330, 335-6, 340, 364, 366, 371, 378-9, 413, 416, 419
4 434, 438-40, 442-5, 451, 452-3, 455-7, 459-61, 464-9, 471-3, 477, 479, 481-2, 485-6, 489-92, 495, 497-8, 501, 504, 510, 515, 518-21, 533-6, 539, 541, 544-7, 549, 551, 555, 569, 571, 577-82, 584-5, 587-93, 596, 598, 601-4, 607-9
Right to Choose 2 153, 158-9, 1614 468
Right to Die 4 442-3, 457, 472, 477-8, 481, 486, 490-1, 558, 581-2, 587-8, 592-3
Right to Information 4 550, 608
SSanctity of Lfe 3 271
4 464, 472, 485, 588, 596
Index Volume 32 No 4 (Continued)
633Medicine and Law
Vol 32 No PageSelective 1 81
3 252, 268-71Self-Control 2 153Social Change 4 568Social Value 2 177, 184-6, 188-9
3 241, 245, 247, 249Solidarity 2 176
3 264, 298, 3204 463, 481, 483, 488-9, 492, 496,
501, 519Sperm 1 96, 98-101, 104-6, 109
3 251-3, 255-60, 262-5, 267-8Survivors 1 9
3 327, 329-30, 335, 337, 341-5
TTerminal Patients 4 550The Right to Die 4 441, 457, 472, 481, 486, 520,
536, 579, 587, 589-90, 592, 598 Therapeutic
Jurisprudence3 373-4, 382
Third-Party Intervention
4 601
Tolerance 1 1, 102 2013 305, 309, 313-4
Torture 1 4, 47
Index Volume 32 No 4 (Continued)
Medicine and Law 634
Vol 32 No PageTorture (continued) 2 139, 197
3 310, 327-30, 335-7, 339, 341-5 4 521, 592
Triage 2 177-8, 180-1, 183-5, 188Trust 1 17, 23, 25-6, 28, 107, 111
2 2103 241-2, 247, 249, 255, 257, 305,
311, 313, 317, 3704 487
UUndergraduate Medical
Education3 288
Unlawful 1 44, 553 252, 2564 439
VVoices of Offspring and
Donors1 95
WWithdrawal of
Mechanical Support of Vital Functions
4 429
Withdrawing Treatment 4 577, 580-1, 583, 585
Wrongful Life 4 441-2Wrongful Birth 4 441-2Wrongful Prolongation
of Life4 441-2, 448, 452-4, 456-8
Index Volume 32 No 4 (Continued)

Medicine and Law
Information for Authors
ManuscriptsArticles intended for publication should not exceed 20 manuscript pages, ideally 3000-4000 words including references. They must be written in grammatically correct English and carefully checked before submission. The use of WORD is essential. The printed text on A4 paper must be double-spaced, justified - using Times Roman sized 11 points type - and printed on a laser printer. There should be a wide margin on the left-hand side of the paper only. All pages, including the title page, must be numbered consecutively. Tables, figures and any annexes must be set out on separate sheets, appended to the article. Please send your manuscript by e-mail as an attachment:[email protected]
Title PageThe first page of a manuscript must contain (a) a concise, informative title, (b) name(s) of each author, (c) institutional affiliation(s), and (d) address for correspondence.
Abstract and KeywordsEach article must be prefaced by an abstract of up to 150 words summarizing the main objectives, findings and conclusions. A maximum of ten keywords should follow the abstract.
Abbreviations Should be clearly defined the first time they are used. Full stops should be omitted.
References and BibliographyReferences should be numbered consecutively in the text with a superscript number, this number correlating with each citation set out in a smaller typeface at the foot of each page. All relevant bibliography should appear within the footnotes included in the article, and no separate list of bibliography is allowed to be attached. Authors may use either the ‘Vancouver’ style or the ‘Harvard Law’ style for citations and references.
Peer ReviewArticles will be sent to one or more experts for review at the discretion of the Editor-in-Chief. In all matters of acceptance and publication of any article, the decision of the Editor-in-Chief is to be regarded as final.

Medicine and Law
TablesEach table must be printed on a separate page, typed double-spaced and clearly headed with the title and number corresponding with that in the text. Footnotes to tables should appear directly below the relevant table.
IllustrationsIllustrations and figures should be numbered consecutively and must be referred to in the text. Each must be printed on a separate sheet, including the author’s name and a clear caption. For clarity of reproduction, line drawings are preferable, and photographs may be transmitted digitally by e-mail, each with a separate caption.
PermissionsAuthors must obtain permission in writing to use previously published material, with the exception of brief quotations. Correspondence about such permission must accompany the manuscript. All authors are required to sign a declaration to this effect.
Copyright Submission of a manuscript implies that the work described has not been published before (except in the form of an abstract or as part of a published lecture, review or thesis); that is not under consideration for publication elsewhere; that its publication has been approved by all co-authors, if any, as well as by the responsible authorities at the institute where the work has been carried out (where such approval is required by the institute itself); that, if and when the manuscript is accepted for publication, the authors agree to automatic transfer of the copyright to the publisher; and that the manuscript will not be published elsewhere in any language without the consent of the copyright holders.All articles published in this Journal are protected by copyright, which covers the exclusive rights to edit, reproduce and distribute the article (e.g. as off-prints), as well as all translation rights. No material published in this Journal may be reproduced photographically or stored on microfilm, in electronic data-bases, video disks, etc., without first obtaining written permission from the publisher.The use of general descriptive names, trade names, trademarks, etc., in this publication, even if not specifically identified, does not imply that these names or trademarks are not protected by the relevant laws and regulations.
Medicine and Law
While the advise and information in this Journal is believed to be true and accurate at the date of its going to press. Neither the authors and editors nor the publishers can accept legal responsibility for any errors or omission that my be made.
EthicsSubmission of a manuscript for publication in this Journal confirms that all standard ethics procedures were conducted; such as but not restricted to, voluntary informed consent of research participants when applicable and approval of the responsible Research Ethics Board(s).
GeneralIf you have a query or need advice about presentation or submission of your paper, the Editor-in-Chief may be able to help you. He may be reached by e-mail via [email protected] are more than welcome to view the above-provided information on:http://ichle.com/87091/informationforauthorshttp://thewaml.com/97918/Informationforauthors
Yours Sincerely,
Dr. Mohammed Saif-Alden Wattad, Adv.
Editor-in-Chief
Copyright: Submission of a manuscript implies that the work described has not been published before (except in the form of an abstract or as part of a published lecture, review or thesis); that is not under consideration for publication elsewhere; that its publication has been approved by all co-authors, if any, as well as by the responsible authorities at the institute where the work has been carried out; that, if and when the manuscript is accepted for publication, the authors agree to automatic transfer of the copyright to the publisher; and that the manuscript will not be published elsewhere in any language without the consent of the copyright holders.
All articles published in this journal are protected by copyright, which covers the exclusive rights to edit, reproduce and distribute the article (e.g. as offprints), as well as all translation rights. No material published in this journal may be reproduced photographically or stored on microfilm, in electronic data-bases, video disks, etc., without first obtaining written permission from the publisher.
The use of general descriptive names, trade names, trademarks, etc., in this publication, even if not specifically identified, does not imply that these names or trademarks are not protected by the relevant laws and regulations.
While the advise and information in this journal is believed to be true and accurate at the date of its going to press, neither the authors and editors nor the publishers can accept legal responsibility for any errors or omission that my be made.
Layout by Probook Ltd, P.O.Box 56055, Tel Aviv 61560, Israel, E-Mail: [email protected]
![Euthanasia: legitimate or illegal? A Comparative Review of Euthanasia Under Iranian and Dutch Laws [in Persian] (joint paper)](https://img.pdfslide.net/doc/110x75/635b5984cbf9b0c333064452/euthanasia-legitimate-or-illegal-a-comparative-review-of-euthanasia-under-iranian.jpg)




























